Embed Size (px)
Citation preview
Laboratory and Pathology Test Menu
and Specimen Collection Guide
ARHS-SC-19.User Field Version = 13
Title Page

Policies and Procedures
Laboratory and Pathology Test Menu and Specimen
Collection Guide
ARHS-SC-19 . 13
LABORATORY SERVICES
Current Version Approved By: ARHS Policy Committee , Aubree Robinson, Bethany Vallangeon
Current Version Approved Date: 06/18/2020
Last Reviewed: 06/18/2020
ARHS-SC-19.User Field
Version = 13
2
1/24/2022 6:01 a1/p1
Approvals - Table of Contents 2
Introduction
3
Laboratory Telephone Numbers
4
Venipuncture Collection
5
Capillary Collection
9
Specimen Labeling Policy
11
Clean Catch Urinalysis Collection Instructions
12
24 Hour Urine Collection Forms/Instructions
13
Stool Collection Instructions
16
Swab Collection
19
Therapeutic Drug Monitoring
22
Test Menu Guide
23

ARHS-SC-19.User Field
Version = 13
3
1/24/2022 6:01 a1/p1
Thank you for allowing ARHS Laboratory and Pathology Services to serve as your resource for laboratory testing. In this collection guide, you will find the pertinent information relating to all tests performed by an ARHS Laboratory, as well as, instructions for the collection of common specimens. Each test in this guide lists which ARHS Laboratory that has the ability to perform the test. For any test requested that is not listed in this collection guide, please contact the ARHS Laboratory you are using to obtain reference laboratory specific information/specimen requirements.
As noted above, ARHS Laboratory and Pathology Services have the ability to perform thousands of tests not listed in this collection guide. However, this requires the need to use multiple reference laboratories to supplement testing not performed in our own laboratories. Each reference laboratory has their specific specimen collection requirements; so again, please contact your ARHS Laboratory to obtain the correct collection information.
This directory is available to all ARHS Laboratory Services users either in print, on
the ARHS Intranet or via the Laboratory Services website (www.apprhs.org)
How to use the guide: Test/Panel Name
Basic Metabolic Panel (BMP)
Lab: WMC/CMH Chemistry Availability: 24 hours TAT: Routine, 4 hours Stat, 1 hour CMH ED - 44 min Test Includes: glucose, BUN, creatinine, sodium, potassium, chloride, CO2, calcium
Specimen: Serum , heparinized plasma Tube: SST, Plain red or Green (Li hep.) Minimum volume: 5 ml Collection: Routine venipuncture Causes for rejection: Gross hemolysis, improper labeling, contamination with IV fluids, serum/plasma not removed from cells within 2 hours, wrong anticoagulant.
Use: to evaluate metabolic status, fluid/electrolyte balance.
1. Lab – Facility performing test 2. Availability – When testing is
performed 3. TAT – average turnaround time for
results 4. Test Includes – tests included in a
panel 5. Special Instructions/Notes
1. Specimen requirements 2. Collection container required 3. Minimum Volume required 4. Pertinent collection information
5. 10. Reasons a sample may be
rejected
6. Uses – background on test use 7. Test limitations if present 8. 13. Additional test information
ARHS-SC-19.User Field
Version = 13
4
1/24/2022 6:01 a1/p1
Watauga Medical Center Telephone Numbers
Main Laboratory 262-4150
Transfusion Services 262-4146
Chemistry 262-4296
Hematology 262-4149
Microbiology 262-4148
Laboratory Fax 262-4147
Pathology Office 262-4106
Pathology Laboratory 268-9401
Histology 265-5028
Cytology 268-8923
Outpatient Laboratory 266-2495
LIS/IT 266-1163
Cardiopulmonary 262-4176
Cannon Memorial Hospital Telephone Numbers
Laboratory 737-7500
Laboratory Fax 737-7501
Pathologists Diagnostic Services
Main Office 336-999-8888

ARHS-SC-19.User Field
Version = 13
5
1/24/2022 6:01 a1/p1
Venipuncture Collection Procedure
Principle
A patient's veins are the main source of blood for laboratory testing as well as a point of entry for IVs.
Since only a few veins are easily accessible to both laboratory and other medical personnel, it is
important that everything be done to preserve their good condition and availability. Correct collection
procedures are the first step to accurate laboratory testing. Collection must be performed on the
correct patient, drawn in the correct tubes, and handled properly after collection to ensure accurate
results.
Procedure
1. Review the request form(s) or labels. See what test(s) have been ordered and that you have the appropriate tubes.
2. When collecting an inpatient, be sure to knock on the patient's door before you enter the room.
3. Cordially greet the patient. Let them know your name, which department you’re from, and the purpose of your visit.
4. Access the patient’s ability to understand. Each inpatient has a Learning Readiness Assessment. If' needed, you may review the nursing assessment found in the patients room chart. You may find it necessary to seek additional assistance before attempting to obtain the sample.
a. What is the patient's primary language? b. What is the patient's education level? Your communication needs to be at a level that the
patient can understand. If the patient asks you questions, keep your response at a level that the patient can understand.
c. Does the patient have any learning impairments? i. Hearing ii. Sight iii. Speech iv. Cognitive Abilities
5. Identify the patient using the two unique identifiers detailed on ARHS-SC-02.
6. Sanitize hands before and after patient contact.
7. If a fasting specimen is required, verify that the patient has not eaten. Food trays are a good sign that the patient has eaten. If you believe that the patient is capable of understanding and answering the question, you may ask the patient if they have eaten within the specified fasting time. In some cases you may need to consult with the nursing department regarding the patients fasting status.
8. Reassure the patient. Be confident and display a positive attitude.
9. Properly position the patient: a. Inpatients should lay on their back in a comfortable position. Add support under the arm
with a pillow if needed. Extend the arm to form a straight fine from the shoulder to the wrist.
b. Outpatients should be comfortably seated in a venipuncture chair. The arm should be positioned on an armrest in a straight line from the shoulder to the wrist. The arm should not be bent at the elbow.
c. Make sure the patient does not have anything in his/her mouth. d. Never perform a venipuncture on a patient who is standing.

ARHS-SC-19.User Field
Version = 13
6
1/24/2022 6:01 a1/p1
10. Prepare your equipment. Assemble your tube(s) and venipuncture supplies, alcohol prep, gauze, tape and tourniquet. Do not place the phlebotomy tray on the patient's bed. Determine the order of tube collection:
1. Blood Cultures 2. Discard tube (necessary if drawing only light blue top tube with a butterfly) 3. Royal blue 4. Light blue (Sodium citrate) 5. Red (no additive) 6. SST 7. Light green (Lithium heparin) 8. Green (Sodium heparin) 9. Lavender (EDTA) 10. Pink (EDTA) 11. White (gel EDTA) 12. Gray (Sodium fluoride) 13. Yellow (ACD)
11. Select site for venipuncture:
a. Do not draw blood above an Intravenous (IV) Infusion. If the patient has an IV in one arm, look for a vein in the other arm. If IV's are located in both arms, blood may be drawn from ABOVE the IV site if the nurse can turn the IV fluids off for at least 2 minutes. Tourniquet use should be avoided in this situation and a discard of 3-5 ml of blood should be drawn before drawing the specimen(s) for testing. Discard waste tube in the biohazard waste.
b. In most cases blood can be drawn from the median cubital vein, located in the Antecubital Fossa. The Cephalic, Basilic, Accessory Cephalic, Median Ante brachial and Radial veins in the arm or the Dorsal Hand Veins may be used. Do not use veins in the Ventral Wrist area. Leg and foot veins should be used only as a last resort and when we have a physician’s written order to draw from the foot or leg. A tourniquet should not be used in these cases.
c. A tourniquet may be applied to help in locating a vein; however it should be left on no longer than 1 minute.
d. You may ask the patient to make a fist to help make the vein more prominent, however in no case should the patient be allowed to pump the fist. Some laboratory results could be altered by the pumping action.
e. Avoid scarred or bruised areas and if possible, the side on which a mastectomy was performed should be avoided.
12. Cleanse the venipuncture site with an alcohol prep using a circular motion from the center to the periphery. For blood cultures, cleanse site in a circular motion for 60 seconds using a chloroprep pad. Allow the area to air dry. While the site is drying, put on a clean pair of gloves. Gloves must always be donned in the presence of the patient.
13. Apply a tourniquet 3 to 4 inches above the venipuncture site. Hold one end taut and tuck a portion of the other end under to form a loop.
14. Perform the Venipuncture - Note, do not attempt to perform more then two venipuncture attempts on a patient. There should be no more than five attempts to collect blood from a patient. If the lab has been unable to collect a specimen, notify the nursing department and document in the LIS.

ARHS-SC-19.User Field
Version = 13
7
1/24/2022 6:01 a1/p1
Vacutainer
a. Holding the vacutainer barrel in your dominant hand, remove the needle cap and position the needle with the bevel up.
b. Pull the skin just below the puncture site tight using either the thumb or index finger of your non-dominant hand. Do not make a "window."
c. Align the needle with the puncture site, keeping the needle at a 15° angle. Use a small quick thrust, puncture the skin and enter the vein in one smooth motion, if possible.
d. Holding the barrel securely, push the first tube fully onto the needle assembly. Blood should flow when the needle punctures the tube cap. If it does not, the needle is either too far in the vein or not in the vein. Back the needle and reposition needle until you feel the needle is in the vein. If blood still does not flow, try another tube.
e. Remove the tube when the blood flow ceases. If multiple tubes are needed, insert them in the order listed above.
f. When all the blood necessary has been collected, release the tourniquet, remove the needle quickly and immediately apply a cotton ball or gauze pad on the puncture site. At the same time, make the needle safe by activating the protective device. Hold pressure to the cotton/gauze. Discard the needle in the sharps container.
Syringe
a. Holding the syringe in your dominant hand, remove the needle cap. Position the needle with
the bevel up.
b. Grasp the patient's arm just below the puncture site with your non-dominant arm and pull the
skin tight with your thumb.
c. Align the needle with a 15-degree angle to the skin. Use a quick, but small, thrust to
penetrate the skin and enter the vein in one motion, if possible.
d. Holding the barrel of the syringe securely, pull back on the syringe plunger until a sufficient
amount of blood fills the syringe.
e. Release the tourniquet, remove the needle quickly and immediately apply a cotton ball or
gauze pad on the puncture site. At the same time, make the needle safe by activating the
safety device. Hold pressure to the cotton/gauze. Discard needle in the sharps container.
f. Using a transfer device, transfer the blood from the syringe to the appropriate tubes
immediately. Fill tubes containing anticoagulants first. Discard of the transfer device and
syringe in the sharps container.
Butterfly
a. Holding the butterfly by the "wings" in your dominant hand, remove the needle cap.
b. Position the needle with the bevel up.
c. Grasp the patient's arm just below the puncture site with your non-dominant arm and pull
the skin tight with your thumb.
d. Align the needle with a 15-degree angle to the skin. Use a quick, but small, thrust to
penetrate the skin and enter the vein in one motion, if possible.
e. Blood will enter the tubing attached to the needle once the needle is in the vein. The
opposite end of the tubing can be attached to a syringe or an adapter can be used and
it can be attached to a vacutainer barrel.
f. When all the blood necessary has been collected, release the tourniquet, remove the
needle quickly and activate the safety mechanism. Immediately apply a cotton ball or
gauze pad on the puncture site. Hold pressure to the cotton/gauze. Discard the butterfly
assembly in the sharps container. Using a transfer device, transfer the blood from the
syringe to the appropriate tubes immediately. Fill tubes containing anticoagulants first.
Discard of the transfer device and syringe in the sharps container.

ARHS-SC-19.User Field
Version = 13
8
1/24/2022 6:01 a1/p1
15. Apply a bandage to the site and advise the patient to leave it on for 1 to 2 hours.
16. In the presence of the patient, label tubes according to ARHS-SC-05.
17. For inpatients, return the patient area to the condition in which you found it - raise side rails,
dispose of trash, lower the bed, etc.
18. Remove gloves and sanitize hands prior to leaving the room.
Adverse Reactions to Phlebotomy
To ensure that any patient that has an adverse reaction such as fainting, seizure, or injury to
phlebotomy will receive immediate care:
Inpatients:
1. The phlebotomist will call the nurse’s station for immediate assistance. 2. The patient’s nurse will be notified. 3. An occurrence report will be completed.
OPIC Outpatients:
1. Basic first aid will be administered. 2. Ammonia and a recliner are available when needed. 3. When indicated 911 will be called per EMTALA Policy.
Main Lab Outpatients:
1. Basic first aid will be administered. 2. Ammonia and a recliner are available when needed. 3. An intercom system is available to obtain assistance. 4. When indicated a CODE Blue will be called.
The following steps can be taken to assist the patient during adverse events:
Fainting:
1. If the patient is sitting, lower head and arms. If lying down, elevate feet. 2. Try to revive patient with ammonia inhalant (draw trays and in draw rooms). 3. Loosen any tight clothing. 4. Apply cold compress to patient’s forehead and back of neck.
Nausea
1. Situate patient comfortably with head lowered. 2. Instruct patient to breathe deeply and slowly. 3. Offer water.
Vomiting
1. Roll prone patients on their side. 2. Give patient a basin. 3. When vomiting ceases, assist patient with towels and water.
Extensive bleeding
1. Apply direct pressure to venipuncture site and note time it takes to cease bleeding.
ORIGINAL AUTHOR: Wendy R. Williams
ORIGINAL EFFECTIVE DATE: 12/30/2010
Venipuncture Collection Procedure

ARHS-SC-19.User Field
Version = 13
9
1/24/2022 6:01 a1/p1
Capillary Collection Procedure
Principle
Capillary blood specimens are especially important for hard to stick patients such as pediatric, obese,
or geriatric patients. This procedure is also used for obtaining blood for bedside glucoses and PKU
newborn screenings. Correct collection procedures are the first step to accurate laboratory testing.
Collection must be performed on the correct patient, drawn in the correct tubes, and handled properly
after collection to ensure accurate results.
Procedure
1. Review the request form(s) or labels. See what test(s) have been ordered and that you have the appropriate tubes.
2. When collecting an inpatient, be sure to knock on the patient's door before you enter the room. 3. Cordially greet the patient and/or patient’s family. Let them know your name, which
department you’re from, and the purpose of your visit. 4. Access the patient’s ability to understand. Each inpatient has a Learning Readiness
Assessment. If' needed, you may review the nursing assessment found in the patients room chart. You may find it necessary to seek additional assistance before attempting to obtain the sample.
a. What is the patient's primary language? b. What is the patient's education level? Your communication needs to be at a level that
the patient can understand. If the patient asks you questions, keep your response at a level that the patient can understand.
c. Does the patient have any learning impairments? i. Hearing ii. Sight iii. Speech iv. Cognitive Abilities
5. Identify the patient using the two unique identifiers detailed on the Patient Identification procedure.
6. Sanitize hands before and after patient contact. 7. If a fasting specimen is required, verify that the patient has not eaten. Food trays are a good
sign that the patient has eaten. If you believe that the patient is capable of understanding and answering the question, you may ask the patient if they have eaten within the specified fasting time. In some cases you may need to consult with the nursing department regarding the patients fasting status.
8. Reassure the patient. Be confident and display a positive attitude. 9. Prepare your equipment. Assemble your tube(s) and collection supplies, alcohol prep, gauze,
and Band-Aid. Do not place the equipment on the patient's bed. 10. Finger stick collections:
a. The preferred site is the middle or ring finger. Stick the palmar surface of the distal phalanx; do not stick the side or tip of the finger.
b. Wash hands and put on gloves. c. If patient’s hand is cold, warm with a heel warmer or a warm wash cloth. d. Clean site with an alcohol pad and let it dry. e. Hold finger to prevent movement and perform puncture with appropriate safety lancet. f. The first drop of blood should be wiped away with gauze. g. To enhance blood flow hold finger downward and apply intermittent pressure. h. Touch collection device to 2nd drop of blood and allow blood to flow into microtainer
tube or place drop on BSG strip. i. Gently tap tube if blood becomes lodged at top of tube.

ARHS-SC-19.User Field
Version = 13
10
1/24/2022 6:01 a1/p1
j. Fill tubes appropriately and invert tubes with anticoagulant. 11. Heel stick collections:
a. The baby should be in a supine position. b. Puncture should be performed on the most medial or most lateral portion of the plantar
surface of the heel. Do not puncture the posterior curvature or the central area of the heel.
c. Wrap the heel in a heel warmer or a warm washcloth for 5 minutes. d. Clean the puncture site with an alcohol pad and allow to air dry. e. Open the tenderfoot blister pack and remove the safety clip from the device. f. Raise the foot above the baby’s heart level and carefully select a safe incision site. g. Place the blade slot surface of the device flush against the heel; both ends should
make light contact. h. Depress the trigger and immediately remove the device. i. Gently wipe away the first drop with a gauze pad. j. Touch collection device to 2nd drop of blood and allow blood to flow into microtainer
tube. k. Gently tap tube if blood becomes lodged at to top of tube. l. Fill tubes appropriately and invert tubes with anti coagulant. m. For PKU screens, allow blood to flow onto the circles on the form. Fill all circles
completely. 12. Apply a bandage to the site and advise the patient to leave it on for 1 to 2 hours. 13. In the presence of the patient, label tubes or PKU form according to Specimen Labeling . 14. For inpatients, return the patient area to the condition in which you found it - raise side rails,
dispose of trash, lower the bed, etc. 15. Remove gloves and sanitize hands prior to leaving the room.
ORIGINAL AUTHOR: Wendy R. Williams
ORIGINAL EFFECTIVE DATE: 12/30/2010
Capillary Collection Procedure

ARHS-SC-19.User Field
Version = 13
11
1/24/2022 6:01 a1/p1
Specimen Labeling
Principle
To ensure that all specimens are labeled in the same manner by all staff and that all necessary
information is supplied with each sample.
Procedure
The primary specimen container for all specimens must be labeled with the following:
1. Patient name (first and last) 2. Patient date of birth 3. Date of collection 4. Time of collection 5. Initials or ARHS employee number of person collecting specimen
Specimens may also include the location of the patient and the facility patient specific identification
number.
Specimens received without date of birth on the label must be accompanied with a requisition or
demographics sheet that includes the required patient identifiers.
Specimens are to be labeled in the presence of the patient at the time of collection.
LIS generated labels are to be placed on specimen tubes with the test names on the left and the
patient name on the right. Labels are also to be placed over the manufacturer label in such a way
that allows the sample to be seen. Specimen cups and tubs may have the label placed over supplied
labeling area. Blood culture tubes should have the label placed at the bottom of the tube making sure
not to cover up the barcode on the bottle. If tubes are labeled with labels other than those generated
by the LIS, the LIS labels should be placed on the tubes in the same manner as above with care
given to keeping the name on the original label visible.
Place the label on the correct tube as indicated on the label. Failure to place the correct labels on the
correct tubes may result in delayed testing. Extra labels may be used to label extra tubes.
In the event of errors/discrepancies in specimen labeling, the best practice is to recollect the sample
and ensure proper specimen labeling at time of recollection. For irreplaceable or difficult-to-obtain
samples, corrections in labeling may be made by the original collector. In addition to the labeling
correction, a Specimen Labeling Discrepancy Form must be completed by the original collector with a
laboratory staff member witnessing the correction.
Cannon Memorial Hospital PKU Labeling
1. Log onto Hearing Link site (wcs.ncpublichealth.com) 2. Choose patient by clicking on patient name in hospital queue. 3. In the green box, click New Specimen.

ARHS-SC-19.User Field
Version = 13
12
1/24/2022 6:01 a1/p1
4. Scan or enter the barcode on the metabolic screening (PKU) form. 5. Fill in
a. Specimen Status b. Date and time of collection c. Collector initials d. Facility
6. Click Submit Data. 7. Return to patient record and click Print Label. 8. Click OK to confirm patient information. 9. Click File then Page Setup then Landscape 10. Set margins at 0.5” for all sides (top/bottom/left/right) 11. Click Printer then Properties then select Labels as the paper type 12. Click OK to print. 13. Inspect label for accuracy. Place one label on each page of the PKU form taking care not to
cover the barcode or the patient medical record number.
ORIGINAL AUTHOR: Wendy R. Williams, MT (AMT)
ORIGINAL EFFECTIVE DATE: 12/30/2010
Specimen Labeling

ARHS-SC-19.User Field
Version = 13
13
1/24/2022 6:01 a1/p1
Clean Catch Urine Collection
Principle
To ensure proper collection from patients for clean catch specimens, the following
instructions are provided to the patient.
Procedure
When presented with an order for a test that requires a clean catch urine specimen,
provide the patient with a specimen cup and a sterile antiseptic pad. If the patient is taking
the container home to collect the specimen, also provide them with a specimen bag to
transport the specimen in. Review the following instructions with the patient or direct them
to the posted instructions in the collection restroom.
Instructions for the female patient:
1. If you are menstruating, first insert a fresh tampon or use cotton to stop the flow. 2. Separate the skin folds around the urinary opening then wash the urinary opening and
its surroundings from front to back with a sterile antiseptic pad. 3. Begin urinating in the toilet, making sure to keep the skin fold apart with the fingers of
one hand. 4. Wait until the urine stream is well established before moving the container to the
genital area but do not touch container to genital area. 5. Replace lid when done collecting sample. 6. Label the container with your name, date of birth and the date and time of collection
and place in the specimen window or deliver to laboratory as soon as possible. Refrigerate specimen if transport to the laboratory will be delayed.
Instructions for the male patient:
1. Wash the end of the penis well with a sterile antiseptic pad and allow to dry. 2. Begin urinating into the toilet. Wait until the urine stream is well established before
moving the container into the path of the stream to catch the rest of the urine. Do not touch the container to the genital area.
3. Replace lid when done collecting sample. 4. Label the container with your name, date of birth and the date and time of collection
and place in the specimen window or deliver to laboratory as soon as possible. Refrigerate specimen if transport to the laboratory will be delayed.
ORIGINAL AUTHOR: Wendy R. Williams, MT (AMT)
ORIGINAL EFFECTIVE DATE: 12/30/2010
Clean Catch Urine Collection

Clinical/Anatomic Pathology Laboratory
Facility/Department: ARHS Laboratory Services
24 Urine Collection Instructions For Use with Boric Acid
Tests Included: Aldosterone, C-peptide, Glucose, Human Growth Hormone (HGH), Hydroxycorticosteriods (17 OHCS), Ketosteriods (17-KS)
Special Patient Preparation:
Aldosterone Avoid diuretics, antihypertensives, estrogen, and licorice. Patient
should be on restricted sodium diet prior to collection (consult MD).
C-peptide Do not collect within 8 hours of last biotin dose.
17 OHCS (Hydroxycorticosteriods) Avoid all medications for 72 hours prior to collection if possible
(Consult MD prior to stopping any medications).
17-Ketosteriods Avoid all medications for 72 hours prior to collection if possible
(Consult MD prior to stopping any medications).
Collection Instructions: *Do Not Urinate Directly into Urine Container*
CAUTION– The container contains a strong acid. Please read precaution instructions on
container.
1. Label urine container with your name and date of birth if not already done.
2. On the first morning when you start collection, urinate as normal in the toilet and discard.
3. Write down the date and time this was done in the space provided below. This is the start of the
collection.
4. Collect all urine your pass for the next 24 hours including the first specimen of the second
morning. All of the urine passed must be added to the container. If any specimens are missed, the
collection must be started over with a new container.
5. Write down the date and time of the last specimen added in the space provided below. This will be the date and time of the first urination on the second morning and is the end of the collection.
6. Take care not to touch the urine with a bowel movement or toilet paper.
7. The urine in the container should be kept cool during the 24 hour collection period. This may be done
by putting the container in a pan with ice.
8. Once collection is completed, bring the container and this sheet to the laboratory.
Questions: Cannon Memorial Hospital 828-737-7500 Watauga Medical Center 828-262-4150
Patient Name:
Date/Time Collection Started:
Date/Time Collection Ended:
Patient Date of Birth:
FA-SC-03.01 Printed: 3/14/2011
Page 1 of 1 Effective Date: 3/14/11

Clinical/Anatomic Pathology Laboratory
Facility/Department: ARHS Laboratory Services
24 Urine Collection Instructions For Use with No Preservative
Tests Included: Protein Electrophoresis, Porphyrines, Porphobilinogen (PGB), Immunofixation, Creatinine Clearance, Sodium, Potassium, Total Protein, Creatinine, Chloride, Heavy Metals*, Amylase, Cadmium*, Chromium*, Cobalt*, Copper*, Histamine, Lead*, Lysozyme, Mercury*, Microalbumin, Nickel*, Osmolality, Selenium*, Urea Nitrogen, Uric Acid, Zinc*, Hydroxyindoleacetic Acid (5-HIAA),
Special Patient Preparation: Calcium Patient should be on low calcium diet for 72 hours prior to collection.
Avoid antacids, phosphates, diuretics, glucocorticoids, carbonic
anhydrase inhibitors, and anticonvulsants (Consult MD before stopping
any medications).
All Heavy Metals* Avoid seafood and red wine for 72 hours prior to collection
Uric Acid Maintain standard diet 24 hours prior to collection.
5-HIAA (Hydroxyindoleacetic acid) Avoid bananas, avocados, plums, eggplant, tomatoes, plantains,
pineapple, and walnuts. Avoid all medications for 72 hours prior to
collection if possible (Consult MD prior to stopping any medications).
Collection Instructions: *Do Not Urinate Directly into Urine Container* 1. Label urine container with your name and date of birth if not already done. 2. On the first morning when you start collection, urinate as normal in the toilet and discard. 3. Write down the date and time this was done in the space provided below. This is the start of the
collection. 4. Collect all urine your past for the next 24 hours including the first specimen of the second
morning. All of the urine passed must be added to the container. If any specimens are missed, the collection must be started over with a new container.
5. Write down the date and time of the last specimen added in the space provided below. This will be the date and time of the first urination on the second morning and is the end of the collection.
6. Take care not to touch the urine with a bowel movement or toilet paper. 7. For all tests ordered other than metals, the urine in the container should be kept cool during the 24
hour collection period. This may be done by putting the container in a pan with ice.
*Collections for metal testing should be maintained at room temperature.
8. Once collection is completed, bring the container and this sheet to the laboratory. Questions:
Cannon Memorial Hospital 828-737-7500 Watauga Medical Center 828-262-4150
Patient Name: Patient Date of Birth: _
Date/Time Collection Started: __________________ Date/ Time Collection Ended:
FA-SC-02.01 Printed: 3/14/2011
Page 1 of 1 Effective Date: 3/14/11

Clinical/Anatomic Pathology Laboratory
Facility/Department: ARHS Laboratory Services
24 Urine Collection Instructions For Use with 6N HCL
Tests Included: Calcium, Catecholamines, Citric Acid, Cortisol (Free), Cystine, Homovanillic Acid (HVA), Hydroxyproline, Magnesium, Metanephrines/Normetanephrine, Oxalate, Phosphorus, Vanillylmandelic Acid (VMA), Ketosteriods (17-KS)
Special Patient Preparation:
17-Ketosteriods Avoid all medications for 72 hours prior to collection if possible (Consult MD prior to
stopping any medications).
Calcium Patient should be on a low calcium diet for 72 hours prior to collection. Avoid antacids,
phosphates, diuretics, glucocorticoids, carbonic anhydrase inhibitors, and
anticonvulsants (Consult MD prior to stopping any medications).
Catecholamines Avoid stress and caffeine. Avoid all medications for 14 days prior to collection if
possible (Consult MD prior to stopping any medications).
Homovanillic Acid
(HVA)
Avoid aspirin, disulfiram, reserpine and pyridoxine for 48 hours and Levodopa for 14
days prior to collection (Consult MD prior to stopping any medications).
Hydroxyproline Patient should be on a collagen-free diet for 24 hours prior to collection. Avoid foods
containing gelatin and meats. Avoid all aspirin-containing drugs (Consult MD prior to
Metanephrines Avoid caffeine before and during collection. Avoid taking monamine oxidase inhibitors
for 7 days prior to collection (Consult MD prior to stopping any medications).
Oxalate Avoid Vitamin C supplements and Vitamin C enriched foods (fruits, broccoli, tomatoes,
peppers, potatoes) for 48 hours prior to collection.
Vanillylmandelic Acid
(VMA)
Avoid all medications for 72 hours prior to collection if possible. Avoid caffeine, tea,
chocolate, fruit (especially bananas) and any vanilla containing substance for 72 hours
prior to collection (Consult MD prior to stopping any medications). Collection Instructions: *Do Not Urinate Directly into Urine Container*
CAUTION– The container contains a strong acid. Please read precaution instructions on container. 1. Label urine container with your name and date of birth if not already done. 2. On the first morning when you start collection, urinate as normal in the toilet and discard.
3. Write down the date and time this was done in the space provided below. This is the start of the
collection.
4. Collect all urine your past for the next 24 hours including the first specimen of the second morning. All of the
urine passed must be added to the container. If any specimens are missed, the collection must
be started over with a new container.
5. Write down the date and time of the last specimen added in the space provided below. This will be the date and
time of the first urination on the second morning and is the end of the collection.
6. Take care not to touch the urine with a bowel movement or toilet paper.
7. For all tests ordered other than metals, the urine in the container should be kept cool during the 24 hour collection
period. This may be done by putting the container in a pan with ice.
8. Once collection is completed, bring the container and this sheet to the laboratory.
Questions: Cannon Memorial Hospital 828-737-7500 Watauga Medical Center 828-262-4150
Patient Name: Patient Date of Birth:
Date/Time Collection Started: Date/Time Collection Ended:
FA-SC-04.01 Printed: 3/14/2011
Page 1 of 1 Effective Date: 3/14/11

Stool Collection
Principle To ensure proper collection from patients for stool specimens, the following instructions are provided to the patient. Two important aspects of collection that must be emphasized are the collection of the specimen before the administration of antimicrobial agents and the prevention of specimen contamination with externally present organisms or normal flora of the body.
Procedure
The following collection and transportation guidelines should be followed in order to
produce the best specimen for microbiology testing:
1. Apply strict aseptic techniques throughout the procedure.
2. Collect the specimen at the appropriate phase of the disease.
3. Make certain that the specimen is representative of the infectious process and is
adequate in quantity for the desired tests to be performed.
4. Collect or place the specimen aseptically in a sterile container.
5. Label and date the container appropriately and complete the requisition with the
patient’s clinical history when appropriate. Place the label on the container, not
the lid.
6. Specify the specimen site or source.
7. Arrange for immediate transportation of the specimen to the laboratory, preferable
within 2 hours of collection.
Outpatients must be given the appropriate sterile collection containers and a biohazard bag for transport of the collection specimen. The patient should also be instructed to label the containers with their name, date of birth and date and time of collection. Para Pak containers should be filled with stool up to the fill line located on the container. Instruct the patient not to overfill.
GI Panel This requires a fresh random stool. Stool specimens should be collected before the patient receives any oil laxative or barium. Specimen must not be contaminated with urine, barium, bismuth or mineral oil. Do not submit in a diaper. Stools collected in sterile containers must be partially transferred to an orange topped Para Pak Enteric container within 2 hours of
collection. S u b m i t b o t h s a m p l e s f o r t e s t i n g .
Ova and Parasite Examination
This requires a fresh random stool. Stool specimens should be collected before the
patient receives any oil laxative or barium. Specimen must not be contaminated with
urine, barium, bismuth or mineral oil. Do not submit in a diaper. Stools collected in sterile
containers must be transferred to a pink topped and a gray topped Para Pak container
(formalin and PVA) within 2 hours of collection.
C. difficile Examination
This requires a fresh random stool. Stool specimens should be collected before the
patient receives any oil laxative or barium. Specimen must not be contaminated with
urine, barium, bismuth or mineral oil. Do not submit in a diaper. Specimen must be
refrigerated or frozen within 2 hours of collection.
Hemoccult
This requires a fresh random stool. Stool specimens should be collected before the

patient receives any oil laxative or barium. Specimen must not be
contaminated with urine, barium, bismuth or mineral oil. Do not submit in a diaper.
Hemoccult cards may be submitted for testing with stool already placed in the testing
areas.
Test Container to Provide to Patient
GI Panel Sterile container and/or Orange Para Pak container
Ova and Parasite Sterile container or Pink and Grey Para Pak container
C. difficile Sterile container
Hemoccult Sterile container
Notes
1. No more than 2 bacteriology specimens and 3 parasitology specimens per
patient are recommended.
2. With the exception of Clostridium difficile, enteric cultures should not be performed after 3 days of hospitalization.
3. Parasitology exams should not be done after 4 days of hospitalization.
4. Physicians are encouraged to increase testing for Clostridium difficile in
appropriate clinical settings (diarrhea and prior antibiotic
administration). ORIGINAL AUTHOR: Wendy R. Williams
ORIGINAL EFFECTIVE DATE: 12/30/2010
Stool Collection

Clinical/Anatomic Pathology Laboratory
Facility/Department: ARHS Laboratory Services
Outpatient Stool Collection Instructions
Your physician has ordered the tests marked below. Please follow the collection instructions below for each test ordered. Bring collected samples back to an ARHS Laboratory or the Outpatient Imaging and Laboratory Center located at 1200 State Farm Road in Boone. The Outpatient Imaging and Laboratory Center is open from 7:00am to 5:00pm Monday through Friday. Watauga Medical Center and Cannon Memorial Hospital Laboratories can accept samples 24 hours a day, 7 days a week.
□ GI Panel Container Color: Orange/White
□ Ova and Parasite (O&P) Container Color: Pink/Gray
Collect stool specimen in a clean, dry container. Do NOT mix urine with the stool sample. Open the Para Pak vial(s). Using the spoon attached to the lid of the vial, place small scoopfuls of stool from areas which appear bloody, slimy, or watery into the vial until the contents reach the red line on the label that reads “Add Specimen to this Line.” DO NOT OVERFILL. If the stool is liquid, carefully pour into the vial until contents reach the red line. If the stool is solid, add portions from the middle and ends to the vial. Replace lid and close tightly. Shake the vial vigorously until the contents are mixed. Label the vial with your name, date of birth, and date and time of collection. Repeat if more than one vial is provided. The sample(s) may remain at room temperature and must be delivered to the laboratory within 24 hours of collection.
*If more than one O&P is ordered, do not collect more than one set of vials per day.
□ C. difficile Toxin/Stool for WBCs/ Container Color: White/Clear
Reducing Substances/Fecal Fat Collect stool specimen in a clean, dry container. Do NOT mix urine with the stool sample. If not collected in the sterile container that was provided, transfer the stool specimen to the sterile container. Label container with your name, date of birth, and date and time of collection. If sample cannot be delivered to the laboratory within an hour, sample must be refrigerated. The sample must be delivered to the laboratory within 24 hours.
FA-SC-01.01 Printed: 3/14/2011
Page 1 of 1 Effective Date: 3/14/11

ARHS-SC-19.03 20
1/24/2022 6:01 a1/p1
Name Color Storage/
Transport Purpose Testing
Method Site
UTM-RT Purple top Pink media
Refrigerate 2-8° Viruses (including
Herpes),
Chlamydia
(including child
abuse) &
Mycoplasma
Culture All
Copan CultureSwab
(red top)
Red Top/ Sponge
Room Temperature
Aerobic bacteria Culture All
BBL CultureSwab
(green top)
Green Top/ Sponge
Room Temperature
Nasopharyngeal Cultures
Culture Nasopharyngeal
fFN White top transport/
swab
Room Temperature
Fetal Fibronectin Immunoassay Posterior formix Vaginal
Cepheid GC (Female)
Pink print Room Temperature
Chlamydia/GC DNA Vaginal/Cervical only
Genprobe (Male)
Blue print Room Temperature
Chlamydia/GC DNA Urethral only
BBL Vacutainer Anaerobic
Collector
Glass collection
kit
Room Temperature
Anaerobic and aerobic bacteria
Culture Anaerobic sites
Swab Collection for Microbiology Principle To ensure proper collection of cultures requiring swab collection, the following procedure is used. Two important aspects of collection that must be emphasized are the collection of the specimen before the administration of antimicrobial agents and the prevention of specimen contamination with externally present organisms or normal flora of the body.
Procedure
The following collection and transportation guidelines should be followed in order
to produce the best specimen for microbiology testing:
1. Apply strict aseptic techniques throughout the procedure.
2. Collect the specimen at the appropriate phase of the disease.
3. Make certain that the specimen is representative of the infectious process and
is adequate in quantity for the desired tests to be performed.
4. Collect or place the specimen aseptically in an appropriate container.
5. Label with two patient identifiers and date and initials of collector. Place the
label on the container, not the lid and complete the requisition with the
patient’s clinical history when appropriate.
6. Specify the specimen site or source.
7. Arrange for immediate transportation of the specimen to the laboratory,
preferable within 2 hours of collection.
8. Refer to the Swab Selection Chart below for collecting a particular specimen for microbiological analysis
9. Swabs are not recommended for collection of sample from significant
infectious process.
10. Swabs must only be touched to the area of collection to avoid contamination.
Swab Type and Usage

Steps for collecting a swab specimen (all except BBL Vacutainer Anaerobic
Collector):
1. Check for expiration date of swab.
2. Peel open the sterile package if required. 3. Remove swab from packaging.
4. Collect sample.
5. Remove lid to transport container and place swab inside. Close container.
6. Label properly with patient’s name, date of birth, date and time of
collection and collector’s initials.
7. Transport to laboratory.
Steps for collecting anaerobic specimen (BBL Vacutainer Anaerobic Collector):
1. Check for expiration date of swab.
2. Peel open the sterile package and remove plunger with sterile swab
attached.
3. Collect sample.
4. Replace swab through holes and into inner tube.
5. While holding at a 45° angle, press down on disc portion of plastic
plunger forcing the inner tube into the outer tube.
6. Gently rotate tube in a swirling motion to facilitate mixing of air in inner tube
and hydrogen in outer tube.
7. Label properly with patient’s name, date of birth, date and time of
collection and collector’s initials.
8. Transport to laboratory.
Ear
Using a sterile swab, gently enter the ear canal, rotate swab before removing.
Avoid contact with other areas of the ear.
Eye
Obtain purulent material from the conjunctiva or cornea. Avoid contact with other
areas of the eye.
Nasal
Gently insert swab into nostril until resistance is met (less than 1 inch). Rotate the
swab then remove it.
Nasopharyngeal
Pass a swab gently through the nostril until it passes the nasopharyngeal wall.
Rotate the swab then remove it.
Throat The swab should be taken from the back of the throat. Keep swab free of saliva; do not touch teeth or tongue. If the isolation of C. diphtheriae is required, please contact the laboratory so that the appropriate transport media/container will be used. If testing for N. gonorrhoeae is desired, please inform the laboratory on the requisition so that the appropriate media can be inoculated.
Wound– Deep
Most often these are specimens from surgical sites; less frequently puncture

wounds and some decubiti may contain anaerobes. These specimens are
suitable for aerobe/anaerobe cultures.
Wound – Surface
Debride area if necessary. Care should be taken not to touch surrounding skin
surface. This is suitable for aerobic culture only.
Sterile Body Fluids
Body fluids for culture should be placed in a sterile container. Do not put fluid into
a swab.
ORIGINAL AUTHOR: Wendy R. Williams
ORIGINAL EFFECTIVE DATE: 12/30/2010
Swab Collection for Microbiology

Therapeutic Drug Monitoring
Recommended collection times for common therapeutic medications:
Drug
Peak
(time after end of
infusion/dose)
Trough
(time before next
dose)
Therapeutic
Range
Aminoglycosides –
Conventional dosing
IM – 1-1.5 hours
IV – 30 min < 30 min
Peak: 4-10
Trough: <2.0
Aminoglycosides –
Extended interval dosing N/A <90 min
Peak: 4-10
Trough: <2.0
Vancomycin IV - 60 min < 30 min Peak: 30-40
Trough: 5-20
Chloramphenicol IV/PO – 2 hours < 30 min Peak: 10-20
Trough: 5-20
Carbamazepine N/A < 30 min 4-12
Phenobarbital N/A < 30 min 10-40
Phenytoin N/A < 30 min 10-20
Valproic Acid N/A < 30 min 50-100
Digoxin N/A < 30 min 0.8-2.0
Lithium N/A < 30 min 0.6-1.2
Theophylline N/A < 30 min 10-20

ABO & Rh
Lab: WMC/CMH Transfusion Service
Availability: 24 Hours
TAT: Routine:, 4 Hours
Stat, 1 Hour
Specimen: Whole Blood Tube: EDTA (lavender/pink)
Minimum Volume: 5ml Collection: Routine venipuncture
Causes For Rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: To determine blood type
and Rh.
Limitations: Certain clinical
conditions may interfere with
typing.
Acetaminophen
Lab: WMC/CMH Chemistry
Availability: 24 Hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li Hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Causes For Rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: monitor therapy, evaluate
toxicity
Additional info: hepatic toxicity
may appear 3-5 days after
ingestion of a toxic dose.
Albumin
Lab: WMC/CMH Chemistry
Availability: 24 Hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep.)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Causes for rejection: Improper labeling, wrong tube,
gross hemolysis, contamination with iv fluids, or
bacteria.
Use: evaluation of nutritional
status, blood osmotic pressure,
renal disease with proteinuria,
and other chronic diseases.
Limitations: hemolysis and high
triglycerides can interfere with
testing.
Alcohol (ETOH, Ethanol)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep.)
Minimum volume: 2 ml
Collection: Routine venipuncture. Do not clean
venipuncture site with alcohol. Transport specimen to
laboratory immediately.
Causes for rejection: Collected from site cleaned
with alcohol.
Storage: transport sample to
laboratory immediately. Keep
tightly closed and store at 4˚C if
testing is delayed.
Use: evaluation of apparently
intoxicated or comatose
patients.
Alkaline Phosphatase (Alk Phos)
Lab: WMC/CMH Chemistry
Availability: 24 Hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep.)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Causes For Rejection: Mislabeled tube, wrong tube,
gross hemolysis, contamination With IV Fluids, or
bacteria.
Use: Evaluation of liver function
and bone disease.
Limitations: Bilirubin,
Methotrexate, & Nitrofurantoin
can interfere with testing.
ALT (SGPT)
Lab: WMC/CMH Chemistry
Availability: 24 Hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparin zed plasma
Tube: SST, Plain red Or Green (Li hep.)
Minimum Volume: 2 ml
Collection: Routine Venipuncture
Causes For Rejection: Mislabeled sample,
wrong tube, gross hemolysis, or
contamination with IV fluids or bacteria.
Use: evaluation of liver function.
Limitations: ALT is less
sensitive to alcoholic liver disease
than AST. High total protein can
interfere with testing.

AmniSure
Lab: WMC/CMH
Microbiology
Availability: 24 Hours
TAT: STAT, 30 hour
Specimen: Vaginal Swab
Collection: non-speculum collection
Causes For Rejection: Mislabeled sample, wrong
swab, specimen not mixed with solvent vial within 1
minute following collection
Use: evaluation for rupture
of fetal membranes
Limitations: Gross hemolysis may
impair tests ability to detect PAMG-1
Ammonia, Venous
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Heparinized plasma
Tube: Green (Li hep.)
Minimum volume: 2 ml
Collection: Routine venipuncture. Fill tube
completely; keep tightly stoppered; place in an ice
slurry; spin and separate within 15 minutes of
collection. If testing is delayed place sample in
refrigerator. Sample may be used up to 3 hours after
collection if collected on ice, centrifuged immediately
and kept on ice or refrigerated.
Causes for rejection: Sample not on ice, wrong
anticoagulant, hemolyzed specimen, mislabeled
sample.
Use: Elevated in liver disease,
inborn errors of metabolism,
indicated in neonates with
neurological deterioration.
Antibody ID (Panel)
Lab: WMC Transfusion Service Availability: As needed TAT: Routine, 4 Hours
Stat, 1 Hour
Note: This test cannot be ordered
individually. It is performed only as a
reflex to a positive antibody screen.
Specimen: Whole blood Tube: EDTA (lavender/pink)
Minimum Volume: 10ml
Collection: Routine venipuncture. Labeling: must have complete patient identification, including full name and MR number.
Causes for rejection: Improper labeling of sample, wrong sample type, hemolysis.
Use: To identify clinically significant unexpected antibodies detected in a positive antibody screen. Limitations: Antibodies to high or low incidence antigens may require referral to a reference lab. A delay in providing compatible blood may occur.
Antibody Screen
Lab: WMC/CMH Transfusion Service
Availability: As needed TAT: Stat: 1 Hour
Routine: 4 Hours
Specimen: Whole blood Tube: EDTA (lavender/pink)
Minimum Volume: 5ml Collection: Routine venipuncture
Causes for rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: To detect unexpected
clinically significant antibodies.

Antibody Titer
Lab: WMC Transfusion Service Availability: As needed TAT: Stat: 1 Hour
Routine: 4 Hours
Specimen: Whole blood Tube: EDTA (lavender/pink)
Minimum Volume: 5ml
Collection: Routine venipuncture Causes for rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: To determine the titer of clinically significant identified antibodies.
Aspirations Of Various Sites for Cytopathology
Lab: Cytopathology
Availability: Mon. – Fri. 5:00 am –
5:00 pm
TAT: 24-48 hours.
Special instructions: please indicate on
requisition if patient has a history of
carcinoma.
Storage: If collected after hours place in
Pathology rack in refrigerator in the main
lab.
Specimen: Aspirates from thyroid, breast, lymph
nodes and other palatable masses.
Minimum volume: Collect as many slides as a
specimen will allow up to 4. Aspirate remaining
aspirate in Cytolyt® solution pull 5 ml of solution back
into syringe and wash out remaining aspirate. Submit
to cytopathology.
Container: Syringes are available from central
supply. Cytolyt available in surgery suite or
Cytopathology lab.
Collection: Label slides w/patient name. Place pea
size aspirate on slide and spread evenly. Let slides air
dry.
Causes for rejection: Improper fixation. Unlabeled
slides or specimen. Coverslips on smears.
Use: To establish the presence
of primary or metastatic
neoplasm. To aid in the
diagnosis of infection.
AST
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum , heparinized plasma
Tube: SST, Plain red or Green (Li hep.)
Minimum volume: 2 ml
Collection: Routine venipuncture
Causes for rejection: Mislabeled sample, wrong
tube, gross hemolysis, or contamination with IV
fluids or bacteria.
Use: Increased AST activity
commonly follows myocardial
infarction, pulmonary emboli,
skeletal muscle trauma,
alcoholic cirrhosis, viral
hepatitis, and drug-induced
hepatitis.
Basic Metabolic Panel (BMP)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
CMH ED - 44 min
Test Includes: glucose, BUN, creatinine,
sodium, potassium, chloride, CO2, calcium
Specimen: Serum , heparinized plasma
Tube: SST, Plain red or Green (Li hep.)
Minimum volume: 5 ml
Collection: Routine venipuncture
Causes for rejection: Gross hemolysis, improper
labeling, contamination with IV fluids, serum/plasma
not removed from cells within 2 hours, wrong
anticoagulant.
Use: to evaluate metabolic
status, fluid/electrolyte
balance.

Bilirubin, Direct
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, plain red or Green (Li hep)
Minimum volume: 2 ml
Collection: Routine venipuncture
Causes for rejection: Gross hemolysis, prolonged
exposure to light.
Use: Liver function test, useful in
diagnosing and monitoring
hepatobiliary obstruction
Bilirubin, Neonatal
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum volume: 2 ml
Collection: Heelstick
Causes for rejection: Gross hemolysis, prolonged
exposure to light.
Use: Increased in hemolytic
disease of the newborn.
Bilirubin, Total
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum volume: 2 ml
Collection: Routine venipuncture
Causes for rejection: Gross hemolysis, prolonged
exposure to light.
Use: To evaluate hepatic
function
Blood Gases, Arterial
(with or without CO-Oximetry analysis)
Lab: CMH Lab/WMC Cardiopulmonary lab
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Test includes: pH, PCO2, PO2,
bicarbonate, base excess, total CO2, O2,
(total hgb, CO saturation, methhgb, and
vol %02, - only measured with co-ox
order).
Specimen: arterial blood
Container: heparinized syringe
Minimum volume: 1ml
Collection: gently agitate syringe to mix the heparin.
Label with the patient’s name and date and deliver
immediately to the cardiopulmonary lab.
Causes for rejection: specimen not aerobic, not
properly labeled, blood clots, air bubbles, insufficient
sample.
Use: evaluate respiratory function
and acid/base balance.
Blood Gases, Venous
Lab: CMH Lab/WMC Cardiopulmonary lab
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Test includes: pH, pCO2, pO2, O2
saturation
Specimen: Venous blood
Container: heparinized syringe
Minimum volume: 1ml
Collection: gently agitate syringe to mix the heparin.
Label with the patient’s name and date and deliver
immediately to the cardiopulmonary lab.
Causes for rejection: specimen not aerobic, not
properly labeled, blood clots, air bubbles, insufficient
sample.
Use: Evaluate respiratory
function, acid/base balance and
estimate cardiac output

Blood Gases, Umbilical Cord Blood
Lab: CMH Lab/WMC Cardiopulmonary lab
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Umbilical cord blood
Minimum volume: 0.3 ml
Collection: gently agitate syringe to mix the heparin.
Label with patient’s name and date and deliver to
the cardiopulmonary lab immediately.
Causes for rejection: specimen not aerobic, not
properly labeled, blood clots, air bubbles, and
insufficient sample.
Use: To evaluate respiratory
status and acid/base balance of
the neonate.
Blood Urea Nitrogen (BUN)
Lab: WMC/CMH Clinical chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum , heparinized plasma
Tube: SST, Plain red or Green top (Li hep)
Minimum Volume: 2mL
Collection: Routine venipuncture or capillary
collection
Causes For Rejection: Improper labeling, gross
hemolysis.
Use: Evaluate renal function and
protein metabolism; to monitor
effectiveness of kidney dialysis
Additional Information:
Elevated BUN levels occur in
chronic glomerulonephritis,
pyelonephritis, and other causes
of chronic renal disease; muscle
wasting may cause increase as
well. Low BUN levels occur in
normal pregnancy, decreased
protein intake, with IV fluids,
some antibiotics, and in some
instances of liver disease.
BNP see (NT-proBNP)
Body Cavity Fluid Cytopathology
Lab: Cytopathology
Availability: Mon.-Fri., 5:00 am – 5:00 pm
TAT: 24-48 hours
Specimen: Fresh body cavity fluid.
Container: Clean 50 ml container or collection
device uses for centesis.
Minimum volume: 50ml
Collection: Gently agitate the bag as fluid is
collected to mix the heparin with the fluid. Label
with patient’s name, hospital number, room number, and
date. Deliver immediately to cytopathology laboratory.
Special instructions: Fluids should be submitted
fresh, unfixed, and heparinized. To provide well
preserved, representative, diagnostic material. Add 3
units of heparin per anticipated 1ml of fluid (each
1ml of fluid contains 1000 units). Include pertinent
clinical information. After hours store in the
Pathology rack in the refrigerator in main lab.
Use: to establish the presence of
primary metastatic neoplasms or
microorganisms. Limitations:
Lack of diagnostic cellular
material or clotted material.
Additional info: Special stains
and immunohistochemistries
will be performed when
appropriate.
Body Fluid Cell Count see (Cell Count Body Fluid)
Body Fluid pH and Occult Blood
Lab: WMC Urinalysis
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Body fluid (synovial, ascetic, pleural, or
pericardial)
Tube: Plain red, or in clean specimen container - or
request Gastroccult card from lab for occult blood
portion.
Collection: usual aseptic collection. Tube must be
properly labeled.
Causes for rejection: mislabeled specimen
Bone Marrow (Aspirate/Biopsy)
Lab: WMC Hematology/surgical
pathology
Availability: Mon.-Fri. 8:00am-5:00pm;
after hours contact the pathologist
TAT: 24-48 hours
Additional info: Clinicians perform all
biopsies. Call the clinical laboratory for
materials and assistance.
Specimen: Bone marrow aspirate and/or biopsy
Minimum volume: 2ml of aspirate, 4cm core of
marrow
Collection: Slides of aspirated marrow and touch
preps of biopsy are made at the bedside by a
technologist. The biopsy core is placed in B Plus
solution and the clot in a separate container of B Plus
solution. Both containers must be properly
labeled with the patient’s information, date and time
specimen was put in the solution.
Causes for rejection: No marrow obtained
Use: To evaluate the bone
marrow morphology;
hematopoesis, myelopoiesis,
myeloid/erythoid ratio,
megakaryocyte, cellularity, and
marrow iron stores. Also to
evaluate platelet dependent
clotting dysfunction, and anemia.
Marrow culture can contribute to
a study of fever of undetermined
origin and possible systemic
infection, in particular
histoplasmosis and TB. Can also
establish presence of, classify,
and serve as a
follow up of neoplasia.
Bronchial Brushing Cytopathology
Lab: Cytopathology
Availability: Mon.-Fri., 5:00 am-5:00 pm
TAT: 24-48 hours
Specimen: Brush from area of lesion obtained by
physician.
Container: Cytolyt® solution vial.
Collection: Place specimen brush in Cytolyt® solution.
Make sure plastic sheath is removed. Label container
and submit all specimens to Cytopathology.
Causes for rejection: Improper fixation. Plastic
sheath left on brush.
Use: To establish the presence
of primary or metastatic
neoplasms. To aid in the
diagnosis of respiratory infections
with herpes virus,
cytomegalovirus, measles virus,
aspergillus, coccidioides,
cryptococcus, histoplasma,
blastomyces, phycomycetes,
pneumecystis carinii,
strongyloides, echinoccus, and
paragonimus. Aid in diagnosis
of lipoid pneumonia,
sarcoidosis, hemosiderosis, and
asbestosis.
Limitations: Allowing brush to
dry before placing in Cytolyt®
will render specimen
unsatisfactory.
Bronchial Washing Cytopathology
Lab: Cytopathology
Availability: Mon.-Fri., 5:00am-
5:00 pm
TAT: 24-48 hours
Special Instructions: Include pertinent
clinical information, ie: previous
carcinomas, on requisition. Indicate need
to evaluate for Pneumocystis carinii or
fungal disease.
Specimen: Obtained by physician.
Container: Cell collection cup on bronchoscopy
tray.
Minimum volume: At least 2 ml of fresh unfixed
material.
Collection: Label bottle with patient name, hospital
number, room number and date. Submit the specimen to
Cytopathology. Be sure to indicate from which side and
lobe the specimen was obtained. After hours place
specimens in the Pathology rack in the refrigerator in
main lab.
Causes for rejection: improper labeling or fixation
Use: To establish the presence of
primary or metastatic neoplasms.
To aid in the diagnosis of
respiratory infections with Herpes
virus, cytomegalovirus, Measles
virus, Aspergillus, Coccidoides,
Cryptococcus, Histoplasma,
Blastomyces, Phycomycetes,
Pneumocystis carinii,
Strongyloides, Lipoid
pneumonitis, Sarcoidosis,
Hemosiderosis, Asbestosis, and
Alveolar proteninosis.
Buprenorphine
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours Stat, 1 hour
Specimen: Freshly voided, untreated urine.
Container: Urine sample cup.
Volume: 10 ml
Storage: Refrigerate up to 24 hours.
Cause for rejection: Improperly labeled
Limitations: Adulterants added to urine specimen may
produce erroneous results. Substances and/or factors
may interfere with the test and cause false results. Drug
levels below the analyte cut off may not be detected
Use: Rapid immunoassay test
to detect a drug of abuse in
urine.
Note: The length of time
following drug use for which a
positive result may occur is
dependent on several factors
including the frequency and
amount of usage, metabolic rate,
excretion rate, drug half- life and
the user's age, weight, activity
and diet. For quantitation or
confirmation a GC/MS should be
ordered.
CA-125

Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 5 ml
Collection: Routine Venipuncture
Causes For Rejection: Gross hemolysis, improper
labeling.
Use: To monitor patients with
various types of malignancies,
evaluate response to therapies,
and as a possible indicator of
recurrence and prognosis.
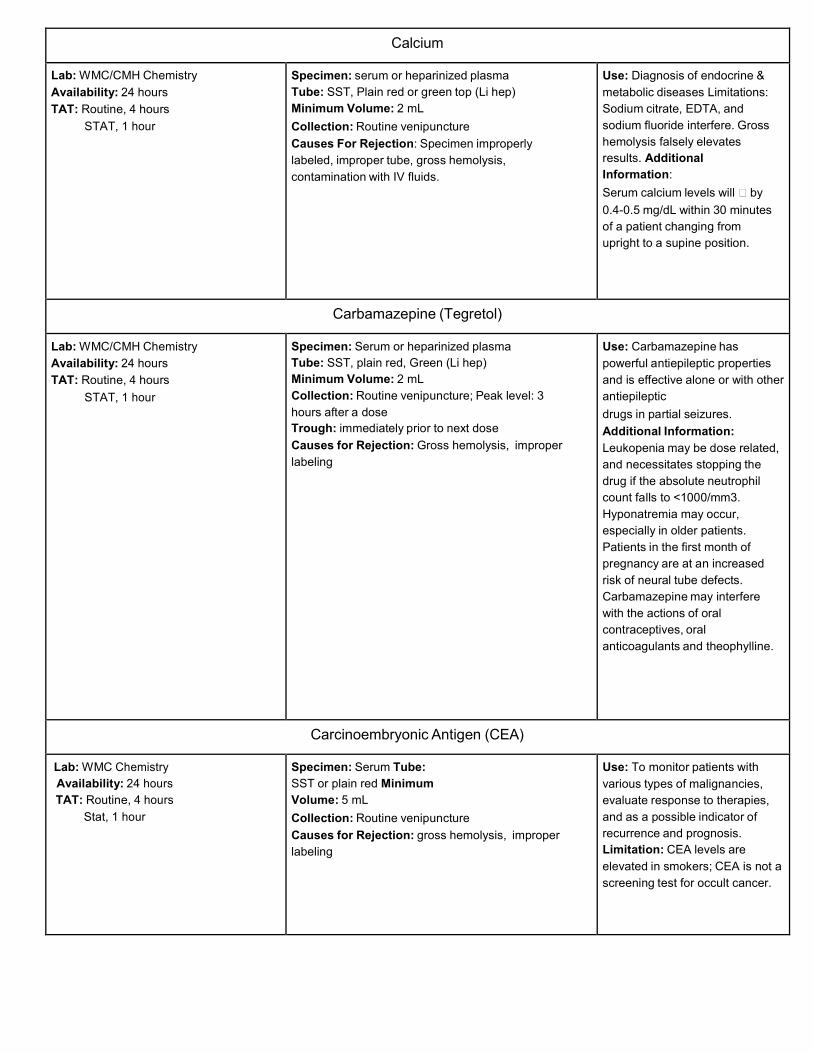
Calcium
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: serum or heparinized plasma
Tube: SST, Plain red or green top (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Specimen improperly
labeled, improper tube, gross hemolysis,
contamination with IV fluids.
Use: Diagnosis of endocrine &
metabolic diseases Limitations:
Sodium citrate, EDTA, and
sodium fluoride interfere. Gross
hemolysis falsely elevates
results. Additional
Information:
Serum calcium levels will by
0.4-0.5 mg/dL within 30 minutes
of a patient changing from
upright to a supine position.
Carbamazepine (Tegretol)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, plain red, Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture; Peak level: 3
hours after a dose
Trough: immediately prior to next dose
Causes for Rejection: Gross hemolysis, improper
labeling
Use: Carbamazepine has
powerful antiepileptic properties
and is effective alone or with other
antiepileptic
drugs in partial seizures.
Additional Information:
Leukopenia may be dose related,
and necessitates stopping the
drug if the absolute neutrophil
count falls to <1000/mm3.
Hyponatremia may occur,
especially in older patients.
Patients in the first month of
pregnancy are at an increased
risk of neural tube defects.
Carbamazepine may interfere
with the actions of oral
contraceptives, oral
anticoagulants and theophylline.
Carcinoembryonic Antigen (CEA)
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum Tube:
SST or plain red Minimum
Volume: 5 mL
Collection: Routine venipuncture
Causes for Rejection: gross hemolysis, improper
labeling
Use: To monitor patients with
various types of malignancies,
evaluate response to therapies,
and as a possible indicator of
recurrence and prognosis.
Limitation: CEA levels are
elevated in smokers; CEA is not a
screening test for occult cancer.

CBC / CBC With Auto Diff + Platelet (Plt)
Lab: WMC/CMH Hematology
Availability: 24 hours
TAT: Routine: 2 hours
Stat: 1 hour
CMH ED: 30 min
Specimen: Whole blood Tube:
EDTA (lavender) only Minimum
Volume: 2 mL Collection: Routine
venipuncture
Causes for Rejection: Wrong sample type, clotted
sample, gross hemolysis, improper labeling, tube not
filled to minimum volume.
Use: To diagnose and monitor
disease states
Limitations: Age and Sex
dependent
Cell Count Body Fluids
Lab: WMC Hematology
Availability: 24 hours
TAT: Routine, 2 hours
Stat, 1 hour
Specimen: Body fluid (synovial, ascitic, pleural, or
pericardial)
Tube: EDTA (lavender)
Minimum Volume: 1 mL
Collection: Usual aseptic collection, DO NOT STORE:
TRANSPORT IMMEDIATELY TO THE LABORATORY
Causes for Rejection: Clotted specimen, improper
labeling, specimens not received in proper tube.
Limitation: Traumatic (bloody)
tap may make interpretation
difficult. Clotted sample will
permit only a qualitative
examination.
Cell Count, CSF ( CSF - Cell Count )
Lab: WMC Hematology
Availability: 24 hours daily
TAT: Routine, 2 hours
Stat, 1 hour
*CSF specimens from patients with
suspected Creutzfeldt-Jakob Disease (CJD)
will be sent to the NC State Lab for testing.
The sample will not be opened prior to
shipping.
Specimen: Spinal Fluid
Container: Sterile plastic tube provided in lumbar kit
Minimum Volume: 1 mL CSF
Collection: Normal lumbar puncture using
established aseptic technique - performed only by
physicians
Storage: CSF must be refrigerated if testing is not
performed immediately.
Use: To aid in diagnosis of
infections of meninges,
subarachnoid hemorrhage,
malignancies of central nervous
system and demyelinating
disorders
Cerebrospinal Fluid (CSF) Cytopathology
Lab: Cytopathology
Availability: Mon.-Fri., 5:00am -
5:00 pm
TAT: 24-48 hours
*CSF specimens from patients with suspected Creutzfeldt-Jakob Disease (CJD) will be sent to the NC State Lab for testing. The sample will not be opened prior to shipping.
Specimen: Fresh fluid.
Container: Sterile tube from lumbar puncture tray.
Minimum Volume: At least 1 ml.
Collection: Label container with patient’s name,
hospital number, room number, date, and time of
collection. Submit specimen to Cytopathology, After
hours, place in Pathology rack in main lab refrigerator.
No anticoagulant or fixative is to be added.
Causes for Rejection: Improper fixation
Use: To establish the presence of
primary or metastatic neoplasms.
Also to establish the presence of
microorganisms such as
Cryptococcus neoformans.

Comprehensive Metabolic Panel (CMP)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
CMH ED - 44 min
Test Includes: glucose, BUN, calcium,
creatinine, total protein, total bilirubin,
alkaline phosphatase, AST, ALT, sodium,
potassium, chloride, CO2
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 5 mL
Collection: Routine venipuncture
Causes for Rejection: Gross hemolysis, improper
labeling, contamination with IV fluids, serum/plasma
not separated from cells within 2 hours of collection,
wrong anticoagulant.
Use: Typically used as a basic
screening panel for nutritional
and metabolic purposes.
Sometimes used to monitor
hyperalimentation therapy.
Chloride
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or Heparinized plasma
Tube: SST, Plain red, or Green(Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Improper labeling,
contamination with IV fluids.
Use: Evaluation of
fluid/electrolyte balance
Additional Information: Chloride
is increased in dehydration, renal
tubular acidosis, and excessive
infusion of normal saline. It is
decreased in over hydration,
CHF, vomiting, chronic
respiratory acidosis, and in some
cases of diuretic therapy.
Limitation: Bromide and
Iodide from therapeutic drugs
can interfere.
Cholesterol
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Specimen: Serum or Heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Improper labeling
Use: Evaluation of lipid status,
nutritional, and metabolic
disorders.
Additional Information: Serum
cholesterol concentration is the
consequence of the relative role of
cholesterol synthesis, clearance, and
dietary intake.
Cholesterol, HDL
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Specimen: Serum or Heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Improper labeling
Use: Helpful in determining the
risk of coronary heart disease.
Limitation: Ascorbic acid,
dipyrone, dopamine, and N-
acetyl cysteine can interfere.

Clostridium difficile (C. diff) Toxin Assay
Lab: CMH/WMC Microbiology
Availability: 24 hours
TAT: 24 hours (Outpatient) 3 hours (Inpatient) Testing performed at WMC/CMH
Specimen: Stool, fresh (< 1 hour old)
Container: Sterile container
Minimum Volume: 5 mL liquid or walnut size
unformed stool
Collection: Collect stool specimen in a clean, dry
container. Specimen must be refrigerated if testing
cannot be performed immediately.
Causes for Rejection: Improper storage, mislabeled
specimen, specimen contaminated with urine, specimen
contaminating outside of container, formed stool,
preserved specimen.
Use: To aid in the diagnosis of
antibiotic associated diarrhea.
Additional Information:
Antibiotic associated diarrhea has
been shown to result from
the toxins produced by C. difficile. It
is recognized that this disease can
be caused by virtually any antibiotic.
The detection of the toxin, rather
than culture of the organism, is
important in the diagnosis of the
disease.
CK (Creatinine Kinase) (CPK)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Hemolysis, wrong sample
type, improper labeling.
Use: To test for occurrence of
myocardial infarction, and for
skeletal muscle damage. CK levels
are elevated in muscular
dystrophy, muscle stress or
trauma, and myocarditis. The
CKMB test will be run if the CK is
found to be greater than 75 IU/L if
performed at WMC. Limitation: IM
injections increase serum CK
activity. CK is elevated following
exercise and normal at onset of
AMI unless patient has been
exercising.
CKMB
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red, Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Hemolysis, wrong sample
type, improper labeling
Use: Diagnosis of AMI, and to
evaluate the extent of AMI
Additional Information: CKMB
increases have been reported with
entities which cause damage to
the myocardium (eg: myocarditis,
malignant hyperthermia, etc.)
however CKMB does not generally
abruptly rise and fall in such no-
acute MI settings as it does in AMI.
Limitation: The diagnosis of AMI
should not be based solely on MB
isoenzyme, but rather should be
supported by other clinical findings.
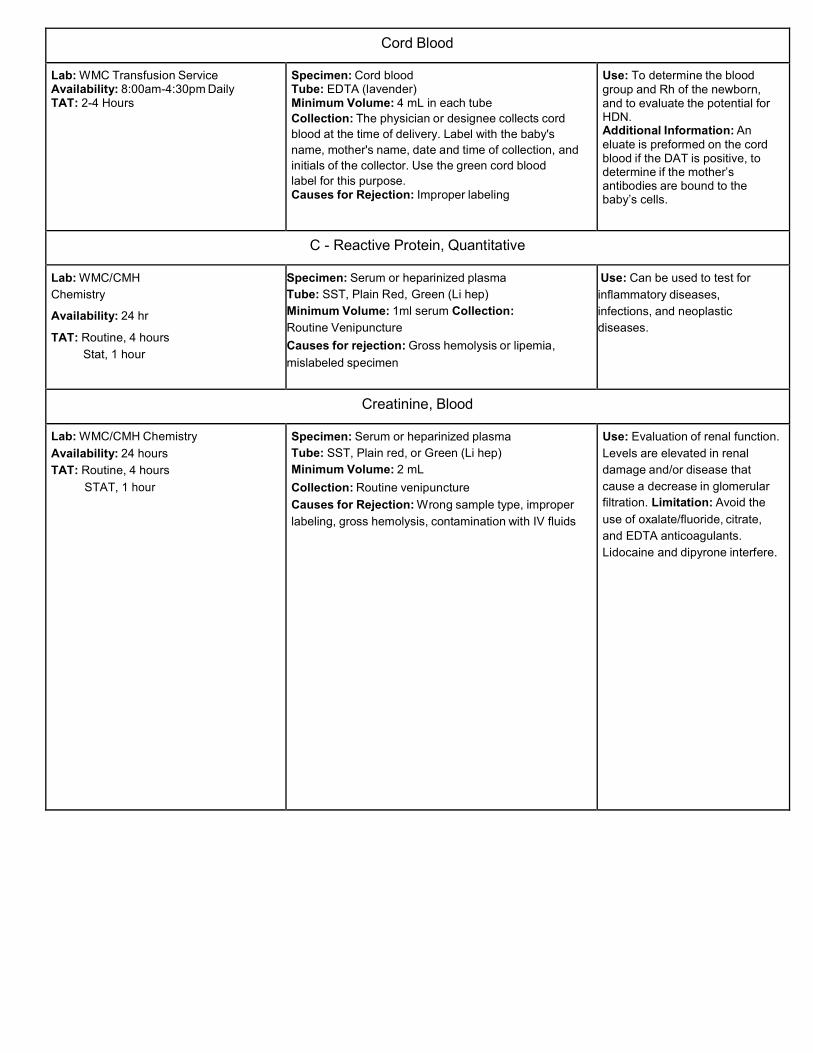
Cord Blood
Lab: WMC Transfusion Service Availability: 8:00am-4:30pm Daily TAT: 2-4 Hours
Specimen: Cord blood Tube: EDTA (lavender) Minimum Volume: 4 mL in each tube
Collection: The physician or designee collects cord
blood at the time of delivery. Label with the baby's
name, mother's name, date and time of collection, and
initials of the collector. Use the green cord blood
label for this purpose. Causes for Rejection: Improper labeling
Use: To determine the blood group and Rh of the newborn, and to evaluate the potential for HDN. Additional Information: An eluate is preformed on the cord blood if the DAT is positive, to determine if the mother’s antibodies are bound to the baby’s cells.
C - Reactive Protein, Quantitative
Lab: WMC/CMH
Chemistry
Availability: 24 hr
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain Red, Green (Li hep)
Minimum Volume: 1ml serum Collection:
Routine Venipuncture
Causes for rejection: Gross hemolysis or lipemia,
mislabeled specimen
Use: Can be used to test for
inflammatory diseases,
infections, and neoplastic
diseases.
Creatinine, Blood
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Wrong sample type, improper
labeling, gross hemolysis, contamination with IV fluids
Use: Evaluation of renal function.
Levels are elevated in renal
damage and/or disease that
cause a decrease in glomerular
filtration. Limitation: Avoid the
use of oxalate/fluoride, citrate,
and EDTA anticoagulants.
Lidocaine and dipyrone interfere.

Creatinine Clearance
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Specimen: Serum/heparinized plasma and aliquot of
24 hour urine collection
Tube: SST, Plain red or Green (Li hep)
Urine: 24 hour urine container without preservative
Minimum Volume: Serum/plasma - 2 mL
Urine - 10 mL aliquot of 24 hour collection
Collection: Serum/plasma- routine venipuncture; Urine-
refer to appropriate 24-hour urine collection form for
collection instructions. Container must be labeled with the
patient’s name, date of birth. date and time collection
started and completed.
Causes for Rejection: No blood creatinine collected,
improperly labeled specimen.
Use: To evaluate renal function,
estimate glomerular filtration rate,
evaluate renal function in small, or
wasted subjects, and
to follow progression of renal
disease.
Limitation: Exercise may cause
increased clearance. The
glomerular filtration rate is
substantially increased in
pregnancy. Ascorbic acid,
ketone bodies, hydration,
numerous cephalosporins, and
glucose might influence
creatinine determinations.
Creatinine, Urine
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Specimen: Urine, 24 hour collection
Container: Clean plastic 24 hour urine container, no
preservative
Minimum Volume: 10 mL aliquot of 24 hour urine
specimen
Collection: Instruct patient to void and discard specimen
at 8:00a and then collect all urine for 24 hours including
the last specimen at 8:00a at the end of the collection
period. Urine should be kept on ice or refrigerated during
collection and until delivery to the lab. Transport urine to
the laboratory immediately after collection is complete.
Container must be labeled with the patient’s name, date
birth, date and time collection was started and
completed. Causes for Rejection: Times not indicated,
improperly labeled specimen
Use: Renal function test when
used as part of creatinine
clearance.
Additional Information: Urine
creatinine is not generally
ordered alone. Creatinine
clearance, which requires a serum
creatinine level, offers useful renal
function data. Serum creatinine
alone is not
an adequate index of
glomerular filtration rate.
Limitation: Completeness of
urine collection requires vigilance
on the part of nursing personnel.
Ingestion of meat may increase
urine as well as serum creatinine
levels. Drugs can interfere with
tubular creatinine secretion.
Creatinine reabsorption occurs
with very low urine flow rates.

Crossmatch
Lab: WMC/CMH Transfusion Service Availability: 24 Hours TAT: Routine, 2-4 Hours
Stat, 1 Hour
Specimen: Whole blood Tube: EDTA (lavender) Minimum Volume: 5 mL
Collection: Routine venipuncture. Specimen must be labeled with Blood Bank Band including patient's full name, Date of Birth, MR number or SS number, date and time of collection, and initials of person collecting the specimen. Blood Bank Band must be completed at time of sample collection.
Causes for Rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: To ensure the compatibility of red blood cells for patients in need of transfusion. Additional Information:
Abnormal proteins and cold or warm auto agglutinins, or unexpected antibodies in the patient's blood may cause delays in the crossmatching process. For routine pre-operative use of type and screen is recommended. In the vast majority of cases this will allow adequate time to rule out any compatibility problems.
GC/Chlamydia (CTNG)
Lab: WMC Microbiology
Availability: 24 hours
TAT: 24 hours (Outpatient) 3 hours (Inpatient) Testing performed at WMC
Specimen: Swab or urine
Container: Sterile container
Minimum Volume: 5 mL urine or single swab
Collection: Use Cepheid CTNG collection kits only.
Causes for Rejection: Improper storage, mislabeled
specimen, sample not sufficient quantity
Use: To aid in the diagnosis of
Neiserria gonorrhoeae or
Chlamydia trachomatis
Additional Information:
Test uses PCR methodologies.
Culture, Anaerobic
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-72 hours
Test Includes: Anaerobic culture,
aerobic culture, and a Gram stain.
Testing performed at WMC.
Specimen: Pus, tissue, or other material properly
obtained from an abscess, biopsy, aspirate, drainage,
exudate, lesion or wound
Collection Device: Sterile container for tissue. Port-
A-Cul vial for pus and aspirate. BD Anaerobic Collection
Device for swabs. If using swabs, you must include an
aerobic swab.
Minimum Volume: Swab in anaerobic device, or 0.5
mL in appropriate anaerobic transport device.
Collection: Disinfect overlying and adjacent areas to
eliminate contamination with indigenous normal flora.
Collection of pus or other fluids through intact skin by
needle aspiration is ideal. Avoid exposure to air. Deliver
immediately to lab.
Causes for Rejection: Specimen not received in
anaerobic transport device, refrigerated specimens,
improper labeling
Use: Isolate and identify
anaerobic and aerobic
pathogens

Culture, Blood
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-72 hours
Negative cultures are incubated for 5
days
Testing performed at WMC.
Specimen: Whole blood
Tube: BacT/Alert blood culture bottles (aerobic and
anaerobic)
Minimum Volume: Optimum sample is 10 mL in each
of two BacT/Alert™ blood culture bottles (aerobic and
anaerobic). If less than 10 mL is collected inoculate
only the aerobic bottle. If more than 10 ml is collected,
inoculate both bottles with equal amounts.
Collection: Remove the plastic cap from blood
culture bottles and cleanse tops with ChloraPrep sponge
or sterile alcohol swab. Select vein of choice in an area
free of skin lesions. Using a ChloraPrep sponge (or
equivalent), scrub venipuncture site with repeated back
and forth strokes for 30 seconds. Allow to dry for 30
seconds. Perform venipuncture. Inoculate appropriate
bottles.
Draw with bottle at downward angle, using a butterfly or
in a syinge. Do not allow liquid in bottle to directly touch
the vacutainer needle due to possible induction of liquid
into bloodstream.
Use: Isolate and identify
potentially pathogenic organisms
causing bacteremia; establish
the diagnosis of endocarditis and
other specific infectious
diseases.
Limitation: Two sets of
negative blood cultures in the
absence of antimicrobial therapy
are usually sufficient to exclude
the presence of
bacteria. One set is seldom
sufficient. Prior therapy may
cause negative cultures or
delayed growth. Improper site
preparation may lead to false
positive blood cultures.
1. For adult patients, two
separate samples (2
venipunctures) are required.
2. For pediatric patients,
smaller samples are
acceptable.
3. For newly admitted patients,
it is desirable to collect all
blood cultures before
antimicrobial therapy is
started. According to QA
protocol this should occur
within 4 hours of patient
arrival.
4. A-lines are in place in many
patients in the Critical Care
areas. It is permissible to
collect one blood culture from
the A-line. It is recommended
that the second culture be
collected by venipuncture.

Culture, Body Fluid
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-72 hours Testing performed at WMC. *CSF specimens from patients with suspected Creutzfeldt-Jakob Disease (CJD) will be sent to the NC State Lab for testing. The sample will not be opened prior to shipping.
Specimen: CSF, synovial fluids, thoracentesis fluids,
etc., collected under aseptic conditions.
Tube: Sterile tube as appropriate, or syringe (with
needle removed)
Minimum Volume: 1 ml
Collection: Disinfect skin over puncture site with 2%
tincture of iodine in concentric circles. Iodine should
remain in contact with skin for at least one minute prior to
puncture to insure complete antisepsis. Immediately
transfer specimen to sterile container and close tightly to
avoid leakage.
Additional Information: If anaerobes are suspected,
order anaerobic culture (listed separately).
Storage: Maintain at room temperature.
Use: Isolate and identify
pathogenic organisms from
normally sterile body fluids.
Culture, Bronchial Washing/ Bronchial Brush
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Testing performed at WMC.
Specimen: Bronchial Washing / Bronchial Brush
Container: Sterile Container
Minimum Volume: 1 ml
Collection: Performed by Physician
Causes for Rejection: Improperly labeled specimen.
Use: Screen for bacterial
growth.
Note: Samples are also
processed for AFB and Fungi.
Culture, Ear
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Testing performed at WMC.
Specimen: Swab or Fluid
Collection Device: BBL Culture Swab (mini-
tip/aluminum shaft) or sterile container
Minimum Volume: 1 Swab or 0.5ml
Collection: Sample usually collected by physician.
Causes for Rejection: Improperly collected or
labeled specimen.
Use: Screen for bacterial
growth.
Culture, Eye
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours Testing performed at WMC.
Specimen: Swab or Plates
Collection Device: BBL Culture Swab (mini-
tip/aluminum shaft) or plates inoculated by MD.
Minimum Volume: 1 Swab or plates
Collection: Sample usually collected by physician.
Causes for Rejection: Improperly collected or
labeled specimen.
Use: Screen for bacterial
growth

Culture, Stool (GI Panel)
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Tests for 14 bacterial pathogens, 4 parasites and 5 viral pathogens.
Specimen: Stool, fresh (<1 hour old); stool in
appropriate transport (available in lab)
Container: Clean, dry plastic container, Meridian Para-
Pak™ Enteric Plus vial or equivalent.. Diapers are not
acceptable.
Minimum Volume: 5 mL or walnut size sample
Collection: Specimen should be collected in a sterile
bedpan, not contaminated with urine, residual soap, or
disinfectants. Those portions of stool which
contain pus, blood, or mucus should be transferred to a
sterile specimen container.
Storage: Refrigerate
Causes for Rejection: Specimens sent on a diaper or
tissue, unlabeled specimen, frozen specimen, specimen
contaminating outside of container.
Use: Screen for pathogenic
bacterial, viral and parasitic
organisms using PCR
technology.
Limitation: GI Panel should not
be done for patients
hospitalized for more than 3
days. See C. difficile toxin.
Culture, Group B Strep
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours Testing performed at WMC.
Specimen: Vaginal/rectal swab.
Collection Device: BBL CultureSwab.
Minimum Volume: One swab
Collection: Using dual swab system, collect vaginal
sample with one swab and rectal sample with the
second swab. Return both swabs to original container.
Storage: Maintain at room temperature.
Use: Isolate and identify group
B beta streptococci.

Culture, Sinus
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours Testing performed at WMC.
Specimen: Swab, Fluid, or Aspirate
Collection Device: Sterile container or BBL Culture
Swab (mini-tip/aluminum shaft)
Minimum Volume: 1 swab or 0.5 ml
Collection: Specimen usually collected by physician.
Causes for Rejection: Specimen not labeled properly.
Use: To determine bacterial
infections of the sinus cavities.
Culture, Sputum
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Test Includes: Culture and Gram stain
Testing performed at WMC.
Specimen: Sputum
Container: Sterile screw cap container
Minimum Volume: 5-10 mL sputum
Collection: Most samples will be collected by the
Cardiopulmonary Department. Expectorated and
induced sputa are screened for quality in the lab.
Causes for Rejection: Contaminated sample,
mislabeled specimen
Use: Isolate and identify
pathogens of the lower
respiratory tract.
Limitation: An adequate
sputum specimen should
contain many WBC’s and few to
no epithelial cells. The latter
are indicative of contamination
with saliva. Results obtained
without proper screening for
contamination may be
misleading.
Culture, Throat (Group A Strep)
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Testing performed at WMC.
Specimen: Material from posterior pharynx, tonsils, or
other inflamed area
Collection Device: Copan Culture Swab sterile culture
collection system or equivalent.
Minimum Volume: One swab
Collection: Swab both tonsillar pillars and the
oropharynx. Do not allow swab to touch the tongue.
Storage: Maintain swab at room temperature
Use: Establish the diagnosis of
strep throat.
Note: Culture will not be done
without a previous negative
Strep Screen.

Culture, Urine
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Testing performed at WMC.
Specimen: Urine
Container: Sterile urine collection container or urine
collection device, which contains boric acid as a
stabilizer.
Minimum Volume: 1 ml urine or properly filled
Boric Acid Tube
Collection: Urine for culture may be midstream clean
voided, from catheter, I/O or indwelling (line only, freshly
voided) or a suprapubic specimen collected via syringe
(by physician only.) Early morning specimens yield
highest bacterial counts from overnight incubation in the
bladder, and are the best specimens for culture.
Storage: Specimen must be refrigerated or placed in
transport device containing boric acid.
Causes for Rejection: Room temperature for more
than two hours or in boric acid tube over 48 hrs,
specimen contaminated with fecal material.
Use: To investigate possible
urinary tract infection (UTI);
monitor treatment for UTI.
Limitation: Hair from the
perineum will contaminate the
specimen. The stream from a
male patient may be
contaminated by bacteria from
beneath the prepuce. Bacteria
from vaginal secretions, vulva, or
distal urethra may contaminate
the specimen, as might bacteria
from the hands or clothing.
Culture, Wound
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: 24-48 hours
Test Includes: Culture and Gram stain
Testing performed at WMC.
Specimen: Aspirates or swabs.
Collection Device: Copan Culture Swab, sterile transport
tube for aspirates. See Culture, Anaerobic if anaerobic
culture is ordered.
Minimum Volume: Swab or 0.5 mL
Collection: Disinfect contiguous areas of skin or
mucus membrane containing resident normal flora
prior to collection of culture material. Collect exudates
from the interior of productive lesions.
Storage: Maintain specimen at room temperature.
Transport to lab immediately.
Reference Range: No growth.
Use: Isolate & identify potentially
pathogenic organisms.
Limitation: Only rapid-growing,
nonfastidious aerobic organisms
can be recovered & identified by
routine methods. Often only
organisms which predominate will
be identified. Anaerobic, fungal, &
mycobacterial pathogens should be
considered, and appropriate
cultures requested if indicated.
Normal skin flora may be
coagulase- negative staphylococci
& Corynebacterium sp
D-Dimer
Lab: WMC/CMH Coagulation
Availability: 24 hours daily
TAT: Routine, 2 hours
Stat, 1 hour
Specimen: Citrated plasma
Tubes: Sodium citrate (blue top) tube
Minimum Volume: fill mark on tube
Collection: Routine venipuncture. Fill tubes until
vacuum is exhausted.
Storage: Citrated plasma may be stored at room
temperature for up to 8 hours, or frozen at -20
degrees Celsius for up to one month.
Causes for Rejection: hemolysis, specimen not
stored properly, specimen improperly labeled,
specimen contaminated with IV fluids.
Use: Elevated levels of D-dimer
are found in such clinical
conditions as deep vein
thrombosis (DVT), disseminated
intravascular coagulation (DIC),
and pulmonary embolism.
Additional Information: D-
dimer levels rise with age,
pregnancy, and in malignancy,
among other conditions.
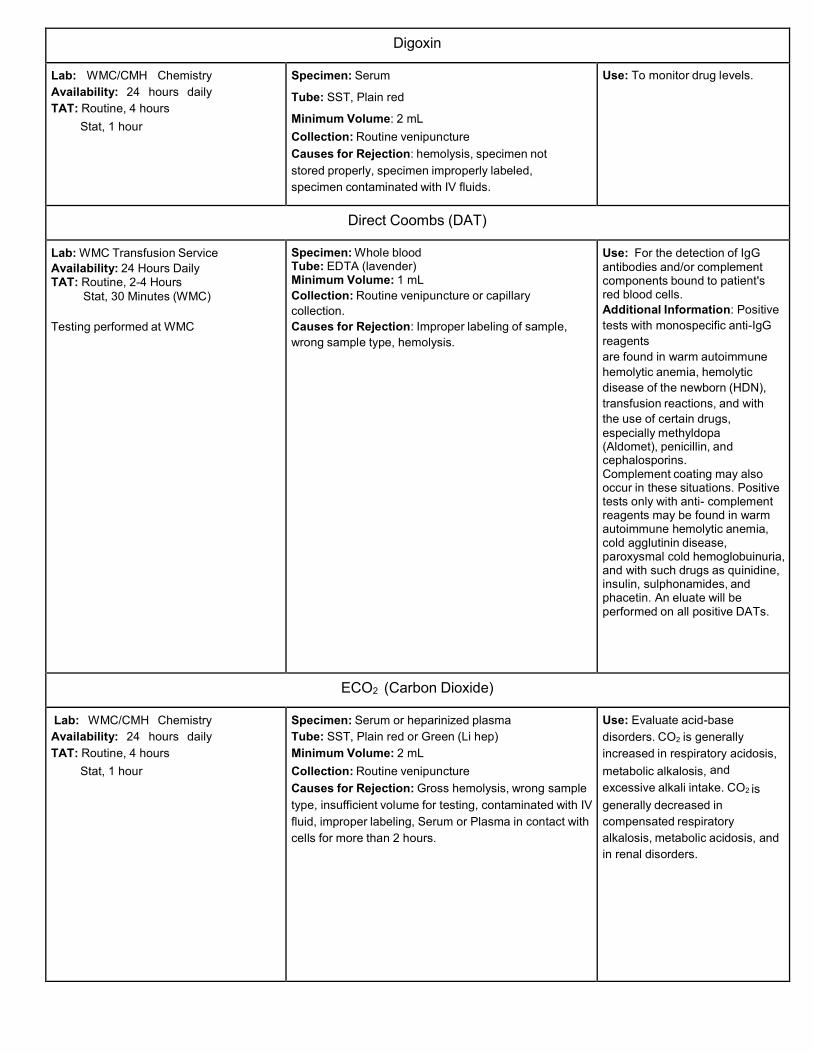
Digoxin
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum
Tube: SST, Plain red
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: hemolysis, specimen not
stored properly, specimen improperly labeled,
specimen contaminated with IV fluids.
Use: To monitor drug levels.
Direct Coombs (DAT)
Lab: WMC Transfusion Service
Availability: 24 Hours Daily TAT: Routine, 2-4 Hours
Stat, 30 Minutes (WMC)
Testing performed at WMC
Specimen: Whole blood Tube: EDTA (lavender) Minimum Volume: 1 mL
Collection: Routine venipuncture or capillary
collection.
Causes for Rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: For the detection of IgG antibodies and/or complement components bound to patient's red blood cells.
Additional Information: Positive
tests with monospecific anti-IgG
reagents
are found in warm autoimmune
hemolytic anemia, hemolytic
disease of the newborn (HDN),
transfusion reactions, and with
the use of certain drugs, especially methyldopa (Aldomet), penicillin, and cephalosporins. Complement coating may also occur in these situations. Positive tests only with anti- complement reagents may be found in warm autoimmune hemolytic anemia, cold agglutinin disease, paroxysmal cold hemoglobuinuria, and with such drugs as quinidine, insulin, sulphonamides, and phacetin. An eluate will be performed on all positive DATs.
ECO2 (Carbon Dioxide)
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Gross hemolysis, wrong sample
type, insufficient volume for testing, contaminated with IV
fluid, improper labeling, Serum or Plasma in contact with
cells for more than 2 hours.
Use: Evaluate acid-base
disorders. CO2 is generally
increased in respiratory acidosis,
metabolic alkalosis, and
excessive alkali intake. CO2 is
generally decreased in
compensated respiratory
alkalosis, metabolic acidosis, and
in renal disorders.

Electrolytes
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Test Includes: sodium, potassium,
chloride, CO2
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: Remove Serum or Plasma from cells if plain
red tube is used; store in plastic transfer tube in
refrigerator if testing is not to be performed immediately.
Causes for Rejection: Gross hemolysis, wrong
sample type, insufficient volume for testing, contaminated
with IV fluid, improper labeling, Serum or Plasma in
contact with cells for more than 2 hours.
Use: Monitor electrolyte status.
Esophageal & Gastric Brushing Cytopathology
Lab: Cytopathology
Availability: Mon-Fri, 5:00-5:00 pm
TAT: 24-48 hours
Specimen: Esophageal and gastric brushing
collected by physician.
Collection: Place brush in Cytolyt® vial. Make sure
plastic sheath is removed. Label with patient name,
hospital number, room, and date. Submit to
Cytopathology. After hours place in Pathology rack in
refrigeratory in main lab
Use: To establish the presence of
primary or metastatic neoplasm,
reactive processes or infectious
disease.
Limitation: Non-diagnostic if
gastric epithelium is not
present or if the specimen is
contaminated with food or
barium sulfate.
Estradiol
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 5 ml
Collection: Routine Venipuncture
Storage: Separate serum from RBC’s; may be stored
up to 2 days at 2-8˚ C
Use: For the evaluation of
normal sexual development,
causes of infertility, and
menopause.

Ferritin
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: 4˚C. If testing is to be delayed and plain tube is
used, separate serum from cells and transfer to a plastic
tube.
Causes for Rejection: Improperly labeled specimen.
Use: Diagnose hypochromic,
microcytic anemias.
Additional Information:
Decreased in iron deficiency
anemia and increased in iron
overload. Ferritin levels
correlate with and are useful in
evaluation of total body iron
stores. In hemochromatosis, both
ferritin and iron saturation are
increased. Limitation: Ferritin
escapes from necrotic
hepatocytes. In the presence of
liver disease, inflammatory
diseases such as rheumatoid
arthritis, malignancy, or iron
therapy, iron deficiency may not
be reflected by low serum ferritin.
Fetal Fibronectin (FFN)
Lab: WMC Hematology
Availability: 24 hours
TAT: Routine, 2 hours
Stat, 1 hour
Specimen: Cervicovaginal Secretions
Tube: Adeza Biomedical Specimen Collection Kit
Minimum Volume: Swab
Collection: Collect during a speculum exam. Lightly
rotate the sterile swab across the posterior fornix of the
vagina for 10 seconds. Place swab in buffer and break
the shaft at the score.
Tips for proper collection:
1. Collect prior to collection of specimen for culture,
digital cervical exam, or vaginal probe ultrasound.
2. Do not contaminate with soaps, lubricants,
disinfectants or Monistat Cream.
3. Do not collect if patient has had sexual intercourse
within 24 hours.
4. Do not use with moderate or gross vaginal
bleeding.
5. Do not collect if membranes are ruptured, placenta
abruption or placenta previa.
Causes for Rejection: Sample not properly labeled.
Expired specimen collection device. Specimens not
properly stored.
Use: It is used as an aid in
assessing the risk of preterm
delivery in less than or equal to
7 to 14 days in pregnant women
with signs of early pre term
labor, intact amniotic
membranes and minimal
cervical dilatation (<3cm),
sampled between 24 weeks, 0
days and 34 weeks, 6 days
gestation.
Limitation: It should not be
interpreted as absolute evidence
for the presence or absence of a
process that will result in delivery
in less than or equal to 7 to 14
days.

Fetal Hemoglobin Stain
Lab: WMC Transfusion Service Availability: 24 Hours TAT: 2-4 Hours
Specimen: Whole blood Tube: EDTA (lavender) Minimum Volume: 2 mL
Collection: Routine venipuncture. Causes for Rejection: mislabeled specimen
Use: To detect the presence of fetal red blood cells in an adult female’s circulation and to determine the post partum dose of RHIG for Rh Negative females with a positive fetal screen.
Fibrinogen
Lab: WMC Hematology
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1hour
Specimen: Plasma, citrated
Tube: Blue (sodium citrate)
Minimum Volume: 4.5 mL or 2.7 mL whole blood,
depending on tube being used for collection. Tube
must be filled to fill line.
Storage: 8 hours at Room Temp. One month in
freezer at -20˚C.
Patient Preparation: The patient should not receive
heparin within 1 hour of collection.
Collection: Routine venipuncture. Collect blue top tube
after Ir tube to prevent the contamination of the specimen
with tissue thromboplastin. Allow tube to fill until vacuum
is exhausted.
Causes for Rejection: Gross hemolysis or clotted
sample, mislabeled specimen
Use: Identify congenital
afibrinogenemia, disseminated
intravascular coagulation (DIC),
and fibrinolytic activity.
Limitation: Increased in patients
on oral contraceptives.
Interpretations of results may be
limited if patient is receiving
anticoagulant therapy, depending
on method of analysis.
Additional Information:
Increased levels may be seen
with inflammation and
pregnancy. Congenital
hypofibrinogenemia may be
responsible for mild
hemorrhagic symptoms;
fibrinogen levels are usually
<100 mg/dL, and screening tests
(PT, PTT) may be normal or only
slightly prolonged.
Folate, Serum (Folic Acid)
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture. Avoid hemolysis
and exposure to light.
Storage: Separate serum from cells and refrigerate at
40C, protected from light.
Causes for Rejection: Hemolysis, prolonged
exposure to light, improperly labeled specimen.
Use: Detect folate deficiency;
monitor folate therapy,
evaluate megaloblastic and
macrocytic anemia.
Limitation: Folate will
deteriorate on exposure to
light.
Additional Information: Serum
folate levels are affected by
dietary intake. Drugs such as
methotrexate and pentamidine,
may induce deficiency. Some
drugs (oral contraceptives,
phenytoin, and ethanol) impair
absorption.

Free T3
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture.
Storage: If plain tube is used, allow to clot and centrifuge
within 45 minutes of collection. Remove serum and store
in a plastic transfer tube at 4° C until testing is performed.
Causes for Rejection: Improper labeling.
Use: A physiologic index of
metabolic activity that
correlates with Free T4 and
TSH.
Free T4
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum (CMH can also accept heparinized
plasma)
Tube: SST or plain red (CMH- green (Li. hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture.
Storage: If plain tube is used, allow to clot and centrifuge
within 45 minutes of collection. Remove serum and store
in a plastic transfer tube at 4° C until testing is performed.
Causes for Rejection: Plasma specimen (except
CMH), improper labeling.
Use: A physiologic index of
metabolic activity that
correlates with TSH.
Frozen Tissue Section
Lab: Surgical Pathology
Availability: Mon-Fri, 8:00am-5:00pm;
after hours call pathologist. Frozen
sections must be scheduled with the
Pathology Department.
TAT: ~20 minutes
Specimen: Fresh tissue with no added fixative.
Container: Plastic specimen container
Collection: Label with patient’s information,
operating room, date and requesting surgeon.
Causes for Rejection: Specimen submitted in
fixative
Limitation: Bone and heavily
calcified tissue cannot be frozen.
Additional Information:
Pathologist calls physician with
diagnosis.

Genital Cytopathology , Routine
Lab: Cytopathology
Availability: Mon-Fri, 5:00am -
5:00 pm
TAT: 24-48 hours
Special Instructions: Submit pertinent
clinical history: age, LMP, history, PMP,
surgery, HRT, abnormal vaginal bleeding,
previous abnormal paps, oral
contraceptives and IUD usage etc.
Notes: Ancillary testing may be ordered
from same ThinPrep PreservCyt® vial i.e.
HPV testing. Call Cytopathology with any
questions about ancillary testing from the
ThinPrep PreservCyt® vial .
Specimen: Endocervical brush, cervical scrap or brush.
Vaginal cuff scrap. For lesions of the vagina or vulva,
scrapings made directly from lesions are desirable.
Container: ThinPrep PreservCyt® vial may be
obtained from the cytopathology department.
Patient Preparation: Patient to avoid douches 48-
72 hours prior to examination. Patient needs to
reschedule if there is excessive menstrual bleeding.
Collection: Label ThinPrep PreservCyt® vial with two
patient identifiers. Submit to cytopathology. Sampling:
1) Endocervix Brush is obtained by inserting brush
into cervical os and rotating, then rinse material into
the ThinPrep PreservCyt® vial. Make sure material
is off the brush.
2) Ectocervical scrape with spatula or broom
thoroughly the entire ectocervix with emphasis on the
squamo-columnar junction. Rinse material into the
ThinPrep PreservCyt® vial . Make sure material is off
the brush.
3) Vaginal specimen obtain specimen by lightly
scraping the vaginal cuff spatula Rinse material
into the ThinPrep PreservCyt® vial. Make sure
material is off the brush.
Causes for Rejection: Fixation in FORMALIN.
Specimen not labeled properly.
Use:
1) To establish the presence
of primary or metastatic
neoplasms.
2) To aid in the diagnosis of
genital infections with HPV,
Herpes virus, Candida,
Trichomonas vaginalis, and
Actiniomyces.
Limitation: Failure to obtain
adequate ectocervical,
enodcervical or vaginal cell
population Ih is suboptimal for
evaluation. Use of lubricating jelly
on the vaginal speculum will
interfere with cytologic
examination.
Gentamicin
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture or capillary
collection. Specimens should be collected prior to the
fourth dose for trough levels and 30 minutes to 1 hour
after fourth dose for peak levels, depending on mode of
administration. See nursing Gentamicin Protocol.
Storage: Refrigerate specimens if testing is not to be
performed immediately.
Causes for Rejection: Improper labeling. Samples
MUST be labeled as peak or trough.
Use: To monitor gentamicin
therapy to maintain effective
levels but avoid toxic side
effects.

Gestational Diabetes Screening (O'Sullivan)
Lab: WMC/CMH Chemistry
Availability: Mon. - Fri. (7a-5p)
TAT: 2-4 hours
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture 1 hour after
glucola.
Patient Preparation: 50 grams of oral glucose given
without regard to time of day or last meal.
Storage: Separate serum / plasma from RBC’s and
maintain specimens at room temperature.
Causes for Rejection: Patient in a stressed condition
(surgery, infection, corticosteroids) or improper labeling.
Use: Investigate the possibility of
Gestational diabetes.
Limitations: A normal result
does not assure that diabetes will
not develop.
GGT (Gamma Glutamyl Transferase)
Lab: WMC Chemistry
Availability: 24 hours TAT:
Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: Separate serum from cells if plain red tube is
used. Refrigerate if testing is not to be performed
immediately.
Causes for Rejection: Improper labeling.
Use: GGT is a biliary enzyme useful
in the diagnosis of obstructive
jaundice, intrahepatic cholestasis,
pancreatitis, and metastatic
carcinoma of the liver. GGT parallels
ALP in liver disease but is not
elevated in bone disease.
Limitation: GGT is elevated in
patients on anticonvulsives and
barbiturates. Acetaminophen can
cause an in-vivo increase. GGT is
sensitive to ethanol intake.
Additional Information: GGT is
more specific for hepatic disease
than ALP. GGT has no origin in
bone or placenta, unlike ALP. GGT
is highest in obstructive liver disease.
Commonly elevated in patients with
cirrhosis, carcinoma of liver and
pancreas, hepatitis, stone,
pancreatitis, and CHF.

GI Panel (see Culture, Stool)
Glucose (Blood Sugar)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: If tube other than SST is used, remove
serum/plasma from cells ASAP and refrigerate if
testing is delayed.
Causes for Rejection: Gross hemolysis, in contact
with cells for prolonged periods of time, collected
above IVs
Use: Diagnosis diabetes mellitus;
evaluate disorders of carbohydrate
metabolism; evaluate acidosis and
ketoacidosis.
Limitation: Mild glucose
impairment can exist with fasting
glucose within normal range.
Specimen not handled properly
can lead to falsely depressed
levels (serum/plasma left in
contact with cells for extended
time.) Additional Information: A
fasting glucose of >140 mg/dL on
more than one occasion is virtually
diagnostic of diabetes mellitus;
likewise a 2-hour post- prandial
glucose level >200 mg/dL is also
virtually diagnostic, obviating the
need for a GTT.

Glucose, CSF
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: 1 hour
*CSF specimens from patients with
suspected Creutzfeldt-Jakob Disease
(CJD) will be sent to the NC State Lab
for testing. The sample will not be
opened prior to shipping.
Specimen: CSF
Tube: Sterile plastic tubes provided in the Lumbar
puncture tray.
Minimum Volume: 1 ml
Collection: CSF specimens are collected only by
physicians or designee using established aseptic
technique.
Storage: CSF specimens are not stored. Testing is
performed immediately to avoid utilization of
glucose in the specimen by bacteria or cellular
components.
Glucose Tolerance (GTT)
Lab: WMC/CMH Chemistry
Availability: Mon-Fri, times set at
scheduling
TAT: Fasting level will be performed
before glucose beverage is given to the
patient (approximately 30 minutes.)
Testing will be completed within 1 hour of
the collection of the final specimen.
Note: Glucose tolerance testing will not be
started after 0900, nor will it be performed
on weekends. Outpatient testing must be
scheduled in advance.
Specimen: Serum or heparinized plasma, whole
blood
Tube: SST or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture, capillary puncture
Patient Preparation: Patient must be fasting. Collect
fasting specimen wait for results. If results of the fasting
specimen are less than 140 mg/dL continue with the
testing. If the fasting results are greater than
140 mg/dL contact the physician for further
instructions. If testing is to continue, have the patient
drink the glucose tolerance beverage according to
the following instructions: non-pregnant adult-75
grams; pregnant female-100 grams; child-1.75g/kg
body weight, not to exceed 75 grams.
Storage: Separate serum/plasma from RBCs and
maintain specimens at room temperature.
Causes for Rejection: Patient not fasting; patient in a
stressed condition (surgery, infection, corticosteroids)
should not have a GTT; improper labeling; fasting results
greater than 140 mg/dL unless physician instructs
otherwise, obvious diabetes mellitus.
Use: Investigate the possibility of
diabetes mellitus.
Limitation: Slight hyperglycemia
is seen in patients on oral
contraceptives. Failure to have
patient on a 3- day high
carbohydrate diet may result in a
false positive GTT. Impaired
glucose tolerance is NOT
equivalent to diabetes mellitus,
neither does a normal result
assure that diabetes will not
develop.
Contraindications: FBS >140
mg/dL on two occasions or
postprandial blood glucose
>200 mg/dL on two occasions in
a non-stressed patient are
indicative of diabetes mellitus and
obviate the need for a GTT. GTT
is also contraindicated in the
presence of obvious diabetes
mellitus.

HCG, Beta Quantitative - Pregnancy Test
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or plasma
Tube: Plain red, SST or Green (Li Hep.)
Minimum Volume: 1.0 mL
Collection: Routine venipuncture.
Cause for Rejection: gross hemolysis, improperly
labeled specimen
Use: To determine the presence
of hCG in patients with gestational
trophoblastic disease, evaluate
and monitor males with testicular
tumors; follow pregnancy. The
quantitative hCG assay should
also be used for non-routine
detection of hCG (eg. ectopic
pregnancy, threatened
miscarriage, or very early
pregnancy).
HCG, Qualitative Serum - Pregnancy Test
Lab: WMC/CMH Hematology
Availability: 24 hours daily
TAT: Routine, 4 hours
STAT, 1 hour
Specimen: Serum Tube:
Plain red or SST Minimum
Volume: 0.5 mL
Collection: Routine venipuncture.
Cause for Rejection: gross hemolysis, improperly
labeled specimen, plasma specimen
Use: Early detection of
pregnancy
Limitations: A number of
conditions other than pregnancy
may cause elevated levels of
hCG. These diagnoses should
be considered if appropriate to
the clinical evidence.
HCG, Qualitative Urine - Pregnancy Test
Lab: WMC/CMH Hematology
Availability: 24 hours daily
TAT: Routine: 4 hours
STAT: 1 hour
Specimen: Urine
Container: any clean, dry plastic or glass container
Minimum Volume: 1.0 mL
Storage: 2-8°C; if testing is to be delayed for more than
48 hours, the specimen should be frozen. Cause for
Rejection: improperly labeled specimen, improper
storage
Use: Early detection of
pregnancy
Limitations: A number of
conditions other than pregnancy
may cause elevated levels of
hCG. These diagnoses should
be considered if appropriate to
the clinical evidence.
Hemoglobin (Hgb)/Hematocrit (Hct)
Lab: WMC/CMH Hematology
Availability: 24 hours
TAT: Routine: 2-4 hours
Stat: 1 hour
Specimen: Whole blood
Tube: EDTA-lavender top
Minimum Volume: 2.7 to 4.5 mL, depending upon
size of tube being used.
Collection: Routine venipuncture. Mix thoroughly
but gently.
Storage: Maintain specimen at room temperature for up
to 24 hours
Causes for Rejection: Clotted specimen, insufficient
quantity, hemolysis, improperly labeled specimen.
Use: Evaluate anemia, blood
loss, hemolysis, polycythemia,
and response to treatment
Limitation: Hyperlipemic plasma
may falsely elevate hemoglobin
result, with corresponding
increase in MCH. Cold agglutinins
may also interfere with
hemoglobin measurement.

Hemoglobin A1C (Hgb A1c)
Lab: WMC Chemistry
Availability: 24 hours TAT:
Routine: 4 hours
Stat: 1 hour
Specimen: Whole blood
Tube: EDTA (lavender)
Minimum Volume: 2.7 to 4.5 mL, depending on size of
tube being used.
Collection: Routine venipuncture. Mix thoroughly but
gently.
Storage: Room temp for up to 24 hours
Causes for Rejection: Clotted specimen, insufficient
quantity, hemolysis, improperly labeled specimen.
Use: The level of hemoglobin
A1C is proportional to the level of
glucose in the blood over a
period of approximately 2
months. Thus, hemoglobin A1C
is accepted as an indicator of the
mean daily blood glucose over
the preceding 2 months. Regular
measurement of hemoglobin A1C
leads to changes in diabetes
treatment and improvement of
metabolic control as indicated by
lowering of hemoglobin A1C
values.
Hepatic Function Panel (LFT / HFP)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Test Includes: albumin, total bilirubin,
direct bilirubin, alkaline phosphatase,
AST, ALT
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green(Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture.
Storage: Remove serum from cells if tube other than
SST is used, store at 4°C in refrigerator, protect from
light.
Causes for Rejection: Prolonged exposure to light,
improper labeling
Use: To evaluate liver function,
investigate abdominal pain.
Hepatitis B Surface Antibody (HBsAb)
Lab: WMC Chemistry
Availability: 24 hours
TAT: 24 hours
Specimen: Serum Tube:
Plain red or SST Minimum
Volume: 5 mL
Collection: Routine venipuncture
Storage: 4˚C. If tube other than SST is used, separate
serum from cells and transfer to a plastic transfer tube
prior to shipping or storing.
Causes for Rejection: Recently administered
isotopes.
Use: Indicator of clinical recovery
and subsequent immunity to
hepatitis B virus. Limitation:
Presence of HBsAb is not an
absolute indicator of resolved
hepatitis infection, nor of
protection from future infection.
Since there are different serologic
subtypes of hepatitis B virus, it is
possible for a patient to have
antibody
to one surface antigen type and
to be acutely infected with a virus
of a different subtype. Thus,
patients may have co- existing
HBsAg and HBsAb. Transfused
patients or hemophiliacs
receiving plasma components
may give false positive results for
HBsAb.

Hepatitis B Surface Antigen (HBsAg)
Lab: WMC Chemistry
Availability: 24 hours
TAT: 24 hours
Note: All indeterminate samples will be
sent to Ref Lab for confirmatory testing.
Specimen: Serum, Plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 5 mL
Collection: Routine venipuncture
Storage: 4˚C. Remove Serum or Plasma from cells if
tube other than SST is used. Test within 48 hrs. Causes
for Rejection: Improperly labeled specimen.
Use: Hepatitis B surface antigen
is the earliest indicator of the
presence of acute infection.
Also indicative of chronic
infection. Useful in the
differential diagnosis of
hepatitis.
Limitation: Patients who are
negative for HBsAg may still
have acute type B viral hepatitis.
There is sometimes a “window”
stage when HBsAg has become
negative and the patient has not
yet Id the antibody.
Hepatitis C Antibody
Lab: WMC Chemistry
Availability: 24 hours
TAT: 24 hours
Note: All indeterminate samples will be
sent to Ref Lab for confirmatory testing.
Specimen: Serum Tube:
Plain red, SST Minimum
Volume: 5 mL
Collection: Routine venipuncture
Storage: If tube other than SST is used, separate
serum from cells and store in a plastic transfer tube.
Causes for Rejection: Insufficient volume, improperly
labeled specimen.
Use: Evaluation panel for
patients with symptoms or
clinical history that suggest
Hepatitis C infection.
Histopathology
Lab: Surgical Pathology
Availability: Mon-Fri, 5:00am-5:00 pm
after hours call pathologist
TAT: 48 hours; tissue requiring
decalcification and/or special stains-48-
72 hours.
Specimen: Fresh tissue or tissue fixed in formalin.
Container: Plastic formalin filled specimen container.
Collection: Container must be properly labeled with
the patient’s information, date and time of collection, and
physician’s name, time placed in formalin. The complete
requisition form should accompany the specimen to
pathology.
Causes for Rejection: Unlabeled or mislabeled
specimen.
Limitation: Fixed tissue cannot
be used for culture and certain
types of histochemistry.
Additional Info: Lymph nodes
suspected of lymphoma should be
submitted on saline moistened
gauze. Muscle biopsies are sent
to lab fresh, without any fixative.

Human Immunodeficiency Virus Screen (Rapid HIV-1/2, p-24 Ag)
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Test Included: HIV antibody screen and
confirmation by Western Blot if indicated by
positive screening result
Specimen: Serum
Tube: SST that has not been opened
Minimum Volume: Full tube
Collection: Routine venipuncture.
Storage: 4˚C
Use: Investigate possible
exposure to human
immunodeficiency virus.
Additional Information: HIV,
the etiologic agent of the
acquired immunodeficiency
syndrome (AIDS) is a cytopathic
retrovirus. Sera which are
repeatedly reactive
in two of three tests are subject
to confirmatory testing by the
Western blot method. Some
individuals may be initially reactive
by the screening and negative or
indeterminate by Western blot.
This may be caused by other viral
antibodies or autoantibodies ,
although this is extremely rare.
Influenza A And B (Flu A / B)
Lab: WMC/CMH Microbiology
Availability: 24 hours daily
TAT: 1 hour
Rapid Antigen Test: Initial test
is performed using rapid antigen
detection
Specimen: Nasal/Nasopharyngeal swab
Minimum Volume: 1 foam tipped or flocked swab
Storage: Room Temperature
Collection: Nasal swab for patients over 3 years old.
Rotate swab against the nasal wall and return to
container. Nasopharyngeal Swab for under age 3. Insert
swab in the posterior nasopharynx and rotate. Remove
and return to container. For nasal wash, flush one nostril
with 1.0 to 2.5mL normal saline. Allow fluid to run out of
nostril into sterile container.
Causes for Rejection: mislabeled specimen
Use: Confirm the diagnosis of
influenza A & B
Additional Information:
Presentation of influenza infection
ranges from mild respiratory
illness to fatal pneumonia. In
addition, secondary infection can
be a serious complication. People
at high risk from infection include
the elderly and patients with
underlying health problems.
Intact PTH (Parathyroid Hormone)
Lab: WMC Chemistry
Availability: 24 hours
Intra-operative Intact PTH scheduled
TAT: OR, 30 minutes
Routine, 4 hours
Specimen: Plasma
Tube: EDTA (full) spin and separate
Storage: 2-8°C if tested within 24 hrs;
Freeze if testing is delayed > 24 hours.
Causes for rejection: Improperly filled, improperly
labeled or collected in wrong tube.
Use: Important marker to
diagnose the disease of the
parathyroid gland and the
kidney. iPTH is used to judge
success or failure of surgery in
the removal of malignant
parathyroid gland, and to
monitor postoperative recovery.

Iron Panel
Lab: WMC Chemistry
Availability: 24 hours TAT:
Routine, 4 hours
Stat, 1 hour
Test Includes:
Total Iron, Total Iron Binding Capacity,
% Saturation [(Fe/TIBC) x 100]
Specimen: Serum Tube:
Plain red or SST Minimum
Volume: 5 mL
Patient Preparation: Specimen should be drawn
fasting in the morning. Specimen should be drawn
before transfusion or before patient is given
therapeutic iron.
Collection: Routine venipuncture.
Storage: 4˚C. If plain red tube is used, allow to clot and
centrifuge within 45 minutes of collection. Remove serum
and store in a plastic transfer tube until testing is done.
Causes for Rejection: Gross hemolysis, plasma
specimen, improperly labeled specimen.
Use: Differential diagnosis of
anemia, especially with
hypochromia and/or low MCV;
work up hemochromatosis in
which iron is increased and
saturation is high; evaluation of
iron poisoning and overload in
renal dialysis patients or patients
with transfusion dependent
anemia.
Ketones (Serum/Plasma)
Lab: WMC/CMH Urinalysis
Availability: 24 hours TAT:
Routine, 4 hours
Stat, 1 hour
Specimen: Serum or Plasma
Tube: SST, green (Li. Hep), or plain red
Minimum Volume: 0.5 mL
Collection: Routine venipuncture
Storage: 4˚C
Causes for Rejection: Improper tube or labeling
Use: To detect ketoacidosis
Lactic Acid
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Heparinized plasma
Tube: Green
Minimum Volume: 2 mL
Collection: Routine venipuncture, drawn on ice.
Plasma must be separated from cells within 15
minutes of collection. Sample may be used up to 3
hours after collection if collected on ice, centrifuged
immediately and kept on ice or refrigerated.
Causes for Rejection: Not collected and or labeled
properly.
Use: Elevated lactate levels can
occur as a result of tissue
hypoxia, diabetes mellitus,
phenformin therapy,
malignancies, glycogen storage
disease, ethanol, methanol or
salicylate ingestion and metabolic
acidosis.
LDH (LD/Lactate Dehydrogenase), Blood
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture. Avoid hemolysis.
Storage: Specimen should be stored at room
temperature.
Causes for Rejection: Hemolysis, wrong sample
type, dilution of sample with IV fluids, improper
storage
Use: Differential diagnosis of
cardiac and liver disorders,
evaluation of hemolytic
disorders.
Limitation: Hemolysis falsely
elevates LDH results. Ascorbic
acid can decrease LDH values.
Elevated total protein >12 g/dL
(associated with Multiple
Myeloma) can interfere with LDH
analysis.

Lipase
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or heparinized plasma
Tube: SST, plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes for Rejection: Improperly labeled specimen.
Use: Evaluate
diseases/disorders of the
pancreas.
Lithium
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum
Tube: Plain red or SST
Minimum Volume: 2 mL blood
Collection: Routine venipuncture.
Storage: Refrigerate. Separate serum from cells if
plain red tube is used; store in plastic transfer tube.
Causes for Rejection: Collection in green lithium
heparin tube, improperly labeled specimen.
Use: Monitor therapeutic drug
level
Lipid Profile
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Test Includes:
Total cholesterol, HDL cholesterol,
triglycerides, LDL cholesterol, VLDL
cholesterol (calculated),
cholesterol/HDL ratio
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 5 mL
Collection: Routine venipuncture.
Storage: 4˚C
Causes for Rejection: Insufficient volume, wrong
sample type, improper labeling.
Use: Evaluation of hyperlipidemia
as an index to coronary heart
disease. Limitation: Triglyceride
levels greater than 400 mg/dL
invalidate the calculations of LDL
and VLDL and a comment must
be made that these parameters
are invalid.
Magnesium (Mg)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture.
Storage: Remove serum from cells if plain tube is
used. Refrigerate at 4oC.
Causes for Rejection: Gross hemolysis,
Use: Magnesium deficiency
produces neuromuscular
disorders. Increased
magnesium levels relate mostly to
patients in renal failure.
Magnesium is used as an
anticonvulsant in pre-eclamptic
patients.
Meningitis Panel
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: Routine, 24 hours
Stat, 4 hours
Testing performed at WMC
Specimen: CSF
Tube: Clear CSF container
Minimum Volume: 1 mL
Collection: Normal lumbar puncture using established
aseptic technique. Lumbar punctures are performed only
by physicians.
Storage: CSF should be refrigerated if testing is not
performed immediately. Be sure to freeze all extra CSF
in reference transfer tube in case more testing is ordered
Use: Screen for pathogenic
bacterial, viral and parasitic
organisms using PCR
technology.

Mono Test (Infectious Mononucleosis)
Lab: WMC/CMH Serology
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or Plasma (WMC)
Whole Blood (CMH)
Tube: Plain red, SST, or EDTA
(WMC), EDTA only (CMH)
Minimum Volume: 0.5 mL
Collection: Routine venipuncture.
Storage: Remove plasma/serum from cells and
refrigerate at 4˚C if testing is to be delayed.
Causes for Rejection: Hemolysis, contamination
with IV fluids, bacteria, etc.
Use: A serological test to
support the diagnosis of
infectious mononucleosis.
MRSA Screening
Lab: CMH/WMC Microbiology
Availability: 24 hours
TAT: 24 hours (Outpatient) 3 hours (Inpatient) Testing performed at WMC/CMH
Specimen: Swab
Container: Sterile container
Minimum Volume: single swab
Collection: Collect by swabbing inside of the nares
Causes for Rejection: Improper storage, mislabeled
specimen, sample not sufficient quantity
Use: To aid in the diagnosis of
or colonization with MRSA
Additional Information:
Test uses PCR methodologies.
Mycoplasma pneumoniae IgM Antibody
Lab: WMC Microbiology
Availability: 24 hours
TAT: 4 hours
Specimen: Serum
Tube: Plain red or SST
Minimum Volume: 0.2 mL
Collection: Routine venipuncture.
Storage: 4˚C
Causes for Rejection: Hemolysis, lipemia, gross
bacterial contamination, improperly labeled
specimen.
Use: Aid in the serodiagnosis of
M. pneumoniae infection.
Additional Info: Mycoplasma
pneumoniae is the cause of the
relatively common “primary
atypical pneumonia.”
Mycoplasma is more difficult to
culture than ordinary bacteria and
the serologic confirmation of the
diagnosis is often desirable.
Nipple Discharge Cytopathology
Lab: Cytopathology
Availability: Mon-Fri 05:00am-
5:00 pm
TAT: 24-48 hours
Special Instructions: Specify nipple
discharge and from which breast.
Include pertinent clinical date, history of
carcinoma on requisition.
Specimen: Nipple discharge
Container: Cytolyt ® Vial
Collection: Gently grip subareolar area and nipple with
thumb and fore finger. When secretion occurs, allow
discharge to drip into the Cytolyt® vial. Label vial and
submit to Cytopathology.
Causes for Rejection: Improper fixation or
mislabeled vial.
Use: To establish the presence
of primary or metastatic
neoplasm.
NT-proBNP
(BNP)

Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Collection: Routine venipuncture. Spin and
separate, Samples may be used up to 3 days.
Causes for rejection: Hemolysis, turbidity,
mislabeled specimen.
Use: The concentration indicates
the prognosis for left ventricular
dysfunction and is useful in
assigning symptoms to cardiac or
non-cardiac causes.

Obstetric Panel
(OB Panel)
Lab: WMC Chemistry, Hematology,
Blood Bank
Availability: 24 hours
TAT: Routine, 4 hours
Panel consists of:
CBC, RPR, Type (ABO/Rh) & Antibody
Screen, Hepatitis B Surface Antigen
Specimen: Serum, EDTA whole blood
Tube: SST, 2 EDTA
Collection: Routine venipuncture. Spin and
separate SST.
Causes for rejection: Hemolysis, incorrectly labeled
specimen, or clotted EDTA specimen.
Use: Prenatal screening
Note: Please refer to individual
tests for additional information.
Occult Blood (Hemoccult)
Lab: WMC/CMH Microbiology
Availability: 24 hours
TAT: Routine, 2 hours
Specimen: Feces (stool)
Container: Hemoccult slide or a clean dry plastic
container.
Minimum Volume: Pea size amount or thin smear of
stool on both boxes of hemoccult slide
Collection: Fresh stool specimen free of gross blood.
When inoculating hemoccult slides use applicator to
apply a thin smear of stool to box A. Reuse applicator to
apply a thin smear of stool from a different part of the
specimen to box B.
Causes for Rejection: Contamination of specimen
with urine or toilet bowel cleaner; mislabeled
specimen.
Storage: Hemoccult slides once inoculated can be
stored at room temp for up to 14 days
Use: It is a qualitative screening
test for the detection of fecal
occult blood which may be
indicative of gastrointestinal
disease.
Limitation: Patient should
avoid red meat and vitamin C in
excess of 250mg for 3 days
before collecting samples. Non-
steroidal anti-inflammatory drugs
should be discontinued for 7 days
prior to collecting samples.
Osmolality, Serum
Lab: WMC Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, Tube:
SST or Plain red Minimum
Volume: 2 mL
Collection: Routine venipuncture.
Storage: Separate serum from cells as soon as clot
forms. Refrigerated samples may be used for up to
three days.
Causes for Rejection: Hemolysis, plasma specimen,
insufficient volume, improper labeling.
Use: Evaluate electrolyte and
water balance, hyperosmolar
status, hydration status; evaluate
seizures; clue to alcoholism,
methanol toxicity, ethylene glycol
ingestion. Additional Info: High
osmolality can result from
hypernatremia, dehydration,
hyperglycemia, mannitol therapy,
azotemia, ingestion of ethanol,
methanol, and ethylene glycol.
Low osmolality may result from
over hydration, hyponatremia.

Osmolality, Urine
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Urine, random or 24-hour
Container: Plastic urine container, no preservative
Minimum Volume: 10 mL
Collection: Centrifuge urine sample after collection for
5 minutes to remove gross particulate matter. Storage:
Refrigerate up to 3 days.
Causes for Rejection: Improper labeling
Use: Evaluation of
concentrating ability of the
kidneys, evaluate electrolyte
and water balance.
Oxycodone Urine Drug Screen
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Freshly voided, untreated urine.
Container: Urine sample cup.
Volume: 10 ml
Storage: Refrigerate up to 24 hours. Cause for
rejection: Improperly labeled, Limitations: Adulterants
added to urine specimen may produce erroneous
results. Substances and/or factors may interfere with the
test and cause false results. Drug levels below the
analyte cut off may not be detected
Use: Rapid immunoassay test
to detect a drug of abuse in
urine.
Note: The length of time
following drug use for which a
positive result may occur is
dependent on several factors
including the frequency and
amount of usage, metabolic rate,
excretion rate, drug half- life and
the user's age, weight, activity
and diet. For quantitation or
confirmation a GC/MS should be
ordered.
Phenytoin (Dilantin)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum or plasma
Tube: SST, Plain red or Green(Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Incorrect tube or improperly
labeled specimen.
Use: To monitor therapeutic
drug level.

Phosphorus
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or green (Li hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Causes For Rejection: Wrong sample type,
improper labeling
Use: Evaluation of phosphorus
metabolism, calcium/
phosphorus balance.
Platelet Count (Plt Count)
Lab: WMC/CMH Hematology
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Whole blood
Tube: Purple (EDTA)
Minimum Volume: 2 ml in EDTA tube, 0.5 in a
Microtainer
Collection: Routine venipuncture or capillary
collection
Storage: Count cannot be performed if sample is
held at room temperature for more than 8 hours or
more than 24 hours refrigerated.
Causes For Rejection: Incorrect specimen
container, clotted specimen, hemolysis, specimen
collected above IV, insufficient volume.
Use: Quantitation of platelets,
evaluation of bleeding disorders,
aid of evaluation of
chemotherapeutic agents in the
management of malignant
disease states, evaluation of
platelet transfusions. Additional
Information: Some patient’s
exhibit clumping of platelets when
the specimen is
collected in EDTA containers. In
these cases, specimens should be
collected in citrate (blue top)
tubes. If a capillary puncture is
performed, large free flowing
drops of blood must be
obtained in order to avoid a
clotted specimen or clumping.
Specimen must be well mixed
during and immediately after
collection.
Platelet Function Screen
Lab: WMC Coagulation
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Whole blood
Tube: 2 Blue - Citrate DO NOT SPIN
Minimum Volume: 2 tubes
Collection: Routine venipuncture
Causes For Rejection: Specimen is over 2 hours old.
Specimen has been spun down. Improperly labeled
specimen or a clotted sample.
Use: Screening test to evaluate
platelet function. Can distinguish
patients on aspirin therapy from
those with a true platelet
dysfunction. Limitations: Low
hemoglobin can interfere with
testing.

Potassium, Blood
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Storage: Separate serum or plasma from cells.
Refrigerate if testing is not to be performed
immediately.
Causes For Rejection: Wrong anticoagulant, gross
hemolysis, sample in contact with cells for more
than 4 hours, diluted with IV fluids, improper
labeling, insufficient volume.
Use: Monitor electrolyte status
Additional Information: Samples
in contact with RBC for prolonged
periods of time will produce
erroneously high
levels of potassium. Some
anticoagulants contain
potassium, e.g., EDTA, which
will lead to falsely elevated
levels.
Potassium, Urine
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Urine, Random or 24 hr
Minimum Volume: 10 ml Collection:
No preservatives, on ice.
Causes For Rejection: Improperly labeled
specimen.
Use: May be elevated with
dietary increase,
hyperaldosteronism, renal
tubular acidosis and at the
onset of alkalosis.
Pregnancy Test - See HCG
Prolactin
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Improperly labeled specimen or
grossly hemolyzed.
Use: To help with the diagnosis
of disease states such as
infertility, gonadial disorders, and
others.
Procalcitonin
Lab: WMC/CMH
Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Improperly labeled specimen or
grossly hemolyzed.
Testing must be performed within 4 hours
after collection.
Use: To help with the diagnosis of
sepsis, septic shock and antibiotic
efficacy.
Note: Same specimen
type must be use for all
serial testing.
Protein, CSF

Lab: WMC Chemistry
Availability: 24 hours
TAT: Stat, 1 hour
*CSF specimens from patients with suspected Creutzfeldt-Jakob Disease (CJD) will be sent to the NC State Lab for testing. The sample will not be opened prior to shipping.
Specimen: Spinal fluid
Container: Sterile plastic transfer tubes provided in
lumbar tray.
Minimum Volume: 1 ml CSF
Collection: Normal lumbar puncture using established
aseptic technique. Lumbar punctures are performed only
by physicians.
Storage: CSF should be refrigerated if testing is not
performed immediately. Be sure to freeze all extra CSF
in reference transfer tube in case more testing is ordered
later.
Causes For Rejection: Improper labeling. See also
Limitations
Use: A reliable, but non-specific
indicator of CNS pathology,
including meningitis, brain
abscess, CVA, MS, and other
degenerative processes causing
neurologic disease.
Limitations: Fresh blood in
specimen will invalidate the
protein result. Turbid samples
may exhibit a positive
interference. Hemolyzed or
xanthochromic samples may
falsely depress results.

Protein, Total Serum/Plasma
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Calculate Globulin:
TP – Albumin = Globulin
A/G Ratio: Albumin divided by globulin
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Storage: Separate serum from cells within 45
minutes. Refrigerate at 4˚ C
Causes For Rejection: Hemolysis, improperly
labeled sample.
Use: Evaluation of nutritional
status, to investigate edema
Additional Information: Causes
of high total protein: dehydration,
some cases of chronic liver
disease, including chronic active
hepatitis and cirrhosis;
neoplasms, especially myeloma.
Causes of low total protein:
pregnancy, IV fluids, cirrhosis or
other liver disease, including
chronic alcoholism;
prolonged immobilization, heart
failure, nephritic syndromes,
glomerulonephritis; neoplasia,
Crohn’s disease and chronic
ulcerative colitis, starvation,
malabsorption or malnutrition,
hyperthyroidism; burns, severe
skin disease; and other chronic
diseases. Very low total protein,
(<4 g/dl) and low albumin cause
edema.
Prothrombin Time (PT)
Lab: WMC/CMH Coagulation
Availability: 24 hours
TAT: Routine, 2-4 hours
STAT, 1 hour
CMH ED, 44 min
Synonyms: INR Protocols for anticoagulants are posted on the ARHS Intranet and are available to all clinicians. Any clinician contacting the laboratory for anticoagulant information will be told the in-house testing available and then referred to the intranet/pharmacy for protocols or to the pathologist for further questions.
Specimen: Citrated plasma
Tube: Sodium citrate (blue top)
Minimum Volume: Full tube , volume depends on
tube
Collection: Routine venipuncture. Fill tube until
vacuum is exhausted.
Storage: Test within 8 hours.
Causes For Rejection: Clotted specimen, hemolysis,
under filled tubes, lipemia, improperly labeled sample.
Use: Evaluation of extrinsic
coagulation; screen for
congenital deficiencies of
factors II, V, VII, X; prothrombin
deficiency, dysfibrinogenemia,
heparin, effect, coumarin effect,
liver failure, DIC, vitamin K
deficiency.
Limitations: Prothrombin
times collected less than 2 hours
after heparin administration will
be prolonged. Many drugs
modify the effect of coumarin,
including salicylates,
barbiturates, quinidine,
antacids, many antidepressants,
and antibiotics.

PTT (APTT)
Lab: WMC/CMH Coagulation
Availability: 24 hours
TAT: Routine, 2-4 hours
STAT, 1 hour
Synonyms: APTT, Activated Partial
Thromboplastin Time
Protocols for anticoagulants are posted on the ARHS Intranet and are available to all clinicians. Any clinician contacting the laboratory for anticoagulant information will be told the in-house testing available and then referred to the intranet/pharmacy for protocols or to the pathologist for further questions.
Specimen: Citrated plasma
Tube: Sodium citrate (blue top)
Minimum Volume: full tube, volume depends on
tube
Collection: Routine venipuncture. Collect blue tube after
another tube. This procedure avoids contamination of
the specimen with tissue thromboplastin. Fill tube until
vacuum is exhausted. Storage: Test within 4 hours at
room temperature. Causes For Rejection: Specimen
older than 4 hours, clotted specimen, hemolysis, under
filled tubes, lipemia, improperly labeled sample
Use: Evaluation of extrinsic
coagulation; screen for
congenital and acquired
deficiencies of factors VIII, IX,
XI, and XII. Also the test used to
monitor heparin therapy.
Limitations: PTT samples
collected less than 2 hours after
heparin administration will be
prolonged.
PSA (Prostate Specific Antigen)
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Storage: Separate serum from cells immediately.
Causes For Rejection: Improper labeling, wrong
sample type.
Use: Used to monitor disease
status in prostate cancer
patients.
Additional Information:
Elevated levels are found in
men with benign prostatic
hypertrophy.
Renal Function Panel (RFP)
Lab: WMC/CMH Chemistry Lab
Availability: 24 Hours
TAT: Routine, 4 Hours
Stat, 1 hour
Test Includes: Albumin, BUN, Calcium,
Chloride, CO2, Creatinine, Glucose,
Phosphorous, Potassium, Sodium
Specimen: Serum or plasma
Tube: SST, Plain red, Green (Li hep)
Minimum Volume: 5 ml
Collection: Routine venipuncture
Causes For Rejection: Gross hemolysis, improperly
labeled specimen
Note: Please refer to individual
tests for additional information.

Respiratory Panel
Lab: WMC/CMH Microbiology Availability:
24 Hours
TAT: Routine, 24 Hours
Stat, 4 hour
Specimen: Nasopharengeal Swab in UTM
Tube: UTM
Collection: Nasopharengeal collection
Storage: Maintain specimen at room
temperature for up to 24 hours
Causes For Rejection:, improperly labeled
specimen, specimen not placed in transport
within 1 hour after collection
Reticulocyte Count
Lab: WMC/CMH
Hematology Availability: 24
Hours TAT: Routine, 4
Hours Stat, 1 hour
Specimen: Whole Blood
Tube: EDTA (lavender
top tube) Minimum
Volume: 2 ml
Collection: Routine
venipuncture
Storage: Maintain specimen at room
temperature for up to 24 hours
Causes For Rejection: Clotted specimen,
hemolysis,
specimens more than 24 hours old,
Use: Evaluate erythropoietic activity.
Increased in acute and chronic hemorrhage
and hemolytic anemias. Evaluate response to
antianemic therapy Limitations:
Reticulocytes may decrease on a dilutional
basis in transfused patients.
RPR - VDRL
Lab: WMC Hematology
Availability: 24 hours TAT:
2 days
Specimen: Serum or Plasma
Tube: SST, plain red, lavender, or green
Minimum Volume: 2
mL Collection:
Routine venipuncture
Storage: 4oC
Causes For Rejection: Hemolysis,
lipemia, gross bacterial contamination,
mislabeled specimen
Use: Screening test for syphilis Note: If
positive reflexes to quantitative RPR and a
confirmatory MHA-TP.
RSV
Lab: WMC/CMH Microbiology
Availability: 24 hours TAT:
Routine, 4 hours Stat, 1 hour
Specimen: Nasopharyngeal swab
Minimum Volume: swab
Collection: Nasal swab - insert swab into
nostril (1 inch), rotate swab against the
nasal wall then remove.. Nasopharyngeal
Swab - insert swab in the posterior
nasopharynx and rotate then remove. For
nasal wash, flush one nostril with 1.0 to
2.5mL normal saline. Allow fluid to run out
of nostril into sterile container.
Storage: Room temp
Causes For Rejection: mislabeled specimen.
Use: For the diagnosis of RSV
infections.

Rubella
Lab: WMC Chemistry
Availability: 24 hours
TAT: 24 hours
Specimen: Serum, heparinized plasma
Tube: SST, Plain red, or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: 4˚C up to 7 days
Causes For Rejection: Hemolysis, lipemia, gross
bacterial contamination
Use: Recommended for immune
status determination. Additional
Information: Rubella virus is the
cause of German measles,
usually a mild exanthema, often
subclinical, however, when
acquired in utero, rubella virus
can cause the congenital rubella
syndrome, deafness, and
mental retardation. For this
reason, it is very important to
immunize women before they
have children. If a woman has
antibodies against rubella, even of
low titer, demonstrated by any of
multiple methods, she need not
worry about infection during
subsequent pregnancy.
If she is not immune, and is not
pregnant, she can receive the
rubella vaccine.
Salicylates, Serum
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum (CMH/WMC), heparinized
plasma (WMC only)
Tube: SST, Plain red (CMH/WMC); Green (Li hep. /
WMC only)
Minimum Volume: 2ml
Collection: Routine Venipuncture
Causes For Rejection: improper labeling.
Use: In the diagnosis of
salicylate overdose and in
monitoring salicylate therapy.
Sedimentation Rate (ESR)
Lab: WMC/CMH Hematology
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
Synonoms: Sed rate, Westergren Sed
Rate, Erythrocyte Sedimentation Rate Note: Best results are from blood less
than 4 hours old.
Specimen: Whole blood
Tube: EDTA (lavender)
Minimum Volume: 4 mL
Collection: Routine venipuncture
Storage: Room temperature for up to four hours;
refrigerate at 4 °C up to 12 hours if testing is to be
delayed
Causes For Rejection: Obvious hemolysis, clotted
specimen, under-filled tube, specimen older than 12
hours, improperly labeled specimen
Use: Evaluate the non-specific
activity of infections, inflammatory
states, autoimmune disorders,
and plasma cell dyscrasias and
autoimmune disorders.
Additional Information:
Elevations in fibrinogen, alpha-
and beta-globulins, and
immunoglobulins increase the
sedimentation of RBCs through
plasma. The test is important
in the diagnosis of temporal
arthritis, as well as its
management.
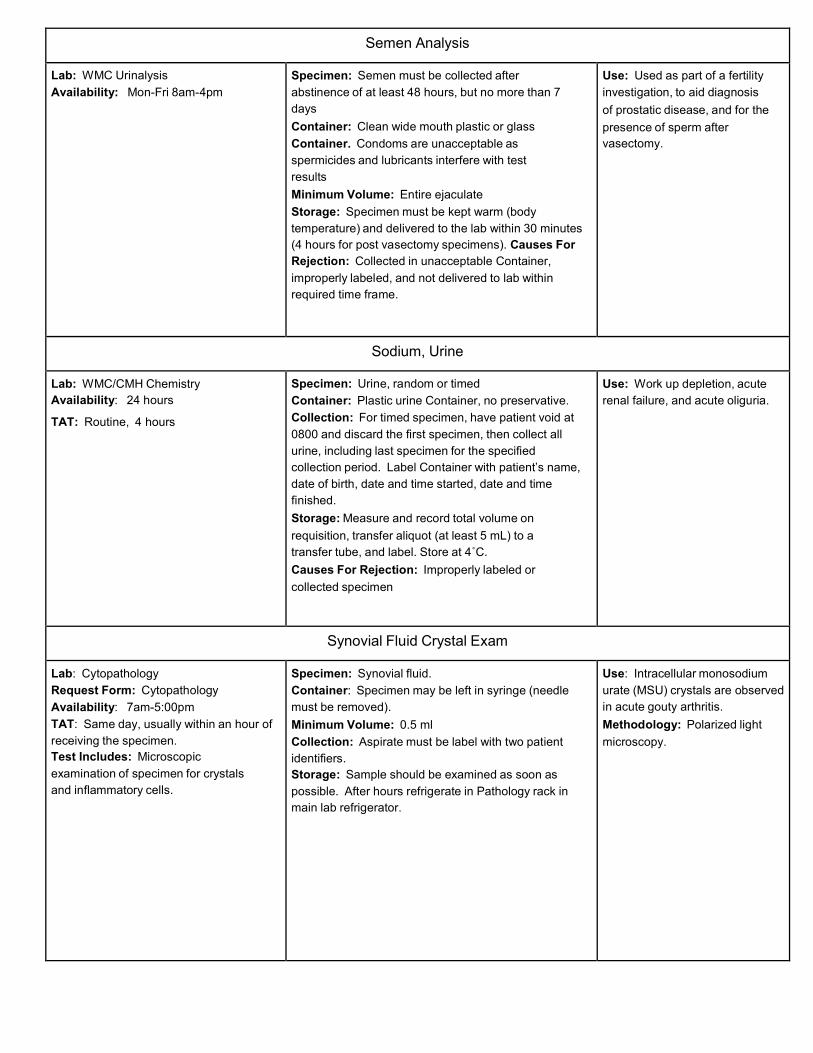
Semen Analysis
Lab: WMC Urinalysis
Availability: Mon-Fri 8am-4pm Specimen: Semen must be collected after
abstinence of at least 48 hours, but no more than 7
days
Container: Clean wide mouth plastic or glass
Container. Condoms are unacceptable as
spermicides and lubricants interfere with test
results
Minimum Volume: Entire ejaculate
Storage: Specimen must be kept warm (body
temperature) and delivered to the lab within 30 minutes
(4 hours for post vasectomy specimens). Causes For
Rejection: Collected in unacceptable Container,
improperly labeled, and not delivered to lab within
required time frame.
Use: Used as part of a fertility
investigation, to aid diagnosis
of prostatic disease, and for the
presence of sperm after
vasectomy.
Sodium, Urine
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Specimen: Urine, random or timed
Container: Plastic urine Container, no preservative.
Collection: For timed specimen, have patient void at
0800 and discard the first specimen, then collect all
urine, including last specimen for the specified
collection period. Label Container with patient’s name,
date of birth, date and time started, date and time
finished.
Storage: Measure and record total volume on
requisition, transfer aliquot (at least 5 mL) to a
transfer tube, and label. Store at 4˚C.
Causes For Rejection: Improperly labeled or
collected specimen
Use: Work up depletion, acute
renal failure, and acute oliguria.
Synovial Fluid Crystal Exam
Lab: Cytopathology
Request Form: Cytopathology
Availability: 7am-5:00pm
TAT: Same day, usually within an hour of
receiving the specimen.
Test Includes: Microscopic
examination of specimen for crystals
and inflammatory cells.
Specimen: Synovial fluid.
Container: Specimen may be left in syringe (needle
must be removed).
Minimum Volume: 0.5 ml
Collection: Aspirate must be label with two patient
identifiers.
Storage: Sample should be examined as soon as
possible. After hours refrigerate in Pathology rack in
main lab refrigerator.
Use: Intracellular monosodium
urate (MSU) crystals are observed
in acute gouty arthritis.
Methodology: Polarized light
microscopy.

Theophylline
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 ml
Collection: Routine venipuncture
Storage: 2-8˚C
Causes For Rejection: Hemolysis, gross lipemia,
improper labeling.
Use: monitor therapeutic drug
level.
Limitations: Troleandomycin &
erythromycin may slow theophylline
elimination. Heart failure, liver
disease, prolonged fever, and
obesity may have similar effects.
Prolonged half-life occurs in
premature infants. By contrast, half
life is shortened in smokers,
variable with Phenobarbital use.
Thyroid Profile
Lab: WMC Chemistry
Availability: 24 hours TAT:
Routine, 4 hours
Stat, 1 hour
Test Includes: Free T4, TSH
Specimen: Serum
Tube: SST or Plain red
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: If plain tube is used, allow to clot and
centrifuge within 45 minutes of collection. Remove
serum and store in a plastic transfer tube at 2-8˚C until
testing is performed.
Causes For Rejection: Plasma specimen , improper labeling
Use: A physiologic index of
metabolic activity that correlates
with free thyroxine (T4).
Tobramycin
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Improperly labeled
specimen.
Use: To monitor drug levels
during therapy.

Triglycerides
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: 4 hours
Specimen: Serum, heparinized plasma
Tube: SST. Plain red or Green (Li hep).
Minimum Volume: 2 mL
Patient Preparation: Patient should be fasting for
12-14 hours prior to specimen collection.
Collection: Routine venipuncture
Storage: 4˚C. Separate serum from cells within 45
minutes of collection.
Causes For Rejection: Non-fasting specimen,
glycerinated tube used for collection, improper
labeling.
Use: Evaluation of
hyperlipidemia
Limitations: The most
common cause of triglyceride
increase is inadequate patient
fasting.
Additional Information: High
concentrations may occur with
hypothyroidism, nephrotic
syndrome, glycogen storage
diseases, and diabetes mellitus.
Extremely high triglycerides
are common in acute
pancreatitis.
Troponin I
Lab: WMC/CMH Chemistry
Availability: 24 hours daily
TAT: Routine, 4 hours
Stat, 1 hour
CMH ED, 50 min
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Incorrect specimen type or
improperly labeled specimen.
Use: As part of the clinical
picture in the diagnosis of AMI.
Limitations: Heterophilic
antibodies are known to cause
interference with immunoassays.
Type And Screen (ABO/Rh and Antibody Screen)
Lab: WMC/CMH Transfusion Service Availability: 24 Hours TAT: Routine, 4 Hours
Stat, 1 Hour
Test Includes: Blood group (ABO), Rh, and Antibody screen.
Specimen: Whole blood Tube: EDTA (lavender) Minimum Volume: 5 mL Collection: Routine venipuncture. Specimen must
be labeled with patient's full name, Date of Birth, MR
number or SS number, date and time of collection, and
initials of person collecting the specimen. Blood Bank
Band must be completed at time of sample collection if sample will be used for crossmatch.
Causes For Rejection: Improper labeling of sample,
wrong sample type, hemolysis.
Use: To determine patient's blood group and Rh and to detect the presence of unexpected clinically significant antibodies, so that blood can be available quickly if a crossmatch is required.
Limitations: Abnormal proteins and cold or warm auto agglutinins, or unexpected antibodies in the patient’s
blood may cause delays in interpretation. May not detect antibodies to low incidence antigens.
Additional Information: If
transfusion is expected the
appropriate number of units
must be ordered to be
crossmatched.

Tzanck Prep for Cytopathology
Lab: Cytopathology
Request Form: Cytopathology
Availability: 5:00 am-5:00 pm
Specimen: Scraping of viral lesion.
Container: Cytolyt® Vial or PreservCyt® ThinPrep vial.
Minimum Volume: 25 ml
Collection: Scrap lesion with plastic applicator and
rinse in Cytolyt® Vial or PreservCyt® ThinPrep vial.
Specimen must be label with two patient identifiers.
Storage: After hours put in Pathology rack in main lab
refrigerator.
Use: In diagnosis of herpes
simplex virus.
Uric Acid
Lab: WMC Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Patient Preparation: At least a 4-hour fast is
preferred for routine testing.
Storage: 2-8˚C. Separate cells from serum prior to
storing.
Causes For Rejection: Improperly labeled
specimen
Use: Uric acid is the end product
of purine metabolism. Elevations
in uric acid occur in renal failure,
prerenal azotemia, gout, lead
poisoning, excessive cell
destruction (e.g.,
chemo), hemolytic anemia, CHF
and after myocardial infarction.
Urinalysis
Lab: WMC/CMH Urinalysis
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Test Includes: Biochemical screening
only. Microscopic examination is
performed if any screening tests are
positive or if otherwise indicated.
Specimen: Urine, random
Container: A clean plastic urine container is
preferred
Collection: A mid-stream, clean-voided specimen is
preferred; catheterization
Storage: Refrigerate if testing is to be delayed more
than 1 hour
Causes For Rejection: Insufficient volume,
bacterial overgrowth, improperly labeled specimen.
Use: Screen for abnormalities
of urine, diagnose and manage
renal disease, urinary tract
infections, and systemic
diseases
Limitations: Insufficient
volume may limit extent of tests
performed. Metabolites of
pyridium may cause color
interference with the dipstick
reactions. High vitamin C
intake may cause an
underestimate of glucosuria, or a
false negative nitrate test.
Low osmolality, alkalinity, and
lack of refrigeration decrease
survival of WBC.

Urinalysis-Complete
Lab: WMC/CMH Urinalysis
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Test Includes: Biochemical screening
and a microscopic evaluation of formed
elements
Specimen: Urine, random
Container: Sterile, plastic urine collection
container.
Minimum Volume: 12 mL is the standard amount used
for testing to insure consistency, and all normal values
are based upon a volume of 12 mL.
Collection: A mid-stream, clean voided specimen is
preferred; catheterization
Storage: Refrigerate if testing is to be delayed more
than 1 hour.
Causes For Rejection: Decomposition or
overgrowth of bacteria, insufficient quantity,
improperly labeled specimen.
Use: Screen for abnormalities of
urine, diagnose and manage renal
disease, urinary tract infection,
systemic diseases Limitations:
Insufficient volume may limit
extent of tests performed.
Metabolites of pyridium may
cause color interference with the
dipstick reactions. High vitamin C
intake may cause an
underestimate of glucosuria, or a
false negative nitrate test. Low
osmolality, alkalinity, and lack of
refrigeration decrease survival of
WBC.
Urine Cytopathology
Lab: Cytopathology
Request Form: Cytopathology
Availability: Mon-Fri 5am-5:00 pm
TAT: 24-48 hours
Special Instructions: Be sure to
indicate on requisition whether
specimen is voided or catheterized,
from bladder, ureter, renal pelvic,
urethra, or bladder washing.
Specimen: Fresh urine or urine in Cytolyt ®
container.
Container: Specimen Container available in
cytopathology or central supply.
Minimum Volume: Not less than 10 ml. Clean
catch voided or cath specimen.
Storage: If collected after hours, place in the
Pathology rack in main lab refrigerator.
Causes For Rejection: Improper fixation, 24 hour
collection.
Use: To establish the presence
of primary or metastatic
neoplasms. To aid in the
diagnosis of infections.
Urine Drug Screen
(Oxycodone ordered separately- see Oxycodone UDS)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Drugs Tested:
WMC : AMP, COC , MTD, OPI, MAMP, PCP, BAR, THC, BZO, OXY, BUP, PPX and TCA
CMH: AMP, BARB, BENZ, COC, OPI, PCP, Methadone and THC
Specimen: Urine
Container: Clean plastic urine cup.
Minimum Volume: 10 ml Collection:
Freshly voided sample
Storage: If not tested immediately refrigerate for up to
48 hours.
Causes For Rejection: Improperly labeled
specimen.
Limitations: Adulterants added to urine specimen may
produce erroneous results. Substances and/or factors
may interfere with the test and cause false results. Drug
levels below the analyte cut off may not be detected.
Use: The detection of drugs of
abuse in urine
The length of time following
drug use for which a positive
result may occur is dependent on
several factors including the
frequency and amount of usage,
metabolic rate, excretion rate,
drug half-life and the user's age,
weight, activity and diet.
For quantitation or confirmation
a GC/MS should be ordered.

Valproic Acid (Depakote)
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Synonyms:
Depakene, Depakote, Valproate
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume:2 mL
Collection: Routine venipuncture. Peak: 1-4 hours
after dose (influenced by meals); Trough:
immediately prior to next dose (possibly more
useful than peak levels).
Storage: Separate serum from cells and refrigerate
at 2-8˚C.
Causes For Rejection: Hemolysis, lipemia
Use: Valproate controls absence,
myoclonic, and tonic-clonic
seizures in generalized, idiopathic,
and symptomatic epilepsy.
Additional Information:
Hepatotoxicity may be fatal, but is
idiosyncratic and not preventable
by routinely monitoring liver
enzymes. Hepatotoxicity occurs in
very young children, usually those
on multiple anticonvulsants.
Valproate cytopenias may be
dose-related and warrant
monitoring of CBCs during
therapy.
Vancomycin
Lab: WMC/CMH Chemistry
Availability: 24 hours
TAT: Routine, 4 hours
Stat, 1 hour
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Causes For Rejection: Improperly labeled
specimen.
Use: To monitor drug therapy
Vitamin B12 Lab: WMC Chemistry
Availability: 24 hours
TAT: 4 hours
Specimen: Serum, heparinized plasma
Tube: SST, Plain red or Green (Li hep)
Minimum Volume: 2 mL
Collection: Routine venipuncture
Storage: Separate serum from cells; store at 4˚C.
Causes For Rejection: Improperly labeled
specimen, wrong specimen type or sample not
properly stoppered.
Use: Detect B12 deficiency as in
pernicious anemia, diagnose folic
acid deficiency, evaluate
hypersegmentation of
granulocyte nuclei, diagnose
macrocytic anemia, diagnose
megaloblastic anemia, evaluate
alcoholism, prenatal care,
evaluate malabsorption,
neurological disorders, or the
elevation of B12 as seen in liver
cell damage or myeloid leukemia.
Limitations: Drugs capable of
interference with B12 and/or folic
acid absorption include
chemotherapeutic agents,
diuretics, antibiotics,
anticonvulsants, sedatives, oral
contraceptives, and many others.

Vitamin D Total (25-OH)
Lab: WMC Chemistry
Availability: 24 hours
TAT: 4 hours
Specimen: Serum
Tube: SST, Plain red
Minimum Volume: 5 mL
Patient Preparation: Fasting specimen preferred;
must collect prior to Schilling’s test, transfusions, or
initiation of B12 therapy
Collection: Routine venipuncture
Storage: Separate serum from cells; store at
4˚C; specimen stable for 24 hours only
Causes For Rejection: Improperly labeled
specimen, wrong specimen type
Clinical Significance:
Vitamin D is synthesized from cholelsterol upon skin exposure to UVB sunlight or through dietary intake. Vitamin D is hydroxylated in the liver to form 25-OH Vitamin D which is further hydroxylated in the kidney to form the biologically active form, 1,25-(OH)2 Vitamin D. The active form is tightly regulated by plasma parathyroid hormone levels and calcium and phosphorous levels. The active form, 1,25-(OH)2 Vitamin D, increases the intestinal absorption of calcium and phosphorous, both are required for regulating bone metabolism. Vitamin D metabolites are bound to vitamin D binding protein and are circulated throughout the body. The concentration of 1,25(OH)2Vitamin D is 1000 times lower than 25-OH Vitamin D and has a half life of 4 hours. Due to its half life of 2-3 weeks, 25-OH Vitamin D is the metabolite that is the most reliable clinical indicator of vitamin D status. Also, 25-OH Vitamin D levels are indicative of the body’s storage levels of vitamin D and correlate with the clinical symptoms of vitamin D deficiency.
Wet Prep / KOH
Lab: CMH Urinalysis/
WMC Micro
Availability: 24 hours
TAT: 4 hours
Specimen: Vaginal swab, nail clippings, hair, skin
scrapings
Collection:
Vaginal Swab - swab the vaginal region and immerse
the swab into a vial containing 2mLs of 0.9% NaCl Nails
- clean with 70% alcohol, scrap away outer portion and
obtain scrapings from the deeper infected areas. Place
in sterile container or on slide. Hair - remove at least 10
intact hairs from infected area. Place in between two
glass slides.
Skin - clean with 70% alcohol. Scrap away the outer
portion and obtain scraping from the deeper infected
areas. Place on a slide.
Causes For Rejection: Improperly labeled
specimen, vaginal swab not received in saline.
Use: Potassium hydroxide
digests or lyses epithelial cells, WBCs, RBCs, mucus, and various other proteinaceous debris, bleaches many pigments and dissolves the “cement” that holds keratinized cells together. This permits detection of fungal elements (yeast and pseudohyphae) that are present in vaginal secretions and keratinized tissue. Most fungi can be demonstrated in the KOH preparation. Wet preps allow for microscopic observation of unfixed “wet mounts” of clinical specimens for the rapid detection of the presence of bacterial, fungal, and parasitic organisms. The presence of white blood cells and “clue cells” may also be identified.





























