Embed Size (px)
Citation preview

[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 1313
ABSTRACTObjective: Systematic review of
the literature pertaining to quality oflife studies in adults suffering frominsomnia, by specifically addressingthe following questions: 1) What isthe impact of insomnia on quality oflife? 2) To what extent do comorbidconditions affect quality of life inpatients with insomnia? 3) What isthe impact of insomnia treatment onquality of life?
Design: Our search wasconducted using theMEDLINE/PubMed and PsycINFOdatabases from the past 25 years(1987–2012), using the keywords“Insomnia” AND “Quality of Life,”“QOL,” “Health-related quality oflife,” or “HRQOL.” Fifty-eight studieswere selected for inclusion by twophysicians who reached a consensusabout the studies to include in thisreview.
Results: The literature revealsthat quality of life is severelyimpaired in individuals with insomnia,comorbid conditions significantlyaffects quality of life negatively, andsleep restoration techniques,including cognitive behavioraltherapy and medications, aresuccessful at improving quality of life.However, restoration of quality of lifeto community levels is still unclear.
Conclusion: Insomnia and itscomorbidities negatively affect anindividual’s quality of life, anddifferent modalities of treatment canproduce improvements in physicaland psychological wellbeing andquality of life. More research isneeded to develop moreinterventions that specifically focuson improving quality of life inpatients suffering from insomnia.
INTRODUCTIONThe World Health Organization
(WHO) defines quality of life (QOL),as individuals’ perception of theirposition in life, in the context ofculture and value systems in whichthey live, and in relation to theirgoals, expectations, standards, andconcerns.1 This conceptualframework is translated into patient-reported ratings of the degree ofsatisfaction one has with health,social, occupational status, and otherlife involvements. Hence, high QOLratings are reflective not only ofsymptom reduction but also anoverall improvement in the self-evaluation of one’s own health. Thisis especially important in assessingwhether interventions haveaccomplished the goal of healthrestoration and not merelysymptomatic treatment. Quality of
Quality of Life in PatientsSuffering from Insomnia
[ R E V I E W ]
by WAGUIH W. ISHAK, MD, FAPA; KARA BAGOT, MD; SHANNON THOMAS; NAIRA MAGAKIAN, MD; DINA BEDWANI, MD; DAVID LARSON, MD; ALEXANDRA BROWNSTEIN; and CHRISTINE ZAKY, MDDr. IsHak, Ms. Thomas, Dr. Magakian, Dr. Bedwani, and Dr. Zaky are rom Cedars-Sinai MedicalCenter; Los Angeles, California; Dr. Bagot is from Yale University School of Medicine, Yale ChildStudy Center, New Haven, Connecticut; Dr. Larson is from University of Southern California KeckSchool of Medicine; and Ms. Brownstein is from University of California Los Angeles.
Innov Clin Neurosci. 2012;9(10):13–26
FUNDING: Dr. IsHak has received grants inassociated research areas as listed below:NARSAD on Quality of Life in MajorDepression, Pfizer Monotherapy in MajorDepression.
FINANCIAL DISCLOSURES: None of theauthors have a conflict of interest in theconduct and reporting of this review.
ADDRESS CORRESPONDENCE TO: WaguihWilliam IsHak, MD, FAPA, Cedars-SinaiMedical Center Department of Psychiatryand Behavioral Neurosciences, DavidGeffen School of Medicine at UCLA, 8730Alden Drive, Thalians W-157, Los Angeles,CA 90048; Phone: (310) 423-3515; Fax:(310) 423-3947; E-mail:[email protected]
KEY WORDS: Insomnia, quality of life, sleepdisorder

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]14
life may be a more reflective lensthrough which to view theconsequences of insomnia; it allowsone to understand the significantimpact this disorder can have on thedaily lives of the people it affects,2–5
as impairments in QOL typically arecited as the impetus for seekingtreatment.6
Insomnia is defined as difficultywith sleep initiation or sleepmaintenance, early morningawakenings or nonrestorative sleep,according to the Diagnostic andStatistical Manual of MentalDisorders, Fourth Edition, TextRevision (DSM-IV-TR) criteria. Suchsymptoms hold the potential todrastically affect the patient’s abilityto maintain a sense of wellbeing andperception of self-satisfaction withhealth, occupational, and socialfunctioning. Consequently, insomniais commonly linked to a diminishedQOL status for both primary(syndromic) and secondary(symptomatic) insomnia.5 Insomniais highly prevalent in the generalpopulation. Research reveals aprevalence of approximately 30percent of insomnia symptoms witha range of 10 to 40 percent,depending on how insomnia isdefined.7 Somewhere between 10and 18 percent of these individualsconsider their difficulties with sleepto be severe and chronic.8 Overall,insomnia is more common in womenthan in men, and its prevalenceincreases with age in both sexes.5
Insomnia may be a primary disorder(a syndrome) or secondary to avariety of physical or psychiatricillnesses (e.g., sleep apnea,depression, anxiety), environmentalfactors (e.g., noise levels,temperature, seasonal changes)and/or psychosocial issues (e.g.,current or upcoming stressors).Identifying and treating potentialunderlying conditions are prioritiesin the management of insomnia.Insomnia is associated with anumber of adverse medical, social,and psychological consequencesleading to QOL impairments.
The World Health Consensusreport on sleep found relatively little
research specifically devoted to thesubject of evaluating QOL ininsomnia.9 The goal of this review isto examine QOL in patients withinsomnia through an in-depth reviewof the topic’s published literature.While recent reviews have focusedon how insomnia affects someaspects of QOL, such as daytimefunctioning, sleep quality,neurocognitive functioning, andsocietal burden,2 QOL generally,3 andQOL within the context of economicand public health consequences,4
information about the extent of therole of comorbidities as well as theimpact of treatment of insomnia onQOL remain largely unaddressed.Additionally there is lack ofinvestigation of studies that comparedifferent treatment modalities andthe differential impact on QOL.
This paper aims to answer thefollowing three questions: 1) What isthe impact of insomnia on QOL? 2)To what extent do comorbidconditions affect QOL in patientswith insomnia? and 3) What is theimpact of insomnia treatment onQOL?
This review will attempt to answerthe above questions via a systematicreview of the published literaturepertaining to QOL in insomnia. It willalso identify knowledge gaps in thefield and propose future areas ofresearch that may deepen ourunderstanding of this topic.
METHODSData sources. A systematic
literature search was conductedusing the MEDLINE/PubMed andPsycINFO databases for the past 25years (1987–2012). We used thekeywords “insomnia” AND “quality oflife,” “QOL,” “health-related qualityof life,” or “HRQOL.” The referencelist of identified papers and priorreviews were manually reviewed foradditional studies. The initial searchyielded 427 articles. The search wasthen narrowed to studies that onlyincluded measurement of quality oflife. This narrowed search yielded150 articles.
Study selection criteria. Twophysicians reviewed the 150
abstracts using the followinginclusion criteria: 1) articles inEnglish or with an availablepublished English translation, 2)publication in a peer-reviewedjournal, 3) studies of humans, 4)studies (of any design) that focusedon insomnia (not other sleepsymptoms), and 5) studies that usedat least one QOL measure ordomains derived from QOLmeasures. Both physicians thenconducted, independently, a focusedreview using the full text articles ofstudies that met the above criteria.The reviewers then reached aconsensus about the studies toinclude in this manuscript.
Data extraction and yield. Thestudy selection process yielded 58articles meeting the aforementionedselection criteria. Researchmethodology and key findings werederived from the full text and thetables of the selected studies. Theliterature search and selectionmethodology are depicted in Figure 1.
QOL measures in insomnia.General QOL measures used ininsomnia. The Medical OutcomesStudy Short Form-36 (SF-36) is avery widely used scale in evaluatinghealth-related QOL (HRQOL) in avariety of medical/psychiatricconditions and in insomnia.10–14 TheSF-36 is a 36-item generic QOLmeasure that assesses eight domainsspecific to HRQOL: 1) physicalfunctioning, 2) role limitation due tophysical health problems (rolephysical), 3) body pain, 4) generalhealth perceptions, 5) vitality, 6)social functioning, 7) role limitationsdue to emotional health problems(role emotional), and 8) mentalhealth.15,16 All health measures arescored on scales of 0 to 100, withhigher scores indicating betterhealth. Community norms are set ata mean score of 50 (SD=10) on eachof its two components: physicalcomponent score (PCS) and mentalcomponent score (MCS). The SF-36has two abbreviated versions: the 12-item SF-12 and the eight-item SF-8.There are several advantages to usingthe SF-36, such as the following:

[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 15
Reliability and validity have beenextensively tested in many differentpopulations; norms have beengenerated for disease-specific andgeneral population; it is easy tocomplete; it allows for comparisonsacross disease states; and it has beenshown to be sensitive to insomnia-related changes.17–19 Limitationsassociated with the SF-36 includedecreased sensitivity at extremes(either good or bad) and its lack ofspecificity to the illness it measures.19
The Quality of Life Enjoyment andSatisfaction Questionnaire Short-Form (Q-LES-Q)is a 16-item scalewith a total score ranging from 0(lowest QOL) to 100 (highest QOL)with established community normsmean score of 78.3 (SD=11.3).20,21 TheQ-LES-Q has been used in a widevariety of research studies ofpsychiatric disorders includinginsomnia.22
The World Health OrganizationQuality of Life—Brief Form(WHOQOL-BREF) is a 24-itemquestionnaire covering four domains(physical health, psychological health,social relationships, andenvironment)23 has been used morecommonly to measure QOL in otherdisorders where insomnia is alsopresent.
The EuroQol-5 (EQ-5D) is a five-item QOL questionnaire covering fivedomains (mobility, self-care, usualactivity, pain and anxiety/ depression)and has been used in comorbiditystudies.24 Other investigators alsoused the QOL inventory, a 31-itemquestionnaire specifically designed forthe study which includes questionsrelated to sleep, cognitive function,daytime performance, social andfamily relationships, and health.4
Details of the psychometricproperties of the general QOLmeasures appear in a previous articleby the authors.25
Insomnia-specific QOLMeasures. Léger et al19 developed ameasurement tool, the Hotel-Dieu-16(HD-16), to specifically evaluate QOLin those with varying severity ofinsomnia. Unlike the aforementionedinstruments, the HD-16 was designedto control for comorbid illness that
may confound the associationbetween QOL and insomnia and wasconstructed based on interviews with20 patients with ‘severe’ insomnia(two or more complaints of insomniain the past month) and validated byapplying the scale to patientsclassified as “good sleepers” (n=391),“mild insomniacs” (n=422), and“severe insomniacs” (n=240). Fivedimensions (physical energy/the willto carry out tasks, cognition, social,and psychological) of QOL areevaluated over 43 questions. Whilethis study has some limitations,including nonspecificity of severalitems (i.e., evaluates symptomatologycommon to many other diseasestates) and only one evaluatedsample, thus the generalizabilityremains unproven; the face validity ofthe study appears sound. The authorsconcluded that an insomnia-specificQOL measurement is better able tocapture the deficits in functioning andQOL directly attributable to insomniaand may better evaluate treatmentoutcome.
The Quality of Life of Insomniacsquestionnaire was developed byRombaut et al26 to specificallyevaluate QOL in insomnia. Thisinstrument has been used in a fewstudies, and it has not been expanded
into clinical or research settings.Other QOL measures used in
insomnia. The Nottingham HealthProfile (NHP, 38-item covering 6domains)27 and the Sickness ImpactProfile (SIP, 136 items covering 12domains), both of which are genericmeasures, have also been used todetect QOL changes associated withinsomnia.18,19 McCall et al22,28 used thedaily living and role functioning(DLRF) and relationship to self andothers (RSO) subscales of theBehavior and Symptom IdentificationScale (BASIS-32) to assess QOL. TheDLRF and RSO subscales have beenshown to differentiate depressedpatients with insomnia from thosewithout insomnia.22
RESULTS WHAT IS THE IMPACTOF INSOMNIA ON QOL?
Insomnia has a large impact on anindividual’s ability to maintain work,physical, and social performance aswell as overall quality of life, asshown by the findings from reviewedstudies (Table 1).
Studies using the SF-36 to assessinsomnia and its impact on QOLshowed that individuals withinsomnia reported poor QOL.10–13,16
Zamitt et al11 used severalinstruments to evaluate the impact
FIGURE 1. Quality of life in insomnia literature search results

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]16
of insomnia on QOL in a sample of261 “insomniacs” compared to acontrol group of 101 good sleepers.Individuals with irregular sleeppatterns, sleep apnea, restless legsyndrome, periodic limb movementdisorders, a history of psychiatricillness, alcohol and substance abuse,epilepsy, and humanimmunodificiency virus infectionwere excluded from the study. Toevaluate QOL, Zamitt et al11 used theSF-36 and the QOL inventory. Theresults showed a significantdifference between the two groups(p<0.0001 MANOVA) on all eight SF-36 subclasses. In comparison to“good sleepers,” individuals withinsomnia reported more healthconcerns that limited physicalactivity, caused more body pain, andcaused more emotional difficulties.
Léger17 explored the effect ofinsomnia on daytime functioningusing the SF-36 to evaluate the QOLof three matched groups of 240subjects with severe insomnia, 422with mild insomnia, and 391 goodsleepers. It was found that thosewith severe insomnia had lower QOLscores in the above eight dimensionsof SF-36 than did those with mildinsomnia and good sleep patterns.Mental status and emotional statewere worse in both the severe andmild insomnia groups compared tothe good sleepers.17 In a study ofinsomnia and quality of life, Katz and
McHorney29 examined 3,445patients diagnosed with chronicmedical and psychiatric conditions.The results showed that patientswith insomnia have lower quality oflife, measured by the SF-36,independent of the presence/absenceof a comorbid chronic illness.Furthermore, the study found thatthe effect of insomnia on quality oflife is equal in severity to the effectof any chronic illness, such ascongestive heart failure or clinicaldepression. Similarly, decreased QOLas a function of insomnia was shownto be comparable to QOL impairmentdue to chronic medical conditions,using the Nottingham Health Profile(NHP)27 and the Sickness ImpactProfile (SIP).18,19
In summary, insomnia negativelyaffects individuals’ quality of life andcould cause increasing impairmentin QOL with increasing severity ofsleep disturbance.3,30–35
WHAT IS THE IMPACT OFCOMORBIDITIES ON QOL ININSOMNIA?
Insomnia commonly exists in thepresence of medical, psychiatric, andpsychosocial stressors.36 Vallieres etal37 found that unemployment,recent death of a friend/familymember, recent end of arelationship, and personal illness arethe most common precipitants forshort-term insomnia (less than onemonth). Underlying stress may beone of the factors contributing toinsomnia and could contributeindependently to impairing anindividual’s quality of life.29 Stressorsmay also exacerbate the severity ofinsomnia as well as other comorbidconditions, which in turn may haveseveral downstream effects on QOLand ability to function. Moreover,studies show that individualssuffering from insomnia have agreater chance of developingdepression and anxiety leading tofurther QOL deterioration.62
Research shows that insomnia wasoften comorbid with chronicillnesses or depression.31
Psychiatric comorbidities. It isestimated that insomnia affectsanywhere from 50 to 80 percent ofthe treatment-seeking psychiatricpopulation,38 highlighting theimportance of psychiatriccomorbidities and/or causes ofpsychopathology. Additionally, 30 to50 percent of the aforementionedpopulation that suffers from chronicinsomnia has one or more of thefollowing psychiatric disorders:major depressive disorder, mania/hypomania, an anxiety disorder(phobias, obsessive-compulsivedisorder, panic disorder, generalizedanxiety disorder) and/or a substanceabuse/dependence disorder.39
Depression. Sleep disturbance isan important component in theclinical presentation of depressivedisorders. Insomnia is a particularly
frequent complaint as it is reportedby nearly 85 percent of depressedpatients.40 Unfortunately, insomniaremains the most commonlyunresolved symptom of depressioneven after mood improvementfollowing selective serotoninreuptake inhibitors (SSRIs)treatment.22 Many depressed patientsattribute low daytime functioning,including poor concentration andmemory, decreased reaction timeand coordination, fatigue, mooddisturbance, and anxiety to inabilityto obtain an adequate amount ofnighttime sleep or sub-par quality ofsleep.
A study performed by McCall etal22 was designed to measure theimpact of insomnia on the quality oflife of inpatients with depression.The results showed lower QOLratings in patients with comorbidinsomnia. This difference wasespecially prominent in those using ameasure of self-report, the BeckDepression Inventory (BDI), ascompared to the clinician-ratedHamilton Rating Scale for Depression(HRSD). In a study of residualsymptoms in depression,approximately 40 percent of patientsreceiving fluoxetine reportedsymptoms compatible withnonrestorative sleep.41 Compared tosleep disturbances related toinitiation or maintenance of sleep,nonrestorative sleep is associatedwith greater daytime functionalimpairment. Therefore, targetinginsomnia in depression may increasedaytime performance and overallQOL.
Anxiety disorders. Generalizedanxiety disorder (GAD) andinsomnia commonly coexist, with atleast 66 percent of patients withGAD experiencing comorbid sleepdisturbances.42 Similarly, GAD is themost common psychiatric disorderamong patients with insomnia.42
Brenes et al43 found that 90 percentof older adults with GAD reportedmoderate to severe insomnia.43
Individuals with significant insomniaoften also experience somaticmanifestations of psychiatric illness,such as elevated physiological

[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 17
TABLE 1. Impact of insomnia on QOL
REFERENCE MEASURE N SUMMARY OF FINDINGS
Zammit et al(1999)11 SF-36
261 insomniasubjects, 101
controlsInsomnia patients had significantly lower SF-36 scores compared to controls (p< 0.0001).
Schubert etal (2002)12 SF-36 2,800
In a population of older adults, 26% reported 1 insomnia symptom, 13% reported 2, and10% reported 3. SF-36 decreased on all 8 domains as the number of reported symptomsincreased (p< 0.0001).
Stein et al(2008)13 SF-36 1,359
Chronic physical illness was associated with poorer HRQOL (p<0.0001). Psychotropicmedications use was associated with lower scores on SF-36 MCS (p=0.0001) and SF-36PCS (p=0.015) in women (controlling for age and number of comorbid illnesses).
Léger et al(2001)17 SF-36
240 insomniasubjects and 391
good sleepers
This study compared good sleepers (GS) to patients with severe insomnia (SI)—Physicianvisit with insomnia complaint: 0% GS v. 18% SI (p<0.0001); regularly taking sleeping pills:0% GS v. 28% SI (p<0.0001); hospitalizations (past 12 mo.): 9% GS v. 18% SI(p=0.0017); on at least 1 medication: 44% GS v. 67% SI (OR=2.59); “Work error that couldhave serious consequences:” 6% GS v. 15% SI (p<0.001).
Katz andMcHorney(2002)29
SF-36 3,445
34% had mild insomnia and 16% had severe insomnia at baseline. 59% (95% CI, 55%-63%) of patients’ with mild insomnia and 83% (95% CI, 78–88%) with severe insomnia atbaseline still had problems at 2-year follow-up. Mild and severe insomnia were associatedwith decreases in physical health perception (mild: OR=2.0; severe: OR=5.1), vitality (mild:OR=2.4; severe: OR=7.4), and mental health (mild: OR=3.5; severe: OR=10.2) domains.
Stein et al(2002)31 SF-36 4,181
Sleep problems were found to be associated with physical (AOR=1.21, 95% CI=1.01–1.45)and mental health problems (AOR=3.58, 95% CI=2.95–4.35) especially in those withcomorbid physical health issues. The co-occurrence of insomnia was independentlyassociated with poorer ratings on the SF-36 PCS (p< 0.001) and increased the odds of 1 ormore days taken off from work in the past 30 days due to physical problems (AOR=1.55,95% CI=1.20–1.98) by 50%.
Hatoum et al(1998)32 SF-36 1,100
Insomnia with reported impairments in daytime functioning was associated with significantQOL deficits across all domains (p<0.001). Compared to patients without insomnia,patients with problems with quality/quantity of sleep (no reported daytime symptoms)demonstrated significantly lower scores on the PCS (p<0.001) and the body pain (p=0.01)subscale.
Guereje et al(2009)34 WHOQOL-Bref 2,152 elderly
NigeriansDifficulty initiating or maintaining sleep and early AM awakening were associated withphysical, psychological, social, and environmental subscales and overall QOL (p<0.05).
Lee et al(2009)35 SF-36 397
Sleep disturbance and daytime fatigue were associated with increased likelihood of lowscores on the following subscales: physical functioning, AOR=6.10; physical healthproblems, AOR=8.28; bodily pain, AOR=6.41; general health, AOR=5.88; vitality,AOR=17.09; social functioning, AOR=5.46; and mental health, AOR=12.83.
QOL: quality of life; SF-36: Medical Outcomes Study Short Form-36; HRQOL: health-related quality of life; MCS: mental component score;PCS: physical component score; OR: odds ratio; CI: confidence interval; AOR: adjusted odds ratio; WHOQOL-Bref: World Health OrganizationQuality of Life—Brief Form

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]18
symptoms of arousal (e.g., dizziness,headache, weakness, fatigue,palpitations, and gastro-intestinaldistress).44 Moreover, patients withinsomnia report more attentiondisorders and memory complaints.45
This may lead to impairedconcentration and increase the riskof traffic accidents as well as fatigueand daytime sleepiness—symptomsassociated with poor QOL.
Veterans returning from combathave been shown to demonstratehigh rates of posttraumatic stressdisorder (PTSD) and traumatic braininjury (TBI),46,47 both of which areassociated with a high prevalence ofinsomnia.48 Additionally, all threediagnostic subcategories of PTSD, re-experiencing, avoidance, and hyper-arousal, may factor into thedevelopment of PTSD as they areassociated with poor sleep hygieneand/or may be the impetus forfrequent awakenings or delayedsleep initiation. In a study by Wallaceet al49 comparing the differentialeffects of PTSD with or withoutcomorbid mild TBI (mTBI) on sleepand daytime functioning, the authorscompared characteristics of sleepbetween healthy sleepers (control),individuals with insomnia plus PTSDplus TBI combined and individualswith insomnia plus PTSD alone.Although those participants withPTSD plus mTBI demonstratedsimilarities in type of insomniaexperienced, short duration of sleep,and severity as compared to PTSDalone participants, the PTSD plusmTBI group indicated greaterdaytime sleepiness although theyspent more of the night sleeping.49
This is an important finding asinsomnia due to decreased durationof sleep has been associated withpoor HRQOL outcomes, such asincreased use of the healthcaresystem, increased morbidity andmortality due to physical illness, andreduced work productivity.49
Childhood-related psychiatricdisorders. Psychiatric illness inchildhood can also have lifelongconsequences on sleep quality andquality of life. Poon and Knight50
investigated the downstream impact
of childhood abuse/neglect onsubjective feelings of sleep difficultyand the secondary effect that thishas on perceived quality of life inadulthood. The authors postulatedthat neglect and abuse in childhoodpromote a neural set-up for poorattachment with hindrance of thedevelopment of positiveinterpersonal relationships later inlife. The anxiety that this engendersin combination with heightenedstress reactivity can contribute toinsomnia secondary to the stress ofpsychosocial issues. This couldfurther impact QOL and the ability tocope with emotional strain as well asdiminish the ability to foster andmaintain social relationships.Parental emotional abuse isassociated with adulthood sleepcomplaints, which is consistent withindices of insomnia associated withemotional and interpersonal stress.
Medical comorbidities.Individuals with insomnia have 60-percent greater healthcare costs ascompared to the general populationdue to over-utilization of thehealthcare system.51 This isevidenced by greater number ofvisits to the emergency departmentand outpatient physicians, increaseduse of pharmacotherapy, and morelaboratory tests ordered,52 proving tobe a great economic and healthcareburden.53 Of patients seen in primarycare settings, approximately 10percent suffer from chronicinsomnia.54
Cancer. Insomnia affects up to 50percent of cancer patients,contributing to feelings of fatigue,and possibly immunosuppression.55,56
In a cross-sectional study of 120elderly patients with cancer, Chengand Lee55 found that those with asymptom cluster of insomnia, pain,and fatigue reported the lowest QOL,based on Functional Assessment ofCancer Therapy (FACT-G) scoresand experienced the greatestdecrements in functioning. Theyconcluded that as 5.5 to 18.8 percentof elderly cancer patients have co-occurrence of the aforementionedsymptom cluster, the combinedimpact of the three serve to decrease
QOL and perceived and actualfunctioning. Further research needsto be done to study the individualimpact of pain, fatigue and insomniaon QOL and functional status in thisunique population.55
Neurological disorders. Insomniamay also exacerbate symptoms ofTBI possibly due to injury to theneural circuitry that regulates sleep,side effects of medications used totreat complications of TBI, orcomorbid psychiatric, pain, ormedical disorders.49 Insomnia mayfurther contribute to worseningsymptoms of TBI by impeding thehealing process that occurs duringsleep. The estimated prevalence ofinsomnia in those with TBI varieswidely from 21 to 93 percent.57,58
Comorbid insomnia is also acommon problem in those withneurodegenerative disorders, such asParkinson’s or Alzheimer’s disease. Incertain neurological conditions,insomnia may be considered a directresult of the disease itself orsecondary to other factors associatedwith it, such as pain, depression, ortreatment medications.59 Caap-Ahlgren and Devlin60 investigated theimpact of insomnia on QOL in apopulation of 102 patients withcomorbid Parkinson’s disease andfound that they had lower scores oneach domain of QOL, as measured bySF-36, as compared to patients withParkinson’s disease with noinsomnia.60
Patients admitted to the ICU.Insomnia is well recognized in theintensive care unit (ICU).61 Despiteexhibiting normal duration of sleep,patients usually demonstrate poorquality and abnormal patterns ofsleep. Poor sleep quality can continuein patients after discharge.62 There isevidence that even the recollection ofthe difficulties experienced while onan ICU can negatively impact sleepsix months after discharge.62 Thesesleep disturbances have been foundto contribute to significant continuingdecrements in HRQOL in all domainsof the EuroQol-5 and to the inabilityto return to prior functioning.62 Lackof treatment may contribute toimpaired QOL.63

[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 19
Congestive heart failure (CHF).In a study conducted by Krakow etal,64 insomnia and sleep-disorderedbreathing (SDB) were the mostcommon causes of sleepdisturbances in patients with CHF.Additionally, Johansson et al65 foundthat in elderly patients with CHF, 42percent demonstrated SDB ascompared to eight percent in thosewithout CHF (p=0.001). In regard toinsomnia, of those with comorbidCHF, 72 percent had difficultymaintaining sleep (as compared to50% in non-CHF patients; p=0.05),and 25 percent exhibited daytimefatigue (as compared to 8% in non-CHF patients; p=0.05).65 The elderlypatients that demonstratedsymptoms of insomnia or SDB andcomorbid CHF had worse QOLscores compared to those withoutCHF. Furthermore, decrements inthe physical composite score of theSF-36 were associated with thefollowing signs of insomnia (p<0.05):difficulty initiating or maintainingsleep, early morning awakening, andnonrestorative sleep. Nonrestorativesleep was also associated with adeficit in the mental healthcomposite score (p<0.05).65 A studyto evaluate the impact of nasaldilator strips (NDS) on sleep quality,SDB, and QOL was done in nonobeseadults with sleep disturbances. Theparticipants consisted of 42 subjectsin the treatment group and 38subjects in the control group. At fourweeks follow-up, the treatmentgroup reported significantimprovements in insomnia severityand sleep quality and improvementin Q-LES-Q (mean d=0.51),compared to small, statisticallyinsignificant changes in the controlgroup.64
Comorbid sleep disorders.Although sleep disorders such asobstructive sleep apnea (OSA), SDB,narcolepsy, snoring and restless legsyndrome/periodic limb movementare considered separate diseaseentities from insomnia, the co-occurrence of the two and theircombined impact on QOL isimportant to consider. To studycharacteristics of insomnia and their
impact on QOL in a population ofpatients with OSA and comorbidinsomnia, Bjornsdottir et al66
evaluated 824 patients with OSA and762 healthy controls. In regard tosymptoms of insomnia, they foundthat compared to their healthycounterparts, those with OSAencountered greater difficulties withsleep maintenance. They also foundthat women with OSA had greatersleep onset latency as compared towomen without OSA. Additionally,increased difficulty initiating and/ormaintaining sleep was associatedwith poorer QOL (SF-12). Individualswith OSA also demonstrated moreimpairment in physical and mentaldomains of perceived QOL.66
WHAT IS THE IMPACT OFTREATMENT OF INSOMNIA ONQOL?
As the impact of insomnia onhealth and wellbeing might be under-recognized, many patients do notseek medical care early in the courseof sleep disturbance, resulting in asignificant amount of under-treatment and inadequatetreatment.67 As 85 to 90 percent ofchronic insomnia is attributable tocomorbidities, including circadianrhythm disorders, physical andpsychiatric illness, concurrentsubstance abuse, and/orpharmacotherapy for comorbidillness,8 cessation of medication/druguse and/or treatment of the primarydisorder may adequately addresssleep disturbances that would lead toa downstream impact on QOL.Behavioral as well as pharmacologicalinterventions play an important rolein treatment and improvement ofdaily functioning and one’sperception of QOL. The details of thereviewed treatment studies areshown in Table 2.
Pharmacological treatments. Ithas been shown that 5 to 8 percentof the general population usemedications to aid in better quality,or greater duration of sleep.8 Thereare three United States Food andDrug Administration (FDA)-approved drug classes for thetreatment of insomnia:
benzodiazepines, benzodiazepinereceptor agonists, and melatoninreceptor agonists.
Benzodiazepines.Benzodiazepines have been shown tobe efficacious in reducing sleep onsetlatency and frequency/amount ofnighttime awakenings. However,benzodiazepines have not beenformally studied for their impact onQOL and their negative effects onnext-day functioning (e.g., decreasedmemory and recall and daytimesleepiness), as well as the risk oftolerance and/or dependence whenused long-term.68
Benzodiazepine receptoragonists (BRAs). BRAs, also knownas nonbenzodiazepine sedative-hypnotics, have also shown efficacyin treatment of insomnia. Theydemonstrate the same hypnoticeffects as benzodiazepines withoutthe high propensity for dependenceand development of tolerance.
There are also severalrandomized, controlled trials (RCTs)that have been conducted toevaluate the efficacy of thesemedications on insomnia and theeffect they have on QOL. In a RCT of458 patients (231 randomized totreatment, 227 randomized toplacebo) studying the impact of a 14-day standing zoplicone regimen withan additional six weeks of medicationper patient request, the patientsrandomized to zolpicone had similarimprovement in the psychologicalwellbeing component and global QOLof the QOLI as compared to theplacebo group. But the treatmentgroup demonstrated significantlygreater improvement in the activity,sleep, social, and work domains.67
These improvements weremaintained at two-month follow-up.
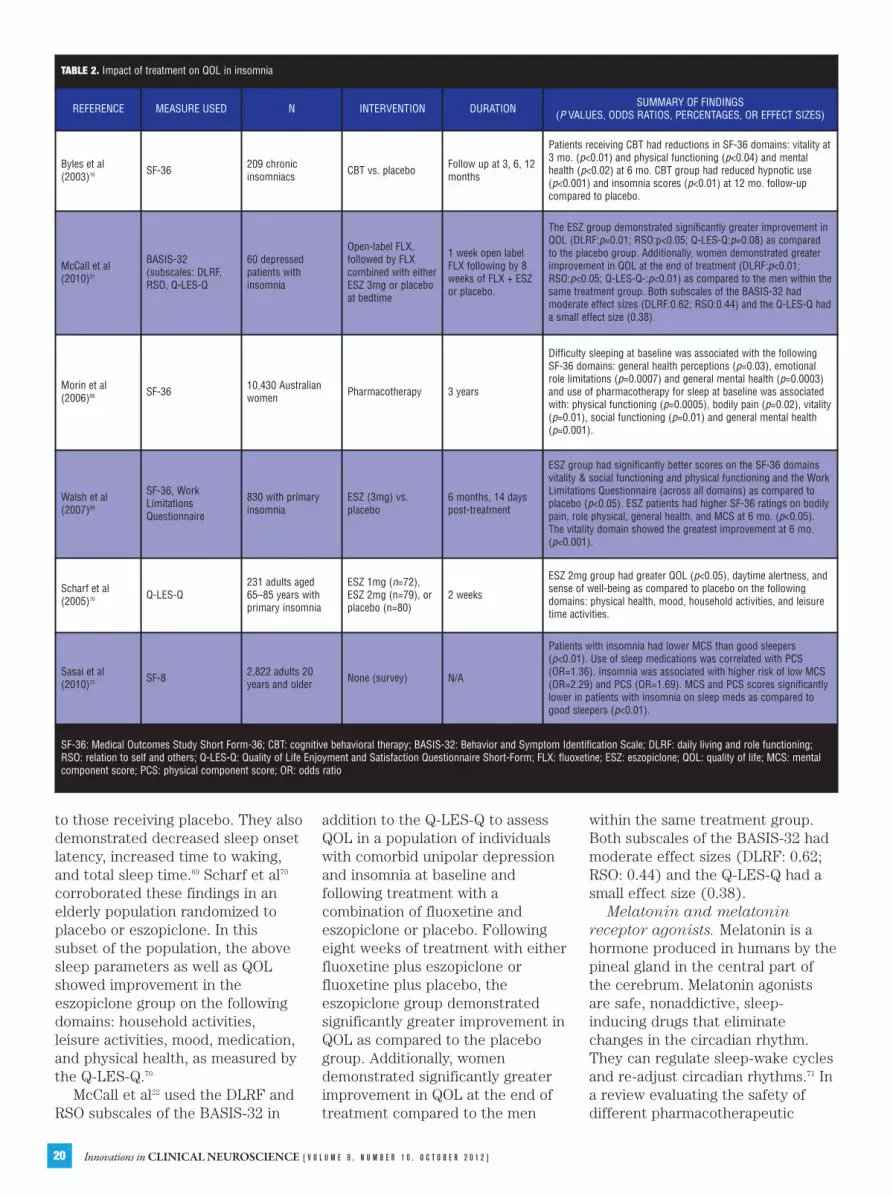
Walsh et al69 evaluated the efficacyof eszopiclone on sleep disturbances(latency of sleep initiation, time towaking after sleep onset, and totalsleep time) and QOL impairments.After six months of study medicationconsumption, the patients receivingeszopiclone demonstrated greaterimprovement in bodily pain, physicaland social functioning, and vitality asmeasured by the SF-36, as compared
Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]20
to those receiving placebo. They alsodemonstrated decreased sleep onsetlatency, increased time to waking,and total sleep time.69 Scharf et al70
corroborated these findings in anelderly population randomized toplacebo or eszopiclone. In thissubset of the population, the abovesleep parameters as well as QOLshowed improvement in theeszopiclone group on the followingdomains: household activities,leisure activities, mood, medication,and physical health, as measured bythe Q-LES-Q.70
McCall et al22 used the DLRF andRSO subscales of the BASIS-32 in
addition to the Q-LES-Q to assessQOL in a population of individualswith comorbid unipolar depressionand insomnia at baseline andfollowing treatment with acombination of fluoxetine andeszopiclone or placebo. Followingeight weeks of treatment with eitherfluoxetine plus eszopiclone orfluoxetine plus placebo, theeszopiclone group demonstratedsignificantly greater improvement inQOL as compared to the placebogroup. Additionally, womendemonstrated significantly greaterimprovement in QOL at the end oftreatment compared to the men
within the same treatment group.Both subscales of the BASIS-32 hadmoderate effect sizes (DLRF: 0.62;RSO: 0.44) and the Q-LES-Q had asmall effect size (0.38).
Melatonin and melatoninreceptor agonists. Melatonin is ahormone produced in humans by thepineal gland in the central part ofthe cerebrum. Melatonin agonistsare safe, nonaddictive, sleep-inducing drugs that eliminatechanges in the circadian rhythm.They can regulate sleep-wake cyclesand re-adjust circadian rhythms.71 Ina review evaluating the safety ofdifferent pharmacotherapeutic
TABLE 2. Impact of treatment on QOL in insomnia
REFERENCE MEASURE USED N INTERVENTION DURATION SUMMARY OF FINDINGS (P VALUES, ODDS RATIOS, PERCENTAGES, OR EFFECT SIZES)
Byles et al(2003)16 SF-36 209 chronic
insomniacs CBT vs. placebo Follow up at 3, 6, 12months
Patients receiving CBT had reductions in SF-36 domains: vitality at3 mo. (p<0.01) and physical functioning (p<0.04) and mentalhealth (p<0.02) at 6 mo. CBT group had reduced hypnotic use(p<0.001) and insomnia scores (p<0.01) at 12 mo. follow-upcompared to placebo.
McCall et al(2010)22
BASIS-32(subscales: DLRF,RSO, Q-LES-Q
60 depressedpatients withinsomnia
Open-label FLX,followed by FLXcombined with eitherESZ 3mg or placeboat bedtime
1 week open labelFLX following by 8weeks of FLX + ESZor placebo.
The ESZ group demonstrated significantly greater improvement inQOL (DLRF:p=0.01; RSO:p<0.05; Q-LES-Q:p=0.08) as comparedto the placebo group. Additionally, women demonstrated greaterimprovement in QOL at the end of treatment (DLRF:p<0.01;RSO:p<0.05; Q-LES-Q-:p<0.01) as compared to the men within thesame treatment group. Both subscales of the BASIS-32 hadmoderate effect sizes (DLRF:0.62; RSO:0.44) and the Q-LES-Q hada small effect size (0.38).
Morin et al(2006)68 SF-36 10,430 Australian
women Pharmacotherapy 3 years
Difficulty sleeping at baseline was associated with the followingSF-36 domains: general health perceptions (p=0.03), emotionalrole limitations (p=0.0007) and general mental health (p=0.0003)and use of pharmacotherapy for sleep at baseline was associatedwith: physical functioning (p=0.0005), bodily pain (p=0.02), vitality(p=0.01), social functioning (p=0.01) and general mental health(p=0.001).
Walsh et al(2007)69
SF-36, WorkLimitationsQuestionnaire
830 with primaryinsomnia
ESZ (3mg) vs.placebo
6 months, 14 dayspost-treatment
ESZ group had significantly better scores on the SF-36 domainsvitality & social functioning and physical functioning and the WorkLimitations Questionnaire (across all domains) as compared toplacebo (p<0.05). ESZ patients had higher SF-36 ratings on bodilypain, role physical, general health, and MCS at 6 mo. (p<0.05).The vitality domain showed the greatest improvement at 6 mo.(p<0.001).
Scharf et al(2005)70 Q-LES-Q
231 adults aged65–85 years withprimary insomnia
ESZ 1mg (n=72),ESZ 2mg (n=79), orplacebo (n=80)
2 weeks
ESZ 2mg group had greater QOL (p<0.05), daytime alertness, andsense of well-being as compared to placebo on the followingdomains: physical health, mood, household activities, and leisuretime activities.
Sasai et al(2010)73 SF-8 2,822 adults 20
years and older None (survey) N/A
Patients with insomnia had lower MCS than good sleepers(p<0.01). Use of sleep medications was correlated with PCS(OR=1.36). Insomnia was associated with higher risk of low MCS(OR=2.29) and PCS (OR=1.69). MCS and PCS scores significantlylower in patients with insomnia on sleep meds as compared togood sleepers (p<0.01).
SF-36: Medical Outcomes Study Short Form-36; CBT: cognitive behavioral therapy; BASIS-32: Behavior and Symptom Identification Scale; DLRF: daily living and role functioning;RSO: relation to self and others; Q-LES-Q: Quality of Life Enjoyment and Satisfaction Questionnaire Short-Form; FLX: fluoxetine; ESZ: eszopiclone; QOL: quality of life; MCS: mentalcomponent score; PCS: physical component score; OR: odds ratio
[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 21
modalities in the elderly,72 theauthors concluded that melatoninagonists are safer to use than thetraditional sedative-hypnotics thatwork on GABA receptors. Theauthors also found that melatoninreceptor agonists also help toimprove mood and quality of sleep inthis population.
Other pharmacologicalinterventions used for insomnia.No information is available on theimpact of sedating medications, suchas antidepressants (e.g., trazodone,mirtazapine, or tricyclics),antipsychotics (e.g., quetiapine,olanzapine, or chlorpromazine), ormood stabilizers (e.g., valproic acid,
lamotrigine, or carbamazepine) onQOL in insomnia.
Potential negative effects ofpharmacological interventions. Incontrast to the above findings, sleepmedications might have negativeeffects on QOL. In a survey of 2,822individuals, Sasai et al73 investigatedthe impact of insomnia and use of
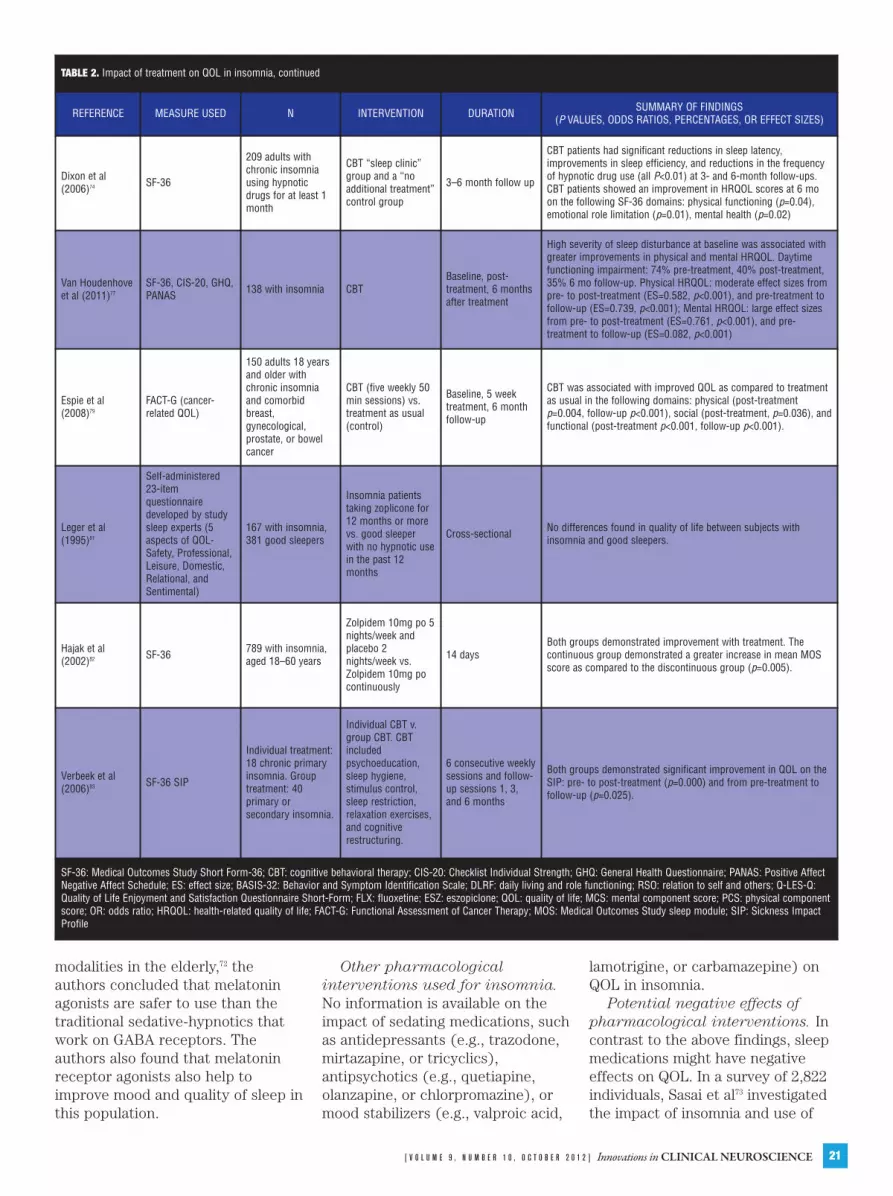
TABLE 2. Impact of treatment on QOL in insomnia, continued
REFERENCE MEASURE USED N INTERVENTION DURATION SUMMARY OF FINDINGS (P VALUES, ODDS RATIOS, PERCENTAGES, OR EFFECT SIZES)
Dixon et al(2006)74 SF-36
209 adults withchronic insomniausing hypnoticdrugs for at least 1month
CBT “sleep clinic”group and a “noadditional treatment”control group
3–6 month follow up
CBT patients had significant reductions in sleep latency,improvements in sleep efficiency, and reductions in the frequencyof hypnotic drug use (all P<0.01) at 3- and 6-month follow-ups.CBT patients showed an improvement in HRQOL scores at 6 moon the following SF-36 domains: physical functioning (p=0.04),emotional role limitation (p=0.01), mental health (p=0.02)
Van Houdenhoveet al (2011)77
SF-36, CIS-20, GHQ,PANAS 138 with insomnia CBT
Baseline, post-treatment, 6 monthsafter treatment
High severity of sleep disturbance at baseline was associated withgreater improvements in physical and mental HRQOL. Daytimefunctioning impairment: 74% pre-treatment, 40% post-treatment,35% 6 mo follow-up. Physical HRQOL: moderate effect sizes frompre- to post-treatment (ES=0.582, p<0.001), and pre-treatment tofollow-up (ES=0.739, p<0.001); Mental HRQOL: large effect sizesfrom pre- to post-treatment (ES=0.761, p<0.001), and pre-treatment to follow-up (ES=0.082, p<0.001)
Espie et al(2008)79
FACT-G (cancer-related QOL)
150 adults 18 yearsand older withchronic insomniaand comorbidbreast,gynecological,prostate, or bowelcancer
CBT (five weekly 50min sessions) vs.treatment as usual(control)
Baseline, 5 weektreatment, 6 monthfollow-up
CBT was associated with improved QOL as compared to treatmentas usual in the following domains: physical (post-treatmentp=0.004, follow-up p<0.001), social (post-treatment, p=0.036), andfunctional (post-treatment p<0.001, follow-up p<0.001).
Leger et al(1995)81
Self-administered23-itemquestionnairedeveloped by studysleep experts (5aspects of QOL-Safety, Professional,Leisure, Domestic,Relational, andSentimental)
167 with insomnia,381 good sleepers
Insomnia patientstaking zoplicone for12 months or morevs. good sleeperwith no hypnotic usein the past 12months
Cross-sectional No differences found in quality of life between subjects withinsomnia and good sleepers.
Hajak et al(2002)82 SF-36 789 with insomnia,
aged 18–60 years
Zolpidem 10mg po 5nights/week andplacebo 2nights/week vs.Zolpidem 10mg pocontinuously
14 daysBoth groups demonstrated improvement with treatment. Thecontinuous group demonstrated a greater increase in mean MOSscore as compared to the discontinuous group (p=0.005).
Verbeek et al(2006)83 SF-36 SIP
Individual treatment:18 chronic primaryinsomnia. Grouptreatment: 40primary orsecondary insomnia.
Individual CBT v.group CBT. CBTincludedpsychoeducation,sleep hygiene,stimulus control,sleep restriction,relaxation exercises,and cognitiverestructuring.
6 consecutive weeklysessions and follow-up sessions 1, 3,and 6 months
Both groups demonstrated significant improvement in QOL on theSIP: pre- to post-treatment (p=0.000) and from pre-treatment tofollow-up (p=0.025).
SF-36: Medical Outcomes Study Short Form-36; CBT: cognitive behavioral therapy; CIS-20: Checklist Individual Strength; GHQ: General Health Questionnaire; PANAS: Positive AffectNegative Affect Schedule; ES: effect size; BASIS-32: Behavior and Symptom Identification Scale; DLRF: daily living and role functioning; RSO: relation to self and others; Q-LES-Q:Quality of Life Enjoyment and Satisfaction Questionnaire Short-Form; FLX: fluoxetine; ESZ: eszopiclone; QOL: quality of life; MCS: mental component score; PCS: physical componentscore; OR: odds ratio; HRQOL: health-related quality of life; FACT-G: Functional Assessment of Cancer Therapy; MOS: Medical Outcomes Study sleep module; SIP: Sickness ImpactProfile

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]22
any sleep medication on the mentalhealth (MCS) and physical health(PCS) composite scores of the SF-8.The authors divided their sampleinto good sleepers, good sleeperstaking sleep medication(s),individuals with insomnia, and thosewith insomnia taking sleepmedication(s). Insomnia was foundto be associated with poorer MCSand PCS (scores <50; 50 is thepopulation average). In regard toboth MCS and PCS, insomniaindividuals taking sleep medicationsscored lower than insomniaindividuals not taking sleep aids.Additionally, good sleepers takingsleep medications demonstratedsignificantly lower scores on the PCSas compared to insomnia individualsnot using sleep medications. As theauthors found that the use ofpharmacotherapy to aid sleep wassignificantly associated withdecrements in perceived physicalhealth QOL, they concluded thatsleep medication is independentlyassociated with poorer physical QOLdue to medication side effects.73 Thisis very important to keep in mind,especially in patients who are takingsleep medications on a long-termbasis.
Non-pharmacologicaltreatments. Cognitive behavioraltherapy (CBT). Several studiesdiscuss the clinical efficacy and costeffectiveness of providing CBT forinsomnia to long-term hypnotic drugusers in general practice.74,75 Thesestudies concluded that CBT couldindeed improve the sleep quality oflong-term hypnotic users withchronic sleep disorders.
Among these was an RCT withtwo treatment arms—a CBT-treated‘sleep clinic’ group and a ‘noadditional treatment’ control group—and post-treatment assessments atthree and six months.75 Two-hundredand nine patients aged 31 to 92 yearswith chronic sleep problems wereenrolled. Among CBT-treatedpatients, SF-36 scores showedsignificant improvements in vitalityat three months (p<0.01). Not onlywas there a notable reduction insymptomatology and health-related
quality of life during active CBT, butalso these reductions weremaintained following the cessation ofCBT.76
In a RCT of 209 patients withchronic insomnia using hypnoticsrandomized to either CBT or control(care as usual in a general medicalpractice), Dixon et al74 found thatover the course of six months, thosereceiving CBT demonstratedsignificant improvement on emotionalrole limitation, mental health, andphysical functioning domains of theSF-36 as compared to controls.
Van Houdenhove et al77
investigated the impact of CBT forinsomnia (CBT-i) on symptoms ofinsomnia and HRQL on 138 patientswith primary insomnia. The authorsfound that CBT-i was effective inimproving sleep disturbances,including sleep onset latency, suchthat percentage of daily use ofpharmacologic sleep aids decreased.Additionally, daytime functioningimproved and HRQOL improved,especially in the emotional domainsuch that scores approachednormative scores. CBT-i appeared tohave the greatest effect on HRQOLand daytime functioning in those withgreater pre-treatment impairment inpsychological QOL and daytimefunctioning and those with severeinsomnia.77
CBT has been also shown toeffective in cancer patients withinsomnia. In 1993, Espie et al78
highlighted practical behavioral andcognitive techniques to manageinsomnia. Based on the sametechniques, the investigatorsevaluated the impact of treatment ofinsomnia on QOL in 150 patientsdiagnosed with cancer who were notundergoing concurrentradiation/chemotherapy for greaterthan one month of the study.79 Theauthors found that the CBT groupdemonstrated significantimprovements on various measures ofsleep, including latency of sleep onsetand waking after sleep onset, as wellas on the physical and functionaldomains of the FACT-G QOLassessment tool as compared to thetreatment as usual group.79
Behavioral therapy. In a studycomparing a three-componentbehavioral intervention (comprisingstimulus control, relaxation and sleephygiene) to sham biofeedback(placebo), Soeffing et al80 found nodifference in SF-36 scores betweengroups at the end of treatment. Alimitation of this study was theevaluation of outcome measure QOLrelatively early after initiation oftreatment, such that effects oftherapy on QOL may not have yetbeen apparent.
Other nonpharmacologicaltreatments. No information isavailable on the effects of lighttherapy, exercise, or nutrition on theQOL of patients suffering frominsomnia.
Treatment limitations. It isimportant to note that a smallnumber of cross-sectional andnoncontrolled studies demonstratedequivocal results of the effect oftreatment of insomnia on QOL inregard to both pharmacological andbehavioral treatments. These resultswere found in regard to “insomniacs”versus “good sleepers” withtreatment with zolpiclone,81 insomniaindividuals treated continuously withnightly zolpidem or discontinuouszolpidem treatment,82 and individualversus group CBT in insomniaindividuals.83 As there were severallimitations in the study design in theaforementioned trials, such as the useof QOL domains instead of a well-validated measure of QOL and lack ofcontrol groups,82,83 the results of thesetrials should be generalized withcaution.
Nonpharmacological approachesfor insomnia management areeffective and can be first-linetherapy.68 However, CBT and othersimilar behavioral interventions arenot readily available and that maylimit their use, thus necessitatingpharmacologic therapy.
Multimodal treatments combiningsleep hygiene and CBT with hypnoticmedications are helpful in relievinginsomnia and improving their QOL.3
More studies are needed to test thefull effects of combined treatmentson QOL in insomnia.

[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 23
DISCUSSIONInsomnia produces clinically
significant impairments in social andoccupational areas of functioning, asevidenced by reduction of workproductivity, frequent absenteeism,decreased cognition and mood, andincreased morbidity of psychologicaland physical illness, accompanied bya greater healthcare burden due tochronicity of illness and direct andindirect costs to society.Furthermore, insomnia may predictfuture episodes of psychiatric illness.An individual’s perception of loss ofor decrements in functioning mayprovide the motivation to seektreatment, thus addressingimpairments in QOL may moreaccurately reflect efficacy oftreatment than indices of disease orillness. As QOL is assessed byquestionnaires investigating personalsatisfaction with physical andpsychological wellbeing, furtherinvestigation into insomnia-specificmeasures is warranted. Severalstudies have shown the sensitivity ofthe generic SF-36 in evaluating ofpatients with insomnia, with aninverse association between degreeof sleep disturbance and QOLratings. These relationships remainafter controlling for comorbidpsychiatric and physical illnesses.Thus a combination of specific andgeneric measurement tools may beindicated to best capture therelationship between insomnia anddomains of QOL. Successfullytreating insomnia may improve apatient’s HRQOL; however,medication side effects may alsonegatively impact perceived QOL.Patients with insomnia andcomorbidities, including mood andanxiety disorders, cardiovascular,renal, respiratory, neurologicaldisorders, cancer, acquiredimmunodeficiency syndrome, andchronic pain have poorer QOL. Aschronic insomnia is associated withincreased healthcare burden,increased morbidity and mortality,and decreased day-to-dayfunctioning, addressing insomnia incomorbid psychiatric and medicalillness is important. Treating both
conditions may improve the outcomefor insomnia, comorbidities, and QOLoverall. Interventions that specificallytarget QOL in insomnia are highlyneeded. Additionally, there remains apaucity of studies that specificallyutilized QOL as primary outcomemeasure, thus further controlledtrials needs to be done to addressrelated gaps in knowledge.
CONCLUSION Quality of life in insomnia is
significantly impaired affectingoverall subjective sense of physicalor psychological well-being. Theeffect of insomnia on QOL may berelated to psychiatric or physicalcomorbidities, medications, and/orvarious psychosocial issues or maybe illustrative of a primary diseaseeffect. Due to the lack of biomarkersto measure disease progression inpsychiatric illnesses, symptomseverity is generally used to measurethe illness activity. However,symptom improvement is not thesole indicator of improvement, asrestoration of QOL remains a keyindicator of wellness. There isevidence to support the positivetreatment effect on QOL in patientssuffering from insomnia. Thesestudies suggest that addressing bothinsomnia and co-morbidities has thepotential of improving bothconditions. However, more work isneeded to enhance ourunderstanding of QOL impairment ininsomnia and to develop moreeffective and specific ways toameliorate it.
REFERENCES1. The World Health Organization
Quality of Life assessment(WHOQOL): position paper fromthe World Health Organization.Soc Sci Med. 1995;41:1403–1409.
2. Wade AG. The societal costs ofinsomnia. Neuropsychiatr DisTreat. 2010;7:1–18.
3. Kyle SD, Morgan K, Espie CA.Insomnia and health relatedquality of life. Sleep Med Rev.2010;14:69–82.
4. Léger D, Bayon V. Societal costs ofinsomnia. Sleep Med Rev.
2010;14:379–389.5. Buysse DJ, Angst J, Gamma A, et
al. Prevalence, course, andcomorbidity of insomnia anddepression in young adults. Sleep.2008;31:473–480.
6. Morin CM, LeBlanc M, Daley M, etal. Epidemiology of insomnia:prevalence, self-help treatments,consultations, and determinants ofhelp-seeking behaviors. SleepMed. 2006;7:123–130.
7. Mai E, Buysse DJ. Insomnia:prevalence, impact, pathogenesis,differential diagnosis, andevaluation. Sleep Med Clin.2008;3:167–174.
8. Ohayon MM. Epidemiology ofinsomnia: what we know and whatwe still need to learn. Sleep MedRev. 2002;6:97–111.
9. Insomnia, an internationalconsensus conference report—Versailles, 13–15 October.Worldwide Project on Sleep andHealth. Geneva: Division of MentalHealth and Prevention ofSubstance Abuse, World HealthOrganization; 1998.
10. Walsh JK, Krystal AD, Amato DA,et al. Nightly treatment of primaryinsomnia with eszopiclone for 6months: effect on sleep, quality oflife, and work limitations. Sleep.2007;30:959–968.
11. Zammit GK, Weiner J, Damato N,et al. Quality of life in people withinsomnia. Sleep.1999;22:S379–S385.
12. Schubert CR, Cruickshanks KJ,Dalton DS, et al. Prevalence ofsleep problems and quality of lifein an older population. Sleep.2002;25:889–893.
13. Stein MB, Belik SL, Jacobi F,Sareen J. Impairment associatedwith sleep problems in thecommunity, relationship tophysical and mental co-morbidity.Psychosom Med.2008;70:913–919.
14. Berger AM, Kuhn BR, Farr LA, etal. Behavioral therapy interventiontrial to improve sleep quality andcancer-related fatigue. Psycho-Oncology. 2009;18:634–646.
15. Lis CG, Gupta D, Grutsch JF. Therelationship between insomnia and

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]24
patient satisfaction with quality oflife in cancer. Support CareCancer. 2008;16:261–2666.
16. Byles JE,Mishra GD,HarrisMA,Nair K.The problems of sleepfor older women: changes inhealth outcomes. Age Ageing.2003;32:154–163.
17. Léger D, Scheuermaier K,Philip P, et al. SF-36: evaluation ofquality of life in severe and mildinsomniacs compared with goodsleepers. Psychosom Med.2001;63:49–55.
18. Reimer MA, Flemons WW. Qualityof life in sleep disorders. SleepMed Rev. 2001;7:335–349.
19. Léger D, Scheuermaier K, RaffrayT, et al. HD-16: a new quality oflife instrument specificallydesigned for insomnia. Sleep Med.2005;6:191–198.
20. Endicott J, Nee J, Harrison W, etal. Quality of Life Enjoyment andSatisfaction Questionnaire: a newmeasure. Psychopharmacol Bull.1993;29:321–326.
21. Schechter D, Endicott J, Nee J.Quality of life of ‘normal’ controls:association with lifetime history ofmental illness. Psychiatry Res.2007;152:45–54.
22. McCall WV, Blocker JN,D’Agostino R, et al. Treatment ofinsomnia in depressed insomniacs:effects of health-related quality oflife, objective and self-reportedsleep, and depression. J ClinSleep Med. 2010;6:322–329.
23. Skevington SM, Lotfy M, O’ConnellKA. The World HealthOrganization’s WHOQOL-BREFquality of life assessment:psychometric properties andresults of the international fieldtrial. A report from the WHO-QOLgroup. Qual Life Res.2004;13:299–310.
24. Mathews WC, May S. EuroQol(EQ-5D) measure of quality of lifepredicts mortality, emergencydepartment utilization, andhospital discharge rates. HealthQual Life Outcomes. 2007;5:5.
25. IsHak WW, Greenberg JM, BalayanK, et al. Quality of life: theultimate outcome measure ofinterventions in major depressive
disorder. Harv Rev Psychiatry.2011;19:229–239.
26. Rombaut N, Maillard F, Kelly F,Hindmarch I. The quality of life ofinsomniacs questionnaire (QOLI).Med Sci Res. 1990;18:845–47.
27. Philip P, Léger D, Quera-Salva MA,et al. Insomniac complaintsinterfere with quality of life butnot absenteeism: respective roleof depressive and organiccomorbidity. Sleep Med.2006;7:585–591.
28. Eisen SV, Dill DL, Grob MC.Reliability and validity of a briefpatient-report instrument forpsychiatric outcome evaluation.Hosp Community Psychiatry.1994;45:242–247.
29. Katz DA, McHorney CA. Therelationship between insomnia andhealth related quality of life inpatients with chronic illness. JFam Pract. 2002;51:229–235.
30. Roth T, Drake C. Evolution ofinsomnia:current status and futuredirection. Sleep Med.2004;5(Suppl 1):S23–S30.
31. Stein MB, Barret-Conner E.Quality of life in older adultsreceiving medications for anxiety,depression or insomnia. Am JGeriatr Psychiatry.2002;5:568–574.
32. Hatoum HT, Kong SX, Kania CM,et al. Insomnia, health relatedquality of life and health careresource consumption.Pharmacoeconomics.1998;14:629–637.
33. Léger D, Guilleminault C, Bader G,et al. Medical and socio-professional impact of insomnia.Sleep. 2002;25:625–629.
34. Gureje O, Kola L, Ademola A,Olley BO. Profile comorbidity andimpact of insomnia in the Ibadanstudy of ageing. Int J GeriatrPsychiatry. 2009;24:686–693.
35. Lee M, Choh AC, Demerath EW, etal. Sleep disturbance in relation toHealth-related quality of life inadults. J Nutr Health Aging.2009;13:576–583.
36. Dikeos DG, Soldatos CR. Thecondition of insomnia:etiopathogenetic considerationsand their impact on treatment
practices. Int Rev Psychiatry.2005;17:255–262.
37. Vallieres A, Ivers H, Bastien CH, etal. Variability and predictability insleep patterns of chronicinsomniacs. J Sleep Res.2005;14:447–453.
38. Smith MT, Perlis ML, Park A, et al.Comparative meta-analysis ofpharmacotherapy and behaviortherapy for persistent insomnia.Am J Psychiatry. 2002;150:5–11.
39. Breslau N, Roth T, Rosenthal L, etal. Sleep disturbance andpsychiatric disorders: alongitudinal epidemiological studyof young adults. Biol Psychiatry.1996;39:411–418.
40. Sunderajan P, Gaynes BN,Wisniewski SR, et al. Insomnia inpatients with depression: aSTAR*D report. CNS Spectr.2010;15:394–404.
41. Nierenburg AA, Keefe BR, LeslieVC, et al. Residual symptoms indepressed patients who respondacutely to fluoxetine. J ClinPsychiatry. 1999;60:221–225.
42. Mahendran R, Subramaniam M,Chan YH. Psychiatric morbidity inpatients referred to an insomniaclinic. Singapore Med J.2007;48:163–165.
43. Brenes GA, Miller ME, StanleyMA, et al. Insomnia in older adultswith generalized anxiety disorder.Am J Geriatr Psychiatry.2009;17:465–472.
44. Kim K, Uchiyama M, Liu X, et al.Somatic and psychologicalcomplaints and their correlateswith insomnia in the Japanesegeneral population. PsychosomMed. 2001;6:441–446.
45. Léger D, Stal V, Guilleminault C,et al. Diurnal consequences ofinsomnia; impact on quality of life.Rev Neurol (Paris).2001;1571270–1278.
46. Lew HL, Vanderploeg RD, MorreDF, et al. Overlap of mild TBI andmental health conditions inreturning OIF/OEF servicemembers and veterans. J RehabilRes Dev. 2008;45:6–11.
47. Pittman J, Goldsmith AA, LemmerJA, et al. Post-traumatic stressdisorder, depression and health-
[ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ] Innovations in CLINICAL NEUROSCIENCE 25
related quality of life in OEF/OIFveterans. Qual Life Res.2012;21:99–103.
48. McLay RN, Klam WP, Volkert SL.Insomnia is the most commonlyreported symptom and predictsother symptoms of post-traumaticstress disorder in U.S. servicemembers returning from militarydeployments. Mil Med.2010;175:759–762.
49. Wallace DM, Shafazand S, RamosAR, et al. Insomnia characteristicsand clinical correlates inOperation EnduringFreedom/Operation Iraqi Freedomveterans with post-traumaticstress disorder and mild traumaticbrain injury: an exploratory study.Sleep Med. 2011;12:850–859.
50. Poon, CY, Knight BG. Impact ofchildhood parental abuse andneglect on sleep problems in oldage. J Gerontol B Psychol SciSoc Sci. 2011;66:307–310.
51. Ozminkowski RJ, Wang S, WalshJK. The direct and indirect costsof untreated insomnia in adults inthe United States. Sleep.2007;30:263–273.
52. Hatoum HT, Kong SX, Kania CM,et al. Insomnia, health-relatedquality of life and healthcareresource consumption: a study ofmanaged care organizationsenrollees. Pharmacoeconomics.1998;14:629–637.
53. Rosekind MR, Gregory KB.Insomnia risks and costs:health,safety, and quality of life. Am JManag Care. 2010;16:617–626.
54. Estivill E, Bov A, Garca-Borreguero D, et al. Consensus ondrug treatment, definition anddiagnosis for insomnia. Clin DrugInvest. 2003;23:351–385.
55. Cheng KK, Lee DTF. Effects ofpain, insomnia, and mooddisturbance on functional statusand quality of life of elderlypatients with cancer. Crit RevOncol Hematol. 2011;78:127–137.
56. O’Donnel JF. Insomnia in cancerpatients. Clin Cornerstone.2004;6:S6–S14.
57. Lew HL, Pogoda TK, Hsu PT, et al.Impact of the “polytrauma clinicaltriad” on sleep disturbance in a
department of veteran affairsoutpatient rehabilitation setting.Am J Phys Med Rehabil.2010;89:437–445.
58. Ouellet MC, Beaulieu-Bonneau S,Morin CM. Insomnia in patientswith traumatic brain injury:frequency, characteristics, andrisk factors. J Head TraumaRehabil. 2006;21:199–212.
59. Dauvilliers Y. Insomnia in patientswith neurodegenerativeconditions. Sleep Med.2007;8:S27–S34.
60. Caap-Ahlgren M, Devlin O.Insomnia and depressivesymptoms in patients withParkinson’s disease-relationship tohealth-related quality of life. Aninterview study of patients livingat home. Arch Gerontol Geriatr.2001;32:23–33.
61. BaHammam A. Sleep in acute careunits. Sleep Breath. 2006;10:6–15.
62. Granja C, Lopes A, Moreira S, etal. Patients’ recollections ofexperiences in the intensive careunit may affect their quality oflife. Crit Care. 2005;9:R96–R109.
63. Lee CM, Herridge MS, Gabor JY, etal. Chronic sleep disorders insurvivors of the acute respiratorydistress syndrome. IntensiveCare Med. 2009;35:314–320.
64. Krakow B, Melendrez D, Sisley B,et al. Nasal dilator strip therapyfor chronic sleep maintenanceinsomnia and symptoms of sleepdisordered breathing. SleepBreath. 2006;10:16–28.
65. Johansson P, Arestedt K, AlehagenU, et al. Sleep disorderedbreathing, insomnia, and healthrelated quality of life: acomparison between age andgender matched elderly with heartfailure or without cardiovasculardisease. Eur J Cardiocasc Nurs.2010;9:108–117.
66. Bjornsdottir E, Janson C, GislasonT, et al. Insomnia in untreatedsleep apnea patients compared tocontrols. J Sleep Res.2011;21:131–138.
67. Goldenberg F, Hindmarch I, JoyceCB, et al. Zopiclone, sleep andhealth-related quality of life.Human Psychopharmacol Clin
Exper. 1994;9:245–251.68. Morin AK. Strategies for treating
chronic insomnia. Am J ManagCare. 2006;12suppl:S230–S245.
69. Walsh JK, Krystal AD, Amtao DA,et al. Nightly treatment of primaryinsomnia with eszopiclone for sixmonths: effect on sleep, quality oflife, and work limitations. Sleep.2007;30:959–968.
70. Scharf M, Erman M, Rosenberg R,et al. A 2-week efficacy and safetystudy of eszopiclone in elderlypatients with primary insomnia.Sleep. 2005;28:720–727.
71. Turek FW, Gillette MU. Melatonin,sleep, and circadian rhythms:rationale for development ofspecific melatonin agonists. SleepMed. 2004;5:523–532.
72. Taylor SR, Weiss JS. Review ofinsomnia pharmacotherapyoptions for the elderly:implications for managed care.Popul Health Manag.2009;12:317–323.
73. Sasai T, Inoue Y, Komada Y, et al.Effects of insomnia and sleepmedication on health-relatedquality of life. Sleep Med.2010;11:452–457.
74. Dixon S, Morgan K, Mathers N, etal. Impact of cognitive behaviortherapy on health-related qualityof life adult hypnotic users withchronic insomnia. Behav SleepMed. 2006;4:71–82.
75. Morgan K, Dixon S, Mathers N, etal. Psychological treatment forinsomnia in the management oflong term hypnotic drug use. Br JGen Pract. 2003;53:923–928.
76. Roth T, Drake C. Evolution ofinsomnia:current status and futuredirection. Sleep Med.2004;5(Suppl 1):S23–S30.
77. Van Houdenhove l, Buyse B,Gabriels L, Van den Bergh O.Treating primary insomnia: clinicaleffectiveness and predictors ofoutcomes on sleep, daytimefunction and health-related qualityof life. J Clin Psychol MedSettings. 2011;18:312–321.
78. Espie CA. ABC of sleep disorders.Practical management ofinsomnia: behavioral and cognitivetechniques. BMJ.

Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 9 , N U M B E R 1 0 , O C T O B E R 2 0 1 2 ]26
1993;306:509–511.79. Espie CA, Fleming L, Cassidy J, et
al. Randomized controlled clinicaleffectiveness trial of cognitivebehavior therapy compared withtreatment as usual for persistentinsomnia in patients with cancer. JClin Oncol. 2008;28:4651–4658.
80. Soeffing JP, Lichstein KL, Nau SD,et al. Psychological treatment ofinsomnia in hypnotic-dependentolder adults. Sleep Med.
2008;9:165–171.81. Léger D, Janus C, Pellois A, et al.
Sleep, morning alertness andquality of life in subjects treatedwith zoplicone and in goodsleepers. Study comparing 167patients and 381 good sleepers.Eur Psychiatry.1995;10:99S–102S.
82. Hajak G, Cluydts R, Declerck A, etal. Continuous versus non-nightlyuse of zolpidem in chronic
insomnia:results of a large-scale,double-blind, randomized,outpatient study. Int ClinPsychopharmacol. 2002;17:9–17.
83. Verbeek IH, Konings GM,Aldenkamp AP, et al. Cognitivebehavioral treatment in clinicallyreferred chronic insomniacs:group versus individual treatment.Behav Sleep Med.2006;4:135–151.





























