Embed Size (px)
Citation preview

For circulation only among the Piramal LDPOC team members
1 QDx Instacheck training: Cortisol, Ferritin & PCT
hsCRP + CRP – All in one
What is CRP and hsCRP?
C-reactive protein (CRP) is protein found in the blood, the levels of which rise in response to
inflammation (i.e. C-reactive protein is an acute-phase protein). Its physiological role is to
bind to phosphocholine expressed on the surface of dead or dying cells (and some types of
bacteria) in order to activate the complement system via the C1Q complex.
CRP is synthesized by the liver in response to factors released by macrophages and fat cells
(adipocytes).
The acute phase response develops in a wide range of acute and chronic inflammatory
conditions like bacterial, viral, or fungal infections; rheumatic and other inflammatory
diseases; malignancy; and tissue injury or necrosis. These conditions cause release of
interleukin-6 and other cytokines that trigger the synthesis of CRP and fibrinogen by the
liver. During the acute phase response, levels of CRP rapidly increase within 2 hours of acute
insult, reaching a peak at 48 hours. With resolution of the acute phase response, CRP declines
with a relatively short half-life of 18 hours. Measuring CRP level is a screen for infectious
and inflammatory diseases. Rapid, marked increases in CRP occur with inflammation,
infection, trauma and tissue necrosis, malignancies, and autoimmune disorders. Because there
are a large number of disparate conditions that can increase CRP production, an elevated
CRP level does not diagnose a specific disease. An elevated CRP level can provide support
for the presence of an inflammatory disease, such as rheumatoid arthritis, polymyalgia
rheumatica or giant-cell arteritis.
The physiological role of CRP is to bind to phosphocholine expressed on the surface of dead
or dying cells (and some types of bacteria) in order to activate the complement system. CRP
binds to phosphocholine on microbes and damaged cells and enhances phagocytosis by
macrophages. Thus, CRP participates in the clearance of necrotic and apoptotic cells.
CRP rises up to 50,000-fold in acute inflammation, such as infection. It rises above normal
limits within 6 hours, and peaks at 48 hours. Its half-life is constant, and therefore its level is
mainly determined by the rate of production (and hence the severity of the precipitating
cause).
Clinical significance
C-reactive protein (CRP) is 1 of the most sensitive acute-phase reactants. Plasma CRP levels
can increase dramatically (100-fold or more) after severe trauma, bacterial infection,
inflammation, surgery, or neoplastic proliferation. Measurement of CRP has been used
historically to assess activity of inflammatory disease, to detect infections after surgery, to
detect transplant rejection, and to monitor these inflammatory processes. While assays for
CRP have been available for many years, the traditional assays lack the sensitivity to measure
basal levels of CRP.
In the mid-1990s, more sensitive methods for measurement of CRP were introduced. These
methods, referred to as high sensitivity CRP (hs-CRP), can accurately measure basal levels of
For circulation only among the Piramal LDPOC team members
2 QDx Instacheck training: Cortisol, Ferritin & PCT
CRP throughout the currently accepted cardiovascular risk assessment range (0.20-10.0
mg/L).
These hs-CRP assays were used to assess outcomes in patients with unstable angina and
showed that hs-CRP values in the upper tertile (>3.0 mg/L) were associated with increased
risk of developing myocardial infarction. Data from prospective studies monitoring hs-CRP
in apparently healthy populations also has been published. All prospective studies reported to
date have been positive, with adjusted relative risks of developing cardiovascular disease or
ischemic events ranging from 2.3 to 4.8 in the highest quartile or quintile of data versus the
lowest quartile or quintile. It also has been shown that hs-CRP is additive with total
cholesterol, LDL and HDL, as well as the Framingham 10-year risk score, with respect to risk
prediction.
When is the hsCRP – All in one test done?
High-sensitivity CRP usually is ordered as one of several tests in a cardiovascular risk
profile, often along with tests for cholesterol and triglycerides, when a person's risk of heart
disease is being evaluated. Some experts say that the best way to predict risk is to combine a
good marker for inflammation, like hs-CRP, along with the lipid profile. When hs-CRP is
evaluated, it may be repeated to confirm that a person has persistent low levels of
inflammation.
CRP is useful for: -
1. Monitoring response to antibiotic therapy in patients with known bacterial infections.
2. Warning of intrauterine infections in obstetric patients with premature rupture of
membranes.
3. Differentiation between active disease and infections in systemic lupus and colitis
ulcerosa.
4. Measure of disease activity and drug response in rheumatoid arthritis.
5. Early detection of complications in postoperative patients.
6. Differentiation between infection and graft-versus-host-disease in bone marrow
transplant patients.
What does the test result mean?
Relatively high levels of hs-CRP in otherwise healthy individuals have been found to be
predictive of an increased risk of a future heart attack, stroke, sudden cardiac death, and/or
peripheral arterial disease, even when cholesterol levels are within an acceptable range.
People with higher hs-CRP values have the highest risk of cardiovascular disease, and those
with lower values have less of a risk. Specifically, individuals who have hs-CRP results at the
high end of the normal range have 1.5 to 4 times the risk of having a heart attack as those
with hs-CRP values at the low end of the normal range.
For circulation only among the Piramal LDPOC team members
3 QDx Instacheck training: Cortisol, Ferritin & PCT
The American Heart Association and U.S. Centers for Disease Control and Prevention have
defined risk groups as follows:
Low risk: less than 1.0 mg/L
Average risk: 1.0 to 3.0 mg/L
High risk: above 3.0 mg/L
These values are only a part of the total evaluation process for cardiovascular diseases.
Additional risk factors to be considered are elevated levels of cholesterol, LDL-C,
triglycerides, and glucose. In addition, smoking, high blood pressure (hypertension), and
diabetes also increase the risk level.
For further information, kindly refer to the pack insert.
For circulation only among the Piramal LDPOC team members
4 QDx Instacheck training: Cortisol, Ferritin & PCT
Procalcitonin (PCT)
What is Procalcitonin?
Procalcitonin (PCT) is a peptide precursor of the hormone calcitonin, the latter being
involved with calcium homeostasis. It is composed of 116 amino acids and is produced by
parafollicular cells (C cells) of the thyroid and by the neuroendocrine cells of the lung and the
intestine.
The level of procalcitonin in the blood stream of healthy individuals is below the limit of
detection (10 pg/mL) of clinical assays. The level of procalcitonin raises in a response to a
proinflammatory stimulus, especially of bacterial origin. In this case, it is produced mainly by
the cells of the lung and the intestine. It does not raise significantly with viral or non-
infectious inflammations. With the derangements that a severe infection with an associated
systemic response brings, the blood levels of procalcitonin may rise to 100 ng/ml. In serum,
procalcitonin has a half-life of 25 to 30 hours. Remarkably the high procalcitonin levels
produced during infections are not followed by a parallel increase in calcitonin or serum
calcium levels.
Clinical significance
Diagnosis and prognosis of sepsis
Measurement of procalcitonin can be used as a marker of severe sepsis caused by bacteria
and generally grades well with the degree of sepsis, although levels of procalcitonin in the
blood are very low. PCT has the greatest sensitivity (85%) and specificity (91%) for
differentiating patients with systemic inflammatory response syndrome (SIRS) from those
with sepsis, when compared with IL-2, IL-6, IL-8, CRP and TNF-alpha. Evidence is
emerging that procalcitonin levels can reduce unnecessary antibiotic prescribing to people
with lower respiratory tract infections. Currently, procalcitonin assays are widely used in the
clinical environment.
Diagnosis of bacteremia
A meta-analysis reported a sensitivity of 76% and specificity of 70%.
Procalcitonin level can help guide antibiotic therapy. Procalcitonin levels may be useful to
distinguish bacterial infections from nonbacterial infections.
When is the Procalcitonin test done?
The procalcitonin test has been approved by the U.S. FDA (Food and Drug Administration)
for use in conjunction with other laboratory findings and clinical assessments to assist in the
risk assessment of critically ill people for progression to severe sepsis and septic shock. For
diagnostic purposes, it is best used during the first day of presentation. It may be used later on
to monitor the response to treatment.

For circulation only among the Piramal LDPOC team members
5 QDx Instacheck training: Cortisol, Ferritin & PCT
Procalcitonin may sometimes be ordered, along with other tests such as a CRP (C-reactive
protein), blood culture, CBC (Complete Blood Count), or CSF (cerebrospinal fluid) analysis
to help detect or rule out sepsis, bacterial meningitis, or bacterial pneumonia in those who are
seriously ill and in children with a fever of unknown origin.
Occasionally, a procalcitonin test may be ordered at intervals to monitor the effectiveness of
antimicrobial treatment.
The procalcitonin test may be ordered along with other tests, when a seriously ill person has
symptoms that suggest that they may have a systemic or severe bacterial infection. When
used, it is typically ordered as an early detection tool, within the first day of hospital
admission.
Complications of sepsis may include:
Chills, fever
Nausea
Rapid breathing, rapid heartbeat
Confusion
Decreased urine output
More severe symptoms include inflammation throughout the body and formation of many
tiny blood clots in the smallest blood vessels. One or more organs may begin to stop working
(multi-organ failure, MOF) and there may be a dangerous drop in blood pressure.
Rarely, it may be ordered at intervals to monitor antimicrobial therapy in persons suspected
of having sepsis.
What does the test result mean?
Low levels of procalcitonin in a seriously ill person represent a low risk of sepsis and
progression to severe sepsis and/or septic shock but do not exclude it. Low concentrations
may indicate a localized infection that has not yet become systemic or a systemic infection
that is less than six hours old. It may also indicate that the person's symptoms are likely due
to another cause, such as transplant rejection, a viral infection, or trauma – post-surgery or
otherwise.
High levels indicate a high probability of sepsis, that is, a higher likelihood of a bacterial
cause for the symptoms. They also suggest a higher risk of progression to severe sepsis and
then to septic shock.
Moderate elevations may be due to a non-infectious condition or due to an early infection
and, along with other findings, should be reviewed carefully. Decreasing procalcitonin levels
in a person being treated for a severe bacterial infection indicate a response to therapy.
For circulation only among the Piramal LDPOC team members
6 QDx Instacheck training: Cortisol, Ferritin & PCT
Cortisol
What is Cortisol?
Cortisol, known more formally as hydrocortisone, is a steroid hormone, more specifically a
glucocorticoid, produced by the zona fasciculata of the adrenal gland. It is released in
response to stress and a low level of blood glucocorticoids. Its primary functions are to
increase blood sugar through gluconeogenesis; suppress the immune system; and aid in fat,
protein and carbohydrate metabolism.
Clinical significance
A cortisol test may be ordered to screen for and help diagnose Cushing syndrome, a group of
signs and symptoms associated with excess cortisol. Blood cortisol testing evaluates both
protein-bound and free cortisol while urine testing evaluates only free cortisol, which should
correlate with the levels of free cortisol in the blood. Sometimes salivary cortisol is also
ordered to help detect Cushing syndrome.
Blood cortisol is also used to help diagnose adrenal insufficiency and Addison disease,
conditions in which the adrenal glands do not function properly.
Multiple blood and/or saliva cortisol levels collected at different times, such as at 8 am and 4
pm, can be used to evaluate both cortisol concentrations and diurnal variation. Normally, the
level of cortisol in the blood rises and falls in a "diurnal variation" pattern, peaking early in
the morning then declining throughout the day and reaching its lowest level about midnight.
A 24-hour urine cortisol sample will not show diurnal variation; it will measure the total
amount of unbound cortisol excreted in 24 hours.
If an abnormal level of cortisol is detected, a doctor will do additional testing to help confirm
the findings and to help determine its cause:
Dexamethasone Suppression
If a person has a high cortisol level, a doctor may perform a dexamethasone suppression test
to help determine whether the cause is related to excess ACTH production by the pituitary.
This test involves analyzing a baseline sample for cortisol, then giving the person oral
dexamethasone (a synthetic glucocorticoid) and measuring cortisol levels in subsequent timed
samples. Dexamethasone suppresses ACTH production and should decrease cortisol
production if the source of the excess is pituitary-related. There are a few variations of this
test. An overnight test may be used to help screen for Cushing syndrome. Longer tests help
confirm initial findings. For these, the medication is usually given (either low or high dose)
every 6 hours for either 2 or 4 days prior to blood or urine collection. Separate 24-hour urine
samples are collected prior to and throughout the testing period and then the blood and urine
samples are measured for cortisol and evaluated.
ACTH Stimulation
If the findings of the initial blood and/or urine tests indicate insufficient cortisol production, a
doctor may order an ACTH stimulation test. This test involves measuring the concentration
of cortisol in a person's blood before and after an injection of synthetic ACTH. If the adrenal
For circulation only among the Piramal LDPOC team members
7 QDx Instacheck training: Cortisol, Ferritin & PCT
glands are functioning normally, then cortisol levels will rise with the ACTH stimulation. If
they are damaged or not functioning properly, then the response will be limited. A longer
version of this test (1-3 days) may be performed to help distinguish between adrenal and
pituitary insufficiency.
When is the Cortisol test done?
A cortisol test may be ordered when a person has symptoms that suggest a high level of
cortisol and Cushing syndrome, such as
High blood pressure (hypertension)
High blood sugar (glucose)
Obesity, especially in the trunk
Fragile skin
Purple streaks on the abdomen
Muscle wasting and weakness
Osteoporosis
Women may have irregular menstrual periods and increased facial hair; children may have
delayed development and a short stature. This test may be ordered when someone has
symptoms suggestive of a low level of cortisol, adrenal insufficiency or Addison disease,
such as:
Weight loss
Muscle weakness
Fatigue
Low blood pressure
Abdominal pain
Dark patches of skin—this occurs in Addison disease, but not secondary adrenal
insufficiency
Sometimes decreased production combined with a stressor can cause an adrenal crisis that
can be life-threatening and requires immediate medical attention. Symptoms of a crisis may
include:
Sudden onset of severe pain in the lower back, abdomen, or legs
Vomiting and diarrhea, resulting in dehydration
Low blood pressure (hypotension)
Loss of consciousness
Suppression or stimulation testing is ordered when initial findings are abnormal. Cortisol
testing may be ordered at intervals after a diagnosis of Cushing syndrome or Addison disease
to monitor the effectiveness of treatment.
What does the test result mean?
Normal values indicated in the following tables pertain to humans. (Normals vary among
species.)
For circulation only among the Piramal LDPOC team members
8 QDx Instacheck training: Cortisol, Ferritin & PCT
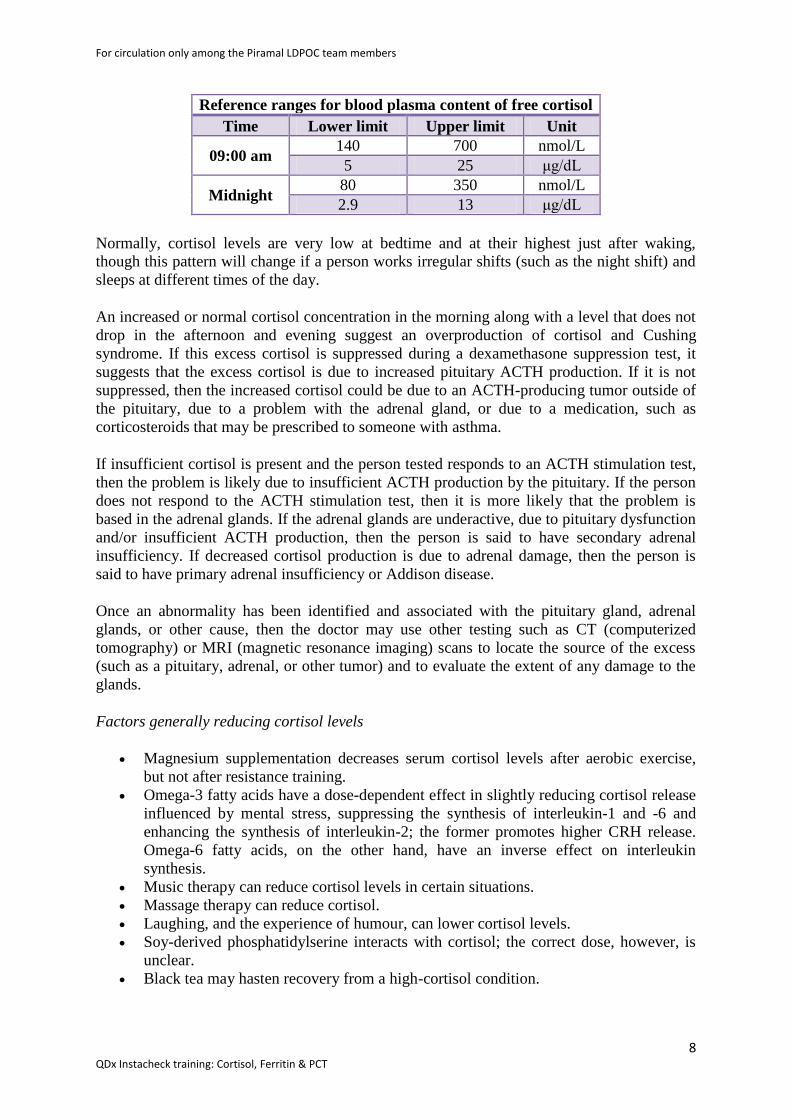
Reference ranges for blood plasma content of free cortisol
Time Lower limit Upper limit Unit
09:00 am 140 700 nmol/L
5 25 μg/dL
Midnight 80 350 nmol/L
2.9 13 μg/dL
Normally, cortisol levels are very low at bedtime and at their highest just after waking,
though this pattern will change if a person works irregular shifts (such as the night shift) and
sleeps at different times of the day.
An increased or normal cortisol concentration in the morning along with a level that does not
drop in the afternoon and evening suggest an overproduction of cortisol and Cushing
syndrome. If this excess cortisol is suppressed during a dexamethasone suppression test, it
suggests that the excess cortisol is due to increased pituitary ACTH production. If it is not
suppressed, then the increased cortisol could be due to an ACTH-producing tumor outside of
the pituitary, due to a problem with the adrenal gland, or due to a medication, such as
corticosteroids that may be prescribed to someone with asthma.
If insufficient cortisol is present and the person tested responds to an ACTH stimulation test,
then the problem is likely due to insufficient ACTH production by the pituitary. If the person
does not respond to the ACTH stimulation test, then it is more likely that the problem is
based in the adrenal glands. If the adrenal glands are underactive, due to pituitary dysfunction
and/or insufficient ACTH production, then the person is said to have secondary adrenal
insufficiency. If decreased cortisol production is due to adrenal damage, then the person is
said to have primary adrenal insufficiency or Addison disease.
Once an abnormality has been identified and associated with the pituitary gland, adrenal
glands, or other cause, then the doctor may use other testing such as CT (computerized
tomography) or MRI (magnetic resonance imaging) scans to locate the source of the excess
(such as a pituitary, adrenal, or other tumor) and to evaluate the extent of any damage to the
glands.
Factors generally reducing cortisol levels
Magnesium supplementation decreases serum cortisol levels after aerobic exercise,
but not after resistance training.
Omega-3 fatty acids have a dose-dependent effect in slightly reducing cortisol release
influenced by mental stress, suppressing the synthesis of interleukin-1 and -6 and
enhancing the synthesis of interleukin-2; the former promotes higher CRH release.
Omega-6 fatty acids, on the other hand, have an inverse effect on interleukin
synthesis.
Music therapy can reduce cortisol levels in certain situations.
Massage therapy can reduce cortisol.
Laughing, and the experience of humour, can lower cortisol levels.
Soy-derived phosphatidylserine interacts with cortisol; the correct dose, however, is
unclear.
Black tea may hasten recovery from a high-cortisol condition.
For circulation only among the Piramal LDPOC team members
9 QDx Instacheck training: Cortisol, Ferritin & PCT
Regular dancing has been shown to lead to significant decreases in salivary cortisol
concentrations.
Factors generally increasing cortisol levels
Caffeine may increase cortisol levels.
Sleep deprivation
Intense (high VO2 max) or prolonged physical exercise stimulates cortisol release to
increase gluconeogenesis and maintain blood glucose. Proper nutrition and high-level
conditioning can help stabilize cortisol release.
The Val/Val variation of the BDNF gene in men, and the Val/Met variation in
women, are associated with increased salivary cortisol in a stressful situation.
Hypoestrogenism and melatonin supplementation increase cortisol levels in
postmenopausal women.
Burnout is associated with higher cortisol levels.
Severe trauma or stressful events can elevate cortisol levels in the blood for prolonged
periods.
Subcutaneous adipose tissue regenerates cortisol from cortisone.
Anorexia nervosa may be associated with increased cortisol levels.
The serotonin receptor gene 5HTR2C is associated with increased cortisol production
in men.
Commuting increases cortisol levels relative to the length of the trip, its predictability
and the amount of effort involved.
Stimuli associated with sexual intercourse can increase cortisol levels in gilts (a young
female pig that has not produced her first litter).
Severe calorie restriction causes elevated baseline levels of cortisol.
Disorders of cortisol production
Hypercortisolism: Excessive levels of cortisol in the blood. (See Cushing's
syndrome.)
Hypocortisolism (adrenal insufficiency): Insufficient levels of cortisol in the blood.
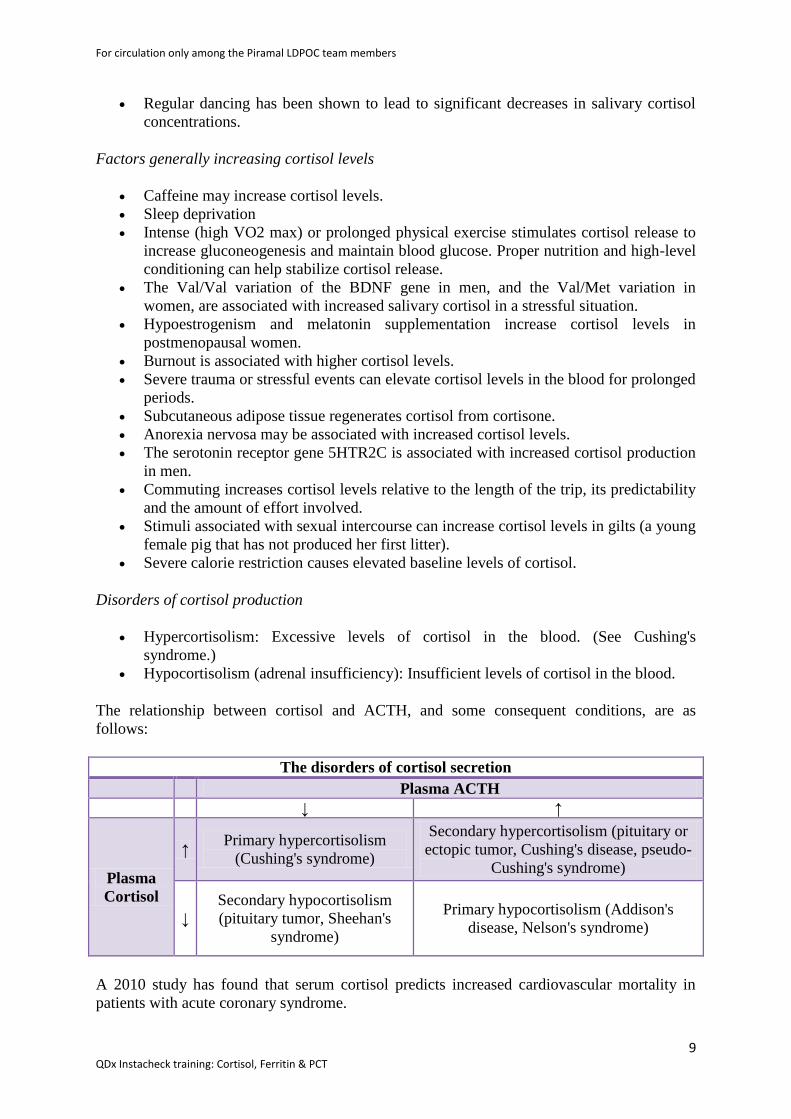
The relationship between cortisol and ACTH, and some consequent conditions, are as
follows:
The disorders of cortisol secretion
Plasma ACTH
↓ ↑
Plasma
Cortisol
↑ Primary hypercortisolism
(Cushing's syndrome)
Secondary hypercortisolism (pituitary or
ectopic tumor, Cushing's disease, pseudo-
Cushing's syndrome)
↓
Secondary hypocortisolism
(pituitary tumor, Sheehan's
syndrome)
Primary hypocortisolism (Addison's
disease, Nelson's syndrome)
A 2010 study has found that serum cortisol predicts increased cardiovascular mortality in
patients with acute coronary syndrome.
For circulation only among the Piramal LDPOC team members
10 QDx Instacheck training: Cortisol, Ferritin & PCT
Ferritin
What is Ferritin?
Ferritin is a ubiquitous intracellular protein that stores iron and releases it in a controlled
fashion. The amount of ferritin stored reflects the amount of iron stored. The protein is
produced by almost all living organisms, including algae, bacteria, higher plants, and
animals. In humans, it acts as a buffer against iron deficiency and iron overload.
Ferritin is a globular protein complex consisting of 24 protein subunits and is the primary
intracellular iron-storage protein in both prokaryotes and eukaryotes, keeping iron in a
soluble and non-toxic form. Ferritin that is not combined with iron is called apoferritin.
Clinical significance
Serum ferritin levels are measured in medical laboratories as part of the iron studies workup
for anemia and for restless legs syndrome. The ferritin levels measured usually have a direct
correlation with the total amount of iron stored in the body. However, ferritin levels may be
artificially high in cases of anemia of chronic disease where ferritin is elevated in its capacity
as an acute phase protein and not as a marker for iron overload.
Normal Ranges
A normal ferritin blood level, referred to as the reference interval is determined by many
testing laboratories. The ranges for ferritin can vary between laboratories but are usually
between 30–300 ng/mL (=μg/L) for males, and 15–200 ng/mL (=μg/L) for females.
Low
If the ferritin level is low, there is a risk for lack of iron, which could lead to anemia.
In the setting of anemia, low serum ferritin is the most specific lab test for iron deficiency
anemia.[19]
However it is less sensitive, since its levels are increased in the blood by infection
or any type of chronic inflammation,[20]
and these conditions may convert what would
otherwise be a low level of ferritin from lack of iron, into a value in the normal range. For
this reason, low ferritin levels carry more information than those in the normal range.
Low ferritin may also indicate hypothyroidism, vitamin C deficiency or celiac disease
In adolescents and teenagers, ferritin levels that are low but yet above those causing anemia
and sickness (12 to 50 ng/mL) may cause symptoms of restless legs syndrome.
A falsely low blood ferritin (equivalent to a false positive test) is very uncommon, but can
result from a hook effect of the measuring tools in extreme cases.
Vegetarianism may contribute to low levels of serum ferritin, with one study finding 40% of
vegetarians tested with low serum ferritin levels.
For circulation only among the Piramal LDPOC team members
11 QDx Instacheck training: Cortisol, Ferritin & PCT
Elevated
If ferritin is high, there is iron in excess or else there is an acute inflammatory reaction in
which ferritin is mobilized without iron excess. For example, ferritins may be high in
infection without signalling body iron overload.
Ferritin is also used as a marker for iron overload disorders, such as hemochromatosis or
hemosiderosis. Adult-onset Still's disease, some porphyrias, and hemophagocytic
lymphohistiocytosis/macrophage activation syndrome are diseases in which the ferritin level
may be abnormally raised.
As ferritin is also an acute-phase reactant, it is often elevated in the course of disease. A
normal C-reactive protein can be used to exclude elevated ferritin caused by acute phase
reactions.
According to a study of anorexia nervosa patients, ferritin can be elevated during periods of
acute malnourishment, perhaps due to iron going into storage as intravascular volume and
thus the number of red blood cells falls.
When is the Ferritin test done?
The ferritin test is ordered to assess a person's iron stores in the body. The test is sometimes
ordered along with an iron test and a TIBC (Total Iron Binding Capacity) to detect the
presence and evaluate the severity of an iron deficiency or overload.
The ferritin test may be ordered, along with other iron tests, when a routine CBC shows that a
person's hemoglobin and hematocrit are low and their red blood cells are smaller and paler
than normal (microcytic and hypochromic), suggesting iron deficiency anemia even though
other clinical symptoms have not yet developed.
Early iron deficiency usually causes no physical effects at all. If a person is otherwise
healthy, symptoms seldom appear before the hemoglobin in the blood drops below a certain
level (10 g per deciliter). However, as the iron-deficiency progresses, symptoms may begin to
develop and a doctor may order ferritin as wells as other iron-related tests. The most common
symptoms of iron deficiency anemia include:
Chronic fatigue/tiredness
Weakness
Dizziness
Headaches
As iron stores continue to be depleted, there may be shortness of breath, ringing in the ears
(tinnitus), drowsiness, and irritability. If the anemia progresses in severity, chest pain,
headaches, leg pains, shock, and even heart failure may occur. Children may develop learning
(cognitive) disabilities. Besides the general symptoms of anemia, there are certain symptoms
that are characteristic of iron deficiency. These include pica (cravings for specific substances,
such as licorice, chalk, dirt, or clay), a burning sensation in the tongue or a smooth tongue,
sores at the corners of the mouth, and spoon-shaped finger- and toe-nails.
For circulation only among the Piramal LDPOC team members
12 QDx Instacheck training: Cortisol, Ferritin & PCT
A ferritin level may also be ordered when iron overload is suspected. Symptoms of iron
overload will vary from person to person and tend to worsen over time. They are due to iron
accumulation in the blood and tissues. Symptoms may include:
Joint pain
Fatigue, weakness
Lack of energy
Abdominal pain
Loss of sex drive
Heart problems
To confirm the presence of iron overload, other iron tests (iron, TIBC) and a genetic test for
hereditary hemochromatosis may be ordered as well.
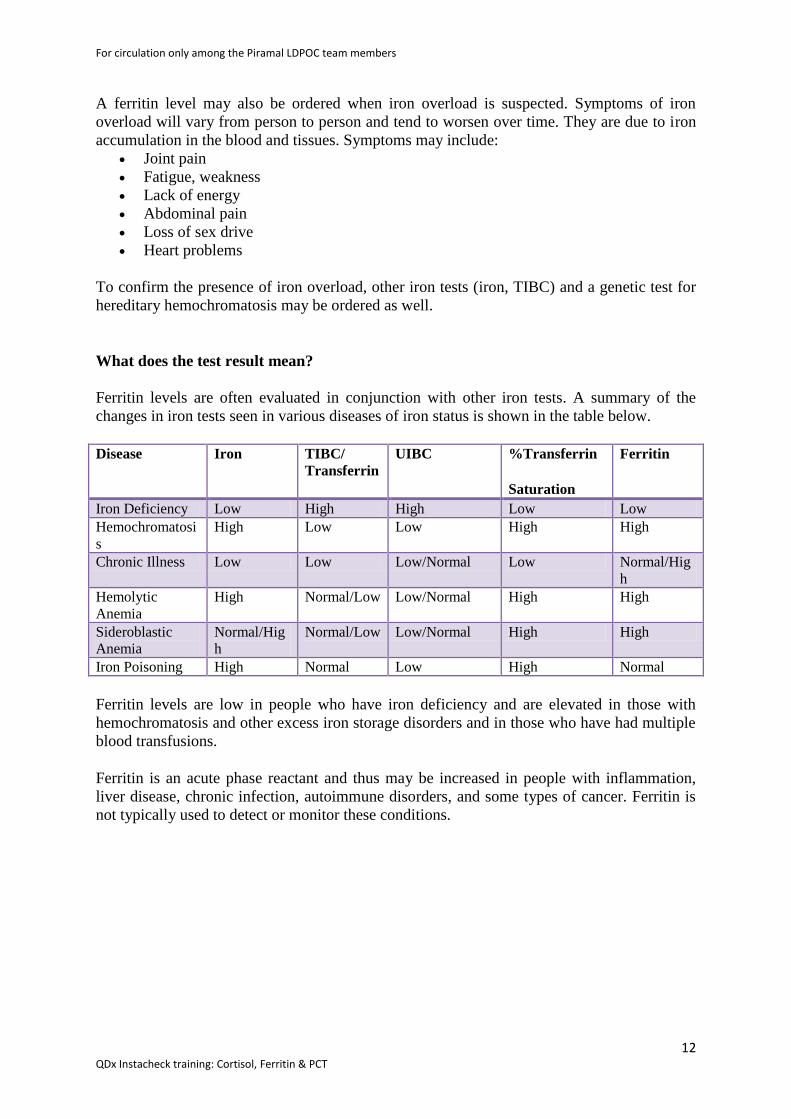
What does the test result mean?
Ferritin levels are often evaluated in conjunction with other iron tests. A summary of the
changes in iron tests seen in various diseases of iron status is shown in the table below.
Disease Iron TIBC/
Transferrin
UIBC %Transferrin
Saturation
Ferritin
Iron Deficiency Low High High Low Low
Hemochromatosi
s
High Low Low High High
Chronic Illness Low Low Low/Normal Low Normal/Hig
h
Hemolytic
Anemia
High Normal/Low Low/Normal High High
Sideroblastic
Anemia
Normal/Hig
h
Normal/Low Low/Normal High High
Iron Poisoning High Normal Low High Normal
Ferritin levels are low in people who have iron deficiency and are elevated in those with
hemochromatosis and other excess iron storage disorders and in those who have had multiple
blood transfusions.
Ferritin is an acute phase reactant and thus may be increased in people with inflammation,
liver disease, chronic infection, autoimmune disorders, and some types of cancer. Ferritin is
not typically used to detect or monitor these conditions.





























