Embed Size (px)
Citation preview
Abel Biesman, DO
John Dinh, DO
FOMA 2020
No actual or potential personal, financial or legal conflict of interest in relation to this program or presentation
All illustrations used in this presentation belong to the public domain. Source material cited either on slide or in notes.

Review of lymph composition
Review of lymphatic system function and purpose
Review of basic anatomy
Indications and contraindications for Osteopathic Manipulative Treatment (OMT) with lymphatic emphasis
Adjunctive OMT treatments for office complaints utilizing the lymphatic system
Research support
Composition
Functions
Anatomy
Composition
Fluid from capillaries
Debris and bacteria from wounds
Circulating Lymphocytes
Macrocytes
Metabolic waste, CO2, O2
Proteins * (low amount but critical)
Fluid Balance
Helps return excess fluid and proteins to circulatory system which cannot be processed by venous system
Immune Support
Production of immune cells
Transport of bacteria to lymph nodes
Fat Transport
Absorption of chylomicrons which are too large for venous system
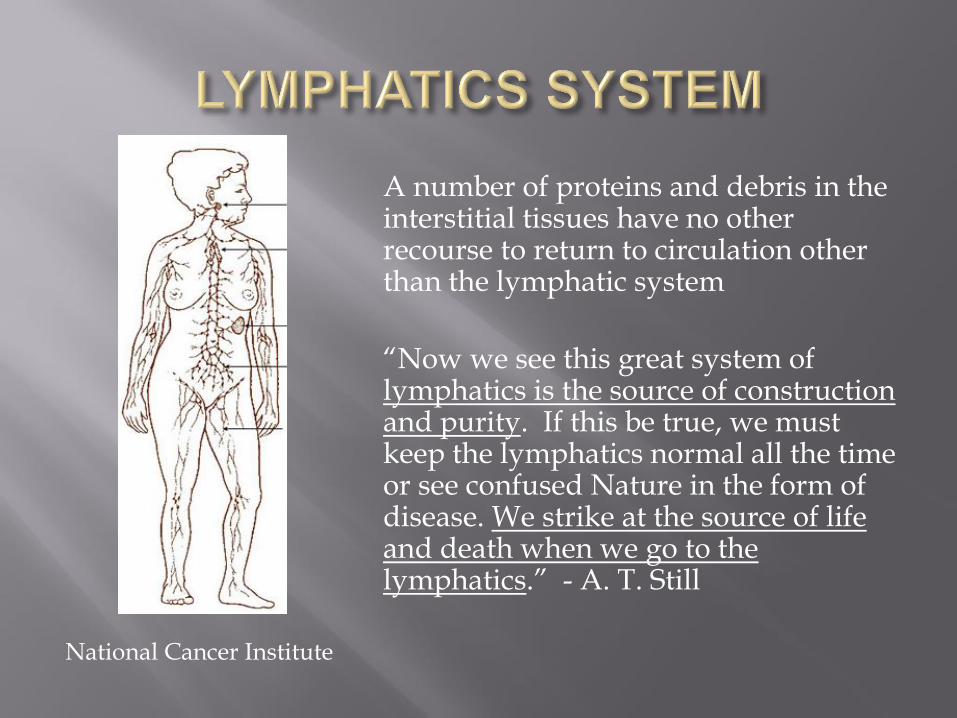
A number of proteins and debris in the interstitial tissues have no other recourse to return to circulation other than the lymphatic system
“Now we see this great system of lymphatics is the source of construction and purity. If this be true, we must keep the lymphatics normal all the time or see confused Nature in the form of disease. We strike at the source of life and death when we go to the lymphatics.” - A. T. Still
National Cancer Institute
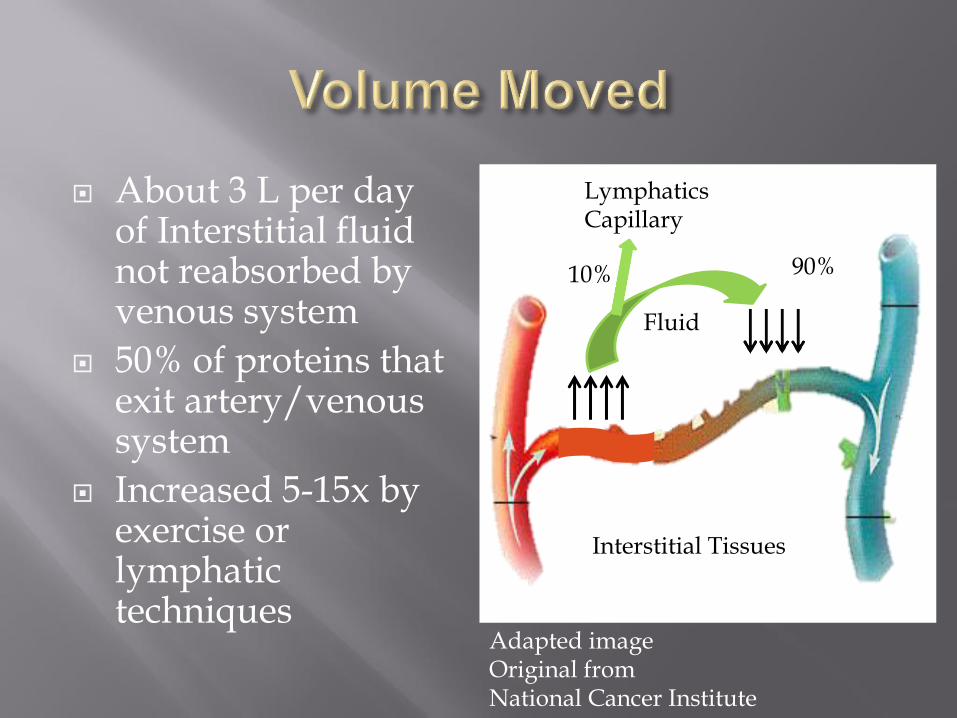
About 3 L per day of Interstitial fluid not reabsorbed by venous system
50% of proteins that exit artery/venous system
Increased 5-15x by exercise or lymphatic techniques
Thieme Atlas of Anatomy Interstitial Tissues
90%
Lymphatics Capillary
10%
Adapted image Original from National Cancer Institute
Fluid
Intrinsic
One way valves
Rhythmic vessel wall contraction
Extrinsic
Muscle contraction squeezing lymphatic vessels
Diaphragm motion and pressure differentials
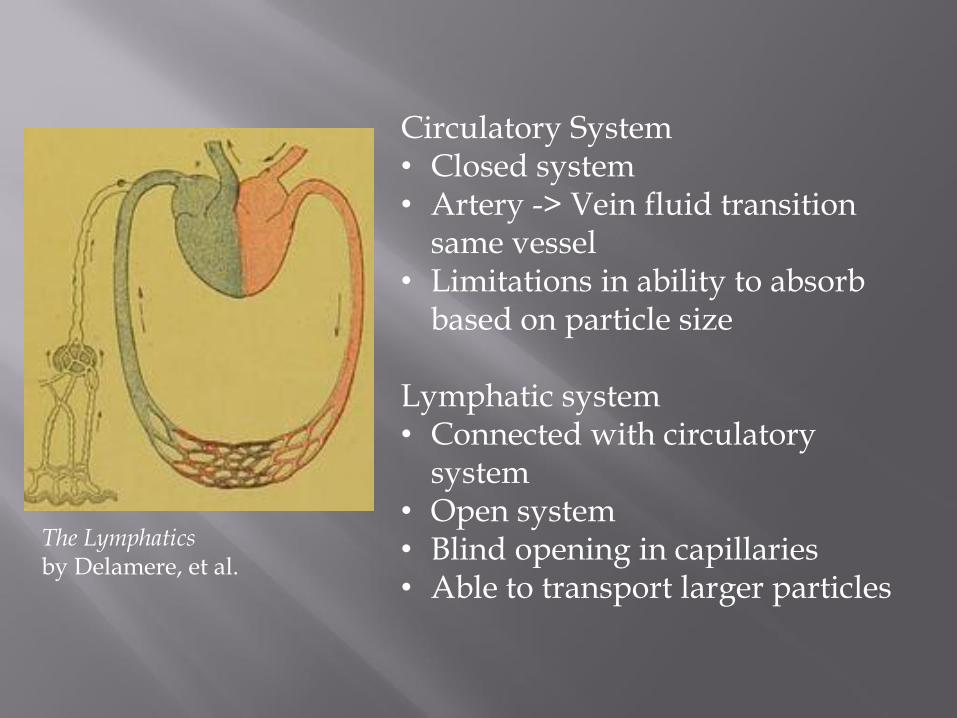
Circulatory System • Closed system • Artery -> Vein fluid transition
same vessel • Limitations in ability to absorb
based on particle size Lymphatic system • Connected with circulatory
system • Open system • Blind opening in capillaries • Able to transport larger particles
The Lymphatics by Delamere, et al.
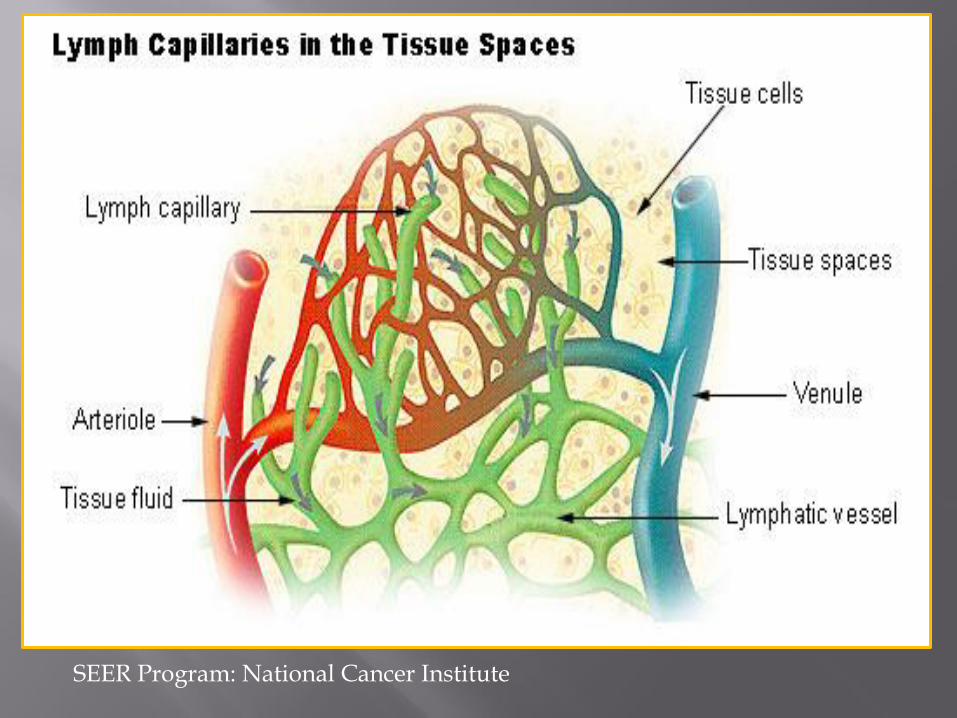
SEER Program: National Cancer Institute
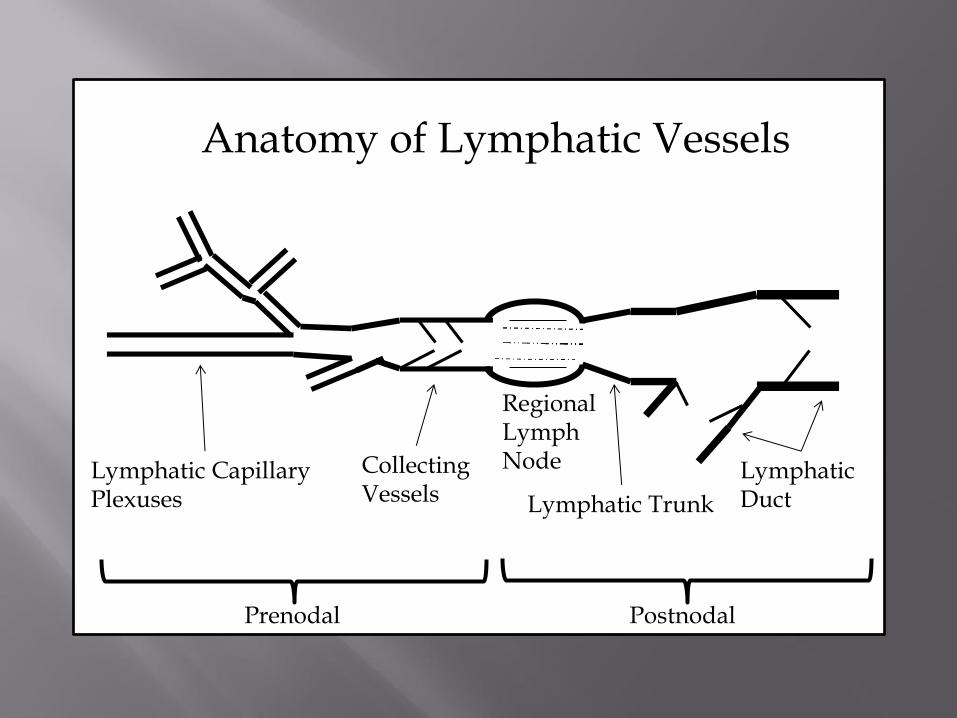
Prenodal Postnodal
Lymphatic Capillary Plexuses
Collecting Vessels
Regional Lymph Node
Lymphatic Trunk
Lymphatic Duct
Anatomy of Lymphatic Vessels
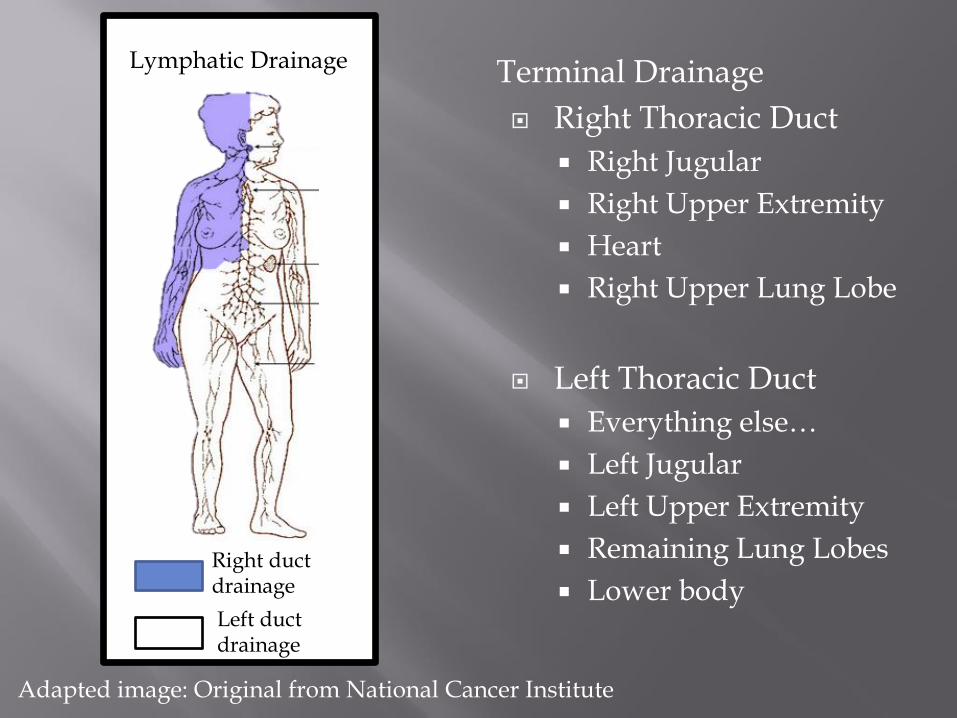
Terminal Drainage
Right Thoracic Duct
Right Jugular
Right Upper Extremity
Heart
Right Upper Lung Lobe
Left Thoracic Duct
Everything else…
Left Jugular
Left Upper Extremity
Remaining Lung Lobes
Lower body
Lymphatic Drainage
Right duct drainage
Left duct drainage
Adapted image: Original from National Cancer Institute
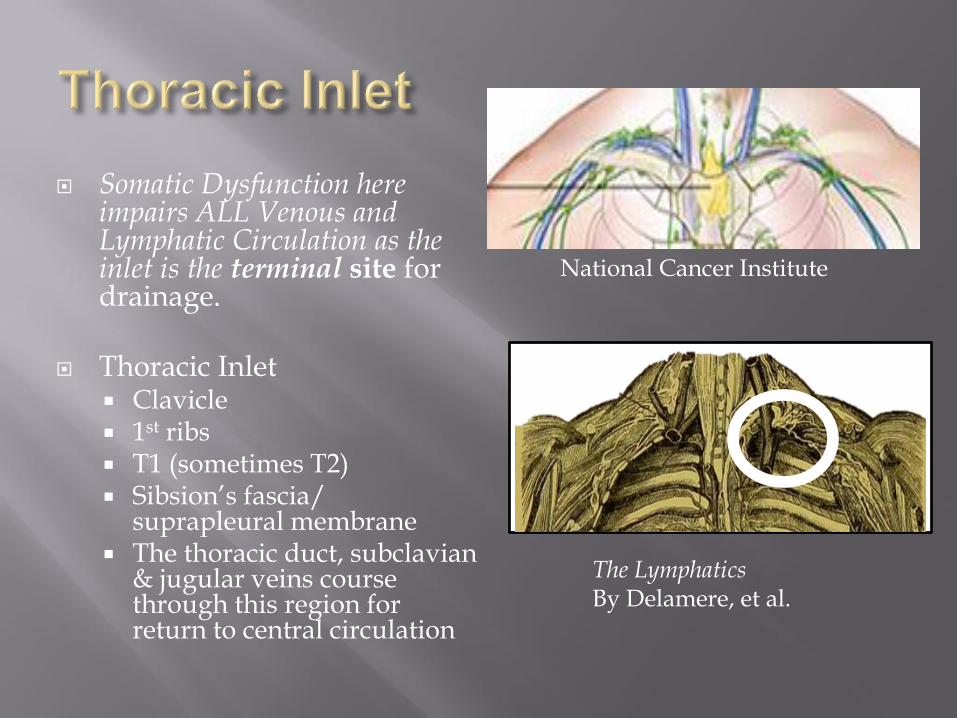
Somatic Dysfunction here impairs ALL Venous and Lymphatic Circulation as the inlet is the terminal site for drainage.
Thoracic Inlet Clavicle 1st ribs T1 (sometimes T2) Sibsion’s fascia/
suprapleural membrane The thoracic duct, subclavian
& jugular veins course through this region for return to central circulation
National Cancer Institute
The Lymphatics By Delamere, et al.
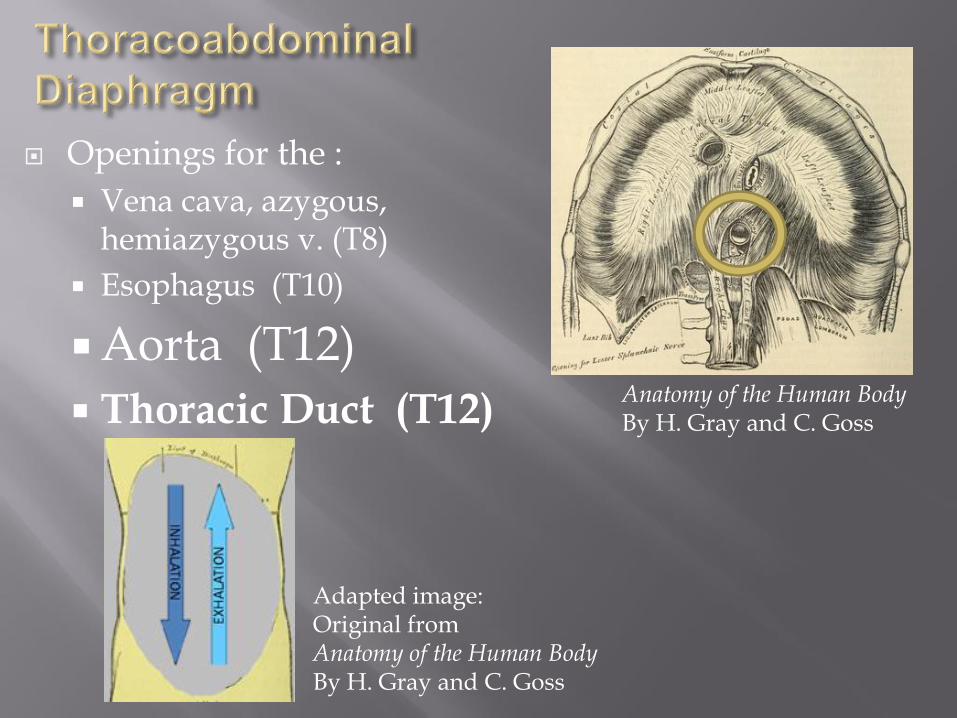
Openings for the :
Vena cava, azygous, hemiazygous v. (T8)
Esophagus (T10)
Aorta (T12)
Thoracic Duct (T12)
Adapted image: Original from Anatomy of the Human Body By H. Gray and C. Goss
Anatomy of the Human Body By H. Gray and C. Goss

Assists transport of low pressure venous / lymphatic fluids from the lower extremities and maintenance of intra-abdominal pressures.
Muscles of the pelvic floor require proper tone for proper function
Venous and lymphatic drainage from the lower extremities must pass under the inguinal ligament
Applied Anatomy of the Lymphatics Millard, F. P., and A. G. Walmsley.
National Cancer Institute
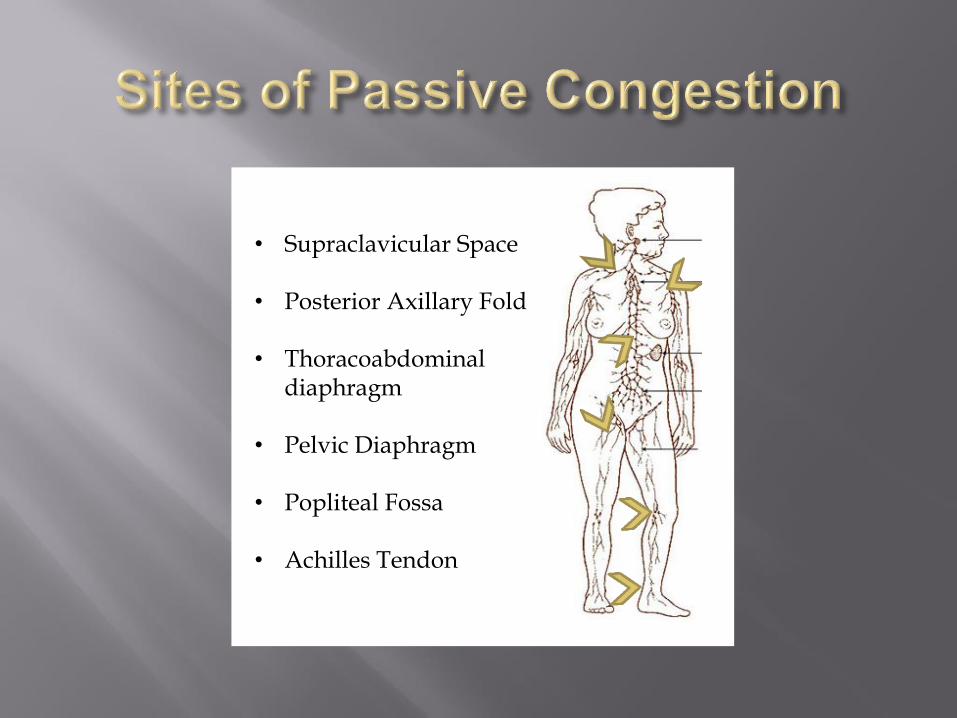
• Supraclavicular Space
• Posterior Axillary Fold
• Thoracoabdominal diaphragm
• Pelvic Diaphragm
• Popliteal Fossa
• Achilles Tendon
INDICATIONS CONTRAINDICATIONS
Edema from any cause
Infection
Atelectasis prevention
Recent Fractures
Open bleeding wounds
DVT
Coagulopathy
Anuresis
Cancer*
Still debated by specialists both among oncologists and neuromusculoskeletal specialists
No research supporting cancer spread from lymphatic techniques in immunocompetent subjects
Research does show that lymphatic techniques and exercise have similar effects on lymphatic flow
79 participants
All received decongestive lymphatic techniques for 8 days
Taught self management techniques
Long term follow up at 38 days
Results
Upper extremity size: 44% reduction
Lower extremity size: 42% reduction
Extremity size reductions maintained at long term follow up (-38% and -41% for upper and lower limbs)

Thoracic duct flow in 4 dogs via a
transonic flow transducer placed just above heart in thoracic duct
Dogs received: Thoracic, Abdominal & Pedal pumps
Exercise defined at 3 mph at 0o incline.
Results displayed similar rise in lymphatic flow from pump techniques and exercise.
• Comparison between lymphatic pump and incentive spirometry in post cholecystectomy patients from 1989-1990
• 21 people in each group
• Results
• In first 4 days, lymphatic pump had higher FVC
• By day 5, incentive spirometry and lymphatic pumps had similar FVC
Conclusion: lymphatic pump helps prevent atelectasis in post surgical patients
Influenza patients treated osteopathically during 1917-1918 had a 0.25% mortality rate, as compared to the national average of 6% (10% for pneumonia patients, compared with 33% to 75% for the national average).
Total mortality 110,120 patients with influenza treated by 2445 Osteopathic physicians was 0.25%.
Mortality in patients receiving traditional medical care was 5% to 6%.
Among patients with influenza pneumonia treated medicinally, mortality was estimated at 33%, and even as high as between 68% and 78% in some large centers.
The death rate due to pneumonia among 6258 patients cared for by osteopathic physicians was 10%.
21-30 million world wide, 23% of U.S. population died!
JAOA • Vol 104 • No 9 • September 2004 • 370–371
Chokepoints:
Thoracic inlet (always)
Thoracoabdominal diaphragm (lungs or below)
Pelvic Diaphragm (pelvis or below)
Popliteal fossa (knees or below)
Condition Specific:
Galbreath, spine, ribs, etc
Lymphatic pump
Chokepoints (start)
Thoracic inlet
Thoracoabdominal diaphragm
Pelvic diaphragm
Popliteal fossa
Pumps (end)
Thoracic pump a.k.a. Miller pump
Abdominal pump
Pedal pump
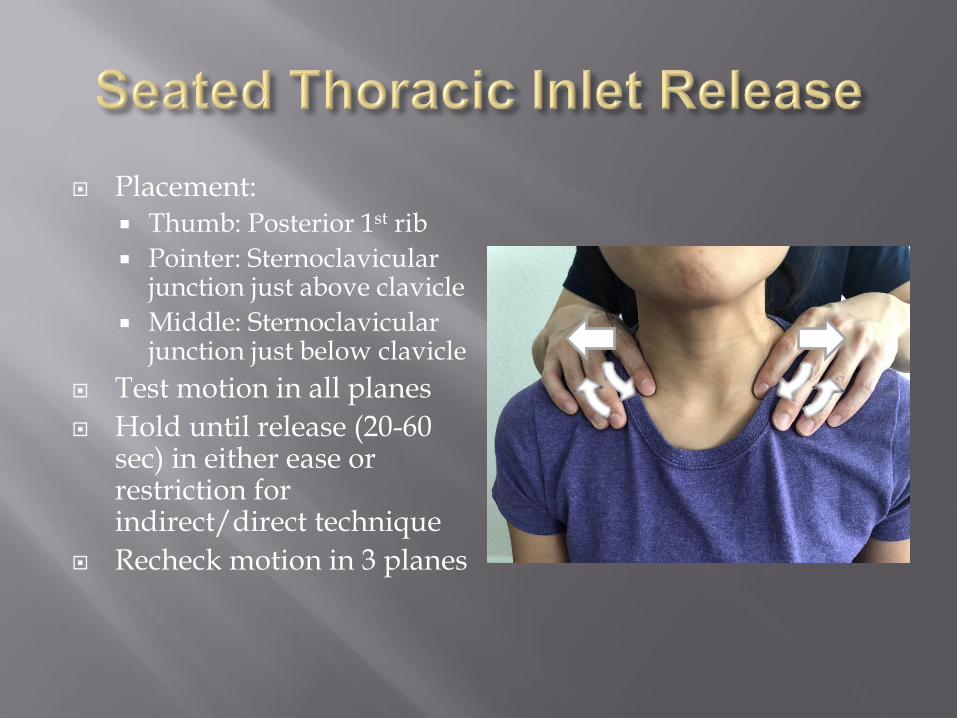
Placement: Thumb: Posterior 1st rib
Pointer: Sternoclavicular junction just above clavicle
Middle: Sternoclavicular junction just below clavicle
Test motion in all planes
Hold until release (20-60 sec) in either ease or restriction for indirect/direct technique
Recheck motion in 3 planes
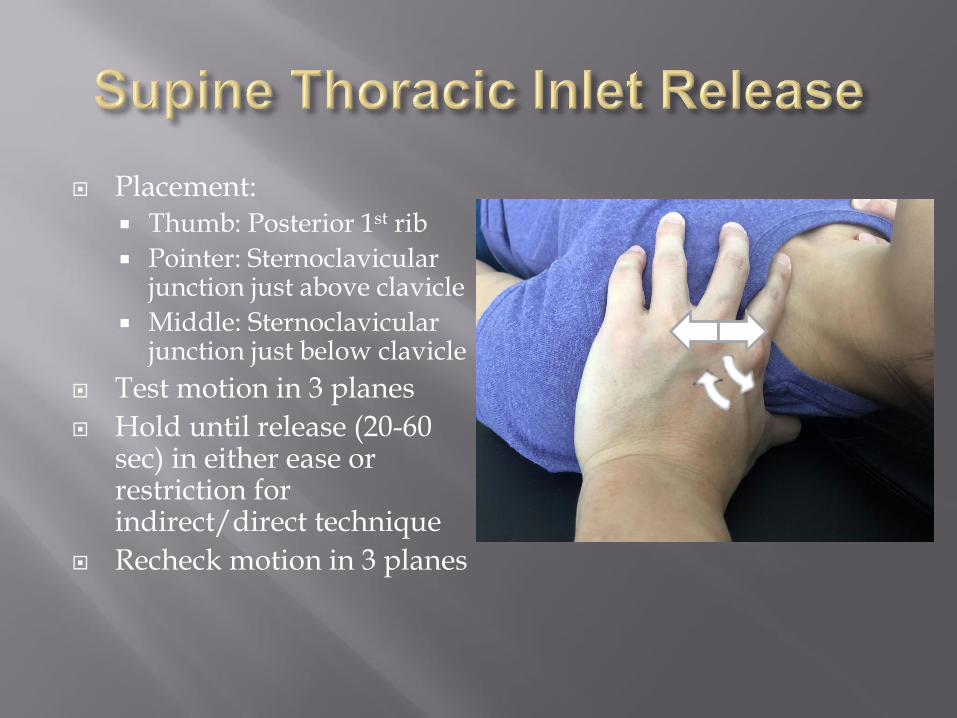
Placement: Thumb: Posterior 1st rib
Pointer: Sternoclavicular junction just above clavicle
Middle: Sternoclavicular junction just below clavicle
Test motion in 3 planes
Hold until release (20-60 sec) in either ease or restriction for indirect/direct technique
Recheck motion in 3 planes
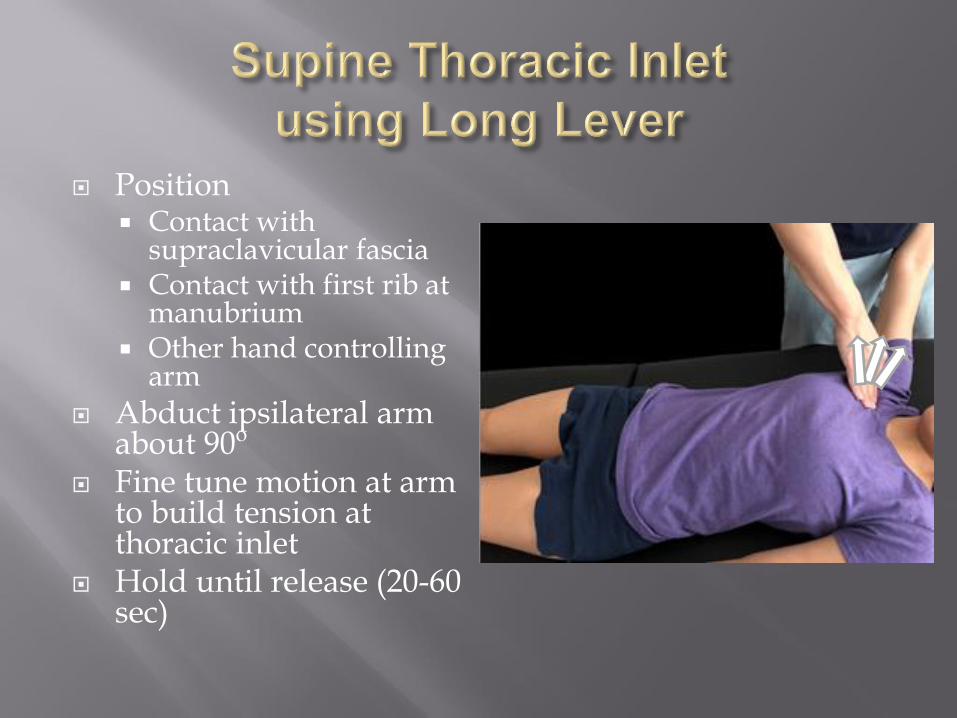
Position Contact with
supraclavicular fascia Contact with first rib at
manubrium Other hand controlling
arm
Abduct ipsilateral arm about 90o
Fine tune motion at arm to build tension at thoracic inlet
Hold until release (20-60 sec)

Position:
Use thumbs or hypothenar eminences
Broad contact along diaphragm just under coastal margin and xiphoid process
Have patient take slow deep breaths
Follow exhalation with additional pressure and resist inhalation
Repeat for 3-5 breaths
Repeat last step if necessary
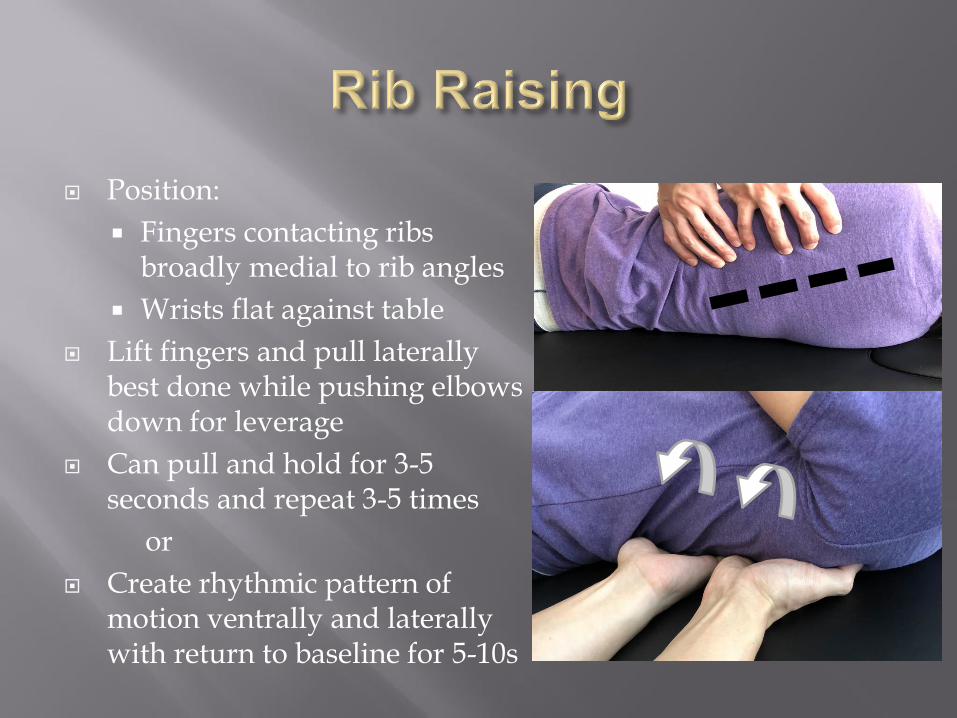
Position:
Fingers contacting ribs broadly medial to rib angles
Wrists flat against table
Lift fingers and pull laterally best done while pushing elbows down for leverage
Can pull and hold for 3-5 seconds and repeat 3-5 times
or
Create rhythmic pattern of motion ventrally and laterally with return to baseline for 5-10s
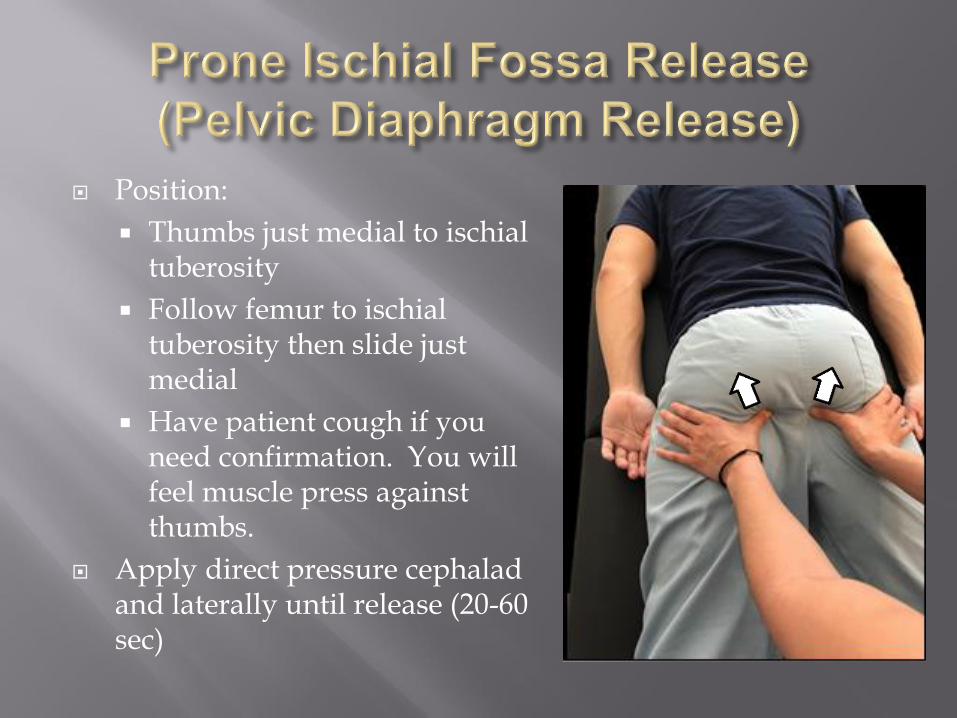
Position:
Thumbs just medial to ischial tuberosity
Follow femur to ischial tuberosity then slide just medial
Have patient cough if you need confirmation. You will feel muscle press against thumbs.
Apply direct pressure cephalad and laterally until release (20-60 sec)
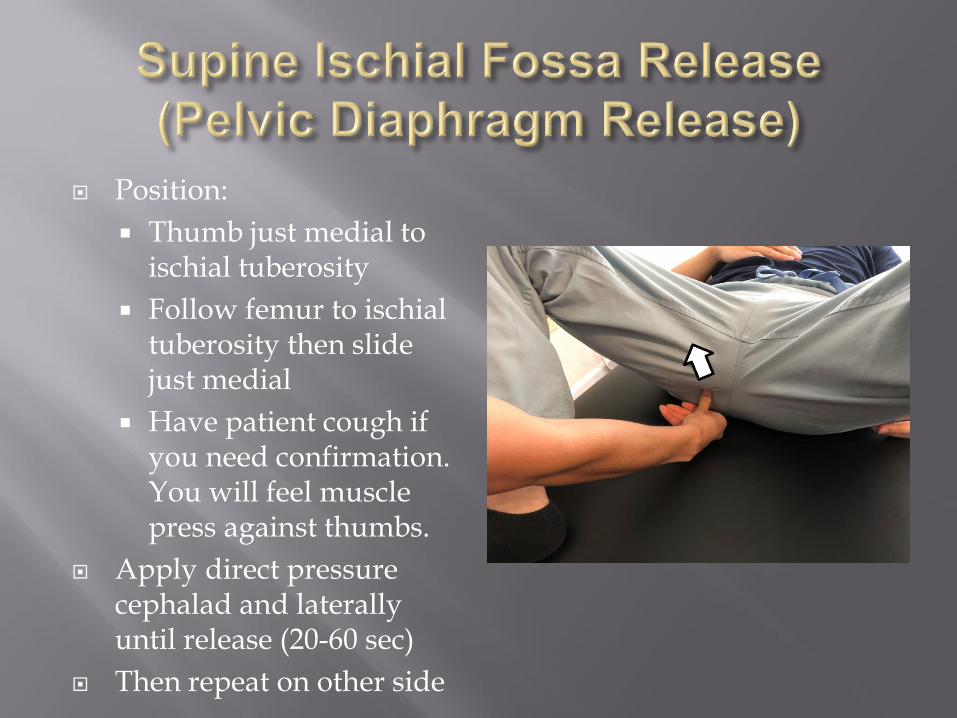
Position:
Thumb just medial to ischial tuberosity
Follow femur to ischial tuberosity then slide just medial
Have patient cough if you need confirmation. You will feel muscle press against thumbs.
Apply direct pressure cephalad and laterally until release (20-60 sec)
Then repeat on other side
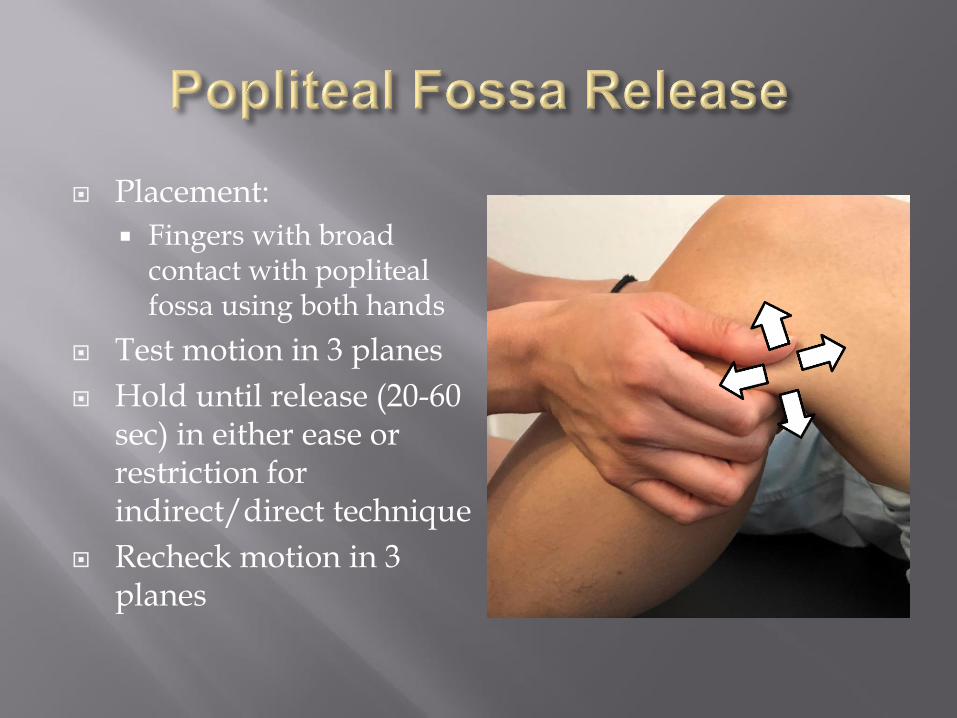
Placement:
Fingers with broad contact with popliteal fossa using both hands
Test motion in 3 planes
Hold until release (20-60 sec) in either ease or restriction for indirect/direct technique
Recheck motion in 3 planes
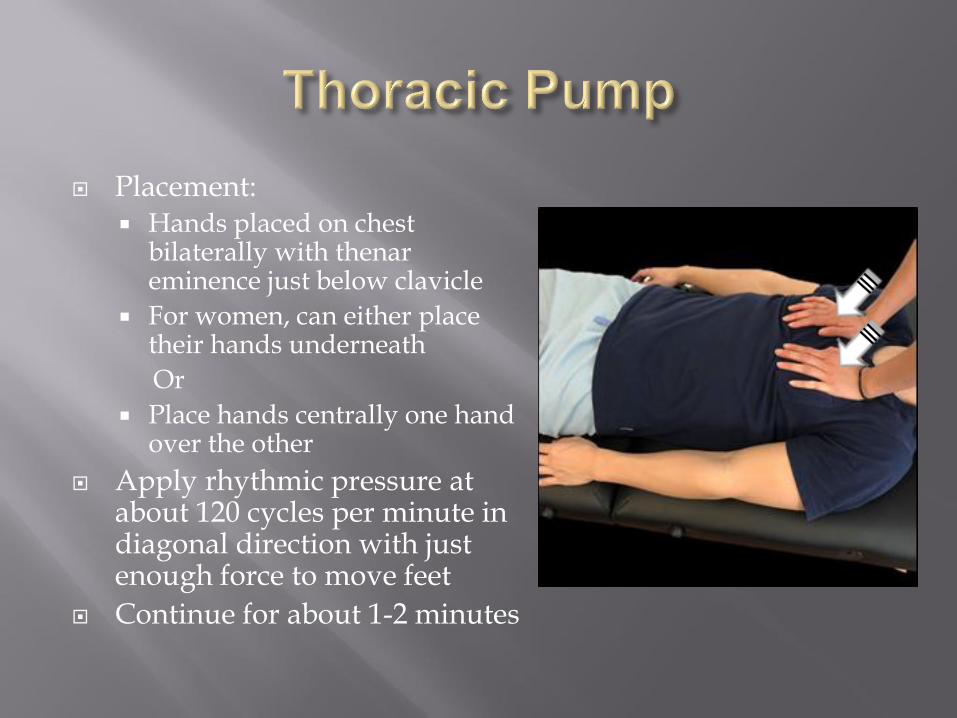
Placement: Hands placed on chest
bilaterally with thenar eminence just below clavicle
For women, can either place their hands underneath
Or
Place hands centrally one hand over the other
Apply rhythmic pressure at about 120 cycles per minute in diagonal direction with just enough force to move feet
Continue for about 1-2 minutes
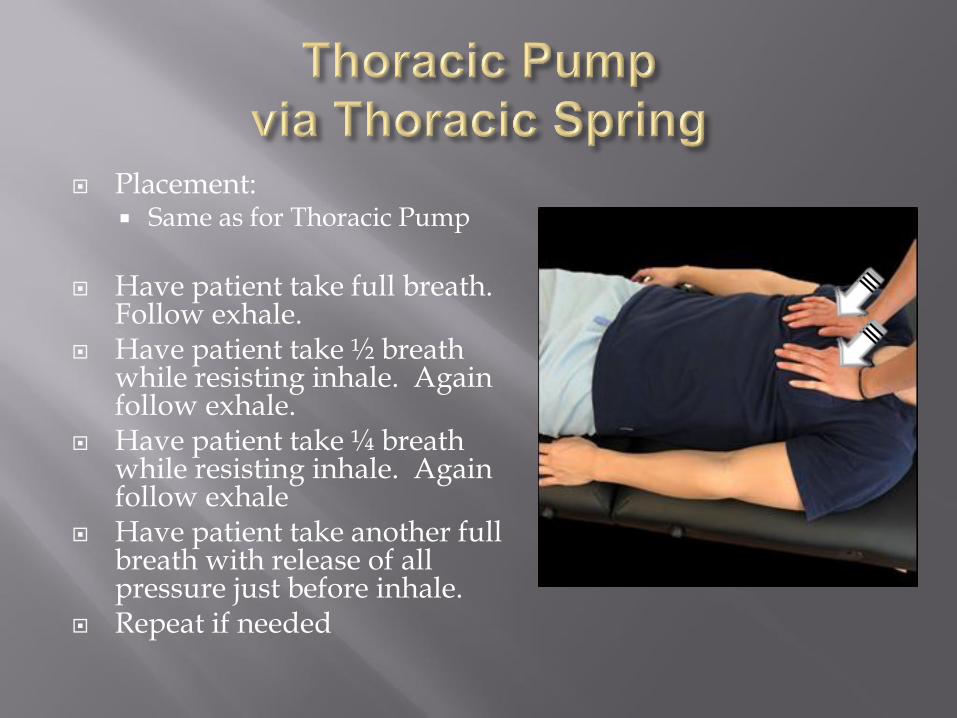
Placement: Same as for Thoracic Pump
Have patient take full breath.
Follow exhale. Have patient take ½ breath
while resisting inhale. Again follow exhale.
Have patient take ¼ breath while resisting inhale. Again follow exhale
Have patient take another full breath with release of all pressure just before inhale.
Repeat if needed
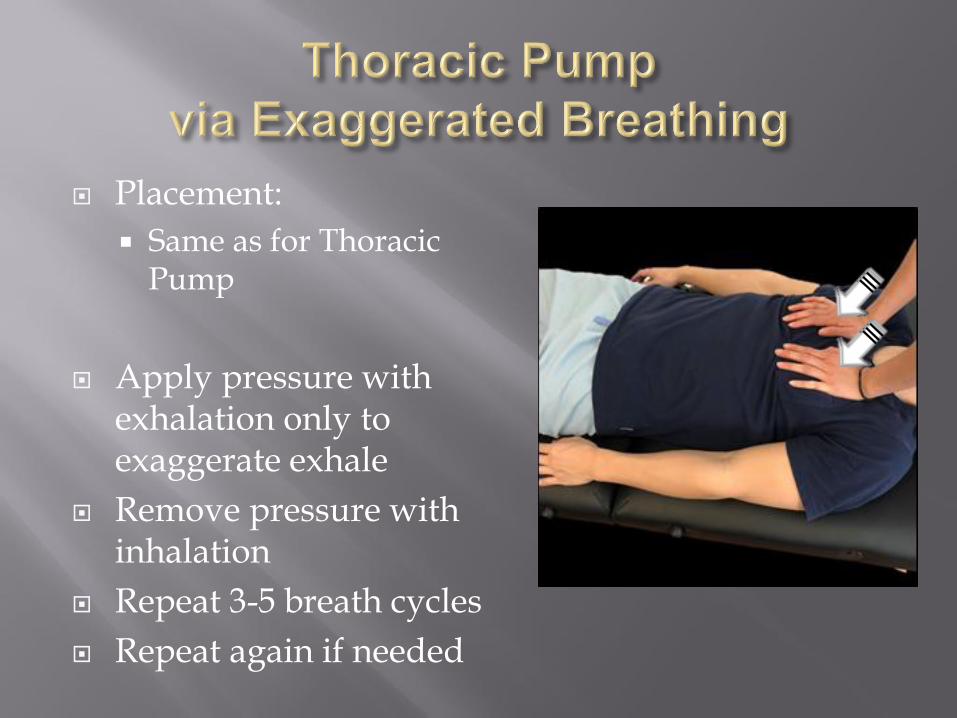
Placement:
Same as for Thoracic Pump
Apply pressure with exhalation only to exaggerate exhale
Remove pressure with inhalation
Repeat 3-5 breath cycles
Repeat again if needed
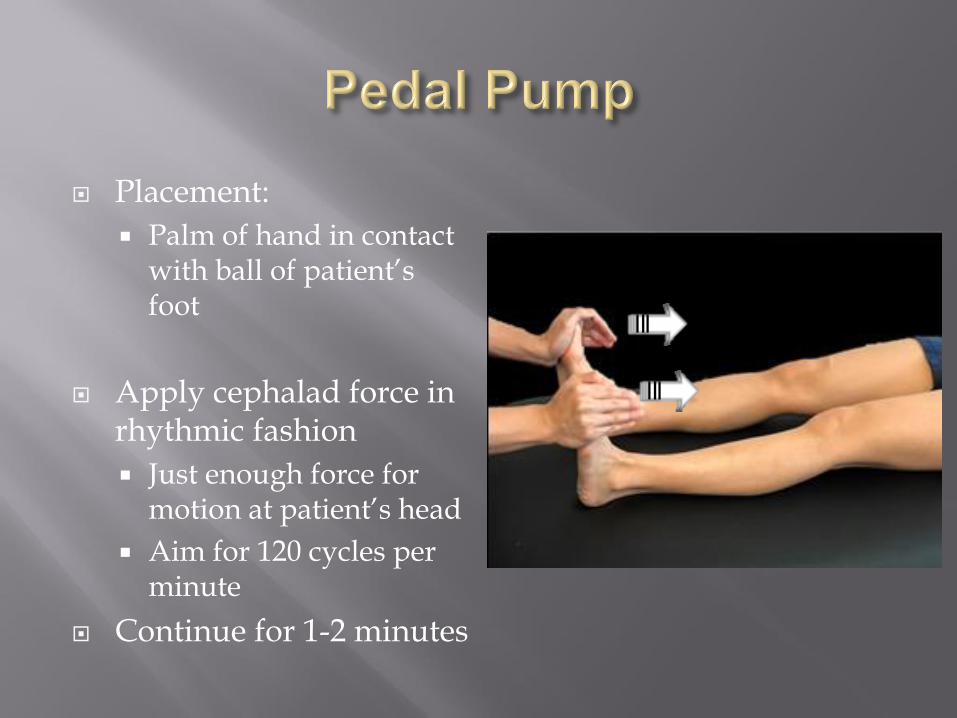
Placement:
Palm of hand in contact with ball of patient’s foot
Apply cephalad force in rhythmic fashion
Just enough force for motion at patient’s head
Aim for 120 cycles per minute
Continue for 1-2 minutes

Employ following techniques as needed after clearing chokepoints yet before performing a lymphatic pump.
These are designed to help lymphatic flow in a more local region.

Gentle stroking maneuver from distal to proximal to “milk” lymphatic back towards thoracic inlet.
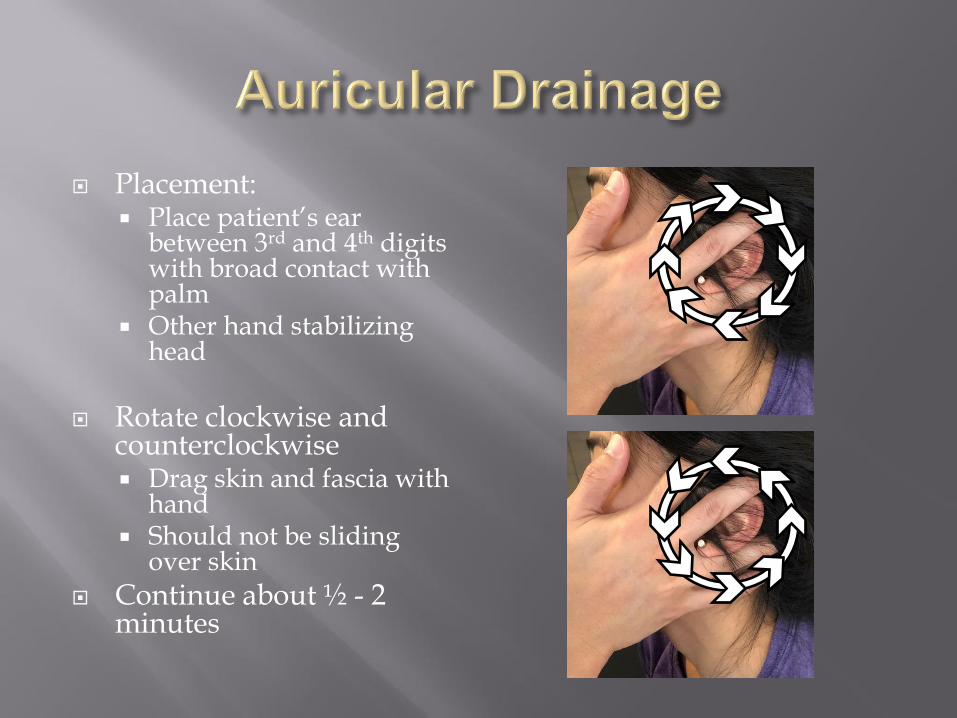
Placement: Place patient’s ear
between 3rd and 4th digits with broad contact with palm
Other hand stabilizing head
Rotate clockwise and counterclockwise Drag skin and fascia with
hand Should not be sliding
over skin
Continue about ½ - 2 minutes

Placement: 3rd, 4th, and 5th fingers
curling behind posterior ramus of the mandible
Hypothenar eminence along body of mandible
Patient mouth slightly open
Other hand stabilizing head
In rhythmic motion draw mandible slightly forward for 3-5 seconds before returning to baseline
Continue 30 sec – 2 min
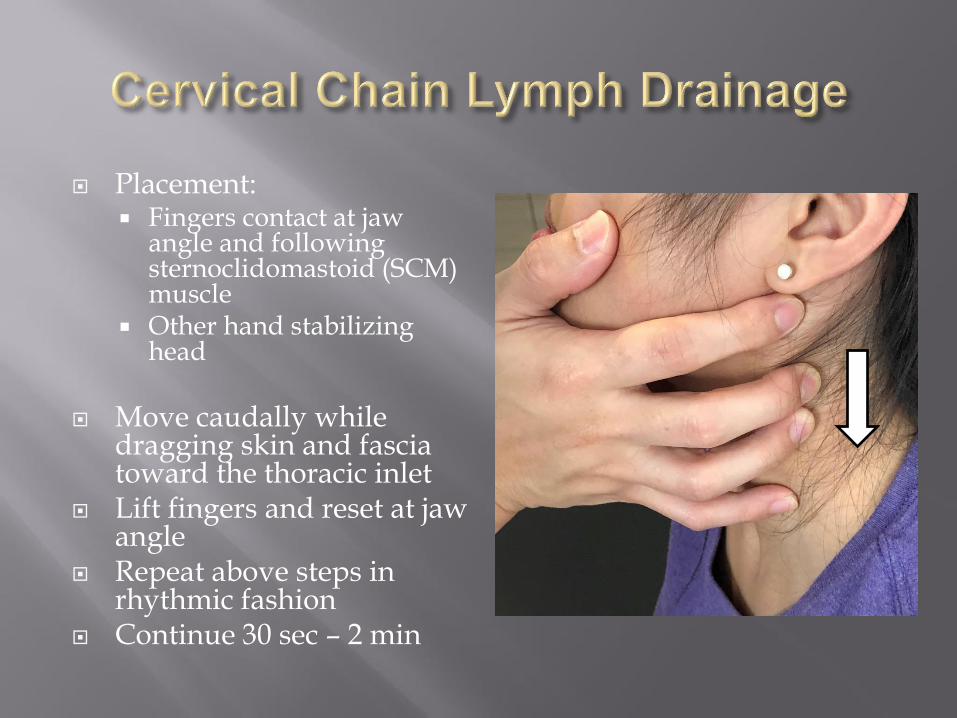
Placement: Fingers contact at jaw
angle and following sternoclidomastoid (SCM) muscle
Other hand stabilizing head
Move caudally while dragging skin and fascia toward the thoracic inlet
Lift fingers and reset at jaw angle
Repeat above steps in rhythmic fashion
Continue 30 sec – 2 min

Focusing on Lymphatic Techniques
Thoracic inlet release
Cervical chain drainage
Galbreath
Auricular drainage
Check for sinus pain and consider effleurage
Thoracic pump

Thoracic inlet release
Cervical chain drainage
Galbreath drainage
Sinus effleurage
Thoracic pump
Thoracic inlet
Abdominal diaphragm
Fix spinal somatic dysfunction
Fix rib somatic dysfunction
Rib raising
Thoracic pump with exaggerated breathing
Thoracic inlet
Abdominal diaphragm
Fix spinal somatic dysfunction (focus T1-4)
Fix rib somatic dysfunction
Liver release
Kidney release
Pelvic diaphragm
Bladder lift
Popliteal fossa
Pedal pump
Thoracic inlet
Abdominal diaphragm
Pelvic diaphragm
Popliteal fossa
Pedal pump
Thoracic inlet
Open appropriate chokepoints
Pump of choice
Cornell, B. (2016). Lymphatic System. BioNinja. Retrieved from Cornell, B. (2016). Lymphatic System. Retrieved from https://ib.bioninja.com.au/higher-level/topic-11-animal-physiology/111-antibody-production-and/lymphatic-system.html
D'Alanzo, G. (2004). Influenza Epidemic or Pandemic? Time to Roll Up Sleeves, Vaccinate Patients, and Hone Osteopathic Manipulative Skills. Journal of the American Osteopathic Association, 104, 9, 370–371. Retrieved from https://jaoa.org/article.aspx?articleid=2093004
Delamere, G., et al. The Lymphatics. Constable, 1903.
Drake, R., Vogl, W., & Mitchell, A. (2005). Grays Anatomy for Students. University of Michigan: Elsevier Churchill Lvgst.
Gray, Henry, and Goss, Charles. Anatomy of the Human Body. Philadelphia and New York : Lea & Febiger, 1858.
Hansen, J. T., & Netter, F. H. (2010). Netters clinical anatomy. Philadelphia, PA: Saunders/Elsevier.
Knott, Marty, B.A., Tune, Johnathan D., Ph.D., Stoll, Scott, D.O., Ph.D., Downey, H. Fred, Ph.D., “Lymphatic Pump Treatments Increase Thoracic Duct Flow,” Osteopathic Research Center News, Vol. 1, issue 2, June 2003.
McCauley, Lyndsey. “The Effect of Lymphatic Pump Treatment on Anti-Tumor Immune Responses.” Theses and Dissertations, University of North Texas Health Science Center, 1 May 2011, unthsc-ir.tdl.org/handle/20.500.12503/26535.
Millard, F. P., and A. G. Walmsley. Applied Anatomy of the Lymphatics. Kirksville, Mo., The Journal Printing Company, 1922.
Nicholas, Alexander S., and Evan A. Nicholas. Atlas of Osteopathic Techniques. 3rd ed., Wolters Kluwer, 2016.
SEER Training Modules, Components of the Lymphatic System. U. S. National Institutes of Health, National Cancer Institute. <https://training.seer.cancer.gov/>.
Schünke, Michael, et al. General Anatomy and Musculoskeletal System. 1st ed., Thieme Medical Publishers, 2014.
Sleszynski SL, Kelso AF, “Comparison of thoracic manipulation with incentive spirometry in preventing postoperative atelectasis,” J Am Osteopath Assoc 1993 Aug; 93(8):834-8, 843-5
Szuba, A, et. al., “Decongestive lymphatic therapy for patients with cancer-related or primary lymphedema,” Am J Med, 2000 Sep; 109(4), pp. 296-300.





























