Embed Size (px)
Citation preview

International Journal of Cardiology xxx (2012) xxx–xxx
IJCA-14676; No of Pages 6
Contents lists available at SciVerse ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Implantable cardioverter defibrillator therapy activation for high risk patients withrelatively well preserved left ventricular ejection fraction. Does it really work?
Konstantinos A. Gatzoulis a,⁎, Dimitris Tsiachris a, Polichronis Dilaveris a, Stefanos Archontakis a,Petros Arsenos a, Apostolis Vouliotis a, Skevos Sideris b, George Trantalis b, Efstathios Kartsagoulis a,Ioannis Kallikazaros b, Christodoulos Stefanadis a
a First Cardiology Department, University of Athens Medical School, Hippokration Hospital, Athens, Greeceb State Department of Cardiology, Hippokration Hospital, Athens, Greece
⁎ Corresponding author at: mail box 175, Drafi Attikis 16944580369; fax: +30 2132088676.
E-mail address: [email protected] (K.A. Gatzouli
0167-5273/$ – see front matter © 2012 Elsevier Irelanddoi:10.1016/j.ijcard.2012.04.005
Please cite this article as: Gatzoulis KA, etwell preserved left ventricular ejection frac
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 7 November 2011Received in revised form 29 December 2011Accepted 1 April 2012Available online xxxxKeywords:Implantable cardioverter defibrillatorLeft ventricular ejection fractionProgrammed ventricular stimulation
Background: Current guidelines for the primary prevention of sudden cardiac death have used a left ventricularejection fraction (LVEF)≤35% as a critical point to justify implantable cardioverter defibrillator (ICD) implanta-tion in postmyocardial infarction patients and in thosewith nonischemic dilated cardiomyopathy.We comparedmortality and ICD activation rates among different ICD group recipients using a cut-off value for LVEF ≤35%.Methods:We followed up for a mean period of 41.1 months 495 ICD recipients (442males, 65.6 years old, 68.9%post myocardial infarction patients, 422 with LVEF≤35%). Prevention was considered primary in patients whofulfilled guidelines criteria or had inducible ventricular arrhythmia during programmed ventricular stimulationfor patients with LVEF >35%.Results: Over the course of the trial, 84 of 495 patients died; 69 experienced cardiac death (6 sudden) and 15 non
cardiac death. ICD recipients with LVEF≤35% compared to those with preserved LVEF (mean LVEF=43%) had agreater incidence of total mortality (18% vs. 11%, log rank p=0.028) and cardiac death (15.4% vs. 5.5%, log rankp=0.005). There was no difference in the incidence for appropriate device therapy between patients with LVEF≤35% and thosewith LVEF>35% (56.9% vs. 65.8%, log rank p=0.93). In themultivariate analysis the presence ofadvanced New York Heart Association stage predicted both total mortality (HR=2.69, 95% CI 1.771–4.086) andcardiac death (HR=3.437, 95% CI 2.163–5.463).Conclusions: ICD therapy may protect heart failure patients at early stages from arrhythmic morbidity andmortality, based on an electrophysiology-guided risk stratification approach.© 2012 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Current guidelines for the prevention of sudden cardiac death (SCD)have used a left ventricular ejection fraction (LVEF) equal to or less than35% as a critical point to justify implantable cardioverter defibrillator(ICD) implantation in post myocardial infarction patients and in thosewith non-ischemic dilated cardiomyopathy [1]. The LVEF used in clini-cal trials assessing the ICD for primary prevention of SCD ranged fromless than 40% in MUSTT to less than 30% in MADIT II, while MADIT Iand SCD-HeFT used LVEFs of less than 35% as entry criteria [2–5].
Much debate though exists concerning the relationship between acertain critical LVEF and the occurrence of lethal ventricular arrhyth-mias [6]. Based on pre-event LVEF estimation alone in patients withlife threatening ventricular arrhythmias (VA), it is demonstratedthat less than one quarter of patients with VAs would have qualifiedfor a prophylactic defibrillator [6]. Moreover, the “sicker” patients
9009, Athens, Greece. Tel.: +30
s).
Ltd. All rights reserved.
al, Implantable cardioverter dtion. Does it really work?, In
are more likely to die of progressive heart failure rather than due toa fatal arrhythmia, since the proportion of SCD is inversely relatedto New York Heart Association (NYHA) functional class [7]. Specifically,even when cardiac patients die suddenly at advanced stages of heartfailure, the mode of SCD is frequently not due to sustained VAs butrather due to asystole or/and electromechanical disssociation, a clinicalsituation that ICD has little or nothing to offer [8]. On the contrary, at theearly stages of heart failure, when most of the dying patients are SCDvictims, the corresponding mode of SCD is due to the unpredictableoccurrence of sustained VAs, a situation where the potential role ofICD is critical [9]. In these patients with preserved LVEF, an electro-physiological (EP) guided approach to select those high risk patientswho may benefit from the ICD implantation may be crucial. However,the ICD appropriate activation rate in this high risk population at earlystages of heart failure remains unknown. Furthermore, meta-analysisof secondary prevention ICD trials has shown no additional benefitfrom the device implantation compared to amiodarone in patient sub-populations with LVEF >35% [10].
Based on the above, the aim of our study was to compare mortalityand ICD activation rates among different ICD group recipients using a
efibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005

Table 1Demographic and clinical characteristics of ICD recipients according to LVEF status.
ICD recipients withEF ≤35% (n=422)
ICD recipients withEF >35% (n=73)
P
Age (years) 65.6±10.2 65.6±11.7 0.98Males (%) 90 84.9 0.19Secondary (%) 21.6 35.6 0.009ICM (%) 69.4 65.8 0.53LVEF (%) 26.9±15.5 43±4.8 b0.001NYHA stage 2.6±0.6 1.8±0.4 b0.001Syncope (%) 27.7 43.8 0.00624 h NSVT (%)⁎ 83.8 80 0.50PVS VT (%)⁎⁎ 73.6 92.7 0.002PVS VF (%)⁎⁎ 4.7 7.3 0.41Months Follow up 39.4±35 50.5±47 0.06
ICD = implantable cardioverter defibrillator, LVEF = Left ventricular ejection fraction,ICM = Ischemic cardiomyopathy, NYHA = New York Heart Association, NSVT = nonsustained ventricular tachycardia, PVS VT/VF = Ventricular tachycardia/ventricularfibrillation induced in programmed ventricular stimulation.⁎ n=353/495.⁎⁎ n=377/495.
2 K.A. Gatzoulis et al. / International Journal of Cardiology xxx (2012) xxx–xxx
cut-off value for LVEF equal to or less than 35%. This LVEF value wasselected to separate the severe from the relatively mild systolic dys-function ischemic and dilated cardiomyopathy patients at risk for SCDin a large database in which selection criteria for ICD implantationwere mostly EP guided.
2. Methods
2.1. Patient population
All patients receiving an ICD at the Hippokration Hospital, University of AthensMedical School, from 1992 up to March 2010 have been included in our ICD database(n=576). Eligibility for ICD implantation was based on the international guidelineswhich, due to their evolving nature, have changed over time, along with the approvalrequirements of the Greek Ministry of Public Health [1]. Specifically, according to thenational guidelines in Greece, an EP induction of a sustained VA is generally but notuniformly required to approve and justify the ICD implantation for the primary preventionof SCD, regardless of the severity of the coexisting LV dysfunction [11]. At the early years ofICD implantation, an EP study was also performed in most of the secondary SCD pre-vention cases when either amiodarone loading or/and some form of revascularizationand hemodynamic procedure were employed as a first therapeutic step. In terms of theprimary prevention of SCD, our post myocardial infarction and dilated cardiomyopathy pa-tients were undergoing periodic LVEF assessment, 24 hourHolter monitor recording and incase of non-sustained ventricular tachycardia (VT) detection or/and syncope occurrence,programmed ventricular stimulation (PVS). Thiswas the case for all primary prevention pa-tients with LVEF>35%. ICD implantation could also be justified in patients with LVEF≤35%by the Greek Ministry of Public Health in cases of recurrent syncope or an indication forbiventricular pacing, regardless of PVSfindings. Patientswith hypertrophic cardiomyopathy(n=63), arrhythmogenic right ventricular cardiomyopathy (n=25), channelopathies andidiopathic ventricular tachycardia (n=12) were excluded.
Secondary prevention refers to the prevention of SCD in those patients who havesurvived a prior cardiac arrest or sustained VT episode (n=117) [1,10,12]. Preventionwas considered primary in patients without a history of cardiac arrest or sustained VTwho fulfilled guidelines criteria or had inducible VT or ventricular fibrillation (VF) duringPVS especially in patients with LVEF >35%. LVEF was assessed with two-dimensionalechocardiography by applying the modified Simpson's rule, using a Hewlett Packard5500 Sonos Ultrasound Machine with a multifrequency transducer (2–5 MHz).
2.2. Electrophysiological study
After written informed consent was obtained, patients underwent PVS. Electrodecatheters were inserted percutaneously from the femoral groin and positioned in theheart under fluoroscopic guidance at the right atrium and at the right ventricular apex.Electrical stimulation of the heart was performed using an external stimulator (Era-His,Biotronik, Berlin, Germany) that produced rectangular impulses 2 ms in duration attwice the diastolic threshold. Bipolar intracardiac electrograms and 12-lead surfaceECGswere simultaneously acquired (BARD Labsystem, Lowell,Massachusetts). Intracardiacelectrograms were amplified, digitized at 1000 Hz, filtered (30 to 500 Hz), and recordedinto an optical disk.
Stimulation protocol consisted of up to triple extrastimuli (S2S3S4) delivered attwo paced cycle lengths (S1S1 550 ms and 400 ms) at the right ventricular apex andat right ventricular outflow tract. Extrastimuli were applied after six-beat drive trainswith a 2-s interdrive pause. Ventricular extrastimuli were introduced beginning late in di-astole andmoved progressively earlier in 10-ms steps until either ventricular refractorinessor a coupling interval of 200 mswas reached. The protocol was terminated prematurelyif a sustained VT (monomorphic or polymorphic) or VF was induced. Unspecific “junkrhythms” and “non-sustained” tachyarrhythmias of b30 s durationwithout hemodynamiccompromise were not considered as VT/VF induction.
In the present study, PVS was performed in 292 out of 331 patients with LVEF≤35%and a primary indication for ICD, and VT/VF was induced in 222 out of 292 (76%). More-over, PVS was performed in 30 out of 91 patients with a secondary indication for an ICDand LVEF ≤35%, since this was required in the early years as above mentioned.
2.3. Device implantation and programming
All implantations were carried out in the catheterization laboratory, and all deviceswere implanted transvenously without thoracotomy. Ventricular and atrial (pacingand shock) leads were positioned conventionally. Implanted systems were manufacturedby Biotronik (Berlin, Germany), Medtronic (Minneapolis, MN, USA), Boston Scientific[Natick, MA, USA, formerly CPI, Guidant (St. Paul, MN, USA)], St. Jude Medical/Ventritex(St. Paul, MN, USA) and ElaMedical (Clamart, France). In the present studywe have includ-ed only patients with ICD capabilities for storing intracardiac electrograms. All deviceswereprogrammed on two consecutive zones: an antitachycardia pacing (ATP) zone (cutoff ratefor VT detectionwas set at amean cycle length of 375±40ms and a detection interval of 16out of 16 or 24 out of 24 beats), and an initial shock zone (VF detection at a mean cyclelength of 300±30ms and a detection interval of 12/16 or 18/24). In the ATP zone, VAswere initially attempted to be terminated by two to five bursts of ATP followed by a similarnumber of ramp ATP runs and, if the arrhythmia continued, by low energy cardioversion
Please cite this article as: Gatzoulis KA, et al, Implantable cardioverterwell preserved left ventricular ejection fraction. Does it really work?, In
and subsequently defibrillator shocks. In the case of VF, device shocks were the initialtherapy.
2.4. Follow-up
Follow-up informationwas obtained at the time of visits at the outpatient arrhythmiaclinic or by telephone contact with patients and patients' private physicians. Patients withICDs were seen at one month after discharge and then at three to six month intervalsthroughout the follow-up and whenever they reported palpitations or shocks. Duringeach follow-up visit, patients were examined and devices interrogated to determine theappropriateness of the delivered therapy (ATP and shocks). ICD therapies were classifiedappropriate when they occurred in response to VT or VF and inappropriate when trig-gered by sinus or supraventricular tachycardia, T-wave over sensing, electrode dysfunc-tion, or other environmental interactions of any cause.
The study end points were death of any cause and development of sustained VAsinterrupted by the device (appropriate ICD activation). Modes of death were establishedfrom written records and by interviewing witnesses and/or attending physicians. SCDwas defined as instantaneous, unexpected death within 1 h of the onset of symptoms orunexpected death during sleep. Non sudden cardiac death was considered to be causedby progressive deterioration of the heart failure symptoms due to worsening myocardialdysfunction. Deaths related to diseases in other systems were considered non cardiacdeaths. The authors of thismanuscript have certified that they complywith the Principlesof Ethical Publishing in the International Journal of Cardiology [29].
2.5. Statistical analysis
Continuous data are expressed as mean±standard deviation; categorical data arepresented as percentages. Differences at baseline were evaluated with the independent-sample t-test for continuous variables and chi-square test for categorical variables. Cumu-lative incidences were analyzed by the method of Kaplan–Meier and compared using thelog-rank test. The relation between baseline characteristics and endpoints was assessedby using Cox regression analysis and described with hazard ratios (HR) and 95% CI. Inthe multivariate Cox regression analysis for all-cause mortality, adjustments were madefor age, gender, LVEF category, NYHA class, type of cardiomyopathy (ischemic andnon-ischemic) and type of prevention (primary and secondary). For all tests, a P-valueof b0.05 was considered significant.
3. Results
Data of follow up were available in 495 (85.8%) ICD recipients(442 males, 65.6 years old, 68.9% ICM). The mean duration of followup was 41.1 months. The study population was grouped accordingto LV function into those with a LVEF ≤35% (n=422) and thosewith a LVEF >35% (n=73).
Patientswith a LVEF>35% received an ICD for secondary preventionat a higher rate compared to those with a LVEF ≤35% (35.6% vs. 21.6%,p=0.009). Similarly, syncope was significantly more frequent in theformer group (43.8% vs. 27.7%, p=0.006), while no difference wasobserved with respect to age, gender and type of cardiomyopathy. Onthe other hand, as expected, NYHA class was higher in ICD recipientswith more severe LV dysfunction (2.6±0.6 vs. 1.8±0.4, pb0.001). Allpatients with a LVEF >35% and a primary indication for ICD (n=47),
defibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005
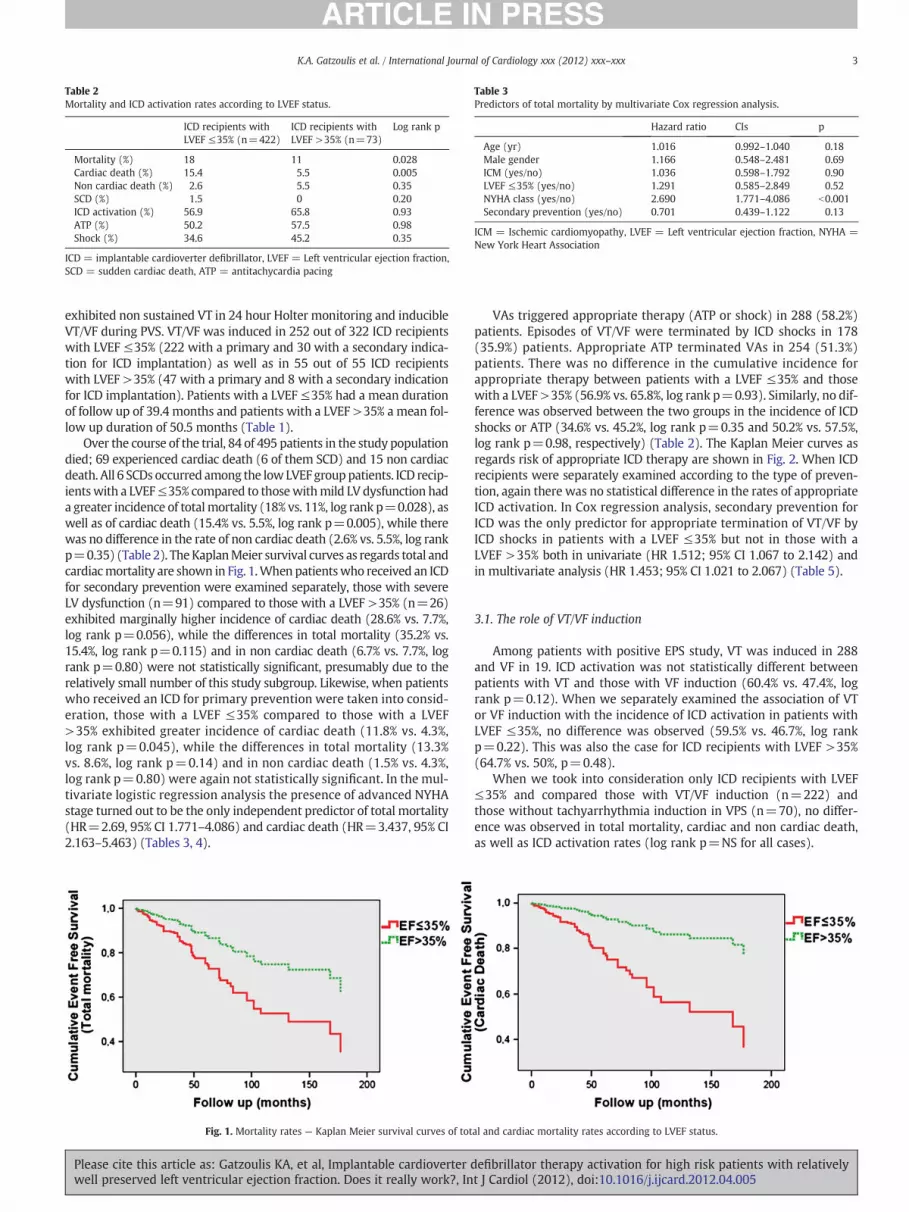
Table 2Mortality and ICD activation rates according to LVEF status.
ICD recipients withLVEF ≤35% (n=422)
ICD recipients withLVEF >35% (n=73)
Log rank p
Mortality (%) 18 11 0.028Cardiac death (%) 15.4 5.5 0.005Non cardiac death (%) 2.6 5.5 0.35SCD (%) 1.5 0 0.20ICD activation (%) 56.9 65.8 0.93ATP (%) 50.2 57.5 0.98Shock (%) 34.6 45.2 0.35
ICD = implantable cardioverter defibrillator, LVEF = Left ventricular ejection fraction,SCD = sudden cardiac death, ATP = antitachycardia pacing
Table 3Predictors of total mortality by multivariate Cox regression analysis.
Hazard ratio CIs p
Age (yr) 1.016 0.992–1.040 0.18Male gender 1.166 0.548–2.481 0.69ICM (yes/no) 1.036 0.598–1.792 0.90LVEF ≤35% (yes/no) 1.291 0.585–2.849 0.52NYHA class (yes/no) 2.690 1.771–4.086 b0.001Secondary prevention (yes/no) 0.701 0.439–1.122 0.13
ICM = Ischemic cardiomyopathy, LVEF = Left ventricular ejection fraction, NYHA =New York Heart Association
3K.A. Gatzoulis et al. / International Journal of Cardiology xxx (2012) xxx–xxx
exhibited non sustained VT in 24 hour Holter monitoring and inducibleVT/VF during PVS. VT/VF was induced in 252 out of 322 ICD recipientswith LVEF ≤35% (222 with a primary and 30 with a secondary indica-tion for ICD implantation) as well as in 55 out of 55 ICD recipientswith LVEF >35% (47 with a primary and 8 with a secondary indicationfor ICD implantation). Patients with a LVEF ≤35% had a mean durationof follow up of 39.4 months and patients with a LVEF >35% a mean fol-low up duration of 50.5 months (Table 1).
Over the course of the trial, 84 of 495 patients in the study populationdied; 69 experienced cardiac death (6 of them SCD) and 15 non cardiacdeath. All 6 SCDs occurred among the lowLVEF group patients. ICD recip-ientswith a LVEF≤35% compared to thosewithmild LV dysfunction hada greater incidence of totalmortality (18% vs. 11%, log rank p=0.028), aswell as of cardiac death (15.4% vs. 5.5%, log rank p=0.005), while therewas no difference in the rate of non cardiac death (2.6% vs. 5.5%, log rankp=0.35) (Table 2). TheKaplanMeier survival curves as regards total andcardiacmortality are shown in Fig. 1.When patientswho received an ICDfor secondary prevention were examined separately, those with severeLV dysfunction (n=91) compared to those with a LVEF >35% (n=26)exhibited marginally higher incidence of cardiac death (28.6% vs. 7.7%,log rank p=0.056), while the differences in total mortality (35.2% vs.15.4%, log rank p=0.115) and in non cardiac death (6.7% vs. 7.7%, logrank p=0.80) were not statistically significant, presumably due to therelatively small number of this study subgroup. Likewise, when patientswho received an ICD for primary prevention were taken into consid-eration, those with a LVEF ≤35% compared to those with a LVEF>35% exhibited greater incidence of cardiac death (11.8% vs. 4.3%,log rank p=0.045), while the differences in total mortality (13.3%vs. 8.6%, log rank p=0.14) and in non cardiac death (1.5% vs. 4.3%,log rank p=0.80) were again not statistically significant. In the mul-tivariate logistic regression analysis the presence of advanced NYHAstage turned out to be the only independent predictor of total mortality(HR=2.69, 95% CI 1.771–4.086) and cardiac death (HR=3.437, 95% CI2.163–5.463) (Tables 3, 4).
Fig. 1. Mortality rates — Kaplan Meier survival curves of tot
Please cite this article as: Gatzoulis KA, et al, Implantable cardioverter dwell preserved left ventricular ejection fraction. Does it really work?, In
VAs triggered appropriate therapy (ATP or shock) in 288 (58.2%)patients. Episodes of VT/VF were terminated by ICD shocks in 178(35.9%) patients. Appropriate ATP terminated VAs in 254 (51.3%)patients. There was no difference in the cumulative incidence forappropriate therapy between patients with a LVEF ≤35% and thosewith a LVEF >35% (56.9% vs. 65.8%, log rank p=0.93). Similarly, no dif-ference was observed between the two groups in the incidence of ICDshocks or ATP (34.6% vs. 45.2%, log rank p=0.35 and 50.2% vs. 57.5%,log rank p=0.98, respectively) (Table 2). The Kaplan Meier curves asregards risk of appropriate ICD therapy are shown in Fig. 2. When ICDrecipients were separately examined according to the type of preven-tion, again there was no statistical difference in the rates of appropriateICD activation. In Cox regression analysis, secondary prevention forICD was the only predictor for appropriate termination of VT/VF byICD shocks in patients with a LVEF ≤35% but not in those with aLVEF >35% both in univariate (HR 1.512; 95% CI 1.067 to 2.142) andin multivariate analysis (HR 1.453; 95% CI 1.021 to 2.067) (Table 5).
3.1. The role of VT/VF induction
Among patients with positive EPS study, VT was induced in 288and VF in 19. ICD activation was not statistically different betweenpatients with VT and those with VF induction (60.4% vs. 47.4%, logrank p=0.12). When we separately examined the association of VTor VF induction with the incidence of ICD activation in patients withLVEF ≤35%, no difference was observed (59.5% vs. 46.7%, log rankp=0.22). This was also the case for ICD recipients with LVEF >35%(64.7% vs. 50%, p=0.48).
When we took into consideration only ICD recipients with LVEF≤35% and compared those with VT/VF induction (n=222) andthose without tachyarrhythmia induction in VPS (n=70), no differ-ence was observed in total mortality, cardiac and non cardiac death,as well as ICD activation rates (log rank p=NS for all cases).
al and cardiac mortality rates according to LVEF status.
efibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005

Table 4Predictors of cardiac death by multivariate Cox regression analysis.
Hazard ratio CIs p
Age (yr) 1.019 0.992–1.046 0.17Male gender 1.705 0.781–3.722 0.18ICM (yes/no) 1.291 0.691–2.410 0.42EF ≤35% (yes/no) 2.159 0.738–6.239 0.16NYHA class (yes/no) 3.437 2.163–5.463 b0.001Secondary prevention (yes/no) 0.777 0.458–1.317 0.34
ICM = Ischemic cardiomyopathy, LVEF = Left ventricular ejection fraction, NYHA =New York Heart Association
4 K.A. Gatzoulis et al. / International Journal of Cardiology xxx (2012) xxx–xxx
3.2. Supplementary analyses
Our study population is heterogeneous based on the fact that in theearly years more secondary compared to primary prevention cases hadbeen included. This is depicted in a graph showing the inclusion ofpatients by year and by indication (Fig. 3). In order to overcomethe heterogeneity of our study population, we have provided supple-mentary analyses dividing the population into 2 periods according toMADIT II publication year.
When ICD recipients in the post-MADIT II era were taken intoconsideration (n=384), there was no difference in the cumulativeincidence for appropriate therapy between patients with a LVEF≤35% (n=333) and those with a LVEF >35% (n=51) (50.5% vs.56.9%, log rank p=0.80). ICD recipients with a LVEF≤35% comparedto those with mild LV dysfunction had a greater incidence of totalmortality (11.4% vs. 2%, log rank p=0.027), as well as of cardiac death(10.5% vs. 0%, log rank p=0.012), while there was no difference inthe rate of non cardiac death (0.9% vs. 2%, log rank p=0.64).
On the other hand, there was no difference in the cumulative inci-dence for appropriate therapy between patients with a LVEF ≤35%(n=89) and those with a LVEF >35% (n=22) in the pre-MADIT II era(80.9% vs. 86.4%, log rank p=0.94). ICD recipients with a LVEF ≤35%compared to those with mild LV dysfunction had a numerically greaterincidence of total mortality (42.7% vs. 31.8%, log rank p=0.23) and car-diac death (33.7% vs. 18.2%, log rank p=0.09), although not statisticallysignificant probably due to inadequate power of the specific analysis.Moreover, there was no difference in the rate of non cardiac death (9%vs. 13.6%, log rank p=0.60).
4. Discussion
The main finding of the present study is that ICD recipients withpreserved ejection fraction experienced appropriate therapy at similarrates to patients with severe LV dysfunction (LVEF ≤35%), while thelong term risk for total and cardiac mortality was significantly higherin the latter group. Our study presents evidence that ICD therapy may
Fig. 2. ICD activation rates — Kaplan Meier curves of ICD
Please cite this article as: Gatzoulis KA, et al, Implantable cardioverterwell preserved left ventricular ejection fraction. Does it really work?, In
protect patients even at early stages of heart failure from arrhythmicmorbidity and mortality based on an EP guided risk stratificationapproach.
Our study is the first to demonstrate a clear cut ICD benefit inpatients with well preserved LVEF (mean LVEF=43%). The similarrates of appropriate ICD activation irrespective of the LVEF status inthe present study might be explained based on the risk stratificationapproach applied and the duration of the follow up period. Specifically,all of the patients with relatively preserved LV function had a wellorganized arrhythmia substrate either on the basis of previous epi-sodes of sustained VAs or on the basis of the coexistence of eithernon-sustained VT on Holter recordings or/and syncope attacks onhistory with inducible VT/VF on PVS. This approach is in line withretrospective analyses of MUSTT, where inducible VT/VF but notlow LVEF could discriminate between modes of death, identifyingpatients at increased arrhythmic death, especially if LVEF was ≥30%[13,14]. Furthermore, an extended period of follow up of 50 months(range from 2 to 192 months) in mildly diseased heart failure patientsallowed time for appropriate ICD activation rate similar to that observedamong ICDpatientswith severe LVdysfunction. The similar incidence ofa high ICD activation rate in both groups of our study patients could berelated to a highly arrhythmogenic state in the group of LVEF>35% inwhom more ICDs were implanted for secondary prevention and/or anincidence of syncope, while a sustained VA was induced on PVS in allcorresponding primary prevention cases.
The study clearly implies that the prognosis of the heart failurepatients can bemarkedly improved by reducing the arrhythmicmor-tality even at early stages with mild LV dysfunction in the content ofeither secondary or primary prevention of SCD provided an ICD isimplanted in truly high risk patients timely. There was also a higherICD activation rate among patients with severe LV dysfunction inwhom the device was implanted for primary prevention of SCDwhen compared to the corresponding observed ICD activation rateof the MADIT II and the SCD-HeFT trial populations, in whom a clearcut ICD benefit was also demonstrated [3,5]. Themost likely explanationfor this observation is the inclusion of an EP guided risk stratificationapproach in our patientswith severe LV dysfunction. Such an EP orientedstrategy may not only increase the number of potential ICD candidatesamong those heart failure patients withmild LV dysfunction but also im-prove arrhythmicmorbidity andmortality in a highly pre-selected groupof those heart failure patients. It is interesting that 6 SCDs occurred inthe low LVEF group (n=6/422, 1.5%) despite the presence of previouslyproperly functioning ICDs, presumably due to bradyarrhythmic mecha-nisms, in contrast to no SCD observed in the corresponding high riskwell preserved LVEF group (n=0/73, 0%). Thus, with the current EPguided risk stratification approach, the ICD implantation resulted inalmost complete elimination of arrhythmic mortality among both ofour high risk group patients.
activation and shocks rates according to LVEF status.
defibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005

Table 5Predictors of ICD shocks in patients with LVEF ≤35% by multivariate Cox regressionanalysis.
Hazard ratio CIs p
Age (yr) 0.994 0.978–1.010 0.47Male gender 1.607 0.800–3.232 0.18ICM (yes/no) 1.020 0.689–1.510 0.92Secondary prevention (yes/no) 1.453 1.021–2.067 0.038
LVEF = Left ventricular ejection fraction, ICM = Ischemic cardiomyopathy.
5K.A. Gatzoulis et al. / International Journal of Cardiology xxx (2012) xxx–xxx
A large number of people die suddenly each year presumably fromsustained VT or VF in most of the cases [1,15]. According to the resultsof multiple clinical trials, LV systolic function, measured as LVEF, iscurrently the main recommended tool to identify patients at higherrisk for SCD thatwould benefit from a prophylactic ICD [1–5]. However,the systematic implementation of current ICD recommendationsresults in a substantial number of inappropriate ICD implantationsand fails to prevent the majority of SCDs in the general population,since LVEF lacks both sensitivity and specificity for prediction ofSCD [16–18]. In the Oregon Sudden Unexpected Death Study, anLVEF >35% was found in 70% of SCD victims who had LVEF measuredbefore their cardiac arrest [9]. Notably, less than 15% of patients afteracute myocardial infarction nowadays have LVEF b40% and only5% have LVEF b30%, in contrast to the pre-reperfusion era whereone-third of patients with acute myocardial infarction had LVEFb40% [17,19].
There are a number of reasons explaining, at least in part, the lackof ICD benefit compared to amiodarone in previous trials in patientswith mild LV dysfunction [10,12]. It has been suggested that in ventri-cles with better LV function, amiodarone is relatively more effective inpreventingmalignant VAs than in patients with moderately to severelyreduced LVEF [12]. Moreover, short time of follow up in most of largeICD trials, in contrast with the present study, did not allow propercomparison according to LVEF status [20]. Finally, in these trialsthere was a predominance of “hard” study end points, namely cardiacdeaths among the “sickest” patients, since expected high event rate inseverely depressed LVEF populations minimized the necessary samplesize [21].
It is clear from large clinical trials that patients with multiple riskfactors are at higher risk than those with only a single risk factor.Specifically, the relative reduction in total mortality associated withICD therapy was 55% in trials that required markers for arrhythmicmortality risk in addition to reduced LVEF, such as inducible VAs. Incontrast, the relative reduction in total mortality in the MADIT-II trial(which only specified an LVEF ≤30% as the enrollment criterion) wasonly 31%, even though used LVEF was significantly lower [3,4,22].There is evidence supporting the implementation of a risk stratification
Fig. 3. A graph showing the inclusion of patients b
Please cite this article as: Gatzoulis KA, et al, Implantable cardioverter dwell preserved left ventricular ejection fraction. Does it really work?, In
approach even at early heart failure stages with relatively well pre-served LV function among patients after “limited” myocardial infarc-tion or with early dilated cardiomyopathy [15,23,24]. In the presentstudy we risk stratified patients based on the history of syncope and/or non sustained VT on Holter recordings, when the LVEF was >35%completing this approach with the results of PVS in the EP laboratory.A sustained VA induction in PVS was required in order to implantan ICD in this group of patients, in contrast to patients with poorLV function. However, there are a number of other non-invasivelyderived electrocardiographic variables such as late potentials, T wavealternans, Holter derived repolarization abnormalities and autonomicdisturbance indices which could be used in a similar approach potential-ly revealing an additional at SCD risk patient population with relativelywell preserved LV function [24–28].
Taken into account that the SCD was adequately suppressed inour patient cohort with the appropriate EP guided risk stratificationapproach leading to a high ICD successful activation rate, it is not sur-prising that the only independent predictor of mortality inmultivariateanalysis was the presence of an advanced NYHA class state. On thisanalysis the low LVEF ≤35%, the type of organic heart disease, the sexand the age as well as the secondary prevention of SCD were not inde-pendent predictors of an increased mortality rate. Indeed, an advancedNYHA class is associated not only with severe myocardial dysfunctionbut also with a detrimental activation of the neurohormonal status, aswell as progressive deterioration of other system states and inflamma-tory responses, all leading to an undesirable final result.
4.1. Limitations
As stated above, our study population is heterogeneous mostly dueto a different approach in ICD candidates during the long follow upperiod. According to the implementation of guidelines by the Greekministry of Public Health an important number of patients withLVEF ≤35% were not implanted with an ICD and we don't knowwhat happened with those patients in terms of arrhythmic events.However, the fact that 67% of our patients with LVEF ≤35% had in-ducible VT/VF enhances arrhythmic risk of these patients as well asthe probability for subsequent ICD activation and strengthens ourstudy findings regarding similar rates of appropriate ICD therapy inboth study subgroups. As regards the vague predictive value of PVSin non-ischemic patients with dilated cardiomyopathy our study is notadequately powered to examine this issue. Moreover, we acknowledgea lack of data regarding the absolute number of ICD activations.
In summary, the present study presents evidence that ICD therapymay protect heart failure patients even at early stages with mild LVsystolic dysfunction from arrhythmic morbidity and mortality, providedan EP guided risk stratification approach is applied early and periodically.
y year and by indication for ICD implantation.
efibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005

6 K.A. Gatzoulis et al. / International Journal of Cardiology xxx (2012) xxx–xxx
This strategymay limit arrhythmicmortality andmarkedly improve longterm prognosis in this particular heart failure population.
Acknowledgments
None declared.
References
[1] Epstein AE, Dimarco JP, Ellenbogen KA, et al. American College of Cardiology;American Heart Association Task Force on Practice Guidelines; American Associationfor Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelinesfor device-based therapy of cardiac rhythm abnormalities. Heart Rhythm 2008;5:e1–62.
[2] Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomizedstudy of the prevention of sudden death in patients with coronary artery disease.Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med 1999;341:1882–90.
[3] Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator inpatients with myocardial infarction and reduced ejection fraction. N Engl J Med2002;346:877–83.
[4] Mushlin AI, Hall WJ, Zwanziger J, et al. The cost-effectiveness of automatic implant-able cardiac defibrillators: results from MADIT. Multicenter Automatic DefibrillatorImplantation Trial. Circulation 1998;97:2129–35.
[5] Mark DB, Nelson CL, Anstrom KJ, et al. Cost-effectiveness of defibrillator therapyor amiodarone in chronic stable heart failure: results from the Sudden CardiacDeath in Heart Failure Trial (SCD-HeFT). Circulation 2006;114:135–42.
[6] Pascale P, Schlaepfer J, OddoM, SchallerMD, Vogt P, FromerM. Ventricular arrhythmiain coronary artery disease: limits of a risk stratification strategy based on the ejectionfraction alone and impact of infarct localization. Europace 2009;11:1639–46.
[7] Uretsky B, Sheahan G. Primary prevention of sudden cardiac death in heart failure:will the result be shocking? J Am Coll Cardiol 1997;30:1589–97.
[8] Luu M, Stevenson WG, Stevenson LW, Baron K, Walden J. Diverse mechanisms ofunexpected cardiac arrest in advanced heart failure. Circulation 1989;80:1675–80.
[9] Stecker EC, Vickers C, Waltz J, et al. Population-based analysis of sudden cardiacdeath with and without left ventricular systolic dysfunction. Two year findingsfrom the Oregon Sudden Unexpected Death Study. J Am Coll Cardiol 2006;47:1161–6.
[10] Connolly S, Hallstrom AP, Cappato R, et al. Meta-analysis of the implantable cardi-overter defibrillator secondary prevention trials. Eur Heart J 2000;21:2071–8.
[11] Manolis AS, Vardas P, Sakantamis G, Gatzoulis K, Manolis AG. Guidelines for theimplantation of cardiac defibrillators. Hellenic J Cardiol 1996;37:165–71.
[12] Domanski M, Saksena S, Epstein A, et al. Relative effectiveness of the implantablecardioverter defibrillator and antiarrhythmic drugs in patients with varyingdegrees of left ventricular dysfunction who have survived malignant ventriculararrhythmias. J Am Coll Cardiol 1999;34:1090–5.
[13] Buxton AE, Lee KL, Hafley GE, et al. Relation of ejection fraction and inducibleventricular tachycardia to mode of death in patients with coronary artery disease:
Please cite this article as: Gatzoulis KA, et al, Implantable cardioverterwell preserved left ventricular ejection fraction. Does it really work?, In
an analysis of patients enrolled in themulticenter unsustained tachycardia trial. Cir-culation 2002;106:2466–72.
[14] Buxton AE, Lee KL, Hafley GE, et al. Limitations of ejection fraction for predictionof sudden death risk in patients with coronary artery disease: lessons from theMUSTT study. J Am Coll Cardiol 2007;50(12):1150–7.
[15] Lloyd-Jones D, Adams R, Brown T, et al. Cardiovascular deaths and sudden deathremain the single most common cause of death in the United States. Heart diseaseand stroke statistics-2010 update. Circulation 2010;121:e1–170.
[16] Buxton AE, Ellison KE, Lorvidhaya P, Ziv O. Left ventricular ejection fraction forsudden death risk stratification and guiding implantable cardioverter-defibrillatorsimplantation. J Cardiovasc Pharmacol 2010;55(5):450–5.
[17] Santangeli P, Dello Russo A, Casella M, Pelargonio G, Di Biase L, Natale A. Leftventricular ejection fraction for the risk stratification of sudden cardiac death:friend or foe? Intern Med J 2011;41:55–60.
[18] Gorgels APM, Gijsbers C, de Vreede-Swagemakers J, Lousberg A, Wellens HJ. Out-of hospital cardiac arrest-the relevance of heart failure. The Maastricht CirculatoryArrest Registry. Eur Heart J 2003;24:1204–9.
[19] Bauer A, Barthel P, Schneider R, et al. Improved stratification of autonomic regulationfor risk prediction in post-infarction patients with preserved left ventricular function(ISAR-Risk). Eur Heart J 2009;30:576–83.
[20] Bokhari F, Newman D, Greene M, Korley V, Mangat I, Dorian P. Long-termcomparison of the implantable cardioverter defibrillator vs amiodarone: 11years follow up of a subset of patients in the Canadian Implantable DefibrillatorStudy (CIDS). Circulation 2004;110:112–6.
[21] Rouleau JL, Talajic M, Sussex B, et al. Myocardial infarction patients in the 1990s—their risk factors, stratification and survival in Canada: the Canadian Assessmentof Myocardial Infarction Study. J Am Coll Cardiol 1996;27:1119–27.
[22] Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibril-lator in patients with coronary disease at high risk for ventricular arrhythmia. NEngl J Med 1996;335:1933–40.
[23] Gatzoulis K, Salourou M, Dilaveris P, et al. Programmed ventricular stimulation asa risk stratifier for the primary prevention of sudden cardiac death among dilatedcardiomyopathy patients. Eur Heart J 2009;30:693 (Abstract Suppl).
[24] Ikeda T, Yoshino H, Sugi K, et al. Predictive value of microvolt T-wave alternans forsudden cardiac death in patientswith preserved cardiac function after acutemyocar-dial infarction: results of a collaborative cohort study. J Am Coll Cardiol 2006;48:2268–74.
[25] Gatzoulis K, Carlson M, Biblo L, et al. Time domain analysis of the signal averagedelectrocardiogram in patients with a conduction defect or a bundle branch block.Eur Heart J 1995;16:1912–9.
[26] Gold MR, Bloomfield DM, Anderson KP, et al. A comparison of T-wave alternans,signal averaged electrocardiography and programmed ventricular stimulationfor arrhythmia risk stratification. J Am Coll Cardiol 2000;36:2247–53.
[27] Arsenos P, Gatzoulis KA, Dilaveris P, et al. The rate-corrected QT interval calculatedfrom 24-hour Holter recordings may serve as a significant arrhythmia risk stratifierin heart failure patients. Int J Cardiol 2011;147(2):321–3.
[28] Arsenos P, Gatzoulis K, Manis G, et al. Decreased scale-specific heart rate variabilityafter multiresolution wavelet analysis predicts sudden cardiac death in heart failurepatients. Int J Cardiol 2011 [Epub ahead of print].
[29] Coats AJS, Shewan LG. Statement on authorship and publishing ethics in the Inter-national Journal of Cardiology. Int J Cardiol 2011;153:257–8.
defibrillator therapy activation for high risk patients with relativelyt J Cardiol (2012), doi:10.1016/j.ijcard.2012.04.005





























