Embed Size (px)
Citation preview
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide PreventionCrisis 2008; Vol. 29(1):20–31© 2008 Hogrefe & Huber Publishers
Research Trends
Self-Reported Suicidal Behaviorand Attitudes Toward Suicide and
Suicide Prevention AmongPsychology Students in Ghana,
Uganda, and NorwayHeidi Hjelmeland1,2, Charity S. Akotia3, Vicki Owens4, Birthe L. Knizek1,
Hilmar Nordvik1, Rose Schroeder5, and Eugene Kinyanda6
1Norwegian University of Science and Technology, Trondheim, Norway, 2Norwegian Institute of PublicHealth, Oslo, Norway, 3University of Ghana, Legon, Accra, Ghana, 4Makerere University, Kampala,
Uganda, 5Austin Community College, Austin, TX, USA, 6MRC/UVRI, Uganda Research Unit on AIDS,Entebbe, Uganda
Abstract. Self-reported suicidal behavior and attitudes toward suicide in psychology students are reported and compared in Ghana,Uganda, and Norway. Small differences only were found in own suicidal behavior. However, experience of suicidal behavior in thesurroundings was more common in Uganda than in Ghana and Norway. Although differences were found between the three countries inattitudes toward suicide, which emphasizes the need for culture-sensitive research and prevention, many of the differences were not asbig as expected. The most pronounced difference was that the Norwegian students were more reluctant to take a stand on these questionscompared to their African counterparts. Some differences were also found between the two African countries. The implications of theresults for suicide prevention in Africa are discussed.
Keywords: suicidal behavior, attitudes, prevention, Africa
After many decades of intensive suicidological research itis clear that there is still a lot we don’t know about themeaning of suicidal behavior. In the article “The meaningof suicide: Implications for research,” Boldt (1988)claimed that “in order to develop valid social scientific the-ories of cause, suicidologists must make a paradigmaticshift from the prevailing universal, invariant definition ofsuicide to systematic research into culture-specific mean-ings of suicide.” Others have also pointed out that we needto obtain a broader view of human behavior than what hasso far been provided by Western-based and ethnocentricgeneralization (e.g., Domino & Perrone, 1993) and that weneed to be cautious in transposing research from one coun-try to another (Leenaars & Domino, 1993). Suicide is in-deed a cultural artefact in that no suicide is committed with-out reference to the prevailing normative standards and at-
titudes of a cultural community (Boldt, 1988). Studyingattitudes toward suicide is one of several gateways in de-veloping an understanding of the meanings of suicidal be-havior in different cultures.
It is also generally contended that attitudes toward suicideare important because they affect the willingness of healthcare staff and/or the willingness of people in general to inter-vene in a suicidal crisis or help those who deliberately harmthemselves (e.g., Bagley & Ramsey, 1989). Moreover, atti-tudes affect both the content and efficiency of the interventionor treatment. Numerous cross-cultural studies have indeedshown that cultural factors do play an important role in atti-tudes toward suicide (e.g., Domino, Niles, & Raj,1993–1994; Domino & Perrone, 1993; Domino & Takahashi,1991; Domino, Lin, & Chang, 1995; Eisler, Wester, Yoshida,& Bianchi, 1999; Eskin, 1995; Leenaars & Domino, 1993).
DOI 10.1027/0227-5910.29.1.20Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers

In these studies, attitudes toward suicide have been comparedbetween European, Asian and American countries. To thebest of our knowledge, only a few studies of attitudes towardsuicide have been undertaken in Africa. Alem, Jacobsson,Kebede, and Kullgren (1999) studied attitudes toward suicid-al people (and not the phenomenon as such) in Ethiopia. Oth-er studies have shown that attitudes toward suicide in Africancountries generally are negative (Lester & Akande, 1994, inNigeria; Peltzer et al., 1998, in South Africa; Eshun, 2003, inGhana).
The present study was conducted in Ghana, Uganda, andNorway. In Ghana, suicide is a crime but since the victimis dead, no prosecution is made. Deliberate self-harm isalso a crime, and thus reported to the police. After the pa-tients are released from hospital, they are prosecuted. Cul-turally, suicide is strongly prohibited, and in certain sub-cultures those who attempt suicide need to go through somepurification rites in an attempt to cleanse the victim and thefamily of the shame and calamity. The stigma suicide car-ries affects not only the individual involved but also fami-lies and even generations. There are no accurate statisticson suicidal behavior in Ghana, so nothing is known aboutthe size of the problem. Suicide is also a crime in Ugandaand it carries enormous stigma. Suicide is considered a badomen for the clan and therefore necessitates cleansing rit-uals. No reliable official statistics on suicidal behavior areavailable in Uganda either. When considering the stigmasuch acts carry, it would be plausible to assume that a num-ber of measures are taken in order to cover up the fact thatsomeone has killed or harmed themselves deliberately inboth these African countries. No official steps have beenmade to start suicide prevention efforts in these countries.Norway, on the other hand, has reliable statistics on suicidalbehavior, and during the last 10 years has had an ongoingnational suicide prevention plan initiated by the Ministryof Health and Social Affairs (Norwegian Board of Health,1996). Suicide might still carry some stigma though.
The main purpose of the present study was thus to pre-sent self-reported suicidal behavior and attitudes towardsuicide and suicide prevention in psychology students inGhana and Uganda, then to compare them with each otherand with a country from the Western part of the world withreliable suicide statistics and a national suicide preventionprogram, namely Norway. Potential gender differences inattitudes were also investigated.
Because not much is known about the prevalence of sui-cidal behavior in Ghana and Uganda, a comparison of suicid-al acts known to students (both their own and others’) can atleast give some indication of the size of the problem when wecompare these figures with figures found in a country withreliable suicide statistics (Norway). Moreover, as pointed outby Eisler et al. (1999) knowledge of attitudes toward suicidein subjects not involved in suicidal behavior can providevaluable predictors of vulnerability and risk factors useful inplanning of prevention programs. Thus, in Ghana and Ugan-da, where virtually nothing officially has been done so far toprevent suicide, the results of the present study may be useful
as a starting point in putting the issue on the agenda andinitiating suicide preventive efforts. Psychology studentswere chosen both because they are future key personnel intreating suicidal persons and working in suicide prevention,and because they are comparable across countries with regardto age and level of education. Previous research has shownthat attitudes are affected by a number of factors, for instance,experiences with suicidal behavior, own mood and knowl-edge (see Schmidtke & Häfner, 1989, for references). Thus,relationships between attitudes and such variables were alsoinvestigated.
Method
Participants
In Ghana, 570 students (274 women, 290 men, 6 nondis-closing gender) filled in the questionnaire, whereas thenumbers in Uganda and Norway were 289 (170 women,116 men, 3 nondisclosing gender) and 217 (154 women and63 men), respectively. Students from all levels of the studywere included. There was a significant difference in genderand age distribution between the three countries. The Gha-naian sample had more men (51%) than women (48%; 1%missing), while the opposite distribution was found in theother two countries (Uganda: 40% men, 59% women, 1%missing; Norway: 29% men, 71% women; χ² = 33.71, p <.001, Cramer’s V = 0.18). The gender distribution in thesamples was representative of the gender distribution in thetotal population of the psychology students in the threecountries. The Norwegian sample was slightly older, meanage 25.9 years, SD = 5.2, than the Ghanaian, mean age 25.1,SD = 6.1, which in turn was older than the Ugandan sample,mean age 24.2, SD = 6.0; F(2, 1040) = 4.31, p < .05, butthe age differences were in fact quite small, although sta-tistically significant (probably due to the relatively largesample size and thus a high statistical power).
Instrument
The Attitudes Toward Suicide questionnaire (ATTS) devel-oped by Salander Renberg and Jacobsson (2003) was em-ployed. The ATTS contains three questions about experienceof suicidal behavior, and 39 items on attitudes toward suicideand suicide prevention. Some of the items in this question-naire were selected from the Suicide Opinion Questionnaire(Domino, Moore, Westlake, & Gibson, 1982) and otherswere added. Most of the items were scored on a 5-point Lik-ert-type scale from strongly agree, with a score of 5, agree(4), undecided (3), disagree (2) to strongly disagree (1). Twoof the attitude questions were scored differently; namely, aquestion of probability of one’s own future suicide (surely not/ hope not but not sure / yes under certain circumstances /surely yes) and to what degree suicide should be prevented
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 21
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31

(in all cases / in all cases, but with few exceptions / in somecases yes / in some cases no / not in any case, if a person wantsto commit suicide, no-one, including medical services, hasthe right to stop him or her). The questionnaire also assessedrespondents’ own life-weariness, death wishes and suicidal-ity (acts and ideation), using questions developed by Paykelet al. (1974) and from the European Values Study (Halman,1993). The questions on death wishes and life-wearinesswere computed into two sum-variables (including 6 itemseach) called Life-Weariness last year (Cronbach’s α = 0.67)and Life-Weariness earlier in life (Cronbach’s α = 0.70). Thequestions included in these sum-variables were: (1) How of-ten have you thought of the meaning of your life? (2) Haveyou ever felt that life was not worth living? (3) Have you everthought of your own death? (4) Have you ever wished youwere dead, for instance that you could go to sleep and notwake up? (5) Have you ever thought of taking your own life,even if you would not really do it? (6) Have you ever reacheda point where you seriously considered taking your life, orperhaps made plans how you would go about doing it? Eachof these questions was scored from often (a score of 4),through sometimes (3), hardly ever (2) to never (1). A ques-tion about the degree of happiness from the European ValuesStudy (Halman, 1993) was included, and was to be scoredfrom “very happy,” through “quite happy,” “not particularlyhappy” to “not at all happy” (scored from 4 to1). Basic de-mographic data were also included in the questionnaire.
In their original study, Salander Renberg and Jacobsson(2003) conducted a factor analysis on the attitude questionsthat resulted in a ten-factor model. They acknowledged thatthe internal consistency for the whole instrument and ofsome of the factors was rather low, indicating that the in-strument measures a very broad area of attitudes towardsuicide. However, they questioned whether an instrumentassessing different attitude domains can yield a high totalinternal consistency, because different attitudes toward sui-cide might be conflicting and instable, reflecting ambiva-lence toward the phenomenon. The face and construct va-lidity of the instrument were found to be satisfactory. Theysuggested that future studies should investigate whether thefactors found in their original study are “universal” orwhether they differ between different groups.
Procedure
The Norwegian data were collected as part of a Europeanmulticenter study on suicide prevention and research (Sa-lander Renberg & Jacobsson, 2001), whereas the Africandata were collected in a separate study. In all three countriesthe data collection procedure was similar in that the ques-tionnaires were distributed, filled in and collected againduring class while someone from the research team waspresent to answer any questions the students might have.The participants were informed of the study both orally andin writing, and it was emphasized in both ways that partic-ipation was voluntary. Students were especially requested
to seek help from a qualified counselor if the questionnairecaused them any discomfort or if they had some relatedissues they would like to discuss. For this reason the name,postal address, phone number and e-mail address for thoseresponsible for the project were written on the informationsheet. None of the students in any of the countries madesuch contact either in class, during, or immediately afterthe data collection, or later.
The questionnaires were only distributed to those stu-dents present in the different classes targeted. No attemptwas made to send the questionnaire to those students notpresent in these classes. The classes chosen for data collec-tion were either those with compulsory attendance or witha traditionally high attendance rate. Because of a very highnumber of students in the first four levels of psychology inGhana, a stratified sampling (by gender) was conducted inthese classes, whereas all the students in the fifth levelfilled in the questionnaire. No students in Ghana and Ugan-da refused to fill in the questionnaire, whereas two studentsin Norway did. There is no reason to believe that there wereany systematic differences between those students attend-ing class and those who did not on the day of the study,since the study was not announced beforehand. The datawere collected during the years 2001 and 2002 in Norwayand in 2002 in Ghana and Uganda.
The Norwegian students filled in the Norwegian versionof the questionnaire (Norwegian is very similar to Swedish),while the Ghanaian and Ugandan students filled in the Eng-lish version. English is the language used in schools in bothGhana and Uganda, so the students are very familiar with it.The questionnaire went through a procedure of translationand back-translation between Swedish and English.
The study was approved by two ethical committees inNorway (both the regional one assessing the Norwegianpart of the study and the one responsible for research indeveloping countries with participation of Norwegian re-searchers), and by the relevant bodies at the University ofGhana, and Makerere University in Uganda.
Data Analyses
Chi-square analyses were used to investigate differencesbetween the countries on self-reported suicidal behaviorand experiences of suicidal behavior from their surround-ings. With regard to the attitude variables, factor analyseswere initially conducted in the three countries separatelyand congruency coefficients calculated in order to investi-gate the structural equivalence of the instrument betweenthe countries (Gorsuch, 1983, p. 285). Congruency coeffi-cients exceeding 0.90 are considered evidence of satisfac-tory congruency between factors (McCrae & Costa, 1997).Furthermore, chi-square analyses, ANOVAs and correla-tion analyses (Pearson’s r) were conducted were relevant.The level of statistical significance was in general set at5%, but because of the relatively high number of analyses,a Bonferroni correction of the α level was employed where
22 H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention
Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers
relevant (see Results section). The strength of the differ-ences was assessed by Cramer’s V.
Results
Self-Reported Suicidal Behavior andLife-Weariness
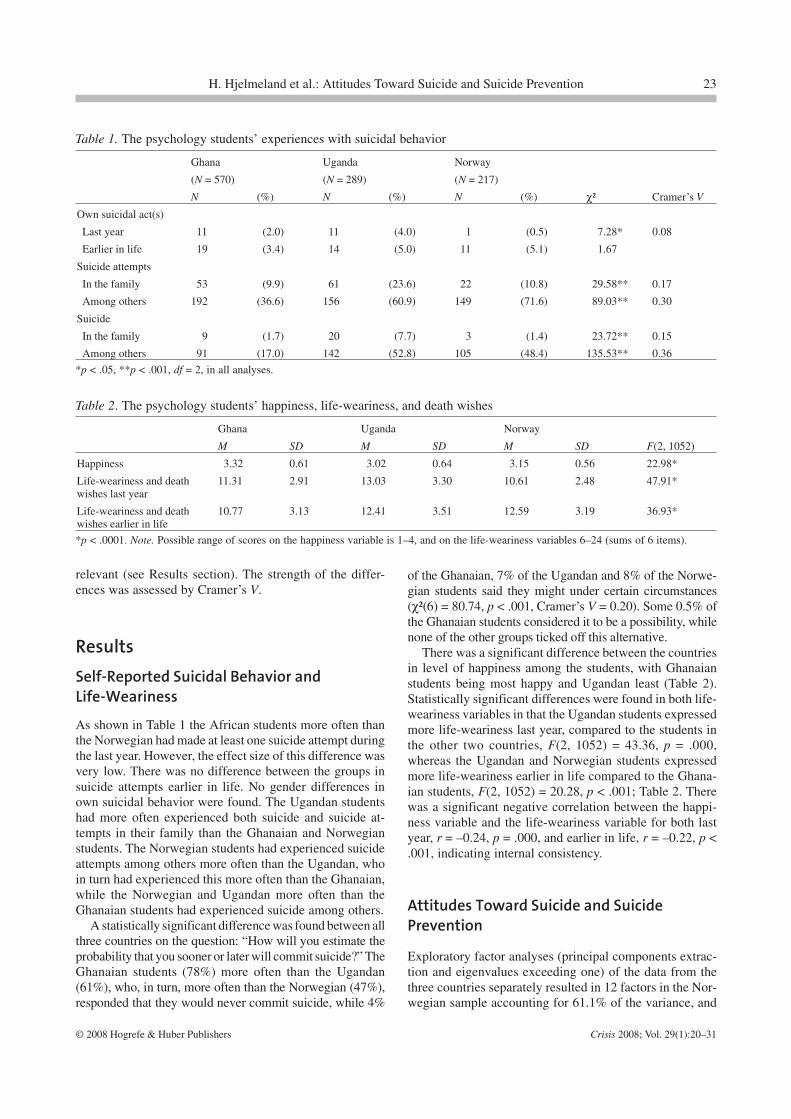
As shown in Table 1 the African students more often thanthe Norwegian had made at least one suicide attempt duringthe last year. However, the effect size of this difference wasvery low. There was no difference between the groups insuicide attempts earlier in life. No gender differences inown suicidal behavior were found. The Ugandan studentshad more often experienced both suicide and suicide at-tempts in their family than the Ghanaian and Norwegianstudents. The Norwegian students had experienced suicideattempts among others more often than the Ugandan, whoin turn had experienced this more often than the Ghanaian,while the Norwegian and Ugandan more often than theGhanaian students had experienced suicide among others.
A statistically significant difference was found between allthree countries on the question: “How will you estimate theprobability that you sooner or later will commit suicide?” TheGhanaian students (78%) more often than the Ugandan(61%), who, in turn, more often than the Norwegian (47%),responded that they would never commit suicide, while 4%
of the Ghanaian, 7% of the Ugandan and 8% of the Norwe-gian students said they might under certain circumstances(χ²(6) = 80.74, p < .001, Cramer’s V = 0.20). Some 0.5% ofthe Ghanaian students considered it to be a possibility, whilenone of the other groups ticked off this alternative.
There was a significant difference between the countriesin level of happiness among the students, with Ghanaianstudents being most happy and Ugandan least (Table 2).Statistically significant differences were found in both life-weariness variables in that the Ugandan students expressedmore life-weariness last year, compared to the students inthe other two countries, F(2, 1052) = 43.36, p = .000,whereas the Ugandan and Norwegian students expressedmore life-weariness earlier in life compared to the Ghana-ian students, F(2, 1052) = 20.28, p < .001; Table 2. Therewas a significant negative correlation between the happi-ness variable and the life-weariness variable for both lastyear, r = –0.24, p = .000, and earlier in life, r = –0.22, p <.001, indicating internal consistency.
Attitudes Toward Suicide and SuicidePrevention
Exploratory factor analyses (principal components extrac-tion and eigenvalues exceeding one) of the data from thethree countries separately resulted in 12 factors in the Nor-wegian sample accounting for 61.1% of the variance, and
Table 1. The psychology students’ experiences with suicidal behavior
Ghana Uganda Norway
(N = 570) (N = 289) (N = 217)
N (%) N (%) N (%) χ² Cramer’s V
Own suicidal act(s)
Last year 11 (2.0) 11 (4.0) 1 (0.5) 7.28* 0.08
Earlier in life 19 (3.4) 14 (5.0) 11 (5.1) 1.67
Suicide attempts
In the family 53 (9.9) 61 (23.6) 22 (10.8) 29.58** 0.17
Among others 192 (36.6) 156 (60.9) 149 (71.6) 89.03** 0.30
Suicide
In the family 9 (1.7) 20 (7.7) 3 (1.4) 23.72** 0.15
Among others 91 (17.0) 142 (52.8) 105 (48.4) 135.53** 0.36
*p < .05, **p < .001, df = 2, in all analyses.
Table 2. The psychology students’ happiness, life-weariness, and death wishes
Ghana Uganda Norway
M SD M SD M SD F(2, 1052)
Happiness 3.32 0.61 3.02 0.64 3.15 0.56 22.98*
Life-weariness and deathwishes last year
11.31 2.91 13.03 3.30 10.61 2.48 47.91*
Life-weariness and deathwishes earlier in life
10.77 3.13 12.41 3.51 12.59 3.19 36.93*
*p < .0001. Note. Possible range of scores on the happiness variable is 1–4, and on the life-weariness variables 6–24 (sums of 6 items).
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 23
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31
24 H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention
Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers

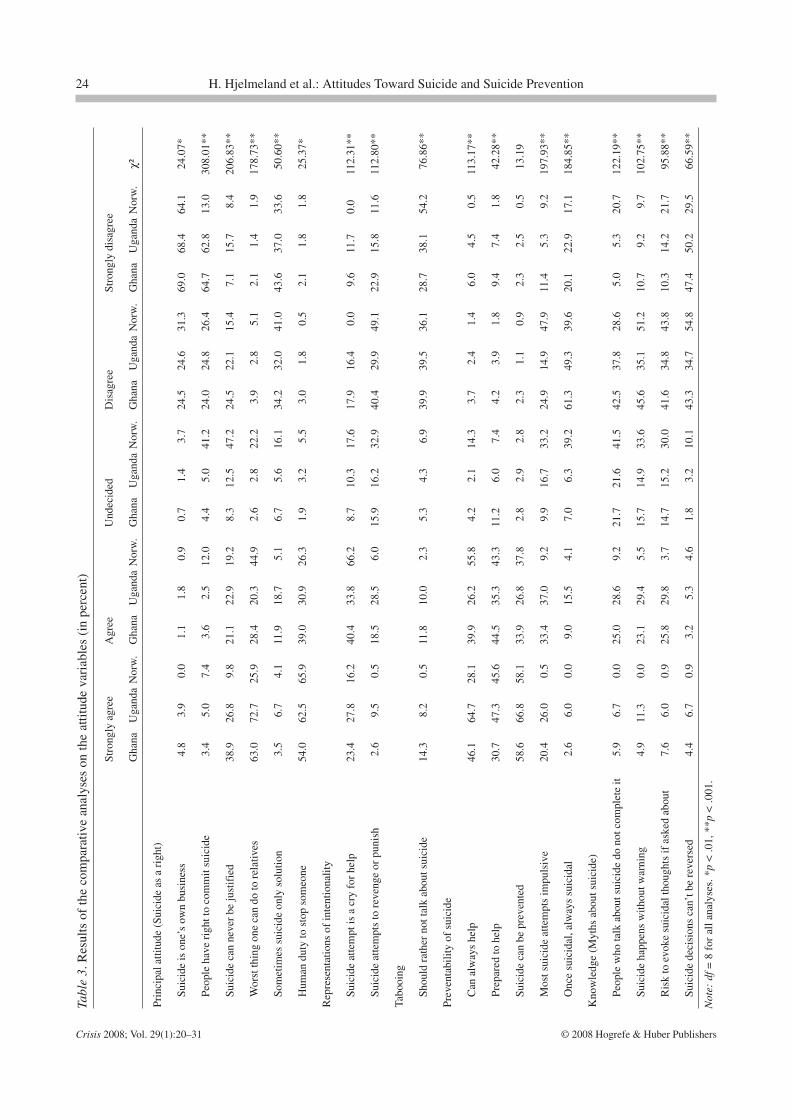
14 factors in both the Ghanaian and Ugandan samples, ac-counting for 56.5% and 58.6% of the variance respectively.At face value, the factor structure in terms of the itemsincluded in the various factors was very different betweenthe three countries. Thus, subsequent factor analyses withthe fixed number of 12 factors were conducted with theGhanaian and Ugandan data so that congruency coeffi-cients could be calculated. None of the congruency coeffi-cients between any of the factors or countries exceeded therequirement of 0.90. Thus comparisons at factor level wereimpossible. The possible explanations and implications ofthis result, as well as the results of confirmatory factor anal-yses, have been discussed elsewhere (Hjelmeland et al.,2006). Because comparisons at factor level turned out to beimpossible, some comparisons at item level were conduct-ed. The items included were those considered to be mostrelevant for suicide prevention and was clustered into fivegroups based on their content to make it easier to followthe analyses (see Table 3 for items included in thesegroups): (1) principal attitude toward suicide (right to com-mit suicide), (2) representations of intentionality, (3) pre-ventability, (4) tabooing, and (5) myths about suicide, re-flecting the knowledge, or lack thereof, on suicide as doc-umented in the literature (from the Western part of theworld; Neuringer, 1987–88; Popenhagen & Qualley, 1998;Shneidman et al., 1994). Since the distribution on some ofthe items was very different between the groups (U shapedin the African countries and A-shaped in Norway), wechose to use χ² analyses instead of t-tests because thatwould present better information on how the studentsscored than just means and standard deviations.
Table 3 shows the results of the comparative analyses.The effect size as measured by Cramer’s V is reported inthe text where statistically significant differences werefound. Statistically significant group differences werefound on all of the statements reflecting a principal attitudeconcerning suicide as a right. The vast majority of studentsin all three countries (93%–95%) did not think that suicideis one’s own business and no one should interfere, so thisdifference was probably statistically significant only be-cause of the large sample size, as also indicated by the loweffect size (Cramer’s V = 0.11). Follow-up analyses re-vealed that the Norwegian differed from the African sam-ples. Nineteen percent of the Norwegian students and7–8% of the African agreed that people have the right totake their lives (Cramer’s V = 0.38), while 29% of the Nor-wegian, 50% of the Ugandan, and 60% of the Ghanaianstudents thought that suicide can never be justified, impli-cating that it cannot be a right people have (Cramer’s V =0.31; significant differences between all three countries).The item “Suicide is the worst thing one can do to one’srelatives” was included in the group of variables implyingsuicide as a right because, according to Battin (1995), hav-ing a right to do something implicates not to cause othersharm. Around 91% of the Ghanaian, 93% of the Ugandan,and 71% of the Norwegian students agreed with this state-ment (Cramer’s V = 0.29; the Norwegian students differed
significantly from the two African student groups). Theitem “Sometimes suicide is the only solution” also indicat-ed that this is something people have a right to do undercertain circumstances, and here the majority in all threecountries disagreed (Ghana: 78%, Uganda: 69%, and Nor-way: 74%; Cramer’s V = 0.15). Follow-up analyses re-vealed statistically significant differences between allcountries. The vast majority in all three countries agreedthat it is a human duty to stop a person from committingsuicide (Ghana and Uganda 93%, Norway 92%; Cramer’sV = 0.11). The Norwegian students were more often unde-cided than the African students on all but one of the vari-ables concerning suicide as a right.
Sixty-four percent of the Ghanaian, 62% of the Ugan-dan and 83% of the Norwegian sample regarded suicideattempt as a cry for help (Cramer’s V = 0.23; Norway dif-fered from the two African countries). Again, a larger pro-portion of the Norwegian sample was undecided. Twen-ty-one percent of the Ghanaian, 38% of the Ugandan and7% of the Norwegian students saw suicide attempts as actsof revenge or punishment (Cramer’s V = 0.23; the differ-ence being statistically significant between all three coun-tries). Ninety percent of the Norwegian and 78% and 69%of the Ugandan and Ghanaian students, respectively, didnot agree that suicide should not be talked about (Cra-mer’s V = 0.19; statistically significant difference betweenall three countries).
There were statistically significant differences betweenthe groups on four of the five items concerning suicidepreventability. Around 91% of the Ugandan, 84% of theNorwegian, and 80% of the Ghanaian students (significantdifference between all three countries) believed that it isalways possible to help a person with suicidal thoughts(Cramer’s V = 0.23). The majority in all three countriesare also prepared to help a person in a suicidal crisis bycontacting him/her (Cramer’s V = 0.14). The item “Mostsuicide attempts are impulsive” implies that it would bedifficult to prevent suicide, and here the majority of boththe Ghanaian (54%) and the Ugandan (63%) studentsagreed, while only 10% of the Norwegian students did(Cramer’s V = 0.31). Follow-up analyses indicated thatthere was also a statistically significant difference be-tween the two African countries on this variable. The item“A person once having suicidal thoughts will never letthem go” indicates that it would be difficult to preventsuicide. Statistically significant differences were foundbetween all three countries (Cramer’s V = 0.29). No dif-ference between the three countries was found on the item“Suicide can be prevented.” While 3% in all three coun-tries were undecided, 93%–96% believed that suicide in-deed can be prevented. Also regarding suicide prevent-ability, the Norwegian students showed greater indeci-siveness than the African (on three of the four variableswhere significant differences were found).
The Ghanaian (81%) and Ugandan (77%) studentsmore often than the Norwegian students (65%) stated thatsuicide should be prevented in all cases, or in all cases
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 25
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31

with a few exceptions (14%, 17% and 31% respectively),whereas one percent of both the Ghanaian and Ugandanand none of the Norwegian students responded that sui-cide should not be prevented in any case, χ²(6) = 36.35, p< .001, Cramer’s V = 0.13.
Statistically significant group differences were found onall four of the knowledge/myth variables. Almost half ofthe students in all three countries (43% in Ghana, 48% inUganda, and 49% in Norway) disagreed with the statement“People who talk about suicide do not commit suicide”(Cramer’s V = 0.24). Follow-up analyses showed that theNorwegian students more often were undecided and lessoften agreed with this statement compared to their Africancounterparts. Around 61% of the Norwegian, 56% of theGhanaian and 44% of the Ugandan students did not thinkthat suicide happens without previous warning (Cramer’sV = 0.22). The apparent difference between the two Africancountries was not statistically significant. About half of theAfrican students (49% in Uganda and 52% in Ghana) andtwo-thirds (66%) of the Norwegian students did not believethat you might evoke suicidal thoughts in a person’s mindif you ask about it (Cramer’s V = 0.21). The vast majorityof students in all three countries disagreed with the state-ment that once a person has made up his mind about com-mitting suicide no one can stop him or her, but the Ghana-ian students disagreed to an even larger degree than theother two groups (Cramer’s V = 0.18). The most pro-nounced difference on all the knowledge/myth variableswas that once again the Norwegian students were undecid-ed more often than their African counterparts.
Gender Differences in Attitudes TowardSuicidal Behavior and Prevention
The gender analyses were conducted for each country sep-arately. No gender differences were found in the knowl-edge/myth, preventability and tabooing variables in any ofthe countries. In the group of statements concerning suicideas a right, two gender differences were found. In Ghanaeven more women (95.2%) than men (92.0%) disagreedthat suicide is one’s own business and no one should inter-fere, χ²(4) = 15.67, p < .01, Cramer’s V = 0.17. In Ugandawomen (95.2%) more often than men (76.8%) disagreedwith people having a right to commit suicide, χ²(4) = 31.75,p < .001, Cramer’s V = 0.34.
Gender differences were found in both statements as-cribing intentionality to suicide attempts. In Ghana, morewomen (71.7%) than men (56.3%) agreed that a suicideattempt is a cry for help, while 11.0% of the women and6.3% of the men were undecided (χ²(4) = 36.92, p < .001,Cramer’s V = 0.26). Also in Norway women (87.6%) moreoften than men (69.0%) agreed that suicide attempts arecries for help, while none of either women or men dis-agreed with this, χ²(2) = 11.98, p < .01, Cramer’s V = 0.24.In Norway, men (14%) more often than women (3%)
agreed that suicide attempts are made because of revengeor to punish someone, χ²(4) = 11.58, p < .05, Cramer’s V= 0.23.
Correlation Analyses
Since the factor structure differed between the countries,indicating cultural differences in associations between at-titude variables, the correlation analyses were conductedfor each of the countries separately. In order to keep thenumber of analyses down to a comprehensible level, wedecided to create one variable as an index of knowledge bysummarizing the scores on the four knowledge/myth vari-ables, and then reverse it so that a high score on this sumvariable indicated a high level of knowledge (that is, dis-belief in the myths). In addition, we let the clearest state-ments on suicide as a right (i.e., “People have the right tocommit suicide”) and preventability of suicide (i.e., “Sui-cide can be prevented”) represent these groups of variablesin the correlation analyses. Thus, correlation analyses(Pearson’s r) were conducted between the knowledge andattitude variables as well as between these variables andrelevant background variables, namely, own suicidal be-havior last year and earlier in life, suicidal behavior in thesurroundings (i.e., in the family and among others), happi-ness and life-weariness last year and earlier in life. Due tothe high number of correlation analyses (each attitude vari-able was correlated with 14 variables), the α level was Bon-ferroni corrected and set at 0.003.
In Ghana the following significant correlations werefound: The knowledge variable correlated negatively withtabooing (r = –0.25, p < .001) and having experienced sui-cide attempts among others (outside of the family; r =–0.15, p < .001). The item “People should have a right totake their own lives” correlated positively with having ex-perienced suicide in the family (r = 0.14, p = < 001), life-weariness last year (r = 0.15, p < .001), life-weariness ear-lier in life (r = 0.21, p < .001), and own suicide attemptearlier in life (r = 0.17, p < .001). The item “Suicide canbe prevented” correlated negatively with having experi-enced suicide in the family (r = –0.19, p < .001). Happinesscorrelated negatively with viewing suicide attempts as criesfor help, whereas life-weariness and death-wishes earlierin life correlated positively with both viewing suicide at-tempts a cries for help (r = 0.13, p < .01) and as revenge orpunishment (r = 0.15, p < .001).
With a Bonferroni correction of the α-level, only onestatistically significant correlation was found in Uganda:The item “People should have a right to take their ownlives” correlated positively with life-weariness and deathwishes last year (r = 0.22, p < .001).
In Norway the following significant correlations werefound: Knowledge about the topic of suicide correlatednegatively with tabooing (r = –0.24, p < .001). The item“People have the right to take their own life” correlatedpositively with experience of suicide among others outside
26 H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention
Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers

the family (r = 0.15, p < .001). Seeing suicide attempts asmade to revenge something or punish someone correlatedpositively with having experienced suicide among others(r = 0.10, p < .001). Happiness correlated positively withbelieving that suicide can be prevented (r = 0.23, p < .001).
Discussion
Self-Reported Suicidal Behavior andLife-Weariness
In terms of own suicidal behavior, the countries differedonly slightly (although statistically significant) whereas theUgandan and Norwegian students almost twice as often asthe Ghanaian had experienced suicide attempts in their sur-roundings. The Ugandan students had experienced com-pleted suicide more often than the Ghanaian and Norwe-gian students. Analyses of the happiness and life-wearinessvariables showed that the Ugandan psychology studentsseem to perceive life as harder than their Ghanaian andNorwegian counterparts. This might be reflecting less hopedue to the specter of AIDS, rebel activities, and atrocitiesthat has been going on in parts of Uganda in most of thesestudents’ lives.
In Norway the suicide rate was approximately13/100,000 at the time of the data collection (NorwegianBureau of Statistics, 2003) which is around the Europeanaverage. Norway does not have a national registration ofattempted suicide, but based on regional registrations, forinstance, the Norwegian part of the WHO/EURO Multi-center Study on Suicidal Behavior (Hjelmeland & Bjerke,1996), it is estimated that the attempted suicide rate (thosemedically treated) is at least ten times higher than the sui-cide rate. Based on the experience with suicidal behaviorfound among the African students compared to the Norwe-gian students, it would be plausible to suggest that suicidalbehavior is a considerable public health problem also in thetwo African countries, especially in Uganda, where the sui-cide rate probably is higher than in Norway, while the Gha-naian suicide rate might be lower. These estimations are,of course, speculations and should be followed by epide-miological studies in these countries.
Alem et al. (1999) found that their respondents in Ethi-opia knew more persons who had completed suicide thanhad attempted suicide, which is in contrast to the knownhigher prevalence of attempted suicide. They explain theirfinding with the fact that, because of the stigma suicidalbehavior carries in African countries, attempts are made toconceal suicidal acts, and it is relatively unusual for suicideattempters to be taken to hospital. Our findings are not con-sistent with the findings of Alem et al. in that our infor-mants do know of more suicide attempts than they do ofsuicides; however, it is nowhere near the approximate 10:1relationship that might be expected, at least in Norway.
Attitude and Knowledge Variables
The lack of structural equivalence shown by the differencesin factor structure might be an indication of lack of validityand/or reliability of the instrument (discussed further inHjelmeland et al., 2006). Furthermore, comparisons at itemlevel are by some considered to be dubious (van de Vijver& Leung, 1997). However, we still know very little aboutwhether suicidal behavior has a different meaning in Afri-can countries compared to Western countries. Thus, wecannot dismiss the possibility that differences in factorstructure, which might indicate different latent variables, isa valid finding indicating differences in meaning (Hjelme-land et al., 2006). Furthermore, we urgently need researchrelevant for suicide prevention in Ghana and Uganda andalthough it is not considered to be methodologically per-fect, comparisons at item level of especially relevant itemswill at least give us some preliminary indications of poten-tial cultural differences in meaning of suicidal behavior. Itis also very useful to know how future gate-keepers in Gha-na and Uganda respond to items like the ones included inthe present study, and how they differ to some of their West-ern counterparts in their views on such issues. The decisionto do comparisons at item level is also supported by thefindings of Seidlitz et al. (1995) showing links betweenparticular risk factors and particular attitudes demonstrat-ing the importance of examining specific attitude itemsseparately rather than combining them into scales.
The results showed that the Norwegian students consid-er suicide to be a right more often than the African, but alsothat the Norwegian students more often seem to lack ability(or will?) to take a stand on such questions. The vast ma-jority in all three groups, however, agreed that suicide isnot one’s own business and that it is a human duty to stopsomeone from committing suicide. Even though the differ-ences mainly are between the Norwegian students, on theone hand, and the African students, on the other hand, thereare also some differences between the two African coun-tries. Ugandans more often than Ghanaians think that sui-cide sometimes can be justified and that it sometimes canbe the only solution.
The Norwegian students more often than the African viewsuicide attempts as cries for help. Apparently the culturalcontext plays a role here. In Norway the current developmentis in the direction of increased fragmentation of social net-works due to family dissolution and reconstruction. For in-stance, almost half of the households today consist of onlyone adult. The responses from the Norwegian students thusmight be reflecting this weakened social network, where pos-sibilities for a suicidal individual to communicate despair arelimited. The same context sensitivity is demonstrated whenthe African more often than Norwegian students believe thatmany suicide attempts are made because of revenge or topunish someone else. In cultures where suicide affects fami-lies and clans in a different way than in the Western part ofthe world, the possibilities of using it as revenge or punish-
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 27
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31

ment might also be completely different. Interestingly, thereis a rather large difference between the two African countries,indicating differences also between African cultures. This un-derlines the danger of assuming similarity between countriesfrom the same continent without investigating if this really isthe case and demonstrates the need for further culture-specif-ic/culture-sensitive research.
Although the majority in all three countries disagreedwith the statement that one should rather not talk aboutsuicide, the topic seems to be most taboo in Ghana, fol-lowed by Uganda and then Norway. As pointed out by Phil-lips (2004), it is important to address such taboos beforesuicide prevention can truly start. It can be questionedwhether this has had any effect on the responses to the ques-tionnaire, and it might be speculated that the relatively lowfrequency of experience with suicidal behavior in the Gha-naian group, compared to the other two, partly can be ex-plained by this taboo. However, the effect of social desir-ability is expected to be smaller in anonymous question-naire studies than in face-to-face interviews.
The majority in all three countries believes that suicidecan and should be prevented. This is followed up by a beliefthat you can always help a suicidal person and a readinessto help by taking contact. At the same time, the majority ofthe Ugandan and Ghanaian students believe that most sui-cide attempts are impulsive, thus indicating that they mightbe difficult to prevent. However, this item is on suicideattempts, not on suicide, and it might be questioned wheth-er the informants differentiate between suicide and suicideattempts. It is worth noting that there are also differencesbetween the two African countries here in that the Ugandanstudents even more often than both the Ghanaian and theNorwegian believe that you can always help a suicidal per-son. The Ghanaian students seem a bit more reluctant tohelp than the Ugandan and Norwegian students. Neverthe-less, these results are promising in terms of suicide preven-tion since suicidal behavior seems to be an even biggerproblem in Uganda than in Ghana.
The Norwegian students had a slightly higher level ofknowledge in suicidology compared to the African stu-dents, as was to be expected since Norway has had somefocus on suicide and suicide prevention during the last cou-ple of decades, first due to a large increase in suicide ratesin the 1970s and 1980s, and subsequently because a Gov-ernmental action plan for suicide prevention was launchedin the 1990s (National Board of Health, 1996). However,based on both the small effect sizes of the differences andthe fact that the Norwegian students to a much higher de-gree than the African students did not know whether tobelieve in the myths or not, the differences were smallerthan what could be expected.
Gender Differences
Few and mostly small gender differences were found in thisstudy. The most pronounced one was found in Uganda,
where most women compared to about 75% of the menbelieved that people do not have the right to commit sui-cide. Previous research has shown mixed results in termsof gender differences in attitudes toward suicide in thatsome studies have found differences (e.g., Domino &Groth, 1997; Domino & Takahashi, 1991), while othershave either not found or found only minor gender differ-ences (e.g., Domino et al., 1993–1994; Domino & Su,1994–1995; Kocmur & Dernovsek, 2003).
Relationship Between Knowledge, Attitudesand Background Variables
More knowledge was associated with less tabooing in bothGhana and Norway, and also with experience of suicidalbehavior in Ghana. The view that people have the right tocommit suicide was associated with life-weariness and/orexperience of suicidal behavior in all three countries, afinding in keeping with previous studies (e.g., Minear &Brush, 1980–1981; Stillion et al., 1986). In addition, expe-rience of suicide was in Ghana associated with a more neg-ative view on the possibility to prevent suicide, happinesswith less, and life-weariness, with more belief in suicidalattempts as cries for help. Life-weariness was also associ-ated with viewing suicide attempts as made in revenge orto punish someone. In Norway, happiness was associatedwith a more positive view on the possibility to prevent sui-cide. Although all the associations found were in the ex-pected directions, they were surprisingly few and the cor-relation coefficients found were relatively small.
General Discussion
As pointed out by Alem et al. (1999) among others, attitudestoward suicide are reflections of its social meaning in a cul-ture, and such attitudes are generally assumed to be ratherpermissive in the developed part of the world, while they areconsidered to be more restrictive in the developing world(e.g., Lester & Akande, 1994; Eshun, 2003). Difficulties lead-ing to suicide occur in a specific cultural and societal settingand the individuals’ possibilities of changing the circum-stances are restricted by local legal and cultural practice. Ac-cordingly, the attitudinal differences between the studentgroups in the present study must also be seen in light of theirspecific ideological environment. For example, the Norwe-gians are more reluctant to take a stand on both knowledgeand attitude issues compared to the Africans. In a society likeNorway’s, where suicide has been on the agenda to a largerdegree than in, for example, Ghanaian and Ugandan socie-ties, such insecurity might reflect a transitional state betweenprejudice and more knowledge-based attitudes. However, itmight also just reflect lack of knowledge among the studentsand if this indecisiveness persists into their professional ca-
28 H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention
Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers

reers, this might have damaging effects on the ability of thesefuture psychologists to prevent suicide in their clients. Basedon previous research on the relationship between attitudestoward suicide and suicidal behavior, it is premature to claimthat some attitudes are wrong and others are right in terms oftheir effectiveness to prevent suicide (Salander Renberg &Jacobsson, 2003). What we do know, however, is that it is ofvital importance for therapists to be conscious of their ownattitudes and the effect such attitudes have on the relationshipwith their clients. Although Maine et al. (2001) found thatonly knowledge, not attitudes, were important, we believethat even if they may not be directly important in interventionor treatment, they are important indirectly as they might af-fect people’s interest in acquiring knowledge (Lang et al.,1989), and also people’s receptivity to different kinds ofknowledge. We also believe that attitudes have an impact ontherapists’ ability or will to talk to suicidal clients and influ-ence the way that suicidality is talked about.
Domino and Takahashi (1991) pointed out that culturaldifferences influence the willingness to share personal in-formation on such a sensitive topic as suicide, and that thismight result in a higher incidence of the “undecided” re-sponse alternative. Since this topic was expected to be moretaboo in the two African countries, as was supported tosome degree in our study, we would have expected to findthat the African students ticked the undecided alternativemore often than the Norwegians. The finding that this wasmore often the case for the Norwegian students, and alsoto a much higher degree compared to the African students,was therefore surprising and is difficult to explain. It canbe speculated that religion might have had an effect on this.We would assume that religion plays a much larger part inthe lives of Ugandans and Ghanaians compared to Norwe-gians in general since Norway in many ways is a moresecular country. Based on their faith and their religious val-ues, it therefore might be easier for the Africans to take astand on questions regarding life or death. Moreover, thegreater emphasis on religion in the two African countriesmight also explain the difference in viewing suicide as aright, in that tolerance of suicide has been found to be neg-atively associated with religiousness (Neeleman et al.,1997). Because religion might be more important in theAfrican students’ life compared to the Norwegians’, reli-gion can be considered as a confounding variable in thisstudy. However, as pointed out by Domino et al.(1993–1994) such differences do reflect the real world andcontrolling for religion would have resulted in nonrepre-sentative samples. Besides, Bagley and Ramsey (1989)have found the influence of religious affiliation on attitudestoward suicidal behavior to be weak.
Methodological Considerations
In addition to the methodological issues discussed else-where in this paper, one other important question in cross-cultural studies like this is whether the respondents in coun-
tries with such different cultures understand the questionsin the same way, or even define suicide attempt and suicidein an equal manner. Attitudes toward suicide appear to bequite complex and, perhaps more than other phenomena,reflect both individual and cultural dynamics. However,Domino and Takahashi (1991) have emphasized that al-though cross-cultural comparisons might be influenced byquite a substantial number of variables and thereby be lim-ited in their generalizability, they still provide a windowinto an important area of human concern, and thus help usto develop our understanding of the meanings of suicidalbehavior.
Implications for Suicide Prevention
Some implications for suicide prevention should be men-tioned. It is clear that the attitudes toward suicide and sui-cide prevention found in this study in general give groundsfor optimism regarding initiation of suicide preventive ef-forts in Ghana and Uganda. No doubt, both the Africancountries have a young generation of upcoming psycholo-gists who do not reflect the generally held negative andcondemning attitudes to the same degree as often seen inthe general population, and who see both the value andpossibility of preventing suicidal behavior. We would alsoassume that mere participation in this study might havesome suicide preventive power in itself, as it made the re-spondents reflect upon a topic that they might not havethought much about previously, and thus will be more alertto problems of suicidality in their surroundings. This viewis supported by the findings of Jenner and Niesing (2000),as well as a number of the comments made on the backpage of our questionnaire (where the participants were en-couraged to give their comments to the study), and orallyas the questionnaires were handed in.
Eisler et al. (1999) pointed out that knowledge and atti-tudes toward suicide in subjects not involved in suicidalbehavior gives valuable information on meanings assignedto suicide in a culture and the results of the present studyindeed indicate that the phenomenon of suicide is assigneddifferent meanings in different cultures. For instance, inNorway the general impression of indecisiveness mightpoint to an understanding of suicide as such a complex phe-nomenon that it is almost impossible to take a clear standon the various aspects connected to it. In those able to takea stand, a tendency toward viewing suicide as a matter ofpersonal rights and/or as a cry for help from an individualunder unbearable circumstances is evident. In Ghana andUganda, on the other hand, suicide is viewed more as a jointmatter with less choice for the individual and huge conse-quences for the family, even though the Ugandan studentsseem a bit more permissive than the Ghanaian. This is alsothe case for the representation of intentionality, where thesuicidal act more often is viewed in terms of influencingothers. This leaves us with a general meaning of suicide asmore of a private matter in Norway compared to the two
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 29
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31

African countries where it is perceived more as a joint mat-ter for the family/clan, reflecting the different family struc-tures in general in these countries, where the extended fam-ily is more common in Africa than in Norway.
Some countries in the Western part of the world, as Nor-way, have had national suicide prevention plans for sometime now, and it might be tempting to just “export” theseplans to developing countries. However, in line with previ-ous authors underlining the dangers of transposing researchfrom one country to another (e.g., Boldt, 1988; Domino &Perrone, 1993; Leenaars & Domino, 1993), the findings ofthe present study emphasize the need for suicide preventionefforts to be culture-sensitive and culture-specific. This hasalso been underlined by Phillips (2004) and Vijayakumaret al. (2004, 2005) who pointed to the fact that there arelarge differences in both risk and protective factors associ-ated with suicidal behavior between developed and devel-oping countries. Moreover, since priorities of preventiveefforts and strategies in developing countries to a large de-gree is ruled by donor money (S. Ndyanabangi, Ministryof Health, Uganda, personal communication, 2003), thismight in some quarters create a backlash against “import-ed” programs. When planning suicide prevention programsin developing countries, it is also important to keep in mindthat, for instance, Africa in general has only 0.34 mentalhealth professional per 100,000 population (Vijayakumar,2004). The results of this study, however, gives grounds foroptimism regarding the possibilities for developing and ini-tiating suicide preventive efforts in Ghana and Uganda, al-though parallel with that, more research is, of course, need-ed. We propose qualitative studies in order to develop ourunderstanding of the meaning(s) of suicidal behavior inthese two countries further. The results of such studies willalso contribute to develop the ATTS into a more culturesensitive instrument.
References
Alem, A., Jacobsson, L., Kebede, D., & Kullgren, G. (1999).Awareness and attitudes of a rural Ethiopian community to-ward suicidal behavior. A key informant study in Butajira,Ethiopia. Acta Psychiatrica Scandinavica, 100, 65–69.
Bagley, C., & Ramsay, R. (1989). Attitudes toward suicide, reli-gious values and suicidal behavior: Evidence from a commu-nity survey. In R.F.W. Diekstra, R. Maris, S. Platt, A. Schmidt-ke & G. Sonneck (Eds.), Suicide and its prevention. The roleof attitude and imitation (pp. 78–90). E.J. Brill: Leiden.
Battin, M.P. (1995). Ethical issues in suicide. Englewood Cliffs,NJ: Prentice-Hall.
Boldt, M. (1988). The meaning of suicide: Implications of re-search. Crisis, 9, 93–108.
Domino, G., & Groth, M. (1997). Attitudes toward suicide: Ger-man and U.S. nationals. Omega, 35, 309–317.
Domino, G., Lin, J., & Chang, O. (1995). Attitudes toward suicideand conservatism: A comparison of Chinese and United Statessamples. Omega, 31, 237–252.
Domino, G., Moore, D., Westlake, L., & Gibson, L. (1982). Atti-tudes toward suicide: A factor analytic approach. Journal ofClinical Psychology, 38, 257–262.
Domino, G., Niles, S., & Raj, S.D. (1993–94). Attitudes towardsuicide: A cross-cultural comparison of Singaporean and Aus-tralian university students. Omega, 28, 125–137.
Domino, G., & Perrone, L. (1993). Attitudes toward suicide: Ital-ian and United States physicians. Omega, 27, 195–206.
Domino, G., & Su, S. (1994–95). Conservatism and attitudes to-ward suicide: A study of Taiwanese-American and U.S. adults.Omega, 30, 131–143.
Domino, G., & Takahashi, Y. (1991). Attitudes toward suicide inJapanese and American medical students. Suicide and Life-Threatening Behavior, 21, 345–359.
Eisler, A.A., Wester, M., Yoshida, M., & Bianchi, G. (1999). At-titudes, beliefs, and opinions about suicide: A cross-culturalcomparison of Sweden, Japan, and Slovakia. In J.-C. Lasry, J.Adair, & K. Dion (Eds.), Latest contributions to cross-culturalpsychology (pp. 176–191). Lisse: Swets & Zeitlinger.
Eshun, S. (2003). Sociocultural determinants of suicide ideation:A comparison between American and Ghanaian college sam-ples. Suicide and Life-Threatening Behavior, 33, 165–171.
Eskin, M. (1995). Adolescents’ attitudes toward suicide, and asuicidal peer: A comparison between Swedish and Turkishhigh school students. Scandinavian Journal of Psychology, 36,201–207.
Gorsuch, R.L. (1983). Factor analysis (p. 285). Hillsdale, NJ: Erl-baum.
Halman, L. (1993, April). Suicidal attitudes and modernizing so-ciety. Some methodological issues and results from the Euro-pean Values Study. Paper presented at the seminar on suicidalbehavior in society: Methodological aspects, Högberga Kurs-gård, Lidingö Sweden.
Hjelmeland, H., & Bjerke, T. (1996). Parasuicide in the county ofSør-Trøndelag, Norway. General epidemiology and psycho-logical factors. Social Psychiatry and Psychiatric Epidemiol-ogy, 31, 272–283.
Hjelmeland, H., Kinyanda, E., Knizek, B.L., Owens, V., Nordvik,H., & Svarva, K. (2006). A discussion of the value of cross-cultural studies in search of the meaning(s) of suicidal behaviorand the methodological challenges of such studies. Archives ofSuicide Research, 10, 15–27.
Jenner, J.A., & Niesing, J. (2000). The construction of the SE-DAS: A new suicide-attitude questionnaire. Acta PsychiatricaScandinavica, 102, 139–146.
Kocmur, M., & Dernovsek, M.Z. (2003). Attitudes toward suicidein Slovenia: A cross-sectional survey. International Journal ofSocial Psychiatry, 49, 8–16.
Lang, W.A., Ramsay, R., Tanney, B.L., & Tierney, R.J. (1989).Caregiver attitudes in suicide prevention: Help for the helpers.In R.F.W. Diekstra, R. Maris, S. Platt, A. Schmidtke, & G.Sonneck (Eds.), Suicide and its prevention. The role of attitudeand imitation (pp. 260–272). Leiden: E.J. Brill.
Leenaars A.A., & Domino, G. (1993). A comparison of commu-nity attitudes toward suicide in Windsor and Los Angeles. Ca-nadian Journal of Behavioral Science, 25, 253–266.
Lester, D., & Akande, A. (1994). Attitudes about suicide amongthe Yoruba of Nigeria. Journal of Social Psychology, 134,851–853.
Maine, S., Shute, R., & Martin, G. (2001). Educating parentsabout youth suicide: Knowledge, response to suicidal state-
30 H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention
Crisis 2008; Vol. 29(1):20–31 © 2008 Hogrefe & Huber Publishers
ments, attitudes, and intention to help. Suicide and Life-Threat-ening Behavior, 31, 320–332.
McCrae, R.R., & Costa, P.T. (1997). Personality trait structure asa human universal. American Psychologist, 52, 509–516.
Minear, J.D., & Brush, L.R. (1980–81). The correlations of atti-tudes toward suicide with death anxiety, religiosity, and per-sonal closeness to suicide. Omega, 11, 317–324.
Neeleman, J., Halpern, D., Leon, D., & Lewis, G. (1997). Toler-ance of suicide, religion and suicide rates: An ecological andindividual study in 19 Western countries. Psychological Med-icine, 27, 1165–1171.
Neuringer, C. (1987–88). The meaning behind popular mythsabout suicide. Omega, 18, 155–162.
Norwegian Board of Health. (1996). The national plan for suicideprevention 1994–1998. Oslo, Norway: Norwegian Board ofHealth.
Norwegian Bureau of Statistics. (2003). Causes of death statis-tics. Retrieved on October 10, 2005, from http://www.ssb.no/dodsarsak.
Paykel, E.S., Myers, J.K., Lindenthal, J.J., & Tanner, J. (1974).Suicidal feelings in the general population: A prevalence study.British Journal of Psychiatry, 124, 460–469.
Peltzer, K., Cherian, V.I., & Cherian, L. (1998). Attitudes towardsuicide among South African secondary school pupils. Psy-chological Reports, 83, 1259–1265.
Phillips, M. (2004). Suicide prevention in developing countries:Where should we start? World Psychiatry, 3, 156–157.
Popenhagen, M.P., & Qualley, R.M. (1998). Adolescent suicide:Detection, intervention, and prevention. Professional SchoolCounseling, 1, 30–36.
Salander Renberg, E., & Jacobsson, L. (2001). A European col-laboration project on prevention of suicide. In O.T. Grad (Ed.),Suicide risk and protective factors in the new millennium(pp. 268–272). Ljubljana: Cankarjev Dom.
Salander Renberg, E., & Jacobsson, L. (2003). Development of aquestionnaire on attitudes toward suicide (ATTS) and its ap-plication in a Swedish population. Suicide and Life-Threaten-ing Behavior, 33, 52–64.
Schmidtke, A.S., & Häfner, H. (1989). Public attitudes toward andeffects of the mass media on suicidal and deliberate self-harmbehavior. In R.F.W. Diekstra, R. Maris, S. Platt, A. Schmidtke, &G. Sonneck (Eds.), Suicide and its prevention. The role of attitudeand imitation (pp. 313–330). Leiden: E.J. Brill.
Seidlitz, L., Duberstein, P.R., Cox, C., & Conwell, Y. (1995). At-titudes of older people toward suicide and assisted suicide: Ananalysis of gallup poll findings. Journal of the American Ge-riatrics Society, 43, 993–998.
Shneidman, E., Farberow, N.L., & Litman, R. (1994). The psy-chology of suicide. A clinician’s guide to evaluation and treat-ment. Northvale: Jason Aronson Inc.
Stillion, J.M., McDowell, E.E., Smith, R.T., & McCoy, P.A. (1986).Relationships between suicide attitudes and indicators of mentalhealth among adolescents. Death Studies, 10, 289–296.
Van de Vijver, F., & Leung, K. (1997). Methods and data analysis ofcomparative research. In J.W. Berry, Y.H. Poortinga, & J. Pandey(Eds.), Handbook of cross-cultural psychology. Volume 1. Theo-ry and method (pp. 257–300). Boston: Allyn and Bacon.
Vijayakumar, L. (2004) Suicide prevention: The urgent need indeveloping countries. World Psychiatry, 3, 158–159.
Vijayakumar, L., John, S., Pirkis, J., & Whiteford, H. (2005). Sui-cide in developing countries (2). Risk factors. Crisis, 26,112–119.
About the authors
Heidi Hjelmeland is Professor of Health Science at the Depart-ment of Social Work and Health Science, Norwegian Universityof Science and Technology in Trondheim, Norway, as well as aresearcher at the Division of Mental Health at the Norwegian In-stitute of Public Health, Oslo, Norway. Her current research fo-cuses on cultural and communicative/intentional aspects of sui-cidal behavior.
Charity S. Akotia is Senior Lecturer at the Department of Psy-chology, University of Ghana, Legon, Accra, Ghana. Her currentresearch focuses on community psychology and suicidal behav-ior.
Vicki Owens is Lecturer at the Department of Mental Health andCommunity Psychology, Makerere University, Kampala, Ugan-da. Her current research interests are development of values andcounseling training.
Birthe L. Knizek is Associate Professor at the Department of Psy-chology, Norwegian University of Science and Technology,Trondheim, Norway. Her current research focuses on various as-pects of suicidal behavior as well as the use of qualitative methodsin cultural studies.
Hilmar Nordvik is Professor of Personality Psychology at the De-partment of Psychology, Norwegian University of Science andTechnology, Trondheim, Norway. His research interests lie in per-sonality traits, vocational psychology, and psychometric method-ology.
Rose Schroeder is Counseling Psychologist and Professor at Aus-tin Community College, Austin, Texas, USA. Her research inter-est is stress among black women.
Eugene Kinyanda is a consultant psychiatrist currently workingas Research Manager with the Medical Research Council/UgandaVirus Research Institute, Uganda Research Unit on AIDS, Enteb-be, Uganda. His current research focuses on suicidality in the highrisk groups of HIV/AIDS and war traumatized populations.
Heidi Hjelmeland
Department of Social Work and Health ScienceNorwegian University of Science and TechnologyN-7491 TrondheimNorwayE-mail [email protected]
H. Hjelmeland et al.: Attitudes Toward Suicide and Suicide Prevention 31
© 2008 Hogrefe & Huber Publishers Crisis 2008; Vol. 29(1):20–31





























