Embed Size (px)
Citation preview
RESEARCH PROPOSAL
THE PREVALENCE OF MENTAL DISORDERS AMONG PRISONERS AT BUTARE
PRISON
By
HABYARIMANA Charles and KANGABE Valentine
Submitted in partial fulfillment of requirement for Advanced
Diploma in
MENTAL HEALTH NURSING
In the
Department of Mental Health
FACULTY OF NURSING SCIENCES
KIGALI HEATH INSTITUTE
i
Supervisor: PROF SIMBA KANANGA
Co-supervisor: Mr. GASOVYA Augustin
Kigali December 2010
ii
DECLARATION
We do hereby declare that this project submitted in partial
fulfillment of the requirement for the Advanced Diploma in
Mental Health, at Kigali Health Institute, is our original
work and has not previously been submitted elsewhere. Also, we
do declare that a complete list of references is provided
indicating all the sources of information quoted or cited.
HABYALIMANA Charles
And
KANGABE Valentine
iii
DEDICATION
We dedicate this research proposal to:
Our Parents,
All our siblings, and
Our best friends.
iv
ACKNOWLEDGEMENT
We deeply thank the Government of RWANDA for the scholarship
provided to help us achieve this level of education.
We highly appreciate the administration of KIH especially the
staff of Mental Health Department, and all lecturers who
provided us with excellent nursing skills.
We would like to thank also the clinical supervisors who
supported us during our practice in different hospitals.
We indeed thank PROF SIMBA KANANGA and Mr. GASOVYA Augustin,
our research project supervisors, for their professional
thoughtfulness and the contribution provided during the
preparation of this research proposal.
v
SUMMARY OF THE STUDY
The purpose of this research project is to evaluate the
Prevalence of Mental Disorders among prisoners population of
Butare Prison. Background: Prisoners are particularly
vulnerable to developing mental health problems. Findings from
recent studies indicate that the prevalence of mental illness
is higher in prisons than in the community, and co-morbidity
is common.
vi
Problem statement: Even though prison population is at high
risk to develop mental disorders, prevalence of mental
disorders in Butare prison is not known. Significance of the
study: The study will help health care givers to promote the
mental health of prisoners, as well as moral and mental health
of prison staff and should therefore be one of the central
objectives of good prison management.
Methodology: This cross sectional study will be carried out at
Butare prison, and selected participants will be observed and
interviewed by researchers. A sample of this study will be
selected by systematic random sampling. The prevalence of
mental disorders among prison population of Butare prison will
be presented according to the categories of mental disorders,
age group and sex of prisoners. The research will take three
months and the total budget will be 3481800 rwfs for period of
four months .
vii
TABLE OF COTANTS
DECLARATION.................................................ii
DEDICATION.................................................iii
ACKNOWLEDGEMENT.............................................iv
SUMMARY OF THE STUDY.........................................v
TABLE OF COTANTS............................................vi
LIST OF SYMBOLE AND ABREVIATIONS/ ACRONYMS..................ix
LIST OF TABLES...............................................x
CHAPITER 1.INTRODUCTION......................................1
1.1DEFINITION OF KEY TERMS PERTINENT TO THE STUDY..........1
1.2 BACKGROUND OF THE STUDY................................1
1.3PROBLEM STATEMENT.......................................3
1.4 OBJECTIVES.............................................4
1.4.1 Main objective......................................4
1.4.2 Specific objective............................4
1.5 RESEARCH QUESTIONS.....................................4
1.7 SIGNIFICANCE OF THE STUDY..............................4
1.8 SUBDIVISION OF THE STUDY...............................5
CHAPITER2. LITERATURE LIVIEW.................................6viii
2.1. THEORY ABOUT MENTAL DISORDERS.........................6
2.2. ETIOLOGY OF MENTAL DISORDERS..........................7
2.3. MENTAL HEALTH OF PRISONERS............................8
2.4. FACTORS CONTRIBUTING TO MENTAL DISORDERS AMONG
PRISONERS..................................................8
2.4.1 The inmates’ social world...........................9
2.4.2 Prison violence.....................................9
2.4.3 Isolation...........................................9
2.4.4 Prison victimization...............................10
2.5 THE LINKAGE BETWEEN MENTAL DISORDERS AND CRIME........11
2.6 FREQUENCY OF MENTAL DISORDES AMONG PRISONERS POPULATION
..........................................................13
CHAPTER 3. RESEARCH METHODOLOGY.............................14
3.1. STUDY AREA...........................................14
3.2 STUDY DESIGN..........................................14
3.3 STUDY POPULATION......................................14
3.5. SAMPLING METHODS.....................................15
3.6. DATA COLLECTION METHODS AND PROCEDURES...............15
3.7 .DATA ANALYSIS........................................16
3.8 PROBLEMS AND LIMITATIONS OF THE STUDY.................16
3.9 ETHICAL CONSIDERATION.................................17
CHAPITER 4.PRESENTATION OF THE RESULTS......................18
4.1. THE PROPORTION OF MENTAL DISORDERS AMONG PRISON
POPULATION OF BUTARE PRISON BY AGE GROUP..................18
ix
LIST OF REFFERENCIES........................................23
WORK PLAN...................................................25
THE GANT CHART..............................................26
BUDGET......................................................27
I. PREPARATION..............................................27
II.THE SURVEY...............................................28
III .THE STUDY SUPPLIES.....................................28
IV.THE PRODUCTION OF THE RAPPORT............................29
V. THE WORKSHOP FOR REPORT VALIDATION......................29
VI. THE BUDGET SUMMARY......................................30
BUDGET JUSTIFICATION........................................30
PROFILE OF APPLICANT AND INSTITUTION........................31
C.PROFILE OF INSTITUTION....................................33
APPENDIX....................................................34
x

xi
LIST OF SYMBOLE AND ABREVIATIONS/ ACRONYMS
%: Percentage
&: And
APA: American Psychiatric association.
BMJ: British medical journal.
DPD: dissocial personality disorder
DSM-IV: Diagnostical and Statistical Manual for mental
disorders Fourth Edition.
e.g: Example
Et al: Et alii or at aliae (and others)
KHI: Kigali Health Institute
Mr.: Mister
Prof: Professor
PTSD: Post traumatic stress disorders.
SHU: Special Housing Unity.
xii
LIST OF TABLES
Table 4.1.a the proportion of mental disorders among prisoners
population aged between 18-24...............................18
Table 4.1.bThe proportion of mental disorder among prison
population aged between 25-31...............................18
Table 4.1.c the proportion of mental disorder among prison
population aged between 32-38...............................19
Table 4.1 d. The proportion of mental disorder among prison
population aged between 39-45...............................19
Table4.1.e The proportion of mental disorder among prison
population aged between 46-52...............................20
Table4.1.f The proportion of mental disorder among prison
population aged between53-59................................20
Table4.1.g The proportion of mental disorder among prison
population aged between 60-66...............................20
Table4.1.h The proportion of mental disorder among prison
population aged between 66-73...............................21
Table 4.2 the proportion of mental disorders among prisoners
population of Butare prison by sex..........................21
Table 4.3 Proportion of prisoner population of Butare prison
without mental disorders by sex.............................22
Table4.4 Prevalence of mental disorders among prisoners
population of Butare Prison according to their categories.. .22
xiii
CHAPITER 1.INTRODUCTION
1.1DEFINITION OF KEY TERMS PERTINENT TO THE STUDY
Prevalence: In an epidemiologic study the prevalence is the
proportion of individuals in a population having disease.
Prevalence is a statistical concept referring to the number of
case of disease that are present in a particular population at
a given time (Medterms, 2010)
Mental disorders: In DSM-IV, each of the mental disorders is
conceptualized as clinical significant behavior or
psychological syndrome or pattern that occurs in an individual
and that associated with present distress (e.g. a painful
symptom) or disability (e.g. impairment in one or more
important areas of functioning) or with significantly
increased risk of suffering death, pain, disability (DSMIV-
2000).
Prison: a correctional institution where persons are confined
while on trial or for punishment. A prison is a place in which
people are confined and deprived of a range of liberties.
Prison is a place in which people are physically confined and,
usually, deprived of a range of personal freedoms (James B, 2004).
Prisoner: One who has been committed to a prison, jail or
penal institution for the purpose of detention until he or she
may be tried for a crime of which he or she is accused, or for
xiv
the purpose of punishment after conviction of such crime. He
is one deprived of freedom of expression or action or one
held in custody, captivity, or a condition of forcible
restraint, especially while on trial or serving a prison
sentence (William H, 2000).
1.2 BACKGROUND OF THE STUDY
Prisoners are particularly vulnerable to developing mental
health problems. Findings from recent studies indicate that
the prevalence of mental illness is higher in prisons than in
the community, and co-morbidity is common. The prison
environment and the rules and regimes governing daily life
inside prison can be seriously detrimental to mental health.
Histories of abuse, deprivation, homelessness, and
unemployment and substance misuse are common. Many prisoners
have numeracy and literacy problems and most prisoners have a
lower than average of intelligent quotient (Singleton et
al ,1998 ).
It is also important to bear in mind that people with mental
disorders are particularly vulnerable to imprisonment, and
initiatives aimed at diverting them from detention are not
always effective (Birmingham, 2001). Women prisoners reported
that imprisonment impacted negatively up on their health. The
initial shock of imprisonment, separation from families and
enforced living with other women suffering drug withdrawal and
xv
serious mental health problems affected their own mental
health (Douglas et al., 2000).
The U.S. prison population, at least as measured by looking at
its largest component, the state prison population,
experiences a prevalence of mental illness very much in line
with that of the general population. Beck and Maruschak in
Mental Health Treatment in State Prisons reported that the
prevalence of mental illness, broadly defined, was between 22%
and 24% in the prison population( Beck &Maruschak, 2000)
The prevalence of psychiatric morbidity among prisoners in
England and Wales were provided by two large-scale point-
prevalence studies carried out in the late 1980s and early
1990s by the Institute of Psychiatry, London (Gunn et al,
1991). Mental disorder (including substance misuse diagnoses)
was found in 37% of sentenced male prisoners, 63% of men on
remand, 57% of sentenced women prisoners and 76% of women
remand prisoners.
In Africa, with reference to Nigeria, Mental health problems
have been observed to be higher among incarcerated inmates
compared to the general population. Common mental health
problems amongst them include substance misuse, personality
disorders and minor (neurotic) symptoms. With these disorders
estimated to be present in 25 to 75% of prisoners, they are
more common than the psychotic disorders, which have been
estimated to account for 2 to 10% of psychiatric morbidityxvi
among them. However, the psychotic disorders have also been
observed to be more common among inmates compared to the
general population. In addition, the frequency of psychosis
tends to be higher in hospital-based studies and the prison
condition has been identified as a potential source of rapid
deterioration in those with preexisting psychosis and
decompensation in vulnerable inmates (Fatoye et al, 2006).
In eastern African with reference to Kenya-Uganda –Tanzania,
95% of criminals in prison were seriously mentally ill. There
was not a single case of psychopathic personality disorder
although this is the one psychiatric disorder that is most
commonly associated with criminal behaviors (Frank, 2002).
Mental health of Rwandan prison population is quit alike of
other prisoners all over the world. The cases of mentally ill
patient received at Neuro-psychiatric Hospitals from different
Central Prisons and some cases of mentally ill prisoners
reported by Prison health services make certain that there are
mental disorders among Rwandan Prison population. Butare
Prison dispensary has reported thirty-two cases of mental ill
prisoners, who were under antipsychotic treatment in March
2010 (Butare prison monthly report, 2010).
1.3PROBLEM STATEMENT
In general, Prison population is more exposed to develop
mental disorders. Their condition of life, deprivation of
liberty, being forced to define themselves as weak, helpless
xvii
and dependent threaten their self concept ,without forgetting
the linking between criminal behaviors and mental disorders.
Even though health care is applied in prisons of Rwanda, there
is an evident lack of data on the prevalence of mental
disorders among prisoners population, while they are more
exposed to stressors which may result in mental disorders.
During our training period at Ndera Neuro-psychiatric Hospital
we have released that there are some cases of mental ill
prisoners who are hospitalized. Skilled mental health
professionals in Rwandan Prisons are still deficient and for
this reason only prisoners who show observable and danger
mental disorders symptoms like agitation, aggressiveness, are
identified as mentally ill and brought to Psychiatric
Hospital, Other patients who do not present stranger symptoms
are ignored. This may lead to further Mental Health problems
to prison population and to all Rwandan society particularly.
With reference to Ndera Neuropsychiatric Hospital, in Rwanda
some kind of mental disorders are more frequent including:
mood disorder, anxiety disorders, psychotic disorders, drugs
and alcohol misuse. This research will determine on which
prevalence the same mental disorders are found in prison
population of Butare prison.
xviii
1.4 OBJECTIVES
1.4.1 Main objective
To evaluate the prevalence of mental disorders within prison
population of Butare Prison. 1.4.2 Specific objective
To identify the more frequent categories of mental disorders
among the prisoner population at Butare prison.
To determine the proportion of mental disorders among
prisoners population of Butare prison by age and sex.
1.5 RESEARCH QUESTIONS
Which categories of mental disorders are more frequent in the
prisoner population of Butare Prison ?
Which is the proportion of mental disorders among prison
population of Butare Prison by age and sex?
1.7 SIGNIFICANCE OF THE STUDY.
a. Scientific interest: The study will help to be aware of
mental health condition and addressing mental health need
among prisoners of Rwandan prisons, as the regained
information will be useful in planning and improving quality
of care for both prisoners with mental disorders and the
prison population as a whole.
b. Professional interest: The presence of prisoners with
unrecognized and untreated mental disorders can complicate and
negatively affect the prison environment, so the study will
help health care givers to promote the mental health care of
xix
prisoners, as well as moral and mental health of prison staff
and should therefore be one of the central objectives of good
prison management.
c. Social interest: Prison health cannot be addressed in
isolation from the health of the general population since
there is a constant inter-change between the prison and the
broader community. This Study will help then Rwandan
community, to avoid and reduce frequent social impairments
caused by some discharged prisoners after the end of their
punishment.
1.8 SUBDIVISION OF THE STUDY
This study is subdivided into 4 main parts: Part one consists
of the introduction which is composed by definition of key
terms, the background, problem statements, objectives,
research questions, research hypothesis and the significance
of the study. Part two consists of the literature review,
which put emphasis on mental health condition, mental
disorders, as well as their causes and their frequency among
prison population, part three consists of methodology, which
also explains the study area, the study designs sampling
strategies, sample size data collection tools, data analysis,
problem and limitation of the study, and the fourth part which
shows how results of the study will be presented.
xx

xxi
CHAPITER2. LITERATURE LIVIEW
2.1. THEORY ABOUT MENTAL DISORDERS
Mental illness, according to American Psychiatric association
[APA], mental disorders is considered as clinically
significant syndrome experienced by a person and marked by
distress, disability or risk of suffering disability or loss
of freedom (Wanda, 2006).
Referring to Pater (2003), Mental illness is any illness
experienced by a person which affect their emotions, thought
or behaviors which is out of keeping with their cultural
believes and personality, and is producing a negative effect
on their life or on the life of their families (Vikram,2003).
DSM-IV-TR Classification of mental disorders
Disorders usually first diagnosed in infancy childhood or
adolescent, Delirium, Dementia, Amnesic and other cognitive
disorders, Mental disorders due to general medical condition
not elsewhere classified, Substance related disorders,
Schizophrenia and other psychotic disorders, Mood disorders,
Anxiety Disorders, Somatoform disorders, Dissociative
disorders, Personality disorder, Sexual and gender identity
disorders ( Katherine et al.,2004).
Brief description of main psychotic disorders
a. Mood disorders: The mood disorders section includes
disorders that have a disturbance in mood as the predominant
xxii
features .The section contains depressive disorders ; manic
and hypo manic episode and bipolar disorders(DSMIV,2000)
b. Anxiety disorders
The anxiety disorders section includes Panic disorders without
agoraphobia; agoraphobia without history of panic disorder;
specific phobia; social phobia; obsessive compulsive disorders
; post traumatic stress disorders, acute stress disorders,
general anxiety disorders; anxiety disorders due to general
medical condition; Substance induced anxiety disorders due to
general medical condition(DSMIV, 2000).
c. Psychotic-disorders: The term psychotic refers to delusion
or prominent hallucinations, with the hallucination occurring
in the absence of insight into their pathological nature. The
disorders in this section include schizophrenia,
schizopreniform Disorders schizoaffective disorders,
delusional disorder, brief psychotic disorders, shared
psychotic disorders, Psychotic disorders due to general
medical condition, and psychotic disorders not otherwise
specified(DSMIV, 2000).
b. Substance –related Disorders: The substance related
disorders include disorders related to the taking of drug of
abuse (including alcohol),to the side effects of medication,
and to the toxin exposure(DSMIV, 2000)
xxiii
2.2. ETIOLOGY OF MENTAL DISORDERS
a. Biological theory
Structural damages to the brain can result from injuries such
as from accidents and from diseases that cause deterioration
(Susan, 2004)
Many of biochemical theories of psychopathology suggest that
too much or too little of certain neurotransmitters in synapse
causes specific types of psychopathology. Psychological
symptoms may be linked to the number of functioning of
receptors for the neurotransmitters on the dendrites. Many
mental illnesses run in families, suggesting that people who
have a family member with a mental illness are more likely to
develop a mental illness. Susceptibility is passed on in
families through genes. Experts believe many mental illnesses
are linked to abnormalities in many genes not just one. That
is why a person inherits a susceptibility to a mental illness
and doesn't necessarily develop the illness. Mental illness
itself occurs from the interaction of multiple genes and other
factors such as stress, abuse, or a traumatic event which can
influence, or trigger, an illness in a person who has an
inherited susceptibility to it (Susan, 2004).
b. Psychological theory.
Psychological theory of abnormality (mental disorders) varies
greatly in factors and processes they say are involved in the
development of abnormal or maladaptive behaviors. Some
theories focus on effect of rewards and punishment in thexxiv
environment, some focus on thought process and some focus on
difficulties human have in striving to realize their full
potentials in capricious world. Others include; severe
psychological trauma suffered as emotional, physical or sexual
abuse. An important early loss, such as the loss of parent,
neglect, poor ability to relate to others, etc...
Psychodynamic theory of mental disorders suggest that all
behaviors, thoughts and emotional whether normal or abnormal
are influenced to a large extend by unconscious process.
(Vakon et al., 2000).
c. Social theory
Psychological theory focus primarily on an individual they
attribute problematic psychological symptoms to unconscious
conflict, negative cognition existential anxiety and other
factors residing largely within the individual. Although these
theories may suggest that the environment plays a great role
in creating these problems.
They still consider the individual as the primary unit of
analysis. These social approaches to abnormality focus more on
the larger social structures within which an individual lives.
Psychological factors that may contribute to mental illness
include: Severe psychological trauma suffered as a child, such
as emotional, physical, or sexual abuse and an important early
loss, such as the loss of a parent or neglect (Vakon, 2000)
xxv
2.3. MENTAL HEALTH OF PRISONERS
According toVikram, mental health of prisoners is important
since some peoples with mental illness get involved in
criminal activities and end in prison. Being in prison can be
stressful experience. The isolation loss of freedom and
anxiety can in some people lead to mental illness. Drug abuse
also may occur in some prisons; thus being in prison can cause
mental disorders. In prison different types of mental
disorders are common. Included are psychotic disorders,
especially in people who are behaving in odd way, speaking to
imaginary people or themselves, restless or agitated. Withdraw
reactions in people with drink or drug problems, very soon
after being put in prison. Depression and anxiety, which are
likely to be the result of imprisonment. Suicide can occur
even in the most highly guarded environment such as prison
(Vikram, 2003).
2.4. FACTORS CONTRIBUTING TO MENTAL DISORDERS AMONG PRISONERS
There are many factors which may contribute to mental disorders
among prisoners, the latter include the treatment prisoners had
in early family life, their community bonding, school
performance, employment history, marital responsibilities,
personality factors, occupational experience, delinquent
activities, psychiatric history, physical health, critical life
events generating stress, and the residual degree of resilience
they retained despite the vicissitudes of life they might have
experienced. The unrelated effects might also include reactivexxvi
mental disturbance from the crimes they committed (Waldron et al.,
2004).
2.4.1 The inmates’ social world
There are a variety of ways to deal with the stress created by
prison life. Some inmates feel they must be active in order to
survive the prison experience. Their activities include
watching television or listening radio or stereo, obtaining
and using a drug, making alcohol beverage, lifting weight or
participating in other activities. Inmates must cope with
physical social and psychological problems that result from
punishment, and the loss of liberty.
The deprivation of goods and services in a society that vary
material procession the deprivation of heterosexual
relationships and result threat to the inmates’
masculinity ,and the deprivation of security in an inmate’s
population that threatens his safety and some time his life
and health.
Everything the inmates do, including the showers they can take
and the hours they can sleep, is regulated by the prison
staff. An individual prison may house up to 2,000 men at a
time, many with violent backgrounds. As of 2004, U.S. prisons
housed over 630,000 inmates who were serving time for a
violent offense (Bureau of Justice Statistics, 2007). Placing
these men together in close quarters may lead to feelings of
hostility, anger, and inevitably violence.xxvii
2.4.2 Prison violence
A common reaction to incarceration is violence including
violence against oneself. Probably the violence among inmates
is underreported; many inmates do not report incidents for
fear of reprisal from other inmates. One way in which inmate
behavior can be explained is the inmates’ criminal tendency or
their inclination to commit crime (Camp et al., 2005).
Prison violence is a product of what Colvin (2000) describes
as dimensions of control. The first type of control seen
in the prison environment is consistent coercion
(intimidation). Consistent coercion occurs when the offender
and victim have an ongoing, highly punitive relationship.
Individuals under this type of control experience high level
of self directed anger and weak social bonds (Colvin, 2000).
Inmates then have a decrease inpro-social behavior and a high
probability of mental health problems.
2.4.3 Isolation
Isolation is the term used when inmates are separated from the
general prison population. There are three situations which
may call for an inmate to be put in isolation. These include
disciplinary segregation, administrative segregation, and
protective custody. According to Singleton et al (1998) , the
level of confinement and isolation experienced by some
prisoners is, in itself, detrimental to their mental health,
but the situation is made worse by the fact that some
prisoners turn to using illicit substances to help them dealxxviii
with long periods of time spent locked up. It is not difficult
to imagine how prisoners with pre-existing psychiatric
problems deteriorate and others who are vulnerable to
developing mental health problems decompensate in these
conditions (Singleton, 1998).Numerous studies have documented
the effects of solitary confinement on prisoners giving them
the name; Special Housing Unit Syndrome or SHU Syndrome. Some
of the many SHU Syndrome symptoms include: visual and auditory
hallucinations, hypersensitivity to noise and touch, insomnia
and paranoia, uncontrollable feelings of rage and fear,
distortions of time and perception, increased risk of suicide,
PTSD.
2.4.4 Prison victimization
Victimization in prison can take many forms:
physical/assaultive, psychological, and sexual. Byrne and
Hummer (2008b) state that while assault does occur in prison,
the extent and severity is unknown. This may be due to the
differences in definitions of assault among correctional
departments.
For example, some departments may or may not include verbal
threats or attempted
assault when reporting levels of assault in their prisons
(Byrne et al., 2008).
Physical Victimization
The most common form of victimization in prisons is physical
abuse. Another influence on inmate violence is the formalxxix
organization of the prison which may include security,
programs, rehabilitation, staff characteristics, and prison
trains (Gaes et al.,2005).
Psychological victimization: According to South et al.,
(2006), Psychological victimization may include bullying which
includes ridiculing, ostracizing, and rumor spreading.
Victimization may take place because the inmate has not
integrated into a social system
such as a gang which would protect inmates from bullying.
Psychological victimization
may also occur when inmates exhibit higher levels of
maladjustment to prison life.
Inmates who are powerless and feel inferior may experience
this type of victimization if
unable or unwilling to conform to prison life.
Impact of Victimization
Inmates who are victims of another inmate’s aggression and
violence are often placed under immense psychological stress.
Victimized inmates often experience clinical Features similar
to Posttraumatic Stress Disorder (PTSD), a mental disorder
that is caused by a (n) extreme traumatic event(s) that
involved physical harm or the threat of physical harm
(National Institute of Mental Health, 2008)
2.5 THE LINKAGE BETWEEN MENTAL DISORDERS AND CRIME
According to Vikram (2003), certain kinds of mental illness
may influence suffers’ behaviors in different ways, so thatxxx
they do things that break the law. Violent behaviors can occur
in people who are suffering from severe mental disorders like
during a psychotic phase they may wander in public places,
shouting at peoples. Rarely, mentally ill person may threat or
attack someone. Stealing is a crime associated with people who
abuse drugs or alcohol. The reason is simple: these people are
stealing in order to get money to pay their drug habits In
adolescent stealing may be the result of conduct disorder.
Dangerous driving is associated with drinking too much alcohol
and severe disorders. However if we look at the issue of
mental illness and crime by asking question Do most people who
commit crimes suffers from mental illness, the answer is no.
Thus it is important that do not treat people with mental
illness as if they are potentially violent or likely to break
the law. The vast majority of people with mental illness are
not violent (Vikram, 2003).
Personality theory suggest that, emotional conflict and
personality deviation characterize many criminals especially
habitual offenders, leading some theorists to conclude that
such deviation cause criminal behavior. The early studies
emphasized the frequency of an association between mental
disorders and crime. According to Michael.D(2000), Antisocial
Personality Disorder is the most highly correlated mental
disorder with crime. An individual with Antisocial Personality
Disorder has a pervasive pattern of disregard for the rights
of others, and violations of them. The disorder is
xxxi
characterized by a lack of conformity or respect for lawful
behavior. They repeatedly carry out acts that are grounds for
their arrest. Borderline Personality Disorders, which is
possibly the most difficult mental disorder to treat, also can
contribute to criminality (Michael, 2000). Paranoid Personality
Disorder is characterized by a pervasive distrust and
suspiciousness of others. An individual with this disorder
will often interpret another motive as malevolent. When a
person feels someone is motivated to harm them in some manner
it is not surprising that the individual would act in a
violent way to either prevent the acts they expect to have
occur or respond aggressively to those they have seem as
hostile( Michael, 2000)
Intelligence and crime
Closely associated with the mental disorder approach is the
linking of crime and intelligence .It is argued that low
intelligence causes crime, this approach has long historically
roots .As noted ,early studies of family histories that found
many people of lower intelligence in a family line of
criminals concluded that the criminal behavior was caused by
low intelligence.
Howard Professionals through their publication of crime and
human nature, started that there is a clear and consistent
link between criminality and low intelligence and critics’
criminology text book for ignoring the research in this area
(Richard et al., 1985).
xxxii
Cognitive development theory
This approach is based on the belief that the way in which
people organize their thoughts about law result in either
criminal behavior or noncriminal behaviors (Lawrence K, 1958).
Psychologist refers to this organization of thoughts as moral
reasoning. When this reasoning is applied to law, it is termed
legal reasoning, although that term has a different meaning to
person trained in law. The stems from the early works of Jean
Piaget, who believed that there are two in development of
moral reasoning. According to Piaget leave the first stage at
about the age of 13, and the second stage lead to more moral
behavior than the first.The believe that the rules are screed
and immutable and the believe that rules are the products of
humans (Sue, 2000).
Psychiatric approach
The psychoanalytic theories of Sigmund Freud and his
colleagues introduced the concepts of the unconscious, along
with techniques for probing that element of personality and
emphasized that human behavior is motivated and purposive.
According to Freud (1856-1939), human have mental conflicts
because of desire and energy that are repressed into
unconscious. The urges, ideas, desires, and instincts are
basic, but they are repressed because of society’s morality.
Freud saw original human nature as assertive and aggressive.
It is not learned but is rooted deeply in early childhood
experiences. According to Freud we all have criminal
xxxiii
tendencies, but during the socialization process, most of us
learn to control them by developing an ability to control
impulses and acts them out or projects them inward. In the
case of the latter, the child may become neurotic, in the case
of the former, delinquent.
2.6 FREQUENCY OF MENTAL DISORDES AMONG PRISONERS POPULATION
According to Luke Birmingham (2003), mental health problems
are the most significant cause of morbidity in prisons. Over
90% of prisoners have a mental disorder.A recently published
systematic review of serious mental disorder among prisoners
gives some insight into the extent of the problem that exists
in prisons in Western countries today. This review suggests
that typically about one in seven prisoners have psychotic
illnesses or major depression, and about half of all male
prisoners and one in five women prisoners have antisocial
personality disorder. These rates, which are considerably
higher than those found in comparable community samples,
reflect a substantial level of treatment need (Faze et al., 2002).
According to Andersen, several studies have directly compared
females and males in similar or identical study designs.
Except for psychoses and alcohol abuse dependence, females
have overrepresentation of disorders with ration of 2-3 in
relation to males in prison sample (Andersen, 2004). In Fazel &
Danesh’s large review of 62 prison surveys 3.7% among male and
4% among female prisoners had ongoing mental disorders. Fazel
xxxiv
et al., 2002) found an average prevalence of 10%major
depression among male prisoners and 12% among female prisoners
with some differences as to the status of the disorder and
dissocial personality disorder (DPD) has been considered. In
1998, data from Correctional Services Canada found 1,000
inmates, out of 14,000 in the prison population, were
diagnosed with mental-health disorders. In 2004, that number
soared to 1,500 in a prison population of 12,500
(Upswing et al., 2005).
Falissard et al conducted a survey on prevalence of mental
disorders in French prisons for men. Prevalence rates for a
diagnosis given independently by both clinicians and for a
consensual diagnosis were respectively: 3.8% (6.2%) for
schizophrenia, 17.9% (24%) for major depressive disorder,
12.0% (17.7%) for generalized anxiety and 10.8% (14.6%) for
drug dependence. (Falissard et al, 2006).
CHAPTER 3. RESEARCH METHODOLOGY
This part describe the methodology which will be used in this
study, it will contain the description of study area, study
design and study population, sampling methods, sample size and
data collection methods and procedure to be used. Ethical
consideration and limitation of the study are also part of
this chapter.
xxxv
3.1. STUDY AREA
This study will be realized at Butare Prison. This area has
been selected as study site because it is one of the national
reference Prisons of Rwanda and its location is accessible
for the researchers and we have some information about the
state of this prison. The Prison is located at Huye District,
Southern Province.
3.2 STUDY DESIGN
This study will be cross sectional study. the cross-sectional
study is the most appropriate to measure the prevalence of
disease and is called “prevalence study”. This measure the
frequency of disease relation to age, sex, ect. The cross
sectional study is done once in a given period of time to
establish the state of affaires (disease, health state) at
particularly time (Stretch et al., 2006).
3.3 STUDY POPULATION
The study population is a collection of individuals with a
common character which interested the study.
The population of this study will include prisoners of Butare
prison and who will voluntarily accept to participate in the
research. This prison contains 9156 including 8335 men and
801women.This population is composed with members who are 18
to 70 age old. 3.4. SAMPLE SIZE
xxxvi
Graham and cook (2009) defined a sample as small group of
cases down from and used to represent some large group. In
this study the sample size will be calculated using the
following formula:
(3; 1)
n= Expected minimum sample size.
z=is a standard value which correspond to 1.96 (at 95%
confidence internal)
p=proportion /problem magnitude
ε=is the margin of error on p =5%
q=100-p, 100-80= 20
(3; 2)
Researchers prefer to use the half population of the sample
size calculated, because of shortage of time and available
budget. So the study will involve 123 participants from whole
prison population of Butare population)
xxxvii
3.5. SAMPLING METHODS
Sampling refers to the process of selecting a proportion of
the population to represent the entire of population.
Participants who would be selected as a sample of this study
will be selected by systematic random sampling. As we have a
population of 9156 by dividing with sample size of 123 we
obtain 74, randomly we will select any number between 1 and 74
so from that number we will select every 75th name from the
list of prisoners until we reach the last one, number 9156.we
will end up with 123 selected prisoners.
3.6. DATA COLLECTION METHODS AND PROCEDURES
For our study we will use mental status examination as main
tools of identification of the presence of any symptom of
mental disorders trough interview. The following techniques
will be used and we hope this study will have efficient
findings.
3.6.1structured observational method
The purpose of an observation is to try to understand a place,
an event or a behavior by watching (and taking note). After
observing you can reflect (think about what you have
seen).From your observation you can draw inferences about the
place, event, or behavior that might lead you to a large or
more general conclusion (Beck et al., 2005).
xxxviii
In our research we will use mental status examination form.
The selected prisoners will be observed during interview; here
different tools of mental disorders will be identified like
mood disorders, affect disturbance, etc.
3.6.2 Semi-structured interview
According to Beck et al., (2005), semi- structured interviews
are conducted on the basis of a free structure consisting of
open ended questions that define the area to be explored, at
least initially, and from which the interview or interviewee
may diverge in order to purse an idea in more detail. The
researchers prepare in advance a written topic guide is a
list question to be covered with each respondent .For our
research, we will prepare an interview guide to be used and
completed while we will be interviewing prisoners concerned
buy this study.
3.7 .DATA ANALYSIS
The data will be collected, entered in the computer from data
capture sheet and will be analyzed using computer software
SPSS (Statistical Package for Social Sciences). Demographic
data will be analyzed with frequencies means and standards
deviations, prevalence will be given in frequencies and
percentages.
xxxix
3.8 PROBLEMS AND LIMITATIONS OF THE STUDY
3.8.1. The problems of the study
a. Financial resources
b. Difficulty in obtaining information on sensitive and/or
private matters.
3.8.2. Limitations
The study population is too large so as limitation the sample
size will be large.
The risk of getting false information.
Communication problem considering the condition of prisoners.
3.9 ETHICAL CONSIDERATIONThe research will be carried out after obtaining permission
from KHI authorities and the Direction of Butare Prison.
The prisoners will participate voluntarily and freely in this
study after clearly explaining to them the significance of the
study in order to obtain their informed consent. The interview
will be done in a safe environment and the interviewers will
respond to all participants’ enquires and show acceptance of
their comments. The confidentiality will be assured to the
prisoners who will participate in the research as they will be
named by using the codes. During the study, the researcher
will consider various rights of the participants, such as
right to privacy, right to information and informed consent,
right to appropriate treatment and care, right to choices,
right to respect, and right to complain.
xl

xli
CHAPITER 4.PRESENTATION OF THE RESULTS
4.1. THE PROPORTION OF MENTAL DISORDERS AMONG PRISON
POPULATION OF BUTARE PRISON BY AGE GROUP
Table 4.1.a the proportion of mental disorders among prisonerspopulation aged between 18-24
Age
Group
Categories of
mental disorders
Frequencies Percentages
18-24 Mood disorders Anxiety disorders Psychotic
disorders Drugs and alcohol
misuse Others
Table 4.1.bThe proportion of mental disorder among prison populationaged between 25-31Age
Group
Categories of
mental disorders
Frequencies Percentages
25-31 Mood disorders Anxiety
disorders Psychotic
disorders Drugs and
alcohol misuse
xlii
Others
xliii
Table 4.1.c the proportion of mental disorder among prison
population aged between 32-38
Age
Group
Categories of
mental disorders
Frequencies Percentages
32-38 Mood disorders Anxiety
disorders Psychotic
disorders Drugs and
alcohol misuse Others
Table 4.1 d. The proportion of mental disorder among prisonpopulation aged between 39-45Age
Group
Categories of
mental disorders
Frequencies Percentages
39-45 Mood disorders Anxiety disorders Psychotic
disorders Drugs and alcohol
misuse Others
xliv

xlv
Table4.1.e The proportion of mental disorder among prison populationaged between 46-52Age
Group
Categories of
mental disorders
Frequencies Percentages
46-52 Mood disorders Anxiety disorders Psychotic
disorders Drugs and alcohol
misuse Others
Table4.1.f The proportion of mental disorder among prison population
aged between53-59
Age
Group
Categories of
mental disorders
Frequencies Percentages
53-59 Mood disorders Anxiety disorders Psychotic
disorders Drugs and alcohol
misuse Others
Table4.1.g The proportion of mental disorder among prison populationaged between 60-66
Age
Group
Categories of
mental disorders
Frequencies Percentages
xlvi
60-66 Mood disorders Anxiety disorders Psychotic
disorders Drugs and alcohol
misuse Others
xlvii
Table4.1.h The proportion of mental disorder among prison populationaged between 66-73
Age
Group
Categories of
mental disorders
Frequencies Percentages
67-73 Mood
disorders Anxiet
y disorders Psycho
tic disorders Drugs and
alcohol misuse Others
Table 4.2 theproportion ofmentaldisorders amongprisonerspopulation ofButare prisonby sex.
xlviii
Sex Categories of
Mental Disorders
Frequency
Male
Mood disorders Mood disorders Anxiety disorders Psychotic
disorders Drugs and
alcohol misuseOthers
Female Mood disorders Mood disorders Anxiety disorders Psychotic
disorders Drugs and
alcohol misuseOthersTotalPercentage

xlix
Table 4.3 Proportion of prisoner population of Butare prison
without mental disorders by sex.
Table4.4 Prevalence of mental disorders among prisoners populationof Butare Prison according to their categories.
l
Sex Freque
ncy Male Female Total Percentage
Mental disorders
detected
frequenc
y
Perce
ntage Mood disorders Anxiety
disorders Psychotic
disorders Drugs and
alcohol misuse Others total
LIST OF REFFERENCIES
African Medical Journal, Vol. 83 No. 10
American Psychiatric Association, 2000. Diagnostic and statistical of
mental disorders, fourth edition.p19
Birmingham L, (2004) Mental disorder and prisons, Psychiatric
Bulletin, p393-397
Butare Prison Dispensary monthly report, March, 2010.
Coid J., Petruckevitch A., Bebbington P. ,et al (2003b)
Psychiatric morbidity in prisoners and solitary cellular
confinement, II: special (‘strip’) cell. Journal of Forensic
Psychiatry and Psychology, 14,320-304.
Commission on Safety and Abuse in America’s Prisons, 2006, p23
Her Majesty’s Inspectorate of Prison, 1997b, 2000a
(http://byprcpch.org/cgi/content/full/9/9)
Hochstetler & Delisi, 2005, Health Services Research Unit,
University of Oxford, UK Department of Public Health, p258
li
Isherwood S. & Parrott, J. (2002) Audit of transfers under the
Mental Health Act from prison the impact of organizational
change. Psychiatric Bulletin, p 368-370
James.B (2004) life inside a supermax security prison,
voyageur press, hardcover p.192
Johnson, 1997, Psychiatric mental health nursing., fouth edition
Johnson,1997, Psychiatric mental health nursing ,fourth edition , p5.
Journal (Advances in Psychiatric Treatment (2003), p 191-199
Kathrine M. F&Patrician A.Holoday worret, 2004, psychiatric mental
health nursing, third edition, page646-652)
L.keltner& L. Schwecke,2003, Psychiatric Nursing,Fourth Edition ,
p188-190
Michael D. (2000), Mental Disorders and Crime: Personality Disorders
Nurse J., Woodcock P. & Ormsby J. (2003) Influence of
environmental factors on mental health within prisons:
focus group study. BMJ, p 480 -485
Rhodes, L. (2005) Psychological effects of the supermax
prison. American Journal of Public Health, 95, 10, 1692-1695.
Routledge, Liebling, 1992, Studies in Prison A., London
scandinavica,volume 110,issues s424,p5-59
lii
Singleton, N., Meltzer, H. & Gatward, R. (1998)Psychiatric Morbidity
among Prisoners in England and Wales(Office for National Statistics),
London: Stationery Office.)
Steve Taylor&David field(2003),Sociology of Health and health care.
ThirdEdition,Blacwell pag42-56
Sue Titus,Reid,2000,Crime and Criminology, 9TH edition. United
States, Mccraw-Hill Higher Education. Pag419-434.
Susan Nolen H.2004, Abnormal psychology 3rd edition, p34-36
The British Journal of Psychiatry (2002) ,p 354-359
(http://byprcpsychorg/misc/terms.shttml)
Upswing: report, Paul Hunter reports, 2005
Vikram P. 2003, Where there is no psychiatrist, p3-5; p 195-197
Wanda K. 2006, Psychiatric Mental Health Nursing, University of
medicine and Detistery of New Jery, Lippincott&Wilkins , 6th
edition p8
TASKS TO BE
PERFORMED
DATES TO BE
COMPLETED
PERSONNEL
ASSIGNED TO
TASK
PERSON DAYS
REQUIRED
1.Finalizing
the research
proposal and
submission
Week 1-9
20th June-26th
August
2
Researchers
+1Superviso
r
3persons×67days
=221
2.Ethical
clearance
Week 10-11
27th Aug-3rd
2
researchers
2
persons×7days=1
liii
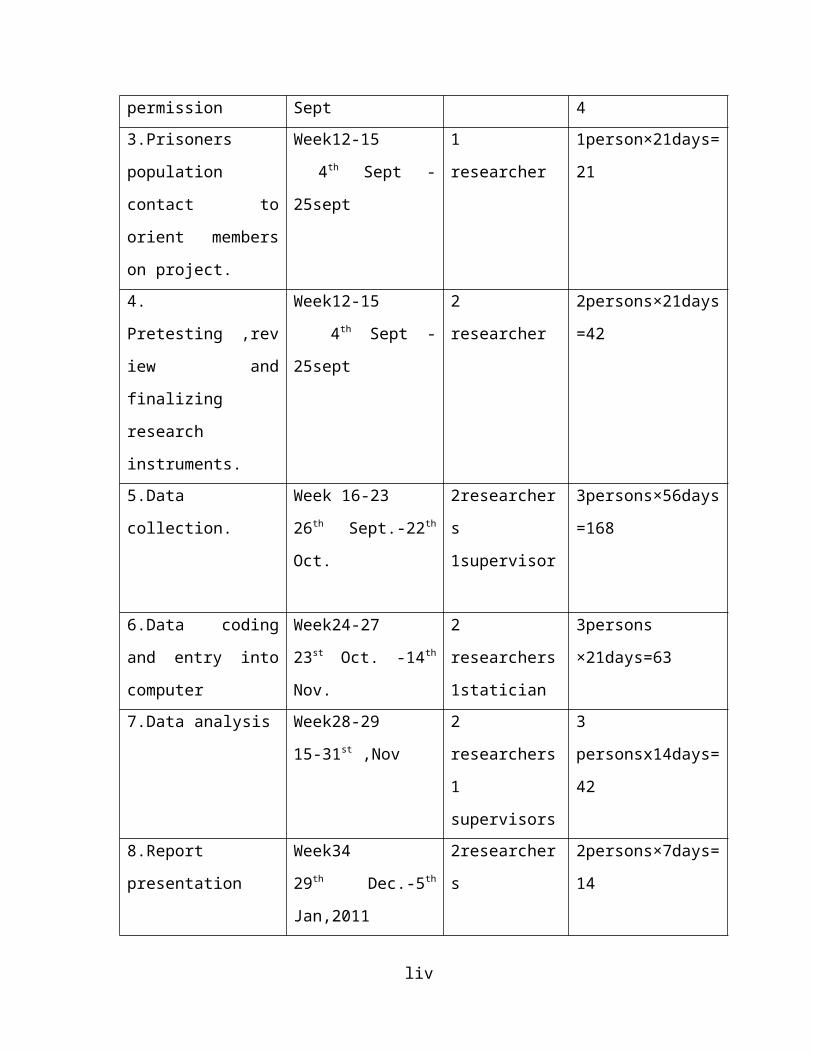
permission Sept 43.Prisoners
population
contact to
orient members
on project.
Week12-15
4th Sept -
25sept
1
researcher
1person×21days=
21
4.
Pretesting ,rev
iew and
finalizing
research
instruments.
Week12-15
4th Sept -
25sept
2
researcher
2persons×21days
=42
5.Data
collection.
Week 16-23
26th Sept.-22th
Oct.
2researcher
s
1supervisor
3persons×56days
=168
6.Data coding
and entry into
computer
Week24-27
23st Oct. -14th
Nov.
2
researchers
1statician
3persons
×21days=63
7.Data analysis Week28-29
15-31st ,Nov
2
researchers
1
supervisors
3
personsx14days=
42
8.Report
presentation
Week34
29th Dec.-5th
Jan,2011
2researcher
s
2persons×7days=
14
liv
9.Report
writing (final
draft)
Week35
6th,Jan-
12th,Jan,2011
2researcher
s
2persons×7days=
14
10.Submission
of final report
Week 36
13th Jan-19th
Jan
2
researchers
2personsx7days=
14
11.feed back to
Butare Prison
staff.
Week 37
20th -26th
,Jan,2010
2
researchers
persons×7days=1
4
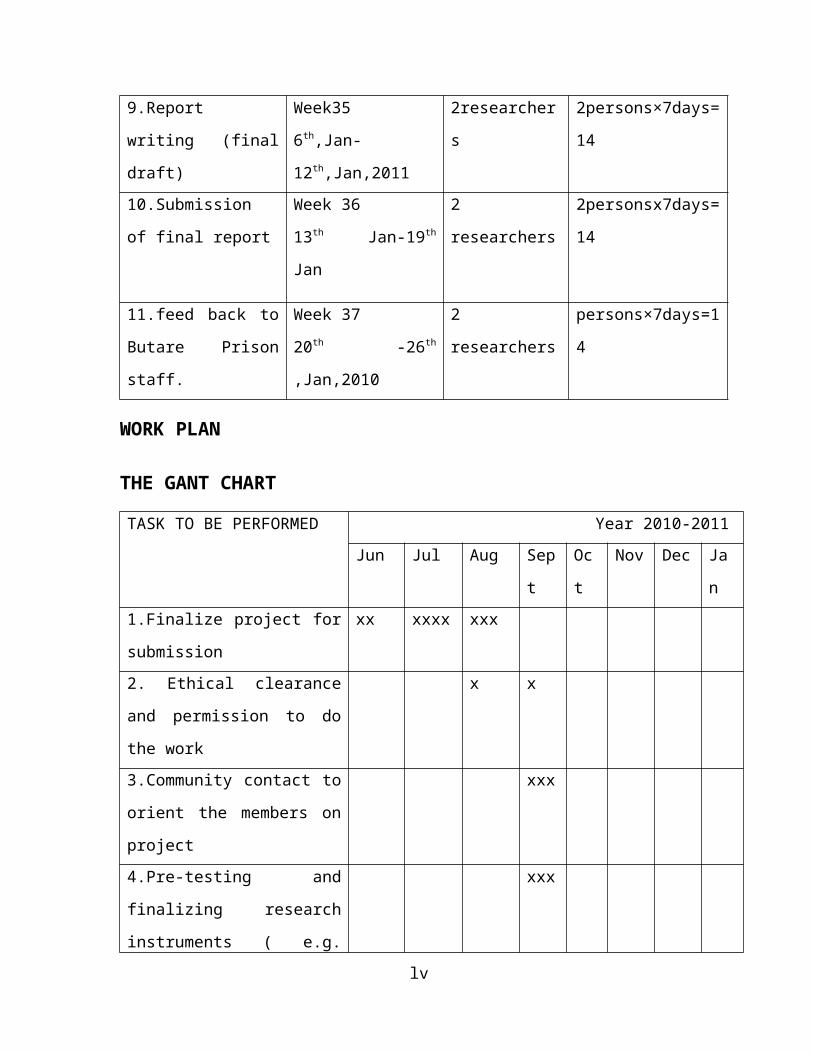
WORK PLAN
THE GANT CHART
TASK TO BE PERFORMED Year 2010-2011Jun Jul Aug Sep
t
Oc
t
Nov Dec Ja
n1.Finalize project for
submission
xx xxxx xxx
2. Ethical clearance
and permission to do
the work
x x
3.Community contact to
orient the members on
project
xxx
4.Pre-testing and
finalizing research
instruments ( e.g.
xxx
lv
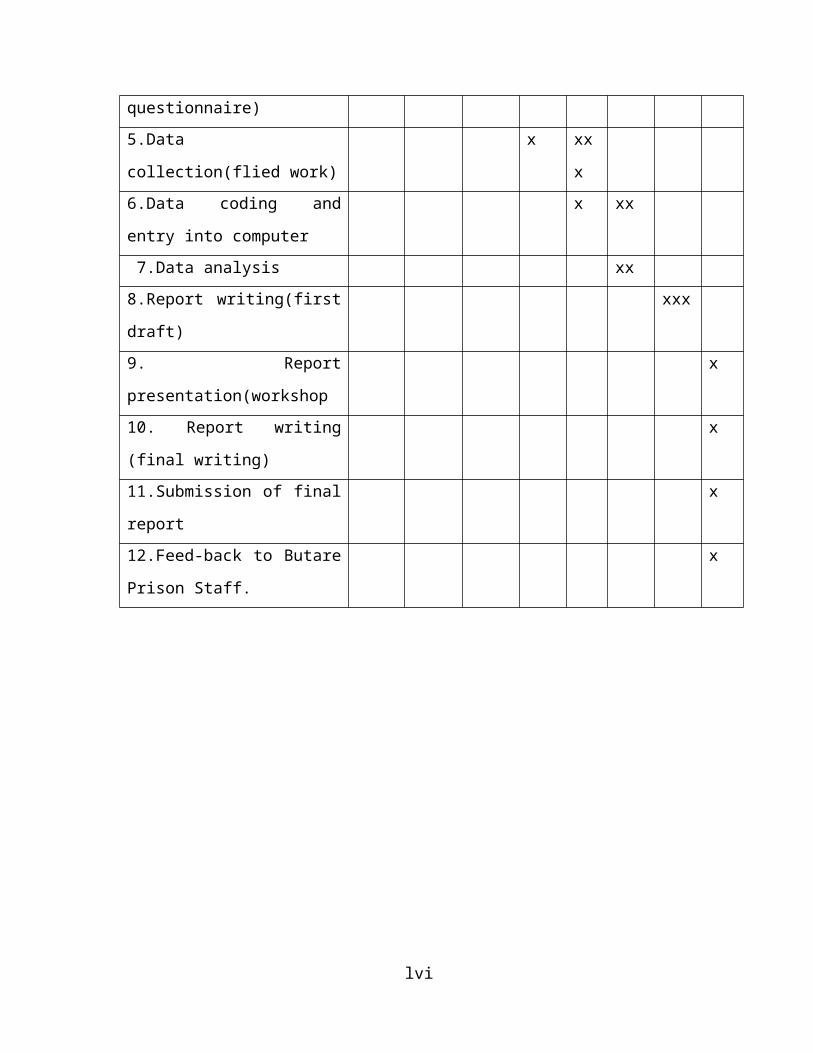
questionnaire)5.Data
collection(flied work)
x xx
x6.Data coding and
entry into computer
x xx
7.Data analysis xx8.Report writing(first
draft)
xxx
9. Report
presentation(workshop
x
10. Report writing
(final writing)
x
11.Submission of final
report
x
12.Feed-back to Butare
Prison Staff.
x
lvi
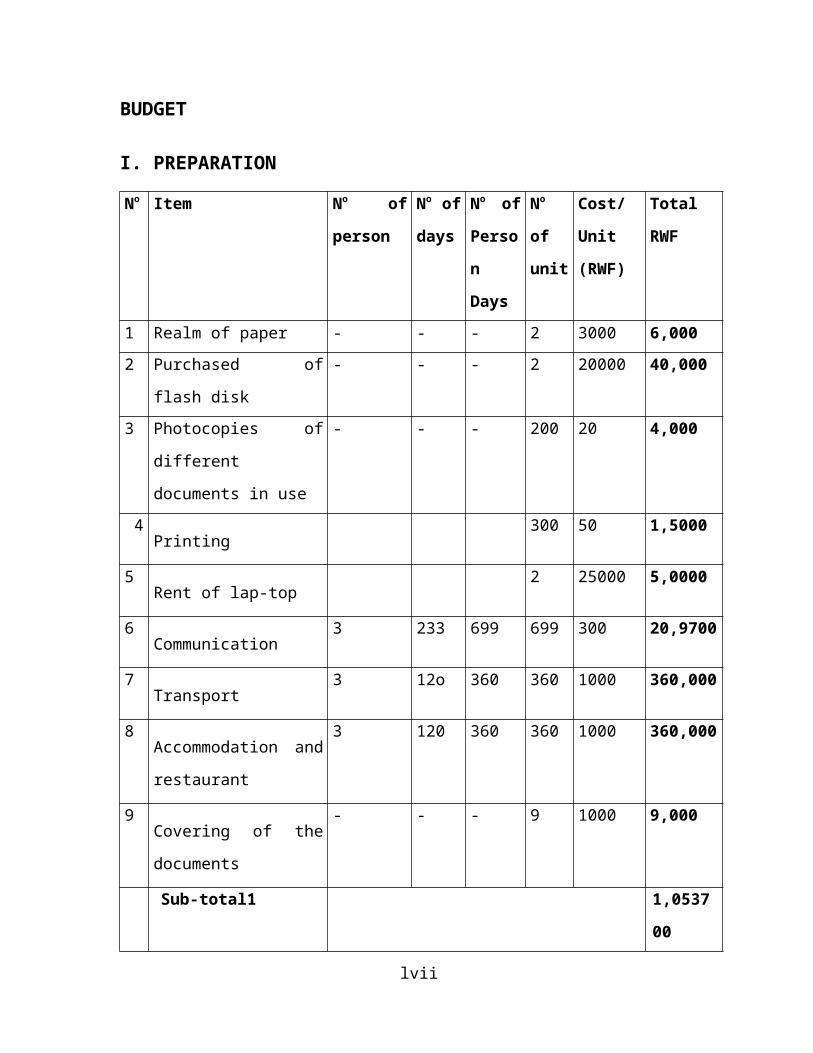
BUDGET
I. PREPARATION
No Item No of
person
No of
days
No of
Perso
n
Days
No
of
unit
Cost/
Unit
(RWF)
Total
RWF
1 Realm of paper - - - 2 3000 6,0002 Purchased of
flash disk
- - - 2 20000 40,000
3 Photocopies of
different
documents in use
- - - 200 20 4,000
4Printing
300 50 1,5000
5Rent of lap-top
2 25000 5,0000
6Communication
3 233 699 699 300 20,9700
7Transport
3 12o 360 360 1000 360,000
8Accommodation and
restaurant
3 120 360 360 1000 360,000
9Covering of the
documents
- - - 9 1000 9,000
Sub-total1 1,0537
00
lvii
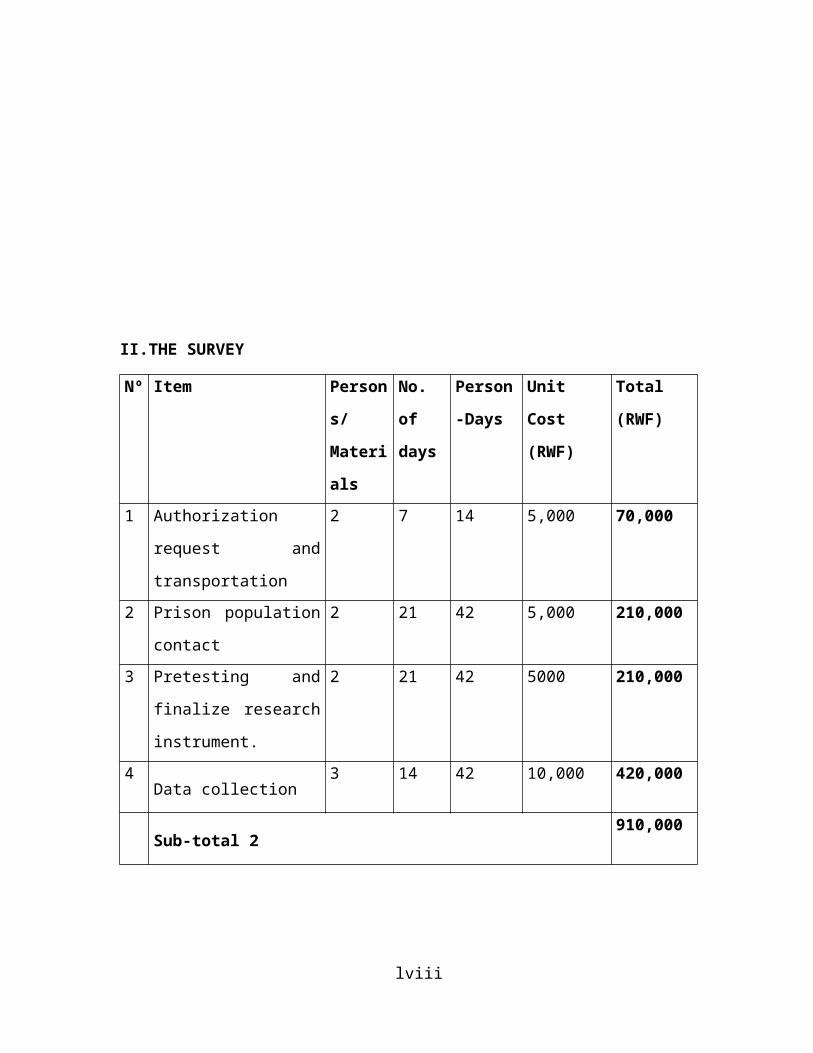
II.THE SURVEY
Nº Item Person
s/
Materi
als
No.
of
days
Person
-Days
Unit
Cost
(RWF)
Total
(RWF)
1 Authorization
request and
transportation
2 7 14 5,000 70,000
2 Prison population
contact
2 21 42 5,000 210,000
3 Pretesting and
finalize research
instrument.
2 21 42 5000 210,000
4Data collection
3 14 42 10,000 420,000
Sub-total 2910,000
lviii
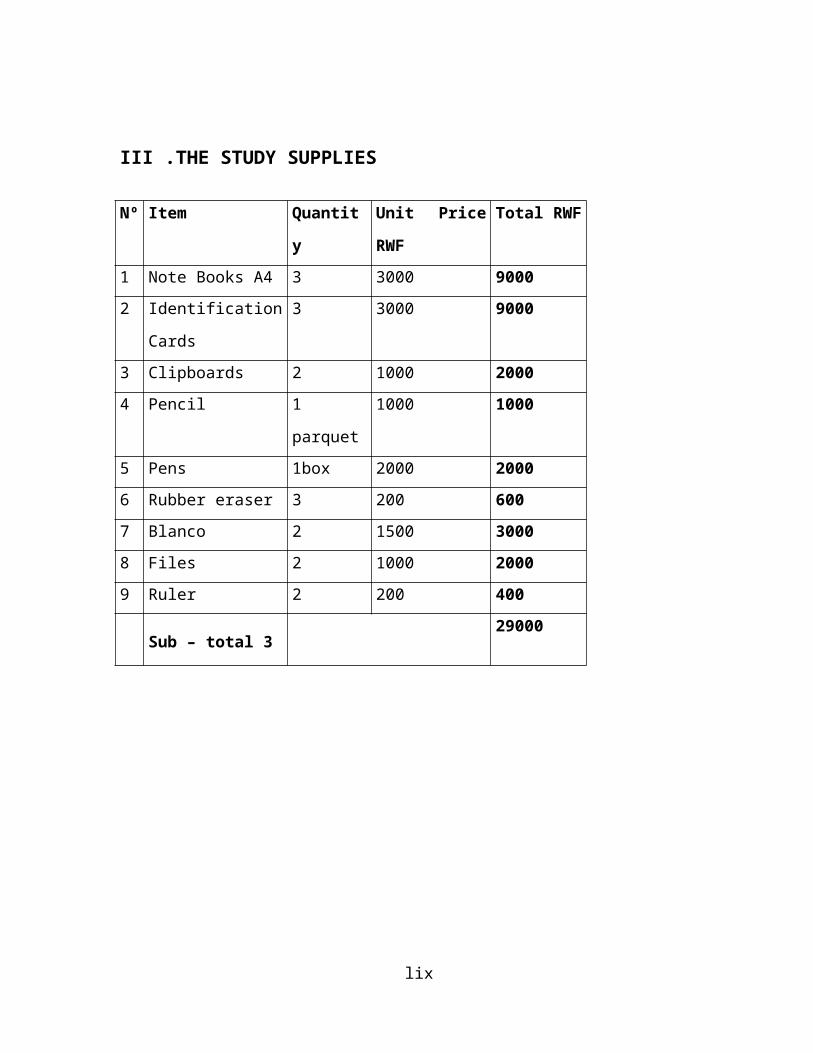
III .THE STUDY SUPPLIES
lix
Nº Item Quantit
y
Unit Price
RWF
Total RWF
1 Note Books A4 3 3000 90002 Identification
Cards
3 3000 9000
3 Clipboards 2 1000 20004 Pencil 1
parquet
1000 1000
5 Pens 1box 2000 20006 Rubber eraser 3 200 6007 Blanco 2 1500 30008 Files 2 1000 20009 Ruler 2 200 400
Sub – total 329000
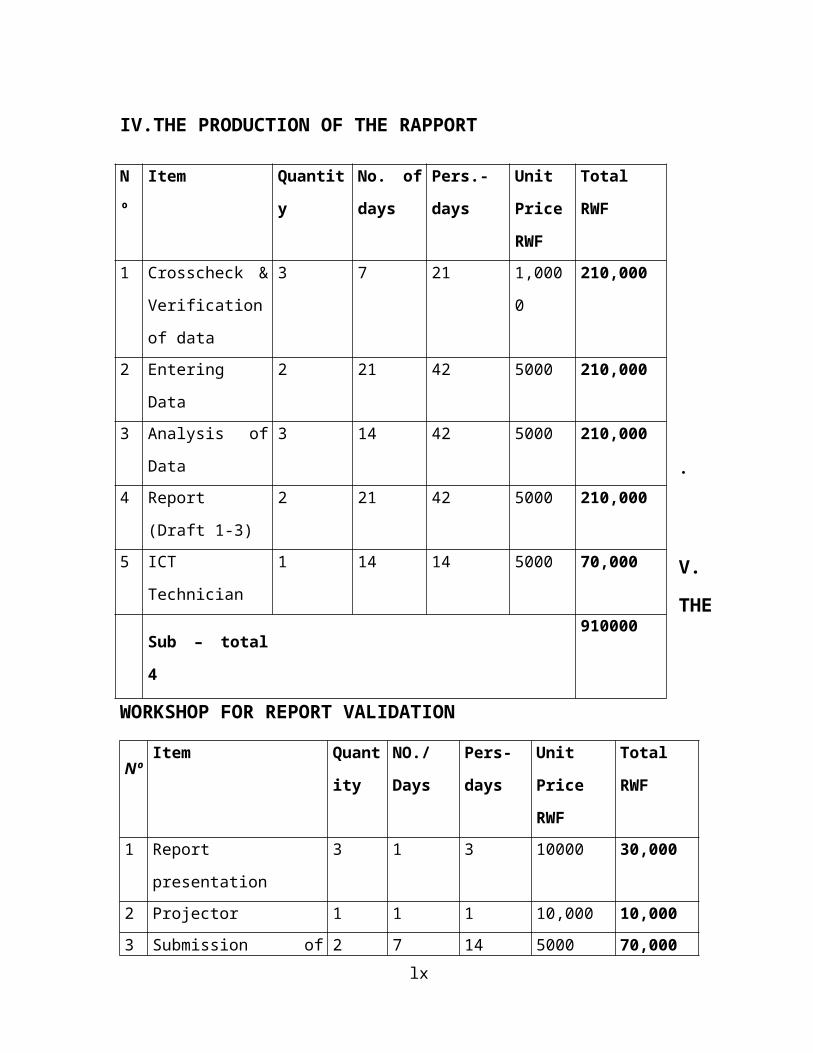
IV.THE PRODUCTION OF THE RAPPORT
.
V.
THE
WORKSHOP FOR REPORT VALIDATION
NºItem Quant
ity
NO./
Days
Pers-
days
Unit
Price
RWF
Total
RWF
1 Report
presentation
3 1 3 10000 30,000
2 Projector 1 1 1 10,000 10,0003 Submission of 2 7 14 5000 70,000
lx
N
º
Item Quantit
y
No. of
days
Pers.-
days
Unit
Price
RWF
Total
RWF
1 Crosscheck &
Verification
of data
3 7 21 1,000
0
210,000
2 Entering
Data
2 21 42 5000 210,000
3 Analysis of
Data
3 14 42 5000 210,000
4 Report
(Draft 1-3)
2 21 42 5000 210,000
5 ICT
Technician
1 14 14 5000 70,000
Sub – total
4
910000
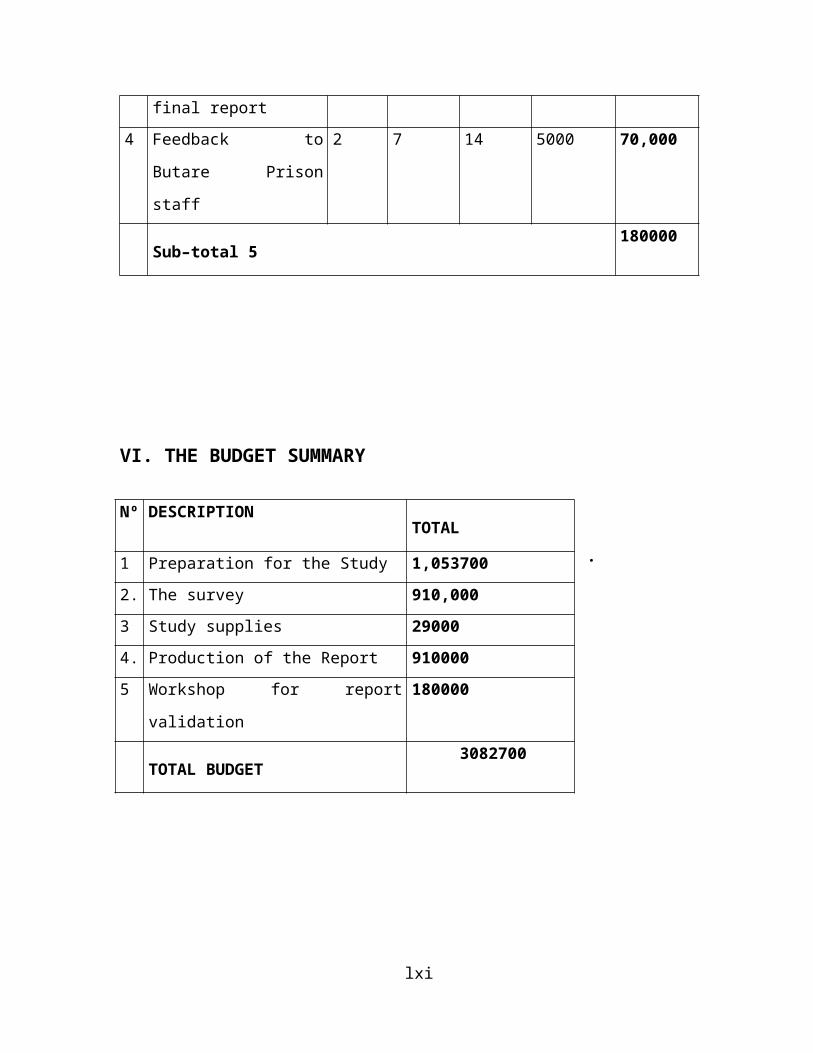
final report4 Feedback to
Butare Prison
staff
2 7 14 5000 70,000
Sub–total 5180000
VI. THE BUDGET SUMMARY
.
lxi
Nº DESCRIPTIONTOTAL
1 Preparation for the Study 1,0537002. The survey 910,0003 Study supplies 290004. Production of the Report 9100005 Workshop for report
validation
180000
TOTAL BUDGET 3082700
BUDGET JUSTIFICATION
One of the factors for success of this survey is financial
availability, our budget is proportional with the following
activities: preparation of the research project requiring
1,053,700; 910,000 for survey;29000 for study
supplies;910,000for production of the study;180,000 for work
shop for report validation and 399,100 for unforeseen.
The total sum will be 3481800 rwfs including all needs for
this study and unforeseen cases which can appear during
implementation of this project.
A.CURRICULUM VITAE OF APPLICANT
I. Identity
Surname: KANGABE Date of
birth: March the 20th ,1987
lxii
Nationality: Rwandese
Fist name: Valentine
II. Academic profile : Qualification; School or
University ;Year
1994-1999:Primary school at Rango Primary school
2000-2006: Secondary school:1-3rd year at Group Scolaire
Notre Dame de Lourdes Byimana
4-6th year at ESI
Rwamagana
2008-2010: Higher education at Kigali Health Institute in
Mental Health Nursing DepartmentIII.Post held: Work experience2006-2007:Served as a nurse at Ruhuha health centerIV.LanguageKinyarwanda : Very good
French : Very good
English : Good
PROFILE OF APPLICANT AND INSTITUTION
lxiii
B.CURRICULUM VITAE OF APPLICANT
I. Identity
Surname: HABYARIMANA Date of
birth: 1st January,1980
Fist name: Charles
Nationality: RwandeseI. Academic profile : Qualification; School or
University ;Year
a. Primary school at Rutonde
b. Secondary school:1-3rd year at Group Scolaire Ste Bernadette
4-6th year at Group Scolaire
official Butare
c.2008-2010 :Higher education at Kigali Health Institute in
Mental Health Nursing DepartmentIII.Post held: Work experience2005-2007:Served as a nurse at Ruhuha health center.IV.LanguageKinyarwanda : Very good
French : Very good
English : Good
Swahili : Good
lxiv
lxv
C.PROFILE OF INSTITUTION
A. Name: Kigali Health Institute (KHI)
B. Address: Po.Box: 3286 Kigali-Rwanda
phone :( +250) 572172 / 571788
Fax: (+250) 571787
e-mail:[email protected]
C. Campuses: KHI has two campuses in different places namely
Kigali and Nyamishaba
D. Faculties: KHI has three faculties: Allied Health Sciences,
General Nursing and Community health sciences.
D.1.Nursing has: General Nursing, Mental Health and Midwifery
departments.
D.2. Allied Health Sciences has: Medical Imaging Sciences,
Dentistry, Physiotherapy, Ophthalmology and Anesthesia
departments, Biomedical Laboratory Sciences.
D.3. Community Health sciences has: Environmental Health
Department
E. Vision of KHI: To be centre of excellence in training and
development of health professionals
G. Mission: “To train and improve the capacity of health
workers”lxvi
In order to realize the above vision and mission, Kigali
Health Institute will have to put special emphasis on the
goals identified in KHI Strategic Plan 2007 - 2012.
H. Budget and resources
H. Administration department.
-Rector: Dr. Ndushabandi Desire
-v/rector in charge of academic affairs and research: Dr.
Kabagabo Chantal
-v/ rector in charge of administration and finance: Mr.Kazige
Eugène
lxvii
APPENDIX
lxviii
1. INFORMED CONSENT LETTER
We, HABYARIMANA Charles and KANGABE Valentine, have the
pleasure to introduce ourselves to you and invite you to
participate in this study: ‘Prevalence of mental disorders
among prisoners of Butare prison’.
The work will be conducted by the researchers and those who
have been chosen to participate will contribute in the
following manner:
They will be observed and interviewed by researchers.
They will also have to respond to some oral questions.
The information gathered during this study will remain
confidential. You do not have to identify your names.
Thank you for your good understanding.
2. INTERVIEW GUIDE (English Version)
2. a. Identification
i. Age distribution
18 to 24 years old
25 to 31 years old
32 to 38 years old
39to 45 years old
46 to 52 years old
53to 59 years old
60 to66 years oldlxix
67 o 73 years old
ii. Gender Male
Female
2. b. Questionnaires for assessment of mental disorders
symptoms trough interview and observation
I. MOOD DISORDERS
Have you ever had the following symptoms for a period of two
weeks?
Depressed mood
Apathy
Pessimism
Sense of loneliness
Suicide ideation
Fatigue/loss of drive
Hypersomnia
Insomnia
Psychomotor retardation
grandiosity
Aggressiveness more
talkative than usual
lxx
Fright of ideas
increase in goal directed activity
Impairment in occupational functioning or in usual social
activities without a known
cause (e.g. drug abuse, a medication or a general medical
condition
Others (specify)
……………. ………….
…………….
…………..
II. PSYCHOTIC DISORDERS
Have you ever had two or more of the following symptoms?
Illusion
Disorganized speech
Hallucination
Affective flattening
Delusion
Other thought disorders
Others (specify)
……………. ………….
…………….
…………..
lxxi
III. ANXIETY DISORDERS
Have you ever had some of the following symptoms?
Restlessness or feeling keyed up or on edge
Being easily fatigued
Difficulty concentrating or mind going blank
Being Irritable
Sleep disturbance
A fear of that you are going mad
Felling of panic
Being detached from oneself
Feeling not in control of your action or detached from your
surrounding
Repeated thoughts or flashbacks of traumatic experiences
Trembling or shaking
Others (specify)
……………. ………….
…………….
…………..
IV. ALCOHOL AND DRUG MISUSE
a. Do you regularly take one or more drugs and/or alcohol
to change or to manage:
lxxii
Your mood
Your emotion
The state of your conscious
b have you ever had the following problems during a period
of 12 months?
Taking a large amount of drug
Physical hazardous
Withdraw syndrome
Failure to fulfill major role obligation because
alcohol or drug
Others ( specify)
……………. ………….
…………….
…………..
UMUGEREKA (Version Kinyarwanda)
1. Amabwiriza
Twebwe HABYARIMANA Charles na KANGABE Valentine, dushimishijwe
no kubibwira tukanabashishikariza kwitabira ubu bushakashatsi
bugamije kugaragaza ubwiganze bw’indwara zo mu mutwe muri
gereza ya Butare. Iki gikorwa tuzagikorana n’abazaba bemeye
kwitabira ubu butumire, kandi bizakorwa mu buryo bukurikira :
Abitabiriye, hari ibibazo bazasubiza imbonankubone.
Amakuru yose azaturuka muri ubu bushakashatsi ni ibanga, niyo
mpamvu udasabwa kugaragaza amzina yawe.
Tubashimiye ubufatanye bwanyu.
2. INTERVIEW GUIDE (Kinyarwanda Version)
lxxiii
a. Irangamimerere
Imyaka
18 - 24
25 - 31
32 - 38
39- 45
46 - 52
53- 59
60 -66
67-73
Igitsina Gabo
Gore
2. b. Ibigaragaza ko umugororwa afite ibibazo byo mu mutwe
binyuze mu kiganiro.
Indwara z’agahinda /ibyishimo birenze.
Waba warigeze ugaragaza bimwe mu bimenyetso bikurikira?
Agahinda
yego oya
lxxiv
Gucika intege
yego oya
Guta icyizere
yego oya
Kumva uri wenyine
yego oya
Gushaka kwiyahura
yego oya
Kunanirwa no kubura ubushake yego
oya
Gusinzira cyane
yego oya
Kudasinzira
yego oya
Kubura intege yego
oya
Kubura amahwemo
yego oya
Kugira amahane
yego oya
Kumva uri umuntu ukomeye Yego
oya
Kugira amagambo menshi bidasanzwe Yego
oya
Kugira ibitekerezo byinshi byisukiranya Yego
oya
lxxv
Kugira ibyishimo birenze urugero Yego o
oya
Gukorana ingufu nyinshi kandi utananirwa Yego
oya
Kutuzuza inshingano zawe no kunanirwa kubana
n’abandi
Yego oya
Ibindi
……………. ………….
…………….
…………..
b. Indwara z’imitekerereze n’ibyumviro.
Waba warigeze ugaragaza bimwe mu bimenyetso bikurikira ?
Kumva (ibyumviro ) bidasanzwe yego
oya
Kumva (ibyumviro ) ibitariho yego
oya
Imitekerereze idasanzwe yego
oya
Izindi ndwara zimitekerereze yego
oya
Kugira amagambo atajyanye yego
oya
Guhindagurika mumaranga mutima yego
oya
lxxvi
Ibindi
……………. ………….
…………….
…………..
c.Indwara z’ ubwoba
Waba warigeze ugaragaza bimwe mu bimenyetso bikurikira ?
Guhorana impungenge
yego oya
Kunanirwa vuba
yego oya
Kumva ufite umushiha
yego oya
Kudasinzira neza
yego oya
Kumva ugiye guta umutwe
yego oya
kunanirwa gufata gahunda
yego oya
Guhorana igihunga
yego oya
lxxvii
Kugarukirana kw’amashusho y’ibyakubayeho.
Yego oya
Ibindi
……………. ………….
…………….
…………..
d. Inzoga n’ibiyobyabwenge
a.Waba ukunze gukoresha inzoga cyangwa ibiyobya bwenge kugira
ngo bigufashe kugenzura:
Ibyishimo cyangwa agahinda
yego oya
Amarangamutima
yego oya
Imitekerereze
yego oya
b.Waba warigeze uhura n’iki kibazo kubera gukoresha inzoga
cyangwa ibiyobyabwenge mu gihe kingana n’umwaka?
Kungero urugero rw’ ikiyobyabwenge wafataga yego
oya
lxxviii
Kubura amahwemo igihe utabonye ikiyobya bwenge yego
oya Kunanirwa kuzuza inshingano zawe zaburi
munsi yego oya
Ibindi
……………. ………….
…………….
…………..
APPLICATION LETTER FOR CARRYING OUT RESEARCH
lxxix
Kigali Health Institute
Faculty of Nursing Sciences
Department of Mental Health
September, the 7th, 2010
To: The General Director Butare Prison
RE: Request for permission to carry out a research
Dear Sir/ Madam,
We would like to conduct a research on “prevalence of mental
disorders among prisoners at Butare prison.”
We humbly request your authorization to carry out our proposed
research study.
We look forward to your favorable response.
Faithfully yours,
lxxx
Students,
Charles HABYARIMANA
And
Valentine KANGABE
Kigali Health Institute
Department of Mental Health
PO.BO 3286
September, the 7th, 2010
To: The President of the KHI research committee.
Re: Requesting for the authorization for conducting a
research.
lxxxi
Dear Sir,
We humbly wish to request your authorization to conduct the
study. In fact, we are finalist students at KHI Department of
Mental Health our study will evaluate “the prevalence of
Mental Disorders among prisoners population at Butare prison”
Your favorable response shall be highly appreciated.
Faithfully yours,
Students,
Charles HABYARIMANA
And
Valentine KANGABE
lxxxii





























