Embed Size (px)
Citation preview
Adv Ther (2009) 26(4):404-424.DOI 10.1007/s12325-009-0021-x
REVIEW
Psychotropic Drugs and Renal Failure: Translating the Evidence for Clinical Practice
Nour T. Baghdady · Suman Banik · Shari A. Swartz · Roger S. McIntyre
Received: February 9, 2009 / Published online: May 4, 2009 / Printed: May 8, 2009 © Springer Healthcare Communications 2009
REVIEW
ABSTRACT
Introduction: The kidney is a primary route of drug elimination; abnormal kidney function is predicted to alter the pharmacokinetics of agents metabolized and/or excreted predomi-nantly through this route. The high preva-lence of mental disorders associated with psychotropic drug use in individuals with deteriorating renal function suggests there is a need to investigate the effects of renal failure on psychotropic pharmacokinetics. The aim
DOI
0021-x
Issue Number:
4of this review is to provide a clinically acces-sible overview of the effect of chronic renal failure on the pharmacokinetics for each of the major classes of prescribed psychotropic agents. Methods: All English language arti-cles published between 1977 and 2008 were searched through PubMed, using the fol-lowing keywords: “renal,” “kidney,” “phar-macokinetics,” “renal impairment,” “renal insufficiency,” and “renal failure.” Each of these search words was cross-referenced with the non-proprietary name of each psychotro-pic agent. The manufacturer’s product insert was also reviewed for some agents for updated dosing. Owing to the lack of adequately pow-ered studies, an inclusive manner was used. Results: Chronic renal failure variably affects the pharmacokinetic parameters of psycho-tropic drugs. A review of each psychotropic drug is provided, with an emphasis on the individual pharmacokinetic parameters and recommended dosing. Conclusions: The adju-dication of safe and effective doses for any psychotropic agent needs to be individual-ized. Tactics including dosage adjustment, slow titration, and careful monitoring for serious adverse events should be incorporated into practice.
Nour T. Baghdady King Abdul-Aziz University, Jeddah, Saudi Arabia, and Mood Disorders Psychopharmacology Unit, University Health Network, Toronto, Ontario, Canada
Suman Banik Royal College of Surgeons in Ireland, Dublin, Ireland, and Mood Disorders Psychopharmacology Unit, University Health Network, Toronto, Ontario, Canada
Shari A. Swartz University of Ottawa, Faculty of Medicine, Ottawa, Ontario, Canada, and Mood Disorders Psychopharmacology Unit, University Health Network, Toronto, Ontario, Canada
Roger S. McIntyre ( ) Department of Psychiatry and Pharmacology, University of Toronto, Toronto, Ontario, Canada, and Mood Disorders Psychopharmacology Unit, University Health Network, 399 Bathurst Street, Toronto, Ontario, Canada M5T 2S8. Email: [email protected]

Adv Ther (2009) 26(4):404-424. 405
Keywords: kidney failure; pharmacokinetics; psychotropic agents; renal disease
INTRODUCTION
The kidney is a primary route of drug elimi-nation; abnormal kidney function is predicted to alter the pharmacokinetics of agents metab-olized and/or excreted predominantly through this route.1 Mental and renal disorders co-occur together, particularly in end-stage renal disease (ESRD). One systematic review showed that the mean prevalence of mental disorders in patients undergoing dialysis was 44% (range 20%-83%) with the most common diagnosis being major depression.2 The co-occurrence of these disorders invites the need for familiar-ity with the safety, pharmacokinetic profile, and efficacy of psychotropic agents in indi-viduals with deteriorating kidney function. Herein, we provide a clinically accessible and pragmatic review of the effect of suboptimal renal function on the handling of the major classes of psychotropic agents with an empha-sis on antidepressants, antipsychotics, and anticonvulsants.
METHODS
All English language articles published between 1977 and 2008 were searched through PubMed using the following keywords: “renal,” “kidney,” “pharmacokinetics,” “renal impair-ment,” “renal insufficiency,” and “renal failure.” Each of these words was cross-referenced with the non-proprietary name of each psychotropic agent. The manufacturer’s product insert was also reviewed for some agents for updated dosing recommendations, ie, GlaxoSmithKline for par-oxetine, Eli-Lilly & Co. for duloxetine, Bristol-Myers Squibb Co. for aripiprazole, Sanofi-Aventis for zolpidem, and Wyeth Pharmaceuticals for
zaleplon. The articles selected for inclusion were decided after discussion amongst the authors.
PSYCHOTROPIC DRUG CLASSES
Antidepressants
Selective Serotonin Reuptake InhibitorsEscitalopram is the (S)-enantiomer of the race-
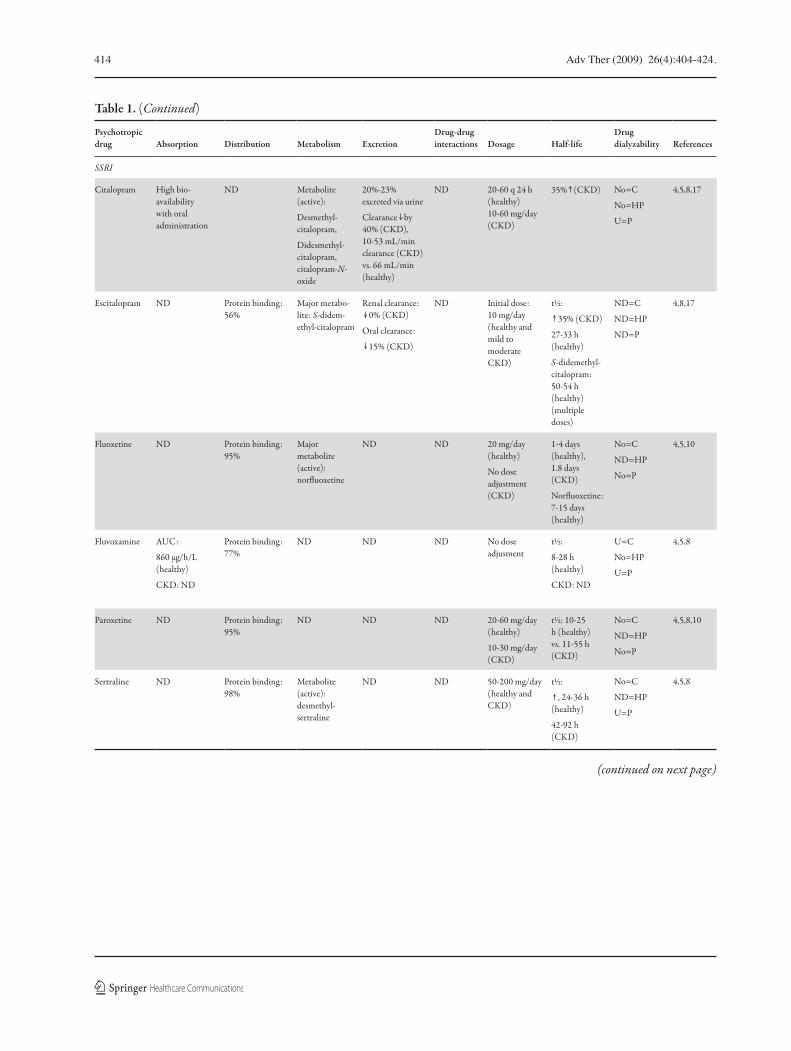
mic antidepressant citalopram. Although the pharmacokinetics of escitalopram have not been extensively studied in patients with compromised renal function, the pharmacokinetics of citalo-pram in diseased kidney states are known to be altered (Table 1; adapted with permission).3 The elimination half-life (t1/2) of citalopram in patients with mild to moderate renal insufficiency (creati-nine clearance [CrCl] 10-53 mL/min) increases by approximately 35%, while the renal clearance decreases by 40%.17 In keeping with these find-ings, patients with mild to moderate kidney dis-ease should initiate treatment at 10-20 mg/day with lower doses (ie, 5 mg) for more severe renal impairment.17,40,41
Fluoxetine is the most studied selective sero-tonin reuptake inhibitor (SSRI) among individ-uals with renal failure.10 Fluoxetine treatment administered to depressed individuals undergo-ing renal dialysis has been proven to be highly efficacious and well tolerated.42 The pharmacoki-netic parameters of fluoxetine and its primary active metabolite, norfluoxetine, were unaltered in patients with renal failure when compared with healthy controls (Table 1). Fluoxetine treat-ment in patients undergoing hemodialysis does not require a change in dose initiation or titra-tion when compared with individuals without kidney disease.8,42
A single study evaluating the effect of renal impairment on fluvoxamine (100 mg/day for 6 weeks) pharmacokinetics in individuals with renal impairment (CrCl <50 mL/min) did not

406 Adv Ther (2009) 26(4):404-424.
observe any significant differences in any kinetic parameter (Table 1).8
Several studies regarding the use of parox-etine in renal failure reported an increase in plasma concentration (Cmax) and t1/2. One study demonstrated a mean t1/2 of 29.7 hours (10.9-54.8 hours) in subjects with impaired renal function (CrCl <30 mL/min) versus a mean t1/2 of 17.3 hours (9.6-25.1 hours) in subjects with normal kidney function (CrCl >100 mL/min) (Table 1).8 Paroxetine should be initiated at a lower dose (ie, 10 mg of paroxetine or 12.5 mg of controlled-release formulations of parox-etine) in patients with severe renal impairment (CrCl <30 mL/min).8,10,43
Like most SSRIs, sertraline has not been extensively studied in individuals with renal fail-ure. A small case series of patients with anuria reported an increase in the t1/2 (ie, 42-92 hours vs. 24-36 hours in healthy controls).8 Interestingly, sertraline has been reported to prevent hypoten-sive reactions to hemodialysis, but the exact mechanism subserving this operation has not been elucidated.44
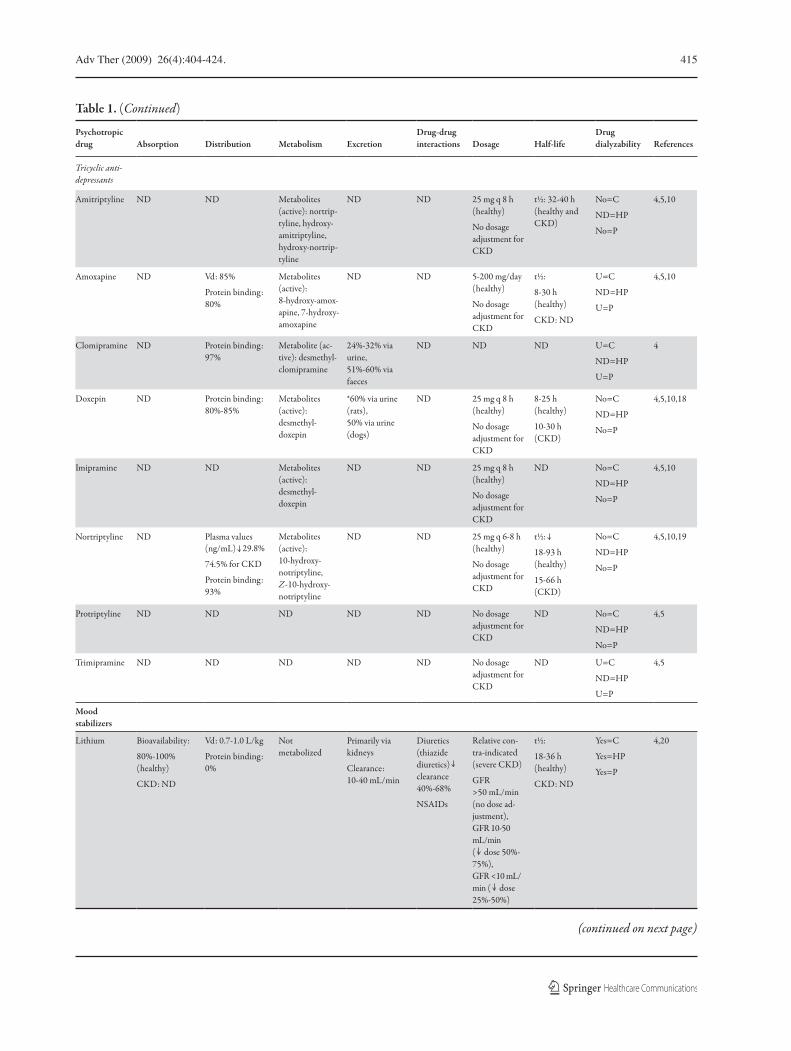
Tricyclic AntidepressantsThe serum concentration and mean t1/2 of
tricyclic antidepressant conjugated hydroxy-lated metabolites are markedly increased in subjects with renal failure; however, no con-siderable increase in unconjugated hydrox-ylated metabolites are reported.8,45 Dose adjustment is not necessary for commonly prescribed tricyclic antidepressants (ie, desip-ramine, imipramine, and nortriptyline); how-ever, caution is advised.8 Therapeutic drug monitoring can be beneficial but is not fre-quently performed as patients may exhibit toxicity despite normal laboratory values.45 Therefore, clinical signs of therapeutic and toxic effects are often used to guide appropri-ate dosing.45
Serotonin and Norepinephrine Reuptake Inhibitors
VenlafaxineVenlafaxine is metabolized in the liver to
O-desmethyl-venlafaxine.46 The major excretion pathway of both the parent drug and metabolite are via the kidney (87% of dose is recovered in the urine).46 Patients with moderate renal insuffi-ciency undergoing dialysis exhibit an increase in t1/2 of venlafaxine and O-desmethyl-venlafaxine; this is in contrast to the pharmacokinetics for venlafaxine in individuals with mild renal impairment, which remained unchanged (Table 1).8,45 In patients with mild renal impair-ment, no alteration of dose is required; further decrements in renal function invite the need for lower dose initiation and slower titration.45 The association between venlafaxine and elevations in blood pressure require increased vigilance for this vital sign in all patients with renal failure who were treated with venlafaxine.10,45,46
DuloxetineDuloxetine was only approved by the US
Food and Drug Administration (FDA) in 2004;13 thus, limited data on the safety of duloxetine in patients with renal failure are available. Duloxetine is highly protein bound (>90%), binding primarily to albumin and alfa1-acid gly-coprotein.13 The binding to plasma proteins does not appear to be significantly affected by renal failure. Duloxetine administered as a single dose results in a 100% increase in Cmax and the area under the concentration-time curve (AUC) in patients with ESRD receiving hemodialysis.47 The major metabolites of duloxetine, 4-hydroxy duloxetine glucuronide, and 5-hydroxy,6-meth-oxy duloxetine sulfate, all of which are primarily excreted via the kidneys, exhibit AUC values seven to nine times higher in patients with renal failure compared with subjects with normal renal function.47 Taken together, duloxetine is

Adv Ther (2009) 26(4):404-424. 407
best avoided in ESRD, patients requiring dialysis, or patients with severe renal impairment (CrCl <30 mL/min).47 Duloxetine seems to be a reason-able alternative in individuals with mild to mod-erate renal impairment (CrCl 30-80 mL/min) as no significant effects on pharmacokinetics are observed (Table 1).47
Serotonin Agonists/AntagonistsTrazodone and NefazodoneLimited data concerning the effect of renal
failure on the pharmacokinetic profile of tra-zodone are available. The t1/2 of the parent drug was reported to be unchanged in patients receiv-ing hemodialysis, although the effect on its metabolites was unknown.8 It has been reported that hemodialysis does not hasten the elimina-tion of trazodone.8 Renal impairment does not seem to considerably alter the pharmacokinetics of nefazodone (Table 1). However, nefazodone is problematic in the fact that it causes acute hepa-totoxicity; based on this, the drug was withdrawn from the Canadian and European markets.8,48
Noradrenergic and Specific Serotonergic Antidepressants
MirtazapineA single-dose study using 15 mg of mir-
tazapine demonstrated that the clearance in mild renal impairment was largely unaffected, whereas it decreased by 33% and 50% in mod-erate and severe renal insufficiency, respectively (Table 1). In addition, time to peak plasma concentration (tmax) and AUC were higher in moderate and severe renal impairment.8,12 The manufacturer (Schering-Plough, Kenilworth, NJ, USA) dosage should be adjusted in patients with renal failure.45,49
Monoamine Oxidase InhibitorsThe use of monoamine oxidase inhibitors
(MAOI) in patients with impaired renal function
is discouraged, due to the lack of efficacy data, as well as tolerability and safety issues in crit-ically ill patients.8 For example, orthostatic hypotension, a common side effect of MAOIs, may augment the drop in blood pressure associ-ated with dialysis therapy.8,50 The use of MAOIs are thus reserved for treatment-resistant and tertiary cases.8,51
Noradrenaline and Dopamine Reuptake Inhibitors
BupropionAlthough bupropion is eliminated almost
entirely by the liver, renal impairment may affect its disposition (Table 1). For example, the AUC ratios of hydroxybupropion:bupropion and hydrobupropion:bupropion were decreased by 66% and 69%, respectively, in patients with renal impairment.9 These changes most likely reflect a decrease in the metabolic clearance of bupro-pion rather than an alteration in protein bind-ing.9 Bupropion may accumulate in individuals with renal failure as the drug may build up and predispose seizure activity.10 Hence, dose adjust-ment should be considered; however, the exact dose recommendation is still not yet available.9
Antipsychotic Drugs
First-Generation AntipsychoticsHaloperidol appears to be safe in ESRD
based on its minimal excretion in urine (<1%).52 The electrolyte imbalances associated with renal failure may portend increased risk for cardiac dysrhythmias (QTc prolongation) when exposed to antipsychotic treatment.10 In this context, piperidine phenothiazines such as mesoridazine and thioridazine should be avoided.10 Furthermore, phenothiazine antipsychotics may intensify vulnerability to hypotension in patients with deteriorated renal function.53

408 Adv Ther (2009) 26(4):404-424.
Second-Generation AntipsychoticsOlanzapineOlanzapine is metabolized in the liver to
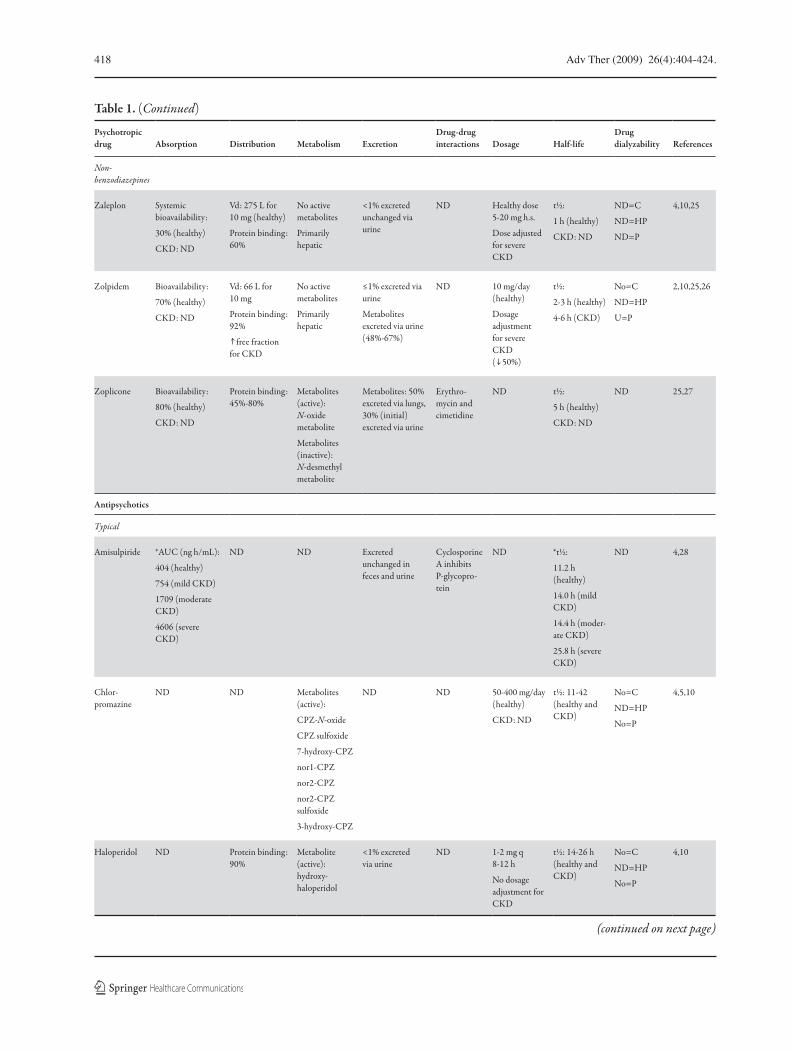
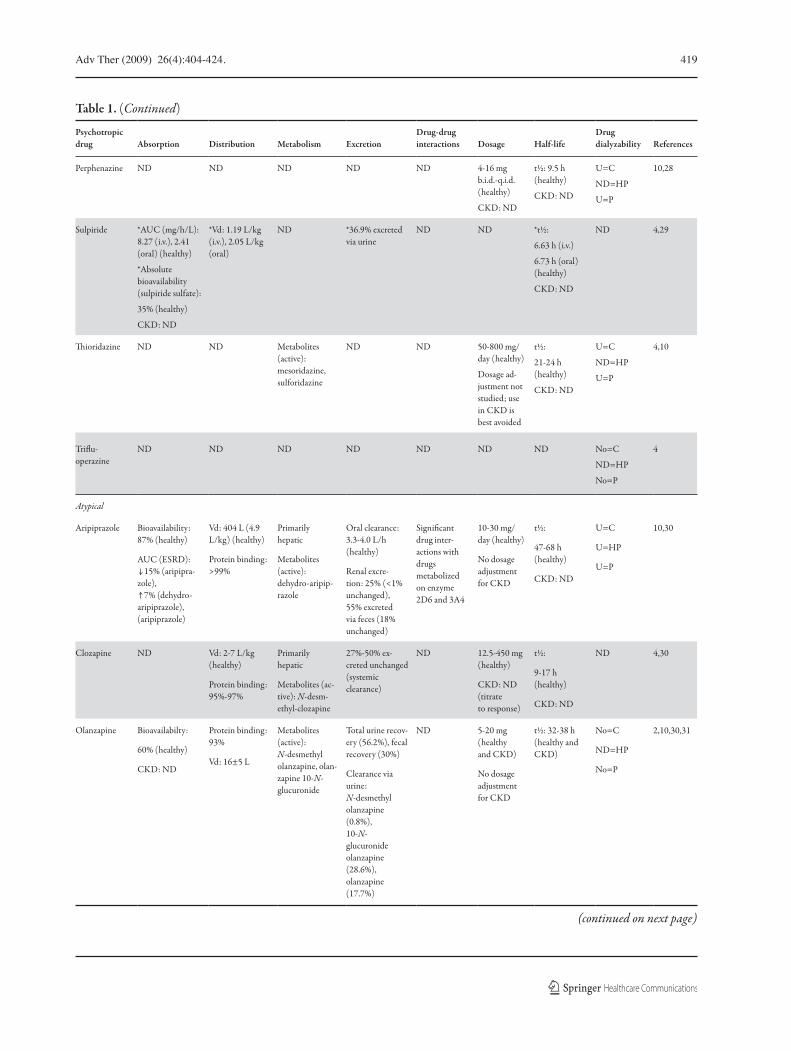
produce metabolites that are cleared via the kidney.10 Multiple-dose studies in renal fail-ure are not yet available; however, single-dose studies illustrate the safe use of olanzapine with no dose adjustment (Table 1). A notewor-thy adverse effect associated with olanzapine therapy is the exacerbation of glucoregula-tory disturbances, a common cause of chronic renal failure.10
QuetiapineA single-dose study evaluated low-dose que-
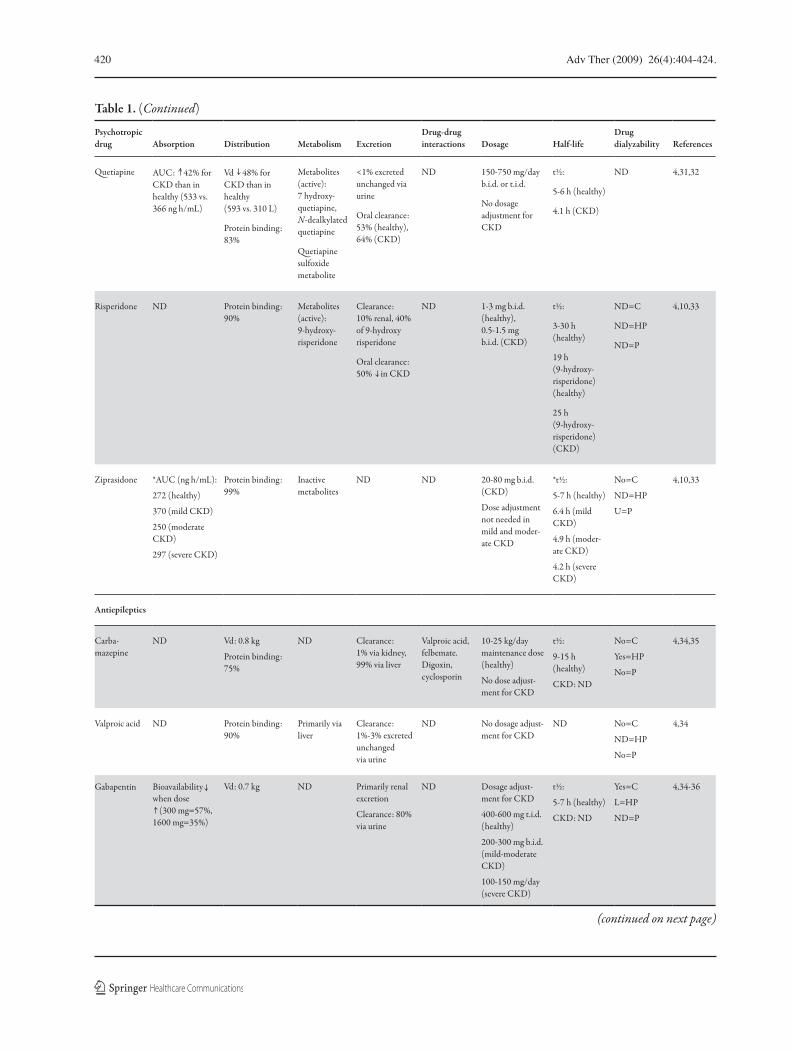
tiapine (ie, 25 mg) in a small case series of individuals with renal disease and a CrCl rang-ing from 8 to 33 mL/min per 1.73 m2 (n=8), and healthy volunteers (n=8).32 A 26% lower-ing in the mean apparent oral clearance and a corresponding 48% reduction in the appar-ent volume of distribution in participants with compromised kidney function were reported relative to the healthy volunteers. The AUC and the mean Cmax were also reported to be higher, with values of 42% and 52%, respec-tively. The mean t1/2 was similar in both groups (Table 1).32,54
Ziprasidone, Risperidone, and PaliperidoneA single study reported that ziprasidone’s
pharmacokinetics are unaltered in patients with impaired renal function.33 The associa-tion of ziprasidone and other antipsychot-ics with electrocardiographic changes requires vigilance for toxicity in individuals with electrolyte disturbances.10
The oral clearance of the primary metabolite of risperidone, 9-hydroxy-risperidone (ie, pali-peridone), was decreased by 50% in individuals with renal failure (Table 1).55 These observa-tions provide the impetus for lower initial
dosing and slower titration in subjects treated with risperidone.33,55
AripiprazoleAripiprazole (15 mg) treatment in patients
with severe renal failure (CrCl <30 mL/min) resulted in a higher Cmax for both aripiprazole and its main metabolite dehydro-aripiprazole by 36% and 53%, respectively.56 Moreover, the AUC of aripiprazole exhibited a 15% decrease, con-trary to dehydro-aripiprazole which increased by 7% (Table 1). Renal excretion for both the parent drug and the metabolite was <1%.56,57
Anxiolytics/Hypnotics
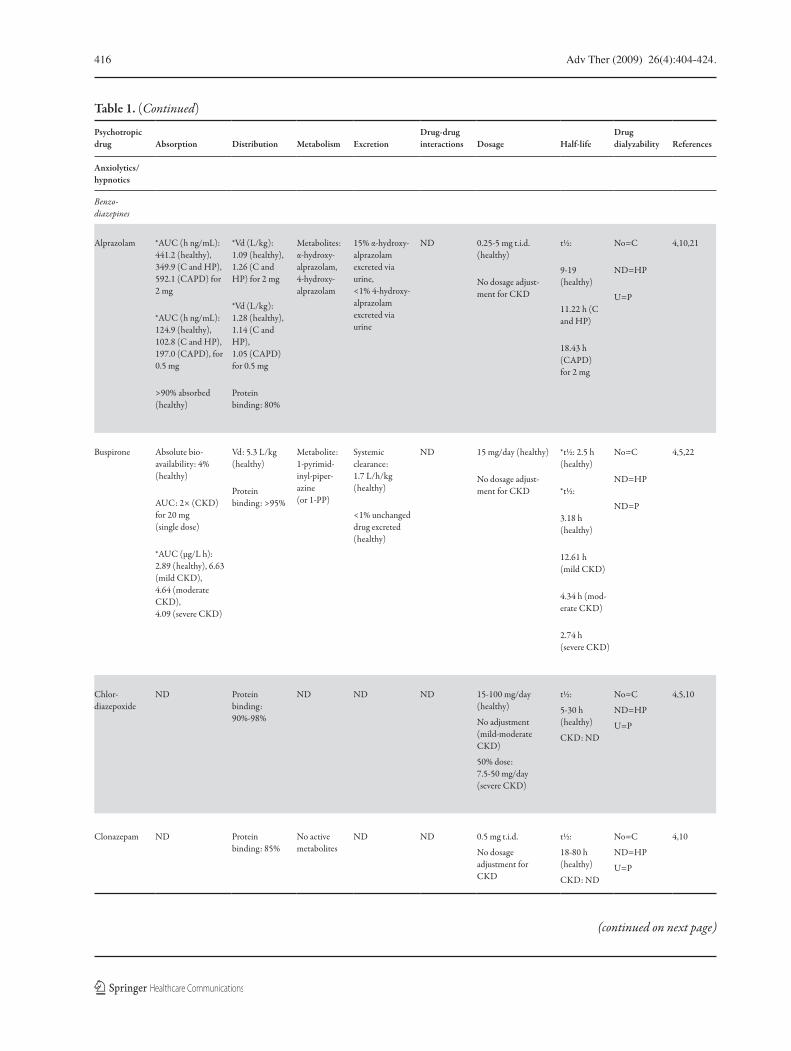
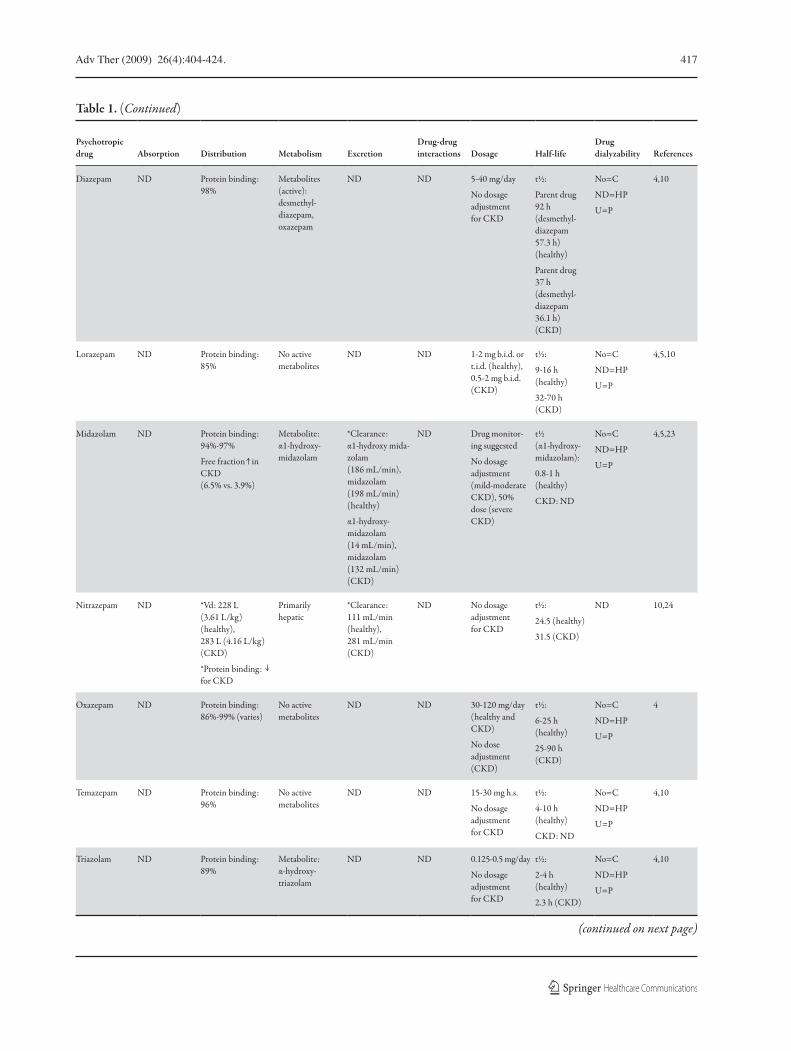
BenzodiazepinesBenzodiazepines (BZD) carry the advantage
of having a wide therapeutic window, allowing flexibility of dosing and the use of various routes of administration.8 They are also solely metab-olized by the liver; consequently, BZDs do not usually require dose adjustment in renal failure (Table 1).10 Selection of a BZD should be based on its pharmacokinetic profile, taking solubil-ity, absorption, and t1/2 into consideration (refer to Table 1 for details on pharmacokinetics). In keeping with this view, the clinician is often able to predict the onset and duration of anxiolytic effect and portend adverse effects.8
Non-BenzodiazepinesZolpidemZolpidem is a novel sedative-hypnotic that
is used for short-term treatment of insom-nia.58 Zolpidem (10 mg/day for 14 or 21 days) was evaluated in a small case series (n=11) in patients with ESRD.58 The results indi-cated that there were no significant changes in medication pharmacokinetics (Table 1). Moreover, this agent is not reliably removed by hemodialysis.58

Adv Ther (2009) 26(4):404-424. 409
ZaleplonZaleplon is a new non-benzodiazepine hyp-
notic agent also used for the short-term treatment of insomnia.10 The pharmacokinetics of zaleplon are unaltered in patients with mild to moderate renal impairment, as <1% of the dose is excreted unchanged in the urine (Table 1). As a result, dos-age adjustment is not necessary. As a cautionary note, however, zaleplon has not been adequately studied in individuals with severe renal failure or those undergoing hemodialysis.10,59
Mood Stabilizers
LithiumA known side effect of lithium is nephro-
toxicity. A review that included data from 14 separate studies reported that the prevalence of reduced glomerular filtration associated with chronic lithium therapy was approximately 15%.60 In patients with renal failure, lithium can be used cautiously where reliably manag-ing the psychiatric and renal condition can be assured.20
The renal clearance of lithium declines pro-portionally with the decline in renal function to a threshold of CrCl 30 mL/min.20 Treatment studies regarding the kinetics of lithium in ESRD are relatively limited. A dose reduction in patients with compromised renal function is of paramount importance in order to avoid toxicity as a result of lithium accumulation.20 Lithium is a small molecule that is largely removed by dialysis.20 Typically, a single supple-mentary dose given post-dialysis would be suffi-cient to maintain steady-state plasma levels.20
Antiepileptics
CarbamazepineCarbamazepine is almost entirely metabo-
lized by the cytochrome P450 enzyme system
in the liver.34 It is first metabolized to the active epoxide metabolite; further metabolism yields inactive metabolites that are excreted by the kidney.34 An insignificant amount of parent or active metabolite is excreted by the kidney.34 Therefore, dose adjustment is not necessary for carbamazepine in renal failure. Although 20%-50% of carbamazepine is extracted by dialysis, a post-dialysis supplement dose is not required.34
Carbamazepine has been associated with hyponatremia and possibly interstitial nephri-tis; however, the mechanisms subserving these adverse events are not well-characterized.34 In patients with severe renal impairment it is rec-ommended that serum sodium levels are mon-itored every 3 months after the initiation of carbamazepine therapy.34
OxcarbazepineOxcarbazepine was developed through
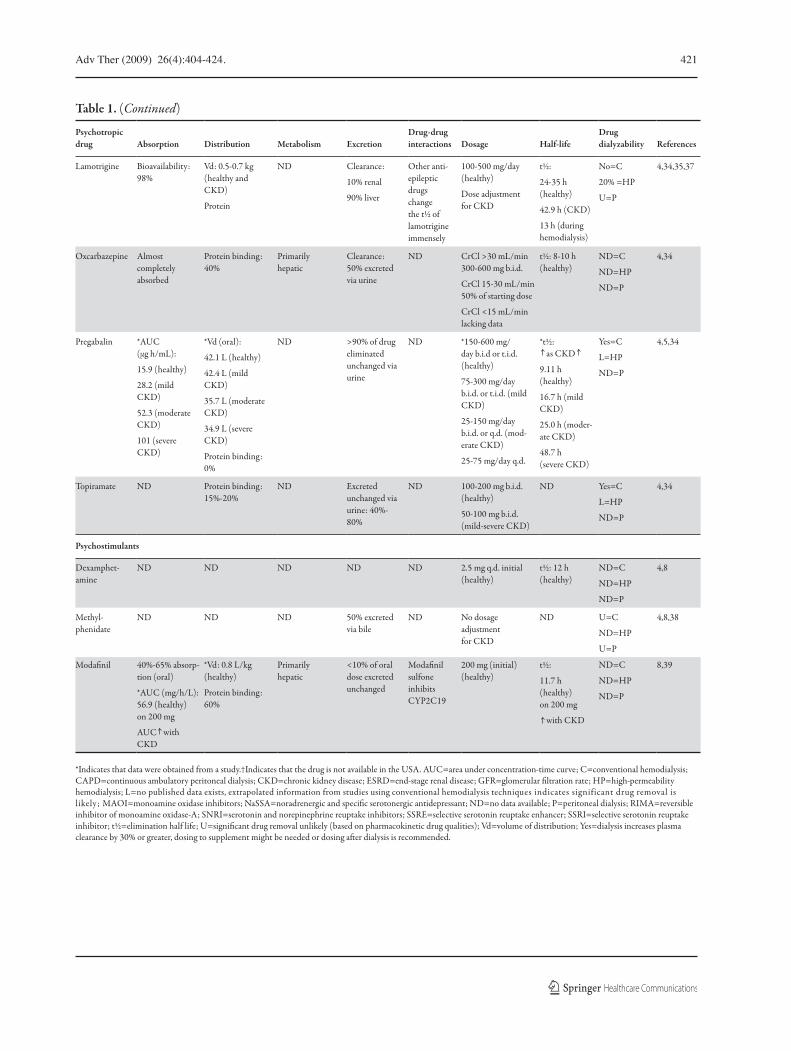
structural alteration of carbamazepine.34 Although similar in structure, both agents are different in their pharmacokinetic profiles.34 In contrast to carbamazepine, oxcarbazepine is excreted largely via the kidney (Table 1), as the parent compound or its metabolite (ie, mono-hydroxy derivatives [MHD]).34 The clearance of MHD is linearly correlated to CrCl.61
A single-dose study involving 20 patients with varying degrees of renal insufficiency com-pared with healthy volunteers was reported.62 All subjects were administered a single 300 mg oral dose of oxcarbazepine. A modest elevation in the plasma concentration of oxcarbazepine and MHD were reported. In keeping with these observations, dose reduction was not essential in patients with CrCl >30 mL/min; however, patients with a CrCl of 15-30 mL/min required a 50% dose reduction and a prolonged titra-tion of the drug.62 In patients with a CrCl <10 mL/min, there is an increased tendency

410 Adv Ther (2009) 26(4):404-424.
for the accumulation of the glucuronides of oxcarbazepine and MHD upon multiple dos-ing.62 The association between oxcarbazepine and hyponatremia warrant close attention to serum electrolyte levels in individuals with renal disease.34
Valproic AcidNo dose adjustment is required for val-
proic acid in patients with impaired renal function owing to its minimal renal excre-tion (1%-3%).34 Hemodialysis, using low effi-ciency dialyzers, removes approximately 20% of plasma valproic acid resulting in a short-term decline in plasma concentrations. A post-dialysis supplementary dose is not nec-essary as the decline in valproic acid levels is temporary and no significant change in mean t1/2 is noted. The use of high efficiency dia-lyzers in cases of valproic acid toxicity has been reported, and has been demonstrated to significantly increase its clearance. With chronic hemodialysis, the effect of high effi-ciency dialyzers on valproic acid clearance is unknown. Rare renal adverse events associated
with the use of valproic acid, including tub-ulointerstitial nephritis, Fanconi syndrome, and hyponatremia, have been reported in a few cases.34,63,64
GabapentinPharmacokinetic studies on gabapentin
have documented that this agent is absorbed by a saturable process; therefore, an increase in dose will lead to a decrease in bioavailabil-ity.34 They also confirmed that gabapentin is not hepatically metabolized and is eliminated entirely unchanged by the kidney.34 Renal fail-ure does not affect the extent of gabapentin absorption.65 On the other hand, the clearance of gabapentin was significantly altered, result-ing in an accumulation with a corresponding increase in t1/2 and the occurrence of dose-dependent toxicity (eg, somnolence, dizziness, ataxia, nystagmus, and tremor). Hemodialysis extracts 35% of gabapentin from the blood.36 As a result, a 200-300 mg dose is suggested after each session. The effect of peritoneal dialysis on the kinetics of gabapentin has not been investigated.34
Adv Ther (2009) 26(4):404-424. 411
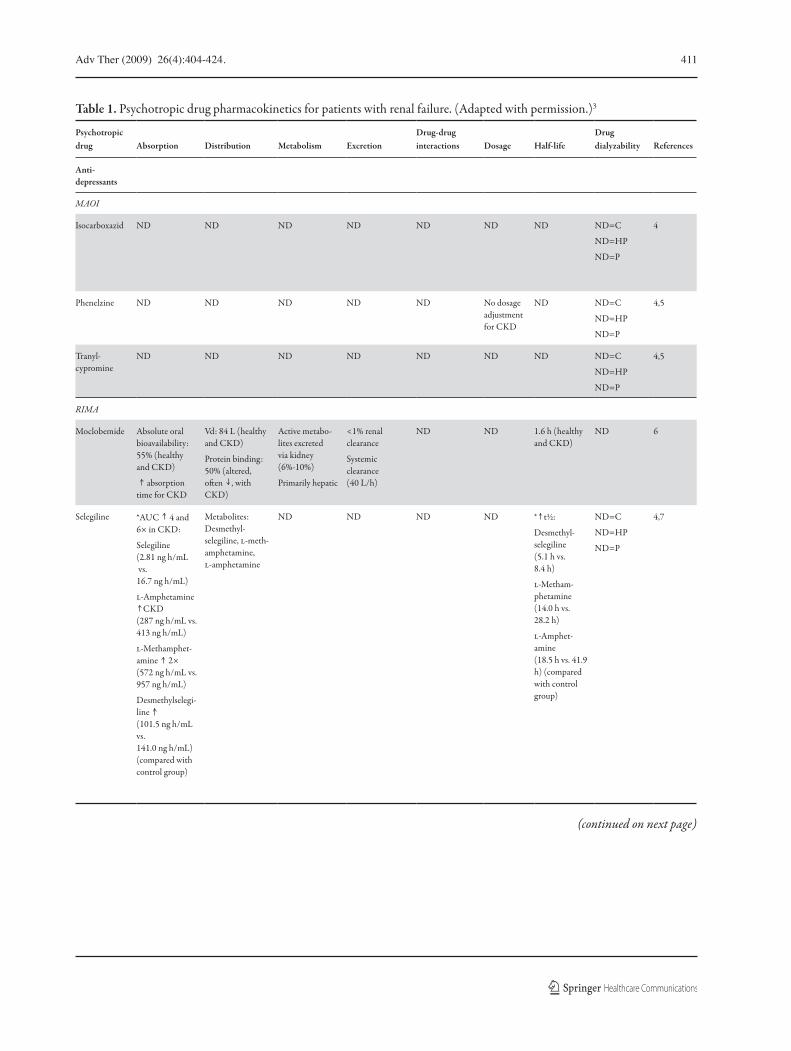
Table 1. Psychotropic drug pharmacokinetics for patients with renal failure. (Adapted with permission.)3
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Anti- depressants
MAOI
Isocarboxazid ND ND ND ND ND ND ND ND=C
ND=HP
ND=P
4
Phenelzine ND ND ND ND ND No dosage adjustment for CKD
ND ND=C
ND=HP
ND=P
4,5
Tranyl-cypromine
ND ND ND ND ND ND ND ND=C
ND=HP
ND=P
4,5
RIMA
Moclobemide Absolute oral bioavailability: 55% (healthy and CKD)
absorption time for CKD
Vd: 84 L (healthy and CKD)
Protein binding: 50% (altered, often , with CKD)
Active metabo-lites excreted via kidney (6%-10%)
Primarily hepatic
<1% renal clearance
Systemic clearance (40 L/h)
ND ND 1.6 h (healthy and CKD)
ND 6
Selegiline *AUC 4 and 6× in CKD:
Selegiline (2.81 ng h/mL vs. 16.7 ng h/mL)
l-Amphetamine CKD
(287 ng h/mL vs. 413 ng h/mL)
l-Methamphet-amine 2× (572 ng h/mL vs. 957 ng h/mL)
Desmethylselegi-line (101.5 ng h/mL vs. 141.0 ng h/mL) (compared with control group)
Metabolites: Desmethyl-selegiline, l-meth-amphetamine, l-amphetamine
ND ND ND ND * t½:
Desmethyl-selegiline (5.1 h vs. 8.4 h)
l-Metham-phetamine (14.0 h vs. 28.2 h)
l-Amphet-amine (18.5 h vs. 41.9 h) (compared with control group)
ND=C
ND=HP
ND=P
4,7
(continued on next page)
412 Adv Ther (2009) 26(4):404-424.
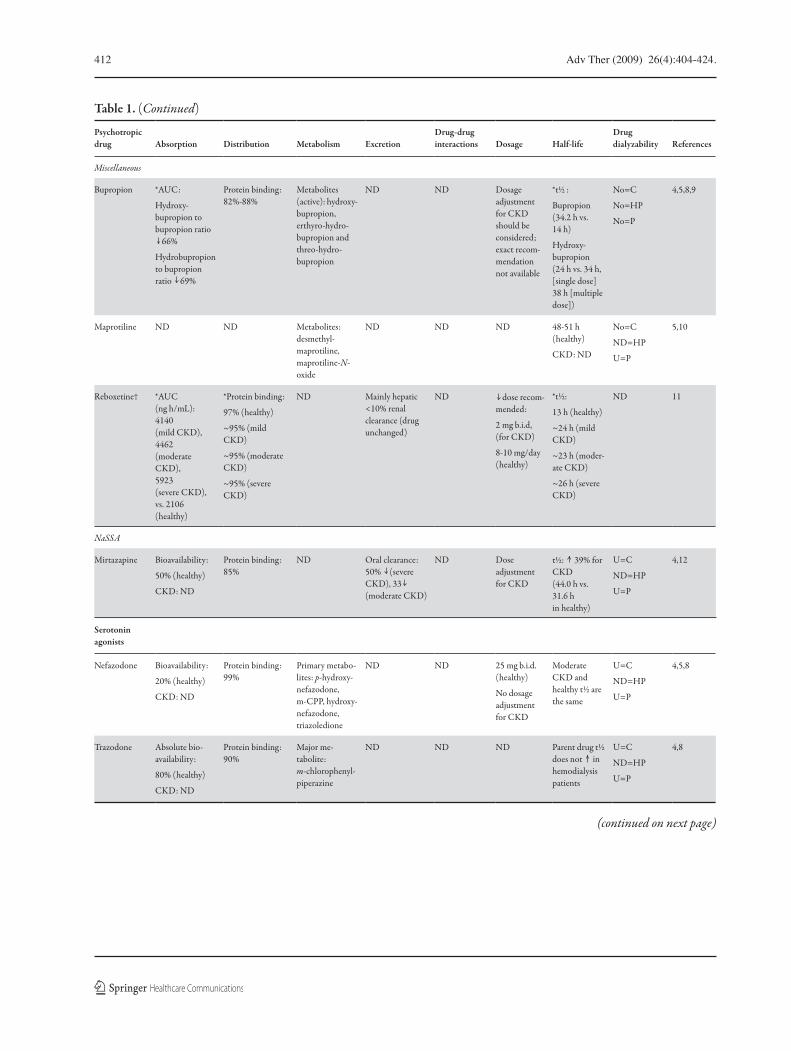
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Miscellaneous
Bupropion *AUC:
Hydroxy-bupropion to bupropion ratio
66%
Hydrobupropion to bupropion ratio 69%
Protein binding: 82%-88%
Metabolites (active): hydroxy-bupropion, erthyro-hydro-bupropion and threo-hydro-bupropion
ND ND Dosage adjustment for CKD should be considered; exact recom-mendation not available
*t½ :
Bupropion (34.2 h vs. 14 h)
Hydroxy-bupropion (24 h vs. 34 h, [single dose] 38 h [multiple dose])
No=C
No=HP
No=P
4,5,8,9
Maprotiline ND ND Metabolites: desmethyl-maprotiline, maprotiline-N-oxide
ND ND ND 48-51 h (healthy)
CKD: ND
No=C
ND=HP
U=P
5,10
Reboxetine† *AUC (ng h/mL): 4140 (mild CKD), 4462 (moderate CKD), 5923 (severe CKD), vs. 2106 (healthy)
*Protein binding:
97% (healthy)
~95% (mild CKD)
~95% (moderate CKD)
~95% (severe CKD)
ND Mainly hepatic <10% renal clearance (drug unchanged)
ND dose recom-mended:
2 mg b.i.d, (for CKD)
8-10 mg/day (healthy)
*t½:
13 h (healthy)
~24 h (mild CKD)
~23 h (moder-ate CKD)
~26 h (severe CKD)
ND 11
NaSSA
Mirtazapine Bioavailability:
50% (healthy)
CKD: ND
Protein binding: 85%
ND Oral clearance: 50% (severe CKD), 33 (moderate CKD)
ND Dose adjustment for CKD
t½: 39% for CKD (44.0 h vs. 31.6 h in healthy)
U=C
ND=HP
U=P
4,12
Serotonin agonists
Nefazodone Bioavailability:
20% (healthy)
CKD: ND
Protein binding: 99%
Primary metabo-lites: p-hydroxy-nefazodone, m-CPP, hydroxy-nefazodone, triazoledione
ND ND 25 mg b.i.d. (healthy)
No dosage adjustment for CKD
Moderate CKD and healthy t½ are the same
U=C
ND=HP
U=P
4,5,8
Trazodone Absolute bio-availability:
80% (healthy)
CKD: ND
Protein binding: 90%
Major me-tabolite: m-chlorophenyl-piperazine
ND ND ND Parent drug t½ does not in hemodialysis patients
U=C
ND=HP
U=P
4,8
(continued on next page)
Adv Ther (2009) 26(4):404-424. 413
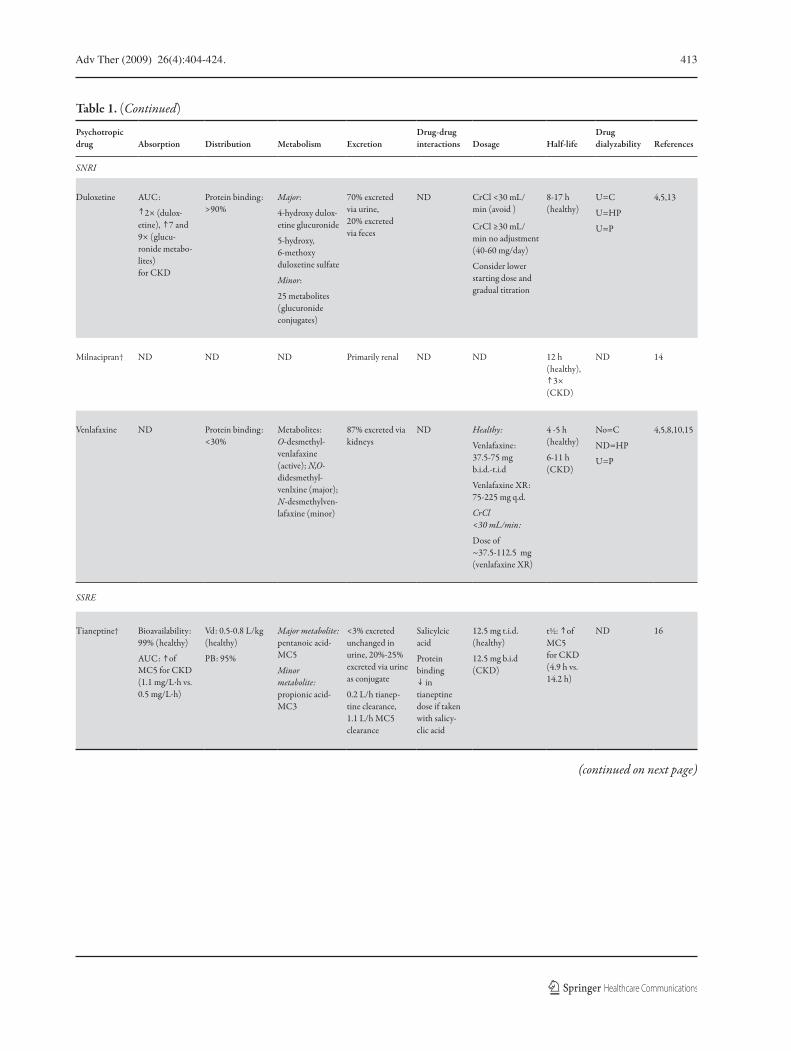
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
SNRI
Duloxetine AUC:
2× (dulox-etine), 7 and 9× (glucu-ronide metabo-lites) for CKD
Protein binding: >90%
Major:
4-hydroxy dulox-etine glucuronide
5-hydroxy, 6-methoxy duloxetine sulfate
Minor:
25 metabolites (glucuronide conjugates)
70% excreted via urine, 20% excreted via feces
ND CrCl <30 mL/min (avoid )
CrCl ≥30 mL/min no adjustment (40-60 mg/day)
Consider lower starting dose and gradual titration
8-17 h (healthy)
U=C
U=HP
U=P
4,5,13
Milnacipran† ND ND ND Primarily renal ND ND 12 h (healthy),
3× (CKD)
ND 14
Venlafaxine ND Protein binding: <30%
Metabolites: O-desmethyl-venlafaxine (active); N,O-didesmethyl-venlxine (major); N-desmethylven-lafaxine (minor)
87% excreted via kidneys
ND Healthy:
Venlafaxine: 37.5-75 mg b.i.d.-t.i.d
Venlafaxine XR: 75-225 mg q.d.
CrCl <30 mL/min:
Dose of ~37.5-112.5 mg (venlafaxine XR)
4 -5 h (healthy)
6-11 h (CKD)
No=C
ND=HP
U=P
4,5,8,10,15
SSRE
Tianeptine† Bioavailability: 99% (healthy)
AUC: of MC5 for CKD (1.1 mg/L·h vs. 0.5 mg/L·h)
Vd: 0.5-0.8 L/kg (healthy)
PB: 95%
Major metabolite: pentanoic acid- MC5
Minor metabolite: propionic acid- MC3
<3% excreted unchanged in urine, 20%-25% excreted via urine as conjugate
0.2 L/h tianep-tine clearance, 1.1 L/h MC5 clearance
Salicylcic acid
Protein binding
in tianeptine dose if taken with salicy-clic acid
12.5 mg t.i.d. (healthy)
12.5 mg b.i.d (CKD)
t½: of MC5 for CKD (4.9 h vs. 14.2 h)
ND 16
(continued on next page)
414 Adv Ther (2009) 26(4):404-424.
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
SSRI
Citalopram High bio-availability with oral administration
ND Metabolite (active):
Desmethyl- citalopram,
Didesmethyl-citalopram, citalopram-N-oxide
20%-23% excreted via urine
Clearance by 40% (CKD), 10-53 mL/min clearance (CKD) vs. 66 mL/min (healthy)
ND 20-60 q 24 h (healthy) 10-60 mg/day (CKD)
35% (CKD) No=C
No=HP
U=P
4,5,8,17
Escitalopram ND Protein binding: 56%
Major metabo-lite: S-didem-ethyl-citalopram
Renal clearance: 0% (CKD)
Oral clearance:
15% (CKD)
ND Initial dose: 10 mg/day (healthy and mild to moderate CKD)
t½:
35% (CKD)
27-33 h (healthy)
S-didemethyl-citalopram: 50-54 h (healthy) (multiple doses)
ND=C
ND=HP
ND=P
4,8,17
Fluoxetine ND Protein binding: 95%
Major metabolite (active): norfluoxetine
ND ND 20 mg/day (healthy)
No dose adjustment (CKD)
1-4 days (healthy), 1.8 days (CKD)
Norfluoxetine: 7-15 days (healthy)
No=C
ND=HP
No=P
4,5,10
Fluvoxamine AUC:
860 µg/h/L (healthy)
CKD: ND
Protein binding: 77%
ND ND ND No dose adjusment
t½:
8-28 h (healthy)
CKD: ND
U=C
No=HP
U=P
4,5,8
Paroxetine ND Protein binding: 95%
ND ND ND 20-60 mg/day (healthy)
10-30 mg/day (CKD)
t½: 10-25 h (healthy) vs. 11-55 h (CKD)
No=C
ND=HP
No=P
4,5,8,10
Sertraline ND Protein binding: 98%
Metabolite (active): desmethyl-sertraline
ND ND 50-200 mg/day (healthy and CKD)
t½:
, 24-36 h (healthy)
42-92 h (CKD)
No=C
ND=HP
U=P
4,5,8
(continued on next page)
Adv Ther (2009) 26(4):404-424. 415
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Tricyclic anti-depressants
Amitriptyline ND ND Metabolites (active): nortrip-tyline, hydroxy-amitriptyline, hydroxy-nortrip-tyline
ND ND 25 mg q 8 h (healthy)
No dosage adjustment for CKD
t½: 32-40 h (healthy and CKD)
No=C
ND=HP
No=P
4,5,10
Amoxapine ND Vd: 85%
Protein binding: 80%
Metabolites (active): 8-hydroxy-amox-apine, 7-hydroxy-amoxapine
ND ND 5-200 mg/day (healthy)
No dosage adjustment for CKD
t½:
8-30 h (healthy)
CKD: ND
U=C
ND=HP
U=P
4,5,10
Clomipramine ND Protein binding: 97%
Metabolite (ac-tive): desmethyl-clomipramine
24%-32% via urine, 51%-60% via faeces
ND ND ND U=C
ND=HP
U=P
4
Doxepin ND Protein binding: 80%-85%
Metabolites (active): desmethyl-doxepin
*60% via urine (rats), 50% via urine (dogs)
ND 25 mg q 8 h (healthy)
No dosage adjustment for CKD
8-25 h (healthy)
10-30 h (CKD)
No=C
ND=HP
No=P
4,5,10,18
Imipramine ND ND Metabolites (active): desmethyl-doxepin
ND ND 25 mg q 8 h (healthy)
No dosage adjustment for CKD
ND No=C
ND=HP
No=P
4,5,10
Nortriptyline ND Plasma values (ng/mL) 29.8%
74.5% for CKD
Protein binding: 93%
Metabolites (active): 10-hydroxy-notriptyline, Z-10-hydroxy-notriptyline
ND ND 25 mg q 6-8 h (healthy)
No dosage adjustment for CKD
t½:
18-93 h (healthy)
15-66 h (CKD)
No=C
ND=HP
No=P
4,5,10,19
Protriptyline ND ND ND ND ND No dosage adjustment for CKD
ND No=C
ND=HP
No=P
4,5
Trimipramine ND ND ND ND ND No dosage adjustment for CKD
ND U=C
ND=HP
U=P
4,5
Mood stabilizers
Lithium Bioavailability:
80%-100% (healthy)
CKD: ND
Vd: 0.7-1.0 L/kg
Protein binding: 0%
Not metabolized
Primarily via kidneys
Clearance: 10-40 mL/min
Diuretics (thiazide diuretics) clearance 40%-68%
NSAIDs
Relative con-tra-indicated (severe CKD)
GFR >50 mL/min (no dose ad-justment), GFR 10-50 mL/min ( dose 50%-75%), GFR <10 mL/min ( dose 25%-50%)
t½:
18-36 h (healthy)
CKD: ND
Yes=C
Yes=HP
Yes=P
4,20
(continued on next page)
416 Adv Ther (2009) 26(4):404-424.
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Anxiolytics/hypnotics
Benzo- diazepines
Alprazolam *AUC (h ng/mL): 441.2 (healthy), 349.9 (C and HP), 592.1 (CAPD) for 2 mg
*AUC (h ng/mL): 124.9 (healthy), 102.8 (C and HP), 197.0 (CAPD), for 0.5 mg
>90% absorbed (healthy)
*Vd (L/kg): 1.09 (healthy), 1.26 (C and HP) for 2 mg
*Vd (L/kg): 1.28 (healthy), 1.14 (C and HP), 1.05 (CAPD) for 0.5 mg
Protein binding: 80%
Metabolites: α-hydroxy-alprazolam, 4-hydroxy-alprazolam
15% α-hydroxy-alprazolam excreted via urine, <1% 4-hydroxy-alprazolam excreted via urine
ND 0.25-5 mg t.i.d. (healthy)
No dosage adjust-ment for CKD
t½:
9-19 (healthy)
11.22 h (C and HP)
18.43 h (CAPD) for 2 mg
No=C
ND=HP
U=P
4,10,21
Buspirone Absolute bio-availability: 4% (healthy)
AUC: 2× (CKD) for 20 mg (single dose)
*AUC (µg/L h): 2.89 (healthy), 6.63 (mild CKD), 4.64 (moderate CKD), 4.09 (severe CKD)
Vd: 5.3 L/kg (healthy)
Protein binding: >95%
Metabolite: 1-pyrimid-inyl-piper-azine (or 1-PP)
Systemic clearance: 1.7 L/h/kg (healthy)
<1% unchanged drug excreted (healthy)
ND 15 mg/day (healthy)
No dosage adjust-ment for CKD
*t½: 2.5 h (healthy)
*t½:
3.18 h (healthy)
12.61 h (mild CKD)
4.34 h (mod-erate CKD)
2.74 h (severe CKD)
No=C
ND=HP
ND=P
4,5,22
Chlor-diazepoxide
ND Protein binding: 90%-98%
ND ND ND 15-100 mg/day (healthy)
No adjustment (mild-moderate CKD)
50% dose: 7.5-50 mg/day (severe CKD)
t½:
5-30 h (healthy)
CKD: ND
No=C
ND=HP
U=P
4,5,10
Clonazepam ND Protein binding: 85%
No active metabolites
ND ND 0.5 mg t.i.d.
No dosage adjustment for CKD
t½:
18-80 h (healthy)
CKD: ND
No=C
ND=HP
U=P
4,10
(continued on next page)
Adv Ther (2009) 26(4):404-424. 417
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Diazepam ND Protein binding: 98%
Metabolites (active): desmethyl- diazepam, oxazepam
ND ND 5-40 mg/day
No dosage adjustment for CKD
t½:
Parent drug 92 h (desmethyl-diazepam 57.3 h) (healthy)
Parent drug 37 h (desmethyl-diazepam 36.1 h) (CKD)
No=C
ND=HP
U=P
4,10
Lorazepam ND Protein binding: 85%
No active metabolites
ND ND 1-2 mg b.i.d. or t.i.d. (healthy), 0.5-2 mg b.i.d. (CKD)
t½:
9-16 h (healthy)
32-70 h (CKD)
No=C
ND=HP
U=P
4,5,10
Midazolam ND Protein binding: 94%-97%
Free fraction in CKD (6.5% vs. 3.9%)
Metabolite: α1-hydroxy-midazolam
*Clearance: α1-hydroxy mida-zolam (186 mL/min), midazolam (198 mL/min) (healthy)
α1-hydroxy-midazolam (14 mL/min), midazolam (132 mL/min) (CKD)
ND Drug monitor-ing suggested
No dosage adjustment (mild-moderate CKD), 50% dose (severe CKD)
t½ (α1-hydroxy-midazolam):
0.8-1 h (healthy)
CKD: ND
No=C
ND=HP
U=P
4,5,23
Nitrazepam ND *Vd: 228 L (3.61 L/kg) (healthy), 283 L (4.16 L/kg) (CKD)
*Protein binding: for CKD
Primarily hepatic
*Clearance: 111 mL/min (healthy), 281 mL/min (CKD)
ND No dosage adjustment for CKD
t½:
24.5 (healthy)
31.5 (CKD)
ND 10,24
Oxazepam ND Protein binding: 86%-99% (varies)
No active metabolites
ND ND 30-120 mg/day (healthy and CKD)
No dose adjustment (CKD)
t½:
6-25 h (healthy)
25-90 h (CKD)
No=C
ND=HP
U=P
4
Temazepam ND Protein binding: 96%
No active metabolites
ND ND 15-30 mg h.s.
No dosage adjustment for CKD
t½:
4-10 h (healthy)
CKD: ND
No=C
ND=HP
U=P
4,10
Triazolam ND Protein binding: 89%
Metabolite: α-hydroxy-triazolam
ND ND 0.125-0.5 mg/day
No dosage adjustment for CKD
t½:
2-4 h (healthy)
2.3 h (CKD)
No=C
ND=HP
U=P
4,10
(continued on next page)
418 Adv Ther (2009) 26(4):404-424.
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Non- benzodiazepines
Zaleplon Systemic bioavailability:
30% (healthy)
CKD: ND
Vd: 275 L for 10 mg (healthy)
Protein binding: 60%
No active metabolites
Primarily hepatic
<1% excreted unchanged via urine
ND Healthy dose 5-20 mg h.s.
Dose adjusted for severe CKD
t½:
1 h (healthy)
CKD: ND
ND=C
ND=HP
ND=P
4,10,25
Zolpidem Bioavailability:
70% (healthy)
CKD: ND
Vd: 66 L for 10 mg
Protein binding: 92%
free fraction for CKD
No active metabolites
Primarily hepatic
≤1% excreted via urine
Metabolites excreted via urine (48%-67%)
ND 10 mg/day (healthy)
Dosage adjustment for severe CKD ( 50%)
t½:
2-3 h (healthy)
4-6 h (CKD)
No=C
ND=HP
U=P
2,10,25,26
Zoplicone Bioavailability:
80% (healthy)
CKD: ND
Protein binding: 45%-80%
Metabolites (active): N-oxide metabolite
Metabolites (inactive): N-desmethyl metabolite
Metabolites: 50% excreted via lungs, 30% (initial) excreted via urine
Erythro-mycin and cimetidine
ND t½:
5 h (healthy)
CKD: ND
ND 25,27
Antipsychotics
Typical
Amisulpiride *AUC (ng h/mL):
404 (healthy)
754 (mild CKD)
1709 (moderate CKD)
4606 (severe CKD)
ND ND Excreted unchanged in feces and urine
Cyclosporine A inhibits P-glycopro-tein
ND *t½:
11.2 h (healthy)
14.0 h (mild CKD)
14.4 h (moder-ate CKD)
25.8 h (severe CKD)
ND 4,28
Chlor-promazine
ND ND Metabolites (active):
CPZ-N-oxide
CPZ sulfoxide
7-hydroxy-CPZ
nor1-CPZ
nor2-CPZ
nor2-CPZ sulfoxide
3-hydroxy-CPZ
ND ND 50-400 mg/day (healthy)
CKD: ND
t½: 11-42 (healthy and CKD)
No=C
ND=HP
No=P
4,5,10
Haloperidol ND Protein binding: 90%
Metabolite (active): hydroxy- haloperidol
<1% excreted via urine
ND 1-2 mg q 8-12 h
No dosage adjustment for CKD
t½: 14-26 h (healthy and CKD)
No=C
ND=HP
No=P
4,10
(continued on next page)
Adv Ther (2009) 26(4):404-424. 419
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Perphenazine ND ND ND ND ND 4-16 mg b.i.d.-q.i.d. (healthy)
CKD: ND
t½: 9.5 h (healthy)
CKD: ND
U=C
ND=HP
U=P
10,28
Sulpiride *AUC (mg/h/L): 8.27 (i.v.), 2.41 (oral) (healthy)
*Absolute bioavailability (sulpiride sulfate):
35% (healthy)
CKD: ND
*Vd: 1.19 L/kg (i.v.), 2.05 L/kg (oral)
ND *36.9% excreted via urine
ND ND *t½:
6.63 h (i.v.)
6.73 h (oral) (healthy)
CKD: ND
ND 4,29
Thioridazine ND ND Metabolites (active): mesoridazine, sulforidazine
ND ND 50-800 mg/day (healthy)
Dosage ad-justment not studied; use in CKD is best avoided
t½:
21-24 h (healthy)
CKD: ND
U=C
ND=HP
U=P
4,10
Triflu-operazine
ND ND ND ND ND ND ND No=C
ND=HP
No=P
4
Atypical
Aripiprazole Bioavailability: 87% (healthy)
AUC (ESRD): 15% (aripipra-
zole), 7% (dehydro-
aripiprazole), (aripiprazole)
Vd: 404 L (4.9 L/kg) (healthy)
Protein binding: >99%
Primarily hepatic
Metabolites (active): dehydro-aripip-razole
Oral clearance: 3.3-4.0 L/h (healthy)
Renal excre-tion: 25% (<1% unchanged), 55% excreted via feces (18% unchanged)
Significant drug inter-actions with drugs metabolized on enzyme 2D6 and 3A4
10-30 mg/day (healthy)
No dosage adjustment for CKD
t½:
47-68 h (healthy)
CKD: ND
U=C
U=HP
U=P
10,30
Clozapine ND Vd: 2-7 L/kg (healthy)
Protein binding: 95%-97%
Primarily hepatic
Metabolites (ac-tive): N-desm-ethyl-clozapine
27%-50% ex-creted unchanged (systemic clearance)
ND 12.5-450 mg (healthy)
CKD: ND (titrate to response)
t½:
9-17 h (healthy)
CKD: ND
ND 4,30
Olanzapine Bioavailabilty:
60% (healthy)
CKD: ND
Protein binding: 93%
Vd: 16±5 L
Metabolites (active): N-desmethyl olanzapine, olan-zapine 10-N-glucuronide
Total urine recov-ery (56.2%), fecal recovery (30%)
Clearance via urine: N-desmethyl olanzapine (0.8%), 10-N-glucuronide olanzapine (28.6%), olanzapine (17.7%)
ND 5-20 mg (healthy and CKD)
No dosage adjustment for CKD
t½: 32-38 h (healthy and CKD)
No=C
ND=HP
No=P
2,10,30,31
(continued on next page)
420 Adv Ther (2009) 26(4):404-424.
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Quetiapine AUC: 42% for CKD than in healthy (533 vs. 366 ng h/mL)
Vd 48% for CKD than in healthy (593 vs. 310 L)
Protein binding: 83%
Metabolites (active): 7 hydroxy-quetiapine, N-dealkylated quetiapine
Quetiapine sulfoxide metabolite
<1% excreted unchanged via urine
Oral clearance: 53% (healthy), 64% (CKD)
ND 150-750 mg/day b.i.d. or t.i.d.
No dosage adjustment for CKD
t½:
5-6 h (healthy)
4.1 h (CKD)
ND 4,31,32
Risperidone ND Protein binding: 90%
Metabolites (active): 9-hydroxy-risperidone
Clearance: 10% renal, 40% of 9-hydroxy risperidone
Oral clearance: 50% in CKD
ND 1-3 mg b.i.d. (healthy), 0.5-1.5 mg b.i.d. (CKD)
t½:
3-30 h (healthy)
19 h (9-hydroxy-risperidone) (healthy)
25 h (9-hydroxy-risperidone) (CKD)
ND=C
ND=HP
ND=P
4,10,33
Ziprasidone *AUC (ng h/mL):
272 (healthy)
370 (mild CKD)
250 (moderate CKD)
297 (severe CKD)
Protein binding: 99%
Inactive metabolites
ND ND 20-80 mg b.i.d. (CKD)
Dose adjustment not needed in mild and moder-ate CKD
*t½:
5-7 h (healthy)
6.4 h (mild CKD)
4.9 h (moder-ate CKD)
4.2 h (severe CKD)
No=C
ND=HP
U=P
4,10,33
Antiepileptics
Carba- mazepine
ND Vd: 0.8 kg
Protein binding: 75%
ND Clearance: 1% via kidney, 99% via liver
Valproic acid, felbemate. Digoxin, cyclosporin
10-25 kg/day maintenance dose (healthy)
No dose adjust-ment for CKD
t½:
9-15 h (healthy)
CKD: ND
No=C
Yes=HP
No=P
4,34,35
Valproic acid ND Protein binding: 90%
Primarily via liver
Clearance: 1%-3% excreted unchanged via urine
ND No dosage adjust-ment for CKD
ND No=C
ND=HP
No=P
4,34
Gabapentin Bioavailability when dose
(300 mg=57%, 1600 mg=35%)
Vd: 0.7 kg ND Primarily renal excretion
Clearance: 80% via urine
ND Dosage adjust-ment for CKD
400-600 mg t.i.d. (healthy)
200-300 mg b.i.d. (mild-moderate CKD)
100-150 mg/day (severe CKD)
t½:
5-7 h (healthy)
CKD: ND
Yes=C
L=HP
ND=P
4,34-36
(continued on next page)
Adv Ther (2009) 26(4):404-424. 421
Table 1. (Continued)
Psychotropic drug Absorption Distribution Metabolism Excretion
Drug-drug interactions Dosage Half-life
Drug dialyzability References
Lamotrigine Bioavailability: 98%
Vd: 0.5-0.7 kg (healthy and CKD)
Protein
ND Clearance:
10% renal
90% liver
Other anti-epileptic drugs change the t½ of lamotrigine immensely
100-500 mg/day (healthy)
Dose adjustment for CKD
t½:
24-35 h (healthy)
42.9 h (CKD)
13 h (during hemodialysis)
No=C
20% =HP
U=P
4,34,35,37
Oxcarbazepine Almost completely absorbed
Protein binding: 40%
Primarily hepatic
Clearance: 50% excreted via urine
ND CrCl >30 mL/min 300-600 mg b.i.d.
CrCl 15-30 mL/min 50% of starting dose
CrCl <15 mL/min lacking data
t½: 8-10 h (healthy)
ND=C
ND=HP
ND=P
4,34
Pregabalin *AUC (µg h/mL):
15.9 (healthy)
28.2 (mild CKD)
52.3 (moderate CKD)
101 (severe CKD)
*Vd (oral):
42.1 L (healthy)
42.4 L (mild CKD)
35.7 L (moderate CKD)
34.9 L (severe CKD)
Protein binding: 0%
ND >90% of drug eliminated unchanged via urine
ND *150-600 mg/day b.i.d or t.i.d. (healthy)
75-300 mg/day b.i.d. or t.i.d. (mild CKD)
25-150 mg/day b.i.d. or q.d. (mod-erate CKD)
25-75 mg/day q.d.
*t½: as CKD
9.11 h (healthy)
16.7 h (mild CKD)
25.0 h (moder-ate CKD)
48.7 h (severe CKD)
Yes=C
L=HP
ND=P
4,5,34
Topiramate ND Protein binding: 15%-20%
ND Excreted unchanged via urine: 40%-80%
ND 100-200 mg b.i.d. (healthy)
50-100 mg b.i.d. (mild-severe CKD)
ND Yes=C
L=HP
ND=P
4,34
Psychostimulants
Dexamphet-amine
ND ND ND ND ND 2.5 mg q.d. initial (healthy)
t½: 12 h (healthy)
ND=C
ND=HP
ND=P
4,8
Methyl-phenidate
ND ND ND 50% excreted via bile
ND No dosage adjustment for CKD
ND U=C
ND=HP
U=P
4,8,38
Modafinil 40%-65% absorp-tion (oral)
*AUC (mg/h/L): 56.9 (healthy) on 200 mg
AUC with CKD
*Vd: 0.8 L/kg (healthy)
Protein binding: 60%
Primarily hepatic
<10% of oral dose excreted unchanged
Modafinil sulfone inhibits CYP2C19
200 mg (initial) (healthy)
t½:
11.7 h (healthy) on 200 mg
with CKD
ND=C
ND=HP
ND=P
8,39
*Indicates that data were obtained from a study.†Indicates that the drug is not available in the USA. AUC=area under concentration-time curve; C=conventional hemodialysis; CAPD=continuous ambulatory peritoneal dialysis; CKD=chronic kidney disease; ESRD=end-stage renal disease; GFR=glomerular filtration rate; HP=high-permeability hemodialysis; L=no published data exists, extrapolated information from studies using conventional hemodialysis techniques indicates significant drug removal is likely ; MAOI=monoamine oxidase inhibitors; NaSSA=noradrenergic and specific serotonergic antidepressant; ND=no data available; P=peritoneal dialysis; RIMA=reversible inhibitor of monoamine oxidase-A; SNRI=serotonin and norepinephrine reuptake inhibitors; SSRE=selective serotonin reuptake enhancer; SSRI=selective serotonin reuptake inhibitor; t½=elimination half life; U=significant drug removal unlikely (based on pharmacokinetic drug qualities); Vd=volume of distribution; Yes=dialysis increases plasma clearance by 30% or greater, dosing to supplement might be needed or dosing after dialysis is recommended.
422 Adv Ther (2009) 26(4):404-424.
CONCLUSIONS
Taken together, deterioration in renal function significantly affects the pharmacokinetic profile of psychotropic agents. The use of these agents in this patient population is not uncommon due to the co-occurrence of mental and renal disor-ders. In this context, caution is warranted when prescribing psychotropic agents to individuals with impaired renal function. Guiding priciples include, but are not limited to, slow titration of doses, low-dose treatment initiation, and careful monitoring of clinical response.
ACKNOWLEDGMENTS
RSM has received research or grants from Stanley Medical Research Institute, and National Alliance for Research on Schizophrenia and Depression (NARSAD). He has also received pharmaceutical research grants from Eli Lilly, Janssen-Ortho, and Shire. He has also served on advisory boards for AstraZeneca, Bristol-Myers Squibb, France Foundation, GlaxoSmithKline, Janssen-Ortho, Solvay/Wyeth, Eli Lilly, Organon, Lundbeck, Biovail, Pfizer, Shire, and Schering-Plough. He has taken part in speaker bureaus for Janssen-Ortho, AstraZeneca, Eli Lilly, Lundbeck, Biovail, and Wyeth; and has taken part in CME activities for AstraZeneca, Bristol-Myers Squibb, France Foundation, I3CME, Solvay/Wyeth, Physicians’ Postgraduate Press, and CME outfitters.
REFERENCES
Sun H, Frassetto L, Benet LZ. Effects of renal fail-1. ure on drug transport and metabolism. Pharmacol Ther. 2006;109:1-11.
Murtagh FE, Addington-Hall J, Higginson IJ. The 2. prevalence of symptoms in end-stage renal dis-ease: a systematic review. Adv Chronic Kidney Dis. 2007;14:82-99.
McIntyre RS, Baghdady NT, Banik S, Swartz 3. SA. The use of psychotropic drugs in patients with impaired renal function. Prim Psychiatry. 2008;15:73-88.
Johnson CA, Simmons WD. 2009 Dialysis of 4. Drugs. Nephrology Pharmacy Associates. Avail-able at: www.ckdinsights.com/downloads/Dialysis-Drugs2009.pdf. Accessed March 2009.
Aronoff GR, Brier ME. Prescribing drugs in renal 5. disease. In: Brenner BM, Rector FC, eds. Brenner & Rector’s The Kidney. Philadelphia, PA: 2004;2849-2870.
Schoerlin MP, Horber FF, Frey FJ, Mayersohn M. 6. Disposition kinetics of moclobemide, a new MAO-A inhibitor, in subjects with impaired renal func-tion. J Clin Pharmacol. 1990;30:272-284.
Anttila M, Sotaniemi EA, Pelkonen O, Rautio A. 7. Marked effect of liver and kidney function on the pharmacokinetics of selegiline. Clin Pharmacol Ther. 2005;77:54-62.
Crone CC, Gabriel GM. Treatment of anxiety and de-8. pression in transplant patients: pharmacokinetic con-siderations. Clin Pharmacokinet. 2004;43:361-394.
Turpeinen M, Koivuviita N, Tolonen A, et al. Effect 9. of renal impairment on the pharmacokinetics of bupropion and its metabolites. Br J Clin Pharma-col. 2007;64:165-173.
Cohen LM, Tessier EG, Germain MJ, Levy NB. Up-10. date on psychotropic medication use in renal dis-ease. Psychosomatics. 2004;45:34-48.
Coulomb F, Ducret F, Laneury JP, et al. Pharmacoki-11. netics of single-dose reboxetine in volunteers with re-nal insufficiency. J Clin Pharmacol. 2000;40:482-487.
Timmer CJ, Sitsen JM, Delbressine LP. Clinical 12. pharmacokinetics of mirtazapine. Clin Pharmaco-kinet. 2000;38:461-474.
Westanmo AD, Gayken J, Haight R. Duloxetine: 13. a balanced and selective norepinephrine- and serotonin-reuptake inhibitor. Am J Health Syst Pharm. 2005;62:2481-2490.
Preskorn SH. Milnacipran: a dual norepinephrine 14. and serotonin reuptake pump inhibitor. J Psychiatr Pract. 2004;10:119-126.
Ereshefsky L, Dugan D. Review of the pharma-15. cokinetics, pharmacogenetics, and drug interac-tion potential of antidepressants: focus on venla-faxine. Depress Anxiety. 2000;12(suppl. 1):30-44.
Adv Ther (2009) 26(4):404-424. 423
Wilde MI, Benfield P. Tianeptine. A review of 16. its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in depres-sion and coexisting anxiety and depression. Drugs. 1995;49:411-439.
Rao N. The clinical pharmacokinetics of escitalo-17. pram. Clin Pharmacokinet. 2007;46:281-290.
Hobbs DC. Distribution and metabolism of dox-18. epin. Biochem Pharmacol. 1969;18:1941-1954.
Rosser R. Depression during renal dialysis and 19. following transplantation. Proc R Soc Med. 1976;69:832-834.
Ward ME, Musa MN, Bailey L. Clinical Phar-20. macokinetics of lithium. J Clin Pharmacol. 1994;34:280-285.
Schmith VD, Piraino B, Smith RB, Kroboth PD. Al-21. prazolam in end-stage renal disease: I. Pharmaco-kinetics. J Clin Pharmacol. 1991;31:571-579.
Mahmood I, Sahajwalla C. Clinical pharmacokinet-22. ics and pharmacodynamics of buspirone, an anxi-olytic drug. Clin Pharmacokinet. 1999;36:277-287.
Spina SP, Ensom MH. Clinical pharmacokinetic 23. monitoring of midazolam in critically ill patients. Pharmacotherapy. 2007;27:389-398.
Ochs HR, Oberem U, Greenblatt DJ. Nitrazepam 24. clearance unimpaired in patients with renal insuffi-ciency. J Clin Psychopharmacol. 1992;12:183-185.
Drover DR. Comparative pharmacokinetics and 25. pharmacodynamics of short-acting hypnoseda-tives: zaleplon, zolpidem and zopiclone. Clin Phar-macokinet. 2004;43:227-238.
Chouinard G, Lefko-Singh K, Teboul E. Metabolism 26. of anxiolytics and hypnotics: benzodiazepines, buspirone, zoplicone, and zolpidem. Cell Mol Neu-robiol. 1999;19:533-552.
Canal M, MacMahon M, Kwan J, Dubruc C. Ami-27. sulpride: kinetics in patients with renal failure. Eu-ropean Neuropsychopharmacology. 2000;10(sup-pl. 3):330-331.
Schmitt U, Abou El-Ela A, Guo LJ, et al. Cy-28. closporine A (CsA) affects the pharmacodynamics and pharmacokinetics of the atypical antipsychotic amisulpride probably via inhibition of P-glycopro-tein (P-gp). J Neural Transm. 2006;113:787-801.
Bressolle F, Bres J, Faure-Jeantis A. Absolute bio-29. availability, rate of absorption, and dose pro-
portionality of sulpiride in humans. J Pharm Sci. 1992;81:26-32.
Mauri MC, Volonteri LS, Colasanti A, et al. Clini-30. cal pharmacokinetics of atypical antipsychotics: a critical review of the relationship between plasma concentrations and clinical response. Clin Pharma-cokinet. 2007;46:359-388.
Shen WW. The metabolism of atypical antip-31. sychotic drugs: an update. Ann Clin Psychia-try. 1999;11:145-158.
Thyrum PT, Wong YW, Yeh C. Single-dose pharma-32. cokinetics of quetiapine in subjects with renal or hepatic impairment. Prog Neuropsychopharmacol Biol Psychiatry. 2000;24:521-533.
Aweeka F, Jayesekara D, Horton M, et al. The phar-33. macokinetics of ziprasidone in subjects with nor-mal and impaired renal function. Br J Clin Pharma-col. 2000;49(suppl. 1):27-33.
Israni RK, Kasbekar N, Haynes K, Berns JS. Use of 34. antiepileptic drugs in patients with kidney disease. Semin Dial. 2006;19:408-416.
Lacerda G, Krummel T, Sabourdy C, Ryvlin P, Hir-35. sch E. Optimizing therapy of seizures in patients with renal or hepatic dysfunction. Neurology. 2006;67(suppl. 4):28-33.
Bassilios N, Launay-Vacher V, Khoury N, et al. 36. Gabapentin neurotoxicity in a chronic haemodialy-sis patient. Nephrol Dial Transplant. 2001;16:2112-2113.
Lamictal [pamphlet]. United States: GlaxoSmith-37. Kline; 2007.
Quinn D, Bode T, Reiz JL, Donnelly GA, Darke AC. 38. Single-dose pharmacokinetics of multilayer-release methylphenidate and immediate-release methylphe-nidate in children with attention-deficit/hyperactiv-ity disorder. J Clin Pharmacol. 2007;47:760-766.
Robertson P Jr., Hellriegel ET. Clinical pharmacoki-39. netic profile of modafinil. Clin Pharmacokinet. 2003;42:123-137.
Bezchlibnyk-Butler K, Aleksic I, Kennedy SH. Cita-40. lopram - a review of pharmacological and clinical effects. J Psychiatry Neurosci. 2000;25:241-254.
Nemeroff CB. Overview of the safety of citalopram. 41. Psychopharmacol Bull. 2003;37:96-121.
Levy NB, Blumenfield M, Beasley CM Jr., et al. 42. Fluoxetine in depressed patients with renal fail-ure and in depressed patients with normal kidney function. Gen Hosp Psychiatry. 1996;18:8-13.
424 Adv Ther (2009) 26(4):404-424.
Paxil CR [pamphlet]. United States: GlaxoSmith-43. Kline; 2008.
Yalcin AU, Sahin G, Erol M, Bal C. Sertraline hydro-44. chloride treatment for patients with hemodialysis hypotension. Blood Purif. 2002;20:150-153.
Beliles K, Stoudemire A. Psychopharmacologic 45. treatment of depression in the medically ill. Psy-chosomatics. 1998;39:2-19.
Holliday SM, Benfield P. Venlafaxine. A review of 46. its pharmacology and therapeutic potential in de-pression. Drugs. 1995;49:280-294.
Cymbalta [pamphlet]. United States: Eli-Lilly and 47. Company; 2009.
Choi S. Nefazodone (Serzone) withdrawn because of 48. hepatotoxicity. Can Med Assoc J. 2003;169:1187.
Remeron - mirtazapine [pamphlet]. United States: 49. Organon; 2008.
Levy NB. Psychopharmacology in patients with re-50. nal failure. Int J Psychiatry Med. 1990;20:325-334.
American Psychiatric Association. Practice guide-51. line for the treatment of patients with major de-pressive disorder (revision). Am J Psychiatry. 2000;157(suppl. 4):1-45.
Fukunishi I, Kitaoka T, Shirai T, et al. Psychiatric 52. disorders among patients undergoing hemodialysis therapy. Nephron. 2002;91:344-347.
Sheehan J, White A, Wilson R. Hazards of phe-53. nothiazines in chronic renal failure. Ir Med J. 1982;75:335.
DeVane CL, Nemeroff CB. Clinical pharmacokinet-54. ics of quetiapine: an atypical antipsychotic. Clin Pharmacokinet. 2001;40:509-522.
Snoeck E, Van PA, Sack M, et al. Influence of age, 55. renal and liver impairment on the pharmacokinet-ics of risperidone in man. Psychopharmacology (Berl). 1995;122:223-229.
Abilify [pamphlet]. United States: Bristol-Myers 56. Squibb Company; 2006.
Winans E. Aripiprazole. Am J Health Syst 57. Pharm. 2003;60:2437-2445.
Ambien CR [pamphlet]. France: Sanofi-Aventis; 58. 2007.
Sonata [pamphlet]. United States: Wyeth Pharma-59. ceuticals; 2006.
Presne C, Fakhouri F, Noel LH, et al. Lithium-in-60. duced nephropathy: rate of progression and prog-nostic factors. Kidney Int. 2003;64:585-592.
Flesch G. Overview of the clinical pharmacoki-61. netics of oxcarbazepine. Clin Drug Investig. 2004;24:185-203.
Rouan MC, Lecaillon JB, Godbillon J, et al. The ef-62. fect of renal impairment on the pharmacokinetics of oxcarbazepine and its metabolites. Eur J Clin Pharmacol. 1994;47:161-167.
Watanabe T, Yoshikawa H, Yamazaki S, Abe Y, Abe 63. T. Secondary renal Fanconi syndrome caused by valproate therapy. Pediatr Nephrol. 2005;20:814-817.
Zaki EL, Springate JE. Renal injury from valproic 64. acid: case report and literature review. Pediatr Neurol. 2002;27:318-319.
Blum RA, Comstock TJ, Sica DA, et al. Pharma-65. cokinetics of gabapentin in subjects with various degrees of renal function. Clin Pharmacol Ther. 1994;56:154-159.












![[Psychotropic drugs in prison]](https://img.dokumen.tips/doc/110x75/6328edb96c3a86e3190a3798/psychotropic-drugs-in-prison.jpg)
















