Embed Size (px)
Citation preview
MRI features of
Nonischemic dilated cardiomyopathies
and its clinical correlation.
PROJECT REPORT
Submitted during the course of DM Cardiology by
Dr. DIBYA RANJAN BEHERA
DM Trainee
DEPARTMENT OF CARDIOLOGY
Jan 2015 – Dec 2017
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY
TRIVANDRUM, KERALA
ii | P a g e
TITLE
MRI features of
Nonischemic dilated cardiomyopathies
and its clinical correlation.
Principal Investigator:
Dr. Dibya Ranjan Behera
Senior Resident,
Department of Cardiology, SCTIMST
Guide:
Dr. Ajit Kumar V.K.,
Professor and Head
Department of Cardiology, SCTIMST
iii | P a g e
DECLARATION
I hereby declare that this thesis titled “MRI features of Nonischemic Dilated
cardiomyopathies and its clinical correlation” has been prepared by me
under the capable supervision and guidance of Dr. Ajit Kumar V. K., Professor
and Head, Department of Cardiology, Sree Chitra Tirunal Institute for Medical
Sciences & Technology, Thiruvananthapuram.
Date: Dr. Dibya Ranjan Behera,
Place: Thiruvananthapuram DM cardiology resident,
Department of Cardiology SCTIMST,
Thiruvananthapuram.
iv | P a g e
CERTIFICATE
This is to certify that this thesis titled “MRI features of Nonischemic Dilated
cardiomyopathies and its clinical correlation”, is a bonafide work of Dr. Dibya
Ranjan Behera, DM Cardiology Resident and has been done under my direct
guidance at Sree Chitra Tirunal Institute for Medical Sciences & Technology,
Thiruvananthapuram. He has shown keen interest in preparing this project.
Date: Dr. Ajit Kumar V.K.,
Place: Thiruvananthapuram Professor and Head
Department of Cardiology,
SCTIMST
v | P a g e
CERTIFICATE
This is to certify that this thesis titled “MRI features of Nonischemic
Dilated cardiomyopathies and its clinical correlation”, is a bonafide work
of Dr. Dibya Ranjan Behera, DM Cardiology Resident and has been done
under my direct guidance at Sree Chitra Tirunal Institute for Medical Sciences
& Technology, Thiruvananthapuram. He has shown keen interest in preparing
this project.
Date: Dr. Ajit Kumar V.K.,
Place: Thiruvananthapuram Professor and Head
Department of Cardiology,
SCTIMST
vi | P a g e
ACKNOWLEDGEMENT
It is a genuine pleasure to express my deep sense of thanks and
gratitude to my mentor and guide Dr. Ajit Kumar V.K., Professor and
head, Department of Cardiology, SCTIMST for his valuable inputs,
expertise knowledge and continued support to accomplish this project.
I owe a deep sense of gratitude to Dr. T.R. Kapilamoorthy and Dr.
Anees T. for their constant guidance, encouragement and immense support
throughout the project.
I am very grateful to Dr. Jagan Mohan Tharakan for his inspiring
attitude, and amicable nature which helped me in shaping up this thesis.
I take this opportunity to record my sincere thanks to all the faculty
members of Department of Cardiology, SCTIMST for their critical review
of the thesis, besides their help in innumerable ways which has made this
thesis possible.
I am thankful to all my fellow colleagues in the Department of
Cardiology, SCTIMST for their help and guidance.
My sincere thanks to technical, nursing, medical records department
and computer division staff of SCTIMST for their extreme co-operation
and support.
I would like to express my gratitude to my parents Mr. Ramesh
Chandra Behera and Mrs. Suhasini Behera for their encouragement, my
supportive wife Dr. Abhilipsa Acharya, who is always at my side when I
needed her, and my son Kousthuv, who served as my inspiration.
Above all, to the Great Almighty, the author of knowledge and
wisdom, for strength and peace of mind he bestowed upon me.
Dibya Ranjan Behera
vii | P a g e
Table of contents
1. Introduction 1
2. Review of literature 2
3. Aim and Objective 18
4. Methods 19
5. Results 24
6. Discussion 55
7. Limitations 64
8. Conclusion 65
9. Bibliography 66
10. Annexure
Abbreviation 75
Proforma 76
1 | P a g e
INTRODUCTION
Non-ischemic dilated cardiomyopathy (NIDCM) is the most common form of
cardiomyopathy. Till now transthoracic echocardiography has been the first line of imaging
modality to diagnose cardiomyopathy. But it has its own limitations. Cardiac MRI (CMR)
is increasingly recognized as a noninvasive test of paramount importance in NIDCM. It
not only helps in accurate diagnosis of NIDCM, also helps in differentiating its from
ischemic cardiomyopathy. It has the ability to differentiate and diagnose various forms of
NIDCM. Observational studies so far has shown that the CMR helps in risk stratification
based on presence of late gadolinium enhancement (LGE). Presence of LGE has been
shown as poor prognostic marker in majority of studies with few exception. Thus LGE-
CMR may help in further risk stratification in NIDCM patients beyond conventional risk
markers, which may have further therapeutic implication.
So the current study was contemplated to prove or disprove the above observations.
Surprisingly, there is no data from our country also regarding this.
2 | P a g e
REVIEW OF LITERATURE
Cardiomyopathies are chronic progressive myocardial disorders with a distinct
pattern of morphological, functional and electrophysiological changes. The expert
consensus panel (2006) of the American Heart Association proposes the following
definition: “Cardiomyopathies are a heterogeneous group of diseases of the myocardium
associated with mechanical and/or electrical dysfunction that usually (but not invariably)
exhibit inappropriate ventricular hypertrophy or dilatation and are due to a variety of causes
that frequently are genetic. Cardiomyopathies are either confined to the heart or are part of
generalized systemic disorders, often leading to cardiovascular death or progressive heart
failure-related disability.” (1)
Dilated cardiomyopathy (DCM) represents the most common cardiomyopathy. (1)
Dilated cardiomyopathy is characterized by dilatation and impaired contraction of the left
ventricle or both ventricles, in which the degree of myocardial dysfunction is not explained
by the abnormal loading conditions or the extent of ischemic damage. Non ischemic DCM
(NIDCM) is defined as depressed systolic function (left ventricular ejection fraction (LV-
EF) <50%) on a non-CMR study in the absence of significant coronary artery disease
(defined as >50% luminal stenosis on coronary angiography and/or a history of coronary
revascularisation or myocardial infarction), valvular disease, hypertensive heart disease
(1995 WHO/International Society and Federation of Cardiology criteria.) (2)
It’s of mainly 2 types.
3 | P a g e
Primary forms - genetic, acquired, or mixed conditions in which the pathological
involvement is predominantly limited to the myocardium and associated with a strong
genetic inheritance in idiopathic cases (≈30%of patients).
In secondary DCM -systemic affections from autoimmune, cytotoxic, infective or
metabolic diseases.
Recognition and differentiation of the underlying pathological substrate leading to
ventricular dilatation may be crucial not only to specifically the target patients therapy
(e.g., treatment of heart failure symptoms versus revascularization versus
immunosuppressive and/or antiviral) but also for better individual risk stratification
because of the extremely variable prognostic implications associated with the different
forms of disease.(3,4)
Routine diagnostic imaging workup of patients with DCM (including
echocardiography, selective coronary angiography, and, when indicated, endomyocardial
biopsy) has been integrated in the last few years with the use of cardiac magnetic resonance
(CMR) which allows identifying and characterizing the presence and location of
myocardial damage in most of the cases combining its unique tissue characterization
capabilities with the assessment of biventricular regional and global function.
Now we will review the role of CMR in the evaluation of DCM, analyzing
respective strengths and limitations in the light of the current literature and technological
developments.
CMR Acquisition Protocol and Features:
4 | P a g e
CMR helps in evaluation and quantification of LV dilatation and systolic
dysfunction and detection of possible underlying tissue abnormalities particularly
myocardial fibrosis. (1,5,6)
A standard imaging protocol in DCM includes a four-chamber horizontal long-axis,
two-chamber vertical long-axis, and short-axis views using breath-hold steady-state free
precession (SSFP) cine sequences with full coverage of both ventricles to provide
assessment of biventricular volumes and global and regional functions (Table 1).
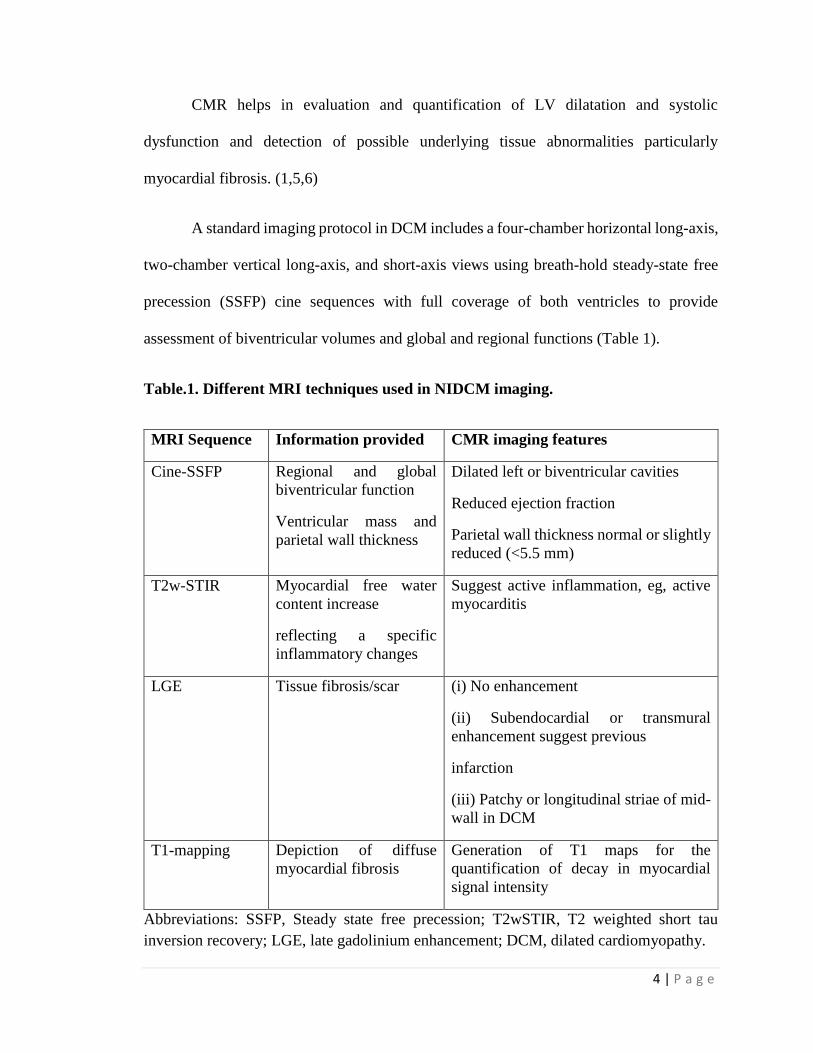
Table.1. Different MRI techniques used in NIDCM imaging.
MRI Sequence Information provided CMR imaging features
Cine-SSFP
Regional and global
biventricular function
Ventricular mass and
parietal wall thickness
Dilated left or biventricular cavities
Reduced ejection fraction
Parietal wall thickness normal or slightly
reduced (<5.5 mm)
T2w-STIR
Myocardial free water
content increase
reflecting a specific
inflammatory changes
Suggest active inflammation, eg, active
myocarditis
LGE
Tissue fibrosis/scar (i) No enhancement
(ii) Subendocardial or transmural
enhancement suggest previous
infarction
(iii) Patchy or longitudinal striae of mid-
wall in DCM
T1-mapping
Depiction of diffuse
myocardial fibrosis
Generation of T1 maps for the
quantification of decay in myocardial
signal intensity
Abbreviations: SSFP, Steady state free precession; T2wSTIR, T2 weighted short tau
inversion recovery; LGE, late gadolinium enhancement; DCM, dilated cardiomyopathy.
5 | P a g e
CMR is now considered the reference technique for the quantification of ventricular
volumes and functional parameters, to measure wall thickness and ventricular mass in
patients with DCM.(7–9) In advanced cases, LV dysfunction may be associated with
diffuse myocardial wall thinning (diastolic wall thickness < 5.5 mm). (10)
T2-weighted short-tau inversion recovery (T2w-STIR) imaging using an ECG-
gated triple inversion recovery (IR) technique is recommended to depict tissue edema when
an overlapping active inflammatory process is suspected such as in myocarditis, acute
myocardial infarction, Takotsubo syndrome, sarcoidosis.(11)
Gadolinium is biologically inert tracer that freely distributes in extracellular space
but does not cross the intact cell membrane. Due to a combination of increased extracellular
volume and slower washout kinetics, there is a relative accumulation of gadolinium in areas
of necrosis, fibrosis, infiltration, and inflammation in the late washout phase Gadolinium
is a paramagnetic substance which shortens the T1 / T2 decay time and hence cause hyper
enhancement.(12) A standard acquisition protocol includes late enhancement imaging with
T1 weighted inversion recovery images acquired 10–20 minutes after contrast
administration (also called late gadolinium enhancement or LGE), usually obtained using
a segmented 2D or 3D inversion recovery gradient-echo breath-hold approach, with
inversion time optimized to null myocardial signal intensity. Phase-sensitive inversion
recovery (PSIR) reference imaging incorporates the phase polarity information that
enhances myocardial tissue contrast. It is also recommended to ensure matching section
position and same slice thickness between IR-CE and cine- SSFP imaging in order to obtain
direct comparison between regional wall motion abnormalities and LGE findings.(13) Use
6 | P a g e
of IR-CE imaging may be helpful to characterize the myocardium and to differentiate DCM
patients from LV dysfunction related to CAD.(14)
LGE has been described as being present in patients with DCM in 12–67% of the
cases.(15) (15–17) The most common pattern being characterized by a mid wall linear
distribution likely representing the intramural layer of septal fibrosis which has been
observed in pathologic samples.(18) Mc Crohon et al. found three different no LGE
patterns in 59% of patients with DCM. Rest 41 % have LGE and two type of patterns of
LGE : (a) subendocardial or transmural enhancement indistinguishable from patients with
previous infarction , and (b) patchy or longitudinal striae of midwall enhancement clearly
different from the distribution in patients with CAD (28%). (14) However, since LGE is
ascribed to relative accumulation of gadolinium in areas of damaged myocardium, LGE-
CMR techniques may miss a diffuse type of fibrosis. (19)
Myocardial T1-mapping techniques have also been recently proposed for the
depiction of diffuse myocardial fibrosis, undetectable with conventional IR-CE CMR
techniques. (20) The basic principle relies on the shortening of T1-relaxation time of
myocardial tissue which directly correlated with the amount of interstitial fibrosis with
collagenous replacement. (21)
Clinical implications of CMR in DCM patients:
Current clinical implication of CMR in DCM patients are
1. evaluation of global biventricular structure and function
2. differential diagnosis in nonischaemic forms
3. differential diagnosis between ischaemic and nonischaemic forms
7 | P a g e
4. detection of intracavitary thrombi
5. prognostic stratification
Evaluation of global biventricular structure and function:
Cine images usually show LV hypokinesia and increased volumes in DCM.
Roughly, the end-diastolic volumes that constitute a DCM are more than 140 mL for the
LV and more than 150 ml for the RV; these data may be more accurate if indexed to the
body surface area. In Cine -SSFP, the normal LV end-diastolic volume (EDV)/BSA
(mL/m2) in males is 82.3 ± 14.7 and in females is 77.7 ± 10.8. So values more than this
are considered as dilated LV. (22)
Evaluation of global biventricular systolic function with cine-SSFP is now regarded
as the gold standard imaging technique. It is not affected by the geometric assumptions
used in 2D echocardiography for the left ventricle (such as the area/length method).
Furthermore, the approximation in delineating endocardial border with CMR approach is
considerably less than with 2D echocardiography minimizing operator dependence and
intra- and inter-observer reproducibility variability(23,24).
In DCM, LV ejection fraction is the strongest predictor of progression to heart
failure, while LV volume and mass are independently correlated with mortality and
morbidity; therefore accurate quantification of all these parameters is essential for adequate
patient’s evaluation and also to monitor progression of disease and response to therapy.(25)
Bourantas et al showed that RV dilatation and dysfunction also significantly predicts
adverse outcome in DCM patients. (26)
8 | P a g e
Chamber enlargement is also associated with valvular insufficiency which can be
assessed with phase-contrast sequences representing an accurate technique for quantifying
the severity of valve regurgitation and for providing information on diastolic function. (27)
Detection of intracavitary thrombi :
CMR is the preferred diagnostic tool to recognize its presence which is depicted as
a soft-tissue intracavitary lesion, nonenhancing on postcontrast IR-CE images and with a
variable signal intensity on either T1 or T2 images.(28) The technique has shown an
excellent sensitivity and specificity for LV thrombus detection and is superior to both
transthoracic and trans esophageal echocardiography. (29)
Differential diagnosis between ischemic and nonischemic forms :
The diagnosis of NIDCM starts with the exclusion of ischemic cardiomyopathy
(ICM). Generally, coronary angiography is routinely performed for the differentiation.
NIDCM Is diagnosed when patients have no obstructive coronary arteries or coronary risk
factors. But, no obstructive coronary artery on angiography is not synonymous with not
having ICM. (14) The spontaneous recanalization after coronary artery occlusion caused
by a rupture of a minimally stenotic unstable plaque, embolization or any spasm may
mask the cause. Conversely, it is not uncommon that patients with DCM have CAD. Isner
et al through an autopsy study in DCM patients has described occurrence of
subendocardial and transmural fibrosis indistinguishable from ischemic lesions.(30)
CMR is currently recognized as a useful tool to know whether the LV dysfunction
is caused by CAD. Cine-SSFP CMR with its excellent spatial and temporal resolution is
9 | P a g e
able to detect regional wall motion abnormalities and wall thinning in a coronary arterial
territory. A subendocardial or transmural LGE in CMR involving a coronary artery
distribution also indicates ischemic cardiomyopathy as the ischemic wave front starts from
subendocardium.
On the other hand, NIDCM mostly show a lack of LGE . The most common
distribution of LGE is mid-wall enhancement, followed by patchy or diffuse striated LGE.
(14) The distribution of LGE is unrelated to any particular coronary arterial territory. This
LGE distribution also shown to correspond to focal fibrosis at autopsy. (31)
The mid wall LGE pattern may also represent the morphological correlate of an
chronic inflammatory process, rather than a focal fibrosis,. De Cobelli et al. found LGE in
70% of patients with chronic heart failure and histologically proven chronic myocarditis.
Mid wall LGE was the most common pattern of LGE distribution found in their series
suggesting that IRCE CMR may noninvasively identify areas of myocardial damage due
to chronic inflammation.(32)
Differential diagnosis of non-ischemic forms :
Differentiation between various forms of non-ischemic DCM is still a complex and
partially investigational issue. The unique tissue characterization ability of CMR offers a
significant additional diagnostic contribution to the conventional diagnostic tools. (33–36)
CMR, in general, allows characterization of acute versus chronic injuries using T2w-
imaging and T2-mapping techniques (T2-STIR). Quantification of intramyocardial iron
deposition can be done with T2∗ techniques in patients with hemochromatosis. LGE –

10 | P a g e
CMR provides data regarding necrosis/fibrosis, which is a valuable noninvasive
alternative to endomyocardial biopsy. (37)
A pattern-based approach of LGE is described in literature based on the concept
that the location (subendocardial, transmural, subepicardial, mid myocardial) and pattern
(focal or diffuse) of abnormal LGE allow differentiation between ischemic and
nonischemic cardiomyopathies as well as differential diagnoses in nonischemic forms.(38)
(Figure1. Patterns of hyperenhancement (HE) with MRI in various disease states, with
localization for ischemic versus nonischemic lesions. HTN = hypertension. (39)
11 | P a g e
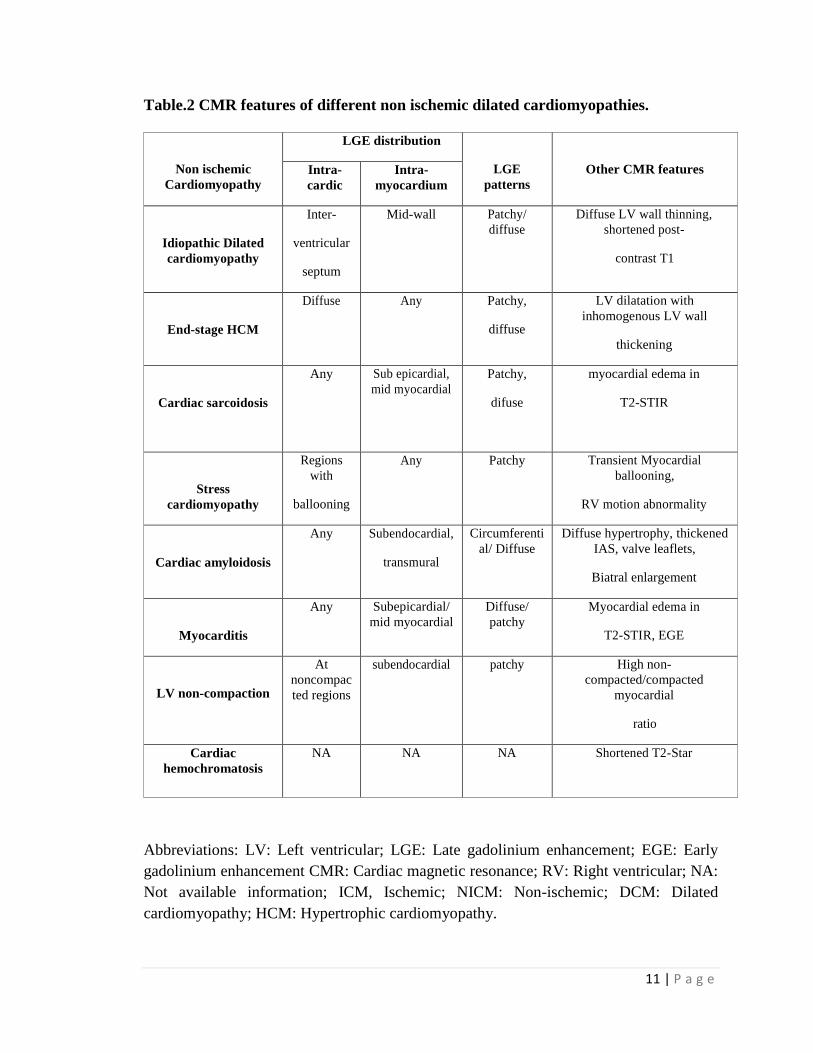
Table.2 CMR features of different non ischemic dilated cardiomyopathies.
Non ischemic
Cardiomyopathy
LGE distribution
LGE
patterns
Other CMR features Intra-
cardic
Intra-
myocardium
Idiopathic Dilated
cardiomyopathy
Inter-
ventricular
septum
Mid-wall Patchy/
diffuse
Diffuse LV wall thinning,
shortened post-
contrast T1
End-stage HCM
Diffuse Any Patchy,
diffuse
LV dilatation with
inhomogenous LV wall
thickening
Cardiac sarcoidosis
Any Sub epicardial,
mid myocardial
Patchy,
difuse
myocardial edema in
T2-STIR
Stress
cardiomyopathy
Regions
with
ballooning
Any Patchy Transient Myocardial
ballooning,
RV motion abnormality
Cardiac amyloidosis
Any Subendocardial,
transmural
Circumferenti
al/ Diffuse
Diffuse hypertrophy, thickened
IAS, valve leaflets,
Biatral enlargement
Myocarditis
Any Subepicardial/
mid myocardial
Diffuse/
patchy
Myocardial edema in
T2-STIR, EGE
LV non-compaction
At
noncompac
ted regions
subendocardial patchy High non-
compacted/compacted
myocardial
ratio
Cardiac
hemochromatosis
NA NA NA Shortened T2-Star
Abbreviations: LV: Left ventricular; LGE: Late gadolinium enhancement; EGE: Early
gadolinium enhancement CMR: Cardiac magnetic resonance; RV: Right ventricular; NA:
Not available information; ICM, Ischemic; NICM: Non-ischemic; DCM: Dilated
cardiomyopathy; HCM: Hypertrophic cardiomyopathy.
12 | P a g e
Idiopathic DCM is diagnosed when NIDCM is present but no cause is made out.
CMR showed dilated LV cavity with thinned walls. Most of them are LGE negative. LGE
positivity varies from 12% to 67% as mentioned earlier. Most commonly LGE is present
in mid myocardial region of IVS.
Familial DCM is defined as DCM in two or more first or second degree relatives.
Without proper screening it may be missed in up to 18% of cases. CMR features resemble
that of idiopathic DCM.(40,41)
Myocarditis is usually viral in origin. Although spontaneous recovery is common,
5-10% of cases may progress to chronic dilated cardiomyopathy. Due to patchy
involvement the use of endomyocardial biopsy (EMB) for diagnostic purpose is limited.
T2-STIR CMR shows focal areas of increased signal intensity, representing active
inflammation/edema. Myocardial necrosis on histology is well correlated with both early
and late gadolinium enhancement. (42)Cine-SSFP CMR may show regional wall motion
abnormalities. The LGE is subepicardial, mostly in lateral wall and in a nonischemic
pattern of distribution.
End stage HCM resembles dilated cardiomyopathy. Matoh et al showed that end
stage HCM patients had more LGE extent than the DCM patients, and LGE volume
correlated to lower global and local LV function. (43) LGE-CMR may be useful to evaluate
myocardial damage in HCM patients, and to differentiate the dilated phase of HCM from
DCM. LGE is also a poor prognostic marker in end stage HCM patients. (44)
Cardiac involvement in amyloidosis leads to thickening of ventricular and atrial
walls and the atrio-ventricular valves. CMR shows above findings along with pleural /
13 | P a g e
pericardial effusion. The thickness of the interatrial septum more than 6 mm is fairly
specific for amyloidosis.(45) On LGE- CMR , a distinctive pattern of LGE is frequently
seen with circumferential hyperenhancement of the subendocardium or a global transmural
pattern often including the interatrial septum and right ventricle. (46)This LGE pattern has
a high diagnostic accuracy for diagnosing cardiac amyloid compared to EMB and also has
been shown as the single best noninvasive imaging parameter for cardiac amyloid. (47,48)
The presence of LGE also has been shown to be associated with poor prognosis. (49)
Cardiac involvement in sarcoidosis occurs in 20-30% of cases. CMR cine-SSFP
shows localized areas of wall thinning and regional wall motion abnormalities due to
underlying disease activity. T2 –STIR images shows high-signal intensity in areas of
active myocardial inflammation. LGE shows areas of myocardial damage and may help
guide the site for endomyocardial biopsy. LGE-CMR shows various non specific LGE
patterns, including patchy, midwall, subepicardial, or subendocardial, distribution with a
predilection for the basal and mid-septal segments. (50) The presence of LGE portends a
nine-fold higher rate for adverse events (death, VT/ defibrillator shock). (51,52)
Peripartum cardiomyopathy arises in the last month of pregnancy or within 5
months postpartum with 75% of the cases manifesting in the first 2 months after delivery.
Mouquet et al found that CMR shows dilated LV dimensions with decreased LV function
and no LGE. (53) But Arora et al found presence of LGE in 25 to 30% of cases , which
also was associated with poor long term prognosis. (34)
Chemotherapy induced cardiomyopathy is mostly described following
anthracyclin based chemotherapy. (54,55)CMR shows dilated LV dimensions with
14 | P a g e
decreased LV function. Role of LGE –CMR in this group of patients is still investigational.
Draft et al , in 53 patients with anthracyclines induced cardiac toxicity showed that changes
in LV end-systolic volumes, LV strain, pulse wave velocity, and LVEF by CMR within 6
months of receiving anthracyclines, but no new LGE. (56)
Prognostic stratification :
As already mentioned above, LGE may also provide intriguing information
regarding patients’ risk stratification. (3)
Several previous studies showed the lack of relationship between the presence of
LGE or LGE volume, and LV volume and function. (43,57) In contrast, Lehrke et al found
that LGE presence is associated with adverse myocardial remodeling and dilated LV
volumes with poor LV function. (25)
In DCM, a series of factors is associated with adverse prognosis, such as age,
gender, LVEF, QRS duration and cardiac biomarkers. (58) Although most of the papers
showed LGE as a poor prognostic marker , still this remains controversial.(59)
The mid-wall LGE in DCM correlates with intraventricular conduction disturbance,
and is independently predictive of sudden cardiac death (SCD) or ventricular tachycardias.
(60) There is a large series of papers in literature reporting that the presence of mid-wall
enhancement is predictive of inducible ventricular tachycardia allowing the stratification
of patient’s risk and the selection of ideal candidate for ICD. LGE-CMR can also help to
identify the arrhythmogenic substrate and plan an appropriate mapping and ablation
strategy. (16,25,61–63)
15 | P a g e
Assomull et al. also correlated LGE with mortality and cardiovascular events (HR,
3.4; CI, 1.4 to 8.7) and found that it was the best predictor of sudden cardiac death (HR,
5.4). (16)
The same observation was found by Wu et al. who reported that LGE predicted
adverse outcomes in patients scheduled for ICD implantation with a higher event rate (heart
failure, appropriate ICD discharge, and cardiac death, 44%versus 8%; 𝑃 = 0.001;HR, 8.2;
CI, 2.2 to 30.9; 𝑃 = 0.002). (64)
In contrast, Hombach et al. did not reproduce the same results and found that mid
wall enhancement was not associated with an independent prognostic impact, highlighting
the prominent still investigational nature of those studies requiring further clinical
validation from large prospective dedicated trials. (59) In this regard, a large prospective
longitudinal study of 472 patients with DCM with a median follow-up of 5.3 years was
recently published providing evidence that the assessment of mid-wall fibrosis with LGE-
CMR imaging was independent prognostic information beyond LVEF in patients with
nonischemic dilated cardiomyopathy (HR, 2.43 (95% CI, 1.50–3.92); 𝑃 < 0.001).(3)
One recent metanalysis has shown that LGE in patients with NIDCM is associated
with increased risk of all-cause mortality, heart failure hospitalization, and SCD.. It also
concluded that detection of LGE by CMR has excellent prognostic characteristics and may
help guide risk stratification and management in patients with NICM. (65)
Not only mere presence of LGE but the amount of LGE volume determines the
adverse outcome. Shimuzu et al (63) visually quantify LGE volume in NIDCM patients
and found that the incidence of cardiac events was significantly higher in group with LGE
16 | P a g e
extent > 10% of LV volume than the group with <10% ( 36% vs 2 % , Log rank , p =
0.0001). Similarly Poyhonen et al, (66)visually quantified LGE in NIDCM patients and
showed that LGE volume > 17% of LV volume was the strongest predictor of bad
prognosis. Similar results from other studies showed that extensive LGE lead to the
impairment of cardiac function, the propensity to ventricular arrhythmias and high
probabilities of cardiac mortality and morbidity. (25,67). Therefore, the analysis of LGE
volume and not only the presence of LGE, may be valuable to predict prognosis and
identify high-risk patients in DCM.
One recent article by Tateshi et al showed added benefit of systolic blood pressure
response (SBPR) during exercise to LGE positivity in DCM patients. Patients with LGE-
positive and SBPR <40 mm Hg had a significantly high cardiac events (HR 2.08, 95% CI
1.06 to 4.11, p=0.034). But, there was no significant difference in the cardiac event-free
survival rate between the LGE positive + SBPR ≥40 mm Hg and LGE-negative +SBPR
<40 mm Hg groups (p=0.736).
LGE also determines the therapeutic response to drugs and devices. Machii et
al,(58) showed that reverse remodeling occurred after treatment in patients with no LGE
and with LGE localized in inter-ventricular septum, but did not in patients with extensively
distributed LGE. Since LV segments with a lower amount of LGE are expected to have
more viable but functionally disturbed cardiomyocytes and reversible matrix fibrosis, they
are more likely to benefit from therapies. Bello et al also showed that myocardial
contractility improved in 56% with no LGE compared to 3% with LGE and concluded
that presence of LGE affects the response of heart failure patients to beta blocker. (17)
17 | P a g e
CMR assesses mechanical dysynchrony. It also provides the location of myocardial
scar and coronary venous anatomy for optimal lead placement , which influence the
likelihood for success of CRT. (68,69) Multiple studies have shown that the extent of
myocardial scar, depicted as LGE is predictive of response to CRT.(70–72) On the above
of that , LV lead placement over the region of scar reduce the effectiveness of CRT. (70)
Bleeker et al demonstared lower response rates to CRT and no change in dysynchrony for
those with posterolateral scar (14% vs. 81%, p < 0.05) compared with those without . (70)
White et al reported that a LGE extent cutoff value of 15% of LV volume provided
sensitivity and specificity of 85% and 90%, respectively, for clinical response to CRT. (71)
Another study have shown that pacing in a site with >50% transmural scar was associated
with poor response to CRT.(72)
18 | P a g e
AIM AND OBJECTIVE
Hypothesis:
1. MRI features of NIDCM helps in assessment ventricular function and also helps in
diagnosis.
2. Myocardial fibrosis, detected by MRI as late gadolinium enhancement (LGE) is a
marker of poor prognosis.
Aim:
To study the MRI features of NIDCM and its clinical correlation.
Study objectives are:
1. Global biventricular structural and functional assessment.
2. Differential diagnosis made out by MRI.
3. Late gadolinium enhancement (LGE) – prevalence and distribution pattern.
4. Clinical correlation of LGE with – Left ventricular (LV) function, Death ,
Sudden cardiac death (SCD), Arrhythmia, heart failure (HF)
hospitalizations
.
19 | P a g e
MATERIAL AND METHODS
Study design :
A retrospective observational study.
Inclusion criteria:
All patients of NIDCM (decreased systolic function, i.e., LVEF < 50%) who
underwent CMR from 1/1/2012 to 31/12/2016 .
Exclusion criteria:
1. significant CAD (>50% luminal narrowing on coronary angiography and/or a
history of coronary revascularisation or myocardial infarction),
2. valvular disease
3. hypertensive heart disease
Follow up:
They were followed prospectively up to 31/6/2017 for clinical end points. Primary
end point was defined as occurrence of major cardiac end points (MACE). It includeed
all-cause mortality, sustained VT/appropriate ICD shock, sudden cardiac death (SCD)/
resuscitated cardiac arrest (RCA), and heart failure hospitalization. Secondary end points
were defined as occurrence of all-cause mortality, cardiac mortality, sudden cardiac death
(SCD)/ resuscitated cardiac arrest (RCA), sustained VT/ ICD shock and HF
hospitalization.
20 | P a g e
Baseline demographic data of all enrolled patients were taken from medical records
including full clinical history, symptomatic status. Chest roentgenogram,
electrocardiogram, echocardiography details and CMR findings were also recorded.
Detailed Echocardiography was done prior to CMR with emphasis on the following
parameters:
1. LV dimensions- LVIDD, LVIDS
2. Ejection fraction – LVEF, RVEF
3. RWMA- present/ absent ; RWMA area
4. Diastolic Dysfunction- present /absent
5. Mitral regurgitation –present/absent
6. Tricuspid regurgitation- present/absent
7. Pulmonary hypertension- present / absent
8. RV dysfunction- present / absent
9. Dysynchrony - present / absent
Cardiac MRI Sequences:
Cardiac MRI was done with SIEMENS 1.5 T machine or a 3 Tesla system
(Discovery 750w; General electric GE healthcare; USA). Following cardiac MRI
sequences were used :
1. Cine – Steady state with free precession (Cine-SSFP) sequences (Short axis,
four chamber and two chamber views). It detects both regional as well as global
biventricular structure and function.
21 | P a g e
2. T2 weighted Short tau inversion recovery (T2w-STIR) – It detects free water in
myocardium, reflecting inflammatory changes.
3. Late gadolinium enhancement (LGE)- Late Gadolinium enhancement
was assessed using PSIR (Phase sensitive Inversion Recovery) sequences with an
inversion time of 200 ms, a repetition time of 8.5 ms, and an echo time of 3.5 ms,
after 20-30 min of intravenous injection of Gadolinium based contrast agent (0.2
mmol/kg body weight)
It detects tissue fibrosis/ scar .
a. There can be -
(i) LGE or no LGE
(ii) LGE pattern: Subendocardial/ midmyocardial/ subepicardial /
transmural enhancement .
(iii) LGE Distribution: focal / global / circumferential
4. Perfusion imaging - It was performed using three parallel short-axis sections in
end-inspiration. A fast GRADIENT echo sequence was used. Perfusion study used
0.05 mmol/kg of gadolinium at 4 mL/s followed by a 25 mL saline flush. Total scan
time was 1.4 mins.
5. T1-mapping – Generation of T1 maps for the quantification of decay in myocardial
signal intensity.
Following CMR the below parameters were studied:
1. LV size and morphology
i. LV ESV, LVESV/ m2
ii. LV EDV, LVEDV/m2
22 | P a g e
iii. LV SV , LV SV/m2
iv. LV EF
v. RVEDV, RVEDV/m2
vi. RVESV, RVESV/m2
vii. RV SV ,RV SV/m2
viii. RVEF
2. T2 w STIR – present/ absent
3. LGE-
i. Present/ absent -
ii. If present -
1. Pattern: Subendocardial/ midmyocardial/ subepicardial /
transmural enhancement
2. Distribution: focal / global / circumferential
LGE Quantification:
LGE was quantified by visual scoring method. (73). In a left ventricular 17-
segment model, each segment, was scored according to the percentage of enhancement
estimated visually. Score 0 was given for no enhancement, score 1 for 0% – 25%
enhancement, score 2 for 26% – 50% enhancement, score 3 for 51% – 75% enhancement
and score 4 for 76% – 100% enhancement. The global extent of LGE, “LGE score” was
calculated by adding scores from all 17 segments. LGE extent (volume) of LGE was
calculated as a percentage of the total score (4 × 17 = 68). So, LGE volume = 100 × (LGE
score) / 68 . It was expressed as % of LV volume.
23 | P a g e
Data collection:
The data was collected from medical records and follow up data was obtained from
their follow up visits in cardiology/cardiac surgery outpatient clinics or by telephonic
enquiry if there was no follow up visit in the last six months. All data was handled with
care to maintain patient confidentiality. Records were maintained in both computer and
paper formats. The closing point for any one patient will be the time of their last visit to
the follow-up clinic during study period.
Data analysis:
The data was analysed by the principal investigator with advice from a statistician.
Descriptive data were analysed by frequencies and categorical data by percentages , and
continuous variables by means and standard deviations. Continuous variables were
compared using Student’s t test (for parametric test) or Mann-Whitney U test (for non
parametric test) as appropriate. Group comparisons were done by χ2 tests. All statistical
analyses were done by the SPSS statistical software (release 23.0, SPSS Inc.; Chicago,Ill).
24 | P a g e
RESULTS
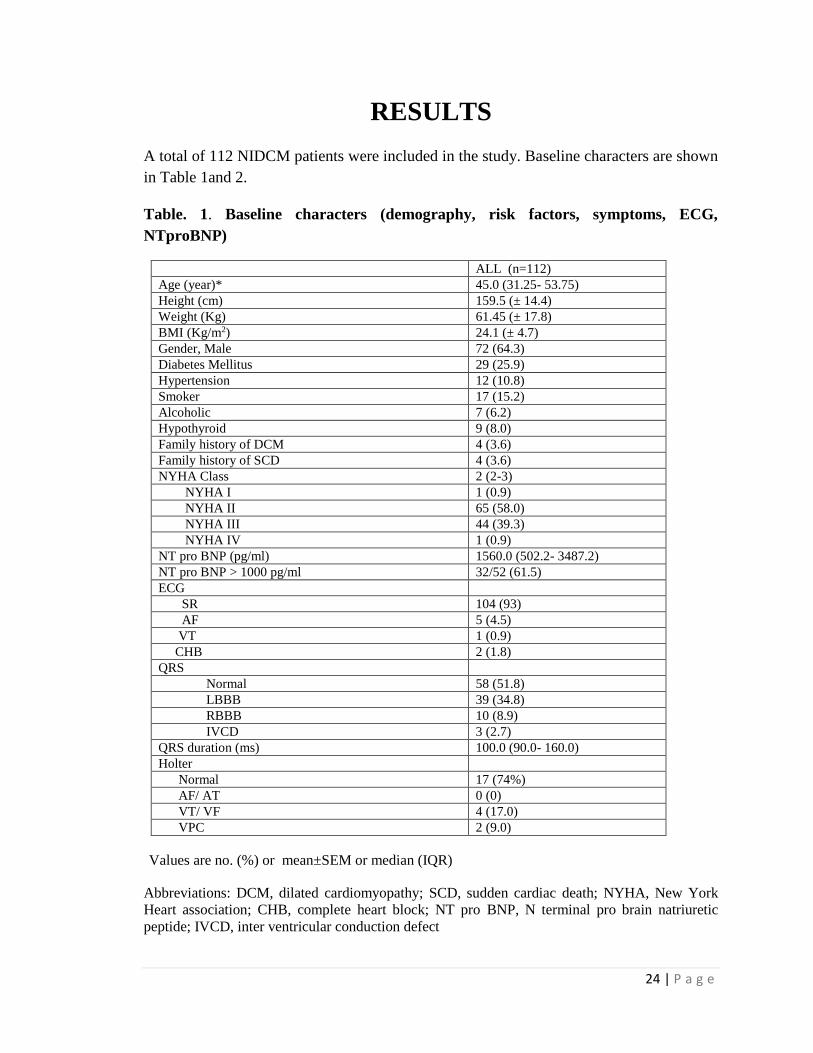
A total of 112 NIDCM patients were included in the study. Baseline characters are shown
in Table 1and 2.
Table. 1. Baseline characters (demography, risk factors, symptoms, ECG,
NTproBNP)
ALL (n=112)
Age (year)* 45.0 (31.25- 53.75)
Height (cm) 159.5 (± 14.4)
Weight (Kg) 61.45 (± 17.8)
BMI (Kg/m2) 24.1 (± 4.7)
Gender, Male 72 (64.3)
Diabetes Mellitus 29 (25.9)
Hypertension 12 (10.8)
Smoker 17 (15.2)
Alcoholic 7 (6.2)
Hypothyroid 9 (8.0)
Family history of DCM 4 (3.6)
Family history of SCD 4 (3.6)
NYHA Class 2 (2-3)
NYHA I 1 (0.9)
NYHA II 65 (58.0)
NYHA III 44 (39.3)
NYHA IV 1 (0.9)
NT pro BNP (pg/ml) 1560.0 (502.2- 3487.2)
NT pro BNP > 1000 pg/ml 32/52 (61.5)
ECG
SR 104 (93)
AF 5 (4.5)
VT 1 (0.9)
CHB 2 (1.8)
QRS
Normal 58 (51.8)
LBBB 39 (34.8)
RBBB 10 (8.9)
IVCD 3 (2.7)
QRS duration (ms) 100.0 (90.0- 160.0)
Holter
Normal 17 (74%)
AF/ AT 0 (0)
VT/ VF 4 (17.0)
VPC 2 (9.0)
Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: DCM, dilated cardiomyopathy; SCD, sudden cardiac death; NYHA, New York
Heart association; CHB, complete heart block; NT pro BNP, N terminal pro brain natriuretic
peptide; IVCD, inter ventricular conduction defect
25 | P a g e
The median age was 45.0 years with inter quartile range of 31.25 years to 53 .7
years. Mean BMI was 24. 1 (± 4.7) kg/m2. Seventy two were male (64.3%). Twenty five
percent had diabetes mellitus while 10% had hypertension. Seventeen percent were
smokers. Nine patients (8%) were hypothyroid on treatment. Seven patients (6.2%) had
history of long term heavy alcohol intake (> 100- 120 mg/day). Family history of DCM
(ie,, two or more than DCM cases in first or second degree relatives ) was present in 4
patients (3.6%). Family history of SCD was present in 4 patients (3.6%).
Most patients had exertional dyspnea as the major symptom. Most of them were in
NYHA class II (58%) followed by NYHA class III (39.3%). One patient presented with
NYHA class IV. NT pro BNP during admission was done in 52 patients. Median NT pro
BNP was 1560 pg/ml. NT pro BNP value more than 1000 pg/ml was found in 32 out of
those 52 patients (61%) of them.
Most of the patients were in sinus rhythm (93%), while five patients had atrial
fibrillation, 2 had complete heart block and one presented with ventricular tachycardia.
LBBB was present in 35% of patients while RBBB in 9% and IVCD in 3% of cases. The
median QRS duration was 100mm (IQR: 90 - 160 mm). Chest X ray showed cardiomegaly
(cardiothoracic ratio >60%) in 74 patients (66.7%). Twenty four hour holter study was
performed in 23 patients, out of which 74% had normal study while 17% had VT and 9%
had VPCs.
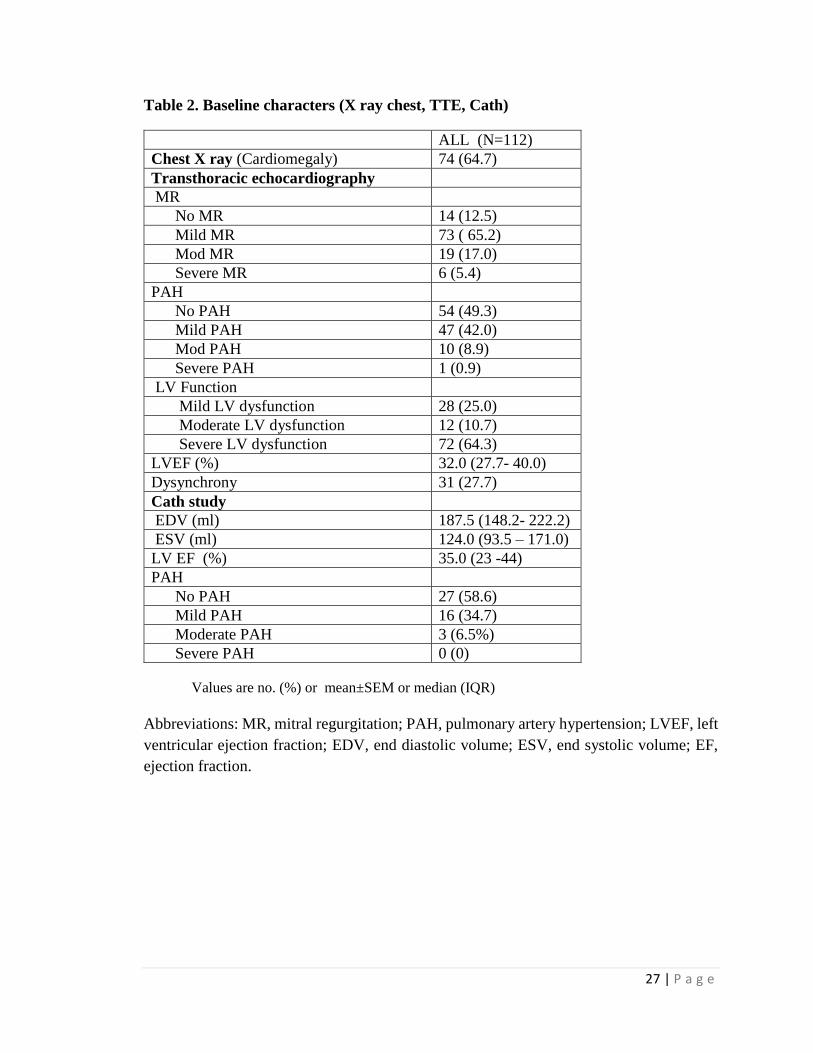
Transthoracic echocardiography (TTE) was done in all cases and all measurements,
grading of lesions were done as per American society of echocardiography (ASE)
guidelines. TTE showed no mitral regurgitation in 12% of cases while mild, moderate and
26 | P a g e
severe mitral regurgitation were found in 65%, 17% and 5% respectively. So, majority of
patients had mild MR by echo. Similarly by transthoracic echocardiography pulmonary
arterial hypertension (PAH) was assessed. PAH was absent in 49% of patients. Fort two
percent had mild PAH , while moderate and severe PAH were present in only 9% and 1%
of patients respectively. Median LV ejection fraction was 32 %. Twenty five percent
patients had mild LV dysfunction (LVEF 40% to 49%), 12% had moderate LV dysfunction
(LVEF 40% to 35%) and 64% had severe LV dysfunction (LVEF < 35%). Both inter-
ventricular and intra-ventricular dysynchrony was present in 27% of patients.
Invasive right heart catheterization was performed in 70 patients. The median end
diastolic volume, end systolic volume and LV ejection fraction by cath study were 187 ml,
124 ml and 35% respectively. Fifty eight percent of patients by cath study had no PAH
while 35% had mild PAH and 7% had moderate PAH.
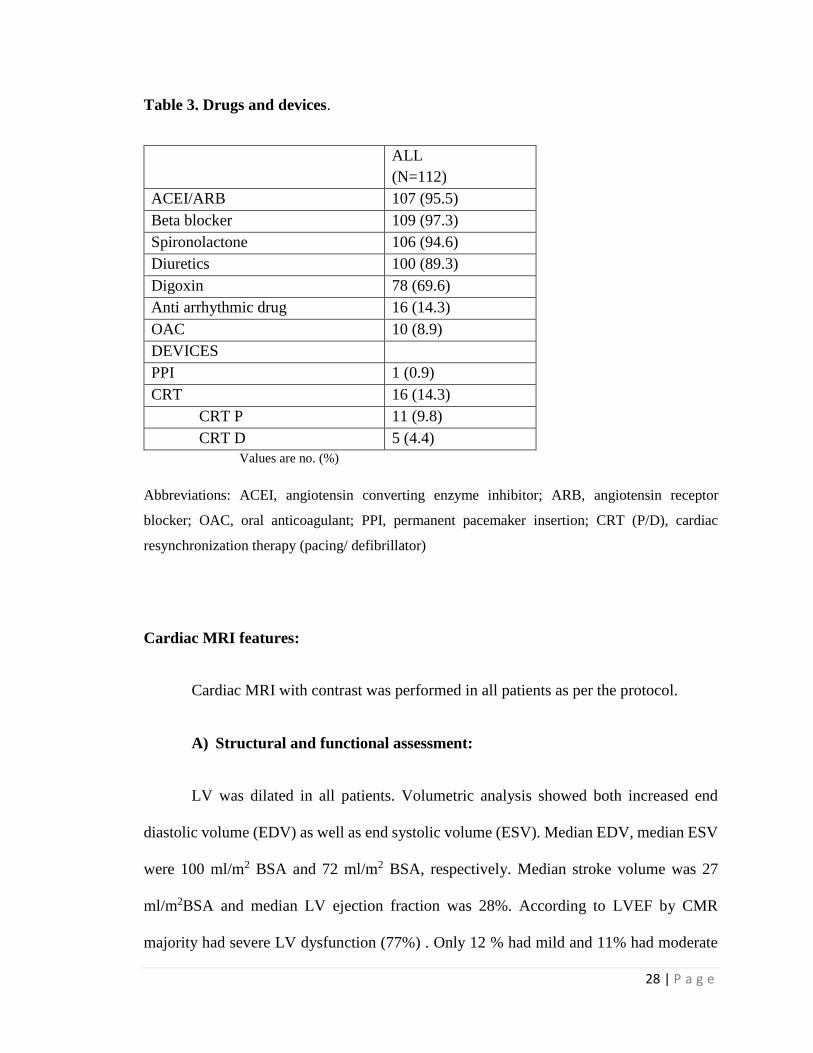
Most of the patients were in cardiac failure and treated according to existing HF
guidelines. (74) (Table 3). More than ninety percent of patients received ACE inhibitor /
ARBs, beta blocker, Mineralocorticoid receptor antagonist and diuretics. Digoxin was
prescribed in 70% of cases. Oral anticoagulant was given in 10 patients with AF and
CHADS2VAS2 >1. Permanent pacemaker inserted in 1 patient with CHB. Sixteen patients
received CRT out of which, 11 received CRT-P and 5 received CRT-D.
27 | P a g e
Table 2. Baseline characters (X ray chest, TTE, Cath)
ALL (N=112)
Chest X ray (Cardiomegaly) 74 (64.7)
Transthoracic echocardiography
MR
No MR 14 (12.5)
Mild MR 73 ( 65.2)
Mod MR 19 (17.0)
Severe MR 6 (5.4)
PAH
No PAH 54 (49.3)
Mild PAH 47 (42.0)
Mod PAH 10 (8.9)
Severe PAH 1 (0.9)
LV Function
Mild LV dysfunction 28 (25.0)
Moderate LV dysfunction 12 (10.7)
Severe LV dysfunction 72 (64.3)
LVEF (%) 32.0 (27.7- 40.0)
Dysynchrony 31 (27.7)
Cath study
EDV (ml) 187.5 (148.2- 222.2)
ESV (ml) 124.0 (93.5 – 171.0)
LV EF (%) 35.0 (23 -44)
PAH
No PAH 27 (58.6)
Mild PAH 16 (34.7)
Moderate PAH 3 (6.5%)
Severe PAH 0 (0)
Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: MR, mitral regurgitation; PAH, pulmonary artery hypertension; LVEF, left
ventricular ejection fraction; EDV, end diastolic volume; ESV, end systolic volume; EF,
ejection fraction.
28 | P a g e
Table 3. Drugs and devices.
ALL
(N=112)
ACEI/ARB 107 (95.5)
Beta blocker 109 (97.3)
Spironolactone 106 (94.6)
Diuretics 100 (89.3)
Digoxin 78 (69.6)
Anti arrhythmic drug 16 (14.3)
OAC 10 (8.9)
DEVICES
PPI 1 (0.9)
CRT 16 (14.3)
CRT P 11 (9.8)
CRT D 5 (4.4)
Values are no. (%)
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor
blocker; OAC, oral anticoagulant; PPI, permanent pacemaker insertion; CRT (P/D), cardiac
resynchronization therapy (pacing/ defibrillator)
Cardiac MRI features:
Cardiac MRI with contrast was performed in all patients as per the protocol.
A) Structural and functional assessment:
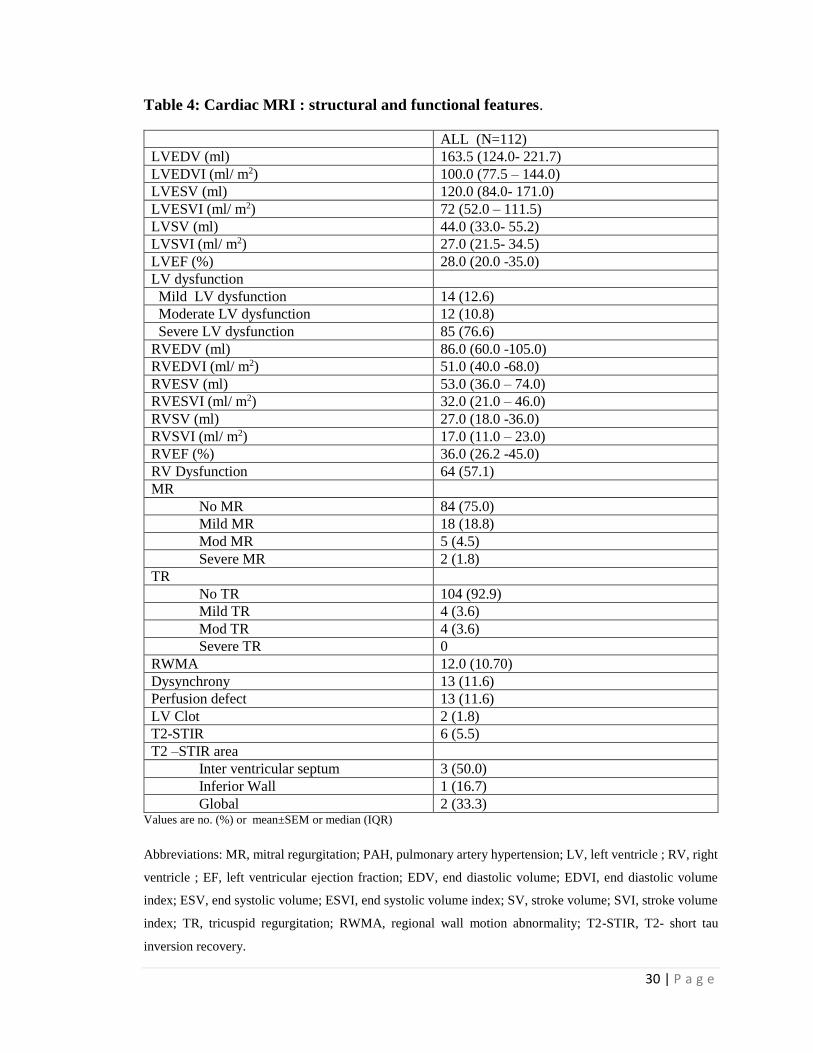
LV was dilated in all patients. Volumetric analysis showed both increased end
diastolic volume (EDV) as well as end systolic volume (ESV). Median EDV, median ESV
were 100 ml/m2 BSA and 72 ml/m2 BSA, respectively. Median stroke volume was 27
ml/m2BSA and median LV ejection fraction was 28%. According to LVEF by CMR
majority had severe LV dysfunction (77%) . Only 12 % had mild and 11% had moderate
29 | P a g e
degree of LV dysfunction. Right ventricle dimensions were dilated in most of the patients.
RVEDV, RV ESV, RV SV, RVEF were 51 ml/m2, 32 ml/m2, 27 ml/m2 , 36%. RV
dysfunction (RVEF <40%) was present in 57% of patients. (Table 4)
Seventy five percent of cases showed no mitral regurgitation, while 19% showed
mild MR, 5% showed moderate MR and 2% showed severe MR. Majority of patients
showed no tricuspid regurgitation ( 93%) while 3.6% each showed mild and moderate TR.
No patients showed pericardial effusion.
Regional wall motion abnormalities, not accounting to any coronary vascular
territory was seen in 12 cases (10%). Dysynchrony was present in 13 cases (11%).
Perfusion defect, not accounting into any particular vascular territory was present in 13
cases (11%). T2-STIR images showing myocardial edema was present in 6 cases (5.5%)
out of which, 3 showed in the region of inter ventricular septum, one in inferior wall and
rest two showed globally. Two cases had organized LV apical clot.
30 | P a g e
Table 4: Cardiac MRI : structural and functional features.
ALL (N=112)
LVEDV (ml) 163.5 (124.0- 221.7)
LVEDVI (ml/ m2) 100.0 (77.5 – 144.0)
LVESV (ml) 120.0 (84.0- 171.0)
LVESVI (ml/ m2) 72 (52.0 – 111.5)
LVSV (ml) 44.0 (33.0- 55.2)
LVSVI (ml/ m2) 27.0 (21.5- 34.5)
LVEF (%) 28.0 (20.0 -35.0)
LV dysfunction
Mild LV dysfunction 14 (12.6)
Moderate LV dysfunction 12 (10.8)
Severe LV dysfunction 85 (76.6)
RVEDV (ml) 86.0 (60.0 -105.0)
RVEDVI (ml/ m2) 51.0 (40.0 -68.0)
RVESV (ml) 53.0 (36.0 – 74.0)
RVESVI (ml/ m2) 32.0 (21.0 – 46.0)
RVSV (ml) 27.0 (18.0 -36.0)
RVSVI (ml/ m2) 17.0 (11.0 – 23.0)
RVEF (%) 36.0 (26.2 -45.0)
RV Dysfunction 64 (57.1)
MR
No MR 84 (75.0)
Mild MR 18 (18.8)
Mod MR 5 (4.5)
Severe MR 2 (1.8)
TR
No TR 104 (92.9)
Mild TR 4 (3.6)
Mod TR 4 (3.6)
Severe TR 0
RWMA 12.0 (10.70)
Dysynchrony 13 (11.6)
Perfusion defect 13 (11.6)
LV Clot 2 (1.8)
T2-STIR 6 (5.5)
T2 –STIR area
Inter ventricular septum 3 (50.0)
Inferior Wall 1 (16.7)
Global 2 (33.3) Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: MR, mitral regurgitation; PAH, pulmonary artery hypertension; LV, left ventricle ; RV, right
ventricle ; EF, left ventricular ejection fraction; EDV, end diastolic volume; EDVI, end diastolic volume
index; ESV, end systolic volume; ESVI, end systolic volume index; SV, stroke volume; SVI, stroke volume
index; TR, tricuspid regurgitation; RWMA, regional wall motion abnormality; T2-STIR, T2- short tau
inversion recovery.
31 | P a g e
B)Gadolinium contrast study:
Late gadolinium enhancement (LGE) was present in 44 cases (39.3%). Rest 68
cases were LGE –ve (60.7%). So, the prevalence of LGE +ve in NIDCM patients in this
cohort is 39%. (Table 5)
Table 5. LGE status.
LGE status
LGE +ve 44 (39.3)
LGE –ve 68 (70.7)
Values are no. (%) ; Abbreviations: LGE, late gadolinium enhancement
In majority of patients LGE distribution was predominantly found in mid
myocardium [33 cases (75%)], followed by sub epicardial not accounting into any coronary
vascular territory [6 cases (13.6%)], transmural [3 cases (6.8%)] and sub epicardial [2 cases
(4.5%)]. (Table 6) Pattern of LGE distribution were regional/ patchy in majority [33 cases
(75%)], followed by global/diffuse in 8 cases (18.2%) and circumferential in 3 cases
(6.8%). Considering the area of distribution, inter ventricular septum was the most common
site of LGE [38 cases (92.7%)], followed by inferior wall [23 cases (56%)], anterior wall
[21 cases (51.2%)], and least common in lateral wall [16 cases (40%)], though considerable
overlap occurred between different regions. If we look from base to apex , then most
common area of LGE distribution was mid part [36 cases (87.8%)] followed by base [27
32 | P a g e
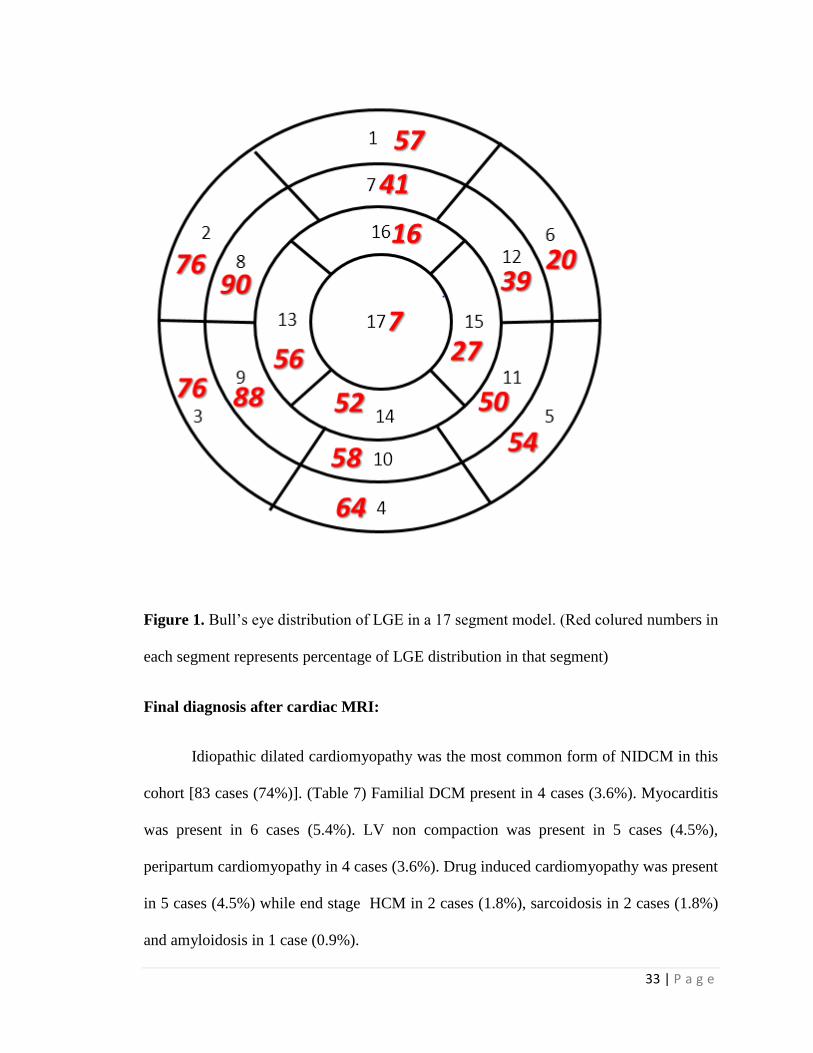
cases (66%)] and apex [17 cases (40.5%)]. Bull‘s eye distribution model consisting of 17
segments showed that most common site of LGE positivity was mid IVS segments
followed by inferior wall , anterior wall and lateral wall. (Figure 1)
Table 6. LGE distribution pattern.
LGE Positive 44 (39.3)
LGE Pattern
Sub endocardial 6 (13.6)
Mid myocardial 33 (75.0)
Subepicardial 2 (4.5)
Transmural 3 (6.8)
LGE distribution
Global/ Diffuse 8 (18.2)
Regional /Patchy 33 (75.0)
Circumferential 3 (6.8)
LGE Area
Anterior wall 21 (51.2)
Inter ventricular septum 38 (92.7)
Inferior wall 23 (56.1)
Lateral wall 16 (36.3)
Base of LV 27 (65.9)
Mid of LV 36 (87.8)
Apex of LV 17 (40.5)
Values are no. (%)
Abbreviations: LGE, late gadolinium enhancement
33 | P a g e
Figure 1. Bull’s eye distribution of LGE in a 17 segment model. (Red colured numbers in
each segment represents percentage of LGE distribution in that segment)
Final diagnosis after cardiac MRI:
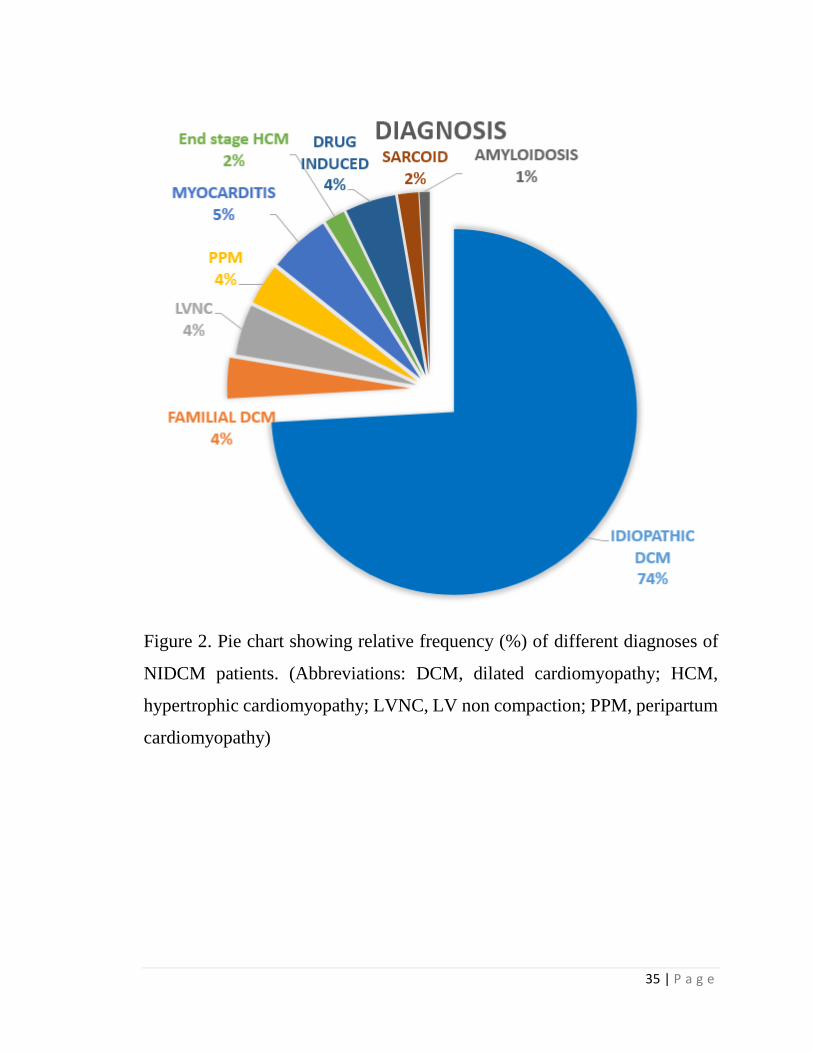
Idiopathic dilated cardiomyopathy was the most common form of NIDCM in this
cohort [83 cases (74%)]. (Table 7) Familial DCM present in 4 cases (3.6%). Myocarditis
was present in 6 cases (5.4%). LV non compaction was present in 5 cases (4.5%),
peripartum cardiomyopathy in 4 cases (3.6%). Drug induced cardiomyopathy was present
in 5 cases (4.5%) while end stage HCM in 2 cases (1.8%), sarcoidosis in 2 cases (1.8%)
and amyloidosis in 1 case (0.9%).
34 | P a g e
Table 7. Differential Diagnosis
Diagnosis No. (%)
Idiopathic DCM 83 (74.1)
Familial DCM 4 (3.6)
Myocarditis 6 (5.4)
LV Noncompaction 5 (4.5)
Drug induced Cardiomyopathy 5 (4.5)
Peripartum cardiomyopathy 4 (3.6)
End stage HCM 2 (1.8)
Sarcoidosis 2 (1.8)
Amyloidosis 1 (0.9)
Values are no. (%)
Abbreviations: DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy.
35 | P a g e
Figure 2. Pie chart showing relative frequency (%) of different diagnoses of
NIDCM patients. (Abbreviations: DCM, dilated cardiomyopathy; HCM,
hypertrophic cardiomyopathy; LVNC, LV non compaction; PPM, peripartum
cardiomyopathy)
36 | P a g e
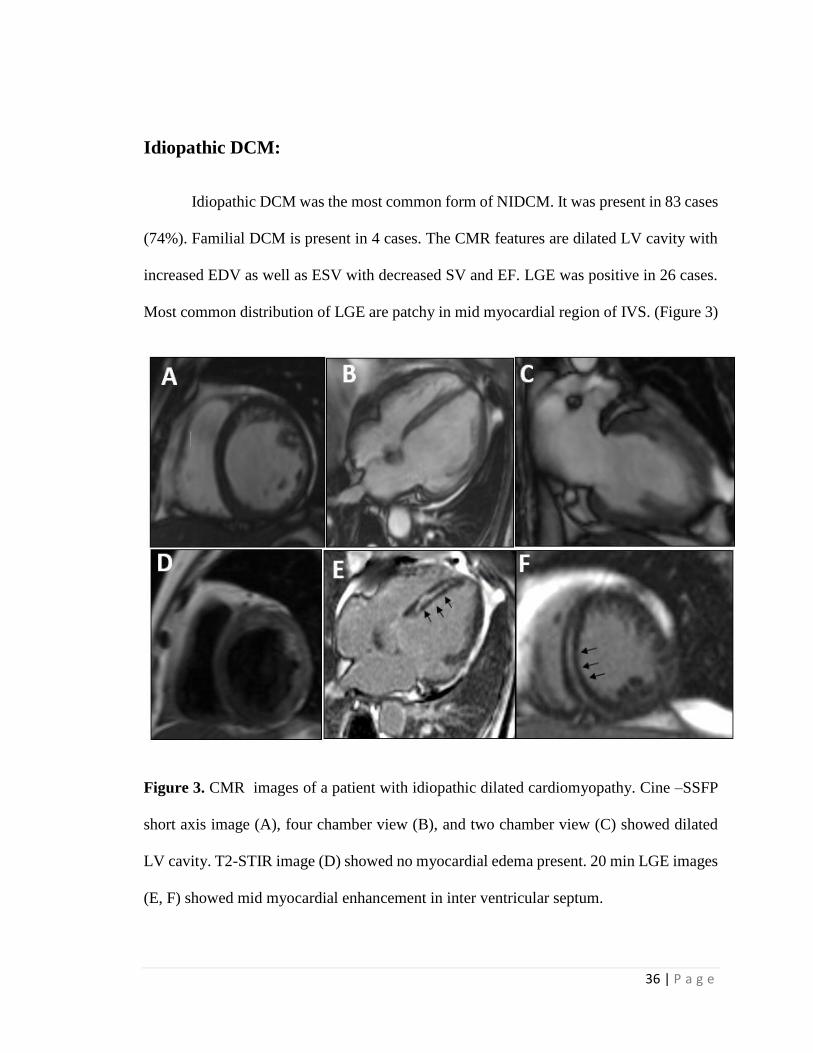
Idiopathic DCM:
Idiopathic DCM was the most common form of NIDCM. It was present in 83 cases
(74%). Familial DCM is present in 4 cases. The CMR features are dilated LV cavity with
increased EDV as well as ESV with decreased SV and EF. LGE was positive in 26 cases.
Most common distribution of LGE are patchy in mid myocardial region of IVS. (Figure 3)
Figure 3. CMR images of a patient with idiopathic dilated cardiomyopathy. Cine –SSFP
short axis image (A), four chamber view (B), and two chamber view (C) showed dilated
LV cavity. T2-STIR image (D) showed no myocardial edema present. 20 min LGE images
(E, F) showed mid myocardial enhancement in inter ventricular septum.
37 | P a g e
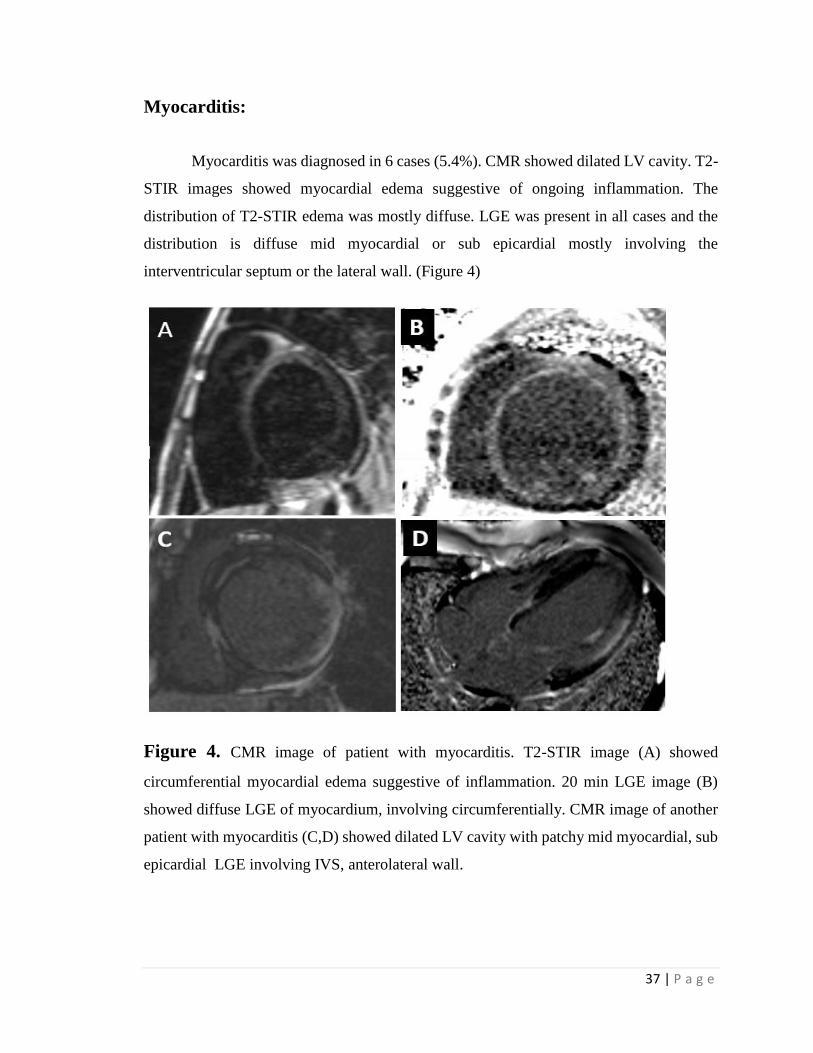
Myocarditis:
Myocarditis was diagnosed in 6 cases (5.4%). CMR showed dilated LV cavity. T2-
STIR images showed myocardial edema suggestive of ongoing inflammation. The
distribution of T2-STIR edema was mostly diffuse. LGE was present in all cases and the
distribution is diffuse mid myocardial or sub epicardial mostly involving the
interventricular septum or the lateral wall. (Figure 4)
Figure 4. CMR image of patient with myocarditis. T2-STIR image (A) showed
circumferential myocardial edema suggestive of inflammation. 20 min LGE image (B)
showed diffuse LGE of myocardium, involving circumferentially. CMR image of another
patient with myocarditis (C,D) showed dilated LV cavity with patchy mid myocardial, sub
epicardial LGE involving IVS, anterolateral wall.
38 | P a g e
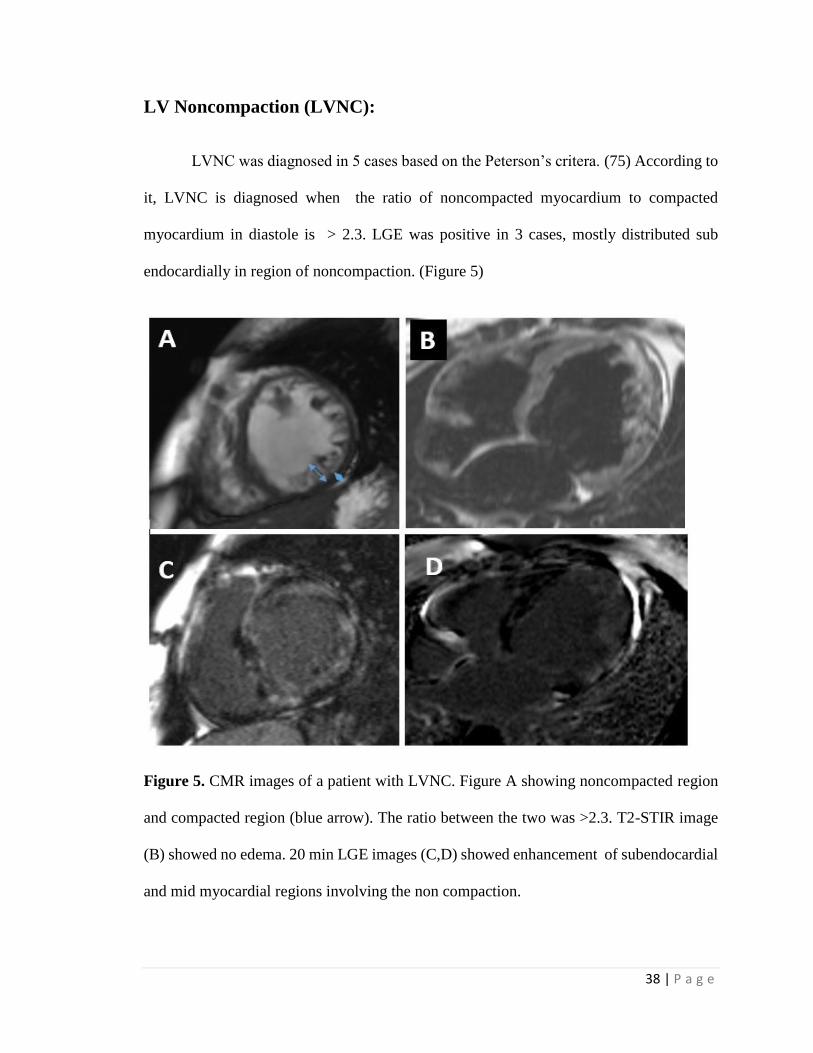
LV Noncompaction (LVNC):
LVNC was diagnosed in 5 cases based on the Peterson’s critera. (75) According to
it, LVNC is diagnosed when the ratio of noncompacted myocardium to compacted
myocardium in diastole is > 2.3. LGE was positive in 3 cases, mostly distributed sub
endocardially in region of noncompaction. (Figure 5)
Figure 5. CMR images of a patient with LVNC. Figure A showing noncompacted region
and compacted region (blue arrow). The ratio between the two was >2.3. T2-STIR image
(B) showed no edema. 20 min LGE images (C,D) showed enhancement of subendocardial
and mid myocardial regions involving the non compaction.
39 | P a g e
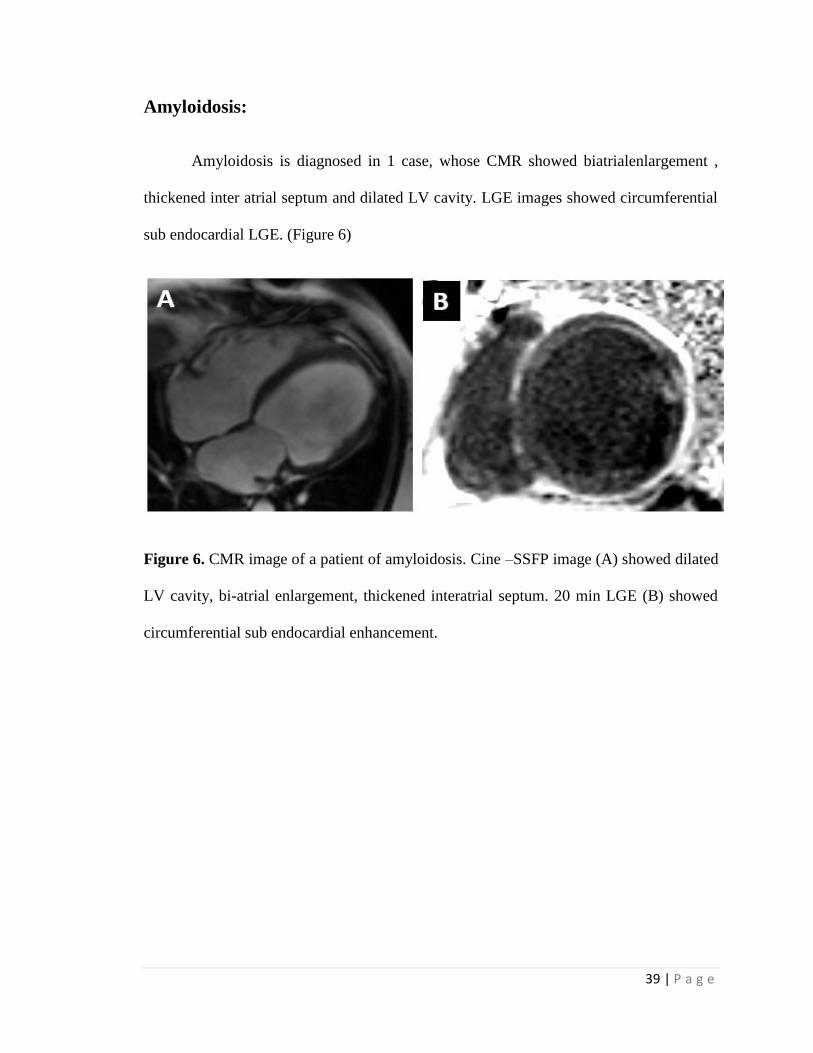
Amyloidosis:
Amyloidosis is diagnosed in 1 case, whose CMR showed biatrialenlargement ,
thickened inter atrial septum and dilated LV cavity. LGE images showed circumferential
sub endocardial LGE. (Figure 6)
Figure 6. CMR image of a patient of amyloidosis. Cine –SSFP image (A) showed dilated
LV cavity, bi-atrial enlargement, thickened interatrial septum. 20 min LGE (B) showed
circumferential sub endocardial enhancement.
40 | P a g e
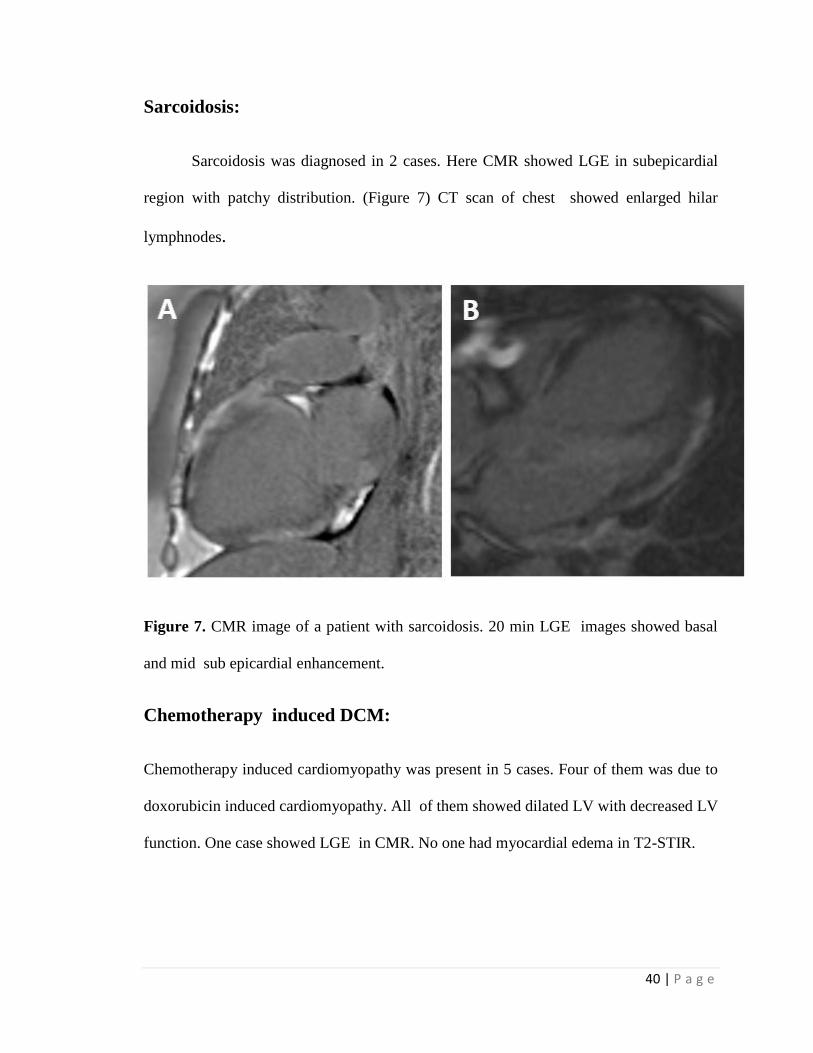
Sarcoidosis:
Sarcoidosis was diagnosed in 2 cases. Here CMR showed LGE in subepicardial
region with patchy distribution. (Figure 7) CT scan of chest showed enlarged hilar
lymphnodes.
Figure 7. CMR image of a patient with sarcoidosis. 20 min LGE images showed basal
and mid sub epicardial enhancement.
Chemotherapy induced DCM:
Chemotherapy induced cardiomyopathy was present in 5 cases. Four of them was due to
doxorubicin induced cardiomyopathy. All of them showed dilated LV with decreased LV
function. One case showed LGE in CMR. No one had myocardial edema in T2-STIR.
41 | P a g e
Peripartum cardiomyopathy:
Four cases had peripartum cardiomyopathy. CMR showed featurs like idiopathic DCM.
Onepatient showed LGE in CMR.
End stage (dilated stage) of HCM:
Two cases had end stage HCM. Their CMR images resemble that of dilated
cardiomyopathy. Both had LGE positivity.
Comparison between LGE +ve and LGE –ve group
The total cohort was divided into two cohorts based upon presence or absence of LGE
,i.e., LGE +ve group and LGE –ve group. They were followed prospectively for a mean of
745 ± 320 days.
Baseline characters:
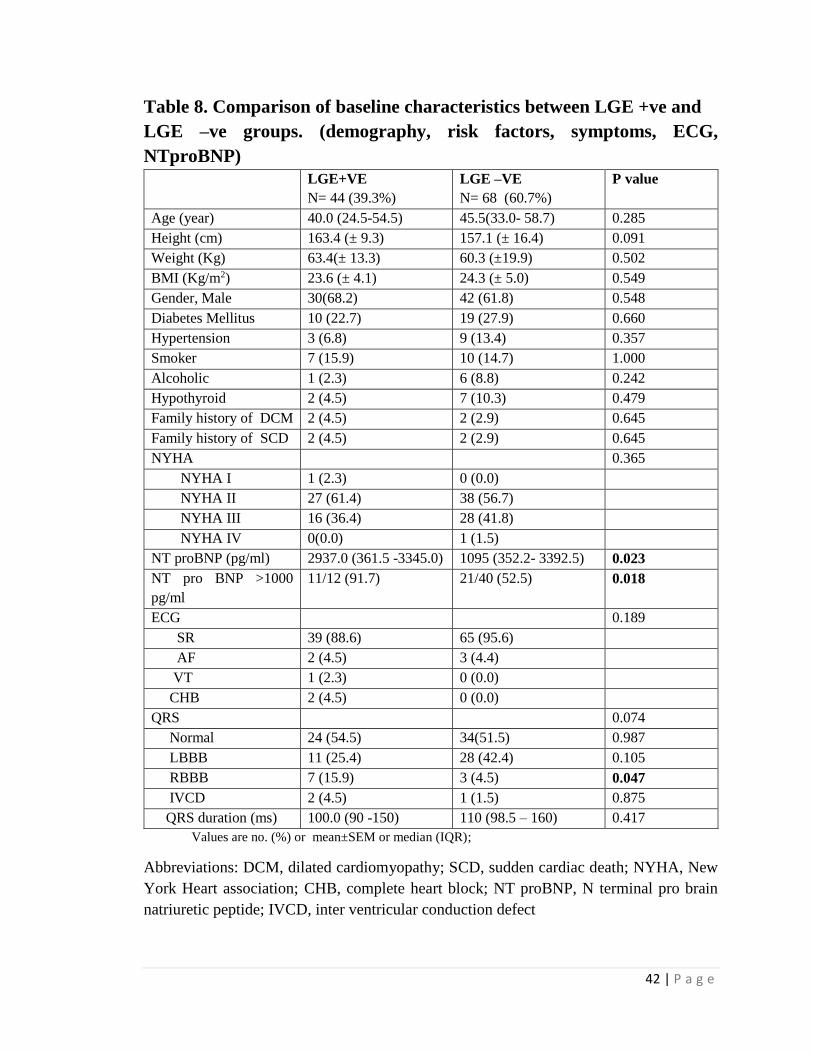
All the base line features were similar in both groups except NT pro BNP values.
(Table 8 and 9) Median NT pro BNP was significantly higher in LGE +ve group (2934.0
pg/ml) compared to LGE –ve group (1095.0 pg/ml), p < 0.023. Similarly, NT pro BNP >
1000 pg/ml was present in significantly higher in LGE +ve group than LGE –ve group (
91.7% vs 52.5% , p= 0.018).
42 | P a g e
Table 8. Comparison of baseline characteristics between LGE +ve and
LGE –ve groups. (demography, risk factors, symptoms, ECG,
NTproBNP)
LGE+VE
N= 44 (39.3%)
LGE –VE
N= 68 (60.7%)
P value
Age (year) 40.0 (24.5-54.5) 45.5(33.0- 58.7) 0.285
Height (cm) 163.4 (± 9.3) 157.1 (± 16.4) 0.091
Weight (Kg) 63.4(± 13.3) 60.3 (±19.9) 0.502
BMI (Kg/m2) 23.6 (± 4.1) 24.3 (± 5.0) 0.549
Gender, Male 30(68.2) 42 (61.8) 0.548
Diabetes Mellitus 10 (22.7) 19 (27.9) 0.660
Hypertension 3 (6.8) 9 (13.4) 0.357
Smoker 7 (15.9) 10 (14.7) 1.000
Alcoholic 1 (2.3) 6 (8.8) 0.242
Hypothyroid 2 (4.5) 7 (10.3) 0.479
Family history of DCM 2 (4.5) 2 (2.9) 0.645
Family history of SCD 2 (4.5) 2 (2.9) 0.645
NYHA 0.365
NYHA I 1 (2.3) 0 (0.0)
NYHA II 27 (61.4) 38 (56.7)
NYHA III 16 (36.4) 28 (41.8)
NYHA IV 0(0.0) 1 (1.5)
NT proBNP (pg/ml) 2937.0 (361.5 -3345.0) 1095 (352.2- 3392.5) 0.023
NT pro BNP >1000
pg/ml
11/12 (91.7) 21/40 (52.5) 0.018
ECG 0.189
SR 39 (88.6) 65 (95.6)
AF 2 (4.5) 3 (4.4)
VT 1 (2.3) 0 (0.0)
CHB 2 (4.5) 0 (0.0)
QRS 0.074
Normal 24 (54.5) 34(51.5) 0.987
LBBB 11 (25.4) 28 (42.4) 0.105
RBBB 7 (15.9) 3 (4.5) 0.047
IVCD 2 (4.5) 1 (1.5) 0.875
QRS duration (ms) 100.0 (90 -150) 110 (98.5 – 160) 0.417
Values are no. (%) or mean±SEM or median (IQR);
Abbreviations: DCM, dilated cardiomyopathy; SCD, sudden cardiac death; NYHA, New
York Heart association; CHB, complete heart block; NT proBNP, N terminal pro brain
natriuretic peptide; IVCD, inter ventricular conduction defect
43 | P a g e
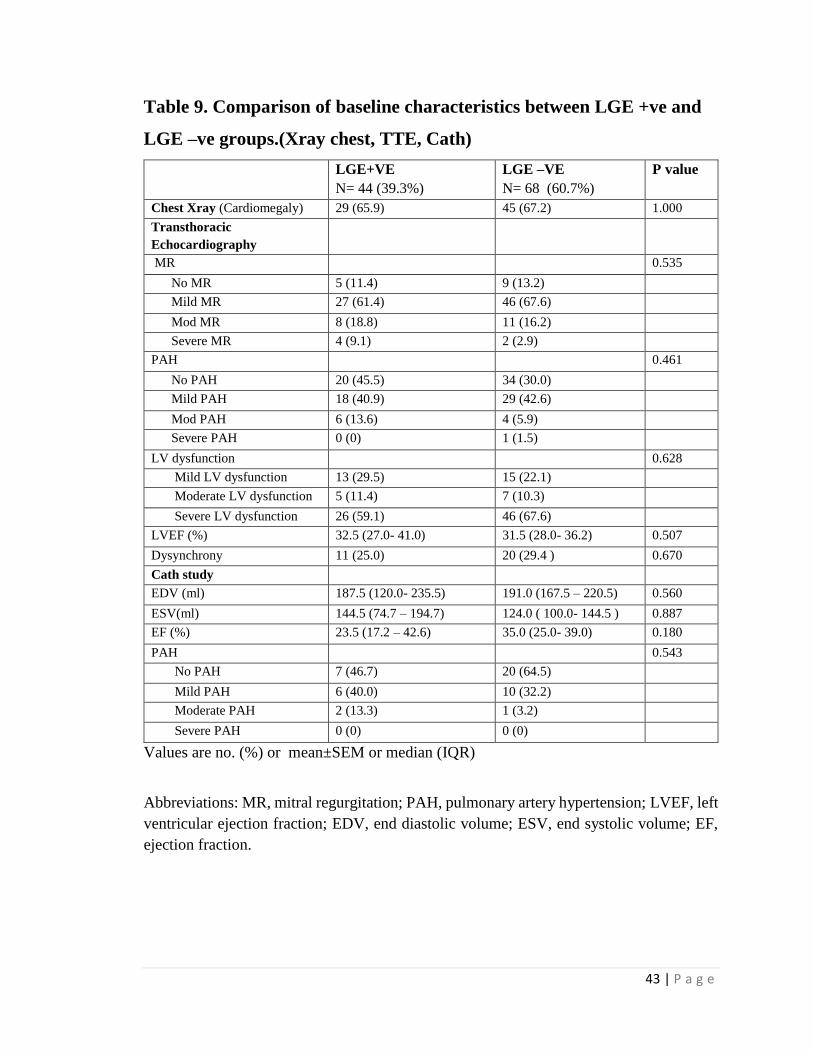
Table 9. Comparison of baseline characteristics between LGE +ve and
LGE –ve groups.(Xray chest, TTE, Cath)
LGE+VE
N= 44 (39.3%)
LGE –VE
N= 68 (60.7%)
P value
Chest Xray (Cardiomegaly) 29 (65.9) 45 (67.2) 1.000
Transthoracic
Echocardiography
MR 0.535
No MR 5 (11.4) 9 (13.2)
Mild MR 27 (61.4) 46 (67.6)
Mod MR 8 (18.8) 11 (16.2)
Severe MR 4 (9.1) 2 (2.9)
PAH 0.461
No PAH 20 (45.5) 34 (30.0)
Mild PAH 18 (40.9) 29 (42.6)
Mod PAH 6 (13.6) 4 (5.9)
Severe PAH 0 (0) 1 (1.5)
LV dysfunction 0.628
Mild LV dysfunction 13 (29.5) 15 (22.1)
Moderate LV dysfunction 5 (11.4) 7 (10.3)
Severe LV dysfunction 26 (59.1) 46 (67.6)
LVEF (%) 32.5 (27.0- 41.0) 31.5 (28.0- 36.2) 0.507
Dysynchrony 11 (25.0) 20 (29.4 ) 0.670
Cath study
EDV (ml) 187.5 (120.0- 235.5) 191.0 (167.5 – 220.5) 0.560
ESV(ml) 144.5 (74.7 – 194.7) 124.0 ( 100.0- 144.5 ) 0.887
EF (%) 23.5 (17.2 – 42.6) 35.0 (25.0- 39.0) 0.180
PAH 0.543
No PAH 7 (46.7) 20 (64.5)
Mild PAH 6 (40.0) 10 (32.2)
Moderate PAH 2 (13.3) 1 (3.2)
Severe PAH 0 (0) 0 (0)
Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: MR, mitral regurgitation; PAH, pulmonary artery hypertension; LVEF, left
ventricular ejection fraction; EDV, end diastolic volume; ESV, end systolic volume; EF,
ejection fraction.
44 | P a g e
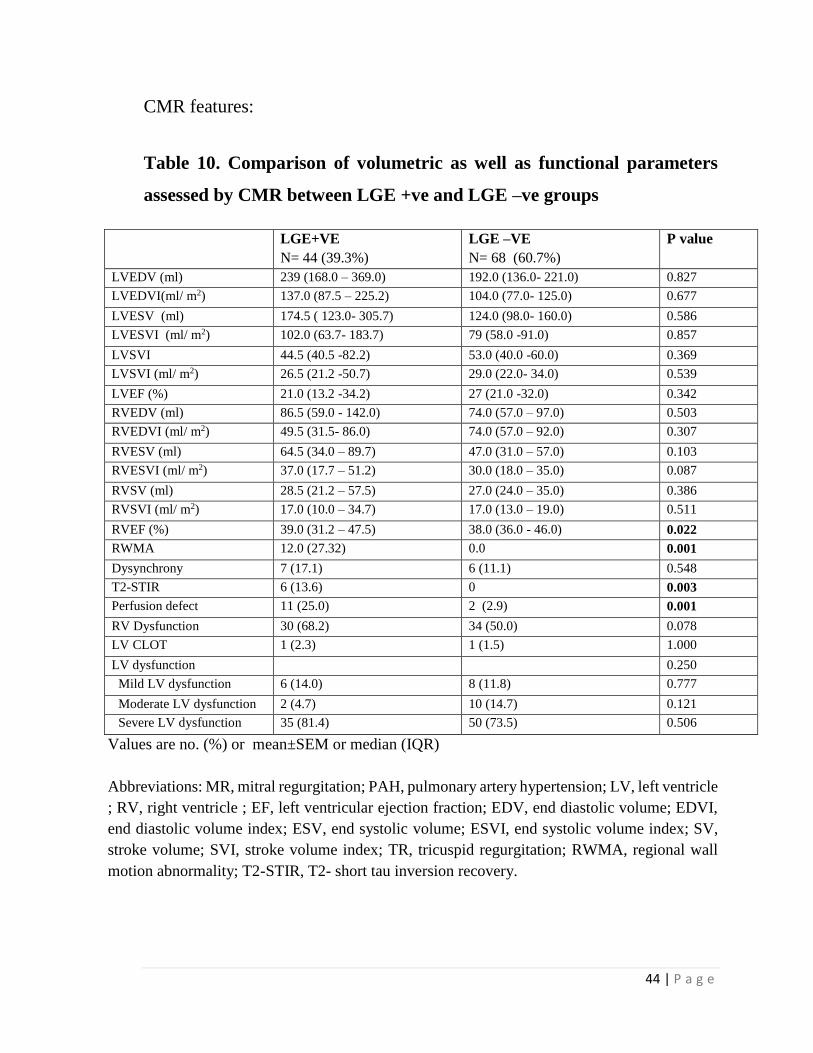
CMR features:
Table 10. Comparison of volumetric as well as functional parameters
assessed by CMR between LGE +ve and LGE –ve groups
LGE+VE
N= 44 (39.3%)
LGE –VE
N= 68 (60.7%)
P value
LVEDV (ml) 239 (168.0 – 369.0) 192.0 (136.0- 221.0) 0.827
LVEDVI(ml/ m2) 137.0 (87.5 – 225.2) 104.0 (77.0- 125.0) 0.677
LVESV (ml) 174.5 ( 123.0- 305.7) 124.0 (98.0- 160.0) 0.586
LVESVI (ml/ m2) 102.0 (63.7- 183.7) 79 (58.0 -91.0) 0.857
LVSVI 44.5 (40.5 -82.2) 53.0 (40.0 -60.0) 0.369
LVSVI (ml/ m2) 26.5 (21.2 -50.7) 29.0 (22.0- 34.0) 0.539
LVEF (%) 21.0 (13.2 -34.2) 27 (21.0 -32.0) 0.342
RVEDV (ml) 86.5 (59.0 - 142.0) 74.0 (57.0 – 97.0) 0.503
RVEDVI (ml/ m2) 49.5 (31.5- 86.0) 74.0 (57.0 – 92.0) 0.307
RVESV (ml) 64.5 (34.0 – 89.7) 47.0 (31.0 – 57.0) 0.103
RVESVI (ml/ m2) 37.0 (17.7 – 51.2) 30.0 (18.0 – 35.0) 0.087
RVSV (ml) 28.5 (21.2 – 57.5) 27.0 (24.0 – 35.0) 0.386
RVSVI (ml/ m2) 17.0 (10.0 – 34.7) 17.0 (13.0 – 19.0) 0.511
RVEF (%) 39.0 (31.2 – 47.5) 38.0 (36.0 - 46.0) 0.022
RWMA 12.0 (27.32) 0.0 0.001
Dysynchrony 7 (17.1) 6 (11.1) 0.548
T2-STIR 6 (13.6) 0 0.003
Perfusion defect 11 (25.0) 2 (2.9) 0.001
RV Dysfunction 30 (68.2) 34 (50.0) 0.078
LV CLOT 1 (2.3) 1 (1.5) 1.000
LV dysfunction 0.250
Mild LV dysfunction 6 (14.0) 8 (11.8) 0.777
Moderate LV dysfunction 2 (4.7) 10 (14.7) 0.121
Severe LV dysfunction 35 (81.4) 50 (73.5) 0.506
Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: MR, mitral regurgitation; PAH, pulmonary artery hypertension; LV, left ventricle
; RV, right ventricle ; EF, left ventricular ejection fraction; EDV, end diastolic volume; EDVI,
end diastolic volume index; ESV, end systolic volume; ESVI, end systolic volume index; SV,
stroke volume; SVI, stroke volume index; TR, tricuspid regurgitation; RWMA, regional wall
motion abnormality; T2-STIR, T2- short tau inversion recovery.
45 | P a g e
Most of the functional and volumetric parameters were similar inboth the groups
with few exceptions. RV ejection fraction was significantly less in LGE +ve group
compared to LGE -ve group. Similarly RWMA, perfusion defect and T2-STIR edema is
significantly more common in the LGE +ve group.
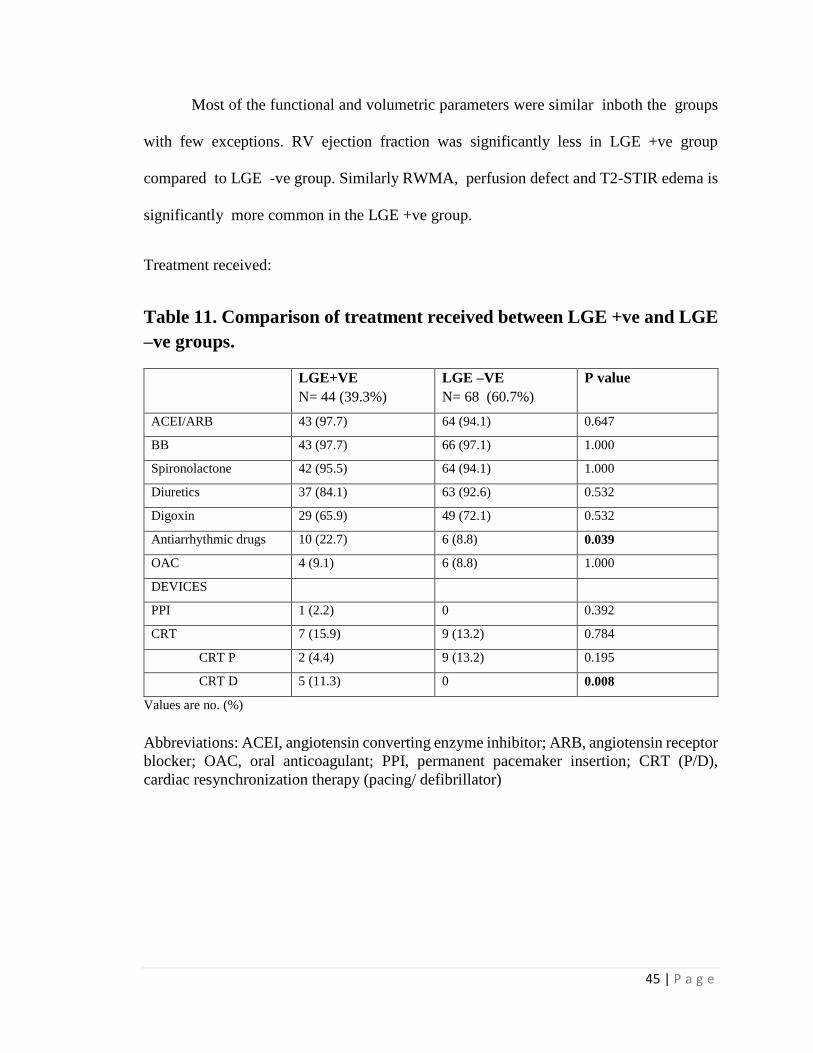
Treatment received:
Table 11. Comparison of treatment received between LGE +ve and LGE
–ve groups.
LGE+VE
N= 44 (39.3%)
LGE –VE
N= 68 (60.7%)
P value
ACEI/ARB 43 (97.7) 64 (94.1) 0.647
BB 43 (97.7) 66 (97.1) 1.000
Spironolactone 42 (95.5) 64 (94.1) 1.000
Diuretics 37 (84.1) 63 (92.6) 0.532
Digoxin 29 (65.9) 49 (72.1) 0.532
Antiarrhythmic drugs 10 (22.7) 6 (8.8) 0.039
OAC 4 (9.1) 6 (8.8) 1.000
DEVICES
PPI 1 (2.2) 0 0.392
CRT 7 (15.9) 9 (13.2) 0.784
CRT P 2 (4.4) 9 (13.2) 0.195
CRT D 5 (11.3) 0 0.008
Values are no. (%)
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor
blocker; OAC, oral anticoagulant; PPI, permanent pacemaker insertion; CRT (P/D),
cardiac resynchronization therapy (pacing/ defibrillator)
46 | P a g e
Treatment received by both groups were not significantly different except
antiarrhythmic medications such as amiodarone , which was more prescribed in LGE +ve
group compared to LGE –ve group (p=0.039). This suggest higher incidence of
arrhythmias in LGE +ve group for which amiodarone was given for secondary prophylaxis.
(Table 11)
Follow up:
The mean follow up period was 745 ± 320 days with no significant difference
between two groups. The primary end point , combined major adverse cardiac event (
MACE, comprising all cause mortality, sustained VT, SCD/ RCA, appropriate ICD shock
and HF hospitalization) was significantly more in LGE +ve group than the LGE –ve group
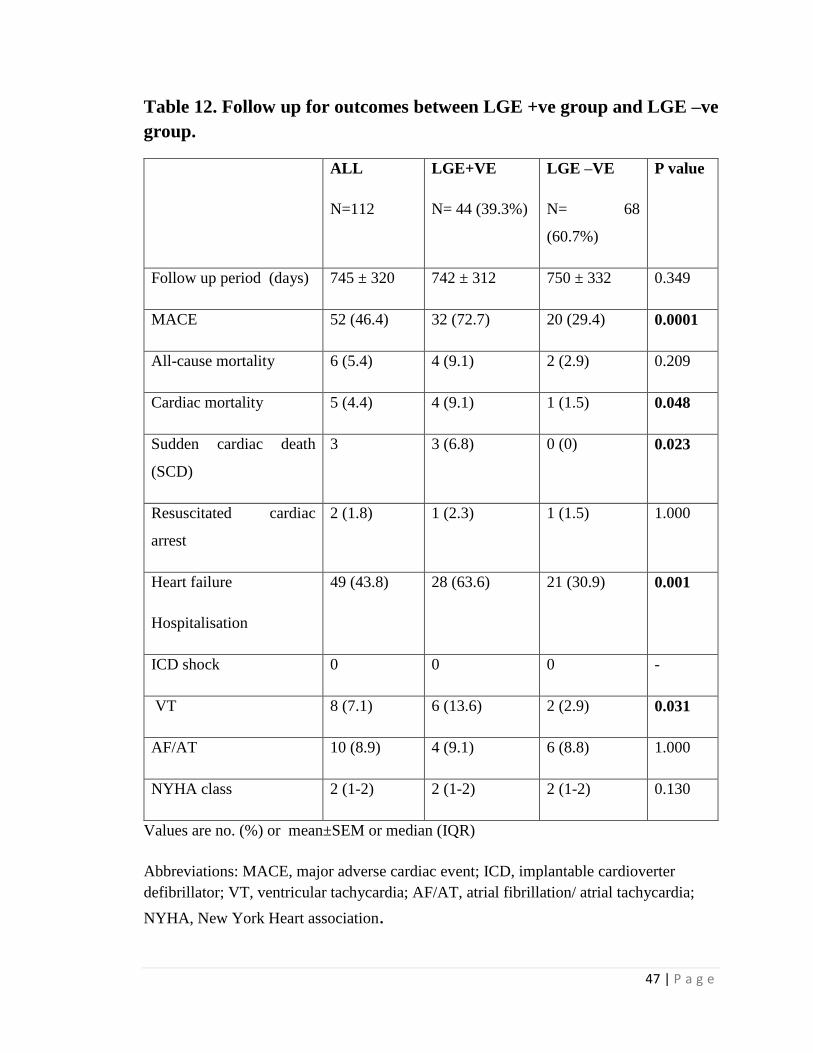
( 72.7% vs 29.4%, p <0.0001). (Table 12).
47 | P a g e
Table 12. Follow up for outcomes between LGE +ve group and LGE –ve
group.
ALL
N=112
LGE+VE
N= 44 (39.3%)
LGE –VE
N= 68
(60.7%)
P value
Follow up period (days) 745 ± 320 742 ± 312 750 ± 332 0.349
MACE 52 (46.4) 32 (72.7) 20 (29.4) 0.0001
All-cause mortality 6 (5.4) 4 (9.1) 2 (2.9) 0.209
Cardiac mortality 5 (4.4) 4 (9.1) 1 (1.5) 0.048
Sudden cardiac death
(SCD)
3 3 (6.8) 0 (0) 0.023
Resuscitated cardiac
arrest
2 (1.8) 1 (2.3) 1 (1.5) 1.000
Heart failure
Hospitalisation
49 (43.8) 28 (63.6) 21 (30.9) 0.001
ICD shock 0 0 0 -
VT 8 (7.1) 6 (13.6) 2 (2.9) 0.031
AF/AT 10 (8.9) 4 (9.1) 6 (8.8) 1.000
NYHA class 2 (1-2) 2 (1-2) 2 (1-2) 0.130
Values are no. (%) or mean±SEM or median (IQR)
Abbreviations: MACE, major adverse cardiac event; ICD, implantable cardioverter
defibrillator; VT, ventricular tachycardia; AF/AT, atrial fibrillation/ atrial tachycardia;
NYHA, New York Heart association.
48 | P a g e
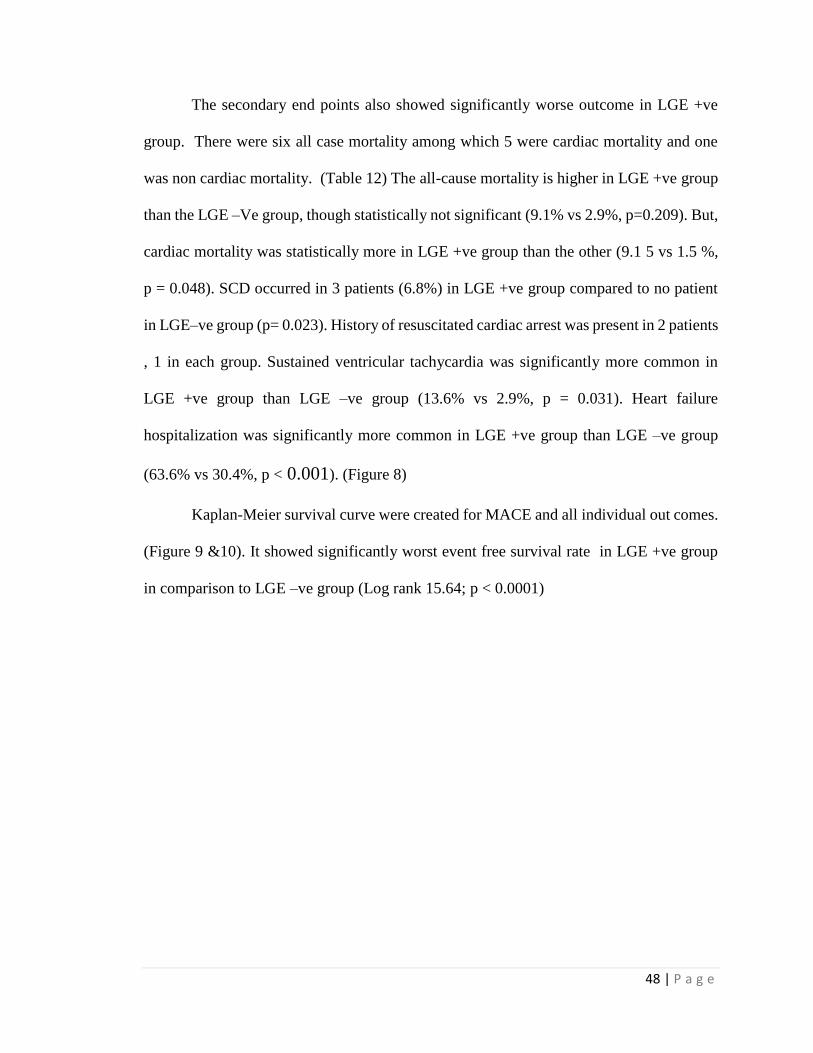
The secondary end points also showed significantly worse outcome in LGE +ve
group. There were six all case mortality among which 5 were cardiac mortality and one
was non cardiac mortality. (Table 12) The all-cause mortality is higher in LGE +ve group
than the LGE –Ve group, though statistically not significant (9.1% vs 2.9%, p=0.209). But,
cardiac mortality was statistically more in LGE +ve group than the other (9.1 5 vs 1.5 %,
p = 0.048). SCD occurred in 3 patients (6.8%) in LGE +ve group compared to no patient
in LGE–ve group (p= 0.023). History of resuscitated cardiac arrest was present in 2 patients
, 1 in each group. Sustained ventricular tachycardia was significantly more common in
LGE +ve group than LGE –ve group (13.6% vs 2.9%, p = 0.031). Heart failure
hospitalization was significantly more common in LGE +ve group than LGE –ve group
(63.6% vs 30.4%, p < 0.001). (Figure 8)
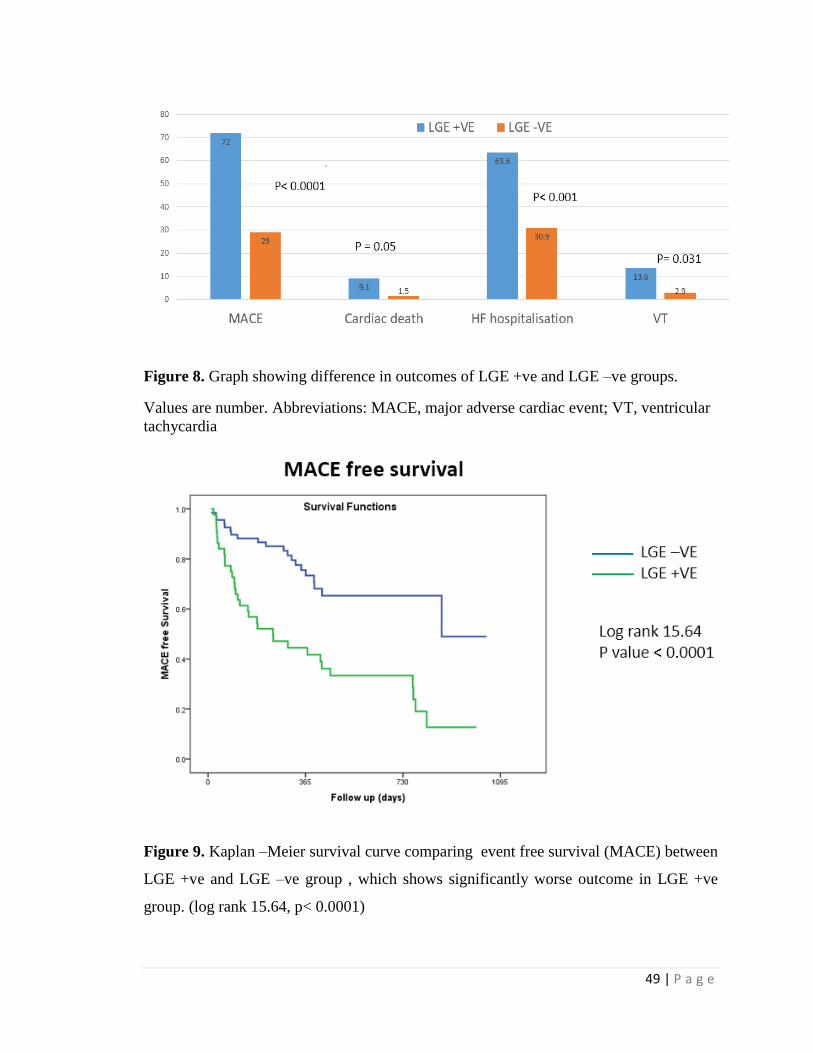
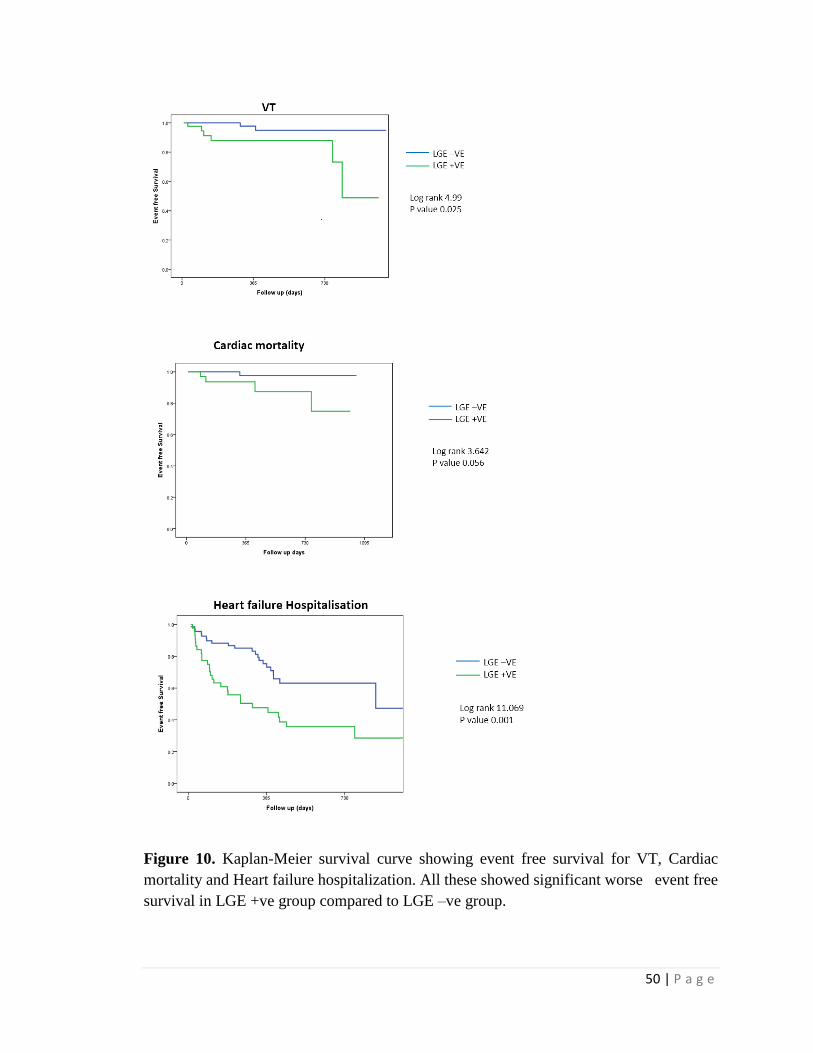
Kaplan-Meier survival curve were created for MACE and all individual out comes.
(Figure 9 &10). It showed significantly worst event free survival rate in LGE +ve group
in comparison to LGE –ve group (Log rank 15.64; p < 0.0001)
49 | P a g e
Figure 8. Graph showing difference in outcomes of LGE +ve and LGE –ve groups.
Values are number. Abbreviations: MACE, major adverse cardiac event; VT, ventricular
tachycardia
Figure 9. Kaplan –Meier survival curve comparing event free survival (MACE) between
LGE +ve and LGE –ve group , which shows significantly worse outcome in LGE +ve
group. (log rank 15.64, p< 0.0001)
50 | P a g e
Figure 10. Kaplan-Meier survival curve showing event free survival for VT, Cardiac
mortality and Heart failure hospitalization. All these showed significant worse event free
survival in LGE +ve group compared to LGE –ve group.
51 | P a g e
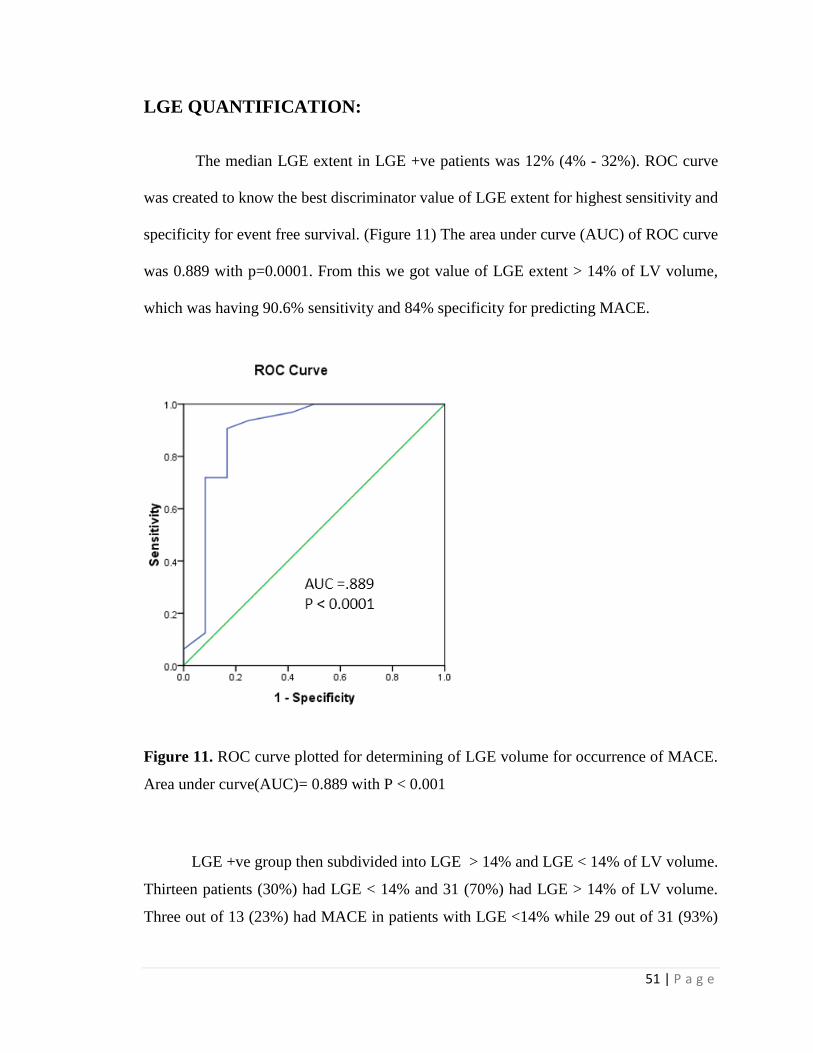
LGE QUANTIFICATION:
The median LGE extent in LGE +ve patients was 12% (4% - 32%). ROC curve
was created to know the best discriminator value of LGE extent for highest sensitivity and
specificity for event free survival. (Figure 11) The area under curve (AUC) of ROC curve
was 0.889 with p=0.0001. From this we got value of LGE extent > 14% of LV volume,
which was having 90.6% sensitivity and 84% specificity for predicting MACE.
Figure 11. ROC curve plotted for determining of LGE volume for occurrence of MACE.
Area under curve(AUC)= 0.889 with P < 0.001
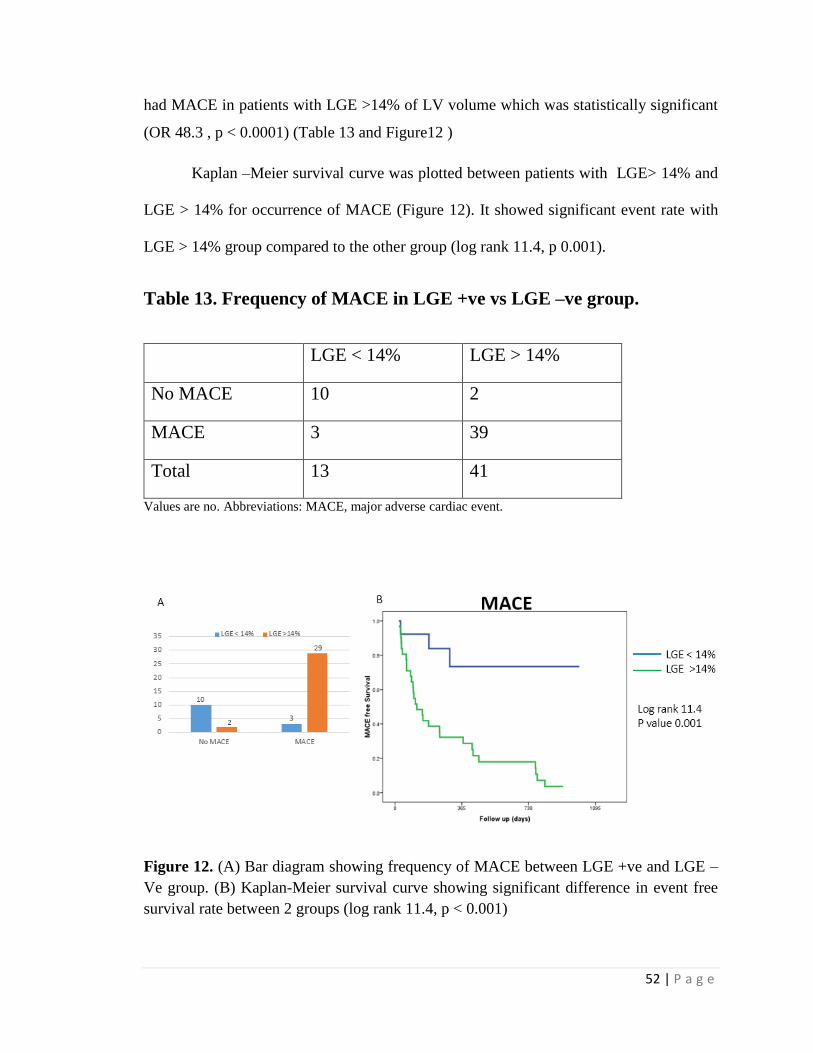
LGE +ve group then subdivided into LGE > 14% and LGE < 14% of LV volume.
Thirteen patients (30%) had LGE < 14% and 31 (70%) had LGE > 14% of LV volume.
Three out of 13 (23%) had MACE in patients with LGE <14% while 29 out of 31 (93%)
52 | P a g e
had MACE in patients with LGE >14% of LV volume which was statistically significant
(OR 48.3 , p < 0.0001) (Table 13 and Figure12 )
Kaplan –Meier survival curve was plotted between patients with LGE> 14% and
LGE > 14% for occurrence of MACE (Figure 12). It showed significant event rate with
LGE > 14% group compared to the other group (log rank 11.4, p 0.001).
Table 13. Frequency of MACE in LGE +ve vs LGE –ve group.
LGE < 14% LGE > 14%
No MACE 10 2
MACE 3 39
Total 13 41
Values are no. Abbreviations: MACE, major adverse cardiac event.
Figure 12. (A) Bar diagram showing frequency of MACE between LGE +ve and LGE –
Ve group. (B) Kaplan-Meier survival curve showing significant difference in event free
survival rate between 2 groups (log rank 11.4, p < 0.001)
53 | P a g e
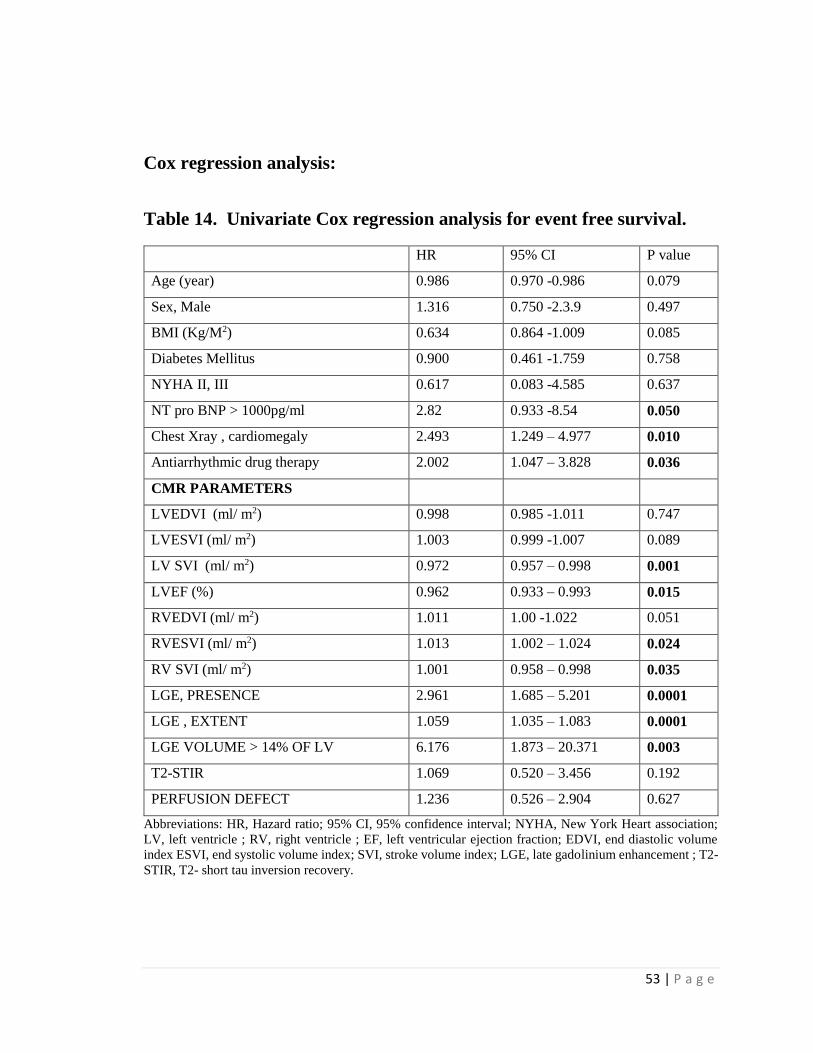
Cox regression analysis:
Table 14. Univariate Cox regression analysis for event free survival.
HR 95% CI P value
Age (year) 0.986 0.970 -0.986 0.079
Sex, Male 1.316 0.750 -2.3.9 0.497
BMI (Kg/M2) 0.634 0.864 -1.009 0.085
Diabetes Mellitus 0.900 0.461 -1.759 0.758
NYHA II, III 0.617 0.083 -4.585 0.637
NT pro BNP > 1000pg/ml 2.82 0.933 -8.54 0.050
Chest Xray , cardiomegaly 2.493 1.249 – 4.977 0.010
Antiarrhythmic drug therapy 2.002 1.047 – 3.828 0.036
CMR PARAMETERS
LVEDVI (ml/ m2) 0.998 0.985 -1.011 0.747
LVESVI (ml/ m2) 1.003 0.999 -1.007 0.089
LV SVI (ml/ m2) 0.972 0.957 – 0.998 0.001
LVEF (%) 0.962 0.933 – 0.993 0.015
RVEDVI (ml/ m2) 1.011 1.00 -1.022 0.051
RVESVI (ml/ m2) 1.013 1.002 – 1.024 0.024
RV SVI (ml/ m2) 1.001 0.958 – 0.998 0.035
LGE, PRESENCE 2.961 1.685 – 5.201 0.0001
LGE , EXTENT 1.059 1.035 – 1.083 0.0001
LGE VOLUME > 14% OF LV 6.176 1.873 – 20.371 0.003
T2-STIR 1.069 0.520 – 3.456 0.192
PERFUSION DEFECT 1.236 0.526 – 2.904 0.627
Abbreviations: HR, Hazard ratio; 95% CI, 95% confidence interval; NYHA, New York Heart association;
LV, left ventricle ; RV, right ventricle ; EF, left ventricular ejection fraction; EDVI, end diastolic volume
index ESVI, end systolic volume index; SVI, stroke volume index; LGE, late gadolinium enhancement ; T2-
STIR, T2- short tau inversion recovery.

54 | P a g e
Univariate Cox regression analysis was performed for detecting significant
unadjusted predictors of MACE (Table14) . Significant predictors of MACE were
cardiomegaly by chest x-ray, NT pro BNP > 1000 pg/ml at the time of admission, LV SVI,
LVEF, RV SVI, RV ESVI, LGE presence and LGE extent. Among these LGE extent> 14%
of LV volume was the strongest predictor of MACE ( HR 6.17, CI: 1.87 – 20.37, p =0.003).
Multivariate Cox regression analysis was performed for detecting the adjusted predictors
of MACE (Table 15). The best overall predictors of MACE were LGE > 14% of LV
volume and presence of LGE.
Table 15. Multivariate Cox regression analysis for event free survival.
HR 95% CI P value
LGE, PRESENCE 2.301 1.346 – 3.974 0.008
LGE VOLUME > 14% OF LV 8.894 2.618 – 28.856 0.0001
Abbreviations: HR, Hazard ratio; 95% CI, 95% confidence interval; LGE, late gadolinium enhancement.
55 | P a g e
DISCUSSION
In our study we included 112 patients of NIDCM after excluding all ischemic DCM
by coronary angiography. The median age is 45 years and majority are male (64%). So it
is a disease affecting young males more than females, in their 3rd and 4th decade. One fourth
of them were diabetic while other coronary risk factors were present in less than 15% of
cases.
History of long term heavy alcohol intake (> 110- 120 mg / day) was present in 7
cases. The exact dose and duration of alcohol intake to cause cardiomyopathy is still not
known. Though, alcoholic cardiomyopathy can have systolic or diastolic dysfunction, with
or without LV dilatation. It mimics idiopathic DCM morphologically.(76) So, in the
absence of any definitive evidence, we preferred them to keep in idiopathic DCM group.
Family history of DCM (at least 2 members in first or second degree relatives have
DCM) is present in 4 cases which were labelled as Familial DCM. They all resemble
morphologically idiopathic DCM.
Majority of patients were in NYHA class II followed by NYHA class III. Most of
the patients were in sinus rhythm while only 5 cases had AF. So, this suggest that incidence
of AF is not high in DCM patients. Thirty five percent showed LBBB and 9% showed
RBBB suggesting high incidence of bundle branch block in DCM patients which also may
aggravate existing LV dysfunction.
Chest X-ray showed that 65% patient had cardiomegaly (CTR >0.6 ). This
emphasizes the role of basic investigations in evaluation of DCM patients. Trans thoracic
56 | P a g e
echocardiography (TTE) is the most commonly performed basal investigation to diagnose
DCM. We found that majority of patients had severe LV dysfunction with EF < 35%.
Mitral regurgitation (MR) was present in 87% but mostly it was mild (65%). MR in DCM
patients is usually due to LV dilatation leading to coaptation defect (secondary MR), which
occurs in hugely dilated LV. Mancuso et al showed limitations of present American society
of Echocardiographic criteria in diagnosing as well as grading secondary MR. (77) By
TTE, 50% had no PAH while 42% had only mild PAH. This suggest that PAH is
uncommon in DCM patients unless in very advanced cases with severe diastolic
dysfunction. Dysynchrony was present in 27% of case signifying one important correctable
cause of LV dysfunction. Invasive right heart catheterization showed also dilated LV
dimension with poor LV function. The prevalence and pattern of MR and PAH matches
with TEE data with good correlation. Majority of patients were on guideline directed
medical therapy.
The “NEED” for CMR in DCM.
TTE is usually the first imaging test done for assessing cardiomyopathies. The
reasons are it is easily available, can be done quickly with good hemodynamic assessment
and also puts light on etiology. The disadvantages are high inter observer variability,
affected by patients body position and clarity of echo window and less role in tissue
characterization. So, CMR is now considered gold standard in the evaluation of
cardiomyopathies.The reason behind this are
57 | P a g e
(1) with highresolution, detailed three-dimensional (3D)images of cardiac and
thoracic anatomy without interference of body habitus
(2) accurate tissue characterization based on various T1W/ T2 W and LGE
techniques which helps in diagnosis as well as prognosis.
CMR features:
The LVEDV and LVESV were more than normal values suggesting dilated LV.
Mean LVEF was 28 %. Seventy six percent had severe LV dysfunction.
Mean RVEF was 36% and 57% of patients had RV dysfunction. So, it shows that
almost half of DCM patients have biventricular dysfunction. RV function carries an
important prognostic significance in DCM patients. Bourant et al showed that poor RV
function leads to increased MACE rates in NIDCM patients.(26)Groote et al ,also showed
RVEF as an independent poor prognostic indicator heart failure patients. (78)We also
found that RV stroke volume asan poor prognosis predictor . These findings also strongly
recommends for doing CMR in all DCM patients as CMR is the gold standard for RV
volume and function assessment which will help in risk stratification.
Regional wall motion abnormality (RWMA), not in any coronary artery territory
distribution was present in 12 cases (10%). Most common location of RWMA was IVS
followed by inferior wall and all of them had LGE. Eight of them were diagnosed as
idiopathic DCM and rest one each as end stage HCM, sarcoidosis, myocarditis and LVNC.
Though, 5 of those 12 cases(42%) had MACE, RWMA was not found to be marker of poor
prognosis both in univariate and multivariate model. Poyhonen et al showed RWMA in
upto 34% of cases and described RWMA as a marker of bad prognosis. (66) This difference
58 | P a g e
in observation can be explained by higher number of patients (39%) in the Poyhonen’s
study have RWMA active myocarditis, whereas in our case only 10% had RWMA and 5%
had active myocarditis.
Dysynchrony was present in 12% of cases which almost half compared to
dysnchrony detected by TTE. The reason can be explained by simultaneous ECG recording
and Doppler analysis in TTE , which is not possible in CMR. T2-STIR showing myocardial
edema was present in 7 cases. Majority had myocarditis and one case had sarcoidosis. This
tool helps in distinguishing active phase from chronic phase of disease. (72)
One important finding we got that perfusion defect was present in 12% of cases.
Most of these cases had LGE and the areas showing perfusion defect matches with the
areas showing LGE.There is not much data on perfusion defect in NIDCM in existing
literature.(79)This may suggest that microvascular abnormality may be an etiology leading
to myocardial damage and fibrosis. This concept is in research phase now. One perfusion
study using SPECT imaging in NIDCM showed that patients with perfusion defect had
poor cardiac outcome than patients who didnot have it. (80)
LGE-CMR:
Prevalence of LGE :
The prevalence of LGE in various studies varies from 12 % to 67%. (14,16,17)
There is no data from India. This study is perhaps the first study from India about CMR in
NIDCM .Prevalence of LGE in NIDCM patients in our study is 39% which is comparable
to the existing data.
Distribution pattern of LGE:
59 | P a g e
The pattern of LGE distribution in CAD ( sub endocardial) is distinct from that seen
in NIDCM , making it an important tool in determining etiology.(39)
Overall LGE most commonly found in mid myocardial location of IVS followed by inferior
wall , though it may vary according to diagnosis. Some groups reported only midwall
enhancement in NICM (16)whereas others , including us , have got different patterns of
enhancement. (59,64) Mc crohon et al (14) found 2 predominant patterns of LGE
distribution in idiopathic DCM. First, Mid myocardial (28%) followed by had
subendocardial or transmural enhancement (13%) not in the territory of a coronary artery.
The reason for this discrepancy is not very clear. Histological examination showed patterns
of fibrosis matching with all pattern of LGE. (81,82).The mid myocardial LGE was
correlated with the focal segmental fibrosis in an autopsy study.(83)
Distribution pattern of LGE helps in diagnosis of different forms of
NIDCM.(38,39). End stage HCM was diagnosed when a patient with h/o HCM presented
with echo/ MRI features s/o DCM. Both the two patients in our series had LGE in IVS,
inferior wall with midmyocardial to transmural involvement. Matoh et al showed that LGE
CMR helps in differentiating end stage HCM patients from DCM and also helps in risk
stratification. (43) Myocarditis showed LGE diffuse and predominantly subepicardial and
mid myocardial LGE. Sarcoidosis showed patchy subepicardial LGE with predilection for
basal segments and amyloidosis showed circumferential subendocardial LGE as described
in literature.(42,48,50)
Though clinical history and TTE helped in suspicion of the underlying condition,
the final diagnosis was only made out after CMR study. This credit goes to the unique
60 | P a g e
tissue characterization ability of CMR which is not there in TTE. (43). That’s why CMR
is now considered the gold standard for diagnosis of cardiomyopathies. (15)
Prognostic importance of CMR in NIDCM:
To know the prognostic significance of LGE we divided the patients based on
presence or absence of LGE. No baseline difference in baseline features, symptoms, CXR,
TTE, ECGwas notedexcept RBBB which is more common in LGE +ve group.NT pro BNP
value at admission was also more in LGE +ve group signifying they were more clinically
sick. Both groups received equal treatments except antiarrhythmic therapy which is more
often prescribed in LGE +ve group. It says that LGE +ve group had more incidence of
arrhythmias than LGE –ve group.
Sixteen patients received CRT. Among these, 5 patients received CRT-D and 11
CRT-P. All patients who received CRT-D were LGE +ve. This signifies that LGE +ve
group had more incidence of VT than the LGE –ve group.
Baseline CMR volumetric data showed, all the LV dimensions including LVEDV,
LVESV were tend to be higher and LVEF tend to be lower in LGE +ve group though
statistically not significant. The existing literature also had differential views regarding
this. Many studies showed increased LV dimensions and decreased LVEF in LGE +ve
group, arguing for more fibrosis leading to more remodeled LV. (3,16,25) But, many other
studies did not show any significant difference in LV dimensions and function between
LGE +ve and LGE –ve group. (64,67)This depends upon the type and extent of fibrosis.
In DCM patients , the previous histopatholgy studies showed fibrosis is of 2 types – either
diffuse ( interstitial) or segmental (replacement) fibrosis.LGE CMR can pick up the
replacement fibrosis with good resolution but, it’s poor in detecting the interstitial fibrosis.
61 | P a g e
All patients with RWMA and T2-STIR edema and majority of patients with
perfusion defect were in LGE +ve group. This suggests that LGE +ve group,which had
wall fibrosis also had more wall motion abnormalities, more myocardial edema and
perfusion defects . These may be different pathological spectrum of the same underlying
etiology.
On follow up, LGE +ve group showed significantly more adverse outcome
compared to LGE –ve group. The primary end point (MACE) and secondary endpoints
(cardiac mortality, sustained VT, HF hospitalization) were significantly more in LGE +ve
group than LGE –ve group. This clearly suggests that LGE in NIDCM patients heralds
poor prognosis. LGE +ve patients not only had more sustained VT, cardiac mortality but
also had more HF hospitalisations. So it increases both mortality and morbidity. In
Univariate analysis, presence of LGE is one of the major determinant of MACE (HR 2.96;
p< 0.00001).
We quantify LGE extent visually and from ROC curve found LGE extent > 14%
as the best discriminator with highest sensitivity and specificity to determine MACE. In
Univariate analysis, LGE volume > 14% of LV volume was the strongest predictor of
MACE (HR 6.176, p =0.003). In Multivariate analysis, after adjusting age, LV function
and other confounders , LGE extent > 14% of LV volume and LGE positivity were the
only two discriminators for MACE. This clearly showed that quantification of LGE adds
to the prognostication value of CMR in NIDCM patients.
In earlier studies the prognostic values of LGE in NIDCM has been clearly
documented.(16,64,3,25,67)Assomull et al.(16)correlated LGE with mortality and adverse
cardiac events and described LGE as the best predictor of SCD with hazard ratio of 5.4.
62 | P a g e
Wu et al. (64) also shown that LGE +ve patients had higher MACE (HF,
appropriate ICD shock, and cardiac mortality; 44%versus 8%; 𝑃 = 0.001;HR, 8.2; 𝑃 =
0.002). One recent metanalysis(65)has shown that LGE +ve NIDCM patients had higher
risk of all-cause mortality, HF hospitalization, and sudden cardiac death. This metanalysis
put foreword the concept of taking LGEas an independent entity for risk stratification of
NIDCM.
Shimuzu et al (63) were one of the earlier investigators to visually quantify LGE
volume in NIDCM patient. They showed that MACE was significantly higher in patients
with LGE extent of > 10% of LV volume compared to the patients with <10% of LV
volume ( 36% vs 2 % , Log rank , p = 0.0001). Similarly Poyhonen et al, (66) also visually
quantified LGE in NIDCM patients and showed that LGE volume > 14% of LV volume
was the best parameter to predict bad prognosis. We also found a LGE volume > of 17%
of LV volume as the best predictor poor prognosis.
LGE denotes focal fibrosis, which may promote re-entry mechanism leading to
ventricular tachycardia. Areas of fibrosis in NIDCM, detected by CMR as LGE were found
as substrates for inducible VT. (61)This concept is also supported by the data from ICD
patients showing more appropriate shock in LGE positive patients.(64)In addition, more
fibrosis also can change the mechanical property of myocardium causing loss of
ventricular compliance leading to increased incidence of heart failure . (84)
Based on our study we can say that LGE presence and quantification helps in
additional risk stratification in NIDCM patients. Currently ICD as a primary prophylaxis
is indicated only based on LVEF criteria.(85)ICD implantation as per LVEF criteria had
63 | P a g e
not shown any significant benefit in DEFINITE study. (86)LVEF, which is usually taken
as a measure of LV function has been accepted as best predictor of mortality in
NIDCM.(87) But LVEF was not found to be a predictor of ICDdischarge. (88) Our study
also showed that lower LVEF, though predicted MACE in univariate model , wasnot an
independent predictor of MACE in multivariate model. For this reasons, the criteria for
ICD implantation needs an urgent revision. LGE in CMR should be taken as an emerging
indication for ICD in NIDCM patients. (89)
64 | P a g e
LIMITATIONS
This is a retrospective but with an observational- follow up study design. It is a
single center study. Only those NIDCM patients who underwent CMR were analysed ,
which may not represent the entire spectrum of NIDCM.
LGE- showed only focal or replacement fibrosis whereas it is poor in detecting
diffuse interstitial fibrosis. Hence LGE determined fibrosis underestimates the presence
and extent of the myocardial in NIDCM.(81) Pre- and post-contrast T1 mapping may
further improve this deficit.(90)
65 | P a g e
CONCLUSION
• Accurate volumetric measurement and functional assessment can be
done by CMR.
• Prevalence of LGE in NIDCM is 39%.
• Cardiac MRI helps in diagnosing various forms of NIDCM based on
distribution pattern of LGE.
• LGE positive patients showed significantly higher combined major
cardiac events including all-cause mortality, VT, SCD, heart failure
hospitalisations. Thus LGE is a poor prognostic marker in NIDCM
patients and LGE extent gives an additional prognostic information
beyond LVEF.
• Further research will be needed to determine whether therapy guided
by CMR findings can lower morbidity and mortality in NIDCM
patients.
.
66 | P a g e
BIBLIOGRAPHY
1 Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, et al.
Contemporary definitions and classification of the cardiomyopathies: an American
Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart
Failure and Transplantation Committee; Quality of Care and Outcomes Research and
Functional Genomics and Translational Biology Interdisciplinary Working Groups;
and Council on Epidemiology and Prevention. Circulation. 2006 Apr
11;113(14):1807–16.
2 Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O’Connell J, et al.
Report of the 1995 World Health Organization/International Society and Federation of
Cardiology Task Force on the Definition and Classification of cardiomyopathies.
Circulation. 1996 Mar 1;93(5):841–2.
3 Gulati A, Jabbour A, Ismail TF, Guha K, Khwaja J, Raza S, et al. Association of fibrosis
with mortality and sudden cardiac death in patients with nonischemic dilated
cardiomyopathy. JAMA. 2013 Mar 6;309(9):896–908.
4 Aukrust P, Yndestad A, Ueland T, Kristian Damås J, S. Frøland S, Gullestad L. The
role of intravenous immunoglobulin in the treatment of chronic heart failure. Int J
Cardiol. 2006 Sep 10;112(1):40–5.
5 Nanjo S, Yoshikawa K, Harada M, Inoue Y, Namiki A, Nakano H, et al. Correlation
Between Left Ventricular Diastolic Function and Ejection Fraction in Dilated
Cardiomyopathy Using Magnetic Resonance Imaging With Late Gadolinium
Enhancement. Circ J. 2009;73(10):1939–44.
6 Kassi M, Nabi F. Role Of Cardiac Mri In The Assessment Of Nonischemic
Cardiomyopathies. Methodist DeBakey Cardiovasc J. 2013;9(3):149–55.
7 Quarta G, Sado DM, Moon JC. Cardiomyopathies: focus on cardiovascular magnetic
resonance. Br J Radiol. 2011 Dec 1;84(special_issue_3):S296–305.
8 Masci PG, Dymarkowski S, Bogaert J. The role of cardiovascular magnetic resonance
in the diagnosis and management of cardiomyopathies. J Cardiovasc Med. 2008
May;9(5):435–449.
9 Semelka RC, Tomei E, Wagner S, Mayo J, Kondo C, Suzuki J, et al. Normal left
ventricular dimensions and function: interstudy reproducibility of measurements with
cine MR imaging. Radiology. 1990 Mar 1;174(3):763–8.
10 Sparrow PJ, Merchant N, Provost YL, Doyle DJ, Nguyen ET, Paul NS. CT and MR
Imaging Findings in Patients with Acquired Heart Disease at Risk for Sudden Cardiac
Death. RadioGraphics. 2009 May 1;29(3):805–23.
67 | P a g e
11 Francone M, Carbone I, Agati L, Ducci CB, Mangia M, Iacucci I, et al. Utility of T2-
weighted short-tau inversion recovery (STIR) sequences in cardiac MRI: an overview
of clinical applications in ischaemic and non-ischaemic heart disease. Radiol Med
(Torino). 2011 Feb 1;116(1):32–46.
12 Lee DH. Mechanisms of contrast enhancement in magnetic resonance imaging. Can
Assoc Radiol J J Assoc Can Radiol. 1991 Feb;42(1):6–12.
13 Breuckmann F, Maderwald S, Buhr C, Bruder O, Schlosser T, Erbel R, et al. Cardiac
MRI: Estimation of Changes in Normalized Myocardial Gadolinium Accumulation
Over Time After Contrast Injection in Patients with Acute Myocarditis and Healthy
Volunteers. RöFo - Fortschritte Auf Dem Geb Röntgenstrahlen Bildgeb Verfahr. 2011
Oct;183(10):933–8.
14 McCrohon JA, Moon JCC, Prasad SK, McKenna WJ, Lorenz CH, Coats AJS, et al.
Differentiation of Heart Failure Related to Dilated Cardiomyopathy and Coronary
Artery Disease Using Gadolinium-Enhanced Cardiovascular Magnetic Resonance.
Circulation. 2003 Jul 8;108(1):54–9.
15 Satoh H, Sano M, Suwa K, Saitoh T, Nobuhara M, Saotome M, et al. Distribution of
late gadolinium enhancement in various types of cardiomyopathies: Significance in
differential diagnosis, clinical features and prognosis. World J Cardiol. 2014 Jul
26;6(7):585–601.
16 Assomull RG, Prasad SK, Lyne J, Smith G, Burman ED, Khan M, et al. Cardiovascular
Magnetic Resonance, Fibrosis, and Prognosis in Dilated Cardiomyopathy. J Am Coll
Cardiol. 2006 Nov 21;48(10):1977–85.
17 Bello D, Shah DJ, Farah GM, Luzio SD, Parker M, Johnson MR, et al. Gadolinium
Cardiovascular Magnetic Resonance Predicts Reversible Myocardial Dysfunction and
Remodeling in Patients With Heart Failure Undergoing β-Blocker Therapy.
Circulation. 2003 Oct 21;108(16):1945–53.
18 Francone M. Role of Cardiac Magnetic Resonance in the Evaluation of Dilated
Cardiomyopathy: Diagnostic Contribution and Prognostic Significance [Internet].
International Scholarly Research Notices. 2014 [cited 2017 Sep 24]. Available from:
https://www.hindawi.com/journals/isrn/2014/365404/ref/
19 Flett AS, Hayward MP, Ashworth MT, Hansen MS, Taylor AM, Elliott PM, et al.
Equilibrium contrast cardiovascular magnetic resonance for the measurement of
diffuse myocardial fibrosis: preliminary validation in humans. Circulation. 2010 Jul
13;122(2):138–44.
20 Liu C-Y, Liu Y-C, Wu C, Armstrong A, Volpe GJ, van der Geest RJ, et al. Evaluation
of Age-Related Interstitial Myocardial Fibrosis With Cardiac Magnetic Resonance
Contrast-Enhanced T1 Mapping: MESA (Multi-Ethnic Study of Atherosclerosis). J Am
Coll Cardiol. 2013 Oct 1;62(14):1280–7.
68 | P a g e
21 Dass S, Suttie JJ, Piechnik SK, Ferreira VM, Holloway CJ, Banerjee R, et al.
Myocardial Tissue Characterization Using Magnetic Resonance Noncontrast T1
Mapping in Hypertrophic and Dilated CardiomyopathyClinical Perspective. Circ
Cardiovasc Imaging. 2012 Nov 1;5(6):726–33.
22 Alfakih K, Plein S, Thiele H, Jones T, Ridgway JP, Sivananthan MU. Normal human
left and right ventricular dimensions for MRI as assessed by turbo gradient echo and
steady-state free precession imaging sequences. J Magn Reson Imaging JMRI. 2003
Mar;17(3):323–9.
23 Bellenger NG, Burgess MI, Ray SG, Lahiri A, Coats AJS, Cleland JGF, et al.
Comparison of left ventricular ejection fraction and volumes in heart failure by
echocardiography, radionuclide ventriculography and cardiovascular magnetic
resonance. Are they interchangeable? Eur Heart J. 2000 Aug 1;21(16):1387–96.
24 Lorenz CH, Walker ES, Morgan VL, Klein SS, Graham TP. Normal Human Right and
Left Ventricular Mass, Systolic Function, and Gender Differences by Cine Magnetic
Resonance Imaging. J Cardiovasc Magn Reson. 1999 Jan 1;1(1):7–21.
25 Lehrke S, Lossnitzer D, Schöb M, Steen H, Merten C, Kemmling H, et al. Use of
cardiovascular magnetic resonance for risk stratification in chronic heart failure:
prognostic value of late gadolinium enhancement in patients with non-ischaemic
dilated cardiomyopathy. Heart. 2011 May 1;97(9):727–32.
26 Bourantas CV, Loh HP, Bragadeesh T, Rigby AS, Lukaschuk EI, Garg S, et al.
Relationship between right ventricular volumes measured by cardiac magnetic
resonance imaging and prognosis in patients with chronic heart failure. Eur J Heart
Fail. 2011 Jan 1;13(1):52–60.
27 Thavendiranathan P, Phelan D, Collier P, Thomas JD, Flamm SD, Marwick TH.
Quantitative Assessment of Mitral Regurgitation: How Best to Do It. JACC Cardiovasc
Imaging. 2012 Nov 1;5(11):1161–75.
28 Paydarfar D, Krieger D, Dib N, Blair RH, Pastore JO, Stetz JJ, et al. In vivo magnetic
resonance imaging and surgical histopathology of intracardiac masses: distinct features
of subacute thrombi. Cardiology. 2001;95(1):40–7.
29 Srichai MB, Junor C, Rodriguez LL, Stillman AE, Grimm RA, Lieber ML, et al.
Clinical, imaging, and pathological characteristics of left ventricular thrombus: A
comparison of contrast-enhanced magnetic resonance imaging, transthoracic
echocardiography, and transesophageal echocardiography with surgical or pathological
validation. Am Heart J. 2006 Jul 1;152(1):75–84.
30 Isner JM, Virmani R, Itscoitz SB, Roberts WC. Clinical pathologic conference. Left
and right ventricular myocardial infarction in idiopathic dilated cardiomyopathy. Am
Heart J. 1980 Feb;99(2):235–42.
31 Roberts WC, Siegel RJ, McManus BM. Idiopathic dilated Cardiomyopathy: Analysis
of 152 necropsy patients. Am J Cardiol. 1987 Dec 1;60(16):1340–55.
69 | P a g e
32 De Cobelli F, Pieroni M, Esposito A, Chimenti C, Belloni E, Mellone R, et al. Delayed
Gadolinium-Enhanced Cardiac Magnetic Resonance in Patients With Chronic
Myocarditis Presenting With Heart Failure or Recurrent Arrhythmias. J Am Coll
Cardiol. 2006 Apr 18;47(8):1649–54.
33 Al-Mallah MH, Shareef MN. The role of cardiac magnetic resonance imaging in the
assessment of non-ischemic cardiomyopathy. Heart Fail Rev. 2011 Jul 1;16(4):369–
80.
34 Arora NP, Mahajan N, Mohamad T, Kottam A, Afonso LC, Danrad R, et al. Cardiac
Magnetic Resonance Imaging in Peripartum Cardiomyopathy. Am J Med Sci. 2014
Feb 1;347(2):112–7.
35 Ntusi NBA, Chin A. Characterisation of peripartum cardiomyopathy by cardiac
magnetic resonance imaging. Eur Radiol. 2009 Jun 1;19(6):1324–5.
36 Crean A, Merchant N. Role of cardiac magnetic resonance imaging in identification of
amyloid cardiomyopathy. Indian Heart J. 2004 Dec;56(6):682–3.
37 Ptaszek LM, Price ET, Hu MY, Yang PC. Early Diagnosis of Hemochromatosis-
Related Cardiomyopathy with Magnetic Resonance Imaging. J Cardiovasc Magn
Reson. 2005 Jan 1;7(4):689–92.
38 Cummings KW, Bhalla S, Javidan-Nejad C, Bierhals AJ, Gutierrez FR, Woodard PK.
A Pattern-based Approach to Assessment of Delayed Enhancement in Nonischemic
Cardiomyopathy at MR Imaging. RadioGraphics. 2009 Jan 1;29(1):89–103.
39 Mahrholdt H, Wagner A, Judd RM, Sechtem U, Kim RJ. Delayed enhancement
cardiovascular magnetic resonance assessment of non-ischaemic cardiomyopathies.
Eur Heart J. 2005 Aug;26(15):1461–74.
40 Goerss JB, Michels VV, Burnett J, Driscoll DJ, Miller F, Rodeheffer R, et al. Frequency
of familial dilated cardiomyopathy. Eur Heart J. 1995 Dec;16 Suppl O:2–4.
41 Ku L, Feiger J, Taylor M, Mestroni L. Familial Dilated Cardiomyopathy. Circulation.
2003 Oct 28;108(17):e118–21.
42 Mahrholdt H, Goedecke C, Wagner A, Meinhardt G, Athanasiadis A, Vogelsberg H, et
al. Cardiovascular Magnetic Resonance Assessment of Human Myocarditis: A
Comparison to Histology and Molecular Pathology. Circulation. 2004 Mar
16;109(10):1250–8.
43 Matoh F, Satoh H, Shiraki K, Saitoh T, Urushida T, Katoh H, et al. Usefulness of
Delayed Enhancement Magnetic Resonance Imaging to Differentiate Dilated Phase of
Hypertrophic Cardiomyopathy and Dilated Cardiomyopathy. J Card Fail. 2007 Jun
1;13(5):372–9.
44 Xiao Y, Yang K-Q, Yang Y-K, Liu Y-X, Tian T, Song L, et al. Clinical Characteristics
and Prognosis of End-stage Hypertrophic Cardiomyopathy. Chin Med J (Engl). 2015
Jun 5;128(11):1483–9.
70 | P a g e
45 Fattori R, Rocchi G, Celletti F, Bertaccini P, Rapezzi C, Gavelli G. Contribution of
magnetic resonance imaging in the differential diagnosis of cardiac amyloidosis and
symmetric hypertrophic cardiomyopathy. Am Heart J. 1998 Nov;136(5):824–30.
46 Maceira AM, Joshi J, Prasad SK, Moon JC, Perugini E, Harding I, et al. Cardiovascular
Magnetic Resonance in Cardiac Amyloidosis. Circulation. 2005 Jan 18;111(2):186–93.
47 Vogelsberg H, Mahrholdt H, Deluigi CC, Yilmaz A, Kispert EM, Greulich S, et al.
Cardiovascular Magnetic Resonance in Clinically Suspected Cardiac Amyloidosis:
Noninvasive Imaging Compared to Endomyocardial Biopsy. J Am Coll Cardiol. 2008
Mar 11;51(10):1022–30.
48 Austin BA, Tang WHW, Rodriguez ER, Tan C, Flamm SD, Taylor DO, et al. Delayed
hyper-enhancement magnetic resonance imaging provides incremental diagnostic and
prognostic utility in suspected cardiac amyloidosis. JACC Cardiovasc Imaging. 2009
Dec;2(12):1369–77.
49 Migrino RQ, Christenson R, Szabo A, Bright M, Truran S, Hari P. Prognostic
implication of late gadolinium enhancement on cardiac MRI in light chain (AL)
amyloidosis on long term follow up. BMC Med Phys. 2009 May 5;9:5.
50 Ichinose A, Otani H, Oikawa M, Takase K, Saito H, Shimokawa H, et al. MRI of
Cardiac Sarcoidosis: Basal and Subepicardial Localization of Myocardial Lesions and
Their Effect on Left Ventricular Function. Am J Roentgenol. 2008 Sep 1;191(3):862–
9.
51 Patel AR, Klein MR, Chandra S, Spencer KT, Decara JM, Lang RM, et al. Myocardial
damage in patients with sarcoidosis and preserved left ventricular systolic function: an
observational study. Eur J Heart Fail. 2011 Nov;13(11):1231–7.
52 Patel MR, Cawley PJ, Heitner JF, Klem I, Parker MA, Jaroudi WA, et al. Detection of
Myocardial Damage in Patients With Sarcoidosis. Circulation. 2009 Nov
17;120(20):1969–77.
53 Mouquet F, Lions C, Groote P de, Bouabdallaoui N, Willoteaux S, Dagorn J, et al.
Characterisation of peripartum cardiomyopathy by cardiac magnetic resonance
imaging. Eur Radiol. 2008 Dec 1;18(12):2765.
54 Tan TC, Scherrer-Crosbie M. CARDIAC COMPLICATIONS OF
CHEMOTHERAPY: ROLE OF IMAGING. Curr Treat Options Cardiovasc Med. 2014
Apr;16(4):296.
55 Zuppinger C, Timolati F, Suter TM. Pathophysiology and diagnosis of cancer drug
induced cardiomyopathy. Cardiovasc Toxicol. 2007 Jun 1;7(2):61–6.
56 Drafts BC, Twomley KM, D’Agostino R, Lawrence J, Avis N, Ellis LR, et al. Low to
Moderate Dose Anthracycline-Based Chemotherapy is Associated with Early
Noninvasive Imaging Evidence of Subclinical Cardiovascular Disease. JACC
Cardiovasc Imaging. 2013 Aug;6(8):877–85.
71 | P a g e
57 Bohl S, Wassmuth R, Abdel-Aty H, Rudolph A, Messroghli D, Dietz R, et al. Delayed
enhancement cardiac magnetic resonance imaging reveals typical patterns of
myocardial injury in patients with various forms of non-ischemic heart disease. Int J
Cardiovasc Imaging. 2008 Aug;24(6):597–607.
58 Machii M, Satoh H, Shiraki K, Saotome M, Urushida T, Katoh H, et al. Distribution of
late gadolinium enhancement in end-stage hypertrophic cardiomyopathy and dilated
cardiomyopathy: differential diagnosis and prediction of cardiac outcome. Magn Reson
Imaging. 2014 Feb;32(2):118–24.
59 Hombach V, Merkle N, Torzewski J, Kraus JM, Kunze M, Zimmermann O, et al.
Electrocardiographic and cardiac magnetic resonance imaging parameters as predictors
of a worse outcome in patients with idiopathic dilated cardiomyopathy. Eur Heart J.
2009 Aug 1;30(16):2011–8.
60 Bogun FM, Desjardins B, Good E, Gupta S, Crawford T, Oral H, et al. Delayed-
enhanced magnetic resonance imaging in nonischemic cardiomyopathy: utility for
identifying the ventricular arrhythmia substrate. J Am Coll Cardiol. 2009 Mar
31;53(13):1138–45.
61 Nazarian S, Bluemke DA, Lardo AC, Zviman MM, Watkins SP, Dickfeld TL, et al.
Magnetic Resonance Assessment of the Substrate for Inducible Ventricular
Tachycardia in Nonischemic Cardiomyopathy. Circulation. 2005 Nov 1;112(18):2821–
5.
62 Okutucu S, Oto A. Risk stratification in nonischemic dilated cardiomyopathy: Current
perspectives. Cardiol J. 2010;17(3):219–29.
63 Shimizu I, Iguchi N, Watanabe H, Umemura J, Tobaru T, Asano R, et al. Delayed
enhancement cardiovascular magnetic resonance as a novel technique to predict cardiac
events in dilated cardiomyopathy patients. Int J Cardiol. 2010 Jul 23;142(3):224–9.
64 Wu KC, Weiss RG, Thiemann DR, Kitagawa K, Schmidt A, Dalal D, et al. Late
Gadolinium Enhancement by Cardiovascular Magnetic Resonance Heralds an Adverse
Prognosis in Nonischemic Cardiomyopathy. J Am Coll Cardiol. 2008 Jun
24;51(25):2414–21.
65 Kuruvilla S, Adenaw N, Katwal AB, Lipinski MJ, Kramer CM, Salerno M. Late
Gadolinium Enhancement on CMR Predicts Adverse Cardiovascular Outcomes in
Non-ischemic Cardiomyopathy: A Systematic Review and Meta-analysis. Circ
Cardiovasc Imaging. 2014 Mar 1;7(2):250–8.
66 Pöyhönen P, Kivistö S, Holmström M, Hänninen H. Quantifying late gadolinium
enhancement on CMR provides additional prognostic information in early risk-
stratification of nonischemic cardiomyopathy: a cohort study. BMC Cardiovasc
Disord. 2014 Aug 27;14:110.
72 | P a g e
67 Neilan TG, Coelho-Filho OR, Danik SB, Shah RV, Dodson JA, Verdini DJ, et al. CMR
Quantification of Myocardial Scar Provides Additive Prognostic Information in
Nonischemic Cardiomyopathy. JACC Cardiovasc Imaging. 2013 Sep;6(9):944–54.
68 Heydari B, Jerosch-Herold M, Kwong RY. Imaging for Planning of Cardiac
Resynchronization Therapy. JACC Cardiovasc Imaging. 2012 Jan;5(1):93–110.
69 Duckett SG, Chiribiri A, Ginks MR, Sinclair S, Knowles BR, Botnar R, et al. Cardiac
MRI to investigate myocardial scar and coronary venous anatomy using a slow infusion
of dimeglumine gadobenate in patients undergoing assessment for cardiac
resynchronization therapy. J Magn Reson Imaging JMRI. 2011 Jan;33(1):87–95.
70 Bleeker GB, Kaandorp TAM, Lamb HJ, Boersma E, Steendijk P, Roos A de, et al.
Effect of Posterolateral Scar Tissue on Clinical and Echocardiographic Improvement
After Cardiac Resynchronization Therapy. Circulation. 2006 Feb 21;113(7):969–76.
71 White JA, Yee R, Yuan X, Krahn A, Skanes A, Parker M, et al. Delayed Enhancement
Magnetic Resonance Imaging Predicts Response to Cardiac Resynchronization
Therapy in Patients With Intraventricular Dyssynchrony. J Am Coll Cardiol. 2006 Nov
21;48(10):1953–60.
72 Chalil S, Foley PWX, Muyhaldeen SA, Patel KCR, Yousef ZR, Smith REA, et al. Late
gadolinium enhancement-cardiovascular magnetic resonance as a predictor of response
to cardiac resynchronization therapy in patients with ischaemic cardiomyopathy. Eur
Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card
Cell Electrophysiol Eur Soc Cardiol. 2007 Nov;9(11):1031–7.
73 Comte A, Lalande A, Walker PM, Cochet A, Legrand L, Cottin Y, et al. Visual
estimation of the global myocardial extent of hyperenhancement on delayed contrast-
enhanced MRI. Eur Radiol. 2004 Dec 1;14(12):2182–7.
74 Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016
ESC Guidelines for the diagnosis and treatment of acute and chronic heart failureThe
Task Force for the diagnosis and treatment of acute and chronic heart failure of the
European Society of Cardiology (ESC)Developed with the special contribution of the
Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016 Jul 14;37(27):2129–
200.
75 Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, Anderson RH,
et al. Left Ventricular Non-Compaction: Insights From Cardiovascular Magnetic
Resonance Imaging. J Am Coll Cardiol. 2005 Jul 5;46(1):101–5.
76 Piano MR, Phillips SA. Alcoholic cardiomyopathy: Pathophysiologic insights.
Cardiovasc Toxicol. 2014 Dec;14(4):291–308.
77 Mancuso FJN, Moisés VA, Almeida DR, Oliveira WA, Poyares D, Brito FS, et al.
Criteria for Mitral Regurgitation Classification were inadequate for Dilated
Cardiomyopathy. Arq Bras Cardiol. 2013 Nov;101(5):457–65.
73 | P a g e
78 de Groote P, Millaire A, Foucher-Hossein C, Nugue O, Marchandise X, Ducloux G, et
al. Right ventricular ejection fraction is an independent predictor of survival in patients
with moderate heart failure. J Am Coll Cardiol. 1998 Oct 1;32(4):948–54.
79 Parsai C, O’Hanlon R, Prasad SK, Mohiaddin RH. Diagnostic and prognostic value of
cardiovascular magnetic resonance in non-ischaemic cardiomyopathies. J Cardiovasc
Magn Reson. 2012 Aug 2;14:54.
80 Sobajima M, Nozawa T, Suzuki T, Ohori T, Shida T, Matsuki A, et al. Impact of
myocardial perfusion abnormality on prognosis in patients with non-ischemic dilated
cardiomyopathy. J Cardiol. 2010 Nov 1;56(3):280–6.
81 Unverferth DV, Baker PB, Swift SE, Chaffee R, Fetters JK, Uretsky BF, et al. Extent
of myocardial fibrosis and cellular hypertrophy in dilated cardiomyopathy. Am J
Cardiol. 1986 Apr 1;57(10):816–20.
82 Beltrami CA, Finato N, Rocco M, Feruglio GA, Puricelli C, Cigola E, et al. The cellular
basis of dilated cardiomyopathy in humans. J Mol Cell Cardiol. 1995 Jan 1;27(1):291–
305.
83 Maehashi et al. The Role of Myocarditis and Myocardial Fibrosis in Dilated
Cardiomyopathy. Analysis of 28 Necropsy Cases [Internet]. PubMed Journals. [cited
2017 Sep 27]. Available from: https://ncbi.nlm.nih.gov/labs/articles/2038116/
84 Choi E-Y, Choi BW, Kim S-A, Rhee SJ, Shim CY, Kim YJ, et al. Patterns of late
gadolinium enhancement are associated with ventricular stiffness in patients with
advanced non-ischaemic dilated cardiomyopathy†. Eur J Heart Fail. 2009 Jun
1;11(6):573–80.
85 Epstein AE, DiMarco JP, Ellenbogen KA, Estes NAM, Freedman RA, Gettes LS, et al.
ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm
Abnormalities. Heart Rhythm. 2008 Jun 1;5(6):e1–62.
86 Kadish A, Dyer A, Daubert JP, Quigg R, Estes NAM, Anderson KP, et al. Prophylactic
Defibrillator Implantation in Patients with Nonischemic Dilated Cardiomyopathy. N
Engl J Med. 2004 May 20;350(21):2151–8.
87 Dec GW, Fuster V. Idiopathic Dilated Cardiomyopathy. N Engl J Med. 1994 Dec
8;331(23):1564–75.
88 Goldberger JJ, Cain ME, Hohnloser SH, Kadish AH, Knight BP, Lauer MS, et al.
American Heart Association/American College of Cardiology Foundation/Heart
Rhythm Society Scientific Statement on Noninvasive Risk Stratification Techniques
for Identifying Patients at Risk for Sudden Cardiac Death: A Scientific Statement From
the American Heart Association Council on Clinical Cardiology Committee on
Electrocardiography and Arrhythmias and Council on Epidemiology and Prevention.
Circulation. 2008 Sep 30;118(14):1497–518.

74 | P a g e
89 Lakdawala NK, Winterfield JR, Funke BH. Dilated Cardiomyopathy. Circ Arrhythm
Electrophysiol. 2013 Feb 1;6(1):228–37.
90 Broberg CS, Chugh SS, Conklin C, Sahn DJ, Jerosch-Herold M. Quantification of
Diffuse Myocardial Fibrosis and Its Association With Myocardial Dysfunction in
Congenital Heart DiseaseClinical Perspective. Circ Cardiovasc Imaging. 2010 Nov
1;3(6):727–34.
75 | P a g e
ABBREVIATIONS
ACEI Angiotensin converting enzyme inhibitor
AF/AT Atrial fibrillation/ atrial tachycardia
ARB Angiotensin receptor blocker
ASE American society of echocardiography
CHB Complete heart block
CI Confidence interval
CMR Cardiac MRI
CRT (P/D) Cardiac resynchronization therapy (pacing/ defibrillator)
DCM Dilated cardiomyopathy
EDV(I) End diastolic volume (index)
EF Ejection fraction
EMB Endomyocardial biopsy
ESV (I) End systolic volume (index)
HCM Hypertrophic cardiomyopathy
HR Hazards ratio
ICD Implantable cardioverter defibrillator
IQR Inter quartile range
IR-CE Inversion recovery- contrast enhanced
IVCD Inter ventricular conduction defect
IVS Inter ventricular septum
LGE Late gadolinium enhancement
LV Left ventricle
76 | P a g e
LVNC LV non compaction
MACE Major adverse cardiac event
MR Mitral regurgitation
NT pro BNP N terminal pro brain natriuretic peptide
NYHA New York Heart association
OAC Oral anticoagulant
PAH Pulmonary artery hypertension
PPI Permanent pacemaker insertion
PSIR Phase sensitive inversion recovery
RV Right ventricle
RWMA Regional wall motion abnormality
SCD Sudden cardiac death
SSFP Steady state free precession
SV (I) Stroke volume (index)
T2- STIR T2- short tau inversion recovery
TR Tricuspid regurgitation
TTE Transthoracic cardiomyopathy
VT Ventricular tachycardia
77 | P a g e
PROFORMA
Age :
Sex:
Hospital No:
Risk factors
DM
HTN
Dyslipidemia
Family h/o CAD
Family h/o SCD
Family h/o DCM
Smoking
Alcohol
Other risk factors (mention)
H/o Arrythmiaa(VT/AF)
Respiratory problem :
Other Systems:
Functional Class – NYHA 1, II, III, IV
ECG
Rhythm- SR/ AF/ VT
PR interval-
BBB- LBBB/ RBBB
QRS – Duration, Axis
78 | P a g e
LVH/ RVH
ST T changes
Q waves-
X-Ray-
CTR
PVH
PAH
Echocardiogram –
LV dimensions-
Ejection fraction -
RWMA
Diastolic Dysfunction
Mitral regurgitation
RV dysfunction
Others-
Holter study( if done):
CAG- Cath study:
Coronary status -
Cath study-
LV SP
LV EDP
PCWP-
PA-
LVangio-
RWMA
79 | P a g e
EDV-
ESV-
EF-
Cardiac MRI
LV size and morphology
LV ESV-
LV EDV
LV SV –
LV EF-
T1 mapping –
T2 w STIR –
LGE-
Present/ absent -
If present,Distrubation-
subendocardial/ midmyocardial/ subepicardial
Regional / Global
Diagnosis:
Idiopathic DCM
Amyloidosis
Sarcoidosis
Peripartum CMP
Takotusbo CMP
Myocarditis
Blood tests-
80 | P a g e
ESR
CRP
Trop T
Pro BNP
Virological markers
Autoimmune markers
Medications:
ACEI/ARB
BB
Aldosterone antagonist
Diuretics
Digoxin
Antiarrtymic ( Amiodarone)
OAC
Date of last visit :
Follow up :
Symptoms : NYHA I/ II/ III/ IV
Mortality: All cause mortality, CVS mortality
Any CHF:
HF hospitalizations
Any SCD/ aborted cardiac arrest
Device implantations – ICD/ CRT-P/ CRT- D
Arrhythmias / ICD/CRT- frequency of shocks
Mortality
Cause of death:
81 | P a g e
Details of death:
Other complications:
LGE +ve Vs LGE –ve:
LGE +VE LGE -VE
LV EDV
LVSDV
LVEF
NYHA CLASS
SCD/ ABORTED SCD
MORTALITY
ARRHYTHMIAS/ SHOCK
HF HOSPITALISATION
82 | P a g e
83 | P a g e
84 | P a g e
Plagiarism Checker X Originality
Report
Similarity Found: 3%
Thesis_dibyaranjan.docx
Date: Tuesday, October 03, 2017
Statistics: 253 words Plagiarized / 8617 Total words
Remarks: Low Plagiarism Detected - Your Document needs Optional
Improvement.
------------------------------------------------------------------------------------------
-
INTERNET SOURCES:
------------------------------------------------------------------------------------------
- 0% - https://link.springer.com/article/10.100
0% - https://jcmr-online.biomedcentral.com/ar
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciedu.ca/journal/index.php/i
0% - http://circimaging.ahajournals.org/conte
0% - http://www.annalsthoracicsurgery.org/art
0% - https://www.scribd.com/document/12412244
0% - http://www.nejm.org/doi/full/10.1056/NEJ
0% - https://quizlet.com/102471856/patho-ch23
0% - http://stroke.ahajournals.org/content/43
0% - http://journals.sagepub.com/doi/10.1177/
0% - http://onlinelibrary.wiley.com/doi/10.11
0% - https://link.springer.com/article/10.118
0% - https://www.researchgate.net/publication
0% - Empty
0% - https://healthcare-in-europe.com/en/manu
0% - http://pubs.rsna.org/doi/full/10.1148/ra
0% - https://link.springer.com/content/pdf/10
0% - https://www.researchgate.net/publication
0% - http://www.sciencedirect.com/science/art
0% - http://europepmc.org/articles/PMC3981528
0% - http://www.massgeneral.org/imaging/news/
0% - https://www.researchgate.net/publication
0% - http://mriquestions.com/uploads/3/4/5/7/
0% - https://rd.springer.com/article/10.1186/
85 | P a g e
0% - http://www.tandfonline.com/doi/full/10.1
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
1% - https://bmccardiovascdisord.biomedcentra
0% - https://www.scribd.com/document/32568023
0% - https://link.springer.com/chapter/10.100
0% - http://www.dartmouth.edu/~library/recmgm
0% - https://link.springer.com/article/10.118
0% - https://bmcmedethics.biomedcentral.com/a
0% - https://link.springer.com/content/pdf/10
0% - https://link.springer.com/content/pdf/10
0% - http://applications.emro.who.int/imemrf/
0% - http://www.sciencedirect.com/science/art
0% - http://www.anmco.it/uploads/u_cms/media/
0% - http://paperity.org/p/74013807/microrna-
0% - http://www.nature.com/jhh/journal/v21/n8
0% - https://link.springer.com/article/10.100
0% - https://www.arcr.niaaa.nih.gov/arcr382/a
0% - https://2768335.r.bat.bing.com/?ld=d3x_X
0% - https://2768335.r.bat.bing.com/?ld=d3HTG
0% - https://link.springer.com/content/pdf/10
0% - https://bmcanesthesiol.biomedcentral.com
0% - http://jasn.asnjournals.org/content/19/9
0% - http://www.sciencedirect.com/science/art
0% - http://paperity.org/p/74815375/associati
0% - https://link.springer.com/content/pdf/10
0% - https://link.springer.com/article/10.100
0% - http://asecho.org/wordpress/wp-content/u
0% - http://europepmc.org/articles/PMC3734881
0% - https://link.springer.com/article/10.100
0% - https://0.r.bat.bing.com/?ld=d3NqjULIwEx
0% - http://www.sciencedirect.com/science/art
0% - https://link.springer.com/chapter/10.100
0% - https://www.researchgate.net/publication
0% - https://www.chemweb.com/articles/SV10554
0% - https://www.uptodate.com/contents/treatm
0% - http://www.internationaljournalofcardiol
0% - http://heart.bmj.com/content/heartjnl/ea
0% - https://link.springer.com/article/10.100
0% - http://onlinelibrary.wiley.com/doi/10.10
0% - https://issuu.com/clinicscardivepublishi
0% - https://www.researchgate.net/publication
0% - https://www.scribd.com/document/22657749
0% - http://www.cardiacep.theclinics.com/arti
0% - https://www.researchgate.net/publication
0% - http://circimaging.ahajournals.org/conte
0% - http://www.scientificoajournals.org/pdf/
0% - https://link.springer.com/article/10.100
0% - https://www.researchgate.net/profile/Jay
0% - https://www.researchgate.net/publication
86 | P a g e
0% - http://www.internationaljournalofcardiol
0% - https://www.ncbi.nlm.nih.gov/pmc/article
0% - http://www.ajronline.org/doi/full/10.221
0% - http://www.sciencedirect.com/science/art
0% - https://www.researchgate.net/publication
0% - https://link.springer.com/article/10.100
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/content/pdf/10
0% - https://www.researchgate.net/publication
0% - http://www.sciencedirect.com/science/art
0% - https://www.researchgate.net/publication
0% - http://www.sciencedirect.com/science/art
0% - https://link.springer.com/content/pdf/10
0% - https://academic.oup.com/europace/articl
0% - https://www.ncbi.nlm.nih.gov/pmc/article
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://www.wjgnet.com/1949-8462/full/v6
0% - https://academic.oup.com/ehjcimaging/art
0% - http://www.sciencedirect.com/science/art
0% - http://www.academia.edu/14506883/Inciden
0% - http://www.insuficienciacardiaca.org/pdf
0% - https://www.wjgnet.com/1949-8462/full/v6
0% - http://www.nature.com/articles/nrcardio.
0% - http://www.nature.com/eye/journal/v2/n1/
0% - https://link.springer.com/chapter/10.100
0% - https://www.researchgate.net/publication
0% - https://www.wjgnet.com/1949-8462/full/v8
0% - https://link.springer.com/article/10.100
0% - http://journals.lww.com/jcardiovascularm
0% - http://circimaging.ahajournals.org/conte
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - https://jcmr-online.biomedcentral.com/ar
0% - http://www.onlinejase.com/article/S0894-
0% - https://www.escardio.org/Journals/E-Jour
0% - http://www.radiologyassistant.nl/en/p4cd
0% - https://link.springer.com/article/10.100
0% - https://www.centrallakesclinic.biz/echoc
0% - https://jcmr-online.biomedcentral.com/ar
0% - http://www.sciencedirect.com/science/art
0% - https://openi.nlm.nih.gov/detailedresult
0% - http://indianheartjournal.com/ihj09/nov_
0% - http://misc.medscape.com/pi/android/meds
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://www.researchgate.net/publication
0% - https://www.scribd.com/document/13081402
0% - http://heart.bmj.com/content/91/suppl_1/
0% - http://heart.bmj.com/content/91/suppl_1/
0% - https://academic.oup.com/ehjcimaging/art
0% - https://www.scribd.com/document/25878812
0% - https://2768335.r.bat.bing.com/?ld=d37Ai
0% - http://paperity.org/p/74013807/microrna-
0% - https://synapse.koreamed.org/Synapse/Dat
0% - https://31004134.r.bat.bing.com/?ld=d3sI
87 | P a g e
0% - http://www.sciencedirect.com/science/art
0% - http://bpl.rajasthan.gov.in/BPL/bpl_list
0% - http://heart.bmj.com/content/heartjnl/ea
0% - https://2648102.r.bat.bing.com/?ld=d3N_6
0% - https://31004134.r.bat.bing.com/?ld=d3Q9
0% - https://www.scribd.com/document/35808717
0% - https://en.wikipedia.org/wiki/Cardiac_va
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/content/pdf/10
0% - https://www.researchgate.net/publication
0% - http://appliedradiology.com/articles/the
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://www.scribd.com/document/22657749
0% - http://circ.ahajournals.org/content/115/
0% - https://issuu.com/amranhajjaj/docs/medst
0% - http://emedicine.medscape.com/article/15
0% - http://clincancerres.aacrjournals.org/co
0% - https://medworm.com/research/angioplasty
0% - http://www.sciencedirect.com/science/art
0% - http://circ.ahajournals.org/content/133/
0% - http://europepmc.org/articles/PMC3952043
0% - https://www.tandfonline.com/doi/full/10.
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://www.researchgate.net/publication
0% - https://www.researchgate.net/profile/Nic
0% - http://www.onlinejacc.org/content/61/24/
0% - https://www.researchgate.net/profile/Ami
0% - http://www.medscape.com/viewarticle/7373
0% - https://academic.oup.com/europace/articl
0% - https://www.cancercare.org/publications/
0% - https://www.researchgate.net/publication
0% - https://update.revolvy.com/topic/Receive
0% - https://www.researchgate.net/publication
0% - http://www.imaging.onlinejacc.org/conten
0% - http://www.cardiov.ox.ac.uk/principal-in
0% - http://onlinelibrary.wiley.com/doi/10.10
0% - https://www.tandfonline.com/doi/full/10.
0% - https://www.researchgate.net/profile/Hei
0% - http://onlinelibrary.wiley.com/rss/journ
0% - https://jcmr-online.biomedcentral.com/ar
0% - http://www.nature.com/pcan/journal/v7/n4
1% - https://bmccardiovascdisord.biomedcentra
0% - https://documents.mx/health-medicine/esc
0% - https://medworm.com/research/radiology.x
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/article/10.118
0% - http://www.sciencedirect.com/science/art
0% - https://pt.scribd.com/document/282951164
0% - http://circep.ahajournals.org/content/9/

88 | P a g e
0% - http://anilaggrawal.com/ij/vol_003_no_00
0% - http://www.rguhs.ac.in/cdc/onlinecdc/upl
0% - https://pubs.niaaa.nih.gov/publications/
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - https://www.nature.com/gimo/contents/pt1
0% - https://2768335.r.bat.bing.com/?ld=d3_oz
0% - http://applications.emro.who.int/imemrf/
0% - https://link.springer.com/chapter/10.100
0% - https://www.researchgate.net/institution
0% - http://www.iasj.net/iasj?func=fulltext&a
0% - http://qims.amegroups.com/article/view/4
0% - http://circimaging.ahajournals.org/conte
0% - http://www.sciencedirect.com/science/art
0% - https://cardiovascularultrasound.biomedc
0% - https://www.clevelandclinicmeded.com/med
0% - https://link.springer.com/article/10.100
0% - https://rd.springer.com/content/pdf/10.1
0% - http://www.sciencedirect.com/science/art
0% - http://www.slideserve.com/tab/how-i-do-c
0% - http://europepmc.org/articles/PMC3782322
0% - http://www.clevelandclinicmeded.com/live
0% - https://link.springer.com/chapter/10.100
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://link.springer.com/chapter/10.100
0% - https://jcmr-online.biomedcentral.com/ar
0% - http://www.freepatentsonline.com/y2017/0
0% - https://www.researchgate.net/publication
0% - http://circ.ahajournals.org/content/117/
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - https://www.scribd.com/document/33858450
0% - https://link.springer.com/article/10.100
0% - http://www.onlinejacc.org/content/67/25/
0% - http://pubs.rsna.org/doi/10.1148/radiol.
0% - http://www.sciencedirect.com/science/art
0% - https://link.springer.com/article/10.100
0% - http://www.onlinecjc.ca/article/S0828-28
0% - https://www.scribd.com/document/82181281
0% - https://academic.oup.com/ehjcimaging/art
0% - http://cinc.mit.edu/archives/2008/pdf/03
0% - http://emedicine.medscape.com/article/41
0% - http://www.sciencedirect.com/science/art
0% - https://www.karger.com/Article/FullText/
0% - http://www.radiologyassistant.nl/en/p4a3
0% - http://www.sciencedirect.com/science/art
0% - http://www.sciencedirect.com/science/art
0% - http://www.who.int/woman_child_accountab
0% - https://academic.oup.com/ehjcimaging/art
0% - http://europepmc.org/articles/PMC3169800
0% - http://circ.ahajournals.org/content/125/
0% - https://www.researchgate.net/publication
0% - http://circ.ahajournals.org/content/108/
0% - https://pubchem.ncbi.nlm.nih.gov/compoun
89 | P a g e
0% - http://circ.ahajournals.org/content/108/
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://link.springer.com/chapter/10.100
0% - https://intarchmed.biomedcentral.com/art
0% - https://link.springer.com/article/10.100
0% - https://link.springer.com/article/10.100
0% - https://www.wjgnet.com/1949-8462/full/v6
0% - http://onlinelibrary.wiley.com/doi/10.11
0% - http://www.imaging.onlinejacc.org/conten
0% - http://www.birpublications.org/doi/pdf/1
0% - http://www.sciencedirect.com/science/art
0% - https://www.brainscape.com/flashcards/qu
0% - https://www.scribd.com/document/33858450
0% - https://pharmaceuticalintelligence.com/t
0% - https://medworm.com/journal/the-american
0% - http://www.apa.org/pi/lgbt/resources/par
0% - https://medworm.com/rss/medicalfeeds/con
0% - https://www.researchgate.net/publication
0% - https://www.regenerativenutrition.com/na
0% - http://heart.bmj.com/content/97/9/727
0% - https://link.springer.com/protocol/10.13
0% - http://www.sciencedirect.com/science/art
0% - https://jcmr-online.biomedcentral.com/ar
0% - https://en.wikipedia.org/wiki/Pathophysi
0% - http://www.academia.edu/13426766/Left_ve
0% - https://www.researchgate.net/publication
0% - http://www.internationaljournalofcardiol
0% - https://link.springer.com/article/10.100
0% - http://www.sciencedirect.com/science/art
1% - https://bmccardiovascdisord.biomedcentra
0% - https://academic.oup.com/ehjcimaging/art
0% - http://www.sciencedirect.com/science/art
0% - https://link.springer.com/content/pdf/10
0% - https://link.springer.com/article/10.118
0% - http://europepmc.org/articles/PMC4045555
0% - http://circimaging.ahajournals.org/conte
0% - https://arthritis-research.biomedcentral
0% - http://fiaiweb.com/wp-content/uploads/20
0% - http://fiaiweb.com/wp-content/uploads/20
0% - http://diabetes.diabetesjournals.org/con
0% - http://onlinelibrary.wiley.com/doi/10.11
0% - https://link.springer.com/article/10.118
0% - https://link.springer.com/article/10.100
0% - https://www.ncbi.nlm.nih.gov/labs/journa
0% - https://link.springer.com/article/10.100
0% - https://academic.oup.com/europace/articl
0% - http://pubmedcentralcanada.ca/pmcc/artic
0% - https://link.springer.com/chapter/10.10





























