Embed Size (px)
Citation preview

Monosialoganglioside GM1 Reduces Ischemia-Reperfusion-Induced Injury in the Rat Retina
Michel Weber,* Saddek Mohand-Said,f David Hicks,^ Henri Dreyfus,\and Jose Alain Sahetf
Purpose. Gangliosides are normal components of cell membranes, contribute to structuralrigidity and membrane function, and have been shown to protect against various insults tothe brain. This study evaluates the effect of exogenously administered monosialogangliosideGM1 on retinal damage induced by transient retinal ischemia and reperfusion.
Methods. Retinal ischemia was induced unilaterally in Long Evans rats by increasing intraocularpressure to 160 mm Hg for 60 minutes. GM1 (30 mg/kg, intraperitoneally) or buffer controlswere administered at 48 hours, 24 hours, and 15 minutes before ischemia, and survivaltime after ischemia was either 8 or 15 days. The degree of retinal damage was assessed byhistopathologic study according to Hughes' quantification of ischemic damage.
Results. Retinal ischemia led to significant reductions in thickness and cell number, principallyin the inner retinal layers (30% to 80%), and to a lesser extent in the outer retinal layers (18%to 42%). Pretreatment with intraperitonealy injected monosialoganglioside GM1 conferredsignificant protection against retinal ischemic damage either 8 or 15 days after ischemicsurvival time. After 8 days reperfusion, the ischemic-induced loss in overall retinal thicknesswas reduced by 70%, and those of the inner nuclear and plexiform layers were reduced by77% and 44%, respectively. Ischemic-induced ganglion cell, inner nuclear, and outer nuclearlayer cell density losses were reduced by 45%, 40%, and 57%, respectively. After 15 days ofreperfusion, approximately the same statistically significant differences could be observed incomparison with the 15-day ischemic-reperfusion group.
Conclusions. Monosialoganglioside GM1 protects the rat retina from pressure-induced ischemicinjury when administered intraperitonealy 2 days before insult. This protection afforded byGM1 can be observed even after 8 days or 15 days of reperfusion. Invest Ophthalmol Vis Sci.1996; 37:267-273.
VFangliosides are naturally occuring glycosphingoli-pids that contain one or more sialic acids and areparticularly abundant in neuronal membranes.' Theyinfluence functional dynamics of the cellular mem-branes on several ways: They contribute to the struc-tural rigidity of the membranes; they are involved inthe transfer of information between neighboring cellsor between cell surfaces and the extracellular environ-ment (neurotransmitters, hormones); and they modu-late cell growth by regulating proliferation and matu-ration processes controlled by polypeptide growth fac-
From the * Department of Ophthalmology, Centre Hospitalo-Universitaire de Nantes,and the ^Laboratory of Retinal Physiopathology, Louis Pasteur University,Strasbourg, France.Submitted for publication August 2, 1995; revised October 27, 1995; acceptedOctober 30, 1995.Proprietary interest category: N.Reprint requests: Jose Alain Saliel, Clinique Ophtabnologique, Centre Hospitalo-Univeisitaire de Strasbourg, 1 place de I'hopilal, 67091 Straslwurg cedex, France.
tors, such as fibroblast growth factor, epidermalgrowth factor, or nerve growth factor.2 In hypoxicbrain, the levels of gangliosides decrease, and this hasbeen correlated with the subsequent impairment ofthe central nervous system.3 It has been shown thatexogenously administered gangliosides can cross dieblood-brain barrier,4 insert into plasma membranes,and be functional after this incorporation. Accord-ingly, exogenously administered gangliosides couldsubstitute functionally for endogenous gangliosideswithin the plasma membrane, a major site of ischemicneuronal injury.
In experimental models of cerebral ischemia, mo-nosialoganglioside GM1 partially reduces ischemicneuronal damage.5"9 The mechanism of action pro-posed for neuroprotection is not completely under-stood. This effect has been attributed, among othermechanisms, to a protective effect on neuronal func-
Investigalive Ophthalmology & Visual Science, February 1996, Vol. 37, No. 2Copyright © Association for Research in Vision and Ophthalmology 267

268 Investigative Ophthalmology 8c Visual Science, February 1996, Vol. 37, No. 2
tion, expressed as maintenance of (Na+,K+) ATPaseactivity10; to blockade of excitatory amino acid-medi-ated neurotoxicity (both prevention of ischemia-in-duced downregulation of protein kinase C and reduc-tion of membrane protein phosphorylation inducedby toxic doses of glutamate that reduces the ischemia-induced intracellular calcium elevation and glutamatetoxicity)""15; and to response potentialization towardneurotrophic factors16"18 produced locally in in-creased quantities as a biochemical response to in-jury.19'20 GM1 also increased regeneration of crush-injured axons of the mammalian optic nerve.21'22
To estimate the protective role of exogenouslyinjected monosialoganglioside GM1, we performedhistopathologic studies on ischemia-induced lesionsin the rat retina, with or without the use of GM1. Weshow that such pretreatments significantly protectedrat retina against ischemic damage.
MATERIALS AND METHODS
Experimental Proposal
Long Evans rats (250 to 350 g) were assigned to oneof three groups:
Group 1 (untreated): No retinal ischemia was in-duced, and no intraperitoneal injections were per-formed (n = 5).
Group 2 (ischemic): Retinal ischemia was in-duced, and the animals received no intraperitonealinjection of GM1 (n = 9) or they received intraperito-neal injections of the phosphate-buffered saline vehi-cle (n = 8); no histopathologic differences were foundbetween these two groups (data not shown).
Group 3 (GM1): Animals were pretreated withmonosialoganglioside GM1 (Fidia Laboratory, Aban-oterme, Italy) (30 mg/kg per day, intraperitoneally)at 48 hours, 24 hours, and 15 minutes before induc-tion of ischemia (n = 8).
All procedures involving rats adhered to theARVO Statement for the Use of Animals in Ophthal-mic and Vision Research.
Ischemia Model and Histologic Procedures
Fifteen minutes after each rat was anesthetized with anintraperitoneal injection of 6% sodium pentobarbital(0.1 ml/100 g), the topical anesthetic oxybuprocainechlorhydrate was applied to the eye. Pupils were di-lated with an eye drop of phenylephrine chlorhydrateand tropicamide. A 3O'/2-gauge needle attached toa manometer-pump assembly was inserted into theanterior chamber and sealed with cyanoacrylate ce-ment. Eye pressure was raised to 160 mm Hg for 60minutes with air. Retinal ischemia was confirmed bywhitening of the fundus. After 60 minutes, the needleand cyanoacrylate cement were removed. The animalswere allowed to recover and survive for 8 days (n =
5, ischemic group; w = 4, GM1 group) or 15 days (n= 4, ischemic and GM1 groups). After 8 or 15 days ofreperfusion, the rats were killed with an overdose ofsodium pentobarbital. The eye of interest was immedi-ately enucleated and fixed by immersion in Bouin'ssolution. After rinsing in a phosphate buffer, the eyewas dehydrated, embedded in paraffin, sectioned witha microtome at 4-/um thickness, and stained with he-matoxylin and eosin. Each section cut along the hori-zontal meridian of the eye contained all of the retinaextending from the ora serrata in the temporal hemi-sphere to the ora serrata in the nasal hemisphere,while passing through the optic nerve head.
Quantification of Ischemic Damage and RescueIt has been demonstrated previously that changes inretinal layer thickness accurately reflect changes incell number.23 To quantify the degree of cell loss fromischemic retinal damage, we measured different thick-nesses (//m) and different linear cell densities (num-ber of nuclei in a 50-//m wide band) according toHughes' quantification of ischemic damage in the ratretina.24
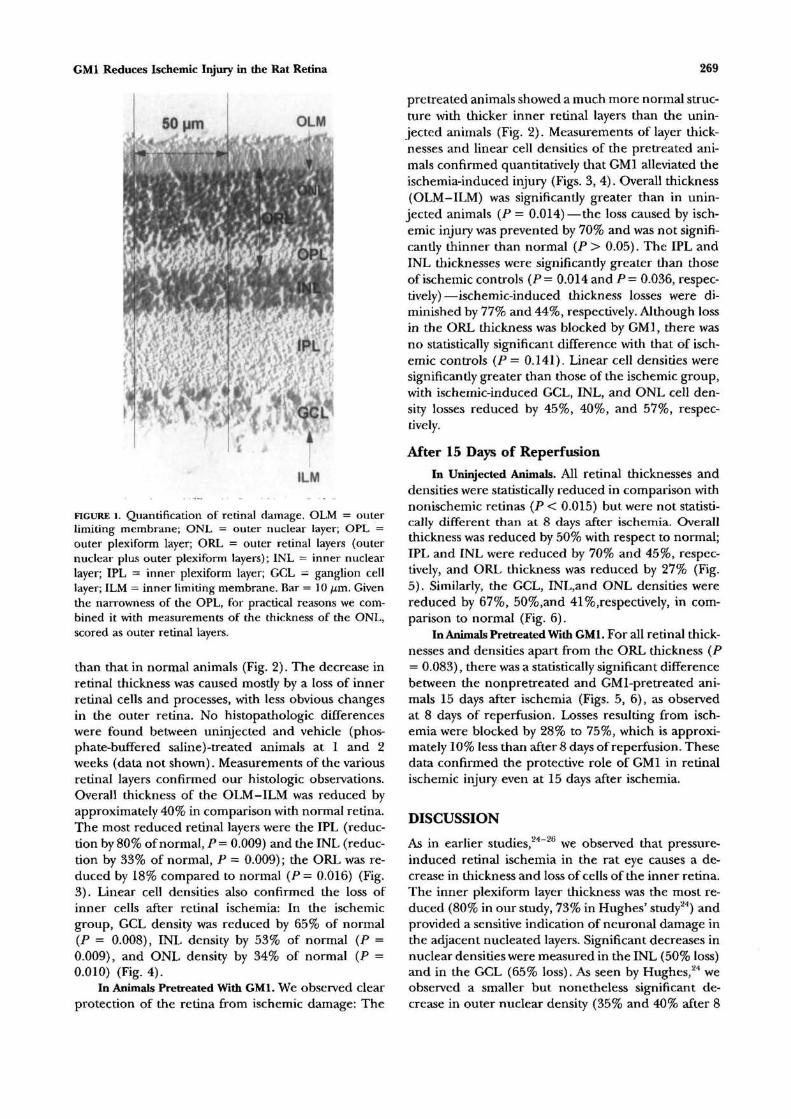
The thickness of the overall retina from the outerto the inner limiting membrane (OLM-ILM), and ofthe outer nuclear layer (ONL) and outer plexiformlayer (pooled together as outer retinal layers [ORL]),inner nuclear layer (INL), and inner plexiform layer(IPL) were measured (Fig. 1). Nuclear cell densitiesincluded the density of cell nuclei along a 50-//mlength of each of the three nucleated layers (ONL,INL, and ganglion cell layer [GCL]).
These parameters were measured, subsequent toa masking procedure, on retinal sections examinedwith an optical microscope (X40 objective) and thendigitalized by a computer-controlled display cameraon a computer screen (Macintosh LC II Ci; Apple,Cupertino, CA) and with the aid of an Optiscan imageanalysis system. For each thickness and density, foursets of three measurements were determined in boththe temporal and nasal hemispheres, giving a total of24 measurements for each parameter. In this way, foreach eye, the entire retinal section was sampled whiletaking into consideration the differences in thicknessand density in the posterior and peripheral regionsof the retina.24 These measurements, evaluated subse-quent to a masking procedure by two authors (MW,SMS), did not differ by more than 5%.
Statistical AnalysisAll data were analyzed with BMDP Statistical Software1993 (University of California Press, Berkeley). Mann-Whitney nonparametric tests were used.
RESULTSAfter 8 Days of Reperfusion
In Uninjected Rats. Histologic examination showedthat the overall thickness of the retina was much less
GM1 Reduces Ischemic Injury in the Rat Retina
OLM
FIGURE l. Quantification of retinal damage. OLM = outerlimiting membrane; ONL = outer nuclear layer; OPL =outer plexiform layer; ORL = outer retinal layers (outernuclear plus outer plexiform layers); INL = inner nuclearlayer; IPL = inner plexiform layer; GCL = ganglion celllayer; ILM = inner limiting membrane. Bar = 10 (im. Giventhe narrowness of the OPL, for practical reasons we com-bined it with measurements of the thickness of the ONL,scored as outer retinal layers.
than that in normal animals (Fig. 2). The decrease inretinal thickness was caused mostly by a loss of innerretinal cells and processes, with less obvious changesin the outer retina. No histopathologic differenceswere found between uninjected and vehicle (phos-phate-buffered saline)-treated animals at 1 and 2weeks (data not shown). Measurements of the variousretinal layers confirmed our histologic observations.Overall thickness of the OLM-ILM was reduced byapproximately 40% in comparison with normal retina.The most reduced retinal layers were the IPL (reduc-tion by 80% of normal, P = 0.009) and the INL (reduc-tion by 33% of normal, P = 0.009); the ORL was re-duced by 18% compared to normal {P = 0.016) (Fig.3). Linear cell densities also confirmed the loss ofinner cells after retinal ischemia: In the ischemicgroup, GCL density was reduced by 65% of normal(P = 0.008), INL density by 53% of normal (P =0.009), and ONL density by 34% of normal (P =0.010) (Fig. 4).
In Animals Pretreated With GM1. We observed clearprotection of the retina from ischemic damage: The
pretreated animals showed a much more normal struc-ture with thicker inner retinal layers than the unin-jected animals (Fig. 2). Measurements of layer thick-nesses and linear cell densities of the pretreated ani-mals confirmed quantitatively that GM1 alleviated theischemia-induced injury (Figs. 3, 4). Overall thickness(OLM-ILM) was significantly greater than in unin-jected animals (P = 0.014)—the loss caused by isch-emic injury was prevented by 70% and was not signifi-cantly thinner than normal (P > 0.05). The IPL andINL thicknesses were significantly greater than thoseof ischemic controls (P= 0.014 and P — 0.036, respec-tively)—ischemic-induced thickness losses were di-minished by 77% and 44%, respectively. Although lossin the ORL thickness was blocked by GM1, there wasno statistically significant difference with that of isch-emic controls (P = 0.141). Linear cell densities weresignificantly greater than those of the ischemic group,with ischemic-induced GCL, INL, and ONL cell den-sity losses reduced by 45%, 40%, and 57%, respec-tively.
After 15 Days of Reperfusion
In Uninjected Animals. All retinal thicknesses anddensities were statistically reduced in comparison withnonischemic retinas (P < 0.015) but were not statisti-cally different than at 8 days after ischemia. Overallthickness was reduced by 50% with respect to normal;IPL and INL were reduced by 70% and 45%, respec-tively, and ORL thickness was reduced by 27% (Fig.5). Similarly, the GCL, INL,and ONL densities werereduced by 67%, 50%,and 41%,respectively, in com-parison to normal (Fig. 6).
In Animals Pretreated With GM1. For all retinal thick-nesses and densities apart from the ORL thickness (P= 0.083), there was a statistically significant differencebetween the nonpretreated and GMl-pretreated ani-mals 15 days after ischemia (Figs. 5, 6), as observedat 8 days of reperfusion. Losses resulting from isch-emia were blocked by 28% to 75%, which is approxi-mately 10% less than after 8 days of reperfusion. Thesedata confirmed the protective role of GM1 in retinalischemic injury even at 15 days after ischemia.
DISCUSSION
As in earlier studies,24"26 we observed that pressure-induced retinal ischemia in the rat eye causes a de-crease in thickness and loss of cells of the inner retina.The inner plexiform layer thickness was the most re-duced (80% in our study, 73% in Hughes' study24) andprovided a sensitive indication of neuronal damage inthe adjacent nucleated layers. Significant decreases innuclear densities were measured in the INL (50% loss)and in the GCL (65% loss). As seen by Hughes,24 weobserved a smaller but nonetheless significant de-crease in outer nuclear density (35% and 40% after 8

Investigative Ophthalmology & Visual Science, February 1996, Vol. 37, No. 2
*>* _
and 15 days of reperfusion, respectively). Accordingto Hughes,24 this outer nuclear density decrease wasassigned to greater evidence of Muller cell expansionspresent after 60 minutes of ischemia but was morenoticeable after 90 or 120 minutes. The apparentlylower threshold for damage to inner retinal neuronsin the rat could be attributed to defects in restorationof the inner retinal circulation in the days after isch-emic insult,*4 to the widespread distribution of gluta-matergic receptors in the inner retina, or both.2728
These reports have shown die expression and distribu-tion of four NMDA, four AMPA, and three high-affin-ity kainate receptor subunits in the adult rat retina.
OLM-ILM ORL INL
FIGURE 3. Measurements of the thickness of different retinallayers (mean ± standard deviation) in (D) control animals(n = 5) and in ischemic (•) nonpretreated (n — 5) rats orffl GM1 pretreated rats (n = 4) after 8 days after ischemia.Significance values above the black column correspond tocomparisons between normal and ischemic conditions,whereas significance values above the gray column refer tocomparisons between GM1-treated and ischemic groups. *P< 0.05).
FIGURE 2. Light micrographsof the posterior pole of adultrat retina. Normal, unin-jected rat (A). One weekafter retinal ischemia in un-injected rat (B) and in GM1-pre treated rat (C). Twoweeks after retinal ischemiain uninjected rat (D) and inGMl-pretreated rat (E). Bar= 10 fj.m.
These results indicate that exogenously adminis-tered monosialoganglioside GM] can reduce signifi-cantly the development of experimental retinal isch-emic injury at 8 and 15 days after ischemia. There wasa statistically significant preservation of overall (OLM-ILM) thickness, INL thickness and density, IPL thick-ness, GCL density, and ONL density. The preventionof ischemic-induced loss by GM1 was observed for allretinal layers varying between 40% and 100% after 8days of reperfusion. This prevention was slightlysmaller after 15 days of reperfusion (28% to 75%).
ONL GCL
FIGURE 4. Measurements of the density of outer and innernuclear and ganglion cell layers (mean ± standard devia-tion) in control D animals (n = 5) and in ischemic • non-pretreated (n = 5) animals or H GMl-pretreated animals~(n = 4) after 8 days after ischemia (see Fig. 3 for explanationof significance values; *P < 0.05).

GMl Reduces Ischemic Injury in the Rat Retina 271
OLM-ILM ORL
FIGURE 5. Measurements of the thickness of different retinallayers (mean ± standard deviation) in control 0 animals (n= 5) and in ischemic • nonpretreated (n = 4) or GM1-pretreated H animals (n = 4) after 15 days after ischemia(see Fig. 3 for explanation of significance values; *P < 0.05).
For the ORL, the combination of only slight ischemicinjury and large sample variation led to a lack of statis-tically significant difference when comparing nonpre-treated and pretreated animals, whereas the averagereduction of loss was the highest for the parametersmeasured. This GMl protective effect observed for allretinal layers with predominance in inner layers couldbe correlated to the GMl blockade of excitatoryamino acid-mediated neurotoxicity. Although the ma-jority of reports on retinal excitotoxicity have shownprincipal damage of the inner retinal layers,29'30 itseems that excitatory amino acids can also injure thephotoreceptor cells.31
Results observed here for the retina are consistentwith the reduction of ischemic-induced neuronal dam-age by exogenously administered GMl observed inexperimental models of brain ischemia5"9: GMl treat-ment decreases mortality at 48 hours after inductionof global ischemia and minimizes the infarct size at24 to 72 hours after focal cerebral ischemia. Ourchoice of GMl ganglioside was justified by numerouspublications on the brain and optic nerve21'22 and bythe fact that among the gangliosides, GMl representsthe species the least susceptible to catabolism, whetherin situ or when added exogenously. Nevertheless, reti-nal ganglioside composition is different from that inthe brain, with much more disialoganglioside GD3 inmammalian retina.32 Further experiments to deter-mine the degree of protection of other gangliosideswill thus be of interest. In other respects, consideringthe neurologically adverse effects observed with sys-temically administered GMl in clinical trials (Guil-lain-Barre syndrome and demyelinative neuropa-thies) y
33'34 further studies will be needed to determine
the most appropriate method of delivery. Althoughwe have used intraperitoneal injections in the currentstudy, intravitreal GM, injections may be preferable.Such an approach could not only avoid adverse sys-temic effects but could increase targeting of GMl di-recdy to the more vulnerable inner retinal layers evenwhen the retinal circulation is interrupted. Finally,protection afforded by GMl injection after ischemiamust be evaluated to broaden the clinical interest ofsuch therapeutic paradigms.
It is widely accepted that ischemia and reperfusionof neuronal tissue lead to the generation of excitatoryamino acids and free radicals that produce neuronaldamage, predominandy through a massive intracellu-lar influx of Ca++. This Ca++ overload leads to celldamage and death through the activation of enzymes,such as Upases, proteases, and endonucleases, whichdegrade cell membranes and organelles. In retinalischemia, the effects of neuronal damage have beenreduced by the application of Ca++-channel antago-nists of excitatory amino acid receptor antago-nists,37"40 by free-radical scavengers41"43 and by growthfactors.26'44 The mechanism (s) by which GMl permitprotection from ischemic injury is unclear, althoughit has been implicated in decreasing die damagecaused by elevated intracellular Ca++ levels from excit-atory amino acids in other systems. Accordingly, al-though the mechanism (s) of protection of GMl inthe context of retinal ischemia remain (s) undefinedby this study, GMl pretreatment restores structural
160
ONL GCL
FIGURE 6. Measurements of the density of outer and innernuclear and ganglion cell layers (mean ± standard devia-tion) in control • animals (n = 5) and in ischemic • non-pretreated (n = 4) or H GMl-pretreated rats (n = 4) after 15days after ischemia (see Fig. 3 for explanation of significancevalues; *P < 0.05).
272 Investigative Ophthalmology 8c Visual Science, February 1996, Vol. 37, No. 2
changes after an ischemic insult to rat retina, sug-gesting that GM1 might be considered a potentialtherapeutic modality for combating retinal ischemia.
Key Words
ganglioside, GM1, ischemia, protection, retina
Acknowledgment
The authors thank J. M. Nguyen for statistical analysis.
References
1. Svennerholm L. Chromatographic separation of hu-man brain gangliosides. / Neurochem. 1963; 10:613-623.
2. Nagai Y. Functional roles of gangliosides in bio-signal-ing. Behav Brain Res. 1995; 66:99-104.
3. Qi Y, Xue QM. Ganglioside levels in hypoxic brainsfrom neonatal and premature infants. Mol Chem Neuro-pathol. 1991; 14:87-97.
4. Tettamanti G, Venerando B, Roberti S, et al. The fateof exogenously administered brain gangliosides. In:Rapport MM, Gorio A, eds. Gangliosides in Neurologicaland Neuromuscular Function, Development and Repair.New York: Raven Press; 1981:225-240.
5. Karpiak SE, Mahadik SP, Wakade CG. Gangliosidesreduction of ischemic injury. Crit Rev Neurobiol.1990; 5:221-237.
6. Lazzaro A, Seren MS, Koga T, Zanoni R, Schiavo N,Manev H. GM1 reduces infarct volume after focal ce-rebral ischemia. Exp Neurol. 1994; 125:278-285.
7. Mazzari S, Karpiak SE, Lipartiti M, et al. Monosialo-ganglioside effects on excitatory amino acid-relatedneurotoxicity and cerebral ischemia. In: Guidotti A,ed. Neurotoxicity of Excitatory Amino Acids. New York:Raven Press; 1990:281-291.
8. Seren MS, Lazzaro A, Yang CL, et al. Orally adminis-tered glycolipid derivative LIGA20 reduces infarct vol-ume and behavioral impairment after focal cerebralischemia. / Pharmacol Exp Ther. 1994; 263:460-465.
9. Simon RP, Chen J, Graham SH. GM1 gangliosidetreatment of focal ischemia: A dose-response and mi-crodialysis study. / Pharmacol Exp Ther. 1993; 265:24-29.
10. Mahadik SP, Hawver DB, Hungund BL, Li YS, KarpiakSE. GM1 ganglioside treatment after global ischemiaprotects changes in membrane fatty acids and proper-ties of Na+, K+-ATPase and Mg2+-ATPase./Afeizros«Res. 1989; 24:402-412.
11. Favaron M, Manev H, Vicini S, Guidotti A, Costa E.Prevention of excitatory amino acid-induced neuro-toxicity by natural and semisynthetic sphingoglycoli-pids. In: Guidotti A, eds. Neurotoxicity of ExcitatoryAmino Acids. New York: Raven Press; 1990:243-258.
12. Lombardi G, Moroni F. GM1 ganglioside reduces isch-emia-induced excitatory amino acid output: Microdi-alysis study in the gerbil hippocampus. Neurosci Lett.1992; 134:171-174.
13. Magal E, Louis J-C, Aguilera J, Yavin E. Gangliosidesprevent ischemia-induced down-regulation of proteinkinase C in fetal rat brain. JNeurochem. 1990; 55:2126-2131.
14. Mahadik SP, Hungund BL, Gokhale VS, et al. Monosi-aloganglioside (GM1) restores membrane fatty acidlevels in ischemic tissue after cortical focal ischemiain rat. Neurochem Int. 1993;23:163-172.
15. Manev H, Favaron M, Vicini S, Guidotti A. Ganglio-side-mediated protection from glutamate-inducedneuronal death. Ada Neurobiol Exp. 1990; 50:381-394.
16. Doherty P, Dickson JG, Flanigan TP, Walsh S. Ganglio-side GM1 does not initiate, but enhances neurite re-generation of nerve growth factor-dependent sensoryneurones. / Neurochem. 1985; 44:1259-1265.
17. Katoh-Semba R, Skaper SD, Varon S. Interaction ofGM1 ganglioside with PC12 pheochromocytoma cells:Serum- and NGF-dependent effects on neuriticgrowth (and proliferation)./ Neurosci Res. 1984; 12:299-310.
18. Leon A, Benvegnu D, Dal Toso R, et al. Dorsal rootganglia and nerve growth factor: A model for under-standing the mechanism of GM effect on neuronalrepair. J Neurosci Res. 1984; 12:277-287.
19. Nieto-Sampedro M, Cotman CW. Growth factor in-duction and temporal order in central nervous systemrepair. In: Cotman CW, ed. Synaptic Plasticity. NewYork: The Guilford Press; 1986:407-455.
20. Kumon Y, Sakaki S, Kadota O, et al. Transient increasein endogenous basic fibroblast growth factor in neu-rons of ischemic rat brains. Brain Res. 1993; 605:169-174.
21. Sautter J, Schwartz M, Duvdevani R, Sabel BA. GM1ganglioside treatment reduces visual deficits aftergraded crush of the rat optic nerve. Brain Res. 1991;565:23-33.
22. Yoles E, Zalish M, Lavie V, et al. GM1 reduces injury-induced metabolic deficits and degeneration in therat optic nerve. Invest Ophthalmol Vis Sci. 1992;33:3586-3591.
23. Michon JJ, Li ZL, Shioura N, Anderson RJ, Tso MOM.A comparative study of methods of photoreceptormorphometry. Invest Ophthalmol Vis Sci. 1991; 32:280-284.
24. Hughes WF. Quantitation of ischemic damage in therat retina. Exp Eye Res. 1990;53:573-582.
25. Biichi ER, Suivaizdis I, Fu J. Pressure-induced retinalischemia in rats: An experimental model for quantita-tive study. Ophthalmobgica. 1991;203:138-147.
26. Unoki K, Lavail M. Protection of the rat retina fromischemic injury by brain-derived neurotrophic factor,ciliary neurotrophic factor, and basic fibroblastgrowth factor. Invest Ophthalmol Vis Sci. 1994; 35:907-915.
27. Hamassaki-Britto DE, Hermans-Borgmeyer I, Heine-mann S, Hughes TE. Expression of glutamate receptorgenes in the mammalian retina: The localisation of Glu.R-1 through Glu.R-7 mKNA. J Neurosci. 1993; 13:1888-1898.
28. Brandstater JH, Hartveit E, Sassoe-Pognetto M, Was-sle H. Expression of NMDA and high-affinity kainatereceptor subunit mRNAs in the adult rat retina. EurJNeurosci. 1994; 6:1100-1112.
29. Abrams L, Politi LE, Adler R. Differential susceptibilityof isolated mouse retinal neurons and photoreceptorsto kainic acid toxicity. Invest Ophthalmol Vis Sci.1989; 30:2300-2308.

GM1 Reduces Ischemic Injury in the Rat Retina 273
30. Siliprandi R, Canella R, Carmignoto G, et al. N-methyl-D-aspartate-induced neurotoxicity in the adultrat retina. Vis Neurosci. 1992;8:567-573.
31. Kanno C, Ishiguro S, Shiono T, Kikuchi M, TamaiM. Decrease of opsin content in the developing ratphotoreceptor cells by systemic administration of L-glutamate. Cell Struct Fund. 1991; 16:399-403.
32. Edel-Harth S, Dreyfus H, Bosch P, et al. Gangliosidesof whole retina and rod outer segments. FEBS Lett.1973; 35:284-288.
33. Diez-Tegedor E, Guttierrez-Riva E, Gil-Peralta A.Gangliosides and Guillain-Barre syndrome: TheSpanish data. Neuroepidemiology. 1993; 12:251-256.
34. Simone IL, Annunciata P, Maimone D, et al. Serumand CSF anti-GMl antibodies in patients with Guil-lain-Barre sydrome and chronic inflammatory demy-elinative polyneuropathy. / Neurol Sci. 1993; 114:49-55.
35. Crosson CE, Willis JA, Potter DE. Effect of the calciumantagonist, nifedipine, on ischemic retinal dysfunc-tion. / Ocul Pharmacol. 1990; 6:293-299.
36. Takahashi K, Lam TT, Edward DP, Buchi ER, TsoMOM. Protective effects of flunarizine on ischemicinjury in the rat retina. Arch Ophthalmol. 1992;110:862-870.
37. Yoon YH, Marmor MF. Dextromethorphan protectsretina against ischemic injury in vivo. Arch Ophthalmol.1989; 107:409-411.
38. Mosinger JL, Price MT, Bai HY, et al. Blockade ofboth NMDA and non-NMDA receptors is required foroptimal protection against ischemic neuronal degen-eration in the in vivo adult mammalian retina. ExpNeurol. 1991; 113:10-17.
39. Weber M, Bonaventure N, Sahel JA. Protective roleof excitatory amino acid antagonists in experimentalretinal ischemia. Graefe's Arch Clin Exp Ophthalmol.1995;233:360-365.
40. El-Asrar AMA, Morse PH, Maimone D, TorczynskiE, Reder AT. MK-801 protects retinal neurons fromhypoxia and the toxicity of glutamate and aspartate.Invest Ophthalmol Vis Sci. 1992;33:3463-3468.
41. Gupta LY, Marmor MF. Mannitol, dextromethorphan,and catalase minimize ischemic damage to the retinalpigment epithelium and retina. Arch Ophthalmol.1993; 111:384-388.
42. Szabo ME, Droy-Lefaix MT, Doly M, Carre C, BraquetP. Ischemia and reperfusion-induced histologicchanges in the rat retina. Invest Ophthalmol Vis Sci.1991;32:1471-1478.
43. Nayak MS, Kita M, Marmor MF. Protection of rabbitretina from ischemic injury by superoxide dismutaseand catalase. Invest Ophthalmol Vis Sci. 1993; 34:2018-2022.
44. Zhang C, Takahashi K, Lam TT, Tso MOM. Effects ofbasic fibroblast growth factor in retinal ischemia. In-vest Ophthalmol Vis Sci. 1994;35:3163-3168.




























