Embed Size (px)
Citation preview
Methadone-related deaths and prescription drug use
By Dr Danielle Clode Dr Raymond Martyres Assoc. Prof. Michael Nicholls Ms Jannine Allan
A report for the Department of Human Services of Victoria

Acknowledgements
We would like to thank the staff at the Victorian Institute for Forensic Medicine, particularly Ms Marde Hoy and Prof. Olaf Drummer for facilitating this research. We would also like to acknowledge the assistance of Peter Thomson, Ken Patterson, Rory King, Simon Low, Leanne Shepherd, Neoni Banks and Jason King at Medicare.
Citation for this report
Clode D, Martyres RF, Nicholls MER and Allan J. (2008) Methadone-related deaths and prescription drug use, De-partment of Human Services, Victoria.
© Danielle Clode
This publication is copyright. Copyright for the entire con-tents is vested in the authors. Apart from any fair dealing for the purposes of private study, criticism or review as permit-ted under the Copyright Act, no part may be reproduced, stored in a retrieval system or transmitted in any form or by any means—electronic, mechanical or otherwise—without prior written permission.
— METHADONE-RELATED DEATHS —
— 3 —
Contents
Acknowledgements................................................................................................2 Citation for this report............................................................................................2
Contents .....................................................................................................................3 Project objective.........................................................................................................4 Researcher’s brief ......................................................................................................4 Summary of findings..................................................................................................5
Heroin addiction and overdose ......................................................................................6 Heroin overdoses .......................................................................................................7 Treatment of heroin addiction....................................................................................8
Pharmacotherapy in Victoria .................................................................................9 Safety of methadone ............................................................................................10
Methadone deaths ....................................................................................................11 Methadone treatment for heroin addiction...........................................................11 Methadone for pain relief.....................................................................................12 Polydrug use.........................................................................................................12 Summary ..............................................................................................................13
Prescription drug abuse............................................................................................14 Prescription drug use and overdose risk ..............................................................14 Risks of prescription drug abuse for heroin addicts.............................................15 Risks of prescription drug abuse for methadone users ........................................15
Study proposal .........................................................................................................16 Methods........................................................................................................................17
Application for data process ....................................................................................17 Victorian Institute of Forensic Medicine .............................................................17 Department of Justice ..........................................................................................17 Medicare ..............................................................................................................17
Confidentiality .........................................................................................................18 Case selection from National Coroners Information System ..................................18
Data extraction method ........................................................................................18 Case selection...................................................................................................18 Removal of duplicates......................................................................................19 Case-matching..................................................................................................19
Toxicology ...............................................................................................................20 Results..........................................................................................................................22
Category characteristics prior to case selection .......................................................22 Selected data from NCIS database...........................................................................23 Toxicology results....................................................................................................24 Breakdown of different drug types detected............................................................25 Medicare data...........................................................................................................27
Prescriptions.........................................................................................................27 Prescribers............................................................................................................28 Pharmacies ...........................................................................................................30 Benzodiazepines and methadone .........................................................................32
Chronic illnesses ......................................................................................................33 Patterns of prescription drug use over time .............................................................35
Changes within individuals prior to death ...........................................................35 The effect of the 2001 heroin drought on prescription drug patterns ..................35
References....................................................................................................................37

— METHADONE-RELATED DEATHS —
— 4 —
Project objective
The objective of this project is to identify trends in the contribution of prescription drugs to methadone- and heroin-related deaths from toxicology reports and the Phar-maceutical Benefits Schedule data. The project will compare rates at which people dying after taking methadone and heroin visited doctors, and obtained and filled pre-scriptions in the years and months prior to death. We will examine patterns over time, across practitioners and pharmacies, and between different patient groups (age, gen-der) compared with control groups of other drug deaths (i.e. excluding heroin and methadone) and non-drug deaths (carbon monoxide poisoning).
Researcher’s brief
‘The objective of the project is to investigate the prescription drug-seeking behaviour prior to death of heroin-related and methadone-related deaths at the State Coroner’s Office.
The project will involve two stages: 1. Identifying cases of heroin-related and methadone-related deaths at the State
Coroner’s Office and determination of the drugs identified by forensic toxicol-ogy examinations; and
2. Linking these records with those for the deceased held by Medicare and the Pharmaceutical Benefits Scheme.
Information about the relationship between prescription drug-seeking behaviour and heroin-related and methadone-related deaths will add to current knowledge about this relationship. Specifically, it will add information about drug-seeking behaviour prior to death by deceased individuals older than the young (15–24 years of age) cohort of heroin-related deaths studied by Martyres et al (2004).
Other opioid-related deaths, specifically methadone-related deaths, will also be inves-tigated. This has the potential to prevent methadone-related deaths and improve the safety of methadone treatment of opioid dependence, by developing counter meas-ures to reduce the diversion and misuse of sedating prescriptions drugs with the po-tential to contribute to central nervous system depression and cause combined drug toxicity and death.
It will also include information about the involvement of pharmacies in the supply chain to prescription drugs sought by drug-seeking individuals who experience her-oin-related and methadone-related deaths.’
Rural and Regional Health and Aged Care Services, Department of Human Services, Request for Quotation, 2005

— METHADONE-RELATED DEATHS —
— 5 —
Summary of findings
Between 2002 and 2007 there were 93 deaths in Victoria in which methadone was implicated as a cause of death. By comparison, 350 deaths were attributed to herion (excluding methadone cases), and 513 cases to drugs other than heroin and metha-done and alcohol. Methadone deaths were more common among males than females (2.2:1) with the deceased’s ages ranging from 16 to 57 years (mean = 34 years).
Medicare data were found for 82 of the 93 methadone deaths. Only five cases had been prescribed methadone from the Pharmaceutical Benefits Schedule (PBS), pre-sumably for pain relief. The remaining cases are assumed to either be on treatment for heroin addiction (which is administered under the Opiate Dependency Treatment Program, not the PBS) or to have obtained methadone illicitly. Eighty-two heroin, other drug and carbon monoxide deaths from the same time period were matched by age and gender to the methadone cases for comparison.
Most methadone deaths were polydrug cases with only three (4%) having only methadone found in their toxicology results. Most methadone deaths also had benzo-diazepines (69%) and/or antidepressants present (45%). By comparison, heroin users were most commonly found to have analgesics in addition to heroin (74%—usually codeine) and benzodiazepines (52%). As expected the Other Drugs group had a wide range of drugs present in toxicology, while the Carbon Monoxide group had few other drugs present, other than alcohol (50%).
Prescription drug use was substantially higher in the Methadone group (mean = 43.96 prescriptions) in the twelve months before death than in the Heroin group (22.88), Other Drugs group (26.33) or Carbon Monoxide group (9.15). Fifteen percent of the Methadone group obtained prescriptions from ten or more different prescribers, which was higher than that for the Heroin (9%), Other Drugs (6%) or Carbon Mon-oxide (1%) groups. The Methadone cases were also the most likely to use ten or more different pharmacies to dispense their prescriptions (20%) compared with the Heroin and Other Drugs groups (12% each). No case in the Carbon Monoxide group used more than ten different pharmacies in the twelve months before death.
There was an association between the presence of antidepressants and benzodiazepi-nes in toxicology results with the prescription of these drugs in the twelve months be-fore death for the Methadone, Heroin and Other Drugs groups.
People who had died from a methadone-related death were significantly more likely to have suffered from chronic disease, particularly cardiovascular disease, than any other group. Chronic illness was listed as contributing to death in 24 Methadone cases, 6 Heroin cases, 14 Other Drugs cases and 1 Carbon Monoxide case.
As was also found in our previous study (Martyres et al. 2004), prescription drug use by heroin users increased in the 24 months prior to death. However, this increase was substantially greater for the Other Drugs group, and even larger in the Methadone group. The increase for the Carbon Monoxide group was relatively slight. This find-ing strengthens the case for investigating proportional increases in prescription drug use as a means of identifying individuals at risk of death from overdose.

— METHADONE-RELATED DEATHS —
— 6 —
Heroin addiction and overdose Drug addiction and the associated deaths from drug overdoses are a ubiquitous and growing international problem. Whilst drug-related deaths may be caused by a wide range of drug types, opioid addiction in particular, including heroin and morphine, as well as benzodiazepines seems to present particular risks. A Western Australian study of drug deaths between 1985 and 1998, for example, found that the risk of death was higher for opiate users than for amphetamine users (Bartu et al. 2004).
Whilst the majority of drug deaths are related to heroin, these deaths cannot be con-sidered in isolation from other drugs. The vast majority of drug-related deaths in-volve a variety of different drug types—a drug cocktail—and are often known as polydrug deaths. In a London audit of drug-related deaths, Hickman et al. (2007) found that most cases involved more than one drug type. Two-thirds of cases (66%) included heroin, 56% included alcohol, 41% included benzodiazepines, 42% in-cluded cocaine and 32% included methadone. Dihydrocodeine and amphetamines were found in 12% and 11% of cases respectively. The presence of opioids in these cocktails seemed to increase the risk of overdose and death.
Opioid deaths in Australia increased from 70 in 1979 to 550 in 1995 (Hall and Darke, 1998). This represents an increase from 10.7 deaths/million people aged 15–44 years to 67 deaths/million people in the same age group, with the increase being more marked in males than females (see also Hall et al. 1999). Opioid deaths increased be-tween 1988 and 1996 across all Australia states. The most deaths occurred in the most populous states of New South Wales and Victoria (Lynskey and Hall, 1998); however, deaths relative to population rose even more in the other states. This in-crease in opioid deaths was greater than that attributed to suicide during the same pe-riod (Lynskey and Hall, 1998).
There are significant gender differences in the patterns of opioid deaths. Hall and Darke (1998) noted that the increasing rates of opioid deaths in Australia from 1970 disproportionately affected males. By 1995, males’ rate of death from opioid over-dose had risen to 104.6 deaths/million people aged 15–44, compared with a rate for females of 27.9. While males reportedly face a higher risk of death from any cause than females (1.79 times higher), they face a substantially increased risk from drug deaths in particular (2.69 times higher than females) (Bartu et al. 2004).
Male and female drug users also exhibit notable differences in drug-taking behaviour. Darke et al. (2000) found that males who had died from heroin-related causes were more likely to have also consumed alcohol, while females were more likely to have also consumed benzodiazepines. Garrick et al. (2000) found that while males pre-dominated in cases of heroin-related deaths (5:1), females were more common in methadone deaths.
Drug-related deaths occur across a wide population demographic, from accidental poisonings in young children to sometimes-intentional prescription drug overdoses in the elderly. However opioid addiction, particularly heroin addiction, tends to occur in a much narrower age range, rarely occurring in individuals younger than 15 years or older than 50 years. Darke et al. (2000) reported that the average age of heroin-related deaths in New South Wales in 1992–96 was 31 years. Similarly, Gerosta-molous et al. (2001) reported an average age of 30 years for males and 29 years for females among Victorian heroin-deaths in 1997–98.
— METHADONE-RELATED DEATHS —
— 7 —
Heroin overdoses
Heroin deaths are the single largest cause of illicit drug deaths in Australia, with 91% of drug deaths in New South Wales between 1995 and 1997 having morphine (the major metabolite of heroin) present at some level (Garrick et al. 2000), and 90% of drug deaths between 1997 and 1999 (Sheedy et al. 2003). Eighty percent of these cases had morphine present at a toxic level. A majority of these cases appeared to be new rather than chronic users, and there was a much higher proportion of males than females (5:1). Heroin is also the leading cause of drug deaths overseas, for example in Germany (Graß et al. 2003).
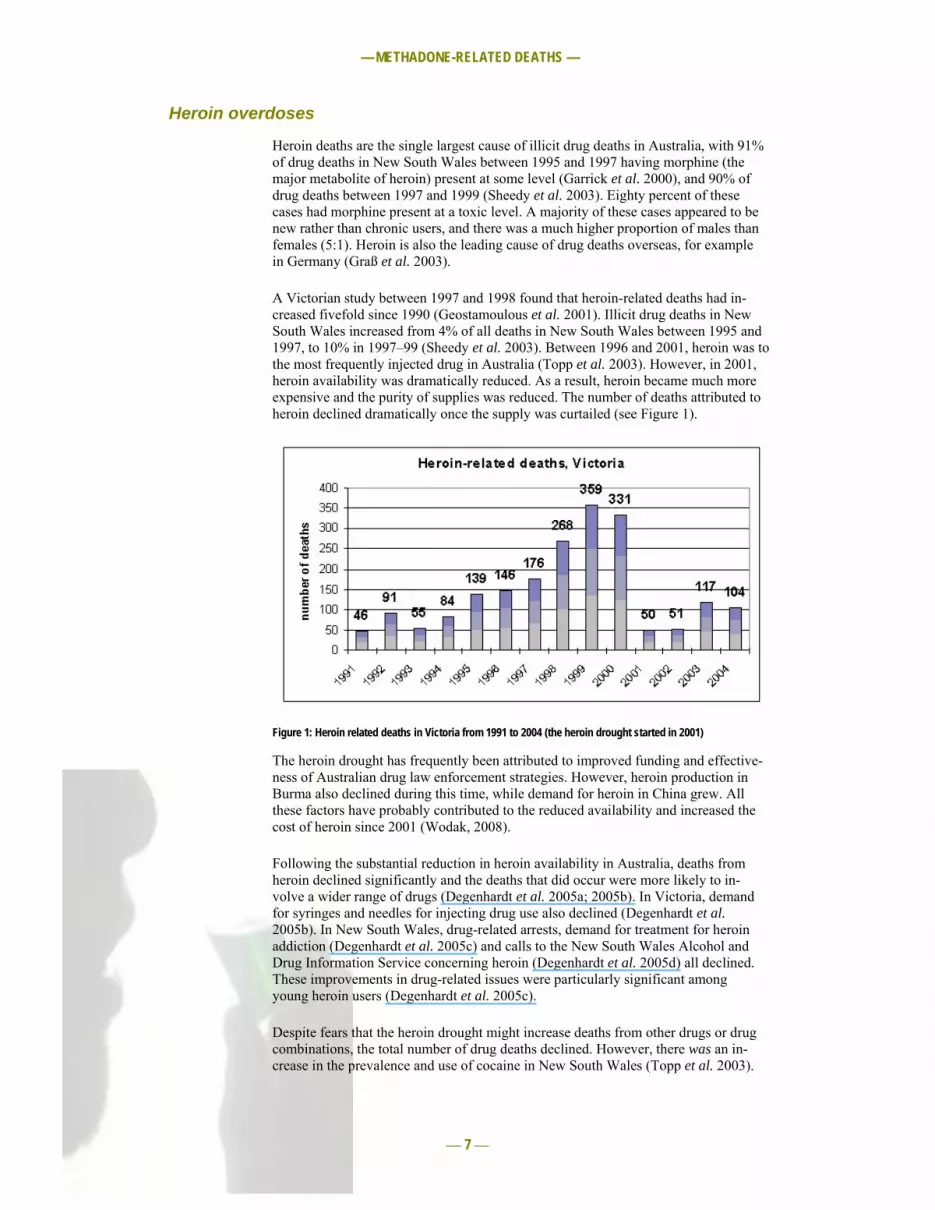
A Victorian study between 1997 and 1998 found that heroin-related deaths had in-creased fivefold since 1990 (Geostamoulous et al. 2001). Illicit drug deaths in New South Wales increased from 4% of all deaths in New South Wales between 1995 and 1997, to 10% in 1997–99 (Sheedy et al. 2003). Between 1996 and 2001, heroin was to the most frequently injected drug in Australia (Topp et al. 2003). However, in 2001, heroin availability was dramatically reduced. As a result, heroin became much more expensive and the purity of supplies was reduced. The number of deaths attributed to heroin declined dramatically once the supply was curtailed (see Figure 1).
Figure 1: Heroin related deaths in Victoria from 1991 to 2004 (the heroin drought started in 2001)
The heroin drought has frequently been attributed to improved funding and effective-ness of Australian drug law enforcement strategies. However, heroin production in Burma also declined during this time, while demand for heroin in China grew. All these factors have probably contributed to the reduced availability and increased the cost of heroin since 2001 (Wodak, 2008).
Following the substantial reduction in heroin availability in Australia, deaths from heroin declined significantly and the deaths that did occur were more likely to in-volve a wider range of drugs (Degenhardt et al. 2005a; 2005b). In Victoria, demand for syringes and needles for injecting drug use also declined (Degenhardt et al. 2005b). In New South Wales, drug-related arrests, demand for treatment for heroin addiction (Degenhardt et al. 2005c) and calls to the New South Wales Alcohol and Drug Information Service concerning heroin (Degenhardt et al. 2005d) all declined. These improvements in drug-related issues were particularly significant among young heroin users (Degenhardt et al. 2005c).
Despite fears that the heroin drought might increase deaths from other drugs or drug combinations, the total number of drug deaths declined. However, there was an in-crease in the prevalence and use of cocaine in New South Wales (Topp et al. 2003).

— METHADONE-RELATED DEATHS —
— 8 —
Treatment of heroin addiction
Heroin is a highly addictive drug, with withdrawal symptoms occurring even after a short period of use. Withdrawal may cause flu-like symptoms including irritation, sweating, and muscle cramps and spasms, with the worst effects occurring two to four days after withdrawal. Although most symptoms disappear after a few weeks, sometimes they can persist for months.
Bartu et al. (2004) found that risk of death was substantially reduced in opiate and amphetamine users who undertook treatment (compared with untreated individuals). However, those who dropped out of treatment increased their risk of death substan-tially.
There are many treatment options for heroin addition. The first step is often a process of detoxification, in which the addict is supported through the initial withdrawal pe-riod, usually in a residential setting. Medication to alleviate withdrawal symptoms may be used. Some patients are able to stay off heroin following detoxification, with-out further treatment (particularly if they have social support or a lifestyle change). Many patients, however, require additional treatment following detoxification.
Naltrexone is an opioid antagonist that blocks the effects of heroin and reduces opioid tolerance. Naltrexone can precipitate the onset of severe withdrawal symp-toms, and drug users are vulnerable to overdose if they use heroin after taking naltrexone.
Buprenorphine is a partial opioid antagonist with a minimal risk of overdose. Patients may experience withdrawal symptoms during use. Buprenorphine is more expensive than methadone, and achieves similar results. It is widely use in France and other countries.
Methadone is a synthetic opioid which is provided as an alternative drug of addiction to heroin. Legally provided methadone offers better control of the addiction, safer in-take of opioids and allows patients to undertake social or behavioural treatments for factors associated with their addiction, before detoxification. Methadone treatment generally continues for one to two years, and is often most effective in older patients. Methadone has been available since 1964.
Connock et al. (2007) completed a systematic review of the evidence for the relative efficacy of methadone and buprenorphine treatment for opioid dependency. They found that methadone patients were more likely to stay on their treatment program, both increasing the efficacy of the treatment and reducing the costs of delivering suc-cessful treatment. However, the review also found that methadone may carry higher risks, although this was not investigated systematically. Morgan et al. (2006) recently attributed the decline in heroin/morphine deaths in the UK since 2000 to the success of methadone treatment programs.

— METHADONE-RELATED DEATHS —
— 9 —
Pharmacotherapy in Victoria
Pharmacotherapeutic treatment for heroin addiction began in Victoria in 1985 with similar programs being operated in other states (see Gaughwin et al. 1993 for a re-view). By 2001, over 7000 people were enrolled in methadone treatment programs (see Figure 2). In 2002, the use of buprenorphine was introduced as an alternative treatment for heroin addiction.
Figure 2: Annual numbers of pharmacotherapy patients in Victoria from 1985 to 2002 by treatment type
The number of people enrolled in the methadone program initially declined with the introduction of buprenorphine (see Figure 3), but has since stabilised with around 40% of pharmacotherapy patients using buprenorphine (4000–5000) and around 60% using methadone (5000–6000).
Figure 3: Quarterly numbers of pharmacotherapy patients in Victoria from January 2000 to April 2005

— METHADONE-RELATED DEATHS —
— 10 —
Safety of methadone
Although heroin remains the major cause of opioid death internationally, both methadone and buprenorphine also carry risks of central nervous system depression, particularly when taken in association with benzodiazepines (Drummer 2005). While buprenorphine is relatively rarely listed in Victoria as contributing to the cause of death, deaths associated with methadone have been more common.
Methadone can cause death through respiratory depression, pulmonary oedema and other cardiac problems. It may also contribute to death through bronchopneumonia, renal failure and aspiration of vomitus (Corkery et al. 2004). Methadone deaths are much less common, however, than heroin deaths. For example, Garrick et al. (2000) found methadone in only 19 cases (13%) of illicit drug deaths in New South Wales between 1995 and 1997 (13 of which were at toxic levels) compared with the pres-ence of heroin (as its metabolite morphine) in 91% of cases.
Pirnay et al. (2004) reported 34 deaths associated with buprenorphine and 35 cases attributed to methadone between 1997 and 2002 in Paris, out of 1600 deaths in total. Gibson and Degenhardt (2007) identified 32 deaths associated with oral naltrexone treatment, one associated with buprenorphine treatment and 282 associated with methadone treatment in Australia between 2000 and 2003. Relative to the numbers treated, however, oral naltrexone actually represented a higher risk of death than methadone (2.8–7.4 times higher). More recently, Gibson et al. (2008) compared the survival rates of individuals randomly assigned to methadone and buprenorphine treatment programs. They found that mortality was significantly reduced in individu-als who undertook treatment for longer than seven days but that there was no differ-ence in mortality risk between the different treatments.
Teichtahl et al. (2005) reported significantly reduced respiratory responses in patients on methadone treatment compared with controls, with decreased hypercapnic ventila-tory response (HCVR) and increased hypoxic ventilatory response (HVR). In their study, sleep apnoea, level of carbon dioxide in the arterial blood (PaCO2), height and alveolar–arterial oxygen pressure gradient were all positively associated with de-creased HCVR in methadone users, and height and PaCO2 were positively associated with HVR. Wang et al. (2005) reported that methadone patients had a significantly higher level of sleep apnoea (30%) compared with controls (0%).
Ernst et al. (2002) noted a high level of pre-existing health conditions in methadone-related deaths, including kidney, lung, cardiac and pancreatic disease, blood-borne viral infections, chronic pain or injury, diabetes and obesity, and various mental and nervous system illnesses.
Methadone treatment has been associated with increased irregularities in heart rate (particularly an increased QT interval in the recovery period of a heart beat) (Ehret et al. 2006). An increased QT interval is associated with heart arrhythmias, such as tor-sades de pointes (Atkinson et al. 2007), and sudden death. Ehret et al. (2006) found that methadone patients were more likely to have prolonged QT intervals, and that liver function also contributed to long QT intervals (but see Justo, 2006). Liver func-tion is frequently compromised in people who abuse alcohol and in intravenous drug users, because of the high incidence of hepatitis. Peles et al. (2007) found no associa-tion between the size of methadone dose and QT interval, although they did report prolonged QT intervals in three of 138 methadone patients. Two of these patients were the only cases to have died in a two-year follow-up, although their deaths were not attributed to cardiac conditions.

— METHADONE-RELATED DEATHS —
— 11 —
Methadone deaths
Methadone deaths fall into three major categories defined by the source of the methadone. Methadone may be obtained legally for addiction treatment or for pain relief. It may also be obtained illegally, where it has been diverted from legitimate sources. There are also occasional cases of accidental poisoning with methadone, such as in children of a patient legally supplied with methadone.
A South Australian study of methadone-related deaths between 1984 and 1994 found that illegal use of methadone accounted for half of all deaths. There was a large in-crease in methadone-related deaths related to prescriptions for pain relief. By con-trast, the number of deaths of patients on opioid treatment programs fell during the study period (Wiliamson et al. 1997). A later review of all methadone-related deaths in South Australia between 1996 and 1999 found 35 cases, 10 of whom were partici-pants in a methadone treatment program (Green et al. 2000).
Similarly, a review of methadone-related deaths in Minnesota, USA found that only 35% of deaths were of individuals on methadone treatment programs. A further 15% were prescribed methadone for the treatment of chronic pain. Thirty-nine percent were identified as illicit drug users (Gagjewski and Apple, 2003). Shah et al. (2005) found that of the 143 methadone deaths in New Mexico, USA, only 68 obtained their methadone through a physician. Twenty-one percent of the total methadone deaths were on a methadone maintenance program, 19% received methadone for pain relief and a further 7% were prescribed methadone for unknown reasons (Shah et al. 2005). A German study found that only 35% of methadone deaths were involved in metha-done treatment programs (Heinemann et al. 2000).
Methadone treatment for heroin addiction
Deaths of individuals starting methadone treatment in Australia first came to light in 1992, when Drummer et al. (1992) reviewed ten cases of individuals who had died of methadone toxicity in Victoria, days after starting methadone treatment. High starting doses were implicated in these cases, particularly for patients with unknown toler-ance to opioids; however, six of the ten cases also had other drugs present, and all ten individuals had hepatitis. Five of the cases also had bronchopneumonia.
Caplehorn and Drummer (1999) reported that methadone deaths of individuals in methadone treatment programs in New South Wales in 1994 were more likely to oc-cur during the first two weeks of treatment, rather than later in the program. In fact, risk of death in the first two weeks of the program are higher than for untreated her-oin users; however, this risk reverses after prolonged treatment.
Zador and Sunjic’s study (2000) of deaths of individuals on methadone maintenance treatment in New South Wales from 1990 to 1995 reported that the most common cause of death was drug overdose (44%), half of which occurred during the first week of treatment. Nearly all of the drug overdose deaths were in patients with a pattern of polydrug use. In an examination of methadone-related deaths in New South Wales in 1996, Zador and Sunjic (2002) reported that only 49% of the individuals were in a methadone treatment program.
In a review of methadone-related deaths in Western Australia between 1993 and 1999, Ernst et al. (2002) found that 43% of deaths were of individuals undertaking methadone treatment, although this high percentage may have been associated with the introduction of treatment programs by new providers. Methadone-related deaths have not increased as the number of people entering methadone treatment programs has increased, suggesting that methods have improved and risks reduced. In a review of the literature on the risks of methadone treatment programs, Bell and Zador (2000) note that despite widespread concerns about the risks, heroin addicts are at less risk of death while on methadone than without treatment, and that the risks associated
— METHADONE-RELATED DEATHS —
— 12 —
with beginning methadone treatment can be mitigated by more careful control at the onset of the program.
Significant differences exist between different countries of the incidence of metha-done deaths in addiction treatment. It seems likely that this is due to differences in the way in which methadone is used, and the treatment systems in place. In the past, methadone-related deaths have been significantly higher in the UK than in Australia, with Hall et al. (2000) attributing this to the less-regulated delivery of methadone in the UK.
A recent review of methadone treatment programs in the UK concluded that the risk of deaths from methadone has declined since 1997, probably due to improvements in clinical training and regulation of treatment delivery (Morgan, 2006). In the UK, ir-regularities in the delivery of methadone for drug addiction were largely associated with private methadone providers rather than National Health Service (Strang and Sheridan, 2001; see also Strang et al. 1996). Private providers were more likely to prescribe twice the recommended daily dose, in an injectable rather than oral form, and in weekly or fortnightly pick-up batches rather than daily treatments. Strang et al. (2007) confirmed that the doubling of opiate substitution treatment (including metha-done) in the UK had been accompanied by significant improvements in the method of delivery.
Similarly, a study in Switzerland reports a substantial decrease in the number of drug overdoses and no change in the number of methadone-related deaths between 1994 and 1998, associated with increasing numbers of participants in methadone treatment programs (Perret et al. 2000). In New Mexico (USA), methadone deaths decreased between 1998 and 2002 (Shah et al. 2005). A recent twelve-year review in Sweden of participants in a methadone treatment program found no drug-related deaths at all up until 2000 (Fugelstad et al. 2007).
Methadone for pain relief
Methadone used for pain relief may be far less regulated than centralised methadone maintenance treatment programs for addiction, thus increasing the risk of overdose. Sims et al. (2007) used multiple public health data sources to survey methadone-related adverse events in an American study. They found that a substantial increase in methadone prescription rates (727%—primarily for pain treatment rather than addic-tion) was accompanied by an even greater increase in population-adjusted metha-done-related deaths (1770%). Wysowski (2007) reports a 55% increase in the number of drug-related deaths in the US from 1999 to 2003, with the largest increase being due to methadone (275%), followed by antidepressants (primarily serotonin specific reuptake inhibitors, 130%) and psychostimulants (117%). Terpening and Johnson (2007) highlight the risks of using methadone for pain relief, suggesting that while methadone may have reduced deaths through the treatment of opioid dependence, its increasing use for pain relief may have increased deaths.
Polydrug use
Methadone alone can cause death; however, in most overdose cases, other drugs are also present and may substantially increase the risk of death. In a review of metha-done deaths in New South Wales in 1994, Caplehorn and Drummer (2002) found that benzodiazepines were more likely to contribute to the deaths of people receiving methadone for legitimate sources (methadone treatment programs and for pain relief) than those obtaining methadone illegally. A study of UK drug users found that indi-viduals who had been prescribed both methadone and diazepam were much more likely to have overdosed than those prescribed either drug in isolation or had not been prescribed drugs (Man et al. 2004). Ernst et al. (2002) identified benzodiazepines as the most significant risk factor associated with methadone-related deaths, with ben-zodiazepines being present in 74% of the 84 methadone-related deaths in their study.

— METHADONE-RELATED DEATHS —
— 13 —
A study of drug-related deaths in Hamburg, Germany between 1990 and 1999 found that more than half of the cases were polydrug deaths in which methadone was pre-sent (Heinemann et al. 2000). Wolf et al. (2004) noted that polydrug use was impli-cated in 54% of methadone-related deaths in a study from Palm Beach, USA. It was noted in their study that polydrug use may contribute to deaths in cases where the amount of methadone present appears to be sub-lethal. A significant increase in the number of methadone-related deaths in Kentucky, USA between 2000 and 2004 was also associated with high levels of polydrug use, particularly antidepressants (39.8% of cases) and benzodiazepines (32.4%) (Shields et al. 2007; see also Sims et al. 2007).
Individuals prescribed methadone were more likely to use several drugs at the time of their last overdose than individuals with no prescriptions or only diazepam prescrip-tions (Man et al. 2004).
Summary
Both deaths of individuals from legally prescribed methadone for opioid dependancy, and also deaths from illegally obtained or diverted sources of methadone raise ques-tions about clinical standards and guidelines. There now appears to be evidence that deaths from legally prescribed methadone are associated with poorly regulated, de-centralised systems with lack of systematic training or guidelines for methadone de-livery. Improved training and guidelines in the use of methadone (for either drug ad-diction or pain relief) appear to substantially reduce the risk of death although the concomitant use of other drugs remains a particular threat. Such increased training and regulation (such as the use of daily supervised doses, and non-injectable forms) also reduce the diversion of methadone onto the black market, in addition to the po-tential to reduce methadone-related deaths (Strang et al. 2005; Zador, 2007).
Despite the controversy surrounding its use, methadone appears to be a relatively safe, well-established treatment option for opioid dependence, which demonstrably saves lives (Wodak 2002). Diverted methadone might pose greater risks (particularly in relation to polydrug use), but the greatest risks appear to arise in the use of metha-done for pain relief.

— METHADONE-RELATED DEATHS —
— 14 —
Prescription drug abuse
Prescription drug abuse and trafficking in medicinal drugs is a significant clinical and public health problem (Dobbin, 1998; USDHHS, 1995). In Australia, drug abuse typically involves polydrug abuse (Ross, 1993; Ross et al. 1996). General practitio-ners write over 15 million prescriptions each year for drugs known to be abused, par-ticularly narcotic analgesics and benzodiazepines (ABCI, 1997).
In addition to being associated with drug overdose and death, prescription drug abuse has been associated with mood disorders, violence and other crimes. Prescription drug abuse contributes to the spread of HIV and hepatitis C and causes injuries due to impaired motor and cognitive function. Trafficking prescribed drugs may also sup-port illicit drug use (see review by Dobbin, 1998). The estimated health care and so-cietal costs associated with prescription drug abuse far outweigh the costs associated with illicit drug use (ABCI, 1997). A Health Insurance Commission (HIC) report, ta-bled in 1995/96, estimated that doctor- and pharmacy-shopping alone, incurred a di-rect cost of $31 million each year through the Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS). Polydrug use is a major clinical and public health problem.
Prescription drug use and overdose risk
Prescription drug abuse, particularly of opioids, is a common feature of heroin abuse. Rosenblum et al. (2007) surveyed previous prescription opioid abuse in patients on an American methadone program and found that 69% had abused prescription opioids prior to treatment. The most commonly reported drugs were oxycodone (79%), hydrocodone (67%), methadone (40%), morphine (29%), heroin (13%), hy-dromorphine (16%), fentanyl (9%) and buprenorphine (1%).
Prescribed benzodiazepines, other opioids (i.e. other than heroin), tricyclic antide-pressants and tranquilisers have all been associated with increased risk of overdose in young heroin users in Victoria (Burns et al. 2004). In a review of heroin-related deaths in New South Wales for 1992–96, Darke et al. (2000) found that 76% in-volved a combination of other drugs, most commonly alcohol (46%), benzodiazepi-nes (27%), antidepressants (7%) and cocaine (7%). Sheedy et al. (2003) attributed an increase in heroin deaths from 1995–97 to 1997–99 to concomitant use of alcohol, benzodiazepines and antidepressants. Similarly, in their Victorian study of heroin deaths from 1997 to 1998, Gerostamalous et al. (2001) found that benzodiazepines were present in 45% of cases and alcohol in 36%.
A German study of methadone deaths found that only 4.5% of cases had only metha-done present. Sixty-one percent also had benzodiazepines present, 40% alcohol, 39% morphine, 35% cannaboids, 28% cocaine, 3% antidepressants and 2% amphetamines (Musshoff et al. 2003).
Benzodiazepines are the most commonly found prescription drug in polydrug deaths (e.g. Darke et al. 2000). In a study of current heroin users, Darke et al. (2003) found that 30% of participants had been prescribed benzodiazepines in the last month. Those who had been prescribed benzodiazepines were more likely to have attended a general practitioner or psychiatrist, and also more likely to have required ambulance attendance.

— METHADONE-RELATED DEATHS —
— 15 —
Risks of prescription drug abuse for heroin addicts
Our previous study on heroin-related deaths and prescription drug use in young Vic-torian heroin users found polydrug use in 75% of toxicology reports and prescription drugs present in 65% of victims (Martyres et al. 2004). Victims accessed medical services six times more frequently than the general population of 15- to 24-year-olds, and more than half of all prescribed drugs were those prone to misuse, such as ben-zodiazepines and opioid analgesics. A dramatic pattern of increasing drug-seeking behaviour in the years prior to death was identified, with doctor visitation rates, num-ber of different doctors seen and rates of prescriptions, particularly for drugs prone to misuse, peaking in the year before death. Increasing ‘doctor-shopping’ in the years before heroin-related death may reflect the increasing misuse of prescription drugs, but also an increasing need for help. The association between heroin use, fatal over-dose and prescription drugs suggests that doctor-shopping should be seen, not merely as an economic cost to subsidised health care systems, but as an opportunity for in-tervention and, potentially, reduction in mortality.
Risks of prescription drug abuse for methadone users
Prescription drug abuse seriously jeopardises the safety of methadone programs. Ap-proximately 15 to 30 methadone-related deaths occur in Victoria each year. Deaths from methadone alone are rare. In Victoria, 68% of methadone-related deaths are due to combined drug toxicity involving prescription drugs, commonly benzodiazepines (Dobbin, 1995).
The proposed study provides the opportunity to extend the generalisability of our ear-lier findings from a young population (younger than 25 years old) to the entire age range of heroin users, and provide an opportunity to test if increasing doctor-shopping prior to death is also observed in methadone users. By comparing the pat-terns of these groups with other deaths (drug-related suicides) and normative data, we will be able to draw much clearer conclusions about the contribution of prescription drugs to drug-related deaths, and what should be appropriate responses from general practitioners to drug-seekers.

— METHADONE-RELATED DEATHS —
— 16 —
Study proposal
We propose to examine patterns of Pharmaceutical Benefits Scheme (PBS)–listed prescription drug use and doctor- and pharmacy-shopping behaviour in Victorians who have recently died of drug-related causes. In particular, we wish to investigate the extent to which prescription drugs are associated with, and possibly contribute to, deaths in three groups—methadone users, heroin users and drug-related suicides. The patterns of prescription drug use, and doctor and pharmacy visitation behaviour of these people prior to their death will be compared with a matched control group of non–drug-related deaths—carbon monoxide deaths. In addition, we would like to compare patterns of prescription drug use during times of high heroin availability (2000) to patterns during the heroin drought (2001–02). By comparing prescription drug use during periods of differing heroin availability, we hope to offer an insight into the dynamics of heroin-related deaths in a fluctuating drug environment.
The purpose of these investigations is to clarify how PBS-listed prescription drugs are associated with or contribute to drug-related deaths, and the extent to which in-formation about drug-seeking behaviour might assist general practitioners to better refer and/or treat patients at high risk of drug-related death.
Drug-related suicides have been selected as a control group in order to distinguish be-tween the ‘plea for help’ hypothesis and the ‘polydrug use’ hypothesis in relation to illicit drug use. Our earlier finding that doctor-shopping increases prior to overdose death can be interpreted in two ways—as either a plea for help or attempt to obtain medical assistance for their declining mental and physical health, or as ‘doctor-shopping’ or an attempt to obtain illicit drugs for abuse. There is a reasonable expec-tation that people who suicide might increase their rate of doctor visits before death (as a ‘plea for help’), but even if they do, their use of prescription drugs of abuse should not increase. The use of drug-related suicides (rather than the larger groups of suicide by hangings and knife wounds) further restricts our comparison to deaths which might involve both prescription drugs and increased doctor visitation. Any dif-ferences between this group (suicides) and the accidental drug death group thus pro-vides stronger evidence of drug-seeking versus help-seeking behaviour. The com-parison with this group potentially gives us a clearer insight into why doctor-shopping occurs, rather than just observing that it does.
— METHADONE-RELATED DEATHS —
— 17 —
Methods
Application for data process
Victorian Institute of Forensic Medicine
Discussions were held with staff at the Victorian Institute of Forensic Medicine on 31 March 2006 to refine the research proposal. In principle support for research was provided on 16 May 2006 pending formal approval. An application for access to the National Coroners Information System (NCIS) was lodged on 31 May 2006. We were notified in September 2006 that to receive access to NCIS, Department of Jus-tice ethics was required. A meeting with Prof. Olaf Drummer, Victorian Institute of Forensic Medicine on 25 September 2006 formalised collaborative research arrange-ments and refined data protocols. Access to the National Coroners Information Sys-tem was obtained for the period January 2007 to January 2008. Additional toxicology reports for all these cases were provided by NCIS staff. NICS staff provided Medi-care with identifying information for all cases on 9 May 2007.
Department of Justice
An application for Department of Justice ethics approval was lodged on 10 October 2006. A request for additional information was received on 31 October and sent on 1 November 2006. Department of Justice ethics was granted and approval for access to the National Coroners Information System gained on 18 January 2007 followed by database training and data selection.
Medicare
A request for data from Medicare was lodged on 27 March 2006. A request for addi-tional information was received on 1 May 2006, which was sent on the same day. A response was expected by 10 May, but it was not until 21 September that we were in-formed that Medicare could not release data without patient consent (and therefore could not release deceased data).
Our request was put to the External Request Evaluation Committee for reconsidera-tion on 26 October 2006 and was been referred to the Minister’s delegate. Dr Mar-tyres and Dr Clode met with the Minister’s delegate in Canberra on 3 January 2007 to further discuss and refine the proposal. At this meeting, the delegate gave in-principle approval for the research to progress in the public interest and that data would be re-leased subject to certain methodological constraints. In particular, we were unable to access Medicare Benefits Schedule or Pharmaceutical Benefits Schedule data prior to 2001 because of changes to the data recording system. We amended our methodology to accommodate this limitation and our data request form was approved on 8 March 2007.
A request for data extraction was made on 9 May 2007. Case-matching required sev-eral iterations as alternative cases were selected to replace non-matched cases. A number of cases also required manual matching. Delays were experienced during June and July because of issues with the coding program used to match the data. By September 2007 the request to extract the data was in progress.
The final data sample was sent in November 2007. When reviewed, the data were found to be incomplete and incorrect. Medicare requested its return, along with a signed Statuary Declaration before they would send the corrected version. During this review, we also identified that archived data needed to be included to complete the data sample.The corrected data sample plus the archived data were extracted in January, reviewed by Medicare in February and received on 10 March 2008.
— METHADONE-RELATED DEATHS —
— 18 —
Confidentiality
Maintaining the confidentiality of cases has been a major component of this research project, particularly in obtaining the release of Medicare details. Access to the Na-tional Coroners Information System (NCIS) was limited to de-identified data, requir-ing toxicology reports to be extracted by NCIS staff separately and provided in a de-identified form. Identifying information was sent directly from NCIS staff to Medi-care staff to allow case-matching to occur. Cases were coded by Coroner’s Court codes and matching data from the Health Insurance Commission was provided using these codes.
Protocols to minimise re-identification of data or cases by other individuals have been followed, including using only grouped data (by year) and not reporting on in-dividual cases. Identifiable traits such as postcode of death have been excluded from the data analysis while other traits such as individual date of death, which are neces-sary for analysis but might potentially lead to identification, will not be reported for individuals.
Case selection from National Coroners Information System
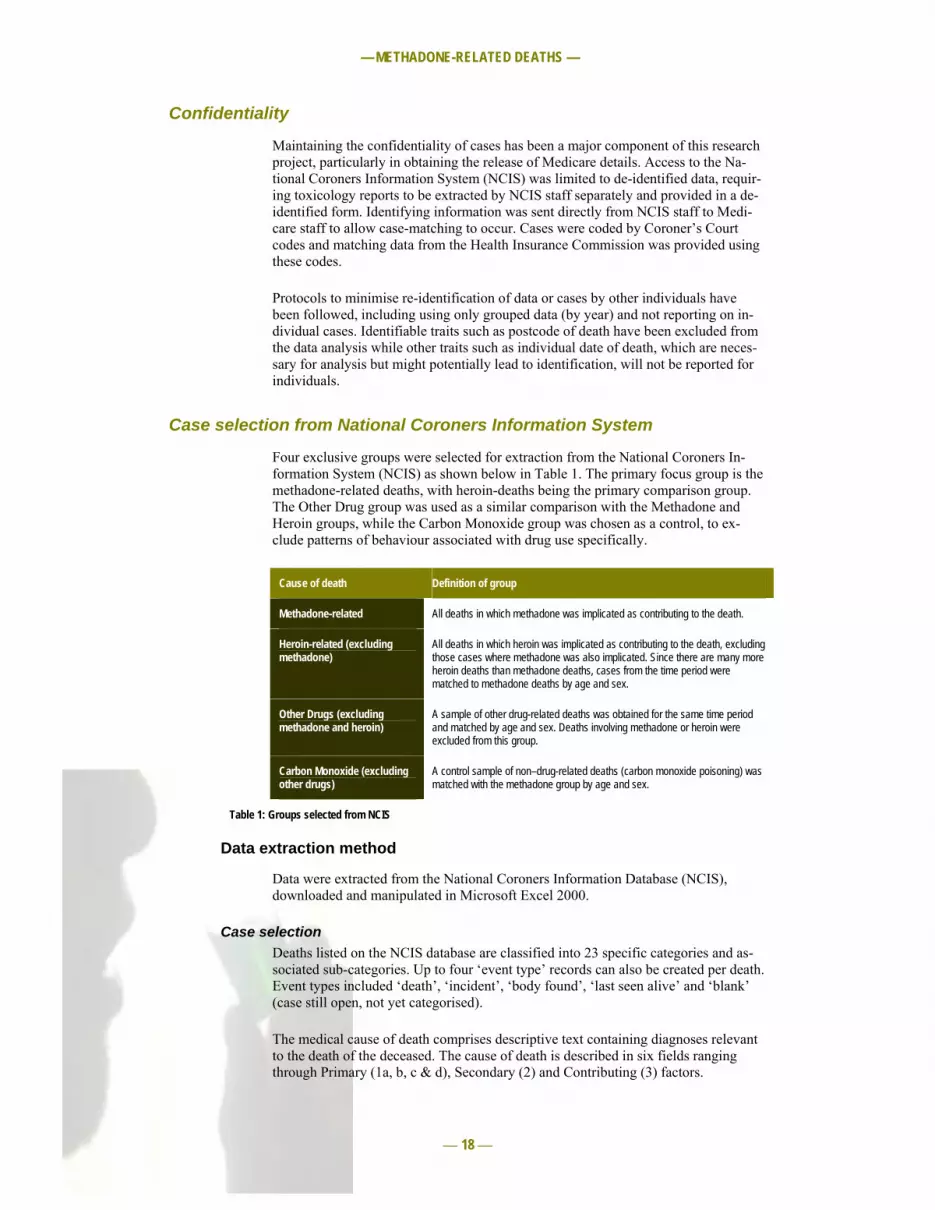
Four exclusive groups were selected for extraction from the National Coroners In-formation System (NCIS) as shown below in Table 1. The primary focus group is the methadone-related deaths, with heroin-deaths being the primary comparison group. The Other Drug group was used as a similar comparison with the Methadone and Heroin groups, while the Carbon Monoxide group was chosen as a control, to ex-clude patterns of behaviour associated with drug use specifically.
Cause of death Definition of group
Methadone-related All deaths in which methadone was implicated as contributing to the death.
Heroin-related (excluding methadone)
All deaths in which heroin was implicated as contributing to the death, excluding those cases where methadone was also implicated. Since there are many more heroin deaths than methadone deaths, cases from the time period were matched to methadone deaths by age and sex.
Other Drugs (excluding methadone and heroin)
A sample of other drug-related deaths was obtained for the same time period and matched by age and sex. Deaths involving methadone or heroin were excluded from this group.
Carbon Monoxide (excluding other drugs)
A control sample of non–drug-related deaths (carbon monoxide poisoning) was matched with the methadone group by age and sex.
Table 1: Groups selected from NCIS
Data extraction method
Data were extracted from the National Coroners Information Database (NCIS), downloaded and manipulated in Microsoft Excel 2000.
Case selection Deaths listed on the NCIS database are classified into 23 specific categories and as-sociated sub-categories. Up to four ‘event type’ records can also be created per death. Event types included ‘death’, ‘incident’, ‘body found’, ‘last seen alive’ and ‘blank’ (case still open, not yet categorised).
The medical cause of death comprises descriptive text containing diagnoses relevant to the death of the deceased. The cause of death is described in six fields ranging through Primary (1a, b, c & d), Secondary (2) and Contributing (3) factors.

— METHADONE-RELATED DEATHS —
— 19 —
We used two key selection criteria for data extraction: Date range 01/01/2002 – 31/12/2007 Medical cause of death keyword
The keyword searched across all categories for all event types and across all the de-scriptive text relevant to the cause of death. The results of the search retrieved all cases (open and closed) containing the specified keyword in any of the medical cause of death text descriptions. The resulting data sets contained multiple events for all closed cases. For some cases, there were multiple entries across categories (i.e. the case had been recorded twice under two different categories). For example, the same person may be found with heroin as the primary cause of death in one entry, and on another entry with vomiting as the primary cause, and heroin as a secondary cause.
Removal of duplicates In order to remove duplicates, the columns containing post code, event code and rank data were removed as these fields were sometimes different across the Events types e.g. postcode for ‘Death’ may be different from postcode for ‘Last seen alive’. In Mi-crosoft Excel we then used: 1. Advance Filtered on unique records, 2. Subtotaled on change of NCIS number, and 3. Physically deleted all remaining duplicated records. These were the records that
had been entered under more than one category.
The records were deleted if the cause of death was attributed to a foreign body (e.g. car, building, tree, fire or plastic bag). In some cases the choice was between the cause of death being methadone/heroin and the cause of death being alcohol or can-nabis. In these cases the alcohol or cannabis records were deleted.
The Heroin and Carbon Monoxide groups were then checked for duplicates (using the VLOOKUP function of Excel) within the Methadone group. Where duplicates were found, they were deleted from the Heroin or Carbon Monoxide group.
Case-matching Once the data samples were unique, each data record was tagged in each extract with a code for the drug (H = Heroin, M = Methadone, CO = Carbon Monoxide and S = Other Drug) and combined. The data were then sorted by age and then by sex. The data set was then manually scrolled through, and for every Methadone record a corre-sponding CO, H and S record in the same age/sex group was manually flagged.
Where a corresponding Heroin, Carbon Monoxide or Other Drug record was not found in the same sex/age group, the nearest age was selected. Where there was a choice between the nearest age being older or younger, the younger was chosen.
Target groups NCIS groups MBS/PBS matches
Methadone-related deaths 100 93 83
Heroin-related deaths (excluding methadone) 100 93 93
Other Drug deaths (excluding methadone and heroin)
100 93 93
Carbon Monoxide poisoning (excluding other drugs)
100 93 92
Total sample size 400 372 361
Table 2: Planned and achieved samples for each group

— METHADONE-RELATED DEATHS —
— 20 —
Toxicology
Toxicology results for each case were extracted by NCIS staff and provided in a de-identified form. For data from 2002–06, results were provided with drug types classi-fied by ‘drug-group’ (see Table 3). Some adjustment of the NCIS drug categories was required to address the specific interests of this research project (e.g. to separate Methadone from the ‘opioid’ group and to group drug types not of interest into a sin-gle Other Drugs group). The recoding is shown in Table 3. Data prior to 2002 were provided in a raw form, and were recoded manually to match the drug categories and format for the later years (see Table 3).
Drug description NCIS drug class
Recoded drug class
Notes
Alcohol(ethanol) Alcohol alcoho
Amphetamines Amphet amphet
Anaesthetics Anaest analge grouped under analgesic
Analgesics Analge "
Anti-depressants Antide antide
Anti-psychotics or major tranquillisers Antips antips
Barbiturates Barbit barbit
Benzodiazepines Benzod benzod
Cannabis Cannab cannab
Carbon monoxide Carbon carbon
Carbon monoxide +/- hydrogen cyanide Chydro " grouped under carbon
Heroin Heroin heroin morphine and morphine deriva-tives inc. in this group
Opioid narcotics Opioid opioid morphine and morphine deriva-tives recoded as heroin
methad methadone, propoxyphene and norpropoxyhene recoded as methadone
Antibiotics Antibi othsub
Anti-convulsants Antico "
Anti-diabetics Antidi "
Anti-histamines Antihi "
Anti-inflammatories Antiin "
Asthma Asthma "
Cardiovascular drugs Cardio "
Diuretics Diuret "
Endogenous substances Endoge "
Muscle relaxants and anti-spastics Muscle "
Other poisons Othpoi "
Other substances classed as drugs Othsub "
Stimulants and anorectics Stimul stimul includes cocaine
Volatile substances Volati volati
Table 3: NCIS and recoded categories for drugs and other substances reported in toxicology results

— METHADONE-RELATED DEATHS —
— 21 —
The opioids in toxicology results are difficult to interpret as heroin rapidly breaks down into morphine and its metabolites, as does codeine. Codeine is a common con-taminant in illicitly manufactured heroin. Morphine may also be taken directly (usu-ally for pain relief, where it is the dominant analgesic—Drummer, 2005).
It is not possible to distinguish these different sources of morphine in the toxicology results. For the purposes of this study, morphine and morphine derivatives have all been subsumed under the category of heroin, as this is the dominant source of mor-phine generally, and particularly in this sample, however it must be noted that this may artificially inflate heroin occurrences slightly (for a discussion of the methodo-logical constraints of post-mortem toxicology for drugs of abuse, see Drummer, 2004).

— METHADONE-RELATED DEATHS —
— 22 —
Results
Category characteristics prior to case selection
A total of 93 methadone-related deaths were identified from the National Coroners Information System (NCIS) between 2002 and 2007. There were more than three times the number of heroin-related deaths (350) during the same period (see Table 4). Other drug toxicity deaths (excluding methadone, heroin and alcohol) accounted for over five hundred deaths, and carbon monoxide deaths were also high (446).
The sex ratio of deaths differed significantly between the groups with twice as many males occurring in the Methadone group as females (2.2:1). Males were four-to-five times more frequent in the Heroin and Carbon Monoxide death groups than females, but were roughly equivalent in the Other Drugs toxicity group.
The mean age and age range for the Methadone deaths and Heroin deaths were very similar (averaging around 32–34 years). Other Drugs deaths included a significantly older demographic ranging to a maximum of 88 (compared with 56 and 57 for the Heroin and Methadone groups). Carbon Monoxide deaths also included this older age range, but also extended into a much younger age group with the youngest recorded death being three years of age.
Matching cases to the age and gender of the methadone group removes variation ap-plicable to these age and gender differences, resulting in a stronger experimental de-sign and basis for comparison.
2002–2007 Total Males Females Sex ratio (M:F)
Age range (years)
Mean age (years)
All Methadone-related deaths (inclusive)
93 64 29 2.2:1 16–57 33.9
Heroin deaths (excluding methadone)
350 287 63 4.6:1 15–56 32.1
Other Drug deaths (exclud-ing methadone, heroin and alcohol)
515 267 246 1.1:1 19–88 44.0
Carbon Monoxide deaths 446 370 76 4.9:1 3–87 38.5
Table 4: Demographic patterns of all cases prior to matching
The distribution of methadone cases over time has remained relatively stable (see Table 5 and Figure 4). As expected from longer time scale data, heroin deaths fluctu-ated over time, depending on market circumstances of drug availability and toxicity. The decline in deaths for all groups in 2006 and 2007 relates to the number of open cases at NCIS and cases for which data had not been completed or entered.

— METHADONE-RELATED DEATHS —
— 23 —
Methadone Heroin Other Drugs Carbon Monox-ide
2002 16 62 122 122
2003 22 95 130 101
2004 17 95 122 112
2005 20 58 104 77
2006 18 37 37 34
2007 (partial) 0 3 0 0
Total 93 350 515 446
Table 5: Trends in drug-related (and control) deaths over time (2002–07) for all cases
0
20
40
60
80
100
120
140
2002 2003 2004 2005Year
Numb
er of
death
s
Methadone HeroinOther Drugs Carbon Monoxide
Figure 4: Trends in drug-related and control deaths over time for years with complete data (2002–05) for all cases
Selected data from NCIS database
Cases from the Heroin, Carbon Monoxide and Other Drugs categories were matched first by age and sex (and then randomly selected) with the methadone cases, resulting in a completed data set. These cases were then matched with Pharmaceutical Benefits Scheme (PBS) and Medicare Benefits Schedule (MBS) data from Medicare. Nine of the 93 Methadone cases had no matching Medicare data sets, reducing the sample size to 82. Where matching data were not available for cases selected in the Heroin, Other Drugs and Carbon Monoxide groups, alternative cases were selected using the above criteria (by gender then age). The final data set characteristics are described in Table 6.
2002–2007 Total Males Females Age range (years)
Mean age (years)
Methadone 82 56 26 16–54 34.02
Heroin 82 56 26 17–53 33.65
Other Drugs 82 56 26 19–57 34.50
Carbon Monoxide 82 56 26 19–54 34.17
Total subjects 328 224 104 16–57 34.09
Table 6: Final matched data set characteristics

— METHADONE-RELATED DEATHS —
— 24 —
Toxicology results
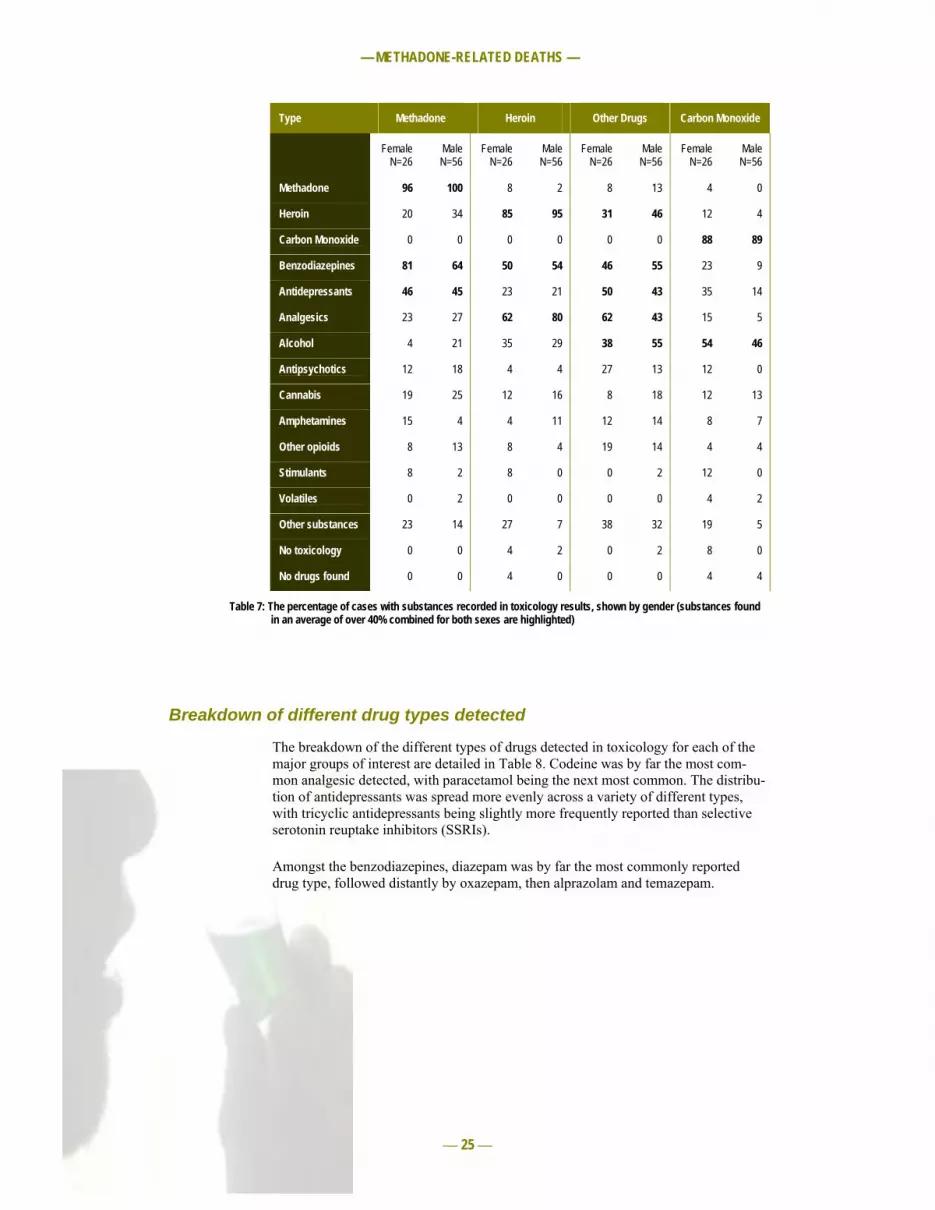
A wide range of substances was reported in the toxicology results of all groups (see Table 7). In only four cases were no substances found in toxicology results, one case in the Heroin group and three in the Carbon Monoxide group. In an additional five cases, no toxicology report was available for the case (two Heroin, one Other Drugs and two Carbon Monoxide). Drugs or substances other than that designated as the cause of death were present in the vast majority of cases.
Methadone was the only drug present in three of cases (4%) in the Methadone group, and heroin was the only drug present in three cases (4%) in the Heroin group. By comparison, carbon monoxide was the only substance present in 25 cases (30%) in the Carbon Monoxide group.
The pattern of drugs present differed between the groups examined. As expected, each group was highly likely to have the drug or substance designated as their cause of death identified in toxicology results. Whilst toxicological results may influence the designation of the cause of death, other factors (such as the circumstances sur-rounding the death, witness accounts etc.) also influence this designation. Thus a case may be designated as a heroin death without heroin being detected in the toxicologi-cal results. Also, heroin (and other drugs) may break down rapidly and be undetected despite having been present at the time of death. In each of the Methadone, Heroin and Carbon Monoxide groups, there were some toxicological results not showing the drug or substance designated as the cause of death.
There are clear patterns present in the types of drugs taken in the different groups. About half of all Carbon Monoxide deaths had also consumed alcohol. A third of women in this group had taken antidepressants, although the level of other drugs taken in this group was relatively low.
Around three-quarters of the Methadone group had also consumed benzodiazepines, a pattern that was stronger in women than in men. This pattern may reflect a particu-lar preference for benzodiazepine consumption by methadone users; however, it is also likely to reflect the particularly high risk of death by combining the use of these two central nervous system depressants. Almost half of the Methadone group also consumed antidepressants.
The Heroin group was more likely to have analgesics (primarily codeine) showing in their toxicology than any other drug type, with the preference stronger in men than women. Codeine is a common contaminant in illicitly produced heroin, which may explain the result. Benzodiazepines were consumed by about half of the heroin group.
As expected, the Other Drugs group revealed a broad spread of drug types, the most common being analgesics (mostly codeine), antidepressants, benzodiazepines and al-cohol, with around a third having taken heroin.
— METHADONE-RELATED DEATHS —
— 25 —
Type Methadone Heroin Other Drugs Carbon Monoxide
Female N=26
Male N=56
Female N=26
Male N=56
Female N=26
Male N=56
Female N=26
Male N=56
Methadone 96 100 8 2 8 13 4 0
Heroin 20 34 85 95 31 46 12 4
Carbon Monoxide 0 0 0 0 0 0 88 89
Benzodiazepines 81 64 50 54 46 55 23 9
Antidepressants 46 45 23 21 50 43 35 14
Analgesics 23 27 62 80 62 43 15 5
Alcohol 4 21 35 29 38 55 54 46
Antipsychotics 12 18 4 4 27 13 12 0
Cannabis 19 25 12 16 8 18 12 13
Amphetamines 15 4 4 11 12 14 8 7
Other opioids 8 13 8 4 19 14 4 4
Stimulants 8 2 8 0 0 2 12 0
Volatiles 0 2 0 0 0 0 4 2
Other substances 23 14 27 7 38 32 19 5
No toxicology 0 0 4 2 0 2 8 0
No drugs found 0 0 4 0 0 0 4 4
Table 7: The percentage of cases with substances recorded in toxicology results, shown by gender (substances found in an average of over 40% combined for both sexes are highlighted)
Breakdown of different drug types detected
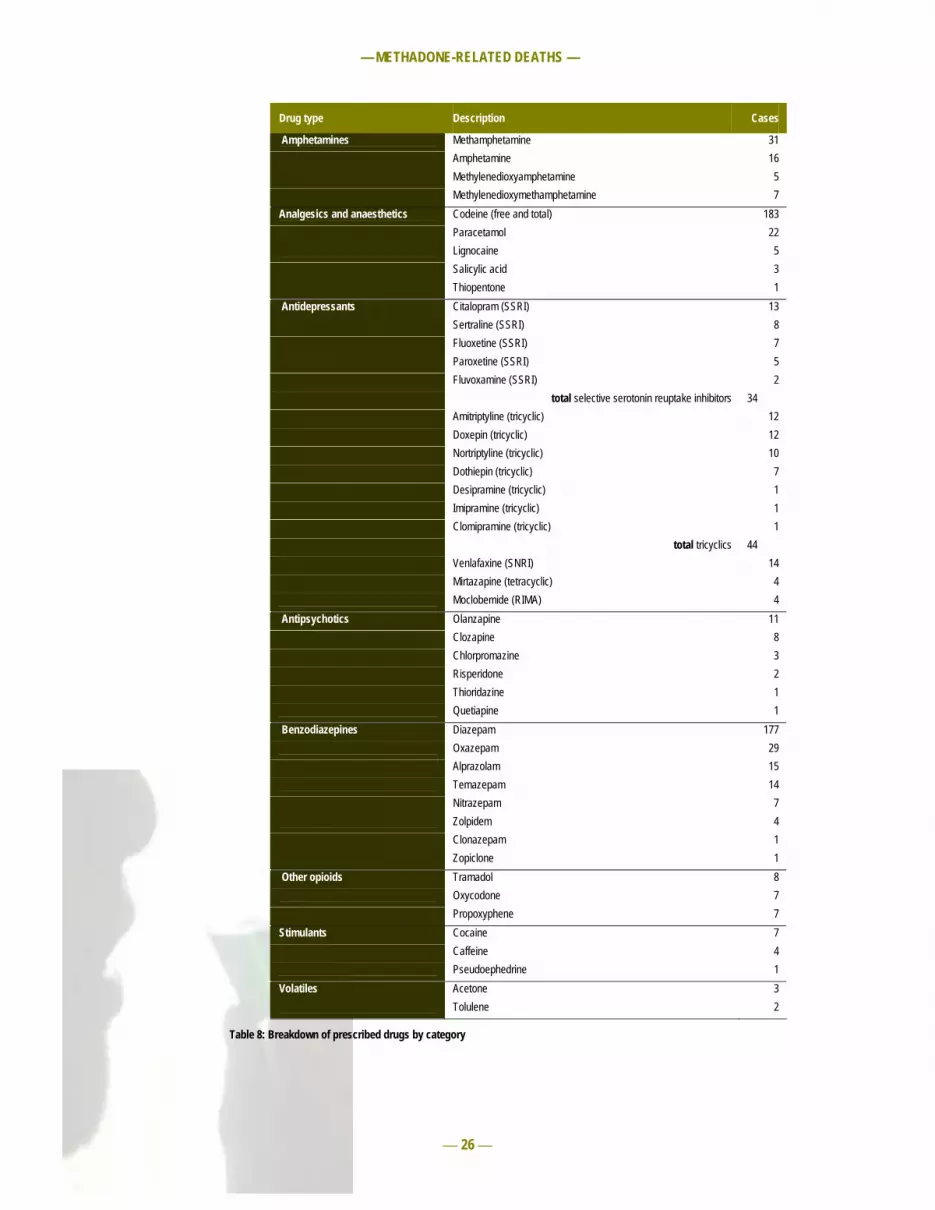
The breakdown of the different types of drugs detected in toxicology for each of the major groups of interest are detailed in Table 8. Codeine was by far the most com-mon analgesic detected, with paracetamol being the next most common. The distribu-tion of antidepressants was spread more evenly across a variety of different types, with tricyclic antidepressants being slightly more frequently reported than selective serotonin reuptake inhibitors (SSRIs).
Amongst the benzodiazepines, diazepam was by far the most commonly reported drug type, followed distantly by oxazepam, then alprazolam and temazepam.
— METHADONE-RELATED DEATHS —
— 26 —
Drug type Description Cases
Amphetamines Methamphetamine 31 Amphetamine 16 Methylenedioxyamphetamine 5 Methylenedioxymethamphetamine 7 Analgesics and anaesthetics Codeine (free and total) 183 Paracetamol 22 Lignocaine 5 Salicylic acid 3 Thiopentone 1 Antidepressants Citalopram (SSRI) 13 Sertraline (SSRI) 8 Fluoxetine (SSRI) 7 Paroxetine (SSRI) 5 Fluvoxamine (SSRI) 2 total selective serotonin reuptake inhibitors 34 Amitriptyline (tricyclic) 12 Doxepin (tricyclic) 12 Nortriptyline (tricyclic) 10 Dothiepin (tricyclic) 7 Desipramine (tricyclic) 1 Imipramine (tricyclic) 1 Clomipramine (tricyclic) 1 total tricyclics 44 Venlafaxine (SNRI) 14 Mirtazapine (tetracyclic) 4 Moclobemide (RIMA) 4 Antipsychotics Olanzapine 11 Clozapine 8 Chlorpromazine 3 Risperidone 2 Thioridazine 1 Quetiapine 1 Benzodiazepines Diazepam 177 Oxazepam 29 Alprazolam 15 Temazepam 14 Nitrazepam 7 Zolpidem 4 Clonazepam 1 Zopiclone 1 Other opioids Tramadol 8 Oxycodone 7 Propoxyphene 7 Stimulants Cocaine 7 Caffeine 4 Pseudoephedrine 1 Volatiles Acetone 3 Tolulene 2
Table 8: Breakdown of prescribed drugs by category

— METHADONE-RELATED DEATHS —
— 27 —
Medicare data
Prescriptions
The Pharmaceutical Benefits Scheme (PBS) does not include all medicines, nor does it cover medicines dispensed outside community pharmacies (e.g. the Highly Specialised Drugs Program, Botulinum Toxin Program, Human Growth Hormone Program, IVF/GIFT program, Opiate Dependence Treatment Program and Special Authority Pro-gram). As a result, non-PBS medical services may be provided for prisoners, hospital inmates and others. Methadone provided for opiate addiction is prescribed under the Opiate Dependence Treatment Program and is therefore not recorded in PBS data. Methadone prescribed for pain relief, however, is included under the PBS. Due to the privacy constraints required by Medicare, we were unable to identify which cases were on a methadone treatment program.
Of the four groups under comparison, Methadone deaths had the highest level of pre-scription drug use, receiving an average of 43.96 prescriptions in the 12 months before death (see Table 9). Heroin and Other Drug deaths obtained similar numbers of prescrip-tions – 22.88 and 26.33 respectively. This rate was still substantially higher than the rate obtained by Carbon Monoxide deaths of 9.15 prescriptions. These rates compare with population averages for 16- to 55-year-olds of approximately 6.7 prescriptions per year in the US (Medical Expenditure Panel Survey, 2002). This rate is considerably higher than the self-reported baseline prescription rate of 2.3 per year reported by Darke et al. (2006). Martyres et al. (2004) reported that cases of young heroin deaths received an av-erage of 17 prescriptions in the year before their death, but fell to just 3.6 per year in the fourth year before their death. In the report of this research (MDGP, 2002), an additional survey of young current heroin users found that they were receiving an average of 13.2 prescriptions per year.
Category Methadone Heroin Other Drugs Carbon Monoxide Total
Benzodiazepine 1536 951 649 170 3306
Antidepressant 424 233 238 222 1117
Opioid 433 126 423 31 1013
Analgesic 220 120 165 43 548
Antipsychotic 227 89 120 99 535
Antibiotic 171 65 100 29 365
Asthma 92 113 70 9 284
Anti-inflammatory 78 44 64 25 211
Cardiovascular 56 17 73 21 167
Endogenous 67 17 7 8 99
Methadone 36 0 0 0 36
Diuretic 20 0 8 2 30
Antidiuretic 10 7 12 0 29
Anticoagulant 10 0 6 8 24
Stimulant 1 0 0 0 1
Other substance 224 94 224 82 624
Total 3605 1876 2159 750 8390
Average/person 43.96 22.88 26.33 9.15 23.31
Table 9: Number of prescriptions obtained for different drug categories in the twelve months before death

— METHADONE-RELATED DEATHS —
— 28 —
Benzodiazepines were the most commonly prescribed (as distinct from non-prescription) drugs for all groups except the Carbon Monoxide group, for whom antide-pressants were more common.
Methadone was prescribed on the PBS (presumably for pain relief) in just five cases (with a total of 36 prescriptions). This suggests that the vast majority of methadone deaths in this sample have received their methadone either illicitly or through a metha-done treatment program.
Prescribers
In the twelve months before death, the 328 subjects obtained a total of 8390 prescrip-tions from 1040 different prescribers Because individuals with more prescriptions (or who see more prescribers) disproportionately influence the calculation of total group av-erages, we have calculated overall averages from the average per person, thus effec-tively weighting the scores per person. This provides more meaningful description data; however, these ‘weighted’ averages do not calculate back to the total number of pre-scriptions.
The weighted average number of prescriptions obtained by each person per prescriber was around six. Subjects saw an average of around four different prescribers in the twelve months before death, with methadone subjects obtaining prescriptions from the highest number of different prescribers and carbon monoxide subjects from the fewest different prescribers (see Table 10).
Summary charac-teristics
Total PBS prescriptions issued
Average number of dif-ferent prescribers
(weighted)
Average number of pre-scriptions/prescriber
(weighted)
Methadone 3605 5.4 7.7
Heroin 1876 4.3 5.2
Other Drugs 2159 3.8 7.7
Carbon Monoxide 750 1.7 3.5
Total 8390 3.8 6.03
Table 10: Prescription and prescriber patterns in the twelve months before death for each group
The average number of different prescribers seen belies the vast variation in individual behaviours. For example, many subjects obtained no prescriptions or only one or two prescriptions during the last twelve months of life, from a single practitioner. Many oth-ers however obtained a large number of prescriptions from a very large number of gen-eral practitioners (see Table 11). In general, the Carbon Monoxide group were most likely to obtain most of their prescriptions from the fewest prescribers, with 84% seeing fewer than three prescribers. This compares with 57% of Other Drugs cases, 40% of Heroin cases and 39% of Methadone cases.

— METHADONE-RELATED DEATHS —
— 29 —
Number of pre-scribers
Methadone Heroin Other Drugs Carbon Monoxide
0 8 12 18 27 1 12 13 13 23 2 12 8 16 19 3 3 4 4 2 4 9 11 4 2 5 6 14 8 4 6 7 4 7 1 7 3 4 6 3 8 7 3 0 0 9 3 3 1 0 10 1 2 0 0 11 1 0 1 0 12 0 2 1 0 13 2 1 0 0 14 0 1 0 0 15 3 0 1 1 16 2 0 0 0 17 1 0 0 0 18 0 0 0 0 19 0 0 0 0 20 0 0 0 0 21 0 0 1 0 22 1 0 0 0 25 1 0 0 0 41 0 1 0 0 43 0 0 1 0 Total 82 82 82 82
Table 11: Distribution of the number of prescribers seen by individuals within each group
The Carbon Monoxide group were the most likely to have received no prescriptions in the last twelve months (33%) while the Methadone group were the least likely to have received no prescriptions in the last twelve months (10%). All cases were successfully matched with individual Medicare records. An absence of records means that the indi-viduals did not access Pharmaceutical Benefits Scheme (PBS) services during this time. This may be because they did not require any medical services, or they may have ob-tained medical services elsewhere (such as in prison or overseas).
The distribution of the number of prescribers seen was somewhat bimodal, probably re-flecting differences between those attending sole practitioner practices and those attend-ing multiple practitioner clinics. The Methadone and Heroin groups seemed to exhibit a slightly stronger second peak at around four and five prescribers than the Carbon Mon-oxide and Other Drugs groups, perhaps reflecting differences in the types of practices utilised.
Carbon Monoxide cases were unlikely to obtain prescriptions from ten or more different prescribers with only one case (1%) doing so. This compares with 6% of the Other Drugs group and 9% of the Heroin group. The Methadone group was most likely to see ten or more different prescribers, with 15% of cases having done so.

— METHADONE-RELATED DEATHS —
— 30 —
Pharmacies
In the twelve months before death, the 328 subjects obtained prescriptions from 572 dif-ferent pharmacies (an average of 14.67 prescriptions per pharmacy). The number of pre-scriptions supplied by medical practitioners in the twelve months before death tallies very closely with the number of prescriptions filled by pharmacies for the same period for all groups.
The Methadone group obtained prescriptions from substantially more pharmacies (322) than the Heroin group (274) and the Other Drugs group (228), both of which were higher again than the Carbon Monoxide group (115). These totals exceed the total num-ber of different pharmacies used because the same pharmacies are being visited within different groups. On average, Methadone subjects visited 5.6 different pharmacies, ob-taining an average of 8.8 prescriptions from each. By comparison, the Heroin group vis-ited slightly fewer pharmacies and obtained almost half as many prescriptions from each pharmacy on average. Individuals in the Other Drugs category visited even fewer differ-ent pharmacies but obtained many more prescriptions from each one (an average of 9.5). As expected, the Carbon Monoxide group visited very few different pharmacies and ob-tained a lower number of average prescriptions (see Table 12).
Total PBS prescrip-tions filled
Average number of pharmacies attended
(weighted)
Average number of prescrip-
tions/pharmacy (weighted)
Methadone 3605 5.6 8.8 Heroin 1878 4.7 4.6 Other Drugs 2159 3.8 9.5 Carbon Monoxide 751 1.7 3.8 Total 8393
Table 12: Pharmacy patterns in the twelve months before death for each group (Note: these figures relate to prescriptions filled, which differ slightly from the number issued, see Table 10)
Patterns similar to those seen with the prescribers were observed in the number of phar-macies visited by the different groups. The cases within the Carbon Monoxide group visited the fewest number of pharmacies with over 85% seeing three or fewer different pharmacies in the twelve months before death (see Table 13). This compares with 66% of the Other Drugs group, 45% of the Heroin group and 49% of the Methadone group.

— METHADONE-RELATED DEATHS —
— 31 —
Number of phar-macies
Methadone Heroin Other Drugs Carbon Monoxide
0 8 11 18 27 1 13 15 16 21 2 11 5 12 15 3 8 6 8 7 4 7 7 5 5 5 6 8 3 2 6 3 11 3 2 7 3 6 2 2 8 2 3 5 0 9 4 0 0 1 10 4 1 2 0 11 0 0 1 0 12 4 1 0 0 13 0 2 3 0 14 0 1 2 0 15 1 1 0 0 16 1 2 1 0 17 3 1 0 0 18 2 0 0 0 20 1 0 0 0 21 0 1 0 0 28 1 0 0 0 33 0 0 1 0 Total 82 82 82 82
Table 13: Distribution of the number of pharmacies seen by individuals within each group
As expected, there was a pattern of association found between the prescription of drugs within the last twelve months and the presence of those drugs in the toxicology reports for all prescription drug types (see Table 14). This analysis is a conservative one, based only on which individuals were prescribed, or not prescribed, certain drugs in the twelve months before death. The analysis does not take into account the quantity of drugs pre-scribed, nor the immediacy of the prescription before death. Due to low sample sizes (particularly for the Carbon Monoxide group), patterns of association (χ2) statistics are presented in Table 12 for descriptive purposes only. The pattern of association is strong-est for benzodiazepines and antidepressants, although, surprisingly, the association for benzodiazepines is weaker for the Methadone group than for Heroin or Other Drugs groups.
Methadone Heroin Other Drugs Carbon Monoxide χ2 cases
prescribed χ 2 cases
prescribed χ 2 cases
prescribed χ 2 cases
prescribed Antipsychotics 21.358 25 3.998 17 5.858 6 1.570 21 Other opioids 0.607 27 0.264 13 8.586 23 8.995 4 Benzodiazepines 3.909 61 23.52 57 12.35 44 0.771 14 Analgesics 1.386 34 0.594 25 3.615 21 7.961 9 Antidepressants 18.189 43 9.807 33 14.233 41 22.391 34
Table 14: The association between drugs prescribed in the last twelve months and presence of those drugs in toxicology results measured by Chi square statistics (significance calculated only for cases with more than five expected cell values [shaded yellow], degrees of freedom (df) = 1, p<0.05 in bold)

— METHADONE-RELATED DEATHS —
— 32 —
Benzodiazepines and methadone
Benzodiazepines emerge as a recurring theme in association with Methadone cases. They are more commonly reported in the toxicology of Methadone cases (69%) than the other three groups (52% for Heroin, 52% for Other Drugs and 13% of Carbon Monoxide deaths) (see Table 7). Almost half of the benzodizepines prescribed in the 12 months be-fore death were prescribed to the Methadone group (compared with 22% for Heroin, 19% for Other Drugs and just 5% for Carbon Monoxide). And yet there is a noticeably weaker association between the prescription of benzodiazepines and the presence of benzodiazepines in the toxicology results for the methadone group than might be ex-pected.
The Methadone group is not a homogenous sample, comprising individuals on heroin treatment, a small number of individuals being prescribed methadone (presumably for pain relief) and others obtaining methadone illicitly.
There are three possible explanation for the higher frequency of benzodiazepine in the toxicology of the Methadone group than in the Heroin and Other Drugs groups:
1) The different drug groups have different preferences for polydrug use (e.g. the Heroin group prefer to use analgesics like codeine because it contributes to the effect of the heroin). Whilst this explains the higher level of analgesics in Heroin toxicology, there seems to be no a priori reason why the Methadone group would have a stronger preference for benzodiazepines over the Heroin or Other Drugs groups.
2) The different drug groups have different levels of access to different drugs. This theory is supported by the higher level of prescription drugs in the Metha-done and Other Drugs groups compared with the Heroin group. Individuals in the Methadone group have an extraordinarily high level of connection with the medical system, obtaining large amounts of prescription drugs, including ben-zodiazepines. And yet, even those who have not been prescribed benzodiazepi-nes are likely to be found, on death, with benzodiazepines in their system. There appears to be no a priori reason why methadone users should be more likely to obtain benzodiazepines from illicit sources than heroin users.
3) The individual or combined effects of benzodiazepines and/or methadone contribute to the deaths of individuals in the Methadone group but not in the Heroin or Other Drugs groups. Our findings cannot rule out the possibility that individuals dying from methadone-related deaths may be more vulnerable to cardiorespiratory depression made worse by benzodiazepines.

— METHADONE-RELATED DEATHS —
— 33 —
Chronic illnesses
Medical causes of death listed on the toxicology results often include chronic illnesses in addition to the cause of death for which the case was selected (drug toxicity and car-bon monoxide poisoning). The additional conditions listed as contributing to the cause of death are summarised in Table 15.
Type Description of condition Methadone Heroin Other Drugs
Carbon Monoxide
Heart disease Coronary artery atherosclerosis/disease 6 3 2 1 Cardiomegaly/cardiac enlargement 4 2 Ischaemic heart disease 3 3 Anomalous coronary artery 1 Myocarditis 1 1 Dilated cardiomyopathy 1 Bacterial endocarditis 1 Total incidence of heart disease 16 5 7 1 Lung disease Asthma 3 2 Broncho-/pneumonia/tracheobronchitis 4 1 2 Sleep apnoea 1 1 Chronic obstructive airways disease 1 Total incidence of lung disease 8 1 5 1 Liver disease Hepatitis 1 1 1 Hepatic microvesicular steatosis 1 Haemochromatosis with cirrhosis 1 Hepatomegaly and steatosis 1 Total incidence of liver disease 3 1 2 0 Mental illness Major depression 1 Anorexia nervosa 1 Epilepsy 1 Schizophrenia 1 Total incidence of mental illness 2 0 1 1 Other diseases Multiple sclerosis 1 Chronic pancreatitis 1 Morbid obesity/obesity 2 2 Diabetes mellitus 1 Pregnancy 1 Total number of cases with chronic
illness 24 6 14 1
Table 15: Incidence and descriptions of disease across the different groups (note disease incidence subtotals include cases with multiple conditions and exceed the total number of cases with chronic illnesses)
Factors associated with the primary cause of death (such as respiratory arrest due to drug overdose, or aspiration of gut contents) are not included. Heart disease was the most com-mon form of chronic illness, followed by various respiratory diseases. The incidence of chronic diseases mentioned as a cause of death within the study population differed dra-matically between the four comparison groups, with the Methadone group suffering from a substantially higher level of chronic illnesses than any other group. Both Methadone and Other Drugs had more cases of chronic illness contributing to their deaths than the Heroin group, while the Carbon Monoxide group had only one case.
Darke et al. (2006) found a similarly high level of systemic disease among opioid deaths in New South Wales between 1998 and 2002, with more than a quarter of cases ex-hibiting disease in more than one organ. They reported that 5.7% of opioid deaths had severe coro-nary artery atherosclerosis, which is similar to findings in our study, where 7.3% of metha-done deaths and 3.7% of heroin deaths had coronary artery atherosclerosis or disease re-corded as contributing to death, a combined rate for opioid deaths of 5.5%. However, Darke et al. (2006) reported much higher levels of liver disease than found in our study.

— METHADONE-RELATED DEATHS —
— 34 —
Many drugs are known to have a negative effect on the cardiorespiratory system, includ-ing amphetamines, heroin and other opioids, methadone, benzodiazepines and antide-pressants. Polydrug use may compound the individual effects of these drugs, leading to unintentional overdose, while the use of prescription drugs with illicit drugs like heroin is also known to increase the risk of overdose. The high prevalence of polydrug use in methadone and heroin users can make it difficult to untangle the contributions of differ-ent drugs to overdose deaths. The high incidence of heart disease in methadone groups in previous studies, for example, has often been attributed to the deceased’s history of il-licit drug abuse, particularly heroin.
The results outlined in Table 15 clearly indicate that high levels of chronic disease (par-ticularly heart disease) in the Methadone group cannot be attributed entirely to past her-oin addiction, because the Heroin group shows much lower levels of chronic disease. The closest group in incidence of chronic disease is the Other Drugs group, which largely comprise prescription, rather than illicit, drugs. This suggests that methadone-related deaths and/or other prescription drug deaths have a stronger association with heart disease than heroin deaths. In order to examine this possible relationship, we ex-amined the patterns of association between the presence or absence of heart disease, with the presence or absence of different drugs in toxicology results.
Only three substances showed any association with the presence or absence of heart dis-ease. There were fewer than expected cases of heart disease in individuals with carbon monoxide in their toxicology results (χ2 = 6.177, df = 1, p<0.05). Similarly, only four individuals with heart disease had consumed alcohol (compared with 25 heart disease cases who had no alcohol present). By contrast, there were more than expected cases of heart disease in those with other substances (χ2 = 6.217, df = 1, p<0.05). As the ‘other substances’ category includes cardiovascular drugs and anticoagulants, this may be the explanation of this association.
The strongest association between heart disease and toxicology was found for metha-done (χ2 = 9.583, df = 1, p<0.05). Individuals with heart disease were significantly more likely to have methadone in their toxicology results than those without heart disease. This contrasts with the complete absence of association between heroin and heart dis-ease in this data set (χ2 = 0.231, df = 1, not significant). There was no association be-tween heart disease and amphetamines, analgesics, benzodiazepines, antidepressants, cannabis, or other opioids in toxicology.
This finding suggests that the relationship between heart disease and methadone is not generically related to drug-taking activity, either prescription or illicit. Rather, these re-sults suggest that there is something specific to methadone use that has an association with heart disease.
As the other groups are matched for both gender and age with the Methadone group in this study, demographic differences are unlikely to explain the differences between the groups, and the different patterns of association within drug types. However, as we have no information on the illicit drug history of the cases under investigation, it is possible that individuals using methadone have a longer history of drug use (irrespective of age) than individuals using heroin or other drugs, which could increase their level of heart disease.
Our findings support other studies which have found an association between methadone consumption and heart disease. This pattern of association, however, does not imply cau-sation. It is possible that methadone contributes to heart disease, or that heart disease is increased by the presence of methadone alone or in combination with other drugs. It is also possible that sick heroin users are more likely to be in contact with general practitio-ners and health services, and so more likely to take up methadone tretament options.

— METHADONE-RELATED DEATHS —
— 35 —
Patterns of prescription drug use over time
Changes within individuals prior to death
Previous research (Martyres et al. 2004) found a rapid increase in the number of pre-scription drugs obtained in the twelve months before death for heroin-related deaths. In this study, we compared the levels of prescription drugs obtained within each group dur-ing six-monthly intervals in the four years before death. Figure 5 reveals a trend towards increasing prescription use for all groups leading up to death, with the strongest trend in the Methadone group and the Other Drugs group and weakest in the Carbon Monoxide group.
Figure 5: Number of prescriptions obtained within each group in six-monthly intervals before death
These results replicate similar findings from Martyres et al. (2004) study of annual pre-scription drug use in heroin users. Martyres et al. (2004) reported an average of 17 pre-scriptions in the first year, 9.5 in the second year, 4.5 in third and 3.6 in the fourth for young heroin-users. The similarity in trends and overall quantities between the two stud-ies supports the robustness of the original study and extends the findings from the sam-ple of young heroin users (age 14–24 years) to a broader age range (age 15–54 years).
Figure 5 also demonstrates that the effect of increasing prescription use (or ‘doctor-shopping’) is even more pronounced in Methadone deaths and Other Drugs deaths, but is not significant in Carbon Monoxide deaths. Escalating prescription drug use is con-firmed as a potentially important predictor of overdose death.
The effect of the 2001 heroin drought on prescription drug patterns
The previous study by the Melbourne Division of General Practitioners (MDGP, 2002) of prescription drug use by young heroin users allows a comparison of prescription drug use by heroin users in 1992–99 with prescription patterns in the current data set in 2002–05 (sample sizes from 1991, 2000, 2001 and 2006 were too small to be reliably representative). These two data sets enable a comparison of the proportion of prescrip-tion drug use patterns prior to the 2001 heroin drought with patterns during and after the heroin drought. We have not compared absolute levels of prescription drug use because of variations in sample size between years and between data sets.
0
5
10
15
20
25
30
0-6m 6-12m 12-18m 18-24m 24-30m 30-36m 36-42m 42-48mPeriod before death
Aver
age n
umbe
r of p
resc
riptio
ns
Methadone Other drugs Heroin Carbon monoxide

— METHADONE-RELATED DEATHS —
— 36 —
0%
20%
40%
60%
80%
100%
1992 1993 1994 1995 1996 1997 1998 1999
OtherAnti-infectionMajor tranquilisersAnti-depressantsNon-opioid analgesicsOpioidsBenzodiazepines
Figure 5: Proportion of different prescriptions provided to young Victorians (15–24) who died of heroin overdose between 1994 and 1999 (M=95, F=60; N=155)
0%
20%
40%
60%
80%
100%
2002 2003 2004 2005
OtherAnti-psychoticsAnti-depressantsAnalgesicsOpioidsBenzodiazepines
Figure 6: Proportion of different prescriptions provided to Victorians (16–54) who died of heroin overdose between 2002 and 2007 (M=56, F=26; N=82)
Despite differences in the coding systems used between the different data sets, overall there appears to have been a general increase in the proportion of prescription drugs prone to abuse (benzodiazepines, opioids, analgesics and antidepressants). In 1992, drugs prone to abuse accounted for 50% of the prescriptions obtained by heroin users. This proportion increased in the mid-1990s to 60%–70% and in 1999 rose again to 80%. After the ongoing heroin drought from 2001, benzodiazepines, opioids and other drugs prone to abuse accounted for between 70% and 85% of prescriptions provided.
The major reduction in heroin availability occurred in 2001 and resulted in a dramatic decrease in the number of deaths attributed to heroin. Concerns were raised that reduced heroin availability might increase prescription drug abuse and deaths from polydrug use. While our data suggests that there has been an increase in the proportion of prescription drugs prone to abuse by heroin users during that time, the increase appears to pre-date the heroin drought, being apparent in the late 1990s and peaking at current levels in 1999.
It must be noted that Medicare made significant changes to data coding in 2001, which might also account for differences between the two data sets; however, it seems unlikely that this would account for the changes in proportions between prescriptions prone to abuse and other types of prescriptions, particularly when the trend appears to occur within the first data set, rather than between data sets.

— METHADONE-RELATED DEATHS —
— 37 —
References ABCI. Australian Illicit Drug Report 1996–1997. Australian Bureau of Criminal Intelli-
gence, Canberra, 1997.
Atkinson D, Dunne A, Parker M. Torsades de pointes and self-terminating ventricular fibrillation in a prescription methadone user. Anaesthesia 2007 Sep;62(9):952–5.
Bartu A, Freeman NC, Gawthorne GS, Codde JP, Holman CD. Mortality in a cohort of opiate and amphetamine users in Perth, Western Australia. Addiction 2004; 99(1):53–60.
Bell J, Zador D. A risk–benefit analysis of methadone maintenance treatment. Drug Saf 2000;22(3):179–90.
Burns JM, Martyres RF, Clode D, Boldero JM. Overdose in young people using heroin: associations with mental health, prescription drug use and personal circum-stances. Med J Aust 2004;181(7 Suppl):S25–8.
Caplehorn JR, Drummer OH. Fatal methadone toxicity: signs and circumstances, and the role of benzodiazepines. Aust N Z J Public Health 2002;26(4):358–62.
Caplehorn JR, Drummer OH. Mortality associated with New South Wales methadone programs in 1994: lives lost and saved. Med J Aust 1999;170(3):104–9.
Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, Fry-Smith A, Day E, Lintzeris N, Roberts T, Burls A, Taylor RS. Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation. Health Technol Assess 2007;11(9):1–171, iii–iv.
Corkery JM, Schifano F, Ghodse AH, Oyefeso A. The effects of methadone and its role in fatalities. Hum Psychopharmacol 2004;19(8):565–76.
Darke S, Kaye S, Duflou J. Systemic disease among cases of fatal opioid toxicity, Ad-diction 2006;101:1299–305.
Darke S, Ross J, Teesson M, Lynskey M. Health service utilization and benzodiazepine use among heroin users: findings from the Australian Treatment Outcome Study (ATOS). Addiction 2003;98(8):1129–35.
Darke S, Ross J, Zador D, Sunjic S. Heroin-related deaths in New South Wales, Austra-lia, 1992–1996. Drug Alcohol Depend 2000; 60(2):141–50.
Degenhardt LJ, Conroy E, Gilmour S, Hall WD. The effect of a reduction in heroin sup-ply on fatal and non-fatal drug overdoses in New South Wales, Australia. Med J Aust 2005a;182(1):20–3.
Degenhardt L, Day C, Dietze P, Pointer S, Conroy E, Collins L, Hall W. Effects of a sustained heroin shortage in three Australian States. Addiction 2005b;100(7):908–20.
Degenhardt L, Day C, Conroy E, Gilmour S, Hall W. Age differentials in the impacts of reduced heroin: effects of a “heroin shortage” in NSW, Australia. Drug Alco-hol Depend 2005c;79(3):397–404.
Degenhardt L, Day C, Gilmour S, Hall W Patterns of illicit drug use in NSW, Australia following a reduction in heroin supply. Int J Drug Policy 2005d;16(5):300–7.
Dobbin M. Methadone-related deaths in Victoria, 1993–1994. The proceedings of the 1995 Autumn School of Studies on Alcohol and Drugs, 1995. Department of Drug and Alcohol Studies, St Vincent’s Hospital, Melbourne.
Dobbin, M. Prescription drug abuse. Report prepared for the Victorian Department of Human Services. 1998.
Drummer OH, Opeskin K, Syrjanen M, Cordner SM. Methadone toxicity causing death in ten subjects starting on a methadone maintenance program. Am J Forensic Med Pathol 1992;13(4):346–50.

— METHADONE-RELATED DEATHS —
— 38 —
Drummer OH. Postmortem toxicology of drugs of abuse. Forensic Sci Int 2004 Jun 10;142(2–3):101–13.
Drummer OH. Recent trends in narcotic deaths. Ther Drug Monit 2005;27(6):738–40.
Ehret GB, Voide C, Gex-Fabry M, Chabert J, Shah D, Broers B, Piguet V, Musset T, Gaspoz JM, Perrier A, Dayer P, Desmeules JA. Drug-induced long QT syn-drome in injection drug users receiving methadone: high frequency in hospital-ized patients and risk factors. Arch Intern Med 2006;166(12):1280–7.
Ernst E, Bartu A, Popescu A, Ileutt KF, Hansson R, Plumley N. Methadone-related deaths in Western Australia 1993–99. Aust N Z J Public Health 2002;26:364–70.
Fugelstad A, Stenbacka M, Leifman A, Nylander M, Thiblin I. Methadone maintenance treatement: the balance between life-saving treatment and fatal poisonings, Ad-diction 2007;102:406–12.
Gagajewski A, Apple FS. Methadone-related deaths in Hennepin County, Minnesota: 1992–2002. J Forensic Sci 2003;48(3):668–71.
Garrick TM, Sheedy D, Abernethy J, Hodda AE, Harper CG. Heroin-related deaths in Sydney, Australia. How common are they? Am J Addict 2000; 9(2):172–8.
Gaughwin M, Kliewer E, Ali R, Faulkner C, Wodak A, Anderson G. The prescription of methadone for opiate dependence in Australia, 1985–1991. Med J Aust 1993;159(2):107–8.
Gerostamoulos J, Staikos V, Drummer OH. Heroin-related deaths in Victoria: a review of cases for 1997 and 1998. Drug Alcohol Depend 2001;61(2):123–7.
Gibson A, Degenhardt L, Mattick RP, Ali R, White J, O’Brien S. Exposure to opioid maintenance treatment reduces long-term mortality. Addiction 2008;103(3):462–8.
Gibson AE, Degenhardt LJ. Mortality related to pharmacotherapies for opioid depend-ence: a comparative analysis of coronial records. Drug Alcohol Rev 2007;26(4):405–10.
Graβ H, Behnsen S, Kilmot H-G, Staak M, Käferstein H. Methadone and its role in drug-related fatalisties in Cologne 1989–2000. For Sc Int 2003; 132(3)195–200.
Green H, James RA, Gilbert JD, Harpas P, Byard RW. Methadone maintenance programs—a two-edged sword? Am J Forensic Med Pathol 2000;21(4):359–61.
Hall W, Darke S.Trends in opiate overdose deaths in Australia 1979–1995. Drug Alco-hol Depend 1998; 52(1):71–7.
Hall W, Linskey M, Degenhardt L, Trends in opiate related deaths in the United King-dom and Australia 1985–1995, Drug Alcohol Depend 2000;57:247–54.
Hall WD, Degenhardt LJ, Lynskey MT. Opioid overdose mortality in Australia, 1964–1997: birth-cohort trends. Med J. Aust 1999; 17(1): 34–7.
Heinemann A, Iwersen-Bergmann S, Stein S, Schmoldt A, Püschel K. Methadone-related fatalities in Hamburg 1990–1999: implications for quality standards in maintenance treatment? For Sci Int 2000;113(1–3):449–55
Hickman M, Carrivick S, Paterson S, Hunt N, Zador D, Cusick L, Henry J. London au-dit of drug-related overdose deaths: characteristics and typology, and implica-tions for prevention and monitoring. Addiction 2007;102(2):317–23.
Justo D. Methadone-induced long QT syndrome vs methadone-induced Torsades de Pointes. Arch Int Med 2006;166:2288.
Lynskey M, Hall W. Jurisdictional trends in opioid overdose deaths, 1988–96. Aust NZ J Public Health 1998;22(7):802–7.
Martyres RF, Clode D, Burns JM. Seeking drugs or seeking help? Escalating “doctor shop-ping” in young heroin users before fatal overdose, Med J. Aust 2004;180:211–14.

— METHADONE-RELATED DEATHS —
— 39 —
Man LH, Best D, Gossop M, Stillwell G, Strang J. Relationship between prescribing and risk of opiate overdose among drug users in and out of maintenance treatment. Eur Addict Res 2004;10(1):35–40.
MDGP, Help Understanding Drug Use, Melbourne Division of General Practice, Mel-bourne, 2002.
Morgan O, Griffiths C, Hickman M. Association between availability of heroin and methadone and fatal poisoning in England and Wales 1993–2004. Int J Epide-miol 2006;35(6):1579–85.
Musshoff F, Lachenmeier DW, Madea B. Methadone substitution: medicolegal prob-lems in Germany. Forensic Sci Int 2003;133(1–2):118–24.
Peles E, Bodner G, Kreek MJ, Rados V, Adelson M. Corrected-QT intervals as related to methadone dose and serum level in methadone maintenance treatment (MMT) patients: a cross-sectional study. Addiction 2007;102(2):289–300.
Perret G, Déglon JJ, Kreek MJ, Ho A, La Harpe R. Lethal methadone intoxications in Geneva, Switzerland, from 1994 to 1998. Addiction 2000;95(11):1647–53.
Pirnay S, Borron SW, Giudicelli CP, Tourneau J, Baud FJ, Ricordel I. A critical review of the causes of death among post-mortem toxicological investigations: analy-sis of 34 buprenorphine-associated and 35 methadone-associated deaths. Ad-diction 2004;99(8):978–88.
Rosenblum A, Parrino M, Schnoll SH, Fong C, Maxwell C, Cleland CM, Magura S, Haddox JD. Prescription opioid abuse among enrollees into methadone mainte-nance treatment. Drug Alcohol Depend 2007;90(1):64–71.
Ross HE. Benzodiazepine use and anxiolytic abuse and dependence in treated alcohol-ics. Addiction 1993;88:209–18.
Ross J, Darke S, Hall W. Benzodiazepine use among heroin users in Sydney: patterns of use, availability and procurement. Drug and Alcohol Review 1996;15:237–43.
Shah N, Lathrop SL, Landen MG. Unintentional methadone-related overdose death in New Mexico (USA) and implications for surveillance, 1998–2002. Addiction 2005;100(2):176–88.
Sheedy DL, Garrick TM, Fortis AH, Harper CG. Changing trends in heroin-related deaths in Sydney, Australia–1995 to 1999. Am J Addict 2003;12(1):52–9.
Shields LB, Hunsaker Iii JC, Corey TS, Ward MK, Stewart D. Methadone toxicity fa-talities: a review of medical examiner cases in a large metropolitan area. J Fo-rensic Sci 2007,52(6):1389–95.
Sims SA, Snow LA, Porucznik CA. Surveillance of methadone-related adverse drug events using multiple public health data sources. J Biomed Inform 2007;40(4):382–9.
Strang J, Manning V, Mayet S, Ridge G, Best D, Sheridan J. Does prescribing for opiate addiction change after national guidelines? Methadone and buprenorphine pre-scribing to opiate addicts by general practitioners and hospital doctors in Eng-land, 1995–2005. Addiction 2007;102(5):761–70.
Strang J, Sheridan J, Barber N. Prescribing injectable and oral methadone to opiate ad-dicts: results from the 1995 national postal survey of community pharmacies in England and Wales. Br Med J 1996;313(7052):270–2.
Strang J, Sheridan J, Hunt C, Kerr B, Gerada C, Pringle M. The prescribing of metha-done and other opioids to addicts: national survey of GPs in England and Wales. Br J Gen Pract 2005;55(515):444–51.
Strang J, Sheridan J. Methadone prescribing to opiate addicts by private doctors: compari-son with NHS practice in south east England. Addiction 2001;96(4):567–76.

— METHADONE-RELATED DEATHS —
— 40 —
Teichtahl H, Wang D, Cunnington D, Quinnell T, Tran H, Kronborg I, Drummer OH. Ventilatory responses to hypoxia and hypercapnia in stable methadone mainte-nance treatment patients. Chest 2005;128(3):1339–47.
Terpening CM, Johnson WM. Methadone as an analgesic: a review of the risks and benefits. W V Med J 2007;103(1):14–18.
Topp L, Day C, Degenhardt L Changes in patterns of drug injection concurrent with a sustained reduction in the availability of heroin in Australia. Med J Aust 1999;171(1):34–7.
USDHHS. Epidemiologic trends in drug abuse. National Institute of Drug Abuse Com-munity Epidemiology Work Group, United States Department of Health and Human Services, 1995.
Wang D, Teichtahl H, Drummer O, Goodman C, Cherry G, Cunnington D, Kronborg I. Central sleep apnea in stable methadone maintenance treatment patients. Ches. 2005;128(3):1348–56.
Williamson PA, Foreman KJ, White JM, Anderson G. Methadone-related overdose deaths in South Australia, 1984–1994. How safe is methadone prescribing? Med J Aust 1997;166(6):302–5.
Wodak A What caused the recent reduction in heroin supply in Australia? Int J Drug Policy 2008;19(4):279–86.
Wodak A. Methadone and heroin prescription: babies and bath water. Subst Use Misuse 2002;37(4):523–31.
Wolf BC, Lavezzi WA, Sullivan LM, Flannagan LM. Methadone-related deaths in Palm Beach County. J Forensic Sci 2004;49(2):375–8.
Wysowski DK. Surveillance of prescription drug-related mortality using death certifi-cate data. Drug Saf 2007;30(6):533–40.
Zador D, Sunjic S. Deaths in methadone maintenance treatment in New South Wales, Australia 1990–1995. Addiction 2000;95(1):77–84.
Zador D. Methadone maintenance: making it better. Addiction 2007;102(3):350–1.
Zador DA, Sunjic SD. Methadone-related deaths and mortality rate during induction into methadone maintenance, New South Wales, 1996. Drug Alcohol Rev 2002;21(2):131–6.





























