Embed Size (px)
Citation preview
EURURO-5656; No. of Pages 8
Platinum Priority – Prostate CancerEditorial by XXX on pp. x–y of this issue
More Extensive Pelvic Lymph Node Dissection Improves Survival
in Patients with Node-positive Prostate Cancer
Firas Abdollah a, Giorgio Gandaglia a, Nazareno Suardi a, Umberto Capitanio a, Andrea Salonia a,Alessandro Nini a, Marco Moschini a, Maxine Sun b, Pierre I. Karakiewicz b, Sharhokh F. Shariat c,Francesco Montorsi a, Alberto Briganti a,*
a Division of Oncology/Unit of Urology, URI, IRCCS Ospedale San Raffaele, Milan, Italy; b Cancer Prognostics and Health Outcomes Unit, University of Montreal
Health Centre, Montreal, Quebec, Canada; c Department of Urology, Medical University of Vienna, Vienna, Austria
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X
ava i lable at www.sc iencedirect .com
journa l homepage: www.europea nurology.com
Article info
Article history:
Accepted May 15, 2014
Keywords:
Neoplasm recurrence
Prostatic neoplasms/pathology
Prostatic neoplasms/surgery
Prostatic neoplasms/mortality
Lymph node invasion
Lymph node dissection
Abstract
Background: The role of extended pelvic lymph node dissection (ePLND) in treatingprostate cancer (PCa) patients with lymph node invasion (LNI) remains controversial.Objective: The relationship between the number of removed lymph nodes (RLNs) andcancer-specific mortality (CSM) was tested in patients with LNI.Design, setting, and participants: We examined data of 315 pN1 PCa patients treatedwith radical prostatectomy (RP) and anatomically ePLND between 2000 and 2012 at onetertiary care centre. All patients received adjuvant hormonal therapy with or withoutadjuvant radiotherapy (aRT).Outcome measurements and statistical analysis: Univariable and multivariable Coxregression analyses tested the relationship between RLN number and CSM rate, afteradjusting to all available covariates. Survival estimates were based on the multivariablemodel; patients were stratified according to RLN number using points of maximumseparation.Results and limitations: The average number of RLNs was 20.8 (median: 19; interquartilerange: 14–25). Mean and median follow-up were 63.1 and 54 mo, respectively. At 10-yr,the CSM-free survival rate was 74.7%, 85.9%, 92.4%, 96.0%, and 97.9% for patients with 8, 17,26, 36, and 45 RLNs, respectively. By multivariable analyses, the number of RLNs inde-pendently predicted lower CSM rate (hazard ratio [HR]: 0.93; p = 0.02). Other predictors ofCSM were Gleason score 8–10 (HR: 3.3), number of positive nodes (HR: 1.2), and aRTtreatment (HR: 0.26; all p � 0.006). The study is limited by its retrospective nature.Conclusions: In PCa patients with LNI, the removal of a higher number of LNs during RPwas associated with improvement in cancer-specific survival rate. This implies that ePLNDshould be considered in all patients with a significant preoperative risk of harbouring LNI.Patient summary: We found that removing more lymph nodes during prostate cancersurgery can significantly improve cancer-specific survival in patients with lymph nodeinvasion.
# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Urology, Urological Research Institute, San RaffaeleHospital, University Vita-Salute, Via Olgettina, 60, Milan 20132, Italy. Tel. +39 02 2643 7790;Fax: +39 02 2643 7298.E-mail address: [email protected] (A. Briganti).
Please cite this article in press as: Abdollah F, et al. More Extensive Pelvic Lymph Node Dissection Improves Survival in Patientswith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.doi.org/10.1016/j.eururo.2014.05.011
http://dx.doi.org/10.1016/j.eururo.2014.05.0110302-2838/# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
EURURO-5656; No. of Pages 8
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X2
1. Introduction
Radical prostatectomy (RP) is one of the most commonly
used treatments for patients with prostate cancer (PCa)
[1,2]. However, the benefit of an extended pelvic lymph
node dissection (ePLND) is still debated. It is generally
accepted that whenever a PLND is indicated, this should be
anatomically extended [3]. Such an extensive approach
represents the only accurate staging procedure for lymph
node invasion (LNI) in PCa [4]. However, the therapeutic
impact of this ePLND (if any) is still unclear [5–13].
Results of a recent randomised clinical trial suggested
that ePLND could significantly decrease the risk of
biochemical recurrence (BCR) after RP in patients with
intermediate- or high-risk tumours [6]. However, although
BCR risk reduction is an important finding, it does not
necessarily translate into better survival. In contrast, several
observational reports failed to demonstrate any beneficial
impact of ePLND on BCR and/or survival [5,9,13]. There may
be two main reasons for this result: (1) use of limited and
nonhomogeneous PLND, which might have artificially
undermined the role of PLND, and (2) selection of patients
at lower risk of dying from PCa. These points are key, since
any therapeutic benefit associated with surgical treatments
of PCa should be tested using a proper surgical approach
(ie, ePLND) in a properly selected population (ie, patients at
higher risk of dying from the disease).
To address this issue, we tested the relationship between
the number of removed lymph nodes (RLNs) and cancer-
specific mortality (CSM) in pN1 patients treated with RP and
ePLND.
2. Materials and methods
We evaluated the data of 315 M0 pN1 PCa patients treated with RP and
ePLND between 2000 and 2012 at one tertiary care centre. Patients were
staged preoperatively with pelvic/abdominal computerised tomography
or abdominal ultrasound, bone scan, and chest x-ray. Seven surgeons
performed RP using a standardised retropubic technique. EPLNDs
consisted of excision of fibrofatty tissue along the external iliac vein,
the distal limit being the deep circumflex vein and the femoral canal.
Proximally, ePLND was performed up to and including the bifurcation of
the common iliac artery. Furthermore, all fibrofatty tissue within the
obturator fossa was removed to completely skeletonise the obturator
nerve. The lateral limit consisted of the pelvic sidewall, and the medial
dissection limit was defined by perivesical fat. In all the patients included
in our cohort, LNs along the internal iliac vessels were dissected. In some
cases, LNs located in the presacral and common iliac areas were also
removed.
Postoperatively, all patients received adjuvant hormonal therapy
(aHT), which was intended to be lifelong. However, given the retrospective
nature of the cohort, it is uncertain whether patients discontinued
treatment after a period of androgen-deprivation therapy. Additionally,
147 (46.7%) patients received aRT. ART was administered based on the
clinical judgment of each treating physician according to patient and
cancer characteristics. Radiation therapy consisted of localised radiation
delivered to the prostate and to the seminal vesicle bed with pelvic LN
irradiation (whole pelvis radiotherapy). Details of the aRT technique used
have been previously published [14]. Adjuvant treatments (both aHT and
aRT) were initiated within 90 d from RP. The institutional review board
approved the study.
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
2.1. Variable definition
All patients included in this study had complete clinical and pathology
data, which consisted of age at surgery, prostate-specific antigen (PSA)
value, D’Amico risk group (low- vs intermediate- vs high-risk) [15],
pathologic Gleason score (2–7 vs 8–10), pathologic tumour stage (pT2 vs
pT3a vs pT3b vs pT4), surgical margin status (negative vs positive),
number of removed LNs (RLNs), number of positive lymph nodes, aRT
status (no aRT vs aRT), and year of surgery.
2.2. Statistical analyses
Descriptive statistics of categorical variables focused on frequencies and
proportions. Means, medians, and interquartile ranges (IQR) were
reported for continuously coded variables. Chi-square and Mann-
Whitney tests were used to compare the statistical significance of
differences in proportions and medians, respectively.
Univariable and multivariable Cox regression analyses were used to
test the relationship between the number of RLNs and CSM rate, after
adjusting for all available covariates. Estimated survival curves were
plotted based on the multivariable model results. Survival curves were
stratified according to the number of RLNs, using the points of maximum
separation, as described by Harrell [16]. The number of RLNs was then
dichotomised according to the most informative cut-off predicting CSM.
This was obtained applying the chi-square test for every possible cut-off
value and choosing the lowest p value. Survival curves were then
stratified according to the most informative cut-off for the number of
RLNs. Finally, predicted 10-yr survival according to the number of RLNs
was plotted for the entire cohort, and after stratification according to
Gleason score and aRT status.
All statistical analyses were performed using the R statistical package
system (R Foundation for Statistical Computing, Vienna, Austria), with a
two-sided significance level set at p < 0.05.
3. Results
3.1. Baseline patient characteristics
Clinical and pathologic demographics of the cohort,
stratified by adjuvant treatment status are reported in
Table 1. The average PSA value was 24.2 ng/ml (median:
11.2 ng/ml; IQR: 6.9–24.4 ng/ml). Most of the patients
included in the study were affected by high-risk disease at
diagnosis (60%). Most patients harboured a pT3b disease
(66%), and had a pathologic Gleason score 8–10 (57%).
Average number of RLNs and positive LNs was 20.8
(median: 19; IQR: 14–25) and 3.3 (median: 2.0; IQR: 1–3),
respectively. For all examined variables, there were no
statistically significant differences between patients treated
with aRT versus without aRT (all p � 0.07).
3.2. Cox regression analyses and survival estimates
At univariable analyses, Gleason score 8–10 (hazard ratio
[HR]: 2.9), pT4 (HR: 6.7), aRT treatment (HR: 0.40), and the
number of positive LNs (HR: 1.1) were the only predictors of
CSM rate (all p � 0.02) (Table 2). At multivariable analyses,
Gleason score 8–10 (HR: 3.3) and a higher number of
positive LNs (HR: 1.2) were independently associated
with higher CSM rate (all p � 0.006) (Table 2). Conversely,
aRT treatment (HR: 0.26) and a higher number of RLNs
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011
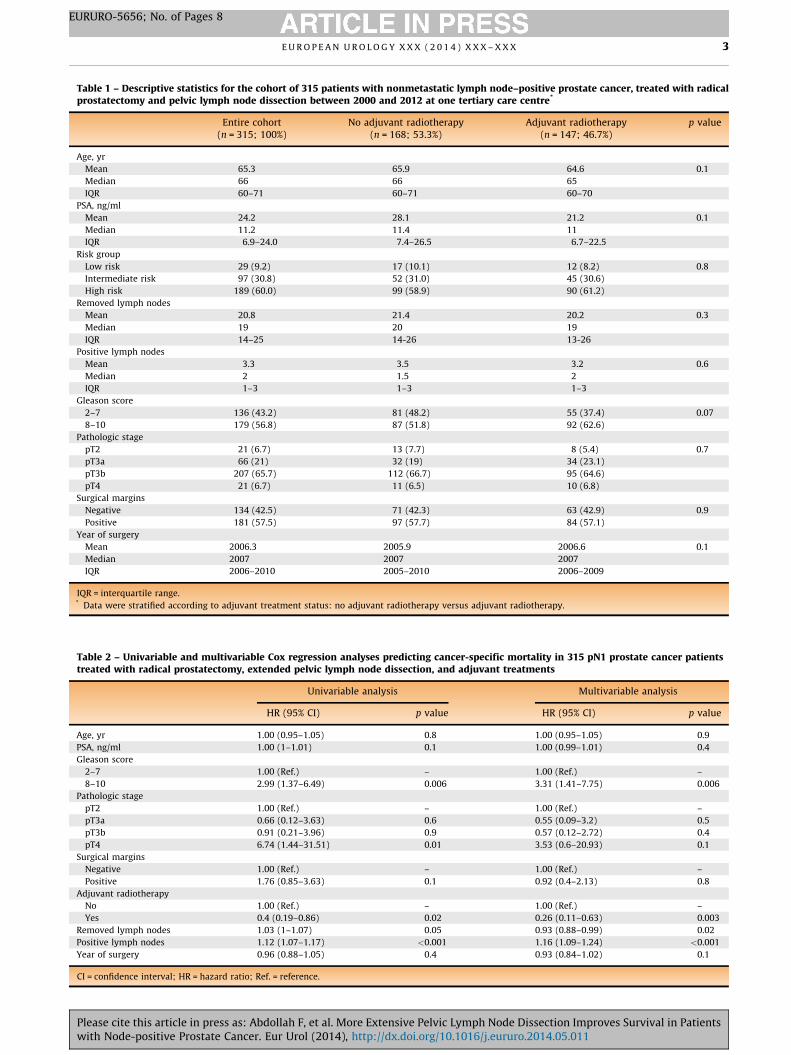
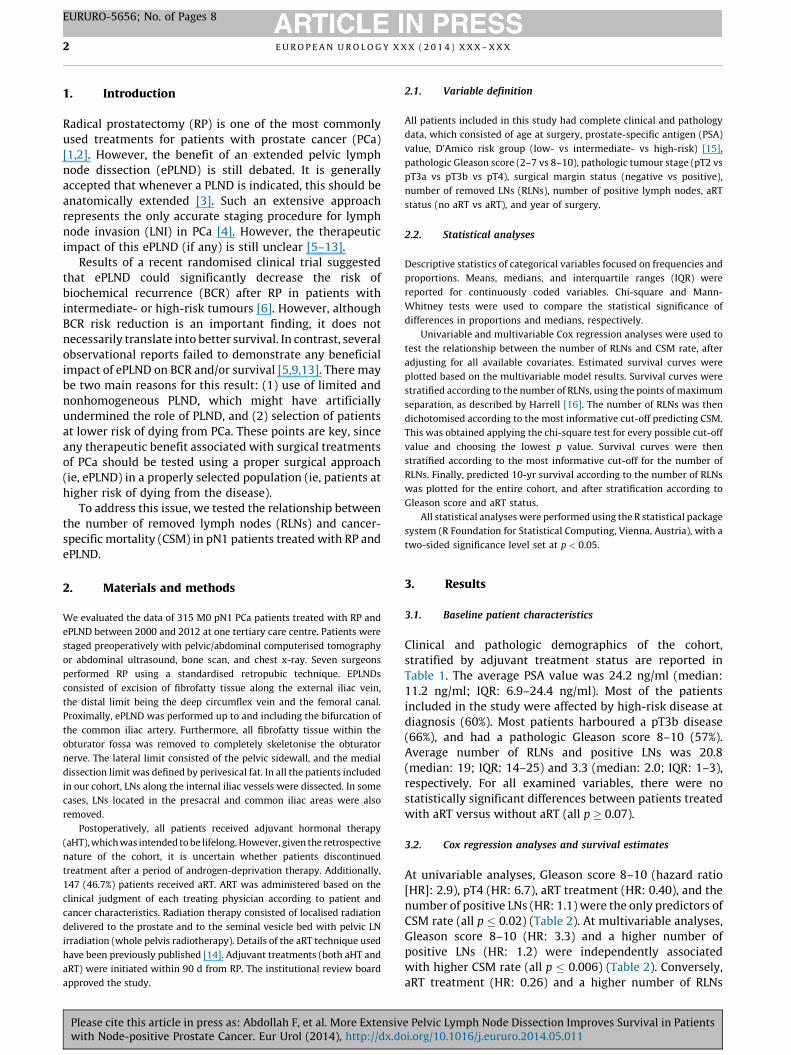
Table 1 – Descriptive statistics for the cohort of 315 patients with nonmetastatic lymph node–positive prostate cancer, treated with radicalprostatectomy and pelvic lymph node dissection between 2000 and 2012 at one tertiary care centre*
Entire cohort(n = 315; 100%)
No adjuvant radiotherapy(n = 168; 53.3%)
Adjuvant radiotherapy(n = 147; 46.7%)
p value
Age, yr
Mean 65.3 65.9 64.6 0.1
Median 66 66 65
IQR 60–71 60–71 60–70
PSA, ng/ml
Mean 24.2 28.1 21.2 0.1
Median 11.2 11.4 11
IQR 6.9–24.0 7.4–26.5 6.7–22.5
Risk group
Low risk 29 (9.2) 17 (10.1) 12 (8.2) 0.8
Intermediate risk 97 (30.8) 52 (31.0) 45 (30.6)
High risk 189 (60.0) 99 (58.9) 90 (61.2)
Removed lymph nodes
Mean 20.8 21.4 20.2 0.3
Median 19 20 19
IQR 14–25 14-26 13-26
Positive lymph nodes
Mean 3.3 3.5 3.2 0.6
Median 2 1.5 2
IQR 1–3 1–3 1–3
Gleason score
2–7 136 (43.2) 81 (48.2) 55 (37.4) 0.07
8–10 179 (56.8) 87 (51.8) 92 (62.6)
Pathologic stage
pT2 21 (6.7) 13 (7.7) 8 (5.4) 0.7
pT3a 66 (21) 32 (19) 34 (23.1)
pT3b 207 (65.7) 112 (66.7) 95 (64.6)
pT4 21 (6.7) 11 (6.5) 10 (6.8)
Surgical margins
Negative 134 (42.5) 71 (42.3) 63 (42.9) 0.9
Positive 181 (57.5) 97 (57.7) 84 (57.1)
Year of surgery
Mean 2006.3 2005.9 2006.6 0.1
Median 2007 2007 2007
IQR 2006–2010 2005–2010 2006–2009
IQR = interquartile range.* Data were stratified according to adjuvant treatment status: no adjuvant radiotherapy versus adjuvant radiotherapy.
Table 2 – Univariable and multivariable Cox regression analyses predicting cancer-specific mortality in 315 pN1 prostate cancer patientstreated with radical prostatectomy, extended pelvic lymph node dissection, and adjuvant treatments
Univariable analysis Multivariable analysis
HR (95% CI) p value HR (95% CI) p value
Age, yr 1.00 (0.95–1.05) 0.8 1.00 (0.95–1.05) 0.9
PSA, ng/ml 1.00 (1–1.01) 0.1 1.00 (0.99–1.01) 0.4
Gleason score
2–7 1.00 (Ref.) – 1.00 (Ref.) –
8–10 2.99 (1.37–6.49) 0.006 3.31 (1.41–7.75) 0.006
Pathologic stage
pT2 1.00 (Ref.) – 1.00 (Ref.) –
pT3a 0.66 (0.12–3.63) 0.6 0.55 (0.09–3.2) 0.5
pT3b 0.91 (0.21–3.96) 0.9 0.57 (0.12–2.72) 0.4
pT4 6.74 (1.44–31.51) 0.01 3.53 (0.6–20.93) 0.1
Surgical margins
Negative 1.00 (Ref.) – 1.00 (Ref.) –
Positive 1.76 (0.85–3.63) 0.1 0.92 (0.4–2.13) 0.8
Adjuvant radiotherapy
No 1.00 (Ref.) – 1.00 (Ref.) –
Yes 0.4 (0.19–0.86) 0.02 0.26 (0.11–0.63) 0.003
Removed lymph nodes 1.03 (1–1.07) 0.05 0.93 (0.88–0.99) 0.02
Positive lymph nodes 1.12 (1.07–1.17) <0.001 1.16 (1.09–1.24) <0.001
Year of surgery 0.96 (0.88–1.05) 0.4 0.93 (0.84–1.02) 0.1
CI = confidence interval; HR = hazard ratio; Ref. = reference.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 3
EURURO-5656; No. of Pages 8
Please cite this article in press as: Abdollah F, et al. More Extensive Pelvic Lymph Node Dissection Improves Survival in Patientswith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.doi.org/10.1016/j.eururo.2014.05.011
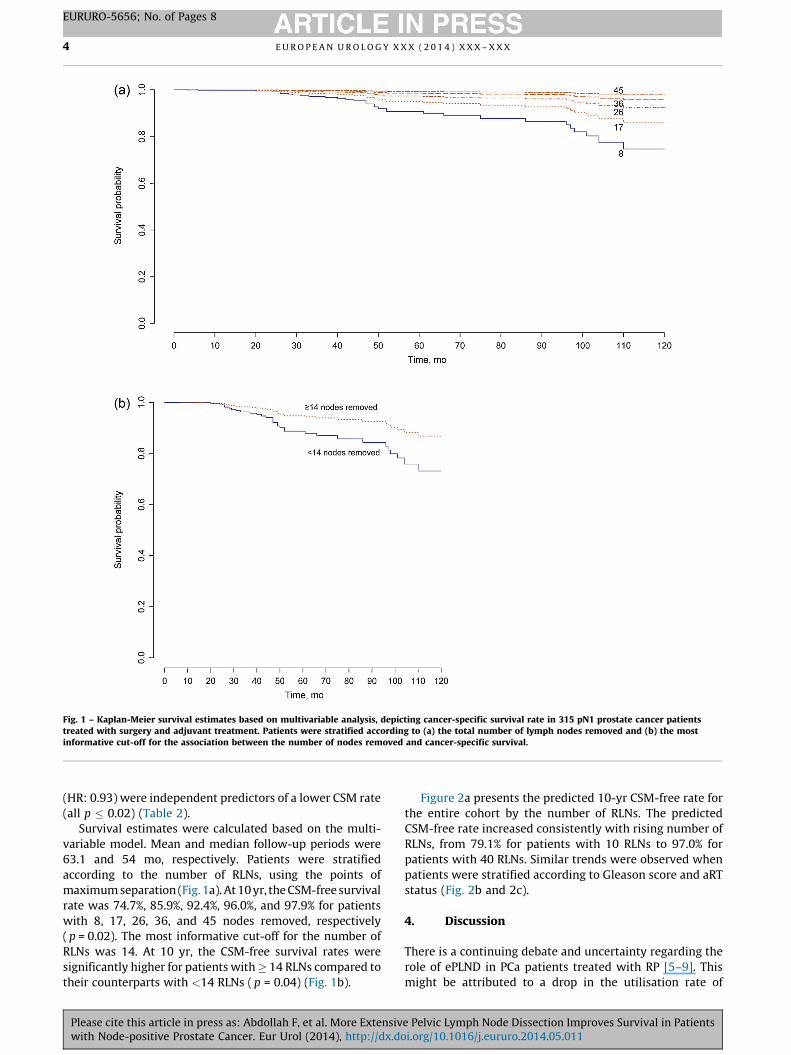
Fig. 1 – Kaplan-Meier survival estimates based on multivariable analysis, depicting cancer-specific survival rate in 315 pN1 prostate cancer patientstreated with surgery and adjuvant treatment. Patients were stratified according to (a) the total number of lymph nodes removed and (b) the mostinformative cut-off for the association between the number of nodes removed and cancer-specific survival.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X4
EURURO-5656; No. of Pages 8
(HR: 0.93) were independent predictors of a lower CSM rate
(all p � 0.02) (Table 2).
Survival estimates were calculated based on the multi-
variable model. Mean and median follow-up periods were
63.1 and 54 mo, respectively. Patients were stratified
according to the number of RLNs, using the points of
maximum separation (Fig. 1a). At 10 yr, the CSM-free survival
rate was 74.7%, 85.9%, 92.4%, 96.0%, and 97.9% for patients
with 8, 17, 26, 36, and 45 nodes removed, respectively
( p = 0.02). The most informative cut-off for the number of
RLNs was 14. At 10 yr, the CSM-free survival rates were
significantly higher for patients with � 14 RLNs compared to
their counterparts with <14 RLNs ( p = 0.04) (Fig. 1b).
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
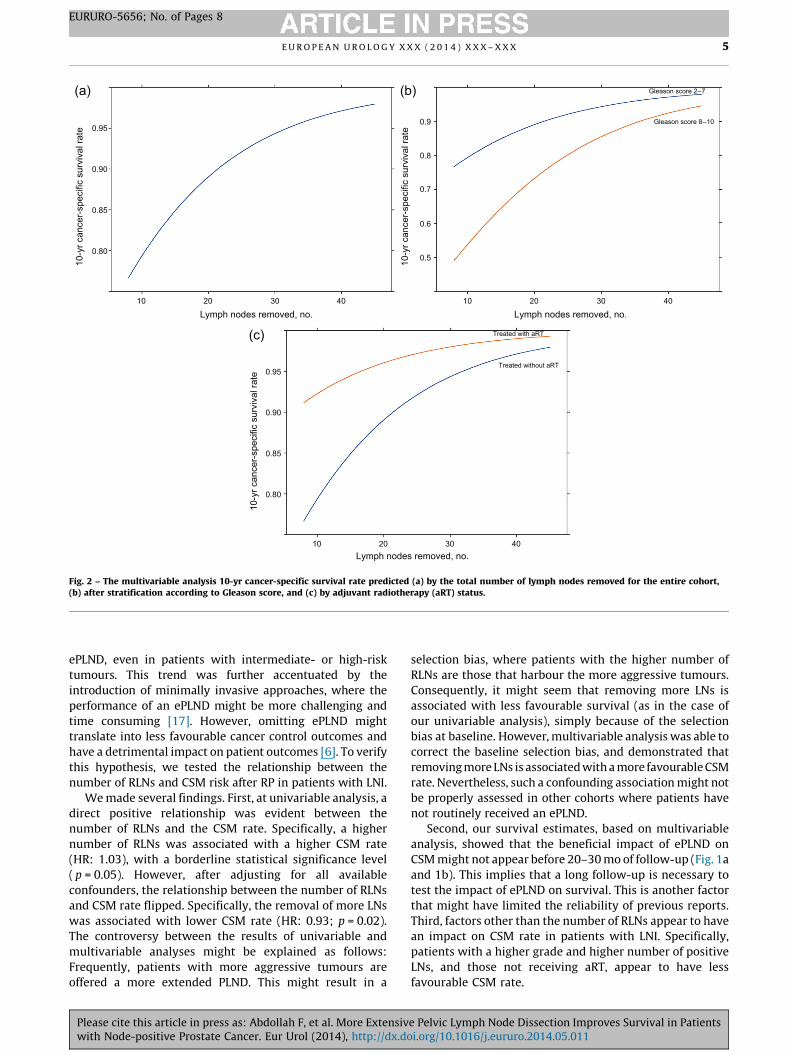
Figure 2a presents the predicted 10-yr CSM-free rate for
the entire cohort by the number of RLNs. The predicted
CSM-free rate increased consistently with rising number of
RLNs, from 79.1% for patients with 10 RLNs to 97.0% for
patients with 40 RLNs. Similar trends were observed when
patients were stratified according to Gleason score and aRT
status (Fig. 2b and 2c).
4. Discussion
There is a continuing debate and uncertainty regarding the
role of ePLND in PCa patients treated with RP [5–9]. This
might be attributed to a drop in the utilisation rate of
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011
Gleason score 8–10
Gleason score 2–7(a) (b)
(c)
Treated without aRT
Treated with aRT
0.95
0.90
0.85
0.80
10 20 30 40 10 20 30 40
0.95
0.90
0.85
0.80
10 20 30 40
0.9
0.8
0.7
0.6
0.5
Lymph nodes removed, no. Lymph nodes removed, no.
Lymph nodes removed, no.
10-y
r can
cer-
spec
ific
surv
ival
rate
10-y
r can
cer-
spec
ific
surv
ival
rate
10-y
r can
cer-
spec
ific
surv
ival
rate
Fig. 2 – The multivariable analysis 10-yr cancer-specific survival rate predicted (a) by the total number of lymph nodes removed for the entire cohort,(b) after stratification according to Gleason score, and (c) by adjuvant radiotherapy (aRT) status.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 5
EURURO-5656; No. of Pages 8
ePLND, even in patients with intermediate- or high-risk
tumours. This trend was further accentuated by the
introduction of minimally invasive approaches, where the
performance of an ePLND might be more challenging and
time consuming [17]. However, omitting ePLND might
translate into less favourable cancer control outcomes and
have a detrimental impact on patient outcomes [6]. To verify
this hypothesis, we tested the relationship between the
number of RLNs and CSM risk after RP in patients with LNI.
We made several findings. First, at univariable analysis, a
direct positive relationship was evident between the
number of RLNs and the CSM rate. Specifically, a higher
number of RLNs was associated with a higher CSM rate
(HR: 1.03), with a borderline statistical significance level
( p = 0.05). However, after adjusting for all available
confounders, the relationship between the number of RLNs
and CSM rate flipped. Specifically, the removal of more LNs
was associated with lower CSM rate (HR: 0.93; p = 0.02).
The controversy between the results of univariable and
multivariable analyses might be explained as follows:
Frequently, patients with more aggressive tumours are
offered a more extended PLND. This might result in a
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
selection bias, where patients with the higher number of
RLNs are those that harbour the more aggressive tumours.
Consequently, it might seem that removing more LNs is
associated with less favourable survival (as in the case of
our univariable analysis), simply because of the selection
bias at baseline. However, multivariable analysis was able to
correct the baseline selection bias, and demonstrated that
removing more LNs is associated with a more favourable CSM
rate. Nevertheless, such a confounding association might not
be properly assessed in other cohorts where patients have
not routinely received an ePLND.
Second, our survival estimates, based on multivariable
analysis, showed that the beneficial impact of ePLND on
CSM might not appear before 20–30 mo of follow-up (Fig. 1a
and 1b). This implies that a long follow-up is necessary to
test the impact of ePLND on survival. This is another factor
that might have limited the reliability of previous reports.
Third, factors other than the number of RLNs appear to have
an impact on CSM rate in patients with LNI. Specifically,
patients with a higher grade and higher number of positive
LNs, and those not receiving aRT, appear to have less
favourable CSM rate.
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X6
EURURO-5656; No. of Pages 8
In a previous report, Joslyn et al. [7] analysed data of
13 020 PCa patients treated initially with RP between 1988
and 1991, within the Surveillance, Epidemiology, and End
Results database. Authors found that removing four or more
LNs was associated with a more favourable survival rate in
both node-negative and node-positive patients. However,
these observations originated from historic patients that
were treated in the early PSA era. In another report,
Masterson et al. [8] examined the data of 4611 PCa patients
treated with RP, and found that the number of RLNs was not
associated with the risk of disease recurrence. However,
when selecting only pN0 patients, a higher number of RLNs
removed was significantly related to a lower BCR risk.
Additionally, Bivalacqua et al. [11] have shown patients
undergoing an ePLND had better oncologic outcomes at
10-yr follow-up compared to their counterparts receiving a
limited PLND. Conversely, other authors found the number
of RLNs was not associated with BCR and/or survival, even in
high-risk patients [5,9,12,13] It is noteworthy that most of
the reports focused exclusively on pN0 patients. This might
have resulted in a selection bias (Will Rogers phenomenon),
where pN0 patients with higher number of RLNs are better
staged and, thus, are more likely to be really free from LNI.
Conversely, pN0 patients with lower number of RLNs are
less probable to be accurately staged, and might actually
harbour an overlooked LNI. The less favourable survival
rates observed in these individuals might largely be
attributable to this. Although such an effect may have also
have partly influenced our results, we tried to minimise it
by focusing only on pN1 patients homogenously treated
with an ePLND. Specifically, one of the strengths of our
study is that it was based on men with LNI receiving
adequate extent of PLND. Given the heterogeneous natural
history of PCa, it is likely that a well-performed ePLND, as
well as any surgical treatment for PCa [18,19], exerts its
maximal effect on those who are at higher risk of dying from
PCa. Selecting individuals who are exposed to higher
cancer-specific risk and lower risk of competing causes of
death may thus maximise the effect of this extensive
surgical approach.
Our study has several clinical implications. Our findings
showed that a more extensive PLND offers better cancer
control outcomes in patients with LNI. It is noteworthy that
the risk for LNI in contemporary PCa patients is still significant
[20,21], and that accurate preoperative staging with imaging
of these individuals is not possible [4]. Consequently, an
ePLND in these men is mandatory to achieve reliable staging
and to improve survival of those with LNI.
Moreover, our results emphasise that it is necessary to be
cautious in interpreting data that originate from cohorts
where patients are not homogenously treated with an
ePLND and/or without long follow-up. Such data might
artificially undermine the benefits of ePLND. However, our
results cannot answer the clinically relevant question
regarding the optimal anatomic extent of ePLND in patients
with LNI. Certainly, all these patients should receive an
anatomic dissection of all lymphatic tissue in the obturator
fossa, as well as along the external and internal iliac vessels.
This should be invariably performed in all patients
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
whenever a PLND is indicated [3]. In addition, our results
seem to support not only a meticulous and careful
dissection of all these areas, but also of the presacral and
common iliac areas in patients with adverse PCa character-
istics, as previously recommended [22,23]. However, such
an approach can be only suggested, but not fully supported,
by our results. Indeed, while our study shows an association
between the number of LNs removed and patient survival,
the lack of data regarding the exact anatomic scheme of LND
in each patient prevents us from giving a clear recommen-
dation about this subject.
Finally, our results showed that patients with LNI might
benefit from maximising local disease control with aRT. This
corroborates our previous findings [24–26] and implies that
not all patients with LNI necessarily harbour a metastatic
disease. Indeed, patients with few positive LNs showed
excellent cancer-specific survival rates after adjusting for
postoperative treatments [12,27]. In this study, we report
the first single-institution series supporting the role of more
extensive PLND, regardless of the extent of nodal invasion.
Our study is not devoid of limitations. First, our results
were derived from retrospective, observational data.
Therefore, our findings should be considered in the context
of retrospective, observational evidence and warrant
prospective, randomised validation. Despite that an an-
atomically ePLND was routinely offered to all RP patients in
our institution, a fluctuation in the number of RLNs was
observed. Indeed, the RLNs ranged between 4 and 83. This
might be derived from individual variability related to
patient characteristics, which is inevitable, especially in
such a large cohort. Moreover, many unobserved confoun-
ders, such as surgical [28], pathologic expertise, and/or
imperceptible changes over time might have affected the LN
count [29]. Likewise, at surgeon discretion, a more extended
PLND that involved presacral and/or common iliac LNs was
performed in some patients. These unobserved confounders
might explain, at least partially, the variability in the LN
count over the study period. In this context, we would like
to highlight that the range of RLNs observed in our series is
in line with what has been reported by other esteemed
authors in large cohorts of patients treated with RP and
anatomically defined ePLND [11,29–32]. However, such
variability allowed us to test the effect between the number
of RLNs and patient survival, since it is likely that some
patients received even more meticulous PLND and a more
careful dissection of pelvic lymphatic tissue, based on the
judgment and expertise of different treating physicians.
Second, a pathology review was not performed. Despite the
variability in surgical technique and pathology reports,
which might have introduced potential biases, our data
benefited from a high expertise and standardised protocols,
given the tertiary care centre nature of our institute. Overall,
seven experienced surgeons (>150 cases each at the time of
study initiation) performed RP and ePLND. Moreover, four
pathologists examined the pathology specimens over the
study period. Although all of them applied a standardised
protocol for nodal evaluation [33], we cannot exclude that a
possible heterogeneity in nodal count may have introduced,
given the retrospective nature of our study. Third, data
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 7
EURURO-5656; No. of Pages 8
regarding complication rate were not available. Fourth, all
patients included in the analyses received aHT. Conse-
quently, our observations might not be applicable in
patients with positive LNs and who received no aHT.
Moreover, the use of aRT was administered based on the
clinical judgment of each treating physician according to
patient and cancer characteristics. Although this might
have introduced a potential bias, it should be highlighted
that multivariable analysis and stratified analysis corrobo-
rate the beneficial impact of an ePLND, regardless of the
adjuvant treatment status.
5. Conclusions
Our results showed that in PCa patients with LNI, the
removal of a higher number of LNs during RP was associated
with an improvement in cancer-specific survival rate.
Particularly, the most informative cut-off for the number
of RLNs was 14. This implies that an ePLND should be
considered in all patients with a significant preoperative
risk of harbouring an LNI.
Author contributions: Alberto Briganti had full access to all the data in
the study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Abdollah, Suardi, Briganti.
Acquisition of data: Gandaglia, Nini, Moschini.
Analysis and interpretation of data: Abdollah, Sun, Gandaglia, Capitano.
Drafting of the manuscript: Abdollah, Briganti.
Critical revision of the manuscript for important intellectual content:
Briganti, Salonia, Karakiewicz, Shariat, Montorsi.
Statistical analysis: Abdollah, Sun, Capitano, Gandaglia.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Briganti, Saloni, Karakiewicz, Shariat, Montorsi.
Other (specify): None.
Financial disclosures: Alberto Briganti certifies that all conflicts of
interest, including specific financial interests and relationships and
affiliations relevant to the subject matter or materials discussed in the
manuscript (eg, employment/affiliation, grants or funding, consultan-
cies, honoraria, stock ownership or options, expert testimony, royalties,
or patents filed, received, or pending), are the following: None
Funding/Support and role of the sponsor: None.
References
[1] Jacobs BL, Zhang Y, Schroeck FR, et al. Use of advanced treatment
technologies among men at low risk of dying from prostate cancer.
JAMA 2013;309:2587–95.
[2] Abdollah F, Sun M, Thuret R, et al. A competing-risks analysis of
survival after alternative treatment modalities for prostate cancer
patients: 1988–2006. Eur Urol 2011;59:88–95.
[3] Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on
prostate cancer. Part 1: screening, diagnosis, and local treatment
with curative intent—update 2013. Eur Urol 2014;65:124–37.
[4] Briganti A, Abdollah F, Nini A, et al. Performance characteristics of
computed tomography in detecting lymph node metastases in
contemporary patients with prostate cancer treated with extended
pelvic lymph node dissection. Eur Urol 2012;61:1132–8.
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
[5] DiMarco DS, Zincke H, Sebo TJ, Slezak J, Bergstralh EJ, Blute ML. The
extent of lymphadenectomy for pTXNO prostate cancer does not
affect prostate cancer outcome in the prostate specific antigen era. J
Urol 2005;173:1121–5.
[6] Ji J, Yuan H, Wang L, Hou J. Is the impact of the extent of lymphadenec-
tomy in radical prostatectomy related to the disease risk? A single
center prospective study. J Surg Res 2012;178:779–84.
[7] Joslyn SA, Konety BR. Impact of extent of lymphadenectomy on
survival after radical prostatectomy for prostate cancer. Urology
2006;68:121–5.
[8] Masterson TA, Bianco FJ, Vickers AJ, et al. The association between
total and positive lymph node counts, and disease progression in
clinically localized prostate cancer. J Urol 2006;175:1320–4, dis-
cussion 1324–5.
[9] Murphy AM, Berkman DS, Desai M, Benson MC, McKiernan JM,
Badani KK. The number of negative pelvic lymph nodes removed
does not affect the risk of biochemical failure after radical prosta-
tectomy. BJU Int 2010;105:176–9.
[10] Schiavina R, Manferrari F, Garofalo M, et al. The extent of pelvic
lymph node dissection correlates with the biochemical recurrence
rate in patients with intermediate- and high-risk prostate cancer.
BJU Int 2011;108:1262–8.
[11] Bivalacqua TJ, Pierorazio PM, Gorin MA, Allaf ME, Carter HB, Walsh
PC. Anatomic extent of pelvic lymph node dissection: impact on
long-term cancer-specific outcomes in men with positive lymph
nodes at time of radical prostatectomy. Urology 2013;82:653–8.
[12] Touijer KA, Mazzola CR, Sjoberg DD, Scardino PT, Eastham JA. Long-
term outcomes of patients with lymph node metastasis treated
with radical prostatectomy without adjuvant androgen-deprivation
therapy. Eur Urol 2014;65:20–5.
[13] Pierorazio PM, Gorin MA, Ross AE, et al. Pathological and oncologic
outcomes for men with positive lymph nodes at radical prostatec-
tomy: The Johns Hopkins Hospital 30-year experience. Prostate
2013;73:1673–80.
[14] Cozzarini C, Montorsi F, Fiorino C, et al. Need for high radiation dose
(�70 gy) in early postoperative irradiation after radical prostatec-
tomy: a single-institution analysis of 334 high-risk, node-negative
patients. Int J Radiat Oncol Biol Phys 2009;75:966–74.
[15] D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical out-
come after radical prostatectomy, external beam radiation therapy,
or interstitial radiation therapy for clinically localized prostate
cancer. JAMA 1998;280:969–74.
[16] Harrell FE. rms: regression modeling strategies (2012). R package
v.3.5-0. http://CRAN.R-project.org/package=rms.
[17] Gandaglia G, Trinh QD, Hu JC, et al. The impact of robot-assisted
radical prostatectomy on the use and extent of pelvic lymph node
dissection in the ‘‘post-dissemination’’ period. Eur J Surg Oncol.
In press. http://dx.doi.org/10.1016/j.ejso.2013.12.016
[18] Wilt TJ, Brawer MK, Jones KM, et al. Radical prostatectomy versus
observation for localized prostate cancer. N Engl J Med 2012;367:
203–13.
[19] Vickers A, Bennette C, Steineck G, et al. Individualized estimation of
the benefit of radical prostatectomy from the Scandinavian Prostate
Cancer Group randomized trial. Eur Urol 2012;62:204–9.
[20] Ploussard G, Briganti A, de la Taille A, et al. Pelvic lymph node
dissection during robot-assisted radical prostatectomy: efficacy,
limitations, and complications-a systematic review of the litera-
ture. Eur Urol 2014;65:7–16.
[21] Abdollah F, Suardi N, Gallina A, et al. Extended pelvic lymph node
dissection in prostate cancer: a 20-year audit in a single center. Ann
Oncol 2013;24:1459–66.
[22] Heidenreich A, Varga Z, Von Knobloch R. Extended pelvic
lymphadenectomy in patients undergoing radical prostatectomy:
high incidence of lymph node metastasis. J Urol 2002;167:1681–6.
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X8
EURURO-5656; No. of Pages 8
[23] Joniau S, Van den Bergh L, Lerut E, et al. Mapping of pelvic lymph
node metastases in prostate cancer. Eur Urol 2013;63:450–8.
[24] Abdollah F, Suardi N, Cozzarini C, et al. Selecting the optimal candi-
date for adjuvant radiotherapy after radical prostatectomy for pros-
tate cancer: a long-term survival analysis. Eur Urol 2013;63:
998–1008.
[25] Briganti A, Karnes RJ, Da Pozzo LF, et al. Combination of adjuvant
hormonal and radiation therapy significantly prolongs survival of
patients with pT2-4 pN+ prostate cancer: results of a matched
analysis. Eur Urol 2011;59:832–40.
[26] Da Pozzo LF, Cozzarini C, Briganti A, et al. Long-term follow-up of
patients with prostate cancer and nodal metastases treated by
pelvic lymphadenectomy and radical prostatectomy: the positive
impact of adjuvant radiotherapy. Eur Urol 2009;55:1003–11.
[27] Briganti A, Karnes JR, Da Pozzo LF, et al. Two positive nodes
represent a significant cut-off value for cancer specific survival
in patients with node positive prostate cancer. A new proposal
based on a two-institution experience on 703 consecutive N+
patients treated with radical prostatectomy, extended pelvic lymph
node dissection and adjuvant therapy. Eur Urol 2009;55:261–70.
[28] Briganti A, Capitanio U, Chun FK-H, et al. Impact of surgical volume
on the rate of lymph node metastases in patients undergoing
Please cite this article in press as: Abdollah F, et al. More Extensivwith Node-positive Prostate Cancer. Eur Urol (2014), http://dx.do
radical prostatectomy and extended pelvic lymph node dissection
for clinically localized prostate cancer. Eur Urol 2008;54:794–804.
[29] Mazzola C, Savage C, Ahallal Y, et al. Nodal counts during pelvic
lymph node dissection for prostate cancer: an objective indicator of
quality under the influence of very subjective factors. BJU Int
2012;109:1323–8.
[30] Eden CG, Zacharakis E, Bott S. The learning curve for laparoscopic
extended pelvic lymphadenectomy for intermediate- and high-risk
prostate cancer: implications for compliance with existing guide-
lines. BJU Int 2013;112:346–54.
[31] Sagalovich D, Calaway A, Srivastava A, Sooriakumaran P, Tewari AK.
Assessment of required nodal yield in a high risk cohort undergoing
extended pelvic lymphadenectomy in robotic-assisted radical pros-
tatectomy and its impact on functional outcomes. BJU Int 2013;
111:85–94.
[32] Seiler R, Studer UE, Tschan K, Bader P, Burkhard FC. Removal of
limited nodal disease in patients undergoing radical prostatectomy:
long-term results confirm a chance for cure. J Urol 2014;191:1280–5.
[33] Briganti A, Larcher A, Abdollah F, et al. Updated nomogram predicting
lymph node invasion in patients with prostate cancer undergoing
extended pelvic lymph node dissection: the essential importance of
percentage of positive cores. Eur Urol 2012;61:480–7.
e Pelvic Lymph Node Dissection Improves Survival in Patientsi.org/10.1016/j.eururo.2014.05.011





























