Embed Size (px)
Citation preview
BioMed CentralBMC Infectious Diseases
ss
Open AcceResearch articleIncreasing the frequency of hand washing by healthcare workers does not lead to commensurate reductions in staphylococcal infection in a hospital wardClive B Beggs1, Simon J Shepherd1 and Kevin G Kerr*2Address: 1School of Engineering, Design and Technology, University of Bradford, Bradford, BD7 1DP, UK and 2Department of Microbiology, Harrogate and District NHS Foundation Trust, Harrogate District Hospital, Lancaster Park Road, Harrogate, HG2 7SX, UK
Email: Clive B Beggs - [email protected]; Simon J Shepherd - [email protected]; Kevin G Kerr* - [email protected]
* Corresponding author
AbstractBackground: Hand hygiene is generally considered to be the most important measure that can be applied to preventthe spread of healthcare-associated infection (HAI). Continuous emphasis on this intervention has lead to the widespreadopinion that HAI rates can be greatly reduced by increased hand hygiene compliance alone. However, this assumes thatthe effectiveness of hand hygiene is not constrained by other factors and that improved compliance in excess of a givenlevel, in itself, will result in a commensurate reduction in the incidence of HAI. However, several researchers have foundthe law of diminishing returns to apply to hand hygiene, with the greatest benefits occurring in the first 20% or so ofcompliance, and others have demonstrated that poor cohorting of nursing staff profoundly influences the effectivenessof hand hygiene measures. Collectively, these findings raise intriguing questions about the extent to which increasingcompliance alone can further reduce rates of HAI.
Methods: In order to investigate these issues further, we constructed a deterministic Ross-Macdonald model andapplied it to a hypothetical general medical ward. In this model the transmission of staphylococcal infection was assumedto occur after contact with the transiently colonized hands of HCWs, who, in turn, acquire contamination only bytouching colonized patients. The aim of the study was to evaluate the impact of imperfect hand cleansing on thetransmission of staphylococcal infection and to identify, whether there is a limit, above which further hand hygienecompliance is unlikely to be of benefit.
Results: The model demonstrated that if transmission is solely via the hands of HCWs, it should, under mostcircumstances, be possible to prevent outbreaks of staphylococcal infection from occurring at a hand cleansingfrequencies < 50%, even with imperfect hand hygiene. The analysis also indicated that the relationship between handcleansing efficacy and frequency is not linear – as efficacy decreases, so the hand cleansing frequency required to ensureR0 < 1 increases disproportionately.
Conclusion: Although our study confirmed hand hygiene to be an effective control measure, it demonstrated that thelaw of diminishing returns applies, with the greatest benefit derived from the first 20% or so of compliance. Indeed, ouranalysis suggests that there is little benefit to be accrued from very high levels of hand cleansing and that in most situationscompliance > 40% should be enough to prevent outbreaks of staphylococcal infection occurring, if transmission is solelyvia the hands of HCWs. Furthermore we identified a non-linear relationship between hand cleansing efficacy andfrequency, suggesting that it is important to maximise the efficacy of the hand cleansing process.
Published: 2 September 2008
BMC Infectious Diseases 2008, 8:114 doi:10.1186/1471-2334-8-114
Received: 20 March 2008Accepted: 2 September 2008
This article is available from: http://www.biomedcentral.com/1471-2334/8/114
© 2008 Beggs et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 11(page number not for citation purposes)

BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
BackgroundHand hygiene is generally considered to be the mostimportant measure that can be applied to prevent thespread of healthcare-associated infection (HAI) [1].Through regular cleansing of hands, healthcare workers(HCWs) reduce the risk to transmitting nosocomial path-ogens between patients and thus reduce the risk of exoge-nously-acquired infection. This has lead to the widespreadopinion that HAI rates can be greatly reduced by increasedhand hygiene compliance alone [2], with the result thathealthcare authorities around the world have vigorouslypromoted hand hygiene as the pre-eminent measure incontrolling HAI. However, this approach assumes that theeffectiveness of hand hygiene is not limited by other fac-tors and that greater compliance will continue to yieldimproved results. While it is undoubtedly the case thatimproved hand hygiene is beneficial [1,3], there is grow-ing evidence that increased compliance may not yield thehoped for results. For example, using dynamic transmis-sion models, Cooper et al [4] and McBryde et al [5] foundthat the law of diminishing returns applies to handhygiene, with the greatest benefits occurring in the first20% or so of compliance. Furthermore, Austin et al [6]and Beggs et al [7] demonstrated that poor cohorting ofnursing staff profoundly influences the effectiveness ofhand hygiene measures. Moreover, Grundmann et al [8]found that during periods of under-staffing, it is necessaryto greatly increase the frequency of hand cleansing inorder to prevent outbreaks of infection. Collectively, thesefindings raise intriguing questions about the limitationsof hand hygiene and the extent to which increasing com-pliance alone can further reduce the spread of infection. Inorder to investigate this issue further, we constructed adeterministic Ross-Macdonald model to analyse thehypothetical general medical ward presented by Cooper etal [4] who found that hand hygiene compliance levels >30% made little impact on the prevalence of Staphylococ-cus aureus infection on the ward. However, in their studythey assumed that each hand cleansing event had an effi-cacy of 100%, – which in "real life" situations on a busyhospital ward is unlikely to be the case. Given this, wedecided to repeat the study of Cooper et al by using amodel that takes into account not only the frequency ofhandwashing but also the efficacy of the hand cleansingprocess. The aim of the study was to evaluate the impactof imperfect hand cleansing on the transmission of sta-phylococcal infection and to identify whether there is alimit, above which further compliance would be unlikelyto yield beneficial results.
Since Ignaz Semmelweis reported in 1847 that the inci-dence of puerperal fever in an obstetric unit could be dras-tically reduced through handwashing [9], cleansing ofhands has been the principal measure employed in hospi-tals to reduce HAI. Until recently, hand cleansing was
achieved through the use of soap and water, a time con-suming [10] and sometimes inefficient process. However,in recent years, new alcohol-based products have becomewidely available. These are more convenient and quickerto use than soap and water and their use is being vigor-ously promoted. Despite this, levels of hand hygiene com-pliance remain low; typically < 50% [11-13]. One reasonfor low compliance appears to be the large number ofhandwashing opportunities that arise during patient care.These make it difficult for HCWs to cleanse their handseffectively, while still carrying out their clinical duties. Forexample, Pittet et al [10] observed an average of 43.4 handhygiene opportunities per hour of patient care on anintensive care unit (ICU), which suggests that busy staffhave very little spare time in which to cleanse their hands.
Although there are relatively few data on the types ofpatient-care activities that result in transmission of patho-gens on the hands of HCWs, there is clear evidence thatsuch transmission does occur. In a study of 'clean' activi-ties, such as lifting patients, palpation of pulses or duringsphygmomanometry, Casewell and Phillips [14] foundthat nurses could contaminate their hands with 100–1000colony forming units (cfu) of Klebsiella spp. Similarly,Ehrenkranz and Alfonso [15] found that nurses readilycontaminated their hands (i.e. 10–600 cfu/mL in glovejuice samples) by touching the groins of patients heavilycolonised with Proteus mirabilis. This suggests that con-tamination of the hands of HCWs is a frequent occur-rence, and that relatively innocuous procedures can resultin transient colonization. This is supported by the resultsof a study undertaken before the use of gloves by HCWsbecame common practice, which reported that 15% ofnurses working in an isolation unit carried a median of104 cfu of S. aureus on their hands and 29% of nursesworking in a general hospital had a median count of 3.8 ×103 cfu [16]. In another study, Daschner [17] found thatS. aureus could be recovered from the hands of 21% ofHCWs on an ICU, and that 21% of doctors and 5% ofnurse carriers had > 1,000 cfu of the organism on theirhands. Collectively, these data reveal that the hands ofHCWs can become heavily contaminated when undertak-ing clinical procedures and they reinforce the need tomaintain good hand hygiene procedures.
Hand cleansing is an imperfect process, the efficacy ofwhich depends on the product used, the techniqueemployed, and the duration of the process. Thus it is likelythat it will not remove all the microorganisms from thehands of HCWs. Girou et al [18], for example, found thathand rubbing with a 75% alcohol-based solution resultedin a median percentage reduction in bacterial contamina-tion of 83% compared with a reduction of only 58%when washing with medicated soap. Similarly, Zaragozaet al [19] found that the use of an alcoholic solution
Page 2 of 11(page number not for citation purposes)

BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
resulted in an average reduction in cfu of 88.2% comparedwith only 49.6% when soap and water was used.
MethodIn order to investigate the impact of sub-optimal handcleansing on the transmission of staphylococcal infection,we modified the model of Cooper et al [4], so that it con-sidered both handwashing frequency and handwashingefficacy (see Appendix) allowing us to simulate the effectof imperfect hand cleansing, something which otherinvestigators had overlooked in their respective studies [3-6,20].
In order to permit direct comparison with Cooper et al [4],we used the same data and simulated the same generalmedical ward as they did. Definitions of the variables usedin our model are presented in Table 1.
In the model the rate of change of colonized patients, y,on the ward is given by:
and the rate of change of contaminated HCWs, y', is:
In the model these differential equations are used to sim-ulate the spread of staphylococcal colonization on theward, with the basic reproductive number, R0, calculatedusing the following expression:
The basic reproductive number, R0, is the average numberof secondary cases of colonization (which precedes infec-
tion) generated by one primary case in the absence of anyinfection control procedures.
Highly transmissible infections exhibit a large R0, whereasthose which are less transmissible have a smaller value ofR0. If the value of R0 is greater than 1, then each colonizedpatient will generate further new cases and it is likely thatan outbreak will ensue. The outbreak will continue untilR0 becomes less than 1, at which point it should begin todie out.
In the model the handwashing frequency, fh, is deter-mined using the following expression derived by Cooperet al [4]:
In the model it was assumed that:
• The transmission of staphylococci is caused by contactwith the transiently colonized hands of HCWs. Contactsbetween transiently colonized HCWs and uncolonizedpatients have a given probability of colonizing thepatient, which is termed the HCW-to-patient transmissi-bility. In the model we did not consider the possibility ofdirect patient-to-patient contacts.
• HCWs acquire transient hand-contamination only bytouching colonized patients. All such contacts betweenuncolonized HCWs and colonized patients have a givenprobability of colonizing the carer, which is termed thepatient-to-HCW transmissibility. In the model we did nottake into account direct HCW-to-HCW transmission orthe possibility of HCWs becoming colonized from exter-nal sources.
dydt
x y y xyn
y= + +( ) +′′
− +σ μ μ γ β μ γ( ) (1)
dydt
yxn
y′
= ′ ′′
− ′ ′ ′β μ λ (2)
Rn
n01= − ′
+ ′ ′ ′( )
( )ββ
μ γ μ λ(3)
fc
nn
h =′
′+′
μ
μ( )(4)
Table 1: Parameters and their default values
Parameter Meaning Default value
N Number of patients 20n' Number of health care workers (HCWs) 3μ Patient removal rate 0.10 per dayμ' Handwashing rate 14.0 per dayλ' Average efficacy of each handwashing event 0.5 (i.e. 50%)γ Detection rate of colonized patients 0.10 per dayσ Proportion of admissions already colonized 0.01c Patient-HCW contact rate 5 per patient per HCW per dayp HCW-patient transmission probability (i.e. transmissibility) 0.1p' Patient-HCW transmission probability (i.e. transmissibility) 0.1β HCW-patient transmission rate (β = cp) 0.5β' Patient-HCW transmission rate (β' = cp') 0.5
Page 3 of 11(page number not for citation purposes)

BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
• The HCW-to-patient transmissibility is assumed to beequal to the patient-to-HCW transmissibility.
• The population of patients is assumed to be homogene-ous, with each patient considered equally likely to be incontact with a HCW in any time interval, equally likely tobecome colonized, and when colonized, equally likely totransmit the pathogen to a HCW on contact.
• The population of HCWs is assumed to be homogene-ous. Variations between HCWs due to differences inbehaviour (such as handwashing) and skin microflora arenot considered.
• The detection of colonized patients is assumed to be arandom process, with the mean detection time dependingonly on a constant level of surveillance activity.
• Once detected, colonized patients are assumed to beremoved from the main ward and thus no longer a sourceof infection. Colonized patients who are not detected areremoved from the ward at the same rate as uncolonizedpatients.
• Each time a HCW washes his or her hands only a portionof the transient microflora present is removed. Theamount removed depends on the efficacy of the handcleansing process.
• The efficacy of the hand cleansing process is assumed tobe the same for all the HCWs on the ward.
In keeping with Cooper et al [4], we assumed the proba-bility of a HCW contaminating their hands, or a patientbecoming colonized, after each HCW-patient contact (i.e.the transmissibility value) to be 0.1. At the start of eachsimulation we assumed that all the patients on the wardwere uncolonized and all HCWs were uncontaminated.Therefore, transmission could only begin once aninfected/colonized patient had been admitted to theward. The various events simulated in the model, togetherwith their rates, are summarized in Table 2.
Where x represents the number of uncolonized patients, yrepresents the number of colonized patients, y' representsthe number of HCWs with contaminated hands, and x'represents the number of HCWs whose hands are uncon-taminated.
Model ScenariosIn our study we modelled the effect of varying the hand-washing frequency on the transmission of staphylococcalinfection within the ward. For each frequency we mod-elled three possible efficacy scenarios (i.e. that each hand-washing event removed 58%, 83% and 100% respectivelyof contaminants from the hands of HCWs). Efficacies of58% and 83% were selected because they represent thevalues found by Girou et al [18] for HCWs using antibac-terial soap and an alcohol-based solution, respectively, ina clinical setting. Having simulated the impact of handcleansing frequency on the prevalence of infection, wethen modelled the impact on R0 of changes in handhygiene efficacy, contact transmissibility, and the HCW-patient contact rate.
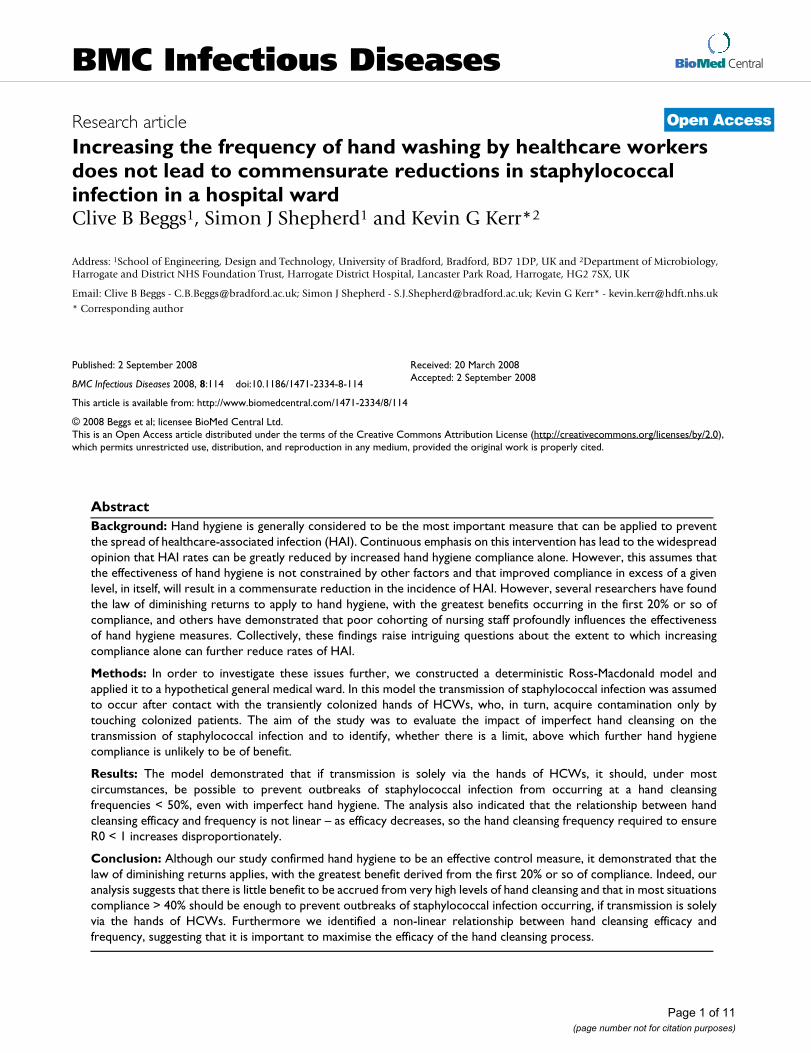
ResultsThe impact of changes in hand cleansing efficacy on wardprevalence are presented in Figure 1. This shows the effectof variations in hand hygiene frequency for mean efficacyvalues of 58%, 83% or 100% respectively. It can be seenthat as efficacy increases, so the frequency required to pre-vent an outbreak reduces. Indeed, under the default con-ditions stated in Table 1, very little benefit is accrued byincreasing the hand cleansing frequency beyond 35%,even when soap and water is used to cleanse hands.
Using equation 3 it is possible to examine the impact thatvariations in hand cleansing efficacy have on basic repro-ductive number, R0. The results of this analysis are pre-sented in Figure 2, which shows R0 curves for fourrepresentative efficacy values (i.e. λ' = 100%, 80%, 60%and 40%). These show that even with very imperfect handhygiene (i.e. λ' = 40%), it should be possible to prevent anoutbreak of staphylococcal infection occurring at a handcleansing frequency of, say 40%. Interestingly, Figure 2
Table 2: Events and their rates
Event Rate of event
Patient removal (when no colonization detected) μ(x + y)Detection of colonized patient and removal γyHCW hand cleaning μ' (x' + y')Removal of contamination from hands of HCWs μ' y'λ'HCW-patient contact c(x + y)HCW-to-patient transmission βxy'/n'Patient-to-HCW transmission β' yx'/n'Admission of uncolonized patient (1 - σ) (μx + μy + γy)Admission of colonized patient σ(μx + μy + γy)
Page 4 of 11(page number not for citation purposes)
BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
suggests that the relationship between hand cleansing effi-cacy and frequency is not linear; rather, as the efficacydecreases, so the hand cleansing frequency required toensure R0 < 1 increases disproportionately. This suggeststhat it is important to maximise the efficacy of the handcleansing process as this will reduce the amount of 'hand-
washing' activity required to prevent an outbreak fromoccurring.
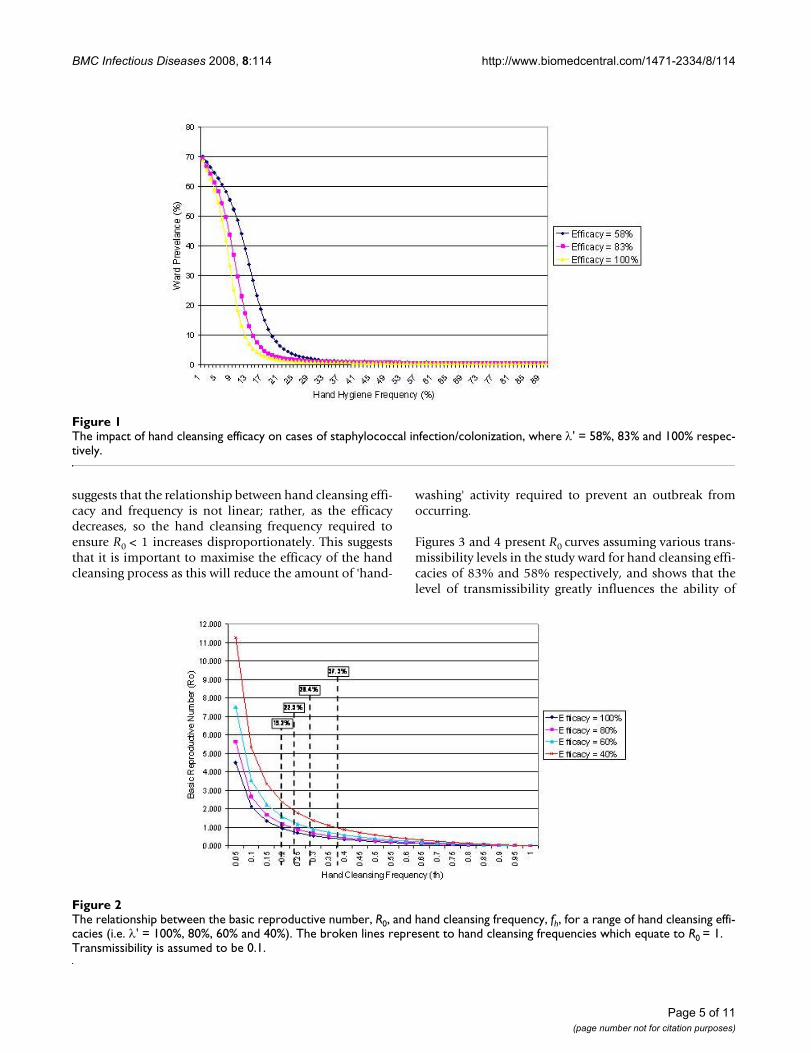
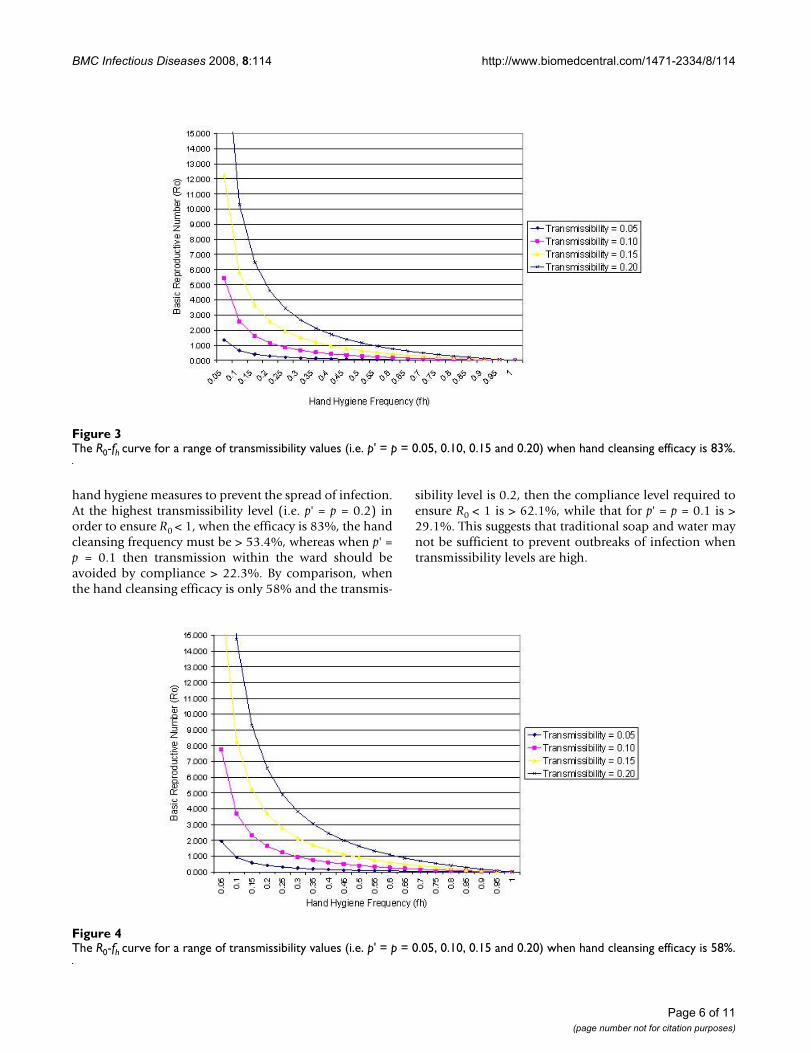
Figures 3 and 4 present R0 curves assuming various trans-missibility levels in the study ward for hand cleansing effi-cacies of 83% and 58% respectively, and shows that thelevel of transmissibility greatly influences the ability of
The impact of hand cleansing efficacy on cases of staphylococcal infection/colonization, where λ' = 58%, 83% and 100% respec-tivelyFigure 1The impact of hand cleansing efficacy on cases of staphylococcal infection/colonization, where λ' = 58%, 83% and 100% respec-tively.
The relationship between the basic reproductive number, R0, and hand cleansing frequency, fh, for a range of hand cleansing effi-cacies (i.e. λ' = 100%, 80%, 60% and 40%)Figure 2The relationship between the basic reproductive number, R0, and hand cleansing frequency, fh, for a range of hand cleansing effi-cacies (i.e. λ' = 100%, 80%, 60% and 40%). The broken lines represent to hand cleansing frequencies which equate to R0 = 1. Transmissibility is assumed to be 0.1.
Page 5 of 11(page number not for citation purposes)
BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
hand hygiene measures to prevent the spread of infection.At the highest transmissibility level (i.e. p' = p = 0.2) inorder to ensure R0 < 1, when the efficacy is 83%, the handcleansing frequency must be > 53.4%, whereas when p' =p = 0.1 then transmission within the ward should beavoided by compliance > 22.3%. By comparison, whenthe hand cleansing efficacy is only 58% and the transmis-
sibility level is 0.2, then the compliance level required toensure R0 < 1 is > 62.1%, while that for p' = p = 0.1 is >29.1%. This suggests that traditional soap and water maynot be sufficient to prevent outbreaks of infection whentransmissibility levels are high.
The R0-fh curve for a range of transmissibility values (i.e. p' = p = 0.05, 0.10, 0.15 and 0.20) when hand cleansing efficacy is 83%Figure 3The R0-fh curve for a range of transmissibility values (i.e. p' = p = 0.05, 0.10, 0.15 and 0.20) when hand cleansing efficacy is 83%.
The R0-fh curve for a range of transmissibility values (i.e. p' = p = 0.05, 0.10, 0.15 and 0.20) when hand cleansing efficacy is 58%Figure 4The R0-fh curve for a range of transmissibility values (i.e. p' = p = 0.05, 0.10, 0.15 and 0.20) when hand cleansing efficacy is 58%.
Page 6 of 11(page number not for citation purposes)
BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
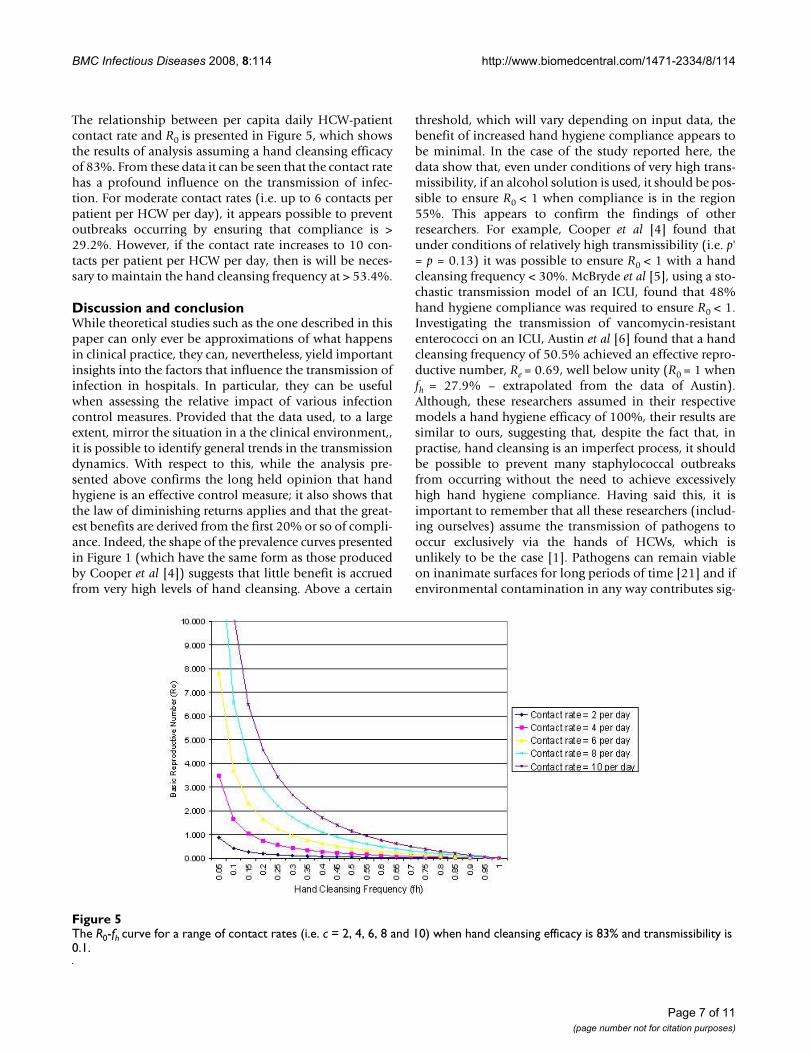
The relationship between per capita daily HCW-patientcontact rate and R0 is presented in Figure 5, which showsthe results of analysis assuming a hand cleansing efficacyof 83%. From these data it can be seen that the contact ratehas a profound influence on the transmission of infec-tion. For moderate contact rates (i.e. up to 6 contacts perpatient per HCW per day), it appears possible to preventoutbreaks occurring by ensuring that compliance is >29.2%. However, if the contact rate increases to 10 con-tacts per patient per HCW per day, then is will be neces-sary to maintain the hand cleansing frequency at > 53.4%.
Discussion and conclusionWhile theoretical studies such as the one described in thispaper can only ever be approximations of what happensin clinical practice, they can, nevertheless, yield importantinsights into the factors that influence the transmission ofinfection in hospitals. In particular, they can be usefulwhen assessing the relative impact of various infectioncontrol measures. Provided that the data used, to a largeextent, mirror the situation in a the clinical environment,,it is possible to identify general trends in the transmissiondynamics. With respect to this, while the analysis pre-sented above confirms the long held opinion that handhygiene is an effective control measure; it also shows thatthe law of diminishing returns applies and that the great-est benefits are derived from the first 20% or so of compli-ance. Indeed, the shape of the prevalence curves presentedin Figure 1 (which have the same form as those producedby Cooper et al [4]) suggests that little benefit is accruedfrom very high levels of hand cleansing. Above a certain
threshold, which will vary depending on input data, thebenefit of increased hand hygiene compliance appears tobe minimal. In the case of the study reported here, thedata show that, even under conditions of very high trans-missibility, if an alcohol solution is used, it should be pos-sible to ensure R0 < 1 when compliance is in the region55%. This appears to confirm the findings of otherresearchers. For example, Cooper et al [4] found thatunder conditions of relatively high transmissibility (i.e. p'= p = 0.13) it was possible to ensure R0 < 1 with a handcleansing frequency < 30%. McBryde et al [5], using a sto-chastic transmission model of an ICU, found that 48%hand hygiene compliance was required to ensure R0 < 1.Investigating the transmission of vancomycin-resistantenterococci on an ICU, Austin et al [6] found that a handcleansing frequency of 50.5% achieved an effective repro-ductive number, Re = 0.69, well below unity (R0 = 1 whenfh = 27.9% – extrapolated from the data of Austin).Although, these researchers assumed in their respectivemodels a hand hygiene efficacy of 100%, their results aresimilar to ours, suggesting that, despite the fact that, inpractise, hand cleansing is an imperfect process, it shouldbe possible to prevent many staphylococcal outbreaksfrom occurring without the need to achieve excessivelyhigh hand hygiene compliance. Having said this, it isimportant to remember that all these researchers (includ-ing ourselves) assume the transmission of pathogens tooccur exclusively via the hands of HCWs, which isunlikely to be the case [1]. Pathogens can remain viableon inanimate surfaces for long periods of time [21] and ifenvironmental contamination in any way contributes sig-
The R0-fh curve for a range of contact rates (i.e. c = 2, 4, 6, 8 and 10) when hand cleansing efficacy is 83% and transmissibility is 0.1Figure 5The R0-fh curve for a range of contact rates (i.e. c = 2, 4, 6, 8 and 10) when hand cleansing efficacy is 83% and transmissibility is 0.1.
Page 7 of 11(page number not for citation purposes)

BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
nificantly to the transmission of staphylococcal infection,then the hand hygiene compliance levels stated abovemay not be adequate.
The results of our study indicate that the level of handhygiene required to ensure R0 < 1 is greatly influenced bythe rate at which HCWs and patients make contact witheach other, and the transmissibility of the contacts made– as these values increase, so the hand cleansing frequencyrequired to prevent an outbreak also increases. Again, thisconfirms the findings of Cooper et al [4] who found trans-missibility to be the single most influential variable intheir study. In our study we assumed, as they did that, foreach contact event, the probability of a HCW colonizing apatient is the same as the probability that the patient willcontaminate the hands of a HCW. We did this to facilitatedirect comparison with the work of Cooper et al [4]. Thishowever, may not be the case, since contamination ofHCWs hands is relatively transient (lasting only for a fewhours), whereas patients tend to remain colonized for thelength of their stay in hospital. Therefore, each colonizedpatient will contaminate many HCWs (Rp >> 1), whereasa contaminated HCW will colonize patients only infre-quently (Rh << 1) [6]. Accordingly, Austin et al [6] usedvalues of p' = 0.40 and p = 0.06, which equates to a com-bined (p' × p) value of 0.024. Similarly, Grundmann et al[8] using the same methodology, adopted values of p' =0.152 and p = 0.01, equating to a combined (p' × p) valueof 0.015. By comparison, we and Cooper et al [4] used acombined (p' × p) value of 0.010, which, although lowerthan that used by the other researchers, is still of the sameorder of magnitude. The default HCW-patient contact rateused in our model was that suggested by Cooper et al [4](i.e. 5 contacts per patient per HCW per day); considera-bly greater than the value of 1.38 contacts per patient perHCW per day reported by Austin et al [6] and somewhatless than the value of 7.6 contacts per patient per HCW perday used by Grundmann et al [8]. Collectively, this givesus confidence that our analysis is valid and that the varia-bles used are realistic.
From the foregoing it can be seen that our results are con-sistent with earlier studies. It can therefore be concludedthat it should be possible to prevent many outbreaks ofstaphylococcal infection through hand hygiene measuresalone, even if high compliance rates are not achieved. Inthe study reported here it appears that compliance rates of40% or so, should be adequate to prevent most outbreaksoccurring. If this is indeed the case, then this raises ques-tions as to why so many outbreaks of staphylococcalinfection continue to occur, despite the fact that recordedhand hygiene compliance rates are generally in the region40% [11-13]. While the reasons for this are unclear, thereappear to be four possible explanations, details of whichare as outlined below:
Hawthorne EffectWhile recorded hand hygiene compliance is typically inthe region 40% [11-13], it may be that the Hawthorneeffect is at work and that observed hand hygiene does notreflect what actually happens in reality – the implicationbeing that general hand washing rates might be consider-ably lower than 40%.
Ward ManagementAnother reason might be the way in which wards areorganized and managed. For example, if a ward is over-crowded or under-staffed, then those nurses on duty willhave to attend to more patients than usual and so theHCW-patient contact rate is likely to rise and with it thehand cleansing frequency required to ensure R0 < 1. Thiswas graphically illustrated by Grundmann et al [8], who,in their study on an ICU, found exposure to relative staffdeficit to be the only factor significantly associated withMRSA transmission. Indeed, they predicted that it wouldrequire an additional 12% improvement in adherence tohand hygiene policies to compensate for staff shortages.Given that during this study, observed hand hygiene com-pliance was on average 59%, the investigators concludedthat under conditions of overcrowding and high work-load, it would be impossible for the nursing staff toachieve the required additional compliance. The HCW-patient contact rate is also influenced by the way in whichnurses are organized. Beggs et al [7] demonstrated that ifnursing staff are allowed to mix freely with patients, thenthe number of potential transmission routes will be high,leading to increased need for hand cleansing. In order tominimise the number of transmission routes it is neces-sary to cohort the nursing staff so that they cannot transferpathogens between different groups of patients. Otherstudies have reached similar conclusions [5,6,12,20,22] –the higher the level of cohorting, the fewer the number ofcontacts between patients.
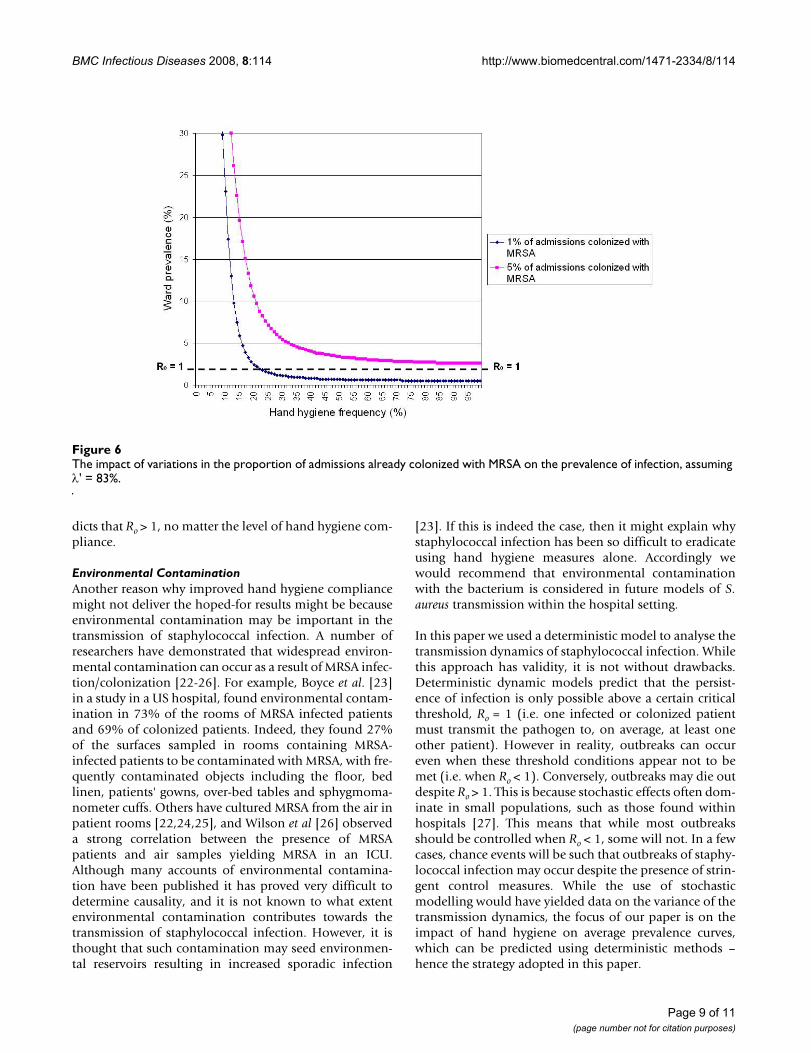
Colonized AdmissionsFigure 5 shows the effect of variations in the proportion ofadmissions already colonized with MRSA on the preva-lence of infection, assuming an average hand cleansingefficacy, λ', of 83%. From this it can be seen that as thenumber of colonized patients entering the ward increases,so the model predicts that it is not possible to completelyeradicate infection through hand hygiene measures alone.No matter the level of hand hygiene compliance, therewill always be a residual level of infection which is diffi-cult to eradicate. Therefore, if the number of colonizedpatients admitted to hospitals is high, then this mightexplain why increased hand hygiene compliance is failingto control the spread of staphylococcal infection. FromFigure 6 it can be seen that when the proportion of MRSAcolonized patients entering hospital is 5%, the model pre-
Page 8 of 11(page number not for citation purposes)
BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
dicts that Ro > 1, no matter the level of hand hygiene com-pliance.
Environmental ContaminationAnother reason why improved hand hygiene compliancemight not deliver the hoped-for results might be becauseenvironmental contamination may be important in thetransmission of staphylococcal infection. A number ofresearchers have demonstrated that widespread environ-mental contamination can occur as a result of MRSA infec-tion/colonization [22-26]. For example, Boyce et al. [23]in a study in a US hospital, found environmental contam-ination in 73% of the rooms of MRSA infected patientsand 69% of colonized patients. Indeed, they found 27%of the surfaces sampled in rooms containing MRSA-infected patients to be contaminated with MRSA, with fre-quently contaminated objects including the floor, bedlinen, patients' gowns, over-bed tables and sphygmoma-nometer cuffs. Others have cultured MRSA from the air inpatient rooms [22,24,25], and Wilson et al [26] observeda strong correlation between the presence of MRSApatients and air samples yielding MRSA in an ICU.Although many accounts of environmental contamina-tion have been published it has proved very difficult todetermine causality, and it is not known to what extentenvironmental contamination contributes towards thetransmission of staphylococcal infection. However, it isthought that such contamination may seed environmen-tal reservoirs resulting in increased sporadic infection
[23]. If this is indeed the case, then it might explain whystaphylococcal infection has been so difficult to eradicateusing hand hygiene measures alone. Accordingly wewould recommend that environmental contaminationwith the bacterium is considered in future models of S.aureus transmission within the hospital setting.
In this paper we used a deterministic model to analyse thetransmission dynamics of staphylococcal infection. Whilethis approach has validity, it is not without drawbacks.Deterministic dynamic models predict that the persist-ence of infection is only possible above a certain criticalthreshold, Ro = 1 (i.e. one infected or colonized patientmust transmit the pathogen to, on average, at least oneother patient). However in reality, outbreaks can occureven when these threshold conditions appear not to bemet (i.e. when Ro < 1). Conversely, outbreaks may die outdespite Ro > 1. This is because stochastic effects often dom-inate in small populations, such as those found withinhospitals [27]. This means that while most outbreaksshould be controlled when Ro < 1, some will not. In a fewcases, chance events will be such that outbreaks of staphy-lococcal infection may occur despite the presence of strin-gent control measures. While the use of stochasticmodelling would have yielded data on the variance of thetransmission dynamics, the focus of our paper is on theimpact of hand hygiene on average prevalence curves,which can be predicted using deterministic methods –hence the strategy adopted in this paper.
The impact of variations in the proportion of admissions already colonized with MRSA on the prevalence of infection, assuming λ' = 83%Figure 6The impact of variations in the proportion of admissions already colonized with MRSA on the prevalence of infection, assuming λ' = 83%.
Page 9 of 11(page number not for citation purposes)

BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
Competing interestsThe authors declare that they have no competing interests.
Authors' contributionsCBB and SJS designed the study. SJS constructed the com-puter model and KGK advised on the clinical aspects ofthe study. CBB wrote the manuscript with major contribu-tions from other authors. All authors have read andapproved the final manuscript.
AppendixIn the model x represents the number of susceptiblepatients and y the number of colonized patients, with thetotal number of patients in the ward being a constant n(i.e. x + y = n). Similarly, the total number of carers is n',with x' representing those HCWs not carrying the patho-gen and y' representing those who are temporarily colo-nized, where x' + y' = n'. The removal rate for uncolonizedpatients is μ, which includes removals due to death, trans-fers to other wards, and discharges. The detection rate ofcolonized patients is γ, which is assumed to be the rate atwhich colonized patients are deliberately removed fromthe ward. With regard to the cleansing of hands, the hand-washing rate is μ' and the average efficacy of each hand-washing event is λ'. The rate at which contamination isremoved from the hands of HCWs on the ward is there-fore μ' y'λ'.
In the model it is assumed that each patient requires acontact from a HCW in a given time interval with a givenprobability and that no superfluous contacts are made.The mean number of contacts required by each patient perday is defined as c, with p being the probability that apatient becomes colonized on contact with a contami-nated HCW, and p' to be the probability that a HCWbecomes contaminated on contact with a colonizedpatient. In the model we let β = cp and β' = cp'. The rates atwhich contacts occur that can potentially result in coloni-zation are therefore βx (for patient colonization) and β' y(for HCW contamination). Since a fraction y'/n' of con-tacts will be with colonized HCWs, and x'/n' with suscep-tible HCWs, the rates for patient and carer colonizationwill be βxy'/n' and β'x'y/n' respectively. The proportion ofpatients admitted to the ward who are colonized orinfected is σ, where(0 ≤ σ ≤ 1).
Based on the above, the model solves the following differ-ential equations to determine the spread of infection/col-onization on the ward.
In the model the rate of change of colonized patients andcontaminated HCWs is given by:
For this system of equations, the basic reproductivenumber, R0, is defined as:
AcknowledgementsThe authors would like to thank Dr Gareth Nisbet for his assistance in obtaining data for the study.
The authors confirm that no funding was received for this study.
References1. Pittet D, Allegranzi B, Sax H, Dharan S, Pessoa-Silva CL, Donaldson L,
Boyce JM: Evidence-based model for hand transmission dur-ing patient care and the role of improved practices. LancetInfect Dis 2006, 6(10):641-652.
2. Teare L, Cookson B, Stone S: Hand hygiene. Bmj 2001,323(7310):411-412.
3. Raboud J, Saskin R, Simor A, Loeb M, Green K, Low DE, McGeer A:Modeling transmission of methicillin-resistant Staphylococ-cus aureus among patients admitted to a hospital. Infect Con-trol Hosp Epidemiol 2005, 26(7):607-615.
4. Cooper BS, Medley GF, Scott GM: Preliminary analysis of thetransmission dynamics of nosocomial infections: stochasticand management effects. J Hosp Infect 1999, 43(2):131-147.
5. McBryde ES, Pettitt AN, McElwain DL: A stochastic mathematicalmodel of methicillin resistant Staphylococcus aureus trans-mission in an intensive care unit: predicting the impact ofinterventions. J Theor Biol 2007, 245(3):470-481.
6. Austin DJ, Bonten MJ, Weinstein RA, Slaughter S, Anderson RM:Vancomycin-resistant enterococci in intensive-care hospitalsettings: transmission dynamics, persistence, and the impactof infection control programs. Proc Natl Acad Sci U S A 1999,96(12):6908-6913.
7. Beggs CB, Noakes CJ, Shepherd SJ, Kerr KG, Sleigh PA, Banfield K:The influence of nurse cohorting on hand hygiene effective-ness. Am J Infect Control 2006, 34(10):621-626.
8. Grundmann H, Hori S, Winter B, Tami A, Austin DJ: Risk factors forthe transmission of methicillin-resistant Staphylococcusaureus in an adult intensive care unit: fitting a model to thedata. J Infect Dis 2002, 185(4):481-488.
9. Semmelweis I: The etiology, concept and prophylaxis of child-bed fever. Pest, Wien und Leipzig , C.A.Hartleben’s Verlag-Expedi-tion; 1861.
10. Pittet D, Mourouga P, Perneger TV: Compliance with handwash-ing in a teaching hospital. Infection Control Program. AnnIntern Med 1999, 130(2):126-130.
11. Pittet D: Improving adherence to hand hygiene practice: amultidisciplinary approach. Emerg Infect Dis 2001, 7(2):234-240.
12. McArdle FI, Lee RJ, Gibb AP, Walsh TS: How much time is neededfor hand hygiene in intensive care? A prospective trainedobserver study of rates of contact between healthcare work-ers and intensive care patients. J Hosp Infect 2006,62(3):304-310.
13. Larson E, Kretzer EK: Compliance with handwashing and bar-rier precautions. J Hosp Infect 1995, 30 Suppl:88-106.
14. Casewell M, Phillips I: Hands as route of transmission for Kleb-siella species. Br Med J 1977, 2(6098):1315-1317.
15. Ehrenkranz NJ, Alfonso BC: Failure of bland soap handwash toprevent hand transfer of patient bacteria to urethral cathe-ters. Infect Control Hosp Epidemiol 1991, 12(11):654-662.
16. Ayliffe GA, Babb JR, Davies JG, Lilly HA: Hand disinfection: a com-parison of various agents in laboratory and ward studies. JHosp Infect 1988, 11(3):226-243.
17. Daschner FD: How cost-effective is the present use of antisep-tics? J Hosp Infect 1988, 11 Suppl A:227-235.
dydt
x y y xyn
y= + +( ) +′′
− +σ μ μ γ β μ γ( ) (1a)
dydt
yxn
y′
= ′ ′′
− ′ ′ ′β μ λ (2a)
Rn
n01= − ′
+ ′ ′ ′( )
( )ββ
μ γ μ λ(3a)
Page 10 of 11(page number not for citation purposes)
BMC Infectious Diseases 2008, 8:114 http://www.biomedcentral.com/1471-2334/8/114
Publish with BioMed Central and every scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
18. Girou E, Loyeau S, Legrand P, Oppein F, Brun-Buisson C: Efficacy ofhandrubbing with alcohol based solution versus standardhandwashing with antiseptic soap: randomised clinical trial.Bmj 2002, 325(7360):362.
19. Zaragoza M, Salles M, Gomez J, Bayas JM, Trilla A: Handwashingwith soap or alcoholic solutions? A randomized clinical trialof its effectiveness. Am J Infect Control 1999, 27(3):258-261.
20. Bonten MJ, Austin DJ, Lipsitch M: Understanding the spread ofantibiotic resistant pathogens in hospitals: mathematicalmodels as tools for control. Clin Infect Dis 2001,33(10):1739-1746.
21. Kramer A, Schwebke I, Kampf G: How long do nosocomial path-ogens persist on inanimate surfaces? A systematic review.BMC Infect Dis 2006, 6:130.
22. Rutala WA, Katz EB, Sherertz RJ, Sarubbi FA Jr.: Environmentalstudy of a methicillin-resistant Staphylococcus aureus epi-demic in a burn unit. J Clin Microbiol 1983, 18(3):683-688.
23. Boyce JM, Potter-Bynoe G, Chenevert C, King T: Environmentalcontamination due to methicillin-resistant Staphylococcusaureus: possible infection control implications. Infect ControlHosp Epidemiol 1997, 18(9):622-627.
24. Shiomori T, Miyamoto H, Makishima K: Significance of airbornetransmission of methicillin-resistant Staphylococcus aureusin an otolaryngology-head and neck surgery unit. ArchOtolaryngol Head Neck Surg 2001, 127(6):644-648.
25. Shiomori T, Miyamoto H, Makishima K, Yoshida M, Fujiyoshi T, UdakaT, Inaba T, Hiraki N: Evaluation of bedmaking-related airborneand surface methicillin-resistant Staphylococcus aureus con-tamination. J Hosp Infect 2002, 50(1):30-35.
26. Wilson RD, Huang SJ, McLean AS: The correlation between air-borne methicillin-resistant Staphylococcus aureus with thepresence of MRSA colonized patients in a general intensivecare unit. Anaesth Intensive Care 2004, 32(2):202-209.
27. Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, MedleyGF, Duckworth GJ, Lai R, Ebrahim S: Systematic review of isola-tion policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literaturewith epidemiological and economic modelling. Health TechnolAssess 2003, 7(39):1-194.
Pre-publication historyThe pre-publication history for this paper can be accessedhere:
http://www.biomedcentral.com/1471-2334/8/114/prepub
Page 11 of 11(page number not for citation purposes)





























