Embed Size (px)
Citation preview

Journal of Consulting and Clinical Psychology1993, Vol. 61, No. 5, 743-750
Copyright 1993 by the American Psychological Association, Inc.0022-006X/93/S3.00
Nicotine Delivery Kinetics and Abuse LiabilityJack E. Henningfield and Robert M. Keenan
It is well established that nicotine meets all criteria of a highly addictive drug. However, as recognizedby the U.S. surgeon general, the nicotine delivery system itself is an important determinant of thetoxic and addictive effects engendered by nicotine use. Therefore, altering the form of nicotine dos-ing may allow for selective therapeutic action in efforts to develop safer and less addictive nicotinereplacement therapies. While it is the case that initial tobacco use often escalates to compulsiveuse accompanied by tolerance and physical dependence, this is not usually observed with nicotinereplacement therapies. These observations are consistent with laboratory data indicating that (a)nicotine polacrilex and transdermal systems deliver nicotine more slowly and at lower dose levelsthan tobacco-based forms, and (b) human data suggesting that the abuse liability of these systems issubstantially lower than that of the tobacco-based nicotine delivery systems. Because the drug dosageform can be systematically manipulated and evaluated, further research in developing alternativenicotine delivery forms may hold substantial promise in the treatment of tobacco dependence. Psy-chological research methods can play an important part in their evaluation.
It is well established that nicotine has significant potential forabuse (Henningfield, Cohen, & Slade, 1991; U.S. Departmentof Health and Human Services [USDHHS], 1988). Nicotine,like cocaine, heroin, and alcohol, is a psychoactive drug thatcan lead to abuse, it serves as a reinforcer of self-administrationbehavior in humans and animals, and it meets criteria for abuseliability on standardized tests in human volunteers (Henning-field & Nemeth-Coslett, 1988). A pharmacologic concept thatis not novel but less widely discussed is that the abuse liabilityof a psychoactive substance is partially related to the bioavail-ability of the drug and the speed of its delivery (i.e., to the kinet-ics of the drug delivery system; Farre & Cami, 1991). For exam-ple, orally ingested preparations of nicotine and cocaine havebeen used (Austin, 1978; Jarvik, Click, &Nakamura, 1970;Jo-hanson & Fischman, 1989) and are not associated with the highpotential for abuse that has been found with preparations suchas nasal insufflation or smoke inhalation, which readily deliversubstantial doses. Unfortunately, there has been little systematiclaboratory study of the importance of the drug delivery systemas a parameter of abuse liability (i.e., its addictive potential). Inthis review, we discuss differences in the pattern of nicotine in-take (kinetics) as a function of the form of delivery, with anemphasis on the influence of these different patterns of intakeon the ability of nicotine and tobacco products to produce de-pendence.
Importance of Drug Intake Pattern on DependenceThe importance of kinetics (i.e., dose and duration of drug
delivery) on abuse liability was demonstrated in a study of co-
Jack E. Henningfield and Robert M. Keenan, National Institute onDrug Abuse Addiction Research Center, Baltimore, Maryland.
Correspondence concerning this article should be addressed to JackE. Henningfield, National Institute on Drug Abuse Addiction ResearchCenter, P.O. Box 5180, Baltimore, Maryland 21224.
caine self-administration by rhesus monkeys (Balster & Schus-ter, 1973). In that study, the effects of cocaine dose and durationof drug delivery as determinants of reinforcing efficacy were ex-amined using response rates generated by fixed-interval sched-ules of reinforcement as the dependent measure. Cocaine dosesof 0.2 or 0.4 mg/kg were delivered at infusion durations rangingfrom 5 to 200 s. Notably, reinforcing efficacy was directly re-lated to cocaine dose and inversely related to the infusion dura-tion. These data are consistent with the clinical observationsthat cocaine use by means of routes of administration withmore rapid delivery are of greater abuse liability than by ad-ministration with slower forms of delivery (Johanson & Fisch-man, 1989). Similarly, deWit, Bodker, and Ambre (1992) foundthat ratings of drug liking by humans were significantly higherwhen similar peak blood levels were produced by giving a singleoral 150-mg dose of pentobarbital than by six doses of 30 mgeach given at 30-min intervals.
There have been no other experimental studies reported inthe literature that have extensively and systematically studiedthe relationship between the kinetics of a drug-delivery prepa-ration and the potential for its abuse. This is unfortunate be-cause of the importance of novel drug delivery preparations (asopposed to novel chemical entities) in patterns of drug abuse aswell as in medications development. The potential importanceof the concept with respect to nicotine was highlighted by thefollowing conclusion of the surgeon general's report on nicotineaddiction (USDHHS, 1988): "The physical characteristics ofnicotine delivery systems can affect their toxicity and addictive-ness. Therefore, new nicotine delivery systems should be evalu-ated for their toxic and addictive effects."
Although a single systematic study of nicotine delivery rateas a determinant of abuse liability has not been reported, sixforms of nicotine delivery that vary widely in their kinetics havebeen studied by the National Institute on Drug Abuse at theAddiction Research Center (ARC) by Henningfield and his col-leagues. These studies included measures of subjective effectssuch as "drug liking," "positive effects," and morphine-benze-
743

744 JACK E. HENNINGFIELD AND ROBERT M. KEENAN
drine-group scores of the ARC Inventory, which are acceptedby the U.S. Food and Drug Administration, the World HealthOrganization, and expert committees as indices of abuse liabil-ity (The Barcelona Conference, 1991; Fischman & Mello,1989). Some of these data, as well as other data from studies ofthe kinetics of various forms of nicotine delivery, will be sum-marized in this article. Taken together, these findings confirmthat the nicotine delivery system is a prominent determinant ofboth kinetics and abuse liability, with slower delivering systemsappearing to be of substantially lower abuse liability than morerapid delivery systems.
These findings have important clinical ramifications in thatnicotine replacement approaches in the form of gum or trans-dermal patches represent a major breakthrough in the fightagainst nicotine dependence (see Hughes, 1993, for a discussionof clinical issues in the use of these treatments). However, theirlimited efficacy has fueled research efforts to develop deliverysystems with kinetic profiles more similar to cigarette smokingwith respect to dosing parameters. Whereas such systems maybe required to enable some people to achieve and maintain ab-stinence from tobacco, it is possible that systems that moreclosely mimic the nicotine delivery characteristics of cigaretteswill be of increased potential to serve as primary addictingagents. Systematically obtained abuse liability data will be re-quired to determine whether such systems will need to be regu-lated differently (e.g., as psychoactive substances) than nicotinepolacrilex (gum) or nicotine transdermal delivery systems.
Reinforcing Effects of NicotineCigarette smoking is a complex behavior that over time be-
comes powerfully conditioned by various conditioning mecha-nisms. First, nicotine directly reinforces smoking behavior, andsuch reinforcement occurs hundreds of times per day and hun-dreds of thousands of times per year. Through this process, thebehaviors of seeking, lighting, and self-administering cigarettesbecome exceedingly entrenched. We may distinguish at leasttwo types of reinforcement that may be obtained from nicotine.Animal studies indicate that nicotine use provides positive rein-forcement through stimulation of nicotinic receptors, which en-genders high rates of self-administration behavior (USDHHS,1988). Furthermore, blocking the effects at these receptors bypretreatments with centrally active nicotine antagonists leadsto extinction of self-administration behavior. Subjective effectssuch as pleasure or "liking," which are assumed to be related toreinforcing effects of nicotine, have also been studied in humansand appear to be directly related to the actions of nicotine inthe brain (Henningfield, Miyasato, & Jasinski, 1985). A secondtype, negative reinforcement, is achieved through the processof relief from the nicotine withdrawal syndrome produced bychronic nicotine use. Thus, the smoker quickly learns that thevarious negative symptoms associated with even a few hours ofnicotine abstinence can be reversed by nicotine use. Researchwith nicotine gum and the transdermal patch delivery systemsconfirms that large and rapid increases in the nicotine concen-tration of the brain are not necessary to alleviate most symp-toms of tobacco withdrawal.
In addition to the direct reinforcing effects obtained fromnicotine use, its administration results in modulation of mood,
appetite, and energy metabolism, and it may provide relief fromstress and boredom (Jarvik, 1991; Perkins, 1992; USDHHS,1988). Also, sensory stimuli associated with the effects of nico-tine use themselves become immediately and powerfully rein-forcing to the user in their own right. These appear to includethe sight, feel, and odor of cigarettes themselves, as well as theeffects of various smoke constituents including nicotine in themouth, nose, and throat (Rose & Levin, 1991; USDHHS,1988). As a result, the control of cigarette smoke over behavioris accomplished by many mechanisms.
Kinetics of Alternative Nicotine Delivery Systems
Nicotine is both a water- and lipid-soluble molecule that isreadily absorbed through the skin and mucosa of the mouth andnose when applied at high concentrations or in a mildly alkalinesolution; the kinetics of several nicotine preparations have beenwell studied (USDHHS, 1988). When nicotine vapor is inhaledalong with tobacco smoke into the lungs, even the acidic smokedelivered by cigarettes is rapidly absorbed because of the con-siderable area for absorption in the alveolar capillary bed of thelung over a wide range of pH values. Nicotine administered inthe form of inhaled cigarette smoke or by rapid intravenousinjection has an initial half-life of approximately 20 min duringwhich time the drug is redistributed throughout blood, muscle,and major organs of the body. Thereafter, the metabolic half-lifeof nicotine appears to be approximately 2 hr (Benowitz, 1988;Benowitz, Jacob, Denaro, & Jenkins, 1991). For transdermallydelivered nicotine preparations, the half-life appears to be closerto 4 hr (Palmer, Bucklet, & Faulds, 1992). This may be due tothe occurrence of some localized nicotine absorption and stor-age by tissue near the patch; small amounts of nicotine are stillreleased for some time after the patch is removed.
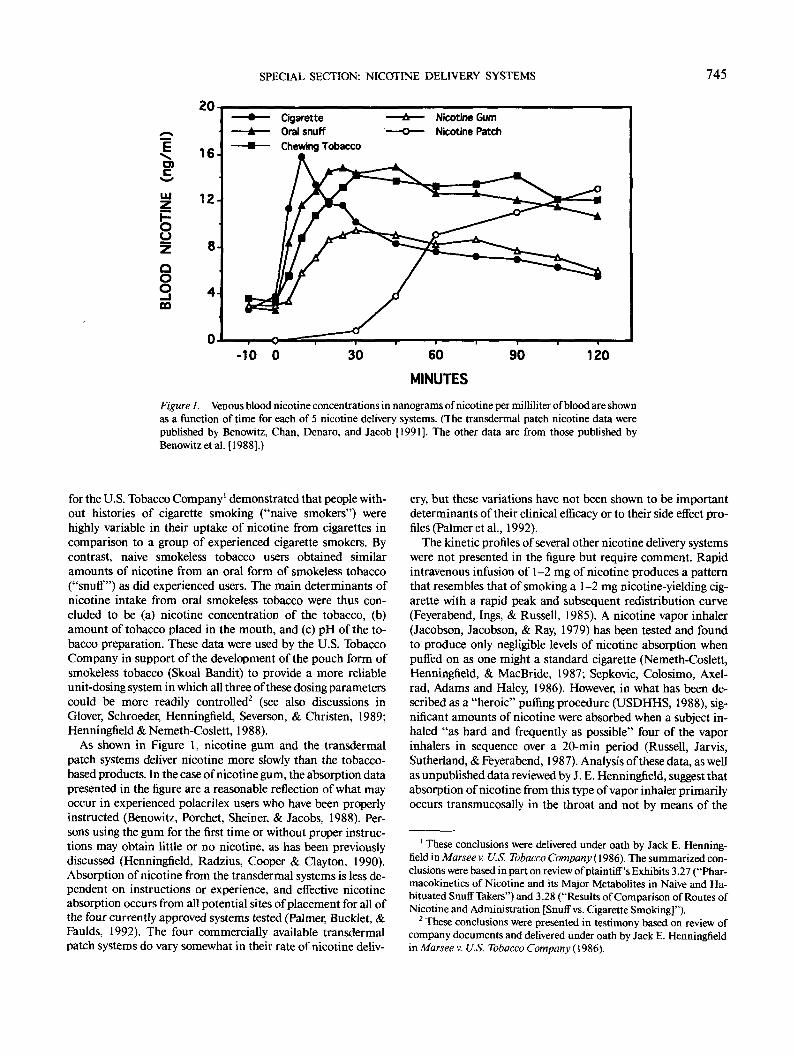
A major distinction between nicotine delivery systems withregard to their kinetic profiles is the rate of initial nicotine up-take and the arterial or venous bolus (i.e., drug concentration)created (Sachs, 1989). In cigarette smoking, inhaled smoke pro-duces a large arterial nicotine concentration relative to the ve-nous concentration, which is immediately delivered to the brainby means of the heart, thereby providing immediate drug rein-forcement that lasts for several minutes. In smokers, the arterialconcentration has been observed to be as high as 10 timesgreater than that of the venous concentration (Henningfield,London, & Benowitz, 1990). Of the various types of nicotineadministration in common use, inhaled nicotine is the onlyroute of administration known to produce a significant arterialconcentration spike that is delivered rapidly to the brain. Figure1 shows the patterns of nicotine absorption across five types ofnicotine delivery systems. Cigarette smoke inhalation producesa rapid spike in the venous blood nicotine concentration that isnot mimicked by the other forms of nicotine delivery.
The two forms of smokeless tobacco that were tested tooksomewhat more time to yield peak blood levels than cigarettesmoke inhalation. One characteristic of smokeless tobacco thatis not evident from Figure 1 may be more important in begin-ning tobacco users than in the experienced users who weretested to produce these data. Two studies that were conducted
SPECIAL SECTION: NICOTINE DELIVERY SYSTEMS 745
20
o>
iu
OO
OO
m
16-
CigaretteOral snuffChewing Tobacco
Nicotine GumNicotine Patch
60
MINUTES
90 120
Figure 1. Venous blood nicotine concentrations in nanograms of nicotine per milliliter of blood are shownas a function of time for each of 5 nicotine delivery systems. (The transdermal patch nicotine data werepublished by Benowitz, Chan, Denaro, and Jacob [1991]. The other data are from those published byBenowitzetal. [1988].)
for the U.S. Tobacco Company1 demonstrated that people with-out histories of cigarette smoking ("naive smokers") werehighly variable in their uptake of nicotine from cigarettes incomparison to a group of experienced cigarette smokers. Bycontrast, naive smokeless tobacco users obtained similaramounts of nicotine from an oral form of smokeless tobacco("snuff") as did experienced users. The main determinants ofnicotine intake from oral smokeless tobacco were thus con-cluded to be (a) nicotine concentration of the tobacco, (b)amount of tobacco placed in the mouth, and (c) pH of the to-bacco preparation. These data were used by the U.S. TobaccoCompany in support of the development of the pouch form ofsmokeless tobacco (Skoal Bandit) to provide a more reliableunit-dosing system in which all three of these dosing parameterscould be more readily controlled2 (see also discussions inGlover, Schroeder, Henningfield, Severson, & Christen, 1989;Henningfield & Nemeth-Coslett, 1988).
As shown in Figure 1, nicotine gum and the transdermalpatch systems deliver nicotine more slowly than the tobacco-based products. In the case of nicotine gum, the absorption datapresented in the figure are a reasonable reflection of what mayoccur in experienced polacrilex users who have been properlyinstructed (Benowitz, Porchet, Sheiner, & Jacobs, 1988). Per-sons using the gum for the first time or without proper instruc-tions may obtain little or no nicotine, as has been previouslydiscussed (Henningfield, Radzius, Cooper & Clayton, 1990).Absorption of nicotine from the transdermal systems is less de-pendent on instructions or experience, and effective nicotineabsorption occurs from all potential sites of placement for all ofthe four currently approved systems tested (Palmer, Bucklet, &Faulds, 1992). The four commercially available transdermalpatch systems do vary somewhat in their rate of nicotine deliv-
ery, but these variations have not been shown to be importantdeterminants of their clinical efficacy or to their side effect pro-files (Palmer etal., 1992).
The kinetic profiles of several other nicotine delivery systemswere not presented in the figure but require comment. Rapidintravenous infusion of 1-2 mg of nicotine produces a patternthat resembles that of smoking a 1-2 mg nicotine-yielding cig-arette with a rapid peak and subsequent redistribution curve(Feyerabend, Ings, & Russell, 1985). A nicotine vapor inhaler(Jacobson, Jacobson, & Ray, 1979) has been tested and foundto produce only negligible levels of nicotine absorption whenpuffed on as one might a standard cigarette (Nemeth-Coslett,Henningfield, & MacBride, 1987; Sepkovic, Colosimo, Axel-rad, Adams and Haley, 1986). However, in what has been de-scribed as a "heroic" puffing procedure (USDHHS, 1988), sig-nificant amounts of nicotine were absorbed when a subject in-haled "as hard and frequently as possible" four of the vaporinhalers in sequence over a 20-min period (Russell, Jarvis,Sutherland, & Feyerabend, 1987). Analysis of these data, as wellas unpublished data reviewed by J. E. Henningfield, suggest thatabsorption of nicotine from this type of vapor inhaler primarilyoccurs transmucosally in the throat and not by means of the
1 These conclusions were delivered under oath by Jack E. Henning-field in Marsee v. U.S. Tobacco Company (1986). The summarized con-clusions were based in part on review of plaintiff's Exhibits 3.27 ("Phar-macokinetics of Nicotine and its Major Metabolites in Naive and Ha-bituated Snuff Takers") and 3.28 ("Results of Comparison of Routes ofNicotine and Administration [Snuff vs. Cigarette Smoking]").
2 These conclusions were presented in testimony based on review ofcompany documents and delivered under oath by Jack E. Henningfieldin Marsee v. U.S. Tobacco Company (1986).
746 JACK E. HENNINGFIELD AND ROBERT M. KEENAN
alveolar capillary bed of the lung as occurs when cigarettesmoke is inhaled. It appears likely that particles such as thosethat comprise cigarette smoke are necessary for deep airwaypenetration of the nicotine vapor particles.
The third system is the device (Premier) developed by theR. J. Reynolds Tobacco Company and patented for use in thedelivery of various pharmacologically active materials, includ-ing nicotine (Cone & Henningfield, 1989; R. J. Reynolds To-bacco Company, 1988). Nicotine absorption following use ofthis device appears to most closely resemble that of cigarettes,although with an even more rapid production of peak nicotinelevels, compared with cigarette smoking. Apparently, the addi-tion of glycerol in amounts roughly equivalent to the "tar" de-livered by a cigarette functioned to enable deep airway penetra-tion of the nicotine vapor. Although this is a viable nico-tine delivery device, widespread use of this product was notachieved, and the device is no longer marketed.
A variety of other systems are currently under developmentfor use as nicotine replacement agents (cf., Russell, 1991). Twoof these involve the delivery of nicotine in the forms of nasalspray and intranasal aerosol to the nasal passages for insuffla-tion (Perkins, Grobe, Stiller, Fonte, & Goettler, 1992; Pomer-leau, Flessland, Pomerleau, & Hariharan, 1992; Sutherland,Russell, Stapleton, Feyerabend, & Ferno, 1992). These devicesdeliver metered doses of nicotine and likely more closely mimicthe kinetics of cigarette smoking. Although these devices arenot approved for use, early findings suggest that these systemsare able to decrease the desire to smoke cigarettes. The results ofearly tests are encouraging, but further testing of these productsneed to be performed to determine their safety, efficacy, andabuse liability.
Nicotine Concentration Produced by Cigarette Smoking
The data shown in Figure 1 illustrate the rapid venous bloodnicotine concentrations that occur after cigarette smoking.However, these measures may greatly underestimate the level ofnicotine that might occur in arterial blood immediately aftersmoke inhalation. The arterial drug concentration determinesthe amount of drug delivered to the brain, the primary site ofnicotine's actions. Because inhaled nicotine is almost immedi-ately absorbed through the alveolar capillary bed of the lungand pumped by means of the left ventricle of the heart directlyto the brain, it has been variously estimated that nicotine dosesfrom a cigarette may reach the brain within 7 to 19 s of puffing(Benowitz, 1992; Russell & Feyerabend, 1978). Moreover, thefindings from a study measuring arterial blood nicotine concen-tration after volunteers smoked cigarettes suggested that arte-rial blood levels would be more concentrated than those in ve-nous blood (Armitageetal., 1975).
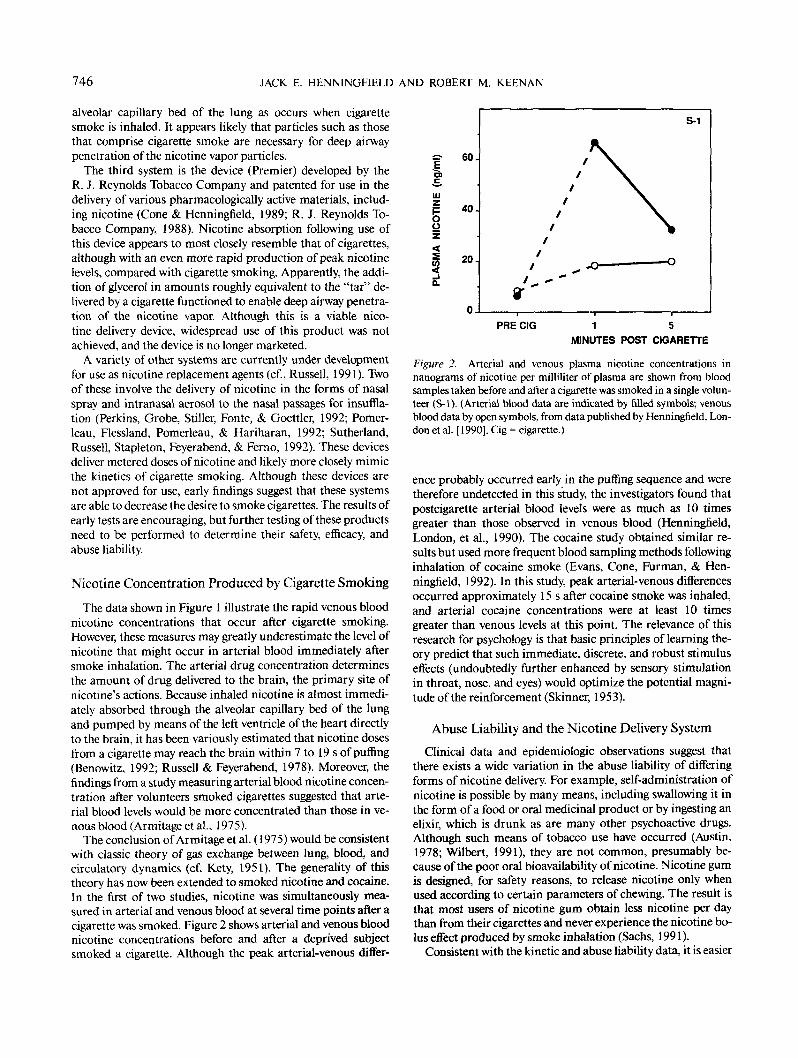
The conclusion of Armitage et al. (1975) would be consistentwith classic theory of gas exchange between lung, blood, andcirculatory dynamics (cf. Kety, 1951). The generality of thistheory has now been extended to smoked nicotine and cocaine.In the first of two studies, nicotine was simultaneously mea-sured in arterial and venous blood at several time points after acigarette was smoked. Figure 2 shows arterial and venous bloodnicotine concentrations before and after a deprived subjectsmoked a cigarette. Although the peak arterial-venous differ-
UJI -oZ<i 20<
S-1
PRE CIG 1 5MINUTES POST CIGARETTE
Figure 2. Arterial and venous plasma nicotine concentrations innanograms of nicotine per milliliter of plasma are shown from bloodsamples taken before and after a cigarette was smoked in a single volun-teer (S-1). (Arterial blood data are indicated by filled symbols; venousblood data by open symbols, from data published by Henningfield, Lon-don et al. [1990]. Cig = cigarette.)
ence probably occurred early in the puffing sequence and weretherefore undetected in this study, the investigators found thatpostcigarette arterial blood levels were as much as 10 timesgreater than those observed in venous blood (Henningfield,London, et al., 1990). The cocaine study obtained similar re-sults but used more frequent blood sampling methods followinginhalation of cocaine smoke (Evans, Cone, Furman, & Hen-ningfield, 1992). In this study, peak arterial-venous differencesoccurred approximately 15 s after cocaine smoke was inhaled,and arterial cocaine concentrations were at least 10 timesgreater than venous levels at this point. The relevance of thisresearch for psychology is that basic principles of learning the-ory predict that such immediate, discrete, and robust stimuluseffects (undoubtedly further enhanced by sensory stimulationin throat, nose, and eyes) would optimize the potential magni-tude of the reinforcement (Skinner, 1953).
Abuse Liability and the Nicotine Delivery SystemClinical data and epidemiologic observations suggest that
there exists a wide variation in the abuse liability of differingforms of nicotine delivery. For example, self-administration ofnicotine is possible by many means, including swallowing it inthe form of a food or oral medicinal product or by ingesting anelixir, which is drunk as are many other psychoactive drugs.Although such means of tobacco use have occurred (Austin,1978; Wilbert, 1991), they are not common, presumably be-cause of the poor oral bioavailability of nicotine. Nicotine gumis designed, for safety reasons, to release nicotine only whenused according to certain parameters of chewing. The result isthat most users of nicotine gum obtain less nicotine per daythan from their cigarettes and never experience the nicotine bo-lus effect produced by smoke inhalation (Sachs, 1991).
Consistent with the kinetic and abuse liability data, it is easier

SPECIAL SECTION: NICOTINE DELIVERY SYSTEMS 747
for most people to abstain from gum than cigarettes, and with-drawal symptoms are of lower magnitude following abstinencefrom nicotine gum or smokeless tobacco (Sachs, 1991;USDHHS, 1988). Similarly, some data suggest that the propor-tion of smokeless tobacco users who are occasional users is sub-stantially higher than that observed for cigarettes. Whereas ap-proximately 10% to 15% of current cigarette smokers smokefewer than 5 cigarettes per day (Evans, Gilpin, et al., 1992;USDHHS, 1988), Ernster et al. (1990) found that approxi-mately 33% of baseball players who actively used smokeless to-bacco during the approximately 8-month training and playingseason abstained during the off-season. Nonetheless, smokelesstobacco is highly addictive (USDHHS, 1986), and the possibil-ity that it is less addictive than cigarettes may be as clinicallyrelevant as the difference between falling from a 20- and a 16-story building. Other characteristics of smokeless tobacco use,including bioavailability profiles and sensory characteristics,appear to maximize its addictive potential (cf. Henningfield &Nemeth-Coslett, 1988).
Laboratory procedures, some borrowed from experimentalpsychology, have been developed to quantify the abuse liabilityof various chemical types and drug dosage forms. These havebeen described in detail in various publications (Fischman &Mello, 1989; Henningfield, Cohen, &Heishman, 1992;Jasinski& Henningfield, 1989). In one type of study, volunteers are per-mitted to self-administer the drug, often under conditions inwhich there is a choice to self-administer the drug under evalu-ation or a control substance such as placebo. Such data permitdirect assessment of the reinforcing effects of the drug (Hen-ningfield, Lukas, & Bigelow, 1986). Another strategy involvesthe assessment of subjective effects produced by drug admin-istration and provides an indirect means of estimating the rein-forcing potential of a drug (Jasinski & Henningfield, 1989). Inbrief under standardized test conditions, a range of doses of thetest compound is administered to individuals with histories ofabuse of a variety of drugs, or at least of the drug type or typesin question. The subjective responses are then evaluated onstandardized test instruments. The most basic is the Drug Lik-ing scale of the Single Dose Questionnaire (Jasinski & Henning-field, 1989), which is sometimes presented as a visual line ana-logue scale of positive effects. A variety of other measures andassessment techniques are used to ensure reliability and validity(Jasinski & Henningfield, 1989).
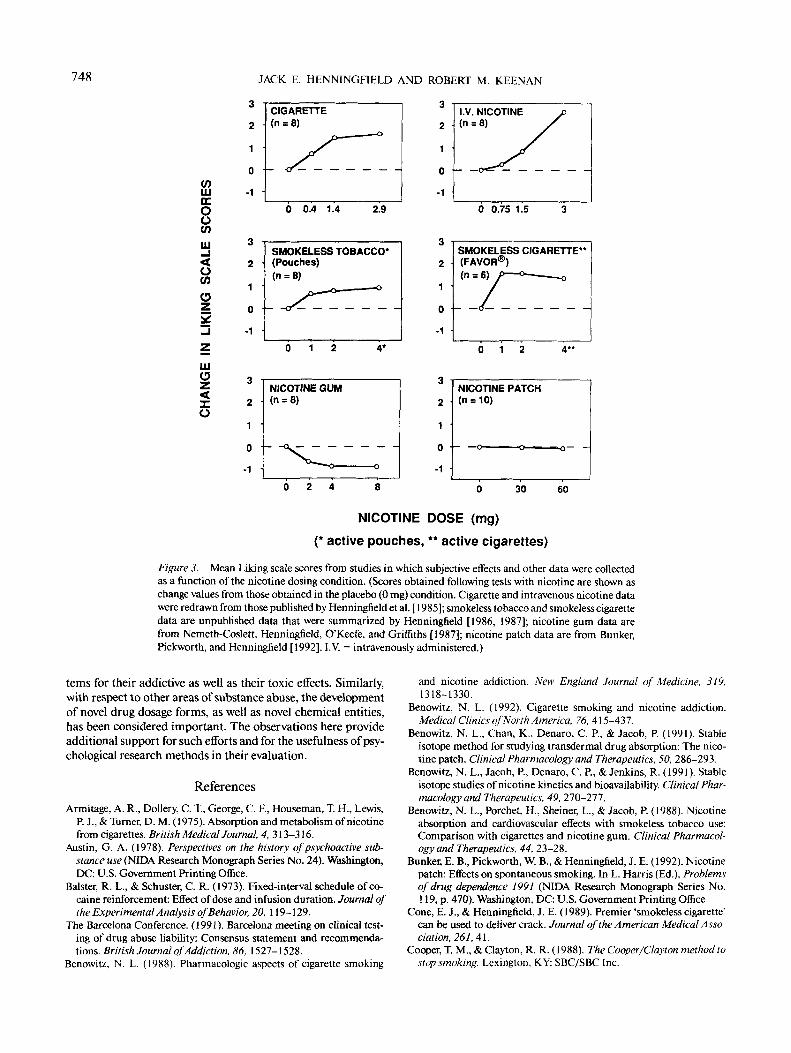
At the ARC, six different forms of nicotine delivery were eval-uated with these subjective effects assessment procedures (un-published). The main findings are summarized in Figure 3. Asshown in Figure 3, Liking scores were elevated by the rapidlydelivering forms of nicotine produced by tobacco consump-tion, as well as by intravenous injection and inhalation of nico-tine vapor. However, scores were unaffected or decreased by nic-otine gum and a transdermal patch system. Such data are con-sistent with the clinical and epidemiological data discussedearlier and may be interpreted as indicating low abuse liabilityof the transdermal and polacrilex systems.
It appears unlikely that intravenous nicotine would ever posea problem of widespread abuse, because desired effects aremore controllable by the user and more readily obtained bysmoke inhalation (also circumventing the safety and comfortproblems produced by intravenous administration). Vapor in-
haler systems will require testing for abuse liability because, al-though they may be low in the dose of nicotine delivered (as theone illustrated in Figure 3), they are high in conditioned andperipheral effects that are considered desirable to cigarettesmokers (Nemeth-Coslett, Henningfield, & MacBride, 1987).As evidenced in Figure 3, even a vapor inhaler system with poornicotine bioavailability may still produce effects characteristicof an abusable substance. Presumably, the inhalation route op-timizes the reinforcing effects of the substance through sensorystimulation. It is also possible that a small amount of nicotinereaching the alveolar bed may produce a nicotine bolus that hasnot been measured in the studies conducted to date (in whichonly venous blood levels have been determined) (Benowitz,1992; Henningfield &Stitzer, 1991; USDHHS, 1988).
As was suggested, it must be emphasized that differences inabuse liability among different drug delivery systems cannot bepredicted only on the basis of their kinetic profiles. Factors suchas ease of use and sensory properties can also affect the abuseliability of a substance. However, bioavailability is a character-istic that was manipulated to the advantage of the smokelesstobacco industry in its development of starter products, the in-dustry term for products low in nicotine, low in pH, and highlyflavored to promote the initiation and spread of smokeless to-bacco addiction (see Footnote 2).
Finally, to determine that certain forms of nicotine deliveryare lower in abuse liability than others is not to conclude thatthey are devoid of abuse liability. Some people do have difficultyin learning to abstain from nicotine polacrilex but may be with-drawn with systematic dose reduction or substitution proce-dures (Cooper & Clayton, 1988; Waranch, Henningfield, & Ed-munds, 1988). Others may require extended, if not lifelong nic-otine replacement therapy when they give up tobacco(Henningfield & Stitzer, 1991). However, it appears that princi-ples of selective medications development can proceed as ra-tionally when the issue is addiction potential as it can when theissue is cardiotoxicity. Both kinds of consequences of nicotineexposure appear to be related to nicotine delivery system andto the kinetics of the drug dosage form (USDHHS, 1988).
ConclusionAll forms of nicotine delivery are not equitoxic or equiaddic-
tive. In fact, a major activity in the development of pharmaceu-tical products to enable people to quit smoking is the develop-ment of nicotine delivery systems with reduced toxicity and ad-dictiveness. As was suggested by the data presented herein,variation in the bioavailability and ease of nicotine extractionappear to be important determinants of the abuse liability ofthe nicotine delivering preparation, whether a tobacco productor a nicotine replacement therapy.
These observations do not imply that all rapid nicotine deliv-ering preparations are without medical value. It is likely that arange of nicotine-delivering types of medications will be neededto help the diverse range of nicotine-dependent tobacco usersachieve and maintain abstinence from the most deadly and ad-dictive forms of nicotine delivery in common use (i.e., cigarettesand smokeless tobacco; Henningfield & Stitzer, 1991). However,the data here do support the recommendation of the surgeongeneral (USDHHS, 1988) to test novel nicotine delivery sys-
748 JACK E. HENNINGFIELD AND ROBERT M. KEENAN
COUlDCOOCOLLJ
OCOCJ5
LLJO
O
3
2
1
0
-1
CIGARETTE(n = 8)
0 0.4 1.4 2.9
3
2
1
0
-1
SMOKELESS TOBACCO*(Pouches)(n = 8)
NICOTINE GUM(n = 8)
-1 •0 0.75 1.5
3
2
1
0
-1
SMOKELESS CIGARETTE'(FAVOR®)
0 1 2 4*
O
2
1
-1
NICOTINE PATCH(n = 10)
30 60
NICOTINE DOSE (mg)(* active pouches, ** active cigarettes)
Figure 3. Mean Liking scale scores from studies in which subjective effects and other data were collectedas a function of the nicotine dosing condition. (Scores obtained following tests with nicotine are shown aschange values from those obtained in the placebo (0 mg) condition. Cigarette and intravenous nicotine datawere redrawn from those published by Henningfield et al. [ 1985]; smokeless tobacco and smokeless cigarettedata are unpublished data that were summarized by Henningfield [1986, 1987]; nicotine gum data arefrom Nemeth-Coslett, Henningfield, O'Keefe, and Griffiths [1987]; nicotine patch data are from Bunker,Pickworth, and Henningfield [1992]. I.V. = intravenously administered.)
terns for their addictive as well as their toxic effects. Similarly,with respect to other areas of substance abuse, the developmentof novel drug dosage forms, as well as novel chemical entities,has been considered important. The observations here provideadditional support for such efforts and for the usefulness of psy-chological research methods in their evaluation.
ReferencesArmitage, A. R., Dollery, C. T., George, C. K, Houseman, T. H., Lewis,
P. J., & Turner, D. M. (1975). Absorption and metabolism of nicotinefrom cigarettes. British MedicalJournal, 4, 313-316.
Austin, G. A. (1978). Perspectives on the history of psychoactive sub-stance use (NIDA Research Monograph Series No. 24). Washington,DC: U.S. Government Printing Office.
Balster, R. L., & Schuster, C. R. (1973). Fixed-interval schedule of co-caine reinforcement: Effect of dose and infusion duration. Journal ofthe Experimental Analysis of Behavior, 20, 119-129.
The Barcelona Conference. (1991). Barcelona meeting on clinical test-ing of drug abuse liability: Consensus statement and recommenda-tions. British Journal of Addiction, 86, 1527-1528.
Benowitz, N. L. (1988). Pharmacologic aspects of cigarette smoking
and nicotine addiction. New England Journal of Medicine, 319,1318-1330.
Benowitz, N. L. (1992). Cigarette smoking and nicotine addiction.Medical Clinics of North America, 76, 415-437.
Benowitz, N. L., Chan, K., Denaro, C. P., & Jacob, P. (1991). Stableisotope method for studying transdermal drug absorption: The nico-tine patch. Clinical Pharmacology and Therapeutics, 50, 286-293.
Benowitz, N. L., Jacob, P., Denaro, C. P., & Jenkins, R. (1991). Stableisotope studies of nicotine kinetics and bioavailability. Clinical Phar-macology and Therapeutics, 49, 270-277.
Benowitz, N. L., Porchet, H., Sheiner, L., & Jacob, P. (1988). Nicotineabsorption and cardiovascular effects with smokeless tobacco use:Comparison with cigarettes and nicotine gum. Clinical Pharmacol-ogy and Therapeutics, 44, 23-28.
Bunker, E. B., Pickworth, W. B., & Henningfield, J. E. (1992). Nicotinepatch: Effects on spontaneous smoking. In L. Harris (Ed.), Problemsof drug dependence 1991 (NIDA Research Monograph Series No.119, p. 470). Washington, DC: U.S. Government Printing Office.
Cone, E. J., & Henningfield, J. E. (1989). Premier 'smokeless cigarette'can be used to deliver crack. Journal of the American Medical Asso-ciation, 261,41.
Cooper, T. M., & Clayton, R. R. (1988). The Cooper/Clayton method tostop smoking. Lexington, KY: SBC/SBC Inc.
SPECIAL SECTION: NICOTINE DELIVERY SYSTEMS 749
deWit, H., Bodker, B., & Ambre, J. (1992). Rate of increase of plasmadrug level influences subjective response in humans. Psychopharma-cology, 107, 352-358.
Ernster, V. L., Grady, D. G., Greene, J. C, Walsh, M., Robertson, P.,Daniels, T. E., Benowitz, N. L., Siegel, D., Gerbert, B., & Hauck,W. W. (1990). Smokeless tobacco use and health effects among base-ball players. Journal of the American Medical Association, 264, 218-224.
Evans, N. J., Gilpin, E., Pierce, J. P., Burns, D. M., Borland, R., John-son, M., et al. (1992). Occasional smoking among adults: Evidencefrom the California tobacco survey. Tobacco Control, 1, 169-175.
Evans, S. M., Cone, E. J., Furman, W., & Henningneld, J. E. (1992).A comparison of the arterial kinetics of smoking and intravenouscocaine. In L. S. Harris (Ed.), Problems of drug dependence 1992(NIDA Research Monograph Series No. 119). Washington, DC: U.S.Government Printing Office.
Farre, M., & Cami, J. (1991). Pharmacokinetic considerations in abuseliability evaluation. British Journal of Addiction, 86, 1601-1606.
Feyerabend, C., Ings, R. M. J., & Russell, M. A. H. (1985). Nicotinepharmacokinetics and its application to intake from smoking. BritishJournal of Clinical Pharmacology, 19, 239-247.
Fischman, M. W, & Mello, N. K. (Eds.). (1989). Testing for abuse lia-bility in humans (NIDA Research Monograph No. 92). Washington,DC: U.S. Government Printing Office.
Glover, E. D., Schroeder, K., Henningneld, J. E., Severson, H. H., &Christen, A. G. (1989). An interpretative review of smokeless tobaccoresearch in the United States: Part II. Journal of Drug Education, 19,1-19.
Henningneld, J. E. (1986). Annual progress report: Biology of depen-dence and abuse potential assessment laboratory. Annual report ofthe addiction research center (p. 37). Rockville, MD: Department ofHealth and Human Services.
Henningfield, J. E. (1987). Annual progress report: Biology of depen-dence and abuse potential assessment laboratory. Annual report ofthe addiction research center (p. 34). Rockville, MD: Department ofHealth and Human Services.
Henningfield, J. E., Cohen, C., & Heishman, S. J. (1992). Quantitativecomparison of drug self-administration in animals and humans. In:J. Cohen-Yanez, J. L. Maezcua-Vastelum, & J. E. Villarei (Eds.),Drug dependence from the molecule to the social level (pp. 25-33).New York: Elsevier Science.
Henningfield, J. E., Cohen, C., & Slade, J. D. (1991). Is nicotine moreaddictive than cocaine? British Journal of Addiction, 86, 565-569.
Henningfield, J. E., London, E. D., & Benowitz, N. L. (1990). Arterio-venous differences in plasma concentration of nicotine after cigarettesmoking. Journal of the American Medical Association, 263, 2049-2050.
Henningneld, J. E., Lukas, S. E., & Bigelow, G. E. (1986). Human stud-ies of drugs as reinforcers. In S. R. Goldberg & I. P. Stolerman (Eds.),Behavioral analysis of drug dependence (pp. 69-112). New \brk: Ac-ademic Press.
Henningfield, J. E., Miyasato, K., & Jasinski, D. R. (1985). Abuse lia-bility and pharmacodynamic characteristics of intravenous and in-haled nicotine. Journal of Pharmacology and Experimental Thera-peutics, 234, 1-12.
Henningfield, J. E., & Nemeth-Coslett, R. (1988). Nicotine depen-dence: Interface between tobacco and tobacco-related disease. Chest,93, 37S-55S.
Henningfield, J. E., Radzius, A., Cooper, T. M., & Clayton, R. R. (1990).Drinking coffee and carbonated beverages blocks absorption of nico-tine from nicotine polacrilex gum. Journal of the American MedicalAssociation, 264, 1560-1564.
Henningfield, J. E., & Stitzer, M. L. (Eds.). (1991). New developments innicotine-delivery systems. New York: Cortland Communications.
Hughes, J. R. (1993). Pharmacotherapy for smoking cessation: Unvali-
dated assumptions, anomalies, and suggestions for future research.Journal of Consulting and Clinical Psychology, 67,751 -760.
Jacobson, N. L., Jacobson, A. A., & Ray, J. P. (1979). Non-combustiblecigarette: Alternative method of nicotine delivery [Abstract]. Chest,76, 355-356.
Jarvik, M. E. (1991). Beneficial effects of nicotine. British Journal ofAddiction, 86, 571-575.
Jarvik, M. E., Glick, S. D., & Nakamura, R. K. (1970). Inhibition ofcigarette smoking by orally administered nicotine. Clinical Pharma-cology and Therapeutics, 11, 574-576.
Jasinski, D. R., & Henningfield, J. E. (1989). Human abuse liabilityassessment by measurement of subjective and physiological effects.In M. W. Fischman & N. K. Mello (Eds.), Testing for abuse liabilityof drugs in humans (NIDA Research Monograph No. 92, pp. 73-100). Washington, DC: U.S. Government Printing Office.
Johanson, C. E., & Fischman, M. W. (1989). The pharmacology of co-caine related to its abuse. Pharmacological Reviews, 41, 3-52.
Kety, S. S. (1951). The theory and application of the exchange of inertgas at the lungs and tissues. Pharmacological Reviews, 3, 1-41.
Marsee v. U.S. Tobacco Company, No. Civ. 84-2777 R (W. D. Okla.,1986).
Nemeth-Coslett, R., Henningfield, J. E., & MacBride, S. (1987). Effectsof inhaled nicotine vapor from smokeless cigarettes. PharmacologyBiochemistry and Behavior, 27, 592.
Nemeth-Coslett, R., Henningfield, J. E., O'Keefe, M. K., & Griffiths,R. R. (1987). Nicotine gum: Dose-related effects on cigarette smok-ing and subjective ratings. Psychopharmacology, 92, 424-430.
Palmer, K. J., Bucklet, M. M., & Faulds, D. (1992). Transdermal nico-tine: A review of its pharmacodynamic and pharmacokinetic proper-ties, and therapeutic efficacy as an aid to smoking cessation. Drugs,44, 498-529.
Perkins, K. A. (1992). Metabolic effects of cigarette smoking. Journal ofApplied Physiology, 72, 401-409.
Perkins, K. A., Grobe, J. E., Stiller, R. L., Fonte, C., & Goettler, J. E.(1992). Nasal spray nicotine replacement suppresses cigarette smok-ing behavior and desire. Clinical Pharmacology and Therapeutics,52, 627-634.
Pomerleau, O. F., Flessland, K. A., Pomerleau, C. S., & Hariharan, M.(1992). Controlled dosing of nicotine via an Intranasal NicotineAerosol Delivery Device (INADD). Psychopharmacology, 108, 519-526.
R. J. Reynolds Tobacco Company (1988). New cigarette prototypes thatheat instead of burn tobacco. Winston-Salem, NC: R. J. ReynoldsTobacco Co.
Rose, J. E., & Levin, E. D. (1991). Inter-relationships between condi-tioned and primary reinforcement in the maintenance of cigarettesmoking. British Journal of Addiction, 86, 605-609.
Russell, M. A. H. (1991). The future of nicotine replacement. BritishJournal of Addiction, 86, 653-658.
Russell, M. A. H., & Feyerabend, C. (1978). Cigarette smoking: A de-pendence on high-nicotine boli. Drug Metabolism Reviews, 80, 29-57.
Russell, M. A. H., Jarvis, M. J., Sutherland, G., & Feyerabend, C.(1987). Nicotine replacement in smoking cessation, absorption ofnicotine vapor from smoke-free cigarettes. Journal of the AmericanMedical Association, 257, 3262-3265.
Sachs, D. P. L. (1989). Nicotine polacrilex: Practical use requirements.Current Pulmonology, 10, 141-157.
Sachs, D. P. L. (1991). Advances in smoking cessation treatment. Cur-rent Pulmonology, 12, 139-198.
Sepkovic, D. W., Colosimo, S. G., Axelrad, C. M., Adams, J. D., &Haley, N. J. (1986). The delivery and uptake of nicotine from an aero-sol rod. American Journal of Public Health, 76, 1343-1344.
Skinnei; B. F. (1953). Science and human behavior. New York: The Free Press.Sutherland, G., Russell, M. A. H., Stapleton, J., Feyerabend, C., &
750 JACK E. HENNINGFIELD AND ROBERT M. KEENAN
Ferno, O. (1992). Nasal nicotine spray: A rapid nicotine delivery sys-tem. Psyehopharmacology, 108, 512-518.
U.S. Department of Health and Human Services. (1986). The healthconsequences of using smokeless tobacco. A report of the advisorycommittee to the surgeon general (DHHS, PHS, NIH Pub. No. 86-2874). Washington, DC: U.S. Government Printing Office.
U.S. Department of Health and Human Services. (1988). The healthconsequences of smoking: Nicotine addiction. A report of the surgeongeneral (DHHS Pub. No. CDC 88-8406). Washington, DC: U.S.Government Printing Office.
Waranch, H. R., Henningfield, J. E., & Edmunds, M. (1988). Elimina-
tion of nicotine gum use following successful replacement therapy forcigarette smoking. Lancet, 2, 49-50.
Wilbert, J. (1991). The ethnopharmacology of tobacco in native SouthAmerica. In F. Aldkofer & K. Thurau (Ed.), Effects of nicotine onbiological systems: Advances in pharmacological sciences. Basel,Switzerland: Birkhauser Verlag.
Received September 25, 1992Revision received December 1, 1992
Accepted February 8, 1993 •
Six Editors Appointed, 1995-2000
The Publications and Communications Board of the American Psychological Associationannounces the appointment of six new editors for 6-year terms beginning in 1995. As ofJanuary 1, 1994, manuscripts should be directed as follows:
• For the Journal of Abnormal Psychology, submit manuscripts to Milton E. Strauss,PhD, Department of Psychology, Case Western Reserve University, 10900 EuclidAvenue, Cleveland, Ohio 44106-7123.
• For the Journal of Applied Psychology, submit manuscripts to Philip Bobko, PhD,Editor, Journal of Applied Psychology, P.O. Box 130, Skillman, New Jersey08558.
• For the Journal of Comparative Psychology, submit manuscripts to Charles T.Snowdon, PhD, Department of Psychology, University of Wisconsin, 1202 WestJohnson Street, Madison, Wisconsin 53706-1696.
• For the Attitudes and Social Cognition section of the Journal of Personality andSocial Psychology, submit manuscripts to Arie W. Kruglanski, PhD, Departmentof Psychology, University of Maryland, College Park, Maryland 20742.
• For Professional Psychology: Research and Practice, submit manuscripts toPatrick H. DeLeon, PhD, JD, Editor, Professional Psychology: Research andPractice, APA, Room 3084, 750 First Street, NE, Washington, DC 20002-4242.
• For Psychological Review, submit manuscripts to Robert A. Bjork, PhD, Psycho-logical Review, Department of Psychology, University of California, Los Angeles,California 90024-1563.
Manuscript submission patterns make the precise date of completion of 1994 volumesuncertain. The current editors, Susan Mineka, PhD; Neal Schmitt, PhD; Gordon G. Gallup,PhD; Abraham Tesser, PhD; Ursula Delworth, PhD; and Walter Kintsch, PhD, respectively,will receive and consider manuscripts until December 31,1993. Should any 1994 volumesbe completed before that date, manuscripts will be redirected to the new editors forconsideration in 1995 volumes.





























