Embed Size (px)
Citation preview
From DEPARTMENT OF CLINICAL NEUROSCIENCE Karolinska Institutet, Stockholm, Sweden
CHARACTERIZATION AND LONG-TERM FOLLOW-UP OF PEDIATRIC ACUTE-
ONSET NEUROPSYCHIATRIC SYNDROME (PANS)
Caroline De Visscher
Stockholm 2021

All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Universitetsservice US-AB, 2021 © Caroline De Visscher, 2021 ISBN 978-91-8016-205-0 Cover illustration: Martha Gromark
CHARACTERIZATION AND LONG-TERM FOLLOW-UP OF PEDIATRIC ACUTE-ONSET NEUROPSYCHIATRIC SYNDROME (PANS)
THESIS FOR DOCTORAL DEGREE (Ph.D.)
By
Caroline De Visscher
The thesis will be defended in public in the lecture hall Inghesalen, Tomtebodavägen 18A, Karolinska Institutet, Stockholm, Sweden and via Zoom on Thursday 3 June, 2021, at 10 am. Due to the ongoing COVID-19 pandemic the lecture hall will only be open to a limited number of pre-registered attendees. https://news.ki.se/dissertation-caroline-de-visscher Principal Supervisor: Prof David Mataix-Cols Karolinska Institutet Department of Clinical Neuroscience Center for Psychiatry Research Co-supervisors: Prof Eva Serlachius Karolinska Institutet Department of Clinical Neuroscience Center for Psychiatry Research Dr Eva Hesselmark Karolinska Institutet Department of Clinical Neuroscience Center for Psychiatry Research Prof Robert Harris Karolinska Institutet Department of Clinical Neuroscience Division of Neuro Dr AnnaCarin Horne Karolinska Institutet Department of Women’s and Children’s Health Division of Clinical Pediatrics
Opponent: Dr Thomas Pollak King’s College Department of Psychosis Studies Examination Board: Dr Janet Cunningham Uppsala University Department of Neuroscience Division of Psychiatry Prof Elisabeth Fernell Gothenburg University Department of Neuroscience and Physiology Division of Psychiatry and Neurochemistry Dr Tatja Hirvikoski Karolinska University Department of Women’s and Children’s Health Division of Neuropsychiatry


To Martha, Harald & Emmanuel.

POPULAR SCIENCE SUMMARY OF THE THESIS In recent years, it has become increasingly clear that disorders of the immune system can initiate or worsen psychiatric symptoms, and that the underlying cause of certain psychiatric diseases may be of inflammatory or autoimmune nature. This opens up for new treatment possibilities of sometimes severe and disabling psychiatric symptoms, if we just knew which patients we could help in this way.
A little more than 20 years ago, Dr. Susan Swedo and colleagues described a sub-group of children and adolescents with neuropsychiatric disorders who had an abrupt onset of severe psychiatric symptoms following a common throat infection, and that the symptoms presented periodically in an atypical way. She called the syndrome Pediatric Autoimmune Neuropsychiatric Syndrome Associated with Streptococcal infections (PANDAS). Since then, a lot of research efforts have been made to clarify the connection between streptococcal infections and the psychiatric syndrome described as PANDAS, yet without being able to find firm scientific evidence. A decade after Dr. Swedo’s first description of PANDAS, the wider syndrome description of Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) was introduced. The main difference is that PANS does not require the presence of a streptococcal infection at onset.
The overall purpose with this research project was to give children and adolescents with suspected PANS access to better care based on research evidence. In order to do that we first needed to increase our understanding. We followed a group of PANS patients over time, described the syndrome in a systematic way and worked with the development of clinical routines. We initiated collaborations with colleagues in neurology and rheumatology, which was necessary for several reasons: firstly, PANS patients often present with both psychiatric symptoms and symptoms from the body, such as movement disorder, pain, urinary problems, skin rashes or joint inflammation; secondly, PANS patients seem to be more vulnerable to other inflammatory or autoimmune diseases and these sometimes present at the same time as the PANS symptoms; and thirdly, medical treatments directed at the immune system should be handled in collaboration with doctors who are specialized in inflammation.
Our research show that PANS can vary a lot between patients, for some resulting in severe and disabling symptoms. We saw that a majority of the patients improved significantly over time, while a third developed more chronic symptoms. This chronic patient group was younger and had more impairment at onset, they needed more psychological and medical treatments and their daily life with school and leisure activities were more impacted. For the whole group, we saw an association with autoimmune disease, which means that a large proportion of the patients had a family history of autoimmune disease, several had autoimmune diseases of their own despite their young age, and some of the inflammatory markers we tested for were abnormal. Because of the wide and varying symptom presentations we concluded that patients should be cared for by medical professionals from several specialties, such as child and adolescent psychiatry, neurology and rheumatology. The measures used in the assessments

should be general enough to capture the patient’s level of functioning, with the addition of symptom-specific measures assessing core psychiatric symptoms such as obsessive-compulsive symptoms, anxiety, depression and behavioral problems.
During the research period the world was heavily impacted by the COVID-19 pandemic. How would the ongoing pandemic affect patients with PANS and their families? We conducted a global survey and found that absence of regular healthcare contacts, school closures, and social distancing had resulted in a lack of everyday support systems for these families, adding to an already strained situation. Even though it was not possible for some patients to access care at all, many reported positive experiences from keeping in touch with healthcare professionals via telephone or video appointments.
In the future, it will be important to focus on much-needed treatment trials including medical and psychological treatments. Another area of importance is to continue the investigation of clinical characteristics, factors influencing disease course and prognosis and laboratory tests in larger patient groups.
ABSTRACT Background
Pediatric acute-onset neuropsychiatric syndrome (PANS) is a cluster of psychiatric and somatic symptoms of proposed autoimmune etiology. It remains a descriptive entity, still of unclear validity and uncertain clinical utility. Further characterizing this patient group, describing its long-term prognosis and reaching a consensus regarding how to best measure its complex phenomenology are therefore important steps towards more efficient assessment, and management of this emerging patient group.
Aims
We aimed to: establish a Swedish cohort of well-characterized patients with PANS and to follow them up longitudinally; propose definitions for different clinical aspects of the syndrome, such as flare and disease course; investigate the suitability of standard clinical measures for following up PANS as well as assessing agreement between informants for these measures. Furthermore, and due to the ongoing COVID-19 pandemic, we wanted to investigate how the pandemic had affected patients with PANS.
Methods
This thesis comprises four studies. Study I was a descriptive study based on the establishment of the PANS cohort (n=45), including detailed clinical assessments, comprehensive laboratory tests and family history of autoimmune disease. Studies II and III were based on the same data collection, from the naturalistic two-to-five year follow-up of patients included in the PANS cohort (n=34). Study IV was a global survey investigating challenges for PANS patients during the ongoing COVID-19 pandemic (n=154).
Results
In study I we showed that PANS was a clinical entity with high variability in psychiatric and somatic symptom presentation and in level of impairment at onset. We also noted a strong association with autoimmunity in the cohort. The results of study II showed that although remission was rare, a majority of patients with PANS was significantly improved two-to-five years after inclusion in the cohort. Approximately one third of the patients had developed a chronic disease course requiring further treatments. These chronic patients had an earlier disease onset and a higher level of impairment at onset. Proposed definitions of flare and disease course seemed to meaningfully distinguish patients regarding impairment and subsequent need of healthcare resources. In study III we showed that ratings on symptom-specific measures varied largely between participants, due to the wide spectrum of PANS symptom presentations. Agreement between informants was excellent on functional scales, fair-to-moderate on global symptom severity scales, and mixed on the symptom-specific scales. Clinician-rated global and functional measures had stronger inter-correlations with parent- and child-rated functional measures than with symptom-specific ones. According to the

survey results in study IV, a third of the parents responded that their child was currently receiving the care they need for their PANS symptoms during the pandemic, while a third perceived a worsening of their children’s psychiatric and somatic symptoms and high stress levels.
Conclusion
The PANS clinical presentation can vary widely between patients, and the symptoms can range from mild to severe and disabling. The combination of psychiatric and somatic symptoms and the association with autoimmune disorders warrants a multi-specialist approach with access to a child and adolescent psychiatrist, psychologist, pediatric neurologist and rheumatologist. While a majority of patients improve significantly over time, a group of patients develop a chronic disease course requiring further treatments and interventions. When assessing and following up patients with PANS, the multi-dimensional clinical presentation of the syndrome should be taken into consideration. Global rather than symptom-specific measures are better suited at a group level, but these should be complemented with an efficient protocol of rating scales assessing core symptoms, such as OCD, anxiety, depression and tics. PANS patients and their families have been affected by the ongoing COVID-19 pandemic. Lack of regular healthcare contacts, school closures, and social distancing, resulting in lack of everyday support systems, have put strain on these families. Future research should focus on further defining the boundaries of the syndrome, prognostic factors, much-needed treatment trials and biomarkers in larger samples with adequate control groups.
LIST OF SCIENTIFIC PAPERS
I. Gromark C, Harris RA, Wickström R, Horne A, Silverberg-Mörse M, Serlachius E & Mataix-Cols D (2019). Establishing a Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic: Baseline Clinical Features of the Pediatric Acute-Onset Neuropsychiatric Syndrome Cohort at Karolinska Institutet. Journal of Child & Adolescent Psychopharmacology, 29(8):625-633.
II. Gromark C, Hesselmark E, Gebel Djupedal I, Silverberg M, Horne A, Harris R, Serlachius E & Mataix-Cols D (2021). A two-to-five year follow-up of a Pediatric Acute-onset Neuropsychiatric Syndrome cohort. Child Psychiatry & Human Development, e-published ahead of print on February 9, 2021, DOI 10.1007/s10578-021-01135-4.
III. De Visscher C, Hesselmark E, Rautio D, Gebel Djupedal I, Silverberg M, Idring Nordström S, Serlachius E & Mataix-Cols D (2021). Measuring clinical outcomes in children with Pediatric Acute-onset Neuropsychiatric Syndrome: Data from a long-term follow-up study. Unpublished manuscript.
IV. De Visscher C, Ringberg H, Serlachius E, Fernández de la Cruz L & Mataix-Cols D (2021). Meeting the specific challenges of children with Pediatric Acute-Onset Neuropsychiatric Syndrome during the COVID-19 pandemic. Unpublished manuscript.

SCIENTIFIC PAPERS NOT INCLUDED IN THE THESIS
1. Pfeiffer Hcv, Wickström R, Skov L, Sörensen CB, Sandvig I, H Gjone, S Ygberg, De Visscher C, Idring Nordström S, Herner LB, Hesselmark E, Hedderly T, Lim M & Debes NM (2021). Clinical guidance for diagnosis and management of suspected Pediatric Acute-onset Neuropsychiatric Syndrome. Acta Paediatrica, e-published ahead of print on April 14, 2021, DOI 10.1111/apa.15875.
2. Isung J, Williams K, Isomura K, Gromark C, Hesselmark E, Lichtenstein P, Larsson H, Fernández de la Cruz L, Sidorchuk A & Mataix-Cols D (2020). Association of primary humoral immunodeficiencies with psychiatric disorders and suicidal behavior and the role of autoimmune diseases. JAMA Psychiatry, 2020 Jun 10;77(11):1-9.
3. Mataix-Cols D, Frans E, Pérez-Vigil A, Gromark C, Isomura K, Fernández de la
Cruz L, Serlachius E, Leckman J, Crowley J, Rück C, Almqvist C, Lichtenstein P & Larsson H (2018). A total-population multigenerational family clustering study of autoimmune diseases in obsessive-compulsive disorder and Tourette’s/chronic tic disorders. Molecular Psychiatry, 23(7):1652-8.
4. Pérez-Vigil A, Fernández de la Cruz L, Brander G, Isomura K, Gromark C &
Mataix-Cols D (2016). The link between autoimmune diseases and obsessive-compulsive and tic disorders: A systematic review. Neuroscience & Biobehavioral Reviews, 71:542-562.
CONTENTS 1 INTRODUCTION.................................................................................................. 1 2 BACKGROUND ................................................................................................... 3
2.1 OCD and related disorders ............................................................................. 3 2.2 PANDAS ...................................................................................................... 3 2.3 From PANDAS to PANS .............................................................................. 4 2.4 Association to autoimmune disease ................................................................ 6 2.5 Clinical assessment........................................................................................ 6 2.6 Clinical management ..................................................................................... 7 2.7 The PANS controversy .................................................................................. 7 2.8 Summary ...................................................................................................... 8
3 RESEARCH AIMS ................................................................................................ 9 3.1 Study I: Establisment of a PANS cohort ......................................................... 9 3.2 Study II: A two-to-five year follow-up of a PANS cohort ............................... 9 3.3 Study III: Measuring clinical outcomes in PANS ............................................ 9 3.4 Study IV: Challenges of children with PANS during the COVID-19
pandemic ...................................................................................................... 9 4 METHODS ...........................................................................................................10
4.1 Clinical setting .............................................................................................10 4.1.1 Establishing a PANS team .................................................................10 4.1.2 The Stockholm clinical routines .........................................................10
4.2 Participants and recruitment ..........................................................................11 4.2.1 The PANS cohort ..............................................................................11 4.2.2 Study I ..............................................................................................11 4.2.3 Studies II and III ...............................................................................11 4.2.4 Study IV ...........................................................................................11
4.3 Measures and assessments used in study I, II and III ......................................11 4.3.1 Structured interview ..........................................................................11 4.3.2 Somatic assessment ...........................................................................12 4.3.3 Laboratory tests ................................................................................12 4.3.4 Measures of global symptom severity and adaptive functioning ..........12 4.3.5 Symptom-specific measures ..............................................................13
4.4 Study procedures ..........................................................................................14 4.4.1 Study I ..............................................................................................14 4.4.2 Study II .............................................................................................15 4.4.3 Study III ...........................................................................................15 4.4.4 Study IV ...........................................................................................15
5 RESULTS .............................................................................................................16 5.1 Study I: Establishment of a PANS cohort ......................................................16 5.2 Study II: A two-to-five year follow-up of a PANS cohort ..............................16 5.3 Study III: Measuring clinical outcomes in PANS ...........................................17
5.4 Study IV: Challenges of children with PANS during the COVID-19 pandemic .....................................................................................................17
6 ETHICAL CONSIDERATIONS ...........................................................................18 6.1 Personal integrity of the study participants ....................................................18 6.2 Informed consent ..........................................................................................18
7 DISCUSSION .......................................................................................................21 7.1 Establishment and characterization of a Swedish PANS cohort ......................21 7.2 Follow-up of a PANS cohort and further definitions of the syndrome.............23 7.3 Suitability of standard clinical measures for the assessment and follow-up
of PANS patients ..........................................................................................25 7.4 Challenges of children with PANS during the COVID-19 pandemic ..............27 7.5 Future directions...........................................................................................28 7.6 Conclusions .................................................................................................28
8 REFLECTIONS ON LEARNING .........................................................................30 9 ACKNOWLEDGEMENTS ...................................................................................31 10 REFERENCES .....................................................................................................33
LIST OF ABBREVIATIONS ADHD
ANA
Attention Deficit Hyperactivity Disorder
Antinuclear Antibodies
ASD
AQ
CAMHS
Autism Spectrum Disorder
Autism Spectrum Quotient
Child and Adolescent Psychiatry Services
CBC
CBT
CGAS
CGI-I
CGI-S
COVID-19
CRP
CTD
CY-BOCS
DSM
ECBI
EEG
ESR
GABHS
ICC
IgA
IgG
IgM
IL
ISI
IVIG
MRI
NSAID
OCD
OCD-RD
Complete Blood Count
Cognitive Behavioral Therapy
Children’s Global Assessment Scale
Clinical Global Impression-Improvement scale
Clinical Global Impression-Severity scale
Coronavirus Disease of 2019
C-reactive Protein
Chronic Tic Disorder
Children’s Yale-Brown Obsessive Compulsive Scale
Diagnostic and Statistical Manual of Mental Disorders
Eyberg Child Behavior Inventory
Electroencephalography
Erythrocyte Sedimentation Rate
Group A Beta-Hemolytic Streptococci
Intraclass Correlation Coefficient
Immunoglobulin A
Immunoglobulin G
Immunoglobulin M
Interleukin
Insomnia Severity Index
Intravenous Immunoglobulin
Magnet Resonance Imaging
Non-Steroidal Anti-inflammatory Drug
Obsessive Compulsive Disorder
OCD-Related Disorders
OCI
ODD
PANDAS
PANS
SAA
SAAI
SDQ
SMFQ
SNAP
SSRI
TD
TNF
WHO
WSAS
YGTSS
Obsessive Compulsive Inventory
Oppositional Defiant Disorder
Pediatric Autoimmune Neuropsychiatric Disorders ass. with Streptococcal infections
Pediatric Acute-onset Neuropsychiatric Syndrome
Serum Amyloid A
Separation Anxiety Avoidance Inventory
Strengths and Difficulties Questionnaire
Short Moods and Feelings Questionnaire
Swanson, Nolan and Pelham Scale
Selective Serotonin Reuptake Inhibitor
Tourette’s Disorder
Tumor Necrosis Factor
World Health Organization
Work and Social Adjustment scale
Yale Global Tic Severity Scale
1
1 INTRODUCTION Increasing evidence of an association between inflammation, autoimmune disease and neuropsychiatric disorders has emerged in recent years.1-3 Clinicians in child and adolescent psychiatry as well as in pediatric rheumatology and neurology meet an increasing number of patients requesting assessment and care for suspected immunopsychiatric symptoms, for which we, when starting this work, lacked a clinical consensus. The most frequently described pediatric immunopsychiatric disorders are pediatric autoimmune neuropsychiatric syndrome associated with streptococcal infections (PANDAS) and pediatric acute-onset neuropsychiatric syndrome (PANS).4,5 These patients often present with obsessive-compulsive and related disorders (OCD-RD) and/or tics associated with a wide range of other psychiatric and somatic symptoms. The onset may be abrupt and severe, resulting in disabling symptoms altering everyday life, not only for the affected child but for the whole family.6,7 Parents often describe intense worry and frustration when seeking help for their affected child or adolescent, realizing that healthcare professionals lack in understanding or knowledge.8
As of today, there is no standardized treatment or care that is scientifically proven to improve the outcome in children with PANS9, but increased knowledge about suspected etiologies of these symptoms may open up for novel treatment approaches. Easily accessible pharmacological treatments such as non-steroidal anti-inflammatory drugs (NSAIDs), and in some cases antibiotics, may be efficient in treating disabling psychiatric symptoms in some children.10,11 For a psychiatrist, this represents a new way of thinking. But we are not there yet. We need to further understand who these patients are, how their symptoms present, prognostic factors, different clinical courses and how to adequately assess a flare or a treatment response. Only then will we be able to conduct important treatment trials that will enable us to decide on efficient treatments, pharmacological or otherwise.
The overall aim of this research project was to further characterize PANS, understand the long-term course of the syndrome and to contribute to the improvement of evidence-based assessment methods.
Stockholm, April 2021
3
2 BACKGROUND 2.1 OCD AND RELATED DISORDERS
OCD-RD include OCD, body dysmorphic disorder, hoarding disorder, skin-picking disorder (dermatillomania), trichotillomania and olfactory reference syndrome.12-14 Although classified in a separate chapter of the Diagnostic and Statistical manual of mental disorders (DSM)-512, tic disorders are frequently considered to be part of this group. OCD and tic disorders are both recurring symptom presentations in PANS.
OCD is characterized by the presence of obsessions and/or compulsions. Obsessions are defined as recurrent, intrusive thoughts, images or urges that cause fear and distress. Compulsions are repetitive behaviors intended to decrease distress or to forestall a feared event or situation.12,13 Approximately 1% of children and 2% of adolescents fulfill the diagnostic criteria for OCD, with an average age of onset around ten years of age, and a higher prevalence in boys during childhood. Without treatment OCD is considered a chronic condition with a poor prognosis.15,16
Tourette’s Disorder (TD) is a neurodevelopmental movement disorder characterized by multiple motor tics and one or more vocal/phonic tics, with duration of longer than one year. Chronic Tic Disorder (CTD) involves either motor or vocal tics lasting longer than one year.13 Collectively, tic disorders (TD/CTD) are more frequent in boys than in girls (3:1 ratio) and typically appear between ages 4-6, being worst around ages 10-12. Tic disorders were previously considered rare, but increased awareness has resulted in revised prevalence figures of approximately 1% of the population.17,18
Among children with OCD and tics 50-75% have one or more co-morbidities, the most prevalent ones being anxiety, depression, attention deficit/hyperactivity disorder (ADHD), depression and oppositional defiant disorder (ODD). OCD and tic disorder have a high comorbidity, with up to 20-40% of children with OCD also having a tic disorder and 20-60% of children with a tic disorder fulfilling the OCD criteria.19,20
The etiology of both OCD and tic disorders is still unclear. Both genetic and environmental factors are thought to be important, but specific genes and environmental risk factors are yet to be identified.21,22 Research into the remaining OCD-RDs lags considerably behind, and little is known about their etiology other than that they are likely heritable and related to one another.23-
26
2.2 PANDAS
PANDAS was first described by Swedo et al. in 1998 as the abrupt, pre-pubertal onset of OCD and/or tics associated with motor abnormalities such as hyperactivity and involuntary movements.5 The onset should be temporally related with a streptococcal infection and the disease course relapsing-remitting. The hypothetical etiology of PANDAS is that antibodies against group A beta-hemolytic Streptococci (GABHS) react to brain tissue in the basal

4
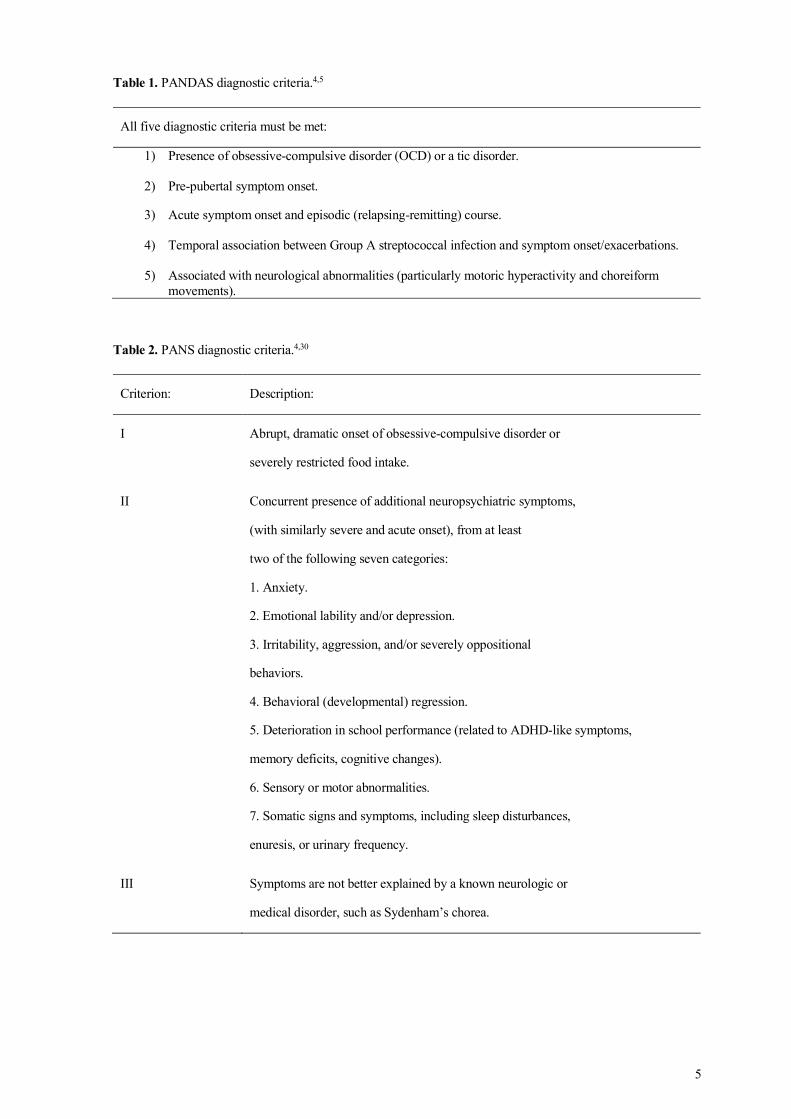
ganglia, causing the psychiatric and neurological symptoms, but this has yet to be clearly demonstrated.27-29 The diagnostic criteria for PANDAS are listed in Table 1.
2.3 FROM PANDAS TO PANS
Because the hypothesized link between streptococcal infections and OCD-related symptoms has been difficult to demonstrate, a reconceptualization of this entity has been proposed. Broader symptom criteria were presented at the 2013 PANS consensus conference.4,30 PANS describes the acute onset of OCD and/or severely restricted food intake in temporal relation with other severe neuropsychological and somatic symptoms including anxiety, emotional lability, irritability/aggression, regression, deterioration in school performance, sensor and motor abnormalities and somatic signs such as enuresis, sleep disturbance and pain.30 The symptoms may result in significant loss of function, severely affecting both the children themselves and their families.6-8 The diagnostic PANS criteria are listed in Table 2.
The main differences from the initial PANDAS criteria include: 1) PANDAS requires neurological findings, but PANS can be diagnosed solely on psychiatric symptoms; 2) PANDAS requires both a specified onset (acute) and course (relapsing-remitting); and 3) PANDAS has a proposed etiology (GABHS).31 Tics are no longer considered a main symptom criterion but are included as a secondary symptom criterion. The PANS criteria do not mention etiology, but infectious agents, e.g. streptococci, mycoplasma and Epstein-Barr virus, as well as autoimmune disease and inflammatory disorders have been proposed as part of the pathogenic mechanism and potential triggers.32,33 Diseases such as Sydenham’s chorea, systemic lupus erythematosus (SLE), TD or other neuroinflammatory encephalitis, e.g. anti-NMDA-receptor encephalitis, need to be ruled out. Throughout this thesis, PANDAS will be considered a sub-group of PANS.
5
Table 1. PANDAS diagnostic criteria.4,5
All five diagnostic criteria must be met:
1) Presence of obsessive-compulsive disorder (OCD) or a tic disorder.
2) Pre-pubertal symptom onset.
3) Acute symptom onset and episodic (relapsing-remitting) course.
4) Temporal association between Group A streptococcal infection and symptom onset/exacerbations.
5) Associated with neurological abnormalities (particularly motoric hyperactivity and choreiform movements).
Table 2. PANS diagnostic criteria.4,30
Criterion: Description:
I Abrupt, dramatic onset of obsessive-compulsive disorder or
severely restricted food intake.
II Concurrent presence of additional neuropsychiatric symptoms,
(with similarly severe and acute onset), from at least
two of the following seven categories:
1. Anxiety.
2. Emotional lability and/or depression.
3. Irritability, aggression, and/or severely oppositional
behaviors.
4. Behavioral (developmental) regression.
5. Deterioration in school performance (related to ADHD-like symptoms,
memory deficits, cognitive changes).
6. Sensory or motor abnormalities.
7. Somatic signs and symptoms, including sleep disturbances,
enuresis, or urinary frequency.
III Symptoms are not better explained by a known neurologic or
medical disorder, such as Sydenham’s chorea.
6
2.4 ASSOCIATION TO AUTOIMMUNE DISEASE
There is increasing evidence for an association between autoimmune disease and a wide range of neuropsychiatric disorders and psychiatric states.1,2,34,35 The detection of anti-NMDA-receptor encephalitis just over ten years ago clarified that an autoimmune brain disease could onset with a severe psychiatric presentation, sometimes in the absence of somatic symptoms.36,37 Similarly, individuals affected by psychiatric disease, such as psychotic and depressive disorders, have been reported to have abnormal immunological phenotypes.1,38-40 Other immune-based illnesses and IgA-deficiency also seem to be more common in the group of patients with OCD and/or tics that fulfill PANS criteria.6,41 Inflammatory markers have been associated with the development or severity of psychosis, bipolar disorder and depression.42-44 Likewise, immunological abnormalities including elevated serum cytokine levels have been noted in patients with tic disorders.45 It remains unclear if the link between autoimmune disease and psychiatric symptoms is stronger in patients fulfilling PANS criteria, even though some evidence suggest that infection-triggered autoimmune disease such as post-streptococcal autoimmune manifestations may represent as PANS symptoms.29,46-48
Large-scale epidemiological studies have shown that individuals with OCD and tic disorders have increased comorbidity with any autoimmune disease (43% and 36%, respectively).49,50 These studies also suggested a familial link between autoimmune diseases in general and both OCD and tics. However, many of the post-infectious autoimmune diseases were excluded and the outcomes were limited to OCD and tic disorders. Primary humoral immunodeficiency, as well as post-infectious inflammatory states, are also associated with psychopathology and suicidal behavior, particularly when also associated with co-occurring autoimmune disease.51-
53
2.5 CLINICAL ASSESSMENT
PANS is a symptom description without objective clinical signs to aid in the diagnostic process. The somatic assessment focuses primarily on excluding other potential causes of the clinical presentation, and assessments (e.g. lumbar puncture, magnetic resonance imaging (MRI) and/or electroencephalography (EEG)) are chosen based on the patient’s symptoms.
The psychiatric assessment should include a developmental history, description of onset and clinical course as well as ratings of current symptoms. Gold-standard measures of core symptoms, such as Children’s Yale-Brown Obsessive Compulsive scale (CY-BOCS)54 for obsessive-compulsive symptoms, are frequently used. At least two clinician-rated instruments or symptom checklists have been developed specifically for PANS, but their administration is time-consuming, their items cannot be easily summed to calculate total scores, and their psychometric properties have not yet been established.55,56
At present there are no biomarkers that unequivocally permit the diagnosis of suspected autoimmune-mediated psychiatric disorders such as the group described within the PANS criteria. Even though there is a clinical test for PANDAS/PANS currently on the market, the Cunningham panel, the reference values of this test are based on a small group of healthy
7
subjects, the comparison of results between other groups of psychiatric illnesses is sparse and the results remain difficult to interpret.57-60 In a recent pilot study comprising a small sample of PANS patients, no neurochemical evidence of neuronal damage or glial activation was found in patient sera.61 The identification of reliable biomarkers that distinguish regular OCD-RD patients from those with PANS-like presentations would represent important progress in the field.
2.6 CLINICAL MANAGEMENT
Proposed pharmacological treatments for PANS include antibiotics, anti-inflammatory and immunomodulatory treatments as well as symptomatic treatments directed at psychiatric symptoms, for instance anti-depressants, anti-psychotics and anxiolytics. Cognitive behavioral therapy (CBT) and parental strategies are also part of the management of symptoms. Proposed treatments are still mainly based on case reports. Few randomized, controlled treatment trials have been conducted, and several suffer from methodological issues due to limited power, open-label treatments and the use of single-symptom outcome measures.9
Antibiotics are frequently used both to treat an infection thought to be a trigger of PANS and to prevent re-infections and relapses. Even though antibiotic prophylaxis is recommended in the case of the rather similar condition rheumatic fever, evidence for long-term antibiotic treatment in PANS is lacking.9,11,28 Immunomodulatory treatments such as intravenous immunoglobulins (IVIG) and therapeutic plasmapheresis have been tried as treatments for patients with PANDAS or PANS, with some success.62-64 Observational data have also indicated that NSAIDs and corticosteroids may improve neuropsychiatric symptoms and shorten flares in patients with PANS.10,65,66 Even though immunomodulatory and/or anti-inflammatory treatments may be beneficial in some cases, the evidence is still inconclusive.9,67
The PANS Research Consortium, an American group of clinicians and researchers, has formulated consensus guidelines regarding the psychiatric and immunomodulatory treatments as well as the treatment of infections for patients fulfilling different stages of PANS severity.68-
70 The consensus guidelines are not evidence-based, but meant to facilitate clinical decision-making while further research is conducted.
2.7 THE PANS CONTROVERSY
PANS is a diagnosis of exclusion and remains a controversial entity. It is important to emphasize that, based on current research, this diagnosis is challenging to distinguish from other DSM-512 diagnoses describing similar psychiatric manifestations. The absence of useful biomarkers has hampered progress in the field. The severe and sometimes debilitating symptoms in combination with a high media-interest may have led to the over-prescription of antibiotics, anti-inflammatory and immunomodulatory treatments. Vague inclusion/exclusion criteria, lack of biomarkers, open-label treatment trials and difficulties in finding validated rating scales for the assessment of responders and non-responders, have resulted in repeated inconclusive clinical trials.9,31 Further characterization of the syndrome is essential to validate PANS as an immunopsychiatric disorder and facilitate adequate treatment.
8
2.8 SUMMARY
PANS is a cluster of psychiatric and somatic symptoms of proposed autoimmune etiology. It remains a descriptive entity, still of unclear validity and uncertain clinical utility. The increased focus on PANS and other proposed immunopsychiatric disorders presents a challenge for both clinicians and researchers in developing evidence-based care. The identification of factors characterizing the sub-group of patients within the OCD-RD spectrum that may have an inflammatory or autoimmune etiology is an important first step, and longitudinal studies are essential to understand the clinical course over time. Identifying distinct clinical traits, together with research efforts directed at identifying precise outcome measures, will enable much-needed treatment trials potentially leading to new and more selective immunopharmacological treatments.
9
3 RESEARCH AIMS The overall aim of this research project was to further characterize PANS through establishing a cohort of PANS patients, to follow them up longitudinally, to describe clinical traits and different clinical courses of the syndrome and to contribute to the improvement of evidence-based assessment with more precise outcome measures, while advancing the establishment of care pathways for PANS patients.
The specific aims of each study are listed below.
3.1 STUDY I: ESTABLISMENT OF A PANS COHORT
Study I aimed to create a Swedish cohort of well-characterized PANS patients, describe their specific clinical characteristics including comorbidities, comprehensive laboratory tests and detailed family history of autoimmune disease.
3.2 STUDY II: A TWO-TO-FIVE YEAR FOLLOW-UP OF A PANS COHORT
Study II aimed to conduct a naturalistic two-to-five year follow-up of the patients included in the PANS cohort, specifically to conduct an assessment of current psychiatric and somatic health status and to investigate clinical characteristics that may influence disease course and prognosis, such as defining the clinical features of a symptom flare and of different clinical courses of the disease.
3.3 STUDY III: MEASURING CLINICAL OUTCOMES IN PANS
Study III aimed to evaluate the suitability of standard clinical measures for the assessment and follow-up of PANS patients, formally assess the agreement between multiple informants (clinician, parent and child) and propose a core battery of measures to use in clinical practice and clinical trials.
3.4 STUDY IV: CHALLENGES OF CHILDREN WITH PANS DURING THE COVID-19 PANDEMIC
Study IV aimed to increase the knowledge about how to best support PANS-affected families during the COVID-19 pandemic, specifically through conducting a global survey.
10
4 METHODS 4.1 CLINICAL SETTING
4.1.1 Establishing a PANS team
In 2014, the specialist pediatric OCD-RD outpatient clinic in Stockholm, Sweden, started accepting referrals of potential PANS cases and, as the demand increased, we established a PANS team within the clinic. Since 2019 the PANS team has further expanded into a separate immunopsychiatric clinic with a broader scope. The clinic primarily receives referrals from Child and Adolescent Psychiatry Services (CAMHS) and pediatric services from throughout the entire Stockholm region, and occasionally from other Swedish regions and Nordic countries. All patients and their parents/legal guardians routinely fill in questionnaires before their first appointment with the multidisciplinary clinical team comprised of child and adolescent psychiatrists, clinical psychologists and nurses. This information is then used to conduct a more focused and efficient face-to-face diagnostic assessment, in which detailed sociodemographic and clinical information is gathered and clinical diagnoses are made according to ICD-10 and DSM-5 criteria.12-14 After this assessment patients are either offered treatment at the clinic or are referred to more appropriate services. For all patients undertaking treatment at the clinic assessments are repeated at post-treatment and at several fixed follow-up times: 3, 6, and 12 months after the end of the treatment. All patients in the clinic are routinely asked for participation in research studies, including long-term follow-up and future linkage to Swedish registers. All participants signed an informed consent form.
4.1.2 The Stockholm clinical routines
We have established close collaborations with the pediatric neuroinflammation team at Karolinska University Hospital, which creates a multi-specialist environment with child and adolescent psychiatry, pediatric rheumatology and pediatric neurology. The collaboration has enabled the development of Sweden’s first clinical routines for the evaluation and management of children and adolescents with PANS, in consensus with pediatric rheumatology, pediatric neurology and CAMHS across Stockholm in April 2018. These routines resemble, but are not identical to, the guidelines previously reported by the PANS Research Consortium in the USA.68,69,71 Since clinical trials are still inconclusive regarding the benefits of long-term antibiotics, the Stockholm clinical routines discourage their use until firmer evidence becomes available. Verified or clinically suspected infections are treated with antibiotics, according to established infectious diseases guidelines and clinical practice. The Stockholm clinical routines also include a requirement for neurological clinical signs, EEG and/or magnetic MRI abnormalities and/or biomarkers (in blood and/or CSF) suggestive of an active inflammation, or traits of primary immunodeficiency, before IVIG treatment is considered.
11
4.2 PARTICIPANTS AND RECRUITMENT
4.2.1 The PANS cohort
The participants in study I, II and III were consecutively referred patients fulfilling strict PANS criteria and consenting to participate in our long-term follow-up study. These patients constitute the PANS cohort.
4.2.2 Study I
Between November 2014 and March 2018, the clinic received 100 referrals regarding suspected PANS, 47 of which met strict PANS criteria. Forty-five of those consented to participation in long-term follow-up. Inclusion criteria were that strict PANS criteria were met and that the patient was under 18 years of age. Attempting to select a strictly defined cohort we made the decision to exclude patients who did not exhibit any somatic symptom or sign. There were no other specified exclusion criteria.
4.2.3 Studies II and III
All patients with a minimum of two years since inclusion in the PANS cohort were eligible for participation, regardless if they were still active patients in the clinic or not. Parents or legal guardians were contacted via an information letter by post followed by a telephone call. Out of the 46 patients eligible for participation, 44 families were reached and 34 active or former patients consented to participate. The main reasons for attrition were that the family no longer wished to participate in research or that they cancelled their participation due to the ongoing COVID-19 pandemic.
4.2.4 Study IV
In order to reach as many PANS affected families as possible we designed a global survey. Information about the survey was spread through information material in the clinic, on social media platforms and through professional networks and patient organizations, both in Sweden and abroad. The parents/guardians of 154 children completed the survey. The main countries represented were Sweden (33%), the United States (32%), the United Kingdom (13%), and Canada (12%). Inclusion criteria were that the child or adolescent was under 18 years of age and with a self-reported PANS diagnosis. Guardians provided information on who had made the diagnosis, but because of the varying access to specialized care, lack of a formal PANS diagnosis from a physician did not constitute an exclusion criterion.
4.3 MEASURES AND ASSESSMENTS USED IN STUDY I, II AND III
The measures were chosen based on our clinical experience and recommendations from the 2013 PANS Consensus Conference.30
4.3.1 Structured interview
The parent and patient interview covered the family history of psychiatric and inflammatory/autoimmune disease, developmental history, school function and daily activities,
12
psychiatric and somatic comorbidities including allergies/sensitivities, vaccination records, onset and current symptoms, potential triggers, unverified (parent-reported) and verified (positive culture or assessed by a clinician) infections, previous and current medications and psychological treatments/interventions. At follow-up, additional focus was given to recently acquired psychiatric and somatic diagnoses, flares and clinical disease course.
4.3.2 Somatic assessment
The medical examination included assessment and documentation of somatic signs. It covered height, weight, heart, lungs, stomach, skin, thyroid, lymph nodes, throat, ears, joints, neurology and motor function.
4.3.3 Laboratory tests
The laboratory protocol was developed for regular clinical use in collaboration with pediatric neurology and rheumatology at Karolinska University Hospital. It included a throat culture and basic blood measurements of hemoglobin, complete blood count (CBC), ferritin, vitamin D levels, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), indicators for liver and kidney disease, thyroid tests, celiac test and several inflammatory and rheumatological markers (protein fractions, immunoglobulin G, A and M, IgG subclasses, antinuclear antibodies (ANAs) and interleukin (IL)-1-b, IL-6, IL-8, IL-10 and tumor necrosis factor (TNF)-a). The reference values used were the ones used by the Karolinska Laboratory in clinical practice (www.karolinska.se/for-vardgivare/karolinska-universitetslaboratoriet).
4.3.4 Measures of global symptom severity and adaptive functioning
The Clinical Global Impressions - Severity scale (CGI-S) is a clinician-rated scale measuring the current global severity of a patient’s psychiatric illness. It is a 7-point single-item scale ranging from ‘normal’ (score 1) to ‘extremely ill’ (score 7).72 The Clinical Global Impressions - Improvement scale (CGI-I) is the equivalence measuring improvement compared to baseline, ranging from ‘very much improved’ (score 1) to ‘very much worse’ (score 7).72 Both CGI-S and CGI-I are a widely used, validated, clinical outcome measures in psychiatry.73 In addition to the original clinician-rated version, the CGI-S was adapted for its use as a self-report measure, resulting in parent- and child-rated versions of the scale.
The Strengths and Difficulties Questionnaire - Parent-/Self-rated version (SDQ-P/S) is a validated, parent- and child-rated, behavioral screening questionnaire consisting of five subscales. Four subscales are measuring difficulties (hyperactivity, emotional symptoms, conduct problems and peer problems) and one is measuring strengths (pro-social behavior). Items are scored from ‘not true’ (score 0) to ‘certainly true’ (score 2), with a maximum total difficulty score of 40. A higher total difficulty score indicates a higher symptom burden and a lower global functioning. A total difficulty score of 14 has been a suggested cut-off in a Swedish sample.74 SDQ-S is adapted for 11-16 year old children and adolescents.75
13
The Children’s Global Assessment Scale (CGAS) is a clinician-rated, extensively validated, single-item measure of general functioning. The scale ranges from 1-100, with higher scores indicating a higher level of general functioning.76 The assessment should be made by a specifically trained child and adolescent psychiatrist or psychologist after a thorough clinical assessment and reflect the most impaired level during a specified time period of one month, regardless of treatment and/or prognosis.77,78
KIDSCREEN-10 - Parent/Youth version is a parent- and child-rated screening instrument measuring well-being and health-related quality of life for children and adolescents. The scale contains 10 items, scored on a 5-point response scale, with a maximum score of 50. A higher score indicates higher health-related quality of life. An additional item measuring general well-being is scored separately, on a 5-point scale, from ‘bad’ (score 1) to ‘excellent’ (score 5).79,80
The Work and Social Adjustment scale - Parent/Youth version (WSAS-P/Y) is a brief and reliable parent- and child-rated measure of educational, work and social adjustment in children and adolescents. The scale includes five items related to everyday activities (school and employment, everyday activities, social activities, leisure time, and family/relationships), scored from ‘not impaired at all’ (score 0) to ‘severely impaired’ (score 8), with a maximum score of 40. A total score above 20 can indicate severe functional impairment. WSAS-P/Y has high internal consistency and is sensitive to change.81,82
4.3.5 Symptom-specific measures
The CY-BOCS and the Yale Global Tic Severity Scale (YGTSS) are clinician-rated instruments to quantify the severity of OCD and tic disorder symptoms, respectively.54,83,84 Both scales have excellent psychometric properties and are routinely employed in clinical practice and clinical trials. Higher total scores indicate a higher symptom burden, and clinically significant levels of OCD and tic symptoms are generally considered to be reached at CY-BOCS >15 and YGTSS >30.54,85,86
The Obsessive Compulsive Inventory - Child Version (OCI-CV) is a 21-item child-rated self-report measure of OCD symptom severity that correlates moderately well with clinician-rated measures of OCD symptoms. It consists of seven sub-scales (doubting/checking, obsessing, hoarding, washing, ordering and neutralizing). Items are scored from ‘never’ (score 0) to ‘always’ (score 2), with a maximum score of 42. A higher score indicates more severe symptoms.87,88
The Short Moods and Feelings Questionnaire - Parent/Child version (SMFQ-P/C) is a 13-item parent- and child-rated screening tool for depressive symptoms in children and adolescents, developed from the longer 34-item version Moods and Feelings Questionnaire (MFQ). Both versions of the scale have been extensively validated in community and clinical samples. Responses are rated on a 3-point scale from ‘not true’ (score 0) to ‘true’ (score 2), with a maximum score of 26. A higher total score indicates more severe depressive symptoms. Suggested cut-offs for girls are >16 and for boys >5 when parent- or self-rated.89,90
14
The Separation Anxiety Avoidance Inventory - Parent/Child version (SAAI-P/C) is a validated 12-item parent- and child-rated measure of avoidance behavior in separation situations. Each item is scored from ‘never’ (score 0) to ‘always’ (score 4), with a maximum score of 48. A higher total score indicates more severe avoidance behavior.91
The Insomnia Severity Index - Child and adolescent version (ISI-C) is a 7-item child-rated measure assessing insomnia severity on a 5-point scale from ‘not at all’ (score 0) to ‘extremely’ (score 4), with a maximum score of 28. A high total score indicates greater insomnia severity, with scores 15 and above indicating clinical insomnia.92,93
The Autism Spectrum Quotient Child/Adolescent version - 10 (AQ-10) is a 10-item parent-rated instrument initially developed as a tool to aid referral decision making for autism spectrum disorder (ASD) evaluation. The maximum score is 10 and scores 6 or above are considered a positive indication of ASD.94 Follow-up data has shown a high incidence of neuropsychiatric symptoms in PANS-patients, highlighting the importance of using an ASD screening tool even for previously assessed patients.95,96
The Swanson, Nolan and Pelham scale (SNAP-IV) is a parent- or teacher-rated scale assessing ADHD-related symptoms and ODD in children and adolescents.97,98 It is a frequently used tool in treatment studies as well as in everyday clinic work following up ADHD treatment. The SNAP-IV exists in different versions depending on items rated. The version most frequently used in Sweden is a 30-item version rating ADHD inattention, ADHD hyperactivity/impulsivity and ODD. Each item is scored from ‘not at all’ (score 0) to ‘very much’ (score 4), with a maximum total score of 120. Mean scores for each sub-section of the scale are also calculated.99
The Eyberg Child Behavior Inventory (ECBI) is a 36-item parent-rated scale of disruptive behavior problems in children, divided in an intensity scale measuring the frequency of a behavior and a problem scale measuring if the parent perceives the behavior as a problem. The maximum score on the intensity scale is 252, and scores >130 are considered clinically significant. The maximum score on the problem scale is 36, with scores >14 indicating significant parental distress.100,101
4.4 STUDY PROCEDURES
4.4.1 Study I
Patients underwent a thorough clinical evaluation carried out by a child and adolescent psychiatrist together with a psychologist or a psychiatric nurse. The assessments included a comprehensive psychiatric and medical evaluation, relevant validated rating scales and a laboratory workup taken either at onset or during a flare. In order to describe baseline characteristics of the cohort a large amount of data was assembled, including developmental and medical history, psychiatric and medical symptoms, somatic signs and results from laboratory tests. Analyses were largely descriptive. Subgroups of patients within the cohort

15
were compared using t-tests for continuous variables and chi-square tests for proportions. P-values below 0.05 were considered to be statistically significant.
4.4.2 Study II
The evaluation at follow-up was a face-to-face assessment with a child and adolescent psychiatrist, focusing on current psychiatric and medical symptoms, school attendance, pharmacological treatments, psychological treatments and/or interventions and somatic signs. Psychiatric and medical diagnoses received during the follow-up time were noted. Participants also underwent a somatic assessment and laboratory tests were conducted.
Based on clinical experience we developed operational definitions of a PANS flare and of different clinical courses of the syndrome. Flare was defined as worsening of PANS-related symptoms and/or loss of function (CGI-S equal to or above 4) for longer than four days, irrespective of treatment given. Clinical course was defined as follows:
1. Remitted: no PANS symptoms for the last 12 months. 2. Relapsing-remitting course: at least one flare during the last 12 months, but in
remission >50% of the time for the last 12 months. 3. Chronic-static/progressive course: fulfilling criteria for flare >50% of the time for the
last 12 months.
Analyses were largely descriptive. For comparative reasons, remitted and relapsing-remitting course groups were merged into a non-chronic group. For simplicity, the chronic-static/progressive course group was renamed the chronic group. Chronic and non-chronic patients were compared using t-tests for continuous variables with parametric distributions and Wilcoxon rank-sum tests or Wilcoxon signed-rank tests for non-parametric distributions. Chi-square tests were employed for proportions. P-values below 0.05 were considered to be statistically significant.
4.4.3 Study III
Analyses were based on data collected as part of the long-term follow-up of the PANS cohort (study II) and included clinician-rated measures of global symptom severity and general functioning and parent- and child-rated measures of specific symptoms and general functioning. The parent- and child-rated measures were submitted prior to the face-to-face assessment at the clinic. Descriptive analyses were calculated for each scale and subscale. Intraclass correlation coefficients (ICCs) were calculated to establish the degree of agreement between clinician-, parent- and child ratings of the same rating scale.102,103 Correlation coefficients were calculated in order to measure the degree of association between measures.104 P-values below 0.05 were considered to be statistically significant.
4.4.4 Study IV
The survey was designed using the online survey platform ‘SurveyGizmo’. Data collection took place between May 5th and June 11th 2020. Analyses were descriptive in nature.
16
5 RESULTS 5.1 STUDY I: ESTABLISHMENT OF A PANS COHORT
Fewer than 50% of the referrals met strict PANS criteria. The median age at intake was 7.2 years (range 3.0-13.1) and 56% were male. The most frequently reported onset symptoms were OCD (89%), anxiety (78%), emotional lability (71%) and sleep disorders (69%). Sixty-two percent had complex tics and almost as many (60%) experienced other motor function abnormalities such as choreiform movements, difficulties in gross motor control and fine motor skills or perception of muscle weakness. ADHD-related symptoms such as attention deficit and hyperactivity were reported in 63% and 43%, respectively. Half of the patients reported school difficulties and deterioration in school performance since the PANS onset. The most common abnormalities documented in the somatic evaluation were signs of ear, nose and throat infections (16%).
The mean CGI-S and CGAS ratings at the time of the assessment were 3.8 (SD 0.9, range 2–6) and 50 (SD 10.1, range 21–70). The wide range in global symptom severity and general function ratings implies that some patients were suffering severe symptoms at onset, while others only presented with mild symptoms, but still fulfilled PANS criteria.
Twenty-four percent had a pre-existing autoimmune disease (e.g. severe asthma, severe atopic eczema, severe and multiple nutritional allergies, celiac disease or post-infectious arthritis) and a slightly smaller proportion (18%) a pre-existing psychiatric/neuropsychiatric diagnosis. Sixteen percent had an onset of an inflammatory or autoimmune disease in temporal relation to the onset of the PANS symptoms. As many as 76% reported having a biological relative with at least one inflammatory or autoimmune disease, while the same number for psychiatric disorders were 64%. Complement activation (37%), leukopenia (20%), positive ANAs (17%) and elevated thyroid antibodies (11%) were the most frequent laboratory findings.
5.2 STUDY II: A TWO-TO-FIVE YEAR FOLLOW-UP OF A PANS COHORT
For the 34 participants who underwent the follow-up assessment, median age at follow-up was 11.5 years (range 6.7-17.1) and median follow-up time was 3.3 years (range 2.3-4.9). The majority of participants were significantly improved over the follow-up period. The median CGAS scores had increased from 53 (range 54–70) to 61 (range 28–80) and the median CGI-S scores had decreased from 4 (range 2–6) to 3 (range 1–6), both representing statistically significant differences (z = − 3.59, p < 0.001 and z = 3.70, p < 0.001, respectively). Fifty-nine percent presented with active PANS-symptoms at the time of the follow-up assessment.
During the follow-up time, a full 38% had received a neuropsychiatric diagnosis, ADHD being the most common one (26%), followed by ASD (9%) and intellectual disability (3%). Twelve percent had a newly diagnosed autoimmune or inflammatory disease during the follow-up time.
At a group level there were significant reductions in global symptom severity and improvement in general function. Sixty-two percent reported OCD-related symptoms at follow-up, but only
17
15% had a CY-BOCS score above 15, suggestive of clinical levels of OCD. The same was true for tics, whereby 50% reported motor or vocal tics, but only 6% scored above 30 on the YGTSS, the equivalent of clinically relevant tic disorder. About a third of the participants reported one or several of the following symptoms: anxiety, hyperactivity/impulsivity, behavioral difficulties, depressive symptoms, sleep disorder and tiredness/fatigue.
Flares and disease course over the last 12 months prior to the follow-up assessment were documented according to our proposed operational definitions. The median number of flares was 1 (range 0-3). Two patients had no flares during the last 12 months prior to the follow-up assessment and were classified as being remitted. Twenty participants were classified as relapsing–remitting and 12 as having a chronic-static/progressive course. The latter group had an earlier PANS onset, greater impairment and had received more pharmacological and psychological treatments. Levels of IL-1-β and TNF-α were both elevated in the chronic compared to the non-chronic course group (χ2 = 7.77, p = 0.01 and χ2 = 11.69, p < 0.001).
5.3 STUDY III: MEASURING CLINICAL OUTCOMES IN PANS
Median and mean scores on most global and specific symptom scales indicated low to moderate symptom severity and a high level of functioning at follow-up, but there was substantial variability in the data. Some participants still experienced impairing symptoms. Specifically, ratings on symptom-specific measures varied largely between participants, reflecting the heterogeneity of symptom presentations and clinical courses that are characteristic of PANS. Agreement between informants was excellent on functional scales, fair to moderate on global symptom severity scales and mixed on the symptom-specific scales. Clinician-rated global symptom severity and functional measures had stronger inter-correlations with parent- and child-rated functional measures than with symptom-specific measures.
5.4 STUDY IV: CHALLENGES OF CHILDREN WITH PANS DURING THE COVID-19 PANDEMIC
Of the 154 participating children and adolescents, 84% were receiving medication and 45% had ongoing psychological treatments and/or interventions. Only 33% of guardians responded that their child was currently receiving the care they need for their PANS symptoms during the pandemic. Approximately one third of guardians perceived a worsening of their children’s psychiatric and somatic symptoms and high stress levels. When asked specifically which symptoms had worsened, 23% indicated obsessive-compulsive symptoms, 22% worry/anxiety, and 20% difficulties in focusing. Lack of regular healthcare contacts, school closures, and physical distancing, resulting in lack of everyday support systems, had resulted in aggravated difficulties for these families.
18
6 ETHICAL CONSIDERATIONS Ethical considerations involved reflecting on all aspects of the research, from planning the project, meeting the patients and their families, handling clinical and research data in a way that safeguarded the integrity of the participants, analyzing and communicating the results, to implementation of the new knowledge into the clinic. Families were generally very positive when asked to participate in the studies. Some had perceived a lack of knowledge regarding suspected immunopsychiatric disorders before they came to the clinic, and some reported feeling misunderstood and frustrated. The families were clearly informed that their child would benefit from the same level of care, regardless of participation in the research studies.
Patients with OCD-RD with suspected PANS are often seriously ill at onset and therefore need to undergo necessary medical examinations including cultures and blood tests, and sometimes also lumbar puncture, EEG and MRI. The study procedures substantially overlapped current regional guidelines for OCD-RD as well as for inflammatory disorders. At the follow-up assessment some of the participants were no longer attending patients at the clinic and their throat cultures and blood tests could thus not fully be considered part of the usual clinical care. The tests represented an additional, but very limited, risk for the participating child. Participants were offered a mild anaesthetic cream before the blood test was taken, but the procedure still involved some discomfort. The risk of physical harm related to the procedure was considered minimal.
The research involving the PANS cohort (studies I, II and III) was approved by the Regional Ethics Review Board in Stockholm (reference number EPN 2015/1977-31/4 (2019-02132)). The survey in study IV was completely anonymous and no personal data were stored and hence according to Swedish law an ethical review was not necessary.
6.1 PERSONAL INTEGRITY OF THE STUDY PARTICIPANTS
PANS is seemingly a rare condition, which increases the risk that a participating individual may be identifiable, even though the data were pseudonymized prior to analysis. All data were handled confidentially, meaning all personal data were handled securely in coded form, and following the European General Data Protection Regulation (GDPR) legislation. Each participant included in the PANS cohort was assigned a study number, and the code key as well as the clinical data was kept separately in a locked cabinet and on a secure data server.
6.2 INFORMED CONSENT
It is important to give special consideration to medical research when children are involved as participants. For patients included in our PANS cohort we took great care to provide relevant information in a manner appropriate for the child’s age and level of maturity. The informed consents were signed by both parents/legal guardians and, if possible, the participating children. The consent forms consisted of several parts: data being saved for research purposes, linkage to national registers, and consent to being contacted for future studies. The families

19
were clearly informed as to their right to end participation at any moment, and how this could be achieved.
Some families also provided video films, in order to facilitate the assessment of motor symptoms. A special consent form was then signed, both for the storage of the film files in the patient records and for their use in research and for educational purposes.

21
7 DISCUSSION The overall aim of this research project was to further characterize PANS, to understand the long-term course of the syndrome and to contribute to the improvement of evidence-based assessment methods. Because the work contained in this thesis took part in the middle of the COVID-19 pandemic, we also wanted to explore how the pandemic may have affected the symptoms and care of patients with PANS.
7.1 ESTABLISHMENT AND CHARACTERIZATION OF A SWEDISH PANS COHORT
We started accepting PANS referrals in 2014, under the umbrella of a specialist child and adolescent psychiatry OCD-RD clinic. As demand increased we developed into a PANS team, building collaborations with pediatric neurology and rheumatology clinicians. At that time there were no clear care systems for PANS patients in Sweden, and no published guidelines for their assessment and treatment. As clinicians meeting these patients, we realized they differed in several aspects from other OCD-RD patients. They tended to be younger, more severe at onset, exhibit a broader spectrum of psychiatric and somatic symptoms, and the disease course was more often waxing and waning. We started to gather consent for these patients to be included in our PANS cohort, based on strict PANS criteria.4,30 However, PANS is a symptom description and a clinical entity that is challenging to distinguish from DSM-5 diagnoses describing similar psychiatric manifestations. Aiming to select a strictly defined cohort, we made the decision to exclude patients who did not exhibit any somatic symptoms. Somatic symptoms are only listed as secondary PANS criteria, so our cohort may differ slightly from other PANS cohorts not having this requirement.
There are no biomarkers that unequivocally guide in the diagnostic process. In order to ensure fulfillment of PANS criteria and exclusion of other treatable conditions that may have influenced the patient’s clinical presentation, we developed a comprehensive assessment protocol based on previous patient records, patient and family history, assessment of current symptoms and somatic signs, and a laboratory workup primarily focusing on inflammatory markers. If the patient did not present with active PANS symptoms at the time of assessment, the laboratory workup was made in temporal relation to a flare, at a later timepoint, in order to capture an active disease state. Similarly to previously published baseline data from the Stanford cohort6, the median time between symptom onset and first assessment at the clinic exceeded one year, further complicating the diagnostic process.
PANS has sometimes been described as affecting primarily healthy children. In our sample, approximately one fifth of the patients had a previous psychiatric diagnosis, and one fourth had a previous autoimmune or inflammatory disease diagnosis. For these children the PANS onset implied an abrupt and severe worsening of psychiatric symptoms. Our clinical experience shows that it is important to continue to treat an underlying, co-morbid, psychiatric disorder, while also focusing on potential anti-inflammatory or immunomodulatory treatments. The PANS diagnosis therefore did not replace previously diagnosed conditions.

22
Compared with reported data from the Stanford cohort30 (n=47) and the Gothenburg cohort105 (n=23), the patients included in our cohort were younger at onset (7.5 vs. 9.6 and 8.5 years, respectively). We observed a similar distribution between males and females as in the Gothenburg cohort (56% males), while 77% males were reported in the Stanford cohort. Complement activation, elevated thyroid antibodies and positive ANAs were among the most common laboratory test abnormalities. The complement system is involved in autoimmune reactions and its activation does not frequently occur in healthy individuals.106 The same is true for elevated anti-TPO antibodies, which is described in only 1-2% of healthy children.107,108 Positive ANAs are more difficult to interpret, as the test has a non-negligible false positive rate. In our sample, 17% had a positive ANA test, while baseline data from the Stanford cohort6 reported a 28% positive rate. Previous studies have shown that as many as 15% of children may have a positive ANA test, with some being healthy, some having an autoimmune disease and some having a non-autoimmune inflammatory disease.109,110
The high rate of autoimmune comorbidity, as well as a family history of autoimmune disease, has also been reported from the Stanford6 and Gothenburg105 cohorts. Together with the abnormal laboratory tests, this indicates an association with autoimmunity. Larger cohorts and an OCD-RD control group would be required in order to determine the value of these clinical traits and tested inflammatory markers. Even though an association between autoimmunity, positive immunological markers and psychiatric manifestations has been previously described,34,44,111 the relevance of these markers in PANS patients has not yet been established. With current knowledge the laboratory protocol should be primarily used to detect other disorders such as autoimmune thyroiditis and celiac disease, rather than to follow a disease course or as a tool in treatment decision-making.
We believe PANS is a rare clinical entity and a thorough multidisciplinary assessment is essential in order to avoid unnecessary treatments. During the study period for study I (November 2014 to March 2018) our OCD-RD clinic received over 1500 referrals, out of which 47 fulfilled criteria for PANS. Many suspected PANS cases were more likely to be regular OCD or TD/CTD patients who would respond well to traditional evidence-based treatments for these conditions. Conversely, strict PANS criteria exclude a significant number of children who may still benefit from anti-inflammatory treatments. Absence of core symptoms, such as OCD and/or anorexia, was the main reason for exclusion from the PANS cohort. Other reasons were insidious symptom onset or spontaneous resolution of symptoms before the assessment took place. Several of the excluded patients exhibited an atypical onset of severe psychiatric symptoms, often influencing behavior, communication or perception, and sometimes also being related to an infection or an autoimmune disease. Despite not including these patients, their symptoms were in many cases clearly disabling. Whether the PANS criteria are too narrow, currently excluding these other psychiatric manifestations, or if PANS would benefit from being merged into a broader immunopsychiatric entity is an important field of enquiry.
23
The main strength of study I was the careful protocol-driven approach of the data collection, the multidisciplinary nature of our team and the close collaborations with pediatric neurologists and rheumatologists. The study generated important knowledge about the variability in symptom presentations, psychiatric and somatic comorbidities and the association to autoimmunity. The main limitation was the modest sample size, resulting in limited power for analyses of patient sub-groups. Furthermore, the data regarding family history were parent-reported and not verified via patient records. The cohort was followed longitudinally and further data were presented in study II.
7.2 FOLLOW-UP OF A PANS COHORT AND FURTHER DEFINITIONS OF THE SYNDROME
We prospectively followed participants included in the PANS cohort for two-to-five years. In order to limit the risk of selectively following-up chronic patients, we conducted the follow-up assessment regardless if the participants were still active patients at the clinic or not. The main finding of study II was that although remission was rare, a large majority of children with PANS significantly improved during the follow-up period. Nonetheless, a non-negligible minority were still experiencing disabling symptoms, needing further pharmacological and psychological interventions.
Another important finding was that 38% of the participants had undergone a neuropsychiatric assessment and been diagnosed with an additional neuropsychiatric diagnosis during the follow-up period, mirroring the previous results from another PANDAS cohort.96 This highlights the importance of repeated psychiatric assessments in this patient group, since a selective focus on PANS symptoms may result in missed opportunities for pharmacological, psychological or adaptive interventions in other areas.
Even though baseline data from study I revealed high levels of somatic findings at intake, these were much rarer at follow-up. To routinely perform an extensive somatic assessment and a comprehensive laboratory workup, which are both time-consuming and costly, may be important at intake to exclude other, potentially treatable conditions, but may have limited value at follow-up. An assessment focusing on signs of current infection (or other somatic symptoms that may have arisen) should be adequate. PANS has clinical similarities to Sydenham’s chorea and rheumatic fever, and, we therefore suggest that heart auscultation is routinely performed in order to detect any murmurs indicative of rheumatic heart disease.
There is limited data published on inflammatory markers in PANS patients, and the level of disease activity (flare, disease course) is rarely rated at the time of testing, making interpretation difficult. In our sample, thyroid abnormalities were more common at follow-up, while positive ANAs were rarer. None of the patients had elevated IL-1-β or TNF-α levels at baseline, but both were significantly elevated in the symptomatic and chronic patients, compared to asymptomatic and non-chronic patients, at follow-up. Until more data, with the addition of adequate control groups, becomes available the results suggest that the laboratory protocol for
24
routine use at follow-up should be limited to a small number of clinically relevant tests, based on current signs of infection, comorbidities or ongoing pharmacological treatments.
Based on our clinical experience working with PANS patients, we proposed operational definitions of flare and disease course. We determined that previous definitions were difficult to use in clinical practice. A flare had been defined by Leon et al. as a noticeable increase in a child’s previous PANDAS symptoms for at least 24 hours,96 and by Brown et al. as an acute neuropsychiatric deterioration meeting strict PANS/PANDAS criteria but without a specified time period.10 These definitions may be problematic because of the risk of capturing the natural waxing and waning of psychiatric symptoms rather than a true PANS flare. Brown et al. also defined clinical courses as follows: relapsing-remitting with flares and an approximate return to baseline without immunomodulatory treatment; chronic-static with unchanging symptoms lasting longer than nine months; and progressive as a chronic course deteriorating over time.10 Defining disease course in this way may be ambiguous. A patient with a flare resolved after administration of an immunomodulatory treatment, such as IVIG or steroids, will be difficult to classify as either relapsing-remitting or chronic-static. We believe our proposed definition of a flare to be more precise and more easily applicable in the clinic, and that our definitions of disease course to enable classification regardless of treatment are essential in both clinical and research settings.
Though limited by the small sample size our definitions of flare and disease course appeared to meaningfully distinguish the non-chronic (remitted and relapsing-remitting groups) and chronic (chronic-static/progressive group) patients at follow-up regarding level of impairment, global symptom severity and subsequent need of medical and psychological healthcare resources. Follow-up time was similar between the two groups, but the more severe chronic course group had an earlier PANS onset. Despite symptom severity ratings being similar at baseline, the chronic course group had significantly lower CGAS scores (more impairment), indicating that early onset and impaired function may be potential predictors of chronicity in PANS patients.
The main strength of study II was that, to our knowledge, it was the first naturalistic long-term follow-up of a well-characterized PANS cohort. The main limitation was the small sample size, impacted even more by the ongoing COVID-19 pandemic as previously consenting participants no longer wished, or had the possibility, to take part in clinical research. We experienced substantial data loss for the laboratory tests due to limited access to the laboratory, also related to the ongoing pandemic. The baseline characteristics of the participants were comparable to those not available at follow-up, which in a way mitigated this limitation.
Studies I and II were naturalistic studies in a clinical setting, in which adaptations in clinical routines were inevitable during the study period. For example, some of the measures administered at follow-up (e.g. CY-BOCS and YGTSS) were not available in the baseline data for some participants, hindering certain longitudinal analyses. Furthermore, even though clinician-rated measures of global functioning, disease severity and improvement all indicated significant improvement at follow-up, families frequently reported persisting PANS symptoms
25
influencing daily life and activities. This discrepancy may suggest that the instruments used did not capture the full extent of the patients’ difficulties, or that clinicians and families interpreted the impact of PANS symptoms differently. The use of appropriate outcome measures is critical and was further investigated in study III.
7.3 SUITABILITY OF STANDARD CLINICAL MEASURES FOR THE ASSESSMENT AND FOLLOW-UP OF PANS PATIENTS
In study III, we analyzed data from the follow-up of the PANS cohort described in studies I and II. The uncertainty in how to best measure the complex symptom presentation that constitutes PANS has implications for both clinical practice and when designing clinical trials. We wanted to investigate the suitability of a range of standard clinical measures for the assessment and follow-up of PANS patients, and to formally assess the degree of agreement between multiple informants (clinician, parent and child).
At a group level the median ratings on measures assessing global symptom severity and adaptive functioning indicated a low symptom burden and a rather high level of everyday functioning. Symptom-specific measures revealed a large variability in the data, reflecting the heterogeneity of clinical presentations and disease courses that are characteristic of PANS. These results extended the findings of study II.
CGI-S is a gold standard, clinician-rated, measure of global symptom severity in psychiatric illnesses. Using the same rating scale as a parent- and child-rated measure showed a rather low agreement between informants, suggesting that it is useful to complement the clinician rating with both parent and child views of the current symptoms. Overall, the agreement between ratings made by parent and child were excellent for functional scales, but only fair-to-moderate for global symptom severity and most symptom-specific scales.
KIDSCREEN-10 and WSAS-P/Y correlated well with clinician-rated global symptom severity and functional scales, and the agreement between parent and child ratings was excellent. One parent- and child-rated functional scale may be enough for both clinic and research purposes, and multiple parents considered that the KIDSCREEN-10 was most easily accessible for a younger patient group. Somewhat surprisingly, SDQ-P/S had weak inter-correlations with global symptom severity and functional scales, and the agreement between informants was only moderate. Even though our results suggest that SDQ-P/S may be less clinically useful for this particular patient group it should be noted that the SDQ impact supplement was not used and therefore not included in the data.
Obsessive-compulsive symptoms are a main PANS criteria, but clinically relevant OCD symptoms were rare in our sample at follow-up. Assessing obsessive-compulsive symptoms with a self-rated scale as a complement to CY-BOCS may therefore not add significant information. At onset OCD is generally a more pervasive part of the PANS symptom presentation, and more time should be devoted to a comprehensive OCD assessment. The agreement between SMFQ-P/C ratings made by parent and child was only fair, indicating the importance of having both parent- and child-ratings to avoid underestimating mood symptoms
26
and depressive traits in PANS patients. Conversely, the agreement between SAAI-P/C ratings made by parent and child was excellent and, if really made individually, either the parent or child rating may be enough for clinical purposes.
Longitudinal data indicate a high comorbidity with neuropsychiatric disorders, combined with intensification of related symptoms during PANS flares.95,96 It is therefore strongly recommended that measures being able to screen for, and assess the severity of, autistic behaviors, inattention, hyperactivity and conduct problems are used when following up PANS. In our sample, ECBI had a very strong association to SNAP-IV, suggesting that the simpler SNAP-IV may sufficiently cover the patients’ oppositional behaviors for clinical purposes. When detecting potentially severe oppositional defiant behaviors, ECBI can be used as a complement.
The main limitation of study III was that our data was limited to a modest sample of patients from a single clinical setting. The age range of our sample was also such that the results from the child-rated measures should be interpreted with caution. Despite our efforts, it is possible that the younger children received help from their parents when completing the questionnaires. Furthermore, since only total scores were available, we were not able to calculate internal consistency of the scales included in study III. We could thus not examine the psychometric properties of the scales in this particular sample. Future studies would benefit from conducting such psychometric analyses.
In summary, our clinical experience and the results from study III suggest that it is important to include clinician, parent and child ratings in the assessment of PANS. A single perspective is unlikely to capture the full complexity of the syndrome. General measures assessing global disease severity and adaptive functioning are well suited but need to be complemented by symptom-specific scales representative of the core symptoms, such as OCD, anxiety, depression and behavioral problems. However, their exclusive use is problematic as the natural course of the syndrome is such that some patients may not have specific symptoms to rate at follow-up. The assessment will also benefit from being straightforward and as brief as possible. Based on our experience, we recommend the use of a core battery of clinician-, parent- and child-rated measures in both clinical practice and in clinical trials, see Box 1.
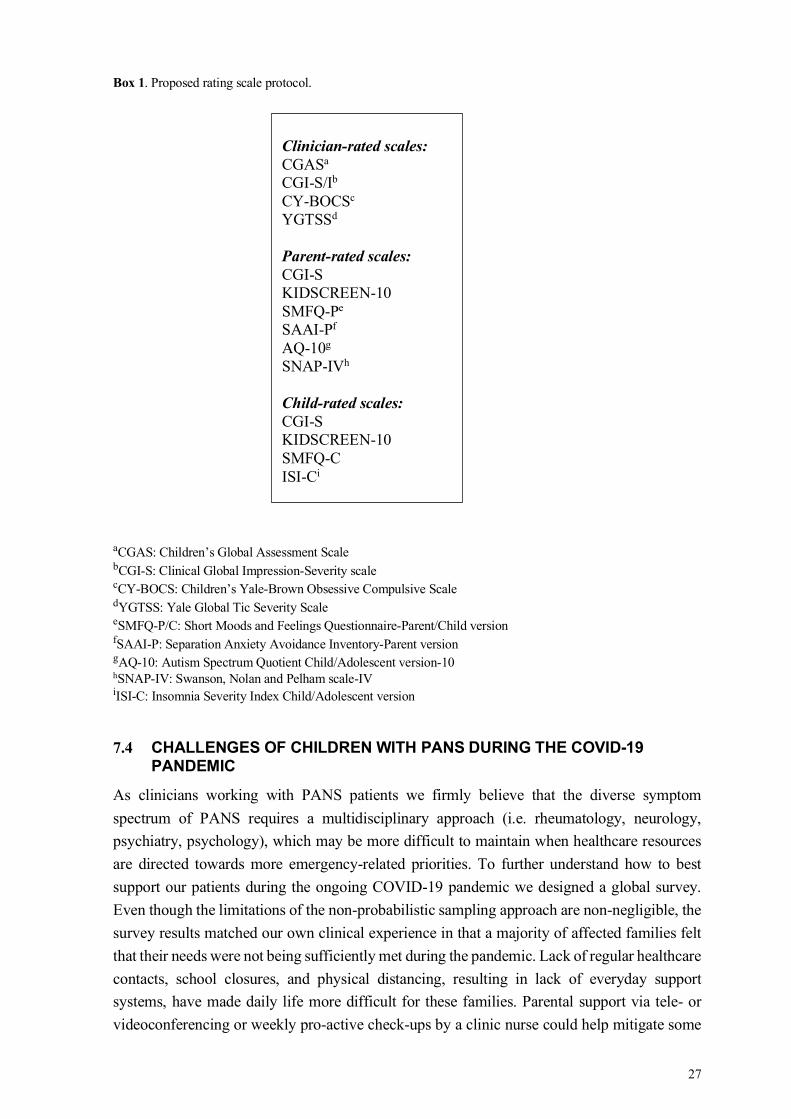
27
Box 1. Proposed rating scale protocol.
aCGAS: Children’s Global Assessment Scale bCGI-S: Clinical Global Impression-Severity scale cCY-BOCS: Children’s Yale-Brown Obsessive Compulsive Scale dYGTSS: Yale Global Tic Severity Scale eSMFQ-P/C: Short Moods and Feelings Questionnaire-Parent/Child version fSAAI-P: Separation Anxiety Avoidance Inventory-Parent version gAQ-10: Autism Spectrum Quotient Child/Adolescent version-10 hSNAP-IV: Swanson, Nolan and Pelham scale-IV iISI-C: Insomnia Severity Index Child/Adolescent version
7.4 CHALLENGES OF CHILDREN WITH PANS DURING THE COVID-19 PANDEMIC
As clinicians working with PANS patients we firmly believe that the diverse symptom spectrum of PANS requires a multidisciplinary approach (i.e. rheumatology, neurology, psychiatry, psychology), which may be more difficult to maintain when healthcare resources are directed towards more emergency-related priorities. To further understand how to best support our patients during the ongoing COVID-19 pandemic we designed a global survey. Even though the limitations of the non-probabilistic sampling approach are non-negligible, the survey results matched our own clinical experience in that a majority of affected families felt that their needs were not being sufficiently met during the pandemic. Lack of regular healthcare contacts, school closures, and physical distancing, resulting in lack of everyday support systems, have made daily life more difficult for these families. Parental support via tele- or videoconferencing or weekly pro-active check-ups by a clinic nurse could help mitigate some
Clinician-rated scales: CGASa CGI-S/Ib CY-BOCSc YGTSSd Parent-rated scales: CGI-S KIDSCREEN-10 SMFQ-Pe SAAI-Pf AQ-10g SNAP-IVh Child-rated scales: CGI-S KIDSCREEN-10 SMFQ-C ISI-Ci
28
of these unwanted consequences. CBT can also be offered via videoconferencing and can be helpful in alleviating worsened anxiety and obsessive-compulsive symptoms. Worsening of psychiatric and somatic symptoms should be taken seriously and be thoroughly assessed within a multidisciplinary team. The survey provides unique information relevant to the current situation.
7.5 FUTURE DIRECTIONS
During conduct of these studies our clinic has developed into a specialized immunopsychiatry clinic with broader inclusion criteria (abrupt onset or worsening of multiple psychiatric symptoms in combination with somatic symptoms, loss of previously established functions, atypical onset or course) than the initial PANS team. Inclusion in the Stockholm Immunopsychiatry cohort started in 2019, and local assessment and treatment protocols for these patients have been developed. PANS patients constitute a fraction of these patients, and their treatment no longer differs from that of other patients with suspected immunopsychiatric etiologies. More research is needed to establish whether PANS in its current form should remain a separate entity, or if the PANS diagnostic criteria are too narrow. However, it is clear that a sub-group of psychiatric patients do benefit from anti-inflammatory or immunomodulatory treatments, and that some of these patients do not fulfill PANS criteria.
Collaborations both within Sweden and abroad are essential in establishing safe, efficient, cost-effective and evidence-based clinical routines. An ongoing collaboration between the Nordic countries and the UK has recently published consensus guidelines for the assessment, treatment and follow-up of PANS patients.112 As more knowledge becomes available, such guidelines need continuous updating.
Several studies have attempted to characterize PANS patients and to define clinical aspects of the syndrome, such as a flare and different clinical courses.5-7,10,95,96,105,113 Efforts now need to be oriented towards the implementation of much needed treatment trials, preferably beginning with current first line treatments such as NSAIDs and CBT and eventually also second- or third-line treatments such as cortisone and IVIG. Treatment trials would benefit from being blinded, randomized, controlled and to include multi-dimensional outcome measures.
Identification of potential biomarkers, predictive and prognostic factors should also be a priority of future research with larger samples and adequately chosen control groups. Work creating an OCD-RD control group within our clinic is ongoing but is paused due to the ongoing COVID-19 pandemic. Furthermore, linkage to Swedish registers will enable a deeper understanding of the course, risk factors and comorbidities of PANS patients.
7.6 CONCLUSIONS
The research work constituting this thesis has generated important knowledge that has been successively introduced into clinical routines, enabling the development from a small team dedicated to PANS patients into a new immunopsychiatric clinic.

29
We have established a cohort of well-characterized PANS patients, described their baseline characteristics, followed them over time, proposed definitions of flare and different clinical courses, and assessed suitability of standard clinical measures for the assessment, determination of treatment response and follow up. Our findings confirm previous research showing that the PANS presentation can vary largely between patients and that the symptoms can be severe and disabling. The combination of psychiatric and somatic symptoms, as well as the multi-dimensional treatment approaches, warrant a multi-specialist program with access to a child and adolescent psychiatrist, psychologist, pediatric neurologist and rheumatologist. Further supporting the need of collaboration with other medical specialties, we found strong indications of an association with autoimmune disease in our cohort. A majority of the participants significantly improved during the follow-up period, even though full remission was rare. Approximately one third of the patients had a chronic course, still exhibiting disabling symptoms. Interestingly, this sub-group had an earlier PANS onset and was more impaired at onset. We found that a large proportion of the participants had received a neuropsychiatric diagnosis during the follow-up period. Neuropsychiatric assessments should therefore be part of routine clinical care for these patients, in order not to miss other important areas in which effective interventions can be made. When assessing and following up patients with PANS, the multi-dimensional aspect of the syndrome should be taken into consideration. Global rather than symptom-specific measures are better suited at a group level, but these should be complemented with an efficient protocol of rating scales assessing core symptoms, such as OCD, anxiety, depression and tics.
Lastly, PANS patients and their families have been affected by the ongoing COVID-19 pandemic, largely because a multi-disciplinary treatment approach has been difficult to maintain, and school and societal support has not been functioning as usual. Digital care, appointments via video or telephone, can ensure continued care contacts and help mitigate some of the impact of the pandemic.
30
8 REFLECTIONS ON LEARNING I always saw myself as a clinician more than a researcher, but starting to meet PANS patients made me realize that the clinical part was no longer sufficient. We inevitably needed to describe this sub-group of OCD-RD patients and our attempts at assessment and treatment, to make sure that the care provided was ‘good enough’ while not risking our patients’ wellbeing. I have met all of my research patients, and been the responsible clinician for most of them. First and foremost, I have learnt that it is very difficult to adapt clinical practice into research or make research out of clinical practice. We have assembled extensive amounts of data in order to be able to draw some, simple statistical conclusions. Successively, I have learnt to have a clearer view of the expected end result of a study. What is it really that we want to know, present in a table, at a conference, in the work with clinical guidelines? Rather than trying to collect all data. Another aspect of clinical research is that the patient’s disorder will not act as we expect it to. The flare will come in the middle of follow-up, interventions that improved function after one flare might be ineffective after the next, a pandemic comes and alter daily life and societal support, or something else happens. Research takes time. Creating a cohort of well-evaluated patients with PANS took several years. Conducting the follow-up assessments and the rating scale protocols another two years. Fortunately, the close linkage between research and clinic made it possible to adapt the clinical routines according to our achieved knowledge, already at an early stage. As our unit has developed into an immunopsychiatric clinic, seeing a wider spectrum of patients, and while including patients into the Stockholm immunopsychiatry cohort, we have a lot of new knowledge, and a lot of mistakes, to learn from.
Illustration: Martha Gromark
31
9 ACKNOWLEDGEMENTS First of all, I would like to thank all the patients and their families for taking part in the research and allowing us to learn more about the group of psychiatric and somatic symptoms described as PANS. I have known some of you for several years, a long time during which a lot has happened in the field of immunopsychiatry. You have put up with me responding ‘I don’t know’ more times than I can count, you have trusted me and my colleagues and questioned us when needed. THANK YOU!
Second, I would like to thank my supervisors. David Mataix-Cols, you have been my principal supervisor through this thesis and guided me through scientific thinking, planning and writing. I have learnt that everything can always be better, and after your constructive criticism it always is. Eva Serlachius, thank you for being my co-supervisor and colleague. I deeply appreciate your advice, guidance and small talks on research, patient work, teaching and life. Robert Harris, as my co-supervisor you guided me through the doctoral process, explained complicated immunological things I needed to know, and just generally cheered me on. Anna Carin Horne, not only my co-supervisor but also my colleague. We have handled many sick patients together, and you have guided me through the treatment of several more, as the super rheumatologist that you are. Eva Hesselmark, you took on the role as my co-supervisor during the last year of my thesis. You have helped me more than I know how to express. Thank you!
I would also like to thank my clinical colleagues at G22. Maria Silverberg-Mörse, you recruited me back in 2014 and we started to build the PANS team together. Like me, always so fascinated by the disorders we do not entirely understand, the patients who do not fit into the expected template, where we might have missed a treatment opportunity or where we just think we can do more. The immunopsychiatry unit is there because of you. My other doctor, nurse, psychologist and administration co-workers, thank you for being the colleagues you are, offering knowledge, support, friendship, knitting moments and, when needed, wine.
I would also like to especially thank Ronny Wickström and the neuroinflammatory group at Astrid Lindgren’s hospital. What a collaboration we have! From specific patients to development of clinical routines and international collaborations.
The research group at G22, what an amazing way to do research! Thank you for collegial support, interesting journal clubs, lab meetings and all the fun parts about being a PhD-student.
My PhD-student colleagues, directors of studies and teachers from the KI research school in epidemiology. I can imagine no better way to study epidemiology, statistics, ethics and writing than the way we had the opportunity to do it. Thank you for the support, networking and friendships!
Jennifer Frankovich, when starting out in 2014, you helped us get on track. You visited us at G22, we saw patients together, you welcomed us to Stanford and you shared your immense knowledge in the field of PANDAS, PANS and immunopsychiatry. You are a true inspiration.
32
Alberto Spalice, you have welcomed me to your lively and lovely clinic in Rome more than once and we have shared many conversations about patients, assessments, treatments, research projects and life in general. No one on the planet answers a WhatsApp message faster than you. Thank you. Your patients are so lucky!
I would like to thank SANE – Förbundet autoimmune encefaliter med psykiatrisk presentation, for the important work that you do in spreading knowledge and supporting families. SANE organized Sweden’s first international PANDAS/PANS conference in 2019, bringing clinicians, researchers and affected families together. I would also like to specifically thank you for spreading our survey for study IV.
This work would not have been possible without the financial contribution from ALF Medicin, Jane and Dan Olsson foundation, Fonden för rehabilitering och medicinsk forskning (FRF-stiftelsen), Drottning Silvias jubileumsfond and Fonden för psykisk hälsa.
Anneli Grundsten, my close friend and very clever colleague. You helped keep me sane through these years.
Lastly, I wish to thank my family. My medical-oriented parents and bonus-parent, Mona Arvidsson, Thomas Arvidsson and Metha Brattwall, for all the support and the non-stop discussions over seafood and wine, believing I would somehow make all this fall into place (if I just focused on life as well, and maybe even rest a bit sometimes). My sister and bonus-siblings. My daughter, Martha, for teaching me about life, looking at me with ‘the eyes’ when I do stupid things, and making sure we always have access to cookies when working from home (and thank you for the illustrations!). My son, Harald, for reminding me about what is important, helping me sort out all the technical stuff that just need to work, and lightening up my writing breaks with your newly constructed robots. Emmanuel, my husband, who loves me for being me, writes me little notes, makes sure I have breakfast, picks me up at work when I’m tired, reads all I write even though it is very far from your area, supports me, talks to me, parties with me, experiences life with me. I love you all very, very much.
33
10 REFERENCES
1. Najjar S, Pearlman DM, Alper K, Najjar A, Devinsky O. Neuroinflammation and psychiatric illness. Journal of neuroinflammation. 2013;10:43.
2. Kayser MS, Dalmau J. The emerging link between autoimmune disorders and neuropsychiatric disease. The Journal of neuropsychiatry and clinical neurosciences. 2011;23(1):90-97.
3. Nicolini H, Lopez Y, Genis-Mendoza AD, Manrique V, Lopez-Canovas L, Niubo E, et al. Detection of anti-streptococcal, antienolase, and anti-neural antibodies in subjects with early-onset psychiatric disorders. Actas espanolas de psiquiatria. 2015;43(2):35-41.
4. Swedo S, Leckman J, Rose N. From research subgroup to clinical syndrome: modifying the PANDAS criteria to describe PANS (pediatric acute-onset neuropsychiatric syndrome). Pediatr Therapeut. 2012;2(2):113.
5. Swedo SE, Leonard HL, Garvey M, Mittleman B, Allen AJ, Perlmutter S, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. The American journal of psychiatry. 1998;155(2):264-271.
6. Frankovich J, Thienemann M, Pearlstein J, Crable A, Brown K, Chang K. Multidisciplinary clinic dedicated to treating youth with pediatric acute-onset neuropsychiatric syndrome: presenting characteristics of the first 47 consecutive patients. J Child Adolesc Psychopharmacol. 2015;25(1):38-47.
7. Gromark C, Harris RA, Wickström R, Horne A, Silverberg-Mörse M, Serlachius E, et al. Establishing a Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic: Baseline Clinical Features of the Pediatric Acute-Onset Neuropsychiatric Syndrome Cohort at Karolinska Institutet. J Child Adolesc Psychopharmacol. 2019;29(8):625-633.
8. Frankovich J, Leibold CM, Farmer C, Sainani K, Kamalani G, Farhadian B, et al. The Burden of Caring for a Child or Adolescent With Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS): An Observational Longitudinal Study. J Clin Psychiatry. 2018;80(1).
9. Sigra S, Hesselmark E, Bejerot S. Treatment of PANDAS and PANS: a systematic review. Neuroscience and biobehavioral reviews. 2018;86:51-65.
10. Brown KD, Farmer C, Freeman GM, Jr., Spartz EJ, Farhadian B, Thienemann M, et al. Effect of Early and Prophylactic Nonsteroidal Anti-Inflammatory Drugs on Flare Duration in Pediatric Acute-Onset Neuropsychiatric Syndrome: An Observational Study of Patients Followed by an Academic Community-Based Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic. J Child Adolesc Psychopharmacol. 2017;27(7):619-628.
11. Burchi E, Pallanti S. Antibiotics for PANDAS? Limited Evidence: Review and Putative Mechanisms of Action. The primary care companion for CNS disorders. 2018;20(3).
34
12. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D. C.2013.
13. World Health Organization. The ICD-10 classification of mental and behavioral disorders: clinical descriptions and diagnostic guidelines. Geneva1992.
14. WHO. International statistical classification of diseases and related health problems (11th Revision). Geneva2018.
15. Flament MF, Whitaker A, Rapoport JL, Davies M, Berg CZ, Kalikow K, et al. Obsessive compulsive disorder in adolescence: an epidemiological study. Journal of the American Academy of Child and Adolescent Psychiatry. 1988;27(6):764-771.
16. Flament MF, Koby E, Rapoport JL, Berg CJ, Zahn T, Cox C, et al. Childhood obsessive-compulsive disorder: a prospective follow-up study. Journal of child psychology and psychiatry, and allied disciplines. 1990;31(3):363-380.
17. Bloch MH, Leckman JF. Clinical course of Tourette syndrome. Journal of psychosomatic research. 2009;67(6):497-501.
18. Leckman JF. Tourette's syndrome. Lancet (London, England). 2002;360(9345):1577-1586.
19. Leonard HL, Freeman J, Garcia A, Garvey M, Snider L, Swedo SE. Obsessive-compulsive disorder and related conditions. Pediatric annals. 2001;30(3):154-160.
20. Coffey BJ, Biederman J, Smoller JW, Geller DA, Sarin P, Schwartz S, et al. Anxiety disorders and tic severity in juveniles with Tourette's disorder. Journal of the American Academy of Child and Adolescent Psychiatry. 2000;39(5):562-568.
21. Leckman JF. Phenomenology of tics and natural history of tic disorders. Brain & development. 2003;25 Suppl 1:S24-28.
22. Mataix-Cols D, Boman M, Monzani B, Ruck C, Serlachius E, Langstrom N, et al. Population-based, multigenerational family clustering study of obsessive-compulsive disorder. JAMA psychiatry. 2013;70(7):709-717.
23. Nordsletten AE, Monzani B, Fernandez de la Cruz L, Iervolino AC, Fullana MA, Harris J, et al. Overlap and specificity of genetic and environmental influences on excessive acquisition and difficulties discarding possessions: Implications for hoarding disorder. American journal of medical genetics Part B, Neuropsychiatric genetics : the official publication of the International Society of Psychiatric Genetics. 2013;162b(4):380-387.
24. Monzani B, Rijsdijk F, Iervolino AC, Anson M, Cherkas L, Mataix-Cols D. Evidence for a genetic overlap between body dysmorphic concerns and obsessive-compulsive symptoms in an adult female community twin sample. American journal of medical genetics Part B, Neuropsychiatric genetics : the official publication of the International Society of Psychiatric Genetics. 2012;159b(4):376-382.
25. Monzani B, Rijsdijk F, Anson M, Iervolino AC, Cherkas L, Spector T, et al. A twin study of body dysmorphic concerns. Psychol Med. 2012;42(9):1949-1955.
26. Monzani B, Rijsdijk F, Harris J, Mataix-Cols D. The structure of genetic and environmental risk factors for dimensional representations of DSM-5 obsessive-compulsive spectrum disorders. JAMA psychiatry. 2014;71(2):182-189.
35
27. Kirvan CA, Swedo SE, Kurahara D, Cunningham MW. Streptococcal mimicry and antibody-mediated cell signaling in the pathogenesis of Sydenham's chorea. Autoimmunity. 2006;39(1):21-29.
28. Cunningham MW. Post-Streptococcal Autoimmune Sequelae: Rheumatic Fever and Beyond. In: Ferretti JJ, Stevens DL, Fischetti VA, eds. Streptococcus pyogenes : Basic Biology to Clinical Manifestations. Oklahoma City (OK): University of Oklahoma Health Sciences Center (c); 2016.
29. Brimberg L, Benhar I, Mascaro-Blanco A, Alvarez K, Lotan D, Winter C, et al. Behavioral, pharmacological, and immunological abnormalities after streptococcal exposure: a novel rat model of Sydenham chorea and related neuropsychiatric disorders. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology. 2012;37(9):2076-2087.
30. Chang K, Frankovich J, Cooperstock M, Cunningham MW, Latimer ME, Murphy TK, et al. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. Journal of Child and Adolescent Psychopharmacology. 2015;25(1):3-13.
31. Gilbert DL, Mink JW, Singer HS. A Pediatric Neurology Perspective on Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infection and Pediatric Acute-Onset Neuropsychiatric Syndrome. The Journal of pediatrics. 2018;199:243-251.
32. Cutforth T, DeMille MM, Agalliu I, Agalliu D. CNS autoimmune disease after Streptococcus pyogenes infections: animal models, cellular mechanisms and genetic factors. Future neurology. 2016;11(1):63-76.
33. Kurlan R, Johnson D, Kaplan EL. Streptococcal infection and exacerbations of childhood tics and obsessive-compulsive symptoms: a prospective blinded cohort study. Pediatrics. 2008;121(6):1188-1197.
34. Graus F, Saiz A, Dalmau J. Antibodies and neuronal autoimmune disorders of the CNS. Journal of neurology. 2010;257(4):509-517.
35. Pollak TA, Lennox BR, Müller S, Benros ME, Prüss H, Tebartz van Elst L, et al. Autoimmune psychosis: an international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin. The Lancet Psychiatry. 2020;7(1):93-108.
36. Dalmau J, Armangué T, Planagumà J, Radosevic M, Mannara F, Leypoldt F, et al. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. The Lancet Neurology. 2019;18(11):1045-1057.
37. Dalmau J, Gleichman AJ, Hughes EG, Rossi JE, Peng X, Lai M, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. The Lancet Neurology. 2008;7(12):1091-1098.
38. Najjar S, Pearlman D, Zagzag D, Golfinos J, Devinsky O. Glutamic acid decarboxylase autoantibody syndrome presenting as schizophrenia. The neurologist. 2012;18(2):88-91.
39. Zandi MS, Irani SR, Lang B, Waters P, Jones PB, McKenna P, et al. Disease-relevant autoantibodies in first episode schizophrenia. Journal of neurology. 2011;258(4):686-688.
36
40. Pollak TA, Rogers JP, Nagele RG, Peakman M, Stone JM, David AS, et al. Antibodies in the Diagnosis, Prognosis, and Prediction of Psychotic Disorders. Schizophrenia bulletin. 2019;45(1):233-246.
41. Murphy TK, Patel PD, McGuire JF, Kennel A, Mutch PJ, Parker-Athill EC, et al. Characterization of the pediatric acute-onset neuropsychiatric syndrome phenotype. Journal of child and adolescent psychopharmacology. 2015;25(1):14-25.
42. Goldstein BI, Lotrich F, Axelson D, Gill MK, Hower H, Goldstein TR, et al. Inflammatory markers among adolescents and young adults with bipolar spectrum disorders. The Journal of clinical psychiatry. 2015;76(11):1556.
43. Khandaker GM, Zammit S, Burgess S, Lewis G, Jones PB. Association between a functional interleukin 6 receptor genetic variant and risk of depression and psychosis in a population-based birth cohort. Brain, behavior, and immunity. 2018;69:264-272.
44. Khandaker GM, Stochl J, Zammit S, Goodyer I, Lewis G, Jones PB. Childhood inflammatory markers and intelligence as predictors of subsequent persistent depressive symptoms: a longitudinal cohort study. Psychological medicine. 2018;48(9):1514-1522.
45. Parker-Athill EC, Ehrhart J, Tan J, Murphy TK. Cytokine correlations in youth with tic disorders. J Child Adolesc Psychopharmacol. 2015;25(1):86-92.
46. Orefici G, Cardona F, Cox CJ, Cunningham MW. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). In: Ferretti JJ, Stevens DL, Fischetti VA, eds. Streptococcus pyogenes : Basic Biology to Clinical Manifestations. Oklahoma City (OK): University of Oklahoma Health Sciences Center (c); 2016.
47. Xu J, Liu RJ, Fahey S, Frick L, Leckman J, Vaccarino F, et al. Antibodies From Children With PANDAS Bind Specifically to Striatal Cholinergic Interneurons and Alter Their Activity. The American journal of psychiatry. 2020:appiajp202019070698.
48. Hyman SE. PANDAS: Too Narrow a View of the Neuroimmune Landscape. The American journal of psychiatry. 2021;178(1):5-7.
49. Mataix-Cols D, Frans E, Perez-Vigil A, Kuja-Halkola R, Gromark C, Isomura K, et al. A total-population multigenerational family clustering study of autoimmune diseases in obsessive-compulsive disorder and Tourette's/chronic tic disorders. Molecular psychiatry. 2018;23(7):1652-1658.
50. Perez-Vigil A, Fernandez de la Cruz L, Brander G, Isomura K, Gromark C, Mataix-Cols D. The link between autoimmune diseases and obsessive-compulsive and tic disorders: A systematic review. Neuroscience and biobehavioral reviews. 2016;71:542-562.
51. Isung J, Williams K, Isomura K, Gromark C, Hesselmark E, Lichtenstein P, et al. Association of Primary Humoral Immunodeficiencies With Psychiatric Disorders and Suicidal Behavior and the Role of Autoimmune Diseases. JAMA psychiatry. 2020.
52. Isung J, Isomura K, Almqvist C, Lichtenstein P, Larsson H, Wester T, et al. Association of chronic and acute inflammation of the mucosa-associated lymphoid tissue with psychiatric disorders and suicidal behavior. Translational psychiatry. 2019;9(1):227.
37
53. Orlovska S, Vestergaard CH, Bech BH, Nordentoft M, Vestergaard M, Benros ME. Association of Streptococcal Throat Infection With Mental Disorders: Testing Key Aspects of the PANDAS Hypothesis in a Nationwide Study. JAMA psychiatry. 2017;74(7):740-746.
54. Storch EA, Murphy TK, Adkins JW, Lewin AB, Geffken GR, Johns NB, et al. The children's Yale-Brown obsessive-compulsive scale: psychometric properties of child- and parent-report formats. Journal of anxiety disorders. 2006;20(8):1055-1070.
55. Swedo S KM, Latimer B, Leckman J. Pediatric Acute Neuropsychiatric Symptom Scale. https://pandasnetwork.org/wp-content/uploads/2018/11/pandas_pans_scale.pdf. Accessed March 11, 2021.
56. Bejerot S, Hesselmark E, Humble M. Abstract # 1786 The PsychoNeuroInflammatory related Signs and Severity Inventory (PNISSI). Brain, Behavior, and Immunity. 2016;57:e23.
57. Moleculera. PANS and PANDAS diagnosis and treatment. http://www.moleculeralabs.com/pandas-pans-diagnosis-and-treatment/ 2016.
58. Shimasaki C, Frye RE, Trifiletti R, Cooperstock M, Kaplan G, Melamed I, et al. Evaluation of the Cunningham Panel™ in pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS) and pediatric acute-onset neuropsychiatric syndrome (PANS): Changes in antineuronal antibody titers parallel changes in patient symptoms. Journal of neuroimmunology. 2020;339:577138.
59. Hesselmark E, Bejerot S. Biomarkers for diagnosis of Pediatric Acute Neuropsychiatric Syndrome (PANS) - Sensitivity and specificity of the Cunningham Panel. Journal of neuroimmunology. 2017;312:31-37.
60. Hesselmark E, Bejerot S. Corrigendum to Biomarkers for diagnosis of Pediatric Acute Neuropsychiatric Syndrome (PANS) - Sensitivity and specificity of the Cunningham Panel [J. Neuroimmunol. 312. (2017) 31-37]. Journal of neuroimmunology. 2017;313:116-117.
61. Johnson M, Fernell E, Gillberg C, Fasth A, Dinkler L, Blennow K, et al. No neurochemical evidence of neuronal injury or glial activation in children with Pediatric Acute-onset Neuropsychiatric Syndrome: An explorative pilot study. The world journal of biological psychiatry : the official journal of the World Federation of Societies of Biological Psychiatry. 2021:1-16.
62. Latimer ME, L'Etoile N, Seidlitz J, Swedo SE. Therapeutic plasma apheresis as a treatment for 35 severely ill children and adolescents with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. J Child Adolesc Psychopharmacol. 2015;25(1):70-75.
63. Barzman DH, Jackson H, Singh U, Griffey M, Sorter M, Bernstein JA. An Atypical Presentation of Pediatric Acute Neuropsychiatric Syndrome Responding to Plasmapheresis Treatment. Case reports in psychiatry. 2018;2018:8189067.
64. Perlmutter SJ, Leitman SF, Garvey MA, Hamburger S, Feldman E, Leonard HL, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet (London, England). 1999;354(9185):1153-1158.
65. Brown K, Farmer C, Farhadian B, Hernandez J, Thienemann M, Frankovich J. Pediatric Acute-Onset Neuropsychiatric Syndrome Response to Oral Corticosteroid
38
Bursts: An Observational Study of Patients in an Academic Community-Based PANS Clinic. J Child Adolesc Psychopharmacol. 2017;27(7):629-639.
66. Spartz EJ, Freeman GM, Jr., Brown K, Farhadian B, Thienemann M, Frankovich J. Course of Neuropsychiatric Symptoms After Introduction and Removal of Nonsteroidal Anti-Inflammatory Drugs: A Pediatric Observational Study. J Child Adolesc Psychopharmacol. 2017;27(7):652-659.
67. Williams KA, Swedo SE, Farmer CA, Grantz H, Grant PJ, D'Souza P, et al. Randomized, Controlled Trial of Intravenous Immunoglobulin for Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections. Journal of the American Academy of Child and Adolescent Psychiatry. 2016;55(10):860-867.e862.
68. Thienemann M, Murphy T, Leckman J, Shaw R, Williams K, Kapphahn C, et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I-Psychiatric and Behavioral Interventions. J Child Adolesc Psychopharmacol. 2017;27(7):566-573.
69. Frankovich J, Swedo S, Murphy T, Dale RC, Agalliu D, Williams K, et al. Clinical management of pediatric acute-onset neuropsychiatric syndrome: part II—use of immunomodulatory therapies. Journal of Child and Adolescent Psychopharmacology. 2017;27(7):574-593.
70. Cooperstock MS, Swedo SE, Pasternack MS, Murphy TK. Clinical management of pediatric acute-onset neuropsychiatric syndrome: Part III—Treatment and prevention of infections. Journal of Child and Adolescent Psychopharmacology. 2017;27(7):594-606.
71. Michael S. Cooperstock SES, Consortium MSPaTKMftPP. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part III—Treatment and Prevention of Infections. Journal of Child and Adolescent Psychopharmacology. 2017;27(7):594-606.
72. Guy W. ECDEU Assessment Manual for Psychopharmacology - Revised. In: U.S. Department of Healt EaW, Public Health Service, Mental Health Administration., ed. Rockville, MD.: NIMH Psychopharmacological Research Branch, Diviosion of Extramural Research Programs.; 1976.
73. Berk M, Ng F, Dodd S, Callaly T, Campbell S, Bernardo M, et al. The validity of the CGI severity and improvement scales as measures of clinical effectiveness suitable for routine clinical use. Journal of evaluation in clinical practice. 2008;14(6):979-983.
74. Malmberg M, Rydell AM, Smedje H. Validity of the Swedish version of the Strengths and Difficulties Questionnaire (SDQ-Swe). Nordic journal of psychiatry. 2003;57(5):357-363.
75. Smedje H, Broman JE, Hetta J, von Knorring AL. Psychometric properties of a Swedish version of the "Strengths and Difficulties Questionnaire". European child & adolescent psychiatry. 1999;8(2):63-70.
76. Schorre BE, Vandvik IH. Global assessment of psychosocial functioning in child and adolescent psychiatry. A review of three unidimensional scales (CGAS, GAF, GAPD). European child & adolescent psychiatry. 2004;13(5):273-286.
39
77. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The global assessment scale. A procedure for measuring overall severity of psychiatric disturbance. Archives of general psychiatry. 1976;33(6):766-771.
78. Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, et al. A children's global assessment scale (CGAS). Archives of general psychiatry. 1983;40(11):1228-1231.
79. Europe TKG. The KIDSCREEN Questionnaires - Quality of life questionnaires for children and adolescents. Lengerich: Pabst Science Publishers; 2006.
80. Ravens-Sieberer U, Erhart M, Rajmil L, Herdman M, Auquier P, Bruil J, et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: a short measure for children and adolescents' well-being and health-related quality of life. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation. 2010;19(10):1487-1500.
81. Mundt JC, Marks IM, Shear MK, Greist JH. The Work and Social Adjustment Scale: a simple measure of impairment in functioning. The British journal of psychiatry : the journal of mental science. 2002;180:461-464.
82. Jassi A, Lenhard F, Krebs G, Gumpert M, Jolstedt M, Andrén P, et al. The Work and Social Adjustment Scale, Youth and Parent Versions: Psychometric Evaluation of a Brief Measure of Functional Impairment in Young People. Child psychiatry and human development. 2020;51(3):453-460.
83. Rapp AM, Bergman RL, Piacentini J, McGuire JF. Evidence-Based Assessment of Obsessive-Compulsive Disorder. Journal of central nervous system disease. 2016;8:13-29.
84. Leckman JF, Riddle MA, Hardin MT, Ort SI, Swartz KL, Stevenson J, et al. The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. Journal of the American Academy of Child & Adolescent Psychiatry. 1989;28(4):566-573.
85. Storch EA, McGuire JF, Wu MS, Hamblin R, McIngvale E, Cepeda SL, et al. Development and Psychometric Evaluation of the Children's Yale-Brown Obsessive-Compulsive Scale Second Edition. Journal of the American Academy of Child and Adolescent Psychiatry. 2019;58(1):92-98.
86. McGuire JF, Piacentini J, Storch EA, Murphy TK, Ricketts EJ, Woods DW, et al. A multicenter examination and strategic revisions of the Yale Global Tic Severity Scale. Neurology. 2018;90(19):1711-1719.
87. Foa EB, Coles M, Huppert JD, Pasupuleti RV, Franklin ME, March J. Development and validation of a child version of the obsessive compulsive inventory. Behavior therapy. 2010;41(1):121-132.
88. Aspvall K, Cervin M, Andrén P, Perrin S, Mataix-Cols D, Andersson E. Validity and clinical utility of the obsessive compulsive inventory - child version: further evaluation in clinical samples. BMC psychiatry. 2020;20(1):42.
89. Kent L, Vostanis P, Feehan C. Detection of major and minor depression in children and adolescents: evaluation of the Mood and Feelings Questionnaire. Journal of child psychology and psychiatry, and allied disciplines. 1997;38(5):565-573.
90. Jarbin H, Ivarsson T, Andersson M, Bergman H, Skarphedinsson G. Screening efficiency of the Mood and Feelings Questionnaire (MFQ) and Short Mood and
40
Feelings Questionnaire (SMFQ) in Swedish help seeking outpatients. PloS one. 2020;15(3):e0230623.
91. In-Albon T, Meyer AH, Schneider S. Separation Anxiety Avoidance Inventory-Child and Parent Version: Psychometric Properties and Clinical Utility in a Clinical and School Sample. Child Psychiatry & Human Development. 2013;44(6):689-697.
92. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep medicine. 2001;2(4):297-307.
93. Chung KF, Kan KK, Yeung WF. Assessing insomnia in adolescents: comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep medicine. 2011;12(5):463-470.
94. Allison C, Auyeung B, Baron-Cohen S. Toward brief “Red Flags” for autism screening: The Short Autism Spectrum Quotient and the Short Quantitative Checklist for Autism in toddlers in 1,000 cases and 3,000 controls [corrected]. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;51(2):202-212.e207.
95. Gromark C, Hesselmark E, Djupedal IG, Silverberg M, Horne A, Harris RA, et al. A Two-to-Five Year Follow-Up of a Pediatric Acute-Onset Neuropsychiatric Syndrome Cohort. Child psychiatry and human development. 2021:1-11.
96. Leon J, Hommer R, Grant P, Farmer C, D'Souza P, Kessler R, et al. Longitudinal outcomes of children with pediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS). European child & adolescent psychiatry. 2018;27(5):637-643.
97. Bussing R, Fernandez M, Harwood M, Wei H, Garvan CW, Eyberg SM, et al. Parent and teacher SNAP-IV ratings of attention deficit hyperactivity disorder symptoms: psychometric properties and normative ratings from a school district sample. Assessment. 2008;15(3):317-328.
98. Swanson JM, Kraemer HC, Hinshaw SP, Arnold LE, Conners CK, Abikoff HB, et al. Clinical relevance of the primary findings of the MTA: success rates based on severity of ADHD and ODD symptoms at the end of treatment. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40(2):168-179.
99. SNAP-IV Swedish version. Available at: http://www.sfbup.se/wp-content/uploads/2020/04/SNAP-IV-SFBUP.pdf. Accessed February 24, 2021.
100. Axberg U, Johansson Hanse J, Broberg AG. Parents' description of conduct problems in their children - a test of the Eyberg Child Behavior Inventory (ECBI) in a Swedish sample aged 3-10. Scandinavian journal of psychology. 2008;49(6):497-505.
101. Burns GL, Patterson DR. Factor structure of the Eyberg Child Behavior Inventory: a parent rating scale of Oppositional Defiant Behavior Toward Adults, Inattentive Behavior, and Conduct Problem Behavior. Journal of clinical child psychology. 2000;29(4):569-577.
102. Ciccheti. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assess- ment instruments in psychology. Psychol Assess. 1994(6(4)):284-290.
103. Fält E, Wallby T, Sarkadi A, Salari R, Fabian H. Agreement between mothers', fathers', and teachers' ratings of behavioural and emotional problems in 3-5-year-old children. PloS one. 2018;13(11):e0206752.

41
104. Akoglu H. User's guide to correlation coefficients. Turkish journal of emergency medicine. 2018;18(3):91-93.
105. Johnson M, Fernell E, Preda I, Wallin L, Fasth A, Gillberg C, et al. Paediatric acute-onset neuropsychiatric syndrome in children and adolescents: an observational cohort study. The Lancet Child & adolescent health. 2019;3(3):175-180.
106. McGeer PL, Lee M, McGeer EG. A review of human diseases caused or exacerbated by aberrant complement activation. Neurobiology of aging. 2017;52:12-22.
107. Harel L, Prais D, Uziel Y, Mukamel M, Hashkes P, Harel G, et al. Increased prevalence of antithyroid antibodies and subclinical hypothyroidism in children with juvenile idiopathic arthritis. The Journal of rheumatology. 2006;33(1):164-166.
108. Kroon MW, Vrijman C, Chandeck C, Wind BS, Wolkerstorfer A, Luiten RM, et al. High prevalence of autoimmune thyroiditis in children and adolescents with vitiligo. Hormone research in paediatrics. 2013;79(3):137-144.
109. Wananukul S, Voramethkul W, Kaewopas Y, Hanvivatvong O. Prevalence of Positive Antinuclear An-tibodies in Healthy Children. Asian Pacific journal of allergy and immunology. 2005;23(2-3):153.
110. Malleson PN, Mackinnon MJ, Sailer-Hoeck M, Spencer CH. Review for the generalist: The antinuclear antibody test in children-When to use it and what to do with a positive titer. Pediatric Rheumatology. 2010;8(1):27.
111. Al-Diwani AAJ, Pollak TA, Irani SR, Lennox BR. Psychosis: an autoimmune disease? Immunology. 2017;152(3):388-401.
112. Pfeiffer H, Wickstrom R, Skov L, Sørensen CB, Sandvig I, Gjone H, et al. Clinical guidance for diagnosis and management of suspected Pediatric Acute-onset Neuropsychiatric Syndrome in the Nordic countries. Acta paediatrica (Oslo, Norway : 1992). 2021.
113. Hesselmark E, Bejerot S. Clinical features of paediatric acute-onset neuropsychiatric syndrome: findings from a case- control study. BJPsych open. 2019;5(2):e25.













![[Neuropsychiatric symptoms in mild cognitive impairment]](https://img.dokumen.tips/doc/110x75/63369389e8daaa60da0ff6fc/neuropsychiatric-symptoms-in-mild-cognitive-impairment.jpg)















