Embed Size (px)
Citation preview
History of Orthodontics

History of OrthodonticsA glance at an exciting path, the oldest specialty
of dentistry has treaded so far…
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTD
New Delhi • London • Philadelphia • Panama
®
Basavaraj Subhashchandra PhulariBDS MDS FAGE FRSH
FormerlyFaculty, Department of Orthodontics and Dentofacial OrthopedicsMauras College of Dentistry, Hospital and Oral Research Institute
Republic of Mauritius
Foreword
US Krishna Nayak
Headquarters
Jaypee Brothers Medical Publishers (P) Ltd
4838/24, Ansari Road, Daryaganj
New Delhi 110 002, India
Phone: +91-11-43574357
Fax: +91-11-43574314
Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
Website: www.jaypeebrothers.com
Website: www.jaypeedigital.com
© 2013, Jaypee Brothers Medical Publishers
All rights reserved. No part of this book may be reproduced in any form or by any means without the prior permission
of the publisher.
Inquiries for bulk sales may be solicited at: [email protected]
This book has been published in good faith that the contents provided by the author contained herein are original, and
is intended for educational purposes only. While every effort is made to ensure accuracy of information, the publisher
and the author specifically disclaim any damage, liability, or loss incurred, directly or indirectly, from the use or
application of any of the contents of this work. If not specifically stated, all figures and tables are courtesy of the author.
Where appropriate, the readers should consult with a specialist or contact the manufacturer of the drug or device.
History of Orthodontics (A glance at an exciting path, the oldest specialty of dentistry has treaded so far…)
First Edition: 2013
ISBN 978-93-5090-471-8
Printed at
®
Overseas Offices
J.P. Medical Ltd.
83, Victoria Street, London
SW1H 0HW (UK)
Phone: +44-2031708910
Fax: +02-03-0086180
Email: [email protected]
Jaypee Brothers Medical Publishers Ltd
The Bourse
111 South Independene Mall East
Suite 835, Philadelphia, PA 19106, USA
Phone: +267-519-9789
Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
Shorakhute, Kathmandu
Nepal
Phone: +00977-9841528578
Email: [email protected]
Jaypee-Highlights Medical Publishers Inc.
City of Knowledge, Bld. 237, Clayton
Panama City, Panama
Phone: +507-301-0496
Fax: +507-301-0499
Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
17/1-B Babar Road, Block-B, Shaymali
Mohammadpur, Dhaka-1207
Bangladesh
Mobile: +08801912003485
Email: [email protected]

Dedicated to
My Dear ParentsSubhashchandra and Shivalingamma Phulari
My BrothersSangamesh BE (USA), Jagadish BE (USA) and Manjunath BE (USA)
My Beloved WifeDr Rashmi GS, Reader (Oral Pathology)
andMy Sons
Yashas and Vrishank

FFFooorrreeewwwooorrrddd
Humanity is passing through the most exciting period in the history of itsexistence, because of rapid technological advancement and increase in theresearch activities, there has been an enormous increase in the informationavailable which has led to better understanding of the respective subjects andareas of specialization.
With the contemporary understanding of orthodontics, it is more apt andimportant for everyone involved in the subject to be aware of how ourforefathers in the subject thought, how the subject evolved in differentcountries, how new concepts evolved providing a trigger to each and everyoneto explore deeper into the subject and make learning more exciting and enjoyable.
Dr Basavaraj Subhashchandra Phulari has made sincere efforts to go intothe depth of each topic providing an exhaustive insight. I am convinced that itwill be a great learning experience for all the readers.
US Krishna Nayak
BDS MDS (Ortho) FFPA FICD FADI FWFO
Dean Academics, AB Shetty Memorial Institute of Dental SciencesKarnataka, India
Past President, Indian Orthodontic SocietyPast President, Indian Dental Association Head Office
Chairman, 8th Asia-Pacific Orthodontic Congress and 47th IOCNew Delhi, India
Chairman, 17th IOS PG Convention-2013Editor, Asia Pacific, HEAL TALK-A Journal of Clinical Dentistry
President Elect, International College of Dentists(India, Sri Lanka and Nepal Section)
Secretary, International College of Continuing Dental Education(India Section).
Immediate Past Chairman, Pierre Fauchard Academy(India Section)

PPPrrreeefffaaaccceee
Knowledge and understanding of the history of a scientific field can enable future practioners of thatfield better to anticipate and respond to the challenges of rapid globalization and be better prepared tomold our future.
Exposure to the history of our specialty helps us think, ask question and explore the concepts andenable us to grasp what the subject is about and how it has evolved over the years.
History of Orthodontics is interesting and same time it is complex. This book is an attempt to glanceand take a note of important milestones in the exciting journey of this fascinating field. It is hoped thatthe book would be useful to all the students of the faculty.
Extensive coverage of important events in the history of orthodontics that shaped what it is today.Separate chapters dedicated to eminent inventors of the field—EH Angle, LF Andrew, James McNamaraand TM Graber.
Evolution of recent advances in orthodontics such as Invisalign and dental lasers are included.Evolution of orthodontic materials, model analysis, cephalometrics and orthodontic appliances areincluded. Exhaustive list of references is given for further reading.
Basavaraj Subhashchandra Phulari

AAAccckkknnnooowwwllleeedddgggmmmeeennntttsss
Writing history of the oldest specialty of dentistry and as fascinating as orthodontics at that, was aherculean task. For writing history of any field, even it requires the author/historian to be present atthat specific time and place of the event that has taken place, which is practically not possible.
An event of today becomes history tomorrow. As we unravel and cherish the history of yester-years, a new history would be shaping today. In the light of this practicality, I do agree that none of thechapters in the book is directly written by me. I have drawn generously from the existing literatureabout the subject in the form of various books, journal articles, research papers and thesis, etc. In manyof the chapters, literature about a specific event or person/researcher is kept as it appears in itsoriginal literature so as to maintain authenticity and also not to inadvertently twist the history. Manyof the illustrations of the orthodontic appliances and photographs of eminent researchers used in thisbook are facsimiles of the pictures that appear in the existing literature about the subject.
I hereby humbly acknowledge all the authors of various orthodontic books, articles, thesis, seminars, etc.,whose works inspired the birth of this project. The list of the literature used for the preparation of this project isgiven at the end of the book under the heading of suggested reading.
I also gratefully acknowledge all the professors, teachers and postgraduate students of the faculty fromvarious dental institutions in India and abroad who have contributed directly or indirectly to this exhaustivepiece of work.
My special thanks to my beloved wife, Dr Rashmi GS, Reader and Postgraduate Guide,Department of Oral Pathology, Manubhai Patel Dental College and Hospital and Oral ResearchInstitute, Vadodara, Gujarat, India, for her valuable critical comments during the preparation ofthe manuscript, editorial assistance and proofreading.
I take this wonderful opportunity to thank Dr Rajendrasinh Rathore, Chairman of Manubhai PatelDental College and Hospital and Oral Research Institute, Vadodara, for his inspirational supportduring this endeavor and throughout my career. I also thank Dr Yashraj Rathore, Trustee, ManubhaiPatel Dental College and Hospital and Oral Research Institute, Vadodara, for encouraging me duringthis project.
I owe a debt of gratitude to Professor (Dr) US Krishna Nayak, Dean Academics, AB Shetty MemorialInstitute of Dental Sciences, Mangalore, Karnataka, India, for his continuous encouragement in all myendeavors and for providing foreword to this book.
I am indebted to Dr Anil Shah for all the help and encouragement I have received from him duringthe formation of the Chapter 7—History of Dental Lasers and their Applications in Orthodontics inthe book.
I extend my heartfelt gratitude to Dr Padmaja Ankit Arora for helping me with important referencesthat were required for writing the chapters on TM Graber, James McNamara and Invisalign.
My heartfelt gratitude goes to Dr Poorya Naik, Assistant Professor, College of Dental Sciences,Davengere, Karnataka, Dr Ramesh GC, Assistant Professor, Sharavati Dental College, Shimoga,Karnataka, and Dr Sujay J, Assistant Professor, SJM Dental College, Chitradurga, Karnataka, whohave helped immensely in this endeavor. Exceptional efforts made the production of this book possible.
I extend my special thanks to Dr Hina Desai for comments and suggestions regarding chapter onDr TM Graber’s Contribution to Orthodontics.
I will be failing in my duty if I do not mention the affection and support I have received fromDr Syed Zakaullah, Chairman, Al Badar Dental College and Hospital, Gulbarga, Karnataka, who hasalways provided that moral boost much needed during compilation of this book.
My heartfelt gratitude goes to Shri Jitendar P Vij (Group Chairman), Mr Ankit Vij (ManagingDirector) and Mr Tarun Duneja (Director-Publishing) of M/s Jaypee Brothers Medical Publishers (P)Ltd, New Delhi, India, whose exceptional efforts made the production of this book possible. I gratefullyacknowledge the contributions made by the talented professional staff at M/s Jaypee Brothers MedicalPublishers; in particular, I would like to thank Mr Venugopal V, Mr KK Raman and Mr Rajesh Sharma,for their untiring efforts in ensuring that every minute detail is taken care of.
I am indebted to my dear parents for all their love and sacrifices that have made me what I am.I thank my dear sons Yashas and Vrishank for being the constant source of inspiration to set andreach new goals in life.
Most of all, I thank God for all the kindness and mercy showered upon me.
xii History of Orthodontics

CCCooonnnttteeennntttsss
1. History of Dentistry 1
Ancient Dentistry 2Dentistry During the Middle Ages 6Dentistry in the Sixteenth and Seventeenth Centuries 7Dentistry in the Eighteenth Century 10
2. Introduction to Orthodontics 14
Definition of Orthodontics 14What is Malocclusion? 15Aims of Orthodontic Treatment 15Branches of Orthodontics 16Orthodontic Appliances 17Timing of Orthodontic Intervention 18Scope of Orthodontics 18Benefits of Orthodontic Treatment 19
3. History of Orthodontics from Ancient Civilization to Twentieth Century 20
Ancient Civilization 20Middle Ages through Seventeenth Century 21Eighteenth Century 22Nineteenth Century 23Twentieth Century 24
4. History of Orthodontics in United States of America 28
Norman Williams Kingsley (1829–1913) 31
5. History of Orthodontics in Great Britain 34
The British Society for the Study of Orthodontics 37
6. History of Orthodontics in Greece and Rome 44
Middle Ages (Fifth to Fifteenth Centuries) to the Eighteenth Century 44European Pioneers of the Early Nineteenth Century 45
7. History of Dental Lasers and their Applications in Orthodontics 47
All Laser Devices 47Properties of Laser Beam 48Focused Versus Defocused Beam 48Types of Laser 49Lasers and their Dental Applications 50Current Clinical Use of Dental Lasers 51Laser Use in Dentistry 51Laser Classification 52Applications of Lasers in Orthodontics 53Laser Safety 58Precautionary Measures 58
xiv History of Orthodontics
8. Angle’s Contribution to the Faculty of Orthodontics 59
Edward Hartley Angle—Dental Graduation 60Angle‘s Dental Practice at Towanda 60Edward Hartley Angle’s Professional Teaching Career 61Edward Hartley Angle‘s School of Orthodontics 65Appliance Contribution by Edward H Angle 66Angle’s Orthodontic Material Invention 69Case-Angle Controversy 70Criticisms 71
9. Dr TM Graber’s Contribution to Orthodontics 76
Thomas M Graber (1917–2007) 76TM Graber’s Contributions 77Graber’s Other Contributions to Orthodontics 85
10. James McNamara’s Contribution to Orthodontics 88
James McNamara Analysis 88Relating the Maxilla to the Cranial Base 89Relating the Mandible to the Maxilla (Midface) 89Relating the Mandible to the Cranial Base 91Dentition Analysis 91Airway Analysis 92Studies on Functional Appliances 93Studies on Rapid Maxillary Expansion 95Studies on TMJ 96
11. Andrews’ Straight Wire Appliance 98
Why “Straight Wire”? 100Variable Bracket Sitting Procedures: Lawrence F Andrew’s Remedy 102Straight Wire Appliance Brackets for Different Clinical Situations 102Straight Wire Appliance (SWA) 103
12. Evolution of Orthodontic Appliances 106
Brackets and Bands 107Archwires 114Properties of Archwire 117Auxiliaries 119History of Orthodontic Materials 120
13. History of Model Analysis 122
Carey’s Analysis 123Pont’s Index 123Linderharth Index 124Korkhaus’ Analysis 124Howe’s Analysis—1954 124Bolton’s Analysis 125Cast Analysis: Symmetry and Space 126Alignment (Crowding), Space Analysis 126Arvey Peck, Sheldon Peck—1972 127Huckaba’s Analysis 127Hixon and Old Father Method—1958 128
xvContents
Marvin M Tanaka, Lystle E Johnston in 1974 128Nance Analysis 129Total Space Analysis—1978 130Wylie 131Kesling Model Analysis 131Martinek Analysis 131Suwannee Luppanapornlarp 1313D Model Analysis 132
14. History of Cephalometrics 133
History Prior to the Advent of Radiography 134Cephalometric Radiography 137Holly B Broadbent’s Contribution 138Other Important Contributions 139Cephalometric Analysis 139Evolution of Cephalometrics 140Patient Orientation 140X-ray Source Position 140Film Position and Enlargement 140Posteroanterior (Frontal) Cephalometry 141Steiner’s Analysis: Cecil C Steiner (1896–1989) 143
15. History of Extraction in Orthodontics 145
Arch-Length Analyses 146Second Premolar Extraction 147Evolution of the Philosophy of Extraction in Conjunction with Orthodontic Therapy 148Need for Extraction 150Choice of Teeth for Extraction 150Serial Extraction 150Historical Perspective 151Tweed’s Method (1966) 152
16. History of Expansion Appliances 154
Wescott’s Expansion Device 154Angell’s Palatal Expansion Device 154Fixed Rapid Maxillary Expansion Appliances 156
17. History of Removable Orthodontic Appliances 160
Development of Removable Orthodontic Appliances 161Components of Removable Orthodontic Appliance 162
18. History of Fixed Orthodontic Appliances 167
E-Arch Appliance 171Pin and Tube Appliance 171Ribbon Arch Appliance 172Edgewise Appliance 172What was Orthodontics before Angle System? 173Evolution and Development of the Edgewise Appliance 173Evolution of Bracket 174Evolution of Edgewise Buccal Tubes 174The Concept of the Ideal Arch 175The Ideal Arch Wire 176
xvi History of Orthodontics
Advantages and Disadvantages of Edgewise Appliance 178Building Treatment into the Edgewise Appliance 178Begg Appliance 179Straight Wire Appliance 180Andrews Six Keys to Optimal Occlusion 180Limitations of Straight Wire Appliance (SWA) 182Lingual Technique 183
19. History of Myofunctional Orthodontic Appliances 186
Activator 187Frankel Appliance 189Bionator 189Class III or Reverse Bionator 190Oral Screen (Vestibular Screen) 190Herbst Appliance 190Twin-Block Appliance 190The Double Plate 191The Tooth Positioner 191
20. History of Surgical Orthodontics 193
Pioneers 195Mandibular Procedures 196
21. History of Cleft Lip and Cleft Palate 197
Demographic Data 199Embryological Aspects 200Classification 200Etiology of Cleft Lip and Palate 201Clinical Features 202Cleft Lip and Palate Associated Problems 203
22. History of Malocclusion Indices 205
Index of Orthodontic Treatment Needs (IOTN) 218Peer Assessment Rating 219Index of Complexity, Outcome and Need 220Dental Aesthetic Index 221
23. History of Interproximal Enamel Reduction in Orthodontics 223
History of Interproximal Enamel Reduction 223Indications 224Contraindications 225
24. History of Invisalign 226
Historical Perspective of Invisalign 227What Exactly the Invisalign Means? 228Developing the Invisalign Brand 228Philosophy of Invisalign 229Fabrication of Invisalign 229Principle of Stereophotolithography 231Summary of the Invisalign Technique 231Indications of Invisalign 232Advantages of Invisalign 232
xviiContents
Disadvantages of Invisalign 232Limitations of Invisalign 232Procedure of Treatment with the Invisalign 232Benefits of Invisalign 233Care of Teeth with Invisalign 233Study 1 233Outcome Assessment of Invisalign and Traditional Orthodontic Treatment
Compared with the American Board of Orthodontics Objective Grading System 233Study 2 234How Well does Invisalign Work? A Prospective Clinical Study Evaluating the Efficacy of
Tooth Movement with Invisalign 234Study 3 235Retaining Alignment Changes with Invisalign 235Study 4 235Structural Conformation and Leaching from In Vitro Aged and Retrieved Invisalign
Appliances 235Study 5 235Cytotoxicity and Estrogenicity of Invisalign Appliances 235Study 6 236Color Fading of the Blue Compliance Indicator Encapsulated in Removable Clear
Invisalign Teen Aligners 236Study 7 236A Comparison of Treatment Impacts between Invisalign Aligner and Fixed Appliance
Therapy during the First Week of Treatment 236Other Studies 237Scientific Studies 237
25. History of Molar Distalization in Orthodontics 238
History of Molar Distalization 238Indications for Molar Distalization 239Contraindications of Molar Distalization 239An Ideal Intraoral Molar Distalization Appliance 240Mechanism of Action of Distalizing Appliances 240Pendulum Appliance 240Pend-X Appliance 241M-Pendulum Appliance 241Pendulum F Appliance 243Jones Jig 243Intermaxillary Class II Malocclusion Correction Appliances 243Vertical Holding Appliance 243Removable Molar Distalization Splint 244Symmetric Distalization with a TMA Transpalatal Arch 244Tube Plates for Distalization of Molars 244Cetlin Appliance 245Anchorage Need 245Extraoral Force 245The Force Applied 245The Lokar Appliance 245K-Loop Molar Distalizer 246The Distal Jet Appliance 246The Crozat Appliance 247
xviii History of Orthodontics
Molar Distalization by Magnets 247The Magnets 248The Klapper Superspring 248Herbst Appliance 248The Mandibular Anterior Repositioning Appliance (MARA) 249Saif Springs 249The ‘Fastback’ Appliance for Molar Distalization 249Features of Fast Back Appliance 250
Suggested Reading 251
Index 259
1HHHiiissstttooorrryyy ooofff DDDeeennntttiiissstttrrryyy
These seems to be little doubt that dentistry insome form has been practiced from the mostancient times, there seems to be but little doubt,since considerable fragmentary evidence stillexists as to the general methods used by theancients. If we stop to enquire who first extractedteeth, made plates or filled carious cavities weshall find that all such information is shroudedin the mists of antiquity along with the historyof the pyramids and other relics of earlycivilization.
Oral disease has been a problem for humanssince the beginning of time. Skulls of the Cro-Magnon people, who inhabited the earth 25,000
years ago, show evidence of tooth decay. Theearliest recorded reference to oral disease is froma Sumerian text (circa 5,000 BC) that describes“tooth worms” as a cause of dental decay.
Dentistry, as a part of the medical art, was firstpracticed by the priests as a sort of religious rite,but later material remedies were added to aid ineffecting cures and help to maintain the prestigeof the priesthood. Later the laity becameinterested, and surgery, including dentistry, wasfor a long period practiced by barbers andtravelling charlatans, who resorted to music andvarious other forms of entertainment to attract the
� Ancient Dentistry
– I-Em-Hetep
– Saracens
– Prof George Ebers
– Hwang-ti
– Ya-tong
– Aesculapius
– Celius Aurelianus
– Hippocrates
– Galen
– The Etruscans
– Dr Guerini
– Saint Apollonia
– Marshall H Saville
� Dentistry during the Middle
Ages
– Abulcasis
– Garriopontus
– John Gaddesden
– Guy de Chauliac
– Giovanni Plateario
� Dentistry in the Sixteenth and
Seventeenth Centuries
– Walter Herman Ryff
– Andreas Vesalius
– Gabrielus Fallopius
– Bartholomeus Eustachius
– Ambro’ise Pare
– Johann Stephan Strobelberger
– Nathaniel Highmore
– William Cowper
– James Drake
– Wilhelm Fabry
– Antoni Van Leeuwenhoek
– Matthias Gottfried Purmann
� Dentistry in the Eighteenth
Century
– Lorenz Heister
– Johann Adolph Goritz
– Pierre Fauchard
– Bourdet
– Thomas Berdmore
– John Hunter
– Robert Bunon

2 History of Orthodontics
Fig. 1.1: GV Black
people. Finally, a few of the more far-seeingmedical and dental practitioners becameconvinced of the necessity for better educatedmen to practice this important speciality, andthus dentistry gradually rose from about thebeginning of the sixteenth century from adesultory trade or calling to the dignity of alearned profession.
However, not until the latter half of thenineteenth century and the first part of thetwentieth century did it really make rapidprogress. It is a notable fact that many worthydentists of modern times began their career in thelaboratory or office of older practitioners. Later,however, they added to this training suchscientific knowledge as was obtainable at the timeand reached an honorable position amongprofessional men. Not until 1840 was a dentalcollege organized to teach systematically thetheory and practice of dental surgery. This, theBaltimore College of Dental Surgery, was charteredFebruary 1, 1840, opened in that year, and is stillin existence.
Perhaps it is within the last thirty-two yearsthat the greatest progress has been made by thisyoung profession, during which time Dr Black(Fig. 1.1) introduced scientific cavity preparationand a balanced alloy, Drs. Callahan, Rhein, Bestet al gave us scientific root-canal work, and DrTaggart perfected and introduced the gold inlay,while silicate fillings have come to occupy animportant place in operative work, and theRoentgen ray has become an indispensable aid indiagnosing pathological conditions. In 1910 Dr.William Hunter, of London, contributed hiscelebrated paper on the “Relation between OralInfection and Systemic Disease,” and woke thedental profession to its responsibilities. Oralprophylaxis has progressed to a point whereunclean mouths are no longer tolerated, and theprosthesis has come to our aid with removablebridge-work and more scientific methods ofdenture-making.
ANCIENT DENTISTRY
In the words of a distinguished writer, “To knowthe history of a profession is to know the professionitself.” It has also been said, “There is nothing newunder the sun;” but be that as it may, it is a fact that
much that is considered new in medicine, dentistryand surgery was known to Hippocrates, Fauchard,Galen and Pare. Sacerdotal Medicine, which waspracticed in remote times by the priesthood, wasmostly derived from the false notion prevalentamong primitive peoples that the afflicted personhad been stricken by the wrath of some divinity.The priests were always ready to treat such cases,as they were well paid, and if the person recovered,their prestige was considerably increased, while ifthe patient did not improve it was because thesupposed offender was not worthy of receiving thedesired pardon.
The first physician of record was I-Em-Hetep(“He who cometh in peace”), who lived in theregion of King Tosher of the Third Dynasty ofEgypt, about 4000 BC. He was evidently a man ofgreat prominence, since the Egyptians constructeda pyramid at Sakkra in his honor, and as manystatuary likenesses of him have been found, it isevident that after his death he was worshippedas the Egyptian God of Medicine. That the earlyEgyptian surgeons had to use great skill in thetreatment of disease is proven by the oldest bookin existence, called The Instruction of Path- Hetep.
Ancient Egypt was the seat of culture andlearning; many students were drawn there fromother lands in search of knowledge, and we aretold that during the time of Herod- Otus, about500 BC, dentistry was practiced as a specialty, so

3History of Dentistry
that “Egypt is quite full of doctors: those for theeyes, those for the head, and some for the teeth,others for the belly or for occult maladies.”
The Saracens invaded Egypt in the seventhcentury, and in 642 A.D., shamefully destroyedthe great library at Alexandria. It is probable thatmuch valuable literature pertaining to earlymedicine and dentistry was thus lost, amongothers the writings of Herophilus and Erasistratus,who, about 300 B.C., were pioneers in dissectionnot only of cadavers but of living men condemnedto death by the kings of Egypt.
Dental art among the ancient Egyptians isdescribed at some length in the papyrus of Ebers aname derived from the material on which it iswritten (papyrus, a form of ancient parchment, orpaper), and the discoverer, Prof George Ebers whofound it at Thebes in 1872. This work, which datesfrom 3500 to 1500 BC, gives many remedies fortoothache and the so-called “Benut blisters in theteeth.” These remedies consisted of dough, honey,oil, fennel seeds, incense, onions and similaringredients used in various combinations, to bemade into a plaster and applied to the achingtooth. One prescription consists of the following:
It is evident that dentistry in some of its cruderforms must have come into being as soon as manbegan to experience trouble with his teeth. Theteeth are likewise largely relied upon to furnishdiagnostic evidence in determining whetherprehistoric skulls found in excavating are ofhuman or animal origin. Prehistoric teeth do not,as a rule, show evidence of caries, and if it bepresent it is said to be an evidence of considerableage, though it is difficult to understand the reasonfor this assumption, since caries is usually mostprevalent among children. Signs of abrasion arequite common, owing to the food habits and longlife of the subject.
The oldest written account of a dentaloperation, other than extraction, is found in astatement by Archigenes, of Rome, who advocatedthe repining of a tooth which ached without therebeing evidence of caries, his idea being that thepain was caused by morbid material in the interiorof the tooth, which by this means could beevacuated.
Among the ancient Hebrews neither the Biblenor the Talmud makes any mention of dentaloperations, though the teeth and their beautiesare often extolled. “An eye for an eye and a tooth
for a tooth” was a part of the law of the land, as,also, “If a man smite out one of his servant’s teethhe shall let him go free.”
The Chinese boast a very ancient civilization,and it is not unlikely that dentistry in some of itscruder forms was known to them at a very earlyperiod in the world’s history. The Chinese “Fatherof Medicine,” was Hwang-ti, who lived about 2700BC.
The celebrated medical works of China referto toothache, which is called “Ya-tong,” anddescribe nine varieties of this malady, and inaddition there to seven distinct diseases of thegums. Puncturing the gums as well as distantparts of the body for the relief of toothache andabscesses was practiced, this being, perhaps, oneof the oldest forms of dental or oral surgery. Thesame method of treatment, known as acupuncture,was applied to many other diseases as well andthe Chinese doctors chose their points of electionin a very scientific and learned manner, havingaltogether three hundred and eighty-eight sitesfor puncturing, twenty-six of which were for therelief of toothache. For this purpose they used gold,silver or steel needles and cauterized the siteafterward with a cone of moxa, a sort of slow-burning vegetable wool applied through a hole ina coin. The moxa is compact and burns slowly,drawing up the epidermis into a blister withoutviolence or excessive heat.
According to Dabry, the Chinese believed therewere worms in the teeth, and among the remediesused therefore arsenic is said to have been madeinto pills, and one placed near the aching tooth orinto the ear on the opposite side from the achingorgan, whereupon the pain would positivelycease. Another favorite prescription used by theChinese read as follows: “Roast a bit of garlic andcrush it between the teeth; mix with choppedhorseradish seeds or saltpeter; make into a pastewith human milk; form pills and introduce oneinto the nostril on the opposite side to where thepain is felt.”
According to the Greeks, Aesculapius, the Godof Medicine, is supposed to have been the son ofApollo. Cicero mentions three deities of this name,the third of which was said to be the son ofArsippus, who was the first to teach tooth-drawingand blood-letting. The instrument used for tooth-drawing is supposed to have been the“odontagogon” of lead mentioned by Celius

4 History of Orthodontics
Aurelianus and exhibited in the temple of Apolloat Delphi, sculapius, who was worshipped by theGreeks as one of their many Gods, was said to havehealed the sick and to have raised the dead as well.As time elapsed there were reputed to be not onlyone, or, as related by Cicero, three sculapii, buttradition gave rise to many Gods of this name towhom numerous temples known as “Asklepeia”were erected, among which was the famous templeof Cos, where Hippocrates gained most of hisknowledge of medicine. The priests or followers ofEsculapius were known as “Asklepiadi.”
To Hippocrates is accorded the honorable titleof Father of Medicine, and even in those early daysthe “oath of Hippocrates” was a solemnobligation to be taken by all who undertook thestudy or practice of medicine. Hippocrates wasborn on the island of Cos about 460 BC and firststudied medicine under his father, but laterdevoted his attention to the medical books in thetemple of Cos. Hippocrates wrote much in regardto dental maladies and their remedial measures,among which were considered extraction andcauterization. He was the inventor of certain crudedental forceps and other dental instruments. Hepracticed the extraction of loose teeth andcauterization of those that ached but were notloose. He also recognized that the first teeth areformed before birth by the nourishment of the fetusin the womb.
In speaking of fracture of the lower jaw,Hippocrates recommended binding the teeth nextto the lesion together. He distinguished betweenthe complete and the incomplete fractures andtreated separately of fractures of the symphysis. Ifthe teeth were loosened he advised bindingseveral together on either side of the fracture untilconsolidation of the bone had taken place, usingfor this purpose either gold wire or linen thread.
At this time lay medicine had begun tosupplant sacerdotal medicine, and healing by thepriests as a religious rite was slowly giving placeto more scientific and rational methods.
Galen, who lived about six hundred years afterHippocrates, was an able writer and commentedon Hippocrates’s work. Galen was a notedanatomist, and although he classified the teethas bones, he said they were unlike other bones.He was the first to recognize nerves (pulps) inthe teeth, and also erroneously believed that the
teeth have something to do with the sense of taste.In his anatomical researches he recognized sevenpairs of cranial nerves and classified thetrigeminal as the third pair. He was also of theopinion that the teeth grow and thus repair thewear on them, basing his opinion on the fact, nodoubt, that a tooth having no opponent becamelonger. In painful Dentition Galen advisedrubbing the gums with the milk of a bitch or thebrains of hare.” He was, in his day, one of themost famous medical men of Rome and theauthor of many works on medicine.
By this time the doctors’ shops were wellsupplied with medicines, bandages and a greatvariety of instruments, showing that the medicalart had made considerable advancement.Dentistry had not yet become a separateprofession, but was practiced by the doctors alongwith medicine and surgery.
The Etruscans, or early Italians inhabiting thatpart of Italy known as Etruria, between the Tiberand Arno, about 1000 to 200 BC, used bridgesmade of gold rings holding ox teeth, for thepurpose of replacing lost dental organs.
Just who these Etruscans or Toshi were, fromwhence they came or what became of them is notdefinitely known, and their language is equallyextinct, no code having been discovered by whichtheir writings can be deciphered.
The Romans have also left us some specimensof bridge-work and other prosthetic appliances,which for the most part are found in tombs or inthe urns containing the ashes of those cremated.It was said to be a custom to remove such piecesfrom the mouth before cremation and afterwardplace them in the urn with the ashes. Accordingto the Law of the Twelve Tables, written in Romeabout 450 BC, it was not unlawful to bury or burncorpses with the gold that was used to bind theteeth together.
At this early period in the world’s history,Rome must have had dentists, though she had asyet no doctors. According to Dr. Guerini andothers a gold crown is now in the museum of PopeJulius, in Rome, which was discovered inexcavating at Satricum, near that city.
This would tend to prove that the Etruscansnot only did bridge-work, but were versed in theart of making crowns also. The appliance foundat Satricum was made of two plates of gold

5History of Dentistry
stamped to represent the labial and lingualsurfaces of the lower central incisor, and werethen soldered together to form the crown of thetooth. It is soldered to a narrow strip of goldwhich is contoured in such manner as to encirclethe neighboring teeth, which act as a support forthe appliance.
Saint Apollonia in the year 300 AD, wascanonized by the Church of Rome, and since thenhas been the patron saint of dentistry. The ninthday of February has been observed by the Churchof Rome in her commemoration. A photograph ofthe painting of this saint was, in 1900, presentedto the Academy of Stomatology of Philadelphia,on behalf of Dr Mary H Stillwell, of Pittsburgh, byDr C N Pierce, together with this historical sketch:
“Longing to obtain the grace of baptism, shemade her way to Saint Leonine, a disciple of St.Anthony of Egypt, and, as he baptized her, hebade her go to Alexandria and preach the faith.So she went forth, and though she was only awoman, young and frail, yet so eloquent were herwords, so fervent her zeal, that she made manyconverts. About this time a tumult had been stirredup in the city against the Christians and the massof the people were enraged at her teaching andcame with bitter complaints to her father, whogave her up to be judged by the governor.
They brought her before the idol temple andbade her worship the graven image. It is reportedthat she made a sign of the cross, and there cameforth from the statue an evil spirit shrieking,‘Apollonia has driven me hence!’ This was morethan could be borne; the people thirsted forvengeance, so they tried by torture to overcomeher constancy. She was bound and one by one herteeth were drawn out, but still she did not flinchor fear, and on her refusal to accede to the demandsof her persecutors and renounce her faith, she wasbrutally clubbed about the head and face, andsubsequently suffered death by fire.
“For a period of nearly fifteen hundred yearsher intercession has been sought for relief from allpain incident to dental diseases, and her relicshave been and are regarded as possessing greatefficacy in the cure of the same.”
Scribonius Largus, writing during the firstcentury of the Christian era, was perhaps the firstauthor to give rise to the belief that worms were
the cause of pain and decay in the teeth. As weshall find later this superstition existedthroughout the Middle Ages, and it was not untilthe early part of the eighteenth century thatFauchard first cast doubt on their existence. As aremedy for these worms, Scribonius Largussuggested that if the seeds of hyoscyamus(henbane) be burned on charcoal and the fumesinhaled they would cause the worms to fall fromthe teeth. It is a noteworthy fact that the seed budsof henbane, when burned, form an ash that muchresembles worms, and as the drug has a narcoticeffect that probably soothed and relieved the pain,it is no wonder that the ignorant populace of thattime readily gave ear to such seemingly plausiblehumbug.
Celius Aurelianus gave an account of theodontagogon of lead found in the temple of Apolloat Delphi, by which it was assumed that teethshould not be extracted unless loose enough to beremoved with a leaden instrument, though somehave contended that this was only a model placedthere, probably by Esculapius, to be reproducedwith an iron instrument by those wishing to copyit, lead being less affected by corrosion, andtherefore more lasting. He also wrote on fracturesand dislocation of the jaw, and described themethods to be used in their reduction.
Celsus gave a prescription for producing sleep inpersons afflicted with toothache. It containedacorns, castoreum, cinnamon, poppy, mandrakeand pepper. When there was a large carioushollow in the tooth to be extracted, Celsusrecommended that it should first be filled eitherwith lint or lead, in order to prevent the tooth frombreaking under the pressure of the instrument. Itis not definitely known that he used fillings as ameans of preserving the teeth or relievingtoothache.
Marshall H Saville, according to an article in theBulletin of the Pan- American Union, reported thefinding of teeth inlaid with gold, turquoise, rockcrystal, red cement and other foreign substancesin skulls of the aborigines who lived in variousparts of North and South America. These teethhad been bored out with some tool and the fillingskillfully placed in the cavity.
This custom was quite common in Mexico,Central America and the province of Esmeraldas,

6 History of Orthodontics
Ecuador. In this latter province he also securedan upper jaw from one of the natives whichcontained not only teeth inlaid with gold, but alsoa right lateral incisor which had beentransplanted to replace a lost central incisor,showing that dentistry had reached a high stageof development as a means of ornamentation atleast. He also discovered in an excavation atCopan a lower jaw with a left lateral incisor thathad been carved from some dark stone andimplanted to take the place of one that had beenlost. In one case several teeth were found boundtogether with gold bands.
There are in the Peabody Museum of HarvardUniversity teeth in which had been placed inlaysof jade, iron pyrites and gold, some of themarranged symmetrically in triangles, also bandedinlays, all of which apparently were used forornamentation (Dental Cosmos, 1916, Iviii, 281).
Among Primitive People, even at the presenttime, some very peculiar customs prevail whichhave, no doubt, been a heritage from ancient times.Most of these people have beautiful strong teethwhich they ornament and embellish in variousways for cosmetic or religious purposes, much tothe detriment of these valuable organs. Thesubstitution of gold teeth for missing ones hasbeen practiced in Java from remote times, andamong the natives in many parts of Asia and thePacific Islands there is prevalent the custom ofdyeing the teeth black. In Sumatra the women filetheir teeth down to the gums or into points, orpartially remove the enamel, so as to be able toapply the dye.
In Japan the married women dye their teethblack in order to distinguish them from the singlewomen, using a dye that is made of urine, ironand a substance called “saki.” It is claimed thatthis dye is very durable and does not wear off formany years. Dr L Ottofy, in an article on “Dentistryin Japan,” says, “The practice of blackening teeth,as a symbol of the marital state, on the part ofwomen is becoming obsolete, yet a number stillcontinue the practice.” Formerly large quantitiesof black artificial porcelain teeth were exportedfrom America to Japan, where artificial plates formen and single women were made with whiteteeth and those for married women with blackteeth. There are on exhibition in the Army MedicalMuseum at Washington, D C, several sets of teethof Japanese origin, carved from wood, that bearout the foregoing statement.
In Eastern India some of the people plane theirteeth down to an even level and dye them red bymasticating areca nuts. It is also said to be acustom in New South Wales for a young man tohave his front teeth knocked out with a stone onreaching the age of virility, this being supposed toenhance his personal appearance. The natives ofthe Hawaiian Islands knock out their front teethas a sacrifice to their god Eatoa.
DENTISTRY DURING THE MIDDLE AGES
Abulcasis (1050–1122), an Arabian author, wholived at Cordova, was one of the most able writersand surgeons of the Middle Ages. He wrote atreatise on medicine, entitled De Chirurgia,consisting of three volumes, the first of which wasdevoted entirely to the subject of cauterization, aform of treatment much practiced at that time. Hismethod of performing this operation was to inserta red-hot cautery through a tube to protect thesurrounding parts.
He was especially interested at that early datein prophylaxis and devoted special attention tothe tartar on the teeth, illustrating and describingfourteen forms of scrapers or sealers for its removal.He was a very religious and devout man, cautiousin the treatment of his patients and firmly opposedto the needless extraction of teeth. When it becamenecessary to extract, he used one form of forcepsto loosen the tooth and another for its removal.Elevators were used if the forceps failed or thetooth was broken. According to this author,replantation was extensively practiced andartificial substitutes were made of ox bone to replaceteeth that had been lost. He advocated replantingteeth that had been removed by mistake or accident,holding them in place with ligatures of gold orsilver wire until they had again become firm.
Garriopontus, an Arabian writer, in 1045 AD, said:“On the island of Delphi a painful molar tooth,which was extracted by an inexperienced physician,occasioned the death of a philosopher, for themarrow of the tooth, which originates from thebrain, ran down into the lungs and killed thatphilosopher.” For all we know this is the first recordof a death resulting from the extraction of a tooth.
John Gaddesden (1400–1450), an English doctorat Oxford, stated that dried cows’ dung or the fatof a green frog would positively cause teeth to fallout when applied to them, and said, “If an ox,peradventure, chewed a little frog with the grass,

7History of Dentistry
its teeth would fall out on the spot”. He is alsoauthority for the statement that “The brains of ahare rubbed on the gums not only facilitatedentition but will make teeth grow again wherethey have been lost”. All of these remedies wererecommended and employed by many laterwriters, who claimed to have performedmarvellous cures by such absurd treatment.
Such statements as the foregoing seemridiculous to us, as anyone could have easilysatisfied himself of their falsity. The applicationof the cautery or arsenical compounds must havemet with some success, as the latter is known toproduce extensive necrosis.
Guy de Chauliac (1300–1368) was the most notedsurgeon of the Middle Ages. He and others of thatperiod wrote extensively of dental ailments andoperations for their relief by both physicians andbarbers. Guy followed in the foot-steps of theArabians, who had made considerable progressbefore him, and referred explicitly to dentators andtheir instruments, thus beginning the recognitionof dentistry as a specialty of medicine. He advisedthat dental operations be performed for greatersecurity under the supervision of doctors, but hadno criticism to make of dentators. This learneddoctor used camphor, sulphur, myrrh andasafcetida as a filling material for carious cavities,and, like his predecessors, lent belief to thesuperstitious idea of worms in the teeth. It isuncertain whether the worms referred to by himwere particles of decaying food, nerves, larvae ofinsects or the burning henbane seed, as previouslyreferred to, but the accepted belief was that theywere responsible for the pain in odontalgia.Fumigations with seeds of leek, onion andhenbane mixed with goats’ tallow were resortedto in order to drive out the worms, after the mannerfirst described by Scribonius Largus.
Guy de Chauliac also refers to medicines whichsend the patient to sleep, among which aredecoctions of opium, hyoscyamus and lettuce. Anew sponge was soaked in these medicines andthen dried, and when sleep was to be produced itwas wet and applied to the patient’s nostrils. Thisform of anesthesia must have been very effective,for it is related that it was used for surgicaloperations, amputations actually being performedin this manner. To awaken the patient from thisdeep slumber, another sponge was wet with
vinegar and applied, or the juice of the rue fennelwas placed in the patient’s nostrils. This fact is ofgreat importance, as it marks the first step ingeneral anesthesia and antedates Horace Wells’sdiscovery by five hundred years, though it isdoubtful if this old method was ever usedextensively. This author is the first to cast doubton the efficacy of the fat of green frogs for thepurpose of causing the teeth to fall out.Superstition being uppermost in the lives of thepeople in those days, it took considerable courageto contradict the old authorities on such a well-established belief.
In 1308, the barbers and surgeons of Londonwere incorporated into one guild and the name ofbarber-surgeon was used to denote practitionersin all branches of surgery. This arrangement lasteduntil 1745 before it was finally dissolved, afterwhich the barbers were only allowed to extractteeth. This should give one a fair conception ofthe low repute into which surgery had fallenduring that period.
The title of Doctor was first bestowed by theuniversities during the twelfth century and wasused to denote a learned man in any profession.The title of Doctor of Medicine was first bestowedon William Gordenia by the College at Asti, inItaly, in 1329. Whether this title was earned orhonorary is not known. The title of SurgeonDentist was first given to Gillies and several othermen in France in 1622, though the title was notfully established for many years afterward.
Giovanni Plateario (1450–1525), a professor atPisa, was the first dentist to use the sitting posturefor performing operations on the teeth, othersbefore him having used the horizontal position.The prevailing custom was to let the patient lieprone on ground and to hold his head betweenoperator’s knees with a vise-like grip.
DENTISTRY IN THE SIXTEENTH AND
SEVENTEENTH CENTURIES
Dentistry, with the other arts and sciences, madeits most notable advancement as a learnedprofession during the sixteenth century, for it wasabout this time that the world as we know it, madeits first rapid strides forward. The invention ofthe printing press in 1436, the taking ofConstantinople by the Turks in 1453 and thediscovery of America in 1492 all led to much

8 History of Orthodontics
migration of peoples and the dissemination ofknowledge, which constituted the beginning of anew era in which dentistry had its part.
In Germany, dentistry had been practiced formany centuries, as shown by artificial teeth in theurns of those who had been cremated, and at thistime the Germans had made considerableprogress. Here, as elsewhere, medicine was firstpracticed as a religious rite combined withwitchcraft and empirical remedies. As early as1460 Heinrich von Pfolsprundt wrote a book onmedicine and surgery in which he describedwounds and fractures and the mode of theirtreatment. Pains of the teeth and gums weretreated by him by the use of beverages, showinghis lack of skill in that direction.
Walter Herman Ryff (died 1570) wrote the firstbook which treated of dentistry independently ofmedicine in 1548. He is conspicuous for the factthat his book was written in German, a livingtongue, instead of the customary Latin, so that hemay be looked upon as the first who attempted todiffuse useful medical knowledge among thecommon people. One of the most interesting thingsabout his writings is that he is the first author torecognize the relation between diseases of the eyesand teeth, declaring that because of their intimaterelation, neither can be healthy without the otherbeing so too. While this reasoning is clearly wrongin the light of our present knowledge, itnevertheless marks a step in the right direction.According to Ryff the principal causes of dentaldiseases are heat, cold, traumatism and thegathering of humors, and he says “The mostatrocious pain is when an apostema ripens in theroot”.
Andreas Vesalius (1514–1564), who at the earlyage of twenty-five years became famous as ananatomist, was the first who dared to correct theerrors in Galen’s work, and gave a much moreaccurate description of the anatomy of the teeththan that given by Galen. His researches in regardto the teeth are incomplete, since he states that thepermanent teeth grow from the roots of thetemporary teeth. This erroneous conclusion wasdue to the fact, no doubt, that the deciduous teethhave no roots when shed.
Gabrielus Fallopius (1523–1562), a pupil ofVesalius, carried out more fully his investigations
of the development of the teeth and correctedVesalius’ error by showing that the permanentteeth do not grow from the roots of the temporaryteeth, but that they are generated twice over, thefirst time in the uterus. He gave the first account ofthe dental follicle, and likened the teeth in theirformation to the feathers of a bird ( De DentibusLibellus, Venice, 1563).
Bartholomeus Eustachius (died in 1574) wasanother great anatomist of the sixteenth century.After long and patient research he brought muchlight to bear on the macroscopic (gross) anatomyof the teeth, the number and variations of the roots,the alveoli, etc,. and gave a very clear descriptionof the ligaments of the teeth and the means bywhich they are held in the alveolus. He also gavean account of the central cavity of the tooth, andstated that it contains blood- vessels and nerves,and not marrow, as was claimed by someanatomists. He also investigated the embryologyof the teeth and confirmed the claim ofHippocrates that the first teeth are formed in theuterus. Eustachius is the first to deny that the teethgrow during a whole lifetime, as was first claimedby Aristotle. Speaking of dental diseases, thisauthor remarked that dental surgery was in hisdays a most abject calling, notwithstanding itshaving had as its initiator no less a person thanAesculapius, the God of Medicine.
Ambro’ise Pare, born in France (1517–1592), isjustly entitled to the credit of being known as the“Father of Modern Surgery.” As an anatomist heis less accurate than either Vesalius or Eustachius,but as a surgeon he gained great renown, havingbeen successively a barber, surgeon- barber, andfinally, in 1562, chief surgeon to the court. In hisworks this surgeon treated of dental maladies verythoroughly, which fact may be attributed to hishaving first been a barber and consequently atooth-puller. He described fractures of the jaw andthe methods of their reduction with considerablethoroughness, and related some interesting caseswhich he had treated. In one instance a friend ofhis had his jaw broken and three teeth knockedout by a blow from a dagger, whereupon Pare soskillfully treated the injury that all the teeth weresuccessfully replaced and made of use.
The Golden Tooth, in 1593 much was said inGermany of a Silesian child, aged seven years, inwhose mouth a golden tooth had erupted. Great

9History of Dentistry
credence was given to this story and the learneddoctors and philosophers speculated upon thephenomenon without the slightest doubt as to itsgenuineness. Many books and papers werewritten to explain the strange occurrence, and onewriter, Jacob Horst, claimed that on the date of thechild’s birth, that is, December 22, 1585, the Sunwas in conjunction with Saturn in the sign ofAries, and in consequence the nutritive force haddeveloped so much that instead of osseoussubstance, golden matter had been secreted. Itappears that the golden tooth was nothing morethan a crown or lamina of gold let down deep intothe gum, and made by a dentist or jeweler for thepurpose of deception, since a fee was charged forseeing the child. Balthasar Camindus, a doctor ofFrankfort, had noted that the boy had not lenthimself to being examined by the learned, whowere likely to expose the fraud, and further relatesthat a certain nobleman, being denied the privilegeof seeing the tooth, struck a dagger into the boy’smouth and wounded him so badly that a surgeonwas called and the fraud exposed.
In the early part of the seventeenth century thedental art was still in a pitiful state of development,as shown by the literature on the subject, onlyabout twenty publications having appeared inEurope during the preceding century.
Johann Stephan Strobelberger, physician to theImperial Baths at Carlsbad, published a book in1630 in which he referred to “Gout in the teeth”,which included all of the diseased humors of theteeth that were supposed to fall by drops into thearticular cavities and surrounding parts. In hiswritings we find that many crude and worthlessremedies were still used for toothache, and theinstruments for extraction consisted for the mostpart of the pelican, named from its likeness to thebeak of that bird, and also some very rude forceps.He was one of the first to cast doubt on the valueof fumigations with hyoscyamus seeds to causeworms to fall from the teeth, though he did not inthe least doubt the existence of the wormsthemselves, suggesting oil of vitriol or a decoctionmade of a frog cooked in vinegar to kill theminstead. Among the remedies he suggested forodontalgia is the American tobacco plant(Nicotiana tabacum).
Nathaniel Highmore (1613–1684) (published atreatise on anatomy in 1651, in which for the first
time the maxillary sinus named for him isaccurately described), though its existence hadlong been known. He pointed out for the first timethe anatomical relation between the teeth andantrum, and related a most amusing incident inconnection with perforation of this sinus. A lady,having much pain in her teeth finally had theupper canine tooth extracted, after which therewas an incessant flow of humors (pus) from theantrum. The patient herself wishing to learn thecause thereof passed a silver probe into the cavityits entire length, which produced the effect of itshaving reached the eye. Much amazed shestripped a long feather and passed it into it sogreat a distance that she concluded that it hadreached her brain, not knowing that the feathersimply curled up in the cavity. He was able toallay her fears by informing her of the cavity inthe bone and the opening produced by theextraction of the canine tooth.
William Cowper (1666–1709) was the first topractise opening the antrum by the extraction ofthe first molar. This was toward the end of theseventeenth century, and he seems to be the firstto recognize antral diseases. This was somethinglike 50 years after Highmore had described theantrum.
James Drake, a contemporary of Cowper,operated in the same manner, and it was thisauthor who made known in a book entitledAnthropologia nova, published in 1707, themethod of Cowper, for which reason the above-mentioned proceeding is sometimes called the“Cowper-Drake operation.”
Wilhelm Fabry, better known under the Latinname of Fabricius Hildanus (1560–1634), chiefdoctor to the city of Berne, gave some veryinteresting clinical reports on the relation betweendental affections and tic douloureux, and citedan instance where a lady who had sufferedatrociously for four years with pain in the headwas completely cured by the extraction of fourdecayed teeth. He also gave an account of aninteresting case of rhinoplasty performed by Dr JGriffon, an eminent surgeon of that day, upon ayoung girl of Geneva, whose nose had been cutoff by the Duke of Savoy’s soldiers in a fit of rage.Fabry testifies to the natural appearance of thenose even for twenty years afterward. He stated

10 History of Orthodontics
that Gaspare Tagliacozzi, of the University ofBologna, was the inventor of this operation.
Antoni Van Leeuwenhoek (1632–1723), aDutchman, was the first to make high-poweredmicroscopes with which, in 1678, he madediscovery of the tubular structure of dentine, andin 1683 he discovered microorganisms in tartarscraped from between the teeth. From a perusal ofhis writings and drawings it appears that thesebodies were bacteria rather than animalcules, ashe supposed. Both Carpenter and Beal state thathis work was done with single lenses, as thecompound microscope did not reach a usefulstage until about 1820 to 1830. It is astonishinghow much was accomplished by such primitivemeans. This in all probability represents the firststep in bacteriology, which was only madepossible by the aid of high-powered lenses.
Matthias Gottfried Purmann (1648–1721) has thehonor of being the first writer to make mention ofwax models in connection with prosthetic work.Whether these models were made from molds ornot is a disputed question, but the supposition isthat they were carved to the desired shape andthen passed on to a craftsman who reproducedthem in bone or ivory.
Many other incidents of considerable interestduring the seventeenth century have to be omittedin a history of this character, and considerationwill now be given to the development of theeighteenth century.
DENTISTRY IN THE EIGHTEENTH CENTURY
In 1700, France took the lead in the dental art andhad recognized the importance of dentistry byrequiring prospective practitioners to take anexamination under the edict of 1699 to show theirqualifications before entering the profession. Thereis abundant evidence that the Germans had alsomade considerable progress during the twopreceding Centuries and they have likewise leftus considerable literature upon dental surgery.Dentistry had already begun to flourish as adistinct specialty of medicine, but it remained, aswe shall see later, for Pierre Fauchard to effect thefinal separation.
Lorenz Heister (1683–1758), of Frankfurt-am-Main, published a treatise on dentistry entitledDe Dentium Dolore in 1711, in which he advised
removing the decayed part of a tooth with a file ortoothpick and filling the cavity with white wax,mastic or gold or lead-foil. In this work he gave avery concise description of removable prostheticpieces made of ivory or hippopotamus tusks andmaintained in position simply by their form.Heister also refers to nasal prosthesis, which wasthen carried out by applying noses of wood orsilver, properly painted. There was at this timemuch contention among dentists as to theadvisability of removing caries by the use of thefile, as practised by Heister and others,because ofthe destruction of the enamel of the tooth. We find,however, that this was practised for a long period,and was advocated in a modified form by sucheminent dentists as Drs. Chapin A. Harris andRobert Arthur more than a century later.
Upto the eighteenth century the clumsy pelicanor rude forceps, used to exert lateral force on thetooth, was still in general use, but this wasmodified about this time into what was known asthe key of Garengeot, named after the man whoperfected, though he did not invent, the instrument.According to some writers this instrument had itsorigin in Germany, not in England. It was a mostefficient instrument for extracting teeth and wasin general use for more than a century, havingbeen extensively used in America, and is muchused in France and other European countries atthe present time.
Johann Adolph Goritz, of Regensburg, writing in1725, opposed too many extractions and also theinsertion of prosthetic pieces, because they causedthe loss of the teeth to which they were attached.This was due to their being wired to the naturalteeth, causing great strain on and consequentloosening of the abutments.
Pierre Fauchard (born in Brittany about 1690 anddied in Paris in 1761) was the founder of moderndentistry. He published a work in 1728 entitledLe Chirurgien Dentiste, which marked a newepoch in the history of the dental art. This bookwas highly commended by the leading medicalauthorities of the day. It was translated intoGerman in 1733, and a second revised Frenchedition was issued in 1746, and a third in 1786. Itconsisted of two volumes in duodecimo, with 40full-page plates, 863 pages in all, and treated ofall branches of dentistry as understood andpracticed at that time. According to Fauchard

11History of Dentistry
dentistry was then an important calling, as herefers to the examination which prospectivepractitioners were compelled to undergo even asearly as 1700, and advises that a dentist beincluded in the board of examiners. He expressedhimself in no uncertain terms as to the need of aschool of surgery in which the theory and practiceof dental surgery could be properly taught.
Fauchard lamented that so little was writtenby able dentists who had preceded him, becausethese men guarded their knowledge with secrecylest someone might profit at the author’s expense.
It is a mistake to think that he created the art ofdentistry, but that he placed it on a higher planeby many valuable inventions and by collectingand publishing all of the available knowledge onthe subject, there is no doubt. To show howconcisely he wrote, it may suffice to quote thefollowing account of work that may be done onteeth :
“They may be cleaned; they may be straightened;they may be made shorter; caries may be removedfrom them; they may be cauterized; they may be filledwith lead; they may be separated; they may be placedin proper position; they may be fastened; they may beremoved from the jaw; they may be replaced in thejaw; or they may be taken out to be placed in anotherperson’s mouth; and at last teeth are artificiallyconstructed, and may be placed instead of those thathave been lost. All of these operations demand askillful, steady and trained hand and a completetheory.”
In this work he refers to the popular idea ofworms in the teeth, which idea had existed formore than one thousand years. He admits thepossibility of them, but states that he has neverseen them, and that if they do exist they are notthe cause of caries, but the eggs of insects mayhave entered carious cavities and there hatchedand produced worms.
Although Andry relates seeing very smallworms with a powerful glass, Fauchard states thathe employed the same means but could not seethem. Thus he sets forever at rest this foolishsuperstition in regard to worms in the teeth as acause of dental ailments so long indulged by thepeople of those times. Perhaps it is only as a matterof courtesy toward the many authors whopreceded him that he admits their presence at all.
Fauchard gave a very accurate description ofthe anatomy of the teeth, their structure, position,
origin, growth and anatomical parts as, body, rootand neck. He described accurately the pulp cavityand root canals, and after a most thoroughmacroscopic description, goes into the histologyof the teeth, following the writings of La Hire in1699. Fauchard agrees with the popular idea ofhis day in regard to caries, and states that it mayhave its origin within the tooth as well as without.
From a passage in the fifth chapter ofFauchard’s work one learns that tooth-brusheswere then already in use, but he says that thosemade of horsehair are too rough and frequentlyhave a destructive action upon the teeth. Headvised using small sponges, with which the teethshould be rubbed up and down, inside andoutside, every morning. Before using the spongesthey were to be dipped in tepid water or preferablyaqua vitae, “the better to fortify the gums andrender the teeth firm.”
He was strong in his condemnation of elixirsand cures by magical means so much practised inhis day, and a reference is made to the large andincreasing number of Charlatans of the day,wherein he exclaimed, “There will shortly be moredentists than persons affected with dentaldiseases.” He laments over the poor quality ofwork done by them, relating a case where adeciduous tooth was extracted without roots,whereupon the dentist in an effort to extract theroots removed the permanent tooth just erupting.
Fauchard advised seating the patient in aneasy arm-chair for the purpose of performingdental operations, and condemned the practice ofseating him on the ground or floor and holdinghis head between the operator’s knees, as wascommonly done, as unskillful and unsanitary, andin the case of pregnant women, as capable of doinggreat harm. He practiced opening the tooth forrelieving abscesses by evacuating the pus. Afterthree months he stopped these teeth to preventtheir getting worse, but no mention of root-canalwork is made, though he placed a little cotton-wool in the cavity with oil of cinnamon andallowed it to remain several weeks before fillingthem.
Fauchard practiced orthodontia, and relates acase in which he used the file and pelican andput a crooked tooth in place, which operationrequired about ten minutes. The most difficultcases he states required from three to ten days,

12 History of Orthodontics
and sometimes several months, to complete. Heused gold and silver plates, which were perforatedwith holes through which he passed a silk threadfor correcting irregularities, and when this wasnot sufficient he forced them in place with thepelican or forceps.
In 1737, Fauchard made a full upper set ofteeth for a lady of high rank, holding the same inplace with springs, and relates that the lady atewith it easily and could not get along without it.He also relates having made a full upper and lowerset for a gentleman, who had worn them for morethan twenty-four years. When a full upper set ofteeth was made, Fauchard used flat springs tohold the piece in place, atmospheric suction notbeing recognized and used until the year 1800.He states, however, that he has been successful inthree cases in placing full upper sets without theaid of springs. He also brought palatine prosthesisto a high degree of perfection and described fivekinds of obturators, which were, however,somewhat-complicated. The materials most in usein dental prosthesis were human teeth,hippopotamus tusks, ivory of the best quality andox bone. Crowns were placed on natural roots (ifhealthy) and held in place with screws or boundto neighboring teeth.
The second edition of Fauchard’s work, whichappeared in 1746, contains (pp. 275-277) the firstaccount of pyorrhea alveolaris, familiarly called“Riggs’s disease,” after the American dentist, DrJohn M Riggs, who, in 1876, introduced themethod of scraping the tartar from the crowns androots for its cure.
In the first edition of Fauchard’s work (vol. ii,p. 30) mention is made of a machine for preparingand drilling into teeth. This machine is illustratedin Siemens d’Odontologie (Jourdain, 1756, p. 207).This was no doubt the beginning of the dentalengine, and antedates the dental engine that theGreenwoods made from an old spinning wheel.
Summing up his writings, we may say that,notwithstanding the falsity of some of his ideas,he was far in advance of his profession and wastruly the founder of modern dentistry, and hasgiven inestimable service to suffering humanity.
During the first part of the nineteenth century,almost all plates were fitted for the attachment ofsprings in case they were needed look natural.Mouton also invented a method of applyingpartial dentures by fixing them to the natural teeth
with springs or clasps. He also practicedtransplantation of teeth as well as the correctionof dental irregularities, and gained great renownthereby. He used subluxation of the teeth for thepurpose of severing the dental nerve as a remedyagainst toothache.
Philip Pfaff, dentist to Frederick the Great,deserves passing mention, since he was the firstGerman to write a real treatise on dentistry. He isthe first author who practised capping an exposednerve before placing a filling in the cavity,Fauchard usually filling the cavity directly overthe exposure. He also described the constructionof artificial teeth in which he made use of not onlyivory, bone and tusks of the hippopotamus andthe sea cow, but also of silver, mother of pearl andeven enameled copper. His most importantcontribution to science was the invention of theplaster model, poured in a beeswax impression.
Bourdet, dentist to the King of France, wrote abook on dentistry in 1757, in which the novel ideawas advanced of extracting carious teeth, fillingthem with gold or lead and then replanting them.If the alveolus was injured he replanted the teethimmediately and performed the operation of fillingafterward. He also used prosthetic pieces madeentirely of gold and covered them with flesh-colored enamel on the outside, showing that somedentists of olden times were even more artisticthan a large proportion of the practitioners of thepresent day who make no pretence of hiding theirglaring gold crowns. He also made use ofprosthetic pieces of hippopotamus tusk, to whichhuman teeth were fastened with rivets.
Thomas Berdmore, who was dentist to George IIIof England and the first dentist to the EnglishRoyal Family, is mentioned as having instructedRobert Wooffendale, by many reputed to havebeen the first dentist in America. Wooffen daleemigrated to America in 1766, and though he waspreceded by several men who practised the art, hewas probably far more efficient than any whopreceded him. In 1768 Berdmore published anexcellent work on dentistry which went throughmany editions three English, two German and thelast an American edition, appearing in Baltimore,the cradle of American dentistry, in 1844, 76 yearsafter the first edition, affording splendid proof ofits value.

13History of Dentistry
John Hunter (the celebrated English surgeon(born February 13, 1728), studied under hisbrother William, who conducted a school ofanatomy in London. In 1771 he published a bookentitled Natural History of the Human Teeth,and in 1776 another work entitled PracticalTreatise on the Diseases of the Teeth. He was agreat lecturer and writer and kept a superbanatomical collection and extensive library. Sogreat did his fame become that he was madeSurgeon-General to the English Army. Hunterwas a strenuous partisan of replanting andtransplanting teeth, and described theseoperations much more fully than had been donebefore. He experimented by transplanting asound tooth drawn from a living person into acock’s comb by making an incision with a lancet.When, some months later, the cock was killedthe head was injected and examined and thetooth was found to be attached and circulationestablished as is found in the natural gums. Ifwe may judge from early writings, transplantingand replanting were far more common at thattime than at present, and also profitable, as maybe judged by the charges of Paul Eurialius Jullion,whose fee was five pounds five shillings fortransplanting a live tooth and two pounds twoshillings for a dead tooth.
Robert Bunon (died 1749), a French dentist bornat the beginning of the eighteenth century, wasone of the first to deny that the eye tooth hasanything to do with the organ of sight, showingthat it is supplied by the infraorbital nerve. Hewas an ardent champion of conservative dentistryand prophylaxis and succeeded in convertingmany medical men, surgeons and priests to hisviews. When Fauchard’s book, Le ChirugienDentiste, appeared he was disappointed to findbut little therein that interested him, and set aboutto write a book of his own. Before publishing hiswork he entered the College of Surgery to undertaketwo years’ practice with a regularly licensedsurgeon, to undergo theoretical and practicalexaminations and to take oath before the ChiefSurgeon of the Realm in accordance with the edictof May, 1699, in order to obtain the diploma ofsurgeon- dentist. He was highly eulogized by theprincipal journals of the time, and by this meanswon much fame and many wealthy clients.
One of the chief merits of his book is that ofhaving ascribed to the deciduous teeth all of theimportance that they really have. In cases ofstomatitis, Bunon advised the complete removalof tartar before administering other treatment. Heused the same measures against mercurialstomatitis in the specific treatment of syphilis.
2IIInnntttrrroooddduuuccctttiiiooonnntttooo OOOrrrttthhhooodddooonnntttiiicccsss
Humans have attempted to straighten teeth forthousands of years before orthodontics became adental specialty in the late nineteenth century.Proper alignment of teeth has long beenrecognized to be an essential factor for esthetics,function and overall preservation of dental health.Malposed/poorly aligned teeth may predisposeto a number of unfavorable sequelae such as poororal hygiene predisposing to periodontal diseasesand dental caries, poor esthetics giving rise topsychosocial problems, increased risk of trauma,abnormalities of function and temporo-mandibular joint (TMJ) problems (Box 2.1).Orthodontics is the branch of dentistry concernedwith the growth of the face, development ofocclusion and the prevention and correction ofocclusal anomalies/abnormalities. The term“orthodontics” comes from Greek: “orthos” meaningright or correct and “odontos” meaning tooth (Flow
chart 2.1). The term orthodontics was first coinedby Le Felon in 1839.
DEFINITION OF ORTHODONTICS
Knowing the definition is often an importantinitial step in understanding any subject. Anumber of definitions have been put forward over
� Definition of Orthodontics
� What is Malocclusion?
� Aims of Orthodontic
Treatment
– Functional Efficiency
– Structural Balance
– Esthetic Harmony
� Branches of Orthodontics
– Preventive Orthodontics
– Interceptive Orthodontics
– Corrective Orthodontics
� Orthodontic Appliances
– Removable Orthodontic
Appliances
– Fixed Orthodontic
Appliances
– Functional Appliances
– Orthopedic Appliances/
Extraoral Force Appliances
� Timing of Orthodontic
Intervention
– Deciduous Dentition
– Early Mixed Dentition
– Late Mixed Dentition/Early
Permanent Dentition
� Scope of Orthodontics
– Monitoring and Assessment
of Developing Dentition
– Correcting Malocclusions of
Dental Origin
– Correcting Malocclusions of
Skeletal Origin
– Adult Orthodontics
– Guards
– Management of Dentofacial
Anomalies
� Benefits of Orthodontic
Treatment
Box 2.1: Unfavorable sequelae of malocclusion
� Poor facial appearance� Poor oral hygiene maintenance� Risk of dental caries� Risk of periodontal diseases� Abnormalities of functions� Psychosocial problems� Risk of trauma to the teeth� TMJ problems.
15Introduction to Orthodontics
the years to explain what orthodontics is. Some ofthe widely followed definitions are given below:
In 1911, Noyes gave the first definition oforthodontics as, “The study of the relation of theteeth to the development of the face and the correctionof arrested and perverted development.”
In 1922, The British Society of Orthodontistsproposed that, “Orthodontics includes the study ofgrowth and development of jaws and faceparticularly and the body generally, asinfluencing the position of the teeth; the study ofaction and reaction of internal and externalinfluences on the development, and the preventionand correction of arrested and perverteddevelopment.”
Later, the American Board of Orthodontics(ABO) and the American Association ofOrthodontists (AAO) stated that, “Orthodontics isthat specific area of dental practice that has as itsresponsibility, the study and supervision of thegrowth and development of the dentition and itsrelated anatomical structures from birth to dentalmaturity, including all preventive and correctiveprocedures of dental irregularities, requiring therepositioning of teeth by functional or mechanicalmeans to establish normal occlusion and pleasingfacial contours.”
WHAT IS MALOCCLUSION?
The term ‘malocclusion’ was first coined byGuilford and it refers to any irregularities inocclusion beyond the accepted range of normal.Malocclusions are caused by hereditary orenvironmental factors or more commonly, by boththe factors acting together. One of the mostcommon causes of malocclusion is adisproportion in size between the jaw and theteeth or between the maxillary and the mandibularjaws. A child who inherits mother’s small jaw
Flow chart 2.1: Derivation of the term orthodontics and father’s large teeth may have teeth that aretoo big for the jaw, causing crowding in the arch.Abnormal oral habits, such as thumb/digitsucking, lip biting and mouth breathing mayalso cause malocclusion by adversely affectingthe normal occlusal development. Malocclusioncan be presented in a number of ways. Some ofthe common characteristics of malocclusioninclude:� Overcrowded teeth� Spacing between the teeth� Improper “bite” between maxillary and
mandibular teeth� Disproportion in the size and the alignment
between the maxillary and the mandibularjaws.It must be appreciated that not all malocc-
lusions need treatment. Treatment of malocclus-ions that are mildly unesthetic and not detrimentalto the health of the teeth and their supportingstructures may not be needed and is not justified.
AIMS OF ORTHODONTIC TREATMENT
Although orthodontic treatment improves facialappearance and is occasionally performed forcosmetic reasons, it should be aimed at restorationof overall dental health.
Jackson has summarized the aims oforthodontic treatment that are popularly knownas Jackson’s triad (Fig. 2.1). They are:
i. Functional efficiencyii. Structural balance
iii. Esthetic harmony.
Functional Efficiency
The teeth along with their surrounding structuresare required to perform certain significantfunctions such as mastication and phonation.Orthodontic treatment should increase theefficiency of the functions performed.
Structural Balance
Orthodontic treatment not only affects teeth butalso the soft tissue envelop and the associatedskeletal structures. The treatment should maintaina balance between these structures and thecorrection of one should not affect the health ofthe other.
16 History of Orthodontics
Fig. 2.1: Aims of orthodontic treatment (Jackson’s triad)
Esthetic Harmony
The orthodontic treatment should enhance theoverall esthetic appeal of the individual. Thismight just require the alignment of certain teeth ormovement of the complete dental arch, includingits basal bone. The aim is to get results which gowell with the patient’s personality and make himor her look more esthetically appealing.
BRANCHES OF ORTHODONTICS
The general field of orthodontics can be dividedinto the following three categories based on thenature and time of intervention:� Preventive orthodontics� Interceptive orthodontics� Corrective orthodontics.
Preventive Orthodontics
Preventive orthodontics is defined as “Action takento preserve the integrity of what appears to be thenormal occlusion at a specific time.” As the nameimplies, preventive orthodontics includes actionsundertaken prior to the onset of a malocclusion,so as to prevent the anticipated development of amalocclusion.
Preventive orthodontics encompasses all thoseprocedures that attempt to ward off untowardenvironmental attacks or anything that would
change the normal course of events. They includethe care of deciduous dentition with restorationof carious lesions that might change the archlength, monitoring of eruption and sheddingtimetable of teeth, early recognition andelimination of oral habits that might interfere withthe normal development of the teeth and jaws;removal of retained deciduous teeth andsupernumeraries which may impede eruption ofpermanent teeth and maintenance of spacefollowing premature loss of deciduous teeth toallow proper eruption of their successors.
Interceptive Orthodontics
Interceptive orthodontics implies that when theaction is taken, an abnormal situation (maloc-clusion) already exists. Certain interceptiveprocedures are undertaken during the earlymanifestation of malocclusion to lessen theseverity of malocclusion and sometimes toeliminate the cause.
Interceptive orthodontics is defined by theAmerican Association of Orthodontists as “Thatphase of the science and art of orthodonticsemployed to recognize and eliminate potentialirregularities and malpositions in the developingdentofacial complex.”
Interceptive procedures include serialextraction, correction of developing anteriorcrossbite, control of abnormal oral habits, removalof supernumeraries and ankylosed teeth andelimination of bony or tissue barriers to eruptingteeth.
Certain procedures undertaken may becommon to both preventive and interceptiveorthodontics. However, the timing of the servicesrendered is different. Preventive orthodonticprocedures are carried out before the manifestationof a malocclusion, while the goal of interceptiveorthodontics is to intercept a malocclusion thathas already been developed or is developing, soas to restore a normal occlusion.
Corrective Orthodontics
Corrective orthodontics, like interceptiveorthodontics, is also undertaken after themanifestation of a malocclusion. It employscertain technical procedures to reduce or correctthe malocclusion and to eliminate the possiblesequelae of malocclusion.
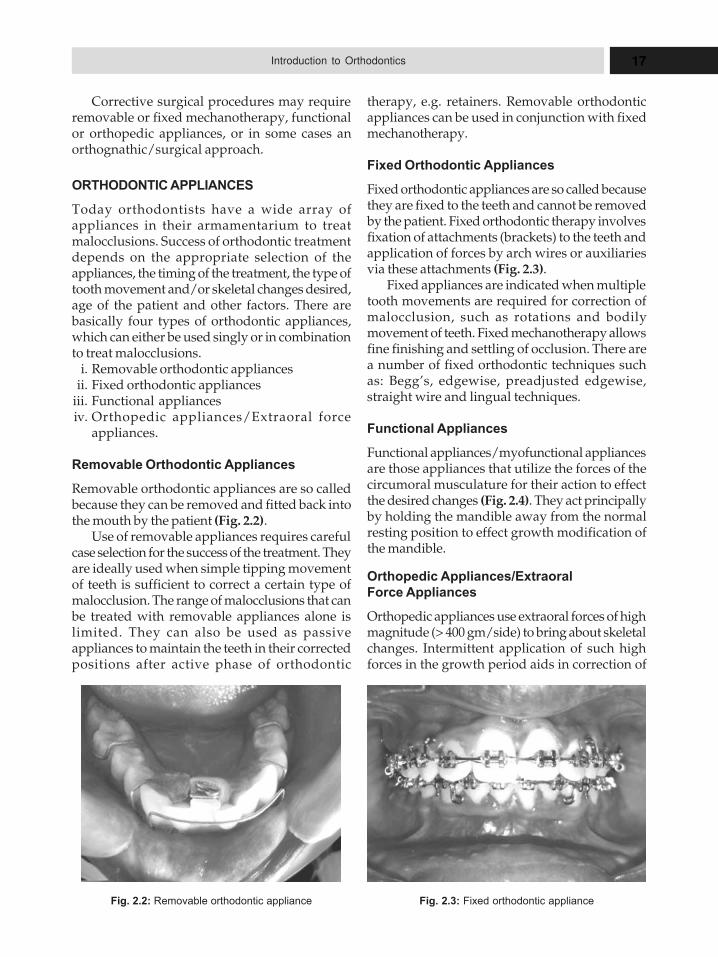
17Introduction to Orthodontics
Fig. 2.2: Removable orthodontic appliance Fig. 2.3: Fixed orthodontic appliance
Corrective surgical procedures may requireremovable or fixed mechanotherapy, functionalor orthopedic appliances, or in some cases anorthognathic/surgical approach.
ORTHODONTIC APPLIANCES
Today orthodontists have a wide array ofappliances in their armamentarium to treatmalocclusions. Success of orthodontic treatmentdepends on the appropriate selection of theappliances, the timing of the treatment, the type oftooth movement and/or skeletal changes desired,age of the patient and other factors. There arebasically four types of orthodontic appliances,which can either be used singly or in combinationto treat malocclusions.
i. Removable orthodontic appliancesii. Fixed orthodontic appliances
iii. Functional appliancesiv. Orthopedic appliances/Extraoral force
appliances.
Removable Orthodontic Appliances
Removable orthodontic appliances are so calledbecause they can be removed and fitted back intothe mouth by the patient (Fig. 2.2).
Use of removable appliances requires carefulcase selection for the success of the treatment. Theyare ideally used when simple tipping movementof teeth is sufficient to correct a certain type ofmalocclusion. The range of malocclusions that canbe treated with removable appliances alone islimited. They can also be used as passiveappliances to maintain the teeth in their correctedpositions after active phase of orthodontic
therapy, e.g. retainers. Removable orthodonticappliances can be used in conjunction with fixedmechanotherapy.
Fixed Orthodontic Appliances
Fixed orthodontic appliances are so called becausethey are fixed to the teeth and cannot be removedby the patient. Fixed orthodontic therapy involvesfixation of attachments (brackets) to the teeth andapplication of forces by arch wires or auxiliariesvia these attachments (Fig. 2.3).
Fixed appliances are indicated when multipletooth movements are required for correction ofmalocclusion, such as rotations and bodilymovement of teeth. Fixed mechanotherapy allowsfine finishing and settling of occlusion. There area number of fixed orthodontic techniques suchas: Begg’s, edgewise, preadjusted edgewise,straight wire and lingual techniques.
Functional Appliances
Functional appliances/myofunctional appliancesare those appliances that utilize the forces of thecircumoral musculature for their action to effectthe desired changes (Fig. 2.4). They act principallyby holding the mandible away from the normalresting position to effect growth modification ofthe mandible.
Orthopedic Appliances/Extraoral
Force Appliances
Orthopedic appliances use extraoral forces of highmagnitude (> 400 gm/side) to bring about skeletalchanges. Intermittent application of such highforces in the growth period aids in correction of
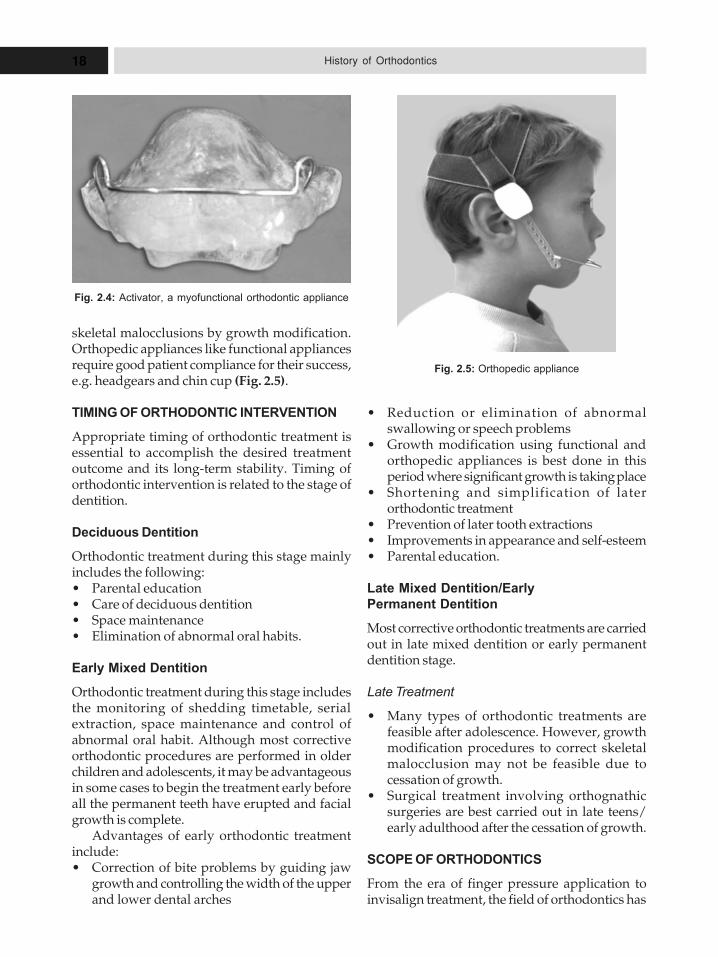
18 History of Orthodontics
Fig. 2.4: Activator, a myofunctional orthodontic appliance
Fig. 2.5: Orthopedic appliance
skeletal malocclusions by growth modification.Orthopedic appliances like functional appliancesrequire good patient compliance for their success,e.g. headgears and chin cup (Fig. 2.5).
TIMING OF ORTHODONTIC INTERVENTION
Appropriate timing of orthodontic treatment isessential to accomplish the desired treatmentoutcome and its long-term stability. Timing oforthodontic intervention is related to the stage ofdentition.
Deciduous Dentition
Orthodontic treatment during this stage mainlyincludes the following:� Parental education� Care of deciduous dentition� Space maintenance� Elimination of abnormal oral habits.
Early Mixed Dentition
Orthodontic treatment during this stage includesthe monitoring of shedding timetable, serialextraction, space maintenance and control ofabnormal oral habit. Although most correctiveorthodontic procedures are performed in olderchildren and adolescents, it may be advantageousin some cases to begin the treatment early beforeall the permanent teeth have erupted and facialgrowth is complete.
Advantages of early orthodontic treatmentinclude:� Correction of bite problems by guiding jaw
growth and controlling the width of the upperand lower dental arches
� Reduction or elimination of abnormalswallowing or speech problems
� Growth modification using functional andorthopedic appliances is best done in thisperiod where significant growth is taking place
� Shortening and simplification of laterorthodontic treatment
� Prevention of later tooth extractions� Improvements in appearance and self-esteem� Parental education.
Late Mixed Dentition/Early
Permanent Dentition
Most corrective orthodontic treatments are carriedout in late mixed dentition or early permanentdentition stage.
Late Treatment
� Many types of orthodontic treatments arefeasible after adolescence. However, growthmodification procedures to correct skeletalmalocclusion may not be feasible due tocessation of growth.
� Surgical treatment involving orthognathicsurgeries are best carried out in late teens/early adulthood after the cessation of growth.
SCOPE OF ORTHODONTICS
From the era of finger pressure application toinvisalign treatment, the field of orthodontics has
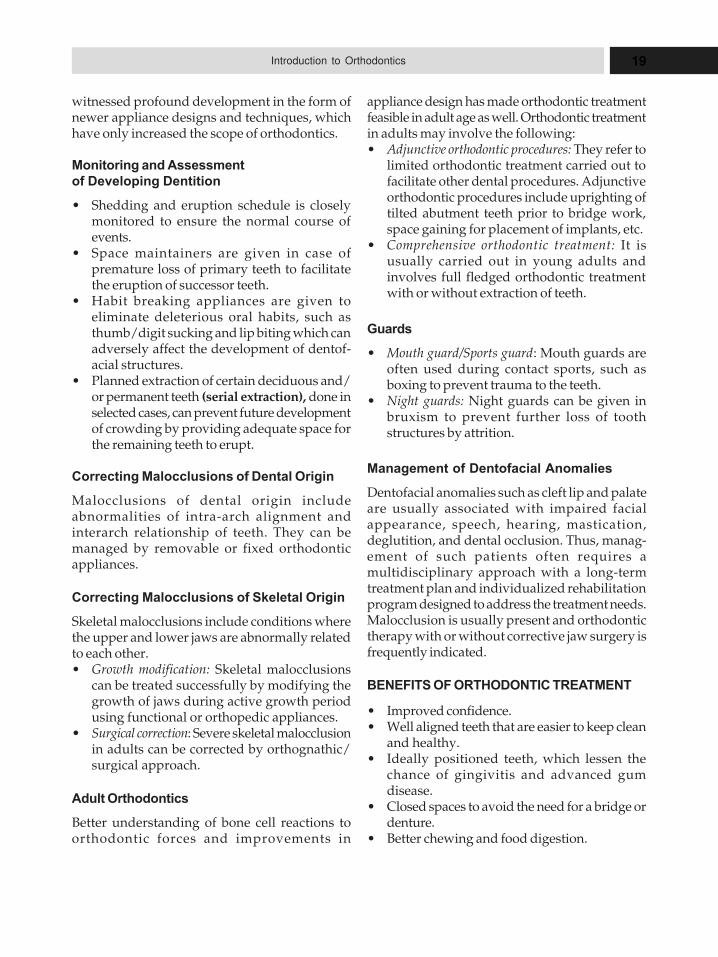
19Introduction to Orthodontics
witnessed profound development in the form ofnewer appliance designs and techniques, whichhave only increased the scope of orthodontics.
Monitoring and Assessment
of Developing Dentition
� Shedding and eruption schedule is closelymonitored to ensure the normal course ofevents.
� Space maintainers are given in case ofpremature loss of primary teeth to facilitatethe eruption of successor teeth.
� Habit breaking appliances are given toeliminate deleterious oral habits, such asthumb/digit sucking and lip biting which canadversely affect the development of dentof-acial structures.
� Planned extraction of certain deciduous and/or permanent teeth (serial extraction), done inselected cases, can prevent future developmentof crowding by providing adequate space forthe remaining teeth to erupt.
Correcting Malocclusions of Dental Origin
Malocclusions of dental origin includeabnormalities of intra-arch alignment andinterarch relationship of teeth. They can bemanaged by removable or fixed orthodonticappliances.
Correcting Malocclusions of Skeletal Origin
Skeletal malocclusions include conditions wherethe upper and lower jaws are abnormally relatedto each other.� Growth modification: Skeletal malocclusions
can be treated successfully by modifying thegrowth of jaws during active growth periodusing functional or orthopedic appliances.
� Surgical correction: Severe skeletal malocclusionin adults can be corrected by orthognathic/surgical approach.
Adult Orthodontics
Better understanding of bone cell reactions toorthodontic forces and improvements in
appliance design has made orthodontic treatmentfeasible in adult age as well. Orthodontic treatmentin adults may involve the following:� Adjunctive orthodontic procedures: They refer to
limited orthodontic treatment carried out tofacilitate other dental procedures. Adjunctiveorthodontic procedures include uprighting oftilted abutment teeth prior to bridge work,space gaining for placement of implants, etc.
� Comprehensive orthodontic treatment: It isusually carried out in young adults andinvolves full fledged orthodontic treatmentwith or without extraction of teeth.
Guards
� Mouth guard/Sports guard: Mouth guards areoften used during contact sports, such asboxing to prevent trauma to the teeth.
� Night guards: Night guards can be given inbruxism to prevent further loss of toothstructures by attrition.
Management of Dentofacial Anomalies
Dentofacial anomalies such as cleft lip and palateare usually associated with impaired facialappearance, speech, hearing, mastication,deglutition, and dental occlusion. Thus, manag-ement of such patients often requires amultidisciplinary approach with a long-termtreatment plan and individualized rehabilitationprogram designed to address the treatment needs.Malocclusion is usually present and orthodontictherapy with or without corrective jaw surgery isfrequently indicated.
BENEFITS OF ORTHODONTIC TREATMENT
� Improved confidence.� Well aligned teeth that are easier to keep clean
and healthy.� Ideally positioned teeth, which lessen the
chance of gingivitis and advanced gumdisease.
� Closed spaces to avoid the need for a bridge ordenture.
� Better chewing and food digestion.
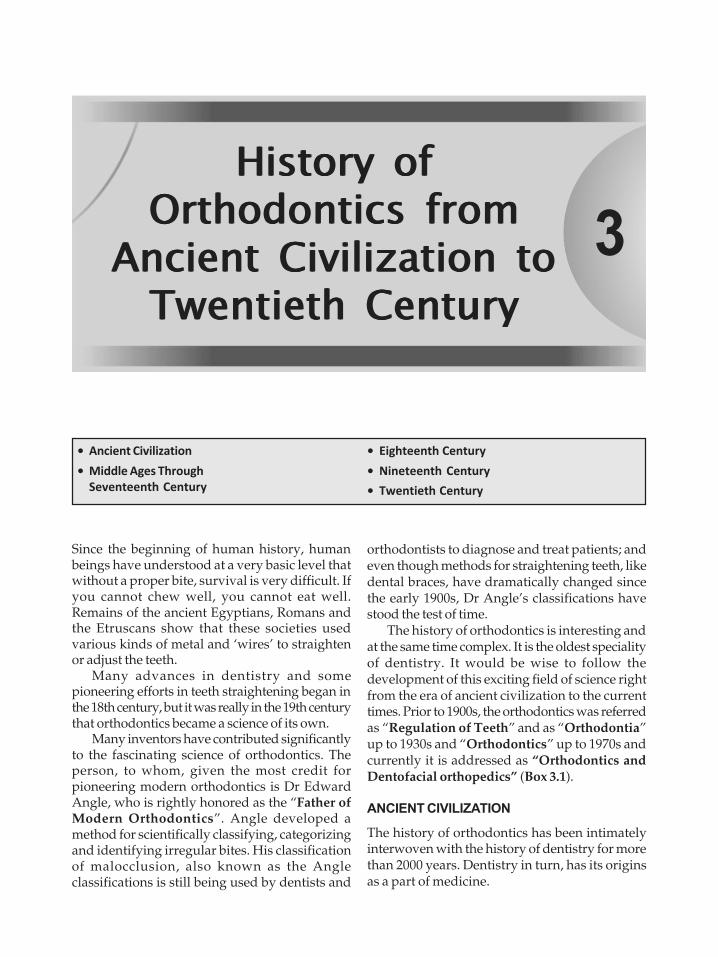
3
HHHiiissstttooorrryyy ooofffOOOrrrttthhhooodddooonnntttiiicccsss fffrrrooommm
AAAnnnccciiieeennnttt CCCiiivvviiillliiizzzaaatttiiiooonnn tttoooTTTwwweeennntttiiieeettthhh CCCeeennntttuuurrryyy
Since the beginning of human history, humanbeings have understood at a very basic level thatwithout a proper bite, survival is very difficult. Ifyou cannot chew well, you cannot eat well.Remains of the ancient Egyptians, Romans andthe Etruscans show that these societies usedvarious kinds of metal and ‘wires’ to straightenor adjust the teeth.
Many advances in dentistry and somepioneering efforts in teeth straightening began inthe 18th century, but it was really in the 19th centurythat orthodontics became a science of its own.
Many inventors have contributed significantlyto the fascinating science of orthodontics. Theperson, to whom, given the most credit forpioneering modern orthodontics is Dr EdwardAngle, who is rightly honored as the “Father ofModern Orthodontics”. Angle developed amethod for scientifically classifying, categorizingand identifying irregular bites. His classificationof malocclusion, also known as the Angleclassifications is still being used by dentists and
orthodontists to diagnose and treat patients; andeven though methods for straightening teeth, likedental braces, have dramatically changed sincethe early 1900s, Dr Angle’s classifications havestood the test of time.
The history of orthodontics is interesting andat the same time complex. It is the oldest specialityof dentistry. It would be wise to follow thedevelopment of this exciting field of science rightfrom the era of ancient civilization to the currenttimes. Prior to 1900s, the orthodontics was referredas “Regulation of Teeth” and as “Orthodontia”up to 1930s and “Orthodontics” up to 1970s andcurrently it is addressed as “Orthodontics andDentofacial orthopedics” (Box 3.1).
ANCIENT CIVILIZATION
The history of orthodontics has been intimatelyinterwoven with the history of dentistry for morethan 2000 years. Dentistry in turn, has its originsas a part of medicine.
� Ancient Civilization
� Middle Ages Through
Seventeenth Century
� Eighteenth Century
� Nineteenth Century
� Twentieth Century

21History of Orthodontics from Ancient Civilization to Twentieth Century
The Greek physician, Hippocrates (460–377BC), was the first to separate medicine from fancyor religion. He established a medical traditionbased on facts and the collected information wasgathered into a text known as the ‘CorpusHippocraticum’. This text of the pre-Christian eracontains many references to the teeth and to thetissues of the jaws as part of the medical text, whichincludes descriptions of irregularity and crowdingof teeth.
Aristotle (384–322 BC), the Greek philosopher wasthe first writer who studied the teeth in a broadmanner. In his work entitled De PartibusAnimalium (On the Parts of Animals), hecompared various dentitions of the known speciesof animals of that time.
Aulius Cornelius Celsus (25 BC–50 AD), theprominent Roman author of the first century,described finger pressure to move teeth in his workDe Re Medicina (on Medicine) (Table 3.1).
When in a child, a permanent tooth appearsbefore the fall of the milk tooth, it is necessary todissect the gum all around the latter and extractit. The other tooth must then be pushed with thefinger, day by day, towards the place that wasoccupied by the one extracted; and this is to becontinued until it reaches its proper position.
The medical art of the Romans reached itszenith under Claudius Galenus, commonlyknown as Galen (AD 130–200). For 15 centurieshe dominated medical thought, and it was not
until the Renaissance that the infallibility of hismedical expertise was questioned. In his medicalwritings, he described dental anatomy andembryology by specifically identifying the origin,growth, and development of the teeth andenumerating the functions of each. He believedthe teeth to be true bones. Because dissection wasperformed on animals rather than on humanbeings, he erroneously applied some of hisfindings to human beings (e.g. the presence of anintermaxillary bone and the insensibility of teeth).
MIDDLE AGES THROUGH SEVENTEENTH
CENTURY
There is little reference to dentition during thisperiod. An Arabic physician Paul of Aegina(Paulus Aegineta 625–690) wrote aboutirregularities in the dental arches caused bysupernumerary teeth. He advised extraction ofsuch teeth.
Ambrose Paré (1517–1590), a French surgeon,paid specific attention to the cleft palate. He wasthe first surgeon to devise an obturator fortreatment of cleft palate.
Renaissance Period
(Fourteenth to Sixteenth Century)
During the Renaissance, one of the greatestgeniuses of history, Leonardo da Vinci (1452–1519), is remembered because he painted a smileon the lips of Mona Lisa. Her smile remains mostprovocative; yet the brush was only one of themany tools he mastered. He was the first artist todissect the human body for the acquisition ofanatomic knowledge and the first to draw accuratepictures of these dissections.
Leonardo was the first to recognize tooth formand the first to realize that each tooth was relatedto another tooth and to the opposing jaw as well,thus perceiving the articulation of the teeth. He
Table 3.1: Ancient civilization
Years Authors Contributions to orthodontics
460–377 BC Hippocrates Description of irregularity “Corpus Hippocraticum”.
384–322 BC Aristotle Comparison of various dentitions of different speciesof animals in his work “On the Parts of Animals”.
25 BC–50 AD Aulius Cornelius Celsus Described finger pressure to move teeth in his work‘De Re Medicina (On Medicine)’.
Box 3.1: Evolution of the term orthodontics
� Orthodontics– “Regulation“ prior to 1900s– “Orthodontia” up to 1930s (“ia” referred to a
medial condition)– “Orthodontics” up to 1970s– Currently “Orthodontics and Dentofacial
orthopedics”

22 History of Orthodontics
described the maxillary and frontal sinuses andestablished their relationship to facial height. Hedetermined and made drawings of the number ofteeth and their root formations. He noted that“those teeth that are the farthest away from theline of the temporomandibular articulation are ata mechanical disadvantage as compared withthose that are nearer.”
Those (teeth) that act most powerfully, themascellari (molars) have broad flattened crownssuitable for grinding the food, but not for tearingor cutting it. Those that act less powerfully, theincisors, are suitable for cutting the food but notfor grinding it. The maestre (canines) areintermediate between these two sets, their functionbeing presumably that of tearing the food.
Andreas Vesalius (1514–1564), a Belgianphysician and anatomist, set a precedent for thestudy of human anatomy when he personallyperformed a dissection. It had been the custom forstudents to do the dissections while the lecturerdescribed the procedure and specimen. He provedGalen wrong in many areas of anatomicknowledge. His classic work, On the Fabric ofthe Human Body, became the foundation thatreconstructed our knowledge of human anatomyand thereby laid the basis for the practice ofmedicine and surgery.
In this book, he described the minute anatomyof the teeth, particularly the dental follicle andsubsequent pattern of tooth eruption:
Gabriele Fallopio (1523–1562), commonly knownas Fallopius, an Italian anatomist, wrote in hisObservationes Anatomica (Anatomic Observ-ations) a detailed description of the dental follicle. Hewrote the terms hard and soft palate.
A membranous follicle is formed inside thebone furnished with two apices, one posterior (thatis to say, deeper down, more distant from thegums), to which is joined a small nerve, a smallartery and a small vein; the other anterior (that is,more superficial) which terminates in a filament.Inside the follicle is formed a special white andtenacious substance, and from this the tooth itself,which at first is osseous only in the part nearestthe surface, while the lower part is still soft, thatis, formed of the above mentioned substance. Eachtooth comes out traversing and widening a narrowaperture, bare and hard; and in process of timethe formation of its deeper part is completed.
Bartholomaeus Eustachio (1520–1574),commonly known as Eustachius, also an Italiananatomist, described the minute structure of manyorgans, especially the tube that connects themiddle ear with the nasopharynx and that bearshis name. He wrote Libellus de Dentibus (Bookon the Teeth) in 1563, which is the first importantspecialized monograph on the anatomy of theteeth. In this book, he collected the writings ofvarious authors from Hippocrates to Vesalius,added the results of his own researches, and gavethe first accurate account of the phenomenon ofthe sequential development of the first and seconddentitions. He described the eruption and thefunction of the teeth, contending that there wasno analogy between the deciduous and permanentdentitions. Eustachius devoted more attention tothe teeth than most anatomists, giving fulldescriptions of the different forms, number andvarieties. He indicated the manner of articulationof the teeth and gave a somewhat ambiguousexplanation of the nature of the attachment of theteeth to the socket and the gingival tissues,comparing the latter to the attachment of the nailsto the skin. His explanation of the internalstructure of the teeth differentiated the two layersand compared the enamel with the bark of trees.
Eustachius described the dental follicle andits blood supply. He refuted the doctrine that rootsof the deciduous dentition served to form thepermanent teeth. He maintained that the germs ofthe permanent teeth are too small to be seen in thefetus. He also mentioned that the teeth arenourished differently than other bones, aswitnessed by their inability to repair whenfractured.
The first book in the German language to havereference to the teeth was entitled “ArzeiBuchlein” (A Book of the Surgical Art) and waspublished in 1530 (author unknown). It containsthe following comment. When teeth begin to dropout push the new one every day toward the placewhere the first one was, until it sits there and fitsamong the others, for if you neglect to attend tothis, the old teeth (deciduous) will remain and theyoung ones (permanent) will be impeded fromgrowing straight.
EIGHTEENTH CENTURY
18th Century witnessed major events in thedevelopment of dental science and dentistry
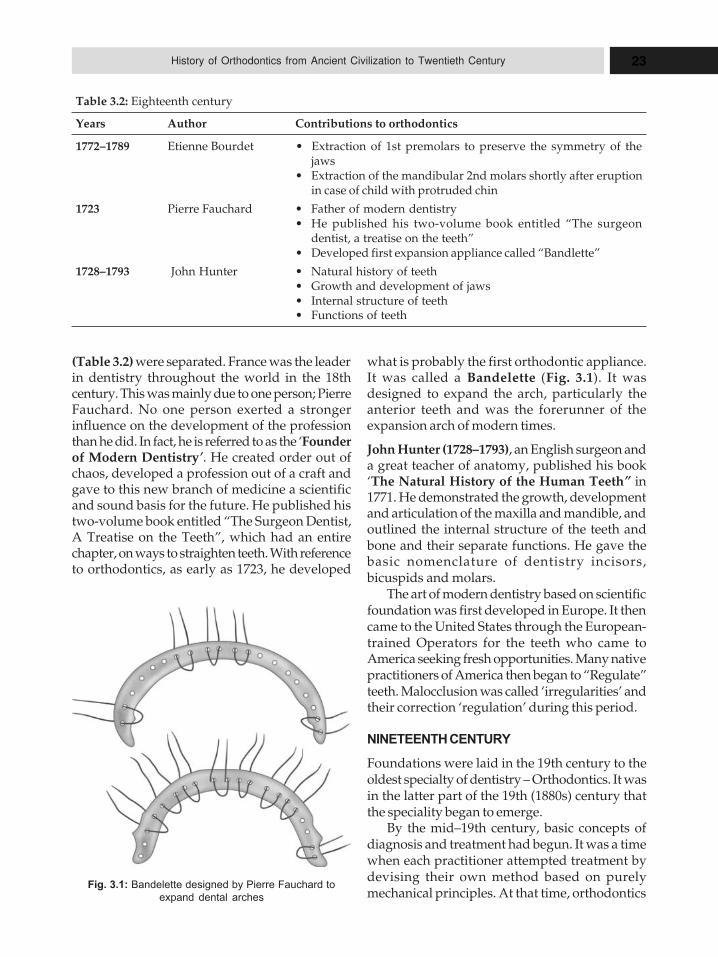
23History of Orthodontics from Ancient Civilization to Twentieth Century
(Table 3.2) were separated. France was the leaderin dentistry throughout the world in the 18thcentury. This was mainly due to one person; PierreFauchard. No one person exerted a strongerinfluence on the development of the professionthan he did. In fact, he is referred to as the ‘Founderof Modern Dentistry’. He created order out ofchaos, developed a profession out of a craft andgave to this new branch of medicine a scientificand sound basis for the future. He published histwo-volume book entitled “The Surgeon Dentist,A Treatise on the Teeth”, which had an entirechapter, on ways to straighten teeth. With referenceto orthodontics, as early as 1723, he developed
what is probably the first orthodontic appliance.It was called a Bandelette (Fig. 3.1). It wasdesigned to expand the arch, particularly theanterior teeth and was the forerunner of theexpansion arch of modern times.
John Hunter (1728–1793), an English surgeon anda great teacher of anatomy, published his book‘The Natural History of the Human Teeth” in1771. He demonstrated the growth, developmentand articulation of the maxilla and mandible, andoutlined the internal structure of the teeth andbone and their separate functions. He gave thebasic nomenclature of dentistry incisors,bicuspids and molars.
The art of modern dentistry based on scientificfoundation was first developed in Europe. It thencame to the United States through the European-trained Operators for the teeth who came toAmerica seeking fresh opportunities. Many nativepractitioners of America then began to “Regulate”teeth. Malocclusion was called ‘irregularities’ andtheir correction ‘regulation’ during this period.
NINETEENTH CENTURY
Foundations were laid in the 19th century to theoldest specialty of dentistry – Orthodontics. It wasin the latter part of the 19th (1880s) century thatthe speciality began to emerge.
By the mid–19th century, basic concepts ofdiagnosis and treatment had begun. It was a timewhen each practitioner attempted treatment bydevising their own method based on purelymechanical principles. At that time, orthodontics
Table 3.2: Eighteenth century
Years Author Contributions to orthodontics
1772–1789 Etienne Bourdet � Extraction of 1st premolars to preserve the symmetry of thejaws
� Extraction of the mandibular 2nd molars shortly after eruptionin case of child with protruded chin
1723 Pierre Fauchard � Father of modern dentistry� He published his two-volume book entitled “The surgeon
dentist, a treatise on the teeth”� Developed first expansion appliance called “Bandlette”
1728–1793 John Hunter � Natural history of teeth� Growth and development of jaws� Internal structure of teeth� Functions of teeth
Fig. 3.1: Bandelette designed by Pierre Fauchard to
expand dental arches
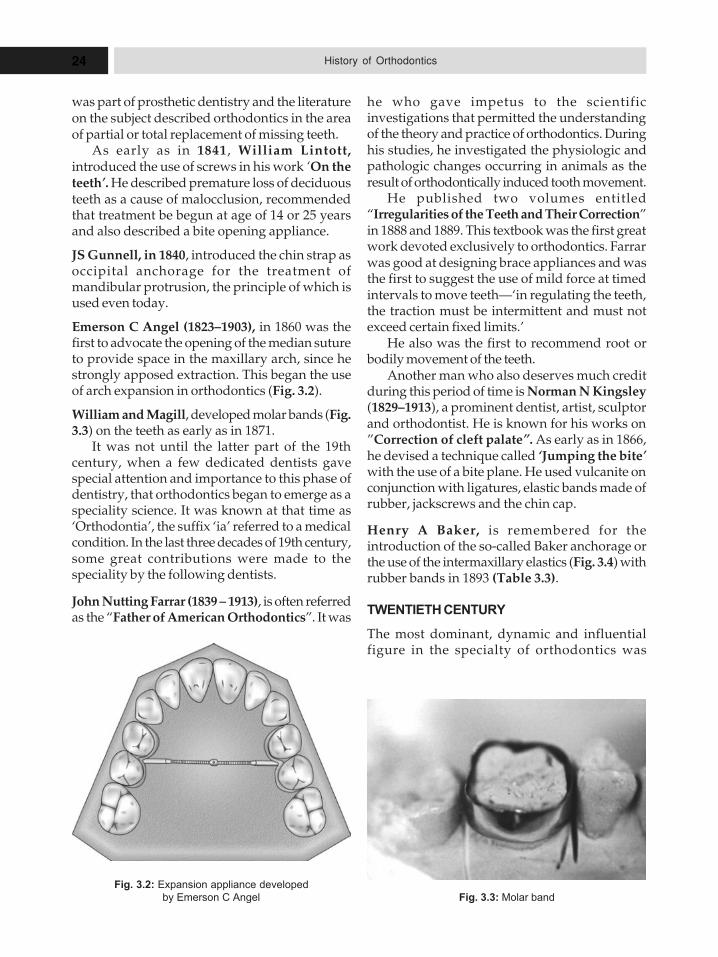
24 History of Orthodontics
was part of prosthetic dentistry and the literatureon the subject described orthodontics in the areaof partial or total replacement of missing teeth.
As early as in 1841, William Lintott,introduced the use of screws in his work ‘On theteeth’. He described premature loss of deciduousteeth as a cause of malocclusion, recommendedthat treatment be begun at age of 14 or 25 yearsand also described a bite opening appliance.
JS Gunnell, in 1840, introduced the chin strap asoccipital anchorage for the treatment ofmandibular protrusion, the principle of which isused even today.
Emerson C Angel (1823–1903), in 1860 was thefirst to advocate the opening of the median sutureto provide space in the maxillary arch, since hestrongly apposed extraction. This began the useof arch expansion in orthodontics (Fig. 3.2).
William and Magill, developed molar bands (Fig.3.3) on the teeth as early as in 1871.
It was not until the latter part of the 19thcentury, when a few dedicated dentists gavespecial attention and importance to this phase ofdentistry, that orthodontics began to emerge as aspeciality science. It was known at that time as‘Orthodontia’, the suffix ‘ia’ referred to a medicalcondition. In the last three decades of 19th century,some great contributions were made to thespeciality by the following dentists.
John Nutting Farrar (1839 – 1913), is often referredas the “Father of American Orthodontics”. It was
he who gave impetus to the scientificinvestigations that permitted the understandingof the theory and practice of orthodontics. Duringhis studies, he investigated the physiologic andpathologic changes occurring in animals as theresult of orthodontically induced tooth movement.
He published two volumes entitled“Irregularities of the Teeth and Their Correction”in 1888 and 1889. This textbook was the first greatwork devoted exclusively to orthodontics. Farrarwas good at designing brace appliances and wasthe first to suggest the use of mild force at timedintervals to move teeth—‘in regulating the teeth,the traction must be intermittent and must notexceed certain fixed limits.’
He also was the first to recommend root orbodily movement of the teeth.
Another man who also deserves much creditduring this period of time is Norman N Kingsley(1829–1913), a prominent dentist, artist, sculptorand orthodontist. He is known for his works on”Correction of cleft palate”. As early as in 1866,he devised a technique called ‘Jumping the bite’with the use of a bite plane. He used vulcanite onconjunction with ligatures, elastic bands made ofrubber, jackscrews and the chin cap.
Henry A Baker, is remembered for theintroduction of the so-called Baker anchorage orthe use of the intermaxillary elastics (Fig. 3.4) withrubber bands in 1893 (Table 3.3).
TWENTIETH CENTURY
The most dominant, dynamic and influentialfigure in the specialty of orthodontics was
Fig. 3.2: Expansion appliance developed
by Emerson C Angel Fig. 3.3: Molar band
25History of Orthodontics from Ancient Civilization to Twentieth Century
Edward H Angle (1855–1930) (Fig. 3.5). He isregarded as the “Father of Modern Orthodontics”.His classification of malocclusion was publishedin the Dental Cosmos, in 1899. Angle developed aclassification of malocclusion based on thisprinciple, which is still used today.
Edward Hartley Angle (1855–1930)
Angle was born on June 1, 1855, in Herrick,Pennsylvania. He graduated from PennsylvaniaCollege of Dentistry, in 1878. It was then that hestarted his first orthodontic case on his preceptor’sson. The problems that arose stimulated him todevote the rest of his life to orthodontics.
He presented his first scientific paper in 1887before the ninth International Medical Congress.In the same year, his first paper bound edition
book on orthodontics was published, and the lastfully revised seventh edition appeared in 1907.He became professor of orthodontics in the year1892.
Angle started the first school of Orthodonticsin St Louis in 1900, independent from anyuniversity. From 1900 to 1928 he was the activehead of his school, first in St Louis, later in NewLondon, Connecticut and finally in Pasadena,California. Under Angle’s aegis, the AmericanSchool of Orthodontists was founded in 1901.
Angle introduced the most universally usedclassification of malocclusion, and even developeda number of appliances such as the E-arch, the
Table 3.3: Nineteenth century
Year Author Contributions to orthodontics
1841 William Lintott Introduced the use of screws1840 JS Gunnell Introduced chin strap1860 Emerson C Angel � First to introduce arch expansion by opening midpalatal
suture� “Father of expansion appliances”.
1871 William and Magill Developed molar bands1888 and 1889 John Nutting Farrar � “Father of American orthodontics”
� Wrote “Irregularities of the Teeth and Their Correction”.This textbook was the first great work devoted exclusivelyto orthodontics
� Laid the foundation for “Scientific orthodontics” (intermittentforces, limits to amount of tooth movements)
1829 to 1913 Norman N Kingsley � “Treatise on Oral Deformities“ worked on correction of cleftpalate
� Extraoral traction1893 Henry A Baker Baker’s anchorage (Intermaxillary elastics)
Fig. 3.4: Baker’s anchorage (Intermaxillay elastics)
Fig. 3.5: Edward Hartley Angle (1855–1930)

26 History of Orthodontics
pin and tube appliance, the ribbon arch applianceand the edgewise appliance.
He has been given the most credit forpioneering modern orthodontics is Dr EdwardAngle. Dr Angle developed a method forscientifically classifying, categorizing andidentifying irregular bites. His malocclusionclassifications, also known as the AngleClassifications are still used by dentists andorthodontists today to diagnose and treat patients.And even though methods for straightening teeth,like dental braces, have dramatically changedsince the early 1900’s, Dr. Angle’s classificationshave stood the test of time.
Although Angle died on August 11, 1930, hisinfluence is still felt very strongly in the orthodonticfield. The whole world still uses his classificationof malocclusion and his excellent descriptions ofocclusion are hardly less important than hisclassification of malocclusion. His strongopposition against extraction of teeth as a part oforthodontic therapy has served as a balance wheelagainst promiscuous tooth removal. Hismechanical genius has provided some of the mostefficient appliances in use at present.
Another distinguished orthodontist wasCalvin S Case [(1847–1923) (Fig. 3.6)]. Hedeveloped a classification of malocclusions thatincluded 26 divisions. Case published his majorwork “A practical treatise on the techniques andprinciple of dental orthopedic and prostheticcorrection of the cleft palate”. Case was a strong
advocate of the relationship of malocclusion tofacial improvement. Facial improvement was aguide to treatment.
1847–1923
One of the great pioneers in orthodontics, CalvinCase, was born in Jackson, Michigan, on April 24,1847. He graduated dentistry and medicine fromOhio Dental College in 1871 and University ofMichigan Medical School in 1884, respectively.
He became Professor of Prosthetics andOrthodontics, at Chicago College of DentalSurgery. He dropped his professorship ofprosthetics in 1896 and later continued in onlyorthodontics throughout his life.
As a prolific writer, Case wrote 123 articles indental literature alone on orthodontic diagnosis,orthodontic appliance, problems of toothmovement, cleft palate and associated speechproblems, and prosthetic restorations of normalspeech and function. He was the second authornext to Angle. His textbook, the Techniques andPrinciples of Dental Orthopedia, was publishedin 1908.
Case was also a pioneer in orthodonticmechanotherapy. He was the first one to stress theimportance of root movement (1892). He was oneof the first to use rubber elastics in treatment (1892),small gauge, and light resilient wires for toothalignment (1917). He pioneered the use of relievesto stabilize orthodontic results. He is regarded asthe outstanding man of his time in the prostheticaspect of rehabilitation of cleft palate deformities.
Charles A Hawley (1861–1929), used a celluloidsheet containing a geometric figure that whenadapted to a model determined the extent ofproposed tooth movement (1905) and introducedthe retainer appliance (Fig. 3.7) that bears his name(1908) (Table 3.4).
In 1931, B Holly Broadbent published anarticle in the first issue of the new AngleOrthodontist entitled. “A New X-ray Techniqueand its Application to Orthodontia”. It was theintroduction to the specialty and to dentistry ofcephalometric roentgenography (Fig. 3.8) and, ofcourse, cephalometric tracing and evaluation.Broadbent devised the roentgenographiccephalometer, which is the instrument thataccurately positions the head relative to the filmFig. 3.6: Calvin S Case (1847–1923)
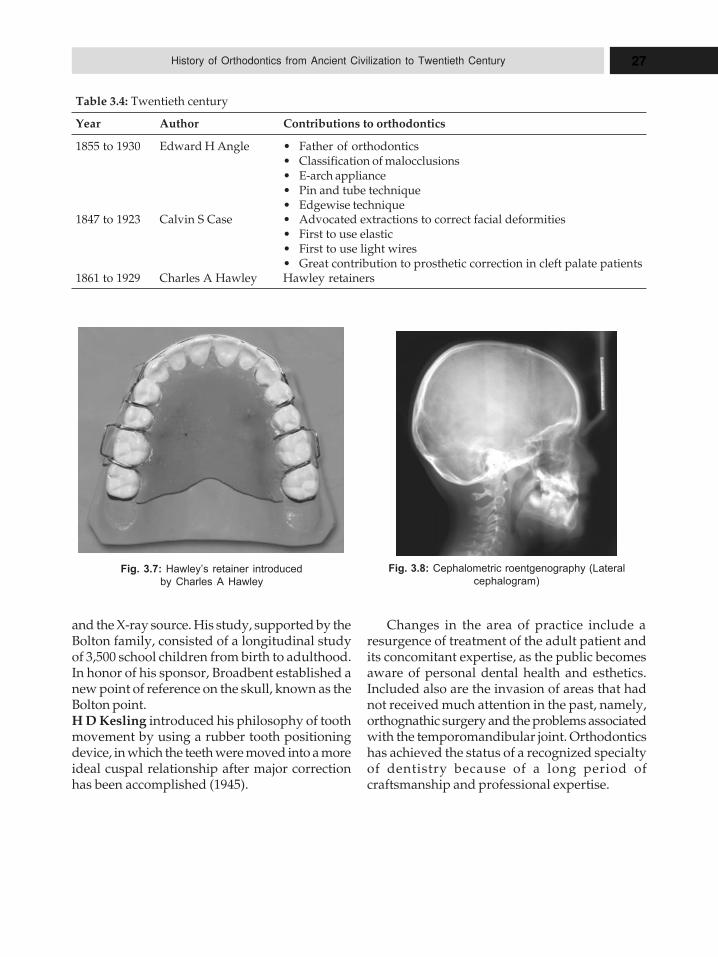
27History of Orthodontics from Ancient Civilization to Twentieth Century
and the X-ray source. His study, supported by theBolton family, consisted of a longitudinal studyof 3,500 school children from birth to adulthood.In honor of his sponsor, Broadbent established anew point of reference on the skull, known as theBolton point.H D Kesling introduced his philosophy of toothmovement by using a rubber tooth positioningdevice, in which the teeth were moved into a moreideal cuspal relationship after major correctionhas been accomplished (1945).
Table 3.4: Twentieth century
Year Author Contributions to orthodontics
1855 to 1930 Edward H Angle � Father of orthodontics� Classification of malocclusions� E-arch appliance� Pin and tube technique� Edgewise technique
1847 to 1923 Calvin S Case � Advocated extractions to correct facial deformities� First to use elastic� First to use light wires� Great contribution to prosthetic correction in cleft palate patients
1861 to 1929 Charles A Hawley Hawley retainers
Fig. 3.8: Cephalometric roentgenography (Lateral
cephalogram)
Changes in the area of practice include aresurgence of treatment of the adult patient andits concomitant expertise, as the public becomesaware of personal dental health and esthetics.Included also are the invasion of areas that hadnot received much attention in the past, namely,orthognathic surgery and the problems associatedwith the temporomandibular joint. Orthodonticshas achieved the status of a recognized specialtyof dentistry because of a long period ofcraftsmanship and professional expertise.
Fig. 3.7: Hawley’s retainer introduced
by Charles A Hawley
4HHHiiissstttooorrryyy ooofff OOOrrrttthhhooodddooonnntttiiicccsss
iiinnn UUUnnniiittteeeddd SSStttaaattteeesss ooofffAAAmmmeeerrriiicccaaa
� American Orthodontics (1800–
1840)
– Benjamin James
– Samuel S Fitch
– M Bourand
� American Orthodontics (1840–
1875)
– Chapin A Harris
– Thomas W Evans
– Emerson C Angell
– O A Marvin
– William E Magill
� American Orthodontics (1875–
1900)
– John H Farrar
– Norman W Kingsley
– Alton H Thompson
– Isaac B Davenport
– Henry A Baker
– Eugene S Talbot
– Simeon H Guilford
– WGA Bonwill
In Colonial America, primitive conditions fordental care existed for almost a century untilEuropean-trained operators for the teeth cameto this country seeking fresh opportunities. Theart of dentistry in America can be said to havehad its origin with the importation of thesepractitioners to the colonies.
One of the most important native practi-tioners was John Greenwood (1760–1819). Hisskills were first learned from his father, who wasan instrument maker. He was apprenticed to DrGamage, who taught him the rudiments of thedental art. Through experience, he becameproficient in the practice.
Other practitioners include Josiah Flagg(1763–1816) of Boston, who advertised that he“regulates teeth from their first teeth, to preventpain and fevers in children, assists nature in theextension of the jaw, for a beautiful arrangementof a second set of teeth.”
In 1798 CW Whitlock of Philadelphia statedthat he supplies the deficiencies of nature files,regulates, and extracts teeth. John Le Tellier, alsoof Philadelphia states, “regulates teeth from their
first cutting in children” (1804). B Fendall ofBaltimore advertised that he “regulates the teethof children” (1784).
Leonard Koecker (1728–1850), practiced inPhiladelphia, advertised that he suppliesligatures to teeth of an irregular position. Hestated this in his published articles in the medicalpress (1826): “Irregularities of the teeth is one ofthe chief predisposing causes of disease, andnever fails even in the most healthy conditionsto destroy, sooner or later, the strongest and bestset of teeth unless properly attended to. It is notonly a most powerful cause of destruction of thehealth and beauty of the teeth but also to theregularity of the features of the face, alwaysproducing, though slowly, some irregularity, butfrequently the most surprising and disgustingappearance. It is, however, a great pleasure toknow that dental surgery is abundantly providedwith a remedy, and in most delicate subjects ifplaced under proper care at an early age, thegreater portion of the teeth of the permanent setmay invariably be preserved to perfect health and

29History of Orthodontics in United States of America
regularity”. A note about his recomm-endationfor extraction is as follows. He advocated theextraction of first molars “since they are generallypredisposed to disease and if these teeth beextracted at any period before the age of twelveyears, all the anterior teeth will grow more orless backwards, and the second and third molarsso move toward the anterior part of the mouth tofill up the vacant space”.
American Orthodontics (1800–1840)
Irregularity of the teeth had been recognized bydental surgeons early in the nineteenth century.Benjamin James (1814) noted that he was “oftencalled upon to cure irregularity, than to preventit.” Levi S Parmly (1819) stated, “whereirregularities are allowed to proceed and becomefixed, it is often a matter of difficulty, andsometimes of impossibile to rectify them.”
Samuel S Fitch, MD, whose book entitled ASystem of Dental Surgery, published in 1829, isconsidered the first definitive work on dentistryin this country, devoted a significant amount ofinformation to irregularities of the teeth. He wasthe first to classify malocclusion, what is asfollows:
‘There are four states of this kind of irregularity.The first when one central incisor is turned in, and theunder teeth come before it, whilst the other centralincisor keeps its proper place, standing before the underteeth. The second is, when both the central incisors areturned in, and go behind the under teeth; but the lateralincisors are placed properly and stand out before theunder teeth. The third variety is when the centralincisors are placed properly but the lateral incisorsstand very much in; and when the mouth is shut, theunder teeth project before them and keep them backward.The fourth is, when all incisors of the upper are turnedin, and those of the under jaw shut before them’.
His treatment consisted of applying “a force whichshall act constantly upon the irregular teeth and bringthem forward; the other force to remove that obstructionwhich the under teeth, by coming before the upper,always occasion.” This is done by “application of aninstrument adapted to the arch of the mouth, fasteninga ligature on the irregular tooth and removing theresistance of the under teeth by placing someintervening substances between the teeth of the upperand under jaw, so as to prevent them from completelyclosing.”
Other practitioners found various forms oftreatment, such as the use of gold or silver plates “toexert a gentle but continued pressure.” ShearjashubSpooner (1809–1859) wrote in his Guide to SoundTeeth (1838), “we have to consider, first, their generalappearance as to regularity to the central circle; and,second, the state of preservation of each individual toothin cases where there is a predisposition to a projectingchin”.
M Bourand from Paris observed that the parentsshould be alerted to the shedding of the deciduous teethand any possible deformity. He stated: “Defects,sometimes, which are of such magnitude, that I haveknown, in my long practice in both hemispheres, someyoung ladies of respectable families and of elegantfeatures who could not observe their smilingcountenances in a looking glass without blushing atthe irregularities of their teeth; when comparing theirmouths with some of their young friends toward whomtheir parents had bestowed all the necessary care toregulate their growth from childhood”.
American Orthodontics (1840–1875)
The correction of irregularities, however, easy intheory, will be found most difficult and delicatein practice; not only will much skill be foundrequisite, but, in equal degree, patience.
Thus, by the mid-nineteenth century basicconcepts of diagnosis and treatment had begun.It was a time when each practitioner attemptedtreatment by devising his own method based onpurely mechanical principles. Orthodontics waspart of prosthetic dentistry, and the literature onthe subject described orthodontics in the area ofpartial and total replacement.
Chapin A Harris (1806–1860), one of the mostinfluential dental surgeons during this period,published the first modern classic book ondentistry, “The Dental Art”, in 1840. In it he givesmuch attention to various orthodontic treatmentprocedures that were adapted from French andEnglish practitioners. His personal techniqueincluded the use of gold caps on molars to openthe bite and knobs soldered to a band for toothrotations.
Materials generally used were cotton or silkligatures, metallic wedged arches, and woodenwedges, but the discovery of vulcanite, a materialused for artificial dentures, permitted the

30 History of Orthodontics
construction of bite plates and other forms ofremovable appliances. In addition, springs thatwere to be attached to the metal frames for usein individual tooth movement were introduced.
As early as 1841, William Lintott introducedthe use of screws. They were described in thechapter entitled “Irregularities of the Teeth”, as:“When any one or more teeth project beyond theright line, and it is desired to move them inwards,a small hole must be drilled through the bar, overagainst the most prominent point of each; ascrew-thread is then to be cut and a short screwintroduced, which working through the bar, will,by a turn or two, each day, keep up such acontinued pressure against each tooth as willquickly force it back as desired.
He described the premature loss of deciduousteeth as a cause of malocclusion, explained thatcrowding was due to faulty growth anddevelopment. He recommended that treatmentshould begin at the age of 14 or 15 years and alsodescribed a bite-opening appliance, whichconsisted of a labial arch of a light bar of gold orsilver passed around the front surfaces of theteeth by means of ligatures (known as Indiantwist), and the necks of the irregular teeth withpressure applied for movement.
In this manner, any required movement ofthe teeth, inwards or outwards may be affectedwith great ease, and in very little time causingno serious annoyance to the patient, the wholeapparatus being removed and cleansed everytwo or three days.
A modification of the screw, called the crib,was introduced by the Frenchman JMA Strangein 1841. Strange also introduced the use of theclamp band. For retention he advised: Of use arubber band attached to some hooks on theappliance surrounding the molars for retention.”The chin strap as occipital anchorage for thetreatment of mandibular protrusion wasintroduced by JS Gunnell in 1840, and theprinciple of this may be seen today. Occipitalanchorage was obtained by the use of headgeardevised by F Christopher Kneisel.
In 1852 the American Society of DentalSurgeons, the first National Dental Association,established in this country (1840), committed toa great interest in this phase of dentistry, formeda committee on dental irregularities. The first
report was given by E J Tucker, a respected dentalsurgeon of Boston, in 1853. He condemned thepractice of early extraction of deciduous teeth andadvocated the use of rubber bands, or tubes, fortooth movement. He said, “The exact position ofthe teeth, the lines of force to be observed, and thetenacity of the power exerted, are allconsiderations requiring study and a carefuljudgment.” This same society sponsored thepublication of the first book on orthodontics,Essay on Regulating the Teeth (1841). It waswritten by Solymon Brown (1790–1876) of NewYork, and was intended to inform parents bystressing the importance of preventingirregularities.
In 1854 Thomas W Evans (1823–1897), anAmerican dentist practicing in Paris, France,published the requirements for an appliance inthe Dental Newsletter, which are as follows:
First: a firm support which shall not loosenor in any way injure the teeth to which it isattached; Second: a steady and sufficientpressure; Third: great delicacy of constructionthat the apparatus may be a light as possible;Fourth: as a mechanism as simple as the case willadmit.
In 1860 Emerson C Angell (1823–1903) wasprobably the first person to advocate the openingof the median suture to provide space in themaxillary arch, since he took a strong standagainst extraction. James D White also perfecteda removable vulcanite appliance with a hinge ina split palate (1860).
OA Marvin (1828–1907), in 1866, outlinedthe objectives of orthodontic treatment–first:the preservation of correct facial expression;second: the restoration of such expression;Third: the proper articulation of the teeth forbetter mastication; Fourth: their orderlyarrangement, with a view to preventingdecay.
As early as 1871 William E Magill (1825–1896) had cemented bands on the teeth.
It may be of interest to know that in 1864George J Underwood of New York presented hisgraduation thesis at the Pennsylvania College ofDental Surgery (Philadelphia) entitled”Orthodontia”.

31History of Orthodontics in United States of America
American Orthodontics (1875–1900)
It was not until the latter part of the nineteenthcentury when a few dedicated dentists gavespecial attention and importance to this phaseof dentistry, that our specialty began to emerge.Known in that time as orthodontia, it requiredspecial mechanical skills and knowledge in suchbasic sciences as anatomy, physiology, andpathology.
The period of the last three decades of thenineteenth century is studied in the frameworkof individual dentists and their contributions.Each practitioner developed his own theory andpractice, some to a greater degree of excellencethan others. Those to be discussed briefly includeJohn H Farrar (1839–1913); Norman W Kingsley(1829–1913); Alton H Thompson (1849–1914);Issac B Davenport (1854–1922); Henry A Baker(1848–1934); Eugene S Talbot (1847–1925);Simeon H Guilford (1841–1919); and WGABonwill (1833–1899).
John H Farrar could be referred to as the Fatherof American Orthodontics. It was he who gaveimpetus to the scientific investigations thatpermitted the understanding of the theory andpractice of orthodontics. He began his studies in1875, during which time he investigated thephysiologic and pathologic changes occurring inanimals as the result of orthodontically inducedtooth movement. As a result of his studies, hepublished a series of articles, between 1881 and1887, in the Dental Cosmos, one of the leadingdental journals, enunciating the principle that “inregulating teeth, the traction must be intermittentand must not exceed certain fixed limits.” He alsopublished “Irregularities of the Teeth and TheirCorrection” (Vol. 1 in 1888 and Vol. 2 in 1889), inwhich he demonstrated the many uses of thescrew as the motivating attachment and the basisof what he referred to as a system of orthodontia.(Copies of these books are in the AmericanAssociation of Orthodontists library in St Louis,Mo). He stressed the “importance of theobservance of the physiologic law which governstissues, during movement of the teeth, the subjectbeing to prevent pain.” Farrar was the originatorof the theory of intermittent force, and the firstperson to recommend root or bodily movementof the teeth.
NORMAN WILLIAMS KINGSLEY (1829–1913)
Norman Williams Kingsley (Fig. 4.1) was born on2nd October 1829. Kingsley was one of thefounders, who served as the first Dean of theNew York University College of Dentistry. Hereceived honorary degree from Baltimore Collegeof Dental Surgery in 1871.
Kingsley was a prolific writer, with over 100articles on cleft palate rehabilitation, theinadequacies of cleft palate surgeries, obturators,orthodontic diagnosis, and orthodonticappliances. He was a prominent dentist, artist,and orthodontist. As early as 1866, heexperimented with appliances for the correctionof cleft palate and is associated with a techniqueknown as jumping the bite with the use of a biteplate. It was the treatment for protrusion of themaxilla, not necessarily with extractions, shapingthe dental arches to be in harmony with eachother. He used vulcanite in conjunction withligatures, elastic bands made of rubber,jackscrews, and the chincap. In 1880 he publishedA Treatise on Oral Deformities, which remaineda textbook for many years. He, too, emphasizedthe importance of the relationship betweenmechanics and biology as the principle on whichorthodontics should be based. His book was thefirst to recommend etiology, diagnosis, andtreatment planning.
Fig. 4.1: Norman W Kingsley (1829–1913)
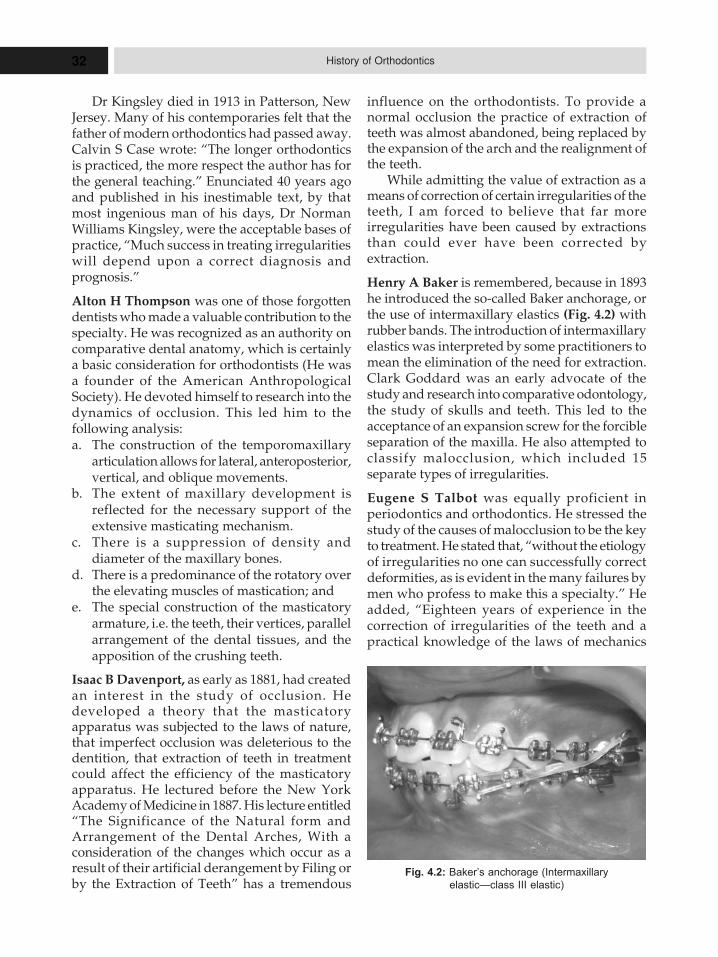
32 History of Orthodontics
Dr Kingsley died in 1913 in Patterson, NewJersey. Many of his contemporaries felt that thefather of modern orthodontics had passed away.Calvin S Case wrote: “The longer orthodonticsis practiced, the more respect the author has forthe general teaching.” Enunciated 40 years agoand published in his inestimable text, by thatmost ingenious man of his days, Dr NormanWilliams Kingsley, were the acceptable bases ofpractice, “Much success in treating irregularitieswill depend upon a correct diagnosis andprognosis.”
Alton H Thompson was one of those forgottendentists who made a valuable contribution to thespecialty. He was recognized as an authority oncomparative dental anatomy, which is certainlya basic consideration for orthodontists (He wasa founder of the American AnthropologicalSociety). He devoted himself to research into thedynamics of occlusion. This led him to thefollowing analysis:a. The construction of the temporomaxillary
articulation allows for lateral, anteroposterior,vertical, and oblique movements.
b. The extent of maxillary development isreflected for the necessary support of theextensive masticating mechanism.
c. There is a suppression of density anddiameter of the maxillary bones.
d. There is a predominance of the rotatory overthe elevating muscles of mastication; and
e. The special construction of the masticatoryarmature, i.e. the teeth, their vertices, parallelarrangement of the dental tissues, and theapposition of the crushing teeth.
Isaac B Davenport, as early as 1881, had createdan interest in the study of occlusion. Hedeveloped a theory that the masticatoryapparatus was subjected to the laws of nature,that imperfect occlusion was deleterious to thedentition, that extraction of teeth in treatmentcould affect the efficiency of the masticatoryapparatus. He lectured before the New YorkAcademy of Medicine in 1887. His lecture entitled“The Significance of the Natural form andArrangement of the Dental Arches, With aconsideration of the changes which occur as aresult of their artificial derangement by Filing orby the Extraction of Teeth” has a tremendous
influence on the orthodontists. To provide anormal occlusion the practice of extraction ofteeth was almost abandoned, being replaced bythe expansion of the arch and the realignment ofthe teeth.
While admitting the value of extraction as ameans of correction of certain irregularities of theteeth, I am forced to believe that far moreirregularities have been caused by extractionsthan could ever have been corrected byextraction.
Henry A Baker is remembered, because in 1893he introduced the so-called Baker anchorage, orthe use of intermaxillary elastics (Fig. 4.2) withrubber bands. The introduction of intermaxillaryelastics was interpreted by some practitioners tomean the elimination of the need for extraction.Clark Goddard was an early advocate of thestudy and research into comparative odontology,the study of skulls and teeth. This led to theacceptance of an expansion screw for the forcibleseparation of the maxilla. He also attempted toclassify malocclusion, which included 15separate types of irregularities.
Eugene S Talbot was equally proficient inperiodontics and orthodontics. He stressed thestudy of the causes of malocclusion to be the keyto treatment. He stated that, “without the etiologyof irregularities no one can successfully correctdeformities, as is evident in the many failures bymen who profess to make this a specialty.” Headded, “Eighteen years of experience in thecorrection of irregularities of the teeth and apractical knowledge of the laws of mechanics
Fig. 4.2: Baker’s anchorage (Intermaxillary
elastic—class III elastic)

33History of Orthodontics in United States of America
have taught me not to rely on any particularappliance. Frequently, though a certainappliance has worked well in one case it maynot have been efficient in another case of similarnature. He advised that close attention todisproportion in the size of the maxilla andmandible, general contour and profile of the face,and the family history including hereditaryfactors important. He was one of the first torecommend the surgical exposure of impactedcanines.
In a paper presented to the Mississippi ValleyAssociation of Dental Surgeons in March 1891,entitled “Scientific Investigation of the Craniumand Jaws,” he demonstrated intraoralmeasurements on cast with such instruments asthe registering calipers and the T-square withgraduated sliding indicator. This was one of theearliest attempts applying specific analysis ofcasts that reflected measurement of the jaws.
Simeon H Guilford, dean of the PhiladelphiaDental College, was regarded as one of the finestpractitioners of that period. At the request of theNational Association of Dental Faculties, hewrote the first textbook for students, Orthodontia:Malposition of Human Teeth, Its Prevention andRemedy, published in 1889. In this, he attemptedto offer a classification of malocclusion. “Thereare two divisions—simple irregularities or themalposition of few teeth with no important facialdisharmony, and complex irregularities, that is,malposition of many teeth having correspondingfacial deformity” (These divisions contain elevenclasses of malposition).
He commented on extraction in treatments:“Probably no operation in the practice oforthodontia is more important, or has associated
with it greater possibilities for good or evil to thepatient than that of extraction”.
WGA Bonwill said, “in vying with nature inmatching the teeth, there must be more than meremechanics, more than being capable of filling atooth or treating an abscess–we must be dentalartists.” He developed what is known as theBonwill equilateral triangle. It is based on themandibular analysis of a tripod arrangement,extending from the center of the condyloid processto the median line at the point where themandibular central incisors touch at the cuttingedge. His measurements of more than 2,000 casesshowed that from the center of one condyloidprocess to the center of the other was four inchesand that from the center to the incisor was alsofour inches. He used this theory in his orthodontictreatment. He advocated a specialty oforthodontics many years before Angle:
“Really, in every city, someone should makeof this a special practice, and the professionshould encourage such by sending cases forinspection and consultation. And such aspecialist should do all he can, in return to teachby example and demonstrations by clinics, toenlighten those who are placed so far from largecities that they are compelled to take such cases.When we can have that understanding betweenus, then we may feel as banded brothers morefully equipped for those hitherto difficult andthankless operations.”
The principles of resorption and depositionof alveolar bone during tooth movement werediscussed by LE Custer (Ohio) in March, 1888,at a meeting of the Mississippi Valley DentalAssociation, in a paper entitled “IntermittentPressure: Its Relation to Orthodontia.”
5HHHiiissstttooorrryyy ooofff
OOOrrrttthhhooodddooonnntttiiicccsssiiinnn GGGrrreeeaaattt BBBrrriiitttaaaiiinnn
� Orthodontics in Britain
– Bell
– Medical Act of 1858
– Tomes
– Sir John Russell Reynolds
– Charles Goodyear
– 1878 Dentists Act
– JA Donaldson
� The British Society for the
Study of Orthodontics
– Badcock
Several eighteenth-century British authors,notably John Hunter, discussed the problemsassociated with irregular dentition. However, thefirst English textbook to be devoted to the subjectmatter of what would later be termedorthodontics appeared in 1803. Joseph Fox’sNatural History of the Human Teeth, subtitled,describing the proper mode of treatment toprevent irregularities of the teeth, detailedseveral practical methods for altering the positionand orientation of teeth in the mouth. In 1829,Thomas Bell published The Anatomy,Physiology and Diseases of the teeth, in whichhe also discussed orthodontic problems andtechniques. Five years later, William Imrie, in hisinterestingly titled Parents’ Dental Guide,attributed irregularity of teeth to “intemperanceof various kinds, combined with artificial modesof living”. James Robinson published, TheSurgical, Mechanical, and Medical Treatment ofteeth in 1846, which contained his ideas onetiology and treatment. It is clear, from thesetexts, that procedures aimed at straightening theteeth were already part of the general dentalsurgeon’s repertoire by the first half of thenineteenth century.
In 1829, Bell, lecturer at Guy’s Hospital on theanatomy and diseases of the teeth, expressed
misgivings regarding the quality of much of thetreatment on offer to “regulation cases”, as theywere then termed.
There is not a subject connected with thatbranch of practice, of which the present workprofesses to treat, which has given rise to suchgross charlatanism, or to so much gratuitouscruelty, as that which regards the treatment orprevention of irregularity in the permanent teeth.
Concerns of this sort were, however, notuncommonly voiced with regard to many aspectsof dentistry at this time. The practice of dentistrywas still unregulated; there were no recognizedtraining programs or prerequisite educationalrequirements. The better-qualified practitioners,such as Bell, MRCS (later FRCS) and FRS, foundmuch to complain about.
In Britain, for much of the nineteenth century,dental work was undertaken by three dissimilargroups of practitioners. The members of the firstgroup, small in number but perhaps the mostinfluential, had recognized medical qualific-ations, which they had augmented by a shortperiod of training in dentistry. These men werebased predominantly in London and some of thelarger provincial cities; most of them, like Bell,held hospital or dispensary appointments atsome stage in their careers. The authors whose

35History of Orthodontics in Great Britain
publications have been discussed above arerepresentative of this group.
The second group had acquired their dentalskills primarily by way of an apprenticeship, ofvariable length and effectiveness, to anestablished dental practitioner. The number ofthis category of practitioners grew as the centuryprogressed. The third group, perhaps the largest,and the most readily available to the generalpopulation, had little formal training and oftencombined their dental work with some otheroccupation, such as druggist or barber.
The forms of treatment offered by thedifferent groups varied. Those who weremedically qualified tending towards a surgicalorientation, which encompassed the whole of thebuccal cavity. The second group, those who hadfollowed the apprenticeship route, generallyadopted a more mechanical approach, with anemphasis on the filling of teeth and the fitting ofprosthesis. They would also perform extractions.The activities of this group most closelyresembled the general dental practitioners oftoday. The services offered by the third groupwere more basic, chiefly involving the extractionof painful teeth.
The Medical Act of 1858 regulated thepractice of medicine, laying down statutoryeducational requirements and establishing aMedical Register, which was administered by theGeneral Medical Council (GMC). The MedicalAct also empowered the Royal College ofSurgeons of England to award, by examination,a License in Dental Surgery. The first diet of thisexamination took place in 1860. Realizing thebenefits of the Medical Act, the leading dentists,many of whom were, as noted above, medicallyqualified, and urged that similar provisions bemade for dentistry. Sir John Tomes, MRCS (laterFRCS) and FRS, was prominent in thesecampaigns.
While Tomes and his peers werecampaigning for the establishment of a regulatedsystem of dental qualification and registration,they were also active in expanding dentistry’sinstitutional base. The Dental Hospital of Londonwas founded in 1858, and it’s associated LondonSchool of Dental Surgery (LDS) in the followingyear. The rival Metropolitan School of DentalSurgery (which later became the National DentalHospital) was also established in 1858, just before
the Royal College of Surgeons of England beganexamining for the newly created LDS. TheEdinburgh Dental Dispensary, run and staffedby surgeons, was founded in 1860. In 1863, theOdontological Society of Great Britain wasformed, from the merger of two older, rivaldental societies, under the leadership of Tomesand Samuel Cartwright, the professor of dentalsurgery at King’s College Hospital.
A long political campaign achieved successin 1878, with the passage of the first Dentists Act,which extended the remit of the GMC to allowsome regulation of dental practice. The Act alsoempowered the surgical colleges of Edinburghand Dublin, and the Faculty of Physicians andSurgeons of Glasgow to offer examinations indentistry similar to that of the London College.While it would be more than a further 40 yearsbefore all unregulated practice was finallycontrolled, the passing of the 1878 Act was anindication of the growing professional and socialstatus of dentistry.
Generalism had been the dominant ideologyof nineteenth-century British medicine. In 1881,Sir John Russell Reynolds, later president of theRoyal College of Physicians and the BritishMedical Association, maintained that“specialism” denoted “miserable retrogressioninstead of evolution (and) the survival not of thefittest, but of the charlatan and the quack”. Aswe shall see, similar views continued to bearticulated by many, well into the twentiethcentury. However, as David Innes Williams haspointed out, the formation of the Royal Societyof Medicine (RSM) in 1907 signaled a new, morepositive, attitude to specialization withinmedicine itself. The RSM was organized intothirteen sections, rather than the traditionaltripartite division of physic, surgery andobstetrics. The Odontological Society wasincorporated into the RSM as one of its originalconstituent sections, which represented anacceptance of the place of dentistry within themedical establishment.
By this time, specialization had little impactwithin general dentistry. However, many of theleading dentists, mostly members of the firstgroup described above, regarded dentistry as adivision within medicine and themselves asmedical practitioners who had taken a specialinterest in dentistry. The meaning of specialism

36 History of Orthodontics
varied, in other words, according to whether oneregarded medicine or dentistry as the parent,generalist discipline.
Meanwhile, the demand for treatment tocorrect irregularities of the teeth and jawscontinued to grow. Earlier in the nineteenthcentury patients undergoing treatment tostraighten their teeth were described as“regulation cases”; references to the fact that theaim of treatment was to correct what were called“irregularities of the teeth”. By the middle ofthe century, however, the term “malocclusion”was coming into common use. This change ofvocabulary signaled a shift of emphasis awayfrom a narrow focus just on the position of thefront teeth, towards the consideration of both therelationship of teeth to each other, and to theteeth in the opposing jaw. The clinical practiceof correcting malocclusion then became knownas “orthodontia”. Later the term “orthodontics”was preferred.
As the nineteenth century proceeded, thematerials available to practitioners of“orthodontia” were improved and new methodswere widely adopted. William Imrie, forexample, made significant changes toorthodontic technique in the 1830s. He usedplaster models of the dentition, made caps forteeth, which were soldered to arches to reinforceanchorage, and introduced gold bite plates to beused over the palate. A treatise by Charles Gaine,of Bath, published in 1856, is interesting in thatit draws on the record of successfully treatedcases. Gaine is credited with the introduction,simultaneously with WH Dwinelle in the USA,of the jackscrew into orthodontics, an innovationthat was to have a great impact on the ability tomove individual teeth and to expand the distancebetween rows of teeth. Gaine also recognized theneed to maintain the teeth in their correctedpositions for a period of time after toothmovement had been completed. Like Bell, heurged that orthodontic treatment be undertakenonly by those competent to do so. Thedevelopment of a technology specific to thecorrection of irregular dentition gave itspractitioners a stronger claim to a distinctive skill,as well as a greater sense of professional identity.
Vulcanite was patented, in 1844, by CharlesGoodyear and rapidly found application indentistry, providing a distinct improvement in
the production of both dentures and regulationplates. In a series of papers published in the1870s, FH Balkwill described a furtherrefinement in the use of the material, wherebythe vulcanite was applied directly to the workingplaster model of the teeth. This avoided the needto construct a model of the appliance in wax. Thenew technique significantly improved accuracy,and drastically reduced workshop time.Balkwill’s papers demonstrate that Britishdentists were actively involved uninnovation inthe field of orthodontics in the second half of thenineteenth century. Although his appliances mayseem crude by modern-day standards, theydemonstrated many ingenious features, andappear to have been effective. Many of thenuances of tooth movement were, evidently, wellappreciated at this time. Moreover, the fact thatBalkwill worked in Plymouth indicates that theprovision of orthodontic treatment was notlimited to the metropolis.
Following the 1878 Dentists Act, the newlycreated dental schools incorporated someteaching of orthodontics into their curricula. The1882 “Student Supplement” of the British Journalof Dental Science listed lectures on irregularitiesof teeth as part of the dental surgery alsopathology courses were offered at both theNational Dental Hospital and the DentalHospital of London. Orthodontic subject matterappeared both in the major general textbooks andin more specific volumes. Of the latter, JamesOakley Coles’ On deformities of the mouth,congenital and acquired, and their mechanicaltreatment, first published in 1868, and J FColyer’s Notes on the treatment of irregularitiesin position of the teeth, are notable. Articles onorthodontics began to appear regularly in thedental periodical literature. The first formalcourse of lectures on “what was later known asorthodontics” was delivered by John HenryBadcock, dental surgeon to Guy’s Hospital,shortly after his appointment in 1900.
JA Donaldson, in his history of The NationalDental Hospital, accurately describes thesituation existing in most dental schools aroundthe turn of the century:
There was an increasing interest inorthodontics, partly as a result of lectures andwritings by practitioners who had studied in theUnited States of America, and partly because it

37History of Orthodontics in Great Britain
was a field soon to be included in therequirements of examining bodies. By 1902, thisled to the adoption by the National DentalHospital of “rules for regulation cases” and thefitting up of a room on the first floor for theirtreatment, but no teacher was appointed at thistime. The treatment of each case was undertakenby a student under the supervision of the dentalsurgeon of the day.
In other words, orthodontic theory andpractice were still being taught as integratedaspects of general dentistry.
Nevertheless, from 1903 onwards, the stafflists of the Manchester Dental Hospital containedthe names of a number of orthodonticdemonstrators or tutors. In 1909, mention is madefor the first time of the existence of a separateOrthodontic Department. In the same year,George G Campion was appointed as lecturer inorthodontics to the Victoria University,Manchester. By 1905 a “Regulation Room” hadbeen established in the Royal Dental Hospital,staffed by the “Regulation Room HouseSurgeon”. By the beginning of the next decade,a number of other hospitals had followed suit.However, no formal postgraduate courses inorthodontics existed and many British dentistsinterested in the subject went to the United Statesfor advanced training. For example, in the firstdecade of the twentieth century, HaroldChapman, Hubert Visick, AC Lockett, David Fyfeand Ernest Sheldon Friel, all attended the schoolrun by the pre-eminent American orthodontist,Edward Angle, originally in St Louis. By thistime, there were several full-time orthodontistsin North America, most notably Angle himself,who had entered dedicated practice in 1892, but,as yet, none at all in Britain. A pupil of Angle,Friel, in Dublin, set up the first such practice inthe British Isles in 1909.
Orthodontics appears to have caught thedental imagination in the early years of thetwentieth century. It is revealing, for instance,that the American, the British, the German, andthe European orthodontic societies were allfounded within ten years of each other. Someauthorities, notably the leading historian oforthodontics BW Weinberger, have attributedthis widespread surge of interest to the impactof Angle’s writings. There is certainly no doubtthat, when compared to the situation in Britain,
the teaching and the practice of orthodontics inNorth America were more established, betterorganized and more sophisticated, or that Anglewas a dominant (if controversial) figure inAmerican orthodontics. It is telling, for instance,that Angle’s pupils from the British Isles, notablyChapman, Friel and Visick, came to occupyleading positions within British orthodontics.Prolific authors of research papers, all three werefounder members of the BSSO, Chapman andFriel serving as president.
Angle’s teaching was predicated upon theassumption that orthodontics should be aspecialty wholly independent of generaldentistry. Part of the rationale for a specialistservice, as he articulated it, was that the aim oftreatment had become more ambitious. Its goalwas now the establishment of “normalocclusion”. The objective was to place all the teethin their correct relation, not only to theirimmediate neighbors, but also to theirantagonists in the opposite jaw, and in aharmonious relation to the whole face. There wasintense debate among orthodontists, in Americaand elsewhere, as to whether or not this idealcould be achieved in all patients and, if so, how.But the fact that this debate took placedemonstrates the rising technical and aestheticaspiration of practitioners of orthodontics.
Angle’s bold assertion that orthodonticsshould be divorced from dentistry met with littlesupport in Britain. An editorial in the BritishDental Journal of 1902 stated:
“Where the specialization of specialities maylead can hardly be foreseen, and we even awaitthe prophesed eminent rhinologist devoted to theleft nostril. That dental speciality admits of muchdivision of labor without detriment isunquestionable, but the swing of the pendulummay well be too far. It appears that theorthodontist has already arrived in America, andthere is a Society.”
In North America, however, the trend toseparate orthodontics from general practice wasgathering pace.
THE BRITISH SOCIETY FOR THE STUDY OF
ORTHODONTICS
It was from within this context of growingprofessional status and confidence, coupled withconsiderably improved technical capability, that

38 History of Orthodontics
the British Society for the Study of Orthodonticssprung up. Practitioners in Britain were awareof the increasing presence of orthodonticspecialists in North America, but did not seekimmediately to emulate them in their advocacyof a separate specialty. There was, in any case,as an editorial in the dental journal Items ofInterest noted, a difference in the interpretationof the word “specialist”, between England andthe USA. In England, a “specialist” was often ageneral practitioner having an interest andexpertise in a particular aspect of dentistry,whereas, in the USA, the term was used todesignate someone who exclusively practiced inthat field. The English interpretation ofspecialization would certainly be formative, aswe shall see, of the first British specialist society.
The driving force behind the creation of theBSSO was, without doubt, George Northcroft,who was a successful London dental practitioner.On 15 October 1907, Northcroft wrote to anumber of his fellow practitioners inviting themto attend a preliminary meeting to discuss thefoundation of a society, the object of which wouldbe the promotion of the study of orthodontia.This meeting was held on 21 October 1907, inhis rooms at 115 Harley Street, London. Elevenpractitioners attended, in addition to North croft.Nine of those practiced in the West End ofLondon, the other two being based in Wimbledonand Eastbourne, respectively. At least seven hadhospital appointments. The founders of the BSSOwere evidently drawn from the upper strata, interms of their institutional, educational and socialstatus, of the British dental profession. They werethe heirs of the group of practitioners who hadcampaigned to raise the professional standing ofdentistry in the second half of the nineteenthcentury. It was agreed to proceed with the planof setting up a society.
An inaugural meeting was held, by generalinvitation, in the room of the Medical Society ofLondon, on 5 December 1907, which thirty-fivepeople attended. Badcock was elected president,with Northcroft, James Sim Wallace, andMontagu Hopson being vice presidents. All foursenior office-bearers held or had recently held,posts in one or other of the London hospitals.
As already noted, Badcock had been, until1905, dental surgeon and lecturer in dentalsurgery at Guy’s Hospital. Northcroft held a
similar appointment at the London HospitalDental School, in the founding of which he hadbeen closely involved. Sim Wallace, the authorof the influential text Essay on the irregularitiesof the teeth (1904), was on the staff of severalLondon hospitals over the course of his career,while Hopson eventually became head of theDental School at Guy’s Hospital.
The social and professional background of theearly leaders of the BSSO is very revealing as tothe character of the society and its aims. As Weiszhas pointed out, in Britain, unlike North Americaor the rest of Europe, specialist expertise cameto be identified as the unique possession of seniorhospital staff. It was to hospital consultants, andonly hospital consultants, that generalpractitioners referred patients in need of anexpert opinion. What was odd and distinctivelyBritish about this arrangement, was that thehospital consultants espoused an ideology ofgentlemanly holism and regarded themselves asmedical generalists, albeit often with somedegree of specific focus in their clinical interests.Thus, even the major beneficiaries of the processof specialization within British medicine did notpresent themselves as specialists per se. Such wasthe authority and prestige of the hospitalconsultant, especially those in the Londonteaching hospitals that this model came to be thedefinitive one for specialization in Britain. As weshall see, this pattern of specialist interest withinan ostensibly generalist framework can be readilyidentified within the agenda of the BSSO.
In his address to the inaugural meeting,Badcock, as president-elected, pointed out “therewas now sufficient demand for a society, “wheremembers could consult and advise each otherupon the problems of the already large butincreasingly important branch of dental surgery,orthodontia”. He felt, “the proposed name forthe society should indicate that it was not theintention to create a group of specialists,practising orthodontia, but to provide anopportunity when everybody who wasinterested in both theory and practice could meetfor mutual benefit”.
The rules of the new society were closelymodeled upon those of the existing Odontol-ogical Section of the Royal Society of Medicine,which were intended to ensure that theorganization was non-political and disengaged

39History of Orthodontics in Great Britain
from controversy. One feature of the rule book,very revealing of the society’s self-image, wasthat members were to be prohibited from holdingany commercial patents relating to dentistry.There was also an injunction against secretremedies, which were regarded as the staple ofthe “quack” specialist. One speaker at theinaugural meeting thought that the prohibitionagainst patents would have an inhibiting effectupon the future development of dentaltechnology. Nevertheless, the gentlemanly ethosof the upper strata of London medicine, with itspronounced antipathy to trade, prevailed and therule was confirmed. This was again in markedcontrast to American practice, where severalorthodontists had taken out patents on technicalinnovations.
The first full meeting of the BSSO took placein January 1908. As president, Badcock presentedthe first official paper. He chose, as his topic, theobjectives of the new society and his views arevery indicative of the state of orthodontics inBritain at this time.
This is a very broad and inclusive remit for aspecial interest in dental or medical society, andis quite different in character from the nearestNorth American equivalent. It is clear that, inoffering membership to all with an interest inorthodontics, regardless of occupational status,the BSSO did not constitute itself, at leastprimarily, as an organization to advance theprofessional interests of orthodontists. Ratherthan, the society defined its mission as the moredisinterested one of encouraging theadvancement of knowledge in the field. Againthere are resonances here with the constitutionof the RSM. As Innes Williams has recentlyargued, while the RSM represented theacceptance of a degree of specialization withinBritish medicine, in presenting itself as a purelylearned society, it effectively recognizedspecialties as categories of knowledge rather thandivisions of practice. While the BSSO sought toencourage the improvement of correctivetechnique as well as the scientific understandingof normal and irregular dentition, the similarityof its aims with those of the RSM is noteworthy.To some extent, as Innes Williams notes, thisemphasis was chosen to avoid engagement inissues relating to competition in the medicalmarketplace. Nevertheless, it is also true, as the
quotation from Badcock indicates, that thefounding figures of the BSSO evidently believedthat development of the scientific and academiccontent of the subject would assist orthodonticsin achieving a much more prominent placewithin dentistry as a whole.
Badcock acknowledged that anxieties hadbeen expressed that the creation of a new society,devoted solely to one particular branch ofdentistry, could be divisive within the dentalprofession. But he regarded this apprehensionas being groundless. He was not, however, inprinciple against specialization in the NorthAmerican sense. He foresaw that eventually, atleast in the larger centers of population, only full-time specialists might provide an orthodonticservice. In his judgment, this development wouldbe beneficial. Interestingly, Badcock comparedthe advantages to be gained from orthodonticspecialization to those that would accrue fromthe administration of anesthetics by specialistanesthetists, as against administration by generalpractitioners with an interest in anesthesia,which, he stated, was the usual practice at thetime. In other words, Badcock was prepared, atleast partially, to repudiate the view, widespreadstill among medical practitioners in Britain, thatfull-time specialization was necessarily to bedeplored.
As mentioned earlier, in the first decades ofthe twentieth century, North American orthod-ontics was riven by acrimonious controversy,relating to both the cause and the treatment ofmalocclusion. The society’s founders were veryanxious that these divisions should not bereplicated within the BSSO. With characteristicmoderation, Badcock emphasized the Council’sdesire to include representatives from all schoolsof thought. Another of the early presidents, HarryBaldwin, described the society as a “model ofseductive humility” and was evidently proudthat the society enjoyed a harmoniousrelationship with the generalist British DentalAssociation.
Some of the controversy which disturbedNorth American orthodontics centered onAngle’s rigid insistence that it was bad practiceto extract healthy teeth to facilitate toothrealignment. This tenet became the governingprinciple of those full-time Americanorthodontists who practised the Angle method.

40 History of Orthodontics
Badcock argued, however, that many potentialorthodontic patients could not afford either themoney or time for prolonged and sophisticatedtreatment, and for those patients extraction wasa necessary part of successful management. Thiswas, effectively, a recognition of the differencesbetween the British and American circumstancesof orthodontic practice. Several of Badcock’saudience would have held appointments involuntary hospitals where they would provideeconomical treatment for charitable patients.Moreover, British orthodontists knew that if theywished to expand the range of patients that theytreated, it was necessary to make available asimplified form of treatment.
On the other hand, Badcock also deploredthose orthodontists who viewed treatmentpurely in empirical, mechanical terms. In hisview, the realignment of the teeth could besuccessful, in the long-term, only if it was basedupon sound biological principles. He admittedthat the profession was still woefully ignorantin the fields of etiology, pathology andprophylaxis. Again the stated purpose of theSociety was to be a disinterested forum, a vehiclefor the advancement, not merely of technique,but of science.
Badcock concluded by outlining the Council’splans for furthering the aims of the Society.Future meetings would consist of the reading anddiscussion of papers, casual communications andclinical evenings of a practical nature. A libraryand museum would be created; investigationcommittees, comprising small groups ofmembers, would be setup to look at selectedtopics. He mentioned normal arch determin-ation, classification and orthodontic terminologyas possible topics for the attention of theseinvestigating committees.
Thus, we can discern, in its first presidentialaddress, some of the distinctive characteristicsof the British Society for the Study ofOrthodontics. Its constitution emulated thegentlemanly ethos of London patrician medicine,with its disdain for trade and its antipathytowards factional enthusiasm. It saw the futureprogress of orthodontics as being best achievedthrough the liberal ideals of the advancement ofknowledge and the improvement of education,rather than by the pursuit of specialization andprofessional organization. Many of its founders
had links with the London teaching hospitalsand/or with socially exclusive private practice,of the Harley Street variety. While not necessarilyor wholly antipathetic to specialist practice, mostof the leading members identified themselves,as we shall see, as generalists with a specialinterest in orthodontics, rather than as specialistpractitioners, per se. The BSSO was, in otherwords, a distinctively British specialist body.
The BSSO met seven or eight times a year.Each meeting usually consisted of thepresentation of a long paper and several shortpapers or demonstrations. Sometimes, papersshared a related theme. Approximately twentypapers or demonstrations were subsequentlypublished in the Society’s annual Transactions.Every year its president addressed the Society,and these addresses, also published in theTransactions, provide a valuable record of theopinions of the leading figures in Britishorthodontics, from 1907 onwards.
It is evident from the Transactions that notall the members of the Society were content withthe first president’s relatively relaxed attitude tothe prospect of full-time practice. In 1910, SimWallace was elected president. His presidentialaddress reaffirmed his commitment togeneralism, in terms with which many of hiscolleagues in metropolitan medicine anddentistry would have been very familiar. Thedanger of specialization was, he argued, that itconfined its practitioners to a narrow route,distorting the sense of proportion and limitingthe large and liberal outlook, which should becharacteristic of a learned profession. Suchrestriction of vision was stigmatized as the curseof specialism. Sim Wallace emphasized that theBSSO had been setup to serve the high ideal ofthe study of orthodontics and not merely toimprove its practice or even its teaching. Theimplication was clear; full-time specialization, bydepriving those interested in orthodontics of abroad intellectual outlook, would hinder ratherthan advance the development of their subject.
But those presidents who concernedthemselves with the quality of the Britishteaching of orthodontics frequently tended to adifferent view. This was particularly true of thosewho contrasted the situation in Britain with thatin North America, to whose specialistinstitutions, as we have seen many British

41History of Orthodontics in Great Britain
prospective practitioners travelled to receivepostgraduate training. For instance, in 1915,Frank Bouquet Bull, a leading member of theSociety and a future president, firmly expressedhis low opinion of the quality of the teaching oforthodontics in Britain. He attributed thisdeficiency to the fact that both lectures andclinical instruction in orthodontics werecombined with dental surgery. With very fewexceptions, the actual teaching was still carriedout by generalists rather than specialistorthodontists. Bull pointed out that theprolonged nature of orthodontic treatment madeit difficult to incorporate within the standardcurricula of general dentistry. Most dentalstudents undertook just over two years of clinicalinstruction but this was rarely long enough tofollow a single orthodontic case to conclusion.Bull also believed that, until students had gainedsome basic knowledge of orthodontics, theycould not fully appreciate its value. Thus manywould-be practitioners, who might otherwisehave been attracted to orthodontics, chose toremain with restorative dentistry.
Bull recommended that orthodonticinstruction should be separated from that ofgeneral dental surgery, and that it should bepostponed until the second year of clinicalstudies. By this stage students would be betterprepared to benefit from the teaching. In thesecond year, a period of three months should beset aside exclusively for orthodontics. Bullapplauded the fact that the London DentalHospital and the Birmingham Dental School hadalready implemented such a system. Hesuggested that independent OrthodonticDepartments be created, each to be under thedirection of someone with a particular interestin orthodontics, preferably assisted by ademonstrator and a specialist orthodontic housesurgeon. This, he believed, would enable bothpatient management to be more effective, andthe standard of teaching to be improved.
Bull was not the only eminent Britishorthodontist concerned about these matters. In1916, Bertram B Samuel gave a short paperentitled ‘Suggestions for the formation of aLondon orthodontic center’. As he saw it,orthodontics in England had two seriousdeficiencies, the dearth of treatment facilities forless well-off children and the absence of
opportunities for postgraduate training. Theestablishment of a dedicated clinical center inLondon would meet both needs. Samuelproposed the Forsyth Institute in Boston as amodel for orthodontic education in Britain.
Bull’s and Samuel’s papers were bothdelivered in the second year of the First WorldWar. The war imposed a hiatus on Britishdentistry as a whole and upon the activities anddevelopment of the BSSO in particular. Manydentists were heavily involved in the war effort,dealing with maxillofacial injuries. Orthodonticwork was substantially curtailed. Even afterpeace returned, orthodontic treatment remainedavailable to only a very small section of thepopulation. The vast majority of the work wasstill carried out by dentists who also practisedother branches of dental surgery. Even theteachers in the orthodontic departments of thedental schools were not necessarily orthodonticspecialists in the North American sense, althoughthey would certainly have had considerableexpertise in the subject. However, the BritishIslands had, as we have already noted, begun toacquire their first full-time orthodontists. Thecase for and against specialization wouldcontinue to be discussed at the meetings of theSociety for many years to come. But when JLPayne gave his presidential address in 1921, heseems to have considered that the principle ofspecialization had become accepted. S Spokes,president in the following year, judged that thedevelopment of orthodontics as a specialty hadnot been detrimental to the general dentalpractitioner but had benefited the profession asa whole.
Throughout the 1920s and 1930s, the technicalrepertoire of the orthodontist continued toimprove and expand. A notable advance was theintroduction of stainless steel, which wasemployed in the construction of bands, archesand springs. Stainless steel was much cheaperand more clinically effective than the previousmetal of choice, gold. However, considerablymore skill was required to work the newmaterial, stainless steel being difficult to weld.Friel was a major pioneer for the introduction ofstainless steel, and several other Britishorthodontists contributed to the realization of itsclinical potential. A further important innovationwas the adoption, with modifications, by British

42 History of Orthodontics
orthodontists of Angle’s pin and tube method ofeffecting tooth movement. This new procedure,together with other similar techniques, againenhanced clinical effectiveness, whiledemanding great precision in its constructionand manipulation.
In 1921, unregistered dental practice wasfinally made illegal in Britain. There was,however, a considerable shortage of dentists, andtherefore little economic incentive for theordinary dentist to diversify his practice. Fromthe 1920s onwards, for a variety of reasons likeawareness of lack of knowledge and equipment,legal considerations, ready availability of otherremunerative work, many general practitionerswere unwilling to undertake orthodontic work.And those who did perform such work tendedto employ the cheaper and easier techniques.They were inclined, for instance, to favorremovable appliances rather than the fixed ones,which were generally more precise and powerfulbut required more skill to fit and took up morechair time. Thus, the gap between the standardsof orthodontic work carried out by the generalpractitioner and that undertaken by the full-timespecialist, or taught within the orthodonticdepartments of the dental hospitals, continuedto widen. British orthodontists, meanwhile,looked across the Atlantic and saw that, if thestandard of the teaching of orthodontics inBritain was to match its American counterpart,then more specialized facilities and specialistteachers were required. Between the wars, callsfor the setting up of a dedicated postgraduatecenter for orthodontics in London were regularlyrepeated. It was even suggested that it could berun under the auspices of the BSSO.
Nothing came of these plans. However, in1931, the Eastman Dental Clinic opened inLondon. This included a separate orthodonticdepartment, which provided both affordabletreatment and postgraduate orthodontic training.After the Second World War, the Eastman wasincorporated into the British PostgraduateMedical Federation. Under the leadership ofClifford Ballard, its orthodontic departmentcame to play a very important role in the furtherdevelopment of the subject in Britain.
The establishment of the National HealthService in 1948 created the conditions for a greatexpansion in the provision of orthodontic care
in Britain. The principle of a state-funded healthcare system seems to have been enthusiasticallyendorsed by the leadership of the BSSO. In 1942,the Society set up a committee to examine theimplications of the Beveridge Report fororthodontics. Faced with the prospect of a need-driven health service, free at the point of deliveryand presumably including orthodontics in itscomprehensive provision, the committeeconsidered what sort of orthodontic care couldbe delivered to the general population, and bywhom. In 1945, giving the first presidentialaddress for six years, tellingly titled ‘Ouropportunity’, Norman Gray welcomed theforthcoming peacetime expansion of health careas providing the prospect of raising the standardsof British orthodontics and increasing thenumbers of its practitioners. Noting that hispredecessors had expressed differing opinionson the subject, Gray affirmed his belief that thetime for specialization had finally arrived. Heenvisaged that the demand for orthodontictreatment would greatly increase once thefinancial obstacles that had excluded poorerchildren, were substantially removed. Thechallenge was to train sufficient numbers ofspecialists to meet the orthodontic needs of thepopulation.
In the same year, Friel also urged his felloworthodontists to embrace the ideal of full-timespecialization as the only way, as he saw it, toraise British orthodontic standards to the levelthat had been achieved in the United States. Frieldeprecated the fact that much treatment inBritain was still undertaken by, as he put it,“skilled amateurs”. He argued that attempts toexpand the provision of treatment without theintroduction of adequate postgraduate educationwould simply prolong this unwelcomecircumstance. His choice of terms is an indicationof how far the discourse surroundingspecialization in British dentistry had changed.Whereas previously the integration oforthodontics within the general practice ofdentistry had been praised as conducive to a“sense of proportion” and a “large and liberaloutlook”, it was now stigmatized as“amateurism”. The “curse of specialism” hadevidently been lifted.
The administrative structure that was chosenfor the NHS imposed a rigid division between

43History of Orthodontics in Great Britain
hospital doctors and community-based generalpractitioners, an arrangement which was veryconducive to the establishment of specialties.Gradually, many more consultants wererecruited in virtually every branch of medicineand dentistry, including orthodontics. At the sametime, the universities became more involved inorthodontic education. The first reader inorthodontics, Corisande Smyth, was appointed in1951 at the Royal Dental Hospital School and thefirst professor, Clifford Ballard, at the Institute ofDental Surgery, University of London, in 1956.Other educational innovations were made. In1949, the Faculty of Physicians and Surgeons ofGlasgow awarded their first Diploma of DentalOrthopedics. The Royal College of Surgeons ofEngland followed suit in 1954.
By the mid-1950s, it was apparent, however,that the impact of the setting up the NHS on theprocess of specialization in orthodontics hadbeen, to an extent, paradoxical. Many morespecialists were being trained but, owing todemand for treatment vastly outstrippingsupply, more orthodontic work was beingundertaken by general practitioners, often usinglimited means of treatment and under great timepressure. The membership of the BSSOcontinued to include a substantial number ofgeneral practitioners, reflecting the dual avenuesof service provision.
The changes that the founding of the NHShad set in train did not come fully into effect untilthe 1960s, when substantial number oforthodontic specialists were appointed, either asconsultant in dental hospitals or with regionalhospital boards. Oddly enough, however, thisexpansion of the specialty was to prove fatal forthe BSSO. As noted above, its founders hadconceived the BSSO rather as a learned societyfor the advancement of orthodontics than as aprofessional body to speak for orthodontists. Thisdirection was taken partly to avoid thefactionalism that had marked orthodonticsocieties in North America. However, the
Society’s constitution was interpreted, bysuccessive meetings of its Council, as precludingits involvement in any discussion or consultationremotely political, even when orthodontic serviceprovision was involved. In 1919, the Parliam-entary Health Committee invited the BSSO tosend a report on its activities. The Secretary wasinstructed to decline, and reply that theiractivities did not extend to political affairs. When,in 1920, the Federation of Medical and AlliedSocieties invited the BSSO to affiliate, theSecretary replied that it was not empowered byits bye-laws to join.
This fastidiousness also prevented the societyfrom exercising its full influence during theplanning and implementation of the NHS. It wasinitially reluctant, for instance, to becomeinvolved in the consideration of specialist titleswithin the service. The BSSO also declined to giveany advice to the British Dental Associationregarding charges for orthodontic appliances. In1962, the Society was invited to submit evidenceto the Standing Dental Advisory Committee, onhospital dental services. It again refused,expressing a wish not to become involved inadministrative problems. This decision waseventually reversed, under pressure from themembership of the Society, but the damage hadbeen done. Widespread dissatisfaction with thealoofness of the BSSO from matters relating toprofessional interest, particularly amongmembers carrying out a significant amount oforthodontic treatment in practice as opposed tothe hospital service, led to the formation of theBritish Association of Orthodontists in 1965. TheBSSO lost a number of members to the new body,whose membership was restricted to those whowere full-time, or nearly full-time orthodonticpractitioners. The British Association soughtactively to articulate its members’ point of viewin the political arena. Eventually, in 1994, theBSSO lost its separate identity, merging with anumber of other orthodontic groups to form theBritish Orthodontic Society.
6HHHiiissstttooorrryyy ooofff
OOOrrrttthhhooodddooonnntttiiicccsss iiinnnGGGrrreeeeeeccceee aaannnddd RRRooommmeee
� Middle Ages (Fifth to Fifteenth
Centuries) to the Eighteenth
Century
– Matthaeus Gottfried
Purmann
– Etienne Bourdet
– John Hunter
� European Pioneers of the Early
Nineteenth Century
– Joseph Fox
– Joachim Lefoulon
– Christophe-François Delabarre
– JM Alexis Schange
– Friedrich Christoph Kneisel
– John Tomes
The earliest description of irregularities of the teethwas given about 400 BC, by Hippocrates (ca 460–377 BC). The first treatment of an irregular toothwas recorded by Celsus (25 BC–AD 50), a Romanwriter, who said, “If a second tooth should happento grow in children before the first has fallen out,that which ought to be shed is to be drawn outand the new one daily pushed toward its place bymeans of the finger until it arrives at its justproportion”. That might still be good advice, butchildren today do not need ancient history to tellthem how to goad a high canine into place.
Probably the first mechanical treatment wasadvocated by Pliny the Elder (AD 23–79), whosuggested filing elongated teeth to bring them intoproper alignment. This method remained inpractice until the 1800s.
MIDDLE AGES (FIFTH TO FIFTEENTH
CENTURIES) TO THE EIGHTEENTH
CENTURY
Progress during the Middle Ages was nil.Dentistry entered a period of marked decline, asdid all sciences. After the 16th century,considerable progress was made, although littlewas written of orthodontics during this period.In France, students of dentistry were admittedto a University, as early as 1580. The first mention
of practicing dentistry exclusively was made byPierre Dionis (1658–1718). He called dentists“operators for the teeth” and stated that they couldalso open or widen the teeth when they are set tooclose together.
Matthaeus Gottfried Purmann (1692) was thefirst to report taking wax impressions. In 1756,Phillip Pfaff used plaster of Paris impressions.Malocclusions were called “irregularities” of theteeth, and their correction was termed“regulating”. It remained for the enlightenmentto reawaken the spirit of scientific thoughtnecessary to advance dentistry and otherdisciplines.
Beginning in the 18th century, the leadingcountry in the field of dentistry was France. Thiswas due, in large measure, to the efforts of oneman: Pierre Fauchard (1678–1761 ) has been calledthe “Father of Orthodontia”. He was the first toremove dentistry from the bonds of empiricismand put it on a scientific foundation. In 1728, hepublished the first general work on dentistry, atwo volume opus entitled The Surgeon Dentist: ATreatise on the Teeth.
Fauchard described, but probably was not thefirst to use, the bandeau, and an expansion archconsisting of a horseshoe-shaped strip of preciousmetal to which the teeth were ligated. This became

45History of Orthodontics in Greece and Rome
the basis for Angle’s E-arch, and even today itsprinciples are used in unraveling a crowdeddentition. He also “repositioned” teeth with aforceps, called “pelican” because of itsresemblance to the beak of that bird, and ligatedthe tooth to its neighbors until healing took place.At that time, little attention was paid to anythingother than the alignment of teeth and then almostexclusively to the maxilla.
Etienne Bourdet (1722–1789)
Fauchard’s bandeau was refined by EtienneBourdet (1722–1789), dentist to the king of France.His was the first record of recommending serialextraction (1757) and of extracting premolars torelieve crowding. He was also the first to practice“lingual orthodontics”, expanding the arch fromthe lingual. There followed a long line of lingualappliances, including the jackscrew, theexpansion plate, and, closer to our time, thelingual arch.
John Hunter (1728–1793)
Although he was not a dentist, John Hunter (Fig.6.1) (1728–1793) made the greatest advances indentistry of his time. An English anatomist andsurgeon, Hunter took a particular interest in the
anatomy of the teeth and jaws. His text, TheNatural History of the Human Teeth (1771),presented the first clear statement of orthopedicprinciples. He was the first to describe normalocclusion, to attempt to classify the teeth. Heestablished the difference between teeth and boneand gave the teeth names like cuspidati andbicuspidati. He was the first to describe the growthof the jaws, not as a hypothesis, but as a soundscientific investigation. His findings have neverbeen successfully challenged.
EUROPEAN PIONEERS OF THE EARLY
NINETEENTH CENTURY
Joseph Fox (1776–1816)
Joseph Fox (1776–1816), a student of Hunter, wasanother Englishman who made notablecontributions to the budding science oforthodontics. He devoted four chapters of hisbook, the “Natural History and Diseases of theHuman Teeth” (1814), to that topic. The first toclassify malocclusion (1803), he was also one ofthe first to observe that the mandible grows mainlyby distal extension beyond the molars, with littleor no increase in the anterior region.
According to Weinberger, Fox was the first togive explicit directions for correcting theirregularities of teeth. He was particularlyinterested in the judicious removal of deciduousteeth, treatment timing, and the use of bite blocksto open the bite. His other appliances included anexpansion arch and a chin cup (about 1802).
Joachim Lefoulon
Joachim Lefoulon, a Frenchman, is probably bestknown for having given the science a name:orthodontosie (1841), which roughly translatesinto orthodontia. He was also the first to combinea labial arch with a lingual arch. In the area ofetiology, he arrived at factors of an entirelydifferent character from those of most authorities.These were based on biologic phenomenacontrolling the growth, form, and dimension oforgans and tissues.
Christophe-François Delabarre (1787–1862)
Christophe-Fraçnois Delabarre (1787–1862;French) introduced the crib and the principle ofthe lever and the screw (1815). He separatedcrowded teeth by means of swelling threads orwooden wedges placed between them.
Fig. 6.1: John Hunter

46 History of Orthodontics
JM Alexis Schange
JM Alexis Schange (1807, French) in 1841published the first work confined to orthodontics.He introduced a modification of the screw, theclamp band, and, in 1842, three years after thevulcanization process had been developed,rubber bands (actually, sections of rubbertubing). He also coined the term anchorage.
Friedrich Christoph Kneisel (1797–1847) and
John Tomes (1812–1895)
Friedrich Christoph Kneisel (1797–1847,German), was the dentist to Prince Charles of
Prussia. He was the first to use plaster models torecord malocclusion (1836). That same year, whenhe fitted his prognathic patient with a chin strap,he became the first to use a removable appliance.Kneisel wrote the first French and German treatisesdevoted exclusively to orthodontics. He and JohnTomes (1812–1895, English) used variousremovable appliances to treat regularities of this.Tomes was also first to demonstrate boneresorption and apposition.
47History of Dental Lasers and their Applications in Orthodontics
7HHHiiissstttooorrryyy ooofff DDDeeennntttaaalll LLLaaassseeerrrsssaaannnddd ttthhheeeiiirrr AAAppppppllliiicccaaatttiiiooonnnsss
iiinnn OOOrrrttthhhooodddooonnntttiiicccsss
Light amplification by the stimulated emission ofradiation. In 1956, American Physicist Townesfirst amplified microwave frequencies by thestimulated emission process and Maser(Microwave Amplification by Stimulated Emissionof Radiation) came into the use. In 1959, Schawlowand Townes discussed extending the Maserprinciple to the optical portion of theelectromagnetic field, laser.
In 1960, Theodore Maiman, Scientist with theHughes Aircraft Corporation developed firstworking laser device, that emitted a deep redcolored beam from a ruby crystal. In 1964, Pateldeveloped CO2 laser. In 1964, Geusic developedNd: YAG Laser.
Einstein, early in the 20th century describedthree possible mechanisms involving protonradiation. Absorption occurs when an atom in alower energy level is raised to a higher energylevel by absorbing a photon of energy.Spontaneous emission is the process in which anatom in a higher level decays to a staler lowerenergy level, releasing a photon.
Stimulated emission occurs when an atomalready in the excited state decays to a stale state,after interaction with a photon corresponding
exactly to the absorption energy. This result in twophotons of light emitted with the same wavelength,with temporal and spatial coordination.
Using Einstein theory laser is produced.
ALL LASER DEVICES HAVE FOLLOWING
COMPONENTS
Laser Medium
This can be solid, liquid or gas. This determinesthe wavelength of emitted light from the laser.
Optical Cavity or Laser Tube
Having two mirrors, one fully reflective and otherpartially transmissive which are located at eitherend of the optical cavity.
An external mechanical, chemical or opticalpower source which excites the atoms in the lasermedium to higher energy levels. Atoms in excitedstate spontaneously emit photons of light whichbounce back and forth between the two mirrors inthe laser tube striking other atoms and causingmore stimulated emissions. Photons of energy ofthe same wavelength and frequency escapethrough the transmissive mirrors and form a laserbeam.
� All Laser Devices have
Following Components
– Laser Medium
– Optical Cavity or Laser Tube
– Clinicians can Control
Several Variables of Laser
Exposure
� Properties of Laser Beam
� Focused versus Defocused
Beam
� Types of Laser
� Lasers and Their Dental
Applications
� Current Clinical use of Dental
Lasers
� Laser use in Dentistry
� Laser Classification
� Applications of Lasers in
Orthodontics
� Laser Safety
� Precautionary Measures
48 History of Orthodontics
Clinicians can Control Several Variables of
Laser Exposure
Wavelength
� Determines the quality or type of reactionbetween laser and tissue
� It is determined by composition and structureof active medium
� It in turn, predominantly influences whetherabsorption occurs.
Power
� Instant measure of energy output.� Optical properties of the tissue including its
water content.� Wave from described the manner in which
laser power is delivered over time. It can be:– Continuous: They deliver the power output
at a constant level over a prolonged periodof time, generally any time span exceeding1 sec, e.g. CO2 laser.
– Chopped/gated beam: It is similar tocontinuous one except beam isalternatively released and interrupted bya shutter mechanism; this chopping canbe either a single chop or series of timedchops.
� Pulsed lasers: In this, energy is emitted inshort bursts according to a set repetitive seriesof pulses. Between the pulses no laser energyis emitted.
� Because the amount of heat generated duringthe procedure translates directly into theamount of collateral damage and thuspostoperative discomfort – it is generallyrecommended that the laser be used at a lowsetting and in pulsed mode for soft tissueprocedures.
PROPERTIES OF LASER BEAM
Coherent: All the photon of light are in spatialand temporal coherence.Mono Chromaticity: Of one particular wavelength.Collimation: No divergence of the beamLaser beam interaction with tissue: Laser beamand tissue interact in four ways:
Reflection
A reflected light bounces off the tissue surface andis directed toward as energy dissipates so
effectively after reflection, there is little danger ofdamage to other parts of the mouth. It limits theamount of energy that enters the tissues.
Scattering
When beam is scattered within the tissue. Whenlight energy bounces from molecule to moleculewithin the tissue. High absorption minimizesscattering. Scattering distributes the energy overa large volume of tissue, dissipating the thermaleffects.
Transmission
Light energy can also travel beyond a given tissueboundary. This is called transmission.Transmission irradiates surrounding tissue andmust be quantified.
Absorption
Refers to how far beam is absorbed within thetissue or whether it is absorbed at all.
FOCUSED VERSUS DEFOCUSED BEAM
Laser beam can be focused through a lens toachieve a converging beam, which increases inintensity to form a focal spot, the most intensepart of the beam. This focused beam cuts the tissue.
In defocused beam, intensity is less, beamdiverges and power decreases. So a largercircumferential area of the beam hits the tissuesurface causing ablation of the tissue. The lasertip cuts soft tissue through ‘ablation’ of tissue. Thismeans that the cellular temperature is raisedrapidly through the absorption of laser energy bythe melanin in the cells and the cells virtuallyexplode. This characteristic is useful in bothcutting and contouring gingival tissues.
The principal effect of laser energy is photo-thermal: This thermal effect of laser energy ontissue depends on degree of temperature rise andcorresponding reaction of interstitial andintracellular water as the laser energy is absorbed,heating occurs.
Hyperthermia occurs when tissue iselevated above normal temperature but is notdestroyed at temperature of approximately60oC. Proteins begin to denature without anyvaporization of the underlying tissue.Coagulation refers to the irreversible damage

49History of Dental Lasers and their Applications in Orthodontics
to tissue, congealing liquid into a soft semisolid mass. Soft tissue edges can be ‘welded’together with a uniform heating to 70–80oCwhere there is adherence of the layers becauseof stickiness due to collagen molecule.
When the target tissue containing water iselevated to temperature of 100oC, vaporization ofwater occurs, process is called ablation. If the tissuetemperature is raised to about 200oC, it isdehydrated and then burned in presence of airwith carbon as end product. If laser energycontinues to be applied, the surface carbonizedlayer absorbs the incident beam, becomes a heatsink and preventing normal tissue ablation. Theheat conduction causes a collateral thermaltrauma to a wide area.
TYPES OF LASER
Soft Lasers
They provide (a thermal) low energy atwavelengths believed to stimulate circulation andcellular activity. Used to promote healing andreduce inflammation, edema and pain, e.g. diodelaser.
Hard Lasers
Have been used for surgical applications, e.g., CO2
laser.Lasers are named according to the lasermedium employed:� Solid state—e.g. ruby laser, neodymium laser� Gas state—e.g. argon laser, CO2 laser� Semiconductor state—e.g. diode laser
CO2 Laser
� CO2 laser were first developed by Patel in 1964.� Have a wavelength of 10.6 microns.� Since the beams of this laser fall into the far
infrared range on the spectrum, they are notvisible. These lasers often use a quartz-fiberincorporating a 630 nm (Red) coaxial helium-neon laser into the device to act as an aimingbeam and thus facilitate use.
� It received safety clearance by the U.S. Foodand drug administration for use in soft tissuesurgery in 1976.
� CO2 lasers have an affinity for wet tissuesregardless of tissue color. Tissue pigment doesnot affect the performance of CO2 laser.
� CO2 laser wavelength is readily absorbed bywater as soft tissue is 75%–90% water, about
98% of the energy is converted to heat andabsorbed at the tissue surface with very littlescatter or penetration (0.2 to 0.3 mm).
� CO2 lasers reflect off mirrors, allowing accessto difficult areas. Unfortunately, they reflectoff dental instruments making accidentalreflection to non target tissue causing concern.
� CO2 laser is absorbed by optical fibers and lackof fiber optic delivery system make CO2 laserdifficult for allows the beam to be deliveredthrough a flexible tube giving access to all areasof oral cavity.
� CO2 laser works in no contact mode with thetissue and no tactile feedback occurs.
� Depth of laser incision is proportional to thepower and duration of exposure. Laser softtissue surgery is performed with power 5–15watts in either pulsed for continuous mode.
� It is the fastest laser in removing tissue for oraluse.
Nd:YAG Laser
� Developed by Geusic in 1964. Refers toneodymium: yttrium-aluminium-garnet, acrystal of yttrium-aluminum-garnet doped withneodymium. Lasers are in infrared range, 1.06microns wavelength and cannot be seen. Theselasers use a red helium-neon laser for aiming.
� It is not well-absorbed by water but is partiallyabsorbed by hemoglobin and melanin. It hasan affinity for pigmented tissues.
� ND: YAG laser light transmits through waterand penetrates wet tissue more deeply thanCO2 laser. Heat build-up, scatter and depth oftissue penetration by the beam remain majorconsiderations.
� They can be delivered by fiber optic technology.Their access into the mouth is unlimited.
� Laser work in either contact or noncontactmode when working on tissue contact modeis recommended by using pulsed rate, a coatedsapphire tip or combination of water and aircooling in contact mode, penetration depth canbe reduced to a point equal to CO2 .
� Contact tip provide surgeon a tactile feedback.� For dental use, it can deliver power up to three
watts in either pulsed or nonpulsed mode.
Erbium– YAG Laser
In 1997, FDA saftey clearance for use on hardtissues such as enamel, cementum and bone.
50 History of Orthodontics
It consists of two wavelengths:� Erbium: yttrium-aluminum-garnet laser at
2940 nm wavelength.� Erbium: chromium-yttrium-scandium-
gallium-garnet at 2780 nm wavelength.� These lasers are delivered by a special optical
fiber or hollow wave guide technology; operatein pulsed mode with an accompanying heliumneon laser as an aiming beam, sincewavelength is invisible.
� Wavelength 2940 nm, is ideal for absorptionby hydroxyapatite and water making it efficientin ablating enamel and dentin.
� It is essential to use a water spray to wet thesurface during laser radiation to achievemaximum efficiency of tissue removal withminimal heat generation.
� They have highest absorption in water andhave shallow penetration into soft tissue ofany wavelength.
� They can be used to cut soft tissue preciselydue to high water content.
� These lasers are well-absorbed by hard tissues;the surgeon must protect adjacent toothstructures in the operative field.
Argon Lasers
� Argon laser light has 2 primary wavelengths,488 and 514.5 nm. These manifest as blue andgreen visible light.
� Argon is highly absorbed by hemoglobin,strongly absorbed by melanin and poorlyabsorbed by water.
� It is absorbed well by oral soft tissue andprovides excellent hemostasis.
� May be well suited for selective destruction ofblood clots and hemangiomas with minimaldamage to adjacent tissues.
� It is not absorbed by hard tissue; no particularcare is needed to protect teeth during lasersurgery.
� Travel fiber optically.� Either an attenuated argon or helium neon red
beam can serve as an aiming beam.� They have the ability to cure composite
resins.
Diode Lasers
� Diode is a solid active medium laser,manufactured from semiconductor crystals
using some combination of aluminum, indium,gallium and arsenic.
� Wavelength 812 nm for active medium-aluminum to 980 nm for active medium-indium,placing them at the beginning of near infraredportion of invisible nonionizing spectrum.
� The laser energy is absorbed by pigmentationin the soft tissues and this makes the diodelaser an excellent haemostatic agent.
� As it is used in contact mode, it provides tactilefeedback during surgical procedure.
� It can be delivered through a flexible quartzfiber optic hand piece in continuous wave andgated pulses modes and is used in contact withsoft tissues for surgery or out of contact fordeeper coagulation.
� These lasers are poorly absorbed by toothstructure so that soft tissue surgery can besafely performed in close proximity to enamel,dentin and cementum.
� It can often be used without anesthesia toperform very precise anterior soft tissueesthetic surgery or surgery in other areas ofthe mouth without bleeding or discomfort.
� It is an excellent soft tissue surgical laser.
LASERS AND THEIR DENTAL APPLICATIONS
Carbon Dioxide Laser
Clinical applications removal of soft tissue byablation. Recommended for gingivectomy,frenectomy and excision of soft tissue pathology(both benign and malignant). Also used for laserde-epithelization of flaps during and after surgery.
Precautions avoid hard tissue contact by laseremission, especially tooth structure. Use expandedmargins when performing a laser excisionalbiopsy to prevent fulguration of diagnostic areas.Tissue penetration from laser irradiation will beapproximately 0.5 mm deep, depending on powerdensity; very little heat damage occurs belowvisual depth of wound.
Neodymium:YAG Laser
Clinical applications: Removal of soft tissue byablation. Recommended for gingivectomy,frenectomy and excision of soft tissue pathologyespecially hemorrhage lesions. Also used for lasersubgingival curettage procedure.
Precautions: Avoid hard tissue contact by laser.Same precautions as listed for CO2 laser. Tissue
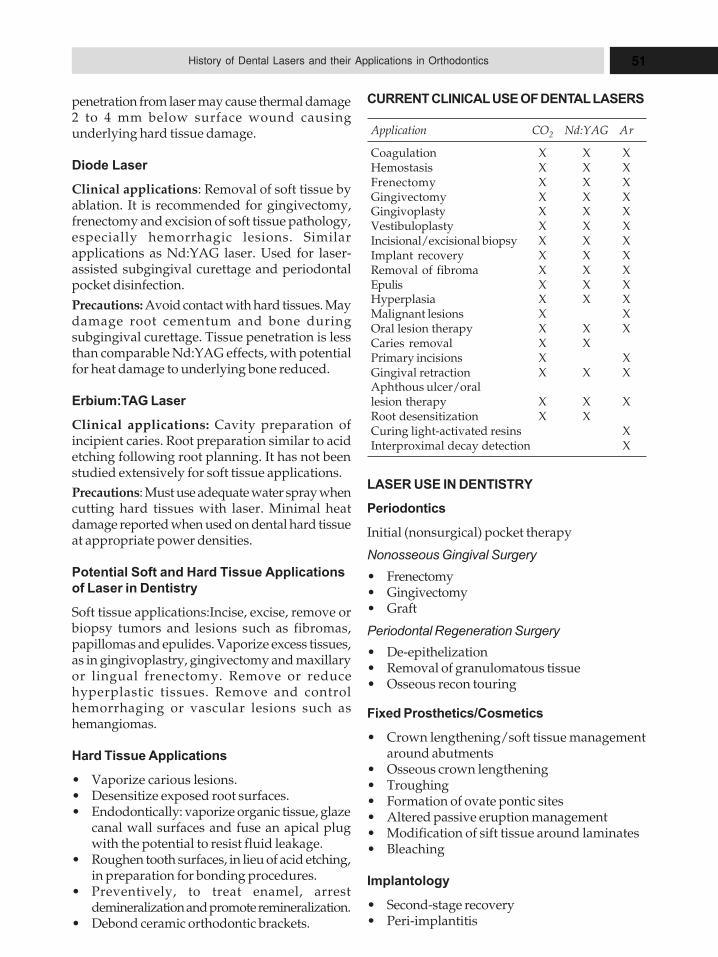
51History of Dental Lasers and their Applications in Orthodontics
penetration from laser may cause thermal damage2 to 4 mm below surface wound causingunderlying hard tissue damage.
Diode Laser
Clinical applications: Removal of soft tissue byablation. It is recommended for gingivectomy,frenectomy and excision of soft tissue pathology,especially hemorrhagic lesions. Similarapplications as Nd:YAG laser. Used for laser-assisted subgingival curettage and periodontalpocket disinfection.
Precautions: Avoid contact with hard tissues. Maydamage root cementum and bone duringsubgingival curettage. Tissue penetration is lessthan comparable Nd:YAG effects, with potentialfor heat damage to underlying bone reduced.
Erbium:TAG Laser
Clinical applications: Cavity preparation ofincipient caries. Root preparation similar to acidetching following root planning. It has not beenstudied extensively for soft tissue applications.
Precautions: Must use adequate water spray whencutting hard tissues with laser. Minimal heatdamage reported when used on dental hard tissueat appropriate power densities.
Potential Soft and Hard Tissue Applications
of Laser in Dentistry
Soft tissue applications:Incise, excise, remove orbiopsy tumors and lesions such as fibromas,papillomas and epulides. Vaporize excess tissues,as in gingivoplastry, gingivectomy and maxillaryor lingual frenectomy. Remove or reducehyperplastic tissues. Remove and controlhemorrhaging or vascular lesions such ashemangiomas.
Hard Tissue Applications
� Vaporize carious lesions.� Desensitize exposed root surfaces.� Endodontically: vaporize organic tissue, glaze
canal wall surfaces and fuse an apical plugwith the potential to resist fluid leakage.
� Roughen tooth surfaces, in lieu of acid etching,in preparation for bonding procedures.
� Preventively, to treat enamel, arrestdemineralization and promote remineralization.
� Debond ceramic orthodontic brackets.
CURRENT CLINICAL USE OF DENTAL LASERS
Application CO2 Nd:YAG Ar
Coagulation X X XHemostasis X X XFrenectomy X X XGingivectomy X X XGingivoplasty X X XVestibuloplasty X X XIncisional/excisional biopsy X X XImplant recovery X X XRemoval of fibroma X X XEpulis X X XHyperplasia X X XMalignant lesions X XOral lesion therapy X X XCaries removal X XPrimary incisions X XGingival retraction X X XAphthous ulcer/orallesion therapy X X XRoot desensitization X XCuring light-activated resins XInterproximal decay detection X
LASER USE IN DENTISTRY
Periodontics
Initial (nonsurgical) pocket therapy
Nonosseous Gingival Surgery
� Frenectomy� Gingivectomy� Graft
Periodontal Regeneration Surgery
� De-epithelization� Removal of granulomatous tissue� Osseous recon touring
Fixed Prosthetics/Cosmetics
� Crown lengthening/soft tissue managementaround abutments
� Osseous crown lengthening� Troughing� Formation of ovate pontic sites� Altered passive eruption management� Modification of sift tissue around laminates� Bleaching
Implantology
� Second-stage recovery� Peri-implantitis
52 History of Orthodontics
Removable Prosthetics
� Epulis fissurate� Denture stomatitis� Residual ridge modification� Tuberosity reduction� Torus reduction� Soft tissue modification
Pediatrics/Orthodontics
� Exposure of teeth� Soft tissue management of orthodontic patients
Oral Surgery/Oral Medicine/Oral Pathology
� Biopsy� Operculectomy� Apicoectomy� Oral soft tissue pathologies
Operative Dentistry
� Deciduous teeth� Permanent teeth
Advantages of Lasers in Soft Tissue Surgery
1. Laser cut is more precise in tissue removal withgreater visibility since it seals off blood vesselsand lymphatic leaving a clear, dry field.
2. Laser sterilizes as it cuts to reduce the risk ofblood borne transmission of disease.
3. Minimal pain and swelling has been reportedafter surgery.
4. Less postoperative infection has been reported,since the wound is sealed with a biologicaldressing.
5. There is less wound contraction duringhealing and mucosal tissue does not scar.
6. Less damage occurs to adjacent normal tissue.7. Access is better to parts of oral cavity,
especially the mandibular, lingual, retromolarand parapharyngeal areas.
8. Better patient acceptance, less operative timeand fewer postoperative adverse squeal.
9. In treatment medically compromised patientHIV +ve and mentally retarded patients.
10. Lasers can be adjusted to cut, vaporize orcoagulate tissue, they offer greater versatilitythan conventional instruments.
11. Pain is reduced to absent 90% of time due tothe sealing of nerve fibers.
Laser Safety
1. Precautions for patients and dental staffduring laser procedures to protect non-targettissues particularly the eyes from stray beams.
2. Reflective surfaces such as instruments, mirrorand even polished restorations have potentialto redirect laser energy.
3. Matte instruments and protective eye glassesfor patients and staff– Green safety glass– Nd: YAG laser– Amber colored glasses– Argon laser– Clear glasses– CO2 laser.
4. Patients eyes should be covered with moist 2 x2 gauze pads.
5. Non target oral tissues should be shielded withwet gauze, packs.
6. Laser plume created when tissue vaporizesshould be considered infectious. Use of anappropriate evacuation system to draw off andfilter the plume is essential.
7. Extreme caution must be used when operatinglaser in vicinity of explosive gases such asanesthetics.
8. Staff who will operate a laser or attend laserprocedures must be thoroughly trained torespect this powerful tool and follow standardprotocol.
9. At some operating powers of CO2 laser can causedamage to dental hard structures, clinicianshave emphasized need for an adequate shieldsuch as flat bladed instrument or silver foilbetween gingival and teeth, so that beam willstrike the instrument rather than the tooth.
LASER CLASSIFICATION
They are based chiefly on the potential of theprimary laser beam or reflected beam to causebiologic damage to the eyes or skin. Higher theclassification number, greater the potential hazard.
Class I
� Lasers working under normal operatingconditions do not pose a health hazard.
� Devices are totally enclosed, beam does notexit housing, e.g. CD player.
Class II
� Lasers emit only visible light with lower poweroutput and do not normally pose a hazard
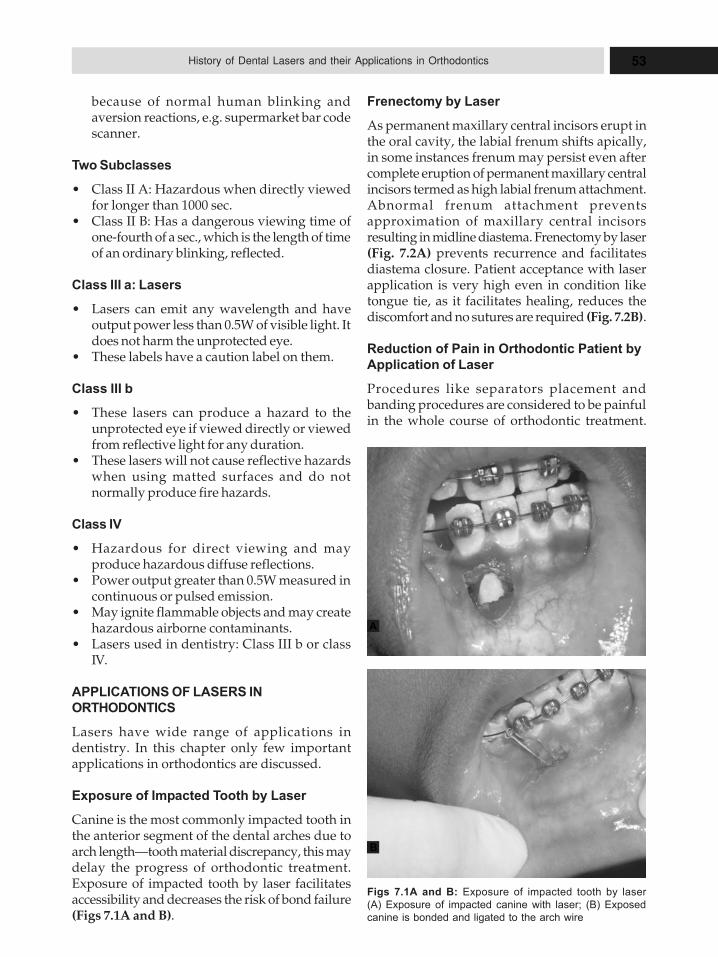
53History of Dental Lasers and their Applications in Orthodontics
because of normal human blinking andaversion reactions, e.g. supermarket bar codescanner.
Two Subclasses
� Class II A: Hazardous when directly viewedfor longer than 1000 sec.
� Class II B: Has a dangerous viewing time ofone-fourth of a sec., which is the length of timeof an ordinary blinking, reflected.
Class III a: Lasers
� Lasers can emit any wavelength and haveoutput power less than 0.5W of visible light. Itdoes not harm the unprotected eye.
� These labels have a caution label on them.
Class III b
� These lasers can produce a hazard to theunprotected eye if viewed directly or viewedfrom reflective light for any duration.
� These lasers will not cause reflective hazardswhen using matted surfaces and do notnormally produce fire hazards.
Class IV
� Hazardous for direct viewing and mayproduce hazardous diffuse reflections.
� Power output greater than 0.5W measured incontinuous or pulsed emission.
� May ignite flammable objects and may createhazardous airborne contaminants.
� Lasers used in dentistry: Class III b or classIV.
APPLICATIONS OF LASERS IN
ORTHODONTICS
Lasers have wide range of applications indentistry. In this chapter only few importantapplications in orthodontics are discussed.
Exposure of Impacted Tooth by Laser
Canine is the most commonly impacted tooth inthe anterior segment of the dental arches due toarch length—tooth material discrepancy, this maydelay the progress of orthodontic treatment.Exposure of impacted tooth by laser facilitatesaccessibility and decreases the risk of bond failure(Figs 7.1A and B).
Frenectomy by Laser
As permanent maxillary central incisors erupt inthe oral cavity, the labial frenum shifts apically,in some instances frenum may persist even aftercomplete eruption of permanent maxillary centralincisors termed as high labial frenum attachment.Abnormal frenum attachment preventsapproximation of maxillary central incisorsresulting in midline diastema. Frenectomy by laser(Fig. 7.2A) prevents recurrence and facilitatesdiastema closure. Patient acceptance with laserapplication is very high even in condition liketongue tie, as it facilitates healing, reduces thediscomfort and no sutures are required (Fig. 7.2B).
Reduction of Pain in Orthodontic Patient by
Application of Laser
Procedures like separators placement andbanding procedures are considered to be painfulin the whole course of orthodontic treatment.
Figs 7.1A and B: Exposure of impacted tooth by laser
(A) Exposure of impacted canine with laser; (B) Exposed
canine is bonded and ligated to the arch wire
A
B
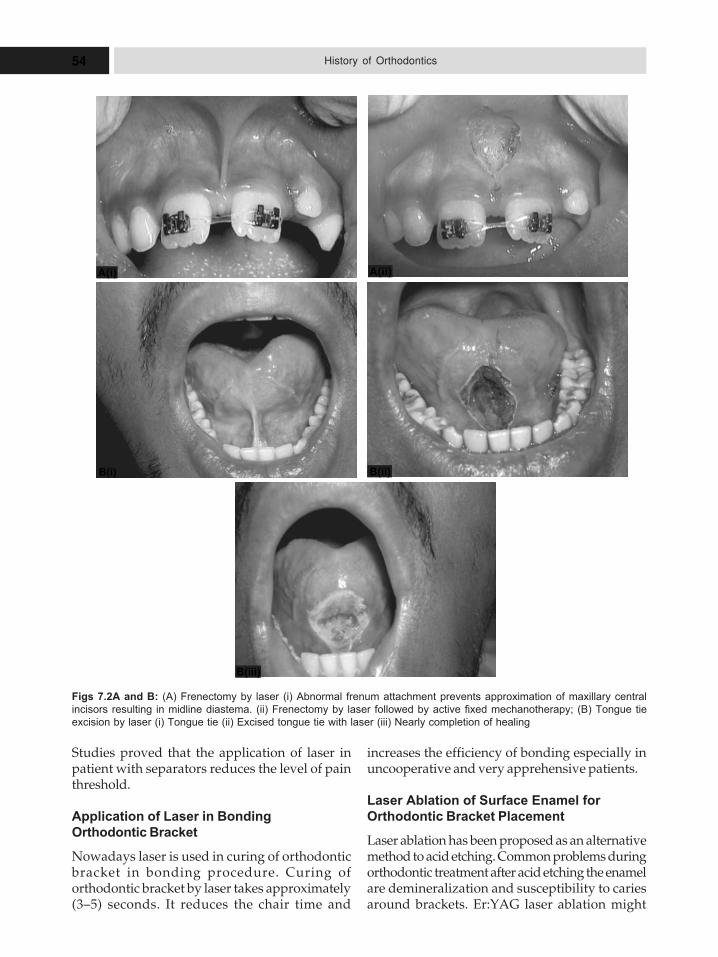
54 History of Orthodontics
Studies proved that the application of laser inpatient with separators reduces the level of painthreshold.
Application of Laser in Bonding
Orthodontic Bracket
Nowadays laser is used in curing of orthodonticbracket in bonding procedure. Curing oforthodontic bracket by laser takes approximately(3–5) seconds. It reduces the chair time and
increases the efficiency of bonding especially inuncooperative and very apprehensive patients.
Laser Ablation of Surface Enamel for
Orthodontic Bracket Placement
Laser ablation has been proposed as an alternativemethod to acid etching. Common problems duringorthodontic treatment after acid etching the enamelare demineralization and susceptibility to cariesaround brackets. Er:YAG laser ablation might
Figs 7.2A and B: (A) Frenectomy by laser (i) Abnormal frenum attachment prevents approximation of maxillary central
incisors resulting in midline diastema. (ii) Frenectomy by laser followed by active fixed mechanotherapy; (B) Tongue tie
excision by laser (i) Tongue tie (ii) Excised tongue tie with laser (iii) Nearly completion of healing
A(i) A(ii)
B(i) B(ii)
B(iii)
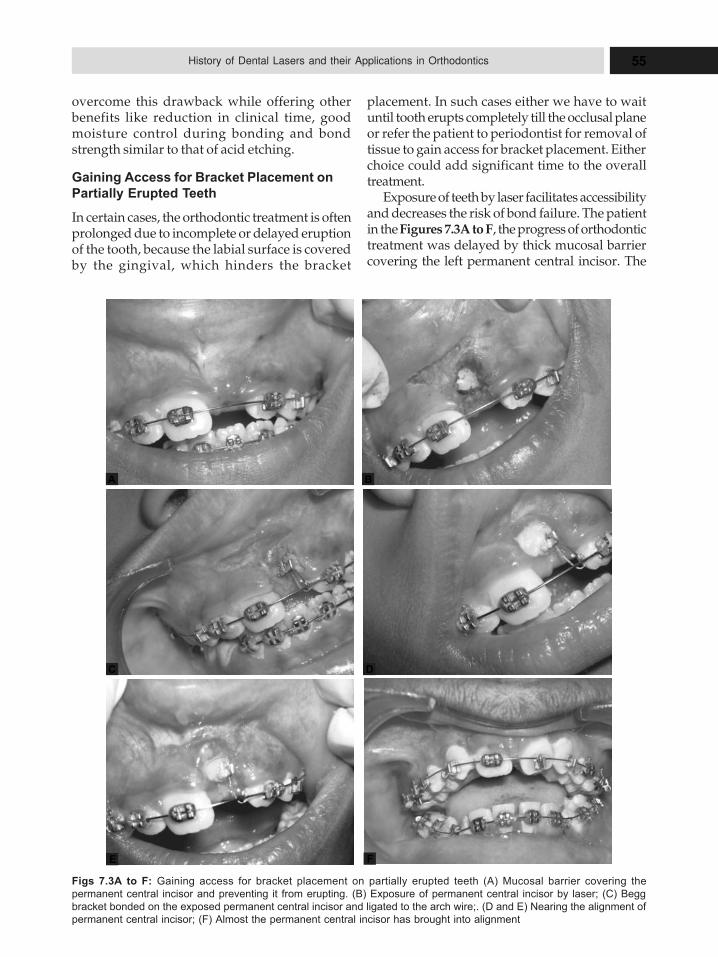
55History of Dental Lasers and their Applications in Orthodontics
overcome this drawback while offering otherbenefits like reduction in clinical time, goodmoisture control during bonding and bondstrength similar to that of acid etching.
Gaining Access for Bracket Placement on
Partially Erupted Teeth
In certain cases, the orthodontic treatment is oftenprolonged due to incomplete or delayed eruptionof the tooth, because the labial surface is coveredby the gingival, which hinders the bracket
placement. In such cases either we have to waituntil tooth erupts completely till the occlusal planeor refer the patient to periodontist for removal oftissue to gain access for bracket placement. Eitherchoice could add significant time to the overalltreatment.
Exposure of teeth by laser facilitates accessibilityand decreases the risk of bond failure. The patientin the Figures 7.3A to F, the progress of orthodontictreatment was delayed by thick mucosal barriercovering the left permanent central incisor. The
Figs 7.3A to F: Gaining access for bracket placement on partially erupted teeth (A) Mucosal barrier covering the
permanent central incisor and preventing it from erupting. (B) Exposure of permanent central incisor by laser; (C) Begg
bracket bonded on the exposed permanent central incisor and ligated to the arch wire;. (D and E) Nearing the alignment of
permanent central incisor; (F) Almost the permanent central incisor has brought into alignment
C D
A B
E F
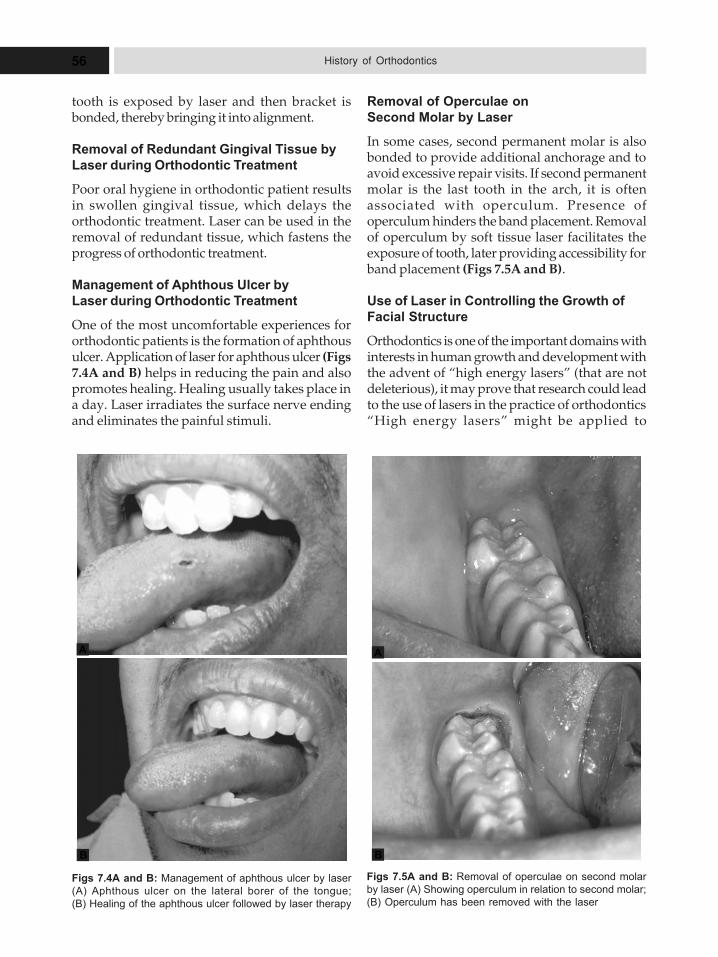
56 History of Orthodontics
Figs 7.4A and B: Management of aphthous ulcer by laser
(A) Aphthous ulcer on the lateral borer of the tongue;
(B) Healing of the aphthous ulcer followed by laser therapy
Figs 7.5A and B: Removal of operculae on second molar
by laser (A) Showing operculum in relation to second molar;
(B) Operculum has been removed with the laser
tooth is exposed by laser and then bracket isbonded, thereby bringing it into alignment.
Removal of Redundant Gingival Tissue by
Laser during Orthodontic Treatment
Poor oral hygiene in orthodontic patient resultsin swollen gingival tissue, which delays theorthodontic treatment. Laser can be used in theremoval of redundant tissue, which fastens theprogress of orthodontic treatment.
Management of Aphthous Ulcer by
Laser during Orthodontic Treatment
One of the most uncomfortable experiences fororthodontic patients is the formation of aphthousulcer. Application of laser for aphthous ulcer (Figs7.4A and B) helps in reducing the pain and alsopromotes healing. Healing usually takes place ina day. Laser irradiates the surface nerve endingand eliminates the painful stimuli.
Removal of Operculae on
Second Molar by Laser
In some cases, second permanent molar is alsobonded to provide additional anchorage and toavoid excessive repair visits. If second permanentmolar is the last tooth in the arch, it is oftenassociated with operculum. Presence ofoperculum hinders the band placement. Removalof operculum by soft tissue laser facilitates theexposure of tooth, later providing accessibility forband placement (Figs 7.5A and B).
Use of Laser in Controlling the Growth of
Facial Structure
Orthodontics is one of the important domains withinterests in human growth and development withthe advent of “high energy lasers” (that are notdeleterious), it may prove that research could leadto the use of lasers in the practice of orthodontics“High energy lasers” might be applied to
A
B
A
B
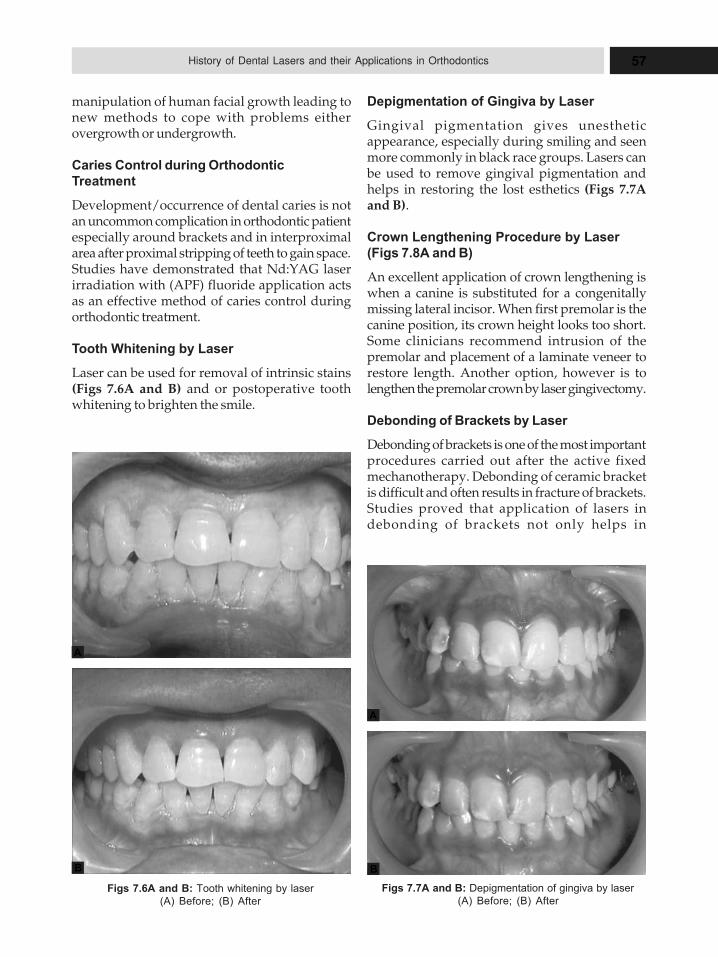
57History of Dental Lasers and their Applications in Orthodontics
manipulation of human facial growth leading tonew methods to cope with problems eitherovergrowth or undergrowth.
Caries Control during Orthodontic
Treatment
Development/occurrence of dental caries is notan uncommon complication in orthodontic patientespecially around brackets and in interproximalarea after proximal stripping of teeth to gain space.Studies have demonstrated that Nd:YAG laserirradiation with (APF) fluoride application actsas an effective method of caries control duringorthodontic treatment.
Tooth Whitening by Laser
Laser can be used for removal of intrinsic stains(Figs 7.6A and B) and or postoperative toothwhitening to brighten the smile.
Figs 7.6A and B: Tooth whitening by laser
(A) Before; (B) After
Figs 7.7A and B: Depigmentation of gingiva by laser
(A) Before; (B) After
A
B
A
B
Depigmentation of Gingiva by Laser
Gingival pigmentation gives unestheticappearance, especially during smiling and seenmore commonly in black race groups. Lasers canbe used to remove gingival pigmentation andhelps in restoring the lost esthetics (Figs 7.7Aand B).
Crown Lengthening Procedure by Laser
(Figs 7.8A and B)
An excellent application of crown lengthening iswhen a canine is substituted for a congenitallymissing lateral incisor. When first premolar is thecanine position, its crown height looks too short.Some clinicians recommend intrusion of thepremolar and placement of a laminate veneer torestore length. Another option, however is tolengthen the premolar crown by laser gingivectomy.
Debonding of Brackets by Laser
Debonding of brackets is one of the most importantprocedures carried out after the active fixedmechanotherapy. Debonding of ceramic bracketis difficult and often results in fracture of brackets.Studies proved that application of lasers indebonding of brackets not only helps in
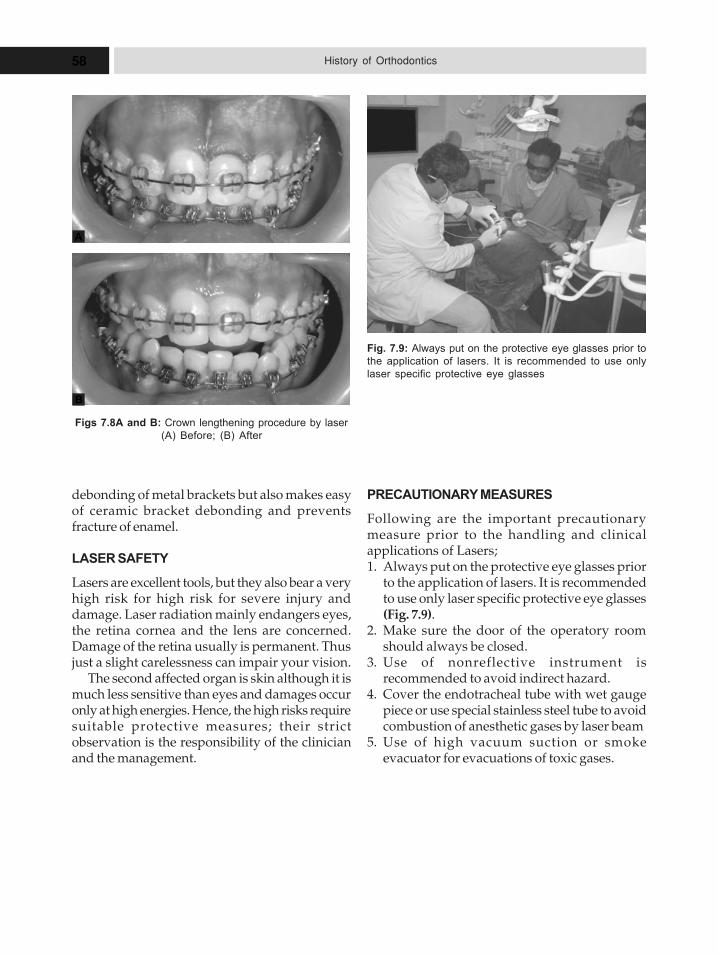
58 History of Orthodontics
Figs 7.8A and B: Crown lengthening procedure by laser
(A) Before; (B) After
Fig. 7.9: Always put on the protective eye glasses prior to
the application of lasers. It is recommended to use only
laser specific protective eye glasses
A
B
debonding of metal brackets but also makes easyof ceramic bracket debonding and preventsfracture of enamel.
LASER SAFETY
Lasers are excellent tools, but they also bear a veryhigh risk for high risk for severe injury anddamage. Laser radiation mainly endangers eyes,the retina cornea and the lens are concerned.Damage of the retina usually is permanent. Thusjust a slight carelessness can impair your vision.
The second affected organ is skin although it ismuch less sensitive than eyes and damages occuronly at high energies. Hence, the high risks requiresuitable protective measures; their strictobservation is the responsibility of the clinicianand the management.
PRECAUTIONARY MEASURES
Following are the important precautionarymeasure prior to the handling and clinicalapplications of Lasers;1. Always put on the protective eye glasses prior
to the application of lasers. It is recommendedto use only laser specific protective eye glasses(Fig. 7.9).
2. Make sure the door of the operatory roomshould always be closed.
3. Use of nonreflective instrument isrecommended to avoid indirect hazard.
4. Cover the endotracheal tube with wet gaugepiece or use special stainless steel tube to avoidcombustion of anesthetic gases by laser beam
5. Use of high vacuum suction or smokeevacuator for evacuations of toxic gases.
8AAAnnngggllleee’’’sss CCCooonnntttrrriiibbbuuutttiiiooonnn
tttooo ttthhheee FFFaaacccuuullltttyyy ooofffOOOrrrttthhhooodddooonnntttiiicccsss
� Edward Hartley Angle –Dental
Graduation
� Angle’s Dental Practice at
Towanda
� Edward Hartley Angle’s
Professional Teaching Career
� Edward Hartley Angle‘s School
of Orthodontics at Pasadena,
California USA
� Appliance Contribution by
Edward H Angle
– E-arch Appliance
– Pin and Tube Appliance
– Ribbon Arch Appliance
– Edgewise Appliance
� Angle’s Orthodontic Material
Invention
� Case-Angle Controversy
� Criticisms
� Edward H Angle’s Publications
and Presentations
Edward H Angle is one of the most dominant,dynamic, and influential figures in the specialtyof orthodontics. He separated orthodontics fromthe other branches of dentistry. Edward HAngle’s early years reflect elements of a classicAmerican success story of his era: a fiercelydetermined young man of no remarkableheritage serendipitously finding hisconsiderable aptitudes and blazing trails inpursuit of his visionary goals. At various timesin his letters, he expressed his admiration for apantheon of archetypes with traits akin to hisown, such as the indomitable messenger in “AMessage to Garcia”, the popular, inspirationalshort story (1899) by Elbert Hubbard, whichbecame required reading for Angle’s students.Samuel L Clemens (Mark Twain), poet-storyteller James Whitcomb Riley, GeorgeCatlin, Benjamin Franklin, and Rembrandt vanRijn were among his favorite heroes. All werecreative achievers and resolute individualists ofhumble birth and with great connection toeveryday people.
Dr Angle never forgot his farm-boy life innortheastern Pennsylvania that helped shape
many of his qualities and quirks in adulthood.From the southern boundary of District no. 1 ofHerrick Township in Bradford County, you couldalmost see the deep, winding chasm of theSusquehanna River valley. This area wasnicknamed “Ballibay” in the 1820s by the newsettlers from the town of Ballybay, CountyMonaghan, Ireland. Edward Hartley Angle wasborn here June 1, 1855 in a modest, white wood-framed house near the crest of a hill on his father’s200-acre dairy farm (Fig. 8.1). He is recorded inthe 1860 Bradford County census book as“Hartly”, the fifth of six children, and third son,to Philip Casebeer Angle and Isabel ErskineAngle. His father’s roots were primarily Dutchand his mother was born in Ireland. Fromchildhood, he was called “Hart” by his familyand close friends. The Angles had a seventh child,William, a bright lad, who died of illness at age11. Teen-aged Hart was hurt terribly by the lossof his younger brother Willie, his favorite sibling.
Hart showed no enthusiasm in school or onthe farm, to the utter dismay of hisunsympathetic father. He was always behind inhis learning, especially mathematics, and he

60 History of Orthodontics
avoided farm work as much as he could. He wasa natural tinkerer, a whittler, a maker of things.In reminiscences, his wife Anna told about hisheavily scarred knees, lifetime reminders ofboyhood knife slips. When his father needed amore efficient hay rake, 11-year-old Hartinvented one. However, he did not get muchappreciation for the new machine, and soonsomeone else applied for and was awarded thepatent for Hart’s instinctively clever work. It wasan early lesson in life’s unfairness that thesensitive boy probably long remembered.
In Angle’s letters, we find a man whocherished his boyhood friendships throughoutlife. He never lost contact with some of hisHerrick chums, like Cyrus Camp, Guy Fuller, andJerry Sanger. His correspondence with them isoften in the playful tones of a kid still horsingaround the farmyard. Angle peppered his lettersto his hometown friends with monikersconcocted from the names of town fathers withwhom the boys occasionally skirted trouble.“Cy” Camp was sometimes referred to as “J.Rufus Avery” or “Gideon Squares” in Hart’sjocular letters to him. Angle also showed his self-deprecating humor to old, dear friends in thevariety of comical aliases he used in signing hisletters: Alexander J Horatio, Alonzo Revellen, BigFoot, Colossus Doc the Great, Flat-nosed Hart,Little Harty Angle, Old Man Friar, Uncle Reuben,and sometimes simply the geometric notation“.
EDWARD HARTLEY ANGLE—DENTAL
GRADUATION
In 1874, at age 18, Edward Hartley Angle wasintroduced to dentistry with coaxing from his
understanding mother Isabel. Recognizing hisnascent mechanical skills, she secured a positionfor Hart with a dentist in nearby Herrick, as anoffice apprentice. He got on well in dentistry—itappealed instantly to his keen manual and visualsenses, his love of tools and his need fororderliness. Two years later, he applied to dentalcolleges. His scratchy, brief letter of inquiry datedSeptember 6, 1876, to the Baltimore DentalCollege is the earliest document extant from hishand. In it, he touted his proficiencies in theindispensable texts of the day: Harris’s ThePrinciples and Practice of Dental Surgery (1863) andPiggot’s Chemistry and Metallurgy, as Applied tothe Study and Practice of Dental Surgery (1854).Although his English constructions and spellingwere rather crude for a schooled 21-year-old,young Angle exuded the restless confidence thatwould mark his entire adult life and would winhim success in many adventures to come. He wasinvited to enroll at Pennsylvania College ofDental Surgery in Philadelphia for their DDSprogram, then arranged in two 6-month termsspaced over a nominal 2 years and located in abuilding at the northwest corner of Twelfth andFilbert Streets. Angle alluded to his collegeexperiences years later in friendly letters withclassmates EL Townsend and Charles J Tibbets.In 1895, Angle completed his MD degree fromMarion Sims College.
ANGLE‘S DENTAL PRACTICE AT TOWANDA
After dental school graduation in 1878, EdwardAngle went to the Bradford County seat,Towanda, and set-up a general practice ofmechanical dentistry in the center of town. Hebecame a boarder in the home of Towanda’sleading physician, Dr David Shepard Pratt, agood strategic decision for the bright new dentistin town. Young Dr Angle advertised in localnewspapers, such as The Sullivan Review, andappeared to be rapidly successful. Here in hisleisure as an unmarried young professional,Angle developed his first interests inmechanisms for tooth alignment or “regulation”,considered the main purpose for moving teethat that time.
In Towanda, Angle experienced declininghealth that was to plague him on and off for the
Fig. 8.1: Angle’s white wood-framed house where he was
born

61Angle’s Contribution to the Faculty of Orthodontics
rest of his life. He was diagnosed with pleuralpneumonia. Today, we may understand thischronic respiratory condition as a consequenceof tuberculosis. One popular treatment of the daywas for the sufferer to move to fresher, cleanerair—to a pristine resort set up for this purposeor to the mountains or the desert. Angle formedspecial bonds throughout his career with thosewho shared the same affliction, former studentAlbert “Leaf” Ketcham being the most prominentamong them.
After 3 years of dental practice in Towanda,in the spring of 1881, 26-year-old Dr Angleabandoned dentistry and took a train toMinneapolis, Minnesota, on a physician’s advice,in search of better health. Within a few months,his condition improved and, with his recovery,came renewed confidence and resolves to makesomething of himself. For his health’s sake, Anglewas considering permanent retirement fromdentistry in favor of work that was less confiningand more outdoors. In Minneapolis, he heardthat sheep farming in Montana was where the“big money” could be made. In the fall, hereturned briefly to Pennsylvania to entice someof his old farm buddies from Herrick to join himin setting up a lucrative sheep-raising business.They signed on excitedly, and the lot of hisBallibay cronies—including his older brotherMahlon and close friend Cy Camp—traveledwith the freewheeling Hart to the fresh air of theMontana wilderness in search of their “pot ofgold” (Fig. 8.2).
Angle invested all his savings into theirsheep-farming venture, all to be undone by thegreat blizzard of 1882, a record-breaking deepfreeze that killed off the entire herd. The empty-handed boys from Ballibay sullenly returned toPennsylvania, except for Hart. A defeated Angle,feeling physically better but mentally depleted,hobbled in to Minneapolis by mid-1882 lookingfor work—again in dentistry.
EDWARD HARTLEY ANGLE’S
PROFESSIONAL TEACHING CAREER
Edward Hartley Angle got back into generaldental practice and soon resumed the creativethinking and tinkering with tooth-regulatingappliances that he began in Towanda. Within acouple of years, Angle inquired at the Dental
Department of the Minnesota Hospital College inMinneapolis regarding faculty employment.Impressed with what he had to offer, the collegeadministrators tailored a position to suit his skillsand their needs. In 1886, 31-year-old EdwardAngle was appointed a professor of histology andlecturer on comparative anatomy andorthodontia. A few years later, after the HospitalCollege merged into the University of Minnesota,he was elevated to professor of orthodontia, arare position in those days when orthodontia wasa neglected part of the prosthetics departmentat dental colleges. At the same time, he quicklyascended through the ranks to become presidentof the Minneapolis City Dental Society in 1888.He also was able to maintain his small privatedental office, where he experimented more andmore with novel approaches in orthodonticmechanisms. In sum, through his resilience,industriousness, and good fortune, Angleseemed to have landed on his feet
Fig. 8.2: Edward Hartley Angle

62 History of Orthodontics
psychologically and financially from the Montanaget-rich-quick debacle a few years earlier.
His big break came in 1887 when Angle waspermitted on the speaking program of the NinthInternational Medical Congress convened inWashington, DC. On the fourth day of thisimportant Congress, Thursday, September 8,1887, the section on “Dental and Oral Surgery”was called to order at 11 AM in the UniversalistChurch at the corner of 13th and L Streets. Thirty-two-year-old Dr Angle was the youngest of thesession’s speakers and was scheduled last on theday’s program. Two prominent authorities onorthodontics directly preceded Angle: ClarkGoddard, professor at University of California,San Francisco, and Eugene Talbot, textbookwriter and professor from Chicago.
A confident Edward Angle presented his talk,entitled “Notes on Orthodontia with a NewSystem of Regulation and Retention”, usinglantern slides—a relatively new visual aid forlecturing. He demonstrated his classification oftooth movements and his novel orthodonticdevices, such as piano wire in a soldered “pipe”(tube) and the jackscrew and traction screw. Theopen discussion that followed was sometimesacrimonious. Many well-known dentists in theaudience, including John N Farrar and Victor HJackson, accused Angle of falsely claimingoriginality. They cited others (includingthemselves) who earlier introduced similarappliances. Angle carefully explained how hisdevices were different and better, indeed “new”,but apparently, he did not prevail. The editedpaper and subsequent inflammatory discussionswere published in the Transactions of the NinthInternational Medical Congress under an imposed,truncated, noncontroversial title, “Notes onOrthodontia”. This 1887 article commonly hasbeen called the “First Edition” of his classictextbook on the treatment of malocclusion.Actually, Angle considered that his first editionwas his 14-page chapter appended to Loomis PHaskell’s new book on dental laboratoryprocedures published in 1887; he titled thisversion of his Congress paper “Extracts of Noteson Orthodontia, with a New System byRegulation and Retention” and it did not containthe discrediting commentaries.
Years later, colleagues observed that thebitterness Angle developed from the
contemptuous treatment he received at this 1887Congress helped harden him for the professional“fights” he was to invite and encounterthroughout his adventurous career. To those whowould challenge him, his style often seemedabrasive, sometimes brutal; to others, those loyalto him and backing his causes, he was ascharming and gentle as a puppy.
The year 1892 was a watershed in Angle’sprofessional development: he announced that hewould be practicing orthodontia to the exclusionof all other dental therapies. With this decision,he became the first acknowledged exclusivespecialist in orthodontics in the world. Until thismoment, none of the authorities on orthodonticsworldwide and in history ever mustered thevision and confidence to limit their dental ormedical practice to only this emerging type oftreatment. Angle was no longer on the faculty atthe University of Minnesota. He resigned toconcentrate his energies on experimentation inorthodontia and the development of marketable,prefabricated (“ready-made” in his vernacular),new treatment appliances. He also needed timeto work on his textbook’s third edition, his firstreal book, a 51-page work, 20 pages longer thanhis 1890 edition, which had been published asan appendix in the second edition of Haskell’sprosthetics laboratory book. He hired AnnaHopkins, a bright young Minneapolis secretarialschool graduate, to help him with his book andpractice. It was the beginning of a life-shapingrelationship for both of them.
Angle‘S Married Life
In March 1887, Edward Hartley Angle married to22-year-old Florence when he was running 31years old. Less than 9 months later their daughterFlorence Isabel Angle (Fig. 8.3) was born inMinneapolis, only 3 months after her father’sdisastrous appearance at the Ninth InternationalMedical Congress in Washington.
Angle’s correspondence a dozen years laterdescribed a disintegration of this marriage fromthe start. The couple was grossly mismatched,he the ambitious idea man and she the day-dreaming reader of romances. Angle graduallylost respect for Florence “Senior”, as he referredto his wife in some letters, and he became bydefault an absentee father to their sickly daughter“Florencie”. By July 1900, his personal confidence

63Angle’s Contribution to the Faculty of Orthodontics
conversationalist. In addition, he was a talentedartist, not only with intricate line drawings andcreations for clinical orthodontics, but also incrafting gold jewelry, such as stickpins set withsemiprecious stones, which he often gave as giftsto friends.
Furthermore, Angle was an avid collector ofthings of the world. He gladly received andstudied valuable arts and crafts from friends andhis grateful foreign correspondents in SouthAfrica, Japan, and elsewhere. Angle asked hiswell-known orthodontist-friends and mentorsfor photographs of themselves and other dentalcelebrities, both earlier and contemporary, to addto his lantern slide collection, which he projectedas a historical prelude to his lectures at variousmeetings. He loved American-Indian artifacts,arrowheads and tomahawk heads which hechallenged his patients and friends to find andtrade to him. He collected animal and humanskulls and osteological materials in plentifulsupply from archeologists excavating the burialmounds around St Louis. He and Annanourished for over three decades an extensivecollection of American-Indian weavings,beadwork, textiles, clothing, and baskets, mostly
in his new directions was strong enough to prompthim to move out of their boarding-houseapartment in St Louis. He had his thrivingpractice, his income-producing books, patentsand appliances, his growing international fame,his prospering proprietary school, and perhapsmost significantly, Anna Hopkins, his secretary,amanuensis, confidante, and sympathetic soulmate (Fig. 8.4). It took Angle another 9 years todeliver an acceptable divorce settlement forFlorence senior in May 1908. Angle’s mother haddied a few months earlier, and the delay andparticular timing of his divorce may well reflectthe determination of a devoted son to shield hisdevout mother from the shame of his brokenmarriage. On June 28, 1908, Hart and Anna weremarried in St Louis (at ages 53 and 36,respectively) and within 2 months thenewlyweds had moved to New York to begin anew chapter in their lives, as retired gentry.
Angle as an Artist
It should not be forgotten that Edward HartleyAngle’s personal vision was wide and deep, notsimply confined to his profession. He was keenobserver of nature in all its forms. The preambleof the citation accompanying the honorary Doctorof Science degree awarded to Dr Angle in 1915by the University of Pennsylvania acknowledgedhis broad intellectual base: “Lover of art andnature, intimate friend of trees and flowers, butpreeminently founder of the science oforthodontia….” Angle exercised hisintellectualism with an active sociability. He wasa worldly man who enjoyed people and places;he was an outgoing celebrant and
Fig. 8.3: Angle’s daughter—Florence Isabel Angle on the
left
Fig. 8.4: Edward Hartley Angle
64 History of Orthodontics
from the tribes of the Plains and Great Basin areasof the United States (Fig. 8.5). Most of theirarcheological and ethnographic collections weredonated to institutions and museums in theirlifetimes. Almost 300 valuable objects ofAmerican–Indian ethnography were given byAnna Hopkins Angle from 1930, the year ofEdward Angle’s death, to 1959, two years afterher death, to the museum of Claremont College,now the Pomona College Museum of Art in LosAngeles. It represents a living testament to thebroad tastes and intellectual vigor of the Angles.
About Anna Hopkins (Angle’s Second Wife)
About 1908, Angle married his longtimesecretary, Anna Hopkins (1872–1957) (Fig. 8.6),who had obtained her DDS degree from theUniversity of Iowa and her orthodontic trainingin his school. “Mother Angle” became secretaryof the American Society of Orthodontists, afounding coeditor of the Angle Orthodontist, andhonorary chair of the Angle Society executivecommittee, but she would be best rememberedas Angle’s amanuensis, editor, foil, and bufferfor many of his downtrodden students. Someobservers have suggested that Anna deservedmuch of the credit for the high quality of Angle’swritten record through her significant literaryinput during typing. There is absolutely noevidence to support this assertion, given theadmirable consistency of Angle’s literary output,handwritten as well as typewritten, even duringperiods when Anna’s absence was known, suchas when she was attending the College of
Dentistry at the University of Iowa from 1900 to1902. Angle’s letters to Anna are just as colorfuland articulate as the rest of his correspondence.However, Anna did provide valuable technicalskills and judgment. She knew how to craft solid,well-spelled, grammatically correct text. Shelikely served as a trusted sounding board for herexuberant boss, and she surely must have wovensome subtle corrections and softened phrases intohis sometimes acerbic commentaries. Dr Angleoften appended his own handwrittencorrections, notes, or comments to the finaltypewritten letters. And to almost all addressees,including some close relatives, he hand-signedhis letters boldly as “Edward H Angle.” Onlywith old friends would he let go and sign acreative or diminutive nickname. At rare timesduring the 1899 to 1910 period, Anna would signhis letters in his absence. Her version of hissignature is rather authentic looking, but stillrecognizably not his own.
For a period in 1901–1902, when AnnaHopkins was away at the University of Iowastudying for her dental degree, Angle’scorrespondence was managed by his youngersister, Lillian, an accountant by occupation. The
Fig. 8.5: Archeological and ethnographic collections of
Angle and his wife Anna Hopkins
Fig. 8.6: Anna Hopkins

65Angle’s Contribution to the Faculty of Orthodontics
technical quality of the letters that “Lillie”attempted to transcribe during that time wasnoticeably weaker and Angle knew it. He had toapologize often to his correspondents for latenessand errors, and he resorted to handwrittencorrections and appended notes more frequently.
Angle as a Writer
Angle’s style of writing was largely verbal: hisletters (and probably his speeches) were dictatedto and transcribed by his talented secretary (andlater, second wife), Anna Hopkins. He was giftedwith the turn of phrase, using colorful languagein original ways, and often waxing effusively ina highly readable way.
Angle became convinced that anomalies ofmolar occlusion were prime factors in the originsof most orthodontic problems, including dentalcrowding. Thus, he took the bold step ofpopularizing the word “mal-occlusion” in thelate 1890s, around the time he was creating hislandmark work “Classification of Malocclusion”.Published in 1899, that article brought order outof chaos, simplicity from existing diagnosticcomplexity, transformations that Angle’s creativemind seemed particularly adept at seeing anddoing. Quickly, he changed the title of histextbook from a prosaic “The Angle system ofregulation and retention of the teeth …” (1890–1899) to the then ground-breaking concept,“Treatment of malocclusion of the teeth …”(1900, 6th edition).
Angle was a perfectionist whose painstakingexactness in his scientific thinking and writingsbecame a hallmark of his lifetime of work inorthodontics. His detailed letters to managersand book editors of the SS White DentalManufacturing Company show him as apolymath with a remarkable understanding ofthe tasks of typesetter, illustrator, and publisher.Angle edited his book six times over, modifyingand adding to it every time, as his own expertisedeveloped and progressed, turning what beganas a 20-page article in 1887 into a 628-page text in1907. He always seemed to be at work on anaddress, an illustrated presentation, orpublication. He prepared by hand many of hisintricate drawings and by 1900 had a library ofover a thousand glass lantern-slides for projection.Besides his well-known textbook editions, Anglewrote around 80 articles for publication in various
professional journals in the United States, Europe,and Australia between 1887 and his death in1930. In addition, during his lifetime, close to 100abstracts and commentaries about his work werepublished. Another 150 articles are recorded inthe indexed scientific literature about EdwardAngle and his legacy, and this number continuesto grow.
In addition to his own writing, Angle’s lettersshow that he served enthusiastically as a mentorin scientific writing and editing, long before theera of peer review. He generously volunteeredideas and topics for former students andcolleagues, including one of his first four students,Milton T Watson, longtime friend William J Brady,and brother-in-law/editor Cy Camp, who wasessential in the final editing and proofing of thesixth edition (1900) of Angle’s textbook. Angleconscripted all of them and three other colleaguesto write popular articles to increase publicawareness of the young specialty of orthodontiain the first decade of the 20th century.
Minneapolis merchants Robert Foster andOtto Keidle remained close friends with theAngles from their formative years there. In theAngle letter archive from 1899 to 1910, “Bob andOtto” (also called “White Child and Baron”)received some of the most entertaining yarns andhomespun dialects from Edward Angle at hischarmingly best. Angle, who no longer used hischildhood name “Hart” with newly acquiredfriends, still often signed off humorously as“Rube” or “Reuben” or the like. In his well-written personal ramblings to friends, Angle’sbroad and deep nonprofessional interests inpeople, poetry, literature, history, and the worldthrough clearly.
EDWARD HARTLEY ANGLE‘S SCHOOL OF
ORTHODONTICS AT PASADENA,
CALIFORNIA, USA
Angle’s attempts at teaching undergraduatedental students at 4 schools had been frustratedby his inability to separate orthodontics from thedental curriculum, although he finallyestablished the first department of orthodonticsin a university (Marion Sims Dental College,Saint Louis, 1897). After the meeting of theNational Dental Association in 1899, severalmembers persuaded Angle to train them in hisoffice. This was the first postgraduate course in
66 History of Orthodontics
orthodontics, as well as the first school devotedexclusively to the specialty, and it was 3 weekslong. In 1908, he gave up his practice in SaintLouis and moved, first to New York, then to NewLondon, and finally to Pasadena, Calif (1916).Wherever he went, the Angle School went withhim. His students erected what was to becomethe first building exclusively devoted to theteaching of orthodontics (1922). In 1924, theschool was chartered as the Angle College ofOrthodontia (Fig. 8.7).
After heading orthodontic departments atseveral dental schools, Angle decided he couldbe more effective by teaching small, select groupsin his Saint Louis office. Thus was founded (1900)the first postgraduate school of orthodontics(Angle School of Orthodontia, Fig. 8.8). He alsofounded the first orthodontic journal, TheAmerican Orthodontist, in 1907, but could notprolong its publication beyond 1912.
Prior to admission, student was thoroughlygrilled in the basic sciences, either by Dr Angleor one of his staff. The applicant was expected toknow the anatomy, embryology and histologyof the head and neck (exclusive of the brain), the
growth, development, and functioning of thedenture. He also expected the applicant to bereasonably familiar with history, general science,and English literature. Filing, soldering, and wirebending had to be mastered before the studentwas permitted to do any appliance manipulation.Only after surviving the rigors of discipline,theory, technique, and case analysis, the studentwas allowed admission to the clinic.
In June 1922, the members of this schoolfounded a formal association: The Edward HAngle Society of Orthodontia (commonly calledthe Angle Society). The meeting of this societyin New London in 1928 was the last meeting thatAngle ever attended.
They had no acrylics, no alginates, no lightwires, no model trimmers and no preformedbands. Impressions were taken in plaster and,because undercuts prevented removing the stonymass in one piece, the operator was obliged toscore the material and pry it off, piece by piece.he poured impression was later trimmed by handwith a plane, a saw, or a huge file.
APPLIANCE CONTRIBUTION BY
EDWARD H ANGLE
Edward H Angle’s correspondence and patentsreveal features of the most dynamic side perhapsof this multidimensional man: the rapt andconsummate inventor, a human wellspring ofnew ideas (Fig. 8.9). During his lifetime, Angleapplied for and received 45 patents (his wifeAnna obtained his 46th patent in 1934, four yearsafter his death). Most were appliances andinstruments related to clinical orthodontics, butthey included laboratory equipment and a novelautomobile wheel. His contemporary rolemodels were likely among the new breed ofinventive, risk-taking industrialists, such asThomas Edison, George Eastman, and CharlesKettering. America led the world by thebeginning of the 20th century in technologicalinnovation and entrepreneurship. In the firstyears of the 1900s, American medicine wasablaze with new light and directions for themedical and dental community. At JohnsHopkins University, William Osler initiatedcreative reforms in clinical education and single-handedly systematized the field of internalmedicine. At Northwestern University, GreeneVardiman Black introduced the nomenclature of
Fig. 8.7: Angle school of orthodontia
Fig. 8.8: Angle School of Orthodontia, first postgraduate
school for orthodontists
67Angle’s Contribution to the Faculty of Orthodontics
tooth anatomy and the modern principles andtools of operative dentistry.
Edward Angle’s rationale for patenting hisinventions was to take legal claim of his ideasand to protect his business interests. However,many of Angle’s colleagues criticized him for thezeal with which he protected his breakthroughappliances and systems for doing “toothregulation” and “orthodontia” more easily.Patent protection certainly makes sense intoday’s high-stakes environment of corporateespionage and intellectual property rights, butin Angle’s time, patenting—particularly inmedicine—was viewed in many circles as selfishand mercenary.
Angle’s enthusiasm for advancing themateria technica of orthodontics was so strongthat he freely mentored, encouraged, andworked with colleagues in their efforts to developnew appliances. This is seen in Angle’s letters toHenry A Baker of Boston in which he praises the“Baker method of anchorage” and later seeks toprotect Baker’s professional reputation as the firstto use inter-maxillary anchorage against equalclaims made by Calvin S Case of Chicago. It isalso apparent in his letters to E L Townsendwhere he encourages Townsend to write andpublish articles concerning Townsend’s idea fora prosthetic bridge appliance. Angle workedcooperatively with several of his former students
to develop orthodontic appliances andinstruments: Jacob Lowe Young, Spencer RAtkinson and Albert H Ketcham each jointly heldpatent rights to one or more inventions withAngle. Furthermore, trusting the biomechanicalacumen of his former student Milton T Watson,Angle asked him to try out competitors’orthodontic appliances and to conduct acomparative study and report back to Angle withhis conclusions.
Angle, the enterprising innovator, workedand reworked designs to develop the bestappliances. As President of the E H AngleRegulating Appliance Company, incorporated inSt Louis in May 1907, he kept track of the work ofother inventors active in the budding field oforthodontia and maintained a folder withrelevant patents filed by others. Within the 11-year record of correspondence covered by theAngle letter archives, he relentlessly houndedthose he perceived as idea stealers, patentinfringers, and plagiarists—Clarence D Lukens,James N MacDowell, and Miland Knapp, andmanufacturers Julius Aderer, Claudius Ash, andBlue Island Specialty Company. In anger, heslapped some with lawsuits and inflammatorydefamations.
The age-old rule that brilliant inventors makepoor business people did not apply to Edward HAngle. He was in fact the consummate, confidentbusinessman, maximizing income and minimizingexpenses. Angle was a demanding taskmaster inhis detailed letters to the machinists to whom heoutsourced appliance manufacture at varioustimes: William Hahn, the Hardinge brothers, andJohn E Canning. They were required to fabricatehis devices with tight tolerances and on tightbudgets. He held the SS White DentalManufacturing Company, which by 1895 becamethe exclusive distributor of the Angle System, toa rigorous Angle-controlled business relationship.His detailed handwritten invoices from the “E HAngle Regulating Appliance Co” show his (andAnna’s) arithmetic accuracy in billing to the penny,making a lie of his schoolboy reputation of beingweak with numbers.
Angle’s Patented Orthodontic Devices, firstpatent in 1889 is push type jackscrew which wasused to increase the width of the arches there bytreating the malocclusions. In 1851, a lingual archsoldered to bands that are cemented on teeth;
Fig. 8.9: Edward Hartley Angle
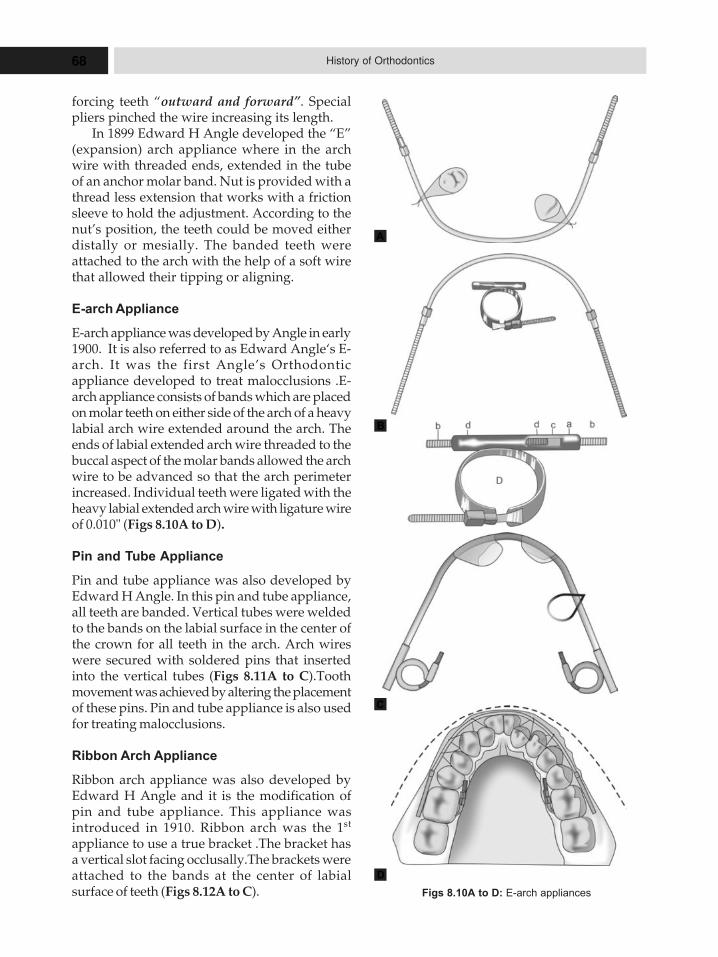
68 History of Orthodontics
forcing teeth “outward and forward”. Specialpliers pinched the wire increasing its length.
In 1899 Edward H Angle developed the “E”(expansion) arch appliance where in the archwire with threaded ends, extended in the tubeof an anchor molar band. Nut is provided with athread less extension that works with a frictionsleeve to hold the adjustment. According to thenut’s position, the teeth could be moved eitherdistally or mesially. The banded teeth wereattached to the arch with the help of a soft wirethat allowed their tipping or aligning.
E-arch Appliance
E-arch appliance was developed by Angle in early1900. It is also referred to as Edward Angle‘s E-arch. It was the first Angle’s Orthodonticappliance developed to treat malocclusions .E-arch appliance consists of bands which are placedon molar teeth on either side of the arch of a heavylabial arch wire extended around the arch. Theends of labial extended arch wire threaded to thebuccal aspect of the molar bands allowed the archwire to be advanced so that the arch perimeterincreased. Individual teeth were ligated with theheavy labial extended arch wire with ligature wireof 0.010" (Figs 8.10A to D).
Pin and Tube Appliance
Pin and tube appliance was also developed byEdward H Angle. In this pin and tube appliance,all teeth are banded. Vertical tubes were weldedto the bands on the labial surface in the center ofthe crown for all teeth in the arch. Arch wireswere secured with soldered pins that insertedinto the vertical tubes (Figs 8.11A to C).Toothmovement was achieved by altering the placementof these pins. Pin and tube appliance is also usedfor treating malocclusions.
Ribbon Arch Appliance
Ribbon arch appliance was also developed byEdward H Angle and it is the modification ofpin and tube appliance. This appliance wasintroduced in 1910. Ribbon arch was the 1st
appliance to use a true bracket .The bracket hasa vertical slot facing occlusally.The brackets wereattached to the bands at the center of labialsurface of teeth (Figs 8.12A to C). Figs 8.10A to D: E-arch appliances
A
B
C
D
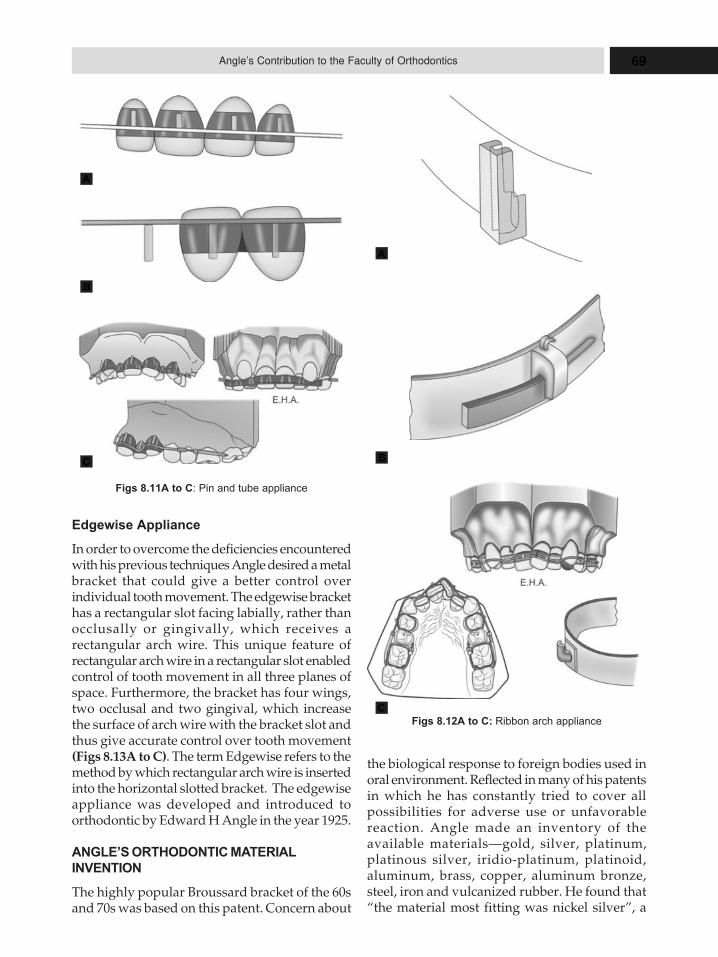
69Angle’s Contribution to the Faculty of Orthodontics
Edgewise Appliance
In order to overcome the deficiencies encounteredwith his previous techniques Angle desired a metalbracket that could give a better control overindividual tooth movement. The edgewise brackethas a rectangular slot facing labially, rather thanocclusally or gingivally, which receives arectangular arch wire. This unique feature ofrectangular arch wire in a rectangular slot enabledcontrol of tooth movement in all three planes ofspace. Furthermore, the bracket has four wings,two occlusal and two gingival, which increasethe surface of arch wire with the bracket slot andthus give accurate control over tooth movement(Figs 8.13A to C). The term Edgewise refers to themethod by which rectangular arch wire is insertedinto the horizontal slotted bracket. The edgewiseappliance was developed and introduced toorthodontic by Edward H Angle in the year 1925.
ANGLE’S ORTHODONTIC MATERIAL
INVENTION
The highly popular Broussard bracket of the 60sand 70s was based on this patent. Concern about
Figs 8.11A to C: Pin and tube appliance
Figs 8.12A to C: Ribbon arch appliance
the biological response to foreign bodies used inoral environment. Reflected in many of his patentsin which he has constantly tried to cover allpossibilities for adverse use or unfavorablereaction. Angle made an inventory of theavailable materials—gold, silver, platinum,platinous silver, iridio-platinum, platinoid,aluminum, brass, copper, aluminum bronze,steel, iron and vulcanized rubber. He found that“the material most fitting was nickel silver”, a
A
B
C
A
B
C
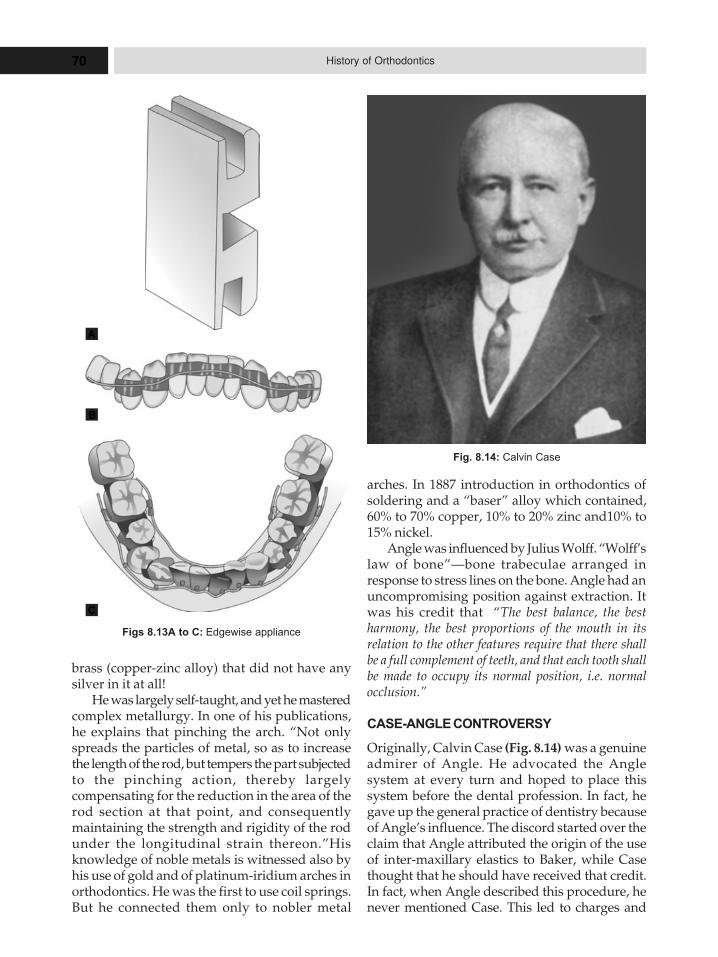
70 History of Orthodontics
brass (copper-zinc alloy) that did not have anysilver in it at all!
He was largely self-taught, and yet he masteredcomplex metallurgy. In one of his publications,he explains that pinching the arch. “Not onlyspreads the particles of metal, so as to increasethe length of the rod, but tempers the part subjectedto the pinching action, thereby largelycompensating for the reduction in the area of therod section at that point, and consequentlymaintaining the strength and rigidity of the rodunder the longitudinal strain thereon.”Hisknowledge of noble metals is witnessed also byhis use of gold and of platinum-iridium arches inorthodontics. He was the first to use coil springs.But he connected them only to nobler metal
arches. In 1887 introduction in orthodontics ofsoldering and a “baser” alloy which contained,60% to 70% copper, 10% to 20% zinc and10% to15% nickel.
Angle was influenced by Julius Wolff. “Wolff’slaw of bone”—bone trabeculae arranged inresponse to stress lines on the bone. Angle had anuncompromising position against extraction. Itwas his credit that “The best balance, the bestharmony, the best proportions of the mouth in itsrelation to the other features require that there shallbe a full complement of teeth, and that each tooth shallbe made to occupy its normal position, i.e. normalocclusion.”
CASE-ANGLE CONTROVERSY
Originally, Calvin Case (Fig. 8.14) was a genuineadmirer of Angle. He advocated the Anglesystem at every turn and hoped to place thissystem before the dental profession. In fact, hegave up the general practice of dentistry becauseof Angle’s influence. The discord started over theclaim that Angle attributed the origin of the useof inter-maxillary elastics to Baker, while Casethought that he should have received that credit.In fact, when Angle described this procedure, henever mentioned Case. This led to charges and
Figs 8.13A to C: Edgewise appliance
Fig. 8.14: Calvin Case
A
C
B
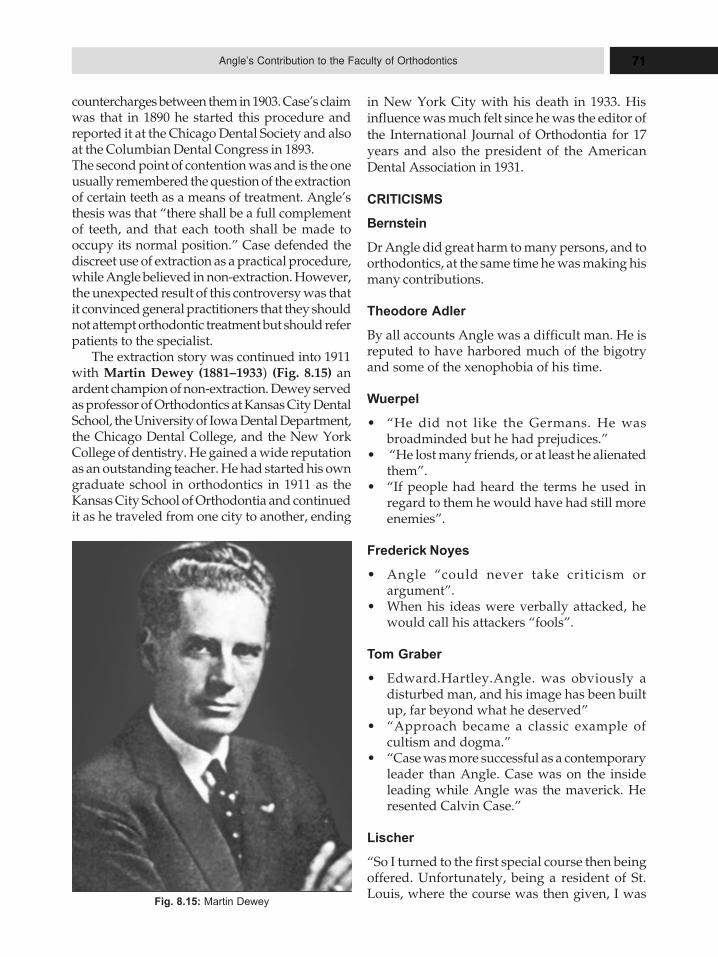
71Angle’s Contribution to the Faculty of Orthodontics
countercharges between them in 1903. Case’s claimwas that in 1890 he started this procedure andreported it at the Chicago Dental Society and alsoat the Columbian Dental Congress in 1893.The second point of contention was and is the oneusually remembered the question of the extractionof certain teeth as a means of treatment. Angle’sthesis was that “there shall be a full complementof teeth, and that each tooth shall be made tooccupy its normal position.” Case defended thediscreet use of extraction as a practical procedure,while Angle believed in non-extraction. However,the unexpected result of this controversy was thatit convinced general practitioners that they shouldnot attempt orthodontic treatment but should referpatients to the specialist.
The extraction story was continued into 1911with Martin Dewey (1881–1933) (Fig. 8.15) anardent champion of non-extraction. Dewey servedas professor of Orthodontics at Kansas City DentalSchool, the University of Iowa Dental Department,the Chicago Dental College, and the New YorkCollege of dentistry. He gained a wide reputationas an outstanding teacher. He had started his owngraduate school in orthodontics in 1911 as theKansas City School of Orthodontia and continuedit as he traveled from one city to another, ending
Fig. 8.15: Martin Dewey
in New York City with his death in 1933. Hisinfluence was much felt since he was the editor ofthe International Journal of Orthodontia for 17years and also the president of the AmericanDental Association in 1931.
CRITICISMS
Bernstein
Dr Angle did great harm to many persons, and toorthodontics, at the same time he was making hismany contributions.
Theodore Adler
By all accounts Angle was a difficult man. He isreputed to have harbored much of the bigotryand some of the xenophobia of his time.
Wuerpel
� “He did not like the Germans. He wasbroadminded but he had prejudices.”
� “He lost many friends, or at least he alienatedthem”.
� “If people had heard the terms he used inregard to them he would have had still moreenemies”.
Frederick Noyes
� Angle “could never take criticism orargument”.
� When his ideas were verbally attacked, hewould call his attackers “fools”.
Tom Graber
� Edward.Hartley.Angle. was obviously adisturbed man, and his image has been builtup, far beyond what he deserved”
� “Approach became a classic example ofcultism and dogma.”
� “Case was more successful as a contemporaryleader than Angle. Case was on the insideleading while Angle was the maverick. Heresented Calvin Case.”
Lischer
“So I turned to the first special course then beingoffered. Unfortunately, being a resident of St.Louis, where the course was then given, I was
72 History of Orthodontics
asked to sign a contract to locate elsewhere oncompletion of the instruction. Angle added: ‘Youknow, Lischer, I can pick the flowers in my gardenmyself.‘
Robert Rubin
Angle possessed many of the personality qualitiesseen in geniuses. They can be difficult, demanding,and unforgiving. They tend to be so devoted totheir field that they fail to develop other aspects oftheir lives. Angle seems to fit that category.”
Wuerpel
It (orthodontics) was his religion and his god. Hewould sacrifice everything for its sake. He couldonly see his life and his work and his devotion interms of orthodontia.”
Edward H Angle’s Publications and
Presentations
Though Angle died 1930, his influence is still feltstrongly in orthodontics. Even his enemiesrecognized the many contributions made byEdward Hartley Angle. His pioneer efforts inorthodontic education, his contribution toorthodontic literature, and his developments ofinnumerable instruments and appliances are notthe accomplishments for which he will beremembered. Long after these have faded intohistory, Angle’s name will be associated with theonward march of biologic science and it will berealized how perceptive was the mind that couldpenetrate the empiricism of his day and proclaimthe significance of normal occlusion. Thisestablished orthodontia as a science and it willremain Angle’s greatest monument. Characteristicof the man was a remark made shortly before hedied: “I have finished my work. It is as perfect as Ican make it.”
Date Event
June 1, 1855 Eward Hartley Angle born toPhilip Casebeer Angle (1820–1907) and Isabel Erskine Angle(1824–1908) in district 1“Ballibay”, Herrick Township,Bardford County, Pennsylva-nia. The fifth of seven children.Demonstrates early talent forusing tools and devising and
constructing machinery, inclu-ding a hay rake (at age 11); at-tends high school in Canton,Pennsylvania.
1874–1876 Apprentices with a local dentistin Herrick.
Fall 1876– Attends the PennsylvaniaFebruary 1878 College of Dental Surgery in
Philadelphia, receiving DDSdegree on February 28, 1878;beings practicing dentistry inTowanda, the county seat ofBradford County, Pennsylva-nia. Here he develops an inter-est in orthodontia.
Spring 1881 Develops a chronic respiratoryailment, called pleural pneu-monia, probably tuberculosis.
Autumn 1881 Moves to Minneapolis, Min-nesota, for health reasons.Within months, his health re-covers and he returns to Penn-sylvania briefly to join his olderbrother Mahlon and friends inplanning a sheep-raising ven-ture in Montana.
Late 1881 Moves to Montana with associ-ates to enter the sheep-ranchingbusiness.
Early 1882 The severe winter of 1882 killstheir sheep flock and dooms theventure financially.
1882–1883 Relocates to Minneapolis andresumes the private practice ofdentistry; continues his interestin orthodontia.
1886 Accepts position as professor ofhistology and lecturer on com-parative anatomy and orth-odontia in the Dental Depart-ment of the Minnesota HospitalCollege in Minneapolis. Twoyear later, it becomes part of theUniversity of Minnesota, and heis elevated to professor of orth-odontia. Maintains his part-timeprivate practice of dentistry.
March 1887 Marries florence A Canning ofMinneapolis, sister of his ma-chinist Hohn E Canning.
September 8, Present of his first major address
73Angle’s Contribution to the Faculty of Orthodontics
1887 describing aspects of the AngleSystem of Regulating Appli-ances before the 9th Interna-tional Medical Congress inWashington, DC. Angle’s origi-nality is challenged in theheated discussion that ensues.Angle later considers a 14 pageextract of this paper, publishedwithout discussion in an 1887textbook by Loomis P Haskell,as the “first edition” of the SerenAmerican editions of his famousbook.
December 3, Daughter Florence Isabel Angle1887 is born in Minneapolis. (She
died in 1970 in Morganton,North Carolina.)
1888 Elected president of the Minne-apolis City Dental Society.
March 5, 1889 Patents a jack-screwmachinism, the first of 46 pat-ents held by angle.
1890 “Second edition” of his book ispublished, as a 30-page appe-ndix to the second edition of adental laboratory handbook byLoomis P Haskell.
1892 Resigns from the faculty at theUniversity of Minnesota; limitshis practice exclusively to orth-odontia, thus becoing ostensiblythe world’s first specialist inorthodontia.
1892 Hires Anna Hopkins (1872–1957) of Minneapolis as his sec-retary and office assistant.
1892 Publishes third edition, a 51-page pamphlet entitled, TheAngle System of Regulation andRetention of the Teeth.
1892–1898 Professor of orthodontia at theAmerican College of Dental Sur-gery (later merging into North-western University School ofDentistry) in Chicago.
1894 Appointed surgeon to the GreatNorthern Railroad for the treat-ment of fractures of the maxil-lae.
1895 Fourth american edition is pub-lished, a 112-page hard-coverbook now titled. The Angle Sys-tem of Regulation and Reten-tion of the Teeth and Treatmentof Fractures of the Maxillae.
1895 Relocates to St Louis, Missouri(with his wife Florence, hisdaughter florence Isabel, and hissecretary-assistant AnnaHopkins; sets up a private prac-tice there limited to orthodontia.
1896–1899 Professor of orthodontia in theDental Department of Marion-Sims College of Medicine, StLouis.
1897–1898 Teaches in the Dental Depart-ment of Washington University,St Louis.
1897 Fifth American edition is pub-lished by SS White,philadelphia; also a Germantranslation of his fourth (1895)American edition is publishedby SS White Co, Berlin.
1897 Is awarded MD degree fromMarion-Sims College of Medi-cine.
1899 Dental Cosmos publishesAngle’s “Classification of Mal-occlusion”, his most importantjournal article to date.
1899 Claudius Ash publishesGustave Darin’s French trans-lation of Angle’s book under thetitle Methode du ProfesseurAngle Pour la Regularisation etle Traitement des Dents et Pourle Traitement des Fractures desMaxillaires.
June 6, 1899 Patents the E-Arch, his expan-sion archwire mechanism.
August 1899 Angle’s paper on orthodontiaprepared for presentation at theNational Dental Associationmeeting at Niagara Falls is by-passed at the last minute by pro-gram officials. This personalslight fuels Angle’s desire tofound a postgraduate school of

74 History of Orthodontics
orthodontia and a professionalsociety devoted to orthodontia.
November 1899Teaches a postgraduate courseon orthodontia in his office inthe Olivia Building, St Louis.Attending are thomas B mercer,Henry E Lindas, Herbert APullen, and Milton T Watson.
December 8, Resigns his appointment of1899 Marion Sims college of medi-
cine.1900 Founds the Angle School of
Orthodontia; first 5-week courseis held from May 1 through earlyjune 1900 in the odeon Build-ing, St Louis.
July 1900 Separates from wife FlorenceCanning Angle.
October 1900 Publishes sixth edition, a 315-page work, Treatment ofMalocclusion of the Teeth andFractures of the Maxillae.Angle’s System.
Early 1901 Founds the Society of Orthod-ontists (antecedent of the Ameri-can Association of Ortho-dontists) and serves as its firstpresident.
Early 1901 Founds the Society of DentalScience of St Louis.
July 1901 First meeting of the Society ofOrthodontists (renamed in 1902,The American Society of Orth-odontists) is held in St Louis,Missouri.
1902 With Angle’s encouragement,Anna Hopkins graduates fromthe University of lowa with aDDS degree.
December Offered the editorship of orth1902 odontia of the international
Dental Journal; Angle declinesthe offer.
August 29– Chairman of Section VISeptember 3, (Orthodontia) of the fourth1904 International Dental Congress,
St Louis.1904 German translation of his fifth
(1895) American edition is pub-lished by SS white Co Berlin.
1905 Contributes chapter on orth-odontia in Edward C Kirk’sAmerican Textbook of Oper-ative Dentistry (also in 1911edition, revised).
Spring 1906 Resigns membership in Ameri-can Society of Orthodontists;encourages establishment of TheAlumni Society of the AngleSchool of Orthodontia (EarliestForer-unner of the Edward HAngle Society of orthodontists).
Winter 1906– Retires from practice of1907 orthodontia in St Louis;
focuses on writing seventhAmerican edition of Treatmentof Malocclusion of the Teeth,Angle’s System (628 pages).
1907 Father Philips Casesbeer Angledies, age 87.
May 1907 Incorporates the EH AngleRegulating Appliance co in StLouis, Missouri.
June 1907 Founds The American Orth-odontist, the first journal in theworld devoted exclusively toorthodontics (discontinued in1912); it is the forerunner of TheAngle Orthodontist.
1908 Mother Isable Erskine Angledies, age 84.
May 1908 Divorces Florence CanningAngle in Minneapolis, Minne-sota.
June 27, 1908 Marries Anna Hopkins in StLouis, Missouri.
Summer 1908 Moves from St Louis with wifeAnna H Angle to Larchmont,New York.
September 15– The Angle School of orthodontiaOctober 31, is in New York City for a 6-week1908 course, in an office building at
rhe corner of West 72nd Streetand Broadway.
Fall 1908 Hemann Muesser publishesJosef Grunberg’s German trans-lation of Angle’s sixth (1900)American edition under the titleBehandlung der Okklusions-anomalien der Zahne.
75Angle’s Contribution to the Faculty of Orthodontics
April 1909 Purchases home at 58 BellevuePlace, New London, Connecti-cut.
July 1909 Wins patent infringement suitagainst appliance manufacturerJulius Aderer.
October – The Angle School of OrthodontiaDecember 1909 moves to New London, conn-
ecticut; course session length-ened to 9 weeks, given in theMunsey Building.
July– Second (final) course session inSeptember New London at the Harbor1911 School, after which Angle closes
Angle School of Orthodontiadue to his declining health.
1913 Revised and expanded Germanedition of Angle’s book (1907American edition) is publishedwith new chapters by JosefGrunberg and AlbinOppenheim (778 pages).
February 22, Awarded Honorary ScD degree1915 by the University of Penns-
ylvania.Late 1916 Angle moves to southern
Califomia for health reason;purchases home at 1025 NorthMadison Avenue, Pasadena.
1917 At request of Hames C Angle (norelation), he reopens the AngleSchool of Orthodontia at hishome in Pasadena.
1922 Edward H Angle Society of orth-odontists is started in Califor-
nia by graduates of the AngleSchool of Orthodontia.
1922–1923 Grateful students fund con-struction of a building in Pasa-dena for the Angle School ofOrthodontia at 550 JacksonStreet, next to Angle’s home; itis dedicated on January 8, 1923.
1924 The Angle College of Orthodon-tia and Infirmary is chartered byCalifornia. No tuition is chargedfor the college’s 12-month pro-gram (which is followed withperiodic faculty supervisionduring the first year of privatepractice). All patients weretreated free of charge.
September 15, Patents the edgewise arch1925 mechanism.Late 1927 The Angle College of Orthodon-
tia closes unofficially due toAngle’s deteriorating health.
August 11, Edward H Angle dies in Santa1930 Monica, California, at age 75
from heart failure; burial atMountain View Cemetery,Altadena, California.
November 17, The Angle Orthodontist, a1930 scientific journal devoted exclu-
sively to orthodontics, isfounded in chicago in DrAngle’s memory by the newlyreorganized Edward H AngleSociety of Orthodontia.
76 History of Orthodontics
9DDDrrr TTTMMM GGGrrraaabbbeeerrr’’’sssCCCooonnntttrrriiibbbuuutttiiiooonnn tttooo
OOOrrrttthhhooodddooonnntttiiicccsss
THOMAS M GRABER (1917–2007)
Dr TM Graber as an Orthodontist,
Researcher, and Dental Educator
Dr Thomas M. “Tom” Graber, known inter-nationally as an orthodontist, researcher, anddental educator, born in St Louis on May 27, 1917and died on June 26 at age 90, in Evanston, Illinois.Dr Thomas M Graber was certainly a pioneeramongst men. His complete devotion and love forthe specialty of orthodontics is reflected in hisextensive works on a myriad of topics, spanningover a period of nearly six decades. As Dr Graber’sfamily friend and colleague Dr Jim McNamaranoted, “Tom’s energy and enthusiasm for ourprofession make him a wonderful role model forfuture generations of orthodontists.” The passingof Dr Thomas M Graber marks the end of an era inorthodontics.
Dr TM Graber’s Dental Graduation
Dr Graber earned a DMD degree in dentistry(Washington University, 1940), an MSD inorthodontics (Northwestern University, 1946),and a PhD in anatomy (Northwestern University,1950).
Dr TM Graber’s Working Experience
Dr TM Graber served as a captain in the UnitedStates Army Dental Corps from 1941–1945. Hewas on the faculty of Northwestern Universityfrom 1946–1958 at the University of Chicago from
1969–1982, where he was the head of the Sectionof Orthodontics; and at the University of Illinoisat Chicago College of Dentistry from 1994 untilhis death. He also served as a visiting professoron the faculties of the University of Michigan. TheUniversity of Freiburg, Germany, and theUniversity of Gothenburg, Sweden. A naturalteacher, he was “one of those people who couldtake complex subjects and explain them clearly tostudents,” said his wife, Doris, a professor ofpolitical science at the University of Illinois atChicago.
A pioneer in orthodontics and craniofacialbiology, Dr Graber did research on craniofacialanomalies, cleft palate, cleft lip, temporomandi-bular joint anatomy and disturbances, orthopedicgrowth guidance of the dentofacial complex, andthe use of magnetic forces in orthodontics anddentofacial orthopedics. His 60 years of researchhave added to our knowledge in these fields andchanged the way they are taught around theworld.
He gave more than 475 continuing educationcourses around the world and was on theAmerican Association of Orthodontists AnnualSession program more than any other person inAAO history. Beginning in 1951, he made annuallecture tours to university departments andmedical and dental societies around the world.He wrote 28 books on orthodontics and dentalanatomy and contributed chapters to 20 otherbooks. He wrote more than 175 scientific articlesin refereed dental and medical journals, not to
� Thomas M Graber (1917–2007)
� TM Graber’s Contributions
� Graber’s Other Contributions
to Orthodontics

77Dr TM Graber’s Contribution to Orthodontics
mention hundreds of book and journal articlereviews and abstracts.
From 1985 to 2000, he served as editor-in-chiefof the American Journal of Orthodontics andDentofacial Orthopedics. He went on to found theWorld Journal of Orthodontics, and he continuedas editor-in-chief of that publication until his death.
Dr Graber’s contributions to organizedorthodontics and orthodontic education wereunsurpassed. He served on the AAO Council onOrthodontic Education from 1962 to 1973;founded the Audiovisual Council of the AAO in1962; was general chairman of the AAO AnnualSession twice; founded the Kenilworth DentalResearch Foundation; was director of ContinuingEducation for the G. V. Black Institute since 1967;was director of Dental Continuing Education forthe University of Chicago Center for ContinuingEducation from 1971 to 1981; founded theNorthwestern University Cleft Lip and PalateInstitute and the Orthodontic Section at theUniversity of Chicago Medical School; was afounding member of the Illinois Society ofOrthodontists; and was a former president of theChicago Society of Orthodontists, the MidwestComponent of the Edward H. Angle Society, andthe Illinois Society of Orthodontists.
Dr Graber held appointments at Children’sMemorial Hospital and Wyler Children’s Hospitalin Chicago. He received honorary doctoral degreesfrom the University of Gothenburg, Sweden, 1989;Washington University, St Louis, 1991; theUniversity of Michigan, 1994; Kunming MedicalUniversity, China, 1996; and Aristotle Universityof Thessaloniki, Greece, 2005. His honorary-degrees from Washington University and theUniversity of Michigan were the first and onlyones ever given to a dentist.
Dr Graber received awards too numerous tolist. He was quite proud to be the first non-Japaneseperson to be inducted as a member of the JapanOrthodontic Society in 1997, and he received theEmperor of Japan’s Order of the Sacred Treasure,the highest Japanese award ever bestowed upona noncitizen of Japan, in 2003.
Active in his community, Dr Graber was amember of the Sons of the American Revolution,Fort Dearborn Chapter; and had been a leader inthe Boy Scouts of America where all four sonsbecame Eagle Scouts.
He was a generous philanthropist, havingendowed a professorship at the University of
Michigan and contributed to the University ofIllinois at Chicago College of Dentistry as well.
Dr Graber enjoyed travel, visiting countriesaround the world and even the North Pole andAntarctica. He enjoyed photography; he skied,played tennis, bicycled, swam, went scuba diving,and sailed—pursuing many of these activities wellinto his 80s.
He is survived by his wife of 66 years, Dr DorisGraber; sons Dr Lee W Graber, Dr Thomas WGraber, Jack D Graber, and Dr Jim M Graber;daughter Dr Susan Graber; and 14 grandchildren.
TM GRABER’S CONTRIBUTIONS
TM Graber’s contribution are listed and explainedbelow;
Physiology of Occlusion
Normal Occlusion
— TM Graber (DCNA, 1968)
In this paper, Dr Graber states that any definitionof normal occlusion cannot be static and merelydescriptive of tooth relationships. Normalocclusion involves not only the teeth, but also theinvesting tissues, the contiguous and motivatingmusculature, curve of Spee, inter-occlusalclearance, and the TMJ morphology and function.He has organized the historical progress in thedevelopment of current concepts of occlusion intothree periods:� Fictional period (before 1900)� Hypothetical period (1900–1930)� Factual period (1930 – present).
Fictional Period
� Concepts were developed from inductiveanalysis.
� Terminology was loose and reflected thepersonal preferences of the authors.
� Authors talked about dental antagonisms,“meeting” or “gliding” of teeth.
� Good descriptions of the morphologic natureof individual teeth existed, but an appreciationof the functioning dentition as a whole waslacking.
Hypothetical Period
It was EH Angle who organized the existingconcepts of occlusion at the time and formulateddefinite principles of diagnosis in treatment.
78 History of Orthodontics
� He gave the ‘key of occlusion’ based on theposition of the upper first molar.
� Angle described normal occlusion using askull that he called ‘Old Glory’.
� Calvin Case developed the concept of “apicalbase”. He also called attention to the effect ofthe nose and chin button on the profile.
� In 1908, Bennett suggested the functionalanalysis or the dynamic approach to occlusionfor the first time. He noted that the mandiblehad a resting position (depended onmusculature) and a functional position(depended on the teeth in maximum contact).
Factual Period
� With the introduction of biometric proceduresand scientific methodology, this period saw atrend toward the dynamic and a de-emphasison the static.
� In 1931, B. Holly Broadbent introducedradiographic cephalometry.
� Occlusion now meant inter-digitation of teethplus the influence of the musculature as wellas that of the temperomandibular joint.
The Developing Occlusion—Orthodontic
Considerations for the Handicapped
— Owen, Graber (DCNA, 1974).
� The authors state that the nature and severityof the handicap in a child may totally dominatethe dental diagnostic and treatmentconsiderations.
� They have described the type of care to berendered according to the severity of thehandicap – mild, moderate, severe.
� Timing, case selection and management arethe main factors in treating or not treating thehandicapped patient.
� It is important to weigh the possible benefitsto the child with the individual’s physical anddental status as affected by his ability tocomprehend and cope with orthodonticprocedures.
The “Three M’s”: Muscles, Malformation
and Malocclusion
— TM Graber (AJO, 1963)
� In this classic article, Dr Graber has analyzedmuscles and their relationship to structural
configuration in Class I, Class II, and Class IIImalocclusions.
� “Whenever there is a struggle between muscleand bone, bone yields.” Muscle function canbe adaptive to morphogenetic pattern.
� A change in muscle function can initiatemorphologic variation in the normalconfiguration of the teeth and supporting bone,or it can enhance an already existingmalocclusion.
� In the latter instance, the inherent structuralmal-relationship calls for compensatory oradaptive muscle activity to perform the dailyfunctions.
� The structural abnormality is increased bycompensatory muscle activity to the extent thata balance is reached between pattern,environment, and physiology.
� It is imperative that the orthodontist appraisemuscle activity and that he conduct hisorthodontic therapy in such a manner that thefinished result reflects a balance between thestructural changes obtained and the functionalforces acting on the teeth and investing tissuesat that time.
The Role of Upper Second Molar Extraction
in Orthodontic Treatment
— TM Graber (AJO, 1955)
� In Class II treatment, the greatest changeproduced by the orthodontic appliances is inthe maxilla. Distal adjustment of tooth positionin the maxilla alone, or in conjunction withmandibular growth, is the basis for correction.
� If space required for the tooth adjustment isgained in the second molar area, only as muchspace as required need be used, with thesubsequent mesio-vertical eruption of themaxillary third molars filling the gap.
� Maxillary 2nd molar removal expeditescorrection of Class II division 1 malocclusion,provided that:
� There is excessive labial inclination of themaxillary incisors, with no spacing.
� Overbite is minimal.� 3rd molars are present in the maxilla, in good
position and of proper shape.� The cases offering the poorest prognosis for
maxillary 2nd molar extraction are severebasal dysplasias with vertically inclined
79Dr TM Graber’s Contribution to Orthodontics
maxillary incisors, no spacing, and severeoverbite.
Maxillary Second Molar Extraction in Class II
Malocclusion
— TM Graber (AJO, 1969)
� In this paper, Dr Graber has again dwelledupon the removal of upper 2nd molars as atherapeutic means for correction of Class IImalocclusion.
� He recommends the extraction of maxillary2nd molars in those instances in which thereare good maxillary 3rd molars and where thereis a significant Class II/1 malocclusion andinvolvement of all 4 tissue systems – teeth, bone,muscle and nerve.
� A fixed lingual arch is used to prevent themandibular 2nd molars from over-erupting.
� The results appear to be stable over a longperiod of time.
� The iatrogenic reaction is minimal or non-existent.
Extraoral Force—Facts and Fallacies
— TM Graber (AJO, 1955)
� Dr Graber studied 150 cases of Class II/1malocclusion treated with extra-oral forceusing the same type of appliance.
� The appliance consisted of molar bands, a .045inch stainless steel labial arch wire withvertical spring loops at the lateral-canineembrasure to receive the cervical gear. This wasa metal tube with a continuous spring insideto provide distal motivating force.
He concluded that:� Class II/1 malocclusions are amenable to
correction by the use of extraoral force. Markedimprovement in the basal relations can beobtained; overbite and overjet problems canbe helped greatly.
� Coordination of treatment with the pubertalgrowth spurt ensures a greater likelihood ofsuccess [10–12 years in girls; 12–17 years in boys].
� Certain untoward sequale may be seen in theuse of extraoral force. These include:
� Incomplete correction of tooth malrelationship,� Excessive distal tipping of maxillary 1st molars,� Possible impaction of maxillary 2nd or 3rd
molars,� Possible excessive lingual tipping of maxillary
incisors,
� Possible unilateral response in correction ofclass II relationship, and
� Difficulty in the control of excessive overbite.
Dentofacial Orthopedics versus Orthodontics
— Graber, Chung, Aoba (JADA, 1967)
� In this paper, the authors have reported thatorthopedic therapeutic measures with heavyand interrupted force against the bone may beused successfully in orthodontics.
� Greater use of this type of extraoral force isrecommended because of its superior abilityto correct basal jaw anteroposterior mal-relationships.
� In addition, there is greater stability, a lowerpercentage of tooth extractions, minimal useof intra-oral appliances, less attendantorthogenic damage (decalcification, rootresorption), minimal chair time, and longerintervals between appointments.
� An occipital base of anchorage is moresatisfactory for correction of Class IIImandibular prognathism.
� In cases of open bite, the direction of restrictiveforce must be as vertical as the design of thecranial cap will permit.
� In Class II/1 malocclusion, a cervical sourceof anchorage is satisfactory.
Heavy Intermittent Cervical Traction in
Class II Treatment: A Longitudinal
Cephalometric Assessment
— Mills, Holman, Graber (AJO, 1978)
Investigated the changes brought about in thedentofacial complex as a result of the use ofheavy cervical traction forces appliedintermittently in the maxilla in growing Class IIdivision 1 patients, and compared withuntreated controls.
Their findings showed that there was:� A stable reduction in the ANB angle is seen.� SNA did not move downward during
treatment; no significant tipping of PPoccurred.
� Less forward progress of point B and Pogoccurred in treated group. Thus, SNB wasconstant.
� Mandible was rotated downward andbackward—slight increase in SN-MP angle.
� Significant decrease in overbite occurredduring treatment.
80 History of Orthodontics
� U1-SN decreased during treatment, butincreased during follow-up.
� Treatment had marked withholding effect onnormal downward and forward eruption ofmaxillary 1st molars. However, in post-treatment period, these teeth erupted more thanin controls, losing some of the treatment effect.
� Distal tipping of upper molars occurred duringtreatment, but relapsed after applianceremoval.
� Distal uprighting of lower molars and incisorsoccurred during treatment. Molar position wasstable, but incisors relapsed followingtreatment.
� Sagittal arch length decreased significantlyduring treatment. This effect was stable.
� Both the downs OP and functional OP tippeddownward anteriorly as a result of treatment,and relapsed insignificantly followingtreatment.
� Anterior facial height increased more thannormally as a result of treatment. Most of thischange took place in the lower facial height.
The Effectiveness of Protraction Face Mask
Therapy: A Meta-analysis
— Kim, Viana, Graber, Omerza and BeGole(AJODO, 1999)
This study examined the effectiveness of maxillaryprotraction with orthopedic appliances inClass III patients. A meta-analysis of relevantliterature was performed to determine whether aconsensus exists regarding controversial issuessuch as the timing of treatment and the use ofadjunctive intra-oral appliances.
The results showed that there was:� No distinct difference between the palatal
expansion group and non-expansion groupexcept for 1 variable, upper incisorangulations, which increased to a greaterdegree in the non-expansion group. Thisfinding implies that more skeletal effect andless dental change are produced in theexpansion appliance group.
� Examination of the effects of age revealedgreater treatment changes in the youngergroup.
� Results indicate that protraction face masktherapy is effective in patients who aregrowing, but to a lesser degree in patients who
are older than 10 years of age, and thatprotraction in combination with an initialperiod of expansion may provide moresignificant skeletal effects.
Craniofacial Features of Patients with
Class III Abnormalities: Growth-related
Changes and Effects of Short-term and
Long-term Chin-cup Therapy
— Deguchi, Kuroda, Minoshima and Graber(AJODO, 2002)
� The craniofacial features of patients withClass III abnormalities, including growth-related changes and effects of short-term andlong-term chin-cup therapy, were studied.
� Twenty female subjects were treated with chin-cups and an orthopedic force of 500 g for 31months (short-term treatment group). Another36 female patients were treated with chin-cupsand a force of 250 to 300 g for 86 months (long-term treatment group).
� Cross-sectional lateral films of 562 skeletalClass III girls served as controls.
Their results showed that:� Short-term treatment resulted in a slight
improvement in ANB angle and Witsappraisal, while long-term treatment resultedin a significant improvement in ANB angleand Wits appraisal.
� Such treatment also resulted in a significantinhibition of the growth of the ramus (2.2 mm)and body length (3.6 mm) of the mandible, abackward rotation of the mandible, and areduction (8.2°) of the gonial angle.
� However, there was no alteration of anyparameter of the maxilla and the cranial base,except the length of S-N and N-S-Ar in the long-term treatment group.
Long-term Application of Chin-cup Force
Alters the Morphology of the Dolichofacial
Class III Mandible
— Deguchi, Kuroda, Hunt and Graber (AJODO, 1999)
� Investigated the immediate and long-termeffects of prolonged use (mean, 7 years 2months) of chin-cup appliances in subjectswith dolichofacial Class III mandibles.
� Thirty six female subjects with severe skeletalClass III malocclusions, associated with largegonial angles, were studied.
81Dr TM Graber’s Contribution to Orthodontics
� At post-treatment (T1, 65 months duration) andpost-retention (T2, 56 months after T1), Ar-Meand Wits appraisal cephalometric parameterswere significantly different between patientsand control subjects (n = 230).
� The Go-Me parameter in treated subjects waslonger than that of the controls at T0 butbecame significantly shorter at T2.
� Ar-Go parameter increased less than thecontrols at T2.
� Results indicate that long-term use of thechin-cup appliance (>5 years) is effective insubjects with severe skeletal Class IIIabnormality.
Rare Earth Magnets and Impaction
— Vardimon, Graber, Drescher and Bourauel (AJO, 1991)
Introduced a new, magnetic attraction system,with a magnetic bracket bonded to an impactedtooth and an intra-oral magnet linked to aHawley-type retainer for stimulating the naturaleruption of an impacted tooth into the oralcavity.� The magnetic system consisted of a magnetic
bracket and an intra-oral magnet.� A miniaturized prism-shaped Nd2Fe14B
magnetic alloy in an un-magnetized form wasground down (width = 2.20 mm × height =2.59 mm × depth = 2.02 mm) to fit into anenlarged intra-bracket space, i.e. into the spacecreated between two machined down-tiewings of a twin bracket.
� Vertical and horizontal magnetic bracketswere designed, with the magnetic axismagnetized parallel and perpendicular to thebase of the bracket, respectively.
� The vertical type is used for impacted incisorsand canines.
� Horizontal magnetic bracket is applied forimpacted premolars and molars.
Rare Earth Magnets
Graber described the potential for the clinicalutilization of rare earth magnets for the followingpurposes:� Space control (space closure/opening)� Open bite therapy (intrusion of posterior teeth)� Palatal expansion� Growth guidance (functional appliances)� De-impaction of canines and molars.
Magnetic versus Mechanical Expansion with
Different Force Thresholds and Points of
Force Application
—Vardimon, Graber, Voss and Verrusio (AJODO, 1987)
Studied the effects of force magnitude (high vslow) and point of force application (tooth vs directpalatal endosseous pins) on palatal expansiontreatment in 4 Macaca fascicularis monkeys.
Animal 1 (IS)
� Received an upper acrylic appliance with anexpansion screw.
� The appliance was bonded bilaterally fromcanine to 1st molar.
� Thus, high forces (2033 g) were transmittedindirectly to the mid-palatal suture via theabutment teeth.
Animal 2 (IM)
� Received two permanent SmCo5 magnets inrepelling configuration.
� The appliance was bonded to the abutmentteeth (canine and 1st molar).
� It transmitted low forces (258 g) indirectly tothe mid-palatal suture.Sliding (A) and stationary (B) acrylic housings
to receive the magnets. (C) Acrylic occlusalextensions to be bonded to dental arch. (D)Horizontal tubes to receive the U-shaped bar (E)Vertical holes (F) to retain the reactivation holders(G) Teflon rings (H) to serve as barriers in thereactivation process.
Animal 3 (DM)
� Received a magnetic unit linked to a plateattached to the palate via 4 endosseous pins.
� It transmitted low forces (258 g) directly to thepalatal shelves.
Animal 4 (control): received a passive shamappliance bonded to abutment teeth.
Their results showed that:� Treatment time was longer in the low force,
magnetically-induced appliances groups – 33days in IS, 135 days in IM and 95 days in DMgroups.
� In animal IS, a diastema developed betweenthe incisors and the force was directed supero-laterally and then transmedially, thus causing
82 History of Orthodontics
fractures in the nasal complex and otheriatrogenic sequelae.
� In the magnetically-induced appliances, theforce radiated supero-laterally, dissipating inthe zygomatico-frontal suture, and the overjetsignificantly increased due to markedwidening of incisive and transverse sutures.
� The palatally pinned magnetic applianceproduced bodily tooth movement, the greatestincrease in inter-molar distance, and asuperior positioning of the maxillo-palatineregion.
� Their results suggested reduction ofconventional forces for palatal expansion byup to eight-fold, through the use of rare earthmagnets.
Stability of Magnetic versus Mechanical
Palatal Expansion
— Vardimon, Graber and Voss (EJO, 1989)
Spatial stability following palatal expansion (PE)treatment was studied longitudinally on 8Macaca fascicular is monkeys.� The sample was divided into short-term and
long-term groups.� The 4 animals in each group received:� An indirect screw (IS) PE appliance (F = 2035 g).� An indirect magnetic (IM) PE appliance (F =
258 g and 360 g).� A direct magnetic (DM) PE appliance (F = 258 g
and 360 g).� A sham appliance.� Direct force transmission was via pinning to
the palatal shelves, indirect transmission wasvia abutment teeth.
This study indicated that:� Transverse stability was greatest in the
skeletally borne appliance.� Inter-canine distance relapse was 53% for IS
and 23% for DM groups.� Inter-molar expansion was more stable than
inter-canine expansion due to selective activityof circummaxillary sutures and rootconfiguration.
� Sagittal advancement and vertical superiortranslation were greater in the magneticappliances with low force PE regimen.
� Clinical implication – low force PE regimencan be of substantial benefit in young skeletalClass III patients with transverse maxillarydeficiency.
Magnetic Strength and Corrosion of
Rare Earth Magnets
— Ahmad, Drummond, Graber, BeGole (AJODO, 2006)
� Evaluated several magnet coatings and theireffects on magnetic flux density.
� Sixty neodymium-iron-boron magnets weredivided into 6 equal groups—polytetra-fluoroethylene-coated (PTFE), parylene-coated, and noncoated.
� They were subjected to 4 weeks of aging insaline solution, ball milling, and corrosiontesting.
� Their results showed a significant decrease inmagnet flux density after applying a protectivelayer of parylene, whereas a slight decreasewas found after applying a protective layer ofPTFE.
� After 4 weeks of aging, the coated magnetswere superior to the non-coated magnets inretaining magnetism.
� The corrosion-behavior test showed nosignificant difference between the 2 types ofcoated magnets, and considerable amounts ofiron-leached ions were seen in all groups.
� The authors concluded that throughout theprocesses of coating, soaking, ball milling, andcorrosion testing, PTFE was a better coatingmaterial than parylene for preserving magnetflux density. However, corrosion testingshowed significant metal leaching in allgroups.
Functional Orthopedic Magnetic Appliance
(FOMA) II—Modus Operandi
— Vardimon, Stutzmann, Graber, Voss, Petrovic(AJODO, 1989)
� Introduced a new functional appliance (FA)to correct Class II dentoskeletal malocclusions.
� The FOMA II uses upper and lower attractingmagnets (Nd2Fe14B) to constrain the lower jawin an advanced sagittal posture.
� In vitro, a special gauge transducer measuredthe magnetic attractive path and forces.
� In vivo, 13 prepubertal female Macacafascicularis monkeys received facial implantsand were treated for 4 months with thefollowing appliances:– Conventional FA (4 subjects)– FOMA II (5 subjects)– Combined FOMA II + FA (2 subjects)– Sham (control) appliance (2 subjects).
83Dr TM Graber’s Contribution to Orthodontics
1. The FOMA II consisted of upper and lowermagnetic plates.� Buccal (solid line) and lingual (dashed
line) 0.035-inch stainless steel arch wiresformed the metal substructure.
� The two arch wires were linked togetherby acrylic overlaying the incisor and molarcrowns.
� The FOMA II was designed with amagnetic inclined plane (25°).
2. The conventional FA (feedback plates) guidedthe mandible to a forward position by using aslanted guide bar attached to the upper plateand a lower oblique plane of the lower plate.
3. The combined FOMA II + FA applianceconsisted of a labial magnetic unit and alingual prong system.
4. The sham appliance with its passive upperand lower plates.
The in vitro results showed the following:� Vertico-sagittally displaced upper and lower
magnets attracted ultimately along an obliqueline with a terminal horizonal slide to becomefully superimposed.
� The functional performance improved whenthe magnetic interface acted as a magneticinclined plane.
� The magnetic force was able to guide andconstrain the mandible toward the constructiveprotrusive closure position.
The in vivo results demonstrated the following:� Functional performance increased in FOMA
II (22%) and in the combined FOMA II + FA(28%) over the conventional FA.
� Mandibular length increased significantly inthe treated animals over the control animals.
� Incisor proclination was lower in magneticappliances than in the conventional FA.
� Mandibular elongation and condylar posteriorinclination resulted from posterosuperiorendochondral growth and by bonyremodeling of the condylar neck.
� No anterior displacement of the post-glenoidspine nor the articular eminence was found.
The Functional Orthopedic Magnetic
Appliance (FOMA) III
— Vardimon AD, Graber TM, Voss LR, Muller(AJODO, 1990)
� Developed an intraoral inter-maxillaryappliance for the treatment of Class III
malocclusions that exhibit midface sagittaldeficiency with or without mandibular excess.
� The FOMA III consists of upper and loweracrylic plates with a permanent magnetincorporated into each plate.
� The upper magnet is linked to a retractionscrew and is retracted periodically (e.g.monthly) to stimulate maxillary advancementand mandibular retardation.
� The upper plate of a FOMA III consists of a0.031-inch stainless steel arch wire formingthe metal substructure. The arch wire bypassesthe premolar-canine segment to permiteruption and crosses the occlusal plane at theM1-M2 embrasure (a).
� The upper magnetic housing (b) is linked to aretraction screw (c).
� The magnetic unit (b + c) is positioned alongthe midpalatal line.
� The screw housing is linked to the plate at theM1-M2 level (d).
� Two guiding bars (e), attached to the plate(lingually to the central incisors and laterallyto the screw housing), and restrains themagnetic unit from vertical deflection viaguiding tubes (f).
Upper Plate of a FOMA III in
an Experimental Animal
� The attractive mode neodymium magnets usedin their study produced a horizontal force of98 g and a vertical force of 371 g.
� The ratio of horizontal to vertical force vectorsis dictated by inclination of magnetic interfacein the sagittal plane.
� The more perpendicular the magnetic interfaceis to the occlusal plane (sin 90° = 1), the greateris the horizontal force vector.The interaction between sutural and condylar
growth sites appeared biphasic, characterized byan immediate and rapid excitation of thecircummaxillary sutures followed by a delayedand slow suppression of the condylar cartilage.
Maxilla
1. The target area of the protractive force wasfound to be localized in the pterygomaxillaryfissure.
2. Three-dimensionally, the separation of thesutures at the PMF was found to diminish ininferosuperior and lateromedial directions.
84 History of Orthodontics
Mandible
The fact that no pathologic change was found inthe condylar cartilage encourages a long-term useof the FOMA III appliance, initiating treatment atan early skeletal age.� A later radiographic and histologic study by
Vardimon, Graber et al (AJODO, 1994), againon nine Macaca fascicularis monkeys who weretreated for 4 months with FOMA III revealedthe following data:1. The growth pattern of the cranial base
(saddle angle) was not altered.2. Midfacial protraction occured along a
recumbent hyperbolic curve with ahorizontal maxillary displacement and ananterosuperior premaxillary rotation.
3. Cumulative protraction of the maxillarycomplex was initiated at the pterygom-axillary fissure with an additionalcontribution provided by othercircummaxillary sutures (zygomaticom-axillary s., transverse s., premaxillary s.).
4. Inhibition of mandibular length wasminimal, but a tendency toward a verticalcondylar growth pattern was observed.
Determinants Controlling Iatrogenic
External Root Resorption and Repair
During and After Palatal Expansion
—Vardimon, Graber, Voss, Lenke (AO, 1991)
� In this study, the mechanisms controllingexternal root resorption (ERR) and repair werestudied on 8 Macaca fascicularis monkeys.
� The animals were treated with jackscrew,magnetic and sham palatal expansion screws.They were divided into short- and long-termgroups.
� SEM morphometric analysis found majorevidence of ERR in the tooth-borne jackscrewappliance, in the long-term group, in themaxillary premolars, on the buccal andfurcation root surfaces, on the mesio-buccalroot and in the apical zone.
� Correspondingly, the ERR mechanism iscontrolled by impulse (F. Δt) and the criticalbarrier of the PDL as primary determinantsand by the environment density as thesecondary determinant.
� ERR is initially regulated by the forcecomponent of the impulse and, with increasedduration, by the time component.
� The impairment/repair dynamics were foundto be dominated by 3 principles: ERR level ofirreversibility, delayed resorption responseand jiggling.
Repair of Orthodontically Induced Root
Resorption by Ultrasound in Humans
— El-Baily, El-Shamy and Graber (AJODO, 2004)
� This study evaluated the effect of low-intensitypulsed ultrasound (LIPUS) on the healingprocess of orthodontically induced tooth-rootresorption in humans.
� Twelve orthodontic patients who were seekingorthodontic treatment that necessitatedextracting the first premolars beforemechanotherapy participated in this study.
� For each patient, buccally activated springswere used to tip the maxillary first premolarsbuccally, with an initial force level of 50 g.
� A short period of LIPUS was applied to 1 sideof each patient’s mouth, with the other sideused as a control.
� After 4 weeks, the experimental premolars ofall patients were extracted, and the premolarsof 6 patients were studied by scanning electronmicroscopy (SEM); the premolars of the other6 patients were studied histologically.
� The SEM study showed a statisticallysignificant decrease in the areas of resorptionand the number of resorption lacunae in theLIPUS-exposed premolars.
� Histologic examination showed healing of theresorbed root surface by hypercementosis.
� The results of this study provide a non-invasive method for reducing root resorptionin humans.
Repair Process of External Root Resorption
Subsequent to Palatal Expansion Treatment
—Vardimon, Graber and Pitaru (AJODO, 1993)
� The repair process of external root resorption(ERR) and the role of retention mechanics inenhancing ERR repair were studied on eightMacaca fascicularis monkeys that were dividedequally into short- and long-term groups. Sixmonkeys received palatal expansionappliances, and 2 received sham appliances.
� The short-term group received activetreatment.
� The long-term group received additionalretention (4 months) and relapse (2 months)
85Dr TM Graber’s Contribution to Orthodontics
treatment periods with biweekly injections ofindividual vital dye per phase, i.e. procion redH-8B and violet H-3R (80 mg/kg B.W.),respectively.
Their results showed that:� The short-term group demonstrated penetrated
resorption with pulp exposure at sites withinitial deficiency of the protecting odontoblasticlayer (apical zone, nutrition canal).
� The long-term group showed two forms of ERRrepair:1. Non-functional retarded repair cementum,
comprised of overlapped incremental linesand deprived of extrinsic fibers, wasdelineated in severe pulp exposure.The pulp/dentin complex showed intenseincorporation of procion dye in thedentinal tubuli, conceivably related to adefense response in the form of scleroticdentin.
2. Functional rapid repair cementum,comprised of discriminated incrementallines mainly of mixed cellular cementum,with a consistent pattern of five sequentialphases: the lag phase (14–28 days), theincipient phase (14 days), the peak phase(14–28 days), the steady phase (42–56 days)and the retreating phase (70 days).Sharpey’s fibers at functional ERR siteswere scarce, never emerging from thedentinocemental junction, and notdeveloping into principal fibers. The pulp/dentin complex showed an increase inpulp stones but no formation of tertiarydentin. The apical area responded byhypercementosis in the form of apicalocclusion and a displaced pulp canal.
GRABER’S OTHER CONTRIBUTIONS TO
ORTHODONTICS
A Cephalometric Analysis of the
Developmental Pattern and Facial
Morphology in Cleft Palate
— TM Graber (AO, 1949)
� Thirty three cleft palate patients (22 males, 11females) were studied cephalometrically.
It was found that:� The maxilla in Cleft palate patient’s cases is
deficient in antero-posterior, lateral, as wellas vertical growth.
� There is an abnormally large contribution ofupper face height to total face height when theteeth are in occlusion, due to vertical maxillarydeficiency.
� There is markedly larger inter-maxillaryclearance or freeway space in CP individualswhen compared to normal. This suggests thatwhile there is a bony insufficiency, the generalmusculature attempts to maintain a normaldevelopmental pattern and relation of parts.
� Mandibular growth on the whole appearsnormal. Values taken with the teeth inocclusion indicate over closure.
� There is excessive lingual axial inclination ofthe lower incisors to the mandibular plane.
� The maxillary 1st molar tends towards a distalposition with reference to craniometricmeasurements outside the maxilla.
� Surgical correction can limit the growthpotential of the maxillary denture.
� The clinical results of orthodontic treatment,while improving the tooth-to-toothrelationship in some cases, does notnecessarily stimulate basal bone development.Therapeutic results are often unstable andhave to be maintained indefinitely.
A Functional Study of the Palatal and
Pharyngeal Structures
— Graber, Bzoch, Aoba (AO, 1959)
� Using high speed roentgenographicequipment, the soft tissue morphology ofnormal subjects was studied during the instantof production of various consonant sounds(p, b, f, w, m).
� Biometric analysis was made.
Following conclusions were drawn:� Soft palate increases significantly in length
from the rest to functional position.� The greatest extent of the upward and
backward movement of the palate takes placeat the midpoint of the posterior superiorsurface of the palate (mean = 16 mm).
� The velopharyngeal valve is consistentlyclosed for all the consonant sounds duringnormal speech production.
� Slight anterior movement of the posteriorpharyngeal wall is seen in 50% of normalcases.The authors concluded that the orthodontist,as well as the prosthodontist and speech
86 History of Orthodontics
therapist, should profit from a betterappreciation of normal speech physiology.
Postmortems in Post-treatment Adjustment
— TM Graber (AJO, 1966)
� In this classic article, Dr Graber stresses theneed for a longer period of orthodonticmanagement in many cases.
� He says that, with the orthodontists’dependence on pattern and growth anddevelopment, it is essential to keep patientsunder observation longer and observe thestatus of the stomatognathic system in itsbiologic continuum.
� The concept of treating the malocclusion onceand then considering it finished is un-physiologic. Thus, the philosophy of a longerorthodontic management and responsibility,with two or three shorter periods of orthodonticmechanotherapy, is more appropriate.
Serial Extraction: A Continuous Diagnostic
and Decisional Process
— TM Graber (AJO, 1971)
� Serial extraction is a guided, progressiveremoval of deciduous teeth ahead of the timethey would normally be shed, to enlist thefundamental phenomena of adaptability andadjustment.
� Dr Graber states that the technique isbiologically sound, proven, and should not beconsidered a compromise.
� In almost all instances of serial extractions,conventional orthodontic therapy is requiredto complete the alignment of teeth, to parallelthe roots, to eliminate overbite and to effectresidual space closure. However, the durationof such mechanotherapy is significantlyshorter, is likely to produce less damage, andthe results are more stable.
Orthosurgical Teamwork
— Olson, Mincey and Graber (JADA, 1975)
� Using the examples of 6 patients with differentmalocclusions, the authors have reported onthe combined orthodontic-surgical approachtowards treatment.
� They state that surgery and orthodontics canseparately, but surely better in combination,
correct a variety of developmental jawdeformities, whether they are hereditary ortraumatic in origin.
� The patient is best served by this teamwork,not only during the actual mechanical andoperative phases, but also during the initialdiagnostic and treatment planning phases,that are every bit as important.
� Proper diagnosis requires a thoroughknowledge of growth and development, ofcephalometric analysis, of occlusion andproper jaw relationships, and of surgical andorthodontic techniques to correct thesedeformities.
� Here, the orthodontist, because of his trainingand experience in these aspects, can beinvaluable to the surgeon.
Post-pharyngeal Lymphoid Tissue in Angle
Class I and Class II Malocclusions
— Sosa, Graber and Muller (AJO, 1982)
� Studied the relationship between the adenoidtissue and type of malocclusion.
� Xeroradiographic lateral cephalograms weremade of 80 Class I and 64 Class II/Imalocclusions.
� The epipharyngeal lymphoid tissue,nasopharyngeal airway, nasopharynx andcertain cephalometric landmarks weremeasured.
Their results showed that:� There is no clear-cut relationship between
either Class I or Class II/I malocclusions andthe total nasopharyngeal area.
� Sexual dimorphism was seen:– Class I males: widening of antero-posterior
dimension of nasopharynx is associatedwith anterior rotation of the mandible,longer maxillas, larger SNB angles,opening of cranial base angle, andincreased distance from sella to PNS. Thus,these patients have more anteriorlypositioned maxilla and mandible.
– No association was present at all for ClassII/I males.
– Class II/I females: larger nasopharyngealarea is associated with longer maxillae andsmaller palatal plane angles, and anteriorrotation of mandible.

87Dr TM Graber’s Contribution to Orthodontics
Orthodontics and Temporomandibular
Disorder: A Meta-analysis
— Kim, Graber and Viana (AJODO, 2002)
� In this meta-analysis, the relationship betweentraditional orthodontic treatment, includingthe specific type of appliance used andwhether extractions were performed, and theprevalence of temporomandibular disorders(TMD) were investigated.
� Their data indicated that traditionalorthodontic treatment did not increase theprevalence of TMD.
Growth Modification of the Rabbit
Mandible Using Therapeutic Ultrasound:
Is it Possible to Enhance Functional
Appliance Results?
— El-Bialy, El-Shamy, Graber (AO, 2003)
� The objective of this study was to evaluate theeffect of therapeutic US on condylar andmandibular growth in the rabbit model.
� Eight growing New Zealand male rabbits werechosen for this study.
� They received therapeutic US on one side ofthe mandible for 20 minutes/day for fourweeks.
� Anthropometrical and histological evaluationsrevealed that US enhances mandibular growthby condylar endochondreal bone growth andconsequently mandibular ramus growth.
� It thus increases the mandibular condylar,ramal, and total mandibular heights ingrowing rabbits.
Dr Thomas M Graber was certainly apioneer amongst men. His complete devotionand love for the specialty of orthodontics isreflected in his extensive works on a myriad oftopics, spanning over a period of nearly sixdecades.
As Dr Graber’s family fr iend andcolleague, Dr Jim McNamara noted, “Tom’senergy and enthusiasm for our professionmake him a wonderful role model for futuregenerations of orthodontists.” The passing ofDr Thomas M Graber marks the end of an erain orthodontics.
88 History of Orthodontics
10JJJaaammmeeesss MMMcccNNNaaammmaaarrraaa’’’sss
CCCooonnntttrrriiibbbuuutttiiiooonnn tttoooOOOrrrttthhhooodddooonnntttiiicccsss
Dr McNamara received his dental andorthodontic education at the University ofCalifornia, San Francisco, and a Doctorate inAnatomy from the University of Michigan. Heserves as the Thomas M and Doris Graberendowed Professor of Dentistry in theDepartment of Orthodontics and PediatricDentistry, Professor of Cell and DevelopmentalBiology in the University of Michigan MedicalSchool and Scientist at the Center for HumanGrowth and Development. He is the author(with artist William L Brudon) of the new text,Orthodontics and Dentofacial Orthopedics. Hehas maintained a private practice in Ann Arborsince 1971. He is a Diplomate of the AmericanBoard of Orthodontics and a Fellow of theAmerican College of Dentists. In addition, DrMcNamara is editor-in-chief of the 40 volumeCraniofacial Growth Monograph Seriespublished through the University of Michigan.He has published over 180 scientific articles inrefereed journals, has written, edited orcontributed to 53 books, and has presentedcourses and lectures in 30 countries. Morerecently, McNamara has focused on clinicalstudies of the effects of orthodontic, orthopedicand surgical interventions on the growth of theface. He serves as the curator of The University
of Michigan Elementary and Secondary SchoolGrowth Study, one of the largest longitudinalstudies of untreated individuals in the world.This unique collection allows the study of facialdevelopment from the early juvenile period tomiddle age in the same group of untreatedsubjects, providing a basis of comparison forongoing clinical investigations.
JAMES McNAMARA ANALYSIS
Presented by Dr James A McNamara as anoriginal article in the December 1984 issue of theAmerican Journal of orthodontics.� He asserts that his analysis method is
presented as a language, which can be usedby the clinician to better identify and describethe structural relationships of the jaws, as wellas to communicate easily with other cliniciansas well as lay persons.
� This method of analysis is derived in part fromthe principles of the Ricketts’ and Harvoldanalyses.
� The James McNamara analysis is useful indiagnosis and treatment planning of theindividual patient when values derived fromthe tracing of the patients’ head film arecompared to established norms; the normsfrom three groups have been derived:
� James McNamara Analysis
� Relating the Maxilla to the
Cranial Base
� Relating the Mandible to the
Maxilla (Midface)
� Relating Mandible to Cranial
Base
� Dentition Analysis
� Airway Analysis
� Studies on Functional
Appliances
� Studies on Rapid Maxillary
Expansion
� Studies on TMJ
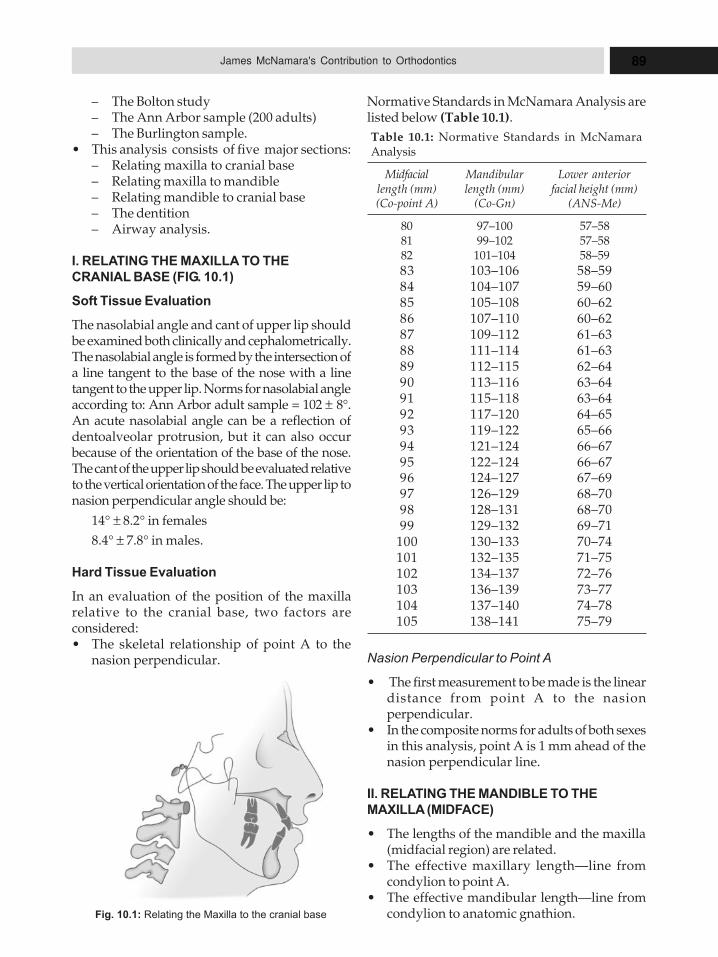
89James McNamara's Contribution to Orthodontics
– The Bolton study– The Ann Arbor sample (200 adults)– The Burlington sample.
� This analysis consists of five major sections:– Relating maxilla to cranial base– Relating maxilla to mandible– Relating mandible to cranial base– The dentition– Airway analysis.
I. RELATING THE MAXILLA TO THE
CRANIAL BASE (FIG. 10.1)
Soft Tissue Evaluation
The nasolabial angle and cant of upper lip shouldbe examined both clinically and cephalometrically.The nasolabial angle is formed by the intersection ofa line tangent to the base of the nose with a linetangent to the upper lip. Norms for nasolabial angleaccording to: Ann Arbor adult sample = 102 ± 8°.An acute nasolabial angle can be a reflection ofdentoalveolar protrusion, but it can also occurbecause of the orientation of the base of the nose.The cant of the upper lip should be evaluated relativeto the vertical orientation of the face. The upper lip tonasion perpendicular angle should be:
14° ± 8.2° in females
8.4° ± 7.8° in males.
Hard Tissue Evaluation
In an evaluation of the position of the maxillarelative to the cranial base, two factors areconsidered:� The skeletal relationship of point A to the
nasion perpendicular. Nasion Perpendicular to Point A
� The first measurement to be made is the lineardistance from point A to the nasionperpendicular.
� In the composite norms for adults of both sexesin this analysis, point A is 1 mm ahead of thenasion perpendicular line.
II. RELATING THE MANDIBLE TO THE
MAXILLA (MIDFACE)
� The lengths of the mandible and the maxilla(midfacial region) are related.
� The effective maxillary length—line fromcondylion to point A.
� The effective mandibular length—line fromcondylion to anatomic gnathion.
Normative Standards in McNamara Analysis arelisted below (Table 10.1).
Table 10.1: Normative Standards in McNamaraAnalysis
Midfacial Mandibular Lower anteriorlength (mm) length (mm) facial height (mm)(Co-point A) (Co-Gn) (ANS-Me)
80 97–100 57–5881 99–102 57–5882 101–104 58–59
83 103–106 58–5984 104–107 59–6085 105–108 60–6286 107–110 60–6287 109–112 61–6388 111–114 61–6389 112–115 62–6490 113–116 63–6491 115–118 63–6492 117–120 64–6593 119–122 65–6694 121–124 66–6795 122–124 66–6796 124–127 67–6997 126–129 68–7098 128–131 68–7099 129–132 69–71
100 130–133 70–74101 132–135 71–75102 134–137 72–76103 136–139 73–77104 137–140 74–78105 138–141 75–79
Fig. 10.1: Relating the Maxilla to the cranial base
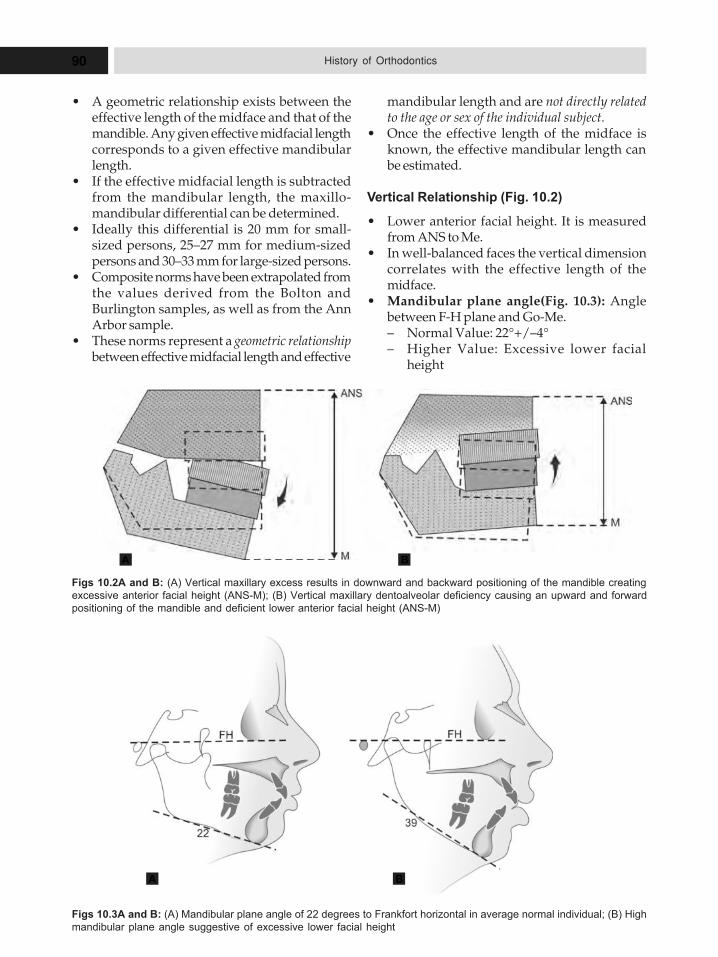
90 History of Orthodontics
� A geometric relationship exists between theeffective length of the midface and that of themandible. Any given effective midfacial lengthcorresponds to a given effective mandibularlength.
� If the effective midfacial length is subtractedfrom the mandibular length, the maxillo-mandibular differential can be determined.
� Ideally this differential is 20 mm for small-sized persons, 25–27 mm for medium-sizedpersons and 30–33 mm for large-sized persons.
� Composite norms have been extrapolated fromthe values derived from the Bolton andBurlington samples, as well as from the AnnArbor sample.
� These norms represent a geometric relationshipbetween effective midfacial length and effective
mandibular length and are not directly relatedto the age or sex of the individual subject.
� Once the effective length of the midface isknown, the effective mandibular length canbe estimated.
Vertical Relationship (Fig. 10.2)
� Lower anterior facial height. It is measuredfrom ANS to Me.
� In well-balanced faces the vertical dimensioncorrelates with the effective length of themidface.
� Mandibular plane angle(Fig. 10.3): Anglebetween F-H plane and Go-Me.– Normal Value: 22°+/–4°– Higher Value: Excessive lower facial
height
Figs 10.2A and B: (A) Vertical maxillary excess results in downward and backward positioning of the mandible creating
excessive anterior facial height (ANS-M); (B) Vertical maxillary dentoalveolar deficiency causing an upward and forward
positioning of the mandible and deficient lower anterior facial height (ANS-M)
A B
Figs 10.3A and B: (A) Mandibular plane angle of 22 degrees to Frankfort horizontal in average normal individual; (B) High
mandibular plane angle suggestive of excessive lower facial height
A B
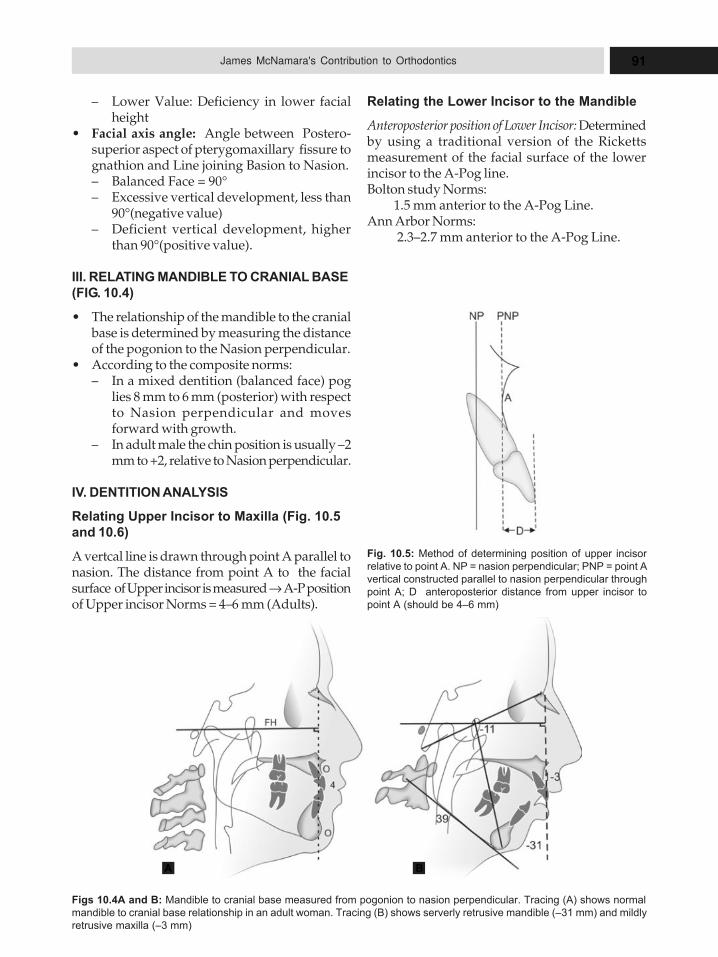
91James McNamara's Contribution to Orthodontics
– Lower Value: Deficiency in lower facialheight
� Facial axis angle: Angle between Postero-superior aspect of pterygomaxillary fissure tognathion and Line joining Basion to Nasion.– Balanced Face = 90°– Excessive vertical development, less than
90°(negative value)– Deficient vertical development, higher
than 90°(positive value).
III. RELATING MANDIBLE TO CRANIAL BASE
(FIG. 10.4)
� The relationship of the mandible to the cranialbase is determined by measuring the distanceof the pogonion to the Nasion perpendicular.
� According to the composite norms:– In a mixed dentition (balanced face) pog
lies 8 mm to 6 mm (posterior) with respectto Nasion perpendicular and movesforward with growth.
– In adult male the chin position is usually –2mm to +2, relative to Nasion perpendicular.
IV. DENTITION ANALYSIS
Relating Upper Incisor to Maxilla (Fig. 10.5
and 10.6)
A vertcal line is drawn through point A parallel tonasion. The distance from point A to the facialsurface of Upper incisor is measured → A-P positionof Upper incisor Norms = 4–6 mm (Adults).
Relating the Lower Incisor to the Mandible
Anteroposterior position of Lower Incisor: Determinedby using a traditional version of the Rickettsmeasurement of the facial surface of the lowerincisor to the A-Pog line.Bolton study Norms: 1.5 mm anterior to the A-Pog Line.Ann Arbor Norms: 2.3–2.7 mm anterior to the A-Pog Line.
Fig. 10.5: Method of determining position of upper incisor
relative to point A. NP = nasion perpendicular; PNP = point A
vertical constructed parallel to nasion perpendicular through
point A; D anteroposterior distance from upper incisor to
point A (should be 4–6 mm)
Figs 10.4A and B: Mandible to cranial base measured from pogonion to nasion perpendicular. Tracing (A) shows normal
mandible to cranial base relationship in an adult woman. Tracing (B) shows serverly retrusive mandible (–31 mm) and mildly
retrusive maxilla (–3 mm)
A B
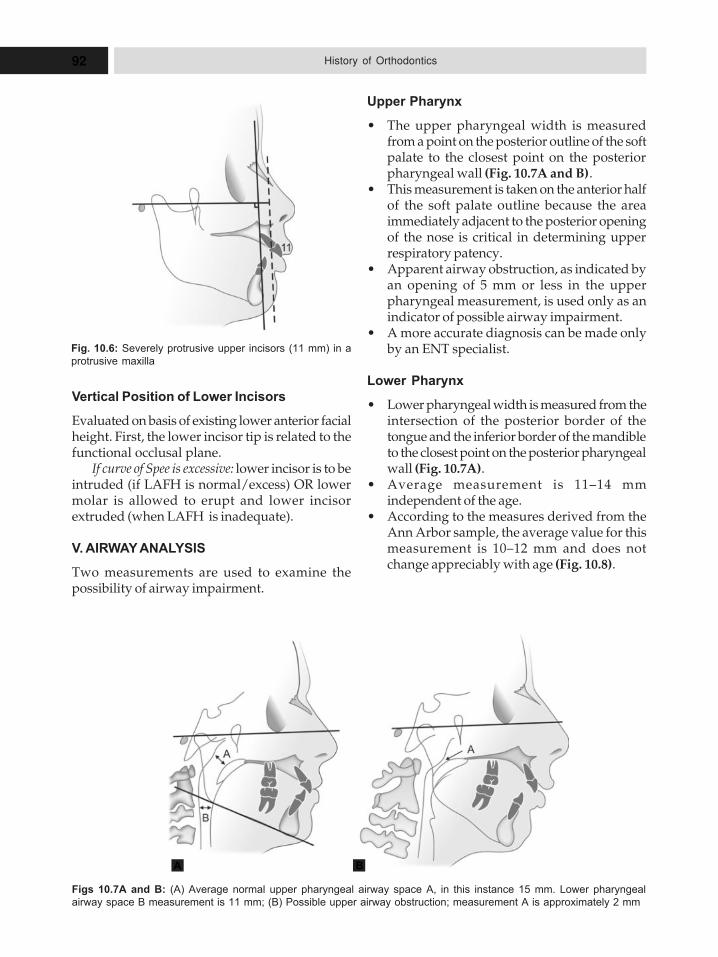
92 History of Orthodontics
Vertical Position of Lower Incisors
Evaluated on basis of existing lower anterior facialheight. First, the lower incisor tip is related to thefunctional occlusal plane.
If curve of Spee is excessive: lower incisor is to beintruded (if LAFH is normal/excess) OR lowermolar is allowed to erupt and lower incisorextruded (when LAFH is inadequate).
V. AIRWAY ANALYSIS
Two measurements are used to examine thepossibility of airway impairment.
Upper Pharynx
� The upper pharyngeal width is measuredfrom a point on the posterior outline of the softpalate to the closest point on the posteriorpharyngeal wall (Fig. 10.7A and B).
� This measurement is taken on the anterior halfof the soft palate outline because the areaimmediately adjacent to the posterior openingof the nose is critical in determining upperrespiratory patency.
� Apparent airway obstruction, as indicated byan opening of 5 mm or less in the upperpharyngeal measurement, is used only as anindicator of possible airway impairment.
� A more accurate diagnosis can be made onlyby an ENT specialist.
Lower Pharynx
� Lower pharyngeal width is measured from theintersection of the posterior border of thetongue and the inferior border of the mandibleto the closest point on the posterior pharyngealwall (Fig. 10.7A).
� Average measurement is 11–14 mmindependent of the age.
� According to the measures derived from theAnn Arbor sample, the average value for thismeasurement is 10–12 mm and does notchange appreciably with age (Fig. 10.8).
Figs 10.7A and B: (A) Average normal upper pharyngeal airway space A, in this instance 15 mm. Lower pharyngeal
airway space B measurement is 11 mm; (B) Possible upper airway obstruction; measurement A is approximately 2 mm
A B
Fig. 10.6: Severely protrusive upper incisors (11 mm) in a
protrusive maxilla
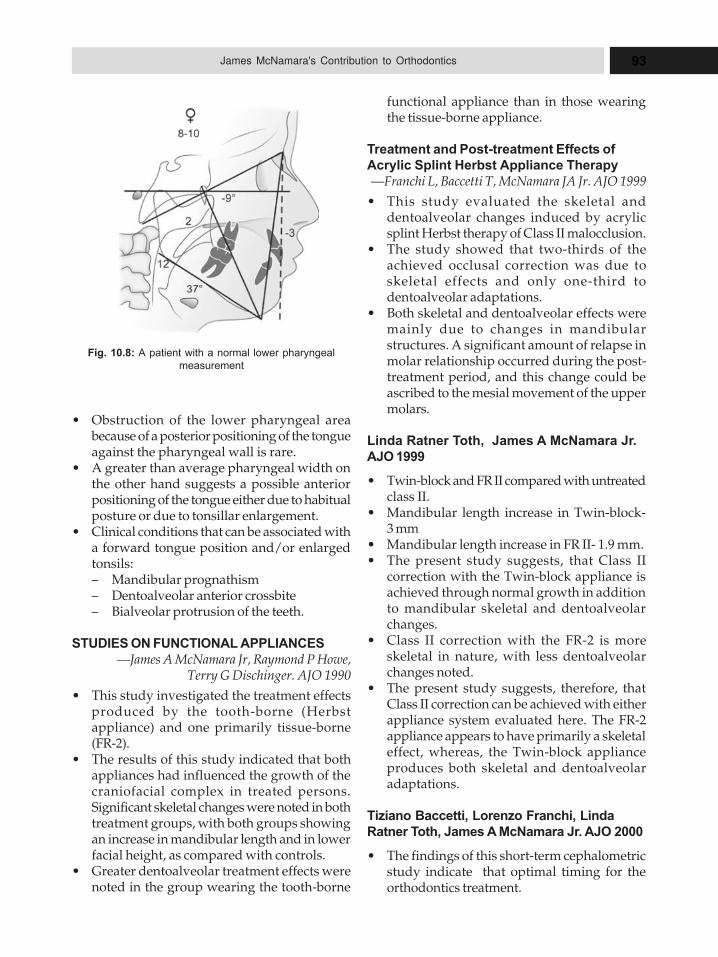
93James McNamara's Contribution to Orthodontics
� Obstruction of the lower pharyngeal areabecause of a posterior positioning of the tongueagainst the pharyngeal wall is rare.
� A greater than average pharyngeal width onthe other hand suggests a possible anteriorpositioning of the tongue either due to habitualposture or due to tonsillar enlargement.
� Clinical conditions that can be associated witha forward tongue position and/or enlargedtonsils:– Mandibular prognathism– Dentoalveolar anterior crossbite– Bialveolar protrusion of the teeth.
STUDIES ON FUNCTIONAL APPLIANCES
—James A McNamara Jr, Raymond P Howe,Terry G Dischinger. AJO 1990
� This study investigated the treatment effectsproduced by the tooth-borne (Herbstappliance) and one primarily tissue-borne(FR-2).
� The results of this study indicated that bothappliances had influenced the growth of thecraniofacial complex in treated persons.Significant skeletal changes were noted in bothtreatment groups, with both groups showingan increase in mandibular length and in lowerfacial height, as compared with controls.
� Greater dentoalveolar treatment effects werenoted in the group wearing the tooth-borne
Fig. 10.8: A patient with a normal lower pharyngeal
measurement
functional appliance than in those wearingthe tissue-borne appliance.
Treatment and Post-treatment Effects of
Acrylic Splint Herbst Appliance Therapy
—Franchi L, Baccetti T, McNamara JA Jr. AJO 1999
� This study evaluated the skeletal anddentoalveolar changes induced by acrylicsplint Herbst therapy of Class II malocclusion.
� The study showed that two-thirds of theachieved occlusal correction was due toskeletal effects and only one-third todentoalveolar adaptations.
� Both skeletal and dentoalveolar effects weremainly due to changes in mandibularstructures. A significant amount of relapse inmolar relationship occurred during the post-treatment period, and this change could beascribed to the mesial movement of the uppermolars.
Linda Ratner Toth, James A McNamara Jr.
AJO 1999
� Twin-block and FR II compared with untreatedclass II.
� Mandibular length increase in Twin-block-3 mm
� Mandibular length increase in FR II- 1.9 mm.� The present study suggests, that Class II
correction with the Twin-block appliance isachieved through normal growth in additionto mandibular skeletal and dentoalveolarchanges.
� Class II correction with the FR-2 is moreskeletal in nature, with less dentoalveolarchanges noted.
� The present study suggests, therefore, thatClass II correction can be achieved with eitherappliance system evaluated here. The FR-2appliance appears to have primarily a skeletaleffect, whereas, the Twin-block applianceproduces both skeletal and dentoalveolaradaptations.
Tiziano Baccetti, Lorenzo Franchi, Linda
Ratner Toth, James A McNamara Jr. AJO 2000
� The findings of this short-term cephalometricstudy indicate that optimal timing for theorthodontics treatment.
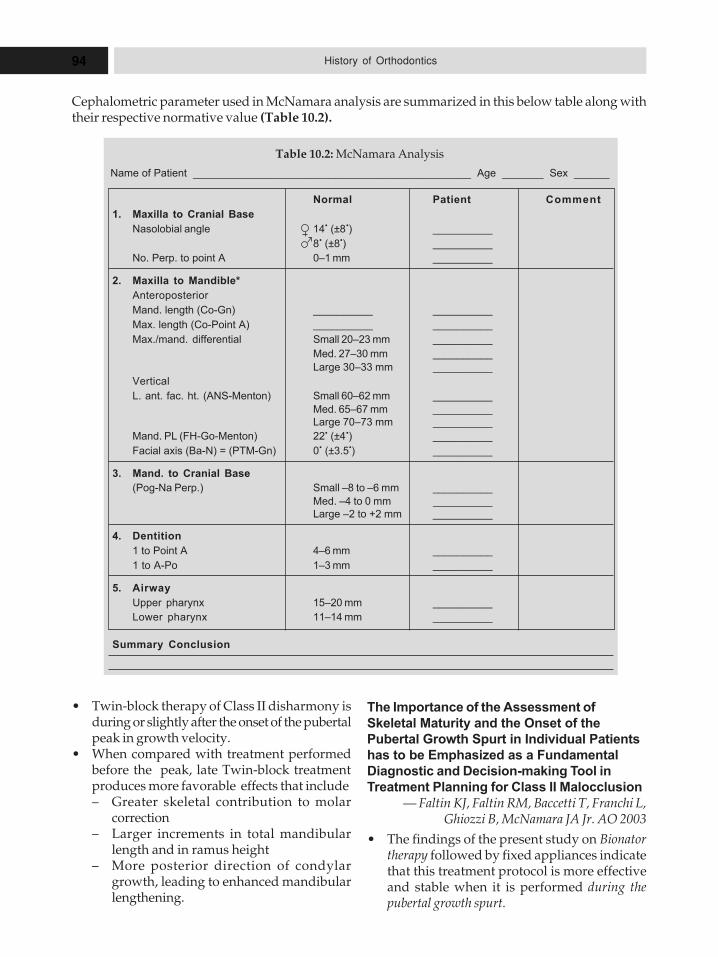
94 History of Orthodontics
� Twin-block therapy of Class II disharmony isduring or slightly after the onset of the pubertalpeak in growth velocity.
� When compared with treatment performedbefore the peak, late Twin-block treatmentproduces more favorable effects that include– Greater skeletal contribution to molar
correction– Larger increments in total mandibular
length and in ramus height– More posterior direction of condylar
growth, leading to enhanced mandibularlengthening.
The Importance of the Assessment of
Skeletal Maturity and the Onset of the
Pubertal Growth Spurt in Individual Patients
has to be Emphasized as a Fundamental
Diagnostic and Decision-making Tool in
Treatment Planning for Class II Malocclusion
— Faltin KJ, Faltin RM, Baccetti T, Franchi L,Ghiozzi B, McNamara JA Jr. AO 2003
� The findings of the present study on Bionatortherapy followed by fixed appliances indicatethat this treatment protocol is more effectiveand stable when it is performed during thepubertal growth spurt.
Normal Patient Comment
1. Maxilla to Cranial Base
Nasolobial angle 14� (±8�) __________
8� (±8�) __________
No. Perp. to point A 0–1 mm __________
2. Maxilla to Mandible*
Anteroposterior
Mand. length (Co-Gn) __________ __________
Max. length (Co-Point A) __________ __________
Max./mand. differential Small 20–23 mm __________
Med. 27–30 mm __________
Large 30–33 mm __________
Vertical
L. ant. fac. ht. (ANS-Menton) Small 60–62 mm __________
Med. 65–67 mm __________
Large 70–73 mm __________
Mand. PL (FH-Go-Menton) 22� (±4�) __________
Facial axis (Ba-N) = (PTM-Gn) 0� (±3.5�) __________
3. Mand. to Cranial Base
(Pog-Na Perp.) Small –8 to –6 mm __________
Med. –4 to 0 mm __________
Large –2 to +2 mm __________
4. Dentition
1 to Point A 4–6 mm __________
1 to A-Po 1–3 mm __________
5. Airway
Upper pharynx 15–20 mm __________
Lower pharynx 11–14 mm __________
Summary Conclusion
Table 10.2: McNamara Analysis
Name of Patient _______________________________________________ Age _______ Sex ______
Cephalometric parameter used in McNamara analysis are summarized in this below table along withtheir respective normative value (Table 10.2).
95James McNamara's Contribution to Orthodontics
� Optimal timing to start treatment with theBionator is when a concavity appears at thelower borders of the second and the thirdcervical vertebrae (CVMS II). In the long-term,the amount of significant supplementaryelongation of the mandible in subjects treatedduring the pubertal peak is 5.1 mm more than inthe controls, and it is associated with abackward direction of condylar growth.
� Significant increments in mandibular ramusheight also were recorded.
de Almeida MR, Henriques JF, de Almeida
RR, Weber U, McNamara JA Jr Angle.
Orthod 2005
� The results indicated that the treatment effectsof Herbst produced in the mixed dentitionpatients were primarily dentoalveolar innature.
� The mandibular incisors were tipped labially,and the maxillary incisors were retruded; asignificant increase in mandibular posteriordentoalveolar height occurred, and there wasa restriction in the vertical development of themaxillary molars.
� There was no difference in the forward growthof the maxilla between the two groups.
� In comparison with the controls, however, theHerbst treatment produced a modest butstatistically significant increase in totalmandibular length.
Paola Cozza, Tiziano Baccetti, Lorenzo
Franchi, Laura De Toffol, and James A
McNamara, Jr. AJO 2006
Two-thirds of the samples in the 22 studiesreported a clinically significant supplementaryelongation in total mandibular length (a changegreater than 2.0 mm ) as a result of overall activetreatment with functional appliances. The amountof supplementary mandibular growth appears tobe significantly larger if the functional treatmentis performed at the pubertal peak in skeletalmaturation. The Herbst appliance showed the highestcoefficient of efficiency (0.28 mm per month) followedby the Twin-block (0.23 mm per month). Thecoefficient for the bionator 0.17 m per month). Forthe activator, it was slightly lower (0.12 mm permonth). The coefficient of efficiency for the Fränkelappliance, was the lowest (0.09 mm per month).
STUDIES ON RAPID MAXILLARY EXPANSION
Joyce Y Chang, James A McNamara
Jr,Thomas A Herberger. AJO 1997
� The purpose of this investigation was toexamine the long-term effect of the Haas-typeRME on bite opening and on the antero-posterior position of the maxilla.
� There was no significant difference amonggroups receiving rapid maxillary expansion,followed by edgewise treatment (RME),standard edgewise therapy alone (SET), or notreatment (CTRL).
� The current investigation of long-termtreatment effects concludes therefore that RMEtherapy used in the treatment of patients withClass I and Class II malocclusions does nothave a significant long-term effect on eitherthe vertical or the anteroposterior dimensionsof the face.
McNamara JA Jr, Baccetti T, Franchi L,
Herberger TA. AO 2003 RME Followed by
Fixed Appliances
� In comparison with controls, a net gain of 6 mmwas achieved in the maxillary arch perimeter,whereas a net gain of 4.5 mm was found for themandibular arch perimeter.
� The amount of correction in both maxillaryand mandibular intermolar widths equaledtwo-thirds of the initial discrepancy, whereastreatment eliminated the initial deficiency inmaxillary and mandibular intercanine widths.
� The amount of correction for the deficiency inmaxillary arch perimeter was about 80%,whereas in the mandible a full correction wasachieved.
Geran RG, McNamara JA Jr, Baccetti T,
Franchi L, Shapiro LM. AJO 2006
� Treatment with an acrylic splint RME followedby fixed appliances produced significantlyfavorable short-term and long-term changesin almost all maxillary and mandibular archmeasurements.
� The amount of change in both maxillary andmandibular intermolar and intercanine widthsfully corrected the initial discrepancies.
� Approximately 4 mm of long-term relative increasein maxillary arch perimeter, and 2.5 mm additional
96 History of Orthodontics
maintenance of mandibular arch perimeter wereobserved in the TG compared with the CG.
� These results suggest that this protocol iseffective and stable for the treatment ofconstricted maxillary arches, and can relievemodest deficiencies in arch perimeter.
Cozza P, Baccetti T, Franchi L, McNamara
JA Jr. Am J Orthod Dentofacial Orthop. 2006
� The aim of this study was to investigate theeffectiveness of a quad-helix/crib (Q-H/C)appliance in a group of growing subjects withthumb-sucking habits and both dental andskeletal open bites.
� The Q-H/C appliance was effective incorrecting the dental open bite in 90% ofgrowing subjects with thumb-sucking habitsand dentoskeletal open bites.
� The average increase in overbite during Q-H/C therapy (3.6 mm more), the maxillary andmandibular incisors had significantly greaterlingual inclinations (about 4.0 degrees)associated with greater extrusion (1.4 and 1.0mm, respectively) in the Q-H/C group.
� The Q-H/C protocol produced a clinicallysignificant improvement in the vertical skeletalrelationships because of downward rotationof the palatal plane. Neuromuscular andskeletal adaptations to altered function in theorofacial region.
James A McNamara, Jr. AJO 1973
� The nature of intrinsic musculoskeletaladaptations resulting from experimentalalterations of the orofacial environment.
� Neuromuscular adaptations.� Mandibular adaptations – changes in the
growth pattern of the condylar head andcompensatory migration of the dentition.(depending on the maturational level).
� Maxillary adaptations – changes in the extentand vector of growth of the skeletal components.
James A McNamara, Jr and Carlson DS.
AJO 1979
� TMJ adaptations to protrusive function.� Significant adaptive responses can occur in
the mandibular condyle of the juvenile rhesusmonkey following alteration in the functionalposition of the mandible.
� Pre-chondroblastic – chondroblastic layershowed responses.
� Initial adaptations along the posterior borderof the condyle followed by changes in theposterosuperior region.
� This study demonstrated that significantadaptive responses can occur in themandibular condyle of the juvenile rhesusmonkey following alteration in the functionalposition of the mandible.
� And that the condyle is highly responsive tochanges in the biomechanical and biophysicalenvironment of the TMJ region during growth.
Kristine S West and James A McNamara, Jr.
AJO 1999
� The purpose of the present study was to evaluatecephalometrically the craniofacial growthchanges and adjustments that occur from lateadolescence to mid adulthood in persons whohad no previous history of orthodontictreatment. Mandibular and midfacial lengths aswell as posterior and lower anterior facial heightshad increased significantly for males andfemales over both time intervals.
� The pattern of expression of these changes wasdifferent in the two genders: males showed ananterior rotation of the mandible, whereasfemales demonstrated a posterior rotation ofthe mandible.
� Soft tissue changes also were somewhatdifferent between genders. In males, the noseand chin grew downward and forward, withthe lips generally moving straightdownward.
� In contrast, females had nasal growth thatprogressed downward and forward, and therewas a slight retrusion of the lips over time.
� Continued tooth eruption was noted in bothgenders as well.
STUDIES ON TMJ
McNamara, Jr. OOO 1997
� The relationship between orthodontictreatment and TMDs has long been of interestto the practicing orthodontist.
� The interest in orthodontics and TMD in partwas prompted in the late 1980‘s after litigationthat alleged that orthodontic treatment was theproximal cause of TMD in orthodontic patients.

97James McNamara's Contribution to Orthodontics
� This resulted in an increased understandingof the need for risk management as well as formethodologically sound clinical studies.The findings of current research investigatingthe relation of orthodontic treatment and TMDare as follows:
Signs and Symptoms of TMD May Occur in
Healthy Persons
� Signs and symptoms of TMD increase withage, particularly during adolescence, untilmenopause and so TMD s that originateduring treatment may not be related to thetreatment.
� Treatment performed during adolescence doesnot increase or decrease the chances of TMDlater in life.
� Extraction of teeth as a part of treatment plandoes not increase the risk of TMD.
� There is no increased risk of TMD associatedwith any particular type of orthodonticmechanics.
� Although a stable occlusion is a reasonableorthodontic treatment goal, not achieving a
specific gnathologic ideal occlusion does notresult in signs and symptoms of TMD.
� Thus far there is little evidence thatorthodontic treatment prevents TMD,although the role of posterior unilateralcrossbite correction in children may warrantfurther investigation.
Conclusion
� The overall goal of McNamara’s researchis to provide a sound biological basis forunderstanding how the face normallygrows and how facial growth can be alteredby experimental and therapeutic interven-tion.
� His past research involved studies of bothnormal and experimental alterations in thegrowth of the facial region in a non-humanprimate, using the rhesus monkey as a modelof human craniofacial development.
� More recently, McNamara has focused onclinical studies of the effects of orthodontic,orthopedic and surgical interventions on thegrowth of the face.
11AAAnnndddrrreeewwwsss’’’ SSStttrrraaaiiiggghhhtttWWWiiirrreee AAAppppppllliiiaaannnccceee
� Why “Straight Wire”?
� Deficiencies in the
Conventional Edgewise Bracket
Design, and How they are
Overcome in the ‘Straight
Wire Brackets’
� Variable Bracket Sitting
Procedures: Lawrence F
Andrew’s Remedy
� Straight Wire Appliance
Brackets for Different Clinical
Situations
� Straight Wire Appliance (SWA)
The ‘straight wire’ appliance is an example ofwhat a motivated person could achieve withdetermination and perseverance. It is afascinating story of a man fully engaged inpractice that carried out outstanding researchextending into numerous projects andculminated in the development of an appliancethat has profoundly affected the practice oforthodontics.
After his graduation in 1959, Laurence FAndrews (Fig. 11.1) was looking for a topic to writea thesis that was required for certification by theAmerican Board of Orthodontics. The theme thathe chosed was the prevalent quality of Americanorthodontic practice with respect to staticocclusion. He started an assessment of post-treatment orthodontic study models exhibited atthe meetings of American Board of Orthodontics,Angle Society and Tweed Foundation. Althoughthe records indicated that the patients’ occlusionhad shown remarkable improvement over theoriginal condition, and there were few commonfindings (such as class I molar occlusion, normaloverjet, absence of cross bites and incisorrotations), many other features like angulationsand inclinations of various teeth and curve ofSpee were quite disparate. These cases had beenjudged as the outcome of excellent treatment by
examiners appointed at these prestigioussocieties, and yet they differed considerably.Therefore, Lawrence F Andrews concluded thatthe then existing criteria for measuring the
Fig. 11.1: Lawrence F Andrew

99Andrews’ Straight Wire Appliance
quality of finishing were ill defined and neededto be revised.
He rightly decided that the answer to hisquestion rested in the nature’s ideal cases. Thusstarted his tryst with the normal, which he latteron called optimal occlusion. He collectedorthodontic study models of 120 non-treatedindividuals whose occlusion was considered tobe ideal by him and his peers. With a keen eyeand logical mind, he picked out the six consistentfeatures related to the clinical crowns, whichwere common to all the study models. He namedthese as the six keys to normal occlusion. Theydescribe the characteristics of best static naturalocclusion as related to molar relation, angulationsand inclinations of the teeth and stipulate thatthere should be no rotations and spaces, and thecurve of Spee should be flat. He published hisresults in the American Journal of Orthodonticsin the year 1972. The article since has attainedthe status of mandatory reading for anyoneaspiring to become an orthodontist.
The uniqueness of Andrews’ study was thatthe tooth positions were referenced fromclinically visible teeth crowns (or, morespecifically, the labial and buccal surfaces ofclinical crowns) and not from the long axis ofthe teeth, which can be judged only from theradiographs. Further, the referents selected weresuch that optimal occlusion based on themobviated the need to use articulating paper tocheck the interfacing of occlusal surfaces or viewthe occlusion from the lingual side. The mostimportant of the referents was the facial axis ofclinical crown, formerly termed long axis of theclinical crown. For all the teeth other than themolars, it is the most prominent ridge on thecrown’s face; while for the molars it is thedominant groove on the crown’s face. From thefacial perspective it appears as a straight line.From the mesial or distal perspective it isperceived as a straight line tangent to themidpoint of the crown’s face. The midpoint offacial axis of clinical crown is named as the facialaxis point (FA point), which is formerly termedlong axis point. It is used for assessing thepositions of the teeth as also for placing thebrackets accurately on the teeth. When all theteeth are correctly positioned, the plane joiningthe FA points of all the teeth is named asAndrews’ plane.
Andrews later stated in his interview that heconsidered finding the facial axis of clinicalcrown as his most significant contribution toorthodontics, because it can be used for bothangulations and inclination. Also it has a reliablecorrelation with planes of crown at all times andwith the mid-transverse planes of all the crownsin an arch when the teeth are correctlypositioned. “Without it there would have beenno six keys and no straight wire appliance.”
Andrews reexamined the treated casesapplying the criteria of the six keys. This studyrevealed that most of them failed to attain many,if not all, keys. The failures were, in a descendingorder of occurrence, errant angulations of theteeth; interarch relations, inclinations of the teeth,rotations of remaining teeth, excess curve of Speeand persistent spaces.
Lawrence F Andrew started analyzing thecauses for the above short comings and came tothe conclusion that the standard edgewiseappliance had too many deficiencies to obtainconsistent results. These were in the followingform:1. Variability in wire bending from operator to
operator and even with the same operator.2. Deficiencies in the standard edgewise bracket
design.3. Variations in the bracket sitting procedures.
Lawrence F Andrew’s next study was aimedat exploring the conceptual feasibility ofdeveloping an appliance, which would facilitateobtaining the six keys consistently in treatedcases. It consisted of numerous measurementson the plaster casts of non-orthodontic normalocclusion. These ascertained the naturalanatomic similarities (earlier named ‘tendencies’by Wheeler) in human dentitions. Specifically,they were related to constancy of position andshape within each tooth type, and consistencyof relative size of crowns within an arch. Theconclusions from this study were:1. Most individuals have normal teeth
regardless of whether they have normalocclusion or malocclusion. Abnormallyshaped crowns in the rest of the persons aregenerally amenable to restorative proceduresto normalize them before orthodontictreatment is started.
2. Each normal tooth type (such as the centralincisors, lateral incisors, cuspids, etc.) is

100 History of Orthodontics
similar in shape from one individual toanother.
3. All the teeth in any individual’s mouth aregenerally proportionate though they mayvary in size from person to person, i.e. all theteeth tend to be large, medium or small.
4. The size of normal crowns within a dentitionhas no effect on the relative prominence oftheir facial surfaces, or the curvatures bothvertical and horizontal of the labiabuccalsurfaces on which the brackets will be placed,or on the location of contacts between twoteeth types. Also, optimal crown angulationor inclination as well as interarch relation arenot related to the size of the crowns and henceare attainable, whatever may be the size ofthe crowns.
5. When the upper and lower jaws areproportionate and properly related, it isalways possible for the teeth to be brought inoptimal occlusion.The study thus paved the way for creating a
new appliance by taking advantage of theanatomic similarities in the human dentition, andby recognizing the fact that similarities exist inthe positions of the normal teeth when they areoptimally occluded. Andrews developed hisappliance to address all the above mentionedproblems with respect to variability in wirebending, deficiency in bracket design andvariable bracket sitting procedures.
WHY “STRAIGHT WIRE”?
The term straight wire in the present contextrefers to an archwire that is given the arch formand often the curvature to open the bite, butwhich is free from the first, second or third orderbends. It is a ‘formed’ but ‘unbent’ archwire.Lawrence F Andrew’s endeavor to develop anappliance that would permit the use of such anarchwire by transferring most of the toothguidance functions from the archwires to thebrackets (by modifying the bracket design), wasbased on the following reasoning:1. Some of the bends in an archwire are needed
for effecting first, second and third ordertooth movements (Lawrence F Andrewstermed these as the primary bends). It isdifficult to make these bends precisely foraffecting the exact amount of toothmovement. Hence, if precise tooth guidance
is built in the brackets instead of dependingon the wire bends, more consistent resultscould be obtained.
2. Other wire bends (secondary bends) arerequired for compensating for faultyplacement of the brackets or the deficienciesin the bracket design. One example is thebuccal root torque in the posterior region ofthe archwire that is needed in theconventional edgewise treatment, which isgiven not to effect any torquing movementbut to avoid unintentional torque. Standardedgewise brackets placed on the curvedbuccal surfaces of the posterior teeth, onreceiving a flat (untorqued) archwire, wouldcreate an unintended torque on the teeth in acrown buccalroot lingual fashion that isgenerally undesirable. Buccal root torque inthe archwire prevents this from happening.These wire bends are needed in all thesuccessive archwires and in almost all thepatients. This repetitive wire bending couldbe eliminated if the bracket designshortcomings are corrected by suitablemodifications (for example, by having built-in torque in the brackets itself to remedy theabove mentioned situation).
3. Even for the same operator, the bends placedin the successive archwires are likely to vary.They will certainly be different for differentoperators. Since every bend in the archwirenot only causes some action but also has areaction, the results from such differing bendsare unpredictable and often lead to undesiredtooth movements. Additional secondary wirebends will be required for overcoming them.
4. Some of the bends influence the actions ofother bends, e.g. torque in the anterior sectionof the archwire negates the tip by a ratio of1:4 (wagon-wheel effect). Accurate wirebending to negate such ill effects is extremelydifficult but provision could be made in thebracket design to overcome them to a largeextent.
However, it should be noted that in only fewcases, the entire treatment could be completedusing ‘straight’ archwires. Andrews stated thatstraight wires in progressively larger dimensionstake the treatment close to the treatmentobjectives, but in many cases would require somewire bending in the final archwires to fine tune

101Andrews’ Straight Wire Appliance
the results. The analogy he gave was of reachingsome destination far away. You need not walkall the distance. The straight wire appliance islike an airplane that takes you to the nearestairport quickly and effortlessly. Final wirebending is like walking the last few kilometers.
Deficiencies in the conventional edgewisebracket design, and how they are overcome inthe ‘straight wire brackets’
The conventional edgewise brackets areidentical for all the teeth except some mesiodistalwidth differences. However, different teeth havedifferent relative prominences, angulations andinclinations. This necessitates giving first, secondand third order bends in the archwire.1. Bracket base is perpendicular to the
faciolingual axis, and the slot is cut parallelto the facio-lingual axis. This leads totargeting the bracket slots to differentinclinations and occlusogingival levels. Whenplaced on different teeth with varyingcurvatures, the latter may result in functionalinterferences.
2. Because the bracket bases are not contouredocclusiogingivally, they can rock on thecurved crown facial surfaces, which furtheraffect the slot inclination and occlusogingivalpositions. Similarly, lack of mesiodistal basecontour could lead to rocking of the brackets,which will affect the rotational control.
3. Because the brackets are not angulated,second order bends in the archwire becomenecessary. Angulating the bracketsthemselves does not solve the problembecause of rocking potential of the bracketbase.
4. Stems of equal prominence necessitate thefirst order bends such as the bends requiredbetween the upper central and lateral incisors.Similarly, because the molar tubes or bracketshave no offset built-in, first order bendsbecome necessary mesial to the molars.Andrews rightly observed that what stands
between the orthodontist and the teeth are thebrackets, and therefore the brackets should bedesigned and affixed on the teeth such that theirplanes should reflect the planes of the teethcrowns. Hence he set about designing a newsystem of edgewise brackets (and a more preciseway of attaching them on the teeth. His brackets
(which he described as fully programmedbrackets) had the following features:1. Every tooth type had a specifically designed
bracket, which had precisely builtinangulations and inclinations to eliminate thesecond and third order bends. The magnitudeof angulations and inclinations for differentteeth (‘prescription’ values in degrees) werederived from his study of normal occlusion.
2. Unlike in the conventional edgewise brackets,in which the slots are perpendicular to thevertical edges of the bracket, the slots werecut at an angle to the vertical edges forattaining the built-in angulation in thebracket. This obviated the need to rotate thebrackets for angulating them.
3. The bases of the brackets were inclined (theangle of inclination precisely matching theinclination of the facial plane of the respectivecrown at the FA point) in order to effect thetorque needed for the particular tooth type;the bracket slots were not torqued within thebracket body. In other words, the torque wasbuilt in the bracket bases and not in the faceof the bracket. This made it possible to makethe mid-transverse planes of each crown andbracket stem and slot, coincide, and also toalign the mid-transverse planes of all thecrowns and bracket slots so that theycoincided with Andrews’ plane when theteeth were correctly positioned.
4. The thickness of the brackets stem was variedaccording to the facial prominence of eachtooth, thus eliminating the need for the firstorder bends. The bracket bases were madesuch that the slot in every bracket wasperpendicular to the mid-sagittal plane of thecrown. This necessitated a built-in offset inthe maxillary molar tubes or brackets.
5. The bracket bases were contoured bothocclusogingivally and mesiodistally,(compound contouring) according to thefacial surface anatomy of each tooth type toeliminate rocking of the brackets on the teeth;since bracket rocking in the occlusogingivaldirection would affect the built-in torque, andbracket rocking in the mesiodistal directionwould affect the rotational control.Thus it became possible to use flat unbent
archwires in the appliance through most part of

102 History of Orthodontics
the treatment. The treatment could be started withsmall diameter wires, which would flex in thebrackets on malpositioned teeth. The resilientwires, while regaining their original shape andform, would correct the malpositions to someextent. As one gradually moves to biggerdiameter archwires, they would progressivelyalign the teeth till a full size ‘straight’ archwire,could passively fit in all the brackets.
Two types of bracket configuration wereoriginally made available. The vertical edgeswere always parallel to the facial axis of clinicalcrown, while the horizontal edges wereperpendicular to the vertical edges in the squaretype brackets and at a different angle in therhomboid shaped or so-called ‘diamond’ -brackets. The latter type bracket became morepopular since the horizontal edges could be wellaligned with the incisal edges.
Some other features called the conveniencefeatures meant for increasing the ease of theoperator such as marking on the brackets toidentify them, and gingival tie wings on theposterior teeth extended laterally for ease ofligation were added to the brackets. Similarly,for comfort of the patients some features wereincorporated, as for example, the facial aspectsof the incisor and canine brackets being curvedand parallel to the crown’s facial surface so as toreduce irritation to the lips. Some more featuresnamed auxiliary features such as power arms,hooks, face-bow tubes, tubes for utility archesand rotation arms were also added.
VARIABLE BRACKET SITTING
PROCEDURES: LAWRENCE F ANDREW’S
REMEDY
Many authors earlier had suggested differentlandmarks for bracket locations on the teeth.Lawrence F Andrews felt that the traditionalreferents for angulation (long axis of the crownor the tooth, incisal edges for incisors and cusptips for other teeth, marginal ridges, contactpoints, etc.) were neither reliable nor practical.Similarly, inclination referents viz. long axis ofcrowns or teeth were unsatisfactory.Additionally, the inclination of the bracket slotsat varying heights on these axis would varybecause of the curvature of the facial surface.Thus, a location of the landmark at a specified
distance from the incisal edge or the cusp tip wouldcause variation of slot inclination depending onthe crown heights of the same type but differentsize teeth.
Lawrence F Andrews emphasized that theaccurate placement of the brackets was anintegral part of the straight wire appliance. Hesuggested a bracket sitting procedure, which wasaimed at targeting the slot within two degreesand 0.5 mm of the precise placement over theslot site (This is the area on a tooth that wouldaccept the bracket such that the bracket slotwould receive a ‘straight’ archwire passivelywhen the tooth gets optimally positioned). Hedemonstrated that most of the people are able tomark the midpoint of a line about 10 mm inlength (a figure close to the length of facial axisof clinical crown of a maxillary central incisor)to the accuracy of within 0.5 mm. Further, theycan also judge the parallelism of two or morelines within the accuracy of two degrees. Hencehe reasoned that it should be possible for anyonewith average skill to draw with a pencil the facialaxis of clinical crown of all the teeth, mark theirmidpoints and align the midpoint of the base ofeach bracket with the facial axis point in such away that the sides of the brackets are parallel withthe facial axis of clinical crown. This is done byplacing the brackets on the crowns straddling thefacial axis of clinical crown with the verticalcomponents of the brackets (viz. the verticaledges of brackets and the tie wings) parallel tothe facial axis of clinical crown and the horizontalmidpoint of the brackets equidistant from the endpoints of the facial axis of clinical crown. Thiswould provide the accuracy needed in using thefull potential of the fully programmed brackets.
STRAIGHT WIRE APPLIANCE BRACKETS
FOR DIFFERENT CLINICAL SITUATIONS
Andrews initially introduced brackets for thetreatment of non-extraction cases, with an ANBdifferential of less than five degrees, which hereferred to as the standard brackets.Subsequently he developed brackets forextraction cases.
There was one standard (non-extraction)bracket for every tooth except for the incisors,that had three, and the maxillary molars, that hadtwo. The differing features were built-in

103Andrews’ Straight Wire Appliance
inclination for the incisor brackets andangulations, and offset angles for the molars. Allother features remained the same. The upper andlower incisor inclinations were different fordifferent skeletal types. For skeletal class I, classII and class III, the upper central incisorinclinations were 7, 2, and 12 degrees, the upperlateral incisor inclinations were 3, -2 and 8degrees, and for all mandibular incisors theinclinations were –1, 4 and –6 degrees,respectively. For maxillary first molars, theangulation and offset were 5 and 10 degrees, forclass I molar finish occlusion, while these were 0and 0 degree for class II molar finish occlusion.
The brackets for extraction cases weredeveloped in a more elaborate fashion. Series ofbrackets were developed for differentcombinations of extractions, ANB differentials,and anchorage requirements. As the teeth aretranslated, they tend to tip mesiodistally androtate into the extraction sites since the force actsat the brackets away from the center of resistance,both in the lateral as well as occlusal perspectives.In addition to these tendencies, the maxillarymolars during translation also tend to tip duringtranslation on account of the drag created by theprominent lingual root. Hence the relevantexisting features of the brackets were altered ornew features were added to counter these effectsto an extent that would overcorrect them.
Depending on the amount of translationrequired, the built-in angulation for the caninesand premolars was varied. For teeth undergoingdistal or mesial translation, 2, 3 and 4 degreeswere added to or subtracted from thecorresponding angulations of the standardbrackets for minimum (up to 2 mm), moderate(2 to 4 mm) and maximum (4 to 6 mm) retractionrespectively. This was meant for giving thecounter mesiodistal tip.
Anti rotation adjustments were built in theextraction series to prevent the teeth fromrotating into the extraction site. This was in theform of deviation of the mesiodistal axis of theslot from its normal (perpendicular to themidsagittal plane) position by 2, 4 and 6 degreesrespectively for minimum (less than 2 mm),moderate (2 to 4 mm) and maximum (4 to 6 mm)retraction.
For maxillary molars needing translation, theinclination values were altered (in addition to
counter rotation and counter mesiodistal tip) toneutralize the buccal crown-tipping tendency.The additional (negative) inclination was four,five and six degrees for minimum, moderate andmaximum translation. For mandibular molars,only counter rotation and counter-mesio-distaltip were added.
The canine, premolar and molar bracketstubes acquired attached ‘power arms’ to movethem in a bodily manner instead of permittingany tipping (The usage of these was originallyenvisaged and the term originally coined byCalvin Case. Andrews retained the name in hishonor). The length of power arm was adjustedsuch that the amount of moment generated fromit, when added to the moment created by thebuilt-in angulation for counter tip, would equalthe moment arising from application of themesially or distally directed force on the tooth,thus nullifying the latter.
All these modifications were bound to createan impression of the necessity of keeping a verylarge inventory of brackets. However, Andrewsargued that there are only 12 treatment planpossibilities for each arch, which are met by amixture of some standard and some translationbrackets. Hence depending on one’s practicerequirements, one could keep the standard andcommonly required translation brackets in stockand order for the remaining as and whenrequired.
STRAIGHT WIRE APPLIANCE (SWA)
Lawrence F Andrews made some interestingremarks when he introduced the straight wireappliance to the profession. He was candid toadmit that he did not consider the appliance asthe ultimate one (“Will there ever be one?”). Hefurther emphasized that although he had his owntreatment philosophy and mechanics, hisappliance was not meant to serve only his wayof treatment, but was for universal use to suitany philosophy and mechanics employingedgewise brackets. He felt that his appliancecould successfully treat about 90 percent of casesleaving out the 10 percent of extreme cases(which would need surgical orthodontics).
As was mentioned earlier, the SWA did notgain universal acceptance instantly. Althoughmajority of the edgewise practitioners changed

104 History of Orthodontics
over to some form of pre-adjusted edgewiseappliance by eighties, there were some whovoiced serious misgivings. Further, manyresearchers critically examined the concept of theSWA, and found several flaws in the conceptitself. The comments/observations of some of theprominent critics is summarized below.
The main drawback of the SWA is that itoverlooks biological variation in the anatomy ofteeth of different individuals (this criticismwould hold true for other versions of pre-adjusted edgewise appliances also). Dellinger,Vardiman, Lamberts, Germane and other havediscussed this aspect. They used moresophisticated gadgets to study the crown surfacecurvatures (‘profile’) of different teeth. Dellingerused an optical comparator. Germane et al usedmagnified projections of the X-ray pictures ofextracted teeth for making the measurements.Dellinger argued that the basic data should havebeen collected from individuals havingmalocclusion and not from ideal occlusion castsas was done by Andrews.
One of the important features of SWA (andother pre-adjusted edgewise appliance) is thetorque built in the brackets, which ideally shouldeliminate third order bends in the archwire. Auniform torque value in the bracket slots for anygiven tooth of all the patients is based on thepremise that individual teeth of any given type(e.g. right upper central incisors or leftmandibular second premolars, etc.) in all thepatients would exhibit identical curvatures offacial surfaces. Only then, at a particular heighton any type of tooth (e.g. at the facial axis point)brackets with properly contoured bases wouldfit in identical manner. The above mentionedauthors have challenged this axiom. Accordingto them this curvature could vary by as much as5.2 0 to 10.40 for teeth with low variation and12.80 to 25.60 for teeth with high variations. Suchvariations are bound to affect the torque valuesin most of the individuals. Therefore, use ofprescribed bracket torque value may improvecare in some patients but not the others.Treatment must be tailored to the biologicvariation presented by each patient. This impliesthat the third order bends will be often requiredin most of the patients.
Andrews had laid great stress on theconsistency of the long axis point (later renamed
as facial axis point). This is also not accepted bythese authors. Dellinger found it erratic andinconsistent. Germane et al also questionedAndrews’ contention that the facial surfacecontour is more consistent when long axis. pointis used to locate the brackets and that theclinicians can place the brackets within an errorof ± 2 degrees torque.
The colum angle, i.e. the angle between thelong axis of crown and the long axis of root differsfrom tooth to tooth and also for the same toothin different persons. In class II division 2 casesthe central incisors have a more acute collumangle than that seen in class II division 1 cases.Hence, even when crowns are correctlypositioned (which is difficult on account of earliermentioned reason) root placement will vary.Teeth with more acute collum angle will beplaced closer to the palatal cortical plate in somecases even pressing against it. What effect thevariation in root placement will have on thehealth of the teeth or stability of the results is notknown yet.
Different vertical growth patterns havedifferent inclines of occlusal plane with respectto the cranium. The inclination value of themaxillary incisors are preadjusted with respectto the occlusal plane. While the angle of U1 toSN remains almost same in all groups, thatbetween U1 to OP varies in high, average or lowmandibular plane angle cases. Hence, a uniformbuilt-in torque value for all the patients wouldplace the upper incisors in positions other thatoptimum in high or low angle case. The upperincisors would be placed more upright or moreproclined respectively in these cases. Such caseswould require different torque values for correctplacement of these teeth.
Dellinger made a scathing attack on SWA. Hestated, “Clinicians are being saved not by whatthe SWA does but by what it does not do” (sinceless than full size wires are used). And further“If full sized unbent archwires are placed in themouth and are allowed to totally work out, theresults would be erratic, inconsistent andclinically unacceptable”.
There is at least some truth in this commentbecause Andrews stated, in his interviewpublished few years later after the above criticismappeared, that his preference is for 0.022 bracketsand that the largest wire he uses in these brackets

105Andrews’ Straight Wire Appliance
is 0.018" X 0.025" (He does not use full size wires,not even the NiTi wires).
Schudy also made comments similar toDillinger- “Placing a lot of torque in the upperincisor brackets and then never using it by notfilling the brackets is an admission that it is notright for some of the patients”. He also pointedout the possibility of abuse of the appliance bythe general dentists. “It (the SWA) does not placethe teeth in their proper position automaticallyas it allegedly is supposed to do. It provides aneasy way for the general dentist to try to doorthodontics, believing that it automaticallyproduces good results” (JCO Aug 92).
Perhaps a balanced view of thecontradictory opinions can be found in the
article of Ross et al that summed up neatly theplace of SWA in modern orthodontics. “Thestraight wire appliance should not beconsidered an inappropriate tool. It is animportant step forward in orthodonticmechanotherapy that has maximumeffectiveness on average or good skeletalpatterns. It is clear that the concept of ‘oneappliance fits all’ defies normal biologicvariation among orthodontic patients. Hence,skilled orthodontic care is still needed in spiteof technologic advances”.
Whatever inventions have occurred from histime to till date in orthodontics is purely on thebasis of Andrews Angle’s keys to normalocclusion.
12EEEvvvooollluuutttiiiooonnn ooofff
OOOrrrttthhhooodddooonnntttiiiccc AAAppppppllliiiaaannnccceeesss
� Brackets
– Metal Brackets
– Plastic Brackets
– Ceramic Brackets
– Weldable Brackets
– Bondable Brackets
– Ribbon Arch Brackets
– Modified Ribbon Arch/
Brackets in Begg Technique
– Tip Edge Brackets
– Edgewise Brackets
– Preadjusted Edgewise
Brackets
– Lingual Brackets
– Self-ligating Brackets
– Single Width Bracket
– Twin Brackets
– Lewis Bracket
– Steiner Bracket
– Broussard Bracket
– Lang Brackets
– Jaraback – 1963
– Roth – 1976
� Bands
� History of Archwires
– Gold
– Stainless Steel
– Nickel–Titanium Alloys
– Beta–Titanium or TMA or Can
Wire
– Cobalt-Chrome-Nickel Alloy
– Optiflex Archwire
– Multistrand Archwires
� Manufacturing of Archwire
� Methods of Straightening of
Orthodontic Wires
� Properties of Archwire
– Pseudoelastic Effect
– Thermoelastic Effect
– Strength of the Wire
– Formability
– Solubility And Weldability
– Friction
– Environmental Stability
– Shape Memory Effect
� Auxiliaries
� History of Orthodontic Materials
– Use in Dentistry
– Uses in Orthodontics
Man has long enhanced his appearance. Evidencedates back some 3000 years. Archaeologists havediscovered mummified remains with crude metalbands wrapped around individual teeth withcatgut thought to have been used to apply forces.Later in 400-500 BC, Hippocrates and Aristotleboth considered ways to straighten teeth. TheEtruscans were using appliances to maintainspace and prevent collapse of the dentition; whilein a Roman tomb in Egypt, a researcher found anumber of teeth bound with a gold wire, theoriginal ligature wire. At the time of Christ,Aurelius Cornelius Celsus first recorded thetreatment of malaligned teeth using fingerpressure.
Despite all this evidence and experimentation,until the 1700s the most aesthetic though noteffective appliance remained the finger. TheFrench surgeon, Pierre Fauchard the “Founder ofModern Dentistry” described procedures foraligning the teeth, including: filing them,manipulating them with forceps, and then tyingthem with thread to a silver or gold “bandeau”.
A contemporary of Fauchard, Etienne Bourdet,dentist to the King of France, went a step furtherand recommended the extraction of first premolarsto maintain symmetry of the jaws. He also usedthe first and more aesthetic lingual appliances.
The discovery of vulcanite, when combinedwith gold wire springs and screws, allowed the
107Evolution of Orthodontic Appliances
use of removable appliances to induce individualtooth movement. By 1937, the discovery of acrylichad allowed translucent acrylic plates to replaceblack vulcanite.
Edward H Angle (1855–1930), the “Father ofModern Orthodontics” developed the firstwidely adopted system for correctingmalocclusions using brackets soldered to thelabial of metal bands. Thus the Edgewise systemwas born.
BRACKETS AND BANDS
Until the early 20th century, 14 to 18 carat goldwas the principle metal used for constructingorthodontic brackets and bands. However, withthe metallurgical developments of World Wars Iand II appropriate forms of stainless steel becameavailable. The introduction of stainless steelallowed the development of progressivelysmaller appliances. The road to smallerappliances had begun and it was significantlyaccelerated with Buonocore’s direct bonding ofresin to enamel and Newman’s use of epoxy resinin 1965 to directly bond brackets to the labialsurface of teeth.
BRACKETS
� Brackets are passive components whichprovide a means of transferring tooth-movingforces from archwires, elastics and otheractive components of fixed orthodonticappliance.
� They can be welded to the bands which arethen cemented onto the teeth (weldablebrackets). Bondable brackets beingincreasingly used in recent years, althoughweldable ones have to be opted in some cases.
� Brackets manufactured from a variety ofmaterials are available and they can be ofvarious designs suitable for differentorthodontic techniques.Brackets can be classified in a number of ways
as listed below:I. Depending on material used for manufacture
1. Metal bracketsa. Goldb. Stainless steelc. Titanium
2. Plastic brackets3. Ceramic brackets
II. Depending on mode of attachment
1. Weldable brackets2. Bondable brackets
III. Depending on technique for which they areused1. Ribbon arch brackets2. Begg modified ribbon arch brackets3. Tip-edge bracket4. Edgewise brackets5. Pre-adjusted edgewise brackets6. Lingual brackets
Metal Brackets
� Metal brackets (Fig. 12.1) are routinely used inorthodontic practice of which steel bracketsare the most frequently used.
� Titanium brackets are recently introducedand have high biocompatibility and lowfriction.
Advantages of Metal Brackets
a. They can be sterilised.b. They can be recycled.c. They resist deformation and fracture.d. Exhibit less friction with the arch wire.e. They are comparatively less expensive.
Disadvantages
a. Easily noticeable, metallic brackets areaesthetically not pleasant.
b. They may corrode and cause staining of theteeth.
Plastic Brackets
Plastic brackets (Fig. 12.2) initially made fromacrylic and later from injection moulded poly-carbonate, were introduced in the 1970s. Theypromised significantly enhanced aesthetics;
Fig. 12.1: Metal brackets
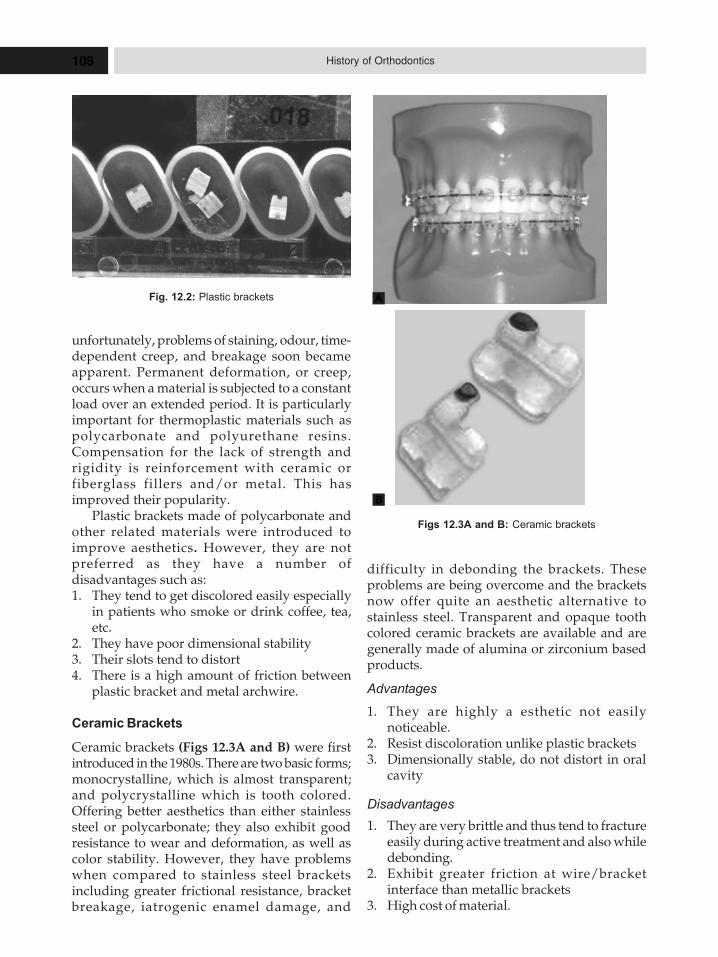
108 History of Orthodontics
unfortunately, problems of staining, odour, time-dependent creep, and breakage soon becameapparent. Permanent deformation, or creep,occurs when a material is subjected to a constantload over an extended period. It is particularlyimportant for thermoplastic materials such aspolycarbonate and polyurethane resins.Compensation for the lack of strength andrigidity is reinforcement with ceramic orfiberglass fillers and/or metal. This hasimproved their popularity.
Plastic brackets made of polycarbonate andother related materials were introduced toimprove aesthetics. However, they are notpreferred as they have a number ofdisadvantages such as:1. They tend to get discolored easily especially
in patients who smoke or drink coffee, tea,etc.
2. They have poor dimensional stability3. Their slots tend to distort4. There is a high amount of friction between
plastic bracket and metal archwire.
Ceramic Brackets
Ceramic brackets (Figs 12.3A and B) were firstintroduced in the 1980s. There are two basic forms;monocrystalline, which is almost transparent;and polycrystalline which is tooth colored.Offering better aesthetics than either stainlesssteel or polycarbonate; they also exhibit goodresistance to wear and deformation, as well ascolor stability. However, they have problemswhen compared to stainless steel bracketsincluding greater frictional resistance, bracketbreakage, iatrogenic enamel damage, and
difficulty in debonding the brackets. Theseproblems are being overcome and the bracketsnow offer quite an aesthetic alternative tostainless steel. Transparent and opaque toothcolored ceramic brackets are available and aregenerally made of alumina or zirconium basedproducts.
Advantages
1. They are highly a esthetic not easilynoticeable.
2. Resist discoloration unlike plastic brackets3. Dimensionally stable, do not distort in oral
cavity
Disadvantages
1. They are very brittle and thus tend to fractureeasily during active treatment and also whiledebonding.
2. Exhibit greater friction at wire/bracketinterface than metallic brackets
3. High cost of material.
Fig. 12.2: Plastic brackets
Figs 12.3A and B: Ceramic brackets
A
B
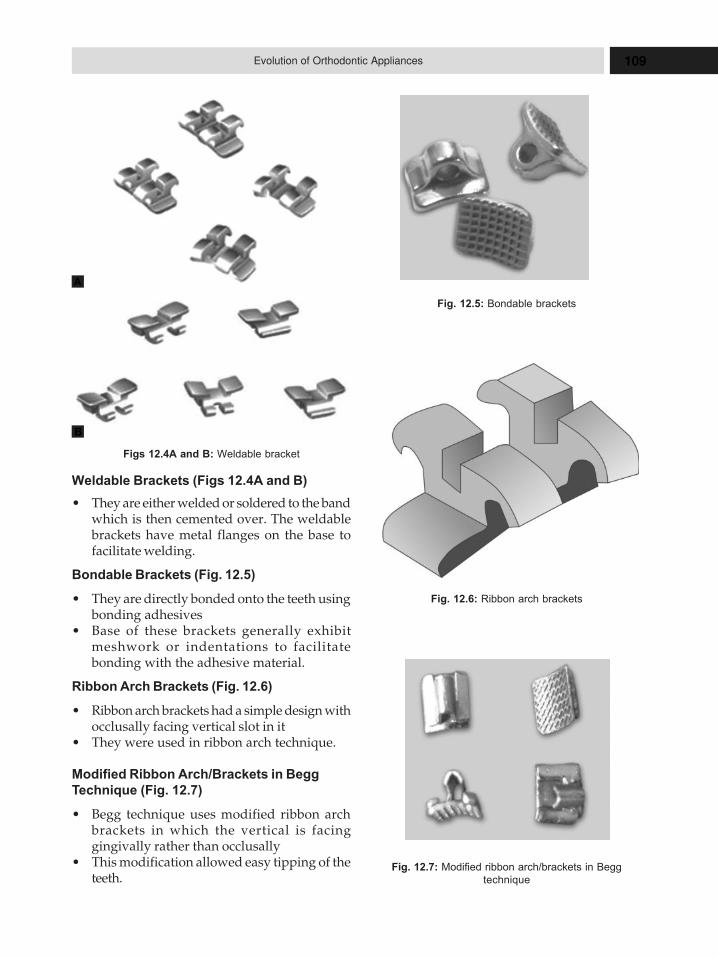
109Evolution of Orthodontic Appliances
Weldable Brackets (Figs 12.4A and B)
� They are either welded or soldered to the bandwhich is then cemented over. The weldablebrackets have metal flanges on the base tofacilitate welding.
Bondable Brackets (Fig. 12.5)
� They are directly bonded onto the teeth usingbonding adhesives
� Base of these brackets generally exhibitmeshwork or indentations to facilitatebonding with the adhesive material.
Ribbon Arch Brackets (Fig. 12.6)
� Ribbon arch brackets had a simple design withocclusally facing vertical slot in it
� They were used in ribbon arch technique.
Modified Ribbon Arch/Brackets in Begg
Technique (Fig. 12.7)
� Begg technique uses modified ribbon archbrackets in which the vertical is facinggingivally rather than occlusally
� This modification allowed easy tipping of theteeth.
Figs 12.4A and B: Weldable bracket
Fig. 12.5: Bondable brackets
Fig. 12.6: Ribbon arch brackets
Fig. 12.7: Modified ribbon arch/brackets in Begg
technique
A
B
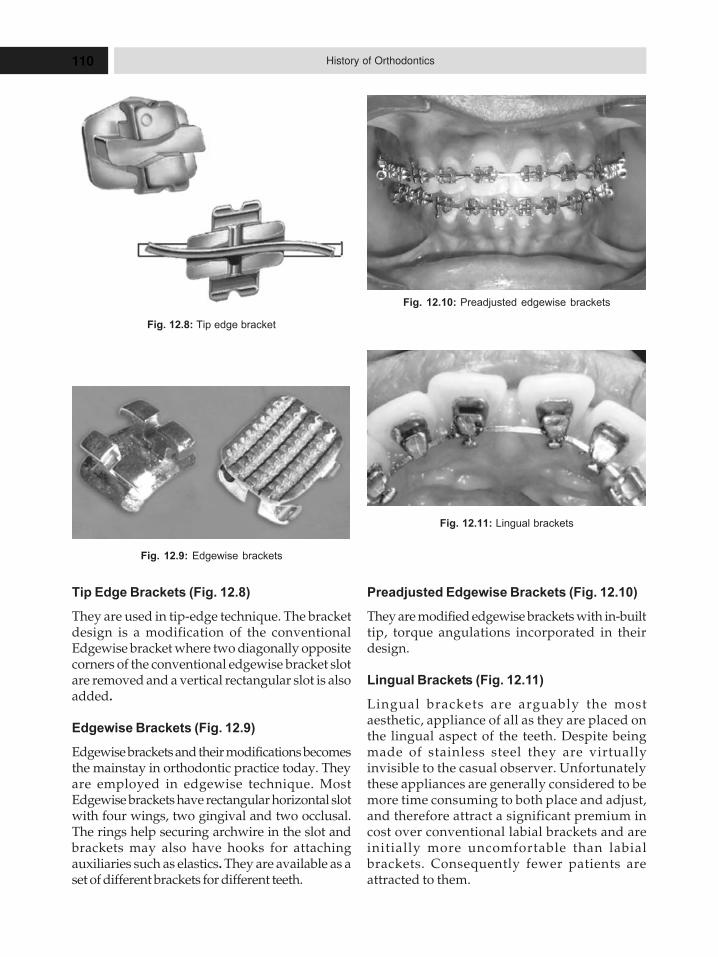
110 History of Orthodontics
Tip Edge Brackets (Fig. 12.8)
They are used in tip-edge technique. The bracketdesign is a modification of the conventionalEdgewise bracket where two diagonally oppositecorners of the conventional edgewise bracket slotare removed and a vertical rectangular slot is alsoadded.
Edgewise Brackets (Fig. 12.9)
Edgewise brackets and their modifications becomesthe mainstay in orthodontic practice today. Theyare employed in edgewise technique. MostEdgewise brackets have rectangular horizontal slotwith four wings, two gingival and two occlusal.The rings help securing archwire in the slot andbrackets may also have hooks for attachingauxiliaries such as elastics. They are available as aset of different brackets for different teeth.
Preadjusted Edgewise Brackets (Fig. 12.10)
They are modified edgewise brackets with in-builttip, torque angulations incorporated in theirdesign.
Lingual Brackets (Fig. 12.11)
Lingual brackets are arguably the mostaesthetic, appliance of all as they are placed onthe lingual aspect of the teeth. Despite beingmade of stainless steel they are virtuallyinvisible to the casual observer. Unfortunatelythese appliances are generally considered to bemore time consuming to both place and adjust,and therefore attract a significant premium incost over conventional labial brackets and areinitially more uncomfortable than labialbrackets. Consequently fewer patients areattracted to them.
Fig. 12.8: Tip edge bracket
Fig. 12.9: Edgewise brackets
Fig. 12.10: Preadjusted edgewise brackets
Fig. 12.11: Lingual brackets
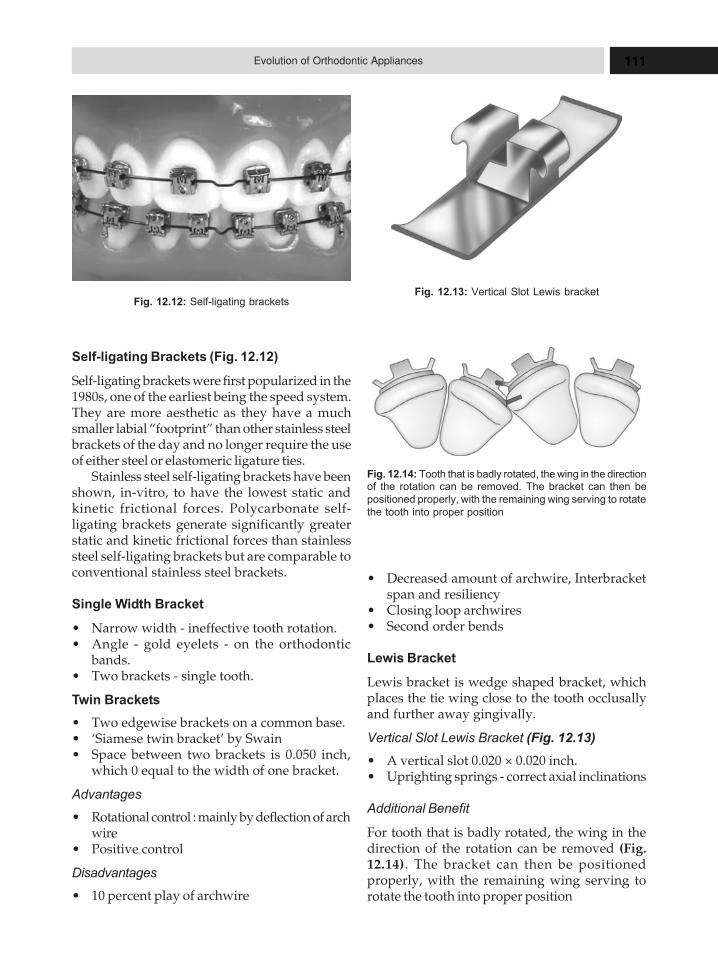
111Evolution of Orthodontic Appliances
Self-ligating Brackets (Fig. 12.12)
Self-ligating brackets were first popularized in the1980s, one of the earliest being the speed system.They are more aesthetic as they have a muchsmaller labial “footprint” than other stainless steelbrackets of the day and no longer require the useof either steel or elastomeric ligature ties.
Stainless steel self-ligating brackets have beenshown, in-vitro, to have the lowest static andkinetic frictional forces. Polycarbonate self-ligating brackets generate significantly greaterstatic and kinetic frictional forces than stainlesssteel self-ligating brackets but are comparable toconventional stainless steel brackets.
Single Width Bracket
� Narrow width - ineffective tooth rotation.� Angle - gold eyelets - on the orthodontic
bands.� Two brackets - single tooth.
Twin Brackets
� Two edgewise brackets on a common base.� ‘Siamese twin bracket’ by Swain� Space between two brackets is 0.050 inch,
which 0 equal to the width of one bracket.
Advantages
� Rotational control : mainly by deflection of archwire
� Positive control
Disadvantages
� 10 percent play of archwire
� Decreased amount of archwire, Interbracketspan and resiliency
� Closing loop archwires� Second order bends
Lewis Bracket
Lewis bracket is wedge shaped bracket, whichplaces the tie wing close to the tooth occlusallyand further away gingivally.
Vertical Slot Lewis Bracket (Fig. 12.13)
� A vertical slot 0.020 × 0.020 inch.� Uprighting springs - correct axial inclinations
Additional Benefit
For tooth that is badly rotated, the wing in thedirection of the rotation can be removed (Fig.12.14). The bracket can then be positionedproperly, with the remaining wing serving torotate the tooth into proper position
Fig. 12.12: Self-ligating bracketsFig. 12.13: Vertical Slot Lewis bracket
Fig. 12.14: Tooth that is badly rotated, the wing in the directionof the rotation can be removed. The bracket can then be
positioned properly, with the remaining wing serving to rotate
the tooth into proper position
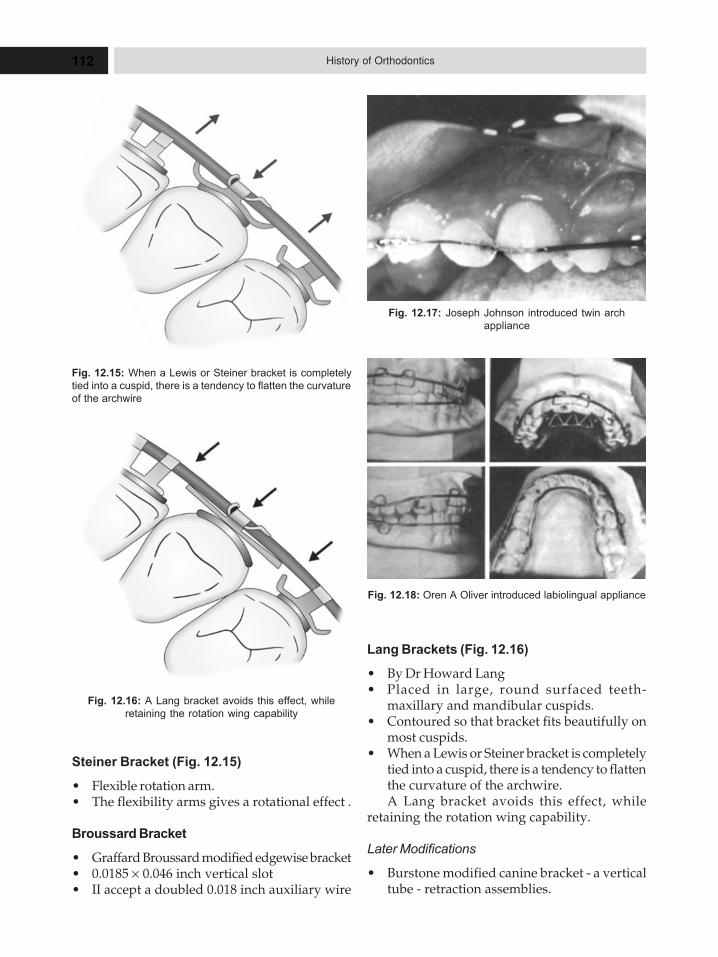
112 History of Orthodontics
Steiner Bracket (Fig. 12.15)
� Flexible rotation arm.� The flexibility arms gives a rotational effect .
Broussard Bracket
� Graffard Broussard modified edgewise bracket� 0.0185 × 0.046 inch vertical slot� II accept a doubled 0.018 inch auxiliary wire
Lang Brackets (Fig. 12.16)
� By Dr Howard Lang� Placed in large, round surfaced teeth-
maxillary and mandibular cuspids.� Contoured so that bracket fits beautifully on
most cuspids.� When a Lewis or Steiner bracket is completely
tied into a cuspid, there is a tendency to flattenthe curvature of the archwire.A Lang bracket avoids this effect, while
retaining the rotation wing capability.
Later Modifications
� Burstone modified canine bracket - a verticaltube - retraction assemblies.
Fig. 12.15: When a Lewis or Steiner bracket is completely
tied into a cuspid, there is a tendency to flatten the curvature
of the archwire
Fig. 12.16: A Lang bracket avoids this effect, while
retaining the rotation wing capability
Fig. 12.17: Joseph Johnson introduced twin arch
appliance
Fig. 12.18: Oren A Oliver introduced labiolingual appliance
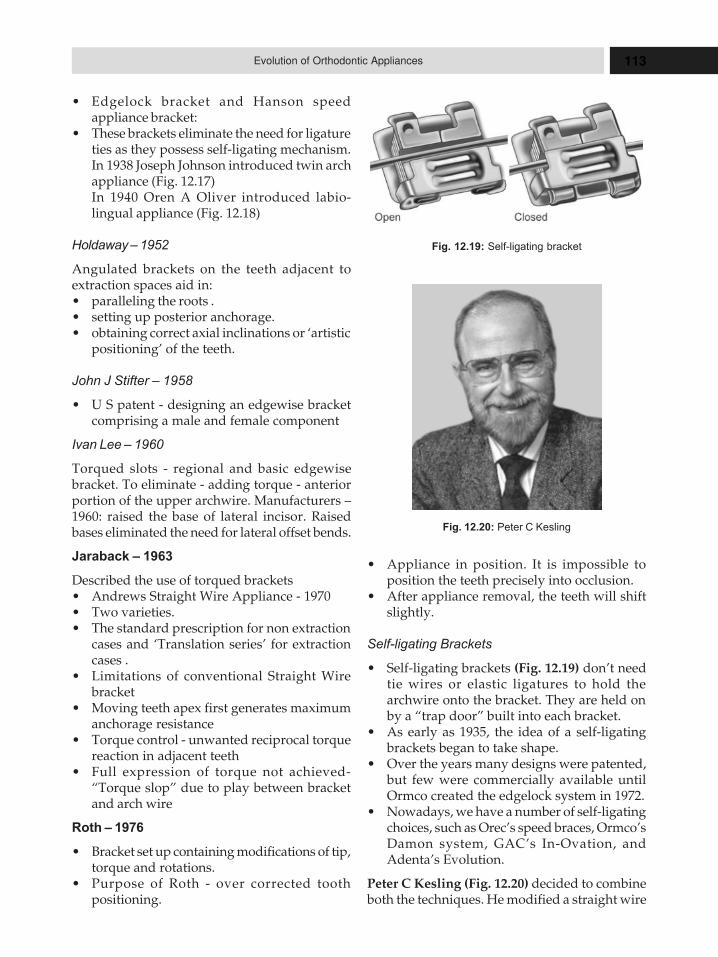
113Evolution of Orthodontic Appliances
� Edgelock bracket and Hanson speedappliance bracket:
� These brackets eliminate the need for ligatureties as they possess self-ligating mechanism.In 1938 Joseph Johnson introduced twin archappliance (Fig. 12.17)In 1940 Oren A Oliver introduced labio-lingual appliance (Fig. 12.18)
Holdaway – 1952
Angulated brackets on the teeth adjacent toextraction spaces aid in:� paralleling the roots .� setting up posterior anchorage.� obtaining correct axial inclinations or ‘artistic
positioning’ of the teeth.
John J Stifter – 1958
� U S patent - designing an edgewise bracketcomprising a male and female component
Ivan Lee – 1960
Torqued slots - regional and basic edgewisebracket. To eliminate - adding torque - anteriorportion of the upper archwire. Manufacturers –1960: raised the base of lateral incisor. Raisedbases eliminated the need for lateral offset bends.
Jaraback – 1963
Described the use of torqued brackets� Andrews Straight Wire Appliance - 1970� Two varieties.� The standard prescription for non extraction
cases and ‘Translation series’ for extractioncases .
� Limitations of conventional Straight Wirebracket
� Moving teeth apex first generates maximumanchorage resistance
� Torque control - unwanted reciprocal torquereaction in adjacent teeth
� Full expression of torque not achieved-“Torque slop” due to play between bracketand arch wire
Roth – 1976
� Bracket set up containing modifications of tip,torque and rotations.
� Purpose of Roth - over corrected toothpositioning.
� Appliance in position. It is impossible toposition the teeth precisely into occlusion.
� After appliance removal, the teeth will shiftslightly.
Self-ligating Brackets
� Self-ligating brackets (Fig. 12.19) don’t needtie wires or elastic ligatures to hold thearchwire onto the bracket. They are held onby a “trap door” built into each bracket.
� As early as 1935, the idea of a self-ligatingbrackets began to take shape.
� Over the years many designs were patented,but few were commercially available untilOrmco created the edgelock system in 1972.
� Nowadays, we have a number of self-ligatingchoices, such as Orec’s speed braces, Ormco’sDamon system, GAC’s In-Ovation, andAdenta’s Evolution.
Peter C Kesling (Fig. 12.20) decided to combineboth the techniques. He modified a straight wire
Fig. 12.19: Self-ligating bracket
Fig. 12.20: Peter C Kesling

114 History of Orthodontics
bracket, to create tip edge bracket and differentialforce technique. In this technique initial crowntipping was done followed by controlled rootuprighting with straight arch wires (differentialtooth movement with straight arch wires).Therefore it is known as the “differential straightarch technique”. Archwire slot permits initialcrown tipping mesially or distally and faceshorizontally, the slot and bracket are termed
Kesling determined that:� It is necessary for each tooth to tip either
mesially or distally but not in both directions� All teeth tip distally except those distal to the
extraction sites, which tip mesially� Anchor molars should remain upright
throughout Rx.� Diagonally opposite corner were removed� Permits desired distal crown tipping� Preadjusted in three dimensions-
� tip, torque, in and out built in� Slot size - 0.022" × 0.028
Alexander – 1983
Vari–simplex discipline:� Vary - variety of bracket types used;� Simplex - KISS principle (Keep it Simple Sir)
Discipline was chosen rather than theappliance.
� Based on edgewise philosophy
Creekmore – 1993
Slot machine onies solution to the� Inaccuracies of bracket placement,� Anatomic and biologic variations, over
correction for tissue rebound and relapse and� Mechanical differences of preadjusted
edgewise orthodontic appliance
� It orients the archwire slot to relative to thefacial surface of each tooth on the model.
BANDS
Bands (Fig. 12.21) are passive components thatprovide space for fixing various attachments ontothe teeth. They are generally made of soft stainlesssteel. The stainless steel strips are available indifferent widths and thickness to suit differentteeth (table 12.1). Weldable brackets, buccal tubesand other auxiliary attachments are soldered orwelded over the bands, which are then cementedaround the intended teeth.
Availability
1. Custom-made bands are fabricated using bandmaterials which are available in the form ofspools.
2. Preformed seamless bands are available indifferent sizes which can be directly cementedaround the tooth. Preformed bands areincreasingly being used in recent years.
ARCHWIRES
History of Archwires
By the 1960s, gold as an archwire had largely beenreplaced. It gave way to thinner, more resilientstainless steel wires such as Wilcox’s Australianwire. However, in 1974, Unitek patented its nitinol(Nickel Titanium Naval Ordnance Laboratory)wire having the lowest modulus of elasticity andmost extensive deactivation range of anyequivalent cross sectional wire of the time. Thisallowed the application of light forces over aprotracted range. By 1986, “superelastic” alloywires that undergo stress induced change in theircrystal form had been developed. These offeredsignificant advantages over nitinol. The range ofwires available to orthodontist has been futherFig. 12.21: Bands
Table 12.1: The stainless steel strips are available indifferent widths and thickness to suit different teeth
Teeth Band Thickness Band Width Figure(Inches)
Incisor 0.003 0.125Canine 0.003 0.150Premolar 0.003 0.150Molar 0.0050.006 0.0180.018

115Evolution of Orthodontic Appliances
extended by the addition of various other elements(Table 12.2) including cobalt-chromimum. Beta-titanium and, in 1994 copper. Copper NiTichanges its crystal form at a specific temperature.Most recently, a nickel free wire, titanium-niobiumhas been introduced. With these new wires,especially the super elastic wires, it is no longernecessary to incorporate multiple loops,significantly enhancing aesthetics as well ascomfort.
A number of manufacturers now offer NiTiand stainless steel archwires coated with toothcolored material to enhance their aesthetics,especially when combined with ceramic brackets.Unfortunately, these coatings tend to wear awaywith time; however, further research should seethis resolved.
The search for improved aesthetics is leadingus down the road of fiber reinforced composites.These materials are not yet clinically useful asarchwires; however, they have been incorporatedinto bis-GMA ribbons and bonded, as strips, tomultiple teeth, to provide retention and alsoanchorage, reducing the number of conventionalbrackets required.
Manufacturing
The manufacture of metal alloy wires involvesmaking an ingot followed by rolling and drawing:1. Making the Ingot: This involves pouring of
molten metal into a mold. The result obtainedis the cast wire to produce an ingot. Amagnified view of this ingot shows crystals orgrains; it is mainly this grain structure, whichultimately controls the significant mechanicalproperties of the final wire. Grain formationdepends on the rate of cooling and the size ofthe ingot.
2. Rolling: The formed ingot is rolled into a longbar. This is done with the help of a devicetermed as the roller. During rolling, theindividual grains retain their identitythroughout this process. Each grain getselongated proportional to the ingot. Thesqueezing and massaging actions of rollerincreases the strength by causing the grains tomesh and interlock. The rolling procedure iscontinued till the crystals are so locked thatthey can no longer adjust. At this point, therolling is interrupted and the metal structureis annealed by heating it to a suitable
temperature. At the annealing temperature,atoms become mobile enough to move aboutand thereby get relieved of some of the internalstresses, which had been introduced duringrolling. When the metal cools down, the grainstructure is seen to be uniform.
3. Drawing: This is the final step, wherein thissmall cross section wire is further drawn intoits final size. This is a more precise step inwhich the wire is pulled through a small holein a die. The hole is slightly smaller than thestarting diameter of the wire; so that the wallis squeezed uniformly from all sides as itpasses through. The cross section of the wiresare the same as the die.
Methods of Straightening of Orthodontic Wires
Following are the two methods of straighteningof wires;1. Spinner straightening.2. Pulse straightening.1. Spinner straightening: In this type of
straightening, the wire is pulled through abronze roller, which torsionally twist thewires. However, this mode does not producewires as mechanically efficient as the the onesproduced by ‘pulse straightening’.Disadvantages: Disadvantages of spinnerstraightening are as listed below� Deformation� Decreased yield stress value.
2. Pulse straightening: This is a recent and moreaccepted method of straightening of wires,which employs special machines to straightenwires which lead to:� Maintenance of the yield strength� Smooth finish, which would be also,
beneficial as it produces less friction.Pulse straightened wires have superior
qualities in comparison to spinner straightenedwires as shall be discussed in the following sectionon stainless steel.
Basic metallurgy: At this juncture, it is mandatoryto understand briefly the metallurgical properties.1. Metal: According to the Metals Handbook
(1992); a metal is defined as ‘an opaquelustrous chemical substance that is a goodconductor of heat and electricity and, whenpolished is a good reflector of light’.
2. Alloy: An alloy is defined as ‘a metal containingtwo or more elements, at least one of which is

116 History of Orthodontics
a metal, and all of which are mutually solublein the molten state’.
3. Alloy system: ‘An alloy system is an aggregateof two or more metals in all possiblecombinations’.
Metallic Bonds and Crystalline Structure
Metallic bonds imply the primary ionic interaction,which holds the metal structure. Atoms with freevalence electrons as the metal atoms are able tolose their outer shell (valence) electrons and forma positive ion. The free electrons are able to moveabout in the metal space lattice and they are termedas an ‘electron cloud’. The electrostatic attractionbetween the positive ions and the electron cloudforms the ‘metallic bond’.
It is this metallic bond that is responsible forluster, conductivity properties and ability of themetal to deform plastically.
A regular crystalline configuration is typicalfor metals. This is referred to as ‘space lattice’ or‘crystal’ (grain).
The common lattice configurations are:1. Simple cubic.2. Body-centered cubic or ‘BCC’, e.g. austenite
NiTi.3. Face-centered cubic or ‘FCC’, e.g. austenite
SS.4. Body-centered Tetragonal ‘BCT’, e.g.
martenisitc SS.5. Close packed Hexagonal, e.g. martensitic
NiTi.It can be inferred from the above examples that
the lattice configurations (in turn, the grainstructure and their orientation) play a significantrole in determining the ultimate mechanicalproperties.
Cast versus Wrought Metals
� Generally, all metals and their alloys originatefrom castings. A cast metal which isplastically deformed, either by machining orworking, is termed as a wrought metal.
� Cast structures are close to equilibriumconditions and are incorporated in somedental applications. However, the orthodonticwires are in the wrought form. Wrought metalshave a fibrous structure with extremelyelongated crystals. Also this structure exhibitsenhanced mechanical properties like increasedtensile strength and hardness.
� Because of this, the strength values could bealtered by the phenomenon of either workhardening or heat treatment. This could be eitherbeneficial (for example: the formation of ‘dead’ligature wires) or could be deleterious (propertiesof a wire may be lost during solderingprocedures) and should be kept in mind.
Solidification of Metals
Liquid state: The liquid or ‘molten state’ representsa multitude of random atoms or moleculessurrounding numerous unstable atomicaggregates. This can be seen in the solidificationcurve as shown in the:
If a metal is allowed to cool, it first cools downuniformly (as shown by the portion A-B). After thisthere is a gradual increase in temperature (till B),also known as the latent heat of solidification. Theportion below the fusion temperature (B-B’) istermed as super cooling. It is during this periodthat the crystallization of the metal begins. Thistakes place around ‘nuclei’; also termed as embryos.
B-B1→ Super cooling
Tf → Fusion temperature
This nucleus formation can either be homog-enous or heterogeneous. This eventually leads to‘grain’ or crystal formation. It is at the Grain bound-ary that the areas of lattice imperfections can exist.
Lattice Imperfections and Dislocations
As would have been seen in the solidification ofmetals:� Crystallization does not occur in a uniform
manner and some lattice positions may be‘vacant’ or ‘overcrowded’. These are termedas “lattice imperfections”. Dislocations aredefects along a particular path in apolycrystalline structure. e.g. edge dislocation.
� Dislocations tend to build up at grainboundaries, greater stress is required toproduce greater slip. Thus, the materialbecomes stronger, harder and less ductile. Thisis termed as the phenomenon of ‘strainhardening’ or ‘work hardening’.
� The ultimate result of strain hardening isfracture.
Heat Treatment
Heat treatment is the thermal processing of analloy for a length of time above room temperaturebut below its solidus temperature.
117Evolution of Orthodontic Appliances
Quenching: A process wherein the metal is cooledrapidly from an elevated temperature.
The Heat treatment procedures are carried outfor the following reasons:a. Preservation of a phase at room temperature,
which is stable usually at highertemperatures.
b. Rapidly terminate a process that only occursat elevated temperature.
Types of Heat Treatment
1. Stress relief: This refers to a ‘low’ temperatureheat treatment to relieve the stresses due tostrain hardening. Cobalt-chromium alloy isvery responsive to stress relief. It also, improvesductility.
2. Annealing heat treatment: This employs aheat treatment at a substantially highertemperature as compared to the stress relief.Consists of three phases: i. Recovery. ii. Recrystallization.iii. Grain growth.
3. Age hardening heat treatment: It is a long termprocess in which the temperature is slightlylesser than the anneal temperature. The metalis then cooled rapidly by quenching.
PROPERTIES OF ARCHWIRE
Different types of archwire, right from gold to tilldate invention in archwire, are explained belowwith their properties.
Archwires are one of the active components offixed orthodontic appliances, which when usedbring about various tooth movements (tipping,bodily, torque, rotational and vertical movements)
through the medium of brackets and weldedbuccal tube on the palatal aspect of the molarbands.
Gold
Before 1950’s, gold and other precious alloycombinations like platinum and palladium withgold and copper were routinely used fororthodontic purposes. Gold and gold alloyarchwire exhibit excellent formability,environmental stability and biocompatibility.Angle’s Ribbon arch appliance utilized a goldplatinum alloy combination as the ‘archwire’.However, their popularity lost ground due to twomain reasons:a. The marginal properties and cost factor
involved.b. Advent of stainless steel or the ‘rust free’ alloys.
Stainless Steel
Stainless steel (Fig. 12.22) was introduced byWilkinson in 1929. Stainless steel archwire (Table
12.2) exhibit adequate strength, high resilience,formability, high stiffness, biocompatibility andeconomic feasibility.
The drawback of these archwires includeshigh modulus of elasticity; more frequentactivations are required to maintain the same forcelevel.
Nickel-titanium Alloys (Fig. 12.23)
Nickel titanium alloyl also known as nitinol,(Nickel titanium Naval Ordnance Laboratory)was invented by William R Buchler at NavalOrdnance Laboratory. The main advantage of this
Table 12.2: Classification of archwires
I. Based on material used1. Gold and gold alloys2. Stainless steel3. Nickel-titanium alloys4. Beta-titanium5. Cobalt–chromium- nickel alloys6. Optiflex archwires
II. Based on cross-section1. Round2. Square3. Rectangular4. Multistranded Fig. 12.22: Stainless steel
118 History of Orthodontics
alloy over others is the high elasticity and shapeback memory. The drawback of these archwires isthat they cannot be neither welded nor soldered,and cannot receive bends or loops or helices.Various phases of NiTi, like the austenitic-active,with pseudoelasticity and the latest beingsuperelastic Cu-NieTi were brought out. Othervarieties like martensitic active alloy orthermoelastic NiTi alloy also evolved. The creditfor introducing the superelastic NiTi goes to FujioMiura and to Dr Rohit Sachdeva for introducingCu-NieTi.
Beta-titanium or TMA or Can Wire
Goldberg and CJ Burrstone invented beta-titaniumand it is also known by TMA or CAN wire. Themain advantage of these arch wires include highrange of action, high spring back, receive bends,loops and helices, and they can be welded orsoldered.
Cobalt-chrome-nickel Alloy
Cobalt- chrome-nickel alloy is also known aselgiloy. These wires exhibit excellent formability,joinability, spring back and biocompatibility.
Optiflex Archwire
Optiflex archwire was invented by MF Talass in1992. Optiflex archwires are composed of clearoptical fibers and are therefore highly aesthetic.The drawback of these archwire is that they cannotreceive sharp bends.
Multistrand Archwires
Multistranded archwires are made up of numberof thinner wires. They can be round or rectangular,
Fig. 12.23: Nickel-titanium alloy
braided or twisted and may have three strands orsix strands. The main advantage of these archwires is that they exhibit increased flexibility.
Physical Properties of Wire
The first group of properties is concerned withthe elastic behavior which represents the internalstress/strain in the wire. This is produced by anexternal force deflecting the wire, the stress beingthe internal load and the strain the internaldistortion.
1. Stiffness/Springiness
i. Pseudoelastic effect: When an austenitic wireis placed in the mouth and deformed byforcing it into the misaligned brackets, thepseudoelastic effect is induced. Thistransforms the austenitic alloy into amartenstic state which, as the teeth align,gradually reverses to the austenitic state.
ii. Thermoelastic effect: Martensitic-active alloysare stable at room temperature, but whenraised to mouth temperature, the materialchanges into an austenitic state which exhibitsshape memory.
iii. Martensitic stabilized alloy (e.g Unitek’s originalnitinol): The alloy, introduced in 1970 byAndreasen.It is stabilized by introducing a certain amountof work hardening during processing and doesnot show true memory shape properties.Austenitic-active Alloy: “Active “ means that itexhibits the shape memory, in this case of thepseudoelastic type, the shape memory effectbeing induced by stress distorting the archwire in malaligned teeth. Examples ofsuperelastic Niti are Titanol from Forestadentand Nitinol SE from Unitek.Martensitic-active Alloy: Again this exhibitsshape memory, but of the thermally activatedvariety. This alloy is stable at low temperaturesbut when is placed in the mouth, and thetemperature increased to mouth temperature,it exhibits the shape memory effect. Examplesof thermally activated Niti are Neo Sentalloyfrom GAC and Nitinol XL from Unitek.
2. Range of Deflection – Spring Back
The range of wire is the distance it will bendelastically before permanent deformation occurs.

119Evolution of Orthodontic Appliances
If the wire is deflected beyond its yield point, itwill not return to its original shape.
3. Strength of the Wire
The strength of a wire is important because itdetermines the maximum force it can deliver.
The above three properties are related by theformula: strength = stiffness X range.
4. Formability
This is the amount of permanent deformation awire can withstand before it breaks.
5. Solubility and Weldability
Stainless steel can be soldered and welded, butNiTi cannot. Miura recently reported a methodof soldering nickel-titanium wires. TMA isweldable as described by Burrstone.
6. Friction
The laboratory understanding of friction is notrelevant to the clinical situation. Because everytime the patient bites together, the tooth is liableto move a small distance in all three planes ofspace. More important is the concept that the twocomponents, bracket and wire, may damage eachother as they moved across their surfaces. This isborne out by the fact that it is difficult to slideteeth with ceramic brackets along a wire, as theabrasiveness of the ceramic notches the surfaceof the metal.
7. Environmental Stability
Any material used for the construction of wiremust be stable in the oral environment. This hasbeen one of the limitation aesthetic.
8. Shape Memory Effect
The shape memory effect exhibited by the morerecent nickel-titanium wires has revolutionizedthe selection of wires for appropriate toothmovement. The wires manufactured fororthodontic purposes are composed of an alloyof nearly equal parts of nickel and titanium. Theshape memory effect is brought about by a changein the internal crystal formation from themartensitic phase with a hexagonal crystalstructure to or from the austenitic phase with acuboids crystal structure (Kusy, AJO Sep 1991).
The shape in crystalline structure can bebrought about by either:a. Stress, as in the pseudoelastic effect in the
Austenitic Active Alloy.
b. Heat, as in the thermoelastic effect in theMartensitic-active alloy where the transitiontemperature is between room and mouthtemperatures.
AUXILIARIES
Brass wire was initially used to ligate the archwire to the band/bracket combination. However,by the 1960s, the thinner and more aestheticstainless steel had replaced it as the ligature tie ofchoice. The advent of polyurethane materials hasseen the introduction of aesthetic coloredelastomeric modules to ligate the arch wire to thebracket. While offering good aesthetics wheninitially placed these modules are prone todiscoloration and breakdown over time and somust be regularly replaced. They also tend toincrease the friction between the bracket and thearchwire. Nevertheless, their ease of placementand appeal to younger patients has ensured theirgeneral use.
The latest innovation to the orthodontist’saesthetic armamentarium is the sequential clearplastic aligner. The principles of this process wereactually developed by kesling in 1945. However,itdid not achieve more widespread use untilinvisalign combined the technique with 3Dcomputer graphic and CAD/CAM technology toallow phased movement of multiple teeth to correctmid to moderate malocclusions. Since invisalignappeared a number of other companies havereleased similar products, including anAustralian company, Clear Smile. Unfortunately,these appliances are not suitable for treating allmalocclusions. Those with significant crowdingor spacing, and/or interarch discrepancies (suchas Class II and III relationships) often cannot betreated properly with these systems alone.Similarly, individuals with very short crowns andyounger adolescents where teeth are not fullyerupted are generally not suitable. Although someextraction treatments are being carried out they arenot normally as suitable as non-extraction cases.Precise alignment and finishing with these systemscan be more difficult compared to traditional fixedappliances so that a compromise result may needto be accepted. Further, they are still somewhatvisible on the labial surface and over the incisaledges. However, clear aligners are considerablymore aesthetic than traditional braces.

120 History of Orthodontics
HISTORY OF ORTHODONTIC MATERIALS
Baptized with a name resulting from thecontraction of the words “elastic” and“polymer”, elastomer is an umbrella term whichencompasses materials which resist distortionand resume their original shape or volume.Classified according to their chemical structure,however, materials which are not necessarilyflexible are still called elastomers.
Their resilience has been exploited since anti-quity. A century and a half after Fauchard’s useof silk, the first elastomer, rubber, allowed theupgrade of simple ties to gradual movements.This started for rubber a career which was notchallenged for another century.
Returning from Columbus’ second voyage,Michele de Cuneo reported in 1495 the strangecustom “Indians” have to milk trees (latex meansmilk in Latin). In 1521, Hernando Cortes reportedthat Aztecs use this coagulated and dried milkto make balls for game and to waterproof textiles.In 1750, Francois Fresneau was the first to describethe tree which is now known as Hevea brasiliensis.The tree was called by the indigenes caa (tears)ochu (wood), i.e. the tree which sheds tears. Thisgave in French its current name, “caoutchouc”.Its name in English came from the famous scientistJoseph Priestley who described the material in1770 as “excellently adapted for wiping frompaper the marks of a black lead pencil”, in otherwords, a good ”rubber”. A similar product is guttapercha, extracted from another tree, Pallaquiumgutta, which grows in Southeast Asia.
The first attempt to commercialize the newmaterial were deterred because it softened whenheated and was partially soluble in water. It wasnot until 1839 when Charles Goodyearaccidentally discovered “sulfur cross-linking”that rubber became a substitute for the omnipresentplastics.
Soon, rubber became precious, and Brazil wasfast to monopolize it. Henry Wickhamsucceeded, however, in smuggling the nuts of thetree to England. Starting 1976, England developedlarge rubber plantations in Ceylon (Sri Lanka) andMalaya (Malaysia, Indonesia). An invention withimportant consequences was that of J Dunlopwho, in 1888, invented the pneumatic tires forbicycles. The extension of this idea by theburgeoning industry of automobiles made
chemists worldwide try to find a substitute forthis natural polymer of isoprene (C5H8)n. Successoccurred in 1910 when Karl Dietrich Harries, inGermany, polymerized with the help of sodium(Na), 2,3 dimethyl Butadiene. This rubbersubstitute, which received the name Buna, wasfollowed by the invention of Buna-S (S standingfor styrene) by K Ziegler in 1927. In the U S, asulfur-substituted elastomer was invented by J CPatrick in 1930, and produced under the nameThiokol. The next year, a chlorine-substituted one,invented by F J A Nieuwland and W H Carothers,was launched by Dupont Company under thename Duprene (name changed today toChloroprene or Neoprene).
Otto Bayer invented polyurethanes, inGermany, in 1937. While the latter may notrepresent a major category of elastomers for thegeneral use, these most interesting fororthodontics. In the recent years, polyurethaneshave become increasingly important due toadvances in telechelic polymers (from tele,distance, and chele, claw, in Greek). Thesepolymers (especially polyols) contain reactiveend groups which can be used to further increasetheir molecular weight (mw), or to generate othercopolymers with a wide range of properties.Usually, as the molecular weight). Increases, themore valuable are the polymers.
The above series of discoveries has led to adiminished share of consumption for naturalrubber (only 35% among all elastomers). Not onlythat the plantations in Southeast Asia are bothexpensive to maintain and subject to weatherconditions, but the substitutes prove to be betterand by far more versatile.
Use in Dentistry
While maxillofacial prostheses were described byAmbroise Pare’ (1517-1590), their massive usewas determined by the two world wars. While theelastomers used years ago were mainly vinylplastisols (plasticized polyvinyl chloride), todaypolyurethanes, as such or modified with acrylics,and silicone rubbers (HTV, high temperaturevulcanized) are preferred.
After minor uses of elastomer, in the makingof dams, cups, points, special filling materials(gutta percha), a major impact was prompted bythe spread of AIDS. This has led to a new

121Evolution of Orthodontic Appliances
assessment of the cross-infection procedures, inwhich gloves were essential. Their routine wearingduring treatment became mandatory in the U Sfollowing OSHA’s regulations and FDA’s alert ofMarch 1991.
Among the elastomeric impression materialsused in large amount are the polysulfides, the“addition” and “condensation” polysiloxanes,and the polyethers. All of these are identified bythe American Dental Association (Specification19) as “non-aqueous elastomeric dentalimpression materials”.
The advantage of these elastomers is relatedto their hydrophobicity, which renders them bothaccurace and physically and chemically stable.Polyethers are less water repellent and thereforeless dimensionally stable in the presence ofhumidity. This reflects also on theirbiocompatibility, since these are not inert and canlead to tissue irritations whenever the material isleft in the sulcus. Likewise, “condensation”polysiloxanes are less accurate due to reasonswhich we will examine later.
Uses in Orthodontics
In addition to the elastomers generally used indentistry, some particular uses anddevelopments are specific to orthodontics. Thus,while water-based alginates are used in dentistryfor study and record models, in orthodontics theseare the preferred impression materials. A similarcase is that of composites, which are used indentistry as restoratives, filling materials, onlaysand inlays, while in orthodontics, as adhesives.
Alginates the insoluble salts rather thanpolymers, alginates are of low cost, convenientand enough accurate for most orthodonticoperations. Their advantage resides in a gelstructure which can resume its shape when theimpression is made over undercuts. Succeedingthe agar-agar impression materials (colloidalsuspensions in water which can be reused),alginates is commonly classified as “irreversiblehydrocolloids”. Both before and after gelation,alginates are altered by heat and water: in waterpresence, these materials expand: in its absence,they contract (syneresis). As a result, alginate
impressions have a limited life, even if kept in“humidors”.
Elastics, elastomeric auxiliaries recalled by thefamous Case-Angle controversy (Angle attributedtheir first use to Baker, instead of Case), the firstuse of intermaxillary elastics has beendocumented to date as early as 1880. Initially usedto exert interarch forces, today elastics are used toclose spaces within the arches, hold archwires inbrackets and act as force-delivery systems forretraction, protraction, tipping, intrusion,extrusion and rotation.
Natural rubber, the first elastomer used forsuch purposes, has lost considerable ground inthe last years. Due to proprietary “secrets”, it isdifficult to make a correct estimate. The chemicalnature of the elastomers used is often withheld,as are some characteristics like the thermalbehavior (thermoset vs thermoplastic). At therecent A A O Annual convention in Denver, noneof the exhibitors selling gloves knew the materialthese were made of (the alternative was “latex” or“non-latex”).
Polyurethanes are now preferred due to theirsuperior properties such as biocompatibility, bettertensile and tear strength, and higher elasticitymodulus and abra-sion resistance than the bestnatural rubber. A review of their properties hasbeen recently published. Unfortunately, allelastomers lose 50 to 70 percent of their initialforce during their first day of application, and afterthree weeks, only 30 to 40 percent of it is left6. Tocompensate for this diminished force, strongerelastics have to be used. To prevent possibledamage, these are prestressed in advance to 50 to100 percent of their length. Unfortunately, thisleads to a lack of certitude when it comes to knowthe force applied.
Functional appliances used as early as 1902for Robins’ monobloc, Vulcanized rubber was forlong time the only material available for functionalappliances. Tooth positioners, bite planes, chincups, oral screens, wedges, cushions and elasticstraps can all be made of elastomers. As it will beshown, that some feels soft or hard is just a matterof cross-linking which is adjustable as needed.
13HHHiiissstttooorrryyy ooofffMMMooodddeeelll AAAnnnaaalllyyysssiiisss
� Carey’s Analysis
– Procedure
– Inference
� Pont’s Index
– Drawback of Pont’s Analysis
� Linderharth Index
� Korkhaus’ Analysis
� Howe’s Analysis—1954
– The Procedure
� Bolton’s Analysis
– Procedure
– Determination of Overall
Ratio
– Determination of Anterior
Ratio
� Cast Analysis: Symmetry and
Space
� Alignment (Crowding), Space
Analysis
– Principles of Space Analysis
� Arvey Peck, Sheldon Peck—
1972
� Huckaba’s Analysis
� Hixon and Old Father
Method—1958
� Marvin M Tanaka, Lystle E
Johnston in 1974
– Short Method—Tanaka-
Johnson
– Procedure in the Maxillary Arch
– Modifications
� Nance Analysis
– Procedure for Mandibular
Arch—1976
– Long Method
– Problems
� Total Space Analysis—1978
– Anterior Area
– Middle Area
– Posterior Area
� Wylie
– Commenting on Model
Analysis
� Kesling Model Analysis
� Martinek Analysis
– Comparative Analysis of
Howes, Rees, Kesling and
Strayer
� Suwannee Luppanapornlarp
� 3d Model Analysis
Orthodontic diagnosis and treatment planning isdone by taking into consideration the toothmaterial, skeletal and muscle balance and growthpotential. Among the various decisions taken, animportant decision is the one taken for or againstextraction of certain teeth to achieve the desiredresults. Model analysis is one of the essentialdiagnostic aids. Study models help us tovisualize the patient’s occlusion from all aspectsand also help us in making the necessarymeasurements of the teeth and the dental archesand basal bone. Most of the model analysissuggested by various authors does not correlatethe findings of model analysis with their
diagnostic aids such as cephalogram and OPGand hence diagnostic value of such independentmodel analysis is questionable.
Model analysis provides us with valuableinformation and when it is correlated with otherdiagnostic aids will help us in diagnosing andplanning treatment for a case. Among otherbenefits, model analysis provides a means ofevaluating the amount of space required forproper alignment of teeth; by allowing accurateassessment of Arch length—Tooth materialdiscrepancy. Various methods of model analysishave been described and appropriate analysismust be selected for a given case.

123History of Model Analysis
CAREY’S ANALYSIS
Arch length—Tooth material discrepancy is oneof the important causative factors ofmalocclusion. Carey’s analysis is aimed atdetermining the extent of the discrepancy.Carey’s analysis is performed on the mandibularcast. If the same analysis carried out on themaxillary arch, then it is called as Arch PerimeterAnalysis.
Procedure
1. Determination of arch length: The arch lengthanterior to the mandibular first molars ismeasured using a 0.012 inch soft round brasswire which adapted to the model of themandibular arch so that one end engaged firstpermanent lower near the marginal ridge.The wire is next passed over the buccal cuspsof the premolars, then over the normal cuspalposition of the cuspid, then over the anteriorteeth at ridge center and finally around thesame course on the opposite side, ending inthe mesiobuccal line angle of the lower firstpermanent molar of the other side. The wireis cut at this point and straightened, and thelength is recorded.� In case of proclined anteriors, the soft
round brass wire is passed along thecingulum of anterior teeth.
� In case of retroclined anteriors the softround brass wire is passed labial to theanterior teeth.
� In case of well aligned anterior teeth, thewire passes over the incisal edges of theanterior teeth.
2. Determination of arch width/tooth material:Tooth material is determined by measuringthe mesiodistal width of the teeth anterior tothe first permanent molars (incisors, caninesand premolars) at the maximum contourusing bow divider.
3. Determination of the discrepancy: Thediscrepancy refers to the difference betweenthe arch length and tooth material.
Inference
1. Non-extraction case: If the discrepancy is 2.5mm or less, it indicates minimal tooth
material excess, which can be managed byproximal stripping.
2. Extraction of second premolar: If the discrepancyis 2.5–5 mm. second premolar may need beextracted.
3. Extraction first Premolar: If the discrepancy ismore than 5 mm, then extraction of firstpremolar is advised.
PONT’S INDEX
Pont in 1909, proposed a method ofpredetermining the ideal arch width which hasbecome to be known as Pont’s index. However,he felt that the method of measuring teeth todetermine arch width was not the only factor toconsider in orthodontic treatment planning. Healso stressed the assessment of facial profile,determination of Angle classification,relationship of upper and lower jaws to oneanother and the midline as important essentialsto be considered.
Pont devised a method of predetermining an“ideal” arch width based on the mesiodistalwidth of the crowns of the maxillary incisors.Pont suggested that the ratio of combinedincisor to transverse arch width (as measuredfrom the center of the occlusal surface of theteeth) was ideally 0.8 in the bicuspid area and0.64 in the first molar area. He also suggestedthat the maxillary arch can be expanded 1 to 2mm more during treatment than the ideal toallow for relapse. In recent years there has beenan unfortunate revival of the use of the Pont’sindex in a most sloppy manner. Its only occlusalguide Researchers at the University ofWashington applied the pont’s index to patientswho had undergone complete orthodontictreatment and were out of retention for at least10 years. No permanent teeth had beenextracted in any of the patients. They found verypoor correlations between the combinedmaxillary incisor width and the ultimate archwidth in the bicuspid and molar areas, andconcluded that measuring the mesiodistal widthof incisors to predetermine maxillary bi-molarand inter bicuspid width is of no value.Mandibular arch form and mandibular inter-canine diameter have been repeatedly found tobe more reasonable treatment guides for bothmandibular and maxillary ultimate arch width

124 History of Orthodontics
than the Pont’s index. It’s of little use in rationaltreatment planning.
In an interesting prelude to the index itself, Pontnoted that the mesiodistal width of the maxillarycentral and lateral incisors could be used to predictthe mesiodistal width of the maxillary canines innormal dental arches. He sugested that half themesiodistal diameter of central plus the mesiodistaldiameter of lateral would generally, equal themesiodistal width of the canine. Pont did notindicate the size of the sample used to determinethe proposed index, but did state that they were ofFrench nationality only.
For each normal dental arch, he suggestedthat a constant relationship existed between thewidth of four upper anterior teeth and the widthof the dental arch in premolar and molar area.All his measurements and predictions wererelated to the maxillary arch and did not includean assessment of the mandibular arch.
Pont determined a constant ratio between1. The width of the four maxillary incisors2. The width of the maxillary arch as measured
from the center of the occlusal surface of thefirst premolars and first molars. In the idealdental arch he concluded that the ratio ofcombined incisors width to transverse archwidth was 0.8 in the premolar area and 0.64in the molar area.In orthodontic procedure Pont suggested that
the maxillary dental arch should be expandedone or two millimeters more than that found innormal occlusion to allow for relapse.
Drawback of Pont’s Analysis
JA Stifter in 1958, tested Pont’s analysis in idealand normal class I dentitions. Cases withslightly slipped contacts, minor rotations andinsignificant deviations from perfect occlusionwere used, but were considered in a groupseparately from ideal sample, a significantcorrelation existed between the combinedmaxillary incisors widths and the inter molarand inter premolar width. No correspondingcorrelation was found for normal group. Thesample consisted of French nationalities. HencePont’s index universal validity is questionableand analysis does not taken into considerationand the alignment of teeth.
Hotz in 1961, suggested that deviations fromPont’s index may be related to long and narrowly
shaped dental arches. He concluded that dueconsideration must be given to the shape of theskull in assessment of arch form and width.
LINDERHARTH INDEX
Linder Harth G in 1961, on a study on Rhinelandpopulation proposed index values of 85 and 64rather than Pont’s values of 80 and 64.
KORKHAUS’ ANALYSIS
Korkhaus used Linder Hart’s measurements andintroduced a third measurement from themidpoint of the inter premolar line of upper archto a point incision between the incisal edges ofupper central incisors. For a particular width ofincisors there is a specific value of the distancefrom the incision to the interpremolar lineaccording to Korkhaus.
If the perpendicular distance frominterpremolar line is more than ideal, then theanterior teeth are proclined, if it lesser than theideal then the teeth are retroclined.
HOWE’S ANALYSIS—1954
Howe devised a formula for determining whetherthe apical bases could accommodate the patient’steeth.
The Procedure
Tooth material (TM) equals the sum of themesiodistal width of the teeth from the firstpermanent molar forward. Premolar diameter(PMD) is the arch width measured at the top ofthe buccal cusps of the first premolars. Premolardiameter to tooth material ratio (PMD:TM) isobtained by dividing the premolar diameter bythe sum of the width of the 12 teeth.
Premolar basal arch width (PMBAW) isobtained by measuring, with the bowed end ofthe boley Gauge, the diameter of the apical baseon the casts at the apical of the first premolars.The ratio of the premolar basal arch width totooth material (PMBAW:TM) is obtained bydividing the premolar basal arch width by thesum of the width of the 12 teeth.
Basal arch length (BAL) is measured at themidline from the estimated anterior limits of theapical base to a perpendicular that is tangent tothe distal surface of 2nd molar. The ratio of BAL

125History of Model Analysis
to tooth material (BAL:TM) is obtained by dividingthe arch length by the sum of the width of the 12teeth.
Howe’s believed that the premolar, basal archwidth (he called it the canine fossa diameter)should equal approximately 44% of themesiodistal width of the 12 teeth in the maxillaif it is to be sufficiently large to accommodate allthe teeth. When the ratio between basal archwidth and tooth material is less than 37%.Howe’s considered that to be a basal archdeficiency necessitating extraction of premolars.If the premolar basal width is greater than thepremolar coronal arch width, expansion of thepremolars may be undertaken safely.
Since this method was introduced, rapidpalatal expansion has came into more commonuse and clinicians have more opportunity to alterthe apical base itself.
Howe’s analysis is useful in planningtreatment of problems with suspected apical basedeficiencies and dividing whether to 1) extractteeth 2) Widen the dental arch or 3) expandrapidly the palate.
Mandibular apical base distance is morecritical than that of maxillary. In the authorsopinion Howe’s analysis is more logical andsuperior to the pont’s Index because the Howe’sanalysis is applicable to each arch and has beenrepresented as an aid to thoughtful diagnosis andplanning while the Pont’s index is often used asa rigid rule and an illogical excuse for notextracting.
BOLTON’S ANALYSIS
Bolton’s analysis gives significance to tooth size.According to Bolton, there exists a ratio betweenthe mesiodistal widths of maxillary andmandibular teeth. Malocclusion occurs whenthere is disparity between the mesiodistaldimensions of maxillary and mandibular teeth.Bolton’s analysis helps in determiningdisproportion in size between maxillary andmandibular teeth.
Procedure
1. Sum of mandibular 12 teeth: The mesiodistalwidth of all the teeth mesial to the mandibular
second permanent molars are measured andsummed up.
2. Sum of maxillary 12 teeth: The mesiodistalwidth of all the teeth mesial to the maxillarysecond permanent molars are measured andsummed up.
3. Sum of mandibular 6 teeth (anteriors): Themesiodistal width of all the teeth mesial tothe mandibular first permanent premolarsare measured and summed up.
4. Sum of maxillary 6 teeth (anterior) : Themesiodistal width of all the teeth mesial tothe maxillary first permanent premolars thatis maxillary anteriors are measured andsummed up.
Determination of Overall Ratio
According to Bolton’s study, the sum ofmesiodistal width of the mandibular teethanterior to second permanent molars is 91.3% ofthe mesiodistal width of maxillary teeth anteriorto the second permanent molar.
Overall Ratio =Sum of mandibular 12 � 100
Sum of maxillary 12
Inferences
If the ratio is less than 91.3%, then it indicatesmaxillary tooth material excess.Amount of maxillary excess is determined by theformula,
Sum of maxillary 12Sum of mandibular 12 by 100
91.3=
×
If the ratio is more than 91.3%, then it indicatesmandibular tooth material excess.Amount of mandibular excess is determined bythe formula,
Sum of mandibular 12Sum of mandibular 12 91.3
100=
×
Determination of Anterior Ratio
According to Bolton’s study, the sum of mesio-distal widths of mandibular anteriors should be77.2% of the mesiodistal width of maxillaryanteriors. The anterior ratio is obtained by theformula,

126 History of Orthodontics
Anterior RatioSum of mandibular 6 100
Sum of maxillary 6=
×
Inferences
If the ratio is less than 77.2%, then it indicatesmaxillary tooth material excess.Amount of maxillary excess is determined by theformula,
Sum of maxillary 6Sum of mandibular 6 100
77.2=
×
If the ratio is more than 77.2%, then it indicatesmandibular tooth material excess.Amount of mandibular excess is determined bythe formula,
Sum of maxillary 6Sum of mandibular 6 77.2
100=
×
CAST ANALYSIS: SYMMETRY AND SPACE
An asymmetric position of an entire arch shouldhave been detected already in the facial/estheticexamination. An asymmetry of arch form alsomay be present even if the face looks asymmetric.
A transparent ruled grid placed over theupper dental arch and oriented to the palatalraphe can make it easier to see a distortion ofarch form. Asymmetry within dental arch, butwith symmetric arch form, also can occur. Itusually results either from lateral drift of incisoror from drift of posterior teeth unilaterally. Theruled grid also helps in seeing where drift of teethhas occurred. Lateral drift of incisors occursfrequently in patients with severe crowding,particularly if a primary canine was lostprematurely on one side. This often results inthe permanent canine being locked out of thearch while the other canine is nearly in its normalposition with all the incisors shifted laterally.Drift of posterior teeth is usually caused by earlyloss of a primary molar, but sometimes developseven when primary teeth were exfoliated on anormal schedule.
ALIGNMENT (CROWDING), SPACE ANALYSIS
It’s important to quantify the amount ofcrowding the arches, because treatment variesdepending in the severity of crowding. Space
analysis using the dental casts is required for thispurpose.
Principles of Space Analysis
Since malaligned and crowded teeth usually resultfrom lack of space, thus analysis is primarily ofspace within the arches. Space analysis requiresa comparison between the amounts of spacerequired to align them properly.� Analysis can be done either directly on the
dental casts or by computer after appropriatedigitization of the arch and tooth dimensions.
� Dental cast analysis is two dimensional.� If a computer method is preferred, it is easier
and more practical to use an office copyingmachine to obtain a 2-D usage of the occlusalview of the dental casts, then digitize from that.
� A readable and surprisingly accurate imagecan be obtained by simply placing the castson the center of the copying machine,avoiding the edges of its image area, wheredistortions often appear.
� Whether done manually or computerized, thefirst step in space analysis is calculation ofspace available. This is accomplished bymeasuring arch perimeter from the 1st molarto the other over the contact points ofposterior teeth and incisal edge of anteriors.
There are two ways to accomplish this.1. By dividing the dental arch into segments that
can be measured as straight line approxim-ations of the arch.
2. Or by contouring a piece of wire (or a curvedline on computerize screen) to the line ofocclusion and then straightening it out formeasurement. The 1st method is preferred formanual calculation because of its greaterreliability.Second step is to calculate the amount of
space required for alignment of teeth. This isdone by measuring the mesiodistal width of eachtooth from contact point to contact point and thensumming the width of the individual teeth. Ifthe sum of the widths of the permanent teeth isgreater than the amount of space available, thereis an arch perimeter space deficiency andcrowding would occur. If available space is largerthan the space required (excess space), gapsbetween some teeth would be expected.
127History of Model Analysis
Space analysis carried out in way is based ontwo important assumptions1. Anteroposterior of the incisors is correct. (i.e.
incisors are neither excessively protrusive norretrusive.
2. The space available will not change becauseof growth; neither assumption can be takenfor granted.
It must be remembered that incisor protrusion isrelatively common and that retrusion thoughuncommon, does occur. There is an interactionbetween crowding of tooth and protrusion ofretrusion.� If the incisors are positioned lingually, this
accentuates crowding but if the incisorsprotrude, the potential crowding will be atleast partially alleviated.
� If there is not enough room to properly alignthe teeth, the result can be crowding,protrusion or some contribution of the two.For this reason, information about how muchthe incisors protrude must be available fromclinical examination to evaluate the results ofspace analysis.
The second assumption, that space available willnot change during growth is valid for adults butmay not be for children. In a child with a wellproportioned face, there is little or no tendencyfor the dentition to the displaced relative to thejaw during growth, but the teeth often shiftanteriorly or posteriorly in a child with a jawdiscrepancy. For this reason, space analysis is lessaccurate and less useful for children with skeletalproblems (Class II, Class III, long and short face)than in those with good facial proportions.
Even in children with well proportionedfaces, the position of the permanent molarschanges when primarly molars are replaced bypremolars. If space analysis is done in the mixeddentition it is necessary to adjust the spaceavailable measurement to reflect the shift inmolar position that can be anticipated.
ARVEY PECK, SHELDON PECK—1972
It has been shown that naturally well alignedmandibular incisors possess distinctive dimensionalcharacteristics; these teeth are significantly smallermesiodistally and significantly larger facial-lingually when compared with average populationtooth dimensions.
The primary sources of facio lingual tooth sizedata for the incisors have been skeletal materialand extracted teeth and not plaster casts.
The index proposed for clinical orthodonticsutilizes an MD/FL ratio. It’s constructed in thefollowing manner.
MD crown diameter in mmIndex = × 100
FL crown diameter in mm
Mandibular incisors of two groups of youngfemale Caucasian adults from North easternregion, i.e. Boston were studied.� One group was designated as group with
perfect mandibular incisors alignment, whilethe other was designated as the “Controlpopulation group”. The members of bothsample were all within same age range(17-27 years).
� For each subject in both groups, themaximum mesiodistal (MD) crown diameterand the maximum FL crown diameter weremeasured directly in the mouth. Themandibular central incisors of the group withperfect alignment has a mean MD/FL indexof 88.4 with a SD of 4.3
� The mandibular lateral incisors of the groupswith perfect alignment had a mean MD/FLindex of 90.4 with a standard deviation of 4.8.
� Take the lower incisor measurements in asequence beginning with the four MDmeasurements, right lateral incisor to left lateralincisor followed by four FL measurements,left lateral incisor to left lateral incisor.
� Male-female differences in MD/FL indicesfor the mandibular incisors appear to thebelow clinical significance.
HUCKABA’S ANALYSIS
� It uses both study casts and radiographs fordetermining the width of unerupted tooth.
� It is necessary to compensate for enlargementof radiographic image. This can be done bymeasuring an object than can be seen both inradiograph and on the cast. A simple propor-tional relationship can then be established asfollows;
Actual width of primary molar (X1)
Apparent width of primaryyy molars (X2)=

128 History of Orthodontics
Actual width of unerupted premolar (Y1)
Apparent width of unnnerupted premolar (Y2)
OR Y 1X1 Y1
X2=
×
This can be used for both arch groups.
HIXON AND OLD FATHER METHOD—1958
They examined the dental casts and periapicalradiographs of 41 children in the mixed dentitionand the casts of the same children takenfollowing the eruption of canines and premolars.Utilizing a 16 inch target film distance they founda weak correlation between the mesiodistalwidths of the primary and permanent teeth. Thecorrelation coefficient between the sum of thewidths of mandibular permanent incisors andthat of mandibular permanent canines andpremolars measured on the casts, was similar toreported by other authors. The strongestcorrelation was between, on the one hand, thesum of the width of the central and lateralincisors in one quadrants, measured on the castsadded to the sum of the width of the twopremolars in the same quadrant, measured onradiographs and on the other, the sum of thewidth of the canines and premolars after theireruption. From these results the authors deviseda table for prediction of mesiodistal width ofunerupted canines and premolars.
MARVIN M TANAKA, LYSTLE E JOHNSTON
IN 1974
Dental casts of 506 orthodontic patients inCleveland area were obtained from theOrthodontic Department of Case WesternReserve University School of Dentistry. To beincluded in the study, patients had to be ofprobable European ancestry and less than 20years old.
Short Method—Tanaka-Johnson
A shorter but less precise method has beendeveloped which is of merit, but does not allowfor sexual dimorphism with equal accuracy.a. Add the width of the mandibular incisors and
divide by two.b. To the value obtained add 10.5 mm to predict
the combined widths of mandibular cuspidand bicuspids and 11.0 mm to predict the
combined width of the maxillary cuspid andbicuspids.
c. Compute the amount of spee to left in the archfor molar adjustment by subtracting theestimated cuspid and bicuspid size from themeasured space available in the arch afteralignment of the incisors. Record these valuesfor each side. From all the values nowrecorded, a complete assessment of the spacesituation in the mandible is possible.
Procedure in the Maxillary Arch
The procedure is similar to that for the lowerarch, with two exceptions: 1) A differentprobability chart is used for predicting the uppercuspid and bicuspid sum. 2) Allowance must bemade for overjet correction when measuring thespace to be occupied by the aligned incisors.Remember width of the lower incisors is used topredict upper cuspid and bicuspid widths.
It is good practice to study the radiographswhen mixed dentition analysis is done in orderto note absence of permanent teeth, unusualmalpositions of development, or abnormalitiesof crown form. For example, mandibular 2nd
premolars sometimes have two lingual cusps,when they are so formed, the crown is larger thanmight be expected from the probability chart;therefore a higher predicator value is used.
Modifications
A technique for mixed dental analysis thatcompensates nicely for radiographicenlargement of tooth images in periapical filmsis available. Its based on the assumption thatthe degree of magnification for a primary toothwill be the same as that for its underlyingpermanent successor on the same film.1. Measure the width of the primary tooth on
the X-ray film (Y1) and the width of itsunderlying permanent successors (X1) on theX-ray film.
2. Measure the primary tooth (Y) directly in themouth or on the dental cast. The width ofthe unerupted permanent totoh (X) can thenbe calculated by simple mathematicalproportion
X : X1 = Y : Y1 or X = X1Y / Y1
X/X1 = Y/Y1
X = X1Y/ Y1

129History of Model Analysis
Inaccuracy in radiographic tooth sizemeasurements is not dentist fault. It occursbecause the developing tooth are not alwaysplaced exactly at right angles to the central ray,therefore, the radiographic image of the tooth,when slightly rotated or tipped, is significantlylarger than the actual size of the tooth.
Ballard and Wylie 1947, conducted aninvestigation to evaluate the assumption thatthere is harmony in tooth size in any oneindividual that is, if the incisors are larger thanaverage, the canines and premolars and molarsare also correspondingly larger than average.
They examined the casts of 441 individualswho had permanent incisors, canines, premolarsand 1st molars fully erupted.
They developed a predictive formula.X = 9.41 + 0.527Y andWhich X = sum of mesiodistal width of
canines and premolars and Y = Sum ofmesiodistal width of mandibular incisors.
NANCE ANALYSIS
Determined the space available in the archfor unerrupted canines and premolars bymeasuring the mesiodistal width of primarymolars and canine as dental casts, and determinedthe space required by measuring the mesiodistalwidth of the unerupted teeth on radiographs.He claimed that this assessment was accurate inmost cases. He also measured total arch lengthfrom mesial surface of one permanent first molarto the other and showed that, in transition frommixed to permanent dentition, molar movemesially on average 1.7 m in lower arch and 0.9m in upper arch.Clinical judgment:� It’s not time consuming� It requires no special equipment or
radiographic projections� Although best done an dental casts, it can be
done with reasonable accuracy in the mouth.� It may be used for both dental arches.Mixed Dentition Analysis have been misused inseveral ways:1. They have been applied mechanically
without proper regard for biologic dynamicsof a critical stage is dentitional development.
2. Naive assumptions have been made (e.g. Auniversal 1.7 mm late mesial shaft).
3. Many have presumed than to have anaccuracy that is not present in any of themethods yet developed.
None of Mixed Dentition Analysis are as preciseas one might like, and all must be used withjudgment and knowledge of development.
Mandibular incisors have been chosen formeasuring since they are erupted into the mouthearly in the mixed dentition, easily measuredaccurately and are directly in the midst of mostspace management problems.
Maxillary incisors are not used in any of thepredictive procedures, since they show too muchvariability in size and their correlations withother groups of teeth are of lower predictivevalue. Therefore, the lower incisors are measuredto predict the size of upper as well as lowerposterior teeth.
Procedure for Mandibular Arch—1976
1. Measure with tooth measuring gauge, thegreatest mesiodistal width of each of the fourmandibular incisors and record the values inmixed dentition analysis form.
2. Determine the amount of space needed foralignment of the incisors. Set the Boley gaugeto a value equal to the sum of the width ofthe left central incisors and left lateral incisors.Place the point of the gauge at the midline ofthe alveolar crest between the central incisorsand set the other point along the line of thedental arch on the left side. Mark on the toothor the cast the precise point where the distalsurface of the lateral incisors will be whenaligned. Repeat this on the right side of thearch. If the cephalometric evaluations showthe mandibular incisors to be too far labially,the Boley guage tip is placed at the midlinebut moved lingually a significant amount tosimulate the expected uprighting of theincisors as dictated by the cephalometricevaluation.
3. Compute the amount of space available afterincisor alignment. To do this, measure thedistance from the point marked in the line ofthe arch. To the mesial surface of the firstpermanent molar. This distance is the spaceavailable for the cuspid and 2 bicuspids andfor any necessary molar adjustment after the

130 History of Orthodontics
incisors have been aligned. Record data forboth sides.
4. Predict the size of the combined widths of themandibular cuspid and bicuspids.
Long Method
Experienced clinicians may choose to use the 50%prediction since it is a more precise estimate.Those who are inexperienced or without the useof cephalometrics and a precision appliancemethod would do well to proceed moreconservatively (i.e. use 75% level of prediction).
Prediction of the combined width of cuspid,first bicuspid and second bicuspid is done by useof probability charts.
The tables used herein are based on sizevariations and relationships in teeth. NorthAmerican whites and may or may not be validfor other ethnic groups.
Problems
A problem arises when considering the space leftfor molar adjustment. If this value in the chart isnegative, that is, the predicted sizes of 3, 4, and 5are greater than the space left after the alignmentof the incisors, then crowding will occur in thearch even without any forward molar adjustmentwhen the first permanent molars are in an endto end relationship (i.e. a flush terminal plane ofthe second primary molars, approximately 3.5mm of space (one half a cusp width) is requiredto convert to a class I molars relationship. Thisneeded 3.5 mm might be acquired, withoutorthodontic intervention, in any of three ways1. 3.5 mm more late mesial shift of the
mandibular first permanent molar than themaxillary.
2. At least 3.5 mm more forward growth of themandible than the maxilla.
3. Some combination of dental adjustment anddifferential skeletal growth. Since we cannotyet predict accurately the amongst ofdifferential skeletal growth that will occur,treatment planning must be based on dentaladjustment factors. If differential skeletalgrowth occurs during this period, in themolar relationship will result and the mixeddentition analysis prediction must be alteredaccordingly. When there is class I molarrelationships in mixed dentition, no part of
the arch perimeter need to be prevented formolar adjustment and all the space can bemade available for incisors, cuspids andbicuspids.Perhaps the most severe termination of mixed
dentition analyzes is their inability to reflect theposition of the incisors with respect to the skeletalprofile. There are a number of crude rules ofthumb for determining how much archperimeter deduction occurs for each degree ormillimeter the incisor edge is changed in thecephalometric visualization of treatment. Forexample, one degree of tipping or 1 mm of lingualdisplacement of the mandibular incisal edge issaid to be equal to 1 mm of arch shortening oneach side.
TOTAL SPACE ANALYSIS—1978
This analysis is developed by Levern Merrifield.This method has divided the lower dental archinto 3 areas. Anterior middle and posterior toanalyze the space requirement in the lower arch.Measurement from study casts and cephalogramsare used in this analysis
Anterior Area
Space Required
� Measure width of mandibular incisors on themodels and width of canine from radiographs.
� Cephalometric correction for incisor positionis calculated according to Tweeds method.FMIA is taken into consideration. The incisorsare then repositioned and the difference is theactual and proposed FMIA is determined.The difference in angulations is multiplied by0.8 mm to get difference in multi meters.
� Soft tissue modification: Upper lip is measuredfrom vermilion border of upper lip to greatestcurvature of labial surface of central incisor.The total chin thickness is measured from softtissue chin point to NB Line.
� If lip thickness is greater than chin thicknessthe difference is determined and multipliedby 2 and added to the space required. If lessno modification is necessary.
� Measure Z angle of Merrifield and add thecephalometric correction to it. If correctedangle is greater than 80°, the mandibularincisor angulations is modified is necessary.

131History of Model Analysis
If the correlate angle is less than 75° additionaluprighting of mandibular incisor is necessary.
Space Available
Measure space availability by using brass wirefrom mesiobuccal line angle of first primarymolar of one side to another.
Middle Area
Space Required
� Measure mesiodistal width of first premolaras the cast and measure width of theunerupted premolar from the radiographs.
� Curve of occlusion: A flat object is placed onthe occlusal surface of mandibular teethcontaining the incisors and first molar. Thedeepest position between the flat surface ismeasured and occlusal surface of primarymolars was measured on both side.
Depth on right side + depth of left side + 0.5 mm
2 mm
Space Available
Using brass wire measure from mesiobuccal lineangle of first primary molar to the distal buccalline angle of first permanent molar on either side.
Posterior Area
Space Required
a. Mesiodistal width of II and III molars isobtained from radiographs as they might beunerupted. If not visible Wheelers method isused for calculation
X = Y-X1/Y1X = Estimated width of 3rd molarY = Actual size if premolar 1 mandibular molarX’ = Wheelers value for 3 molars.Y’ = Wheelers value for 1 molars.
Space Available
Amount of space available consists of spacepresently available on casts and estimatedincrease.a. Space presently available; obtained by
measuring the distance on occlusal plane todistal surface of I molar to anterior border oframus on lateral cephalogram
b. Estimated increase: The increase is 3 mm peryear, i.e. 1.5 on either side until 14 years ofage in girls and 16 years in boys.
Total space deficit: This is arrived by comparingthe space required and space available inanterior, middle and posterior. Thus we canknow where the discrepancy is present.
WYLIE
Commenting on Model Analysis
In the year 1959, Commenting on model analysismethods point out “first of all, it is next toimpossible to measure bone dimension fromeven the best plaster cast.”Teeth, yes with greataccuracy. But no one can arrive a reliable ratiowithout measuring the both componentsaccurately. As a matter of fact, only the procedureof Howe’s Pretends to measure anything buttooth-size and between teeth. Second, one oversimplifies the problem when he Presumes thatcrowding can be analyzed completely. When heknows the size of teeth basal bone. But admitsthat we cannot ignore the abundant Empiricalevidence that such procedures work, becausethrough trial and error, we have discovered thedimensions which we should accept as timingfactor.
KESLING MODEL ANALYSIS
In the year 1945, he reported his analysis. Keslinggave a method of analysis, which was so-called“diagnostic setup”. Aim of this analysis is todetermine the needs of reducing tooth material.
MARTINEK ANALYSIS
Comparative Analysis of Howes, Rees,
Kesling and Strayer
Martinek, in the year 1957, presented aninteresting paper on comparing the analysis ofHowes, Rees, Kesling, Strayer on five treatedcases.
SUWANNEE LUPPANAPORNLARP
In the year 1993, Suwannee luppanapornlarp,studied the long-term comparative effects ofpremolar extraction in clear-cut extraction andnon extraction class-2 patients. He concluded thatpremolar extraction produced a significantlygreater reduction in hard and soft tissue protrusion

132 History of Orthodontics
both treatments produced the mandibular mesialdisplacement—extraction significantly more thannon-extraction. However, at recall the two groupsdid not differ with respect to signs and symptomsof dysfunction.
3D MODEL ANALYSIS
In the current age, where today’s technologicalbarrier is tomorrow’s technological breakthrough,we are continuously reinventing industries,manufacturing and design practices and findinginnovative applications of new technological
breakthroughs for tried and true practices. Thefirst time 3D modeling technologies were appliedto the dental industry was in 1987 by Dr Mormann.The 3D modeling technology, at this point andtime, allowed Dr Mormann to revolutionize thereconstructive dental industry. Over the years,as 3D modeling technologies improved, theapplication became ever more revolutionary. Hereis a partial list of currently available treatmentsdesigned with the aid of 3D modeling software:Bending ART system Invisalign® treatment,Suresmile process Orthocad, E-models, etc.
133History of Cephalometrics
14HHHiiissstttooorrryyy ooofff
CCCeeeppphhhaaalllooommmeeetttrrriiicccsss
� History Prior to the Advent of
Radiography
– Classifying Physiques
– Measurements and
Proportions
– Renaissance to the
Twentieth Century
- Leonardo da Vinci
- Albrecht Durer
- Spigel
- Pieter Camper
- Deschamps
- Johann Friedrich
Blumenbach
- Anders Retzius
- Thomas Huxley
- Broca
- Paul Topinard
- Ihering
� Cephalometric Radiography
– Wilhelm Conrad Roentgen
– Wilhem Koening and Dr Otto
Walkhoff
– Van Loon
– AJPacini and Carrera
– Atkinson
– Simpson
– Dewey and Riesner
� Holly B Broadbent’s
Contribution
– Paul Simon
– Charles Bingham Bolton
� Other Important Contributions
– Allan G Brodie
– Thompson and Brodie
– Margolis
– Wylie
� Cephalometric Analysis
� Evolution of Cephalometrics
� Patient Orientation
� X-ray Source Position
� Film Position and Enlargement
� Posteroanterior (Frontal)
Cephalometry
– Down’s Analysis
– Steiner Analysis
– Tweed’s Triangle
– Wit’s Appraisal
Ever since God created man in his image, manhas been trying to change man into his image.Attempts to change facial appearance arerecounted throughout recorded history. Thequestion of what is a normal face, as that of whatconstitutes beauty, will probably never beanswered in a free society.
Orthodontists, in their attempts to changefacio-orodental deviations from accepted norms,have adopted cephalometric measurement, amethod long employed in physical anthropology.With the introduction of roentgenography, it wasinevitable that this procedure should be employedas a medium for the purpose of roentgenographiccephalometrics. Cephalometric radiography wasintroduced into orthodontics during the 1930s.
Cephalometry had its beginning incraniometry. Craniometry is defined in theEdinburgh encyclopedia of 1813 as “the art ofmeasuring skulls of animals so as to discover theirspecific differences”. For many years, anatomistsand anthropologists were confined to measuringcraniofacial dimensions using the skull of deadindividuals. Although precise measurementswere possible, craniometry has the disadvantagefor growth studies.
Cephalometry is concerned with measuringthe head inclusive of soft tissues, be it living ordead. However, this procedure had its limitationsowing to the inaccuracies that resulted fromhaving to measure the skulls through varyingthickness of soft tissues.

134 History of Orthodontics
With the discovery of X-rays by Roentgen in1895, radiographic cephalometry came intobeing. It was defined as the measurement of headfrom bony and soft tissue landmarks on theradiographic image (Krogman and Sassouni 1957).This approach combines the advantages ofcraniometry and anthropometry. The disadv-antage is that it produces two-dimensional imageof a three-dimensional structure.
HISTORY PRIOR TO THE ADVENT OF
RADIOGRAPHY
Classifying Physiques
History prior to the advent of radiographyshould begin with the mention of attempt of thescientists to classify the human physiques. In 500BC, the Greek physician and Father of medicine,Hippocrates, designated two physical types —habitus phithicus with a long thin body subject totuberculosis, and habitus applecticus— a shortthick individual susceptible to vascular diseasesand apoplexy. The search was continued byAristotle, Galen (200 AD) and Rostan (1828).Rostan was the first to include muscle mass as acomponent of physique. Viola’s (1909)morphological index recognizes threemorphological types. Kretschmer (1921) adheredto the three Greek terms: the pyknic (compact),aesthetic (without strength), and athletic.Kretshmer also included dysplastic physiquewhich was taken up by Sheldon again in 1940.
The long historic thread extended into thetwentieth century when Sheldon introduced hismethod of somatotyping, based on threecomponents of physiques, each rated on a sevenpoint scale and expressed as a three digit numbercalled somatotype. It also included a rating ofdysplasia in the five regions of the body.“Dysplasia is literally bad shape or form. Insomatotyping, it refers to disharmony or unevendistribution of a component or components indifferent parts of the body,” according to Carterand Heath.
Moreover their definition of a somatotypequantifies relative fatness or endomorphy, relativemusculoskeletal robustness or mesomorphy andrelative linearity or ectomorphy. The somatotypethen stands as a “measuring of overall appraisalof body shape and composition, an anthropologicalidentification tag and a useful description ofhuman physique.”
Sheldon’s temperamental components,viscerotonia, somatotonia, and cerebrotonia,convey behavioral traits commonly associatedwith physique. With a seven-point scale for eachsomatotype component, there is a widedistribution in the dense midrange around the4-4-4 type; a close relation between somatotypeand temperament becomes tenuous.Nonetheless, common knowledge suffices torecognize dominant behavioral trait in manyinstances, and that information can be revealingabout the people in general. It may also give someclues relating to the orthodontic treatment byproviding an insight to the character of thepatients—their expectations concerning thetreatment’s contribution to their well being, eventheir understanding and willingness to accept thediscipline of cooperation needed for successfulconclusion of therapy.
Measurements and Proportions
Early History—the Canons
Portrayal of human form demands not onlyartistic talent and technical ability but alsodisciplined and consistent style. To ensure thesestipulations when images of royalty and deitywere commissioned and executed, the ancientEgyptians developed an intricate quantitativesystem that defined the proportions of the humanbody. It became known as the Canon. The theoryof proportions according to Panofsky is a systemof establishing the mathematical relationsbetween the various members of the livingcreature, in particular of the human being. Themathematical relation can be expressed by thedivision of a whole as well as by themultiplication of the unit; the effort to determinethem could be guided by the desire for beauty aswell as interest in the norms, or finally by theneed for establishing a convention.
Initially the canons were enclosed in a gridsystem of equalized squares with 18 horizontallines, line 18 drawn through hairline. Later it wasincluded in a grid system of 22 horizontal lines,line 21 drawn through the upper eyelid.
After the outline of the human figure, wasdrafted on papyrus leaves the iconographicnorms or canon, served to insert the figure into anetwork of equal squares. The image could betransferred to any required size by first drawinga coordinate system to proper size; into this

135History of Cephalometrics
system the image can then be drawn readily andaccurately for displaying in a tomb or on a wall.This procedure is still universally used to enlargeor reduce any kind of illustration.
Indian econometric studied extensively byRuelius, was transmitted through sanskritliterature and extensively reviewed in Indiantexts of architecture. The proportional canons ofthat system were already detailed in oldersources and did not materially change with time.Face height was used as the module of both theSariputra and Alekhyalakshana proportionalsystem, which closely reflected the naturalrelation of the parts of the body with each other.The Sariputra system, dated 1200 AD are knownfor the sculptures honoring the God Buddha.
Renaissance to the Twentieth Century
Fifteenth century saw the advent of specificmeasurements being made to compare thefeatures of different skulls and heads. Leonardoda vinci (1452–1519 AD) was probably one ofthe earliest people of note to apply the theory ofhead measurement to good effect in practice.
He used a variety of lines related to specificstructures in the head to assist in his study of thehuman form. His drawings included a study offacial proportions in natural head position.According to the notes, the profile was dividedinto seven parts by eight horizontal lines.Subdivision is made with vertical lines. In hisstudy of horse and horse men, he used a schemeof facial measurement within a grid system withfive horizontal and six vertical lines and thesubject in natural head position. The joining ofthe lower lip and the chin and the tip of the jawand the upper tip of the ear with the temple formsa perfect square; and each face is half a head.
Albrecht Durer (1471–1528 AC) was abrilliant, unusually productive and an exuberantartist of great virtuosity. He published a treatisein 1528 on cranial measurements whichcomprised “Vier Bucher von menschlicherProportion” dealing with the proper proportionof human form in the first two books, theproportions according to mathematical rules inthird book, the human figure in motion in thefourth book. Durer’s four books mark a climax,which the theory of proportions had neverreached before or was to reach ever after.
Using strictly geometrical methods, heprovided a proportionate analysis of theleptoprosopic (long) face and euryprosopic(broad) face in coordinate system, where thehorizontal and the vertical lines were drawnthrough the same landmarks or facial features.His drawings attest continuous efforts to definevariations in the facial morphology. One of thisis significant as the key to cephalometric analysis.In the difference between the retroclined and theproclined, facial profile is shown by a change ofangle between the vertical and the horizontalaxes of a rectangular coordinate system tocharacterize the facial configuration of eachsubject.
Sixteenth century saw the first truly scientificattempt in cranial measurement and theintroduction by Spigel (1578–1625 AD) of the“lineae cephalometricae” . Spigel’s linearcephalometricae consisted of four lines: the facial,occipital, frontal and sincipital lines. Hedescribed these lines as follows:� Facial: from the most inferior point of the chin
to the most superior point on the forehead.� Occipital: from the crown of the head to the
atlas.� Frontal: from one temple to the other.� Sincipital: from the lowest part of the ear, in
the region of the mastoid process, to thehighest part of the sinciput, sinciput being theanterior part of the head or skull fromforehead to the crown.According to him, in a well proportioned
skull, these lines should all be equal.The Dutchman Pieter Camper (1722–1789
AD) was credited with the introduction of facialangle and for famous publication “Dissertationsur les varietes naturelles de la physionomie”which appeared posthumously in 1791. The keyto his methodology was to orient crania in space,horizontal from the middle of the porusacusticus to a point below the nose. Camper’shorizontal became the reference line for theangular measurements used to characterizeevolutionary trends in studies of facialmorphology and aging.
The facial angle as he described, was formedby the intersection of a facial line and a horizontalplane. The facial line was a line tangential to themost prominent part of the frontal bone and tothe slight convexity anterior to the upper teeth.

136 History of Orthodontics
The horizontal plane passes through the lowerpart of the nasal aperture, backwards along theline of the zygomatic arch and through the centerof the external auditory meatus.
Camper’s facial angle was readily acceptedas standard measurement in craniology. Theterms prognathic and orthognathic introducedby Retzius are tied to Camper’s illustrations offacial form in man and primates. As a result, theangle between a horizontal line and the line fromnasion to prosthion became the time-honoredanthropological method to determine the facialtype. The term prognathism refers to theprominence of the face or jaws, relative to theforehead, and a straight facial profile becamelabeled as orthognathous.
The drawbacks of Camper’s facial angle were:� It ignores the contribution made by the lower
jaw to facial forms.� He did not adhere strictly to his location of
posterior reference point for the horizontalplane.
� The direct comparison of skull of differentages was not possible because the locatingpoint might alter in position relevant to otherbony structures with advancing age.Shortly after this, Deschamps (1740–1824
AD) introduced the cephalic triangle made upof facial, occipital, and coronal angles. The facialangle was the lesser angle formed by theintersection of a horizontal line that passes fromthe external auditory meatus to the base of thenose, which crossed a profile line. This is similarto Camper’s facial angle. Fortunately, the use ofexternal auditory meatus as a reference pointenabled a rough comparison to be made betweendifferent skulls.
In the same period as Camper, there was aFrench man, Daubenton who was veryconcerned with the relative position of theforamen magnum in man and lower animals. Hemade use of new angles, including the occipitalangle to make measurements. Although hismeasurements were not very reliable, a similarangle was later used by another craniologist,Pierre Broca.
Daubenton’s occipital angle is formed by twolines, the first line passes along the level ofopening of the foramen magnum, from the initialedge of the foramen along the surface of theoccipital condyles and anteriorly for short
distance. The second line passes from the posteriormargin of the foramen magnum to the tip of thenasal spine. Broca’s occipital angle was formedby two different lines giving alternative angles,originating from the posterior and anteriormargins of the foramen magnum and passinganteriorly through the junction of frontal and nasalbones. The magnitude of occipital angle decreasesas the habitual posture of the animal tend moretowards upright.
An antagonist of Camper, Johann FriedrichBlumenbach (1752–1840 AD) rejected themethod of lines and angles as a test of nationalcharacteristics and proposed a minute survey ofthe skull particularly the frontal and maxillarybones. In 1795, he described a method ofpositioning the cranium which has to bemeasured in a standard reproducible manner.His method was simple, consisting of resting theskull on its base and looking down verticallyupon its vault. The points to be noted were, theprojection of the maxilla anterior to the frontalarch, the direction, of the jaws and cheek bones(outward, forward, etc.) and the proportionalbreadth or narrowness of the head.
Anders Retzius (1796–1860 AD) correlatedthe two schemes, i.e. of Camper and Blumenbach,thereby providing a basis for the methods ofcraniology used today. He is also credited withthe introduction of cephalic index, the ratio ofbreadth to length of the skull expressed as apercentage.
Nineteenth century produced three greatmen in the history of craniology: Huxley, Brocaand Topinard.
Thomas Huxley (1825–1895 AD) wrote in1876, “the so-called facial angle, in the fact, doesnot simply express the development of jaws inrelation to face, but is the product of two factors,facial and cranial, which vary independently. Theface remaining the same, prognathism may beindefinitely increased or diminished, by rotationof the frontal region of the skull, backward orforward, upon the anterior end of the basicranialaxes”. He also introduced two new angles, thesphenomaxillary and spheno- ethmoidal angles.He preferred the spheno- maxillary angle toCamper’s angle when comparing the degree ofprognathism in different skulls. This angle isformed by the two lines drawn from basion andprosthion to prosphenion. The other angle,

137History of Cephalometrics
sphenoethmoidal tends to be less than 180° inman.
Broca (1824–1880 AD) who is the founder ofthe Paris society of anthropology believed thatthe great variability of the cranial formconstituted a principal difficulty for thecraniologist. He was the first craniologist toinstitute a precise and accurate technique whichcould be used to compare crania so that it wasmade possible to discriminate between thevariation in racial types among human skulls.He introduced a base line “plan alveolo-condylien” which passes through the alveolarpoint and tangential to the inferior surfaces ofthe two occipital condyles. He also developed acraniostat, mainly constructed of wood forpositioning the skull.
It was generally accepted at this time that theangles were best determined on projecteddrawings of the skull. Broca devised a simplemethod to trace the outline of the skull on to apiece of paper by fixing the skull in the craniostatand positioning a drawing board with paperattached to it parallel to the midsagittal plane anda pencil held in a frame perpendicular to thepaper. The resultant tracing was equivalent to atracing of the peripheral, as depicted on a lateralskull radiograph.
Paul Topinard (1830–1912 AD) used a similarcraniostat with some additional modifications.Topinard wrote in 1890 “the craniometersubstitutes the mathematical data for theuncertain data founded on judgment andopinion. Moreover it studies the skeleton of theensemble, the cranium and the face separatelyand each of the plates as well”.
During nineteenth century, the need forstandardization of methods used in craniometrybecame an important issue and since then, manybodies have met to better define those points andplanes in use. The most important meeting as faras the dental profession is concerned was heldin Frankfurt-am-Main in August 1882. This wasthe 13th General congress of the germananthropological society and it is to this congressthat the Frankfurt horizontal plane owes itsname.
Earlier in 1859, a horizontal plane followingthe zygomatic arches was suggested by a Russiancraniologist, Von Baer. Later, the plane wasdefined more precisely as line drawn from the
center of each auditory meatus to the lower pointon the inferior margin of each orbit by VonIhering (1850–1930). The Frankfurt agreementmodified Von Ihering’s definition such that theplane passes through the upper border of thebony meatus vertically above their centers.However, the reproducibility of this plane on anintact skull is less than Broca’s condyloalveolarplane. Subsequent to the agreement, thedefinition of the horizontal plane has beenaltered so that it is now taken as passing throughthe right and left porion and left orbitale.Thereby, reducing the problems incurred byasymmetrical skulls.
CEPHALOMETRIC RADIOGRAPHY
In 1895, Professor Wilhelm Conrad Roentgenmade a remarkable contribution in the field ofscience with the discovery of x-rays. On December28, 1895, he submitted a paper “On a new kindof rays, A Preliminary Communication” to theWurzburg Physical Medical Society for publicationin its journal.
Professor Wilhem Koening and Dr OttoWalkhoff simultaneously made the first dentalradiograph in 1896. It was clear that the use ofX-rays provided the means of obtaining adifferent perspective on the arrangement andrelation of bones, thus expanding the horizonsof craniometry and cephalometry.
The evolution of cephalometry in thetwentieth century is universally linked toEdward Hartlay Angle’s publication of hisclassification of malocclusion. But the dogmaticinferences of the new school were criticized forfailing to include differential diagnosis of facialprofile in patients with class III and class IImalocclusion.
Van Loon was probably the first to introducecephalometry to orthodontics, when he appliedanthropometric procedures in analyzing facialgrowth by making plaster casts of face into whichhe inserted oriented casts of the dentition.Hellman used cephalometric techniques anddescribed their value beginning with 1920s.
The first X-ray picture of skull in the standardlateral view was taken by AJ Pacini and Carrerain 1922. Pacini received a research award fromthe American Roentgen Ray Society for a thesisentitled “Roentgen ray anthropometry of theskull”. Pacini introduced a teleroentgenographic

138 History of Orthodontics
technique for standardized lateral headradiography and thereby opened a way, whichproved to become a tremendous advance incephalometry, as well as in measuring thegrowth and development of face. His method,which was rather primitive, involved a largefixed distance from the X-ray source to thecassette. The head of the subject, placed adjacentto a standard holding the cassette, wasimmobilized with a gauze bandage wrappedaround both the face and the cassette after thepatient’s midsagittal plane was carefully orientedparallel to the cassette.
He identified the following anthropometriclandmarks on the roentgenogram: gonion,pogonion, nasion, and anterior nasal spine. Healso located the center of the sella turcica andthe external auditory meatus. He measured thegonion angle and the degree of maxillaryprotrusion.
Atkinson in 1922 advocated the use ofroentgenograms in locating the ‘key ridge’ and thesoft tissue relations to the face and jaws. In 1923McCowen reported on profile roentgenograms thathe used for orthodontic purposes to visualize therelationship between the hard and soft tissues andto note the changes in profile which occur duringtreatment.
Simpson presented a method for obtainingprofile roentgenograms in 1923 before AmericanSociety of Orthodontists. In 1927, Ralph Waldronof Newark, NJ made mention of measuring thegonion angle from a roentgenogram taken at 90o
to the facial profile. Waldron was the first toconstruct a cephalometer, which differed littlefrom those used today.
In 1928, Dewey and Riesner published anarticle, “A Radiographic study of facialdeformity”. Dewey and Riesner immobilized thepatients head in a head clamp and placed thecassette against the patient’s face. They tookprofile roentgenograms by aligning the eye to earplane by a right angle leveling technique. Theyused a target distance of three feet.
In 1931, the methodology of cephalometricradiography came into full function when BHolly Broadbent in USA and H Hofrath inGermany simultaneously published methods toobtain standardized head radiographs in theangle orthodontist (A new X-ray technique andits application to orthodontia) and inFortschritte der Orthodontie, respectively.
This development enabled orthodontists tocapture the field of cephalometry from theanatomists and anthropologists who hadmonopolized craniometric studies, particularlyin nineteenth century.
HOLLY B BROADBENT’S CONTRIBUTION
Broadbent’s interest in craniofacial growth beganwith his orthodontic education under E H Anglein 1920. He continued to pursue that interestalong with his orthodontic practice, workingwith a leading anatomist J Wingate Todd.
The idea of diagnosing dental deformities bymeans of planes and angles was first proposedin 1922 by Paul Simon of Germany in his book,“Fundamental principles of a systematic
diagnosis of dental anomalies”. Although his“Law of the canines” was later disproved byBroadbent, his theories stimulated the latter toapply the principles of craniometry to livingsubjects.
The uncertainty of locating landmarks in theskull of the living child by approaching throughskin and soft tissues led him to search for a meansof recording craniometric landmarks on theliving child accurately as done with a craniostatin measuring the dead skull.
During 1920’s, Broadbent refined thecraniostat into craniometer by the addition ofmetric scales. This proved to be the first step inthe evolution of craniostat into a radiographiccephalostat. It did not take him much longer toconvert the direct measuring instrument into aradiographic craniometer.
Meanwhile, the course of Broadbent’sorthodontic practice corrected the malocclusionof Charles Bingham Bolton, son of Chester andFrancis P Bolton. His discussions of facial growthwith Congress woman, Bolton led to the additionof Bolton study of facial growth to the long listof Bolton philanthropies. As Charles grew toadulthood, this study became a major personalas well as financial commitment.
Cephalometrics was neither developed as atechnique looking for an application nor was itdeveloped as a diagnostic tool. Broadbent’s singlegoal was the study of craniofacial growth. TheBroadbent’s technique for cephalometricradiography was one of the tools which hedeveloped for the implementation of that study.
139History of Cephalometrics
The technique and apparatus perfected for theBolton fund study of the normal developmentalgrowth of the face, eliminated practically all ofthe technical difficulties encountered in previousmethods of recording dentofacial changes, andproved to be a convenient as well as scientificmethod of measuring orthodontic procedures.
According to Broadbent, the patient’s headwas centered in the cephalostat with the superiorborders of the external auditory meatus restingon the upper parts the two ear rods. The lowestpoint on the inferior bony border of the left orbit,indicated by the orbital marker, was at the levelof the upper parts of the ear rods. The nose clampwas fixed at the root of the nose to support theupper part of the face. The focus film distancewas set at five feet (152.4 cm) and the subject filmdistance could be measured to calculate imagemagnification. With the two X-ray tubes at rightangles to each other in the same horizontal plane,two images (lateral and posteroanterior) couldbe simultaneously produced.
Germany’s Hofrath’s technique differed fromBroadbent’s technique in this way of the centralray was not fixed in relation to the head and noplan was suggested for super-positioningsubsequent X-rays.
OTHER IMPORTANT CONTRIBUTIONS
In 1937, using serial records of twins; Broadbentshowed how growth or its lack was the greatestlimiting factor in clinical success. In 1943, hestipulated that, eruption of the third molars hadno ill effect on the denture, particularly the lowerincisors.� In 1938, Allan G Brodie at the University of
Illinois presented a cephalometric appraisalof orthodontic results:1. The use of elastic causes a disturbance in
the Bolton plane-occlusal plane angle;2. Axial inclinations of orthodontically-
moved teeth tend to return to theiroriginal inclinations.
3. Bone changes during treatment arerestricted to the alveolar process.
� Brodie, in a landmark study (1941) used forhis PhD in anatomy, corroboratedBroadbent’s contention that the growthpattern of the normal child’s face developsin an orderly fashion downward and forward
and the pattern once attained at an early age,did not change.
� Thompson and Brodie (1942) in a report onthe rest position of the mandible, concludedthat:1. Morphogenetic pattern of the head was
established ata early age and did notchange,
2. Presence or absence of teeth has little bearingon the rest position of the mandible and
3. Vertical facial proportions are constantthroughout life.
Margolis (1943) wrote on the relationshipbetween the inclination of the lower incisor andthe incisor-mandibular plane angle and was thefirst to corroborate Tweed’s clinical observationthat, in normal occlusions, the lower incisors are90° to the mandibular basal bone.
In 1947, Wylie produced a method ofassessing anteroposterior dysplasias and thatsame year, Margolis contributed his maxillo-facial triangle.
CEPHALOMETRIC ANALYSIS
The major use of radiographic cephalometry is incharacterizing the patient’s dental and skeletalrelationships. This led to the development of anumber of cephalometric analyzes to compare apatient to his or her peers, using populationstandards. William B Downs (Fig. 14.1 ) in 1948
Fig. 14.1: William B Downs (1899–1996)
140 History of Orthodontics
developed the first cephalometric analysis. Itssignificance was that, it presented an objectivemethod of portraying many factors underlyingmalocclusion and there could be a variety ofcauses of malocclusion exclusive to teeth. Thiswas followed by another analyzes by Cecil CSteiner (1953), CH Tweed (1953) , RM Ricketts(1958), V Sassouni (1969), HD Enlow (1969), JRJaraback (1970), Alex Jacobson (1975), etc.
EVOLUTION OF CEPHALOMETRICS
The thoroughness of Broadbent’s approach to thedesign of the cephalometric method is evidentfrom the fact that the basic technique hassurvived almost unchanged for over seventyyears.
In about two decades time, the instrumen-tation had evolved to a form more suitable forthe individual practitioner through thepioneering efforts of Margolis (Fig. 14.2), Higleyand others.
PATIENT ORIENTATION
The ears were established as the basis fororientation and fixation in the beam axis.Frankfurt plane was adopted for horizontalorientation with nasion for stabilization. TheFrankfort horizontal plane (FHP) was chosenbecause this was approximate the natural headposition (NHP). But the FHP also had itsdrawbacks and those were:1. Some individuals show a variation of their
FHP to the true horizontal to an extent of ±10°.
2. The landmarks to locate the FH plane, orbitaleand porion, especially the latter, are difficultto identify on a cephalogram.An alternative to overcome this problem was
to use a functionally derived NHP. According toMorrees and Kean, it was obtained by askingthe subject to look at the image of their eyes inthe mirror located at eye level. A frame ofreference was originally intended as a reliableprocedure for orienting facial profiles so that,same orientation could be established ondifferent occasion by different investigators.Although the functionally derived NHP wasmore accurate, its reproducibility was less thanFHP (anatomic approximation of NHP). Lateraland posteroanterior views perpendicular to eachother in the horizontal plane were specified forthree-dimensional analyses.
Bjork’s studies of facial prognathismillustrated the unreliability of intracranialreference lines in cephalograms.
Kroagman and Sassouni (1957) conducted anexhaustive survey of roentgenographiccephalometry in which the FHP (Frankforthorizontal plane) coincided with the physiologicor true horizontal.
Sassouni made an attempt to standardize theorientation of cephalograms by means of anoptical plane advocated in 1862 by Broca, whostated that “when a man is standing and whenhis visual axis is horizontal, his head is in naturalposition”.
X-RAY SOURCE POSITION
The X-ray source is positioned five feet (152.4 cm)from the subject’s midsagittal plane. A changeto 150 cm has been adopted by some as aconveniently round metric number, but thedifference is negligible. A major improvementin lateral cephalostats is, the capability of takinglateral and posteroanterior views with a singleX-ray source instead of two.
FILM POSITION AND ENLARGEMENT
The other significant change from the originaltechnique is adjustability of film position. Theoriginal cephalostat was based on the design ofthe anthropometric craniometer and cassettes wereattached to these mechanisms. The disadvantage
Fig. 14.2: Herbert I Margolis (1900–1984)

141History of Cephalometrics
of this very efficient mechanical design is that itmakes cassette position and resultant enlargementdepended on head size. Evaluation of serialchanges by direct superimposition is madeunreliable by this variable enlargement.
The relative immunity of angularmeasurements to enlargement distortions ledmany researchers to opt for angular over linearvalues whenever possible. Also newer instrumentshave been developed that can over come thisdrawback of variable enlargement by providingindependent adjustments for head holdingmechanisms and cassette.
POSTEROANTERIOR (FRONTAL)
CEPHALOMETRY
Since the introduction of a standardized methodfor obtaining skull radiographs, cephalometricshas become one of the major diagnostic tools inorthodontics. The posteroanterior cephalogramcontains diagnostic information not readilyavailable from other sources. This informationallows the practitioner to evaluate the width andangulation of the dental arches in relation to theirosseous bases in the transverse plane; evaluatethe width and transverse positions of the maxillaand mandible, evaluate the relative verticaldimensions of bilateral osseous and dentalstructures; assess nasal cavity width, and analyzevertical and/or transverse facial asymmetries.
Malocclusions and dentofacial deformitiesconstitute three-dimensional conditions orpathologies. Although all orthodontic patientsdeserve an equally comprehensive threedimensional diagnostic examinations,assessment of posteroanterior cephalometricviews are of particular importance in cases of:1. Dentoalveolar and facial asymmetries2. Dental and skeletal cross bites3. Functional mandibular displacements.
The same equipment that is used for thelateral cephalometric projections is utilized. Theinitial unit described by Broadbent consisted ofa set up in which two X-ray sources with twocassettes were simultaneously used, so thatlateral and frontal cephalograms were taken atthe same time. Although precise-three-dimensional evaluations are possible using thistechnique, it has now been almost abandoned
since it requires rather large equipment with twoX-ray sources.
Modern equipment uses one X-ray source.Therefore, following lateral cephalometricregistration, the patient must be repositioned ifa posteroanterior cephalogram has to beproduced. A head holder or cephalostat that canbe rotated 90° is used, so that the central X-raybeam penetrates the skull of the patient in aposteroanterior direction and bisects thetransmeatal axis perpendicularly. Maintainingthe identical horizontal orientation from lateralto the posteroanterior projection is critical whencomparative measurements are made on eachother (Moyers et al, 1988).
In using natural head position for postero-anterior cephalometric registrations, somepractical problems are encountered. The patient’shead is facing the cassette; which makes itdifficult for the patient to look into a mirror toregister natural head position (Solow andTallgren, 1977). Furthermore, space problemsmake it impossible to place a nose piece in frontof nasion to establish support in a vertical plane.
For better evaluation of patients withcraniofacial anomalies that require specialattention to the upper face, the patient headshould be positioned with the tip of the nose andforehead lightly touching the cassette holder.(Chierci, 1981)
In cases of suspected significant mandibulardisplacement, the posteroanterior cephalogramshould be taken with the mouth of the patientslightly open in order to differentiate betweenfunctional mandibular displacements anddentoskeletal facial asymmetry (Faber, 1985). Asfar as exposure conditions and considerations areconsidered, more exposure is needed for postero-anterior cephalograms than lateral views (Enlow,1982).
Cephalometric radiography, which came intowidespread use after the Second World War,enabled orthodontist to measure the changes intooth and jaw positions produced by growth andtreatment. Among other findings, these radiog-raphs revealed that many class II and Class IIImalocclusions resulted from faulty jaw relation-ships, not just malposed teeth. By the use of cephal-ometrics, it was also possible to see that jaw growthcould be altered by orthodontic treatment.

142 History of Orthodontics
According to Salzmann, cephalometricradiograph can show following features;1. Show dimensional relationship of the
craniofacial components.2. Reveal manifestations of growth and
developmental abnormalities.3. Helps in treatment planning.4. Helps in diagnosing the patient, especially of
skeletal origin.5. Helps in evaluating the dentofacial growth
changes during and after the orthodontictreatment.The goal of cephalometric analysis is to
estimate the relationship, in all three planes thatis in anteroposterior, vertical and transverserelationship of the jaws to the cranial base andto other, the relationship of the teeth to theirsupporting bone, and the effect of the teeth onthe profile.
In the 16th century, artists Durer and Da Vincisketched a series of human faces with straightlines joining homologous anatomic structures.Variations in these lines highlighted the structuraldifference among the faces. These facialproportions were basically an artist’s attempt,with beauty and harmony as the guidingprinciples, to quantify the basic structures of thehuman face.
Much later, the anthropologists invented aninstrument—the craniostat, which helped inorienting dry skulls and facilitating standardizedmeasurement. This improved the art ofcomparisons as the instrument improvedreproducibility but this also did not allow thestudy of skulls of living humans. The discoveryof the X-rays in 1895 by Sir William ConradRoentgen, proved to be a boon in this direction.
Orthodontic diagnosis and treatmentplanning for growth children must involvegrowth prediction. The pubertal growth spurt isconsidered to be an advantageous period forcertain types of orthodontic treatment andshould be taken into account together withorthodontic treatment planning.
Because of the wide individual variation inthe timing of the pubertal growth spurt,chronological age is an unreliable guide forassessment of children development status.Other parameters such as, growth velocity,secondary sex changes, dental development and
skeletal ossification, have proven to be moreaccurate.
The standard method to evaluate skeletalmaturity has been the use of hand-wristradiographs, matching the overall pattern of thesubject’s maturation to a set of reference patterns,available in an atlas. Skeletal maturation isgenerally determined by evaluating either thestage of ossification of bones of the hand andwrist, due to the large number of different typesof bones available in these areas, or theossification onset of the ulnar sesamoid.However, to avoid taking additional radiographs,the cervical vertebrae, as seen on routine lateralcephalograms, have been used to determine theskeletal maturity.
It is well known that the lateral view ofcervical vertebral bodies change with growth. In1972, Lamparski stated that the cervicalvertebrae were as statistically and clinicallyreliable in assessing skeletal age as the hand-wristtechnique. In recent years, evaluation of cervicalvertebrae has been increasingly used todetermine skeletal maturation. Several authorshave reported a high correlation between cervicalvertebrae maturation and skeletal maturation ofthe hand-wrist. It has been found that cervicalvertebrae could offer an alternative method forassessing maturity without the need of hand-wrist radiographs. However, cervical vertebraewere used to evaluate growth in a subjectivemanner because the method consisted of aqualitative comparison between the patientradiographs and the images contained in theatlas.
Mito et al (2002) established a new methodfor objectively evaluating skeletal maturation oncephalometric radiographs. A regression formulawas determined to obtain cervical vertebral boneage based on ratios of measurements of the thirdand fourth cervical vertebral bodies. However,the population used to derive the formulaconsisted of Japanese girls only.
The study of facial form as revealed in theanalysis of lateral skull radiographs. In additionto clinical examination, analysis of a lateralcephalogram permits a more detailed evaluationof facial and dentoskeletal structures to aiddiagnosis and treatment planning, especially incases with a skeletal discrepancy. Also provides
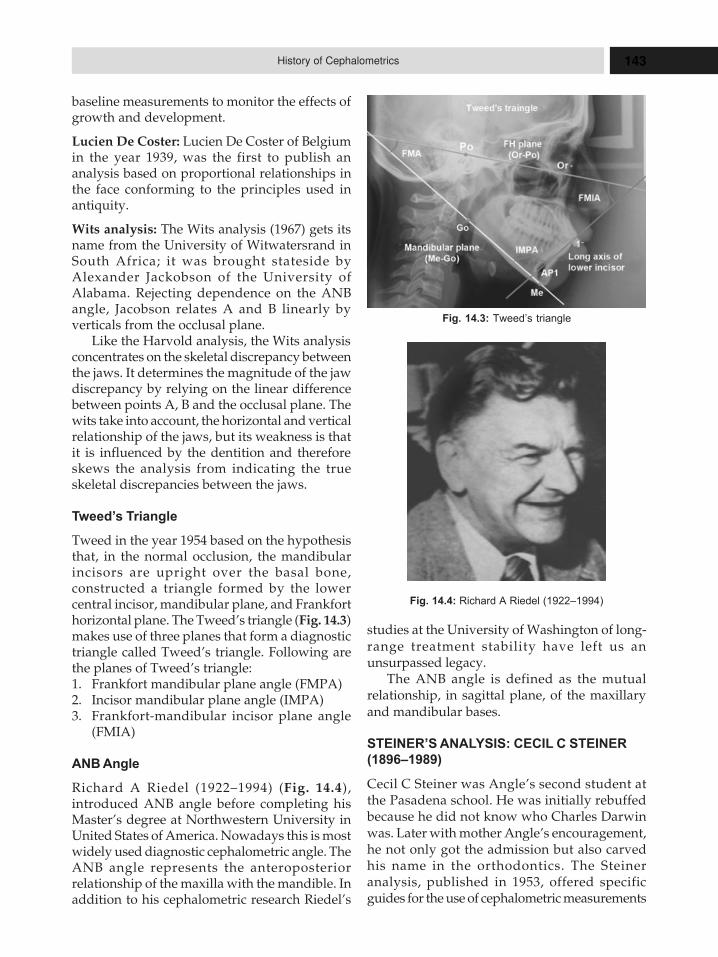
143History of Cephalometrics
baseline measurements to monitor the effects ofgrowth and development.
Lucien De Coster: Lucien De Coster of Belgiumin the year 1939, was the first to publish ananalysis based on proportional relationships inthe face conforming to the principles used inantiquity.
Wits analysis: The Wits analysis (1967) gets itsname from the University of Witwatersrand inSouth Africa; it was brought stateside byAlexander Jackobson of the University ofAlabama. Rejecting dependence on the ANBangle, Jacobson relates A and B linearly byverticals from the occlusal plane.
Like the Harvold analysis, the Wits analysisconcentrates on the skeletal discrepancy betweenthe jaws. It determines the magnitude of the jawdiscrepancy by relying on the linear differencebetween points A, B and the occlusal plane. Thewits take into account, the horizontal and verticalrelationship of the jaws, but its weakness is thatit is influenced by the dentition and thereforeskews the analysis from indicating the trueskeletal discrepancies between the jaws.
Tweed’s Triangle
Tweed in the year 1954 based on the hypothesisthat, in the normal occlusion, the mandibularincisors are upright over the basal bone,constructed a triangle formed by the lowercentral incisor, mandibular plane, and Frankforthorizontal plane. The Tweed’s triangle (Fig. 14.3)makes use of three planes that form a diagnostictriangle called Tweed’s triangle. Following arethe planes of Tweed’s triangle:1. Frankfort mandibular plane angle (FMPA)2. Incisor mandibular plane angle (IMPA)3. Frankfort-mandibular incisor plane angle
(FMIA)
ANB Angle
Richard A Riedel (1922–1994) (Fig. 14.4),introduced ANB angle before completing hisMaster’s degree at Northwestern University inUnited States of America. Nowadays this is mostwidely used diagnostic cephalometric angle. TheANB angle represents the anteroposteriorrelationship of the maxilla with the mandible. Inaddition to his cephalometric research Riedel’s
Fig. 14.3: Tweed’s triangle
Fig. 14.4: Richard A Riedel (1922–1994)
studies at the University of Washington of long-range treatment stability have left us anunsurpassed legacy.
The ANB angle is defined as the mutualrelationship, in sagittal plane, of the maxillaryand mandibular bases.
STEINER’S ANALYSIS: CECIL C STEINER
(1896–1989)
Cecil C Steiner was Angle’s second student atthe Pasadena school. He was initially rebuffedbecause he did not know who Charles Darwinwas. Later with mother Angle’s encouragement,he not only got the admission but also carvedhis name in the orthodontics. The Steineranalysis, published in 1953, offered specificguides for the use of cephalometric measurements

144 History of Orthodontics
in treatment planning, based on whatcompromised incisor positions would benecessary to achieve normal occlusion when theANB angle was not ideal. It I also incorporatedarch length and other considerations, such as theprofile, enabling even the neophyte orthodontist
to determine, for example, if extractions werenecessary. Through this step-by step approach,the Steiner analysis has been instrumental in“popularizing“ cephalometrics. At one time,southern California was known cephalomtricallyas Steiner Territory”.
145History of Extraction in Orthodontics
15HHHiiissstttooorrryyy ooofff EEExxxtttrrraaaccctttiiiooonnn iiinnnOOOrrrttthhhooodddooonnntttiiicccsss
� Arch-Length Analyses
� Second Premolar Extraction
� Evolution of the Philosophy of
Extraction in Conjunction with
Orthodontic Therapy
– Case or Angle Controversy
� Need for Extraction
� Choice of Teeth for Extraction
� Serial Extraction
� Historieal Perspective
– Dewel’s Method 1978
– Tweed’s Method (1966)
– Nance Method
– Grewe’s Method
Extraction of one or more teeth is sometimesnecessary to establish normal functionalocclusion, especially when jaws are not largeenough to accommodate all the teeth. Toothextraction may also be needed to correct theanteroposterior dental arch relationships. Thespace gained by extraction is utilized to relievecrowding or to retract the proclined anteriors.
The decision of extraction should always bebased on sound judgment, taking patient’s age,development and amount of space needed fortooth alignment into consideration. The decisionto opt for extraction should be made only aftercareful clinical evaluation, cephalometric andmodel analysis to assess the need and outcome ofsuch extraction. First premolars are mostfrequently extracted as a part of orthodontictreatment followed by the second premolars.Injudicious extractions may lead to undesirableconsequences such as arch collapse, deep overbite,spacing and tissue damage.
By the 1930s, the relatively common extractionpractices of the late 19th century, dictated largelyby technique limitations, had given way toAngle’s non-extraction dogma. Although a moretempered position continued to be held by Caseand others, the word “extraction” had becomeall but unmentionable. Thus, when it wasmentioned in the literature, it was frequently
described euphemistically as “reduction in thetotal number of dental units”. According toLischer, “The extraction of one or morepermanent teeth to facilitate an orthodontictreatment dates back at least to Fauchard (1728),and has been resorted to ever since. . . . Thenarrow, orthodox view that extraction of a toothis never justified is being discarded. . . . The profileof a growing child must never be regarded as afixed line, but one in which further changes willcontinue to take place.” As early as 1920, GeorgeW Grieve (1870–1950, Angle School, 1907; Fig.15.1), considered the dean of Canadianorthodontists, recommended the removal ofpermanent teeth. However, the increase inextractions that took place in the mid-1940s wasdue, in large part, to the influence of CharlesTweed, whose teachings had become widelyaccepted. He advocated positioning themandibular incisors upright over basal bone(approximately 90° to the mandibular planeangle) and argued that expansion of dental unitsoff this bone led to instability. Extractions in thepermanent dentition rapidly became the mostcommon treatment strategy for the correction ofClass I and II malocclusions, and, as Allan Brodieruefully remarked, “soon the air was filled withbicuspids”. The prevalence of extractions soaredfrom a modest 30% in 1953 to 76% in 1968.
146 History of Orthodontics
Tweed did not extract indiscriminately, but, intoo many patients, practitioners looked on theremoval of 4 premolars as the easy way out of anarch-length problem. Conservative leaders,although acknowledging that extraction had itsplace, were reluctant to endorse it publicly, outof fear that it would lead to abuses. Brodie, whobecame Angle’s torchbearer, said, “If I say it’sOK to extract, the first thing you know,everybody’s going to be extracting instead ofmaking a proper diagnosis. Doctor Angle toldme that and it’s true”.
By the 1980s, the pendulum had swung backtoward non-extraction as orthodontists beganusing new appliances and technologies toincrease arch length and width, making it easierto treat crowded dentitions without extractions.Several other factors were responsible for thisshift, including some negative ones.� Relapses (including the return of rotations
and overbite) and the reopening of extractionspaces.
� Gingival depressions at extraction sites.� The finding that extraction is no guarantee
of stability.� Flattened lips—”aged” look. The general
public often prefers fuller and more
prominent lips. Abraham Goldstein studiedpatients 21 years after retention and found thatnon-extraction patients looked better.� Lack of incisor prominence.� Narrowed maxillary arch.� Desire to avoid extended treatment.� The increased fear of malpractice
litigation. In the 1980s, claims were madethat temporomandibular disorderproblems could be attributed to theremoval of maxillary premolars. But therewere also some positive factors.
� Increased use of extraoral traction andfunctional appliances to take advantageof growth.
� More arch length gained by the use ofbonded brackets.
� Better understanding of retention.� Reproximation (e.g. air-rotor stripping,
“slenderizing”).� Increased use of removable appliances
(which rely mainly on a full complementof teeth).
� Revival of “arch development”14 (lateralexpansion, rotation or distalization ofmolars, and controlled proclination ofmandibular incisors). By 1993, theprevalence of extraction had returned to1950s levels (28%). Proffit and Fieldsbelieve that nonextraction is once againbeing carried to an extreme.
ARCH-LENGTH ANALYSES
In the 1950s, to a considerable extent a result ofSilas J Kloehn’s (1902–85, Fig. 15.2) revival ofcervical traction and Nance’s arch-length analysis,there was increased interest in mixed-dentitiontreatment and serial extraction. Perceiving a needfor improvement in mixed-dentition tooth-sizemeasurement, Hixon and Oldfather in 1958developed an analysis based on the widths of themandibular permanent incisors and the X-raymeasurements of the unerupted canines andpremolars, using a 16-in cone. This contributionproved to be the most popular of its kind to date;however, it was later revised because it was learnedthat this analysis often under predicted the widthsof unerupted teeth. Moyers’ analysis (1973), basedon linear regression equations and the widths ofthe mandibular incisors, achieved widespread
Fig. 15.1: George W Grieve

147History of Extraction in Orthodontics
clinical acceptance because of its simplicity andease of application. Offering insight into why someocclusions did not “fit”, Wayne Bolton devisedan analysis based on average measurements todetermine tooth-size discrepancies between themaxillary and mandibular arches. This analysismade it possible to determine whether themaxillary or the mandibular teeth (commonly,the 6 anterior teeth) have deficient or excessivemesiodistal diameters. His analysis immediatelybecame a standard part of the complete diagnosticanalysis of malocclusion, although, in 2000, Smithet al, examining the validity of Bolton’s ratios forvarious ethnic groups, concluded that the ratiosapply only to white women and should not beused arbitrarily for white men, Hispanics, or blacks.Peck and Peck, believing that tooth shape (ratherthan tooth width) might be a factor in determiningwhether crowding of the mandibular incisorswould occur, devised an index based on the ratiobetween the mesiodistal and faciolingual widths.With this and Bolton’s ratios, it became possibleto determine the need for re-proximation. In
extreme cases, a mandibular incisor might requireextraction.
SECOND PREMOLAR EXTRACTION
A borderline patient presents the dilemma ofextracting first premolars when the amount ofcrowding does not warrant the 14 or 15 mm perarch thus gained, or the alternative of non-extraction, which might be equally undesirablefor reasons of esthetics or stability. The idea ofextracting teeth other than the first premolarsmust have occurred to early clinicians, and somemight very well have done so. Surely, many hadto deal with congenitally missing secondpremolars. But it was well into the 20th centurybefore it is mentioned the literature. One of thefirst authors to spell it out was Clarence W (Clu)Carey (1904–2003, Fig. 15.3). Carey was aninnovator whose many contributions toorthodontics include laminated arches, the Bi-Potoothbrush, and the tooth-size dental calculator.He was nevertheless more cautious when headvocated (1947) extracting 4 second premolarsif the discrepancy is more than 2.5 mm and if theoperator is willing to accept a compromisedresult. In 1949, Nance spoke of removing thesecond rather than the first premolars to keepthe incisors over basal bone. Perhaps the mostdefinitive description of second-premolarextraction procedures during those years waswritten by B F (Tod) Dewel (1902–99, Fig. 15.4 ),who emphasized that closure of extraction spacesrequires “a delicate balance . . . between anterioranchorage and posterior resistance”. Hereminded us that “extraction of second premolarsdecreases by 2 teeth the resistance the buccalsegments present when the spaces are beingclosed”. In 1964, Ricketts (1920–2003) advocatedplacing the mandibular incisors within 1standard deviation of the Point A-pogonionplane. That same year, Schoppe suggested that adiscrepancy of 7.5 mm or less should be thecriterion for considering second premolarremoval, if there is no need for incisor retraction.He offered these advantages for the option:� Permits more rapid mesial movement of
molars.� Permits less lingual movement of incisors.� Is probably the best means of gaining space
when a minimum of space is necessary.
Fig. 15.2: Silas J Kloehn
148 History of Orthodontics
� Tends to alter the profile less.� Tends to hasten closure of the extraction
space.Reminiscent of Tweed’s “100 cases”, Logan
showed 100 case records of patients treated withsecond premolar extractions at the 1970 annualPacific Coast Society of Orthodontists’ meeting.In a 1973 article, he listed these advantages ofsecond-premolar extraction, over and abovethose proffered by Schoppe.� Eliminates problems of rotated, tipped, or
late-erupting second premolars.� Facilitates closure of anterior open bite by
reducing posterior vertical dimension.� Eliminates need to bond mandibular second
premolars, which are less-than-idealcandidates for bonding.
� Gains additional space for second and thirdmolars.
� Makes it easier to control rotations, axialinclinations, and anterior torque.
� Requires less Class II elastic force andheadgear.
� Produces fewer end-to-end bites because ofthe comparative widths of maxillary andmandibular premolars.
� Maintains the maxillary first premolar, whichis usually stronger than the second premolar.
EVOLUTION OF THE PHILOSOPHY OF
EXTRACTION IN CONJUNCTION WITH
ORTHODONTIC THERAPY
The role of extractions in orthodontic treatmenthas been a matter of controversy for years.Although John Hunter recognized the role ofextraction as early as 1771 in his book Naturalhistory of the teeth, it was not until mid 20th centurythat extraction of teeth in conjunction withorthodontic therapy became more acceptable.
Case-Angle Controversy
Originally, Calvin Case (Fig. 15.5) was a genuineadmirer of Angle. He advocated the Anglesystem at every turn and hoped to place thissystem before the dental profession. In fact, hegave up the general practice of dentistry becauseof Angle’s influence. The discord started over theclaim that Angle attributed the origin of the useof inter-maxillary elastics to Baker, while Case
Fig. 15.3: Clarence W (Clu) Carey
Fig. 15.4: BF Dewel

149History of Extraction in Orthodontics
thought that he should have received that credit.In fact, when Angle described this procedure, henever mentioned Case. This led to charges andcounter charges between them in 1903. Case’sclaim was that in 1890 he started this procedureand reported it at the Chicago Dental Society andalso at the Columbian Dental Congress in 1893.
The second point of contention was—and isthe one usually remembered—the question of theextraction of certain teeth as a means oftreatment. Angle’s thesis was that “there shallbe a full complement of teeth, and that each toothshall be made to occupy its normal position”.Case defended the discreet use of extraction as apractical procedure, while Angle believed in non-extraction. However, the unexpected result ofthis controversy was that it convinced generalpractitioners that they should not attemptorthodontic treatment but should refer patientsto the specialist.
The extraction story was continued into 1911with Martin Dewey (1881–1933) (Fig. 15.6) anardent champion of non-extraction. Deweyserved as professor of Orthodontics at KansasCity Dental School, the University of Iowa Dental
Fig. 15.5: Calvin Case Fig. 15.6: Martin Dewey
Department, the Chicago Dental College, and theNew York College of dentistry. He gained a widereputation as an outstanding teacher. He hadstarted his own graduate school in orthodonticsin 1911 as the Kansas City School of Orthodontiaand continued it as he traveled from one city toanother, ending in New York City with his deathin 1933. His influence was much felt since he wasthe editor of the International Journal ofOrthodontia for 17 years and also the presidentof the American Dental Association in 1931.
The climax of this conflict was a debate in1911 at the annual meeting of the National DentalAssociation (former name of the ADA). Bitternessand animosity were rampant. It took many yearsafter this episode for the problem to become amatter of calm and objective evaluation andrespectful appreciation of various points of view,each of which has made its contribution toorthodontics.
The first decade of the twentieth century wasan era of the manufacture of standardizedappliances. These appliances were made as setsof various kinds mounted on cards and sold bydental supply companies. By the use of a few
150 History of Orthodontics
simple soldering techniques, the dentist couldmake a required “fitting”, as it was called.
William J Brady (Iowa City) advertised as aconsulting specialist in orthodontia:
Advice by mail upon regulating cases of allkinds. Appliances fitted to models with fullinstructions for handling from beginning to end.Instructions: send good models of both upperand lower, with thin wax bite. Give age and sex.Pack carefully. After examination, an estimateof the cost of instructions of appliance will besubmitted free of charge. If satisfactory, remit theamount by bank draft or money order.
George C Ainsworth patented a regulatingappliance that used vertical tubes and theprinciple of the loop wire in 1904.Varney Barnespatented the so-called Barnes posterior tubeconsisting of a soldered band that held severalteeth together, with vertical tubing applying rootpressure to individual teeth.
Many innovative ideas and procedures wereintroduced. Victor H Jackson (1850–1929) wasexperienced in mechanics and devised a speciallydesigned appliance known as the Jackson crib,which incorporated the use of an auxiliary spring(finger) as an aid in tooth movement. His appliancewas one of the first “systems” of treatment toinfluence the development of modernorthodontics. Jackson published Orthodontia andOrthopaedia of the Face in 1904. In it, he claimedthat with his method a large number of patientscould be cared for as contrasted to the highlysophisticated techniques in vogue at the time thatlimited the number of patients.
Another contribution was reintroduction ofthe maxillary suture opening by Herbert APullen (1874–1938) in 1902. Charles A Hawley(1861–1929) used a celluloid sheet containing ageometric figure that, when adapted to a modeldetermined the extent of proposed toothmovement (1905) and introduced the retainerappliance that bears his name (1908).
Scientific studies included research in dentalhistology, particularly by Frederick B Noyes(1904); the influence of heredity and environmenton dental structures (1905); emphasis onrhinology, which brought the medical fraternityinto cooperation (1907); the study of thedeciduous dentition vis-a-vis nasodental growth,especially by Edward A. Bogue (1838–1921); and
the diagnosis of “mouth breathing”, which tookon special meaning (1907).
In 1907 Benno Lischer (1876–1959)(Figure14.7), dean and professor of dental orthopedics atWashington University Dental School in St. Louis,founded the International School of Orthodontia,and in 1912, he published Principles and Methodsof Orthodontia. He was an advocate of earlytreatment. Lischer wrote: “It is my firm belief thatirreparable damage is done by oft repeated advice towait until the permanent teeth are all erupted beforebeginning operations for correction of malocclusion.”Other publications included the first separatejournal entitled American Orthodontist, whichstarted in 1907 and ceased publication in 1912. In1909 CN Johnson (Chicago) edited a work entitledA Textbook of Operative dentistry, whichcontained a chapter, “Orthodontia”, written byHerbert A Pullen covering over 275 pages of text.It contained not only etiology, diagnosis, andtreatment modalities but also instruction inlaboratory procedures.
NEED FOR EXTRACTION
Extraction of teeth in orthodontic treatment isnecessary in two main circumstances:1. For the relief of crowding caused by arch
lengthtooth material discrepancy2. For the correction of anteroposterior dental
arch relationship.
CHOICE OF TEETH FOR EXTRACTION
The choice of teeth for extraction should becarefully made with consideration to thefollowing factors:� The amount of tooth material excess in
relation to arch length, degree and site ofcrowding.
� The anteroposterior inter-arch relationship.� Profile of the patient.� Age of the patient and his/her dental
developmental status.� The direction of jaw growth.� Carious status of the teeth.� General health status of the dentition.
SERIAL EXTRACTION
Serial extraction is an interceptive orthodonticprocedure undertaken in the (early) mixed

151History of Extraction in Orthodontics
dentition period that involves planned removalof certain primary and permanent teeth in aprogrammed sequence, so as to relieve crowdingin the arches and to guide the remaining eruptingpermanent teeth into a more favorable position.
A thorough understanding of the dynamics oforofacial growth and development and that of thestomatognatic system is essential for the successof serial extraction procedures. When executedproperly in carefully selected patients with theproper assessment, skilled timing and carefulmonitoring, programmed serial extractionprocedures can produce best possible and moststable results with minimal or in some cases nofurther need of corrective mechanotherapy at alater stage when all permanent teeth erupt.
Although occasionally used to intercept ClassII and Class III malocclusions, serial extractionprocedure is mainly used to intercept and/ortreat Class I malocclusions with crowdingresulting from severe tooth size arch lengthdiscrepancy.
Definition
� Tweed: Serial extraction as ‘the planned andsequential removal of the primary andpermanent teeth to intercept and reducedental crowding problems.’
� Iondon: The correctly timed, plannedremoval of certain deciduous and permanentteeth in mixed dentition cases withdentoalveolar disproportion.
HISTORICAL PERSPECTIVE
Robert Bunon in the early 1743 advised extractionof primary teeth to achieve a better alignment ofpermanent teeth in his diseases of teeth (Table15.1).
Later several authors like Bourdet (1757),Hunter (1771), Robinson (1846) and Harris(1855) advocated removal of primary canines andthe premolars when permanent incisorscrowded.
The term “serial extraction” was first coinedby Kjellgren in 1929. However it was Nance whopopularized the procedure in 1940’s in Englandand is considered as the Father of SerialExtraction technique practiced today.
Although popular, the term “serial extraction”does not stress the importance of thoroughknowledge of growth and development, compre-hensive analysis based on investigative recordsrequired to execute the procedure properly andthus may be misleading.
Hotz (1970) recommended the term “guidanceof eruption”. It is also sometimes referred to as“guided extraction”, while other authors preferto call the procedure “Guidance of Occlusion”.
Dewel’s Method 1978
Dewel’s has proposed a three step serial extractionprocedure in 1978 (Table 15.2).Step 1: In this step the deciduous canines areextracted to create space for the alignment of theincisors (Fig. 15.7A). The main objective ofextracting primary canines is to establish theintegrity of upper and lower incisors. Thisprevents development of lingual cross bite ofmaxillary laterals and resultant mesial migrationof maxillary canines.Step 2: In this step deciduous first molars areextracted at 8-9 years of age. The objective of
Table 15.1: Authors and their inventions
Authors Diseases of teeth
Robert Bunon (1743) First reference to extractionof primary teeth to facilitatealignment of permanentteeth
Kjellgren (1929) First coined the term SerialExtraction
Nance (1940s) Popularized the procedureconsidered father of serialextraction technique
Hotz (1970) Argued against the termserial extraction to call itguidance of eruption
Table 15.2: Dewel’s method
Steps Tooth extracted Purpose
Step 1 Extraction of Alignment ofdeciduous canines incisors
Step 2 Extraction of To facilitate the eruptiondeciduous first of first premolars aheadmolars of permanent canines
Step 3 Extraction of first To facilitate eruptionpremolars of permanent canines
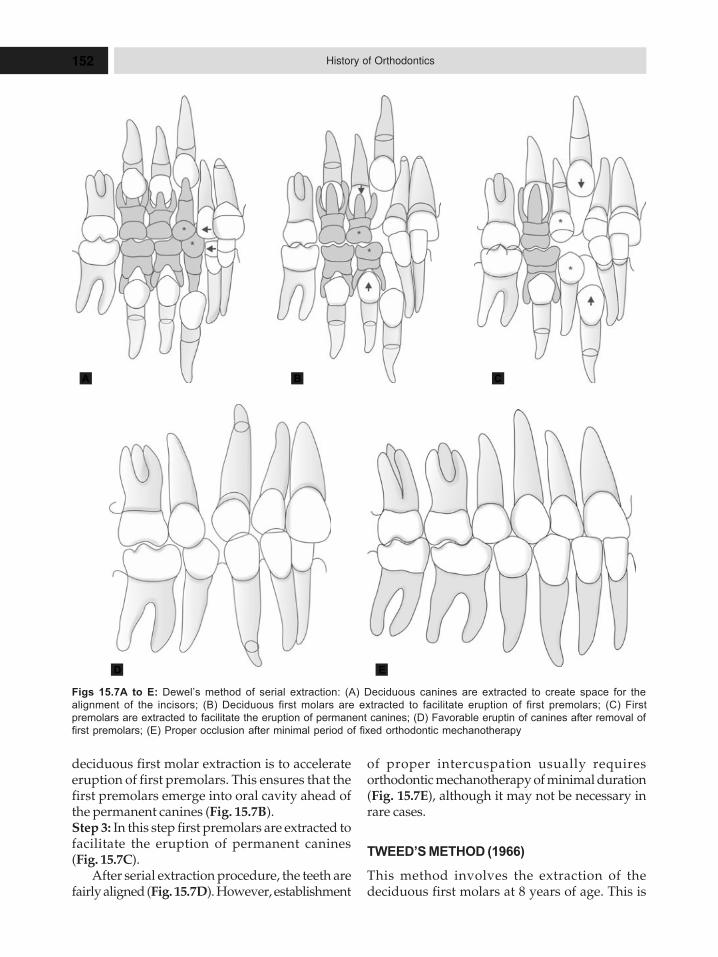
152 History of Orthodontics
deciduous first molar extraction is to accelerateeruption of first premolars. This ensures that thefirst premolars emerge into oral cavity ahead ofthe permanent canines (Fig. 15.7B).Step 3: In this step first premolars are extracted tofacilitate the eruption of permanent canines(Fig. 15.7C).
After serial extraction procedure, the teeth arefairly aligned (Fig. 15.7D). However, establishment
Figs 15.7A to E: Dewel’s method of serial extraction: (A) Deciduous canines are extracted to create space for the
alignment of the incisors; (B) Deciduous first molars are extracted to facilitate eruption of first premolars; (C) First
premolars are extracted to facilitate the eruption of permanent canines; (D) Favorable eruptin of canines after removal of
first premolars; (E) Proper occlusion after minimal period of fixed orthodontic mechanotherapy
of proper intercuspation usually requiresorthodontic mechanotherapy of minimal duration(Fig. 15.7E), although it may not be necessary inrare cases.
TWEED’S METHOD (1966)
This method involves the extraction of thedeciduous first molars at 8 years of age. This is
A B C
D E

153History of Extraction in Orthodontics
followed by the extraction of the first premolarsand the deciduous canines simultaneously.
Nance Method
Nance method of serial extraction is amodification of Tweed’s method which involvesthe extraction of the deciduous first molarsfollowed by the extraction of the first premolarsand the deciduous canines.
Grewe’s Method
Grewe’s method of serial extraction is based onthe planning of extraction sequence for differentclinical conditions.1. Class 1 malocclusion with premature loss of
a mandibular deciduous canine.Class 1 malocclusion with premature loss of amandibular deciduous canine will result inmidline shift, when the arch lengthdiscrepancy is 5–10 mm/arch, then theremaining deciduous canines should beextracted the deciduous first molars areextracted next, if the first premolar have theirroots more than half formed. If the roots of thefirst premolars are not developed more thanhalf then extractions of the deciduous first
molar is delayed. The first premolars shouldbe extracted as they emerge.
2. Class 1 malocclusion with severe mandibularanterior crowding.Deciduous Canines are extracted when thereis arch length deficiency and more than 5 mmper quadrant. The deciduous first molars areextracted next on completion of at least half offirst premolar root formation and the extractionof first premolars follow as the erupt into theoral cavity.
3. Class 1 malocclusion where minimalmandibular anterior crowding is 6–10 mmarch deficiency.In such conditions the first premolars areextracted. The deciduous first molars areextracted when the roots of the premolars aremore than half formed, as this would in turnresult in premature loss or eruption of the firstpremolar as soon as the first premolars eruptinto the oral cavity; these are extracted followedby deciduous canines. If this is bound to beeruption of permanent canines before that offirst premolar, then the deciduous canine isextracted first followed by the extraction of thedeciduous first molar and encleation of thefirst premolar.
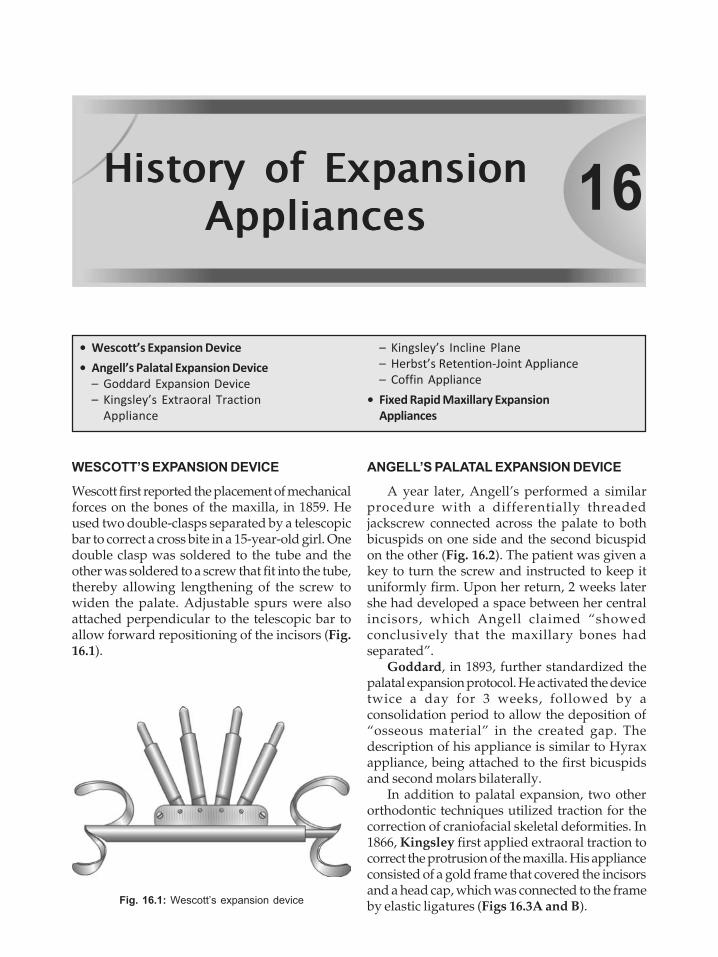
16HHHiiissstttooorrryyy ooofff EEExxxpppaaannnsssiiiooonnnAAAppppppllliiiaaannnccceeesss
� Wescott’s Expansion Device
� Angell’s Palatal Expansion Device
– Goddard Expansion Device
– Kingsley’s Extraoral Traction
Appliance
WESCOTT’S EXPANSION DEVICE
Wescott first reported the placement of mechanicalforces on the bones of the maxilla, in 1859. Heused two double-clasps separated by a telescopicbar to correct a cross bite in a 15-year-old girl. Onedouble clasp was soldered to the tube and theother was soldered to a screw that fit into the tube,thereby allowing lengthening of the screw towiden the palate. Adjustable spurs were alsoattached perpendicular to the telescopic bar toallow forward repositioning of the incisors (Fig.16.1).
ANGELL’S PALATAL EXPANSION DEVICE
A year later, Angell’s performed a similarprocedure with a differentially threadedjackscrew connected across the palate to bothbicuspids on one side and the second bicuspidon the other (Fig. 16.2). The patient was given akey to turn the screw and instructed to keep ituniformly firm. Upon her return, 2 weeks latershe had developed a space between her centralincisors, which Angell claimed “showedconclusively that the maxillary bones hadseparated”.
Goddard, in 1893, further standardized thepalatal expansion protocol. He activated the devicetwice a day for 3 weeks, followed by aconsolidation period to allow the deposition of“osseous material” in the created gap. Thedescription of his appliance is similar to Hyraxappliance, being attached to the first bicuspidsand second molars bilaterally.
In addition to palatal expansion, two otherorthodontic techniques utilized traction for thecorrection of craniofacial skeletal deformities. In1866, Kingsley first applied extraoral traction tocorrect the protrusion of the maxilla. His applianceconsisted of a gold frame that covered the incisorsand a head cap, which was connected to the frameby elastic ligatures (Figs 16.3A and B).Fig. 16.1: Wescott’s expansion device
– Kingsley’s Incline Plane
– Herbst’s Retention-Joint Appliance
– Coffin Appliance
� Fixed Rapid Maxillary Expansion
Appliances
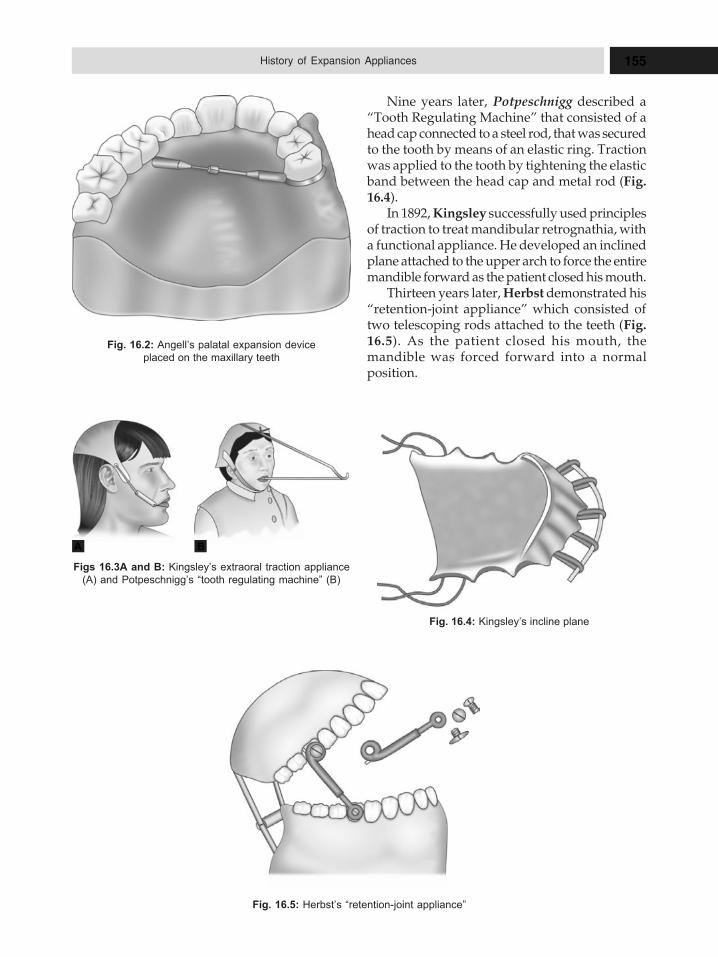
155History of Expansion Appliances
Nine years later, Potpeschnigg described a“Tooth Regulating Machine” that consisted of ahead cap connected to a steel rod, that was securedto the tooth by means of an elastic ring. Tractionwas applied to the tooth by tightening the elasticband between the head cap and metal rod (Fig.16.4).
In 1892, Kingsley successfully used principlesof traction to treat mandibular retrognathia, witha functional appliance. He developed an inclinedplane attached to the upper arch to force the entiremandible forward as the patient closed his mouth.
Thirteen years later, Herbst demonstrated his“retention-joint appliance” which consisted oftwo telescoping rods attached to the teeth (Fig.16.5). As the patient closed his mouth, themandible was forced forward into a normalposition.
Fig. 16.2: Angell’s palatal expansion device
placed on the maxillary teeth
Figs 16.3A and B: Kingsley’s extraoral traction appliance
(A) and Potpeschnigg’s “tooth regulating machine” (B)
Fig. 16.5: Herbst’s “retention-joint appliance”
Fig. 16.4: Kingsley’s incline plane
A B

156 History of Orthodontics
Arch expansion is one of the methods ofgaining space in orthodontics. The concept of archexpansion was explained for the first time byEmerson C Angel. Hence, he is considered asfather of expansion appliances. Arch expansioncan be slow or rapid, removable or fixed. Slowarch expansion brings about mainly dentoalveolarexpansion whereas rapid maxillary expansionbrings about both skeletal as well as dentoalveolarexpansion.
Rapid maxillary expansion appliances are thebest appliances of the orthopedic expansion. Inthis, changes are produced mainly in theunderlying skeletal structures rather than by themovement of teeth through the alveolar bone.Rapid maxillary expansion not only separates themidpalatal suture but also affects the circum-zygomatic and circummaxillary sutural systems.
Rapid maxillary expansion is also calledpalatal expansion or split palate. Rapid maxillaryexpansion is a skeletal type of expansion, whichproduces skeletal changes by separation of midpalatal suture.
Rapid maxillary expansion device was firstused by Emerson C Angel in the year 1860. Heused a jackscrew type of rapid maxillaryexpansion device between two premolars inmaxillary arch on palatal side in a 14-year-oldgirl and achieved arch expansion by ¼ inch in 14days. For this significant valuable contribution tothe expansion in orthodontics, he is consideredas the Father of rapid maxillary expansion.
Walter Coffin in 1877, developed a spring forthe purpose of arch expansion which has come tobe known as Coffin spring. This spring alsoproduces arch expansion by separation of midpalatal suture, when used in young patients. Thisexpansion device was of gained popularity by
orthodontic community at that time. Later in 1956,this expansion device was reintroduced toorthodontics by Andrew Hass, in the United Statesof America.
Removable expansion appliance may be asimple expansion appliance with incorporatedjackscrew or Coffin appliance. Fixed archexpansion appliances are toothborne expansionappliance (Hyrax, Isacson) or tooth and tissueborne expansion appliance (Derichsweiler Haasexpansion appliance). How much to expand andwhen to expand are evaluated by model analysis.
FIXED RAPID MAXILLARY EXPANSION
APPLIANCES
Fixed rapid maxillary expansion appliances arefixed expanders and cannot be removed by thepatient. These fixed expanders can be classifiedinto tooth and tooth tissue-borne appliances.
Tooth and tissue borne appliances are:� Derichsweiler type� Haas type.
Most commonly used fixed expander of toothborne appliances are:� Hyrax type� Isaacson type.
Derichsweiler-type expander: Derichsweilerexpansion appliance consists of molar bands onright and left permanent first molars and firstpremolars with wire tags soldered into the palatalsurface of all molar and premolar bands. The outerfree ends of wire tags are inserted into split palatalacrylic incorporating a jack expansion screw inits center (Fig. 16.6).
Haas-type expander: Haas expander wasdesigned and popularized by Andrew Hass inthe year 1961. This appliance consist of molarbands on right and left permanent molars andpremolars. A jackscrew is incorporated in themidline into the two acrylic pads that closelycontact the palatal mucosa. Support wires alsoextend anteriorly from the molars along the buccaland lingual surface of the posterior teeth, to addrigidity to the appliance (Fig. 16.7).
Haas states that, more bodily movement andless dental tipping is produced when acrylicpalatal coverage is added to support the appliancethus permitting the forces to be generalized notonly against the teeth but also against theunderlying soft and hard palatal tissuesFig. 16.6: Derichsweiler type expander
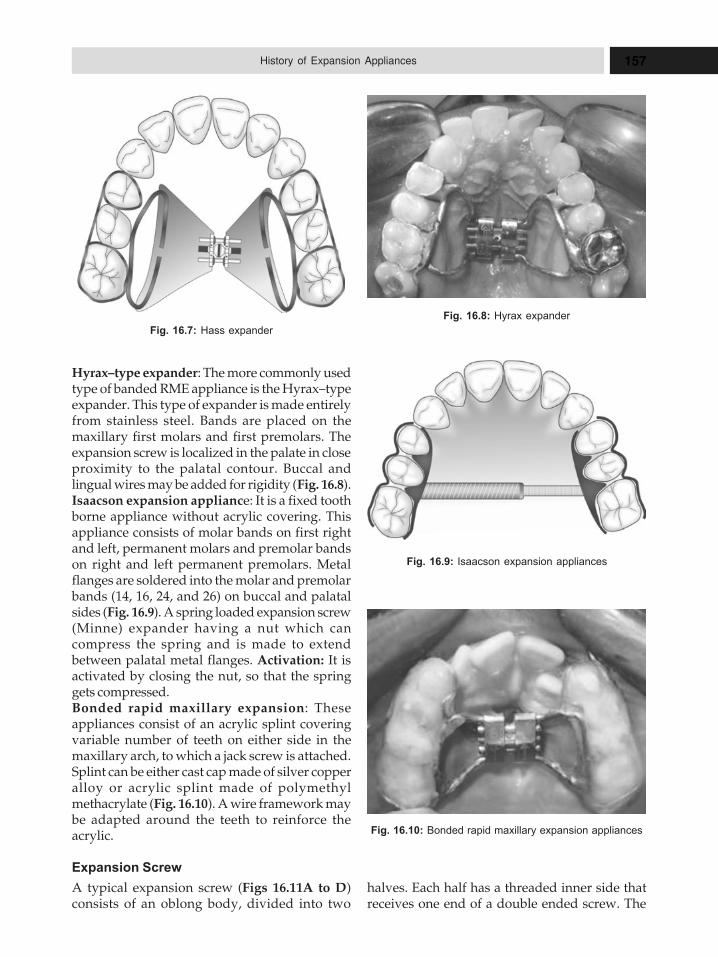
157History of Expansion Appliances
Fig. 16.7: Hass expander
Hyrax–type expander: The more commonly usedtype of banded RME appliance is the Hyrax–typeexpander. This type of expander is made entirelyfrom stainless steel. Bands are placed on themaxillary first molars and first premolars. Theexpansion screw is localized in the palate in closeproximity to the palatal contour. Buccal andlingual wires may be added for rigidity (Fig. 16.8).Isaacson expansion appliance: It is a fixed toothborne appliance without acrylic covering. Thisappliance consists of molar bands on first rightand left, permanent molars and premolar bandson right and left permanent premolars. Metalflanges are soldered into the molar and premolarbands (14, 16, 24, and 26) on buccal and palatalsides (Fig. 16.9). A spring loaded expansion screw(Minne) expander having a nut which cancompress the spring and is made to extendbetween palatal metal flanges. Activation: It isactivated by closing the nut, so that the springgets compressed.Bonded rapid maxillary expansion: Theseappliances consist of an acrylic splint coveringvariable number of teeth on either side in themaxillary arch, to which a jack screw is attached.Splint can be either cast cap made of silver copperalloy or acrylic splint made of polymethylmethacrylate (Fig. 16.10). A wire framework maybe adapted around the teeth to reinforce theacrylic.
Expansion Screw
A typical expansion screw (Figs 16.11A to D)consists of an oblong body, divided into two
Fig. 16.8: Hyrax expander
Fig. 16.9: Isaacson expansion appliances
halves. Each half has a threaded inner side thatreceives one end of a double ended screw. The
Fig. 16.10: Bonded rapid maxillary expansion appliances
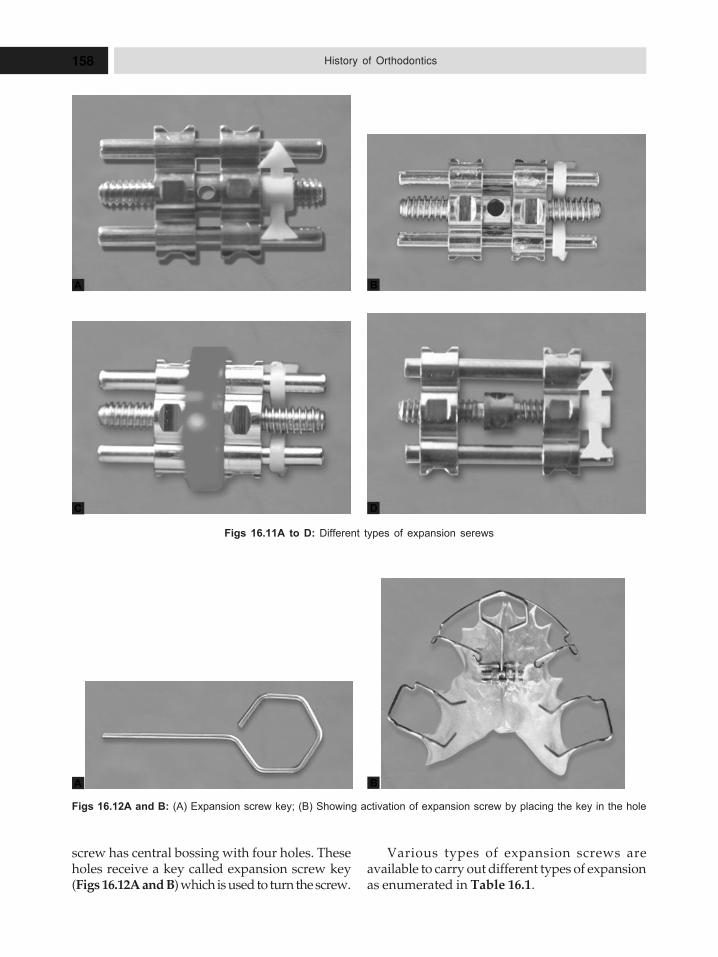
158 History of Orthodontics
screw has central bossing with four holes. Theseholes receive a key called expansion screw key(Figs 16.12A and B) which is used to turn the screw.
Figs 16.11A to D: Different types of expansion serews
Various types of expansion screws areavailable to carry out different types of expansionas enumerated in Table 16.1.
Figs 16.12A and B: (A) Expansion screw key; (B) Showing activation of expansion screw by placing the key in the hole
A B
C D
A B

159History of Expansion Appliances
Table 16.3: Expansion orthodontic appliances
Author Contributions toorthodontics
S.No. Type of expansion appliance Developed by
1 Derichweiler expansion Derichweilerappliance
2 Isaacson’s expansion Isaacsonappliances
3 Haas expansion appliance Haas4 Coffin spring Walter coffin5 Jack expansion screw Jack
Table 16.1: Different types of expansion screws
Expansion screw type Use
Symmetrical bilateral Bilateral expansionexpansion screw
Traction screw Closing spaces
Expansion screw with Separate expansion ofsplit activator maxilla or mandible
Three-dimensional Anterior and bilateralscrew expansion
Expansion Screw Activation Schedule
Schedule by Timms
See Table 16.2.
Expansion Orthodontic Appliances
Expansion orthodontic appliances (Table 16.3)are used to relieve crowding in cases of archlength—tooth material discrepancy. Following arethe researchers involved in the development ofvarious type of expansion appliances.
Table 16.2: Timm’s schedule of activation ofexpansion screw
Age of the patient Degree of Number ofactivation activation in a day
Up to 15 years 90o 2 times in a day
More than 45o 4 times in a day15 years
17HHHiiissstttooorrryyy ooofff RRReeemmmooovvvaaabbbllleee
OOOrrrttthhhooodddooonnntttiiiccc AAAppppppllliiiaaannnccceeesss
� Development of Removable
Orthodontic Appliances
– Victor Hugo Jackson
– George Crozat
– Robin
– Andersen
– Adam
– Martin Schwartz
– Indications
– Contraindications
– Advantages
– Disadvantages
� Components of Removable
Orthodontic Appliances
– Retentive Components
– Active Components
– Base Plate
Removable orthodontic appliances are so-calledbecause they are designed to be fitted andremoved by the patient. Removable orthodonticappliances are limited to tipping and simplerotatory movements of teeth, which are sufficientfor many orthodontic treatments. They dependon cooperation and a certain degree of skill onthe part of patient. Removable orthodonticappliances may be active or passive.
The use of removable orthodontic applianceswas always more popular in Europe than theUnited States, but even there, the use of fixedappliances [using (generally metal) bands andbrackets] has largely become the primary methodof treatment. Nevertheless, as the authors ofRemovable Orthodontic Appliances point out,removable appliances are often an effectivemeans of addressing many patients’ needs andin some cases have considerable advantages overfixed appliances.
Use of removable appliances also requirescareful case selection for, success of the treatment.They are ideally used when simple tippingmovement of teeth is sufficient to correct a certain
type of malocclusion. The range of malocclusionsthat can be treated with removable appliancealone is limited. They can also be used as passiveappliances to maintain teeth in their correctedpositions after active phases of orthodontictherapy, e.g. retainers. Removable orthodonticappliance is often used in conjunction with fixedmechanotherapy.
The most familiar removable device is theretainer, specifically the Hawley or Begg device.Its function, however, is retention—keeping teethin their place after the desired tooth-movementhas been achieved.
The main drawback of removable orthodonticappliances is that they can only apply a tippingforce (whereas fixed appliances can also apply arotating force), this means they are not suitablefor the complete treatment of some cases(specifically, serious class II and III cases). Amongthe big advantages of removable orthodonticappliances are in the area of anchorage (since thepalatal area is also used for this), significant sincefixed appliances must generally rely on adjacentteeth (As the authors note, the use of removable
161History of Removable Orthodontic Appliances
appliances generally involves the upper arch;lower arch treatment with them is limited bydifficulties with retention and bulk, as well asthe limited space available for active componentson the appliances themselves).
DEVELOPMENT OF REMOVABLE
ORTHODONTIC APPLIANCES
Removable orthodontic appliances begin with abrief general introduction, and then discusses the‘Biomechanics of tooth movement’, variousactive components that can be utilized, and howthey function and are integrated into devices,including a variety of springs, bows, and screws.
The next survey ‘Appliance retention’, ‘Thebaseplate’, and ‘Anchorage’, discussing thefactors that should be taken into considerationwhich designing the device, both generally(going so far as to note: “Removable appliancesshould ideally be fitted within two weeks of theimpression being taken”) and also in tailoring itto the individual case. Anchorage issues, inparticular, must be closely monitored from visitto visit, and as the authors point out: “if space iscritical, it may be wise to plan for extraoral anchoragefrom the start”. Clearly, the use of extraoralanchorage headgear, which in the case ofremovable appliances cannot be cervical (sincethe pull must be upwards so as not to displacethe appliance) allows for much greater flexibilityin treatment, as headgear can be used as the solesource of anchorage or to reinforce intraoralanchorage, as well as extraoral traction be anactive component for tooth movement.
Victor Hugo Jackson
Victor Hugo Jackson is from United States ofAmerica. He was the chief proponent ofremovable appliances.� At that time, neither the modern plastics for
base plate material nor stainless steel wire-clasp, springs were available.
� Appliances are fabricated with bases andprecious metal or nickel silver wires.
� In early 20th centuries.
George Crozat
In early 1900s, Crozat developed a removableappliance fabricated entirely of precious metal
that is still used occasionally. Crozat applianceconsists of:
– Modified Jackson’s clasp.– Heavy gold wire framework.– Lighter gold finger springs to produce
desired tooth movement.
Robin
In the year 1900, forerunner of all functionalappliances, the monobloc was developed byRobin.
Andersen
In the 1920s, andersen developed activator inNorway. He was the first person to developfunctional appliance.
Adam
In the 1921s, Adam developed a clasp calledAdam’s clasp.
Martin Schwartz
� He developed split plate appliance.
Indications of Removable Orthodontic
Appliances
Use of removable orthodontic appliancesrequires careful selection. They should not beused in circumstances where fixed orthodonticappliance therapy would be more appropriate.May be used as an adjunct to fixed orthodonticappliance treatment.
Contraindications of Removable
Orthodontic Appliances
Removable orthodontic appliances arecontraindicated in case, where bodily movementis required.
Advantages of Removable Appliances
Advantages of removable orthodontic appliancesare listed below:1. Removable appliances permit easy cleaning.2. They need less chair side time.3. They are good for overbite reduction.4. They can tip the teeth efficiently.5. They eliminate occlusal interferences.
162 History of Orthodontics
Disadvantages of Removable
Orthodontic Appliances
Disadvantages of removable orthodonticappliances are listed below:1. Removable orthodontic appliances can bring
about only a limited type of tooth movement.2. Anchorage of tooth movement is sometimes
difficult, since anchor teeth cannot beprevented from tilting.
3. Retention with removable orthodonticappliance is more difficult than with fixedappliances.
4. A high degree of cooperation and a certainamount of skill is required from the patient,who has to remove, clean and replace theappliance at frequent interval.
5. Limited scope on lower arch.6. They affect speech.
Advantages of Removable Appliances
a. They are removable and therefore easier toclean.
b. They can provide increased vertical andhorizontal anchorage due to palatal coverage.
c. They can produce efficient over-bitereduction in a growing child.
d. They can transmit forces to blocks of teeth.
Disadvantages of Removable Appliances
a. The appliances can be left out.b. Only tilting movements are possible.c. They affect speech.d. A technician’s input is required to make the
appliances.e. Intermaxillary traction is more difficult.f. They are inefficient for multiple tooth
movements.g. Lower removable appliances are more
difficult to tolerate.
COMPONENTS OF REMOVABLE
ORTHODONTIC APPLIANCE
Removable orthodontic appliance consists offollowing three components:1. Retentive components2. Active components3. Base plate.
Retentive Components
Evolution of Clasp Design
� Jackson describes the construction of a cribclasp which has a square form and is designednot only to grasp the tooth buccally but, byrunning forward and backward and turningsharply at a right angle, to grasp the toothanteroposteriorly. The next real advance inclasp design was the introduction of thearrowhead type of clasp, usually attributedto Schwarz and introduced in England byTischler.
� The arrowheads depend on the use of thespaces below the point of contact betweentwo teeth. Several arrowheads are usuallyembodied in a clasp.
� The modified arrowhead clasp, introduced byAdam in 1949 and today widely referred toas the Adam clasp, makes use of the mesialand distal undercuts of a single tooth onlyand can in practice be applied to any tooth,deciduous or permanent.The success of a removable orthodontic
appliance mainly depends upon good retentionof the appliance. Adequate retention of aremovable orthodontic appliance is achieved byincorporating certain wire components, gotengaged the undercuts on the teeth. These wirecomponents that help in retention of a removableappliance are called clasps. Following are thedifferent type of clasps which aids in retentionto the appliance:
i. ‘C’clasp or Circumferential claspii. Jackson’s clasp or Full clasp
iii. Adam’s claspiv. Schwartz claspv. Crozat clasp
vi. Triangular claspvii. Ball end clasp
viii. Resta claspix. Eyelet claspx. Southend clasp.
Modifications of Adam’s Clasp and its Use
Adam’s clasp offers a unique feature that, itsdesign can be modified in a number of ways suitvaries clinical requirements. The following aresome of the modifications of Adam’s clasp.
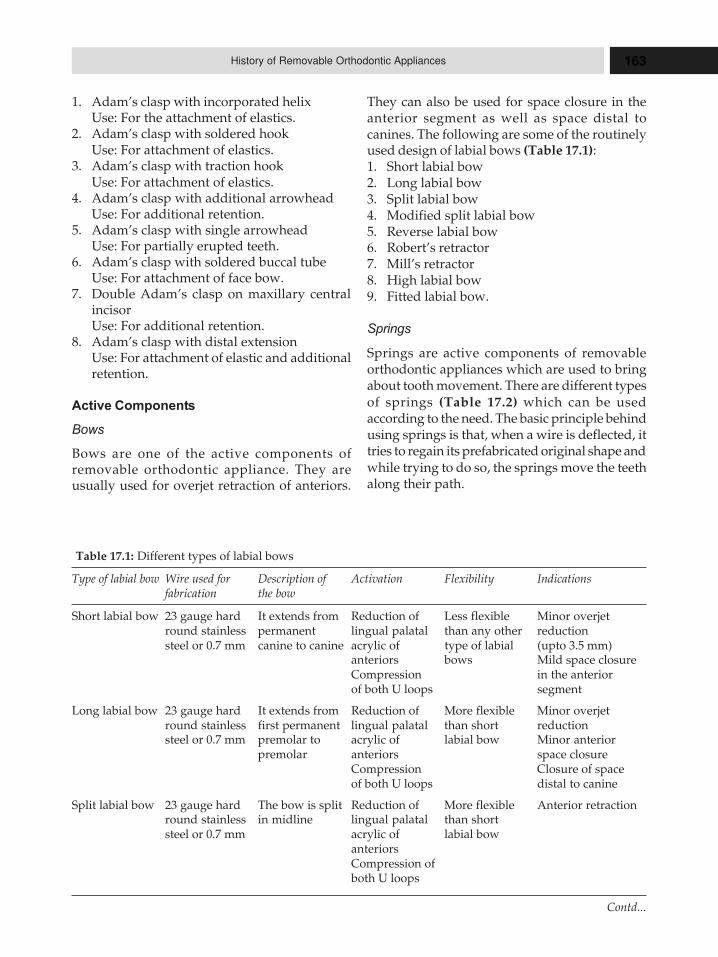
163History of Removable Orthodontic Appliances
1. Adam’s clasp with incorporated helixUse: For the attachment of elastics.
2. Adam’s clasp with soldered hookUse: For attachment of elastics.
3. Adam’s clasp with traction hookUse: For attachment of elastics.
4. Adam’s clasp with additional arrowheadUse: For additional retention.
5. Adam’s clasp with single arrowheadUse: For partially erupted teeth.
6. Adam’s clasp with soldered buccal tubeUse: For attachment of face bow.
7. Double Adam’s clasp on maxillary centralincisorUse: For additional retention.
8. Adam’s clasp with distal extensionUse: For attachment of elastic and additionalretention.
Active Components
Bows
Bows are one of the active components ofremovable orthodontic appliance. They areusually used for overjet retraction of anteriors.
They can also be used for space closure in theanterior segment as well as space distal tocanines. The following are some of the routinelyused design of labial bows (Table 17.1):1. Short labial bow2. Long labial bow3. Split labial bow4. Modified split labial bow5. Reverse labial bow6. Robert’s retractor7. Mill’s retractor8. High labial bow9. Fitted labial bow.
Springs
Springs are active components of removableorthodontic appliances which are used to bringabout tooth movement. There are different typesof springs (Table 17.2) which can be usedaccording to the need. The basic principle behindusing springs is that, when a wire is deflected, ittries to regain its prefabricated original shape andwhile trying to do so, the springs move the teethalong their path.
Table 17.1: Different types of labial bows
Type of labial bow Wire used for Description of Activation Flexibility Indicationsfabrication the bow
Short labial bow 23 gauge hard It extends from Reduction of Less flexible Minor overjetround stainless permanent lingual palatal than any other reductionsteel or 0.7 mm canine to canine acrylic of type of labial (upto 3.5 mm)
anteriors bows Mild space closureCompression in the anteriorof both U loops segment
Long labial bow 23 gauge hard It extends from Reduction of More flexible Minor overjetround stainless first permanent lingual palatal than short reductionsteel or 0.7 mm premolar to acrylic of labial bow Minor anterior
premolar anteriors space closureCompression Closure of spaceof both U loops distal to canine
Split labial bow 23 gauge hard The bow is split Reduction of More flexible Anterior retractionround stainless in midline lingual palatal than shortsteel or 0.7 mm acrylic of labial bow
anteriorsCompression ofboth U loops
Contd...
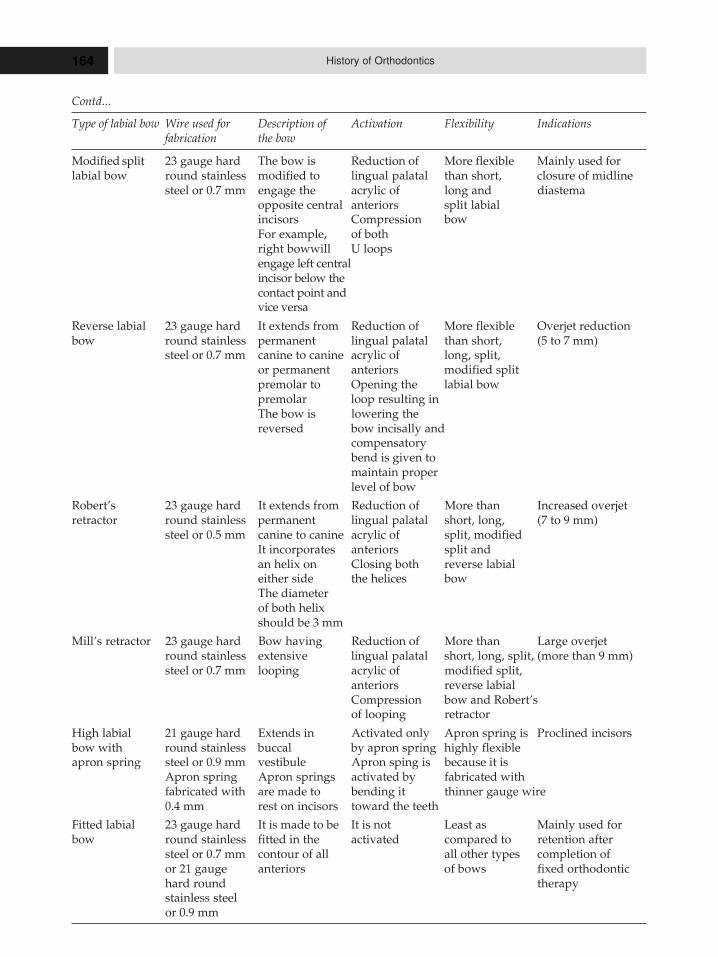
164 History of Orthodontics
Modified split 23 gauge hard The bow is Reduction of More flexible Mainly used forlabial bow round stainless modified to lingual palatal than short, closure of midline
steel or 0.7 mm engage the acrylic of long and diastemaopposite central anteriors split labialincisors Compression bowFor example, of bothright bowwill U loopsengage left centralincisor below thecontact point andvice versa
Reverse labial 23 gauge hard It extends from Reduction of More flexible Overjet reductionbow round stainless permanent lingual palatal than short, (5 to 7 mm)
steel or 0.7 mm canine to canine acrylic of long, split,or permanent anteriors modified splitpremolar to Opening the labial bowpremolar loop resulting inThe bow is lowering thereversed bow incisally and
compensatorybend is given tomaintain properlevel of bow
Robert’s 23 gauge hard It extends from Reduction of More than Increased overjetretractor round stainless permanent lingual palatal short, long, (7 to 9 mm)
steel or 0.5 mm canine to canine acrylic of split, modifiedIt incorporates anteriors split andan helix on Closing both reverse labialeither side the helices bowThe diameterof both helixshould be 3 mm
Mill’s retractor 23 gauge hard Bow having Reduction of More than Large overjetround stainless extensive lingual palatal short, long, split, (more than 9 mm)steel or 0.7 mm looping acrylic of modified split,
anteriors reverse labialCompression bow and Robert’sof looping retractor
High labial 21 gauge hard Extends in Activated only Apron spring is Proclined incisorsbow with round stainless buccal by apron spring highly flexibleapron spring steel or 0.9 mm vestibule Apron sping is because it is
Apron spring Apron springs activated by fabricated withfabricated with are made to bending it thinner gauge wire0.4 mm rest on incisors toward the teeth
Fitted labial 23 gauge hard It is made to be It is not Least as Mainly used forbow round stainless fitted in the activated compared to retention after
steel or 0.7 mm contour of all all other types completion ofor 21 gauge anteriors of bows fixed orthodontichard round therapystainless steelor 0.9 mm
Contd...
Type of labial bow Wire used for Description of Activation Flexibility Indicationsfabrication the bow
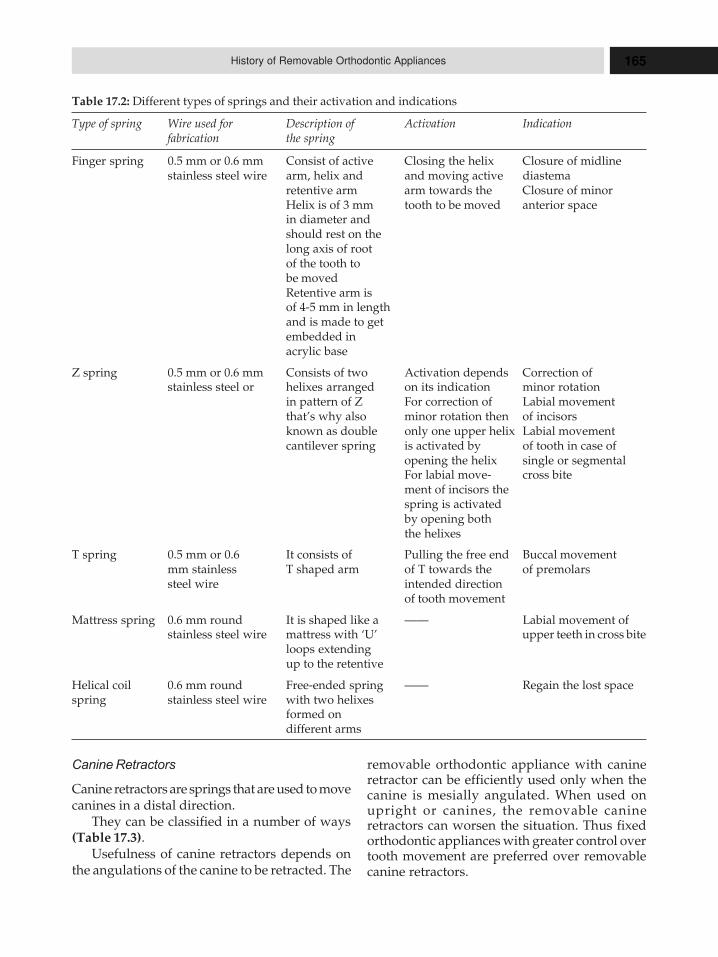
165History of Removable Orthodontic Appliances
Table 17.2: Different types of springs and their activation and indications
Type of spring Wire used for Description of Activation Indicationfabrication the spring
Finger spring 0.5 mm or 0.6 mm Consist of active Closing the helix Closure of midlinestainless steel wire arm, helix and and moving active diastema
retentive arm arm towards the Closure of minorHelix is of 3 mm tooth to be moved anterior spacein diameter andshould rest on thelong axis of rootof the tooth tobe movedRetentive arm isof 4-5 mm in lengthand is made to getembedded inacrylic base
Z spring 0.5 mm or 0.6 mm Consists of two Activation depends Correction ofstainless steel or helixes arranged on its indication minor rotation
in pattern of Z For correction of Labial movementthat’s why also minor rotation then of incisorsknown as double only one upper helix Labial movementcantilever spring is activated by of tooth in case of
opening the helix single or segmentalFor labial move- cross bitement of incisors thespring is activatedby opening boththe helixes
T spring 0.5 mm or 0.6 It consists of Pulling the free end Buccal movementmm stainless T shaped arm of T towards the of premolarssteel wire intended direction
of tooth movement
Mattress spring 0.6 mm round It is shaped like a —— Labial movement ofstainless steel wire mattress with ‘U’ upper teeth in cross bite
loops extendingup to the retentive
Helical coil 0.6 mm round Free-ended spring —— Regain the lost spacespring stainless steel wire with two helixes
formed ondifferent arms
Canine Retractors
Canine retractors are springs that are used to movecanines in a distal direction.
They can be classified in a number of ways(Table 17.3).
Usefulness of canine retractors depends onthe angulations of the canine to be retracted. The
removable orthodontic appliance with canineretractor can be efficiently used only when thecanine is mesially angulated. When used onupright or canines, the removable canineretractors can worsen the situation. Thus fixedorthodontic appliances with greater control overtooth movement are preferred over removablecanine retractors.
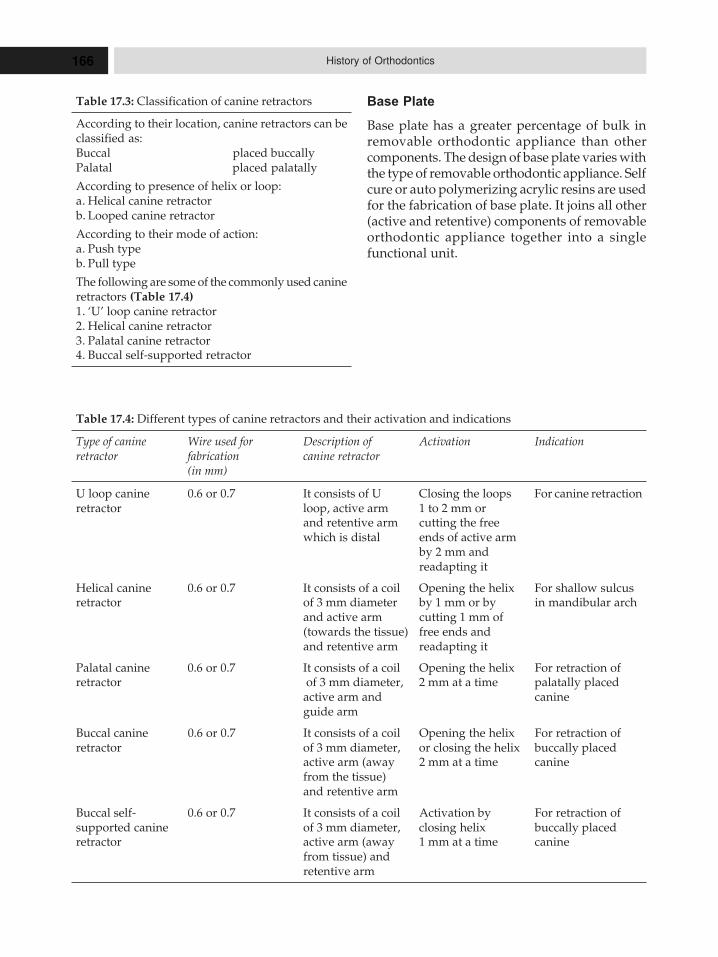
166 History of Orthodontics
Table 17.4: Different types of canine retractors and their activation and indications
Type of canine Wire used for Description of Activation Indicationretractor fabrication canine retractor
(in mm)
U loop canine 0.6 or 0.7 It consists of U Closing the loops For canine retractionretractor loop, active arm 1 to 2 mm or
and retentive arm cutting the freewhich is distal ends of active arm
by 2 mm andreadapting it
Helical canine 0.6 or 0.7 It consists of a coil Opening the helix For shallow sulcusretractor of 3 mm diameter by 1 mm or by in mandibular arch
and active arm cutting 1 mm of(towards the tissue) free ends andand retentive arm readapting it
Palatal canine 0.6 or 0.7 It consists of a coil Opening the helix For retraction ofretractor of 3 mm diameter, 2 mm at a time palatally placed
active arm and canineguide arm
Buccal canine 0.6 or 0.7 It consists of a coil Opening the helix For retraction ofretractor of 3 mm diameter, or closing the helix buccally placed
active arm (away 2 mm at a time caninefrom the tissue)and retentive arm
Buccal self- 0.6 or 0.7 It consists of a coil Activation by For retraction ofsupported canine of 3 mm diameter, closing helix buccally placedretractor active arm (away 1 mm at a time canine
from tissue) andretentive arm
Table 17.3: Classification of canine retractors
According to their location, canine retractors can beclassified as:Buccal placed buccallyPalatal placed palatally
According to presence of helix or loop:a. Helical canine retractorb. Looped canine retractor
According to their mode of action:a. Push typeb. Pull type
The following are some of the commonly used canineretractors (Table 17.4)1. ‘U’ loop canine retractor2. Helical canine retractor3. Palatal canine retractor4. Buccal self-supported retractor
Base Plate
Base plate has a greater percentage of bulk inremovable orthodontic appliance than othercomponents. The design of base plate varies withthe type of removable orthodontic appliance. Selfcure or auto polymerizing acrylic resins are usedfor the fabrication of base plate. It joins all other(active and retentive) components of removableorthodontic appliance together into a singlefunctional unit.
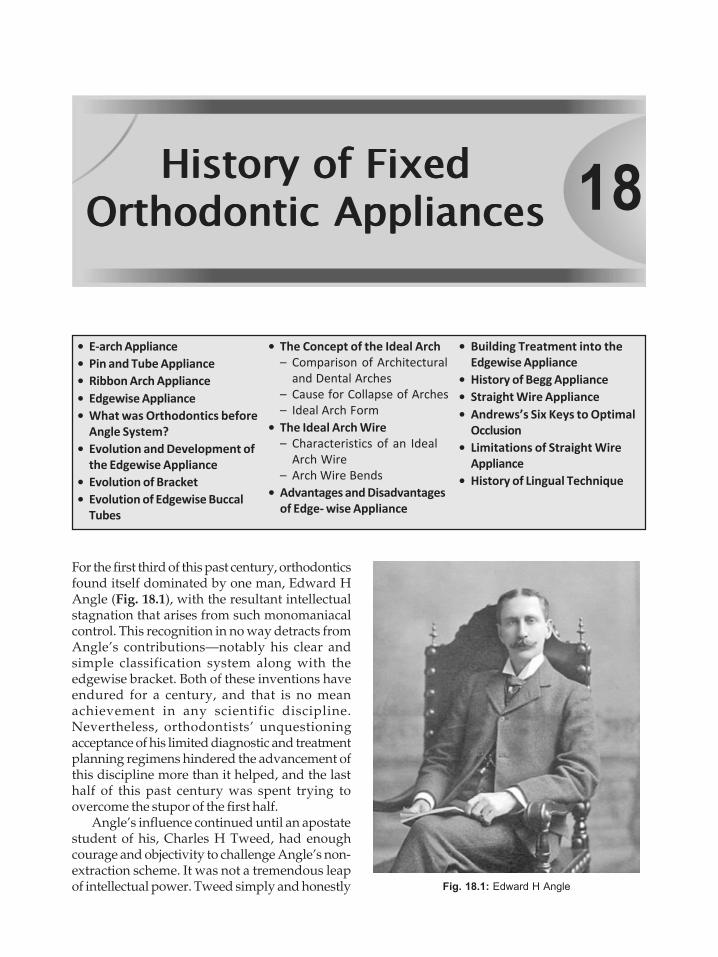
18HHHiiissstttooorrryyy ooofff FFFiiixxxeeeddd
OOOrrrttthhhooodddooonnntttiiiccc AAAppppppllliiiaaannnccceeesss
� E-arch Appliance
� Pin and Tube Appliance
� Ribbon Arch Appliance
� Edgewise Appliance
� What was Orthodontics before
Angle System?
� Evolution and Development of
the Edgewise Appliance
� Evolution of Bracket
� Evolution of Edgewise Buccal
Tubes
� The Concept of the Ideal Arch
– Comparison of Architectural
and Dental Arches
– Cause for Collapse of Arches
– Ideal Arch Form
� The Ideal Arch Wire
– Characteristics of an Ideal
Arch Wire
– Arch Wire Bends
� Advantages and Disadvantages
of Edge- wise Appliance
� Building Treatment into the
Edgewise Appliance
� History of Begg Appliance
� Straight Wire Appliance
� Andrews’s Six Keys to Optimal
Occlusion
� Limitations of Straight Wire
Appliance
� History of Lingual Technique
For the first third of this past century, orthodonticsfound itself dominated by one man, Edward HAngle (Fig. 18.1), with the resultant intellectualstagnation that arises from such monomaniacalcontrol. This recognition in no way detracts fromAngle’s contributions—notably his clear andsimple classification system along with theedgewise bracket. Both of these inventions haveendured for a century, and that is no meanachievement in any scientific discipline.Nevertheless, orthodontists’ unquestioningacceptance of his limited diagnostic and treatmentplanning regimens hindered the advancement ofthis discipline more than it helped, and the lasthalf of this past century was spent trying toovercome the stupor of the first half.
Angle’s influence continued until an apostatestudent of his, Charles H Tweed, had enoughcourage and objectivity to challenge Angle’s non-extraction scheme. It was not a tremendous leapof intellectual power. Tweed simply and honestly Fig. 18.1: Edward H Angle

168 History of Orthodontics
recognized that when 100 percent of your patientsrelapsed, there might be something wrong withthe diagnosis and/or treatment planning.
Dr Tweed (Fig. 18.2) acted appropriately inthe face of this challenge—quite unlike the ancientdentist who chided a young colleague who wasdescribing his meticulous technique ofendodontic filling to the monthly assembly ofdentists. The old man explained his owntechnique that used a simple matchsticksharpened with a pocketknife and then jammedinto the canal. When the young dentist asked ifa lot of these root canal fillings did notsubsequently fail, the older man replied, “Everydamn time!”
Tweed tired of those orthodontic abscessesand, unlike his peers, sought to correct thedeficiencies he saw in Angle’s philosophy. Somewould say that he overcorrected, but that said,we must pay homage to anyone who has the skilland temerity to successfully challenge a mentorand his minions. Tweed’s success brings to mindthe remark of C S Lewis, who said, “No genius isso fortunate as he who has the skill and ability todo well that which others have been doingpoorly”.
Nevertheless, I do not think that Tweed wouldhave ever been able to deliver his paperdescribing his extraction technique if Angle hadstill been alive. Angle’s influence over the society
that bore his name was too immense to permitsuch hubris from a young upstart. But asSamuelson, the MIT economist, once noted:“Science progresses slowly—funeral byfuneral.” And so it was and is in orthodontics.
Non-extraction Philosophy
Aside from the edgewise bracket and theclassification system, Angle’s most enduringlegacy has been his belief in non-extractiontherapy. Angle had unsuccessfully experimentedwith premolar extractions while using his ribbonarch appliance, but he never solved the problemof paralleling the roots to prevent the extractionspaces from opening. If he could not do it, then,ergo, no one else could, and this resulted in avirulent opposition to any extractions and aninsistence upon enlarging the arches toaccommodate all of the teeth.
This dogma stayed dominant for severaldecades until Tweed advocated the extraction ofpremolars based on his diagnostic triangle, whichwas the first systematic treatment planningstratagem orthodontists had. Tweed receivedcorroboration simultaneously from anotherformer Angle protégé in Australia, RaymondBegg, who had studied aborigines and concludedthat nature intended for enamel to wear. Hedecided that orthodontists could mimic natureby extracting teeth prior to orthodontic therapy.The Tweed and Begg extraction philosophieseventually prevailed and remained uncontestedfor some time.
Several years passed before Holdaway ,
published his articles that suggested the softtissue as the determining feature of diagnosis.This disputed Tweed’s narrow diagnosticregimen that focused on the mandibular incisorand totally neglected the soft tissue. Tweed’striangle set in motion a trend that emphasizedmore prudence in the extraction of teeth. Soonothers added their discoveries regarding soft tissueand the maxillary incisors as main determinantsof diagnosis and treatment planning.
From the inception of this specialty, with Angle,diagnosis never had too much importance becauseeveryone received the same non-extractiontreatment with the same expansive appliance. Themarvel of it is all that the collection of orthodonticrecords never became important. A few monthsFig. 18.2: Dr Tweed

169History of Fixed Orthodontic Appliances
ago an orthodontist boasted that since invoking adifferent treatment regimen, he was treating 98percent of his patient non-extraction usingtreatment. One was tempted to ask if he still tookrecords because with diagnostic certainty suchas that, records are clearly redundant.
Orthodontists should not waste patients’ timeand money taking impressions, cephalometricX-rays or doing treatment simulations, if alltreatment plans are essentially the same. One doesnot need orthodontic records to come to such apreconceived conclusion.
Obviously, this one-size-fits-all treatmentplanning did not benefit patients a hundred yearsago, and it does not in our own age, but suchsimplicity continues to hold enormous appeal formany orthodontists. Orthodontists pridethemselves in being scientists, and without doubtthey receive good training in the scientific method;but it takes very little anecdotal information toeclipse the scientific judgment of many in theprofession. Albert Szent-Györgyi was probablymore right than he knew when he said, “The brainis not an organ of thinking but an organ of survivallike a claw and fang. It is made in such a way soas to make us accept as truth that which is onlyadvantage.”
No matter how spectacularly orthodontictherapy changes, it will benefit our patientsminimally if we do not have a concomitantimprovement in our diagnostic and prognosticknowledge. This remains the number oneimperative for those who practice orthodontics.Orthodontists should view any new therapyunaccompanied by equally sophisticateddiagnostic knowledge suspiciously. Patients havealready received far too much orthodontictreatment but diagnosis.
Instrumentation
The first attempts to correct malocclusions usedsimple large arch wires ligated to the malposedteeth. Pierre Fauchard of France developed theprecursor of the modern appliance — expansionarch.
This arrangement gave only tipping control,in one dimension, and soon proved inadequatefor controlling rotations. In 1887 Edward H Angle
introduced the E arch, i.e. expansion arch thatused a labial wire supported by clamp bands onthe molar teeth which ligated to the other teeth.
Metallurgical developments by the early 20thcentury allowed clinicians to encase all of theteeth with bands and solder attachments thatcould control the horizontal rotations. Angledeveloped a popular attachment known as thepin and tube attachment in 1911, and it satisfiedmany of the requirements of clinicians; but thisdemanded unusual dexterity, patience and skill,so dental clinicians evolved to a ribbon-archbracket, which Angle introduced in 1918. Itprovided good control in two-dimensions andbecame popular quickly. The ribbon archattachment also marked the first time orthodonticattachments gained the name bracket.
When Angle launched the ribbon-arch bracket,he had already started work on the edgewisebracket primarily as a supplement to his ribbon-arch appliance. Nevertheless, the edgewisebracket did not suddenly spring full-grown fromAngle’s fertile mind, but slowly evolved withseveral iterations. When Angle realized that thisbracket could deliver three-dimensional controlof the teeth with horizontal, one directionalplacement and simultaneous engagement of allthe teeth, he changed the bracket several timesuntil he achieved it in 1928. It received early andenthusiastic endorsement from dental cliniciansthroughout the United States and eventuallyeclipsed other useful orthodontic appliances suchas the McCoy open tube appliance, the Atkinsonuniversal appliance and the Johnson twin wireattachment.
The universal application and durability ofthe edgewise bracket confirmed Angle’s immodestclaim that it offered the “latest and best inorthodontic mechanisms”. Innovators have addedminor but practical trimmings such as rotatingwings, twin brackets, different dimensions,preadjusted appliances, lingual applications, etc.,but the essence has remained edgewise. For anyinstrument, particularly in the health sciences, toremain virtually unchanged (and almost as usefulfor close to a century) approaches unbelievability.In the automobile industry, this would be equivalentto the Model T Ford remaining as the epitome ofmotoring sophistication.

170 History of Orthodontics
Other than adding wings and doubling thebracket to make the popular twin edgewise bracket,Angle’s invention has remained basicallyunchanged. Holdaway suggested angulations forbrackets to help set anchorage, parallel roots andartistically position teeth, while Lee had built someanterior brackets with the ability to torque incisors.But it was Andrews who was to develop anappliance that would apply first, second and thirdorder movements to the teeth without makingchanges in the wire—hence the Straight WireAppliance. Preadjusted orthodontic applianceshave dominated the profession for the past 30 years,and the belief in them shows little sign of abating,even though many have questioned the one-size-fits-all idea.
And back again...
The publication of Frankel’s work with functionalappliances illustrated significant enlargement ofdental arches and reawakened an interest in non-extraction therapy. Nevertheless, Frankelmechanics required the use of removableappliances, and that did not resonate well withmany orthodontists or their patients. After a briefflurry of interest in the United States, few clinicianscontinued to use the Frankel appliance on aregular basis.
Nevertheless, the successful use of orthopedicappliances alerted orthodontists to the possibilityof increasing arch widths and arch perimeterswith minimum forces. Although mandibularcanines offer significant resistance to expansion,mandibular premolars and first molars oftendemonstrate substantial and stable expansion.Brader hinted at this with his work on the tri-focal ellipse arch form, but he did not followthrough about how this might give wider andmore accommodating arch forms.
Low-force titanium coil expanders haveshown their ability to develop arches laterally,and recently Damon has suggested that low archwire forces, coupled with a passive tube and asmall wire-to-lumen ratio, enable teeth and theiraccompanying dentoalveoli to expand in allplanes of space. Damon feels that using small,low-force wires such as those of Copper Ni-Ti™(Ormco Corporation, Orange, CA) achieves theideal biological forces proposed long ago byseveral investigators.
Self-ligating brackets that essentially form atube, developed several decades ago with theOrmco Edgelok 26 being the first, closely followedby the speed bracket. Both of these early self-ligating systems suffered from the fact that thestraight-wire appliance phenomenon debuted atapproximately at the same time, plus a lack ofappreciation for what the newer titanium wirescould achieve.
Damon has persisted since 1995 with hisversion of a self-ligating bracket and hasfundamentally changed the types of arch wiresand the sequence in which clinicians use them.His experience has shown that with manypatients he can often eliminate distalization ofmolars, extractions (excluding those needed toreduce bimaxillary protrusions) and rapid palatalexpansion. He offers compelling clinical evidenceof doing this with consistency.
The Damon bracket is essentially a tubedesigned with the right dimensions to fostersliding mechanics where needed and enoughplay in the system for torque and rotationalcontrol using the larger cross section wires.Damon starts cases with a large lumen arch wireslot and 0.014 or smaller diameter hi-technologyarch wires. Starting cases with a large dimensionpassive arch wire slot and small diameter wiresdiminishes the divergence of the angles of theslots. This lowers the applied force and bindingfriction.
The most logical questions readers couldpropose would be why has Damon shownsuccessful expansion whereas Angle did not?The quantity of expansion probably differs little,but the quality of expansion offers a quantumchange. Mollenhauer has suggested as muchwith his appeal for light forces. Even thoughAngle used a ribbon arch, (which suggests a thin,delicate wire) the actual size of the wire had thedimension of 0.036 × 0.022 inches. Ligating to thiswire would overwhelm the periodontium andprevent the development of a supportingdentoalveolus. Rather than forming new bone, thesupporting dentoalveolus would simply bend andupon completion of treatment quickly return.Astute clinicians often see this with molardistalization from headgear use and over treatsuch movement in order to compensate for thisregressive bone bending.
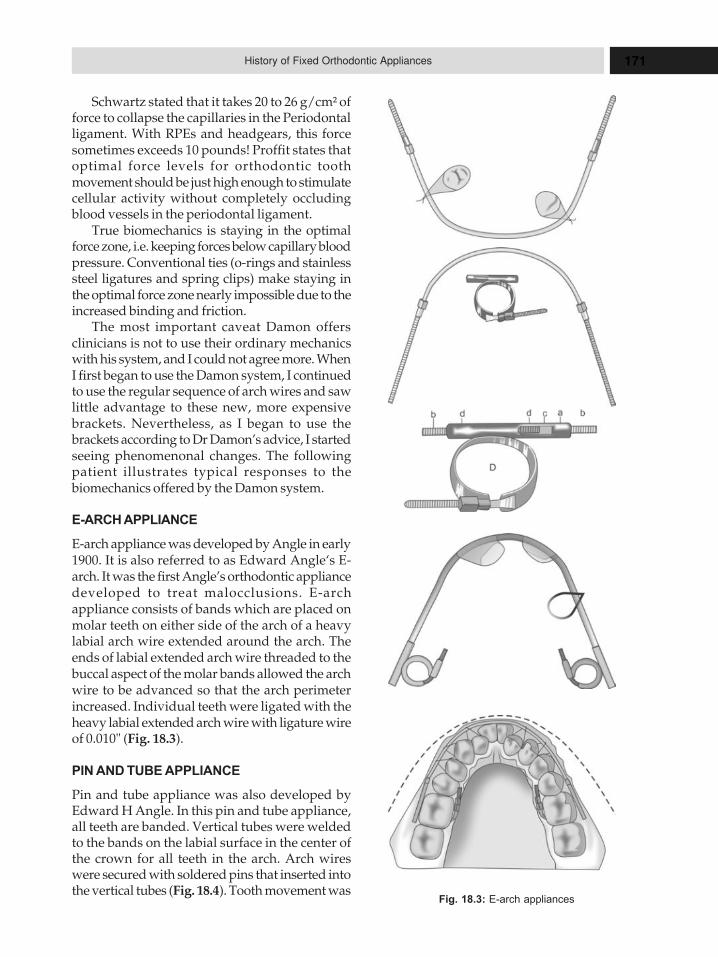
171History of Fixed Orthodontic Appliances
Schwartz stated that it takes 20 to 26 g/cm² offorce to collapse the capillaries in the Periodontalligament. With RPEs and headgears, this forcesometimes exceeds 10 pounds! Proffit states thatoptimal force levels for orthodontic toothmovement should be just high enough to stimulatecellular activity without completely occludingblood vessels in the periodontal ligament.
True biomechanics is staying in the optimalforce zone, i.e. keeping forces below capillary bloodpressure. Conventional ties (o-rings and stainlesssteel ligatures and spring clips) make staying inthe optimal force zone nearly impossible due to theincreased binding and friction.
The most important caveat Damon offersclinicians is not to use their ordinary mechanicswith his system, and I could not agree more. WhenI first began to use the Damon system, I continuedto use the regular sequence of arch wires and sawlittle advantage to these new, more expensivebrackets. Nevertheless, as I began to use thebrackets according to Dr Damon’s advice, I startedseeing phenomenonal changes. The followingpatient illustrates typical responses to thebiomechanics offered by the Damon system.
E-ARCH APPLIANCE
E-arch appliance was developed by Angle in early1900. It is also referred to as Edward Angle‘s E-arch. It was the first Angle’s orthodontic appliancedeveloped to treat malocclusions. E-archappliance consists of bands which are placed onmolar teeth on either side of the arch of a heavylabial arch wire extended around the arch. Theends of labial extended arch wire threaded to thebuccal aspect of the molar bands allowed the archwire to be advanced so that the arch perimeterincreased. Individual teeth were ligated with theheavy labial extended arch wire with ligature wireof 0.010" (Fig. 18.3).
PIN AND TUBE APPLIANCE
Pin and tube appliance was also developed byEdward H Angle. In this pin and tube appliance,all teeth are banded. Vertical tubes were weldedto the bands on the labial surface in the center ofthe crown for all teeth in the arch. Arch wireswere secured with soldered pins that inserted intothe vertical tubes (Fig. 18.4). Tooth movement was
Fig. 18.3: E-arch appliances
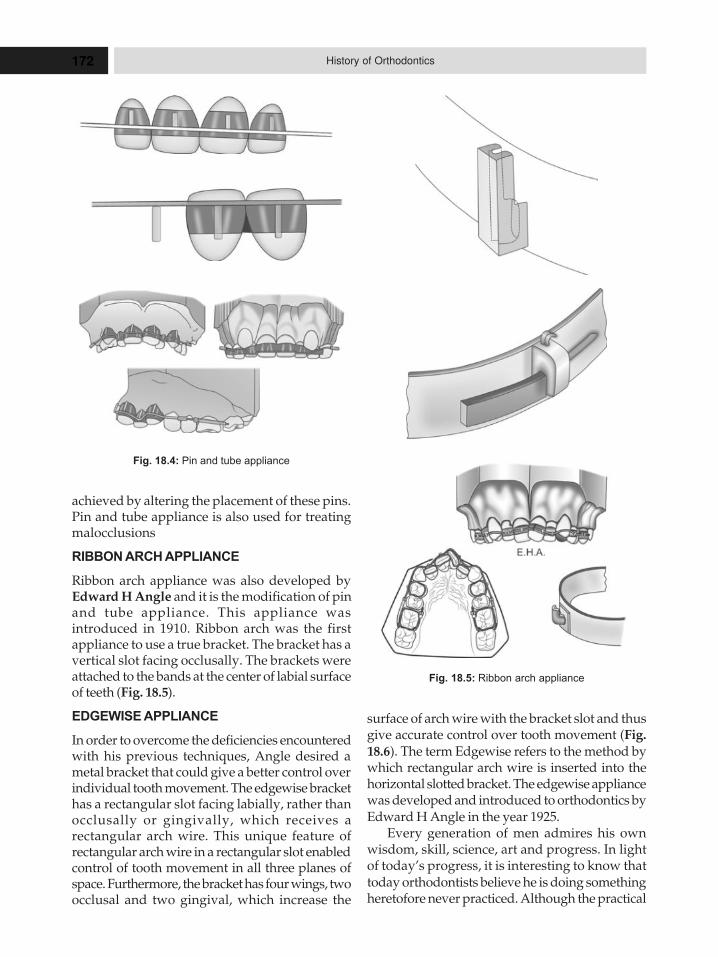
172 History of Orthodontics
surface of arch wire with the bracket slot and thusgive accurate control over tooth movement (Fig.
18.6). The term Edgewise refers to the method bywhich rectangular arch wire is inserted into thehorizontal slotted bracket. The edgewise appliancewas developed and introduced to orthodontics byEdward H Angle in the year 1925.
Every generation of men admires his ownwisdom, skill, science, art and progress. In lightof today’s progress, it is interesting to know thattoday orthodontists believe he is doing somethingheretofore never practiced. Although the practical
Fig. 18.5: Ribbon arch appliance
achieved by altering the placement of these pins.Pin and tube appliance is also used for treatingmalocclusions
RIBBON ARCH APPLIANCE
Ribbon arch appliance was also developed byEdward H Angle and it is the modification of pinand tube appliance. This appliance wasintroduced in 1910. Ribbon arch was the firstappliance to use a true bracket. The bracket has avertical slot facing occlusally. The brackets wereattached to the bands at the center of labial surfaceof teeth (Fig. 18.5).
EDGEWISE APPLIANCE
In order to overcome the deficiencies encounteredwith his previous techniques, Angle desired ametal bracket that could give a better control overindividual tooth movement. The edgewise brackethas a rectangular slot facing labially, rather thanocclusally or gingivally, which receives arectangular arch wire. This unique feature ofrectangular arch wire in a rectangular slot enabledcontrol of tooth movement in all three planes ofspace. Furthermore, the bracket has four wings, twoocclusal and two gingival, which increase the
Fig. 18.4: Pin and tube appliance
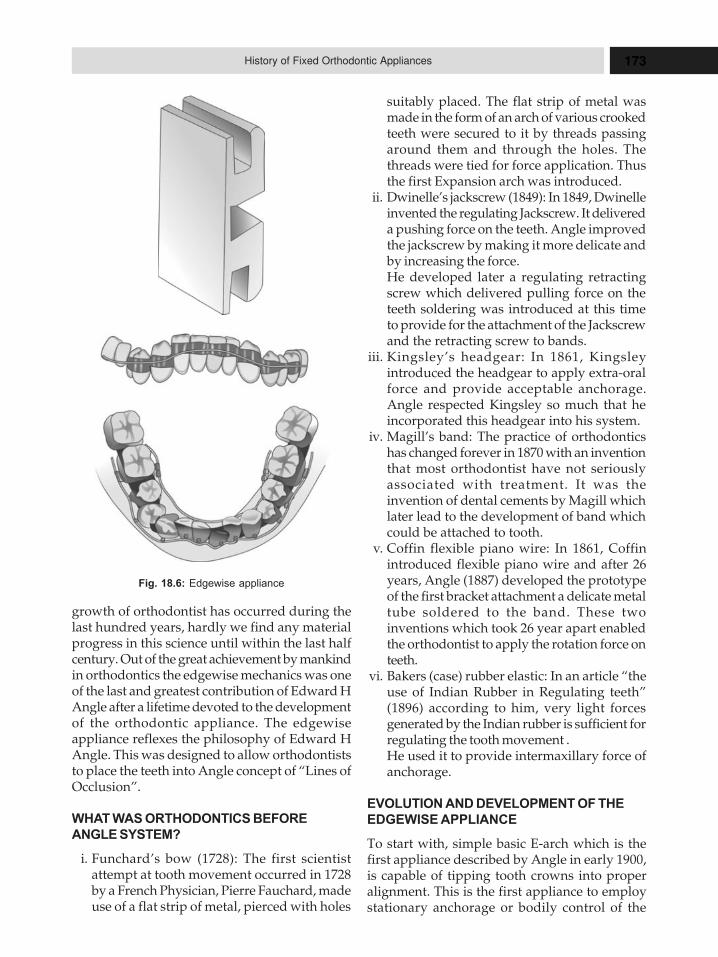
173History of Fixed Orthodontic Appliances
growth of orthodontist has occurred during thelast hundred years, hardly we find any materialprogress in this science until within the last halfcentury. Out of the great achievement by mankindin orthodontics the edgewise mechanics was oneof the last and greatest contribution of Edward HAngle after a lifetime devoted to the developmentof the orthodontic appliance. The edgewiseappliance reflexes the philosophy of Edward HAngle. This was designed to allow orthodontiststo place the teeth into Angle concept of “Lines ofOcclusion”.
WHAT WAS ORTHODONTICS BEFORE
ANGLE SYSTEM?
i. Funchard’s bow (1728): The first scientistattempt at tooth movement occurred in 1728by a French Physician, Pierre Fauchard, madeuse of a flat strip of metal, pierced with holes
suitably placed. The flat strip of metal wasmade in the form of an arch of various crookedteeth were secured to it by threads passingaround them and through the holes. Thethreads were tied for force application. Thusthe first Expansion arch was introduced.
ii. Dwinelle’s jackscrew (1849): In 1849, Dwinelleinvented the regulating Jackscrew. It delivereda pushing force on the teeth. Angle improvedthe jackscrew by making it more delicate andby increasing the force.He developed later a regulating retractingscrew which delivered pulling force on theteeth soldering was introduced at this timeto provide for the attachment of the Jackscrewand the retracting screw to bands.
iii. Kingsley’s headgear: In 1861, Kingsleyintroduced the headgear to apply extra-oralforce and provide acceptable anchorage.Angle respected Kingsley so much that heincorporated this headgear into his system.
iv. Magill’s band: The practice of orthodonticshas changed forever in 1870 with an inventionthat most orthodontist have not seriouslyassociated with treatment. It was theinvention of dental cements by Magill whichlater lead to the development of band whichcould be attached to tooth.
v. Coffin flexible piano wire: In 1861, Coffinintroduced flexible piano wire and after 26years, Angle (1887) developed the prototypeof the first bracket attachment a delicate metaltube soldered to the band. These twoinventions which took 26 year apart enabledthe orthodontist to apply the rotation force onteeth.
vi. Bakers (case) rubber elastic: In an article “theuse of Indian Rubber in Regulating teeth”(1896) according to him, very light forcesgenerated by the Indian rubber is sufficient forregulating the tooth movement .He used it to provide intermaxillary force ofanchorage.
EVOLUTION AND DEVELOPMENT OF THE
EDGEWISE APPLIANCE
To start with, simple basic E-arch which is thefirst appliance described by Angle in early 1900,is capable of tipping tooth crowns into properalignment. This is the first appliance to employstationary anchorage or bodily control of the
Fig. 18.6: Edgewise appliance

174 History of Orthodontics
anchor molar teeth. But Dr Angle realized the shortcomings in this approach and thereafter developedthe pin and tube appliance in 1910, by which thetooth roots could be brought into proper axialrelationships. But the difficulties encounteredwith this mechanism involved the high degree ofskill necessary to obtain proper parallelismbetween the tubes and the arch wire and also thenecessity to unsolder the pins every time. It wasdesigned to move teeth in different locations onthe arch wire and also correction of rotations.
The next step in the evolutionary process wasthe development of the ribbon arch appliance in1915. The ribbon arch bracket was actually thefirst bracket as such, to be used in an appliance. Itis obvious, therefore this was a great step forwardin the development of orthodontic appliances. Thechief advantage of the ribbon arch appliance wasthe fact that rotations were easily accomplished.It is also offered buccolingual and incisogingivalmovements. Gingivo-incisal and gingivo byocclusal movements are also possible.
The main disadvantage was that mesiodistalaxial movement was difficult to obtain, seconddisadvantage is the difficulty in obtaining distaltipping movements of the buccal segments, thirdthe size of ribbon arch itself did not offer thestability thought necessary for stabilization oranchorage of the posterior teeth.
Dr Angle’s final achievement was presentedshortly before his death. The edgewise appliancewas introduced to the dental profession in 1925.The edgewise arch mechanism was designed toallow the orthodontist to place the teeth intoAngle’s concept of “Line of occlusion”. Theoriginal bracket was designed with slot 0.022 by0.028 inch. Over the years, many changes andmodifications have been made in the basicappliance itself.
Gold alloy arch wires were used exclusivelyin the formative years of the appliance. AlthoughDr Angle intended the edgewise appliance to beused only for treatment without the removal ofteeth, to fit into is concept of the line of occlusion,the mechanical principles of this original thinkingwere so sound that the basic philosophy is still inuse today. It will probably have considerable valuein orthodontics for many years to come.
Over the years, new principles of forceapplication and control have been evolved by
orthodontists who have conscientiously studiedthe possibilities and potentials of this appliance.It is interesting to note, that in 1943 Dr RobertStrang made the statement that he was certainthat undiscovered possibilities are still to bebrought forth, from this device to aid the specialistin difficult corrective procedures. However, it isnecessary to constantly bearing mind the basicphilosophy and concepts of the edgewiseappliance as originally presented by Dr Angle.The basic concepts are still the key success withits use.
EVOLUTION OF BRACKET
The evolution of edgewise bracket is the studythat has to be heard and read and never to beforgotten. This story started in 1916 in the form ofribbon-arch bracket as devised by Dr E H Angle.Although it became very popular at that time thebracket could not mask its deficiencies. Some ofthe highlighting faults of these brackets were:a. It could not control tooth movement in all three
planes.b. Root control was not upto expectations.
Hence, Angle decided to modify this bracketand the year 1925 the “edgewise bracket” was bornto overcome the deficiencies of the ribbon arch.Angle reoriented the soft from vertical to horizontaland inserted to rectangular wire rotated 90 degreesto the orientation. It had with the ribbon arch, thusthe name “edgewise”. The bracket was referred toinitially as “open face” or “tie bracket”.
The edgewise bracket by Angle was madewith soft gold with a 0.022 × 0.028" slot that wasreadily deformed by the forces of occlusion andby tying ligature wires to the bracket. The originaledgewise bracket was redesigned into the crosssection that is used today. The original designhas been modified to provide a slightly largerbracket and one with greatly increased tying areaunder the wings; this increased area makes theplacement and tying of ligature wires much easy.
The brackets are modified in so many ways.For examples, single width bracket, twin bracket,curved base twin bracket, twin bracket toothrotation, etc.
EVOLUTION OF EDGEWISE BUCCAL TUBES
The last tooth in the arch that is banded, which isusually a molar, has been commonly referred to

175History of Fixed Orthodontic Appliances
as the anchor tooth. A section of tubing instead ofsome type of edgewise bracket is placed on thebuccal surface of the anchor molar and as is calledthe buccal tube. In edgewise appliance, theoriginal buccal tube was a piece of 0.22 × 0.028"gold or nickel silver tubing soldered to the molarband. The buccal tube is for insertion andstabilization of the arch wire, which is insertedinto the tube horizontally and is thereforecompletely encased in the sheath like structure.
THE CONCEPT OF THE IDEAL ARCH
At an early stage in his development, manrecognized in the arch, a strong, stable frame workupon which to build structures. The igloos of theArctic and the mud huts of the plains are examplesof structures employing the keystone andbalancing effect of arches and domes.
An excellent comparison of the orthodonticarch with other natural arch formations was madesome time ago by Dr Mathew Lasher. He notedthat the shell of an egg has extreme strength inspot of its delicate structure and that the curvedwalls and ceilings of caves maintain their integrityfor millions of years. Dr Lasher went to comparethe architectural arch with the dental arch, acomparison, with slight modification, that isworth reviewing.
Comparison of Architectural
and Dental Arches
To appreciate the concept of the ideal dental arch,it is necessary to describe the basic principleswhich lead stability to the architectural formationknown as the voussoir arch. A series of wedge—shaped units usually made from blocks of stoneare arranged to form a structure with a curvedouter surface and a curved inner surface. This archwill be self supporting even without and joiningmaterial and it is possible to determine thedistribution of forces which tend to maintain andsupport it.
The top block [A] is known as the keystone. BlockB, resting on the ground itself or the structure uponwhich the arch rests is called the abutment. Blocks Cknown as haunches. The curved inner surface iscalled the intrados and the curved outer surface iscalled the extrados. The height of the arch is calledthe rise, and the width is called the span.
The architect must determine geometrically, thecurvature of the arch and the weight is to bemaintained, because each unit of an arch is anactive, working component tending to maintainits own position and to give support to itsadjacent component. There is a central distributionof force between the various blocks that maintainthis structure in equilibrium.
The same principle applies in a dental arch;consider each of the teeth as supportingstructures, each maintaining itself against thepressures transmitted from the adjacent teeth. Theline of force resistances which maintains the teethare properly positioned anatomically ormechanically to produce a balanced arrangement.Therefore, it is imperative that each unit in a dentalarch be in a precise anatomical relationship to itsneighbors and that each contact relationship besuch that forces are distributed through the centerof mass of the crown in the horizontal plane.
There is arch integrity along a smooth curve,through the center of mass in the mesiodistal planein the anterior teeth. These may be termed the“haunches” of the arch. The basis of this smoothcurve is the cuspids, which may be called the“Springers”. The bicuspids and molars aresupports and may be termed the “pillars”. Thisstructure is buttressed or reinforced laterally bythe cheek on the outside and the tongue on theinside. Theoretically the dental arch will maintainitself if the bicuspids and molars are not disturbedby lateral force. If such forces are present, then theentire arch may lose its continuity and its integritywill be destroyed.
Cause for Collapse of Arches
Four basic reasons for failure of arches:1. Slipping of the voussoirs: The curvature of
the arch is either too flat or too pointed andthe haunches or side blocks are more in orout because they cannot take the strain, e.g.Irregular arrangement of teeth.
2. Rotation of voussoirs: The line of action orresistance passes to the outer or inner thirdof the blocks, rather than through the middle,creating a tendency in part of the blocks torotate in the arch and to cause failure.
3. Crushing: The weight imposed on the arch isgreater than the strength of the material toresist.

176 History of Orthodontics
4. Failure of the buttresses: If lateral stressesexceed the limits of the additional support,the buttress will fail, and the entire structurewill collapse.The similarity of problems of the anatomical
arrangement of teeth to those of the architecturalarch has been noted for many years. In dentalarches, only slipping and rotations will cause thecollapse of arches. Slipping is mainly becausewhich irregular arrangement of the teeth androtations of the teeth occurs when the line of forcedoes not pass through the center of mass of thetooth. Crushing of the voussoir arch, does notoccur in the dental arch.
Failure of buttresses: The buttressing effect of thecheeks and tongue against bicuspids and molarsis demonstrated clearly by the integrity andstability of this area when arch widths are notchanged during treatment.
Ideal Arch Form
A consideration of the causes of failure of thedental arch automatically gives an insight intothe primary objectives of orthodontic treatmentfor maximum stability, it is essential that archintegrity be established of ideal arrangement ofthe teeth. The teeth should be positioned asindicated by Edward H Angle to conform to the“line of occlusion”.
Accepting this it is also necessary to acceptthe concept of the ideal arch as essential to a wellbalanced tooth arrangement, that isfundamentally stable and will more likelymaintain its integrity, with this objective all archwires made, and towards it all planned toothmovements are predicted.
The variation in dimension and shape of thedifferent teeth in each arch makes theirrelationship which each of them unique andprecise, if arranged in an ideal arch form. Sincethere is a variation in anatomical dimension in alabiolingual direction of various teeth at thebracket level, it is necessary to consider severalanatomical demands that determine thearrangement of teeth in an ideal arch form, themaxillary arch, the central incisor is a thickertooth than the lateral incisor, and so as the cuspid.
Since the maxillary anterior teeth contact themandibular anterior teeth, it is safe to assume that
the curvature of the lingual surfaces of themaxillary anterior teeth should conform to acontinuous smooth arch. This being the case, thelabial outline of the maxillary anterior teeth at thebrackets will vary according to the differences inthickness of the teeth themselves. The generalposition of all the maxillary anterior teeth mustrelate to the labial contour of the mandibularanterior arch.
In the mandibular arch, arch wireconfiguration again is governed by tooth shapeand size. The variation of the labial outline willbe governed by the dimensions of the individualteeth at bracket level. Consequently, there is adifference between the labial outlines of themaxillary incisal teeth and of the mandibularincisal teeth which relate to the labial contour ofthe mandibular incisal teeth. In the mandibulararch, the labiolingual dimensions of the fouranterior teeth are the same, so that a continous arcis contoured. The smaller labiolingual dimensionsof the mandibular canine reduce the effect in thisarea.
In its normal position, the mesiobuccal cuspin the maxillary and mandibular molar is muchmore prominent than rest of the tooth. Therefore,an offset, or a step out, as it is sometimes called isnecessary to make the wire conform to the buccalsurface of maxillary and mandibular molars.
The general form assumed by the arch wire ineach arch, therefore, must be a curve in the anteriorsection and a general tapering distally,progressively increasing in arch width.
THE IDEAL ARCH WIRE
The purpose of an ideal arch wire is: to transmitto the brackets through the contour of the wire,the ideal arch form of the teeth, for particularpatient.
Forming the arch wire: There are differentmethods of forming an arch wire as well asdifferent techniques for different wires, i. e. goldalloys and stainless steel. Arches are made in oneof the three ways.1. By indirect measurement
a. The Angle methods—using graphb. The Bonwill-Hawley method
2. By direct measurement—patient mouth (Chairside)
3. By adaptation: on a plaster, model

177History of Fixed Orthodontic Appliances
The ideal arch wire can be made by any one ofthose three methods, depending upon theunderstanding and skill of the operator. The“Angle” and “Bonwill-Hawley” methods providea means of obtaining perfect arch symmetry byintermittent checking during the formation of thearch wire.
Characteristics of the Ideal Arch Wire
An ideal arch wire has certain identifyingcharacteristics. It is flat and without bends in itsvertical plane other than the curve of speed. It isbilaterally symmetrical and has the followingbends in the horizontal plane.
The anterior bend: This is the arch that extendsaround the labial of the teeth from cuspid to cuspid.
The lateral set-back bends: Because of thelabiolingual thickness of central and cuspids ascompared to the lateral incisors known as thelateral set-back bends.
The mesial cuspid bends: The demarcationbetween the cuspid eminence bends and the lateralset-backs is made at the mesial of the cuspid andis known as the mesial cuspid bend.
The buccal sweep: The part of the arch wire thatextends distally from the cuspid eminence is nota straight line, but instead it has a slight or gentlecurve running from the cuspid to the end of thearch wire. This gentle curve forms an arch that isat least equal to the thickness of the archwire.
The molar bayonet bends: The first and secondmolars usually extend buccally out from the lineof the cuspid and bicuspid surfaces due to thebuccolingual thickness of those teeth. Tocompensate, the arch wire is bent abruptlyoutward by a double bend called the bayonet bend.
Arch Wire Bends
All bends placed in arch wires during treatmentof the various types of malocclusions with theEdgewise arch mechanism may by classified intothree general types.1. Primary or first order bends: Are those bends
placed in the arch wire that do not alter thehorizontal plane of the wire.Examples: The various bends used to form theideal arch wire when properly placed, permitthe arch wire to lie tangent to a glass slab in itsentirety.
2. Secondary or second order bends : Are alsoknown as tip back bends are bends placed inthe arch wire in the vertical plane. They areutilized to tip the teeth in the buccal segmentsof both dental arches either mesially or distally.In edgewise appliance, three types of secondorder bends are there;i. Tip back bendsii. V bendsiii. Artistic positioning bendsi. Tip back bends: Tip back bends for
preparing anchorage in edgewiseappliance. It is an upward and downwardbend. These bends are placed between IIbicuspid, first molar, and in between Imolar and II molar. The degree of tip backin the terminal molar is such that, whenthe arch wire is placed in the buccal tubes,it will cross the cuspid teeth at the dento-enamel junction.The arch wire when raised and ligated tothe two brackets on the first molars aredepressed. At this point, the arch wire willlie gingival to the brackets of the secondpremolar teeth.
ii. V bend: These V bends are placed betweenthe lateral and cuspid teeth. The apex ofthe V is pointed gingival.Significance: It separates anterior segmentand posterior segment. It differentiatestorque in anterior and posterior segment.
iii. Artistic positioning bends: Are importantfor the finishing phase of treatment. Thesebends are necessary because the long axisof each tooth is inclined relative to the planeof a continuous arch wire. Withoutadequate artistic positioning bends, theincisor teeth are positioned straight up anddown with the roots too close togetherproducing an effect sometimesdisparagingly called “orthodontic look”.
3. Tertiary or third order bends: Better knownas torque are placed in the arch wire to effectbuccolingual or labiolingual root and crownmovements in single teeth or groups of teeth.Torque is a twist in the wire in the horizontalplane. In upper anterior teeth the torque valuein positive means palatal root torque or labialcrown torque and in upper/lower in posteriorteeth torque given in negative is buccal roottorque.

178 History of Orthodontics
ADVANTAGES AND DISADVANTAGES OF
EDGEWISE APPLIANCE
The edgewise appliance was invented by Angleand introduced to the dental profession in 1925.It was then far the advance of any other appliancein the control that it give the orthodontist overthe movement of the teeth, and it has never lostthat position.
From mechanical viewpoint, the best appliancewould be one that offers the most complete controlof the teeth in all three planes of space with theleast amount of material. Edgewise is an exactingappliance, requiring thorough understandingand skill in its manipulation. It is a labial archtechnique offering excellent control in thelabiolingual, mesiodistal and vertical directions.It is possible with one rectangular arch wore tomove teeth in three planes of space. Otherappliances may be able to achieve a comparabledegree of control, but not without auxillaryattachments to the main arch wire.1. The ability to obtain tooth movements in all
three planes of space with a single arch wire.This is true for all the teeth in both arches.
2. The philosophy of treating to an ideal archor the Angle’s concept of the line of occlusion.
3. The use of rectangular or square edgewisearches which, if properly used; control archwidths, arch form, buccolingual crowninclinations, axial root inclinations and incisorcrown and torque.
Disadvantages
1. Operator skill is required. Bends incorporatedin the arch wire should be accurate to getproper finishing of the case.
2. Heavy forces generated: Causes paindiscomfort to the patients, damage to toothroots.
3. Anchorage control or extraoral anchorage:Edgewise mechanism was designed to achieveuniversal tooth movements. But the forcesdelivered by it are much too high. Theseexcessive forces limit its tooth movingefficiency because, high forces prevent toothmovements from being kept under control.When force is applied with the edgewisemechanism, there is movement of the anchorteeth as well as of the teeth which are to bemoved.
4. More chair side time.
5. Tipping of tooth crown is impossible withrectangular wires. It is most important incertain stage of the treatment of almost everypatient, to produce no tooth movement otherthan tipping of tooth crowns. For example,bidentoalveolar potrusion.
6. Patient cooperation: Heavy forces cause pain,as well as for anchorage using headgears.
7. Anterior movement of dental arches: It hasbeen found that, soon after edgewise archwires are fully engaged in tie brackets on all ormost of the teeth their is in most patients, someanterior movements of the dental arches as awhole. The explanation for this anteriormovement is that the sum of the forces exertedby the arch wires and transmitted through thetie brackets to the roots of teeth is to producean anterior thrust on the dental arches. It isbecause tie brackets have a significantmesiodistal dimension arch wires exert forcemesially or distally on tooth roots whenengaged in the brackets.
BUILDING TREATMENT INTO THE EDGEWISE
APPLIANCE
There are several basic principles of applianceconstruction that have been referred to asbuilding treatment into the appliance in thisinstances is defined as the basic components thatare cemented to the teeth—the bends with theirrespective attachments. The shape andmanipulation of arch wire and auxiliaries aredirectly related to the basic appliance that is fixedupon the teeth. Many of the adjustments andtooth movements that require highlycomplicated arch wire bends can be producedwithout these time consuming adjustments, ifsome of the treatment is built into the appliance,by placing the brackets and tubes in such aposition that they become unnecessary. Thefollowing principles will result in more consistentresults with far less effort. The time spent inincorporation of these details into the basicappliance construction will pay large dividends.
Bracket angulations: Angle described howedgewise brackets were soldered to band stripes,with the bracket slot parallel to the band strip, atthe same time, he suggested angulated posteriorbrackets to produce desired tooth movements. Thegeneral rule in the earlier days of the edgewiseappliance was to place the band strip on the teeth
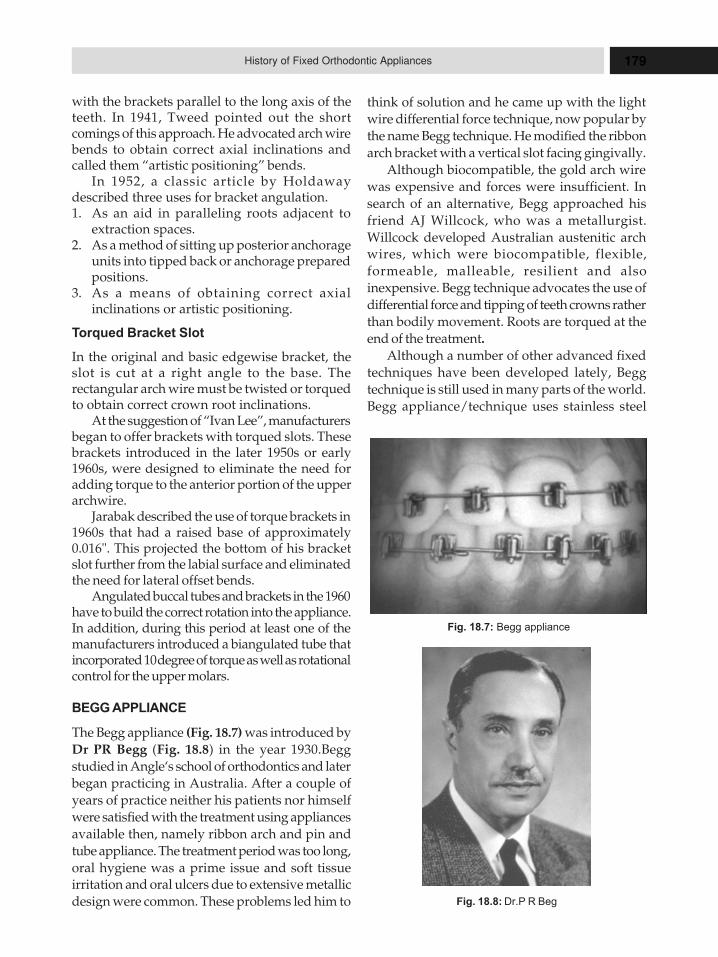
179History of Fixed Orthodontic Appliances
with the brackets parallel to the long axis of theteeth. In 1941, Tweed pointed out the shortcomings of this approach. He advocated arch wirebends to obtain correct axial inclinations andcalled them “artistic positioning” bends.
In 1952, a classic article by Holdawaydescribed three uses for bracket angulation.1. As an aid in paralleling roots adjacent to
extraction spaces.2. As a method of sitting up posterior anchorage
units into tipped back or anchorage preparedpositions.
3. As a means of obtaining correct axialinclinations or artistic positioning.
Torqued Bracket Slot
In the original and basic edgewise bracket, theslot is cut at a right angle to the base. Therectangular arch wire must be twisted or torquedto obtain correct crown root inclinations.
At the suggestion of “Ivan Lee”, manufacturersbegan to offer brackets with torqued slots. Thesebrackets introduced in the later 1950s or early1960s, were designed to eliminate the need foradding torque to the anterior portion of the upperarchwire.
Jarabak described the use of torque brackets in1960s that had a raised base of approximately0.016". This projected the bottom of his bracketslot further from the labial surface and eliminatedthe need for lateral offset bends.
Angulated buccal tubes and brackets in the 1960have to build the correct rotation into the appliance.In addition, during this period at least one of themanufacturers introduced a biangulated tube thatincorporated 10 degree of torque as well as rotationalcontrol for the upper molars.
BEGG APPLIANCE
The Begg appliance (Fig. 18.7) was introduced byDr PR Begg (Fig. 18.8) in the year 1930.Beggstudied in Angle‘s school of orthodontics and laterbegan practicing in Australia. After a couple ofyears of practice neither his patients nor himselfwere satisfied with the treatment using appliancesavailable then, namely ribbon arch and pin andtube appliance. The treatment period was too long,oral hygiene was a prime issue and soft tissueirritation and oral ulcers due to extensive metallicdesign were common. These problems led him to
think of solution and he came up with the lightwire differential force technique, now popular bythe name Begg technique. He modified the ribbonarch bracket with a vertical slot facing gingivally.
Although biocompatible, the gold arch wirewas expensive and forces were insufficient. Insearch of an alternative, Begg approached hisfriend AJ Willcock, who was a metallurgist.Willcock developed Australian austenitic archwires, which were biocompatible, flexible,formeable, malleable, resilient and alsoinexpensive. Begg technique advocates the use ofdifferential force and tipping of teeth crowns ratherthan bodily movement. Roots are torqued at theend of the treatment.
Although a number of other advanced fixedtechniques have been developed lately, Beggtechnique is still used in many parts of the world.Begg appliance/technique uses stainless steel
Fig. 18.7: Begg appliance
Fig. 18.8: Dr.P R Beg
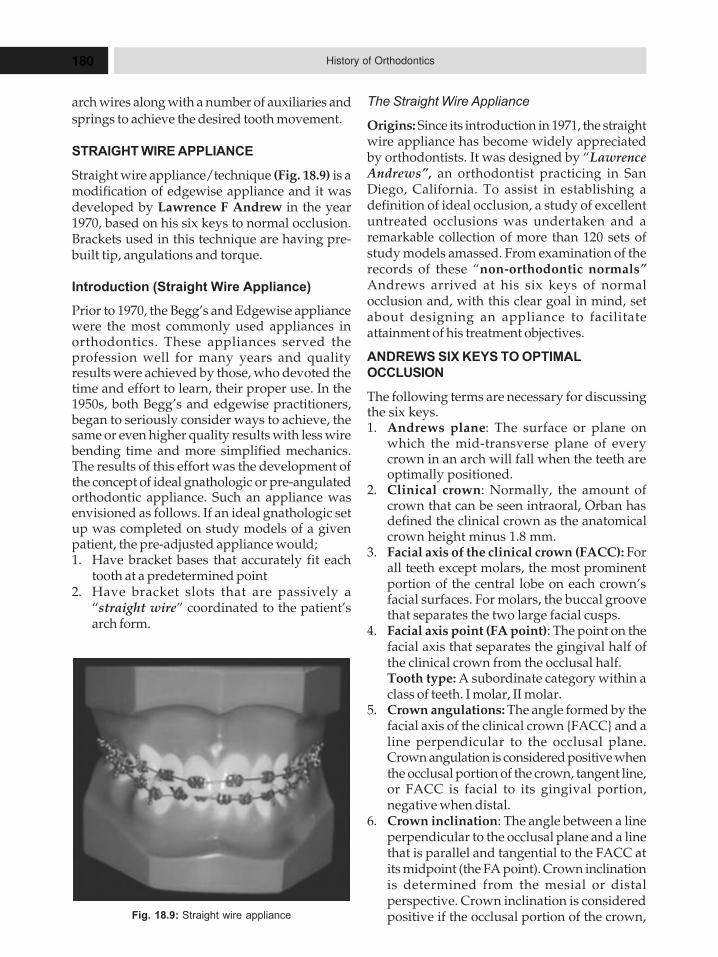
180 History of Orthodontics
arch wires along with a number of auxiliaries andsprings to achieve the desired tooth movement.
STRAIGHT WIRE APPLIANCE
Straight wire appliance/technique (Fig. 18.9) is amodification of edgewise appliance and it wasdeveloped by Lawrence F Andrew in the year1970, based on his six keys to normal occlusion.Brackets used in this technique are having pre-built tip, angulations and torque.
Introduction (Straight Wire Appliance)
Prior to 1970, the Begg’s and Edgewise appliancewere the most commonly used appliances inorthodontics. These appliances served theprofession well for many years and qualityresults were achieved by those, who devoted thetime and effort to learn, their proper use. In the1950s, both Begg’s and edgewise practitioners,began to seriously consider ways to achieve, thesame or even higher quality results with less wirebending time and more simplified mechanics.The results of this effort was the development ofthe concept of ideal gnathologic or pre-angulatedorthodontic appliance. Such an appliance wasenvisioned as follows. If an ideal gnathologic setup was completed on study models of a givenpatient, the pre-adjusted appliance would;1. Have bracket bases that accurately fit each
tooth at a predetermined point2. Have bracket slots that are passively a
“straight wire” coordinated to the patient’sarch form.
The Straight Wire Appliance
Origins: Since its introduction in 1971, the straightwire appliance has become widely appreciatedby orthodontists. It was designed by “LawrenceAndrews”, an orthodontist practicing in SanDiego, California. To assist in establishing adefinition of ideal occlusion, a study of excellentuntreated occlusions was undertaken and aremarkable collection of more than 120 sets ofstudy models amassed. From examination of therecords of these “non-orthodontic normals”Andrews arrived at his six keys of normalocclusion and, with this clear goal in mind, setabout designing an appliance to facilitateattainment of his treatment objectives.
ANDREWS SIX KEYS TO OPTIMAL
OCCLUSION
The following terms are necessary for discussingthe six keys.1. Andrews plane: The surface or plane on
which the mid-transverse plane of everycrown in an arch will fall when the teeth areoptimally positioned.
2. Clinical crown: Normally, the amount ofcrown that can be seen intraoral, Orban hasdefined the clinical crown as the anatomicalcrown height minus 1.8 mm.
3. Facial axis of the clinical crown (FACC): Forall teeth except molars, the most prominentportion of the central lobe on each crown’sfacial surfaces. For molars, the buccal groovethat separates the two large facial cusps.
4. Facial axis point (FA point): The point on thefacial axis that separates the gingival half ofthe clinical crown from the occlusal half.Tooth type: A subordinate category within aclass of teeth. I molar, II molar.
5. Crown angulations: The angle formed by thefacial axis of the clinical crown {FACC} and aline perpendicular to the occlusal plane.Crown angulation is considered positive whenthe occlusal portion of the crown, tangent line,or FACC is facial to its gingival portion,negative when distal.
6. Crown inclination: The angle between a lineperpendicular to the occlusal plane and a linethat is parallel and tangential to the FACC atits midpoint (the FA point). Crown inclinationis determined from the mesial or distalperspective. Crown inclination is consideredpositive if the occlusal portion of the crown,Fig. 18.9: Straight wire appliance

181History of Fixed Orthodontic Appliances
tangent line, or FACC is facial to its gingivalportion, negative to lingual.
Key I : Interarch Relationships: Key I patients tothe occlusion and the interarch relationships ofthe teeth. This key consists of seven parts:� The mesiobuccal cusp of the permanent
maxillary first molar occludes in the groovebetween the mesial and middle buccal cuspsof the permanent mandibular first molar.
� The distal marginal ridge of the maxillary firstmolar occludes with the mesial marginal ridgeof the mandibular second molar.
� The buccal cusps of the maxillary first molarocclude in the central fossa of the mandibularsecond molar.
� The buccal cusps of the maxillary premolarshave a cusp embrasure relationship with themandibular premolars.
� The lingual cusps of the maxillary premolarshave a cusp fossa relationship with themandibular premolars.
� The maxillary canine has a cusp-embrasurerelationship with the mandibular canine andfirst premolar. The tip of its cusp is slightlymesial to the embrasure.
� The maxillary incisor overlaps the mandibularincisors and the midlines of the arches match.
Key II: Crown angulations: Essentially all crownsin the sample have a positive angulation.
Key III: Crown inclination:� Most maxillary incisors have a positive
inclination, mandibular incisors havenegative inclination.
� Canines and premolars are negativeinclination. I and II molars have morenegative inclination.
Key IV: Rotations: The fourth key to optimalocclusion is an absence of tooth rotations.
Key V: Tight contacts: Contact points shouldabout unless a discrepancy exits in mesiodistalcrown diameter.
Key VI: Curve of spee: The depth of the curve ofspee ranges from a flat plane to a slightly concavesurface.
Additional Keys
Key VII: Intercuspal position: Intercuspalposition and retruded jaw relation should becoincident.
Key VIII: Anterior guidance: In mandibularprotrusion, opening should be guided by theincisors. There should be disocclusion of all otherteeth.
Key IX: Canine guidance: Lateral movements ofthe mandible should guided by the working sidecanines. There should be disocclusion of all otherteeth on both working and non-working sides.
Key X: Cusp embrasure contact: The intercuspalposition should be even throughout both buccalsegments.
Historical Background
Until the mid 1970s, most fixed appliance therapywas carried out using the standard edgewisebracket, either in single or twin form, having a 90o
bracket base and bracket slot angulations. Archwire bending by the orthodontist was required inorder to achieve adequate results.
Two major disadvantages resulted from thistreatment method:
Arch wire bends were time consuming andtedious. Even in the hands of experienced operator,adjustments were imprecise and hard workrequiring hours of additional chairside attention.
The short comings of the bracket system andthe extreme skill required of the orthodontist,resulted in many undertreated cases which led tothe second disadvantage. Molars were not in atrue class I relationship, lacked torque. In effectthe resulting occlusion, had the appearance of a“nice orthodontic result” rather than a pleasingnatural dentition. Equally important, the long-termstability of tooth alignment was compromised byfailing to establish ideal tooth relationships.
The Straight Wire Appliance
Prior to the 1970s, there were minor applianceadjustments made in the direction of preadjustedappliances (i.e. tipping of the brackets to minimizethe need for II order bends), but it was not untilLawerence F Andrews evaluation andmeasurement of the non-orthodontic normal studymodels, followed by his development of theAndrews’ straight wire appliance that thepreadjusted appliance became a sophisticatedthree-dimensional system commercially availableto the orthodontist.
It was hailed by clinicians as a radical stepforward offering the dual advantage of less wirebending, coupled with an improved quality of

182 History of Orthodontics
finished cases. For the first time, a system secondto offer an escape from the drudgery of wirebending. If the finished stage of treatment wasless taxing on the patient and orthodontist thenperhaps, the quality of the completed case wouldbe greatly enhanced.
The old mechanics and heavy force levels weredeveloped for standard edgewise brackets. Simplydid not transfer to the new sophisticated bracketsystem. Operators found that many unwantedchanges occurred early in treatment in responseto the heavy forces in particular. A “Rollercoaster” effect was frequently observed, withrapid, undesirable deepening of the bite.
Another frequent observation was in the areaof the premolars and canines which tended to tipand rotate into the extraction sites. Suchunwanted tooth movement retarded treatment tosuch a great extent, that the theoretical advantageoffered by the new system was dramaticallycompromised.
The Late 1970s
There was two possible ways to proceed. The routetaken by Andrews (and later by Roth) was tomaintain the same force levels and treatmentmechanics, but introduce features into thebracket system to prevent undesirable changes.Hence extra torque was introduced into incisorbrackets and anti-tip and anti-rotation featureswere added to canine, premolar and molarbrackets. There was the extraction of translationseries of brackets, some of which were altergrouped together to produce the definitive Rothappliance.
Today the straight wire concept has beenmodified by Roth, Ricketts and Alexander. Theadvantages of straight wire appliance include:1. Precise control of premolar and molar torque.2. Bilateral symmetry of buccolingual
inclination.3. Bilateral symmetry of arch form.4. Use of straight arch wires with few or no
bends. This reduces chairside time. Inaddition, the results are not compromised dueto clinicians wire bending limitations.
5. Precise control of finishing in both areas in allthree planes of space.
6. Elastic use is very minimal and confined tolast stage of treatment.
7. Self limitations of movement. Hence, even ifthe patient misses one or two appointmentsnothing untoward can happen.
8. Finishing is excellent, not only is the estheticsenhanced but it is possible to producemutually protected occlusion. The stability ofresult is thereby guaranteed.
LIMITATIONS OF STRAIGHT
WIRE APPLIANCE (SWA)
It is wrong to assume that no wire bending at all isnecessary with Single wire appliance (SWA).While no bending is necessary in the initial stagesof treatment, finishing required some wire bendingin almost every case. First, because the applianceprescriptions are based on averages, they cannotpossibly account for all the variations of tooth sizeand shape. This means that detailing bends wouldbe needed in finishing wires of some patients.
Second, bracket placement is such an exactingrequirement of preadjusted appliance that whenbrackets are not properly positioned, they mustbe repositioned or compensatory bends must bemade. Wire bending may be necessary for overcorrection.
Other criticism that have been leveled againstthe SWA include:1. The higher forces that may be needed2. Torque values3. Attempt to confirm each patient arch to the
same basic arch form.Not withstanding these limitations, the SWA
is a significant step forward in rendering“Quality orthodontic treatment and has come tostay at the end of the treatment, a stage offinishing and detailing is required. Rectangularfinishing arch wires must incorporate a complexseries of adjustments to compensate for labio-lingual crown position (first order bends)mesiodistal root position or tip (second-orderbends) and labiolingual root position or torque(third order bends)”.
Straight wire attachments incorporateindividual adjustments for each tooth, thethickness of the base of each bracket and tubevaries so that ideal alignment can be obtained froma simplified arch form, omitting the inset and offsetbends required with traditional edgewiseappliance. The angle at which the arch wireintersects the long axis of the labial faces of the

183History of Fixed Orthodontic Appliances
teeth is also predetermined in such a way so as tobuild in the optimum tip for each tooth. Finallythe angle at which the slot is set into theattachment is adjusted to provide the ideal torque.
LINGUAL TECHNIQUE
Since the earliest fixed lingual orthodonticappliances appeared in the mid to late 1970s, theyhave been subject to significant vicissitudes.Beginning in 1979, an initial wave of popularityoccurred when the first mass-manufacturedlingual brackets were released in the United States.At that time, the media and public had been madeaware, rather suddenly, of a new technique thatwould allow straightening of teeth, without therequirement for traditional labial “outsidebraces”. No matter how vigorously esthetic labialbrackets (e.g. plastic, polycarbonate, vinyl andceramic brackets) or other moderately effectivealternatives (e.g. Invisalign [Align TechnologyInc., Santa Clara Calif.]) have been promoted overthe years, many adults do not seek orthodontictreatment because of the perceived embarrassmentof wearing braces.
The earliest consistently documented work onlingual appliances began around 1975, when 2orthodontists working independently in Japanand the United States started developing theirown systems to place braces on the inside surfacesof the teeth. The early prototypes were based onmodified, traditional “outside” braces. Muchcredit has been given to late Dr Craven Kurz ofCalifornia, who with co-workers developed theearly Kurz/Ormco lingual bracket system.However, over the same period, significantdevelopment was made by Professor Kinya Fujita,of Kanagawa Dental University in Japan, whocontinues to make great advances in this clinicaldiscipline.
Why Lingual Orthodontics Developed
Slowly in North America
Clinical protocols had not been fully elucidatedin those early days, resulting in many cliniciansfeeling impelled to begin lingual orthodontic caseswithout being fully prepared. Orthodontistsfound that the new lingual technique requiredmuch more rigorous attention in detail, as well asa fundamentally different approach to treatmentplanning and biomechanics. Postural challenges
associated with potential back pain and relateddiscomfort may have discouraged manyoperators— although these difficulties wereovercome with practice and enhanced efficiencyof clinical technique — resulting in theabandonment of many early lingual orthodontictreatments, which were completed with labialappliances. An early generation of frustratedclinicians came to believe that accurate, efficientlingual orthodontic treatment was an inherentparadox — much like earlier views that, achievingmanned flight was impossible. Many negativeperspectives continue to be propagated,particularly in North America. Thus, much of thelong-term development of lingual orthodontictherapy has occurred in other parts of the world,including Japan, Italy, France, Korea, Germany,Singapore and Australia, Turkey, Israel and SouthAfrica, although there are a few dedicatedpractitioners in the United States.
The lingual technique (Fig. 18.10) wasintroduced by Craven kurz in 1976. Dr Craven kurz,
Fig. 18.10: Lingual technique

184 History of Orthodontics
an assistant professor at UCLA school of dentistry,realized that many of his patients were adults.
This led to the development of the concept ofthe lingually bonded appliance, consisting ofplastic Lee Fisher brackets bonded to the lingualaspect of the anterior dentition and metal bracketsbonded to the lingual aspect of the posteriordentition. The plastic brackets were used for theinherent ease of recontouring and reshaping themto avoid direct contact with the opposing teeth.
Dr Fujita of Japan published cases treated withhis modification of the Begg light wire appliance.He had bonded the Begg brackets lingually orpalatally and used the same AJ WillcockAustralian austenitic arch wires contoured to thelingual aspect of the teeth. He explained the archform which resembled a mushroom (when viewedocclusally) and advocated the same basic stepsas in the conventional Begg technique to be usedwith the Begg brackets with a modified base.
The 1970s was an exciting decade fororthodontics. The straight wire appliance wasdeveloped, treatment demands had increased, andadults were seeking treatment in greater numbers.This increasing demand for adult treatmentbrought unique concerns to the profession.Esthetics was then and continues to be a primaryconcern of patients. Adult patients present withunique challenge, of wanting to look good evenduring orthodontic treatment. They havedemands of their work and broader social needsto consider. They think that braces are normallymeant for kids. In an effort to provide solution tothese esthetic problems, tooth colored brackets andwires were also introduced. But these bracketswere invisible only from a distance and stainingof the bracket and the tooth presented a significantproblem. The search for improved estheticalternatives to metal or clear brackets continued.Some orthodontists thought of placing braces onthe lingual side, leaving the labial surfaceretouched.
During the evolution of lingual appliancetherapy, the technique has moved in and out ofpublic and professional favor. Over the years, theappliances and techniques have improveddramatically and as a result, a reliable system hasemerged.
Research has shown that physically attractivepeople achieve higher levels of success in many
aspects of life than unattractive people.Improvement in one’s physical appearance, as iscommon with orthodontic treatment, canpositively affect social and professionalinteractions. The use of unattractive labialorthodontic practice can negatively affect one’sself-esteem. Many patients, if given the choice,would opt for an appliance that was not visible,provided the course and treatment and qualityof results were the same as with a conventionaltreatment. Thus was born the methodology oflingual orthodontics.
Even before the development of true lingualappliance, the orthodontic company Ormco inconjunction with Dr Wildman, had attempted todevelop a system to align the dentition using thelingual approach. This system consisted of apedicle positioner, rather than a multibracketedsystem. Although innovative, the inherentlimitations of this system prevented it from gainingwidespread popularity in orthodontic community.
It was only in early 1970s that Dr Craven Kurz,an assistant professor at UCLA school of dentistry,realized that a major portion of his privateorthodontic practice was dominated by adultpatients. Dr Kurz developed the first true lingualappliance, consisting of plastic Lee Fisher bracketsbonded to lingual aspect of the anterior dentitionand metal brackets bonded to lingual aspect ofposterior dentition. The plastic brackets were usedfor the inherent case of recontouring andreshaping them to avoid direct contact withopposing teeth. Around the same time Dr K Fujitaof Japan published cases treated with hismodification of the Begg light wire appliance. Hehad bonded the Begg bracket lingually and usedthe same Australian A J Wilcock wire contouredto lingual aspect of teeth. He explained the archform which resembled a mushroom and advocatedthe same basic steps as in conventional Beggtechnique to be used with Begg bracket withmodified base. Further, research was carried outby individuals and group of individualsassociated together, with financial finding fromorthodontic manufacturing companies. Thelingual task force was setup by Ormco to developa commercially viable lingual appliance.
The lingual task force pioneers Dr Kurz,Gorman and Smith were the first to conductcourses on the edgewise lingual appliance, Dr
185History of Fixed Orthodontic Appliances
Vince Kelly of Oklahoma and Dr Steve Paige ofFlorida were the first to start giving courses usingBegg appliance lingually.
Dr Dilier Fillon of France is the onlyorthodontist to have restricted his practice tolingual orthodontics exclusively.
Some of the drawbacks encountered duringthe development of lingual orthodontics were :1. Tissue irritation and speech difficulty2. Gingival improvement3. Occlusal interference4. Appliance control5. Base pad adaptation6. Appliance placement and bonding7. Appliance prescription8. Wire placement.Generation 1 1976 Flat maxillary occlusal bite
plane from C-C the lowerincisor and PM bracket werelow profile and half round.No hooks.
Generation 2 1980 Hooks were added to caninebrackets.
Generation 3 1981 Hooks added to all anteriorand PM brackets the firstmolar had a bracket withinternal hook.
Generation 4 1982–84 Addition of low profileanterior inclined plane, hooksoptional.
Generation 5 1985–86 Anterior inclined planebecause pronounced,increase in labial torque inmaxillary anterior regionTPA attachment.
Generation 6 1987–90 Inclined plane because moresquare in shape. Hooks onanteriors and premolarswere elongated. Hooks on allbrackets.
Generation 7 1990– Maxillary anterior inclinedPresent plane is now heart-shaped with
short hooks. The lower ante-rior brackets have larger incli-ned plane with short hooks.The premolars brackets werewidened mesiodistally andhooks were shortened, the
increased width of PM bracketallows better angulation androtation control.
9. Ligation.10. Attachment.
Modifications were done from time to timeto correct these drawbacks :
Drawbacks of Lingual
1. Discomfort to the tongue.2. Difficulty in speech, which usually improves
after two to three weeks of applianceplacement.
3. Extended chairside time needed for applianceplacement and adjustments.
4. Expensive.
Advantages
� The labial enamel surface of anterior teethplays an important esthetic role.
� In labially placed brackets, the susceptibilityof enamel surface to chemical results andplaque accumulation with poor oral hygieneis increased.
� Permanent and unsightly decalcificationmarks can result in labial.
� Easy access for routine oral hygieneprocedures on the labial surfaces.
� Clinical judgment of treatment progress canbe enhanced.
� Evaluation of individual tooth position can beeasily accomplished by having labial surfacefree of distracting metal or plastic brackets.
� Soft tissue responses of the lips and cheeks totreatment can be judged accurately becausethere is no distortion of shape or irritationcaused by labial appliance.Four distinct situations exist where lingual
appliances may be more effective than labialappliances because of their unique mechanicalcharacteristics.� Intrusion of anterior teeth� Maxillary arch expansion� Combining mandibular repositioning
therapy with orthodontic movements� Distalization of maxillary molars.
19HHHiiissstttooorrryyy ooofff
MMMyyyooofffuuunnnccctttiiiooonnnaaalllOOOrrrttthhhooodddooonnntttiiiccc AAAppppppllliiiaaannnccceeesss
� History of Activator
� History of Frankel Appliance
� History of Bionator
� History of Oral Screen
� History of Herbst Appliances
� History of Twin-Block Appliance
� History of Double Plate
� History of Tooth Positioner
The term “Functional appliance” means thatwhen the appliance is fully seated in the mouth,the mandible is forced into an eccentric/Non-ecentric relation position. Any such mandibularposture causes the musculature to try to move themandible toward a centric position. This resultsin force systems being exerted whenever theappliance is mounted on the teeth or soft tissuesof the mouth.
Although functional appliances have been usedthroughout the century in Europe and in the last40 years in the United States, it was not until thelate 1960s that scientific data were available toevaluate the empiric rationalization for their clinicaleffectiveness. This early data consisted of animalexperiments demonstrating histologic andradiographic evidence of increased growth of thecondylar cartilage when the mandible was heldin a forward position. Breitner’s early monkeystudies and Alexander Petrovic and coworker’sinitial findings and usually rats as models werecomplemented by later primates and rat studiesconducted by number of independent investigators.Petrovic suggested that the unique characteristicof the condylar cartilage, including cell divisionof the prechondroblast (as opposed to thechondroblast in epiphyseal cartilage of his longbones or cartilage in the synchondroses of thecranial base) make this cartilage more responsive
to orthopedic devices. The animal studies of the1960s and 1970s created enormous enthusiasmin the professional community and played animportant role in the rapid acceptance and use offunctional appliances in the United States thathas been largely ignored up till that time.
There were two important considerations thatwere left unanswered. First, would the increasein overall mandibular length achieved withorthopedic devices placed in growing rats andmonkeys also occur in growing children? Second,was the quantitative increase in condylar growthdemonstrated at a cellular level enough of anincrease to make a relevant clinical difference inhumans? In response to these issues, variousinvestigators in the 1970s and 1980s conductedretrospective clinical studies. This was occurringat the same time that many clinicians wereembracing functional appliances as the answerof mandibular deficient patient. A number of theseretrospective studies demonstrated some averagemodest increases in mandibular growth (2–4 mmper year) during treatment with functionalappliances. Other investigators did not considerthe effect of functional appliance on quantitieslengthening of the mandible to be clinicallysignificant. In addition, it became clear that therewas much greater variability in the mandibulargrowth response of humans to functional

187History of Myofunctional Orthodontic Appliances
appliance that in the animal models. Also thevariability of growth potential in response toorthopedic treatment was much greater for themandible than for the maxilla.
The enthusiasm for functional appliance inthe United States during the 1980s considerablymoderated in the 1990s in the light of the lessimpressive results of the retrospective clinicalstudies complemented by clinical experiences.Although a modest mean increase in mandibulargrowth may occur for a group of patients beingtreated with functional appliances, the increaseis not predictable because of the great variabilityin patient’s response. In addition, there still isuncertainty whether discernible mandibulargrowth acceleration is nearly temporal and doesnot result in an absolute final gain in mandibularlength. In other words, it is possible that theultimate length of the mandible may not be alteredappreciably in spite of accelerated growth duringtreatment. There still has been no cleardemonstration that the observed treatment effectsrepresent true growth stimulation beyond the limitof human growth variation. In spite of thecontinued controversy around the reliability ofgains in mandibular length from functionalappliance treatment, there are the effects thatcontribute to the correction of Class IImalocclusion.
ACTIVATOR
Viggo Andresen(1870–1950) (Fig. 19.1) in 1908in Denmark designed a loose filling appliancewhich he first used on his daughter. He made amodified Hawley type of retainer on the maxillaryarch to which he added a lower lingual horse-shoe shaped flange which helped in positioningthe mandible forward. Viggo Andersen removedhis daughter’s fixed appliances before she left forher summer vacation, as was customary at thetime, and placed a Hawley-type maxillaryretainer. On the mandibular teeth, he placed alingual horseshoe flange that guided the mandibleforward about 3 to 4 mm in occlusion. Andresen,a Danish dentist, did not start specializing inorthodontics until 1919. On his daughter’s return,he was surprised to see that nighttime wearing ofthe appliances had eliminated her Class IImalocclusion, and it was stable. Applying thistechnique to other patients resulted in significant
sagittal corrections that he could not produce withconventional fixed appliances. The originalAndresen activator was a tooth-borne, looselyfitting passive appliance consisting of a block ofplastic covering the palate and the teeth of botharches, designed to advance the mandible severalmillimeters for Class II correction and open thebite 3 to 4 mm. The original design had facetsincorporated into the body of the appliance todirect erupting posterior teeth mesially or distally,so, despite the simple design, dental relationshipsin all 3 planes of space could be changed. Indesigning an inert appliance that fitted loosely inthe mouth and, because of its mobility, transferredmuscular stimuli to the teeth, jaws, andsupporting structures, Andresen had taken adecisive step in orthodontic treatment. Althoughhe had effectively redesigned Robin’s monoblocto correct Class II Division 1 malocclusions, hedeclared that he had no knowledge of Robin’swork at the time. Andresen’s novel device wasnot initially well received. First, removableappliances were not much accepted at that time.Second, the profession was under the influence of
Fig. 19.1: Viggo Andersen
188 History of Orthodontics
Martin Schwarz, whose active plate was then acommon form of removable not functionalappliance. Finally, Andresen advocatedextractions, although not necessarily inconnection with activator treatment. And, incontrast to Angle’s concept of ideal occlusion thatwas then prevalent, Andresen advocated a morerealistic “individual and functional gnathologicaloptimum”. Thus he was subjected to the same typeof ridicule that Tweed endured years later. In 1925,Andresen, then director of the orthodonticdepartment at the University of Oslo, begandeveloping for the government a simple methodof treating Norwegian children. He modified hisretainer into an orthodontic appliance, using awax bite to register the mandible in an advancedposition. At the university, Karl Häupl (1893–1960)(Fig. 19.2), an Austrian pathologist andperiodontist, saw the possibilities of the applianceand became an enthusiastic advocate of what heand Andresen called the “Norwegian system”.Häupl’s theories were inadvertently strengthenedby the findings of Oppenheim, who showed thepotential tissue damage caused by the heavyorthodontic forces of fixed appliances. At that time,
there was no mention of “growth stimulation”.Activator use became so widespread amongEuropean practitioners that there was concern thatproper diagnosis was being neglected.Unfortunately, reminiscent of Angle’s following,“functional jaw orthopedics became a professionof faith, a religion, beside which no other opinionwas tolerated”. Furthermore, Reitan, in his 1952doctoral thesis, questioned Roux’s hypothesisand demonstrated that no special histologicpicture emerged from the use of functionalappliances. His findings were supported by laterresearchers. Andresen and Häupl latercollaborated on a textbook (Funktions-kieferorthopädie) about their system in 1936. Thesixth edition included Leopold Petrik as coauthor.Although Häupl’s complete rejection of fixedappliances led the profession astray for a time,had it not been for his promotional efforts, theactivator might have languished in obscurity. Theadvantages of the activator include:1. Treatment in the deciduous and early or late
mixed dentition is possible and successful,2. Appointments can be spread out to 2 months
or more3. Tissues are not easily injured4. The appliance is worn at night only and is
acceptable from an esthetic and hygienicstandpoint
5. It helps eliminate pressure habits, mouthbreathing, and tongue thrusting.
Its disadvantages include:1. Success depends on patient compliance2. Activators are of little value in marked
crowding, so that patients must be selected3. The appliance does not obtain a good
response in older patients4. Forces on individual teeth cannot be
controlled with the same degree of exactnessas in fixed appliances.
During the time of Viggo Andresen and Häuplthe appliances were made of vulcanized rubber,but this gave way to acrylic in the 1950s. Over theyear, various modifications have been made tothe original design of Andresen’s appliance suchas:1. The bow activator of AM Schwartz2. Wunderer’s modification3. The propulsor4. Cutout or palate free activatorFig. 19.2: Karl Häupl
189History of Myofunctional Orthodontic Appliances
5. The reduced activator or cybernator ofSchmuth
6. Kawetzky modification7. Herren’s modification of the activator.
Most of the modifications of Andresenappliance were based on Andresen’s concepts.There can be advantages to using a simple designin terms of patient cooperation, case of adjustmentand freedom from breakages.
Graber Observed That
“Numerous modifications have been made to theAndresen—Häupl monobloc and have beendescribed in texts and periodical contributions byPetrik, Eschler, Hoffer, Grossman and others. Theseare surprisingly effective at times but generally asimpler design of appliance is performed.”
FRANKEL APPLIANCE
A more recent innovation in functional appliancedesign, the functional corrector or functionalregulator or Frankel Appliance was designed byRolf Frankel (Fig. 19.3) in Germany and wasintroduced to orthodontics in 1966. This appliancewas unique in that, it was principally tissue-borne,mostly supported in the vestibule rather thansupported by teeth. There are five types of Frankelappliances and are used for management ofAngle’s class I, Class II and class III malocclusionsand even it is used in bimaxillary protrusion.Types and their indication in specificmalocclusion is explained below.
Types of Frankel Appliance
There are five types of Frankel’s Appliances a areas follows:1. FR-I is further divided into 3 types:
FR-I aFR-I bFR-Ic
2. FR-II3. FR-III4. FR-IV5. FR-V
Indications of Various Types of Frankel
Appliance
FR-I a appliance of Frankel: Treating Angle’sclass I malocclusion with deep bite.FR-I b appliance of Frankel: Indicated for treatingcases of Angle’s class II division 1 malocclusionwhere the overjet does not exceed 5 mm.FR-I c appliance of Frankel: Indicated for treatingcases of the Angle’s class II division I maloccl-usion where the overjet is more than 7 mm.FR-II appliance of Frankel: Indicated for treatingcases of Angle’s class II division 1 malocclusionand class II malocclusion.FR-III appliance of Frankel: Indicated for Angle’sclass III malocclusionFR-IV appliance of Frankel: Indicated for treatingbimaxillary protrusion and open bite.FR-V appliance of Frankel: It is used with head-gear.
BIONATOR
The Bionator was developed in Germany byWilhelm Balter in the early 1950s to increasepatient’s comfort and facilitate daytime wear toincrease the functional use of the appliance. Balteraccomplished this by drastically reducing acrylicbulk of the appliance. There are three types ofBionators ,1. Standard bionator2. Class III or Reverse bionator and3. Open bite bionator.
Standard Bionator
Standard bionator is used for the treatment of classII division 1 malocclusion and Angle’s class I malo-cclusion having constricted (narrow) dental arch.Fig. 19.3: Rolf Frankel
190 History of Orthodontics
Class III or Reverse Bionator
Class III bionator is also known as reversebionator and is used for the treatment of Angle’sClass III malocclusion caused due to mandibularprognathism.
Open Bite Appliance
This type of bionator is used in open bite cases.
Uses of Bionatar
1. Class II malocclusion.2. Class III malocclusion.3. Deep bite cases.4. Open bite cases.
ORAL SCREEN (VESTIBULAR SCREEN)
Newell in 1912 introduced oral screen. It iscomposed of acrylic base material which fits inthe buccal/labial vestibule of the mouth.
Indications
Indications for oral screen includes1. Oral habits such as
a. Thumb sucking or Mouth breathingb. Tongue thrustingc. Lip biting.
2. In cases of mild proclination of maxillaryanterior teeth.
HERBST APPLIANCE
The Herbst bite jumping mechanism wasdeveloped by Emil Herbst in the early 1900s.Theoriginal banded design of this appliance wasintroduced at the International Dental Congressin Berlin (Germany) by Herbst in 1905.It wasintroduced by Pancherz. Pancherz (Fig. 19.4) useda banded Herbst design that involved the� Placement of bands on molar
and premolarMaxilla� Bands are connected by copper
lingual wire� Bands on lower right first premolar
and lower right first premolarMandible� Bands are connected by a
lower lingual arch wireThe Herbst appliance is a fixed functionalorthopedic appliance having passive tube andplunger system with the exact length of the tube
determining the amount of anterior mandibulardevelopment. The tube is attached to a maxillaryposterior root, whereas the plunger is fixedanteriorly to the mandibular dentition and slidesthrough the tube during opening and closingmovements.
TWIN-BLOCK APPLIANCE
Twin-block appliance is a functional jaworthopedic appliance developed by Scottishorthodontist William Clark in the year 1977.
The Twin-block appliance is composed ofmaxillary and mandibular retainers that fit tightlyagainst the teeth, alveolus, and adjacentsupporting structures. Delta clasps are usedbilaterally to anchor the maxillary appliance tothe first permanent molars and 0.030 inch ballclasps are placed in the interproximal areasanteriorly. The precise clasp configurationdepends on the type of deciduous or permanentteeth and number of teeth present at the time ofappliance construction.
Various designs are available for the lowerpart of the twin block appliance. The originaldesign advocated by Clark and it consists of ahorse shoe of acrylic that extends anteriorly fromthe mesial of the first permanent molars.
The acrylic covers the lingual aspect of thepremolar/deciduous molars and the canines andincisors. In this design, delta clasps are used toanchor the appliance to the first premolar/firstdeciduous molar and ball clasp are present betweenthe canines and lateral incisors, additional ballclasps can be placed between the incisors if
Fig. 19.4: Pancherz

191History of Myofunctional Orthodontic Appliances
appliance retention is thought to be a problem.There should not be any acrylic material touchingthe lower molars, this allows the lower molar toerupt vertically if the acrylic on the maxillary blockis trimmed to increase the vertical dimension.
The Twin-block appliance has been shown toproduce increase in mandibular length, incisorproclination and variations in lower anteriorfacial height.
The posterior bite blocks of the twin-blockappliance can be trimmed to facilitate the eruptionof the lower posterior teeth in patient with a deepbite and an accentuated curve of spee. The blocksalso can be left untouched to prevent the eruptionof the posterior teeth in patients with a tendencytoward an anterior open bite.
Indications
Twin-block appliance most commonly used in thetreatment of class II malocclusions.
Duration of Treatment
Full time wearing of twin block applianceincluding during eating and the duration oftreatment usually is about (9–12) months.
Just as Andresen’s discovery of the activatorwas an accidental outgrowth of his retainer, sowas Hans Peter Bimler’s (1916–2003) (Fig. 19.5)Elastischer Gebissformer (elastic bite former) afortuitous development. As a surgeon treating jawinjuries during World War II, Bimler had deviseda maxillary splint for a patient who had lost hisleft gonial angle. The splint provided a guide into
which the patient could insert the remainder ofhis mandible. In so doing, however, the pull ofscar tissue led to a slight widening of the maxillaryarch. Bimler reasoned that it might be possible toexpand the arch by means of crosswisemandibular movements, and the Bimler appliancewas born. Bimler also developed, about 1938, the“roentgenphotogramm,” by superimposing aphotograph on a head plate, to show therelationship between the skull, the teeth, and thesoft tissues something done today by computer.World War II brought European orthodonticprogress almost to a standstill. Nevertheless,functional appliances got a boost because preciousmetals were no longer available for fixedappliances. In Germany, dentists were ordered tospecialize in functional jaw orthopedics. Still, thewar brought its own brand of progress. Afterseveral modifications, the Bimler applianceachieved its final form in 1949. Compared withprevious functional appliances, its reduced sizemade it possible to wear all day, its elasticityallowed muscular movements to translate moreeffectively to the dentition, and, because the upperand lower parts were connected by a wire, gradualforward positioning of the mandible becamepossible. Also like Andresen, Bimler was attackedby the functional establishment, in particularHäupl, for his new ideas, but every functionalappliance subsequently developed hasincorporated at least one of his innovations.
THE DOUBLE PLATE
A Martin Schwarz (1887–1963) (Fig. 19.6) beganhis career as an ear, nose, and throat physicianbut was diverted into dentistry by famedhistologist Bernhard Gottlieb. He became directorof Kieferorthopaedia, Vienna Polyclinic, and thejaw orthopedics division of the Viennesegovernment in 1939, where he expandedorthodontic service from 100 to more than 3000patients. In 1956, Schwarz attempted to combinethe advantages of the activator and the active plateby constructing separate mandibular andmaxillary acrylic.
THE TOOTH POSITIONER
In 1944, Harold D Kesling (1901–79) (Fig. 19.7)developed the tooth positioner. The techniqueinvolved taking impressions of a patient nearingFig. 19.5: Hans Peter Bimler
192 History of Orthodontics
Fig. 19.6: A Martin SchwarzFig. 19.7: Harold D Kesling
completion, denuding the plaster of appliances,and resetting the teeth into ideal positions (the“diagnostic setup”). From the new models, arubber positioner was made that, if worn enoughhours, acted as a finishing appliance. It could also
be used as a retainer or a recovery appliance. Laterversions were made of other materials, includingclear plastic. Out of these innovations developedT(ooth) P(ositioner) Orthodontics (LaPorte, Ind),which now markets them as Pre-Finishers.
20HHHiiissstttooorrryyy ooofff SSSuuurrrgggiiicccaaalllOOOrrrttthhhooodddooonnntttiiicccsss
� Hullihen
� Blair
� Brown
� Bruhn and Linderman
� Eiselberg and Pehr Gadd
� Rosenthal
� Kazanjian
� Mowlem Appliance
� Pionears
� Mandibular Procedures
Children with congenital malformations suchas cleft lip and palate often require surgicalprocedures along with orthodontic treatment fortheir rehabilitation.
In recent times, new approaches have beenadapted in orthodontic treatment such asimplant placement to gain anchorage anddistraction osteogenesis for advancement ofmaxilla or mandible.
Although orthodontic treatment provides ameans of correcting maxilla-mandibular skeletaldiscrepancies, it is limited to actively growingchildren. In non-growing individuals, surgicalintervention has been implemented tocircumvent this limitation.
The first surgical procedure for the correctionof a craniofacial deformity was reported in 1848,at which time Hullihen successfully performeda partial osteoplastic resection of a prognathicmandible. The subapical osteotomy of theanterior mandible was followed by the removalof a wedge-shaped section of bone from each sideof the mandibular body. The anterior segmentwas then setback into the new position.
Surgical treatment of mandibularretrognathia, however, was not reported until the1st decade of the 20th century, when Blairdemonstrated the use of a bilateral horizontalramus osteotomy to advance the mandible.
Oral and maxillofacial surgical procedures aresometimes necessary to optimize the results oforthodontic treatment. Surgical orthodonticsencompasses all those surgical procedures thatare carried out as an adjunct to, or in conjunctionwith orthodontic treatment. These proceduresmay range from minor surgeries such as toothextraction to major procedures such asorthognathic surgeries of maxilla and/ormandible.
In cases of crowding due to arch length -toothmaterial discrepancy, it may be necessary toextract some teeth to obtain proper alignment ofteeth. Unerupted teeth may require surgicalexposure to facilitate bracket placement and theirsubsequent alignment.
Adult patients with narrow maxilla may needsurgically assisted rapid maxilla expansion tocorrect malocclusion in transverse plane.
Cases with significant skeletal discrepanciesand dentofacial deformities cannot be treatedsatisfactorily by orthodontic management alone.In such cases, surgical correction by means oforthognathic surgeries of maxilla and mandiblemay be indicated to obtain optimal occlusal andesthetics results. Adult patients with significantskeletal malocclusion may also benefit fromorthognathic surgery in whom, growthmodification procedures cannot be carried out.

194 History of Orthodontics
Two years later, Babcock suggested a similarosteotomy for mandibular prognathism .
Osteotomy of the mandibular corpus has alsobeen advocated for advancement of theretrognathic mandible. According to Limberg,Brown in 1918 and Bruhn and Linderman in 1921performed a vertical osteotomy of the mandibularbody followed by acute advancement of theanterior segment. The ensuing defect usuallyhealed by new bone in growth. However, theamount of advancement with these osteotomieswas limited and often associated with instabilityof bone segment fixation.
In an attempt to increase the contact surfacearea between divided bone segments andprovide greater stability of bone fixation,different modifications of mandibularosteotomies were developed. For example, inorder to obtain broader contact surfaces, Cryerand Limberg performed C-shaped arcing andL-shaped oblique osteotomies, respectively,concentric with the desired movement of themandible. Likewise, Eiselberg and Pehr Gadddeveloped step-like sliding osteotomies forlengthening or widening the mandible.
According to Wassmund, in 1927 Rosenthalperformed the first mandibular osteodistractionprocedure by using an intraoral tooth-borneappliance that was gradually activated over aperiod of one month.
In 1937, Kazanjian also performedmandibular osteodistraction by using gradualincremental traction instead of acuteadvancement. After performing modifiedL-shaped osteotomies in the corpus, he attacheda wire hook to the symphysis, thereby providingdirect skeletal fixation to the bone segment to bedistracted. Three days postoperatively, an “overthe face” appliance was placed and activatedwith an elastic band, thereby exerting tractionon the chin and gradually pulling the mandibularanterior segment forward. Seventeen days later,the elastic force was removed. Occlusal splints,connected by rigid bars, remained in place for11 weeks at which time complete consolidationof the jaw had taken place.
Kazanjian’s “over the face” appliance forgradual advancement of the mandible. Eventhough the first distraction osteogenesisprocedures applied gradual traction to the bonesegments and surrounding soft tissues, this
technique did not gain immediate acceptance. Thiswas primarily due to the lack of control over bonesegment manipulation, inadequacy of distractionappliances, and the instability of osseous fixation.Instead, corrective osteotomies remained aprincipal treatment modality for the managementof mandibular deformities, especially after theintroduction of the sagittal split osteotomy byTrauner and Obwegeser.
Although acute bone segment movementsremained the treatment of choice, the adaptationof orthopedic external skeletal fixation to themandible rekindled interest in osteodistraction.The application of external skeletal fixation forcraniofacial fractures was first reported byHaynes, in 1939. Using a number of pinsconnected to a rigid bar, he applied this techniqueto a comminuted, compound fracture of themandible.
Based on external skeletal fixators for thelower extremities, two other external mandibularfixation devices were developed in 1941. TheMowlem appliance and the Converse andWaknitz appliance were similarly designed andconsisted of three main parts: two pairs offixation pins with locking plates located on eitherside of the fracture, and an interveningtelescoping fixation bar.
Stader, in 1942, further modified themandibular external fixator by adding double-plane-joint elements and a threaded rod to connectboth pin fixation clamps (Shaar and Kreuz, 1942).Stader’s fixation appliance was the firstmandibular device that allowed angularadjustments in two planes as well asanteroposterior incremental compression ordistraction.
The early 1950s began a period of rapiddevelopment in orthognathic surgery. In 1954,Caldwell and Letterman developed a verticalramus osteotomy technique, which had theadvantage of minimizing trauma to the inferioralveolar neurovascular bundle. This method couldbe used instead of a body ostectomy to correctmandibular excess. Europe then became the centerof progress. Pupils of the Vienna School ofmaxillofacial surgery, Richard Trauner and HugoObwegeser (1957), introduced the intraoralbilateral sagittal split ramus osteotomy, allowingcorrections in all three planes of space without aneed for bone grafting. Even so, it was not until

195History of Surgical Orthodontics
the early to middle 1960s that mandibular surgeriesbecame popular in the United States. MarshRobinson and SM Moos developed a reliableextraoral procedure for prognathism: the verticalsubsigmoid or vertical ramus osetotomy with abone cut posterior to the inferior dental nerve.Spectacular changes in the midface resulted fromthe treatment of craniofacial deformities and theorbital areas by Paul Tessier in France during the1960s and 1970s. Derek Henderson also developedappropriate planning techniques using acombination of photocephalometry and accuratemodel surgery. He emphasized anticipating soft-tissue changes. Alveolar surgeries were the nextprocedures to gain popularity in the United Statesafter being pioneered in Europe. In 1959, HeinzKöle, a student of Obwegeser, introducedsubapical dentoalveolar osteotomies in the anteriormandible. In 1960, Obwegeser began performingmaxillary surgery and, by 1969, had describedmany LeFort I osteotomies, marking the beginningof a new era in the correction of dentofacialdeformities: before the mid-1960s, maxillarydeficiency was typically treated by mandibularsurgery. Obwegeser also performed the first total2-jaw surgery (1970), facilitating the correctionof extensive aberrations in a single operation.Advances in mandibular surgery includedintraoral vertical oblique osteotomy (foradvancement or setback), total mandibularsubapical osteotomy, and refinement of lowerborder osteotomy. Again, Europeans led the way.In 1972, Paul Tessier came to New York todemonstrate the surgeries he had perfected inthe 1960s, and it was not until then that Americansurgeons, concerned as they were about bloodsupply and total or partial loss of the osteotomizedfragment, could be convinced of the possibilitiesof moving the midface skeleton. In 1974, theEuropean literature featured 104 LeFort Iosteotomies that demonstrated remarkablestability and predictability. In the mid-1970s, Belland Epker started to popularize the procedure,now commonplace in the surgeon’s repertoire.About that time, orthodontists and oral surgeonsbegan to realize that, contrary to current practice,orthodontists, having aligned the separate arches,could better detail the occlusion if the applianceswere left inplace during surgery. Improvementsin the stiffness of orthodontic wire helped make
this possible, even after the introduction of bonding.At the same time, training of oral surgeons startedto include orthognathic procedures. Until about1975, the prevailing concept of facial deformitieswas that they existed only the sagittal plane, but,as diagnosis became more thorough, surgeonsacquired a measure of control over the verticaland transverse dimensions. Plating techniques(1983) and screws for the fixation of jaw fragmentsreduced the risk of relapse and allowedintermaxillary fixation to be dispensed within manypatients. By the 1990s, the use of rigid fixationhad become routine, increasing precision andpatient comfort (eliminating 6 to 8 weeks of wiredjaws, liquid diets, inability to brush lingually, and“claustrophobia”). More recently, the use ofresorbable bone plates in Helsinki and Groningenreduced the risk of leaving plates permanentlyin situ or the necessity of a second operation. Othertechnological improvements have included freeze-dried bone, bovine bone, and autogenous bone;biodegradable osteosynthesis material;hypotensive general anesthesia (to reduce bloodloss); smaller instruments with better intraoraldesigns; computer-aided treatment planning; andcomputerized axial tomography scans(3-dimensional reconstruction).
PIONEERS
Wescott first reported placing mechanical forceson the bones of the maxilla in 1859. He used 2double clasps separated by a telescopic bar tocorrect a crossbite in a 15-year-old girl. However,the entire expansion procedure was slow andtedious, lasting several months. A year later,Angell performed a similar procedure with adifferentially threaded jackscrew connected tothe premolars. Palatal expansion was achievedrapidly in 2 weeks by the separation of themaxillary bones at the midpalatal suture.Goddard, in 1893, further standardized thepalatal expansion protocol. He activated thedevice twice a day for 3 weeks followed by astabilization period to allow the deposition of“osseous material” in the created gap. Codivilla,who lengthened a femur to correct limb lengthdeficiencies, first reported bone lengthening byDO in 1905. Abbot then reported lengthening thetibia and the fibula in 1927. These early efforts

196 History of Orthodontics
were complicated by edema, skin necrosis,infection, and delayed ossification of theexpanded bone.
MANDIBULAR PROCEDURES
Osteotomy of the mandibular corpus was alsoadvocated for advancement of the retrognathicmandible. According to Limberg, Brown in 1918and Bruhn- Linderman in 1921, each performeda vertical osteotomy of the mandibular bodyfollowed by acute advancement of the anteriorsegment. The ensuing defect usually healed bynew bone ingrowth. However, the amount of
advancement with these osteotomies was limitedand often associated with instability of bonesegment fixation. In 1927, Rosenthal performedthe first mandibular osteodistraction procedureby using an intraoral tooth-borne appliance thatwas gradually activated over a month. In 1937,Kazanjian also performed mandibularosteodistraction using gradual incrementaltraction instead of acute advancement. Afterperforming modified L-shaped osteotomies in thecorpus, he attached a wire hook to the symphysis,thereby providing direct skeletal fixation to thebone segment to be distracted.
21HHHiiissstttooorrryyy ooofff CCCllleeefffttt LLLiiipppaaannnddd CCCllleeefffttt PPPaaalllaaattteee
� Demographic Data
� Embryological Aspects
� Classification of Cleft Lip and Palate
� Etiology of Cleft Lip and Palate
� Clinical Features of Cleft Lip and
Palate
� Lip and Palate
Associated Problems
The history of surgery of cleft lip and palatesreaches as far backwards as the pre-christian erato 390 BC when for the first time a cleft lip wasclosed successfully in China. Although Egyptianand Greek medicines developed to a remarkabledegree, no descriptions of cleft operations havesurvived. In the middle ages operations on cleftlip have been several times described. A successfuloperation on a cleft palate did however not occuruntil 1816. This can be explained by the fact thatcleft palates were thought to be secondary tosyphilis, but also because without anesthetic thisoperation was extremely painful and difficult.Graefe in 1816 and Roux in 1819 published thefirst satisfactory results. After the introduction ofchloroform cleft surgery made remarkableprogress. The development of cleft surgery hasbeen chronologically described and finally thepresent state of affairs is discussed.
Long before dentists held the notion that theycould give patients pretty smiles, innovativesurgeons were coping with a challenge far morefundamental: how to give certain unfortunateinfants new faces. Many children born with cleftpalates, unable to nurse, failed to survive becauseof malnutrition. Others were left to die eitherbecause of superstition or because the anomalywas too hideous to contemplate. The term“harelip”, now considered demeaning, is believedto have come from the cleft lip’s resemblance to a
rabbit’s mouth. It was once believed that childrenwith cleft lips were born to women who, whenpregnant, were frightened by the devil, who hadassumed the shape of a hare. The incidence ofcleft lip and palate—the single most commondefect affecting orofacial structures isapproximately 1 in 1000 births; for cleft palateonly, 1 in 200; isolated cleft lips occur in 20% ofall clefts. Cosmetic surgery began in the ancientworld. The Romans performed simple techniquessuch as repairing damaged ears. Physicians inancient India used skin grafts for reconstructivework as early as 800 BC. However, the early historyof cleft lip and palate surgery describes onlyunilateral procedures.
The first report of surgical cleft lip repairappears in Chin Annals, involving repair of anapparently congenital cleft in 390 BC. Thetreatment consisted of cutting and stitching theedges of the cleft together, followed by 100 days ofcomplete bed rest, when the patient could eat onlythin gruel and was not allowed to smile or talk.Hippocrates (400 BC) and Galen (150 AD)mentioned cleft lips, but not cleft palates, in theirwritings. The first exact description in the westernworld of cleft lip surgery was given by JohanYperman, who practiced in the 14th century. Heperformed a 2-layer operation with waxed,twisted thread. In 1552, Houlier proposed suturingpalatal clefts; 12 years later, Ambroise Paré

198 History of Orthodontics
illustrated obturators for palatal perforations. Forcenturies, perforations of the palate wereconsidered to be secondary to syphilis, and cleftpalate was not recognized as a congenital disorderuntil 1556, when Pierre Franco, along with Paré,described in detail the principles and techniquesof cleft palate surgery.
Franco has been called the “father of cleft palatesurgery”. Hendrik van Roonhuyze of theNetherlands (1625–1672) advised that a cleft lipshould be repaired when the baby was between 3and 4 months of age, because if done earlier, theresults would be unfavorable. James Cook ofWarwick (1614–1688) was the first to warn againstremoval of the pre-maxilla because of the dangerof interfering with subsequent growth. PierreFauchard, in his book Le Chirurgien Dentiste,described several different obturators to close thecleft palate defect. The first successful closure of asoft palate defect was reported in 1764 by LeMonnier, a French dentist, using sutures alongwith cautery of the edges (the first palatorrhaphy).In the United States, Matthew Wilson, practicingin the 18th century, was the first to publish anaccount of a cleft lip surgery. Because of the dangersassociated with surgery in any form, especiallythat involving the head or face, it was not untilthe 19th and 20th centuries that such surgeriesbecame commonplace. A successful operation ona cleft palate finally occurred in 1816 when C vonGraefe published the first satisfactory results(Philbert J Roux, called by many the founder ofmodern cleft lip and palate surgery, did so in 1819).Von Graefe cauterized the margins before suturingthem together. When the wound failed to heal, hefreshened the wound margins and fastened themto the cheeks, so that they could not rip out. Roux’soperation is well known because the first patientto undergo this procedure, medical student JohnStephenson, wrote a thesis about it to completehis degree in medicine. After the introduction ofchloroform, cleft surgery made remarkableprogress. In 1820, Jonathan C Warren was probablythe first American surgeon to perform reconstructiverhinoplasty and close a palate successfully. In 1828,he performed a successful closure of a soft palate,noting that, after closure, the width of the hardpalate cleft also diminished. Thus, Warren becamean early pioneer in preoperative orthopedicrepositioning of the pre-maxilla. The first plasticsurgeon in the United States was John PeterMettauer. He performed the first cleft palate
operation in 1827 with instruments that he designedhimself. In 1828, Johann F Dieffenbach enhancedcleft palate surgery by elevating the hard palatalmucosa to allow closure of the hard palate cleft.He also performed the first closure of both hardand soft palates in 1834. The introduction of generalanesthesia in the late 1840s led to great advancesin cleft palate surgery. In the 1840s, Simon PHullihen (1810–1857) advocated surgical repairin infancy before eruption of the dentition andused an adhesive strap from cheek to the otherbefore surgery. In 1861, von Langenbeck was thefirst to use a mucoperiosteal flap, which wasseparated from the hard palate. This method isstill used in many centers. Norman W Kingsley’sTreatise on Oral Deformities as a Branch of MechanicalSurgery in 1880 was the first recognized work onorthodontic and prosthetic treatment of cleft palates.In the field of cleft lip surgery, Hagedorn was aleading pioneer (1884). He used a quadrangularflap to increase the thickness of the medial part ofthe lip. The first attempts at bone grafting in patientswith clefts were performed by von Eiselberg in1901 and Lexer in 1908. Drachter in 1914 reportedclosure of a cleft with tibial bone and periosteum.The 1930s were an important decade fordevelopments in both cleft palate and cleft lip.Blair and Brown (1930) attempted to correct theanterior nares by shifting the tissues toward themidline. Also that year, V Veau, a leading figurein cleft surgery, advised that bilateral cleft lipscould be closed in 2 to 3 stages, depending on thewidth of the gap. His name was perpetuated whenhe devised a 4-part classification of clefts. Later inthe decade, Kilner and Wardill independentlydeveloped the “pushback” procedure (in whichtissue from the palate is moved back to lengthenit). The first cleft palate clinic in the United Stateswas established in 1939 when Herbert Cooperopened the Lancaster (Pa) Cleft Palate Clinic.Cooper’s recognition of the need formultidisciplinary involvement resulted in theformation of a clinic that had all the necessarydental and surgical specialists in one location.He was also among the first to use cineradiographyto evaluate velopharyngeal function. In a patientwith a bilateral cleft palate, the surgical closure ofthe lip is different from that of a unilateral conditionbecause of the position of the pre-maxilla, the shortcolumella, and the absence of the muscles in theprolabium. Surgeons who excised the pre-maxillato suture the gap in the lip did not realize the

199History of Cleft Lip and Cleft Palate
damage being done to maxillary growth with thisoperation. Elastic traction to reposition the pre-maxilla in bilateral cleft lip and palate patients isstill being practiced. In 1950, C Kerr McNeil, oftencalled the founder of modern-day, pre-maxillaryorthopedic treatment, described the use of acrylicappliances to reposition bony cleft segments, inaddition to traction. Also in 1950, TM Graber, inhis PhD dissertation, was the first to document adisturbance in facial growth as a result of palatalsurgery. His work led to the alteration and stagingof surgical procedures. About that time, surgeonsin Europe were inserting bone grafts as a primaryprocedure. In the 1960s, Sheldon W Rosenstein,working with surgeons, introduced the techniqueof placing a plate in the maxilla of a newbornbefore surgical lip closure to guide the maxillarysegments into proper alignment. After lip closure,the aligned segments helped guide the teeth intobetter positions and reduced the incidence andseverity of cross-bite and segment malalignment.The late 1960s and early 1970s was a period whenprimary bone grafting and maxillary orthopedicswere in vogue, but by the 1970s many who hadpreviously advocated the bone-graft procedure hadabandoned it because their results had negativeeffects on the growth of the maxilla and themidface. Others, including Hugo Obwegeser,recommended the LeFort I osteotomy withsecondary bone grafting after development of theadult dentition, especially as an aid to orthodonticand prosthetic reconstruction. Additionally, muchdiscussion has occurred over the role and the timingof pre-surgical appliances. Both the hard palateand the alveolus can be molded with passive moldsand active devices, with the shared ultimate goalsof facilitating surgical repair and providing animproved long-term outcome in both facial formand palatal function.
The word ‘cleft’ literally means a crack, splitor a gap. Orofacial clefts are congenital deformities,which manifest at birth. Cleft lip and cleft palateare the most common congenital malformationsof the head and neck region. The term cleft lip andcleft palate is commonly used to represent twotypes of malformation which are embryologicallydistinct that, is,1. Cleft lip with or without associated cleft palate
(CL ± CP).2. Isolated cleft palate (CP).
The term harelip often used to denote cleft lipshould be discouraged. Cleft lip and cleft palateexhibit wide range of presentation with varyingdegrees of severity; from a small notch in the lipvermillion to a complete bilateral cleft of lip andcleft palate. Cleft may occur in isolation or as partof a syndrome.
Management of these patients is quitechallenging since clefts of lip and palate are usuallyassociated with impaired facial appearance,speech, hearing, mastication, deglutition, dentalocclusion and treatment should address theseproblems. Thus, management of cleft lip and palaterequires a multidisciplinary approach with a longterm treatment plan and individualizedrehabilitation program designed to address thetreatment needs have given patient. Malocclusionis usually present and orthodontic therapy withor without corrective jaw surgery is frequentlyindicated.
The defects generally have profoundpsychosocial implications on the afflicted childrenand their patents. It is reassuring that, with a teamapproach, the defects are fairly correctable andneed not adversely affect the child’s future.
DEMOGRAPHIC DATA
Race
The reported incidence of clefts of the lip andpalate varies from 1 in 500 to 1 in 2500 live birthsdepending on geographic origin, racial and ethnicbackgrounds. The incidence of cleft lip and palateis reported to be highest in Asians (Mongoloids -1 in 500), intermediate in Caucasians and least inNegroid populations (1 in 2000 to 2500).� Jones C (2000) estimated the occurrence of oral
clefts in UK to be 1 in 700 births.� Fough-Anderson (1956) cited 1 in 665 as
incidence of cleft lip and palate in Denmark.� Overall incidence of cleft lip and palate in
human appears to be 1:700 live births.
Sex
Males are more commonly affected by orofacialclefts, than females by a ratio of 3:2.
Cleft lip with or without cleft palate is morecommon in males than in females (2:1),whereasisolated cleft palate is observed to be more commonin female.

200 History of Orthodontics
Type and Side
� Cleft lip with or without cleft palate is morecommon than isolated cleft palate.
� Unilateral clefts are more common ascompared to that of bilateral clefts (pre-alveolar clefts) .
� Unilateral clefts account for 75% of all cleftseen, while bilateral clefts account for theremaining 25%.
� In cases of unilateral clefts, left side is morecommonly affected than the right side. Thereason why left side is more frequentlyinvolved is unknown.
Syndromic and Nonsyndromic
As stated earlier orofacial clefts can occur alone(nonsyndromic) or as part of syndrome withcongenital deformities of other parts of the body(syndromic). Over 300 syndromes are known tobe associated with orofacial clefts. However,clefting syndromes are rare and make up only 5 %of all clefts.
EMBRYOLOGICAL ASPECTS
An understanding of the embryologicaldevelopment of these structures is essential so asto appreciate the etiology of these clefts.
The embryonic development of palate takesplace between 6th and 9th weeks of intrauterinelife. The entire palate develops from twostructures:� Primary palate (premaxilla) and� Secondary palate.
Primary Palate
� The primary palate is the triangular shapedpart of the palate anterior to the incisiveforamen. It is developed from frontonasalprocess by fusion of two medial nasalprocesses; primary palate forms the premaxillawhich carries the incisor teeth.
Secondary Palate
� The secondary palate gives rise to the hardand soft palate posterior to the incisiveforamen. It develops from the fusion of threeparts as follows:
♦ Two palatine shelves, which extend fromleft and right maxillary process towardsthe midline.
♦ Nasal septum which grows downwardsfrom the frontonasal process along themidline.
After the descent of the tongue, the elongatedpalatine shelves become horizontally orientedand are in close proximity to each other by 8thweek. They fuse with each other in the midlineand is represented by the median palatine raphe.The palatine shelves also fuse with primary palateand the nasal septum.
Incisive foramen is present at the junction ofprimary and secondary palates. Fusion betweenpalatine shelves and nasal septum proceeds fromincisive foramen in a posterior direction endingat uvula; whereas, fusion between the primarypalate and anterior borders of the palatine shelvesprogresses in an anterior direction towards thelip.
Cleft Lip and Palate Formation
Cleft lip and palate occur when mesenchymalconnective tissues from various embryologicalstructures fail to merge with each other.� Cleft lip— Arises from failure of fusion between
medial nasal processes and the maxillaryprocess. It can be unilateral or bilateral; andcan be extended into the alveolar process(CL + CP).
� Cleft palate— Arises from failure of palatineshelves to fuse with each other, or with thenasal septum or with the primary palate.
CLASSIFICATION
There are many classifications of clefts. Fewcommonly used ones are given below.
I. Embryologic Classification
Patients with cleft lip and palate can be dividedinto two groups which are embryologically distinct.1. Cleft lip with or without cleft palate (CL ± CP)
Include:♦ Patients with cleft lip and cleft palate (CL
+ CP)♦ Patients with cleft lip without cleft palate
(CL)

201History of Cleft Lip and Cleft Palate
2. Isolated cleft palate (CP) include: Patient withcleft palate alone
II. Classification by the International
Confederation for Plastic and
Reconstructive Surgery (1968)
This classification has three main groups.
Group 1—Cleft of Anterior Primary Palate
a. Lip:♦ Right side♦ Left side♦ Both
b. Alveolus:♦ Right side♦ Left side♦ Both.
Group 2—Clefts of Anterior and Posterior Palate
a. Lip:♦ Right side♦ Left side♦ Both
b. Alveolus:♦ Right side♦ Left side♦ Both
c. Hard palate:♦ Right side♦ Left side♦ Both.
Group 3—Clefts of Posterior Secondary Palate
a. Hard palate:♦ Right side♦ Left side
b. Soft palate : Median.
III. Veau’s Classification
This classification is morphological and describedas four types of clefts:Group I Clefts of the soft palate only.Group II Clefts of the hard and soft palate
extending up to the incisive foramen.Group III Complete unilateral clefts involving
the soft palate, hard palate, alveolarridge and the lip on one side.
Group IV Complete bilateral clefts of the softand hard palate, alveolar ridge andthe lip.
IV. Kernahan’s Stripped ‘Y’ Classification
Kernahan proposed a symbolic classification ofcleft lip and palate deformity using a stripped ‘Y’having numbered blocks. The incisive foramen isrepresented symbolically by a small circle withthe dividing pointing between the primary andsecondary palates.
Each right and left limb is divided into threeportions representing respectively the lip, alveolusand area between alveolus and incisive foramen.The stem of the Y is similarly divided into threeportions representing hard palate and soft palate.Each block represents a specific area of the oralcavity:Block 1 and 4 — lipBlock 2 and 5 — alveolusBlock 3 and 6 — hard palate anterior to the
incisive foramenBlock 7 and 8 — hard palate posterior to the
incisive foramenBlock 9 — soft palate
Each individual can be diagrammaticallyrepresented by stippling appropriate areas ofclefting. In submucous cleft of palate theappropriate section is cross hatched.
ETIOLOGY OF CLEFT LIP AND PALATE
Despite numerous clinical and experimentalinvestigations, the etiology of cleft lip and palatesin humans is still largely unknown palate. In mostcleft cases, no single factor can be identified as thecause. Heredity with superimposedenvironmental factors is considered to be the mostprobable cause of cleft formation.
It is important here to distinguish between twoforms of clefts; Non-syndromic clefts with no otherrelated health problem and syndromic cleftsassociated with other birth disorders orsyndromes.
Syndromic Cleft Cases
In syndromic cases, cleft occurs by monogenicmode of transmission, i.e. by a single mutant geneproducing a large effect. Over 300 syndromes havebeen reported in the literatures which haveassociated clefts along with other defects. Most ofthese syndromes are rare. Some of the relativelycommon syndromes associated with cleft lip andpalate are listed in Box 21.1.
202 History of Orthodontics
Velocardiofaial syndrome (velum=palate, cardia= heart, facies = face) is the most commonsyndrome to exhibit clefts. The features includethe following—� Cleft palate� Cardiac defects� Characteristic facial appearance� Learning problems and speech� Feeding problems.
Nonsyndromic Clefts
Recent investigations show that both heredity andenvironmental factors act together in causation ofnon-syndromic clefts. Such a mode of transmi-ssion of a defect/trait caused by interaction ofmultiple genes and multiple environmentalfactors is known as multifactorial inheritance.
Heredity (Genetic Predisposition)
In contrast to syndromic clefts caused by singlemutant gene, clefts in non-syndromic patients arecaused by multiple genes (polygenic), eachproducing small effects which together create thiscondition.
Every individual carries some genetic liabilityfor clefting, but there is no cleft formation until thethreshold level for expression is reached. Whenthe total genetic liability of an individual reachesa certain level, the threshold for expression isreached and cleft occurs.
Genetic basis of cleft lip and palate issignificant but not predictable. Studies reveal that,less than 40% of cleft lip with or without cleft
palate is genetic in origin; less than 20% of isolatedcleft palates (CP) are genetically determined.
Environmental Factors
Earlier, heredity was thought be single mostimportant causative factor. However, recentstudies have shown that, environmental factorsplay a significant contributory role at the criticaltime of embryogenic development when lip andpalate shelves are fusing.
A number of environmental factors have beensuggested as causative factors including:1. A defective vascular supply to the area
involved during critical time of embryonicdevelopment.
2. A mechanical disturbance in which, size ofthe tongue may prevent union of parts.
3. Excessive concentration of circulatingsubstances such as alcohol, certain drugs(antibiotics, steroids, insulin) and toxins.
4. Viral infections.5. Exposure to radiation.6. Hypoxia.7. Vitamin deficiencies and excesses.8. Stress.
Risk of Producing a Child with Cleft Deformity
1. Every parent has approximately a 1 in 700 riskof having a child with a cleft.
2. Parents having a child with a cleft haveincreased risk of having the 2nd child affected-2% to 5%.
3. If more than one person in immediate familyhas a cleft→ risk rises to 10% to 12%.
4. A parent having a cleft→ has 2% to 5% chanceof producing a child with a cleft.
5. If a syndrome is involved, the risk forrecurrence within a family can be as high as50%
6. Maternal age→ increased risk of clefting isobserved when age of conceiving is late.
CLINICAL FEATURES
Oral clefts commonly affect the upper lip, alveolarridge and hard and soft palates.� The clefting anterior to the incisive foramen is
defined as the cleft of primary palate.� The clefting posterior to the incisive foramen
is defined as a cleft of secondary palate.
Box 21.1: Common syndromes associated with cleftlip and palate� Craniofacial Syndromes� Velocardiofacial syndrome� Apert’s syndrome� Crouzon’s syndrome� Carpenters syndrome� Down syndrome� Encephalocele� Goldenhar syndrome� Hypertelorism� Pfeiffer syndrome� Pierre robin syndrome� Saethre-Chotzen syndrome� Treacher Collins syndrome� Van der Woude’s syndrome
203History of Cleft Lip and Cleft Palate
� A patient may have clefting of primary palate,secondary palate or both.
� The clefts can be complete, i.e. extending theentire distance from the lip to the soft palate orincomplete.
� CL ± CP can e unilateral or bilateral; isolatedcleft palate occurs in midline.
� Severity of CL ± CP may range from a smallnotch on the edge of the vermilion border to awide cleft extending into the nasal cavity.
� Isolated cleft palate may also present withvarying degrees of severity. Mildest form is thebifid uvula. A more severe form is a cleft of thesoft palate. A complete cleft palate constitutesa cleft of the hard palate, soft palate and cleftuvula.
CLEFT LIP AND PALATE ASSOCIATED
PROBLEMS
Most patients with cleft lip with cleft palate (CL +CP) and isolated cleft palate (CP) present with amyriad associated problems.1. Dental problems2. Occlusal problems (malocclusion and
impaired facial aesthetics)3. Feeding problems4. Nasal deformity5. Ear problems6. Speech difficulties7. Psychological problems.
Dental Problems
Cleft involving alveolus often affects thedevelopment of primary and permanent teeth andthe jaw. The cleft usually extends between thelateral incisor and canine area. Teeth may becongenitally absent in the area of cleft or evensupernumerary teeth may also be present. Teethpresent near the region of cleft may bemorphologically deformed or hypomineralized.Crowding or severe displacement of the teeth nearthe region is a common finding. The patient withcleft lip and palate shows the following features .� Lateral incisor on the cleft side may be absent.� Presence of supernumerary teeth� Fusion of teeth� Enamel hypoplasia� Multiple missing teeth� Ectopically erupting teeth� Anterior and/or posterior cross bite
� Periodontal complications� Crowding may be seen� Spacing may be present.
Occlusal Problems
� Clefts involving alveolus and palateinvariably show malocclusion. Patients withclefts especially of the palate, showdiscrepancies in size, shape and position oftheir jaws.
� Most patients exhibit class III malocclusionwith hypoplastic maxilla and relativeprognathism of the mandible.
� Along with missing teeth or supernumeraryteeth, retardation of maxillary growthsignificantly contributes to the developmentof malocclusion. Scar contracture followingearly closure of cleft palate significantlyretards the growth and development of maxillain all three planes of space. Narrow high archpalate with constricted and retruded maxillais a common finding.
Feeding Problems
Structural defects of cleft lip and palate preventnegative oral pressure required for effectivesucking. Feeding is a major problem in thesepatients as food and liquids regurgitate throughthe nose. Thus, breast or bottle feeding by suckingis difficult. However, babies can swallownormally, if they are fed directly toward the hypo-pharynx. The problem can be overcome throughthe use of specially designed nipples that areelongated and have bigger opening which extenddirectly into the hypopharynx. Child may swallowlot of air during swallowing and need frequentburping.
Nasal Deformity
Patients with cleft lips often exhibit deformities ofnasal architecture, especially when the cleftextends into the floor of the nose. Plastic surgeryof nose is usually done at later stage and treatmentafter correction of all clefts and associatedproblems.
Ear Problems
Clefts involving soft palate predispose to middleear infections. This is because the levator and

204 History of Orthodontics
tensor veli palatine, the muscles of soft palate areleft unattached in case of soft palate clefts. Thesemuscles have their origins near the auditory tubeand under normal circumstances allow openingof the auditory tube into the nasopharynxfacilitating equilibrium and the pressure.
In palatine clefts this function is disrupted,the middle ear becomes a closed space without adrainage mechanism. When tube openingmechanism is impaired, there is greatersusceptibility of middle ear infections.Accumulation of serious fluids and then bacteriacan lead to serous otitis media. Chronic otitismedia causes hearing impairment, that is commonin patients with cleft palate.
Speech Difficulties
During normal speech, the tongue, lips, lower jawand soft palate work together in a highlycoordinated fashion to produce the sounds. Thesoft palate is raised during the speech, preventingair from escaping from the nose. The soft palatefunctions as a valve to control the distribution ofescaping air between oropharynx and
nasopharynx. This is called valopharyngealmechanism. (Valo = softpalate).
During speech and deglutition, soft palate iselevated towards the posterior pharyngeal wallby contraction of its muscles. Valopharyngealmechanism cannot function when a soft palate isinvolved by the cleft. The soft palate cannot elevateto make contact with the pharyngeal wall andthis result in escape of air into the nasal cavityproducing hyper nasal speech.
Hearing impairment may further aggravate thespeech problem. Retardation of consonant sounds(i.e. p, b, t, d, k, g) is the most common problem.Speech problem should be addressed at theearliest, and several years of speech therapy maybe needed to achieve intelligible speech.
Psychosocial Problems
Impaired facial aesthetics, hearing and speechproblems often produce psychosocial problemsin these patients. Support of the family,professional help and social worker are allnecessary to the normal well being of thesepatients.
22HHHiiissstttooorrryyy ooofff MMMaaallloooccccccllluuusssiiiooonnnIIInnndddiiiccceeesss
� Index of Orthodontic Treatment Needs
� Peer Assessment Rating
� Index of Complexity, Outcome and Need
� Dental Aesthetic Index
Traditional orthodontic thinking has emphasizedthe major benefits of orthodontic treatment on:the ‘improvement of physical functions, theprevention of tissue destruction and thecorrection of aesthetic impairment’. (StandardDental Advisory Committee, 1973). In times oflimited resources, it is important that patientswho need treatment should be treated and that,when treatment is undertaken, the malocclusionshould be corrected to an appreciable extent.Many studies in the UK and Scandinavia haveassessed the success of treatment by recordingthe various occlusal traits before treatment, andafter treatment.
British Studies
Over recent years, the standard of orthodontictreatment undertaken within the general dentalservices has given cause for concern. Severalreports have suggested that British orthodonticresults are not as good as Northern Europeancountries (Cousins, 1973; Shaw, 1983; Haynes,1979; British Orthodontic Standards WorkingParty, 1986).
A report on child dental health in Englandand Wales (Todd and Dodd, 1985) found that 30percent of 15-year-olds who had previouslyreceived orthodontic treatment were in need offurther treatment. The occlusal index (Summers,1971) was used by Elderton and Clark, (1983) to
record treatment need in a sample of 256 patientsin the Scottish Dental Service, most of thetreatment being undertaken with removableappliances. Some reduction was seen in 88 percent of cases. However, 30 percent of cases wereminimally improved or made worse, and in thosecases which started with a marked malocclusiononly about one-third showed a sizeableimprovement. Sixty-five percent of cases fallingin the ‘No treatment need’ category at the startof treatment showed a sizeable improvement.Thirty-five percent of cases falling in the ‘notreatment need’ category at the start of treatmentshowed no improvement and, in fact, 15 percentwere made worse.
In a further survey of 51 cases with a class IIdivision 1 malocclusion treated with removableappliances (Elderton and Clark 1984), 41 percentof cases finished in the two best categories andsubstantial improvement was found for onequarter of the whole sample. However, 20 percentof the cases showed no improvement at all.
In a study undertaken by the DentalReference Service in 1984 (DHSS 1986), for 59percent of the estimate references (852), thedental officer disaggreed substantially orfundamentally with the proposed treatment. In49 percent of the completed treatments, thedental officer considered the treatment unsatis-factory to a major or fundamental extent.

206 History of Orthodontics
During the year 1986—87, 35,800 orthodonticcases treated within the General Dental serviceswere reported as discontinued (14 percent of allnon-prior approval cases and 26 percent of prior-approval cases).
Scandinavian Studies
Myrberg and Thilander, (1973) assessedtreatment results in 1486 cases. In 60 percent,removable appliances were used, whilst theremainders were treated with fixed appliances.In 54 percent of the cases the result was goodand in 1 percent treatment had no effect.However, the criteria for assessing the successof treatment were not stated.
Berg, (1979) analyzed 246 consecutivelytreated cases, the majority having undergonefixed appliance treatment. The author looked atboth dental cast and radiographic records. Hefound that the objectives were only achieved in43 percent of all cases. Root resorption waspresent in 14 percent of all cases and overjet wasnot eliminated in 13 percent of Class II cases. theobjectives were not achieved in a substantialpercentage of class I, class II, and class IIImalocclusions. Although all the objectives hadnot been attained, substantial improvement hadbeen achieved and the author coined the phrase‘partial success’.
In a further study, Berg and Fredlund, (1981)used the Treatment Priority Index, TPI (Grainger,1967) on 60 cases randomly selected from 329consecutively treated patients in two privatepractices. At the end of treatment, 36 cases (60percent) achieved normal or near normalocclusion. They found the greater reduction inthe TPI score resulted from an improvement inoverjet. It was suggested that the degree ofimprovement was more important than the‘success’ of treatment.
Post-retention Survey
There have been several investigations involvingthe prevalence of malocclusions over 20 years ofage (Ingervall et al 1978 ; Mohlin, 1982 ; Bernholdand Lindquist, 1981). These studies indicate thatthe prevalence of malocclusion in men andwomen is similar to that found in children,although 10 percent of men and 25 percent ofwomen had previously received orthodontic
treatment. Mohlin suggested that the need wasstill high as much of the orthodontic treatmentwas provided 20-30 years ago, probably as acompromise owing to limited orthodonticresources, removable appliances having beenused in two-thirds of the treatments. Thetreatments had probably reduced the severity ofmalocclusions, but had not eliminated them.However, Myrberg and Thilander (1973), havereported mild to severe relapse in 24 percent oforthodontically treated children, 1–5 years aftertreatment.
The long-term stability of orthodontictreatment has been reported for a group of 96patients treated 12–35 years previously(Sadowsky and Sakols, 1982), the majority ofcases having been treated with both upper andlower Edgewise appliances. The authorsrevealed that 72 percent of cases still haddeviations outside the ‘ideal’ range. There wasa tendency for overjet and overbite to increase,as well for the development of lower anteriorcrowding.
Other studies have shown that even whenoptimal treatment results had been achieved,imperfection in alignment and occlusion oftendeveloped in the long-term (Water, 1953; Simonsand Joondeph, 1973; Little et al 1981, 1988; Udheet al 1983; Shields et al 1985). The constraintsimposed by underlying skeletal discrepancieswhich could not be changed by orthodontictreatment alone were highlighted in a review of50 consecutively treated patients with an originaloverjet of 10–15 mm. As few as 6 percentdisplayed an overjet within the normal range(less than 4 mm) on follow-up (Nashed andReynolds, 1989). However, 60 percent of all thepatients had their overjets reduced to less than 5mm as a result of treatment.
Some studies have attempted to determinethe effectiveness of the orthodontic treatmentprovision by the hospital orthodontic service,using recently developed occlusal indices asmeasures of outcome and assessed the influenceof operator, treatment methods, and individualdepartments upon treatment outcome in termsof dento-occlusal change. Pickering and Vig,(1974) in the first application of an index to assessthe effectiveness of orthodontic treatment usedSummer’s Occlusal Index (Summers, 1971) as anoutcome measure to evaluate the effectiveness

207History of Malocclusion Indices
of treatment provided for 351 patients treated inone London hospital. This study revealed that aproportion of patients did not benefit fromtreatment and that fixed appliances were themost effective treatment method. Berg, (1979)used a criterion based approach to assess asample of consecutive cases treated in hispractice. He found that optimal treatment resultswere achieved in only 43 percent of cases. In asimilar evaluation, Berg and Fredlund, (1981)concluded that 60 percent of a sample of casescollected form two private practices had normalocclusions following treatment. While bothinvestigations produced favorable results, ananalysis of 256 completed cases at the ScottishDental Estimates Board using Summer’s OcclusalIndex (Summers, 1971) revealed that treatmentchange was inadequate and the standard oftreatment required improvement (Elderton andClark, 1984). More recently, Jones (1988), carriedout an extensive study using a three- dimensionalassessment of occlusal change of 109 patients. Heconcluded that the overall success of treatmentwas high. This was influenced by the method oftreatment; two arch fixed appliances being moreeffective than removable appliances.
The only large scale study has been carried outby Richmond (1991). He assessed 1210 patients’records obtained from the Dental Practice Boardof England and Wales for orthodontic treatmentneed and treatment standards with the Index ofOrthodontic Treatment Need (Brooke and Shaw,1989) and the Peer Assessment Rating (Richmondet al 1992) respectively. He concluded that thestandard of treatment was poor and many patientsdid not receive an improvement in occlusionfollowing a course of orthodontic treatment.Again, two arch fixed appliance therapy was themost effective treatment method.
There are very few recorded studies dealingwith the evaluation of treatment results in largesamples or in randomly selected cases. In manypublished studies, only successful cases areanalyzed and the frequency with which thedemonstrated results could be achieved is oftennot considered. However, Myrberg andThilander (1973) examined 1486 treated casesand graded the treatment results. In their clinicaljudgment, good results were obtained in 54% ofthe cases.
Petterson and Andren (1978) found that themajority of orthodontic patients were satisfiedwith their treatment results. Although most ofthe patients had found treatment to be‘troublesome’ 76 percent would have been willingto go through the same procedure again. About94 percent would have had their children treatedif they had developed a similar malocclusion.
Fredlund in 1977 (unpublished material)examined the treatment results in all of the 209cases he had started in 1973. Berg (1979) examinedthe treatment results in 264 consecutively treatedcases. Both Fredlund and Berg found thereproducibility of criteria such as ‘good’,‘acceptable‘, etc. to be questionable and theytherefore based their observations on whether ornot so-called ‘text-book’ normal occlusion hadbeen achieved. The results of the two independentstudies were similar : text-book normal occlusionwas achieved in less than 50 percent of the cases.
While many practitioners are convinced thatorthodontic treatment influences the soft tissueprofile, controversy remains concerning theprecise soft tissue response to changes in toothposition. A positive correlation between incisormovement and soft tissue changes has beenreported (Roos, 1977). On the other hand, thestudies of Angelle (1973) and Hershey (1972)showed that changes in tooth position are notsystematically followed by proportional softtissue profile changes. Variables such as lipmorphology, type of treatment (extraction versusnon extraction therapy, choice of extraction),patient gender, and age have been heldresponsible for individual differences in softtissue response (Wisth, 1972, 1974).
Extraction decisions have to be made not onlyby considering the among of crowding but alsothe eventual influence of orthodontic toothdisplacement on the soft tissue surface of the face.No information concerning the correlationbetween the initial among of crowding and thechanges in profile during orthodontic treatmentwas found in the literature. In nonextractiontherapy without extraoral traction, one canassume that tooth alignment protrudes theanterior teeth and the facial profile. In extractiontherapy, tooth alignment partly consumes theextraction spaces. Closing the remaining spaces

208 History of Orthodontics
could retrocline the anterior teeth and retracts thefacial profile.
Williams and Hosila (1976) found thatorthodontic treatment with extraction ofpremolars was accompanied by changes of thesoft tissue profile. In some cases these changesimproved the facial aesthetics; in others anundesired profile outcome could be seen. Forthis reason, a carefully studied extraction policy,accounting for all possible changes, would bevery valuable. The same study indicated thatorthodontic treatment with extraction of four firstmolars results in less incisor retraction than casestreated with extraction of four-first premolarsor maxillary first premolars and mandibularsecond premolars. Clinical observation pointsin the same direction: therapy with moreposteriorly situated extraction seems to result inless incisor retroclination. De Castro (1974)recommended extraction of second premolars incases where retraction of anterior teeth has to beavoided. By this choice, the closing of extractionspaces after alignment would be mainly realizedby mesial movement of posterior teeth insteadof distal movement of anterior teeth.
An important motivation factor fororthodontic treatment is improved dentofacialappearance (Gosney, 1986 ; Birkeland et al 1999).The relationship between physical appearanceand perception of an aesthetic deviation, and theimpact of such a deviation on self-esteem andbody image are important issues in determiningthe benefits from orthodontic treatment.Attention should be given to the specific occlusaland aesthetic deviations that cause concern to thepatients, and assumptions based purely on thegeneral occlusal condition should be avoided(Gosney, 1986). A variety of social, cultural, andpsychological factors, and personal normsinfluence perception of physical attractiveness(Jenny, 1975; Baldwin, 1980). Studies in socialpsychology indicate that physical attractivenessplays a major role in social interaction andinfluence the impression of an individual’s socialskill (Baldwin, 1980; Shaw, 1981).
As orthodontic treatment improves facialappearance, it is assumed to increase self-worth.However, this hypothesis has been difficult toverify. One study on self-concept changes duringorthodontic treatment showed no long-lastingeffect on self-esteem (Korabit, 1994). Another
indicated that a high self- esteem could be relatedto orthodontic concern (Birkeland et al 1996).
Whilst many indices exist to recordmalocclusion, it is important to distinguish thosethat classify malocclusions into types (Angle,1899) and those that record prevalence inepidemiological studies (Bjork et al 1964), fromthose indices that attempt to record treatmentneed for priority. Furthermore, indices used torecord treatment success and treatment difficultywill have differing requirements.
Many indices have been developed with theintention of categorizing malocclusions intovarious groups, according to the urgency andneed for treatment (Summers, 1971; Salzmann,1968; Linder-Aroson, 1974; Lundstrom, 1977;Grainger, 1967; Draker, 1960). Individuals withgreatest treatment need can then be assignedpriority when orthodontic resources are limitedand when the availability of treatment isunevenly spread. Similarly, individuals withlittle need for treatment can be safeguarded fromthe potential risks of treatment (Shaw, 1988).
The early efforts to design indexes were theproduct of workers in the public health field, tryingto establish data about pathologic or handicappingdental conditions. Thus, Klein et al developedthe DMF (decayed, missing, filled) scale that wasand is the ultimate in simplicity is measuring dentalconditions for large numbers of people. Earlyefforts to quantify the extent of malocclusion werebased on the assumptions about ideal occlusionpreviously outlined. As a result, researchers likeGraineger produced data on that basis. From thisdata, he developed the Orthodontic TreatmentPriority Index. Salzmann published theHandicapping malocclusion Assessment (theSalzmann index) that also measures variationsfrom this arbitrary standard. Others working onthis vein of thought include Massler and Frankel,VanKirk and Pennell, Bjork et al, Summers, Freerand Adkin, Ingervall and Ronnerman, and Helm.
Experience made it apparent to someobservers that variation from a very narrow idealoften failed to equitably identify the trulyhandicapping malocclusions. Because of theCHAMPUS program, the Armed forces of theUnited States in 1976 contracted with theNational Research Council to organize a workforce to define “Seriously handicappingorthodontic conditions”. An excellent committee

209History of Malocclusion Indices
of highly qualified workers in the field labored forsome time but was unable to produce such adefinition.
HL Draker Suggested a different approachin which selected deviations from ideal werescored and weighted. He called it theHandicapping Labiolingual Deviation index orHLD Index. Careful reading of the original articlemakes it clear that he made some of themwanting. Then he suggested some changes butnever reported any more test results in his article.A number of indices have been introduced,however, based on his suggestions and have beencalled an HLD Index.
Cons et al approached the index problemfrom purely the appearance standpoint anddeveloped the Dental Aesthetic Index. Theygenerally used the opinions of the lay public asto what constituted unacceptable dentalarrangements from the aesthetic standpoint. TheDental Index has been accepted by the WorldHealth Organization as a screening tool.
Meanwhile in Europe, probably because ofgovernment pressure, much effort was spent ondefining which patients qualified as needingorthodontic treatment to be paid for by thegovernment. It would be helpful to rememberthe extent to which dentistry is socialized inmany of those countries. Brook and Shaw in 1989developed the Index of Treatment Need used inthe United Kingdom. Richmond et al alsodeveloped the PAR (Peer Assessment Rating)Index (1990, 1992) as a tool to measure the resultsof orthodontic treatment and not the need.Espeland et al produced a new approach inNorway for their mixture of public and privatefunding of treatment.
Draker HL, Albany NY in 1960 proposed theHandicapping Labiolingual Deviation (HLD)index which was an attempt to obtain a methodwhich would complement and perhaps substitutefor clinical judgment which, although useful to adegree, is vulnerable because it is entirelysubjective. The three planes commonly used fororthodontic orientation, i.e. the sagittal plane;frankfurt plane and orbital plane are the basisfor HLD measurements. The intention was tomeasure the presence or absence, and the degree,of the handicap caused by the components of theindex, and not to diagnose “malocclusion”. Hefound that labiolingual deviations from a fictitiousnorm rather than the state of occlusion are of
epidemiological importance in establishingprevalence rates for physically handicappingorthodontic defects, and degree of the physicalhandicap. These deviations are measurable indefinite units.
Fastlicht J in 1970 did a study to compare thedegree of crowding of the anterior teeth in caseswhich were treated orthodontically years beforewith those which were not treated, in order todetermine whether treatment had an influencethrough time on the crowding of the incisors. Heconcluded that the crowding of the incisors wasan anatomic-physiologic phenomenon ofadaptation observed in orthodontically treatedcases, as well as in untreated cases, whichresulted from the combination of several factors,such as sex, anatomic predisposition ofdolichocephalic or long-faced persons, tooth-sizediscrepancies, exaggerated overbite, extrusion ofthe canines, reduction of the intercanine width,age, muscle function, and, in some cases,imperfect mechanotherapy. There was lesscrowding of the incisors in the treated group.Thus, it was assumed that treatment had afavorable influence over the stability of the dentalarches.
Summers CJ in 1971 developed the OcclusalIndex (OI) Nine characteristics were scored inthe occlusal index: dental age, molar relation,overbite, overjet, posterior cross-bite, posterioropen-bite, tooth displacement (actual andpotential), midline relations and missingpermanent teeth. The purpose of describing thesescoring procedures in detail are as follows : tostandardize scoring procedures, to indicate howeach scoring procedure is mutually exclusive andenable investigators to apply subjectiveclassification to the objective measurements. TheOI was tested for validity, validity during time,and intraexaminer reliability. The OI appears tocorrelate highly (rs = 0.920) with the clinicalstandard indicating high validity; the OI alsoappears to be valid during time, since the averagegroup scores did not decrease during time. Intra-examiner reliability was very high (rs = 0.963).
Little RM in 1975 proposed the Irregularityindex, a scoring method which involvedmeasuring the linear displacement of theanatomic contact points (as distinguished fromthe clinical contact points) of each mandibularincisor from the adjacent tooth anatomic point,the sum of these five displacements representing

210 History of Orthodontics
the relative degree of anterior irregularity. Perfectalignment from the mesial aspect of the left canineto the mesial aspect of the right canine wouldtheoretically have a score of 0, with increasedcrowding represented by greater displacementand, therefore, a higher index score. Rather thanmeasuring from contact point to ideal arch formor to another subjective point, the actual lineardistance between adjacent contact points isdetermined. Such a measure represents thedistance that anatomic contact points must bemoved to gain anterior alignment.
Eismann in 1980 carried out an investigationon pre-treatment, post-retention and follow-upcasts of 200 patients treated with removableorthodontic appliances to assess changesresulting from orthodontic treatment. He foundthat the extent of abnormal criteria between theinitial casts and the post-treatment casts wasreduced on average to about one-fifth and thisimprovement generally remained constant overthe follow-up period, apart from slight furtherimprovements resulting from reduction ofextraction spaces.
Berg R, Fredlund A in 1981 tried to evaluatethe degree of morphological improvementachieved during treatment. 30 cases wereselected; the recordings were made on pre- andpost-treatment plaster models. The degree ofimprovement, or change during treatment, wasassessed by means of a treatment priority indexworked out by a study-group of Norwegianorthodontists. The findings indicated thatevaluation of treatment results by an index scoresystem may be a contribution to the quantificationof the changes achieved; may relate the degreeof change to the condition before treatment andperhaps to the need for treatment; and may alsopermit comparison of the effects of differenttreatment methods.
Shaw WC in 1983 compared the orthodonticmanpower, finance and training in England andWales, the Netherlands, Norway, Sweden andDenmark to find out the criteria for generalacceptance of an adequate orthodontic service.The following criteria were concluded: (a)treatment should be available to all those in need,(b) the cost should be reasonable, (c) treatmentshould be of a satisfactory standard. Theprinciples emerging from the comparison thatseemed to be relevant to these criteria were—(a)acceptance of the principle that the majority of
treatment be undertaken or at least supervised byspecialists, (b) improvement in the ratio ofspecialists to susceptible age groups bymaximizing training capacity, (c) extension of therole of dental surgery assistants, (d) guidelinesto eliminate unnecessary treatment of acceptablemalocclusions.
Brook PH, Shaw WC in 1989 conducted astudy to formulate a valid and reproducibleindex of orthodontic treatment priority using 222patients referred to a regional orthodontic centerfor advice or treatment. To simulate the use ofthe indices in a screening program, 333, 11–12year old school children were also examined. Thefunctional and dental health component of theindex was based on the index of treatmentpriority used by Swedish Dental Board with fivegrading, grade 1 representing little or no needfor treatment and grade 5 representing greatneed of treatment. The second part of the overallassessment of treatment priority, the aestheticcomponent was based on the SCAN index(Standardized Continuum of Aesthetic Need).The dental photographs of the patients wereevaluated on a 10-point scale in the aestheticcomponent. Satisfactory levels of intra- and inter-examiner agreement was obtained and it wasproposed that the main benefit by use of thisindex to the patient of orthodontic treatmentwould be in improved aesthetics and social-psychological well-being and additionally theeffect this may have on attitudes to dental health.
Richmond S, Shaw WC, O’Brien KD,Buchanan IB, Jones R, Stephens CD, et al in1992 developed the PAR (Peer AssessmentRating) index to assign a score to various occlusaltraits which make up a malocclusion. Theindividual scores were summed to obtain anoverall total, representing the degree a casedeviates from normal alignment and occlusion.The score of zero indicated good alignment andhigher scores (rarely beyond 50) indicatedincreased levels of irregularity. The overall scorewas recorded on the pre- and post-treatmentdental casts. The difference between these scoresrepresented the degree of improvement as aresult of orthodontic intervention and activetreatment. After all 272 cases were evaluated by74 examiners and they concluded that the PARindex provided a single summary score for allthe occlusal anomalies and may be used for alltypes of malocclusions, treatment modalities and

211History of Malocclusion Indices
extraction/non-extraction cases. The scoreprovided an estimate of how far a case deviatesfrom normal and the difference in scores for pre-and post-treated cases reflected the perceiveddegree of improvement and therefore the successof treatment.
Richmond S, Shaw WC, Roberts CT,Andrews M in 1992 developed a method forrelating numerical change in the weighted PARscores to consensus professional judgments inorder to express the degree of improvementresulting from treatment. A panel of 74examiners was asked to examine 128 pairs ofdental casts. Using this index, it was revealed thatat least 30 percent reduction was needed for acase to be judged ‘improved’ and a change inscore usually of 22 to bring about a change judgedto be ‘greatly improved’. It was concluded thatfor a practitioner to demonstrate high standards,the proportion of an individual’s case load lyingin the ‘worse or no different’ category should benegligible and the mean percentage reductionshould be as high as possible (greater than 70percent). The greater the mean percentagereduction in weighted PAR scores the higher thestandard of orthodontics achieved. If the meanpercentage reduction is high and the proportionof cases that have been ‘greatly improved’ is alsohigh, this indicates that the practitioner is treatinga great proportion of cases with a clear need fortreatment, to a high standard.
Richmond S, Andrews M in 1993 assessedthe outcome of treatment provided by a sampleof Norwegian orthodontists using objectivemeasures of assessment. A sample of 220 caseswas collected from Norwegian specialistorthodontists who had agreed to participate inthis study. The index of orthodontic treatmentneed and the PAR index were applied to the pre-and post-treatment cases. They concluded thatthe indices could be used to identify differencesnot only between individual practitioners, butalso health care systems in different countries. Itwas confirmed that the Norwegian orthodontistswere producing a high standard of orthodontictreatment.
Buchanan IB, Shaw WC, Richmond S,O’Brien KD, Andrews M in 1993 compared therelative merits of the PAR index and Summer’sOcclusal Index in terms of validity and reliability.A panel of 74 examiners rated 256 sets of study
models. They found that the occlusal index wasfairly complicated in use and incorporatedseveral weighting mechanisms appropriate toeach developmental stage. The PAR index wasa simple, easy to grasp method of assessingtreatment standards as opposed to the morecomplicated approach of Summer. On the basisof this study it was found that the PAR index isas reliable and as valid a method of assessingorthodontic treatment outcome as is the occlusalindex.
O’Brien KD, Shaw WC, Roberts CT in 1993studied the effectiveness of orthodontictreatment provided by a sample of 17 hospitalbased orthodontic departments. They used indexof orthodontic treatment need and the PAR indexas a measure of orthodontic treatment need andstandard of treatment respectively, in 120consecutively started patients from eachdepartment. The influence of operator, treatmentmethods and individual departments upontreatment outcome in terms of dento-occlusalchange was also assessed. They found that thehospital orthodontic service provided treatmentof a high standard. It was also seen that thegreatest influence upon the standard of treatmentwas the choice of treatment methods andoperator experience. Two arch fixed applianceswere found to be more effective than singlearched fixed appliances and removableappliances. Single arch fixed appliances weremore effective than removable appliances. Therewas also an additional effect arising from theaspirations of the consultant and supportingstaff.
Kerr WJS, Buchanan IB in 1993 used PeerAssessment Rating Index to assess theimprovement produced is a series of 150 casestreated with removable appliances and toascertain in which circumstances they performedmost successfully. The pre- and post-treatmentstudy models were used to assess theeffectiveness of the appliance. As measured bythe PAR index 89.3 percent of a group of patientsselected as suitable for treatment with removableappliances were either ‘improved’ or ‘greatlyimproved’. Of 10.7 percent cases which wereclassified as being ‘worse, no different’, six weremixed dentition cases where the treatmentobjectives were limited to the alignment of oneincisor tooth and only seven were judged as

212 History of Orthodontics
being unsuitable for removable appliances on theground of their malocclusion.
Richmond S, Roberts CT, Andrews M in1994 assessed the need for orthodontic treatmentbefore and after treatment, on a systematicsample of 1225 cases, using the Index ofOrthodontic Treatment Need (IOTN). Theresults showed that the number of patientsneeding orthodontic treatment on aestheticgrounds after appliance treatment fell by 27percent for non-prior approval cases and 45percent for prior approval cases. The number ofpatients needing orthodontic treatment on dentalhealth grounds fell by 36 percent for non-priorapproval cases and 45 percent for prior approvalcases. They also found that upper and lower fixedappliances had the greatest influence or outcomeof treatment in terms of aesthetics and dentalhealth.
Shaw WC, Richmond S, O’Brien KD in 1995published an article describing the developmentand validation of two indices, IOTN (an indexof treatment need) and PAR (an index oftreatment outcome). To assess the extent towhich the indices reflect current orthodonticopinion, a validation exercise was carried out.A panel of 74 dentists was enlisted. Each memberof the panel recorded a personal opinion on theneed for orthodontic treatment and the changedue to treatment of 234 starts and finish studycasts, with standardized rating scales. Themodels were independently scored with theIOTN and the Index of Treatment Outcome (PARindex) by the investigating team. Experiencewith their use in Europe suggested they have auseful role in resource allocation and planning,monitoring and promoting standards, betteruniformity in patient identification and referral,and informed consent.
DeGuzman L, Vig PS, O’Brien K in 1995conducted a study to evaluate the relationshipbetween the subjective estimates of severity ofmalocclusion and treatment difficulty by usinga panel of American Orthodontists and toevaluate the relationship between severity anddifficulty, and the PAR index. A group of 11orthodontists examined the 200 study casts. Theresults of this study made it possible to derive aset of weightings for the PAR index and tocalculate scores that would represent groupingsof malocclusion’s severity and treatment
difficulty, according to the perceptions of a panelof orthodontists. As a result, the PAR index maybe considered to represent a good approximationof malocclusion severity and treatment difficulty,and may be used as an outcome measure for theassessment of dento-occlusal change.
Jenny J, Cons NC in 1996 modified the DentalAesthetic Index (DAI), an orthodontic index thatprovides a single score linking the public’sperceptions for dental aesthetics with objectivemeasurements associated with malocclusion. Itnow had decision-points along the DAI scaledefining specified case severity levels. DAI scoresof 25 and below represent normal or minormalocclusion with no treatment needed or slighttreatment need. DAI scores of 26 to 30 representdefinite malocclusion with treatment elective.DAI scores of 31 to 35 represent severemalocclusion with treatment highly desirable.DAI scores of 36 and higher represent very severeor handicapping malocclusion with treatmentconsidered mandatory.
Turbill EA, Richmond S, Wright JL in 1996conducted a study in which subjective gradingof cases at the Dental Practice Board of Englandand Wales was compared to the Peer AssessmentRating Index (PAR) and Index of OrthodonticTreatment Need (IOTN) in assessing 1505 casessampled at the Board between late 1990 and mid-1991. They concluded that some cases rated as‘greatly improved’ or ‘improved’ by PAR stillhad substantial residual malocclusion (weightedPAR at finish) and/or residual need for treatmentand that the dental advisers disliked PAR’s lowweighting of buccal occlusion and residual buccalspaces.
Turbill EA, Richmond S, Wright JL in 1996used the Index of Treatment Need and PeerAssessment Rating index to assess targeting, useof appliances, and standards of outcome forGeneral Dental Service orthodontic cases collectedbetween 1990 and 1991 and compared them witha sample of cases from an earlier study, collectedbetween 1987 and 1988. The samples of casesused in this study were sub-samples from twoparent samples, each of around 1500 cases. Theyconcluded that since the 1988 study, there hadbeen a trend to acceptance of more cases withlower need for treatment, but no increase intreatments previously defined as ‘unnecessary’.The standard of completed cases had improved

213History of Malocclusion Indices
slightly in terms of both residual need for treatmentand residual malocclusion (IOTN and weightedPAR scores at finish). These limited improvementswere apparently associated with increased useof fixed appliances.
Buchanan IB, Russell JI, Clark JD in 1996did a study to investigate the usefulness of thePAR index as a means of differentiating betweenresults achieved by two different fixed appliancetechniques: the preadjusted Edgewise and theBegg appliance. A group of 41 cases treated usingthe Begg appliance and 41 cases treated usingthe preadjusted Edgewise appliance weregathered. Comparison of results using themonogram and percentage reduction on the twoappliance system groups indicated that the casestreated by the preadjusted Edgewise appliancehad a better outcome. This comparison showedthat there was a significant difference betweenthe two appliance types in terms of treatmentsuccess when the monogram, percentagereduction and comparison of the actual PARscores were considered. Preadjusted Edgewisecases being more successful than the Begg. Thisdifference was much more marked in the caseswith low start PAR score than it was in the highstart group, where the appliance type seemed tobe of less relevance.
Birkeland K, Furevik J, Boe OE and WisthPJ in 1997 used the Peer Assessment Rating indexto assess the treatment results in a postgraduateclinic and to assess the occlusion at a 5 yearfollow-up control, in relation to the originalmalocclusions, and the changes occurring in thefollow-up period. 224 cases were selected andthe treatment result was a 76.9 percent PAR scorereduction. The treatment success was greatest forAngle Class II division 2 with 80.8 percent PARscore reduction, closely followed by Angle ClassII division 1 (78.4 percent). Extractions did notsignificantly influence treatment success andneither did the sex difference.
Saelens NA, deSmit AA in 1998 did a study toinvestigate (in extraction and non-extractiontherapy), the initial amount of crowding, thechanges in the position of the incisors and molars,the changes in the soft tissue profile, and the clinicaloutcome. Three groups of 30 patients wereinvestigated. In all cases, the orthodontic treatmentmoved the molars mesially. The lower incisorsremained in about the same position in the
extraction groups but then proclined in the non-extraction group. The upper incisors wereretroclined approximately 2 mm in the extractiongroups. A change in lip protrusion was found inthe non-extraction group, where tooth alignmentwas accompanied by proclination. It was concludedthat within the appropriate indications, extractionof first or second premolars, or non-extractiontherapy with light-wire appliances and no extra-oral anchorage, leads to good occlusal resultswithout unfavorable changes in the facial profile.
Parker WS in 1998 discussed theHandicapping Labiolingual Deviation Index(CalMod), a lawsuit-driven modification of some1960 suggestions by Dr Harry L Draker, whichproposed to identify the worst lookingmalocclusions as handicapping and offered a cut-off point to identify them. The HLD (CalMod)index went into official use late in 1991, and asof January 1 1998, 135,655 patients had beenexamined orally by qualified orthodontists andscreened using this index. Of this number, 49,537were found to have a score of 26 or greater, andstudy models of these patients were producedand screened by board-qualified orthodontistsfor the fiscal intermediary. The HLD (CalMod)index proved to be a successful tool to identify alarge number of very disfiguring malocclusionsand two known destructive forms of mal-occlusion (deep destructive impinging bites anddestructive individual anterior cross bites). Thesewere all then certified as medically necessaryhandicapping malocclusions.
Firestone AR, Hasler RU, Ingervall B in 1999did a study to investigate the objective need fortreatment and the treatment results for twogroups of patients who were treated in a dentalschool orthodontic clinic approximately 10 yearsapart and to investigate factors predictive ofchange in PAR score and the length of treatment.They concluded that changes in treatmenttechniques and the introduction of new materialshave had a significant positive effect ontreatment outcome in a postgraduate dentalschool orthodontic clinic and improvement inocclusion and alignment was primarily the resultof a reduction in overjet, an increase in thealignment of the maxillary anterior teeth, and areduction in overbite.
Hamdan AM, Rock WP in 1999 did a studyto re-test the validity of the PAR index against

214 History of Orthodontics
assessments by West Midland ConsultantOrthodontists, to compare the validity of threenew weighting systems and to apply the best newweighting system to unweighted PAR scores andexamine the effect for each malocclusion class.Eighty sets of pre- and post-treatment dentalcasts, representing equal numbers of Class I,Class II division 1, Class II division 2, and ClassIII cases were randomly selected. The resultssupported the hypothesis that it is inappropriateto group all orthodontic cases together to derivea generic weighting formula and that weightingsshould be derived separately for eachmalocclusion class. The most valid PAR indexweightings were derived by multiple regressions,modified by the addition to base weights forbuccal occlusion and lower anterior displa-cements. Assessments of treatment outcomeusing point and percentage reductions weremore valid than using the original PARmonogram.
Arnett GW, Jelic JS, Kim J, Cummings DR,Beress A, Worley M et al in 1999 presented atechnique for soft tissue cephalometric analysis.Forty-six adult white models comprised thecephalometric database for this analysis. Theyconcluded that, (a) natural head position mustbe adjusted for some patients using clinicaljudgment,(b) the Soft Tissue CephalometricAnalysis (STCA) is a facial diagnostic tool, (c)STCA diagnosis is used for cephalometrictreatment planning(CTP), (d) clinical facialanalysis is used to augment cephalometricinformation, (e) absolute projection values forimportant soft tissue structures are measured tothe true vertical reference line, (f) the true verticalreference line is placed through subnasal and (g)the true vertical reference line is moved forwardfrom subnasale when maxillary retrusion isindicated by clinical and cephalometric findings.
Birkeland K, Boe OE, Wisth PJ in 2000 did astudy to measure aesthetic and occlusal changesfrom 11 to 15 years of age using the Index ofOrthodontic Treatment Need (IOTN) and PeerAssessment Rating (PAR) Index, to comparetreated and untreated groups using the sameindices. Out of a sample of 359 children simpletreatment with removable appliances was usedin 23.8 percent. They found that children wereless critical in their aesthetic evaluationcompared with that noted by the examiners. The
post-treatment mean PAR scores of 5.8 in thisstudy with 6.0 in the former showed a highstandard of treatment results.
Cooper S, Mandall NA, Dibiase D, ShawWC in 2000 did a study to establish whetherIOTN was reliable over time, between the age of11 and 19 years old, for subjects who had notreceived orthodontic treatment and to investigatethe changes over time in the occlusal traits thatcomprise the dental health component of IOTN.Study casts of a longitudinal sample of 11 yearold (n = 314), 15 year old (n = 314) and 19 yearold (n = 142) subjects were examined. They foundthat the dental health component of IOTN isreliable between 11 and 19 years despitetemporal changes in the separate occlusal traitsthat comprise the index and IOTN DHC gradingat the age of 11 years is likely to be similar whenthe patient reaches 19 years. They also found thatmost of the occlusal traits contributing to IOTNDHC improved over time except posterior crossbite and displacement of contact points thatworsened between 11 and 19 years.
Fastlicht J in 2000 developed a visualcephalometric analysis based on two geometricconstructs the “Tetragon”, a polygon thatrepresents the maxillo-dento-mandibularcomplex, made up of reliable and familiarcephalometric landmarks—the palatal plane, themandibular plane, and the axes of the maxillaryand mandibular central incisors, the “Trigon”, acomplementary triangle situated above theTetragon and formed by one plane that isintrinsic to the Tetragon—the palatal plane(PNS-ANS)—and two that are extrinsic – thepterygo-palatal plane (Pt-PNS). He concludedthat the Tetragon and the Trigon provide a clearpicture of the position of the maxillo-dento-mandibular structures within the craniofacialcomplexes and that this visual cephalometricanalysis could be a useful diagnostic tool fortreatment planning, surgical preparation, andevaluation of growth, treatment progress, andpost-treatment results.
Pinto N, Woods M, Crawford E in 2000conducted a study, designed to determine theinfluence of the pretreatment vertical facialpattern on post-treatment occlusal change (asassessed with the PAR index) occuring afterfixed-appliance orthodontic treatment of patientsmanaged by one orthodontist with consistent

215History of Malocclusion Indices
aims and methods. Pretreatment, post-treatmentand follow-up casts of 60 patients were assessedby the PAR index. The pretreatment verticalfacial pattern for each subject was establishedusing the Jarabak Facial Height Quotient. Theresults of this study suggested that thepretreatment vertical facial pattern, at least onits own, is not likely to be predictive of theamount of post-treatment occlusal change.
Beatrice M, Woods M in 2000 conducted astudy designed to assess whether or notrotational changes occurring during or aftertreatment, in one accepted indicator of verticalfacial dimension, the Facial Axis, are in any wayrelated to post-treatment occlusal changes. Thepretreatment, post-treatment and follow-upcephalograms of 55 cases were assigned numbersand arranged in random order by anindependent observer before being traced anddigitized by one examiner. The pretreatmentvertical facial pattern for each subject wasestablished using the Jaraback Facial HeightQuotient. Occlusal assessment using thepretreatment (T1) post-treatment (T2) andfollow-up (T3) models was undertaken using thePAR index. They concluded that the facial axistends to change in the long-term followingroutine, comprehensive orthodontic treatment.A change in the Facial Axis does not seem to bedirectly related to the underlying vertical facialtype. Long-term post-treatment Facial Axischanges and long-term changes occurring in theocclusion are not directly related.
Wijayaratne D, Harkness M, Herbison P in2000 conducted study to determine in childrenwith Class II, division 1 malocclusions treatedwith functional appliances, first, if lower incisorproclination affects the assessment of treatmentoutcome using the PAR index and, second toevaluate the effectiveness of functionalappliances after adjusting the PAR score for anylower incisor proclination. The subjects in thisstudy were 43 consecutively treated childrenwho were assigned to either an untreated group,a group treated with Frankel function regulators,or a group treated with Harvold activators. ThePAR index showed that improvements weremade during treatment with functionalappliances in 50 percent of the cases in this study;however, cephalometric analysis, which is notpart of the PAR assessment, showed that in a
proportion of cases the overjet reduction wasachieved by lower incisor proclination, which isconsidered by some authorities to be unstable.
Daniels C, Richmond S in 2000 formulateda study to propose orthodontic indices to assesstreatment need, complexity, treatmentimprovement, and outcome based oninternational professional opinion, intended foruse in the context of specialist practice, and tocompare treatment thresholds in differentcountries and serve as a basis for qualityassurance standards in orthodontics. Aninternational panel of 97 orthodontists from ninecountries was asked to judge 240 dental casts forassessment of treatment need and 98 pairedpretreatment and post-treatment cases forassessment of treatment outcome. The outcomewas a new index, Index of Complexity, Outcomeand Need (ICON) which was based on theaverage opinion of a large panel of internationalorthodontic opinions. For the first time thedesign of the index had been specificallydeveloped to enable assessments of treatmentneed and outcome using one set of occlusal traits.The accuracy of the index to reflect professionalopinion for a diverse sample of cases wasestimated at 84 percent for decisions of treatmentneed and 68 percent for treatment outcomes. Themethod was heavily weighted by aesthetics.
Kim JC, Mascarenhas AK, Joo BH, Vig KWL,Beck FM, Vig PS in 2000 conducted a study toassess the value of cephalometric variables inpredicting orthodontic outcomes for patients withClass II malocculusions and variables that are mostuseful as predictors of pre-PAR, post-PAR, percentPAR reduction, and treatment duration. This studyevaluated selected cephalometric variables withthe intention of identifying predictors of theocclusal outcome of orthodontic treatment in 223patients with Class II malocclusions. The resultsshowed that Cephalometric variables explained39.2 percent of the variation in the pre-PAR scores;they suggested that cephalometrics may be morevaluable as a diagnostic tool than a prognostictool. The selected cephalometric variablesexplained only 18 percent of the variance of thepost-treatment occlusal result (post-PAR). Sixteenpercent of the variance in improvement of themalocclusion (percent PAR reduction) could beexplained by cephalometric variables.
Mascarenhas AK, Vig K in 2002 did a studyto compare the quality of orthodontic treatment

216 History of Orthodontics
provided by orthodontists in private practice(experts) with that of graduate orthodonticresidents (novice). The sample consisted of 143cases treated by private practice orthodontistsand 165 cases treated at the graduate orthodonticclinic. The results of study showed that althoughthere was no difference in the final occlusaloutcome there was a difference in the treatmentduration between the graduate educationalsetting and private practice, favoring the GOC.These results indicated that the clinicalproficiency of graduate orthodontic program wascomparable to that of highly experienced privatepractice orthodontists.
Yang-Powers LC, Sadowsky C, RosensteinS, BeGole EA in 2002 conducted a study todetermine whether dental relationships at theend of orthodontic treatment in a universitypostgraduate clinic are within the ABO’s limitfor passing the phase III examination, to assessthe contribution of each of the 8 components ofthe OGS to the total OGS score, to determinewhether treatment outcome is different for thevarious malocclusion categories, and toinvestigate treatment outcome in a sample ofcases that passed ABO certification comparedwith cases treated in a university clinic. Thesample used in this retrospective study consistedof records of 96 patients treated in the graduateorthodontic clinic at the University of Illinois atChicago. They concluded that there was astatistically significant difference (P < 0.05) inoverall treatment outcome (OGS score) betweenthe university group (average total score 45.54)and the ABO group (total score 33.88). Significantdifferences in treatment outcome (using OGSscores) were found between the university andthe ABO groups for the components of rootparalleling (panorex), occlusal contact, andoverjet. Occlusal contact and overjet weresignificantly higher (worse) in the universitysample. Panorex was significantly higher(worse) for the ABO group. The ABO groupexhibited better finishing details in the anteriorsegment and in the second molar region than didthe university group.
Cassinelli AG, Firestone AR, Beck MF, VigKWL in 2003 did a study to test whether objectivecriteria can be used to identify difficult andcomplex cases before treatment, and to determinewhether objective measures of malocclusion
severity (e.g. the PAR index) or an index oforthodontic treatment need (e.g., the IOTN)could be used to differentiate between easy anddifficult cases. A further aim was to investigatewhether factors related to the treatment or thepatients were associated with orthodontists’evaluations of cases as easy or difficult aftertreating the patients. Ten orthodontists practicingin Ohio were selected by telephone solicitation,and each orthodontist was asked to identify thecomplete records of 10 treated cases he or shejudged as having been easy to treat and 10 casesas having been difficult to treat. The casesselected were to be chosen from the last 100patients the orthodontist had treated. This studyshowed that complexity, or difficulty inachieving an ideal occlusion, increases as theseverity of the initial malocclusion increases.Complex cases are associated with patients whoare seen more often and receive repeatedwarnings about compliance problems. Easycases have less severe malocclusions initially, areassociated with compliant patients, and are morelikely to have 2-phase treatment.
Weerakone S, Dhopatkar A in 2003conducted a study to demonstrate the potentialof a new software package, clinical outcomesmonitoring program (COMP), for use in clinicalresearch by carrying out a limited audit forillustration. The program can collect data fromPAR, IOTN, and ICON indexes with built-in“Wizards” capable of calculating all 3 scoresautomatically. The COMP database containedinformation on 205 consecutively finished casesover a period of approximately 1 year after theintroduction of the COMP. This studydemonstrated that this approach is useful incomparing outcomes from various providers andmonitoring the general quality of treatment in apractice with many orthodontists.
Lieber WS, Carlson SK, Baumrind S,Poulton DR in 2003 tested the reliability andsubtraction frequency of the study model—scoring system of the American Board ofOrthodontists (ABO). Thirty-six post-treatmentstudy models were selected from six differentorthodontic offices. They found that the greatestlimitation of the ABO index, its dependence onlandmark identification. Most of the scoringinvolved measuring “landmark-to-landmark”linear distances using the ABO scoring tool.

217History of Malocclusion Indices
Reliability was lower than expected, suggestingthat the ABO index may still be overly subjective.Subtraction frequency revealed a significantemphasis on second molars.
Cangialosi TJ, Riolo ML, EdOwens S,Dykhouse VJ, Moffitt AH, Grubb JE et al in2004 have discussed criteria for determining theacceptability of a case presented for the AmericanBoard of Orthodontics (ABO) Phase III clinicalexamination which is case difficulty. Casedifficulty can often be subjective; however, it isrelated to case complexity, which can bequantifiable. Over the past 5 years, the ABO hasdeveloped and field-tested a discrepancy index,made up of various clinical entities that aremeasurable and have generally accepted norms.These entities summarize the clinical features ofa patient’s condition with a quantifiable,objective list of target disorders that representthe common elements of an orthodonticdiagnosis: overjet, overbite, anterior open bite,lateral open bite, crowding, occlusion, lingualposterior crossbite, buccal posterior crossbite,ANB angle, IMPA, and SN-Go-Gn angle. Thegreater the number of these conditions in apatient, the greater the complexity and thegreater the challenge to the orthodontist.
Read MJF, Deacon S, O’Brien K in 2004conducted a prospective cohort study. Thirty-twochildren were included in the study over a 2-yearperiod. Study casts were analyzed with the PeerAssessment Rating (PAR index), weighted withthe UK weights. Cephalometric radiographswere analyzed with the Pancherz analysis. Thisprospective cohort study showed that themodification of the Twin-block appliance was aneffective method of treating Class II malocclusionin terms of the morphological effects on thedental and skeletal tissues; and the maintheoretical advantages of this appliances over theremovable twin-block were that patientcooperation is enhanced and the appliance isactive for 24 hours a day, there is no transitionphase between the functional and fixedappliances phases, and it is less bulky.
Fogle LL, Southard KA, Southard TE, CaskoJS in 2004 conducted a retrospective study toprovide soft and hard tissue cephalometricanalysis of treatment effects after correcting ClassII malocclusions in growing patients withmoderate to severe mandibular retrognathia and
to examine the outcomes for growing patients witha range of skeletal anteroposterior and verticaldysplasias, who were treated with orthodonticsand growth modification techniques.Pretreatment and post-treatment cephalograms of100 growing Class II division 1 patients withmandibular skeletal retrusion were divided into5 groups depending on initial vertical andanteroposterior measurements. Post-treatmentsoft and hard tissue measurements were assessedand compared between the groups. Theyconcluded that conventional orthodontic therapysuccessfully correct and Class II division 1malocculusions in growing patients through acombination of skeletal and dentoalveolarchanges, with the greatest changes occurring inpatients who initially had the most severe skeletaldysplasias.
Janson G, de Souza JEP, Henriques JFC,Cavalcani CT in 2004 did a study to comparethe occlusal changes of the FRI and the eruptionguidance appliance, using the Peer AssessmentRating (PAR) index. From the treated-patientsrecords of the Orthodontic Department, BauruDental School, and two samples of Class IIpatients were retrospectively drawn. Group 1consisted of 25 patients treated with the FRI.Group 2 included 30 patients treated with the Gseries of the eruption guidance appliance knownas Occlus-o-Guide. The results of this researchshowed that there was a similar effectiveness inproducing occlusal changes in the twoinvestigated appliances, regardless of treatmenttime. The main shortcoming of the Frankelappliance was its large size and the initialdiscomfort and the eruption guidance appliancepresented advantages because it was smaller butpresented a slightly greater mean treatment time.
Abei Y, Nelson S, Amberman BD, Hans MGin 2004 conducted a study to compareorthodontic treatment outcome in a sample ofpatients divided on the basis of orthodonticprovider education by using 2 outcomemeasures. The first measure was the patient’sperception of the improvement in his or hersmile. A visual analog scale (VAS) was used toestimate this variable. Second, we used the ABOIto compare the alignment of the teeth. The goalwas to obtain evidence to support the commonlyheld belief that orthodontic specialists providebetter orthodontic care than do general dentists.

218 History of Orthodontics
Survey data were obtained from 280 students. Inthis sample, significantly lower ABOI scores werefound per patients treated by orthodonticspecialists compared with patients treated bygeneral dentists.
Malocclusion is a common oral disorderwhich manifests itself during childhood and thecorrection of malocclusion (orthodontictreatment) is frequently carried out duringchildhood. With the growing demand fororthodontic treatment a variety of clinician-basedindices have been developed to classify varioustypes of malocclusion and determine theirorthodontic treatment need. These indices canbe used in estimating orthodontic treatmentneed, prioritizing of treatment need in patientsreferred for orthodontics particularly wherethere are limited resources for orthodonticsamong public health care services, andsafeguarding for the patients.
The most commonly employed malocclusionindices are the Dental Aesthetic Index (DAI),Index of Orthodontic Treatment Need (IOTN),Peer Assessment Rating and Index ofComplexity, Outcome and Need (ICON).
Generally, among the commonly used indices,IOTN (AC, DHC), DAI and ICON are used toassess the orthodontic treatment needs whileICON and PAR are used to assess the treatmentoutcome. In some ways, the indices of IOTN, DAIand ICON are similar. All include twocomponents-morphological and esthetic. Thedifference is that for the IOTN, the estheticcomponent is separated from the dental healthcomponent. All the three indices measure similartraits such as overjet, reverse overjet, open bite,overbite, anteroposterior molar relationship, anddisplacement. However, the weights of thesetraits are rated differently by each index. The fourindices are described below.
INDEX OF ORTHODONTIC TREATMENT
NEEDS (IOTN)
Brook and Shaw in 1989, developed a valid andreproducible index (Index of orthodontictreatment need—IOTN) to determine orthodontictreatment need. This index attempts to rankmalocclusion in terms of the significance ofvarious occlusal traits for an individual’s dental
health and perceived aesthetic impairment. It intendsto identify those individuals who would most likelybenefit from orthodontic treatment. The index hastwo components, the aesthetic and dental healthcomponents, which rank malocclusion in increasingpriority according to aesthetic considerations anddental health implication.
Aesthetic Component
Aesthetic component (AC) consists of a scale often color photographs showing different levelsof dental attractiveness. The dental attractivenessof prospective patients can be rated withreference to this scale. Grade 1 represents themost and grade 10 the least attractivearrangement of teeth. The score reflects theaesthetic impairment. Aesthetic Componentvalue indicates patient’s esthetic concern andreflects sociopsychological needs.Grade 1, 2, 3 and 4 — no or slight need for
treatment,Grade 5, 6 and 7 — moderate or borderline
need for treatment,Grade 8, 9 and 10 — need for orthodontic
treatment.
Dental Health Component
Dental health component (DHC) involves featuresthat might impair the health and function of thedentition. DHC records the various occlusal traitsof a malocclusion that would increase themorbidity of the dentition and surroundingstructures. The traits of malocclusion are: overjet,reverse overjet, overbite, open bite, crossbite,displacement of teeth, impeded eruption of teeth,buccal occlusion, hypodontia and defects of cleftlip and palate. Functional disturbances are alsorecorded which included lip competency,mandibular displacement, traumatic occlusion andmasticatory or speech difficulties. Only the worstocclusal feature is recorded. The components ofDHC are shown in Table22.1. There are five grades.Grade 1 and 2 – no need or slight need for
treatment,Grade 3 – moderate or borderline
need for treatment,Grade 4 and 5 – need for orthodontic
treatment.
219History of Malocclusion Indices
Table 22.1: The dental health component is usuallyrecorded at the chair side by direct examination ofthe subject but can also be recorded from dentalcasts need (IOTN) (Shaw et al, 1989)
Grade 5 (Need treatment)5.a Impeded eruption of teeth (except for third
molars) due to crowding, displacement,presence of supernumerary teeth, retaineddeciduous teeth and any pathological cause
5.b Extensive hypodontia with restorativeimplications (more than 1 tooth missing in anyquadrant) requiring pre-restorative orthodo-ntics
5.c Increased overjet greater than 9 mm5.d Reverse overjet greater than 3.5 mm with
reported masticatory or speech difficulties5.e Defects of cleft lip and palate and other
craniofacial anomalies5.f submerged deciduous teeth
Grade 4 (Need treatment)4.a Less extensive hypodontia requiring pre-
restorative orthodontic or orthodontic spaceclosure to obviate the need for prosthesis
4.b Increased overjet greater than 6 mm but lessthan or equal to 9 mm
4.c Reverse overjet greater than 3.5 mm with nomastieatory or speech difficulties
4.d Reverse overjet greater than 1mm but less than3.5 mm with reported masticatory or speechdifficulties
4.e Anterior or posterior crossbites with greaterthan 2 mm discrepancy between retrudedcontact position and intercuspal position
4.f Posterior lingual crossbite with no functionalocclusal contact in one or both buccal segments
4.g Severe contact point displacements greaterthan 4 mm
4.h Extreme lateral or anterior open bite greaterthan 4 mm.
4.i Increased and completed overbite withgingival or palatal trauma
4.j Partially erupted teeth, tipped and impactedagainst adjacent teeth
4.k Presence of supernumerary teeth.Grade 3 (Borderline need)
3.a Increased overjet greater than 3.5 mm but lessthan or equal to 6 mm with incompetent lips
3.b Reverse overjet greater than 1mm but less thanor equal to 3.5 mm.
3.c Anterior or posterior crossbites with greaterthan 1 mm but less than or equal to 2mmdiscrepancy between retruded contact positionand intercuspal position
3.d Contact points displacements greater than 2mm but less than or equal to 4 mm
3.e Lateral or anterior open bite greater than 2mm but less than or equal to 4 mm.
3.f Deep overbite complete on gingival or palataltissues but no trauma.
Grade 2 (Little need)2.a Increased overjet greater than 3.5 mm but less
than or equal to 6 mm with incompetent lips2.b Reverse overjet greater than 0 mm but less than
or equal to 1 mm2.c Anterior or posterior crossbites with less than
or equal to 1 mm discrepancy betweenretruded contact position and intercuspalposition
2.d Contact point displacements greater than 1mm but less than or equal to 2 mm
2.e Anterior or posterior open bite greater than 1mm but less than or equal to 2 mm
2.f Increased overbite greater than or equal to 3.5mm without gingival contact
2.g Pre-normal or post-normal occlusions with noother anomalies (includes up to half a unitdiscrepancy)
Grade 1 (None)1. Extremely minor malocclusions including contact
points displacements less than 1 mm
Limitations
Aesthetic component cannot be used accuratelyin mixed dentition. There is a shortage ofscientific information regarding the long-termeffects of malocclusion. Nonetheless the DHC ofIOTN provides a structured method forassessment of malocclusion.
PEER ASSESSMENT RATING
The Peer assessment rating (PAR) index,previously refered to as the index of treatmentstandards, was described by S Richmond, W CShaw, K D O’Briene, I B Buchaman, R Joes, C DStephens and M Andrew in 1992.The PAR indexis a quantitative occlusal index measuring howmuch a patient deviates from normal alignmentand occlusion. This index is designed to measurethe efficacy or the outcome of orthodontictreatment by comparing the severity of occlusionon pretreatment and post-treatment casts. ThePAR index has five components.1. Upper and lower anterior segments: Scores are
recorded for both upper and lower anteriorsegment alignment. The features recorded arecrowding, spacing and impacted teeth.

220 History of Orthodontics
2. Buccal occlusion: The buccal occlusion isrecorded for both left and right sides. Therecording zone is from the canine to the lastmolar. All discrepancies are recorded whenteeth are in occlusion.
3. Overjet: Positive overjet as well as teeth incrossbite is recorded. The most prominentaspect of any one incisor is recorded. If thetwo lateral incisors are in crossbite while thecentred incisors are with increased overjet of4 mm, the score will be 3 for crossbite and 1for the positive overjet, 4 in total.
4. Overbite: The vertical overlap or open bite ofthe anterior teeth is recorded.
5. Centerline assessment: The centerlinediscrepancy between the upper and lowerdental midline is recorded in relation to lowercentral incisors.
The PAR index is applied to an individual’s pre-and post-treatment study casts. Scores areassigned to each component. The individualscores are calculated in each component andmultiplied by a weight of each component. Scoresare summed to obtain a total score that representsthe degree a case deviates from normal alignmentand occlusion. The degree of improvement as aresult of orthodontic intervention is obtained bycalculating the difference between the pre- andpost-treatment PAR scores. The degree ofimprovement can be assessed using two differentmethods:1. Nomogram: The degree of change is
separated into 3 sections:a. Worse or no difference,b. Improved andc. Greatly improved
2. Percentage improvement: This method givesa more sensitive assessment than thenomogram which only provides three broadbands of treatment change. A change of scorefrom 40 to 10 would represent an 80%improvement as would a change from 15 to3. However, the actual reduction in PARscores is also relevant as in the first case wherethere has been a much greater change with a30 point reduction as opposed to the secondcase in which the degree of change is less withonly a 12 point reduction.
INDEX OF COMPLEXITY, OUTCOME AND
NEED
The Index of Complexity, Outcome and Need(ICON) has been developed recently and claimsamong other things, to evaluate orthodontictreatment complexity. ICON is based on thesubjective judgments of 97 orthodontists fromnine countries. It is a single assessment methodto quantify orthodontic treatment complexity,outcome and need. The ICON consists offollowing five weighted components, Table 22.2:1. The Aesthetic Component (AC): The dental
aesthetic component of the IOTN is used.Once this score is obtained it is multiplied bythe weighting of 7.
2. Crossbite: Crossbite is deemed to be present ifa transverse reaction of cusp to cusp or worseexists in the buccal segment. This includesbuccal and lingual crossbites consisting of oneor more teeth with or without mandibulardisplacement.
3. Anterior vertical relationship: This trait includesboth open bite (excluding developmentconditions) and deep bite. If both traits arepresent only the highest scoring raw score iscounted. Scoring protocol is given in Table22.2.
4. Upper arch crowding/spacing: The sum of themesiodistal crown diameters is compared tothe available arch circumference, mesial to thelast standing tooth on either side.
Buccal segment anteroposterior relationship: Theanteroposterior cuspal relationship is scoredaccording to the protocol given in Table 22.2 foreach side in turn. The raw scores for both sidesare added together.
Calculation of the Final Scores
Once all of the raw scores have been obtainedand multiplied by their respective weights, theyare added together to yield a weighted summaryscore for a particular cast. The summed score isinterpreted as following: pre-treatment scoresgive the treatment needs and complexity grades;end of treatment scores gives the acceptability;while (pre-treatment scores)—(4 × post-treatmentscores) gives the degree of improvement.
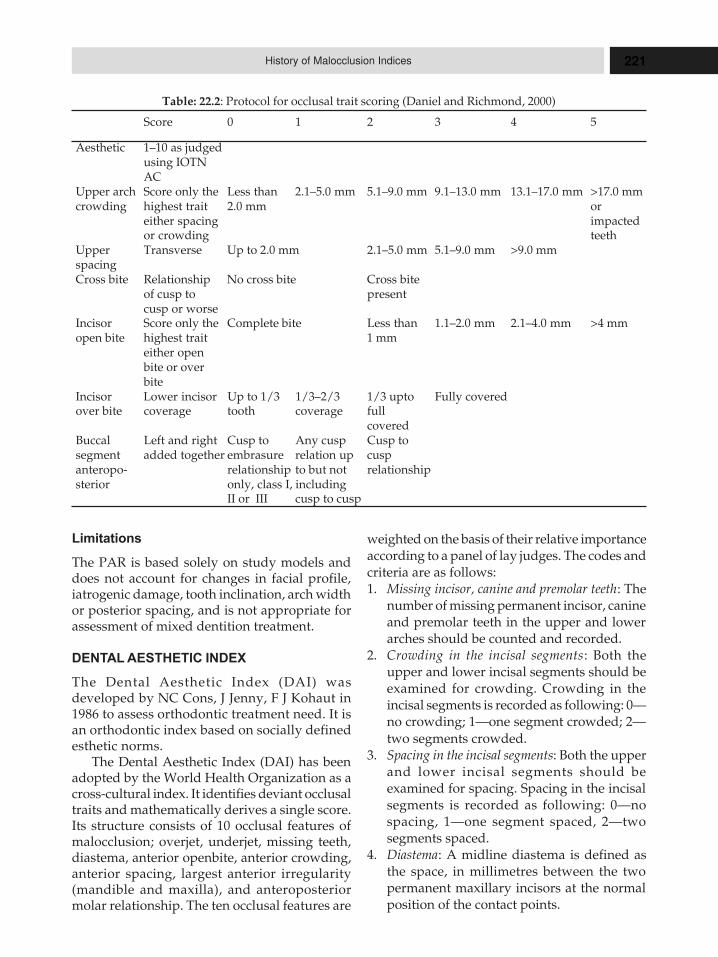
221History of Malocclusion Indices
Limitations
The PAR is based solely on study models anddoes not account for changes in facial profile,iatrogenic damage, tooth inclination, arch widthor posterior spacing, and is not appropriate forassessment of mixed dentition treatment.
DENTAL AESTHETIC INDEX
The Dental Aesthetic Index (DAI) wasdeveloped by NC Cons, J Jenny, F J Kohaut in1986 to assess orthodontic treatment need. It isan orthodontic index based on socially definedesthetic norms.
The Dental Aesthetic Index (DAI) has beenadopted by the World Health Organization as across-cultural index. It identifies deviant occlusaltraits and mathematically derives a single score.Its structure consists of 10 occlusal features ofmalocclusion; overjet, underjet, missing teeth,diastema, anterior openbite, anterior crowding,anterior spacing, largest anterior irregularity(mandible and maxilla), and anteroposteriormolar relationship. The ten occlusal features are
weighted on the basis of their relative importanceaccording to a panel of lay judges. The codes andcriteria are as follows:1. Missing incisor, canine and premolar teeth: The
number of missing permanent incisor, canineand premolar teeth in the upper and lowerarches should be counted and recorded.
2. Crowding in the incisal segments: Both theupper and lower incisal segments should beexamined for crowding. Crowding in theincisal segments is recorded as following: 0—no crowding; 1—one segment crowded; 2—two segments crowded.
3. Spacing in the incisal segments: Both the upperand lower incisal segments should beexamined for spacing. Spacing in the incisalsegments is recorded as following: 0—nospacing, 1—one segment spaced, 2—twosegments spaced.
4. Diastema: A midline diastema is defined asthe space, in millimetres between the twopermanent maxillary incisors at the normalposition of the contact points.
Table: 22.2: Protocol for occlusal trait scoring (Daniel and Richmond, 2000)
Score 0 1 2 3 4 5
Aesthetic 1–10 as judgedusing IOTNAC
Upper arch Score only the Less than 2.1–5.0 mm 5.1–9.0 mm 9.1–13.0 mm 13.1–17.0 mm >17.0 mmcrowding highest trait 2.0 mm or
either spacing impactedor crowding teeth
Upper Transverse Up to 2.0 mm 2.1–5.0 mm 5.1–9.0 mm >9.0 mmspacingCross bite Relationship No cross bite Cross bite
of cusp to presentcusp or worse
Incisor Score only the Complete bite Less than 1.1–2.0 mm 2.1–4.0 mm >4 mmopen bite highest trait 1 mm
either openbite or overbite
Incisor Lower incisor Up to 1/3 1/3–2/3 1/3 upto Fully coveredover bite coverage tooth coverage full
coveredBuccal Left and right Cusp to Any cusp Cusp tosegment added together embrasure relation up cuspanteropo- relationship to but not relationshipsterior only, class I, including
II or III cusp to cusp
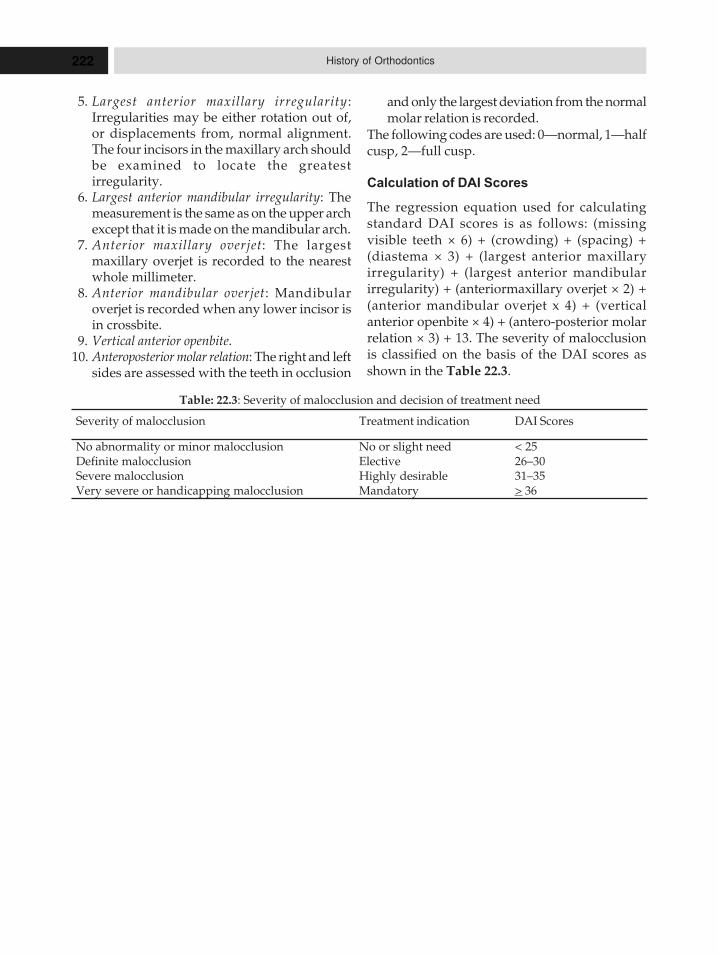
222 History of Orthodontics
5. Largest anterior maxillary irregularity :Irregularities may be either rotation out of,or displacements from, normal alignment.The four incisors in the maxillary arch shouldbe examined to locate the greatestirregularity.
6. Largest anterior mandibular irregularity: Themeasurement is the same as on the upper archexcept that it is made on the mandibular arch.
7. Anterior maxillary overjet: The largestmaxillary overjet is recorded to the nearestwhole millimeter.
8. Anterior mandibular overjet: Mandibularoverjet is recorded when any lower incisor isin crossbite.
9. Vertical anterior openbite.10. Anteroposterior molar relation: The right and left
sides are assessed with the teeth in occlusion
and only the largest deviation from the normalmolar relation is recorded.
The following codes are used: 0—normal, 1—halfcusp, 2—full cusp.
Calculation of DAI Scores
The regression equation used for calculatingstandard DAI scores is as follows: (missingvisible teeth × 6) + (crowding) + (spacing) +(diastema × 3) + (largest anterior maxillaryirregularity) + (largest anterior mandibularirregularity) + (anteriormaxillary overjet × 2) +(anterior mandibular overjet x 4) + (verticalanterior openbite × 4) + (antero-posterior molarrelation × 3) + 13. The severity of malocclusionis classified on the basis of the DAI scores asshown in the Table 22.3.
Table: 22.3: Severity of malocclusion and decision of treatment need
Severity of malocclusion Treatment indication DAI Scores
No abnormality or minor malocclusion No or slight need < 25Definite malocclusion Elective 26–30Severe malocclusion Highly desirable 31–35Very severe or handicapping malocclusion Mandatory > 36
23HHHiiissstttooorrryyy ooofff IIInnnttteeerrrppprrroooxxxiiimmmaaalll
EEEnnnaaammmeeelll RRReeeddduuuccctttiiiooonnn iiinnnOOOrrrttthhhooodddooonnntttiiicccsss
� History of Interproximal
Enamel Reduction
– Ballard
– Hudson
– Bolton
– Kelsten
– Paskow
– Shillingbourg and Grace
– Tuverson
– Doris, Bernard and Kuftinec
– Sheridan
– Zachrisson
� Indications of Interproximal
Enamel Reduction
� Contraindications of
Interproximal Enamel
Reduction
Interproximal enamel reduction (IER) isunderstood to be the clinical act of removing partof the dental enamel from the interproximalcontact area. The aim of this reduction is to createspace for orthodontic treatment and to give teetha suitable shape whenever problems of shape orsize requires attention. In the literature, this clinicalact is normally referred to as “stripping”, althoughother names can be found, such as “slendering”,“slicing”, “Hollywood trim”, “selective grinding”,“mesiodistal reduction”, “reapproximation”,“interproximal wear”, and “coronoplastia”. IERis a critical procedure. Therefore, planning andexecution need to be carefully assessed. Thistreatment should be considered as an exactreduction of interproximal enamel and not just asa simple method to solve problems.
HISTORY OF INTERPROXIMAL
ENAMEL REDUCTION
Interproximal dental stripping has been used byorthodontists for many years. It was initially usedto gain space when correcting mandibular incisorcrowding or to prevent such crowding.
In 1944, Ballard recommended a carefulstripping of the interproximal surfaces, mainlyfrom the anterior segment, when a lack of balanceis present. In 1954, Begg published his study of
Stone age man’s dentition, where he referred tothe shortening of the dental arch over time, whichoccurred through abrasion. Although the degreeof shortening of the dental arch found by Beggwas contested, the existence of this naturalreduction led to the publication anddevelopment of the technique for interproximalenamel reduction.
In 1956, Hudson stated that mesiodistalreduction of the mandibular incisors is onlyoccasionally referred to in the literature, andlisted just three previous articles with directreference to the mesiodistal reduction ofmandibular incisors. In his study, Hudson statedthat stripping should be carried out with mediumand fine metallic strips, followed by finalpolishing and topical application of fluoride. Hestated that it was possible to gain 3 mm of spacebetween mandibular canines, and presented anenamel thickness table for incisor andmandibular canine contact points.
In 1958, Bolton published his seminal studytitled “Disharmony in tooth size and its relationto the analysis and treatment of malocclusion”.This study, together with Ballard’s study,supported the need in dental dimensiondiscrepancy problems, to use interproximalstripping to correct problems of dental balance.

224 History of Orthodontics
In 1969, Kelsten recommended the use ofmechanical means to carry out stripping andrecommended prior alignment of teeth. Heposited that, only after alignment stripping couldbe simply and accurately achieved. That sameyear, Rogers and Wagner described an in vitrostudy that used teeth extracted for orthodonticreasons. These extracted teeth were subjected tostripping and polishing. It was found that if theextracted teeth were treated with fluoride afterstripping, they offered greater resistance to acidattacks, mainly in the 48 to 96 hours after theprocedure. This scientifically justified theimportance, already highlighted by Hudson, oftopical fluoride application after stripping andpolishing.
In 1971, Paskow published an article thatrecommended the use of mechanical methods ofIER (interproximal enamel reduction).
In 1973, Shillingbourg and Grace wrote anarticle entitled “Thickness of enamel and dentin”,which was an important study on enamel anddentin thickness. The results of this study laterserved as the scientific basis for work on strippingand allowed the amount of enamel that could besafely removed from each dental face to beaccurately determined. Also in the 70s, Peck andPeck published articles, on crowding of themandibular incisors and presented the Peckindex. They advised stripping whenever themesiodistal dimension of the mandibular incisorsdid not fall within acceptable figures calculablefrom their index. They claimed that anything inexcess would constitute predisposition towardcrowding.
In 1980, Tuverson published “Anteriorinterocclusal relations: Part 1”, which presenteda highly, detailed description of the strippingtechnique using a back angle and abrasive disks.
In 1981, Doris, Bernard, and Kuftinecconcluded that one of the strongest determiningfactors for dental crowding is the dimension ofteeth in the arch. In 1981, Betteridge presentedthe results of stripping on the anterior andinferior segment after 1 year without retention.She observed some relapse, but concluded thatesthetics were clearly acceptable afterobservation by a panel of three dentists, threeorthodontists, and three non-dentists.
In 1985, Sheridan published his article “Air-rotor stripping” and, in 1987, “Air-rotor stripping
update”. These articles totally revolutionized thetechnique and aims of interproximal enamelreduction. He recommended:1. Use of a turbine with carbide drill, instead of
diamond disks and strips.2. Stripping on buccal sectors; in other words,
distally on canines or mesially on the secondmolars on both arches. This achieves greaterspace and allows the preservation of incisors.
3. Use of stripping procedures to achieve space(up to 8 mm per arch) for the correction ofmoderate dentomaxillary disharmony,without recourse to extraction or excessiveexpansion.In 1986, Zachrisson proposed a new direction
for stripping: improvement of the shape of theteeth, mainly for incisors and reduction of theblack triangular space above the papilla.
INDICATIONS
The IER (Interproximal enamel reduction)technique has evolved over the years; it was firstused only for stripping mandibular incisors, withthe aim of preventing and correcting crowding.Areas of application have continued to grow:1. Tooth size discrepancy: In 1944, Ballard
recommended careful stripping of theproximal surfaces of the anterior teeth whenthere was imbalance.
2. Crowding of mandibular incisors: Stripping wasfirst used to obtain space for the correctionand prevention of crowding.
3. Tooth shape and dental esthetics: Stripping canand should be used for the reshaping ofenamel on some teeth, thus contributing toan improved finishing of orthodontictreatment and dental esthetics.
4. Normalization of gingival contour andelimination of triangular spaces above thepapilla, thus greatly improving esthetics andsmile.
5. Moderate dentomaxillary disharmony: This is aprimary area of application for interproximalenamel reduction in the technique developedby Sheridan in 1985 and 1987, which allowedspace to be obtained for the correction ofmoderate dental crowding; up to 8 mm perarch could be achieved without the need forextraction or excessive expansion.

225History of Interproximal Enamel Reduction in Orthodontics
6. Reduced expansion and premolar extraction.7. Camouflage of class II and III malocclusions: The
use of mandibular stripping can be beneficialin camouflaging slight to moderate class IIIconditions and overjet. In orthodontic treatmentto camouflage class II with the extraction oftwo maxillary premolars, correcting thecrowding and inclination of the mandibularincisors with stripping is an ideal solution.
8. Correction of the curve of spee: For the correctionof an exaggerated curve of spee, it is necessaryto create a few millimeters of space in thearch. This can be achieved through moderatestripping.
CONTRAINDICATIONS
There are several contraindications for theapproximation technique:1. Severe crowding (more than 8 mm per arch): With
application of IER, it would be hazardous tocarry out orthodontic correction. There wouldbe risk of excessive loss of enamel and all ofthe ensuing consequences.
2. Poor oral hygiene and/or poor periodontalenvironment: IER should not be used when
there is active periodontal disease or lack ofdental stability. Although little scientificevidence exists linking IER and increaseddental mobility, it is prudent to avoid thistechnique in these situations. In addition, IERshould not be used when there is poor oralhygiene, the orthodontist could be heldresponsible for all subsequent iatrogenicactivity. Vanarsdall has called attention to thepotential deleterious consequences.
3. Small teeth and hypersensitivity to cold :Stripping should not be used in thesesituations, as the risk of the appearance of oran increase in dental sensitivity is great.
4. Susceptibility to decay or multiple restorations:There is a risk of causing imbalance inunstable oral situations, although thestripping of restorations, instead of enamelsurfaces, is an option to consider.
5. Shape of teeth: Stripping should not be carriedout on “square” teeth—teeth with straightproximal surfaces and wide bases—as theseshapes produce broad contact surfaces, andcould potentially cause food impaction andreduce interseptal bone.
24HHHiiissstttooorrryyy ooofff IIInnnvvviiisssaaallliiigggnnn
As far back as 1945, orthodontists realized that asequence of removable plastic appliances couldmove teeth toward a predetermined result. Someorthodontists even made simple plastic “alignertrays” in their offices for minor adjustments. Butit took an adult who’d just had braces to take theconcept a step further.
Invisalign was the brainchild of Zia Chishtiand Kelsey Wirth, graduate students in StanfordUniversity’s MBA program. Wirth hadtraditional braces in high school (she reportedlyhated them). Chishti had finished adult treatmentwith traditional braces and now wore a clearplastic retainer. He noticed that if he didn’t wearhis retainer for a few days, his teeth shiftedslightly — but the plastic retainer soon movedhis teeth back the desired position. In 1997, heand Wirth applied 3D computer imaginggraphics to the field of orthodontics and createdAlign Technologies and the Invisalign method.With a boost from ample Silicon Valley venturefunding, Align soon took the orthodonticindustry by storm. Dentists and other dentalcompanies were skeptical at first, because neither
Chishti nor Wirth had any professional dentaltraining. Invisalign braces were first madeavailable to the public in May, 2000 and provedextremely popular with patients. Soon similarproducts began appearing on the market, madeby GAC, 3-M Unitek, Ormco, OrthoClear, andothers.
Manufactured by American dental productmanufacturer Align Technology, Inc., thesealigners are based on the suggestions of dentistDr H.D. Kessling, who first proposed the removabletray alternative to braces in 1945. Of greatimportance was Dr Kessling’s idea that theremovable tray be part of a series of trays, witheach tray forcing teeth to maneuver one step furtherinto line. In 1998, Align Technology received fullFDA approval for Invisalign as a Class II medicaldevice. Align Technology continues to get FDAtesting and approval for modifications made inthe years since. Nearly one million patients haveused Invisalign under the guidance of theirdentists, orthodontists and cosmetic surgeons.When used properly, these aligners get the sameor similar results as traditional braces.
� Historical Perspective of
Invisalign
� What Exactly the Invisalign
Means?
� Developing the Invisalign Brand
� Philosophy of Invisalign
� Fabrication of Invisalign
� Principle of
Stereophotolithography
� Summary of the Invisalign
Technique
� Indications of Invisalign
� Advantages of Invisalign
� Disadvantages of Invisalign
� Limitations of Invisalign
� Procedure of Treatment with
the Invisalign
� Benefits of Invisalign
� Care of Teeth with Invisalign
� Study 1
� Study 2
� Study 3
� Study 4
� Study 5
� Study 6
� Study 7
� Other Studies

227History of Invisalign
HISTORICAL PERSPECTIVE OF INVISALIGN
The movement of teeth through sequential stages,individually planned by a set up in casts, and theuse of elastomeric appliances was initiallysuggested by:
Remensyner (1926) when he introduced theFLEX-O-LITE gum massaging appliance, throughwhich reported minor tooth movements andKesling (1945) by introducing a vulcaniteappliance called the Tooth Positioner.
Though thermoplastic sheets weremanufactured as far back as 1896, thermoformingas a process was not known until a little before1950.
The Dental Contour Appliance wasmanufactured using an industrial grade vacuumformer and reported by Nahoum (1964).
Modlin (1974) reported realignment of teethusing vacuum formed appliances.
Ponitz (1971), McNamara et al (1985)described the use and efficacy of invisibleretainers.
The Essix System was described bySHERIDAN et al. for fabricating retainers in 1993.
Rinchuse and Rinchuse described activetooth movement with the same in 1997.
Lindor and Schoff (1998), Hilliard (2000),Armbruster (2003), Giancotti (2004) and othershave contributed to the treatment possibilitieswith the Essix System. The limitations of all Essixappliances were the small magnitude of changesachieved, associated with the technicaldifficulties, to manually subdivide, in stages, amovement, desired in several small progressivemovements.
The Invisalign System was developed in 1998by Align Technology. This was the first techniqueto be based on 3D Digital Technology. A series ofalgorithm stages were produced to move teeth into0.015–0.025 mm, successive precise movementsusing computer programmes that manipulate thevirtual images of the individual malocclusion.
Chisti and Wirth, 2 MBA Students fromStanford University were credited with theformation of Align Technology.
Boyd et al (2000) published the first clinicalstudy carried out in the Pacific university,California reporting successful treatmentoutcomes in cases with mild crowding andspacing between 3–6 mm.
Boyd and Vlaskalic(2001), Womack (2002),Norris(2002), Miller(2002), Christianson (2002),Joffe (2003), Faltin (2003) have documentedsuccessful treatment outcomes and deliberated onthe finer nuances of Invisalign therapy.
Lagravere (2005) conducted a systematicreview on the system. The authors could make noconclusion from the same about the indicationsfor, limitations of and outcomes of use of theInvisalign system because the author found nostudy that quantified treatment effects oraccomplishment of treatment goals using it.
Djeu et al (2005) assessed the treatmentoutcome of Invisalign and traditional orthodontictreatment compared with the American Board ofOrthodontics objective grading system and foundtreatment effects with Invisalign deficient incertain respects. Tuncay (2006) edited apublication on the Invisalign concept and itsclinical management.
BOYD (2006, 2008) demonstrated use ofInvisalign in a surgical case, and reviewedprevious Invisalign studies showing significantlimitations for complex tooth movement withcurrent case reports showing successful treatmentof moderate to severe malocclusions, attributingit to technological advancements in the systemduring a decade of its existence.
The Clear Aligner concept and branding ofan alternative low-cost orthodontic appliancesystem to both orthodontists and general dentistswas introduced by TAE WEON KIM (2004).Thesystem uses digital aid combined with manualmanipulation to fabricate aligners.
Kim (2007) authored the Clear AlignerManual.
The Orthoclear system introduced itself as analternative to Invisalign.CHISTI, WEN &
Riepenhausen (2005) were the founders of thesame.
Miller, Crawford and Nanda (2006) describedcase reports with the Orthoclear system.
Orthoclear was involved in a legal battle overpatents with Invisalign and a settlement wasreached in 2006 wherein Orthoclear decided tostop operations in the US.
3D Ortholine was established as a systemoffering aligner therapy by Abouhassan (2006)and inculcated an advanced system of virtual setups and appliance design where special emphasiswas placed on the sequential division of tooth

228 History of Orthodontics
movement to enhance patient comfort andincrease the scope of tooth movements with alignertherapy.
Vaid and Abouhassan (2008) reported clinicalreports and technological parameters of thesystem, designed to provide efficacy. Long-termresults were still awaited.
Profit (2007) described a role for AlignerTherapy in treating complex malocclusions withlimitations in specific scenarios and predicted afuture for this method of treatment.
Namiranian (2008) studied the effect of alignerthickness on stress production and concluded thatthick and medium aligners were more likely toproduce effective tooth movement compared tomedium aligners.Different Systems of Plasticaligners differ in the clinical and laboratory stepsand the modifications possible, that they offer theoperator. A lot of the published data is “systembased “rather than “therapy based” and hascommercial or system specific allegiance to it. Theliterature on the therapy is definitely encouraging,but is mostly anecdotal including case reports orclinician’s innovations.
Randomized clinical trials that follow theCONSORT statement are needed to evaluate thetreatment effects of Aligners. Technologicalanalysis of the biomechanical properties of thematerials used and the permutation of toothmovements effectively possible, with anorganized classification of stages involved willand should be the trend of future research.
WHAT EXACTLY THE INVISALIGN MEANS?
Invisalign refers to a series of clear, removableheavy-duty plastic aligners that gradually correctminor crookedness and gaps, overcrowded teeth,overbites and/or minor underbites. Whenconsidering your options, there are a number ofreasons to select this procedure over other choicessuch as metal braces, crowns, veneers andimplants.
DEVELOPING THE INVISALIGN BRAND
So where does Invisalign fit into this picture? TheInvisalign brand was first launched in Americain 1999. Invisalign products work in much thesame way as conventional brackets in thatappliances are fitted to your teeth, and thoseappliances then move the teeth slowly and gently
towards their optimum positions. But whereasconventional braces are built from stainless steeland metal wire, Invisalign products are clearplastic aligners that are less than one millimeterthick. They are also removable, which makeseveryday tasks such as eating much easier—asyou can probably imagine.
One of the reasons why Invisalign has grownin recent years is because orthodontic work foradults is becoming much more popular. In thepast, most people believed that braces could onlyreally make a difference to your teeth as a teenager,when your teeth were still growing. But that is amyth. Braces can still move your teeth as an adultand you can still achieve the smile you want laterin life. As more adult orthodontic treatments arebecoming available, more people are keen to learnabout the options available to them.
The growth in adult orthodontic treatment hasled to greater consumer demand for more flexibleproducts that can be adapted to suit a customer’slifestyle. For example, conventional braces mayget just the same results as Invisalign aligners.But if you’ve got a big presentation with your bossnext week, what would you rather be wearing: anold-fashioned metal and wire bracket or avirtually invisible aligner that you can evenremove if you need to? In a nutshell, that’s whymost adults choose Invisalign.
Over the years, Invisalign has developed intoa successful brand with a number of products inits portfolio. There is the original, definitiveInvisalign program, which this site covers in detailfrom treatment through to costs. Recently,however, Invisalign has also released modifiedversions of the original system to exploit newopportunities within the dental market.
Invisalign Express is a new version of theInvisalign system which is designed to correctminor orthodontic issues in short timescales.
Invisalign Teen is the program that Invisalignhas designed specifically for teenagers. It includesa number of modifications that make it easier forteenagers and parents to manage the treatmentand therefore achieve the desired results.
For a long time now Orthodontists and patientshave wanted to correct teeth inconspicuously andwithout the use of fixed dental brackets. Newtechnology has turned this dream into reality; thenew type of treatment is called Invisalign (Fig.24.1) (Invisible/Align) Technique.
229History of Invisalign
Align Technologies introduced Invisalign(invisible/align) in 1999. Invisalign incorporatesa series of invisible (clear) plastic aligners that fitcomfortably over teeth and are designed to moveteeth gradually into the desired position.Invisalign aligners are manufactured at the aligntechnologies dental laboratory using computer-aided design/computer-aided manufacturing(CAD/CAM) processes.
PHILOSOPHY OF INVISALIGN
Invisalign takes the principles of Kesling,Nahoum, and Raintree Essix even further,using cter-aided-design-computer-aided-manufacture (CAD-CAM) technology combinedwith laboratory techniques to fabricate a series ofcustom appliances that are esthetic andremoveable, and that can move teeth frombeginning to end.
The Invisalign system has been tested inuniversity clinical trials and is available to public.There are currently certain limitations to thisappliance in terms of cost, case selection,experienced required for computer treatmentplanning, difficulty obtaining certain toothmovements and lack of potential in cases involvingmixed dentition or impacted teeth. However as thenumber of clinicians using this appliance increasesmore information will be available to evaluate therisks and benefits of this system.
A great help in the future will be to use one ofthe emerging intraoral scanning devices to replace
the PVS impressions and to record treatmentchangesor modifications immediately in a digitalformat. Adding the other 3D compartments(skeletal, facial, jaw movements and animation tothe current surface map of the teeth) will greatlyenhance the diagnostic and treatment capabilitiesof this appliance. Thus the clinician must haveindepth understanding of the biomechanics,biology, periodontal concerns and optimaltherapeutic occlusion achieved duringorthodontic treatment to successfully plan anduse this appliance.
FABRICATION OF INVISALIGN
The orthodontist submits the following to aligntechnology:� A set of a polyvinyl siloxane impressions� A centric occlusion bite registration� A panaromic radiograph� A lateral cephalometric radiograph� Photographs.
The impressions are poured up in dentalplaster and then placed in a tray and encased withepoxy and urethane. The impressions areinspected by the laboratory to ensure that thepatients dentition has been fully captured. The trayis placed into a destructive scanner (Figs 24.2Aand B) using computed tomography. The scannersrotating blades makes numerous passes over theepoxy encased models removing a thin layer witheach pass. A computer linked with a scanner thenassembles the scanned information to create athree-dimensional rendering of the models.
After the bite has been established, based onthe clinician’s treatment plan technicians generatea virtual correction of malocclusion that is thenreviewed by the clinician this process is calledthe Clin-Check. The software cuts the virtualmodels and separates the teeth allowing them tobe move individually (Fig. 24.3). A virtual gingivalis placed along the gingival line of the clinicalcrown to serve as the margin for the manufacturingof the aligners (Fig. 24.4).
After final approval the treatment sequence isdivided into a series of algorithmic stages. Eachstage has maximum tooth movement potential of0.25 mm/appliance. Models of each stage oftreatment are made by having the computer directtheir fabrication in a process calledStereolithography (Figs 24.5A to C).
Fig. 24.1: Invisalign appliance
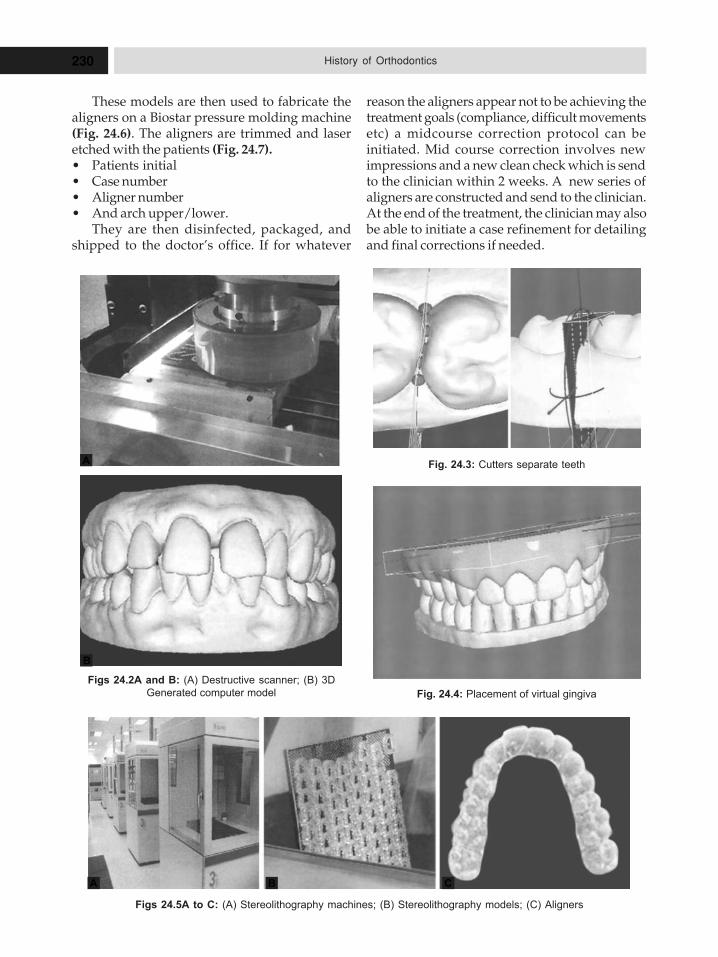
230 History of Orthodontics
These models are then used to fabricate thealigners on a Biostar pressure molding machine(Fig. 24.6). The aligners are trimmed and laseretched with the patients (Fig. 24.7).� Patients initial� Case number� Aligner number� And arch upper/lower.
They are then disinfected, packaged, andshipped to the doctor’s office. If for whatever
Fig. 24.3: Cutters separate teeth
Fig. 24.4: Placement of virtual gingiva
Figs 24.2A and B: (A) Destructive scanner; (B) 3D
Generated computer model
A
B
reason the aligners appear not to be achieving thetreatment goals (compliance, difficult movementsetc) a midcourse correction protocol can beinitiated. Mid course correction involves newimpressions and a new clean check which is sendto the clinician within 2 weeks. A new series ofaligners are constructed and send to the clinician.At the end of the treatment, the clinician may alsobe able to initiate a case refinement for detailingand final corrections if needed.
Figs 24.5A to C: (A) Stereolithography machines; (B) Stereolithography models; (C) Aligners
A B C
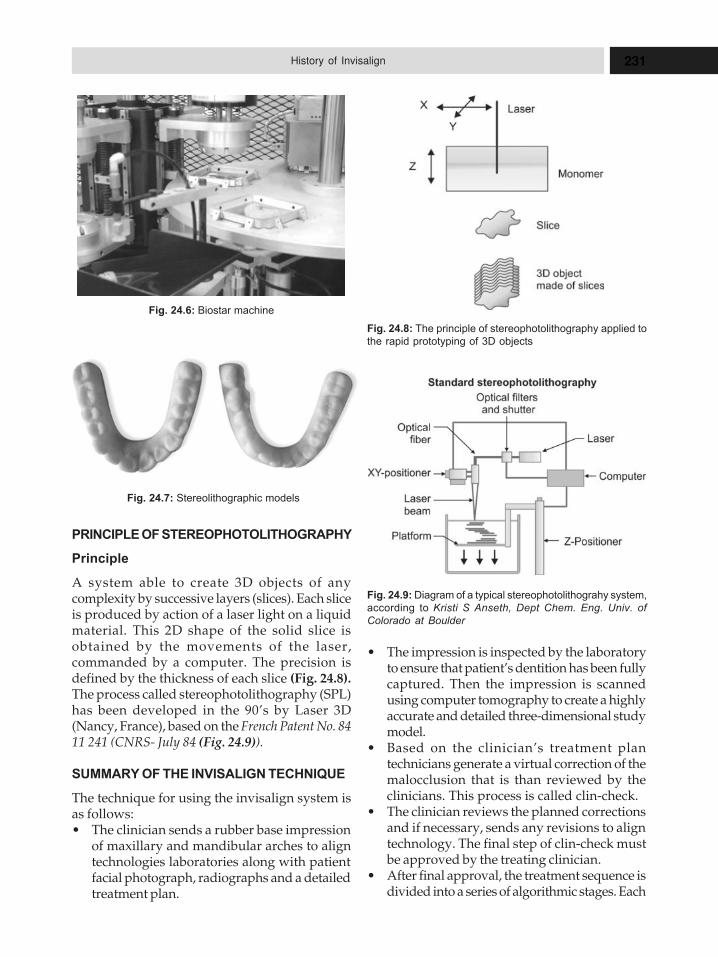
231History of Invisalign
PRINCIPLE OF STEREOPHOTOLITHOGRAPHY
Principle
A system able to create 3D objects of anycomplexity by successive layers (slices). Each sliceis produced by action of a laser light on a liquidmaterial. This 2D shape of the solid slice isobtained by the movements of the laser,commanded by a computer. The precision isdefined by the thickness of each slice (Fig. 24.8).The process called stereophotolithography (SPL)has been developed in the 90’s by Laser 3D(Nancy, France), based on the French Patent No. 8411 241 (CNRS- July 84 (Fig. 24.9)).
SUMMARY OF THE INVISALIGN TECHNIQUE
The technique for using the invisalign system isas follows:� The clinician sends a rubber base impression
of maxillary and mandibular arches to aligntechnologies laboratories along with patientfacial photograph, radiographs and a detailedtreatment plan.
� The impression is inspected by the laboratoryto ensure that patient’s dentition has been fullycaptured. Then the impression is scannedusing computer tomography to create a highlyaccurate and detailed three-dimensional studymodel.
� Based on the clinician’s treatment plantechnicians generate a virtual correction of themalocclusion that is than reviewed by theclinicians. This process is called clin-check.
� The clinician reviews the planned correctionsand if necessary, sends any revisions to aligntechnology. The final step of clin-check mustbe approved by the treating clinician.
� After final approval, the treatment sequence isdivided into a series of algorithmic stages. Each
Fig. 24.8: The principle of stereophotolithography applied to
the rapid prototyping of 3D objects
Fig. 24.9: Diagram of a typical stereophotolithograhy system,
according to Kristi S Anseth, Dept Chem. Eng. Univ. of
Colorado at Boulder
Fig. 24.6: Biostar machine
Fig. 24.7: Stereolithographic models
232 History of Orthodontics
stage has a maximum tooth movementpotential of 0.25 mm per appliances.
� Models of each stage of treatment are made byprocess called stereolithography Individualappliances (aligners) are made from thecomputer-generated models of each stage.
� A typical invisalign treatment requires 20 to30 aligners for the maxillary and mandibulararches.
� In most of the cases, treatment with invisalignis done in less than a year; however, treatmenttime depends on the specific alignmentproblem.
INDICATIONS OF INVISALIGN
According to researchers and align technologies,invisalign can be used to correct the followingtypes of mild malocclusions:1. Malocclusion with mild crowding cases.2. Malocclusion with mild spacing case.3. In cases mild relapse – after traditional braces
have been removed, when some relapsingtooth movement has occurred.
ADVANTAGES OF INVISALIGN
1. Improved esthetics compared to fixedorthodontic appliance and ability to removethe appliance.
2. Invisalign patients showed no measurable rootresorption.
3. It gives the patient an esthetic choice in theirorthodontic treatment.
DISADVANTAGES OF INVISALIGN
1. Fabrication of the aligners is a very timeconsuming and tedious process that probablywould not be practical day to day orthodonticpractice.
2. Severe derotations, complex extrusions andlarge translations are less predictable withinvisalign and may require auxiliarytreatment.
LIMITATIONS OF INVISALIGN
1. All permanent teeth should be fully eruptedfor treatment using invisalign as it is difficultto achieve retention of the appliance on shortclinical crowns.
2. The treatment procedures do not allow forcontinued eruption of teeth, or significantdental arch changes during growth that mayoccur during the mixed dentition phase.
3. There is currently no capability to incorporatebasal orthopedic change with this appliancesystem, thus restricting it to malocclusionsrequiring pure dental movements.
4. Unlike fixed or removable appliances, thetreatment plan cannot be changed once theappliance series has begun. If change intreatment is desired the current series may becompleted and a new plan and appliances aremade or the current series may be stopped.
5. The inability to integrate hard and soft tissuesof the head into the computer treatment thusthere is no direct indication of where teeth arein relation to basal bone or in relation to thelips or other soft tissues of head.
6. Invisalign is generally not recommended intreating more complicated malocclusions suchas severe deep bite, anterior-posteriorcorrections greater than 2mm, uprightingseverely tipped teeth and closure of premolarextraction spaces.
PROCEDURE OF TREATMENT WITH THE
INVISALIGN
First Evaluation
� Orthodontist evaluates and creates a programof treatment.
� Records and impressions of arches are taken.
Invisalign Aligners Made and Delivered
� A CT-scan (Computed Tomography or CAT-scan), is made from your dental impressionsthat produces an extremely accurate, 3Ddigital model of your teeth.
� CAD (Computer-aided design) software isthen used to simulate the movement of yourteeth during treatment.
� The treatment plan are reviewed, modified,and approved before the aligners are created.
� Invisalign then uses advanced stereo-lithography (SLA) technology to build precisemoulds of teeth at each stage of treatment.
� Individualized, custom-created clear alignersare made from these models and sent toorthodontist.
233History of Invisalign
Wearing of Invisalign (Fig. 24.10)
� Visits are made to orthodontist for adjustmentsand to check progress on a monthly basis.
� At regular intervals, a new set of custom-molded clear aligners are received to continuethe straightening process.The total number of clear aligners is specific to
you, determined by orthodontist for the course oftreatment.
BENEFITS OF INVISALIGN
1. Invisible thus no unwarranted attention toyour mouth.
2. Removable thus easy to eat, brush and floss.3. No brackets to catch food or plaque.4. Healthier gums from properly aligned teeth
that help gums to “fit” tighter around eachtooth.
5. Easier cleanings in maintaining a good oralhygiene program that reduce chances ofplaque build-up, tooth decay and periodontaldisease.
CARE OF TEETH WITH INVISALIGN
1. Teeth and the aligners would need to be keptcleaned every day if the teeth and gums are tobe healthy during and after orthodontictreatment.
2. Follow orthodontist directions on how oftento brush, how often to floss and use of othercleaning aids to help maintain good dentalhealth.Like brackets and arch wires are to braces,
Invisalign aligners move teeth through theappropriate placement of controlled force on
the teeth. The principal difference is thatInvisalign not only controls forces, but alsocontrols the timing of the force application. Ateach stage, only certain teeth are allowed tomove, and these movements are determined bythe orthodontic treatment plan for thatparticular stage. This results in an efficientforce delivery system.
STUDY 1
OUTCOME ASSESSMENT OF INVISALIGN AND
TRADITIONAL ORTHODONTIC TREATMENT
COMPARED WITH THE AMERICAN BOARD OF
ORTHODONTICS OBJECTIVE GRADING
SYSTEM
Garret Djeu,a Clarence Shelton,b and AnthonyMaganzinic
New York, NY
Introduction
This treatment-outcome assessment objectivelycompares Invisalign (Align Technology, SantaClara, Calif) treatment with braces.
Methods
This study, a retrospective cohort analysis, wasconducted in New York, NY, in 2004. Records from2 groups of 48 patients (Invisalign and bracesgroups) were evaluated by using methods from theAmerican Board of Orthodontics Phase IIIexamination. The discrepancy index was used toanalyze pretreatment records to control for initialseverity of malocclusion. The objective gradingsystem (OGS) was used to systematically gradeposttreatment records. Statistical analyses evaluatedtreatment outcome, duration, and strengths andweaknesses of Invisalign compared with braces.
Results
The Invisalign group lost 13 OGS points more thanthe braces group on average, and the OGS passingrate for Invisalign was 27% lower than that forbraces. Invisalign scores were consistently lowerthan braces scores for buccolingual inclination,occlusal contacts, occlusal relationships, andoverjet. Invisalign’s OGS scores were negativelycorrelated to initial overjet, occlusion, and buccalposterior crossibite. Invisalign patients finishedFig. 24.10: Wearing invisalign appliance

234 History of Orthodontics
4 months sooner than those with fixed applianceson average. P _ .05 was used to determinestatistically significant differences.
Conclusion
According to the OGS, Invisalign did not treatmalocclusions as well as braces in this sample.Invisalign was especially deficient in its ability tocorrect large anteroposterior discrepancies andocclusal contacts. The strengths of Invisalign wereits ability to close spaces and correct anteriorrotations and marginal ridge heights. This studymight help clinicians to determine which patientsare best suited for Invisalign treatment (Am JOrthod Dentofacial Orthop 2005;128.
STUDY 2
HOW WELL DOES INVISALIGN WORK? A
PROSPECTIVE CLINICAL STUDY EVALUATING
THE EFFICACY OF TOOTH MOVEMENT WITH
INVISALIGN
Neal D. Kravitz,a Budi Kusnoto,b Ellen BeGole,cAles Obrez,d and Brent Agrane
South Riding, Va, White Plains, Md, andChicago, Ill
Introduction
The purpose of this prospective clinical study wasto evaluate the efficacy of tooth movement withremovable polyurethane aligners (Invisalign,Align Technology, Santa Clara, Calif).
Methods
The study sample included 37 patients treatedwith Anterior Invisalign. Four hundred oneanterior teeth (198 maxillary and 203 mandibular)were measured on the virtual treat models. Thevirtual model of the predicted tooth position wassuperimposed over the virtual model of theachieved tooth position, created from theposttreatment impression, and the 2 models weresuperimposed over their stationary posterior teethby using Tooth Measure, Invisalign’s proprietarysuperimposition software. The amount of toothmovement predicted was compared with theamount achieved after treatment. The types ofmovements studied were expansion, constriction,intrusion, extrusion, mesiodistal tip, labiolingualtip, and rotation.
Results
The mean accuracy of tooth movement withInvisalign was 41%. The most accurate movementwas lingual constriction (47.1%), and the leastaccurate movement was extrusion (29.6%)—specifically, extrusion of the maxillary (18.3%) andmandibular (24.5%) central incisors, followed bymesiodistal tipping of the mandibular canines(26.9%). The accuracy of canine rotation wassignificantly lower than that of all other teeth, withthe exception of the maxillary lateral incisors. Atrotational movements greater than 15°, theaccuracy of rotation for the maxillary canines fellsignificantly. Lingual crown tip was significantlymore accurate than labial crown tip, particularlyfor the maxillary incisors. There was no statisticaldifference in accuracy between maxillary andmandibular teeth of the same tooth type for anymovements studied.
Conclusion
In this prospective clinical study evaluating theefficacy of tooth movement with Invisalign, thefollowing conclusions were made:1. The mean accuracy of tooth movement with
Invisalign was 41%. The most accurate toothmovement was lingual constriction (47.1%).The least accurate tooth movement wasextrusion (29.6%). The mandibular canine wasthe most difficult tooth to control.
2. Maxillary and mandibular canines achievedapproximately one-third of the predictedrotation. The accuracy of canine rotation wassignificantly lower than the rotation of all otherteeth, with the exception of the maxillary lateralincisors. At rotational movements greater than15°, the accuracy for the maxillary canines wassignificantly reduced.
3. With the exception of canine rotation, no toothwas significantly less accurate in movement.
4. Lingual crown tip was significantly moreaccurate than labial crown tip, particularly forthe maxillary incisors.
5. The severity of pretreatment overjet mightinfluence the accuracy of anterior toothmovement with Invisalign.
6. There was no statistical difference in accuracybetween maxillary and mandibular teeth ofthe same type for any tooth movement studied.These results indicate that we still have muchto learn regarding the biomechanics and
235History of Invisalign
efficacy of the Invisalign system. Clinicianswho prescribe Invisalign treatment shouldfully recognize its limitations and committhemselves to providing the gold standard ofcare for their patients. Providing quality care,regardless of the treatment modality, is onlyway to truly be a premiere provider.
STUDY 3
RETAINING ALIGNMENT CHANGES WITH
INVISALIGN
Kuncio D, Maganzini A, Shelton C, et al: Invisalignand traditional orthodontic treatmentpostretention outcomes compared using theAmerican Board of Orthodontics objective gradingsystem. Angle Orthod 77:864-869, 2007.
Relapse of orthodontic cases, while extensivelystudied, remains poorly understood. In this study,while both techniques produced acceptable initialresults, cases treated with conventional braceswere more stable over time. Retention times werecomparable but changes in resultant treatmentforces were more frequent with Invisalign thanwith fixed appliances.
STUDY 4
STRUCTURAL CONFORMATION AND
LEACHING FROM IN VITRO AGED AND
RETRIEVED INVISALIGN APPLIANCES
Susan Schuster, DDS,a George Eliades, DDS,DrDent,b Spiros Zinelis, PhD,c Theodore Eliades,DDS, MS, DrMed, PhD,d and T. Gerard Bradley,BDS, MSe
Milwaukee, Wis, and Athens, Greece
The objectives of this study were to investigate thestructure of Invisalign appliances (AlignTechnology, Santa Clara, Calif) after intraoralexposure, and to qualitatively and quantitativelycharacterize the substances leached from the alignersafter accelerated in vitro aging. Samples of Invisalignappliances were randomly selected from 10 patientsbefore intraoral placement and after retrieval, andthe prepared specimens were subjected to (1) bright-field optical reflection microscopy to study thesurface morphology; (2) Fourier transform infraredmicrospectroscopy to characterize the in vivochanges in molecular composition induced onappliance surfaces, (3) scanning electron
microscopy and energy dispersive X-raymicroanalysis to identify the elemental compositionof integuments formed on the surface, and (4) Vickershardness (HV200) testing. Another set of referenceand retrieved appliances was subjected to artificialaging for 2 weeks, and the extracts were subjected togas chromatography-mass spectroscopy. Theretrieved appliances demonstrated substantialmorphological variation relative to the as-receivedspecimens involving abrasion at the cusp tips,adsorption of integuments, and localizedcalcification of the precipitated biofilm at stagnationsites. Buccal segments of retrieved appliancesshowed an increase in hardness, which might beattributed to mastication-induced cold work;however, the clinical implication of this effect onmechanotherapy is unknown. In vitro aged andretrieved appliances were found to leach notraceable amount of substances in an ethanol agingsolution. (Am J Orthod Dentofacial Orthop2004;126:725-8).
Conclusion
Retrieved Invisalign appliances demonstratesubstantial morphological variation in relationto new specimens, involving abrasion at the cusptips, adsorption of integuments at stagnation sites,and localized calcification of the biofilmdeveloped during intraoral service. An increasein hardness of the buccal segments of the retrievedappliances was found; this could mainly beattributed to cold work during mastication. Theclinical implication of this effect in the forcedelivery of the appliance requires further study.In vitro aged appliances were found not to releasetraceable monomers or byproducts afterimmersion in an ethanol-water solvent. The agingpattern of these appliances intraorally involvesabrasive wear arising from mastication, and, thus,no definitive consensus on their reactivity andbiological properties can yet be established.
STUDY 5
CYTOTOXICITY AND ESTROGENICITY OF
INVISALIGN APPLIANCES
Theodore Eliades,a Harris Pratsinis,b AthanasiosE. Athanasiou,c George Eliades,d and DimitrisKletsase
Thessaloniki and Athens, Greece

236 History of Orthodontics
Introduction
Our purpose was to study the in-vitro cytotoxicand estrogenic properties of Invisalign appliances(Align Technology, Santa Clara, Calif). Methods:Three sets, each consisting of a maxillary and amandibular appliance, of as-received alignerswere immersed in normal saline solution for 2months. Samples of eluents were diluted to 3concentrations (5%, 10%, and 20% vol/vol) andtested for cytotoxicity on human gingivalfibroblasts and estrogenicity by measuring theireffect on the proliferation of the estrogen-responsive MCF-7 breast cancer cells. All assayswere repeated 4 times for each maxillary andmandibular set, and the results were analyzedwith 2-way analysis of variance (ANOVA) withappliance and concentration serving as predictorsat the .05 level of significance; differences amonggroups were investigated with the Tukey test.
Results
There was no evidence of cytotoxicity on humangingival fibroblasts and no stimulation ofproliferation of the MCF-7 cell line at anyconcentration, indicating no estrogenicity of alignereluents. Conclusions: The use of Invisalignappliances did not seem to induce estrogenic effectsunder the conditions of this experiment. (Am JOrthod Dentofacial Orthop 2009;136:100-3).
Conclusion
No cytotoxic or estrogenic activity of Invisalignappliances was documented in this in-vitro assay,which used a standard model for the assessmentof estrogenicity of materials.
STUDY 6
COLOR FADING OF THE BLUE COMPLIANCE
INDICATOR ENCAPSULATED IN REMOVABLE
CLEAR INVISALIGN TEEN ALIGNERS
Timm Cornelius Schotta; Gernot Go¨ zb
Objective
To evaluate the color fading in aqueous solutionsof the blue dot wear-compliance indicators of theInvisalign TeenH System outside the oral cavity.
Materials and Methods
The compliance indicators in the Invisalign Teenaligners were tested for color resistance in variousaqueous models with no saliva involved.
Results
Color fading was observed as a function of time,pH, and temperature while complianceindicators were stored in drinking water or soursoft drinks and in conjunction with the use ofcleaning tablets and a dishwasher. The findingsof color fading were consistent with the colorchanges observed when the aligners were beingworn by patients. Color fading, notably asobserved in connection with acidic soft drinksand cleaning techniques, introduces uncertaintyinto the assessment of actual patient compliance,as reflected by the fading colors of complianceindicators.
Conclusion
Compliance indicators are not immune to simpleintentional or unintentional manipulations.Therefore, they can best show an estimate of weartime but cannot be recommended as objectivewear-time indicators. (Angle Orthod.2011;81:185–191).
STUDY 7
A COMPARISON OF TREATMENT IMPACTS
BETWEEN INVISALIGN ALIGNER AND FIXED
APPLIANCE THERAPY DURING THE FIRST
WEEK OF TREATMENT
Kevin B. Miller,a Susan P. McGorray,b RandyWomack,c Juan Carlos Quintero,d MarkPerelmuter,e Jerome Gibson,f Teresa A. Dolan,gand Timothy T. Wheelerh
Rock Hill, SC, Gainesville and Miami, Fla,Glendale, Ariz, Louisville, Ky, and
San Antonio, Tex
Introduction
The aim of this study was to evaluate thedifferences in quality of life impacts betweensubjects treated with Invisalign aligners (AlignTechnology, Santa Clara, Calif) and those with

237History of Invisalign
fixed appliances during the first week oforthodontic treatment. Methods: A prospective,longitudinal cohort study involving 60 adultorthodontic patients (33 with Invisalign aligners,27 with fixed appliances) was completed by usinga daily diary to measure treatment impactsincluding functional, psychosocial, and pain-related outcomes. A baseline survey wascompleted before the start of treatment; diaryentries were made for 7 consecutive days tomeasure various impacts of the subjects’orthodontic treatment over time. The data werethen analyzed for differences between treatmentmodalities in terms of the subjects’ reportedimpacts from their orthodontic treatment.
Results
The baseline mean values did not differ betweengroups for pain reports (P _ .22) or overall qualityof life impact (P _ .51). During the first week oftreatment, the subjects in the Invisalign groupreported fewer negative impacts on overall qualityof life (P _.0001). The Invisalign group alsorecorded less impact in each quality of lifesubscale evaluated (functional, psychosocial, andpain-related, all P _.003). The visual analog scalepain reports showed that subjects in the Invisaligngroup experienced less pain during the first weekof treatment (P _.0001). The subjects in the fixedappliance group took more pain medications thanthose in the Invisalign group at days 2 and 3 (bothP _.007).
Conclusion
Adults treated with Invisalign alignersexperienced less pain and fewer negative impactson their lives during the first week of orthodontictreatment.
OTHER STUDIES
SCIENTIFIC STUDIES
In a systematic review of the literature, publishedin the Journal of the American Dental Association in2005.Drs. Manual Lagravere and Carlos Flores-Mir were unable to draw strong conclusions about
the effectiveness of the Invisalign system. Theypointed to the need for randomized clinical trials.Since this paper, more studies about the clinicaleffectiveness have been published; for example inthe UK, Dr Paul Humber has analyzed 100 back-to-back Invisalign cases. Assessing the patientsafter two sets of aligners, he found that 94% of thedentitions had achieved the objectives set. In theUSA, Akhlaghi and colleagues comparedtreatment with the invisalign system withtreatment with conventional braces andconcluded that “conventional fixed appliancesachieved better results in the treatment of Class Imild crowding malocclusions” In a comparisonof outcomes between the two approaches, Kuncioet al reported that the Invisalign group displayedgreater relapse saying “the mean alignment of theInvisalign group was superior to the Braces groupbefore and after the retention phase, but thesedifferences were not statistically significant.Therefore, even though the Invisalign casesrelapsed more, they appear to have the same, ifnot better, overall alignment scores.” In a largerstudy Djeu and colleagues had similar findingsto Akhlaghi above and concluded that “Invisalignwas especially deficient in its ability to correctlarge anteroposterior discrepancies and occlusalcontacts”. They felt that “The strengths ofInvisalign were its ability to close spaces andcorrect anterior rotations and marginal ridgeheights.” They added “Invisalign patientsfinished 4 months sooner than those with fixedappliances on average.” Furthermore, work atNYU/Buffalo University by Dr Omar Fetouh waspublished in 2009 where 67 patients were studied,half of whom were treated with Invisalign andhalf with fixed appliances. He concluded that‘There was no statistical significant differencebetween the scores of the Invisalign group andBraces group for Alignment, OcclusalRelationship and Interproximal Contacts. TheInvisalign group had higher scores in Marginalridges, Bucco-lingual inclination, OcclusalContacts, and Overjet than the Braces group.’ Hisconclusion was that Invisalign can treat mildmalocclusions ‘as efficiently, if not better, asbraces.’
25HHHiiissstttooorrryyy ooofff MMMooolllaaarrrDDDiiissstttaaallliiizzzaaatttiiiooonnn iiinnnOOOrrrttthhhooodddooonnntttiiicccsss
Whenever there is space deficiency, the methodsof gaining space that strikes to our mind first are,extraction, expansion and stripping. Angle,proposed expansion of dental arches for nearlyevery patient and extraction for orthodonticpurpose was not necessary for stability of resultsor for aesthetics. He believed that when teeth couldbe saved by dental treatment, extraction of teethfor orthodontic purpose seemed particularlyinappropriate unacceptable.
In 1930’s, Charles Tweed observed relapse afternon-extraction expansion treatment and decidedto retreat with extraction. In recent years, thepercentage of patients having extraction as a partof orthodontic treatment has decreasedconsiderably as experiments has shown thatpremolar extraction does not necessarilyguarantee stability of teeth alignment. Proximalstripping also has its own limitation.
HISTORY OF MOLAR DISTALIZATION
The concept of ‘distal driving’ of the maxillaryposterior teeth has a long orthodontic history in1920s. Class II elastic treatment was thought to bean easy and effective tool but early cephalometricstudies in 1940s showed little or no distalmovement of upper molars. Thus headgears werereintroduced as means of moving upper molarsback. These extra oral appliances were heavilydependent on patient cooperation, forcesgenerated were high and intermittent causingsevere patient discomfort and prolongedtreatment time.
To overcome these difficulties, more recentlyseveral intra oral appliances employing palatalanchorage have been used to produce distalmovement of upper molars. Distalizationmechanics has found many supporters in its
� History of Molar Distalization
� Indications for Molar
Distalization
� Contraindications of Molar
Distalization
� An Ideal Intraoral Molar
Distalization Appliance should
meet the following Criteria
� Mechanism of Action of
Distalizing Appliances
� Pendulum Appliance
� Pend-X Appliance
� M-pendulum Appliance
� Pendulum F Appliance
� Jones Jig
� Intermaxillary Class II
Malocclusion Correction
Appliances
� Vertical Holding Appliance
� Removable Molar Distalization
Splint
� Symmetric Distalization with a
TMA Transpalatal Arch
� Tube Plates for Distalization of
Molars
� Cetlin Appliance
� Anchorage Need
� Extraoral Force
� The Force Applied
� The Lokar Appliance
� K-loop Molar Distalizer
� The Distal Jet Appliance
� The Crozat Appliance
� Molar Distalization by Magnets
� The Magnets
� The Klapper Superspring
� Herbst Appliance
� The Mandibular Anterior
Repositioning Appliance
(MARA)
� Saif Springs
� The ‘Fastback’ Appliance for
Molar Distalization
� Features of Fast Back Appliance
239History of Molar Distalization in Orthodontics
quarters since it provides the arch with increaselength which may correct arch relationship as wellas do away with extraction and loss of tooth. Insome cases the operator gets bonus of achievingexpansion or molar derotation also.� Molar distalization, in recent years is evolved
as an alternative method of gaining space toconventional methods where ever is indicated.
� Kingsley was the first person to try to move themaxillary teeth backwards in 1892 by meansof headgear.
� Oppenheim advocated that position ofmandibular teeth as being the most correct forindividual and use of occipital anchorage formoving maxillary teeth distally into correctrelationship without disturbing mandibularteeth. In 1944, he treated a case with extra-oralanchorage for distalizing maxillary molar.
� Renfroe (1956) reported that lip bumperprimarily devised to hold hypertonic lower lipcaused a distal movement of lower molarssufficient to change class I to Class II.
� Gould (1957) was first person to discuss aboutunilateral distalization of molars with extra-oral force.
� Kloehn (1951) described the effects of cervicalpull headgear.
� Graber T-M. (1969) extracted the maxillary IImolar and distalized the first molar to correctclass II div.1.Non-extraction treatment plans for angle class
II malocclusions often require the distal movementof maxillary molars in the initial stage of treatmentto convert the class II molar relationship to a classI molar relationship.
Most traditional approaches to molardistalization including extra-oral tractionthrough use of a headgear, Wilson distalizingarches, spring appliances and inter-maxilalryelastics with sliding jigs, require considerablepatient compliance to be successful.
With heightened awareness of balance andharmony of the facial profile combined with a needto treat patients with marginal spacediscrepancies, a variety of methods have beenproposed to move molars distally with reduceddependence on patient co-operation. Morerecently, the subjectivity and problems ofpredicting patient behavior have led manyclinicians to devise appliances that minimizedreliance on the patient and that are under the
control of the clinician. Relying on the patient’swillingness to wear an appliance consistentlymay result in increased treatment time, a changeof treatment plan or both.
In recent years, appliances largelyindependent of patient compliance increasinglyhave been used for maxillary molar distalization.
INDICATIONS FOR MOLAR DISTALIZATION
In a Growing Child
� To relieve mild crowding� Causes permanent increase in arch-length of
about 2 mm on each side.
Late Mixed Dentition
� When lower E space – utilized for relief ofanterior crowding
� Upper molars distalized to get a class I relation� Class I malocclusion—with highly/labially
placed canine/impacted canine� Lack of space for eruption of premolars due to
mesial migration of permanent first molars� Good soft tissue profile� Borderline cases� Mild-to-moderate space discrepancy with
missing 3rd molars/2nd molars not yet erupted� Axial inclination : Mesially angulated upper
molars� Normal or hypodivergant growth pattern� Late mixed dentition with mild crowding of
anteriors.
CONTRAINDICATIONS OF MOLAR
DISTALIZATION
� Profile:– Retrognathic profile.
� Functional:– Numerous signs and symptoms of
temperomandibular joint– Posteriorly and superiorly displaced
condyles.� Skeletal:
– Class II skeletal– Skeletal open– Excess lower face height– Constricted maxillary arch– Dolicocephalic growth pattern.
� Dental:Class I or III molar relation.
240 History of Orthodontics
� Dental open biteMaxillary first molar distally inclined.
AN IDEAL INTRAORAL MOLAR
DISTALIZATION APPLIANCE SHOULD
MEET THE FOLLOWING CRITERIA
1. Minimal need for patient compliance.2. Acceptable esthetics and comfort.3. Minimal loss of anterior anchorage (as
evidenced by axial proclination of the incisors.4. Bodily movement of molars to avoid
undesirable side-effects, lengthening oftreatment and unstable results.
5. Minimal chair time for placement andreactivations.
Advantage
No patient cooperation was necessary to obtainmolar movement.
MECHANISM OF ACTION OF DISTALIZING
APPLIANCES
� Passive 0.016 × 0.22 inch wire with stops thatabut the distal wings of premolar brackets isinserted, and the coils are placed on the wirebetween first premolars and molars. The coilsare activated 8 to 10 mm by compressing andmaintaining them against the molars bycrimpable hooks.
� Since the reaction force of the coil moves thewire anterior, the function of the stop againstpremolar bracket is to ensure that the wirecannot move past first premolars, thus placingreaction force on Nance appliance. To enhanceanchorage, 0.018 inch uprighting spring isplaced in the vertical slot of the premolarbrackets directing the crowns distally.
� When class II elastics are attached, rectangularwire with 10 degree of incisor lingual root torqueis inserted in the mandibular arch to maintainlower incisor position. Molar position ismaintained by inserted of 0.016 x 0.022 inchwire with stops that about the molar tubes.Various types of molar distalization
appliances in orthodontics are listed below andfew of them are described in this chapter:� Headgears� Wilson Bimetric arch design� ACCO
� Crozat appliance� Crickett appliance� CETLIN appliance� Removable molar distalization splint� Modified Nance Lingual appliance� Non-extraction treatment (lip bumper)� Molar distalization with magnets� Transpalatal arch� Use of Super elastic NiTi� Double loop niti� The Pendulum appliance� Jones Jig� C-space regainer� Lokar appliance� Intra oral bodily molar distalizer (IBMD)� Maillary distalizing system (MDS)� Fixed piston appliance� The K-loop appliance� The distal jet� Using Implants� Fixed functional appliances.
PENDULUM APPLIANCE
This appliance first described by Hilgers in 1992uses a large Nance button in the palate foranchorage and 0.032-inch TMA springs (OrmcoCorporation) that delivers a distalizing force tothe upper molars. The springs insert into lingualsheaths on the palatal surface of the band. Theanterior portion of the appliance is retained withpremolar bands, which are joined to the applianceusing a retaining wire. Occlusally-bonded restson the primary molars or second premolars addto the retention. If expansion of the upper arch isindicated, then a midline screw can be added tothe appliance. This version of the appliance isknown as the Pend-X appliance.
Byloff and Darendeliler (1997) showed thatthe appliance moved molars distally withoutcreating bite opening, but the molars did tend totip. At the incisal edge was the anchorage losswas measured at 0.92 mm (SD ±0.67). Secondpremolar anchorage loss was measured at amean of 1.63 mm (SD ±1.23), but distal movementof the molar represented 71 per cent of the spaceopened. If molar uprighting bends wereincorporated into the appliance it reduced thetipping, but increased the anchorage loss at thepremolars by 0.61 mm and the incisal edge by0.62 mm (Byloff et al., 1997).

241History of Molar Distalization in Orthodontics
Ghosh and Nanda (1996) also found that thependulum appliance is a reliable method fordistalizing maxillary molars at the expense ofmoderate anchorage loss. The advantages of theappliance lies in its minimal dependence onpatient’s compliance, ease of fabrication, onetime activation, adjustment of the springs, ifnecessary to correct minor transverse and verticalmolar positions, and patient’s acceptance. Themean maxillary molar movement was 3.4 mmwith a distal tipping of 8.4 degrees. There was,however, 2.5 mm mesial movement of the firstpremolar, which represents some anchorage loss.Thus, for every millimeter of distal molarmovement, the premolar moved mesially0.75 mm.
Hilgers (1992) reports that when theappliance is placed before the eruption of thesecond molars, two-thirds of the tooth movementis molar distalization, one-third is experiencedas forward shift of the anchor bicuspids. If placedafter eruption of the second molars, theexperience tends to be reversed, one-third distalmovement of the first molar, and two-thirdsanchorage slip.
Advantages
� Minimal dependence on patient compliance� Ease of fabrication� One time activation� Adjustment of the springs if necessary to
correct minor transverse and vertical molarpositions.
� Patient’s acceptance.� Unilateral class II corrections.� Used to regain space lost through mesial
drifting of the upper first molars because ofeither early loss of second deciduous molarsor impaction of first molars under distal crowncontour of the deciduous molars. Rapiddistalization of upper first molars andstabilization with an insta Nance providespace for the erupting second bicuspids.
Disadvantages
James J Hilgers in 1992 introduced an appliancefor class II correction in non-compliant patients.The “pendulum appliance” is a hybrid that useslarge Nance acrylic button in the palate for
anchorage along with 0.032" TMA springs thatdeliver light, continuous force to the upper firstmolars without affecting the palatal button. Thus,the appliance produces a broad swinging orpendulum of force from the midline of the palateto the upper molars.
PEND-X APPLIANCE
� In cases with severe narrowing of maxillaryposterior segments, if expansion of upper archis needed, a mid palatal jack screw can beincorporated into the center of the Nancebutton.
� The screw is activated one-quarter turn everythree days, after a week or so for patientadjustment, to produce a slow, stableexpansion.
� The resulting activation is usually sufficientnot only to correct any transversediscrepancies, but also to control molarrotation during distalization.
M-PENDULUM APPLIANCE
Giuseppe Scuzzo in 1999 introduced M-pendulum:� In this horizontal pendulum loops are
inverted, it will allow bodily movement ofboth the roots and crowns of the maxillarymolars. Once the distal molar movement hasoccurred, the loop can be activated simply byopening it.
� The activation produces buccal/distal uprighting of the molar roots and thus a truebodily movement rather than a simple tippingor rotation.
� Pendulum springs are activated to 40–45o,resulting in about 125 g of force on each side.This activation is repeated until the desireddistalization of the molars is obtained.
Advantages
� True bodily molar movement� Minimal dependence on patient compliance� Ease of fabrication� Little need for reactivation� Patient’s acceptance.
An intra-maxillary anchorage unit is neededto counteract the reactive forces and moments inmolar distalization.
242 History of Orthodontics
Anchorage Design of the M-pendulum
Appliance
� The anchorage block consists of a Nancepalatal button and anchoring teeth in the samedental arch. The acrylic button fits tightlyagainst the palatal mucosa in the region of thepalatal rugae and is linked to the teeth withocclusally bonded onlays. After placement ofthe pre-activated pendulum springs, theanchorage unit is designed to counteract thereactive forces and moments.
� The anchorage effect of the anterior palatalplate to the resilient palatal mucosa might bedue to hydrodynamic interactions. Additionalvertical stabilization might result from tonguepressure while swallowing. Anchorage valueof the soft tissue supported Nance holdingarch should not be overestimated.
� The anchorage mainly depends on the dentalanchorage quality of the teeth. The resistancepotential of these anchorage teeth isdetermined by the size of the anchoragerelevant surfaces and thus by the number ofteeth involved, by root topography and theattachment level and by the bone structure andthe desmodontal reactive state.
� The bone structure and attachment level isconstant among children and adolescentstreated with pendulum appliance butdifferences might occur with respect to thenumber of teeth, root topography anddesmodontal reactive state.
Number of Anchorage Teeth
� Hilgers used only anterior part of theappliance, using bands on maxillary firstpremolars or deciduous molars and a holdingarch to the Nance button. He observed thatafter placing the springs, Nance buttonstended to lift. So the recommended thatsupporting elements should be bondedocclusally to the maxillary second premolarsor second deciduous molars for additionalstability. Additional bonding of occlusal onlays to the canines to obtain additionalanchorage support is also recommended.
� The reactive segment should consist of asmany anchorage teeth as possible, which arecombined to form a multi-rooted anterioranchorage unit with occlusal onlays and the
Nance button and permit uniform periodontalpressure distribution.
Anchorage Quality of Deciduous Molars and
Premolar Root Topography
� The desmodontal anchorage quality of theanchoring teeth depends largely on their rootsurfaces and root topography.
� Even if root surface of deciduous molars andpremolars are identical, anchorage quality ofdeciduous molars undergoes a constantdecrease during physiologic resorptionresulting in imbalance in the favor of thepremolars.
� The results of this study show that extent andquality of molar distalization are better andside-effects are less pronounced in theanchorage and the incisor region if premolarsalone are used for anchorage.
� It is advisable to perform an initial test forincreased tooth mobility when using dec.molars for anchorage, to avoid having toremove the appliance prematurely when theanchorage quality is overestimated.
� A panoramic radiograph providesinformation on the extent of root resorption ofdec. molars and indirectly quality of such teethfor anchorage purposes during pendulumappliance therapy.
Desmodontal Reactive State, Potential
Causes of Reduced Anchorage
� The primarily unmoved tooth in a desmodontalresting state offers the best tissue resistance.
� Initial leveling increases the proliferation rateof cells relevant to the remodeling process inthe anchorage unit and increases readinessfor reactive movement. Therefore initialleveling should not be performed in the regionof the anchorage unit when placing pendulumappliance.
� Omission of Nance anterior palatal plate alsoleads to increased loss of anchorage.
Potential Measures for Increased
Anchorage
When an end osseous implant is used in the regionof the hard palate or miniscrews, stationary intra-oral anchorage can be achieved without teeth beingincorporated. The fixing of pendulum appliance
243History of Molar Distalization in Orthodontics
to an Osseo integrated palatal implant of the orthosystem not only represents a significantimprovement in anchorage quality during molardistalization but also permits stationary anchoragewith a transpalatal arch during the subsequentdistal guidance of premolars and canines. Theyare used in exceptional cases such as adults withproblematic periodontal anchorage or in mixeddentitions with early loss of the decidduous molars.
PENDULUM F APPLIANCE
Favero modified pendulum appliance for lingualtechnique. Acrylic portion of the Nance buttonhas a larger dimension than in other pendulumappliances and can accommodate in the anteriorregion a segmented wire, which is inserted in thelingual brackets of the incisors.
An increase in biological anchorage quality ispossible. Occlusal forces can be usedtherapeutically for increased anchorage if thecomposite on lays to which the wires are attachedwere formed with an occlusal relief.
This method can be applied only ifmandibular arch has sufficient teeth which arein stable position (i.e. no orthodontic treatmentis performed simultaneously in the mandible).
Drawbacks
1. Lingual tipping of molars.2. Difficult to fabricate.
JONES JIG
The Jones Jig was first introduced by Richard D.Jones and J. Michael White. Jones Jig is one of theappliances which accomplish tooth movementwithout the need for patient compliance. Theappliance uses an open coil Nickel titaniumspring to deliver 70–75 g. Over a compressiverange 1–5 mm to the molars.
Advantages
The advantages of the Jones Jig appliance are that,it can achieve class I relationship even when:� 2nd motors erupted or unerupted� In mixed and permanent dentition� Unilateral as well as bilateral distalization� Growing and non-growing patients.
The appliance is also said to be a predictable,painless sand rapid method of correcting class IIrelationship with minimum patient co-operation.
INTERMAXILLARY CLASS II MALOCCLUSION
CORRECTION APPLIANCES
Several intermaxillary fixed non-complaintappliances have been proposed and used overthe past two decades.
Advantages
� Forward displacement of the mandible.� Backward displacement of the maxilla� Anterior force on the mandibular dentition.
All above three actions and movements willbring about the correction of class IImalocclusion.
Disadvantages
The common disadvantage of intermaxillaryappliances is undesirable steepening of theocclusal plane with concomitant flaring of thelower incisors and distal tipping along withextrusion of the maxillary incisors.
VERTICAL HOLDING APPLIANCE
Vertical Holding Appliance is a fixed functionalintra-oral distalizing appliance, as it is activatedfrom the functional activity of the tongue.
Wire used for the fabrication of thisappliance: 0.040 inch wire is used for thefabrication of this appliance.
Helices of Vertical Holding Appliance
� Vertical holding appliance consist of fourhelices in its design
� The two helices are placed just distal to eachmaxillary first molar
� Other two helices are placed at the center ofthe appliance.
V-Bend
� V-bend is fabricated using 0.040 inch wire� V-bend separates the helices of VHA which
are placed at the center of the appliance� V-bend portion of the wire is embedded in the
acrylic button.
Acrylic Button
� Acrylic button is composed of self –cure acrylicmaterial
� Size of the acrylic button—size of a dime
244 History of Orthodontics
� Thickness of the button—the acrylic buttonshould be 2–5 mm away from the palate
� Acrylic button contributes greater proportionas compared to the any other portion of theappliance.
Action
Vertical holding appliance results in intrusionand distally directed force.
REMOVABLE MOLAR DISTALIZATION SPLINT
The removable molar distalization appliance wasput forward by Dr A. Korrodi Ritto, to overcomethe drawbacks of patient co-operation, neededwith other removable appliances like theremovable plates and headgears.
Advantages
1. It is smaller than conventional removable plates.2. It is comfortable.3. Esthetics.4. Better patient co-operation.
Disadvantage
There is more amount of molar tipping seen ratherthan bodily, molar distalization. Therefore the bestcases for treatment with this appliance are thosewhere the molars are already messily tipped.
SYMMETRIC DISTALIZATION WITH A TMA
TRANSPALATAL ARCH
The intra-oral distalization methods can allproduce bodily distal movement of the maxillarymolars, but can also cause a mesial movement ofthe maxillary premolars and canines, or aproclination of the mandibular incisors when classII elastics are used. In addition, the loss of anterioranchorage often leads to relapse of the maxillarymolars during the correction of caninerelationship, overbite and over jet.
According to Cetlin’s method, maxillarymolars can be distalized unilaterally by using aGoshgarian transpalatal arch in conjunction withextra-oral traction. A toe-in-bend in thetranspalatal arch applies a mesiobuccal rotationto the molar on the side of the bend and a distallydirected force against the molar on the oppositeside. This procedure does not cause a loss ofanterior anchorage.
Advantages
This method has several advantages:1. ‘TMA’ has better shape memory and resilience
than stainless steel.2. The arch is simple to construct.3. The system is hygienic and economic.4. This is no anterior anchorage loss; the
premolars and canines spontaneously followthe molar distally.
Drawbacks
1. Because the ‘TMA’ is more fragile thanstainless steel, the arch must be bent carefully,and fractures in the mouth are more common.
2. Since the ‘TMA’ arch rotates the anchor molarmore mesiobuccally than a conventional archdoes. It should be combined with a fixedorthodontic appliance using a rectangulararch-wire or a passive stainless steel wiresegment between the second molar and canineon the anchor side.
3. The system can only distalize one molar at atime, and therefore is recommended for usewith unilateral or slight bilateral class II molarrelationships.
4. An extra-oral appliance should be worn atnight to reinforce anchorage.
TUBE PLATES FOR DISTALIZATION OF
MOLARS
Lain Benauwt explained the use of a removableappliance for distalizing the molars. Theseappliances were introduced as the applianceswith wires sliding in tubes.
Advantages
1. Retention of the appliance is very good, as themovable parts contribute to the retention (dueto incorporation of Adam’s clasp).
2. It is very helpful in mixed dentition, whendeciduous molars are not too retentive or arebroken down or missing.
3. Unwanted displacement of teeth is minimizeddue to the Adam’s Clasp who holds the molarand avoids rotation.
4. An extra-oral appliance can be used alongwith this appliance to support and reinforcethe stationary part or indirectly theanchorage.
245History of Molar Distalization in Orthodontics
5. Expansion is also possible all the same timeas the distalization of the molar, and isachieved by changing the angulations of thetubes in relation to the sagittal plane.
6. Repair is easy.
Disadvantage
It is a delicate appliance. The two wires must holdthe movable part without binding.
CETLIN APPLIANCE
The appliance involves a combination of anextra-oral force in the form of headgear and aninfra oral force in the form of a removableappliance. In molar distalization, bodily distalmovement rather than distal tipping of themaxillary molars is essential. When there is onlya distal tipping, the molars relapse messily,uprighting under their apices to comeback to itsoriginal position.
To overcome these drawbacks, the Cetlinappliance utilizes a removable appliance intraorally to tip the crowns distally and then anextra oral force to upright the roots. So the intra-oral removable appliance can be called thecrown mover while the extra-oral force, is theroot mover.
ANCHORAGE NEED
The anchorage for the removable appliance is byproper adaptation to the palate, an acrylic shieldaround the four maxillary incisors and a modifiedAdam’s Clasp on the first premolars.
EXTRAORAL FORCE
� The extraoral appliance is a headgear, whichis inserted into the molar tube. The headgearused in generally a cervical or a high pull type,depending on the usual consideration ofskeletal pattern.
� The removable appliance is worn 24 hours aday. The appliance also contains a bite planeto disengage the molars (to aid in rapid molarmovements).
THE FORCE APPLIED
� In the removable appliance, the spring isactivated only 1 to 1.5 mm, measured alongthe occlusal surface of the molar and It
supplies only 30 g of force on the molars. Thesprings are placed as far gingivally as possibleto minimize crown tipping and to cause molarmovement without Irritation.
� The removable appliance exerts a force, whichmoves the molar crowns distally, with relativeease.
� The extra oral headgear on the other handexerts a force of 150 g per tooth and is used tocontrol root position. The headgear is advisedto be worn for 12–14 hours/day.
� When using a cervical headgear, it is generallynecessary to elevate the outer bow to producean appropriate “force couple” that will movethe roots distally, by directing the line of forceabove the outer of mass of the molar.
THE LOKAR APPLIANCE
The Lokar appliance was developed by Dr LoterIn 1894.
Components of Lokar Appliance
The appliance consists of two basic components,and they are:� A mesial sliding component� A component which inserts Into arch wire tube
of the molar.
Design of the Lokar Appliance
� The distalizer is inserted into arch wire tubeof the first molar and the application isadapted such that it is parallel to the plane ofocclusion and as close to the teeth as possibletor patient comfort.
� A 0012" S.S. ligature wire hand twisted aroundthe premolar bracket before the Lokar is fixedto the molar tube. This ligature wire is engagedaround the mesial sliding component of thedistalizer and tightened to activate theappliance.
Force Applied and Activation of the
Appliance
The force is delivered by NiTi Coil spring, whichgets compressed during activation.
Anchorage
The anchorage is by a Nance appliance, solderedto the premolars.
246 History of Orthodontics
Activation
A 0.012" S.S. ligature wire is hand twisted twicearound the premolar bracket, such that the freeends of the ligature face distally. One of the freeends is then passed over the mesial slidingcomponent of the mainframe and tightened toactivate the appliance. The force is delivered bythe NiTi Coil spring, which gets compressedduring activation. The best activation is achievedby compressing the spring by 2–3 mm.
Re-activation of the Appliance
Re-activation is done at 5–6 weeks interval.
K-LOOP MOLAR DISTALIZER
The K-loop molar distalizer was developed byVamn Kalra. The K-loop molar distalizer consistsof:� A K-loop—to provide the forces and moments� A Nance button—to resist anchorage.
– The K-loop is made of 0.017- x 0.025" TMAwire. Which can be activated twice as muchas stainless steel before it undergoespermanent deformation. A loop made of‘TMA’ also produces less than half the forceof one made with stainless steel.
– Each loop of the ‘K’ should be 8 mm longand 1.5 mm wide. The legs of the ‘K’ arebent down 20° and inserted into the molartube and the premolar bracket. The wire ismarked at the mesial of the molar tube andthe mesial of the premolar bracket. Stopsare bent into the wire ‘1 mm’ distal to thedistal mark and ‘1 mm’ mesial to the mesialmark. Each stop should be well-definedand about 1.5 mm long. These bends helpkeep the appliance away from themucobuccal fold, allowing a 2 mmactivation of the K-loop.
– The 120° bends in the appliance legsproduce moments that counteract thetipping moments created by the force of theappliance, and these moments arereinforced by the moment of activation asthe loop is squeezed into place. Thus, themolar undergoes a translatory movementinstead of tipping. Root movementcontinues even after the force hasdissipated. If an extrusive or intrusive forceagainst the molar is not desired, it is
important to center the K-loop between thefirst molar and the pre molar.
– For additional molar movement, theappliance is reactivated 2 mm after 6-Sweeks. The loop is easy to remove from themolar tube, since the distal end of the wireis not bent. In most cases, one reactivation,producing a total of as much as 4 m of distalmolar movement is sufficient.
– The palatal Nance button, held in place bywires extending from bands on the firstpremolars or first deciduous molars, isprimarily responsible for preventing anteriormovement of the first premolars. The buttonshould be large enough to, provide adequateanchorage and prevent tissue impingement,but should be kept away from the teeth. Theacrylic should not be built up so that thebutton acts as a bite plane.
– The premolars moved forward by about ‘1mm’ during ‘4 mm’ of molar distalization.If necessary, the anchorage can bereinforced by attaching a straight pull orhigh-pull headgear with a force of 150 g tothe premolars.
Advantages
The K-loop molar distalizing appliance has thefollowing advantages:� Simple yet efficient� Controls the moment-to-force ratio to produce
bodily movement, controlled tipping oruncontrolled tipping as desired
� Easy to fabricate and place� Hygienic and comfortable for the patient� Requires minimal patient co-operation low-
cost.
THE DISTAL JET APPLIANCE
The distal jet was designed by Akto Carano andMiiuro Testa in 1996.
Appliance Design
� The appliance consists of bilateral tubes of0.036" internal diameter which are attachedto an acrylic name button. NiTi Coil springand screw clamps are slide over each tube.
� The wire extending from the acrylic, througheach tube ends in a bayonet bend that isinserted into the lingual sheath of the first
247History of Molar Distalization in Orthodontics
molar band. An anchor wire from the Nancebutton is soldered to the bands on the 2ndpremolars.
Components
1. The transpalatal connectors—rigidlyimmobilize the premolars and provide asupport to the Nance button.
2. The Bayonet director unit: Lumen of the tubeportion supports the molar bayonet, while itsoutside diameter supports the spring and theactivation lock.
3. The molar bayonet: It is drawn out of thebayonet director unit during distalization andinserted into the lingual sheath. The distal stepprevents the spring from riding on the verticalarm of the molar bayonet while activating theappliance.
4. NiTi springs: NiTi coil springs of 150 gm areused for children and 250 gm used for adults.
5. Stainless steel springs: The appliance can alsobe fabricated with stainless steel springs.
6. Activation locks—to compress and activate thesprings.
7. Lock wrench: To engage and tighten (the screwof the activation lock).
Activation
� The distal jet is activated by sliding the dampcloser to the first molar once a month.
� Once the distalization is complete, theappliance can be converted to a Nance retainersimply by replacing the clamp-springassemblies with light-cured or cold cure acrylicand cutting off the arms or the promoters.
Advantages
The advantages of the distal-jet appliance arelisted below:� Minimal patent discomfort� Minimal or no molar tipping� Ease of fabrication� Ease of insertion� Esthetically acceptable� Well-tolerated by patients� Ease of conversion to a Nance holding arch to
maintain the distalized molar position� It can be used with a full-fixed appliance
There are several modifications to the distal-jet appliance, for different purposes. They are:
1. Conversion to Nance holding arch.2. Double set screw distal Jet appliance.3. Incorporation of helical loops into bayonet
wire far molar rotation and up-fighting.4. Incorporation of Jack screws for maxillary
expansion.
THE CROZAT APPLIANCE
The crozat appliance is similar to the crickettappliance but has palatal and lingual bars insteadof stainless steel wire components.
Dr Crozat viewed the appliance as acting in atruncated cone or funnel. As the molars are beingtranslated distally in a divergent direction,expansion must be placed in the appliance to avoidthe more roots striking the lingual cortical plate,blocking movement. Over-expansion can alsoimpede distal movement by emerging the rootsagainst the buccal plate.
Treatment of a bilateral class II malocclusionwith a good lower arch is begun with rotationadjustments of the upper molars. First themeasurement is made between the lingual arms;and each crib clasp complex is rotated to increasethis measurement ½ mm per side. Once therotation adjustment is begun every third rotationadjustment, the molars are expanded to keep theteeth tracking back into a more divergent portionof the arch. Once the molars are derotatad, class IIelastics are added to continue distal movement.Similar unilateral class II can also treated, withcrozat appliance.
Dr Crozat introduced this appliance in 1919.Dr Crozat’s goal was to solve crowding by thedistal movement of molars. As he moved molarsdistally, expansion of the appliance wasnecessary because the bony dental arch itself iswider in the posterior regions.
MOLAR DISTALIZATION BY MAGNETS
� Magnets have been used intra-orally for avariety of reasons. More often for retention ofprosthesis. In contemporary orthodontics,light continuous force (75 to 100 g) arecommonly used to correct malocclusion withtypical tooth movement of 0.5 mm/week.
� Miniature Samarium-cobalt (Sm-Co) magnetsare used and they have been proved to beeffective and efficient force delivery systems.Ferrite, Ainico or platinum cobalt have been

248 History of Orthodontics
tried but left out due to their very low magneticstrength and hence larger size.
� The magnets can either be used in the attractiveor the repelling state. The repelling state ispreferred. It was found that the Sm-Co magnet;when used, exert very high forces of more than200 omi at small separations, while optimumorthodontic forces were generated (75 to180 g), when separation was 0.5 to 1.00 mm.
� Magnetic Force = (Separation)n = (d)n
� The force exerted by the magnets decrease from200 gms at contact to about 409 gms at 2mm,with a rapid decrease of force at greaterseparations.
� The magnets used showed goodbiocompatibility when they were coated.
� The stainless steel coated samarium-cobaltmagnets can be recycled and showed goodbiocompatibility.
THE MAGNETS
� The magnets are four in number and they areencased in a steel sleeve with a finely machinedhole in the center and coated with abiocompatible polymer to avoid leaching outof products.
� Two of the magnets are pre-set in regulation(on each wire) for easy insertion bilaterally.Both repelling magnets on each wire areclamped together to avoid possible loss ofmagnet.
THE KLAPPER SUPERSPRING
This appliance is an auxiliary which is fitted tofully banded upper and lower fixed appliances(ORTHO design, 744 Falls Circle, Lake Forest,Illinois 60045, USA).
Design of the Appliance
The appliance consists bilaterally of a lengthmulti-flex nickel-titanium which is bent back on itattaching to the upper first molar tube andattaching to the lower arch wire by means of ahelical loop. The springs lie in the buccal vestibule.The effect of the spring is to place a distalizingand intrusive force to the upper first molar.
Latest Design of Klapper Super Spring
The latest design of the spring requires a specialoval tube to be fitted to the upper first molars. This
facilitates buccolingual adjustment of the springsin the vestibule and aids patient comfort. Thesprings can be readily removed for adjustment oractivation. There have been no studies to datedocumenting results achieved with this appliance.
Availability of the Appliance
The appliance comes in two sizes:� 27 mm primarily designed for extraction cases
and� 40 mm for non-extraction cases.� The springs are paired for left and right sides.
Indications
1. Dental Class II malocclusion.2. Deep bite with retroclined mandibular incisors.
Contraindications
1. Cases predisposed to root resorption.2. Dental and skeletal open bites.3. Vertical growth with high mandibular plane
angle and excess lower facial height.
HERBST APPLIANCE
The Herbst bite jumping mechanism wasdeveloped by Emil Herbst in the early 1900’s.Theoriginal banded design of this appliance wasintroduced at the international dental congressin Berlin (Germany) by Herbst in 1905. It wasintroduced by Pancherz. Pancherz used a bandedHerbst design that involved the:
� Placement of bands on molarand premolar
Maxilla� Bands are connected by copperlingual wire
� Bands on lower right first premolarand lower right first premolar
Mandible� Bands are connected by alower lingual arch wire
Herbst Appliance
The Herbst appliance is a fixed functionalorthopedic appliance having passive tube andplunger system with the exact length of the tubedetermining the amount of anterior mandibulardevelopment. The tube is attached to a maxillaryposterior root, whereas the plunger is fixedanteriorly to the mandibular dentition and slidesthrough the tube during opening and closingmovements.

249History of Molar Distalization in Orthodontics
THE MANDIBULAR ANTERIOR
REPOSITIONING APPLIANCE (MARA)
The Mandibular Anterior RepositioningAppliance (MARA, Allesee OrthodonticsAppliances, PO Box 725, Sturtevant, WI 53177,USA) MARA consists of cams made from 0.060square wire attached to tubes (0.062 square) onupper first molar bands or stainless steel crowns.A lower first molar crown has a 0.059 armprojecting perpendicular to its buccal surface,which engages the cam of the upper molar. Theappliance is adjusted so that when the patientcloses, the cam on the upper first molars guidesthe lower first molars and repositions themandible forwards into a Class I relationship.There have been no studies to date documentingresults achieved with this appliance. Thedevelopers of the appliance recommend a 12-month treatment time to achieve a bite jumping ororthopaedic effect. Stabilization of the lowermolars is assisted by the fitting of a lingual archand on the upper arch a transpalatal bar tostabilize the upper molars is placed. Thisappliance does not require the placement ofattachments on teeth other than the first molars.
Indication
Skeletal Class II with mandibular deficiency.
Contraindications
1. Dolichofacial growth pattern.2. Cases predisposed to root resorption.3. Dental and skeletal open bites.4. Vertical growth with high mandibular plane
angle and excess lower facial height.
SAIF SPRINGS
Design of the Appliance
These are long nickel-titanium closed coil springsthat are used to apply Class II inter-maxillary tractionwhen fully banded fixed appliances are in place(Saif Springs, Pacific Coast Manufacturing Inc, 18506142nd Ave, NE Woodinville, WA 98072, USA). Thesprings are tied in place with steel ligatures and areworn in place of inter-maxillary elastics.
Availability of the Saif Spring
The springs are available in two lengths:
� 7 and� 10 mm.
Pre-requisites of the Spring
No longitudinal research studies on this auxiliaryare available in the literature to date. Starnes(1998) recommends that for successful treatmentto be carried out the prerequisites are as follows:� Prior correction of deep bites;� Stabilization of each arch with a large
rectangular arch wire;� Direction of force as horizontal as possible;� Sufficient resistant torque (lower incisor
lingual crown torque);� Perfect fit of bands;� Proper placement of hooks for spring
attachments.
THE ‘FASTBACK’ APPLIANCE FOR MOLAR
DISTALIZATION
Modern Orthodontic Science is constantlyexploring new non-extraction therapies throughresearch carried out employing appliances thatwill allow the Orthodontist to gain space bothtransversally and distally. Consequentially, inrecent times we have observed an increase in thenumber of appliances for the distalization of theupper molars. Italians have been particularlyprolific in this area, probably on account of manyof our young patients being reluctant to followthe therapeutic indications that come with extra-oral tractions. The common goal for all thoseinvolved in developing new distalizingappliances appears to be the ability to provide adental movement that is bio-mechanicallycontrolled and generated by adequate forces, whilekeeping undesired contramovements to aminimum., the ideal Distalizer should occupy thesmallest possible space, interfere as little aspossible with function and provide bodily distalmovement of the dental elements involved withminimal (or absence of) patient compliance. Distalmovement should occur in the patient withminimal damage to the surrounding tissues andfunction, generating minimal (or absence of)contra-movements. The appliance used should beengineered in such a way that would maketherapy management easy and safe.
The ‘Fastback’ Molar Distalizer is now fullyestablished as a ‘reference’ appliance in the
250 History of Orthodontics
Orthodontic field. A growing number ofProfessionals, having had the opportunity to fullyevaluate and appreciate the ease and safety of useas well as the bio-mechanical developmentprovided by this device, are now prescribing itregularly whenever they need to gain space in theposterior region. At the time of writing, 6 yearshave passed since the initial prototypes of‘Fastback’ devices were introduced.
FEATURES OF FAST BACK APPLIANCE
Fast back features are as follows:� Easy to plan and assemble� Reduced bulk� Minimal patient discomfort� Good aesthetics� Continuous, constant forces are at work at all
times� Intensity and direction of the forces applied
can be� Accurately controlled
� Reduced or minimal loss of anchorage� Reduced or minimal contra-movements� Bodily Distalization occurs, no risk of
undesired movements� Easy, non-frequent Activation� Checks every 4/6 weeks, cost-effective patient� management� Spherical or long ends ensure the appliance
stops� when not activated, should the patient skip
one or more appointments� The ‘Fastback’ can be used in conjunction with
fixed� Buccal appliances (brackets).
There are three versions of the ‘Fastback’appliance:� FB1 (Monolateral FB with ‘Tripod’ Anchorage
unit) with or without ‘Nance’ button� FB2 (Bilateral FB ) with ‘Nance’ button� FB3 (Bilateral FB ) with ‘Nance’ button and
Extensions, or Rests, to the Canines.

SSSuuuggggggeeesssttteeeddd RRReeeaaadddiiinnnggg
1. A practical guide to the management of the teeth.1819:198.
2. Ackerman JL, Profitt WR. The characteristics ofmalocclusion: A modern approach toclassification and diagnosis. Am J Orthod1969;56:443-54.
3. Adams CP. The modified arrowhead clasps. DentRecord, 1950; 70:I43.
4. Adams. Removable appliances yesterday andtoday. Am J Orthod, 1969;202-18
5. Ahmad KA, Drummond JL, Graber TM, BeGoleE. Magnetic strength and corrosion of rare earthmagnets. Am J Orthod Dentofacial Orthop2006;130:275 e11-15.
6. Ainsworth GC. Some thoughts regardingmethods and a new appliance for movingdislocated teeth into position. Int Dent J, 1904;24:481.
7. Alexander D. Vardimon AD, Graber TM,Drescher D, Bourauel C. Rare earth magnets andimpaction. Am J Orthod Dentofac Orthop. 1991;100: 494-512.
8. Allan G Brodie. Orthodontic concepts prior tothe death of Edward H Angle. AO, 1956; Vol. 26,Page 144-54.
9. Andressen V. The Norwegian system of functionalgnathoorthopedics. Acta Gnathol 1936;1:4.
10. Andrews lF. The keys for normal occlusion . AJO,1972; Vol.62, Page 296.
11. Angel EC. Treatment of irregularities of thepermanent teeth. Dent Cosmos 1860;1:540. DentCosmos, 1860; 1:281.
12. Angle CP. The modified arrowhead clasp—somefurther considerations. Dent Record, 1953; 73,332-3.
13. Angle EH. Evolution of orthodontia—recentdevelopments. Dent Cosmos. Reprint August,1912:5.
14. Asbell MB. Bicentenary of a dental classic: JohnHunter’s “Natural History of the Human Teeth.”J Am Dent Assoc, 1972;84:1311-4.
15. Asbell MB. The American Association ofOrthodontists: a history, 1965-90 [unpublishedmanuscript]. p. 68-71.
16. Atkinson SA. Albin Oppenheim. Am J Orthod,1957; 43:46-51.
17. Badcock JH. The screw expansion plate. Trans.Brit Soc Orthop, pp 1911;3-8.
18. Barrer, HG. Treatment timimg of borderlinecases. J Clin Orthodont, 1971;5:191-9.
19. Bates v. State Bar of Arizona, 433 U S 350, 364,1977.
20. Baty DL, Storie DJ, von Fraunhofer JA. Syntheticelastomeric chains: a literature review Am JOrthop Dentofac Orthop, 1994;105:536-42
21. Baumrind S, Korn EL, Boyd RL, Maxwell R. Thedecision to extract: part 1. Am J Orthod Dento-facial Orthop, 1996;109:297-309.
22. Begg PR, KeslingPC. Begg orthodontic theoryand technique (3 Edn). (W.B. Saunders).
23. Begg PR. Begg orthodontic theory and techn-ique. Philadelphia; WB Saunders: 1965.
24. Bernhard Schwaninger. Evaluation of the straightarch wire concept. AJO, 1978; Vol. 74,188-96.
25. Bishara SE, Staley RN. Mixed-dentitionmandibular arch length analysis. Angle Orthod1984;36:130-5.
26. Björk A. The face in profile, an anthropologicalX-ray investigation on Swedish children andconscripts. Svensk Tandl Tidskr 1947;40 Suppl.
27. Bogue EA. Orthodontia of the deciduous teeth.Dent Digest 1912;13:671-7;1913;19:9-14; 1919;25:193-210.
28. Bolton WA. Disharmony in tooth size and itsrelation to the analysis and treatment ofmalocclusion. Angle Orthod 1958; 28: 113-30.
252 History of Orthodontics
29. Bonham ManessW. The straight wire concept.AJO, 1978; Vol.73, 541-50.
30. Breece GL, Nieberg LG. Motivations for adultorthodontic treatment. J Clin Orthod, 1986;20(3):166-71.
31. Brodie AG. On the growth pattern of the humanhead from the third month to the eighth year oflife. Am J Anat, 1941;68:209-62.
32. Buonocore MG. A simplified method ofincreasing the adhesion of acrylic filling materialsto enamel surfaces. Journal of Dental Research.1955;63/S.I Abstract No. 556, p232
33. Cacciafesta V, Sfondrini MF, Ricciardi A, ScribanteA, Klersy C, Auricchio F. Evaluation of frictionand stainless steel aesthetic self-ligating bracketsin various bracket-archwire combin-ations. AmJ Orthod Dentofac Orthop, 2003; 124:395-402.
34. Caniklioglu MC, Ozturk Y. Guray bite raiser: itsclinical use in lingual orthodontic treatment. JLingual Orthod, 2002; 2(3):71-7.
35. Carey CW. Linear arch dimensions and toothsize. AJO, 1949;35:764-6.
36. Carey CW. Linear arch dimensions and toothsize. AJO, 35:764-6,194.
37. Carey CW. Lower arch dimension and tooth size.Am J Orthod, 1949;35:762-75.
38. Carroll-Ann Trotman, James A. McNamara Jr.Association of lip posture and the dimensions ofthe tonsils and sagittal airway with facialdimensions. AO 1997;67:425-32.
39. Carter RN. Clinical management of ceramicbrackets. J Clin Orthod, 1989;23(12):807–9.
40. Castro FM. The trend of orthodontic treatment.Proceedings of the American Society of Orthod-ontists, 1930 and 1932;119-23.
41. Castro FW. A historical sketch of orthodontia.Dent Cosmos, 1934;66:112.
42. Cetlin NM, Ten Hoeve AJ. Nonextractiontreatment. J Clin Orthod, 1983;17:396-413.
43. Charles H Tweed. Clinical orthodontics, 1st Edn,Vol.1 (The C.V. Mosby Company).
44. Columbia. Sentinel, June 4, 1796.45. Coreil MN. Uncompromising aesthetic
treatment—dispelling the myths about ceramicbrackets. Clinical Impressions, 2004;13(1):4-11.
46. Cozza P, Baccetti T, Franchi L, McNamara JA Jr.Treatment effects of a modified quad-helix inpatients with dentoskeletal open bites. AJO2006Jun;129(6):734-9.
47. Creekmore T. Lingual orthodontics—Its renai-ssance. Am J Orthod Dentofacial Orthop, 1989;96(2):120–37.
48. Curtis EK. Orthodontics at 2000. St Louis:American Association of Orthodontists; 2000. pp.27.
49. Curtner RM. Personal communication.November 1, 1995.
50. de Almeida MR, Henriques JF, de Almeida RR,Weber U, McNamara JA Jr. Short-term treatmenteffects produced by the Herbst appliance in themixed dentition. Angle Orthod. 2005 Jul;75(4):540-7.
51. De Medicina, Edition of Pincius for Fontana,Venice, 6 May 1497. Library #131881(incunabula), College of Physicians, Philadelphia.For English translation see Foster EW. “Celcus”.Dent Cosmos, 1879;21:235-41.
52. Deguchi T, Kuroda T, Hunt NP, Graber TM.Long-term application of chin-cup force altersthe morphology of the dolichofacial Class IIImandible. Am J Orthod Dentofacial Orthop1999;116:610-5.
53. Deguchi T, Kuroda T, Minoshima Y, Graber TM.Craniofacial features of patients with Class IIIabnormalities: Growth-related changes andeffects of short-term and long-term chin-cuptherapy. Am J Orthod Dentofacial Orthop2002;121:84-92
54. Deguchi T, Takano-Yamamoto T, Kanomi R,Hartsfield JK Jr, Roberts WE, Garetto LP. Theuse of small titanium screws for orthodonticanchorage. J Dent Res, 2003;82:377-81.
55. Dent Cosmos 1887;29:275.56. Dental Register, 1891;45:369.57. Dewel BF. A question of terminology. Am J
Orthodont, 1970;58:78-9.58. Dewel BF. Orthodontics: midcentury
recollections. Eur J Orthod, 1981;3:77-8.59. Dewel BF. Prerequisites in serial extraction. Am.
J Orthodont, 1969; 55:633-9.60. Dewel BF. Second premolar extraction in
orthodontics: principles, procedures, and caseanalysis. Am J Orthod, 1955;441:107-20.
61. Dewel BF. Serial extraction—its limitationssandcontraindications. Arizona Dent J, Sept 15, 1968;14:14-30.
62. Dewel BF. The Case-Dewey-Cryer extractiondebate: a commentary. Am J Orthod, 1964;50:862-5.
63. Dewel, BF. Precautions in serial extraction. Am JOrthodont, 1971;60:615-8.
64. DJ Bowells. The straight wire appliance : Dentalup date, 1986; Vol.13, 367-76.
65. Dougherty HL, Allergy to rubber, Am J OrthopDentofac Orthop, 1993;104:23A-24A.
66. Downs, William B, 1899-1966 (Obituary), AngleOrthod, 1983;53:1.
67. Dwinnell WH. Priority in the use of steel jack-screws. Dent Cosmos, 1886;28;171-2.
68. Earl W Renfroe. Edgewise (Lea and Febiger 1975).
253Suggested Reading
69. Einleitung zur Nötigen Wissenschaft einesZahnarztes, (Introduction to the importantscience of dentistry), Wien, 1766:182.
70. Eitzen C. Implant anchorage in orthodontics. In:Technology spotlight. Available at: http://www.dentalcompare.com/spotlight.asp?spotlighted_8. Accessed December 25, 2006.
71. El-Bialy T, El-Shamy I, Graber TM. Repair oforthodontically induced root resorption byultrasound in humans. Am J Orthod DentofacialOrthop 2004;126:186-93.
72. El-Bialy T, El-Shamy I, Graber TM. Growthmodification of the rabbit mandible usingtherapeutic ultrasound: is it possible to enhancefunctional appliance results? Angle Orthod. 2003;73:631–639.
73. Evans TW. Dental Newsletter, 1854;8:30.74. Eveleth PB, Tanner JM. World wide variation in
human growth (2nd edn), Cambridge, Mass.Cambridge University Press, 1990.
75. Everelt Shapiro. Broukline Mass. Currentconcepts and clinical applications of the edgewisearch mechanics, AJO, 1957; Vol.43, 174-91.
76. Faltin KJ, Faltin RM, Baccetti T, Franchi L, GhiozziB, McNamara JA Jr. Long-term effectiveness andtreatment timing for Bionator therapy. AngleOrthod. 2003 Jun;73(3):221-30.
77. Fauchard P. The surgeon dentist or treatise onthe teeth. (Translated from second edition of 1746by Lilian Lindsay) London: Butterworth and Co,1946:130.
78. Federal Gazette, Philadelphia, June 14, 1797.79. Ferris T, Alexander RG, Boley J, Buschang PH.
Long-term stability of combined rapid palatalexpansion-lip bumper therapy followed by fullfixed appliances. Am J Orthod DentofacialOrthop, 2005;128:310-25.
80. Fillion D. The resurgence of lingual orthodontics.Clinical Impressions, 1998; 7(1):2-9.
81. Fletcher GGT. The Begg appliance and technique(wright).
82. Fogel MS. Borderline malocclusions, differentialdiagnosis. Part one, J Clin Orthodont, 1971;5;248-59. Part two. 1971;5:305-20.
83. Foster TD. A Textbook of Orthodontics, St Louis,Blackwell Scientific Publications, 1982.
84. Fujita K. Multilingual bracket and mushroomarch wire technique. A clinical report. Am JOrthod 1982; 82(2):120-40.
85. Fujita K. New orthodontic treatment with lingualbracket and mushroom archwire appliance. AmJ Orthod, 1979;76(6):657-75.
86. Fulmer DT, Kuftinec MM. Cephalometricappraisal of patients treated with fixed lingualorthodontic appliances: historic review and
analysis of cases. Am J Orthod DentofacialOrthop, 1989;95(6):514-20.
87. Furstman LL. Interview. December 6, 1987.88. Geran RG, McNamara JA Jr, Baccetti T, Franchi
L, Shapiro LM. A prospective long-term studyon the effects of rapid maxillary expansion in theearly mixed dentition. AO 2006 May;129(5):631-40.
89. Glasgold AI, Silver FH, Applications ofbiomaterials in facial plastic surgery. CRC Press,1991, Boca Raton, FL.
90. Goldstein A. The clinical testing of orthodonticresults. Am J Orthod 1965;51:723-55.
91. Goren S, Zoizner R, Geron S, Romano R. Lingualorthodontics versus buccal orthodontics:biomech-anical and clinical aspects. J LingualOrthod, 2003; 3(1):1-7.
92. Gorman JC, Smith RJ. Comparison of treatmenteffects with labial and lingual fixed appliances.Am J Orthod Dentofacial Orthop, 1991; 99(3):202-9.
93. Gorman JC. Treatment of adults with lingualorthodontic appliances. Dent Clin North Am,1988;32(3):589-620.
94. Gottlieb, EL. Orthodontics in the year 2000. J ClinOrthod, 2000;34:9-10.
95. Graber TM, B Neumann. Removable orthodonticappliance. WB Saunders Co. Philadelphia, 1977.
96. Graber TM, Bzoch KR, Aoba T. A functional studyof the palatal and pharyngeal structures. AngleOrthod. 1959; 29(1): 30-40.
97. Graber TM, Chung DDB, Aoba JT. Dentofacialorthopedics vs orthodontics. J Am Dent Assoc.1967; 75: 1145-66.
98. Graber TM, Neumann B. Removable OrthodonticAppliances. Philadelphia. WB Saunders, 1984.
99. Graber TM, Neumann B: Removable orthodonticAppliances. WB Saunders, Philadelphia, 1984.
100. Graber TM, Vanarsdall RL, et al. Orthodontics,Current Principles and Techniques. Diagnosis andTreatment Planning in Orthodontics. Mosby,2000.
101. Graber TM. A cephalometric analysis of thedevelopmental pattern and facial morphologyin cleft palate. Angle Orthod. 1949; 19(2): 91-100.
102. Graber TM. An orthodontic perspective after 75years. Am J Orthod. 1976; 69(5): 572-83.
103. Graber TM. Auxiliary personnel – pillars ofpractice procedure. Am J Orthod. 1965; 51(6): 412-36.
104. Graber TM. Books for the dentist. J Am DentAssoc. 1974; 88: 1322-42.
105. Graber TM. Ch. 4 - Current status of magneticforces in orthodontics (Biomechanics in clinicalorthodontics) W.B. Saunders Co. 1997.
254 History of Orthodontics
106. Graber TM. Extraoral force – facts and fallacies.Am J Orthod. 1955; 41: 490-505.
107. Graber TM. Maxillary second molar extractionin Class II malocclusion. Am J Orthod. 1969; 56(4):331-53.
108. Graber TM. Normal occlusion. Dent Clin NorthAm. 1968; Jul.: 273-90.
109. Graber TM. Notes and comments. DentalAbstracts 1976; 21(12): 712-13.
110. Graber TM. Occlusal splints (Letter to Editor). JAm Dent Assoc. 1980; 100: 171a.
111. Graber TM. On thumbsucking (Letter to Editor).J Am Dent Assoc. 1970; 81: 805.
112. Graber TM. Orthodontics: Principles and Practice.WB Saunders, 1998.
113. Graber TM. Postmortems in post-treatmentadjustment. Am J Orthod. 1966; 52(5): 331-52.
114. Graber TM. Pride in orthodontics. Am J OrthodDentofac Orthop. 2000 May;117(5):618-20.
115. Graber TM. Serial extraction: A continuousdiagnostic and decisional process. Am J Orthod.1971; 60(6): 541-75.
116. Graber TM. The “three M’s”: Muscles,malformation and malocclusion. Am J Orthod.1963; 49(6): 418-50.
117. Graber TM. The role of upper second molarextraction in orthodontic treatment.Am J Orthod.1955; 41: 354-361.
118. Guerini V. A history of dentistry from the mostancient times until the end of the eighteenthcentury. Philadelphia: Lea and Febiger, 1909.
119. Gunnell JS. A remedy for the protrusion of thelower jaw. Am J Dent Soc, 1841;2:65.
120. Hall RR, Hill DW, Beach AD. A carbon dioxidesurgical laser Ann R coll Surg Engl 19771;48;181-8.
121. Harradine N. Current products and practices.Self-ligating brackets: Where are we now?.Journal of Orthodontics. 2003; 30, pp262-73.
122. Hawley CA. Determination of normal arch andits application to orthodontia. Dent Cosmos,1905;47;541-52.
123. Hellman M. An introduction to growth of thehuman face from infancy to adulthood. Int JOrthod, 1932;18:777-98.
124. Hellman M. The face in its developmental career.Dent Cosmos, 1935;75:685-9.
125. Hicks MJ, Flaitz CM, Westernman GH, BlakenauRJ, Powell GL, Berg JH. Enamel caries initiationand progression following low energy. ArgonLaser J Clin Dent 1995;20(1):9-13.
126. Hitchcock HP. Pitfalls of the Crozat appliance.Am J Orthod, 1972;62:461-8.
127. Hixon EH, Oldfather RE. Estimation of the sizesof unerupted cuspid and bicuspid teeth. AngleOrthod, 1958;48:236-40.
128. Hong RK, Soh BC. Customized indirect bondingmethod for lingual orthodontics. J Clin Orthod,1996;30(11):650-2.
129. Hong RK. Tandem archwire technique in theFujita lingual bracket treatment. J LingualOrthod, 2002;2(4):100-4.
130. Hower AE. A polygon portrayl of coronal andbasal arch dimensions in the horizontal plane.Am J orthod, 1954; 40:811.
131. Hower AE: A polygon portrayl of coronal andbasal arch dimensions in the horizontal plane.Am J orthod. 1954 ; 40:811.
132. Int J Orthod, 1924;10:471.133. Items Interest, 1899;41:151.134. Items Interest, 1899;41:178.135. Items Interest, 1900;42:43.136. Jackson VH. Some methods in regulating. Dent
Cosmos, 1886;28:372-5.137. James A McNamara Jr, Carlson DS. Quantitative
analysis of TMJ adaptations to protrusivefunction. AJO 1979:76,6593-610.
138. James A McNamara Jr. Neuromuscular andskeletal adaptations to altered function in theorofacial region. AJO 1973;64;6;578-605.
139. James A McNamara Jr. Orthodontic treatmentand temporomandibular disorders. OOO1997:83:107-17.
140. James A McNamara. Influence of respiratorypattern on craniofacial growth. AO 1981;51:269-300.
141. James A McNamara. Maxillary transversedeficiency. AJO may 2000:117:5-568-70.
142. James A. McNamara Jr, Raymond P. Howe, TerryG. Dischinger A comparison of the Herbst andFränkel appliances in the treatment of Class IImalocclusion. AJO 1990;98:134-44.
143. JC Bennet, PR Mclaughlin: Orthodontic treatmentmechanics and the preadjusted appliance. 1st edn.(Wolfe).
144. Johnson JE. The twin-wire appliance. Am JOrthod Oral Surg, 1938;24:303.
145. Jost-Brinkman PG, Stien H, et al. Histologicalinvestiga-tion of the human pulp afterthermodebonding of metal and ceramic brackets.Am J Orthod 1992;102:410.
146. Joyce Y. Chang James A. McNamara Jr. ThomasA. Herberger A longitudinal study of skeletalside effects induced by rapid maxillary expansion.AJO 1997:112:330-37.
147. K Calman, Hospital doctors: training for thefuture, London, HMSO, 1993; Dentists Register,London, General Dental Council, 1999.
148. Kesling HD. Coordinating the predeterminedpattern and tooth positioner with conventionaltreatments. Am J Orthod Oral Surg, 1946; 32:285-93.
255Suggested Reading
149. Ketcham A. Treatment by orthodontistssupplementing that by the rhinologist. DentCosmos, 1914;54:1312-21.
150. KG. Issacson; J.K. Williams: An introduction tofixed appliances: III Edn, Page 1 (Wright).
151. Kim JH, Viana MAG, Graber TM, Omerza FF,BeGole EA. The effectiveness of protraction facemask therapy: A meta-analysis. Am J OrthodDentofac Orthop 1999;115:675-85.
152. Kim MR, Graber TM, Viana MA. Orthodonticsand temporomandibular disorder: A meta-analysis. Am J Orthod Dentofacial Orthop2002;121:438–46.
153. Kingsley NW. A treatise on oral deformities, 1880.Republished in classics in dentistry library,Birmingham, Alabama, 1980.
154. Kingsley NW. Dent Cosmos, 1934;66:131.155. Kingsley NW. Jumping the bite. Dent Cosmos,
1892;33:788.156. Kjellgren, B. Serial extraction as a corrective
procedure in dental orthopedic therapy. ActaOdont. Scandinav, 8:17-43, 1948; abst, Am JOrthoddont, 1949;35:471-6.
157. Kristine S. West and James A. McNamara, Jr.Changes in the craniofacial complex fromadolescence to midadulthood: A cephalometricstudy. AJO 1999;115:521-32.
158. Krogman WM. Child Growth, Ann Arbor, Mich.The University of Michigan Press, 1972.
159. Krogman WM. Forty-years of growth, researchand orthodontics. Am J Orthod, 1973; 63:357-65.
160. Kurz C, Romano R. Lingual orthodontics:historical perspective. In: Romano R, editor.Lingual orthodontics. Hamilton (ON): BC Decker;1998; pp3-20.
161. Kurz C, Swartz ML, Andreiko C. Lingual ortho-dontics: a status report. Part 2: Research anddevelopment. J Clin Orthod, 1982; 16(11):735-40.
162. Kusy R. Orthodontic biomaterials: From the Pastto the present. Angle Orthodontist, 2002, 72:6, p-501-12.
163. Lew KK. Initial alignment with .008" pulsestraightened supreme Wilcock wire in lingualorthodontics. Aust Orthod J, 1991;12(1):53-4.
164. Li ZZ, Code JE, Van De Merwe WP. Er: YAGlaser ablation of enamel and dentin of humanteeth. Determination of ablation rates at variousinfluences and pulse repetition rates.Laser surgMed 1992;12:625-30.
165. Linda Ratner Toth, James A. McNamara Jr.Treatment effects produced by the Twin-blockappliance and the FR-2 appliance of Fränkelcompared with an untreated Class II sample. AJO1999;116:597-609.
166. Lischer BE. Time to tell. New York: Vantage; 1950.
167. Lischer BE. What are the requirements oforthodontic diagnosis? Int J Orthod, 1933;19:377-85.
168. Logan LR. Second premolar extraction in Class Iand Class II. Am J Orthod, 1973;63:115-47.
169. Lundstrom A. Malocclusion of the teeth regardedas a problem in connection with the apical base.Svensk Tandl-Tidskr Supp, 1923. Reprinted in IntJ Orthod, 11:591, 724, 793, 933, 1022, 1109, 1925.
170. Martinek Edward E. A comparison of varioussurvey’s on the adequacy of basal bone.AJO,1956;42:244-254.
171. Martinek, Edward E. A comparison of varioussurvey’s on the adequacy of basal bone. AJO,1956;42:244-254.
172. Mayne WR. Serial extraction in orthodontics atthe crossroads. D Clin North America, July 1968.
173. Mc Namara JA Jr, Brudon WL. Orthodontics anddentofacial orthopedics. Needham Press. 2ndedition. 2002.
174. Mc Namara JA Jr. A method of cephalometricevaluation. Am J Orthod. 1984; 86: 449-469.
175. McCoy JD. Applied orthodontics. 6th ed.Philadelphia: Lea and Febiger, 1946.
176. McNamara JA. A method of cephalometricevaluation. Am J Orthod, 1984;86:449.
177. Mershon JV. The removable lingual arch as anappliance for the treatment of malocclusion ofthe teeth. Int J Orthod, 1918;41:478;1920;12:1002;Dent Cosmos, 1920;62:698.
178. Michal Meyer. Pre adjusted edgewise appliances.Theory and Practice: AJO, 1978; Vol. 73, 485-498.
179. Midda M. The use of laser in periodontology.Curr opin Dent 1992;2;104-8.
180. Mills CM, Holman RG, Graber TM. Heavyintermittent cervical traction in Class II treatment:A longitudinal cephalometric assessment. Am JOrthod. 1978; 74(4): 361-79.
181. Moorrees CFA. The dentition of the growingchild, Cambridge, Harvard University Press,1959.
182. Nakai TT. The influence of serial extractionprocedures on the soft tissues: profiles in class 2,division 1 malocclusions; a cephalommetric study.Am J Orhodont, 1968; 54:154.
183. Nance HN. The removal of second premolars inorthodontic treatment. Am J Orthod, 1949;35:685-95.
184. National Gazette, April 11, 1826.185. National Research Council, Polymer Science and
Engineering, National Academy Press,Washington DC, 1994.
186. New York Daily Advertiser, Aug. 2, 1797.187. Newman GV. Epoxy adhesives for orthodontic
attachments. American Journal of Orthodontics.1965;51:12. p901-12.
256 History of Orthodontics
188. Noyes FB, Schour I, Noyes H. A textbook ondental histology and embryology includinglaboratory directions. Philadelphia: Lea andFebiger: 1938.
189. Numbers in superscript in this article refer torelated Angle letters (volume:page) as publishedin the comprehensive archival publication cited:Peck S, ed. The World of Edward Hartley Angle,MD, DDS: His Letters, Accounts and Patents. 4Volumes. Boston, Mass: E H Angle Educationand Research Foundation; 2007. ISBN 978-0-9779524-0-3; available on a non-profit basis [email protected].
190. Oliver RG. The effect of different methods ofbracket removal on the amount of residualasdhesive. Am J Orthod Dentofacial Orthop1988;93:196-200.
191. Olson RE, Mincey DL, Graber TM. Orthosurgicalteamwork. J Am Dent Assoc. 1975; 90: 998-1011.
192. Oppenheim A. Human tissue response to ortho-dontic intervention of short and long duration.Am J Orthod Oral Surg, 1942;28:263-301.
193. Owen D, Graber TM. The developing occlusion –orthodontic considerations for the handicapped.Dent Clin North Am. 1974; 18(3): 711-21.
194. Paige SF. A lingual light-wire technique. J ClinOrthod, 1982;16(8):534-44.
195. Paola Cozza, Tiziano Baccetti, Lorenzo Franchi,Laura De Toffol, and James A. McNamara, Jr.Mandibular changes produced by functionalappliances in Class II malocclusion: A systematicreview. AJO 2006:129:599.
196. Paredes V, Gandia JL, Cibrian R. A new, accurateand fast digital method to predict uneruptedtooth size. Angle Orthod, 2006;76:14-9.
197. Peck H, Peck S. An index for assessing tooth-shape deviations as applied to the mandibularincisors. Am J Orthod, 1972;61:384- 401.
198. Pfeiffer JL. The emergence of man, New York:Harper and Row, 1967.
199. Philadelphia Gazette, Jan. 1, 1813. Quoted byWeinberger BW, Historical Resume of theEvolution and Growth of Orthodontia. J AmDent Assoc, 1934;22:2006.
200. Pick RM, Pecaro BC, Silberman CJ. The lasergingivec-tomy. The use of the CO2 laser forremoval of phytoin hyperplasia.
201. Pont A. Der Zahn Index, Orthodontics Zeitshrifffor zahnartizliche orthopeadic, 1909;3:306-321.
202. Pont A. Der Zahn Index, orthodontics Zeitshrifffor zahnartizliche orthopeadic, 1909;3:306-21.
203. Poon KC, Taverne AA. Lingual orthodontics: areview of its history. Aust Orthod J, 1998;15(2):101-4.
204. Portrait. J Can Dent Assoc, 1950;16:100-1.205. Proffit WR, Fields HW, editors. Contemporary
orthodontics. 3rd ed. St Louis: Mosby; 2000.
206. Proffit WR. Concepts of growth anddevelop-ment. In: Contemporary Orthodontics,(2nd edn.) St Louis: Mosby Yearbook, 1999;24-62.
207. Proffit WR. Forty-year review of extractionfrequencies at a university orthodontic clinic.Angle Orthod, 1994;64:407-14.
208. Profitt WR, Ackerman JL. Rating thecharacteristics of malocclusion: A systematicapproach for planning treatment. Am J Orthod1973;64(3):258-69.
209. Profitt Wr: Contemporary Orthodontics, st louis,CV Mosby, 1986.
210. Pullen HA. Expansion of dental arches andopening maxillary suture in relation to develo-pment of the internal and external face. DentCosmos, 1912;54:509-28.
211. Raymond C Thurow. Edgewise orthodontics, 4thEdn. (The CV Mosby Company)
212. Reed A Holdaway. Bracket angulation as appliedto the edgewise appliance. AO. 1952;227-36.
213. Reish MS, Rubber consumption is rising, Chem.and Eng News, August 14,1995.
214. Richard A Hocevar. Why edgewise? AJO, Vol.No.80; 237-55.
215. Ricketts RM. Keystone triad. Part 2. Am J Orthod,1964;50:728-50.
216. Ringenberg, QM. Serial extraction: stop, look,and be certain. Am J Orthodont, 1964;50:327-36.
217. Robert HW Strang, 1881-1982 (Obituary). AngleOrthod, 1983;53:1.
218. Rogers AP. Evolution, development, and applic-ation of myofunctional therapy in orthodontia.Am J Orthod Oral Surg, 1939;25:1-19.
219. Rossman JA, Cobb CM, Laser in periodontaltherapy. Periodontology 2000;1995:150-64.
220. Rufenacht CR. Fundamentals of esthetics.Chicago; quintessence; 1990.
221. Rupertogonzalez-Giralda. Dental specializationin spain. BJO, Feb, 1908 .
222. Russell JS. Current products and practices.Aesthetic Orthodontic Brackets. Journal ofOrthodontics. 2005; 32, pp146-63.
223. Salzmann JA. Handicapping malocclusionassessment to establish treatment priority. Am JOrthod, 1968;54:749-65.
224. Salzmann JA. Principles of orthodontics, 2nd ed.Philadelphia: JB Lippincott, 1950:721.
225. Sarver DM, yanosky M, Principles of cosmeticdentistry in orthodontics; part 3. Laser treatmentfor tooth eruption and soft tissue problems. AmJ Orthod Dentofacial Orthop 2005; in press.
226. Schoppe RJ. An analysis of second premolarextraction procedures. Angle Orthod, 1964;34:292-302.
227. Schwab DT. The borderline patient and toothremoval. Am J Orthodont, 1971;59:126-45.
257Suggested Reading
228. Schwarz AM, M Gratzinger. RemovableOrthodontic Appliances. WB Saunders Co.Philadelphia, 1966.
229. Scuzzo G, Takemoto K. Lingual straight-wiretechnique. In: Scuzzo G, Takemoto K, editors.Invisible orthodontics. Berlin: QuintessenceVerlag; 2003. pp145-56.
230. Shankland WM. The American Association ofOrthodontists. St. Louis: CV Mosby: 1971.
231. Sheldon Peck. A Biographical Portrait of EdwardHartley Angle, the First Specialist in Orthodontics,Part 1. The Angle Orthodontist: November 2009,Vol. 79, No. 6, pp. 1021-7.
232. Sheldon Peck. A Biographical Portrait of EdwardHartley Angle, the First Specialist in Orthodontics,Part 2. The Angle Orthodontist: November 2009,Vol. 79, No. 6, pp. 1028-33.
233. Sheldon Peck. A Biographical Portrait of EdwardHartley Angle, the First Specialist in Orthodo-ntics, Part 3. The Angle Orthodontist: November2009, Vol. 79, No. 6, pp. 1034-6.
234. Silver FH. Biomaterials, medical devices and tissueengineering: an integrated approach. Chapmanand Hall, 1993, London.
235. Simon PW. On gnathostatic diagnosis inorthodontics. Int J Orthod, 1924;10:755-77.
236. Sinclair PM, Cannito MF, Goates LJ, Solomos LF,Alexander CM. Patient responses to lingualappliances. J Clin Orthod, 1986; 20(6):396-404.
237. Smith SS, Buschang PH, Watanabe E. Interarchtooth size relationship of 3 populations. Am JOrthod Dentofacial Orthop, 2000;117:169-74.
238. Sung JH. History of skeletal anchorage anddevelopment of microimplants for orthodonticanchorage. Unpublished manuscript; via e-mail;December 26, 2005.
239. Suwannee. The effect of premolar extraction: Along-trem comparison of outcomes in “clear cut”Extraction and non-extraction class 2 patients.
240. Swinehart EW. Orthodontic bands. In: DeweyM, Anderson M, eds. Practical Orthodontia. St.Louis: CV Mosby: 1955, p. 201. Dent Cosmos1864;5:503.
241. Tanaka MM, Johnston LE. The prediction of thesize of the unerupted canines and premolars in acontemporary orthodontic Population. J AmDent Assoc 1974;88:798
242. Tanaka MM, Johnston Le. The prediction of thesize of the unerupted canines and premolars in acontemporary orthodontic Population. J AmDent Assoc, 1974;88:798.
243. Tanner JM, Whitehouse RH, Takaishi M.Standards from birth to maturity for height,weight, height velocity and weight velocity inBritish children, Arch Dis Child. 1966;41:454-71.
244. Terwilliger. The development of the edgewisearch mechanism and its place in contemporaryorthodontics. A J O, 1951;Vol.37,670-8.
245. This paper is based on a larger study, G S Taylor,‘Review of the Transactions of the British Societyfor the Study of Orthodontics, 1907–1971’, DDSThesis, University of Glasgow, 2004.
246. Thomas M Graber, Brainerd F Swain. Currentorthodontic concepts and technique (II Edn.)Vol.No:5, 453-74.
247. Thomas M Graber, Brainerd F Swain.Orthodontics current principles and techniques(LV Mosby company) 1st Indian edition.
248. Tiziano Baccetti, Lorenzo Franchi, Linda RatnerToth, James A McNamara Jr. Treatment timingfor Twin-block therapy. AJO 2000;118:159-70.
249. Todd TW. Heredity and environment, facts infacial development. Int J Orthod, 1932;18:799-808.
250. Tucker EJ. Irregularities of the teeth. DentNewsletter, 1853;6:95.
251. Tulley Wj, AC Campbell. A Manual of practicalOrthodontics. J Wright and Sons, Bristol, 1960.
252. Vaden JL, Dale JG, Klontz HA. The Tweed-Merrifield Edgewise appliance: philosophy,diagnosis, and treatment. In: Graber TM,Vanarsdall RL, editors. Orthodontics—currentprinciples and techniques. St Louis: Mosby YearBook Inc.; 1994. pp. 627-84.
253. Valiathan A, Siddhartha D. Fibre reinforcedcomposite arch-wires in Orthodontics: Functionmeets aesthetics. Trends Biomaterials. Artif.Organs, 2006;20:1pp.16-19.
254. Vardimon AD, Graber TM, Drescher D, BourauelC. Rare earth magnets and impaction. Am JOrthod Dentofacial Orthop 1991; 100:494-512.
255. Vardimon AD, Graber TM, Pitaru S. Repairprocess of external root resorption subsequentto palatal expansion treatment. Am J OrthodDentofac Orthop 1993;103:120-30.
256. Vardimon AD, Graber TM, Stutzman J, Voss L,Petrovic AG. Reaction of the pterygomaxillaryfissure and the condylar cartilage to intermaxillaryClass III magnetic mechanics. Am J OrthodDentofac Orthop 1994;105:401-13.
257. Vardimon AD, Graber TM, Voss LR, Lenke J.Determinants controlling iatrogenic external rootresorption and repair during and after palatalexpansion.Angle Orthod. 1991; 61(2): 113-22.
258. Vardimon AD, Graber TM, Voss LR, Muller TP.Functional orthopedic magnetic appliance(FOMA) III-Modus operandi. Am J OrthodDentofac Orthop.1990; 97(2): 135-48.
259. Vardimon AD, Graber TM, Voss LR, Verrusio E.Magnetic versus mechanical expansion withdifferent force thresholds and points of
258 History of Orthodontics
application. Am J Orthod Dentofacial Orthop1987;92: 455-66.
260. Vardimon AD, Graber TM, Voss LR. Stability ofmagnetic vs. mechanical palatal expansion. Eur.J Orthod. 1989; 11(2): 107-15.
261. Vardimon AD, Stutzmann JJ, Graber TM, VossLR, Petrovic AG. Functional orthopedicmagnetic appliance (FOMA) II-Modusoperandi. Am J Orthod Dentofac Orthop1989;95:371-87.
262. Von Fraunhofer JA, Allen DJ, Orbell GM. Laseretching of enamel for direct bonding. AngleOrthod 1993;63:73-6.
263. Wachman C. Treatment of the teeth—Andressenmethod. Am J Orthod, 1949; 33:61
264. Wahl N. A short history of the Pacific CoastSociety of Orthodontists. Part 1. PCSO Bull,2000;72:30-4.
265. Walsh LJ, Abood D, Brockhurst PJ. Bonding ofresin composites to carbon dioxide laser—modified human enamel. Dent Mater1994;10:162-6.
266. Wayne A Bolton. The clinical evaluation of toothsize analysis. AJO. 1962;48:504-529.
267. Wayne A Bolton. The clinical evaluation of toothsize analysis. AJO, 1962; 48:504-29.
268. Wayne Allen Bolton. Dishormony in toothsize,and its relation to the analysis and treatmentof malocclusion. Angle ortho, 1958; 28:113-130.
269. Weinberger BW. [citing EJ Tucker]. Importanceof regulating the teeth and employment of gumelastics. Am J Dent Soc, 1850;11:28-31.
270. Weinberger BW. Orthodontics, and historicalreview of its origin and evolution. St. Louis: CVMosby; 1926.
271. Weinberger BW. The contribution of orthod-ontia to dentistry. Dent Cosmos, 1936;78:849.
272. Weinberger BW. The contribution of orthodontiato dentistry. Dent Cosmos, 1936;78:844-53.
273. Wiechmann D. Modulus-driven lingual ortho-dontics. Clinical Impressions, 2001;10(1):2-7.
274. William R Profit: Contemporary orthodontics ,II Edn (Mosby) Page 357-62.
275. Wilton Marion Krogman. The creativity ofEdward.H. Angle retrospect and prospect; A O1976;Vol.46; 209-18.
276. Wylie Wendell L. 1913–1966, (Obituary), AngleOrthod, 1960;36:177.
277. Zachrisson BU. Bonding in orthodontics. InGraber Tm, Vanarsdall RL(Eds). Orthodontics:current principles and Techniques, Ed 3, st Louis,Mosby.
IIInnndddeeexxx
A
Adam’s clasp 162with incorporated helix 163with soldered hook 163with traction hook 163
Adult orthodontics 19Advantages of
lasers in soft tissue surgery 52metal brackets 107removable appliances 161,
162Aesthetic component 218Aims of orthodontic treatment
15, 16fAlignment of incisors 152fAltered passive eruption
management 51American
Board of Orthodontics 15Orthodontics 29, 30
Anchorage design ofM-pendulum appliance 242
Andrews’ straight wire appliance98
Angell’s palatal expansion deviceplaced on maxillary teeth155f
Anterior movement of dentalarche 178
Apert’s syndrome 203Aphthous ulcer 51, 56fApicoectomy 52Application of laser in
bonding orthodontic bracket54
orthodontics 53
Archlength analyses 146wire 114
bends 177Argon lasers 50Artistic positioning bends 177
B
Baker’s anchorage 25f, 33fBall end clasp 162Base plate 162, 166Begg appliance 179fBenefits of orthodontic treatment
19Bleaching 51Bolton’s
analysis 125study 125
Bondable brackets 109, 109fBonded rapid maxillary
expansion appliances 157,157f
Branches of orthodontics 16British Society
for Study of Orthodontics 37tof Orthodontists 15
Broca’s occipital angle 136Broussard bracket 112Buccal
self-supported retractor 166sweep 177
C
Calculation ofDAI scores 222final scores 220
Page numbers followed by f refer to figure and t refer to table
Camper’s angle 136Canine
guidance 181retractors 165
Carbon dioxide laser 50Care of deciduous dentition 18Carey’s analysis 123Caries
control during orthodontictreatment 57
removal 51Carpenters syndrome 203Case-angle controversy 70, 148Cast versus wrought metals 116Cephalometric
analysis 139of developmental pattern
and facial morphologyin cleft palate 85
radiography 137roentgenography 27f
Ceramic brackets 108, 108fCetlin appliance 245Characteristic
facial appearance 202of ideal arch wire 177
Choice of teeth for extraction 150Circumferential clasp 162Classification of
archwires 117tcanine retractors 166tmalocclusions 27
Cleftlip and palate formation 200of anterior
and posterior palate 201primary palate 201
260 History of Orthodontics
of posterior secondary palate201
palate 202Cobalt-chrome-nickel alloy 118Common syndromes associated
with cleft lip and palate203
Components of removableorthodontic appliance 162
Comprehensive orthodontictreatment 19
Contraindications ofmolar distalization 239removable orthodontic
appliances 161Correcting malocclusions of
dental origin 19skeletal origin 19
Correction ofcleft palate 24, 25curve of Spee 225
Corrective orthodontics 16Craniofacial
anomalies 219syndromes 203
Craniometry 133Crouzon’s syndrome 203Crowding of mandibular incisors
224Crown
angulations 180, 181inclination 180, 181lengthening procedure 57, 58f
Crozatappliance 247tclasp 162
Curing light-activated resins 51Current clinical use of dental
lasers 51Curve of Spee 181Cusp embrasure contact 181
D
Debonding of brackets by laser57
Deciduousdentition 18teeth 52
Deficient lower anterior facialheight 90f
Definition of orthodontics 14Dental
aesthetic index 221and skeletal cross bites 141contour appliance 227health component 218
Dentistry ineighteenth century 10sixteenth and seventeenth
centuries 7Dentoalveolar and facial
asymmetries 141Dentofacial orthopedics versus
orthodontics 79Denture stomatitis 52Depigmentation of gingiva 57,
57fDesign of
appliance 248, 249Lokar appliance 245
Destructive scanner 231fDetermination of
anterior ratio 125arch
length 123width 123
discrepancy 123overall ratio 125
Development of removableorthodontic appliances 161
Dewel’s method 151, 151tof serial extraction 152f
Different types ofcanine retractors 166texpansion screws 158f, 159tlabial bows 163t
Diode laser 50, 51Disadvantages of removable
appliances 162orthodontic appliances 162
Distal jet appliance 246tDown syndrome 203Drawback of
lingual 185Pont’s analysis 124
E
E-arch appliance 27, 68, 68f, 171,171f
Earlymixed dentition 18permanent dentition 18
Ectopically erupting teeth 203Edgewise
appliance 69, 70f, 172, 173fbrackets 110, 110ftechnique 27
Edward Hartley angle 67fElimination of abnormal oral
habits 18
Enamelhypoplasia 203reduction in orthodontics 223
Encephalocele 203Erbium-YAG laser 49Esthetic harmony 15, 16Etiology of cleft lip and palate 201Evolution of
bracket 174cephalometrics 140clasp design 162edgewise buccal tubes 174orthodontic appliances 106
Expansionorthodontic appliances 159,
159tscrew 157, 159
Exposure ofimpacted tooth 53teeth 52
Extensive hypodontia 219External skeletal fixation 194Extraction of second premolar
123Extraoral
force 79, 245appliances 17
traction 25Eyelet clasp 162
F
Fabric of human body 22Facial
angle 135axis
angle 91of clinical crown 180point 180
deformities 27Factual period 77, 78Failure of buttresses 176Fastback appliance for molar
distalization 249Father of
American Orthodontics 24,25, 31
expansion appliances 25modern
dentistry 23orthodontics 20
orthodontics 27Features of fast back appliance
250Fictional period 77
261Index
Film position and enlargement140
Fixedorthodontic appliance 17, 17fprosthetics/cosmetics 51rapid maxillary expansion
appliances 156Focused versus defocused beam
48Force applied and activation of
appliance 245Founder of modern dentistry 23Frankel appliance 189Frankfort mandibular
incisor plane angle 143plane angle 143
Frenectomy 51Functional
mandibular displacements141
orthopedic magneticappliance 82, 83
study of palatal andpharyngeal structures 85
Functions of teeth 23Fusion of teeth 203
G
Gaining access for bracketplacement on partiallyerupted teeth 55
Gingivalcontact 219fretraction 51
Gingivectomy 51Gingivoplasty 51Goldenhar syndrome 203Grewe’s method 153Growth and development of
jaws 23
H
Haas expansion appliance 159Hard
lasers 49tissue
applications 51evaluation 89
Healing of aphthous ulcer 56Heavy gold wire framework 161Helical canine retractor 166Helices of vertical holding
appliance 243Herbst’s
appliance 190, 248
retention-joint appliance 155High labial bow 163History of
arch wires 114cephalometrics 133cleft lip and cleft palate 197dental lasers 47dentistry 1expansion appliances 154extraction in orthodontics 145fixed orthodontic appliances
167interproximal enamel
reduction 223malocclusion indices 205model analysis 122molar distalization in
orthodontics 238orthodontic materials 120orthodontics in
Greece and Rome 44united states of america 28
removable orthodonticappliances 160
surgical orthodontics 193Hixon and old father method
128Howe’s analysis—1954 124Huckaba’s analysis 127Hyperplasia 51Hypothetical period 77
I
Impeded eruption of teeth 219Incisor mandibular plane angle
143Index of
complexity 220orthodontic treatment needs
218Indications of
removable orthodonticappliances 161
various types of Frankelappliance 189
Interceptive orthodontics 16Intercuspal position 181Intermaxillary elastics 25, 25fInternal structure of teeth 23Interproximal
decay detection 51enamel reduction 223
Irregularities of teeth 30, 36Isaacson expansion appliances
157f
J
Jack expansion screw 159Jackson’s
clasp or full clasp 162triad 16
James McNamara analysis 88Jumping bite 24
K
Kernahan’s stripped ‘Y’classification 201
Kesling model analysis 131Kingsley’s
extraoral traction appliance155f
incline plane 155fKorkhaus’ analysis 124
L
Labiolingual appliance 112fLack of incisor prominence 146Lang brackets 112Laser
ablation of surface enamel fororthodontic bracketplacement 54
beam interaction with tissue48
classification 52medium 47safety 52, 58use in dentistry 51
Late mixed dentition 18, 239Lateral
borer of tongue 56fset-back bends 177
Latest design of Klapper superspring 248
Lattice imperfections anddislocations 116
Law of canines 138Limitations of straight wire
appliance 182Linder Hart’s measurements 124Linderharth index 124Lineae cephalometricae 135Lingual
brackets 110ftechnique 183, 183f
Lokar appliance 245Long
axis of root 165labial bow 163
Looped canine retractor 166Lower pharynx 92
262 History of Orthodontics
M
Magnetic strength and corrosionof rare earth magnets 82
Management ofaphthous ulcer 56, 56fdentofacial anomalies 19
Mandibularplane angle 90procedures 196
Martensiticactive alloy 118stabilized alloy 118
Maxilla 83McNamara analysis 94tMechanism of action of
distalizing appliances 240Mesial cuspid bends 177Metal brackets 107, 107fMetallic bonds and crystalline
structure 116Method of
determining position of upperincisor 90f
straightening of orthodonticwires 115
Mill’s retractor 163, 164Modification of Adam’s clasp 162Modified
Jackson’s clasp 161ribbon arch 109fsplit labial bow 163
Molarband 24fbayonet bends 177distalization 239
Mouth guard 19M-pendulum appliance 241Multiple missing teeth 203Multistrand archwires 118Myofunctional orthodontic
appliance 18f
N
Nanceanalysis 129method 153
Narrowed maxillary arch 146Nasal
deformity 203septum 200
Natural history of human teeth23, 34, 45
Nd:YAG laser 49, 50Nickel-titanium alloy 117, 118fNight guards 19
Non-aqueous elastomeric dentalimpression material 121
Non-extraction philosophy 168Nonosseous gingival surgery 51Nonsyndromic clefts 202Normal lower pharyngeal
measurement 93fNormalization of gingival
contour 224Normative standards in
McNamara analysis 89tNumber of anchorage teeth 242
O
Occlusal interference 185Open bite appliance 190Opening midpalatal suture 25Optiflex archwire 117, 118Oral
lesion therapy 51screen 190soft tissue pathologies 52
Orthodontia and orthopaedia offace 150
Orthodonticand dentofacial orthopedics
20and temporomandibular
disorder 87appliances 17, 186
Orthopedic appliance 17, 18fOrthosurgical teamwork 86Osseous recon touring 51Overcrowded teeth 15
P
Palatal canine retractor 166Pallaquium gutta 120Paris Society of Anthropology
137Pend-X appliance 241Periodontal regeneration
surgery 51Periodontics 51Permanent teeth 52Pfeiffer syndrome 203Pierre Robin syndrome 203Pieter camper 135Pin and tube
appliance 68, 69f, 171, 173ftechnique 27
Placement of virtual gingiva 231fPlastic brackets 107, 108fPont’s index 123
Poorfacial appearance 15oral hygiene 225
maintenance 15Posteroanterior cephalometry
141Post-retention survey 206Potential soft and hard tissue
applications of laser indentistry 51
Preadjusted edgewise brackets110, 110f
Premolarbasal arch width 124diameter 124
Primaryincisions 51palate 200
Principles ofspace analysis 126steriophotolithography 231
Properties ofarchwire 117laser beam 48
Protrusive upper incisors 92fPulse straightening 115Pulsed lasers 48Pyorrhea alveolaris 12
R
Radiographiccephalometry 134study of facial deformity 138
Range of Deflection 118Re-activation of appliance 246Reflection 48Removable
molar distalization splint 244orthodontic appliance 17, 17fprosthetics 52
Removal offibroma 51granulomatous tissue 51redundant gingival tissue 56
Residual ridge modification 52Retentive components 162Reverse labial bow 163Ribbon arch
appliance 68, 69f, 172, 172fbrackets 109, 109f
Risk ofdental caries 15periodontal diseases 15
Roentgen ray anthropometry ofskull 137
263Index
Role of upper second molarextraction in orthodontictreatment 78
Root desensitization 51
S
Saethre-Chotzen syndrome 203Scandinavian studies 206Schwartz clasp 162Scope of orthodontics 18Second premolar extraction 147Secondary palate 200Self-ligating bracket 111, 111f,
113, 113fSevere crowding 225Shape of teeth 225Short labial bow 163Single width bracket 111Size of acrylic button 243Soft
lasers 49tissue
evaluation 89modification 52
Solidification of metals 116Southend clasp 162Spheno-ethmoidal angles 136Split labial bow 163Sports guard 19Steiner bracket 112, 112fStereolithographic models 230f,
231fStraight wire 180
appliance 103, 180, 181, 181f
Strength of wire 119Structural balance 15Studies on
functional appliances 93rapid maxillary expansion 95TMJ 96
Submerged deciduous teeth 219Supernumerary teeth 219System of dental surgery 29
T
Temporomandibular joint 14Thickness of button 244Timing of orthodontic
intervention 18Timm’s schedule of activation of
expansion screw 159tTooth
shape and dental esthetics 224size discrepancy 224whitening 56f, 57
Total space analysis 130Treacher-Collins syndrome 203Triangular clasp 162Tube plates for distalization of
molars 244Tuberosity reduction 52Tweed’s
method 152triangle 143, 143f
Twinarch appliance 112fblock appliance 190brackets 111
Two palatine shelves 200Types of
Frankel appliance 189heat treatment 117laser 49
U
Unfavorable sequelae ofmalocclusion 15
Upper pharynx 92Uses
in orthodontics 121of bionatar 190
V
Van der Woude’s syndrome203
Variable bracket sittingprocedures 102
Veau’s classification 201Velocardiofacial syndrome 203Vertical
holding appliance 243position of lower incisors 92
Vestibular screen 190Vestibuloplasty 51
W
Wearing invisalign appliance233f
Weldable brackets 109Wescott’s expansion device 154,
154f





























