Embed Size (px)
Citation preview
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Journal of Behavioral Medicine, Vol. 24, No. 4, 2001
Heterogeneity in the Social Networks of Youngand Older Adults: Prediction of Mental Healthand Cardiovascular Reactivity During Acute Stress
Bert N. Uchino,1,2 Julianne Holt-Lunstad,1 Darcy Uno,1
and Jeffrey B. Flinders1
Accepted for publication: February 9, 2001
We examined the utility of a broad framework that separated positive, negative,and ambivalent social network members. One hundred thirty-three young andolder participants completed the social relationships index, measures of men-tal health, and a cardiovascular reactivity protocol. Results replicated priorresearch on the beneficial influence of positive (supportive) ties on psycho-logical outcomes. More important, analyses also revealed that the number ofambivalent network ties predicted age-related differences in depression andsympathetic control of heart rate reactivity during stress. The statistical inter-actions between age and ambivalent ties on cardiovascular responses duringstress were not changed when statistically controlling for other social networkcategories, demographic variables, and various personality factors. These datasuggest that social network ambivalence was a relatively unique predictor ofcardiovascular reactivity and highlight the utility of separating the variancedue to positive, negative, and ambivalent network ties. Implications for thestudy of social relationships, physiological processes, and health outcomes arealso discussed.
KEY WORDS: social networks; cardiovascular reactivity; age; health.
1Department of Psychology and Health Psychology Program, University of Utah, Salt LakeCity, Utah 84112-0251.
2To whom correspondence should be addressed; e-mail: [email protected].
361
0160-7715/01/0800-0361$19.50/0 C© 2001 Plenum Publishing Corporation
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
362 Uchino, Holt-Lunstad, Uno, and Flinders
INTRODUCTION
The quality and quantity of one’s social relationships have been reliablyrelated to morbidity and mortality (Berkman, 1995; Cohen, 1988; Houseet al., 1988). In a review of large prospective studies, House et al. (1988)found strong evidence indicating that all-cause mortality rates were higheramong individuals with relatively poor social relationships. These data areoften taken as evidence for the health benefits of close, confiding relation-ships. However, even close relationships are not uniformly positive (Braikerand Kelly, 1979). Research from the Terman Life Cycle study suggests thatpast negativity in social relationships predicted greater mortality (Friedmanet al., 1995). These findings highlight the importance of considering bothpositivity and negativity in examining the health-related consequences of so-cial relationships (Brown, 1987; Orden and Bradburn, 1968; Weissman et al.,1971).
The joint contribution of positivity and negativity in the study of socialrelationships and health has not been adequately examined (Barrera, 1980;Major et al., 1997; Rook, 1984). This is noteworthy because positive andnegative aspects of social relationships tend to be statistically independentand/or separable dimensions (Finch et al., 1989; Fiore et al., 1983; Ruehlmanand Karoly, 1991). Even when moderate negative correlations have beenfound, positive and negative aspects of social relationships still appear to rep-resent distinct, separable factors (Pierce et al., 1991; Ruehlman and Karoly,1991).
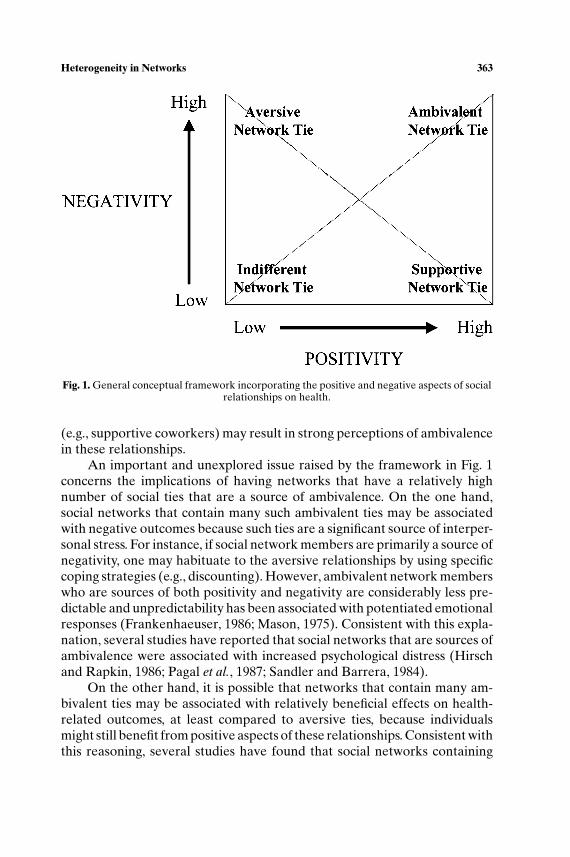
The separability of positive and negative aspects of social relationshipsmay have significant conceptual implications for their joint study. As illus-trated in Fig. 1, such data suggest that any given social network member maydiffer in their underlying positive and negative basis (Cacioppo and Berntson,1994). As depicted in the high positivity/low negativity corner, there maybe social network members that are primarily sources of social support orother pleasant interpersonal experiences (e.g., supportive coworkers). Thelow positivity/high negativity corner reflects a network tie that is primar-ily a source of negativity or what we label a socially aversive tie (e.g., anunreasonable work supervisor). The low positivity/low negativity cornerwould be a socially indifferent tie and may represent network members thatare characterized by relatively low levels of social interactions (e.g., casualcoworkers). A relatively unique aspect of this conceptualization for the socialrelationships and health literature is represented in the high positivity/highnegativity corner or what we label a network member who is a source ofambivalence. It refers specifically to network members that are a sourceof both positivity and negativity. For instance, negative interactions withnetwork ties that in the past have been sources of positive interactions
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 363
Fig. 1. General conceptual framework incorporating the positive and negative aspects of socialrelationships on health.
(e.g., supportive coworkers) may result in strong perceptions of ambivalencein these relationships.
An important and unexplored issue raised by the framework in Fig. 1concerns the implications of having networks that have a relatively highnumber of social ties that are a source of ambivalence. On the one hand,social networks that contain many such ambivalent ties may be associatedwith negative outcomes because such ties are a significant source of interper-sonal stress. For instance, if social network members are primarily a source ofnegativity, one may habituate to the aversive relationships by using specificcoping strategies (e.g., discounting). However, ambivalent network memberswho are sources of both positivity and negativity are considerably less pre-dictable and unpredictability has been associated with potentiated emotionalresponses (Frankenhaeuser, 1986; Mason, 1975). Consistent with this expla-nation, several studies have reported that social networks that are sources ofambivalence were associated with increased psychological distress (Hirschand Rapkin, 1986; Pagal et al., 1987; Sandler and Barrera, 1984).
On the other hand, it is possible that networks that contain many am-bivalent ties may be associated with relatively beneficial effects on health-related outcomes, at least compared to aversive ties, because individualsmight still benefit from positive aspects of these relationships. Consistent withthis reasoning, several studies have found that social networks containing
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
364 Uchino, Holt-Lunstad, Uno, and Flinders
both positive and negative aspects predicted lower levels of psychologicaldistress (Abbey et al., 1985; Lepore, 1992; Tilden et al., 1990). It is importantto note, however, that many studies that have found the co-occurrence ofpositivity and negativity in social relationships to predict decreased distressutilized global assessments such that individuals may have been thinkingabout different network members when providing these assessments (Majoret al., 1997). Therefore, it is unclear whether or not these studies are ade-quately assessing ambivalence within any specific network member.
The main aim of this study was to investigate these competing hypothe-ses in terms of relevant psychological and physiological processes. We realizethat the categories of social ties depicted in Fig. 1 may differ in terms of poten-tially interesting variables such as relationship type, importance, and contact(Berschied and Reis, 1998). As we discuss later, these factors have impli-cations for the mechanisms by which these different categories of relation-ships may influence health-related outcomes. A crucial first step, however,would be to determine if these different relationship categories indeed pre-dict health-related outcomes. In fact, the primary measures in this study werechosen because they are implicated in disease processes. For instance, ourmain psychological measure was depression as it has been linked to higherrates of mortality (Smith and Gallo, 2001; Wulsin et al., 1999).
We also examined these competing hypotheses in predicting cardiovas-cular reactivity during acute stress. Although definitive data are needed, ev-idence suggests that cardiovascular reactivity during stress may predict thedevelopment and expression of cardiovascular disorders (Karmarck et al.,1997; Krantz et al., 1991; Manuck, 1994). If indeed ambivalent ties are as-sociated with significant interpersonal stress this may lead to alterations inautonomic responsiveness that result in greater cardiovascular reactivity tostressful situations. For instance, Fleming et al. (1987) found that individu-als with relatively high levels of interpersonal stress (i.e., crowding) showedincreased cardiovascular reactivity to a laboratory stressor. The authors sug-gested that chronic interpersonal stressors might be associated with morefrequent surges in catecholamines that prime individuals to respond morestrongly to additional stressors. It is also possible that such interpersonalstress might deplete an individual’s coping resources such that additionalstressors are appraised as more threatening (Fleming et al., 1987). Thesedata suggest that the interpersonal stress associated with ambivalent tiesmay potentiate cardiovascular reactivity to stressful situations.
We believe that the health-related correlates of social relationshipsmight also be more evident by examining such differences across the lifespan(Uchino et al., 1992, 1999a). It is possible that the health effects of social re-lationships may be more evident in older adults because these social networkprocesses impose additional (perhaps excess) demand on physiological
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 365
systems that are already showing functional age-related changes (Timiras,1994). As a result, we predicted that age should moderate the pattern ofhealth-related outcomes associated with social relationships, with these as-sociations being more evident in older individuals.
Because of the cross-sectional nature of our study, we also examinedthe association between differing categories of social relationships such asambivalent ties and related factors that might plausibly influence such net-work assessments. For instance, personality factors such as trait-positive andtrait-negative affectivity may influence perceptions of support, whereas hos-tile individuals may elicit interpersonal transactions that impede effectiverelationship maintenance (Smith and Gallo, 2001). If network ties that aresources of ambivalence predict cardiovascular reactivity, it becomes impor-tant to begin investigating whether or not this construct is a unique pre-dictor of these outcomes, especially given the relative lack of research onthis network type. Therefore, we also examined the association betweenour social network measures and related personality measures, and whetherany such associations could explain the pattern of results obtained in ourstudy.
METHOD
Participants
Sixty-four men and 69 women between the ages of 30 and 70 (M = 47.2)participated in this study. Approximately equal numbers of men and womenwere recruited from each decade group (e.g., 30–39) through advertise-ments placed in local newspapers. Individuals were paid $35.00 for approxi-mately 2.5 h of participation. Consistent with our prior research (Cacioppoet al., 1995), the following self-reported inclusion criteria were used to selecthealthy participants: no existing hypertension, no cardiovascular prescrip-tion medication use, no past history of chronic disease with a cardiovascularcomponent (e.g., diabetes), no recent history of psychological disorder (e.g.,major depressive disorder), no tobacco use, and no consumption of morethan 10 alcoholic beverages a week.
An examination of additional demographic information provided byparticipants revealed that most participants were White (84%), Asian/PacificIslander (7%), or Hispanic/Latino (4.5%). The ethnic composition of ourremaining participants was Native American (3.5%) or African American(1%). In terms of education level, 40.5% reported partial college experiencewhile an additional 26.5% graduated from college. Some of our participantsalso had partial graduate/professional school experience (10%) and some had
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
366 Uchino, Holt-Lunstad, Uno, and Flinders
completed graduate/professional school (23%). The median yearly incomeof our sample was between $20,000 and $29,000.
Procedure
Potential participants were recruited through advertisements in the localpapers. All interested individuals were first screened by telephone accord-ing to the criteria detailed earlier. Qualifying individuals were scheduled foran appointment, and upon arrival completed an informed consent documentand a demographic background questionnaire. Participants’ self-reports wereagain checked for reliability against the inclusion criteria. Following comple-tion of these questionnaires, the participant’s height and weight were ob-tained using a standard medical scale from which body mass index (BMI)was calculated (i.e., weight in kg and height in meters2).
Participants were then escorted to a separate sound attenuated roomwhere four mylar bands were placed in the tetrapolar configuration forimpedance cardiograph recordings according to published guidelines(Sherwood et al., 1990). An occluding cuff of appropriate size was placedon the upper left arm. In order to allow time for contact resistance of themylar bands to stabilize, individuals were seated in a comfortable chair andwere asked to start completion of a questionnaire packet (discussed later).Following this adaptation period of approximately 20 min, participants wereinstructed to relax for the next 12 min while resting measures of cardiovascu-lar function were obtained. During the final 5 min of the resting assessment,cardiovascular assessments of systolic blood pressure (SBP), diastolic bloodpressure (DBP), and mean arterial pressure (MAP) were obtained onceevery 90 s, whereas impedance cardiograph readings were recorded contin-uously. Participants also completed a baseline measure of state anxiety at theend of the rest period.
Following the resting assessments, participants performed a speech taskand mental arithmetic task developed by Cacioppo et al. (1995). Basic agedifferences in cardiovascular activity and reactivity to this protocol are de-tailed in an earlier report (Uchino et al., 1999b). The order of the stressorswas counterbalanced. The speech task was based on the following scenario:they were in a department store shopping when a security guard falsely ac-cuses them of shoplifting a belt. Participants were given 3 min to prepareand 3 min to present their speeches while impedence cardiography measureswere recorded continuously throughout the task. Blood pressure readingswere obtained during Minutes 1 and 3 of the preparation and actual speechperiods. As a measure of task performance, the number of speech promptsgiven to participants was recorded. State anxiety was again assessed at theend of the speech task.
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 367
The mental arithmetic task consisted of six 1-min serial subtractionproblems. Participants were given a new subtraction problem each minute,with each subsequent problem adjusted for difficulty so that effort was rela-tively constant across participants (i.e., approximately 10 serial subtractionsper minute). Impedance cardiography measures were recorded continuouslythroughout the task, whereas blood pressure was assessed during Minutes 1, 3,and 5 of the task. Performance during the task was measured as the percentof incorrect serial subtractions. At the end of the math task, participantscompleted the state anxiety measure. Upon completion of both psychologi-cal stressors, participants completed the packet of questionnaires (discussedlater). Participants were then compensated, debriefed, and thanked for theirparticipation.
Cardiovascular Measures
A Dinamap Model 8100 monitor (Critikon corporation, Tampa, Florida)was used to measure SBP, DBP, and MAP. The Dinamap used the oscillo-metric method to estimate blood pressure. Blood pressure assessments wereobtained via a properly sized occluding cuff positioned on the upper left armof the participant according to the manufacturer’s specifications. Mean SBP,DBP, and MAP for each epoch were averaged across minutes to increase thereliability of these assessments (Kamarck et al., 1992).
A Minnesota Impedance Cardiograph Model 304B was used to mea-sure the ECG, basal thoracic impedance (Z0), and the first derivative of theimpedance signal (dZ/dt). Four mylar bands were placed in the tetrapolarconfiguration according to published guidelines (Sherwood et al., 1990). A4 mA AC current at 100 kHz was passed through the two outer bands, andZ0 and dZ/dt were recorded from the two inner bands. The ECG, Z0, anddZ/dt signals were digitized at 500 Hz. The impedance data were ensemble-averaged within 1-min epochs and each waveform was verified or edited priorto analyses. Stroke volume (SV) was estimated using the Kubicek equation(Sherwood et al., 1990) and the subsequent cardiac output (CO) in L/minwas calculated by multiplying heart rate by (SV/1000). Total peripheral re-sistance (TPR) was measured in resistance units (dynes-second · cm−5) basedon MAP and CO (i.e., TPR = MAP/CO × 80). Pre-ejection period (PEP)was calculated as the time interval in ms between the Q-point of the ECGand the B-point of the dZ/dt signal. PEP was of particular interest in thepresent study because it provides a sensitive index of sympathetic controlof the heart (Cacioppo et al., 1994). These minute-by-minute impedance-derived measures of heart rate, CO, TPR, and PEP were averaged acrossminutes within each epoch (e.g., baseline, task) to increase measurementreliability.

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
368 Uchino, Holt-Lunstad, Uno, and Flinders
Respiratory sinus arrhythmia (RSA) provided a noninvasive measureof parasympathetic control of the heart and was calculated based on thedigitized interbeat intervals that were checked and edited for artifacts usingthe detection algorithm of Berntson et al. (1990). Following linear detrending(Berntson et al., 1995; Litvack et al., 1995), the heart-period time series wasband-pass–filtered from 0.12 to 0.40 Hz (Neuvo et al., 1984). The powerspectrum of the heart-period time series was calculated using a Fast FourierTransform and scaled to ms2/Hz. RSA was calculated as the natural log of thearea under the heart-period power spectrum within the corner frequenciesof the band-pass filter (Litvack et al., 1995). RSA was calculated on a minute-by-minute basis and aggregated across minutes within each epoch to increasemeasurement reliability.
Questionnaires
Social Relationships Index (SRI)
The SRI was developed as a self-report version of the social supportinterview (Fiore et al., 1983; Kiecolt-Glaser et al., 1991; Uchino et al., 1992).The SRI instructed individuals to list the initials of up to 10 importantnetwork members with whom they have contact. These network memberswere then rated in terms of how helpful and upsetting they were (1 – notat all, 6 – extremely) when the participant needed different types of assis-tance (i.e., emotional, tangible, and informational). For the present study, theCronbach’s alphas for the SRI were comparable to our pilot work (alphasof 0.76–0.87). Therefore, in order to increase reliability through aggregation,for each network member an index of positivity and negativity was calculatedby averaging across support components.
Consistent with Barrera (1980) and Rook (1984), we operationalizeddifferent categories of social relationships as the number of individuals inone’s network who were only sources of positivity (i.e., supportive ties),only sources of negativity (i.e., aversive ties), or sources of both positivityand negativity (i.e., ambivalent ties). Thus, a socially supportive networkmember was an individual rated as greater than 1 on positivity and only a1 on negativity and an aversive network tie was an individual rated as onlya 1 on positivity and greater than 1 on negativity. An ambivalent networkmember was an individual rated as greater than 1 on both positivity andnegativity. In our pilot work, these network measures were temporally stablewith significant 2-week test-retest correlations of r = 0.69 (p < 0.001)for the number of supportive ties, r = 0.75 (p < 0.001) for the numberof aversive ties, and r = 0.51 (p < 0.001) for the number of ambivalentties. Because of our interest in important social relationships, the SRI did
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 369
not provide a broad enough assessment to sample socially indifferent ties.However, our primary hypotheses regarded the relative impact of the threerelationship categories represented earlier.
Interpersonal Support Evaluation List (ISEL)
The ISEL contained 40 questions and assessed total social support andthe specific dimensions of appraisal, self-esteem, belonging, and tangiblesupport. Cohen et al. (1985) reported that the internal consistencies of thescales range from 0.60 to 0.92; with a 4-week test-retest reliability of 0.87for the total scale. The reliability of the ISEL has also been established overa 6-month period (Cohen et al., 1985). In the present study, the internalconsistency of the ISEL was 0.92.
Test of Negative Social Exchanges (TENSE)
The TENSE contained 18 questions and assessed global interpersonalstress (e.g., insensitivity, interference). The TENSE appeared to be statisti-cally independent from measures of social support and has been associatedwith increased psychological distress. The test-retest reliability of the TENSEranged from 0.65 to 0.80 (Ruehlman and Karoly, 1991). The internal consis-tency of the TENSE in the present study was high (0.89).
Beck Depression Inventory (BDI)
The BDI contained 21 clinically derived items and appears to be a re-liable and valid measure of depression (Beck, 1974; Beck et al., 1961). Becket al. (1961) reported a split-half correlation of 0.86 for the BDI. In addition,the BDI is related to clinical ratings of depth of depression. In our study, theBDI was internally consistent (α = 0.80) with a mean score of 6.5 (SD= 5.1).
Satisfaction With Life Scale (SWLS)
The SWLS contained five items and assessed global life satisfaction.Diener and colleagues (Diener et al., 1985) reported an internal consistencyof 0.87 and retest correlation of 0.82. The internal consistency of the SWLSin the current study was similarly high (0.88).
Positive and Negative Affect Scale (PANAS)
The PANAS contained 20 items and measured the independent affec-tive dimensions of trait-positive and trait-negative affect (Watson et al., 1988).
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
370 Uchino, Holt-Lunstad, Uno, and Flinders
The PANAS is characterized by adequate test-retest reliability (e.g., 8 weekstability of 0.68 and 0.71 for trait-positive and trait-negative affectivity, re-spectively). Consistent with prior research, the internal consistency of thePANAS was high in our study for both trait-positive affect (0.84) and trait-negative affect (0.84).
Aggression Questionnaire (AQ)
The 29-item AQ assessed the cognitive, affective, and behavioral aspectsof trait aggression. Confirmatory factor analyses revealed evidence for thedimensional structure of the AQ (Buss and Perry, 1992). The AQ has good2-month test-retest reliabilities (rs = 0.72–0.80) and is characterized by goodinternal consistencies of 0.72–0.89 (Buss and Perry, 1992). In the presentstudy, the internal consistency of the AQ was 0.89.
State Anxiety Scale
The short form of the Spielberger State-Trait Anxiety Scale was ad-ministered to participants prior to and following each psychological stressor(Marteau and Bekker, 1992). Participants were asked to rate their currentfeelings on a 4-point scale, ranging from 1 (not at all) to 4 (very much). Con-sistent with prior work, the internal consistency of the scale in our study washigh (Chronbach’s alpha of 0.78–0.80).
RESULTS
Preliminary Analyses
We first performed repeated measures analyses of variance (Epoch:baseline, speech task, math task) on state anxiety scores and the cardio-vascular measures to examine the efficacy of the stress protocol. As detailedin an earlier report (Uchino et al., 1999b), the stress protocol led to significantincreases in state anxiety, SBP, DBP, CO, and heart rate. In addition, PEPwas shortened, and RSA decreased in response to the stress protocol. Consis-tent with our prior work (Cacioppo et al., 1995), few significant effects werefound as a function of task order and the patterns of results reported herewere similar when statistically controlling for task order. Therefore, in orderto increase the reliability and generalizability of our reactivity assessment weaggregated across tasks (Kamarck et al., 1992).
We first examined the association between our social network mea-sures of supportive ties, aversive ties, and ambivalent ties with the ISEL and
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 371
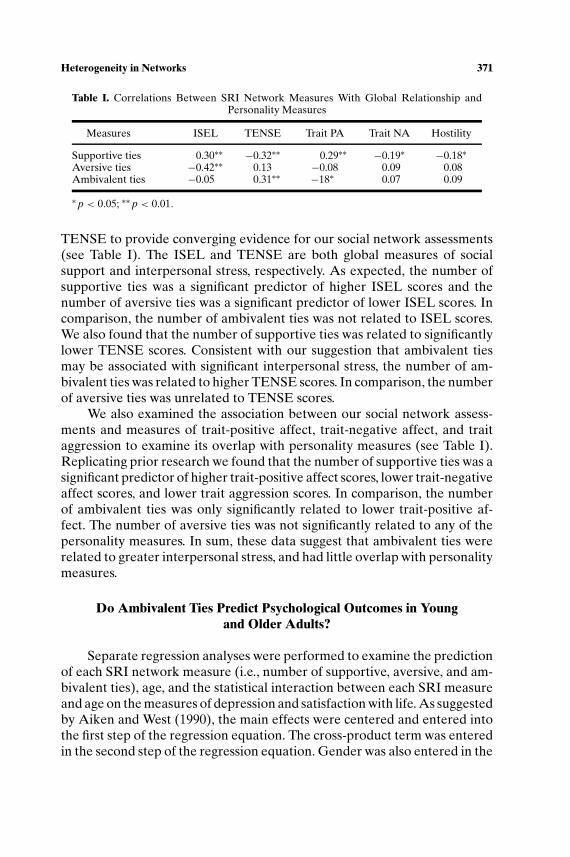
Table I. Correlations Between SRI Network Measures With Global Relationship andPersonality Measures
Measures ISEL TENSE Trait PA Trait NA Hostility
Supportive ties 0.30∗∗ −0.32∗∗ 0.29∗∗ −0.19∗ −0.18∗Aversive ties −0.42∗∗ 0.13 −0.08 0.09 0.08Ambivalent ties −0.05 0.31∗∗ −18∗ 0.07 0.09
∗ p < 0.05; ∗∗ p < 0.01.
TENSE to provide converging evidence for our social network assessments(see Table I). The ISEL and TENSE are both global measures of socialsupport and interpersonal stress, respectively. As expected, the number ofsupportive ties was a significant predictor of higher ISEL scores and thenumber of aversive ties was a significant predictor of lower ISEL scores. Incomparison, the number of ambivalent ties was not related to ISEL scores.We also found that the number of supportive ties was related to significantlylower TENSE scores. Consistent with our suggestion that ambivalent tiesmay be associated with significant interpersonal stress, the number of am-bivalent ties was related to higher TENSE scores. In comparison, the numberof aversive ties was unrelated to TENSE scores.
We also examined the association between our social network assess-ments and measures of trait-positive affect, trait-negative affect, and traitaggression to examine its overlap with personality measures (see Table I).Replicating prior research we found that the number of supportive ties was asignificant predictor of higher trait-positive affect scores, lower trait-negativeaffect scores, and lower trait aggression scores. In comparison, the numberof ambivalent ties was only significantly related to lower trait-positive af-fect. The number of aversive ties was not significantly related to any of thepersonality measures. In sum, these data suggest that ambivalent ties wererelated to greater interpersonal stress, and had little overlap with personalitymeasures.
Do Ambivalent Ties Predict Psychological Outcomes in Youngand Older Adults?
Separate regression analyses were performed to examine the predictionof each SRI network measure (i.e., number of supportive, aversive, and am-bivalent ties), age, and the statistical interaction between each SRI measureand age on the measures of depression and satisfaction with life. As suggestedby Aiken and West (1990), the main effects were centered and entered intothe first step of the regression equation. The cross-product term was enteredin the second step of the regression equation. Gender was also entered in the
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
372 Uchino, Holt-Lunstad, Uno, and Flinders
first step of the regression equation to account for its potential influence onpsychological outcomes.
Results of these regression analyses revealed main effects for our socialnetwork measures. Replicating prior research, the number of supportive tieswas associated with lower levels of depression (b = −0.44, t = 2.32, p <
0.03) and higher satisfaction with life (b = 0.17, t = 2.96, p < 0.01). In com-parison, the number of aversive ties predicted greater levels of depression(b = 2.46, t = 2.70, p < 0.01) and lower satisfaction with life (b = 0.69, t =2.50, p < 0.01).
We also found a significant interaction between age and the number ofaversive ties for depression (b = −0.25, t = 2.41, p < 0.02). Follow-up testswere conducted to examine the pattern associated with this significant statis-tical interaction (Aiken and West, 1990). Results of these follow-up analysesrevealed that depression was lower as a function of age for individuals with arelatively high number of aversive ties (b = −0.15, t = 2.01, p < 0.05). How-ever, depressive symptoms were higher as a function of age for individualswith a relatively low number of aversive ties (b = 0.13, t = 1.98, p < 0.05).These results were unchanged while statistically controlling for (a) the num-ber of supportive and ambivalent ties or (b) the total number of listed networkmembers. Although this statistical interaction was not expected, these dataappear to indicate that older individuals may be more effective at psycho-logically coping with aversive ties.
No significant main effects of ambivalent ties were found on the mentalhealth measures. However, the age× ambivalent ties interaction for depres-sion was significant (b = 0.03, t = 2.15, p < 0.04). Follow-up analyses of thisstatistical interaction revealed that depression was greater as a function ofage for individuals with a relatively high number of ambivalent network ties(b = 0.11, t = 1.89, p = 0.06). In comparison, depression was unchangedas a function of age for individuals with a relatively low number of ambiva-lent network ties (b = −0.05, t = 1.13, n.s.). Importantly, further analysesrevealed that the age× ambivalent ties interaction for depression remainedsignificant while statistically controlling for the number of supportive andaversive ties. In addition, statistically controlling for the total number oflisted network members did not alter these findings.
Do Ambivalent Ties Predict Cardiovascular Reactivity DuringStress in Young and Older Adults?
Separate regression analyses were again performed to examine the pre-diction of each social network measure (i.e., number of supportive, aversive,and ambivalent ties), age, and the statistical interaction between each net-work measure and age on cardiovascular reactivity during stress. We utilized
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 373
the following analysis strategy informed by the basic physiology of the cardio-vascular system. First, we examined the prediction of traditional measuresof heart rate and blood pressure reactivity by these social network cate-gories. Any significant associations with these measures were followed up byan analysis of their underlying autonomic (i.e., PEP and RSA) or hemody-namic (i.e., CO and TPR) determinants. In these analyses, gender, baselinemeasures of cardiovascular activity, BMI, and parental history of hyperten-sion were entered in the first step of the regression equation to also accountfor their potential influence on cardiovascular reactivity.
No significant simple (main) effects of supportive ties, aversive ties, orambivalent ties were found on measures of heart rate and blood pressurereactivity. However, consistent with our predictions regarding potential in-teractions between age and social ties, we found a significant age× support-ive ties interaction for heart rate reactivity during stress (b = −0.05, t =2.12, p = 0.04). Results of follow-up analyses (Aiken and West, 1990) re-vealed that individuals with a relatively high number of supportive ties did notshow differences in heart rate reactivity as a function of age (b = −0.06, t =0.85, n.s.). However, individuals with a relatively low number of supportiveties showed greater heart rate reactivity to stress as a function of age (b =0.16, t = 2.18, p = 0.03). This statistical interaction was unchanged whilestatistically controlling for the number of aversive and ambivalent ties (p =0.03) or the total number of listed network members (p = 0.04) and is con-sistent with the potential health-promoting role of social support. Analysesof the underlying autonomic determinants of this association failed to reveala parallel significant interaction on the measures of PEP and RSA reactivity.
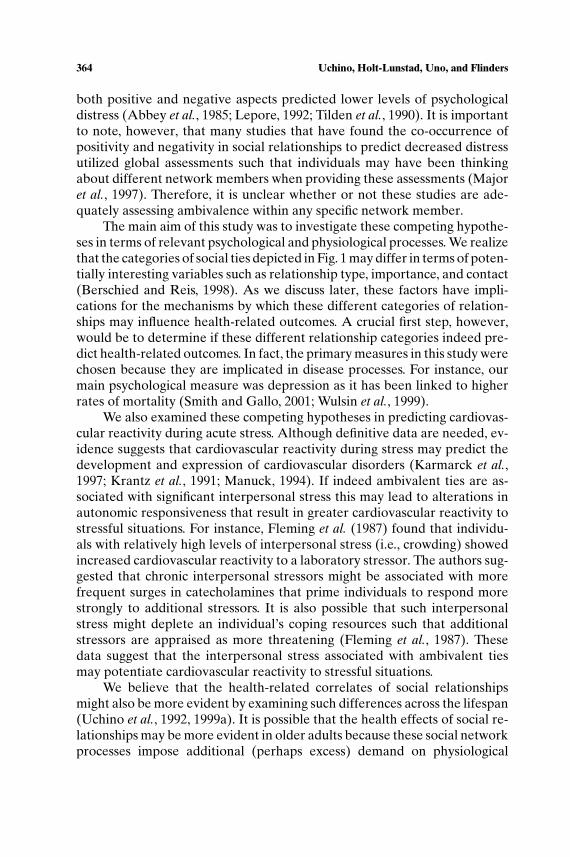
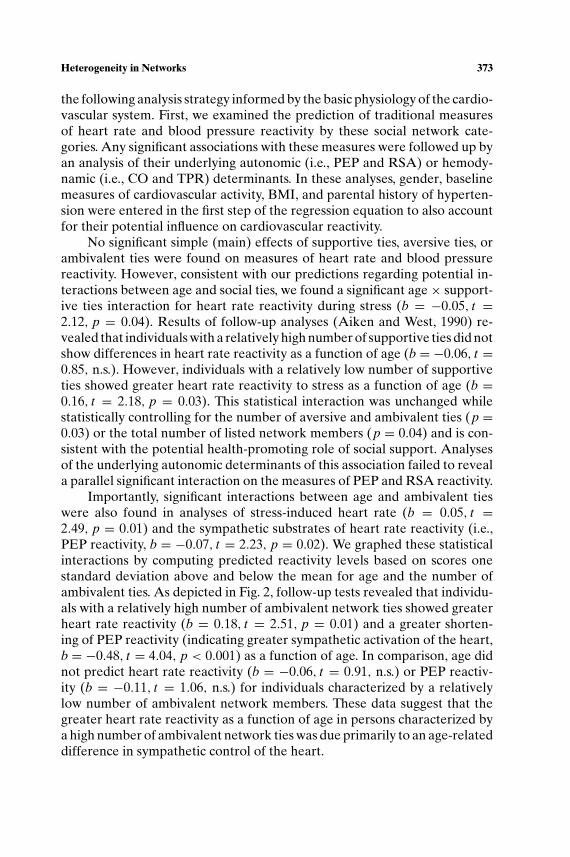
Importantly, significant interactions between age and ambivalent tieswere also found in analyses of stress-induced heart rate (b = 0.05, t =2.49, p = 0.01) and the sympathetic substrates of heart rate reactivity (i.e.,PEP reactivity, b = −0.07, t = 2.23, p = 0.02). We graphed these statisticalinteractions by computing predicted reactivity levels based on scores onestandard deviation above and below the mean for age and the number ofambivalent ties. As depicted in Fig. 2, follow-up tests revealed that individu-als with a relatively high number of ambivalent network ties showed greaterheart rate reactivity (b = 0.18, t = 2.51, p = 0.01) and a greater shorten-ing of PEP reactivity (indicating greater sympathetic activation of the heart,b = −0.48, t = 4.04, p < 0.001) as a function of age. In comparison, age didnot predict heart rate reactivity (b = −0.06, t = 0.91, n.s.) or PEP reactiv-ity (b = −0.11, t = 1.06, n.s.) for individuals characterized by a relativelylow number of ambivalent network members. These data suggest that thegreater heart rate reactivity as a function of age in persons characterized bya high number of ambivalent network ties was due primarily to an age-relateddifference in sympathetic control of the heart.

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
374 Uchino, Holt-Lunstad, Uno, and Flinders
Fig. 2. Top panel: Predicted heart rate reactivity as a function of age and ambivalent ties (oneSD above and below the mean). Bottom panel: Predicted PEP reactivity as a function of ageand ambivalent ties (one SD above and below the mean).
Importantly, further analyses revealed that the statistical interactionsbetween age and ambivalent ties were not altered when statistically con-trolling for the number of supportive and aversive ties for both heart ratereactivity (p = 0.02) and PEP reactivity (p = 0.02). These statistical interac-tions were also unchanged when statistically controlling for the total numberof listed network ties. These data suggest that the number of ambivalent tieswas a relatively independent predictor of these age-associated cardiovasculardifferences during stress.
Are Ambivalent Ties a Unique Predictor of CardiovascularReactivity in Young and Older Adults?
Because of the cross-sectional nature of these data, it was importantto evaluate several plausible alternative explanations for our findings. Forinstance, age is typically associated with differences in basic demographicvariables. Thus, we first examined whether social network differences indemographic factors might be responsible for the age × ambivalent ties(and supportive ties) interactions for cardiovascular reactivity obtained inthis study. Inconsistent with this possibility, statistically controlling for the

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 375
additional demographic factors of education level and household incomedid not statistically alter any of our social network differences in reactivityreported earlier.
It was also possible that the statistical interactions between age andnumber of ambivalent or supportive ties were due to greater task-specific af-fective responses, perhaps because of differences in task performance. If thiswere true, the effects reported earlier may be more reflective of the currentsituation and may not necessarily represent how these individuals respondphysiologically to stress in their everyday lives. To examine this possibility,we repeated the analyses reported earlier while statistically controlling forchanges in state anxiety or the percent of incorrect math problems and thenumber of speech prompts. Importantly, none of our statistical results werealtered in these reanalyses.
Finally, we examined the potential influence of personality factors onour results linking supportive and ambivalent ties to age-related differencesin cardiovascular reactivity. Importantly, statistically controlling for trait-positive and trait-negative affect did not alter the age× ambivalent ties inter-action for heart rate reactivity (p = 0.01) or PEP reactivity (p = 0.02). In ad-dition, the age× supportive ties interaction was not influenced by statisticallycontrolling for trait-positive and trait-negative affect (p = 0.02). Statisticallycontrolling for trait hostility produced similar results as for trait-positive andtrait-negative affect. In sum, it appears as if the prediction of age-related dif-ferences in cardiovascular reactivity by ambivalent and supportive ties werenot explained by demographic, task-specific, and personality factors.
DISCUSSION
Prior research has provided strong evidence that social relationships in-fluence mental and physical health outcomes (Berkman, 1995; Cohen, 1988;House et al., 1988; Sarason et al., 1989). Much of the focus in prior studieshas been on the health-promoting role of social support. Consistent withthis research, we found that the number of supportive ties predicted bet-ter psychological outcomes and a lower age-related difference in heart ratereactivity during acute stress. Also consistent with prior research we foundthat the number of aversive ties predicted lower levels of mental health (e.g.,Rook and Pietromonaco, 1987).
A major aim of this study, however, was to evaluate if ambivalent tiespredicted health-related outcomes. Results of this study were consistent withthe utility of separating out such network ties as a high number of ambivalentties predicted greater age-related differences in depression and sympatheticcontrol of heart rate reactivity during acute stress. These data are importantbecause much of the prior research on social relationships and health has only

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
376 Uchino, Holt-Lunstad, Uno, and Flinders
assessed one dimension (typically positivity or social support). As outlined inFig. 1, however, high positivity includes both supportive and ambivalent ties,whereas high negativity includes both aversive and ambivalent ties. Thus, ex-amining either positive or negative dimensions of social networks in isolation(i.e., by assessing only a single dimension or statistically controlling for onedimension) may mask the different health profiles of these network types andobscure reliable associations between social relationships and health-relatedoutcomes.
At a broad level we also evaluated competing predictions about thenature of the association between a high number of ambivalent networkties and health-relevant outcomes. Results of this study were inconsistentwith the notion that individuals might benefit from the positivity associatedwith ambivalent ties and instead suggest that such ties may have negativeconsequences. As noted earlier, studies that have found positive aspects ofrelationships to buffer the distress associated with negative aspects of re-lationships utilized global assessments. This procedure raises the possibilitythat individuals may have been thinking about different network memberswhen providing these assessments (Major et al., 1997). Therefore, it is unclearwhether or not these studies were adequately assessing ambivalence withinany given network member. We avoided this potential conceptual problemby assessing positivity and negativity from specific network ties, and comput-ing an index of ambivalence at the level of each network member. Studiesthat have utilized similar approaches have tended to support the notion thatnetwork ties that are sources of ambivalence have negative influences on psy-chological outcomes (Hirsch and Rapkin, 1986; Pagal et al., 1987). However,this is the first study to suggest that such ambivalent ties may predict measuresof cardiovascular reactivity during stress.
Given that social ambivalence appears to predict negative consequences,it is important to discuss more specific mechanisms potentially responsiblefor these findings. There are at least two reasons why networks with a highnumber of ambivalent ties may be detrimental. First, social networks with ahigh number of ambivalent network ties may be associated with significantlevels of interpersonal stress (Coyne and DeLongis, 1986). Consistent withthis hypothesis, we found that the number of ambivalent ties was relatedto increased interpersonal difficulties as assessed by the TENSE. If socialnetwork members are primarily a source of negativity, one may habituate tothe aversive relationships by using adaptive coping strategies such as ignoringtheir behavior. However, ambivalent network members are sources of bothpositivity and negativity and thus relatively less predictable compared toaversive or supportive ties. This unpredictability may in turn be associatedwith potentiated emotional responses and increased ruminative thinking.There is also a relatively large body of literature on how unpredictability may

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 377
heighten biological stress responses (Frankenhaeuser, 1986; Mason, 1975).As suggested by Fleming et al. (1987), interpersonal stressors may primeindividuals to respond more strongly to other stressful situations at both thepsychological (e.g., appraisals) and biological levels of analysis. Research isnow being conducted to more precisely evaluate this potential mechanism bydirectly assessing the interactional stress associated with ambivalent networkmember (e.g., ambulatory blood pressure recordings in everyday life).
A second reason why having networks filled with ambivalent ties may berelated to adverse health consequences is because they do not allow access toeffective social support during times of need (Sandler and Barrera, 1984). Wefound that the number of ambivalent ties was unrelated to global perceptionsof social support. However, given that the ISEL provides data on generalizedperceptions of support, it is possible that individuals were also thinking aboutdifferent subsets of individuals when providing such an assessment. Researchthat directly examines this question by having an ambivalent network tieproviding support during stressful laboratory tasks would provide compellingdata for or against this hypothesis.
It is possible that ambivalent network ties may not universally be relatedto negative health outcomes. For instance, if individuals can avoid contactwith ambivalent network ties then its effects might be more limited. However,it may be the nature of ambivalent ties that makes this possibility difficultbecause of co-occurring positive aspects of the relationships. If this is the case,however, we might expect that the frequency of contact with such ties mightbe a moderator of the results found in this study. Future research examiningsuch relationship variables should help to delineate the boundary conditionsassociated with such network ties.
These data also highlight the potential importance of examining thehealth-related consequences of social relationships across the lifespan(Antonucci and Jackson, 1987; Carstensen, 1992). We proposed that thehealth effects of social relationships may be more evident in older adultsbecause these social network processes impose excess demands on physi-ological systems that are showing functional age-related changes (Timiras,1994). It is also important to note that many of the health outcomes pre-dicted by social relationships have a long-term etiology and develop slowlyover time (e.g., cardiovascular disease). Because of the stability of importantsocial relationships (e.g., familial ties, spouse), the health effects of socialrelationships might also be more evident in older individuals because ofthe cumulative influences of such network interactions over an appreciableperiod of time (Hansson et al., 1990). Thus, network ties that are sources ofambivalence may play a role in both the development and exacerbation ofhealth problems. Long-term prospective data would be necessary to defini-tively address these questions.

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
378 Uchino, Holt-Lunstad, Uno, and Flinders
One complex question that arises from these age-related differences iswhether ambivalent relationships are qualitatively different in young andolder adults. Ancillary analyses revealed that age was uncorrelated with thenumber of ambivalent ties. Thus, it does not appear that older individuals hadmore ambivalent ties in their social network. However, it is possible that theambivalent ties in older individuals’ social networks were more important orconsequential to them if they are indeed forged by many years of nurturanceor selectivity (Carstensen, 1992; Hansson et al., 1990). It is interesting tospeculate that this greater emotional bond and/or reliance of older adults ontheir social networks may make it more difficult to minimize contact withsuch individuals and hence exacerbate the influence of socially ambivalentties in older individuals.
Because of the cross-sectional nature of our data we also examined alter-native explanations for our data including the contribution of trait-positiveaffect, trait-negative affect, and trait aggression. Our data indicated thatsocial relationships continued to predict cardiovascular reactivity after ac-counting for these personality processes. These results are consistent withresearch indicating that social relationships predict more objective indicesof health (e.g., cardiovascular function, immune function) even after consid-ering personality factors or their proposed confounding mechanism (Houseet al., 1988; Kiecolt-Glaser et al., 1991; Uchino et al., 1999a). Of course, ourdata do not indicate that personality processes are unimportant to the studyof social relationships and physical health outcomes. On the contrary, per-sonality factors clearly predict health outcomes in their own right (Matthews,1988; Smith and Gallo, 2001). Our study suggests that more complex modelsmay be necessary to fully understand health-related associations betweenpersonality factors and social relationships.
We did not expect, nor find, the number of socially aversive ties to pre-dict cardiovascular reactivity during stress. As mentioned earlier, it may bethat individuals habituate to the interpersonal stress of having primarily neg-ative network members. Alternatively, individuals may choose to minimizecontact with such relationships so its effects may be limited, at least at thephysiological level of analysis. Consistent with prior research (Rook, 1984),it should also be noted that ratings of negativity were relatively low in ourstudy. It is possible that higher ratings of negativity may result in more ad-verse influences for aversive ties (and ambivalent ties). A broad, explicitassessment of differing relationships (e.g., coworkers, neighbors) would beuseful to examine this issue.
There are important limitations of the present study that should benoted. First, as discussed earlier we utilized a cross-sectional design. Althoughwe examined several plausible alternative explanations, well-designed lon-gitudinal studies will be necessary to more definitively address this question.

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 379
Because of the homogeneous ethnic composition of our sample and its rela-tively high education level, future research using a broader sample of partic-ipants would also be needed to establish the generality of these findings. Itis important to note, however, that we were able to replicate prior researchon social support and psychological outcomes as well as age-related differ-ences in cardiovascular reactivity (Jennings et al., 1997; Uchino et al., 1999b).This gives us some confidence in the comparability of our sample with priorresearch. Finally, a priori power analyses revealed that the present samplesize would only allow us to detect a moderate effect size (r = 0.30). Theuse of larger samples in future research may be beneficial for the statisticaldetection of smaller effect sizes.
Finally, it is worth discussing the health implications of our measures aswe found that a high number of ambivalent ties predicted greater age-relateddifferences in depression and stress-induced cardiac sympathetic control ofheart rate reactivity. Although more evidence is needed, evidence does existlinking these specific measures to disease processes. For instance, depressionhas been linked to decrements in immunity and increased mortality (Herbertand Cohen, 1993; Smith and Gallo, 2001). Animal models also suggest thathigh heart rate reactivity during stress is associated with increased coronaryartery atherosclerosis (Manuck et al., 1983), an effect that appears mediatedby activation of the sympathetic nervous system (Kaplan and Manuck, 1989).Although we did not find these social network ties to predict blood pressurereactivity, age is typically associated with increased blood pressure reactivityduring stress (e.g., Jennings et al., 1997). This decreased vascular complianceseen in older individual may have made detection of any additional variancein these measures difficult with the present sample size.
The data linking ambivalent ties to age-related difference in heart rateand PEP reactivity may also have implications for immune-related diseaseprocess as extensive interactions exist between the autonomic, endocrine,and immune systems (Ader et al., 1991). Consistent with this possibility, PEPreactivity to the same stress protocol has been linked to a poorer immuneresponse to an influenza vaccination in older adults (Cacioppo, 1994). Thesedata highlight the importance of future research modeling the independentand interactive biological pathways by which differing social relationshipsmay influence health outcomes.
ACKNOWLEDGMENTS
This research was generously supported by a James A. ShannonDirector’s Award 1 R55 AG13968 from the National Institute on Aging,Grant 1 R01 MH58690-01 from the National Institute of Mental Health, anda University Research Committee Grant 21560 from the University of Utah
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
380 Uchino, Holt-Lunstad, Uno, and Flinders
awarded to the first author. We would like to thank David Lozano, DanielLitvack, John T. Cacioppo, Robert Kelsey, and William Guethlein for theirexpert technical assistance and for providing us with copies of their dataacquisition and reduction software (i.e., ANS suite and ENSCOREL).
REFERENCES
Abbey, A., Abramis, D. J., and Caplan, R. D. (1985). Effects of differential sources of socialsupport and social conflict on emotional well-being. Basic Appl. Soc. Psychol. 6: 111–129.
Ader, R., Felton, D., and Cohen, N. (1991). Psychoneuroimmunology, Academic Press, NewYork.
Aiken, L. S., and West, S. G. (1990). Multiple Regression: Testing and Interpreting Interactions,Sage, London.
Antonucci, T. C., and Jackson, J. S. (1987). Social support, interpersonal efficacy, and health: Alife course perspective. In Carstensen, L., and Edelstein, B. A. (Eds.), Handbook of ClinicalGerontology, Pergammon Press, New York, pp. 291–311.
Barrera, M. (1980). A method for the assessment of social support networks in communitysurvey research. Connections 3: 8–13.
Beck, A. T. (1974). Depression: Clinical, Experimental, and Theoretical Aspects, Harper andRow, New York.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., and Erbaugh, J. (1961). An inventory formeasuring depression. Arch. Gen. Psychiatry 4: 561–571.
Berkman, L. F. (1995). The role of social relations in health promotion. Psychosom. Med. 57:245–254.
Berntson, G. G., Cacioppo, J. T., and Quigley, K. S. (1995). The metrics of cardiac chronotropism:Biometric perspectives. Psychophysiology 32: 162–171.
Berntson, G. G., Quigley, K. S., Jang, J., and Boysen, S. (1990). An approach to artifact identifi-cation: Application to heart period data. Psychophysiology 27: 586–598.
Berschied, E., and Reis, H. T. (1998). Attraction and close relationships. In Gilbert, D. T., Fiske,S. T., and Lindzey, G. (Eds.), The Handbook of Social Psychology, McGraw-Hill, New York,pp. 193–281.
Braiker, H. B., and Kelly, H. H. (1979). Conflict in the development of close relationships. InBurgess, R. L., and Huston, T. L. (Eds.), Social Exchange in Developing Relationships,Academic Press, New York, pp. 135–168.
Brown, G. W. (1987). Social factors and the development and course of depressive disorders inwomen. Br. J. Soc. Work 17: 615–634.
Buss, A. H., and Perry, M. (1992). The aggression questionnaire. J. Pers. Soc. Psychol. 63: 452–459.
Cacioppo, J. T. (1994). Social neuroscience: Autonomic, neuroendocrine, and immune responsesto stress. Psychophysiology 31: 113–128.
Cacioppo, J. T., and Berntson, G. G. (1994). Relationship between attitudes and evaluative space:A critical review, with emphasis on the separability of positive and negative substrates.Psychol. Bull. 115: 401–423.
Cacioppo, J. T., Berntson, G. G., Binkley, P. F., Quiqley, K. S., Uchino, B. N., and Fieldstone, A.(1994). Autonomic cardiac control II: Basal response, noninvasive indices, and autonomicspace as revealed by autonomic blockade. Psychophysiology 31: 586–598.
Cacioppo, J. T., Malarkey, W., Kiecolt-Glaser, J. K., Uchino, B. N., Sgoutas-Emch, S. A.,Sheridan, J. F., Berntson, G. G., and Glaser, R. (1995). Heterogeneity in neuroendocrineand immune responses to brief psychological stressors as a function of autonomic cardiacactivation. Psychosom. Med. 57: 154–164.
Carstensen, L. L. (1992). Social and emotional patterns in adulthood: Support for socioemotionalselectivity theory. Psychol. Aging 7: 331–338.

P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
Heterogeneity in Networks 381
Cohen, S. (1988). Psychosocial models of the role of social support in the etiology of physicaldisease. Health Psychol. 7: 269–297.
Cohen, S., Mermelstein, R. J., Kamarck, T., and Hoberman, H. M. (1985). Measuring the func-tional components of social support. In Sarason, I. G., and Sarason, B. (Eds.), Social Support:Theory, Research, and Application, Martinus Niijhoff, The Hague, Holland, pp. 73–94.
Coyne, J. C., and DeLongis, A. (1986). Going beyond social support: The role of social relation-ships in adaptation. J. Consult. Clin. Psychol. 54: 454–460.
Diener, E., Emmons, R. A., Larsen, R. J., and Griffin, S. (1985). The satisfaction with life scale.J. Pers. Assess. 49: 71–75.
Finch, J. F., Okun, M. A., Barrera, M., Zautra, A. J., and Reich, J. W. (1989). Positive and negativesocial ties among older adults: Measurement models and the prediction of psychologicaldistress and well-being. Am. J. Community Psychol. 17: 585–605.
Fiore, J., Becker, J., and Coppel, D. B. (1983). Social network interactions: A buffer or a stress?Am. J. Community Psychol. 11: 423–439.
Fleming, I., Baum, A., Davidson, L. M., Rectanus, E., and McArdle, S. (1987). Chronic stress asa factor in psychologic reactivity to challenge. Health Psychol. 6: 221–238.
Frankenhaeuser, M. (1986). A psychobiological framework for research on human stress andcoping. In Appley, M. H., and Trumbull, R. (Eds.), Dynamics of Stress: Physiological, Psy-chological, and Social Perspectives, Plenum, New York, pp. 101–116.
Friedman, H. S., Tucker, J. S., Schwartz, J. E., Tomlinson-Keasey, C., Martin, L. R., Wingard,D. L., and Criqui, M. H. (1995). Psychosocial and behavioral predictors of longevity: Theaging and death of the “Termites”. Am. Psychol. 50: 69–78.
Hansson, R. O., Jones, W. H., and Fletcher, W. L. (1990). Troubled relationships in later life:Implications for support. J. Soc. and Pers. Rel. 7: 451–463.
Herbert, T. B., and Cohen, S. (1993). Depression and immunity: A meta-analytic review. Psychol.Bull. 113: 472–486.
Hirsch, B. J., and Rapkin, B. D. (1986). Social networks and adult social identities: Profiles andcorrelates of support and rejection. Am. J. Community Psychol. 14: 395–412.
House, J. S., Landis, K. R., and Umberson, D. (1988). Social relationships and health. Science241: 540–545.
Jennings, J. R., Kamarck, T., Manuck, S., Everson, S., Kaplan, G., and Salonen, J. (1997). Agingor disease? Cardiovascular reactivity in Finnish men over the middle years. Psychol. Aging12: 225–238.
Kamarck, T., Everson, S., Kaplan, G., Manuck, S., Jennings, R., Salonen, R., and Salonen, J.(1997). Exaggerated blood pressure responses during mental stress are associated withenhanced carotid atherosclerosis in middle-aged Finnish men. Circulation 96: 3842–3848.
Kamarck, T. W., Jennings, J. R., Debski, T. T., Glickman-Weiss, E., Johnson, P. S., Eddy, M. J., andManuck, S. B. (1992). Reliable measures of behaviorally-evoked cardiovascular reactivityfrom a PC-based test battery: Results from student and community samples. Psychophysi-ology 29: 17–28.
Kaplan, J. R., and Manuck, S. B. (1989). The effects of propanolol on behavioral interactionsamong adult male Cynomolgus monkeys (Macaca fascicularis) housed in disrupted socialgroupings. Psychosom. Med. 51: 449–462.
Kiecolt-Glaser, J. K., Dura, J. R., Speicher, C. E., Tras, J. O., and Glaser, R. (1991). Spousalcaregivers of dementia victims: Longitudinal changes in immunity and health. Psychosom.Med. 53: 345–362.
Krantz, D. S., Helmers, K. F., Bairey, N., Nebel, L. E., Hedges, S. M., and Rozanski, A. (1991).Cardiovascular reactivity and mental stress-induced myocardial ischemia in patients withcoronary artery disease. Psychosom. Med. 53: 1–12.
Lepore, S. J. (1992). Social conflict, social support, and psychological distress: Evidence of cross-domain buffering effects. J. Pers. Soc. Psychol. 63: 857–867.
Litvack, D., Oberlander, T., Carney, L., and Saul, J. (1995). Time and frequency domain methodsfor heart rate variability: A methodological comparison. Psychophysiology 32: 492–504.
Major, B., Zubek, J. M., Cooper, M. L., and Richards, C. (1997). Mixed messages: Implicationsof social conflict and social support within close relationships for adjustment to a stressfullife event. J. Pers. Soc. Psychol. 72: 1349–1363.
P1: FYJ
Journal of Behavioral Medicine [jobm] PP207-342431 June 26, 2001 20:43 Style file version Feb 25, 2000
382 Uchino, Holt-Lunstad, Uno, and Flinders
Manuck, S. B. (1994). Cardiovascular reactivity in cardiovascular disease: “Once more unto thebreach”. Int. J. Behav. Med. 1: 4–31.
Manuck, S. B., Kaplan, J. R., and Clarkson, T. B. (1983). Behavioral induced heart rate reactivityand atherosclerosis in Cynomolus monkeys. Psychosom. Med. 45: 95–108.
Marteau, T. M., and Bekker, H. (1992). The development of a six-item short form of the statescale of the Spielberger state-trait anxiety inventory (STAI). Br. J. Clin. Psychol. 31: 301–306.
Mason, J. W. (1975). Emotion as reflected in patterns of endocrine integration. In Levi, L. (Ed.),Emotions: Their Parameters and Measurement, Raven Press, New York, pp. 143–181.
Matthews, K. A. (1988). CHD and Type A behaviors: Update on an alternative to the Booth-Kewley and Friedman quantitative review. Psychol. Bull. 104: 373–380.
Neuvo, Y., Cheng-Yu, D., and Mitra, S. (1984). Interpolated finite impulse response filters. IEEETrans. ASSP 32: 563–570.
Orden, S. R., and Bradburn, N. M. (1968). Dimensions of marital happiness. Am. J. Sociol. 73:715–731.
Pagal, M. D., Erdly, W. W., and Becker, J. (1987). Social networks: We get by with (and in spiteof) a little help from our friends. J. Pers. Soc. Psychol. 53: 793–804.
Pierce, G. R., Sarason, I. G., and Sarason, B. R. (1991). General and relationships-specific per-ceptions of social support: Are two constructs better than one? J. Pers. Soc. Psychol. 61:1028–1039.
Rook, K. S. (1984). The negative side of social interaction: Impact on psychological well being.J. Pers. Soc. Psychol. 46: 1097–1108.
Rook, K. S., and Pietromonaco, P. (1987). Close relationships: Ties that heal or ties that bind.Adv. Pers. Rel. 1: 1–35.
Ruehlman, L. S., and Karoly, P. (1991). With a little flak from my friends: Development andpreliminary validation of the test of negative social exchange (TENSE). Psychol. Assess. 3:97–104.
Sandler, I. N., and Barrera, M. (1984). Towards a multidimensional approach to assessing theeffects of social support. Am. J. Community Psychol. 12: 37–52.
Sarason, B. R., Sarason, I. G., and Pierce, G. R. (1989). Social Support: An Interactional View,Wiley, New York.
Sherwood, A., Allen, M., Fahrenberg, J., Kelsey, R., Lovallo, W., and Van Doornen, L. (1990).Methodological guidelines for impedance cardiography. Psychophysiology 27: 1–23.
Smith, T. W., and Gallo, L. C. (2001). Personality traits as risk factors for physical illness. InBaum, A., Revenson, T., and Singer, J. (Eds.), Handbook of Health Psychology, LawrenceErlbaum, Hillsdale, NJ, pp. 139–172.
Tilden, V. P., Nelson, C. A., and May, B. A. (1990). The IPR inventory: Development andpsychometric characteristics. Nurs. Res. 39: 337–343.
Timiras, P. S. (1994). Physiological Basis of Aging and Geriatrics, CRC Press, London.Uchino, B. N., Holt-Lunstad, J., Uno, D., Betancourt, R., and Garvey, T. S. (1999a). Social
support and age-related differences in cardiovascular function: An examination of potentialmediators. Ann. Behav. Med. 21: 135–142.
Uchino, B. N., Kiecolt-Glaser, J. K., and Cacioppo, J. T. (1992). Age-related changes in cardio-vascular response as a function of a chronic stressor and social support. J. Pers. Soc. Psychol.63: 839–846.
Uchino, B. N., Uno, D., Holt-Lunstad, J., and Flinders, J. B. (1999b). Age-related differences incardiovascular reactivity during acute psychological stress in men and women. J. Gerontol.Psychol. Sci. 54: P339–P346.
Watson, D., Clark, L. A., and Tellegen, A. (1988). Development and validation of brief measuresof positive and negative affect: The PANAS scale. J. Pers. Soc. Psychol. 54: 1063–1070.
Weissman, M., Klerman, G. L., and Paykel, E. S. (1971). Clinical evaluation of hostility indepression. Am. J. Psychiatry 128: 261–266.
Wulsin, L. R., Vaillant, G. E., and Wells, V. E. (1999). A systematic review of the mortality ofdepression. Psychosom. Med. 61: 6–17.

Copyright of Journal of Behavioral Medicine is the property of Springer Science & Business Media B.V. and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.





























