Embed Size (px)
Citation preview
Review Paper: AbsorbablePolymeric Surgical Sutures:
Chemistry, Production, Properties,Biodegradability, and Performance
CHENNAKKATTU KRISHNA SADASIVAN PILLAI AND
CHANDRA P. SHARMA*Division of Biosurface Technology, Biomedical Technology Wing,
Sree Chitra Tirunal Institute for Medical Sciences & Technology,
Poojappura, Thiruvananthapuram 695 012, India
ABSTRACT: Among biomaterials used as implants in human body, suturesconstitute the largest groups of materials having a huge market exceeding$1.3 billion annually. Sutures are the most widely used materials in woundclosure and have been in use for many centuries. With the development of thesynthetic absorbable polymer, poly(glycolic acid) (PGA) in the early 1970s, a newchapter has opened on absorbable polymeric sutures that got unprecedentedcommercial successes. Although several comparative evaluations of suturematerials have been published, there were no serious attempts of late on acomprehensive review of production, properties, biodegradability, and perfor-mance of suture materials. This review proposes to bring to focus scattered dataon chemistry, properties, biodegradability, and performance of absorbablepolymeric sutures.
KEY WORDS: polymeric sutures, absorbable, chemistry, properties,biodegradation.
*Author to whom correspondence should be addressed.E-mail: [email protected] 2–5 and 9 appear in color online: http://jba.sagepub.com
JOURNAL OF BIOMATERIALS APPLICATIONS Vol. 25 — November 2010 291
0885-3282/10/04 0291–76 $10.00/0 DOI: 10.1177/0885328210384890� The Author(s), 2010. Reprints and permissions:http://www.sagepub.co.uk/journalsPermissions.nav
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

INTRODUCTION
A suture is a biomaterial device, either natural or synthetic, used toligate blood vessels and approximate tissues together [1]. Thus, its
major functions are to bring and hold tissues together followingseparation by surgery or trauma. It can also denote the method usedfor mechanical wound closure. The goals of wound closure includeobliteration of dead space, even distribution of tension along deep suturelines, maintenance of tensile strength across the wound until tissuetensile strength is adequate, and approximation of the epithelial portionof the closure. Although there are other methods for mechanical woundclosure such as staples, tape, and adhesive [2], sutures are the mostwidely used materials in wound closure. Sutures have registeredtremendous growth during the last two decades and have become thelargest group of biomaterials having a huge market exceeding$1.3 billion annually [3–7]. Although several evaluations of suturematerials have been published [8–18], there were no serious attempts oflate on a comprehensive review of production, properties, biodegrad-ability, and performance of suture materials. The purpose of this articleis, therefore, to systematically and comprehensively review all availableinformation generated in recent times covering all aspects on thedevelopments on chemistry, production, properties, biodegradability,and performance of absorbable polymeric sutures. Comparative evalua-tions with other sutures have also been made at appropriate placeswherever it is required.
A comparative evaluation in general on various closure materials usedin vascular devices was published by Hon et al. [10] in 2009. Theyprovided an overview of sutures used in vascular devices, focusing onhow they work, their efficacy in achieving hemostasis, any risksassociated with their use, and indications as to which should be usedfor particular indications. Li and Yuan [8] brought out a review in 2006on research progresses on synthetic absorbable polymeric sutures. In2002, Gassner [12] reviewed the area of wound closure materials.
A review with substantial input on biodegradability and emergingtrends on sutures was published by Singhal et al. in 1988 [4]. They havebrought out the salient features of absorbable sutures based onpoly(glycolic acid) (PGA) and its copolymers and mentioned thecoming of the promising polydioxanone (PDO; certain authors usePDS to indicate polydioxanone suture) and poly(trimethylene carbonate)(PTMC) based absorbable sutures.
Horacek [9] indicated that the absorbable sutures are based mostly onthe lower �-hydroxycarboxylic acids and copolydioxanes. Some of the
292 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
properties and uses of suture materials have been reviewed by Yu andCavaliere [11]. Otherwise, one depends mostly on the classic book onclosure materials published in 1996 by Chu et al. for reference [1].Benicewicz and Hopper [15] and later Jodar et al. [16–18] discussed thenature of synthetic suture materials.
Guidelines for choice in regard to wound healing, location of incision,and surgical needles and the difference between various absorbable andnonabsorbable sutures are discussed in the review by Swanson andTromovitch [19]. Vogt et al. [20] summarized the current experimentaland clinical bases of surgical scar management in a recent review.
CHARACTERISTICS OF SUTURE MATERIALS
The ideal suture would be totally biologically inert and should notcause any tissue reaction. It would be easy for the surgeon to handle andknot it reliably. An ideal suture should have the following characteristics[1,4,5,9–11]:
1. easy to handle2. elicit minimal tissue reaction3. does not support bacterial growth4. possess high tensile strength5. easy to sterilize6. elicit no allergic reaction7. elicit no carcinogenic action8. absorbed after serving its function
Thus, a suture should not only be very strong but also be able tosimply dissolve in body fluids and lose strength at the same rate that thetissue gains strength. It would neither cause nor promote complications[21]. In short, sutures should provide the most secure woundapproximation for an adequate time with minimal adverse effect onthe normal wound healing process. Additional factors such as presenceof infection, tissue characteristics, and wound location, tension onwound edges, age, and medical condition of patient, cosmoses, color,speed, and cost are considered by Bennett [22].
Obviously, there is no single suture material which can fulfill all thesecriteria [1]. The surgeon should choose the right suture for the type ofsurgery that he/she is performing because different tissues havediffering requirements for suture support (some needing only a fewdays, e.g., muscle, subcutaneous tissue, skin, while others require weeksor even months, e.g., fascia and tendon). In addition, healing rates ofvarious tissues also will differ depending on various factors such as
Absorbable Polymeric Surgical Sutures 293
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
infection, debility, respiratory problems, obesity, collagen disorders,malnutrition, malignancy, drugs, for example cytotoxics and steroids [1].The present surgeon has several choices of suture material available andhe may choose them based on availability and his familiarity. There aresome characteristics which are essential for all sutures. They include:sterility, uniform diameter and size, pliability for ease of handling andknot security, uniform tensile strength by suture type and size, andfreedom from contaminants that would elicit tissue reaction. To make itexplicit, the various terms used to characterize suture materials aredescribed in Table 1 [1,5,15,16,19,21,22]. Proper suturing technique isessential for obtaining good cosmetic results and avoiding scarring andpoor wound healing. Techniques that must be mastered include goodeversion of skin edges, avoiding suture marks, maintaining uniformtensile strength along the skin edges, and precise approximation alongskin edges [5].
HISTORY OF SUTURE MATERIALS
Suturing is not a new technique but is a known procedure sinceancient era. This is the branch basically evolved for the purpose ofwound healing and its management [23]. Physicians have been usingsutures for at least 4000 years [24]. Archaeological records from ancientEgypt and India show the use of linen, animal sinew, flax, hair, grass,cotton, silk, pig bristles, and animal gut to close wounds [24,25]. Thefamed Sushruta is reported to have used suture materials of bark,tendon, hair, and silk as sutures in surgery [26–30].
The first detailed description of a wound suture and the suturematerials used in it is described by Sushruta in Sushruta Samhita,written in 500 BCE. Since he was the author of the earliest systematicreport, it is assumed that in the case of Egyptian, Babylonian, Greek,and Arab surgeries, all have their origins in India [30]. The ancientGreek physician Claudius Galen (131–211 CE) was the first to describethe chorda or gut string as a suture material. The surgeon Antyllus (300CE) performed bone and joint resections, tracheotomies and the firstoperations on traumatic aneurysms, using chorda material [31]. The useof dried sheep intestine (for ligatures in surgical operations) is advised inVagbhataratha Kaumudi (700 AD), a commentary by Harikrishna onAstanga Hridaya of Vaghbhata-II [32] and in similar works [33–36]. InEurope, Salerno and Rogerio recommended gut strings as suturematerial, especially for wounds at the large abdominal viscera.Abulcasim (second half of the 10th century), the famous Arab surgeon,produced a detailed description of suture techniques. The Frenchman
294 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Ambroise Pare (1510–1590), who originally was a barber, became one ofthe greatest surgeons of all times, used fine linen strips and silk forvascular ligatures [14–19,22,37]. Joseph Lister introduced the firstcatgut suture sterilized with carbolic acid in 1860 and the chromiccatgut (CG) in 1880 [38,39]. To avoid a detailed historical descriptionwhich is not intended in this review, a time scale of the appearance ofvarious suture materials in use is shown in Tables 2–4 [5,22,31,38–45].
Table 1. Terms describing the various characteristics related to suture materials[1,5,15,16,19,21,22].
No. Term Description
1. Absorbable Progressive loss of mass and/or volume of suture material;does not correlate with initial tensile strength
2. Breaking strength Limit of tensile strength at which suture failure occurs3. Capillarity Extent to which absorbed fluid is transferred along the
suture4. Elasticity Measure of the ability of the material to regain its original
form and length after deformation5. Fluid absorption Ability to take up fluid after immersion6. Knot-pull tensile
strengthBreaking strength of knotted suture material (10–40%
weaker after deformation by knot placement)7. Knot strength Amount of force necessary to cause a knot to slip (related
to the coefficient of static friction and plasticity of a givenmaterial)
8. Memory Inherent capability of suture to return to or maintain itsoriginal gross shape (related to elasticity, plasticity, anddiameter)
9. Nonabsorbable Surgical suture material that is relatively unaffected by thebiological activities of the body tissues and is thereforepermanent unless removed
10. Plasticity Measure of the ability to deform without breaking and tomaintain a new form after relief of the deforming force
11. Pliability Ease of handling of suture material; ability to adjust knottension and to secure knots (related to suture material,filament type, and diameter)
12. Straight-pull tensilestrength
Linear breaking strength of suture material
13. Suture pullout value The application of force to a loop of suture located wheretissue failure occurs, which measures the strength of aparticular tissue; variable depending on anatomic siteand histological composition (fat, 0.2 kg; muscle,1.27 kg; skin, 1.82 kg; fascia, 3.77 kg)
14. Tensile strength Measure of a material or tissue’s ability to resistdeformation and breakage
15. Wound breakingstrength
Limit of tensile strength of a healing wound at whichseparation of the wound edges occurs
Absorbable Polymeric Surgical Sutures 295
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

These tables also provide trade names and the firms that manufacturethe sutures.
By 1900, the catgut industry was firmly established in Germany dueto the use of sheep intestines in their sausage industry. Many methods ofsterilizing were used but the introduction of iodine sterilization byClaudius in 1902 established what was to become the standard methodof preparation for nearly half a century [46]. Buckskin and silver wirewere developed in the 18th century whereas chemical modificationswere effected on catgut during the 19th century. Cotton and treatednatural materials were used in the 20th century as suturing materials.The introduction of steel wire and synthetic nonabsorbable fibers likenylon, polyester, and polypropylene (PP) during World War II greatlyexpanded the chemical composition of suture materials. The year 1906witnessed the development of the first truly sterile catgut sterilized bysporicidal treatment with iodine following the suggestion of the Germansurgeon Franz Kuhn (1866–1929) and Braun [31], Melsungen, Germanystarted the industrial-scale production of Kuhn Catgut in 1908. Catgutand silk dominated the suture market until 1930. The time scale of theappearance of absorbable sutures after the discovery of PGA in 1968/1970 is given in Table 3 [5,22,31,41–45]. Catgut is phased out in manycountries, because the risk of Creutzfeldt–Jakob Disease (CJD) infectionis still higher than with modern synthetic suture materials, even withimproved sterilization processes.
Table 2. Absorbable natural sutures [31,38,39].
Year Name of suture Trade name Manufacturer
16th century Catgut, plain,Surgigut�
Catgut or surgicalcatgut, twistedmultifilament
Astra, Ethicon, D/G, SSC,Kollsut, DemeTech
1880 Chromic catgut Catgut or surgicalcatgut, twistedmultifilament
Astra, Ethicon, D/G, SSC,Kollsut, DemeTech,Sutures India PrivateLimited, Bangalore,Futura Surgicare Pvt.Ltd., Bangalore,MedSurge Ind Pvt Ltd,Chennai
Surgigut� Twisted multifilament,plain and chromic
USS
Softgut� Glycerin coated D/G1950–1960 Collagen sutures Collagen, twisted
multifilament, plainand chromic.
Ethicon
296 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
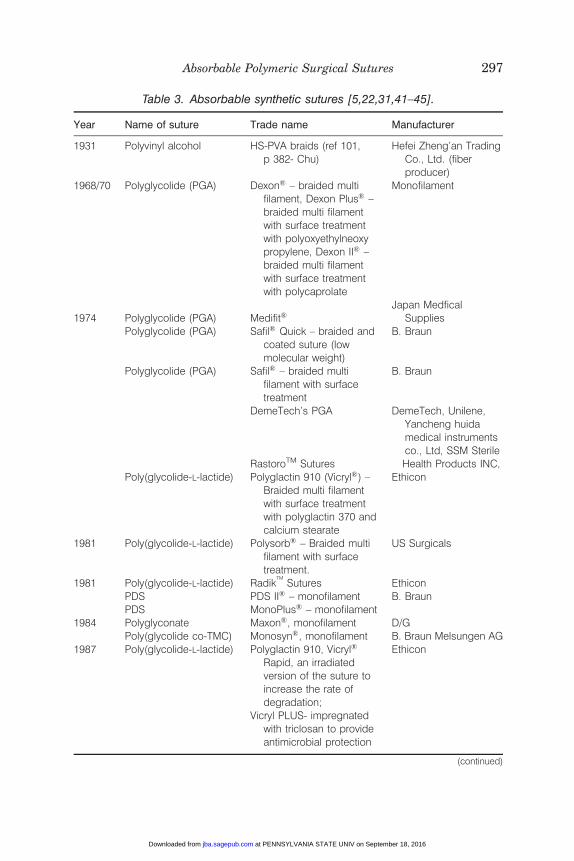
Table 3. Absorbable synthetic sutures [5,22,31,41–45].
Year Name of suture Trade name Manufacturer
1931 Polyvinyl alcohol HS-PVA braids (ref 101,p 382- Chu)
Hefei Zheng’an TradingCo., Ltd. (fiberproducer)
1968/70 Polyglycolide (PGA) Dexon� – braided multifilament, Dexon Plus� –braided multi filamentwith surface treatmentwith polyoxyethylneoxypropylene, Dexon II� –braided multi filamentwith surface treatmentwith polycaprolate
Monofilament
1974 Polyglycolide (PGA) Medifit�Japan Medfical
SuppliesPolyglycolide (PGA) Safil� Quick – braided and
coated suture (lowmolecular weight)
B. Braun
Polyglycolide (PGA) Safil� – braided multifilament with surfacetreatment
B. Braun
DemeTech’s PGA DemeTech, Unilene,Yancheng huidamedical instrumentsco., Ltd, SSM Sterile
RastoroTM Sutures Health Products INC,Poly(glycolide-L-lactide) Polyglactin 910 (Vicryl�) –
Braided multi filamentwith surface treatmentwith polyglactin 370 andcalcium stearate
Ethicon
1981 Poly(glycolide-L-lactide) Polysorb� – Braided multifilament with surfacetreatment.
US Surgicals
1981 Poly(glycolide-L-lactide) RadikTM
Sutures EthiconPDS PDS II� – monofilament B. BraunPDS MonoPlus� – monofilament
1984 Polyglyconate Maxon�, monofilament D/GPoly(glycolide co-TMC) Monosyn�, monofilament B. Braun Melsungen AG
1987 Poly(glycolide-L-lactide) Polyglactin 910, Vicryl�
Rapid, an irradiatedversion of the suture toincrease the rate ofdegradation;
Ethicon
Vicryl PLUS- impregnatedwith triclosan to provideantimicrobial protection
(continued)
Absorbable Polymeric Surgical Sutures 297
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
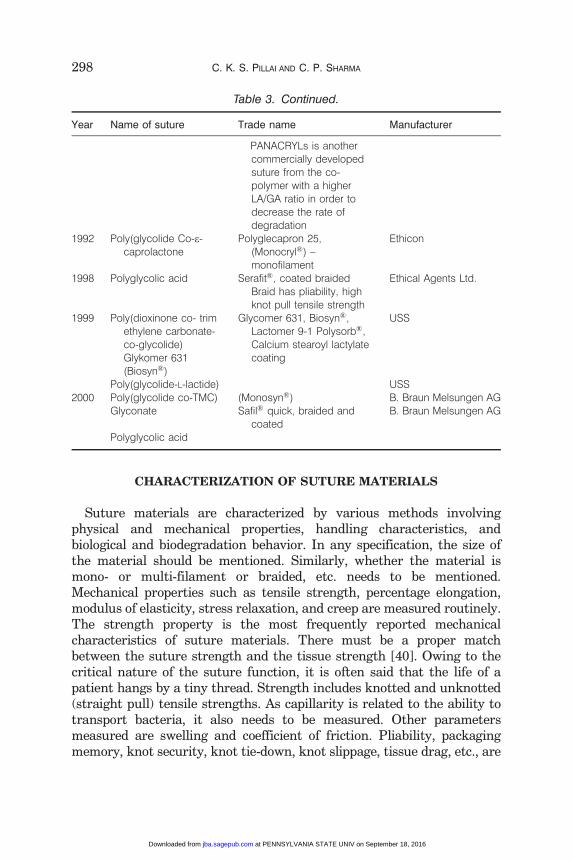
CHARACTERIZATION OF SUTURE MATERIALS
Suture materials are characterized by various methods involvingphysical and mechanical properties, handling characteristics, andbiological and biodegradation behavior. In any specification, the size ofthe material should be mentioned. Similarly, whether the material ismono- or multi-filament or braided, etc. needs to be mentioned.Mechanical properties such as tensile strength, percentage elongation,modulus of elasticity, stress relaxation, and creep are measured routinely.The strength property is the most frequently reported mechanicalcharacteristics of suture materials. There must be a proper matchbetween the suture strength and the tissue strength [40]. Owing to thecritical nature of the suture function, it is often said that the life of apatient hangs by a tiny thread. Strength includes knotted and unknotted(straight pull) tensile strengths. As capillarity is related to the ability totransport bacteria, it also needs to be measured. Other parametersmeasured are swelling and coefficient of friction. Pliability, packagingmemory, knot security, knot tie-down, knot slippage, tissue drag, etc., are
Table 3. Continued.
Year Name of suture Trade name Manufacturer
PANACRYLs is anothercommercially developedsuture from the co-polymer with a higherLA/GA ratio in order todecrease the rate ofdegradation
1992 Poly(glycolide Co-e-caprolactone
Polyglecapron 25,(Monocryl�) –monofilament
Ethicon
1998 Polyglycolic acid Serafit�, coated braidedBraid has pliability, highknot pull tensile strength
Ethical Agents Ltd.
1999 Poly(dioxinone co- trimethylene carbonate-co-glycolide)Glykomer 631(Biosyn�)
Glycomer 631, Biosyn�,Lactomer 9-1 Polysorb�,Calcium stearoyl lactylatecoating
USS
Poly(glycolide-L-lactide) USS2000 Poly(glycolide co-TMC) (Monosyn�) B. Braun Melsungen AG
Glyconate Safil� quick, braided andcoated
B. Braun Melsungen AG
Polyglycolic acid
298 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
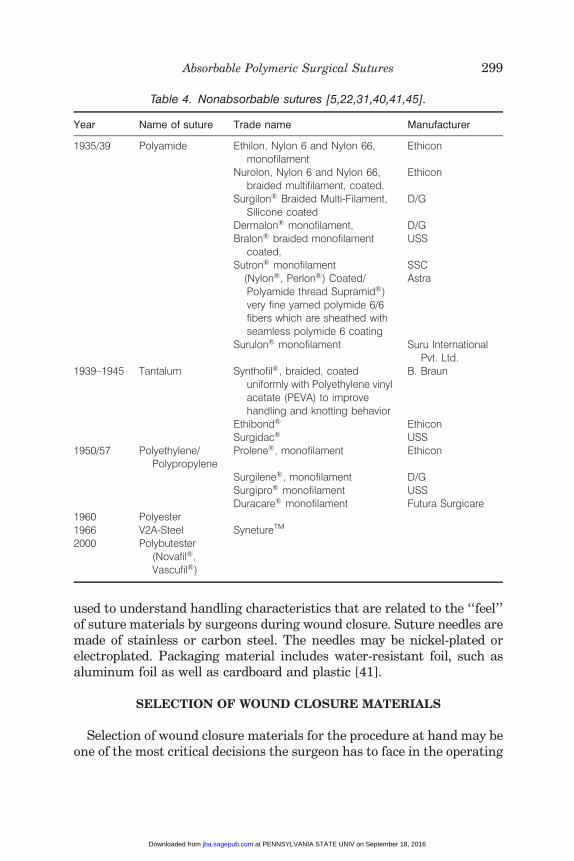
used to understand handling characteristics that are related to the ‘‘feel’’of suture materials by surgeons during wound closure. Suture needles aremade of stainless or carbon steel. The needles may be nickel-plated orelectroplated. Packaging material includes water-resistant foil, such asaluminum foil as well as cardboard and plastic [41].
SELECTION OF WOUND CLOSURE MATERIALS
Selection of wound closure materials for the procedure at hand may beone of the most critical decisions the surgeon has to face in the operating
Table 4. Nonabsorbable sutures [5,22,31,40,41,45].
Year Name of suture Trade name Manufacturer
1935/39 Polyamide Ethilon, Nylon 6 and Nylon 66,monofilament
Ethicon
Nurolon, Nylon 6 and Nylon 66,braided multifilament, coated.
Ethicon
Surgilon� Braided Multi-Filament,Silicone coated
D/G
Dermalon� monofilament, D/GBralon� braided monofilament
coated,USS
Sutron� monofilament SSC(Nylon�, Perlon�) Coated/Polyamide thread Supramid�)very fine yarned polymide 6/6fibers which are sheathed withseamless polymide 6 coating
Astra
Surulon� monofilament Suru InternationalPvt. Ltd.
1939–1945 Tantalum Synthofil�, braided, coateduniformly with Polyethylene vinylacetate (PEVA) to improvehandling and knotting behavior
B. Braun
Ethibond� EthiconSurgidac� USS
1950/57 Polyethylene/Polypropylene
Prolene�, monofilament Ethicon
Surgilene�, monofilament D/GSurgipro� monofilament USSDuracare� monofilament Futura Surgicare
1960 Polyester1966 V2A-Steel SynetureTM
2000 Polybutester(Novafil�,Vascufil�)
Absorbable Polymeric Surgical Sutures 299
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

room [5,22]. Apart from personal preferences, the final choice willdepend upon various patient factors that influence the healing process,the characteristics of the tissues involved, and potential post-operativecomplications [42,47–49]. Both optimal wound closure and as unob-structive scars as possible are of high significance after plastic-reconstructive surgeries. Untearable, absorbable, as thin as possible,monophile sutures with atraumatic needle-suture combinations asoffered by various manufactures should be preferred. A perfecttechnique closing the wound intracutaneously in two layers should betaken for granted today. The task of suture selection is complicated bythe wide variety of suturing materials available. Selection of suturesinappropriate in size or number may increase the risk of complicationand delay healing [50,51].
Certain guiding principles for selecting a suture material for a giventask have emerged [22,43,48,51,52]. When a wound reaches maximalstrength, sutures are no longer needed. Therefore, it would be better toclose slow-healing tissues (skin, fascia, and tendons) with nonabsorbablesutures or long-lasting absorbable sutures or close fast healing tissues(stomach, colon, and bladder) with absorbable sutures. Foreign bodies inpotentially contaminated tissues may convert contamination intoinfection. This indicated that one has to avoid multifilament sutureswhich may convert contaminated wound into an infected one or usemonofilament sutures or absorbable sutures which resist harboringinfection. Where cosmetic results are important, close and prolongedapposition of tissues and avoidance of irritants will produce the bestresults. In such situations, use the smallest inert monofilament suturematerials (nylon, PP) and avoid using skin sutures alone and closesubcuticularly whenever possible. Similarly, foreign bodies in thepresence of fluids containing high crystalloid concentrations maycause precipitation and stone formation. Then, it is advised to useabsorbable sutures in the urinary and biliary tracts. For selecting suturesize, use the finest sized suture commensurate with the natural strengthof the tissue to be sutured and use retention sutures to reinforceappropriately sized primary sutures if the patient is at risk of producingsudden strains on the suture line post-operatively. Remove the retentionsutures as soon as that risk is reduced.
The characteristics of commonly used suture materials and needlesare discussed by Bennet [22]. Grisham and Zukin [48] provideenough information to make an informed choice of sutures whenrepairing pediatric lacerations. Moy et al. [5] have discussed in detailthe scientific basis of selection of suture materials and they point outthat a proper suturing technique is essential for obtaining good
300 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
cosmetic results and avoiding scarring and poor wound healing.Hochberg et al. [44], who reviewed the available materials for skinclosure, and their biomechanical properties, advantages, and dis-advantages, proposed a pattern for better understanding of thelimitations, indications, and numerous choices to be consideredbefore choosing a suture material. Cost-effective and practicalsolutions are discussed by Williams and Armstrong [53]. There iswidespread consensus among cutaneous surgeons regarding optimalsuture selection and closure technique by anatomic location. Adamset al. [54] point out that more experienced surgeons tend to repairlarger defects but, possibly because of their increased confidence andskill, rely on less complicated repairs.
CLASSIFICATION
Sutures are, in general, categorized according to the type of material(natural or synthetic), the lifetime of the material in the body(absorbable or nonabsorbable), and the form in which they weremade (braided, twisted, and monofilament) [1,5]. Suture manufactur-ing comes under the regulatory control of the Food and DrugAdministration (FDA) because sutures are classified as medicaldevices. Manufacturing guidelines and testing for the industry isprovided by a nonprofit, non-governmental agency called United StatesPharmacopeia (USP), located in Rockville, MD. The USP system wasestablished in 1937 for standardization and comparison of suturematerials, corresponding to metric measures. The three classes ofsutures are collagen, synthetic absorbable, and nonabsorbable. Theyare as follows:
. Class I – Silk or synthetic fibers of monofilament, twisted, or braidedconstruction.
. Class II – Cotton or linen fibers or coated natural or synthetic fibersin which the coating contributes to suture thickness without addingstrength.
. Class III – Metal wire of monofilament or multifilament construction.
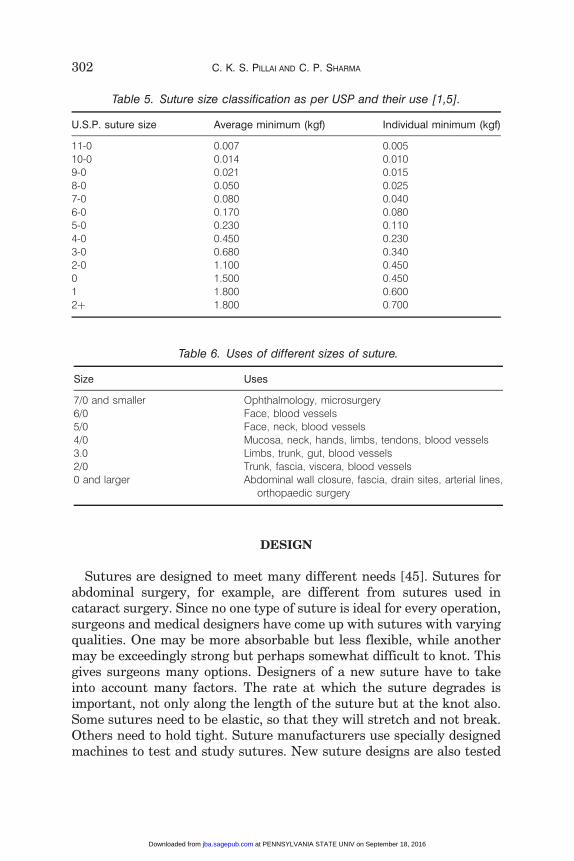
Size refers to the diameter of the suture strand and is denoted aszeroes. The more zeroes characterizing a suture size, the smallerthe resultant strand diameter (e.g., 4-0 is larger than 5-0). The smallerthe suture, the lesser the tensile strength of the strand. These sizedetails are provided in Table 5 and the uses of different sizes of suture inTable 6 [1,5].
Absorbable Polymeric Surgical Sutures 301
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
DESIGN
Sutures are designed to meet many different needs [45]. Sutures forabdominal surgery, for example, are different from sutures used incataract surgery. Since no one type of suture is ideal for every operation,surgeons and medical designers have come up with sutures with varyingqualities. One may be more absorbable but less flexible, while anothermay be exceedingly strong but perhaps somewhat difficult to knot. Thisgives surgeons many options. Designers of a new suture have to takeinto account many factors. The rate at which the suture degrades isimportant, not only along the length of the suture but at the knot also.Some sutures need to be elastic, so that they will stretch and not break.Others need to hold tight. Suture manufacturers use specially designedmachines to test and study sutures. New suture designs are also tested
Table 5. Suture size classification as per USP and their use [1,5].
U.S.P. suture size Average minimum (kgf) Individual minimum (kgf)
11-0 0.007 0.00510-0 0.014 0.0109-0 0.021 0.0158-0 0.050 0.0257-0 0.080 0.0406-0 0.170 0.0805-0 0.230 0.1104-0 0.450 0.2303-0 0.680 0.3402-0 1.100 0.4500 1.500 0.4501 1.800 0.6002þ 1.800 0.700
Table 6. Uses of different sizes of suture.
Size Uses
7/0 and smaller Ophthalmology, microsurgery6/0 Face, blood vessels5/0 Face, neck, blood vessels4/0 Mucosa, neck, hands, limbs, tendons, blood vessels3.0 Limbs, trunk, gut, blood vessels2/0 Trunk, fascia, viscera, blood vessels0 and larger Abdominal wall closure, fascia, drain sites, arterial lines,
orthopaedic surgery
302 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
by subjecting them to chemical tests, such as soaking them in varioussolutions, and testing on animals.
The surface of a monofilament is very smooth and passes easilythrough tissue. However, they can be difficult to handle and tie as theyare less flexible than multifilament construction. Most monofilamentsalso have ‘‘memory’’. This memory results in a suture that holds theshape it had in the package, making it more difficult to work with. Somememory can be relaxed, but is not effective in all sutures. Inmultifilaments, construction involves several filaments or strandsbeing braided or twisted together. This results in a strong suture thatis flexible and easy to handle. Multifilament sutures pass less easilythrough tissue than smooth monofilaments and the resulting ‘‘tissuedrag’’ can cause tissue trauma [45]. These problems are significantlyreduced by using ‘‘coated’’ braided materials.
COATING MATERIALS
Suture materials are frequently coated, especially braided or twistedsutures, to facilitate their handling properties, particularly a reductionin tissue drag when passing through the needle tract and the ease ofsliding knots down the suture during knotting. Traditional coatingmaterials used are bees wax, paraffin wax, silicone, poly(tetrafluor-oethylene) (PTFE), etc. The trend is toward a coating material that hasa chemical property similar to the suture to be used. The coatingsused depend on whether the suture is absorbable or nonabsorbable.Absorbable coatings include Poloxamer 188 and calcium stearatewith a copolymer of glycolic acid (GA) and lactic acid (LA)[55]. Nonabsorbable sutures may be coated with wax, silicone,fluorocarbon, etc.
Sutures may also be dyed to make them easy to see during surgery.Only FDA-approved dyes and coatings may be used. Some allowable dyesare: logwood extract, chromium–cobalt–aluminum oxide, ferric ammo-nium citrate, pyrogallol, D&C Blue No. 9, D&C Blue No. 6, D&C GreenNo. 5, and D&C Green No. 6. Suture needles are made of stainless orcarbon steel. The needles may be nickel-plated or electroplated.Packaging material includes water-resistant foil, such as aluminumfoil as well as cardboard and plastic.
THE PROCESS OF WOUND HEALING
The implantation of biomaterials initiates both an inflammatoryreaction to injury as well as processes to induce healing [56–58].
Absorbable Polymeric Surgical Sutures 303
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
The healing of wounds is a complex dynamic process that can beseparated into a series of phases. Phase I of wound healing involves aninflammatory response over 1–5 days that induces an outpouring oftissue fluids into the wound, an increased blood supply and cellular andfibroblast proliferation. In Phase II of wound healing, covering a periodof 5–14 days, there is an increased collagen formation and depositionwithin the wound, together with formation of fibrin and fibronectinthrough fibroblastic activity, and wound closure/contraction com-mences. Phase II gradually merges to Phase III, from day 14 onward,and there is reorganization and maturation (cross-linking) of collagenfibers together with deposition of fibrous connective tissue, the latterresulting in scar formation. This healing process occurs when there is noinfection, minimal edema (swelling), or fluid discharge. Complications inwould healing and their attendant delays commonly result from twoprimary causes, infection and mechanical effects [59].
ABSORBABLE NATURAL SUTURE MATERIALS
Sutures are, in general made up of fibers from natural or syntheticpolymers. Metallic fibers such as steel fibers are also used extensively.Polymeric fibers could be absorbable or nonabsorbable. Natural suturesare made of catgut or reconstituted collagen (RC), or from cotton, silk, orlinen. Synthetic nonabsorbable sutures may be made of PP,poly(ethylene glycol terephthalate) (PET), poly(butylene glycol terephtha-late) (PBT), polyamide (PA), different proprietary Nylons, or Goretex�.
Catgut and regenerated collagen are the two absorbable naturalsutures available in the market. The term ‘catgut’ was first mentionedin 1599, in J.A. Murray’s English Dictionary, where ‘kit’ or ‘cat’ was notlisted as describing the animal, cat, but ‘violin, stringed instrumentscollectively.’ Consequently, ‘catgut’ meaning something like ‘lute string’has arisen through a mistaken inference that ‘kit’ referred to ‘cat’ [60].Another view is based on its source. Catgut is prepared from theintestines of the sheep or goat, or in general from ‘cattle’ whichoriginally denoted not only cows but all types of livestock. So, the ‘cat-’in‘‘catgut’’ might not refer to cat, but it is an abbreviation for ‘cattle.’
Catgut was the staple absorbable suture material through the 1930s,while physicians used silk and cotton where a nonabsorbable materialwas needed. Catgut sutures are well known for their great toughnessand tenacity. Catgut is sold as plain catgut (untreated) and CG (tannedby chromium trioxide, the yellow shade of plain catgut then turn to adarker shade of brown). The chromium trioxide treatment, firstdeveloped by Joseph Lister, makes CG more resistant to absorption
304 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
and causes less tissue reaction than plain catgut suture [61]. Its uniformchromic properties allow a slow and safe absorption with minimal tissuereaction.
The basic constituent of catgut is collagen, which is the mainconstituent of skin and hides and is used as source of gelatin and glueand leather. Collagen is the major structural protein found in allmulticellular organisms.
Catgut sutures are packaged in alcohol solution like ethanol orisopropanol to retain their flexibility and packages are sterilized eitherby 60Co g-ray irradiation or ethylene oxide (EO) treatment. Glycerinecoating (Softgut�) is adopted to eliminate the need of alcohol packing.The coating also improves handling characteristics. However, somecomplications have been reported on its use [62,63].
Degradation Behavior of Absorbable Natural Suture Materials
Typically, sutures made from catgut are readily absorbed by thehuman body mainly due to the actions of the proteolytic enzymes ofphagocytes and other cells [64–66]. Cellular collagenase and proteaseseventually degrade and remove catgut and reconstituted collaged basesutures giving rise to a rapid loss of strength during the most criticalperiod of wound healing and higher than average level of tissuereactions [64–68]. Catgut sutures retain tensile strength during thefirst 4–5 days only and after 2 weeks, the tensile strength is essentiallygone [22]. On the other hand, in a comparative study of PDO, PGA(Dexon�), Polyglactin 910 (Vicryl� Rapid, an irradiated form of Vicryl�
to increase the rate of hydrolysis), and CG suture materials for closureof skin incision in rats, Aslan et al. [69] showed that the macroscopicappearance of all specimens was not statistically different. CG,however, retains strength for 2–3 weeks. Fast-absorbing gut(Ethicon) is the newer form that dissolves fast and can be used inchildren. Catgut sutures elicit far more intense tissue reaction thansynthetic absorbable sutures, because of their foreign protein struc-tures. Areas of catgut suture degradation contain dense accumulationof macrophages, lymphocytes, and foreign body giant cells. Aftercomplete absorption, these are replaced by a dense mass ofmacrophages [70]. The tissue reactions are far more intense withplain catgut sutures giving rise to exudates with some tissue necrosis[71]. Most studies indicate that catgut sutures are completely absorbedbetween 35 and 60 days [70,72].
Postlethwait and Smith [73] used a new synthetic suture, XLG�
which is a copolymer derived from LA and GA through lactide (LL) and
Absorbable Polymeric Surgical Sutures 305
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
glycolide (GL) intermediates. Determinations of the rate of loss ofstrength in various sites in experiments on dogs show that XLG� losesstrength slightly more rapidly than does CG. An exception is suturessuspended in the stomach, where CG quickly loses strength, whereasXLG� maintained strength similar to that at other implantation sites[73]. In a comparative study with Vicryl� suture, Reul Jr. concluded(after a study in 53 patients subjected to a wide range of generalabdominal and cardiovascular procedures) that Vicryl� suture may beused wherever catgut or other absorbable sutures are normally used andhas the advantage of greater reliability of strength retention and rate ofabsorption than is observed with CG [74]. Sanz et al. [75] report after acomparative study of standard absorbable sutures, that Maxon� andPDS elicited a lower degree of chronic inflammation when comparedwith Vicryl� and CG. In developing a standardized readily reproducibleexperimental model, Edlich et al. [76] showed that among theabsorbable sutures, Dexon� sutures evoked the least inflammatoryresponse and that the infection rate of contaminated tissues containingDexon� was significantly lower than the incidence of infection of tissuecontaining catgut sutures. Similar studies on comparative evaluations ofvarious fibers have shown that that the catguts cause more intensetissue reaction than the other fibers [77,78].
Shishatskaya et al. [79] implanted polyhydroxyalkanoate (PHA)sutures [polyhydroxybutyrate (PHB) and a copolymer of hydroxybuty-rate and hydroxyvalerate (PHV)] to test animals intramuscularly, andtissue reaction was investigated and compared with the reaction to silkand catgut. The reaction of tissues to the polymeric implants was similarto their reaction to silk and was less pronounced than the reaction tocatgut.
Sharp et al. [80] addressed the problem of common bile duct stricturesby systematically investigating the healing canine end-to-end choledo-chal anastomosis sutured with monofilament polyglyconate (PG)absorbable suture and comparing with braided Vicryl� and CG sutures.Seventy-six canines, randomized to control versus sutured groups,underwent either mobilization (controls) or transection of the mid-common bile duct and were allowed to heal 5, 10, 15, or 50 days post-operatively before sacrifice. PG suture caused significantly lessperianastomotic inflammation than did chronic suture, with Vicryl�
sutures evoking an intermediate inflammatory response.In a study involving the comparative evaluation of the effects of CG,
Vicryl�, PDO, and PTMC suture on urothelial healing in a rabbit modelsimulating pyeloplasty, Wainstein et al. [81] performed pyelouretero-tomies on 8-week-old rabbits (12 rabbits (24 renal units) and 3 control
306 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

rabbits) and closed with interrupted 7-0 sutures. Histologic evidence ofacute and chronic inflammation and foreign body reaction was mostsevere at 10 days and 5 weeks in pyeloureterotomies closed with CG.There was mild inflammation in those closed with Vicryl� at 10 days,but it was minimal in those closed with Vicryl�, PDO, and PTMC at5 and 12 weeks. Reabsorption of PGA was complete by 5 weeks, but wasincomplete with the other three sutures at that time. By 12 weeks, therewas persistent suture in 50% of the renal units closed with PDO and in100% of those closed with PTMC. No animal developed a renal calculus.Because of the mild inflammatory response and rapid tissue reabsorp-tion of Vicryl� in this animal model, this suture appears to be the bestsuture for pyeloplasty.
In another study involving a comparative evaluation of plain catgutand CG with Dexon�, Dexon Plus�, and MaxonTM (incubated inhuman gastric juice, bile, pancreatic juice, and their mixture), Tianet al. [82] reported that plain catgut rapidly lost its strength in each ofthese digestive fluids. CG was susceptible to digestion although itretained most of its strength in bile for 2 weeks. Synthetic absorbablesutures, PGA or its derivatives (Dexon�, Dexon Plus�, and MaxonTM),maintained most of their strength for 2 weeks, disintegrating onlyafter 5–8 weeks. Although catgut is widely used, the study suggeststhat it disintegrates too rapidly, at least under the conditions tested, tobe appropriate for alimentary tract surgery, whereas the syntheticsutures maintained their integrity rather well for 2–3 weeks needed forvisceral wound healing. The data suggest that slowly absorbedsynthetic sutures may be particularly useful in pancreatic or biliaryanastomoses where a single layer is preferable and where anonabsorbable suture offers inherent disadvantages. A similar com-parative study between the copolymer, poly(lactide-co-glycolide)(PLGA) and CG in corneal surgery by Dunlap et al. [83] showed thatthe 8/0 copolymer showed 30% greater initial strength than 8/0chromic collagen. At the end of 1 week, the copolymer retained over90% of its initial rupture strength while chromic collagen had lostnearly 50% of its strength. After 10 days, the strength of the copolymertended to fall rapidly and by day 21 the suture had negligible strengthand began to absorb, completely disappearing by 7 weeks. Chromiccollagen tended to remain in situ for many weeks although possessingnegligible rupture strength. These sutures were used in suturingcorneoscleral wounds of 45 consecutive patients undergoing routinecataract surgery.
Comparing suture strengths for clinical applications, Vasanthan et al.[84] evaluated three suture materials CG, Vicryl�, and Vicryl� fast
Absorbable Polymeric Surgical Sutures 307
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

absorbing (Vicryl� Rapid) in 4-0 and 5-0 gages. The authors found thatthat CG sutures could sustain their strength better than Vicryl� Rapidafter 2 weeks. The 4-0 sutures are stronger and have greater tensilestrength than 5-0 sutures. Vicryl� Rapid may not be a desirable suture iftensile strength is required after 10 days. Appropriately designed clinicalstudies are necessary to confirm this finding in an in vivo environment.Table 7 provides a comparative evaluation of natural absorbable sutureswith those of natural nonabsorbable sutures [22,69,70,72,75,82–84].
CG is suitable for all surgical procedures, especially for tissues thatregenerate faster. It is not generally recommended for an incision thatrequires sustaining of the tissues for a prolonged period of time. It isabsorbed much faster when used in the mouth and in the vagina, due tothe presence of microorganisms. Special precautions should be taken forcardiovascular surgery, due to the continued heart contractions. Specialprecautions should also be taken in patients with cancer, anemia, andmalnutrition conditions. They tend to absorb this suture at a higherrate. Although synthetic alternatives are available, catgut sutures arestill used in hospitals throughout the world [84].
Reconstituted Collagen
RC, having been shown previously to be biodegradable and to have lowimmunologic activity, is prepared either by enzymatic digestion of nativecollagen-rich tissues or by the extraction of the tissues with salt
Table 7. Chemical and physical properties of PGA [1,5,9,11,15,16,18,85,86].
Melting temperature 224–2268C, 215–2178CGlass transition temperature 368CDensity 1.5–1.64 g/cm3
Specific volume (1/density) 0.5952 cm3/gSpecific gravity (100% crystalline) 1.548Specific gravity (100% amorphous) 1.707Specific gravity (100% crystalline) 1.50Heat of fusion (100% crystalline) 49.34 cal/gCrystallinity (%) 35–37Solvent Hexafluoroisopropanol (HFIP)Molecular weight 20–145,000Inherent viscosity 0.5–0.6 dL/gIntrinsic viscosity 0.6–1.6 dL/gDiameter 15–25mmTenacity 5–10 g/denier
100–200,000 psiKnot/straight tenacity 50–80%Elongation 15–35%
308 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
solutions. RC sutures prepared from bovine long flexor tendons aresimilar in appearance to catgut and are almost exclusively used inmicrosurgery. The mechanical and thermal stability of RC fibrils can beincreased by maturation in vitro when incubated in air at 378C [87–89].RC sutures are used in ophthalmic surgery as well as for otherapplications [90–92]. Plain collagen (PC) sutures were, however,shown to act as relatively inert bodies when used to close experimentalcataract incisions [93]. In a study on tissue reactions produced by thesesutures, Regan and Dunnington showed that in cataract incisions theabsorption of these sutures did not occur until wound healing was wellestablished. They concluded that collagen appeared to be a satisfactorysuture material for ocular surgery [93].
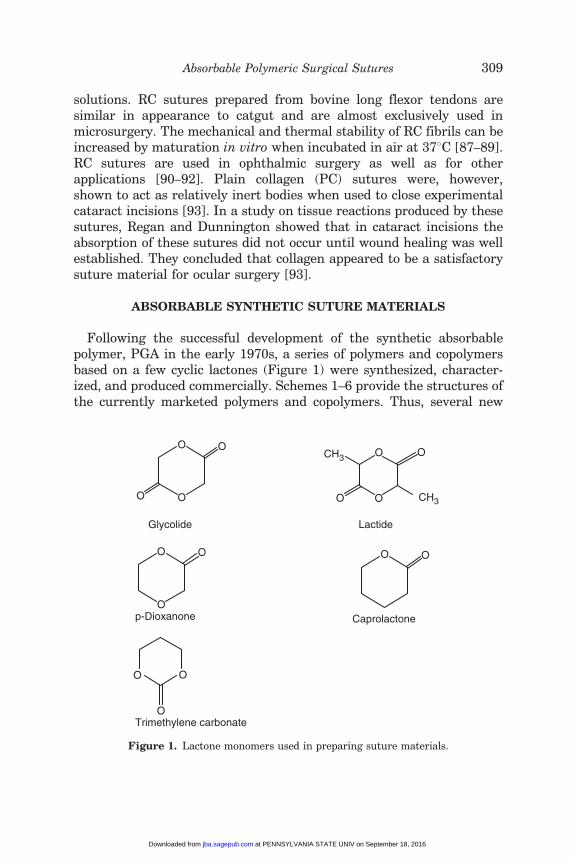
ABSORBABLE SYNTHETIC SUTURE MATERIALS
Following the successful development of the synthetic absorbablepolymer, PGA in the early 1970s, a series of polymers and copolymersbased on a few cyclic lactones (Figure 1) were synthesized, character-ized, and produced commercially. Schemes 1–6 provide the structures ofthe currently marketed polymers and copolymers. Thus, several new
O
O
O
O OO CH3
OCH3 O
Glycolide Lactide
O
O
O O O
p-Dioxanone
O
O O
Trimethylene carbonate
Caprolactone
Figure 1. Lactone monomers used in preparing suture materials.
Absorbable Polymeric Surgical Sutures 309
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
OO
O
O
O
Ring opening Polymerization
n
O
O
HO
OH
Lactic acid
Lactide
Polylactide (PLA)
( (
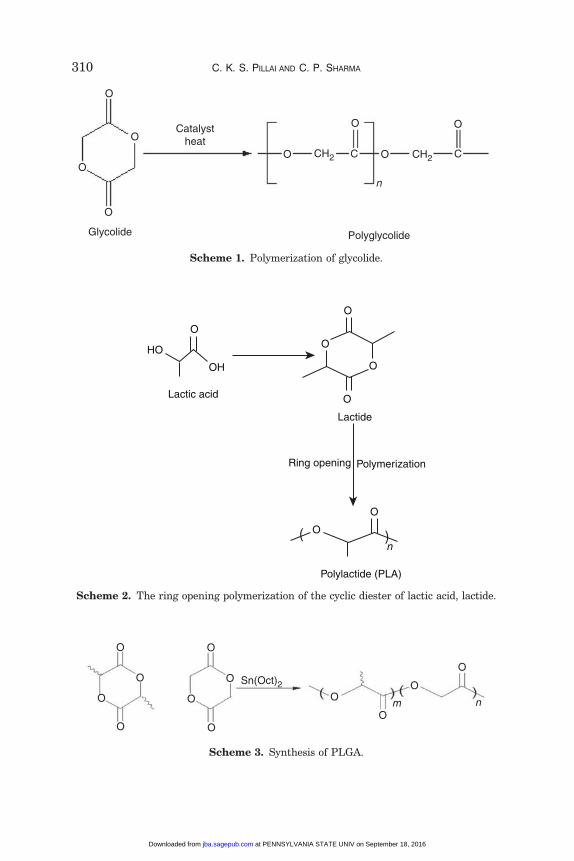
Scheme 2. The ring opening polymerization of the cyclic diester of lactic acid, lactide.
CH2
n
Glycolide Polyglycolide
Catalystheat
O
O
O
O
O
O
O
O
C CCH2
Scheme 1. Polymerization of glycolide.
O
O
O
O
O
O Sn(Oct)2O
O
O
O
nm
O
O
Scheme 3. Synthesis of PLGA.
310 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
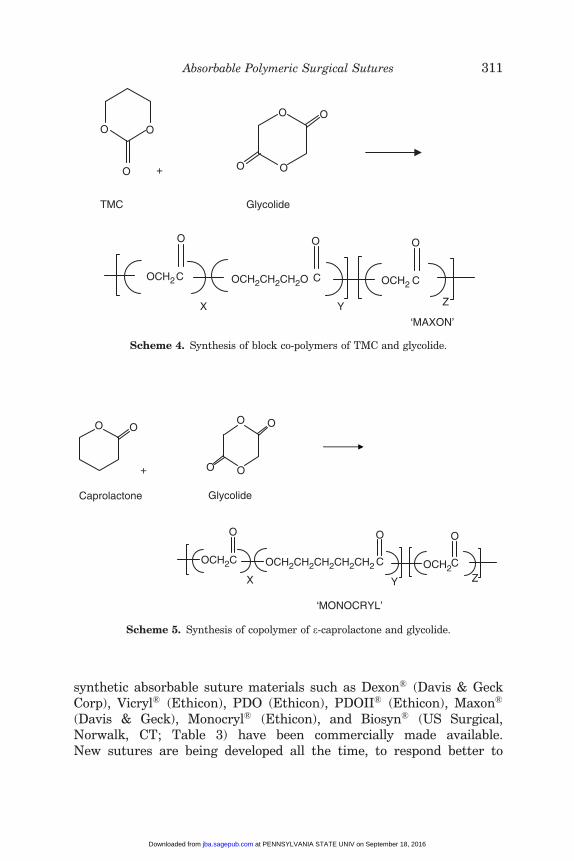
synthetic absorbable suture materials such as Dexon� (Davis & GeckCorp), Vicryl� (Ethicon), PDO (Ethicon), PDOII� (Ethicon), Maxon�
(Davis & Geck), Monocryl� (Ethicon), and Biosyn� (US Surgical,Norwalk, CT; Table 3) have been commercially made available.New sutures are being developed all the time, to respond better to
O
O +
O
O
O
O
TMC
OCH2C
O
X
C
O
Y
OCH2CH2CH2O OCH2 C
O
Z
‘MAXON’
O
Glycolide
Scheme 4. Synthesis of block co-polymers of TMC and glycolide.
O O
+
O
O
O
O
OCH2C
O
X
C
O
Y
OCH2CH2CH2CH2CH2 OCH2C
O
Z
‘MONOCRYL’
Caprolactone Glycolide
Scheme 5. Synthesis of copolymer of e-caprolactone and glycolide.
Absorbable Polymeric Surgical Sutures 311
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
particular surgical needs. The spectrum of suture material propertiesis researched through laboratory experiments, whose results arevalidated in extensive studies and trials [15,94]. Absorbablesutures are now well known to behave favorably in vitro and in ananimal model [95].
Owing to their precisely controlled manufacturing processes anduniform and reproducible properties, these absorbable biomaterials havereceived a great deal of attention in the medical field [1,85]. The mostimportant advantage of synthetic absorbable sutures is their reprodu-cible degradability inside a biological environment. This property willenable the sutures to minimize chronic undesirable tissue reactionsafter the sutures have lost their function. Due to the development ofthese synthetic fibers, they have replaced some natural fibers likecotton, linen, and catgut for wound closure purposes. Today, surgeonshave the option to choose among a large number of suture materials(Tables 3 and 4) with various chemical, physical, mechanical, andbiological properties.
Vicryl� is a braided suture produced from a copolymer of GA/LA at a90/10 mol/mol composition [96,97]. Polisorb� and XLG� are based upona combination of GA and LA but with a different composition. Dexon�
[96,97] is a braided suture based upon the homopolymer of GA.Maxon� [98], the most pliable monofilament suture to date, is formedfrom a segmented block copolymer of GL and e-caprolactone(e-CL). Recently, Biosyn� [99], a monofilament suture based on a
O
O
O
+
O
O +
O
O
O
O
PDO
OCH2 CH2 CH2O C
O
X
OCH2 C
O
ZC
O
Y
OCH2 CH2 OCH2
‘BIOSYN’
O
TMC Glycolide
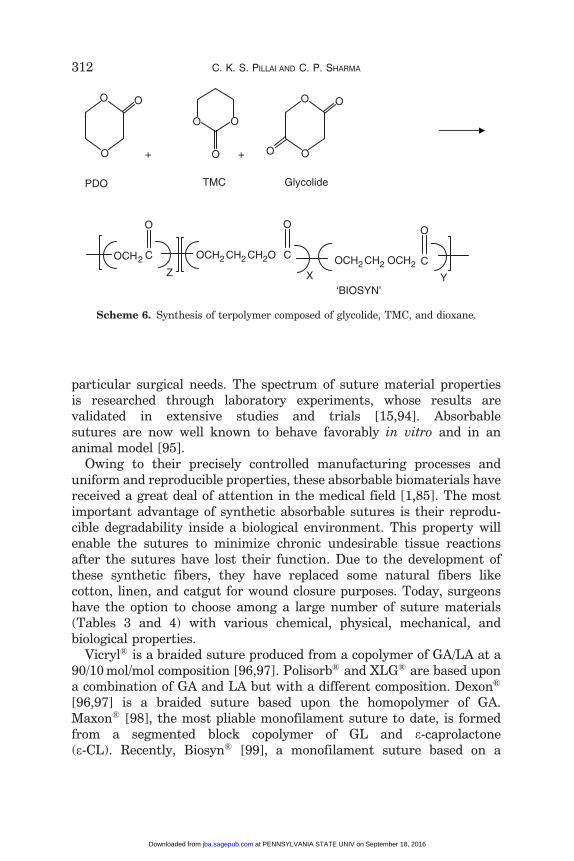
Scheme 6. Synthesis of terpolymer composed of glycolide, TMC, and dioxane.
312 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
nonrandom terpolymer of p-dioxanone, trimethylene carbonate (TMC)and GA, was introduced. A modified version of the suture, Vicryl�
Rapid, is currently on the market, which is an irradiated version of thesuture to increase the rate of degradation. Panacryl� is anothercommercially developed suture from the copolymer with a higher LA/GA ratio in order to decrease the rate of degradation. Severalcopolymers have subsequently been developed for the fabrication ofmonofilament sutures [100–103].
The general criteria for selecting a polymer for use as a suture are tomatch the mechanical properties and the time of degradation to theneeds of the application [104–116]. Claude et al. [117] compared theperformance of nonabsorbable sutures, commonly used for vascularanastamoses in microsurgery, with absorbable sutures, rarely evaluatedin this type of surgery. The reported results from macroscopic,histologic, and functional evaluations revealed no significant differ-ences between the two types of sutures. However, local giant-cellinflammatory reaction was more important with the nonabsorbablesuture. The use of nonabsorbable sutures such as PP usually causeslate-occurring wound sinus formation in mass closure of midlineincisions in general surgery and gynecology patients with a reportedsmall incidence of fascial dehiscence. Gallup et al. [118] showed thatthe closure technique is safe and expedient and distributes tensionequally over a continuous line with PGA filaments. Yang and Pastorino[119] state that monofilament absorbable sutures are at least as goodas steel wires to close the sternum after complete or partial sternotomy.In a study carried by Andrade et al. [120] on evaluating the suturematerial modifications resulting from its interaction with tissues, itwas observed that absorbable suture materials induced differentiatedtissue reactions and morphologic surface changes suggesting thatindications should be individualized. A comparison of absorbable versusnonabsorbable sutures was done by Tan et al. for subcuticular skinclosure of a transverse suprapubic incision [121]. Ferguson et al. [122]noted that saliva appears to enhance degradation rates in bothsynthetic and natural absorbable sutures. Riddick et al. [123] evaluatedthe effect of absorbable sutures in reproductive tissue and concludedthat (1) the magnitude of tissue response to suture material varies fordifferent tissues, (2) the degree of tissue wall fibrosis does notnecessarily correspond to external tissue adhesions, and (3) adhesionsare maximal at the surgical knots regardless of the suture materialused. De Persia et al. [100] may be referred for obtaining data oncomparative evaluation of properties and performance of a number ofsutures.
Absorbable Polymeric Surgical Sutures 313
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

Polyglycolide or Poly(Glycolic Acid) (PGA)
Poly(�-ester)s are thermoplastic polymers with hydrolytically labilealiphatic ester linkages in their backbone. Although all polyesters aretheoretically degradable, only aliphatic polyesters with reasonably shortaliphatic chains between ester bonds can degrade over the time framerequired for suture materials [124]. PGA is the simplest linear aliphaticpolyester. Owing to its controllable hydrolytic degradation, PGA and itscopolymers with LA, e-CL, and TMC are widely used as materials for thesynthesis of absorbable sutures and are being evaluated in thebiomedical field [104,108,112].
Synthesis and Properties of PGA
PGA can be obtained through several different processes starting withdifferent materials: polycondensation of GA, ring-opening polymeriza-tion (ROP) of GL (Scheme 1), solid-state polycondensation (SSP) ofhalogenoacetates, acid catalyzed reaction of carbon monoxide, formal-dehyde, etc. The ROP of GL obtained by heating GA is the most commonsynthetic method adopted to produce the high molecular weight (MW)product. Stannous octoate, approved by the FDA as a food stabilizer,is the most commonly used initiator [86,125,126]. PGA of MW20,000–140,000 is suitable for fiber extrusion and suture manufacturing.Tables 7 and 8 list the properties of the polymer and its fiber.
SSP is employed in another procedure where sodium chloroacetate isheated at a temperature between 1608C and 1808C, continuously passingnitrogen through the reaction vessel. The sodium chloride whichprecipitates within the polymeric matrix can be conveniently removedby washing the product of the reaction with water [128]. In anothermethod, the acid catalyzed reaction of carbon monoxide, formaldehyde,or one of its related compounds like paraformaldehyde or trioxane isemployed to prepare PGA [129].
PGA is a highly crystalline (around 45–55%) polymer having glasstransition temperature between 358C and 408C and its melting point inthe range 225–2308C (Tables 7 and 8). It is soluble only in highlyfluorinated solvents like hexafluoroisopropanol and hexafluoroacetonesesquihydrate that can be used to prepare solutions of the high MWpolymer for melt spinning and film preparation. Fibers of PGA exhibithigh strength and modulus. PGA shows excellent mechanical propertiesdue to its high crystallinity. A self-reinforced form composed of PGA isstiffer than any other degradable polymeric system used clinically [24]
314 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
and has been shown to exhibit a modulus of approximately 12.5 GPa[25].
Due to its excellent fiber-forming ability and biodegradability, PGAwas investigated for developing resorbable sutures [130]. This resultedin the development of Dexon� series of commercial sutures. [Dexon�
was the first FDA approved (1969) synthetic suture.] Among the Dexon�
series of commercial PGAs, Dexon� S is uncoated and Dexon� Plus andDexon� II are coated to improve handling properties, knot performance,and smooth passage through tissues. After Dexon, several grades haveappeared in the market under different trade names [131]. Caprosyn�
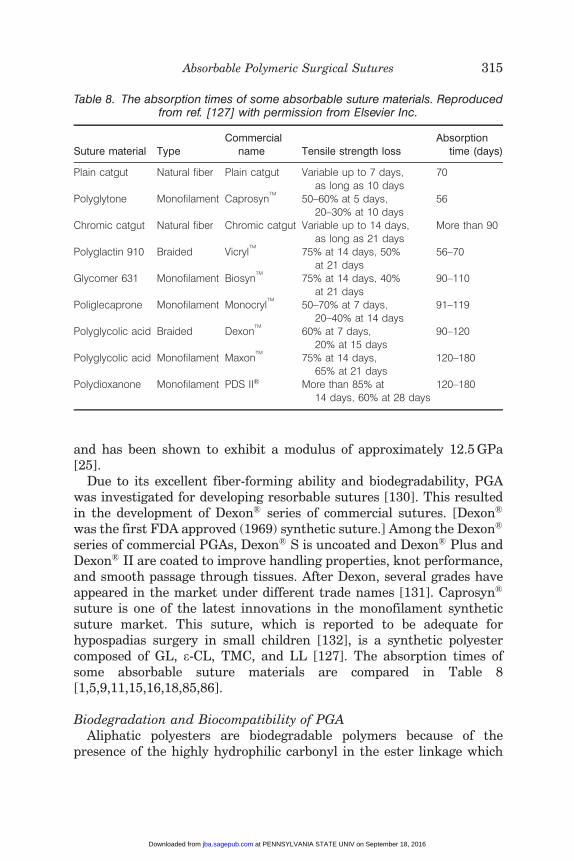
suture is one of the latest innovations in the monofilament syntheticsuture market. This suture, which is reported to be adequate forhypospadias surgery in small children [132], is a synthetic polyestercomposed of GL, e-CL, TMC, and LL [127]. The absorption times ofsome absorbable suture materials are compared in Table 8[1,5,9,11,15,16,18,85,86].
Biodegradation and Biocompatibility of PGAAliphatic polyesters are biodegradable polymers because of the
presence of the highly hydrophilic carbonyl in the ester linkage which
Table 8. The absorption times of some absorbable suture materials. Reproducedfrom ref. [127] with permission from Elsevier Inc.
Suture material TypeCommercial
name Tensile strength lossAbsorption
time (days)
Plain catgut Natural fiber Plain catgut Variable up to 7 days,as long as 10 days
70
Polyglytone Monofilament CaprosynTM
50–60% at 5 days,20–30% at 10 days
56
Chromic catgut Natural fiber Chromic catgut Variable up to 14 days,as long as 21 days
More than 90
Polyglactin 910 Braided VicrylTM
75% at 14 days, 50%at 21 days
56–70
Glycomer 631 Monofilament BiosynTM
75% at 14 days, 40%at 21 days
90–110
Poliglecaprone Monofilament MonocrylTM
50–70% at 7 days,20–40% at 14 days
91–119
Polyglycolic acid Braided DexonTM
60% at 7 days,20% at 15 days
90–120
Polyglycolic acid Monofilament MaxonTM
75% at 14 days,65% at 21 days
120–180
Polydioxanone Monofilament PDS II� More than 85% at14 days, 60% at 28 days
120–180
Absorbable Polymeric Surgical Sutures 315
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
undergoes hydrolytic and/or enzymatic chain cleavage to �-hydroxy-acids, which in most cases are ultimately metabolized in human body.The parameters that control the hydrolysis rates are the temperature,molecular structure, and ester group density as well as the species ofenzyme used. The degree of crystallinity may be a crucial factor, sinceenzymes attack mainly the amorphous domains of a polymer [133].
PGA undergoes hydrolytic degradation through the nonspecificscission of the ester backbone [85]. The degradation process is erosiveand appears to take place in several steps during which the polymer isconverted back to its monomer GA: the first step involves diffusion ofwater into the amorphous (noncrystalline) regions of the polymermatrix, cleaving the ester bonds; the second step starts after theamorphous regions have been eroded, leaving the crystalline portion ofthe polymer susceptible to hydrolytic attack. Upon collapse of thecrystalline regions, the polymer chain dissolves.
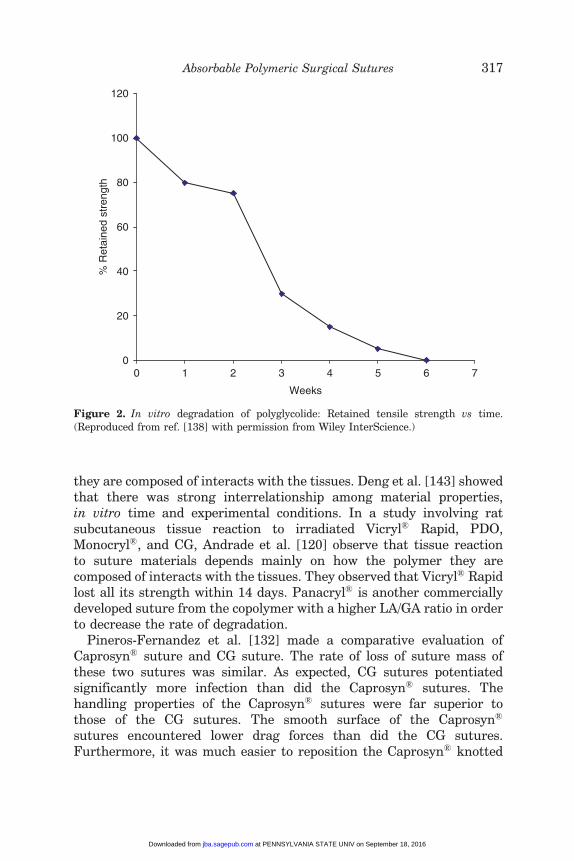
When exposed to physiological conditions, PGA is also broken down bycertain enzymes, especially those with esterase activity [112,134–138].The degradation product, GA, is nontoxic and it can enter thetricarboxylic acid cycle after which it is excreted as water and carbondioxide. A part of the GA is also excreted by urine [112,134]. Studiescarried out using sutures made from PGA have shown that the materialloses half of its strength after 2 weeks and 100% after 4 weeks. Thepolymer is completely resorbed by the organism in a timeframe of 4–6months [105,108]. Figure 2 shows the in vitro degradation of PGA.
The absorption of water and its penetration into the interior of PGA,PLA, and their copolymers initiate hydrolytic fragmentation degrada-tion followed by the reduction of mechanical properties [139,140]. Thedegradation of PGA is faster than that of PLA. Unlike PLA,extracellular enzymes are also thought to have a role in in vivodegradation of PGA. The glycolate generated from PGA during finalhydrolysis is either excreted directly in the urine or is oxidized toglyoxylate that gets converted to glycine, serine, and pyruvate [141].Debus et al. [131] studied four different braided absorbable surgicalmaterials (Dexon�, Dexon II Bicolor�, Vicryl�, and Polysorb�) in vitroand in vivo with regard to their physical properties as well as tissuecompatibility and surgical handling and found that they basically sharethe same indications. The authors concluded that all features andproperties of braided suture material reached a high level of quality withPolysorb�.
The tensile tests on co/terpolymers of LL, e-CL, and GL showed thatthe tensile strength was strongly dependent on the draw ratio [142].Tissue reaction to suture materials depends mainly on how the polymer
316 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
they are composed of interacts with the tissues. Deng et al. [143] showedthat there was strong interrelationship among material properties,in vitro time and experimental conditions. In a study involving ratsubcutaneous tissue reaction to irradiated Vicryl� Rapid, PDO,Monocryl�, and CG, Andrade et al. [120] observe that tissue reactionto suture materials depends mainly on how the polymer they arecomposed of interacts with the tissues. They observed that Vicryl� Rapidlost all its strength within 14 days. Panacryl� is another commerciallydeveloped suture from the copolymer with a higher LA/GA ratio in orderto decrease the rate of degradation.
Pineros-Fernandez et al. [132] made a comparative evaluation ofCaprosyn� suture and CG suture. The rate of loss of suture mass ofthese two sutures was similar. As expected, CG sutures potentiatedsignificantly more infection than did the Caprosyn� sutures. Thehandling properties of the Caprosyn� sutures were far superior tothose of the CG sutures. The smooth surface of the Caprosyn�
sutures encountered lower drag forces than did the CG sutures.Furthermore, it was much easier to reposition the Caprosyn� knotted
0
20
40
60
80
100
120
0 1 2 5 6 7
Weeks
% R
etai
ned
stre
ngth
3 4
Figure 2. In vitro degradation of polyglycolide: Retained tensile strength vs time.(Reproduced from ref. [138] with permission from Wiley InterScience.)
Absorbable Polymeric Surgical Sutures 317
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
sutures than the knotted CG sutures. These biomechanical perfor-mance studies demonstrated the superior performance of syntheticCaprosyn� sutures compared to CG sutures and provide compellingevidence of why Caprosyn� suture is an excellent alternative to CGsuture.
Hong et al. [144,145] compared the biodegradability of Monocryl�
monofilaments with poly(trimethylene carbonate-e-caprolactone)-block-poly(p-dioxanone) [poly(TMC-e-CL)-block-PDO] copolymers. The biode-gradability of PDO homopolymer is much slower compared with that ofthe copolymer, Monocryl�. The lower rate of degradation of Monocryl�
may be due to the presence of the GL content in it. The release of anantimicrobial agent like triclosan added to the surface of PGA threadswas studied by Zurita et al. [146] in different media with high-performance liquid chromatography.
The efficacy of five synthetic absorbable suture materials in intestinalanastomoses in rats, together with their interference with the normalphysiopathological cicatrization process was investigated by de Werraet al. [147]. The materials analyzed were PGA, Dexon�, Maxon�, PDO,Vicryl�, and Biosyn�. An anatomopathological study, performed in threegroups of rats undergoing postmortem examinations after 6, 20, and 90days showed that the least interference was caused by Biosyn�, whilePGA and Vicryl� yielded very good results though giving rise to agreater fibrous component [147]. In another comparative study, Aslanet al. [69] did not find any difference in the macroscopic appearance ofall specimens of the histopathological cross-sections from the skinincision sites under light microscope. A prospective, randomized trialcompared PGA subcuticular skin closure with interrupted silk skinclosure in 152 patients [148]. There was no significant difference in theincidence of wound infection.
Absorbable monofilaments, such as the monofilament sutures such asPDO� II and Maxon� eliminate many of the concerns raised by braidedsutures, but generally monofilaments do not handle as well as braids.These sutures provide an in vivo breaking strength retention ofapproximately 20–30% after 2 weeks, considered by many to be thecritical wound healing period [149]. Monofilament sutures of blockterpolymers of LL, e-CL, and GL also showed potential for use asabsorbable surgical sutures [150]. In another study on Monocryl�, silk,and Vicryl� sutures in oral surgery, Arcuri et al. [151] noted that theclinical healing at 90 days was the same for all the different threads,different from what happened in the critical post-operative period(within 3 weeks). Moy and Kaufman studied 584 repairs of surgicaldefects using two different synthetic absorbable sutures, Vicryl�, and
318 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

Maxon�. No difference in scar width or post-operative complications wasfound between the two sutures, but Maxon� demonstrated preferablehandling and tying characteristics [152].
Several authors [153–155] studied the effect of coatings such aspoloxamer 188 on the handling characteristics of synthetic sutures.Poloxamer 188 was chosen because it does not damage the tissuedefenses of the host and invite infection. Since poloxamer 188 is readilysoluble in aqueous solutions, it is rapidly absorbed in the tissueenvironment resulting in an uncoated suture that displays increasedknot security. The increased knot security, thus, observed with thecoated PGA suture after implantation, was considered to be a distinctclinical advantage over that of the coated Vicryl� Rapid sutures [153]. Inanother study, uncoated Dexon-S� was found to be superior to coatedVicryl� with respect to knot reliability [154]. Dexon� was reported tooffer a favorable alternative for catgut since this synthetic absorbablesuture material produced fewer early tissue reactions in a study on 123patients undergoing neck surgery with respect to wound complications[155]. Dexon� appears to offer a favorable alternative since thissynthetic, absorbable suture material produces fewer early tissuereactions.
Edlich et al. [156] showed that the chemical structure of the sutureappeared to be the most important factor in the development of surgicalinfection and PGA sutures were found to evoke the least inflammatoryresponse among the absorbable sutures. After evaluating the use of PGAsutures in 126 operations performed upon 118 unselected patients,Dardik et al. [157] reported that PGA exhibited excellent behavior sothat it could be termed a ‘‘universal’’ suture material. PGA appears tocompare favorably with other sutures with respect to handling, tensilestrength, knot security, lack of toxicity, and minimal tissue reaction.PGA did not interfere with the process of wound healing, and thematerial was well tolerated in both clean and contaminated operations.Similar results are reported by other groups as well [158–160]. The useof absorbable sutures such as Dexon� in corneolimbal incision techniquewas reported to be seemingly safe [161].
The Vicryl� suture was assessed in 72 surgical patients whounderwent follow-up observation for at least 30 days, and it proved tobe an excellent inert absorbable synthetic suture [162]. In order torapidly assess the performance of a suture material, Weir and Buchananshowed that increasing the test temperature may be an effective methodfor accelerating the degradation rate of bioabsorbable polymers as apotential means to rapidly assess processing, sterilization, and storagevariables [163].
Absorbable Polymeric Surgical Sutures 319
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Liu et al. [164] compared Vicryl�, PP, and Vicryl� Plus fibrin gluesutures in the closure of pharyngeal wounds in experimental animals.There was a significant difference in the rates of pharyngo-cutaneousfistula formation between rats having Vicryl� and PP sutures. Thefibrin glue-treated group had the highest fibroblast activity and collagendeposition. PP produced minimal tissue reaction, which facilitated thehealing process.
Sutures are generally sterilized by EO. However, it was shown byBezwada et al. [165] that PGA braided sutures could be sterilizedwithout damage by Gama radiation.
PGA is particularly useful in subcutaneous and intracutaneousclosures, abdominal, and thoracic surgeries. With its high initial tensilestrength, it has guaranteed holding power through the critical woundhealing period. This suture being absorbable should not be used whereextended approximation of tissue is required. Special precautionsshould be taken in elderly patients and patients with history of anemiaand malnutrition conditions. As with any suture material, adequateknot security requires the accepted surgical technique of flat andsquare ties.
Polylactide or Poly(Lactic Acid) (PLA)
PLA polymers are leading biomaterials having applications inbiomedical and pharmaceutical industries as resorbable implantmaterials, wound closure, bone fixation devices and as vehicles forcontrolled drug delivery [166–168]. They are characterized by theirinherent biodegradability and biocompatibility with high mechanicalstrength. However, their clinical applications are sometimes affected bythe high hydrophobic behavior and consequent poor water uptake,which results in a slow hydrolytic degradation rate [169].Copolymerization of LL with other comonomers is used to modify theproperties of PLA and to control its degradation behavior suitable forthe specific applications in the field [170–173].
The synthesis of PLAs can be carried out by the ring openingpolymerization of the cyclic diester (LL) of LA (Scheme 2) [174–176].PLA of high MW for suture applications is produced from the LLmonomer by ROP using most commonly a stannous octoate catalyst[174]. Due to the chiral nature of LA, several distinct forms ofpolylactide exist: poly-L-lactide (PLLA or PLA in common use) is theproduct resulting from polymerization of L-lactide. Polymerization of aracemic mixture of LL and D-lactides (DL) usually leads to the synthesis
320 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

of poly-DL-lactide (PDLLA) which is not crystalline but amorphous.It is reported that the PLA produced using silica-supported alkoxidecatalysts had a higher MW weight and Tm than those produced with thehomogeneous catalyst [175]. PLA has a crystallinity of around 37%, aglass transition temperature between 508C and 808C and a meltingtemperature between 1738C and 1788C.
There are several patents that report the production of sutures fromPLA polymer [177–184]. Reinforced PLA fibers can be made by a dry-spinning/hot-drawing process [185]. The initial tensile strength of thePLA fibers is lower than that of the commercially available sutures suchas PDO, Vicryl�, silk, and Ethilon� (Ethilon� refers to Nylon 6 andNylon 66 monofilament suture marketed by Ethicon). The handlingcharacteristics of PLA sutures were found to be superior to those of themonofilament sutures such as PDO and Ethilon� and comparable withthe multifilament sutures such as Vicryl� and silk. A compositeconsisting of PDLA and bioglass was used as a coating for degradablesutures such as Vicryl� by Chen et al. [186]. Scanning electronmicroscopy (SEM) observations indicated a homogeneous coating onthe surface. The results suggest that the bioglass/PDLA/Vicryl�
composite sutures are promising bioactive materials for wound healingand tissue engineering applications. Histological studies on thedegradation of 14C tagged PLA polymer in vivo conducted by Kulkarniet al. indicated that PLA was nontoxic, nontissue reactive, andbiodegradable. The degradation studies also point out that the polymeror its degradation products are not retained in any of the vital organs ofthe animals. The polymer implant, however, degrades slowly in vivo,losing 12–14% in 3 months. Their study indicated that PLA could be avery suitable material for sutures, vascular grafts, and other surgicalimplants [176].
Kangas et al. compared the strength properties of PDLA and Maxon�
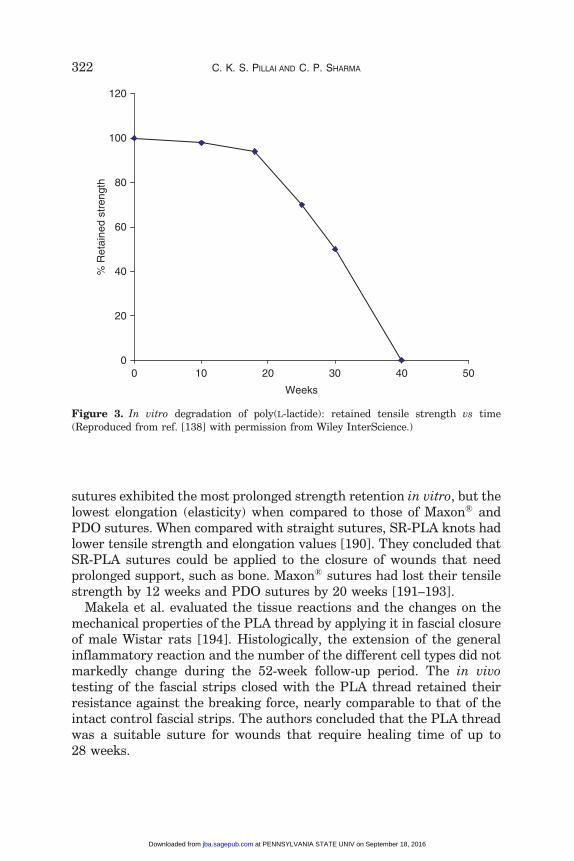
sutures in vitro, in the subcutis, and in the achilles tendon of rabbits andshowed that although PDLA had a lower initial tensile strength thanMaxon�, PDLA showed more prolonged tensile strength retention (TSR)than Maxon� [187]. The authors concluded that PDLA offered analternative to Maxon� in the repair of the Achilles tendon. Lou et al.[188] reported that when PLA sutures of size 5-0 were exposed tophysiological saline (0.9 wt% NaCl aqueous solution) at 378C, the knot-pull strength decreased by 12% after 28 days. Figure 3 shows thatduring hydrolytic degradation of PLA, molecular mass decreases andMW distribution becomes broader continuously with an increase in thedegradation time [189]. In a comparative evaluation of mechanicalproperties, Makela et al. showed that self-reinforced PLA (SR-PLA)
Absorbable Polymeric Surgical Sutures 321
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
sutures exhibited the most prolonged strength retention in vitro, but thelowest elongation (elasticity) when compared to those of Maxon� andPDO sutures. When compared with straight sutures, SR-PLA knots hadlower tensile strength and elongation values [190]. They concluded thatSR-PLA sutures could be applied to the closure of wounds that needprolonged support, such as bone. Maxon� sutures had lost their tensilestrength by 12 weeks and PDO sutures by 20 weeks [191–193].
Makela et al. evaluated the tissue reactions and the changes on themechanical properties of the PLA thread by applying it in fascial closureof male Wistar rats [194]. Histologically, the extension of the generalinflammatory reaction and the number of the different cell types did notmarkedly change during the 52-week follow-up period. The in vivotesting of the fascial strips closed with the PLA thread retained theirresistance against the breaking force, nearly comparable to that of theintact control fascial strips. The authors concluded that the PLA threadwas a suitable suture for wounds that require healing time of up to28 weeks.
0
20
40
60
80
100
120
0
Weeks
% R
etai
ned
stre
ngth
10 20 30 40 50
Figure 3. In vitro degradation of poly(L-lactide): retained tensile strength vs time(Reproduced from ref. [138] with permission from Wiley InterScience.)
322 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Poly(Lactide-co-Glycolide) (PLGA)
Copolymers of GL with both LL and DL have been developed for bothdevice and drug delivery applications. For suture applications, LL-co-GLcopolymer must have a high concentration of GL for achieving propermechanical and degradation properties. PLGA is synthesized by meansof random ROP of two different monomers (Scheme 3), the cyclic dimersof GA and LA. Depending on the ratio of LL to GL used for thepolymerization, different forms of PLGA can be obtained. Multifilamentbraided Vicryl� sutures developed by Ethicon contain 90/10 molar ratioof GA to LA and they are coated with 2–10% of a 50:50 mixture of anamorphous polyglactin 370 (a 65/35 mole ratio of PLGA copolymer) andcalcium stearate [1]. All PLGAs are amorphous rather than crystallineand show a glass transition temperature in the range 40–608C. Unlikethe homopolymers of LA and GA which show poor solubilities, PLGAcan be dissolved by a wide range of common solvents, includingchlorinated solvents, tetrahydrofuran, acetone, or ethyl acetate.
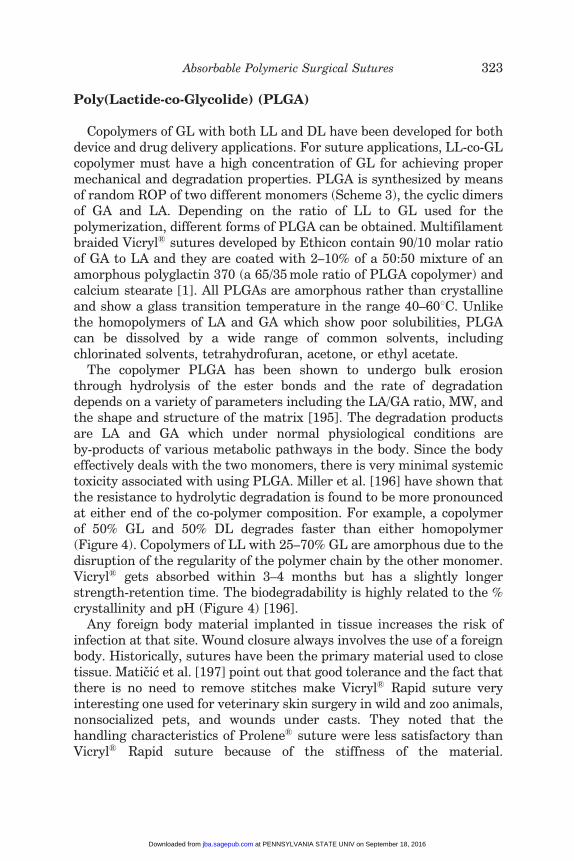
The copolymer PLGA has been shown to undergo bulk erosionthrough hydrolysis of the ester bonds and the rate of degradationdepends on a variety of parameters including the LA/GA ratio, MW, andthe shape and structure of the matrix [195]. The degradation productsare LA and GA which under normal physiological conditions areby-products of various metabolic pathways in the body. Since the bodyeffectively deals with the two monomers, there is very minimal systemictoxicity associated with using PLGA. Miller et al. [196] have shown thatthe resistance to hydrolytic degradation is found to be more pronouncedat either end of the co-polymer composition. For example, a copolymerof 50% GL and 50% DL degrades faster than either homopolymer(Figure 4). Copolymers of LL with 25–70% GL are amorphous due to thedisruption of the regularity of the polymer chain by the other monomer.Vicryl� gets absorbed within 3–4 months but has a slightly longerstrength-retention time. The biodegradability is highly related to the %crystallinity and pH (Figure 4) [196].
Any foreign body material implanted in tissue increases the risk ofinfection at that site. Wound closure always involves the use of a foreignbody. Historically, sutures have been the primary material used to closetissue. Maticic et al. [197] point out that good tolerance and the fact thatthere is no need to remove stitches make Vicryl� Rapid suture veryinteresting one used for veterinary skin surgery in wild and zoo animals,nonsocialized pets, and wounds under casts. They noted that thehandling characteristics of Prolene� suture were less satisfactory thanVicryl� Rapid suture because of the stiffness of the material.
Absorbable Polymeric Surgical Sutures 323
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Additionally, Vicryl� Rapid showed better control of knotting thanProlene�. However, it should be noted that Vicryl� was shown to elicitpronounced inflammatory reaction (Figure 5(a) and (c)) compared tochiotosan gels (Figure 5(a) and (b)), which elicited very minimalinflammatory response [198]. In the case of infectious wounds,Pineros-Fernandez et al. showed that the closure of contaminatedwounds with the InsorbTM staples (a copolymer of LA and GA ofunknown composition, produced by Incisive Surgical, Inc., USA) is asuperior choice to Vicryl� suture because they have a significantly lowerincidence of infection [199]. Figure 6 gives a photograph of theelectrospun fiber of the copolymer [200].
The major popularity of these biocompatible copolymers can beattributed in part to their approval by the FDA for use in humans, itsgood processibility which enables fabrication of a variety of structuresand forms, controllable degradation rates and their success asbiodegradable sutures compared to the earlier suture materials.
Polyglyconate
Copolymers of GA with TMC have been prepared (Scheme 4) as bothsutures (Maxon�, by Davis and Geck) and as tacks and screws.
0
2
4
6
0 7525 50 100
PLA (%)
Mon
th
Figure 4. The effect of glycolide to lactide composition on the in vivo degradation of rateof polygalactin implanted under the dorsal skin of rat. (Reproduced from ref. [195] with
permission from Wiley InterScience.)
324 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

Typically, these are prepared as A–B–A block copolymers in a 2:1GL:TMC ratio, with a GL–TMC center block (B) and pure GL end blocks(A). These materials have better flexibility than pure PGA and areabsorbed in approximately 7 months. GL has also been copolymerizedwith TMC and p-dioxanone to form a terpolymer suture (Biosyn�) thatabsorbs within 3–4 months and offers reduced stiffness compared withpure PGA fibers [201].
Martin and Motbey [202] reported the use of Maxon� suture inpediatric gastrointestinal surgery because it has a low coefficient offriction and very low tissue drag and is stronger (straight pull andknot strength) than corresponding gages of braided syntheticabsorbable sutures. It is slowly absorbed, its half-life (in relation
Figure 6. Electrospun fiber of PLGA copolymer. (Reproduced from ref. [197] withpermission from Wiley InterScience.)
Figure 5. (a)–(c) Histological sections demonstrating minimal tissue response in the
surrounding tissues: (a) SDG implant, (100�), (b) FDG implant (100�), and (c) chronicforeign body reaction in the tissues surrounding surgical sutures (200�). FDG – gels with
lower cross-linking density SDG – gels with higher cross-linking density. (Reproduced
from ref. [198] with permission from Wiley InerScience.)
Absorbable Polymeric Surgical Sutures 325
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
to strength) being 5 weeks and complete disappearance occurringin 6–7 months. The authors report that Maxon� is superior toother currently available sutures for pediatric gastrointestinalsurgery.
The hydrolytic degradation of PG has been studied in vitro byFarrar and Gillson [203]. They report that the observed relationshipbetween strength and MW was more complex than expected.However, the data could be modeled using an empirically derivedrelationship between tensile strength and number average molecularweight (Mn). Changes in other mechanical properties, such as strainat break, were also found to be strongly dependent Mn. Flyger et al.[204] showed that an absorbable monofilament suture such as PGcan be used safely in a single layered continuous colonic anasto-mosis. Of the 105 patients in the study, 1 developed an anastomoticleak. None of the patients had symptoms of anastomotic stricture atfollow-up.
The effectiveness of Biosyn�, PDO, and Maxon� monofilamentsutures in healing musculoaponeurotic incisions in rats was studied byRodeheaver et al. The authors recommended all the three syntheticabsorbable sutures in clinical use in laparotomy incisions because theyprovided secure closure of laparotomy incisions [205].
The slowly absorbing nature of PG suture was tested to determine itssuitability for use in microarterial anastomoses under ordinary tensionand under undue tension by Huang et al. [206]. The results showed thatPG suture retains tensile strength for an adequate period to allowvascular healing and causes a less pronounced tissue response thannonabsorbable Nylon suture. Complete absorption of the suturematerial was followed by a complete regeneration of the vessel wall.These results demonstrated that absorbable PG suture might besuitable for microvascular anastomosis of arteries under ordinarytension and under tension to a certain degree.
Poly(L-Lactide-co-e-Caprolactone)
The copoloymer of LL with e-CL exhibited good strength andflexibility suitable for monofilament sutures. It also showed improvedhandling characteristics. This was established by Tomihata et al. [207]in a comparative study involving six types of other monofilamentsutures (two of these were nonabsorbable) for comparisons. Suturesconsisting of GL were the strongest among all the sutures examined. Onthe other hand, Prolene� (PP) and poly(L-lactide-co-e-caprolactone)(PLA-e-CL) sutures showed high knot-pull strength despite low straight
326 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
pull strength. A good correlation between tan � and bending plasticityindex was observed and the PLA-e-CL sutures exhibited high tan �, highbending plasticity, and good resistance against untying.
Co/terpolymers of LL, e-CL, and GL are biodegradable in the humanbody and, as such, have considerable potential for use in biomedicalapplications such as surgical sutures, nerve guides, bone fixationdevices, and drug delivery systems [143,208]. Baimark et al. [208]reported that the monofilament fiber of the block copolymer of LL ande-CL had a tensile strength 4400 MPa and recommended that thismaterial has potential to be developed further as a lower cost alternativeto the current commercial monofilament surgical sutures.Monofilaments of the block terpolymer of LL, e-CL, and GL have beenmelt spun for potential use as absorbable surgical sutures. As-spunfibers of the terpolymers produced by melt spinning were elastic,amorphous, and isotropic and could be promising materials for use asmonofilament sutures [150,209].
Polydioxanone (PDO or PDS)
Resorbable multifilament sutures such as PLA and PGA develop agreater amount of friction when penetrating tissues and have a higherrisk of infection. So, monofilament sutures based on PDO having smoothand soft surface were introduced in the 1980s [209]. PDO suture hashandling properties that are acceptable for use in vascular applications,and it provides adequate mechanical support for sutured vessels to heal[210]. In addition, PDO provides good flexibility owing to the presence ofan ether oxygen group in the backbone of the polymer chain.
PDO is prepared by the ROP of p-dioxanone to get a colorless, semi-crystalline polymer with a very low glass transition temperature rangingfrom �108C to 08C (see Table 9 for mechanical properties). Being analiphatic polyester, it undergoes degradation by the nonspecific scissionof the ester bond. PDO can be considered a slow to moderately degradingpolymer due to the high crystallinity and hydrophobicity of the polymer.In the body, PDO is broken down into glycoxylate and excreted in theurine or converted into glycine and subsequently into carbon dioxide andwater [124,211]. PDO has demonstrated no acute or toxic effects onimplantation. The monofilament loses 50% of its initial breakingstrength after 3 weeks and is absorbed within 6 months, providing anadvantage over Dexon� or other products for slow-healing wounds.
Sutures are prepared by extrusion into fibers at the lowest possibletemperatures to avoid depolymerization back to the monomer. Severalpublications exist on the synthesis [108,150,210,212], fiber formation
Absorbable Polymeric Surgical Sutures 327
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
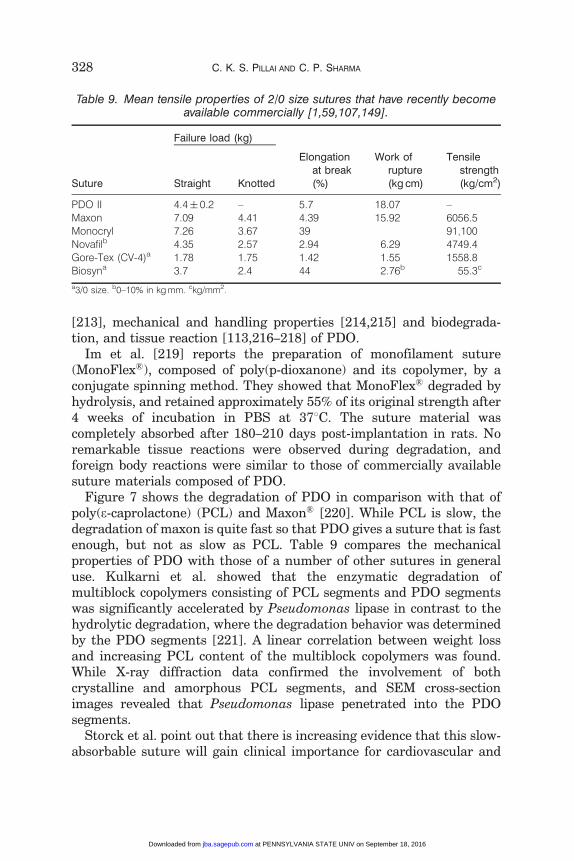
[213], mechanical and handling properties [214,215] and biodegrada-tion, and tissue reaction [113,216–218] of PDO.
Im et al. [219] reports the preparation of monofilament suture(MonoFlex�), composed of poly(p-dioxanone) and its copolymer, by aconjugate spinning method. They showed that MonoFlex� degraded byhydrolysis, and retained approximately 55% of its original strength after4 weeks of incubation in PBS at 378C. The suture material wascompletely absorbed after 180–210 days post-implantation in rats. Noremarkable tissue reactions were observed during degradation, andforeign body reactions were similar to those of commercially availablesuture materials composed of PDO.
Figure 7 shows the degradation of PDO in comparison with that ofpoly(e-caprolactone) (PCL) and Maxon� [220]. While PCL is slow, thedegradation of maxon is quite fast so that PDO gives a suture that is fastenough, but not as slow as PCL. Table 9 compares the mechanicalproperties of PDO with those of a number of other sutures in generaluse. Kulkarni et al. showed that the enzymatic degradation ofmultiblock copolymers consisting of PCL segments and PDO segmentswas significantly accelerated by Pseudomonas lipase in contrast to thehydrolytic degradation, where the degradation behavior was determinedby the PDO segments [221]. A linear correlation between weight lossand increasing PCL content of the multiblock copolymers was found.While X-ray diffraction data confirmed the involvement of bothcrystalline and amorphous PCL segments, and SEM cross-sectionimages revealed that Pseudomonas lipase penetrated into the PDOsegments.
Storck et al. point out that there is increasing evidence that this slow-absorbable suture will gain clinical importance for cardiovascular and
Table 9. Mean tensile properties of 2/0 size sutures that have recently becomeavailable commercially [1,59,107,149].
Failure load (kg)
Suture Straight Knotted
Elongationat break(%)
Work ofrupture(kg cm)
Tensilestrength(kg/cm2)
PDO II 4.4� 0.2 – 5.7 18.07 –Maxon 7.09 4.41 4.39 15.92 6056.5Monocryl 7.26 3.67 39 91,100Novafilb 4.35 2.57 2.94 6.29 4749.4Gore-Tex (CV-4)a 1.78 1.75 1.42 1.55 1558.8Biosyna 3.7 2.4 44 2.76b 55.3c
a3/0 size. b0–10% in kg mm. ckg/mm2.
328 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
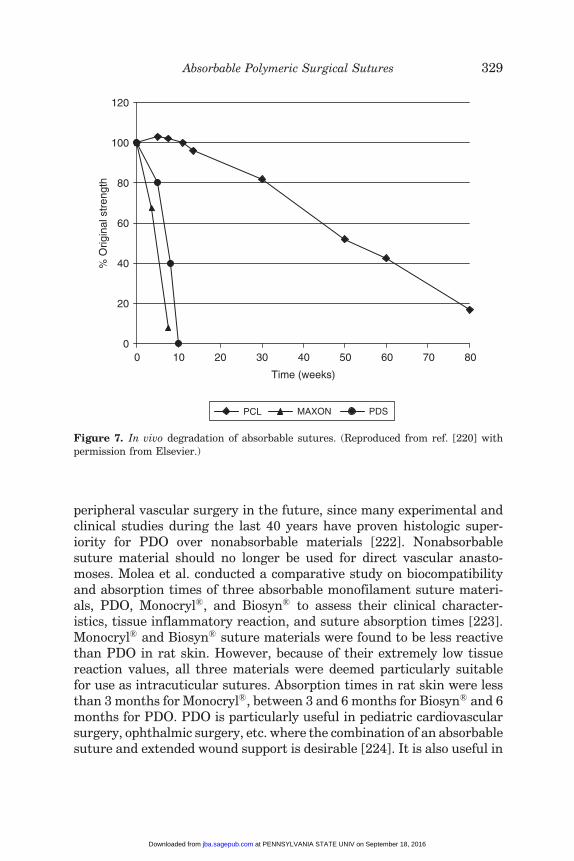
peripheral vascular surgery in the future, since many experimental andclinical studies during the last 40 years have proven histologic super-iority for PDO over nonabsorbable materials [222]. Nonabsorbablesuture material should no longer be used for direct vascular anasto-moses. Molea et al. conducted a comparative study on biocompatibilityand absorption times of three absorbable monofilament suture materi-als, PDO, Monocryl�, and Biosyn� to assess their clinical character-istics, tissue inflammatory reaction, and suture absorption times [223].Monocryl� and Biosyn� suture materials were found to be less reactivethan PDO in rat skin. However, because of their extremely low tissuereaction values, all three materials were deemed particularly suitablefor use as intracuticular sutures. Absorption times in rat skin were lessthan 3 months for Monocryl�, between 3 and 6 months for Biosyn� and 6months for PDO. PDO is particularly useful in pediatric cardiovascularsurgery, ophthalmic surgery, etc. where the combination of an absorbablesuture and extended wound support is desirable [224]. It is also useful in
0
20
40
60
80
100
120
0
Time (weeks)
% O
rigin
al s
tren
gth
PCL MAXON PDS
10 20 30 40 50 60 70 80
Figure 7. In vivo degradation of absorbable sutures. (Reproduced from ref. [220] withpermission from Elsevier.)
Absorbable Polymeric Surgical Sutures 329
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
preparing barbed sutures that can anchor securely in tissues and obviatethe need for surgical knots [225, 226].
Hong et al. [145] investigated the mechanical properties andbiodegradability of [poly(TMC-e-CL)-block-PDO] copolymers in compar-ison with PDO and Monocryl� monofilaments in vivo and in vitro.Poly(TMC-e-CL)-block-PDO copolymer was prepared by using ringopening polymerization reaction [144]. The implantation studies ofabsorbable suture strands performed in gluteal muscle of rats showedthat these polymers, poly(TMC-e-CL)-block-PDO, PDO, and Monocryl�,were semi-crystalline with 27%, 32%, and 34% crystallinity, respectively.The mechanical properties of poly(TMC-e-CL)block-PDO were compara-tively lower than those of the other polymers. The biodegradability ofPDO was the lowest among these polymers.
PDO and Maxon� sutures are known to reduce complications in thehealing of the wound significantly. Vracko and Pegan [227] analyzed thefrequency of the complications in the healing of the operative wound on114 and 108 patients upon the biliary tract with a subcostal incision andclosed in one layer with PDO and Maxon� sutures. The difference in thedevelopment of complications in the healing of the surgical woundbetween the two drained groups was not statistically significant.
The longer dissolution time of PDO was utilized by Anderson et al.[228] to prevent local sepsis and anastomotic leakage developing fromshort dissolution time and multifilament structure of sutures such asVicryl�. In a study of 98 rat colonic anastomoses, no difference wasfound in complication rates or cellular reaction to the suture materialbetween Vicryl� and PDO [228]. PDO sutures were also shown tomaintain their strength in a 28-day observation period in a repairoperation involving 36 canine flexor digitorum profundus tendons using5-0 Maxon� or PDO monofilament [229]. All the tendons healed withoutrupture or formation of gaps of more than 2 mm. Maxon� repairs wereinitially superior in gap and ultimate strength to PDO repairs. However,the gap and ultimate tensile strength of Maxon� repairs had decreasedsignificantly at day 14. PDO was shown to be a safe alternative tostandard sternotomy closure after pediatric open cardiac surgery byKeceligil et al. [230].
The ease of handling and knot performance of sutures are parametersthat concern the surgeon during surgery [231]. Studies on threemonofilament sutures, Prolene�, Biosyn�, and PDO, and one braidedpolyester suture (Surgidac�) showed that Prolene� and Biosyn� suturesgave improvements in loop elongation and loop-holding capacity overPDO, with the Snyder knots being consistently superior to Duncanknots. Biosyn� gave no improvement over PDO. Both Prolene� and
330 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Surgidac� sutures gave superior knot performance to PDO, but onlyProlene� gave equivalent ease of manipulation. As a result, there may beclinical advantages in replacing PDO with Prolene� or Surgidac�
sutures for certain arthroscopic procedures. The PDO suture, however,was found significantly better than catgut in terms of pliability, ease ofpassage through tissue, ease of tying, strength, fray resistance, andoverall handling properties.
PDO would appear to be particularly useful in situations requiringextended wound support, in potentially infected wounds in which amonofilament suture would have lessened tendency to harbor patho-genic bacteria, and in cases where ease of passage through tissue,smooth tie-down, and precise knot placement are important [232].Various sizes of undyed monofilament PDO surgical suture wereassessed in 52 surgical patients who underwent plastic surgery. With asingle exception, follow-up observations were carried out for at least40 days. Clinical results were judged satisfactory in 13 patients andexcellent in 39 patients.
PDO was shown to lose its shape totally within 2 months in a studyinvolving foreign body reaction, capsule formation, and mechanicalproperties [233]. In another study, Sasaki et al. investigated thedurability of plain catgut and CG, Vicryl� Rapid, PGA, PDO,Prolene�, and silk sutures in human pancreatic juice and bile [234].Plain catgut and CG disintegrated in pancreatic juice and pancreaticjuice plus bile mixture. PGA and Vicryl� Rapid suture materials werevulnerable to pancreatic juice within 7 days. PDO retained most of itsinitial strength in pancreatic juice and bile. Prolene� and silk retained84% and 92% of their initial strength, respectively. The authors foundthat PDO was the strongest suture material in pancreatic juice. PDOsutures are, however, reported to undergo bending, curling, or strippingaway (the barbs) from the suture body after extraction in anexperimental study [235].
Poly(e-Caprolactone) (PCL)
PCL is produced by the ROP of e-CL. It is a semi-crystalline polymerwith a melting point of 59–648C and a glass-transition temperature of�608C. The polymer has been regarded as tissue compatible and used asa biodegradable suture in Europe. The polymer undergoes hydrolyticdegradation due to the presence of hydrolytically labile aliphatic esterlinkages in physiological conditions (such as in the human body) [124].Because the homopolymer has a degradation time on the order of2 years, copolymers have been synthesized to accelerate the rate of
Absorbable Polymeric Surgical Sutures 331
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
bioabsorption. For example, copolymers of e-CL with DLL have yieldedmaterials with more-rapid degradation rates. The introduction ofmonofilament sutures of e-CL and GL (Monacryl�; Scheme 5) solvedmany of the problems with braided sutures that relate to tissue drag andthe trauma as well as the possible potentiation of infection through theinterstices of the braid structure. Another bioresorbable (SynBiosys�)multiblock copolymer composed of e-CL, GL, LL, and poly(ethyleneglycol) units has been developed as a drug delivery vehicle for small andmedium sized biologically active molecules. PCL has low tensile strength(approximately 23 MPa) but an extremely high elongation at break(4700%) [196]. PCL is also an FDA approved material.
Bezwada et al. [149] showed that Monocryl� sutures displayedexcellent handling properties, minimal resistance during passagethrough tissue, and excellent tensile properties. Absorption data onthese sutures indicate that absorption is complete between the 91st and119th days of implantation, with slight or minimal tissue reaction [149].The biodegradability of Monocryl� sutures is much better than that ofPDO [144].
A copolymer of LL, e-CL, and TMC was used as a suture coating for aPGA suture that could contain an antimicrobial agent like triclosan. Atotal release of triclosan is attained after a few days of exposure to aDulbecco’s based medium, whereas equilibrium concentrations arereached when a Sorensen hydrophilic medium is used [146].
Poly(Trimethylene Carbonate) (PTMC)
ROP of TMC gives high MW weight flexible PTMC. Unlike thepreviously described polyesters, PTMC undergoes surface degradation.The rate of in vivo degradation was found to be much higher thanin vitro degradation. This is presumably due to the contribution ofin vivo enzymatic degradation process [124]. The low mechanicalperformance of the homopolymer led to the development of severalco/terpolymers such as Maxon� and Biosyn� (Schemes 6) with othercyclic lactones. A comparison of mechanical properties of Maxon� andBiosyn� is given in Table 10 [98,99,114,208,216,222].
Maxon� was formulated to combine predictable in vivo performance ofsynthetic absorbable suture with the handling characteristics of amonofilament suture [94,98,101,114,227]. The studies carried out inrats showed cumulative strength retention of 81% at 14 days, 59% at28 days, and 30% at 42 days [98]. Histologic assessment of absorptionobtained from serial sections at intervals of 3–9 months showed that, insizes 00 and 4-0, complete absorption occurred between 6 and 7 months.
332 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
The authors believe that the absorption of these sutures was achievedthrough the action of mononuclear and multinuclear macrophageswhich were confined to the implant and sequestered by a fibrousconnective tissue capsule. The results of studies of radiolabeled suturescarried out in the subcutaneous tissues of rats revealed urine andexpired CO2 to be the major excretory routes of the metabolites. Thesesutures thus were shown to maintain good strength with little or noabsorption during the critical wound healing period with minimal tissuereaction. Hydrolytic degradation studies showed that changes inmechanical properties of the copolymer were found to be stronglydependent on changes in the value of Mn [203].
Biosyn� has, however, been shown to exhibit more problems onsuturing after childbirth in a comparative study with the multifilamentsuture Dexon II� [236]. Women who required suturing by midwiveswere allocated for repair with either the multifilament suture Dexon II�
or with a new monofilament of Biosyn�. The results at follow-up after8–12 weeks indicated that more women in the monofilament groupreported problems with the sutured area.
Polyhydroxyalkanoates
PHAs are polyesters produced by micro-organisms (like Alcaligeneseutrophus or Bacillus megaterium) as energy storage materials [237–239]. The most common PHA, poly(3-hydrobutyrate) (PHB), is a semi-crystalline polyester (Figure 8) that undergoes hydrolytic degradation bysurface erosion, making it an attractive material for controlled releaseapplications. It has relatively high melting point and crystallizes rapidly,making entrapment of drug technically difficult. The related copolymerswith 3-hydroxyvalerate, P(3HB-co-3HV)s, have similar semi-crystallineproperties though their slower rates of crystallization result in matriceswith different properties. PHB and P(3HB-co-3HV) matrices lose mass
Table 10. A comparison of mechanical properties of Biosyn and Maxon sutures[99,99,208,217,222].
Physical property Biosyn (3/0) Maxon (3/0)
Diameter (mm) 0.29 0.293Knot pull strength (kg) 2.4 2.9Young’s modulus (kpsi) 145 425Straight-pull strength (kg) 3.7 3.9Elongation (%) 44 30Tensile strength (kg/mm2) 55.3 56.2
Absorbable Polymeric Surgical Sutures 333
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
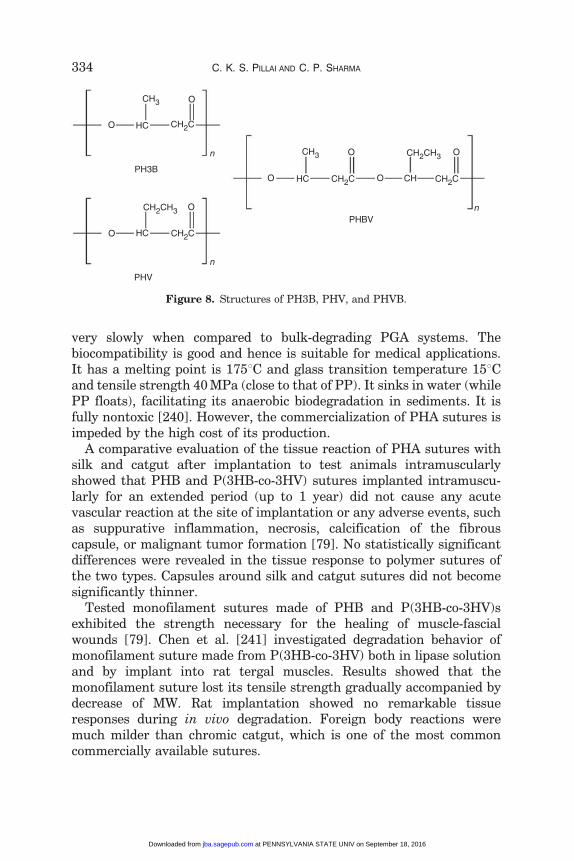
very slowly when compared to bulk-degrading PGA systems. Thebiocompatibility is good and hence is suitable for medical applications.It has a melting point is 1758C and glass transition temperature 158Cand tensile strength 40 MPa (close to that of PP). It sinks in water (whilePP floats), facilitating its anaerobic biodegradation in sediments. It isfully nontoxic [240]. However, the commercialization of PHA sutures isimpeded by the high cost of its production.
A comparative evaluation of the tissue reaction of PHA sutures withsilk and catgut after implantation to test animals intramuscularlyshowed that PHB and P(3HB-co-3HV) sutures implanted intramuscu-larly for an extended period (up to 1 year) did not cause any acutevascular reaction at the site of implantation or any adverse events, suchas suppurative inflammation, necrosis, calcification of the fibrouscapsule, or malignant tumor formation [79]. No statistically significantdifferences were revealed in the tissue response to polymer sutures ofthe two types. Capsules around silk and catgut sutures did not becomesignificantly thinner.
Tested monofilament sutures made of PHB and P(3HB-co-3HV)sexhibited the strength necessary for the healing of muscle-fascialwounds [79]. Chen et al. [241] investigated degradation behavior ofmonofilament suture made from P(3HB-co-3HV) both in lipase solutionand by implant into rat tergal muscles. Results showed that themonofilament suture lost its tensile strength gradually accompanied bydecrease of MW. Rat implantation showed no remarkable tissueresponses during in vivo degradation. Foreign body reactions weremuch milder than chromic catgut, which is one of the most commoncommercially available sutures.
CH3
CH3
HC
HC
CHHCPH3B
PHBV
PHV
CH2C
CH2C
CH2C CH2C
CH2CH3
CH2CH3
O
O
O
O
O
O O
O
n
n
n
Figure 8. Structures of PH3B, PHV, and PHVB.
334 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
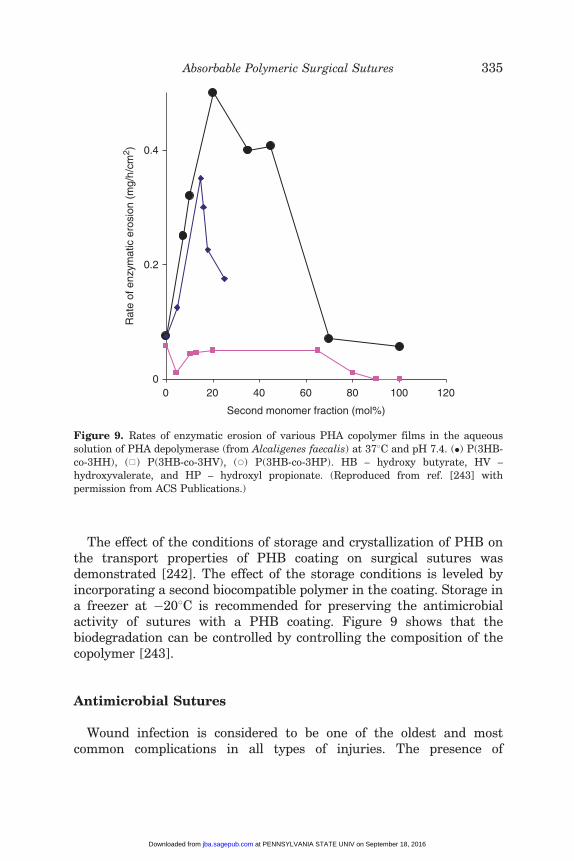
The effect of the conditions of storage and crystallization of PHB onthe transport properties of PHB coating on surgical sutures wasdemonstrated [242]. The effect of the storage conditions is leveled byincorporating a second biocompatible polymer in the coating. Storage ina freezer at �208C is recommended for preserving the antimicrobialactivity of sutures with a PHB coating. Figure 9 shows that thebiodegradation can be controlled by controlling the composition of thecopolymer [243].
Antimicrobial Sutures
Wound infection is considered to be one of the oldest and mostcommon complications in all types of injuries. The presence of
0
0.2
0.4
0
Second monomer fraction (mol%)
Rat
e of
enz
ymat
ic e
rosi
on (
mg/
h/cm
2 )
20 40 60 80 100 120
Figure 9. Rates of enzymatic erosion of various PHA copolymer films in the aqueous
solution of PHA depolymerase (from Alcaligenes faecalis) at 378C and pH 7.4. (�) P(3HB-
co-3HH), (h) P(3HB-co-3HV), (*) P(3HB-co-3HP). HB – hydroxy butyrate, HV –hydroxyvalerate, and HP – hydroxyl propionate. (Reproduced from ref. [243] with
permission from ACS Publications.)
Absorbable Polymeric Surgical Sutures 335
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

foreign materials in wound has been known to enhance thesurrounding tissues to wound infection. Suture materials are theprobably the most important biomaterials in wound infection becausethe infection begins along or near suture lines. The use ofantimicrobial sutures is expected to provide protection from woundinfection. Several approaches have been reported in developingantimicrobial sutures. The incorporation of silver metal on thesurface of sutures is one of the approaches adopted to impartantimicrobial activity to sutures [244].
Sutures Based on ChitinOne of the most promising biomaterials that can accelerate wound
healing is the natural polysaccharide known as chitin that containsN-acetyl glucosamine (NAGA) moiety as repeating unit. Chitin is, thus,poly(N-acetylglycosamine), the linear polymeric structure of which isexpected to give rise to fiber formation and film-forming ability similarto those of cellulose [245]. NAGA can be found in certain essentialhuman glycoproteins in connective tissues like hyaluronic acid andkeratin sulfate. The glucosamine moiety in chitin has been shown toexhibit a variety of biological functions, such as anti-inflammatory,hepatoprotective, antireactive, and antihypoxic activities. The NAGAderivatives are also shown to exhibit antitumor effect [246]. In additionto its potential antitumor effect, chitin, and its derivatives have beenreported as possible wound healing accelerators. Chitosan (CS), thedeacetylated form of chitin, has been reported to have antimicrobialactivity against Gram-positive pathogens like Staphylococcus aureus,Staphylococcus epidermidis, and Staphylococcus haemolyticus[247–250]. A possible mode of action for chitin derivatives in woundhealing is one in which glycosaminoglycans play a role in the structuralorganization of collagen [251].
Although chitin fibers could be made into textile materials, chitinsutures have remarkable properties over other fibers for biomedicalapplications [252–255]. One study reports that chitin fibers havecomparable properties to those of collagen and lactide fibers [256]. Bythe mid-1950s, chitin-coated sutures were being used, which enhancedhealing time by 35–50%. Chitin sutures resist attack in bile urine andpancreatic juice, which are problem areas with other absorbable sutures[257].
The preparation of chitin threads for use in the fabrication ofabsorbable suture materials, dressings, and biodegradable substrates forthe growth of human skin cells has been reported [258,259]. Thewet-spinning process has been employed to prepare chitin sutures.
336 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

The process used strong polar protic solvents such as trichloroacetic acid(TCA), dichloroacetic acid (DCA), etc. to dissolve chitin. Kifune et al.[260] reported a process for the production of chitin fibers having hightensile strength and flexibility, suitable particularly for the preparationof absorbable surgical sutures. In the 1970s, Brine and Austin developeda method to spin pure chitin filaments. A Japanese firm bought thepatent rights, and suture materials are now manufactured in Japan[261,262]. A number of similar patents and processes have also beenreported wherein various highly polar solvents and solvent mixers wereused [263–268]. Although dry tenacities of above 3 g/denier wereobtained, the low wet tenacities were still undesirable. In addition,chlorohydrocarbons are solvents that are increasingly becoming envir-onmentally unacceptable.
Spun chitin filaments developed in the 1970s for sutures were shownto enhance healing time by 35–50% and are fully absorbed by the body[78,269,270]. It is reported that chitin is a suitable material forabsorbable, flexible sutures for use in contact with bile, urine, andpancreatic juices, which are problem areas with other absorbablesutures [271]. The sutures developed from chitin with sufficientstrength and flexibility were absorbed in about 4 months in rat muscleswithout any adverse effect [251].
Chitin is, thus, an absorbable suture material with suitablemechanical properties. Tissue reaction is not specific and the goodhealing which ensued provided evidence for a satisfactory biocompat-ibility. Toxicity tests, including acute toxicity, pyrogenicity, mutageni-city, etc. were negative in all respects. The chitin suture was absorbedin about 4 months in rat muscles. The persistence of the tensilestrength of the chitin was better than Dexon� or catgut in bile, urine,and pancreatic juice but weakening occurred early in the presence ofgastric juice [78]. Application in 132 patients proved satisfactory interms of tissue reaction and good healing indicating satisfactorybiocompatibility [272]. In a study of the comparative evaluation of fourabsorbable suture materials, chitin, PGA, plain catgut, and CG,Tachibana et al. observed that the TSR of chitin in muscle was 45%at 14 days and 7% at 25 days, which was similar to that of PGA. TheTSR of chitin was maintained by 35% in gastric juice, 97% in bile, and100% in pancreatic juice after immersion for 30 days. The correspond-ing values for PGA were 54%, 0%, and 0%, respectively, whereas bothcatguts had dissolved within 30 days. The tissue reaction of chitin wassimilar to that of PGA [77].
The importance of chitin suture materials is on the increase as can bewitnessed by several publications [78,273–280]. Biodegradable
Absorbable Polymeric Surgical Sutures 337
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
polyurethane (PU) elastomers with potential for biomedical applicationas nonabsorbable sutures with improved hydrophobic properties weresynthesized by modification of chitin by the reaction of CL and 4,40-diphenylmethane diisocyanate, extended with different mass ratios ofchitin and/or 1,4-butanediol (BDO) [280]. The results of different testsdemonstrated that the synthesized products are potential candidates asnonabsorbable sutures as previously investigated into their in vitrobiocompatibility and nontoxicity [281–284]. Optimum hydrophobicitywas obtained from elastomer extended with chitin in comparison toelastomers extended with BDO. The surface free energy was alsoaffected by chemical composition of the final PU. Structure–propertyrelationship for the prepared elastomers showed that the maindetermining factors were hydrogen bonding, hydrophobicity, andcontent of chitin in PU backbone. Xiong et al. [285] have shown thatchitin suture has a potential to construct tissue engineering skeletalmuscle. When chitin was cultured with myoblast L6 of rats in vitro, theyobserved a parallel arrangement of scaffold that can control thedirectivity of tissue engineering skeletal muscle fibers.
Chitin with enhanced tensile strength (4 g/denier) and modulus (100 g/denier) was produced from chitin or CS acetate/formate polymer[286,287]. Fibers spun from lyotropic liquid crystalline solution possesshighly oriented chains both in amorphous as well as crystalline regionsand thus offer higher breaking strength and modulus [288]. Knaul et al.showed that the properties of chitin produced by microwave-medicatedreaction are at par with those derived from conventional chemicallymodified ones [289,290]. A blend of CS konjac glucomannan (KGM)fibers showed good antibacterial activity to S. aureus. The structureanalysis by Fourier transform infra red (FTIR) spectrometry, SEM, andX-ray diffraction (XRD) methods indicated that there were stronginteraction and good miscibility between the CS and KGM moleculewhich resulted from strong intermolecular hydrogen bonds [291]. Novelbioactive cellulosic-CS fibers could be developed by coating cellulose withCS [292].
Biodegradation of Chitin FibersChitin is considered to be highly biodegradable and easily excreted in
urine [293]. When attacked by natural fungi, CS films have a built-insource of nitrogen to enhance biodegradation. It is generally believedthat lysozyme is mainly responsible for CS degradation in the humanbody [294–298].
The biocompatibility and safety of CS has been revealed throughtests involving mutagenicity, acute and subacute toxicity, hemolysis,
338 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
and sensitization [299,300]. The US FDA considers CS as a foodadditive in animal feed when used as a precipitating agent forproteineceous materials [298]. No abnormal symptoms were observedwhen CS was orally administrated to rabbits, broilers, and hens at adosage of 0.7–0.8 g/kg body weight/day for upto 239 days [299,300].Rabbits also did not exhibit any abnormal symptom when CS wasintravenously injected. It was also observed that the presence of CSenhanced the absorption of drugs when administrated orally [301–306].The characteristic property of an ideal surgical suture consists of easybiointegration and tissue adaptation until healing occurs withoutdisturbing the healing process. It should also disappear on completionof healing. The currently available absorbable sutures such as alginate,collagen, catgut, and branan ferulate have limitations and not alwayssatisfactory. On the other hand, chitin as a wound healing acceleratorhas great potentialities from the point of view of absorbable surgicalsutures.
Recent Developments in Antibacterial SuturesThis is an area that is fast developing as can be seen from the
worldwide interest shown by several groups [307–326]. Anti-microbialsurgical sutures, which for a long period provide the wound with theantibiotics settled in their structure, can be of considerable use forprecautions and treatment of surgical sepsis [309]. Tsai et al. [307]studied the antibacterial property of a newly made, silver compoundcoated braided Nylon suture. It was observed that the antibacterialproperty of the suture was depended upon the type of bacterial species.For example, a difference of almost 103 in the number of Pseudomonasaeruginosa was observed within a period of 6 h when tested on threerepresentative bacterial species, S. aureus, Escherichia coli, andP. aeruginosa. The responses of S. aureus and E. coli to the silvercompound coated Nylon thread, however, were not as drastic asP. aeruginosa [244].
Blaker et al. [310] have used antimicrobial coatings of silver-dopedbioactive glass (AgBG) on resorbable Vicryl� and nonresorbableMersilk� surgical sutures and compared their thermal properties. Theresults showed that the bioactive glass coating did not affect thedynamic mechanical and thermal properties of the sutures [310].Rozzelle et al. [311] showed that the use of antimicrobial suture forcerebrospinal fluid shunt surgery wound closure is safe, effective, andmay be associated with a reduced risk of post-operative shunt infection.
Incorporation of antibacterials such as triclosan is used to impartantimicrobial activity. In a randomized prospective clinical study
Absorbable Polymeric Surgical Sutures 339
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
comparing the use of two absorbable sutures, Vicryl� Rapid versusVicryl�, Al-Qattan reported that Vicryl� Rapid sutures were moresuitable than Vicryl� ones in pediatric hand surgery [312]. It was alsodemonstrated by Storch et al. [313] that Vicryl� Rapid suture withtriclosan inhibits bacterial colonization of suture after direct in vivochallenge with S. aureus in a guinea pig model. Marco et al. also studiedthe efficacy of a new antibacterial suture coated Vicryl� Plus suture(Vicryl� containing triclosan) and compared it with the traditionalbraided suture, Vicryl�, in a validated animal model of orthopedicinfection [314]. No clinical signs of infection were observed. They foundpredominant polymorphonuclear neutrophil populations in four samplesin the Vicryl� group versus two in the Vicryl� Plus with triclosan group.Under simulated conditions of severe intraoperative contamination, theantibacterial suture reduced the number of positive cultures aftersurgery by 66.6%. The authors concluded that judging from the availableclinical information, its use might contribute to reducing the number ofinfected implants by 25.8%.
Suture materials are also chemically treated to introduce groups suchas carboxyl groups for antimicrobial drug immobilization [315]. Thiswas demonstrated by preparing PP-graft-polyacrylonitrile (PP-g-PAN)sutures by graft copolymerization of acrylonitrile onto PP monofilamentusing a pre-irradiation method. The grafted PP monofilaments weresubsequently hydrolyzed to introduce carboxyl groups for antimicrobialdrug immobilization. In general, the hydrolysis did not cause anysignificant variation in crystalline structure.
In another work, antimicrobial activity was imparted to weavedpolyester fiber based sutures by coating PHB, containing the anti-microbial agent furazolidone (FZ) [316]. The prolonged FZ effect (7–14days) is achieved by two-step application of a sheath, constituting 10% ofthe suture weight and containing 2–6% FZ. The sheath structure andantimicrobial activity of sutures can be modified by the introduction ofother biocompatible and biodegradable polymers.
Bide et al. studied the interaction of an antibiotic compound withcommon suture materials such as silk, Nylon, and polyester andcompared its uptake, release, and subsequent long-term antimicrobialeffectiveness [317]. Dye-like incorporation provides infection resistancethat persists over days or weeks as opposed to hours for the dippedmaterial. Gupta et al. reports the development of antimicrobial PPsutures by graft copolymerization of 1-vinylimidazole onto PP mono-filament sutures [318,319]. They are subsequently immobilized with anantimicrobial drug, ciprofloxacin. The modified suture releases the drugover a period of 4–5 days.
340 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

Capromed� threads are demonstrated to have high strength char-acteristics and resolve in the body within 8–9 months [320].Experimental studies of antibacterial properties revealed that theirimplantation in animal tissues induced active desorption of antibiotics.Antibiotic desorption from the Capromed� suture material facilitateswound healing, prevents ligature fistulas, and reduces the rate of post-operative complications by a factor of 4. Contaminated wounds closedwith sutures had higher infection rates compared with those repairedwith topical tissue adhesive [321].
The Emerging Perspectives
The scope and future perspectives for surgical suture materials appearto be vast as can be noted from several new publications emerging in thearea. Suture application varies for different tissues, different patients,and different circumstances. The availability of a large array of newsutures, staples, tapes, and topical adhesives can make the proper choicefor closure a challenge. The present day user qualities of biologicallyinert, synthetic, absorbable, and nonabsorbable threads have approach-ing the limit of the requirements imposed by modern surgery. Thisnecessitates further progress in this area which can be noted from therenewed interest in developing novel concepts and designs for theproduction and manufacturing of strong and elastic threads made ofbiocompatible absorbable natural (e.g., chemical modifications of PHAs,collagen, chitin, alginate, etc.) or synthetic polymers.
With the increasing complexity and technical requirements of internalsurgery, absorbable sutures that get gradually degraded and absorbedwith the healing of wounds are required. Absorbable sutures such asPGLA and PDO have tremendous development value and have brightapplication prospects because of excellent biocompatibility, absence oftissue reaction, high strength and toughness, moderate stretchability,lack of toxicity and irritation, and controllable degradability. Owing tothese excellent properties and extensive application sectors, they earnedwidespread attention as medical-care materials in the textile sectorglobally. PDO and its copolymers having good workability and strongpenetration enable accurate joining of tissues without damage, thusmaking it possible for them to be used in surgeries using continuousstitching.
One of the most interesting developments in recent times is the smartsuture that can be used to seal difficult wounds where access is limited[322]. The suture contracts to its permanent shape when heated and itsself-knotting action occurs when it is heated a few degrees above normal
Absorbable Polymeric Surgical Sutures 341
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

body temperature. It uses a shape memory polymer (SMP) that containsa hard segment and a ‘switching’ segment, both having differentthermal properties. One segment melts, or makes another kind oftransition, at a higher temperature than the other. By manipulating thetemperature and stress applied to the overall material, Langer andLeindlin [322] end up with a material that forms a temporary shape atone temperature, and a permanent shape at a higher temperature. Afterincreasing the temperature, the suture material shrinks, creating a knotwith just the right amount of tension on the surrounding tissue. It isdifficult to create such a knot in the confined spaces associated withendoscopic surgery. They demonstrated this by creating the first ‘smart’degradable suture.
Novel bioactive materials have been prepared by coating violetresorbable Vicryl� sutures with a bioactive glass powder derived froma co-precipitation method [323]. With the first wave of bioactive suturesalready in the market place, research is directed to the development offuture products such as sutures that could potentially demonstrate notonly antimicrobial activity but also anesthetic and antineoplasticfunctions [324]. A suturing material that serves not to prevent infection,but to combat bacteria introduced from other sources and to promotewound healing would represent a significant improvement overcurrently used materials.
After resection and repair of the intestines, tissue degradation leadsto weakening of the repair site and risk of post-operative leakage.Matrix metalloproteinases (MMPs) are thought to be responsible forcollagenolysis in the direct vicinity of surgical sutures in many tissues.Several experimental studies show that MMP inhibitors administeredsystemically alleviate post-operative weakening of intestinal anasto-moses. This has led to the development of the exciting discovery ofdrug delivery by means of MMP inhibitor-coated sutures to improvetissue integrity during anastomotic repair and to reduce post-operativecomplications. Pasternak et al. coated sutures with a cross-linkedfibrinogen film and bound the MMP inhibitor doxycycline into this film[325]. The sutures were then used in a standard rat model forevaluating mechanical properties of colonic anastomoses 3 days aftersurgery. The breaking strength of the anastomoses on the critical thirdday after operation was 17% higher with doxycycline-coated suturescompared to controls.
The formation of bacterial biofilms on the surface of implantedmaterials is a critical factor that may lead to chronic microbial infectionand tissue necrosis. In an interesting study, Harnet et al. [326]established the great potential of using antibacterial sutures to
342 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
combat the menace. They investigated the stability of polyelectrolytemultilayer (ML) films on suture materials and the antibacterial effectobtained with chlorhexidine (CHX)-functionalized films built ondifferent types of suture materials such as silk, polyester, and PLGA[326]. They compared E. coli culture on glass coverslips and glasscoverslips with ML and CHX films and observed inhibition of thebacterial relative luminescence.
Zhukovskii [273] in a recent review has discussed the problems andprospects for development and production of surgical suture materials.According to him, the assortment and user qualities of biologically inert,synthetic, absorbable, and nonabsorbable threads have approached thelimit of the requirements imposed by modern surgery. He anticipatesbetter manufacturing processes for production of strong and elasticthreads made of absorbable natural polymers – PHAs and theircopolymers, collagen, chitin, CS, alginate, etc. The attention ofinvestigators is increasingly focusing on suture materials with bothindividual and comprehensive biological activity [307–327]. Creation ofthread containing native biological structures (cell growth factor, bloodplasma proteins, cells of different organs and tissues, and other cells,including those that increase biocompatibility) and self-regulatingmaterials with biologically active molecules in their structure capableof markedly altering their properties under small external physical orchemical effects is promising.
With the introduction of new clinical methods to carry out surgicaloperations such as minimally invasive vascular surgery (also calledlaparoscopy) [328], it has become imperative that the suture cannot behandled with fingers and the use of stainless-steel needle holders isrequired. In a farsighted experiment, Tremblay et al. investigated themechanical and microstructural effects of the manipulations withlaparoscopic needle holder on polymeric suture monofilament [329].Surgipro� (PP), Teflene� (polyvinylidene fluoride), and Gore-Tex�
(polytetrafluoroethylene) monofilament sutures were pinched with astandard clinical protocol by a surgeon. Teflene� and Gore-Tex�
monofilament sutures were shown to be unaffected even after severepinching with laparoscopic needle holders whereas the propertiesdecreased significantly for Surgipro� sutures.
As knotting induces decrease in mechanical properties, bettermethods of selection and tying of suture materials are required toensure maintenance of the tensile and knot security properties.Introduction of mechanical tying method was found to be a usefulalternative to hand tying and provided reproducible test results[330,331]. The mechanical properties of damaged suture are important
Absorbable Polymeric Surgical Sutures 343
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

to all surgeons who use suture arthroscopically. So, Wright et al. [332]measured the mechanical properties of damaged sutures. They notedthat the newer polyethylene core sutures (FiberWire and Orthocord)have superior mechanical properties which are maintained evenwhen cut.
Clinicians are often faced with the challenging task of distinguishingbetween accidental and inflicted pediatric head trauma. Studies by Coatsand Margulies [333] showed sizeable difference between pediatric boneand suture material properties that underscored the crucial role thatsutures play in the unique response of the pediatric head to impact inlow height falls. The large strains in the pediatric bone and suture resultin a skullcase that can undergo dramatic shape changes before fracture,potentially causing substantial deformation in the brain. These dataprovide necessary information to enhance our understanding ofmechanisms of head injury in young children.
The combination of sutures and techniques of suturing are expected toplay greater role in future as the awareness on the influence of theseparameters apart from the properties of suture materials on sutureperformance is established. Yotsumoto et al. [334] who repaired thegastrocnemius tendons of 24-week-old cattle (diameter 14–16�9–11 mm2) with application of a single locking, multiple locking, singlegrasping, or multiple grasping technique concluded that mechanicalproperties of each tendon suture depended on the particular combina-tion of suture materials and repair techniques.
Great expectations are raised on the new polyblend sutures thatappear to fill a void in the armamentarium of the surgeon. Wust et al.made a comprehensive comparison of the mechanical properties of fourtypes of braided polyblend sutures with widely used braided polyesterand monofilament PDO sutures [335]. The ultimate strength ofpolyblend suture material was 2–2.5-fold greater than that of polyesteror PDO sutures, but the resistance to fraying was up to 500-fold greaterthan that of polyester or PDO sutures. With regard to strength, thismakes polyblend sutures particularly advantageous for use with metallicedges of anchors or prostheses or with absorbable anchor eyelets.
Great developments are expected in the manufacturing processes forthe production of strong and elastic absorbable and nonabsorbablesutures [132,336,327]. Special technology has been developed for theproduction of PP surgical monofilaments to meet medical needs for asuture material meeting tight specifications for physical and mechanicalproperties [336]. Alternate off-line hot-drawing and annealing (threecycles) were carried out by Chooprayoon et al. to develop the orientedsemi-crystalline morphology in block copolymer of LL and e-CL
344 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

[208,337]. Several new varieties of monofilaments are discussed by DeBreuck [338]. The suture configuration and the nature of suturematerial have profound influence on the biomechanical characteristicsof single-row repair in comparison to double-row repair. Baums et al.[339] have shown that double-row suture anchor repair with arthro-scopic Mason-Allen/medial mattress stitches provides initial strengthsuperior to single-row repair with arthroscopic Mason-Allen stitchesunder isometric cyclic loading as well as under ultimate loadingconditions.
CONCLUSIONS
Over the years, surgical suture materials have matured as coreproducts of a mature industry. New sutures are being developed all thetime, to better respond to particular surgical needs. Basic materials aremodified depending on their intended application to provide the surgeonwith a suture material of optimal quality. The present day user qualitiesof biologically inert, synthetic, absorbable, and nonabsorbable threadshave approaching the limit of the requirements imposed by modernsurgery. This necessitates further progress in this area which can beanticipated if manufacturing processes for production of strong andelastic thread made of biocompatible absorbable natural polymers –polyoxyalkanoates, collagen, chitin, alginate, etc., are developed. Theattention of researchers is increasingly focusing on suture materialswith potential not only for antimicrobial activity but also anesthetic andantineoplastic functions.
ACKNOWLEDGMENTS
We thank Dr K. Mohandas, Director and Dr G. Bhuvaneswar, Head,BMT Wing, SCTIMST for encouragement and for providing facilities.We also thank Mrs Minimol for rendering help in the preparation of thisarticle.
REFERENCES
1. Chu, C.-C., von Fraunhofer, J.A. and Greisler, H.P. (eds) (1996). WoundClosure Biomaterials and Devices, Boca Raton, Florida, CRC Press, Inc.
2. Wikipedia, the free encyclopedia. Available at: http://library.sccsc.edu/surgtech/sutures1.htm (accessed December 23, 2009).
3. Barber, F.A., Boothby, M.H. and Richards, D.P. New Sutures and SutureAnchors in Sports Medicine, Sports Med. Arthrosc., 2006: 14: 177–184.
Absorbable Polymeric Surgical Sutures 345
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

4. Singhal, J.P., Singh, H. and Ray, A.R. Absorbable Suture Materials:Preparation and Properties, Polym. Rev., 1988: 28: 475–502.
5. Moy, R.L., Waldman, B. and Hein, D.W. A Review of Sutures and SuturingTechniques, J. Dermatol. Surg. Oncol., 1992: 18: 785–795.
6. Bloom, B.S. and Goldberg, D.J. Suture Material in Cosmetic CutaneousSurgery, J. Cosmet. Laser Ther., 2007: 9: 41–45.
7. Ajmeri, J.R. and Ajemri, C.J. (2006). Surgical Sutures: The Largest TextileImplant Material, In: Anand, S.C., Kennedy, J.F. and Rajendran, S. (eds),Medical Textiles and Biomaterials for Health Care, Boca Raton, Boston, NewYork, Woodhead Publishing Ltd.; Cambridge, England, CRC Press, pp. 432–440.
8. Li, J. and Yuan, X.-Y. Research Progresses on Synthetic Absorbable Sutures,J. Tianjin Polytechnic University, 2006: 25: 18–21.
9. Horacek, I. Survey of the Present Knowledge on Biodegradable Polymers forResorbable Sutures, Chemicke Vlakna, 1989: 39: 214–222.
10. Hon, L.-Q., Ganeshan, A., Thomas, S.M., Warakaulle, D., Jagdish, J. andUberoi, R. Vascular Closure Devices: A Comparative Overview, Curr. Probl.Diagn. Radiol., 2009: 389: 33–43.
11. Yu G.V. and Cavaliere R. Suture Materials. Properties and Uses, J. Am.Podiatry. Assoc., 1983: 73: 57–64.
12. Gassner, R. Wound Closure Materials, Oral Maxillofac. Surg. Clin. NorthAm., 2004: 14: 95–104.
13. Edlich, R.F., Drake, D.B., Rodeheaver, G.T. et al. SynetureTM StainlessSTEEL Suture. A Collective Review of its Performance in Surgical WoundClosure. J. Long Term Eff. Med. Implants, 2006: 16: 101–110.
14. Guttman, B. and Guttmann, H. (1994). Properties, Uses and ClinicalInvestigation, In: Dumitriu, S. (ed.), Polymeric Biomaterials, New York, NY,Marcel Dekker, Ch. 10, pp. 321–356.
15. Benicewicz, B.C. and Hopper, P. Polymers for Absorbable Surgical Sutures,Part I, Bioact. Compat. Polym. 1990: 5: 543.
16. Jodar, M.R., Bel, P.E. and Sune, A.J.M. Synthetic Absorbable SutureMaterials I. Properties and Thread Length, Ciencia Pharm., 1992: 2: 47.
17. Jodar, M.R., Bel, P.E. and Sune, A.J.M. Synthetic Absorbable SutureMaterials II Test of the Diameter and Caliber, Ciencia Pharm., 1992: 2: 292.
18. Jodar, M.R., Bel, P.E. and Sune, A.J.M. Synthetic Absorbable SutureMaterials III. Tension Strength, Ciencia Pharm., 1992: 2: 88.
19. Swanson, N.A. and Tromovitch, T.A. Suture Materials, 1980s: Properties,Uses, and Abuses. Int. J. Dermatol., 1982: 21: 373–378.
20. Vogt, P.M., Altintas, M.A., Radtke, C. and Meyer-Marcotty, M. Bases andMethods of Suturing [Grundlagen und Techniken der chirurgischen Naht],Chirurg, 2009: 80: 437–447.
21. ASJOG�. Available at: http://www.asjog.org/Journal/Issue%202%20Final/018%20I%20&%20T.pdf (accessed December 15, 2009).
22. Bennett, R.G. Selection of Wound Closure Materials, J. Am. Acad.Dermmatol., 1988: 18: 619.
23. AyurvedaForYou.Availableat:http://ayurveda-foryou.com/archive/surgery1.html (accessed December 28, 2009).
346 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

24. Mukherjee, D.P. Sutures. In: Kroschwitz, J.I. (eds) (1989). Polymers:Biomaterials and Medical Applications, New York, NY, John Wiley &Sons, pp. 535–545.
25. Planck, H., Dauner, M. and Renardy, M. (eds) (1990). Medical Textiles forImplantation, Berlin, Springer-Verlag.
26. Tewari, M. and Shukla, H.S. Sushruta: The Father of Indian Surgery,Indian J. Surg., 2005: 67: 229–230.
27. Kansupada, K.B. and Sassani, J.W. Sushruta: The Father of Indian surgeryand Ophthalmology, Doc. Ophthalmol., 1997: 93: 159–167.
28. Raju, V.K. Sushruta of Ancient India, Indian J. Ophthalmol., 2003: 51: 119–122.
29. Chari, P.S. Sushruta and our Heritage, Indian J. Plastic Surg., 2003: 36: 4–13.
30. Bhishagratna, K.L. (1907). Sushruta Samhita, An English Translation ofthe Sushruta Samhita. Based on Original Sanskrit Text in three volumes.Calcutta, No. 10, Kasi Ghose’s Lane.
31. Animal Gut String. Available at: http://www.sutures-bbraun.com/index.cfm?B99330432A5AE626642C24642369CCA0 (accessed December 5,2009).
32. Medicine Meets Millenium. Available at: http://www99.mh-hannover.de/aktuelles/projekte/mmm/germanversion/d_fs_programme/speech/Sharma_V.html (accessed December 16, 2009).
33. Jaggi, O.P. (1973). History of Science and Technology in India, Vol.-IV:Indian System of Medicine, Delhi, Atma Ram & Sons.
34. Sharma, P.V. (1972). History of Medicine in India, New Delhi, IndianNational Science Academy.
35. Sharma, P.V. (1972). Indian Medicine in the Classical Age, Varanasi,Chaukhamba Amarabharati Prakashan.
36. Ambekar, A.P. A Review on Spider Silk: New Biomaterial, Colourage, 2008:55: 66–72.
37. Answersingenesis.org. Available at: http://www.answersingenesis.org/creation/v14/i2/scientists.asp (accessed December 12, 2009).
38. Lamont, A. Joseph Lister: Father of Modern Surgery, Creation, 1992: 14:48–51.
39. Pubmedcentral. Available at: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid¼1081445&blobtype¼pdf (accessed December 5, 2009).
40. Patel, KA. and Thomas, W.E.G. Sutures, Ligatures and Staples, Surgery,2008: 26: 48–53.
41. Taylor, B. and Bayat, A. Basic Plastic Surgery Techniques and Principles:Choosing the Right Suture Material, Stud. BMJ, 2003: 11: 140–141.
42. Brissot, H. Current Suture Materials in Surgery [Les sutures chirurgicales,aujourd’hui], Prat Med Chir de l’Ani Cie, 2002; 37: 469–474.
43. Dunn, D.L. (1994). Wound Closure Manual, Ethicon Inc, Somerville, NewJersey, Johnson & Johnson Co.
44. Hochberg, J., Meyer, K.M. and Marion, M.D. Suture Choice and OtherMethods of Skin Closure, Surg. Clin. North. Am., 2009: 899: 627–641.
45. DemeTECH. Available at: http://www.demetech.us/suture-specs.php(accessed December 28, 2009).
Absorbable Polymeric Surgical Sutures 347
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

46. Chu, C.C. Mechanical Properties of Suture Materials: An ImportantCharacterisation, Ann. Surg., 1981: 193: 365.
47. Heyl, V. Plastic and Reconstructive Surgery: Suture Technique and ScarIssues [Nahttechnik und Narbenprobleme bei plastischen und rekonstruk-tiven Operationen], Gynakol. Prax., 2007: 31: 701–706.
48. Grisham, J.E. and Zukin, D.D. Suture Selection for the Pediatrician,Pediatr. Emerg. Care, 1990: 6: 301–314.
49. O’Neal, R.B. and Alleyn, C.D. Suture Materials and Techniques, Curr. Opin.Periodontol., 1997: 4: 89–95.
50. Awadein, A., Sharma, M., Bazemore, M.G., Saeed, H.A. and Guyton, D.L.Adjustable Suture Strabismus Surgery in Infants and Children, J AAPOS,2008: 12: 585–590.
51. SURU. Available at: http://www.suru.com/frmsut.htm/http://www.medicine.usask.ca/surgery/surgical-skills-lab/Suture%20Lab%20Handout (accessedDecember 23, 2009).
52. Szarmach, R.R., Livingston, R.N.J., Rodeheaver, G.T., Thacker, G.J.and Edlich, R.F. An Innovative Surgical Suture and Needle Evaluation andSelection Program, J. Long Term Eff. Med. Implants, 2002: 12: 211–229.
53. Williams, R.L. and Armstrong, D.G. Wound Healing: New Modalities for aNew Millennium, Clin. Podiatr. Med. Surg., 1998: 15: 117–128.
54. Adams, B., Levy, R., Rademaker, A.E., Goldberg, L.H. and Alam, M.Frequency of Use of Suturing and Repair Techniques Preferred byDermatologic Surgeons, Dermatol. Surg., 2006: 32: 682–689.
55. Rodeheaver, G.T., Shimer, A.L., Boyd, L.M., Drake, D.B. and Edlich, R.An Innovative Absorbable Coating for the Polybutester Suture, J. LongTerm Eff. Med. Implants, 2001: 11: 41–54.
56. Cotton, R.S., Kumar, V. and Robin, S.L. (1989). Inflammation andRepair, In: Robin’s Pathologic Basis of Diseases, Philadelphia, WBSaunders, p. 39.
57. Callin, J.I., Goldstein, I.M. and Sydrmman, R. (1992). Inflammation:Basic Principles and Clinical Correlations, 2nd edn, New York, Raven Press.
58. Cohen, I.K., Diegelmmann, R.F. and Lindblad, W.J. (eds) (1992). WoundHealing: Biochemical and Clinical Aspects, Philadelphia, WB Saunders.
59. Lin, P.H., Hirko, M.K., von Fraunhofer, J.A. and Greisler, H.P. (1996). WoundHealing and Inflammatory Response to Biomaterials, Ch 2., In: Chu, C.C., vonFraunhofer, J.A. and Greisler, H.P. (eds), Wound Closure Biomaterials andDevices, Boca Raton, Florida, USA, CRC Press, Inc, pp. 7–24.
60. Catgut. Available at: http://en.wikipedia.org/wiki/Catgut (accessedDecember 12, 2009).
61. Francoeur, J.R. Joseph Lister: Surgeon Scientist (1827–1912), J. Invest.Surg., 2000: 13: 129–132.
62. Stone, I.K., von Fraunhofer, A.J. and Masterson, B.A. A Comparative Studyof Suture Materials: CG and CG Treated with Glycerine, Am. J. Obstet.Gynecol., 1985: 151: 1087.
63. Grant, A. Dyspareunia Associated with the Use of Glycerol-ImpregnatedCatgut to Repair Perennial Trauma-Report of a Three Year Follow upStudy, Br. J. Obstet. Gynecol., 1989: 96: 741.
348 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
64. Salthouse, T.N., Williams, J.A. and Williams, D.A. Relationship of CellularEnzyme Activity to Catgut and Collagen Suture Activity, Surg. Gynecol.Obstet., 1969: 129: 691–696.
65. Jenkins, H.P., Hrdina, L.S., Owens, F.M. and Swisher, F.M. Absorption ofSurgical Gut (catgut): Duration in Tissues after Loss of Tensile Strength,Arch. Surg., 1942: 45: 74.
66. Okada, T., Hayashi, T. and Ikada, Y. Degradation of Collagen Suture InVitro and In Vivo, Biomaterials 1992: 13: 448.
67. Walton, M. Strength Retention of CG and Monofilament Absorbable SutureMaterials in Joint Tissues, Clin. Orthop. Relat. Res., 1989: 242: 303–310.
68. Rhoads, J.E., Tabata, Y. and Nakajima A. The Decline in Strength of Catgutafter Exposure to Living Tissues, Arch. Surg., 1937: 34: 377–397.
69. Aslan, M., Buyukkurt, M.C. and Yildirim U. Comparison of DifferentAbsorbable Suture Materials in Skin Closure: An Experimental Study inRats, Pain Clin., 2005: 17: 81–88.
70. Katz, A.R. and Turner, R.J. Evaluation of Tensile and Absorption Propertiesof PGA Sutures, Surg. Gynecol. Obstet., 1970: 131: 701.
71. Lawrie, P., Angus, G. and Reese, A.J.M. The Absorption of Surgical Catgut,Br. J. Surg., 1959: 46: 638.
72. Lawrie, P., Angus, G. and Reese, A.J.M. The Absorption of Surgical Catgut.II. The Influence of Size, Br. J. Surg., 1960: 47: 551–555.
73. Postlethwait, R.W. and Smith, B.M. A New Synthetic Absorbable Suture,Surg. Gynecol Obstet., 1975: 140: 377–380.
74. Reul Jr, GJ. Use of Vicryl� (Polyglactin 910) Sutures in General Surgicaland Cardiothoracic Procedures, Am. J. Surg., 1977: 134: 297–299.
75. Sanz, L.E., Patterson, J.A., Kamath, R., Willett, G., Ahmed, S.W. andButterfield, A.B. Comparison of Maxon suture with Vicryl, Chromic Catgut,and PDS Sutures in Fascial Closure in Rats, Obstet. Gynecol., 1988: 71:418–422.
76. Edlich, R.F., Panek, P.H. and Rodeheaver, G.T. Physical and ChemicalConfiguration of Sutures in the Development of Surgical Infection, Ann.Surg., 1973: 77: 679–688.
77. Tachibana, M., Yaita, A., Taniura, H., Fukasawa, K., Nagasue, N. andNakamura. The Use of Chitin as a New Absorbable Suture Material: AnExperimental Study, N. Surg. Today, 1988: 18: 533–539.
78. Nakajima, M., Atsumi, K. and Kifune, K. Chitin is an Effective Material forSutures, Jpn. J. Surg., 1986: 16: 418–424.
79. Shishatskaya, E.I., Volova, T.G., Puzyr, A.P., Mogilnaya, O.A. and Efremov,S.N. Tissue Response to the Implantation of BiodegradablePolyhydroxyalkanoate Sutures, J. Mater. Sci. Mater. Med., 2004: 15:719–728.
80. Sharp, K.W., Ross, C.B., Tillman, V.N. and Dunn, J.F. Common Bile DuctHealing. Do Different Absorbable Sutures Affect Stricture Formation andTensile Strength?, Arch. Surg., 1989: 124: 408–414.
81. Wainstein, M., Anderson, J. and Elder, J.S. Comparison of Effects of SutureMaterials on Wound Healing in a Rabbit Pyeloplasty Model, Urology, 1997:49: 261–264.
Absorbable Polymeric Surgical Sutures 349
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
82. Tian, F., Appert, H.E. and Howard, J.M. The Disintegration of AbsorbableSuture Materials on Exposure to Human Digestive Juices: An Update, Am.Surg., 1994: 60: 287–291.
83. Dunlap, W.A., Purnell, W.D. and McPherson Jr, S.D. Laboratory andClinical Evaluation of a New Synthetic Absorbable Suture for OphthalmicSurgery, Adv. Ophthalmol., 1976: 33: 49–61.
84. Vasanthan, A., Satheesh, K., Hoopes, W., Lucaci, P., Williams, K. andRapley, J. Comparing Suture Strengths for Clinical Applications: A Novel InVitro Study, J. Periodontol., 2009: 80: 618–624.
85. Perrin, D.E. and English, J.P. (1997). PGA and Polylactide, In: Domb, A.J.,Kost, J. and Wiseman D.M. (eds), Handbook of Biodegradable Polymers, TheNetherlands, Harwood Academic Publishers, pp. 3–27.
86. Lowe, C.E. Preparation of High Molecular Weight Polyhydroxyacetic Ester,US Patent 2,668,162, 1954.
87. Al-Abdullah, T., Plint, A.C. and Fergusson, D. Absorbable Versus Non-absorbable Sutures in the Management of Traumatic Lacerations andSurgical Wounds: A Meta-Analysis, Pediatr. Emerg. Care, 2007: 23:339–344.
88. Danielsen, C.C. Reconstituted Collagen Fibrils, Fibrillar and MolecularStability of the Collagen upon Maturation In Vitro, Biochem. J., 1984: 222:663–668.
89. Danielsen, C.C. Mechanical Properties of Reconstituted Collagen Fibrils.A Study on Reconstitution Methodology and Influence of In VitroMaturation, Connect. Tissue Res., 1981: 9: 51–57.
90. Klopper, P.J. Collagen in Surgical Research, Eur. Surg. Res., 1986: 18:218–223.
91. Alder, R.H., Montes, M., Dayer, R. and Harrod, D. A Comparison ofReconstituted Collagen Suture for Colon Anstmoses, Surg. Gynecol Obstet.,1967: 124: 1245–1252.
92. Brumback, G.F. and McPherson Jr, S.D. Reconstituted Collagen Sutures inCorneal Surgery: An Experimental and Clinical Evaluation, Am. J.Opthalmol., 1967: 64: 222–227.
93. Regan, E.P. and Dunnington, J.H. Collagen Sutures in Cataract Surgery:Clinical and Experimental Observations, Trans. Am. Ophthalmol. Soc.,1966: 64: 39–49.
94. Benicewicz, B.C. and Hopper, P.K. Polymers for Absorbable SurgicalSutures – Part II, J. Bioact. Compat. Polym., 1991: 6: 64–94.
95. Caulfield, R.H., Maleki-Tabrizi, A., Patel, H., Coldham, F., Mee, S. andNanchahal, J. Comparison of Zones 1 to 4 Flexor Tendon Repairs UsingAbsorbable and Unabsorbable Four-Strand Core Sutures, J. Hand Surg.Eur., 2008: 33: 412–417.
96. Craig, P.H., Williams, J.A., Davis, K.W. et al. A Biologic Comparison ofPolyglactin 9910 and PGA Sutures, Surg. Gynecol. Obstet., 1995: 141: 1–10.
97. Reed, A.M. and Gilding, A.K. Biodegradable Polymers for Use in Surgery:PGA – Polylactic Acid Homo and Copolymers: 2. In Vitro Degradation,Polymer, 1981: 22: 494–498.
350 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
98. Katz, A., Mukherjee, D.P., Kaganov, A.L. and Gordon, S. A New SyntheticMonofilament Absorbable Suture made from Polytrimethylene Carbonate,Surg. Gynecol. Obstet., 1992: 161: 213–222.
99. Roby, M.S., Bennet, S.L. and Liu, C.K. (1995). Absorbable BlockCopolymers and Surgical Articles Fabricated from Them, US Patent5,403,347 (to United States Surgical Corporation).
100. De Persia, R., Guzman, A., Rivera, L. and Vazquez, J. (2005). Mechanics ofBiomaterials: Sutures After the Surgery. Applications of EngineeringMechanics in Medicine, Mayaguez, GED – University of Puerto Rico.
101. Laufman, H and Rubel, T. Synthetic Absorbable Sutures, Surg. Gynecol.Obstet., 1977: 145: 597–608.
102. Biber, B.L. and Kuzmina, N.L. Man-Made Yarns for Reabsorbable SurgicalSuture Materials, Fibre Chem., 1992: 23: 229–235.
103. Shalaby, S.W. and Burg, K.J.L. (2003). Absorbable and BiodegradablePolymers, Boca Raton, Florida, CRC.
104. Talor, B. and Bayat, A. Basic Plastic Surgery Techniques andPrinciples: Choosing the Right Suture Material, Stud. BMJ, 2003: 11:140–141.
105. Middleton, J.C. and Tipton, A.J. Synthetic Biodegradable Polymers asOrthopedic Devices, Biomaterials, 2000: 21: 2335–2346.
106. Daniels, A.U., Chang, M.K.O., Andriano, K.P. Mechanical Properties ofBiodegradable Polymers and Composites Proposed for Internal Fixation ofBone, J. Appl. Biomater., 1990: 1: 57–78.
107. von Fraunhofer, J.A., Storey, R.J. and Masterson, B.J. Tensile Propertiesof Suture Materials, Biomaterials, 1988: 9: 324–327.
108. Middleton, J.C. and Tipton, A.J. Synthetic Biodegradable Polymers asMedical Devices, Med. Plast. Biomater., 1998; 30. Available at: http://www.mddionline.com/article/synthetic-biodegradable-polymers-medical-devices (accessed December 12, 2009).
109. U.S. Absorbable and Erodible Biomaterials Products Markets, Chap. 10,Mountain View, CA, Frost & Sullivan, 1995.
110. Goupil, D. (1996). Sutures, In: Ratner, B.D., Hoffman, A.S., Schoen, F.J.and Lemons, J.E. (eds), Biomaterials Science: An Introduction to Materialsin Medicine, New York, Academic Press, pp. 356–360.
111. Barrows, T.H. Degradable Implant Materials: A Review of SyntheticAbsorbable Polymers and their Applications, Clin. Mat., 1986: 1: 233.
112. Gilding, D.K and Reed, A.M. Biodegradable Polymers for Use in Surgery-Polyglycolic/Poly(lactic acid) Homo- and Copolymers, Polymer 1979: 20:1459–1484.
113. Kohn, J. and Langer, R. (1996). Bioresorbable and Bioerodible Materials,In: Ratner, B.D., Hoffman, A.S., Schoen, F.J. and Lemons, J.E. (eds),Biomaterials Science: An Introduction to Materials in Medicine, New York,Academic Press, pp. 64–72.
114. Pietrzak, W.S, Sarver, D.R. and Verstynen, M.L. Bioabsorbable FixationDevices: Status for the Craniomaxillofacial Surgeon, J. Craniofac. Surg.,1997: 8: 87.
Absorbable Polymeric Surgical Sutures 351
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
115. Pietrzak, W.S., Verstynen, M.L. and Sarver, D.R. BioabsorbablePolymer Science for the Practicing Surgeon, J. Craniofac. Surg., 1997:8: 92.
116. Shalaby, S.W. (ed.) (1994). Biomedical Polymers, Designed to DegradeSystems, New York, Hanser.
117. Claude, O., Gregory, T., Montemagno, S., Bruneval P. and Masmejean,E.H. Vascular Microanastomosis in Rat Femoral Arteries: ExperimentalStudy Comparing Non-absorbable and Absorbable Sutures, J. Reconstr.Microsurg., 2007: 23: 87–91.
118. Gallup, D.G., Nolan, T.E. and Smith, R.P. Primary Mass Closure of MidlineIncisions with a Continuous Polyglyconate Monofilament AbsorbableSuture, Obstet. Gynecol., 1990: 76: 872–875.
119. Yang, X.N. and Pastorino, U. Are Absorbable Sutures Inadequate to Closethe Sternum? J. Thorac. Cardiovasc. Surg., 2006: 132: 1503.
120. Andrade, M.G.S., Weissman, R. and Reis, S.R.A. Tissue Reaction andSurface Morphology of Absorbable Sutures after In Vivo Exposure,J. Mater. Sci. Mater. Med., 2006: 17: 949–961.
121. Tan, P.C., Mubarak, S. and Omar, S.Z. Absorbable Versus Non-AbsorbableSutures for Subcuticular Skin Closure of a Transverse Suprapubic Incision,Int. J. Gynecol. Obstet., 2008: 103: 179–181.
122. Ferguson Jr, R.E.H., Schuler, K., Thornton, B.P., Vasconez, H.C. andRinker, B. The Effect of Saliva and Oral Intake on the Tensile Properties ofSutures, Ann. Plast. Surg., 2007: 58: 268–272.
123. Riddick, D.H., DeGrazia, C.T. and Maenza, R.M. Comparison of Polyglacticand Polyglycolic Acid Sutures in Reproductive Tissue, Fertil. Steril., 1977:28: 1220–1225.
124. Nair, L.S. and Laurencin, C.T. Biodegradable Polymers as Biomaterials,Prog. Polym. Sci., 2007: 32: 762–798.
125. Stridsberg, K.M., Ryner, M. and Albertsson, A.-C. Controlled Ring-OpeningPolymerization: Polymers with Designed Macromolecular Architecture,Adv. Polym. Sci. (Springer), 2002: 157: 41–65.
126. Kaihara, S., Matsumura, S., Mikos, A.G. and Fisher, J.P. Synthesis ofPoly(L-lactide) and Polyglycolide by Ring-Opening Polymerization, Nat.Protoc., 2007: 2: 2767–2771.
127. Pineros-Fernandez, A., Drake, D.B., Rodeheaver, P.A., Moody, D.L.,Edlich, R.F. and Rodeheaver, G.T. Caprosyn, Another Major Advance inSynthetic Monofilament Absorbable Suture, J. Long Term Eff. Med.Implants, 2004: 14: 359–368.
128. Matthias, E. A Detailed Characterization of PGA Prepared by Solid-statePolycondensation Reaction, Macromol. Chem. Phys., 1999: 200:2221–2229.
129. Masuda, T., Matsuda, A., Murata, K. and Yamazaki, S. (1993).Biodegradable Plastic Composition, US Patent 5,227,415.
130. Devi, K.S. and Vasudevan, P. Absorbable Surgical Sutures, Polym. Rev.,1985: 25: 315–324.
131. Debus, E.S., Geiger, D., Sailer, M., Ederer, J. and Thiede, A.Physical, Biological and Handling Characteristics of Surgical Suture
352 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

Material: A Comparison of Four Different Multifilament AbsorbableSutures, Eur. Surg. Res., 1997: 29: 52–61.
132. Guarino, N., Vallasciani, S.A. and Marrocco, G.J. Urology, 2009: 181:1318–1323.
133. Vieira, A.C., Vieira, J.C., Guedes, R.M. and Marques, A.T. DegradationCharacterization of Aliphatic Polyesters – In Vitro Study, AIP Conf. Proc.,2008: 1042: 309–311.
134. Gunatillake, P.A. and Adhikari, R. Biodegradable Synthetic Polymers forTissue Engineering, Eur. Cell. Mater., 2003: 5: 1–16.
135. Tormala, P. Biodegradable Self-reinforced Composite Materials:Manufacturing Structure and Mechanical Properties, Clin. Mater., 1992:10: 29–34.
136. Madras, G. (2005). Enzymatic Degradation of Polymers, In: Smith, R. (ed.),Biodegradable Polymers for Industrial Applications, Boca Raton, Boston,New York, Washington DC, CRC Press, pp. 406–426.
137. Piskin, E. Biodegradable Polymers as Biomaterials, J. Biomat. Sci. Polym.Ed., 1995: 6: 775–795.
138. Ginde, R.M. and Gupta, R.K. In Vitro Chemical Degradation of PGAPellets and Fibres, J. Appl. Polym. Sci., 1987: 33: 2411–2429.
139. Chu, C.C. (1983). Survey of Clinically Important Wound Closure, In:Szycher, M. (ed.), Biomaterials in Biocompatible Polymers, Metal andComposites, Lancaster, PA, USA, Tecnomic Publishing, pp. 477–523.
140. Amecke, B., Bendix, D. and Entenmann, G. Resorbable Polyesters:Composition, Properties, Applications, Clin. Mater. 1992: 10: 47–50.
141. Holliger, J.O. and Battistone, G.C. Biodegradable Bone Repair Materials,Clin. Orthop. Relat. Res., 1986: 207: 290–305.
142. Siripitayananon, J., Molloy, R., Bunkird, S., Kleawkla, A., Panjakha, R. andChooprayoon, P. Effects of Hot-Drawing and Annealing on the Morphologyand Mechanical Properties of Biodegradable Polyester MonofilamentFibers, Int. Polym. Process., 2008: 23: 161–167.
143. Deng, M., Chen, G., Burkley, D. et al. A Study on In Vitro DegradationBehavior of a Poly(Glycolide-co-L-Lactide) Monofilament, Acta Biomater.,2008: 4: 1382–1391.
144. Hong, J.-T., Cho, N.-S., Yoon, H.-S., Kim, T.-H., Koh, M.-S. and Kim, W.-G.Preparation and Characterization of BiodegradablePoly(Trimethylenecarbonate-e-Caprolactone)-Block-Poly( p-Dioxanone)Copolymers, J. Polym. Sci. Part A Polym. Chem., 2005: 43: 2790–2799.
145. Hong, J.-T., Cho, N.-S., Yoon, H.-S., Kim, T.-H., Koh, M.-S., Kim, W.-G.Biodegradable Studies of Poly(Trimethylenecarbonate-e-Caprolactone)-Block-Poly(p-Dioxanone), Poly(Dioxanone), and Poly(Glycolide-e-Caprolactone) (Monocryl�) Monofilaments, J. Appl. Polym Sci., 2006:102: 737–743.
146. Zurita, R., Puiggalı, J. and Rodrıguez-Galan, A. Triclosan Release fromCoated PGA Threads, Macromol. Biosci., 2006: 6: 58–69.
147. de Werra, C., Rendano, F., D’Armiento, F., Somma, P. and Forestieri, P.Comparison of Five Synthetic Absorbable Suture Materials in IntestinalAnastomosis: Experimental Study in Rats [Confronto tra cinque materiali
Absorbable Polymeric Surgical Sutures 353
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
di sutura sintetici riassorbibili nelle anastomosi intestinali: studiosperimentale nel ratto.], Chir. Ital., 2003: 55: 227–233.
148. Clough, J.V. and Alexander Williams, J. Surgical and Economic Advantagesof Polyglycolic-Acid Suture Material in Skin Closure, Lancet, 1975: 7900:194–195.
149. Bezwada, R.S, Jamiolkowski, D.D., Lee, I.-Y. et al. Monocryl� Suture, ANew Ultra-Pliable Absorbable Monofilament Suture, Biomaterials, 1995:16: 1141–1148.
150. Channuan, W., Siripitayananon, J., Molloy, R. and Mitchell, G.R. Definingthe Physical Structure and Properties in Novel Monofilaments withPotential for Use as Absorbable Surgical Sutures Based on a LactideContaining Block Terpolymer, Polymer, 2008: 49: 4433–4445.
151. Arcuri, C., Cecchetti, F., Dri, M., Muzzi, F. and Bartuli, F.N. Suture in OralSurgery. A Comparative Study, Minerva Stomatol., 2006: 55: 17–31.
152. Moy, R.L. and Kaufman, A.J. Clinical Comparison of Vicryl� (Vicryl�) andPolytrimethylene Carbonate (Maxon) Suture Material, J. Dermatol. Surg.Oncol., 1991: 17: 667–669.
153. Rodeheaver, G.T., Foresman, P.A., Brazda, M.T. and Edlich, R.F.A Temporary Nontoxic Lubricant for a Synthetic Absorbable Suture,Surg. Gynecol. Obstet., 1987: 164: 17–21.
154. Trimbos, J.B. and Klopper, P.J. Knot Security of Synthetic AbsorbableSuture Material: A Comparison of PGA and Polyglactin-910, Eur. J. Obstet.Gynecol Reprod. Biol., 1985: 19: 183–190.
155. Solhaug, J.H. and Heimann, P. PGA (PGA, Dexon) Sutures in NeckSurgery, Acta Chir. Scand., 1975: 141: 326–328.
156. Edlich, R.F., Panek, P.H. and Rodeheaver, G.T. Surgical Sutures andInfection: A Biomaterial Evaluation, J. Biomed. Mater. Res., 1974: 8:115–126.
157. Dardik, H., Dardik, I. and Laufman, H. Clinical Use of PGA Polymer as aNew Absorbable Synthetic Suture, Am. J. Surg., 1971: 121: 656–660.
158. Bergman, F.O., Borgstrom, S.J. and Holmlund, D.E. Synthetic AbsorbableSurgical Suture Material (PGA). An Experimental Study, Acta Chir.Scand., 1971: 137: 193–200.
159. Tanabe, T, Nakajima, S., Matsunami, S, Tamura, K. and Shiono, T. NewSurgical Suture: Synthetic Absorbable PGA Suture, Shujutsu, 1971: 25:273–279.
160. Dardik, H., Dardik, I., Katz, A.R. and Laufman, H. A New AbsorbableSynthetic Suture in Growing and Adult Primary Vascular Anastomoses:Morphologic Study, Surgery, 1970: 68: 1112–1121.
161. Nielsen, N.V., Hojbjerg, J.C. and Westerlund, E. Absorbable Sutures(Dexon and Vicryl�) in the Corneolimbal Incision, Used in LensImplantation Surgery, Acta Ophthalmol. 1980: 58: 48–55.
162. Martyn, J.W. Clinical Experience with a Synthetic Absorbable SurgicalSuture, Surg. Gynecol. Obstet, 1975: 140: 747–748.
163. Weir, N. and Buchanan, F.J. (2000). Accelerated Test Methods for theEvaluation of Bioabsorbable Suture Materials, In: Nephew International
354 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Symposium – Tissue Engineering: Advances in Tissue Engineering,Biomaterials and Cell Signalling, University of York, York, England, p. 144.
164. Liu, S.-A, Tung, K.-C, Cheng, C.-C. and Chiu, Y.-T. The Impact ofDifferent Closure Materials on Pharyngeal Wound Healing: AnExperimental Animal Study, Eur. Arch. OtoRhinoLaryngol., 2008: 265:227–231.
165. Bezwada, R.S., Jamiolkowski, D.D. and Shalaby, S.W. (1991). RadiationSterilizable Bioabsorbable Sutures, In: Transactions of the Annual Meetingof the Society for Biomaterials in Conjunction with the InternationalBiomaterials Symposium, Scottsdale, Arizona, USA, p. 186.
166. Albersson, A.C. and Varma, I.K. Recent Developments in Ring OpeningPolymerization of Lactones for Biomedical Applications,Biomacromolecules, 2003: 4: 1466–1486.
167. Li, S., Tenon, M., Garreau, H., Braud, C. and Vert, M. EnzymaticDegradation of Stereocopolymers Derived from L-, DL- and Meso-Lactides,Polym. Degrad. Stab., 2000: 67: 85–90.
168. Zhou, S., Deng, X., Li, X., Jia, W. and Liu, L. Synthesis andCharacterization of Biodegradable Low Molecular Weight AliphaticPolyesters and Their Use in Protein-Delivery Systems, J. Appl. Polym.Sci., 2004: 91: 1848–1856.
169. Bergsma, J.E., Rozema, F.R., Bos, R.R.M., Boering, G., Bruijn W.C. andPennings, A.J. In Vivo Degradation and Biocompatibility Study of In VitroPre-Degraded As-Polymerized Polylactide Particles, Biomaterials, 1995:16: 267–274.
170. Lim, L.-T., Auras, R. and Rubino, M. Processing Technologies forPoly(Lactic Acid), Prog. Polym. Sci., 2008: 33: 820–852.
171. Jalabert, M., Fraschini, C. and Prud’Homme, R.E. Synthesis andCharacterization of Poly(L-Lactide)s and Poly(D-Lactide)s of ControlledMolecular Weight, J. Polym. Sci. Part A Polym. Chem., 2007: 5: 1944–1955.
172. Takizawa, K., Nulwala, H., Hu, J., Yoshinaga, K. and Hawker, C.J.Molecularly Defined (L)-Lactic Acid Oligomers and Polymers: Synthesisand Characterization, J. Polym. Sci. Part A Polym. Chem., 2008: 46: 5977–5990.
173. Penning, J.P., Dijkstra, H. and Pennings, A.J. Preparation and Propertiesof Absorbable Fibres from L-Lactide Copolymers, Polymer, 1993: 34:942–951.
174. Mehta, R., Kumar, V., Bhunia, H. and Upadhyay, S.N. Synthesis ofPoly(Lactic Acid): A Review, J. Macromol. Sci. Polym. Rev., 2005: 45:325–349.
175. Kim, E., Shin, E.W., Yoo, I.-K. and Chung, J.S. Characteristics ofHeterogeneous Titanium Alkoxide Catalysts for Ring-OpeningPolymerization of Lactide to Produce Polylactide, J. Mol. Catal.A Chem., 2009: 298: 36–39.
176. Kulkarni, R.K., Pani, K.C., Neuman, C. and Leonard, F. Polylactic Acid forSurgical Implants, Arch. Surg., 1966: 93: 839–843.
177. Kaplan, D.S. (1982). Surgical Suture Derived from Segmented Polyether-Ester Block Copolymers, US Patent 4,314,561.
Absorbable Polymeric Surgical Sutures 355
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
178. Baptist, J.N. and Ziegler, J.B. (1965). Method of Making AbsorbableSurgical Sutures from Poly Beta Hydroxy Acids, US Patent 3,225,766.
179. Schmitt, E.E. and Polistina, R.A. (1967). Surgical Sutures, US Patent3,297,033.
180. Schneider, A.K. (1972). Polylactide Sutures, US Patent 3,636,956.
181. Gogolewski, S. and Pennings, A.J. (1992). Filament Material PolylactideMixtures, US Patent 5,110,852.
182. Schneider, A.K. (1974). Polylactide Fabric Graphs for SurgicalImplantation, US Patent 3,797,499.
183. Gogolewski, S. and Pennings, A.J. (1990). Method of Preparing PolyesterFilament Material, US Patent 4,915,893.
184. Tomihata, K., Sasaki, I. and Suzuki, M. (1998). Surgical Suture andMethod for Preparation Thereof, US Patent 5,797,962.
185. Lam, K.H., Nijenhuis, A.J., Bartels, H. et al. Reinforced Poly(L-Lactic Acid)Fibres as Suture Material, J. Appl. Biomater., 1995: 6: 191–197.
186. Chen, Q.Z., Blaker, J.J. and Boccaccini, A.R. Bioactive and MechanicallyStrong Bioglass�-Poly(D,L-Lactic Acid) Composite Coatings on SurgicalSutures, J. Biomed. Mater. Res. B Appl. Biomater., 2006: 76: 354–363.
187. Kangas, J., Paasimaa, S., Makela, P. et al. Comparison of StrengthProperties of Poly-L/D-Lactide (PLDLA) 96/4 and Polyglyconate (Maxon�)Sutures: In vitro, in the Subcutis, and in the Achilles Tendon of Rabbits,J. Biomed. Mater. Res., 2001: 58: 121–126.
188. Lou, C.-W, Yao, C.-H., Chen, Y.-S, Hsieh, T.-C, Lin, J.-H and Hsing, W.-H.Manufacturing and Properties of PLA Absorbable Surgical Suture, Text.Res J., 2008: 78: 958–965.
189. Zhou, Z.H., Liu, X.P., Liu, Q.Q. and Liu, L.H. Morphology, Molecular MassChanges, and Degradation Mechanism of Poly-L-Lactide in Phosphate-Buffered Solution, Polym. Plast. Technol. Eng., 2009: 48: 115–120.
190. Makela, P., Pohjonen, T., Tormala, P., Waris, T. and Ashammakhi, N.Strength Retention Properties of Self-Reinforced Poly L-Lactide(SR-PLLA) Sutures Compared with Polyglyconate (Maxon�) andPolydioxanone (PDO) Sutures. An In Vitro Study, Biomaterials, 2002:23: 2587–2592.
191. Tormala, P. Ultra-High Strength, Self-Reinforced Absorbable PolymericComposites for Applications in Different Disciplines of Surgery, Clin.Mater., 1993: 13: 35–40.
192. Vainionpaa, S., Rokkanen, P. and Tormala, P. Surgical Applications ofBiodegradable Polymers in Human Tissues, Prog. Polym. Sci., 1989: 14:679–716.
193. Ikada, Y. and Tsuji, H. Biodegradable Polyesters for Medical and EcologicalApplications. Macromol. Rapid Commun., 2000: 21: 117–132.
194. Heino, A., Naukkarinen, A., Kulju, T., Tormala, P., Pohjonen, T. andMakela, E.A. Characteristics of Poly(L-)Lactic Acid Suture Applied toFascial Closure in Rats, J. Biomed. Mater. Res., 1996: 30: 187–192.
195. Gunatillake, P., Mayadunne, R. and Adhikari, R. Recent Developments inBiodegradable Synthetic Polymers, Biotechnol. Annu. Rev., 2006: 12:301–347.
356 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
196. Miller, R.A., Brady, J.M. and Cutright, D.E. Degradation Rates of OralResorbable Implants (Polylactates and Polyglycolates: Rate ModificationWith Changes in PLA/PGA Copolymer Ratios, J. Biomed. Mater. Res.,1977: 11: 711–719.
197. Maticic, D., Kreszinger, M., Pirkic, B., Vnuk, D., Radisic, B. and Gracner,D. Comparative Study of Skin Closure in Dogs with Polypropylene andPolyglactin 910, Veterinarski Arhiv., 2005: 75: 383–390.
198. Azab, A.K., Doviner, V., Orkin, B. et al. Biocompatibility Evaluation ofCrosslinked Chitosan Hydrogels After Subcutaneous and IntraperitonealImplantation in the Rat, J. Biomed. Mater. Res. A, 2007: 83A: 414–422.
199. Pineros-Fernandez, A., Salopek, L.S., Rodeheaver, P.F., Drake, D.B.,Edlich, R.F. and Rodeheaver, G.T. A Revolutionary Advance in SkinClosure Compared to Current Methods, J. Long Term Eff. Med. Implants,2006: 16: 19–27.
200. Katti, D.S., Robinson, K.W., Ko, F.K., Laurencin, C.T. BioresorbableNanofiber-Based Systems for Wound Healing and Drug Delivery:Optimization of Fabrication Parameters, J. Biomed. Mater. Res. B Appl.Biomater., 2004: 70: 286–296.
201. Astete, C.E. and Sabliov, C.M. Synthesis and Characterization of PLGANanoparticles, J. Biomater. Sci. Polym. Ed., 2006: 17: 247–289.
202. Martin, H.C.O. and Motbey, J. Use of Polyglyconate Suture in PaediatricGastrointestinal Anastomosis, Aust. N. Z. J. Surg., 1993: 63: 883–887.
203. Farrar, D.F. and Gillson, R.K. Hydrolytic Degradation of Polyglyconate B:The Relationship Between Degradation Time, Strength and MolecularWeight, Biomaterials 2002: 23: 3905–3912.
204. Flyger, H.L., Hakansson, T.U. and Jensen, LP. Single Layer ColonicAnastomosis with a Continuous Absorbable Monofilament PolyglyconateSuture, Eur. J. Surg., 1995: 161: 911–913.
205. Rodeheaver, G.T., Salopek, L.S., Green, C.W. et al. Effectiveness ofGlycomer 631 Monofilament Sutures in Closing MusculoaponeuroticIncisions, J. Long Term Eff. Med Implants, 1998: 8: 225–231.
206. Huang, G.-K., Li, H.-Q. and Wu, X.-M. Study on MicrovascularAnastomosis of Arteries with Absorbable Polyglyconate Suture,Microsurg., 1995: 16: 505–509.
207. Tomihata, K., Suzuki, M. and Tomita, N. Handling Characteristics ofPoly(L-lactide-Co-e-Caprolactone) Monofilament Sutures, Biomed. Mater.Eng., 2005: 15: 381–391.
208. Baimark, Y., Molloy, R., Molloy, N., Siripitayananon, J., Punyodom, W. andSriyai, M. Synthesis, Characterisation and Melt Spinning of a BlockCopolymer of L-Lactide and “-Caproactone for Potential Use as anAbsorbable Monofilament Surgical Suture, J. Mater. Sci. Mater. Med.,2005: 16: 699–707.
209. Yang, K.-K, Li, X.-L. and Wang Y.-Z. Poly(p-Dioxanone) and itsCopolymers, J. Macromol. Sci. Polym. Rev., 2002: 42: 373–398.
210. Merrell, S.W. and Lawrence, P.F. Initial Evaluation of AbsorbablePolydioxanone Suture for Peripheral Vascular Surgery, J. Vasc. Surg.,1991: 14: 452–457.
Absorbable Polymeric Surgical Sutures 357
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
211. Maurus, P.B. and Kaeding, C.C. Bioabsorbable Implant Material, Review.Oper. Tech. Sports Med., 2004: 12: 158–160.
212. Ray, J.A., Doddi, N. and Regula, D. Polydioxanone (PDO), A NovelMonofilament Synthetic Absorbable Suture, Surg. Gynecol. Obstet., 1981:153: 497–507.
213. Boland, E.D., Coleman, B.D., Barnes, C.P., Simpson, D.G., Wnek, G.E. andBowlin, G.L. Electrospinning Polydioxanone for Biomedical Applications,Acta Biomater., 2005: 1: 115–123.
214. Mazzarese, P.M., Faulkner, B.C., Gear, A.J.L, Watkins, F.H., Rodeheaver,G.T. and Edlich, R.F. Technical Considerations in Knot Construction. PartII. Interrupted Dermal Suture Closure, J. Emerg. Med., 1997: 15: 505–511.
215. Brown, R.P. Knotting Technique and Suture Materials, Br. J. Surg., 1992:79: 399–400.
216. Metz, S.A., Chegini, N. and Masterson, B.J. In Vivo and In VitroDegradation of Monofilament Absorbable Sutures, PDO� and Maxon�,Biomaterials, 1990: 11: 41–45.
217. Rodeheaver, G.T., Beltran, K.A., Green, C.W. et al. Biomechanical andClinical Performance of a New Synthetic Monofilament Absorbable Suture,J. Long-Term Eff. Med., 1996: 6: 181–198.
218. Van Rijssel, E.J.C., Brand, R., Admiraal, C., Smit, I. and Trimbos, J.B.Tissue Reaction and Surgical Knots: The Effect of Suture Size, KnotConfiguration, and Knot Volume, Obstetr. Gynecol., 1989: 74: 64–68.
219. Im, J.N., Kim, J.K., Kim, H.-K., In, C.H., Lee, K.Y. and Park, W.H. In vitroand In vivo Degradation Behaviors of Synthetic Absorbable BicomponentMonofilament Suture Prepared with Poly(p-dioxanone) and its Copolymer,Polym. Degrad. Stabil., 2007: 92: 667–674.
220. Barber, F.A. and Click, J.N. The Effect of Inflammatory Synivial Fluid onthe Breaking Strength of New Long Lasting Sutures, J. Arthrosc. Relat.Surg., 1992: 8: 437–411.
221. Kulkarni, A., Reiche, J., Hartmann, J., Kratz, K. and Lendlein, A. SelectiveEnzymatic Degradation of Poly(e-caprolactone) Containing MultiblockCopolymers, Eur. J. Pharm. Biopharm., 2008: 68: 46–56.
222. Storck, M., Orend, K.-H. and Schmitz-Rixen, T. Absorbable Suture inVascular Surgery, Vasc. Surg., 1993: 27: 413–424.
223. Molea, G., Schonauer, F., Bifulco, G. and D’Angelo, D. Comparative Studyon Biocompatibility and Absorption Times of Three AbsorbableMonofilament Suture Materials (Polydioxanone, Poliglecaprone 25,Glycomer 631), Brit. J. Plast. Surg., 2000: 53: 137–141.
224. Song, C.X., Cui, X.M. and Schindler, A. Biodegradable Copolymers Basedon p-Dioxanone for Medical Application, Med. Biol. Eng. Comput., 1993:31: S147–S150.
225. Ingle, N.P., King, M.W., Leung, J.C. and Batchelor, S. (2006). BarbedSuture Anchoring Strength: Applicability to Dissimilar PolymericMaterials, In: Transactions – 7th World Biomaterials Congress, CurranAssociates, Inc., Sydney, Australia, 17–21 May, 2004, p. 1260.
358 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
226. Murtha, A.P., Kaplan, A.L., Paglia, M.J., Mills, B.B., Feldstein, M.L. andRuff, G.L. Evaluation of a Novel Technique for Wound Closure Using aBarbed Suture, Plast. Reconstr. Surg., 2006: 117: 1769–1780.
227. Vracko, J. and Pegan, V. Single-layer Closure of a Subcostal Incision Usinga Monofilament Absorbable Suture Material – Comparison ofPolydioxanone (PDO) and Polyglyconate [Jednoslojno zatvaranje supkos-talnih incizija monofilamentnim apsorpcijskim savnim materijalom–uspor-edba polidioksanona (PDO) i poliglikonata]. Acta Chir. Iugosl., 1989: 36:15–25.
228. Anderson, E., Sondenaa, K. and Holter, J. A Comparative Study ofPolydioxanone (PDO�) and Polyglactin 910 (Vicryl
��) in Colonic
Anastomoses in Rats, Int. J. Colorectal Dis., 1989: 4: 251–254.
229. Ahmed, H.A. and Goldie, B.S. Comparison of the Mechanical Properties ofPGA-Trimethylene Carbonate (Maxon) and Polydioxanone Sutures(PDO2) Used for Flexor Tendon Repair and Active Mobilization, J. HandSurg., 2002: 27B: 329–332.
230. Keceligil, H.T., Kolbakir, F., Akar, H., Konuralp, C., Demir, Z. andDemirag, M.K. Sternal Closure with Resorbable Synthetic Loop SutureMaterial in Children, J. Pediat. Surg., 2000: 35: 1309–1311.
231. Li, X., King, M. and MacDonald, P. Comparative Study of KnotPerformance and Ease of Manipulation of Monofilament and BraidedSutures for Arthroscopic Applications, Knee Surg. Sport Traumatol.Arthrosc., 2004: 12: 448–452.
232. Chusak, R.B. and Dibbell, D.G. Clinical Experience with PolydioxanoneMonofilament Absorbable Sutures in Plastic Surgery, Plast. Reconstr.Surg., 1983: 72: 217–221.
233. Kontio, R., Ruuttila, P., Lindroos, L. et al. Biodegradable Polydioxanoneand Poly (L/D) Lactide Implants: An Experimental Study on Peri-implantTissue Response, Int. J. Oral Max. Surg., 2006: 34: 766–776.
234. Muftuoglu, M.A., Ozkan, E. and Saglam, A. Effect of Human PancreaticJuice and Bile on the Tensile Strength of Suture Materials, Am. J. Surg.,2004: 188: 200–203.
235. Sasaki, G.H., Komorowska-Timek, E.D., Bennett, D.C. and Gabriel, A.An Objective Comparison of Holding, Slippage, and Pull-out Tensions forEight Suspension Sutures in the Malar Fat Pads of Fresh-frozen HumanCadavers, Aesthet. Surg. J., 2008: 28: 387–396.
236. Dencker, A., Lundgren, I. and Sporrong, T. Suturing After Childbirth - ARandomised Controlled Study Testing a New Monofilament Material,BJOG: Int. J. Obstetr. Gynaecol., 2006: 113: 114–116.
237. Jacquel, N., Lo, C.-W., Wei, Y.-H., Wu, H.-S. and Wang, S.S. Isolation andPurification of Bacterial Poly(3-hydroxyalkanoates), Biochem. Eng. J.,2008: 39: 5–27.
238. Rocha, R.C.S., Silva, L.F., Taciro, M.K. and Pradella, J.G.C. Production ofPoly(3-hydroxybutyrate-co-3-hydroxyvalerate) P(3HB-co-3HV) with aBroad Range of 3HV Content at High Yields by Burkholderia sacchariIPT 189, World J Microbiol Biotechnol., 2008: 24: 427–431.
Absorbable Polymeric Surgical Sutures 359
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
239. Anderson, A.J. and Dawes, E.A. Occurrence, Metabolism, Metabolic Role,and Industrial Use of Bacterial Polyhydroxyalkonoates, Microbiol. Rev.,1990: 54: 450–472.
240. Steinbuchel, A. (2002). Biopolymers, Weinheim, Wiley-VCH, Vol. 10.
241. Chen, X., Yang, X., Pan, J., Wang, L. and Xu, K. Degradation Behaviors ofBioabsorbable P3/4HB Monofilament Suture, In Vitro and In Vivo, 2010:92B: 447–455.
242. Fedorov, M.B., Vikhoreva, G.A., Kil’deeva, N.R., Kechek’Yan, A.S.,Gerasimov, V.I. and Gal’braikh, L.S. Structural Changes in Films andProperties of Surgical Sutures with Polyhydroxybutyrate Coating, FibreChem., 2008: 40: 118–122.
243. Doi, Y., Tamaki, A., Kunioka, M. and Saito, T. Biodegradation Of MicrobialCopolyesters: Poly(3-hydroxybutyrate-co-3-hydroxyvalerate) and Poly(3-hydroxybutyrate-co-3-hydroxybutyrate), Macromolecules, 1990: 23: 26–31.
244. Chu, C.C. (1991). Recent Advancements in Suture Fibres for WoundClosure, In: Vigo, T.L. and Turbak, A.F. (eds), High-tech FibrousMaterials, Washington, DC, ACS Symposium Series 457, pp. 167–211.
245. Rathke, T.D. and Hudson, S.M. Review of Chitin and Chitosan as Fiber andFilm Formers, J. Macromol. Sci – Rev. Macromol. Chem. Phys., 1994: C34:375–437.
246. Muzzarelli, R.A.A. and Muzzarelli, C. Chitosan Chemistry: Relevance tothe Biomedical Sciences, Adv. Polym. Sci., 2005: 186: 151–209.
247. Kumar, M.N.V.R., Muzzarelli, R.A.A., Muzzarelli, C., Sashiwa, H., Domb,A.J. Chitosan Chemistry and Pharmaceutical Perspectives, Chem. Rev.,2004: 104: 6017–6084.
248. Pillai, C.K.S., Paul, W. and Sharma, C.P. (2010). Chitosan: Manufacture,Properties & Uses, In: Columbus, F. (ed.), Chitosan: Manufacture, Properties& Uses, Hauppauge, NY, Nova Science Publishers, Inc. (in press).
249. Nishimura, K., Nishimura, S., Seo, H., Nishi, N., Tokura, S. and Azuma, I.Macrophage Activation with Multi-porous Beads Prepared from PartiallyDeacetylated Chitin, J. Biomed. Mater. Res., 1986: 20: 1359–1372.
250. Zikakis, J.P. (1984). Chitin, Chitosan and Related Enzymes, New York,Academic.
251. Singh, D.K. and Ray, A.R. Biomedical Applications of Chitin, Chitosan, andtheir Derivatives, Polym. Rev., 2000: 40: 69–83.
252. Kurita, K. Chitin and Chitosan: Functional Biopolymers from MarineCrustaceans, Mar. Biotechnol., 2006: 8: 203–226.
253. Hirano, S. Chitin Biotechnology Applications, Biotechnol. Ann. Rev., 1996:2: 237–258.
254. Rinaudo, M. Main Properties and Current Applications of SomePolysaccharides as Biomaterials, Polym. Int., 2008: 57: 397–430.
255. Pillai, C.K.S., Paul, W. and Sharma, C.P. Chitin and Chitosan Polymers:Chemistry, Solubility and Fiber Formation, Progr. Polym. Sci., 2009: 4:641–678.
256. Desai, A.A. Biomedical Implantable Materials Sutures, Asian Text. J.,2005: 14: 54–56.
360 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from

257. Austin, P.R., Brine, C.J., Castle, J.E. and Zikakis, J.P. Chitin: New Facetsof Research, Science, 1981: 212: 749–753.
258. Mikhailov, G.M. and Lebedeva, M.F. Procedures for Preparing Chitin-based Fibers, Russ. J. Appl. Chem., 2007: 80: 685–694.
259. Daly, W.H. and Macossay, J. An Overview of Chitin and Derivatives forBiodegradable Materials Applications, Fibres Text East Eur., 1997: 5: 22–27.
260. Kifune, K., Inoue, K. and Mori, S. (1984). Process for the Production ofChitin Fibers, US Patent 4,431,601.
261. Brine, C.J. and Austin, P.R. (1975). Renaturated Chitin Fibrils, Films andFilaments, In: Church, T.D. (ed), Marine Chemistry in CoastalEnvironment, Washington, DC, ACS Symposium Series, Vol. 18, p. 505.
262. Austin, P.R. (1975). Solvents for and Purification of Chitin, US Patent3,892,731 and Purification of Chitin, US Patent 3,879, 377.
263. Tokura, S. and Seo, H. (1984). Manufacture of Chitosan Fiber and Film,Japanese Patent 59,116,418.
264. Unitika Co. Ltd. (1982). Chitin Powder and its Production, JapanesePatent 57,139,101.
265. Unitika Co. Ltd. (1983). Production of Chitin Yarn, Japanese Patent58,214,513.
266. Unitika Co. Ltd. (1983). Prodcution of Chitin Yarn, Japanese Patent58,214,512.
267. Tokura, S., Nishi, N. and Noguchi, J. Studies on Chitin III: Preparation ofChitin Fibres, Polym. J., 1979: 11: 781–786.
268. Austin, P.R. and Brine, C.J. (1976). Chitin Films and Fibers, US Patent4,029,727.
269. Nakajima, M., Atsumi, K. and Kifune, K. (1984). Development ofAbsorbable Sutures from Chitin, In: Zikakis, J.P. (ed.), Chitin, Chitosanand Related Enzymes, New York, Harcourt Brace Janovich, p. 407.
270. Yano, H., Iriyama, K., Nishiwaki, H. and Kifune, K. Effect of N-acetyl-D-glucosamine on Wound Healing in Rats, Mie. Med. J., 1985: 35: 53–56.
271. Minami, S., Okamoto, Y., Matsuhashi, A. and Shigemasa, Y. (1992).Production, Properties, and Some New Applications of Chitin and itsDerivatives, In: Tokura, S. and Azuma, I. (eds), Chitin Derivatives of LifeSciences, Sapparo, Jpn. Chitin Soc, pp. 333–351.
272. Kifune, K., Yamaguchi, Y. and Kishimoto, S. Wound Healing Effect ofChitin Surgical Dressings, Trans. Soc. Biomater., 1988: 11: 216–218.
273. Zhukovskii, V.A. Problems and Prospects for Development and Productionof Surgical Suture Materials, Fibre Chem., 2008: 40: 208–216.
274. Mikhailov, G.M. and Lebedeva, M.F. Procedures for Preparing Chitin-based Fibers, Russ. J. Appl. Chem., 2007: 80: 685–694.
275. Paluch, D., Szosland, L., Staniszewska-Kus, J., Solski, L., Szymonowicz, M.and Gebarowska, E. The Biological Assessment of the Chitin Fibres, Polim.Med., 2000: 30: 3–31.
276. Hirano, S., Zhang, M., Nakagawa, M. and Miyata, T. Wet Spun Chitosan-Collagen Fibers, their Chemical N-modifications, and Blood Compatibility,Biomaterials, 2000: 21: 997–1003.
Absorbable Polymeric Surgical Sutures 361
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
277. Pillai, C.K.S. and Sharma, C.P. Electrospinning of Chitin and ChitosanNanofibres, Trends Biomater. Artif. Organs, 2009: 23: 175–197.
278. Machinami, R., Kifune, H., Kawaide, A. and Tsurutani, R. A HistologicalStudy of the Fate of Chitin Suture Material after Intramuscular Suturing,Med. Sci. Res., 1991: 19: 391–392.
279. Nakajima, M., Atsumi, K. and Kifune, K. (1984). Development of the NewAbsorbable Suture by Chitin, In: Transactions of the Annual Meeting of theSociety for Biomaterials in Conjunction with the InternationalBiomaterials Symposium, Washington, DC, USA, p. 28.
280. Zia, K.M., Barikani, M., Zuber, M., Bhatti, I.A. and Barmar, M. SurfaceCharacteristics of Polyurethane Elastomers Based on Chitin/1,4-butanediol Blends, Int. J. Biol. Macromol., 2009: 44: 182–185.
281. Zia, K.M., Zuber, M., Bhatti, I.A., Barikani, M. and Sheikh, M.A.Evaluation of Biocompatibility and Mechanical Behavior of PolyurethaneElastomers based on Chitin/1,4-butane diol Blends, Int. J. Biol. Macromol.,2009: 44: 18–22.
282. Zia, K.M., Zuber, M., Bhatti, I.A., Barikani, M. and Sheikh, M.A.Evaluation of Biocompatibility and Mechanical Behavior of Chitin-basedPolyurethane Elastomers. Part-II: Effect of Diisocyanate Structure, Int. J.Biol. Macromol., 2009: 44: 23–28.
283. Zia, K.M., Bhatti, I.A., Barikani, M., Zuber, M. and Sheikh, M.A. XRDStudies of Chitin-based Polyurethane Elastomers, Int. J. Biol. Macromol.,2008: 43: 136–141.
284. Zia, K.M., Barikani, M., Zuber, M., Bhatti, I.A. and Sheikh, M.A. MolecularEngineering of Chitin based Polyurethane Elastomers, Carbohydr. Polym.,2008: 74: 149–158.
285. Xiong, S.-H., Yu, L., Liao, H. et al. Morphological Study on Myoblast L6 ofRats Co-cultured with Chitin Suture In Vitro, Chin. J. Clin. Rehab., 2006:10: 46–48.
286. Lucca, G.V., Kezar III, H.S. and O’Brien, J.P. (1991). High Strength Fibersfrom Chitin Derivatives, US Patent 5,021,207.
287. Dutaa, P.K. and Ravi Kumar, M.N.V. (1997). Waste Utilization: ChitosanFibres by Direct Dissolution, In: Indian Chemist Convention, New Delhi,17–20 December.
288. Phongying, S., Aiba, S.-I. and Chirachanchai, S. Direct ChitosanNanoscaffold Formation via Chitin Whiskers, Polymer, 2007: 48: 393–400.
289. Knaul, J., Hooper, M., Chanyi, C. and Creber, K.A.M. Improvements in theDrying Process for Wet-spun Chitosan Fibers, J. Appl. Polym. Sci., 1998:69: 1435–1444.
290. Knaul, J.Z. and Creber, K.A.M. Coagulation Rate Studies of SpinnableChitosan Solutions, J. Appl. Polym. Sci., 1997: 66: 117–127.
291. Fan, L., Zheng, H., Xu, Y., Huang, J. and Zhang, C. Preparation andProperties of Chitosan/Konjac Glucomannan Blend Fibers, J. Macromol.Sci. Part A: Pure Appl. Chem., 2007: 44: 439–443.
292. Rahbaran, S., Redlinger, S. and Einzmann, M. New Bioactive CellulosicFibers, Chem. Fibers Int., 2006: 56: 25–29.
362 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
293. Onishi, H. and Machida, Y. Biodegradation and Distribution of Water-soluble Chitosan in Mice, Biomaterials, 1999: 20: 175–182.
294. Varum, K.M., Myhr, M.M., Hjerde, R.J.N. and Smidsrod, O. In vitroDegradation Rates of Partially N-acetylated Chitosans in Human Serum,Carbohydr. Res., 1997: 299: 99–101.
295. Sashiwa, H., Saimoto, H., Shigemasa, Y., Ogawa, R. and Tokura, S.Lysozyme Susceptibility of Partially Deacetylated Chitin, Int. J. Biol.Macromol., 1990: 12: 295–296.
296. Shigemasa, Y., Saito, K., Sashiwa, H. and Saimoto, H. EnzymaticDegradation of Chitins and Partially Deacetylated Chitins, Int. J. Biol.Macromol., 1994: 16: 43–49.
297. Shigemasa, Y. and Minami, S. Applications of Chitin and Chitosan forBiomaterials, Biotechnol. Genet. Engg. Rev., 1996: 17: 413–420.
298. McCurdy, J.D. (1992). FDA and the Use of Chitin and ChitosanDerivatives, In: Brine, C.J., Sanford, P.A. and Zikakis, J.P. (eds),Advances in Chitin and Chitosan, London, New York, Elsevier AppliedScience, pp. 659–662.
299. Seo, H. Processing and Utilization of Chitin and Chitosan. Sen-iGakkaishi, 1990: 46: 564–569
300. Amano, K. and Ito, E. The Action of Lysozyme on Partially DeacetylatedChitin, Eur. J. Biochem., 1978: 85: 97–104.
301. Pangburn, S.H., Trescony, P.V. and Heller, J. Lysozyme Degradation ofPartially Deacetylated Chitin its Films and Hydrogels, Biomaterials, 1982:3: 105–108.
302. Tomihata, K. and Ikada, Y. In Vitro and In Vivo Degradation of Filmsof Chitin and its Deacetylated Derivatives, Biomaterials, 1997: 18:567–575.
303. Muzzarelli, R. Depolymerization of Methyl Pyrrolidinone Chitosan byLysozyme, Carbohydr. Polym., 1992: 19: 29–34.
304. Berscht, P.C., Nies, B., Liebendorfer, A. and Kreuter, J. In VitroEvaluation of Biocompatibility of Different Wound Dressing Materials, J.Mater., Sci.: Mater. Med., 1995: 6: 201–220.
305. Chung, L.Y., Schmidt, R.J., Hamlyn, P.F., Sagar, B.F., Andrews, A.M. andTurner, T.D. Biocompatibility of Potential Wound Management Products:Hydrogen Peroxide Generation by Fungal Chitin/Chitosans and TheirEffects on the Proliferation of Murine L929 Fibroblasts in Culture,J. Biomed. Mater. Res., 1998: 39: 300–307.
306. Ohkawa, K., Tatehata, H. and Yamamoto, H. Formation andBiodegradation of Natural Polymer Hydrogels, Fibers, and Capsules,Kobunshi Ronbunshu, 1999: 56: 583–596.
307. Tsai, W.C., Chu, C.C., Chiu, S.S. and Yao, J.Y. In Vitro Quantitative Studyof Newly Made Antibacterial Braided Nylon Sutures, Surg. Gynecol.Obstetr., 1987: 165: 207–211.
308. Kovtun, E.A., Plygan, E.P., Gudz, O.V. and Sergeev, V.P.Creation of Sutures with Antimicrobial Properties, Fibre Chem., 2000:32: 287–292.
Absorbable Polymeric Surgical Sutures 363
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
309. Blaker, J.J., Boccaccini, A.R. and Nazhat, S.N. Thermal Characterizationsof Silver-containing Bioactive Glass-coated Sutures, J. Biomater. Appl.,2005: 20: 81–98.
310. Blaker, J.J., Nazhat, S.N. and Boccaccini, A.R. Development andCharacterisation of Silver-doped Bioactive Glass-coated Sutures forTissue Engineering and Wound Healing Applications, Biomaterials, 2004:25: 1319–1329.
311. Rozzelle, C.J., Leonardo, J. and Li, V. Antimicrobial Suture Wound Closurefor Cerebrospinal Fluid Shunt Surgery: A Prospective, Double-blinded,Randomized Controlled Trial, J. Neurosurg.: Pediatr., 2008: 2: 111–117.
312. Al-Qattan, M.M. Vicryl� Rapide� versus Vicryl��
Suture in Skin Closure ofthe Hand in Children: A Randomized Prospective Study, J. Hand Surg.,2005: 30: 90–91.
313. Storch, M.L., Rothenburger, S.J. and Jacinto, G. ExperimentalEfficacy Study of Coated Vicryl� plus antibacterial suture in GuineaPigs Challenged with Staphylococcus aureus, Surg. Infect., 2004: 5:281–288.
314. Marco, F., Vallez, R., Gonzalez, P., Ortega, L., De La Lama, J. and Lopez-Duran, L. Study of the Efficacy of Coated Vicryl� Plus� AntibacterialSuture in an Animal Model of Orthopedic Surgery, Surg. Infect., 2007: 8:359–365.
315. Gupta, B., Jain, R., Anjum, N. and Singh, H. Preparation of AntimicrobialSutures by Preirradiation Grafting of Acrylonitrile onto PolypropyleneMonofilament. III. Hydrolysis of the Grafted Suture, J. Appl. Polym. Sci.,2004: 94: 2509–2516.
316. Fedorov, M.B., Vikhoreva, G.A., Kil’deeva, N.R., Mokhova, O.N.,Bonartseva, G.A. and Gal’braikh, L.S. Antimicrobial Activity of Core-sheath Surgical Sutures Modified with Poly-3-hydroxybutyrate, Appl.Biochem. Microbiol., 2007: 43: 611–615.
317. Bide, M., Bachuwar, A., Phaneuf, M. et al. Fiber-Antibiotic Interactions in theDevelopment of Infection-resistant Sutures, AATCC Rev., 2007: 7: 44–48.
318. Anjum, N., Gulrez, S.K.H., Singh, H. and Gupta, B. Development ofAntimicrobial Polypropylene Sutures by Graft Polymerization. I. Influenceof Grafting Conditions and Characterization, J. Appl. Polym. Sci., 2006:101: 3895–3901.
319. Gupta, B., Anjum, N., Gulrez, S.K.H. and Singh, H. Development ofAntimicrobial Polypropylene Sutures By Graft Copolymerization.II. Evaluation of Physical Properties, Drug Release, and AntimicrobialActivity, J. Appl. Polym. Sci., 2007: 103: 3534–3538.
320. Volenko, A.V., Germanovich, ChS., Gurova, O.P. and Shvets,R.A. Capromed is an Antibacterial Sutural Material, Med. Tekh., 1994: 2:32–34.
321. Quinn, J., Maw, J., Ramotar, K., Wenckebach, G. and Wells, G.Octylcyanoacrylate Tissue Adhesive Versus Suture Wound Repair in aContaminated Wound Model, Surgery, 1997: 122: 69–72.
322. Lendlein, A. and Langer, R. Biodegradable, Elastic Shape Memory Polymersfor Potential Biomedical Applications, Science, 2002: 296: 1673–1676.
364 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
323. Bretcanu, O., Verne, E., Borello, L. and Boccaccini, A.R. Bioactivity ofDegradable Polymer Sutures Coated with Bioactive Glass, J. Mater. Sci.:Mater. Med., 2004: 15: 893–899.
324. Neligan, P.C. Bioactive Sutures, Plast. Reconstr. Surg., 2006: 118:1645–1647.
325. Pasternak, B., Rehn, M., Andersen, L. et al. Doxycycline-coated SuturesImprove Mechanical Strength of Intestinal Anastomoses, Int. J. ColorectalDis., 2008: 23: 271–276.
326. Harnet, J.-C., Le Guen, E., Ball, V. et al. Antibacterial Protection of SutureMaterial by Chlorhexidine-functionalized Polyelectrolyte Multilayer Films,J. Mater. Sci.: Mater. Med., 2009: 20: 185–193.
327. Zhukovskii, V.A., Khokhlova, V.A. and Korovicheva, S.Yu. SurgicalSuture Materials with Antimicrobial Properties, Fibre Chem., 2007; 39:136–143.
328. Scott, D.J. and Goova, M.T. (2004). New and Evolving LaparoscopicInstrumentation, In: Soper, N.J., Swanstrom, L.L. and Eubanks, W.S.(eds), Mastery of Endoscopic and Laparoscopic Surgery, 2nd edn,Lippincott, Williams & Wilkins, pp. 24–33
329. Tremblay, S., El Maliki, A., Fiset, M. and Mantovani, D. LaparoscopicSurgical Manipulations Affect the Mechanical Properties and theMicrostructure of Polymeric Sutures, Mater. Sci. Forum., 2007: 539–543:161–166.
330. Kim, J.-C., Lee, Y.-K., Lim, B.-S., Rhee, S.-H. and Yang, H.-C. Comparisonof Tensile and Knot Security Properties of Surgical Sutures, J. Mater. Sci.:Mater. Med., 2007: 18: 2363–2369.
331. Im, J.N., Kim, J.K., Kim, H.-K., Lee, K.Y. and Park, W.H. Effect of TyingConditions on the Knot Security of Suture Materials, J. Appl. Polym. Sci.,2008: 109: 918–922.
332. Wright, P.B., Budoff, J.E., Yeh, M.L., Kelm, Z.S. and Luo, Z.-P.Strength of Damaged Suture: An In Vitro Study, Arthroscopy, 2006: 22:1270–1275.
333. Coats, B. and Margulies, S.S. Material Properties of Human Infant Skulland Suture at High Rates, J. Neurotrauma, 2006: 23: 1222–1232.
334. Yamagami, N., Mori, R., Yotsumoto, T., Hatanaka, H., Takao, M. andUchio, Y. Biomechanical Differences Resulting from the Combination ofSuture Materials and Repair Techniques, J. Orthopaed. Sci., 2006: 11:614–619.
335. Wust, D.M., Meyer, D.C., Favre, P. and Gerber, C. Properties ofBraided Polyblend Polyethylene Sutures in Comparison to BraidedPolyester and Monofilament Polydioxanone Sutures, Arthroscopy, 2006:22: 1146–1153.
336. Zhukovskii, V.A., Voronova, I.G., Khokhlova, V.A., Gridneva, A.V. andFilipenko, T.S. Technological Developments in Making PolypropyleneSurgical Monofilaments, Fibre Chem., 2008: 40: 322–329.
337. Chooprayoon, P., Siripitayananon, J., Molloy, R., Bunkird, S.,Soywongsa, T. and Tariyawong, A. Processing, MechanicalProperty Development and In Vitro Hydrolytic Degradation Studies of a
Absorbable Polymeric Surgical Sutures 365
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from
Poly(L-lactide-co-e-caprolactone) Monofilament Fibre for Potential Use asan Absorbable Surgical Suture, Adv. Mater. Res., 2008: 55–57: 693–696.
338. De Breuck, H. Monofilaments for Medical Applications, Unitex, 2009: 1:13–15.
339. Baums, M.H., Buchhorn, G.H., Spahn, G., Poppendieck, B., Schultz, W.and Klinger, H.-M. Biomechanical Characteristics of Single-row Repair inComparison to Double-row Repair with Consideration of the SutureConfiguration and Suture Material, Knee Surg. Sports Traumatol.Arthrosc., 2008: 16: 1052–1060.
366 C. K. S. PILLAI AND C. P. SHARMA
at PENNSYLVANIA STATE UNIV on September 18, 2016jba.sagepub.comDownloaded from





























