Embed Size (px)
Citation preview

Long-term outcomes from a multiple-risk-factor diabetes trial forLatinas: ¡Viva Bien!
Deborah J Toobert, Ph.D1, Lisa A Strycker, M.A1, Diane K King, Ph.D2, Manuel Barrera Jr.,Ph.D3, Diego Osuna, M.D., M.P.H4, and Russell E Glasgow, Ph.D5
1 Oregon Research Institute, 1715 Franklin Blvd, Eugene, OR 97403- 1983, USA2 Institute for Health Research Address Kaiser Permanente Colorado, P.O. Box 378066, Denver,CO 80237-8066, USA3 Psychology Department, Arizona State University, Box 871104, Tempe, AZ 85287-1104, USA4 University of Colorado Health Sciences Center, Institute for Health Research, KaiserPermanente Colorado, P.O. Box 378066, Denver, CO 80237-8066, USA5 Dissemination and Implementation Science, Division of Cancer Control and PopulationSciences, National Cancer Institute, 6130 Executive Blvd., Room 6144, Rockville, MD 20852,USA
AbstractLatinas with type 2 diabetes are in need of culturally sensitive interventions to make recommendedlongterm lifestyle changes and reduce heart disease risk. To test the longer-term (24-month)effects of a previously successful, culturally adapted, multiple-healthbehavior- change program,¡Viva Bien!, 280 Latinas were randomly assigned to usual care or ¡Viva Bien!. Treatment includedgroup meetings to promote a culturally adapted Mediterranean diet, physical activity, supportiveresources, problem solving, stress-management practices, and smoking cessation. ¡Viva Bien!participants achieved and maintained some lifestyle improvements from baseline through 24months, including significant improvements for psychosocial outcomes, fat intake, social–environmental support, body mass index, and hemoglobin A1c. Effects tended to diminish overtime. The ¡Viva Bien! multiple-behavior program was effective in improving and maintainingsome psychosocial, behavioral, and biological outcomes related to heart health across 24 monthsfor Latinas with type 2 diabetes, a high-risk, underserved population (ClinicalTrials.gov number,NCT00233259).
KeywordsLatina; Diabetes; Multiple behavior change Self-management; Randomized controlled trial
INTRODUCTIONLatinas with type 2 diabetes are an underserved population at high risk for coronary heartdisease. Hispanic Americans, the fastest-growing ethnic population in the USA—andparticularly Hispanic women (Latinas)—have a greater prevalence of type 2 diabetes andmore diabetes complications than Anglos [1]. By 2050, the Hispanic population will triple,and this population is among the least affluent of US ethnic groups. Disparities in the
Correspondence to: D J Toobert [email protected] authors have no potential conflicts of interest relevant to this article.
NIH Public AccessAuthor ManuscriptTransl Behav Med. Author manuscript; available in PMC 2011 October 19.
Published in final edited form as:Transl Behav Med. 2011 September ; 1(3): 416–426. doi:10.1007/s13142-010-0011-1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
distribution of health and health care in North America are largely attributable to race/ethnicity and socioeconomic status [2, 3], and their effects on the social determinants ofhealth and health-related behaviors places low-income Latinas at greater risk for chronicdiseases such as diabetes [4, 5]. Mexican-American adults are twice as likely as non-Hispanic whites to be diagnosed with diabetes [6]. Studies controlling for social economicstatus find reduced disparities for some health outcomes, but not for diabetes in Latinos [7,8]. Emerging public health models advocate an appropriate response to diabetes disparitiesin health care, such as delivering culturally sensitive diabetes interventions [9].
The ¡Viva Bien! study was a multiple-behavior, coronary-heart-disease-risk-factorintervention designed for Latinas with type 2 diabetes. Prior research has identified the hearthealth benefits of “Mediterranean Diet”-style eating practices [10], being physically active[11–16], managing stress [17–19], and utilizing social–environmental support to initiate andsustain health-supporting behaviors [20–24]. Most US adults, including Latinas, engage inmultiple risk behaviors [25], but multiple-risk-factor intervention studies are rare [26–28].Studies investigating maintenance of multiple health behaviors are expensive, complicated,and infrequently reported. Yet, for individuals with type 2 diabetes, sustaining multiplehealthful behaviors over a lifetime is critical for improving risk factors [29] and avoidingadverse consequences of illness progression, such as coronary heart disease [30].
Practical strategies and theoretical mechanisms for sustaining health behaviors over longerperiods are not well established or understood. Just as medication for chronic illnessesgenerally is prescribed for long periods and may require periodic changes and doseadjustments to retain efficacy, health-behavior interventions may require long activetreatment and similar dose adjustments to retain effects [31, 32]. Of the maintenance studiesavailable, there is clear evidence that few improvements are sustained long-term [33–37],and this research area is characterized by conflicting findings [15, 38, 39].
The purpose of this paper is to advance scientific knowledge and improve clinical practiceregarding the long-term effects of multiple-behavior-change programs in an underserved andhigh-risk Latina population. The study documents the extent to which the ¡Viva Bien!intervention helped Latinas with type 2 diabetes make simultaneous changes in psychosocialfactors and multiple lifestyle behaviors that were hypothesized to result in improvedbiologic and quality of life outcomes from baseline to 24 months.
METHODSStudy Design
The ¡Viva Bien! program was a cultural adaptation and evaluation of an established,evidence-based lifestyle change program for an underserved population at high risk for heartdisease: Latinas with type 2 diabetes [40]. Specific cultural adaptations are described in theappendix. The efficacy of this program was demonstrated previously in mostly non-Hispanicwhite women [41, 42]. The adaptation of ¡Viva Bien! addressed sociocultural, economic, andenvironmental contexts important for Latinas [40].
Patients were recruited from nine Kaiser Permanente clinics in the Denver, Colorado,metropolitan area, and one large community health center, the Salud Family Health Center,in Commerce City near Denver. Kaiser Permanente is a managed-care organization thatserves about 450,000 patients in the Denver metropolitan area, about 17% of whom areLatino. Salud is a community health center that provides comprehensive primary healthservices to low-income patients. About 65% of Salud’s patients are Latinos whose primarylanguage is Spanish.
Toobert et al. Page 2
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Inclusion criteria were self-identified Latina ethnicity, 30–75 years of age, diagnosis of type2 diabetes for at least 6 months identified by electronic medical record codes and using theWelborn criteria [43], living independently, having a telephone, and the ability to read ineither English or Spanish. Exclusion criteria included being on an insulin pump, beingdevelopmentally disabled, or having end-stage renal disease. Participants were recruited [44;Fig. 1) in four waves, with roughly one fourth of the sample participating in each wave.
Letters in English and Spanish, signed by the project’s Latino physician, were mailed topotential participants, along with self-addressed stamped postcards that could be returned todecline further contact or request information. Women who did not return postcards weretelephoned by bilingual project recruiters, who described the program, confirmed eligibility,and invited qualified candidates to participate. Those who agreed were scheduled forbaseline assessments. Those in the usual care condition received $25 gift cards forassessment completion; those in ¡Viva Bien! received the intervention at no cost to them andwere not paid for assessment completion or for their time in the study.
Research procedures followed were approved by the Kaiser Permanente Denver, Colorado,and Oregon Research Institute institutional review boards, and were in accordance with theHelsinki Declaration of 1975, as revised in 2000. All participants gave written informedconsent. Data were collected from 2006 through 2009 and analyzed for this report in 2010.
Treatment ProtocolParticipants who completed baseline assessments (N=280) were randomized to enhancedusual diabetes care or to the ¡Viva Bien! intervention. The ¡Viva Bien! program included a2½-day retreat followed by meetings that were weekly for the first 6 months, semi-monthlyfor months 6–12, monthly for months 12–18, and bi-monthly for months 18–24. Theprogram encouraged participants to (a) follow the Mediterranean diet adapted for Latinonationality subgroups, (b) practice stress-management techniques daily, (c) engage in 30 minof daily physical activity, (d) stop smoking, and (e) participate in problem- solving-basedsupport groups. The purpose of the retreat was to introduce the program and practice newskills. The intervention continued with 4-h facilitatorled meetings, providing 1 h each ofinstruction and practice of the above components except for smoking, which was addressedindividually due to the small number of smokers. The usual medical care condition at KaiserPermanente Denver, Colorado, consisted of management of complications associated withdiabetes, monitoring of other health factors, and specified frequencies of laboratory assaysand specialty exams in compliance with the American Diabetes Association standards ofcare. The enhancement included a choice of one free Kaiser-Permanente Denver, Coloradoclass covering the areas targeted in ¡Viva Bien!.
MeasuresAssessments were conducted at baseline and at 6, 12, and 24 months for all participants. Theabbreviated form of the ARSMA-II [45] was used to measure bidirectional acculturation. Inaddition, questions about participant nativity and nativity of parents were asked to determinegenerational status. Problem-solving ability was assessed using the Diabetes Problem-Solving Interview [46]. Self-efficacy was measured with the Confidence in OvercomingChallenges to Self-Care instrument [47]. Social support was assessed using the UCLASocial Support Inventory [48]. The semi-quantitative food frequency questionnaire [49] wasused to document percent of calories from saturated fat. Stress-management practice wasassessed using a self-monitoring log to track daily minutes of yoga stretches, breathingexercises, progressive relaxation, and meditation and visualization. The stress-managementpractice score was the summed minutes across 7 days of these activities (square-roottransformed for analyses) [41]. The Modified International Physical Activity Questionnaire
Toobert et al. Page 3
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
was used to calculate the number of days per week participants engaged in exercise [50].This measure has been previously validated [50] and in the present study correlated 0.34(p=0.007) at baseline in a subset of participants (n=60) wearing ActiGraph (MTI HealthServices) accelerometers for 7 days. The Brief Chronic Illness Resources Survey [51]provided frequencies of an individual’s perceived social–environmental support for diseasemanagement. Measures of height and weight were taken on a sensitive digital scale (DetectoElectronics). Hemoglobin A1c assays were performed at the Kaiser Permanente Denver,Colorado Regional Reference Laboratory in Aurora, CO, and measured on a Bio-RadVariant II Turbo liquid by high-pressure liquid chromatography. Ten-year coronary heartdisease risk was assessed using the United Kingdom Prospective Diabetes Study logisticequation [52]. Hemoglobin A1c values and the coronary heart disease 10-year risk scorewere square-root transformed for analyses.
AnalysesDescriptive analyses were used to determine whether transformations were needed. Chi-square or t tests were used to evaluate differences in participant characteristics between thetwo treatment conditions and between dropouts and those who completed the study at 24months.
Long-term effects—Generalized estimating equations models [53] were used to comparelong-term treatment effects on outcome measures from baseline to 24 months. Models werespecified using a first-order autoregressive correlation structure, and separate models wereconducted to examine treatment group interactions with both linear and quadratic trends.Linear-trend results are presented here, as model results were similar for linear and quadratictrends. Wave was covaried in all analyses, as was age, which was found in univariatecorrelational analyses to be significantly associated with outcomes at baseline. Effect sizes(d) were calculated on the difference between the two treatment conditions at all followuptime points.
Missing data—Mean percent (averaged across ten measures) of total observations missingat each assessment point were as follows: 10% usual care vs. 9% ¡Viva Bien! at baseline;25% usual care vs. 27% ¡Viva Bien! at 6 months; 32% usual care vs. 39% ¡Viva Bien! at 12months; and 39% usual care vs. 43% ¡Viva Bien! at 24 months. Generalized estimatingequations analyses were performed two ways. First, a complete-case approach was used, inwhich participants with missing follow-up data on the outcome variable of interest wereexcluded from the analysis. Identical analyses were conducted after missing data wereimputed using multiple imputation procedures via the expectation-maximization algorithmwith NORM software [54]. The results were similar; therefore, only intent-to-treat (imputed)results are presented in the tables (with superscripts indicating differences from complete-case results).
Statistical analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL).
RESULTSParticipants
Recruitment results have been reported previously [44]. The study recruited a diverse,relatively highrisk sample of Latina women (N=280). About 51% of those confirmedeligible agreed to participate.
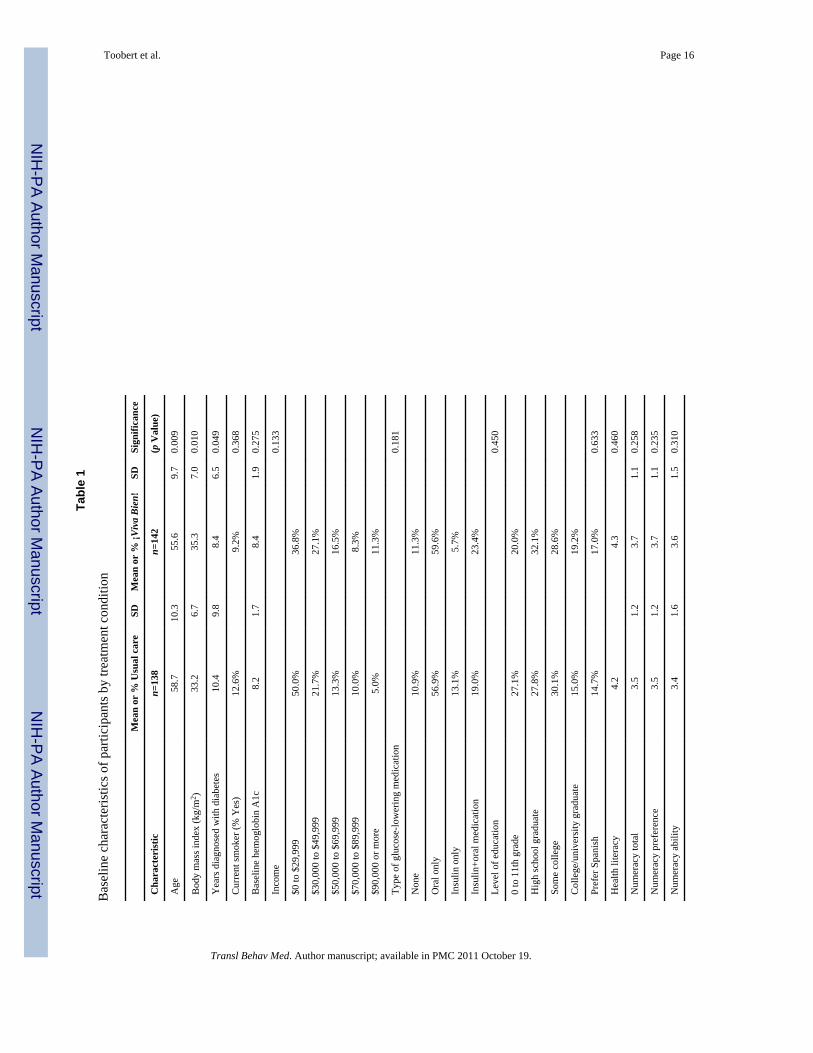
Participant characteristics are presented in Table 1. On average, participants were about 57years of age, had been diagnosed with diabetes for almost 10 years, were obese, and had a
Toobert et al. Page 4
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
baseline hemoglobin A1c level greater than 8. Approximately two thirds reported an annualfamily income of less than $50,000. The recruited sample varied by acculturation, with40.8% mostly Anglo-oriented, 24.3% somewhat Anglo-oriented, 17.6% mixed Latino-and-Anglo-oriented, 4.8% somewhat Latino-oriented, and 12.5% mostly Latino-oriented [40].Sixteen percent preferred Spanish to English, and health literacy scores were considerablylower than in our prior primary care-based diabetes projects. Most participants were born inthe USA (79.6%) or Mexico (15.8%), with one to two women each reporting their birthcountry as El Salvador, France, Morocco, Brazil, Peru, Panama, Cuba, Puerto Rico,Guatemala, or Honduras. The participants’ parents were also born primarily in the USA(mother= 72.1%; father=69.8%) and Mexico (mother=21.6%; father=23.7%), with smallpercentages in many other European, Asian, and Latin American countries. Acculturationlevel was not significantly associated with outcomes at baseline. Despite randomization,there were significant baseline differences between conditions on age, body mass index, andyears diagnosed with diabetes (which significantly correlated with age). Usual careparticipants were older, had diabetes longer, and had lower bodymass index than ¡Viva Bien!participants.
Attendance at ¡Viva Bien! sessions varied. Weekly meeting attendance during the first 6months averaged 65%, declined to 48% for meetings between 6 and 12 months, andaveraged 46% for meetings between 12 and 24 months.
Attrition rates were 22.5% at 6 months, 30.0% at 12 months, and 38.6% at 24 months, withno significant differences between treatment conditions in attrition at any time point.
Relative to dropouts, study completers were older (mean years at baseline=59.0 years[SD=8.9] vs. 54.1 [SD=11.1]; t(189)=3.76, p<.001), had higher health literacy (mean scoreat baseline=4.4 [SD=0.8] vs. 4.1 [SD=0.9]; t(196)=2.65, p=.009), had higher numeracyscores (mean score at baseline=3.7 [SD=1.2] vs. 3.4 [SD=1.2]; t(217)=2.21, p=.028), had alower prevalence of smoking (7.1% vs. 17.0%; χ2(1)=6.6, p=.01), and had a lowerproportion of taking insulin (24.0% vs. 41.0%; χ2 (1)=9.2, p=.01). Dropouts and completersdid not differ significantly on body mass index, years diagnosed with diabetes, income,education, language preference, or acculturation.
Psychosocial OutcomesThere were large and consistent differences between conditions on improvement in thepsychosocial variables hypothesized to be influenced by the intervention (Table 2). The¡Viva Bien! condition improved considerably more than the usual care condition by the 6-month follow-up on measures of problem solving, self-efficacy, and perceived supportiveresources. Gains were essentially maintained at 12- and 24-month follow-ups, with 24-month follow-up effect sizes ranging from no effect for self-efficacy to 0.75 for problemsolving and perceived support.
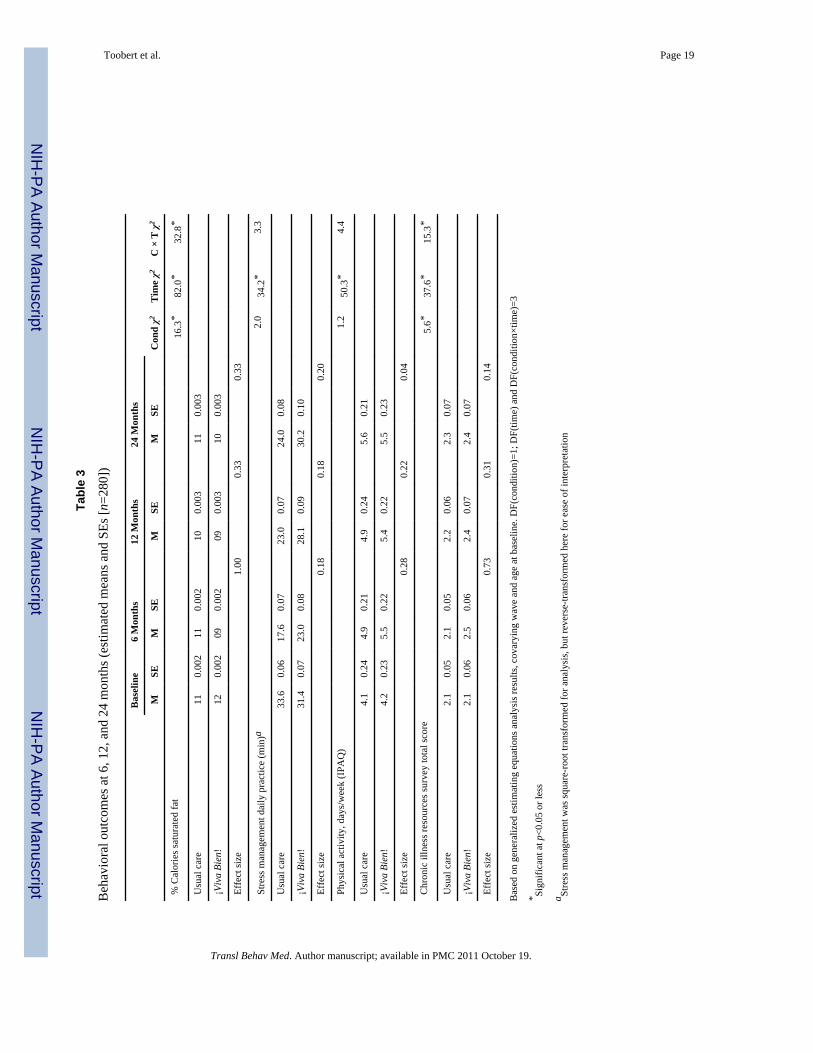
Behavior ChangeBetween-condition effects were found across 24 months on two of the targeted behavioraloutcomes (Table 3): percent calories from saturated fat and engagement in social–environmental support activities. Effect sizes ranged from 0.04 (for physical activity) to 0.33(for percent calories from saturated fat) at the 24-month follow-up. The ¡Viva Bien!participants did not maintain their initial 6-month significant improvements relative to theusual care condition on practice of stress management. For physical activity, initial 6-monthsignificant improvements relative to usual care also were not maintained, in part because theusual care condition improved on this outcome.
Toobert et al. Page 5
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
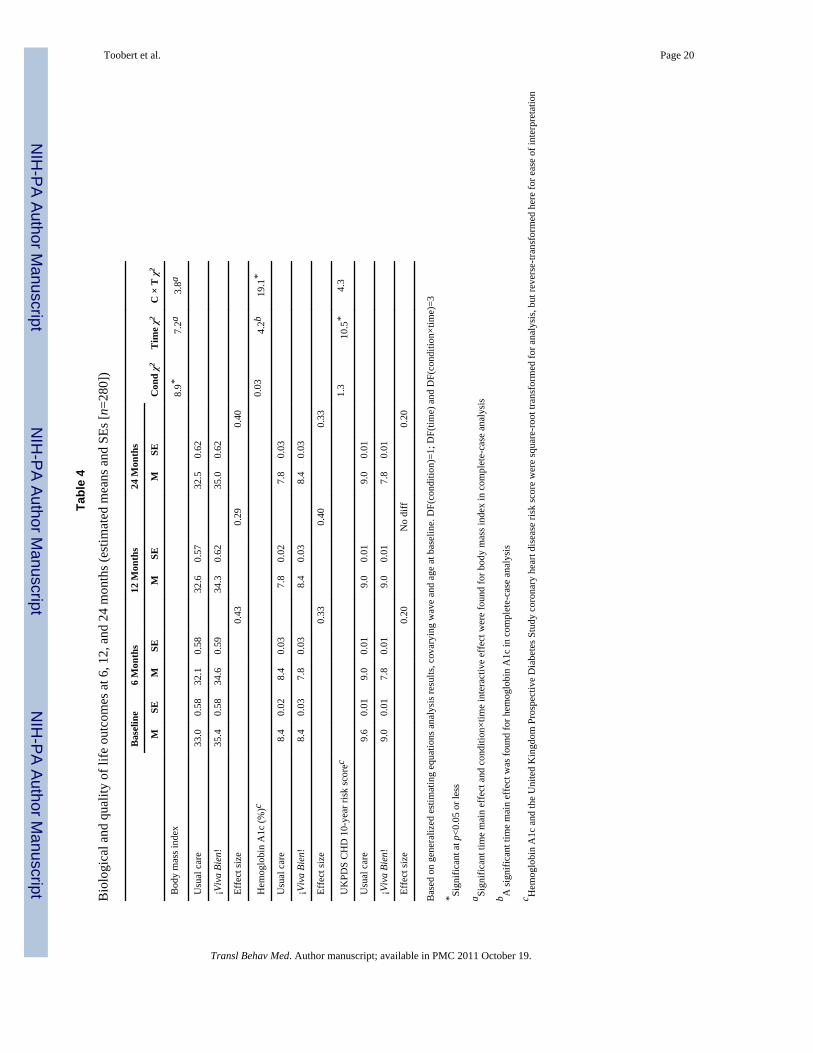
Biological OutcomesBiological outcomes across 24 months were inconsistent (Table 4). The ¡Viva Bien!condition improved significantly more than the usual care condition on body mass index, butearly improvement in hemoglobin A1c was not maintained. Coronary heart disease risk asmeasured by the United Kingdom Prospective Diabetes Study logistic equation was notsignificantly improved. Biologic improvements generally decreased across the 2-yearperiod.
DISCUSSIONThere is a paucity of information on the long-term effects of multiple-risk-factor trials,especially in high-risk populations [15, 38]. The primary goal of this paper was to evaluatewhether the effects of a multiple-behavior-change program, ¡Viva Bien!, adapted for anunderserved and high-risk Latina population, sustained improvements on targeted diabetesself-management, psychosocial variables, and biologic outcomes after the interventionfaded.
The ¡Viva Bien! intervention was initially intense, with a 2½-day retreat followed by 6months of weekly 4-h meetings, but the study was also designed to maximize participantreach and generalizability of the outcomes. Few exclusion criteria were employed, andpatients were recruited from two different health systems. The intervention componentswere delivered by a mix of bilingual clinical staff and community professionals and wereevaluated systematically for their appropriateness and appeal to Latina participants in focusgroups, a review by Latino/a professionals, and pilot testing prior to the intervention trial[40]. Cultural appropriateness was assured by systematically giving participantsopportunities to inform and influence intervention components to ensure cultural fit whilemaintaining fidelity to the original intervention. The finding that attrition rates were notassociated with language preference or acculturation suggests that the program wasculturally relevant to most Latinas in the sample.
While the 38.6% 24-month dropout rate was disappointing, attrition did not differsignificantly by treatment condition or key participant characteristics, and attrition analysesindicated that those unavailable for the 24-month follow-up were generally similar to thosewho continued participation. Compared with our previous lifestyle-change study withmostly Anglo women [55], the Mediterranean Lifestyle Program (MLP), from which ¡VivaBien! was adapted, program attendance was higher (65% for 0–6 months and 47% for 6–24months in ¡Viva Bien! vs. 54% for 0–6 months and 31% for 6– 24 months). The ¡Viva Bien!attendance rates are in line with those reported in similar studies with this population, suchas those reported in a review of multifactorial lifestyle interventions to prevent chronicillness (diabetes and coronary heart disease) by Angermayr et al. [56]. All studies in thereview contained a stress-management component. In eight of the studies that explicitlyreported attendance rates, most reported that participants attended more than 60% of thescheduled sessions.
The 24-month retention rate in ¡Viva Bien! was lower than in the MLP (61.4% in ¡VivaBien! vs. 85.3% in the MLP). There are few studies with which to compare the ¡Viva Bien!retention rates directly (i.e., multiple-risk-factor programs with Latinas having type 2diabetes, at 24-month followup). Somewhat comparable studies report retention ratesranging from 56% to 100%, although mostly for much shorter follow-up times (with anotable exception [57]). Silberman et al. [58] reported that 78.1% of the participantsremained enrolled in the program at the end of 1 year. In the Angermayr et al. review [56],the proportion of participants terminating study interventions prematurely varied from 0% to44%, depending on length of follow-up. At 24 months in the Diabetes Prevention Program
Toobert et al. Page 6
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Outcome Study [57], 81% of participants were still enrolled. In a program by Eakin et al.[59] targeting urban Latinos with multiple chronic conditions, the retention rate at 6 monthswas 81%. However, this intervention was much lower in intensity than either the MLP or¡Viva Bien!. A dietary intervention targeting Latinas [60] found that at 12 months 79% ofthe original 357 study participants were available for follow-up analyses. Brown, Garcia,Kouzekanani, and Hanis [61] reported a 12-month retention rate of 90% in their studyinvolving a culturally competent lifestyle intervention targeting Mexican- Americans withtype 2 diabetes. Poston et al. [62] reported a 12-month retention rate of 66% in a study of108 Mexican-American women testing a culturally tailored lifestyle modificationintervention.
¡Viva Bien! employed a number of methods to maximize attendance and retention. Theseincluded family member involvement, expert presentations, practical, and relevant skill-based intervention components, friendly competitions, and active involvement. Socialconnection with staff and peers was strongly encouraged. Staff and peers made phone callsand sent cards to participants who missed sessions. Health benefits experienced in theprogram also exerted a strong influence to remain in the study. Transportation barriers wereminimized by the provision of taxi service and by locating meetings in convenientcommunity settings. Of those giving a reason for non-attendance, the most frequent wasillness (9.9%), followed by work-related conflicts (4.5%), being on vacation (4.2%), orhaving a social conflict (3.7%). Anecdotal evidence from exit interviews suggested that asthe in-person intervention sessions faded, intervention condition participants felt adiminished responsibility to themselves and to the program. Future studies in this populationmight improve adherence/retention by introducing maintenance strategies from thebeginning of the program, maintaining the level of intensity throughout the interventionperiod and offering greater incentives for follow-up assessment participation.
Despite missing data arising from attrition, results of generalized estimating equationanalyses using complete-case and imputed data were similar. ¡Viva Bien! participantscompared with usual care significantly improved by the 6-month follow-up on thepsychosocial measures of problem solving, selfefficacy, and perceived support, and thesegains were maintained at 12- and 24-month follow-ups. Between-condition effects werefound across 24 months on dietary patterns (percent calories from saturated fat) and use ofsocial–environmental resources to support chronic disease self-management. Improvementsin stress management and days per week exercised were sustained by ¡Viva Bien!participants; however, there were improvements in these factors by usual care participantsby the end of 24 months as well, thus diminishing the longitudinal intervention effect.Effects of ¡Viva Bien! on biological outcomes were initially promising. These effects werenot maintained, however, as participants in both conditions approached baseline levels by 24months.
Although the treatment condition improved across the 24-month intervention, the challengein sustaining physical activity is well documented [63, 64], and sustaining stressmanagement over long periods is virtually undocumented. For behaviors that are notcurrently part of daily living, such as physical activity or stress management (as opposed toeating) to become habitual, it may be that the intervention must address not only individualbehaviors, but also the home, neighborhood, job, and social environments, which mayincrease stress and promote sedentary lifestyles. While these environments may alsoencourage unhealthful eating, it is possible that changing eating habits (e.g., modifying foodpreparation techniques to reduce saturated fat) requires less effort to sustain, once mastered,than a daily walk or stress-management practices [65]. Recent evidence suggests that peoplewith diabetes experience greater perceived exertion than those without diabetes,necessitating greater motivational and supportive resources than the general population to
Toobert et al. Page 7
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
maintain physical activity [66]. And, in general, participation in regular physical activityamong Hispanics tends to be lower than in non- Hispanic whites [67]. Thus, an ecologicalapproach that includes personal, intrapersonal, organizational, and environment/policychanges to support healthful lifestyles, particularly among populations with increased riskand disproportionate burden for chronic conditions such as diabetes, may be required forsustained change in multiple health behaviors.
This practical trial has both methodological strengths and weaknesses, as well asimplications for practice, policy, and research [68, 69]. Strengths include an interventionthat addressed a multiple-risk-factor problem with a previously tested multiple-behavior-change intervention, cultural adaptation for a Latina population, a reasonably large anddiverse Latina sample, use of multiple measures, multiple imputation procedures forhandling missing data, and generalized estimating equation analyses across 24 months.
A possible limitation of our study was the use of primarily self-report measures forbehavioral outcomes. Most of these measures have been validated against more objectivestandards in previous studies, but it is not known whether possible self-reportinginaccuracies influenced the observed results. The correlation (r=0.34) in this study betweenthe Modified International Physical Activity Questionnaire and accelerometer data, thoughmoderate, is similar to findings of other studies correlating self-reports of activity and moreobjective indicators (e.g., our study [70] correlating 7-day pedometer step counts 0.31 with a7-day diary physical activity in a sample of older women). Such results suggest that the twomodes of physical activity measurement (self-report and pedometer/accelerometers) provideboth common and unique information. Another limitation was that the comprehensivelifestyle intervention cannot be easily disentangled to understand the contribution of discreteelements. The efficacy of the core components of the lifestyle intervention (diet, physicalactivity, stress management, and social support) have been well established in the literature;less understood is how they work in concert.
Future DirectionsThe short-term effectiveness of multibehavioral interventions, such as ¡Viva Bien!, isencouraging, but the inability of behavioral interventions to sustain behavior change orimprovements in biologic or quality-of-life outcomes over time continues to be a challenge[71]. More research is needed to develop and test novel and cost-effective interventions thatcan sustain the motivation and support needed to accomplish successful, lifelong diabetesself-management. Research that investigates characteristics of social and physicalenvironments associated with sustaining multiple-health-behavior change is sorely needed[72].
The ¡Viva Bien! program succeeded in changing multiple key health behaviors. As contactfaded after 6 months, so did the intervention effects. For people with chronic conditions,maintenance interventions that provide ongoing social, motivational, and problem-solvingsupport may be as important as addressing long-term medication adherence. Suchinterventions may be best delivered through community organizations (e.g., faith-based,worksites, schools), neighborhoods (e.g., infrastructures that support activity; neighborhoodgroups that support norms for health), and technology (e.g., phone, social media, internet).
AcknowledgmentsWe acknowledge the invaluable contributions of the assessment and intervention staffs of the ¡Viva Bien! project,including Cristy Geno Rasmussen, Alyssa Doty, Fabio Almeida, Sara Hoerlein, Carmen Martin, Angela Casola,Eve Halterman, and Breanne A. Griffin. We are deeply indebted to the 280 dedicated and committed women whoparticipated in the study.
Toobert et al. Page 8
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Funding disclosure: This research was supported by grant number R01- HL077120 from the National Heart, Lung,and Blood Institute.
References1. Narayan KMV, D’Agostino RB, Kirk JK, et al. Disparities in A1C levels between Hispanic and
non-Hispanic white adults with diabetes. Diabetes Care. 2008; 31:240–246. [PubMed: 17977939]2. Livingston, G.; Minushkin, S.; Cohn, D. [Accessibility verified August 6, 2010] Hispanics and
health care in the United States: access, information and knowledge. 2008. Available athttp://pewhispanic.org/reports/report.php?ReportID=91
3. Ward MM. Access to care and the incidence of end-stage renal disease due to diabetes. DiabetesCare. 2009; 32:1032–1036. [PubMed: 19460914]
4. Gallo LC, de los Monteros KE, Ferent V, Urbina J, Talavera G. Education, psychosocial resources,and metabolic syndrome variables in Latinas. Annals of Behavioral Medicine. 2007; 34:14–25.[PubMed: 17688393]
5. DeNavas-Walt, C.; Proctor, BD.; Smith, JC. US Census Bureau, current population reports,P60-236, income, poverty, and health insurance coverage in the United States: 2008. Washington,DC: U.S. Government Printing Office; 2008. 2009
6. National Center for Health Statistics. [Accessibility verified August 6, 2010] Health, United States,2008 with chartbook. Available at http://www.cdc.gov/nchs/data/hus/hus08.pdfTBM page 9 of 11
7. Whitfield KE, Clark R, Weidner G, Anderson NB. Sociodemographic diversity and behaviormedicine. Journal of Consulting and Clinical Psychology. 2002; 70:463–481. [PubMed: 12090363]
8. Saydah S, Cowie C, Eberhardt MS, De Rekeneire N, Narayan KM. Race and ethnic differences inglycemic control among adults with diagnosed diabetes in the United States. Ethnicity & Disease.2007; 17:529–535. [PubMed: 17985509]
9. Sarkisian CA, Brown AF, Norris KC, Wintz RL, Mangione CMA. Systematic review of diabetesselfcare interventions for older, African American, or Latino adults. The Diabetes Educator. 2003;29:467–479. [PubMed: 12861963]
10. de Lorgeril M, Renaud S, Mamelle N, et al. Mediterranean alpha-linolenic acid-rich diet insecondary prevention of coronary heart disease. Lancet. 1994; 343:1454–1459. [PubMed:7911176]
11. Wing RR, Hill JO. Successful weight loss maintenance. Annual Review of Nutrition. 2001;21:323–341.
12. Crawford D, Jeffery RW, French SA. Can anyone successfully control their weight? Findings of athree-year community-based study of men and women. International Journal of Obesity andRelated Metabolic Disorders. 2000; 24:1107– 1110. [PubMed: 11033978]
13. Schoeller DA, Shay K, Kushner RF. How much physical activity is needed to minimize weightgain in previously obese women? The American Journal of Clinical Nutrition. 1997; 66:551–556.[PubMed: 9280172]
14. Mekary RA, Feskanich D, Hu FB, Willett WC, Field AE. Physical activity in relation to long-termweight maintenance after intentional weight loss in premenopausal women. Obesity. 2010;18:167–174. [PubMed: 19498346]
15. Elfhag K, Rossner S. Who succeeds in maintaining weight loss? A conceptual review of factorsassociated with weight loss maintenance and weight regain. Obesity Reviews. 2005; 6:67–85.[PubMed: 15655039]
16. Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. A descriptive study of individualssuccessful at long-term maintenance of substantial weight loss. The American Journal of ClinicalNutrition. 1997; 66:239–246. [PubMed: 9250100]
17. Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology,pathophysiology, and management of psychosocial risk factors in cardiac practice: the emergingfield of behavioral cardiology. Journal of the American College of Cardiology. 2005; 45:637–651.[PubMed: 15734605]
Toobert et al. Page 9
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

18. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated withmyocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet.2004; 364:937–952. [PubMed: 15364185]
19. Gonder-Frederick LA, Cox DJ, Ritterband LM. Diabetes and behavioral medicine: the seconddecade. Journal of Consulting and Clinical Psychology. 2002; 70:611–625. [PubMed: 12090372]
20. White AM, Philogene GS, Fine L, Sinha S. Social support and self-reported health status of olderadults in the United States. American Journal of Public Health. 2009; 99:1872– 1878. [PubMed:19696390]
21. Anderson ES, Winett RA, Wojcik JR, Williams DM. Social cognitive mediators of change in agroup randomized nutrition and physical activity intervention: social support, self-efficacy,outcome expectations and self-regulation in the Guide-to-Health Trial. Journal of HealthPsychology. 2010; 15:21–32. [PubMed: 20064881]
22. Beverly EA, Miller CK, Wray LA. Spousal support and food-related behavior change in middle-aged and older adults living with type 2 diabetes. Health Education & Behavior. 2008; 35:707–720. [PubMed: 17456857]
23. Vrazel J, Saunders RP, Wilcox S. An overview and proposed framework of social-environmentinfluences on the physical-activity behavior of women. American Journal of Health Promotion.2008; 23:2–12. [PubMed: 18785368]
24. Leifheit-Limson EC, Reid KJ, Kasl SV, et al. The role of social support in health status anddepressive symptoms after acute myocardial infarction: evidence for a stronger relationship amongwomen. Circulation: Cardiovascular Quality and Outcomes. 2010; 3:143–150. [PubMed:20160162]
25. Fine LJ, Philogene S, Gramling R, Coups EJ, Sinha S. Prevalence of multiple chronic disease riskfactors: 2001 National Health Interview Survey. American Journal of Preventive Medicine. 2004;27:18–24. [PubMed: 15275670]
26. Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease?The Lifestyle Heart Trial. Lancet. 1990; 336:129–133. [PubMed: 1973470]
27. Toobert DJ, Glasgow RE, Radcliffe JL. Physiologic and related behavioral outcomes from theWomen’s Lifestyle Heart Trial. Annals of Behavioral Medicine. 2000; 22:1–9. [PubMed:10892523]
28. Prochaska JJ, Nigg CR, Spring B, Velicer WF, Prochaska JO. The benefits and challenges ofmultiple health behavior change in research and in practice. Preventive Medicine. 2010; 50:26–29.[PubMed: 19948184]
29. Wing RR, Epstein LH, Nowalk MP, Koeske RH. Behavior change, weight loss, and psychologicalimprovements in type II diabetic patients. Journal of Consulting and Clinical Psychology. 1985;53:111–122. [PubMed: 3980816]
30. Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention andcardiovascular disease in patients with type 2 diabetes. The New England Journal of Medicine.2003; 348:383–393. [PubMed: 12556541]
31. Norris SL, Nichols PJ, Caspersen CJ, et al. The effectiveness of disease and case management forpeople with diabetes. American Journal of Preventive Medicine. 2002; 22:15–38. [PubMed:11985933]
32. Turk MW, Yang K, Hravnak M, Sereika SM, Ewing LJ, Burke LE. Randomized clinical trials ofweight loss maintenance: a review. The Journal of Cardiovascular Nursing. 2009; 24:58–80.[PubMed: 19114803]
33. Kumanyika SK, Bowen D, Rolls BJ, et al. Maintenance of dietary behavior change. HealthPsychology. 2000; 19(Suppl 1):42–56. [PubMed: 10709947]
34. Pavlou KN, Krey S, Steffee WP. Exercise as an adjunct to weight loss and maintenance inmoderately obese subjects. The American Journal of Clinical Nutrition. 1989; 49(Suppl 5):1115–1123. [PubMed: 2655416]
35. Wing RR, Fava JL, Phelan S, et al. Maintaining large weight losses: the role of behavioral andpsychological factors. Journal of Consulting and Clinical Psychology. 2008; 76:1015–1021.[PubMed: 19045969]
Toobert et al. Page 10
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
36. Wing RR, Tate DF, Gorin AA, Raynor HA, Fava JL. A self-regulation program for maintenance ofweight loss. The New England Journal of Medicine. 2006; 355:1563–1571. [PubMed: 17035649]
37. Wing RR, Jakicic J, Neiberg R, et al. Fitness, fatness, and cardiovascular risk factors in type 2diabetes: Look AHEAD Study. Medicine and Science in Sports and Exercise. 2007; 39:2107–2116. [PubMed: 18046181]
38. Pi-Sunyer FX. How effective are lifestyle changes in the prevention of type 2 diabetes mellitus?Nutrition Reviews. 2007; 65:101–110. [PubMed: 17425061]
39. Martinson BC, Sherwood NE, Crain AL, et al. Maintaining physical activity among older adults:24-month outcomes of the Keep Active Minnesota Randomized Controlled Trial. PreventiveMedicine. 2010; 51:37–44. [PubMed: 20382179]
40. Osuna D, Barrera M Jr, Strycker LA, et al. Methods for the cultural adaptation of a diabeteslifestyle intervention for Latinas: an illustrative project. Health Promotion Practice. 2010 in press.
41. Toobert DJ, Strycker LA, Glasgow RE, Barrera M, Angell K. Effects of the MediterraneanLifestyle Program on multiple risk behaviors and psychosocial outcomes among women at risk forheart disease. Annals of Behavioral Medicine. 2005; 29:128–37. [PubMed: 15823786]
42. Toobert DJ, Glasgow RE, Strycker LA, et al. Biologic and quality of life outcomes from theMediterranean Lifestyle Program: a randomized clinical trial. Diabetes Care. 2003; 26:2288–2293.[PubMed: 12882850]
43. Welborn TA, Garcia-Webb P, Bonser A, et al. Clinical criteria that reflect c-peptide status inidiopathic diabetes. Diabetes Care. 1983; 6:315–316. [PubMed: 6347586]
44. Toobert DJ, Strycker LA, Glasgow RE, et al. ¡Viva Bien!: overcoming recruitment challenges in amultiple-risk-factor diabetes trial. American Journal of Health Behavior. 2010 in press.
45. Cuellar I, Arnold B, Maldanado R. Acculturation Rating Scale for Mexican Americans-II: arevision of the original ARSMA scale. Hispanic Journal of Behavioral Sciences. 1995; 17:275–304.
46. Glasgow RE, Toobert DJ, Barrera M, Strycker LA. Assessment of problem solving: a key tosuccessful diabetes self-management. Journal of Behavioral Medicine. 2004; 27:477–490.[PubMed: 15675636]
47. Glasgow RE, Toobert DJ, Gillette CD. Psychosocial barriers to diabetes self-management andquality of life. Diabetes Spectrum. 2001; 14:33–41.
48. Schwarzer R, Dunkel-Schetter C, Kemeny ME. The multidimensional nature of received socialsupport in gay men at risk of HIV infection and AIDS. American Journal of CommunityPsychology. 1994; 22:319–339. [PubMed: 7879745]
49. Patterson RE, Kristal A, Tinker LF, et al. Measurement characteristics of the Women’s HealthInitiative Food Frequency Questionnaire. Annals of Epidemiology. 1999; 9:178–187. [PubMed:10192650]
50. Craig CL, Marchall AL, Sjostrom M, et al. International Physical Activity Questionnaire: 12-country reliability and validity. Medicine and Science in Sports and Exercise. 2003; 35:1381–1395. [PubMed: 12900694]
51. Glasgow RE, Strycker LA, Toobert DJ, Eakin E. A social-ecologic approach to assessing supportfor disease self-management: the Chronic Illness Resources Survey. Journal of BehavioralMedicine. 2000; 23:559–583. [PubMed: 11199088]
52. Stevens RJ, Kothari V, Adler AI, Stratton IM, Holman RR. The UKPDS risk engine: a model forthe risk of page 10 of 11 TBM coronary heart disease in type II diabetes (UKPDS 56). ClinicalScience. 2001; 101:671–679. [PubMed: 11724655]
53. Veger SL, Liang KY. The analysis of discrete and continuous longitudinal data. Biometry. 1986;42:121–130.
54. Schafer, JL. [Accessibility verified March 1, 2010] NORM: multiple imputation of incompletemultivariate data under a normal model, software for Windows 95/98/NT, 1999, version 2.03.1999. Available from www.stat.psu.edu/~jls/misoftwa.html
55. Toobert DJ, Glasgow RE, Strycker LA, Barrera M, Ritzwoller DP, Weidner G. Long-term effectsof the Mediterranean Lifestyle Program: a randomized clinical trial for postmenopausal womenwith type 2 diabetes. International Journal of Behavioral Nutrition and Physical Activity. 2007;4:1–12.10.1186/1479-5868-4-1 [PubMed: 17229325]
Toobert et al. Page 11
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
56. Angermayr L, Melchart D. Multifactorial lifestyle interventions in the primary and secondaryprevention of cardiovascular disease and type 2 diabetes meillitus: a systematic review ofrandomized controlled trials. Annals of Behavioral Medicine. 2010; 40:49–64. [PubMed:20652464]
57. Knowler W, Fowler S, Hamman R, et al. 10-year follow-up of diabetes incidence and weight lossin the Diabetes Prevention Program Outcomes Study. Lancet. 2009; 374:1677–1686. [PubMed:19878986]
58. Silberman A, Banthia R, Estay IS, et al. The effectiveness and efficacy of an intensive cardiacrehabilitation program in 24 sites. American Journal of Health Promotion. 2010; 24:260–266.[PubMed: 20232608]
59. Eakin EG, Riley KM, Bull SS, Reeves MM. Resources for health: a primary-care based diet andphysical activity intervention targeting urban Latinos with multiple chronic conditions. HealthPsychology. 2007; 26:392–400. [PubMed: 17605558]
60. Elder JP, Ayala GX, Campbell NR, et al. Long-term effects of a communication intervention forSpanish-dominant Latinas. American Journal of Preventive Medicine. 2006; 31:159–166.[PubMed: 16829333]
61. Brown SA, Garcia AA, Kouzekanani K, Hanis CL. Culturally competent diabetes self-management education for Mexican Americans: the Starr County Border Health Initiative.Diabetes Care. 2002; 25:259–268. [PubMed: 11815493]
62. Poston WSC, Reeves RS, Haddock CK, et al. Weight loss in obese Mexican Americans treated for1-year with Orlistat and lifestyle modification. International Journal of Obesity. 2003; 27:1486–1493. [PubMed: 14634679]
63. Marcus BH, Williams DM, Dubbert PM, et al. Physical activity intervention studies: what weknow and what we need to know: a scientific statement from the American Heart AssociationCouncil on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity);Council on Cardiovascular Disease in the Young; and the Interdisciplinary Working Group onQuality of Care and Outcomes Research. Circulation. 2006; 114:2739–2752. [PubMed: 17145995]
64. Merrill RM, Aldana SG, Greenlaw RL, et al. Can newly acquired healthy behaviors persist? Ananalysis of health behavior decay. Preventing Chronic Disease. 2008; 5:A13. [PubMed: 18082002]
65. Watson JF, DuFord S. Perceived and actual knowledge of diet by individuals with noninsulin-dependent diabetes. The Diabetes Educator. 1992; 18:401–406. [PubMed: 1296889]
66. Huebschmann AG, Reis EN, Emsermann C, et al. Women with type 2 diabetes perceive hardereffort during exercise than nondiabetic women. Applied Physiology, Nutrition, and Metabolism.2009; 34:851–857.
67. Adabonyan I, Loustalot F, Kruger J, Carlson SA, Fulton JE. Prevalence of highly active adults–Behavioral Risk Factor Surveillance System, 2007. Preventive Medicine. 2010; 51:139– 143.[PubMed: 20561970]
68. Glasgow RE. Translating research to practice: lessons learned, areas for improvement, and futuredirections. Diabetes Care. 2003; 26:2451–2456. [PubMed: 12882877]
69. Tunis SR, Stryer DB, Clancey CM. Practical clinical trials. Increasing the value of clinical researchfor decision making in clinical and health policy. Journal of the American Medical Association.2003; 290:1624–1632. [PubMed: 14506122]
70. Strycker LA, Duncan SC, Chaumeton NR, Duncan TE, Toobert DJ. Reliability of pedometer datain youth and older women. International Journal of Behavioral Nutrition and Physical Activity.2007; 4:4.10.1186/1479-5868-4-4 [PubMed: 17306031]
71. Soloman S, Kingston R. National efforts to promote behavior change research: views from theoffice of behavioral and social sciences research. Health Education Research. 2002; 17:495–499.[PubMed: 12408194]
72. Sallis JF, Saelens BE, Frank LD, et al. Neighborhood built environment and income: examiningmultiple health outcomes. Social Science & Medicine. 2009; 68:1285–1293. [PubMed: 19232809]
Toobert et al. Page 12
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Appendix
Cultural adaptations of ¡Viva Bien! intervention components1. Intervention Component: Initial 2½-Day Retreat
The kickoff retreat started the program and built camaraderie between participants and staff.The retreat consisted of introductions and practice of all ¡Viva Bien! program pieces:
Mediterranean diet meals (catered)
Physical activity (aerobic and strength training)
Stress management
Social support groups
Smoking cessation
Cultural Adaptations—The Mediterranean Diet was adapted to the tastes of the Latinoculture (see below). Bilingual staff gave presentations in English and Spanish. English andSpanish PowerPoint slide shows and program pamphlets were provided, illustrated withphotographs of Latina women.
2. Intervention Component: MeetingsWeekly 4-h meetings were held for the first 6 months. Meetings were bimonthly for months7–12 and further tapered from months 12–24. Meetings featured of 1 h each of:
Mediterranean diet (potluck)
Physical activity
Stress management
Social support groups
Cultural Adaptations—After 6 months, family nights were added to involve familymembers in participants’ activities and to celebrate their achievements. Family Nights wereintended to increase the families’ support for participants’ intervention engagement. At thesuggestion of participants who wanted to ask questions they were unable to ask theirpersonal health care providers, we added presentations and question–answer sessions withthe project’s Latino physician.
3. Intervention Component: Mediterranean DietParticipants were encouraged to follow the Mediterranean diet emphasizing vegetables,fruits, legumes, nuts, cereals, olive oil, limited animal fat, and portion control.
Cultural Adaptations—Latin American recipes were altered by the Latina projectdietitian to conform to the ¡Viva Bien! diet. The goal was to lower the fat and calories whilemaintaining flavor with traditional ingredients and spices. Latinas represent a diverse group,and there is no typical “Latino diet,” so recipes from specific Latin American countries weremodified using common staples. In this way, the program covered the wide range of ethnicLatin American foods. Potluck dinners were key to the diet component. The Latina dietitianconducted cooking demonstrations to show new methods for preparing typical foods.Participants were shown how to modify their favorite recipes by incorporating the principlesof the Mediterranean diet into their usual foods. Attention was paid to acceptance andsupport from family members who might benefit from dietary changes. To help participants
Toobert et al. Page 13
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
follow the diet, colorful pamphlets were created in English and Spanish and includedphotographs of common Latino foods and Latina women.
4. Intervention Component: Physical ActivityThe program recommended 30 min of moderate aerobic activity most days per week and theperformance of ten strength-training exercises two times per week.
Cultural Adaptations—At physical activity sessions during the retreat and meetings,participants could choose to walk outside or follow a trained instructor in an aerobics classled in both English and Spanish, with Latin (for example, salsa) style steps and music. Thus,women could determine for themselves which physical activities were culturallyappropriate. Colorful pamphlets, available in English and Spanish, were created to supportthe physical activity component. The pamphlets included photographs of Latina women.Take-home exercise DVDs/CDs available in English and Spanish also were created for theprogram.
5. Intervention Component Stress ManagementParticipants were encouraged to practice stress-management techniques for at least 1 h perday, consisting of: 20 min of yoga stretches, 15 min of progressive deep relaxation, 15 minof meditation, and 5 min of directed or receptive imagery.
Cultural Adaptations—Take-home stress-management CDs were created for the programin English and Spanish. The research team considered adapting the stress-managementcomponent out of concern that yoga and meditation practices may be seen as religiousactivities incongruent with Latina participants’ cultural experiences. But, focus groupparticipants did not raise objections, and the yoga and meditation components were retained.
6. Intervention Component: Social SupportGroup support constituted 1 h at each meeting. Support group sessions included structuredmini units (for example, pleasant activities, goal setting, social support, problem solving,negative thoughts) and less-structured “check-in” sessions so that participants could discusssuccesses and barriers to making lifestyle changes.
Cultural Adaptations—Participants were offered groups conducted primarily in Englishor Spanish to accommodate language preferences. Because the support-group structure wasflexible, participants could choose topics that were culturally appropriate and personallyrelevant. Handout materials were available in English or Spanish.
7. Intervention Component: Smoking CessationParticipants who used tobacco were encouraged to set a quit date and stop.
Cultural Adaptations—To help participants stop smoking, colorful pamphlets werecreated for the program in English and Spanish and featuring Latina women. Smokingcessation sessions were led by a bilingual facilitator.
Toobert et al. Page 14
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 1.CONSORT diagram of ¡Viva Bien! study participation
Toobert et al. Page 15
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Toobert et al. Page 16
Tabl
e 1
Bas
elin
e ch
arac
teris
tics o
f par
ticip
ants
by
treat
men
t con
ditio
n
Mea
n or
% U
sual
car
eSD
Mea
n or
% ¡V
iva
Bien
!SD
Sign
ifica
nce
Cha
ract
eris
ticn=
138
n=14
2(p
Val
ue)
Age
58.7
10.3
55.6
9.7
0.00
9
Bod
y m
ass i
ndex
(kg/
m2 )
33.2
6.7
35.3
7.0
0.01
0
Yea
rs d
iagn
osed
with
dia
bete
s10
.49.
88.
46.
50.
049
Cur
rent
smok
er (%
Yes
)12
.6%
9.2%
0.36
8
Bas
elin
e he
mog
lobi
n A
1c8.
21.
78.
41.
90.
275
Inco
me
0.13
3
$0 to
$29
,999
50.0
%36
.8%
$30,
000
to $
49,9
9921
.7%
27.1
%
$50,
000
to $
69,9
9913
.3%
16.5
%
$70,
000
to $
89,9
9910
.0%
8.3%
$90,
000
or m
ore
5.0%
11.3
%
Type
of g
luco
se-lo
wer
ing
med
icat
ion
0.18
1
Non
e10
.9%
11.3
%
Ora
l onl
y56
.9%
59.6
%
Insu
lin o
nly
13.1
%5.
7%
Insu
lin+o
ral m
edic
atio
n19
.0%
23.4
%
Leve
l of e
duca
tion
0.45
0
0 to
11t
h gr
ade
27.1
%20
.0%
Hig
h sc
hool
gra
duat
e27
.8%
32.1
%
Som
e co
llege
30.1
%28
.6%
Col
lege
/uni
vers
ity g
radu
ate
15.0
%19
.2%
Pref
er S
pani
sh14
.7%
17.0
%0.
633
Hea
lth li
tera
cy4.
24.
30.
460
Num
erac
y to
tal
3.5
1.2
3.7
1.1
0.25
8
Num
erac
y pr
efer
ence
3.5
1.2
3.7
1.1
0.23
5
Num
erac
y ab
ility
3.4
1.6
3.6
1.5
0.31
0
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Toobert et al. Page 17p
valu
es re
porte
d in
the
tabl
e w
ere
deriv
ed fr
om c
hi-s
quar
e te
sts (
for n
omin
al v
aria
bles
) or t
test
s (fo
r ord
inal
, int
erva
l, or
ratio
var
iabl
es) c
ondu
cted
to c
ompa
re g
roup
diff
eren
ces
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Toobert et al. Page 18
Tabl
e 2
Psyc
hoso
cial
out
com
es a
t 6, 1
2, a
nd 2
4 m
onth
s (es
timat
ed m
eans
and
SEs
[n=2
80])
Bas
elin
e6
Mon
ths
12 M
onth
s24
Mon
ths
Con
d χ2
Tim
e χ2
C ×
T χ
2M
SEM
SEM
SEM
SE
Qua
lity
of p
robl
em so
lvin
g st
rate
gies
27.5
*7.
8*19
.9*
Usu
al c
are
4.3
.03
4.2
0.04
4.2
0.04
4.2
.05
¡Viv
a Bi
en!
4.3
0.04
4.4
0.04
4.4
0.04
4.5
0.03
Effe
ct si
ze0.
500.
500.
75
Self-
effic
acy
2.3a
21.4
*15
.8*
Usu
al c
are
3.2
0.06
3.2
0.07
3.3
0.07
3.4
0.07
¡Viv
a Bi
en!
3.1
0.06
3.5
0.06
3.4
0.07
3.4
0.07
Effe
ct si
ze0.
460.
14N
o di
ff
UC
LA p
ositi
ve su
mm
ary
scor
e41
.7*
127.
2*55
.5*
Usu
al c
are
2.4
0.06
2.6
0.06
2.5
0.07
2.6
0.07
¡Viv
a Bi
en!
2.5
0.06
3.2
0.07
3.1
0.07
3.2
0.09
Effe
ct si
ze1.
000.
850.
75
Bas
ed o
n ge
nera
lized
est
imat
ing
equa
tions
ana
lysi
s res
ults
, cov
aryi
ng w
ave
and
age
at b
asel
ine.
DF(
cond
ition
)=1;
DF(
time)
and
DF(
cond
ition
×tim
e)=3
* Sign
ifica
nt a
t p<0
.05
or le
ss
a A si
gnifi
cant
con
ditio
n m
ain
effe
ct w
as fo
und
for s
elf-
effic
acy
in c
ompl
ete-
case
ana
lysi
s
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Toobert et al. Page 19
Tabl
e 3
Beh
avio
ral o
utco
mes
at 6
, 12,
and
24
mon
ths (
estim
ated
mea
ns a
nd S
Es [n
=280
])
Bas
elin
e6
Mon
ths
12 M
onth
s24
Mon
ths
Con
d χ2
Tim
e χ2
C ×
T χ
2M
SEM
SEM
SEM
SE
% C
alor
ies s
atur
ated
fat
16.3
*82
.0*
32.8
*
Usu
al c
are
110.
002
110.
002
100.
003
110.
003
¡Viv
a Bi
en!
120.
002
090.
002
090.
003
100.
003
Effe
ct si
ze1.
000.
330.
33
Stre
ss m
anag
emen
t dai
ly p
ract
ice
(min
)a2.
034
.2*
3.3
Usu
al c
are
33.6
0.06
17.6
0.07
23.0
0.07
24.0
0.08
¡Viv
a Bi
en!
31.4
0.07
23.0
0.08
28.1
0.09
30.2
0.10
Effe
ct si
ze0.
180.
180.
20
Phys
ical
act
ivity
, day
s/w
eek
(IPA
Q)
1.2
50.3
*4.
4
Usu
al c
are
4.1
0.24
4.9
0.21
4.9
0.24
5.6
0.21
¡Viv
a Bi
en!
4.2
0.23
5.5
0.22
5.4
0.22
5.5
0.23
Effe
ct si
ze0.
280.
220.
04
Chr
onic
illn
ess r
esou
rces
surv
ey to
tal s
core
5.6*
37.6
*15
.3*
Usu
al c
are
2.1
0.05
2.1
0.05
2.2
0.06
2.3
0.07
¡Viv
a Bi
en!
2.1
0.06
2.5
0.06
2.4
0.07
2.4
0.07
Effe
ct si
ze0.
730.
310.
14
Bas
ed o
n ge
nera
lized
est
imat
ing
equa
tions
ana
lysi
s res
ults
, cov
aryi
ng w
ave
and
age
at b
asel
ine.
DF(
cond
ition
)=1;
DF(
time)
and
DF(
cond
ition
×tim
e)=3
* Sign
ifica
nt a
t p<0
.05
or le
ss
a Stre
ss m
anag
emen
t was
squa
re-r
oot t
rans
form
ed fo
r ana
lysi
s, bu
t rev
erse
-tran
sfor
med
her
e fo
r eas
e of
inte
rpre
tatio
n
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Toobert et al. Page 20
Tabl
e 4
Bio
logi
cal a
nd q
ualit
y of
life
out
com
es a
t 6, 1
2, a
nd 2
4 m
onth
s (es
timat
ed m
eans
and
SEs
[n=2
80])
Bas
elin
e6
Mon
ths
12 M
onth
s24
Mon
ths
Con
d χ2
Tim
e χ2
C ×
T χ
2M
SEM
SEM
SEM
SE
Bod
y m
ass i
ndex
8.9*
7.2a
3.8a
Usu
al c
are
33.0
0.58
32.1
0.58
32.6
0.57
32.5
0.62
¡Viv
a Bi
en!
35.4
0.58
34.6
0.59
34.3
0.62
35.0
0.62
Effe
ct si
ze0.
430.
290.
40
Hem
oglo
bin
A1c
(%)c
0.03
4.2b
19.1
*
Usu
al c
are
8.4
0.02
8.4
0.03
7.8
0.02
7.8
0.03
¡Viv
a Bi
en!
8.4
0.03
7.8
0.03
8.4
0.03
8.4
0.03
Effe
ct si
ze0.
330.
400.
33
UK
PDS
CH
D 1
0-ye
ar ri
sk sc
orec
1.3
10.5
*4.
3
Usu
al c
are
9.6
0.01
9.0
0.01
9.0
0.01
9.0
0.01
¡Viv
a Bi
en!
9.0
0.01
7.8
0.01
9.0
0.01
7.8
0.01
Effe
ct si
ze0.
20N
o di
ff0.
20
Bas
ed o
n ge
nera
lized
est
imat
ing
equa
tions
ana
lysi
s res
ults
, cov
aryi
ng w
ave
and
age
at b
asel
ine.
DF(
cond
ition
)=1;
DF(
time)
and
DF(
cond
ition
×tim
e)=3
* Sign
ifica
nt a
t p<0
.05
or le
ss
a Sign
ifica
nt ti
me
mai
n ef
fect
and
con
ditio
n×tim
e in
tera
ctiv
e ef
fect
wer
e fo
und
for b
ody
mas
s ind
ex in
com
plet
e-ca
se a
naly
sis
b A si
gnifi
cant
tim
e m
ain
effe
ct w
as fo
und
for h
emog
lobi
n A
1c in
com
plet
e-ca
se a
naly
sis
c Hem
oglo
bin
A1c
and
the
Uni
ted
Kin
gdom
Pro
spec
tive
Dia
bete
s Stu
dy c
oron
ary
hear
t dis
ease
risk
scor
e w
ere
squa
re-r
oot t
rans
form
ed fo
r ana
lysi
s, bu
t rev
erse
-tran
sfor
med
her
e fo
r eas
e of
inte
rpre
tatio
n
Transl Behav Med. Author manuscript; available in PMC 2011 October 19.





























