Embed Size (px)
Citation preview
Bladder Cancer
Molecular and Immunohistochemical Analysis of thePrognostic Value of Cell-Cycle Regulators in UrothelialNeoplasms of the Bladder
Andriy O. Yurakh a,*, David Ramos b, Silvia Calabuig-Farinas b,Jose Antonio Lopez-Guerrero c, Jose Rubio d, Eduardo Solsona d,Alina M. Romanenko a, Alexander F. Vozianov a, Antonio Pellin b,Antonio Llombart-Bosch b
a Institute of Urology, Academy of Medical Science of Ukraine, Kyiv, UkrainebDepartment of Pathology, School of Medicine, University of Valencia, Valencia, SpaincUnit of Molecular Biology, Instituto Valenciano de Oncologıa, Valencia, SpaindDepartment of Urology, Instituto Valenciano de Oncologıa, Valencia, Spain
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted March 13, 2006Published online ahead ofprint on March 31, 2006
Keywords:Bladder cancerCyclin D1Disease progressionp14ARFp15INK4Bp16INK4Ap21Waf1p27kip1p53MDM2RecurrenceRetinoblastoma Protein
Abstract
Objective: To evaluate the prognostic and predictive value of molecular andimmunohistochemical markers related to cell-cycle control in terms of recur-rence, progression, and survival in urothelial neoplasms of the bladder (UNB).Patients and Methods: Clinical and pathological findings of 84 patients with UNBwere assessed. Homozygous deletion (HD) and promoter methylation of p14ARF,p15INK4B, p16INK4A, loss of heterozygosity of the locus 9p21, p53 mutations, andimmunohistochemical expression of p53, p16, p14, p21, p27, pRb, Ki67, MDM2,and cyclin D1 proteins were evaluated in relation to overall survival (OS),recurrence-free survival (RFS), and progression-free survival (PFS).Results: In the univariate analysis, RFS was shorter in cases with p14ARF
( p = 0.006), p15INK4B (p = 0.003), p16INK4A (p = 0.03) HD, low p14 immunoreactivityindex (IRI) ( p = 0.01) and high Ki67 IRI ( p = 0.04); HD of the 9p21 locus genes andp14 IRI remained as independent prognostic factors for early UNB recurrence(p = 0.006) whereas tumour stage (p = 0.00001) and cyclin D1 IRI ( p = 0.049) wererelated to worse PFS in the multivariate analysis. In the univariate analysis, IRI forKi67 (p = 0.002), cyclin D1 ( p = 0.06), p53 (p = 0.00008), p16 (p = 0.02), p27(p = 0.0005) MDM2 (p = 0.01) and p53 mutations (p = 0.03) were related to poorOS, and only the Ki67 IRI retained their independent value in the multivariateanalysis.Conclusion: : 9p21 HD and p14 IRI constitute independent predictive factors forUNB recurrence and cyclin D1 IRI and tumour stage for progression. In addition,Ki67 IRI and tumour stage are independent prognostic factors for overallsurvival in UNB.# 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Institute of Urology 9a, Yu. Kotsubinsky Str. 04053, Kiev, Ukraine.Tel. +380 44 4866731; Fax: +380 44 2551565.E-mail address: [email protected] (A.O. Yurakh).
0302-2838/$ – see back matter # 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.03.027
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5 507
Table 1 – Antibodies used in the study
Antigen Clone Source Retrieval Dilution
p53 DO7 DAKO yes 1/50
Ki67 MIB1 DAKO yes 1/50
p14ARF AB-4 Neomarkers yes 1/100
p16INK4A F-12 Santa Cruz yes 1/500
p21WAF1 F-5 Santa Cruz yes 1/50
p27KIP1 SX53G8 Novocastra yes 1/50
pRb 1F8 Neomarkers yes 1/25
MDM2 1B-10 Novocastra yes 1/50
Cyclin D1 P2D11F11 Novocastra yes 1/20
1. Introduction
Molecular alterations of genes implicated in cellcycles are important molecular events in carcino-genesis of urothelial neoplasm of the bladder (UNB).The prognostic significance of alterations of the 9p21chromosomal region, where p15INK4B, p16INK4A, andp14ARF genes are located, as well as alteration ofp21Cip, p27Kip1, p53, MDM2, and CCND1 genes andproteins have been intensively studied during thelast decade. Numerous studies show them as aprognostic markers of UNB clinical outcomes, butvery often results of studies are dissimilar and thecomparative prognostic value of these proteins andgenes are not clear.
Alterations of 9p21 locus, especially p16INK4A/ARF
gene, are very promising prognosticators of clinicaloutcomes because they affect both the p53 and pRbcell-cycle regulatory pathways [1]. The significanceof this locus for tumourigenesis was shown withanimal models of cancer [2].
The aim of the present study was to evaluate thesignificance of alterations in 10 cell-cycle regulatorsto predict recurrence, progression, and overallsurvival (OS) in a series of patients with UNB.
2. Materials and methods
We analyzed material from 84 patients with UNB who had
been treated in the Fundacion Instituto Valenciano de
Oncologıa (I.V.O.), Valencia, Spain. The classification of
tumour stage and grade was defined according to Interna-
tional Society of Urological Pathology and World Health
Organization criteria [3]. No special patient selection was
performed, but many Ta tumours were too small to obtain
adequate samples and were not included in the study. For the
molecular study, fresh-frozen material from the tumour and
from bladder urothelium of normal appearance were used.
The frozen sections were studied with hematoxylin and eosin.
The immunohistochemical (IHC) study was carried out on
formalin-fixed, paraffin-embedded tumoural tissues from the
same samples.
Tumour progression was defined as: (a) progression from
superficial UNB when it becomes a muscle-infiltrating tumour
during follow-up; (b) progression from muscle-infiltration
UNB when after treatment (cystectomy) the disease has
spread to lymph nodes, metastasis, or has had local
recurrence.
2.1. Immunohistochemical study
An IHC study for p53, MDM2, pRb, Cyclin D1, Ki67, p14ARF,
p16INK4A, p21WAF1/Cip1, and p27Kip1 proteins was performed
with the standard avidin-biotin peroxidase complex (ABC)
method with the LSAB kit (DAKO, Denmark). The antibodies
used are listed in Table 1. As controls, known positive tissue
sections were used, and for negative controls, exposure to the
primary antibody was omitted. Colour was developed with
30,30-aminobenzidine and counter-stained with Mayer’s
hematoxylin.
To evaluate the extent of immunostaining we used the
immunoreactivity index (IRI), which was calculated as the
percentage of stained cells by counting 1000 cells per slide.
2.2. DNA extraction
DNA was extracted from 0.10–0.15 g of fresh frozen tissue.
Lysis solution that contained proteinase K (Life Technologies)
in 100 mg/ml concentration was used with subsequent
incubation at 37 8C for 16 h. Standard phenol/chloroform
protocol, followed by precipitation with ethanol, was used for
DNA purification [4]. DNA was quantified by spectrophoto-
metry at 260 nm and quality was checked by measuring the
ratio between the 260 nm and 280 nm values.
2.3. Homozygous deletions of p15INK4B, p16INK4A andp14ARF genes
Differential polymerase chain reaction (dPCR) was used to
detect homozygous deletions (HD) of 9p21 locus genes. PCR
parameters and primer sequences were designed as pre-
viously described by our group [5,6]. The PCR products were
visualized and photographed in ultraviolet light after electro-
phoresis in 1.5% agarose (Fig. 1). The gel image was then
analyzed by 1D Image Analysis Software (Eastman Kodak). The
intensities of the target band and the control band (b-globin)
were compared. The presence of HD was determined by
decreasing the ratio of target band intensity to b-globin band
intensity compared with the normal control samples analysed
in the same gel.
2.4. Methylation-specific PCR
The methylation status of the 50CpG islands in genes promoter
regions was determined by following the procedure described
by Herman et al. [7]. The primer used and the PCR parameters
have been described by our group in previous studies [5,6]. PCR
products were analyzed in 2% ethidium-bromide stained gel.
We confirmed the presence of hypermethylation by identify-
ing the PCR bands in the samples amplified with the
methylated primers. The presence of bands in cases that
were amplified with unmethylated primer was used to
confirm the quality of the modified DNA.
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5508
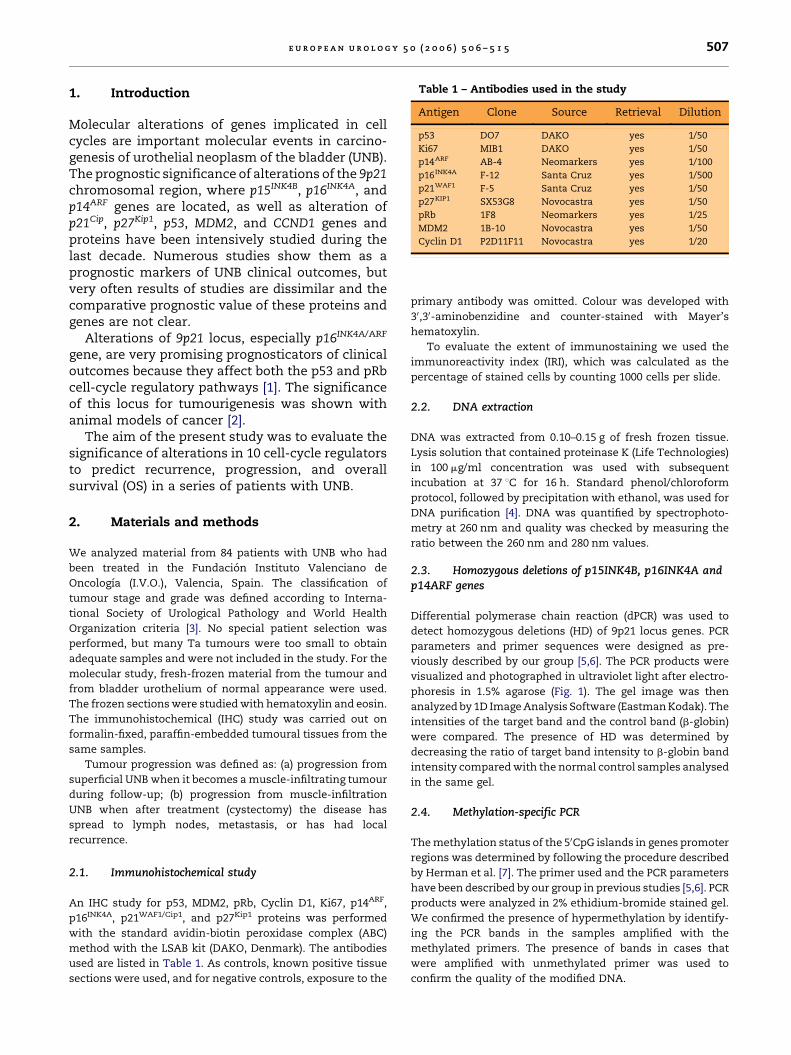
Fig. 1 – dPCR analysis of HDs of genes p15INK4B (exon 1),
p16INK4A (exon 1a and 2), and p14ARF (exon 1b). Cases #1, #2,
and #6 have all investigated exons deleted, which was
common for most cases with deletions. NC – negative
control.
2.5. p53 Mutation analysis
We used the non-radioisotopic method of single-strand
conformation polymorphism (SSCP) described by Ainsworth
et al. [8] to screen mutations in exons 5–8 of p53 with primers
previously described [6].
All SSCP positive cases underwent sequencing analysis to
confirm the presence of a mutation. PCR products were
purified with Centricon columns (Amicon) and sequenced
with the Big Dye terminator kit v1.1 (Applied Biosystem)
according to standard protocol on an automatic sequencer ABI
Prism 310 (Applied Biosystem). Sequences obtained were
compared with a consensus p53 sequence (GeneBank acces-
sion number: AF307851).
2.6. Loss of heterozygosity
For the lossofheterozygosity (LOH) analysis of the9p21region, a
small tandem repeat testing of DNA from tumoural and
corresponding normal tissue was used by employing fluores-
cent-labelled primers for the following microsatellite markers:
D9S162 (forward: 50AGCAAGGCA AGCCACATTTC 30; reverse: 50
TGGGGGATGCCCAGATAACTATATC 30), D9S942 (forward: 50
GCAAGATTCCAAACAGTA 30; reverse: 50 CTCATCCTGCG-
GAAACCA TT 30), D9S157 (forward: 50 AGCAAGGCAAGCCA-
CATTTC 30; reverse: 50 TGGGGA TGCCCAGATAACTATATC 30).
After DNA amplification, the PCR products were electrophor-
esed in an ABI Prism 310 sequencer with a subsequent
quantitative evaluation of the allele ratio with Gene Scan and
Geno Typer software (Applied Biosystem). Loss of one allele in
the tumour sample was estimated as LOH, and loss of both
alleles, when present in the normal sample, as HD. Cases that
presented an additional peak (allele) in a tumour sample were
considered as having microsatellite instability.
2.7. Statistical analysis
The STATISTICA version 6.0 (Stat Soft Inc.) statistical software
package was used for statistical analysis. We applied the
Pearson Chi-square test for statistical analysis between
qualitative variables. The nonparametric ANOVA Mann-
Whitney U Test or, depending on the number of groups, the
Kruskal-Wallis test, was used between qualitative and
quantitative variables.
All pathological, molecular, and IHC data were analyzed in
relation to tumour recurrence and progression as end point
variables, and to findings of the three-month control cysto-
scopy, as we had previously found this to be an important
prognostic factor for recurrence and progression [9]. Survival
analysis, including OS, progression-free survival (PFS), and
recurrence-free survival (RFS) was performed in relation to
clinical, pathological, molecular, and IHC data. The Kaplan-
Meier proportional risk model with the log-rank test for
comparing survival between groups was used. Optimal cut-
points of immunostaining extent, which predict tumour
recurrence or progression with the smallest quantity of
false-positive and false-negative results (Table 2), were
calculated with ROC-analysis. Multivariate Cox proportional
regression analysis was performed to reveal independent
survival predictors. All markers that showed a relationship
with survival in the univariate analysis were included in the
regression model. Models were then adjusted by using forward
and backward stepwise methods.
3. Results
Clinical and pathological data of the patients arepresented in Table 3. Positive results at the three-month cystoscopy in 21.8% (12 of 55 patients) andtumour recurrence in 29.8% (25 of 63 patients) wereobserved. Disease progression occurred only in19.1% (16 of 84 patients) patients because of highfrequency of superficial tumours in the series.Fourteen of 84 patients (16.7%) died of tumourprogression. Median follow-up was 36.4 months(range: 1.3–49.2).
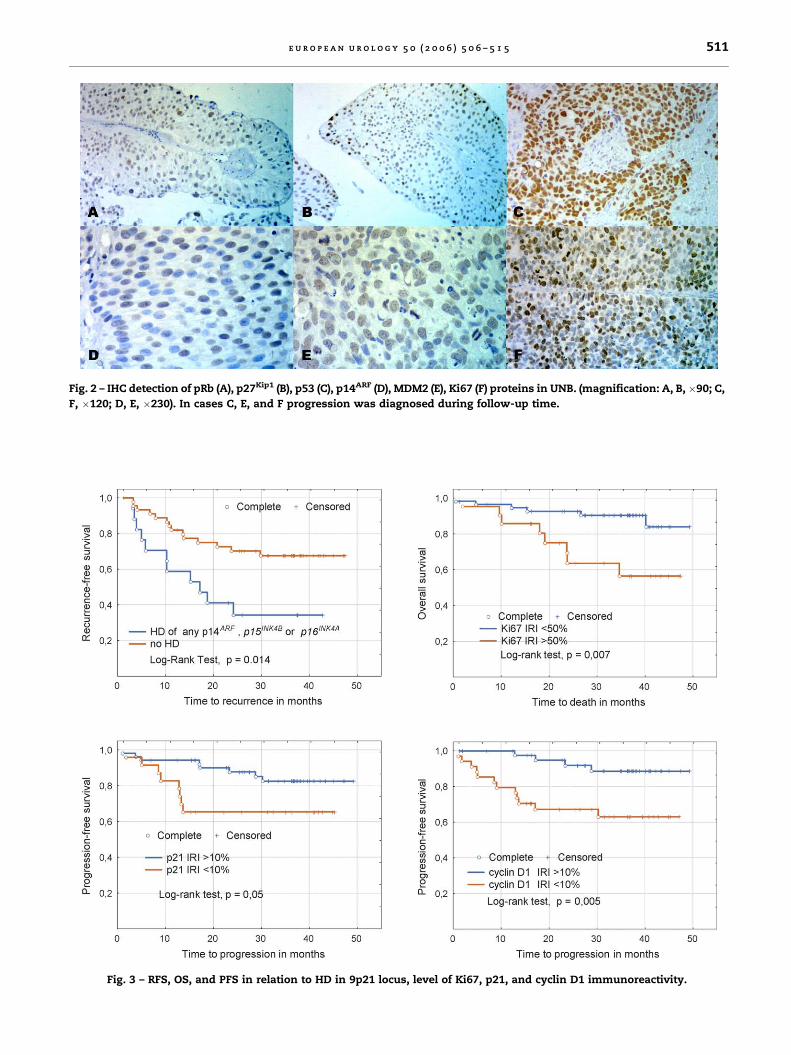
Some pathological parameters show relationshipwith RFS, PFS, and OS (Table 4). Patterns of IHCstaining of UNB are illustrated in Fig. 2. Afterunivariate analysis, we found no relationshipbetween tumour recurrence and IRI of investigatedproteins, excluding Ki67 and p14 expression. Asignificant relationship between all IRI of investi-gated proteins and both PFS and OS was founded,except p14ARF and pRb for PFS and p14ARF for OS(Table 2 and Fig. 3).
Deletion of p15INK4B or p16INK4A/ARF (exons 1a, 1b,and 2) genes was present in 23.8% (20 of 84) tumours.Furthermore, 85% (17 of 20) cases with HD had allinvestigated exons deleted (Fig. 1). Recurrence wasdiagnosed in 64.7% (11 of 17) tumours with HD of atleast one of the investigated genes. Patients with HD
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5 509
Table 3 – Baseline clinical and pathological data of thestudy group
Gender Male 72 (85.7%)
Female 12 (14.3%)
Tumour type Single 46 (54.8%)
Multicentric 38 (44.2%)
Papillary 63 (75.0%)
Sessile 21 (25.0%)
Primary 57 (67.9%)
Recurrent 27 (32.1%)
Stage pTa 8 (9.5%)
pT1 55 (65.5%)
pT2-4 21 (25.0%)
Grade G1 15 (17.6%)
G2 43 (51.2%)
G3 26 (31.0%)
Tumour size <1 cm 5 (6.0%)
1–3 cm 41 (48.8%)
>3 cm 38 (45.2%)
CIS simultaneous yes 8 (9.5%)
no 76 (90.5%)
Ta
ble
2–
Un
iva
ria
tea
na
lysi
so
fth
ece
ll-c
ycl
ep
rote
ins
imm
un
ore
act
ivit
yin
dex
es
wit
hR
FS
,P
FS
,a
nd
OS
Pro
tein
RFS
PFS
OS
Cu
t-p
oin
t3-y
ea
rsu
rviv
ala
log-
ran
kte
stp
Cu
t-p
oin
t3-y
ea
rsu
rviv
ala
log-
ran
kte
stp
Cu
t-p
oin
t3-y
ea
rsu
rviv
ala
log-
ran
kte
stp
p53
25%
47.1
/67.1
1.4
70.1
460%
82.9
/40.1
�2.8
50
.00
460%
89.8
/46.0
�3.9
60
.00
00
8
Ki6
710%
75.2
/51.1
�2.0
10
.04
435%
94.3
/61.1
�2.9
40
.00
335%
97.2
/71.2
�3.1
50
.00
16
p14
AR
F30%
20.0
/65.7
2.5
70
.01
50%
81.5
/70.5
�1.1
00.2
750%
84.5
/92.3
0.1
50.8
7
p16
INK
4A
10%
75.0
/53.6
1.0
10.3
110%
56.8
/85.1
2.5
10
.01
210%
68.8
/86.5
2.3
00
.02
2
p21
Wa
f150%
51.1
/73.4
0.7
80.4
310%
64.4
/82.3
1.9
30
.05
10%
59.6
/93.9
2.9
50
.00
32
p27
Kip
150%
49.2
/59.7
0.7
40.4
620%
24.6
/84.6
3.7
40
.00
02
20%
35.8
/90.3
3.4
50
.00
05
5
pR
b5%
75.0
/53.6
�1.0
90.2
720%
67.9
/80.0
1.4
10.1
510%
68.5
/88.5
2.0
10
.04
4
MD
M2
25%
58.7
/55.5
�0.4
40.6
515%
63.5
/82.5
1.9
60
.05
15%
62.7
/91.8
2.5
40
.01
1
Cy
clin
D1
8%
76.2
/52.9
�1.5
40.1
210%
62.4
/88.3
2.7
90
.00
53
10%
71.5
/92.4
2.7
80
.00
55
Nega
tiv
elo
g-r
an
kv
alu
es
resu
ltfr
om
inv
ers
ere
lati
on
ship
betw
een
IRI
an
dsu
rviv
al.
aP
rop
ort
ion
surv
ivin
gin
gro
up
wit
hIR
Ilo
wer/
hig
her
tha
ncu
t-p
oin
t.
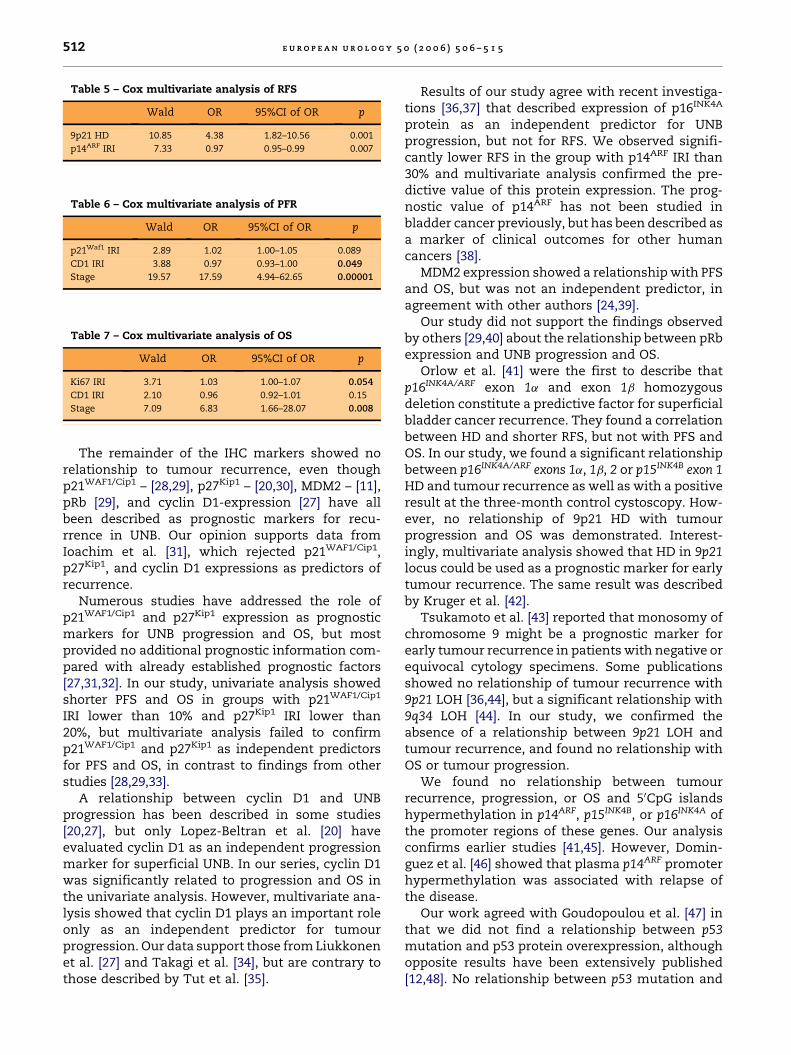
in the 9p21 locus showed a significantly higher rateof positive results at the three-month controlcystoscopy: 46.7% (7 of 15) vs. 12.5% (5 of 40)( p = 0.006). Risk of disease recurrence was signifi-cantly higher in patients with 9p21 HD compared topatients without HD of these genes (p = 0.01) (Fig. 3).Univariate analysis showed no significant relation-ship between HD and OS or PFS (Table 4).
No relationship between LOH in locus 9p21 andOS, PFS and RFS was found.
Promoter hypermethylation of the 50CpG islandswas observed in six (7.1%) cases for p15INK4B, 22(26.1%) for p14ARF, and 5 (6%) for p16INK4A. Simulta-neous hypermethylation of p15INK4B and p14ARF wasobserved in one (1.2%) case, whereas p16INK4A andp14ARF were simultaneously hypermethylated inthree cases (3.6%). No differences in OS, PFS, andRFS between groups and p14ARF promoter methyla-tion were found. The same was observed for p16INK4A
and p15INK4B promoter methylation (Table 4).Progression was found in 44.4% (4 of 9 patients)
with p53 mutation, higher than in the group with awild-type p53—16.0% (12 of 75 patients) ( p = 0.04).Patients with mutated p53 showed a worse three-year OS and PFS when compared to patients withoutp53 mutation ( p = 0.03 and p = 0.05 respectively); norelationship was found regarding RFS ( p = 0.81).
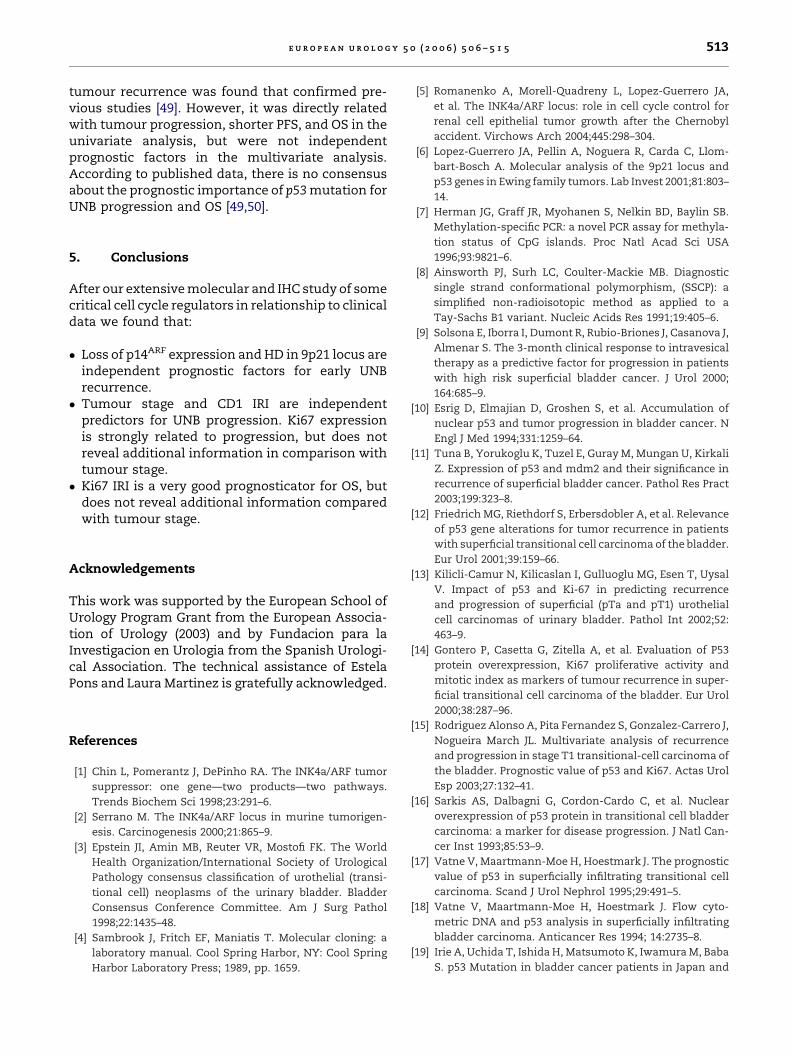
Cox proportional regression analysis showedloss of p14 expression and HD in 9p21 locus asindependent prognostic factors for a shorterrecurrence-free interval (Table 5). Both tumourstage and cyclin D1 expression were independentmarkers for PFS (Table 6) and tumour stage and
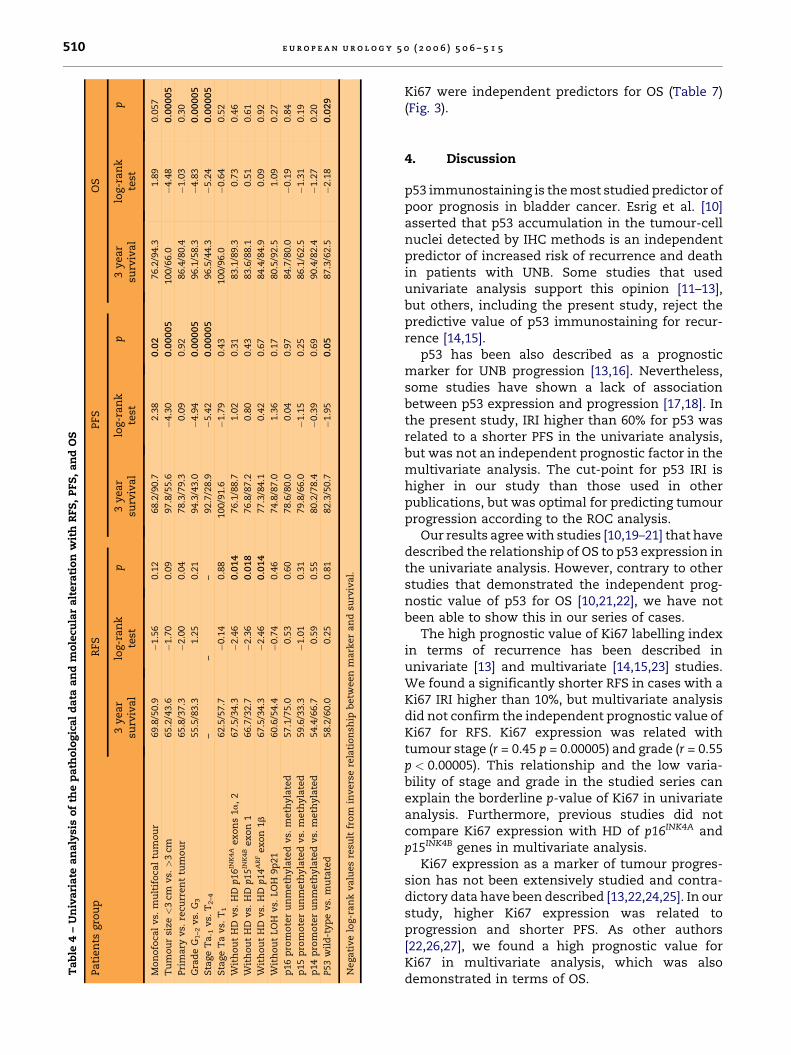
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5510
Ta
ble
4–
Un
iva
ria
tea
na
lysi
so
fth
ep
ath
olo
gic
al
da
taa
nd
mo
lecu
lar
alt
era
tio
nw
ith
RFS
,P
FS
,a
nd
OS
Pa
tien
tsgro
up
RFS
PFS
OS
3y
ea
rsu
rviv
al
log-r
an
kte
stp
3y
ear
surv
iva
llo
g-r
an
kte
stp
3y
ea
rsu
rviv
al
log-r
an
kte
stp
Mo
no
foca
lv
s.m
ult
ifo
cal
tum
ou
r69.8
/50.9
�1.5
60.1
268.2
/90.7
2.3
80
.02
76.2
/94.3
1.8
90.0
57
Tu
mo
ur
size
<3
cmv
s.>
3cm
65.2
/43.6
�1.7
00.0
997.8
/55.6
�4.3
00
.00
00
5100/6
6.0
�4.4
80
.00
00
5
Pri
ma
ryv
s.re
curr
en
ttu
mo
ur
65.8
/37.3
�2.0
00.0
478.3
/79.3
0.0
90.9
286.4
/80.4
�1.0
30.3
0
Gra
de
G1–2
vs.
G3
55.5
/83.3
1.2
50.2
194.3
/43.0
�4.9
40
.00
00
596.1
/58.3
�4.8
30
.00
00
5
Sta
ge
Ta
-1v
s.T
2–4
––
–92.7
/28.9
�5.4
20
.00
00
596.5
/44.3
�5.2
40
.00
00
5
Sta
ge
Ta
vs.
T1
62.5
/57.7
�0.1
40.8
8100/9
1.6
�1.7
90.4
3100/9
6.0
�0.6
40.5
2
Wit
ho
ut
HD
vs.
HD
p16IN
K4A
ex
on
s1
a,
267.5
/34.3
�2.4
60
.01
476.1
/88.7
1.0
20.3
183.1
/89.3
0.7
30.4
6
Wit
ho
ut
HD
vs.
HD
p15IN
K4B
ex
on
166.7
/32.7
�2.3
60
.01
876.8
/87.2
0.8
00.4
383.6
/88.1
0.5
10.6
1
Wit
ho
ut
HD
vs.
HD
p14ARF
ex
on
1b
67.5
/34.3
�2.4
60
.01
477.3
/84.1
0.4
20.6
784.4
/84.9
0.0
90.9
2
Wit
ho
ut
LO
Hv
s.LO
H9p
21
60.6
/54.4
�0.7
40.4
674.8
/87.0
1.3
60.1
780.5
/92.5
1.0
90.2
7
p16
pro
mo
ter
un
meth
yla
ted
vs.
meth
yla
ted
57.1
/75.0
0.5
30.6
078.6
/80.0
0.0
40.9
784.7
/80.0
�0.1
90.8
4
p15
pro
mo
ter
un
meth
yla
ted
vs.
meth
yla
ted
59.6
/33.3
�1.0
10.3
179.8
/66.0
�1.1
50.2
586.1
/62.5
�1.3
10.1
9
p14
pro
mo
ter
un
meth
yla
ted
vs.
meth
yla
ted
54.4
/66.7
0.5
90.5
580.2
/78.4
�0.3
90.6
990.4
/82.4
�1.2
70.2
0
P53
wil
d-t
yp
ev
s.m
uta
ted
58.2
/60.0
0.2
50.8
182.3
/50.7
�1.9
50
.05
87.3
/62.5
�2.1
80
.02
9
Nega
tiv
elo
g-r
an
kv
alu
es
resu
ltfr
om
inv
ers
ere
lati
on
ship
betw
een
ma
rker
an
dsu
rviv
al.
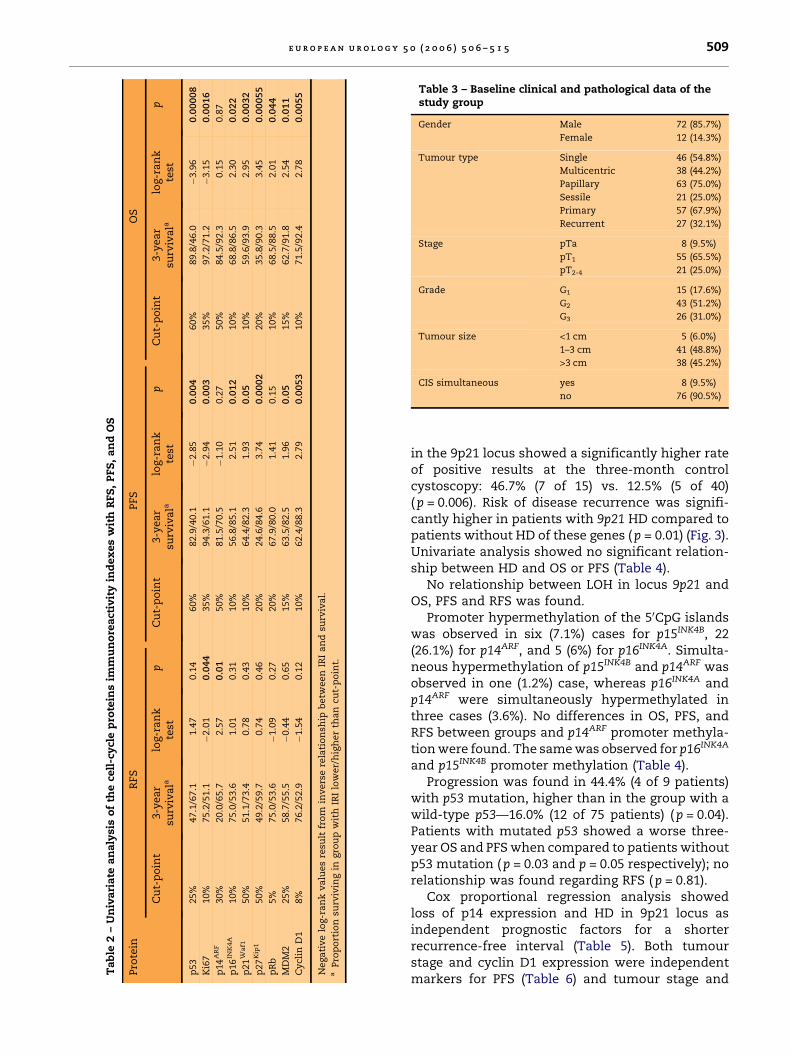
Ki67 were independent predictors for OS (Table 7)(Fig. 3).
4. Discussion
p53 immunostaining is the most studied predictor ofpoor prognosis in bladder cancer. Esrig et al. [10]asserted that p53 accumulation in the tumour-cellnuclei detected by IHC methods is an independentpredictor of increased risk of recurrence and deathin patients with UNB. Some studies that usedunivariate analysis support this opinion [11–13],but others, including the present study, reject thepredictive value of p53 immunostaining for recur-rence [14,15].
p53 has been also described as a prognosticmarker for UNB progression [13,16]. Nevertheless,some studies have shown a lack of associationbetween p53 expression and progression [17,18]. Inthe present study, IRI higher than 60% for p53 wasrelated to a shorter PFS in the univariate analysis,but was not an independent prognostic factor in themultivariate analysis. The cut-point for p53 IRI ishigher in our study than those used in otherpublications, but was optimal for predicting tumourprogression according to the ROC analysis.
Our results agree with studies [10,19–21] that havedescribed the relationship of OS to p53 expression inthe univariate analysis. However, contrary to otherstudies that demonstrated the independent prog-nostic value of p53 for OS [10,21,22], we have notbeen able to show this in our series of cases.
The high prognostic value of Ki67 labelling indexin terms of recurrence has been described inunivariate [13] and multivariate [14,15,23] studies.We found a significantly shorter RFS in cases with aKi67 IRI higher than 10%, but multivariate analysisdid not confirm the independent prognostic value ofKi67 for RFS. Ki67 expression was related withtumour stage (r = 0.45 p = 0.00005) and grade (r = 0.55p < 0.00005). This relationship and the low varia-bility of stage and grade in the studied series canexplain the borderline p-value of Ki67 in univariateanalysis. Furthermore, previous studies did notcompare Ki67 expression with HD of p16INK4A andp15INK4B genes in multivariate analysis.
Ki67 expression as a marker of tumour progres-sion has not been extensively studied and contra-dictory data have been described [13,22,24,25]. In ourstudy, higher Ki67 expression was related toprogression and shorter PFS. As other authors[22,26,27], we found a high prognostic value forKi67 in multivariate analysis, which was alsodemonstrated in terms of OS.
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5 511
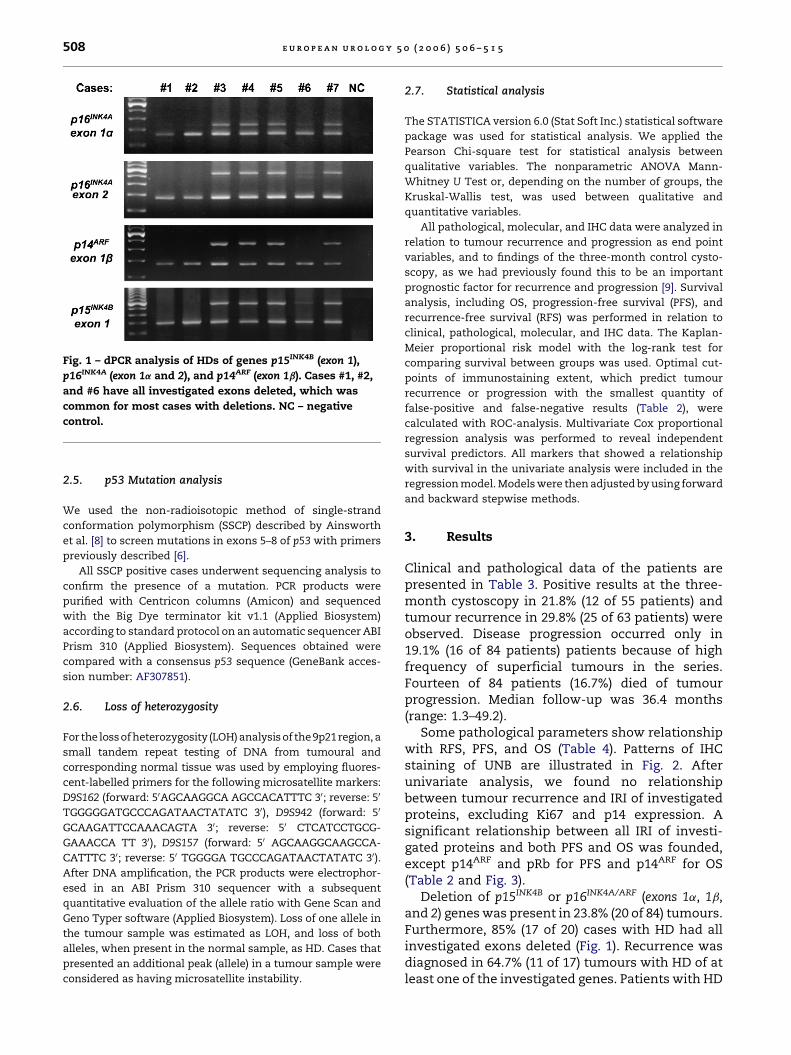
Fig. 2 – IHC detection of pRb (A), p27Kip1 (B), p53 (C), p14ARF (D), MDM2 (E), Ki67 (F) proteins in UNB. (magnification: A, B, �90; C,
F, �120; D, E, �230). In cases C, E, and F progression was diagnosed during follow-up time.
Fig. 3 – RFS, OS, and PFS in relation to HD in 9p21 locus, level of Ki67, p21, and cyclin D1 immunoreactivity.
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5512
Table 7 – Cox multivariate analysis of OS
Wald OR 95%CI of OR p
Ki67 IRI 3.71 1.03 1.00–1.07 0.054
CD1 IRI 2.10 0.96 0.92–1.01 0.15
Stage 7.09 6.83 1.66–28.07 0.008
Table 5 – Cox multivariate analysis of RFS
Wald OR 95%CI of OR p
9p21 HD 10.85 4.38 1.82–10.56 0.001
p14ARF IRI 7.33 0.97 0.95–0.99 0.007
Table 6 – Cox multivariate analysis of PFR
Wald OR 95%CI of OR p
p21Waf1 IRI 2.89 1.02 1.00–1.05 0.089
CD1 IRI 3.88 0.97 0.93–1.00 0.049
Stage 19.57 17.59 4.94–62.65 0.00001
The remainder of the IHC markers showed norelationship to tumour recurrence, even thoughp21WAF1/Cip1 – [28,29], p27Kip1 – [20,30], MDM2 – [11],pRb [29], and cyclin D1-expression [27] have allbeen described as prognostic markers for recu-rrence in UNB. Our opinion supports data fromIoachim et al. [31], which rejected p21WAF1/Cip1,p27Kip1, and cyclin D1 expressions as predictors ofrecurrence.
Numerous studies have addressed the role ofp21WAF1/Cip1 and p27Kip1 expression as prognosticmarkers for UNB progression and OS, but mostprovided no additional prognostic information com-pared with already established prognostic factors[27,31,32]. In our study, univariate analysis showedshorter PFS and OS in groups with p21WAF1/Cip1
IRI lower than 10% and p27Kip1 IRI lower than20%, but multivariate analysis failed to confirmp21WAF1/Cip1 and p27Kip1 as independent predictorsfor PFS and OS, in contrast to findings from otherstudies [28,29,33].
A relationship between cyclin D1 and UNBprogression has been described in some studies[20,27], but only Lopez-Beltran et al. [20] haveevaluated cyclin D1 as an independent progressionmarker for superficial UNB. In our series, cyclin D1was significantly related to progression and OS inthe univariate analysis. However, multivariate ana-lysis showed that cyclin D1 plays an important roleonly as an independent predictor for tumourprogression. Our data support those from Liukkonenet al. [27] and Takagi et al. [34], but are contrary tothose described by Tut et al. [35].
Results of our study agree with recent investiga-tions [36,37] that described expression of p16INK4A
protein as an independent predictor for UNBprogression, but not for RFS. We observed signifi-cantly lower RFS in the group with p14ARF IRI than30% and multivariate analysis confirmed the pre-dictive value of this protein expression. The prog-nostic value of p14ARF has not been studied inbladder cancer previously, but has been described asa marker of clinical outcomes for other humancancers [38].
MDM2 expression showed a relationship with PFSand OS, but was not an independent predictor, inagreement with other authors [24,39].
Our study did not support the findings observedby others [29,40] about the relationship between pRbexpression and UNB progression and OS.
Orlow et al. [41] were the first to describe thatp16INK4A/ARF exon 1a and exon 1b homozygousdeletion constitute a predictive factor for superficialbladder cancer recurrence. They found a correlationbetween HD and shorter RFS, but not with PFS andOS. In our study, we found a significant relationshipbetween p16INK4A/ARF exons 1a, 1b, 2 or p15INK4B exon 1HD and tumour recurrence as well as with a positiveresult at the three-month control cystoscopy. How-ever, no relationship of 9p21 HD with tumourprogression and OS was demonstrated. Interest-ingly, multivariate analysis showed that HD in 9p21locus could be used as a prognostic marker for earlytumour recurrence. The same result was describedby Kruger et al. [42].
Tsukamoto et al. [43] reported that monosomy ofchromosome 9 might be a prognostic marker forearly tumour recurrence in patients with negative orequivocal cytology specimens. Some publicationsshowed no relationship of tumour recurrence with9p21 LOH [36,44], but a significant relationship with9q34 LOH [44]. In our study, we confirmed theabsence of a relationship between 9p21 LOH andtumour recurrence, and found no relationship withOS or tumour progression.
We found no relationship between tumourrecurrence, progression, or OS and 50CpG islandshypermethylation in p14ARF, p15INK4B, or p16INK4A ofthe promoter regions of these genes. Our analysisconfirms earlier studies [41,45]. However, Domin-guez et al. [46] showed that plasma p14ARF promoterhypermethylation was associated with relapse ofthe disease.
Our work agreed with Goudopoulou et al. [47] inthat we did not find a relationship between p53mutation and p53 protein overexpression, althoughopposite results have been extensively published[12,48]. No relationship between p53 mutation and
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5 513
tumour recurrence was found that confirmed pre-vious studies [49]. However, it was directly relatedwith tumour progression, shorter PFS, and OS in theunivariate analysis, but were not independentprognostic factors in the multivariate analysis.According to published data, there is no consensusabout the prognostic importance of p53 mutation forUNB progression and OS [49,50].
5. Conclusions
After our extensive molecular and IHC study of somecritical cell cycle regulators in relationship to clinicaldata we found that:
� L
oss of p14ARF expression and HD in 9p21 locus areindependent prognostic factors for early UNBrecurrence.� T
umour stage and CD1 IRI are independentpredictors for UNB progression. Ki67 expressionis strongly related to progression, but does notreveal additional information in comparison withtumour stage.� K
i67 IRI is a very good prognosticator for OS, butdoes not reveal additional information comparedwith tumour stage.Acknowledgements
This work was supported by the European School ofUrology Program Grant from the European Associa-tion of Urology (2003) and by Fundacion para laInvestigacion en Urologia from the Spanish Urologi-cal Association. The technical assistance of EstelaPons and Laura Martinez is gratefully acknowledged.
References
[1] Chin L, Pomerantz J, DePinho RA. The INK4a/ARF tumor
suppressor: one gene—two products—two pathways.
Trends Biochem Sci 1998;23:291–6.
[2] Serrano M. The INK4a/ARF locus in murine tumorigen-
esis. Carcinogenesis 2000;21:865–9.
[3] Epstein JI, Amin MB, Reuter VR, Mostofi FK. The World
Health Organization/International Society of Urological
Pathology consensus classification of urothelial (transi-
tional cell) neoplasms of the urinary bladder. Bladder
Consensus Conference Committee. Am J Surg Pathol
1998;22:1435–48.
[4] Sambrook J, Fritch EF, Maniatis T. Molecular cloning: a
laboratory manual. Cool Spring Harbor, NY: Cool Spring
Harbor Laboratory Press; 1989, pp. 1659.
[5] Romanenko A, Morell-Quadreny L, Lopez-Guerrero JA,
et al. The INK4a/ARF locus: role in cell cycle control for
renal cell epithelial tumor growth after the Chernobyl
accident. Virchows Arch 2004;445:298–304.
[6] Lopez-Guerrero JA, Pellin A, Noguera R, Carda C, Llom-
bart-Bosch A. Molecular analysis of the 9p21 locus and
p53 genes in Ewing family tumors. Lab Invest 2001;81:803–
14.
[7] Herman JG, Graff JR, Myohanen S, Nelkin BD, Baylin SB.
Methylation-specific PCR: a novel PCR assay for methyla-
tion status of CpG islands. Proc Natl Acad Sci USA
1996;93:9821–6.
[8] Ainsworth PJ, Surh LC, Coulter-Mackie MB. Diagnostic
single strand conformational polymorphism, (SSCP): a
simplified non-radioisotopic method as applied to a
Tay-Sachs B1 variant. Nucleic Acids Res 1991;19:405–6.
[9] Solsona E, Iborra I, Dumont R, Rubio-Briones J, Casanova J,
Almenar S. The 3-month clinical response to intravesical
therapy as a predictive factor for progression in patients
with high risk superficial bladder cancer. J Urol 2000;
164:685–9.
[10] Esrig D, Elmajian D, Groshen S, et al. Accumulation of
nuclear p53 and tumor progression in bladder cancer. N
Engl J Med 1994;331:1259–64.
[11] Tuna B, Yorukoglu K, Tuzel E, Guray M, Mungan U, Kirkali
Z. Expression of p53 and mdm2 and their significance in
recurrence of superficial bladder cancer. Pathol Res Pract
2003;199:323–8.
[12] Friedrich MG, Riethdorf S, Erbersdobler A, et al. Relevance
of p53 gene alterations for tumor recurrence in patients
with superficial transitional cell carcinoma of the bladder.
Eur Urol 2001;39:159–66.
[13] Kilicli-Camur N, Kilicaslan I, Gulluoglu MG, Esen T, Uysal
V. Impact of p53 and Ki-67 in predicting recurrence
and progression of superficial (pTa and pT1) urothelial
cell carcinomas of urinary bladder. Pathol Int 2002;52:
463–9.
[14] Gontero P, Casetta G, Zitella A, et al. Evaluation of P53
protein overexpression, Ki67 proliferative activity and
mitotic index as markers of tumour recurrence in super-
ficial transitional cell carcinoma of the bladder. Eur Urol
2000;38:287–96.
[15] Rodriguez Alonso A, Pita Fernandez S, Gonzalez-Carrero J,
Nogueira March JL. Multivariate analysis of recurrence
and progression in stage T1 transitional-cell carcinoma of
the bladder. Prognostic value of p53 and Ki67. Actas Urol
Esp 2003;27:132–41.
[16] Sarkis AS, Dalbagni G, Cordon-Cardo C, et al. Nuclear
overexpression of p53 protein in transitional cell bladder
carcinoma: a marker for disease progression. J Natl Can-
cer Inst 1993;85:53–9.
[17] Vatne V, Maartmann-Moe H, Hoestmark J. The prognostic
value of p53 in superficially infiltrating transitional cell
carcinoma. Scand J Urol Nephrol 1995;29:491–5.
[18] Vatne V, Maartmann-Moe H, Hoestmark J. Flow cyto-
metric DNA and p53 analysis in superficially infiltrating
bladder carcinoma. Anticancer Res 1994; 14:2735–8.
[19] Irie A, Uchida T, Ishida H, Matsumoto K, Iwamura M, Baba
S. p53 Mutation in bladder cancer patients in Japan and
e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5514
inhibition of growth by in vitro adenovirus-mediated
wild-type p53 transduction in bladder cancer cells. Mol
Urol 2001;5:53–8.
[20] Lopez-Beltran A, Luque RJ, Alvarez-Kindelan J, et al. Prog-
nostic factors in stage T1 grade 3 bladder cancer survival:
the role of G1-S modulators (p53, p21Waf1, p27kip1,
Cyclin D1, and Cyclin D3) and proliferation index (ki67-
MIB1). Eur Urol 2004;45:606–12.
[21] Rodriguez-Alonso A, Pita-Fernandez S, Gonzalez-Carrero
J, Nogueira-March JL. p53 and ki67 expression as prog-
nostic factors for cancer-related survival in stage T1 tran-
sitional cell bladder carcinoma. Eur Urol 2002;41:182–8,
discussion 8–9.
[22] Popov Z, Hoznek A, Colombel M, et al. The prognostic
value of p53 nuclear overexpression and MIB-1 as a pro-
liferative marker in transitional cell carcinoma of the
bladder. Cancer 1997;80:1472–81.
[23] Rodriguez-Alonso A, Pita-Fernandez S, Gonzalez-Carrero
J, Nogueira-March JL. Multivariate analysis of survival,
recurrence, progression and development of mestastasis
in T1 and T2a transitional cell bladder carcinoma. Cancer
2002;94:1677–84.
[24] Shiina H, Igawa M, Shigeno K, et al. Clinical significance of
mdm2 and p53 expression in bladder cancer. A compar-
ison with cell proliferation and apoptosis. Oncology
1999;56:239–47.
[25] Tsuji M, Kojima K, Murakami Y, Kanayama H, Kagawa S.
Prognostic value of Ki-67 antigen and p53 protein
in urinary bladder cancer: immunohistochemical analy-
sis of radical cystectomy specimens. Br J Urol 1997;79:
367–72.
[26] Lopez-Beltran A, Luque RJ, Alvarez-Kindelan J, et al.
Prognostic factors in survival of patients with stage Ta
and T1 bladder urothelial tumors: the role of G1-S mod-
ulators (p53, p21Waf1, p27Kip1, cyclin D1, and cyclin D3),
proliferation index, and clinicopathologic parameters.
Am J Clin Pathol 2004;122:444–52.
[27] Liukkonen T, Lipponen P, Raitanen M, et al. Evaluation of
p21WAF1/CIP1 and cyclin D1 expression in the progres-
sion of superficial bladder cancer. Finbladder Group. Urol
Res 2000;28:285–92.
[28] Stein JP, Ginsberg DA, Grossfeld GD, et al. Effect of
p21WAF1/CIP1 expression on tumor progression in blad-
der cancer. J Natl Cancer Inst 1998;90:1072–9.
[29] Chatterjee SJ, Datar R, Youssefzadeh D, et al. Combined
effects of p53, p21, and pRb expression in the progression
of bladder transitional cell carcinoma. J Clin Oncol
2004;22:1007–13.
[30] Del Pizzo JJ, Borkowski A, Jacobs SC, Kyprianou N. Loss
of cell cycle regulators p27(Kip1) and cyclin E in transi-
tional cell carcinoma of the bladder correlates with
tumor grade and patient survival. Am J Pathol 1999;155:
1129–36.
[31] Ioachim E, Michael M, Stavropoulos NE, et al. Expression
patterns of cyclins D1, E and cyclin-dependent kinase
inhibitors p21(Waf1/Cip1) and p27(Kip1) in urothelial car-
cinoma: correlation with other cell-cycle-related proteins
(Rb, p53, Ki-67 and PCNA) and clinicopathological fea-
tures. Urol Int 2004;73:65–73.
[32] Santos LL, Amaro T, Pereira SA, et al. Expression of cell-
cycle regulatory proteins and their prognostic value in
superficial low-grade urothelial cell carcinoma of the
bladder. Eur J Surg Oncol 2003;29:74–80.
[33] Shariat SF, Tokunaga H, Zhou J, et al. p53, p21, pRB, and
p16 expression predict clinical outcome in cystectomy
with bladder cancer. J Clin Oncol 2004;22:1014–24.
[34] Takagi Y, Takashi M, Koshikawa T, Sakata T, Ohshima S.
Immunohistochemical demonstration of cyclin D1 in
bladder cancers as an inverse indicator of invasiveness
but not an independent prognostic factor. Int J Urol
2000;7:366–72.
[35] Tut VM, Braithwaite KL, Angus B, Neal DE, Lunec J, Mellon
JK. Cyclin D1 expression in transitional cell carcinoma of
the bladder: correlation with p53, waf1, pRb and Ki67. Br J
Cancer 2001;84:270–5.
[36] Friedrich MG, Blind C, Milde-Langosch K, et al. Frequent
p16/MTS1 inactivation in early stages of urothelial carci-
noma of the bladder is not associated with tumor recur-
rence. Eur Urol 2001;40:518–24.
[37] Kruger S, Mahnken A, Kausch I, Feller AC. P16 immuno-
reactivity is an independent predictor of tumor progres-
sion in minimally invasive urothelial bladder carcinoma.
Eur Urol 2005;47:463–7.
[38] Kwong RA, Kalish LH, Nguyen TV, et al. p14ARF protein
expression is a predictor of both relapse and survival in
squamous cell carcinoma of the anterior tongue. Clin
Cancer Res 2005;11:4107–16.
[39] Schmitz-Drager BJ, Kushima M, Goebell P, et al. p53 and
MDM2 in the development and progression of bladder
cancer. Eur Urol 1997;32:487–93.
[40] Grossman HB, Liebert M, Antelo M, et al. p53 and RB
expression predict progression in T1 bladder cancer. Clin
Cancer Res 1998;4:829–34.
[41] Orlow I, LaRue H, Osman I, et al. Deletions of the INK4A
gene in superficial bladder tumors. Association with
recurrence. Am J Pathol 1999;155:105–13.
[42] Kruger S, Mess F, Bohle A, Feller AC. Numerical aberra-
tions of chromosome 17 and the 9p21 locus are indepen-
dent predictors of tumor recurrence in non-invasive
transitional cell carcinoma of the urinary bladder. Int J
Oncol 2003;23:41–8.
[43] Tsukamoto M, Matsuyama H, Oba K, Yoshihiro S, Taka-
hashi M, Naito K. Numerical aberrations of chromosome 9
in bladder cancer. A possible prognostic marker for
early tumor recurrence. Cancer Genet Cytogenet 2002;
134:41–5.
[44] Edwards J, Duncan P, Going JJ, Watters AD, Grigor KM,
Bartlett JM. Identification of loci associated with putative
recurrence genes in transitional cell carcinoma of the
urinary bladder. J Pathol 2002;196:380–5.
[45] Maruyama R, Toyooka S, Toyooka KO, et al. Aberrant
promoter methylation profile of bladder cancer and its
relationship to clinicopathological features. Cancer Res
2001;61:8659–63.
[46] Dominguez G, Carballido J, Silva J, et al. p14ARF promoter
hypermethylation in plasma DNA as an indicator of dis-
ease recurrence in bladder cancer patients. Clin Cancer
Res 2002;8:980–5.

e u r o p e a n u r o l o g y 5 0 ( 2 0 0 6 ) 5 0 6 – 5 1 5 515
[47] Goudopoulou A, Saetta A, Korkolopoulou P, et al. p53
mutations detection in urinary bladder cancer in the
Greek population: application of the NIRCA assay. J Exp
Clin Cancer Res 2003;22:99–105.
[48] Cordon-Cardo C, Dalbagni G, Saez GT, et al. p53 mutations
in human bladder cancer: genotypic versus phenotypic
patterns. Int J Cancer 1994;56:347–53.
Editorial Comment
Antonio Lopez-Beltran, Cordoba, [email protected]
This interesting paper deals with the molecularevaluation of cell cycle regulators in bladderurothelial carcinoma. It emphasises alterations atthe INK4 gene, cyclin D1, and tumour proliferation.The topic of cell cycle alterations in bladder canceris expanding rapidly, since some of these proteinsmight represent therapeutic targets in the nearfuture. Yurakh et al. found 9p21 homozygousdeletion and p14 immunoreactivity index-independent predictors of bladder cancer recur-rence. Although this is not an unexpected finding,the methodological approach that combines mole-cular genetic and phenotypic findings with knownclinical predictors give more consistency to theresults.
The role of tumour suppressor genes in cell cycleregulation is complex. The 9p21 gene locus lies atthe centre of the two major tumour suppressorpathways identified in bladder cancer, p53 andpRb.
The 9p21 locus is crucial in the regulation of thecell cycle because of the unusual situation in whichtwo functionally different genes, p16INK4A andp14ARF, are transcribed from the same locus. Thep16INK4A is a cyclin-dependent kinase inhibitorthat functions upstream of pRb to block cyclin-Ddirected phosphorylation of pRb, which induces G1arrest. Inactivation of p16INK4A by mutation,promoter methylation, or, as found in the currentstudy, by homozygous deletion will lead to phos-phorylation of pRb and subsequent cell prolifera-tion. The other gene product at 9p21 is p14ARF,which acts upstream of p53 to stimulate p21WAF1expression, but also plays a role in the regulation of
[49] Lorenzo Romero JG, Salinas Sanchez AS, Gimenez Bachs
JM, et al. p53 Gene mutations in superficial bladder can-
cer. Urol Int 2004;73:212–8.
[50] Oyasu R, Nan L, Szumel RC, Kawamata H, Hirohashi S. p53
gene mutations in human urothelial carcinomas: analysis
by immunohistochemistry and single-strand conforma-
tion polymorphism. Mod Pathol 1995;8:170–6.
the level of p53 by interacting with the proto-oncogene product MDM2; p14ARF can cause cellcycle arrest at any point in the cell cycle through itseffect on p21WAF1. Homozygous deletions of theINK4A gene at 9p21 resulted in lower recurrence-free survival, similar to the findings by Yurakhet al.
In line with recent studies, Yurakh et al. foundthe cyclin D1 immunoreactivity index to be anindependent predictor of progression. Cyclin D1 isan upstream regulator of the cell cycle progressionthrough the G1-S checkpoint. The cyclin D familyforms complexes with CDK 4 and 6 and promotesphosphorylation and inactivation of the pRb,which releases the promoter factor E2F-1 andmediates the progression of cells from the G1 tothe S phase. These authors also found that theKi-67 immunoreactivity index as an independentpredictor of overall survival. Ki-67 is a promisingprognostic biomarker in bladder cancer and awaitsvalidation in clinical trials. Noteworthy in thisstudy, stage remains the most significant singlepredictor of progression and overall survival, andsupports the value of conventional prognosticmarkers in bladder cancer. Despite limitations inthe study (sample size, stage selection, and shortfollow-up) this paper provides superior clinicallyuseful information by combining biomarker infor-mation with conventional clinical parameters.
Understanding the molecular mechanisms thatunderlie cell cycle alterations in bladder cancershould provide important insights into how nor-mal cells become tumourigenic, and how newtherapeutic strategies can be devised. The knowl-edge about cell cycle related markers as predictorsof local and systemic therapy will continue toexpand in the near future, but remains unsettled atpresent.





























