Embed Size (px)
Citation preview

Schizophrenia Research xxx (2015) xxx–xxx
SCHRES-06503; No of Pages 7
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r .com/ locate /schres
Paliperidone palmitate versus oral antipsychotics in recentlydiagnosed schizophrenia
Andreas Schreiner a,⁎, Kaire Aadamsoo b, A. Carlo Altamura c, Manuel Franco d, Philip Gorwood e,Nikolaj G. Neznanov f, Juan Schronen g, Alp Ucok h, Mathias Zink i, Adam Janik j, Pierre Cherubin k,Marjolein Lahaye l, Ludger Hargarter a
a Medical Affairs, Janssen Cilag EMEA, Neuss, Germanyb North Estonia Medical Centre Foundation, Tallinn, Estoniac Department of Psychiatry, University of Milan, Fondazione IRCCS Ca' Granda, Ospedale Maggiore Policlinico, Milan, Italyd Psychiatric Department, Zamora Hospital, Zamora, Spaine Hôpital Sainte-Anne, Paris Descartes University (INSERM U894), Francef St Petersburg V.M. Bekhterev Psychoneurological Research Institute, St Petersburg, Russiag Welgemoed Medical Centre, Cape Town, South Africah Istanbul Medical Faculty, Istanbul, Turkeyi Central Institute of Mental Health, Department of Psychiatry and Psychotherapy, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germanyj Global Clinical Operations, Janssen-Cilag, Warsaw, Polandk Medical Affairs, Janssen Cilag EMEA, Issy-les-Moulineaux, Francel Biostatistics, Janssen Cilag Benelux, Tilburg, The Netherlands
⁎ Corresponding author.E-mail address: [email protected] (A. Schreiner).
http://dx.doi.org/10.1016/j.schres.2015.08.0150920-9964/© 2015 Janssen Pharmaceutica NV. Published b
Please cite this article as: Schreiner, A., et al.Res. (2015), http://dx.doi.org/10.1016/j.schr
a b s t r a c t
a r t i c l e i n f oArticle history:Received 24 February 2015Received in revised form 10 August 2015Accepted 11 August 2015Available online xxxx
Keywords:SchizophreniaPaliperidone palmitateLong-acting injectable and oral antipsychoticsRandomized controlled trialRecently diagnosedRelapse prevention
Objective:Relapse and acute exacerbation are common in schizophrenia andmay impact treatment response andoutcome. Evidence is conflicting in respect to superiority of long-acting injectable antipsychotic therapies versusoral antipsychotics in relapse prevention. This randomized controlled study assessed the efficacy of paliperidonepalmitate versus oral antipsychotics for relapse prevention.Method: Eligible patients with a recent diagnosis of schizophrenia (within 1–5 years) were randomized 1:1 topaliperidone palmitate (n = 376) or oral antipsychotic monotherapy (n = 388) and entered a 2-week initialacute oral treatment phase. Patients who met predefined response criteria were eligible to enter the 24-monthrater-blinded core treatment phase. Patients were evaluated for relapse, symptoms, functioning, quality of life,treatment satisfaction, and tolerability.Results: In the core treatment phase, time to relapse was significantly longer in the paliperidone palmitate(n= 352) comparedwith the oral antipsychotics arm (n=363): 85% of patientswere relapse-free at 469 versus249 days (P = 0.019). Significantly fewer patients receiving paliperidone palmitate met the relapse criteria(52 [14.8%] versus 76 [20.9%, oral antipsychotics]; P = 0.032), representing a 29.4% relative risk reduction. Forpaliperidone palmitate, a significantly greater improvement in Positive and Negative Syndrome Scale totalscore on Day 8 (P = 0.021) and a trend at endpoint (P = 0.075) were observed. Functioning improvementswere comparable between treatment arms. No new safety signals were identified.Conclusion: The observed time to relapse superiority of paliperidone palmitate over oral antipsychotics providesfurther evidence for the value of long-acting injectable antipsychotic therapies in the treatment of schizophrenia,including during the early stages of illness.© 2015 Janssen Pharmaceutica NV. Published by Elsevier B.V. This is an open access article under the CC BY-NC-
ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Despite the availability of effective treatment for schizophrenia, re-lapse and acute exacerbations are common (Emsley et al., 2013a). Re-sponse to treatment after relapse is variable; some patients display
y Elsevier B.V. This is an open access a
, Paliperidone palmitate versues.2015.08.015
emergent refractoriness following relapse even when the interval be-tween onset of first relapse symptoms and initiation of treatment isbrief (Emsley et al., 2013b).
Evidence regarding the superiority of long-acting injectable antipsy-chotic therapies (LATs) over oral antipsychotics in terms of relapse pre-vention is conflicting (Leucht et al., 2011; Kishimoto et al., 2013;Kishimoto et al., 2014), with long-term comparisons scarce (Kaneet al., 2010; Rosenheck et al., 2011). Hence, naturalistic and
rticle under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.

2 A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
appropriately designed studies are needed to compare these treatmentoptions (Kirson et al., 2013; Alphs et al., 2014), particularly in recentlydiagnosed patients with schizophrenia. The Prevention of Relapsewith Oral Antipsychotics versus Injectable Paliperidone Palmitate(PROSIPAL) study was a randomized controlled, open-label, rater-blinded study that assessed the efficacy of paliperidone palmitate (PP)(Janssen-Cilag International NV, 2015), an atypical LAT, comparedwith oral antipsychotic monotherapy, in recently diagnosed patientswith schizophrenia.
2. Methods
2.1. Study design
This multicenter, randomized, prospective, active-controlled, open-label, rater-blinded, international 24-month study in recently diagnosed(within 1–5 years) patients with schizophrenia (NCT01081769) wasconducted in 141 centers across 26 countries (Appendix); it compriseda 2-week initial acute oral treatment phase and a 24-month core treat-ment phase.
Patients expected by the investigator to benefit from switching toone of the study medications were eligible to enter the initial acuteoral treatment phase; patients were eligible for the core treatmentphase if they then met all predefined response criteria:
• A score of ≤4 for at least four of the following Positive and NegativeSyndrome Scale (PANSS) items: P1 (delusions), P2 (conceptual disor-ganization), P3 (hallucinatory behavior), P6 (suspiciousness/persecu-tion), P7 (hostility), and G8 (uncooperativeness) and
• Clinical Global Impression-Severity (CGI-S) score ≤ 4, and• No intolerable side effects of study medication.
Patients were maintained on PP or on the same oral antipsychotic(aripiprazole, quetiapine, olanzapine, paliperidone extended-release[ER], risperidone, or haloperidol as clinically indicated by the investiga-tor) until the end of the core treatment phase, or until relapse or with-drawal from study.
The protocol was reviewed and approved by the Independent EthicsCommittee/Institutional Review Board in each participating country.The studywas conducted in accordancewith the Declaration of Helsinki(2008) and Good Clinical Practice (International Conference onHarmonisation). Eligible patients were informed of the risks and bene-fits of the trial and were required to provide written informed consentfor participation during an initial screening visit (Visit 1 [Day −14]).Standard medical and psychiatric assessments were completed to con-firm the patients' clinical history and current symptomatology.
2.2. Subjects
2.2.1. Key inclusion criteriaPatients experiencing an acute episode of schizophrenia with a
PANSS total score of 70–120 at screening were eligible for this study ifaged 18–65 years, with a diagnosis of schizophrenia according to theDiagnostic and Statistical Manual of Mental Disorders (Fourth edition)criteriamade 1–5 years previously and a history of ≥2 relapses requiringpsychiatric hospitalization in the preceding 24 months; this may haveincluded the current acute episode.
2.2.2. Key exclusion criteriaPatients were not eligible if they were antipsychotic-naive, consid-
ered by the investigator to be treatment-resistant or unsuitable fortreatment with an atypical oral antipsychotic or oral haloperidol mono-therapy, or had received clozapine within the previous 3 months. Otherexclusion criteria included use of LATs within three injection cycles be-fore screening, starting a psychotherapy program within 2 months
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
preceding baseline, a history or current symptoms of tardive dyskinesiaor a history of neuroleptic malignant syndrome, or involuntaryhospitalization.
2.3. Treatment
2.3.1. Initial 2-week acute oral treatment phaseAfter screening, patients were randomized (1:1) to either PP or oral
antipsychotic treatment and immediately entered the 2-week initialacute oral treatment phase. Patients randomized to PP had their previ-ous oral antipsychotic replaced with oral paliperidone ER (dose range:3–12 mg once daily). Patients randomized to oral antipsychotics hadtheir previous oral antipsychotic (Supplementary Table 1) replacedwith an oral antipsychotic different to the one they were using whenthey relapsed, as clinically indicated by the investigator. In both treat-ment arms, previous oral antipsychotics were tapered off over a maxi-mum of 7 days.
A maximum of five, from a possible six, different oral antipsychotics(haloperidol plus four out of five oral atypical antipsychotics) were avail-able to each study site; investigators could choose to prescribe any to thefirst randomized patient at their site. Subsequent patients were each pre-scribed a different oral antipsychotic at the investigator's discretion, to en-sure equal distribution ofmedications. If ≥4 patientswere allocated to theoral antipsychotic arm at a single site, all treatments were again madeavailable to that site such that for the fifth patient the investigator wasagain able to choose from five oral antipsychotics. Oral antipsychoticswere dispensed for self-administration and at each visit; patients werereminded to take their medication. The investigator or designated studypersonnel maintained a log of all drugs dispensed and returned (pillcounts) at each visit; no routine blood level tests were conducted. Drugsupplies for each patient were inventoried and accounted for throughoutthe study.
2.3.2. 24-month core treatment phasePatients randomized to PP received intramuscular PP 150 mg eq. on
Day 1 (deltoid), 100 mg eq. on Day 8 (deltoid), 75 mg eq. on Day 38(deltoid or gluteal), and once monthly thereafter with flexible dosing25–150 mg eq. (deltoid or gluteal). Patients randomized to the oral an-tipsychotic arm continued on the same drug that they had been pre-scribed in the initial acute oral treatment phase, at the dose defined bythe investigator. Dose adjustments were permissible throughout thestudy within the locally-approved dose range. Assessments wereperformed on Day 1, Day 8, and then monthly for the first 4 months,at 6 months and quarterly thereafter until Month 24. Adverse eventsand concomitant medications were recorded continuously. Upon re-lapse, treatment with study medication was terminated; an alternativeantipsychotic could be started at the investigator's discretion.
2.4. Efficacy assessments
The primary efficacy outcome was time to relapse per criteria de-scribed by Csernansky et al. (2002) (Appendix). Secondary outcomesincluded the proportion of patients with relapse at endpoint, PANSStotal and subscale scores, Marder factor scores (Marder et al., 1997),percentage of treatment responders (≥30% decrease in PANSS totalscore from baseline to last observation carried forward endpoint[LOCF, 24months or at early discontinuation]), CGI-S and Clinical GlobalImpression-Change (CGI-C) (Guy, 1972), Personal and Social Perfor-mance (PSP) scale (Morosini et al., 2000), Short Form (36) Health Sur-vey (SF-36) (Ware and Sherbourne, 1992, Ware and Gandek, 1994),European Quality of Life-5 Dimensions (EQ-5D) (EuroQol Group,1990), Subjective Well-Being under Neuroleptics Scale (SWN-S)(Naber, 1995), patient treatment satisfaction (Treatment SatisfactionQuestionnaire for Medication; TSQM) (Atkinson et al., 2004), andphysician's treatment satisfaction (7-point categorical scale).
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.

3A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
2.5. Safety and tolerability
Safety and tolerability assessments included treatment-emergentadverse events (TEAEs), extrapyramidal symptoms (using the Abnor-mal Involuntary Movement Scale [AIMS], Barnes Akathisia RatingScale [BARS], and Simpson Angus Rating Scale [SAS]), and changes inbody weight and body mass index. No protocol-based laboratory testswere obligatory.
2.6. Data analysis.
The whole intent-to-treat (ITT) population included all randomizedpatients who received ≥1 dose of study medication during the 2-weekinitial acute oral treatment phase. The core ITT population comprisedpatients who responded to the 2-week initial acute oral treatmentphase and received ≥1 dose of study medication in the 24-month coretreatment phase. Efficacy and safety analyses were performed on coreITT patients who had at least one post-baseline (Day 1 of the 24-month core treatment phase [Visit 2, responder assessment]) efficacyor safety measurement, respectively, in the 24-month core treatmentphase.
The sample size was calculated based on the primary efficacy vari-able ‘time to a relapse event’, assuming that the proportion of patientsexperiencing a relapse event during the core treatment phase wouldbe 20% in patients receiving PP and 30% in those receiving oral antipsy-chotics. In total, 296patients per treatment armand143 eventswere re-quired to detect this difference, with a power of 80% and two-tailedsignificance level of 5%. Assuming that 3% of subjects would not be in-cluded in the survival analysis, 306 subjects per treatment group (1:1randomization ratio) were required in the 24-month core treatmentphase.
Descriptive statistics were computed for efficacy and safety assess-ments when appropriate. All statistical analyses were two-tailed; con-clusions were based on 5% significance. Two-sided 95% confidence
Fig. 1. Flow and outcomes of the study population.*Of the study completers, 62.5% (PP) and 55.9% (oral APs) of patients completed their Month 2
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
intervals were computed where applicable. Time to relapse was ana-lyzed using standard methods including Kaplan–Meier product-limitsurvival curve estimates for the 85th percentile, representing the lowestpercentile for which estimates for both treatment arms were available,log-rank tests, and proportional hazard regression models. For second-ary efficacy assessments, change from baseline at each visit and atLOCF endpoint were analyzed using theWilcoxon signed-rank test; dif-ferences between treatment groups were analyzed using the Wilcoxontwo-sample test. Categorical variables, e.g. response rates,were evaluat-ed using Fisher's exact test. Unless otherwise stated, all efficacy assess-ments reported at endpoint refer to LOCF endpoint.
3. Results
3.1. Baseline demographics and patient disposition
Overall, 775 patients provided informed consent; of these, 769wererandomized and entered the 2-week initial acute oral treatment phase(Fig. 1). No significant differences were observed between the twoarms for any baseline demographic (Table 1).
Overall, 91.5% of patients randomized to PP received the drug asspecified per protocol; mean average dose from the fourth injection in-clusive (i.e. during the flexible dosing period onwards) was 101.7 ±29.3 mg eq. Mean modal daily doses of the oral antipsychotics are de-scribed in Table 2.
3.2. Efficacy outcomes
Time to relapse (primary outcome) was significantly longer inpatients receiving PP comparedwith those receiving oral antipsychotics(P= 0.019; hazard ratio 1.5; 95% confidence interval 1.1, 2.2). The 85th
percentile for time to relapse was 469 days for PP versus 249 days fororal antipsychotics. Significantly fewer patients receiving PP met the
4 visit. AP = antipsychotic, ITT = intent-to-treat, PP = paliperidone palmitate.
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.

Table 1Patient demographics and baseline characteristics in the core ITT population.
CharacteristicPaliperidone palmitate(n = 352)
Oral APs(n = 363)
Total(N = 715)
Mean age, years (SD) 32.6 (10.7) 32.6 (10.1) 32.6 (10.4)Sex, n (%)
MaleFemale
213 (60.5)139 (39.5)
201 (55.4)162 (44.6)
414 (57.9)301 (42.1)
Mean weight, kg (SD)⁎ 74.8 (15.4) 75.7 (14.8) 75.3 (15.1)Mean BMI, kg/m2 (SD)⁎ 25.5 (4.7) 25.8 (4.4) 25.7 (4.6)Psychiatric history
Paranoid subtype, n (%) 308 (87.5) 308 (84.8) 616 (86.2)Mean age at diagnosis, years (SD) 30.1 (10.6) 30.1 (10.1) 30.1 (10.4)Mean age at start of first AP treatment, years (SD)* 29.1 (10.5) 29.2 (10.0) 29.1 (10.2)Mean time from diagnosis to study entry, years (SD) 3.0 (1.7) 2.9 (1.5) 2.9 (1.6)
Mean time from start of first AP treatment to study entry, years (SD)⁎ 4.0 (3.0) 3.8 (2.4) 3.9 (2.7)Ever been hospitalized, n (%)⁎
Previous hospitalizations, mean (SD)†
Currently hospitalized, n (%)‡
Suicide attempts since diagnosis, n (%)1≥2
328 (93.2)3.1 (2.1)106 (32.3)
12 (3.4)10 (2.8)
332 (91.7)3.1 (2.2)108 (32.5)
18 (5.0)9 (2.5)
660 (92.4)3.1 (2.2)214 (32.4)
30 (4.2)19 (2.7)
Baseline PANSS total score, mean (SD)§ 82.5 (12.0) 81.5 (11.7) –Baseline CGI-S, mean (SD)§ 3.9 (0.4) 3.8 (0.4) –Baseline PSP total score, mean (SD)¶ 55.3 (11.3) 55.3 (11.1) –Previous antipsychotic medications used by ≥5% patients‖, n (%)
Haloperidol 43 (12.2) 42 (11.6) 85 (11.9)Olanzapine 36 (10.2) 21 (5.8) 57 (8.0)Risperidone 62 (17.6) 64 (17.6) 126 (17.6)Trifluoperazine 13 (3.7) 25 (6.9) 38 (5.3)
Comorbidities in N10% of patients, n (%)Cardiovascular 37 (10.5) 38 (10.5) 75 (10.5)Eyes, ears, nose and throat 36 (10.2) 44 (12.1) 80 (11.2)Gastrointestinal 43 (12.2) 47 (12.9) 90 (12.6)Neurologic 33 (9.4) 38 (10.5) 71 (9.9)Psychiatric 35 (9.9) 44 (12.1) 79 (11.0)
AP= antipsychotic, BMI= bodymass index, CGI-S= Clinical Global Impression-Severity, ITT= intent-to-treat, n= number of patients, PANSS=Positive and Negative Syndrome Scale,PSP = Personal and Social Performance, SD = standard deviation.⁎ n = 352 (PP), n = 362 (oral APs).† n = 325 (PP), n = 331 (oral APs).‡ n = 328 (PP), n = 332 (oral APs).§ n = 350 (PP), n = 360 (oral APs), Day 1 visit.¶ n = 346 (PP), n = 355 (oral APs), Day 1 visit.‖ Prior to the initial acute phase of treatment.
4 A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
relapse criteria (52 [14.8%] versus 76 [20.9%, oral antipsychotics]; P =0.032), representing a 29.4% relative risk reduction (Fig. 2).
Secondary outcomes are described in Supplementary Table 2. A sta-tistically significantly greater improvement in PANSS total scorewas ob-served on Day 8 (mean change−4.8 versus−3.7 [oral antipsychotics];P = 0.021); a trend in favor of PP was observed at endpoint (meanchange−16.6 versus−14.1 [oral antipsychotics]; P= 0.075) (Supple-mentary Fig. 1). At endpoint, a ≥30% improvement in PANSS total scorewas observed in 75.6% (PP) versus 69.4% (oral antipsychotics) of pa-tients (P=0.079). Both treatment arms showed comparable significant
Table 2Dosing (daily dose in mg) and drug exposure information for the core ITT oral APs group.
Aripiprazole(n = 81)
Haloperidol(n = 34)
Ola(n =
First dose (acute phase), n 81 34 49Mean (SD) 14.4 (5.8) 7.1 (5.2) 9.5Range 5, 30 1, 20 5, 2
Baseline dose, n 81 34 49Mean (SD) 17.9 (7.0) 8.3 (5.1) 12.0Range 10, 30 2, 20 5, 2
Modal dose, n 81 34 49Mean (SD) 19.1 (7.7) 8.2 (4.6) 12.9Range 10, 30 2, 15 5, 2
Last dose, n 81 34 49Mean (SD) 19.6 (7.7) 7.4 (4.3) 13.3Range 10, 30 2, 15 5, 2
AP = antipsychotic, ER = extended release, ITT = intent-to-treat, SD = standard deviation.
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
improvements at every time point for PANSS total score. Significantlygreater improvements were observed in favor of PP for the PANSSGeneral Psychopathology subscale score at Day 8 (P = 0.018) andendpoint (P = 0.045), and for the Marder factors ‘disorganizedthoughts’ (Day 8, P = 0.042) and ‘uncontrolled hostility/excitement’(Day 8, P = 0.033, endpoint, P = 0.008).
At endpoint, 65.4% of patients receiving PP and 65.0% receiving oralantipsychotics were rated mildly or less severely ill, compared with14.0% and 16.1%, respectively, at baseline (CGI-S total score). Changesin CGI-S from baseline to endpoint were statistically significant within
nzapine49)
Paliperidone ER(n = 77)
Quetiapine(n = 65)
Risperidone(n = 57)
77 65 57(4.2) 6.6 (2.4) 284.6 (174.3) 3.7 (1.6)0 3, 12 100, 800 2, 8
76 64 57(4.7) 7.7 (2.5) 453.1 (184.3) 4.2 (1.4)
0 3, 12 100, 800 2, 677 65 57
(5.2) 7.5 (2.7) 489.2 (188.0) 4.3 (1.6)5 3, 15 100, 800 2, 8
77 65 57(5.3) 7.8 (3.1) 501.5 (204.3) 4.3 (1.5)
5 3, 15 100, 900 2, 8
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.

Fig. 2. Kaplan–Meier plot of time to relapse*.*Relapse was defined by any of the following: psychiatric hospitalization; an increase in the level of psychiatric care (e.g. significant crisis intervention needed to avert hospitalization,clinically notable increases in the frequency or intensity of patient contact required to maintain outpatient status) and an increase of 25% from BL in the Positive and Negative SyndromeScale total score (or an increase of 10 points if the BL score was ≤40); deliberate self-injury; suicidal or homicidal ideation that was clinically significant in the investigator's judgment;violent behavior resulting in clinically significant injury to another person or property damage; substantial clinical deterioration, defined as a change score of 6 (much worse) or 7(very much worse) on the CGI-C scale; the required dose of AP exceeds the maximum approved dose. AP = antipsychotic, BL = baseline, CGI-C = Clinical Global Impression-Change,PP = paliperidone palmitate.
5A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
each group; they did not reach statistical significance between groups(P = 0.4837 [Supplementary Fig. 2]).
PSP total score improved significantly from baseline to endpoint inboth groups (mean change 9.8 [PP] versus 8.7 [oral antipsychotics];both P b 0.0001 within groups); these improvements were not signifi-cant between groups (P = 0.2831 [Supplementary Fig. 3]). Significantimprovements in SF-36, EQ-5D, and SWN-S scores were observed inboth treatment arms (Supplementary Table 2). No significant differ-ences were observed between groups except for a significantly greaterimprovement in EQ-5D index score in favor of oral antipsychotics atMonth 12 (P = 0.017).
In the PP arm, TSQM significantly improved across all domains(P b 0.05) except the ‘side effects’ subscale score. Significantlygreater improvements in the TSQM ‘convenience’ subscale scorewere observed in favor of PP (Month 24 [P b 0.01], Month 12, andendpoint [P b 0.0001]). There were no significant differences inpatients' treatment satisfaction in favor of oral antipsychotics(Supplementary Table 2) except for mean improvement from baselinein the ‘effectiveness’ subscale score at Month 24 (P b 0.05). Greater im-provements in physician's treatment satisfaction were observed for PPversus oral antipsychotics in scores for ‘safety’ (Month 12, P b 0.01),‘mode of administration’ (Months 12, 24, endpoint, P b 0.0001), and‘overall satisfaction’ (Months 12, 24, endpoint, P b 0.05).
3.3. Safety and tolerability
The most common TEAE reported was increase in body weight(Table 3); the proportion of patients reporting a ≥7% increase isshown in Table 4. No new safety signals were observed in either studyarm.
In the safety ITT population (n = 715), ≥1 serious TEAEs were re-ported in 11.6% (PP) and 12.7% (oral antipsychotics) of patients. Four-teen (4.0%) and 11 (3.0%) patients withdrew from the study due to aTEAE in the PP and oral antipsychotics arms, respectively. Two deathsoccurred: one of cardiac arrest (PP), considered unrelated to studydrug; and one of sudden death (oral olanzapine), considered doubtfullyrelated to study drug (Appendix).
The proportion of patientswith a TEAEof hyperprolactinemia and/orat least one potentially prolactin-related TEAE was similar betweentreatment arms (6.3% [PP] versus 5.0% [oral antipsychotics])
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
(Supplementary Table 3). There were no statistically significant differ-ences between treatment arms in changes from baseline to endpointfor extrapyramidal symptom rating scales (Table 3).
4. Discussion
This study aimed to provide robust evidence as to the role of LATs inthe early stages of schizophrenia. Time to relapse was significantly lon-ger for patients receiving PP compared with those receiving oral anti-psychotics. The observed reduction in relative risk of relapse iscomparable with recent clinical studies and meta-analyses (Leuchtet al., 2011; Grimaldi-Bensouda et al., 2012). A recent study of injectablearipiprazole failed to demonstrate an advantage on relapse rates overthe oral formulation (Fleischhacker et al., 2014). However, patientswere only followed for 38 weeks; an advantage may have become ap-parent in the longer term, as observed in the present study. The relapserate reported herein for patients receiving PP is comparable with thatfound in one of the few long-term studies of LATs in early illness,where 8% of patients with recent-onset psychosis who showed a clinicalresponse to long-acting injectable risperidone (LAI-R) relapsed over2 years (Emsley et al., 2008). Another study (Rosenheck et al., 2011)found similar times to hospitalization between unstable patients withschizophrenia receiving oral antipsychotics and those receiving LAI-R.However, several factors may have contributed to this outcome, includ-ing the smaller sample size compared with that originally planned, bi-weekly frequency of study visits, and the chronicity and illness severityof included patients.
In the present study, the greater observed improvement in symptomcontrol at Day 8, and a trend toward better symptom control at end-point in patients receiving PP compared with oral antipsychotics, isconsistent with a 2-year, active-controlled study of patients withschizophrenia or related disorders, in which patients randomized toLAI-R had a significantly greater improvement in symptomcontrol com-paredwith those receiving oral quetiapine (Gaebel et al., 2010). Similar-ly, a more robust reduction in psychotic symptoms was observed inpatients receiving LAI-R than in oral second generation antipsychotics(Buckley et al., 2015). However, there was no advantage in time to re-lapse; the authors noted that frequent clinical contact may have re-duced relapse in both groups and the power to detect between-groupdifferences. Nevertheless, the absence of significant differences
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.

Table 3Safety outcomes in the core ITT population for safety.
Paliperidonepalmitate(n = 352)
Oral APs(n = 363)
Proportion of patients reporting ≥1 TEAE, n (%) 251 (71.3) 225 (62.0)Number of TEAEs rated as possibly, probably orvery likely related to study drug, n (%)
448 (50.3) 294 (43.8)
TEAEs occurring in ≥5% of patients, n (%)Injection-site pain 24 (6.8) 0 (0.0)Nasopharyngitis 25 (7.1) 18 (5.0)Increase in weight 56 (15.9) 63 (17.4)Headache 39 (11.1) 31 (8.5)Tremor 18 (5.1) 8 (2.2)Anxiety 20 (5.7) 16 (4.4)Insomnia 34 (9.7) 29 (8.0)Schizophrenia 29 (8.2) 35 (9.6)Suicidal ideation 16 (4.5) 20 (5.5)
Patients reporting a potentiallyprolactin-related TEAE without a TEAE ofhyperprolactinemia or blood prolactinincreased reported, n (%)
21 (6.0) 15 (4.1)
Frequency of reportedhyperprolactinemia/blood prolactinincreased without any other potentiallyprolactin-related TEAE, n (%)
2 (0.6) 4 (1.1)
Potentially prolactin-related TEAEs occurringin ≥1% ofpatients, n (%)Amenorrhea 11 (3.1) 7 (1.9)Galactorrhea 6 (1.7) 1 (0.3)
Glucose-related TEAEs, n (%)Diabetes mellitus inadequate control 0 (0.0) 1 (0.3)
EPS-related TEAEs occurring in ≥1% ofpatients, n (%)Akathisia 15 (4.3) 14 (3.9)Dyskinesia 5 (1.4) 2 (0.6)Muscle rigidity 8 (2.3) 4 (1.1)Parkinsonism 3 (1.1) 4 (1.1)Restlessness 4 (1.1) 1 (0.3)Tremor 18 (5.1) 8 (2.2)
AIMS total score, Mean (SD)Baseline 0.4 (1.3) 0.4 (1.4)Endpoint LOCF 0.3 (0.9) 0.3 (1.4)Change from baseline to endpoint LOCF −0.1 (1.2) −0.1 (1.4)P value⁎ 0.1183 0.2025P value† 0.8800
BARS total score, Mean (SD)Baseline 0.4 (0.9) 0.4 (1.0)Endpoint LOCF 0.3 (1.0) 0.2 (0.8)Change from baseline to endpoint LOCF −0.1 (1.2) −0.2 (1.0)P value⁎ 0.1772 0.0003P value† 0.6615
SAS Global score, Mean (SD)Baseline 0.1 (0.2) 0.2 (0.3)Endpoint LOCF 0.1 (0.2) 0.1 (0.2)Change from baseline to endpoint LOCF −0.1 (0.2) −0.1 (0.2)P value⁎ b0.0001 0.0001P value† 0.1525
Patient weight, kg, Mean (SD)Baseline 74.8 (15.2) 76.1 (14.8)Endpoint LOCF 77.1 (15.6) 78.0 (14.8)Change from baseline to endpoint LOCF 2.3 (5.9) 1.9 (6.2)P value⁎ b0.0001 b0.0001P value† 0.2648
BMI, kg/m2, Mean (SD)Baseline 25.5 (4.7) 25.9 (4.4)Endpoint LOCF 26.3 (4.8) 26.6 (4.4)Change from baseline to endpoint LOCF 0.8 (2.0) 0.7 (2.1)P value⁎ b0.0001 b0.0001P value† 0.2748
AIMS = Abnormal Involuntary Movement Scale, AP = antipsychotic, BARS = BarnesAkathisia Rating Scale, BMI = body mass index, EPS = extrapyramidal symptoms, ITT =intent-to-treat, LOCF = last observation carried forward, n = number of patients, SAS =
Simpson Angus Scale, SD= standard deviation, TEAE= treatment-emergent adverse event.⁎ P value for within-group difference measured by Wilcoxon signed-rank test.† P value for between-group difference measured by Wilcoxon two-sample test.
6 A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
between groups in other objective symptommeasurements, despite themore frequent occurrence of relapse of patients in the oral treatmentarm, may reflect the now-recognized view that transition to relapsecan be abrupt with few/no early warning signs (Emsley et al., 2013a).
Due to the comprehensive examination of prolactin changes associ-ated with paliperidone ER and PP in their development programs, mea-surement of prolactin plasma levels was not required in this study. Theproportion of patients receiving PP reporting a potentially prolactin-related TEAE in this study was similar to that reported in the develop-ment program (107/3173; 3.4%) (Einarson et al., 2012).
Strengths of this study include the active comparator arm, 2-yearduration, randomized controlled, rater-blinded design, treatmentchoice of oral AP for the investigator, high completion rates (77.3% inthe PP group and 73.3% in the oral AP group), flexible dosing accordingto the label, and a more naturalistic study population compared withthe pivotal studies (inclusion/exclusion criteria).
Protocol-required activities may have enhanced patient adherencein the oral treatment arm due to the number of assessments and treat-ment delivery controlled directly by the prescriber, including pill-count.In particular, the discontinuation rate for patients randomized to oralantipsychotics in this study (26.7%) was lower than that observed inother studies of patients with early schizophrenia (Kahn et al., 2008;McEvoy et al., 2007). Moreover, patients for whom LATs are typicallyused (i.e. those who are partially or non-adherent with oral antipsy-chotics) may be under-represented, leading to under-estimation ofthe value of LATs in non-adherent patients. Nevertheless, it may be pos-sible that some patients were not adherent to treatment e.g. discardingmedication prior to the pill count. Other limitations include the non-blinding of medication (consequent to the required complexity of thestudy design), potential bias favoring the oral arm (patients in the PParm had to switch treatments whereas those in the oral arm remainedon their current medication), any potential selection bias betweenLATs and oral psychotics somehow inherent in the clinician's choice,and lack of control of other non-pharmacological treatment variablesbetween sites. In this study, in the oral treatment arm the six most fre-quently prescribed oral antipsychotics were offered; in order to main-tain a balance between oral treatments, investigators were not alwaysable to choose among all six oral APs for individual patients. Overall,pragmatic open-label studies are considered valuable because theyadd clinically relevant information on treatment effectiveness,complementing the evidence provided by RCTs (Kirson et al., 2013).
Despite their potential advantages, most treatment guidelines ad-vise limiting the use of LATs to multiple-episode or non-adherent pa-tients, with controversy in relation to their role in early schizophrenia(Kim et al., 2012). Nevertheless, less equivocal recommendations advo-cating their use in early illness are emerging, not least during the criticalperiod of the first 2–5 years following diagnosis, when important deci-sions in social and vocational role functioning are made (Malla et al.,2013; Altamura et al., 2012). The superiority of PP over oral antipsychot-ic monotherapy in time to relapse in recently diagnosed patients ob-served in this study may help to bring greater clarity to the role ofLATs, as well as to dispel some of the reticence by psychiatrists towardtheir use in the treatment of patients with schizophrenia, includingthe early stages of illness. Further research in patients early in the courseof their illness is recommended.
Role of the funding source
The study sponsor was involved in the conception and design of thestudy, and in the collection, analysis and interpretation of data.
Authors' contributions
Andreas Schreiner, Ludger Hargarter, andMarjolein Lahayewere in-volved in study design. Ludger Hargarter was the responsible medicalofficer of the sponsor and was involved in study conduct. Pierre
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.
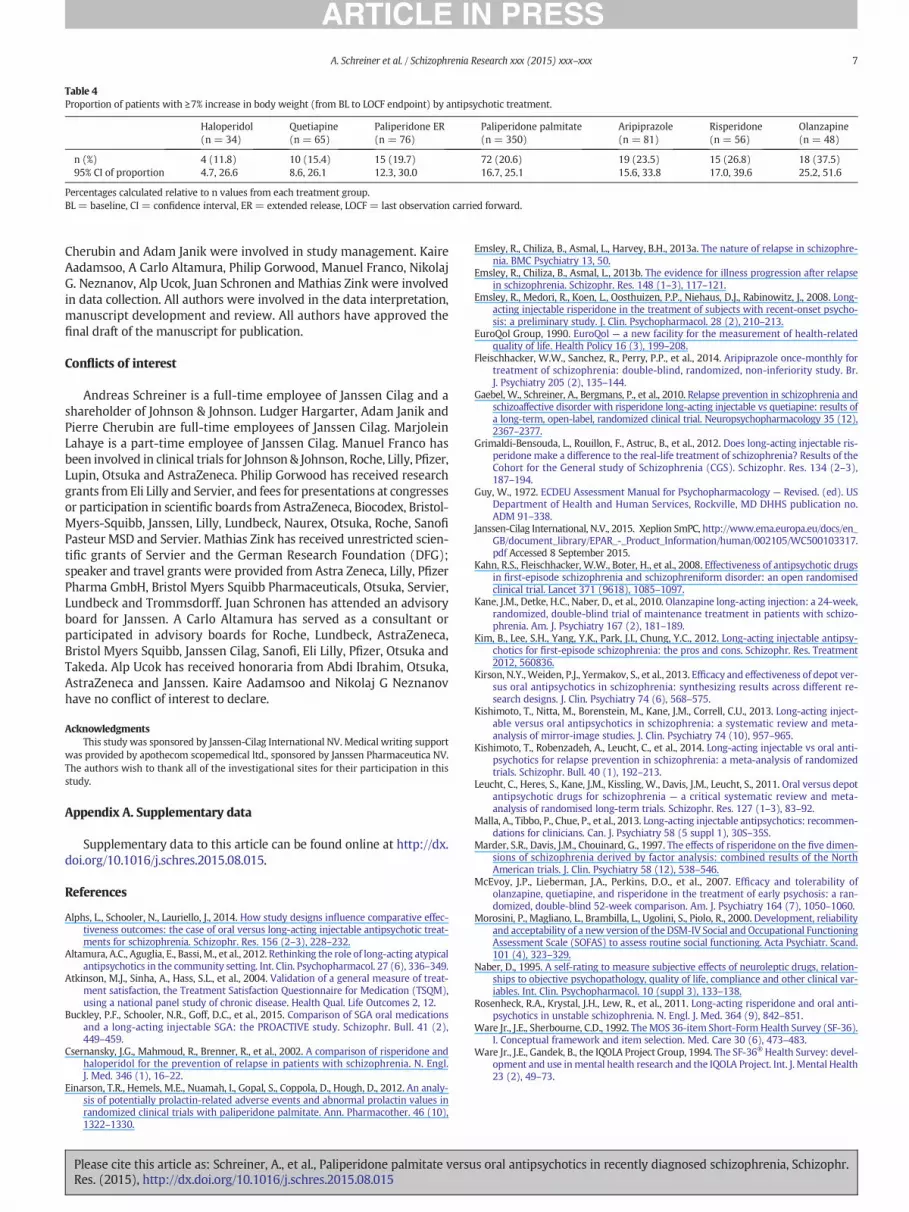
Table 4Proportion of patients with ≥7% increase in body weight (from BL to LOCF endpoint) by antipsychotic treatment.
Haloperidol(n = 34)
Quetiapine(n = 65)
Paliperidone ER(n = 76)
Paliperidone palmitate(n = 350)
Aripiprazole(n = 81)
Risperidone(n = 56)
Olanzapine(n = 48)
n (%) 4 (11.8) 10 (15.4) 15 (19.7) 72 (20.6) 19 (23.5) 15 (26.8) 18 (37.5)95% CI of proportion 4.7, 26.6 8.6, 26.1 12.3, 30.0 16.7, 25.1 15.6, 33.8 17.0, 39.6 25.2, 51.6
Percentages calculated relative to n values from each treatment group.BL = baseline, CI = confidence interval, ER = extended release, LOCF = last observation carried forward.
7A. Schreiner et al. / Schizophrenia Research xxx (2015) xxx–xxx
Cherubin and Adam Janik were involved in study management. KaireAadamsoo, A Carlo Altamura, Philip Gorwood, Manuel Franco, NikolajG. Neznanov, Alp Ucok, Juan Schronen and Mathias Zink were involvedin data collection. All authors were involved in the data interpretation,manuscript development and review. All authors have approved thefinal draft of the manuscript for publication.
Conflicts of interest
Andreas Schreiner is a full-time employee of Janssen Cilag and ashareholder of Johnson & Johnson. Ludger Hargarter, Adam Janik andPierre Cherubin are full-time employees of Janssen Cilag. MarjoleinLahaye is a part-time employee of Janssen Cilag. Manuel Franco hasbeen involved in clinical trials for Johnson & Johnson, Roche, Lilly, Pfizer,Lupin, Otsuka and AstraZeneca. Philip Gorwood has received researchgrants from Eli Lilly and Servier, and fees for presentations at congressesor participation in scientific boards from AstraZeneca, Biocodex, Bristol-Myers-Squibb, Janssen, Lilly, Lundbeck, Naurex, Otsuka, Roche, SanofiPasteur MSD and Servier. Mathias Zink has received unrestricted scien-tific grants of Servier and the German Research Foundation (DFG);speaker and travel grants were provided from Astra Zeneca, Lilly, PfizerPharma GmbH, Bristol Myers Squibb Pharmaceuticals, Otsuka, Servier,Lundbeck and Trommsdorff. Juan Schronen has attended an advisoryboard for Janssen. A Carlo Altamura has served as a consultant orparticipated in advisory boards for Roche, Lundbeck, AstraZeneca,Bristol Myers Squibb, Janssen Cilag, Sanofi, Eli Lilly, Pfizer, Otsuka andTakeda. Alp Ucok has received honoraria from Abdi Ibrahim, Otsuka,AstraZeneca and Janssen. Kaire Aadamsoo and Nikolaj G Neznanovhave no conflict of interest to declare.
AcknowledgmentsThis study was sponsored by Janssen-Cilag International NV. Medical writing support
was provided by apothecom scopemedical ltd., sponsored by Janssen Pharmaceutica NV.The authors wish to thank all of the investigational sites for their participation in thisstudy.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.schres.2015.08.015.
References
Alphs, L., Schooler, N., Lauriello, J., 2014. How study designs influence comparative effec-tiveness outcomes: the case of oral versus long-acting injectable antipsychotic treat-ments for schizophrenia. Schizophr. Res. 156 (2–3), 228–232.
Altamura, A.C., Aguglia, E., Bassi, M., et al., 2012. Rethinking the role of long-acting atypicalantipsychotics in the community setting. Int. Clin. Psychopharmacol. 27 (6), 336–349.
Atkinson, M.J., Sinha, A., Hass, S.L., et al., 2004. Validation of a general measure of treat-ment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM),using a national panel study of chronic disease. Health Qual. Life Outcomes 2, 12.
Buckley, P.F., Schooler, N.R., Goff, D.C., et al., 2015. Comparison of SGA oral medicationsand a long-acting injectable SGA: the PROACTIVE study. Schizophr. Bull. 41 (2),449–459.
Csernansky, J.G., Mahmoud, R., Brenner, R., et al., 2002. A comparison of risperidone andhaloperidol for the prevention of relapse in patients with schizophrenia. N. Engl.J. Med. 346 (1), 16–22.
Einarson, T.R., Hemels, M.E., Nuamah, I., Gopal, S., Coppola, D., Hough, D., 2012. An analy-sis of potentially prolactin-related adverse events and abnormal prolactin values inrandomized clinical trials with paliperidone palmitate. Ann. Pharmacother. 46 (10),1322–1330.
Please cite this article as: Schreiner, A., et al., Paliperidone palmitate versuRes. (2015), http://dx.doi.org/10.1016/j.schres.2015.08.015
Emsley, R., Chiliza, B., Asmal, L., Harvey, B.H., 2013a. The nature of relapse in schizophre-nia. BMC Psychiatry 13, 50.
Emsley, R., Chiliza, B., Asmal, L., 2013b. The evidence for illness progression after relapsein schizophrenia. Schizophr. Res. 148 (1–3), 117–121.
Emsley, R., Medori, R., Koen, L., Oosthuizen, P.P., Niehaus, D.J., Rabinowitz, J., 2008. Long-acting injectable risperidone in the treatment of subjects with recent-onset psycho-sis: a preliminary study. J. Clin. Psychopharmacol. 28 (2), 210–213.
EuroQol Group, 1990. EuroQol — a new facility for the measurement of health-relatedquality of life. Health Policy 16 (3), 199–208.
Fleischhacker, W.W., Sanchez, R., Perry, P.P., et al., 2014. Aripiprazole once-monthly fortreatment of schizophrenia: double-blind, randomized, non-inferiority study. Br.J. Psychiatry 205 (2), 135–144.
Gaebel, W., Schreiner, A., Bergmans, P., et al., 2010. Relapse prevention in schizophrenia andschizoaffective disorder with risperidone long-acting injectable vs quetiapine: results ofa long-term, open-label, randomized clinical trial. Neuropsychopharmacology 35 (12),2367–2377.
Grimaldi-Bensouda, L., Rouillon, F., Astruc, B., et al., 2012. Does long-acting injectable ris-peridone make a difference to the real-life treatment of schizophrenia? Results of theCohort for the General study of Schizophrenia (CGS). Schizophr. Res. 134 (2–3),187–194.
Guy, W., 1972. ECDEU Assessment Manual for Psychopharmacology — Revised. (ed). USDepartment of Health and Human Services, Rockville, MD DHHS publication no.ADM 91–338.
Janssen-Cilag International, N.V., 2015. Xeplion SmPC, http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002105/WC500103317.pdf Accessed 8 September 2015.
Kahn, R.S., Fleischhacker, W.W., Boter, H., et al., 2008. Effectiveness of antipsychotic drugsin first-episode schizophrenia and schizophreniform disorder: an open randomisedclinical trial. Lancet 371 (9618), 1085–1097.
Kane, J.M., Detke, H.C., Naber, D., et al., 2010. Olanzapine long-acting injection: a 24-week,randomized, double-blind trial of maintenance treatment in patients with schizo-phrenia. Am. J. Psychiatry 167 (2), 181–189.
Kim, B., Lee, S.H., Yang, Y.K., Park, J.I., Chung, Y.C., 2012. Long-acting injectable antipsy-chotics for first-episode schizophrenia: the pros and cons. Schizophr. Res. Treatment2012, 560836.
Kirson, N.Y.,Weiden, P.J., Yermakov, S., et al., 2013. Efficacy and effectiveness of depot ver-sus oral antipsychotics in schizophrenia: synthesizing results across different re-search designs. J. Clin. Psychiatry 74 (6), 568–575.
Kishimoto, T., Nitta, M., Borenstein, M., Kane, J.M., Correll, C.U., 2013. Long-acting inject-able versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J. Clin. Psychiatry 74 (10), 957–965.
Kishimoto, T., Robenzadeh, A., Leucht, C., et al., 2014. Long-acting injectable vs oral anti-psychotics for relapse prevention in schizophrenia: a meta-analysis of randomizedtrials. Schizophr. Bull. 40 (1), 192–213.
Leucht, C., Heres, S., Kane, J.M., Kissling, W., Davis, J.M., Leucht, S., 2011. Oral versus depotantipsychotic drugs for schizophrenia — a critical systematic review and meta-analysis of randomised long-term trials. Schizophr. Res. 127 (1–3), 83–92.
Malla, A., Tibbo, P., Chue, P., et al., 2013. Long-acting injectable antipsychotics: recommen-dations for clinicians. Can. J. Psychiatry 58 (5 suppl 1), 30S–35S.
Marder, S.R., Davis, J.M., Chouinard, G., 1997. The effects of risperidone on the five dimen-sions of schizophrenia derived by factor analysis: combined results of the NorthAmerican trials. J. Clin. Psychiatry 58 (12), 538–546.
McEvoy, J.P., Lieberman, J.A., Perkins, D.O., et al., 2007. Efficacy and tolerability ofolanzapine, quetiapine, and risperidone in the treatment of early psychosis: a ran-domized, double-blind 52-week comparison. Am. J. Psychiatry 164 (7), 1050–1060.
Morosini, P., Magliano, L., Brambilla, L., Ugolini, S., Piolo, R., 2000. Development, reliabilityand acceptability of a new version of the DSM-IV Social and Occupational FunctioningAssessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr. Scand.101 (4), 323–329.
Naber, D., 1995. A self-rating to measure subjective effects of neuroleptic drugs, relation-ships to objective psychopathology, quality of life, compliance and other clinical var-iables. Int. Clin. Psychopharmacol. 10 (suppl 3), 133–138.
Rosenheck, R.A., Krystal, J.H., Lew, R., et al., 2011. Long-acting risperidone and oral anti-psychotics in unstable schizophrenia. N. Engl. J. Med. 364 (9), 842–851.
Ware Jr., J.E., Sherbourne, C.D., 1992. TheMOS 36-item Short-FormHealth Survey (SF-36).I. Conceptual framework and item selection. Med. Care 30 (6), 473–483.
Ware Jr., J.E., Gandek, B., the IQOLA Project Group, 1994. The SF-36® Health Survey: devel-opment and use inmental health research and the IQOLA Project. Int. J. Mental Health23 (2), 49–73.
s oral antipsychotics in recently diagnosed schizophrenia, Schizophr.





























