Embed Size (px)
Citation preview
Predicting Anxiety Among Patients In LPU Clinical Dispensary During Dental Treatment: Towards Student’s Clinical
Performance Enhancement
By: Maribel D. Mayuga-Barrion, D.D.M., M.A.T.
Dental anxiety is very common in dental procedures. Anxiety can come
from many different sources. Most of the time, patients become anxious during
tooth extraction and other dental procedures that needs needle injection of
anesthetic solution. Patients also differ in degree of anxiety.
Reasons for anxiety are as different as people, but some are more
common than others. The most common sources is a past bad experience. This
is most often from childhood experiences before modern anesthesia and
techniques. Another source is phobias of the sights and sounds of the dental
office. Many patients do not like the sounds of drills but unfortunately, they are a
necessity. Some patients are simply afraid of needles, and this is very
understandable.
One of the primary reasons that most people avoid visiting the dentist and
seeking dental care, is dental anxiety. Whether this stems from a previous bad
experience, the media, or friends who have told them horror stories, the result is
that they neglect to maintain their dental health by avoiding visits to the dentist,
and in turn create more problems.
As we know, the key factor for good oral hygiene is prevention – stopping
problems before they arise. Unfortunately, phobic patients who suffer from
2
severe anxiety do not visit the dentist for regular care. This results in more
complex problems.(www.floss.com)
Like reasons for anxiety, degrees also differ from person to person. Some
folks are simply a bit nervous anytime they walk into a dental office. They can
have slightly elevated blood pressures once they pull into the parking lot which
goes down as fast as they exit the front door.(Eddelmen, 2012)
Other patients get uncomfortable when they see a needle or hear the drill.
Many patients are nervous about the anesthetics. Some patients can be so
uncomfortable that they have an increased risk for stroke or heart attack due to
the spike in blood pressure that anxiety can produce. Many of these patients
avoid dental work altogether which only worsens their problems later
Other patients, with severe dental fear, cannot sit still when the dentist is
working which endangers them due to the instruments in close proximity to the
face/eyes/mouth. This also makes work extremely difficult for the dentist not
allowing him to do a good job.
According to Dr. Neipris, (2010), it's common to feel some anxiety about
going to the dentist. A phobia is a much stronger feeling. People with dental
phobia are terrified of seeing a dentist. They may never see a dentist, even when
they are suffering from bleeding gums or a broken tooth. What's more, there is no
clear boundary between dental anxiety and a phobia.
You may have dental anxiety or phobia if: the thought of going to the
dentist makes you ill, you have trouble sleeping the night before a dental visit,
3
you feel like crying when you have to see a dentist, you panic when objects are
placed in your mouth during a dental exam.
Bad experiences, usually reaching back to childhood, are a major source
of dental anxiety. Keep in mind, though, that dental care has improved
dramatically over the last 20 years. Pain-free treatments and techniques other
than drilling are commonplace today.
Sitting in the dental chair - just like flying in an airplane - is a situation
where you have little control over what is going to happen. It's common to
be anxious about that.
If you haven't seen a dentist in a while, you may be embarrassed about
the appearance of your teeth. You may become self-conscious and insecure and
you may avoid smiling. In extreme cases, a person's personal and professional
lives may start to suffer. (Neipris, 2010).
It is very important to have a dentist who understands your fears, takes
them seriously, and works with you to overcome them.
If you fear pain, ask for a topical anesthetic to minimize the discomfort of
cleanings and minor gum treatments. A local anesthetic numbs your mouth
completely for a few hours and blocks out all pain.
If the sound of the dentist's tools bothers you, bring a music player with
you to the appointment and wear headphones. Music also helps in different
relaxation techniques. Guided imagery can take your mind off the things going on
around you. Imagine yourself in a pleasant place. For example, imagine the feel
4
of the gentle breeze on your face and the sound of ocean waves breaking
against the shore.
Most importantly, get regular checkups. You'll become familiar with the
dentist and you'll be able to catch problems early, before they become major.
Little is known about the anxiety of patients experience before attending
for dental treatment. The aim of this study is to determine, in dentally phobic
patients.
Self-reported dental fear measures seldom are used in clinical practice to
assess patients’ fears. This examined how well dental fear measures predicted
anxious behaviors displayed during dental treatment.
One of the most prevalent fears is the fear of dentistry. According to the
Diagnostic and statistical manual of mental disorders (DSM-IV), severe dental
anxiety should be considered a specific phobia. This is defined as a clinically
significant anxiety provoked by exposure to a specific feared object or situation,
often leading to avoidance behavior and/or significantly interfering with the
person’s normal routines, occupational functioning, social activities or
relationships (DSM-IV, 1994). Thus, dental fear is a widespread problem, which
can have significant impact on the individual’s health and daily life. It has been
suggested that dental anxiety creates its own vicious circle in which the phobic
patients’ inability to accept dental treatment leads to a real or perceived
deterioration of oral health, which in each turn can create feelings of shame, guilt
and inferiority, subsequently reinforcing fear and anxiety (Berggren, 1994).
Moore et al. (1991) proposed that feelings of powerlessness and embarrassment
5
in the dental situation were important social determinants in the acquisition and
maintenance of dental anxiety. They referred to the “vicious circle” suggesting
that with the passing time of avoidance, social conflicts reinforce anxiety and
result in further avoidance of dental care. In addition, it has been proposed that
the social factors appear to contribute strongly to the maintenance of dental fear ,
especially in long-term avoiders (Berggren, 1994). Berggren found that a majority
of dental phobic patients felt that they had to curtail their social relations, and
many reported widespread negative social life effects. This included family
relations and perceived social support and provides further support to the vicious
circle (Berggren, 1993).
With the aforementioned, the researcher believes that dental anxiety
causes patients to refuse dental treatments that lead to deterioration of their oral
health. Student clinicians had difficulties in handling anxious patients. Thus, the
researcher had an idea of conducting this research to investigate the patient’s
anxiety during dental treatments so that it can help the student clinicians to
improve their clinical practice and to render dental services to patients without
anxiety.
Furthermore, the researcher believed that this study will have significant to
the patients, clinicians and clinical instructors by providing an insight in
increasing the emphasis of anxiety management in health education. On the
other hand, student clinicians would have more insights on how to be more
responsible for the anxiety their patients experience and would have better
6
understanding on the role of anxiety management to enhance their clinical
performance.
Objectives of the Study
In this study, the researcher was anchored by the following objectives: 1)
to determine the respondents’ profile in terms of age, gender, frequency of
dental visit, and type of patient whether dental phobic or not; 2) to determine the
dental anxiety of patients in LPU dental dispensary; 3) to identify the causes and
severity of anxiety of the patients in LPU dental dispensary; 4) to determine if
there is a significant difference between the respondents’ demographic profile
and their level of anxiety; and lastly, 5) to propose a program that will help the
patients cope with dental anxiety and a program that will enhance the students’
clinical performance.
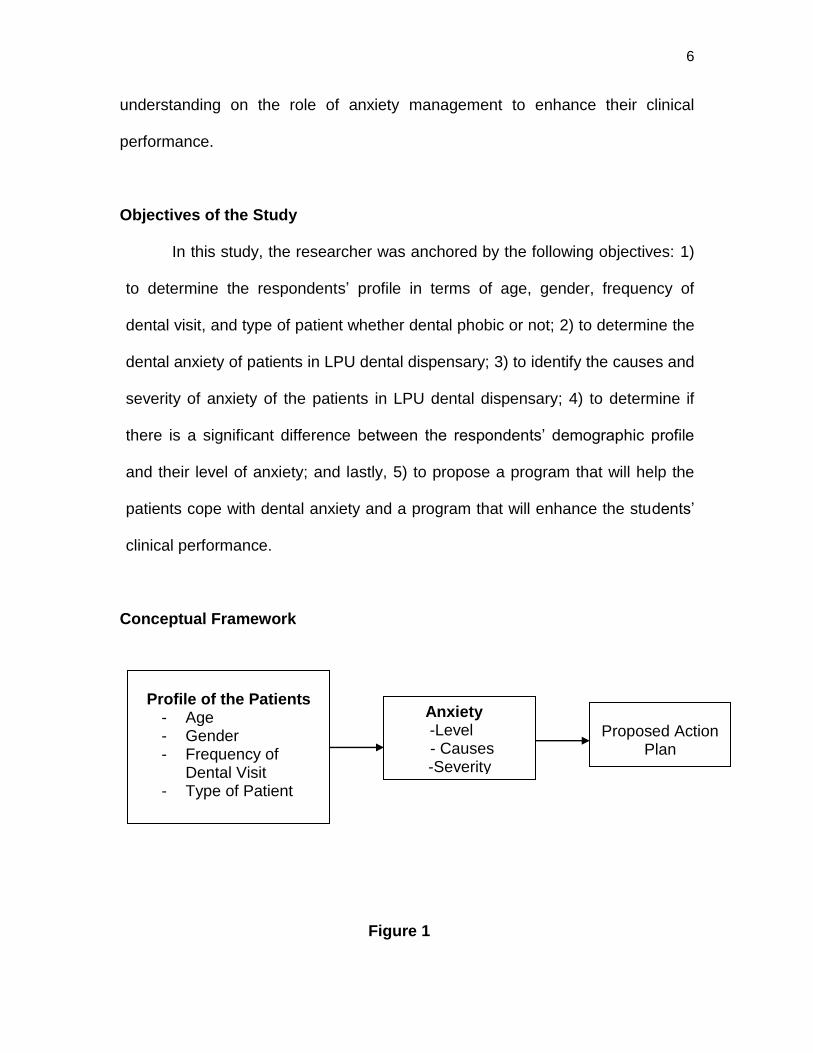
Conceptual Framework
Figure 1
Profile of the Patients
- Age - Gender - Frequency of
Dental Visit - Type of Patient
Anxiety -Level
- Causes -Severity
Proposed Action
Plan
7
Dental anxiety is a multidimensional complex phenomenon, and no one
single variable can exclusively account for its development. A number of factors
that have consistently been linked with a greater incidence of dental anxiety,
including: personality characteristics, fear of pain, past traumatic experiences
particularly in childhood, blood-injury fears and the influence of dentally anxious
family members or peers which elicit fear in a person.
Fear of pain has been linked strongly to the development of dental anxiety
and to avoidance of dental treatment. Highly anxious patients tended to
overestimate the pain experienced when asked to recall it.
The restorative dentistry procedures deliver the most potent triggers for
dental anxiety, namely, the sight, sound and vibrational sensation of rotary dental
drills, coupled with the sight and sensation of a dental local anesthetic injection.
It is for this reason that anxious patients who must undergo restorative
procedures are often managed using the “4S” rule (sight, sound, sensations, and
smell), which aims to reduce the triggers of stress. A patient’s expectation of
experiencing pain, being hurt, and choking or gagging during treatment can also
act as a major trigger for dental anxiety.
It is also important to recognize other factors which can trigger anxiety or
increase it. Aspects of dentist-patient interactions are particularly important.
These include statements made by the operator, in particular when they are
angry or if they make comments. Furthermore, dentally anxious patients have
complained that dentists made them feel guilty for being anxious.
8
The period of time spent waiting for dental treatment is cited commonly by
patients as being anxiety-provoking, as it increases the time to think about what
will happen, and to ponder the worst-case outcomes. This emphasizes the need
for support staff in the dental practice to be aware of an anxious patient and to
actively take measures to reduce their concerns.
Literature Review
In the field of dentistry, knowledge and technical skills are not the only
prerequisites for good practice. An ability to communicate effectively with patient-
in particular, to use active listening skills, to gather and impart information
effectively, to handle patient emotions sensitively, and to demonstrate sympathy,
rapport, ethical awareness, and professionalism—is crucial. Among the benefits
noted when dentists/clinicians demonstrate effective communication skills are
increased patient satisfaction, improved patient adherence to dental
recommendations, decreased patient anxiety, and lower rates of formal
complaints and malpractice claims. (Hannah, et. al 2004)
Dental Anxiety or Dental Fear
Dental fear refers to the fear of dentistry and of receiving dental care. A
severe form of this fear (specific phobia) is variously called dental phobia,
odontophobia, dentophobia, dentist phobia, or dental anxiety. However, it has
been suggested not to use the term "dental phobia" for people who do not feel
their fears to be excessive or unreasonable and resemble individuals with post-
9
traumatic stress disorder, caused by previous traumatic dental experiences.
(Bracha, et. Al, 2006)
Dental anxiety is common and affects people of all ages. There are
different levels of dental anxiety, ranging from slight nervousness to a severe
phobia (an out-of-proportion fear that makes you steer clear of certain situations).
Being nervous about going to the dentist affects people in different ways.
Some people are anxious about specific aspects of dental treatment. Others may
dislike being in close contact with someone they don't know very well. Many
people had unpleasant experiences as a child and are frightened that these will
be repeated. However, nervous or fearful one is when having dental treatment,
there are a number of things one can do to help you overcome your anxiety.
There are also different levels of dental anxiety, ranging from slight
nervousness to a severe phobia (an out-of-proportion fear that makes you avoid
a certain situation). However anxious one may be, it's likely there will be ways of
dealing with the problem one step at a time.
The first step is to get in touch with one’s dentist and talk about his/her
anxiety. It is important to remember that he or she will understand if the patient is
anxious about having treatment.
One way of finding a supportive dentist is by word of mouth. One may be
able to get a recommendation from friends or family. Or one could make some
phone calls to find out which dentists in your area specialize in treating people
with anxiety. When one call, be open about one’s worries so that the staff can
10
arrange the support he/she needs. One may be able to book an appointment with
his/her dentist just to discuss all the worries he/she has.
According to Rocha (2010), one of the difficulties encountered by the
clinician during dental care is the fear that some patients express with respect
to procedures which will take place during their visit. Coming to their dental
appointments may represent a major problem for these patients.
Fear is a primary and powerful emotion which alerts us about imminent
danger, with respect to an object or situation. When danger is recognized, the
individual reacts with a set of behavioral and neurovegetative responses which
are accompanied by a disagreeable sensation.
When danger is not evident, but presents itself in a vague and persistent
manner, or when signs of imminent danger are not consciously perceived, it is
denominated a state of apprehension, in which the existence of anxiety may be
verified. It is not consciously controlled, that is, people do not have the capacity
to interrupt it. Anxiety also aggravates psychological suffering caused by pain.
Childhood is the critical period for the development of anxiety.
Approximately one fourth of the adult American population regularly avoids
dental treatment due to traumatic experiences which occurred during this period.
(Anderson, 1997). People who suffer from intense dental fear are known to be
more difficult patients among dentists and dental students. (Kaakko, et. Al, 1999)
Almost 7% of the general population state they suffer from intense fear of
dentistry, while another 13% state they feel some degree of fear. In Brazil, there
is a 15% prevalence of dental anxiety. (Rocha, 2010)
11
While assessing a short version of the Dental Anxiety Inventory,
Aartman(1998) found that highly anxious dental patients were most anxious
about tooth extraction, followed by drilling.
Rosa & Ferreira, (1997) also stated there was an association between fear
and poor oral health. This could be the result of less frequent attendance to
dental services by patients who fear treatment.
Usually, patients who suffer from dental anxiety wait longer periods of time
before scheduling an appointment and often cancel it. Among the major reasons
given for avoiding dental visits are costs (75.4%) and fear (36.9%) of treatment.
Twenty-three percent of the people who did not regularly attend dental services,
stated that fear was the reason for non-attendance. (Haugejorden, et. Al, 2000)
According to Milgrom et al (1998), patients under forty years old may be
1.5 times more anxious than those over forty. Another finding mentioned in the
literature is that women tend to report higher levels of anxiety than men.(Liddel,
1997)
In emergency dental services, both in private and in dental school clinics,
the reason for attendance is, in the majority of cases, a complaint of pain.
Clinical practice suggests that levels of anxiety and fear among emergency
patients coming to a clinic are greater than in the general population.
Since a delay in seeking care may be due to dental anxiety or fear, this
study proposed to assess the frequency of anxious patients attending a dentistry
school’s emergency clinic, associating anxiety to the undertaken procedure,
time elapsed since the last visit to the dentist, time since the symptoms
12
appeared, previous history of trauma and socio-economic characteristics of the
sample. (Haugejorden, et. Al, 2000)
Persons with special health care needs due to physical and cognitive
impairment can be at increased risk for dental disease which can be attributed
to, as well as exacerbate, existing medical conditions. This study assessed the
nature of perceived barriers to obtaining oral health care among a special-needs
population and the influence of these factors (in particular, fear and anxiety) on
utilization of dental services. A total of 27.9% of the sample reported fear/anxiety
about dental visits, with approximately half of those reporting to be very nervous
or “terrified”. There was an inverse relationship between the frequency of dental
visits and the proportion of respondents reporting themselves as very nervous or
terrified, and between the perception of oral health status and the level of dental
fear/anxiety (P < 0.001). A large difference was reported between patient
preference for pharmacologic modalities for anxiety control and those received
at dental visits, with 40% of the youngest age group indicating that they would
go to the dentist more frequently if sedation or general anesthesia were offered.
The levels of self-reported fear/anxiety and the high proportion of respondents
indicating an unmet need for adjunctive anesthesia services suggest that
fear/anxiety acts as a barrier to dental care among this special-needs group
which could be ameliorated with greater use of these services. (Dionne, et. Al,
2008)
The 1998 Adult Dental Health Survey (Kelly et al., 1998) found that 64% of
respondents were nervous about some form of dental treatment, and 49% were
13
anxious about simply going to the dentist. This fear can then lead to avoidance of
dental treatment (Mellor, 1992), dental neglect (Hakeberg et al., 1993), and a
reduced general quality of life (Locker, 2003; McGrath and Bedi,
2004; Mehrstedt et al., 2004). Eventually, dental neglect can lead to pain, when
many patients seek treatment. This is often undertaken at a referral hospital
under conscious sedation.
Conscious sedation is a technique used to reduce anxiety while
undertaking dental treatment. However, little is known about the patient’s anxiety
in the period before attending for treatment under sedation. A study of Cohen,
et.al, (2000) discusses the impact of dental anxiety on quality of life in the days
leading up to treatment; however, due to the fact that the data are qualitative, the
frequency or severity of these quality-of-life effects is not reported. More
objective research is required to assess anxiety and quality of life in anxious
dental patients.
When fears arise that are considered out of proportion to the demands of
the situation, cannot be explained or reasoned away, are beyond voluntary
control, and lead to avoidance of the feared situation, then a phobia is said to
exist (Marks, 1969). The aims of this study were to determine, in phobic dental
patients scheduled to undergo dental treatment under conscious sedation, (a) the
temporal relationship of experienced anxiety levels in the days prior to the dental
procedure, and (b) the level of disruption to daily life activities
Little is known about the anxiety patients experience before attending for
dental treatment. The aim of this study was to determine, in dentally phobic
14
patients, the temporal relationship of pre-operative anxiety levels, and the
disruption to daily life caused by this. Twenty-four phobic and 19 comparison
(non-phobic) dental patients were recruited. Four validated questionnaires were
used to assess anxiety and quality of life, which each patient completed for 5
days prior to, and on the day of, treatment. Those in the experimental group were
found to have significantly greater levels of dental and general anxiety, and a
significantly lower quality of life compared with those in the comparison group.
Significant temporal relationships were found with all of the questionnaires.
Dental and general anxiety scores were significantly correlated with quality-of-life
measures. This study suggests that phobic dental patients are experiencing
significant increased anxiety, and significant negative quality-of-life effects, in this
period.
Phobic dental patients are experiencing significant increased anxiety, and
significant negative quality-of-life effects, before attending for dental treatment.
It is estimated that as many as 75% of US adults experience some degree
of dental fear, from mild to severe. Approximately 5 to 10 percent of U.S. adults
are considered to experience dental phobia; that is, they are so fearful of
receiving dental treatment that they avoid dental care at all costs. Many dentally
fearful people will only seek dental care when they have a dental emergency,
such as a toothache or dental abscess. People who are very fearful of dental
care often experience a “cycle of avoidance,” in which they avoid dental care due
to fear until they experience a dental emergency requiring invasive treatment,
which can reinforce their fear of dentistry. (Armfield, JM, et.al 2007)
15
Women tend to report more dental fears than men, and younger people
tend to report being more dentally fearful than older individuals. People tend to
report being more fearful of more invasive procedures, such as oral surgery, than
they are of less invasive treatment, such as professional dental cleanings,
or prophylaxis. (Stabholz, et.al 1999)
Dental phobia is the serious, often paralyzing fear of seeking dental care.
It has been reliably reported that 50% of the American population does not seek
regular dental care. An estimated 9-15% of all Americans avoid much needed
care due to anxiety and fear surrounding the dental experience.
In terms of your dental health and overall well-being, this can have serious
ramifications. Besides chronically infected gums and teeth which can affect your
medical status, your ability to chew and digest can be seriously compromised.
Without healthy gums and teeth, your speech can be affected as well. Your self
confidence can be compromised if you are insecure about your breath and smile.
This can lead to serious limitations in both your social and business
environments. (Nicholas, et. al., 2008)
Causes of Dental Anxiety
It has been found that there are two main causes of dental fear in patients:
Direct Experiences and Indirect Experiences.
Direct experience is the most common way people develop dental fears.
We’ve found that a majority of people report that their dental fear began after a
traumatic, difficult, or painful dental experience. These reasons of course are not
the only explanations of dental anxiety. Another contributing factor is simply the
16
perceived manner of the dentists as “impersonal”, “uncaring”, “Uninterested” or
“cold” whereas dentists who are perceived as warm and caring actually
counterbalance the fear caused by painful procedures.
Indirect experience can include vicarious learning, mass media, stimulus
generalization, helplessness and perceived lack of control. Through vicarious
learning one may develop an anxiety simply by hearing of other peoples painful
and traumatic experiences at their dentist’s office. Mass media has negative
portrayal of dentistry in television shows and children’s cartoons. (Dental Fear
Central, 2007)
Stimulus generalization is another indirect experience causing a patient to
develop a fear as a result of a previous traumatic experience in a non-dental
context. A major contributor of stimulus generalization is a patient’s traumatic
experience at hospitals or general practice doctors that wear white coats and
have antiseptic smells throughout their practices. A way that a lot of dental
practicioners have been combating this perception is by wearing clothing that
isn’t so “lab coatish”.
Helplessness and perceived lack of control occurs when a person believes
that they have no means of influencing a negative event. Research has shown
that a perception of lack of control leads to fear whereas a perception of having
control lessens fear greatly. For example, a dentist that tells a patient to raise
their hand during a procedure to signal pain so that the dentist or hygienist can
stop during the procedure will generate a much less fearful and anxious patient
17
thus creating a more pleasant general experience influencing the patient to
continue to come back for additional treatment.
Dental phobias and anxiety stem from various sources. These can lead to
a strongly conditioned fear response. The following are the most common origins
of dental fear:
1. Previously painful or negative experiences during visits to a
dentist’s office. This can even include careless comments made by a dentist or
hygienist during a past examination.
2. A severe discomfort with feeling helpless and/or out of control in the
dental situation.
3. A sense of embarrassment of your dental neglect and fear of
ridicule and/ or belittlement when you present to the dental office.
4. Scary anecdotes of negative dental experiences learned vicariously
from family and friends.
5. Negative, menacing portrayals of dentists in movies, TV,
newspapers and magazines.
6. A sense of depersonalization in the dental process, intensified by
today’s necessity for the use of barrier precautions, such as masks, latex gloves
and shields.
7. A general fear of the unknown.
The first thing you can do is to realize that your dental fear can be overcome.
Fear is a learned behavior which, therefore, can be unlearned. Patient-centered
behavior modification that treats you as a whole person, not as a set of teeth can
18
help you overcome your fears. This will obviously take a team approach between
you and your dentist and his/her staff. Communication is the key. You must feel
comfortable expressing your fears and concerns and have a sense that you are
being listened to. If you feel that the Dr. and/or staff is not genuinely concerned
and listening, then absolutely feel comfortable with seeking out referrals to other
offices.
Specific questions that explore the main categories of dental anxiety will
provide a wealth of information to both the dentist and the often the patient that
will facilitate treatment. The main categories of dental anxiety include: specific
anxieties, generalized reactions, mistrust and catastrophe.
Specific anxieties related to dentistry include questioning about the
individual components that cause anxiety. Needles are often a specific concern
for anxious patients. Problems with needles can include the inability to accept a
dental injection (needle phobia); fainting when a needle is used (Blood Injury
Injection phobia); fear of the needle including fear of pain associated with the
injection; fear that the needle will slip or move or break; fear that the needle will
not provide sufficient anaesthesia and there will be pain. Other specific fears
include fear of the drill. This includes fear of the noise, vibration or pain
associated with the drill if there is insufficient local anaesthetic. Insufficient local
anaesthetic resulting in pain during dental treatment is a common fear. Often the
patient has experienced pain during dental treatment. They have either not
informed the dentist or have informed the dentist and been told that they have
had sufficient local anaesthetic and treatment has continued despite their pain. It
19
is common that with additional local anaesthetic or additional time following the
administration of local anaesthetic that profound anaesthesia can be obtained
eliminating pain during treatment. (Buchanan, et. al, 2007)
Generalized anxiety assessment begins by asking about sleep
disturbances the night before a dental appointment. This gives a better indication
of the level of anxiety associated with dental treatment. An assessment of the
body’s reactions to dental anxiety that a person experiences while in the dental
chair provides additional information about the extent of dental anxiety. Body
reactions can include pounding heart, sweaty palms, shaking, butterflies in the
stomach and nausea. Treatment can be tailored to address these specific
reactions.
Mistrust is a different faucet of dental anxiety that also needs to be
explored. Sometimes a patient has been inappropriately spoken to by a dentist,
hygienist or other member of staff. Remarks about a patient’s dental condition or
at home dental care or simply a condescending attitude can make a patient feel
embarrassed or ashamed. Additionally, if there have been problems during
dental treatment such as pain, unexpected changes to the dental treatment
required, or errors or omissions on the dentists behalf can make a patient very
wary of future dental treatment.
Catastrophising is a type of thought process that can undermine a
patient’s ability to accept dental treatment. Thoughts or beliefs that involve
catastrophic events can paralyze a dental patient. For example some patients
hold the belief that they may have a heart attack during dental treatment or may
20
suffer a serious allergic reaction, be unable to breath or may die as a result of
dental treatment.
The discussion of these different categories of dental treatment usually
identifies the specifics of the patient’s dental anxiety. Anxiety may involve only
one category of dental anxiety or may involve elements of a number or all of the
categories of dental anxiety. Once the specifics of dental anxiety have been
identified specific tools and pathways are used to address the anxiety. (Levitt,
2012)
Severity of Dental Anxiety
Many people have a high level of anxiety and avoid visiting the dentist.
This can cause future dental problems. It is important to note, however, that
many new, wonderful products and procedures are available that can make the
dental visit a pleasant experience. (www.floss.com)
According to a recent study in the British Dental Journal (2011), dental
phobia is initiated by a bad experience that unknowingly has become associated
with dentistry.
The study has found that despite the advancement of modern techniques
and the use of very effective anesthetics, patients still seem to maintain the same
level of anxiety as they did years ago. The proportion was shown to be the same
today as it was in the 1930′s,
Dr. Freeman of Queens University Dental School in Belfast (2012), wrote
the article and explains that if all dental phobia were related to painful
experiences from a patient’s life, the condition should have gotten better over the
21
years because of all the advanced techniques available today. This however is
not the case and it suggests that dental phobia is brought on by outside
experiences which are then related to dental experiences.
There are some techniques for relaxation that a dentist can put into
practice for people with such trauma. Patients may be given sedation and be
informed about pain control and they may be given the advantage of being able
to control their own pain by stopping and starting treatment using hand signals.
Evidence exists regarding the use of dental-specific anxiety measures as
valuable clinical tools. Moore and colleagues found good reliability and validity for
a number of dental anxiety measures when used with a sample of highly anxious
subjects. Dailey and colleagues reported a significantly greater decrease in post
treatment anxiety for patients whose dentists knew their pretreatment dental
anxiety scores in comparison with subjects whose dentists did not know their
scores. Consequently, self-reported dental anxiety measures can provide
valuable information to clinicians interested in evaluating and reducing their
patients’ anxiety levels.
The use of formal dental anxiety measures in general clinical practice,
however, is limited. A survey of British dentists who identified themselves as
specifically treating anxious people revealed that only 20 percent of the sample
used dental anxiety assessments with their adult patients; fewer than 17 percent
used them with pediatric patients. In a PubMed search of the literature, we found
no comparable studies of providers in the United States. The authors who
surveyed the British dentists speculated that dentists may worry that rapport with
22
patients could suffer by focusing on previous negative dental experiences. In
addition, practitioners may avoid the use of such measures owing to perceived
time constraints for patients within the clinical practice, lack of familiarity with the
measures, or an assumed burden regarding scoring and interpreting the results
of complicated formal measures. Thus, the use of dental anxiety assessments
primarily has been limited to research purposes and, in general, has not
extended to clinical practice.
Previous research using dental-specific measures found that, although a
painful or traumatic prior dental experience commonly has been reported among
people with dental anxiety, the impact of previous experience with a particular
type of treatment or a specific dental provider has been a challenge to determine.
Wong and Lytle reported less self-reported anxiety with regard to treatment for
patients who previously had undergone endodontic treatment or oral surgery
than for patients who had not undergone such treatment. Peretz and Moshonov
(2007), however, found no difference in dental anxiety between endodontic
patients experienced with this type of treatment and naive patients.
The relationship between familiarity with the treating practitioner and fear,
too, is equivocal. One study suggested that previous "harsh and painful" dental
treatment from "poorly qualified dentists" increased dental anxiety in a sample of
people living on a kibbutz. It is unclear, however, whether the results from this
homogeneous sample would generalize to a more heterogeneous dental school
sample in the United States.
23
The purpose of this study was to determine which measures best
predicted patients’ ratings of subjects’ anxiety exhibited during dental treatment.
We included both dental-specific measures (Modified Dental Anxiety Scale
[MDAS], Dental Fear Survey [DFS], Gatchel’s 10-point single-item dental anxiety
scale2) and general anxiety scales (State-Trait Anxiety Inventory [STAI], Fear of
Pain Questionnaire-III [FPQ] to assess subjects’ anxiety. We hypothesized that
including general anxiety measures would increase the predictive validity of the
assessment battery. (www.bda-findadentist.org.uk, 2011)
In addition, we expected that a patient’s familiarity with the specific
treatment and the clinician would affect both self-reported and observed anxiety.
Specifically, we predicted that subjects who had undergone the treatment
scheduled for the day of the study would report lower anxiety levels than
treatment-naive subjects. Similarly, we predicted that subjects who were familiar
with the dentist who was scheduled to treat them would report experiencing less
anxiety than subjects who had not been treated by the dentist.
A limitation of the research on dental anxiety is that there is a lack of
studies describing dental fear with the patients, own words and from their
perspective. Most previous research has been performed using psychometric
instruments modified from general psychology and adapted to the field of dental
anxiety. However, there is always a risk that valuable information is lost when
using quantitative instruments. (www.mind.org.uk, 2009)
24
Method
Research Design
The study will use the descriptive research design with the combination of
content analysis of documents and related materials. The respondents of the
study will be the patients in the dental dispensary unit of the LPU-Batangas,
College of Dentistry who receive dental treatments from dental clinicians.
Subjects
Patients who received dental treatments in the dental dispensary unit of
LPU College of Dentistry in SY 2011-2013 had a total population of 234. Using
the Slovin’s formula with 7% margin of error, one hundred nine (109)
respondents were randomly selected to answer the questionnaires and predict
the level, severity and causes of their anxiety.
Instruments
The researcher utilized the following instruments and data gathering
techniques in conducting the study, particular in collecting the data.
Survey data were collected from dental patients in Lyceum of the
Philippines University- Batangas, College of Dentistry. Prior to their
administration, the questionnaire and research methodology will be reviewed and
approved by the Research Department of the university.
A modified version of the Dental Anxiety Survey (MDAS) will be used in
this study. The Cohra’s Dental Anxiety Scale (CDAS) was modified by adding a
fifth question relating to local anaesthetics as it is a major cause of anxiety for
25
many individuals. The answer options were also modified so that the same
options were available for all five questions, and they were rephrased to be in a
more clear order of anxiety. The MDAS is now the most frequently used dental
anxiety questionnaire in the United Kingdom.
Each item scored as follows:
1= Not anxious
2= Slightly anxious
3= Fairly anxious
4= Very anxious
5= Extremely anxious
Total score is a sum of all five items, range 5 to 25: Cut off is 19 or above
which indicates a highly dentally anxious patient, possibly dentally phobic.
( www.sitalchauhan.pwp.blueyonder.co.uk/dentalanxiety)
Data Collection Procedures
In determining the instrument’s validity, the researcher will present the
questionnaire she constructed to her colleagues and dean for comments and
suggestions. The researcher will include all the suggestions in modifying the said
questionnaire for further improvement. Dry-run of the questionnaire will also be
conducted and the necessary revisions will be made for more clarity and
exactness before finally administering the survey.
For the research design of this study, the questions will be revised so that
they will be applied to the clinical and didactic aspects of dental school training.
26
To accomplish this task, questions that pertain to dental training will be changed
to reflect a neutral health care setting. The essential purpose of the question will
remain intact.
Data Analysis
The research questions, methods, and appropriate statistical design for
this study are: ANOVA, t-test, Pearson's r correlation and descriptive statistics
will be used to answer the research questions.
ANOVA and individual t-test will be used to determine the differences exist
by gender, by age, by race, and by year in school for perceived levels of stress,
sources of stress and for methods of managing stress.
Pearson’s r correlation will be used to know if there is a relationship
between the major sources of stress and the levels of perceived stress among
college students.
It will also be used to know if there is a relationship between the amount of
stress perceived by college students and the amount of time they spend involved
in stress reducing or relaxing activities.
Descriptive Statistics includes means, standard deviation, ranges and
percentage. These will also be used to determine the major sources of stress the
college students perceive and the methods they actively participate in to reduce
stress.
27
Results and Discussion
This presents an analysis of the data collected according to the methods
and procedures described in the Method. This analysis includes a reiteration of
the purpose of the study and the results of the demographic data collected on the
sample of dental patients in the clinical dispensary of Lyceum of the Philippines
University who responded to the survey.
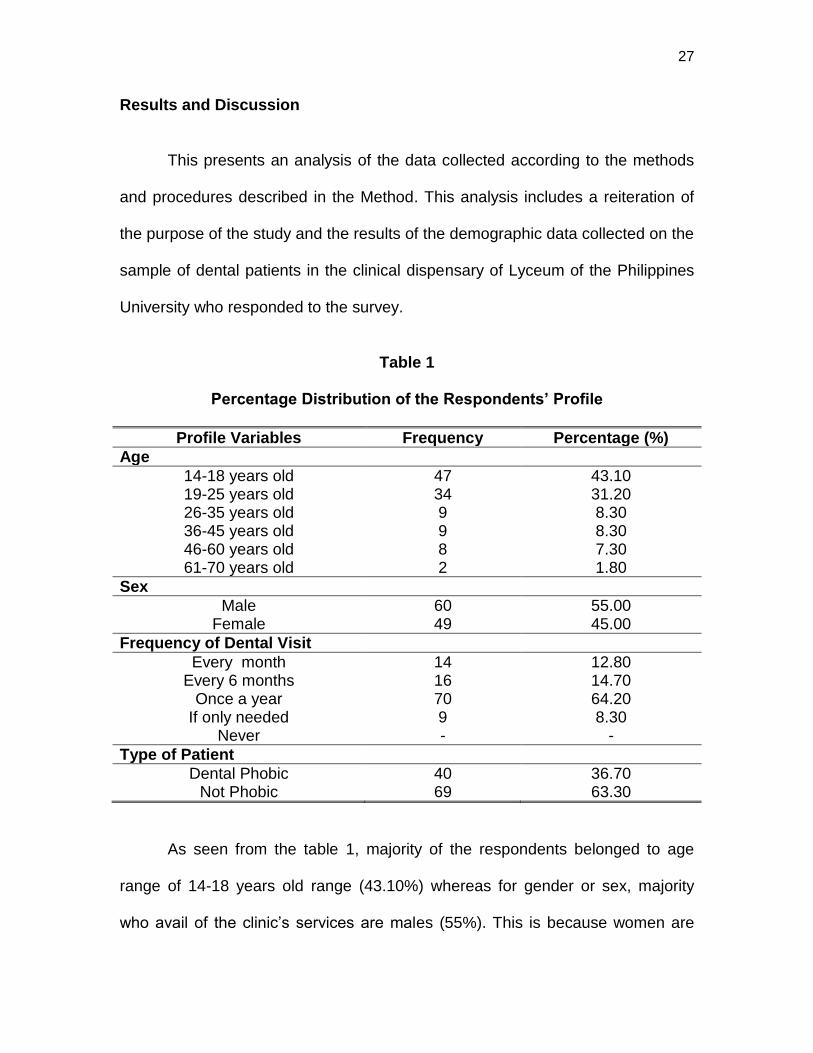
Table 1
Percentage Distribution of the Respondents’ Profile
Profile Variables Frequency Percentage (%)
Age
14-18 years old 47 43.10 19-25 years old 34 31.20 26-35 years old 9 8.30 36-45 years old 9 8.30 46-60 years old 8 7.30 61-70 years old 2 1.80
Sex
Male 60 55.00 Female 49 45.00
Frequency of Dental Visit
Every month 14 12.80 Every 6 months 16 14.70
Once a year 70 64.20 If only needed 9 8.30
Never - -
Type of Patient
Dental Phobic 40 36.70 Not Phobic 69 63.30
As seen from the table 1, majority of the respondents belonged to age
range of 14-18 years old range (43.10%) whereas for gender or sex, majority
who avail of the clinic’s services are males (55%). This is because women are
28
more afraid than men in terms of dental problems. Further, younger people are
more afraid than older ones.
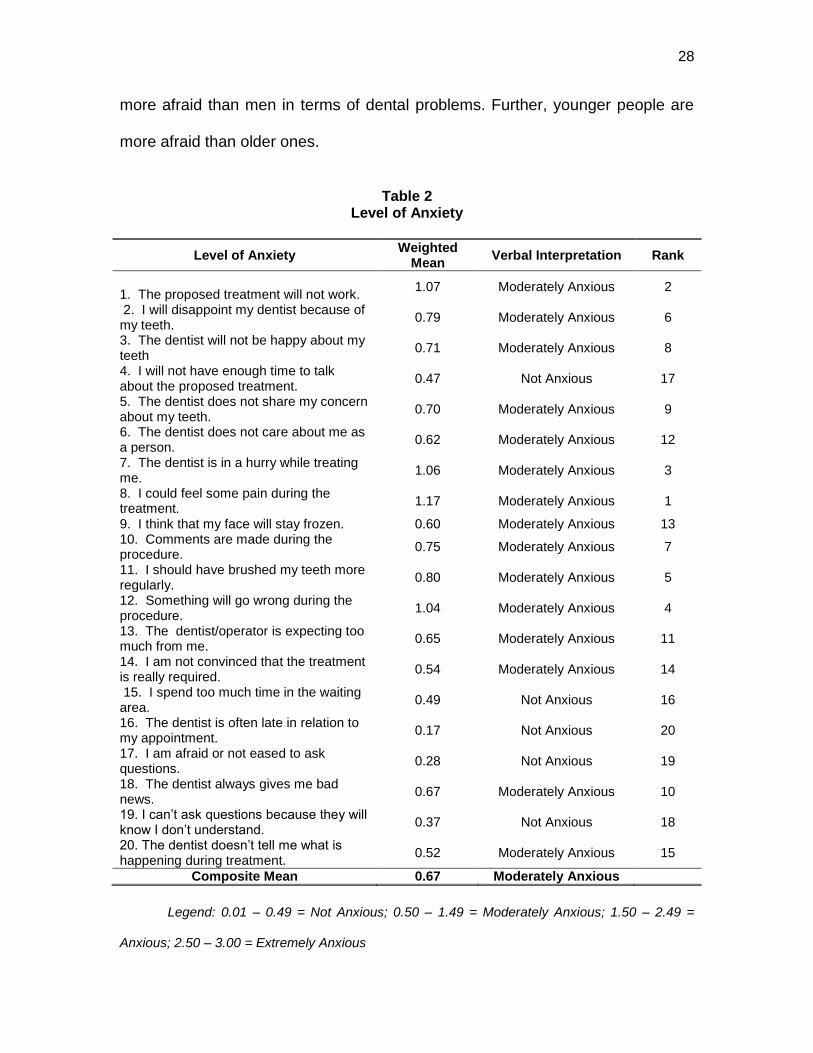
Table 2 Level of Anxiety
Level of Anxiety Weighted
Mean Verbal Interpretation Rank
1. The proposed treatment will not work.
1.07 Moderately Anxious 2
2. I will disappoint my dentist because of my teeth.
0.79 Moderately Anxious 6
3. The dentist will not be happy about my teeth
0.71 Moderately Anxious 8
4. I will not have enough time to talk about the proposed treatment.
0.47 Not Anxious 17
5. The dentist does not share my concern about my teeth.
0.70 Moderately Anxious 9
6. The dentist does not care about me as a person.
0.62 Moderately Anxious 12
7. The dentist is in a hurry while treating me.
1.06 Moderately Anxious 3
8. I could feel some pain during the treatment.
1.17 Moderately Anxious 1
9. I think that my face will stay frozen. 0.60 Moderately Anxious 13 10. Comments are made during the procedure.
0.75 Moderately Anxious 7
11. I should have brushed my teeth more regularly.
0.80 Moderately Anxious 5
12. Something will go wrong during the procedure.
1.04 Moderately Anxious 4
13. The dentist/operator is expecting too much from me.
0.65 Moderately Anxious 11
14. I am not convinced that the treatment is really required.
0.54 Moderately Anxious 14
15. I spend too much time in the waiting area.
0.49 Not Anxious 16
16. The dentist is often late in relation to my appointment.
0.17 Not Anxious 20
17. I am afraid or not eased to ask questions.
0.28 Not Anxious 19
18. The dentist always gives me bad news.
0.67 Moderately Anxious 10
19. I can’t ask questions because they will know I don’t understand.
0.37 Not Anxious 18
20. The dentist doesn’t tell me what is happening during treatment.
0.52 Moderately Anxious 15
Composite Mean 0.67 Moderately Anxious
Legend: 0.01 – 0.49 = Not Anxious; 0.50 – 1.49 = Moderately Anxious; 1.50 – 2.49 =
Anxious; 2.50 – 3.00 = Extremely Anxious
29
Marya, CM, et. al (2012) supports the analysis. Their study mentioned that
age factor was seen to be significantly related to dental anxiety. The anxiety
levels of younger age groups ('less than 20' and 20-30 years) were significantly
higher than the older age groups (51-60 and 'above 60' years). The anxiety levels
of the 51-60-year age group were significantly lower than the other age groups.
Kanegane, et. al (2009), also stated that older patients have often
undergone more dental care in their lifetime, possibly facilitating habituation and
enabling favorable reevaluation of the experience.
In a study of Moore, et. al., 2002, women were better regular attenders
than men. Specialist treated regular attenders were significantly less anxious and
had more positive beliefs.
Majority of the respondents only seek dental treatments once a year
(64.20%) and they are not dental phobic (63.30%).
This only showed that patients that came in the dental dispensary of LPU
College of Dentistry were already educated with regards to proper oral care and
they were already familiar with different dental treatments.
As shown in Table 2, the level of anxiety of patients varies on moderately
to not anxious. Feeling or experiencing pain during dental treatment ranked first
with a weighted mean of 1.17 followed by the fear or worry of not working the
proposed treatment with a weighted mean of 1.07. The dentist is in a hurry while
30
treating also made the patients moderately anxious with a weighted mean of
1.06.
These were followed by the thought of something that may go wrong
during the procedure (1.04), brushing teeth more regularly (0.80), disappointing
the dentist (0.79), comments made during the procedure (0.75), dentist will not
be happy about the patients’ teeth (0.71), dentist does not share concern on
patients’ teeth(0.70), and giving bad news by the dentist (0.67).
Other variables like dentist expecting too much from patients with a mean
of 0.65, dentist does not care about patients as a person (0.62), thinking that the
face will stay frozen (0.60), not being convinced that the treatment is really
required (0.54), and dentist does not tell what is happening during treatment
(0.52) also made the respondents moderately anxious.
People fear what they do not understand and they also, logically, dislike
pain. If someone has had one or more painful past experiences in a dental office
then their fear is completely rational and they should be treated supportively.
(Dental Fear Central, 2004)
Sufferers from fear of pain, in terms of dental health, are unable to visit
dentists because of a prior painful memory when these patients were young.
Fearful patients remember the visit as a particularly painful one. This memory
manifests later in life as an unconscious desire not to visit the dentist resulting in
dental appointments being constantly delayed or missed entirely.
31
Most people prefer not to suffer pain. For dental phobics, however, just the
mere idea of pain is far worse than the actual pain itself. Ironically, because
these patients are unable to regularly visit dentists, they suffer almost constant
pain from their neglected teeth.
It is important to note that the fear of pain from visits to the dentist is often
from memories of long ago. These memories tend to become warped over time.
Modern dental practices have reduced the pain involved in dental procedures
from what they were even as recently as a decade ago.
People afflicted with this type of phobia often do not receive suitable levels
of dental care. By not having any sense of relationship with the dentist, these
people are unable to articulate fears or get any kind of professional reassurance.
By staying away from dentist, these patients further increase fears since nobody
is able to provide information that will counterbalance the imaginations and are
stuck with a mental picture of the dentist based on painful childhood memories.
www.dentalfearcentral.org, (2010)
According to the study of Kanegane, et. al, (2003), fear is a primary
emotion that indicates that a dangerous situation was recognized, leading the
individual to concentrate all his attention on this event. Anxiety represents a fear
which was transferred from a real to an imaginary situation, resulting from similar
facts or that recall a previous situation.
Once patient seats on the dental chair, they were already anxious and
different thoughts came to their minds. The level of anxiety increased when these
32
patients feel any discomforts and pain, and will thought that the proposed
treatment will not work because of the severity of the case. Phobic patients were
also anxious if they feel or see that the dentists were in a hurry in doing the
treatment because they were afraid that the said treatment may fail or the dentist
may hurt or injured them.
Table 3.1
Causes of Dental Anxiety with Regards to Pre-operative Procedure
Pre-Operative Procedure Weighted Mean Verbal
Interpretation Rank
1. I think I have a problem with my teeth. 1.15 Slightly Anxious 1 2. I think that I have to go to the dentist 1.08 Slightly Anxious 2 3. I call to make an appointment. 0.64 Slightly Anxious 11.5 4. I arrive at the dental office 0.72 Slightly Anxious 10 5. I am in the waiting room. 0.59 Slightly Anxious 15 6. I smell various odors in the dental office.
0.49 None 18
7. I heard sounds of instruments in the dental office.
0.64 Slightly Anxious 11.5
8. I sit in the dental chair. 0.94 Slightly Anxious 7 9. The dentist examined my teeth. 1.04 Slightly Anxious 4 10. I don’t understand what the dentist is explaining a needle is used to freeze me
0.46 None 20
11. I feel numbness in my mouth from freezing.
0.62 Slightly Anxious 13.5
12. I feel the scratching on my teeth by the instrument.
0.95 Slightly Anxious 5.5
13. The drill is making high pitch sound. 0.95 Slightly Anxious 5.5 14. The dental instruments are used in my mouth.
1.07 Slightly Anxious 3
15. I think I could choke during dental instrument.
0.62 Slightly Anxious 13.5
16. The rubber dam is used. (because I am afraid to choke or gag.)
0.48 None 19
17. I realize that I will not see the work being done in my mouth.
0.52 Slightly Anxious 17
18. I feel the vibration of the drill. 0.91 Slightly Anxious 8 19. I hear the staff converse during the procedure
0.56 Slightly Anxious 16
20. During treatment, I am afraid to move because of the precision of the work done by the dentist.
0.77 Slightly Anxious 9
Composite Mean 0.76 Slightly Anxious
33
Legend: 0.01 – 0.49 = None; 0.50 – 1.49 = Slightly Anxious; 1.50 – 2.49 = Very Anxious; 2.50 – 3.00 = Extremely Anxious
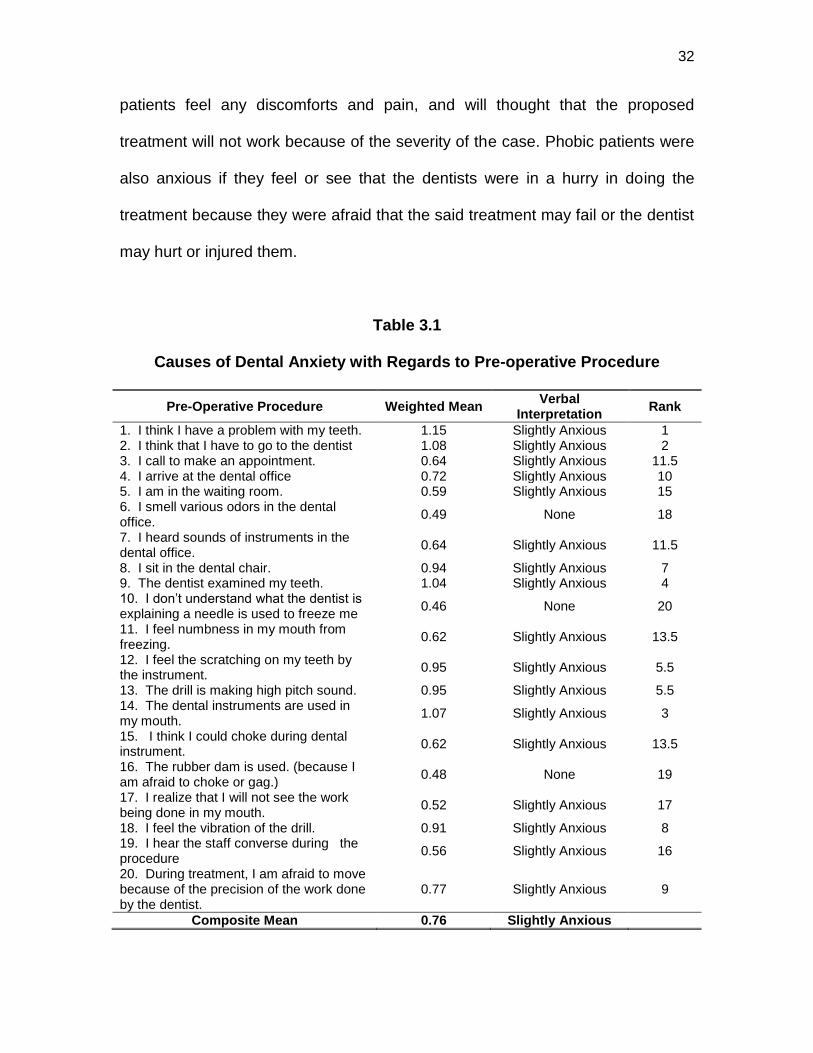
Table 3.1 showed that the thought of having problems with their teeth
(1.15), going to the dentists (1.08), and the dental instruments that are being
used in their mouth (1.07) were the top three causes of dental anxiety with
regards to preoperative procedures which obtained a rating of “slightly anxious.”
Other causes like examination of teeth by the dentist (1.04), scratching of
instruments on teeth (0.95), high pitch sound of drills (0.95), sitting in the dental
chair (0.94), feeling of vibration of drill (0.91), being afraid to move because of
the precision of the work done by the dentist during treatment (0.77), and arriving
at the dental office (0.72) made also the respondents slightly anxious.
According to Levitt (2012), the thought of going to dentists to have dental
treatments make patients already anxious. Thoughts or beliefs that involve
catastrophic events can paralyze a dental patient.
Sometimes a patient has been inappropriately spoken to by a dentist,
hygienist or other member of staff. Remarks about a patient’s dental condition or
at home dental care or simply a condescending attitude can make a patient feel
embarrassed or ashamed.
Some people have had painful encounters with the dental “drill”. Thinking
of the sound alone will make patients feel very anxious. Many people are scared
of the sight of instruments being put into the mouth. Many people find that
having a better look at “the drill” aka the handpiece, and having it demonstrated
on finger, takes a lot of the fear away. Or else, some people find that simply
closing the eyes works while receiving dental care. On the other hand, there are
34
people who like to see exactly what is going on, in which case he can ask his
dentist to show him what he is doing with the help of mirrors.
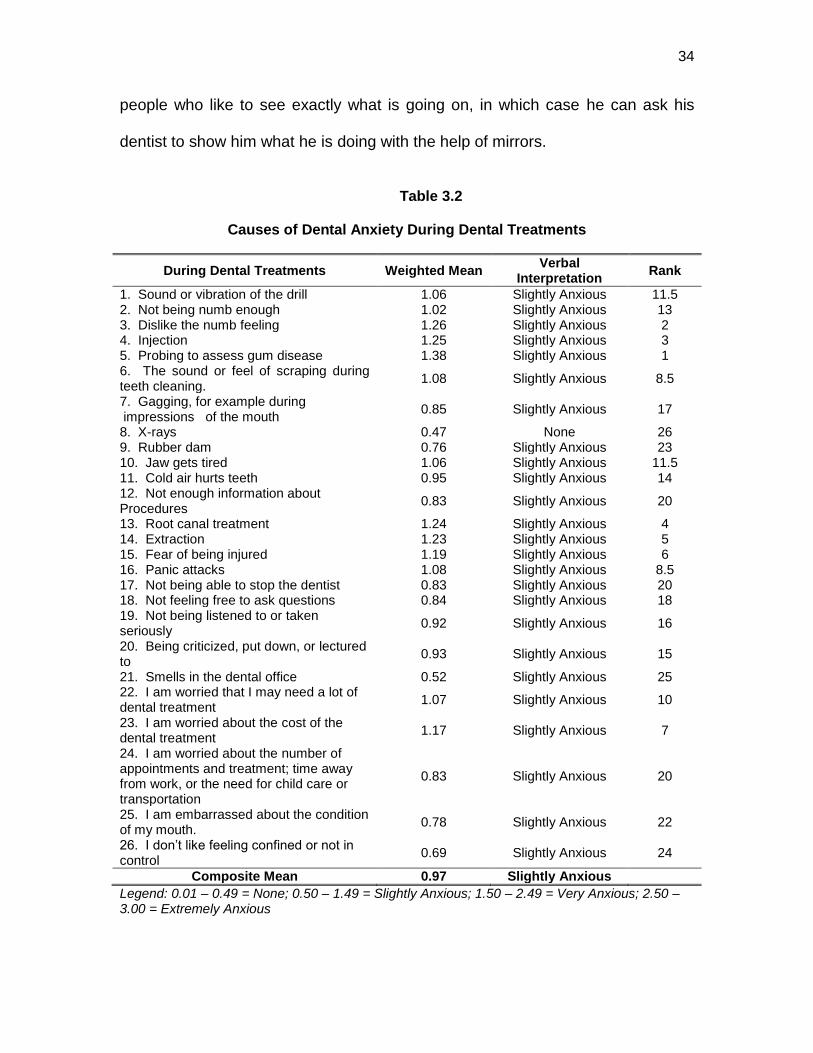
Table 3.2
Causes of Dental Anxiety During Dental Treatments
During Dental Treatments Weighted Mean Verbal
Interpretation Rank
1. Sound or vibration of the drill 1.06 Slightly Anxious 11.5 2. Not being numb enough 1.02 Slightly Anxious 13 3. Dislike the numb feeling 1.26 Slightly Anxious 2 4. Injection 1.25 Slightly Anxious 3 5. Probing to assess gum disease 1.38 Slightly Anxious 1 6. The sound or feel of scraping during teeth cleaning.
1.08 Slightly Anxious 8.5
7. Gagging, for example during impressions of the mouth
0.85 Slightly Anxious 17
8. X-rays 0.47 None 26 9. Rubber dam 0.76 Slightly Anxious 23 10. Jaw gets tired 1.06 Slightly Anxious 11.5 11. Cold air hurts teeth 0.95 Slightly Anxious 14 12. Not enough information about Procedures
0.83 Slightly Anxious 20
13. Root canal treatment 1.24 Slightly Anxious 4 14. Extraction 1.23 Slightly Anxious 5 15. Fear of being injured 1.19 Slightly Anxious 6 16. Panic attacks 1.08 Slightly Anxious 8.5 17. Not being able to stop the dentist 0.83 Slightly Anxious 20 18. Not feeling free to ask questions 0.84 Slightly Anxious 18 19. Not being listened to or taken seriously
0.92 Slightly Anxious 16
20. Being criticized, put down, or lectured to
0.93 Slightly Anxious 15
21. Smells in the dental office 0.52 Slightly Anxious 25 22. I am worried that I may need a lot of dental treatment
1.07 Slightly Anxious 10
23. I am worried about the cost of the dental treatment
1.17 Slightly Anxious 7
24. I am worried about the number of appointments and treatment; time away from work, or the need for child care or transportation
0.83 Slightly Anxious 20
25. I am embarrassed about the condition of my mouth.
0.78 Slightly Anxious 22
26. I don’t like feeling confined or not in control
0.69 Slightly Anxious 24
Composite Mean 0.97 Slightly Anxious
Legend: 0.01 – 0.49 = None; 0.50 – 1.49 = Slightly Anxious; 1.50 – 2.49 = Very Anxious; 2.50 – 3.00 = Extremely Anxious
35
Many people equate the sound of the drill with pain. The logic behind this
is simple: if he had a painful dentistry experience in the past which was
accompanied by the sound of a dental tool, he has come to associate the sound
with pain. Just hearing the sound may evoke a “perception” of pain.
www.dentalfearcentral.org. (2010)
The causes of dental anxiety during dental treatment vary mainly on
slightly anxious having a composite mean of 0.97 as shown in Table 3.2. Among
the causes given, probing to asses gum disease (1.38), dislike the numb feeling
(1.26) and injection (1.25) were the top three causes of dental anxiety.
Root canal treatment, extraction, fear of being injured, cost of dental
treatment, sound or feel of scraping during teeth cleaning, panic attacks, and the
need of having lots of dental treatment were also noted as causes of anxiety
during dental treatment with a weighted mean of 1.24, 1.23, 1.19, 1.17, 1.08,
1.08, and 1.07 with a verbal interpretation of “slightly anxious”.
Levitt (2012), stated that patients were slightly anxious in probing their
gums maybe because they had no idea about the procedure and they were
afraid that their gums may be injured or bleeds. Needles are often a specific
concern for anxious patients. Problems with needles can include the inability to
accept a dental injection.
The fear of the needle including fear of pain associated with the injection;
fear that the needle will slip or move or break; fear that the needle will not provide
sufficient anaesthesia and pain increases the patient’s anxiety.
36
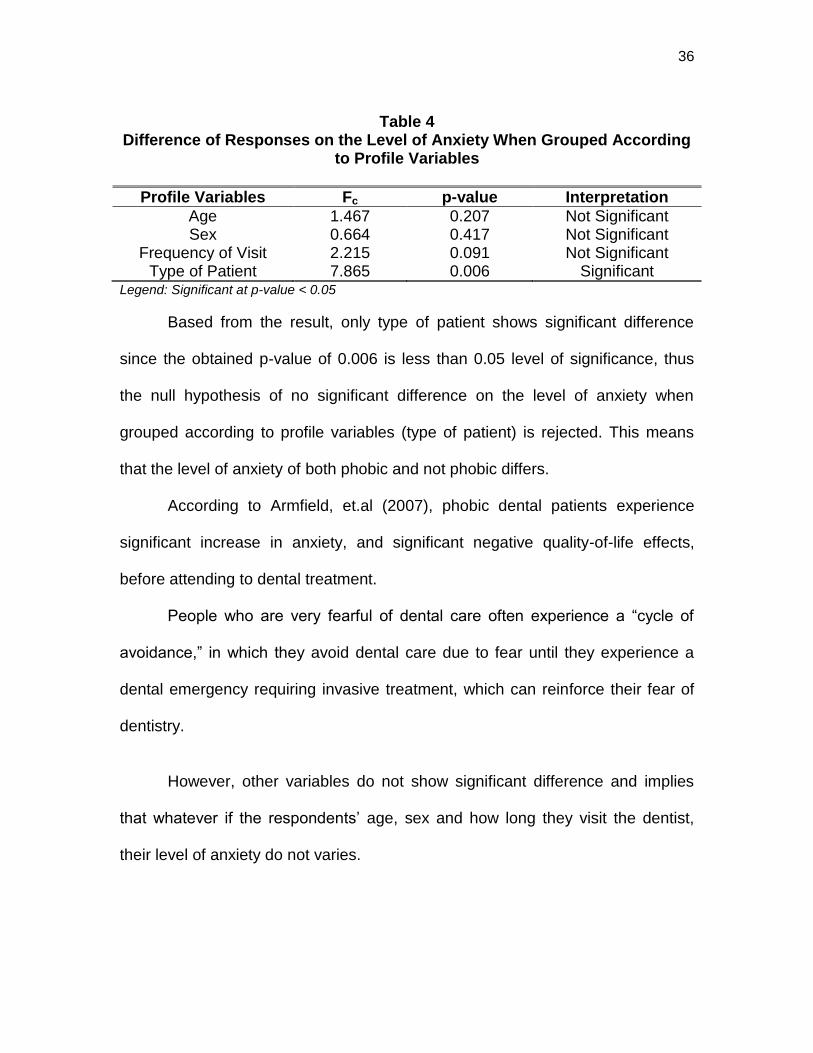
Table 4 Difference of Responses on the Level of Anxiety When Grouped According
to Profile Variables
Profile Variables Fc p-value Interpretation
Age 1.467 0.207 Not Significant Sex 0.664 0.417 Not Significant
Frequency of Visit 2.215 0.091 Not Significant Type of Patient 7.865 0.006 Significant
Legend: Significant at p-value < 0.05
Based from the result, only type of patient shows significant difference
since the obtained p-value of 0.006 is less than 0.05 level of significance, thus
the null hypothesis of no significant difference on the level of anxiety when
grouped according to profile variables (type of patient) is rejected. This means
that the level of anxiety of both phobic and not phobic differs.
According to Armfield, et.al (2007), phobic dental patients experience
significant increase in anxiety, and significant negative quality-of-life effects,
before attending to dental treatment.
People who are very fearful of dental care often experience a “cycle of
avoidance,” in which they avoid dental care due to fear until they experience a
dental emergency requiring invasive treatment, which can reinforce their fear of
dentistry.
However, other variables do not show significant difference and implies
that whatever if the respondents’ age, sex and how long they visit the dentist,
their level of anxiety do not varies.
37
Conclusions
Based on the data analyses the following conclusions were drawn:
1. Sex, age and the frequency of dental visit appear to be important factors
linked to dental anxiety, with males being particularly common within the dentally
anxious group in the population.
2. Patients receiving dental treatments in the Clinical Dispensary of the
College of Dentistry were slightly anxious of the different dental procedures.
3. Dental anxiety is a multidimensional complex phenomenon, which is
influenced by characteristics like fear of pain, past traumatic dental experiences
in childhood, and dentally anxious family members or peers.
4. Severe dental anxiety is a major barrier to seeking professional dental
care, and the implications of this in terms of dental disease are significant in
terms of deterioration of their dentition, and a range of psychosocial problems.
5. Observed anxiety and self-reported anxiety were not related to previous
experience with either the patient or the particular treatment.
Recommendations
Based on the findings of the study, the following recommendations were
given:
1. Dental clinicians, clinical instructors and school administration may continuously
provide dental education and extend programs to the community in order for them to be
aware of the oral diseases that they may experience because of their anxiety.
2. A continuous study and upliftment of skills and knowledge must be acquired by
dental clinicians to be able to share and render the best dental service to their patients.
38
3. The dental clinicians should establish good rapport with their patients for efficient
treatment.
4. Dental clinicians should acquire good communication skills so they can explain
well the procedures, treatments, dental materials that will be used in the treatment as
well as the cost of the said treatment to their patients.
5. The dental dispensary of LPU College of dentistry should be equipped with
Virtual Reality- like glasses that provide both visual and auditory distraction by allowing
the patients to view videotapes through these glasses while having dental work done.
6. Clinicians should provide patients with walkman, books and magazines while
they are waiting in the dental dispensary to relax their minds and lessen their anxiety.
39
Bibliography
Aartman IHA. Reliability and validity of the short version of the Dental Anxiety Inventory. Comm Dent Oral Epidemiology, 1998.
Al-Harasi S, et al. Hypnosis for children undergoing dental treatment. Cochrane Database of Systematic Reviews, 2010.
Anderson JW. Fear in dental chair. Oral Health,1997.
Armfield JM, et.al, "The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear", (2007).
Bracha HS, et.al, "Posttraumatic dental-care anxiety (PTDA): Is "dental phobia" a misnomer?". Hawaii Dent J, 2006.
Buchanan H, et. al, "Accessing dental anxiety online support groups: an exploratory qualitative study of motives and experiences". Patient Educ Couns, June 2007.
Berggren U. Assessment of dental fear: a comparison of two psychometric instruments. Acta Odontol Scand, 1992
British Dental Journal, 2011.
Cohen, SM, et al. The impact of dental anxiety on daily living., British Dental Journal, 2000.
Coldwell SE, et al. "Combining alprazolam with systematic desensitization therapy for dental injection phobia". J Anxiety Disord, 2007.
Dental Fear Central. "Tips for Abuse Survivors and Their Dentist (2007)
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 1994.
Dionne, S., et.al. Dental Fear and Anxiety as a Barrier to Accessing Oral Health Care Among Patients with Special Health Care Needs. Published online: 28 JUN 2008.
Eddleman, L., DDS. Family Dentistry, Monroe, L.A., 2012.
Freeman, R. Queens University Dental School, Belfast, 2012.
40
Hannah, et.al. A communication Skill Course for Undergraduate Dental Students, Journal of dental Education, 2004.
Haugejorden O, et.al. Avoidance of dental visits: the predictive validity of three dental anxiety scales. Acta Odontol Scand, 2000.
Jerome, L. "The Art and Science of Distraction, 2004.
Kaakko T, MD, et.al. Dental anxiety among new patients attending a dental schoolemergency clinic. J Dent Educ 1999.
Kanegane, K, et. al. Dental Anxiety and Salivary Cortisol Levels before Urgent Dental Care. Journal of Oral Science, 2009.
Levitt, J., DDS. Dental anxiety Assessment, Fear of Dentist, Ontario, 2012.
Liddell A, et.al. Gender and Age Differences in Attitudes to Dental Pain
and Dental Control. Community Dent Oral Epidemiology, 1997. Lundgren J, et. al. "Relaxation versus cognitive therapies for dental fear—
a psychophysiological approach".Health Psychol, 2006. Marya, CM., et.al. Dental Anxiety Among Patients Visiting a Dental
Institute in Faridabad, India. West Indian Medical Journal, 2012.
Milgrom P, et.al. The prevalence and practice management consequences of dental fear in a major US city. J Am Dent Assoc , May, 2006.
Moore, et. al. A 3-year comparison of dental anxiety treatment outcomes: hypnosis, group therapy and individual desensitization vs. no specialist treatment. Europe Journal of Oral Science, 2002.
Neipris, L., MD., Dealing With Dental Phobia, My Optimum Health, 2010.
Nicholas, E, et.al. Dental difficulty for adult patients undergoing different dental procedures according to level of dental anxiety. France: 2008.
Peretz, B., et.al. Dental Anxiety Among Patients Undergoing Endodontic Therapy, Published online: 1 Jun 2007.
Rocha RG, et. Al. Dental Anxiety in an Emergency Dental Service. SP, Brazil, 2000.
Rosa AL, et. Al. Dental Anxiety in Patients Undergoing a Routine Dental Treatment. SP, Brazil, 1997.
41
Sarvela,et al. Evaluation and Measurement: A Practitioner’s Perspective, 2nd ed., 2010.
Stabholz, A. et.al. "Dental anxiety among patients prior to different dental treatments". Int Dent J, 1999.
Understanding Anxiety Mind. www.mind.org.uk, published 2009.
www.bda-findadentist.org.uk, 2011.
www.dentalfearcentral.org., 2010.





























