Embed Size (px)
Citation preview

Psychosocial Interventions and Immune System FunctionA Systematic Review and Meta-analysis of Randomized Clinical TrialsGrant S. Shields, PhD; Chandler M. Spahr, MA; George M. Slavich, PhD
IMPORTANCE Recent estimates suggest that more than 50% of all deaths worldwide arecurrently attributable to inflammation-related diseases. Psychosocial interventions mayrepresent a potentially useful strategy for addressing this global public health problem, butwhich types of interventions reliably improve immune system function, under whatconditions, and for whom are unknown.
OBJECTIVE To address this issue, we conducted a systematic review and meta-analysis ofrandomized clinical trials (RCTs) in which we estimated associations between 8 differentpsychosocial interventions and 7 markers of immune system function, and examined 9potential moderating factors.
DATA SOURCES PubMed, Scopus, PsycInfo, and ClinicalTrials.gov databases weresystematically searched from February 1, 2017, to December 31, 2018, for all relevant RCTspublished through December 31, 2018.
STUDY SELECTION Eligible RCTs included a psychosocial intervention, immune outcome, andpreintervention and postintervention immunologic assessments. Studies were independentlyexamined by 2 investigators. Of 4621 studies identified, 62 were eligible and 56 included.
DATA EXTRACTION AND SYNTHESIS Data were extracted and analyzed from January 1, 2019, toJuly 29, 2019. The Preferred Reporting Items for Systematic Reviews and Meta-analyses(PRISMA) guideline was followed. Data were extracted by 2 investigators who were blind tostudy hypotheses and analyses, and were then analyzed using robust variance estimation.Analysis included 8 psychosocial interventions (behavior therapy, cognitive therapy, cognitivebehavior therapy [CBT], CBT plus additive treatment or mode of delivery that augmented theCBT, bereavement or supportive therapy, multiple or combined interventions, otherpsychotherapy, and psychoeducation), 7 immune outcomes (proinflammatory cytokine ormarker levels, anti-inflammatory cytokine levels, antibody levels, immune cell counts, naturalkiller cell activity, viral load, and other immune outcomes), and 9 moderating factors(intervention type, intervention format, intervention length, immune marker type, basal vsstimulated markers, immune marker measurement timing, disease state or reason fortreatment, age, and sex).
MAIN OUTCOMES AND MEASURES The primary a priori outcomes were pretest-posttest-control (ppc) group effect sizes (ppc g) for the 7 immunologic outcomes investigated.
RESULTS Across 56 RCTs and 4060 participants, psychosocial interventions were associatedwith enhanced immune system function (ppc g = 0.30, 95% CI, 0.21-0.40; t50.9 = 6.22;P < .001). Overall, being randomly assigned to a psychosocial intervention condition vs acontrol condition was associated with a 14.7% (95% CI, 5.7%-23.8%) improvement inbeneficial immune system function and an 18.0% (95% CI, 7.2%-28.8%) decrease in harmfulimmune system function over time. These associations persisted for at least 6 monthsfollowing treatment and were robust across age, sex, and intervention duration. Theseassociations were most reliable for CBT (ppc g = 0.33, 95% CI, 0.19-0.47; t27.2 = 4.82;P < .001) and multiple or combined interventions (ppc g = 0.52, 95% CI, 0.17-0.88;t5.7 = 3.63; P = .01), and for studies that assessed proinflammatory cytokines or markers (ppcg = 0.33, 95% CI, 0.19-0.48; t25.6 = 4.70; P < .001).
CONCLUSIONS AND RELEVANCE These findings suggest that psychosocial interventions arereliably associated with enhanced immune system function and may therefore represent aviable strategy for improving immune-related health.
JAMA Psychiatry. 2020;77(10):1031-1043. doi:10.1001/jamapsychiatry.2020.0431Published online June 3, 2020.
Editorial page 996
Supplemental content
Author Affiliations: Center for Mindand Brain, University of California,Davis (Shields); Department ofPsychology, San Diego StateUniversity, San Diego, California(Spahr); Cousins Center forPsychoneuroimmunology andDepartment of Psychiatry andBiobehavioral Sciences, University ofCalifornia, Los Angeles (Slavich).
Corresponding Author: George M.Slavich, PhD, Cousins Center forPsychoneuroimmunology andDepartment of Psychiatry andBiobehavioral Sciences, University ofCalifornia, Los Angeles, UCLA MedicalPlaza 300, Room 3156, Los Angeles,CA 90095 ([email protected]).
Research
JAMA Psychiatry | Original Investigation
(Reprinted) 1031
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022

A large body of research demonstrates that theimmune system is involved in a wide variety of men-tal and physical health problems that cause substan-
tial morbidity and mortality,1,2 including anxiety disorders,depression, suicide, schizophrenia, cardiovascular disease,certain cancers, stroke, and autoimmune and neurodegen-erative disorders.3-6 Indeed, a recent analysis of mortalitydata collected from 195 countries from 1980 to 20177 indi-cated that more than 50% of all deaths in the world todaya re att r i b u t a b l e to i n fl a m m at i o n - re l ate d d i s e a s econditions.8 Although pharmacological interventions repre-sent a logical choice for addressing this serious public healthproblem, such interventions can be costly and have adversebiobehavioral and clinical effects. As a result, several promi-nent groups, including the World Health Organization,National Academy of Medicine, and National Institutes ofHealth, have recently emphasized the goal of reducingglobal disease burden using psychosocial interventionswhen possible.9-11
The ability of psychosocial interventions to enhanceimmunity and improve immune-related health outcomes isgrounded in research showing that immune system pro-cesses are influenced by social, neurocognitive, and behav-ioral factors.12,13 Indeed, although immune system functionwas historically thought to be regulated primarily by patho-gen exposure, physical injury, and internal physiologicalprocesses, numerous studies have now shown that immu-nologic activity is also related to psychosocial factors, suchas life stress, negative emotions, and social support.14-17
Whereas chronic stress has been reported to suppress cellu-lar and humoral immunity18 and to increase nonspecificinflammation,5 for example, psychosocial resilience factors,such as social support and connection, have been found tomitigate the negative effect that life stress has on immunefunction and health.16,19-21
Given these findings, numerous studies have examinedwhether interventions that reduce stress or bolster psycho-logical resources can improve immune system function.However, research on this topic has been mixed: althoughsome studies have found that psychosocial interventionsclearly enhance immunity,22 others have not.23 Meta-analyses have made some progress in identifying factorscontributing to these mixed results, but this work has alsohad several limitations. First, rather than comparing find-ings across different types of interventions, existing reviewsand meta-analyses have primarily focused on only 1 inter-vention type, such as cognitive behavior therapy (CBT),24
meditation,25,26 mind-body interventions,27 lifestyleinterventions,28 mind-body therapies,29 stress managementinterventions,30 or non–therapy-specific interventions.31
Consequently, it remains unknown whether certain inter-ventions are more reliably associated with improved immu-nity than others, which is critical for informing policy. Sec-ond, existing meta-analyses have been largely restricted topopulations with specific disorders, such as HIV-positiveadults,24,30 adults with depression,32 patients with breastcancer,33 or populations with other chronic illnesses.29 Theresulting data are therefore informative but do not address
the important question of whether the effectiveness of vari-ous psychosocial interventions differs across disease condi-tion or patients’ reasons for seeking treatment. Finally,rather than examining a variety of immune markers, exist-ing meta-analyses have either collapsed across differentmarkers, thus obscuring potential marker-specific effects,or have evaluated only a few markers, thus preventing anexamination of whether different psychosocial interven-tions are associated with some immunologic markers moreconsistently than others.30,32,33
To address these issues, we conducted what we believeis the first systematic review and meta-analysis of random-ized clinical trials (RCTs) that have examined the effects of apsychosocial intervention on immune system outcomes. Wefocused on 8 psychosocial intervention types: behaviortherapy, cognitive therapy, CBT, CBT plus additive treat-ment or mode of delivery that augmented the CBT (eg, CBTplus benzodiazepines or phone/video sessions), bereave-ment or supportive therapy, multiple or combined interven-tions, other psychotherapy, and psychoeducation. In addi-tion, we examined 7 immune outcomes that could beinfluenced by these interventions: proinflammatory cyto-kines (eg, interleukin-6) and markers (eg, C-reactive pro-tein), anti-inflammatory cytokines (eg, interleukin-10), anti-bodies (eg, IgA), immune cell counts (eg, CD4), natural killercell activity (eg, cytotoxicity), viral load (eg, HIV RNA), andother immune outcomes (eg, blastogenesis, number of post-operative infectious diseases). Finally, we investigated 9factors that could potentially moderate associationsbetween psychosocial interventions and immune systemfunction: type of psychosocial intervention, interventionformat (no group vs group sessions), intervention length,type of immune marker, whether the immune marker repre-sented basal or stimulated levels, time from treatment ces-sation to immune marker measurement, participants’ dis-ease state or reason for receiving treatment, age, and sex.This meta-analysis thus addresses the critical question of
Key PointsQuestion How consistently are psychosocial interventionsassociated with changes in immune system function, and whichimmunologic, demographic, or clinical factors moderate theseassociations?
Findings In this systematic review and meta-analysis of 56 uniquerandomized clinical trials and 4060 participants, psychosocialinterventions were associated with positive changes in immunityover time, including improvements in beneficial immune systemfunction and decreases in harmful immune function that persistedfor at least 6 months following treatment for participantsrandomly assigned to a psychosocial intervention vs a controlgroup. These associations were most reliable for cognitivebehavior therapy and multiple or combined interventions and forstudies that assessed proinflammatory cytokines or markers.
Meaning These findings suggest that psychosocial interventionsmay enhance immune system function and may thus represent aviable strategy for improving immune-related health.
Research Original Investigation Psychosocial Interventions and Immune System Function
1032 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022

which types of psychosocial interventions are most consis-tently associated with enhanced immune system function,under what conditions, and for whom, which may in turninform research efforts and public policy aimed at usingpsychosocial interventions to improve immune-relatedhealth.
MethodsLiterature ReviewWe performed a comprehensive search of articles publishedin PubMed, Scopus, PsycInfo, and ClinicalTrials.gov, follow-ing the recommended Meta-analysis of Observational Stud-ies in Epidemiology (MOOSE) guidelines34 and using the searchstring presented in the eMethods in the Supplement. The searchwas performed from February 1, 2017, to December 31, 2018,and included all articles published through December 31, 2018.Consistent with recommended procedures and priormeta-analyses,34,35 2 independent reviewers (including C.M.S.) who were blind to study hypotheses and analyses screenedtitles and abstracts from each database, and each reviewer thenread the full text of each study that included a potentiallyrelevant effect (eg, the study was an RCT that included apsychosocial intervention or immune outcome). If an articledid not include sufficient information for analysis, the articlewas marked as such, and after all databases were searched byboth reviewers, we contacted the corresponding authors ofthose articles to obtain the necessary details. In addition, wereviewed the reference lists of all relevant articles to identifyother potentially eligible trials. Given the early start date of thisresearch (June 1, 2016), this protocol was not preregistered. Themeta-analysis was conducted and is reported following thePreferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Inclusion CriteriaEach relevant study was independently examined by allauthors. To be included, studies had to have randomizedparticipants to a psychosocial intervention condition or acontrol condition (ie, any condition lacking a psychosocialintervention component, such as a treatment as usual orwaitlist control condition). In addition, studies had to haveassessed immune system function and have included bothpreintervention and postintervention immunologic assess-ments. These inclusion criteria yielded a data set of RCTsassessing the effects of 8 different psychosocial interven-tions on 7 immune system outcomes. No studies wereexcluded based on any participant characteristics, althoughall of the RCTs included sampled adults.
Coding of Studies and ModeratorsWe coded for several intervention, immunologic, andparticipant-based factors that could potentially moderatethe association between psychosocial interventions andimmune system function. Categorical moderators weredummy coded with appropriate reference groups, and con-
tinuous moderators were centered for analyses at the lowestobtained value to make the interpretation of the intercept(ie, the effect size) for the association between psychosocialinterventions and immune system function at that lowestvalue of the covariate. If the mean participant age was notreported, the median participant age was used if available; ifneither of these statistics were reported, the midpoint of thereported participant age range was used.
Intervention type was coded based on the interventiontype description provided by the study authors, with 3exceptions. First, we coded a study as “CBT plus additive”whenever it included CBT and an additional treatment ormode of delivery that augmented standard CBT (but notanother psychosocial intervention). Second, we coded astudy as “multiple interventions” whenever several differ-ent psychosocial interventions were administered. Third,we coded a study as “other psychotherapy intervention”when a study included an unambiguous psychotherapeuticintervention that was not covered by the other categories(ie, nonspecific stress management therapies, internal fam-ily systems therapy, narrative exposure therapy, and non-specific counseling). Psychoeducation was not included inthis category because it is not a form of psychotherapy. Allrecognized psychotherapies were considered; therefore, if aparticular psychotherapy is not represented (eg, psycho-analysis), it means that the literature review did not yieldany RCTs that have examined how those psychotherapiesare associated with changes in immune system function. Allstudy information was coded by 2 independent reviewers(including C.M.S.), and disagreements were resolved by aconsensus discussion led by a third reviewer (G.M.S.).
Effect Size CalculationTo examine how consistently psychosocial interventionswere associated with changes in immune system function,we calculated the pretest-posttest-control (ppc) group effectsize (ppc Cohen d),36 which increases the statistical powerand precision of effect size estimates relative to estimates ofeffect size from posttest measurement alone.36 We thenconverted effect sizes from ppc Cohen d to ppc Hedges gusing the standard transformation. We used baselinesamples as the pretest values and follow-up samples as theposttest values for each follow-up time point that was avail-able. This effect size provides a relatively unbiased index ofhow immune system function changes in an intervention vsa control group. The ppc group effect size incorporates thepretest-posttest correlation in calculating the variance ofthis effect size, which we obtained from the studies thatreported it and all the authors we contacted for data. Assuch, we set the pretest-posttest correlation as the meta-analytic point estimate of the pretest-posttest correlationfor calculation of the ppc effect sizes (see below). Impor-tantly, sensitivity analyses using the lower and upperbounds of the 95% CI of the estimated pretest-posttest cor-relation indicated no differences in reported results withhigh or low correlations that were used to derive the vari-ance of the effect sizes.
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1033
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022

Analytic StrategyData were analyzed from January 1, 2019, to July 29, 2019, andare available on the Open Science Foundation website (https://osf.io/xcz7s). The primary a priori effect size outcome of interestwas the standardized mean difference between the psychosocialintervention and control groups from preintervention topostintervention. We used ppc g rather than ppc d as the effectsize for analysis because ppc g is a less biased estimate of thepopulation-standardized mean difference effect size than ppcd. Whenever possible, we calculated ppc g from the means, SDs,andsamplesizesthatwerereported.Pretest-posttestcorrelationsbetween time points for each immune marker were provided inseveral studies and by some authors over email. Correlationswere transformed to z scores using the Fisher z transformation,meta-analyzed to obtain a point estimate and 95% CI, and thenback-transformed to a correlation using the Fisher z-to-rtransformation. This back-transformed correlation coefficient ofpretest with posttest immune markers was used as the pretest-posttest correlation for all calculated effect sizes. If the meansand SDs were not reported but graphed, we used the figureextraction program DataThief to extract data from figures with1 × 1-pixel accuracy. If none of this information was available, werequested the required statistics from the relevant correspondingauthor. If the corresponding author did not respond (5 studies),the study was excluded.
Many studies reported more than 1 type of immunologicoutcome, which poses a challenge for conventional meta-analytic methods because calculating mean effect sizes withinstudies without accounting for their correlations can alter orobscure true effect size estimates.37,38 In addition, because onlya limited number of studies have examined the effects of psy-chosocial interventions on immune system function, analyz-ing each immune system outcome separately would substan-tially reduce power because the studies differ in the outcomesassessed. To address these issues, we used the meta-analytictechnique of robust variance estimation, a random-effectsmeta-regression that accounts for dependence between ef-fect size estimates.39,40 This technique robustly estimates ef-fect size weights and standard errors for the given effects, al-lowing for multiple outcomes within studies. We used therobumeta package in R, version 3.6.0 (R Project for StatisticalComputing), to conduct these analyses using the correlatedweights given by Hedges et al,39 with analyses using the smallsample corrections suggested by Tipton.41 To partially ac-count for this dependency, ρ was set to the recommended0.80.40 Heterogeneity was quantified as τ2, which representsbetween-study variance in this meta-analytic method.39,40
Degrees of freedom for all primary analyses were esti-mated using the Satterthwaite approximation, where df = 2/cv2 and cv represents the coefficient of variation, because simu-lation studies have indicated that this method of estimatingdegrees of freedom is most analytically valid with study setsizes of 40 or less (which was the case in moderator analyses)using the robust variance estimation meta-analytic technique.41
Because of how the degrees of freedom are estimated, if df<4,then the risk of type I error is increased and the analysis re-sults cannot be trusted to represent population values.41 How-ever, because this estimation of degrees of freedom is very sen-
sitive to outliers (since degrees of freedom are a function ofthe coefficient of variation), one can be relatively confident thatwhen df>4, outlying studies are not driving observed signifi-cant effects. To assess publication bias, we conducted the Eggertest for funnel plot asymmetry42 as well as a risk of bias as-sessment for each study (described below).
For all analyses, positive effect sizes indicate that a psy-chosocial intervention was associated with improved im-mune function relative to the control condition (eg, by reduc-ing circulating proinflammatory cytokine levels or increasinganti-inflammatory cytokine levels, immune cell counts, natu-ral killer cell activity or cytotoxicity, or lymphocyte or anti-body responses to antigens). In contrast, negative effect sizesindicate that an intervention was associated with impaired im-mune function relative to the control condition (eg, by increas-ing circulating proinflammatory cytokine levels or decreas-ing immune cell counts, natural killer cell toxicity, stimulatedanti-inflammatory cytokine production, or lymphocyte or an-tibody responses to antigens).
To further investigate any significant main findings, we ex-amined the extent to which the following 9 a priori–selectedfactors moderated associations between psychosocial inter-ventions and immune system function: intervention type, in-tervention format, intervention length, type of immune marker,whether the immune marker represented basal or stimulatedlevels, immune marker assessment timing, participants’ dis-ease state or reason for receiving treatment, age, and sex. Be-cause the outcome of these analyses is the standardized meandifference between groups (ie, the effect size), a significant con-tinuous moderator means that the effect size estimate differsbased on the levels of that continuous moderating factor. Giventhat most studies used CBT, secondary analyses parallelingthose described above were conducted to examine this inter-vention type in greater detail. All of the t tests conducted wereunpaired, 2-tailed t tests.
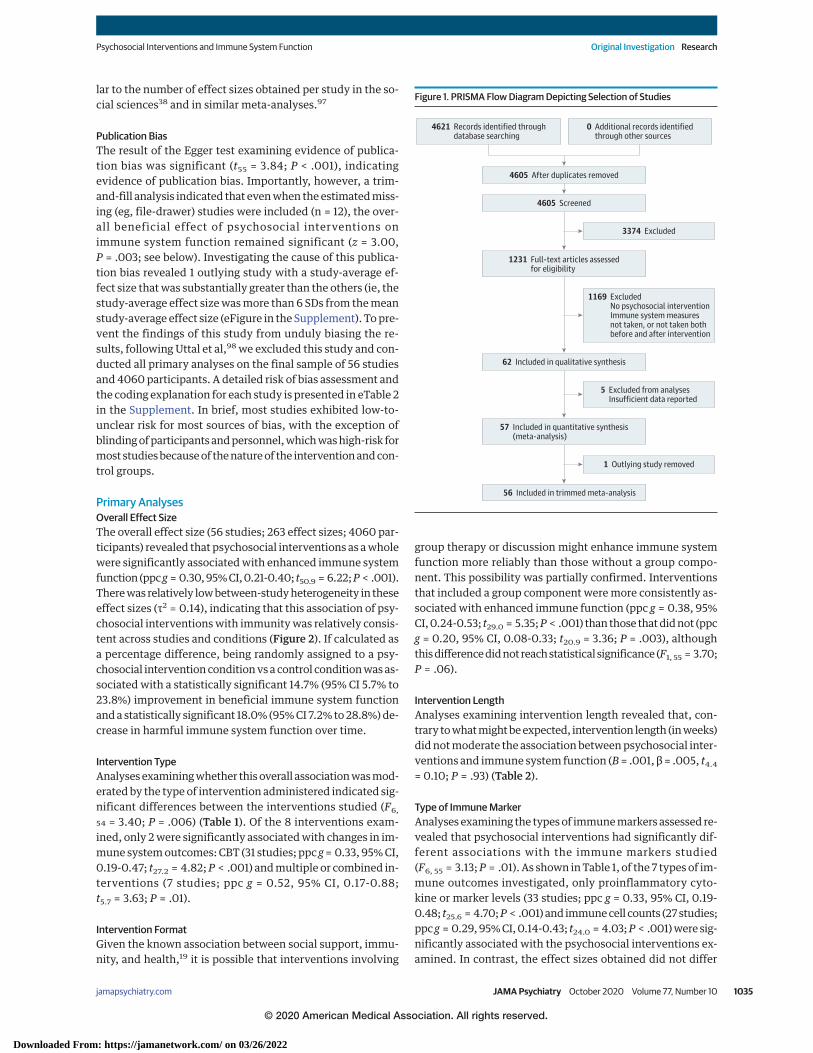
ResultsSearch ResultsThe search of PubMed returned 2941 results; Scopus, 537 re-sults; PsycInfo, 515 results; and ClinicalTrials.gov, 628 re-sults. Of these studies, our inclusion criteria yielded 62 RCTs.Five studies did not present means and standard errors, SDs,or 95% CIs from both preintervention and postintervention inthe text, a table, or a figure, and the authors did not respondto emails requesting these data, leaving 57 studies availablefor preliminary analysis. The publication bias analysis re-vealed that 1 study should be excluded because of potentialbias, leaving a final sample of 56 RCTs23,43-96 available for allprimary analyses. The PRISMA flow diagram is presented inFigure 1, and the included RCTs are described in eTable 1 in theSupplement.
Preliminary AnalysesStudy CharacteristicsThe initial sample included 57 studies and 4076 participants.From these studies, we obtained 265 effect sizes, which is simi-
Research Original Investigation Psychosocial Interventions and Immune System Function
1034 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
lar to the number of effect sizes obtained per study in the so-cial sciences38 and in similar meta-analyses.97
Publication BiasThe result of the Egger test examining evidence of publica-tion bias was significant (t55 = 3.84; P < .001), indicatingevidence of publication bias. Importantly, however, a trim-and-fill analysis indicated that even when the estimated miss-ing (eg, file-drawer) studies were included (n = 12), the over-all beneficial effect of psychosocial interventions onimmune system function remained significant (z = 3.00,P = .003; see below). Investigating the cause of this publica-tion bias revealed 1 outlying study with a study-average ef-fect size that was substantially greater than the others (ie, thestudy-average effect size was more than 6 SDs from the meanstudy-average effect size (eFigure in the Supplement). To pre-vent the findings of this study from unduly biasing the re-sults, following Uttal et al,98 we excluded this study and con-ducted all primary analyses on the final sample of 56 studiesand 4060 participants. A detailed risk of bias assessment andthe coding explanation for each study is presented in eTable 2in the Supplement. In brief, most studies exhibited low-to-unclear risk for most sources of bias, with the exception ofblinding of participants and personnel, which was high-risk formost studies because of the nature of the intervention and con-trol groups.
Primary AnalysesOverall Effect SizeThe overall effect size (56 studies; 263 effect sizes; 4060 par-ticipants) revealed that psychosocial interventions as a wholewere significantly associated with enhanced immune systemfunction (ppc g = 0.30, 95% CI, 0.21-0.40; t50.9 = 6.22; P < .001).There was relatively low between-study heterogeneity in theseeffect sizes (τ2 = 0.14), indicating that this association of psy-chosocial interventions with immunity was relatively consis-tent across studies and conditions (Figure 2). If calculated asa percentage difference, being randomly assigned to a psy-chosocial intervention condition vs a control condition was as-sociated with a statistically significant 14.7% (95% CI 5.7% to23.8%) improvement in beneficial immune system functionand a statistically significant 18.0% (95% CI 7.2% to 28.8%) de-crease in harmful immune system function over time.
Intervention TypeAnalyses examining whether this overall association was mod-erated by the type of intervention administered indicated sig-nificant differences between the interventions studied (F6,
54 = 3.40; P = .006) (Table 1). Of the 8 interventions exam-ined, only 2 were significantly associated with changes in im-mune system outcomes: CBT (31 studies; ppc g = 0.33, 95% CI,0.19-0.47; t27.2 = 4.82; P < .001) and multiple or combined in-terventions (7 studies; ppc g = 0.52, 95% CI, 0.17-0.88;t5.7 = 3.63; P = .01).
Intervention FormatGiven the known association between social support, immu-nity, and health,19 it is possible that interventions involving
group therapy or discussion might enhance immune systemfunction more reliably than those without a group compo-nent. This possibility was partially confirmed. Interventionsthat included a group component were more consistently as-sociated with enhanced immune function (ppc g = 0.38, 95%CI, 0.24-0.53; t29.0 = 5.35; P < .001) than those that did not (ppcg = 0.20, 95% CI, 0.08-0.33; t20.9 = 3.36; P = .003), althoughthis difference did not reach statistical significance (F1, 55 = 3.70;P = .06).
Intervention LengthAnalyses examining intervention length revealed that, con-trary to what might be expected, intervention length (in weeks)did not moderate the association between psychosocial inter-ventions and immune system function (B = .001, β = .005, t4.4
= 0.10; P = .93) (Table 2).
Type of Immune MarkerAnalyses examining the types of immune markers assessed re-vealed that psychosocial interventions had significantly dif-ferent associations with the immune markers studied(F6, 55 = 3.13; P = .01). As shown in Table 1, of the 7 types of im-mune outcomes investigated, only proinflammatory cyto-kine or marker levels (33 studies; ppc g = 0.33, 95% CI, 0.19-0.48; t25.6 = 4.70; P < .001) and immune cell counts (27 studies;ppc g = 0.29, 95% CI, 0.14-0.43; t24.0 = 4.03; P < .001) were sig-nificantly associated with the psychosocial interventions ex-amined. In contrast, the effect sizes obtained did not differ
Figure 1. PRISMA Flow Diagram Depicting Selection of Studies
4621 Records identified throughdatabase searching
4605 After duplicates removed
1231 Full-text articles assessedfor eligibility
57 Included in quantitative synthesis(meta-analysis)
56 Included in trimmed meta-analysis
62 Included in qualitative synthesis
4605 Screened
0 Additional records identifiedthrough other sources
3374 Excluded
1 Outlying study removed
5 Excluded from analysesInsufficient data reported
1169 ExcludedNo psychosocial interventionImmune system measuresnot taken, or not taken bothbefore and after intervention
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1035
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
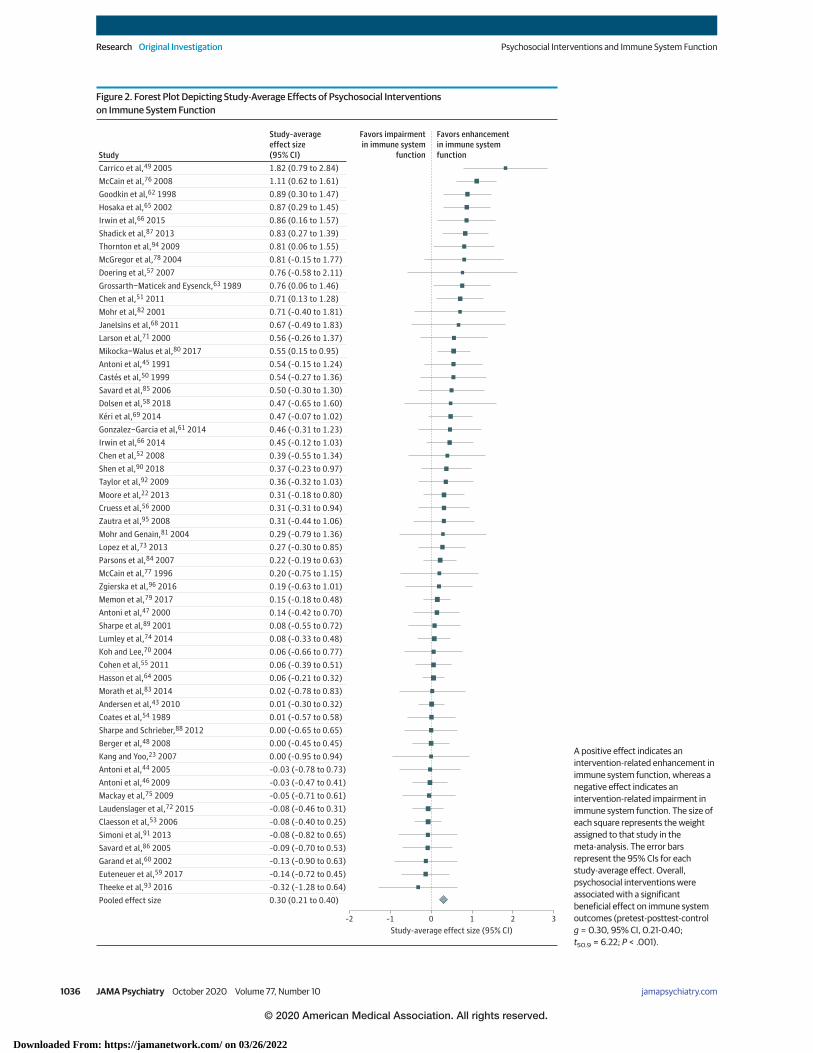
Figure 2. Forest Plot Depicting Study-Average Effects of Psychosocial Interventionson Immune System Function
–2 1 30 2Study-average effect size (95% CI)
–1
Favors impairmentin immune system
function
Favors enhancementin immune systemfunctionStudy
Study–averageeffect size(95% CI)
Carrico et al,49 2005McCain et al,76 2008Goodkin et al,62 1998Hosaka et al,65 2002Irwin et al,66 2015Shadick et al,87 2013Thornton et al,94 2009McGregor et al,78 2004Doering et al,57 2007Grossarth−Maticek and Eysenck,63 1989Chen et al,51 2011Mohr et al,82 2001Janelsins et al,68 2011Larson et al,71 2000Mikocka−Walus et al,80 2017Antoni et al,45 1991Castés et al,50 1999Savard et al,85 2006Dolsen et al,58 2018Kéri et al,69 2014Gonzalez−Garcia et al,61 2014Irwin et al,66 2014Chen et al,52 2008Shen et al,90 2018Taylor et al,92 2009Moore et al,22 2013Cruess et al,56 2000Zautra et al,95 2008Mohr and Genain,81 2004Lopez et al,73 2013Parsons et al,84 2007McCain et al,77 1996Zgierska et al,96 2016Memon et al,79 2017Antoni et al,47 2000Sharpe et al,89 2001Lumley et al,74 2014Koh and Lee,70 2004Cohen et al,55 2011Hasson et al,64 2005Morath et al,83 2014Andersen et al,43 2010Coates et al,54 1989Sharpe and Schrieber,88 2012Berger et al,48 2008Kang and Yoo,23 2007Antoni et al,44 2005Antoni et al,46 2009Mackay et al,75 2009Laudenslager et al,72 2015Claesson et al,53 2006Simoni et al,91 2013Savard et al,86 2005Garand et al,60 2002Euteneuer et al,59 2017Theeke et al,93 2016Pooled effect size 0.30 (0.21 to 0.40)
–0.32 (–1.28 to 0.64)–0.14 (–0.72 to 0.45)–0.13 (–0.90 to 0.63)–0.09 (–0.70 to 0.53)–0.08 (–0.82 to 0.65)–0.08 (–0.40 to 0.25)–0.08 (–0.46 to 0.31)–0.05 (–0.71 to 0.61)–0.03 (–0.47 to 0.41)–0.03 (–0.78 to 0.73)0.00 (–0.95 to 0.94)0.00 (–0.45 to 0.45)0.00 (–0.65 to 0.65)0.01 (–0.57 to 0.58)0.01 (–0.30 to 0.32)0.02 (–0.78 to 0.83)0.06 (–0.21 to 0.32)0.06 (–0.39 to 0.51)0.06 (–0.66 to 0.77)0.08 (–0.33 to 0.48)0.08 (–0.55 to 0.72)0.14 (–0.42 to 0.70)0.15 (–0.18 to 0.48)0.19 (–0.63 to 1.01)0.20 (–0.75 to 1.15)0.22 (–0.19 to 0.63)0.27 (–0.30 to 0.85)0.29 (–0.79 to 1.36)0.31 (–0.44 to 1.06)0.31 (–0.31 to 0.94)0.31 (–0.18 to 0.80)0.36 (–0.32 to 1.03)0.37 (–0.23 to 0.97)0.39 (–0.55 to 1.34)0.45 (–0.12 to 1.03)0.46 (–0.31 to 1.23)0.47 (–0.07 to 1.02)0.47 (–0.65 to 1.60)0.50 (–0.30 to 1.30)0.54 (–0.27 to 1.36)0.54 (–0.15 to 1.24)0.55 (0.15 to 0.95)0.56 (–0.26 to 1.37)0.67 (–0.49 to 1.83)0.71 (–0.40 to 1.81)0.71 (0.13 to 1.28)0.76 (0.06 to 1.46)0.76 (–0.58 to 2.11)0.81 (–0.15 to 1.77)0.81 (0.06 to 1.55)0.83 (0.27 to 1.39)0.86 (0.16 to 1.57)0.87 (0.29 to 1.45)0.89 (0.30 to 1.47)1.11 (0.62 to 1.61)1.82 (0.79 to 2.84)
A positive effect indicates anintervention-related enhancement inimmune system function, whereas anegative effect indicates anintervention-related impairment inimmune system function. The size ofeach square represents the weightassigned to that study in themeta-analysis. The error barsrepresent the 95% CIs for eachstudy-average effect. Overall,psychosocial interventions wereassociated with a significantbeneficial effect on immune systemoutcomes (pretest-posttest-controlg = 0.30, 95% CI, 0.21-0.40;t50.9 = 6.22; P < .001).
Research Original Investigation Psychosocial Interventions and Immune System Function
1036 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
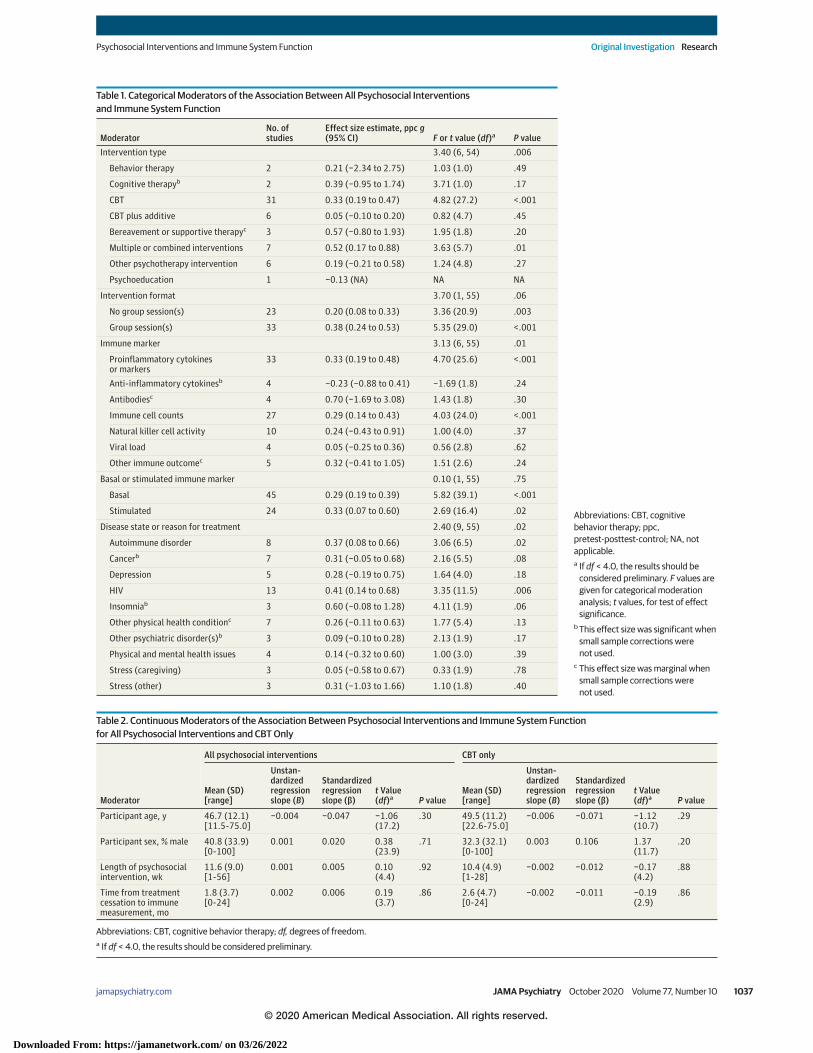
Table 1. Categorical Moderators of the Association Between All Psychosocial Interventionsand Immune System Function
ModeratorNo. ofstudies
Effect size estimate, ppc g(95% CI) F or t value (df)a P value
Intervention type 3.40 (6, 54) .006
Behavior therapy 2 0.21 (−2.34 to 2.75) 1.03 (1.0) .49
Cognitive therapyb 2 0.39 (−0.95 to 1.74) 3.71 (1.0) .17
CBT 31 0.33 (0.19 to 0.47) 4.82 (27.2) <.001
CBT plus additive 6 0.05 (−0.10 to 0.20) 0.82 (4.7) .45
Bereavement or supportive therapyc 3 0.57 (−0.80 to 1.93) 1.95 (1.8) .20
Multiple or combined interventions 7 0.52 (0.17 to 0.88) 3.63 (5.7) .01
Other psychotherapy intervention 6 0.19 (−0.21 to 0.58) 1.24 (4.8) .27
Psychoeducation 1 −0.13 (NA) NA NA
Intervention format 3.70 (1, 55) .06
No group session(s) 23 0.20 (0.08 to 0.33) 3.36 (20.9) .003
Group session(s) 33 0.38 (0.24 to 0.53) 5.35 (29.0) <.001
Immune marker 3.13 (6, 55) .01
Proinflammatory cytokinesor markers
33 0.33 (0.19 to 0.48) 4.70 (25.6) <.001
Anti-inflammatory cytokinesb 4 −0.23 (−0.88 to 0.41) −1.69 (1.8) .24
Antibodiesc 4 0.70 (−1.69 to 3.08) 1.43 (1.8) .30
Immune cell counts 27 0.29 (0.14 to 0.43) 4.03 (24.0) <.001
Natural killer cell activity 10 0.24 (−0.43 to 0.91) 1.00 (4.0) .37
Viral load 4 0.05 (−0.25 to 0.36) 0.56 (2.8) .62
Other immune outcomec 5 0.32 (−0.41 to 1.05) 1.51 (2.6) .24
Basal or stimulated immune marker 0.10 (1, 55) .75
Basal 45 0.29 (0.19 to 0.39) 5.82 (39.1) <.001
Stimulated 24 0.33 (0.07 to 0.60) 2.69 (16.4) .02
Disease state or reason for treatment 2.40 (9, 55) .02
Autoimmune disorder 8 0.37 (0.08 to 0.66) 3.06 (6.5) .02
Cancerb 7 0.31 (−0.05 to 0.68) 2.16 (5.5) .08
Depression 5 0.28 (−0.19 to 0.75) 1.64 (4.0) .18
HIV 13 0.41 (0.14 to 0.68) 3.35 (11.5) .006
Insomniab 3 0.60 (−0.08 to 1.28) 4.11 (1.9) .06
Other physical health conditionc 7 0.26 (−0.11 to 0.63) 1.77 (5.4) .13
Other psychiatric disorder(s)b 3 0.09 (−0.10 to 0.28) 2.13 (1.9) .17
Physical and mental health issues 4 0.14 (−0.32 to 0.60) 1.00 (3.0) .39
Stress (caregiving) 3 0.05 (−0.58 to 0.67) 0.33 (1.9) .78
Stress (other) 3 0.31 (−1.03 to 1.66) 1.10 (1.8) .40
Abbreviations: CBT, cognitivebehavior therapy; ppc,pretest-posttest-control; NA, notapplicable.a If df < 4.0, the results should be
considered preliminary. F values aregiven for categorical moderationanalysis; t values, for test of effectsignificance.
b This effect size was significant whensmall sample corrections werenot used.
c This effect size was marginal whensmall sample corrections werenot used.
Table 2. Continuous Moderators of the Association Between Psychosocial Interventions and Immune System Functionfor All Psychosocial Interventions and CBT Only
Moderator
All psychosocial interventions CBT only
Mean (SD)[range]
Unstan-dardizedregressionslope (B)
Standardizedregressionslope (β)
t Value(df)a P value
Mean (SD)[range]
Unstan-dardizedregressionslope (B)
Standardizedregressionslope (β)
t Value(df)a P value
Participant age, y 46.7 (12.1)[11.5-75.0]
−0.004 −0.047 −1.06(17.2)
.30 49.5 (11.2)[22.6-75.0]
−0.006 −0.071 −1.12(10.7)
.29
Participant sex, % male 40.8 (33.9)[0-100]
0.001 0.020 0.38(23.9)
.71 32.3 (32.1)[0-100]
0.003 0.106 1.37(11.7)
.20
Length of psychosocialintervention, wk
11.6 (9.0)[1-56]
0.001 0.005 0.10(4.4)
.92 10.4 (4.9)[1-28]
−0.002 −0.012 −0.17(4.2)
.88
Time from treatmentcessation to immunemeasurement, mo
1.8 (3.7)[0-24]
0.002 0.006 0.19(3.7)
.86 2.6 (4.7)[0-24]
−0.002 −0.011 −0.19(2.9)
.86
Abbreviations: CBT, cognitive behavior therapy; df, degrees of freedom.a If df < 4.0, the results should be considered preliminary.
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1037
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
between basal and stimulated immune system markers(F1, 55 = 0.10; P = .75).
Immune Marker Assessment TimingAnalyses examining the amount of time that transpired be-tween treatment cessation and when immune markers wereassessed revealed that, contrary to what might be expected, ashorter follow-up period (in months) was not associated witha larger effect size (B = .002, β = .006, t3.7 = 0.19; P = .86)(Table 2). On the other hand, sensitivity analyses examiningthe temporal persistence of these associations revealed thatpsychosocial interventions were associated with enhance-ments in immune system function that lasted for at least 6months following treatment cessation (ppc g = 0.31, 95% CI,0.17-0.45; t8.4 = 5.10; P < .001).
Disease State or Reason for Receiving TreatmentAnalyses examining whether participants’ disease state or rea-son for seeking treatment moderated the association be-tween psychosocial interventions and immune system func-tion revealed that disease state or reason for seeking treatmentwas a significant moderator (F9, 55 = 2.40; P = .02). As shownin Table 1, the most reliable intervention-based associationswere found for individuals receiving treatment for HIV, auto-immune disorders, cancer, and insomnia.
Demographic CharacteristicsAnalyses examining whether associations between psycho-social interventions and immune system function were mod-erated by participants’ age or sex revealed no moderating ef-fects for age (t17.2 = −1.06; P = .30) or sex (t23.9 = 0.38; P = .71)(Table 2).
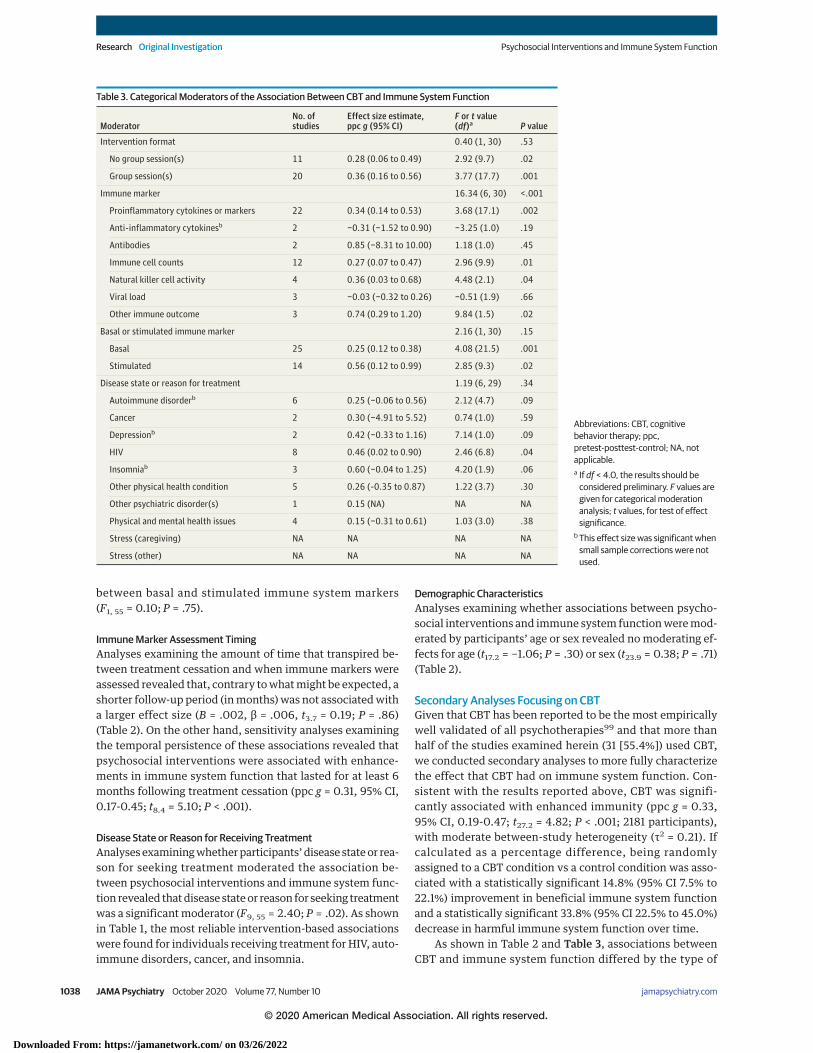
Secondary Analyses Focusing on CBTGiven that CBT has been reported to be the most empiricallywell validated of all psychotherapies99 and that more thanhalf of the studies examined herein (31 [55.4%]) used CBT,we conducted secondary analyses to more fully characterizethe effect that CBT had on immune system function. Con-sistent with the results reported above, CBT was signifi-cantly associated with enhanced immunity (ppc g = 0.33,95% CI, 0.19-0.47; t27.2 = 4.82; P < .001; 2181 participants),with moderate between-study heterogeneity (τ2 = 0.21). Ifcalculated as a percentage difference, being randomlyassigned to a CBT condition vs a control condition was asso-ciated with a statistically significant 14.8% (95% CI 7.5% to22.1%) improvement in beneficial immune system functionand a statistically significant 33.8% (95% CI 22.5% to 45.0%)decrease in harmful immune system function over time.
As shown in Table 2 and Table 3, associations betweenCBT and immune system function differed by the type of
Table 3. Categorical Moderators of the Association Between CBT and Immune System Function
ModeratorNo. ofstudies
Effect size estimate,ppc g (95% CI)
F or t value(df)a P value
Intervention format 0.40 (1, 30) .53
No group session(s) 11 0.28 (0.06 to 0.49) 2.92 (9.7) .02
Group session(s) 20 0.36 (0.16 to 0.56) 3.77 (17.7) .001
Immune marker 16.34 (6, 30) <.001
Proinflammatory cytokines or markers 22 0.34 (0.14 to 0.53) 3.68 (17.1) .002
Anti-inflammatory cytokinesb 2 −0.31 (−1.52 to 0.90) −3.25 (1.0) .19
Antibodies 2 0.85 (−8.31 to 10.00) 1.18 (1.0) .45
Immune cell counts 12 0.27 (0.07 to 0.47) 2.96 (9.9) .01
Natural killer cell activity 4 0.36 (0.03 to 0.68) 4.48 (2.1) .04
Viral load 3 −0.03 (−0.32 to 0.26) −0.51 (1.9) .66
Other immune outcome 3 0.74 (0.29 to 1.20) 9.84 (1.5) .02
Basal or stimulated immune marker 2.16 (1, 30) .15
Basal 25 0.25 (0.12 to 0.38) 4.08 (21.5) .001
Stimulated 14 0.56 (0.12 to 0.99) 2.85 (9.3) .02
Disease state or reason for treatment 1.19 (6, 29) .34
Autoimmune disorderb 6 0.25 (−0.06 to 0.56) 2.12 (4.7) .09
Cancer 2 0.30 (−4.91 to 5.52) 0.74 (1.0) .59
Depressionb 2 0.42 (−0.33 to 1.16) 7.14 (1.0) .09
HIV 8 0.46 (0.02 to 0.90) 2.46 (6.8) .04
Insomniab 3 0.60 (−0.04 to 1.25) 4.20 (1.9) .06
Other physical health condition 5 0.26 (-0.35 to 0.87) 1.22 (3.7) .30
Other psychiatric disorder(s) 1 0.15 (NA) NA NA
Physical and mental health issues 4 0.15 (−0.31 to 0.61) 1.03 (3.0) .38
Stress (caregiving) NA NA NA NA
Stress (other) NA NA NA NA
Abbreviations: CBT, cognitivebehavior therapy; ppc,pretest-posttest-control; NA, notapplicable.a If df < 4.0, the results should be
considered preliminary. F values aregiven for categorical moderationanalysis; t values, for test of effectsignificance.
b This effect size was significant whensmall sample corrections were notused.
Research Original Investigation Psychosocial Interventions and Immune System Function
1038 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022

immune marker assessed (F6, 30 = 16.34; P < .001). In brief,CBT was significantly associated with enhanced immunesystem function as indexed by lower proinflammatory cyto-kine or marker levels (t17.1 = 3.68; P = .002), higher immunecell counts (t9.9 = 2.96; P = .01), higher natural killer cellactivity (t2.1 = 4.48; P = .04), and improved other immuneoutcomes (eg, blastogenesis, number of postoperative infec-tious diseases; t1.5 = 9.84; P = .02). These associations werenot moderated by whether the CBT intervention included agroup component (F1, 30 = 0.40; P = .53), nor were theymoderated by treatment duration (t4.2 = −0.17; P = .88;although only 1 CBT study assessed immune system out-comes with a treatment duration of less than 4 weeks). Inaddition, the benefits of CBT did not differ as a function ofwhether the immune markers represented basal or stimu-lated levels (F1, 30 = 2.16; P = .15), by participants’ diseasestate or reason for treatment (F6, 29 = 1.19; P = .34), by par-ticipants’ age (t10.7 = −1.12; P = .29) or sex (t11.7 = 1.37;P = .20), or by the amount of time (in months) betweentreatment cessation and immune marker assessment(t2.9 = −0.19; P = .86). Even at 6 months posttreatment, CBTwas significantly associated with enhanced immunity (ppcg = 0.32, 95% CI, 0.14-0.51; t9.5 = 3.88; P = .003).
Finally, to examine the potential utility of group CBT forimproving physical health conditions that CBT is not specifi-cally designed to benefit (eg, autoimmune disorders), themodel-estimated effect size associating CBT with a group com-ponent and markers of proinflammatory activity was moder-ate in magnitude in patients with autoimmune disorders (ppcg = 0.41, 95% CI, 0.07-0.76; t7.4 = 2.80; P = .02) when there wasno delay between treatment cessation and immune marker as-sessment.
DiscussionOne of the most important recent discoveries in the healthsciences involves the realization that the immune system isinvolved in the pathophysiology of not just a few disordersbut several major health problems that cause substantialdisease burden and mortality.1,2 Given growing evidenceshowing that psychosocial factors play a role in shapingimmunity,3-6,8,12-20,100,101 we conducted what we believe isthe first systematic review and meta-analysis of RCTs exam-ining how 8 different psychosocial interventions affect 7common immune outcomes that have broad clinical rel-evance. This comprehensive review of 56 RCTs revealedthat psychosocial interventions were significantly associ-ated with enhanced immune system function, as indexedmost consistently by intervention-related decreases in lev-els of proinflammator y c y tokines or markers (eg,interleukin-6, C-reactive protein) and, secondarily, byincreases in immune cell counts (eg, CD56, CD4) over time.These associations were most consistent for CBT and forinterventions incorporating multiple psychotherapies.Moreover, they did not differ by participants’ age, sex, orintervention duration. Finally, we found that these associa-tions persisted for at least 6 months following treatment
cessation. Considered together, these results suggest thatpsychosocial interventions in general—and especially CBTa n d m u l t i p l e o r c o m b i n e d p s y c h o t h e r a p e u t i cinterventions—enhance immune system function andmay thus represent a viable strategy for improvingimmune-related health outcomes.
Converted to percentages, these data reveal that, rela-tive to the control group, psychosocial interventions wereassociated with an 18.0% (95% CI, 7.2%-28.8%) reduction inharmful immune system function as indexed, for example,by proinflammatory cytokine activity. In comparison, anRCT102 found that, relative to a control group, treatmentwith a 40-mg dose of darapladib for reducing cardiovasculardisease risk decreased interleukin-6 levels by 7.8% andC-reactive protein levels by 6.0%, whereas a 160-mg dose ofdarapladib decreased interleukin-6 levels by 12.3% andC-reactive protein levels by 13.0%. Psychosocial interven-tions thus appear to reduce systemic inflammatory activityin a manner that is similar to using darapladib for treatingatherosclerosis.
In addition to being effective, psychosocial interventionsmay represent a relatively affordable strategy for improving im-mune-related health. For example, the mean CBT trial length inthis meta-analysis was 10.4 weeks. Assuming that these CBT ses-sions took place once a week and that a therapist would nor-mally charge $150 per session, the cost of using CBT to induce apersistent (eg, 6-month posttreatment) improvement in im-mune system function would be $1560 per patient. By compari-son, the cost of using infliximab to reduce inflammation in per-sons with an autoimmune disorder is approximately $25 000 perpatient per year.103 Moreover, the functional improvement in im-munity associated with CBT is approximately the same as theimprovement achieved by adding a 10-mg/kg dose of inflixi-mab every 4 weeks (ie, the maximum dose and frequency) to amethotrexate treatment regimen in individuals with rheuma-toid arthritis (ie, estimated effect of CBT on proinflammatorymarkers: ppc g = 0.41; estimated effect of infliximab on C-reactive protein: ppc g = 0.46).104 Finally, whereas the presentmeta-analysis revealed that the association between CBT and im-mune system function was significant for at least 6 months fol-lowingtherapycessation,theeffectsofinfliximabareshorterlast-ing and decay more quickly in patients who take the medicationfor inflammation-related health problems.105 Cognitive behav-ior therapy may thus represent an affordable and relatively lon-ger-lasting adjunctive treatment option for reducing inflamma-tion-related disease risk.
Strengths and LimitationsThe main strengths of this meta-analysis include its focus onRCTs with both preintervention and postintervention immu-nologic assessments, examination of most major psychoso-cial interventions and many different immune outcomes, andexamination of several potential immunologic, demo-graphic, and clinical moderating factors. However, several limi-tations should also be noted. First, the shortest interventionconsidered was 1 week, and all but 3 of the interventions ex-amined were at least 4 weeks in duration. Therefore, our abil-ity to detect differences in short-duration treatments was
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1039
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022

limited. Relatedly, because studies do not regularly report ses-sion frequency, we were not able to consider differences insession frequency as a potential moderator. Second, sensitiv-ity analyses indicated that the psychosocial interventions ex-amined were associated with improvements in immune sys-tem function that persisted for at least 6 months followingtreatment, but there were too few studies with follow-up pe-riods longer than 6 months to obtain reliable estimates fromthose studies. Third, as with any meta-analysis, it is possiblethat unpublished studies could have influenced the results.
Fourth, the control groups in the studies examined variedconsiderably, and it can be difficult to blind participants to theircondition assignment in a psychotherapy RCT. Therefore, pla-cebo and expectancy effects are possible. Fifth, although ran-dom assignment should equate intervention and control groupparticipants on factors such as comedication and cotreatment,some study groups could have differed in the extent to whichparticipants took some forms of medication or received otherformsoftreatment.Sixth,someeffectsizesestimatedinthemod-erator analyses may have been nonsignificant because of low sta-tistical power. This is especially true for the analyses involvingintervention type and disease state or reason for seeking treat-ment. Finally, although these data indicate that psychosocial in-terventions are associated with enhanced immune system func-tion, they do not elucidate the mechanisms underlying theseassociations. It has been suggested that reductions in stress-related neural or psychological processes may help explain suchassociations,3-6,106 butpsychosocial interventionscanhavewide-ranging effects on human cognition and behavior, and addi-
tional research is needed to identify exactly how such interven-tions influence immune system activity and health.
ConclusionsIn conclusion, recent research has shown that the immune sys-tem plays an integral role in many serious disease conditionsand that psychosocial factors can modulate immune systemfunction.3-6,8,107-113 The present meta-analysis extends thiswork by identifying for the first time the types of psychoso-cial interventions that have the most robust associations withimmune system function, the immune system outcomes thatare most consistently associated with these interventions, andthe various factors that moderate these associations. Specifi-cally, we found that psychosocial interventions were associ-ated with improvements in immune system function overtime—in particular, with decreased proinflammatory cyto-kines or markers and increased immune cell counts—and thatthese associations were most consistent for interventions thatincorporate CBT or multiple interventions. Given the effec-tiveness and relative affordability of psychosocial interven-tions for treating chronic disease, we suggest that psychoso-cial interventions may represent a viable strategy for reducingdisease burden and improving human health. Looking for-ward, additional research is needed to elucidate the mecha-nisms through which psychosocial interventions exert rela-tively long-lasting, beneficial effects on the immune systemand health.
ARTICLE INFORMATION
Accepted for Publication: January 17, 2020.
Published Online: June 3, 2020.doi:10.1001/jamapsychiatry.2020.0431
Author Contributions: Drs Shields and Slavich hadfull access to all of the data in the study and takeresponsibility for the integrity of the data and theaccuracy of the data analysis.Concept and design: Shields, Slavich.Acquisition, analysis, or interpretation of data:All authors.Drafting of the manuscript: All authors.Critical revision of the manuscript for importantintellectual content: All authors.Statistical analysis: Shields.Obtained funding: Slavich.Administrative, technical, or material support:All authors.Supervision: Shields, Slavich.
Conflict of Interest Disclosures: None reported.
Funding/Support: This research was supported bya Society in Science–Branco Weiss Fellowship (DrSlavich), National Alliance for Research onSchizophrenia and Depression Young InvestigatorGrant 23958 from the Brain & Behavior ResearchFoundation (Dr Slavich), and grant K08 MH103443from the National Institutes of Health (Dr Slavich).
Role of the Funder/Sponsor: The sponsors had norole in the design and conduct of the study;collection, management, analysis, andinterpretation of the data; preparation, review, orapproval of the manuscript; or decision to submitthe manuscript for publication.
Additional Contributions: We thank Patrick S.Thomas Jr, MD, PhD, at The Menninger Clinic forassisting with the literature review(uncompensated).
REFERENCES
1. Couzin-Frankel J. Inflammation bares a dark side.Science. 2010;330(6011):1621. doi:10.1126/science.330.6011.1621
2. Slavich GM. Understanding inflammation, itsregulation, and relevance for health: a top scientificand public priority. Brain Behav Immun. 2015;45:13-14. doi:10.1016/j.bbi.2014.10.012
3. Miller GE, Chen E, Parker KJ. Psychological stressin childhood and susceptibility to the chronicdiseases of aging: moving toward a model ofbehavioral and biological mechanisms. Psychol Bull.2011;137(6):959-997. doi:10.1037/a0024768
4. O’Donovan A, Neylan TC. Associations of traumaand posttraumatic stress disorder withinflammation and endothelial function: on timing,specificity, and mechanisms. Biol Psychiatry. 2017;82(12):861-863. doi:10.1016/j.biopsych.2017.10.002
5. Slavich GM, Irwin MR. From stress toinflammation and major depressive disorder:a social signal transduction theory of depression.Psychol Bull. 2014;140(3):774-815. doi:10.1037/a0035302
6. Slavich GM, Auerbach RP. Stress and itssequelae: depression, suicide, inflammation, andphysical illness. In: Butcher JN, Hooley JM, eds. APAHandbook of Psychopathology: Psychopathology:Understanding, Assessing, and Treating Adult
Mental Disorders. Vol 1. American PsychologicalAssociation; 2018:375-402. doi:10.1037/0000064-016
7. GBD 2017 Causes of Death Collaborators. Global,regional, and national age-sex-specific mortality for282 causes of death in 195 countries and territories,1980-2017: a systematic analysis for the GlobalBurden of Disease Study 2017. Lancet. 2018;392(10159):1736-1788. doi:10.1016/S0140-6736(18)32203-7
8. Furman D, Campisi J, Verdin E, et al. Chronicinflammation in the etiology of disease across thelife span. Nat Med. 2019;25(12):1822-1832. doi:10.1038/s41591-019-0675-0
9. World Health Organization and InternationalInitiative for Impact Evaluation. An evidence map ofsocial, behavioural and community engagementinterventions for reproductive, maternal, newbornand child health. World Health Organization; 2017.
10. Institute of Medicine. PsychosocialInterventions for Mental and Substance UseDisorders: A Framework for EstablishingEvidence-Based Standards. National AcademiesPress; 2015.
11. National Institute of Mental Health. NationalInstitute of Mental Health Strategic Plan for Research.National Institute of Mental Health; 2015.
12. Sternberg EM. Neural regulation of innateimmunity: a coordinated nonspecific host responseto pathogens. Nat Rev Immunol. 2006;6(4):318-328.doi:10.1038/nri1810
Research Original Investigation Psychosocial Interventions and Immune System Function
1040 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
13. Slavich GM, Cole SW. The emerging field ofhuman social genomics. Clin Psychol Sci. 2013;1(3):331-348. doi:10.1177/2167702613478594
14. Irwin MR. Human psychoneuroimmunology: 20years of discovery. Brain Behav Immun. 2008;22(2):129-139. doi:10.1016/j.bbi.2007.07.013
15. Fagundes CP, Way B. Early-life stress and adultinflammation. Curr Dir Psychol Sci. 2014;23:277-283.doi:10.1177/0963721414535603
16. Kiecolt-Glaser JK, McGuire L, Robles TF, GlaserR. Emotions, morbidity, and mortality: newperspectives from psychoneuroimmunology. AnnuRev Psychol. 2002;53:83-107. doi:10.1146/annurev.psych.53.100901.135217
17. Rohleder N. Stress and inflammation: the needto address the gap in the transition between acuteand chronic stress effects. Psychoneuroendocrinology.2019;105:164-171. doi:10.1016/j.psyneuen.2019.02.021
18. Segerstrom SC, Miller GE. Psychological stressand the human immune system: a meta-analyticstudy of 30 years of inquiry. Psychol Bull. 2004;130(4):601-630. doi:10.1037/0033-2909.130.4.601
19. Uchino BN, Trettevik R, Kent de Grey RG,Cronan S, Hogan J, Baucom BRW. Social support,social integration, and inflammatory cytokines:a meta-analysis. Health Psychol. 2018;37(5):462-471.doi:10.1037/hea0000594
20. Kiecolt-Glaser JK, Wilson SJ. Lovesick: howcouples’ relationships influence health. Annu RevClin Psychol. 2017;13:421-443. doi:10.1146/annurev-clinpsy-032816-045111
21. Miller GE, Brody GH, Yu T, Chen E. Afamily-oriented intervention reduces inflammationin low-SES African American youth. Proc Natl AcadSci U S A. 2014;111(31):11287-11292. doi:10.1073/pnas.1406578111
22. Moore RC, Chattillion EA, Ceglowski J, et al. Arandomized clinical trial of behavioral activation(BA) therapy for improving psychological andphysical health in dementia caregivers: results ofthe Pleasant Events Program (PEP). Behav Res Ther.2013;51(10):623-632. doi:10.1016/j.brat.2013.07.005
23. Kang HY, Yoo YS. Effects of a bereavementintervention program in middle-aged widows inKorea. Arch Psychiatr Nurs. 2007;21(3):132-140.doi:10.1016/j.apnu.2006.12.007
24. Crepaz N, Passin WF, Herbst JH, et al; HIV/AIDSPrevention Research Synthesis Team. Meta-analysisof cognitive-behavioral interventions onHIV-positive persons’ mental health and immunefunctioning. Health Psychol. 2008;27(1):4-14. doi:10.1037/0278-6133.27.1.4
25. Black DS, Slavich GM. Mindfulness meditationand the immune system: a systematic review ofrandomized controlled trials. Ann N Y Acad Sci.2016;1373(1):13-24. doi:10.1111/nyas.12998
26. Pascoe MC, Thompson DR, Jenkins ZM, Ski CF.Mindfulness mediates the physiological markers ofstress: systematic review and meta-analysis.J Psychiatr Res. 2017;95:156-178. doi:10.1016/j.jpsychires.2017.08.004
27. Bower JE, Irwin MR. Mind-body therapies andcontrol of inflammatory biology: a descriptivereview. Brain Behav Immun. 2016;51:1-11. doi:10.1016/j.bbi.2015.06.012
28. Deng W, Cheung ST, Tsao SW, Wang XM, TiwariAF. Telomerase activity and its association with
psychological stress, mental disorders, lifestylefactors and interventions: a systematic review.Psychoneuroendocrinology. 2016;64:150-163. doi:10.1016/j.psyneuen.2015.11.017
29. Morgan N, Irwin MR, Chung M, Wang C. Theeffects of mind-body therapies on the immunesystem: meta-analysis. PLoS One. 2014;9(7):e100903. doi:10.1371/journal.pone.0100903
30. Scott-Sheldon LA, Kalichman SC, Carey MP,Fielder RL. Stress management interventions forHIV+ adults: a meta-analysis of randomizedcontrolled trials, 1989 to 2006. Health Psychol.2008;27(2):129-139. doi:10.1037/0278-6133.27.2.129
31. O’Toole MS, Bovbjerg DH, Renna ME, LekanderM, Mennin DS, Zachariae R. Effects of psychologicalinterventions on systemic levels of inflammatorybiomarkers in humans: a systematic review andmeta-analysis. Brain Behav Immun. 2018;74:68-78.doi:10.1016/j.bbi.2018.04.005
32. Cristea IA, Karyotaki E, Hollon SD, Cuijpers P,Gentili C. Biological markers evaluated inrandomized trials of psychological treatments fordepression: a systematic review and meta-analysis.Neurosci Biobehav Rev. 2019;101:32-44. doi:10.1016/j.neubiorev.2019.03.022
33. Qi L, Wang J, Zhang HL. Meta-analysis ofpsychological interventions on breast cancerpatients’ immune function. In: Proceedings of the2nd International Conference on SustainableDevelopment; December 2-4, Xi’an, China. AtlanticPress; 2017. doi:10.2991/icsd-16.2017.93
34. Stroup DF, Berlin JA, Morton SC, et al.Meta-analysis of observational studies inepidemiology: a proposal for reporting:Meta-analysis of Observational Studies inEpidemiology (MOOSE) Group. JAMA. 2000;283(15):2008-2012. doi:10.1001/jama.283.15.2008
35. Dickerson SS, Kemeny ME. Acute stressors andcortisol responses: a theoretical integration andsynthesis of laboratory research. Psychol Bull.2004;130(3):355-391. doi:10.1037/0033-2909.130.3.355
36. Morris SB. Estimating effect sizes frompretest-posttest-control group designs. Organ ResMethods. 2008;11:364-386. doi:10.1177/1094428106291059
37. Borenstein M, Hedges LV, Higgins JPT,Rothstein HR. Introduction to Meta-analysis. JohnWiley & Sons, Ltd; 2009. doi:10.1002/9780470743386
38. Scammacca N, Roberts G, Stuebing KK.Meta-analysis with complex research designs:dealing with dependence from multiple measuresand multiple group comparisons. Rev Educ Res.2014;84(3):328-364. doi:10.3102/0034654313500826
39. Hedges LV, Tipton E, Johnson MC. Robustvariance estimation in meta-regression withdependent effect size estimates. Res Synth Methods.2010;1(1):39-65. doi:10.1002/jrsm.5
40. Tanner-Smith EE, Tipton E. Robust varianceestimation with dependent effect sizes: practicalconsiderations including a software tutorial inSTATA and SPSS. Res Synth Methods. 2014;5(1):13-30. doi:10.1002/jrsm.1091
41. Tipton E. Small sample adjustments for robustvariance estimation with meta-regression. PsycholMethods. 2015;20(3):375-393. doi:10.1037/met0000011
42. Egger M, Davey Smith G, Schneider M, MinderC. Bias in meta-analysis detected by a simple,graphical test. BMJ. 1997;315(7109):629-634.doi:10.1136/bmj.315.7109.629
43. Andersen BL, Thornton LM, Shapiro CL, et al.Biobehavioral, immune, and health benefitsfollowing recurrence for psychological interventionparticipants. Clin Cancer Res. 2010;16(12):3270-3278.doi:10.1158/1078-0432.CCR-10-0278
44. Antoni MH, Cruess DG, Klimas N, et al.Increases in a marker of immune systemreconstitution are predated by decreases in 24-hurinary cortisol output and depressed mood duringa 10-week stress management intervention insymptomatic HIV-infected men. J Psychosom Res.2005;58(1):3-13. doi:10.1016/j.jpsychores.2004.05.010
45. Antoni MH, Baggett L, Ironson G, et al.Cognitive-behavioral stress managementintervention buffers distress responses andimmunologic changes following notification of HIV-1seropositivity. J Consult Clin Psychol. 1991;59(6):906-915. doi:10.1037/0022-006X.59.6.906
46. Antoni MH, Lechner S, Diaz A, et al. Cognitivebehavioral stress management effects onpsychosocial and physiological adaptation inwomen undergoing treatment for breast cancer.Brain Behav Immun. 2009;23(5):580-591. doi:10.1016/j.bbi.2008.09.005
47. Antoni MH, Cruess DG, Cruess S, et al.Cognitive-behavioral stress managementintervention effects on anxiety, 24-hr urinarynorepinephrine output, and T-cytotoxic/suppressorcells over time among symptomatic HIV-infectedgay men. J Consult Clin Psychol. 2000;68(1):31-45.doi:10.1037/0022-006X.68.1.31
48. Berger S, Schad T, von Wyl V, et al. Effects ofcognitive behavioral stress management on HIV-1RNA, CD4 cell counts and psychosocial parametersof HIV-infected persons. AIDS. 2008;22(6):767-775.doi:10.1097/QAD.0b013e3282f511dc
49. Carrico AW, Antoni MH, Pereira DB, et al.Cognitive behavioral stress management effects onmood, social support, and a marker of antiviralimmunity are maintained up to 1 year inHIV-infected gay men. Int J Behav Med. 2005;12(4):218-226. doi:10.1207/s15327558ijbm1204_2
50. Castés M, Hagel I, Palenque M, Canelones P,Corao A, Lynch NR. Immunological changesassociated with clinical improvement of asthmaticchildren subjected to psychosocial intervention.Brain Behav Immun. 1999;13(1):1-13. doi:10.1006/brbi.1999.0551
51. Chen HY, Cheng IC, Pan YJ, et al.Cognitive-behavioral therapy for sleep disturbancedecreases inflammatory cytokines and oxidativestress in hemodialysis patients. Kidney Int. 2011;80(4):415-422. doi:10.1038/ki.2011.151
52. Chen HY, Chiang CK, Wang HH, et al.Cognitive-behavioral therapy for sleep disturbancein patients undergoing peritoneal dialysis: a pilotrandomized controlled trial. Am J Kidney Dis. 2008;52(2):314-323. doi:10.1053/j.ajkd.2008.03.012
53. Claesson M, Birgander LS, Jansson JH, et al.Cognitive-behavioural stress management does notimprove biological cardiovascular risk indicators inwomen with ischaemic heart disease:a randomized-controlled trial. J Intern Med. 2006;260(4):320-331. doi:10.1111/j.1365-2796.2006.01691.x
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1041
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
54. Coates TJ, McKusick L, Kuno R, Stites DP. Stressreduction training changed number of sexualpartners but not immune function in men with HIV.Am J Public Health. 1989;79(7):885-887. doi:10.2105/AJPH.79.7.885
55. Cohen L, Parker PA, Vence L, et al. Presurgicalstress management improves postoperativeimmune function in men with prostate cancerundergoing radical prostatectomy. Psychosom Med.2011;73(3):218-225. doi:10.1097/PSY.0b013e31820a1c26
56. Cruess S, Antoni M, Cruess D, et al. Reductionsin herpes simplex virus type 2 antibody titers aftercognitive behavioral stress management andrelationships with neuroendocrine function,relaxation skills, and social support in HIV-positivemen. Psychosom Med. 2000;62(6):828-837. doi:10.1097/00006842-200011000-00013
57. Doering LV, Cross R, Vredevoe D,Martinez-Maza O, Cowan MJ. Infection, depression,and immunity in women after coronary arterybypass: a pilot study of cognitive behavioraltherapy. Altern Ther Health Med. 2007;13(3):18-21.
58. Dolsen MR, Soehner AM, Harvey AG.Pro-inflammatory cytokines, mood, and sleep ininterepisode bipolar disorder and insomnia.Psychosom Med. 2018;80:87-94. doi:10.1097/PSY.0000000000000529
59. Euteneuer F, Dannehl K, Del Rey A, Engler H,Schedlowski M, Rief W. Immunological effects ofbehavioral activation with exercise in majordepression: an exploratory randomized controlledtrial. Transl Psychiatry. 2017;7(5):e1132. doi:10.1038/tp.2017.76
60. Garand L, Buckwalter KC, Lubaroff D,Tripp-Reimer T, Frantz RA, Ansley TN. A pilot studyof immune and mood outcomes of acommunity-based intervention for dementiacaregivers: the PLST intervention. Arch PsychiatrNurs. 2002;16(4):156-167. doi:10.1053/apnu.2002.34392
61. Gonzalez-Garcia M, Ferrer MJ, Borras X, et al.Effectiveness of mindfulness-based cognitivetherapy on the quality of life, emotional status, andCD4 cell count of patients aging with HIV infection.AIDS Behav. 2014;18(4):676-685. doi:10.1007/s10461-013-0612-z
62. Goodkin K, Feaster DJ, Asthana D, et al. Abereavement support group intervention islongitudinally associated with salutary effects onthe CD4 cell count and number of physician visits.Clin Diagn Lab Immunol. 1998;5(3):382-391. doi:10.1128/CDLI.5.3.382-391.1998
63. Grossarth-Maticek R, Eysenck HJ. Length ofsurvival and lymphocyte percentage in women withmammary cancer as a function of psychotherapy.Psychol Rep. 1989;65(1):315-321. doi:10.2466/pr0.1989.65.1.315
64. Hasson D, Anderberg UM, Theorell T, ArnetzBB. Psychophysiological effects of a web-basedstress management system: a prospective,randomized controlled intervention study of IT andmedia workers [ISRCTN54254861]. BMC PublicHealth. 2005;5:78. doi:10.1186/1471-2458-5-78
65. Hosaka T, Matsubayashi H, Sugiyama Y, Izumi S,Makino T. Effect of psychiatric group interventionon natural-killer cell activity and pregnancy rate.Gen Hosp Psychiatry. 2002;24(5):353-356. doi:10.1016/S0163-8343(02)00194-9
66. Irwin MR, Olmstead R, Carrillo C, et al.Cognitive behavioral therapy vs tai chi for late lifeinsomnia and inflammatory risk: a randomizedcontrolled comparative efficacy trial. Sleep. 2014;37(9):1543-1552. doi:10.5665/sleep.4008
67. Irwin MR, Olmstead R, Breen EC, et al.Cognitive behavioral therapy and tai chi reversecellular and genomic markers of inflammation inlate-life insomnia: a randomized controlled trial.Biol Psychiatry. 2015;78(10):721-729. doi:10.1016/j.biopsych.2015.01.010
68. Janelsins MC, Davis PG, Wideman L, et al.Effects of tai chi chuan on insulin and cytokinelevels in a randomized controlled pilot study onbreast cancer survivors. Clin Breast Cancer. 2011;11(3):161-170. doi:10.1016/j.clbc.2011.03.013
69. Kéri S, Szabó C, Kelemen O. Expression oftoll-like receptors in peripheral blood mononuclearcells and response to cognitive-behavioral therapyin major depressive disorder. Brain Behav Immun.2014;40:235-243. doi:10.1016/j.bbi.2014.03.020
70. Koh KB, Lee Y. Reduced anxiety level bytherapeutic interventions and cell-mediatedimmunity in panic disorder patients. PsychotherPsychosom. 2004;73(5):286-292. doi:10.1159/000078845
71. Larson MR, Duberstein PR, Talbot NL, CaldwellC, Moynihan JA. A presurgical psychosocialintervention for breast cancer patients:psychological distress and the immune response.J Psychosom Res. 2000;48(2):187-194. doi:10.1016/S0022-3999(99)00110-5
72. Laudenslager ML, Simoneau TL, Kilbourn K,et al. A randomized control trial of a psychosocialintervention for caregivers of allogeneichematopoietic stem cell transplant patients: effectson distress. Bone Marrow Transplant. 2015;50(8):1110-1118. doi:10.1038/bmt.2015.104
73. Lopez CR, Antoni MH, Pereira D, et al. Stressmanagement, depression and immune status inlower income racial/ethnic minority womenco-infected with HIV and HPV. J Appl Biobehav Res.2013;18(1):37-57. doi:10.1111/jabr.12003
74. Lumley MA, Keefe FJ, Mosley-Williams A, et al.The effects of written emotional disclosure andcoping skills training in rheumatoid arthritis:a randomized clinical trial. J Consult Clin Psychol.2014;82(4):644-658. doi:10.1037/a0036958
75. Mackay GM, Forrest CM, Christofides J, et al.Kynurenine metabolites and inflammation markersin depressed patients treated with fluoxetine orcounselling. Clin Exp Pharmacol Physiol. 2009;36(4):425-435. doi:10.1111/j.1440-1681.2008.05077.x
76. McCain NL, Gray DP, Elswick RK, et al. Arandomized clinical trial of alternative stressmanagement interventions in persons with HIVinfection. J Consult Clin Psychol. 2008;76(3):431-441.doi:10.1037/0022-006X.76.3.431
77. McCain NL, Zeller JM, Cella DF, Urbanski PA,Novak RM. The influence of stress managementtraining in HIV disease. Nurs Res. 1996;45(4):246-253. doi:10.1097/00006199-199607000-00009
78. McGregor BA, Antoni MH, Boyers A, Alferi SM,Blomberg BB, Carver CS. Cognitive-behavioralstress management increases benefit finding andimmune function among women with early-stagebreast cancer. J Psychosom Res. 2004;56(1):1-8.doi:10.1016/S0022-3999(03)00036-9
79. Memon AA, Sundquist K, Ahmad A, Wang X,Hedelius A, Sundquist J. Role of IL-8, CRP andepidermal growth factor in depression and anxietypatients treated with mindfulness-based therapy orcognitive behavioral therapy in primary health care.Psychiatry Res. 2017;254:311-316. doi:10.1016/j.psychres.2017.05.012
80. Mikocka-Walus A, Bampton P, Hetzel D,Hughes P, Esterman A, Andrews JM.Cognitive-behavioural therapy for inflammatorybowel disease: 24-month data from a randomisedcontrolled trial. Int J Behav Med. 2017;24(1):127-135.doi:10.1007/s12529-016-9580-9
81. Mohr DC, Genain C. Social support as a buffer inthe relationship between treatment for depressionand T-cell production of interferon gamma inpatients with multiple sclerosis. J Psychosom Res.2004;57(2):155-158. doi:10.1016/S0022-3999(03)00601-9
82. Mohr DC, Goodkin DE, Islar J, Hauser SL,Genain CP. Treatment of depression is associatedwith suppression of nonspecific andantigen-specific TH1 responses in multiple sclerosis.Arch Neurol. 2001;58(7):1081-1086. doi:10.1001/archneur.58.7.1081
83. Morath J, Gola H, Sommershof A, et al. Theeffect of trauma-focused therapy on the altered Tcell distribution in individuals with PTSD: evidencefrom a randomized controlled trial. J Psychiatr Res.2014;54:1-10. doi:10.1016/j.jpsychires.2014.03.016
84. Parsons JT, Golub SA, Rosof E, Holder C.Motivational interviewing and cognitive-behavioralintervention to improve HIV medication adherenceamong hazardous drinkers: a randomizedcontrolled trial. J Acquir Immune Defic Syndr. 2007;46(4):443-450. doi:10.1097/QAI.0b013e318158a461
85. Savard J, Simard S, Giguère I, et al. Randomizedclinical trial on cognitive therapy for depression inwomen with metastatic breast cancer:psychological and immunological effects. PalliatSupport Care. 2006;4(3):219-237. doi:10.1017/S1478951506060305
86. Savard J, Simard S, Ivers H, Morin CM.Randomized study on the efficacy ofcognitive-behavioral therapy for insomniasecondary to breast cancer, part II: immunologiceffects. J Clin Oncol. 2005;23(25):6097-6106. doi:10.1200/JCO.2005.12.513
87. Shadick NA, Sowell NF, Frits ML, et al. Arandomized controlled trial of an internal familysystems-based psychotherapeutic intervention onoutcomes in rheumatoid arthritis:a proof-of-concept study. J Rheumatol. 2013;40(11):1831-1841. doi:10.3899/jrheum.121465
88. Sharpe L, Schrieber L. A blind randomizedcontrolled trial of cognitive versus behavioralversus cognitive-behavioral therapy for patientswith rheumatoid arthritis. Psychother Psychosom.2012;81(3):145-152. doi:10.1159/000332334
89. Sharpe L, Sensky T, Timberlake N, Ryan B,Brewin CR, Allard S. A blind, randomized, controlledtrial of cognitive-behavioural intervention forpatients with recent onset rheumatoid arthritis:preventing psychological and physical morbidity. Pain.2001;89(2-3):275-283. doi:10.1016/S0304-3959(00)00379-1
90. Shen X, Zhu X, Wu Y, et al. Effects of apsychological intervention programme on mentalstress, coping style and immune function inpercutaneous coronary intervention patients. PLoS
Research Original Investigation Psychosocial Interventions and Immune System Function
1042 JAMA Psychiatry October 2020 Volume 77, Number 10 (Reprinted) jamapsychiatry.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022
One. 2018;13(1):e0187745. doi:10.1371/journal.pone.0187745
91. Simoni JM, Wiebe JS, Sauceda JA, et al. Apreliminary RCT of CBT-AD for adherence anddepression among HIV-positive Latinos on theUS-Mexico border: the Nuevo Día study. AIDS Behav.2013;17(8):2816-2829. doi:10.1007/s10461-013-0538-5
92. Taylor CB, Conrad A, Wilhelm FH, et al. Doesimproving mood in depressed patients alter factorsthat may affect cardiovascular disease risk?J Psychiatr Res. 2009;43(16):1246-1252. doi:10.1016/j.jpsychires.2009.05.006
93. Theeke LA, Mallow JA, Moore J, McBurney A,Rellick S, VanGilder R. Effectiveness of LISTEN onloneliness, neuroimmunological stress response,psychosocial functioning, quality of life, andphysical health measures of chronic illness. Int JNurs Sci. 2016;3(3):242-251. doi:10.1016/j.ijnss.2016.08.004
94. Thornton LM, Andersen BL, Schuler TA, CarsonWE III. A psychological intervention reducesinflammatory markers by alleviating depressivesymptoms: secondary analysis of a randomizedcontrolled trial. Psychosom Med. 2009;71(7):715-724.doi:10.1097/PSY.0b013e3181b0545c
95. Zautra AJ, Davis MC, Reich JW, et al.Comparison of cognitive behavioral andmindfulness meditation interventions onadaptation to rheumatoid arthritis for patients withand without history of recurrent depression.J Consult Clin Psychol. 2008;76(3):408-421. doi:10.1037/0022-006X.76.3.408
96. Zgierska AE, Burzinski CA, Cox J, et al.Mindfulness meditation and cognitive behavioraltherapy intervention reduces pain severity andsensitivity in opioid-treated chronic low back pain:pilot findings from a randomized controlled trial.Pain Med. 2016;17(10):1865-1881. doi:10.1093/pm/pnw006
97. Shields GS, Bonner JC, Moons WG. Doescortisol influence core executive functions? ameta-analysis of acute cortisol administration
effects on working memory, inhibition, andset-shifting. Psychoneuroendocrinology. 2015;58:91-103. doi:10.1016/j.psyneuen.2015.04.017
98. Uttal DH, Meadow NG, Tipton E, et al. Themalleability of spatial skills: a meta-analysis oftraining studies. Psychol Bull. 2013;139(2):352-402.doi:10.1037/a0028446
99. Roth A, Fonagy P. What Works for Whom:A Critical Review of Psychotherapy Research. 2nd ed.Guilford Press; 2005.
100. Herbert TB, Cohen S. Stress and immunity inhumans: a meta-analytic review. Psychosom Med.1993;55(4):364-379. doi:10.1097/00006842-199307000-00004
101. Steptoe A, Hamer M, Chida Y. The effects ofacute psychological stress on circulatinginflammatory factors in humans: a review andmeta-analysis. Brain Behav Immun. 2007;21(7):901-912. doi:10.1016/j.bbi.2007.03.011
102. Mohler ER III, Ballantyne CM, Davidson MH,et al; Darapladib Investigators. The effect ofdarapladib on plasma lipoprotein-associatedphospholipase A2 activity and cardiovascularbiomarkers in patients with stable coronary heartdisease or coronary heart disease risk equivalent:the results of a multicenter, randomized,double-blind, placebo-controlled study. J Am CollCardiol. 2008;51(17):1632-1641. doi:10.1016/j.jacc.2007.11.079
103. Bonafede MMK, Gandra SR, Watson C, PrincicN, Fox KM. Cost per treated patient for etanercept,adalimumab, and infliximab across adultindications: a claims analysis. Adv Ther. 2012;29(3):234-248. doi:10.1007/s12325-012-0007-y
104. Lipsky PE, van der Heijde DM, St Clair EW,et al; Anti-Tumor Necrosis Factor Trial inRheumatoid Arthritis With Concomitant TherapyStudy Group. Infliximab and methotrexate in thetreatment of rheumatoid arthritis. N Engl J Med.2000;343(22):1594-1602. doi:10.1056/NEJM200011303432202
105. De Bie CI, Hummel TZ, Kindermann A, et al.The duration of effect of infliximab maintenance
treatment in paediatric Crohn’s disease is limited.Aliment Pharmacol Ther. 2011;33(2):243-250.doi:10.1111/j.1365-2036.2010.04507.x
106. Slavich GM, Way BM, Eisenberger NI, TaylorSE. Neural sensitivity to social rejection isassociated with inflammatory responses to socialstress. Proc Natl Acad Sci U S A. 2010;107(33):14817-14822. doi:10.1073/pnas.1009164107
107. Slavich GM, Giletta M, Helms SW, et al.Interpersonal life stress, inflammation, anddepression in adolescence: testing social signaltransduction theory of depression. Depress Anxiety.2020;37(2):179-193. doi:10.1002/da.22987
108. Antoni MH. Psychosocial intervention effectson adaptation, disease course and biobehavioralprocesses in cancer. Brain Behav Immun. 2013;30(suppl):S88-S98. doi:10.1016/j.bbi.2012.05.009
109. Kiecolt-Glaser JK, Glaser R. Psychoneuroim-munology: can psychological interventionsmodulate immunity? J Consult Clin Psychol. 1992;60(4):569-575. doi:10.1037/0022-006X.60.4.569
110. Miller GE, Cohen S. Psychologicalinterventions and the immune system:a meta-analytic review and critique. Health Psychol.2001;20(1):47-63. doi:10.1037/0278-6133.20.1.47
111. Irwin MR, Slavich GM. Psychoneuroimmu-nology. In: Cacioppo JT, Tassinary LG, Berntson GG,eds. Handbook of Psychophysiology. 4th ed.Cambridge University Press; 2017:377-398. doi:10.1017/9781107415782.017
112. Slavich GM, Sacher J. Stress, sex hormones,inflammation, and major depressive disorder:extending social signal transduction theory ofdepression to account for sex differences in mooddisorders. Psychopharmacology. 2019;236(10):3063-3079. doi:10.1007/s00213-019-05326-9
113. Slavich GM. Psychoneuroimmunology of stressand mental health. In: Harkness KL, Hayden EP, eds.The Oxford Handbook of Stress and Mental Health.Oxford University Press; 2020:519-546. doi:10.1093/oxfordhb/9780190681777.013.24
Psychosocial Interventions and Immune System Function Original Investigation Research
jamapsychiatry.com (Reprinted) JAMA Psychiatry October 2020 Volume 77, Number 10 1043
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ on 03/26/2022





























