Embed Size (px)
Citation preview
Complex Strabismus:Restriction, Paresis,
Dissociated Strabismus,and Torticollis
Kenneth W. Wright
This chapter on complex strabismus reviews the evaluationand management of incomitant strabismus associated
with rectus muscle paresis and ocular restriction. Other topicsinclude dissociated strabismus complex, torticollis, and nystag-mus. Incomitant strabismus is a deviation that changes in different fields of gaze. Incomitance can be caused by ocularrestriction, extraocular muscle paresis, or oblique muscle dys-function or can be associated with a primary A- or V-pattern.The diagnosis and treatment of oblique muscle dysfunction(palsy and overaction), Brown’s syndrome, and A- and V-patternsare covered in Chapter 9.
PARALYTIC RECTUS MUSCLES ANDRESTRICTIVE STRABISMUS: GENERAL PRINCIPLES
If an eye has limited ductions, there are only two basic causes:extraocular muscle paresis or ocular restriction. Therefore, astrabismus associated with limited ductions is secondary toextraocular muscle paresis, ocular restriction, or both.
ParesisExtraocular muscle paresis means weak muscle pull, whereaspalsy indicates a complete lack of muscle function. Cranial
10
323
nerve paresis and primary muscle disease are obvious reasonsfor a weak muscle that can cause limited ocular rotations. Amuscle paresis can also be caused by ineffective muscle pull onthe eye, or mechanical disadvantage of muscle pull. Clinicalexamples of conditions that cause mechanical disadvantage ofmuscle pull include:
• A scarred or tethered muscle preventing transmission ofmuscle pull to the globe (e.g., floor fracture with entrappedinferior rectus muscle)
• A posteriorly displaced rectus muscle (e.g., slipped muscle)• A muscle shifted out of its appropriate plane, thus dimin-
ishing the vector force in the field of action of the muscle(e.g., high myopia with displaced lateral rectus muscle)
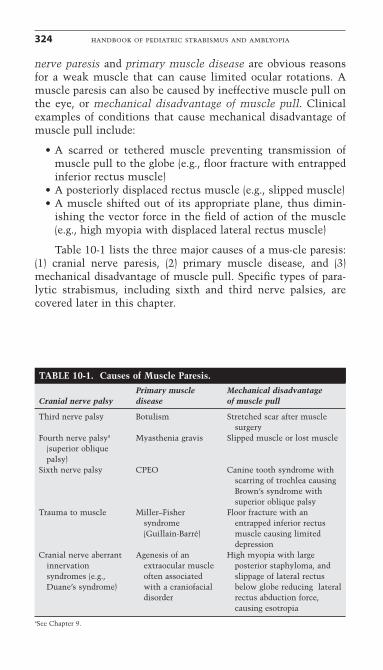
Table 10-1 lists the three major causes of a mus-cle paresis:(1) cranial nerve paresis, (2) primary muscle disease, and (3)mechanical disadvantage of muscle pull. Specific types of para-lytic strabismus, including sixth and third nerve palsies, arecovered later in this chapter.
324 handbook of pediatric strabismus and amblyopia
TABLE 10-1. Causes of Muscle Paresis.Primary muscle Mechanical disadvantage
Cranial nerve palsy disease of muscle pull
Third nerve palsy Botulism Stretched scar after muscle surgery
Fourth nerve palsya Myasthenia gravis Slipped muscle or lost muscle(superior oblique palsy)
Sixth nerve palsy CPEO Canine tooth syndrome with scarring of trochlea causing Brown’s syndrome with superior oblique palsy
Trauma to muscle Miller–Fisher Floor fracture with an syndrome entrapped inferior rectus (Guillain-Barré) muscle causing limited
depressionCranial nerve aberrant Agenesis of an High myopia with large
innervation extraocular muscle posterior staphyloma, and syndromes (e.g., often associated slippage of lateral rectus Duane’s syndrome) with a craniofacial below globe reducing lateral
disorder rectus abduction force, causing esotropia
aSee Chapter 9.
Ocular Restriction
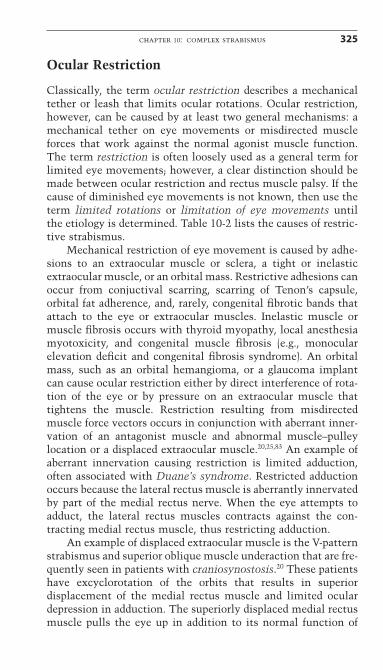
Classically, the term ocular restriction describes a mechanicaltether or leash that limits ocular rotations. Ocular restriction,however, can be caused by at least two general mechanisms: amechanical tether on eye movements or misdirected muscleforces that work against the normal agonist muscle function.The term restriction is often loosely used as a general term forlimited eye movements; however, a clear distinction should bemade between ocular restriction and rectus muscle palsy. If thecause of diminished eye movements is not known, then use theterm limited rotations or limitation of eye movements untilthe etiology is determined. Table 10-2 lists the causes of restric-tive strabismus.
Mechanical restriction of eye movement is caused by adhe-sions to an extraocular muscle or sclera, a tight or inelasticextraocular muscle, or an orbital mass. Restrictive adhesions canoccur from conjuctival scarring, scarring of Tenon’s capsule,orbital fat adherence, and, rarely, congenital fibrotic bands thatattach to the eye or extraocular muscles. Inelastic muscle ormuscle fibrosis occurs with thyroid myopathy, local anesthesiamyotoxicity, and congenital muscle fibrosis (e.g., monocular elevation deficit and congenital fibrosis syndrome). An orbitalmass, such as an orbital hemangioma, or a glaucoma implantcan cause ocular restriction either by direct interference of rota-tion of the eye or by pressure on an extraocular muscle thattightens the muscle. Restriction resulting from misdirectedmuscle force vectors occurs in conjunction with aberrant inner-vation of an antagonist muscle and abnormal muscle–pulleylocation or a displaced extraocular muscle.20,25,83 An example ofaberrant innervation causing restriction is limited adduction,often associated with Duane’s syndrome. Restricted adductionoccurs because the lateral rectus muscle is aberrantly innervatedby part of the medial rectus nerve. When the eye attempts toadduct, the lateral rectus muscles contracts against the con-tracting medial rectus muscle, thus restricting adduction.
An example of displaced extraocular muscle is the V-patternstrabismus and superior oblique muscle underaction that are fre-quently seen in patients with craniosynostosis.20 These patientshave excyclorotation of the orbits that results in superior displacement of the medial rectus muscle and limited oculardepression in adduction. The superiorly displaced medial rectusmuscle pulls the eye up in addition to its normal function of
chapter 10: complex strabismus 325
326 handbook of pediatric strabismus and amblyopiaT
AB
LE 1
0-2.
Cau
ses
of O
cula
r R
estr
icti
on.
Mec
hani
cal
rest
rict
ion
Tig
ht e
xtra
ocul
ar m
uscl
eSt
ruct
ural
adh
esio
nsO
rbit
al m
ass
Mis
dire
cted
mus
cle
forc
es
Th
yroi
d: G
rave
s di
seas
eFa
t ad
her
ence
to
mu
scle
or
scle
ra
Hig
h m
yopi
a w
ith
lar
ge
Con
gen
ital
cra
nia
l n
erve
abe
rran
t (e
.g.,
afte
r st
rabi
smu
s su
rger
y,
post
erio
r st
aph
ylom
ain
ner
vati
onre
tin
al d
etac
hm
ent
surg
ery,
(D
uan
e’s
syn
drom
e)or
per
iocu
lar
trau
ma)
Con
gen
ital
fibr
osis
syn
drom
eC
onge
nit
al fi
brot
ic b
and
Orb
ital
tu
mor
cau
sin
gC
onge
nit
al e
ctop
ic e
xtra
ocu
lar
mu
scle
m
ass
effe
ct o
n g
lobe
inse
rtio
n a
nd
or p
ull
ey
mov
emen
t(c
ran
iosy
nos
tosi
s, e
xtor
ted
orbi
t)C
onge
nit
al B
row
n’s
syn
drom
e: i
nel
asti
c A
cqu
ired
Bro
wn
’s s
yndr
ome:
G
lau
com
a ex
plan
t w
ith
Iatr
ogen
ic d
ispl
aced
mu
scle
in
sert
ion
;SO
mu
scle
ten
don
sc
arri
ng
or i
nfl
amm
atio
n
larg
e bl
eb c
ausi
ng
anti
elev
atio
n a
fter
in
feri
or o
bliq
ue
com
plex
(see
Ch
apte
r 9)
arou
nd
the
troc
hle
am
ass
effe
ct o
n g
lobe
ante
rior
izat
ion
wit
h J
-def
orm
ity,
an
d m
ovem
ent
or d
ispl
ace
lim
ited
dep
ress
ion
aft
er a
nte
rior
SO
ten
don
(acq
uir
eddi
spla
cem
ent
of S
O t
endo
n b
y B
row
n’s
syn
drom
e)re
tin
al b
and
En
trap
ped
mu
scle
aft
er o
rbit
al f
ract
ure
(in
feri
or r
ectu
s m
ost
com
mon
)Fi
bros
is a
fter
loc
al a
nes
thet
ic i
nje
ctio
n
Hig
h m
yopi
a w
ith
lar
ge p
oste
rior
in
to a
mu
scle
(in
feri
or m
ost
com
mon
)st
aph
ylom
a an
d sl
ippa
ge o
f la
tera
l re
ctu
s be
low
glo
beFa
t ad
her
ence
to
extr
aocu
lar
mu
scle
(e.g
., af
ter
stra
bism
us
surg
ery,
ret
inal
su
rger
y,or
per
iocu
lar
trau
ma)
Mon
ocu
lar
elev
atio
n d
efici
t sy
ndr
ome
cau
sed
by a
fibr
otic
in
feri
or r
ectu
s
SO, s
upe
rior
obl
iqu
e.
adduction and limits depression in the field of action of the supe-rior oblique.20 A rare example of restriction caused by a displacedmuscle–pulley was reported by Oh et al.83 They described apatient with limitation of elevation in adduction, or a pseudo-Brown’s syndrome, caused by a congenitally inferiorly displacedlateral rectus muscle and its pulley. These authors hypothesizedthat the infraplaced lateral rectus muscle and pulley act to pullthe eye down, limiting elevation on adduction. Iatrogenic dis-placement of extraocular muscles during strabismus surgery canalso cause limited eye movements. Inferior oblique muscle anteriorization anterior to the inferior rectus insertion can alsocause active restriction and limited elevation (see Chapter 2, Fig. 2–17).15,43,114,135 In some cases, restriction and paresis coexist,such as with paretic lateral rectus muscle and secondary con-tracture of its antagonist medial rectus muscle. It is importantto diagnoses the cause of limited ductions to formulate an effec-tive surgical plan. The next section describes methods for diag-nosing extraocular muscle paresis and ocular restriction.
Diagnosing Restriction Versus ParesisThe principal diagnostic tests that differentiate paresis fromrestriction include saccadic velocity measurements, forced duc-tions, and forced-generation test. Other signs influencing diag-nosis include intraocular pressure changes in various fields ofgaze and lid fissure changes in sidegaze.
SACCADIC VELOCITY MEASUREMENTS
Saccadic velocity measurements can help differentiate restric-tion from paresis by observation, without touching the eye.Therefore, this method is useful in young children as well asadults. Saccadic movements are fast, jerk-like eye movementsthat require normal rectus muscle function. The rectus musclesare the major movers of the eye and are responsible for saccadiceye movements. The presence of a saccadic eye movement indi-cates normal rectus muscle function whereas the inability tostimulate a saccade suggests a rectus muscle palsy. A pareticrectus muscle does not have the power to generate a saccadiceye movement, and the eye drifts slowly to the intended field of gaze. Strabismus associated with limited ductions and diminished saccadic velocity is caused by a rectus muscleparesis, not an oblique muscle palsy.
chapter 10: complex strabismus 327
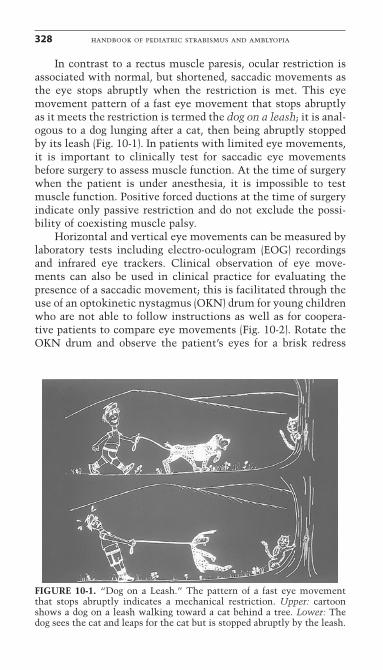
In contrast to a rectus muscle paresis, ocular restriction isassociated with normal, but shortened, saccadic movements asthe eye stops abruptly when the restriction is met. This eyemovement pattern of a fast eye movement that stops abruptlyas it meets the restriction is termed the dog on a leash; it is anal-ogous to a dog lunging after a cat, then being abruptly stoppedby its leash (Fig. 10-1). In patients with limited eye movements,it is important to clinically test for saccadic eye movementsbefore surgery to assess muscle function. At the time of surgerywhen the patient is under anesthesia, it is impossible to testmuscle function. Positive forced ductions at the time of surgeryindicate only passive restriction and do not exclude the possi-bility of coexisting muscle palsy.
Horizontal and vertical eye movements can be measured bylaboratory tests including electro-oculogram (EOG) recordingsand infrared eye trackers. Clinical observation of eye move-ments can also be used in clinical practice for evaluating thepresence of a saccadic movement; this is facilitated through theuse of an optokinetic nystagmus (OKN) drum for young childrenwho are not able to follow instructions as well as for coopera-tive patients to compare eye movements (Fig. 10-2). Rotate theOKN drum and observe the patient’s eyes for a brisk redress
328 handbook of pediatric strabismus and amblyopia
FIGURE 10-1. “Dog on a Leash.” The pattern of a fast eye movementthat stops abruptly indicates a mechanical restriction. Upper: cartoonshows a dog on a leash walking toward a cat behind a tree. Lower: Thedog sees the cat and leaps for the cat but is stopped abruptly by the leash.
movement opposite to the direction of the drum rotation.Compare eye to eye and look for asymmetry of the OKNresponse. An inability to generate a saccadic movement indi-cates a paretic rectus muscle.
FORCED DUCTIONS
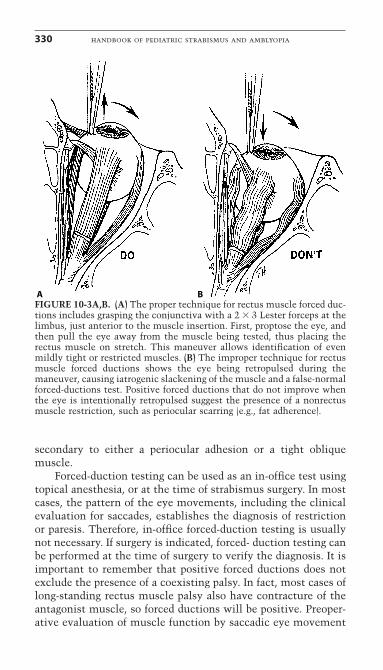
Forced ductions identify the presence of a mechanical restric-tion to ocular rotation; these are performed by grasping the eyewith a forceps and then passively moving the eye into the fieldof limited ocular rotation. If the eye shows a resistance to rota-tion with the forceps (positive forced ductions), then there is amechanical restriction. When performing forced ductions forpossible rectus muscle restriction, proptose the eye to stretchthe rectus muscles. This maneuver will allow identification ofrestriction caused by a tight rectus muscle. If the examiner inad-vertently retropulses the eye, the rectus muscles slacken andproduce a negative forced-duction test, even if the rectus muscleis tight (Fig. 10-3). The opposite holds true for oblique muscleforced ductions, because retropulsing the eye will stretch theoblique muscles and accentuate a tight oblique muscle. If arestriction is worse with retropulsion of the eye, then the res-triction is not caused by a tight rectus muscle but, instead, is
chapter 10: complex strabismus 329
FIGURE 10-2. Photograph of a child being examined with an optokineticnystagmus (OKN) drum. The saccadic movement will be in the directionopposite to the drum rotation. This is a good clinical method to estimateif a saccade is present.
secondary to either a periocular adhesion or a tight obliquemuscle.
Forced-duction testing can be used as an in-office test usingtopical anesthesia, or at the time of strabismus surgery. In mostcases, the pattern of the eye movements, including the clinicalevaluation for saccades, establishes the diagnosis of restrictionor paresis. Therefore, in-office forced-duction testing is usuallynot necessary. If surgery is indicated, forced- duction testing canbe performed at the time of surgery to verify the diagnosis. It isimportant to remember that positive forced ductions does notexclude the presence of a coexisting palsy. In fact, most cases oflong-standing rectus muscle palsy also have contracture of theantagonist muscle, so forced ductions will be positive. Preoper-ative evaluation of muscle function by saccadic eye movement
330 handbook of pediatric strabismus and amblyopia
A BFIGURE 10-3A,B. (A) The proper technique for rectus muscle forced duc-tions includes grasping the conjunctiva with a 2 � 3 Lester forceps at thelimbus, just anterior to the muscle insertion. First, proptose the eye, andthen pull the eye away from the muscle being tested, thus placing therectus muscle on stretch. This maneuver allows identification of evenmildly tight or restricted muscles. (B) The improper technique for rectusmuscle forced ductions shows the eye being retropulsed during themaneuver, causing iatrogenic slackening of the muscle and a false-normalforced-ductions test. Positive forced ductions that do not improve whenthe eye is intentionally retropulsed suggest the presence of a nonrectusmuscle restriction, such as periocular scarring (e.g., fat adherence).
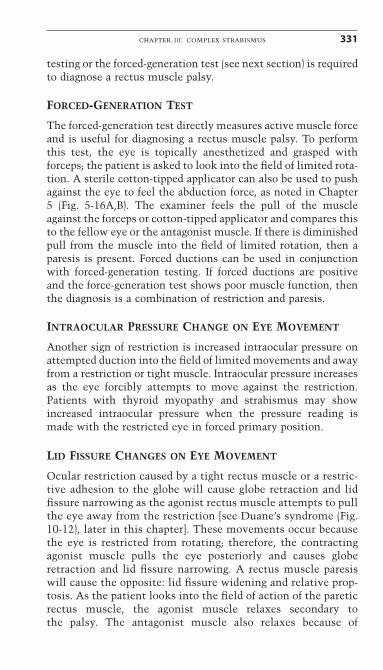
testing or the forced-generation test (see next section) is requiredto diagnose a rectus muscle palsy.
FORCED-GENERATION TEST
The forced-generation test directly measures active muscle forceand is useful for diagnosing a rectus muscle palsy. To performthis test, the eye is topically anesthetized and grasped withforceps; the patient is asked to look into the field of limited rota-tion. A sterile cotton-tipped applicator can also be used to pushagainst the eye to feel the abduction force, as noted in Chapter5 (Fig. 5-16A,B). The examiner feels the pull of the muscleagainst the forceps or cotton-tipped applicator and compares thisto the fellow eye or the antagonist muscle. If there is diminishedpull from the muscle into the field of limited rotation, then aparesis is present. Forced ductions can be used in conjunctionwith forced-generation testing. If forced ductions are positiveand the force-generation test shows poor muscle function, thenthe diagnosis is a combination of restriction and paresis.
INTRAOCULAR PRESSURE CHANGE ON EYE MOVEMENT
Another sign of restriction is increased intraocular pressure onattempted duction into the field of limited movements and awayfrom a restriction or tight muscle. Intraocular pressure increasesas the eye forcibly attempts to move against the restriction.Patients with thyroid myopathy and strabismus may showincreased intraocular pressure when the pressure reading ismade with the restricted eye in forced primary position.
LID FISSURE CHANGES ON EYE MOVEMENT
Ocular restriction caused by a tight rectus muscle or a restric-tive adhesion to the globe will cause globe retraction and lidfissure narrowing as the agonist rectus muscle attempts to pullthe eye away from the restriction [see Duane’s syndrome (Fig.10-12), later in this chapter]. These movements occur becausethe eye is restricted from rotating; therefore, the contractingagonist muscle pulls the eye posteriorly and causes globeretraction and lid fissure narrowing. A rectus muscle paresiswill cause the opposite: lid fissure widening and relative prop-tosis. As the patient looks into the field of action of the pareticrectus muscle, the agonist muscle relaxes secondary to the palsy. The antagonist muscle also relaxes because of
chapter 10: complex strabismus 331
Sherrington’s law, and pressure from orbital fat pushes the eye forward. A patient with a sixth nerve palsy, for example,will show lid fissure widening on attempted abduction (see Fig. 10-10, later in this chapter). This change occurs becausethe medial rectus muscle relaxes on attempted abduction(Sherrington’s law) and, along with the paretic lateral rectus, itis loose; therefore, the posterior pressure of the orbital fatpushes the eye forward.
MANAGEMENT OF INCOMITANTSTRABISMUS: GENERAL PRINCIPLES
Management begins with understanding why the deviation isincomitant. For example, if an incomitant strabismus is associ-ated with severe limitation of ductions, determine whether thelimitation is caused by restriction or paresis. If a significantrestriction is the cause of limited adduction, then one mustrelease the restriction. If severe limitation of ocular rotations issecondary to poor rectus muscle function, then one has toaddress the muscle weakness.
In cases in which the incomitance is associated with littleor no limitation of eye movements, the incomitance can bemanaged by operating on the good eye to match ocular rotationsof the deviated eye. Determine where the deviation is greatestand operate to achieve alignment in primary position whilereducing the incomitance. Use this strategy: recession proce-dures have their greatest effect in the field of action of therecessed muscle, and resections produce a leash with the great-est effect occurring when the eye rotates away from the resectedmuscle (see Chapter 11). Recessing the right medial rectusmuscle will produce an exodeviation greater in leftgaze andalmost no effect in rightgaze, and resecting the right lateralrectus muscle produces an exodeviation that increases in left-gaze. With this strategy in mind, determine what surgery wouldbest correct the following strabismus.
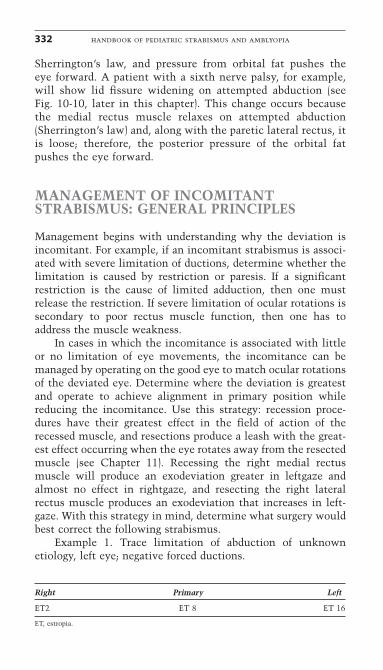
Example 1. Trace limitation of abduction of unknown etiology, left eye; negative forced ductions.
Right Primary Left
ET2 ET 8 ET 16
ET, estropia.
332 handbook of pediatric strabismus and amblyopia
The surgical plan is to recess the right medial rectus muscle 4.0to 5.0mm, as this will match the right medial rectus muscle toits underacting yoke muscle, the left lateral rectus muscle.Weakening the right medial rectus muscle will slightly reduceadduction but will not affect abduction; this reduces the largeesotropia in leftgaze without causing an exotropia in rightgaze.Do not recess the left medial rectus muscle because this surgeryhas little effect in leftgaze where the esotropia is largest and willproduce an exo-deviation in rightgaze. Also, avoid a left lateralrectus resection as this will not strengthen the weak lateralrectus. Instead, it will cause a tight lateral rectus muscle thatalso has little effect in leftgaze where the esotropia is greatestand will cause an exodeviation in rightgaze. For an incomitantesodeviation that is greater than 10 to 15 prism diopters (PD) inprimary position and increases in leftgaze, two-muscle surgerywill be required to correct the deviation in primary position.Consider asymmetrical bilateral medial rectus recessions, witha larger recession on the right medial rectus muscle.
The Faden operation has also been suggested to reduceincomitance. Adding a Faden to a recession of the medial rectusmuscle increases the weakening effect of the recession in adduc-tion and improves the incomitance. The use of the Faden is con-troversial. If it is used, it is most effective on the medial rectusmuscle, as the medial rectus has the shortest arc of contact. The-oretically, the Faden weakens the muscle mostly in the field ofaction of the muscle, with little effect in primary position; there-fore, it may be helpful in reducing incomitance (see Chapter 11).A report on the effect of the Faden procedure on the medialrectus muscles in reducing the AC/A ratio concluded there wasa beneficial effect; however, the table of data in this studyshowed no change of the AC/A ratio. It is likely the Faden pro-cedure has little effect, except in extreme fields of gaze.35
If the limitation is severe, recessing the yoke muscle tomatch the limitation will not work, as operating on the goodeye will not improve the ability of an eye with limited ductionsto come to midline. In these cases of moderate to severe limi-tation of ductions, one must release the restriction or, in the caseof a palsy, transpose muscle forces to bring the eye to midline.Recessing the contralateral yoke muscle only works if the lim-itation is slight, such as a trace to �1 limitation of ductions.
Vertical incomitance can be treated with the same strategyas described previously for horizontal strabismus. One specialsituation that occurs with Grave’s disease and floor fractures is
chapter 10: complex strabismus 333
that of a patient with orthotropia in primary position and ahypotropia in upgaze secondary to a tight inferior rectus muscle.In this case, recess both inferior rectus muscles, with a largerrecession on the side with the restriction. The diagnosis andmanagement of specific types of restrictive and paralytic stra-bismus follow.
SPECIFIC TYPES OF RESTRICTIVESTRABISMUS
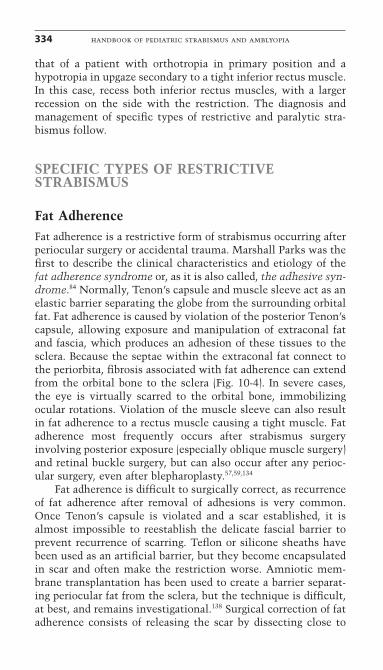
Fat AdherenceFat adherence is a restrictive form of strabismus occurring afterperiocular surgery or accidental trauma. Marshall Parks was thefirst to describe the clinical characteristics and etiology of thefat adherence syndrome or, as it is also called, the adhesive syn-drome.84 Normally, Tenon’s capsule and muscle sleeve act as anelastic barrier separating the globe from the surrounding orbitalfat. Fat adherence is caused by violation of the posterior Tenon’scapsule, allowing exposure and manipulation of extraconal fatand fascia, which produces an adhesion of these tissues to thesclera. Because the septae within the extraconal fat connect tothe periorbita, fibrosis associated with fat adherence can extendfrom the orbital bone to the sclera (Fig. 10-4). In severe cases,the eye is virtually scarred to the orbital bone, immobilizingocular rotations. Violation of the muscle sleeve can also resultin fat adherence to a rectus muscle causing a tight muscle. Fatadherence most frequently occurs after strabismus surgeryinvolving posterior exposure (especially oblique muscle surgery)and retinal buckle surgery, but can also occur after any perioc-ular surgery, even after blepharoplasty.57,59,134
Fat adherence is difficult to surgically correct, as recurrenceof fat adherence after removal of adhesions is very common.Once Tenon’s capsule is violated and a scar established, it isalmost impossible to reestablish the delicate fascial barrier toprevent recurrence of scarring. Teflon or silicone sheaths havebeen used as an artificial barrier, but they become encapsulatedin scar and often make the restriction worse. Amniotic mem-brane transplantation has been used to create a barrier separat-ing periocular fat from the sclera, but the technique is difficult,at best, and remains investigational.138 Surgical correction of fatadherence consists of releasing the scar by dissecting close to
334 handbook of pediatric strabismus and amblyopia
sclera and removing the adhesions without repenetrating theorbital fat. (Perform forced ductions after freeing adhesions toevaluate improvement of the restriction.) Dissect carefully withdirect visualization, as posterior dissections can be dangerous.
chapter 10: complex strabismus 335
A
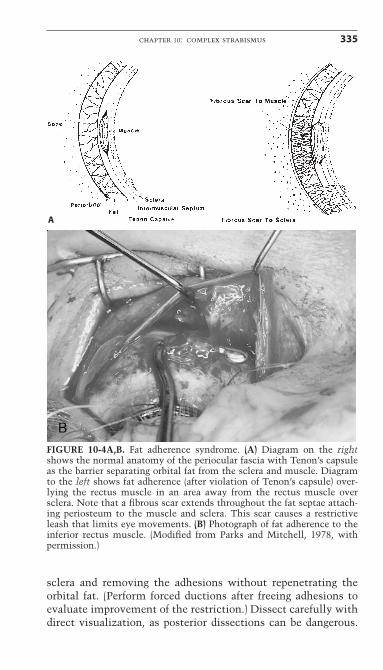
FIGURE 10-4A,B. Fat adherence syndrome. (A) Diagram on the rightshows the normal anatomy of the periocular fascia with Tenon’s capsuleas the barrier separating orbital fat from the sclera and muscle. Diagramto the left shows fat adherence (after violation of Tenon’s capsule) over-lying the rectus muscle in an area away from the rectus muscle oversclera. Note that a fibrous scar extends throughout the fat septae attach-ing periosteum to the muscle and sclera. This scar causes a restrictiveleash that limits eye movements. (B) Photograph of fat adherence to theinferior rectus muscle. (Modified from Parks and Mitchell, 1978, with permission.)
Cases of inadvertent optic nerve transection have occurred,although they are rarely reported. If fat and scar are adherent toa rectus muscle, remove a small amount of the anterior scar,then recess the tight muscle en bloc with the scar rather thantrying to dissect all the scar off the muscle. Avoid extensive dis-section of scar off the muscle, as this usually results in furtherfat manipulation and worsening of the adherence. Medical treat-ment with mitomycin-C has not been effective in reducing post-operative fibrosis and may even increase scarring.17 Injection ofperibulbar corticosteroids also fails to prevent postoperativescarring. The best treatment for fat adherence syndrome is prevention: avoid penetration of posterior Tenon’s capsuleduring the initial surgery. During strabismus surgery, performminimal dissection of muscle fascia and, when dissecting,dissect close to the muscle to stay away from surroundingorbital fat. If Tenon’s capsule is inadvertently torn so fat isexposed, cover the exposed fat by repairing the Tenon’s tear with7-0 vicryl suture.
Grave’s OphthalmopathyGrave’s ophthalmopathy is an autoimmune disease associatedwith inflammation of the extraocular muscles. Initially, there isan acute phase during which there is a lymphocytic infiltrationof the extraocular muscles, resulting in extraocular muscleenlargement and proptosis. This active phase usually lastsseveral months to more than a year. Orbital imaging studiesshow thickened extraocular muscles, especially posteriorly. Thesecond phase is a cicatricial phase with quiescence of inflam-mation and secondary contracture of the muscles. All musclesare usually involved, but the inferior rectus and medial rectusare most severely affected.91 Strabismus is caused by tightfibrotic muscles and can develop in both phases but is most pro-nounced in the cicatricial phase. A restrictive hypotropia causedby tight inferior rectus muscles is the most common type of strabismus, followed by esotropia associated with tight medialrectus muscles.
The management of Grave’s ophthalmopathy is carefulobservation during the acute inflammatory phase. Treatmentwith systemic steroids and even external beam radiation may beindicated for severe disease; however, radiation therapy is noteffective for treatment of the strabismus.126 Orbital decompres-sion is indicated for severe proptosis and visual loss associated
336 handbook of pediatric strabismus and amblyopia
with optic nerve compression from inflamed extraocularmuscles. In most cases, it is better to perform strabismus surgeryafter the active phase has subsided and strabismus measure-ments have stabilized. A report on eight patients whose eyeswere operated on during the active phase of thyroid ophthal-mopathy noted that all eight patients achieved successful long-term alignment (�16 months follow-up); however, half thepatients required more than one operation.
Regarding the timing of surgery, strabismus surgery isusually performed after orbital decompression surgery, becauseorbital surgery can alter eye alignment.21,75 The strategy for thetreatment of Grave’s ophthalmopathy strabismus is to releasethe restriction from the tight rectus muscle, with a rectusmuscle recession being the procedure of choice. It is not advis-able to use rectus muscle resections, as this tightens an alreadystiff, inelastic muscle. A right hypotropia less than 15 PD witha tight right inferior rectus muscle can be surgically addressedwith a right inferior rectus recession, with or without anadjustable suture technique (Fig. 10-5).8,68 If the deviation inprimary position is greater than 18 to 20PD with severe restric-tion, recess the tight inferior rectus muscle more than 5.0mmand add a recession of the contralateral superior rectus muscle.As a rule, expect 3PD of vertical correction for each millimeterof vertical rectus muscle recession.135
One common problem with correcting thyroid strabismushas been late overcorrection after inferior rectus recession,which occurs in up to 50% of cases.24,56,80 Initially after surgery,there is a successful result. Then, at 4 to 6 weeks after the infe-rior rectus recession, a consecutive hypertropia on the side ofthe recession occurs, with underaction of the recessed inferiorrectus muscle and ipsilateral lower eyelid retraction.132 R.Friedman suggested that performing asymmetrical bilateral inferior rectus recessions avoids late overcorrection. A report byCruz and Davitt on eight patients who underwent asymmetri-cal bilateral inferior rectus recessions showed no overcorrec-tions; however, 25% of these patients were undercorrected.24
Ludwig has suggested that a stretched scar at the new insertionis the cause of the overcorrection. It is hypothesized that, at 4to 6 weeks after surgery, the absorbable suture loses its strength.The muscle–scleral attachment stretches and causes the tightmuscle to retract posteriorly. This author has now switched tononabsorbable sutures (6-0 Mersiline), and preliminary resultshave been good, even when using an adjustable suture.
chapter 10: complex strabismus 337
338 handbook of pediatric strabismus and amblyopia
A
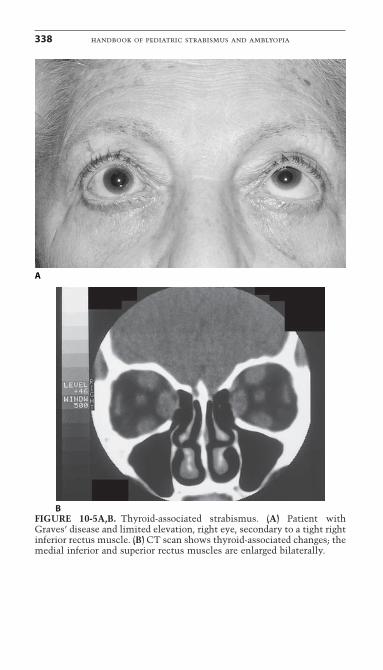
BFIGURE 10-5A,B. Thyroid-associated strabismus. (A) Patient withGraves’ disease and limited elevation, right eye, secondary to a tight rightinferior rectus muscle. (B) CT scan shows thyroid-associated changes; themedial inferior and superior rectus muscles are enlarged bilaterally.
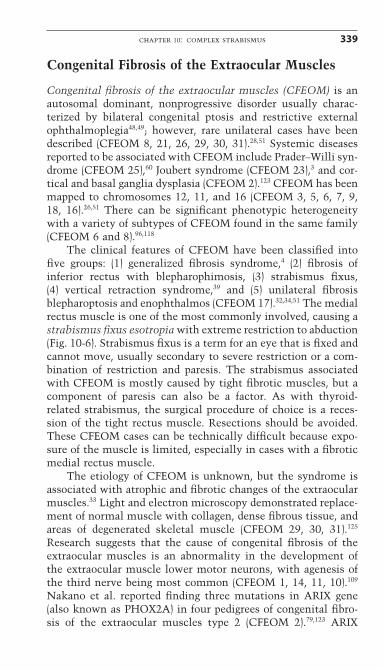
Congenital Fibrosis of the Extraocular Muscles
Congenital fibrosis of the extraocular muscles (CFEOM) is anautosomal dominant, nonprogressive disorder usually charac-terized by bilateral congenital ptosis and restrictive externalophthalmoplegia48,49; however, rare unilateral cases have beendescribed (CFEOM 8, 21, 26, 29, 30, 31).28,51 Systemic diseasesreported to be associated with CFEOM include Prader–Willi syn-drome (CFEOM 25),60 Joubert syndrome (CFEOM 23),3 and cor-tical and basal ganglia dysplasia (CFEOM 2).123 CFEOM has beenmapped to chromosomes 12, 11, and 16 (CFEOM 3, 5, 6, 7, 9,18, 16).26,51 There can be significant phenotypic heterogeneitywith a variety of subtypes of CFEOM found in the same family(CFEOM 6 and 8).96,118
The clinical features of CFEOM have been classified intofive groups: (1) generalized fibrosis syndrome,4 (2) fibrosis of inferior rectus with blepharophimosis, (3) strabismus fixus, (4) vertical retraction syndrome,39 and (5) unilateral fibrosis blepharoptosis and enophthalmos (CFEOM 17).32,34,51 The medialrectus muscle is one of the most commonly involved, causing astrabismus fixus esotropia with extreme restriction to abduction(Fig. 10-6). Strabismus fixus is a term for an eye that is fixed andcannot move, usually secondary to severe restriction or a com-bination of restriction and paresis. The strabismus associatedwith CFEOM is mostly caused by tight fibrotic muscles, but acomponent of paresis can also be a factor. As with thyroid-related strabismus, the surgical procedure of choice is a reces-sion of the tight rectus muscle. Resections should be avoided.These CFEOM cases can be technically difficult because expo-sure of the muscle is limited, especially in cases with a fibroticmedial rectus muscle.
The etiology of CFEOM is unknown, but the syndrome isassociated with atrophic and fibrotic changes of the extraocularmuscles.33 Light and electron microscopy demonstrated replace-ment of normal muscle with collagen, dense fibrous tissue, andareas of degenerated skeletal muscle (CFEOM 29, 30, 31).125
Research suggests that the cause of congenital fibrosis of theextraocular muscles is an abnormality in the development of the extraocular muscle lower motor neurons, with agenesis ofthe third nerve being most common (CFEOM 1, 14, 11, 10).109
Nakano et al. reported finding three mutations in ARIX gene(also known as PHOX2A) in four pedigrees of congenital fibro-sis of the extraocular muscles type 2 (CFEOM 2).79,123 ARIX
chapter 10: complex strabismus 339
encodes a homeodomain transcription factor protein shown tobe required for development of cranial nerves III and IV in mouseand zebrafish. These findings confirm the hypothesis thatCFEOM 2 results from the abnormal development of cranialnerves III and IV and emphasize a critical role for ARIX in thedevelopment of these midbrain motor nuclei.37,79
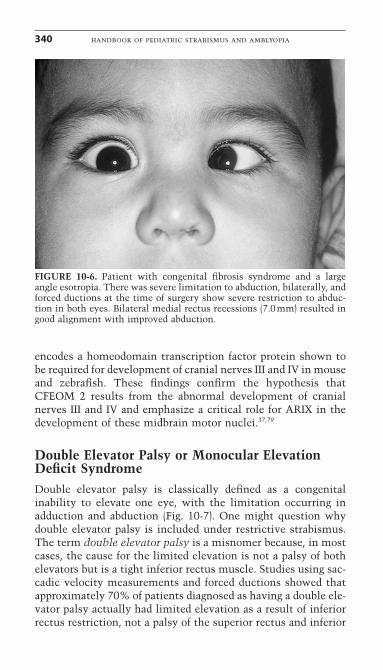
Double Elevator Palsy or Monocular ElevationDeficit SyndromeDouble elevator palsy is classically defined as a congenitalinability to elevate one eye, with the limitation occurring inadduction and abduction (Fig. 10-7). One might question whydouble elevator palsy is included under restrictive strabismus.The term double elevator palsy is a misnomer because, in mostcases, the cause for the limited elevation is not a palsy of bothelevators but is a tight inferior rectus muscle. Studies using sac-cadic velocity measurements and forced ductions showed thatapproximately 70% of patients diagnosed as having a double ele-vator palsy actually had limited elevation as a result of inferiorrectus restriction, not a palsy of the superior rectus and inferior
340 handbook of pediatric strabismus and amblyopia
FIGURE 10-6. Patient with congenital fibrosis syndrome and a largeangle esotropia. There was severe limitation to abduction, bilaterally, andforced ductions at the time of surgery show severe restriction to abduc-tion in both eyes. Bilateral medial rectus recessions (7.0mm) resulted ingood alignment with improved abduction.
oblique muscles.73,106 A more descriptive term now used ismonocular elevation deficit syndrome (MED). MED may bemistaken for Brown’s syndrome, although the limited elevationis worse in adduction than abduction in the latter. Patients withMED present with a hypotropia, a chin elevation, and, often, anipsilateral ptosis. True congenital ptosis is present in 25% ofcases whereas pseudo-ptosis may occur in almost all patientswith a large hypotropia.2 In those cases with a true double ele-vator palsy and a lack of an upgaze saccade, forced ductions attime of surgery usually reveal a tight inferior rectus musclecoexisting with the superior rectus palsy.
An interesting finding in approximately 25% of patientswith double elevator palsy and congenital ptosis is the MarcusGunn jaw-winking phenomenon.133 This association indicates acongenital misdirection syndrome involving the oculomotornerve. It is possible that, as with congenital fibrosis syndrome,the cause of the tight inferior rectus and, in some cases, supe-rior rectus and inferior oblique palsy, is abnormal developmentof cranial nerves (including the oculomotor nerve) with second-ary muscle fibrosis.
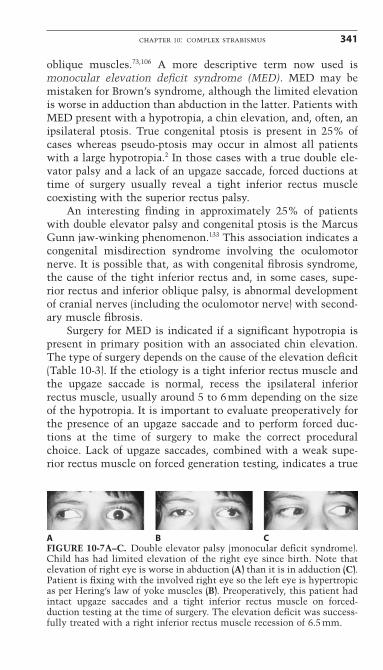
Surgery for MED is indicated if a significant hypotropia ispresent in primary position with an associated chin elevation.The type of surgery depends on the cause of the elevation deficit(Table 10-3). If the etiology is a tight inferior rectus muscle andthe upgaze saccade is normal, recess the ipsilateral inferiorrectus muscle, usually around 5 to 6mm depending on the sizeof the hypotropia. It is important to evaluate preoperatively forthe presence of an upgaze saccade and to perform forced duc-tions at the time of surgery to make the correct proceduralchoice. Lack of upgaze saccades, combined with a weak supe-rior rectus muscle on forced generation testing, indicates a true
chapter 10: complex strabismus 341
A B CFIGURE 10-7A–C. Double elevator palsy (monocular deficit syndrome).Child has had limited elevation of the right eye since birth. Note thatelevation of right eye is worse in abduction (A) than it is in adduction (C).Patient is fixing with the involved right eye so the left eye is hypertropicas per Hering’s law of yoke muscles (B). Preoperatively, this patient hadintact upgaze saccades and a tight inferior rectus muscle on forced-duction testing at the time of surgery. The elevation deficit was success-fully treated with a right inferior rectus muscle recession of 6.5mm.
double elevator palsy. In these cases, a recession of the ipsilat-eral inferior rectus will not correct the hypotropia. Treatment ofa true double elevator palsy with weak superior rectus muscleis to perform a transposition of the ipsilateral medial and lateralrectus muscles up to the superior rectus muscle. In patients withthe superior rectus palsy type of MED, forced ductions are oftenpositive, and the ipsilateral inferior rectus muscle should berecessed. This author prefers the partial tendon transfer (Hummelsheim) instead of the full-tendon transposition (Knapp)to avoid the possible complication of anterior segment ischemiathat can occur up to 20 years after strabismus surgery. In severecases of hypotropia over 15PD, consider adding a recession ofthe contralateral superior rectus muscle.
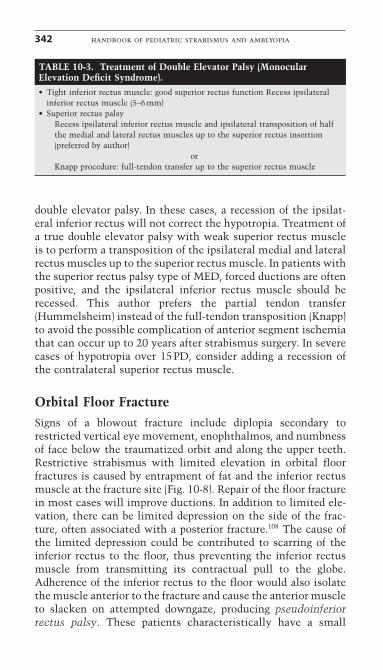
Orbital Floor FractureSigns of a blowout fracture include diplopia secondary torestricted vertical eye movement, enophthalmos, and numbnessof face below the traumatized orbit and along the upper teeth.Restrictive strabismus with limited elevation in orbital floorfractures is caused by entrapment of fat and the inferior rectusmuscle at the fracture site (Fig. 10-8). Repair of the floor fracturein most cases will improve ductions. In addition to limited ele-vation, there can be limited depression on the side of the frac-ture, often associated with a posterior fracture.108 The cause ofthe limited depression could be contributed to scarring of theinferior rectus to the floor, thus preventing the inferior rectusmuscle from transmitting its contractual pull to the globe.Adherence of the inferior rectus to the floor would also isolatethe muscle anterior to the fracture and cause the anterior muscleto slacken on attempted downgaze, producing pseudoinferiorrectus palsy. These patients characteristically have a small
342 handbook of pediatric strabismus and amblyopia
TABLE 10-3. Treatment of Double Elevator Palsy (MonocularElevation Deficit Syndrome).• Tight inferior rectus muscle: good superior rectus function Recess ipsilateral
inferior rectus muscle (5–6 mm)• Superior rectus palsy
Recess ipsilateral inferior rectus muscle and ipsilateral transposition of halfthe medial and lateral rectus muscles up to the superior rectus insertion(preferred by author)
orKnapp procedure: full-tendon transfer up to the superior rectus muscle
hypertropia in primary position, underaction of the inferiorrectus muscle, and a large hypertropia in downgaze.
The key to the diagnosis of a pseudoinferior rectus palsy isnormal inferior rectus muscle function and normal saccadeswhen the eye moves from upgaze to primary position, with infe-rior rectus muscle weakness and slow ocular movements fromprimary position to downgaze. Treatment of pseudoinferiorrectus palsy is to repair the floor fracture. If this does not relievesymptoms, then strabismus surgery is indicated. This author hasfound that a small (3–4 mm) ipsilateral inferior rectus muscletightening procedure (Wright plication or resection) helps toeliminate the anterior muscle slack. A contralateral inferiorrectus recession works well and produces only a slight limita-tion of elevation. If the muscle is captured in a trap-door frac-ture, direct damage to the inferior rectus muscle occurs and can truly weaken the inferior rectus muscles. Small trap-doorfloor fractures can pinch and strangle the inferior rectus muscle,causing necrosis and muscle damage.11 Because of the potentialfor permanent damage, some advocate immediate repair withinthe first few days if there is imaging evidence that the inferiorrectus is entrapped.29 Strabismus surgery should be performedafter reconstructive orbital surgery. If orbital reconstruction is not indicated, and the patient has persistent diplopia 4 to 8 weeks after the trauma, then strabismus surgery is indicated.The strabismus surgical plan depends on the pattern of the strabismus. Table 10-4 lists patterns of strabismus and theirassociated treatment.
Myotoxic Effect of Local AnestheticsInjection of local anesthetics such as lidocaine and marcaineinto an extraocular muscle can result in myotoxic damage to themuscle and cause strabismus.19,40,46 Elderly patients are espe-cially susceptible to the myotoxic effects of local anesthetics.Immediately after the injection of a local anesthetic into anextraocular muscle, there is an acute paresis of the muscle thatlasts for one to several days. Over the next few weeks, localizedsegmental intramuscular fibrosis occurs secondary to localmyotoxicity of the anesthetic. The fibrosis results in a tight andcontracted muscle. What is particularly interesting is that, insome cases, the injected muscle overacts, producing a deviationthat increases in the field of action of the injected muscle.8,13
This deviation is in contrast to the restriction pattern usually
chapter 10: complex strabismus 343
344 handbook of pediatric strabismus and amblyopia
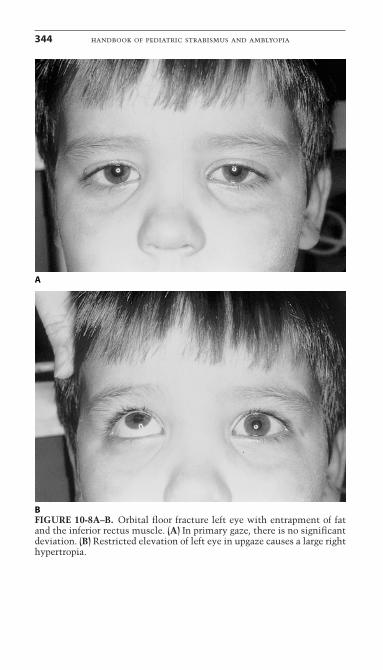
A
BFIGURE 10-8A–B. Orbital floor fracture left eye with entrapment of fatand the inferior rectus muscle. (A) In primary gaze, there is no significantdeviation. (B) Restricted elevation of left eye in upgaze causes a large righthypertropia.
chapter 10: complex strabismus 345
expected with a tight muscle, where the deviation is greatest inthe gaze opposite to the field of the muscle’s action. The causeof the muscle overaction is thought to be secondary to intra-muscular fibrosis, with stretching of the Z-bands and enhancing
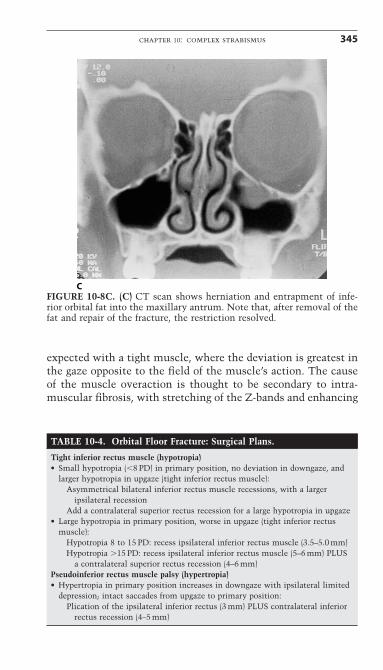
CFIGURE 10-8C. (C) CT scan shows herniation and entrapment of infe-rior orbital fat into the maxillary antrum. Note that, after removal of thefat and repair of the fracture, the restriction resolved.
TABLE 10-4. Orbital Floor Fracture: Surgical Plans.
Tight inferior rectus muscle (hypotropia)• Small hypotropia (�8 PD) in primary position, no deviation in downgaze, and
larger hypotropia in upgaze (tight inferior rectus muscle):Asymmetrical bilateral inferior rectus muscle recessions, with a larger
ipsilateral recessionAdd a contralateral superior rectus recession for a large hypotropia in upgaze
• Large hypotropia in primary position, worse in upgaze (tight inferior rectusmuscle):
Hypotropia 8 to 15 PD: recess ipsilateral inferior rectus muscle (3.5–5.0 mm)Hypotropia �15 PD: recess ipsilateral inferior rectus muscle (5–6 mm) PLUS
a contralateral superior rectus recession (4–6 mm)Pseudoinferior rectus muscle palsy (hypertropia)• Hypertropia in primary position increases in downgaze with ipsilateral limited
depression; intact saccades from upgaze to primary position:Plication of the ipsilateral inferior rectus (3 mm) PLUS contralateral inferior
rectus recession (4–5 mm)
the action and myosin interaction.19 The fibrosis acts to stretchthe muscle fibers that subsequently increases their force, per theStarling’s length tension curve.19 For example, inadvertent injec-tion of the inferior rectus muscle associated with a retrobulbarinjection of anesthetic initially results in an ipsilateral hyper-tropia because of an inferior rectus paresis. Over a few weeks,this changes into an ipsilateral hypotropia with overaction of the inferior rectus muscle, resulting in the hypertropia beinggreatest in downgaze.
Any of the extraocular muscles can be infiltrated during aretrobulbar or peribulbar injection of local anesthetics, with thesuperior and inferior rectus muscles most commonly affected.One of the findings is segmental enlargement of the injectedmuscle seen on orbital imaging. Hamed and Mancuso46 reportedon eight patients with an ipsilateral hypotropia after a retrobul-bar injection of anesthetic, with three patients showing seg-mental enlargement of the inferior rectus muscle. The treatmentis to recess the tight or overacting muscle. This method has pro-duced excellent results, especially in the cases involving anoveracting injected muscle, with the deviation larger in the fieldof action of the muscle. One can help prevent intramuscularinjection injury by injecting into the orbital quadrant away fromthe extraocular muscles, using a blunt cannula and limitinganesthetic volume. The incidence of strabismus after cataractsurgery has diminished dramatically since the widespread use oftopical anesthesia during surgery.
Strabismus After Retinal SurgeryStrabismus can occur virtually after every known retinal surgi-cal procedure.38,57,71,72,103,111,114 The strabismus is usually tran-sient; however, persistent strabismus occurs in approximately7% of scleral buckling procedures.71,117 Common causes of stra-bismus after retinal detachment surgery include fat adherenceand restriction, a lost or slipped muscle, a displaced superioroblique tendon, a large explant under a rectus muscle, andectopic fovea.38,47,57,85,110 Other causes of strabismus after retinalsurgery include patients with preexisting strabismus before theretinal surgery who then experience sensory strabismus sec-ondary to loss of vision.92,130 Of all the causes of persistentrestriction after retinal detachment surgery, fat adherence andperiocular scarring is by far the most common and most diffi-cult to treat.1,57,134 Fat adherence is difficult to treat because there
346 handbook of pediatric strabismus and amblyopia
is no synthetic substitute to recreate the natural boundarybetween the orbital fat and the eye and muscle once Tenon’scapsule is violated.
Occasionally, a lost muscle is associated with postretinalsurgery, as can occur when the traction sutures around themuscle are pulled to gain posterior exposure during the retinalsurgery. In elderly patients, the muscle is relatively weak, andoverzealous traction on the rectus muscle can result in a split-ting of the muscle; this has been termed pulled-in-two syn-drome (PITS). Spontaneous disinsertion and posterior slippage of a rectus muscle behind an encircling buckle can also occur,without removal of the muscle at the time of retinal surgery.47,57
In these cases, the silicone band will cheese-wire through themuscle insertion over several months postoperatively, resultingin late slippage of the muscle behind the buckle and causing anunderaction of the slipped muscle. The slipped rectus musclecan almost always be found attached to sclera at the posterioredge of the encircling buckle or connected to sclera by a pseudo-tendon. Appropriate treatment is to advance the muscle andreattach the muscle with nonabsorbable suture.
Another cause for strabismus after retinal surgery is anoblique muscle that has been displaced anteriorly by an encir-cling band.57,72 Placement of the band behind the superioroblique tendon pulls the superior oblique tendon anteriorly tothe nasal aspect of the superior rectus insertion. The superioroblique tendon now inserts at the nasal side of the superiorrectus insertion, anterior to the equator. The new anterior inser-tion of the superior oblique tendon changes the action of thesuperior oblique muscle from a depressor to an elevator. Thesepatients typically present with a hypertropia and limitation ofdepression of the involved eye. Forced ductions, however, showrelatively mild restriction to depression as compared to the lim-itation on ductions and versions. Treatment is to release theentrapped superior oblique tendon from the buckle or, if thereis severe scarring, perform a superior oblique tenotomy. If the hypertropia is greater than 5PD in primary position, alsoperform a recession of the contralateral inferior rectus muscle(consider adjustable suture). The inferior oblique muscle canalso be entrapped by an encircling element.57 In this case, theelement is passed behind, or splits, the inferior oblique muscle.When the band is tied in place, the muscle is pulled anteriorly,resulting in a hypotropia and excyclotropia. The hypotropiaoccurs because the inferior oblique is displaced anteriorly to the
chapter 10: complex strabismus 347
equator, pulling the front of the eye down. The excyclotropia iscaused by the increased tension on the inferior oblique muscle.Torsional diplopia after retinal surgery is not always associatedwith an entrapped oblique muscle.23 Metz and Norris found twoof four patients with torsional diplopia after retinal surgery tohave no identifiable abnormality of the oblique muscle.72 Thecomplications of oblique muscle entrapments can be diminishedby passing the encircling elements anteriorly, just behind therectus insertions. Extreme posterior passage of the muscle hookmay result in inadvertent hooking of an oblique muscle, espe-cially when working on the superior rectus and lateral rectusmuscles.
The placement of a retinal explant sponge or buckle is oftenidentified as a primary cause for strabismus after retinal surgery.Transient strabismus after a retinal encircling procedure is fre-quent, occurring in approximately 20% of cases. In our experi-ence, however, a retinal encircling element by itself rarelycauses persistent strabismus. Persistent strabismus after retinalsurgery usually results from secondary scarring or a displacedmuscle, as stated previously.78 Infrequently, however, a retinalexplant may be the primary cause of restriction; this occurswhen a large explant is placed directly under a rectus muscle.The explant causes the muscle to deviate from its normalcourse, thus tightening the muscle. For example, a large retinalsponge placed directly under the medial rectus will cause a tight-ening of the medial rectus, as the medial rectus courses over thelarge sponge and produces an esotropia. Low-profile encirclingelements, such as 240 bands that indent the sclera, do not inter-fere with the course of the rectus muscle and, therefore, do notproduce strabismus.
Foveal ectopia occurs in association with macular pucker,peeling of the epiretinal membrane, and retinal translocationsurgery. Acquired foveal ectopia produces an interesting type ofstrabismus and diplopia. These patients will observe that objectsin the central visual field appear double, with one image beingdistorted by metamorphosia. Objects in the peripheral field,however, will often be fused, as the peripheral retina may notbe involved with the ectopia. Thus, patients who undergo mem-brane peeling for a macular pucker may experience postopera-tive diplopia because of foveal ectopia. The image disparitiestend to be small with this condition, and prism glasses have beenfound to be effective in treating this problem.
348 handbook of pediatric strabismus and amblyopia
Retinal translocation surgery can result in severe torsionaldiplopia that prisms cannot correct. Instead, oblique musclesurgery is required to treat the problem.38 Extorsion is inducedfrom macular inferior translocation, and intorsion is secondaryto superior macular translocation. Extorsion can be corrected bya large Harada–Ito procedure, possibly with an inferior obliqueweakening procedure, whereas intorsion can be corrected witha weakening surgery of the superior oblique muscle, perhapswith a tuck of the inferior oblique muscle. Vertical offset of therectus muscle can also change torsion, but one must considerthe risk of anterior segment ischemia in this group of patients.
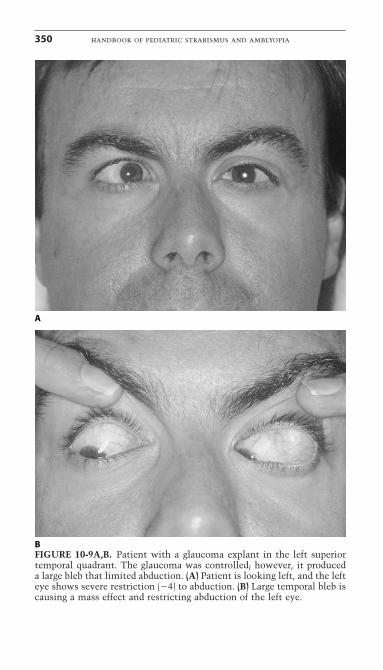
Glaucoma Explants and StrabismusThe incidence of strabismus after glaucoma explant surgeryranges from 10% to 70%, depending on the study.7,90,112 Thecause of the strabismus is, for the most part, the large blebcreated by the glaucoma explant. Strabismus associated with alarge filtering bleb may be caused by the following mechanisms:(1) orbital mass, which displaces the eye (Fig. 10-9); (2) a massdirectly under a muscle or tendon; or (3) scarring or adhesionssecondary to the surgical dissection during placement of theglaucoma explant. The old Baerveldt implant had been associ-ated with the highest incidence of strabismus; however, modi-fications of the Baerveldt implant (fenestrated Baerveldt) havereduced the bleb size and subsequently reduced the incidence ofstrabismus. Valved implants have also reduced the size of thefiltering blebs and have subsequently produced the lowest inci-dence of strabismus.
A large explant in the superior nasal quadrant may cause apseudo-Brown’s syndrome with restricted elevation in adduc-tion, as the bleb displaces and tightens the superior obliquetendon.7,90 Placement of glaucoma explants should be super-otemporal rather than superonasal to avoid the problem of a secondary Brown’s syndrome. The treatment of a bleb-inducedstrabismus is to reduce the size of the bleb by suturing the blebwall to the explant so it cannot expand. Additionally, the oldexplant can be replaced with a newer valved explant.
An interesting observation of some patients with strabismusand severe glaucoma is that they do not experience diplopia but,instead, have visual confusion.57 Visual confusion is the simul-taneous perception of two different foveal images in a patient
chapter 10: complex strabismus 349
350 handbook of pediatric strabismus and amblyopia
A
BFIGURE 10-9A,B. Patient with a glaucoma explant in the left superiortemporal quadrant. The glaucoma was controlled; however, it produceda large bleb that limited abduction. (A) Patient is looking left, and the lefteye shows severe restriction (�4) to abduction. (B) Large temporal bleb iscausing a mass effect and restricting abduction of the left eye.
with strabismus. These patients see the superimposed imagesfrom each fovea. Patients with end-stage glaucoma have tunnelvision and lose their peripheral visual field. If these patientsacquire strabismus, they may experience confusion rather thana true diplopia, as they only have central vision and are forcedto use the fovea of each eye.
High Myopia and Esotropia (Myopic Strabismus Fixus)High myopia, usually greater than 20 diopters, can be associatedwith an acquired large-angle esotropia along with limited abduc-tion and a hypotropia9,25,50,63,116; this is a form of acquired stra-bismus fixus and can be either monocular or binocular. Anotherterm for the high myopia esotropia syndrome is heavy eye syndrome, with hypotropia and limited eye movement.116
Restricted abduction is dramatic, and there is limited elevationof the hypotropic eye. Orbital imaging shows an extremely largeglobe with a posterior staphyloma that fills the orbit, a large infe-rior displacement of the lateral rectus muscle, and a mild nasaldisplacement of the superior rectus muscle. The cause of theesotropia and hypotropia is a combination of restriction, becauseof the massive expansion of the posterior globe against a tightmedial rectus muscle, and displaced lateral and superior rectusmuscles that change the normal vector forces. Displacement ofthe lateral rectus muscle inferiorly and superior rectus musclesnasally is most likely caused by the massive expansion of theposterior aspect of the globe into the superior temporal quad-rant.64 The lateral rectus muscle shows the most displacement,probably due to the laxity of its pulley system. Slippage of thelateral rectus muscle below the globe weakens the abductionvector and pulls the eye down, thus contributing to the esotropiaand hypotropia. The nasally displaced superior rectus musclealso contributes to the esotropia and hypotropia by pulling theeye nasally and diminishing the elevation vector force.
Treatment is aimed at realigning the lateral rectus muscleand releasing the medial rectus muscle, which is inevitablytight. This author prefers a large recession of the medial rectusmuscle, at least 7 to 8mm on a hang-back suture, and a supe-rior transposition of the lateral rectus muscle with a small resec-tion. The posterior sclera is thin in these cases, and access tothe posterior globe is difficult because of the large eye. The hang-back suture of the medial rectus allows for a large recession
chapter 10: complex strabismus 351
without passing a posterior suture. Union of the superior andlateral rectus has also been described.
SPECIFIC TYPES OF PARALYTICSTRABISMUS
Sixth Nerve PalsyA persistent, isolated, congenital sixth nerve palsy is extremelyrare; however, newborns may have a transient sixth nerve palsythat resolves spontaneously over a few days to a few weeks. Acommon cause of isolated acquired sixth nerve palsy in earlychildhood is postviral inflammatory neuropathy, which mayoccur 1 to 3 weeks after a viral illness or immunization or spon-taneously without obvious cause. These patients should be fol-lowed closely to monitor their improvement and watch for thedevelopment of amblyopia. Improvement usually occurs within6 to 10 weeks. After viral or idiopathic causes, the next mostcommon causes of acquired sixth nerve palsy in children andyoung adults include closed head trauma and intracranial neo-plasms. Neuroimaging is indicated for acquired sixth nerve palsyif the palsy does not improve rapidly or if other neurologicalsigns are present. Other causes of an acquired sixth nerve palsyinclude Gradenigo’s syndrome (mastoiditis and sixth nervepalsy), meningitis, myasthenia gravis, and cavernous sinusdisease.
Sixth nerve palsy is typically associated with limited abduc-tion and an esotropia that increases upon gaze to the side of thepalsy (Fig. 10-10). On attempted abduction, there is relative lidfissure widening because both the medial and lateral rectusmuscles are relaxed on attempted adduction and the posteriororbital pressure proptoses the eye. Remember that, on attemptedabduction, the medial rectus muscle is inhibited (Sherrington’slaw). Mild sixth nerve paresis may allow relatively good lateralrectus function and show only a trace limitation of abduction.These patients, however, will have a pattern of divergenceparesis with an esotropia that is greater in the distance than atnear. The divergence paresis pattern should alert the examinerto the possibility of a sixth nerve paresis.
Initial therapy of a traumatic or vascular sixth nerve palsyis observation for 6 months while monitoring the patient forspontaneous recovery. Spontaneous recovery of traumatic sixth
352 handbook of pediatric strabismus and amblyopia
nerve palsy is approximately 80% for unilateral cases and 40%for bilateral cases.53 A complete palsy at the initial presentationand bilateral involvement indicate a poor prognosis for recov-ery.52 During the observation period, alternate monocular occlu-sion or press-on prisms can be used to eliminate diplopia if aface turn does not allow fusion. To prevent secondary contrac-ture of the medial rectus muscle and increase the chances forrecovery, some advocate the use of botulinum injection into theipsilateral medial rectus muscle.10,74 Botulinum paralyzes themuscle for 3 to 6 months, thus preventing contracture. The hopeis that preventing secondary contracture of the medial rectusmuscle will increase the chances of recovery without strabis-mus surgery. The use of botulinum remains controversial,however. Studies comparing botulinum to conservative treat-ment for the management of nerve palsy have shown no sig-nificant difference in recovery rates.53,65 Holmes et al., in aprospective multicenter study of acute traumatic sixth nervepalsy or paresis, reported that patients treated either with botu-linum or conservatively had similarly high recovery rates.53 Itshould be noted that, after a botulinum injection into the medialrectus muscle for a complete sixth nerve palsy, both the medialand lateral rectus will be paralyzed, resulting in essentially nohorizontal movement of the paretic eye. Therefore, the patient
chapter 10: complex strabismus 353
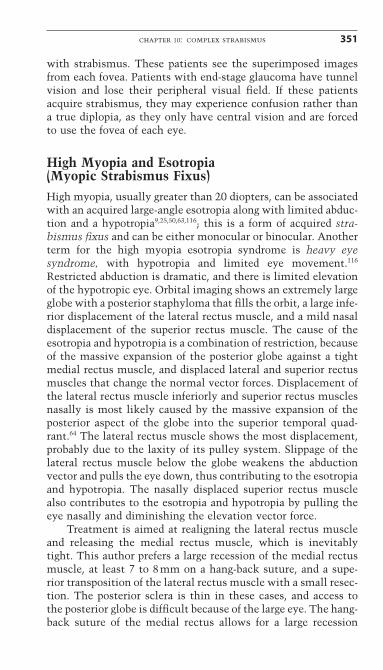
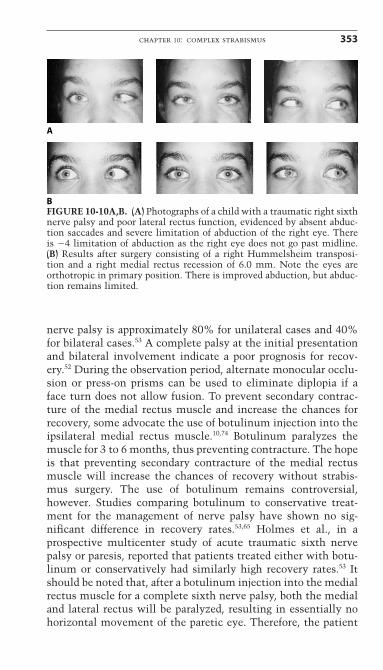
A
BFIGURE 10-10A,B. (A) Photographs of a child with a traumatic right sixthnerve palsy and poor lateral rectus function, evidenced by absent abduc-tion saccades and severe limitation of abduction of the right eye. Thereis �4 limitation of abduction as the right eye does not go past midline.(B) Results after surgery consisting of a right Hummelsheim transposi-tion and a right medial rectus recession of 6.0 mm. Note the eyes areorthotropic in primary position. There is improved abduction, but abduc-tion remains limited.
should be warned that the paretic eye may have decreased move-ment after the injection. In addition, the surgeon should beaware that the effects of botulinum can last more than 6 months,and surgery should be delayed until the botulinum has dissipated.
After the 6-month observation period, lateral rectus musclefunction should be evaluated, as this is critical for determiningthe surgical plan. Lateral rectus muscle function can be assessedby saccadic velocity testing and the active forced-generationtest. If the saccadic velocities are less than 60% of normal or theactive forced-generation test is estimated to be half of thenormal fellow eye, a vertical rectus muscle transposition proce-dure is indicated.
Transposition procedures act by moving innervated verticalrectus muscles to the lateral rectus insertion to provide lateralforce. The lateral force of the transposition does not appropri-ately activate on attempted abduction but, instead, provides aconstant lateral force. Transposition of vertical rectus musclescan involve the full muscle (full-tendon transfer) or the muscle can be split longitudinally and only half the muscle istransferred (partial-tendon transfer). In addition to a transposi-tion, patients with significant residual paresis almost alwaysrequire an ipsilateral medial rectus recession to reduce adduc-tion forces.
The vertical rectus muscles provide substantial circulationto the anterior segment. Older adult patients, especially thosewith arteriosclerotic disease or hyperviscosity syndromes, are atrisk for developing anterior segment ischemia after vertical rectitransposition, particularly those receiving full-tendon transfers.A partial-tendon transfer procedure should be considered inthese patients to maintain anterior circulation and prevent anterior segment ischemia. Modifications of the Hummelsheimpartial-tendon transposition include suturing the transposed vertical muscle to the lateral and resecting a few millimeters ofthe transposed vertical muscle halves.18,82 An important aspect ofthe partial-tendon transfer is to fully mobilize the muscle beingtransferred by splitting the vertical rectus muscles for at least14mm posterior to their insertions.135 If carefully performed, apartial-tendon transfer procedure results in long-term good post-operative eye alignment while reducing the risk of anteriorsegment ischemia. Other options include full-tendon transposi-tion with injection of botulinum toxin to the medial rectus
354 handbook of pediatric strabismus and amblyopia
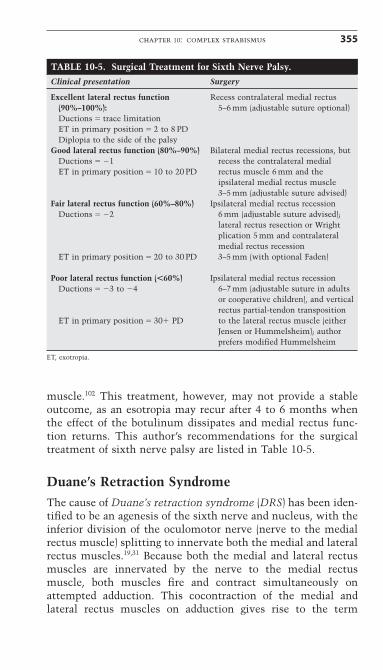
muscle.102 This treatment, however, may not provide a stableoutcome, as an esotropia may recur after 4 to 6 months whenthe effect of the botulinum dissipates and medial rectus func-tion returns. This author’s recommendations for the surgicaltreatment of sixth nerve palsy are listed in Table 10-5.
Duane’s Retraction SyndromeThe cause of Duane’s retraction syndrome (DRS) has been iden-tified to be an agenesis of the sixth nerve and nucleus, with theinferior division of the oculomotor nerve (nerve to the medialrectus muscle) splitting to innervate both the medial and lateralrectus muscles.19,31 Because both the medial and lateral rectusmuscles are innervated by the nerve to the medial rectusmuscle, both muscles fire and contract simultaneously onattempted adduction. This cocontraction of the medial andlateral rectus muscles on adduction gives rise to the term
chapter 10: complex strabismus 355
TABLE 10-5. Surgical Treatment for Sixth Nerve Palsy.Clinical presentation Surgery
Excellent lateral rectus function Recess contralateral medial rectus (90%–100%): 5–6 mm (adjustable suture optional)Ductions � trace limitationET in primary position � 2 to 8 PDDiplopia to the side of the palsy
Good lateral rectus function (80%–90%) Bilateral medial rectus recessions, but Ductions � �1 recess the contralateral medial ET in primary position � 10 to 20 PD rectus muscle 6 mm and the
ipsilateral medial rectus muscle 3–5 mm (adjustable suture advised)
Fair lateral rectus function (60%–80%) Ipsilateral medial rectus recession Ductions � �2 6 mm (adjustable suture advised);
lateral rectus resection or Wright plication 5 mm and contralateral medial rectus recession
ET in primary position � 20 to 30 PD 3–5 mm (with optional Faden)
Poor lateral rectus function (�60%) Ipsilateral medial rectus recession Ductions � �3 to �4 6–7 mm (adjustable suture in adults
or cooperative children), and vertical rectus partial-tendon transposition
ET in primary position � 30� PD to the lateral rectus muscle (either Jensen or Hummelsheim); author prefers modified Hummelsheim
ET, exotropia.
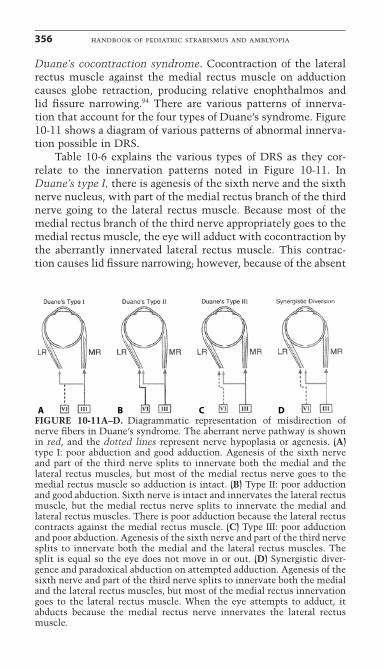
Duane’s cocontraction syndrome. Cocontraction of the lateralrectus muscle against the medial rectus muscle on adductioncauses globe retraction, producing relative enophthalmos and lid fissure narrowing.94 There are various patterns of innerva-tion that account for the four types of Duane’s syndrome. Figure10-11 shows a diagram of various patterns of abnormal innerva-tion possible in DRS.
Table 10-6 explains the various types of DRS as they cor-relate to the innervation patterns noted in Figure 10-11. InDuane’s type I, there is agenesis of the sixth nerve and the sixthnerve nucleus, with part of the medial rectus branch of the thirdnerve going to the lateral rectus muscle. Because most of themedial rectus branch of the third nerve appropriately goes to themedial rectus muscle, the eye will adduct with cocontraction bythe aberrantly innervated lateral rectus muscle. This contrac-tion causes lid fissure narrowing; however, because of the absent
356 handbook of pediatric strabismus and amblyopia
A B C D FIGURE 10-11A–D. Diagrammatic representation of misdirection ofnerve fibers in Duane’s syndrome. The aberrant nerve pathway is shownin red, and the dotted lines represent nerve hypoplasia or agenesis. (A)type I: poor abduction and good adduction. Agenesis of the sixth nerveand part of the third nerve splits to innervate both the medial and thelateral rectus muscles, but most of the medial rectus nerve goes to themedial rectus muscle so adduction is intact. (B) Type II: poor adductionand good abduction. Sixth nerve is intact and innervates the lateral rectusmuscle, but the medial rectus nerve splits to innervate the medial andlateral rectus muscles. There is poor adduction because the lateral rectuscontracts against the medial rectus muscle. (C) Type III: poor adductionand poor abduction. Agenesis of the sixth nerve and part of the third nervesplits to innervate both the medial and the lateral rectus muscles. Thesplit is equal so the eye does not move in or out. (D) Synergistic diver-gence and paradoxical abduction on attempted adduction. Agenesis of thesixth nerve and part of the third nerve splits to innervate both the medialand the lateral rectus muscles, but most of the medial rectus innervationgoes to the lateral rectus muscle. When the eye attempts to adduct, itabducts because the medial rectus nerve innervates the lateral rectusmuscle.
sixth nerve, there is no abduction (Fig. 10-12). If the medialrectus nerve equally innervates the medial and lateral rectusmuscles, then the cocontraction of the lateral rectus muscle willequal the appropriate contraction of the medial rectus muscle,and the eye will have limited adduction in addition to limitedabduction because of the sixth nerve agenesis. This pattern ofpoor adduction and abduction is typical of Duane’s type III (Fig.10-13). In the rare Duane’s type II syndrome, abduction is intactbut is limited because part of the sixth nerve innervates thelateral rectus muscle and part of the medial rectus nerve inner-vates the lateral rectus muscle. Another rare form of Duane’ssyndrome is synergistic divergence. In this syndrome, most ofthe third nerve that should innervate the medial rectus muscleaberrantly innervates the lateral rectus muscle, causing theDuane’s eye to paradoxically abduct on attempted adduction.124
chapter 10: complex strabismus 357
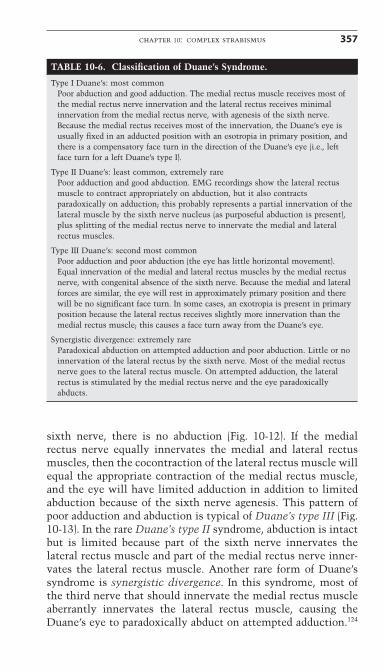
TABLE 10-6. Classification of Duane’s Syndrome.
Type I Duane’s: most commonPoor abduction and good adduction. The medial rectus muscle receives most ofthe medial rectus nerve innervation and the lateral rectus receives minimalinnervation from the medial rectus nerve, with agenesis of the sixth nerve.Because the medial rectus receives most of the innervation, the Duane’s eye isusually fixed in an adducted position with an esotropia in primary position, andthere is a compensatory face turn in the direction of the Duane’s eye (i.e., leftface turn for a left Duane’s type I).
Type II Duane’s: least common, extremely rarePoor adduction and good abduction. EMG recordings show the lateral rectusmuscle to contract appropriately on abduction, but it also contractsparadoxically on adduction; this probably represents a partial innervation of thelateral muscle by the sixth nerve nucleus (as purposeful abduction is present),plus splitting of the medial rectus nerve to innervate the medial and lateralrectus muscles.
Type III Duane’s: second most commonPoor adduction and poor abduction (the eye has little horizontal movement).Equal innervation of the medial and lateral rectus muscles by the medial rectusnerve, with congenital absence of the sixth nerve. Because the medial and lateralforces are similar, the eye will rest in approximately primary position and therewill be no significant face turn. In some cases, an exotropia is present in primaryposition because the lateral rectus receives slightly more innervation than themedial rectus muscle; this causes a face turn away from the Duane’s eye.
Synergistic divergence: extremely rareParadoxical abduction on attempted adduction and poor abduction. Little or noinnervation of the lateral rectus by the sixth nerve. Most of the medial rectusnerve goes to the lateral rectus muscle. On attempted adduction, the lateralrectus is stimulated by the medial rectus nerve and the eye paradoxicallyabducts.
358 handbook of pediatric strabismus and amblyopia
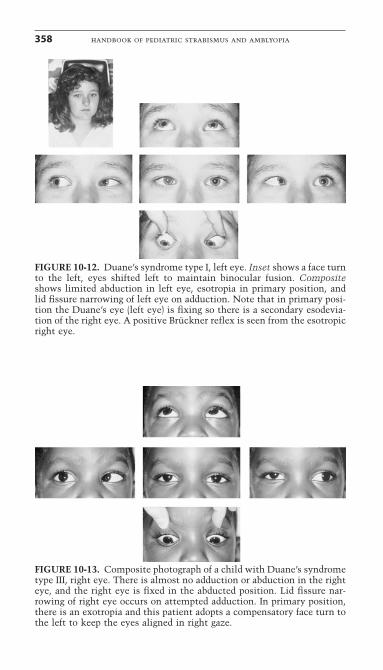
FIGURE 10-12. Duane’s syndrome type I, left eye. Inset shows a face turnto the left, eyes shifted left to maintain binocular fusion. Compositeshows limited abduction in left eye, esotropia in primary position, andlid fissure narrowing of left eye on adduction. Note that in primary posi-tion the Duane’s eye (left eye) is fixing so there is a secondary esodevia-tion of the right eye. A positive Brückner reflex is seen from the esotropicright eye.
FIGURE 10-13. Composite photograph of a child with Duane’s syndrometype III, right eye. There is almost no adduction or abduction in the righteye, and the right eye is fixed in the abducted position. Lid fissure nar-rowing of right eye occurs on attempted adduction. In primary position,there is an exotropia and this patient adopts a compensatory face turn tothe left to keep the eyes aligned in right gaze.
A patient with right synergistic divergence will diverge and havea large exotropia on attempted leftgaze.124
Duane’s syndrome is present at birth and is usually unilat-eral, but it can be bilateral.54 If there is a deviation in primaryposition, patients with DRS will adopt a compensatory face turnto obtain binocular fusion. The face turn is determined by theresting position of the Duane’s eye. If the medial and lateralrectus muscles receive comparable innervation from the splitoculomotor nerve and the eye is centered in primary position,there will be no significant face turn (Duane’s type III). If,however, the medial rectus muscle receives most of the inner-vation from the oculomotor nerve, then the affected eye will restin adduction and the patient will have an esotropic DRS with aface turn toward the side of the affected eye (Duane’s type I).Less commonly, the lateral rectus will receive most of the inner-vation from the oculomotor nerve. In these cases, the Duane’seye will be abducted, causing an exotropia (XT) in primary posi-tion and a face turn toward the opposite side of the Duane’s eye(Duane’s type III with an XT).94
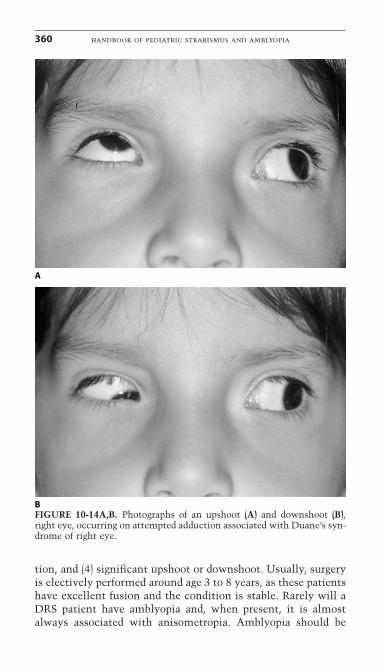
Duane’s syndrome may be associated with an upshoot or adownshoot on attempted adduction, which may resemble infe-rior oblique and superior oblique overaction (Fig. 10-14). Studiesutilizing EMGs have identified a variety of aberrant innerva-tion patterns that explain the vertical movements on adduc-tion.55,107,115 In some cases, the upshoot and downshoot arecaused by strong, inappropriate firing of the lateral rectus muscleon adduction. This leash effect pulls the eye up or down, as theeye rotates slightly up or down past the horizontal plane. Inother cases, the vertical recti are aberrantly innervated by part of the medial rectus nerve, so the vertical muscle fires onadduction.
Other oculomotor misdirection syndromes are associatedwith Duane’s syndrome, such as Marcus Gunn jaw-winking.Duane’s syndrome is associated with numerous systemic syndromes including Goldenhar’s syndrome, Klippel–Feil syn-drome, maternal thalidomide ingestion, fetal alcohol syndrome,and oculocutaneous albinism.31
SURGICAL EVALUATION
Indications for surgery in DRS include (1) significant misalign-ment of the eyes in primary position, (2) noticeable abnormalhead position, (3) narrowing of palpebral fissure due to retrac-
chapter 10: complex strabismus 359
tion, and (4) significant upshoot or downshoot. Usually, surgeryis electively performed around age 3 to 8 years, as these patientshave excellent fusion and the condition is stable. Rarely will aDRS patient have amblyopia and, when present, it is almostalways associated with anisometropia. Amblyopia should be
360 handbook of pediatric strabismus and amblyopia
A
BFIGURE 10-14A,B. Photographs of an upshoot (A) and downshoot (B),right eye, occurring on attempted adduction associated with Duane’s syn-drome of right eye.
the first priority in these unusual cases. In general, muscle resec-tions should be avoided in DRS, because resections can makethe cocontraction and lid fissure narrowing worse.
SURGERY FOR DRS TYPE I WITH ESOTROPIA ANDIPSILATERAL FACE TURN
In cases with esotropia and Duane’s type I, the Duane’s eye is inan adducted position and there is a face turn toward the Duane’seye. The medial rectus muscle is usually contracted and tight.The simplest, most effective treatment for Duane’s type I withesotropia is an ipsilateral medial rectus recession (between 5.0and 7mm). In adult patients, place the medial rectus muscle onan adjustable suture and adjust to a 5° to 10° overcorrection sothere is a small exotropia in primary position; this results instable long-term correction of the face turn. Remember, thelateral rectus muscle is not denervated, as in the case of a sixthnerve palsy, but has innervation provided by part of the medialrectus nerve. This tonic innervation provides stabilizing abduc-tion force, so a muscle transposition procedure is not required.Some have advocated a transposition of the vertical rectusmuscles laterally for DRS and esotropia. This procedure is more invasive and has the risk of producing anterior segmentischemia. The transposition procedure also has a risk of induc-ing a vertical deviation in approximately 15% of patients. Thisauthor prefers the simple and effective ipsilateral medial rectusrecession for Duane’s type I with esotropia.
SURGERY FOR DRS TYPE III WITH EXOTROPIA ANDCONTRALATERAL FACE TURN
In a patient with Duane’s and exotropia, it is almost always aDuane’s type III. The eye is resting in abduction, and the faceturn is away from the Duane’s eye. There is usually a tightlateral rectus muscle, and these patients require an ipsilaterallateral rectus recession. If there is an upshoot or downshoot asso-ciated with the Duane’s type III, then consider a Y-split proce-dure with the lateral rectus recession.
TREATMENT OF GLOBE RETRACTIONGlobe retraction can be diminished by recessing both the ipsi-lateral medial rectus and lateral rectus muscles. In patients withesotropic DRS and severe globe retraction, add a lateral rectusrecession, but recess the medial rectus muscle more than thelateral rectus to compensate for the esotropia. In exotropic DRS,
chapter 10: complex strabismus 361
recess the lateral rectus more than the medial rectus muscle or,for a large exotropia, recess only the lateral rectus muscle (largerecession). For orthotropic DRS without a face turn, recess themedial and lateral rectus muscles the same amount.
TREATMENT OF UPSHOOT AND DOWNSHOOTTwo approaches to reduce upshoot and downshoot associatedwith DRS include these:
1. Y-splitting with recession of the lateral rectus muscle2. Posterior fixation suture (Faden) of the lateral rectus and
appropriate recession of horizontal recti
The Y-splitting procedure of the lateral rectus muscle works byplacing some of the lateral rectus muscle above and below thehorizontal midline, thus preventing an upshoot or downshootwhen the eye is in adduction.95,100 By combining a recession ofthe lateral rectus muscle with the Y-split, one can treat both anexotropia Duane’s type III with an upshoot and downshoot. Inpatients with orthotropic DRS and a severe upshoot and down-shoot, recess the ipsilateral medial rectus muscle along with arecession and Y-split of the ipsilateral lateral rectus muscle. Theposterior fixation suture acts to stop slippage of the lateral rectusmuscle when the eye rotates up or down, and a concurrent reces-sion reduces cocontraction. The authors have found the Y-splitting procedure is more effective than the posterior fixationsuture.
Fourth Nerve Palsy (Superior Oblique Palsy)See Chapter 9.
Third Nerve PalsyThird nerve palsy involves all the extraocular muscles exceptthe lateral rectus and the superior oblique. The strabismus ischaracterized by the eye being “down and out” with a smallhypotropia and a large exotropia (Fig. 10-15). There is limiteddepression, elevation, and adduction, along with preservation ofabduction (intact innervation lateral rectus muscle) and intor-sion seen on attempted eye movement down and in (intactinnervation superior oblique muscle). Ptosis, pupillary dilata-tion, and hypoaccommodation are also present in a completethird nerve palsy. A congenital third nerve paresis is often
362 handbook of pediatric strabismus and amblyopia
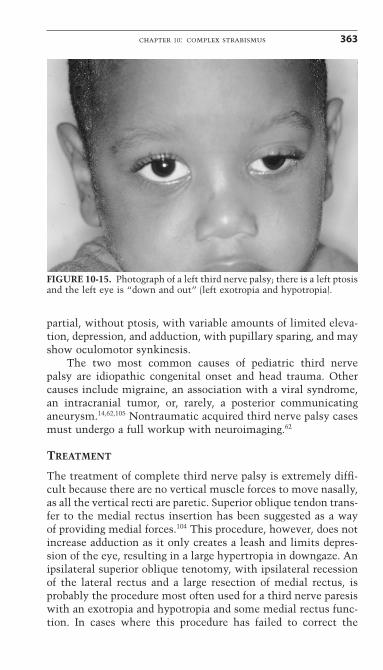
partial, without ptosis, with variable amounts of limited eleva-tion, depression, and adduction, with pupillary sparing, and mayshow oculomotor synkinesis.
The two most common causes of pediatric third nerve palsy are idiopathic congenital onset and head trauma. Othercauses include migraine, an association with a viral syndrome,an intracranial tumor, or, rarely, a posterior communicatinganeurysm.14,62,105 Nontraumatic acquired third nerve palsy casesmust undergo a full workup with neuroimaging.62
TREATMENT
The treatment of complete third nerve palsy is extremely diffi-cult because there are no vertical muscle forces to move nasally,as all the vertical recti are paretic. Superior oblique tendon trans-fer to the medial rectus insertion has been suggested as a wayof providing medial forces.104 This procedure, however, does notincrease adduction as it only creates a leash and limits depres-sion of the eye, resulting in a large hypertropia in downgaze. Anipsilateral superior oblique tenotomy, with ipsilateral recessionof the lateral rectus and a large resection of medial rectus, isprobably the procedure most often used for a third nerve paresiswith an exotropia and hypotropia and some medial rectus func-tion. In cases where this procedure has failed to correct the
chapter 10: complex strabismus 363
FIGURE 10-15. Photograph of a left third nerve palsy; there is a left ptosisand the left eye is “down and out” (left exotropia and hypotropia).

exotropia, this author has split the lateral rectus and transposedthe halves to the nasal border of the superior and inferior rectusmuscles. This procedure has worked in centering the eye;however, horizontal excursions are minimal.
In addition to the difficulty in treating the strabismus,patients with a third nerve palsy and ptosis with poor or absentlevator function, are at risk for developing corneal exposure ifthe ptosis is repaired. Ptosis should be managed with a siliconefrontalis sling procedure, aiming for intentional undercorrectionof the lid position if there is a poor Bell’s phenomenon. The sil-icone sling procedure has an advantage of being reversible ifcorneal exposure becomes a problem. Patients should be warnedabout the risk of corneal exposure and that their diplopia maybe worse after lifting the eyelid, as this removes the occlusion.Many wise patients and physicians opt for leaving the ptosisalone if associated with a poor superior rectus muscle functionevidenced by a poor Bell’s phenomenon.
Inferior Oblique ParesisSee Chapter 9.
Möbius SyndromeMöbius syndrome is characterized by a combination of facialpalsy, sixth nerve palsy, partial third nerve palsy, and distal limbabnormalities such as syndactyly, club foot, or even amputationdefects.23 There is some degree of intellectual impairment in75% of patients.23,131 The Möbius infant typically presents withesotropia, limited abduction, lack of facial expression, and diffi-culty feeding caused by a poor sucking reflex. Craniofacialanomalies can occur and include micrognathia, tongue abnor-malities, and facial or oral clefts. Ocular motility abnormalitiesinclude limited abduction in more than 90% of cases and limitedadduction in 65% of cases.23,66,86 Some patients have globe retrac-tion on adduction and failure to abduct, typical of Duane’s syn-drome. The inheritance pattern of Möbius syndrome is usuallysporadic, and there is great variability of findings,44 suggestingthat the syndrome represents a heterogeneous group of neuro-muscular disorders.87 Prenatal exposure to misoprostol, the abortion-inducing drug, has been implicated as a risk factor.23,41,120
Treatment of the strabismus is tailored to the individual situa-tion. Patients with a large esotropia, tight medial rectus
364 handbook of pediatric strabismus and amblyopia
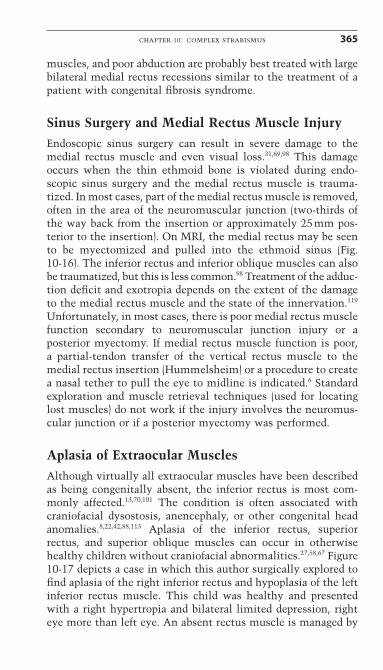
muscles, and poor abduction are probably best treated with largebilateral medial rectus recessions similar to the treatment of apatient with congenital fibrosis syndrome.
Sinus Surgery and Medial Rectus Muscle InjuryEndoscopic sinus surgery can result in severe damage to themedial rectus muscle and even visual loss.31,69,98 This damageoccurs when the thin ethmoid bone is violated during endo-scopic sinus surgery and the medial rectus muscle is trauma-tized. In most cases, part of the medial rectus muscle is removed,often in the area of the neuromuscular junction (two-thirds ofthe way back from the insertion or approximately 25mm pos-terior to the insertion). On MRI, the medial rectus may be seento be myectomized and pulled into the ethmoid sinus (Fig. 10-16). The inferior rectus and inferior oblique muscles can alsobe traumatized, but this is less common.98 Treatment of the adduc-tion deficit and exotropia depends on the extent of the damageto the medial rectus muscle and the state of the innervation.119
Unfortunately, in most cases, there is poor medial rectus musclefunction secondary to neuromuscular junction injury or a posterior myectomy. If medial rectus muscle function is poor, a partial-tendon transfer of the vertical rectus muscle to themedial rectus insertion (Hummelsheim) or a procedure to createa nasal tether to pull the eye to midline is indicated.6 Standardexploration and muscle retrieval techniques (used for locatinglost muscles) do not work if the injury involves the neuromus-cular junction or if a posterior myectomy was performed.
Aplasia of Extraocular MusclesAlthough virtually all extraocular muscles have been describedas being congenitally absent, the inferior rectus is most com-monly affected.13,70,101 The condition is often associated withcraniofacial dysostosis, anencephaly, or other congenital headanomalies.8,22,42,88,113 Aplasia of the inferior rectus, superiorrectus, and superior oblique muscles can occur in otherwisehealthy children without craniofacial abnormalities.27,58,67 Figure10-17 depicts a case in which this author surgically explored tofind aplasia of the right inferior rectus and hypoplasia of the leftinferior rectus muscle. This child was healthy and presentedwith a right hypertropia and bilateral limited depression, righteye more than left eye. An absent rectus muscle is managed by
chapter 10: complex strabismus 365
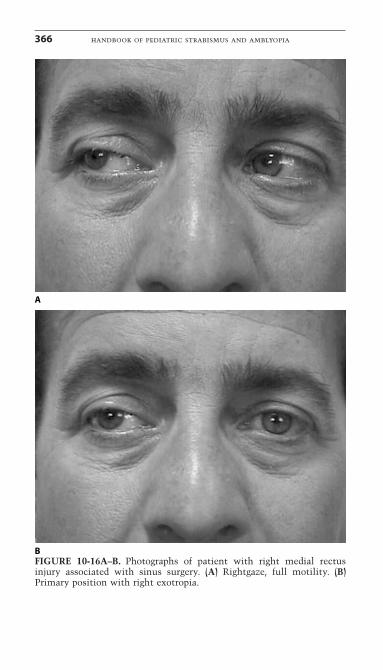
366 handbook of pediatric strabismus and amblyopia
A
BFIGURE 10-16A–B. Photographs of patient with right medial rectusinjury associated with sinus surgery. (A) Rightgaze, full motility. (B)Primary position with right exotropia.
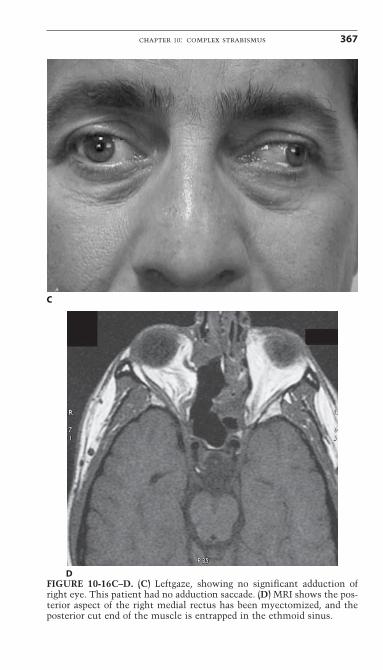
chapter 10: complex strabismus 367
C
DFIGURE 10-16C–D. (C) Leftgaze, showing no significant adduction ofright eye. This patient had no adduction saccade. (D) MRI shows the pos-terior aspect of the right medial rectus has been myectomized, and theposterior cut end of the muscle is entrapped in the ethmoid sinus.
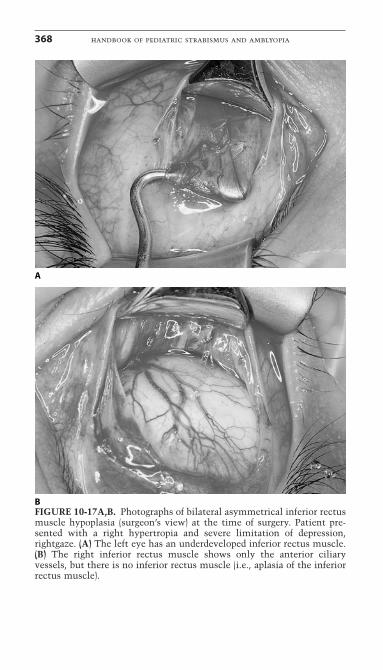
368 handbook of pediatric strabismus and amblyopia
A
BFIGURE 10-17A,B. Photographs of bilateral asymmetrical inferior rectusmuscle hypoplasia (surgeon’s view) at the time of surgery. Patient pre-sented with a right hypertropia and severe limitation of depression,rightgaze. (A) The left eye has an underdeveloped inferior rectus muscle.(B) The right inferior rectus muscle shows only the anterior ciliaryvessels, but there is no inferior rectus muscle (i.e., aplasia of the inferiorrectus muscle).
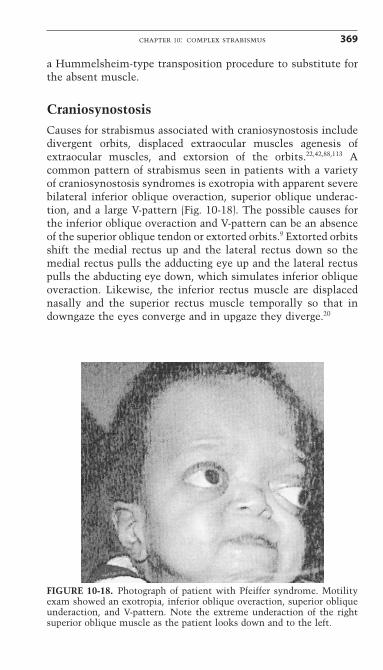
a Hummelsheim-type transposition procedure to substitute forthe absent muscle.
CraniosynostosisCauses for strabismus associated with craniosynostosis includedivergent orbits, displaced extraocular muscles agenesis ofextraocular muscles, and extorsion of the orbits.22,42,88,113 Acommon pattern of strabismus seen in patients with a varietyof craniosynostosis syndromes is exotropia with apparent severebilateral inferior oblique overaction, superior oblique underac-tion, and a large V-pattern (Fig. 10-18). The possible causes forthe inferior oblique overaction and V-pattern can be an absenceof the superior oblique tendon or extorted orbits.9 Extorted orbitsshift the medial rectus up and the lateral rectus down so themedial rectus pulls the adducting eye up and the lateral rectuspulls the abducting eye down, which simulates inferior obliqueoveraction. Likewise, the inferior rectus muscle are displacednasally and the superior rectus muscle temporally so that indowngaze the eyes converge and in upgaze they diverge.20
chapter 10: complex strabismus 369
FIGURE 10-18. Photograph of patient with Pfeiffer syndrome. Motilityexam showed an exotropia, inferior oblique overaction, superior obliqueunderaction, and V-pattern. Note the extreme underaction of the rightsuperior oblique muscle as the patient looks down and to the left.
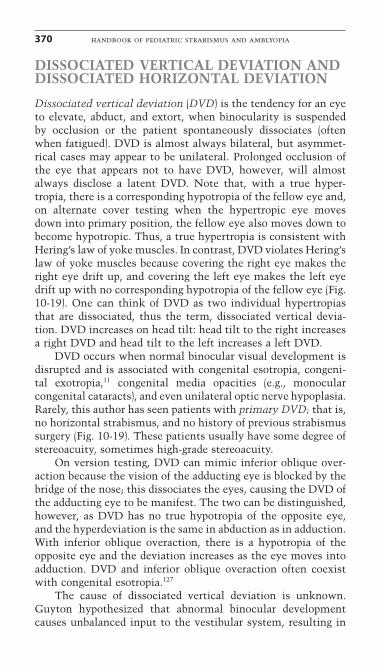
DISSOCIATED VERTICAL DEVIATION ANDDISSOCIATED HORIZONTAL DEVIATION
Dissociated vertical deviation (DVD) is the tendency for an eyeto elevate, abduct, and extort, when binocularity is suspendedby occlusion or the patient spontaneously dissociates (oftenwhen fatigued). DVD is almost always bilateral, but asymmet-rical cases may appear to be unilateral. Prolonged occlusion ofthe eye that appears not to have DVD, however, will almostalways disclose a latent DVD. Note that, with a true hyper-tropia, there is a corresponding hypotropia of the fellow eye and,on alternate cover testing when the hypertropic eye moves down into primary position, the fellow eye also moves down tobecome hypotropic. Thus, a true hypertropia is consistent withHering’s law of yoke muscles. In contrast, DVD violates Hering’slaw of yoke muscles because covering the right eye makes theright eye drift up, and covering the left eye makes the left eyedrift up with no corresponding hypotropia of the fellow eye (Fig.10-19). One can think of DVD as two individual hypertropiasthat are dissociated, thus the term, dissociated vertical devia-tion. DVD increases on head tilt: head tilt to the right increasesa right DVD and head tilt to the left increases a left DVD.
DVD occurs when normal binocular visual development isdisrupted and is associated with congenital esotropia, congeni-tal exotropia,11 congenital media opacities (e.g., monocular congenital cataracts), and even unilateral optic nerve hypoplasia.Rarely, this author has seen patients with primary DVD; that is,no horizontal strabismus, and no history of previous strabismussurgery (Fig. 10-19). These patients usually have some degree ofstereoacuity, sometimes high-grade stereoacuity.
On version testing, DVD can mimic inferior oblique over-action because the vision of the adducting eye is blocked by thebridge of the nose; this dissociates the eyes, causing the DVD ofthe adducting eye to be manifest. The two can be distinguished,however, as DVD has no true hypotropia of the opposite eye,and the hyperdeviation is the same in abduction as in adduction.With inferior oblique overaction, there is a hypotropia of theopposite eye and the deviation increases as the eye moves intoadduction. DVD and inferior oblique overaction often coexistwith congenital esotropia.127
The cause of dissociated vertical deviation is unknown.Guyton hypothesized that abnormal binocular developmentcauses unbalanced input to the vestibular system, resulting in
370 handbook of pediatric strabismus and amblyopia
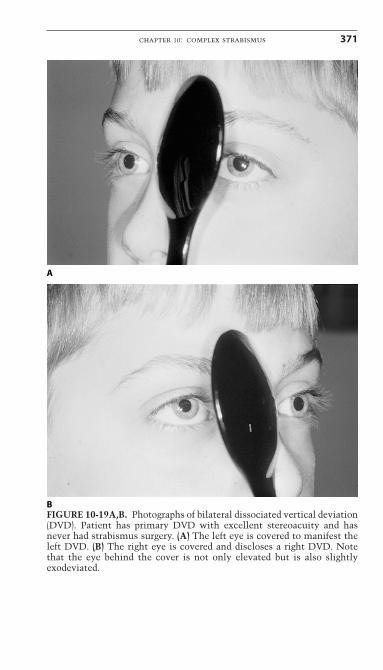
chapter 10: complex strabismus 371
A
BFIGURE 10-19A,B. Photographs of bilateral dissociated vertical deviation(DVD). Patient has primary DVD with excellent stereoacuity and hasnever had strabismus surgery. (A) The left eye is covered to manifest theleft DVD. (B) The right eye is covered and discloses a right DVD. Notethat the eye behind the cover is not only elevated but is also slightlyexodeviated.
latent nystagmus with a cyclovertical movement. Cycloversion/vertical vergence is invoked to damp the cyclovertical nystagmus(a cyclovertical “nystagmus blockage” phenomenon), aidingvision in the fixing eye. Unfortunately, this mechanism also pro-duces unavoidable and undesirable elevation and extorsion ofthe fellow eye that results in DVD.45
This author has a theory about the neurophysiological basisfor DVD. It is interesting that DVD is associated with disrup-tion of early binocular visual development. The interstitialnucleus of Cajal is a brainstem nucleus that regulates cyclover-tical movements. The interstitial nucleus of Cajal receivesinhibitory input from binocular cells in the occipital cortex, andthese inhibitory pathways act to control this nucleus. Lesionsaround the interstitial nucleus of Cajal that interrupt the binoc-ular inhibitory input result in nucleus disinhibition, which isclinically manifested as seesaw nystagmus. Seesaw nystagmusis a dissociated cyclovertical/horizontal nystagmus. Whenseesaw nystagmus occurs in infancy, it can look quite similar toDVD. Infantile strabismus or a dense monocular congenitalcataract disrupts binocular visual development and reducesbinocular cortical cells. Perhaps the lack of binocular corticalcells associated with congenital strabismus or a unilateralblurred retinal image in infancy, results in reduced binocularinhibitory input to the interstitial nucleus of Cajal or similarcyclovertical brainstem nuclei. Reduced binocular inhibitoryinput would cause disinhibition of these cyclovertical nuclei,giving rise to what we see clinically as DVD.
If early surgery for infantile esotropia improves binocular-ity, then children who have had early surgery should have lessDVD. Recent reports on the incidence of DVD in children whohave had early surgery for infantile esotropia, however, remainunchanged from reports 30 years previous.81,136 Even though theincidence may be the same, the severity of DVD seems to havediminished over the past few decades. It is this author’s opinion,along with the observations of senior expert strabismologists,that the incidence of severe DVD requiring surgery hasdecreased. Performing surgery for a large, cosmetically obviousDVD in the 1970s and early 1980s was commonplace. As a res-ident in ophthalmology, this author remembers operating everymonth on several DVD patients. Over the past several years,there have only been a few cases requiring surgery, and usuallyon older adults with DVD. The author’s visits to countrieswhere surgeons continue to operate late, after 2 years of age,have disclosed that a very high prevalence of big, surgically
372 handbook of pediatric strabismus and amblyopia
significant DVD persists. Perhaps, with the advent of early inter-vention of infantile esotropia in this country, our children withinfantile esotropia have been able to establish better binocularfusion, thus reducing the severity, but not the incidence, of theDVD. In this author’s report on very early surgery for congeni-tal esotropia (surgery between 13 and 19 weeks of age), four ofseven patients had DVD on last examination (2–8 years; mean,4 years).136 This DVD, however, was very small and could only be demonstrated by prolonged cover testing. None of thepatients required DVD surgery, although one had surgery forinferior oblique overaction. M cell afferent pathway develop-ment is responsible for motor fusion and control. Because M celldevelopment starts very early, around 6 weeks to 2 months ofage, perhaps our “very early surgery” is not early enough toestablish strong motor fusion and eliminate DVD.137
The treatment of DVD is surgical, and surgery is indicatedif the DVD exists to the point that it becomes a cosmeticproblem. DVD is most often bilateral, and bilateral surgery isusually performed. An exception is with amblyopia, wheresurgery is performed only on the amblyopic eye. With ambly-opia of 2 lines or more, the patient will always fixate with thesound eye, and the sound eye will not manifest the DVD. Mostconsider superior rectus recessions as the treatment choice forpure DVD without inferior oblique overaction. If DVD and infe-rior oblique overaction coexist, then an anterior transposition ofthe inferior oblique is indicated, as this will address both prob-lems with one procedure.12,43,93,121 Strabismus surgery rarely, ifever, cures DVD.
Dissociated horizontal deviation (DHD), which may be unilateral or bilateral, is a subtype of DVD that often occurs in patients who have had previous strabismus surgery for con-genital esotropia.129 This is a dissociated condition like DVD,but the exocomponent of DVD is exaggerated. Cover/uncovertesting may show no shift or a small esotropia, but prolongedocclusion produces an exodeviation. Think of DHD when exam-ining patients with a small residual esotropia, who also have adissociated exodeviation. The treatment of DHD is recession ofthe ipsilateral lateral rectus muscle.128
Torticollis and Face TurnsThis section covers the approach to patients who present withan abnormal head posture. Abnormal head posturing includestorticollis (head tilt), chin elevation and depression, and face
chapter 10: complex strabismus 373
turn. These forms of head posturing can occur independently orin combination, as a patient with a superior oblique palsy willoften have both a head tilt and a face turn. Torticollis can besecondary to a musculoskeletal abnormality of the neck or to anocular problem compensated by head posturing. A simple initialtest to determine the cause is to ask the patients to close theireyes and observe for several seconds to see if the head posturingspontaneously improves. If the face turn improves when theeyes are closed, this suggests an ocular cause. Next, passivelymove the patient’s head from side to side with the patient’s eyesclosed. If the range of motion of the head and neck is normal,this verifies that the head posturing is an ocular torticollis;however, a stiff neck indicates a musculoskeletal problem.
By far the most common ocular causes of abnormal headposturing are nystagmus with a null point and incomitant strabismus with compensatory head posturing to allow fusion.A face turn is often identified by observing the patient’s headposture. A better way to evaluate the presence of a face turn isto observe the position of the eyes. Normal patients withstraight eyes and no face turn will have both eyes centeredwithin the palpebral fissures. If a face turn is present, there willbe a gaze preference with the eyes constantly shifted opposite tothe face turn. For example, a face turn to the right is associatedwith eyes shifted to the left (Fig. 10-20), and a chin elevationwill have the eyes shifted down. When examining a patient fora face turn, first observe the position of the eyes and the pres-ence of a gaze preference. Next, turn or tilt the head opposite tothe compensatory position to place the eyes into the non-preferred field of gaze. If there is a face turn to the right, turn thehead to the left; if there is a head tilt to the right, tilt the headto the left. While the head is held opposite to the compensatoryposition, observe for nystagmus or strabismus. If nystagmusoccurs or increases with a forced face turn to the opposite side,then a compensatory face turn is present to keep the eyes in thearea of the null point. If strabismus is produced by forced headtilt, or turns the eye in with a previously fusing patient, thenthe compensatory head posturing is adopted to maintain fusion,keeping the eyes in the field of gaze where the eyes are aligned.In addition to face turns and head tilts, chin elevations or depres-sions can be compensatory for nystagmus or strabismus, andchin elevations compensate for ptosis.
The degree of face turn can be measured by using an ortho-pedic goniometer placed on the head. Any protractor will work
374 handbook of pediatric strabismus and amblyopia
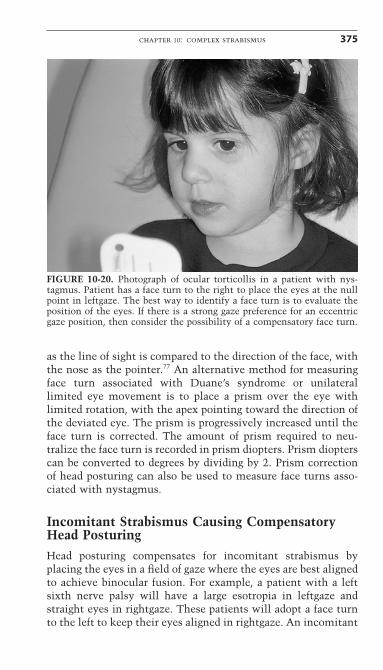
as the line of sight is compared to the direction of the face, withthe nose as the pointer.77 An alternative method for measuringface turn associated with Duane’s syndrome or unilaterallimited eye movement is to place a prism over the eye withlimited rotation, with the apex pointing toward the direction ofthe deviated eye. The prism is progressively increased until theface turn is corrected. The amount of prism required to neu-tralize the face turn is recorded in prism diopters. Prism diopterscan be converted to degrees by dividing by 2. Prism correctionof head posturing can also be used to measure face turns asso-ciated with nystagmus.
Incomitant Strabismus Causing CompensatoryHead PosturingHead posturing compensates for incomitant strabismus byplacing the eyes in a field of gaze where the eyes are best alignedto achieve binocular fusion. For example, a patient with a leftsixth nerve palsy will have a large esotropia in leftgaze andstraight eyes in rightgaze. These patients will adopt a face turnto the left to keep their eyes aligned in rightgaze. An incomitant
chapter 10: complex strabismus 375
FIGURE 10-20. Photograph of ocular torticollis in a patient with nys-tagmus. Patient has a face turn to the right to place the eyes at the nullpoint in leftgaze. The best way to identify a face turn is to evaluate theposition of the eyes. If there is a strong gaze preference for an eccentricgaze position, then consider the possibility of a compensatory face turn.
strabismus where the eyes are aligned in an eccentric field ofgaze can cause an abnormal head posture; this includes cranialnerve palsies, restrictive strabismus, A- or V-patterns, andprimary oblique dysfunction. For example, patients with fusionand an A-pattern exotropia or V-pattern esotropia will show achin depression (eyes straighter in upgaze), whereas an A-patternesotropia or V-pattern exotropia will show a chin elevation (eyesstraighter in downgaze).
The treatment of an abnormal head posture caused byincomitant strabismus is simply to correct the strabismus inprimary position and provide a large field of single binocularvision. If the fixing eye has limited ductions, then move the eyewith limited movements to primary position, and the normaleye will follow.
Nystagmus Causing Compensatory Head PosturingA compensatory head posture can stabilize nystagmus byplacing the eyes at the null point. If the null point is to the right,the patient will shift the eyes to the right and have a face turnto the left. Head posturing associated with nystagmus can takethe form of a face turn, chin elevation or depression, or a headtilt.
A compensatory face turn associated with congenital nys-tagmus can be treated using eye muscle surgery to move the eyeposition from the null point to primary position.77 The generalsurgical principles for correcting a face turn are as follows5:
1. Kestenbaum–Anderson–Parks (Kestenbaum) procedure:With a compensatory face turn to the right, the eyes will beshifted to the left. Therefore, to correct the face turn, move theeyes to the right into primary position (Fig. 10-21), which is doneby moving the right eye out (right medial rectus recession–rightlateral rectus resection) and moving the left eye in (left lateralrectus recession and a left medial rectus resection). The amountof surgery for a specific amount of face turn is listed in Table10-7. Note, Parks Poker Straight 5-6-7-8 (medial recession 5mm,medial resection 6 mm, lateral recession 7 mm, and lateral resec-tion 8mm) is a way of remembering the amount of surgery fora small face turn. In most cases, however, larger amounts ofsurgery are needed.77 Large recessions and resections are neededfor a face turn associated with nystagmus. Postoperative
376 handbook of pediatric strabismus and amblyopia
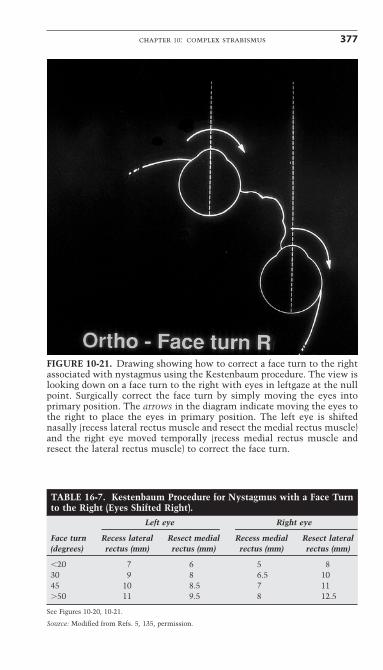
chapter 10: complex strabismus 377
FIGURE 10-21. Drawing showing how to correct a face turn to the rightassociated with nystagmus using the Kestenbaum procedure. The view islooking down on a face turn to the right with eyes in leftgaze at the nullpoint. Surgically correct the face turn by simply moving the eyes intoprimary position. The arrows in the diagram indicate moving the eyes tothe right to place the eyes in primary position. The left eye is shiftednasally (recess lateral rectus muscle and resect the medial rectus muscle)and the right eye moved temporally (recess medial rectus muscle andresect the lateral rectus muscle) to correct the face turn.
TABLE 16-7. Kestenbaum Procedure for Nystagmus with a Face Turnto the Right (Eyes Shifted Right).
Left eye Right eye
Face turn Recess lateral Resect medial Recess medial Resect lateral (degrees) rectus (mm) rectus (mm) rectus (mm) rectus (mm)
�20 7 6 5 830 9 8 6.5 1045 10 8.5 7 11�50 11 9.5 8 12.5
See Figures 10-20, 10-21.
Source: Modified from Refs. 5, 135, permission.
limitation of ocular movements is to be expected, deemed to bean acceptable trade-off.
2. Vertical head posturing: Chin depression (eyes up) istreated with large bilateral superior rectus recessions (8–9mm)and inferior rectus resections (6–7mm). For large chin depres-sions, this can be combined or performed in stages, the superiorrectus recessions first, then inferior rectus resections later if nec-essary. Chin elevations (eyes down) can be treated similarly byrecessing the inferior rectus muscles (7–8mm) and resecting thesuperior rectus muscles (6–7mm).99
Surgical therapy should be based on the greatest amount of abnormal head posture measured at distance and near. Forexample, if the face turn is obvious at distance and not at near,full correction directed at the face turn in the distance shouldbe undertaken. When strabismus coexists with nystagmus, the head posture can be corrected by moving the fixing eye toprimary position. Then adjust the fellow eye to compensate forthe residual strabismus.
Compensatory head tilts are also associated with nystag-mus, which can be corrected by rotating the eyes back toprimary position. A head tilt to the right can be treated by sur-gically extorting the right eye and intorting the left eye.122
SURGICAL TREATMENT OF NYSTAGMUS: NO FACE TURN
Although the Kestenbaum–Anderson–Parks procedure isdirected toward eliminating the abnormal horizontal face turnassociated with nystagmus, another approach has been describedto damp nystagmus in patients without a face turn. Simultane-ous retroequatorial recessions of all four horizontal rectusmuscles have been reported to decrease the amplitude of nys-tagmus and improve visual acuity.30,36,97 The precise mechanismresponsible for damping the nystagmus is not known, and thelong-term effect remains unknown. Vision improves only incases of motor nystagmus, not in patients with sensory nystag-mus who have an abnormal afferent pathway.
Additional Causes of Ocular TorticollisLess common mechanisms for head posturing do exist. Rarely,a patient with diplopia adopts a head posture that inducesmaximal image separation rather than fusion, thus making sup-pression of the diplopic image easier. Other reasons for abnor-
378 handbook of pediatric strabismus and amblyopia
mal head posturing include compensation for visual fielddefects, restriction of the good eye in monocular patients, man-ifest latent nystagmus with a face turn to keep the fixing eye inadduction, ptosis with chin elevation, tilting for monoculartorsion, and cosmetic reasons. Other causes include asymmet-rical dissociated vertical deviation, refractive error in which thepatient adopts a face turn presumably to partially block thepupil, inducing a pinhole effect that provides better visual acuity.
References1. Amemiya T, Yoshida H, Harayama K, et al. Long-term results of
retinal detachment surgery. Ophthalmologica 1978;177:64–69.2. Anderson RL, Baumgartner SA. Strabismus and ptosis. Arch Oph-
thalmol 1980;98:1062–1067.3. Appleton RE, Chitayat D, Jan JE, Kennedy R, Hall JG. Joubert’s syn-
drome associated with congenital ocular fibrosis and histidinemia.Arch Neurol 1989;46(5):579–582.
4. Apt L, Axelrod RN. Generalized fibrosis of the extraocular muscles.Am J Ophthalmol 1978;85(6):822–829.
5. Archer SM. Strabismus surgery planning. In: Del Monte MA, ArcherSM (eds) Atlas of pediatric ophthalmology and strabismus surgery.New York: Churchill Livingstone, 1993:14.
6. Awad AH, Shin GS, Rosenbaum AL, Goldberg RL. Autogenous fasciaaugmentation of a partially extirpated muscle with a subperiostealmedial orbitotomy approach. J AAPOS. 1997;1(3):138–142.
7. Ball SF, Ellis GS, Herrington RG, Liang K. Brown’s superior obliquetendon syndrome after Baerveldt glaucoma implant. Arch Ophthal-mol 1991;110:1368.
8. Barnes RJ. Anencephaly with absence of superior oblique tendon.Surv Ophthalmol 1972;16:371–374.
9. Bagshaw J. The ‘heavy eye’ phenomenon. A preliminary report. Br JOphthalmol 1966;23:73–78.
10. Biglan AW, et al. Management of strabismus with botulinum Atoxin. Ophthalmology 1989;96:935–943.
11. Biglan AW, Davis JS, Cheng KP, Pettapiece MC. Infantile exotropia.J Pediatr Ophthalmol Strabismus 1996;33(2):79–84.
12. Black BC. Results of anterior transposition of the inferior obliquemuscle in incomitant dissociated vertical deviation. JAAPOS 1997;1(2):83–87.
13. Brady AP, Stack JP, O’Keeffe M. Congenital absence of extraocularmuscles: MR demonstration. J Comput Assist Tomogr 1992;16(3):490–491.
14. Branley MG, Wright KW, Borchert MS. Third nerve palsy due to cerebral artery aneurysm in a child. Aust NZ J Ophthalmol 1992;20:137–140.
chapter 10: complex strabismus 379
15. Bremer DL, Rogers GL, Quick LD. Primary-position hypotropia afteranterior transposition of the inferior oblique. Arch Ophthalmol1986;104:229–232.
16. Brodsky MC. Hereditary external ophthalmoplegia synergistic diver-gence, jaw winking, and oculocutaneous hypopigmentation: a congenital fibrosis syndrome caused by deficient innervation toextraocular muscles. Ophthalmology 1998;105(4):717–725.
17. Brooks SE, Ribeiro GB, Archer SM, Elner VM, Del Monte MA. Fatadherence syndrome treated with intraoperative mitomycin-C: arabbit model. J Pediatr Ophthalmol Strabismus 1996;33(1):21–27.
18. Brooks SE, Olitsky SE, de Ribeiro G. Augmented Hummelsheim procedure for paralytic strabismus. J Pediatr Ophthalmol Strabismus2000;37(4):189–195; quiz 226–227.
19. Capo H, Guyton DL. Ipsilateral hypermetropia after cataract surgery.Ophthalmology 1996;103:721–730.
20. Cheng H, Burdon MA, Shun-Shin GA, Czypionka S. Dissociated eyemovements in craniosynostosis: a hypothesis revisited. Br J Oph-thalmol 1993;77:563–568.
21. Coats DK, Paysse EA, Plager DA, Wallace DK. Early strabismussurgery for thyroid ophthalmopathy. Ophthalmology 1999;106(2):324–329.
22. Coats DK, Ou R. Anomalous medial rectus muscle insertion in achild with craniosynostosis. Binoc Vis Strabismus Q 2001;16(2):119–120.
23. Cronenberger MF, de Castro Moreira JB, Brunoni D, et al. Ocular andclinical manifestations of Möbius’ syndrome. J Pediatr OphthalmolStrabismus 2001;38(3):156–162.
24. Cruz OA, Davitt BV. Bilateral inferior rectus muscle recession forcorrection of hypotropia in dysthyroid ophthalmopathy. JAAPOS1999;3(3):157–159.
25. Demer JL, von Noorden GK. High myopia as an unusual cause of restrictive motility disturbance. Surv Ophthalmol 1989;33:281–284.
26. Doherty EJ, Macy ME, Wang SM, Dykeman CP, Melanson MT, EngleEC. CFEOM3: a new extraocular congenital fibrosis syndrome thatmaps to 16q24.2–q24.3. Investig Ophthalmol Vis Sci 1999;40(8):1687–1694.
27. Drummond GT, Keech RV. Absent and anomalous superior obliqueand superior rectus muscles. Can J Ophthalmol 1989;24(6):275–279.
28. Effron L, Price RL, Berlin AJ. Congenital unilateral orbital fibrosiswith suspected prenatal orbital penetration. J Pediatr OphthalmolStrabismus 1985;22(4):133–136.
29. Egbert J, May K, Kersten R, Kulwin D. Pediatric orbital floor frac-ture: direct extraocular muscle involvement. Ophthalmology 2000;107:1875–1879.
30. Egbert JE, Anderson JH, Summers CG. Increased duration of lowretinal slip velocities following retroequatorial placement of hori-zontal recti. J Pediatr Ophthalmol Strabismus 1995;32(6):359–363.
380 handbook of pediatric strabismus and amblyopia
31. Eitzen JP, Elsas FJ. Strabismus following endoscopic intranasal sinussurgery. J Pediatr Ophthalmol Strabismus 1991;28(3):168–170.
32. Engle EC, Goumnerov BC, McKeown CA, et al. Oculomotor nerveand muscle abnormalities in congenital fibrosis of the extraocularmuscles. Ann Neurol 1997;41(3):314–325.
33. Engle EC, Marondel I, Houtman WA, et al. Congenital fibrosis of theextraocular muscles (autosomal dominant congenital external ophthalmoplegia): genetic homogeneity, linkage refinement, andphysical mapping on chromosome 12. Am J Hum Genet 1995;57(5):1086–1094.
34. Engle EC, Kunkel LM, Specht LA, Beggs AH. Mapping a gene for con-genital fibrosis of the extraocular muscles to the centromeric regionof chromosome 12. Nat Genet 1994;7(1):69–73.
35. Brodsky MC, Fray KJ. Surgical management of intermittentexotropia with high AC/A ratio. J Am Assoc Pediatr OphthalmolStrabismus 1998;2:330–332.
36. Fioretto M, Burtolo C, Fava GP. New surgical method for nystagmuswithout null point. Ophthalmologica 1991;203(4):180–183.
37. Flaherty MP, Grattan-Smith P, Steinberg A, Jamieson R, Engle EC.Congenital fibrosis of the extraocular muscles associated with cor-tical dysplasia and maldevelopment of the basal ganglia. Ophthal-mology 2001;108(7):1313–1322.
38. Fujii GY, Kah-Guan AE, Pieramici DJ, et al. Macular translocation:unifying concepts, terminology, and classification. Am J Ophthal-mol 1992;114:72–80.
39. Gillies WE, Harris AJ, Brooks AM, Rivers MR, Wolfe RJ. Congeni-tal fibrosis of the vertically acting extraocular muscles. A new groupof dominantly inherited ocular fibrosis with radiologic findings.Ophthalmology 1995;102(4):607–612.
40. Grimmet MR, Lambert S. Superior rectus overcorrection aftercataract extraction. Am J Ophthalmol 1992;114:72–80.
41. Goldberg AB, Greenberg MB, Darney PD. Misoprostol and preg-nancy. N Engl J Med 2001;344(1):38–47.
42. Greenberg MF, Pollard ZF. Absence of multiple extraocular musclesin craniosynostosis. J Am Assoc Pediatr Ophthalmol Strabismus1998;2(5):307–309.
43. Guemes A, Wright KW. Effect of graded anterior transposition of theinferior oblique muscle on versions and vertical deviation in primaryposition. J Am Assoc Pediatr Ophthalmol Strabismus 1998;2(4):201–206.
44. Gusek-Schneider GC, Langenbucher A, Seitz B. Association of keratoconus and Möbius’ syndrome. J Pediatr Ophthalmol Strabismus2001;38(1):47–48.
45. Guyton DL. Dissociated vertical deviation: etiology, mechanism,and associated phenomena. Costenbader lecture. J Am Assoc PediatrOphthalmol Strabismus 2000;4(3):131–144.
46. Hamed, Mancuso. Inferior rectus muscle contracture syndrome afterretrobulbar anesthesia. Ophthalmology 1991;98:1506–1512.
chapter 10: complex strabismus 381
47. Hamlet YJ, Goldstein JH, Rosenbaum JD. Dehiscence of lateralrectus muscle following intrascleral buckling procedure. Ann Oph-thalmol 1982;14:694–697.
48. Harley RD, Rodrigues MM, Crawford JS. Congenital fibrosis of theextraocular muscles. J Pediatr Ophthalmol Strabismus 1978;15(6):346–358.
49. Harley RD, Rodrigues MM, Crawford JS. Congenital fibrosis of theextraocular muscles. Trans Am Ophthalmol Soc 1978;76:197–226.
50. Hayashi T, Iwashige H, Maruo T. Clinical features and surgery foracquired progressive esotropia associated with severe myopia. ActaOphthalmol Scand 1999;77(1):66–71.
51. Hertel RW, Katowitz JA, Young PL, et al. Congenital unilateral fibro-sis, blepharoptosis, and enophthalmos syndrome. Ophthalmology1992;99:347–355.
52. Holmes JM, Beck RW, Kip KE, Droste PJ, Leske DA. Predictors ofnonrecovery in acute traumatic sixth nerve palsy and paresis. Oph-thalmology 2001;108(8):1457–1460.
53. Holmes JM, Beck RW, Kip KE, Droste PJ, Leske DA. Botulinum toxintreatment versus conservative management in acute traumatic sixthnerve palsy or paresis. J Am Assoc Pediatr Ophthalmol Strabismus2000;4(3):145–149.
54. Hotchkiss MG, Miller NR, Clark AW, et al. Bilateral Duane’s retrac-tion syndrome: a clinical-pathologic case report. Arch Ophthalmol1980;98:870–874.
55. Huber A. Electrophysiology of the retraction syndromes. Br J Oph-thalmol 1974;58:293–300.
56. Hudson HL, Feldon SE. Late overcorrection of hypotropia in Grave’sophthalmopathy. Ophthalmology 1992;99:356–360.
57. Hwang JM, Wright KW. Combined study on the causes of strabis-mus after retinal surgery. Korean J Ophthalmol 1994;8(2):83–91.
58. Ingham PN, McGovern ST, Crompton JL. Congenital absence of theinferior rectus muscle. Aust NZ J Ophthalmol 1986;14(4):355–358.
59. Jameson NA, Good WV, Hoyt CS. Fat adherence simulating inferioroblique palsy following blepharoplasty. Arch Ophthalmol 1992;110(10):1369.
60. Kalpakian B, Bateman JB, Sparkes RS, Wood GK. Congenital ocularfibrosis syndrome associated with the Prader–Willi syndrome. JPediatr Ophthalmol Strabismus 1986;23(4):170–173.
61. Kanski JJ, Elkington AR, Davies MS. Diplopia after retinal detach-ment surgery. Am J Ophthalmol 1973;76:38–40.
62. Kodsi SR, Younge BR. Acquired oculomotor, trochlear, and abducentcranial nerve palsies in pediatric patients. Am J Ophthalmol 1992;114(5):568–574.
63. Krzizok TH, Kaufmann H, Traupe H. New approach in strabismussurgery in high myopia. Br J Ophthalmol 1997;81:625–630.
64. Krzizok TH, Schroeder BU. Measurement of recti eye muscle pathsby magnetic resonance imaging in highly myopic and normal sub-jects. Investig Ophthalmol Vis Sci 1999;40(11):2554–2560.
382 handbook of pediatric strabismus and amblyopia
65. Lee J, et al. Results of a prospective randomized trial of botulinumtoxin therapy in acute unilateral sixth nerve palsy. J Pediatr Oph-thalmol Strabismus 1994;31:283–286.
66. Lengyel D, Zaunbauer W, Keller E, Gottlob I. Mobius syndrome: MRIfindings in three cases. J Pediatr Ophthalmol Strabismus 2000;37(5):305–308.
67. Lin PY, Yen MY. Congenital absence of bilateral inferior rectusmuscles: a case report. J Pediatr Ophthalmol Strabismus 1997;34(6):382–384.
68. Lueder GT, Scott WE, Kutschke PJ, Keech RV. Long-term results ofadjustable suture surgery for strabismus secondary to thyroid oph-thalmopathy. Ophthalmology 1992;99(6):993–997.
69. Mark LE, Kennerdell JS. Medial rectus injury from intranasalsurgery. Arch Ophthalmol 1979;97(3):459–461.
70. Mets MB, Parks MM, Freeley DA, Cornell FM. Congenital absenceof inferior rectus muscle: report of three cases and their manage-ment. Binoc Vis 1987;2(2):77–86.
71. Mets MB, Wendell ME, Gieser RG. Ocular deviation after retinaldetachment surgery. Am J Ophthalmol 1985;99:667–672.
72. Metz HS, Norris A. Cyclotorsional diplopia following retinal detachment surgery. J Pediatr Ophthalmol Strabismus 1987;24(6):287–290.
73. Metz HS. Double elevator palsy. Arch Ophthalmol 1979;97:901–909.
74. Metz HS, Dickey CF. Treatment of unilateral acute sixth nerve palsywith botulinum toxin. Am J Ophthalmol 1991;112:381–384.
75. Michel O, Oberlander N, Neugebauer P, Neugebauer A, RussmannW. Follow-up of transnasal orbital decompression in severe Graves’ophthalmopathy. Ophthalmology 2001;108(2):400–404.
76. Miller NR, Kiel SM, Green WR, Clark AW. Unilateral Duane’sretraction syndrome. Arch Ophthalmol 1982;100:1468–1472.
77. Mitchell PR, Wheeler MB, Parks MM, Kestenbaum surgical proce-dure for torticollis secondary to congenital nystagmus. J PediatrOphthalmol Strabismus 1987;24(2):87–93.
78. Munoz M, Rosenbaum AL. Long-term strabismus complications fol-lowing retinal detachment surgery. J Pediatr Ophthalmol Strabismus1987;24(6):309–314.
79. Nakano M, Yamada K, Fain J, et al. Homozygous mutations in ARIX(PHOX2A) result in congenital fibrosis of the extraocular musclestype 2. Nat Genet 2001.
80. Nardi M, Barca L. Hypercorrection of hypotropia in Graves’ oph-thalmopathy. Ophthalmology 1993Jan;100(1):1–2.
81. Neely DE, Helveston EM, Thuente DD, Plager DA. Relationship ofdissociated vertical deviation and the timing of initial surgery forcongenital esotropia. Ophthalmology 2001;108(3):487–490.
82. Neugebauer A, Fricke J, Kirsch A, Russmann W. Modified transpo-sition procedure of the vertical recti in sixth nerve palsy. Am J Oph-thalmol 2001;131(3):359–363.
chapter 10: complex strabismus 383
83. Oh SY, Clark RA, Velez F, Demer JL. Magnetic resonance imagingdemonstration of instability of rectus pulleys as cause of incomitantstrabismus. Investig Ophthalmol Vis Sci 2001;167:42–44.
84. Parks MM. Causes of the adhesive syndrome In: Symposium on stra-bismus. Transaction of the New Orleans Academy of Ophthalmol-ogy. St Louis: Mosby, 1978:269–279.
85. Pearlman JT, Christensen RE. Motility problems following retinaldetachment surgery. Am Orthopt J 1972;22:64–67.
86. Pedraza S, Gamez J, Rovira A, et al. MRI findings in Möbius syndrome: correlation with clinical features. Neurology 2000;55(7):1058–1060.
87. Peleg D, Nelson GM, Williamson RA, Widness JA. Expanded Möbiussyndrome. Pediatr Neurol 2001;24(4):306–309.
88. Pinchoff BS, Sandall G. Congenital absence of the superior obliquetendon in craniofacial dysostosis. Ophthalmic Surg 1985;16(6):375–377.
89. Porter JD, Baker RS. Absence of oculomotor and trochlear motoneurons leads to altered extraocular muscle development in the Wnt-1 null mutant mouse. Dev Brain Res 1997;100(1):121–126.
90. Prata JA, Minckler DS, Green RL. Pseudo-Brown’s syndrome as acomplication of glaucoma drainage implant surgery. OphthalmicSurg 1993;24:608–611.
91. Prendiville P, Chopra M, Gauderman WJ, Feldon SE. The role ofrestricted motility in determining outcomes for vertical strabismussurgery in Graves’ ophthalmology. Ophthalmology 2000;107(3):545–549.
92. Price RL, Pederzolli A. Strabismus following retinal detachmentsurgery. Am Orthopt J 1982;32:9–17.
93. Quinn AG, Kraft SP, Day C, Taylor RS, Levin AV. A prospective eval-uation of anterior transposition of the inferior oblique muscle, withand without resection, in the treatment of dissociated vertical devi-ation. J Am Assoc Pediatr Ophthalmol Strabismus 2000;4(6):348–353.
94. Raab EL. Clinical features of Duane’s syndrome. J Pediatr Ophthal-mol Strabismus 1986;23:64–68.
95. Raina J, Wright KW, Lin MM, McVey JH. Effectiveness of lateralrectus Y split surgery for correcting the upshoot and downshoot inDuane’s retraction syndrome, Type III. Binoc Vis Strabismus 1997;12(4):233–238.
96. Reck AC, Manners R, Hatchwell E. Phenotypic heterogeneity mayoccur in congenital fibrosis of the extraocular muscles. Br J Oph-thalmol 1998;82(6):676–679.
97. Reinecke RD. Retroequatorial placement of horizontal recti. JPediatr Ophthalmol Strabismus 1996;33(3):201–202.
98. Rene C, Rose GE, Lenthall R, Moseley I. Major orbital complicationsof endoscopic sinus surgery. Br J Ophthalmol 2001;85(5):598–603(review).
384 handbook of pediatric strabismus and amblyopia
99. Roberts EL, Saunders RA, Wilson ME. Surgery for vertical head posi-tion in null point nystagmus. J Pediatr Ophthalmol Strabismus1996;33(4):219–224.
100. Rogers GL, Bremer DL. Surgical treatment of the upshoot and down-shoot in Duane’s retraction syndrome. Ophthalmology 1984;91(11):1380–1383.
101. Romano PE. Absent or hypoplastic extraocular muscles? J MedGenet 1989;26(3):216.
102. Rosenbaum A, Kushner BJ, Kirschen D. Vertical rectus muscle trans-position and botulinum toxin (oculinum) to medial rectus forabducens palsy. Arch Ophthalmol 1989;107:820.
103. Roth AM, Sypnicki BA. Motility dysfunction following surgery forretinal detachment. Am Orthopt J 1975;25:118–121.
104. Saunders RA, Rogers CT. Superior oblique transposition for thirdnerve palsy. Ophthalmology 1982;89:310.
105. Schumacher-Feero LA, Yoo KW, Solari FM, Biglan AW. Third cranial nerve palsy in children. Am J Ophthalmol 1999;128(2):216–221.
106. Scott WE, Jackson OB. Double elevator palsy: the significance ofinferior rectus restriction. Ophthalmology 1977;27:5–10.
107. Scott AB, Wong GY. Duane’s syndrome: an electromyographic study.Arch Ophthalmol 1972;87:142–147.
108. Seiff SR, Good WV. Hypertropia and the posterior blowout fracture:mechanism and management. Ophthalmology 1996;103(1):152–156.
109. Sener EC, Lee BA, Turgut B, Akarsu AN, Engle EC. A clinicallyvariant fibrosis syndrome in a Turkish family maps to the CFEOM1locus on chromosome 12. Arch Ophthalmol 2000;118(8):1090–1097.
110. Sewell JJ, Knobloch WH, Eifrig DE. Extraocular muscle imbalanceafter surgical treatment for retinal detachment. Am J Ophthalmol1974;78:321.
111. Smiddy WE, Loupe D, Michels RG, et al. Extraocular muscle imbal-ance after scleral buckling surgery. Ophthalmology 1989;96:1485–1490.
112. Smith SL, Starita RJ, Fellman RL, Lynn JR. Early clinical experiencewith the Baerveldt 350-mm2 glaucoma implant and associatedextraocular muscle imbalance. Ophthalmology 1993;100:914–918.
113. Snir M, Gilad E, Ben-Sira I. An unusual extraocular muscle anomalyin a patient with Crouzon’s disease. Br J Ophthalmol 1982;66(4):253–257.
114. Stager DR, Weakley DR, Stager D. Anterior transposition of the infe-rior oblique: anatomic assessment of the neurovascular bundle. ArchOphthalmol 1992;110:360–362.
115. Strachan IM, Brown BH. Electromyography of extraocular musclesin Duane’s syndrome. Br J Ophthalmol 1972;56:594–599.
116. Taylor R, Whale K, Raines M. The heavy eye phenomenon: orthop-tic and ophthalmic characteristics. Ger J Ophthalmol 1995;4:252–255.
chapter 10: complex strabismus 385
117. Theodossiadis G, Nikolakis S, Apostolopoulos M. Immediate post-operative muscular disturbance in retinal detachment surgery. ModProbl Ophthalmol 1979;20:367–372.
118. Traboulsi EI, Lee BA, Mousawi A, Khamis AR, Engle EC. Evidenceof genetic heterogeneity in autosomal recessive congenital fibrosisof the extraocular muscles. Am J Ophthalmol 2000;129(5):658–662.
119. Trotter WL, Kaw P, Meyer DR, Simon JW. Treatment of subtotalmedial rectus myectomy complicating functional endoscopic sinussurgery. J Am Assoc Pediatr Ophthalmol Strabismus 2000;4(4):250–253.
120. Vargas FR, Schuler-Faccini L, Brunoni D, et al. Prenatal exposure tomisoprostol and vascular disruption defects: a case-control study.Am J Med Genet 2000;95(4):302–306.
121. Varn MM, Saunders RA, Wilson ME. Combined bilateral superiorrectus muscle recession and inferior oblique muscle weakening fordissociated vertical deviation. J Am Assoc Pediatr Ophthalmol Stra-bismus 1997;1(3):134–137.
122. von Noorden GK, Jenkins RH, Rosenbaum AL. Horizontal transpo-sition of the vertical rectus muscles for treatment of ocular torti-collis. J Pediatr Ophthalmol Strabismus 1993;30(1):8–14.
123. Wang SM, Zwaan J, Mullaney PB, et al. Congenital fibrosis of theextraocular muscles type 2, an inherited exotropic strabismus fixus,maps to distal 11q13. Am J Hum Genet 1998;63(2):517–525.
124. Wilcox LM, Gittinger JW, Breinen GM. Congenital adduction palsyand synergistic divergence. Am J Ophthalmol 1981;91:1–7.
125. Wilder WM, Williams JP, Hupp SL. Computerized tomographic find-ings in two cases of congenital fibrosis syndrome. Comput MedImaging Graph 1991;15(5):361–363.
126. Wilson WB, Prochoda M. Radiotherapy for thyroid orbitopathy.Effects on extraocular muscle balance. Arch Ophthalmol 1995;113(11):1420–1425.
127. Wilson ME, Parks MM. Primary inferior oblique overaction in congenital esotropia: accommodative esotropia and intermittentexotropia. Ophthalmology 1989;96:952–957.
128. Wilson ME, Saunders RA, Berland JE. Dissociated horizontal devia-tion and accommodative esotropia: treatment options when an eso-and an exodeviation co-exist. J Pediatr Ophthalmol Strabismus 1995;32(4):228–230.
129. Wilson ME, McClatchey SK. Dissociated horizontal deviation. JPediatr Ophthalmol Strabismus 1991;28(2):90–95.
130. Wolff SM. Strabismus after retinal detachment surgery. Trans AmOphthalmol Soc 1983;81:182–192.
131. Wolff JE, Koutsandreou AC. Analysis of psychomotor developmentof ten children with Möbius syndrome. Dev Med Child Neurol 2001;43(1):71–72.
132. Wright KW. Late overcorrection after inferior rectus recession. Oph-thalmology 1996;103(9):1503–1507.
386 handbook of pediatric strabismus and amblyopia
133. Wright KW, Liu GY, Murphree AL, et al. Double elevator palsy,ptosis and jaw-winking. Am Orthopt J 1989;39:143–150.
134. Wright KW. The fat adherence syndrome and strabismus after retinasurgery. Ophthalmology 1986;93:411–415.
135. Wright KW. Color atlas of strabismus surgery: strategies and tech-niques. Torrance, CA: Wright, 2000.
136. Wright KW, Edelman PM, McVey JH, Terry A, Lin M. High-gradestereoacuity after early surgery for congenital esotropia. Arch Oph-thalmol 1994;112:913–919.
137. Wright KW. Clinical optokinetic nystagmus asymmetry in treatedesotropes. J Pediatr Ophthalmol Strabismus 1996;33(3):153–155.
138. Yamada M, Shinoda K, Hatakeyama A, Nishina S, Mashima Y. Fatadherence syndrome after retinal surgery treated with amnioticmembrane transplantation. Am J Ophthalmol 2001;132(2):280–282.
chapter 10: complex strabismus 387





























