Embed Size (px)
Citation preview
PARTICIPATORY ACTION RESEARCH FORENVIRONMENTAL HEALTH: ENCOUNTERING
FREIRE IN THE URBAN BARRIO
ERUALDO ROMERO GONZALEZ, RAUL P. LEJANO,GUADALUPE VIDALES, ROSS F. CONNER
University of California, Irvine
YUKI KIDOKORO, BAHRAM FAZELI, AND ROBERT CABRALESCommunities for a Better Environment
ABSTRACT: The community-based approach to health research and intervention is a model ofinquiry rooted in Freire’s participatory action research (PAR). We need to show, in concept andpractice, what it is about PAR that may be well suited for the types of health issues we encounter ininner-city environments. What type of learning results, how does this respond to particular healthissues in the urban context, and what are the particular challenges faced in translating Freire’smodel into today’s urban setting? To investigate these questions, we describe a recent PAR project inSoutheast Los Angeles, California—an area known to some as “Asthmatown.” One salient findingof the research is that PAR allows the integration of complex and multiple forms of knowledge,and this is a necessary response to the complex and multiplex nature of cumulative impacts. Thereare challenges to translating the model to the urban setting, however, such as the difficulties ofparticipation in today’s urban milieu. The research leads to some lessons for practitioners, such asthe need to build “constant” elements into PAR projects. Lastly, we reflect on implications of thismodel for institutional reform.
INTRODUCTION
There has been an important turn toward community-based approaches to health researchand intervention in the United States (Annett & Nickson, 1991; Fraser, 2005; George, Green, &Green, 1999; Israel, Eng, Schulz, & Parker, 2005; Israel, Schulz, Parker, & Becker, 1998; Minkler,2000; Minkler & Wallerstein, 2003; Schulz, Israel, Selig, Bayer, & Griffin, 1998; Swindell, 2000).Part of this trend stems from efforts by the state to devolve itself of responsibilities for healthand other services in local communities (Dillinger, 1994; Manor, 1999). Another reason includesthe hope that community-based approaches might better respond to the health needs of com-munities. There is a gap in the literature, however—namely, the need to show that this modeldoes fit the particular needs of present-day urban communities. In particular, how does the type
Direct Correspondence to: Professor Raul P. Lejano, Department of Planning, Policy, and Design, 202 Social Ecology I,University of California, Irvine, California 92697-7075. Email: [email protected]
JOURNAL OF URBAN AFFAIRS, Volume 29, Number 1, pages 77–100.Copyright C© 2007 Urban Affairs AssociationAll rights of reproduction in any form reserved.ISSN: 0735-2166.
78 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
of learning involved meet the health challenges in today’s inner-cities and urban peripheries?Another gap in the literature is its tendency to characterize community-centered approaches ty-pologically, in a generalized fashion, whereas the real need is to enter more deeply into thecomplex particulars of this model of action. This article attempts to bridge some of these gapsin the literature by linking the complexity of real-world experience to theory. Specifically, weshow how multifaceted forms of community knowledge are necessary to respond to the com-plex and multiplex nature of cumulative impacts in vulnerable communities. Conceptually, thismode of engagement draws its origins from the model of participatory action research (PAR)espoused by Paolo Freire and others (Chambers, 1983; Freire, 1973; Korten, 1983), which orig-inated among agricultural households in rural Brazil and which, in its time, addressed issuessomewhat removed from those in today’s urban setting. The questions that we pose concern themanner by which this model might (or might not) fit the particular issues found in today’s urbancontext:
1. How does the PAR model address knowledge needs for effective health intervention intoday’s lower-income inner cities and urban peripheries?
2. In terms of practice, what are the particular challenges faced in translating the Freireanmodel to the urban setting?
We begin by examining the model in concept and reviewing some of the literature on PAR.Using the Southeast Los Angeles (SELA) PAR Project as a case study, we then examine how PARmight fit the general condition of many of today’s urban communities. We will contrast PAR witha more classic model of health research, epidemiology, in order to underscore the distinguishingfeatures of the former. We then analyze how the SELA PAR Project is practiced in order to learnwhat the challenges are in fitting the model to the urban experience. The case study was in an areathat has been dubbed by some as Asthmatown (Bansal, Bacon, & Davis, 1998). As we discussbelow, our findings have important implications for the practice of PAR for health research andintervention in urban environments. While the insights arrived at in this research directly pertainto the specific context of SELA, we feel that the findings may, to some extent, be transferable toother settings.
THE PAR MODEL: CONCEPTUAL FOUNDATIONS AND PRINCIPLES
PAR draws from a long intellectual history, beginning in the early 20th century, when therearose a phenomenological view of knowledge. Heidegger (1927/1962), Husserl (1900/1970),and Merleau-Ponty (1945/1989) claimed that the essence of meaning was to be found not inobservation of the object by the subject, as is in classical scientific analysis, but in subjectiveexperience. The essence of phenomenology was the edict that we should tend “to the thingsthemselves” and enter into pure descriptions of the experience. This epistemology, which isimplicit in PAR, is not primarily about a subject observing an object, but a community of subjectsreflecting on themselves and their experiences (Sullivan, Kone, Senturia, Chrisman, Ciske, &Krieger, 2001; Van Vlaenderen, 2004). Closer to the realm of practice were the writings of thepragmatist, John Dewey, who maintained that learning came not out of objective measurement,but practical engagement (Dewey, 1925). Most centrally, it was Paolo Freire (1973), a Brazilianpedagogist, who sought to reverse the traditional directionality of education (and the positivisttradition), which was that of:

II Research for Environmental Health II 79
expert → lay person;technocrat → peasant;academic → community
and, instead, build a richer model:
practitioner/expert ←→ practitioner/expert
practitioner/expert
—in other words, building a community of grounded or indigenous experts. This reversal is alsoechoed in the later, Habermasian theorization of knowledge and rationality as intersubjective(Habermas, 1987). Freire’s conceptualization greatly influenced the field of learning in areassuch as rural development (Chambers, 1983; Korten, 1983), neighborhood planning (Checkoway,1984), public health (Giachello et al., 2003; Israel et al., 2005; Minkler, 2000; Wilcox & Knapp,2000), popular epidemiology (Brown, 1997, 2000), and environmental health and risk perception(Kroll-Smith & Floyd, 2000; Tesh, 2000). While we may use the terms “PAR” and “Freirean”interchangeably, we note that they are not simply synonymous. PAR also draws from other linesof applied research, such as Kurt Lewin’s work on Action Research (Lewin, 1946) wherein hedevelops a theory of “learning by doing.” This line of work has since been taken up by numerousresearchers (Susman, 1983; Trist, 1985; Winter, 1989) as well as Argyris and Schon (1974).Reflective practice is probably most clearly manifested in the Freirean process of conscientizationor critical reflection. Epistemologically, critical reflection by community is needed to access acomplex phenomenon, such as health and quality of life, which is wrought by the intersection ofsocial, historical, and physical determinants and not amenable to pure observation.
PAR is defined by Green, George, & Daniel (2003), cited in Minkler, as “systematic inquiry,with the collaboration of those affected by the issue being studied, for the purpose of educationand taking action or effecting social change” (Minkler, 2000, p. 192). A number of academics haveattempted to expound the principles of PAR. PAR is linked by six different but not necessarilyexclusive principles:
1. Community participation, allowing access to local knowledge regarding determinants ofhealth and quality of life,
2. Broad epistemological orientation, recognizing that there are multiple ways of knowing andacquiring knowledge,
3. Linking knowledge to action,4. Empowerment, whereby participants, researchers, and other collaborators share decision
making in the design, implementation, interpretation, and dissemination of data,5. Capacity building, through which the strengthening of bonds and assets among participants
contributes to sustained health monitoring and intervention activities,6. Balance between abstract process outcomes (e.g., community and social capital) and more
distal and/or concrete accomplishments (e.g., reducing disease prevalence and improvingquality of life) (Bansal et al., 1998; Israel et al., 1998; Minkler, 2000; Mora & Diaz, 2005;Wilcox & Knapp, 2000).
EXAMPLES OF PAR PROJECTS
The social and health sciences literature provides case studies of PAR wherein researchersand residents jointly investigate and act upon a variety of urban issues, such as chronic diseases,
80 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
environmental health hazards and risks, inadequate access to health care, social determinants ofhealth, mental health, economic development, housing, and social capital (Brown, 2000; Cagan,Hubinsky, Goodman, Deitcher, & Cohen, 2001; Corburn, 2003; Gittell & Vidal, 1998; Israelet al., 2005; Lasker & Weiss, 2003; Metzler et al., 2003; Minkler, 2000; Mullings & Wali,2001; Tesh, 2000; Wood, 2002). Each of these projects adapted the PAR approach accordingto local conditions, and as a result modes of engagement and methodologies varied from onesetting to another. For instance, the Woburn, Massachusetts case is a classic example of popularepidemiology that utilized lay experiential knowledge of health effects of exposure to toxic hazardsand pollutants as a basis for advocating policy change (Brown, 1987; Brown, Kroll-Smith, &Gunter, 2000). In the Tribal Efforts Against Lead (TEAL) population-based biomedical study, thefocus of the collaboration was the development of educational material and outreach programs toaddress childhood lead poisoning (O’Fallon & Dearry, 2002). As another example, the HealthyEnvironments Partnership (HEP) incorporated resident participation in combining a population-based survey with a neighborhood observational instrument investigating the contributions ofsocial and physical environments to risk factors for cardiovascular disease in Detroit, Michigan(Zenk, Schulz, House, Benjamin, & Kannan, 2005). Yet a different mix of methods was foundin the Healthy Neighborhoods Project (HNP) of West Contra Costa, California, a multisectorcollaboration that involved residents in researching community quality-of-life needs using door-to-door interviews, asset mapping, and community forums (Minkler, 2000). While these PARprojects differ in the nature of resident involvement and collaborative research methods, eachattempts to reverse the traditional directionality between “observer” and “subject” by having acommunity of subjects reflecting on themselves and their experiences.
In the following discussion, we will reflect on how the PAR model fares against the complexityof urban health issues. What this requires is what Geertz (1973) called “thick description,” a modeof inquiry that aspires toward analyses of a complex and grounded nature to match the phenomenonbeing studied. This need for multiple descriptives is seen in PAR through the employment ofdiverse data collection methodologies.
CONTEXT AND METHODOLOGY
The case study is based on the recent SELA PAR Project initiated by Communities for a BetterEnvironment (CBE), a non-profit environmental justice organization in Southeast Los Angeles(SELA). CBE has a long history of activist engagement in communities of color, resulting in thecessation of noxious land uses (e.g., a power plant in Santa Fe Springs, California). CBE’s activistmodel utilizes a three-pronged strategy: (a) grassroots activism; (b) environmental research, and(c) legal assistance. Boundaries between community and CBE blur, since CBE’s communityorganizers are people who grew up and reside in SELA—this strengthens CBE’s ability to representthe community (Swindell, 2000).
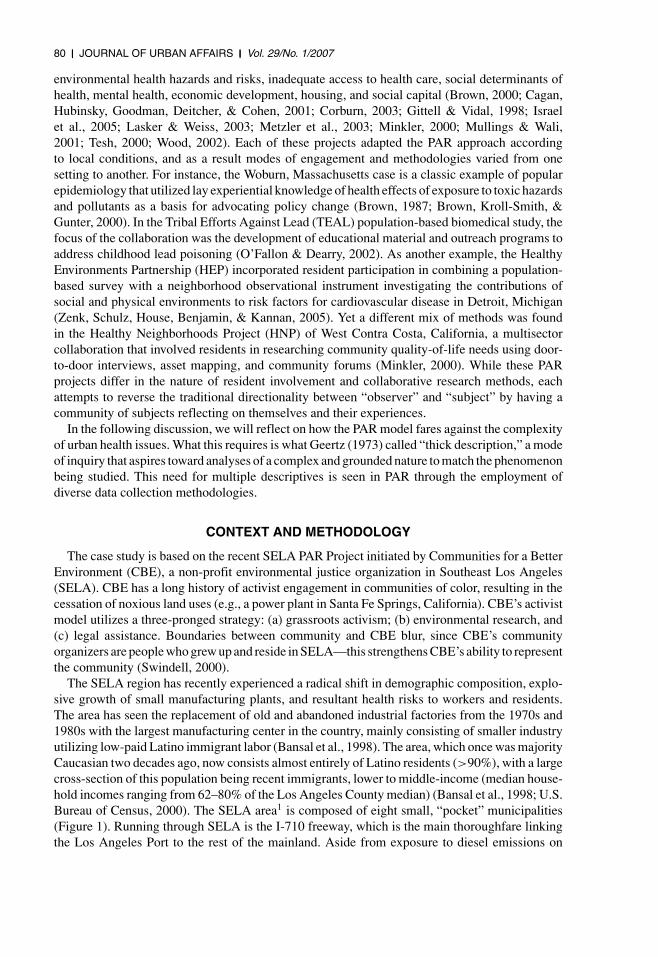
The SELA region has recently experienced a radical shift in demographic composition, explo-sive growth of small manufacturing plants, and resultant health risks to workers and residents.The area has seen the replacement of old and abandoned industrial factories from the 1970s and1980s with the largest manufacturing center in the country, mainly consisting of smaller industryutilizing low-paid Latino immigrant labor (Bansal et al., 1998). The area, which once was majorityCaucasian two decades ago, now consists almost entirely of Latino residents (>90%), with a largecross-section of this population being recent immigrants, lower to middle-income (median house-hold incomes ranging from 62–80% of the Los Angeles County median) (Bansal et al., 1998; U.S.Bureau of Census, 2000). The SELA area1 is composed of eight small, “pocket” municipalities(Figure 1). Running through SELA is the I-710 freeway, which is the main thoroughfare linkingthe Los Angeles Port to the rest of the mainland. Aside from exposure to diesel emissions on
II Research for Environmental Health II 81
FIGURE 1
Map of Southeast Los Angeles, California
I-710, residents in SELA are beleaguered by the confluence of hundreds of small, rail-relatedlight industries that collectively generate nuisance conditions and cumulative health risks. Somerefer to SELA as “Asthmatown,” though the perception of high prevalence of pulmonary andother illnesses in SELA is largely anecdotal.
SELA can be seen as a classic environmental justice situation where lower-income communitiesof color are beleaguered by multiple environmental hazards, that is, cumulative risk (for earlytreatments of environmental justice, see Been & Gupta, 1997; Bullard, 1990; USGAO, 1983;UCC, 1987). The literature has, by now, clearly delineated the “recipe” for cumulative risk, whichis incompatible land use and socioeconomic vulnerability. The particular form in which theseissues manifest themselves in Southern California have been well documented in the literature(see Houston, Ong, & Winer, 2004; Lejano & Iseki, 2001; Lejano, Piazza, & Houston, 2002;Morello-Frosch, Pastor, & Sadd, 2001; Pastor, Sadd, & Hipp, 2001; Pulido, Sidawi, & Vox, 1996).
In 2003, CBE received funding from First 5 Los Angeles, an initiative of the Proposition10 Commission. The grant called for building community “capacity to use research to createsustainable, grassroots strategies to improve the lives of children of ages 0–5, their families, andthe communities that they live in” (First 5 LA, 2002). CBE then approached the University ofCalifornia, Irvine (UCI) as a research partner. The authors of this article were the same personsthat were contacted to form the CBE/UCI project team.
We used process mapping methods (Huff & Jenkins, 2002) and participant–observer modes ofinquiry (Yin, 2003) to study the project. As an aid to analyzing the PAR process, some participantsmaintained journal notes throughout the project. Process mapping involves organizing projectevents through various logics—by ordering them chronologically, then grouping activities bythemes. Participant–observer methods involve reflection on the experience of PAR on the partof the project participants. This included reviewing project meeting notes, participant–observerjournal notes, workshop tapes, and interviews with key stakeholders. These different sourcesof information were categorized, and elements in them were linked to themes that emergedfrom these artifacts, in a process akin to content analysis, performed with multiple types ofartifacts. We derived conceptual models from the PAR experience in a process of pattern-matching(Yin, 2003), in this case against both the conceptual Freirean template, as well as the classic
82 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
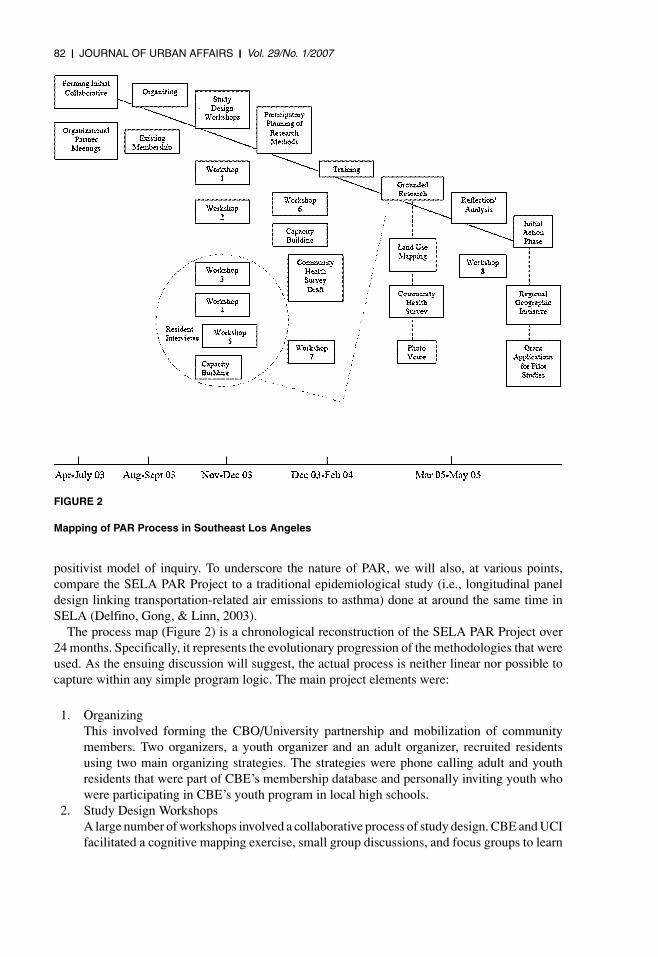
FIGURE 2
Mapping of PAR Process in Southeast Los Angeles
positivist model of inquiry. To underscore the nature of PAR, we will also, at various points,compare the SELA PAR Project to a traditional epidemiological study (i.e., longitudinal paneldesign linking transportation-related air emissions to asthma) done at around the same time inSELA (Delfino, Gong, & Linn, 2003).
The process map (Figure 2) is a chronological reconstruction of the SELA PAR Project over24 months. Specifically, it represents the evolutionary progression of the methodologies that wereused. As the ensuing discussion will suggest, the actual process is neither linear nor possible tocapture within any simple program logic. The main project elements were:
1. OrganizingThis involved forming the CBO/University partnership and mobilization of communitymembers. Two organizers, a youth organizer and an adult organizer, recruited residentsusing two main organizing strategies. The strategies were phone calling adult and youthresidents that were part of CBE’s membership database and personally inviting youth whowere participating in CBE’s youth program in local high schools.
2. Study Design WorkshopsA large number of workshops involved a collaborative process of study design. CBE and UCIfacilitated a cognitive mapping exercise, small group discussions, and focus groups to learn
II Research for Environmental Health II 83
about the main elements of the project design that were important to residents. The mainelements included defining the scope of health issues to be examined (e.g., environmentalexposures, quality of life, violence), the primary study population (children aged 0–5 years,families), and construction of the resident interview guide and the community health survey.Resident participation in the workshops generally ranged from 3 to 10 adult residents andfrom 4 to 10 youth, with youth having the most consistent attendance.
3. Resident InterviewsParticipating community members decided to interview other residents in their homes abouttheir health concerns. The resident interview guide was open ended and obtained insights intowhat factors in the local neighborhood affected children’s health, especially young children.These factors ranged from the immediate household environment to the broader community.The interviews were audio taped, transcribed, and analyzed in succeeding workshops. Theresults of the analysis were used to construct some of the questions for the community healthsurvey.
4. Land Use MappingBased on preliminary input from the workshops, wherein residents spoke of a large numberof problematic land uses, a team started logging and mapping land use patterns in HuntingtonPark. This was subsequently translated into a “risk mapping” (Lejano & Smith, 2006). Therisk mapping was developed by utilizing TRI (Toxics Release Inventory) data to obtain percapita emission estimates for the list of toxic pollutants regulated in California for each ofthe relevant SIC codes in the study area. The per capita emission rates were then multipliedby employee counts for each business in the SELA area to obtain estimates of emissionsfor these small sources. Employee figures were obtained from the Dunn and Bradstreetcommercial business database.
5. Community Health SurveyThe community health survey (n = 109) obtained quantitative and qualitative data that in-cluded the following topics: child and adolescent health, insurance coverage, and perceptionsof neighborhood problems. The non-random survey was administered in SELA neighbor-hoods where CBE had a previous working relationship. This involved collecting data fromhouseholds and residents who were visiting local parks and self-identified as living in theSELA area. The survey team consisted of eight members, which typically involved oneresident paired with one UCI undergraduate student. In the planning meetings, the residentsand CBE representatives thought it was not necessary to use a more rigid randomizationtype design. The data were later mapped using GIS (Geographic Information System).
6. Photo-voiceThe photo-voice project was designed to photograph some of the problems that residentsbelieved existed in their community. Residents (five adult female mothers and five teenagers)participated in the project. The residents attended photo-voice planning meetings held atCBE and learned about participatory theory, the ethics of photography in the public space,and the basics of photographic composition. Participants were provided with disposablecameras and notebooks to annotate the photographs that were taken in a 2-week time period.The photographs were subsequently developed and transferred to compact discs (CDs). Atsubsequent planning meetings, participants were asked to discuss their experiences takingphotographs and to reflect on the photos as a group. Participants arranged the photographson easels according to four themes: air quality, health, children, and open space. Participantsalso wrote personal statements that described each photograph.
7. Reflection/AnalysisThe final element involved ongoing reflection workshops for interpreting data and develop-ing intervention (e.g., asthma surveillance, risk reduction).
84 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
ANALYSIS AND DISCUSSION
How the PAR Model of Learning Addresses the Issues in SELA
We observed how the PAR model allowed the community a point of entry into environmentalhealth issues in the neighborhood—this had implications for the health research. We discuss thefindings below.
1. PAR is suited for environmental health issues of a high degree of complexity, since it enablesthe integration of multiple lines of evidence and multiple ways of knowing. This allows usto discover new sources of risk in the urban setting.
The very first activity of the Study Design Workshops was a cognitive mapping exercise, inwhich residents drew sketches about issues in their neighborhood. These early workshops led theparticipants to a deeper understanding of the complexity of environmental health issues in SELA.Through these exercises, it became clear that the origins of environmental health concerns inSELA arose from a bewildering array of sources—including traditional polluters, small industries,mobile sources, railway and other hazards, congested schools, ill-maintained housing, etc.
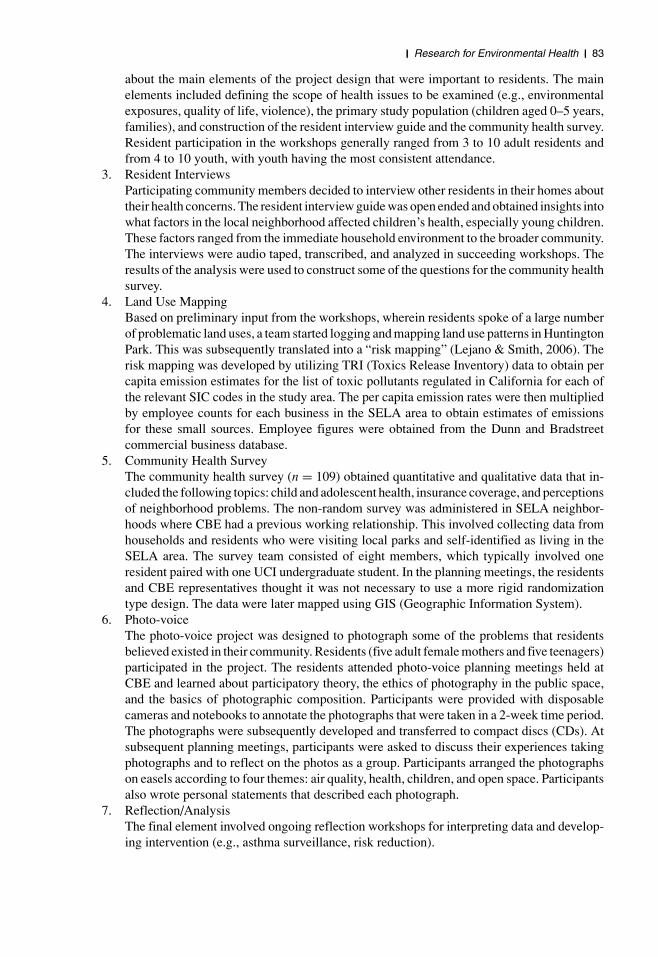
The cognitive mapping exercise brought up questions which motivated the study team to takea closer look at land use, including the northern part of Huntington Park. The cognitive mappingexercises and workshops only provided part of the information sought in PAR, most specificallyqualitative data about sources of pollution and social determinants of health (e.g., lack of insurance,work patterns). This prompted the use of diverse methodologies to understand land use problems,including residents’ interviews, the community health survey, photo-voice, and GIS mapping. Thediverse methodologies allowed the discovery of new sources of vulnerability due to the present-day urban experience. Figure 3 shows how residences and small sources of toxics are intertwined.
Figures 1 and 3, taken together, speak to the complexity of environmental health risks foundin SELA. These communities sit alongside the I-710 freeway and Alameda Avenue, which aremain transportation corridors from the Los Angeles/Long Beach Ports to the rest of California.This gives rise to air emissions, hazardous waste spills, and other risks from diesel truck andother vehicular traffic. Moreover, proximity to these corridors, along with the balkanized politicaldynamic arising from having eight small municipalities competing for land uses has created thetype of complex land use pattern seen in Figure 3. The effect of carving up SELA into eight pocketmunicipalities resulted in some competition for industries that gravitate toward the railway andAlameda corridor (as documented in Broome & Modarres, 1999). This presented a race-to-the-bottom scenario wherein these cities catered to these dirtier industries with more lax standardsand zoning laws than the nearby City of Los Angeles. The degree to which risk facilities andresidences sit side-by-side in SELA is part of the complex nature of risk.
Why might PAR be a suitable mode of research in SELA? The classic, statisti-cal/epidemiological model of research requires already defined hypotheses. These hypotheses,moreover, need to be specified narrowly enough so that fairly precise answers to specific questionscan be arrived at. None of these are possible in SELA, however, since the possible sources ofrisk are myriad enough and possible routes of exposure complex enough, that we cannot yet formsharp hypotheses. Rather, PAR allows one to enter into a discovery-based mode of inquiry thatencourages the identification of multiple hypotheses, using knowledge from different sources. Infact, the first few meetings of the Study Design Workshops revolved around generating questionsthat residents considered important. Knowledge about what problems SELA residents face goesbeyond simple hypotheses regarding the toxicology of environmental exposures—since PAR
II Research for Environmental Health II 85
FIGURE 3
Close-up of a Portion of Huntington Park (SELA)
requires linking knowledge discovery to new avenues for action, we needed to ask questionsabout what processes cause such land use patterns, regulatory laxity, and other phenomena, inthe first place. All of these require the multiple modes of inquiry found in PAR, instead of theunimodal methodology of the classic model. Contrast this to the narrow hypothesis that a classicepidemiological research design generates in the case of SELA—that is, that proximity to theI-710 freeway causes pulmonary disease (Delfino et al., 2003).
86 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
The workshops brought up another area of complexity: the different elements of vulnerabilitythat made up the community “etiology” of environmental health in SELA. By vulnerability,we mean the overlapping of health outcomes, lack of health access, proximity to sources ofair toxics, and others (Pastor, Morello-Frosh, & Sadd, 2005). While there is much literatureon general linkages between neighborhood characteristics and health (e.g., Ellen, Mijanovich,& Dillman, 2001), we need a closer look at actual patterns of movement and land use in acommunity to see specific mechanisms at work. For example, risks from exposure to air toxicsare exacerbated by the lack of daycare facilities inasmuch as parents are increasingly forced to takeinfants on day trips, and exposures to pollutants such as diesel particulates may primarily occurin transit between home and other sites. These are aspects of the complexity of vulnerability thatseems particular to today’s urban condition, especially given dwindling job security and benefits,globalization of traditional industries, and technology-enabled industrial diffusion. On the otherhand, these risks are mitigated by the widespread use, in SELA, of extended family networks forchildcare.
PAR in Contrast to Traditional Research
It is somewhat fortuitous that we find, in SELA, both epidemiological and PAR-centered re-search projects occurring almost concurrently. In portraying epidemiology and PAR in contrastingterms, we do not mean to imply that these research models should be considered as mutually ex-clusive alternatives. In fact, as we will show toward the end of the article, the complexity of healthrisks in SELA necessitates employment of both in complementary fashion. Our point is that PARfills knowledge gaps in epidemiology, and vice versa. As we will see, epidemiology invariablyoperates on homogenous bodies of data—that is, the ideal is to get data of the same form for asufficiently large sample size. PAR, on the other hand, operates on a richer set of information,often existing in varying forms.
This is not to say that the gulf between the two is necessarily unbridgeable. In fact, the growingarea of social epidemiology is increasingly considering more complex, community pathways tohealth and disease and, in the process, gradually bringing more diverse types of knowledge intothe analysis (e.g., socioeconomic stratification, social networks and support, and discrimination).For example, Kawachi and Berkman (2000) discuss how social cohesion and social capital mayinfluence health behaviors and access to health services. Krieger (2000) argues that discrimina-tion harms health among subordinate populations. Marmot (2000) suggests that the prevalence ofpoor health in both men and women could be largely explained by a myriad of influences frompreschool, school age, and working life. The aforementioned authors often draw from multiplelines of information, including the qualitative. The complexity and uncertainty surrounding thephenomena they investigate requires the use of multiple lines of information. PAR is instrumentalin this regard, since it emphasizes the employment of different modes of learning and their inte-gration into a thick description of community health. The multipronged PAR approach respondsto needs brought up in the literature for community-based approaches that can respond to thecomplexity of real-world community problems (Lasker & Weiss, 2003).
The SELA PAR Project used multiple data collection instruments: resident interviews, com-munity health surveys, and photo-voice. Since there is no environmental or industrial monitoringof small sources, we relied on the residents’ perceptions of nuisance effects (i.e., noise, odor) andassociated symptoms (e.g., nausea, headaches, throat irritation) and had to combine quantitativeand qualitative information. The most distinctive contrast is the manifold nature of informationgenerated by PAR (photographs, testimonials, statistical data, and others) versus the unimodaldata of epidemiology. The community health survey itself combined multimodal information,including standard health outcomes (e.g., a prevalence of childhood asthma of 16.7% was found
II Research for Environmental Health II 87
in SELA, as compared to 6.5% over all of Los Angeles County), measures of vulnerability (e.g.,21.8% reported transportation a major barrier to health care access), and qualitative information onresidents’ concerns. For example, the interviews provided narratives that suggested how residentslive with the ubiquity of risk, as in the following excerpt:
. . . When the school children are coming, the train is passing, it seems very dangerous. Andthere are some factories that are . . . they are some factories that are right here . . . I think thatthey are hurtful for . . . because of the fumes that come out for the children . . . for the children’shealth . . . Oh yes . . . well, I think the dust from the fabrics or something comes out . . . I think.That could be something . . . Oh yes, because when I sometimes pass by there, I feel that Icough a lot.
Whereas epidemiology provides uniform information and a high degree of statistical confidencewithin a limited scope, PAR provides multimodal data of a high degree of closeness to the actualscope of experience of the resident. The multimodal nature of knowledge in PAR brings upthe need for integration and, ultimately, linkage to action. In contrast, epidemiology does notrequire an explicit integration and intervention stage. This is because integration occurs muchearlier, when the epidemiological model is adopted and data constrained to the unimodal formthat epidemiology can treat. In contrast to the assumed objective nature of epidemiological data,knowledge in PAR is subject to reflection and interpretation. For the purpose of health interventionand organizing, PAR can be a more powerful mode of inquiry. We see that PAR responds to themultidimensionality of environmental health in SELA—in other words, it implicitly adheres to asocial–ecological model of health in communities (Stokols, Allen, & Bellingham, 1996).
2. In PAR, the integration of multiple lines of knowing gives us confidence in the authenticityof the findings—thus suggesting that resulting action will have greater chance of beingeffective.
Merely having multiple sets of information will not suffice—in fact, without some mode ofintegration, they can remain a disorganized set of random information. How does integrationhappen in PAR? First, the different sets of data can overlap/triangulate, providing a “thick de-scription” of environmental health. The community health survey results were mapped on GISand corroborated results from the photo-voice, resident interviews, and secondary data that thereare hotspots of vulnerability in SELA, one being the northernmost portion of Huntington Park.We learned about vulnerability, which is the overlapping of health outcomes, lack of health ac-cess, proximity to sources of air toxics, and others (Pastor et al., 2005). This integration resultsin a multidimensional picture of health, utilizing quantitative, qualitative, narrative, and visualinformation. To summarize:
• The different types of data helped us triangulate vulnerable “hotspots” in the community(e.g., the northern edge of Huntington Park).
• Integration of multiple types of information provided a multidimensional picture of vulner-ability, describing multiple pathways and factors that make residents in SELA particularlyvulnerable to environmental health injuries.
• Triangulation or overlapping of the interviews and survey data corroborated our suspicionthat asthma prevalence may be significantly elevated all throughout SELA.
• Interviews suggested that parents are most concerned with safety and violent crime outsidethe home, as well as nuisance effects (odor, noise, dust) and transportation barriers to healthcare.
88 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
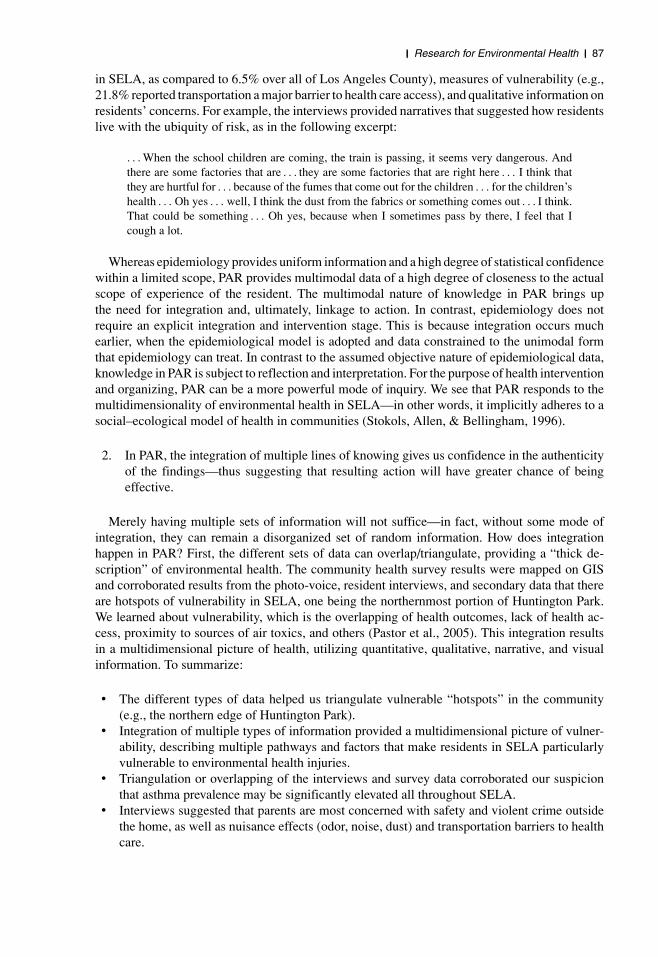
FIGURE 4
Risk ‘Mapping’ of SELA (due to local point sources)
Source: Lejano and Smith (2006)
• Discussions led to some initial research into regulatory processes in SELA, and these havegiven insights into how a more lax mode of regulation, coupled with gaps in scope of authorityof different agencies, allow the presence of toxic industries, such as the chromeplating plantsnext to the Suva schools in Huntington Park (LADHS, 1989; see Lejano & Fazeli, 2007 foran account).
To illustrate the method of triangulation mentioned above, let us consider how knowledge aboutthe distribution of risk in SELA overlapped. In Figure 4, we show a risk “mapping” that portraysthe density of risk-producing land uses across SELA. The figure clearly shows that the northernportion of SELA (the northern boundary of Huntington Park) may bear a higher profile of riskthan elsewhere in the area. This is corroborated by analyses of the health survey that showeda higher prevalence of asthma in the cluster of households sampled in the northern versus thesouthern part of SELA (specifically, 1.49 cases per household on average versus 1.15, p = 0.06in a one-way ANOVA test). The verification of findings through multiple lines of investigation isseen as strengthening the knowledge created within the PAR process.
Integration also occurs in the reflection stage, where participants link knowledge to action(see Figure 2). This also occurs as residents work knowledge into institutions and processes intheir neighborhood. In the case of the SELA PAR Project, intervention is being considered thatresponds to those elements of vulnerability that were identified. As an example, the SEA PARproject led to the Geographic Regional Initiative, a project drawing community advocates andagencies together to discuss ways to make multiple agency databases more accessible to resi-dents. Finally, one other mode of integration occurs in the embedding of this knowledge and
II Research for Environmental Health II 89
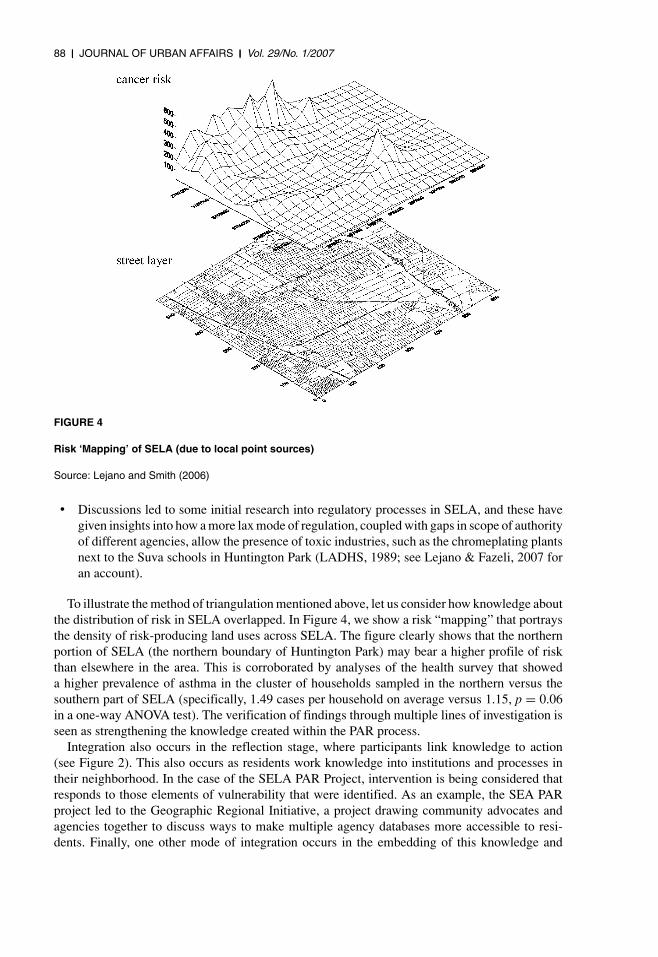
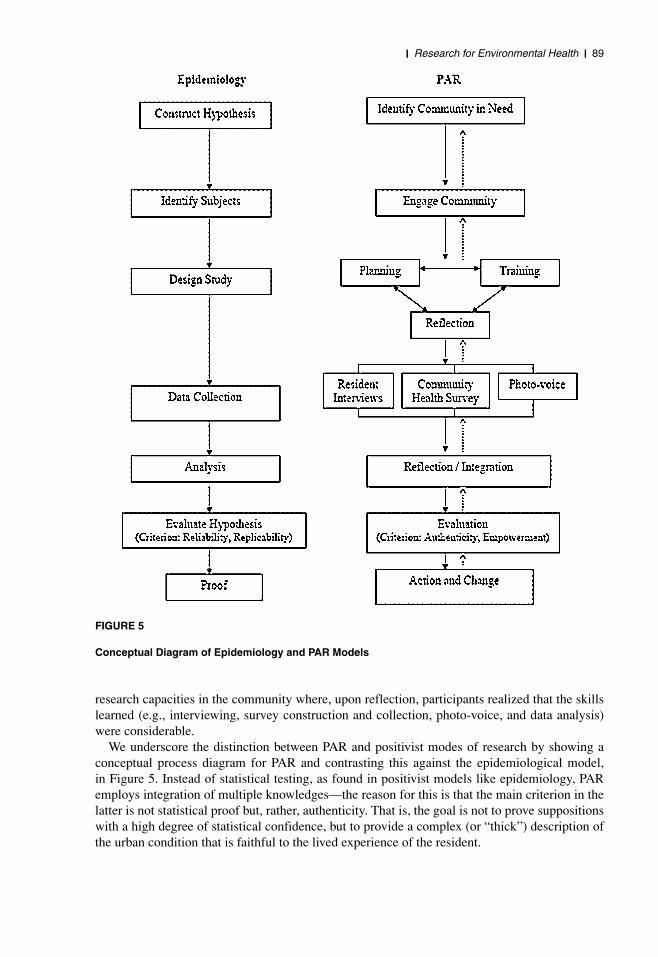
FIGURE 5
Conceptual Diagram of Epidemiology and PAR Models
research capacities in the community where, upon reflection, participants realized that the skillslearned (e.g., interviewing, survey construction and collection, photo-voice, and data analysis)were considerable.
We underscore the distinction between PAR and positivist modes of research by showing aconceptual process diagram for PAR and contrasting this against the epidemiological model,in Figure 5. Instead of statistical testing, as found in positivist models like epidemiology, PARemploys integration of multiple knowledges—the reason for this is that the main criterion in thelatter is not statistical proof but, rather, authenticity. That is, the goal is not to prove suppositionswith a high degree of statistical confidence, but to provide a complex (or “thick”) description ofthe urban condition that is faithful to the lived experience of the resident.
90 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
3. PAR allows for a learning process that is discovery based and allows for capacity building.This is a response to the needs of underserved communities.
In a situation of high uncertainty, there is a need for a model that can uncover new hypotheses,rather than test predetermined ones—something which PAR is designed to do. This is seen clearlyin Figure 5. In particular, we note the elements of learning in the PAR model that are discoverybased, meaning that learning has a capacity-building component and that hypotheses are not fixedbeforehand. This is needed because of the complexity of environmental health problems in thisurban context, and the need for community capacity building.
We have contrasted PAR with epidemiology in order to point out how the participatory modelmight better respond to the demands being set by residents in order to initiate a community-basedresearch effort. In this community, participants were keenly aware of the bottom line: how totranslate the research to improved conditions in SELA. Indeed, during the discussions aroundthe community health survey, we began wondering what might be achievable were we to use aclassic, epidemiological model of research, requiring randomization, controls, and fairly narrowhypotheses. One insight was that, with a classic model, we can answer a question like “Doesproximity to the freeway lead to increased prevalence of childhood asthma?” The group responded,however, by asking: “But didn’t we already know that?” and “But how would such a finding helpthese residents, specifically?” The conclusion was that basic epidemiological data regarding whatsymptoms result from specific exposures could already be had from the literature, and that to dosuch a study in SELA would be interesting to the medical and public health fields in general,but not to SELA specifically. The question the group was more concerned about was: “Whatconditions lead to such exposures, and what areas of intervention should we target first?” Thisprecluded studying the community simply “for study’s sake,” which CBE members made clearat the onset of the project. More generally, PAR departs from the traditionally radical separationbetween the subject (the researcher) and the object (the community) and, instead, includes thecommunity in a model of research that involves the subject reflecting on itself. However, thisreflective mode of research is at odds with the classic scientific method where the objects of studydo not participate in designing and conducting the research (as is consistent with an “objective”model of inquiry).
4. PAR allows the optimization of intervention vis-a-vis the complexity of health risk in thecommunity.
Just as PAR allows us to examine the phenomenon of risk in SELA from many angles, so, too,does it allow us to construct points of intervention from many points of attack. This idea movedCBE to reflect on their present mode of action. The issue began to look less and less like thetypical campaign, which usually focused on single, large sources of pollution. Rather, we findthe agglomeration of small sources, none of them large enough to garner regulators’ attention,creating a daunting cumulative risk problem—as illustrated in Figure 3. As one CBE staffer said:
. . . You’re talking about gas stations, dry cleaners, small chromeplaters—this is where people inthe community work, this is intertwined in people’s lives . . . it . . . requires a lot of participationby the community . . . that develops the capacity of the community to find solutions, fromthings like correlating pollution to health outcomes, to learning to interact with policy decision-makers . . . (personal communication with author).
The approach is to match intervention to the nature of the risk. Since cumulative risk arises froma multitude of sources and routes of exposure, so then intervention should also attack the problemfrom a multitude of directions. The classic model of research, being constrained to fairly narrowhypotheses, can lead to strategies that are unimodal. This might mean, for example, improving

II Research for Environmental Health II 91
ventilation inside homes, but not inquiring as to why homes are so inadequately maintained, tobegin with. PAR can be an appropriate approach since it integrates multiple sources of knowledgeand filters strategies through community priorities for action.
Outcomes of Research
We now return to a point made earlier, which is the complementary nature of epidemiologyand PAR. As discussed, each is well suited to its own particular fields of knowledge. All of thisinformation, whether statistical or narrative, was used to paint a deep picture of environmentalhealth issues in SELA. Epidemiological results showed widely persisting patterns that showedup strongly in the numbers (e.g., association of proximity to the freeway with a few chronichealth conditions). On the other hand, PAR shed light on the particular conditions, found in eachzone, by which risk occurs and is experienced. Moreover, PAR provided deep information onthe mechanisms by which residents were rendered more vulnerable by social conditions. Forexample, the degree to which health risks are embedded (because of a highly heterogeneous landuse) in residential areas emerged early on in the study.
The outcomes of the two analyses are also of interest. Epidemiological results can be extrap-olated outside the study site and used for regional policy. The Delfino study and others seem tohave been considered (e.g., see CARB, 2005) when the California Legislature set a minimumseparation distance of 500 feet (152.4 m.) between new schools and freeways (Senate Bill 352,Chapter 668, Statutes of 2003). Epidemiology, as seen in this case, is extremely useful for settingblanket standards. This is not to say that epidemiology cannot be used to generate local actions,though such has not occurred as of yet. In fact, CBE was not even aware of the Delfino study,reflecting a gap between traditional research and community—something PAR addresses directly.
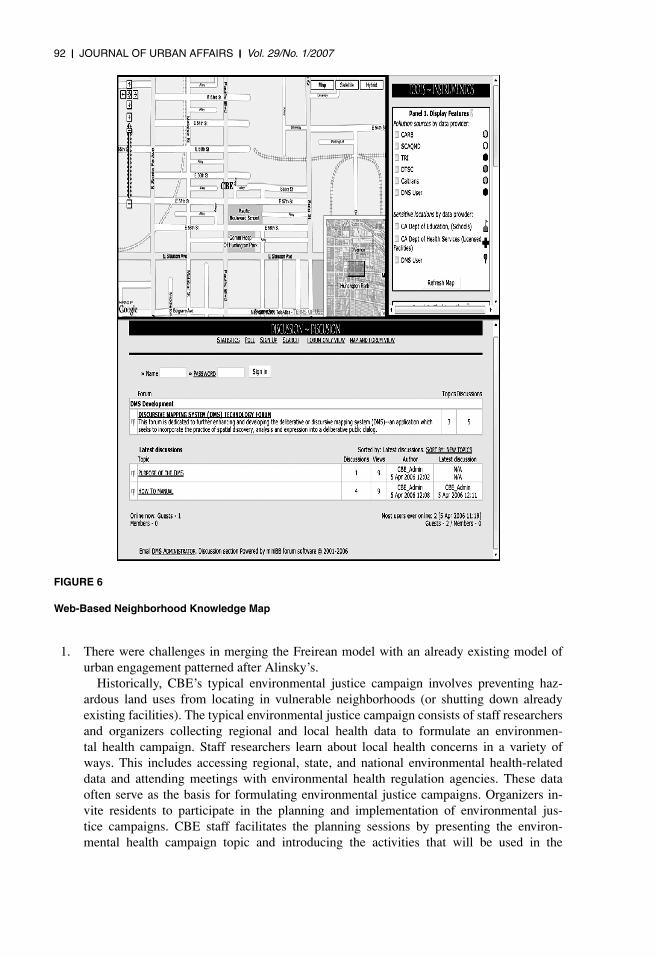
The SELA PAR Project is eminently local and aims for directly local action. Moreover, theoutcomes of the SELA PAR Project are linked to action in the community. Specifically, the SELAPAR Project led to the formation of a coalition among three agencies (AQMD, ARB, and EPARegion IX), CBE, and neighborhood groups who worked with CBE. The SELA PAR Projectshowed the need to integrate different forms of knowledge in arriving at a more broadly sharedand comprehensive understanding of risk in SELA. The distal objective of the coalition wasto share knowledge and, then, to link this to joint pilot studies at intervention. The immediateobjective was to create a common platform for integrating knowledge. One such vehicle is shownin Figure 6, the web-based neighborhood “knowledge map” that the coalition could use (found athttp://www.transecology.info/maps/ accessed April 18, 2006).
The idea is to use the map to integrate knowledge among coalition members. The agencieshave already pooled their databases on the web map. Moreover, residents have started learningto use the operations allowed by the knowledge map. For example, a resident can add his or herown point to indicate where trucks are illegally parked, idling. If a resident sees a violation in abuilding permit, he or she should be able to click on that facility and initiate an online conversationwith the AQMD inspector or building inspector for that facility. Presently, SELA residents areusing the tool for online discussions of specific campaigns. We see, then, that PAR generatesoutcomes that are immediately linked to local action. There is, however, another “side benefit”of this effort that is not local, and that is the fact that AQMD’s new web database (found athttp://www.aqmd.gov/webappl/fim/default.htm accessed August 10, 2006) was reportedly influ-enced by the SELA RGI project.
Challenges of Translating PAR to the Urban Setting
While the PAR model has numerous merits, it also poses serious challenges for practitionersattempting to translate the original Freirean ideal into the urban context.
92 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
FIGURE 6
Web-Based Neighborhood Knowledge Map
1. There were challenges in merging the Freirean model with an already existing model ofurban engagement patterned after Alinsky’s.
Historically, CBE’s typical environmental justice campaign involves preventing haz-ardous land uses from locating in vulnerable neighborhoods (or shutting down alreadyexisting facilities). The typical environmental justice campaign consists of staff researchersand organizers collecting regional and local health data to formulate an environmen-tal health campaign. Staff researchers learn about local health concerns in a variety ofways. This includes accessing regional, state, and national environmental health-relateddata and attending meetings with environmental health regulation agencies. These dataoften serve as the basis for formulating environmental justice campaigns. Organizers in-vite residents to participate in the planning and implementation of environmental jus-tice campaigns. CBE staff facilitates the planning sessions by presenting the environ-mental health campaign topic and introducing the activities that will be used in the
II Research for Environmental Health II 93
campaign. During this process, the entire group also engages in a strengths, weaknesses,opportunities, and threats (SWOT) analysis to identify the group’s collective abilities todo for itself what outside institutions or decision makers do not, and to target individuals,organizations, or institutions that may jeopardize the group’s campaign. The implemen-tation of the campaigns typically consists of assembling protests, marches, petitions, andproviding local testimony at regulatory/legislative proceedings.
CBE’s organizing model draws much from that described by Alinsky (1946, 1972). TheAlinsky model consists of developing a pressure group from within neighborhoods andto confront the “enemy” who is causing a neighborhood problem. According to Alinsky,the neighborhood contains four important types of organizations (churches, ethnic groups,political organizations, and labor unions), even though they may not be organized as aholistic unit. The Alinsky model stresses obtaining participation from these four sectors ina broad-based political action group. This requires grassroots organizing through politicaleducation and progressive tactics, such as protests, marches, and legal suits.
CBE’s model of organizing, however, is not entirely derived from Alinsky’s. While Alin-sky’s model strongly revolves around labor and faith communities, these organizations arenot a focus of the CBE model. Yet, we see similarities to the Alinskyite model in CBE’sfocus on ethnic communities and political activity (both legal and extra-legal defense). In itsstrategy sessions, CBE identifies “threats,” which is similar to Alinsky’s idea of “targets.”What is different from these “targets” or “threats” is that unlike the Alinsky model’s needto identify a palpable, local threat, CBE often identifies threats that are not always visibleor local. For instance, health risks to workers and residents in the region largely arise frompoor regulation of manufacturing industries, and while these industries may be local, thedecision makers responsible for them may not be within the SELA region.
In the SELA PAR Project, CBE was entering into a different mode of action than thatto which it was accustomed, wherein the objective was not the development of politicalaction campaigns or the rapid mobilization of protest, but the engagement of residents incommunity-based knowledge development. Freire’s model requires a slower, more evolu-tionary learning process than CBE’s Alinsky-inspired model, and CBE experienced growingpains in trying to combine them. CBE’s ideal of the community organizer, who typicallyworked on multiple campaigns simultaneously, was not the most suited for PAR. In sub-sequent discussions, CBE staffers suggested that the project could have used a dedicatedproject manager to focus solely on the PAR project on a daily basis—something that reflectsthe steady and studied process that characterizes Freire’s model.
The very word CBE uses for its work, “campaign,” is indicative of the single-issuenature of their projects, in contrast to Freire’s description of his model, “pedagogy.” Theforums involved are also different (i.e., small discussion groups to discuss communityhealth issues versus planning meetings to validate campaign topics), as are the nature ofcommunity involvement (i.e., long-term, progressive commitment versus intense, sporadicaction). Lastly, to some extent, the Alinskyite model already assumes what the problemis and concentrates on seeking avenues for political action. The Freirean model, on theother hand, is more disposed to generating new or alternative causal hypotheses about theproblem.
2. The urban experience presents profound difficulties for effective, long-term participation.It is one thing to mobilize a busload of people for a one-day mass action, and quite another
to mobilize a small group for a 2-year process of collaborative research, and the demandson these publics are also different. This may be part of the reason that the workshops drewdifferent people each time, especially the adults. The most constant element of participa-tion in these workshops was the youth group—high school students for whom a learning
94 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
process is part of their everyday routine. The time requirements for a PAR process are oftenvirtually impossible for adults. Many adults in this heterogeneous, urban setting (in con-trast to the rural context of Freire’s early work), have multiple jobs just to meet basic needs,possibly leaving little to no time or energy to participate for the community good. Practicallyspeaking, participation required about 2 to 3 hours every 2 weeks in meetings, and severalhours each week working on related research projects on their own, over several years. Inaddition, on a number of occasions, interviewees would allude to the perceived lack of socialcohesion, which hurts participation. It may be that today’s urban conditions (excess labor,transitory nature of residence and employment, lack of security) force households to engagein mainly individual survival strategies. While it is too strong a generalization to say thatsocial “apartness” is a common condition in today’s urban setting, it seems to be the casein SELA. Even just the nonuniform conditions of work and other social patterns in SELAmade it hard to even schedule workshops.
Indeed, one of the goals of the SELA PAR Project was to engage those who have mostintimate knowledge of particular stressors in the community. With regard to childhoodexposures to environmental stressors, we sought to find out more about infants and early-school age children of lower-income households. And, so, our desire was to engage mothersin an extended process of inquiry because the collective group believed mothers were themost appropriate subgroup to speak about childhood concerns. This subgroup was, however,the least likely to attend, relative to other subgroups, such as teens. As we found out, mothersattended when they could, which was irregular, and they were generally not able to keep upwith the meeting schedule, which was, at times, every other week.
This poses difficulty for the PAR process, which is evolutionary. Participants start buildingknowledge and insight from session to session. While difficulty of regular participation isundoubtedly an issue in any context, it seems to be particularly challenging in today’s urbansetting, and daunting in the particular case of SELA where, as mentioned, there is a highpercentage of lower-income households.
The changing dynamics of participation in an urban setting, the dynamic and improvisa-tional nature of PAR, and shifting and evolving problems with community health, all point tothe need for practitioners to build some elements of constancy into the design of the SELAPAR study. One such constant element would have been the assignment of an organizerdedicated to the SELA PAR Project on a full-time, everyday basis. Stability of process,which may have been the case in the rural origins of PAR, can be particularly challengingin today’s urban setting.
3. The evolutionary, nonlinear nature of PAR, coupled with the high complexity of urbancontexts, makes the model impossible to blueprint.
In contrast to the more predictable, even conditions (i.e., agricultural) and communities(i.e., smallholders, lifetime residents) found in PAR’s origins, today’s urban context exhibitsprofound diversity. Since PAR draws its design and process from the priorities and char-acter of its particular community, the actual form of PAR becomes highly contextual. Thecomposition of the community participants will vary significantly from place to place. PARis inherently nonlinear, involving numerous changes in plan, trial-and-error, and discovery,reflecting double-loop learning (Argyris & Schon, 1974) as seen in the feedback loops inFigure 2. For example, the community health survey was designed around special healthfair events to collect data, but was later changed to a door-to-door/one-on-one promotoratype design. This type of data collection lent itself to unique challenges that reflected theurban setting. For example, one community member reported that low participating rateswere partly due to the fact that the survey team went out to collect surveys on Saturday
II Research for Environmental Health II 95
afternoons, which is when most people have previous engagements. Much of the projecthad an experimental, improvisational feel to it, and things were being attempted by partici-pants for the first time.
4. PAR challenged the organization through exposure to a broader community agenda.One challenge was the realization that the community’s conceptualization of health prob-
lems (which also included domestic violence, physical infrastructure, and school crowded-ness) was broader than CBE’s (environmental health issues, particularly from air toxics).This created prolonged discussions on project scope, which finally ended up closer to thatoriginally envisioned by CBE. If the mismatch between community prioritization (a neces-sary component of Freire’s conscientization process) and the community-based organiza-tion’s (CBO’s) organizational mandate is serious enough, this can impact the sustainabilityof the PAR process.
The significantly broader notion of health that residents brought to the SELA PAR studywas clearly evident in the earliest workshops. It is perhaps most graphically seen, later on,in the results of the photo-voice project, which entailed residents taking pictures of theirneighborhood that speak to their experience of health and environmental degradation. Thehundreds of photos were thematically arranged, using a mode of visual content analysis,and pictures pertaining to each theme were mounted on a large easel and discussed. To theresident participants, health goes much beyond air pollution and clean water and includesbroken streets, litter, graffiti, and poor facilities maintenance.
5. Given the complexity of participation in the urban setting, moving health advocacy beyondthe CBO-led entrepreneurial model can be difficult or impossible.
The difficulty of establishing a constant base of participating community members sug-gests the need to embed PAR within different institutions in SELA other than the CBO—e.g.,schools, clinics, and local government. There are other reasons, however, for one centralplayer to take ownership of the whole process, since so much of it is constantly in flux. Thismakes it harder to leave the model of the CBO as entrepreneur, especially in SELA. The needfor a permanent CBO-led process can be problematic, however, especially as organizationalconstraints (e.g., grant funding) to long-term action can be severe.
CONCLUSION
By examining PAR, in concept and in practice, we begin to understand why PAR’s model oflearning may be appropriate to the particular problems in much of today’s urban context. On theother hand, we also see how its implementation is particularly difficult in these same situations.We end the article with lessons for practitioners that emerge from this analysis:
1. We should not hypostatize an idealized notion of community, to the extent of alienating ordisrespecting those members of community who do show up. Rather, we need to start andwork with the community as it is at that time and place.
2. We have to remember that PAR is a model of learning-in-action, which can be evolutionaryand improvisational. We must learn when to leave the idealized model of PAR, be flexible,and improvise.
3. The complexity of health issues in the urban setting requires explicitly conducting multiplelines of inquiry, using multiple sources of information. In response to the vagaries of par-ticipation in today’s cities, we need to create multiple mechanisms to allow different people
96 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
to participate. For example, in the SELA initiative, the group decided to have residentsinterview others who could not attend workshops.
4. We need to be creative in combining and prioritizing the array of health outcomes generatedby community, particularly when definitions of community health do not align perfectlywith the organization’s mission.
5. The fluid, unpredictable, and complex nature of the urban experience can make a PARproject difficult to manage, and we need to design “constant” elements into the PAR project,for example, having a dedicated organizer or project manager assigned to the project on afull-time basis.
6. Planning should be conscious about having “float” time up front. For example, it took abouta year to establish a routine vis-a-vis working groups, participation, and a scope of workfor the collaborative. We did not expect such a long time lag, in the beginning. We couldalso have saved time by working with an epidemiologist who could have helped much inplanning the data collection strategies for the survey. This would have helped us avoid somelost time due to the experimental nature of our protocol (e.g., finding out how low therate of response would be or the need to standardize how teams approach households). Inhindsight, we should also have been clearer, earlier on, about the time commitments expectedof potential participants. The truth is that, this being largely an experimental venture, theteam was not sure, in the beginning, how much time it would require of the participants.
We also reflect on the promise this model has for institutional processes at mitigating andreducing health risks in lower-income communities. Whereas traditional regulatory and admin-istrative regimes involve single-jurisdiction approaches (e.g., health service agencies dedicatedto disease monitoring, environmental agencies dedicated to pollution control), PAR points to theneed for new forums in which multiple knowledges, practices, strategies, and stakeholders cancome together in integrative fashion. Perhaps the persistent, intractable nature of cumulative riskand vulnerability in these communities is the clearest indication of the need for institutional re-forms. As an initial impetus to reform, we suggest that there is a need for forums, perhaps withinthe environmental permitting process or city council deliberations, within which multiple publicscan come together and co-design health intervention strategies. These strategies should include,among others, ways to mitigate or redirect land use patterns that contribute to the cumulative riskproblem described herein.
As a final note, we point out that the findings to this study have the potential to be transferredto similar urban settings. Researchers interested in understanding the practice and challenges ofimplementing the PAR model in other urban communities should decide whether or not some ofthe findings of this study could be transferred. In PAR, we find a mode of study that is highlycontextual and, as such, can only be fully understood by studying actual practice in actual places.
ACKNOWLEDGMENT: The authors thank Antonio Figueroa, Jennifer Ramirez, Ciro Aguilar, Violeta Gonzalez,Alma Montes, and Josias Gonzalez for their great work on the community-health surveys, land use mapping,and statistical analysis. We are also grateful to Jorge Villanueva and the SELA residents who participated in thePAR project. The project was funded through a grant from the First Five Foundation–Los Angeles (subcontractto UCI through CBE). Lastly, we thank Professors Sora Park Tanjasiri and Celina Su for their particularly helpfulsuggestions and insights into the challenges of participatory planning.
ENDNOTE
1 Note that we did not include Vernon in these statistics, since this municipality is an industrial enclave with only91 residents.
II Research for Environmental Health II 97
REFERENCES
Alinsky, S. (1946). Reveille for radicals. Chicago: University of Chicago Press.Alinsky, S. (1972). Rules for radicals. New York: Vintage Books.Annett, H., & Nickson, J. P. (1991). Community involvement in health: Why is it necessary? Tropical Doctor, 21,
3–5.Argyris, C., & Schon, A. D. (1974). Theory in practice: Increasing professional effectiveness. San Francisco:
Jossey-Bass.Bansal, S., Bacon, D., & Davis, S. (1998). Holding our breath: The struggle for environmental justice in Southeast
Los Angeles. Los Angeles: Communities for a Better Environment.Been, V., & Gupta, F. (1997). Coming to the nuisance or going to the barrios? A longitudinal analysis of environ-
mental justice claims. Ecology Law Quarterly, 24, 1–56.Broome, C., & Modarres, A. (1999). Creating a toxic neighborhood in Los Angeles County: A historical exami-
nation of environmental equity. Urban Affairs Review, 35(2), 163–187.Brown, P. (1987). Popular epidemiology: Community response to toxic waste-induced disease in Woburn,
Massachusetts. Science, Technology, and Human Values, 12, 78–85.Brown, P. (1997). Popular epidemiology revisited. Current Sociology, 45(3), 137–156.Brown, P. (2000). Popular epidemiology and toxic waste contamination: Lay and professional ways of knowing.
In S. Kroll-Smith, P. Brown, & V. J. Gunter (Eds.), Illness and the environment: A reader in contestedmedicine (pp. 364–383). New York: New York University Press.
Brown, P., Kroll-Smith, S., & Gunter, V. J. (2000). Knowledge, citizens, and organizations: An overview ofenvironments, disease, and social conflict. In S. Kroll-Smith, P. Brown, & V. J. Gunter (Eds.), Ill-ness and the environment: A reader in contested medicine (pp. 9–25). New York: New York UniversityPress.
Bullard, R. (1990). Dumping in Dixie: Race, class, and environmental quality. Boulder, CO: Westview Press.Cagan, E. R., Hubinsky, T., Goodman, A., Deitcher, D., & Cohen, N. L. (2001). Partnering with communities to
improve health: The New York City turning point experience. Journal of Urban Health: Bulletin of the NewYork Academy of Medicine, 78(1), 176–180.
California Air Resources Board (CARB) (2005). Air quality and land use handbook: A community health perspec-tive. Sacramento: California Environmental Protection Agency.
Chambers, R. (1983). Rural development: Putting the last first. London: Longman.Checkoway, B. (1984). Two types of planning in neighborhoods. Journal of Planning, Education, and Research,
3, 102–109.Corburn, J. (2003). Bringing local knowledge into environmental decision making: Improving urban planning for
communities at risk. Journal of Planning, Education, and Research, 22, 420–433.Delfino, R. J., Gong, H. Jr., & Linn, W. S. (2003). Children’s health-asthma symptoms in Hispanic children and
day ambient exposures to toxic and criteria air pollutants. Environmental Health Perspectives, 4(111), 647–656.
Dewey, J. (1925). Experience and nature. Chicago: Open Court.Dillinger, W. (1994). Decentralization and its implications for urban service delivery (Urban management pro-
gramme discussion paper 16). Washington, DC: World Bank.Ellen, I. G., Mijanovich, T., & Dillman, K. (2001). Neighborhood effects on health: Exploring the links and
assessing the evidence. Journal of Urban Affairs, 23(3/4), 391–408.First 5 LA (2002). Neighborhood data use collaborative concept paper. Los Angeles: First 5 LA.Fraser, H. (2005). Four different approaches to community participation. Community Development Journal, 40,
286–300.Freire, P. (1973). Pedagogy of the oppressed. New York: Seabury Press.Geertz, C. (1973). The interpretation of cultures. New York: Basic Books.George, A. M., Green, M. D., & Green, W. L. (1999). Appraising and funding participatory research in health
promotion. International Quarterly of Community Health Education, 21, 19–27.Giachello, A., Arrom, J., Davis, M., Sayad, J., Ramirez, D., Nandi, C., & Ramos, C. (2003). Reducing diabetes
health disparities through community-based participatory action research: The Chicago Southeast diabetescommunity action coalition. Public Health Reports, 118(4), 309–324.
98 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
Gittell, R., & Vidal, A. (1998). Community organizing: Building social capital as a development strategy. ThousandOaks, CA: Sage Publications.
Green, W. L., George, A. M., & Daniel, M. (2003). Guidelines for participatory research in health promotion. In M.Minkler & N. Wallerstein (Eds.), Community-based participatory research (pp. 419–428). San Francisco:Jossey-Bass.
Habermas, J. (1987). The theory of communicative action: Vol. 2. Lifeworld and system: A critique of functionalistreason. Boston: Beacon Press.
Heidegger, M. (1962). Being and time (J. Macquarrie & E. Robinson, Trans.). New York: Harper. (Originallypublished 1927.)
Houston, D. W., Ong, J., & Winer, P. A. (2004). Structural disparities of urban traffic in Southern California: Im-plications for vehicles-related air pollution exposure in minority and high-poverty neighborhoods. Journalof Urban Affairs, 26(5), 565–592.
Huff, A., & Jenkins, M. (2002). Mapping strategic knowledge. Thousand Oaks, CA: Sage.Husserl, E. (1970). Logical investigations: Vol 1 (J. N. Findlay, Trans.). London: Routledge. (Original work
published 1900.)Israel, B. A., Eng, E., Schulz, A. J., & Parker, E. A. (2005). Introduction to methods in community-based participa-
tory research for health. In B. Israel, E. Eng, A. J. Schulz, & E. A. Parker (Eds.), Methods in community-basedparticipatory research for health (pp. 3–26). San Francisco: Jossey-Bass.
Israel, B. A., Schulz, A. J., Parker, E. A., & Becker, A. B. (1998). Review of community-based research: Assessingpartnership approaches to improve public health. Annual Review of Public Health, 19, 173–202.
Kawachi, I., & Berkman, L. (2000). Social cohesion, social capital, and health. In L. F. Berkman & I. Kawachi(Eds.), Social epidemiology (pp. 174–190). Oxford: Oxford University Press.
Korten, D. C. (1983). Social development: Putting people first. In D. C. Korten & F. B. Alfonso (Eds.), Bureaucracyand the poor: Closing the gap. West Hartford, CT: Kumarian Press.
Kreiger, N. (2000). Discrimination in health. In L. F. Berkman & I. Kawachi (Eds.), Social epidemiology(pp. 36–75). Oxford: Oxford University Press.
Kroll-Smith, S., & Floyd, H. H. (2000). Environmental illness as a practical epistemology and a source of profes-sional confusion. In S. Kroll-Smith, P. Brown, & V. J. Gunter (Eds.), Illness and the environment: A readerin contested medicine (pp. 72–91). New York: New York University Press.
LADHS, Los Angeles County Department of Health Services (1989). Final report of health effects (excluding preg-nancy outcome rates) for Suva Elementary and Intermediate School Staffs, Toxics Epidemiology Program,April 6, 1989.
Lasker, R. D., & Weiss, E. S. (2003). Broadening participation in community problem solving: A multidisciplinarymodel to support collaborative practice and research. Journal of Urban Health: Bulletin of the New YorkAcademy of Medicine, 80(1), 14–60.
Lejano, R., & Fazeli, B. (2007). Cumulative risk, incompatible land uses, and environmental justice: Reforminginstitutions around an ethic of care (working paper).
Lejano, R., & Iseki, H. (2001). The question of environmental justice: The spatial distribution of hazardous wasteTSDs in Los Angeles. Journal of Urban Planning and Development, 127(2), 51–62.
Lejano, R., Piazza, B., & Houston, D. (2002). Rationality as social justice and the spatial-distributional analysisof risk. Environment and Planning C, 20, 871–888.
Lejano, R., & Smith, S. C. (2006). Incompatible land uses and the topology of cumulative risk. EnvironmentalManagement, 37(2), 230–246.
Lewin, K. (1946). Action research and minority problems. Journal of Social Issues, 2, 34–46.Manor, J. (1999). The political economy of democratic decentralization. Washington, DC: IBRD.Marmot, M. (2000). Multilevel approaches to understanding social determinants. In L. F. Berkman & I. Kawachi
(Eds.), Social epidemiology (pp. 349–367). Oxford: Oxford University Press.Merleau-Ponty, M. (1989). Phenomenology of perception (C. Smith, Trans.). London: Routledge. (Originally
published 1945.)Metzler, M. M., Higgins, D. L., Beeker, C. G., Freudenberg, N., Lantz, P. M., Senturia, K. D., Eislinger, A. A.,
Viruell-Fuentes, E. A., Gheisar, B., Palermo, A., & Softley, D. (2003). Addressing urban health in Detroit,New York City, and Seattle through community-based participatory research partnerships. American Journalof Public Health, 93(5), 803–811.
II Research for Environmental Health II 99
Minkler, M. (2000). Using participatory action research to build healthy communities. Public Health Reports, 115,191–197.
Minkler, M., & Wallerstein, N. (2003). Introduction to community based participatory research. In M. Minkler& N. Wallerstein (Eds.), Community based participatory research for health (pp. 3–26). San Francisco:Jossey-Bass.
Mora, J., & Diaz, R. D. (2005). Participatory action research: A new vision and practice in Latino communities. InJ. Mora & R. D. Diaz (Eds.), Latino social policy: A participatory research model (pp. 1–21). New York:The Haworth Press.
Morello-Frosch, R., Pastor, M., & Sadd, J. (2001). Environmental justice and Southern Californian’s ‘riskcape’:The distribution of air toxics exposures and health risks among diverse communities. Urban Affairs Review,36(4), 551–578.
Mullings, L., & Wali, A. (2001). Stress and resilience: The social context of reproduction in central Harlem. NewYork: Kluwer Academic/Plenum Publishers.
O’Fallon, L. R., & Dearry, A. (2002). Community-based participatory research as a tool to advance environmentalhealth sciences. Environmental Health Perspectives, 110(2), 155–159.
Pastor, M., Morello-Frosch, R., & Sadd, J. L. (2005). The air is always cleaner on the other side: Race, space, andambient air toxics exposures in California. Journal of Urban Affairs, 27(2), 127–148.
Pastor, M., Sadd, J., & Hipp, J. (2001). Which came first? Toxic facilities minorities move-in and environmentaljustice. Journal of Urban Affairs, 23(1), 1–21.
Pulido, L., Sidawi, S., & Vox, R. (1996). An archeology of environmental racism in Los Angeles. Urban Geography,17(5), 419–439.
Schulz, A. J., Israel, B. A., Selig, S., Bayer, I., & Griffin, C. B. (1998). Development and implementation ofprinciples for community-based research. In R. H. MacNair (Ed.), Research strategies for communitypractice (pp. 83–110). New York: Haworth Press.
Stokols, D., Allen, J., & Bellingham, R. (1996). The social ecology of health promotion: Implications for researchand practice. American Journal of Health Promotion, 10(4), 247–251.
Sullivan, M., Kone, A., Senturia, K. D., Chrisman, N. J., Ciske, S. J., & Krieger, J. W. (2001). Researcher andresearched—community perspectives: Toward bridging the gap. Health Educational Behavior, 28(2), 130–149.
Susman, G. I. (1983). Action research: A sociotechnical systems perspective. In G. Morgan (Ed.), Beyond method:Strategies for social research (pp. 95–113). London: Sage Publications.
Swindell, D. (2000). Issue representation in neighborhood organizations: Questing for democracy at the grassroots.Journal of Urban Affairs, 22(2), 123–137.
Tesh, N. S. (2000). Uncertain hazards: Environmental activists and scientific proof . Ithaca, NY: Cornell UniversityPress.
Trist, E. (1985). Intervention strategies for interorganizational domains. In United Church of Christ (UCC), Toxicwastes and race in the United States: A national report on the racial and socioeconomic characteristics ofcommunities with hazardons waste sites. New York: Commission for Racial justice.
UCC (United Church of Christ) (1987). Toxic wastes and race in the United States: A national report on the racialand socioeconomic characteristics of communities with hazardous waste sites. New York: Commission forRacial justice.
United States General Accounting Office (USGAO) (1983). Siting of hazardous waste landfills and their correlationwith racial and economic status of surrounding communities. Washington, DC: Author.
U. S. Bureau of Census (2000). Census 2000 Summary file 1 – East Los Angeles [online]. Retrieved August 16,2005 from http://factfinder.census.gov.
Van Vlaenderen, H. (2004). Community development research: Merging communities of practice. CommunityDevelopment Journal, 39(2), 135–143.
Wilcox, R., & Knapp, A. (2000). Building communities that create health. Public Health Reports, 115, 139–143.
Winter, R. (1989). Learning from experience: Principles and practice in action research. Philadelphia: The FalmerPress.
Wood, R. L. (2002). Faith in action: Religion, race, and democratic organizing in America. Chicago: Universityof Chicago Press.
100 II JOURNAL OF URBAN AFFAIRS II Vol. 29/No. 1/2007
Yin, R. (2003). Case study research: Design and methods. Thousand Oaks, CA: Sage.Zenk, S. N., Schulz, A. J., House, J. S., Benjamin, A., & Kannan, S. (2005). Application of CBPR in the design
of an observational tool: The neighborhood observational checklist. In B. Israel, E. Eng, A. J. Schulz, &E. A. Parker (Eds.), Methods in community-based participatory research for health (pp. 167–187). SanFrancisco: Jossey-Bass.





























