Embed Size (px)
Citation preview
C. Pathology
PATHOLOGY OF ANGIOSARCOMA OF THE LIVER
CHLORIDE WORKERS AMONG VINYL CHLORIDE-POLYVINYL
Louis B. Thomas
National Cancer Institute National Institutes of Health
Bethesda, Maryland 20014
Hans Popper*
The Mount Sinai School of Medicine City University of New York New York, New York 10029
INTRODUCTION The first reports indicating that angiosarcoma of the liver may be causally re-
lated to employment in the manufacture of polyvinyl chloride (PVC) resins were published early in 1974.’-* Also the animal studies of Maltoni, which are being reported in detail at this conference, support the idea that vinyl chloride (VC) or some metabolic product of VC may be the carcinogenic agent causing hepatic angiosarcomas in some of the VC-PVC workers. The reports of these observations in experimental animals and in VC-PVC workers led to intensive studies of clinical and epidemiologic factors in populations of present and past workers in PVC plants in the United States and in other countries. As a part of these current studies, we have reviewed pathologic materials from a limited num- ber of VC-PVC workers, some of whom had angiosarcomas of the liver. This preliminary report includes our observations on the gross and microscopic features of the hepatic angiosarcomas in these workers. The material was col- lected from various hospitals and we acknowledge particularly the assistance of Dr. Henry Falk and Dr. 1. J. Selikoff whose reports are presented at this confer- ence. In a separate report, also presented at this conference, we have described fibrosis and other pathologic changes in the liver of VC-PVC workers who have not developed angiosarcoma. Similar changes in parts of the liver free of angio- sarcoma were seen in the liver of several of the workers who had developed angiosarcomas. The histologic progression of these hepatic lesions and their re- lationship to the development of angiosarcomas will be of major importance as these studies continue and additional pathologic material from other workers in the VC and PVC industries is collected and reviewed.
VC-PVC WORKERS WITH ANGIOSARCOMA OF THE LIVER The histologic features of angiosarcoma of the liver included in this report are
based on our review of material from 13 patients. Twelve of them worked in four different polyvinyl chloride manufacturing plants in the United States and one was a VC-PVC worker in Great Britain. An additional VC-PVC worker who
* Fogarty Scholar in Residence, Fogarty International Center, National Institutes of Health, Bethesda, Maryland 20014.
268
Thomas & Popper: Pathology of Liver Angiosarcoma 269
probably has angiosarcoma of the liver is not included in our report of the patho- logic features of angiosarcoma because the only material available for histologic review consisted of minute needle-biopsy fragments of hepatic tissue which were insufficient for a definite diagnosis.
A correlation of all the clinical and epidemiologic factors associated with each of the angiosarcoma cases had not been completed at the time of our review and preparation of this report. Reports presented at this conference by Dr. Creech and Dr. Heath include detailed clinical and epidemiologic information about seven of the angiosarcoma patients whose sections we have reviewed. Based on the information they furnished us and the information obtained about the other cases,’% is apparent that each of the 13 VC-PVC workers with hepatic angiosarcomas included in our review had worked in close contact with the polymerization of VC to PVC for many years.
PATHOLOGIC MATERIAL Ten of the 13 patients with angiosarcoma of the liver had died and we have
reviewed sections of the liver obtained at autopsy from 9 of them. In addition, we reviewed sections of liver tissue obtained by needle biopsy or by surgical biopsy at the time of laparotomy from 7 patients. Included were 2 patients who were alive at the time of the review and 1 patient who had a liver biopsy and sub- sequently died but was not subjected to autopsy. In 1 patient who is still alive our review was based on photomicrographs of the biopsy of the hepatic angio- sarcoma because histologic slides were not available.
Gross Lesions in the Liver The weights of the livers of 7 of the 9 patients with angiosarcoma who had died
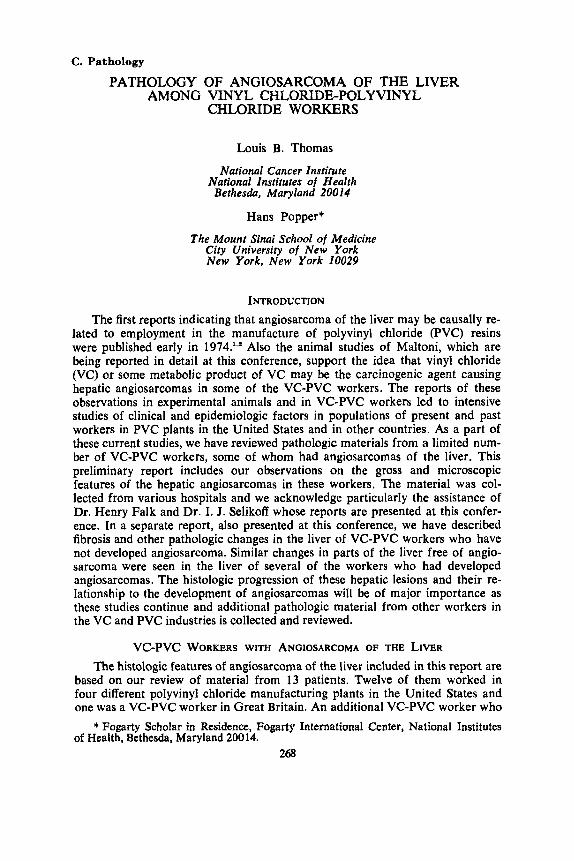
and had been autopsied ranged from 1860-7300 g. The average weight was 4236 g. All were described as being massively involved with cystic, blood-filled tumors which replaced most of the liver. In the larger specimens some of the cystic spaces were several centimeters in diameter and were associated with large areas of fibrosis, hemorrhage, and necrosis. These angiosarcomas often produced bulging masses on the surface of the liver. Rupture of these large cavernous cysts resulted in massive hemorrhage between the diaphragm and the liver or into the peritoneal cavity and was the immediate anatomical cause of death in several patients. The gross appearance of the cut surface of one of the hepatic angiosarcomas is shown in FIGURE 1.
Microscopic Features of Angiosarcomas of the Liver The complex histologic features observed in the hepatic angiosarcomas and
their apparent pathogenesis from multicentric, precursor lesions in the liver are presented diagrammatically in TABLE 1 . The principal aspects of these lesions will be described briefly.
Areas of hemorrhage, necrosis, and marked fibrosis were seen microscopically in sections from most of the specimens. These secondary changes were frequently encountered in parts of the angiosarcoma characterized by the largest blood-filled cavernous spaces which were separated by thick trabecular bands of dense fibrous connective tissue. Although 9 of the 13 angiosarcomas were found to be partially circumscribed by a pseudocapsule of compressed hepatic tissue, none of them was completely encapsulated. Microscopically, they all showed irregular infiltra- tion of angiosarcoma into adjacent hepatic tissue with envelopment of hepatic
270 Annals New York Academy of Sciences
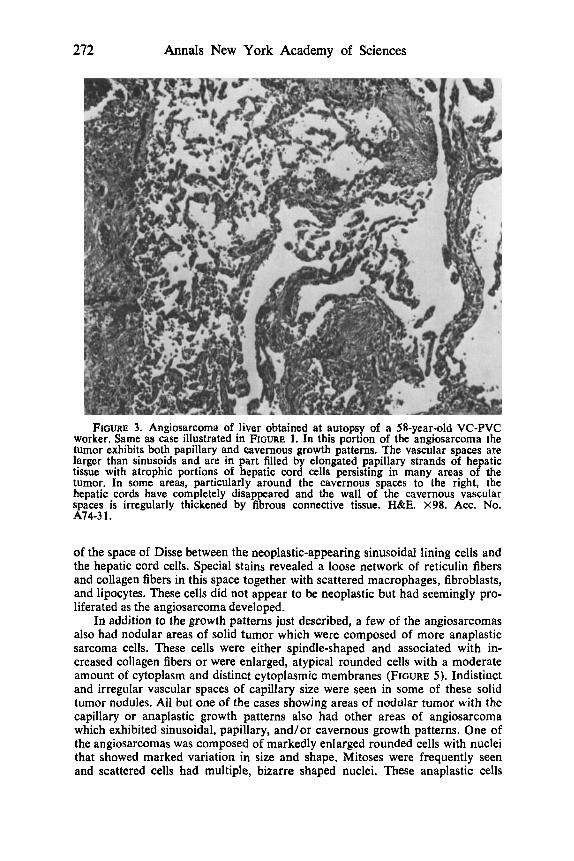
FIGURE 1. Cut surface of liver. Approximately 75 percent of the liver, which weighed 1860 g, has been replaced by angiosarcorna which is partially necrotic and hemorrhagic. The cystic and cavernous spaces of the tumor are irregular in shape and vary from 1-2 mrn, up to nearly 1 cm, in diameter. A few of the spaces are filled with thrombi, particularly in and adjacent to areas of necrosis, but most of them are filled with fresh blood. The left-hand portion of the liver is not involved grossly by angiosarcorna but is involved by irregular, variable sized areas of fibrosis. The inter- vening hepatic tissue is dark green due to bile stasis.
TABLE 1 PATHOGENESIS OF HEPATIC ANGIOSARCQMA IN VC-PVC WORKERS
Sinusoidal dilatation and + Piling up and + Angiosarcoma “stimulation” of sinus- atypia of si- oidal lining cells nusoidal lin- Infiltrative tumor (envelop-
ing cells ing liver cells & bile
Hemorrhage 13/13 Sinusoidal pattern 11/13 Necrosis 13/13 Papillary pattern 7/13 Marked fibrosis 10/13 Cavernous pattern 5/13 Pseudocapsule 9/13 Nodular tumor
Capillary pattern 5/13 Anaplastic pattern 3/13
Secondary changes in angiosarcomas: ductules)
cord cells and, less so, proliferating bile ducts. The characteristic, irregular and indistinct margin between the angiosarcoma and the apparently uninvolved liver is illustrated in FIGURE 1. Sections from most of the specimens showed multi- centric foci of angiosarcoma at the margins of the grossly identifiable angiosar- coma and in some specimens the infiltration by the multicentric angiosarcoma was so diffuse that none of the liver was entirely free of angiosarcoma.
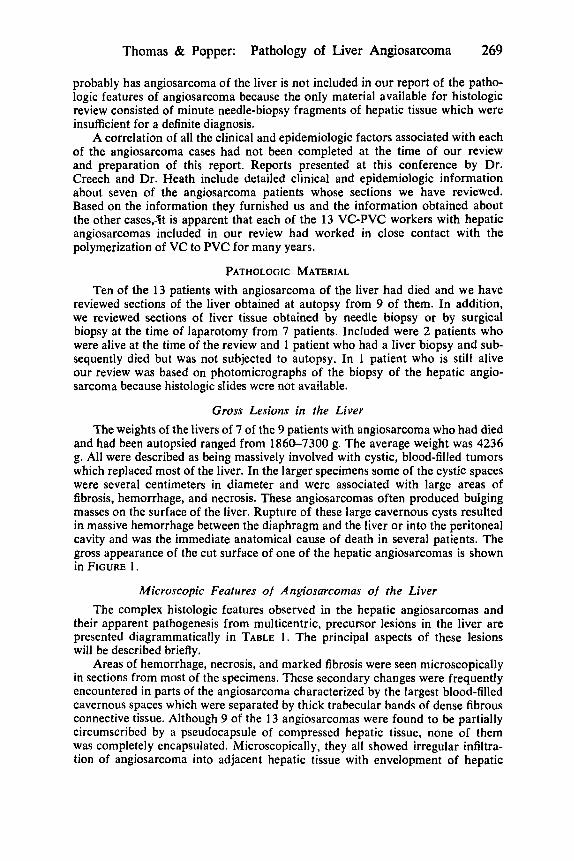
Microscopically the angiosarcomas showed several structural patterns. The sinusoidal pattern was observed in 1 1 of the 13 specimens and is illustrated in FIGURE 2. This pattern is characterized by the envelopment of the hepatocytes in cord arrangement by the neoplastic cells which have variable sized, irregular, hyperchromatic nuclei. Their elongated cytoplasmic processes cover the surface of the hepatic cells and form a lining for the widened hepatic sinusoids. Occa- sionally these sarcomatous, sinusoidal lining cells were detached and multilayered groups of cells partially filled the sinusoidal lumen. The hepatocytes were well preserved and, in fact, were hypertrophied and hyperplastic. They exhibited
Thomas & Popper: Pathology of Liver Angiosarcoma 271
FIGURE 2. Liver obtained by surgical biopsy several months before patient died of angiosarcoma. The sinusoidal pattern of the angiosarcoma is characterized by neo- plastic-appearing sinusoidal lining cells and dilated sinusoids. The hepatic cord cells are hyperplastic. A small bile plug in a dilated bile canaliculus is present in the center of the field. H&E. X392. Acc. No. S74-415.
neither necrosis nor degeneration in the areas of the angiosarcoma which ex- hibited only the sinusoid pattern of growth.
With increased proliferation of the angiosarcoma cells the hepatocytes atrophy and eventually disappear so that larger, cavernous spaces within the tumors were formed. Irregular papillary strands of hepatic cord cells covered by angiosarcoma cells projected into these larger spaces. A low power view of the papillary and cavernous growth patterns is illustrated in FIGURE 3. Thus from our studies of these angiosarcomas the sinusoidal, papillary, and cavernous growth patterns appeared to represent progressive changes caused by continued proliferation and growth of the sarcomatous sinusoidal lining cells. Initially, the angiosarcomas seemed to develop along the hepatic sinusoids and were associated with hypertrophy and hyperplasia of adjacent hepatocytes. Later these angiosar- comas produced a neoplastic caricature of the sinusoidal pattern of the liver by forming larger spaces which often contained papillary projections of atrophic hepatic tissue covered by a layer of angiosarcoma cells. Finally, the largest cav- ernous spaces had thickened, fibrotic walls from which all normal hepatic tissue had disappeared. Some of these largest spaces were incompletely lined by the angiosarcoma cells and it was in these same areas where hemorrhage, necrosis, and thrombosis were most frequently encountered.
FIGURE 4 illustrates an additional histologic feature, namely, an enlargement
272 Annals New York Academy of Sciences
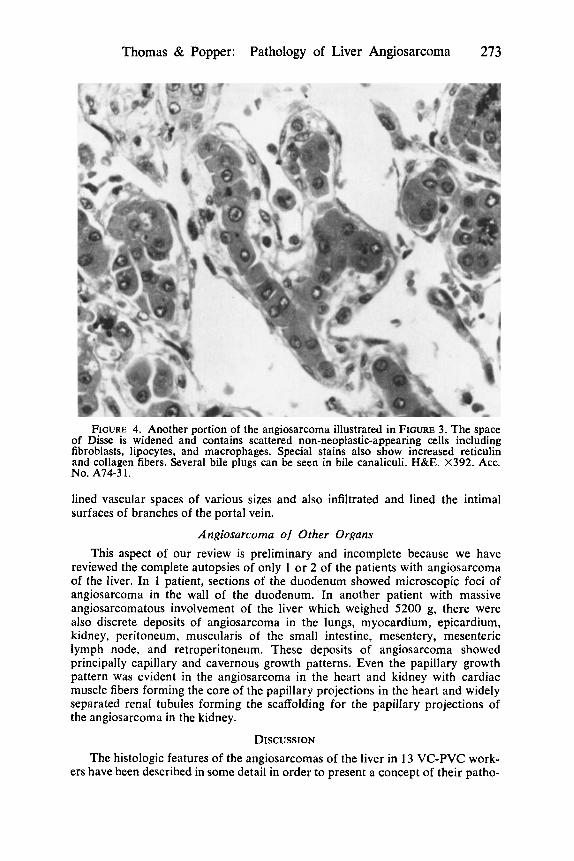
FIGURE 3. Angiosarcoma of liver obtained at autopsy of a 58-year-old VC-PVC worker. Same as case illustrated in FIGURE 1. In this portion of the angiosarcoma the tumor exhibits both papillary and cavernous growth patterns. The vascular spaces are larger than sinusoids and are in part filled by elongated papillary strands of hepatic tissue with atrophic portions of hepatic cord cells persisting in many areas of the tumor. In some areas, particularly around the cavernous spaces to the right, the hepatic cords have completely disappeared and the wall of the cavernous vascular spaces is irregularly thickened by fibrous connective tissue. H&E. X 9 8 . Acc. No. Al4-31.
of the space of Disse between the neoplastic-appearing sinusoidal lining cells and the hepatic cord cells. Special stains revealed a loose network of reticulin fibers and collagen fibers in this space together with scattered macrophages, fibroblasts, and lipocytes. These cells did not appear to be neoplastic but had seemingly pro- liferated as the angiosarcoma developed.
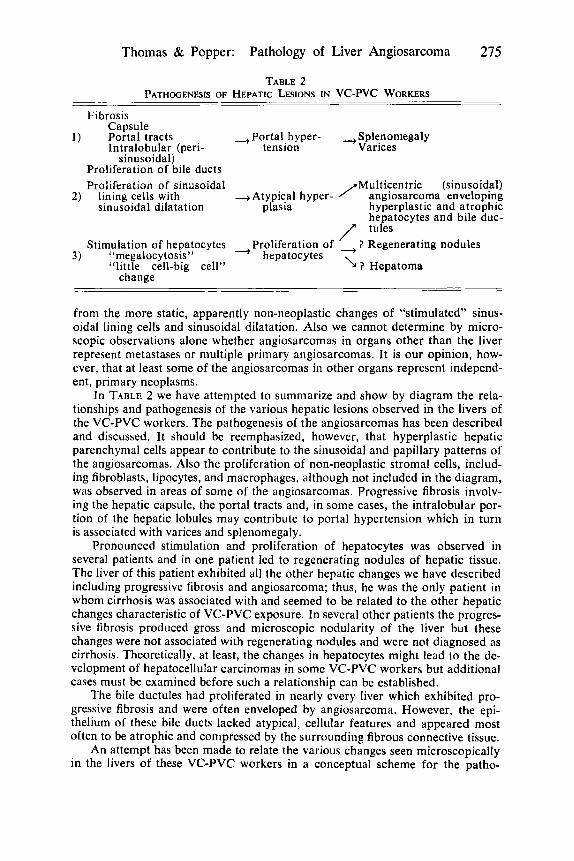
In addition to the growth patterns just described, a few of the angiosarcomas also had nodular areas of solid tumor which were composed of more anaplastic sarcoma cells. These cells were either spindle-shaped and associated with in- creased collagen fibers or were enlarged, atypical rounded cells with a moderate amount of cytoplasm and distinct cytoplasmic membranes (FIGURE 5) . Indistinct and irregular vascular spaces of capillary size were seen in some of these solid tumor nodules. All but one of the cases showing areas of nodular tumor with the capillary or anaplastic growth patterns also had other areas of angiosarcoma which exhibited sinusoidal, papillary, and/or cavernous growth patterns. One of the angiosarcomas was composed of markedly enlarged rounded cells with nuclei that showed marked variation in size and shape. Mitoses were frequently seen and scattered cells had multiple, bizarre shaped nuclei. These anaplastic cells
Thomas & Popper: Pathology of Liver Angiosarcoma 273
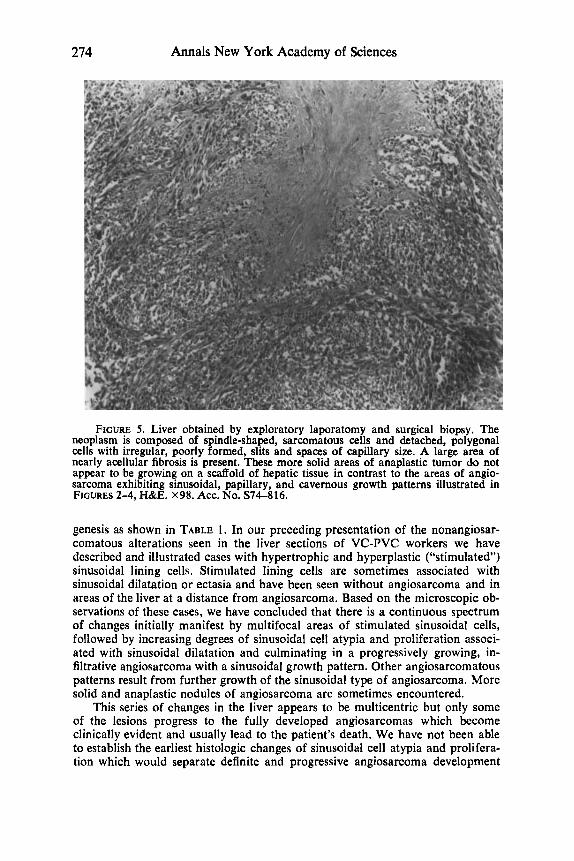
FIGURE 4. Another portion of the angiosarcoma illustrated in FIGURE 3. The space of Disse is widened and contains scattered non-neoplastic-appearing cells including fibroblasts, lipocytes, and macrophages. Special stains also show increased reticulin and collagen fibers. Several bile plugs can be seen in bile canaliculi. H&E. X392. Acc. NO. A74-3 1 .
lined vascular spaces of various sizes and also infiltrated and lined the intimal surfaces of branches of the portal vein.
Angiosarcoma of Other Organs This aspect of our review is preliminary and incomplete because we have
reviewed the complete autopsies of only 1 or 2 of the patients with angiosarcoma of the liver. In 1 patient, sections of the duodenum showed microscopic foci of angiosarcoma in the wall of the duodenum. In another patient with massive angiosarcomatous involvement of the liver which weighed 5200 g, there were also discrete deposits of angiosarcoma in the lungs, myocardium, epicardium, kidney, peritoneum, muscularis of the small intestine, mesentery, mesenteric lymph node, and retroperitoneum. These deposits of angiosarcoma showed principally capillary and cavernous growth patterns. Even the papillary growth pattern was evident in the angiosarcoma in the heart and kidney with cardiac muscle fibers forming the core of the papillary projections in the heart and widely separated renal tubules forming the scaffolding for the papillary projections of the angiosarcoma in the kidney.
DISCUSSION The histologic features of the angiosarcomas of the liver in 13 VC-PVC work-
ers have been described in some detail in order to present a concept of their patho-
274 Annals New York Academy of Sciences
FIGURE 5. Liver obtained by exploratory laporatomy and surgical biopsy. The neoplasm is composed of spindle-shaped, sarcomatous cells and detached, polygonal cells with irregular, poorly formed, slits and spaces of capillary size. A large area of nearly acellular fibrosis is present. These more solid areas of anaplastic tumor do not appear to be growing on a scaffold of hepatic tissue in contrast to the areas of angio- sarcoma exhibiting sinusoidal, papillary, and cavernous growth patterns illustrated in FIGURES 2-4, H&E. x98. Acc. No. S74-816.
genesis as shown in TABLE 1. In our preceding presentation of the nonangiosar- comatous alterations seen in the liver sections of VC-PVC workers we have described and illustrated cases with hypertrophic and hyperplastic (“stimulated”) sinusoidal lining cells. Stimulated lining cells are sometimes associated with sinusoidal dilatation or ectasia and have been seen without angiosarcoma and in areas of the liver at a distance from angiosarcoma. Based on the microscopic ob- servations of these cases, we have concluded that there is a continuous spectrum of changes initially manifest by multifocal areas of stimulated sinusoidal cells, followed by increasing degrees of sinusoidal cell atypia and proliferation associ- ated with sinusoidal dilatation and culminating in a progressively growing, in- filtrative angiosarcoma with a sinusoidal growth pattern. Other angiosarcomatous patterns result from further growth of the sinusoidal type of angiosarcoma. More solid and anaplastic nodules of angiosarcoma are sometimes encountered.
This series of changes in the liver appears to be multicentric but only some of the lesions progress to the fully developed angiosarcomas which become clinically evident and usually lead to the patient’s death. We have not been able to establish the earliest histologic changes of sinusoidal cell atypia and prolifera- tion which would separate definite and progressive angiosarcoma development
Thomas & Popper: Pathology of Liver Angiosarcoma 275
TABLE 2 PATHCGENESIS OF HEPATIC LESIONS IN VC-PVC WORKERS
Fibrosis Capsule
1 ) Portal tracts --$Portal hyper- ,Splenomegaly Intralobular (peri- tension Varices
sinusoidal) Proliferation of bile ducts Proliferation of sinusoidal fMulticentric (sinusoidal)
2) lining cells with --$Atypical hyper- angiosarcoma enveloping sinusoidal dilatation plasia hyperplastic and atrophic
hepatocytes and bile duc- /* tules Stimulation of hepatocytes +Proliferation of ~ ? Regenerating nodules
3) “megalocytosis” hepatocytes “little cell-big cell” I ? Hepatoma
change
from the more static, apparently non-neoplastic changes of “stimulated” sinus- oidal lining cells and sinusoidal dilatation. Also we cannot determine by micro- scopic observations alone whether angiosarcomas in organs other than the liver represent metastases or multiple primary angiosarcomas. It is our opinion, how- ever, that a t least some of the angiosarcomas in other organs represent independ- ent, primary neoplasms.
I n TABLE 2 we have attempted to summarize and show by diagram the rela- tionships and pathogenesis of the various hepatic lesions observed in the livers of the VC-PVC workers. The pathogenesis of the angiosarcomas has been described and discussed. I t should be reemphasized, however, that hyperplastic hepatic parenchymal cells appear to contribute to the sinusoidal and papillary patterns of the angiosarcomas. Also the proliferation of non-neoplastic stromal cells, includ- ing fibroblasts, lipocytes, and macrophages, although not included in the diagram, was observed in areas of some of the angiosarcomas. Progressive fibrosis involv- ing the hepatic capsule, the portal tracts and, in some cases, the intralobular por- tion of the hepatic lobules may contribute to portal hypertension which in turn is associated with varices and splenomegaly.
Pronounced stimulation and proliferation of hepatocytes was observed in several patients and in one patient led to regenerating nodules of hepatic tissue. The liver of this patient exhibited all the other hepatic changes we have described including progressive fibrosis and angiosarcoma; thus, he was the only patient in whom cirrhosis was associated with and seemed to be related to the other hepatic changes characteristic of VC-PVC exposure. In several other patients the progres- sive fibrosis produced gross and microscopic nodularity of the liver but these changes were not associated with regenerating nodules and were not diagnosed as cirrhosis. Theoretically, at least, the changes in hepatocytes might lead to the de- velopment of hepatocellular carcinomas in some VC-PVC workers but additional cases must be examined before such a relationship can be established.
The bile ductules had proliferated in nearly every liver which exhibited pro- gressive fibrosis and were often enveloped by angiosarcoma. However, the epi- thelium of these bile ducts lacked atypical, cellular features and appeared most often to be atrophic and compressed by the surrounding fibrous connective tissue.
An attempt has been made to relate the various changes seen microscopically in the livers of these VC-PVC workers in a conceptual scheme for the patho-
276 Annals New York Academy of Sciences
genesis of portal hypertension and splenomegaly and the development of hepatic angiosarcomas. Chronic exposure to VC in the production of PVC resins, or perhaps some metabolic product of VC, caused stimulation and proliferation of both the parenchymal cells and the stromal cells of the liver. Whether the toxic material accumulates in or effects only one type of cell or all of these cells simul- taneously is unknown. Studies of the pharmacologic and metabolic effects pro- duced by VC on these various cells will be necessary to answer these questions. Further studies of the hepatic changes and angiosarcomas produced by Thoro- trast* and by arsenical compounds' should evaluate the similarities and dissimilari- ties between the lesions produced by these materials and the hepatic lesions in the VC-PVC workers.
SUMMARY We described the histologic features of 13 hepatic angiosarcomas which de-
veloped in workers engaged in the polymerization of vinyl chloride to polyvinyl chloride. Although the histologic features varied considerably in different portions of the angiosarcoma in the same liver and in the angiosarcomas of the liver from different patients, many features were similar such as sinusoidal, papillary, and cavernous growth patterns coincident with the precursor lesions of proliferation and atypia of sinusoidal lining cells.
ACKNOWLEDGMENTS The authors wish to thank the several pathologists who were completely co-
operative in lending slides for review and who also provided representative paraffin blocks to cut additional sections for special stains.
REFERENCES 1. CREECH, J. L., JR. & M. N. JOHNSON. 1974. Angiosarcoma of liver in manufacture
of polyvinyl chloride. J. Occupational Med. 16: 150-151. 2. CREECH, J. L., JR., M. N. JOHNSON & B. BLOCK. 1974. Angiosarcoma of the liver
among polyvinyl chloride workers-Kentucky. Morbidity Mortality Weekly Rep. 23: 49-50. Department of Health, Education and Welfare, Center for Disease Control Publication No. (CDC) 74-8017.
3. SWARM, R. L., E. MILLER & H. J. MICHELITCH. 1962. Malignant vascular tumors in rabbits injected intravenously with colloidal thorium dioxide. Pathol. Microbiol. 25: 27-44.
4. ROTH, F. 1957. Arsen-Leber-Tumoren (Hemangioendotheliom). Z. Krebsforsch. 61: 468-503.
DISCUSSION DR. S. DAUM (Mount Sinai School of Medicine, New York): I noticed that
Dr. Popper included in his description of cases one case of hepatocellular car- cinoma-primary carcinoma of the liver-in which he described focal areas of hepatocellular activation other than in the tumor. I believe I was clinical con- sultant on this case, in which the hepatic tumor was resected at Mount Sinai Hospital prior to the news in the Wall Street Journal of January 24th (1974).
This man worked in a polyvinyl chloride fabrication plant making shower curtains for 17 years prior to the onset of his tumor. I want to ask whether Dr. Popper considers this a tumor from the occupational exposure to vinyl chloride fumes which emanated from the lamination of the plastic in this process?
Thomas & Popper: Pathology of Liver Angiosarcoma 277
DR. H. POPPER (Mount Sinai School of Medicine, New York): I don’t know. DR. FAIRCHILD: Do you see progression of the development of liver cell
change before you see the lining cell effect? Do these occur at the same time or one before the other?
DR. L. B. THOMAS (Nationnl Cancer Institute, Bethesda, Md.): We definitely have seen in many of the biopsies of patients, including those who did not have angiosarcoma, rnegalocytosis or change in the hepatocytes, and the very earliest changes associated with the fibrosis before sinusoidal dilatation and activation of sinusoidal lining cells.
DR. D. MARLOW (Environmental Protection Agency, Durham, N.C.): Dr. Thomas, the implication from your talk was that wherever connective tissue exists there is the potential for the involvement of the organ with these effects, for angiosarcoma. Would you say that is correct?
DR. L. B. THOMAS: No, I would not say that it is correct. Now, I should qualify that “no” by saying that our total experience in looking at various tissues of the body is fairly small.
DR. POPPER: I think one key point should come out which Dr. Thomas and I cannot prove but have good reason to believe. The proliferation of the hepato- cytes has some influence in the development of angiosarcoma. That may sound a little bizarre, but similar situations exist in pathology. I suspected, and we learned today, that we might find fibrosis in the lung. In the spleen, there is primarily stimulation and not much fibrotic change, primarily endothelial stimula- tion, mesenchymal stimulation.
I have a feeling that activation of the hepatocyte almost runs parallel with the proliferation of the fibroblast. The problem is: Does the hepatocyte play some role in the development of the malignant stage?
DR. N. WILLIAMS: I get the impression that you feel that the angiosarcomas are multicentric. If so, this would rule out the possibility of any surgical treat- ment for this condition. One would have to rely entirely on chemotherapy. Am I right in interpreting your views this way?
DR. THOMAS: Unfortunately, I think that is the implication of what we have seen. Obviously, one or another of the nodules becomes the predominant one and the mass that makes the clinical nodule that can be felt, or the hemorrhagic tumor that causes hepatic failure. But other lesions are present, in other areas of the liver.
DR. POPPER: Maybe there is a ray of hope. In view of the fact that the hepatocytes are still functioning, and since many of the chemotherapeutic agents are metabolized in the liver, chemotherapy could be particularly effective.



![A solid phase extraction procedure for Fe3+, Cu2+ and Zn2+ ions on 2-phenyl-1H-benzo[d] imidazole loaded on Triton X-100-coated polyvinyl chloride](https://img.dokumen.tips/doc/110x75/635e2aa9676af2c2c70c08d4/a-solid-phase-extraction-procedure-for-fe3-cu2-and-zn2-ions-on-2-phenyl-1h-benzod.jpg)

























