Embed Size (px)
Citation preview
Psychology in the Schools, Vol. 36(5), 1999© 1999 John Wiley & Sons, Inc. CCC 0033-3085/99/050379-11
SCHOOL-BASED MENTAL HEALTH SERVICES: THE BALTIMORE MODELS
LOIS T. FLAHERTY AND MARK D. WEIST
Center for School Mental Health Assistance. University of Maryland School of Medicine
Through a variety of state and local funding and administrative arrangements. expanded schoolmental health (ESMH) programs have been developed in nearly half of the 176 Baltimore Cityschools over the past decade. These programs augment existing services provided by the schooland help to ensure that a comprehensive range of services (assessment, prevention. case manage-ment. treatment) are available to youth in special and regular education. Baltimore's leadership inthe emerging ESMH field led to the development of the Center for School Mental Health Assis-tance (CSMHA). one of two national centers that provide support and technical assistance to pro-mote comprehensive mental health programs for youth in schools. This paper shares experiencesassociated with the growth of ESMH programs in Baltimore and activities and initiatives of theCSMHA. © 1999 John Wiley & Sons. Inc.
Baltimore has been recognized as a leader in the development of expanded school mental health(ESMH) programs. These programs, which involve comprehensive mental health services includingassessment, therapy (individual, family, group), staff consultation, and prevention activities, aug-ment services provided by school-hired mental health professionals such as school psychologists(Flaherty, Weist, & Warner, 1996; Weist, 1997). In Baltimore City, ESMH programs came about asa result of a confluence of factors in the 1980s. The creative leadership of many individuals in thestate and local health, mental health, and education systems was involved in responding to perceivedunmet needs of children and adolescents for mental health care.
These programs are part of a national movement given impetus by the realization that adoles-cents were not being served by the existing health care system and by concern about rising rates ofteen pregnancy, sexually transmitted diseases, drug and alcohol use, homicide, and suicide. All ofthese problems have behavioral origins, so there was an obvious need to incorporate a counselingcomponent if they were to be addressed successfully. In 1985, the Baltimore City Health Department(BCHD) opened seven school-based health centers in high schools in the city. The main focus ofthese centers was on basic health care, with limited mental-health services provided. Once thecenters opened, the experience was similar to that nationwide, in that 22% of visits were' for psy-chosocial reasons, such as stress in families (e.g., substance abuse, neglect), violence exposure, oranxiety. The Medicaid revenues generated by these centers in excess of what was needed to main-tain them were used to hire mental health professionals. The hiring and training of the mental healthprofessionals was by arrangement with the two medical schools in Baltimore, Johns Hopkins Uni-versity and the University of Maryland. Multiple City and State agencies collaborated to develop andsupport the placement of mental health services in these and other schools so that over a lO-year pe-riod, one-third ofthe 176 schools in Baltimore gained these services (Weist, 1997). Currently, in Bal-timore, almost one half of the city schools contain ESMH programs (Bruns, Glass-Siegel, Walrath,Anderson, & Weist, 1999).
MULTIPLE MODELS
Although the first mental health programs were adjuncts to school health centers, subsequent-ly other models were added in schools which did not have school based health centers (SBHCs).Within a year of the SBHC projects, a demonstration project involving coordinated mental health
Supported by project # MCJ24SH02-01-0 from the Office of Adolescent Health, Maternal and Child Health Bureau (Ti-tle V, Social Security Act), Health Resources and Services Administration, Department of Health and Human Services. Weexpress appreciation to Susan Hill for assistance in organizing information on the School Mental Health Program.
Correspondence to: Lois Flaherty, M.D., 770 Lantern Lane, Blue Bell, PA 19422.
379
380 Flaherty and Weist
and social services from the Departments of Juvenile Justice and Socia'l Services in addition to theHealth and Police Departments began at Booker T. Washington Middle School. This program in-cluded a mental health clinic which was actually a satellite program of a community mental healthcenter, with staff hired by the CMHC placed in the school.
A third model involves the placement of a single clinician in a school; this clinician is hired byand reports to the mental health "Lead Agency" responsible for the area in which the school is lo-cated. Lead agencies are institutions responsible for providing mental health services to given ser-vice areas, in a sense, the community mental health center catchment area model. This "stand-alone"model has actually become the most prevalent one in the Baltimore City Schools. Please note thatwhile individual clinicians are placed in schools, our program places the impetus on them to devel-op relationships with other mental health professionals in the building to ensure that additional ser-vices are coordinated and complementary.
Regardless of specific model, these programs are financed by blending of funds from manysources, including Medicaid fee for service revenues and grants from public and private agencies andfoundations. Medicaid revenues generated by services to special education students delivered as partof the Individualized Education Plan or Individual Family Service Plan form a significant portion ofthe total funding for these programs. The school system has supported the use of these special fundsfor children who are being mainstreamed in regular classes with the rationale that mental health ser-vices can help them to succeed in regular education and keep them from going into more restrictivesettings. These funds have also been allocated to provide services to students in regular education,with the goal that such services would help to reduce inappropriate referrals into special education.
THE BALTIMORE MODELS' FORMULA FOR SUCCESS
Creative Leadership in the Public Sector
School mental health programs in Baltimore would not have developed without individuals whohad a passionate commitment to improve the health of adolescents, the ability to think creatively andflexibly about how to develop programs to help them, and the skills to negotiate agreements betweenagencies. John Santelli, a pediatrician and former Baltimore City Health Commissioner, the lateMaxie Collier, an African American psychiatrist who served as head of mental health, John Birkmayer,a social worker with consummate negotiating skills, and Bernice Rosenthal, with a background in pub-lic health and a long career in the City Health Department, were all instrumental in bringing about theprograms. These individuals exemplified how social activism can effect system change.
Effective Interagency Collaboration
ESMH programs in Baltimore have been developed on the strong foundation of interagencycollaboration. Key agencies in this collaboration have been the Baltimore City Public School Sys-tem, the Baltimore City Health Department, the Baltimore Mental Health Systems (representing pub-lic mental health), the State Department of Health and Mental Hygiene, and universities (the Uni-versity of Maryland and Johns Hopkins University, in particular). Notably, as ESMH programs inBaltimore have gained momentum and visibility, opportunities for networking with agencies andprograms in other states, and at the federal level have increased. This national dialogue has been rec-iprocally beneficial as the city has gained valuable information while it has shared its experiences asa clear leader in the ESMH movement (Han, Rosenthal, Fink, & Weist, 1999).
Creative Approaches to Funding
Related to committed leadership and a priority on bringing needed mental health services to un-der- and un-served youth, a variety of creative funding strategies have been used to support ESMH

Baltimore Models 381
programs in Baltimore. These include: 1) Medicaid dollars from special education services (asabove) to contract out to community mental health providers to expand services in the school andprevent inappropriate referrals into special education; 2) funds from school budgets to augment ser-vices provided by school-hired mental health professionals; 3) grants from the state of Maryland; 4)contracts to provide services for youth at risk; for example, through the City Mayor's Office and theOffice of Employment Development; 5) federal grants; 6) foundation grants; and 7) support fromMental Health Lead Agencies in using surplus dollars from adult services to support ESMH pro-grams for children.
Direct Service Orientation
In contrast to a consultative model, ESMH programs in Baltimore have from the outset focusedon direct service delivery. That is, clinicians see children individually, in groups, or with their par-ents, performing all of the services traditionally provided within community mental health centers.Because of the easier access to school staff, there is consultation provided to teachers and other staff,but this is not usually formalized and generally occurs on an as needed basis.
This focus is in keeping with evolving models of mental health consultation. Originally con-ceptualized as a "hands off" experience in which the consultant diluted his or her effectiveness byactually seeing clients, consultation has evolved into a more complex activity which involves skillat functioning at multiple levels (Erchul & Martens, 1997). In addition to providing an obvious ben-efit to the student, the direct service provision acts as a focus around which consultation and educa-tion can be done for teachers and other staff. The result is a deeper understanding of the reasons fora student's behavior and/ or learning problems as well as of the role mental health interventions canplay in ameliorating problems.
Tie-In With a Parent Program
All of the clinicians working in the schools are hired and supervised by mental health profes-sionals in an affiliated organization. The parent organizations include the departments of psychiatryin-the two medical schools in Baltimore, the University of Maryland and the Johns Hopkins Uni-versity, and community mental health centers. This allows for supervision of front line staff, cover-age on the days when the clinician is not in the school, facilitation of referrals for more intensive ser-vices, and back-up for emergencies.
The availability of supervision from more experienced clinicians has been particularly impor-tant as many of the staff hired to work in the schools have needed further training in order to devel-op the skills necessary for effective functioning within a school setting (Flaherty et al., 1998; Wax-man, Weist, & Benson, 1999). The single most common concern voiced by school-based clinicianshas been the degree to which they feel isolated in the school; having a supervisor available by tele-phone and for weekly face to face meetings serves to decrease this sense of isolation.
The fact that the sponsorship for most of the ESMH programs comes from academic centers isimportant in many ways. It allows for the use of the university's resources in providing staff train-ing. By incorporating experience in the school-based programs into the professional training pro-grams sponsored by the university, more mental health professionals are trained to work in these set-tings. Finally, the graduates of the training programs have been hired to fill positions created byexpansion of the school-based programs and by the inevitable staff turnover.
In cases where the primary sponsor is not a community mental health center (CMHC), there isa need for such connection to address more serious mental health issues in youth (especially thoseinvolving risk of harm to self or others). This affiliation is simplified in our program because theCMHCs in the areas where the school-based programs are located are also affiliated with the Uni-versity of Maryland, which is actually responsible for their operations. In the few cases where the
382 Flaherty and Weist
schools are not in the catchment area for our university, we establish connections with the appropri-ate CMHC. This link between the school programs and the CMHCs is particularly important becausehistorically there has been little connection between them (Burns & Friedman, 1990; Weist, Myers,Hastings, Ghuman, & Han, 1999).
Concern About Rising Numbers of Youngsters in Special Education
The allocation of special funds to schools based on the numbers of special education studentsthey had inevitably led to dramatic rises in special education students. Baltimore was no exceptionto this trend. When it became possible to use the funding designated to educate handicapped studentsto help them remain in regular classrooms with additional support rather than be segregated into spe-cial classes, the opportunity to provide mental health services on a preventive basis to youngsters atrisk of special educational placement arose. Anecdotal data from our program has suggested reduc-tions in special education referrals once the ESMH program is in the school (Flaherty et aI., 1996).We are in the process of more formally documenting this relationship in an ongoing study of ESMHprograms in the city (Bruns et aI., 1999).
HISTORY AND DESCRIPTION OF THE UNIVERSITY OF MARYLAND PROGRAM
Our ESMH program at the University of Maryland began in 1989 with clinicians placed in fourschools-three high schools and one middle school. Each year, the number of schools served wasexpanded to the point that there are now 20 schools, ranging from elementary through high school.The fact that they started small and grew gradually enabled us to learn from our experience and gen-eralize it to new locations. For example, over time we have learned that is absolutely essential forstaff who are new in a school to take the time to develop relationships with teachers, school-hiredmental health professionals, school health providers, and administrators. While time spent in devel-oping these relationships, may be perceived as detracting from early clinical productivity, such timeis critically important. This is because relationships will ultimately determine whether the program
. will succeed or not succeed in the school. Description of work in developing such relationships in. the context of truly interdisciplinary teams is beyond the scope of this paper (but please see Flaher-ty et aI., 1998; Waxman et aI., 1999).
Staffing
Each program is staffed by at least one clinician. Minimum requirements for the positions area master's degree in psychology or social work and training or experience in working with childrenand adolescents. Experience in school settings is desirable but not required. Postdoctoral fellows inpsychology and experienced master's level social workers have filled the majority of the positions.While they have ready access to supervisors, clinicians must be able to work independently. Whileon site, supervision is provided occasionally, in general, clinicians receive supervision at the uni-versity and not the school. As there is typically only one staff member from our program in eachschool, we encourage staff members to form close relationships with other mental health profes-sionals in the building (e.g., school psychologists, counselors, and social workers) to promote peersupport, collegial feedback and problem solving, and informal supervision.
Child and adolescent psychiatrists provide limited on-site consultation and are available by tele-phone when not in the schools. Two senior child and adolescent psychiatrists provide consultationabout clinical issues for staff wishing additional clinical consultation in the form of biweekly officehours.
Service Delivery
The modal service provided is individual psychotherapy. However, this is not the traditionalscheduled weekly 50-minute session. The usual length of individual therapy sessions is 30 minutes;
Baltimore Models 383
groups are 45 minutes to an hour. On average, clinicians schedule 15 or more students in a day(e.g., one group and a number of individual and family sessions) and actually see 8 to 10 students.Some clinicians consistently see 15 or more children per day. Although appointments are scheduled,vacant time can easily be filled with other students who are waiting for appointments. The timeof a given student's therapy session often varies from week to week because the schools do not liketo have youngsters absent from the same subject consistently. However, we have learned that it isbetter to have group therapies at a consistent time each week. But it is emphasized to students thatthey should not attend the group when important activities are occurring in the class they are miss-ing (such as tests). Students often drop in for brief contacts outside their regularly scheduled hours.During most days, each clinician sees at least one student referred because of a crisis, such as hav-ing thoughts of self- or other-harm, experiencing abuse or neglect, or a problem involving a livingsituation.
An assessment is done on every youngster seen; however, this is not the kind of extensive eval-uation done in order to determine eligibility for special educational placement or the intensive socialhistory and diagnostic evaluation typical in community settings. Instead, clinicians conduct focusedevaluations on referred youth. These normally take between one and two sessions and involve ask-ing the student (and his/her parent whenever possible) to provide information on: a) academic func-tioning (past and present); b) family history, constellation, and current functioning; c) life goals,strengths, and operating resilience factors; d) peer relations; and e) mental status. The program was'initially funded to provide proactive, flexible, and more preventive services to all youth with mentalhealth needs. As such, we have strived to keep paperwork and other administrative demands on staffto the necessary minimum, to avoid having a school-based service characterized by barriers to care.This allows for maximal effort to be expended in helping troubled or stressed children directly.
As mentioned, to be able to provide services to more youth in need, all clinicians in our pro-gram run a number of groups. Generally groups at the elementary and middle school levels focus onskill training with youth and include topics such as Social Skills.Anger Management, Avoiding Con-flicts, Coping with Violence, and Coping with the Loss of a Loved One. Groups at the high schoollevel usually include some discussion of these topics, but are more process oriented. For example,in one of our high schools there are process oriented groups for males and for females (in general,we believe having same-gender groups at this age level is advisable). In both groups, students agreeto respect one another and maintain confidentiality. Each week, those who have "issues" (e.g., prob-lems in school, home, dating relationships, at work), share them, group members listen, and providesupport and ideas for handling the issue. We view many of our groups as preventive in nature, asmost of the youth who participate in them are encountering significant life stress, but not necessari-ly presenting frank emotional or behavioral problems. As such, the goal for the group is to help themto avoid the development of these problems and show general success in school and in life.
We have become increasingly interested in manualized interventions. These are typically struc-tured and time limited therapies which can be standardized across settings and taught to new clini-cians relatively easily, provided they have sufficient training and experience. They also allow forevaluation of effectiveness. Examples include cognitive-behavioral treatments for depression, anx-iety, and impulsive behavior. Philip Kendall of Temple University has developed a number of man-ualized interventions that are easily integrated into clinical practice in the schools. For example, aprogram to train impulsive children in cognitive and self-control skills includes manuals for use bythe child, the teacher, the therapist, and the parent, with step-by-step procedures described for eachsession (Kendall, 1992).
We do not set a limit on number of sessions and this is extremely variable, ranging from onevisit to spanning over more than one academic year. In the planning for the programs, we proposedto provide only short-term interventions, reasoning that youngsters in need of long-term treatmentcould be better served in CMHCs mental health outpatient clinics. However, we quickly learned that
384 Flaherty and Weist
this was an unrealistic expectation. Even with the CMHCs and the school-based programs under thesame administrative leadership (i.e., associated with the University of Maryland), it is often difficultto get youth and their families to go from the school to the CMHC, and even when this initial con-nection is made, youth often drop out from these centers prematurely. The upshot of this is that theschool-based program often becomes the only provider, even with rather serious cases (e.g., youthwho present suicidal ideation; Weist, 1997; Weist et al., 1999).
Training Aspects
There is a shortage of mental health professionals of various disciplines trained to work specif-ically in schools (Flaherty et al., 1998). Since the early 1990s, our program has served as a trainingsite for interns and post-doctoral fellows in psychology, social work students, and child and adoles-cent psychiatry residents. Most of these trainees come from the University of Maryland in Baltimore,which is the site of professional schools of medicine, nursing, social work, and law. For social workstudents, the programs have served as a field placement. For psychology interns they are an electiveplacement, and for the child and adolescent psychiatry residents they are a required rotation. For alltrainees, school placements are for the entire school year. This allows them to establish relationships,become a part of the school, and work on a long-term basis with some youth. It is noteworthy thatmany of these trainees choose ESMH as the major focus of their career, and many of them remainwith us. For example, in the past four years, we have eight interns in clinical psychology working inour program. Three of them went on to postdoctoral fellowships in the program, and two have joinedthe faculty.
DEVELOPING AN EVALUATION AND RESEARCH COMPONENT."
Services research is essential to generate new knowledge in the emerging expanded school men-tal health field. Research may involve evaluation of the process of providing services as well as eval-uation of the outcome of services. Without knowing who is being served, how and what services arebeing delivered, and by whom, it is impossible to understand what is happening in the school basedsetting. At·the same time, services research is "challenging and murky," not to mention relativelypoorly funded.
As is the general case with publicly funded programs, funding has not been provided specifi-cally for program evaluation and funding from other sources is limited. The university affiliation ofthe program and the fact that postdoctoral psychology fellowships are offered are undoubtedly strongcontributing factors to the success of research efforts. We are also able to draw on resources withinthe Department of Psychiatry for research support. Finally, grants available through the School ofMedicine for new investigators and pilot projects have been extremely valuable.
We have focused on methodologies that can be incorporated into day to day operations withminimal intrusion into the clinical work. In the beginning, the primary program evaluation was donebased on our annual reports to the funding source and the Department of Psychiatry. This continuesto serve an important function. This process involves the compilation of end-of-year statistics byeach clinician and the preparation of a brief report of activities during the year. The statistics are re-viewed at a retreat held in June soon after the end of the school year and used asa basis for pro-gramming for the next year.
In the early years of the program, the statistics gathered annually from each clinician workingin a school served to document the fact that the programs were filling unmet needs (Flaherty et al.,1996). Subsequently, grants from the School of Medicine allowed us to move forward with projectsthat demonstrated more systematically that we were serving underserved populations who were verymuch in need of mental health services and that these services were effectively addressing unmetneeds. The following section describes these projects.
Baltimore Models 385
Needs Assessment
Needs assessment is fundamental to the development of new programs and refinement of ex-isting programs. Needs assessment involves obtaining information from stakeholders, or potentialconsumers, about perceived needs. The success of a program can be measured against goals gener-ated by the needs assessment process. The initial programs in Baltimore were placed in schools de-termined to be most in need of them on the basis on health and educational statistics routinely ob-tained by the city schools and health department. Thus certain high schools were determined to be"high risk" because of their rates of drop out, pregnancy, and sexually transmitted diseases. How-ever, as programs developed rapidly in Baltimore in the 1990s (associated with increasing fundingopportunities), such careful analyses of where to place programs did not occur. Nationally, there isincreasing recognition of the need for prioritizing the allocation of resources for ESMH programs toyouth in the greatest need, and now, in the late 1990s, this is occurring in Baltimore (Weist, 1998).
In 1996, we undertook a survey of key school personnel in urban and rural areas in four statesto assess their perceptions of their students' problems and needs (Weist et al., in press). Findings re-lated to youth age indicated that elementary schools were confronted primarily with acting out prob-lems in youth. As youth entered middle school, internalizing problems like depression and anxietybecame more evident. Substance abuse was rated as serious concern in high school and to a lesserextent, in middle school. Interestingly, inner-city school administrators rated substance abuse to bemore of a problem in middle school than rural or suburban school administrators. However, by highschool age, rural and suburban school administrators rated it as more of a problem than urban schooladministrators. Notably, this survey underscored that there were more physical health services foryouth in schools than mental health services. This is in contrast with basic epidemiology, which in-dicates that significant emotional/behavioral issues in youth are far more frequent than significantsomatic health issues in youth. This disparity points to the need for capacity building to increase thenumber of well trained mental health providers to work with-youth in schools (Weist, 1998).
Characteristics of Students Seen
One of our early studies looked at high school students who used school-based health servicesversus those who did not. On the whole, users and non-users were similar with respect to self-reportmeasures of life stress, emotional-behavioral disturbance, family environment, locus of control, andself-concept. There was a trend in findings indicating that health center use was a positive indicator(associated with better grades and attendance) for boys, but not for girls. Notably, a small group ofhigh intensity clinic users was found to have high levels of self-reported emotional distress, but sur-prisingly, most of these youth were not receiving mental health services. These findings alerted usto the need for outreach to students who use the health center intensively (Weist, Proescher, Freed-man, Paskewitz, & Flaherty, 1995).
In a subsequent study, we evaluated psychosocial functioning in youth served in the school-based programs with those seen in CMHCs in the same communities. Findings indicated that youthfrom the two settings presented comparable levels of emotional and behavioral problems. However,youth. seen in the schools reported higher levels of exposure to violence and were less likely thanyouth seen in the CMHCs to have past histories of mental health intervention (Weist et al., 1999).Findings from this study supported the idea that the school-based programs were reaching youth inneed who otherwise might not be reached, as well as reaching youth under stress and with internal-izing problems (e.g., anxiety related to violence exposure). These findings are similar to the resultsof an analogous study of youth and mental health services in New Haven, Connecticut (Armbruster,Gerstein, & Fallon, 1997) and provide additional evidence that there are significant barriers to treat-ment for underserved youth in community mental health centers.
386 Flaherty and Weist
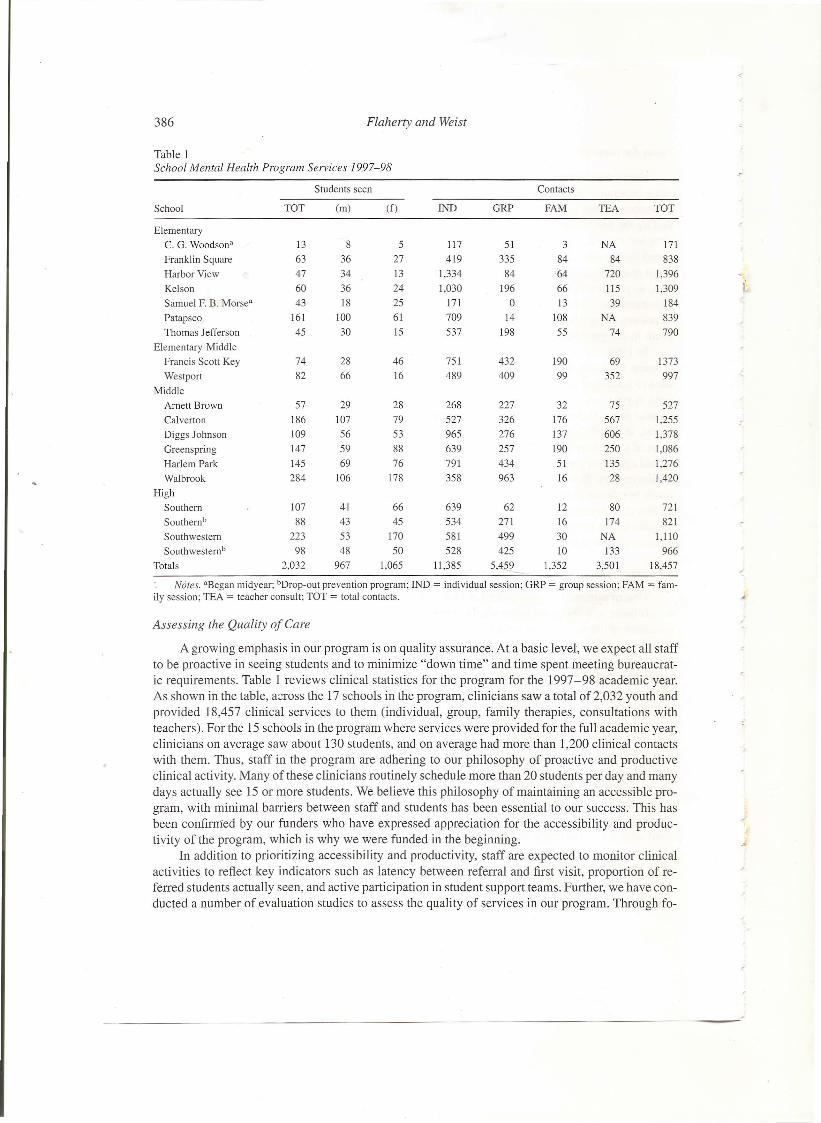
Table 1School Mental Health Program Services 1997-98
Students seen Contacts
School TOT (m) (f) IND GRP FAM TEA TOT
ElementaryC. G. Woodson" 13 8 5 117 51 3 NA 171Franklin Square 63 36 27 419 335 84 84 838Harbor View 47 34 13 1,334 84 64 720 1,396Kelson 60 36 24 1,030 196 66 115 1,309Samuel F. B. Morse" 43 18 25 171 0 13 39 184Patapsco 161 100 61 709 14 108 NA 839Thomas Jefferson 45 30 15 537 198 55 74 790
Elementary-MiddleFrancis Scott Key 74 28 46 751 432 190 69 1373Westport 82 66 16 489 409 99 352 997
MiddleArnett Brown 57 29 28 268 227 32 75 527Calverton 186 107 79 527 326 176 567 1,255Diggs Johnson 109 56 53 965 276 137 606 1,378Greenspring 147 59 88 639 257 190 250 1,086Harlem Park 145 69 76 791 434 51 135 1,276Walbrook 284 106 178 358 963 16 28 1,420
HighSouthern 107 41 66 639 62 12 80 721Southern" 88 43 45 534 271 16 174 821Southwestern 223 53 170 581 499 30 NA 1,110Southwestern" 98 48 50 528 425 10 133 966
Totals 2,032 967 1,065 11,385 5,459 1,352 3,501 18,457Notes. =Began midyear; bDrop-out prevention program; IND = individual session; GRP = group session; FAM = fam-
ily session; TEA = teacher consult; TOT = total contacts. ..Assessing the Quality of Care
A growing emphasis in our program is on quality assurance. At a basic level, we expect all staffto be proactive in seeing students and to minimize "down time" and time spent meeting bureaucrat-ic requirements. Table I reviews clinical statistics for the program for the 1997-98 academic year.As shown in the table, a:::rossthe 17 schools in the program, clinicians saw a total of 2,032 youth andprovided 18,457 clinical services to them (individual, group, family therapies, consultations withteachers). For the 15 schools in the program where services were provided for the full academic year,clinicians on average saw about 130 students, and on average had more than 1,200 clinical contactswith them. Thus, staff in the program are adhering to our philosophy of proactive and productiveclinical activity. Many of these clinicians routinely schedule more than 20 students per day and manydays actually see 15 or more students. We believe this philosophy of maintaining an accessible pro-gram, with minimal barriers between staff and students has been essential to our success. This hasbeen confirmed by our funders who have expressed appreciation for the accessibility and produc-tivity of the program, which is why we were funded in the beginning.
In addition to prioritizing accessibility and productivity, staff are expected to monitor clinicalactivities to reflect key indicators such as latency between referral and first visit, proportion of re-ferred students actually seen, and active participation in student support teams. Further, we have con-ducted a number of evaluation studies to assess the quality of services in our program. Through fo-
Baltimore Models 387
cus groups and surveys, we have polled various stakeholder groups (e.g., youth, families, health cen-ter staff, school administrators) on the most serious problems confronted by youth in the school, rec-ommendations on ways to address these problems, and ways to improve our program. Findings fromthese efforts are helping us to improve services for youth. For example, students have provided ideason the types of group therapies they are interested in have underscored their expectations about con-fidentiality and have provided us with tips on stylistic issues in therapy (such as minimizing note tak-ing during sessions; Nabors, Weist, Tashman, & Myers, in press).
Outcome Evaluation
Outcome studies are considerably more difficult to implement and labor intensive than thosedescribed above. Typically, they involve pre- and post-test measures and control groups. In the schoolsetting, randomized assignment to treatment versus control conditions is difficult and may be im-possible given the mandates of a service program. In our one published study of treatment outcome,we compared high school students who received mental health services with those who did not, outof a total population of students who were seen in the health clinic. We used abbreviated measuresand there was no set number of treatment sessions beyond a minimum of four with a minimum timecourse of one month between the beginning and end of treatment (either mental health or health treat-ment). The mental health treatment group showed significant decreases in depression and increasesin self-concept compared to the comparison group who received physical health services (Weist,Paskewitz, Warner, & Flaherty, 1996).
Nationally, there is increasing pressure for child mental health programs to demonstrate ac-countability and effectiveness, and programs in Baltimore City are under these same pressures. Inour program, we are currently in the middle of a significant evaluation study, involving completionof measures of emotional and behavioral functioning, and tracking of grades, attendance, and disci-pline encounters for students before and after they receive services. Preliminary findings from thisstudy are documenting that indeed students are showing improvements in grades, attendance, schoolbehavior, and general functioning following intervention. But while this effort is promoting programaccountability and we are optimistic about findings from it, we are also aware of the increasing de-mands we are placing on staff in the program. A real challenge for us has become maintaining theflexible, proactive, and productive aspect of services, while negotiating demands to bring in fundsand show accountability.
National Center to Support Expanded School Mental Health Programs
Since 1995, the Maternal and Child Health Bureau of the Health Resources and Services Ad-ministration has funded the Center for School Mental Health Assistance (CSMHA) in our Depart-ment at the University of Maryland. The CSMHA is one of two such national centers which aim toprovide technical assistance and support to school mental health programs nationwide; the other cen-ter-the Center for Mental Health in Schools is located at the University of California, Los Angeles(directed by Howard Adelman and Linda Taylor). The five objectives of the CSMHA are to: 1) pro-vide technical assistance; 2) provide national training and education; 3) analyze critical issues in thefield and make recommendations on addressing them; 4) develop and disseminate appropriate re-sources; and 5) promote networking between people and programs interested in or involved inESMH.
Importantly, the national center and local program are mutually supportive. Clearly, our op-portunity to apply for the grant that developed the national center was based on our experiences inthe local program. Since we have established the center, it has provided support to the program inthe form of resources and training opportunities. In turn, the program has supported the centerthrough sharing of ideas and experiences and providing volunteer staff support at key times (e.g., be-
1I
388 Flaherty and Weist
fore the center's annual conference). Staff from the program and center work well together, and ithas been gratifying to achieve a critical mass of energetic people who are genuinely committed toimproving mental health care for youth.
CHALLENGES AND FUTURE DIRECTIONS
Maintaining Excellence and Moving Forward ~.
" ... the test of a program is its sustainability, both in its original form and later when otherstry to reproduce it" (Dryfoos, 1998).
As our school mental health program has moved into a more mature phase, one of the chal-lenges facing us is to retain high level support at each of the schools we work in. School adminis-trations undergo changes every few years. Principals retire or move on. ESMH programs are subjectto cost-cutting measures and are in danger of being seen as expensive frills in a "back to basics" push.The programs must continually strive to demonstrate their effectiveness and cost-effectiveness.Health care outcomes research is increasingly focused on demonstrating economic benefit of inter-ventions, not simply benefit to health or well-being. Academic medical centers are faced with de-clining patient care revenues and pressures to cut faculty and staff and/or their salaries. We are for-tunate to have support from school principals, teachers, and school health staff, in our departmentand medical school, and at multiple local and state levels. Maintaining this support, however, entailskeeping these various stakeholders informed of activities in the program, seeking and listening totheir input, and participating in other initiatives that aim to improve health and educational systemsfor youth.
Documentation of the success of the programs and dissemination of information remain veryhigh priorities. To date, nearly 40 publications have been produced by the CSMHA, most of these inpeer-reviewed journals. Technical assistance is available to those to call a toll-free number or writefor help with various aspects of ESMH. The CMHSA also publishes a newsletter and sponsors anannual national conference on Advancing School-Based Mental Health Services. Through its Advi-sory Board, the CMHSA enjoys the support of national and local leaders from academia, child ad-vocacy, and government.
Advent of Managed Care
The heavy dependence on ESMH programs on Medicaid funding has meant that they are verymuch affected by the movement of Medicaid into managed health care plans in states across the coun-try. Maryland is no exception as it undergoes the conversion to managed Medicaid. States have lim-ited expertise in negotiating contracts with managed care organizations and are not able to negotiatefrom a position of knowledge and experience. The challenge for ESMH programs is to demonstratecost savings while increasing access to mental health care. Such cost savings may be in other sys-tems, such as the educational or juvenile justice systems, and not directly realized by managed careorganizations (MCOs), however. We are attempting to maintain a dialogue with the leadership inMCOs through critical issues focus groups and the annual CSMHA national conference which hasfeatured presentations on this issue.
Despite the dramatic growth of ESMH programs in Baltimore, the majority of city schools donot have them. Given that we are in an era of uncertainty regarding funding, continued rapid growthis unlikely using the same revenue sources. Other potential sources of revenue are through alloca-tions from school budgets and the new State Children's Health Insurance Program (CHIP). At theCSMHA, we are also exploring the viability of funding programs by documenting cost savings, suchas reduced special education referrals, or referrals for high intensity mental health services such asoutpatient care, residential treatment, or hospitalization. Further, on a national level, there is in-

Baltimore Models 389
creasing recognition that prevention does in fact payoff. But efforts need to be made to more ex-plicitly connect prevention activities of ESMH programs to proximal positive outcomes in schools(e.g., decreased behavioral problems, increased graduation rates), and more distal outcomes in soci-ety (e.g., increased home ownership).
Having an Impact in the Face of Overwhelming Problems
The problems encountered in everyday practice can be truly overwhelming and humbling. It isnot uncommon for new staff to have to deal with suicidal youngsters, victims of sexual and physi-cal abuse, teen gang members, or children dealing with parental substance abuse in the first days orweeks of their work. Decisions about maintaining confidentiality, reporting suspected abuse, and en-suring safety of students and staff have to be made on a day to day basis. Schools lack basic items,like enough new textbooks, and are often dreary buildings in disrepair. Teachers can easily feel un-supported, overwhelmed, and hopeless. Yet we have all experienced the fact that children and ado-lescents, in spite of so many barriers, given the right help, can emerge strong and healthy, ready totake on the tasks of adulthood. Our challenge is to uphold this opportunity for all our youth.
REFERENCES
Armbruster, P., Gerstein, S.H., & Fallon, T (1997). Bridging the gap between service need and service utilization: A school-based mental health program. Community Mental Health Journal, 33. 199-21l.
Bruns, E., Glass-Siegel, M.G., Walrath, e., Anderson, K., & Weist, M.D. (1999). Expanded school mental health programsin Baltimore: A survey of providers. Unpublished manuscript.
Burns, BJ. & Friedman, R.M. (1990). Examining the research base for child mental health services and policy. Journal ofMental Health Administration. 257, 3390-3395.
Dryfoos, J.G. (1998). Safe passage: Making it through adolescence in a risky society (p. 93). New York: Oxford UniversityPress.
Erchul, W.P., & Martens, B.K. (1997). School consultation: Conceptual and empirical bases in clinical practice. New York:Plenum.
Flaherty, L.T, Garrison, E., Waxman, R., Uris, P., Keyes, S., Siegel, M.G., & Weist, M.D. (1998). Optimizing the roles ofschool mental health professionals. Journal of School Health, 68, 162-164.
Flaherty, L.T, Weist, M.D., & Warner, B.S. (1996). School-based mental health services in the United States: History, cur-rent models, and needs. Community Mental Health Journal, 32, 341-352.
Han, Y., Rosenthal, B., Fink, L., & Weist, M.D. (1999). The development of school-based mental health services in Balti-more. Unpublished manuscript.
Kendall, P.e. (.1992). Cognitive-behavioral therapy with impulsive children, 2nd Edition. Ardmore, PA: Workbook Publish-ing.
Nabors, L.A., Weist, M.D., Tashman, N.A., & Myers, CP (In press). Quality assurance and school-based mental health ser-vices. Psychology in the Schools.
Waxman, R.P., Weist, M.D., & Benson, D.M. (1999). Toward collaboration in the growing education-mental health inter-face. Clinical Psychology Review, 19,239-253.
Weist, M.D. (1997). Expanded school mental health services: A national movement in progress. In TH. Ollendick, & RJ.Prinz (Eds.), Advances in clinical child psychology, Volume 19 (pp. 319-352), New York: Plenum Press.
Weist, M.D. (1998). Mental health services in schools: Expanding opportunities. In H. Ghuman, & R. Sarles (Eds.), Hand-book of child and adolescent outpatient. day treatment and community psychiatry (pp. 347-358), Philadelphia: Brun-ner/Maze!.
Weist, M.D .. Myers, C.P., Danforth, J.S., McNeil, D., Ollendick, TH., & Hawkins, R.P. (In press). Expanded school mentalhealth: Assessing needs related to school level and locale. Community Mental Health Journa!.
Weist, M.D., Myers, CP, Hastings, E., Ghuman, H., & Han, Y. (1999). Psychosocial functioning of youth receiving mentalhealth services in the schools vs. community mental health centers. Community Mental Health Journal, 35, 69-81.
Weist, M.D., Paskewitz, D.A., Warner,B.S., & Flaherty, L.T (1996). Treatment outcome of school-based mental health ser-vices for urban teenagers. Community Mental Health Journal, 32, 149-157.
Weist, M.D., Proescher, EJ., Freedman, A.H., Paskewitz, D.A., & Flaherty, L.T (1995), School-based health services for ur-ban adolescents: Psychosocial characteristics of clinic users versus nonusers. Journal of Youth and Adolescence, 24, 251-265.

























![[Cooperation between primary care and mental health services]](https://img.dokumen.tips/doc/110x75/63510236137c5d3168039ebe/cooperation-between-primary-care-and-mental-health-services.jpg)



