Embed Size (px)
Citation preview
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002 59
Model-Based Processing Scheme for Quantitative4-D Cardiac MRI Analysis
George Stalidis, Nicos Maglaveras, Member, IEEE, Serafim N. Efstratiadis, Member, IEEE, Athanasios S. Dimitriadis,and Costas Pappas, Member, IEEE
Abstract—In this paper, we present an integrated model-basedprocessing scheme for cardiac magnetic resonance imaging (MRI),embedded in an interactive computing environment suitable forquantitative cardiac analysis, which provides a set of functionsfor the extraction, modeling, and visualization of cardiac shapeand deformation. The methods apply four-dimensional (4-D)processing (three spatial and one temporal) to multiphase mul-tislice MRI acquisitions and produce a continuous 4-D modelof the myocardial surface deformation. The model is used tomeasure diagnostically useful parameters, such as wall motion,myocardial thicking, and myocardial mass measurements. Theproposed model-based shape extraction method has the advantageof integrating local information into an overall representation andproduces a robust description of cardiac cavities. A learning seg-mentation process that incorporates a generating-shrinking neuralnetwork is combined with a spatiotemporal parametric modelingmethod through functional basis decomposition. A multiscaleapproach is adopted, which uses at each step a coarse-scale modeldefined at the previous step in order to constrain the boundarydetection. The representation accuracy starts from a coarsebut smooth estimation of the approximate cardiac shape and isgradually increased to the desired detail. The main advantagesof the proposed methods are efficiency, lack of uncertainty aboutconvergence, and robustness to image artifacts. Experimentalresults obtained from application to clinical multislice multiphaseMRI examinations of normal volunteers and patients with medicalrecord of myocardial infarction were satisfactory in terms ofaccuracy and robustness.
Index Terms—Cardiacanalysis,deformable representation,mul-tiphase magnetic resonance imaging (MRI), parametric modeling,shape extraction.
I. INTRODUCTION
I N THE last decade, the growing use of the magneticresonance imaging (MRI) modality to cardiac diagnosis
is mainly due to its noninvasive operation, excellent tissuecontrast, and spatial resolution in three dimensions (3-D).Apart from multislice acquisitions, multiphase electrocardio-
Manuscript received February 2, 2000; revised November 5, 2001. This workwas supported in part by the Greek Secretariat of Research and Technology,Ministry of Industry and Development, under the IPER-266 program and in partby the European Commission under the Integration and Communication for theContinuity of Cardiac Care (I4C) project.
G. Stalidis, N. Maglaveras, and C. Pappas are with the Lab of Medical Infor-matics, The Medical School, Aristotle University, 54006 Thessaloniki, Greece(e-mail: [email protected]; [email protected]; [email protected]).
S. N. Efstratiadis is with the Lab of Medical Informatics, The Medical School,Aristotle University, 54006 Thessaloniki, Greece, and the Department of Elec-tronics, Technological Education Institute, 54639 Thessaloniki, Greece (e-mail:[email protected]).
A. S. Dimitriadis is with AHEPA General Hospital, Department of Radiology,The Medical School, Aristotle University, 54006 Thessaloniki, Greece.
Publisher Item Identifier S 1089-7771(02)02013-7.
gram (ECG)-gated acquisitions offer valuable informationon the cardiac motion with good resolution. The geometricaland functional value of this information requires processingmethods that make use of the MRI multidimensional natureand are not restricted to two-dimensional (2-D) processing. Acomplete representation of cardiac chambers is provided by afour-dimensional (4-D) cardiac model. Such a model providesvaluable diagnostic information for both visualization [1],[2] and quantitative evaluation of useful parameters, such asregional wall thickness, curvature, and their dynamics [3]–[6].
A number of techniques have been reported in the literaturemaking use of mathematical models for detection and represen-tation of organ boundaries in medical images. Reference [7] useda Fourier parametrically deformable model in order to detectobject boundaries in 2-D images and then applied the methodto cardiac MRI. While this model is in principle similar to thatpresented here, the difference lies in the model-fitting approachto the image data, which uses optimization in the parameterspace based on their probability distribution. Similar Fourierdescriptors were presented in [8]. In previous reports [9]–[11],active contour models were used to determine borders of struc-tures. These models are attracted by external forces determinedby the image data. An extension of the active contours to 3-Dsurface models is the 3-D balloon model reported in [12], whichhas been applied to the detection of the left ventricular chamberin cardiac MRI data. Graph search and dynamic programmingmethods that minimize an overall path cost function were alsoreported in [13]–[16]. Recently, Niessenet al. [17] presented amodification to the geodesic deformable model and applied itto the segmentation of cardiac computed tomography and MRI.
The study of cardiac motion using geometrical models hasbeen proposed by several researchers. In [1], the presented de-formable model approximates the left ventricle using a few pa-rameters corresponding to physical properties, which vary lo-cally as functions of position. The model is fit using forcesexerted by detected points derived from magnetically taggeddata (MRI-SPAMM). Thomaset al. [18] adopted a multidi-mensional stochastic model containing prior functional infor-mation and used tagged MRI data for estimating the displace-ment field of the moving myocardium. A different approach[2] combined surface construction using minimal area triangu-lation of segmented MRI based on the Bezier tensor product.The left ventricular motion was also studied in [19] using op-tical flow methods. Point-to-point myocardial registration be-tween different phases, without magnetic tagging in 2-D imagesequences [20] and 4-D images [21], was addressed using ge-ometrical surface characteristics (e.g., curvature). Recently, a
1089-7771/02$17.00 © 2002 IEEE

60 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
curvature-based approach was adopted for studying shape de-formation characteristics of cardiac motion [22]. The latter wasalso studied for diagnostic purposes by employing multimodalimage processing techniques and 3-D volume rendering imple-mented on a single-instruction multiple-data parallel machine,achieving real-time processing and visualization [23].
In this paper, we present an integrated processing scheme forcardiac MRI, embedded in an interactive computing environ-ment suitable for quantitative cardiac analysis. The proposedscheme provides a set of functions for the extraction, modeling,and visualization of cardiac geometrical shape and deformation.The methods apply 4-D processing (three spatial and one tem-poral) to multiphase multislice MRI acquisitions and produce acontinuous 4-D model of the myocardial surface deformation.The use of deformable models for studying the cardiac shapeand motion, in contrast to directly applying measurement algo-rithms to the data, is justified as follows. First, deformable mod-eling is a powerful tool for discriminating objects from their sur-roundings due to the integration of incomplete local informationderived from properties, such as pixel intensity, edge strength,and texture, into an overall shape description. In this way, a ro-bust object representation is produced, a property particularlyimportant in medical images, where discontinuities in shapeare often caused by low contrast, artifacts, and noise. Second,the adopted approach is more general since many measurementtypes can be readily obtained based on the mathematical objectdescription, allowing further enhancement of the analysis. In ad-dition, the model is useful for visualization and distributed pro-cessing purposes. The proposed model-based shape extractionmethod produces a robust description of cardiac cavities usedto measure diagnostically useful parameters, such as wall mo-tion, myocardial thicking, and myocardial mass measurements.The detection of myocardial borders was based on a segmenta-tion process with learning features, which incorporated a neuralnetwork classifier with generating-shrinking capabilities [33].The classifier was combined with a boundary detection method,which models cardiac cavities with parametric functions andthen applies decomposition to a Fourier or wavelet functionalbasis. A multiscale approach is adopted, which uses at each stepa coarse-scale model defined at the previous step in order to con-strain the boundary detection. The representation accuracy startsfrom a coarse but smooth estimation of the approximate cardiacshape and is gradually increased to the desired detail. This ap-proach results in improved efficiency, lack of uncertainty aboutconvergence, and robustness to image artifacts.
An important characteristic of the proposed scheme is its en-hanced interactivity with the user. However, the required guid-ance regarding representative point locations of the differentclasses in the MRI is minimal due to the learning classifier,which allows the automated operation based on certain initialassumptions. If the modeling progress is not satisfactory, theuser can provide additional guidance in order to correct theprocess. The proposed algorithm was successfully applied to alarge number of multislice multiphase MRI data sets, obtainedwith conventional protocols.
In the following, the modeling approach for representing theextracted information is presented in Section II. The methodsused by the cardiac analysis system, including preprocessing,
segmentation, model fitting, and measurement, are describedin Section III. Experimental results and their evaluation byclinicians are given in Section IV. Conclusions are discussed inSection V.
II. CARDIAC INFORMATION REPRESENTATION
A. Parametric Representation
The choice of the representative functional formulation ofthe cardiac information is important for cardiac analysis. In ourwork, the cardiac surface is represented by a deformable para-metric model, which employs decomposition to basis functions.The spatial coordinates of the surface points are represented bythree real functions: , , and .The free parameters, , and provide the three degrees offreedom required and are conveniently selected to correspondto specific directions for a straightforward reconstruction. Morespecifically, if one considers a cylindrical shape for the ventric-ular myocardial surface, is assigned to the circular directionaround the cylinder, to the longitudinal direction from top tobottom, and to the temporal direction. The functions repre-senting the cardiac surface undergo an appropriatetransformation by decomposition to a set of multidimensionalbasis functions. A selected set of the resulting coefficients formsthe model parameters. The two decomposition approaches con-sidered are the Fourier and wavelet transforms.
The Fourier decomposition approach, also used in computergraphics, represents shapes by their Fourier descriptors [8] andis analogous to storage of coordinate values by their harmoniccontent rather than their spatial position. Coarse shape char-acteristics are captured by low-order harmonics, while higherorder harmonics represent increasing detail. Expanding this ideato deforming shapes by adding the temporal dimension, cardiacsurfaces are modeled by their predominant spatiotemporal fre-quency components instead of position information. The recon-struction of the cardiac surface is continuous based on the in-terpolation properties of the trigonometric basis functions. Thewavelet-based representation is similar to the Fourier-based onesince it uses the same set of parametric functions to represent thedeforming surface. However, these functions are decomposedinto a multidimensional wavelet basis instead of a trigonometricbasis. While Fourier transform coefficients express the shapefrequency content, the wavelet transform coefficients expressthe shape detail content, defined as the additional informationneeded to produce a higher resolution representation from alower one. The motivation behind the use of wavelets lies ontheir ability to provide a multiresolution representation of thesignal local properties. This is particularly desirable in appli-cations where increased accuracy is required in certain areasof interest. Note that the model parameters using Fourier orwavelet transform do not correspond to any physical propertyof the surface, such as size, rotation, or curvature, apart fromthe zero-order coefficients that correspond to global translation.
B. Deformable Modeling
The above model is fit to the examination data using a numberof surface points extracted from the images. The model parame-ters are estimated using the surface point coordinates as samples

STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 61
of the original functions. The number of samples considered isrestricted by the size of the original data set, with the greatest re-striction in the temporal resolution, since the number of phasesin multiphase MRI is usually 16 (35 ms time step) or smaller.In 2-D multislice acquisitions, the interslice distance (usually 4mm or larger) also limits the number of samples in the verticaldimension. On the other hand, the intraslice image resolution istypically adequate. The size of the parameter set is reduced byrejecting the least important coefficients while ensuring a satis-factory level of representation accuracy. The rejection of coef-ficients reduces the effect of detail and controls the smoothnessof the resulting cardiac surface according to the quality of theoriginal data. In the case of good-quality high-resolution data,accuracy can be increased. However, for noisy low-resolutionor low-contrast original data, a low approximation order shouldbe selected so that the resulting model is robust to noise andrepresents the overall organ shape as reliably as possible. Thefinal number of model coefficients, which defines the modelorder or complexity, depends on the above selections. For ex-ample, a typical choice of eight in all dimensions results in 2048floating-point coefficients per 4-D deformable surface. Consid-ering that these coefficients fully describe a continuously de-formable 3-D surface with all the required anatomical detail,they form a quite compact representation of the cardiac informa-tion when compared to the original 4-D data size. The optimalmodel order is derived experimentally by studying the meanerror of the final representation and the modeling performance.This procedure was carried out with the help of a radiologistby manually tracing the endocardial and epicardial contours inthree 4-D data sets. The resulting data were then used as a ref-erence surface for error measurements.
The deformable model considers an appropriate ordering andassignment mode of the available surface points into a set of 3-Dtransformation matrices. The model properties are determinedby the ordering and assignment mode (Section III-E), as well asthe underlying adopted transform. Regarding the adopted trans-form, the Fourier and wavelet approaches have different prop-erties that make each one of them suitable to application caseswith different requirements. While the wavelet-based model al-lows the preservation of local detail even at low model orders,the Fourier-based model allows the preservation of the overallshape and smooths out detail uniformly over the entire range.Although, the Fourier transform is applied directly to the orig-inal data, the wavelet decomposition is implemented in a hierar-chical fashion by convolving successive approximations of theinitial function with the appropriate quadrature mirror filters.The surface reconstruction is performed by the inverse trans-form, which may be implemented hierarchically using the cor-responding inverse filter. The reconstruction quality dependson the interpolation properties of the corresponding basis func-tions. The Daubechies class of wavelets was used in our work,offering a large scale of functions from very localized in spaceto very smooth. Their important characteristic is separability re-sulting in great computational efficiency when applied to multi-dimensional data. An acceptable compromise between localiza-tion and smoothness is provided by the sixth-order Daubechiesfilters (DAUB6). The described deformable modeling was im-plemented in an interactive computing scheme (Section III),
where the two transforms are used according to their inherentproperties for best results.
III. M ODEL-BASED MRI PROCESSING ANDANALYSIS
A. Method Outline
The problem in question is the accurate and robust extractionof the endocardial and epicardial surfaces of cardiac cavitiesfrom MRI data. Their shape and deformation is then modeledto be used for measuring quantities of diagnostic value. Partic-ular focus is placed on the left ventricle, which is clinically mostimportant. However, the proposed method may be applied withno restriction to other cavities, after certain necessary adjust-ments related to different expected size and shape complexityare made. We consider a 4-D model that is smooth and con-tinuous in both space and time, thus allowing the measurementof myocardial surface motion. Cardiac motion is quite compli-cated since it involves translation, rotation, and, most important,deformation. Therefore, its study in two dimensions is rather in-adequate since the same slice image in different phases does notusually correspond to the same tissue. The proposed method isapplied to multislice multiphase MR images or 3-D multiphasedata acquired by either bright blood or dark blood conventionalprotocols.
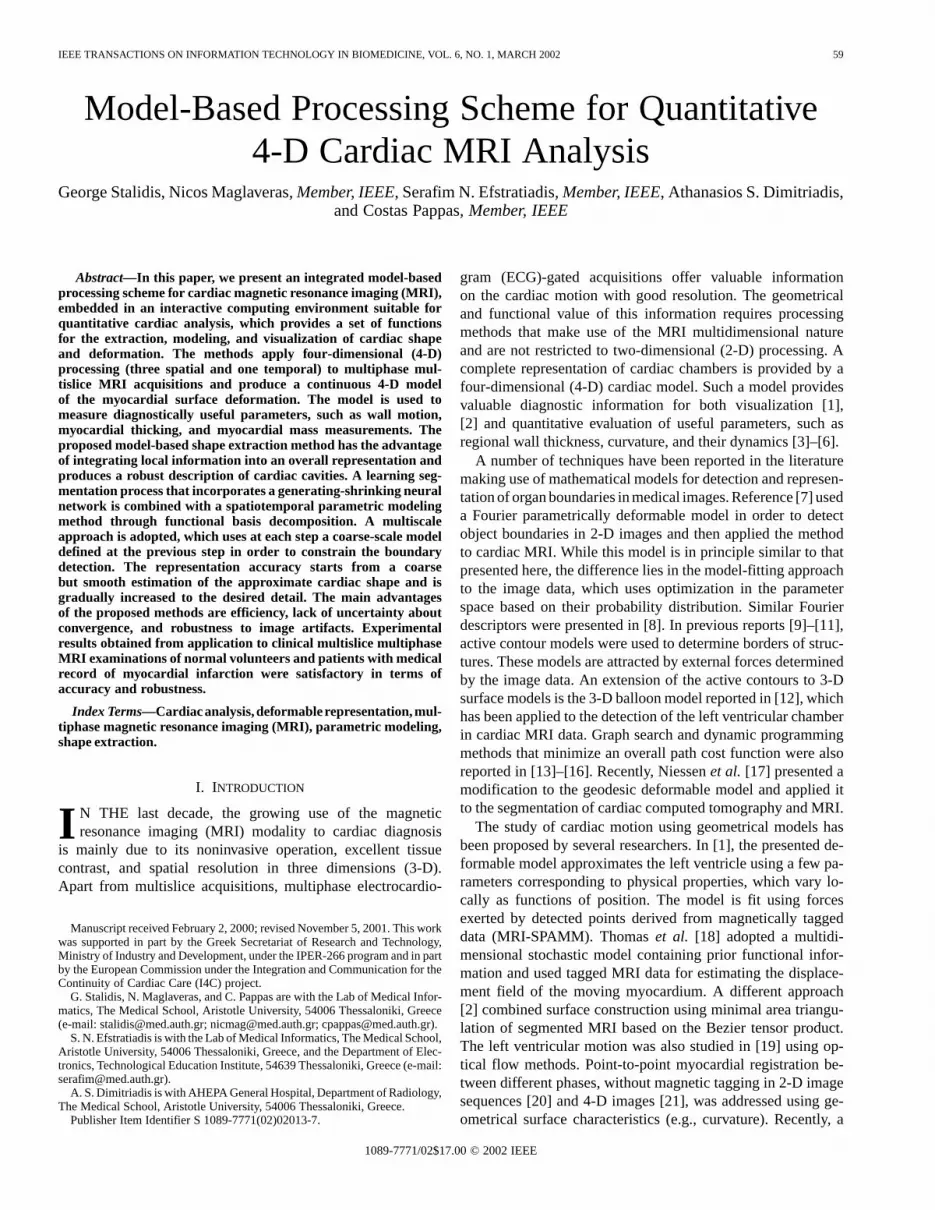
In Fig. 1, a block diagram depicts the flow of the proposedmethod. A multiscale fitting process is followed, where in eachstep the rough version of the model produced by the previousstep is used in deriving a more detailed model. The procedureis initiated by the user, who indicates the rough position of thecavity, as well as reference samples of myocardium, blood, andlung. The size of a predefined coarse cardiac surface model is setaccording to the user input and is used as an initial reference bythe subsequent stages of the algorithm. The sensitive task of dis-criminating the tissue type is handled by a trained neural network(NN)-based classifier. Initial training is performed with minimaluser guidance and can be improved (if necessary) by user inter-action. The classifier output, the coarse model, and the image in-tensity gradient are combined bya radial searchalgorithm, whichidentifies endocardial and epicardial points at a finer scale. Then,the model fitting task is performed by inserting lexicographicallythe coordinates of the detected points in 3-D matrices and by cal-culating the model parameters using an appropriate transform.The resulting model is used to guide the detection and model-fit-ting process at a higher scale, until the required accuracy levelis reached. The above iterative method requires a fairly smallnumber of steps (typically three or four ) and relatively low com-putational cost. As a result, the method is efficient and consider-ably faster than alternative techniques reported in the literature,such as optimization methods and graph searching.
B. Image Preprocessing Stage
Initially, the acquired 4-D MRI data, using conventional MRequipment and protocols, are transferred from the MR unit to agraphics workstation for processing. Modern MR systems pro-duce images with resolution from 80 80 to 256 256 and anumber of 20 or more locations, or isotropic 3-D data with reso-lution of the same order in all three spatial dimensions. This spa-tial resolution is considered adequate for our application. The
62 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
Fig. 1. Method outline.
number of temporal phases ranges from six to 24 per cardiaccycle, corresponding to a minimum time step of 20 ms.
As a first step of the modeling method, the user visualizes thedata and determines the approximate position of the left ven-tricle using a mouse-driven interface. In the case of 2-D mul-tislice data, for each phase, the user selects the slice closest tothe cavity base and the one closest to the cavity apex, assumingaxial acquisition. Then, the cavity center in both slice images,identifying the approximate centroid, is indicated. The line con-necting the two selected points roughly defines the long axis ofthe ventricle and is used as reference for its size and orientation.In practice, we found that the above procedure alone is suffi-cient to indicate the long axis at diastole and systole and doesnot need to be repeated for each phase. Note that accurate selec-tion of the above centroids and exact definition of the ventriclelong axis is not necessary and does not affect the performanceof the method. In the case of 3-D data, a similar procedure isperformed by the user for selecting sections of the volume datainstead of slices. User interaction with 3-D data is very sim-ilar to the 2-D multislice case. Instead of viewing images on
a slice-by-slice basis, which is the default way of viewing rawmultislice data, the user is viewing sections of 3-D data. Sincethe resolution of volume data, which defines the number ofplanes available, is much larger than the number of slices avail-able at multislice acquisitions, the user is also given the possi-bility to skip unnecessary planes of the 3-D data by selecting anintersection distance.
In addition to the above position information, an approximatesmall set of samples from the myocardium, blood (intracavity),and surrounding regions needs to be indicated by the operatorin order to be used in the segmentation phase described below.
C. Classification-Based Segmentation
The extraction of the cardiac surfaces requires the segmen-tation of the MRI data into myocardium, intracavity region(blood), and the cavity surrounding area based on the pixelintensity values, since MRI typically retains good contrastamong myocardium, blood, lung, and fat. The large number ofsuitable segmentation approaches in the literature, particularlyapplied to cardiac MRI, employ, among other techniques,statistical analysis, multiresolution, and fuzzy methods or NNs[29]–[32]. More recently, the cardiac ventricle boundaries weredefined by refining the segmentation threshold according to alearning algorithm [28]. In our method, we adopt an efficientNN-based classifier [33] that was successfully applied to ECGsignal processing [34]. The proposed segmentation networkis trained on a small number of representative tissue pointsand is used to segment image points into three classes: lung,myocardium, and blood. In selecting the above classifier, weconsidered its efficiency when compared to alternative, morecomputationally intensive techniques, which are prohibitive touse in practice due to the large size of typical 4-D data sets.The generating-shrinking neural network classifier (GSNNC),shown in Fig. 2, is based on supervised feedforward NNs andgenerates a three-layer network to classify random patterns inthe -dimensional Euclidean space [33]. This approach ispreferred over the backpropagation algorithm because 1) it canseparate the training patterns very fast (about 1000 times fasterthan backpropagation); 2) its behavior is analytically described;and 3) the learning of a new pattern does not induce loss ofprevious training (on-line training).
More specifically, let us consider the problem of separatingnumber of classes and a three-NN-layer architecture. The
first (input) layer receives information from an-dimensionalvector, which is the input pattern. Given a reference constant,an ( 1)-dimensional vector is formed. The input layer has asmany neurons as the trained patterns and its output is
for (1)
where is the weight of the connection between theth inputcomponent and theth neuron, is the -dimensional vector,and is the total number of training patterns. Thesecond-layer neurons receive input only from the input layer and formthe following output:
for (2)

STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 63
Fig. 2. The generating-shrinking neural network classifier.
where
(3)
The third layer consists of neurons and its output is deter-mined by
for (4)
where is the weight of the to connection. Finally, theweighting factors and are defined as follows:
for
forfor (5)
if is the class for pattern
otherwisefor
(6)
The processing of input vectors by the NN actually involvesnormalization of magnitude [see (5)], which could lead to anextremely scattered decision region, depending on the inputvalues. For this reason, the constantis used as an additionalelement in the input vector, ensuring a minimum vector magni-tude. As a consequence, the morphology of the decision regionis dependent on the value of. The connection between theconstant and the performance of the classifier is mentioned in[33]. It is worth noting that the sensitivity of the performanceon the exact value is very small, due to the learning feature ofthe NN. It can thus be safely selected to be comparable (sameorder of magnitude) with the mean of the other input elements.
The GSNNC algorithm is trained by input patterns using itson-line feature. The NN input is in general a set of statistical in-dexes associated with the image intensity, texture, and structurearound each pixel. Clearly, the consideration of several param-eters allows a more robust clustering. On the other hand, an un-necessary increase of input pattern dimension enlarges the com-putational requirements. The dimensionof the input vectorthus results from the number of input values that play a usefulrole in the intended classification.
In our case, pixel intensity alone was sufficient for tissue dis-crimination due to the good MRI contrast between tissue types.However, the NN input pattern also needed to include positioninformation in order to deal with the standard problem of in-tensity gradients. This artifact involves considerable changesin the intensity scale, such as interslice differences or possible
large intraslice intensity variations around the myocardium, sur-rounding area, or blood. In our approach, the NN classifier tookadvantage of the rather consistent behavior of this artifact overa significant number of successive slices and used position in-formation to create appropriate decision regions that took intoaccount the intensity gradients. Specifically, we concluded to athree-dimensional input pattern, consisting of
1) pixel intensity (range 0 to 255);2) position in the image, measured as angle around the cen-
troid of the cavity (range 0 to 359);3) slice location (range 0 to 35).
Including the temporal phase as an additional parameter did notresult in any significant improvement, for the data we used maybe a straightforward modification in the case of data with inter-phase intensity gradients.
NN training is performed on-line, simultaneously with theinput pattern selection stage by the user. This means that when-ever the user selects a new training pattern through the graphicalinterface, the corresponding node is created in the second NNlayer and the weight matrices are updated. This process is com-putationally very fast and practically carried out instantaneouslybefore the next training pattern is selected. Moreover, it is pos-sible to provide additional training patterns at any time withoutdiscarding the previous training. This property allows the inter-active design of the method, including possible corrective in-tervention by the user. The classification process may start withminimal user guidance, e.g., one point from each class. Alterna-tively, a fully automated method for identifying an initial patternper class can be used. We introduce ahard rule,which derivestraining patterns for class using the histogram of one repre-sentative image, such as predefined bounds forthe intensity values. Although this provided satisfactory initialsegmentation results in most cases, it is not guaranteed to workin a wide range of MRI data sets. Thus, successful unsupervisedNN training requires prior information of the cardiac structureand texture by developing a knowledge base used for selectinggood initial training sets and bound values (intelligent training).The success of the method improves with its extended clinicaluse on sufficient number of different examination cases. Userintervention may be necessary only in certain atypical cases, re-sulting in unsuccessful performance of the initial segmentationstage. Within this work, this was implemented in a preliminaryform in order to save time during our experiments. An initial setof training samples, as they were selected by the user, gave sat-isfactory segmentation results without additional guidance. Theset was used to form the “knowledge” regarding the selection oftraining samples.
The set comprised 32 points, spread into different classesand slice locations in end diastole. From the intensity valuesof these points, a lookup table was formed with the mean in-tensity for each class. An automatic procedure was then imple-mented which scans of eight slices in end diastole to find onesample point from each class in each slice (24 points in total).The criteria for selecting these points are to have intensity closeto the corresponding value in the lookup table and to belong ina uniform region with similar intensities and size of at least 5
5 pixels. It is noted that the technique in this form was only
64 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
(a) (b) (c)
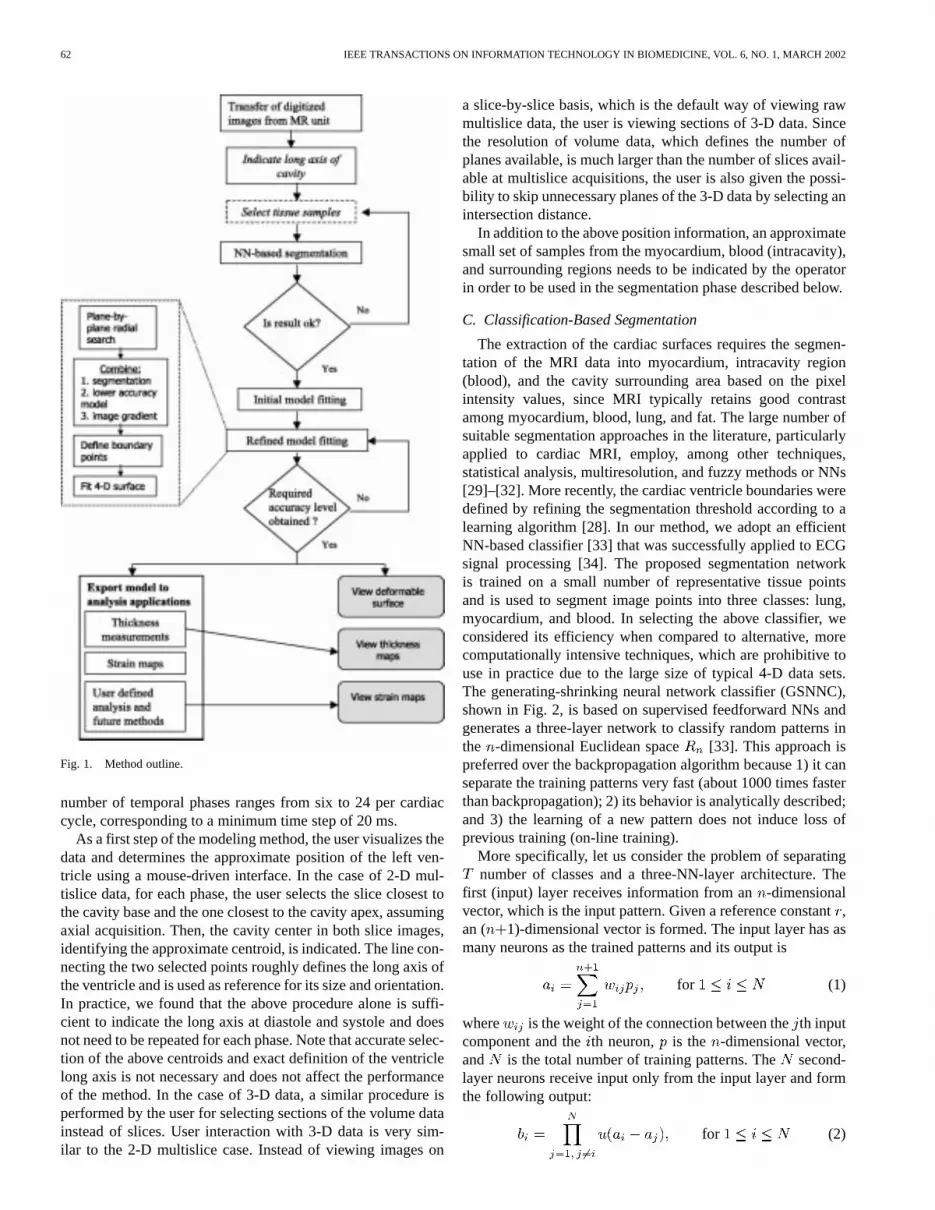
Fig. 3. Application of the GSNNC algorithm for segmenting an axial systolic slice. (a) Original image. (b) Segmented image using automatically derived trainingpatterns. (c) Segmented image using additional training pattern for myocardium. Segmentation labeling: blood (white), myocardium (gray), lung (black).
a crude approach toward intelligent training. However, it wasfound useful in practice in terms of saving user interaction timeand depicted the advantage of the segmentation method to allowprogressive training.
Given the training input, the GSNNC reduces its size by re-jecting nodes, according to a certain shrinking rule, and classi-fies input patterns representing image points and their propertiesinto myocardium, blood, or lung. Due to the GSNNC shrinkingproperty and feed-forward structure, its output is calculated veryefficiently. In case of unsatisfactory results, the user may selectadditional training points, indicating the desirable behavior ofthe classifier at the dubious locations or phases at a negligibleadditional computational cost.
User intervention is possible through a graphical interface,which allows the viewing of slice-by-slice segmentation resultsin parallel with the original data and the selection of additionaltraining samples. The user is able to view selected segmenta-tion results and to decide if he wants to intervene in the trainingbefore or after the execution of the boundary detection algo-rithm. It is also possible to ask for the automatic selection of aninitial training set or to reset the training process. In a typicalexamination, the number of neurons created in the second layeris on the order of 20 to 100. The number of nodes rejected bythe shrinking property can be minimum (e.g., one or two nodes)when the number of samples is small, and a reduction to half canbe reached when the samples contain significant redundancy.
Finally, a nonlinear filtering operation, based on the majorityof labels within a window, is applied to the segmented image inorder to filter out very small isolated regions attributed to noise.Specifically, for each pixel , given a rectangular window ofsize centered around pixel, we have
if is in class
otherwise(7)
For each class, we have
(8)
(9)
If and pixel is classified to class and, then pixel is classified to the majority class ,
which corresponds to . In other words, the above filtercomputes the majority of the labels within a specified rectan-gular window around the working point. If this point is labeleddifferently than the majority and the number of all points in thewindow with different labels than the majority is smaller thana predetermined threshold, then the center point is changed tothe majority class. This threshold and the filter support size areselected so that the filter has maximal effect only on small re-gions that are attributed to noise and produces minimal (almostzero) undesirable distortion to the tissue boundaries. The bestresults were obtained for a 5 5 size window and a thresholdvalue equal to four. Fig. 3(b) and (c) shows the GSNNC seg-mentation results with no user guidance and with an additionaltraining pattern for the myocardium, respectively, when appliedto the axial systolic slice of Fig. 3(a). Note the drastic improve-ment in the GSNNC output quality in Fig. 3(c).
D. Endocardial–Epicardial Border Detection
The output of the classification algorithm, along with acoarse reference 4-D surface model and the image intensitygradient, are considered in the identification of the endocardialand epicardial boundary points. This operation is performedslice-by-slice over the entire 4-D set. In the case of 3-D datasets, 2-D slice images are used instead of 3-D image sections.The search is initiated from the user-defined points, whichapproximately determine the location and orientation of theleft ventricle. These points are used to derive the approximatecentroid of the left ventricle cavity for each location and phaseusing linear interpolation in space and time. More specifically,the border detection method consists of the following steps.
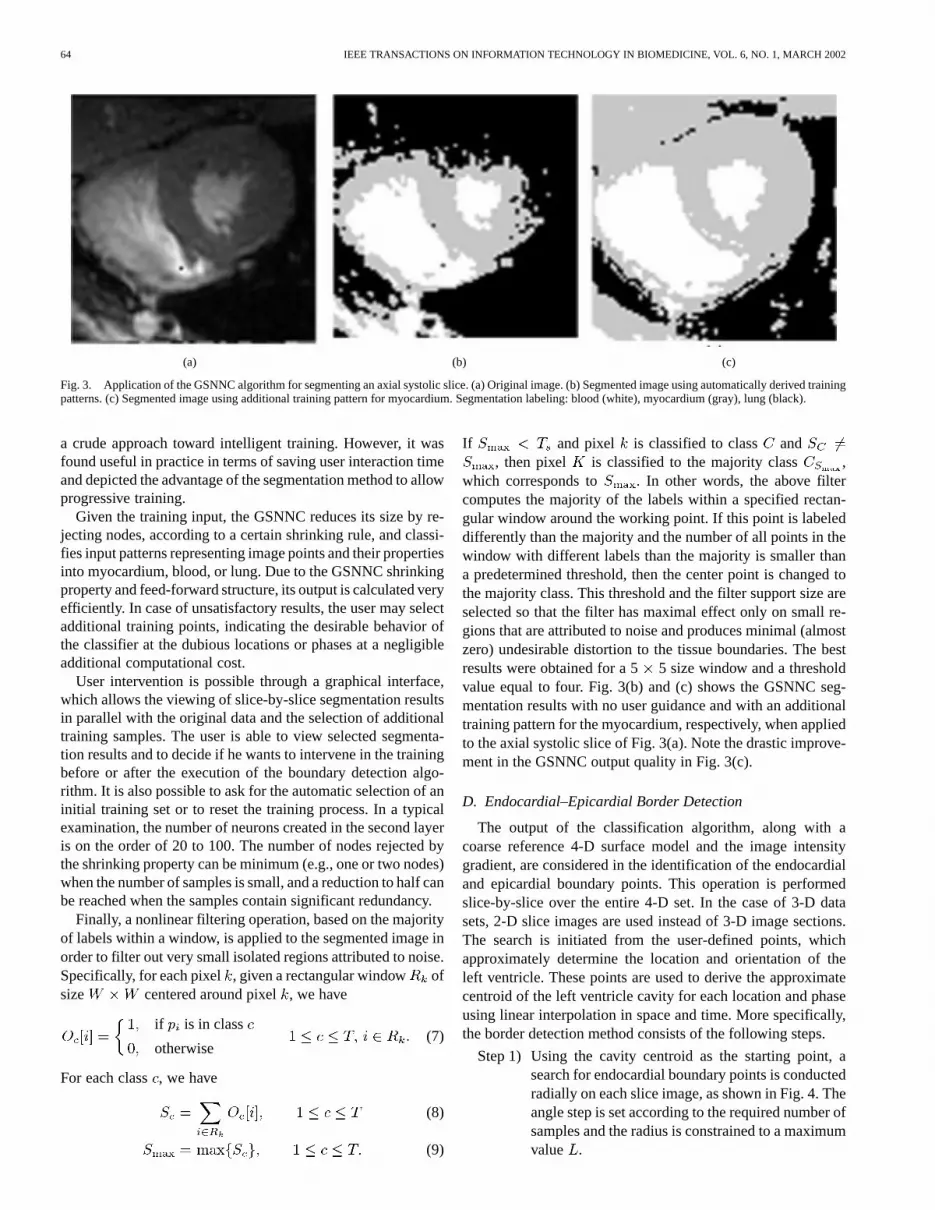
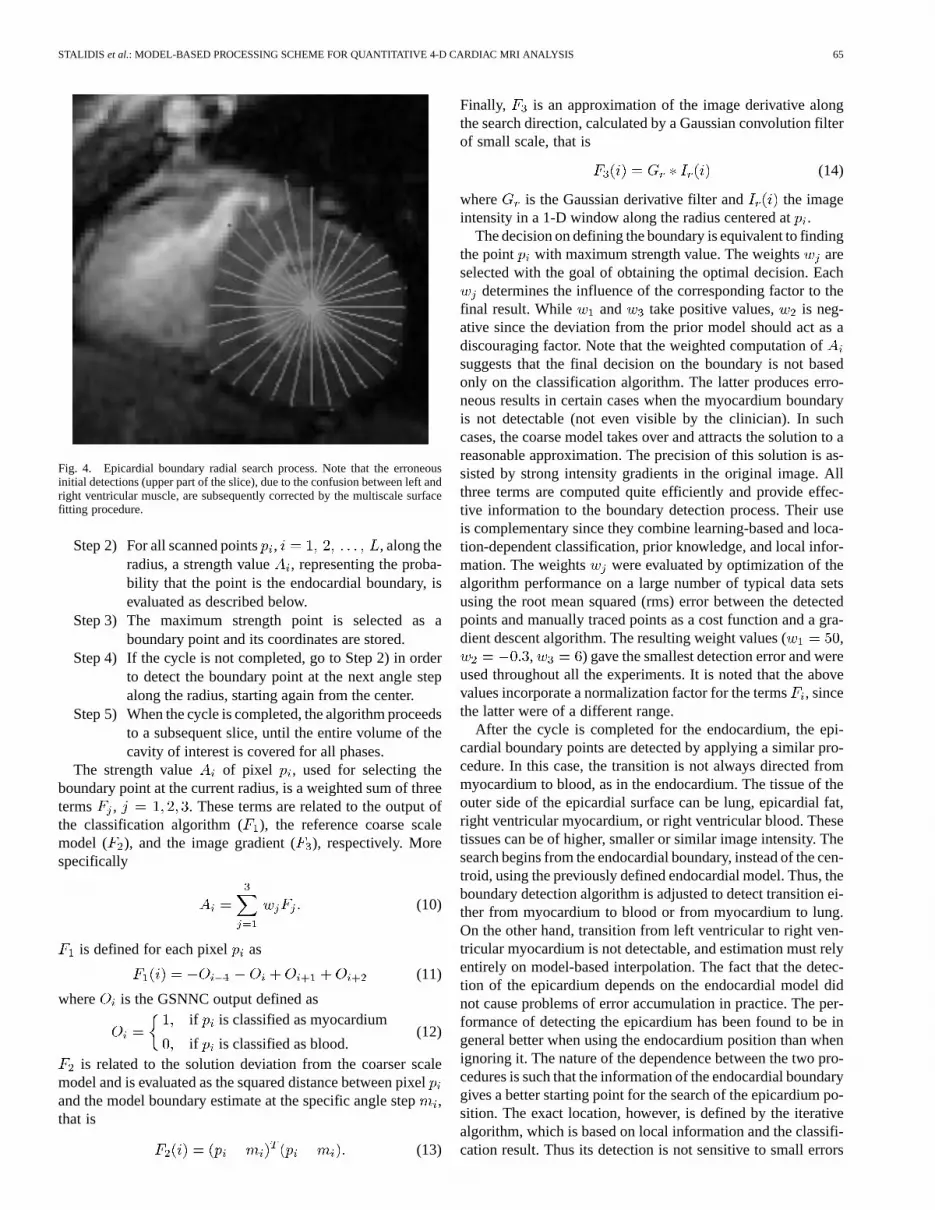
Step 1) Using the cavity centroid as the starting point, asearch for endocardial boundary points is conductedradially on each slice image, as shown in Fig. 4. Theangle step is set according to the required number ofsamples and the radius is constrained to a maximumvalue .
STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 65
Fig. 4. Epicardial boundary radial search process. Note that the erroneousinitial detections (upper part of the slice), due to the confusion between left andright ventricular muscle, are subsequently corrected by the multiscale surfacefitting procedure.
Step 2) For all scanned points, , along theradius, a strength value , representing the proba-bility that the point is the endocardial boundary, isevaluated as described below.
Step 3) The maximum strength point is selected as aboundary point and its coordinates are stored.
Step 4) If the cycle is not completed, go to Step 2) in orderto detect the boundary point at the next angle stepalong the radius, starting again from the center.
Step 5) When the cycle is completed, the algorithm proceedsto a subsequent slice, until the entire volume of thecavity of interest is covered for all phases.
The strength value of pixel , used for selecting theboundary point at the current radius, is a weighted sum of threeterms , . These terms are related to the output ofthe classification algorithm ( ), the reference coarse scalemodel ( ), and the image gradient (), respectively. Morespecifically
(10)
is defined for each pixel as
(11)
where is the GSNNC output defined asif is classified as myocardium
if is classified as blood.(12)
is related to the solution deviation from the coarser scalemodel and is evaluated as the squared distance between pixeland the model boundary estimate at the specific angle step,that is
(13)
Finally, is an approximation of the image derivative alongthe search direction, calculated by a Gaussian convolution filterof small scale, that is
(14)
where is the Gaussian derivative filter and the imageintensity in a 1-D window along the radius centered at.
The decision on defining the boundary is equivalent to findingthe point with maximum strength value. The weights areselected with the goal of obtaining the optimal decision. Each
determines the influence of the corresponding factor to thefinal result. While and take positive values, is neg-ative since the deviation from the prior model should act as adiscouraging factor. Note that the weighted computation ofsuggests that the final decision on the boundary is not basedonly on the classification algorithm. The latter produces erro-neous results in certain cases when the myocardium boundaryis not detectable (not even visible by the clinician). In suchcases, the coarse model takes over and attracts the solution to areasonable approximation. The precision of this solution is as-sisted by strong intensity gradients in the original image. Allthree terms are computed quite efficiently and provide effec-tive information to the boundary detection process. Their useis complementary since they combine learning-based and loca-tion-dependent classification, prior knowledge, and local infor-mation. The weights were evaluated by optimization of thealgorithm performance on a large number of typical data setsusing the root mean squared (rms) error between the detectedpoints and manually traced points as a cost function and a gra-dient descent algorithm. The resulting weight values ( ,
, ) gave the smallest detection error and wereused throughout all the experiments. It is noted that the abovevalues incorporate a normalization factor for the terms, sincethe latter were of a different range.
After the cycle is completed for the endocardium, the epi-cardial boundary points are detected by applying a similar pro-cedure. In this case, the transition is not always directed frommyocardium to blood, as in the endocardium. The tissue of theouter side of the epicardial surface can be lung, epicardial fat,right ventricular myocardium, or right ventricular blood. Thesetissues can be of higher, smaller or similar image intensity. Thesearch begins from the endocardial boundary, instead of the cen-troid, using the previously defined endocardial model. Thus, theboundary detection algorithm is adjusted to detect transition ei-ther from myocardium to blood or from myocardium to lung.On the other hand, transition from left ventricular to right ven-tricular myocardium is not detectable, and estimation must relyentirely on model-based interpolation. The fact that the detec-tion of the epicardium depends on the endocardial model didnot cause problems of error accumulation in practice. The per-formance of detecting the epicardium has been found to be ingeneral better when using the endocardium position than whenignoring it. The nature of the dependence between the two pro-cedures is such that the information of the endocardial boundarygives a better starting point for the search of the epicardium po-sition. The exact location, however, is defined by the iterativealgorithm, which is based on local information and the classifi-cation result. Thus its detection is not sensitive to small errors
66 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
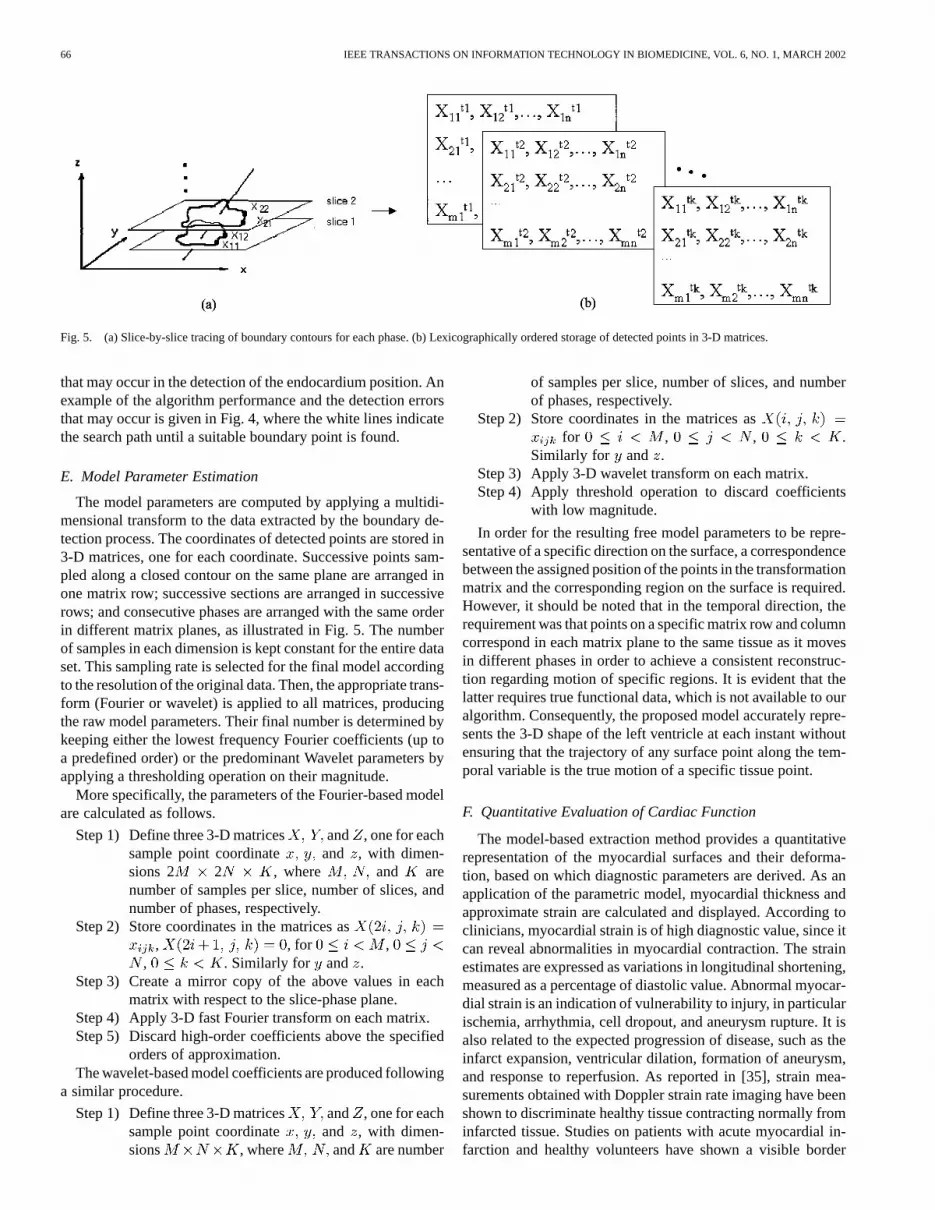
Fig. 5. (a) Slice-by-slice tracing of boundary contours for each phase. (b) Lexicographically ordered storage of detected points in 3-D matrices.
that may occur in the detection of the endocardium position. Anexample of the algorithm performance and the detection errorsthat may occur is given in Fig. 4, where the white lines indicatethe search path until a suitable boundary point is found.
E. Model Parameter Estimation
The model parameters are computed by applying a multidi-mensional transform to the data extracted by the boundary de-tection process. The coordinates of detected points are stored in3-D matrices, one for each coordinate. Successive points sam-pled along a closed contour on the same plane are arranged inone matrix row; successive sections are arranged in successiverows; and consecutive phases are arranged with the same orderin different matrix planes, as illustrated in Fig. 5. The numberof samples in each dimension is kept constant for the entire dataset. This sampling rate is selected for the final model accordingto the resolution of the original data. Then, the appropriate trans-form (Fourier or wavelet) is applied to all matrices, producingthe raw model parameters. Their final number is determined bykeeping either the lowest frequency Fourier coefficients (up toa predefined order) or the predominant Wavelet parameters byapplying a thresholding operation on their magnitude.
More specifically, the parameters of the Fourier-based modelare calculated as follows.
Step 1) Define three 3-D matrices and , one for eachsample point coordinate and , with dimen-sions 2 2 , where and arenumber of samples per slice, number of slices, andnumber of phases, respectively.
Step 2) Store coordinates in the matrices as, , for ,
, . Similarly for and .Step 3) Create a mirror copy of the above values in each
matrix with respect to the slice-phase plane.Step 4) Apply 3-D fast Fourier transform on each matrix.Step 5) Discard high-order coefficients above the specified
orders of approximation.The wavelet-based model coefficients are produced following
a similar procedure.
Step 1) Define three 3-D matrices and , one for eachsample point coordinate and , with dimen-sions , where and are number
of samples per slice, number of slices, and numberof phases, respectively.
Step 2) Store coordinates in the matrices asfor , , .
Similarly for and .Step 3) Apply 3-D wavelet transform on each matrix.Step 4) Apply threshold operation to discard coefficients
with low magnitude.
In order for the resulting free model parameters to be repre-sentative of a specific direction on the surface, a correspondencebetween the assigned position of the points in the transformationmatrix and the corresponding region on the surface is required.However, it should be noted that in the temporal direction, therequirement was that points on a specific matrix row and columncorrespond in each matrix plane to the same tissue as it movesin different phases in order to achieve a consistent reconstruc-tion regarding motion of specific regions. It is evident that thelatter requires true functional data, which is not available to ouralgorithm. Consequently, the proposed model accurately repre-sents the 3-D shape of the left ventricle at each instant withoutensuring that the trajectory of any surface point along the tem-poral variable is the true motion of a specific tissue point.
F. Quantitative Evaluation of Cardiac Function
The model-based extraction method provides a quantitativerepresentation of the myocardial surfaces and their deforma-tion, based on which diagnostic parameters are derived. As anapplication of the parametric model, myocardial thickness andapproximate strain are calculated and displayed. According toclinicians, myocardial strain is of high diagnostic value, since itcan reveal abnormalities in myocardial contraction. The strainestimates are expressed as variations in longitudinal shortening,measured as a percentage of diastolic value. Abnormal myocar-dial strain is an indication of vulnerability to injury, in particularischemia, arrhythmia, cell dropout, and aneurysm rupture. It isalso related to the expected progression of disease, such as theinfarct expansion, ventricular dilation, formation of aneurysm,and response to reperfusion. As reported in [35], strain mea-surements obtained with Doppler strain rate imaging have beenshown to discriminate healthy tissue contracting normally frominfarcted tissue. Studies on patients with acute myocardial in-farction and healthy volunteers have shown a visible border
STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 67
zone between ischemic and nonischemic tissue. Longitudinalstrain (peak shortening) in normal left ventricular myocardiumtypically has negative values in the area of10 to 14 (%),while infarcted areas are not contracting and give positive strainvalues.
In our experiments, myocardial thickness was measuredduring the entire cardiac cycle and was used to estimate radialstrain as the difference in thickness of a specific region betweensystole and diastole (measured as a percentage of full length).Myocardial thickness was measured using the followingalgorithm.
Step 1) For a specific position along the long axis, the en-docardial boundary at diastole is reconstructed as acurve on the plane vertical to the long axis that passesfrom this position.
Step 2) For each boundary point on the curve, the directionnormal to the surface is calculated, using a smootherreconstruction by further decreasing the modelorder.
Step 3) The myocardial thickness is measured by searchingthe point at which the normal vector intersects theepicardial surface.
Step 4) The resulting thickness value and the coordinates ofthe corresponding endocardial point are stored.
Step 5) Steps 1) to 4) are iterated for successive positions onthe long axis until the endocardial surface is covered.
Step 6) Steps 1) to 5) are iterated at successive time instancesuntil the entire cardiac cycle is covered. A set ofthickness measurements is thus acquired for eachtemporal phase.
The number of surface points to be measured is selectableby the user, according to the desirable resolution in the calcula-tions. The produced values are color coded on the endocardialsurface and displayed in CINE mode, together with the surfacedeformation. This view is suitable for qualitative evaluation ofcardiac motion. Since it requires no registration, each phase isaccurately displayed.
Furthermore, thickness measurements are used to derive my-ocardial strain maps. Strain is estimated as the difference inthickness from diastole to systole, expressed as a percentage ofdiastolic value. The produced values are displayed as gray levelscoded on the endocardial surface. The results are approximate,since there is no real functional information in the original datato accurately measure myocardial displacement. However, theprovided accuracy was satisfactory for important diagnostic ap-plications, such as detection of hypokinetic tissue.
IV. CLINICAL APPLICATION AND RESULTS
The proposed methods were applied to 2-D multislice multi-phase and 3-D multiphase cardiac MRI data. In the case of 2-Ddata, the image size was 8080 with a field of view 11.2 cmand interslice distance of 6 mm. The number of slices variedfrom 16 to 24 and the number of phases from 16 to 20 phasesper location. The 2-D data were acquired with a 3.5-T systemfrom three different patients. The images were axial, ECG gated,and T2 weighted. The 3-D acquisitions were also T2-weighted.The data size was 256 145 85 for each phase, and a total
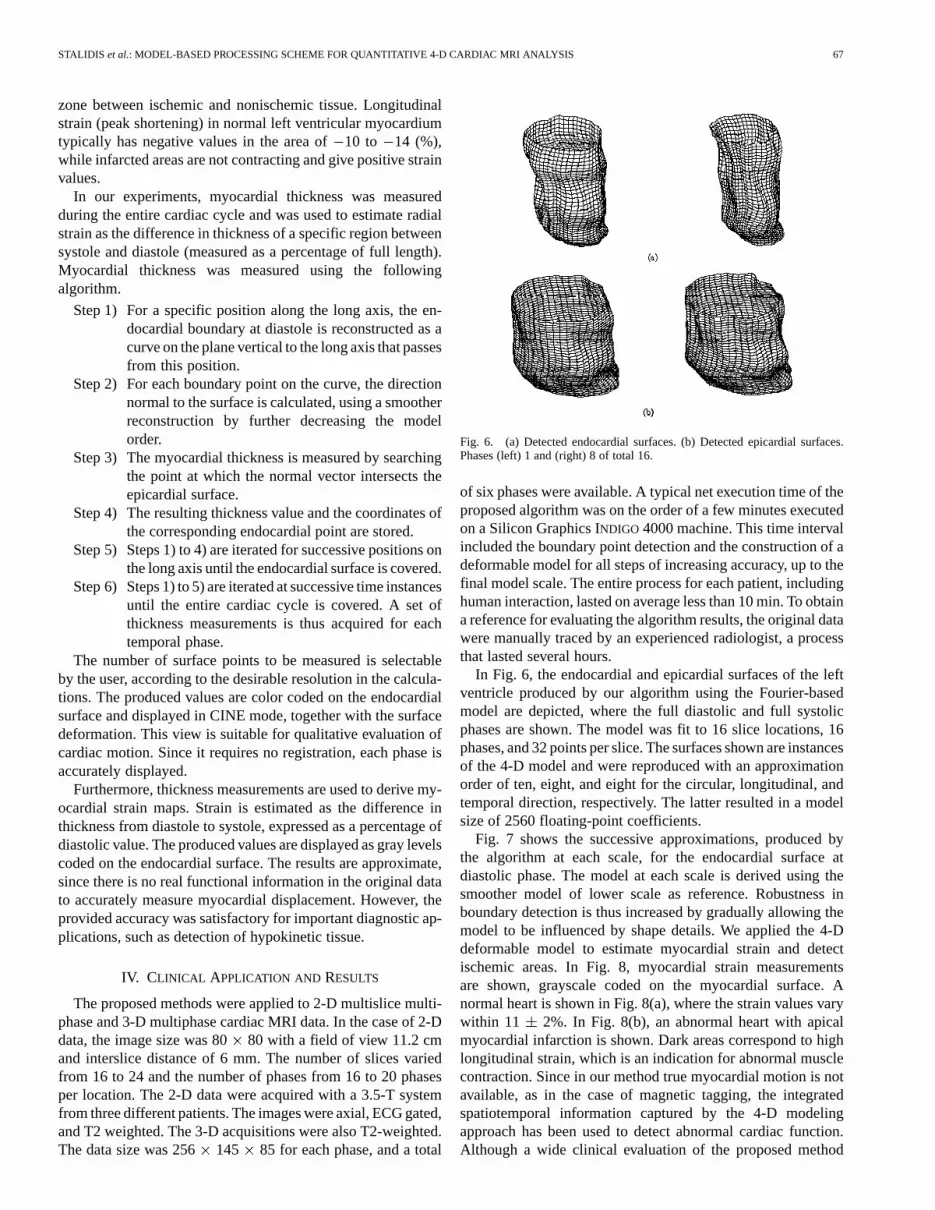
Fig. 6. (a) Detected endocardial surfaces. (b) Detected epicardial surfaces.Phases (left) 1 and (right) 8 of total 16.
of six phases were available. A typical net execution time of theproposed algorithm was on the order of a few minutes executedon a Silicon Graphics INDIGO 4000 machine. This time intervalincluded the boundary point detection and the construction of adeformable model for all steps of increasing accuracy, up to thefinal model scale. The entire process for each patient, includinghuman interaction, lasted on average less than 10 min. To obtaina reference for evaluating the algorithm results, the original datawere manually traced by an experienced radiologist, a processthat lasted several hours.
In Fig. 6, the endocardial and epicardial surfaces of the leftventricle produced by our algorithm using the Fourier-basedmodel are depicted, where the full diastolic and full systolicphases are shown. The model was fit to 16 slice locations, 16phases, and 32 points per slice. The surfaces shown are instancesof the 4-D model and were reproduced with an approximationorder of ten, eight, and eight for the circular, longitudinal, andtemporal direction, respectively. The latter resulted in a modelsize of 2560 floating-point coefficients.
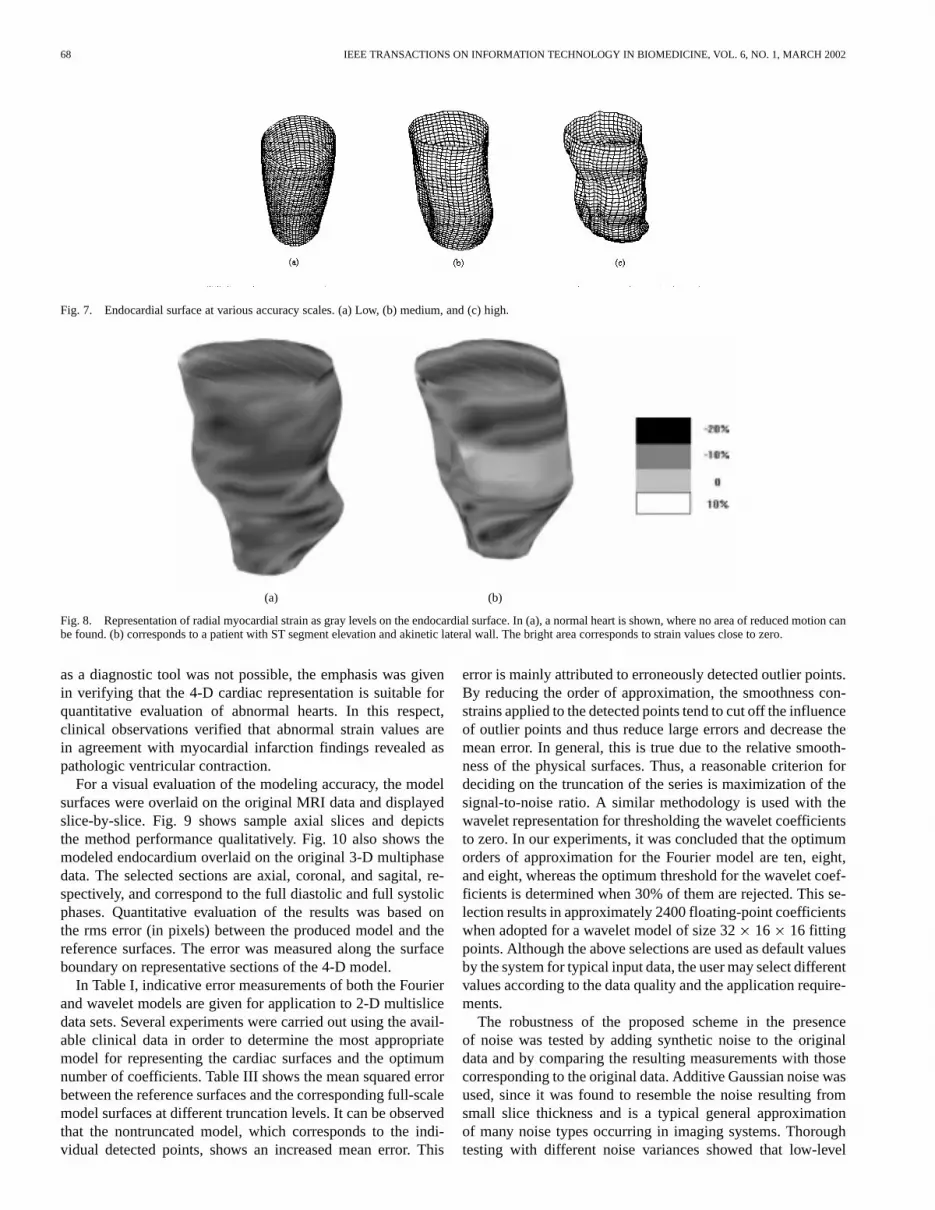
Fig. 7 shows the successive approximations, produced bythe algorithm at each scale, for the endocardial surface atdiastolic phase. The model at each scale is derived using thesmoother model of lower scale as reference. Robustness inboundary detection is thus increased by gradually allowing themodel to be influenced by shape details. We applied the 4-Ddeformable model to estimate myocardial strain and detectischemic areas. In Fig. 8, myocardial strain measurementsare shown, grayscale coded on the myocardial surface. Anormal heart is shown in Fig. 8(a), where the strain values varywithin 11 2%. In Fig. 8(b), an abnormal heart with apicalmyocardial infarction is shown. Dark areas correspond to highlongitudinal strain, which is an indication for abnormal musclecontraction. Since in our method true myocardial motion is notavailable, as in the case of magnetic tagging, the integratedspatiotemporal information captured by the 4-D modelingapproach has been used to detect abnormal cardiac function.Although a wide clinical evaluation of the proposed method
68 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
Fig. 7. Endocardial surface at various accuracy scales. (a) Low, (b) medium, and (c) high.
(a) (b)
Fig. 8. Representation of radial myocardial strain as gray levels on the endocardial surface. In (a), a normal heart is shown, where no area of reduced motion canbe found. (b) corresponds to a patient with ST segment elevation and akinetic lateral wall. The bright area corresponds to strain values close to zero.
as a diagnostic tool was not possible, the emphasis was givenin verifying that the 4-D cardiac representation is suitable forquantitative evaluation of abnormal hearts. In this respect,clinical observations verified that abnormal strain values arein agreement with myocardial infarction findings revealed aspathologic ventricular contraction.
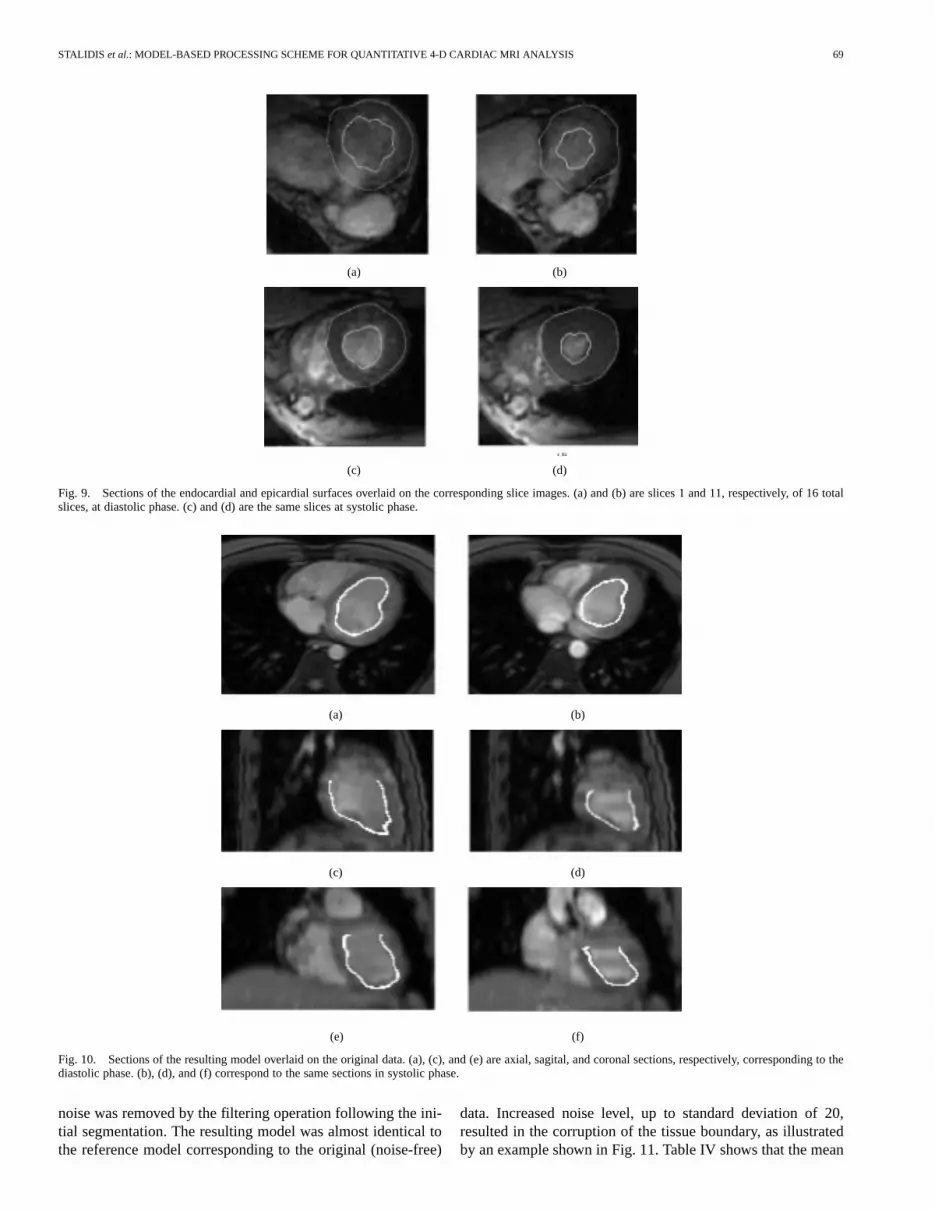
For a visual evaluation of the modeling accuracy, the modelsurfaces were overlaid on the original MRI data and displayedslice-by-slice. Fig. 9 shows sample axial slices and depictsthe method performance qualitatively. Fig. 10 also shows themodeled endocardium overlaid on the original 3-D multiphasedata. The selected sections are axial, coronal, and sagital, re-spectively, and correspond to the full diastolic and full systolicphases. Quantitative evaluation of the results was based onthe rms error (in pixels) between the produced model and thereference surfaces. The error was measured along the surfaceboundary on representative sections of the 4-D model.
In Table I, indicative error measurements of both the Fourierand wavelet models are given for application to 2-D multislicedata sets. Several experiments were carried out using the avail-able clinical data in order to determine the most appropriatemodel for representing the cardiac surfaces and the optimumnumber of coefficients. Table III shows the mean squared errorbetween the reference surfaces and the corresponding full-scalemodel surfaces at different truncation levels. It can be observedthat the nontruncated model, which corresponds to the indi-vidual detected points, shows an increased mean error. This
error is mainly attributed to erroneously detected outlier points.By reducing the order of approximation, the smoothness con-strains applied to the detected points tend to cut off the influenceof outlier points and thus reduce large errors and decrease themean error. In general, this is true due to the relative smooth-ness of the physical surfaces. Thus, a reasonable criterion fordeciding on the truncation of the series is maximization of thesignal-to-noise ratio. A similar methodology is used with thewavelet representation for thresholding the wavelet coefficientsto zero. In our experiments, it was concluded that the optimumorders of approximation for the Fourier model are ten, eight,and eight, whereas the optimum threshold for the wavelet coef-ficients is determined when 30% of them are rejected. This se-lection results in approximately 2400 floating-point coefficientswhen adopted for a wavelet model of size 3216 16 fittingpoints. Although the above selections are used as default valuesby the system for typical input data, the user may select differentvalues according to the data quality and the application require-ments.
The robustness of the proposed scheme in the presenceof noise was tested by adding synthetic noise to the originaldata and by comparing the resulting measurements with thosecorresponding to the original data. Additive Gaussian noise wasused, since it was found to resemble the noise resulting fromsmall slice thickness and is a typical general approximationof many noise types occurring in imaging systems. Thoroughtesting with different noise variances showed that low-level
STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 69
(a) (b)
(c) (d)
Fig. 9. Sections of the endocardial and epicardial surfaces overlaid on the corresponding slice images. (a) and (b) are slices 1 and 11, respectively,of 16 totalslices, at diastolic phase. (c) and (d) are the same slices at systolic phase.
(a) (b)
(c) (d)
(e) (f)
Fig. 10. Sections of the resulting model overlaid on the original data. (a), (c), and (e) are axial, sagital, and coronal sections, respectively, corresponding to thediastolic phase. (b), (d), and (f) correspond to the same sections in systolic phase.
noise was removed by the filtering operation following the ini-tial segmentation. The resulting model was almost identical tothe reference model corresponding to the original (noise-free)
data. Increased noise level, up to standard deviation of 20,resulted in the corruption of the tissue boundary, as illustratedby an example shown in Fig. 11. Table IV shows that the mean
70 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
TABLE IRMS ERROR(IN PIXELS) OF FOURIER AND WAVELET MODEL APPLIED TO2-D MULTISLICE DATA, MEASURED AT DIASTOLE AND SYSTOLE
(a) (b)
(c) (d)
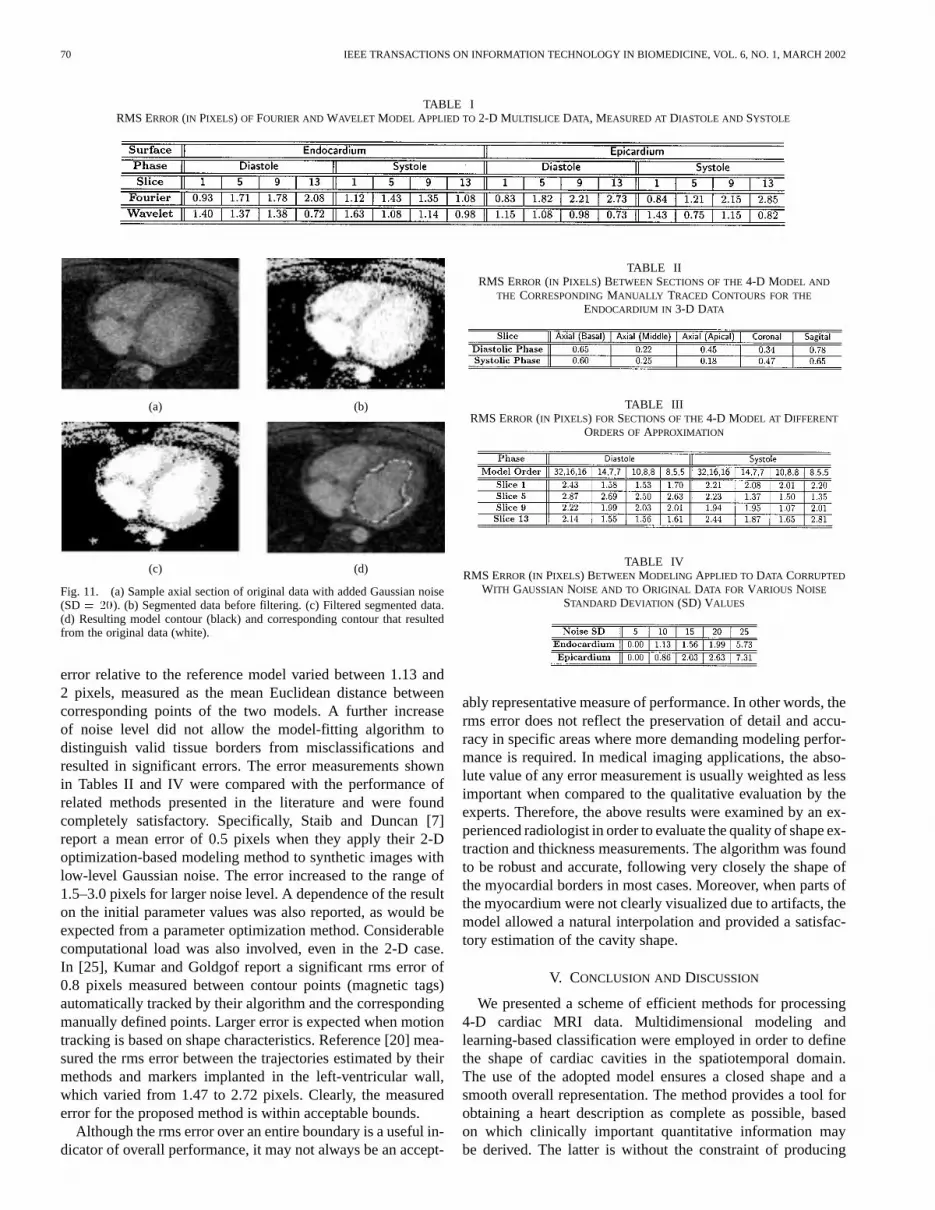
Fig. 11. (a) Sample axial section of original data with added Gaussian noise(SD= 20). (b) Segmented data before filtering. (c) Filtered segmented data.(d) Resulting model contour (black) and corresponding contour that resultedfrom the original data (white).
error relative to the reference model varied between 1.13 and2 pixels, measured as the mean Euclidean distance betweencorresponding points of the two models. A further increaseof noise level did not allow the model-fitting algorithm todistinguish valid tissue borders from misclassifications andresulted in significant errors. The error measurements shownin Tables II and IV were compared with the performance ofrelated methods presented in the literature and were foundcompletely satisfactory. Specifically, Staib and Duncan [7]report a mean error of 0.5 pixels when they apply their 2-Doptimization-based modeling method to synthetic images withlow-level Gaussian noise. The error increased to the range of1.5–3.0 pixels for larger noise level. A dependence of the resulton the initial parameter values was also reported, as would beexpected from a parameter optimization method. Considerablecomputational load was also involved, even in the 2-D case.In [25], Kumar and Goldgof report a significant rms error of0.8 pixels measured between contour points (magnetic tags)automatically tracked by their algorithm and the correspondingmanually defined points. Larger error is expected when motiontracking is based on shape characteristics. Reference [20] mea-sured the rms error between the trajectories estimated by theirmethods and markers implanted in the left-ventricular wall,which varied from 1.47 to 2.72 pixels. Clearly, the measurederror for the proposed method is within acceptable bounds.
Although the rms error over an entire boundary is a useful in-dicator of overall performance, it may not always be an accept-
TABLE IIRMS ERROR(IN PIXELS) BETWEEN SECTIONS OF THE4-D MODEL AND
THE CORRESPONDINGMANUALLY TRACED CONTOURS FOR THE
ENDOCARDIUM IN 3-D DATA
TABLE IIIRMS ERROR(IN PIXELS) FOR SECTIONS OF THE4-D MODEL AT DIFFERENT
ORDERS OFAPPROXIMATION
TABLE IVRMS ERROR(IN PIXELS) BETWEENMODELING APPLIED TODATA CORRUPTED
WITH GAUSSIAN NOISE AND TO ORIGINAL DATA FOR VARIOUS NOISE
STANDARD DEVIATION (SD) VALUES
ably representative measure of performance. In other words, therms error does not reflect the preservation of detail and accu-racy in specific areas where more demanding modeling perfor-mance is required. In medical imaging applications, the abso-lute value of any error measurement is usually weighted as lessimportant when compared to the qualitative evaluation by theexperts. Therefore, the above results were examined by an ex-perienced radiologist in order to evaluate the quality of shape ex-traction and thickness measurements. The algorithm was foundto be robust and accurate, following very closely the shape ofthe myocardial borders in most cases. Moreover, when parts ofthe myocardium were not clearly visualized due to artifacts, themodel allowed a natural interpolation and provided a satisfac-tory estimation of the cavity shape.
V. CONCLUSION AND DISCUSSION
We presented a scheme of efficient methods for processing4-D cardiac MRI data. Multidimensional modeling andlearning-based classification were employed in order to definethe shape of cardiac cavities in the spatiotemporal domain.The use of the adopted model ensures a closed shape and asmooth overall representation. The method provides a tool forobtaining a heart description as complete as possible, basedon which clinically important quantitative information maybe derived. The latter is without the constraint of producing

STALIDIS et al.: MODEL-BASED PROCESSING SCHEME FOR QUANTITATIVE 4-D CARDIAC MRI ANALYSIS 71
directly interpretable parameters or diagnostic informationon the expense of computational complexity. Cardiac motionis incorporated into the model in a way that accounts for3-D motion and deformation and is not restricted to the 2-Dcase. In this way, enhanced robustness properties are inherentwhen compared to motion analysis methods, which typicallyrely on measurements between two successive phases [19],[20]. Although no true functional data were used for accurateregistration between different phases of myocardial regions, theachieved performance is considered quite adequate for manyimportant applications. The shape of myocardial surfaces isconsistently represented in 3-D and at each temporal instant.In this way, measurements of various clinical factors (e.g.,myocardial thickness and strain) in important areas (e.g.,ischemic) can be performed and studied during the cardiaccycle. In case detailed point-to-point registration is needed foraccurate motion analysis measurements, our method may becombined with algorithms tracking either magnetic tags [24],[25] or geometrical markers [20]. This allows an economicaland global representation of the produced information into acompact model.
Unlike optimization techniques, dynamic models, or graphsearch methods, our model-based shape extraction method usesefficient boundary detection and direct fitting processes. There-fore, an important advantage for the system user is the compu-tational efficiency, which allows an improved interactive per-formance. This feature is particularly important when the ex-amination involves 4-D data. At the same time, robustness andinsensitivity to noise, without sacrifice in accuracy, is achievedby gradually reducing the model smoothness. A coarse initialmodel captures the approximate surface shape, independentlyof detail and noise. This information is then used to constraina new boundary extraction step of increased accuracy. Despitethe iterative nature of the method, the small number of requiredsteps and the efficiency of both boundary detection and modelfitting ensure a fast execution time. The latter is also enhancedby the selection of the generating-shrinking neural network al-gorithm for tissue classification, with the additional advantageof its adaptivity to different MRI data types due to its learning-based nature. The problem of undesirable intensity gradientswithin the data set, either within the same slice or of intersliceform, is effectively eliminated. Also, the performance can be im-proved by providing supplementary user guidance to the system.
Experimental results showed that the combination of modelconstraints, image gradient, and learning-based classificationdealt with the most important problems of boundary detectionencountered in practice, without uncertainty about convergence.Moreover, the final surface is represented by a 4-D continuousmodel of controlled smoothness. Abrupt intra- and interslicechanges are smoothed by the surface function and discontinu-ities are interpolated, thus providing a realistic representation ofthe myocardial surfaces. The latter was appreciated very favor-ably by clinical radiologists when applied to real cases. The con-clusion was that the presented cardiac data-processing methodsare a useful tool for cardiac diagnosis. When compared to otherexisting methods, they provide a more compact and readily re-producible representation of the left ventricle, which may be ei-ther displayed or used for quantitative calculations.
REFERENCES
[1] J. Park and D. Metaxas, “Deformable models with parameter functionsfor left ventricle 3-D Wall motion analysis and visualization,” inCom-puters in Cardiology. New York: IEEE Computer Society Press, 1995,pp. 241–244.
[2] J. K. Johnstone and K. R. Sloan, “Visualization of LV wall motion andthickness from MRI data,” inComputers in Cardiology. New York:IEEE Computer Society Press, 1995, pp. 249–252.
[3] J. Lessick, Y. Fisher, R. Beyar, S. Sideman, M. L. Marcus, and H. Azhari,“Regional three-dimensional geometry of the normal human left ven-tricle using cine computed tomography,”Ann. Biomed. Eng., vol. 24,pp. 583–594, 1996.
[4] H. Azhari, I. Gath, R. Beyar, M. L. Marcus, and S. Sideman, “Discrim-ination between healthy and diseased hearts by spectral decompositionof their left ventricular three-dimensional geometry,”IEEE Trans. Med.Imag., vol. 10, no. 2, pp. 207–215, 1991.
[5] A. A. Young, R. Orr, B. H. Smaill, and L. J. Dell’Italia, “Three-dimen-sional changes in left and right ventricular geometry in chronic mitralregurgitation,”Amer. J. Physiol., vol. 271, pp. H2689–H2700, 1996.
[6] N. E. Doherty, N. Fujita, G. R. Caputo, and C. B. Higgins, “Measure-ment of right ventricular mass in normal and dilated cardiomyopathicventricles using cine magnetic resonance imaging,”Amer. J. Cardiol.,vol. 69, pp. 1223–1228, 1992.
[7] L. H. Staib and J. S. Duncan, “Boundary finding with parametricallydeformable models,”IEEE Trans. Pattern Anal. Machine Intell., vol. 14,pp. 1061–1075, 1992.
[8] R. Tello, “Fourier descriptors for computer graphics,”IEEE Trans. Syst.,Man, Cybern., vol. 25, pp. 861–865, 1995.
[9] S. Lobregt and M. A. Viergever, “A discrete dynamic contour model,”IEEE Trans. Med. Imag., vol. 14, pp. 12–24, 1995.
[10] C. A. Davatzikos and J. L. Prince, “An active contour model for mappingthe cortex,”IEEE Trans. Med. Imag., vol. 14, pp. 65–80, 1995.
[11] I. N. Bankman, T. Nizialek, I. Simon, O. B. Gatewood, I. N. Weinberg,and W. R. Brody, “Segmentation algorithms for detecting microcalcifi-cations in mammograms,”IEEE Trans. Inform. Technol. Biomed., vol.1, no. 2, pp. 141–149, 1997.
[12] L. D. Cohen and I. Cohen, “Finite-element methods for active contourmodels and balloons for 2-D and 3-D images,”IEEE Trans. PatternAnal. Machine Intell., vol. 15, pp. 1131–1147, 1993.
[13] D. R. Thedens, D. J. Skorton, and S. R. Fleagle, “Methods of graphsearching for border detection in image sequences with applications tocardiac magnetic resonance imaging,”IEEE Trans. Med. Imag., vol. 14,pp. 42–55, 1995.
[14] D. Geiger, A. Gupta, A. Costa, and J. Vlontzos, “Dynamic programmingfor detecting, tracking and matching deformable contours,”IEEE Trans.Pattern Anal. Machine Intell., vol. 17, pp. 294–302, 1995.
[15] T. Gustavson and S. Molanderet al., “A model-based procedure for fullyautomated boundary detection and 3D reconstruction from 2D echocar-diograms,” inComputers in Cardiology. New York: IEEE ComputerSociety Press, 1994, pp. 209–212.
[16] K. P. Philipet al., “Automatic detection of myocardial contours in cine-computed tomographic images,”IEEE Trans. Med. Imag., vol. 13, pp.241–253, 1994.
[17] W. J. Niessen, B. M. Romeny, and M. A. Viergever, “Geodesic de-formable models for medical image analysis,”IEEE Trans. Med. Imag.,vol. 17, pp. 634–641, 1998.
[18] S. Thomas, J. Denney, and L. Jerry, “Reconstruction of 3-D left ventric-ular motion from planar tagged cardiac MR images: An estimation the-oretic approach,”IEEE Trans. Med. Imag., vol. 14, pp. 625–635, 1995.
[19] M. A. Gutierrez, L. Moura, C. P. Melo, and N. Alens, “3-D analysisof left ventricle dynamics,” inComputers in Cardiology. New York:IEEE Computer Society Press, 1994, pp. 201–204.
[20] J. C. McEachen and J. S. Duncan, “Shape-based tracking of left ventric-ular wall motion,”IEEE Trans. Med. Imag., vol. 16, no. 3, pp. 270–283,1997.
[21] J. S. Duncan and P. Shiet al., “Toward reliable, noninvasive measure-ment of myocardial function from 4-D images,”SPIE Med. Imag., vol.2168, pp. 149–161, 1994.
[22] P. Clarysse, D. Friboulet, and I. E. Magnin, “Tracking geometrical de-scriptors on 3-D deformable surfaces: Application to the left-ventric-ular surface of the heart,”IEEE Trans. Med. Imag., vol. 16, no. 4, pp.392–404, 1997.
[23] M. F. Santarelli, V. Positano, and L. Landini, “Real-time multimodalmedical image processing: A dynamic volume rendering application,”IEEE Trans. Inform. Technol. Biomed., vol. 1, no. 3, pp. 171–178, 1997.
[24] M. A. Guttman, J. L. Prince, and E. R. McVeigh, “Tag and contour de-tection in tagged MR images of the left ventricle,”IEEE Trans. Med.Imag., vol. 13, no. 1, pp. 74–88, 1994.

72 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 6, NO. 1, MARCH 2002
[25] S. Kumar and D. Goldgof, “Automatic tracking of SPAMM grid and theestimation of deformatiom parameters from cardiac MR images,”IEEETrans. Med. Imag., vol. 13, no. 1, pp. 122–132, 1994.
[26] A. A. Young, Z. A. Fayad, and L. Axel, “Right ventricular midwall sur-face motion and deformation using magnetic resonance tagging,”Amer.J. Physiol., vol. 271, pp. H2677–H2688, 1996.
[27] E. A. Ashton, K. J. Parker, M. J. Berg, and C. W. Chen, “A novel vol-umetric feature extraction technique with applications to MR images,”IEEE Trans. Med. Imag., vol. 16, no. 4, pp. 365–371, 1997.
[28] J. Weng, A. Singh, and M. Y. Chiu, “Learning-based ventricle detectionfrom cardiac MR and CT images,”IEEE Trans. Med. Imag., vol. 16, no.4, pp. 378–391, 1997.
[29] J. C. Bezdek, L. O. Hall, and L. P. Clarke, “Review of MR image seg-mentation techniques using pattern recognition,”Med. Phys., vol. 20,no. 4, 1993.
[30] Z. Liang, J. R. MacFall, and D. P. Harrington, “Parameter estimation andtissue segmentation from multispectral MR images,”IEEE Trans. Med.Imag., vol. 13, no. 3, pp. 441–449, 1994.
[31] M. R. Rezaee, C. Nyqvist, P. M. J. van der Zwet, E. Jansen, and J. H. C.Reiber, “Segmentation of MR images by a fuzzy C-mean algorithm,” inComputers in Cardiology. New York: IEEE Computer Society Press,1995, pp. 21–24.
[32] S. C. Amartur, D. Piraino, and Y. Takefuji, “Optimization neural net-works for the segmentation of magnetic resonance Images,”IEEE Trans.Med. Imag., vol. 11, no. 2, pp. 215–220, 1992.
[33] Y. Q. Chen, D. W. Thomas, and M. S. Nixon, “Generating-shrinkingalgorithm for learning arbitrary classification,”Neural Networks, vol. 7,no. 9, pp. 1477–1489, 1994.
[34] N. Maglaveras, T. Stamkopoulos, C. Pappas, and M. G. Strintzis, “ECGprocessing techniques based on neural networks and bidirectional asso-ciative memories,”J. Med. Eng. Technol., vol. 22, no. 3, pp. 106–111,1998.
[35] T. Edvardsen, B. Gerber, J. Garot, D. A. Bluemke, J. A. C. Lima, andO. A. Smiseth, “Doppler derived strain measures myocardial deforma-tion—Validation versus magnetic resonance imaging with tissue tag-ging,” Eur. Heart J. (Abstract Suppl.), vol. 21, p. 30, 2000.
George Stalidisreceived the diploma in electrical engineering from the Aris-totelian University of Thessaloniki (AUTH), Greece, in 1991, the M.Sc. degreein control and information technology from UMIST, U.K., in 1992, and thePh.D. degree in medical informatics from the Medical School, AUTH, in 1999.
He participated in numerous research projects in biomedical engineering andin particular in medical image processing and artificial neural networks. He wasExecutive of the technical support office for SMEs, providing consultancy aboutinvestment opportunities in Eastern Europe and EU funding programs. Since1998, he has been teaching postgraduate classes at the Medical School, AUTH,and the Technical Institute of Thessaloniki on computer programming and net-works. He is currently with the R&D Department, Pouliadis Associates Corpo-ration, as Technical Manager of European and national telematic programs. Hehas participated in ten projects in the area of health informatics. He has morethan 15 publications in the areas of medical image processing, neural networks,control, and telemedicine.
Nicos Maglaveras (S’80–M’87) received theBachelor’s degree (diploma) in electrical engineeringfrom the Aristotelian University of Thessaloniki,Macedonia, Greece, in 1982 and the M.Sc. and Ph.D.degrees from Northwestern University, Evanston,IL, in 1985 and 1988, respectively, in electrical engi-neering with emphasis in biomedical engineering.
He is currently an Assistant Professor in the Labof Medical Informatics, Aristotelian University,Thessaloniki, Greece. His current research interestsare in nonlinear biological systems simulation,
cardiac electrophysiology, medical expert systems, ECG analysis, physiologicalmapping techniques, parallel processing, medical imaging, medical informatics,telematics, and neural networks. He has published more than 100 papers inrefereed international journals and conference proceedings. He has developedgraduate and undergraduate courses in the areas of medical informatics,computer architecture and programming, biomedical signal processing, andbiological systems simulation. He has served as a Reviewer in CEC AIMtechnical reviews and in a number of international journals. He has participatedas Coordinator or Core Partner in national research projects and the HEALTHTELEMATICS, LEONARDO, TMR, IST, and ESPRIT programs of the CEC.
Dr. Maglaveras is a member of the Greek Technical Chamber, the New YorkAcademy of Sciences, CEN/TC251, and Eta Kappa Nu.
Serafim N. Efstratiadis (S’85–M’91) received the diploma from Aristotle Uni-versity, Thessaloniki, Greece, in 1986 and the M.S. and Ph.D. degrees fromNorthwestern University, Evanston, IL, in 1988 and 1991, respectively, all inelectrical engineering.
He has been a Teaching and Research Assistant in the Electrical and Com-puter Engineering Department, Northwestern University (1987–1991). He wasfirst Assistant and Head of the digital TV group at the Signal Processing Lab ofthe Swiss Federal Institute of Technology in Lausanne (1991–1992). He servedin the Greek military as a Technical Advisor (1993–1994). He has been a Re-search Associate at the Information Processing Lab (1993–1996) and the Labof Medical Informatics (1996–present) of Aristotle University. He was AdjunctProfessor at the American College of Thessaloniki (1995–1997). Since 1997, hehas been a Professor in the Department of Electronics, Technological Institute ofThessaloniki (1997–present). In 1995, he coorganized the International Work-shop on Stereoscopic and Three-Dimensional Imaging in Santorini, Greece, andcoedited the proceedings. He is a Technical Reviewer of several internationaljournals and conferences. Since 1985, he has participated in various govern-ment and privately funded projects and coauthored many journal and conferencearticles. His research interests include multidimensional signal processing, mo-tion estimation, monocular and stereo image/video coding, medical image pro-cessing and analysis, and multimedia applications.
Dr. Efstratiadis is a member of the Technical Chamber of Commerce ofGreece. He was a member of the Organizing Committee of the IEEE 2001International Conference on Image Processing, Thessaloniki, Greece.
Athanasios S. Dimitriadis received the M.D. andPh.D. degrees from the Aristotelian University ofThessaloniki, Macedonia, Greece, in 1968 and 1975,respectively. In 1972, he received his specialty inradiology.
Since 1972, he has been with the Faculty of theMedical School, the Department of Radiology,Aristotelian University of Thessaloniki, where heis currently an Associate Professor. Since 1994, hehas been Chairman of the Radiology Department.He has authored or coauthored more than 30 peer-
reviewed international journal papers. His research interests are in the areas ofneuroradiology and the head and neck.
Prof. Dimitriadis is a member of the American College of Radiology, theEuropean Society of Radiology, the European Society of Neurobiology, and theRadiological Society of North America.
Costas Pappas(M’98) received the diploma in medicine from the MedicalSchool of the Aristotelian University of Thessaloniki (AUTH), Thessaloniki,Macedonia, Greece, in 1971 and the Ph.D. degree and “Yfigesia” thesis fromthe same university in 1975 and 1980, respectively.
He has served in the Medical School of AUTH since 1964 as a Teaching As-sistant, Assistant Professor, Associate Professor, and since 2000, Professor ofmedical informatics. Since 1985, he has been responsible for the medical infor-matics courses. Since 1990, he has been Director of the Laboratory of MedicalInformatics, Medical School of AUTH. Since May 2001, he has been the localHealth Minister in the region of West Macedonia. His current research interestsinclude health information systems and biomedical signal and image processing.




























