Embed Size (px)
Citation preview
edicine and Rehabilitation
Archives of Physical M journal homepage: www.archives-pmr.orgArchives of Physical Medicine and Rehabilitation 2015;96:799-808
ORIGINAL RESEARCH
Novel Risk Factors Associated With Current SuicidalIdeation and Lifetime Suicide Attempts in IndividualsWith Spinal Cord Injury
Cheryl B. McCullumsmith, MD, PhD,a,c Claire Z. Kalpakjian, PhD, MS,b
J. Scott Richards, PhD,c Martin Forchheimer, MPP,b Allen W. Heinemann, PhD,d,e
Elizabeth J. Richardson, PhD,c Catherine S. Wilson, PsyD,d,f Jason Barber, MS,g
Nancy Temkin, PhD,g Charles H. Bombardier, PhD,g,h Jesse R. Fann, MD, MPH,g,h for thePRISMS Investigators
From the aDepartment of Psychiatry and Behavioral Neurobiology, University of Cincinnati, Cincinnati, OH; bDepartment of Physical Medicineand Rehabilitation, University of Michigan, Ann Arbor, MI; cSpain Rehabilitation Center, University of Alabama at Birmingham, Birmingham,AL; dDepartment of Physical Medicine and Rehabilitation, Feinberg School of Medicine, Northwestern University, Chicago, IL; eRehabilitationInstitute of Chicago, Chicago, IL; fDepartment of Physical Medicine and Rehabilitation, James A. Haley Veterans’ Hospital, Tampa, FL;gDepartment of Psychiatry and Behavioral Sciences, University of Washington, Seattle, WA; and hDepartment of Rehabilitation Medicine,University of Washington, Seattle, WA.
Abstract
Objective: To determine unique associations of suicidal ideation (SI) and lifetime suicide attempts (SAs) in individuals with spinal cord
injury (SCI).
Design: Cross-sectional analysis.
Setting: Outpatient.
Participants: Individuals with SCI (NZ2533) who were 18 years or older with a history of traumatic SCI.
Interventions: None.
Main Outcome Measures: Any SI in the past 2 weeks (9-item Patient Health Questionnaire) and any lifetime SA.
Results: Three hundred twenty-three individuals (13.3%) reported SI in the past 2 weeks and 179 (7.4%) reported lifetime SA. After controlling
for other factors, both lifetime SA and current SI were associated with study site and current level of depression. In addition, SA was associated
with less education, younger age at injury, having current or past treatment of depression, and having bipolar disorder or schizophrenia. SI was
associated with more years since injury and lifetime SA. Several psychological factors were associated with current SI and lifetime SAs, including
lower environmental reward and less positive affect. In addition, control of one’s community activities and spiritual well-being were associated
with current SI. In bivariate comparisons, severity of SCI was also associated with the 47% of the SAs that occurred after injury.
Conclusions: Several unique associations of SI and lifetime SA in individuals with SCI were identified, including level of environmental reward and
control, spiritual well-being, and severity of SCI. These factors bear further investigation as prospective risk factors for suicidal behavior after SCI.
Archives of Physical Medicine and Rehabilitation 2015;96:799-808
ª 2015 by the American Congress of Rehabilitation Medicine
Supported by the National Institute on Disability and Rehabilitation Research (grant nos.
H133A060107-06A and H133N060033).
Clinical Trial Registration No.: NCT00592384.
Disclosures: none.
0003-9993/15/$36 - see front matter ª 2015 by the American Congress of Re
http://dx.doi.org/10.1016/j.apmr.2014.12.017
Suicide risk after spinal cord injury (SCI) is 3 or more times thatin the general population,1 yet prediction of those with SCI at riskfor suicidal behavior remains elusive. The identification of specificrisk factors in those with SCI may provide critical insights intoprevention strategies. Individuals with SCI have high rates of
habilitation Medicine

Table 1 Exploratory psychological function scales used
Psychological Function Scales
Scale
Abbreviation Psychometric Properties Assessed No. of Questions
No. of
Subjects
Reference
No.
Posttraumatic growth questionnaire PTG Positive psychological change after
a traumatic event
5 905 24
International Physical Activity
Questionnaire
IPAQ Intensity and frequency of physical
activity; modified for wheelchair users
4 566 25, 26
Modified Lorig Chronic Disease
Self-Management Scale
Self-efficacy Confidence in one’s ability to manage
pain, fatigue, and emotional distress
associated with chronic illness
6 662 27
Environmental Reward Observation
Scale
EROS Enjoyment of daily activities and
accomplishments
10 661 28, 29
Functional Assessment of Chronic
Illness TherapieseSpiritual Well-
Being: Meaning Peace and Faith
subscales
FACIT-Sp12 Importance of spirituality in day-to-day
functioning with questions on the
level of peacefulness, sense of purpose,
and strength of spiritual beliefs
12 585 30
Community Participation Inventory
dcontrol and involvement
CPI Individual’s feelings of control over
community participation and sense
of involvement in life situations
Control: 13
Involvement: 14
570 31-34
Positive and Negative Affective
Schedule
PANAS 10 positive and 10 negative emotions
experienced in the previous week
20 210 35
Neurological Quality of Life Neuro-QOL Positive affect and general well-being 9 210 36-38
800 C.B. McCullumsmith et al
established risk factors for suicidal ideation (SI) and suicidalbehavior, including depression, anxiety, post-traumatic stressdisorder, social stress and isolation, chronic medical illness, anddisability.2-8 Furthermore, a subset of individuals with SCI have ahistory of high-risk suicidal behaviors and increased impulsivity,characteristics also associated with suicidal behavior.9-11 Howev-er, unique risk factors for suicidal behavior are not yet wellestablished for individuals with SCI.
Several studies have demonstrated an increased risk of suicideafter SCI compared to the general population.1,12-14 A 10-yearstudy of more than 9000 people from 13 SCI centers found astandardized mortality ratio of 4.9 for suicide, with the highestrisk between 1 and 5 years after SCI and with complete para-plegia.12 Both a 40-year retrospective Danish study and a 30-yearretrospective examination of data from the National Spinal CordInjury Statistical Database found the highest rates of suicide inthose with the least severe disabilities.1,15 However, little is knownabout risks of common antecedents to suicide: SI and suicide at-tempts (SAs), which have some shared and many distinct risksfrom death by suicide.16-21 For example, SI and SAs are both moreprevalent in women, yet death by suicide is more prevalent inmen. Both SI and SAs are significant risk factors for future SI,SAs, and death by suicide and probably account for much of thepredictive value of psychiatric illness in suicidal behavior.22 At-tempts and ideation carry their own morbidity, with decreased
List of abbreviations:
EROS Environmental Reward Observation Scale
FACIT-Sp12 Functional Assessment of Chronic Illness
TherapieseSpiritual Well-being scale
Neuro-QOL Neurological Quality of Life
PHQ-9 9-item Patient Health Questionnaire
SA suicide attempt
SCI spinal cord injury
SI suicidal ideation
functioning, hospital admissions, and short- and long-term medi-cal consequences.
We examined factors associated with current SI and lifetimeattempts in a general population of individuals with SCI. Inparticular, we were interested in whether different characteristicswere associated with SAs and SI in individuals with SCI than hadbeen shown in the population without SCI. We also examinedfactors associated with SAs that occurred before versus after SCI,with the hypothesis that SCI characteristics such as more severeinjury or more violent etiology might differentially increase SAs.Risk factors determined from this study can help guide practi-tioners to identify and treat individuals with SCI at risk ofsuicidal behavior.
Methods
Participants
A total of 2533 participants were recruited between July 2007 andMay 2012 from 4 National Institute on Disability and Rehabili-tation Researchefunded SCI Model System sites and 2 additionalsites as part of the Project to Improve Symptoms and Mood afterSCI23: Rehabilitation Institute of Chicago (nZ874), University ofWashington (nZ417), University of Michigan (nZ517), Univer-sity of Alabama at Birmingham (nZ434), Baylor RehabilitationInstitute (nZ233), and University of Miami (nZ58). Study in-clusion criteria were as follows: individuals 18 years or older witha history of traumatic SCI. We excluded persons who were noneEnglish speakers, too cognitively impaired to comprehend studymaterials, and referrals based on clinical status of depressionrather than screened on a nonselected basis. All participants gaveinformed consent, and each site obtained approval from its localinstitutional review board. The 6 sites had statistically significantdifferences in frequencies of all demographic and baseline char-acteristic measures: mean age, 39 years at Baylor Institute of
www.archives-pmr.org
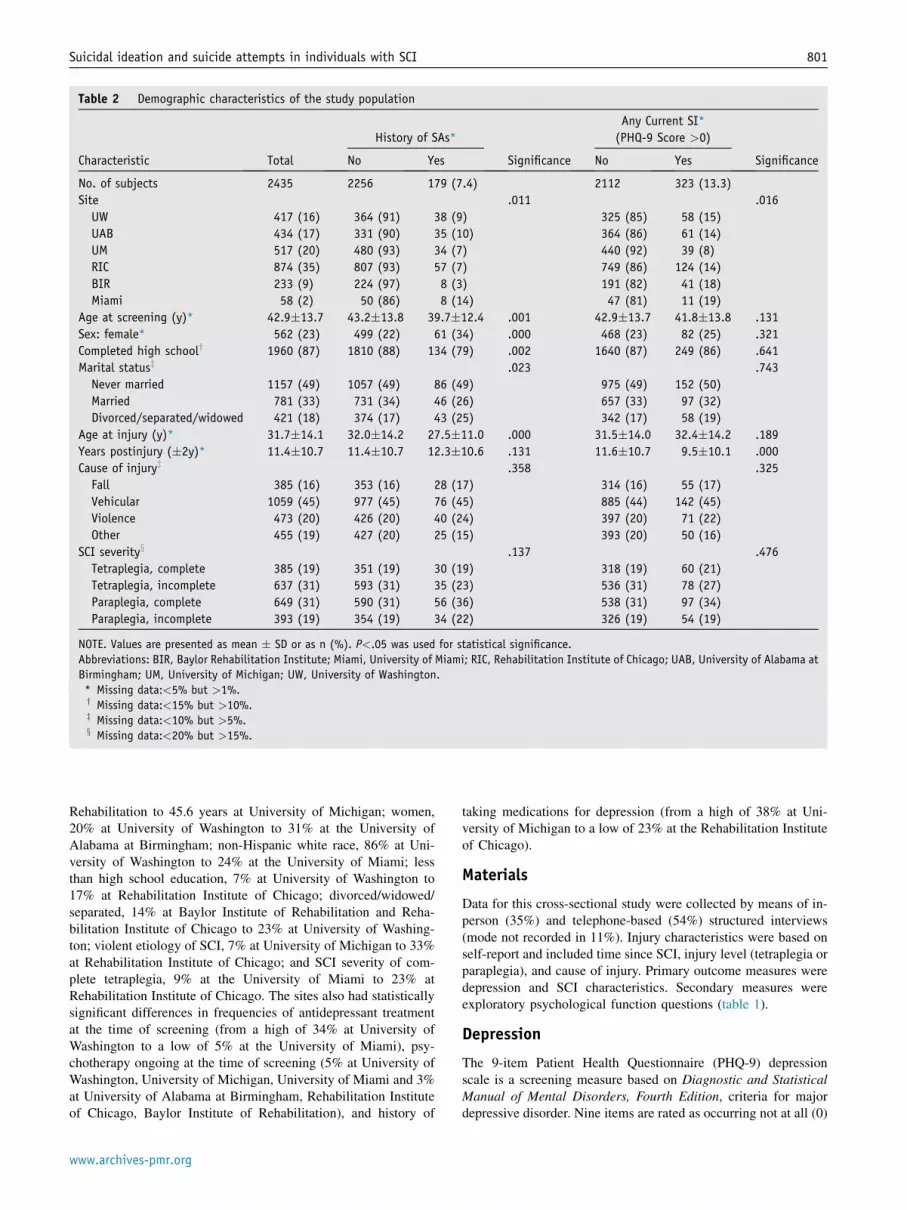
Table 2 Demographic characteristics of the study population
Characteristic Total
History of SAs*
Significance
Any Current SI*
(PHQ-9 Score >0)
SignificanceNo Yes No Yes
No. of subjects 2435 2256 179 (7.4) 2112 323 (13.3)
Site .011 .016
UW 417 (16) 364 (91) 38 (9) 325 (85) 58 (15)
UAB 434 (17) 331 (90) 35 (10) 364 (86) 61 (14)
UM 517 (20) 480 (93) 34 (7) 440 (92) 39 (8)
RIC 874 (35) 807 (93) 57 (7) 749 (86) 124 (14)
BIR 233 (9) 224 (97) 8 (3) 191 (82) 41 (18)
Miami 58 (2) 50 (86) 8 (14) 47 (81) 11 (19)
Age at screening (y)* 42.9�13.7 43.2�13.8 39.7�12.4 .001 42.9�13.7 41.8�13.8 .131
Sex: female* 562 (23) 499 (22) 61 (34) .000 468 (23) 82 (25) .321
Completed high schooly 1960 (87) 1810 (88) 134 (79) .002 1640 (87) 249 (86) .641
Marital statusz .023 .743
Never married 1157 (49) 1057 (49) 86 (49) 975 (49) 152 (50)
Married 781 (33) 731 (34) 46 (26) 657 (33) 97 (32)
Divorced/separated/widowed 421 (18) 374 (17) 43 (25) 342 (17) 58 (19)
Age at injury (y)* 31.7�14.1 32.0�14.2 27.5�11.0 .000 31.5�14.0 32.4�14.2 .189
Years postinjury (�2y)* 11.4�10.7 11.4�10.7 12.3�10.6 .131 11.6�10.7 9.5�10.1 .000
Cause of injuryz .358 .325
Fall 385 (16) 353 (16) 28 (17) 314 (16) 55 (17)
Vehicular 1059 (45) 977 (45) 76 (45) 885 (44) 142 (45)
Violence 473 (20) 426 (20) 40 (24) 397 (20) 71 (22)
Other 455 (19) 427 (20) 25 (15) 393 (20) 50 (16)
SCI severityx .137 .476
Tetraplegia, complete 385 (19) 351 (19) 30 (19) 318 (19) 60 (21)
Tetraplegia, incomplete 637 (31) 593 (31) 35 (23) 536 (31) 78 (27)
Paraplegia, complete 649 (31) 590 (31) 56 (36) 538 (31) 97 (34)
Paraplegia, incomplete 393 (19) 354 (19) 34 (22) 326 (19) 54 (19)
NOTE. Values are presented as mean � SD or as n (%). P<.05 was used for statistical significance.
Abbreviations: BIR, Baylor Rehabilitation Institute; Miami, University of Miami; RIC, Rehabilitation Institute of Chicago; UAB, University of Alabama at
Birmingham; UM, University of Michigan; UW, University of Washington.
* Missing data:<5% but >1%.y Missing data:<15% but >10%.z Missing data:<10% but >5%.x Missing data:<20% but >15%.
Suicidal ideation and suicide attempts in individuals with SCI 801
Rehabilitation to 45.6 years at University of Michigan; women,20% at University of Washington to 31% at the University ofAlabama at Birmingham; non-Hispanic white race, 86% at Uni-versity of Washington to 24% at the University of Miami; lessthan high school education, 7% at University of Washington to17% at Rehabilitation Institute of Chicago; divorced/widowed/separated, 14% at Baylor Institute of Rehabilitation and Reha-bilitation Institute of Chicago to 23% at University of Washing-ton; violent etiology of SCI, 7% at University of Michigan to 33%at Rehabilitation Institute of Chicago; and SCI severity of com-plete tetraplegia, 9% at the University of Miami to 23% atRehabilitation Institute of Chicago. The sites also had statisticallysignificant differences in frequencies of antidepressant treatmentat the time of screening (from a high of 34% at University ofWashington to a low of 5% at the University of Miami), psy-chotherapy ongoing at the time of screening (5% at University ofWashington, University of Michigan, University of Miami and 3%at University of Alabama at Birmingham, Rehabilitation Instituteof Chicago, Baylor Institute of Rehabilitation), and history of
www.archives-pmr.org
taking medications for depression (from a high of 38% at Uni-versity of Michigan to a low of 23% at the Rehabilitation Instituteof Chicago).
Materials
Data for this cross-sectional study were collected by means of in-person (35%) and telephone-based (54%) structured interviews(mode not recorded in 11%). Injury characteristics were based onself-report and included time since SCI, injury level (tetraplegia orparaplegia), and cause of injury. Primary outcome measures weredepression and SCI characteristics. Secondary measures wereexploratory psychological function questions (table 1).
Depression
The 9-item Patient Health Questionnaire (PHQ-9) depressionscale is a screening measure based on Diagnostic and StatisticalManual of Mental Disorders, Fourth Edition, criteria for majordepressive disorder. Nine items are rated as occurring not at all (0)

Table 3 Psychiatric characteristics of suicide attempters and those with SI
Characteristic N Total
History of SAs
Significance
Any Current SI
SignificanceNo Yes No Yes
No. of subjects 2435 2256 180 2116 334
PHQ-9 score 6.3�5.8 6.0�5.7 10.4�6.5 .000 5.1�4.9 13.7�5.7 .000
Antidepressant at screening 353 (24) 313 (23) 39 (40) .000 272 (22) 69 (37) .000
Lithium at screening 22 (1) 16 (1) 6 (6) .002 17 (1) 4 (2) .510
Psychotherapy for depression at screening 96 (4) 72 (3) 24 (13) .000 65 (3) 27 (8) .000
History of medication for depression 432 (30) 370 (28) 61 (62) .000 332 (27) 89 (47) .000
Ever treated for bipolar/manic 67 (3) 39 (2) 26 (15) .000 41 (2) 22 (7) .000
Ever treated for schizophrenia 26 (1) 14 (1) 12 (7) .000 20 (1) 4 (1) .762
Psychological factors
Posttraumatic growth (PTG) 905 12.3�6.9 12.2�6.9 13.7�6.9 .084 12.3�7.0 12.3�6.7 .911
Physical activity (IPAQ) 566 2.10�0.94 2.10�0.93 2.20�0.97 .471 2.12�0.93 2.02�0.98 .425
Self-efficacy (Lorig) 662 7.35�2.04 7.42�2.01 6.42�2.37 .004 7.56�1.95 6.07�2.14 .000
Environmental reward (EROS) 661 27.7�5.6 27.9�5.5 24.9�6.6 .000 28.6�5.2 22.8�5.6 .000
Community participation
(CPIecontrol)
570 53.3�10.3 53.7�10.2 47.6�10.5 .001 54.4�9.7 44.6�12.0 .000
Community participation
(CPIeinvolvement)
585 42.7�13.4 43.0�13.4 38.3�12.9 .073 43.6�13.5 35.3�11.8 .000
Negative affect (PANAS) 210 32.8�9.6 33.4�9.6 26.0�6.4 .001 33.8�9.4 28.1�9.1 .000
Positive affect (PANAS) 210 19.2�8.2 18.3�7.4 29.1�9.7 .000 18.0�7.6 24.8�8.9 .000
Spiritual well-being (FACIT SP-12) 210 34.1�10.4 35.1�10.3 23.9�4.9 .000 36.2�9.3 24.1�10.2 .000
Positive affect and well-being (Neuro-QOL) 210 33.8�8.5 34.6�8.2 25.4�6.4 .000 35.5�7.3 25.6�9.1 .000
NOTE. Values are presented as mean � SD or as n (%). P<.05 was used for statistical significance.
Abbreviations: CPI, Community Participation Inventory; IPAQ, International Physical Activity Questionnaire; PANAS, Positive and Negative Affect
Schedule; PTG, post-traumatic growth questionnaire; Self-efficacy, Modified Lorig Chronic Disease Self-Management Scale.
802 C.B. McCullumsmith et al
to nearly every day (3) during the past 2 weeks. The PHQ-9 hasgood internal consistency and construct validity39 and has beenvalidated for use in the population with SCI.40 To assess the as-sociation of depression with SI, we used the PHQ-8, a well-validated version of the scale that does not include the 9th itemmeasuring SI.41-43
Suicidal ideationCurrent SI was evaluated by a nonzero answer to question 9 of thePHQ-9: “Over the last 2 weeks, how often have you been botheredby.thoughts that you would be better off dead or of hurtingyourself in some way?”
SA historySA history was determined by the following questions: 1) Hasthere ever been a suicide attempt? 2) How many times? 3) Lastattempt? 4) What was the age at first attempt. Timing of an SArelative to SCI was determined by comparing the date of firstreported SA to the date of SCI. In 32 of 180 (17.8%) cases, thetiming of the SA relative to SCI could not be determined becauseof either lack of information or unclear dates. In 8 of 180 (4.4%)cases, study participants had SAs both before and after SCI.Neither those cases in which timing was indeterminate or caseswith SAs before and after SCI were included in analysescomparing factors associated with SAs only before SCI to thosethat occurred only after SCI.
Psychological function questionsExploratory psychological function questions were selected toexplore specific topics related to depression but not necessarilysuicidal behavior and were administered during screening in
successive blocks of screened patients (see table 1) duringscreening sequentially over the course of the study.
Psychiatric history/mental health treatmentSubjects were asked whether they had ever been diagnosed ortreated for depression, bipolar disorder, or schizophrenia.
Statistical analyses
All bivariate relationships with SI and SA history were evaluatedusing t tests, Mann-Whitney tests, and Fisher exact tests, asappropriate. Row percentages are reported for all categoricalvariables, and means and SDs are reported for continuous vari-ables. Missing data rates are reported in footnotes for each table.Multivariate logistic regression was used to assess the relationshipbetween screening measures and each of SI and SA history. First abase model was constructed from a pool of bivariate significantcovariates using a forward stepwise algorithm, and then theremaining explanatory significance of each screening measure wasdetermined by adding it to the base model. For the psychologicalfactors that were given only to subgroups of individuals, third-order modeling was performed, where each psychological factorwas individually tested with the significant factors from the basemodel for the entire population, using only the subjects whoreceived that test of psychological function in that wave. All an-alyses were performed using SPSS version 17.0.a
Results
Of 2435 individuals with SCI screened for depression, 179 (7.4%)reported a lifetime SA and 323 (13.3%) reported any SI in the past2 weeks (table 2). Factors associated with current SI included
www.archives-pmr.org
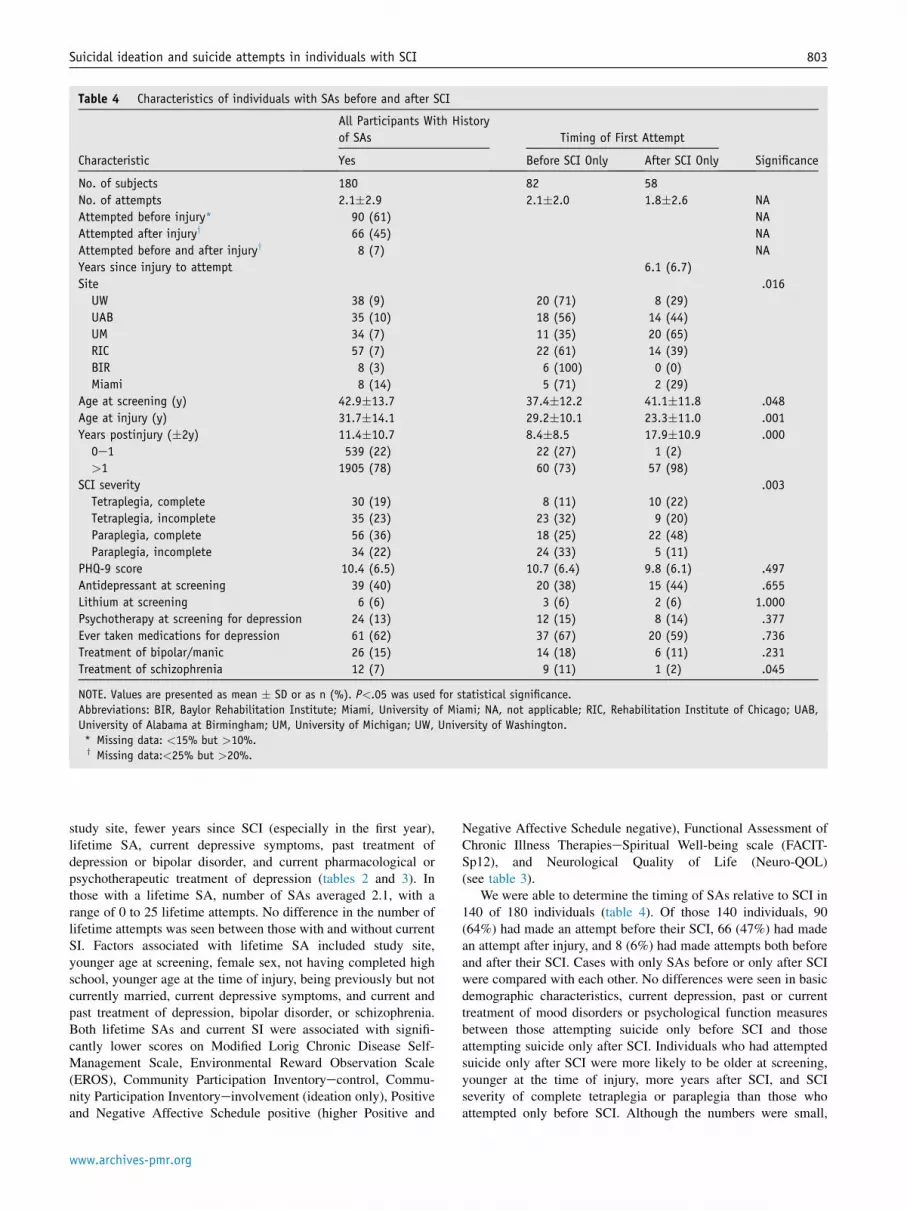
Table 4 Characteristics of individuals with SAs before and after SCI
Characteristic
All Participants With History
of SAs Timing of First Attempt
SignificanceYes Before SCI Only After SCI Only
No. of subjects 180 82 58
No. of attempts 2.1�2.9 2.1�2.0 1.8�2.6 NA
Attempted before injury* 90 (61) NA
Attempted after injuryy 66 (45) NA
Attempted before and after injuryy 8 (7) NA
Years since injury to attempt 6.1 (6.7)
Site .016
UW 38 (9) 20 (71) 8 (29)
UAB 35 (10) 18 (56) 14 (44)
UM 34 (7) 11 (35) 20 (65)
RIC 57 (7) 22 (61) 14 (39)
BIR 8 (3) 6 (100) 0 (0)
Miami 8 (14) 5 (71) 2 (29)
Age at screening (y) 42.9�13.7 37.4�12.2 41.1�11.8 .048
Age at injury (y) 31.7�14.1 29.2�10.1 23.3�11.0 .001
Years postinjury (�2y) 11.4�10.7 8.4�8.5 17.9�10.9 .000
0e1 539 (22) 22 (27) 1 (2)
>1 1905 (78) 60 (73) 57 (98)
SCI severity .003
Tetraplegia, complete 30 (19) 8 (11) 10 (22)
Tetraplegia, incomplete 35 (23) 23 (32) 9 (20)
Paraplegia, complete 56 (36) 18 (25) 22 (48)
Paraplegia, incomplete 34 (22) 24 (33) 5 (11)
PHQ-9 score 10.4 (6.5) 10.7 (6.4) 9.8 (6.1) .497
Antidepressant at screening 39 (40) 20 (38) 15 (44) .655
Lithium at screening 6 (6) 3 (6) 2 (6) 1.000
Psychotherapy at screening for depression 24 (13) 12 (15) 8 (14) .377
Ever taken medications for depression 61 (62) 37 (67) 20 (59) .736
Treatment of bipolar/manic 26 (15) 14 (18) 6 (11) .231
Treatment of schizophrenia 12 (7) 9 (11) 1 (2) .045
NOTE. Values are presented as mean � SD or as n (%). P<.05 was used for statistical significance.
Abbreviations: BIR, Baylor Rehabilitation Institute; Miami, University of Miami; NA, not applicable; RIC, Rehabilitation Institute of Chicago; UAB,
University of Alabama at Birmingham; UM, University of Michigan; UW, University of Washington.
* Missing data: <15% but >10%.y Missing data:<25% but >20%.
Suicidal ideation and suicide attempts in individuals with SCI 803
study site, fewer years since SCI (especially in the first year),lifetime SA, current depressive symptoms, past treatment ofdepression or bipolar disorder, and current pharmacological orpsychotherapeutic treatment of depression (tables 2 and 3). Inthose with a lifetime SA, number of SAs averaged 2.1, with arange of 0 to 25 lifetime attempts. No difference in the number oflifetime attempts was seen between those with and without currentSI. Factors associated with lifetime SA included study site,younger age at screening, female sex, not having completed highschool, younger age at the time of injury, being previously but notcurrently married, current depressive symptoms, and current andpast treatment of depression, bipolar disorder, or schizophrenia.Both lifetime SAs and current SI were associated with signifi-cantly lower scores on Modified Lorig Chronic Disease Self-Management Scale, Environmental Reward Observation Scale(EROS), Community Participation Inventoryecontrol, Commu-nity Participation Inventoryeinvolvement (ideation only), Positiveand Negative Affective Schedule positive (higher Positive and
www.archives-pmr.org
Negative Affective Schedule negative), Functional Assessment ofChronic Illness TherapieseSpiritual Well-being scale (FACIT-Sp12), and Neurological Quality of Life (Neuro-QOL)(see table 3).
We were able to determine the timing of SAs relative to SCI in140 of 180 individuals (table 4). Of those 140 individuals, 90(64%) had made an attempt before their SCI, 66 (47%) had madean attempt after injury, and 8 (6%) had made attempts both beforeand after their SCI. Cases with only SAs before or only after SCIwere compared with each other. No differences were seen in basicdemographic characteristics, current depression, past or currenttreatment of mood disorders or psychological function measuresbetween those attempting suicide only before SCI and thoseattempting suicide only after SCI. Individuals who had attemptedsuicide only after SCI were more likely to be older at screening,younger at the time of injury, more years after SCI, and SCIseverity of complete tetraplegia or paraplegia than those whoattempted only before SCI. Although the numbers were small,

Table 5 Multivariate logistic regression for current suicidal ideation
Stepwise Model* B Odds Ratio Significance
Site .015
UAB (vs UW) �0.15 0.87 .545
UM (vs UW) �0.75 0.47 .003
RIC (vs UW) �0.10 0.90 .614
BIR (vs UW) 0.16 1.17 .536
Miami (vs UW) �0.22 0.80 .602
Years postinjury �0.02 0.98 .023
Previous suicide attempt 0.76 2.13 .000
PHQ-8 (without the ideation item) 0.19 1.21 .000
Constant �3.21 0.04 .000
Abbreviations: BIR, Baylor Rehabilitation Institute; Miami, University of Miami; PHQ-8, 8-item Personal Health Questionnaire; RIC, Rehabilitation
Institute of Chicago; UAB, University of Alabama at Birmingham; UM, University of Michigan; UW, University of Washington.
* Only considering covariates with <15% missing.
804 C.B. McCullumsmith et al
schizophrenia diagnosis was associated more with those who hadattempted suicide only before SCI than those attempting suicideonly after SCI.
In multivariate logistic regression, the following variablesremained independently significantly associated with currentSI: study site, fewer years after SCI, current depressivesymptoms, and lifetime SA (table 5). For the model in Table 5,NZ2340 and R2Z15.6%. In third-order modeling (table 6),each of the psychological factor assessments was addedindividually to the model containing the above significantassociations for that subpopulation (adjusted N values in thetable). The EROS, Community Participation Inventoryecon-trol, FACIT-Sp12, and Neuro-QOL added significantly to theexplanation of the variance (R2) for the model. In multivariatelogistic regression, the following variables remained signifi-cantly associated with lifetime SAs: study site, younger age atthe time of injury, not completing high school, currentdepressive symptoms, current treatment of depression, andpast treatment of bipolar or schizophrenia (table 7). For themodel in Table 7, NZ2103 and R2Z8.1%. Female sex lostindependent association when controlling for current depres-sive symptoms. In third-order modeling (table 8), where thepsychological factors were added individually to the modelcontaining the above significant associations for each sub-population (N values reported in the table), the EROS and
Table 6 Effect of psychological factors on the base model logistic reg
Psychological Factor B Od
Self-efficacy (Lorig) �0.10 0.9
Environmental reward (EROS) �0.12 0.8
Community participation (CPIecontrol) �0.04 0.9
Community participation (CPIeinvolvement) �0.02 0.9
Negative affect (PANAS) �0.02 0.9
Positive affect (PANAS) 0.04 1.0
Spiritual well-being (FACIT-Sp12) �0.09 0.9
Positive affect and well-being (Neuro-QOL) �0.12 0.8
NOTE. P<.05 was used for statistical significance.
Abbreviations: CPI, Community Participation Inventory; PANAS, Positive and
Self-Management Scale.
* Applying each psychological factor individually to the base model in tab
Neuro-QOL each added significantly to the explanation of thevariance (R2) for the model.
Discussion
In our study population, individuals with SCI had high rates of SIand SAs than did the general population. The 7.4% lifetimeprevalence of SAs is much higher than the 4.6% lifetime preva-lence reported for the general US population.20 The 13.3% prev-alence of SI occurring in just the last 2 weeks before screening ismuch higher than even the annual prevalence of 3.3% reported inthe US general population44,45 but is more consistent with a 34.8%past-year SI prevalence in Korean persons with SCI.46 Risk factorsassociated with current SI largely paralleled those found in thegeneral population: current depression and history of an SA withsome notable negative findings of age, sex, race, marital status,and educational level.19,47 In our study, risk factors for lifetimeSAs also paralleled those found in the general population,including past treatment of bipolar disorder or schizophrenia,current treatment of depression, current depression severity, andhaving less than high school education.19,20,45,48 The associationof female sex with lifetime SAs drops out after controlling forcurrent depressive symptoms.
Some unique factors associated with current SI and lifetimeSAs emerged in this study. Current SI was independently
ression for current SI*
ds Ratio Significance N Cox-Snell R2 (%)
0 .146 631 20.5
8 .000 630 22.5
7 .022 548 14.3
9 .247 562 13.6
8 .407 206 17.3
4 .185 206 17.7
1 .000 206 23.3
8 .000 206 24.8
Negative Affect Schedule; Self-efficacy, Modified Lorig Chronic Disease
le 5.
www.archives-pmr.org

Table 7 Multivariate logistic regression for lifetime SAs
Second-Order Stepwise Model* B Odds Ratio Significance
Site .032
UAB (vs UW) 0.06 1.06 .840
UM (vs UW) �0.23 0.80 .432
RIC (vs UW) �0.38 0.68 .158
BIR (vs UW) �1.76 0.17 .003
Miami (vs UW) �0.03 0.97 .953
Age at injury �0.04 0.96 .000
Sex: maley �0.36 0.70 .072
Completed high school �0.47 0.62 .044
Current psychotherapy for depression 0.99 2.70 .002
Treatment for bipolar 2.01 7.43 .000
Treatment for schizophrenia 1.59 4.89 .002
PHQ-9 0.10 1.10 .000
Constant �1.50 0.22 .000
Abbreviations: BIR, Baylor Rehabilitation Institute; Miami, University of Miami; RIC, Rehabilitation Institute of Chicago; UAB, University of Alabama at
Birmingham; UM, University of Michigan; UW, University of Washington.
* Adding variables <15% missing.y Sex left in the model despite nonsignificance.
Suicidal ideation and suicide attempts in individuals with SCI 805
associated with less time after SCI, especially for the first yearafter SCI, but was not associated with any severity or etiology ofSCI. Nam et al46 also did not find a relationship between SCIcharacteristics and SI in individuals with SCI in Korea. Previouswork has found a decreased risk of suicide with increased timefrom SCI, and our findings provide further support for moreintensive suicide screening and preventive interventions earlyafter SCI.1,12 The association of younger age at the time of SCIwith lifetime SAs bears further examination, but the cause andeffect is not clear. For example, impulsive young adults might bemore likely to have both SCI and SAs. Alternatively, an earlyserious life-changing event such as an SCI might increase therisk of SA.
As might be expected, mental health factors predicted bothSAs known to occur only before SCI and those occurring onlyafter SCI. Only schizophrenia was more strongly associated withSAs occurring before SCI, whereas completeness of SCI injury,older age at screening, and younger age at the time of injurywere more strongly associated with SAs that occurred only after
Table 8 Effect of psychological factors on the base model logistic reg
Third-Order Modelingy B Od
Self-efficacy (Lorig) �0.20 0.8
Environmental reward (EROS) �0.11 0.9
Community participation (CPIecontrol) �0.03 0.9
Community participation (CPIeinvolvement) �0.02 0.9
Negative affect (PANAS) �0.04 0.9
Positive affect (PANAS) 0.08 1.0
Spiritual well-being (FACIT-Sp12) �0.09 0.9
Positive affect and well-being (Neuro-QOL) �0.14 0.8
Abbreviations: PANAS, Positive and Negative Affect Schedule; Self-efficacy, M
* Applying each psychological factor individually to the base model in taby Adding each screening measure individually.
www.archives-pmr.org
SCI. The high association of schizophrenia with SAs before SCIbears further investigation; however, the number of subjects withschizophrenia was small. Severity of SCI was associatedsignificantly more with SAs occurring after SCI, which parallelsfindings on death by suicide by DeVivo and coworkers,1 butcontrasts with 2 studies showing decreased risk of death bysuicide in the most severely injured individuals, perhaps becausethe risk factors for SAs do not always overlap with risk factorsfor suicide.16,21,49,50 Our work, combined with that by DeVivoet al and others, suggests a need for careful monitoring of SI andsuicidal behavior in individuals with complete tetraplegia orcomplete paraplegia.12,15
Rates of both current SI and lifetime SAs were significantlydifferent among the 6 study sites. As delineated in the Methodssection, the 6 study sites did differ significantly in the fre-quencies of all demographic variables tested, but there were noclear patterns in these differences that clearly correlate withelevated suicide risk. For example, the University of Miami sitehas the highest prevalence of lifetime SAs and current SI but
ression for current SI*
ds Ratio Significance N Cox-Snell R2 (%)
2 .081 478 12.3
0 .010 478 13.0
7 .202 543 9.0
9 .419 556 8.9
6 .487 203 25.6
8 .211 203 26.0
2 .130 203 26.4
7 .024 203 27.8
odified Lorig Chronic Disease Self-Management Scale.
le 7.

806 C.B. McCullumsmith et al
was not the highest in traditional demographic risk factors forsuicidal behavior including age, female sex, non-Hispanic whiterace, less education, and previously but not currently married.The 6 study sites also differed significantly in frequencies ofcurrent and historical treatment of depression, with suggestionof effect. For example, the University of Miami had the lowestcurrent use of antidepressants (but second highest historical useof antidepressants) and the highest prevalence of both current SIand lifetime SAs. However, Rehabilitation Institute of Chicagoand Baylor Institute of Rehabilitation each had the 2 lowest ratesof historical use of antidepressant medications and also thelowest rates of lifetime SAs. Examination of the psychologicalfactors provides insights into some additional questions thatmight be of use in assessing suicide risk in the population withSCI. Significantly, the EROS, Community Participation In-ventoryecontrol, FACIT-Sp12, and Neuro-QOL all indepen-dently significantly increased the predictive models for currentSI. Similarly, the EROS and Neuro-QOL also independentlysignificantly increased the predictive models for lifetime SAs.These questionnaires all focus on different aspects of sense ofpurpose, enjoyment of daily activities, and general well-being.The EROS asks questions such as “A lot of activities in my lifeare pleasurable” and “Other people seem to have more fulfillinglives,” and it has been associated with depression and scoresimprove with behavioral activation therapy.28,51 The Commu-nity Participation Inventoryecontrol asks questions such as “Iam in control of my own life” and “I have choices about theactivities I do.” Although community enfranchisement measuredby the Community Participation Inventory has been shown to besignificantly affected by depression in this population, ourfinding suggests that the level of control of involvement incommunity activities is an additive risk factor for SI on top ofdepressive symptoms.52 The FACIT-Sp12 asks agreement withstatements such as “I have a reason for living” and “I findcomfort in my faith or spiritual practice,” and it has beenassociated with less distress and more emotional well-being inpatients with cancer.53 The positive affect and well-being scalefor the Neuro-QOL asks agreement with statements such as “Mylife was peaceful” and “Many areas of my life were interestingto me.”36 Taken together, these findings strongly suggest that thelack of ability to engage in one’s environment and pursue ac-tivities that one chooses may significantly add to depression increating risk of SI and SAs. The additive predictive value ofthese questions suggests a need to develop further questionsfocused on daily life engagement and enjoyment as well assense of purpose in the evaluation of suicidal risk in individualswith SCI.
Study limitations
Limitations of this study include its cross-sectional nature, bias ofindividuals who are presenting to SCI centers, recall bias frompatient self-report, lack of multiple comparison testing, and theexploratory nature of the psychological function questions(including these not being administered to all subjects). Althoughseveral exploratory psychological variables tested demonstratedstatistically significant associations with SI and SAs, the clinicalsignificance of these differences is not known. Further informationabout specific timing of SCI relative to SAs would have allowed amore nuanced understanding of our findings.
Our findings echo the high association of depression and mooddisorders with SI and SAs, a concern especially appropriate in the
population with SCI, where depression may not be adequatelyrecognized or treated. Previous work done by our group hasdemonstrated that only 29% of those with depression in the popula-tion with SCI receive pharmacotherapy and 11% receive psycho-therapy, but only half or less of these interventions meet standardguidelines for adequate antidepressant treatment.54 Our work sug-gests that patients with lifetime SAs and current SI have receivedmore care than those with depression only, but might not havereceived adequate treatment to fully treat their illness. This finding,combined with recent work in the general population that demon-strated highest suicide risk for those with most time spent indepressive episodes,55 suggests a need for dramatic increases inscreening and treatment efforts for depression and especially for SIand SAs in SCI.
Conclusions
This cross-sectional study of prevalence of lifetime SAs andcurrent SI suggests further work to be done in recognition andtreatment of those at highest risk of suicidal behavior after SA.Certainly, all individuals with current or past mood disorder,psychosis, or lifetime SAs should be carefully evaluated andtreated to remission. Furthermore, individuals with recent SCI,young age at SCI, and the most severe SCI classi-ficationsdcomplete tetraplegia and paraplegiadshould receiveregular monitoring of suicidal ideation and plans as well astreatment of depression. Further work needs to be done to exploremethods for assessing suicide risk and the temporal associationsbetween engagement in community activities, quality of life,depression, and SI and SAs in the population with SCI.
Supplier
a. SPSS, Inc.
Keywords
Depression; Rehabilitation; Spinal cord injuries; Suicide; Suicide,attempted; Suicidal ideation
Corresponding author
Cheryl B. McCullumsmith, MD, PhD, Department of Psychiatryand Behavioral Neuroscience, University of Cincinnati, 260Stetson St, Suite 3200, Cincinnati, OH 45219. E-mail address:[email protected].
References
1. Cao Y, Massaro JF, Krause JS, Chen Y, Devivo MJ. Suicide mortality
after spinal cord injury in the United States: injury cohorts analysis.
Arch Phys Med Rehabil 2014;95:230-5.
2. Craig A, Tran Y, Middleton J. Psychological morbidity and spinal
cord injury: a systematic review. Spinal Cord 2009;47:108-14.
3. Elliott TR, Frank RG. Depression following spinal cord injury. Arch
Phys Med Rehabil 1996;77:816-23.
4. Peter C, Muller R, Cieza A, Geyh S. Psychological resources in
spinal cord injury: a systematic literature review. Spinal Cord 2012;
50:188-201.
www.archives-pmr.org

Suicidal ideation and suicide attempts in individuals with SCI 807
5. Peter C, Rauch A, Cieza A, Geyh S. Stress, internal resources and
functioning in a person with spinal cord disease. NeuroRehabilitation
2012;30:119-30.
6. Muller R, Peter C, Cieza A, Geyh S. The role of social support and
social skills in people with spinal cord injuryda systematic review of
the literature. Spinal Cord 2012;50:94-106.
7. Krause JS, Carter RE. Risk of mortality after spinal cord injury:
relationship with social support, education, and income. Spinal Cord
2009;47:592-6.
8. Krause JS, Carter R, Zhai Y, Reed K. Psychologic factors and risk of
mortality after spinal cord injury. Arch Phys Med Rehabil 2009;90:
628-33.
9. Krause JS, Carter RE, Pickelsimer E. Behavioral risk factors of
mortality after spinal cord injury. Arch Phys Med Rehabil 2009;90:
95-101.
10. Berry JW, Elliott TR, Rivera P. Resilient, undercontrolled, and
overcontrolled personality prototypes among persons with spinal
cord injury. J Pers Assess 2007;89:292-302.
11. Turner C, McClure R, Pirozzo S. Injury and risk-taking behaviorda
systematic review. Accid Anal Prev 2004;36:93-101.
12. DeVivo MJ, Black KJ, Richards JS, Stover SL. Suicide following
spinal cord injury. Paraplegia 1991;29:620-7.
13. Soden RJ, Walsh J, Middleton JW, Craven ML, Rutkowski SB,
Yeo JD. Causes of death after spinal cord injury. Spinal Cord 2000;
38:604-10.
14. Geisler WO, Jousse AT, Wynne-Jones M, Breithaupt D. Survival in
traumatic spinal cord injury. Paraplegia 1983;21:364-73.
15. Hartkopp A, Brønnum-Hansen H, Seidenschnur AM, Biering-
Sørensen F. Survival and cause of death after traumatic spinal cord
injury: a long-term epidemiological survey from Denmark. Spinal
Cord 1997;35:76-85.
16. Borges G, Angst J, Nock MK, Ruscio AM, Walters EE, Kessler RC.
A risk index for 12-month suicide attempts in the National Comor-
bidity Survey Replication (NCS-R). Psychol Med 2006;36:1747-57.
17. Borges G, NockMK, Haro Abad JM, et al. Twelve-month prevalence of
and risk factors for suicide attempts in the World Health Organization
World Mental Health Surveys. J Clin Psychiatry 2010;71:1617-28.
18. Bruffaerts R, Demyttenaere K, Borges G, et al. Childhood adversities
as risk factors for onset and persistence of suicidal behaviour. Br J
Psychiatry 2010;197:20-7.
19. Kessler RC, Berglund P, Borges G, Nock M, Wang PS. Trends in
suicide ideation, plans, gestures, and attempts in the United States,
1990-1992 to 2001-2003. JAMA 2005;293:2487-95.
20. Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and
risk factors for suicidal ideation, plans and attempts. Br J Psychiatry
2008;192:98-105.
21. Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Sui-
cide and suicidal behavior. Epidemiol Rev 2008;30:133-54.
22. Borges G, Angst J, Nock MK, Ruscio AM, Kessler RC. Risk factors
for the incidence and persistence of suicide-related outcomes: a 10-
year follow-up study using the National Comorbidity Surveys. J
Affect Disord 2008;105:25-33.
23. Bombardier CH, Fann JR, Wilson CS, et al. A randomized controlled trial
of venlafaxine XR for major depressive disorder after spinal cord injury:
methods and lessons learned. J Spinal Cord Med 2014;37:247-63.
24. TedeschiR,CalhounL.ThePosttraumaticGrowth Inventory:measuring
the positive legacy of trauma. J Trauma Stress 1996;9:455-71.
25. Craig CL, Marshall AL, Sjostrom M, et al. International Physical
Activity Questionnaire: 12-country reliability and validity. Med Sci
Sports Exerc 2003;35:1381-95.
26. Washburn RA, Zhu W, McAuley E, Frogley M, Figoni SF. The
physical activity scale for individuals with physical disabilities:
development and evaluation. Arch Phys Med Rehabil 2002;83:
193-200.
27. Middleton J, Tran Y, Craig A. Relationship between quality of life
and self-efficacy in persons with spinal cord injuries. Arch Phys Med
Rehabil 2007;88:1643-8.
www.archives-pmr.org
28. Armento ME, Hopko DR. The Environmental Reward Observation
Scale (EROS): development, validity, and reliability. Behav Ther
2007;38:107-19.
29. Niven K, Totterdell P, Stride C, Holman D. Emotion Regulation of
Others and Self (EROS): the development and validation of a new
individual difference measure. Curr Psychol 2011;30:53-73.
30. Peterman AH, Fitchett G, Brady MJ, Hernandez L, Cella D.
Measuring spiritual well-being in people with cancer: the functional
assessment of chronic illness therapydSpiritual Well-being Scale
(FACIT-Sp). Ann Behav Med 2002;24:49-58.
31. Hammel J, Magasi S, Heinemann A, Whiteneck G, Bogner J,
Rodriguez E. What does participation mean? An insider
perspective from people with disabilities. Disabil Rehabil 2008;30:
1445-60.
32. Heinemann AW, Lai JS, Magasi S, et al. Measuring participation
enfranchisement. Arch Phys Med Rehabil 2011;92:564-71.
33. Heinemann AW, Magasi S, Bode RK, et al. Measuring enfranchise-
ment: importance of and control over participation by people with
disabilities. Arch Phys Med Rehabil 2013;94:2157-65.
34. Magasi S, Hammel J, Heinemann A, Whiteneck G, Bogner J.
Participation: a comparative analysis of multiple rehabilitation
stakeholders’ perspectives. J Rehabil Med 2009;41:936-44.
35. Watson D, Clark LA, Tellegen A. Development and validation of
brief measures of positive and negative affect: the PANAS scales. J
Pers Soc Psychol 1988;54:1063-70.
36. Salsman JM, Victorson D, Choi SW, et al. Development and vali-
dation of the positive affect and well-being scale for the neurology
quality of life (Neuro-QOL) measurement system. Qual Life Res
2013;22:2569-80.
37. Cella D, Nowinski C, Peterman A, et al. The neurology quality-of-
life measurement initiative. Arch Phys Med Rehabil 2011;92:
S28-36.
38. Cella D, Lai JS, Nowinski CJ, et al. Neuro-QOL: brief measures of
health-related quality of life for clinical research in neurology.
Neurology 2012;78:1860-7.
39. Kroenke K, Spitzer RL, Williams JB, Lowe B. The Patient Health
Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: a
systematic review. Gen Hosp Psychiatry 2010;32:345-59.
40. Bombardier CH, Kalpakjian CZ, Graves DE, Dyer JR, Tate DG,
Fann JR. Validity of the Patient Health Questionnaire-9 in assessing
major depressive disorder during inpatient spinal cord injury reha-
bilitation. Arch Phys Med Rehabil 2012;93:1838-45.
41. Tektonidou MG, Dasgupta A, Ward MM. Suicidal ideation among
adults with arthritis: prevalence and subgroups at highest risk: data
from the 2007-2008 National Health and Nutrition Examination
Survey. Arthritis Care Res (Hoboken) 2011;63:1322-33.
42. Walker J, Hansen CH, Hodges L, et al. Screening for suicidality in
cancer patients using Item 9 of the nine-item patient health ques-
tionnaire; does the item score predict who requires further assess-
ment? Gen Hosp Psychiatry 2010;32:218-20.
43. Wells TS, Horton JL, LeardMann CA, Jacobson IG, Boyko EJ. A
comparison of the PRIME-MD PHQ-9 and PHQ-8 in a large military
prospective study, the Millennium Cohort Study. J Affect Disord
2013;148:77-83.
44. Crosby AE, Han B, Ortega LA, Parks SE, Gfroerer J; Centers for
Disease Control and Prevention (CDC). Suicidal thoughts and be-
haviors among adults aged �18 yearsdUnited States, 2008-2009.
MMWR Surveill Summ 2011;60:1-22.
45. Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for
lifetime suicide attempts in the National Comorbidity Survey. Arch
Gen Psychiatry 1999;56:617-26.
46. Nam HS, Kim HR, Ha TH, Shin HI. Suicidal ideation in Korean
persons with spinal cord injury. Spinal Cord 2013;51:789-93.
47. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE.
Prevalence, severity, and comorbidity of 12-month DSM-IV disor-
ders in the National Comorbidity Survey Replication. Arch Gen
Psychiatry 2005;62:617-27.

808 C.B. McCullumsmith et al
48. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR,
Walters EE. Lifetime prevalence and age-of-onset distributions of
DSM-IV disorders in the National Comorbidity Survey Replication.
Arch Gen Psychiatry 2005;62:593-602.
49. Nock M, Hwang I, Sampson N, Kessler R. Mental disorders, co-
morbidity and suicidal behavior: results from the National Comor-
bidity Survey Replication. Mol Psychiatry 2010;15:868-76.
50. Nock MK, Green JG, Hwang I, et al. Prevalence, correlates, and
treatment of lifetime suicidal behavior among adolescents: results
from the National Comorbidity Survey Replication Adolescent
Supplement. JAMA Psychiatry 2013;70:300-10.
51. Carvalho J, Trent LR, Hopko DR. The impact of decreased envi-
ronmental reward in predicting depression severity: support for
behavioral theories of depression. Psychopathology 2011;44:242-52.
52. Wong AW, Heinemann AW, Wilson CS, et al. Predictors of partici-
pation enfranchisement following spinal cord injury: the mediating
role of depression and moderating role of demographic and injury
characteristics. Arch Phys Med Rehabil 2014;95:1106-13.
53. Johannessen-Henry CT, Deltour I, Bidstrup PE, Dalton SO,
Johansen C. Associations between faith, distress and mental adjust-
mentda Danish survivorship study. Acta Oncol 2013;52:364-71.
54. Fann JR, Bombardier CH, Richards JS, et al. Depression after
spinal cord injury: comorbidities, mental health service use,
and adequacy of treatment. Arch Phys Med Rehabil 2011;92:
352-60.
55. Holma KM, Haukka J, Suominen K, et al. Differences in incidence of
suicide attempts between bipolar I and II disorders and major
depressive disorder. Bipolar Disord 2014;16:652-61.
www.archives-pmr.org





























