Embed Size (px)
Citation preview
RAPHNDJD
cdaapdpH
ubtou
iasmvlPs
NnC[g
lvp
A
PS
AHM
©P
AD
ULT
CA
RD
IAC
ight Heart Dysfunction After Left Ventricularssist Device Implantation: A Comparison of theulsatile HeartMate I and Axial-FloweartMate II Devices
ishant D. Patel, BA, Eric S. Weiss, MD, Justin Schaffer, MS, Susan L. Ullrich, RN,ennis C. Rivard, MA, Ashish S. Shah, MD, Stuart D. Russell, MD, and
ohn V. Conte, MD
ivisions of Cardiac Surgery and Cardiology, The Johns Hopkins Medical Institutions, Baltimore, MarylandsoooHrHraaw((
cpivdHds
Background. Right heart dysfunction confers signifi-ant morbidity and mortality after left ventricular assistevice i m plantation and historically occurs in as manys a third of patients. It is unknown whether newerxial flow pumps have a different impact on postim-lant right heart dysfunction. We compared the inci-ence of right heart dysfunction after implantation of theulsatile HeartMate I (XVE) and the continuous floweartMate II left ventricular assist device.Methods. We retrospectively reviewed patients who
nderwent HeartMate I or HeartMate II implantationetween June 2000 and March 2007. Right heart dysfunc-
ion was defined as inotropic/vasodilator support for 14r more consecutive days or the need for a right ventric-lar assist device, or both.Results. Seventy-seven patients underwent HeartMate
mplantation; 43 received a HeartMate I and 34 received HeartMate II, for a mean left ventricular assist deviceupport time of 202 and 160 days, respectively. Operativeortality was lower for HeartMate II patients (28%
ersus 15%; p � 0.26). The HeartMate II patients hadower preoperative right ventricular stroke work index.ulmonary vascular resistance index, right ventricular
troke work index, and pulmonary and right atrial pres-ba
stMHiep4
opkins Medical Institutions, Blalock 618, 600 N Wolfe St, Baltimore,D 21287; e-mail: [email protected].
2008 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ures improved and were similar between groups post-peratively. Overall, right heart dysfunction devel-ped in 35% of HeartMate I patients (15 of 43) and 41%f HeartMate II patients (14 of 34; p � 0.63). FewereartMate II patients (2) than HeartMate I patients (5)
equired 7 or more days of epinephrine, whereas moreeartMate II patients (7) than HeartMate I patients (5)
equired 7 or more days of milrinone. Six HeartMate Ind 3 HeartMate II patients required right ventricularssist device implantation for right heart failure. Survivalas similar (p � 0.7) between groups at, respectively, 3
63% versus 62%), 6 (58% versus 58%), and 12 months49% versus 48%).
Conclusions. Right heart dysfunction is a persistentlinical problem after left ventricular assist devicelacement. We report the first study comparing the
ncidence of right heart dysfunction after HeartMate Iersus HeartMate II implantation. Although the inci-ence of right heart dysfunction was similar, fewereartMate II patients required right ventricular assistevice placement and fewer required pure inotropicupport for right heart failure.
(Ann Thorac Surg 2008;86:832– 40)
© 2008 by The Society of Thoracic Surgeonsearly 5 million Americans suffer from congestiveheart failure (CHF) [1]. With 550,000 new cases diag-
osed annually and cost estimates exceeding $10 billion,HF continues to be a significant public health concern
1, 2]. Survival remains poor, with a 1-year mortality ratereater than 50% for patients with severe CHF [3].Survival, quality of life, and functional capacity are
imited for patients with CHF despite significant ad-ancements in medical therapy. Currently, cardiac trans-lantation is the gold standard for the treatment of CHF,
ccepted for publication May 5, 2008.
resented at the Forty-fourth Annual Meeting of The Society of Thoracicurgeons, Fort Lauderdale, FL, Jan 28–30, 2008.
ddress correspondence to Dr Conte, Division of Cardiac Surgery, Johns
ut it is donor limited, requires immunosupression ther-py, and has many exclusions to candidacy.Left ventricular assist devices (LVAD) have been
hown to successfully support patients awaiting cardiacransplantation [4 –12]. The Randomized Evaluation of
echanical Assistance for the Treatment of Congestiveeart Failure (REMATCH) trial showed that LVADs may
mprove survival and quality of life for those with severend-stage CHF who are not candidates for cardiac trans-lantation [13, 14]. The REMATCH trial demonstrated a8% reduction in the risk of death for LVAD recipients
Drs Conte and Russell disclose that they have a finan-
cial relationship with Thoratec Corp.0003-4975/08/$34.00doi:10.1016/j.athoracsur.2008.05.016
vs
itstldt
CaUiatovoHtpL
M
SWuLMIF
l
T
AMI
DHHSCP
P
O
833Ann Thorac Surg PATEL ET AL2008;86:832–40 HEARTMATE II VERSUS I LVAD
AD
ULT
CA
RD
IAC
ersus patients receiving optimal medical therapy de-pite using an LVAD with limited durability.
Right heart dysfunction (RHD) is a concern after LVADmplantation and occurs historically in as many as onehird of patients [15]. First-generation pulsatile devices,uch as the HeartMate XVE, have been causally related tohe incidence of RHD owing to the mechanical effects ofeft ventricular unloading [15]. The impact of recentlyeveloped axial flow [16–19] LVADs on right heart func-
ion is unknown. The HeartMate II LVAD (Thoratec
ig 1. (Left) The HeartMate II and (right) the HeartMate I (XVE)
Abbreviations and Acronyms
CHF � congestive heart failureCVP � central venous pressureLVAD � left ventricular assist devicemPAP � mean pulmonary artery pressureNYHA � New York heart associationPCWP � pulmonary capillary wedge
pressureREMATCH � Randomized Evaluation of
Mechanical Assistance for theTreatment of Congestive HeartFailure
RHD � right heart dysfunctionRVAD � right ventricular assist deviceRVSWI � right ventricular stroke work index
peft ventricular assist devices.
orporation, Pleasanton, California) is a promising newxial-flow pump that is currently in clinical trials in thenited States (Fig 1). Complete left ventricular unloading
s avoided with this device and other second-generationxial flow pumps. Our sense and that of other investiga-ors is that there is less RHD with the axial flow pumpswing to maintenance of left ventricular end-diastolicolume, maintained septal position, and preservationf right ventricular mechanics. We began using theeartMate II in January of 2005 and sought to compare
he incidence of RHD and right heart failure after im-lantation with the HeartMate II versus HeartMate IVAD.
aterial and Methods
tudy Designe conducted a retrospective review of all patients who
nderwent either HeartMate II or HeartMate I (XVE)VAD implantation at our institution from June 2000 toarch 2007 after Institutional Review Board approval.
ndividual waiver for consent was granted. For analysis,
able 1. Baseline Characteristics
HeartMate II(n � 34)
HeartMate I(n � 43)
pValue
ge (years) 51.4 � 14.5 48.7 � 13.2 0.40ale sex (%) 27 (79.4) 36 (83.7) 0.62
ndicationsIdiopathic
cardiomyopathy (%)16 (47.1) 15 (34.9) 0.35
Ischemiccardiomyopathy (%)
13 (38.2) 15 (34.9) 0.81
Valvular disease (%) 0 (0) 2 (4.7) 0.50Familial
cardiomyopathy (%)2 (5.9) 4 (9.3) 0.69
Postpartumcardiomyopathy (%)
0 (0) 2 (4.7) 0.50
Radiation induced (%) 0 (0) 1 (2.3) 1.00Adriamycin
cardiomopathy (%)1 (2.9) 1 (2.3) 1.00
Myocarditis (%) 1 (2.9) 1 (2.3) 1.00Rheumatic disease (%) 0 (0) 1 (2.3) 1.00Accelerated
atherosclerosispost-OHT (%)
0 (0) 1 (2.3) 1.00
Congenital (%) 1 (2.9) 0 (0) 0.44iabetes mellitus (%) 9 (26.5) 13 (30.2) 0.71yperlipidemia (%) 16 (47.1) 23 (53.5) 0.57ypertension (%) 19 (55.9) 24 (55.8) 0.99moking (%) 17 (50.0) 17 (39.5) 0.35ardiogenic shock (%) 8 (24.2) 8 (21.6) 0.79revious myocardial
infarction (%)13 (38.2) 18 (41.9) 0.74
reoperative intra-aorticballoon pump (%)
11 (32.4) 20 (46.5) 0.20
HT � orthotopic heart transplantation.
atients were grouped into those who underwent
HHa
d(tvwait1v
SSsauu
FHcP
TF
H
R
Cpps
T
H
H
a
Cp
834 PATEL ET AL Ann Thorac SurgHEARTMATE II VERSUS I LVAD 2008;86:832–40A
DU
LTC
AR
DIA
C
eartMate II implantation versus those who hadeartMate I implantation. Relevant baseline, operative,
nd postoperative data were collected. Hemodynamic
able 2. Baseline Hemodynamics, Renal and Hepaticunction, and Hematologic Data
HeartMate II(n � 34)
HeartMate I(n � 43)
pValue
emodynamicsHeart rate (beats/min) 90.1 � 20.3 86.6 � 20.0 0.45Systolic blood pressure
(mm Hg)100.1 � 12.4 99.2 � 16.6 0.80
Ejection fraction (%) 14.2 � 6.7 12.6 � 6.2 0.28PCWP (mm Hg) 25.3 � 10.5 25.5 � 7.6 0.93mPAP (mm Hg) 34.2 � 12.2 35.9 � 9.2 0.52CVP (mm Hg) 12.2 � 6.5 12.4 � 5.9 0.87PVRI
(dynes/sec*cm�5/m2)433 � 269 512 � 435 0.38
Cardiac index(L · min�1 · m�2)
1.8 � 0.5 1.9 � 0.47 0.47
RVSWI (g*m/m2) 5.7 � 2.3 8.2 � 3.9 0.002enal and hepatic
functionBlood urea nitrogen
(mg/dL)42.4 � 24.4 37.0 � 21.1 0.30
Creatinine (mg/dL) 1.7 � 0.8 1.7 � 0.9 0.87Total bilirubin (mg/dL) 1.5 � 1.1 1.9 � 1.5 0.20Alanine
aminotransferase(IU)
92.1 � 221.3 82.3 � 96.0 0.79
Aspartateaminotransferase(IU)
48.9 � 63.8 72.1 � 90.6 0.21
VP � central venous pressure; mPAP � mean pulmonary arteryressure; PCWP � pulmonary capillary wedge pressure; PVRI �ulmonary vascular resistance index; RVSWI � right ventriculartroke work index.
able 3. Preoperative and Postoperative Hemodynamic Indexe
Preoperative
eartMate I hemodynamicsPCWP (mm Hg) 25.5 � 7.6mPAP (mm Hg) 35.9 � 9.2CVP (mm Hg) 12.4 � 5.9PVRI (dynes/sec*cm�5/m2) 512 � 435Cardiac index (L · min�1 · m�2) 1.9 � 0.47RVSWI (g*m/m2) 8.2 � 3.9eartMate II hemodynamicsPCWP (mm Hg) 25.3 � 10.5mPAP (mm Hg) 34.2 � 12.2CVP (mm Hg) 12.2 � 6.5PVRI (dynes/sec*cm�5/m2) 433 � 269Cardiac index (L · min�1 · m�2) 1.8 � 0.5RVSWI (g*m/m2) 5.7 � 2.3
p � 0.05 versus preoperative.
VP � central venous pressure; mPAP � mean pulmonary artery preulmonary vascular resistance index; RVSWI � right ventricular stroke wo
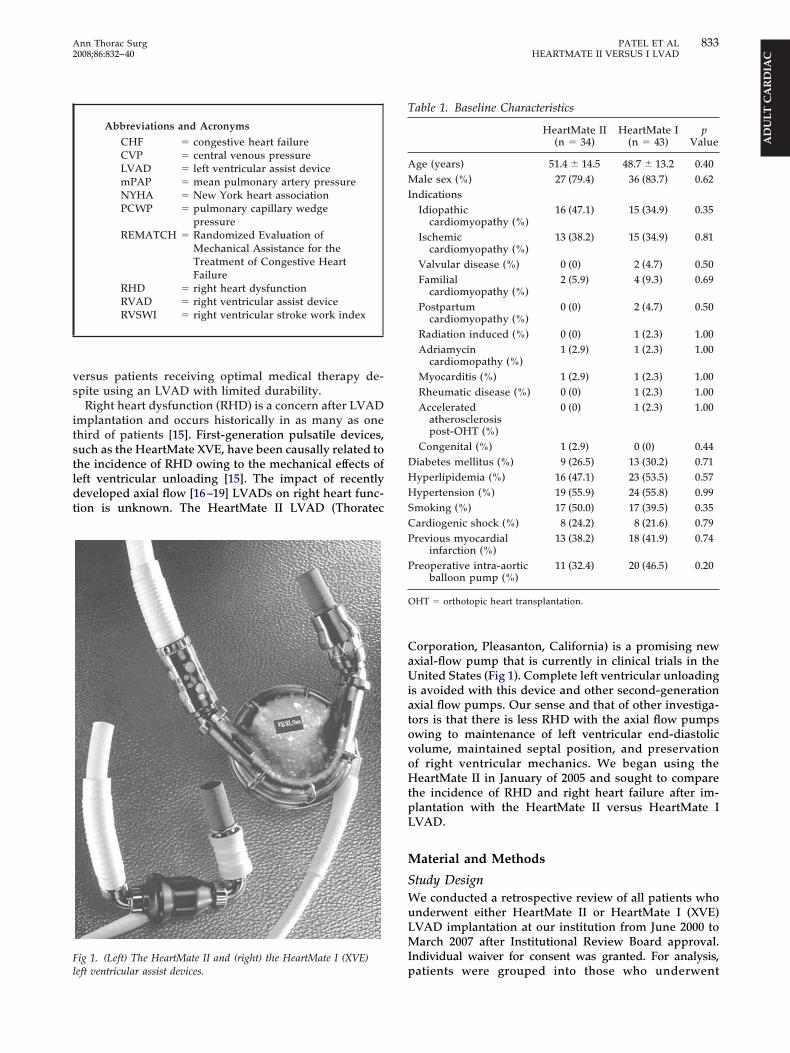
ata included pulmonary capillary wedge pressurePCWP), mean pulmonary artery pressure (mPAP), cen-ral venous pressure (CVP), cardiac index, pulmonaryascular resistance index, and right ventricular strokeork index (RVSWI) collected preoperatively and 1, 3,
nd 6 months after LVAD implantation. Study endpointsncluded survival, the incidence of right heart dysfunc-ion, defined as the need for inotropes or vasodilators for4 or more consecutive days, or the need for a rightentricular assist device (RVAD).
tatistical Analysistatistical analyses were performed using SPSS 12.0oftware (SPSS, Chicago, Illinois). All data are presenteds HeartMate II versus HeartMate I and as mean � SDnless otherwise noted. Fisher’s exact test and t test weresed for qualitative and quantitative variable analyses,
ig 2. Preoperative and postoperative hemodynamic data foreartMate I (solid lines) and HeartMate II (dashed lines). (CVP �
entral venous pressure; mPAP � mean pulmonary artery pressure;CWP � pulmonary capillary wedge pressure.)
1 Month 3 Months 6 Months
10.2 � 6.6a 13.4 � 7.6a 10.6 � 3.0a
20.9 � 7.1a 24.0 � 7.8a 21.5 � 4.2a
9.9 � 5.7 10.8 � 8.1 8.6 � 4.0334 � 184 303 � 74 322 � 662.8 � 0.8a 2.9 � 0.8a 2.7 � 0.7a
4.8 � 2.7a 5.6 � 2.1 5.6 � 3.1
8.6 � 5.6a 11.9 � 4.7a 11.2 � 8.6a
19.0 � 6.8a 22.7 � 7.5a 20.0 � 9.3a
8.8 � 6.5 9.7 � 4.9 9.7 � 8.2290 � 131a 345 � 211 276 � 1523.0 � 0.5a 2.8 � 0.5a 2.69 � 0.7a
5.4 � 2.6 5.4 � 1.9 4.2 � 2.4
s
ssure; PCWP � pulmonary capillary wedge pressure; PVRI �rk index.
rpHhmp
OPmtbawtccitittg
f
mtbtappgrt
R
Dtt4bt2csaA((
fwPHiv
OMmmnot
Tf
E
M
T
H
H
a
835Ann Thorac Surg PATEL ET AL2008;86:832–40 HEARTMATE II VERSUS I LVAD
AD
ULT
CA
RD
IAC
espectively. Kaplan-Meier and log-rank analyses wereerformed to compare survival for HeartMate II versuseartMate I patients. We conducted Cox proportionalazards regression modeling to assess for predictors ofortality and logistic regression analysis to assess for
redictors of right heart dysfunction.
perative Techniqueatients receiving the HeartMate II LVAD underwentedian sternotomy. The outflow graft was anastomosed
o the ascending aorta without bypass whenever possi-le. After the institution of cardiopulmonary bypass, anpical ventriculotomy was made and the inflow cannulaas placed in the left ventricular apex. The pump was
hen activated; after deairing, patients were weaned fromardiopulmonary bypass. Our patients routinely come offardiopulmonary bypass on epinephrine, milrinone, andnhaled nitric oxide in various combinations. The con-inuation of inotropes was made based on clinicalnterpretation of the hemodynamic data. Those pa-ients requiring protracted inotropes typically had ino-rope-dependent LVAD flow as well as echocardio-raphic evidence of right ventricular dysfunction.The HeartMate I LVAD is implanted in a similar
ashion. HeartMate I patients were weaned off cardiopul-
able 4. Postoperative Consecutive Days Requiring Inotropesor HeartMate I and HeartMate II Patients
Number of Patients
HeartMate II HeartMate I
pinephrine� 0.05 �g · kg�1 · min�1
� 14 days 1 0� 7 days 2 5ilrinone� 0.50 �g · kg�1 · min�1
� 14 days 1 0� 7 days 7 5
able 5. Preoperative and Postoperative Renal and Hepatic D
Preoperative
eartMate I renal/hepatic functionBlood urea nitrogen (mg/dL) 37.0 � 21.1Creatinine (mg/dL) 1.7 � 0.9Total bilirubin (mg/dL) 1.9 � 1.5Alanine aminotransferase (IU) 82.3 � 96.0Aspartate aminotransferase (IU) 72.1 � 90.6eartMate II renal/hepatic functionBlood urea nitrogen (mg/dL) 42.4 � 24.4Creatinine (mg/dL) 1.7 � 0.8Total bilirubin (mg/dL) 1.5 � 1.1Alanine aminotransferase (IU) 92.1 � 221.3Aspartate aminotransferase (IU) 48.9 � 63.8
p � 0.05 versus preoperative.
onary bypass in a fixed rate mode, as recommended byhe manufacturer, and once stable off cardiopulmonaryypass, switched to automatic mode. Patients with severe
ricuspid regurgitation underwent concomitant tricuspidnnuloplasty. This decision was made based on thereoperative echocardiogram in most cases. In someatients, intraoperative transesophageal echocardio-rams that showed significant worsening of tricuspidegurgitation prompted repair. Tricuspid repair was rou-inely performed before apical ventriculotomy.
esults
uring the study period, 77 patients underwent implanta-ion with a HeartMate LVAD. Since January 2005, 34 pa-ients have received a HeartMate II LVAD. The remaining3 patients in this study received a HeartMate I LVADetween June 2000 and October 2006. Mean LVAD support
ime was 160.5 � 173.4 days for the HeartMate II group and02.3 � 258.9 days for the HeartMate I group. Baselinelinical characteristics were similar between groups and arehown in Table 1. An ischemic cause of CHF occurred inpproximately one third of patients in each group (p � 1.00).ll HeartMate II patients and 97.6% of HeartMate I patients
42 of 43) were in preoperative New York Heart AssociationNYHA) class IV.
Baseline hemodynamic indices, renal and hepaticunction, and hematologic data are shown in Table 2 andere similar between HeartMate II and I patients.reoperative RVSWI was significantly lower for theeartMate II group (5.7 versus 8.2 g*m/m2; p � 0.002),
ndicating worse right heart function in the HeartMate IIersus HeartMate I group.
perative Dataean cardiopulmonary bypass time was 76.7 � 34.9inutes for the HeartMate II group and 96.2 � 37.5inutes for the HeartMate I group (p � 0.04). Twenty-
ine percent of HeartMate II patients (10 of 34) and 4.7%f HeartMate I patients (2 of 43) underwent concomitantricuspid valve annuloplasty (p � 0.004).
1 Month 3 Months 6 Months
23.7 � 21.1a 18.6 � 9.5a 19.2 � 7.3a
1.4 � 0.9 1.2 � 0.5a 1.1 � 0.4a
2.9 � 7.21 1.0 � 1.8a 0.5 � 0.3a
30.8 � 40.8a 21.1 � 13.4a 23.6 � 17.0a
50.3 � 68.8 28.0 � 16.2a 33.7 � 28.6
27.1 � 17.1a 22.6 � 15.1a 25.5 � 13.4a
1.4 � 0.8 1.1 � 0.5a 1.3 � 0.72.2 � 3.2 1.1 � 1.1 0.8 � 0.5a
70.1 � 165.6 38.8 � 43.0 25.6 � 14.4101.8 � 230.5 55.4 � 90.2 31.1 � 20.0
ata
HCcHmeCtPpisaops
IRovg
If
rcfvfep
RSdSawnuaomtafm
LTI0tHipb
orfH
Fbl
T
B
P
F
PD
DS
a
FHl
836 PATEL ET AL Ann Thorac SurgHEARTMATE II VERSUS I LVAD 2008;86:832–40A
DU
LTC
AR
DIA
C
emodynamicshanges in hemodynamic indices while on mechanical
irculatory support with either the HeartMate II oreartMate I LVAD are shown in Table 3. Mean PCWP,PAP, and cardiac index significantly improved postop-
ratively for the HeartMate II group, whereas the meanVP and pulmonary vascular resistance index trended
oward improvement. For the HeartMate I group, meanCWP, mPAP, CVP, and cardiac index significantly im-roved postoperatively; pulmonary vascular resistance
ndex trended toward improvement, but did not reachtatistical significance. When comparing HeartMate IInd HeartMate I patients, both groups had similar post-perative PCWP, mPAP, and CVP at 1, 3, and 6 monthsostoperatively (Fig 2). Postoperative RVSWI was alsoimilar between groups at 6 months.
notropic/Vasodilator Requirement and RHDight heart dysfunction, defined as 14 consecutive daysf inotropic or vasodilator support or the need for a rightentricular assist device (RVAD), was similar betweenroups (41.2% versus 34.9%; p � 0.63). Three HeartMate
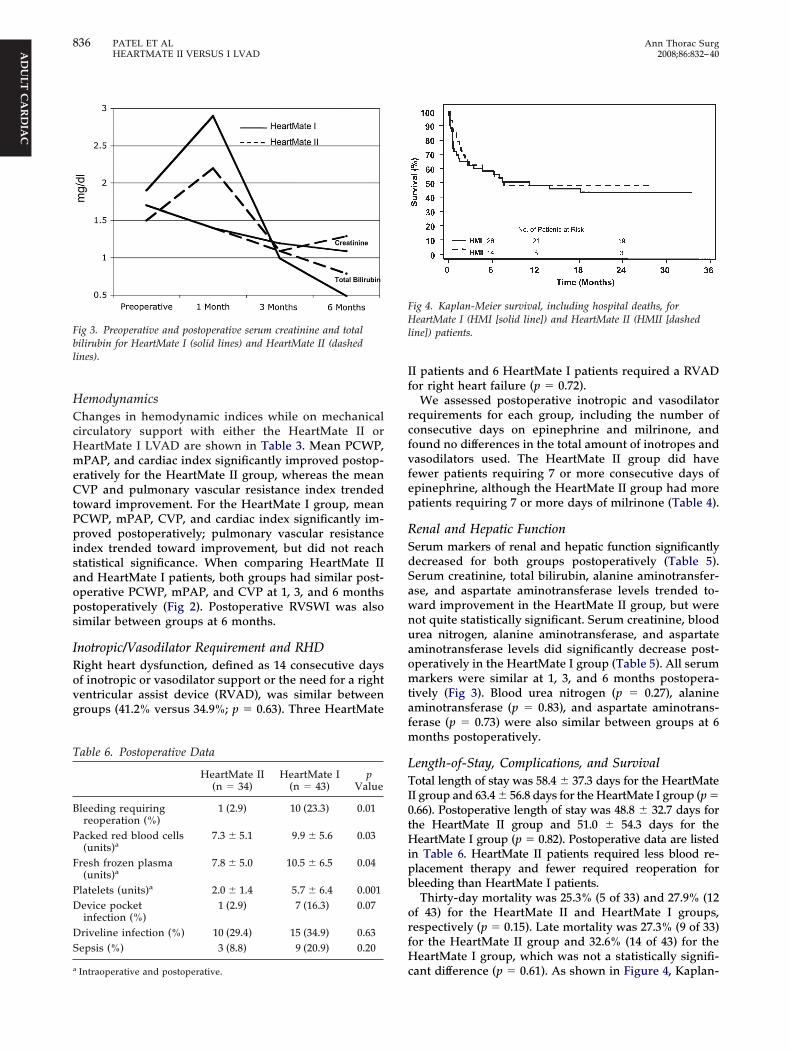
ig 3. Preoperative and postoperative serum creatinine and totalilirubin for HeartMate I (solid lines) and HeartMate II (dashedines).
able 6. Postoperative Data
HeartMate II(n � 34)
HeartMate I(n � 43)
pValue
leeding requiringreoperation (%)
1 (2.9) 10 (23.3) 0.01
acked red blood cells(units)a
7.3 � 5.1 9.9 � 5.6 0.03
resh frozen plasma(units)a
7.8 � 5.0 10.5 � 6.5 0.04
latelets (units)a 2.0 � 1.4 5.7 � 6.4 0.001evice pocketinfection (%)
1 (2.9) 7 (16.3) 0.07
riveline infection (%) 10 (29.4) 15 (34.9) 0.63epsis (%) 3 (8.8) 9 (20.9) 0.20
cIntraoperative and postoperative.
I patients and 6 HeartMate I patients required a RVADor right heart failure (p � 0.72).
We assessed postoperative inotropic and vasodilatorequirements for each group, including the number ofonsecutive days on epinephrine and milrinone, andound no differences in the total amount of inotropes andasodilators used. The HeartMate II group did haveewer patients requiring 7 or more consecutive days ofpinephrine, although the HeartMate II group had moreatients requiring 7 or more days of milrinone (Table 4).
enal and Hepatic Functionerum markers of renal and hepatic function significantlyecreased for both groups postoperatively (Table 5).erum creatinine, total bilirubin, alanine aminotransfer-se, and aspartate aminotransferase levels trended to-ard improvement in the HeartMate II group, but wereot quite statistically significant. Serum creatinine, bloodrea nitrogen, alanine aminotransferase, and aspartateminotransferase levels did significantly decrease post-peratively in the HeartMate I group (Table 5). All serumarkers were similar at 1, 3, and 6 months postopera-
ively (Fig 3). Blood urea nitrogen (p � 0.27), alanineminotransferase (p � 0.83), and aspartate aminotrans-erase (p � 0.73) were also similar between groups at 6
onths postoperatively.
ength-of-Stay, Complications, and Survivalotal length of stay was 58.4 � 37.3 days for the HeartMate
I group and 63.4 � 56.8 days for the HeartMate I group (p �.66). Postoperative length of stay was 48.8 � 32.7 days forhe HeartMate II group and 51.0 � 54.3 days for the
eartMate I group (p � 0.82). Postoperative data are listedn Table 6. HeartMate II patients required less blood re-lacement therapy and fewer required reoperation forleeding than HeartMate I patients.Thirty-day mortality was 25.3% (5 of 33) and 27.9% (12
f 43) for the HeartMate II and HeartMate I groups,espectively (p � 0.15). Late mortality was 27.3% (9 of 33)or the HeartMate II group and 32.6% (14 of 43) for the
eartMate I group, which was not a statistically signifi-
ig 4. Kaplan-Meier survival, including hospital deaths, foreartMate I (HMI [solid line]) and HeartMate II (HMII [dashed
ine]) patients.
ant difference (p � 0.61). As shown in Figure 4, Kaplan-

Myf
f1a0mi[idmniamnpnpt
C
Mafc2awicdiwflhrrm
iitn[b
pmulhhthh
iefFwf
ptOthrsMiim[cbtmvnfciui
tatdwhtuwu
HdwwnglevHstdi
vu
837Ann Thorac Surg PATEL ET AL2008;86:832–40 HEARTMATE II VERSUS I LVAD
AD
ULT
CA
RD
IAC
eier survival, including hospital deaths, was 50% at 1ear for both groups; 2-year survival was 44% and 48%or the HeartMate I and II groups, respectively (p � 0.70).
When analyzing all patients in this series for riskactors for mortality, increasing age (hazard ratio [HR].07; 95% confidence interval [CI]: 1.02 to 1.12; p � 0.004)nd lower preoperative RVSWI (HR 0.75; 95% CI: 0.57 to.98; p � 0.03) were associated with mortality. The lonearker for right heart dysfunction was preoperative
ntra-aortic balloon pump counterpulsation (odds ratioOR] 6.21; 95% CI: 1.01-38.0; p � 0.04). Variables includedn the analyses were age, sex, race, type of HeartMateevice, preoperative inotropes, cause of CHF, diabetesellitus, cardiogenic shock, chronic obstructive pulmo-
ary disease, previous myocardial infarction, body massndex, preoperative intra-aortic balloon pump, preoper-tive creatinine, preoperative PCWP, preoperativePAP, preoperative cardiac index, preoperative pulmo-
ary vascular resistance index, preoperative CVP, andreoperative RVSWI. The type of HeartMate device wasot associated with mortality (HR 0.3; 95% CI: 0.1 to 1.0;� 0.06) or right heart dysfunction (OR 1.3; 95% CI: 0.36
o 5.12; p � 0.64) in our models.
omment
any studies have successfully shown that LVADs aren excellent option for patients with end-stage CHF andor those awaiting cardiac transplantation, with signifi-ant improvements in survival and quality of life [13, 14,0–23]. The REMATCH trial has shown that LVAD ther-py improves survival in end-stage heart failure patientsho are not transplant candidates compared with med-
cally managed patients [13, 14]. The two most frequentauses of death in the LVAD group were sepsis andevice failure [24]. Nearly 50% of the device malfunctions
nvolved implantable components, the most common ofhich was inflow conduit malfunctions resulting in in-ow valve incompetence. The newer axial-flow LVADsave been designed in an effort to minimize operativeisk, improve durability, and lower the risk of device-elated adverse events, in part by reducing the number ofoving parts in the device [16–19].The HeartMate II, developed by Thoratec Corporation,
s a continuous, axial-flow LVAD with a spinning rotor asts lone moving part, an inflow cannula with a sintereditanium surface, an impeller powered by an electromag-etic motor, and a single driveline that exits the abdomen
18, 19, 25–28]. Early results have been excellent in theridge to transplant population [28].Right heart dysfunction is a concern after LVAD im-
lantation and contributes significantly to postoperativeorbidity and mortality. In a study of 108 patients
ndergoing HeartMate I implantation, Dang and col-eagues [15] reported that 38.9%, or 42 patients, had righteart failure postoperatively. Of the 42 patients with righteart failure, 14 required a RVAD. The authors found
hat female patients were more likely to develop righteart failure than male patients, and patients with right
eart failure had a higher early mortality rate, longer sntensive care unit length of stay, higher rates of reop-ration for bleeding, and a greater incidence of renalailure than those who did not have right heart failure.urthermore, the authors found that intraoperative CVPas a significant predictor of postoperative right heart
ailure.Many theories as to the etiology of RHD have been
roposed [29–33]. Experimental models have been usedo try and discern the genesis of LVAD-associated RHD.moto and colleagues [29] found a Frank-Starling rela-
ion for the right ventricular free wall in an isolated righteart canine model. The authors demonstrated a linearelationship between right ventricular systolic peak pres-ure and end-diastolic length or end-diastolic pressure.
oon and coworkers [30] have shown a global decreasen right ventricular systolic function with a concomitantncrease in right ventricular end-diastolic volume to
aintain right ventricular output. Farrar and colleagues31] in an early work found reduced right ventricularontraction in normal dogs during LVAD support. El-eery and colleagues [32], on the other hand, observed
hat right ventricular function during LVAD support wasaintained and the systolic interaction with the left
entricle was of minimal consequence in the mainte-ance of right heart function. Finally, an earlier work
rom Miyamoto and colleagues [33] showed that in-reases in the amount of left ventricular unloading led toncremental decreases in the derivative of right ventric-lar pressure (right ventricular dP/dt), effectively reduc-
ng right ventricular function.A valid criticism of these experimental studies is that
hey are performed in normal hearts and not hearts innimals with CHF. The finding of increased right ven-ricular end-diastolic pressure experimentally, however,oes correlate with what is seen clinically in those heartsith RHD after LVAD implantation. They are enlarged,ypocontractile, and need an increased preload to main-
ain adequate LVAD flows. Many of the LVAD modelssed in these animal experiments are pulsatile pumps,hich do not necessarily reflect what occurs with contin-ous flow devices.In our study, 14 HeartMate II patients and 15eartMate I patients met our definition of right heartysfunction postoperatively. The most significant findingas that 3 HeartMate II and 6 HeartMate I patients under-ent RVAD placement for right heart failure. While theeed for RVAD support was lower in the HeartMate IIroup, this did not reach statistical significance. The
ength of inotrope and vasodilator use is a much softerndpoint. Our more recent tendency to leave patients onasodilators until diuresed may bias the data. TheeartMate II patients did require less pure inotropic
upport and more vasodilators than HeartMate I pa-ients. A larger patient cohort and longer follow-up mayemonstrate true differences in the need for RVAD and
notropic support after HeartMate II implantation.The HeartMate I device mechanically unloads the left
entricle, which may result in bowing of the interventric-lar septum away from the right ventricle. Bulging of the
eptum into the left ventricle may reduce the efficiency of
ruMtfislLo
wirtifdTatra
RHlfotuwaiohiab
flsp
cnMatshis
a2DHHssNihv
TBI
R
1
1
1
Fa
838 PATEL ET AL Ann Thorac SurgHEARTMATE II VERSUS I LVAD 2008;86:832–40A
DU
LTC
AR
DIA
C
ight ventricular contraction by destabilizing the fulcrumpon which the right ventricle contracts (Fig 5) [15].oreover, the right ventricle may receive a venous re-
urn beyond its capacity owing to the LVAD’s effectiveorward flow through the systemic circulation, resultingn right ventricular dysfunction [34]. Maintaining theeptal midline position requires maintenance of someeft ventricular volume. This results in less than maximalVAD flow, which prevents overcirculation that couldverwhelm the functional capacity of the right ventricle.In our early experience with the HeartMate II LVAD,e became more aggressive with performing a concom-
tant tricuspid annuloplasty, and our current policy is toepair the valve in patients with moderate or worsericuspid regurgitation. That may be important, as exper-mental evidence suggests diminished right ventricularunction requires an increased right ventricular end-iastolic pressure to maintain comparable forward flow.his increased right ventricular end-diastolic pressurend right ventricular end-diastolic dimension can causericuspid valve chordal tethering and increase tricuspidegurgitation. Tricuspid valve repair can correct thisbnormality and help maintain flow.Our early clinical impression is that there is less
HD after HeartMate II implantation. We do find thateartMate II patients come off bypass easier, require
ower peak doses of inotropes, and recover relativelyaster than their HeartMate I counterparts. When comingff cardiopulmonary bypass, we monitor the position ofhe septum and attempt to maintain enough left ventric-lar volume to keep the septum in a midline position,hich may lead to less RHD. On logistic regression
nalysis, the only predictor of RHD was preoperativentra-aortic balloon pump counterpulsation, which dem-nstrates that preoperative acuity is a predictor of righteart dysfunction. Although preoperative hemodynamic
ndices were not predictive of RHD in our model, wegree with Dang and colleagues [15] that perhaps theest predictor of postimplant RHD is preoperative RHD.The implications of continuous versus pulsatile blood
ow are currently unknown and have been a matter ofignificant debate [35]. While some argued that pulse-
ig 5. Echocardiogram showing septal bowing into the left ventriclefter HeartMate XVE implantation.
ressure is necessary for maintaining the integrity of the
irculation and end-organ function, others argue thatonpulsatile flow allows for normal end-organ function.any have used animal studies of nonpulsatile flow to
ddress the issue [35–41], but few studies are availablehat describe outcomes in humans supported by nonpul-atile LVADs. Our early results indicate that renal andepatic function after HeartMate II implantation is sim-
lar to the HeartMate I group at 1, 3, and 6 months afterurgery.
Recent years have seen considerable advancement inxial-flow LVADs with the development of the Jarvik000 (Jarvik Heart, New York, New York), the MicroMedeBakey LVAD (MicroMed, Houston, Texas), theeartMate II LVAD, and others. We have shown that theeartMate II continuous, axial-flow LVAD adequately
upports the systemic circulation and arguably demon-trates a lower incidence of right heart dysfunction.evertheless, longer follow-up is necessary to determine
f the HeartMate II LVAD can continue to minimize righteart dysfunction and lower the need for RVAD supportersus older generation pulsatile devices.
his study was supported in part by the Mildred and Carmontlitz Cardiac Research Fund. Doctor Weiss is an Irene Piccinini
nvestigator in Cardiac Surgery.
eferences
1. 2001 Heart and stroke statistical update. Dallas: AmericanHeart Association, 2000.
2. O’Connell JB, Birstow MR. Economic impact of heart failurein the United States: time for a different approach. J HeartLung Transplant 1994;13(Suppl):107–12.
3. Califf RM, Adams KF, McKenna WJ, et al. A randomizedcontrolled trial of epoprostenol therapy for severe conges-tive heart failure: the Flolan International Randomized Sur-vival Trial (FIRST). Am Heart J 1997;134:44–54.
4. Goldstein D, Oz M, Rose E. Implantable left ventricularassist devices. N Engl J Med 1998;339:1522–33.
5. Frazier O, Rose E, Macmanus Q, et al. Multicenter clinicalevaluation of the HeartMate 1000 IP left ventricular assistdevice. Ann Thorac Surg 1992;53:1080–90.
6. Pennington D, McBride L, Peigh P, et al. Eight years’experience with bridging to cardiac transplantation. J ThoracCardiovasc Surg 1994;107:472–81.
7. Korfer R, El-Banayosy A, Arusoglu L, et al. Single-centerexperience with the Thoratec ventricular assist device. J Tho-rac Cardiovasc Surg 2000;119:596–600.
8. McBride LR, Naunheim KS, Fiore AC, et al. Clinical experi-ence with 111 Thoratec ventricular assist devices. Ann Tho-rac Surg 1999;67:1233–9.
9. Portner P, Oyer P, Pennington D, et al. Implantable electricalventricular assist system: bridge to transplantation and thefuture. Ann Thorac Surg 1989;47:142–50.
0. Moskowitz A, Weinberg A, Oz M, Williams D. Quality of lifewith an implanted left ventricular assist device. Ann ThoracSurg 1997;64:1764–9.
1. Catanese K, Goldstein D, Williams D, et al. Outpatient leftventricular assist device support: a destination rather than abridge. Ann Thorac Surg 1996;61:646–53.
2. Mehta S, Aufiero T, Pae W, et al. Combined registry for theclinical use of mechanical ventricular assist pumps and thetotal artificial heart in conjunction with heart transplanta-
tion: sixth official report. J Heart Lung Transplant 1994;14:585–93.
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
D
DiiI
htasodot
MW
839Ann Thorac Surg PATEL ET AL2008;86:832–40 HEARTMATE II VERSUS I LVAD
AD
ULT
CA
RD
IAC
3. Rose E, Gelijns A, Moskowitz A, et al. Long-term mechanicalleft ventricular assistance for end-stage heart failure. N EnglJ Med 2001;345:1435–43.
4. Park SJ, Tector A, Piccioni W, et al. Left ventricular assistdevices as destination therapy: a new look at survival.J Thorac Cardiovasc Surg 2005;129:9–17.
5. Dang NC, Topkara VK, Mercando M, et al. Right heartfailure after left ventricular assist device implantation inpatients with chronic congestive heart failure. J Heart LungTransplant 2006;25:1–6.
6. Frazier OH, Myers TJ, Westaby S, Gregoric ID. Clinicalexperience with an implantable, intracardiac, continuousflow circulatory support device: physiologic implicationsand their relationship to patient selection. Ann Thorac Surg2004;77:133–42.
7. Noon GP, Morley DL, Irwin S, Abdelsayed SV, BenkowskiRJ, Lynch BE. Clinical experience with the MicroMed De-Bakey ventricular assist device. Ann Thorac Surg 2001;71(Suppl):133–8.
8. Griffith BP, Kormos RL, Borovetz HS, et al. HeartMate II leftventricular assist system: from concept to first clinical use.Ann Thorac Surg 2001;71(Suppl):116–20.
9. Frazier OH, Delgado RM, Kar B, Patel V, Gregoric ID, MyersTJ. First clinical use of the redesigned HeartMate II leftventricular assist system in the United States. Tex Heart InstJ 2004;31:157–9.
0. Grady KL, Meyer PM, Dressler D, et al. Longitudinal changein quality of life and impact on survival after left ventricularassist device implantation. Ann Thorac Surg 2004;77:1321–7.
1. Dang NC, Topkara VK, Kim BT, et al. Clinical outcomes inpatients with chronic congestive heart failure who undergoleft ventricular assist device implantation. J Thorac Cardio-vasc Surg 2005;130:1302–9.
2. Frazier OH, Rose EA, Oz MC, et al. Multicenter clinicalevaluation of the HeartMate vented electrical left ventricularassist system in patients awaiting heart transplantation.J Thorac Cardiovasc Surg 2001;122:1186–95.
3. Koul B, Solem JO, Steen S, Casimir-Ahn H, Granfeldt H,Lonn UJ. HeartMate left ventricular assist device as bridge toheart transplantation. Ann Thorac Surg 1998;65:1625–30.
4. Dembitsky WP, Tector AJ, Park S, et al. Left ventricular assistdevice performance with long-term circulatory support: les-sons from the REMATCH trial. Ann Thorac Surg 2004;78:2123–30.
5. Long JW. Advanced mechanical circulatory support with theHeartMate left ventricular assist device in the year 2000. AnnThorac Surg 2001;71(Suppl):176–82.
6. Burke DJ, Burke E, Parsaie F, et al. The HeartMate II: designand development of a fully sealed axial flow left ventricular
assist system. Artif Organs 2001;25:380–5.e agree with what you are saying. We believe that improve-
mh
Dnutpteoiptso
7. Butler K, Thomas D, Taylor L, et al. The HeartMate II axialflow LVAS: journey toward clinical trial. ASAIO J 2000;46:195.
8. Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flow device in patients awaiting heart transplantation.N Engl J Med 2007;357:885–96.
9. Omoto T, Tanabe H, LaRia PJ, Guererro J, Vlahakes GJ. Rightventricular performance during left ventricular unloadingconditions: the contribution of the right ventricular free wall.Thorac Cardiov Surg 2002;50:16–20.
0. Moon MR, Castro LJ, De Anda A, et al. Right ventricularassistance in closed chest dogs. Ann Thorac Surg 1993;56:54–67.
1. Farrar DJ, Compton PG, Dajee H, Fonger JD, Hill JD. Rightheart function during left heart assist and the effects ofvolume unloading in a canine preoparation. Circulation1984;70:708–16.
2. Elbeery JR, Owen CH, Savitt MA, et al. Effects of the leftventricular assist device on right heart function. J ThoracCardiovasc Surg 1990;99:809–16.
3. Miyamoto AT, Tanaka S, Matloff JM. Right ventricular func-tion during left heart bypass. J Thorac Cardiovasc Surg1983;85:49–53.
4. Waldenberger F, Kim YI, Laycock S, Meyns B, Flameng W.Effects of failure of the right side of the heart and increasedpulmonary resistance on mechanical circulatory supportwith use of the miniaturized HIA-VAD displacement pumpsystem. J Thorac Cardiovasc Surg 1996;112:484–93.
5. Song X, Throckmorton AL, Untaroiu A, et al. Axial flowblood pumps. ASAIO J 2003;49:355–64.
6. Saito S, Westaby S, Pigott D, et al. Reliable long-termnonpulsatile circulatory support without anticoagulation.Eur J Cardiothorac Surg 2001;19:678–83.
7. Valdes F, Takatani S, Jacobs BG, et al. Comparison ofhaemodynamic changes in a chronic non-pulsatile biven-tricular bypass and total artificial heart. Trans ASAIO 1980;26:455.
8. Tatsumi E, Toda K, Taenaka Y, et al. Acute phase responsesof vasoactive hormones to nonpulsatile systemic circulation.ASAIO J 1995;41:460–5.
9. Golding LR, Jacobs G, Murakami T, et al. Chronic nonpul-satile blood flow in an alive awake animal: 34 days survival.Trans ASAIO 1980;26:251.
0. Saito S, Westaby S, Pigott D, et al. End-organ functionduring chronic non-pulsatile circulation. Ann Thorac Surg2002;74:1080–5.
1. Nojiri C, Kijima T, Maekawa J, et al. Terumo implantable leftventricular assist system: results of long-term animal study.
ASAIO J 2000;46:117–22.ISCUSSION
R EVGENIJ POTAPOV (Berlin, Germany): This is a verymportant study because there is a fairy tale about an increasedncidence of right heart failure in patients with axial flow pumps.have some questions.You showed that there are no significant differences in right
eart dysfunction between the two groups. You showed also thathere are no significant differences in need of right ventricularssist devices. And you reported that in the first period of yourtudy you used mostly pulsatile pumps and in the second periodf your study you used mostly axial flow pumps. My question is,o you think that this fact and the improvement in the selectionf patients over time may contribute to a decrease or to the trendoward a decrease of right heart failure in your study?
R PATEL: Thank you very much for that important question.
ent in patient selection has lowered our incidence of righteart failure.
R ROBERT F. KORMOS (Pittsburgh, PA): Nice work, veryicely presented, and I think it emphasizes the progression ofnderstanding of managing the right ventricle very nicely across
he board, and I think your comments about patient selectionrobably are relevant. My question relates to the methodology
hat you used to try and prevent right heart dysfunction, whichssentially is to not try to run the device at the highest possibleutput that you can achieve but prevent septal shift. I agree that
s an important step. But do you think this is achievable with theulsatile devices, because my sense is that we are kind of doing
hat already with the pulsatile systems; we are doing the sametrategy. So is it the strategy or the type of device that will impact
n prevention of right ventricular dysfunction?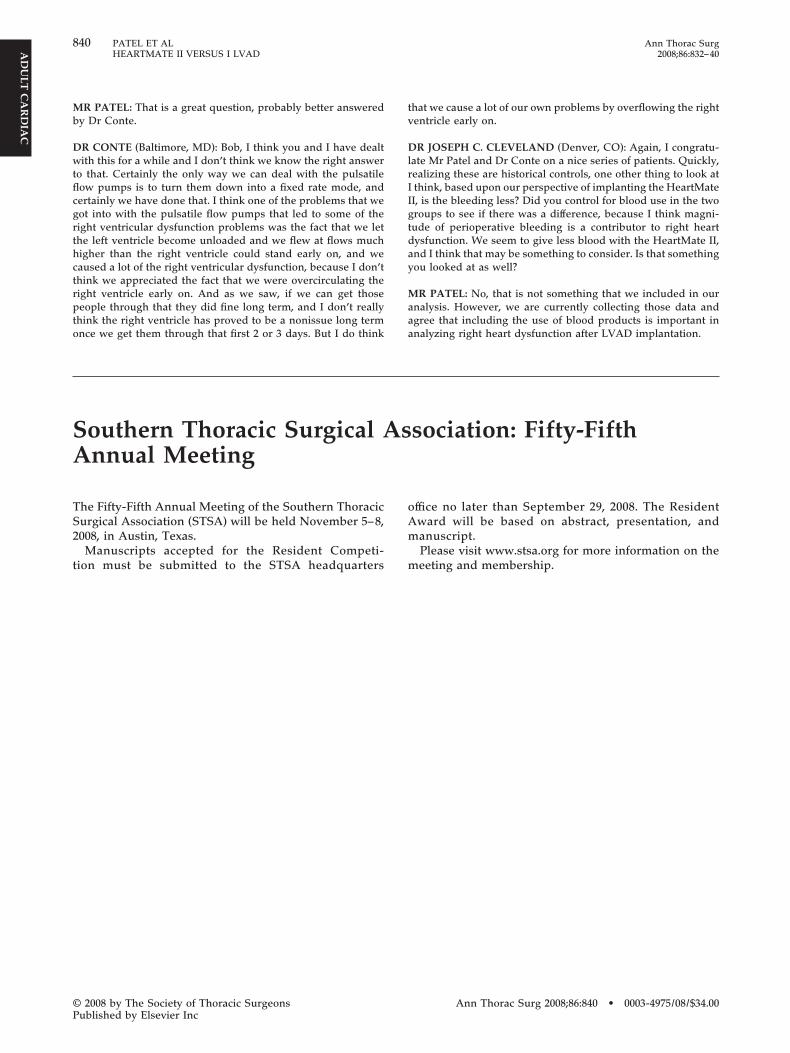
Mb
Dwtflcgrthctrpto
tv
DlrIIgtday
Maa
SA
TS2
t
840 PATEL ET AL Ann Thorac SurgHEARTMATE II VERSUS I LVAD 2008;86:832–40
©P
AD
ULT
CA
RD
IAC
R PATEL: That is a great question, probably better answeredy Dr Conte.
R CONTE (Baltimore, MD): Bob, I think you and I have dealtith this for a while and I don’t think we know the right answer
o that. Certainly the only way we can deal with the pulsatileow pumps is to turn them down into a fixed rate mode, andertainly we have done that. I think one of the problems that weot into with the pulsatile flow pumps that led to some of theight ventricular dysfunction problems was the fact that we lethe left ventricle become unloaded and we flew at flows muchigher than the right ventricle could stand early on, and weaused a lot of the right ventricular dysfunction, because I don’think we appreciated the fact that we were overcirculating theight ventricle early on. And as we saw, if we can get thoseeople through that they did fine long term, and I don’t really
hink the right ventricle has proved to be a nonissue long term
nnual Meeting
ion must be submitted to the STSA headquarters
oAm
m
2008 by The Society of Thoracic Surgeonsublished by Elsevier Inc
hat we cause a lot of our own problems by overflowing the rightentricle early on.
R JOSEPH C. CLEVELAND (Denver, CO): Again, I congratu-ate Mr Patel and Dr Conte on a nice series of patients. Quickly,ealizing these are historical controls, one other thing to look atthink, based upon our perspective of implanting the HeartMateI, is the bleeding less? Did you control for blood use in the tworoups to see if there was a difference, because I think magni-ude of perioperative bleeding is a contributor to right heartysfunction. We seem to give less blood with the HeartMate II,nd I think that may be something to consider. Is that somethingou looked at as well?
R PATEL: No, that is not something that we included in ournalysis. However, we are currently collecting those data andgree that including the use of blood products is important in
nce we get them through that first 2 or 3 days. But I do think analyzing right heart dysfunction after LVAD implantation.
outhern Thoracic Surgical Association: Fifty-Fifth
he Fifty-Fifth Annual Meeting of the Southern Thoracicurgical Association (STSA) will be held November 5–8,008, in Austin, Texas.Manuscripts accepted for the Resident Competi-
ffice no later than September 29, 2008. The Residentward will be based on abstract, presentation, andanuscript.Please visit www.stsa.org for more information on the
eeting and membership.Ann Thorac Surg 2008;86:840 • 0003-4975/08/$34.00





























