Embed Size (px)
Citation preview
Health NetINTERNATIONAL
MALARIA AND LEISHMAINIASIS CONTROL PROGRAM
Published Research Articles
11 - A Circular Lane, P.O. Box 889, University Town, Peshawar, PakistanTel: (92) 91 - 844474 & 42551 Fax: (92) 91 - 840379
E -mail: hnipesh rcpes.comsats.net . pkWebsite: www. healthnetinternational. org
Io
II
i1
oi
ii
io
oi
oo
oo
i1
Ano
phel
ine
bree
ding
site
s: b
orro
w p
itsan
d ric
e fie
lds
-11
11
11
11
i1
11
11
1
45.0
40.0
35.0
.
°30
.0
25.0
0 020
.00 0
15.0
10.0 5.0
0.0
1
Mal
aria
Inci
denc
e A
mon
g A
Rs
in P
akis
tan
1J
JJ
JJ
JJ
9091
9293
9495
- 96
9798
990
01
DA
VI
AFI
.:` C' C C.r, CY
1.1;0C
VI : C,14
MIPIlh;"UJ
11
11
11
11
11
Insecticide treated tents
Spraying of inner surfaces w
ith permethrin or deltam
ethrin forvector control.
Residues persist for 6 m
onths on single sheeted and 12 months
on double sheeted tents
Effective against indoor resting m
osquitoes since mosquitoes
rest on the inner surface after feeding ( -80% m
ortality).
Has controlled epidem
ics in Afghan refugees
Provides com
munity protection: 60%
reduction in falciparumincidence in S
.Asia - they have not been tested elsew
here.
Their effectiveness against exophilic vectors (e.g. S
E A
sia) orhighly anthropophilic vectors (e.g. in A
frican situations) isunknow
n.
Spraying tents with residual pyrethroid
11
1i
i1
1J
11
I1
11
11
11
1l
11
1
Plastic sheeting for refugee camps
What prospect for insecticide treatm
ent of plastic sheeting,used
increasingly for refugeeshelter in A
frica?
Entom
ological trialsof im
pregnated laminated
sheeting scheduledin
2001 -2002.
11
11
11
11
11
11
11
1i
1
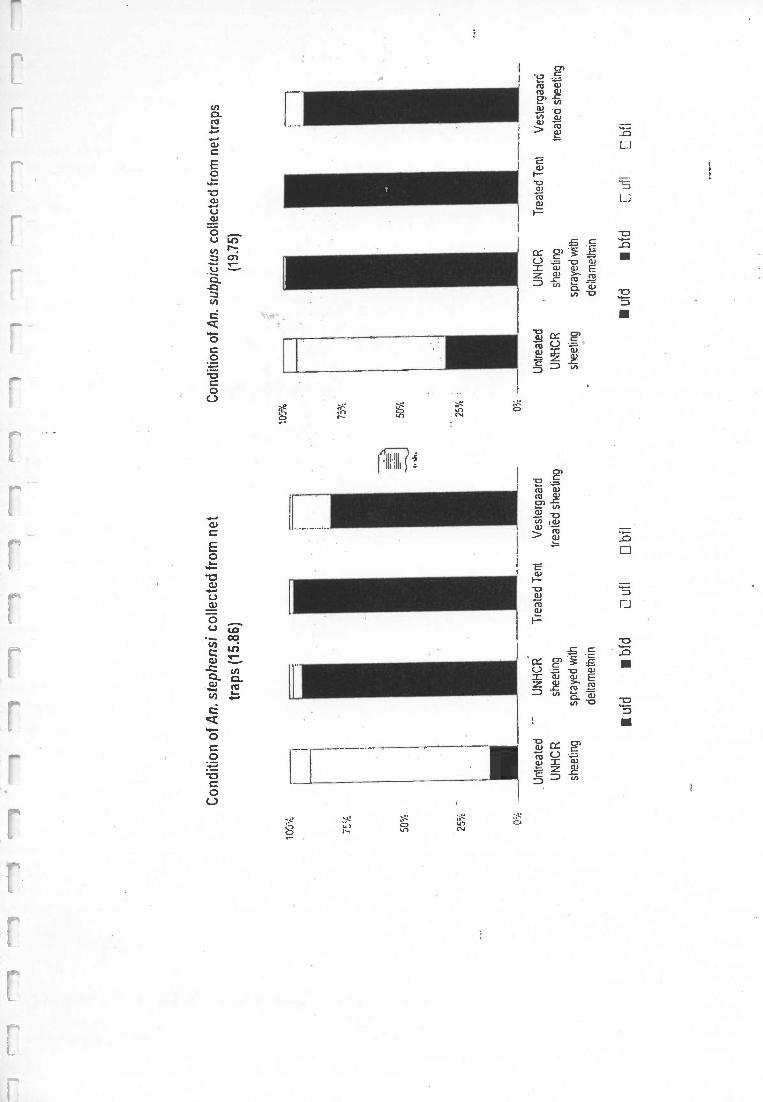
Con
ditio
n of
An.
ste
phen
si c
olle
cted
from
net
trap
s (1
5.86
)
100% 75
%
50%
25%
-
0 =
.
Con
ditio
n of
An.
sub
pict
us c
olle
cted
from
net
trap
s
(19.
75)
.U
ntre
ated
UN
HC
RT
reat
ed T
ent
Ves
terg
aard
UN
HC
Rsh
eetin
g
shee
ting
spra
yed
with
delta
met
hrin
trea
ted
shee
ting
ufd
bfd
D u
flC
l bfl
Unt
reat
edU
NH
CR
UN
HC
Rsh
eetin
g
shee
ting
spra
yed
with
delta
met
hrin
Tre
ated
Ten
tV
este
rgaa
rd
trea
ted
shee
ting
ufd
bfd
CO
bfl
11
)1
11
11
1l
11
1
Mal
aria
res
earc
h an
d co
ntro
lin
Com
plex
Em
erge
ncie
sM
alar
ia a
ssoc
iate
d w
ith c
onfli
ct o
r th
eaf
term
ath
of c
onfli
ct:
flour
ishe
s in
con
ditio
ns o
f cris
is a
ndpo
pula
tion
disp
lace
men
t
Mas
s po
pula
tion
mov
emen
t or
conc
entr
atio
n of
peo
ple
with
in h
igh
risk
area
s-
incr
ease
d ris
k of
epi
dem
ics
Ope
ratio
nal o
r ep
idem
iolo
gica
l diff
eren
ces
com
pare
d to
sta
ble
situ
atio
ns:
-un
stab
le g
over
nmen
t or
no g
over
nmen
t
-U
N o
rgan
isat
ions
and
NG
Os
prov
ide
heal
th s
ervi
ces
-in
secu
rity
or c
onfli
ct m
ake
long
-te
rmpl
anni
ng im
poss
ible
-br
eakd
own
in s
yste
ms,
pro
blem
s of
sup
ply
offo
od o
r m
edic
ine
-di
fficu
lty in
gai
ning
acc
ess
to th
ere
fuge
e po
pula
tion-
- po
orsi
te s
elec
tion,
env
ironm
enta
l det
erio
ratio
n en
cour
ages
vect
or b
reed
ing
-in
crea
sed
vuln
erab
ility
: mal
nutr
ition
or
lack
of i
mm
unity
Str
ateg
ies
for
stab
le s
ituat
ions
mus
tbe
ada
pted
for
com
plex
emer
genc
ies.
}1
11
11
11
11
11
11
11
Pre
vent
ion
1
Acu
te p
hase
Dep
ends
on
type
of s
helte
r av
aila
ble
-pe
rman
ent h
ousi
ng,
tent
s, p
last
ic s
heet
ing
Hum
an s
leep
ing
prac
tices
Vec
tor
beha
viou
r
Pos
sibl
e op
tions
:
...In
sect
icid
e tr
eate
d te
nts.
Per
met
h rin
trea
ted
blan
kets
As
prot
ectiv
e as
trea
ted
nets
in R
CT
ove
r sh
ort p
erio
ds (
62%
prot
ectio
n ag
ains
t Pf,
46%
aga
inst
Pv)
Sui
tabl
e fo
r ep
idem
ics
Cos
t effe
ctiv
e-
outla
y on
inse
ctic
ide
only
)1
11
11
}1
11
1
m d > ti a,
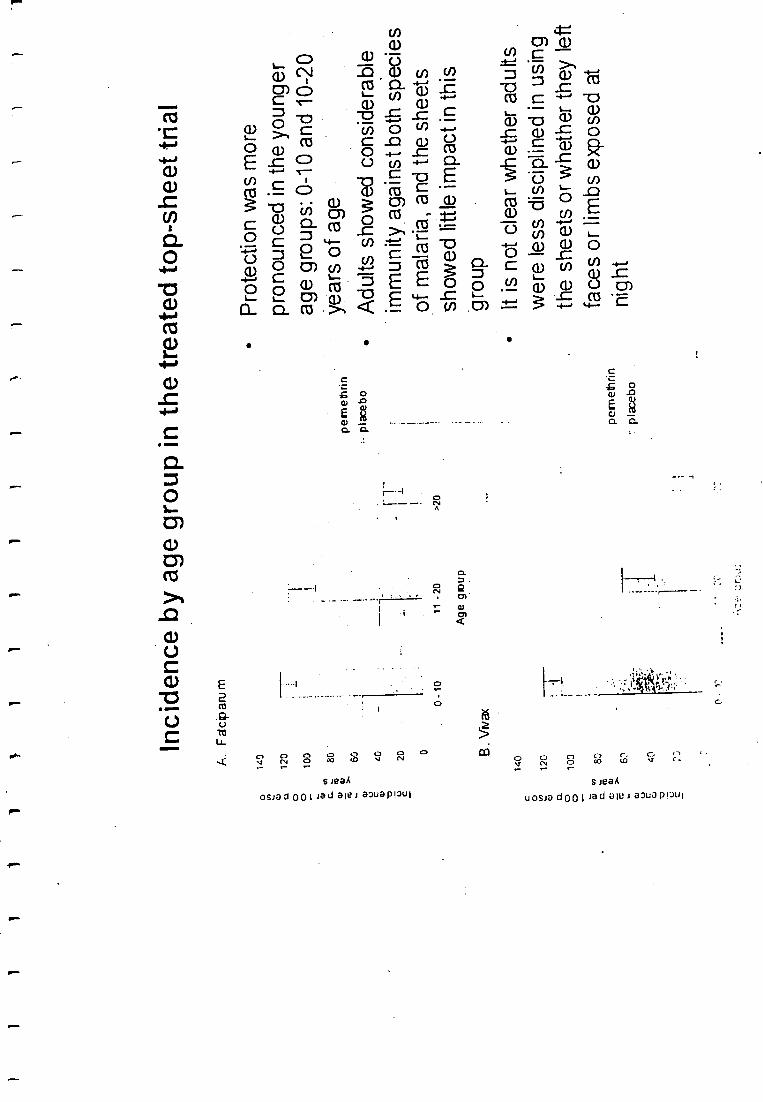
Inci
denc
e by
age
gro
up in
the
trea
ted
top
-she
et tr
ial
A. F
alci
paru
m
140
120
100 80 60 40 20
0
0-10
B. W
ax
140
120
100 80 60 40
o
11 -
20
>20
Age
gro
up
pem
elhr
in
plac
ebo
pem
eeiri
n
-: p
lace
bo
Pro
tect
ion
was
mor
epr
onou
nced
in th
e yo
unge
rag
e gr
oups
: 0 -
10 a
nd 1
0 -2
0ye
ars
of a
ge
Adu
lts s
how
ed c
onsi
dera
ble
imm
unity
aga
inst
bot
h sp
ecie
sof
mal
aria
, and
the
shee
tssh
owed
littl
e im
pact
in th
is*g
roup
It is
not
cle
ar w
heth
er a
dults
wer
e le
ss d
isci
plin
ed in
usi
ngth
esh
eets
or
whe
ther
they
left
face
sor
limbs
exp
osed
at
nigh
t
%of total catch CD
o
suogww fr4
o o s» o en = (D (D
O (1) m 0 -1 -73:- @ 3. M
E.(ou) n,
(2. , 0 c o. a) --I IN- -: gi a (A0 St CD u) w
CD FD` a CD CD =8
CD al al Cn .15 < - a) a) 1A. * 12 =
. Cl) o 0 -I ir. ,-..5. FL * 0 2:
. .44, =
M: CD pia -I
= CD
vu 5 ¡Di (7) SO
co 3 rDeL = al 2Q. o o co 0 C) o so g) "Z Q CD Cli
<D. c -I u,
o R. a it-,. = = U)
* 1:» w = u) 0.
411110
> > i 1 1 1 1 1 1 1 1
Insecticide treated nets - acute phase
Uncertain suitability during acute phase of emergency
Suitable if previously used by refugee population, and structuresallow nets to be hung.
If people unused to nets, less likely to use appropriately -behaviour change, compliance, and education
High initial costs.
Frequent delays in delivery.
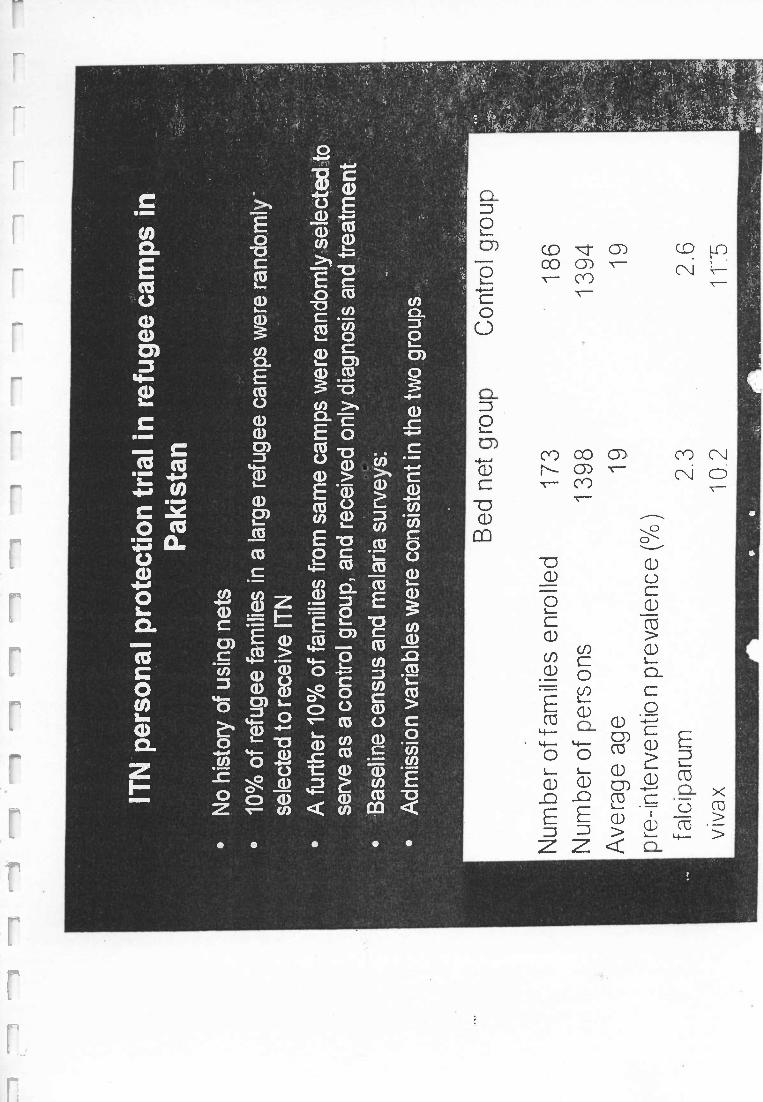
ITN
per
sona
lpr
otec
tion
tria
l in
refu
gee
cam
psin
Pak
ista
n
No
hist
ory
of u
sing
net
s
10%
of r
efug
ee fa
mili
es in
a la
rge
refu
gee
cam
ps w
ere
rand
omly
-
sele
cted
to r
ecei
ve IT
N
A fu
rthe
r 10
% o
f fam
ilies
from
sam
e ca
mps
wer
e ra
ndom
ly s
elec
ted
tose
rve
as a
con
trol
grou
p, a
nd r
ecei
ved
only
dia
gnos
is a
nd tr
eatm
ent
Bas
elin
e ce
nsus
and
mal
aria
surv
eys:
Adm
issi
on v
aria
bles
wer
e co
nsis
tent
inth
e tw
ogr
oups
.
Bed
net
grou
pC
ontr
olgr
oup
Num
ber
of fa
mili
es e
nrol
led
173
Num
ber
ofpe
rson
s13
98
Ave
rage
age
19
pre
-inte
rven
tion
prev
alen
ce(
%)
f alc
ipar
um2.
3vi
vax
10.2
186
1394 19 2.
6
115
1
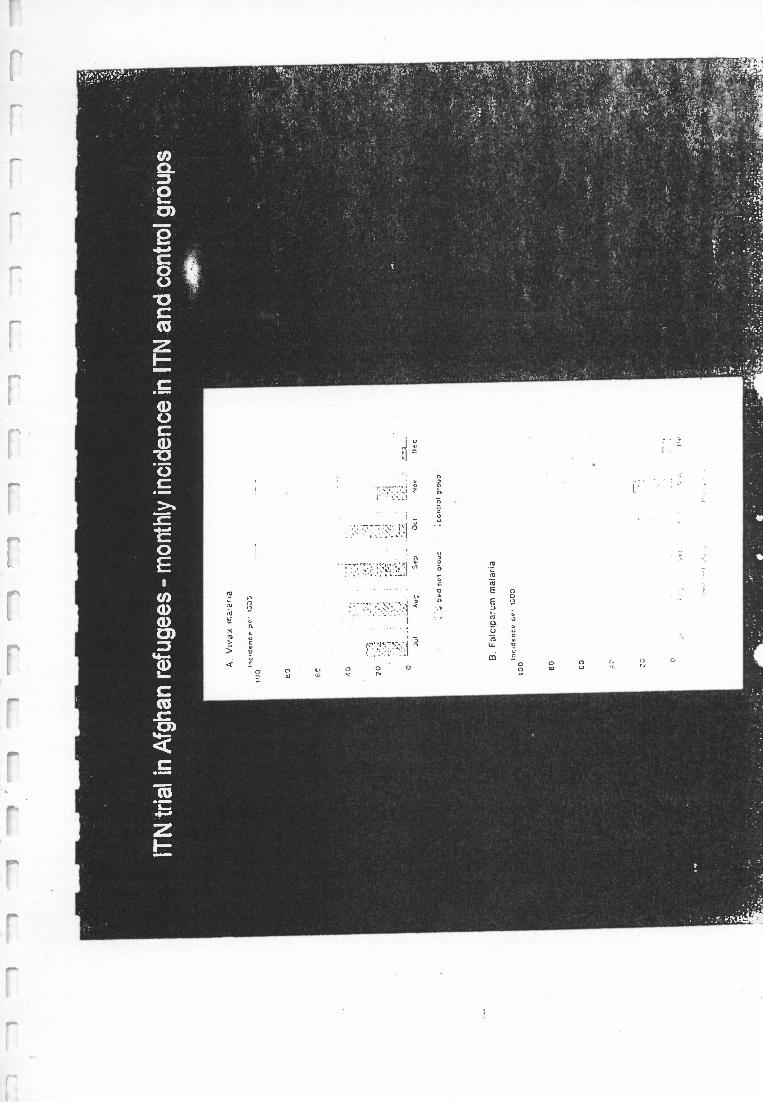
ITN
tria
l in
Afg
han
refu
gees
- m
onth
ly in
cide
nce
in IT
N a
nd c
ontr
ol g
roup
s
e a
ve c
oso
-an
ing
an r
e ug
ee p
rogr
amm
e
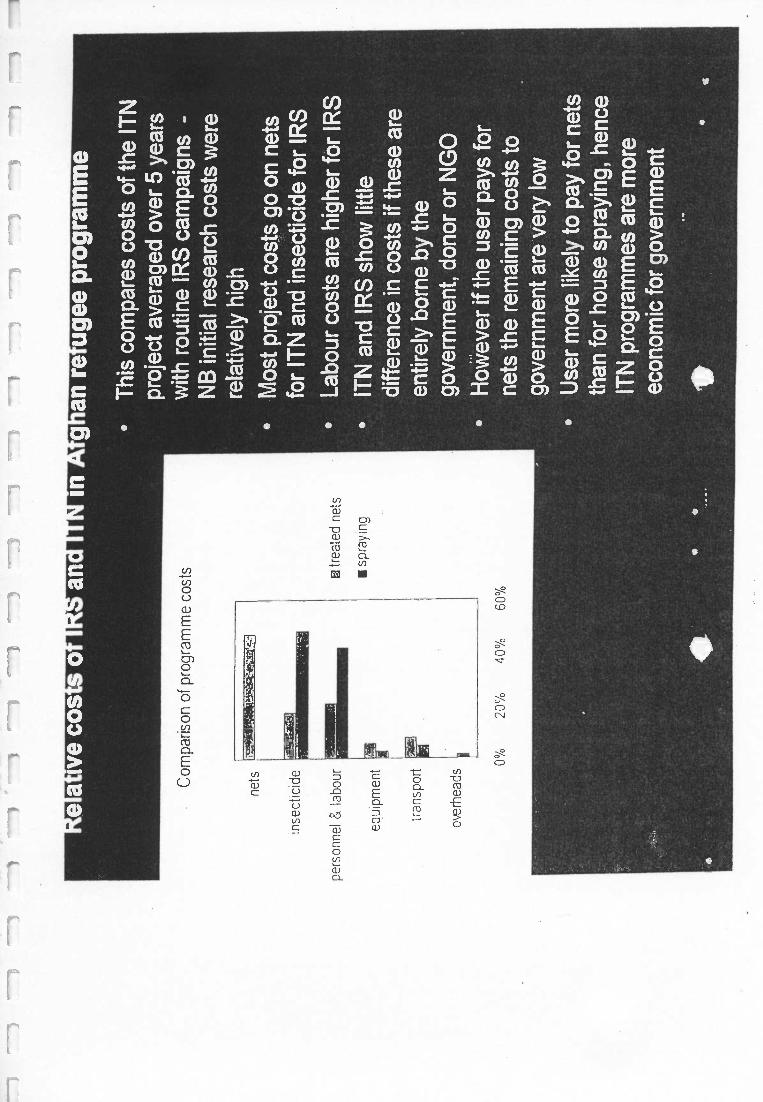
Com
paris
on o
f pro
gram
me
cost
s
nets
inse
ctic
ide
pers
onne
l & la
bour
equi
pmen
t
tran
spor
t
over
head
s
0%20
%40
%60
%
® tr
eate
d ne
ts
spra
ying
Thi
sco
mpa
res
cost
sof
the
ITN
proj
ect a
vera
ged
over
5 y
ears
with
rou
tine
IRS
cam
paig
ns-
NB
initi
al r
esea
rch
cost
sw
ere
rela
tivel
y hi
gh
Mos
t pro
ject
cos
tsgo
on
nets
for
ITN
and
inse
ctic
ide
for
IRS
Labo
ur c
osts
are
hig
her
for
IRS
ITN
and
IRS
sho
w li
ttle
diffe
renc
e in
cos
ts if
thes
e ar
een
tirel
y bo
rne
by th
ego
vern
men
t, do
nor
or N
GO
How
ever
if th
e us
erpa
ysfo
rne
ts th
e re
mai
ning
cos
ts to
gove
rnm
ent a
re v
ery
low
Use
r m
ore
likel
y to
pay
for
nets
than
for
hous
e sp
rayi
ng, h
ence
ITN
prog
ram
mes
are
mor
eec
onom
ic fo
r go
vern
men
t
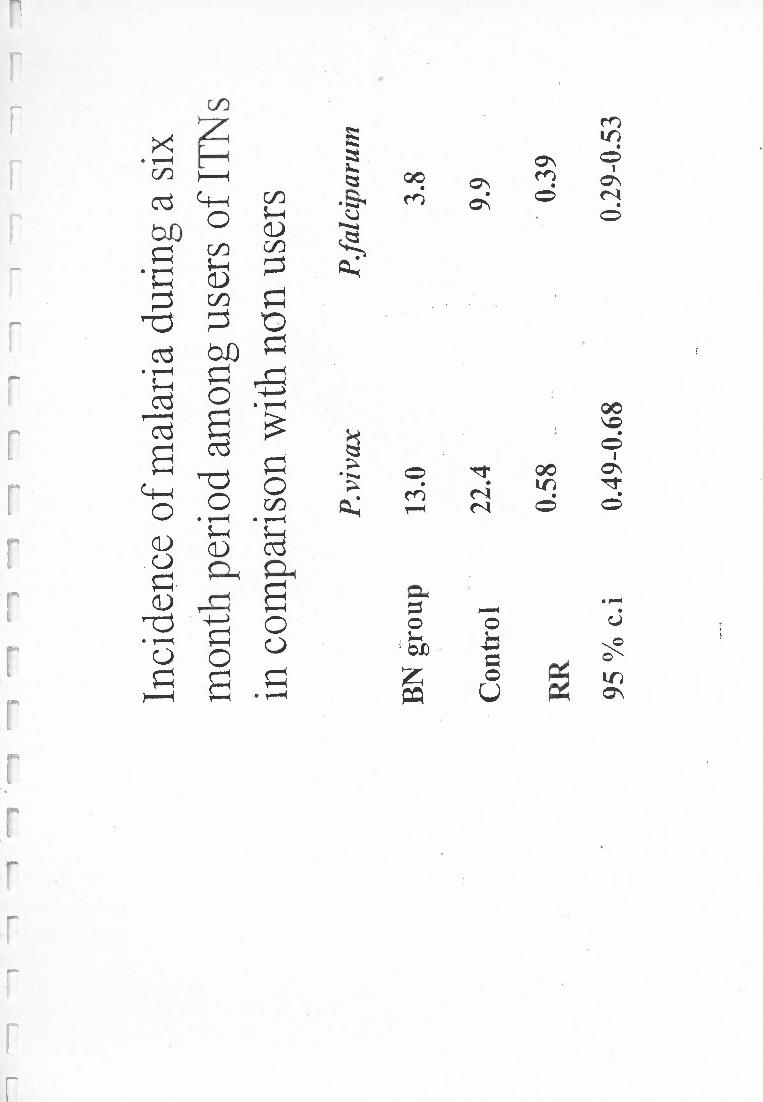
Inci
denc
e of
mal
aria
dur
ing
a si
xm
onth
peri
odam
ong
user
sof
IT
s
in c
ompa
riso
n w
ith n
on u
sers
P. v
i vax
P. f
al c
ipar
um
BN
gro
up13
.03.
8
Con
trol
22.4
9.9
RR
0.58
0.39
95 %
c. i
0.49
-0.6
80.
29-0
.53
t
s
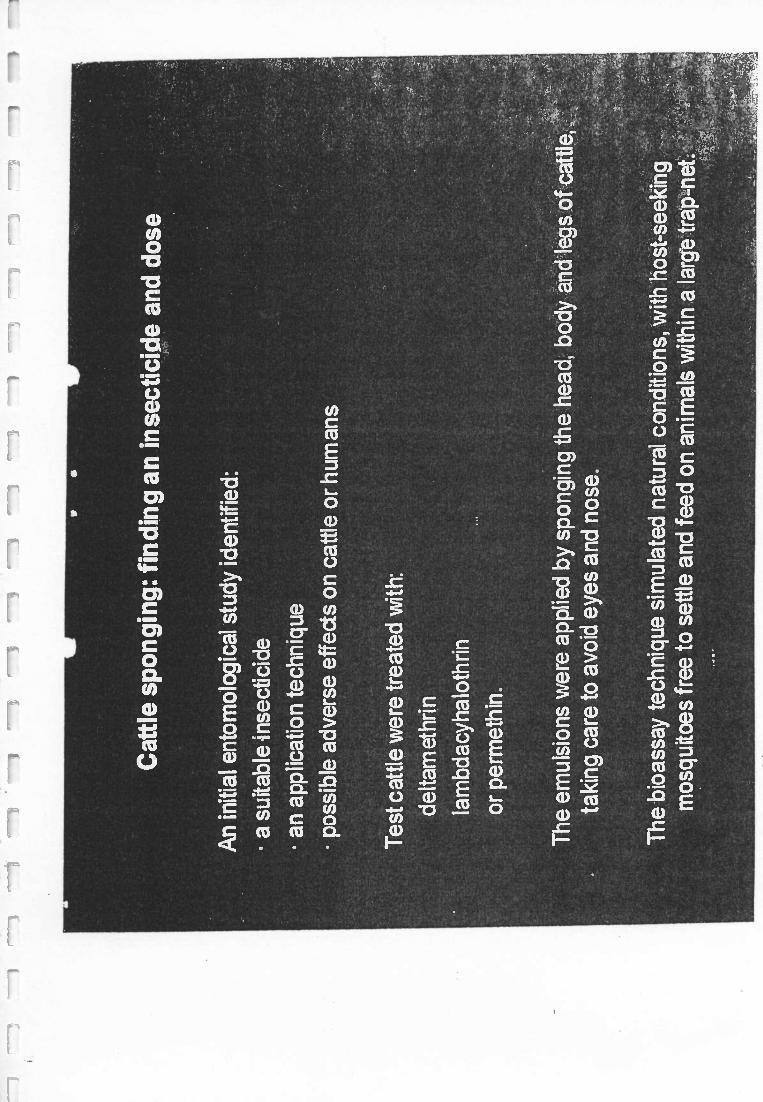
Cattle sponging: finding
an insecticide and dose
An initial entom
ological study identified:
a suitable insecticide
an application techniquepossible adverse effects on cattle or hum
ans
Test cattle w
ere treated with:
deltamethrin
lambdacyhalothrin
or permethin.
The em
ulsions were applied by sponging the head,
body and legs of cattle,taking care to avoid eyes and nose.
The bioassay technique sim
ulated natural conditions, with host- seeking
mosquitoes free to settle and feed on anim
als within a large trap -net.
1L-
11
11
11
11
11
11
11
11
11
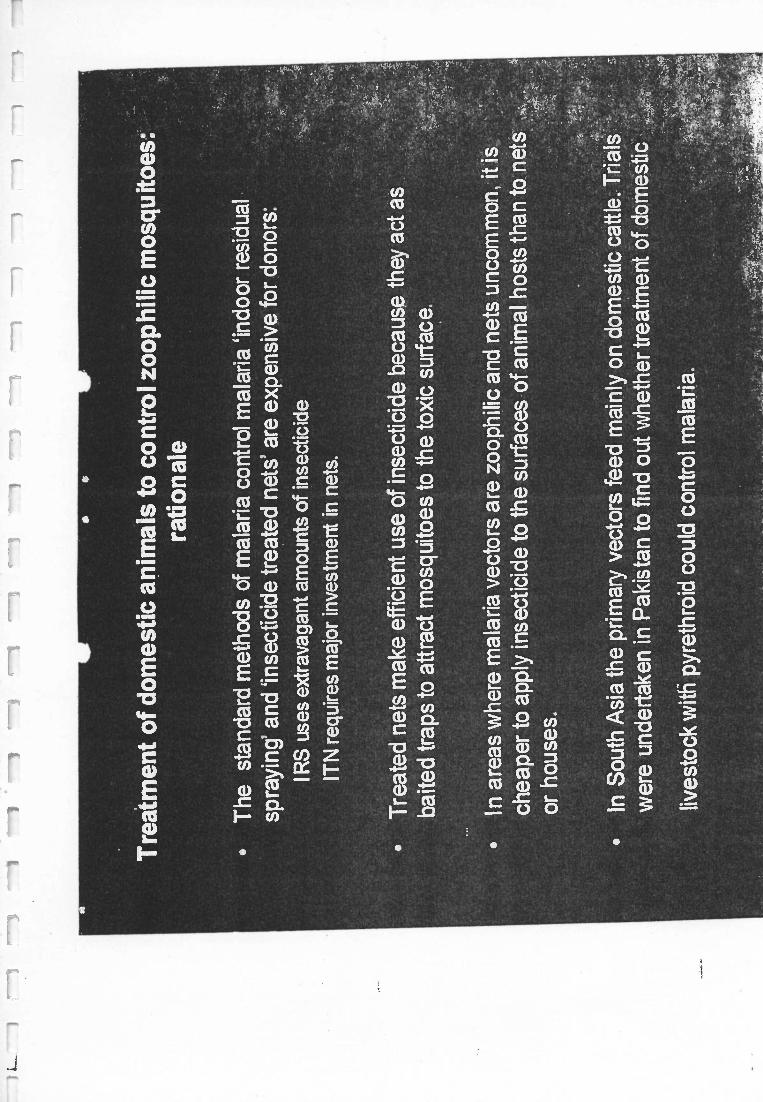
Treatm
ent of domestic anim
als to controlzoophilic mosquitoes:
ration ale
The standard m
ethods of malaria control m
alaria `indoor residualspraying' and `insecticide treated nets' are expensive for donors:
I RS
uses extravagant amounts of insecticide
ITN
requires major investm
ent in nets.
Treated nets m
ake efficient use of insecticide because they act asbaited traps to attract m
osquitoes to the toxic surface.
In areas where m
alaria vectors are zoophilic and nets uncomm
on, it is.
cheaper to apply insecticide to the surfaces of animal hosts than to nets
or houses.
In South A
sia the primary vectors feed m
ainly on domestic cattle. T
rialsw
ere undertaken in Pakistan to find out w
hether treatment
of domestic
livestock with pyrethroid could control m
alaria.
Sponging cattle with deitamethrin insecticide
i-,,
.
r........ - ::-.
1 1 l 1 1 1 1 1 1 1 1 I 1 1
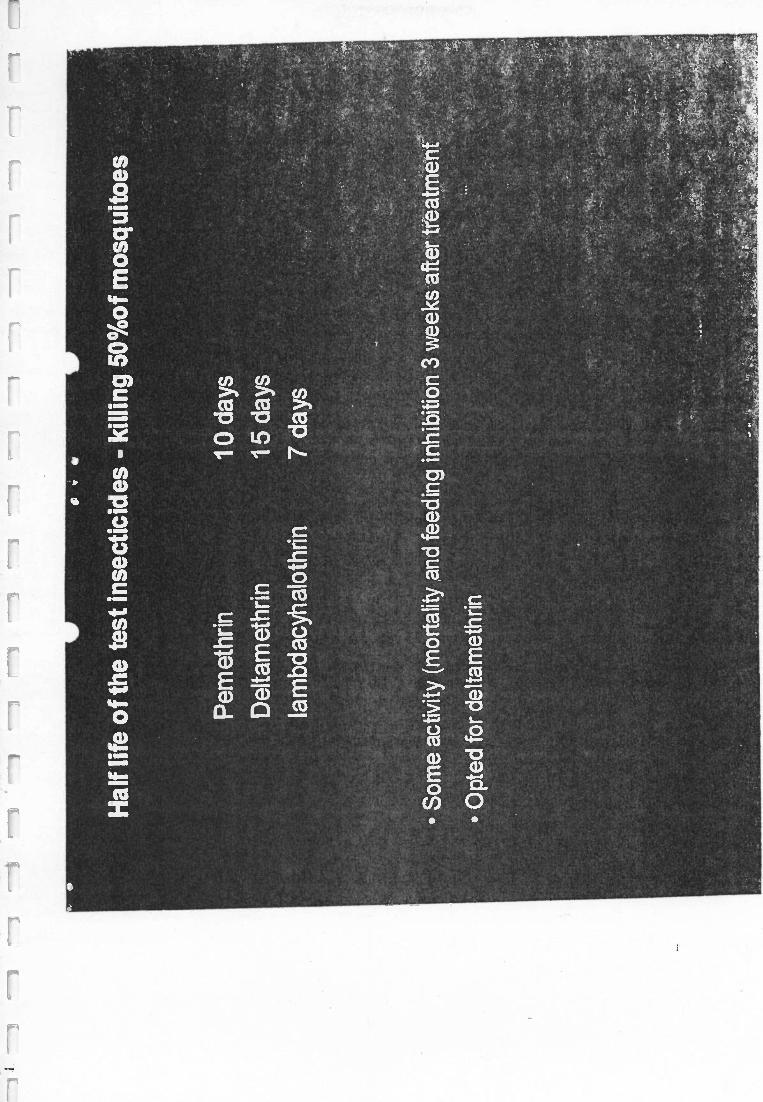
Half life of the test insecticides - killing 50 %of mosquitoes
Pemethrin 10 days
Deltamethrin 15 days
lambdacyhalothrin 7 days
Some activity (mortality and feeding inhibition 3 weeks after treatment
Opted for deltamethrin
M o
4 b
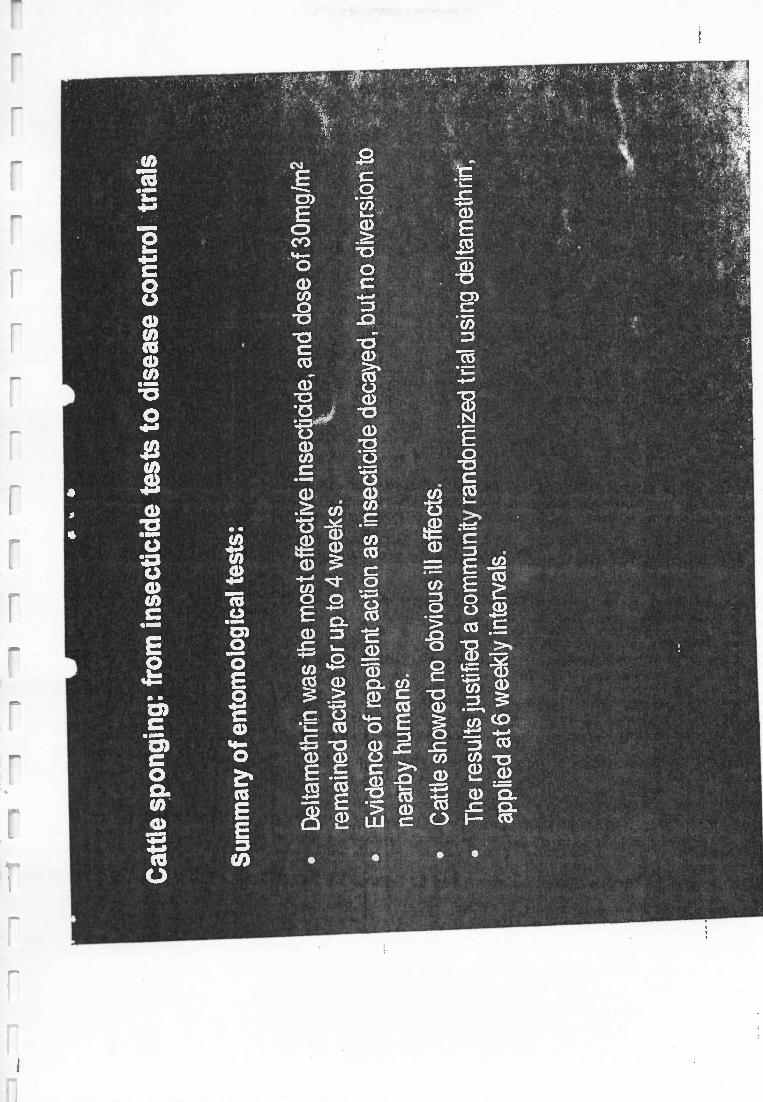
Cattle sponging: from insecticide tests to disease control trials
Summary of entomological tests:
Deltamethrin was the most effective insectidde, and dose of 30mg /m2
remained active for up to 4 weeks.
Evidence of repellent action as insecticide decayed, but no diversion to
nearby humans.
Cattle showed no obvious ill effects.
The results justified a community randomized trial using deltamethrir
applied at 6 weekly intervals.
;t
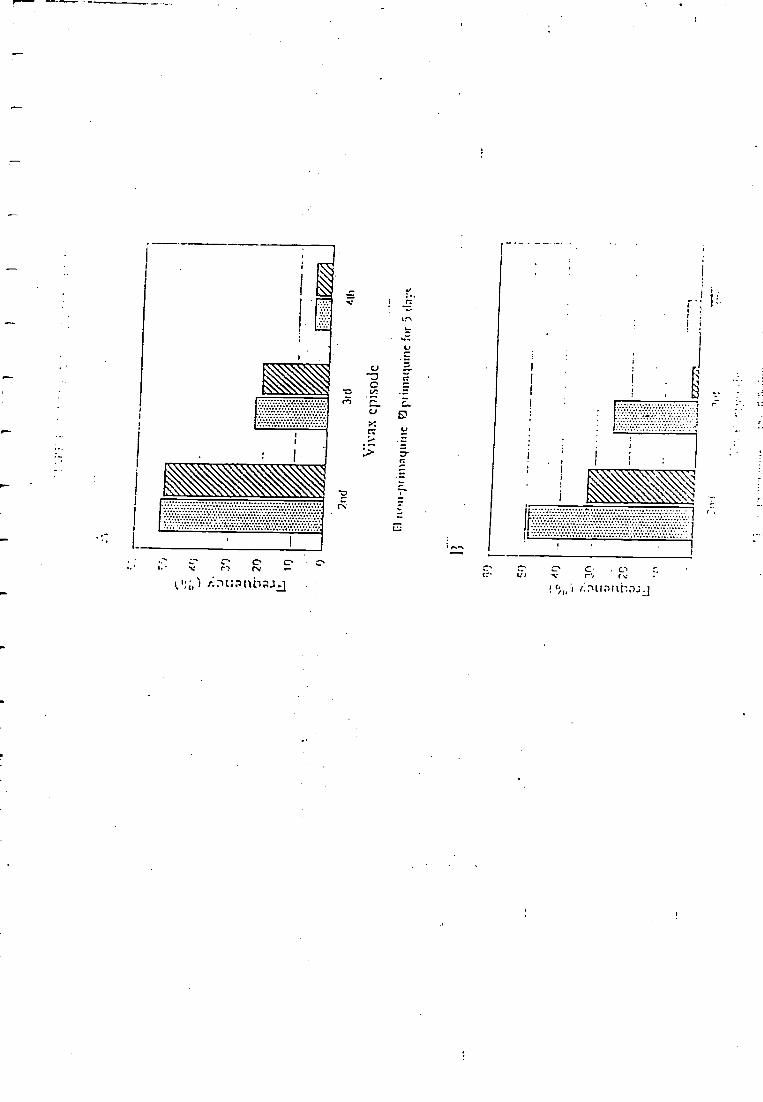
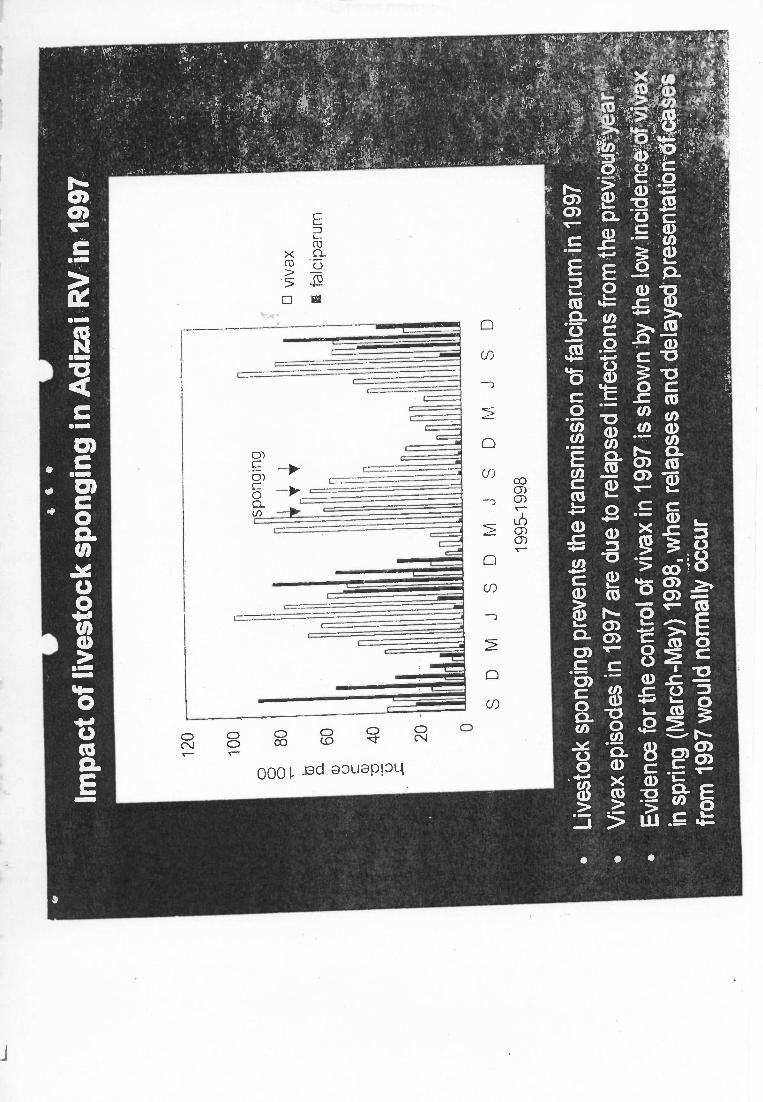
Impactof livestock sponging inAdizai RV in 1997
Livestock sponging prevents the
tran
smis
sion
of f
alci
paru
min
1997
Viv
ax e
piso
des
in19
97 a
re d
ue to
rel
apse
d in
fect
ions
from
the
previous-
Evi
denc
e fo
r th
eco
ntro
l of v
ivax
in 1
997
is s
how
n by
the
low
incidence".
in s
prin
g (M
arch
-M
ay)
1998
, whe
n re
laps
es a
nd d
elay
ed p
rese
ntat
ion
ofca
from
199
7 w
ould
nor
mal
lyoc
cur
1
Cattle sponging trial: conclusions
An effective new
way to control m
alaria in regions wherevectors
are zoophilic.e
y
Sim
ple technologythat can be im
plemented by the, com
mute ty.
Popular because
the benefits in animal productivity an
control are apparent to owners.
ectoparasite copp
Mo re cost- effective than house spraying or
treáted es.r
Rapid effect on
transmission indicates a role
- in epidemic
control
- controlling re- emerging
malaria (e.g. C
entral Asian statesrhéré
use of netsis uncom
mon).
As w
ith indoor residual spraying,cattle treatm
ent cam
should be undertaken judiciously to preventundue selection
insecticide resistance or anthropophilic feedingbehaviour.
1
Relative efficacy of different interventions
In S.A
sia, pyrethroid treated nets and indoor spraying of houses are
equally effective against malaria (giving about 60%
protection againstfalciparum
attacks).T
reated blankets and clothing are effective for shorter period thantreated nets because w
ashing and wear &
tear removes insecticide.
In endemic A
frica, ITN
are the most effective intervention (reducing
malaria deaths by 42%
and morbidity by 45%
in the Gam
bian trials).
IT clothing cheaper than IT
N since only insecticide is needed.
House spraying (IR
S) cheaper than IT
N if done only 2 or 3 tim
es But if
users contribute pay for ITN
, ITN
cheaper than IRS
.
Cost
per person protected* per yearis:
- ITN
$1.5 ($0.25 thereafter)- IT
blankets$0.25 ( cost of blankets excluded)
- IRS
$0.5
1)
1
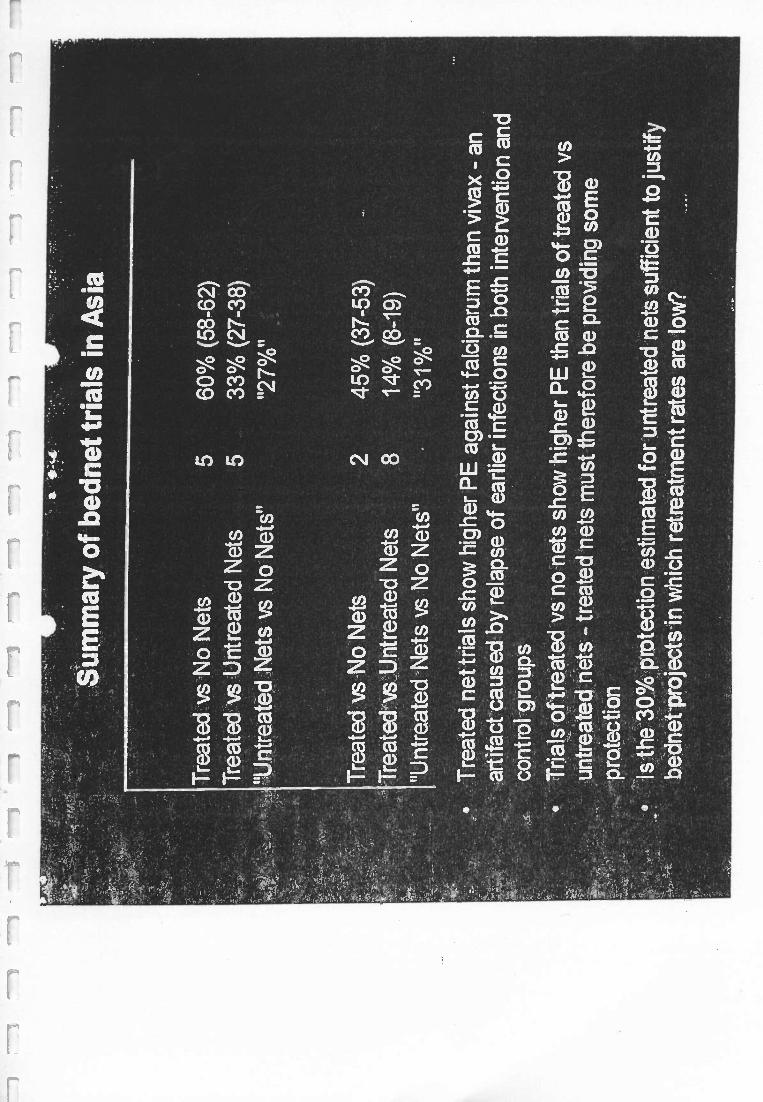
Summ
ary of bednet trials in Asia
Treated
vsN
o Nets
560%
(58 -62)T
reated vs Untreated N
ets5
33% (27 -38)
'Untreated N
ets vs No N
ets""27 %
"
Treated vs N
o Nets
245%
(37 -53)T
reatedvsU.ntreated N
ets8
14% (8 -19)
"Untreated N
ets vs No N
ets""31%
"
Treated net trials show
higherPE
against falciparum than vivax - an
artifact caused by relapse of earlier infections in both intervention andcontrol groups
Trials of treated vs no nets show
higherPE
than trials of treated vsuntreated nets - treated nets m
ust therefore be providing some
protectionIs the 30%
protection estimated for untreated nets sufficient to justify
bednet- projects in which retreatm
ent rates arelow
?
11
11
11
11
11
11
11
i1
Mal
aria
and
Com
plex
Em
erge
ncie
s
Mal
aria
is o
ften
asso
ciat
ed w
ith c
onfl
ict
or th
e af
term
ath
ofco
nflic
t as
the
dise
ase
flou
rish
es in
con
ditio
nsof
cri
sis
and
popu
latio
n di
spla
cem
ent.
Com
plex
em
erge
ncy
defi
nitio
n:"s
ituat
ions
affe
ctin
g la
rge
civi
lian
popu
latio
ns w
ith w
ar o
r ci
vil s
trif
ean
dpo
pula
tion
disp
lace
men
t,re
sulti
ng in
exc
ess
mor
talit
y an
d m
orbi
dity
'.O
pera
tiona
l dif
fere
nces
com
pare
d to
sta
ble
situ
atio
ns:
- un
stab
le g
over
nmen
tor
no
gove
rnm
ent
- M
any
part
ners
- U
Nor
gani
satio
ns a
nd N
GO
s(i
nter
natio
nal
and
loca
l) ta
kere
spon
sibi
lity
for
prov
idin
ghe
alth
ser
vice
s-
inse
curi
ty a
nd o
ngoi
ng c
onfl
ict
mak
e lo
ng -
term
plan
ning
impo
ssib
le-
brea
kdow
n in
sys
tem
sca
use
diff
icul
ties
for
heal
thca
re d
eliv
ery
and
dela
ys in
acce
ss to
sup
plie
sSt
rate
gies
use
d in
sta
ble
situ
atio
nsm
ust b
e ad
apte
d fo
rco
mpl
ex e
mer
genc
ies.
LL
R...: eg`ionFaf IT
Nprogram
me in A
fghanistan:
An IT
N sales projectw
as startedin A
fghanistan in 1992and has
continued to the presentday.
Nets are
'sold by móbile team
s of healtheducators or by the health
staffof fixed N
GO
clinics.
The lead agenc;y;is an N
GO
, HealthN
etInternational
(HN
I), who takes
responsibility for co-ordination ofim
plementing partner. agencies
(WH
O,
locarNG
Os; M
OH
),; staff:training, procurement and
distril4ution of nets-and: insecticide,
monitoring and evaluation of im
plementation.
Revenue is
recycled to procure further nets and insecticide.H
owever
the project could not surviveon such revolving funds: A
donoris
.required to cover orsupport operational costs.
The functions-presently
carried out by HN
I could beborne by district
health services oran MC
P w
erepolitical conditions
more stable or
government funding available
By this m
ethod fabout-400,000 family size nets
have been sold,ço vering 1.5 m
illion people in eastern and=soúthern
Afghanistan, about
20% of the popuatn.
..
..,.N
...
.
'N have the potentral:to becom
ethe prim
árym
ethod-.of1Drevention in
SóuthA
sia:
_,H
EA
LTH
NE
T IN
TE
RN
AT
ION
AL
AF
GH
AN
IST
AN
DIS
TR
IBU
TIO
N O
F M
OS
QU
ITO
NE
TS
UP
UN
TIL
EN
O O
F 2
000
795
322
770
406
3564
1'10
2325
695
0
2480
--
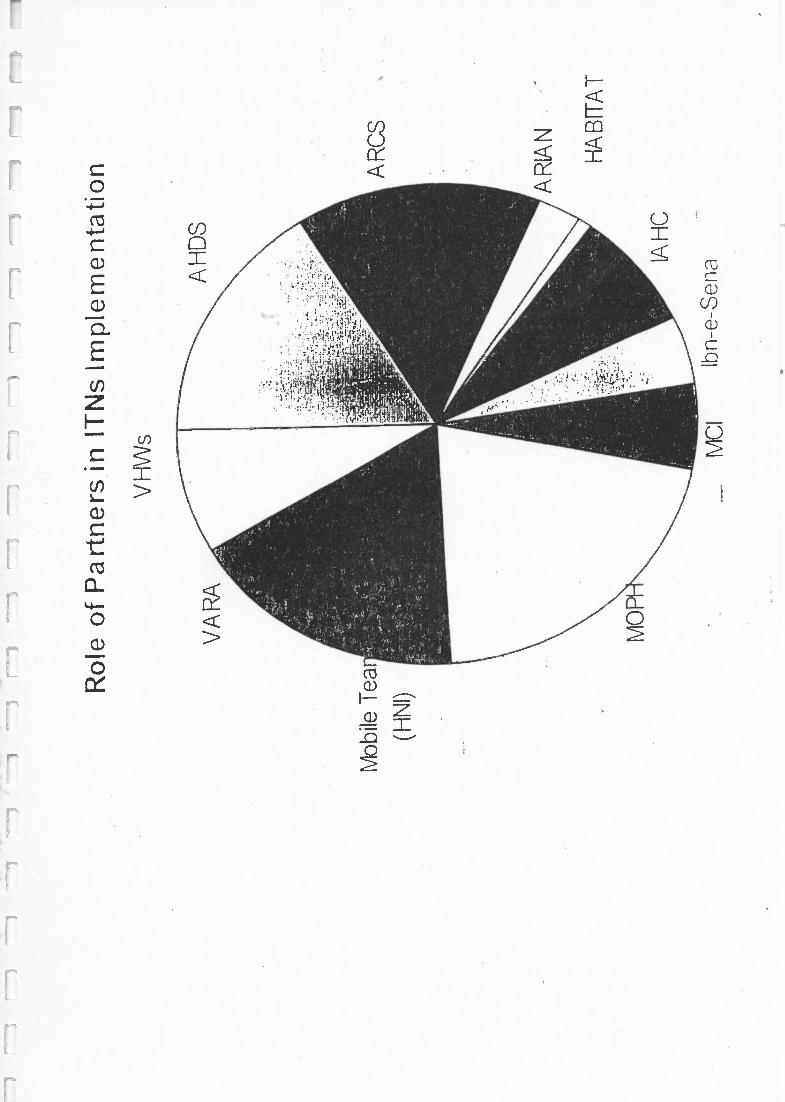
Role of Partners in ITNs Implementation
Mobile Tea
(HNI)
vHws MCI
Ibn -e -Sena
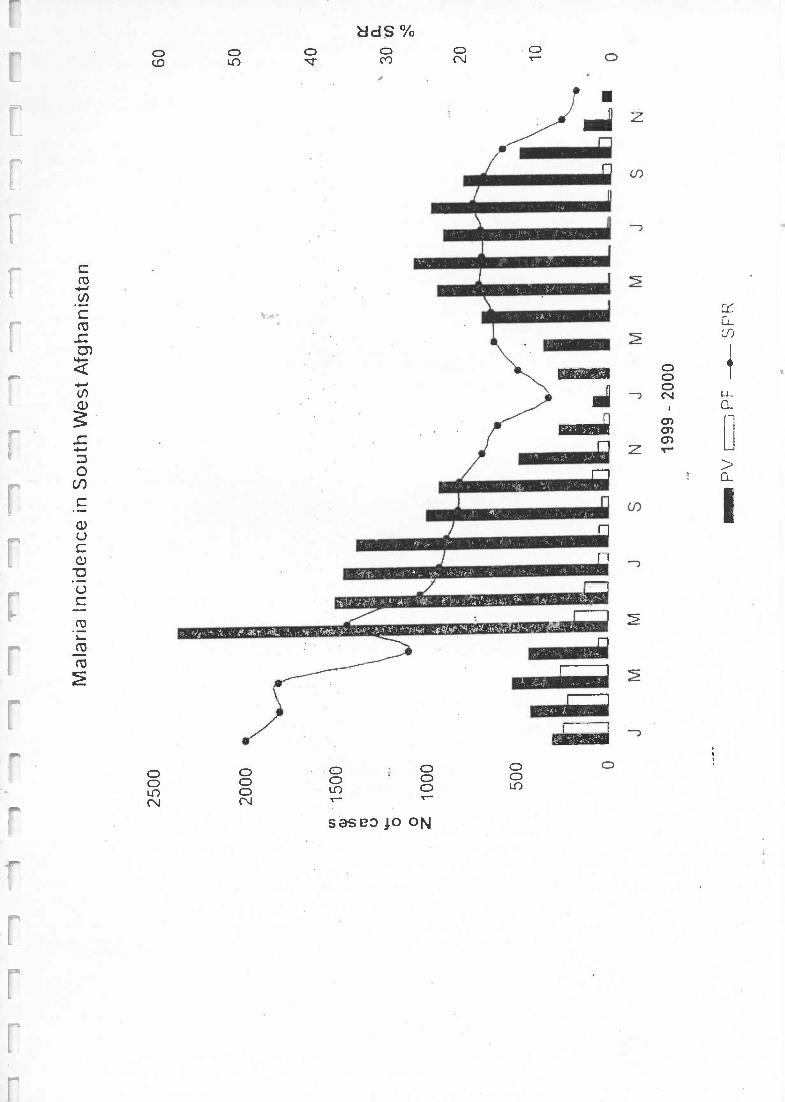
Mal
aria
Inci
denc
e in
Sou
th W
est A
fgha
nist
an
2500
60 50 40
2000
JM
M
ILJ
SN
JM
MJ
SN
1999
- 2
000
® P
V (
, P~
SP
;
30 20 10 0
11
11
11
11
11
11
11
1j
11
1
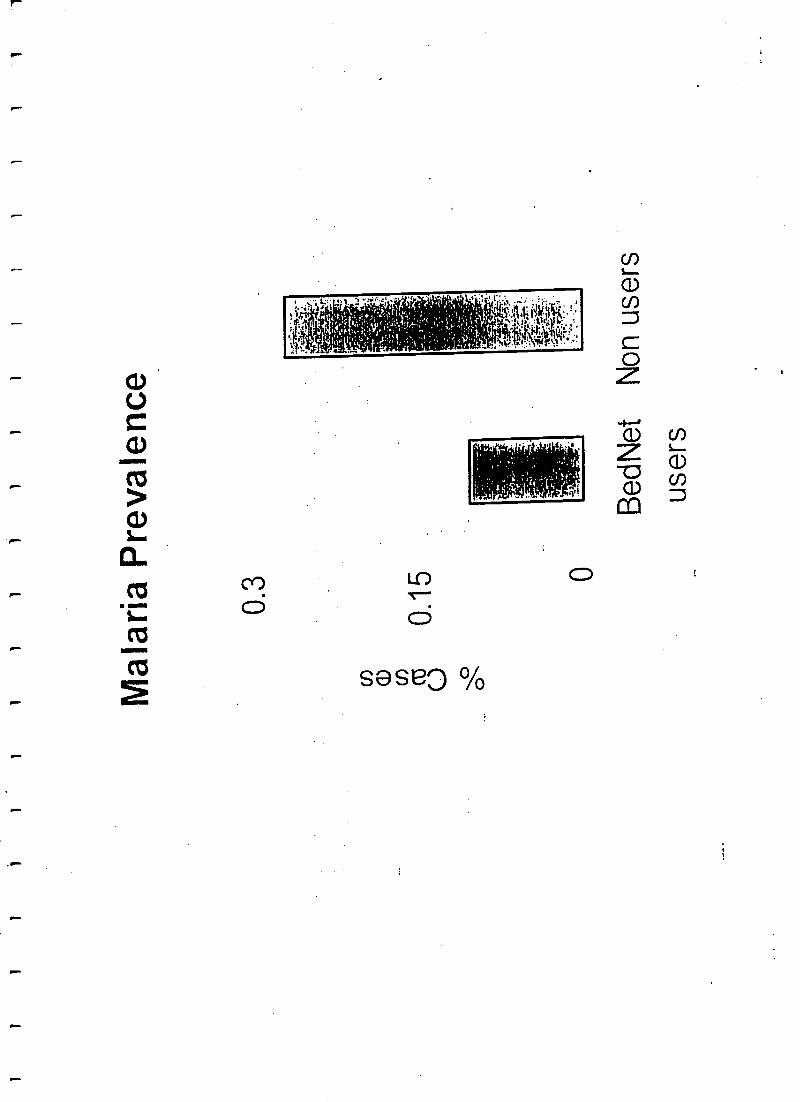
Malaria Prevalence
0.3 0
BedNet
Non users
users
úu3
70")
n
V0Ju
0u
tl
C'
a0
O
O01
>_
q:.
oO
M0000coöóöö.ööoO ci O O O O O O O O O O
Cri
Nr;óót.
O O O Or.orninnTrorinMoon
O O ci O O O O O 0 0 0 o 0
r
0
..-a.,zz.
o 000000000000M011100NNO 0 0 0 0 0 Ci O O O O O ci .-i O o 0 0
O.-,0 0 0
.-+'-+.i0 0 0 0
O.M0 0
O r+000 0 0
1-
d O
o>a
000OOOOo000000NO N O
OoNNO O
OMr'1 VO o d O d O 0
V0
CD
0(1
0QMOOrd 0 0 0 G G
IoáÓÓÓÓÓCiÓOrvrtÓ.-looiÓÓÓ.-;ivÓÓr,iuicó
0
o O r M o 0 0 ó ln all r o Mn rn o r o ln o 0 0 o M N
,,.00OO00000r.000rOMO000000NóÓÓÓÓÓÓÓÓÓÓÓÓÓÓIPtr1ÓÓÓÓÓÓÓÓÓÓkDo
OONON CG
Ó
]oOOr.óÓÓÓÓ0
M0000tT00vrOrNÓCi uirJ,,ÓÓ.-iuriÓÓÓÓrvarÓÓ,-iui.-i
V1DO1
000MOOOMMUI rn-
C17
rT0á
-
>u1010M000OOOMOOOOOtCOCilrV0000ÓÓ0
V'ririr'v1Ñ,MMV'
;
NOhOOO000áÓÓÓÓOÓÓÓÓr,.rV,-rÓÓtf.;00fV
CL! M0000oNU1.-1 t0M
,
Mrv
]NOOMOOOOONMO000)NNCL Or:N ci ci ci ci ci ci v5NN.-t ri ci h.-t
oO
t^
r;:,
.
CO
1Tro
>c.o3rrroccruoc?tn:.-vlJOirZZZÚÚÚQtJiIQ.ÚÚÚÚEÚÚÚÚÚÚÚÚÚ
Cr9
O Ñ ro
ora
N10
v1t0
rTt_ .
a.
N2.?
t0Yc
r+EC.va
ro Nx ß
Q
vLtn
E!0zL
t_ t_ t_ C7 L.
, a+ 112 r0 a.+CCCC cCCCCCCCL..+ ti_
t0 Ñ a-. i,_ oL
°
`O
rEErcoccctxoto333c'c^aivto2a,ñv!aÑo33t-Q,Q`OOOYYEEEááiñíLntLirf
L.
rororovtarororaw.L t0 N N 'ID
c,
cflLc
Q).
ñúE-°c3..,xÑmtac'QmC7C7zO0'Ol7zZÑQ
úC5pL.:
L(13 r0UDUU27ßUUTaUCta r0Y
t L2rfl
C CIV
Y Y
r0
Cr0 r0Y
2N taC
t0
L
Cto
Ltv
C
L10
Cta
t0
Ct0 r0
Lta
C
Ca
Cta
tt0
CN t0
L0
C
C Lt0 t0 la
C Cno t0 to
L210
Cr0
Y
LCO
C Ct0
Y Y
L C C C C gt0 rt t0 r0 t0 _EEEEDC O OMt0 Gl aJ Ñ ßJ t_ taY I I I IDD r0
NtL
r̀p.0 C0 t0
ECto ÑY I
C0E4JI
Cr0
E41I
N LO r0
E Cr0
Z YO(-I
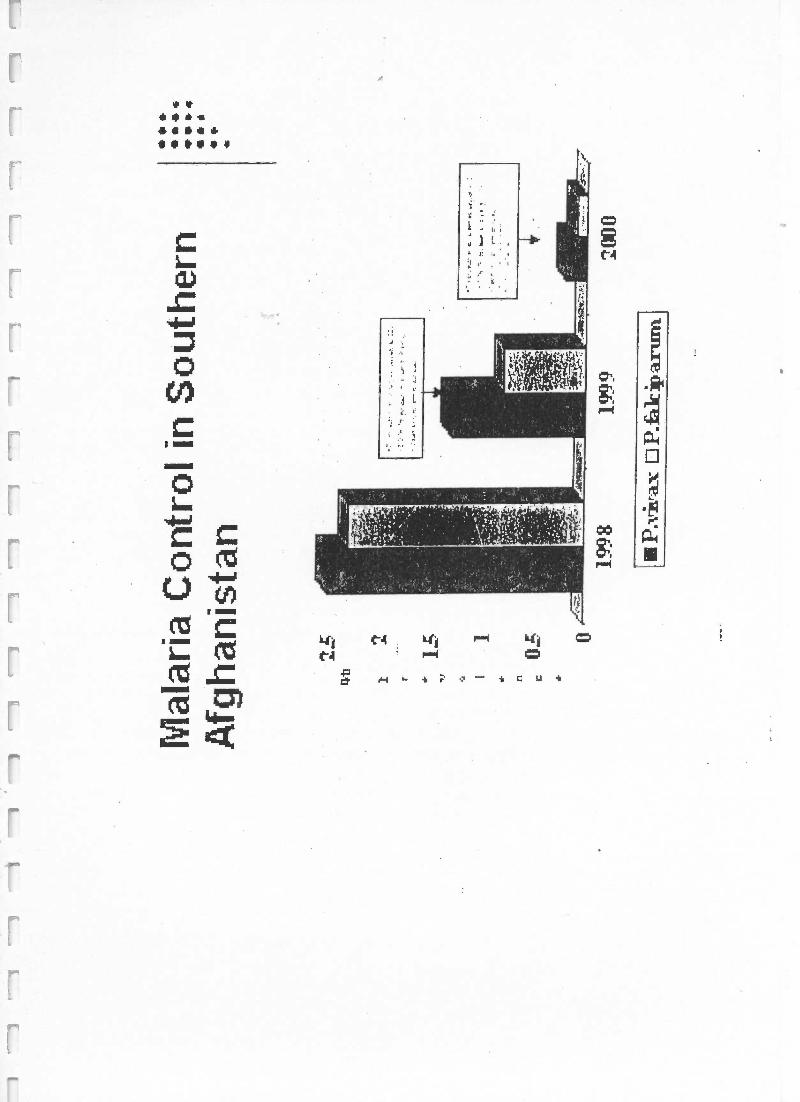
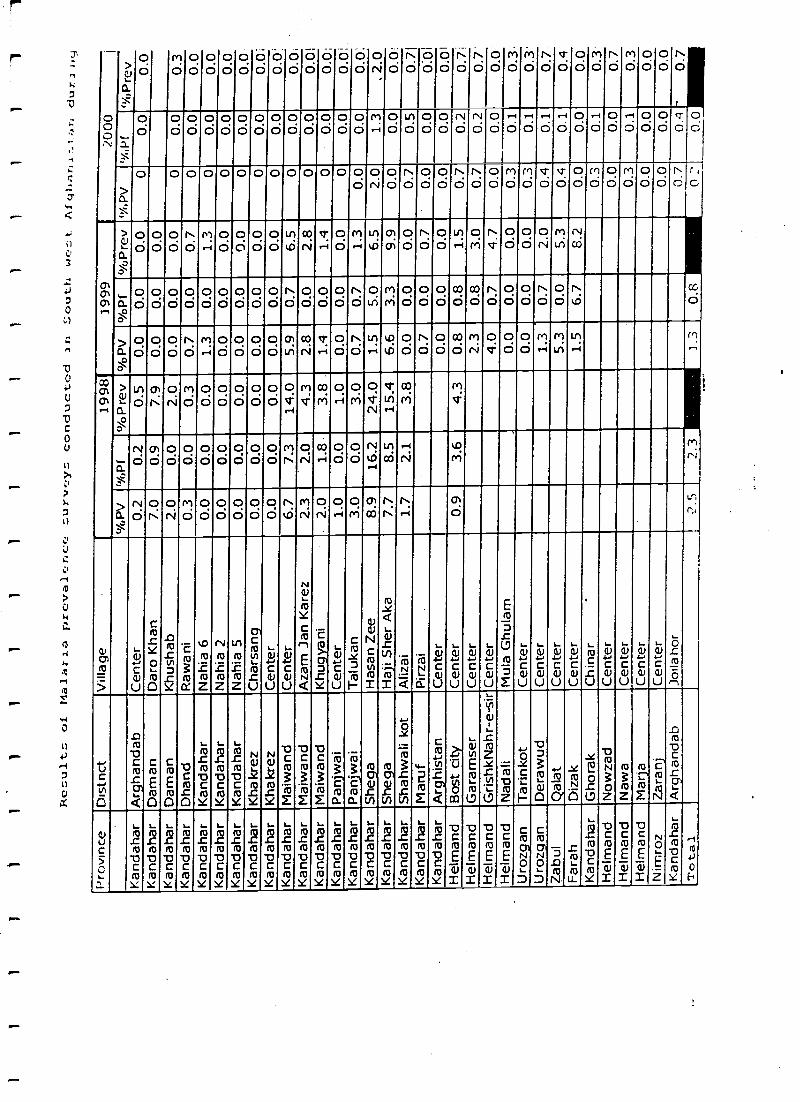
Mal
aria
Con
trol
inS
outh
ern
Afg
hani
stan 19
9819
99
PArá
r:ax
P.fa
k ip
:aru
m.
2000
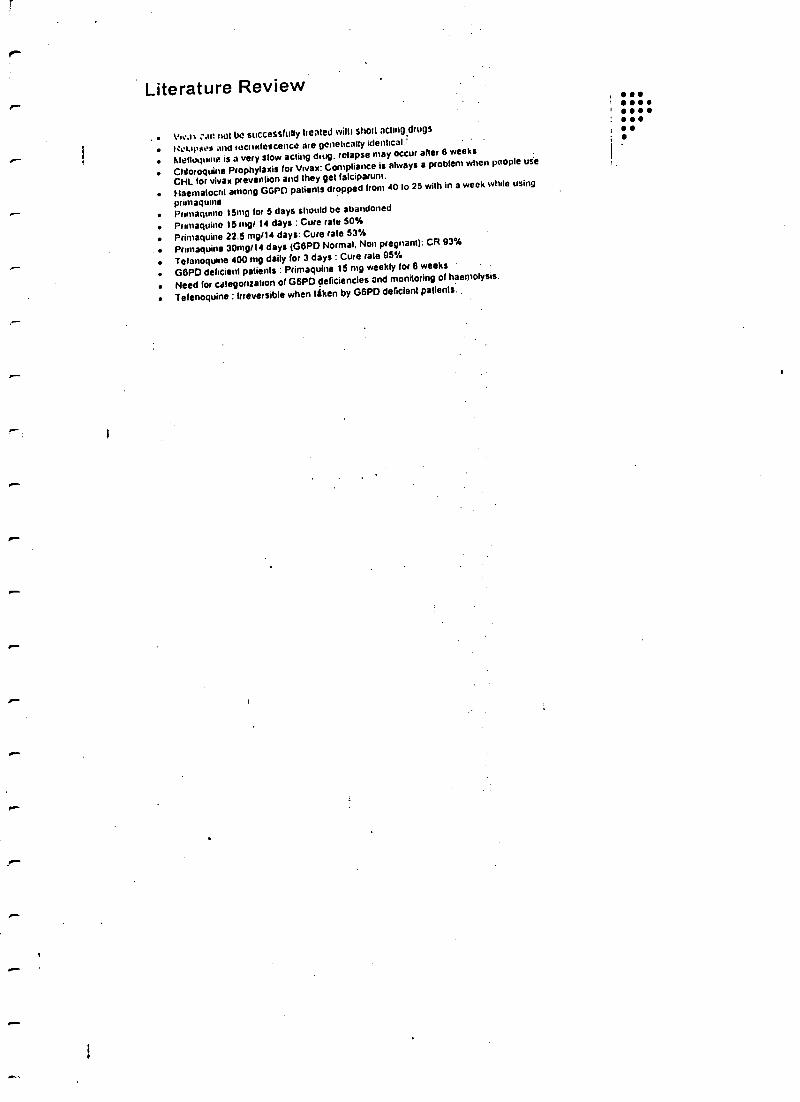
Literature Review ... not be successfully Healed will) shat acbnO.drugs
WWClrrdescence are genetically identrcal.i
Atehuquuue is a very slow acting dung. relapse may occur after 6 weeks
Chloroquine Prophylaxis for Vrvax: Compliance is always a problem when people use
CHL for vivax prevention and they get falciparum.
Haematocnt among G6PD patients dropped from 40 lo 25 with in a week while using
primaqusnePrimaquine 15mg for 5 days should be abandoned
Primaquine 15 mg/ 14 days : Cure rate 50%
Primaquine 22.5 mg/14 days: Cure rate 53%
.. Prmaquine 30mg /)4 days (GGPD Normal. Non pregnant): CR 93%
Telanoquine 400 mg daily for 3 days : Cure rale 95%
G6PD deficient patients : Primaquine 15 mg weekly for 8 weeks
Need for categorization of G6PD deficiencies and monitoring of haemolysis.
Tefenoquine : Irreversible when liken by G6PD deficient patients.
)1
11
11
?1
11
11
11
11
11
1
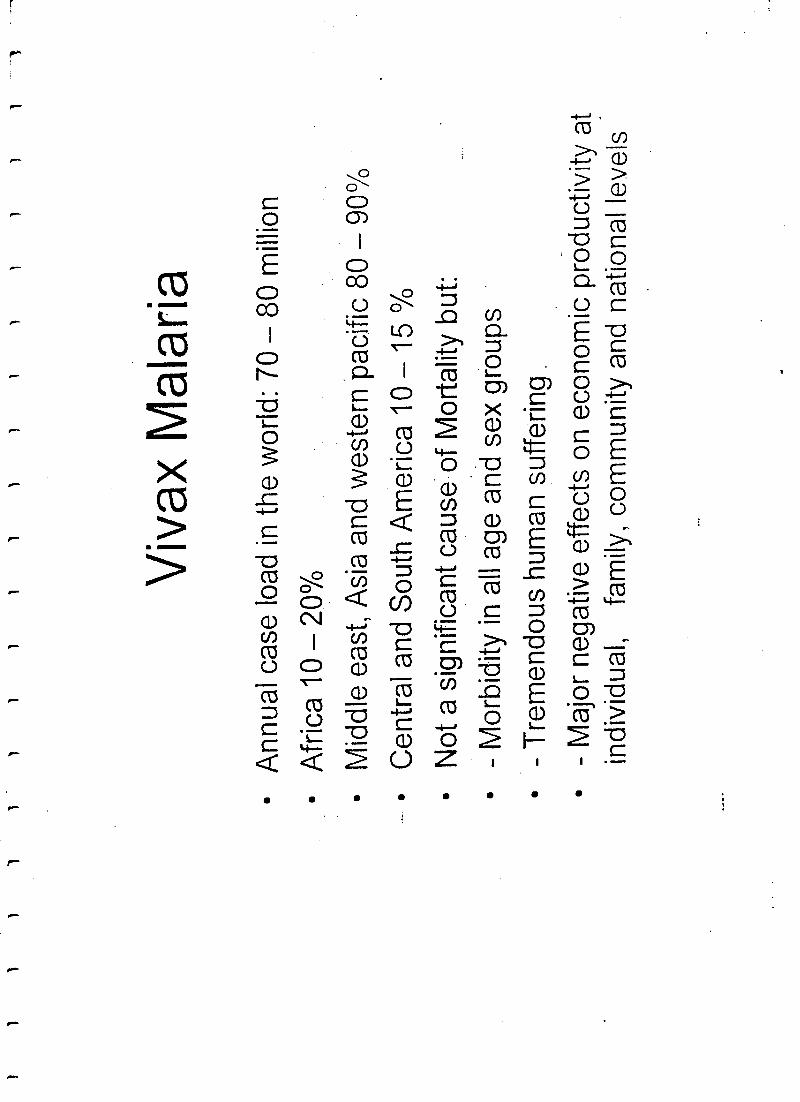
Viv
ax M
alar
ia
Ann
ual c
ase
load
in th
e w
orld
: 70
- 80
mill
ion
Afr
ica
10 -
20 %
0
Mid
dle
east
, Asi
a an
d w
este
rnpa
cifi
c 80
- 9
0%C
entr
al a
nd S
outh
Am
eric
a 10
-15
Not
a s
igni
fica
nt c
ause
of
Mor
talit
y bu
t:-
Mor
bidi
ty in
all
age
and
sex
grou
psT
rem
endo
us h
uman
suff
erin
g.
- M
ajor
neg
ativ
e ef
fect
s on
eco
nom
ic p
rodu
ctiv
ity a
tin
divi
dual
,fa
mily
, com
mun
ity a
nd n
atio
nal l
evel
s
)1
11
1l
11
11
11
11
11
11
1
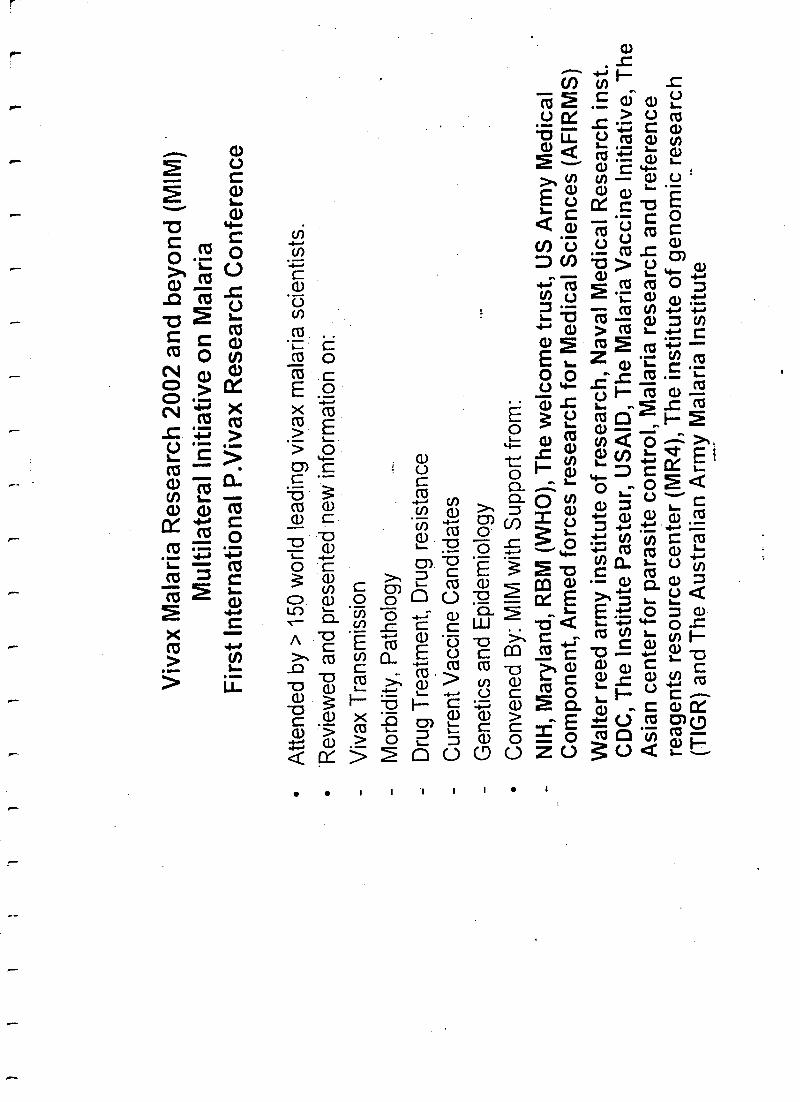
Viv
ax M
alar
ia R
esea
rch
2002
and
bey
ond
(MIM
)M
ultil
ater
al In
itiat
ive
on M
alar
iaF
irst I
nter
natio
nal P
.Viv
ax R
esea
rch
Con
fere
nce
Atte
nded
by
> 1
50 w
orld
lead
ing
viva
x m
alar
ia s
cien
tists
.
*Rev
iew
ed a
nd p
rese
nted
new
info
rmat
ion
on:
Viv
ax T
rans
mis
sion
Mor
bidi
ty, P
atho
logy
Dru
g T
reat
men
t, D
rug
resi
stan
ce
Cur
rent
Vac
cine
Can
dida
tes
Gen
etic
s an
d E
pide
mio
logy
Con
vene
d B
y: M
IM w
ith S
uppo
rt fr
om:
NIH
, Mar
ylan
d, R
BM
(W
HO
), T
he w
elco
me
trus
t, U
S A
rmy
Med
ical
Com
pone
nt, A
rmed
forc
es r
esea
rch
for
Med
ical
Sci
ence
s (A
FIR
MS
)W
alte
r re
ed a
rmy
inst
itute
of r
esea
rch,
Nav
al M
edic
al R
esea
rch
inst
.C
DC
, The
Inst
itute
Pas
teur
, US
AID
, The
Mal
aria
Vac
cine
Initi
ativ
e, T
heA
sian
cen
ter
for
para
site
con
trol
, Mal
aria
res
earc
h an
d re
fere
nce
reag
ents
res
ourc
e ce
nter
(M
R4)
, The
inst
itute
of g
enom
ic r
esea
rch
(TIG
R)
and
The
Aus
tral
ian
Arm
y M
alar
ia In
stitu
te
}1
}
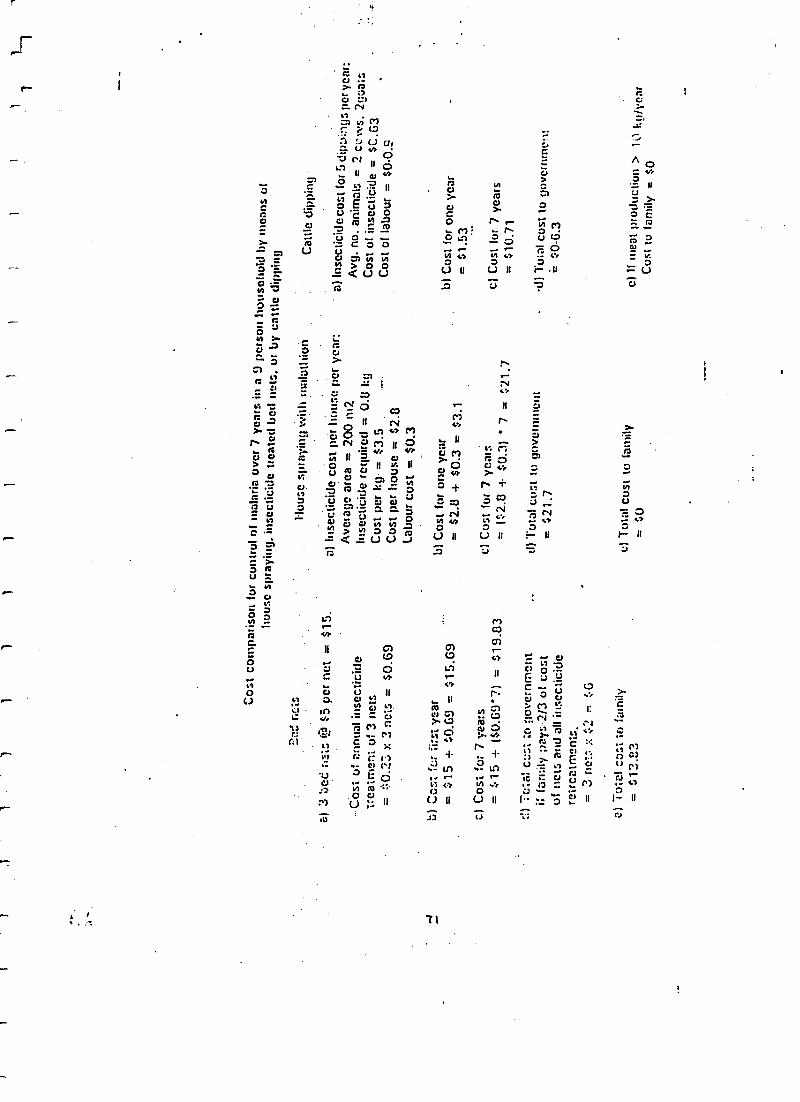
Cos
t com
paris
on fo
r co
ntro
l of m
alar
ia o
ver
7ye
ars
in a
9 p
erso
n ho
useh
old
bym
eans
of
hous
e sp
rayi
ng, i
nsec
ticid
etr
eate
d be
d ne
ts. o
r by
cattl
e cl
ippi
ng
al 3
;,et
. ;,_
is 0
23 5
5 pe
r ne
t=
515
.
Cos
t of a
nnua
l ins
ectic
ide
trea
tmen
t of 3
nEtS
= =
:C.2
3 r.
3 n
ets
= $
0.69
b) ..
c :i
::.r
fi:si
yea
r=
S15
y50.
fì9=
515.
69
;) C
os: f
or 7
,.ea
rs=
$15
y (
$0.6
9'7)
= $
19.8
3
Tet
a: c
ri :o
gov
ernm
ent
if fa
mily
;ray
s -2
/3 o
f cos
tof
net
a an
d al
l ins
ectic
ide
retr
eetm
enis
. $23
= $
6= -.
,net
...,
--
e) T
otal
cos
t to
fam
ilyr,
13.2
3J.
2J )
Hou
se s
pray
ing
Via
l mal
athi
oit
a) In
sect
icid
e co
st p
er lo
ose
per -
year
:A
vera
ge a
rea
= 2
00 n
i?.
Inse
ctic
ide
requ
ired
= 0
.0 k
gC
ost p
er k
g =
$3.
5.
---
Cos
t per
hou
se=
$2.
8La
bour
cos
t = $
0.3
L) C
ost f
or o
neye
ar=
52.íl
4.$0
.3 =
$3.1
c) C
ost f
or 7
yea
rs=
($2
.8 -
1-$0
.3)
' 7 =
$21
.7
tl) T
otal
cos
t to
gove
rnm
ent
= 5
21.7
Cat
tle d
ippi
ng
l
]
a) I
nsec
ticid
eco
st f
or5
dipv
:ags
per
year
:A
vg. n
o. a
nim
als
= 2
cc
ws.
2gu
ats
Cos
t of i
nsec
ticid
e=
5C
.û3
Cos
t of l
abou
r=
50
-0.9
b) C
ost f
or o
neye
ar=
$1.
53
c) C
ost f
or 7
year
s=
510
.71
.d)
Tot
al c
ost t
ogo
vern
mt v
.=
$0
-6.3
el T
otal
cos
t to
fanc
ilye)
If m
eat p
rodu
ctio
n>
1kg
/yea
r=
$0
Cos
t to
fam
ily =
$0
r_
)
r-
r^
4,
I KANSACt'lttNS Ol'7'tIL Rt)YAI, tiOCllrl'Y t)IJ'morn :At .MI?ItICINI: At ,': tttl:Nti (1999) vJ, Ir.s 172
Perinethrin- treated chaddars and top -sheets: appropriate technology for
protection against malaria in Afghanistan and other complex emergencies
Mark ltowhurd''', Nnecnt 1)urrnni', Senn Hewitt', Nnsir Mohammed', Menno Houma', Donn Caruciru', Jan
lirzcndnnl' and Alltot Schnpira' 'lleahhNet luternuriarral, I', f). /lax X89, Uaitrcrxity 7irtos,, !'cshatear, Pakistan;
i '!..',,dorr .School of 1It Klette and 'I mpicu! Ale,licirte, l.rosdnn, ir"(: / li 7117; UK; 'liwapea,, Orion Afalaria Gnom! l 'r,qr. r,
Phnom Penh, Cambodia; 'Office oldie World !!cult!, Organisation Represcrutuite, I'. O. Ilex 52, Hanoi, Vier N
AbstractInsecticide-treated mosquito nets (1'l'N)pruvide excellent protection against malaria; however, they have n
number ufahortcontings that are particularly evident in politically unstable countries or countries at war: :ia
everyone at risk can necessarily afford n net, nets may he difficult to obtain or import, nets may not be
suitnblc for ntigrnnts or refugees steeping under tents or plastic shclier. '!'here is a need in develop cleaner,
locally appropriate alternatives for the most impoverished and for victims of cnnaticx emergencies. Afghan
women, in common with many Muslim peoples of Asia, wear u veil or wrap known as a chaddur to cover the
head and upperbody.'f7tiacloth doubles 03n sheet at night, when they are used by both sexes. A randomized
controlled trial was undertaken in which 10% atilt families ants Afghan refugee camp (population 3950)
ill north- western Pakistan Ind their chaddor's and top-sheets treated with permcthrin insecticide at a dosage
of 1 g /m' while a further 10%1W their thetdrlars treated with placebo formulation. Malaria episodes were
recorded by.passive case detection at the ennui's health centre. From August to November the odds of
having a falciparum or vivax malaria episode were reduced by 64% in children aged 0- I 0 years and by 38%
in refugees aged <20 years in the group using permcthrin -trentcd choddart and top -sheets. incidence in
refugees over 20 years of age Was not significantly reduced. The cost claw permcthrin treatment per persists
bprotected (USi0.I7) was similar to that for treating bedneta (anti cost only 10 -20% of the price of n new
ednct). An entomological study simulating real-life conditions indicated that bust seeking mosalniur.%
were up to 70% lessaucceasful at feeding on then sleeping under treated rhaddurs and siontc were killed by plc
insecticide. Permcthrin-trentcd tap -sheets and blankets should provide appropriate and effective pi otectiun
from malaria in complex emergencies. In Islamic and non -Islamic countries in Asia, treated cheddars and
top -sheets should offer a satisfactory solution for the most vulnerable who cannot afford treated nets.
Keywords: malaria, malaria control, .
tulh,es, inset..lilide treated nt.iterinls, permethrin, refuµus, c pies
emergencies, Pakistan, Afghanistan
IntroductionInsectieídeIrcated nets (ITN) show potential forpreventing malaria moronity nid murbllity (At A)NMI et
al., 1991; (;111)1 a al., 1995; I)'AI.I ?.SANI )Itt 1 et al., 1995;
DINKA et at, 1996; Nt ?V11.1. et al , 1996), and are making
a significant cnniribution to the renaissance in control
initiatives such as 'Roll Back Malaria' (NAIARIto &
TAft.tplt, 19911). Social marketing projects are underway
in several countries in Africa and Asia, including Afgha-
nistan (Pin!.la)N, 1996; I.1NI?S, 1996; itt)wtsmii) et al.,
1997a). Unfortunately thepopulations most at risk from
malaria in Asia me often among the poorest. There is s
need to develop cheaperalternatives to l'i'N for the mostvulnerable wilco arc unable to bear the costs involved
(Ittltc't.l:t', I997).Malaria can he n major prohiern during war or complex
entergcnclea towing to population dlspluccment and thebreakdown of henhh services (111011/4480N, 1995; NA-
JltRA, 1996; l'l't'r et al, 1998). Logistical or culturalconstraints often preclude the 'wort or tame of ITNagainst malaria. '!here is need for simple, effectiveinterventions suitable for refugees or internally displacedpopulationa living outdoors that tin not, as n prerequisite,
require n drastic change in sleeping behaviour.Insecticide-treated wraps, tap -shccts, or blankets may
meet the needs ofboth the poverty stricken and victims of
war. Blankets arc often supplied by nid agencies duringthe acute phase of an emergency and might give protdc-
(inn against malaria if treated with a repellent insecticide.One of the most characteristic features of-Islamic socie-
ties in West and South Asia is the use of chat/days by
women to cover the head and torso when in public.
Virtually all women are veiled since this is expected by
their faith. Economic necessity often requires that chad-
dars duublc as a sheet or blanket at night for warmth or us
Address fior emirs' dame: Mork Rowland, London School of
I lygicne and Tropical Medicine, Keppel Street, London Wc; I I?
711í', UK; e-mail m.ruwlantll itlshun.nc,uki
n partial barrier against biting insects (and are also Ilse.'
by men and children for this purpose). The stsuli.%
presented here describe (i) a randomized controlledof peruletImrin trentcd e-
radd,n.e anal la p- sloets for )u..
Ieclion against tstnlaria in an Afghan refugee camp III
north -western Pakistan, aid (ii) n field experiment win linvestigates how treated ehaddars might give proles.'
against mosquitoes.
Materials anti MethodsSiutlt aras and populations
111e randomizedcontrolled trial was car led out in ti,e
Adiznl refugee settlement(population 3950) and dae
entomological study took place nt the I IcaliI Na t lut ea-
nntinnl (IINI) field centre (IItiwrrl' ei id., 1907) auAzakhel refugee settlement
(population 14 500) near
Peshawar, in north -western l'akisinit. !huh actilenrcinsore sited un waterlogged ground near the lank% ..f the
Kabul river, have existed for giver 16 years, and are highly
malariuus. I louses arc built front nmd, surrounded by :u1
open courtyard and high perimeter wall. in u style tarait al
of rural Pakistan and Afghanistan. I INI runs a hcalhcentre in Adlzai, and provides free microscopy tliattnosis
and treatment. All 510 refugee families living in Mti..ai
are registered at the centre.
ChaddarsChnildarx are uied by all refugees and serve a va iet y , f
functions during the day and night. The primary rune
for females is purdah. Chaddars arc also used as a shield
against the hot sun, for warmth ut night, and as a partial
barrier against biting insects, A typical r/rarldar is rnaaie
from cotton and measures about 3.5 m'. Around thehouse an Afghan woman may wear a dupuua, wlick is a
head scarf made of thinner material that does nut have a
purdah function. In colder months, a thin wooltiablanket (patna) is used. I'or the sake of economy many
men and women use n cotton chaddur of mediumthickness that can be used in all seasons. During the trial
all types of chat/dar, puma, and top-sheet were treated.
hua
lru,r rawnb,r .cnrc(v deign and pnicedutwThe study took place from July to Noveutlicr 1996.
Clinic records from 1495 indicated that 30% of thepopulation suffered at least one malaria episode per year(malaria case defined as a febrile, parasitacrmic episodeidentified by passive case detection). It was anticipatedthat the intervention would give less protection thantreatett nets which Have about 60'%, protection against
7a.omr,liurn,/alcipa,vre malaria in a previous study (Ruv'-IANI) ei al., 1496). On the basis of these results, we
calculated that n study involving 800 individuals inintervention and control groups would give AO% powerit, detect, ns significant at the 5 %. level, a 3O "< reductionill the incidence risk per year.'i'o achieve this stunplc size,201 of refugee households were selected using a randomnumber generator against the list of health centre familyregistration cards. It was considered that an interventiongroup of 10 % would not affect transmis ' rates in aplacebo g p of similar size nor in the remainder of thecamp population.
1meal community health workers assisted 1IN1 staffwith the field work. Family elders were invited to meet-ings where the technique was explained and the proce-dure for treating chaddars was demonstrated. It wagexplained that the treatments would protect againstmosquito biting and reduce the risk of malaria. It wascniphasiretl that treated chaddars should be kept awayfrom direct sunlight and should be washed leas frequentlythan normal, as washing reduces the potency of thetreatment.
Selected households were randomlydivided into inter-vention anti placebo groups, and if more than one familylived in a single house all families therein were allocatedto the saute treatment group. Field teams visited theselected households in the first week of August to updatethe census records and clinic registers.
The teams explained the health messages tti familymembers, treated nil char/den and top-ghetto with assis-tance from fancily members, and gave instruction on coreof treated materials. Materials of the intervention groupwere treated with permeihrin ('Imperator' 25% íìC,7-enecs, Elnstctttere, UK) to give an estimated targetdose of I.O g /ms (0 I mg /erns). Materials of the controlgroup were treated with a placebo liC formulationsupplied by Zencca that lacked the active ingredient.Field workers were under the assumption that lothplacebo and permetlrrin were effective. health centrestaff did not know which families were in which group.
Prior to treatment, samples of chaddars were tested forwater absorbency. On the basis of titis, 2 dilutions ofinsecticide were used, one for coUan (0.15 1. /rnr) andline far woollen materials (02 L /ens). ChadJurx come invarious sizes, 'Fit avoid the need to measure individualsurface areas, chaddars were dipped in un excess ofinsecticide solution in plastic washing -up bowls, endthe excess was simply wrung out.
'Friel families were encouraged to use the health centrehut were not treated any differently from other membersof the camp. All suspected malaria cases were given apresumptive dose of chloruquine (10 mg/kg body -weight) while awaiting the microacopist's verdict. Con-firmed cases were treated with a total of 25 tagchluroquine /kg butlyweight over 3 days. Falcipantmmalaria treatment failures were re- treated with sulfadox-ine - pyrintethantine.
'l'wu.montits after the insecticide treatment, the fieldteams revisited the trial families to re-emphasize thehealth messages and to maintain a spirit of involvement.The trial finished at the end ofNovember after 16 weeksof passive surveillance.
Sriol tun, ySurveys on the experiences and practices of the trial
families were carried out in December using a structuredquestionnaire. An adult male or female was interviewedfrom each of the 102 trial fatuities.
MAKI:. It, V:'I ANO Li
liruonrologicnl studiosThe principal experiment was an attempt to simulate
man- vector contact during the summer when peoplesleep outdoors in their compound courtyards. It wasconducted under 4 giant net traps (length 6 in x width5 m X height 2 m), similar to those described by Stitt.%twit (1993), into which mosquitoes could he reicnged.The net traps were suspended over ant-free platforms sothat the sides would form o good seal when lowered to theground. The idea behind the net traps was to preventmosquitoes from escaping after attempting to feed.Scavenging ants were kept out by a water-filled humai
(0.2 in wide) surrcninding each test platlinnn. The plat-forms were spaced 10 in apart. Adjacent to each piatfo. nh
was a pen fur holding a cow.A week before the start of the experiment, roman
chaddars (length 2.5 in, width 1.5 rn) were dipped in
placebo or perniethrin ('imperator' 25% 1 C) solution togive target hoses of0,0.5, 1.0 end 2.0 g active ing'edicntper mis.
The sleeping arrangement* during time experimentresembled normal practice. At each platform shortlyafter dusk 2 Wren took up their positions, lying onwooden -framed beds known as charpois, and coveredthemselves with a chaddar from head to foot. Beneath thechaddars they wore their normal clothes (shalwar che-mises). The floors of the platforms were cnvercd withwhite sheets.'iltc sides of the net traps were then loweredto the ground. Cows were positioned in the nearby penswhich were then covered with untreated mosquito nets.Host -seeking mosquitoes were collected with aspiratorsthroughout the night from the outside orate net trapa andcattle -baitcd nets and intermittently released into the nettraps. At dawn dead mosquitoes were collected from thefloor sheets while live mosquitoes werecollected front theinner surfaces of the net traps and kept in humidifiedcages for a 6 -h holding period before separation into dead
anti alive. The coliecuuns were then sorted into hluodfedand unfelt groups, and the nuophciines identified tospecies.
The experiment was conducted over 16 nights duringSeptember 1997. Each of the 4 treatments was evaluatedat each of the 4 sites on 4 separate occasions using 4 pairsof men in rotation.
At the end of the simulation experiment, cone bioassaytesta were undertaken using wild -caught /his/Arks arc -pinuisi to aasces the toxicity attic treated fabrica. Fifteenmosquitoes were exposed it each cone, and the timetaken to knock down the median mosquito was recorded.The bioassay was replicated 5 times on a single day ondifferent parts of the chaddars.
Statistical analysisData were analysed using Epiisifu 6 and Stara 5.
Entomological data were converted to propanions,arcsin transformed, and subjected to analysis of varianceand multiple range tests. Cases ofmicrhscopy- confirmedmalaria recorded in the clinic registers were analysedusing logistic regression. Only the lint reported episodeof vivax and falciparum malaria for each person wasincluded in the analysis since many individuals reportedmore than once id a result of relapsed infections.
Results .
Malaria preventionin alt, 102 households and 825 individuals were
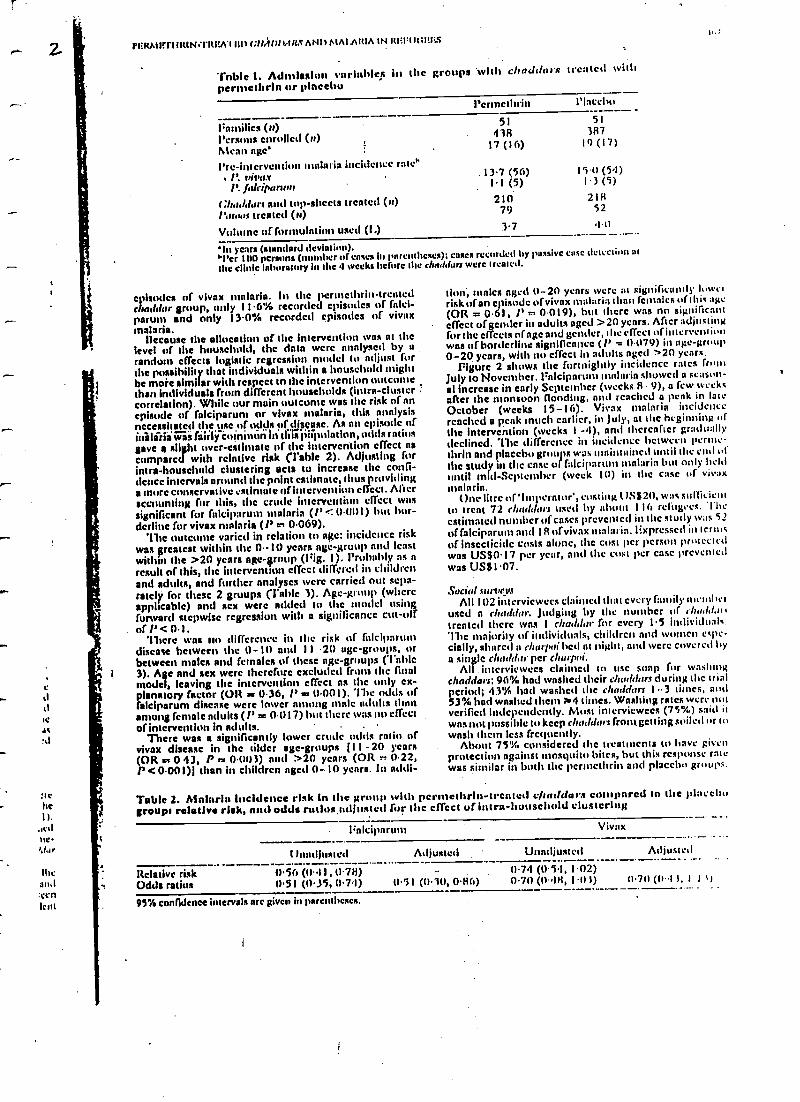
enrolled. The admission variables were similar in theperniethrin treated and placebo groups (Table 1).
Analysis of health centre microscopy records confirmedthat the incidence of malaria was similar in the pernte-thrin and placcbó groups i{i the month preceding chaddartreatment.
The microscopy records showed that 20.7% of theplacebo group recorded one or more symptomatic andparasitacntic episodes of falciparum miliaria betweenAugust and November, and 17.6% recorded equivalent
t'EItM1lfrluRtt4- 11tr(AY tat (.11,41111.111S AND Al/VAR:A IN RI!IRt;l!)i.S
Table 1. Admission nrinhleR in the groups with clraddor:s treated withperntcthrin or placebo
l'crtncthrin Placebo
I ;amities (n)Persons enrolled (n)
51438
51387
Mean age' 17 (16) 19 (17)
Pre-intervention malaria incidence rate". P. vivax . 13.7 (56) 150(54)
1' falcipars ni 1.1 (5) I3 (5)
Chad/dun and top -sheets trcntcd (n) 210 218
Mow treated (n) 79 52
Volume of fi,nnulntion usent (14 3.7 4.41
'In years (standard deviation).'l'er 100 persona (manlier of cases in parentheses); cases recorded by passive ease detection at
the clinic laboratory in like 4 weeks before the chrtd fars were treated.
c +)sodas of vivax malaria. M the pernethrin- treatedchat6lar group, only 11.6% recorded episodes of fnlei-parum and only 13.0% recorded episodes of vivaxmalaria.
Ileesuse the allocation of the intervention was nt thelevel of the household, the data were analysed by nrandom effects logistic mires ' model to adjust forthe possibility that individuals within a household mightbe more similar with respect to the intervention outcomethan individuals from different households (infra- clustercorrelation). While our main outcome was the risk of anepisode of falciparum or vivax malaria, this analysisnecessitated the use of otitis of dlsçuse. As an episode ofinòläri wa (áíríÿ coininon in this Ambition, odds ratiosgave a slight over -estimate of the intervention effect nscompared with relative risk (Table 2). Adjusting forinfra -household clustering acts to increase the confi-dence intervals around the point estimate, thus providinga more conservative estimate of intervcnt' effect. Mieraccounting for this, the crone intervention effect wassignificant for falciparum malaria (P 0.001) hut bor-derline for vivax malaria (!' 0.069).
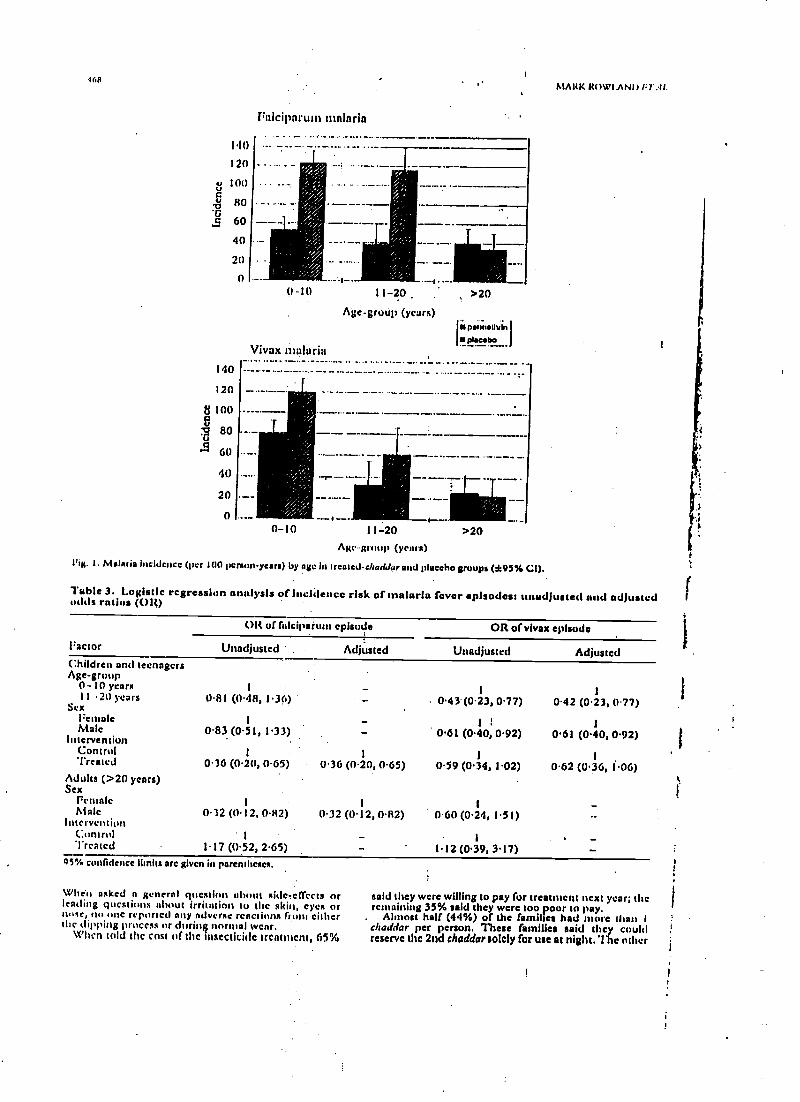
'the outcome varied in relation to age: incidence riskwas greatest within the 0.- 10 years age -group and leastwithin the >20 years age-group (Pig. I). Probably as nresult of this, the intervention effect differed in childrenand adults, and further analyses were carried out scpa-rately for these 2 groups (fable 3). Age-group (whereapplicable) and sex were added to the model usingforward stepwise regression with a significance cut-offof P < 0.1.
'there was lin difference in the risk of falciparumdiscace between the 0-10 and I I 20 age- groups, orbetween males and females of these age- groups ('Table3). Age and sex were therefore excluded from the finalmodel, leaving the intervention effect as the only ex-planatory factor (OR as 0.36, P = 0.001). The odds offalciparum disease were lower n g male adults thanamong female adults (1' = 0.017) but there was no effectof intervention in adults. .
There was a significantly lower crude odds ratio ofvivax disease in the older age- groups j I i - 20 years(OR et 0 43, P == 0.0(13) and >20 years (OR ' 0.22,P <0.001)I titan in children aged 0 -10 years. in addi-
tl.
lion, nudes aged 0-20 years were at significantly luwrtrisk of an episode of vivax malaria than females of this :,Kc(OR = 0.61, 1' Ir. 0.019), but there was no significanteffect of gender in adults aged >20 years. After adjustingfor the cheats nfagc and gender, the effect of interventionwas of borderline significance (/' = 0.079) in age -group0 -20 years, with no effect in adults aged "20 years.
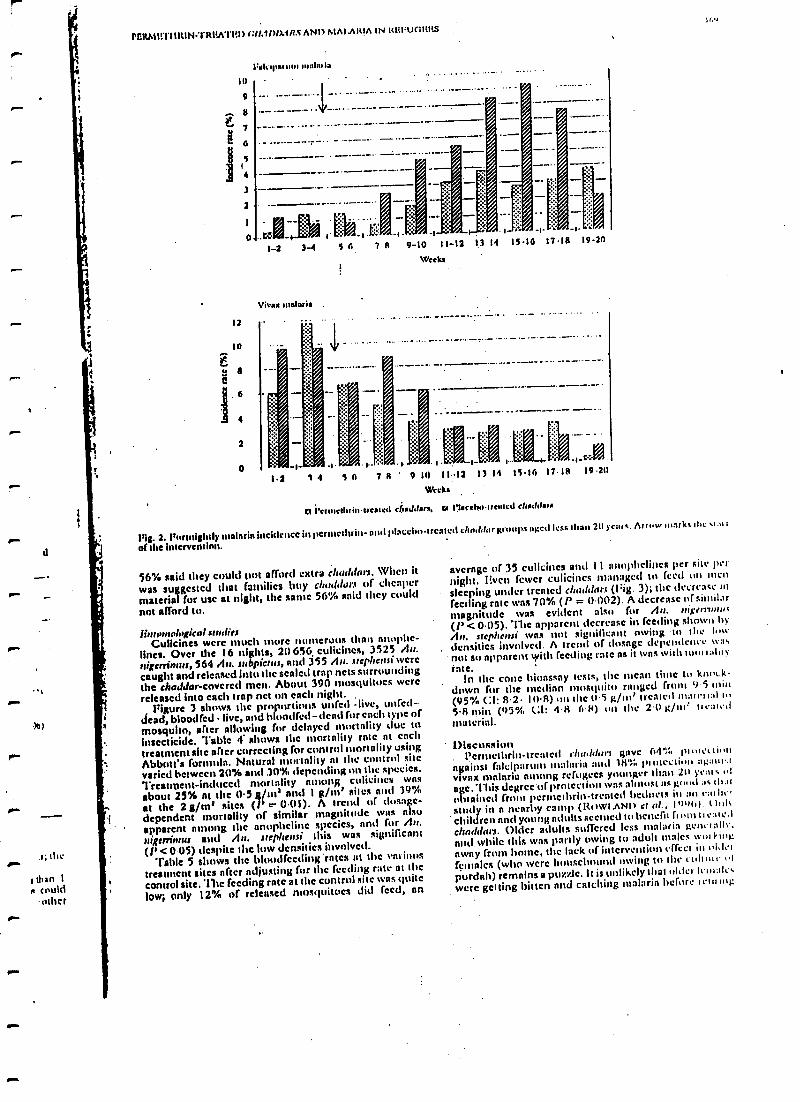
Figure 2 shows the fortnightly incidence rotes fromJuly to November. Fnlciparum malaria showed a scason-al increase in Burly September (weeks 8 9), a few weeksafter the monsoon flooding, and reached a peak in late
October (weeks 15 -16). Vivax malaria incidencereached a peak much earlier, in July, at the beginning ofthe intervention (weeks 1 -4), and thereafter graduallydeclined. The difference in incidence between venne-thrin and placebo sumps was maintained until the end ofthe study in the case of !McMartin' malaria but only helduntil rid -September (week 10) it the case of vivaxmalaria.
One litre of'Itnpernieir', east Mg 1/S820, teat sullit lean
to treat 72 cluuldurs trsetl by about 116 relti evt. Theestimated ntunhcr (daises prevented w the study wars 52
of falciparum and 18 of vivax maim in. Expressed in tenusof insecticide costs alone, the cost per person protectedwas US$0.17 per year, and the cost per case preventedwas US$I.07.
Social lurvevsAll 102 ititcrviewces claimed that every fancily nu. other
used n churldor. Judging by the number of thodd,n,treated there was I clraddur for every 1.5 individuals.The majority of individuals, children and women espe-cially, shared a rhur/,ui bed at night, and acre covered bya single clraddar per chupoi.
All . interviewees claimed to use snap fur washingchar/dam: 96 %, had washed their chuddart during the trialperiod; 43'% had washed the clurddars I -3 tintes, nod53 %, had washed them P.4 dines. Washing rates were nutverified independently. Most interviewees (75'%,) said itwas not possible to keep chadduts front getting soiled or towash them less frequently.
About 75% considered the treatments to have givenprotection against mosquito bites, but this response ratewas similar in both the permethrin and placebo groups.
Table 2. Malaria incidence risk in the group with perntethrltt- trcntcd c /iaddas compared to the placebogroups relative risk, and odds rutlos,m1Jostctl for the effect of infra- houschultl clustering
I;alcipnrum
l /mullioned Adjusted
Viva x
Unadjusted Adjusted
Relative riskOdtls ratios
(pi(' (0)I, I)711)llS 1 (1)15, 0.74) 051 (0.10, 086)
074 (054, I.02)0.70 (1í.4K, I.01) 07(1 ((1 4S, 1 11)
95% confidence intervals are given in parentheses.
1611
I4O
I20
100
8O
60
40
20
140
120
100
G 80
S 60
40
20
0
0
Itnlcil)arum malaria
O -10
Vivax malaria
11-20
Age -group (years)
>20
IIS psùnauu4,
spaesbo
0-10 11 -20
Age-group (years)
l'ig. I. Malaria Incidence (per 100 person- years) by age in heated- chaddar and placebo groups (f95% Cl).
>20
MAItK It()1K'I .ANI
Table 3. Logistic regression nnalysis of incidence risk of malaria fever episodes: unadjusted and adjustedodds ratios (Olt)
Olt of fa lciparwn episode OR of vivax episode
Factor Unadjusted Adjusted Unadjusted AdjustedChildren and teenagersAge -group
0-10 years1 1
I I 20 years 0.81 (0.48, 1.36) 0.43(0.23, 0.77) 0.42 (0.23, 077)SexFemale 1 11 1Malc 0-83 (0.51, 1.33) 0.61 (0.40, 0.92) 0.61 (0.40, 0.92)InterventionControl
1 1 1Treated 0.36 (0.20, 0-65) 0.36 (0-20, 0.65) 059 (0.34, 1.02) 0-62 (0.36, i 06)Adults ( >20 years)Sex
Female 1 1
Male 0.32 (0 12, 0.82) 0.32 (0.12, 0-82) 0.60 (0.24, 1.51)Intervention
Control iTreated 1.17 (0.52, 2.65) 1.12 (0.39, 3.17)
Q5"% confidence limits arc given in parentheses.
When asked n general question cd sicle-ef)eets orleading questions about irritation to the skin, eyes orwise, no line reported any adverse reactions front eitherthe dipping process or during normal wear.
When told the cost of the insecticide treatment, 65%
said they were willing to pay for treatment next year; theremaining 35% said they were too poor to pay.
. Almost half (44 %) of the families had More than 1
chaddar per person. These families said they couldreserve the 2nd chaddar solely for use at night. The other
pm.
r
P".
lol
00.
d
thes..I than 1s could
otherto.
P1?RMlrlI11tIN= IRI£ATI£n) r:lf.11)1)AH.tANI)MAI ARIA IN Itl£I UC)I£t'.S
12
10
a
4
2
o
I:aIripatum matarla
1 -2 3 -4 $ 6 7s 9-10 11-12 1,1 11
Wee kí
15 16
1.2 14 S6 7R 9 11 12 3 14 IS 16
Weeks
n l'eunethriu.treated chaddars. so l'lacebnueotcJ cludde,
7.18 19 20
1::
1118 19.20
Fia. 2. Fntwialuly malaria incidence in itermethrin- and placebo -treated chnddargroups aged less than 21) ycate. Armes nt rk. il e.i: i t
of the intervention.
56% said they could not afford extra cheddars. When it
was suggested that families buy cbuddems of cheaper
material for use at night, the same 56% sold they could
not afford to.
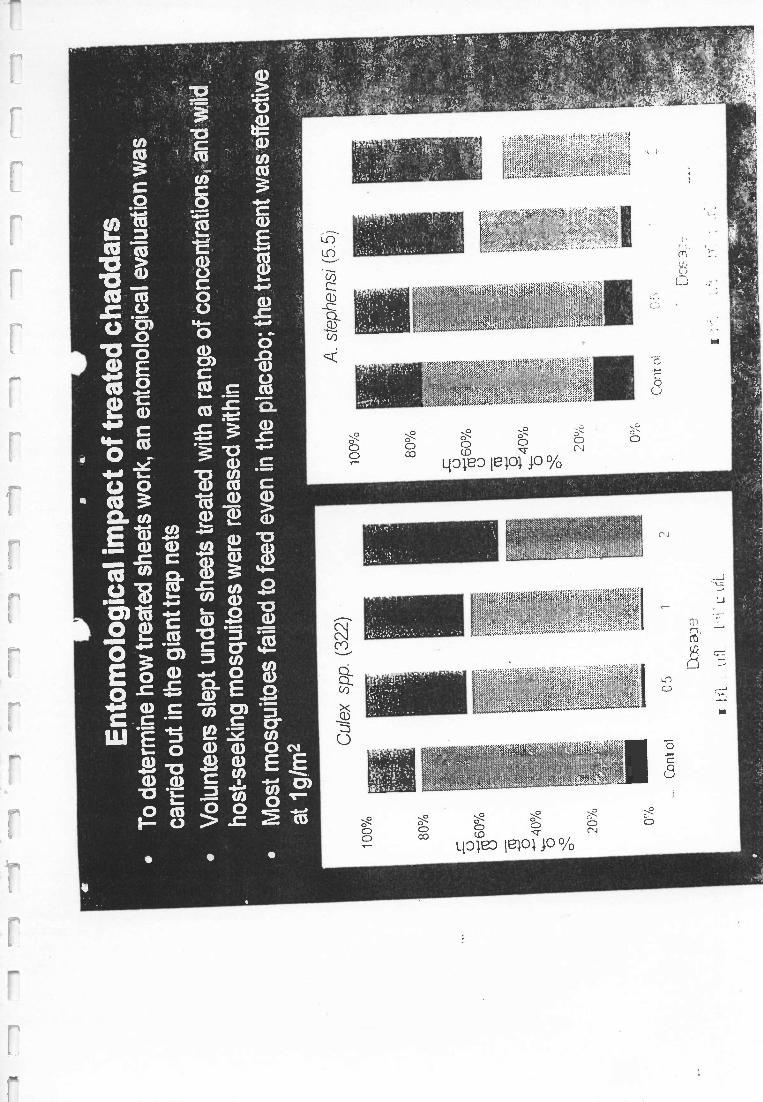
lint logical undiesCulicines were much More numerous than nnophe-
lines. Over the 16 nights, 20 656 culicincs, 3525 An.nigerri)n es, 564 An. subpicnr.y end 355 An. srcphcnsi wcrccaught and released into the sealed trap netssurroundingthe cheddar-covered men. About 390 mosquitoes werereleased into each trap net on each night.
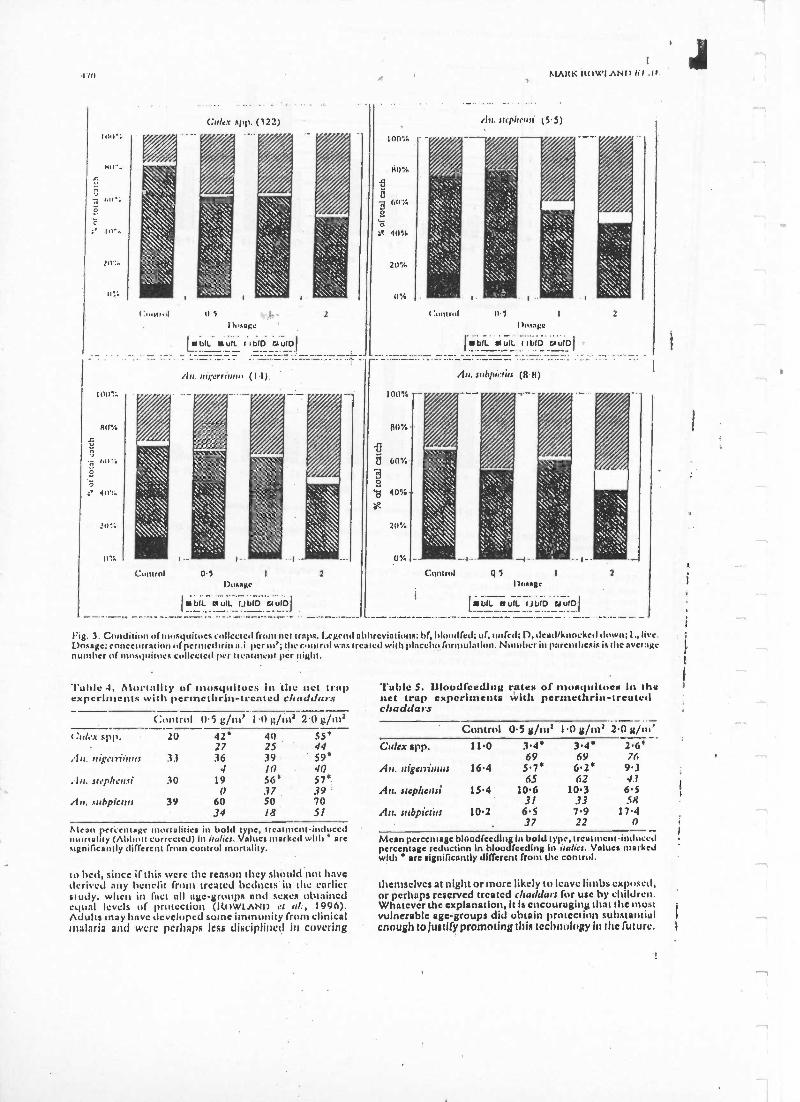
Figure 3 shows the proportions unreel -live, unreeldead, bloodied live, and bloodied - denti for each iypc ofmosquito, after allowing for delayed mortality due toinsecticide. Table 4 shows the mortality rate at eachtreatment site after correcting for control mortality usingAbbott's formula. Natural mortality at Ilse control sitevaried between 20% and .30% depending on the species.
Treatment- induced mortality ninon$ culicincs wits
about 25% at the 0.5 guns' and 1 g /m' sites and 39%at the 2 g /in' sites (' _- 0,11). A trend of dosage -dependent mortality of similar magnitude was alsoapparent among the anophcline species, and for An.nigerrinms and An. srcphersi this was significnnt
(l' <005) despite the low densities involved.'Cable 5 shows the bloodfceding 'rates at the various
treatment Bites after ndjusting for the feeding rate at thecontrol site. The feeding rate at the control site was quitelow; only 12% of released nmsquitcres did feed, on
average of 35 culicincs and 11 nnuphcliucs per site pernight. [?Nett fewer culicincs managed to feed on mensleeping under treated cheddars (Fig. 3); the decrease infeeding rate was 70% (P = 0.002). A decrease of similar
magnitude was evident also for An. rtige,rinm:t
(l' < 0.05). The apparent decrease in feeding shown byAn. srephettsi was not significant owing to the lowdensities involved. A trend of clnsngc dcpcndcnrc tua.not so apparent with feeding rate as it was with tutti alit y
true.In the cone bioassay tests, the mean time tu knock-
down for the median mosquito ranged from 9 5 tain(95'}f C:1: R -2 I0-8) art the 0.5 glut' treater) mtatrr, :tl5.8 min (t)5", Cl: 4R 68) on the 2.0 gin': 11eal.tImaterial.
1)iscussion.
¡'erntelhrin- treated chutldur) gave 641:, ptolcti ii
evillest falcip:trum malaria anti 18'1;,'nowt: i )u ag:nm.tvivnx mnlnrin among refugees younger than 211 veins ttl
age. This degrec'ofprotection was almost as good :tc (lr,u
obtained films peruteihrin- treated hednets in an eaiht.,study in n nearby camp (Rowl Am) ci rr!., 11)í)u) t )nitchildren and young adultsseen)cd to benefit from atonedchnerdan. Older adults suffered less malaria gencrall,and while this was partly owing to adult males taut lingaway from home, the lack of intervention effect in lido(annies (who wcre housebound roving to the ctill nIr of
purdah) remains a puzzle. It is unlikely that older Icuialr.were getting bitten and catching malaria before ietí,tng
170
Ino":(:nlex spp. (122)
AtAIIK ItO\4'IANI) fil .II.
il,l. üipß¡nll (5.5)
o^.
I ()11".6
2
ntgerriwu, (1'1) /l a. suhpirrirs (H H)
Control 05Dosage
bIL auulL--tJ bID Gulf)]
2 QiDnsage
bIL aulL (Jb1O Gil WO
2
Fig. 3. Condition of mosquitoes collected from net traps. Legend abbreviations; bf, Hundred; uf, wired; I), dead /knocked down; 1., live.Dosage: concentration ofperntclhrin a i per nt; Ille control was treated Itlt placebo formulation. Number in parenthesis is the aver: Kenumber of mosquitoes collected per 1Ie /11110111 per night.
Tuttle 4. Mortality of mosquitoes in the net trapexperiments with perntethrin-lrcntcd clraddur.c
Control 05 g/m' 1.0 g/m= 20 g/ms(.tth.t spp. 20 42' 41) 55'
27 25 44, LI. n,glnü,u,s 33 36 39 59'
4 1() 40srlylh.v,.ti 30 19 56' 57'
0 .?7 39 'An. s,rhpicua 39 60 50 70
34 18 51
Mean perretllaKe mot talkies in hold _type, ireaumcnt -inducednl1I iIity (Ahhott corrected) in italics. ViIIICS!Harked with' UI Csignificantly different from control mortality.
to bed, since if this were the reason they should not havederived any henelit front treated bedncts in the earlierstudy, when in fact all age- groups and sexes obtainedequal levels of protection (IttWLANI) et al., I996).Adults may have developed some immunity front clinicalmalaria and were perhaps less disciplined in covering
'fable S. liloudfcedlig rate» of mosquitoes in thenet trap experiments whit pet- meths-in- treatedch addars
2.0 g /nt'Control 0.5 g /ntt I.0 g /nts
Crrlcx app. 11.0 3.4* 3.4' 2.6'69 69 76
nigenilnus 16.4 5.7' 6.2' 9.365 62 4?
An. step/ions( 15.4 10.6 10.3 6.531 33 58
An. subpictirs 10.2 6.5 7.9 17.437 22 n
Mean percentagebloodfecding lit bold type,trc *Imcnt inducedpercentage reduction in hloudfeeding in italics. Values markedwith ' are significantly different front the control.
themselves at night or more likely to leave limbs exposed,or perhaps reserved treated cltaddars for use by children.Whatever the explanation, it Is encouraging that the mostvulnerable age- groups did obtain protection substantialenough to Justify promoting this technology hi the future.
J
rI:RMI: l'11RIN=1'Itl?A'I'lil)(3/. u')).1lt.0 ANI
MALARIA IN ItlEl,ll(;lil?S
That the intervention 'effect was lower agninst vivnx
than against falciparum malariais likely to he n conse-
quence iof relapsed vivnx infections transmitted before
the commencementof the trial
(ROWIANI) el al., 1994,
1996). lice lack of a significant intervention effect for
vivax malaria cony be duc to the peak vivclx transmission
having finished early in the trial, resulting in fewer vivnx
episodes andTherefore less power to detect no effect.
The permethrin treatment provided protection by
inhibitingbluodfccding and, to a lesser extent, by killing
mosquitoes. 71íc effectiveness of insect repellents or
repellent insecticideapplied to combat
uniforms by the
armed forces to protect against nuisance mosquitoes,
sandflies, and lice is well documented (SCI II(I(K el al.,
1982, 1984;GUPTA el al., 1987; SI11)1.DT et al., 1984)),
and there is evidence tint permethrin-impregnateduni-
forms give protection aggninstmalaria nod Iclshmnniasis
in Colombiansoldiers (Solo etal., I 995). Previous work
with permethrin-treated nets in Afghan rcfugcc camps
showed that uncovered individualssleeping nearby did
mot suffer from increasedbiting or from more malnria
episodes as a result of insecticide repellency(1Zo \I AND
et al., 1 996; HBWITT el al., I997), and this is nisi, likely to
hold truc if somemembers of the
household fail to use
treated chuddarr.When a technology is new, good habits may be instilled
though health education. llut when an old technology is
being adapted, it is less easy to break had habits. In
Afghan society, where the use of bedneta is fairly novel, it
was possible to persuade users not to wash the nets
during the malaria transmission season(Wu/LAND et al.,
I996). the of electrician in Afghan society is an ancient
custom and, in contrast tohcdncts, it was not possible to
dissuade refugees from washing them. Against this back-
ground of normal washing practices,the trial still sumo-
aged to demonstrate a substnntial health impact agninst
falciparum malaria. The falciparum season is only 4
months long but the vivnx season starts cnrlicr, in April
(RowlANI) et d., Igg7h).'l'rentetlrhaddarc are unlikely
to cover the entire sensunfrom April In Nnveniln r unless
re- treated. Pew refugees were abld to nlfnnl at second
chaddar or to reserve one solely for use nt night. The
solution to this might he to mnke nvailnble n cheap
material-muslin cloth for cxnntple -that gives protec-
tion when treated but is unsuitable for anytime use. One
treatment might then last an entire season.
Pcrtnethrin is the least irritant and safest of the
synthetic pyrethroids will respect to dermal toxicity
and when skin application is necessary,such as for
scabies or headlice treatment, it Is the insecticide of
choice (I-Ar1.IN & MI(INKINaI, 1990). No negative side -
effects were reported among users of treated chaddar. A
transient irritation is sometimesexperienced when dip-
ping nets in permethrin solution for prolonged periods or
when using permethrin ointment for acnbics treatment
(ANDRI(WS et al., 1992). l'crmethrin-treated ntntcrinla
have an outstanding safety record (SNont)RAss, 1992)
but until we have several years' experience, with treated
chaddar and top-sheets, we wouldrecommend thnt use
be restricted to the main falciparum malaria transmission
season from August to November.
The entomological studyindicated that the dosage
used in the intervention, 1 g/m2, might he reduced to
0.5 g /m2 and still retaineffectiveness. Even nt I g/m2 the
cost per personprotected and cost per case prevented, as
derived from insecticide costs alone, were nlmnst iden-
tical to the costs of insecticide treatment during the
earlier permethrin- treated beano trial (US80.I8 and
US : 1.29, respectively'). The chaddar study gives hope
that the poorest sections of society - -Islamic or other-
wise -may gain protection from malnrin without having
the expense ofbuying beclncts. An nitcrnativc color inn to
the equity problem would be to provide subsidized nets
to means-tested poor, but this would be difficult to
manage or monitor and is liable to corruption.
Single -dose sachets of insecticide, on sale in shops and
plmarmncics for home treatment of nets, are gaining
popularity in Pakistan and Afghanistan. 'These might
be adapted for treating chadrlats or top-sheets.
Treated top-shccts and blankets should provide a
solution to the operational and logistical problems
inherent with conventional forms of malaria cmttrul in
complex emergencies.Blankets provided by aid agencies
might be sprnycd or pre-treated with pernetluin tt
provide protectionfrom malaria ns well as warmth and
shelter.
AcknowledgementsWe arc grateful to
Zenccn for providing the placebo foi nds
!Ion nod to Professors DavidBradley nid Winn (irccnwt,n,I 6,r
their insights and comments on the nmnuscript. Ile:atlthet
International's Malaria and LeishmaninsisConnoi l'rhptanune
Is supported by the EuropeanCommission (DM ) and the
United Nations I Ugh Commissioner forRefugees. The resent'. It
study wassupported by WI IU /UNDI'Ar'lt Special Programme
for Research and Training in Tropical Diseases (Project ID):
960662), the I)cpnrunent for InternationalDevelopment if the
UK, nod I IcalthNet International.
ReferencesAlcamo, P. L., Lindsay, S. \V., Armstrong, J. It., Crouch, A1.,
I lill, A. G., David, I'. I I., Fcgan, G., dc Francisco, A , I Iall.
A., Shcnton, F. C., Chant, K. & Greenwood, II. A1. (1491).
-Iltc effect of insecticide-treated bed nets un omrtahty of
Gambian children. Lancet, 337; 1499-1502.
Andrews, H. II., Joseph, M. C., Mngeuhcim, M. J., 'ninon. I I.
11., Doi, P. A. & Schultz, M. \V. (1992). l'ostmnnrkcting
surveillance study of permethrin creme rinse. lhnnui,.,
Journal a I Public 1lcahh, 82, 857 -861.
[links, F. N., Kubajc, A., Adjuik,M., Williams, I .. A., tangelo,
C., Maude, G. I l., Annals, GAL Knjiharn, li., Adiom:th, J. I I.
& Smith, I'. G. (1996). Impact of permctlnin impregnated
bedneta on child tutortnlity in Kossenn-N.nknna district,
Ghana: a randomizedcontrolled trial. Tropical Atedtchte and
Intonational heath, I, 147 -154.
Choi, l I. \V., Itrcman, J.G.,I'cutach, S. M., Liu, S. , I lightotvcr,
A. W. & Sexton, J. D. (I 903). The effectivenessofinsccticidc
impregnated bed fiels in reducing cases of malaria infection. a
mew- of publishedresults. ; I trtr
tiraa-7oautal o/ I ,.'ft
rat Afelirinr I Hygiene, 52, 177 182.
1)'Alcssnndrn, U , ()lalcyc, II. O., McGuire,W., I angetI t k, l' .
Bennett, S., Alikins, M.K.,'l'hintso,,, M. (:., Chant, Ai. K ,
Chant, il. A. & Greenwood, I1. M. (1995). Atonality and
Ishii!), from malaria in (iambizut children Starr in(r,nhi;
111111 of nnimpregnated bed net progrrttnntc. Lawret, 145.
479 -481.lrcildcn, R. M. (199íi). lixpericnccsofimplementation
In: 1'.t
Gain: a New Method /0r NI tenting ,1 litho ia Deaths. I cogita,
C., Cattnni, J. & tic Savigny, I). (cditnts). hurt national
DevelopmentResearch Centre, Geneva: World IIcahh
Organization. pp. 55 -1 10.
Gupta, It. K., Sweeney, A. W., Rutledge, L. C., Choper, It. D.,
Trances, S. I'. & West , I). It. (1987). liffectiveness of
controlled -release personal-usearthropod repellents nod
permethrin -Impregnatedclothing in the field. ,7eraunl of the
America,' Mosquito Cwurol Assoriarion, 3, 556 560.
I lcwitt, S., Ford, R., Urhnman, I I., Nasir, M. & Rowland, At.
(1997). The effect of bcd nets on unprotected people: open.
air studies In an Afghan rcfugcc village. Bulletin n/ ldntnnto-
I'giral lìroratrh, 87, 455 -.459.
Lines, J. (1996).Review of mosquito nets and insecticides for
nei treatment: a discussion of existing and phlential distribu
lion systems in Africa. Ïrupical Medicine and Internal .d
¡leal:!,, 1, 616 -632.Nnbarro, D. N. & Taylor, It. M. (I 998). The 'Roll Back Malaria'
campaign. Seieare, 280, 2067 -2068.
Najern, J. (1996).Malaria control among
refugees and displaced
.
populations. Geneva:World I leant, Organization, documtcnt
no. CFI) /MAI /96.6.Nevin, C. G., Some, l ?. S., NI a ng'als, V. O., Mutcnti, \Lits, Nt *V.
L., &bush, K.,I.engcler, C. & S , It. W. (1996). Insect'
cidc- ircnted hcdncts reduce i ntrinlity and severe morbidity
from malaria amongchildren on the Kenyan coast. 7'toptro/
Atediciti' and hnrrhatioaal I/nihh, I, I )9 1.16.
Pitt, S., l'corey, I . 14., Stcvc11s, It. 1 I., Shay ipuv,A.. Satana . IC
& Banatvnln, N. (1908). War in I ajikistnn snit se- ewert;cm e
of l' /a.unod tat ipatnnt. l..tnrrt, 152, I270.
Ruwlnnd, M., I Iewitt, S. A4 Durrnni, N. (1991). Pi Imalaria in Afghan refugee villages in Pakistan sprayed ,t,th
972h1AItKRUsS'I.APt1s I1
lanthdacyh+(1ulhtin or malathlnn. Tnnoa riuut of the Ronal.Cnc sety of 7'rnpseal A letlirine and Hygiene, 88, 378 - 179.
Rt.wland, M., IhtunIa, M., Uucorncz, D., Durrnni, N., Rozcn-daal, J , Schapiro, A. & Sundorp, 11. (1996). l'yrcthroid-intpregnntcd lied nets for self protection against malaria forAfghan refugees. 7iasuurriuns of the Royal Society of '1 iopicu!Alydtcine and hygiene, 90, 357 361.
nits, land, M., I Icwitl, S., Durrani, N., Solch, P., Bounto, M. &Sundorp, E. (1997a). Sustainnhility of pyrcrhruid impreg-nated bed nets for malaria control In Afghan communities./lut /ran al she troth/ Health Orgwsi: arion, 75, 23 29.
Ito 1:.11(1, A1., Ilcwiu, S., Durrani, N., llano, N. & Wily, R.(199710. ansmission and control ofvivax malaria in AfghanI (ogee settlements in Pakistan. TiatltortioI15 of the Royalso, ¡qv J Tropism/ AL-Mt- Ieandhygiene,9I,252 255.
Rowley, J. (1997). Affordability. In: iS.ceedings ssj the 'sucnus-riossa! Cmsferenee ass lleduet.t and Other insecticide-TreatedA!arena!, far the llcvention aj Ala/olio, Washington, 1)C,USA, October 2931. USAID. pp. 19 -21.
Schreck, C. 1 ., Kline, I). I.., Cltnniutis, Il. N., Wilkinson, N.,McGovern, T. P. & Weidlusas, D. E. (1982). Evaluation ofpersonal protection methods against phlcbuuuuine watt flicsincluding vccous of leishntuuiasis in Panama. AnscririnJaunud of 7hspicu/ Aledicine and hygiene, 31, 1046 I053.
Schrock, C. E., Haile, D. G. & Kline, 1). L. (1984). The
effectiveness ofperntethrin and 1)lìli"l', alone or in cunshiu.tfirm, for protection against 'Met tacuinrltruchu.t. ellnennusJournal of Tropical Medicine and Hygiene, 33, 7 25 - 7 l0.
Service, M. W. (1993). Mosquito Ecology, Field.Sasuphug Anethads, 2nd edition. Barking, Essex: Elsevier Science l'uhlish.rs.
Shuldt, L. L., Rogers, E. J., Gerber,, E. J. & Schreck, C. li(1989). Effectiveness of pernuthrin- trcutcd military uuilunnfabric against human body lice. Military Alsdicitte, 154.
90 -93.Snodgrass, II. L. (1992). Pcrmcthrin transfer front treated cloth
to the skin surface: potential for exposure in Iturnans Jwrn,.,IuJ Toxico /u &p and Environmental Health, 35, 91-105.
Soto, J., Medina, P., !)ember, N. & Berman, J. (1995). Efficacyof permeihrin- impregnnted uniforms in the preventduu ofmalaria and leishtnaniasis in C:ulosnhinn &oldies s. Cluur!htfeuhnu Ditrate.s, 21, 599 602.
laplin, I). & Mcinkingg, T. L. (1990). l'yrcthrins sural pyre -throids in dermatology. Archives of Unsnutvinr, 126,
213 -221.Thomson, M. C. (1995). Disease Preventive 11 gh Ne, roe
Control: Guidelines for Relief Organisations. Oxford: OXFAM.
Received 1 March 1999; revised 14 Muy 1999; accepted Jarpublication 2 June 1999
Books Receive]
flow to Report Statistics In Medicine: AnuotntedGuidelines for Authors, Editors, and Reviewers.-f. A. Lang & M. Sccic. Philadelphia: American Collegeof Physicians, 1 997. xxvi I 367pp. Price UIS$40 (NorthAmerica); USS55 in Europe (includes shipping). ISBN0- 943126 -44 -4.
'lltis pnper- bucked honk is arranged in 3 parts.!'ant I , Antonin (iuidclincv for Reportinl(Siatisijcnl
John/nation, is ingunizctl jilt() 15 clutptets Ihat corrc-spund Iu 15 general applications of bjuslatistics.
Part 2, Guide to Statistical Terms and Tests, isdesigned to help rcadcrs of scientific articles understandstmistical inforntntion.
Part 3, An Unnnnotnted, Referenced 1.ist of Guide-lines, is supplied for readers already familiar with statis-tical concepts, who will use the book primarily as areference tool in writing, editing, and reviewing scientificarticles.
Host Response to International Parasitic Zoonoses.I I. Ishikurn (editor -in- chief), M. Aikawn, Il. hokum &K. Kikuchi (editors). Tokyo: Springer- Vcrlag, 1998.viii I I22pp. l'rice £69.00. ISBN 4 -431- 71)217 -2.
1 his ntuturgraph includes the contents of a symposiumheld in Sapporo ( Japan), in June 1997, on the pathologyof international parasitic zoonoses, together with addi-tional material on important current prohlenns in para-sitic diseases from a global point of view. Many of theFigures are in colour.
Antibes et Flagellés Intcstinnux, Amibes oculnires:leur diagnostic microscopique. Cahier dc Forma-tion Biologic médicale, 1998, no. II. 255pp [InDrench(.
'Ibis hook contains numerous coloured photomicro-graphs and a bibliography of 214 references.
SEAMIC Health Statistics 1997. Tokyo: Interna-tional Medical Foundation of Jnpan, 1998. 266pp. Price mendation by the Society, Editorial Board, or Editor.
r
not statétl. ISBN 4- 930783 -R -X. SEAMIC Publicationno. 81. [Obtainable front 1MFJ, Ynesu- Ichigaya Bldg, 17Ichigayatantachi 2- chonre, Shinjuku -ku, Tokyo 162 -0843, Japan.]
SEAM1C !kaki' Statistics 1998. Tokyo: Inlet na-00110l Medical Foundation of Japan, 1999. 274pp. !'ricenot stated. ISBN 4- 930783 -82 -8. SEAMIC Publicationnu. 82. [Obtainable from IMF), Yaesu- Ichignya Bldg, 17Jchignyatamachi 2- shunts, Shinjuku -ku, Tokyo 162-0843, Japan.!
World Animal Health in 1997: Reports on the AnimalHealth Status und Disease Control Methods and Tableson incidence of List A Diseases (Part 1) and Tables on theAnimal I4calth Status and Disease Control Methods(Port 2). Paris: Office International des U(tizooties,1998. 754pp. Price Fr.fr. 600 /USS 100 (air stall postageis included for all countricaj. ISBN: l'art 192-90,14-454-1/92-9044-457-6 and l'art 2 92- 9044 -454 -192- 9(1441-460-6. ISSN 1017 -3102. (Obtainable frutti OIE, 12 ruedc Prony, 75017 Paris, France; phone -l-33 1 44151/038,fax -I.33 1 42670987, c -mail pub.salcs(ìoic.int.)
The Economics of Annual Disease Control. O11'Scientific and Tcchuifal Review, 18(2), 289 -561. B. D.Perry (Co- ordinator). Paris: Office International deslipizootics, 1999 (August). 276pp. Price Euro 40. (airmail postage is Included for all countries(. ISBN 92 -9044-488-6. ISSN 0253 -1933. (Obtainable from 0111, 12 ruedc Prony, 75017 l'aris, France; phone -1.33 144I5I8H8,fax 133 1 42670987, c -mail pub.salcs(rilttic. inn.)
The book is divided into two sections. the firstcomprises a practical guide, followed by eight compre-hensive reviews on the diverse aspects of the relationshipbetween economics and animal health. The secondpresents six case studies, ranging from font anti moudhdisease in South -East Asia to rabies control in wildlife.
'Inclusion of titles in this list does not necessarily imply reconr
-- --- ,..a.,K : ,,.- ---- --: ---_ . ..... _.
3I12v7.51ccML4 3 i
SSM : 2557Prod.Type;com ED:BinnyR
pp.1-11(col.flg.:NIL) PAGN: evk SCAN: SHOBHA.V.M
3PERGAMON
Social Science & Medicine I (1111) 11h111
5 Discussion
Afghan refugees and the temporal and spatial distribution of9 malaria in Pakistan
Mark Rowland"t", Mohammad Abdur Rab", Tim Freeman", Naeem Durrani ",
13 Naveeda Rehmanc
7
SOCIALSCIENCE
MEDICINE
www.clscvicr.cum/lucatc/sucscuued
11
IS
17
19
21
23
25
27
29
"Heal:hWet Internatiunal, Uuifersitp Tutvn. Pechawar. Pakistan
bLondon Se!uul.ofHygiene and Tropical Medicate. Londua WCIE7HT. UK
United Nations uIi! /le Cumnrissi r for Re :rt/ees, Islamabad.. Pakistan
Abstract
Influx of refugees and establishment of camps or settlements in malaria endemic areas can affect the distribution and
burden of malaria in the host country. Within a decade of the Soviet invasion of Afghanistan and the arrival of 2.3
million Afghan refugees in Pakistan's North West Frontier Province, the annual burden of malaria among refugees had
risen ten fold from 11.200 cases in 1981 to 118,000 cases in 1991, a burden greater than the one reported by the Pakistan
Ministry of Health for the entire Pakistani population. Politicaldevelopments in,the 1990s led to over half the refugee
population repatriating to Afghanistan, and the Afghan Refugee Health Programme (ARHP) was scaled down
proportionately. Districts in which the ARHI' recorded u reduced incidence of malaria begun to show an increased
incidence in the statistics of the Pakistan government !teak h.progranlinu. This and other evidence painted to a change in
r health seeking practices of the refugees who remained in Pakistan, with many turning from A RI II' to Pakistani health
services as aid declined. Comparison of the two sources of data produced no evidence for the spatial distribution of
malaria in NWFP having changed during the 1990s. Nor was there any evidence for the presence of refugees having
increased the malaria burden in the Pakistani population, 'us is sometimes alleged. This highlights the risk of
r misinterpreting health trends when parallel health services are operating. Over the decade incidence in the refugee
camps decreased by 25% as a result of control activities, and by 1997 the burden amongremaining refugees had fallen
31to 26,856 cases per annum. These trends indicate that the burden would continue to fall if political conditions in
Afghanistan were to improve and more refugees returned to their homeland. Q 2001 Published by Elsevier Science Ltd.
31
33
r
en.
33
39
41
43
45
Äesicaids: M1talareu; Refugees; Pakistan; AI hunistun
Introduction
Migration of refugees from one country to another
can affect the distribution and incidence of malaria in
47 various ways. When coming from a malaria endemic
area, refugees may transport malaria parasites or new
49 strains of parasite to the host country. The parasites
may stimulate outbreaks if the new environment is
5I suitable for transmission (Najcru, 1996). When coming
53 'Corresponding author. London School or Hygiene und
Tropical Medicine. London WOE 71-IT. UK. Tel.: +44.20-
55 7299-4719; NE +44-20-72994720.E -nail address:
murk.rnwlrndtte%Ishtm.uc.uk (M. Rowland).
from u non -endemic urea Io an endemic area, refugees
may be more vulnerable to local transmission than the.
host population, since refugees will luck natural
immunity to native strains und have added problems
of mainburishment and stress to compound the risk
(Toole & Waldman, 1990; Boss, Brink, & Dondero,
1987). Epidemic conditions arise when the health
infrastructure of the host country is over -stretched und
non -immune immigrants are settled onto sites capable of
supporting mosquito breeding.When two and a half million Afghan refugees fled to
Pakistan between 1979 and 1982 to escape the war with
the Soviet Union, they were leaving u country which
0277. 9536 /01)S sec front matter l; 2001 Published by [Elsevier Science Ltd..
PII:50277.9536(01)00341.0
57
59
a,I
63
65
67
69
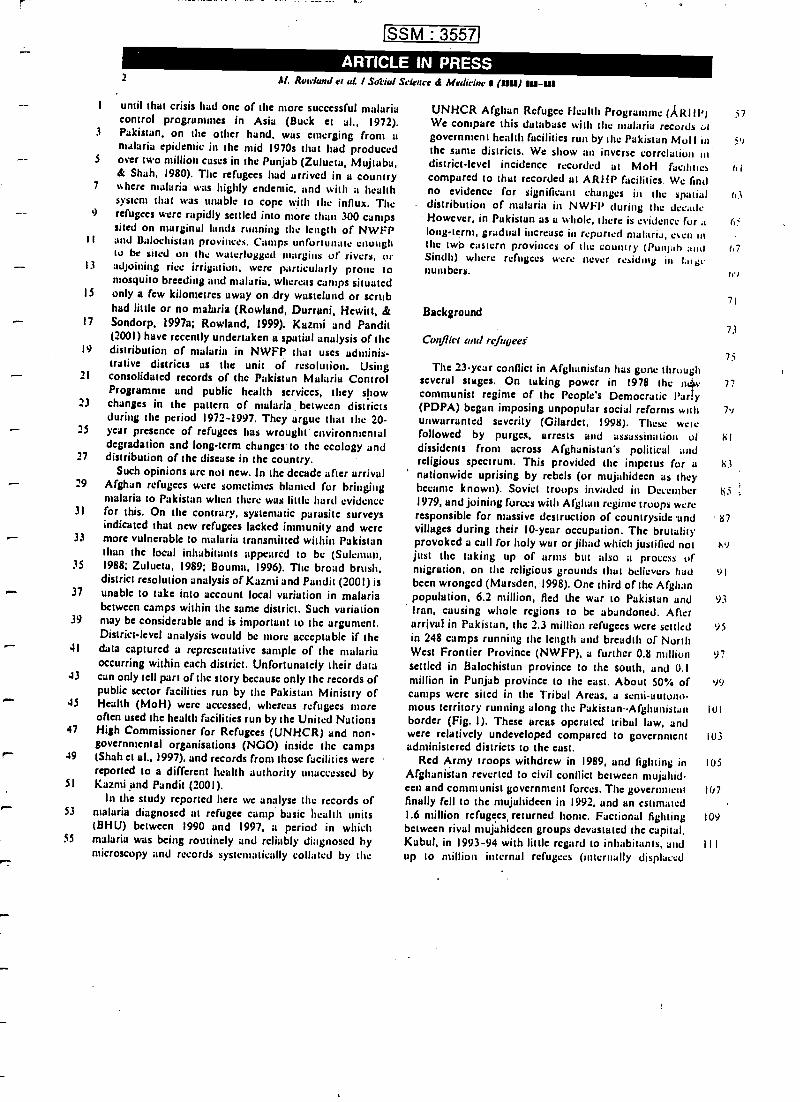
ISSM : 3557
ARTICLE IN PRESSbf. Ruavlunrl er at I SdFiul Science d Medicine s(UU)
I until that crisis had one of the more successful malariacontrol programmes in Asia (Buck et al., 1972).
3 Pakistan. on the other hand, was emerging front amalaria epidemic in the mid 1970s that had produced
5 over two million cases in the Punjab (Zulueta, Mujtaba,& Shah, 1980). The refugees had arrived in a country
7 %%here malaria was highly endemic. and with a healthsystem that was unable io cope will] the influx. The
9) refugees were rapidly settled into more than 300 campssited on marginal lands running the length of NWFP
ll and Baluchistan provinces. Camps unfortunate enoughto be sited on the waterlogged nsargins of rivers, or
13 adjoining rice irrigation, were particularly prone tomosquito breeding and malaria, whereas camps situated
15 only a few kilometres away on dry wasteland or scrubhad little or no malaria (Rowland, Durrani, Hewitt, &
17 Sondorp, 1997a; Rowland, 1999). Kazmi and Pandit(2001) have recently undertaken a spatial analysis of the
19 distribution of malaria in NWFP that uses adminis-trative districts as the unit of resolution. Using
21 consolidated records of the Pakistan Malaria ControlProgramme and public health services, they show
23 changes in the pattern of malaria. between districts
during the period 1972 -1997. They argue that the 20-- 25 year presence of refugees has wrought environmentaldegradation and long -term changes to the ecology and
27 distribution of the disease in the country.Such opinions arc not new. In the decade after arrival
29 Afghan refugees were sometimes blamed for bringingmalaria to Pakistan when there was little hard evidence
31 for this. On the contrary, systematic parasite surveysindicated that new refugees lacked, immunity and were
33 more vulnerable to malaria transmitted within Pakistanthan the local inhabitants appeared to be (Suleman,
35 1988; Zulueta, 1989; Houma, 1996). The broad brush,district resolution analysis of Kazmi and Pundit (2001) is
37 unable to take into account local variation in malariabetween camps within the same district. Such variation
39 may be considerable and is important to the argument.District -level analysis would be more acceptable if the
41 data captured a representative sample of the malariaoccurring within each district. Unfortunately their data
43 can only tell part of the story because only the records ofpublic sector facilities run by the Pakistan Ministry of
45 Health (MoH) were accessed, whereas refugees moreoften used the health facilities run by the United Nations
47 High Commissioner for Refugees (UNHCR) and non-governmental organisations (NGO) inside the campsr- 49 (Shah et al.. 1997), and records from those facilities werereported to a different health authority unaccessed by
51 Kaznti and Pandit (2001).In the study reported here we analyse the records of
53 malaria diagnosed at refugee camp basic health units(BHU) between 1990 and 1997, a period in which
55 malaria was being routinely and reliably diagnosed bymicroscopy and records systematically collated by the
UNHCR Afghan Refugee Health Programme (ARM')We compare this database whit the malaria records utgovernment health facilities run by the Pakistan Moll inthe sanie districts. We show an inverse correlation iodistrict -level incidence recorded ut MoH facilitiescompared to that recorded at ARIIP facilities. We findno evidence for significant changes in the spatialdistribution of malaria in NWFP during the decade.However, in Pakistan as a whole, there is evidence fur a
long -tern], gradual increase in reported malaria, teen inthe twb eastern provinces of the country (Punjab andSindh) where refugees were never residing in 1.1ibcnumbers.
Background
Conflict and refugees'
57
5V
rl
63
6
67
71
73
75The 23-year conflict in Afghanistan has gone through
several stages. On taking power in 1978 the myv 77communist regime of the People's Democratic Parry(PDPA) begun imposing unpopular social reforms with 79unwarranted severity (Gilardet, 1998). These wetsfollowed by purges, arrests and assassination of 81dissidents from across Afghanistan's political andreligious spectrum. This provided tite impetus for u 83nationwide uprising by rebels (or mujahidecn as theybecame known). Soviel troops invaded in December h51979, and joining forces with Afghan regime troops wereresponsible for massive destruction of countryside -and 87villages during their 10 -year occupation. The brutalityprovoked u cull for holy war or jihad which justified not x ijust the taking up of arms but also a process ofmigration, on the religious grounds That believers had 91
been wronged (Marsden, 1998). One third of the Afghanpopulation, 6.2 million, fled the war to Pakistan and 93Iran, causing whole regions to be abandoned. Afterarrival in Pakistan, the 2.3 million refugees were settled 95in 248 camps running the length and breadth of NorthWest Frontier Province (NWFP), a further 0.8 million 97settled in Bulochistan province to the south, and 0.1million in Punjab province to the cast. About 50% of 99camps were sited in the Tribal Areas, a semi- autono-mous territory running along the Pakistan- Afghanistan lulborder (Fig. I). These areas operated tribal law, andwere relatively undeveloped compared to government 103administered districts to the east.
Red Army troops withdrew in 1989, and fighting in 105
Afghanistan reverted to civil conflict between mujahid-een and communist government forces. The government 107
finally fell to the mujahideen in 1992, and an estimated1.6 million refugees, returned home. Factional fighting 109between rival mujahideen groups devastated the capital,Kabul, in 1993 -94 with little regard to inhabitants, and I I I
up to million internal refugees (internally displaced
3
1
7
9
11
13
15
17
19
l
23
25
27
29
31
33
ti
37
i9
41
43
45
47
49
51
53
jj
SSM : 3557
ARTICLE IN PRESS
IRAN
At Rowland t7 u!. / Suciuf S'iknce á Medicine 1 (1111) 111-111
CHINA
(5-1? \.t ....
AFGHANISTAN N ."'. ?FAT'. \;.) ,S /PUNJAa -r..d.« ,.7 tu..
.. +'' tJwr '
~`aALOCHISTAN
/!
(SINDH t 1_. ..-ARABIAN SEA
w .g rar.
i INDIA
North
Mansehrá fAbbolabao/
100 kmf--#
rig. 1. North test Frontier Province. Pakistan ('tribal Areas shown in darker shade). Map of Pakistan shoving position of tic
provinces and Afghanistan.
persons) fled to otter parts of the country (by then thePakistan government was Tess supportive and the borderwas closed to new refugees). Meanwhile another 1.3
mullion refugees returned to peaceful rural areas of thecountry. The continued anarchy in the country providedan opportunity to the Taliban who emerged as a strongpolitical and military force in 1994. Starting front theirbase, the southern city of Kandaltar, they were able tobring almost 90 °ó of the country under their controlwithin 3-4 years. But the Taliban were unable to presshome their early advantage, us the social and civilstructure of the society remains torn, national develop-ment is at a standstill and fighting still continues in somecentral and north eastern regions. The refugee popula-tion exiled in Pakistan remains at 1 -2 million, beingunwilling to return while such difficult social andeconomic conditions persist.
When the refugees first arrived in Pakistan they wctcprovided with tents, food, and fuel. They quickly builttheir own mud homes on site, and found casual work tosupplement their rations (Christensen & Scott, 1988)Schools, clinics, and water supply systems were estab-lished. Over time rations were reduced and finallybrought to an end in the mid 1990s when refugees weredeemed self -sufficient at the level of the poorest inPakistan. A significant proportion of families live at avery marginal level, going for long periods without workand dependent on the charity of neighbours in the cumps(Marsden, 1996).
Malaria epidemiology
3
G3
67
71
71
75.
77
7')
il
.;
Y,i
Ius
107
1u9
An average camp contained I0,000 people but larger 1 I 1
camps might house over 30,000. Camps were mostly
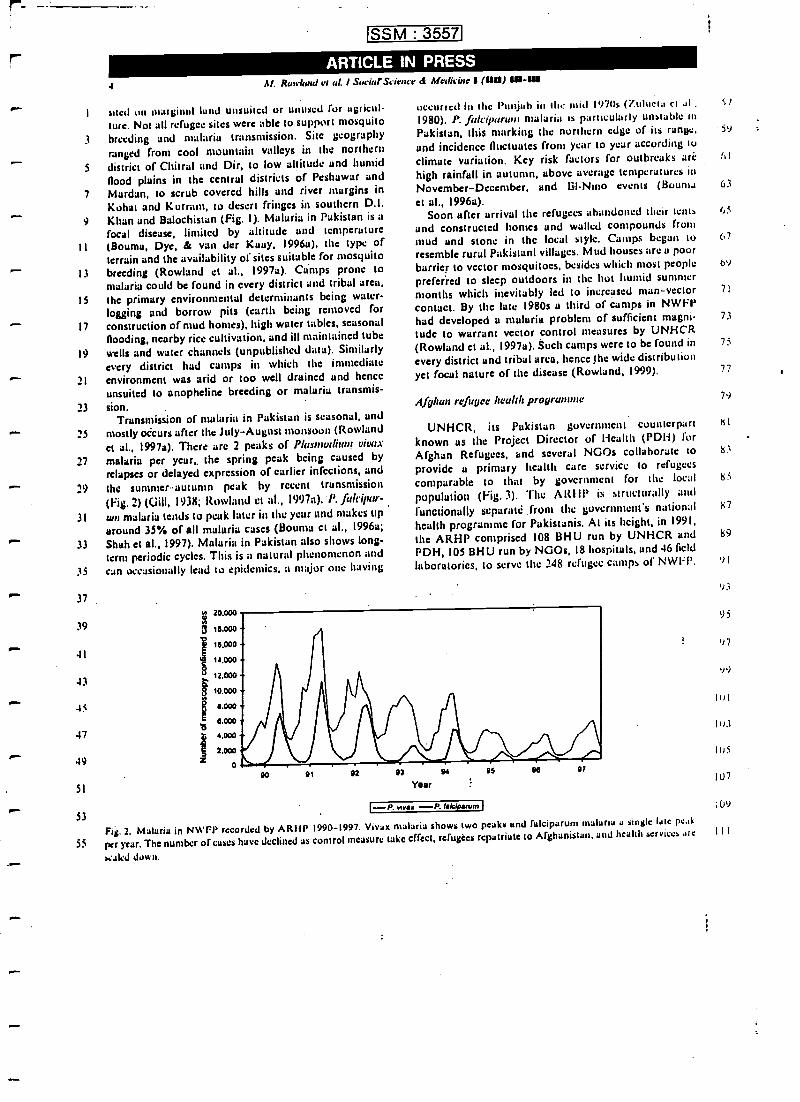
)-P. vivi+ --P. rak/prum i
SSM : 3557
ARTICLE IN PRESS4 dl. Ruufand rr ai I SuriarScicrrcr d Medicine 1(g111 111-/I/
I sited un marginal lund unsuited or unused for agricul-ture. Not all refugee sites were able to support mosquito
3 breeding and malaria transmission. Site geographyranged front cool mountain valleys in the norlhcrn
3 district of Chitral and Dir, to low altitude and humidflood plains in the central districts of Peshawar und
Mardan, to scrub covered hills und river margins inKohut and Kurru m, to desert fringes in southern D.I.Khan and Balochistan (Fig. I). Malaria in Pakistan is u
focal disease, limited by altitude und temperature(Bouma, Dye, & van der Kuuy, 1996u). the type ofterrain and the availability of sites suitable for mosquitobreeding (Rowland et al., 1997a). Camps prone tomalaria could be found in every district und tribal area,the primary environmental determinants being water-logging and borrow pits (earth being removed forconstruction of mud homes), high water tables, seasonalflooding. nearby rice cultivation, and ill maintained tubewells and water channels (unpublished data). Similarly
every district had camps in which the immediateenvironment was arid or too well drained and hence
unsuited to anopheline breeding or malaria transmis-
sion.Transmission of malaria in Pakistan is seasonal, and
mostly occurs after the July- August monsoon (Rowland
et al., 1997a). There are 2 peaks of Plusmodiuni vivatmalaria per year,. the spring peak being caused by
relapses or delayed expression of earlier infections, und
the summer-autumn peak by recent transmission
(Fig. 2) (Gill, 1938; Rowland et al., I')97a). P. fir/rip/Ir-
ani malaria tends to peak later in the year und makes tiparound 35% of all malaria cases (Bouma et al., 1996u;
Shah et al., 1997). Malaria in Pakistan also shows long-term periodic cycles. This is a natural phenomenon and
can occasionally lead to epidemics, a major one having
1
9
II
13
IS
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
53
N 20.000
1L000.-
.
16.000 -
kx 14.000
12.000 -
g 10.000 -
a
z
1.000 -
5.000 -
4.000
2.000
o
occurred in the Punjab in the mid 1970s (T.ulucia ct .r1 . S I
1980). P. faic:parnnt malaria is particularly unstable inPakistan, this marking the northern edge of its range,and incidence fluctuates from year to year according to
climate variation. Key risk factors for outbreaks are !, I
high rainfall in autumn, above average temperatures in
November -December, and C'I -Nino events (Houma 63
et al., I996a).Soon after arrival the refugees abandoned their tents 65
and constructed homes and welled compounds frommud and stone in the local style. Camps began to 67
resemble rural Pakistani villages. Mud houses are a poorbarrier to vector mosquitoes, besides which most people 6)preferred to sleep outdoors in the hot humid summermonths which inevitably led to increased man- vectorcontact. By the lute 1980s u third of camps in NWFPhad developed a malaria problem of sufficient magni-tude to warrant vector control measures by UNHCR(Rowland et al., 1997a). Such camps were to be found in
every district and tribal urea, hence the wide distributionyet focal nature of the disease (Rowland, 1999).
5`l
Afghan refugee health programme
UNHCR, its Pakistan government counterpart
known as the Project Director of Health (PDH) forAfghan Refugees, and several NGOs collaborate to
provide u primary health care service to refugees
comparable to that by government for the local
population (Fig. 3). The ARIII' is structurally and
functionally scparatt:.front the government's national
health programme for Pakistanis. At its height, in 1991,the ARHP comprised 108 BHU run by UNHCR andPDH, 105 BHU run by NGOs, 18 hospitals, and 46 field
laboratories, to serve the 248 refugee camps of NWFP.
03 94
Year
1s N 97
Fig. 2. Malaria in NWFP recorded by ARHP 1990 -1997. Vivax malaria shows two perks and fulciparum malaria u single late peak
per year. The number of rases have declined as control measure take effect. refugees repatriate to Afghanistan. and health services arc
waled down.
71
73
75
77
7)
KI
lr?
85
95
97
..1)
lui
11,3
lus
1U7
;09
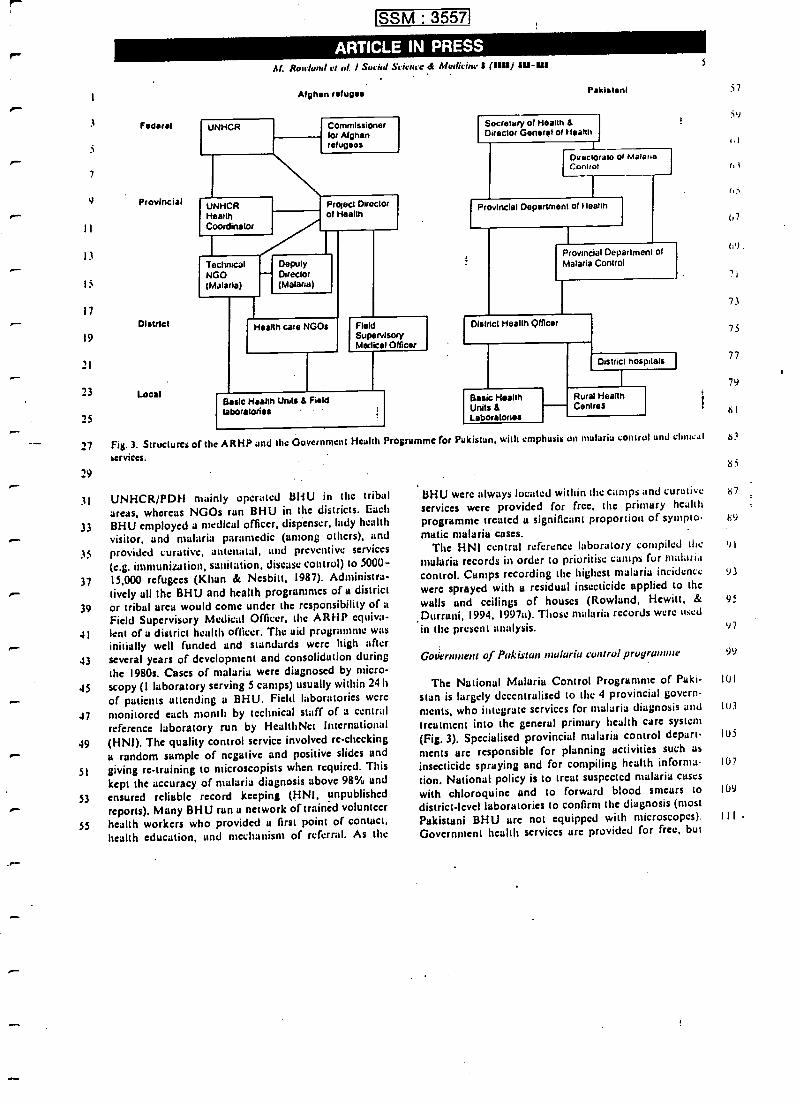
3
r>-
Federai
7
9 ProvincialrII
13
15
17
19
21
23
25
District
Local
SSM : 3557
Al. Rowland et al. I Sacia! Science d Mrrlictne IOM) III-YI
UNHCR
Afghan refugee
UNHCRHealthCoordinator
Commissionerfor Afghanrefugees
TechnicalNGO(Mala ia)
Project Directorof Health
DeputyDirector(Malaria)
Health care NGOs FieldSupervisoryMedical Officer
Basic Health Units & Fieldlaboratories
Pakistani
Secretary of Health &Director Generel of Health
I piado ate of MalaraControl
Provincial Department of Leann
Provincial Department ofMalaria Control
District Health Officer
Bas'c HealthUnits 8Laboratories
District hospitals
Rural HealthCentres
27 Fig. 3. Structures of the ARHP and the Government Health Programme for Pakistan, with emphasis on malaria control and clinical
services.
29
31 UNHCR /PDH mainly operated BHU in the tribalareas, whereas NGOs ran BHU in the districts. Each
33 BHU employed a medical officer, dispenser, lady health
visitor, and malaria paramedic (among others), and35 provided curative, antenatal, and preventive services
(e.g. immunization, sanitation, disease control) ío.5000 -
37 15,000 refugees (Khan & Nesbitt, 1987). Administra-Lively all the BHU and health programmes of a district
39 or tribal area would conte under the responsibility of aField Supervisory Medical Officer, the ARHP equiva-
41 lent of a district health officer. The aid programme wasr-- initially well funded and standards were high after
43 several years of development and consolidation duringthe 1980s. Cases of malaria were diagnosed by micro-
45 scopy (I laboratory serving 5 camps) usually within 24 h
of patients attending a BHU. Field laboratories were47 monitored each month by technical staff of a central
reference laboratory run by HealthNet International49 (HNI). The quality control service involved re- checking
a random sample of negative and positive slides and
51 giving re- training to microscopists when required. This
kept the accuracy of malaria diagnosis above 98% and53 ensured reliable record keeping (HNI, unpublished
reports). Many BHU run u network of trained volunteer
55 health workers who provided u first point of contact,health education, and mechanism of referral. As the
57
59
r,i
67
119 .
7I
73
75
77
79
ti l
ti?
ë?
BHU were always located within the camps and curative s7
services were provided for free, the primary healthprogramme treated a significant proportion of sympto-
matic malaria cases.The HNI central reference laboratory compiled Mc 9
malaria records in order to prioritise camps for malaria
control. Camps recording the highest malaria incidence 93
were sprayed with a residual insecticide applied to thewalls and ceilings of houses (Rowland, Hewitt, & 95
Durruni, 1994, I 997a). Those malaria records were used
in the present analysis. 97
fi rl
Government of Pakistan muluriu control programme 99
The National Malaria Control Programme of Paki- 101
stan is largely decentralised to the 4 provincial govern-ments, who integrate services for malaria diagnosis and 1U3
treatment into the general primary health care system(Fig. 3). Specialised provincial malaria control depart- 105
mente are responsible for planning activities such asinsecticide spraying and for compiling health informa- 107
fion. National policy is to treat suspected malaria caseswith chloroquinc and to forward blood smears to 109
district -level laboratories to confirm the diagnosis (mostPakistani BHU are not equipped with microscopes). III .
Government health services are provided for free, but
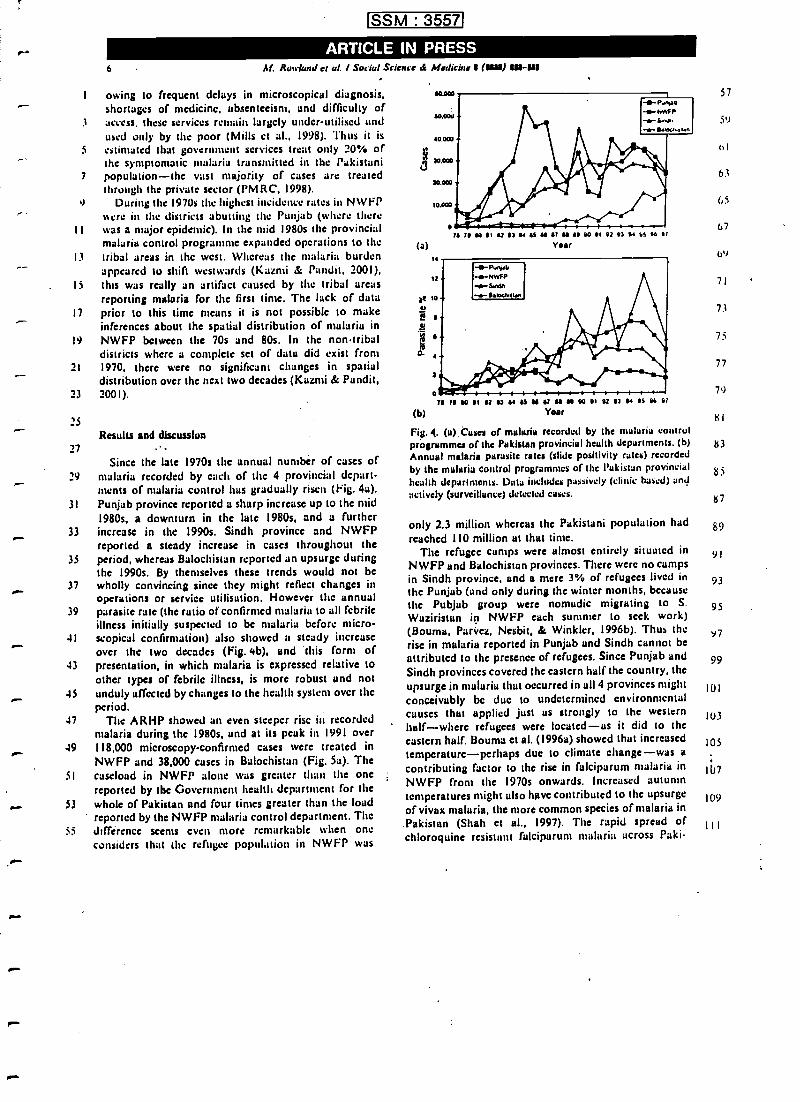
SSM : 3557
ARTICLE IN PRESS6 M. Roa (and et al. I Socia! Science & Medicine a (atad su -UUI
I owing to frequent delays in microscopical diagnosis,shortages of medicine, absenteeism, and difficulty of
3 access. these services remain largely under -utilised andused only by the poor (Mills et al., 1998). Thus it is
5 estimated that government services treat only 20% ofthe symptomatic malaria transmitted in the Pakistani
7 population -the vast majority of eases are treatedthrough the private sector (PMRC, 1998).
,t During the 1970s the highest incidence rates in NWFP%sere in the districts abutting the Punjab (where there
11 was a major epidemic). In the mid 1980s the provincialmalaria control programme expanded operations to the
13 tribal areas in the west. Whereas the malaria burdenappeared to shift westwards (Kazmi & Pandit, 2001),
15 this was really an artifact caused by the tribal areasreporting malaria for the first time. The hick of data
17 prior to this time means it is not possible to makeinferences about the spatial distribution of malaria in
19 NWFP between the 70s and 80s. In the non -tribaldistricts where a complete set of data did exist from
21 1970, there were no significant changes in spatial-distribution over the next two decades (Kazrni & Pandit,
23 2001).
25
Results and discussion27
Since the late 1970s the annual number of cases of29 malaria recorded by each of the 4 provincial depart-
ments of malaria control has gradually risen (Fig. 4a).31 Punjab province reported u sharp increase up to the mid
1980s, a downturn in the late 1980s, and a further33 increase in the 1990s. Sindh province and NWFP
reported a steady increase in cases throughout the35 period, whereas Balochistan reported an upsurge during
the )990s. By themselves these trends would not be37 wholly convincing since they might reflect changes in
operations or service utilisation. However the annual39 parasite rate (the ratio of confirmed malaria to all febrile
illness initially suspected to be malaria before micro41 scopical confirmation) also showed a steady increase
over the two decades (Fig. 413), and this form of43 presentation, in which malaria is expressed relative to
other types of febrile illness, is more robust and not45 unduly affected by changes to the health system over the
period..17 The ARHP showed an even steeper rise in recorded
malaria during the 1980s, and at its peak in 1991 over49 118,000 microscopy -confirmed cases were treated in
NWFP and 38,000 cases in Balochistan (Fig. 5a). The51 caseload in NWFP alone was greater than the one
reported by the Government health department for the53 whole of Pakistan and four times greater than the loud
reported by the NWFP malaria control department. The55 différence seems even more remarkable when one
considers that the refugee population in NWFP was
20 20 14 0t 02 03 14 Si N 02 41 0 00 01 02 03 14 01 00 01Year
70 70 e0 01 02 02 14 0S M R N g 00 01 02 N 14 0S 06 0!
(b) Year
Fig. 4. (a).Cusea of malaria recorded by the malaria controlprogramma of the Pakistan provincial health departments. (b)Annual malaria parasite rates (slide positivity rates) recordedby the malaria control programmes of the Pakistan provincialhealth departments. Data includes passively (clinic based) andactively (surveillance) detected rases.
only 2.3 million whereas the Pakistani population hadreached I IO million at that time.
The refugee camps were almost entirely situated inNWFP and Balochistan provinces. There were no campsin Sindh province, and a mere 3% of refugees lived inthe Punjab (und only during the winter months, becausethe Pubjub group were nomadic migrating to S.
Waziristan in NWFP each summer to seek work)(Bouma, Parvez, Nesbit, & Winkler, I996b). Thus therise in malaria reported in Punjab and Sindh cannot beattributed to the presence of refugees. Since Punjab andSindh provinces covered the eastern half the country. theupsurge in malaria that occurred in all 4 provinces mightconceivably be duc to undetermined environmentalcauses that applied just us strongly to the westernhalf -where refugees were located -us it did to theeastern half. Bouma et al. (1996a) showed that increasedtemperature- perhaps due to climate change -was acontributing factor to the rise in falciparum malaria inNWFP front the 1970s onwards. Increased autumntemperatures might also have contributed to the upsurgeof vivax malaria, the more common species of malaria inPakistan (Shah et al., 1997). The rapid spread ofchloroquine resistant falciparum malaria across Paki-
57
59
(t l
63
(, 5
67
6v
71
73
75
77
79
KI
83
85
tS 7
89
91
93
95
97
99
lUl
I U3
105
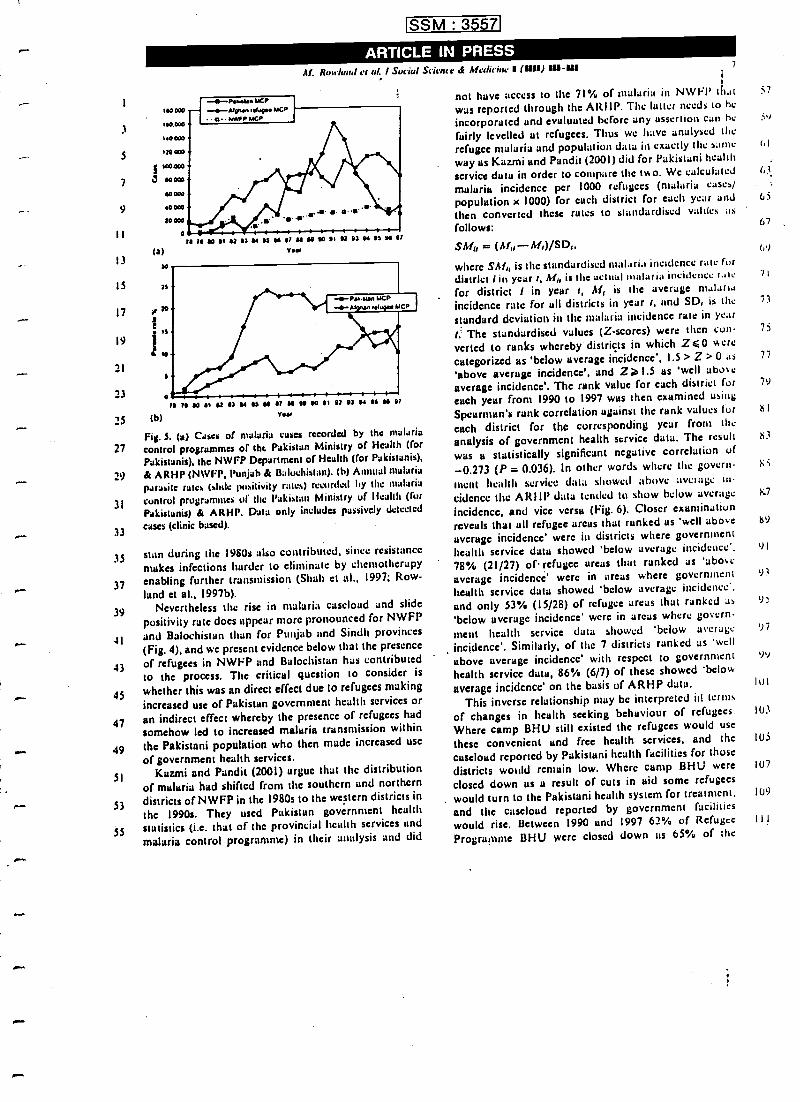
1
3
5
7
9
II
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
SSM : 3557
ARTICLE IN PRESS
J
(a)
AI. Rnw(und et al. I Social Scion( d Mrdicinc ti (Op) SU-sU
19 /9 M 91 92 93 N M M p M M 90 91 92 91 N 93 W 9/Year
(b)
/9 ra M 91 at N M 99 M Q M 99 90 91 at at N M MYa«
Fig. 3. (a) Cases of malaria cases recorded by the malaria
control programmes of the Pakistan Ministry of Health (for
Pakistanis), the NWFP Department of Health (for Pakistanis),
& ARHP (NWFP, Punjab & Baluchistan). (b) Annual malaria
parasite rates (slide positivity rates) recorded by the malaria
control programmes of the Pakistan Ministry of Health (forPakistanis) & ARHP, Data only includes passively detected
erses (clinic bused).
stan during the 1980s also contributed, since resistance
makes infections harder to eliminate by chemotherapyenabling further transmission (Shah et al., 1997; Row-
land et al., 1997b).Nevertheless the rise in malaria caseload and slide
positivity rate does appear more pronounced for NWFP
and Balochistan than for Punjab and Sindli provinces(Fig. 4), and we present evidence below that the presence
of refugees in NWFP and Balochistan has contributedto the process. The critical question to consider is
whether this was an direct effect due to refugees making
increased use of Pakistan government health services or
an indirect effect whereby the presence of refugees had
somehow led to increased malaria transmission withinthe Pakistani population who then made increased use
of government health services.Kazmi and Pandit (2001) argue that the distribution
of malaria had shifted from the southern and northerndistricts of NWFP in the 1980s to the western districts in
the 1990s. They used Pakistan government health
statistics (i.c. that of the provincial health services and
malaria control programme) in their analysis and did
7
ti
not have access to the 71% of malaria in NWEP thatwas reported through the ARHP. The latter needs to heincorporated und evaluated before any assertion can he
fairly levelled at refugees. Thus we have analysed the
refugee malaria and population data in exactly the wane
way as Kazmi and Pandit (2001) did for Pakistani healthservice data in order to compare the two. We calculated
malaria incidence per 1000 refugees (malaria cases/population x 1000) for each district for each year and
then converted these rates to standardised valt(cs as
follows:
SMrr = (Ma- M,) /SDr.
where SAf is the standardised malaria incidence rate fur
district i in year r, Af is the actual mutaria incidence r.1te 7I
for district i in year r, AI, is the average malariaincidence rate for all districts in year r, and SD, is the 73
standard deviation in the malaria incidence rate in year
The standardised values (Z- scores) were then con- 75
verted to ranks whereby districts in which Z <0 werecategorized us 'below average incidence', 1.5 > Z > 0 as 77
'above average incidence', and Z2I.S as 'well aboveaverage incidence'. The rank value for each district for 79
euch year from 1990 to 1997 was then examined using
Spearman's rank correlation against the rank values for h I
each district for the corresponding year from the
analysis of government health service data. The result h3
was a statistically significant negative correlation of-0.273 (P = 0.036). In other words where the govern-
ment health service data showed :shove average tncidencc the ARIIF' data tended to show below average h.7
incidence, and vice versa (Fig. 6). Closer examinationreveals that all refugee areas that ranked us 'well above h9
overage incidence' were in districts where governmenthealth service data showed 'below average incidence'. 91
78% (21/27) of refugee areas that ranked us 'aboveaverage incidence were in areas where government 93
health service data showed 'below average incidence',
and only 53% (15/28) of refugee areas that ranked as 9'below average incidence' were in areas where govern-
ment health service data showed 'below average 97
incidence'. Similarly, of the 7 districts ranked as 'wellabove average incidence' with respect to government 99
health service data, 86% (6/7) of these showed 'below
average incidence' on the basis of ARHP data. lul
This inverse relationship may be interpreted it! terms
of changes in health seeking behaviour of refugees. 103
Where camp BHU still existed the refugees would usethese convenient and free health services, and the I05
caseload reported by Pakistani health facilities for thosedistricts would remain low. Whcrc camp BHU were 107
closed down us u result of cuts in aid some refugees
would turn to the Pakistani health system for treatment. 109
and the caseload reported by government facilities
would rise. Between 1990 and 1997 62% of Refugee 111
Programme BHU were closed down as 65% of the
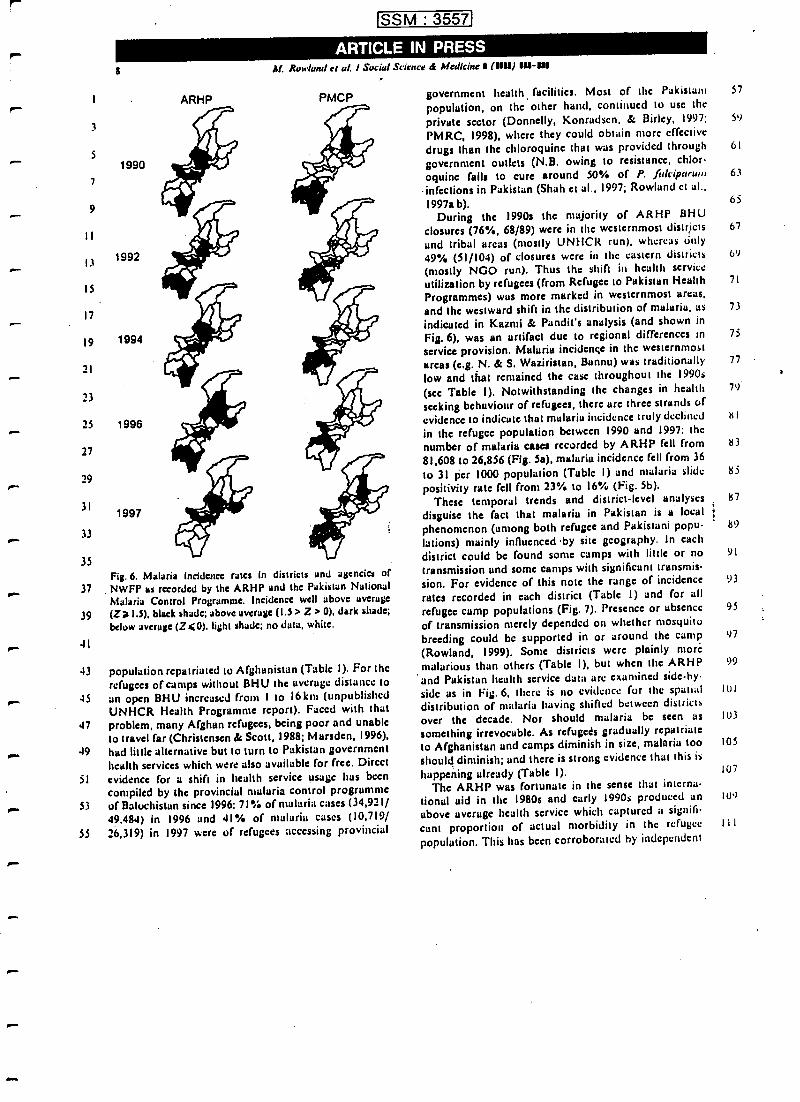
r-1
3
5
7
9
8
1990
pm.
d-
It
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
1992
1994
1996
1997
ARHP
SSM : 3557
Al. Rowland ci d.. I Socia! Science & Medicine I (11111)11U-S111
PMCP
Fig. 6. Malaria incidence rates in districts and agencies ofNWFP as recorded by the ARHP and the Pakistan NationalMalaria Control Programme. Incidence well above average(Z)1.5), black shade; above average (1.5 > Z > 0), dark shade;below average (Z40), light shade; no data, white.
43 population repatriated to Afghanistan (Table 1). For therefugees of camps without BHU the average distance to, 45 an open BHU increased from 1 to 16km (unpublishedUNHCR Health Programme report). Faced with that
47 problem, many Afghan refugees, being poor and unableto travel far (Christensen & Scott, 1988; Marsden, 1996),
.. 49 had little alternative but to turn to Pakistan governmenthealth services which were also available for free. Direct
51 evidence for a shift in health service usage has beencompiled by the provincial malaria control programme
,.- 53 of Baluchistan since 1996: 71% of malaria cases (34,921/49,484) in 1996 und 41% of malaria cases (10,719/
55 26,319) in 1997 were of refugees accessing provincial
government health, facilities. Most of the Pakistani 57
population, on the other hand, continued to use theprivate sector (Donnelly, Konradsen. & l3irley, 1997; 59
PMRC, 1998), where they could obtain more effectivedrugs than the chloroquine that was provided through 61
government outlets (N.B. owing to resistance, chlor-
oquine fails to cure around 50% of P. falclparum 63
infections in Pakistan (Shah et al., 1997; Rowland et al.,1997a b). 65
During the 19901 the majority of ARHP BHUclosures (76 %, 68/89) were in the westernmost districts 67
and tribal areas (mostly UNHCR run), whereas only
49% (51/104) of closures were in the eastern districts 69
(mostly NGO run). Thus the shift in health serviceutilization by refugees (from Refugee to Pakistan Health 71
Programmes) wus more marked in westernmost areas,and the westward shift in the distribution of malaria, as 73
indicated in Kazmi & Pundit's analysis (and shown in
Fig. 6), was an artifact due to regional differences in 75
service provision. Malaria incidençe in the westernmostareas (e.g. N. & S. Waziristan, Bannu) was traditionally 77
low and that remained the case throughout the 1990s
(sec Table I). Notwithstanding the changes in health 79
seeking behaviour of refugees, there are three strands ofevidence to indicate that malaria incidence truly declined i< I
in the refugee population between 1990 and 1997: the
number of malaria cases recorded by ARHP fell from K3
81,608 to 26,856 (Fig. Sa), malaria incidence fell from 36to 31 per 1000 population (Table I) and malaria slide 85
positivity rate fell from 23°/. to 16% (Fig. 5b).These temporal trends and district -level analyses 87
disguise the fact that malaria in Pakistan is a localphenomenon (among both refugee and Pakistani popu- 89
lutions) mainly influenced by site geography. In eachdistrict could be found some camps with little or no 91
transmission and some camps with significant transmis-sion. For evidence of this note the range of incidence 93
rates recorded in each district (Table 1) and for allrefugee camp populations (Fig. 7), Presence or absence 95
of transmission merely depended on whether mosquitobreeding could be supported in or around the camp(Rowland, 1999). Some districts were plainly more
malarious than others (Table I), but when the ARHP 99
and Pakistan health service data are examined side -hy
side as in Fig. 6, acre is no evidence for the spatial 101
distribution of malaria having shifted between districts
over the decade. Nor should malaria be seen as 103
something irrevocable. As refugees gradually repatriate
to Afghanistan and camps diminish in size, malaria too 105
should diminish; and there is strong evidence that this is
happening already (Table 1). 107
The ARHP was fortunate in the sense that interna-
tional aid in the 1980s and early 1990s produced an IO')
above average health service which captured a signifi-
cant proportion of actual morbidity in the refugee 111
population. This has been corroborated by independent
97
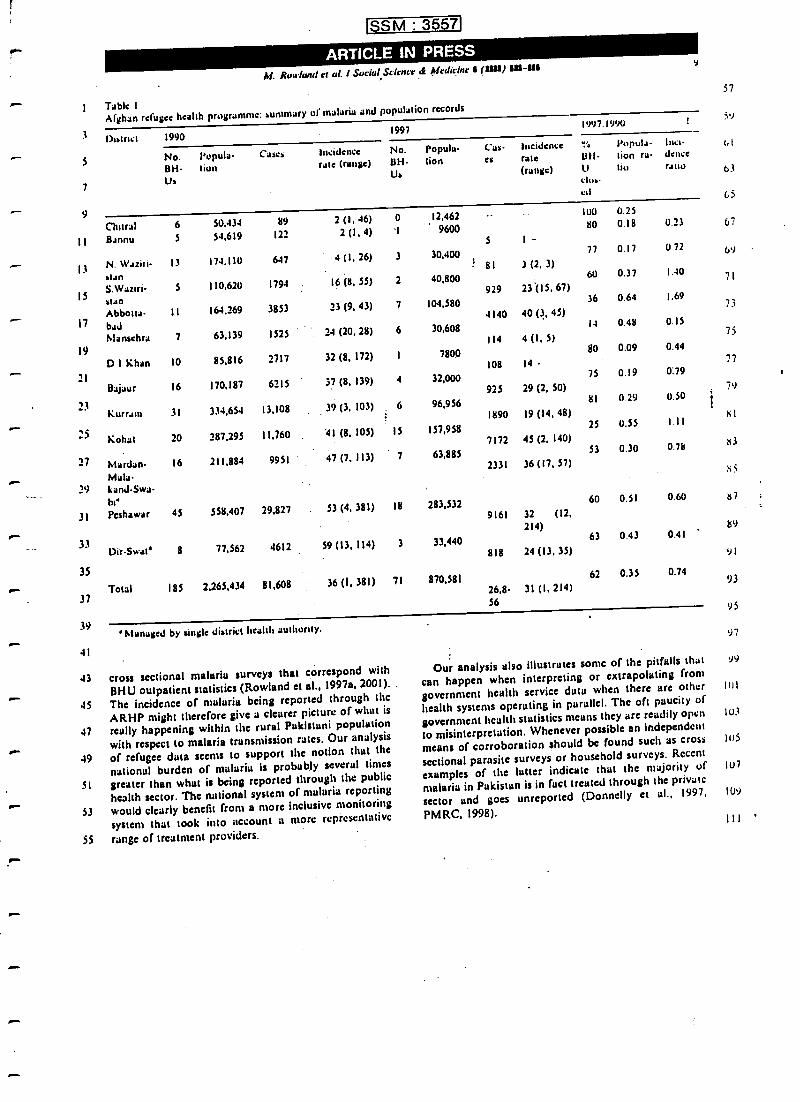
SSM : 3557
M. Rowland et al. l Social Scicncr 4 Afrdirrnc 11 (UU) IU-UI
1 Table IAfghan refugee health programme: summary or malaria and population records
3
5
7
9
II
13
15
17
19
23
.-
21
25
27
29
.31
33
35
37
39
41
District 1990
No. Isupula Cases
BH tionUs
19971997: /990
Incidence No.rate (range) BH.
Us
Popula Cas-
lion esIncidencerile(range)
Ull-Utim-ed
Popula-tion ra-tio
lucidamaratio
Chitral 6 50.434 89 2 (1, 46) 0 12,462 100 0.25
Bannu 5 54,619 122 2(1,4) I 9600 80 0.18 0.23
S I-N. Waziri 13 174,110 647 4 (1, 26) 3 30,400
77 0.17 072
Ilan8I 3 (2, 3)
S. Waziri- 5 110,620 1794 . 16 (8, SS) 2 40,800 60 0.37 1.40
Ilan929 23.(IS, 67)
Abbotta 11 164.269 3853 23 (9, 43) 7 104,58036 0.64 1.69
bad4140 40 (3, 45)
Mansehra 7 63.139 1525 24 (20, 28) 6 30,60814 0.48 0.15
114 4 (1, 5)
D l Khan 10 85,816 2717 32 (8, 172) I 7800 80 0.09 0.44
108 14 -
Bajaur 16 170,187 6215 37 (8, 139) 4 32,000 75 0.19 0:79
925 29 (2, 50)
Kurrant 31 334.654 13,108 39 (3, 103) G 96,956 81 0.29 0.50
1890 19 (14, 48)
Kohut 20 287,295 11,760 41 (8, 105) 15 157,95825 0.55 1.11
7172 45 (2, 140)
Mardrn 16 211,884 9951 47 (7, 113) 7 63,885 53 0.30 0.78
Mala-kandSwabt'
2331 36 (17, 57)
Peshawar 45 558,407 29.827 . 53 (4, 381) 18 283,53260 0.51 0.60
9161 32 (12,214)
Dir -Swat 8 77,562 4612 59 (13, 114) 3 33,44063 0.43 0.41
818 24 (13, 35)
Total 185 2,265,434 81,608 36 (1, 381) 71 870,58162 0.35 0.74
26,8 31 (I, 214)56
'Managed by single district health authority.
43 cross sectional malaria surveys that correspond with
BHU outpatient statistics (Rowland et al., 1997a, 2001).
45 The incidence of malaria being reported through the
ARHP night therefore give a clearer picture of what is
47 really happening within the rural Pakistani population
with respect to malaria transmission rates. Our analysis
49 of refugee data seems to support the notion that thenational burden of malaria is probably several times
51 greater than what is being reported through the public
health sector. The national system of malaria reporting
53 would clearly benefit from a more inclusive monitoring
system that took into account a more representative
55 range of treatment providers.
Our analysis also illustrates some of the pitfalls that
can happen when interpreting or extrapolating from
government health service data when there are other
health systems operating in parallel. The oft paucity of
government health statistics means they are readily open
to misinterpretation. Whenever possible an independent
means of corroboration should be found such as cross
sectional parasite surveys or household surveys. Recent
examples of the latter indicate that the majority of
malaria in Pakistan is in fact treated through the private
sector and goes unreported (Donnelly et al., 1997;
PM RC, 1998).
b I
63
65
67
b`l
71
73
75
77
79
I+ I
83
r5
87
89
91
93
95
97
99
IUI
103
105
107
109
II1 '
1
3
5
i
9
II
13
15
17
19
21
SSM : 3557
ARTICLE iN PRESSAl. Rowland et al. 1 Social Science á Medicine 1 (U11) í1t11 -W
Mills, D., Rowland. M., Shah, I.. Mujahid, C., Hyder, K.,Mackay, H., & Hari. F. (1998). Review of the notionsdniu/uriu prugru . Pakistan. London: Malaria Consor-tium.
Najera, J. A. (1996). Alaloria control sip refiigces anddisplaced populations. CTD /MAL /96.6. Geneva: WHO.
PM RC. (1998). Health survey of Pakistan: Heath profile of thepeople of Pakistan. Islamabad, Pakistan: Pakistan MedicalResearch Council, 19Ipp.
Rowland. M. (1999). Malaria control: Hcdncts or spraying!Malaria control in the Afghan refugee camps of westernPakistan. Transactions of the Royal Society of TropicalMedicine ana! Hygiene, 93, 458 -439.
Rowland. M., Durrrni, N.. Hewitt, S., & Sondorp. E. (19974.Resistance of falciparum malaria to chloroyuine andsulfadoxinepyrimethamine in Afghan refugee settlementsin western Pakistan: Surveys by the general health servicesusing a simplified in vivo test. Tropical Medicine utn!International Health. 2, 1049 -1056.
Rowland. M.. Hewitt. S.. & Durrrni, N. (1994). Malariaprevalence surveys in refugee camps sprayed with malathionand lambdaeyhalothrin. Transactions of the Royal Society ofTropical Medicine and Hygiene. 88, 378 -379.
II
Rowland, M.. Hewitt. S., & Durrasii, N. (1997b). Transnnssionand control of vivo* malaria in Afghan refugee villages inPakistan. Transactions of the Ru!ia! Society of TropuulMedicine und Hygiene, 9!, 252.255.
Shah, L. Rowland, I4., Mehmood, P.. Mujahid, C., Raziyuc.F., Hewitt, S., dc Durrani. N. (1997). Chloroyuine resistancein Pakistan und the upsurge of falciparum malaria in
Pakistani and Afghan refugee populations. Annals ,a!
Tropical Medicine and Parasitology. 91, 591 -602.Sideman. M. (1988). Malaria in Afghan refugees in Pakistan
Transactions of the Royal Sudety of Tropical Medicine undHygiene, 82, 44-47.
Toole, M. J., & Waldman, R. J. (1990). Prevention of excessmortality in refugee and displaced populations in develop.ing countries. Journal of the American Medico! Assucial:on,263, 3296 -3302.
Zulueta, J. De. (1989). Malaria in Afghan refugees. Utipubfished UNHCR report.
Zulueta, J. De, Mujtabu, S. M., & Shah. I. H. (1980). Malariacontrol and long -term periodicity of the disease in Pakistan.Transactions of the Royal Society of Tropical Medicine undHygiene, 7i, 624 -632.
2;
25
27
_J
31
31
36
37
39
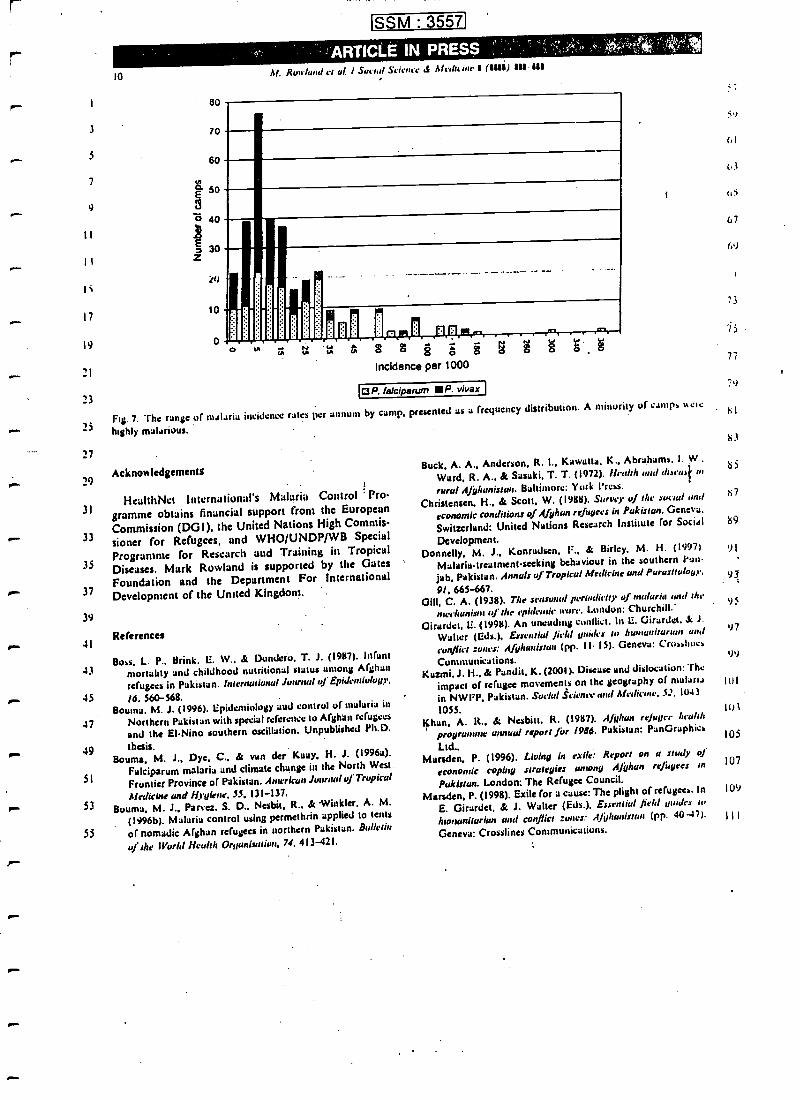
SSM : 3557]
t_
--
1,11=.
1
3
3
7
9
II
11
t
17
19
71
23
25
27
29
31
33
35
37
39
10
80
70
60
É 50
ao 40
30Z
[U
10
o
, -R k
Af. Rowland er al. I Social Science dc Afcdutnc I(11111 UI 111
O
I1rls+p%
41O O O ei O O O
Incidence per 1000
OP. falciparum P. vivax
g Ó S
Fog. 7. The range of malaria incidence rates per annuno by camp, presented as a frequency distribution. A minority of campa acue
highly malarious.
Acknowledgements
HealthNet international's Malaria Control ' Pro-gramme obtains financial support from the EuropeanCommission (DGI), the United Nations High Commis-
sioner for Refugees, and WHO/UNDP /WB SpecialProgramme for Research and Training in TropicalDiseases. Mark Rowland is supported by the GatesFoundation and the Department For InternationalDevelopment of the United Kingdom.
.- 41References
43Boss. L. P.. Brink. E. W.. & Dandero. T. J. (1987). Infant
morality and childhood nutritional status among Afghan
refugees in Pakistan. international Journal of Epidemiology,
- 45 /6.560 -568.Bouma. M. J. (1996). Epidemiology and control of malaria in
47 Northern Pakistan with special reference to Afghan refugees
and the EI -Nino southern oscillation. Unpublished Ph.D.
49 thesis.Boums, M. J., Dye, C., & van der Kaay, H. J. (1996a).
Falciparum malaria and climate change in the North West.
Frontier Province of Pakistan. American Journal of Tropical
53Aedicine and Hygiene, 55. 131 -137.
Bouma. M. J.. Panez. S. D.. Nesbit, R., & 'Winkler. A. M.
(1996b). Malaria control using permethrin applied to tents
53 of nomadic Afghan refugees in northern Pakistan. Buiktin
of the World Hculth Organisation, 74, 413 -421.
51
Buck, A. A., Anderson, R. 1., Kawutta, K., Abrahams, I. W.,
Ward, R. A., & Sasaki, T. T. (1972). Ilealth aid discus# ut
rural Afghanistan. Baltimore: York Press.
Christensen, H., & Scott. W. (1988). Survey of the social und
economic conditions of Afghan refugees in Pakistan. Geneva.
Switzerland: United Nations Research Institute for Social
Development.Donnelly, M. J., Konrudsen, 1., & Birley, M. H. (1997) 91
Malaria- treatment -seeking behaviour in the southern Pun.
jab, Pakistan. Annals of Tropical Medicine and Purasit logs,
9/, 66S -667.6111, C. A. (1938). The seasonal periodicity of Luria I ,hr
mechanism of the c dde ' wore. London: Churchill.Girardet, IL (1998). An unending conflict. In L. Girardet, & 1.
Walter (Eds.). Essential field limites ru humanitarian and
c o n f l i c t :unes A f gh a n i s t a n (pp. 1 I --15). Geneva: Craa»Itocs
Communications.Kazrrti. J. H., & Pandit. K. (2001). Disease and dislocation: The
impact of refugee movements on the geography of marna
in NWT, Pakistan. Sucia! Science und Medicine. 52, 1043
1055.Khan. A. It., & Nesbitt. R. (1987). Afghan re /uuec health
programme annual report for 1986. Pakistan: PsnGraphics
Ltd..Marsden. P. (1996). Living in exile: Report on a study of
economic coping strategies among Afghan refugees to
Pakistan. London: The Refugee Council.Marsden, P. (1998). Exile for a cause: The plight of refugees. In
E. Gírarde'. & J. Walter (Eds.). Essentiul field guides ta
humanitarian and conflict :onus :: Afghatristtor (pp. 40 -47).
Geneva: Crosslines Communications.
iY
1,1
t.3
6i
67
69
73
93
95
97
99
It)I
1113
!05
107
109
TRANSACTIONS OP THE ROYAL. SÓCiETY OF TROPICAL MEDZCINU AND HYGIENE(2001) 95, 125 -12o
Refugee health in the tropics
Malaria control in Afghan refugee camps: novel solutions
Mark Rowland HealthNet International, P. O. Box 889, University Town, Peshawar, Pakistan; and London School of
Hygiene and Tropical Medicine, London WCIE 7HT, UK
Abstract ,
Malaria is one of the major communicable diseases to occur in refugee'camps. Prevention of mortality by
establishing good case management is always the priority. Various types of personal protection or vector
control measures maybe applied depending on local transmission conditions and stage of the emergency.
The range ofinterventiorisapplied In Afghan refugee camps, the factors influencing choice and the relevance
w emergencies in other parts of the world are described.
Keywords* malade refugees, vector control, mosquitoes, Pakistan, Afghanistan
Malaria Is a disease that flourishes in conditions of warand population displacement. Exposure to transmissionIs often several times greater among refugees than amonglocal people (NA>$RA,1996). Several factors can give rise
to a high malaria burden, including breakdown of healthsetvkas, concentration of non -immune refugees in ma-laria risk areas, malnourishment siting of refugee campson marginal land prone to flooding and vector breeding,and problems in gaining access or supplying medicine to'the displaced population (WHO, 2000). Conventionalmalaria control strategies need to be adapted to refugeesituations accordingly.
Complex emergencies usually evolve from acute -emergency to post -emergency phases. The acute phaseis characterized by sudden population displacement andhigh mortality, and may last only a few months. Duringthe post- emergency phase the health situation is broughtunder control and basic needs arc met. Chronic emer-gencies are characterized by political deadlock; someareas of the country stay locked in an acute phase whileother areas may progress towards post-conflict stability.
Afghanistan provides examples of all 3 phases. Thecountry has been at war for over 20 years. Refugees firstcame to Pakistan in the early 1980s, and over a millionremain settled there. The war continues in the north ofAfghanistan, but most of the country Is at peace.
In refugee camps case management may not besufficient 'response to contain malaria. If incidence ormortality continues to rise personal protection andvector control interventions need to be applied. Somemethods are more suitable for the acute phase, others forthe post -emergency phase. The choice of interventionwill depend on local factors such as the type of shelteravailable, human habits, and vector behaviour.
Indoor residual spraying (IRS) is the method mostoften used In acute and chronic emergencies If displacedpopulations inhabit regular housing and vectors areindoor resting. It can work well when there is goodorganization. If coordination between agencies is lack-ing, or insecticide consignments are delayed, spraycampaigns are often completed too late to be effectiveagainst seasonal malaria ( ROWLAND, 1999).
it is not clear whether insecticide- treated nets (ITNs)are an effective intervention during acute emergencies.ITNs are beguilingly attractive to agencies and donorsbecause they are technically simple, proven to be effec-tive in peaceful settings, and because of much iecentgood publicity. This may be deceptive. In acute emer-gencies free distribution of nets may lead to re- selling orblack marketing lithe refugeepopulation has no previousexperience of using nets. Experience shows that if ITNs
Address for correspondence: Dr Mark Rowland, Disease Con-trol and Vector Biology Unit, London School of Hygiene andTropical Medicine, Keppcl street, London WC IE 711T, UK;phone +44 (0)20 7927 2333, fax +44 (0)7580 9075, e-mail
arc distributed like any other relief item (as they may have
to be), with little or no health education, they may not he
used properly or looked after. Also there is presently no.international stockpiling for emergency use, the numberof mass producers is limited, and consignments oftenarrive too late for the acute phase. The initial investmentrequired may seem too much jf the future of the camp is
uncertain.There are other, possibly better, alternatives to ITNs
in the acute phase. Where canvas tents are issued,spraying of inner surfaces with a residual pyrethroid will
give year -long protection against malaria vectors
(HEWITT et al., 1995). Recurrent outbreaks of malaria
among nomadic Afghan refugees were finally controlled
by spraying tents with permethrin (litttJMA a al., I 9')o)
Treatment of blankets or outer sheets with permcthrinis a promising option for refugees sleeping under plasticsheeting or other makeshift materials. A recent study inan Afghan refugee camp showed over 60% protectionagainst falciparum infection for 3 months, and no side -effects (ROWLAND a al., 1999). This new approach isideal in short, acute emergencies because blankets arealways distributed and treatment with permethrin willgive protection in all types of shelter. The cost is only afraction of that required for ITNs. A recent study hasshown that treated blankets are equally effective againstcutaneous leishmaniasis (Leishmania in:pica) in Afghani-stan (REYBURN et al., 2000).
In the post -emergency phase refugees will constructhouses, allowing Increased use of IRS or ITN,. AnnualIRS campaigns can become an expensive drain on therefugee health budget. This is a good moment to changetack and introduce cost recovery. As refugees becomemore self -sufficient some are able and willing to pay forITN' ( ROWLAND or al., 1997). However, most may stillrequire assistance.
Are there cheaper alternatives to 1TNs and IRS thatcan be applied in chronic refugee settings? In the Afghanrefugee camps HealthNet International is pioneering anew method involving the treatment of domestic live-stock pyrethroid Insecticide (ligwrry & Rowt-AND,1999). This approach would not be applicable when titevectors are highly anthropophilic, e.g., Anopheles gaibia.
s.s in Africa or An. dins: in South -East Asia. However,vectors in South Asia arc highly'zoophilie and domesticcattle can therefore act as bait to attract mosquitoes to atoxic surface. A recent study of treated cattle demon-strated a level of control better than that shown by ITNsor IRS, and at a fraction of the cost. The project waspopular with refugees because cattle ectoparasites werevisibly controlled.
Finally we must consider the conditions facing refu-gees when they return home after the conflict. Thegovernment health system may be in no state to providemalaria control. This is the stage where 1TNs havegreatest potential.
A lead agency may coordinate an ITN programme and
12a -. M. kt,vt9 ANI)
provide training and commodities to non -specializednon -governmental organizations (NGOs) working atcommunity level. ITNs and re- treatments may be soldthrough NGO clinics or by teams of community health.workers. The NGO network may be the best way toachieve good coverage if government or private sectordistribution systems are absent in the immediate post-conflict phase. Revenue from sales may serve as arevolving fund for purchase of further nets and 'insecti-cide.
Although no method of malaria prevention is perfect,uppropriute methods do now exist which can amelioratethe situation at different stages of the emergency. Con-certed application of these over several years can have amarked effect on transmission rates. Guidelines arebeing produced by 'Roll Back Malaria' and these willenable agencies to select and apply the appropriatemethod according to the situation.
AcknowledgementsThis work was supported by WHO/UNDP/World Bank
Special Programme for Research and Training in TropicalDiseases (Project ID: 960662), the Department for Interna-tional Development of the UK, and HealthNet International.
Refer sBouma, M. J., Paves, S. D., Nesbit, R. & Winkler, A. M.
(1996). Malaria control using permcthrin applied to tents ofnomadic Afghan refugees in northern Pakistan. Bulletin of duWorld Health Organisation, 74, 413 -421.
Hewitt, S. & Rowland, M. (1999). Control of zoophilic malariavectors by applying pyrethroid insecticides to cattle.. Tropical.1laiei,re anti IntenIJIIJnol Health, 4, 481 -486. .
Hewitt, S., Rowland, M., Nat¡ir, M., Kama1, M. & Kemp, E.(1995). Pyrethroid sprayed tents for malaria control: anentomological evaluation in Pakistan's Nonh West FrontierProvince. Medical and Veterinary Bnioarob , 9, 394 -352.
Najera, J. (1996). Malaria control aprons ogees and displacedpupulario,u. Geneva, Switzerland: Worl Health Organiza-tion. CTD /MAU96.6.
Rcyburn, H., Ashford, R., Mohsen, M., Hewitt, S. & Rowland,M. (2000). A randomized controlled trial of insecticide-crested bednets and cheddars or top sheets, and residualspraying of Interior rooms for the prevention of cutaneousleishmaniasia in Kabul, Afghanistan. Transactions (Mc RoyalSociety of Tropical Medicine and Hygiene, 94, 361-366.
Rowland, M. (1999). Malaria control: bednets or spraying?
t Malaria control in the Afghan refugee camps of weiten,Pakistan. Transaaioru of the Royal Socury of Tn piculAledi. irae
and Hygiene, 93, 458 -459.Rowland, M., Hewitt, S., Durrani, N., Sikh, P., Bouma, M. &
Sondorp, B. (1997). Sustainability ofpyrcthroid impregnatedbed nets for malaria control in Afghan communities. Bulletinof the World Health Orranisation,7S, 23 -29.
Rowland, M., Durranit N., Hewitt, S., Mohammed, N.,Houma, M., Cameiro, I, Roundest, J. & Schapira, A.(1999). Petmethrin- treated ehaddan and top -sheets: appro-priate technology for protection against malaria in Afghani -atan and other complex emergencies. Tnvut:aims of the RoyalSociety of Tropical Medicine and Hygiene, 93, 465 -472.
WHO (2000). Outline strategy for malaria control in complexemergencies. Geneva, Switzerland: World Health Organiza-tion. swow. wlso. intisha /moumlamarivali/gwidefinei/ nalarw
Received 1 March 2000; revised 31 March 2000; accepted forpublication 16 August 2000
Announcement
ROYAL SOCIETY OF TROPICAL MEDICINEAND HYGIENEGamham Fellowships
Professor Cyril Gamham was one of the UK's leading parasitologists in the 20th century and his work was
characterized by outstanding achievement as both laboratoryscientist and field worker in the tropics. The special
place that Gamham occupies among his colleagues is recognized by the Fund set up in his memory to establish
research fellowships for young scientists.
The aim of.the Gamham Fellowship is to encourage young scientists to carry out short -term field projects.Suitable applicants arc invited to apply to the Fund, which is administered by the Royal Society of Tropical
Medicine and Hygiene. .
There are no restrictions by nationality or agé, and fellowship of the Royal Society of Tropical Medicine and
Hygiene is not a requirement. Applications from non-Fellows should be supported by a Fellow who can attest to the
value of the project and to the competence of the Applicant to carry out the work,
One Gamham Fellowship of up to £2000 will be awarded annually .
The Gamham Fellowship is to be used for short -term field projects of up to 2 years' durationPreference will be given to topics in parasitology or medical entomology and to applicants with less than 5 years'
postdoctoral experience .
Applicants are required to submit a detailed project, with costing of the work proposed, and a supporting
statement from their head of department Or supervisor, at least 6 months before the date of commencement
A short report should be submitted within 3 months of completion of the study
Application forms may be obtained from the Administrator, Royal Society of `Tropical Medicine and Hygiene,
Manson House, 26 Portland Place, London, W1B 1EY, UK; fax +44 (0)20 7436 1389, e-mail mail jrstmh.org
The closing date for receipt of applications is 15 September annually.1
Annals uf Tropical Aledicinc & Parasitology, Vol. 95, No. 1, 41-16 (2001)
Resistance of .Plasmodium falciparum malaria
to chloroquine is widespread in easternAfghanistanBY M. A. RAW, T. W. FREEMAN, N. DURRANI,. D. DE POERCK
HealthNet Intirnational, 11-r1 Cirrrdar Latte, University Toma, P.O. Box 889, Peshawar,
Pakistan
AND M. W. ROWLANDHealthNet International and London School of Hygiene and Tropical Medicine, i eppcl Street,
London WC! 7111', U.K.
Received 27 October 2000, Revised 22 November 2000,
Accepted 23 November 2600
Afler two decades of war and conflict in Afghanistan, the public- health system is in disarray and malaria
has re- emerged as a major di , with 'Plasmodium falripanrm malaria becoming increasingly common.
The limited healthcare services that arc available arc mainly delivered by non -governmental organizations
in collaboration with the Ministry of health. Although chloroquine (CO) rcttaains the official first -line
treatment against P. falriparutn malaria, there is little information on the severity or distribution of
resistance to this drug in Afghanistan. In -vivo surveys, co- ordinated by the Malaria Reference Centre in
Jalalabad, were therefore performed to determine the frequency and grades of CQresistance in the three
eastern provinces of Kunar, Nángarhar and Iaghman. Of the 142 cases enrolled in the study, only 47
(33 %) were sensitive. Most of the cases (55'1ít) showed RI resistance but Kii/Kiil resistance was not
uncommon (11 %). The prevalence of resistance appeared similar in children and adults, in malts and
females, and in each of the three provincesinvestigated. Gametocyte carriage post -treatment was elevated
in the resistant cases. M in neighbouring Pakistan, the resurgence of P. fa /riparum in Afghanistan is
probably associated with the transmission and spread of chloroquine-resistant strains. The first -line
therapy used against P. fälriparu,n malaria must be changed in order to reverse this trend.
Ileaith and healthcare in Afghanistan arc in a
grievous state. Twenty years of war and
conflict have led to economic collapse, de-. struction of government health services and
infrastructure, and emigration of manyqualified health workers. Health status and lifeexpectancy are the worst in the region (Anon.,1998). Malaria has re- emerged as a majorpublic -health problem in several areas.. Un-published clinic monitoring reports, produced
by HealthNct International, indicate that morethan 67 0(K) microscopically confirmed cases%ere reported in 1995 from just 83 hospitals
E-mail: inarah(ti?pcs.contaats.net.pk; fax: +92 91
840379.
and clinics (run by international mm- govern-mental organizations in collaboration with theMiniséry of Health) in six eastern provinces.The overall slide positivity rate, based on theexamination of over a quarter of a millionslides, was 19 %. Although most malaria inAfghanistan (90'36 of cases) is the result ofinfection with P. viva. ;, l'. firldrarron predom-inates from September to November, cross -scctional surveys carried out during thisperiod revealing more cases of P. fa/riparummalaria than of P. vivax malaria (unpubl.ohs.). The incidence of P. fii /riparum malaria
appears to be increasing rapidly, with 2U'!.1more cases reported in 1999 than in 1998
(unpubl. obs.). 'Ibis rise has been attributed to
ISSN 0003 -4983 (print) ISSN 1364 -8394 (online)/01/010041-06 m 2001 l.hcrpool School of Tropical Alcdicinc
Cartes PublishingDUI: 10.1080/00034911002(X1.15966
42 RAI! LT .11..
the development and spread of chloraquine(C:Q) resistance (Shah a al., 1997). The pre-vailing crisis in Afghanistan has prevented thecollection of data on CQ resistance, *althoughthe first case known in the country, a maleresident of Kunar province, in the cast of thecountry, occurred in 1986 (Delphini, 1989).More is known about such resistance inAfghan refugees in neighbouring Iran andPakistan than in those still resident in
Afghanistan. Although resistance was
observed in Afghan patients in Iran, thesewere suspected of being imported eases from
Pakistan (I:drissian, 1989). In nine refugeecamps in the North West Frontier. andBaluchistan provinces of Pakistan, the. fre-quency of resistance ranged from 18% to 86%(Rowland et al., 1997; Shah et al., ,1997).However, malaria among refugees in Pakistanis mostly the result of local transmission(Suleman, 1988; Bouma and Rowland, 1994)and the prevalences of CQ resistance' seen in.Afghan refugees are similar to those observedin local Pakistani communities (Shah et al.,1997). Surveys in the refugees therefore revealfew clues about the status of CQ resistance inP. faleiparuut infections transmitted withinAfghanistan. The need for surveys of CQresistance in Afghanistan was recognized by aconsultant of the World l lcalth Organization(WIIO), Professor H. M. Gilles, in 1998
(unpuhl. ohs.). In consequence, the presentstudy was undertaken to determine the extentul resistance to C:Qin the indigenous parasitesof the eastern region of the country.
SU11J1iC: f :S AND METHODS1IOI)S
'ulie study was carried tout su the regionalMalaria Reference Centres in three provincesof eastern Afghanistan -two in Nangarharand one each in Kunar and Laghman- duringOctober and November 1999 (see .Fig.). MIoutpatients presenting with suspected malariawere screened, and those hound to have P.Juli iparuat infections who were not pregnant,aged <7 years, or showing signs of compli-cated malaria were enrolled. After obtaininginformed consent, each enrolled subject was
given supervised treatment with oral CQ(sup-plied by the World Health Organization) atthe standard dosage of 10 mg base /kg body -weight, followed by 15 mg /kg during the next24 h.
In -vivo, 28 -day tests were then carried outusing the method described by Rowland et al.(1997). Briefly, all subjects were requested toreturn each week far 4 weeks so that follow -up, thick and thin smears could he prepared.Each smear was stained with Giemsa's sol-ution. A thick smear was considered negativeif no asexual parasites could, he found in I00fields. All positive smears we're re- examined atthe main HcalthNet reference centre in Jalala-bad, where parasitacmias (parasites /pt) wereestimated by counting parasites /200 Ieueu-cy'tes and assuming that each subject had 8000leucocytes/pl. Subjects showing f. fit/d'art/ontrophozoites at any time during the follow -upperiod were treated with sulfadoxinc-pyrimethamine.
Infections were classified as sensitive ifthere was no trophozoite recrudescence aftertreatment, as RI if trophozoites recrudesced2-4 weeks after CQ treatment, and as Rll/RIII if trophozoites were present I week post-treatment. Discrete variables were analysed
using Xt tests.
RESULTS
Overall, 142 cases of microscopicallyconfirmed P. Jaleiparum malaria were enrolledand followed' up during the course of thestudy. The mean age of cases on enrollmentwas 22 years, with an age range of 7-55 year'sand a male:female ratio of 1:2.
!Forty -seven cases (33%) showed no evi-dence of parasite recrudescence during the4 -week follow -up period, and wuru thusclassified as sensitive to chloroggine. Seventy-nine cases (5596) recrudesced between the 2ndand 4th week of follow -up, thus exhibiting Rlresistance, and the other 16 cases (i I%) werepositive for P. Jdlriparunt trophozoites I weekafter the start of treatment and thereforeclassified as RII /RIII (Table 1).
No significant difference in the
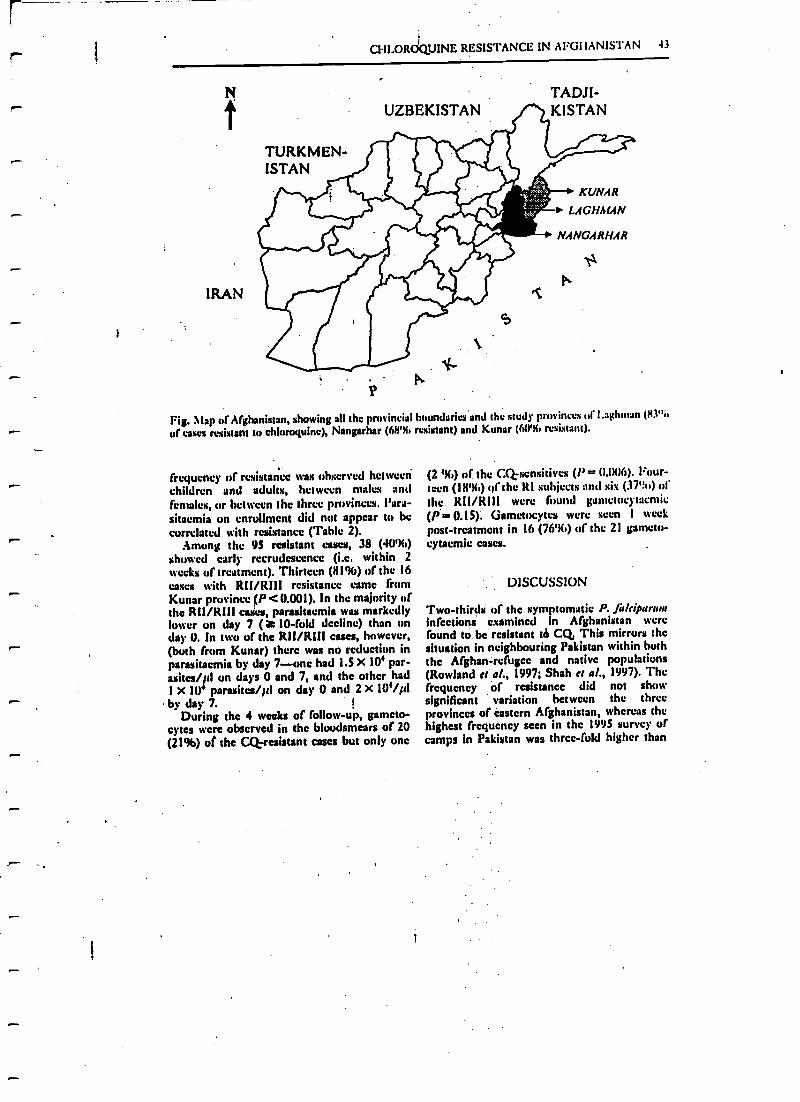
C1ILOROQUINE RESISTANCE IN AFGIIAN!STAN 43
IRAN
TURKMEN-ISTAN
TADJI-UZBEKISTAN KISTAN
P
KUNAR
LACHMdN
NANCARi/.fR
Pi1
Fig. \lap of Afghanistan, showing all the provincial boundaries and the study provinces of l.aghntan (83" b
of cases resistant to chlornquinc), Nangarhar (68% resistant) and Kunar (6(Y% resistant).
frequency Of resistance was observed hetwcetichildren and adults, between males and
females, or between the three provinces. Para -sitaemia on enrollment did not appear to becorrelated with resistance (Table 2).
Among the 95 resistant cases, 38 (40 %)showed early recrudescence (i.e. within 2weeks of treatment). Thirteen (81%) of the 16eases with RU /Rill resistance came fromKunar province (P<0.001). In the majority ofthe Rll /Rill cwki, parasitacmia was markedlylower on day 7 (a 10 -fold decline) than onday U. In two of the Rll /RIII cues, however,(both from Kunar) there was no reduction inparasitaemia by day 7--one had 1.5 X 104 par -asites /id on days 0 and 7, and the other had1 X Ur parasites /Id on day U and 2 X 104/p1by day 7.
During the 4 weeks of follow -up, gameto-cytes were observed in the bloodsmears of 20
(21%) of the Cl resistant cases but only one
(2 96) or the CQ sensitives (/' = 0.006). Four-teenen (1896) ttf the RI subjects and sis (3799) ofthe RII /RI11 were found gametocytacntic
(P 0.I S). Gametocytes were seen 1 week
post -treatment in 16 (76%) of the 21 gameto-cytacmic cases.
DISCUSSION
Two -thirds of the symptomatic P. /a/(sparwninfections examined in Afghanistan werefound to be resistant tb CQ This mirrors thesituation in neighbouring Pakistan within boththe Afghan-refugee and native populations(Rowland et al., 1997; Shah et al., 1997). Thefrequency of resistance did not show
significant variation between the threeprovinces of eastern Afghanistan, whereas thehighest frequency seen in the 1995 survey ofcamps in Pakistan was three -fold higher than
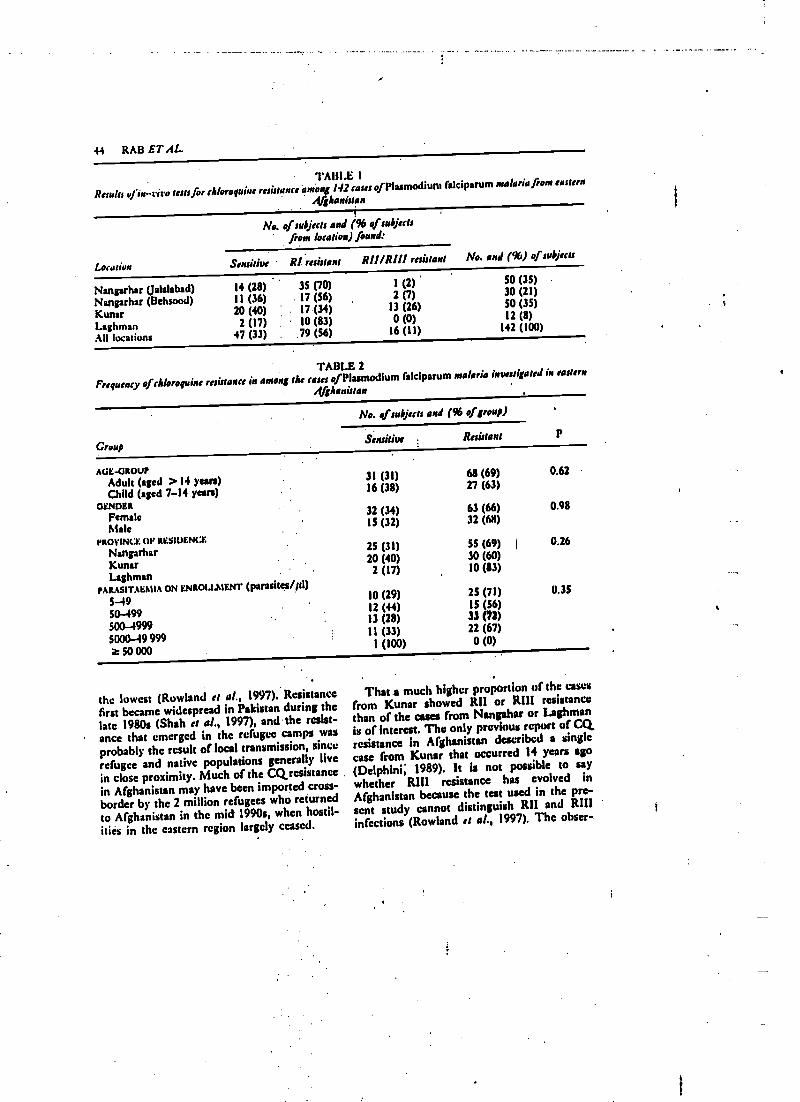
44 RAB ET AL.
TABLE I
Results of in -vit o troffer chloroquine resistance àniong 1.12 eases ofPlasmodium falciparum malaria from eastern
4/jhanistan
No. of subjects and (96 of subjectsfrom location) found:
Location Sensitiv R! resistant RI/ /R/I1 resistant No. and (96) ofsubjects
Nangarhar (Jalalabad) 14 (28) 35 (70) 1 (2) SO (3S)
Nangarhar (Behsood) 11 (36) 17 (56) 2 (7) 30 (21)
Kunar 20 (40) : . 17 (34) 13 (26) SO (35)
Laghman 2 (17) 10 (83) 0 (0) 12 (8)
All locations 47 (33) . 79 (56) 16 (11) 142 (100)
TABLE 2Frequency of chloroquine resistance in among the eases of Plasmodium falciparum malaria investigated in eastern
Afghanistan
Croup
No. of subjects and (96 of group)
PSensitive Resistant
AGE -GROUPAdult (aged > 14 years) 31 (31) 68 (69) 0.62
Child (aged 7 -14 years) 16 (38) 27 (63)
GENDERFemale
32 (34) 63 (66) 0.98
Male1S (32) 32 (68)
PROVINCE (W RESIDENCE
Nangarhar25 (31) SS (69) t 0.26
Kunar . 20 (40) 30 (60)
Laghman2 (17) 10 (83)
PARASITAEMIA ON ENROLLMENT (parasites /p1)
5--4910 (29) 25 (71) (1.35
50-49912 (44) IS (56)
500 -499913 (28) 33 (72)
5000-49 99911 (33) 22 (67)
50 0001 (100) 0 (0)
the lowest (Rowland et al., 1997). Resistancefirst became widespread in Pakistan during thelate 1980: (Shah et al., 1997), and the resist-ance that emerged in thc refugee camps wasprobably thc result of local transmission, sincerefugee and native populations generally live
in close proximity. Much of the CQrcsistancein Afghanistan may have been imported cross -
border by the 2 million refugees who returnedto Afghanistan in the mid 1990s, when hostil-ities in the eastern region largely ceased.
That a much higher proportion of the casesfrom Kunar showed R11 or R111 resistancethan of the cues from Nangaltar or Laghmanis of interest. The only previous report of CQresistance in Afghanistan described a single
case from Kunar that occurred 14 years ago( Delphini; 1989). h is not possible to saywhether Rh resistance has evolved in
Afghanistan because the test used in the pre-sent study cannot distinguish RH and R111infections (Rowland et al., 1997). The obser-.
r-
r
r-
r'
r
r
1
CIII.OROQUINE RESISTANCE IN AFG1IANISTAN 45
vation that, In two of the present subjects,
parasitaemia apparently failed to decline
within 7 days of CQtherapy may indicate that
Rill resistance is common. This might be
confirmed by use of the ;WHO's standard
7 -day test (WHO, 1973) or extended 14 -day
test (WHO, 1994). However, both of thesetests require more frequent collection of fol-low-up smears (which is likely to be difficult
in Afghanistan) than the 28-day test andwould have missed the many resistant infec-
tions that recrudesced between days 14 and 28
in the present study. As RITZ infections have
no greater clinical significance than RII, con-tinued deployment of the 28 -day test seemsmore useful in the current circumstances.
Clinical symptoms were not documented in
any detail. As in the recent surveys in the
refugee camps (Rowland e: W. 1997),
recrudescence was usually associated with a
resumption of fever and other symptoms war-
ranting second -line therapy (data not shown).
The present results indicate an early
increase in gametocytacmia among resistant
cases. Typically gametocytes appear within 14
days of treatment in resistant cased (Price et
al., 1999), peaking around day 7 post- treat-
ment (Robert et al., 2000). Mosquitoes feedingon CQ-resistant infections post- treatment arcfour -fold mure likely to become infected thanthose feeding on sensitive strains (Robert ei
al., 2000). The increased gamctocytogencsis in
P. falriparum caused by CQtherapy (Buckling
ei al., 1999), and other factors, such asanaemia, delay in seeking treatment, and pres-
entation with recrudescent infections (Price et
al., 1999), can therefore potentially hasten the
spread of resistant strains in a country such asAfghanistan, where malaria is hypo -endemic
and transmission seasonal (and hence rather
low).The official treatment guidelines for P. fa!-
riparian malaria in Afghanistan advocate CQ
as first -line treatment and the use of sulfadox-
ine-pyrimethamine for treatment failures.
The present evidence of widespread CQ
resistance indicates that alternative and
effective first -line treatments-perhaps sulfa -
doxine- pyrimcthaminc on its own or in
combination with an artcmisinin derivative -should be made available, at least in the east
of the country. Mapping of CQ resistance
should also be extended to the rest of
Afghanistan.
ACKNOWLEDGEMENTS. We are indebted to M.
Aminulla, technician trainer, and the micro-scopists of the Malaria Reference Centres inNangahar, Kunar and I.aghman provinces fur
collecting and examining bhwdsmears. The
study obtained support from W110
(Afghanistan). FlealthNet International's
Malaria Control Programme in Afghanistan isfinancially supported by the European Com-
mission. M.R. is partly supported by theDepartment for International Development of
the United Kingdom. None of the organiza-tions supporting the study take responsibility
for the views expressed in this article.
REF ERENCES
AMIN. (1998). 1998 Consolidated 'Ippeal j» ilfghanislan. New. York: United Nations Children's Fund
(UNICEF).IIUC1 I.INO, A., RANVORD-
CART1t'IlirE, L. C., Mills, A. & READ, A. P. (1999). Maroquine increases Plas-
modium falriporwan gamctogenesis invitro. Parasitology, 118, 339 -346.
llou iA, M. & ROwt.AND, M. (1994). Failure of passive zooprophylasis: malaria is associated with cattle
ownership In Pakistan. Transaction: of thr Royal Society of Tropical Medicine and Hygiene, 89,351.453.
I)t.I.PlONt, t.. P. (1989). The first case of Plaunodiwm falriparam resistance to chloroquine treatment discov-
ered in the Republic of Afghanistan. Transaction: of the Royal Society ol'Tropical Medirinr and / /ygirne,
83, 316.Euatssi. x, G. H. (1989). Status of the response of Plasmodium falriparum to chioroquinc and mefoquine in
Iran. Tropical and Geographical Medicine, 41, 297 -303.
46 Rrlll Er.lL.
RuuEKr, V., Av(NU- AMIIWVR, H. P., t.r: I1v.si&N, J. Y. & TRAMS. F. (2000). Gametocytemia and infcctih icy
tu mosquitoes of patients with tinc'omplicated P/asmod /aar falciparum malaria attacks monad with
chluroquine or sulfadoxine plus pyrimethamine. American Journal of Trópite! Medicine and Hygiene,
62, 210 -216. .
Roni..tw, M., l)uiuuNt, N., llewrrr, S. .fit SONIX)RP, E. (1997). Resistance of falciparum malaria tu
chluruquine and sulfaduxine- pyrimethamine in Afghan refugee settlements in western Pakistan:
surveys by general health services using a simplified in -vivo 10p. Tropical and latenaatiaaal lleahh,
2, 1019 -1056.Silts. 1., RowI..tNi), M., Alt.Thumu, P., MICjAnu). C., RAZIgUE, h., HEwrr, S. & 1)URRANI, N. (1997).
chloroquine resistance in Pakistan and *1w upsurge of falciparum malaria in Pakistani and Afghan
refugee populations. of T rapital Medicine and Paratitoloxy, 91, 591 -602.
SI:LE IAN, Al. (1988). Malaria in Afghan refugees in Pakistan. Transaction: of Ike Royal Sourly rf Tropical
Medicine and Hygiene, 82, 44 -47. .
PRICE, R., NOS1'EN, F., SIAIPSON, J. A., I.uXEIIERGER, C., PIIAIPUN, L., TER KUII.E, P., VAN VI;G r,
AI.,Chungsuphajaisiddhi, T. k White, N. J. (1999). Risk of gametocyte carriage in uncomplicated
falciparum malaria. American Journal of Tropical Medicine and Hygiene, 60, 1019 -1023.
%VORLu I IEAI: I'1I ORGANIZATION (1973). Chr nosheraAy of Malaria and Resistance to Atlanra /arials. Technical
Report Series Na. S29. Geneva: WHO.WORLD HEALTH ORGANIZATION (1994). Antimalarial Drug PMliciet: Data Requirements. 7itukuvnt of
Uncomplicated Malaria und ,1lanageaient g/'Malaria in Pregnancy. Document WHO /,MALI /94.11070.
Geneva: W1-10.
Annals of Tropical Medicine At Parasitology, Vol. 95, No. I, 41-46 (2001)
Resistance of .Plasmodium falciparum malariato chloroquine is widespread in easternAfghanistanBY M. A. RAB, T. W. FREEMAN, N. DURRANI,. D. DE POERCK
HealthNet lntirnatianal, 1l -A Circular Lane, University Town, P.O. Box 889, Peshawar,
Pakistan
AND M. W. ROWLAND .
Health Net International and London School of Hygiene and Tropical Medicine, K ppcl Street,
London IVCI7HT, U.K.
Received 27 October 2000, Revised 22 November 2000,
Accepted 23 November 2000 ..
After two decades of war and conflict in Afghanistan, the public- health system is in disarray and malaria
has re-emerged as a major disease, with Plasmodium falcipanan malaria becoming increasingly common.
The limited healthcare services that are available are mainly delivered by non-governmental organisations
in collaboration with the Ministry of Health. Although chloroquine (CQ) remains the official first -line
treatment against P. falciparum malaria, there is little information on the severity or distribution of
resistance to this drug in Afghanistan. In-vivo surveys, co-ordinated by the Malaria Reference Centre in
Jalalabad, were therefore performed to determine the frequency and grades of CQresistance in the three
eastern provinces of Kunar, Nangarhar and laghman. Of the 142 cases enrolled in the study, only 47
(33%) were sensitive. Most of the cases (55%) showed R1 resistance but RIi /KIII resistance was not
uncommon (11%). The prevalence of resistance appeared similar in children and adults, in males and
females, and in each of the three provinces investigated. Gametocyte carriage post -treatment was elevated
in the resistant cases. As in neighbouring Pakistan, the resurgence of P. faleiparum in Afghanistan is
probably associated with the tranamisaiun and spread of chloroquinc- resistant strains. The first -line
therapy used against P. fulciparum malaria must he changed in order to reverse this trend.
d icalth and healthcare in Afghanistan arc in agrievous state. Twenty years of war and
conflict have led to economic collapse, de-struction of government health 'services andinfrastructure, and ' emigration of manyqualified health workers. Health status and lifeexpectancy are the worst in the region (Anon.,199$). Malaria has re-emerged as a majorpublic -health problem in several areas.. Un-published clinic monitoring reports, producedby HealthNet International, indicate that morethan 67 000 microscopically confirmed caseswere reported in 1995 from just 83 hospitals
E- -mail: inarai4 pes.contsats.net.p1; fax: + 92 91
1140.179.
and .clinics (run by international non- govern-mental organizations in collaboration with theMinistry of Health) in six eastern provinces.The overall slide positivity rate, based on theexamination of over a quarter of a millionslides, was 19%. Although most malaria inAfghanistan (9(1% of cases) is the result ofinfection with P. viva.r, A Jirlciparturt prcdet »-inatca from September to November, cross-sectional surveys carried out during thisperiod revealing more cases of P. Jakiparuenmalaria than of P. v vox malaria (unpuhl.ohs.). The incidence of P. Jalriparuat ntaiariaappears to be increasing rapidly, with 211"ißmore cases reported in 1999 than in 1198
(unpubl. obs.). This rise has been attributed to
ISSN 11003 -4903 (print) ISSN 1364 -$594 (online) /01/010041.06 O 2001 Liverpool School of Tropical Medicine
Carias PublishingDOL: 10.10110 /t013491tt10200.15vtk,
42 RAH B7'.41..
the development and spread of chloroquine(CQ) resistance (Shah a at, 1997). The pre-vailing crisis in Afghanistan has prevented thecollection of data on CQ resistance,'althoughthe first rase known in the country, a maleresident of Kunar province, in the east of thecountry, occurred in 1986 (Delphini, 1989).More is known about such resistance inAfghan refugees in neighbouring Iran and
Pakistan than in those still resident in
Afghanistan. Although resistance was
observed in Afghan patients in Iran, these
%crc suspected of being imported cases from
Pakistan (Edrissian, 1989). In nine refugeecamps in ' the North West Frontier. andllalochistan provinces of Pakistan, the . fre-quency of resistance ranged from 18% to 86%(Rowland et u/., 1997; Shah el al., .1997).I luwe cr, malaria among refugees in Pakistan
is mostly the result of local transmission(Suleman, 1988; Bouma and Rowland, .1994)
and the prcvalences of CQ resistance' seen in.Afghan refugees arc similar to those observedin Zonal Pakistani communities (Shah et al.,1997). Surveys in the refugees therefore revealfew clues about the status of CQresistancc in
P. fit/ripening infections transmitted withinAfghanistan. The need for surveys of CQresistance in Afghanistan was recognized by aconsultant of the World Health Organization(WHO), Professor H. M. Gilles, in 1998
(unpubl. ohs.). In consequence, the presentstudy was Undertaken to determine the extentof resistance to Coin the indigenous parasitesof the eastern region of the country.
SUBJECTS ANI) METHODS
The study was carried out at the regionalMalaria Reference Centres in three provincesof eastern Afghanistan -two in Nangarharand one each in Kunar and Laghman- duringOctober and November 1999 (see. Fig.). Alloutpatients presenting with suspected malariawere screened, and those found to have P.Jaleiparauu infections who were not pregnant,aged < 7 years, or showing signs, of compli-cated malaria were enrolled. After obtaininginformed consent, each enrolled subject was:
given supervised treatment with oral CQ(sup-plied by the World Health Organization) atthe standard dosage of 10 mg base/kg body -weight, followed by 15 mg /kg during the next
24 h.In -vivo, 28 -day tests wcrc then carried out
using the method described by Rowland et al.(1997). Briefly, all subjects were requested to
return each week for 4 weeks so that follow -up, thick and thin smears could be prepared.Each smear was stained with Gicmsa's sol-ution. A thick smear was considered negative
if no asexual parasites could he found in 1(X)
fields. All positive smears were re- examined at
the main HealthNet reference centre in Jalala-bad, where parasitacmias (parasites/01) wereestimated by counting parasites /200 laueo-
cytcs and assuming that each subject had 84)00
leucucytes /id. Subjects showing 1'. fn /ciperumtrophozoitcs at any time during the follow -upperiod were treated with sulfadoxinc-pyrimethamine.
Infections were classified as sensitive ifthere was no trophozoite recrudescence after
treatment, as RI if trophozoites recrudesced2-4 weeks after CQ treatment, and as Rll/RIII if trophozoitcs were present 1 week post -
treatment. Discrete variables were analysed
using x2 tests.
RESULTS
Overall, 142 cases of microscopicallyconfirmed P. falciparun malaria were enrolledand follower up during the course of thestudy. 'l'ho mean age of cases on enrollmentwas 22 years, with an age range of 7 -55 yearnand a male:female ratio of 1:2.
Forty -seven cases (33%) showed no evi-dence of parasite recrudescence during the4 -week follow -up period, and were thusclassified as sensitive to chlorogyine. Seventy -nine cases (S596) recrudesced between the 2ndand 4th week of follow -up, thus exhibiting RIresistance, and the other 16 ensue (11e!) werepositive for P. fuldparw ss trophozoites 1 week
after the start of treatment and thereforeclassified as RII /Rl1I (Table 1).
No significant difference in the
lhgncrl .Medicine Anti Inarn. .tl I e.Jeh
tut RNl, t w; re 47z-.4x1 mix s000
Indoor residual spraying with alphacypermethrin controlsmalaria in Pakistan: a community- randomized trial
r Mark Rowland", Parvals Mahmood', Jt.vad Igbat'', Ilona Carnafro' and Desmond Chavassr.'
I It...at/Wet I lcrn.aivaal, t'csb.urrr. Paklrtan2 1.n,,lu,r \:buuf uf lIpt;,cnr and Trnpii.d Alydiiiui.l. luse, Uf:
i 1 be Nauu,,.rl 1stu,tr u f llalaria Rrsrar,li .u,.I Training. I..rhurr, I:,kist,ur
OM.
r
Summary We conducted a commitnity- r:uiJomized controlled trial in Pakistan td determine the efficacy of indoor
residual spraying with .iii liacypersuethrin ('I eiidona', Cyanamid, NJ, USA), applied at 25 n,;/m , to inctcm
falciparum and vivax malaria. Wettable powder (WP) and suspension concentrate (SC) formulations were
tested against an unsprayed control in AO irrigated rice -growing area of Sheikhupur. district, Punjab
province. The study area di 80 km= was Divided into nine sectors, which were assigned at random to control.
\\'I. or SC treatments in replicates of 3. Sentinel villages were selected frail, each sector for entomological
and disease mind turing. AlaI.ria was monitored by fortnightly active case deice (ACI)) and by ern...-
sectional parasite surveys on .schoolchildren. Mosquito populations were monitored by space spraying of
rooms and by cattle-landing catches. The spray campaign conk place in June 1997 and covered 96'%, of emu-
pounds. During the 7 months after spraying, the incidence of falciparum malaria was 9.5% lower and that of
vivax malaria 80% (uwei in WP- sprayed than unsprayed sectors. Similar results were uhtaineJ for sector,
sprayed with the SC formulation. Cross- sectional surveys gaveestimates of efficacy comparable to tluuse
obtained by ACp: Anopheles culicifacies was 8096 less abundant and A.stepbensi, the predominant .uu.p1te
line, was up to 68% kiss abundant in sprayed areas over the 7-month period. Reductions in anopheline
pantos rates indicated that the single -spray treatment was effective for the entire transmission season.
Sprayed surfaces lacked odour, which contributed to' the popularity of the campaign. Alphacypermethrin is .a
promising insecticide for the control of malaria in Pakistan and South Asia generally
keywords alphacypernaethrin, pyre liui.l, intuir residual spraying, malaria, vector control, mostit uu,
Pakistan
correspondence Ahrk 'Lowland, I.ondcna School of Hygiene and Trupic,tl Aledicine. Keppcl Strcct.
I.unclun 1ti'C:IIs 711.1; tll;
IntroductionFalciparum and vivax malaria are major health problems in
Pakistan. In the last decade there has been a'sixfold increase
in falciparum- malaria, which now comprises 42% of all
malaria eases recorded by the National Malària Control
Programme (Shah et al. 1997). Factorsassuci.ted.with the
upsurge include the spread of chIoroquine resistanceaerossthe country (Rowland et al. 1997a; Shah et 4.1997), Wanner
autumns favouring prolonged transntissiun.(Bouma et al.
1996), and a chronic decline in vector control at;tivities.
Indoor spraying of residual insecticide is the primary method
of malaria control in Pakistan and South Asia, and has been
shown to prevent morbidity and economic losses (Dezulueta
r` et al. 1980; Mills 1991; Rowland et al. 1994; 1997h). The
472
organophosphorus insecticide malathion has been the main-
stay of malaria control in Pakistan over the past 25 years .mJ
still gives adequate control if campaigns arc properly targeted
and managed (Rowland et al. 1997h), despite malathion re-
sistance in several species of anopheline (Rathor et al. 1985;
Suleman 1993). The only synthetic pyrethroid to he evaluated
in Pakistan is Iambdacyhalothrin, which performed better
than malathion in Afghan refugee camps in North -west
Frontier Province (Rowland et al. 1994). Further trials an
pyrethroids as house -spraying agents are warranted.
The National Institute of Malaria Research and Training
(NIMRT) has conducted several efficacy and safety trials of
new candidate insecticides under the WHO Pesticide Evalu-
ation Scheme. Alphacypermethrin ('Fenduna', CyanainiJ), .111aiphacyano pyrethroid, is being proposed as a new agent fur
® 200084kr.rx St.crtv
1
t,upiaa) Alaviieine and International I lealth tnI.U\11. n Nt17 l'1'472-4%1 11.11 2_7
M. Rowland et al. Indoor residual spraying with alphacypermethrin
indoor residual spraying and treatment of bedncts (WHO1998). We describe a community-randomized controlled trialinvolving two formulations of alphacypermcthrin for indoorresidual spraying undertaken in Sheikhupura district, Punjabpnnince.
Materials and methods
Study area
The wcetahle powder (5'%. WP) and suspension concentrate( Ill% SC) formulations of 'Fendana' were tested against a notreattncnt amend. 'Me study area incorporated thnr UCouncils and covered 180 km' of Sheikhupura district, abode60 km west of Lahore, the provincial capital. Thearea wasnapped b> NIMRT, divided into nine sectors of approxi-mately equal population size and area, and them each sectorwas assigned at random to untreated, WP, or SC spraying inreplicates of three. All 60 villages within the ìtudy area wereincluded in the trial. The study area was a flat, irrigated, agri-cultural plain, with rice as the main crop during the malariaseason (June -November). The area appeared environmentallyhomogeneous. At night, cattle, water buffalo, and otherdomestic animals were kept in the villagcsin owners' com-pounds, and hence almost all sources of blood meals andindoor resting sites were situated in the villages. House com-e--pounds were constructed from mud and brick and separatedby hitch perimeter walla.
r Gems surveys and spray operations
Village elders attended meetings to learn about the study andto give their consent to the project. Twu or three sentinel vil-lages totalling 2000 population were selected frost each sector
I for Disease and entomological monitoring and enumerated.The population and number of houses in sentinel villageswere, respectively. 6017 and 1206 in WP sectors, 5677 and 1 124in SC sectors, and 6567 and 1328 in control sectórs; Bencesentinel villages were consistent between treatment groups.Sentinel villages were chosen carefully so that the distance tovillages in a different treatment group was at Last 1.5 km.r Supervised spray operations were completed within 24 daysin June 1997. The target Jose was 25 nog alphacypermethrinper m'. Spraymen used Hudson X-pert spray pumps (Hudson,'I1.. IISAI to spray living quarters, storage rooms and animal
P". shelters. Each sprayman sprayed 9-10 compounds per day.Spray coverage was 96% of compounds (2665 compoundssprayed) in WI' sectors and 97% (1991 sprayed) in SC sectors.
Active ease detection
To measure a reduction in malaria incidence of 50 %, given
O 21100 Slaü,ves Sciente Ltd
o
an incidence of SO episodes per 1000 person years, we esti-mated that X000 people in cash of the nine sectors should hefollowed by ACI This required the survey teams to visit -toohouse: iii each sector every fortnight. Any member of .0
household reporting fever during the previous .3 days had a
blood smear taken and was treated presumptively withchloroquine. Confirmed cases were given a full course of25 leg chloroquine per kg body weight over 3 days. Adi) sur-veys weir: started in April, 2 months before the spray cam -
paign, and e iuucd 'I J:uour»
Cross -sectional surveys
Crois - sectional surveys were undertaken in April -May andSeptember, i.e. before and after spraying. One or two schuld.were selected from sentinel villages in each sector and 'hie':and thin smears were taken from 200 to 300 children aged5-I5 present on the day. Smears were stained with Gienus.t,and 200 fields were examined before any smear was classifiedas negative. Children positive for parasites were given a fullcourse of chloroquine.
Entomological monitoring
Space spray catches were undertaken fortnightly in tutu sleep-ing rooms, two storage rooms, anti two animal shelters ineach sector. The monitoring mounts were deliberately leftunsprayed, and the sane rooms were used throughout thestuds l'etiu:le anuphelines wore identified to specie. level andscored. 'lit determine pantos rotes, up to I11í1 Mosel .Indfreshly fed specimens were dissected per night; if the numbercaught exceeded 100, the dissections were done according tothe proportion of each species in the overall catch.
One night of buffalo bait collection was carried out fromdusk to dawn, inside and outside an animal shelter, in eachsector each month. Buffalo were {referred to humans as bof-falo landing catches were easier to do, presented nu healthhazard, and yielded more mosquitoes. The same animalswere used throughout. Catching stations were sprayed at thesane time as the rest of the village.
Residual 'activity un mud, wood, thatch, brick, and cementwas monitored every 2 weeks using standard WHO bioassaycone techniques. Forty-five mosquitoes were exposed for.30 min in each test. Susceptibility to alphacypermcthriutwas monitored using standard WHO resistance test kits.Exposure was to 25 mg/m' for I h, and mortality was Iotter 24 h recovery. Climatic variables were recorded daily atthe Lahore Meteorological Station.
Analysis
Overall incidence rates were calculated for each treatment
473
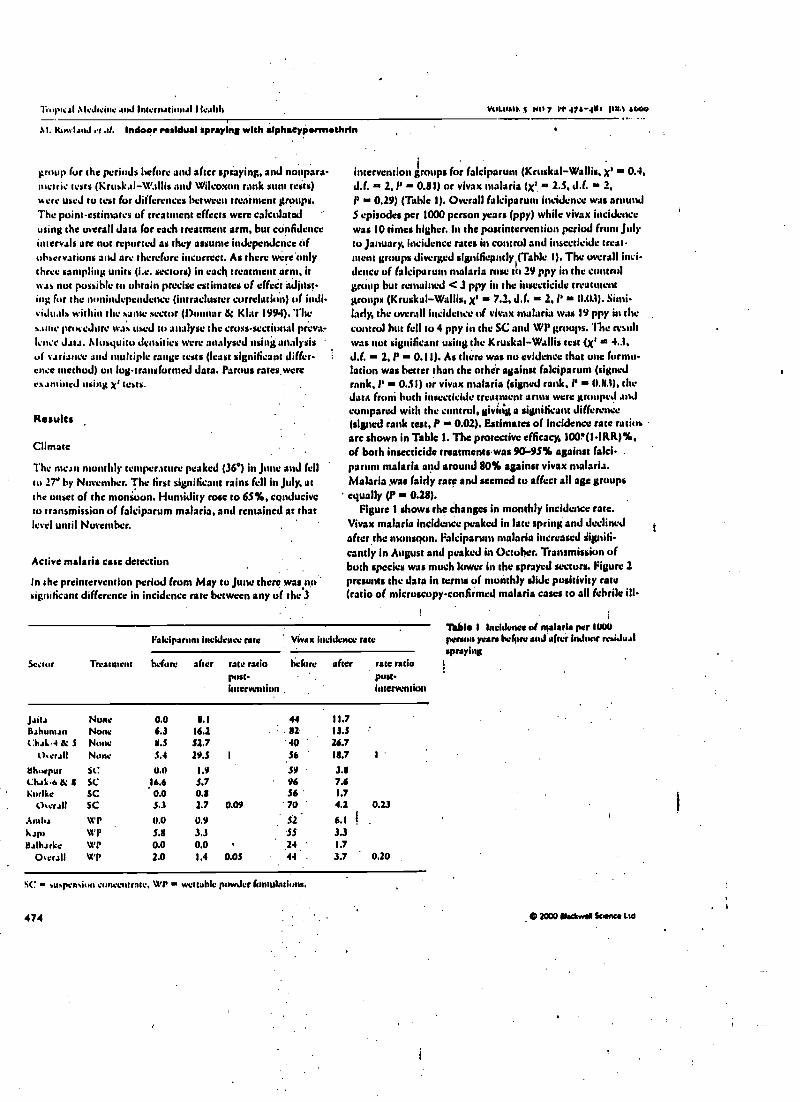
II upical \IeJ'aiue and International Health VQLtMt+ f N" 7 11 47ary0' iull a000
\t. Wiwi-m.1 et .rl. Indoor residual spraying with alphacypa nsathrin
group for the periods before and after spraying, and nonpara-n'cnn: tests (Kruskal- Wallis :und Wilcoxon rank stint sects)were used to test for differences between treatment groups.The point-estimates of treatment effects were calculatedusing the overall data for each treatment arm, hut confidenceintervals are not reported as they assume independence ofobservations and are therefore incorrect. As there wcreunlythree sampling units (i.e. sectors) in each treatment arm, itwas not possible to obtain precise estimates of effect adjust-ing; for the nonindependencc (intracluster correlation) of indi-iduals within the same sector Mannar á Klar 1994). Thes.,nte procedure leas used to analyse the cross-sectional prove-!dice Jata. Ilusyuitu densities were analysed using analysisof vvriance and multiple range tests (least significant differ-ence method) on log- transformed data. Parous ratcswereermined using gz tests.
Results
Climate
The mean monthly temperature peaked (361 in June and fellto ìT' by November. The first significant rains fell in July, atthe onset of the monsoon. Humidity rose to 65 %, cenducivcto transmission of falciparum malaria, and remained at thatIelrl until November. .
Active malaria case detection
In the preintervention period from May to June there wasp*significant difference in incidence rate between any of the 3
intervention groups for falciparum (Kruskal -Wallis, x' is 0.4,d.f. - 2,1' - 011) or vivax malaria (ye i 2. S, d.f. 2,
P - 0.29) (Table 1). Overall falciparum incidence was aroundS episodes per 1000 person years (ppy) while vivax incidencewas 10 tines higher. In the postintervcntion period front Julyto January, incidence rates in control and insecticide treat-ment groups diverged significpntly (Table I). The overall inci-dence of falciparum malaria rose to 29 ppy in the controlgroup but remained < .3 ppy in the insecticide treatmentgroups (Kruskal -Wallis, xt - 7.2, d.f. - 2, i' is 11.03). Simi-larly, the overall incidence of vivax malaria was 19 ppy in thecontrol but fell to 4 ppy in the SC and WI' groups. 'Ille resultwas not significant using the Kruskal -Wallis test {xt - 4.3,J.f. - 2, P - 0.11). As there was no evidence that one formu-lation was better than the other against falciparum (signedrank, l' - 0.51) or vivax malaria (signed rank, P - 0.83), theJata front both insecticide treatment arms were grouped andcompared with the control, giving a significant difference(signed rank test, P - 0.02). Estimates of incidence rate ratiosare shown in Table 1. The protective efficacy, 100'(1- IRR)%,of both insecticide treatmeneswas 90 -9S% against falci-parum malaria and around 80% against vivax malaria.Malaria was fairly rare and seemed tu affect all age groupsequally (P - 0.28).
Figure 1 shows the changes in monthly incidence rate.Vivax malaria incidence peaked in late spring and declinedafter the monstlttn. Falciparunt malaria increased tigoi6-candy in August and peaked in October. Transmission ofboth species was much lower in the sprayed sectors. Figure 2presents the data in ternis of monthly slide positivity rate(ratio of microscopy- confirmed malaria cases to all febrile ill-
Segur Treatment
Faieiparum Incidence rawliable 1 Incidence of malaria per 1000
Vivax incidence rate person years hefnre and after indoor residual
before after raw ratiopost-intervention
I><fore afterspraying
rate ratiopost-intervention
Jaita None 0.0 8.1 44 11.7Bahunun None 6.3 16.1 : 82 13.5C:hal41l' 5 None 8.5 52.7 40 ' 26.7
U,erall None 3.4 29.S 1 56 18.7 1
Bhuepur SC: 0.0 1.9 59 31Chal63; ta SC 16.6 S.7 96 7.6KurIke SC 0.0 0.8 56 ' 1.7
Clcerall SC 5.3 2.7 0.09 70 41 0.23
AInha WP 0.0 0.9 52 6.1
Kap' Vi'P 5.8 3.3 55 3.3
Balharkc WP 0.0 0.0 24 1.7
Oierall WP 2.0 1.4 0.05 44 3.7 0.20
SC: suspemiun concentrate. WI' w wettable powder fontulatiuns.
474 O 2000 Otattwer Sown. Ltd
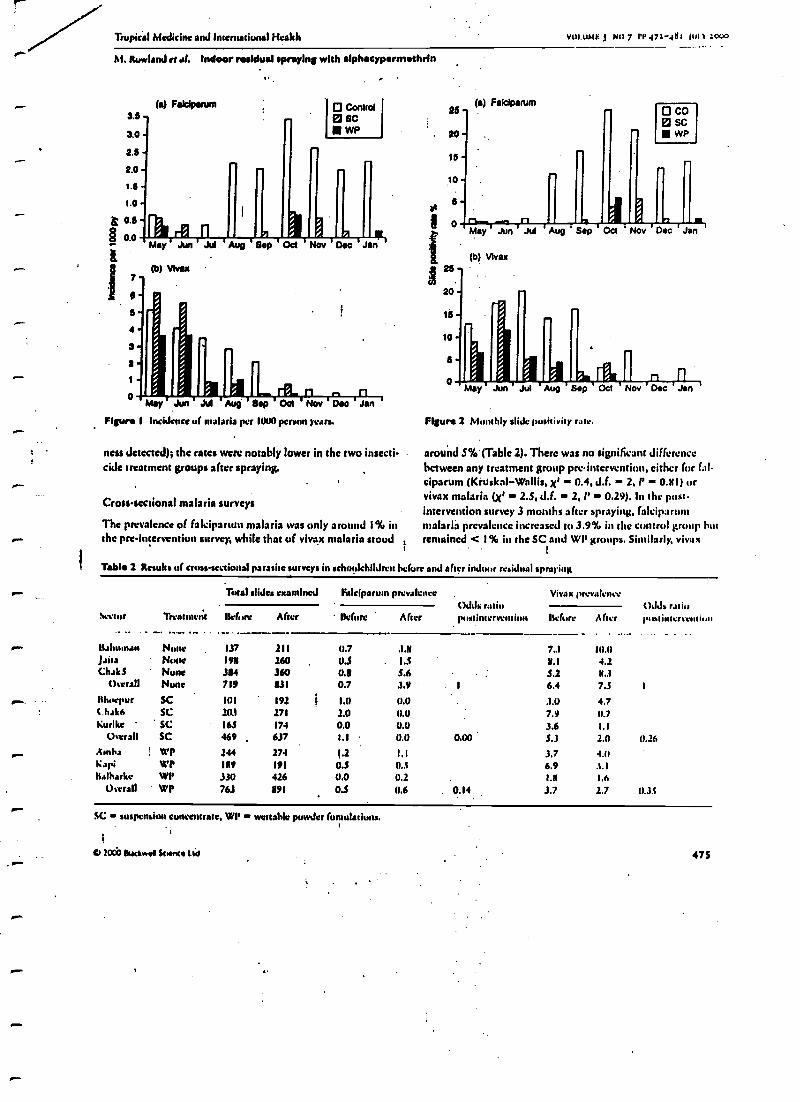
Tropic's' Medicine and International Health VUI.UMt: j NCI PP 47/-4111 11111 3000
M. Rowland rr ell. Indoor residual spraying with alphaeypermethrin
t.
3.5
3.0
3.5
2.0
t.a
1.0
çs0.5
tS 0.0
ä
1
(a) Faklparum O Control0 sCwP
May Jun Jul Aug Bap Oct Nov Dec Jan
(b) Vlvax
4
3
a
oMay Jun Jul Aug Bap Oct Nov
Figure 1 Incidence of malaria per 1000 person ,Mars.
Dec Jan
nets detected); the rates were notably lower in the two insecti-cide treatment groups after spraying.
Cross -sectional malaria surveys
The prevalence of falciparunt malaria was only around I % inthe pre-intervention survey, while that of vivax malaria stood
O COsc
a WP
lay Jun Jul Aug Sep Oct Nov Dec Jan
Figure 2 Monthly slide positivity rate.
around 5% (Table 2). There was no significant differencebetween any treatment group pre-intervention, either for fall-ciparum (Kiuskai- Wallis, x' = 0.4, d.f. = 2,1 - 0311) orvivax malaria (x' = 2.5, J.F. - 2, 1' 0.29). In the post-intervention survey 3 months after spraying, falciparunlmalaria prevalence increased to .3.9% in the control group butremained < 1% in the SC and WI' groups. Similarly, vivax
Table 2 Resuhs of cross- sectional parasite surveys in schoolchildren before and after indoor residual spraying
Sector
i- llahumanJaitaChakS
Overall
Hhoepurt.hak6Kurlke
Overall
.- eYlnha
KapiKalharke
Overall
"p-
Treaunetit
Total slides examined Fatciparunt prevalenceOJds ratiopustinterve
Viral( preva i:1ovt)JJi r.11iopustintcrvcmionBefore After liefine Aher Before After
None . 137 211 11.7 3.8 7..1 111.11
None 198 260 U.S 1.5 8.1 4.2Nunc 354 360 0.5 5.6 S.2 N..1
None 719 831 0.7 3.9 6.4 7.5 1
SC 101 191 It 1.0 0.0 3.0 4.7SC 10.1 171 2.0 0.0 7.9 0.7SC 165 174 0.0 0.0 3.6 1.1
SC 469 637 1.1 0.0 0.00 S.3 2.0 0.26
É WP 144 274 1.2 1.1 3.7 4.0WP 189 191 0.5 0.5 6.9 3.1WP 330 426 0.0 0.2 1.11 1.6WP 763 891 U.S 0.6 0.14 3.7 2.7 0.35
SC suspension concentrate, WI' wettahle powder (emulations.
02063 tuckwoo Schot Ltd 475
Tropical Medicine and International Health votaiMF. 5 Nil 7 PP 471-01 1 ior.
1i. ItowlanJ et .tf. Indoor residual spraying with alphacypermethrin
(b) A. atsphensl (a) A. pulchanYnus
14
12
10
May Jun Jul Aug Sep Oct Nov Dad Jan
(e) A. annularis
May Jun Jul Aug Sep Oct Nov Dec Jan
2
May Jun Jul Aug Sep Oct Nov Ma Jan May Jun Jul Aug gap Oct Nov Dec Jan
Figure 3 rlu.yuitu 'abundance as Jaen mincJ hy'inJtxtr rcuinµ (apaerspray) tioileetiuns from remind rooms.
malaria prevalence remained at 7.5% in the control group butfell to < 3% in the SC and WP groups. Both results were ofborderline significance using Kruskal- Wallis (P 0.06), but ifthe data are regrouped to compare hdth insecticide treat-malts (n Iv 6) against the control (n + 3), the result is signifi-
i
cant fortboth falciparum (signed rank, P 0.02) and vivaxmalaria (signed rank, P w 0.04). Odds ratios fur treatmenteffects are shown in Table 2. The protectivu'efficacy, 11101 I-OR)%, of the spray intervention indicates that faleiparummalaria prevalence was reduced by 100% in the SC and by
476 C 2000 Btackwed Suene uc
rTropical Medicine and International Health
. vu.UAtF f No 7 IT 47: 48t ¡Ili :cvwM. Rowland rt at Indoor residual spraying with alphacyparms hrin
. l
Table 3 Geometric mean density of mosquitoes per sector from space spray collections Inside sentinel living rooms and animal sheds over thepustintertentk,n period from July to Januarg Six rooms were space sprayed In each sector every two weeks. Meansfolttnttid by s tare signifi-cantly different from untreated sectors.
Untreated
Anophr/ro
Wettahle powder Suspen.iva euncentrate
Densityspecies Akan (95% C.1.) Mean (95% C.I.) nductiau Mean
rNl4ik/n 4.7 (3.4, 6.3) 1.0 s (0.6, 1.6) 0.78 0.11sstrplrrnsi 29 (24.33) 9 s (4, 19) 0.68 14rnnrrl,rdi 4.9 (2.9, 7.6) 2.0 s (1.8, 2.1) 0.39 3.2prrlchrdntNS 3.6 (1.4, 7.2) 2.9 (2.3, 3.5) 0.20 2.9sNbpktus 6.4 (3.4, 11.0) 2.2 s (1.2, 3.7) . 0.65 2.8 sCNlrx spp. 47 (34, 63) 26 (12, 53) 0.45 20 s
(95% C.1.)U 1.redor
(0.6, 1.0) 0.x4(S, 33) 0.51(1.5, 3.7) 0.34(0.3, 3.51 0.19(1.4. 5.0) 0.5c(e, 47) 0. St,
proportional reduction in geometric mean density in treated eosupmcd to untreatedsectors.
(a) A. stephensl
1.0
".0.80.60.40.20.0
1.00.80.60.40.20.0May Jun Jul Aug Sap Oct Nov Dec May Jun Jul Aug Sep Oct Nov Dec
(b) A. cuilcllac/es
(c) A. annularls
May Jun Jul Aug Sep Oct Nov Dec
(e) A. pulchemmus
r
1.00.80.60.40.20.0
O
May Jun Jul Aug Sep Pct Nov DecFlaw* 4 Porous rates in anophelines hum indoor resting (spacespray) catches.
(d) A. subp/ctus
at 1.0 -0.8 -0.6 -
0.4 .-+0.2 -0.0
2000 dackwea Science ltd
I IMay Jun Jul Aug Sep Oct Nov Dec
Control® SC
WP
477
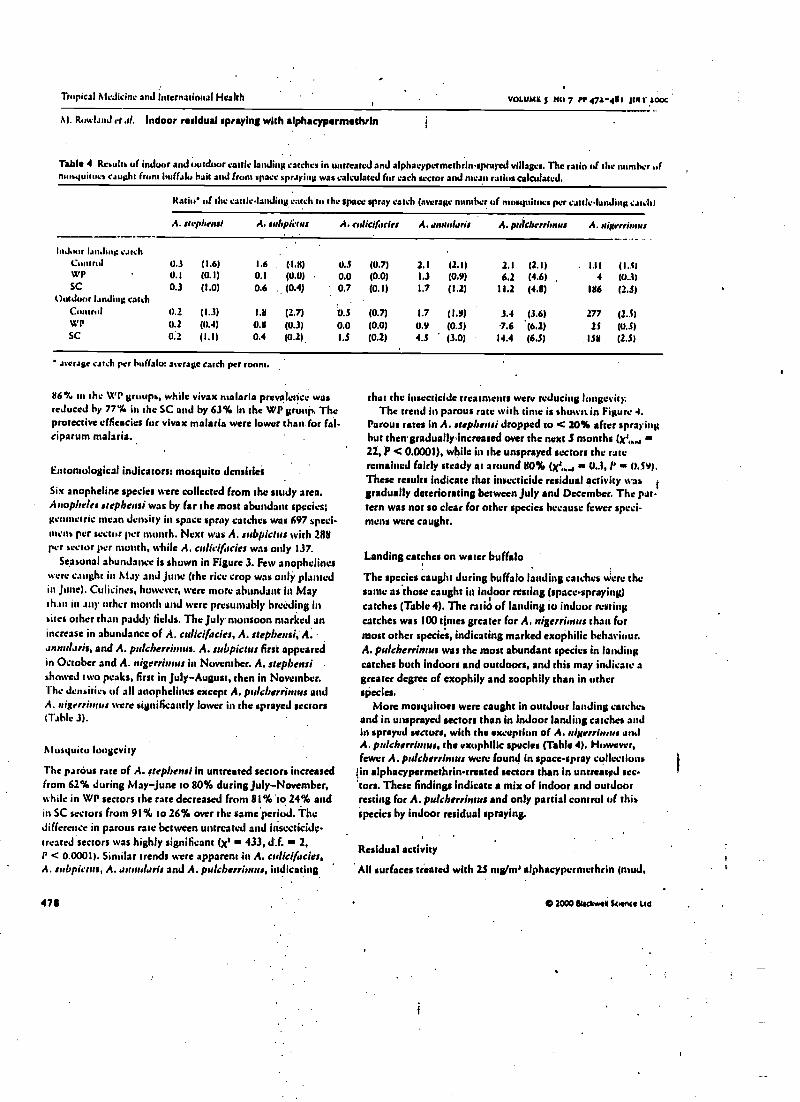
Tropical Medicine and international Health VOLUME 5 NO 7 PP 47a-01 pn.r aooc
NI. Rowland rtal. Indoor residual spraying with a(phacypermethrin
Table 4 Rcaulta of indoor and outdoor cattle landing catches in untreated and alphacypermcthrinsprayed villages. The ratio of the number ofmuayuitova caught from buffalo hait and f pact. apra) Mg was calculated for each sector and mean ratios calculated.
Ratio* of the cattle- landing catch tu the space spray catch (average number of mosquitoes per cauleIanJing ranch)
A. nrpbrns/ A. urlrpüvus A. calicif.rdrs A. rrund.rris A. pr)cbrrr'r t r A. aigrrriorIts
hidoor landing catchControl 0.3 (1.6) 1.6 (1.N) U.S (0.7) 2.1 (I.1) II (2.1) . 131 (1.51WP 0.1 (0.1) 0.1 (O.(1) 0.0 (0.0) 1.3 (0.9) 6.2 (4.6) , 4 (0.3)SC 0.3 (1.0) 0.6 ., (0.4) 0.7 (0.1) 1.7 (1.2) 11.2 (41) 186 (2.S)
Outdoor landing catchControl 0.2 (1.3) 1.11 (2.7) 0.S (0.7) 1.7 (1.9) 3.4 (3.6) 277 (2.5)
(1.2 (0.4) 0.8 (0.3) 0.0 (0.0) 0.9 (0.5) 7.6 .(6.2) 25 (O.S)Sc 0.2 (1.1) 0.4 (0.2) 1.5 (0.2) 4.3 '(3.0) 14.4 (6.S) ISN (2.5)
as crap catch per buffalo: average catch per room.
116% in the WP groups. while vivax malaria prevalence wasreduced by 77% in the SC and by 63% in the WP group. Theprotective efficacies for vivax malaria were lower than for fal-ciparum malaria.
Entomological indicators: mosquito densities
Six anopheline species were collected from the study area.Anopheles stephensi was by far the most abundant species;geometric scan density in space spray catches was 697 speci-nnana per sector per month. Next was A. subpielus with 288per sector per month, while A. ettlicifacies was only 137.
Seasonal abundance is shown in Figure 3. Few anophelineswere caught in Alay and June (the rice crop was only plantedin June). Culicincs, however, were more abundant in Maythan in any other month and were presumably breeding insites other that' paddy fields. The July monsoon marked anincrease in abundance of A. culicifacies, A. stephensi; A..rnnstl.tris, and A. pulcherritttus. A. sabpictus first appearedin October and A. nigerrinnts in November. A. stephensishowed two peaks, first in July- August, then in November.The Densities of all anophelines except A. pulcberüntus andA. nigrrris nss were significantly lower in the sprayed sectors(Table 3).
Mosquito longevity
The partius rate of A. steplensi in untreated sectors increasedfrom 62% during May June to 80% during July- November,while in WP sectors the rate decreased from 81 %to 24% andin SC sectors from 91% to 26% over the same period. Thedifference in parous rate between untreated and insecticide -treated sectors was highly significant (x' - 433, d.f. - 2,P < 0.0001). Similar trends were apparent in A. crrlicifacies,A. subpichrs, A. arrnularis and A. pulcherrimus, indicating
471
that the insecticide treatments were reducing longevity:The trend in parous rate with time is shown.in Figure 4.
Parous rates in A. stephensi dropped to < 20% after sprayingbut then.graduallyincreased over the next S months (x',,,y22, P < 0.0001), while in the unsprayed sectors the rateremained fairly steady at around 80% (x', ,, 0.3, P N. 0.59).These results indicate that insecticide residual activity was
Igradually deteriorating between July and December. The pat-tern was not so clear for other species because fewer speci-mens were caught.
Landing catches on water buffalo
The species caught during buffalo landing catches were thesaute as.those caught in indoor resting (space- spraying)catches (Table 4). The rata) of landing to indoor restingcatches was 100 tjmes greater for A. nigerrimus than furmost other species, indicating marked exophilic behaviour.A. pulcherrintus was the most abundant species in landingcatches both indoors and outdoors, and this may indicate agreater degree of exophily and zoophily than in otherspecies.
More mosquitoes were caught in outdoor landing catchesand in unsprayed sectors than in indoor landing catches andin sprayed sectors, with the exception of A. teigerriams onJA. pulcherrimus, the exophilic species (Table 4). However,fewer A. puleberrimus were found in space -spray collectionstin alphacypermethrin- treated sectors than in untreated sec-tors. These findings indicate a mix of indoor and outdoorresting for A. pulcherrimus and only partial control of titisspecies by indoor residual spraying.
Residual activity
All surfaces treated with 25 mg/m' alphacypurmuthrin (mud.
O 2000 BlttkwsM SCNnrt Ltd
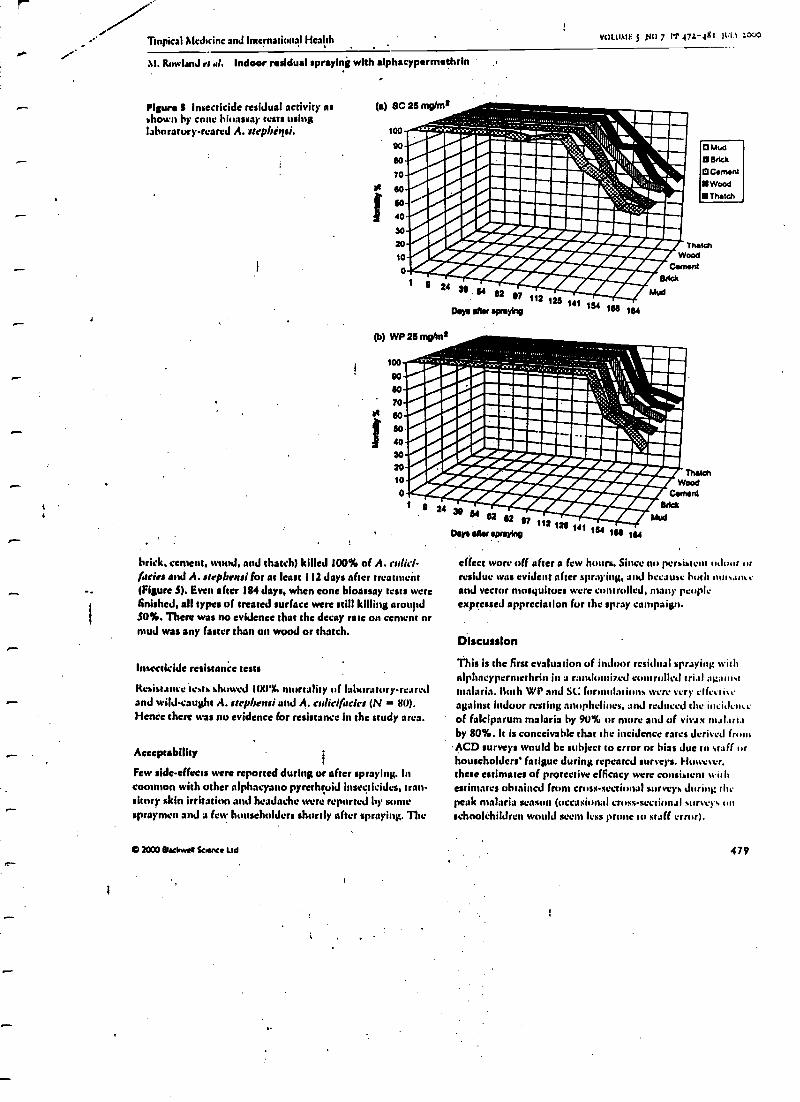
Tropical Medicine and International Health VOLUMES ,t40 7 Pt' 47L-48i 0111 1000
M. Rowland er al. Indoor residual spraying with alphacypermethrin
Figure B Insecticide residual activity asshown by cone bioassay tests usinglaboratory -reared A. strpbigsi.
f
(a) SC 26 myms
í
100 wti. 1x I..../ ::>I,I e/ ;::,, `I `:,°''';.. Il,l,``ìn_:----=:rti¡%Ii'I'''I_I_,- Wood''I''.IIIi- CementI' '' Back
Y
24 J9 7 112 126II Mud
DIP aAM spraying /06 161
70
6o
60
40
30
20
10
0
O Mud
Brick
O Cema.0
Wood
Thatch
(b) WP 26 mphns
Í
100;¡i--'--- `;`% 1:
1:1111111.111
.//i:::';7a//%¡¡< !/// ¡ii;Fo
.//// i///\,i "o o/i20 i iieis `/¡-i,i¡2t/'/_10
o
brick. cement. wood, J, and thatch) killed 100% of A. errlic(-lacks and A. s rpbrstsi for at least 112 days after treatment(Figure S). Even after 184 days, when cone bioassay tests werefinished, all types of treated surface were still killing arou'td50 %. There was no evidence that the decay rate on cement ormud was any faster than an wood or thatch.
Insecticide resistance tests
Resistancc'tests shuw+LJ 100'%. tality of laboratory- rearedand wild- caught A. strpbensi and A. culicif airs (N = 80).Hence there was no evidence for resistance In the study area.
Acceptability
Few side -effects were reported during or after spraying. Incommon with other alphacyano pyrethruid insecticides, tran-sitory skin irritation and headache were reported by somespraymen and a few I schuldcrs shortly after spraying. The
O 2000 Blackwel Science Ltd
Days alter spraying'112 126 141 1
166 164
TltetehWood
CementBrick
Mud
effect ware off after a few hours. Since no persistent 11,100r ..rresidue was evident after spraying. and because both nut..uneand vector mosquitoes were controlled, many peupleexpressed appreciation for the spray campaign.
Discussion
This is the first evaluation of indoor residual spraying withalphacypermethrin in a randomized controlled trial ag,ki,ktmalaria. Both WI' and SC (ormolatinns were very c(fe.ti.tagainst indoor resting anophcliues, and reduced the incidenceof faiciparum malaria by 90% or more and of vivax malariaby 80 %: It is conceivable that the incidence rates derived from
ACD surveys would be subject to error or bias duc to staff orhouseholders' fatigue during repeated surveys. However.these estimates of protective efficacy were consistent withestimates obtained front cross -sectional surveys during sitepeak malaria season (occasional cross -sectional survey. nnschoolchildren would seem less pr to staff error).
479
liop.cal ¡IcJicincand International Health vun.usnn: s NU 7 PP 471-4tt i µus Lou,
M. R.nt ImnJ et al. Indoor residual spraying wich alphacypermethrin
Alphacypermcthrin appeared to have leis effect againstvivax malaria. This result is misleading because relapses ofviva malaria front pre-trial infections would occur at equalfrequency in insecticide-treated and untreated sectors andcould nut be distinguished from new infections. 11w relapserate is high during the spring in Pakistan, just before theusrnsackus. and coincides with a growth in anopheline popula-tions (lox & Strickland 1989; Rowland et al. 19976). Thephenomenon of relapse makes it more difficult to eliminateiv.ta malaria front subtropical areas by vector control emu-
pared to falcipartm malaria, which does not relapse. Severalyears of indoor spraying campaigns in Afghan refugee campsof North -west Frontier Province have brought to an end thepublic health problem of falciparum malaria, but vivaxmalaria still persists (Rowland 1999).
For the last .3 decades, malathion has been the insecticide ofchoice for 'malaria control in Pakistan (Dezulucta et al. 1980;Shah et al. 1997). Recent field trials in North -western Pakistanhave demonstrated that malathion can still reduce malaria inci-dence by up to SS% if campaigns arc properly supervised(Rowland et al. 1997b). Pyrethroids arc now being regularlyused for malaria control in Pakistan (Rowland et al.-1994; Shahet al. 1997), although there have been few evaluation. and noneagainst a control group. A comparative study of lántbdacy-haluthrin and malathion in Afghan refugee camps in FrùntierProvince showed that lambdacyhelothrin was twice as effectivein controlling falciparum malaria but only equal to malathionin controlling vivax malaria (Rowland et al. 1994). 11w resultspresented here indicate that alphacypermethrin is as good aslamhdacyhalothrin in controlling falciparum and superior toI. ntbdacyhalothrin in controlling vivax malaria. However, cau-tion must be exercised when drawing conclusions from trialsconducted in different provinces, as conditions might not havebeen the sane. Where aphacypermcthrin and lambdacy-halothrin have been compared side -by -side (in experimentalhut studies in West Africa), they showed equal toxicity againstfree -living anophelines (Darriet 1991). By contrast, bioassaytests indicated that aphacypermcthrin was more persistentthan lantbdacyhalothrin on mud, wool, çement and thatchsurfaces (Durse et al. 1993í Suleiman at al. 1996). Mphacyper-methrin's notable residual life was confirmed in bioassay testsin Pakistan: mortality began to decline only after 3 months.Under natural conditions, where free flying anophelincs mayremain in sprayed rooms for 2 -3 Jays (Mahntoud & Reiser1981), residues may be lethal for much longer. In India restingdensities of Culex quitsquefasciatus and Aedes subpictuswere reduced for at least 27 weeks after alphacypermethrin-spraying of huts (Antalraj et al. 1987).
The gradual increase in parous rate in the sprayed areas indi-cated a gradual deterioration of residual activity; Btit evert bythe end of the year the parous rates between sprayed andunsprayed sectors had still not fully converged. That sprayed
480
surfaces remained toxic several months after spraying was indi-cated by the lower abundance of A. subpictsu in sprayed areas.This species did not make a significant appearance untilNovember, .S months after the spray campaign, and yet wascontrolled even then. The only anuphcline whose density wassimilar in sprayed and untreated areas was A. nigerr nt Is. anexophilic species (Reiser & Milky 1986) that was 'midi lesslikely to come into contact with treated surfaces.
A. calicif scies, the purported i ' :try vector in the Punjab(Reiser & Boreh4nt 1982), had more or less disappeared bySeptember, and yet falciparum malaria did tug reach its peakuntil October. A. stepbrnsi was five times more prevalent in thestudy area and still abundant in November. In North -westFrontier Province, A. stephrnsi is also more common thanA. culicifacies, and circumsporozuite antigen positivity rateswere found to he about the sane in the two species (Rowlandet al. I997h). Sheikhupunt'stay N. an exceptional area of thePunjab, but circumstantial evidence points to A. stepbrnsibeing the more significant vector there.
Alphacypermcthrin appears highly suited for the controli of malaria in Pakistan and South Asia. It is highly toxic to
vector:, requires only one treatment per year, and was ap-predated by the comnnnits The absence of odour meansit is more acceptable to householders than standard organo-phosphoratu insecticides. In international tenders it is price -competitive tígafnst'its main rivals dultumuthrin, lansbdacy-halothrin and cyfluthin.
Acknowledgements
We thank the staff of the National Ins col MalariaResearch and Training for their hard work and productivity;particularly Mr M. Sarwar and Mr M. Yasin. Mr AlantdarShirazi of Cyanamid provided logistic support wheneverrequired. The field study was funded by Cyanamid, with tech-nical support from WHOPES. HealthNet'International'sMalaria Control Programme is supported by the EuropeanCommisslorj (DGI) and the United Nations High Com-missioner for Refugees. Research costs were partly covered bythe Department for International Development of the UnitedKingdom and by HealthNet International.
References
Amain) D, Ramaiah KD, Rajaval Aker al. (1987) Evaluation ofslphicypermethrin for insecticidal 'activity against mosquitoes.Indian Journal of Medical Research 86, 601 -609.
Bouma MJ, Dye C ec van der Kaay HJ (1996) Falciparum malaria andclimate change In the Nor4 Wont Frontier Province of Pakistan.American Journal of Tropical Medicine and Hygiene SS. 131 -1.17.
Darriet P (1991) Evaluation sut le terrain de l'efficacité du sodspyrethrinoides dans le cadre de la lute contre les vecteurs du palud-isme. Parassisologia 33, 111 -119.
O 2000 Blackwell Sconce Ltd
1
'topical AlcJiciuc and Internatitntal I Icalth vuutsn t ao 7 er 472-481 pn t:c
M. Rowland et .rl. Indoor residual spraying with slphsrypirmsthrin
Desulucu J. Alluj aba SM & Shah IH (1980) Malaria control andlong-term periodicity of the Disease in Pakistan., Transactions ofthe Royal Society of Tropical Medicine and Hygiene 74,624-632.
Donnas A 8: Klar N (1994) MithuJs fur comparing estnt ratas ininterscntiun studies when the unit of allocation is a cluster.r American Journal o(Epidemiology 140, 279 -289.
Dona M\; Vasuki V & Raj.wel A (1993) Evaluation of ursanc,phuschorus and synthetic pyrethwid insecticides against six vector mos-yuitu species. RteirlJ Jr &Mile Pública 27,39I-J97.
Fos E & Strickland GT (1989) The interrelationship of Plas,nadI kiparan. and P. pis'ax in the Punjab. Transactions ()jibe RoyalSociety of Tropical Medicine and Hygiene 83. 471-473.
Alahmood F & Raisin WK (1981) Duration of thc'gano*ruphic cyclesof Anopheles culici(acies gilts and Anopheles soldier's' liston. withobservations on reproductive activity and survivorship during win-ter in Punjab province, Pakistan. Mosquito Net's 41,41-50.
N ills A (1991) The economics Of malaria c rol. Iu Malaria.Waiting for the Vaccine (J. G Targets). \G'r'ey & Sims. Chichester.pp. 141 -168.
Rathor HR, Task G & Rashid S (1985) Pattern of otalathiun cross -resistance tu (enitrothiun in Anopheles stephensi and Anopheles
Pakistan Journal of Medical Research 24, 115 -I 20.!Wiwi" VPK &.Butihant PFL (19112) Estimates of malaria vectorial
capacity fur AnupbvIes .sli. ifacies and An. stepbensi in ruralPunjab province, Pakistan. Jumna! of Medical tntumolugY 19,98 -101.
Rriwn WK & Milby MM (1986) Population dynatnics of somePakistani mosyuitucst Changes in adult relative abundance overtime and space. Annals of Tropical Medicine and Parasitology 80, .
S3 -t,8.
r-
v2t 2000 BtackwW Science Ltd
RrnvlanJ M, Hewitt S & Durrani N (1994) Prevalence ul nulina utAfghan rcfugce camps in Pakistan sprayed with malathi.o or Limb.Jacyhalothrin. Transactions of the Royal Society of TropicalMedicine and Hygiene 88.378 -379.
Rowland M. Durrani N, I lewiu S & Suctdorp E (1997.t) Reviva.oc,c ..ifalciparum malaria tu chlurttyuine and sulLmJuxincyvvrintrAn.unutein Afghan actuate sestlamems in w.. wr n Pakistan: Burn y, by thegeneral health services using a simp(itjed ici visu test. T ru/n. al'Medicine and International Health 11049-1056.
Rowland M, Hewitt S. Durrani N. ¡brit N 8: Wirt: K (19976)Tranimiuion and control of vivax malaria in Afghan refugee vil-lages in Pakistan. Transactions of for Royal Society of TropicalMedicine and Hygiene 91.252 -255.
Rowland M (1999) Malaria control in Afghan refugee camps: indoorresidual spraying ur insecticide treated nuts? Transactions 44 sheRoyal Society of Tropical Medicine and Hygiene 93, 4 S8- 39.
Shah I, Rowland AI. MehnutiI Pei al. (1997) Chluruvptine reviviauvein Pakistan and the upsurge of falcip.trum ntalari.t in Pakistani andAfghan refugee ptgtulatioii. Annals 4-tropical Medicine andParasitology 91, 591 -602.
Sulaiman S, Powanchee ZA, Ghauth I et al. (1996) The residual effect,of alphacypernteshrin and permcthrin against die Dengue vr:nUrArdis allupictus in wowlin huts in Alalaysia. Journal of Ve. forEcology 21, 85 -88.
Solemn M (1993) Pesticide resistance g auJ safe and juJi
cious use of pesticides in Pakistan. Journal o /Scie'nce.undTechnology of the University of Peshawar 14.85 -91.
WHO (1996) Report of for sec i W/ working group meeting:raviraiujalpbacype ibrivanalty/brbrin. WI 1t) /\C'IItWI-AY98.10, Geneva.
481
rf
p.m
Ttupieal MeJicine anJ International HcaIth
vot ut.tr s Nu 7 rr sst-sxd will' 1909
Control of zoophilic malaria vectors by applying pyrethroidinsecticides to cattleSean Hewitt' and Mark Rowland"
1 HealthNet h ernational, University Town. Peshawar. Pakistan
2 London School of Hygiene and Tropical Medicine. London. UK
Summary The principal method of malaria control in South and West Asia - indoor residual spraying - is extravagant
with insecticide. A more efficent way of deploying insecticide might be to apply it on livestock since he
malaria vectors in the region arc jtighly zoophilic. A series of investigations assessed Ow potential oftcattle
treated with pyrethroid to control zoophilic mosquitoes. Perrnethrin, dcltamethrin, and lambdacyhalorhrin
were applied to cattle using a sponge at concentrations of 0.5 g/ns', 0.025 Wm', and 0.025 gins', respectively.
*Whole animal' insecticide bioassays that simulated natural mosquito -host contact were used to measure
insecticidal and behavioural effects on wild host- seeking mosquitoes. The bioassays were performed on bath
sheltered and outdoor grazing animals for up w 4S days post- treatment. The possibility that treatments
might cause diversion of host -seeking vectors from cattle to people nearby was -also investigated. At the
doses tested dcltamethrin had the most pronounced and longest -lasting effect, reducing the proportion of
bloodied survivor.: by over 50% for the first two weeks: The majority of mosquitoes affected by the insecti-
cide were killed before feeding. Insecticidal impact was generally lower on grazing than on sheltered animals.
There was no diversion of host -seeking mosquitoes from treated cattle to nearby humans at any stage after
treatment. The application of insecticide to livestock using campaign approach may prove an effective
means of controlling malaria in the region. M the doses tested dcltamethrin is the most appropriate insecti-
cide for this purpose.
keywords malaria, Pakistan, Afghanistan, refugee camps, pyrcthroids, permerhrin, dcltamethrin, lambda -
cyhalothrin, livestock, cattle, bioassay, insecticidal ear tags
correspondenci Mark Rowland, London School of Hygiene and *Dopiest Medicine, Koppel Street,
London WC1E 7HT, UK. E -mail: [email protected]
IntroductionAlthough house spraying still forms the .Mainstay of vectorcontrol activities in west and south Atria, it is far from idealand the search for a more economical and socially acceptable
strategy continues. The region's Malaria vectors are highlyzoophilic: blood meal analyses conducted by Reisen andBonham (1982) in Pakistan's Punjab revealed lust 196 ofblood meals in Anopheles stepbensi and 3% In An. calici-ficies to be of human origin. Livestock are thought to belargely responsible for generating the high mosquito densitiesin the region, and Bouma and Rowland (1995) have shown a
strong positive correlation between cattle:man ratio and
malaria incidence in NW Pakistan. One might thereforeexpect a strategy of livestock 'dipping' to reduce malaria inci-
dence. Indeed a study conducted in Tajikistan In the 1950s
e 19/9 ¡Wood Science Lie
(Lysenko et al. 1957 showed that treatment of livestock with
DDT could reduce die density and longevity of the vectorpopulation (Anopheles superpictus). But the formulationsavailable at that time ptcant that DDT treatments had to be
applied every 10 days and as a result the strategy proved more
expensive than indoor spraying. Use of modern, better adher-Ing insecticide formulations such as emulsifiable or suspen-sion concentrates, and synthetic pyrcthroids with lowmammalian toxicity and high insecticidal activity, could make
all the difference.An earlier evaluation of pyrethroid-impregnated ear tags
failed to show any effect (unpublished observation). A study
of biting site preferences was conducted and this revealed t11at
95% of anophelines and 90% of culicines were feeding below
the cow's mid line. The failure of ear tags can probably be
attributed to poor translocation of the insecticide to these
411
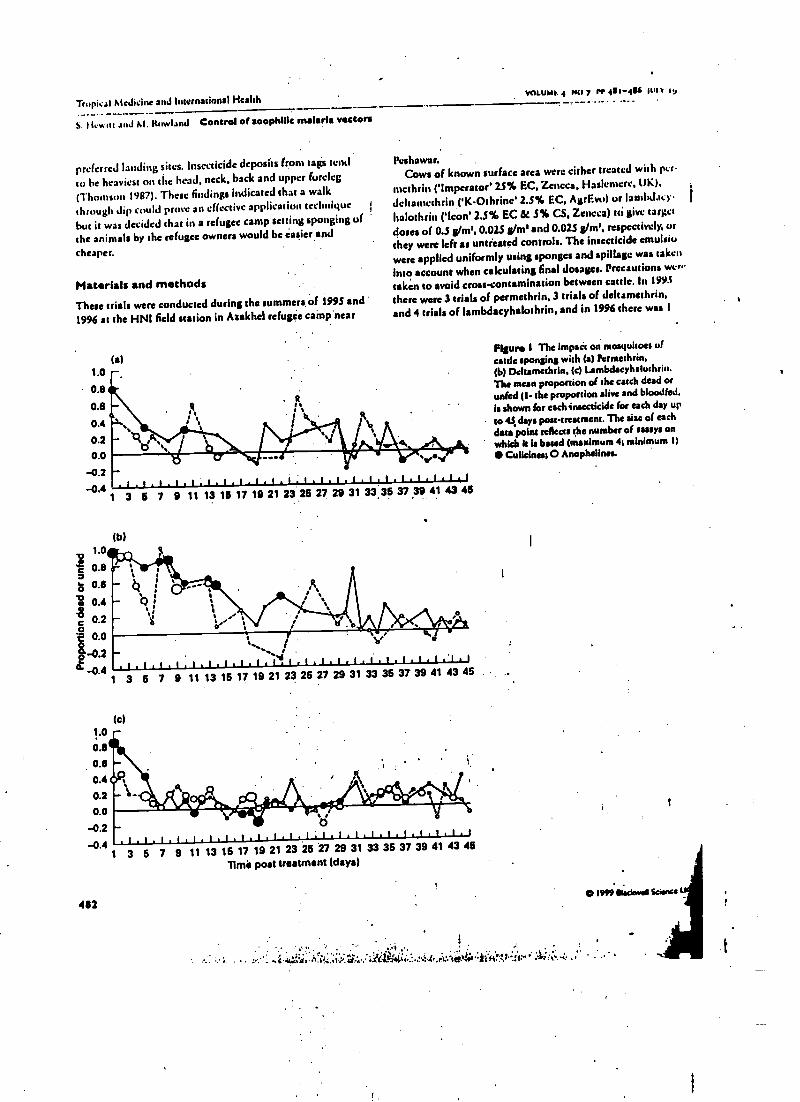
Tropical Medicine and International HealthVOi.UMR 4 NO 7 rr 4114/4 Iut.v ,g
S. 1 t. N ttt and M. *owlauJ Control of aoophillc malaria vectors
preferred landing sites. Insecticide deposits from tags tend
to be heaviest on the head, neck, back and upper foreleg
(Thomson 1997). These findings indicated that a walk
through dip could prove an effective application technique
but it was decided that in a refugee camp setting sponging of
the animals by the refugee owners would be easier and
cheaper.
Materials and methods
These trials were conducted during the summers of 1995 and
1996 at the HNI field station in Azakhel refugee camp near
(a)1.0
0.8
0.8
0.4
0.2
0.0
-0.2-0.4
1 3 5 7 9 11
/.00.8
ais 0.6
: 0.4ec 0.2ot. 0.0
-0.2-0.4
1
.
f'.
Peshawar.Cows of known surface area were either treated with per
mcthrin (' Imperator' 25% EC, Zeneca, Haslcmcre, tIN),
deltamethrin ('K- Othrine 2.S% EC, AgrEvo) or (asnbd.ley
halothrin ('Icon' 2.S% EC & 3% CS, Zencca) tti give target
doses of 0.S g/m3, 0.025 g/m1 and 0.02S g/nt', respectively, or
they were (eft as untreated controls. The insecticide emulsiu
were applied uniformly using sponges and spillage was taken
into account when calculating final dosages. Precautions wow
taken to avoid cross-contamination between cattle. In 1995
there were 3 trials of permethrin, 3 trials of deltsmethrin,
and 4 trials of Iambdacyhalorhrin, and in 1996 there was I
(bi
13 16 17 19 21 23 26 27 29 31 33_35 37 39 41 43 46
(c)1.0
0.8
0.4
0.2
0.0
-0.2
-0.41 3
482
3 5 7 9 11 13 16 17 19 21 23 26 27 29 31 33 36 37 39 41 43 45
.:a .¡ ..t j.. ,.o
.1,1.1,1 1.l.l,l.l,l.l,l : l.t , l . l . l.11l.l,l 1
5 7 9 11 13 16 17 19 21 23 25 27 29 31 33 35 37 39 41 43 4511mii post treatment (days)
Figure I The impact on mosquitoes ofcattle sponging with (a) l'ermethrin.(b) Deltamethrin, (e) t.ambdacyhaluthrin.The mean proportion of the catch dead orunfed (I- the proportion alive and bloodied,is shown for each insecticide for each day up
to 4. days pou -treatment. The size of eachdata point reflects the number of assays onwhich h is baud (maximum 41 minimum 11
Culkines1 O Anophelines.
O 1999 tlyckw ll Scone u
.4 íi:; t:.i.i+:..ti+.if.. :írCis`i+i._:.¿: G.r+.fbv;M Í'[fi.':ir':1'' .4i:a: i ,
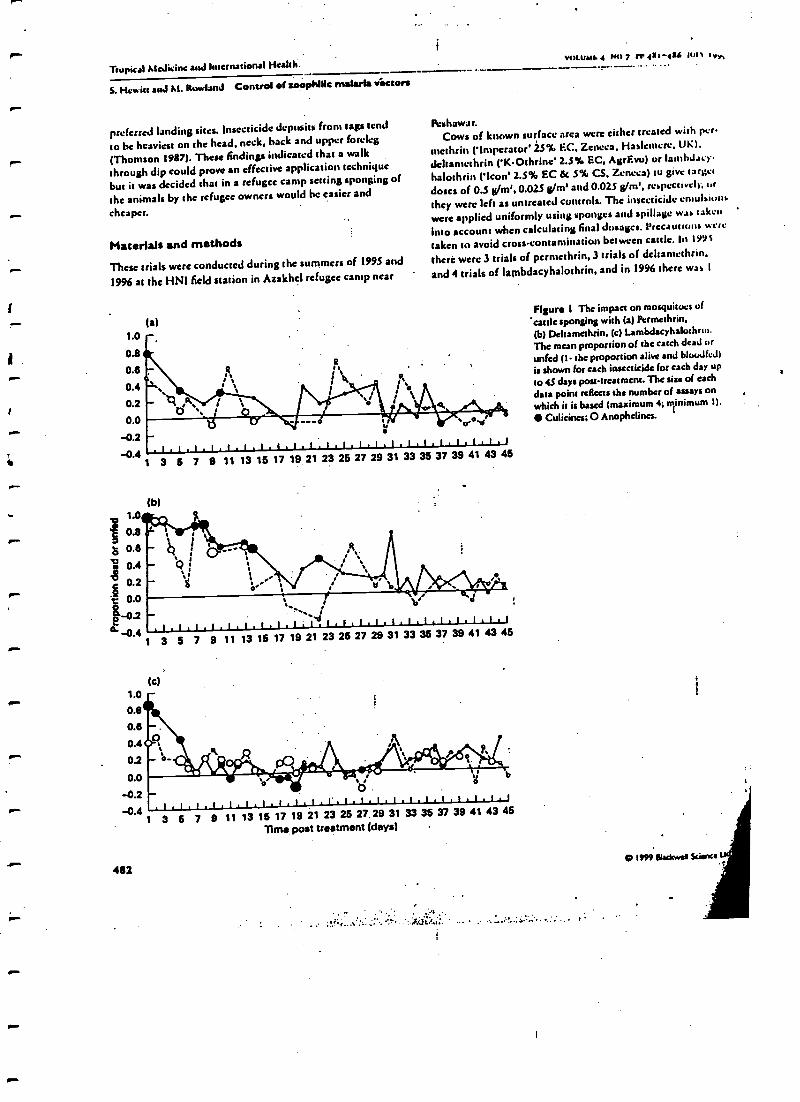
Tropical Medicine and International Health.VOLUMI. 4 No 7 rr 1-4a6 vv,
S. Hewitt and M. Rowland Control of zoophiiic matarla tractors
preferred landing sites. Insecticide deposits from tags tend
co he heaviest on the head, neck, hack and upper foreleg
r (Thomson 1987). These findings indicated that a walk
through dip could prow an effective application technique
but it was decided that in a refugee camp setting sponging of
the animals by the refugee owners would he easier and
cheaper.
Materials and methods
These trials were conducted during the summers of 1995 and
1996 at the HNI field nation in Azakhcl refugee camp near
la)1.0 -0.8
0.6
0.4
0.0
-0.2 -
9:
Peshawar.Cows of known surface area were either treated with per.
ntethrin (' Imperator' 2.5% EC. Zeneca. Haslcmcre. UK).dcltamethrin ('K- Othrine 2.5% EC, AgrEvo) or lamhdacy-
halothrin ('loon' 2.5% EC et 5% CS, Zeneca) to give target
doses of 0.5 g/m', 0.025 g/m' and 0.025 g/m', respectively, or
they were left as untreated controls. The insecticide cmulaiuns
were applied uniformly using sponges and spillage was taken
into account when calculating final dosages. Precautions went
taken to avoid cross -contamination between cattle. In 199S
there were 3 trials of permethrin, 3 trials of deltantethrin,
and 4 trials of lambdacyhalothrin, and in 1996 there was I
f
--.o Nev.'
-0.4 '1,1.l.1.! .I,I.I.I.I.I.I.1.1.1,1.I.1.1.1.1
1.0
0.8
0.6
s 0.4ç 0.2I 0.0
2-0.2d -0.4
1
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45
(b)
,
- 4- Q
,_ e
V
,I.I.I.1. 1.I.1.1.1:Lb1.1,L.1 1 L . 1 , 1 . 1.1.1
tc)1.0 -0.8
0.8
0.4
0.2
0.0
-0.2
3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45
a b-04 .1.1.1.1.1.1.I.t.t,t 1,LiL.1 1.í.1.1.1.1.L1
1 3 5 7 9 11 13 16 17 19 21 23 26 27.29 31 33 35 37 39 41 43 46
Time post treatment (days) .
482
Figue 1 The impact on mosquitoes of
cattle sponging with (a) Pcrtnethrin,(b) Dekamethrin. (c) l.ambdacyhalochrtn.The mean proportion of the catch dead or
unfed (1- the proportion alive and bloodied)
is shown for each insecticide for each day up
to 43 days post -treatment. The size of each
data point reflects the number of assays onwhich is is based (maximum 4; ojinimum 1).
Culicincs; O Anophelines.
.. ...: á' .. .
01999 tsacin es Stirnre
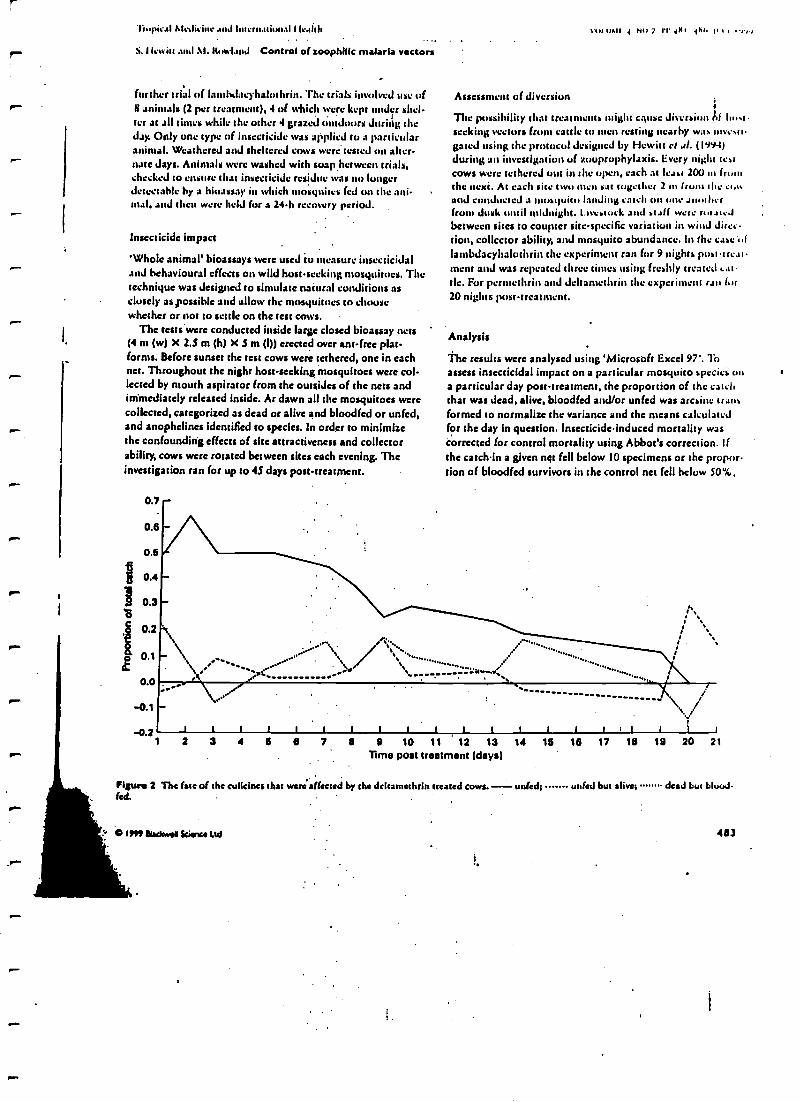
i
'l iupia sI ht Cal ieinc .111,1 lilt eru.uiun.11 I IC.11111
S. I lewitt .nul At. Howland Control of zoophilie malaria vectors
further triad of Iantlseiacyhalothrin. The trials ¡,ivolvcd use ofti animals (2 per treatment), 4 of which were kept under shel-ter at all times while the other 4 graze) Outdoors Juritig theJay. Only one type of insecticide was applied to a particularanimal. Weathered and sheltered cows were tested on alter-nate days. Animals were washed with soap hetwccn trials,checked to ensure that insecticide residue was no longerJetectable by a bioassay in which mosquitos fed on the ani-mal, and then were held for a 24 -h recovery period.
Insecticide impact
'Whole animal' bioassays were used to measure insecticidaland behavioural effects on wild host -seeking mosquitoes. Thetechnique was designed to simulate natural conditions asclosely aspossihle and allow the mosquitoes to choosewhether or not to settle on the test cows.
The tests were conducted inside large closed bioassay nets(4 nt (w) X 2.5 m (h) X S m (I)) erected over ant -free plat-forms. Before sunset the test cows were tethered, one in eachnet. Throughout the night host -seeking mosquitoes were col-lected by mouth aspirator from the outsides of the nets andimmediately released inside. At dawn all the mosquitoes werecollected, categorized as dead or alive and bloodied or unfed,and anophelines identified to species. In order to minimizethe confounding effects of site attractiveness and collectorability, cows were rotated between sites each evening. Theinvestigation ran for up to 45 days post -treatment.
0.7
0.8
0.5
0.4
0.3
0.2
0.1
0.0
0.1
0.2
vIJ111A11 { N117 11{Bh
Assessment of diversion{
The possibility that treatments might cause divers' a( hostseeking vectors front cattle to men resting nearby was inves11gated using the protocol designed by Hewitt et al. (1994)during an investigation of zooprophylaxis. Every night testcows were tethered ont in the open, each at least 200 In fromthe next. At each site two men sat together 2 in frum the GUNand conducted a quite landing catch on one anotherfrom dusk until midnight. l-ivcstock and sh(( were n,hte.Ibetween sites to coupter site specific variation in wind direc-tion, collector ability, and mosquito abundance. In the case 't,flambdacyhalothrin the experiment ran for 9 nights post-
and was repeated three times using freshly treated cat-tle. For perntethrin and deltamethrin the experiment ran for20 nights post- treatment.
Analysis
The results were analysed using 'Microsoft Excel 97'. Toassess insecticidal impact on a particular mosquito species ona particular day post -treatment, the proportion of the catchthat was dead, alive, bloodied and/or unfed was aresinc trans-formed to normalize the variance and the means calculatedfor the day in question. Insecticide induced mortality wascorrected for control mortality using Abbot's correction. ifthe catchin a given ngt fell below 10 specimens or the propor-tion of bloodied survivors in the control net fell below 50 %,
1 1 I t t 1 rj_ I 1 1 I 1 h l 1 I 1
2 3 4 5 8 7 8 9 10 11 ' 12 13 14 16 18 17 18 19 20 21
Time post treatment (days)
Figure 2 The (steal the culicines that were affected by the deltamethrin treated cows. - wiled;led .
C 1999 elsdtwaa Science Ud
tinted but alive; dead but blood-
483
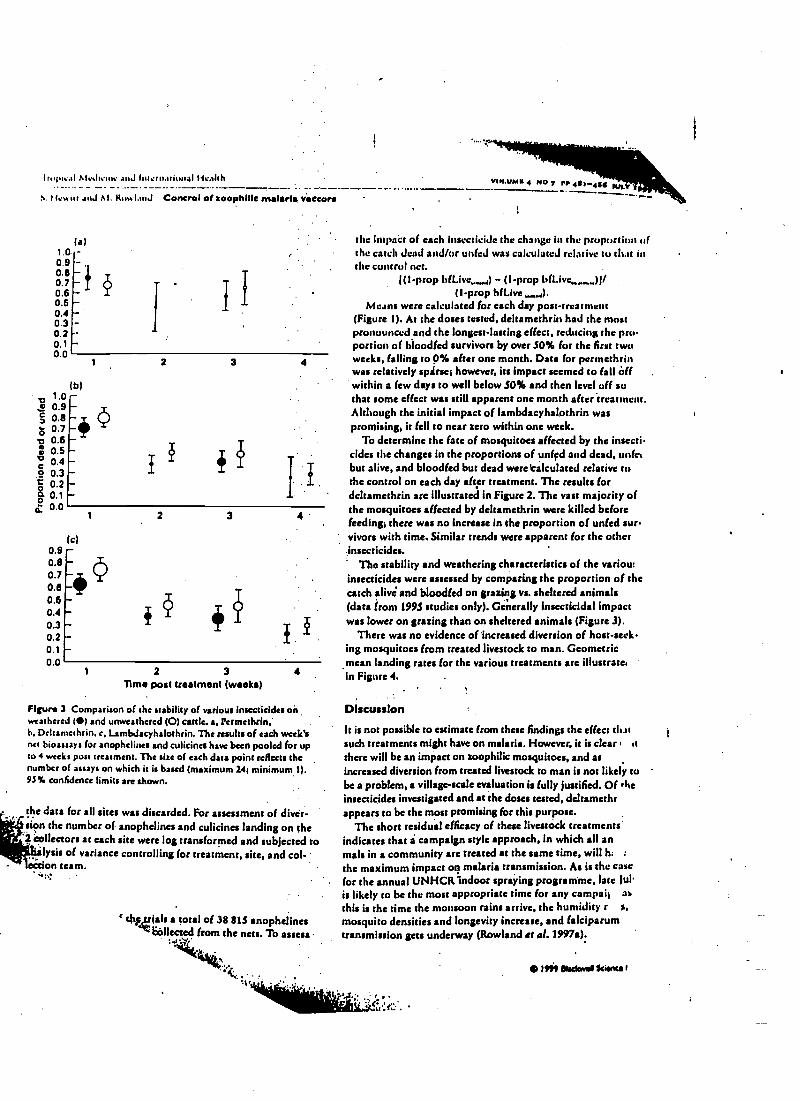
I opi:al Mc.l,:un anJ lntrrn. I Ncahh
S. 11rw itt anJ !11 IttKatttJ Control of zoophIlle malaria. vieeora
1.00.90.80.70.60.50.40.30.20.10.0
1.0c 0.9g 0.8
`00.7
c 0.6ó 0.5° 0.4ó 0.3r 0.2
a 0.1d 0.0
0.90.80.70.60.60.40.30.20.10.0
la)
(b)
-4
I
1
2 3
I
1 2 3
2 3
Time post treatment (weeks)4
Figure 3 Comparison of the stability of various insecticides onweathered (l) and unweathered (0) cattle. a, Permethrin,h, Deltamcthrin, c, Lambdacyhalothrin. The results of each week'snet bioassays for anophelines and culicines have been pooled for upto 4 weeks post treatment. The sire of each data point reflects thenumber of assays on which it is based (maximum 24; minimum 1).95% confidence limits are shown.
the data for all sites was discarded. For assessment of diver-..sipn the number of anophelines and culicines landing on the
collectors at each site were log transformed and subjected to'lysis of variance controlling for treatment, site, and col -'
e ie on team.
` tivrials a total of 38 81.3 anophelineslióllected from the nets. To assess
k4:'1! ' . ..
VIn.UMa 4 NO 7 rr etar-NS14.11.7 Y'
the Impact of each insecticide the change in the proportion ofthe catch dead and /or unfed was calculated relative to that inthe control net.
((1 -prop bfLive,,,,,) - (I -prop bfLivc,,,,,,,,)j/(1 -prop bfLive,,,,,,r).
Means were calculated for each day post -treatment(Figure 1). M the doses tested, deltamcthrin had the mostpronounced and the longest-lasting effect, reducing the pro-portion of b)oodfed survivors by over SO% for the first twoweeks, falling to 0% after one month. Data for pertnethrinwas relatively spsirse; however, its impact seemed to fall tiffwithin a few days to well below 30% and then level off sothat some effect was still apparent one month after treatment.Although the initial impact of lambdacyhalothrin waspromising, it fell to near zero within one week.
To determine the fate of mosquitoes affected by the insecti-cides the changes in the proportions of unfpd and dead, wife(but alive, and bloodied but dead were calculated relative tothe control on each day after treatment. The results fordeltamcthrin are illustrated in Figure 2. The vast majority ofthe mosquitoes affected by deltamcthrin were killed beforefeeding; there was no increase in the proportion of unfed sue,vivors with time. Similar trends were apparent for the otherinsecticides.
The stability and weathering characteristics of the variou:insecticides were assessed by comparing the proportion of thecatch alivé and bloodied on grazing vs. sheltered animals(data lrom199S studies only). Generally insecticidal impactwas lower on grazing than on sheltered animals (Figure 3).
There was no evidence of Increased diversion of host -seeking mosquitoes from treated livestock to man. Geometricmean landing rates for the various treatments are illustrate,in Figure 4.
Discussion .
It is not possible to estimate from these findings the effect thatsuch treatments might have on malaria. However, it is clear: it
there will be an impact on zoophilie mosquitoes, and asincreased diversion from treated livestock to man is not likely tobe a problem, a village -scale evaluation is fully justified. Of rteinsecticides investigated and at the doses tested, deltamethrappears to be the most promising for this purpose.
The short residual efficacy of these livestock treatmentsindicates that i campaign style approach, in which all anmals in a community are treated at the same time, will h: :
the maximum impact on malaria transmission. As is the casefor the annual UNHCR'indoor spraying programme, law )ulis likely to be the most appropriate time for any campail as
this is the time the monsoon rains arrive, the humidity r s,
mosquito densities and longevity increase, and falciparumtransmission gets underway (Rowland et al. 1997.):
..
Sit :i:
ItM 8lackwas Scianca t
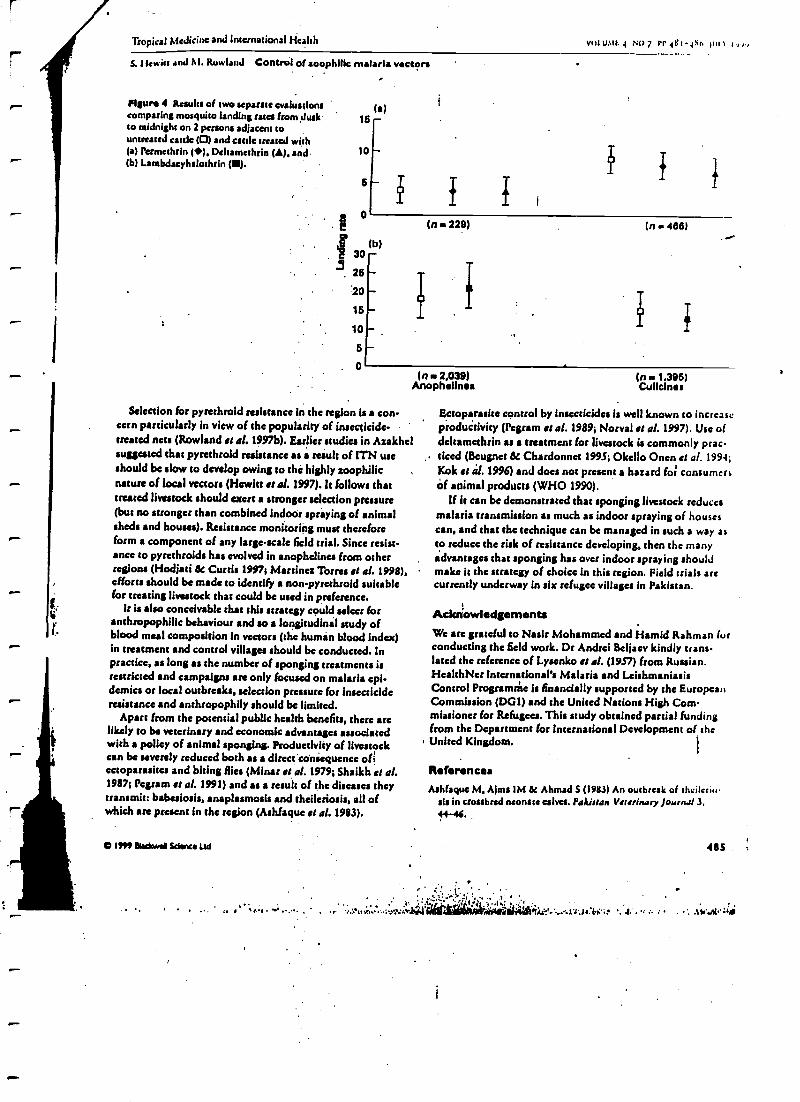
.
Tropical Medicine and International Health vut.uait. 4 NO 7 rr itt-a tir; hin i: vv,
S. Hewitt and M. Rowland Control of zoophilic malaria vectors
Figure 4 Results of two separate evaluationscomparing mosquito landing rates horn duskto midnight on 2 persons adjacent tountreated cattle (0) and cattle treated with(a) Permethrin (4/), Deltamethrin (A), and(b) Lambdacyhalothrin (e).
le)16 -
10
6
0(n 229)
(b)
3.30 -26
-
15
10 -
6
. 0
in ow 466)
(n . 2,039) In . 1,396)Anophelines Cullcinas
Selection for pyrethroid resistance In the region is a con-cern particularly in view of the popularity of insecticide-treated nets (Rowland et al. 1997b). Earlier studies in Azakhelsuggested that pyrethroid resistance as result of ITN useshould be slow to develop owing to the highly zoophilienature of local vectors (Hewitt it al. 1997). h follows thattreated livestock should exert a stronger selection pressure(but no stronger than combined indoor spraying of animalsheds and houses). Resistance monitoring must thereforeform a component of any large -scale field trial. Since resist-ance to pyrethroids has evolved in anophelines from otherregions (Hodjati & Curtis 1997; Martinez Torres et al. 1998),efforts should be made to identify a non- pyrethroid suitablefor treating livestock that could be used in preference.
It is also conceivable that this strategy could select foranthropophilic behaviour and so a longitudinal study ofblood meal composition in vectors (the human blood index)in treatment and control villages should be conducted. Inpractice, as Iong as the number of sponging treatments isrestricted and campaigns are only focused on malaria epi-demics or local outbreaks, selection pressure for Insecticideresistance and anthropophily should be limited.
Apart from the potential public health benefits, there arelikely to be veterinary and economic advantages associatedwith a policy of animal sponging. Productivity of livestockcan be severely reduced both as a direct'coñiequence ofiectoparasites and biting flies (Minar et 01. 1979; Shaikh et al.1987; Pegram et al. 1991) and as a result of the diseases theytransmit: babesiosis, snaplasmosis and theileriosis, all ofwhich arc present in the region ( Ashfaque et al. 1983).
O H!! dsdawal Wants Ltd
Ectoparasite control by Insecticides Is well known to increaseproductivity ( Pegram st al. 1989; Norval st al. 1997). Use ofdeltamethrin as a treatment for livestock is commonly pratdeed (ßeugnct & Chardonnet 1995; Okello Onen et al. 1994;Kok st al. 1996) and does not present a hazard foi consumersof animal products (WHO 1990).
If it can be demonstrated that sponging livestock reducesmalaria transmission as much as indoor spraying of housescan, and that the technique can be managed in such a way asto reduce the risk of resistance developing, then the manyadvantages that sponging has over indoor spraying ahoulJmake it the strategy of choice in this region. Field trials arecurrently underway in six refugee villages In Pakistan.
Acks owledgernents
We are grateful to Nasir Mohammed and Hamid Rahman furconducting the field work. Dr Andrei Beljaev kindly trans-lated the reference of Lysenko st al. (1957) from Russian.HealthNet International's Malaria and LeishmaniasisControl Programdte is financially supported by the EuropeanCommission (DG1) and the United Nations High Com-missioner for Refugees. This study obtained partial fundingfrom the Department for International Development of the
I United Kingdom.
ReferencesAshfaque M, Alma IM at Ahmad S (1983) An outbreak of theilcnu
sis in crossbred neonate calves. Pakistan Veterinary Jot/rnaf 3,4{-46.
/, s,1 . . . / 'tiit.Nl., .::-i .r''
485
üeAn'.+idMir+liiálRüt' ..at't.tlan . . .. . :v:Ai':i%
Tropical McJi.inc and Interna al Health
S. Hewitt and M. Rowland Control of zoophilie malaria vectors
Itcuo wt 1: (:h.trJunoa L (1995) Tick resistance to prrethruids inNew Caledonia. Veterinary l'.tr,tsitulogy S6, .12S -.138. '
Ituu.na \I & Rowland \1 (1995) Failure of passive zuuprtiph)Ltxis;cattle ins ncrship ill Pakistan is associated with .t higher prevalenceof malaria. S rarasactions u/ she Royal Society u% TropicalMedicine and Hygiene 89,351-333. .
I le.. itt S, Ford F. Muhammad N, Urhantan H & Rowland M (1997)The effect u( heJ,oets tin unprotected people: open air attidics in anAfghan refugee siliap:. Bulletin a /Eat (ugfcal Research 87,
4SS -1S9.
I lewitt S, Kemal M. Muhammad N tk Rowland AI (1994) An enm-logical in.zstiga ' f the likely impact of cattle ownership 01 '1
in an Afghan refugee camp in the North West frontierProvince of Pakistan. Medical and Veterinary Ent logy 8,
160 -164.H,.Jiati AIH & Curtis CF (1997) Dosage Differential effects of per -
methrin impregnated into bednets on pyrethruid resistant and sus-ceptible genotypes of the mosquito Anopheles stephensi Medicaland Veterinary Enturrto logy 11,368-372-
Kuk DJ, Fuurie LJ, Lnumcs MD & Oberem PT (1996) Interbreed dif-ferences in the efficacy of 1% dcltamethrin pour -on to protectsmall livestock against infestation with Ixodes rubicundus ( Acari:Ixodidoe). Veterinary Parasitology 63, 109 -117. '
Lysenko A, Lavrenko E et al. (1957) DDT livestock 'dipping' inTajikistan ¡Antimalarial efficacy of treatment of farm animals byDDT in a mountainous region of TajikistanJ. MeditsinskayaParositologiya 1 Parazitarnye Boleynis 26, 212 -218.
Martinez Torres D, Chandra F, Williamson MS et al. (1998) .
Molecular characterization of pyrethro(d knockdown resistance(kdr) in the major malaria vector Anopheles gambles s.s. InsectAl oiecular Biology 7, 179 -184.
Molar J. Riha J & Lamatova Z (1979) Losses In milking qualities ofdairy cattle caused by mosquitoes and horseflies and reduction of
such losses due to use of dicthylttluamide repellent. Folia-
486
..-
W11.11411, .4 Nil er e-.06 µnY 1499
t'arasiruhngit 26,285-288.Norval R. Sutherst KW. Kurki J. Kerr Jt) & Gibson JD (1997) The
effects of the brown ear tick. R. appendiculatter. un milk pr;. ii;tien of San(.; cattle. Alydi,:rl and1Veterinary Erttuuudugy 1 I,
148 -154.Okcllu Once J. Heinunctt R. Sackittu C \1, Mwayi WT, Kakaire 1)
Kabarema Al (1994) Control of tsetse flics in Uganda by dippingcattle in dcltamethrin. Tropical Animal Health and Productivity26, 21 -27.
l'cgram RG, Jans Al), Ousterwijk GPM et al. (1991) StuJves un the
ecunrrmics of ticks in Zambia. Experimental and AppliedAcarulugy 18, 9 -26.
Pvgra.n $.G, 1.emche J. Chizyuka HGIS et al. (1989) Effect of tick con-trol on liveweight gain of cattle in central Zambia. Medical andVeterinary Entomology 3, 313 -320.
Reisen WK e: Burehan) PFL (198I) Estimates of malaria vectorial
capacity for Anopheles culicifacies and An. stephensi in ruralPunjab province, Pakistan. Journal of Medical Entomology 19,
98 -101.Rowland M, Hewitt S, Durrani N, Bano N tl: Wirtz R (1997a)
Transmission' and control of vivats malaria in Afghan refugee
.scttléments in Pakistan. Transactionso /the Royal Society ofTropical Medicine and Hygiene 91, 232 -253.
Rowland M, Hewitt S, Durrani N, Saleh P Bouma M & Sondorp E
((997h) Sustainability of pyrethroid- impregnated bednets for
malaria control in Afghan communities. Bulletin of the World
Health Organization 75.23 -29.Shaikh AG, Issani GB & Soomro GH (1987) Defects in hides in
Pakistan. Pakistan Journal of Agricultural Research 8, 335 -337.Thomson Mt (1987) The effect on tsetse Aies (Glossine app.) of
dcltamethrin applied to cattle either as a spray or incorporated
into car -tags. Tropical Pest Management 33,329-335.WHO (1990) Drltamcthrin. Emlronnuntal Health Criteria 97. World
Health Organization, Geneva.
TRANSACTIONS OF ME ROYAL SOCIETY OF TROPICAL. MEDICINE AND HYGIENE (1999) 93, 641 -64
Randomized controlled trials of 5- and 14 -days primaquine therapy againstrelapses of vivax malaria in an Afghan refugee settlement in Pakistan
Mark Rowland'-' and Naeein Ourrnnit HeolrhNer lurentariotral, University Taunt, Peshawar, Pakistan 'Lo» ónn
School of JIvgiruc and Tropical Medicine, London IVCIL- 7HT, UK
AbstractPrimaquine is the only drug available that can eliminate hypnozoites from the liver and prevent relapses ofvivax malaria. The World Health Organization recommends a course of 14 -21 dams depending on regionand strain. The National Malaria Control and Eradication Programmes of Pakistan and India have adheredto a 5 -day course as their standard as it is deemed more practical to implement and because facility for
detecting lucose 6-phosphate dehydrogenase (G6PD) deficiency is seldom available at the periphen.Evidence for the efficacy of the 5 -day regimen is controversial or lacking. Two, year -long, randomizedcontrolled trials were undertaken in an Afghan refugee camp in north -western Pakistan using a process ofpassive case detection and treaunent at the camp's clinic: the first trial compared treatment with chloroquinealone versus chloroquine plus 5 -days pritnaquine, the second trial compared chloroquine alone versuschloroquine plus 14 -days primaquine. Chioroquine is not hypnozoitocidal and was administered toeliminate the erythrocytic stages and to alleviate clinical symptoms. The daily primaquine dose was0.25 ntg /kg bodyweight and the total chloroquine dose was 25 mg /kg over 3 days. During the first trial 52%(129/250) of the non -primaquine group recorded a 2nd clinical-parasitsemic episode and 23% recorded a3rd, whereas 51% (128/250) of the 5 -days primaquine group reported a 2nd episode and 21% recorded a3rd. During the second trial 49°.6 (49/100) of the non -primaquine group recorded a 2nd episode and 25%recorded a 3rd, whereas only 32% (32/100) of the 14 -days primaquine group recorded a, 2nd and only 2%,
recorded a 3rd. The 5 -days primaquine regimen has no value es an anti- relapse therapy- and should begOandoned. In extended tests in vivo in which vivax cases (n s 31) were treated with chloroquine 25 mg /kgand 14 -days primaquine, there was no parasite recrudescence within 28 days and hence no evidence ofresistance to chloroquine.
Keywords: malaria, /Venom/ vivax, chemotherapy. primaquine, relapse, refugees, Pakistan
IntroductionPrimaquine is the only drug available that can dims.
nace hypnozoites of vivax malaria from the liver andprevent relapses of the disease (GILLES & WARRELL,1993). The World Health Organization recommends a14 -day course (0.25 mg /kg daily) as the standard ther-apy and longer courses against more tolerant strains fromSouth -East Asia and the Pacific (WHO, 1990). TheNational Malaria Control Programme of Pakistan hasadopted a truncated 5 -day course as their standardbecause of the risk of haemolyaia in glucose 6- phosphatedehydrogenase (G6PD) -deficient cases and becausefacility to detect this genetic condition is seldom availablein clinics at the periphery. India and other Asiancountries have the same policy as Pakistan and considerthe 5-day- course to be more practical and economical(BASAVARAI. 1960; SHARMA a al., 1973; ROY er al.,1977). Evidence for the clinical efficacy of the 5 -dayregimen is controversial or lacking (ROY el' al, 1977;SHARAtA er al., 1900; SINOH et al., 1990; BAIRD, 1998;
1TAY & KSHIRSAGAR, 1998; GOGTAY er al., 1998). a call for randomized placebo- controlled trials has
recently been made (BAIRD. 1991).This concern is shared by the agencies responsible for
the health care of Afghan refugees in Pakistan. Vivaxmalaria is a major problem in this population with over100 000 episodes being treated each year at clinics run bythe United Nations High Commissioner for Refugees(UNHCR), the Pakistan Ministry of Health, and non-governmental organizations (ROwtAND er al., 1 994).Many patients given a 5 -day course return to clinics with2nd or 3rd episodes within months of treatment (Row-' LAND et al., 1997; Stint/ er al., 1997). With the seemingfailure of primaquine therapy to significantly reduceannual incidence rates, and with GOP D deficiency beinga common condition among Afghan (1556) and Pakistani(7%) Pathan (BOUMA er al., 1995), more evidence is
Author for correspondence: Mark Rowland. Disease Controland Vector Biology Unit, London School of hygiene andTropical Medicine, Keppel Street, London \VCiE MT, UK:phone +44 020 7427 2333, fax ;4.020 7580 9075,e -mail m.rnalandtñ'Ishun.ac.uk
needed to justify continuing with the 5 -day regimen.Between 1996 and 1998, 2 randomized controlled trialsof primaquine were undertaken at an Afghan refugeecamp. The first compared the standard 5 -day course ofprimaquine versus no anti- relapse therapy. When thusfailed to demonstrate a differential impact, a 2nd trial wasundertaken to examine the efficacy of the WHO- recom-mended 14 -day course since resistance to primaquinemay, conceivably, have evolved. All cases were treatedconcurrently with chloroquine to eliminate erythrocyticstages and to alleviate clinical symptoms. Since chlor-oquine- resistant vivax malaria was becoming quite pre-valent in Asia (BAIRD a al., 1991; SCHUURRAMP et al.,1992; MYAT- PIIONE -KYAW er at, 1993; GARG cr al.,1995), it seemed prudent to also carry out a 26 -day in-vivo test on Plasmodium vivax infections ('VERNSDOR-FER & PAYNE, 1988) in the same refugee camp.
Materials and MethodsPatients with vivax malaria were recruited by a process
of passive case detection at the clinic and microscopy unitgun by HealthNet International in Adizai refugee camp(population 3950) near Charaadda in North West Fron-tier Province. All families within the camp were regis-
tered at the clinic, cenaused each year, and received freediagnostic and treatment services. Clinical, parasitaennecases with temperature >37.5 C or history of fever wererecruited in July and August at the onset of the maintransmission season (RO\r'LAND et al., 1997), tested forG6PD deficiency (Sigma Diagnostics, Poole, Dorset,UK), and allocated at random to either the placebo or theprimaquine group. Cases not admitted to the studyincluded patients with mixed infections or with evidenceof recent antimalarial intake, cases of G6PD deficiencyor .severe anaemia, children aged <3 years, pregnantwomen, and the very elderly. Each case was followed -upeach day by outreach workers who provided supcn'isedtreatment until the course had been completed.
All caseswere treated with 25 mg .chloroquine (Nita-quine -P', Rhone -Poulenc, France) per kg body'veightin divided doses over 3 days. Cases allocated to the non -primaquine groups were given no further treatment.Cases allocated to the primaquine groups were given a
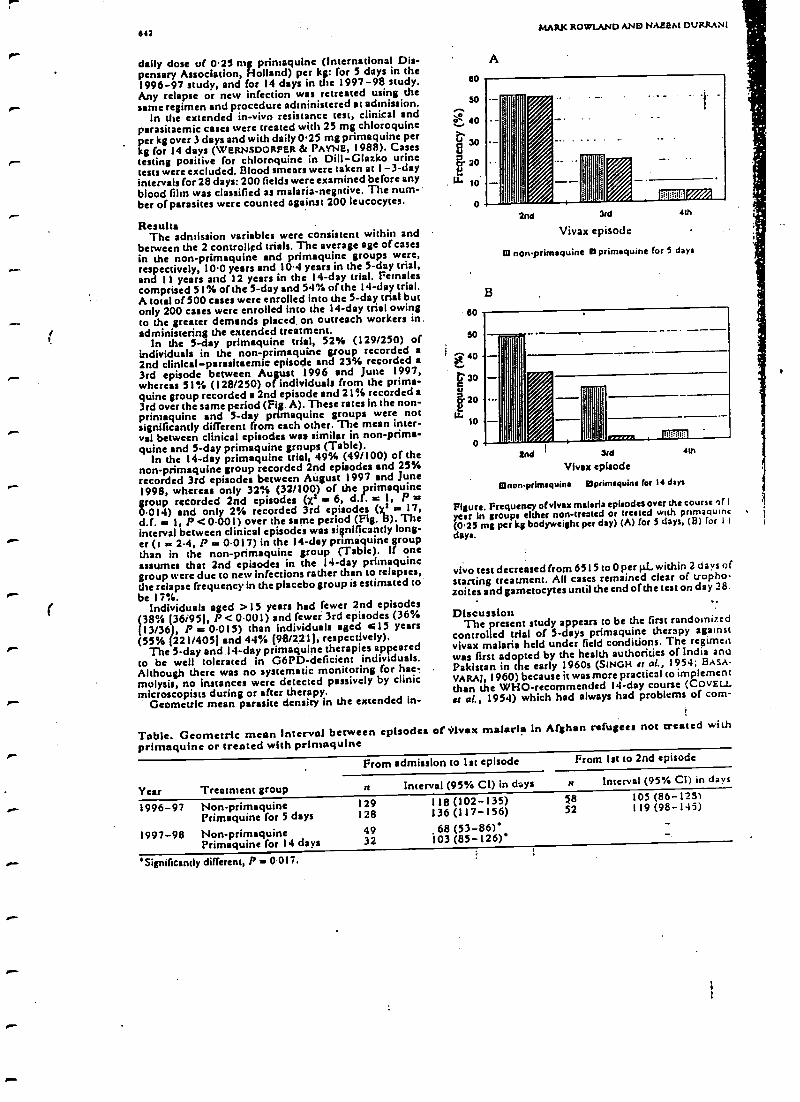
642
daily dose of 0.25 mg rimaquine (International Dis-pensary Association, Holland) per kg: for 5 days in the1996 -97 study, and for 14 days in the 1997 -98 study.Any relapse or new infection was retreated using thesame regimen and procedure administered at admission.
In the extended in -vivo resistance test, clinical andparasitaemic cases were treated with 25 mg chloroquineper kg over 3 days and with daily 0.25 mg primaquine perkg for 14 days (WERNSDORFER & PAYNE, 1988). Casestesting positive for chloroquine in Dill -Glazko urinetests were excluded. Blood smears were taken at 1 -3 -dayintervals for 28 days: 200 fields were examined before anyblood film was classified as malaria- negntive. The num-ber of parasites were counted against 200 leucocytes.
ResultsThe admission variables were consistent within and
between the 2 controlled trials. The average age of casesin the non -primaquine and primaquine groups were,respectively, 10.0 years and 10.4 years in the 5 -day trial,and I I years and 12 years in the 14 -day trial. Femalescomprised 51% of the 5 -day and 54% of the I 4-day trial.A total of 500 cases were enrolled into the 5 -day trial butonly 200 cases were enrolled into the 14 -day trial owingto the greater demands placed on outreach workers in.administering the extended treatment.
In the 5 -day primaquine trial, 52% (129/250) ofindividuals in the non -primaquine group recorded a
2nd clinical -parasitaemic episode and 23% recorded a
3rd episode between August 1996 and June 1997,whereas 51% (128/250) of individuals from the prima-quine group recorded a 2nd episode and 21% recorded a3rd over the same period (Fig. A). These rates in the non -primaquine and 5 -day primaquine groups were notsignificantly different from each other. The mean inter-val between clinical episodes was similar in non -prima-quine and 5 -day primaquine groups (Table).
In the 14 -day primaquine trial, 49% (49/100) of thenon -primaquine group recorded 2nd episodes and 25%recorded 3rd episodes between August 1997 and June1998, whereas only 32% (32/100) of the primaquinegroup recorded 2nd episodes (x2 = 6, d.f. = 1, P =0.014) and only 2% recorded 3rd episodes (x2 a 17,d.f. as ), P <0.001) over the same period (Fig. B). Theinterval between clinical episodes was significantly long-er (t a 2.4, P as 0.017) in the 14-day primaquine groupthan in the non -primaquine group (Table). If oneassumes that 2nd episodes in the 14-day primaquinegroup were due to new infections rather than to relapses,the relapse frequency in the placebo group is estimated tobe 17 %.
Individuals aged >13 years had fewer 2nd episodes(38% 36i951, P <0.001) and fewer 3rd episodes (36%(13/36), P = 0.015) than individuals aged =l5 years(55% (221/405) and 44% (98/221(, respectively).
The 5 -day and 14-day primaquine therapies appearedto be well tolerated in G6PD-deficient individuals.Although there was no systematic monitoring for heelmulysis, no instances were detected passively by clinicmicroscopists during or after therapy.
Geometric mean parasite density in the extended in-
Table. Geometric mean interval between episodesprimaquine or treated with primaquine
60
50
a
60
50
A
MARK ROWIAND AND NAEEM DURRAN1
B
2nd 3rd
Vivax episode
W non - primaquine D primaquine for 5 days
4th
Snd 3rd 4th
Vivax episode
ninon- primaquine Dprimaquine for 14 days
Figure. Frequency ofvlvax malaria episodes over the course of 1year In groups either non -treated or treated with primaquine(0.25 mg per kg bodyweight per day) (A) for 5 days, (e) for ! t
days.
vivo test decreased from 6515 to 0 per pi-within 2 days ofstarting treatment. All cases remained clear of tropho-zoites and gametocytes until the end of the test on day 28.
DiscussionThe present study appears to be the first randomized
controlled trial of 5 -days primaquine therapy againstvivax malaria held under field conditions. The regimenwas first adopted by the health authorities of India andPakistan in the early 1960s (SINGH et al., 1954; BAsA-VARAJ, 19 60) because it was more practical to implementthan the WHO -recommended 14 -day course (COVED.It al., 1954) which had always had problems of corn-
!
of vivax malaria in Afghan refugees not treated with
Year Treatment group
From admission to 1st episode From 1st to 2nd episode
n Interval (95% CI) in days n Interval (95% CI) in days
1996 -97
1997 -98
Non -primaquinePrimaquine for 5 days
Non -primaquinePrimaquine for 14 days
l29128
4932
118 (102 -135)136 (117-156)68(53 -86)'
103 (85 -126)'
5852
105(86 -1251119 (98-145)
'Significantly different, P 0017.
RANDOMIZED CONTROLLED TRIALS OF 5- AND 14 -DAYS PRIMAQUINE THERAPY
pliance (WHO, 1966). Relapse rates in those early as wellas in later studies (SHARMA et al., 1973; ROY st al., 1977)never exceeded 7% in the 0.5 -2 years of follow -up, andthis observation has been used to justify the 5 -day policyever since (GOGTAY a al., 1998) even though a relapserate of under 7% may have been entirely natural (BAIRD,1998). Both SINOII er of. (1990) and SHARMA et al.(1990) compared the 5 -day course of primaquine (pluschloroquine) against non -primaquine treatment (chlor-oquine given alone) in consecutive years. SINGH st al.( I 090) obtained similar rates of 2nd infections (around10%) in both primaquine and non -primaquine groupswhereas SHARAtA et al. (1990) found fewer 2nd infec-tions in the 5 -days primaquine group. The problem withthis method is that relapses cannot be distinguished fromnew infections, the rate of which may vary from year toyear owing to unstable transmission. Where the 5 -dayregimen has been tested against a placebo simulta-neously, and this had only been done under artificialconditions in the USA on J O non -Immune volunteers,the rate of relapse was 100% in both roups (CONTACOSes al., 1974). TTte absolute failure of the 5-day regimen toprevent relapses is confirmed by the present field study inPakistan. There is no Justification to continue with it, andas BMRD (1998) has emphasized, continued use of sub-optimal doses invites selection of resistance to the onlydrug available for anti -relapse therapy.
It is not proposed to switch to 14 -days primaquinetherapy since this is only justified where vivax transmis-sion is under control or where patient compliance with.the I4 -day regimen can be assured (WHO, 1990).Haemolytic reaction to primaquine can be particularlysevere in Asian and Mediterranean variants of G6PD-deficiency (CLYDE, 1981). Because daily medical super-vision for 14 days is unfeasible in areas of Pakistan wheremalaria is most common, the only sensible policy is toabandon use of primaquine until conditions for effectiveand safe use can be met.
AcknowledgementsWe arc grateful to the staff of the HealthNet clinic in Adizel for
their work, and to Dr Naveeda Bano of UNHCR for encoura-ging this study. HealthNct International's Malaria ControlProgramme is supported by the European Commission (DG I )and UNHCR. This research was partly supported by theDepartment for International Development of the United King-dom and by HealthNct International.
ReferencesBaird, J. K. (1998). Primaquine as anti -relapse therapy for
Plaunodium viva:. Transactions of the Royal Society of 7 topicalMedicine and Hygiene, 92, 687.
Baird, J. K., Bann, H. Purnomo, Bangs. M. J. Sublanto, B.,Paschen, L. C. & Hoffman, S. L. (1991). Resistance sochloroquine by Plasmodium vivax in Irian Jaya, Indonesia.American Journal of Tropical Medicine and Hy giene, 44,547 -552.
Basavarai, H. R. (1960). Observations on the treatment of 678malaria eases with primaquine in an area free from malariatransmission in Mysore State, India. Lndiaa Journal of Molar-idea. )4, 269 -281.
Bouma, M. J., Gods, M., Akhtar, T., Khan, N. & Kits, E.(1995). Prevalence and clinical presentation of glucose -6-phosphate dehydrogenate deficiency in Pakistani Pautan andAfghan refugee communities in Pakistan: implications for theuse of primaquine in regional malaria control programmes.Transactions of the Royal Society of Tropical Medicine andH}yietss, 89, 62 -64.
Clyde, D. P. (1981). Clinical problems associated with the useof primaquine as a tissue schisontocidal and ametocidaldrug. Bulletin of the World Health Organization, 59, 391 -395.
643
Contacos, P. G., Coatney, G. R., Collins, W. E., Briesch, P. E. &Jeter, M. H. (1974). Pive day primaquine therapy -anevaluation of radical curative activity against vives malariainfection. American J al of Tropical Medicine and Hirene,22, 693 -695.
Covell, G., Coatney, G. R., Field, J. W. & Singh, J (1954).Chemotherapy of Malaria. Geneva: World Health Organiza-tion Monograph Series, no. 27.
Gar`, M., Gopinathan, N., Bodht, P. 6 I;sh,rsagar, t:. II 995)Vivex malaria resistant to chloroquine: case reports nomBombay. Transactions of the Royal Saver). of Tropical Al edui,rand Hygiene, 89, 656 -657.
Gilles, H. M. bt Watrell, D. A. (1993). Druce- Chwatt'i Estonia.'Afalanology, 3rd edition. London: Edward Arnold.
Gogtay, N. & Kshirsagar, N. A. (1998). Primaquine as anti -relapse therapy for Plasmodium vivais a reply. rauacnoru ofthe Royal Soeieo, of Tropical Medicine and Hygiene, 92, 687.
Go`tay, N., Garg, M., Kadam, V, Kamtekar, K. k Kshusaçar,N. A. (1998). A S days primaquine regimen as anti-relapsetherapy for Plasmodium vivax. Traruacuoru of the Royal Societyof Tropical Medicine and Hygiene, 92, 341.
Myat- Phone -Kyaw, Myint -Oo, Myint -Lwin, Thaw -Zin, Kyin-HIa -Ave & Nwe -Nwe -Yin (1993). Emergence of chloro-qquine- resistant Plasmodium vivax in Myanma (Burma).Transactions of the Royal Society of Tropical Medicine andHasiens, 87, 687.
Rowland, M., Hewitt, S. & Durrsni, N. (1994). Prevalence ofmalaria In Afghan refugee villages sprayed with lambdacyhalothrin or malathion. Transactions of she Raval Society gfTropical Medicine and Hygiene, 88, 378 -379.
Rowland, M., Hewitt, S., Durrani, N., Deno, N. & Wirtz, R.(1997). Transmission and control of vivax malaria in Afghanrefugee settlements in Pakistan. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 91, 252 -255.
Roy, R. G., Chakrapani, K. P., Dhinagaran, D., Sitaraman, NL. & Gosh, R. B. (1977).. Efficacy of 5 -day treatment ofPlasmodium vivax infection in Tamil Nadu. Indian Journal ofMedical Research, 65, 652 -656.
Schuurkamp, G. J. Spicer, Pi E., Kareu, R. K., Bulungol. P. K.& Rieckmann, K. H. (1992): Chloroquine- resistant Plasmo-dium vivax in Papua New Guinea. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 86, 121 -122.
Shah, I., Rowland, M., Mehmood, P., Mujahid, C., Raziq, F.,Hewitt, S. & Durrani N. (1997). Chloroquine resistance inPakistan and the upsurge of falciparum malaria in Pakistaniand Afghan refugee populations. Annals of Tropical Medicineand Parasitology, 91, 591 -602.
Sharma, M. i: D., Schaal, P. N., Vaid, B. K., Dubey, R. C..Nagendra, S., Paithne, P. K. & Joshi, M. L. (1973). Effec-tiveness of drug schedule hein? followed under the NationalEradication Programme, India, for radical cure of vivarmalaria cases. Journal of Conunwricable Diseases, S. 167 -174.
Sharma, R. C., Gautam, A. S., Orlor, V. & Sharma, V. P.(1990). Relapse pattern of Plasmodium vivax in KhedaDistrict, Gujerat. Indian Journal o(Aloiarialo , 27, 95 -99.
Singh, J., Ray, A. P., Mistra, B. G. le Nair, C. P. (1954). Anti-relapse treatment with primaquine and pyrimethamine.Indian Journal gfMalariokjy 8, 127 -136.
Singh, N., Miahra, A. K. de Sharma, V. P. (1990). Radicaltreatment of vivax malaria in Madhya Pradesh, India. LydianJournal of Malanolnp, 27; 55 -56.
Wemsdorfer, W. li. & Payne, D. (1988). Drug sensitivity testsIn malaria parasites. in: Malaria-Principles and Practice ofMalariology, Wemsdorfer, W. H. & McGregor, I. (editors).Edinburgh: Churchill Livingstone, pp. I765 -1800.
WHO (1966). Irodd Heahh Organization Expert Committee onMalaria. Tuejfikrepon.,Geneva; World Health Organization,Technical Report Series, no. 324.
WHO (1990). Practical Chemotherapy of Malaraa. Geneva.World Health Organization, Technical Repon Series, no.805.
Received 1 Slane 1999; revised 12 August 1999; accepted forpublication 23 August 1999
1
n
SIM AMA tAN I IU t.: I1Ii11t41E I S I.11( il'I(Al ItJ(:r
the health structure was destroyed by the war, a policybased tin provision of personal protection seemed theonly sensible way forward. Attltnugh there was littletraditi of using hedncls in Afghanistan, n field trialcarried out in refugee camps in Pakistan in 199I byI IeaItI1Nei 11W:11ß(1011 l cl red th:u mist Afghans %%ertready to adopt the technique and that treatment withpennethrim could give up to 61'Y. protection againstfalcipatrunt and 42%. protection against viva)/ malaria(the trial was undertaken in refugee camps rather than inAfghanistan itself for security reasons) (ROM AND ct al.,1996). l' he trial involved giving treated nets to I fl%u ofthe community while a further 10"(, served as a cumrulgroup. Incidence rotes were particularly Might in the yearof the trial and it sin ayìngg campaigns had to beresumed aftenvnrds to protect the majority tvho lackednets. Ucdnet coverage was increased to 30% in 1992. By1994 the dual control strategy had caused incidence tofall by almost 90%, to only 711 cases per 1000 per annum,while in unsprayed camps incidence fell by only 15%(RoWlANU et al., 1997a, 1947b). A case control studywas undertaken in 1994 to sec whether Afghans were stillusing the acts to good effect despite the reducedtransmission rates. Patients presenting at the 111f Us withsymptoms of malaria and who were slide positive weretaken to he cases, while patients with symptoms ofmalaria but with a negative slide were taken as controls.By comparing cases with controls we calculated addsratios for protection by bedncts.'l'he l'ti was (u t% againstfalciparurn and 52% against vivax malaria (Rom AND etal., 1997b). These values were almost identical to thoseof the prospective trial of 1991 and suggest that P13 oftreated nets may be similar at high and low levels oftransmission.
The level of prulectian obtained from treated nets in1991 and 1994 was suit significantly different from that ofthe indoor spraying campaigns with malathiun held inthe same 2 years in mutt around the sane district. Indoorspraying does not require a change in sleeping habits andprovides passive protection to everyone in the camp. Useof nets requires self -discipline and those who cláimcd touse them (and 70% did) obtained an extra 10% ofprotection (ROW LAND et al., 1996, 1997b). Interest-ingly, the adoption of the pyretlnoid lambda cyhalothrinby the UNI -1C12 indoor spraying programme gave asimilar degree (10"/.) of extra protection over malathiun(Itt'sIANI) et al., 1994). In short there is nothing tochoose between indoor spraying and treated nets in termsof efficacy.
On the basis of these encouraging results a majorprogramme of senora treated nets was started in Afghani-stan by a consortium of NGUs coordinated by I Ieatlh-Nrt International with support from \K/110 andI ì1:11(;1l
ft. bell, debut thy (ulule .Ituttcgy ut Pakistan antiAfghanistan, a health economics analysis was under-taken of the bednet trial and indoor spraying programme(L. Guinness, unpublished report). The total cost of thespraying programme in North West Frontier Provincefrom 1990 to 19115 was 1.1S52.2 minim t. Insecticide cost81.1 Million, nearly half of all vector control costs, Theannual cost per person protected by the indoor sprayingproganume was 80(11. 'Ile cost per malaria infectionaverted was 820, which compared favourably with that ofother malaria control programmes (M11.1S, 199 I).
In the bednet project from 1991 to 1994, only 18% ofcosts went on insecticide while 47:i, went on nets (this
calculation assumes a life-span of 7 years fur nets). 'Ilttannual cost per persnn protected was 81.5 I . Il the cu.r ,:Inets could he placed vi direly un the user, the annual cu.tfor the progr. e would he 81)71) per person I'Eutcri,vlwhich is still no cheaper than the indoor sin twangprogramme.mme. IIttt prices or luci. have fallen by a tpna itt rsince I994 and new pyrethroitls such as deli. Iht in aI,thrill the price mf the perntethrin used iu the efficacy snail .The spraying pr/lgraltlltle icIso Ieitt'Iitcd from vcnnnuuie.of scale while the bednet project was n research trial withhigh monitoring costs. A full -scale bednet developmentproject, integrated into the health system, would be mat ecost- effective, especially if the culnutunily were to pro-vide vuhutIccr labour.
One should Ida° consider the suc,.tl ill gwucnts. Atmalaria declined in the rumps the spraying turugralulne,like any control programme, became less cost -effectiveand harder to justify or sustain. Many refugees are willingto pay for something tangible like n bednet (RutrvANI I etal., 1997h) but few would payfor something as ephem-eral as having their house sprayed (results of unjuuhlishettsurveys). A switch from spraying to nets in central andsouth Asia may not reap any economic benefits to cunt alprogrammes, but it would encourage self -reliance andmay not require the maintenance of a sophisticateddelivery system) or he so deprendcnt'un international aitlas indoor spraying campaigns.
Ack vledp(culeits1lenIrhNct International's Malaria Control l'rugrumnlc is
supported by she liurupcau Commission, the United NationsIligh Commissioner fur Refuges -s, the WIIOIUNI)l'/Wu:IdBank Special l'rogrnnune(or Research and Training in TropicalDiseases (!'inject 11): 961)662), the Department for Intcrna-tionatl Development of the UK, and I IealthNct International
itefcrenccsPox, C. h Strickland, G. '1'. (1989). The interrelationship of
Plasrnod' fulriparuul and P. uivux in the Punjab. Transa,noon uf the !loyal Society of 7íupícal Afe,h'ciue and 1QA'rerte, 83,471-473.
Mills, A. (1991). The erilnonlics uf mulada cuntrol. In: Ala/aria,tVuiringf,lrt,e Vu.:cine,'l'argett, U. (editor). (.:hitltester: Wileyh Sons, pp. 141-168.
Rathur, ll. lt., 'l'oqir, C,. Is ltnshtd, S. (19H5). Pnucnt ufulalsthion croes-resistanee to fenitruthiun irr Anuphclrt ,t:p/,tu.li nnd Annpl,elcs culirifucicr. Pakistan journal ,f AfadaulJ(escruYh, 24,115-.120.
Rowland, M., Itewitt, S. & I)urrnni, N. (1994). Prevalente nlmalaria in Afghaul refugee comps in l'uk,stan sprayed withhuuhdneyhnluthrin or lualud,iun 'li,un,,,too', .J ihrSueic(r a/Tropical Medicine I Ilrsirur, NH, 37H 379.
Itowltuul, M., Ouunut, M., Uueurnez, 1)., I)urrani, N , Itmrndual, J., Schnpira, A. & Sundurp, h. (1996). l'yretluui.t -impregnated lied nets l'ut sell ptulcctian (run, nudaria In,
'Afghan refugees 7iY,IlrUriipnr u1 nc, /1.91r1 tiorirn' uJ I1p,.,dAlerlicine raid llygirnr, 911, 357 361.
Ituwluml, lv1., I lcwitt, S., 1)urtan,, N, 11....n", N. & Wut/, It( I997a).'I'runsanissiun and eunuul uf vivas malaria in All;lr:u,refugee settlements in Pakistan. Transactions of Ihe lho,,!Sncic(v nf 7'rnpiad A(cdiriuc,unl Ilrgicur, 41,252. 255..
Rowland, 111., Hewitt, S., 1)tlrrani, 1V., Salclt, l'., Iluulna. At &Suntlnrp, lì. (19971)). Susrp,inabiliry uf pyvcahrnid imr,rtt;nntcd heel nets for alalnria control in Afghan euutnun,iuesIlrrlleu Ware IVra/d lfcuft, (hgonir.nuin,, 75,2 t 29.
Sulcmnn, M. (19RR). Malaria in Afghan refugees in l'ak,vanJiaruur,iaur a1 Ike Biwa! Society of 'I).,pirn/ Alyd,an. uu,fHygiene, 82,44-47.
Received 27- rr]a,rary 1999; reni.cetl ?3 Ala). 1999; (ICI epic./firr prrGlicatirrrr 101uue 1999
Annals of Tropical \icdicine & Parasitology, Vol. 91, Na. 6, 591-602 (1997)
Chloroquine resistance in Pakistan and theupsurge of falciparum malaria in Pakistaniand Afghan refugee populationsBy 1. S1U1Ali, M. RO\1'LANDf I, P. Ml ?l-IAlOOD, C. ntUJAl ttu §, F. RAZIQUI':11,
S. HR11r1'1" I't .NU N. DURRANIte National Institute of Malaria Research and Training, Lahore, Pakistant HealthNe! International, P.O. Box 889, Peshawar, Pakistan§ Directorate of Malaria Control, Islamabad, Pakistan .
I North West Frontier Department of Malaria Control, Peshawar, Pakistan
Received 12 March 1997, Revise/ 30 June 1997,Accepted 1 July 1997
Surveys conducted in Pakistan during the last decade show that falciparum malaria has.bccome resistant
to chloroquine in Pakistani and Afghan .refugee populations throughout :the country. :Although Riresistance is common everywhere .(with' a frequency of 30°k- 84'Ií,), RII is rarer (2 %- 3691,), and Rillresistance has yet to be detected. The national policy is to prescribe chloroquine as Irst -line treatment ofmalaria. A repeated in -vivo surrey in a sentinel village indicated that prescription of chloroquine can lead
to a IS'lí, increase in the frequency of resistance in a single year, and similar trends were observed in other
districts.Coinciding with the spread of resistance is a 6 -fold increase in the number of falciparum cases recorded
nationally between 1982 and 1992 and a parallel, 5-fold increase in the number of cases recorded in theAfghan refugee population. Resistance contributes to this trend in various ways. Firstly, patients withresistant malaria make repeated visits to health centres. In the sentinel village, for example, whereresistance was measured at 71%, recrudescent infections inflated by 669(h the genuine incidence of new
infections recorded at the health centre. Secondly, owing to ineffective treatment, resistant infections are
often still patent during the post -transmission season: This may enlarge the 'oven%intering' parasite
reservoir, leading to a surge of new cases when transmission resu,ncÑ. Other factors potentially contribut-ing to the upsurge in falciparum include the decreased availability of insecticide for indoor spraying.
Despite the problems posed by resistance for case management, the evidence from the vector -controlprogramme among the refugees .is that malaria control through well -targeted campaigns of insecticidespraying is still able to reduce the incidence of falciparum malaria to a level that existed before the adventof resistance.
Transmission or vivax and falciparum malariain Pakistan is seasonal, and mostly occurs inthe. second half of the year after the July -August monsoon (Strickland et al., 1987;Rowland et al., 1997h). A discernible trend inPakistan is for malaria to show. long -termperiodic cycles, the last major epidemic,havingoccurred in the mid -1970s (Zulueta et al.,
Author to whom correspondence should be addressed.E-mail: [email protected]: fax: 4- 92 321
840379.
0001-198.1/91/060391-12 59.00Crfas Publishing l.td
1980). Falciparum malaria is particularly un-stable at the northern end of its range, and canfluctuate markedly from year to year depend-ing on climatic variation. Iligh rainfall inautumn and temperatures above average inNovember and December are notable risk fac-tors that can .enhance or prolong the trans-mission. season, a perceptible trend in recentyears (Bouma, 1995). Compounding the prob-lem is the development of chloroquine resist-ance, which vas first reported in Pakistan in
1997 Liverpool School of 'l'ropieal .l lcdicinc
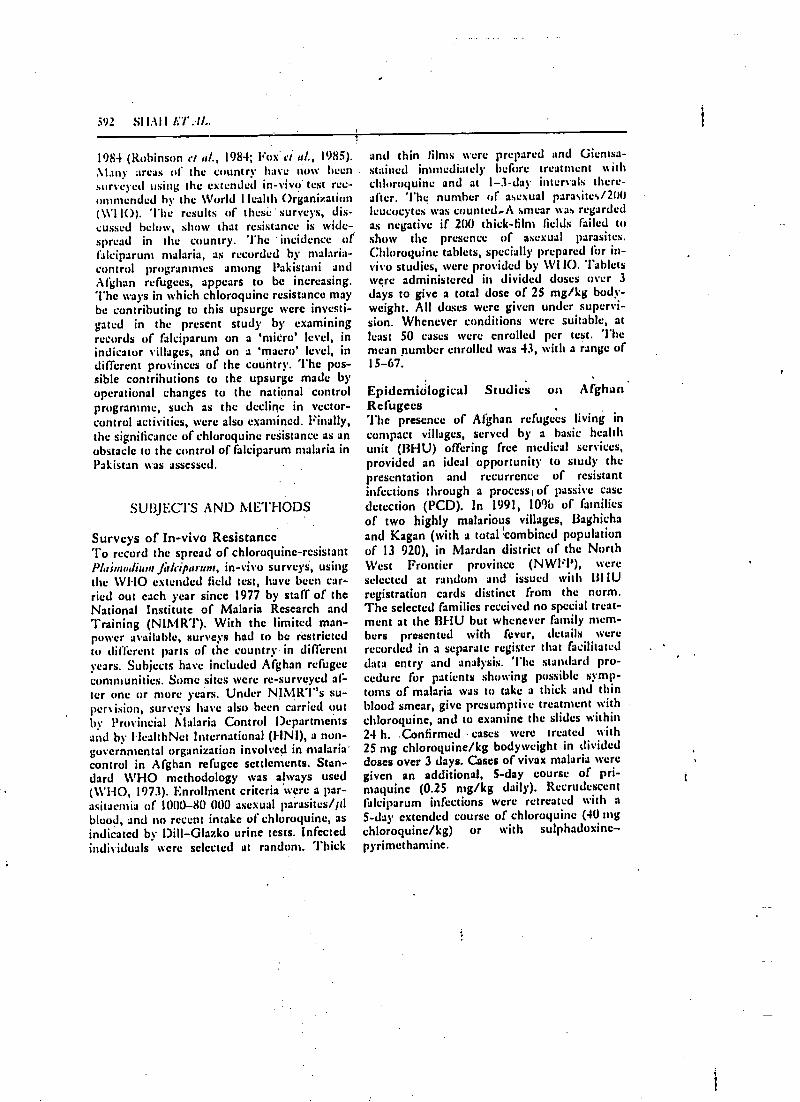
392 SI IAI I ET Al..
1984 (Robinson et al., 1984; Fox' ei al. 1985).
!any arras of the country have now beensurveyed using the extended in -vivo test rec-ommended by the World I Icalth Organization(WHO).IO). The results of these surveys, dis-cussed heIus, show that resistance is wide-spread in the country. The incidence offalciparum malaria, as recorded by malaria -control programmes among Pakistani andAfghan refugees, appears to be increasing.The ways in which chloroquine resistance maybe contributing to this upsurge were investi-gated in the present study by examiningrecords of falciparum on a `micro' level, inindicator villages, and on a 'macro' level, indifferent provinces of the country. The pos-sible contributions to the upsurge made byoperational changes to the national 'controlprogramme, such as the decline in vector -control activities, were also examined. Finally,the significance of chloroquine resistance as anobstacle to the control of falciparum malaria inPakistan was assessed.
SUBJECTS AND METHODS
Surveys of In -vivo ResistanceTo record the spread of chloroquine-resistantP/asnw /iu» r f rliiparum, in -vivo surveys, usingthe 1V1-IO extended field test, have been car-ried out each year since 1977 by staff of theNational Institute of Malaria Research and'!'raining (NIMR'I'). With the limited man-power available, surveys had to be restrictedto different parts of the country in differentyears. Subjects have included Afghan refugeecommunities. Some sites were re- surveyed af-ter one or more years. Under NIMR -1 "s su-pervision, surveys have also been carried outby Provincial Malaria Control Departmentsand by FlealthNet International (FINI), a non-governmental organization involved in malaria'control in Afghan refugee settlements. Stan-dard WHO methodology was always used(11'1-1O, 1973). Enrollment criteria were a par -asitaenua of I(1011 -80 000 asexual parasites /ftlblood, and no recent intake of chloroquine, asindicated by Dill -Glazko urine tests. Infectedindividuals tvere selected at random. Thick
and thin films were prepared and Giemsa-stained immediately before treatment withchloroquine and at 1 -3 -day intervals there-after. The number of asexual Para' ite,./200leucocytes 'as counted.A smear was regardedas negative if 200 thick -film fields failed toshow the presence of asexual parasites.Chloruquine tablets, specially prepared for in-vivo studies, were provided by 1V1 IO. Tabletswere administered in divided doses over 3days to give a total dose of 25 mg /kg body -weight. All doses were given under supervi-sion. Whenever conditions were suitable, atleast 50 cases were enrolled per test. Themean number enrolled was 43, with a range of15 -67.
!'epidemiological Studies on AfghanRefugeesThe presence of Afghan refugees living incompact villages, served by a basic healthunit (BHU) offering free medical services,provided an ideal opportunity to study thepresentation and recurrence of resistantinfections through a processi of passive casedetection (PCD). In 1991, 10% of familiesof two highly malarious villages, 13aghichaand Kagan (with a total I.combined populationof 13 920), in Mardan district of the NorthWest Frontier province (NWFP), were
selected at random and issued with IIIIUregistration cards distinct from the norm.The selected families received no special treat-ment at the BI-lU but whenever family mem-bers presented with fever, details wererecorded in a separate register that facilitateddata entry and analysis. The standard pro-cedure for patients showing possible symp-toms of malaria was to take a thick and thinblood smear, give presumptive treatment withchloroquine, and to examine the slides within24 h. .Confirmed cases were treated with25 mg chloroquine /kg bodyweight in divideddoses over 3 days. Cases of vivax malaria weregiven an additional, S -day course of pri-maquine (0.25 mg /kg daily). Recrudescentfalciparum infections were retreated with a5 -day extended course of chloroquine (40 mgchloroquine /kg) or with sulphadoxine-pyrimcthamine.
r
pm.
"MM.
"Ma
Om"
0
r
pm.
r
r
Mr11.ARIA IN PAKISTAN 593
A survey of malaria prevalence among theselected families was carried out in late De-cember, during the post -transmission season,to assess the success of the earlier drug treat-ments. Families were visited in their homesand blood smears were taken from all willingmembers.
t
Also in December, inhabitants of 13aghichaacre subjected to a survey' of in -vivochloroquine resistance, conducted by staff ofNIAMRT. Exactly I year later, a follow -up,in -vivo survey was carried out, this time byHNI.
National and Refugee Malaria StatisticsGovernment -run rural health centres andI3HU provide free medical services for thelocal Pakistani population and are comparablewith the UHU in the refugee camps. 'l'heProvincial Departments of Malaria Controlcompile the malaria -case records from thesefacilities and earmark the localities where inci-dence is high for focal spraying with residualinsecticide the following year. The UnitedNations High Commission for Refugees (UN-!JCR) is responsible for malaria control in theAfghan refugee villages, and adopts the policyof the national malaria -control programme(MCP), but delegates responsibility for datacollection, analysis and planning to FINI. An-nual malaria data for the last one or twodecades are re- analysed here to show trends infalciparum incidence, slide -positivity rates(SPR), and falciparum:vivax ratios.
Rt:SUi.'1:S
In -vivo Resistance Surveys'l'he consolidated results of 20 years work arepresented in Fig. 1. Resistance was first de-tected in 1981 in Sheikhupura in the Punjab(Figs 1 and 2). Surveys 2 -3 years later inother districts showed that RI resistance wasbecoming widespread in the Punjab and in-creasing in frequency. RII resistance was com-paratively rare at that time, occurring in onlya few percent of cases and in only two of thelive districts surveyed. In 1983 resistance wasrecorded in NWFP. Over the next decade RII
resistance increased in frequency, reaching anational maximum of 36'oí, in Alianwali on thePunjab-NW/FP border in 1992. Only one sur-vey was ever carried out in Baluchistan prov-ince, and this showed a resistance frcyucnc} of52 %. Some localities were re- surveyed afteran interval of several years: in Sheikhupuraresistance increased from 3'%t, to 37';x, between1981 and 1990; in Mardan (N1\ FP) it in-creased from 64' b to 9 -'3i, between 1985 and1987; and in 13annu (Nl1'hl') it increased from56% to 92í%u between 1986 and 1992. Afghanrefugee villages showed levels of resistancesimilar to those in Pakistani villages. Despitethe increase in 'frequency of RII resistance inrecent years, no cast of R1lI resistance has )etbeen recorded in Pakistan.
Studies on Afghan refugeesAccording to BI-lU records, 10% (138/1392)of refugees in 13aghicha and Kagpn contractedfalciparum malaria between July and Decem-ber 1991 (Fig. 3). Of these cases, 49 "n (68/138) recurred once and 17 'ii, (23/138)recurred again, producing an overall incidenceof 16°ií, (229/1392) for the 6 -month period.The mean interval between recurrences was18 days. If chloruquine resistance was absentfrom these villages, the probability of a suc-cessfully treated patient contracting a newinfection of falciparum would be around 1i)(approximately I3/138) or lice tintes less thanthe observed frequency of first recurrences.An in -vivo survey conducted in Decemberrevealed that 7I'4ó of falciparum cases inllaghicha were, in fact, chloruyuine -resistant(Fig. 1). Thus one of the effects of resistanceat the observed lrequcne) was to inflate thereported incidence ut'falciparum l 66 "o userthe period of observation, from the predicted11'41, should resistance not have been present(i,c (138.1. 13)/13921 to 16"0 (229/1392). Incontrast, the proportion of the population prestinting with vivax malaria was, at 22'b (3111/1392), double that which presented withfalciparum, and yet only 25"ís (77/310) ofthese infections recurred after treatment andonly l'h) (5/310) recurred a second time (Fig.3). If the proportion of the population thatbecomes re- infected with vivax is assumed to
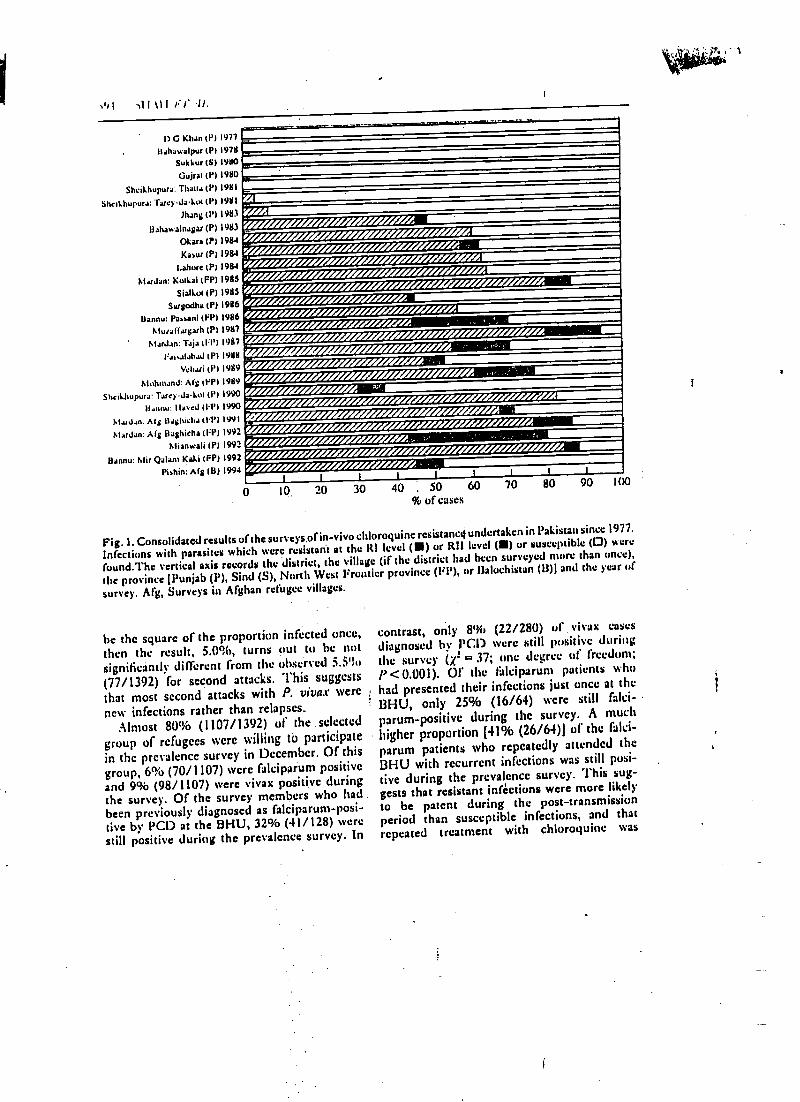
ÍD G Khan (P) 1977
Bahawalpuf (P) 197NSukkur (SI 19110
Gujrat (P) 1980
Sheikhupura: Than.; (P) 1981
Shnkhupura:'racyJaklK (P) 1981
Mang (P11983
Bahawalnaga(P) 1983
Okan 1P) 1984
Kawr W11984t.ahure (P) 1984
Madan: Kutui (FP) 1985Sialkot (P) 1985
Sargodha (P) 1986
Bannu: Piani (FP) 1986C,Iura((iusah (P) 1987
AIarJ.m: Taja (11') 19117
1a1,alahaJ (P) 1988
Vehai (P11989
1.IohnianJ: A(s (FP) 19119
ShciUwpura: Taeydakul (P) 1990
Ilaonu: Havcd 111'11990
hLuJn. Al s llashicha (14'1 1991
Alardan: A(g Bashkha (IP) 1992
Alianwali 1P11992
Bannu: Mir Qalam Kaki (FP) 1992Póhin: A(g (B) 1994
'----- ---- --
AO'^-r /<Ui1i .//i/l1ZfUUili/&:/i,t
Z./4V/Ad/iiiiiiiiliiiii lini/iiiii/17' iiiiiiiii /iii tar/!//.U/!/.f///!/!///!///////// AP/ //. .
:. ,: ,. ;,:
////////////////l!/////////!////!////////
////¡/II1/7/j/.MIESI
///////////////////////////L//////////l!/!/i!,
/ Age/ A'.6% A 11111.11111
////!/!!////!!/!//!/!////////.. ; _',, . .. c, ' ` 1111111111111111111111111
////////////////!//ll//////l///l///////// AV//////!//////.,liii, I/ií/Tii¡ill¿1.///¡ttl
I
0 10 20 30 40 . 50 60% of cases
1 1 1
70 80 90 1(10
Fig. 1. Consolidated results of the surveys.ofin -vivo chloroquine resistance( undertaken in Pakistan since 1977.
Infections with parasites which were resistant at the ltI level (III) or RIZ level (111) or susceptible (0) were
fuund.The vertical axis records the district, the village (if the district had been surveyed mure than unce),
the province !Punjab (P), Sind (S), North West Frontier province (FP), or Baluchistan (13)l and the year of
survey. Mg, Surveys in Afghan refugee villages.
be the square of the proportion infected once,then the result, 5.0 %, turns out to be notsignificantly different from the observed 5.5';u
(77/1392) for second attacks. This suggests
that most second attacks with P. vivax were
new infections rather than relapses..
Almost 80% (1107/1392) of the selected
group of refugees were willing to participatein the prevalence survey in December. Of thisgroup, 6% (70/1107) were falciparum positiveand 9% (98/1107) were vivax positive duringthe survey. Of the survey members who hadbeen previously diagnosed as falciparurn-posi-live by PCD at the BI-11-J, 32% (41/128) werestill positive during the prevalence survey. In
contrast, only 8% (22/280) of ,viva: cases
diagnosed by PCI) were still positive duringthe survey (x2= 37; One degree of freedom;P<0.001). Of the fálciparum patients who
had presented their infections just once at the
131-lÚ, only 25% (16/64) were still falci-
parum -positive during the survey. A much
higher proportion [41% (26/64)) of the falci-
parum patients who repeatedly attended the
131-IU with recurrent infections was still posi-tive during the prevalence survey. This sug-gests that resistant inactions were more likelyto be patent during the post -transmission
period than susceptible infections, and that
repeated treatment with chloroquine was
MALARIA IN PAKISTAN 595
Fig. 2. Map of Pakistan showing districts where surveys of in -vivo chioroquine resistance have been carried
out () and malaria endemicity in 1992, at levels of < 1000 (0), 1000 -1999 (0), 20(X) -2999 ( ®) or > 3000
(®) cases /year in each district.
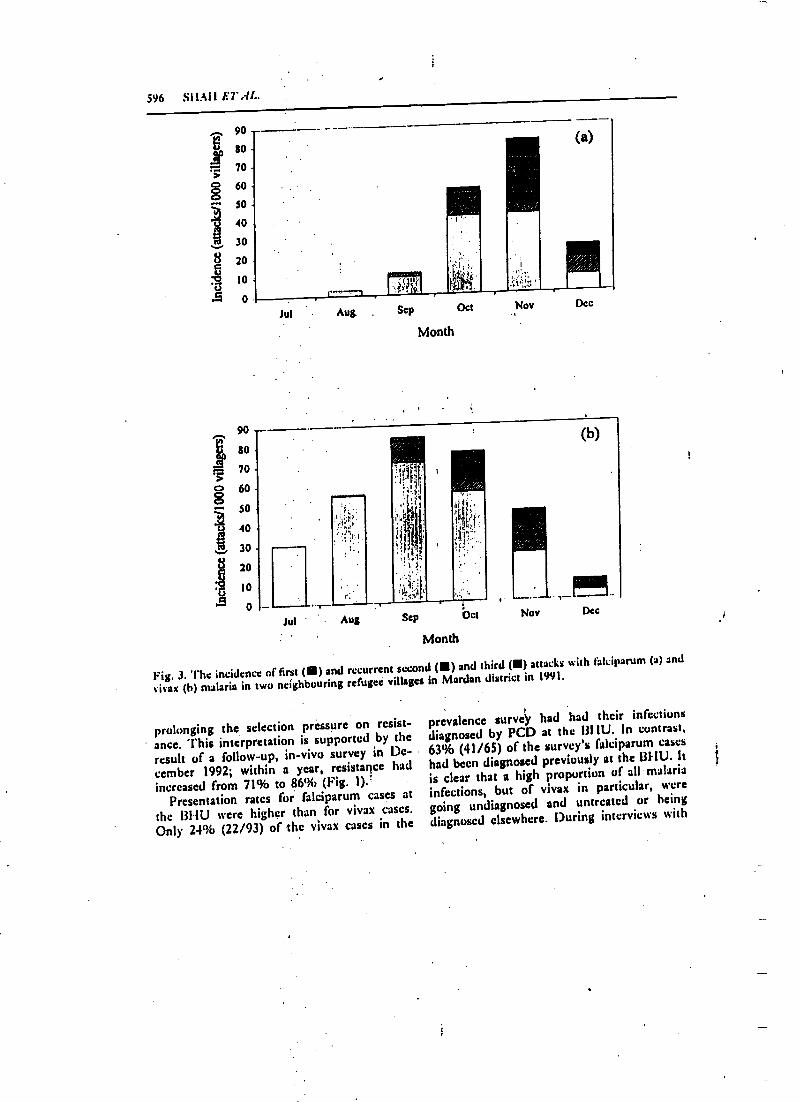
596 SIIAIl E7'AL.
J
';
90
80
70
60
.» 30
40
30
8 20
ti 10
r=
ó...
ú
5
90
80
70
60
so
40
30
20
10
0
Jul
"r-
Aug Sep Oct
Month
Nov Dec
Jul Aug Sep bct
Month
Nov Dec
Fig. 3. The incidence of first (I) and recurrent second (III) and third (II) attacks with falciparum (a) and
vivax (h) malaria in two neighbouring refugee villages in Mardan district in 1991.
prolonging the selection pressure on resist-
. ance. This interpretation is supported by the
result of a follow -up, in -vivo survey in De-cember 1992; within a year, resistance hadincreased from 71% to 86% (Fig. 1).'
Presentation rates for falciparum cases at
the 1311U were higher than for vivax cases.Only 24% (22/93) of the vivax cases in the
prevalence surveÿ had had their infectionsdiagnosed by PCD at the DI IU. In contrast,63% (41/65) of the survey's falciparum caseshad been diagnosed previously at the Bl-IU. It
is clear that a high proportion of all malariainfections, but of vivax in particular, weregoing undiagnosed and untreated or being
diagnosed elsewhere. During interviews with
"
r
pa.
r-
MALARIA IN PAKISTAN 5ï7
HNI, 92% of refugee families claimed to Ilsethe village 13HU in preference to private clin-ics; these claims cannot be confirmed, but itwas certainly the case that private clinics andpharmacies were not permitted within therefugee villages. It seems likely that manycases were clinically asymptomatic, particu-larly those of vivax malaria. The difference inpresentation rate between vivax and falci-parum cases (x2.= 27; one degree of freedom;P<0.001) may be attributable to the greaterseverity of falciparum's clinical symptoms. In-terviews held during the prevalence surveyrevealed that only 4% (4/98) of vivax casesand 23% (16/70) of falciparum cases weresymptomatic at the close of the transmissionseason (symptomatic patients were defined asthose who complained of recent fever, bodypain, headache and vomiting). While these'actual values may not represent the clinicalsituation existing during the height of thetransmission season, the relative values sup-port the proposed explanation for the differ-ence in presentation rate between vivax andfalciparum.
National Records on Malaria in PakistanSince the late 1970s there has been a gradualincrease in the number of recorded cases offalciparum in the Pakistani population; only3630 cases were recorded in 1980 but thisincreased to 56 885 in 1992, even thoughsimilar numbers of slides had been examinedeach year (3 006 624 in 1980 and 2 692 135 in1992). An increase in the number of falci-parum cases has also been observed in theAfghan refugee population, from only 7572'recorded cases in 1987 to 38 359 in 1992.These trends are presented in Fig. 4(a) aschanges in annual falciparum SPR. Analternative presentation, expressed in terms ofannual falciparum incidence, was not favouredsince this would require an accurate estintoleof population size, and this was not availablefor the Pakistani population. Use of SPR as anindicator is not wholly reliable either, becauseover the last decade there has been a gradualswitch from active case detection (ACD) topassive in Pakistan (from 12% P,CD in 1982 to25% PCD in 1991) and PCD `tends to pro-
duce higher SPR. This potentially confound-.
ing factor can be circumvented by presentingthe falciparum data with reference to vivaxdata, since P. fticiparuat and P. viva.r wouldbe equally affected by the switch from ACI)to l'CD. falciparum malaria is thereforeshown as a ' percentage of all malaria( %falciparum) in Fig. 4(b). Data for the Pun-jab are presented separately from data for therest of Pakistan because the Punjab was sub-ject to a major epidemic in the mid- 1970s,which distorts the pattern observed in the restof the country.
Linear regression was used to analyse thechanges in falciparum SPR and (N)falciparumover time. The results (sec 'fable) reveal asignificant increase in both falciparum SPRand %falciparum in every province except thePunjab. However, if the data collected fromthe Punjab from 1980 onwards (i.e. after theepidemic in the 1970s) are analysed,.a positivecorrelation, similar to that in the rest of thecountry, emerges. To test whether the up-surge in falciparum was an artifact caused bythe switch from ACD to PCD in the nationalcontrol programme, the ACD and PC1) data -sets were analysed separately. 'l'he two meth-ods of case detection showed nearly identicalrates of increasing %falciparum with time,and both showed significant increases in falci-parum SPR with time (sec Table). The up-surge was therefore not an artifact caused byprogramme reform. The falciparum SPR and%falciparum in the Afghan refugee popu-lation show a positive correlation over time,similar to that in the Pakistani population (see'fable).
Figure 4 shows that the upsurge in falci-parum started in the early to mid- 1980s,around the same time that chloroquinc resist-ance was becoming widespread in Pakistan.Falcipartim SPR increased about 11) -fold from0.5'%l, to around 5'!íi during the next decade[Fig. 4(a)ß. lalciparuin as a percentage or allmalaria increased 5-fold, from 10')b to 50'!b inthe Pakistani population and from 3'!b to 25%in the refugee population [Fig. 4(b)Ì. Whilethis trend still continues in the local popu-lation, the number of falciparum cases in therefugee population has decreased dramatically
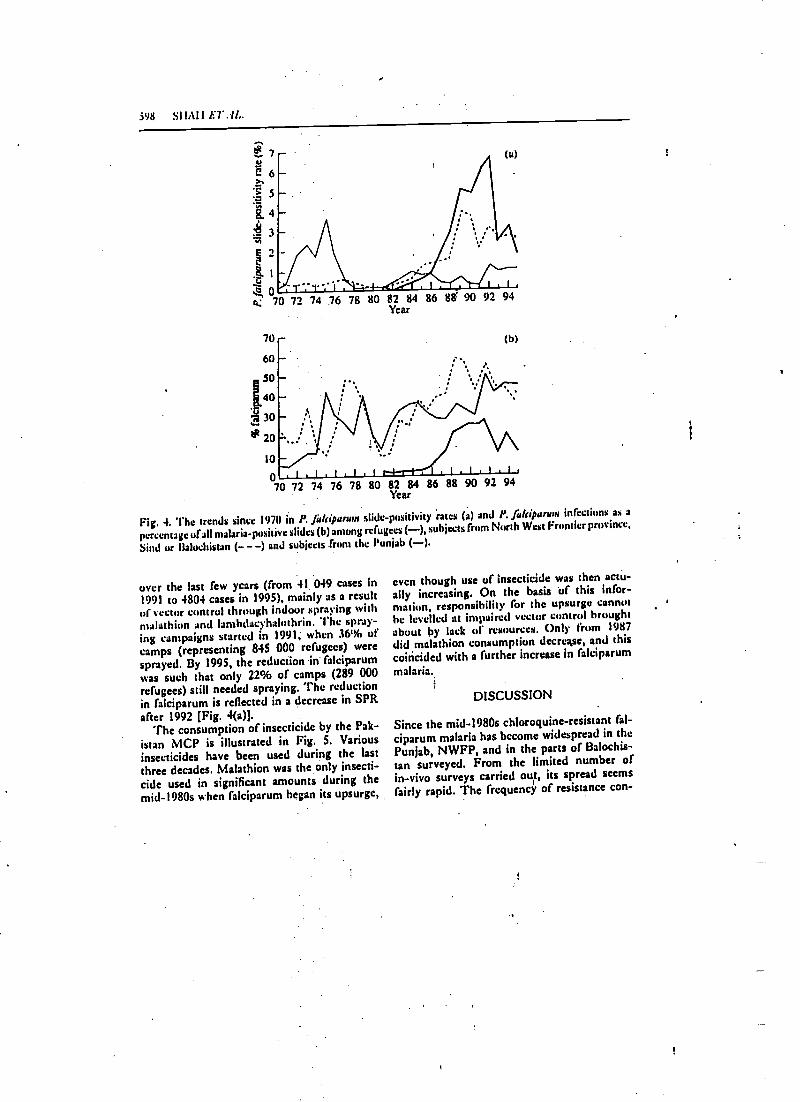
598 SII.UI6TAL.
70
60
SO
[4030
20
IO
070 72 74 76 78 80 82 84 86 88 90 92 94
Year
Fig. 4. The trends since 1970 in P. fulripururn slide- positivity rates (a) and P. Jdriparwn infections as a
percentage ufall malaria -positive slides (b) among refugees (--), subjects from North West Frontier province,
Sind or Baluchistan (- - -) and subjects from the Punjab ( -).
over the last few years (from 41 049 cases In
1991 to 4804 cases in 1995), mainly as a resultof vector control through indoor spraying withmalathion and lambtlacyhalnthrin. The spray-ing campaigns started in 1991, whim 36% ofcamps (representing 845 000 refugees) weresprayed. By 1995, the reduction in falciparumwas such that only 22% of camps (289 000refugees) still needed spraying. The reductionin falciparum is reflected in a decrease in SPRafter 1992 [Fig. 4(a)].
The consumption of insecticide by the Pak-istan MCP is illustrated in Fig. 5. Variousinsecticides have been used during the lastthree decades. Malathion was the only insecti-cide used in significant amounts during themid -1980s when falciparum began its upsurge,
even though use of insecticide was then actu-ally increasing. On the basis Of this infor-mation, responsibility for the upsurge cannothe levelled at impaired vector control broughtabout by lack of resources. Only from 1987did malathion consumption decrease, and thiscoincided with a further increase in falciparum
malaria.
DISCUSSION
Since the mid -1980s chloroquine-resistant fal-ciparum malaria has become widespread in thePunjab, NWFP, and in the parts of Balochis-tan surveyed. From the limited number ofin -vivo surveys carried out, its spread seemsfairly rapid. The frequency of resistance con-
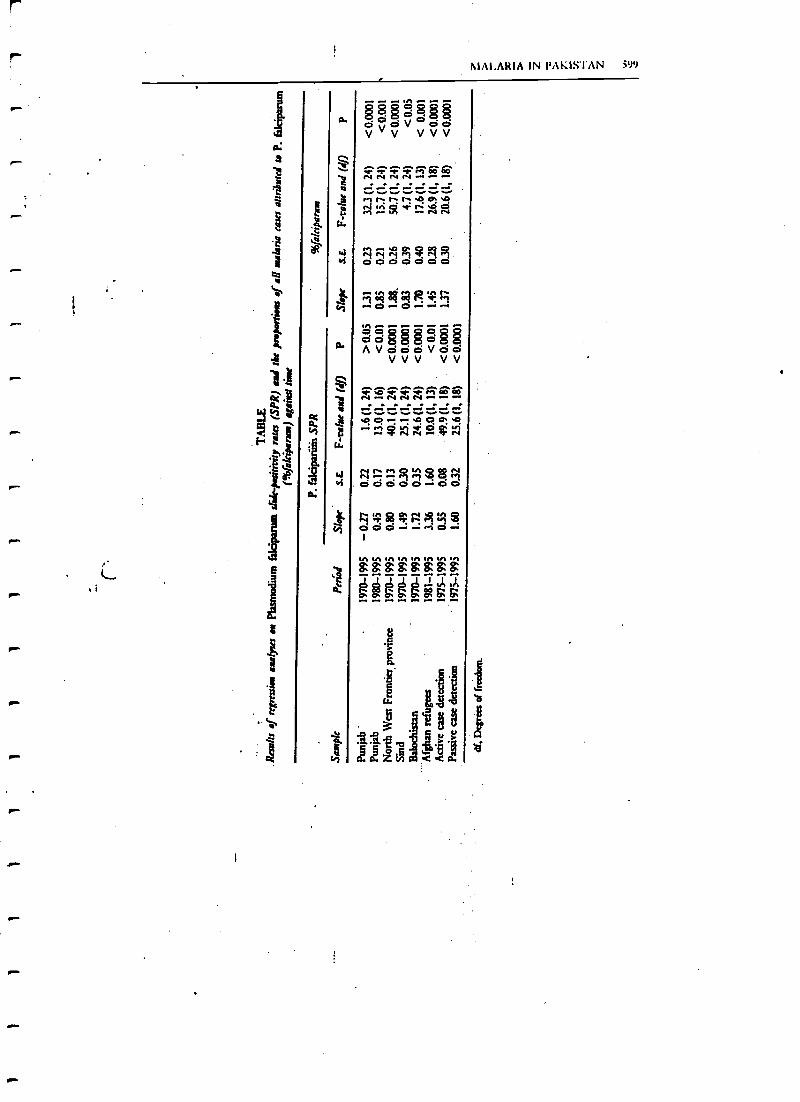
MALARIA IN PAKISTAN 51P9
Ñ
ççç.-.n--çç
2525ó25250°0v°00V V V V V V
ihÑ Ñ Ñ Ñ M+CO
ER iha.oM1 ÑÑ
óó$$$óeAVóddVdoVVV VV
400M-+Ñ Ñ Ñ Ñ
40 0 p-1 -v 0 0 0I 0...^rV4 CiP1'fV
q=-1$4110ó000-d0
qi-t001rM415D
ggágá:ááá^^ wv ^^P P O¡¡ P P P
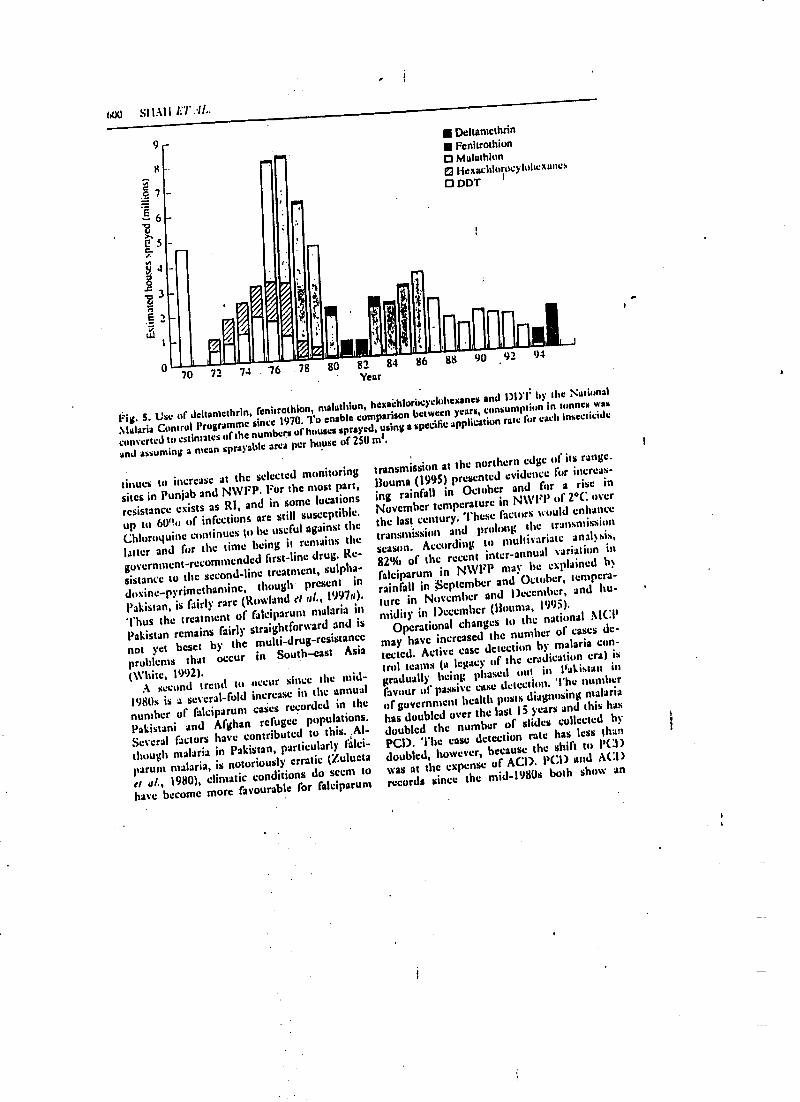
u,80 82
Year
600 S I l.a l l ET .!!..
9
070
%
l
72 74 76
. r
78
B
DeltamethrinFcnitrothion
O Malathion0 ttexachlon>cyhthexane+O DDT
finfiffnmit84 86 88 90 92 94
Fig. S. Use of dcltamcthrin, fenitrothion, malathion,hexachluricyclohexanes and
1)l)'t' by the National
Malaria ControlProgramme since 1970. To enable comparison
between years,consumption in tonnes was
converted to estimates of the numbers of houses sprayed,using a specific
application rate for each insecticide
and assuming a meansprayable area per house of 250 mt.
tinues to increase at the selected monitoring
sites in Punjab and NWFP. For the most part,
resistance exists as RI, and in some locations
up to &Po of infections arc still susceptible.
Chloroyuine continues to he useful against the
latter and for the time being it remains the
government-recommended first-line drug. Re-
sistance to the second -line treatment, sulpha -
doxine- pyrimethamine, though present in
Pakistan, is fairly rare (Rowland ei al., 1997a).
Thus the treatment of falciparumt malaria in
Pakistan remains fairly straightforward and is
not yet beset by the multi- drug -resistance
problems that occur in South -east Asia
(White, 1992).A second trend to occur Since the mid -
1980s is a several-fold increase in the annual
number of falciparum casesrecorded in the
Pakistani and Afghan refugee. populations.
Several factors have contributed to this. .A1-
though malaria in Pakistan, particularly falci-
parum malaria, is notoriously erratic (Zulueta
ei al., 1980), climaticconditions do seem to
have become more favourable for falciparum
transmission at the northern edge of its range.
Houma (1995) presented evidence for increas-
ing rainfall in October and fur a rise in
November temperaturein N\1'FP of 2°C over
the last century. 'l'hese factors would enhance
transmission and prolong the transmission
season. According to multivariate analysis,
82% of the recent inter -annual variation in
falciparum in NWFP may be explained b
rainfall in September. and October, tempera-
ture in November and December, and hu-
midity in December (Houma, 1995).
Operational changes to the national A(CP
may have increased the number of cases de-
tected. Active casedetection by malaria con-
trol teams (a legacy of the eradication era) is
gradually being phased out in Pakistan in
favour of passive case detection. The number
of government health posts diagnosing malaria
has doubled overthe last 15 years and this has
doubled the number of slides collected by
PCI). The case detection rate has less than
doubled, however,because the shift to PC1)
was at the expense of ACD. PCI) and ACI)
records since the mid -1980s both show an
MAI.ARIA IN PAKISTAN
increase in falciparum SPR and Talci-parum:vivax ratios. At best, programme. re-form can only partly explain the upsurge in
falciparum.Vector control though indoor spraying has
had a major impact on malaria in Pakistan in
the past. The epidemic in the Punjab in themid- 1970s, for example, coincided with the
development of resistance in vectors to DDTand 1-ICH (hexachlorocyclohcxanes), and wasfinally brought under control by spray cam-paigns with' malathion (sec Figs 4 and 5;Zuleta et al., 1980). However, during the up-
4 surge in malaria in the mid- 1980s, use ofmalathion by the national programme wasactually increasing, suggesting that factors un-related to vector- control operations were re-sponsible for the upsurge. The evolution ofmalathion resistance has had only a minorrole; although one of the primary vectors in
Pakistan, .4stnphries step / tenti (Pervcr, and
Shah; I989), became widely resistant to
malathion during the mid -1980s (Rathor et al.,1985), recent evidence suggests that spraycampaigns with malathion arc still effective incontrolling malaria in areas where vectors arcmalathion -resistant (Rowland a al., 1997b).
The area under insecticide coverage has de-creased in recent years (Fig. S) and this mayhave contributed to the persisting high levels
of falciparum.The advent and rapid spread of chloroquinc
resistance in the mid -1980s coincided with the
initial falciparum upsurge and may have con-tributed to it in two ways. Firstly, re-
01 crudescent infections lead to patients makingrepeated visits to health posts. This can inflatethe true incidence of new infections (e.g. by
66%, in the present sentinel village). Sec-ondly, inadequately treated infections may
persist into the post -transmission period and
enlarge the `ovcrwintcring' parasite reservoir,leading to a rapid increase in new cases when
transmission resumes. Evidence suggests that
chloroquinc resistance may have initiated thefalciparum, upsurge in the mid -1980s and now
helps to maintain it.Thus there are many factors potentially
or actually contributing to the upsurge infalciparum. To quantify the contributionmade by chloroquinc resistance (or by anyother biological or operational factor) wouldrequire the analysis of local data that aresimply not available, such as those on local
increases in falciparum incidence when
chloroquinc resistance first developed in anarca, or when malathion spraying first becamerestricted (Schoitens el al., 1990), or when
local anophelines : became' resistant to
malathion (Lewis, 1990). Despite the inade-quacies in the data, the evidence from theUNHCR malaria- control programme is that
campaigns of selective spraying withmalathion and lambdacyhalothrin have suc-cessfully reduced the incidence of falciparum
to a tenth of former levels in the Afghanrefugee population of Pakistan (Rowland a al.,1994, 1997b; Bouma, 1995). 'l'Ius the upsurgein chloroquinc- resistant falciparum malaria inPakistan is by no means insurmountable.
ACKNOWLEDGEMENTS. We arc indebted to themicroscopists and technical staff of NIMRTand HNI for carrying out the many fieldsurveys over the years, and thank M. 110umafor kindly commenting on the manuscript.The tINI Malaria Control Programme is
supported by the European Commission,UNHCR and WIIO /TDR.
REFERENCES
13oust.À, NI. J. (1995). Epidemiology and control ,f maUniversity.
Fux, E., Kama% A. A., S.iRWAR, M. ti Srtutaa..{Ntt,falciparum: now in Pakistani l'unjab. Lancet, i, 14
LEtus, A. N. (1990). An rluestneat of now Resisnanre!widener of Malaria in Pakistan. V13C Report No.ation International.
!aria in np,rthera Pakistan. l'h.i). thesis, Leiden
G. T. (1985). Chloroquinc- resistant Plasmodnaa
32- 1434.'lo Malathion by Anopheles stephcnsi .( /furs the81228. Arlington, VA: Medical Service Corpor-
(I(12 S 11.111 ET AL.
P).RVEZ, S. D. & S11111, 1. II. (1989). The rule of Anopheles siephensi asmalaria vector in rural areas of
Pakistan. Pakistan Journal of Health, 26, 73-84.
R.trntt, IL R., TotIpt, G. & RAsum), S. (1985). Pattern of malathion cross-resistance to fenitrvthion in
,ieopiteles stephensi and .hmphrirs nJkifuitr. Pakistan journal of Medical Research, 24, 115-120.
RttuixsoN, D. S., 11.0I.Ev- IIR)UN, hl., EpI.E, O. A. & ROIIINSON, P. S. (1984). C:hh)roquine resistant
malaria in Pakistan. Lancet, 1, 987.
Rimt..ND, M., 11t.w'rrr, S. & DURRANI, N. (1994). Prevalence of malaria in Afghan refugee village in
Pakistan sprayed withlambdacyhalothrin or malathion. Transactions of the Royal Society 4. Tropism!
.Mrdi,iur and Hygiene, 88, 378 -379.
Rol.AXI), M., DCRRAN', N., IIiwrrr, S. & S r tx)Ru, E. (1997a). Resistance of falciparum malaria tu
t:hluroquine and sulfadoxinc-pyrin)cthaminc in Afghan refugee settlements in ;western Pakistan:
surveys by the general health services using a simplified in vivo test. Tropical Medicine und
International Health, in press.Rent t.ANl), M., I hiwt rr, S., DURRANI, N., RAN°, N. & Wuc z, R. A. (19974. Transmission and control of
vicar malaria in Afghan refugee settlements in Pakistan. Transactions of the Royal Society of Tropical
.Medicine und Hygiene, in press.
5< a to t..11. R., 0mm:it, I.., DRAT %, N. Ci., i (Asi í, G. & VAN DIX, W. (1990). Report of an l titnsal Review
of'the Pakistan 'Malaria Control Programme. VIIC Report No. 81126. Arlington, VA: Medical Service
Corporation International.Sr *mcta.tvl), O. 1., LVAR- 1,.1m, A., Fux, E., MI mil, A. A. & Ctunv,»tees, I. A. (1987). Endemic
malaria in four villages of the Pakistani lino hive ul' Punjab. Transactions or th Royal ,tio,iety of
Tropical ,lleJichne and Hygiene, 81; 36-41:
WHITE, N. J. (1992). Antimalarial drug resistance: the pace quickens. Journal of Antimicrobial Chemo-
therapy, 30, 571 -585.11'ORLl) l IEALTJ I ORGANIZATION (1973).
Chemotherapy of Malaria and Resistance to dntinnalariah. Technical
Report Series No. 529. Geneva: WHO.
Zut.UI :TA, J. 1W, MUJTAAA, S. M. & SHAG, I. H. (1980). Malaria control and long -term periodicity at the
disease in Pakistan. Transactions of the Royal Saciégy of Tropical Medicine and hygiene, 74, 624 -632.
Tropical Medicine and international Health
VOLUMI a NO It PP 104y+1056 NovaMSaa 1997
Resistance of falciparum malaria to chloroquine and
sulfadoxine-pyrimethamine in Afghan refugee settlements
in western Pakistan: surveys by the general health services
using a simplified in vivo test
Mark Rowland', Naeem Durranl', Sean Hewitt' and Egbert Sondorp'
HealthNet International, !Whams', Pakistan
Heald:Net international.Amsterdam, The Netherlands.
Summary Surveys of drug resistant falciparum malaria were conducted in several Afghan refugee
settlements, distributed over a 70o km range in western Pakistan, during the transmission seasons
of 1994 and t995. Symptomatic malaria patients were recruited by a process of passive case
detection st the refugees' basic health units. To facilitate follow -up by local health workers, a
modified version of the WHO extended in vivo test was adopted in which blood smears were taken
from each subject, and clinical symptomsrecorded, at weekly intervals. Resistance to chloroquine
and sulfadoxine-pyrimethamine was identified in every settlement. The frequency of chloroquine
resistance ranged from 18% to 6a%. Resistance occurred mostly as RI, with RII resistance never
exceeding :196. Resistance to sulfadoxine-pyrimethamine occurred at much lower frequencies,
ranging from 4% to as%. There was a resumption of clinical symptoms at the onset of parasite
recrudescence in over 9o% of cases. The policy of using chloroquine as first -line treatment might
be changed in favour of sulfadoxine-pyrimethamine in most camps and areas of western Pakistan.
The modified in vivo test was almost as accurate as the normal WHO in vivo test in identifying the
grade of resistance, and should prove a useful tool for the monitoring of resistance to common
antimalarial, by district health services.
keywords chloroquine, resistance, falciparum malaria, sulfadoxine- pyremethamine
correspondeneb Mark Rowland, HealthNet International,PO Box 889; University Town,
Peshawar, Pakistan.
Introduction
Chloroquine- resistant falciparum malaria was first
identified in Pakistan in 1984 (Fox et al. x983). Over the
last decade, resistance surveysconducted by the
National Institute for Malaria Research and Training
using the WHO extended in vivo test (WHO ¡973) have
shown that chloroquine resistance is widespread in
many areas oÉ the Punjab and North -west Frontier
Province (Shah et al. z997). Resistance to sulfadoxine-
pyrimethamine has not been monitored or reported. The
Pakistan Ministry of Health currently recommends the
1 049 C 1997 Iltackwes Scienze Ltd
use of chloroquine as first -line treatment for the
treatment of falciparum malaria. This guideline ntay n .
longer be appropriate.Since the early :98os up to ; million Afghan re(u)re.
.
have settled in camps - often in malarious areas - in
western Pakistan (Rowland et al. 1997). The United
Nations High Commissioner for Refugees presently
adopts the same treatmentguidelines for falciparum
malaria as the Pakistan Ministry of Health. To develop
focally effective treatmentguidelines for the refugee
communities, it is necessary to map the type, level, anti
distribution of drug resistance to chloroquine and
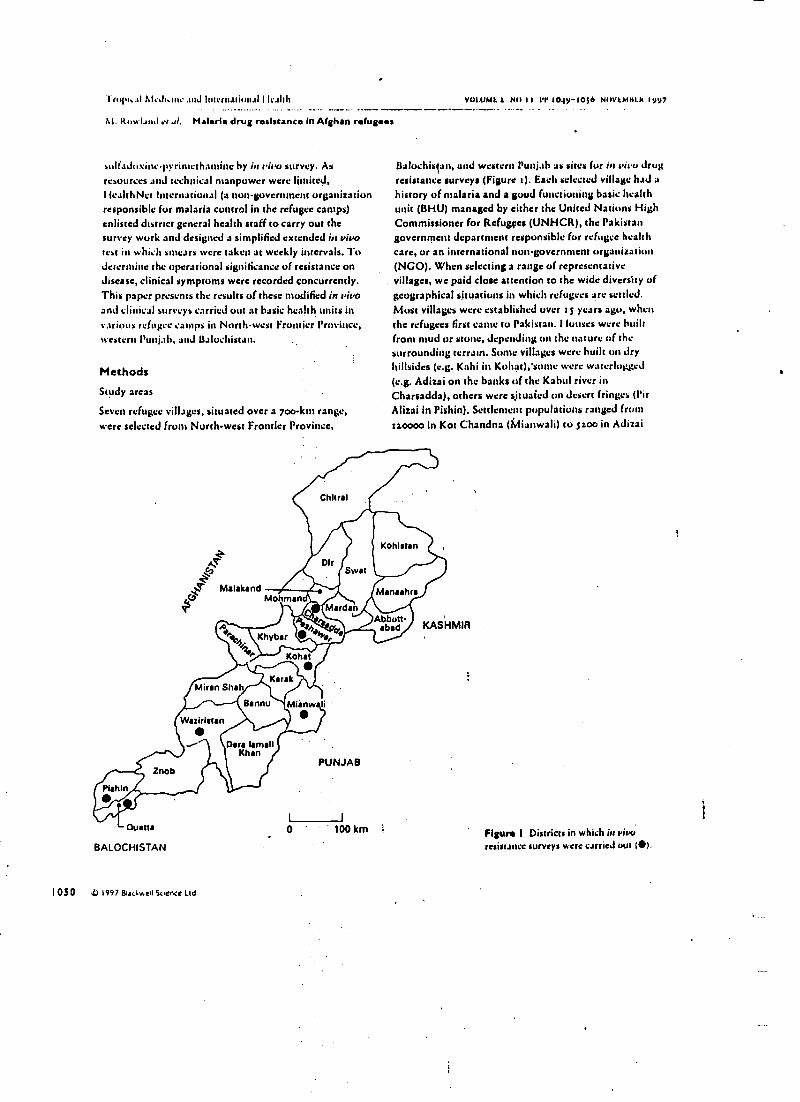
l'rupi:al AL.h.ute.ntJ Inlcrualiun.11 I IC.111I1
hi. Rowland et .d. Malaria drug resistance In Afghan refugees
sulfadoxine- pyrinleth3mine by in vivo survey. Asresources and technical manpower were Binned,I iealthNet International (a nun- government organizationresponsible for malaria control in the refugee camps)enlisted district general health staff to carry out thesurvey work and designed a simplified extended in vivoteat itt which smears were taken at weekly intervals. Todetermine the operational significance of resistance ondisease, clinical symptoms were recorded concurrently.This paper presents the results of these modified in vivoand clinical surveys carried out at basic health units invarious refugee camps in North -west Frontier Province,svestern Punjab, and Baluchistan.
Methods
Study areas
Seven refugee villages, situated over a loo -km range,
were selected from North -west Frontier Province,
Malakand
Miran Shah
Waziristan
Znob
Pishin
Mama
BALOCHISTAN
1050 D 1997 &ukwell Suene Ltd
Mohman
Khyber
Chitral
DirSwat
Minden
'+lt, d1a,
Kohat
Karak
Bannu
Dora IsmailKhan
Miinw li
PUNJAB
0 * 100 km
V01.1/M3 3 NO 11 1'1' 1o49-1o56 NUV3M81k
Baluchistan, and western Punjab as sites for in vivo drugresistance surveys (Figure t). Each selected village had ahistory of malaria and a good functioning basic healthunit (BHU) managed by either the United Nations HighCommissioner for Refugees (UNHCR), the Pakistangovernment department responsible for refugee healthcare, or an international nun -government organization(NCO). When selecting a range of representativevillages, we paid close attention to the wide diversity ofgeographical situations in which refugees are settled.Most villages were established over a S years ago, when
the refugees lirst carte to Pakistan. Houses were builtfrom mud or stone, depending on the nature of thesurrounding terrain. Some villages were built on dryhillsides (e.g. Kahi in Kahat),'sonte were waterlogged(e.g. Adizai on the banks of the Kabul river inCharsadda), others were situaied on desert fringes (l'irAlizai in Pishin). Settlement populations ranged fromzz0000 in Kot Chandna (Mianwali) to zoo in Adizai
Kohlstan
Mansehra
Abbott-abad KASHMIR
Figure I Districts in which in ',hot;resistance surveys were carried out Mi.
Tropical Medicine and International HealthVOLUMB z NO t l Pr 1049--1o5 6 KOt't.NCt h i yy`
M. Rowland et rl. lialatiia drug resistance In Afghan réfugees
( Charsadda). Altitude ranged front ago m in Baglicha
(Mudan) to 1380 m in Main Warsak (Waziristan).
Some settlements were peri-urban (e.g. Badaber in
Peshawar) while most were rural (e.g. Adizai in
Charsadda). Surrounding agriculture sometimes
included rice (e.g. in Mardan), orchardi (in Waziristan),
maize (e.g. in Kohat), wheat or sugar (e.g. in
Charsadda). Local mosquito breeding sites were equally
diverse, and included water -tilledborrow pits in Adizai
(Charsadda), irrigated rice fields in Baghicha (Martian),
reservoir tanks in Azam Warzak (Waziristan), seasonal
rivers in Badaber (Peshawar), and springs in Pir Alizai
(Pishin). Most settlements remained densely populated
even though many Afghans had repatriated voluntarily.Settlements were often situated within a few km of local
Pakistani villages, and malaria prevalence rates in
neighbouring local and refugee communities were often
homologous, suggesting a degree of 'parasite exchange'
(Suleman 7988; Bouma et Rowland 1994). Because
hostilities have mostly ceased in eastern and southern
Afghanistan, cross -border movement of adult males was
frequent, leading to import and export of malaria.
Women and children were much less mobile, and hence
only a small proportion of malaria cases recorded in the
BHUs was acquired in Afghanistan (Rowland el al.
1996).
Survey procedures
The medical officer, malaria supervisor, and
microscopist from each BHU were trained by IlealthNet
International (HNI) in survey methodology. Special
attention was paid to calculation of drug dose according
to body weight, to supervision of treatment, to
recording of clinical symptoms, and to patitint follow -
up. The microscopists had been previously trained by
HNI and were highly proficient. Chloroquine resistance
was surveyed in 7994 and sulfadoxine- pyrintethamine
resistance in 5995. Subjects were recruited by passive
case detection during the transmission season front
\upu'{ (t CAM' tldt:l W.I% {'Ctütt)t'Ll l'i{
standard loi ins and printed registers provided by I INl.
A thick and thin blood smear was taken from any
patient presenting with fever or malaria -like symptoms.
Axillary temperature was taken with an electronic
thermometer and clinical symptoms were recorded
against a checklist. The patient was then given
presumptive treatment with chloroquinc (so mg per kg
I OS I O i947 &ackwet Sc.ence LW
body weight) or sulfadoxine-pyrimethatnine (at mg
sulfadoxine and 1.21 mg pyrintcthantinc per body
weight). The chloroquinc was provided by WI IO, the
sulfadoxine- pyrimethamine (Fansidar) was
manufactured by Roche. Patients were monitored fur
3o min in case they vomited. Patients were requested to
return the next day by which time their swears had been
read by the microscopist. Confirmed falciparum cases,
enrolled into the chloroquinc resistance survey, were
given an additional t3 mg chloroquinc per kg body
weight during the next 2.4 h (total intake zs nlg/kg body
weight). Cases enrolled into the sulfadoxine-
pyrimcthamine resistance survey were given no
additional treatment since the presumptive dose was
equivalent to a radical dose.All subjects wcrc requested to return a week after the
start of radical treatment so that staff could take a
follow -up smear and record clinical symptoms. Tins
procedure was repeated cads week for 4 weeks for
subjects in the chloroquinc resistance survey and each
week for 7 weeks for subjects in the sulfaduxine-
pyrintethamine resistance survey. If a subject (ailed to
report, the health worker visited him in his hunte,
usually that same day, to obtain the blood smear.
All slides were stained with Cictnsa's solution. A
smear was regarded as negative if zoo thick films failed
to show the presence of asexual parasites. Parasites were
initially scored using the plus system (Gilles & Warrell
1993). Unlike in the normal extended test, patients were
not excluded if their parasitaentias were less than
t000/mi of blood, and Dill- Claaku urine tests fur
detection of prior intake of chloroquinc were notperformed. If a chioroquine- treated patient became
falciparum -positive during the follow -up period, he was
retreated with sulfadoxinepyrimcthantine, and tic e
versa. I INI monitors paid impromptu spot checks on
BHU survey staff, and questioned a number of subjet.
in their hontes to contirm iliac survey procedures had
been correctly followed. In order to verify diagnoses, all
slides were retained for re- examination by HNI's
microscopists.
WHO extended in vivo tests
In r993, une year before the modified test surveys, I IN1
staff carried out z normal WHO extended in vivo tests
(WHO 073) in refugee villages in the Charsadda and
Mardan districts. During these, blood smears were
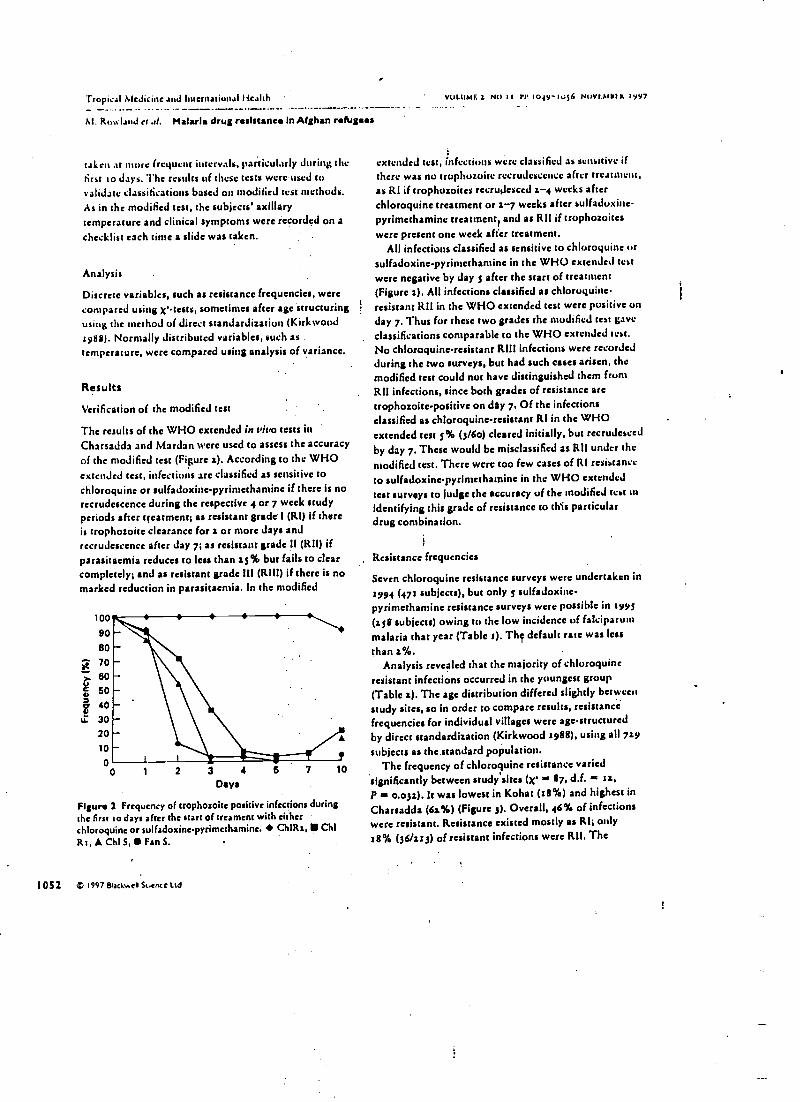
Tropical Medicine and International Health
M. Rowland er al. Malaria drug resistance In Afghan refugees
taken at more frequent intervals, particularly during thefirst to days. The results of these tests were used tovalidate classifications based on modified test methods.
As in the modified rest, the subjects' axillarytemperature and clinical symptoms were recorded on achecklist each time a slide was taken.
Analysis
Discrete variables, such as resistance frequencies, were
compared using x'-tests, sometimes after age structuringusing the method of direct standardization (Kirkwood1y88). Normally distributed variables, such astemperature, were compared using analysis of variance.
Results
Verification of the modified test
The results of the WHO extended in vivo tests inCharsadda and Mardan were used to assess the accuracyof the modified test (Figure 1). According to the WHOextended test, infections arc classified as sensitive tochloroquine or sulfadoxine- pyrintetharnine if there is norecrudescence during the respective 4 or 7 week studyperiods after treatment; as resistant grade I (RI) if thereis trophozoite clearance for a or more days andrecrudescence after day 7; as resistant grade II (RI!) ifparasitaemia reduces to less than as% but fails to clearcompletely; and as resistant grade III (RUI1) if there is nomarked reduction in parasitaemia. In the modified
100
90
80
70
60
g50
. 4030
20
10
00 1 2 3 4
Days
Figure 2 Frequency of trophozoite positive infections duringthe first to days after the start of tremens with eitherchloroquine or sulfadoxinc.pyrimethamine. ChIR:, tg ChiRt,ChIS,FsnS.
10
1 052 D 1997 Blackwell Suence Ltd
VOLUMF.1 NO It 1'P I04y-IVl6 NnVt.alYtk 19y7
extended test, infections were classified as sensitive ifthere was no trophozoite recrudescence after treatment,as RI if trophozoites reirutaesced a -4 weeks afterchloroquine treatment or a -7 weeks after sulfaduxine-pyrimethaminc treattnentl and as RIl if trophozoiteswere present one week after treatment.
All infections classified as sensitive to chloroquine orsulfadoxine -pyrimethamine in the WHO extended testwere negative by days after the start of treatment(Figure a). All infections classified as chloroquine -resistant 1211 in the WHO extended test were positive onday 7. Thus for these two grades the modified test gaveclassifications comparable to the WHO extended test.No chloroquine -resistant RIII infections were recordedduring the two surveys, but had such cases arisen, themodified test could not have distinguished them frumRI[ infections, since both grades of resistance aretrophozoite -positive on day 7. Of the infectionsclassified as chloroquine -resistant RI in the WHOextended ten s% (3/6o) cleared initially, but recrudescedby day 7. These would be misclassified as RII under themodified test. There were too few cases of RI resistance
to sulfadoxine- pyrinsethatnine in the WHO extended
test surveys to judge the accuracy of the modified test inidentifying this grade of resistance to this particulardrug combination.
Resistance frequencies
Seven chloroquine resistance surveys were undertaken in1994 (471 subjects), but only s sulfadoxine -pyrimethamine resistance surveys were possible in syys
(ss8 subjects) owing to the low incidence of falciparurnmalaria that year (Table t). The default rate was lessthan z %.
Analysis revealed chat the majority of chloroquineresistant infections occurred in the youngest group(Table a). The age distribution differed slightly betweenstudy sites, so in order to compare results, resistancefrequencies for individual villages were age -structuredby direct standardization (Kirkwood 1988), using all 7zy
subjects as the standard population.The frequency of chloroquine resistance varied
'significantly between study'sites (X' is 87, d.f. - ra,P - o.o3a). It was lowest in Kohat (18 %) and highest inCharsadda (6a %) (Figure 3). Overall, 46% of infectionswere resistant. Resistance existed mostly as RI; only
28% (36/113) of resistant infections were Rll. The
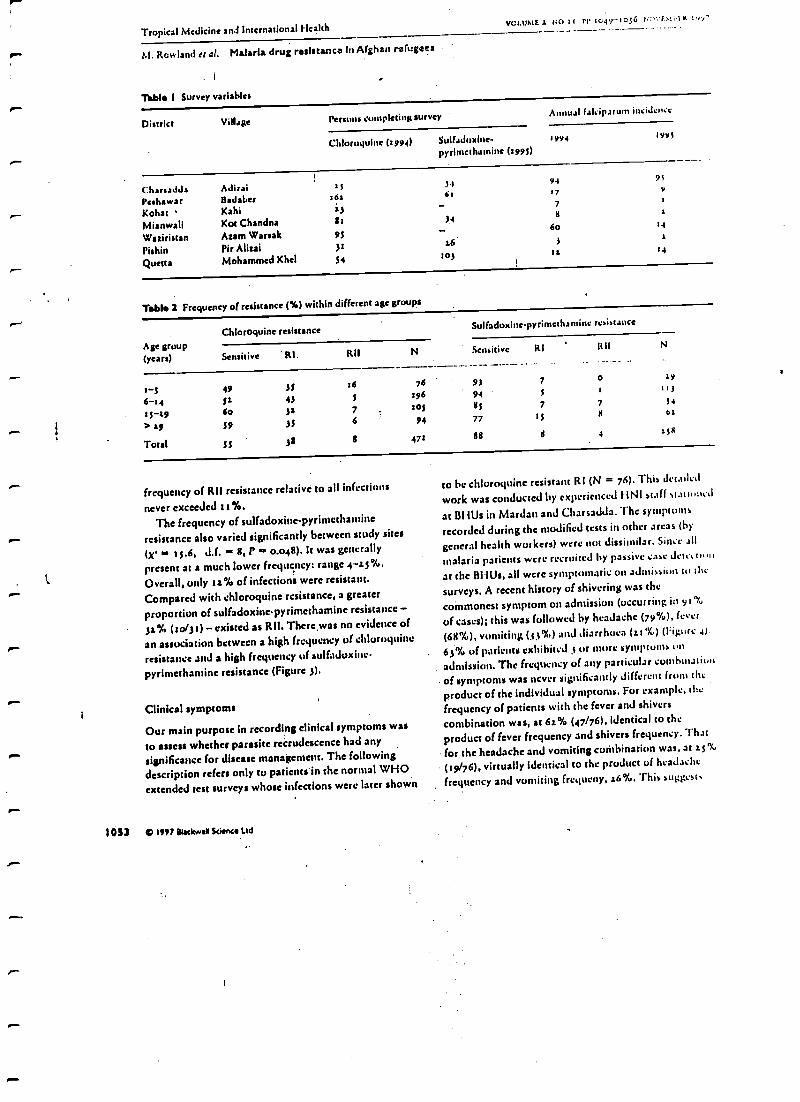
Tropical Medicine and International HealthVCLUMEI NO 73 PP 764--1056
M. Rowland et al. Malaria. drug resistance In Afghan refugaea
.i
Table I Survey variables
Di 'ct Village Persans pleting survey Annuat falciparum inciJcn.c
Chloruquinc (1994) SuI(aduXlnc 3994
pyritnethumine (1990
r9vf
CharsaJJ, Adirai 15
Peshawar !Walser 16a
Kohat Kahl ifMianwali Kot Chandna St
Waziristan Asam Warsak 95
Pishin Pie Alizai 3i
Quetta Mohammed Khel S4
3461
34
s6
9417
7
s
60
3
103 t1
92
Y
1
34
r4
Table 1 Frequency of resistance (%) within different age groups
Age group(years)
Chooroquine resistanceSulfadoxine-pyrimethamine resistance
Sensitive ' RI. Kil N Sensitive RI Itil N
3-s 49 3, 16 76 93 7 o 19
6-t4 St 43196 94 f
t1J
ts-s9 6o 3s 7 lof 6s 7 7 54
> *9 59 35 6 94 77 tf 11 61
Total SS 32 g 473 88 4 158
frequency of RII resistance relative to all infections
never exceeded i z%.
The frequency of sulfadoxinc-pyrinicthamine
resistance also varied significantly between study sites
(x' t 5.6, d.f. - 8, F 0.048). It was generally
present at a much lower frequency: range 4 -sj %.
Overall, only zx% of infections were resistant.
Compared with chloroquine resistance, a greater
proportion of sulfadoxine- pyrimethamine resistance -
3s% (io/3 t) - existed as RH. There was no evidence of
an association between a high frequency of chloroquine
resistance and a high frequency of sutfaduxiuc-
pyrinletharnine resistance (Figure 3).
Clinical symptoms
Our main purpose in recording clinical symptoms was
to assess whether parasite recrudescence had any
significance for disease management. The followingdescription refers only to patients in the normal WHO
extended test surveys whose infections were later shown
I0á3 if) 1997 Blackwell Science Ltd
to he chloroquine resistant RI (N = 76). This detailed
work was conducted by experienced F1141 staff slat ula,l
at BHUs in Mardan and Charsadda. The symptoms
recorded during the modified tests in other areas (by
general health workers) were not dissimilar. Since .ell
malaria patients were recruited by passive case deed u.,n
at the BHUs, all were symptomatic on admission to clic
surveys. A recent history of shivering was the
commonest symptom on admission (occurring in 9 t %
of cases), this was followed by headache (79 %), fever
(68 %), vomiting (33"/.) and diarrhoea (st "lu) (i :igurc 4i.
63% of patients exhibited s or inure symptoms on
admission. The frequency of any particular conlb:natiotc
of symptoms was never significantly different from the
product of the individual symptoms. For example, the
frequency of patients with the fever and shivers
combination was, at 6s% (47/76), identical to the
product of fever frequency and shivers frequency. That
for.the headache and vomiting combination was, at s 5%
(39/76), virtually identical to the product of headache
frequency and vomiting frequcny, s6%. This suggests
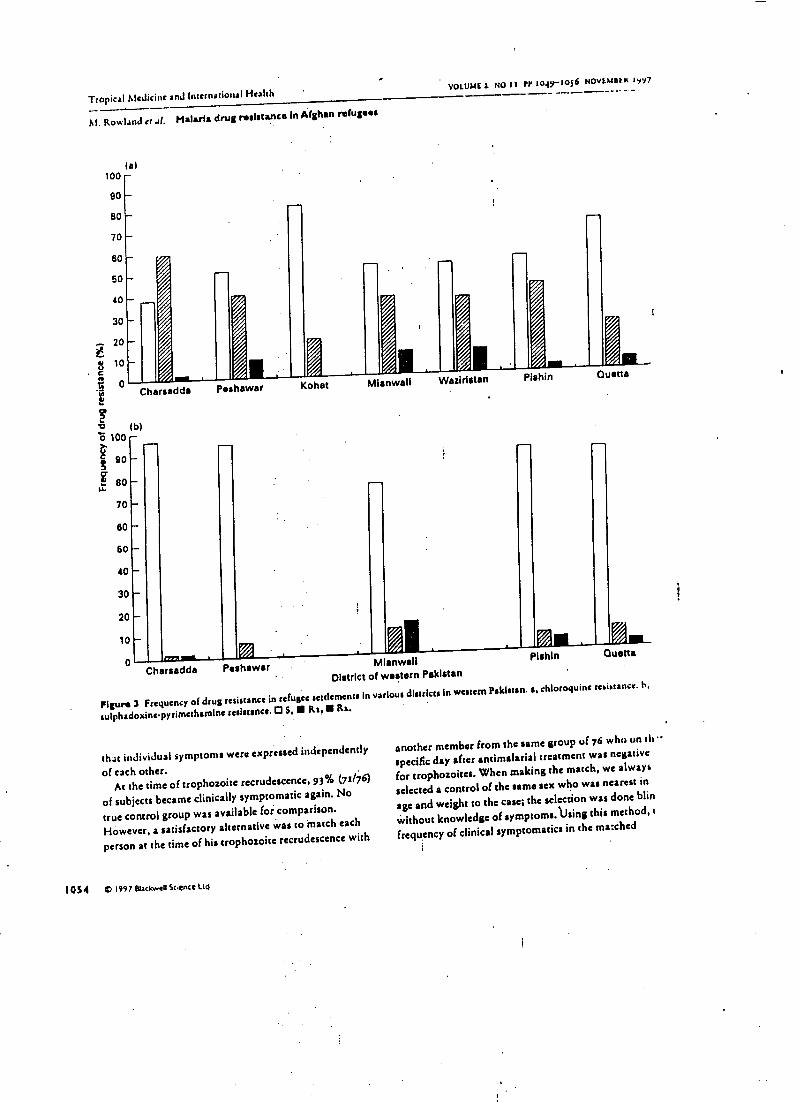
Tropical Alcdicine anJ Intetnatioii l HealthVOLUME I NO II PP tOay-tos6 NOVtMSEK 1y97
M. Rowland et al. Malaria drug realatance In Afghan refugees
is)
70
60
60
40
30
20
10
0.n1...
Charsadda Peshawar MianwallDistrict of western Pakistan
Figura 3 Frequency of drug resistance in refugee settlements in various districts In western Pakistan. a, chloroquine resistance. h.
sulphadoxinepyrimethamine resistance. O S, Rs, Ra.
.
PishIn
Mi..Quetta
that individual symptoms were expressed independently
of each other.At the time of trophozoite recrudescence, 93 D/ (71/76)
of subjects became clinically symptomatic again. No
true control group was available for comparison.
However, a satisfactory alternative was to match each
person at the time of his trophozoite recrudescence with
1054 m 1997 Blackwell Sc.ence Ltd
another member from the same group of 76 who on eh
specific day after antimalarial treatment was negative
for trophozoites. When making the match, we always
selected a control of the same sex who was nearest in
age and weight to the case; the selection was done blip
without knowledge of symptoms.Using this method, i
frequency of clinical symptomatic: in the marched
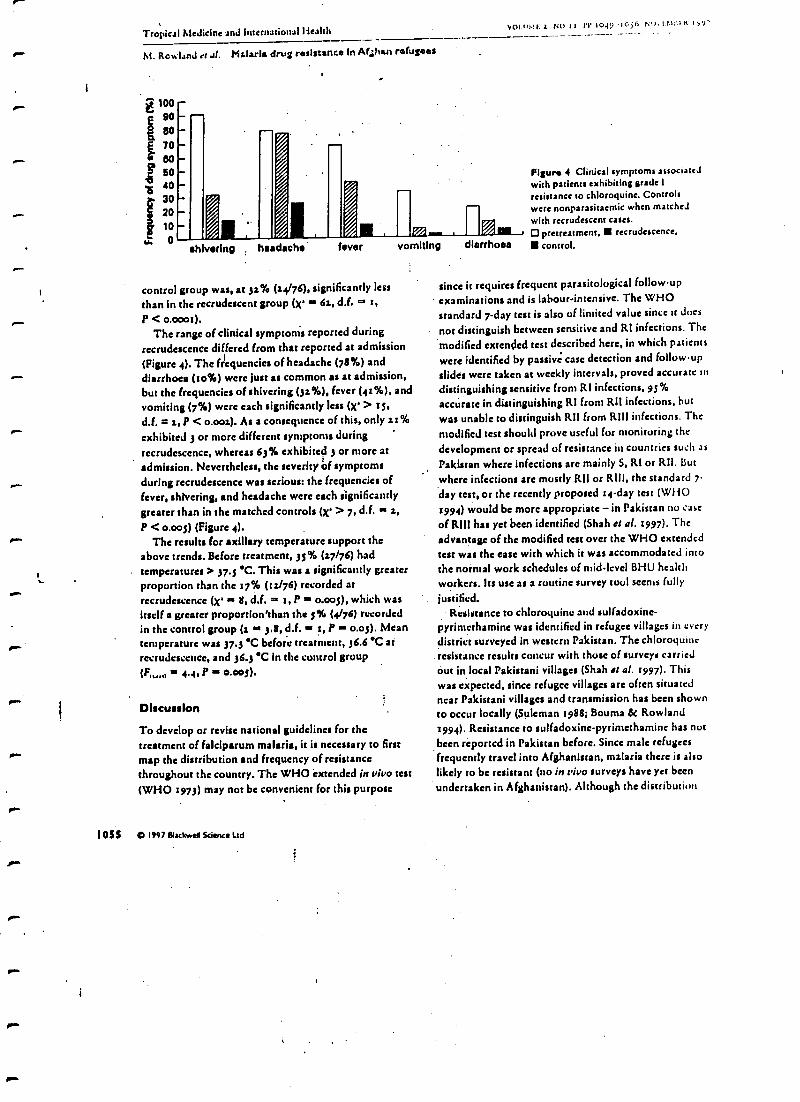
r-
"M.
n-
palm
1^
r
/0.
/F.
elm
s
Tropical Medicine and International HealthVOLII1.1r. i NO 11 N. 1049 '1056 Nu,1.1.1;t111 Iyy'
M. Rowland et u1. Mslarla drug resistance In Ar ¡hen refugees
á 870
8060
.B 40
30
2010
I. 0sh vs Iry . headache fever vomiting diarrhoea
control group was, at 3z% 4.4/76), significantly lessthan in the recrudescent group (X' 6., d.f. r,
P < o.000t).The range of clinical symptoms reported during
recrudescence differed from that reported at admission(Figure 4). The frequencies of headache (78%) anddiarrhoea (5o%) were just as common as at admission,but the frequencies of shivering (3z%), fever (45%), andvomiting (7%) were each significantly less (X' > ts,d.f. = a, P < o.00.). As a consequence of this, only 2r 96
exhibited ; or more different symptoms duringrecrudescence, whereas 63% exhibited ; or more atadmission. Nevertheless, the severity óf symptomsduring recrudescence was serious: the frequencies offever, shivering, and headache were each significantlygreater than in the matched controls (x' > 7, d.f. a a,P < o.00s) (Figure 4).
The results for axillary temperature support theabove trends. Before treatment, 35% 47/76) hadtemperatures > 37.5 T. This was a significantly greaterproportion than the 17% (ía/76) recorded atrecrudescence (X' s 8, d.f. m z, P o.00s), which wasitself a greater proportion'than the s% (4/76) recordedin the control group (z in 3.8, d.f. - 5, P - o.os). Meantemperature was 37.3'C before treatment, 36.6 'C atrecrudescence, and 36.3 'C in the control group(FIN,.1 re 4.4, P - o.00s).
Discussion
To develop or revise national guidelines for thetreatment of falciparum malaria, it is necessary to firstmap the distribution and frequency of resistancethroughout the country. The WHO 'extended in vivo test(WHO 1973) may not be convenient for this purpose
loss O 1997 Blackwell Science Ltd
Figure 4 Clinical symptoms associatedwith patients exhibiting grade 1resistance to chloroquine. Controlswere nonparasitaemic when matchedwith recrudescent cases.O pretreatment, recrudescence,
control.
since it requires frequent parasitological follow -upexaminations and is labour -intensive. The WHOstandard 7 -day rest is also of limited value since u does
not distinguish between sensitive and RI infections. The
'modified extended test described here, in which patients
were identified by passivi case detection and follow -up
slides were taken at weekly intervals, proved accurate indistinguishing sensitive from RI infections, 95%accurate in distinguishing RI from RII infections, hutwas unable to distinguish R11 from RIII infections. The
modified test should prove useful for monitoring thedevelopment or spread of resistance in countries such asPakistan where infections arc mainly S, Rl or Rll. Butwhere infections are mostly RII or RIII, the standard 7-
day test, or the recently proposed r4 -day test (WHO1994) would be more appropriate - in Pakistan no case
of RIII has yet been identified (Shah et al. 1997). Theadvantage of the modified test over the WHO extendedtest was the ease with which it was accommodated intothe normal work schedules of mid -level BHU healthworkers. Its use as a routine survey tool seems fully
justified.Resistance to chloroquine and sulfadoxine-
pyrinwthamine was identified in refugee villages in everydistrict surveyed in western Pakistan. The chloroquineresistance results concur with those of surveys carriedout in local Pakistani villages (Shah et a1. 5997). Thiswas expected, since refugee villages are often situatednear Pakistani villages and transmission has been shown.to occur locally (Suleman 1988; Bouma et Rowland1994). Resistance to sulfadoxine- pyrimethamine has notbeen reported in Pakistan before. Since male refugeesfrequently travel into Afghanistan, malaria there is alsolikely to be resistant (no in vivo surveys have yet beenundertaken in Afghanistan). Although the distribution
Tropical Medicine and International Health vMusts i NO II PP 104,-1016 NOVRMetia IVY7
M. Rowland et al. Malaria drug resistance In Afghan refugees
of resistance was significantly heterogeneous betweenthe 7 study sites, it showed no obvious geographicalgradation or pattern. Ins of the 7 sites, chloroquineresistance exceeded 45%. New infection may beconfused with recrudescence if transmission is intense,and thereby exaggerate the true frequency of resistance.However, in the refugee settlements the low incidence offalciparum in ,994 -91 would seem to rule out newinfections as a significant source of error. The estimatesof resistance frequency are therefore consideredreasonably accurate. Since parasite recrudescence isassociated with a resumption of clinical symptoms, it isbecoming difficult to justify the use of chloroquine asfirst line treatment in the majority of refugeesettlements. A recent WHO report considered itunreasonable to maintain a drug as first-line treatment ifclinical failures exceed as% (WHO 1994). To notchange the first -line drug may lead to a loss of faith inthe refugee health services, and to refugees seekingprivate treatment with expensive or unnecessary drugs(Guinness do Rowland, unpublished), as seems to be the
response of the Pakistani public to its own health
services (M. Donnelly, personal communication).Sulfadoxine- pyrimethamine resistance, though presentin every locality, was comparatively rare and theadoption of this drug as the first -line treatment would bemore efficacious. Indeed one NGO has already switched
from chloroquine to sulfadoxinepyrimethamisie to
reduce the burden of remissions on outpatient clinics(Shah et al. 1997). A more rapid selection ofsulfadoxine- pyrimethamine resistance would, however,be inevitable should this become official policy.
Acknowledgements
We thank the BHU health staff for carrying out thesurveys and the initial microscopy, and HealthNet field
staff for monitoring work. We are grateful to Professor
I OS 6 C 1997 Blackwell Science Ltd
H. M. Gilles for his constructive criticisms. TheHealthNet malaria control programme is supported bythe United Nations High Commissioner for Refugeesand is funded by the European Commission.
References
Boums M bt Rowland M (1994) Failure of passivezooprophylaxis: maliria is associated wish cattle ownershipin Pakistan. Transactions of the Royal Society of Tropical
Medicine and Hygiene g9, 3f s-ltf.Fox E, Khaliq AA, Samar M St Strickland GT Opts)
Chooroquine- resistant Plasmodium falciparum: Now inPakistani Punjab. The Lancet I, 1435 -1434.
Gilles HM & Warren DA (5993) Bruce- Chwats's EssentialMalariology. Edward Arnold, London.
Kirkwood BR 400 Essentials of Medical Statistics. BlackwellScientific Publications. Oxford.
Rowland M, Bouma M, Ducornea D, Durrani N, Rozendaal J.Schapira A it al. (59y6) Pyrethroid impregnated bed nets forpersonal protection against malaria for Afghan refugees.Transactions of the Royal Society of Tropical Medicine and
Hygiene 98,397-96:.Rowland M, Hewitt S, Durrani N, Wins RA & Bano N 0997)
Transmission and control of viva* malaria in Afghanrefugee Settlements. Transactions of the Royal Society of
Tropical Medicine and Hygiene, 9/, sja -sss.
Shah I. Rowland M, Mehmood P, Mujahid C, Raziq F, HewittS et al. (5997) Chloroquine resistance in Pakistan and the
upsurge of falciparum malaria in Pakistani and Afghan
refugee populations. Annals of Tropical Medicine and
Parasitology, in press.Suleman M (spit) Malaria in Afghan refugees in Pakistan.
Tranaatriona of the Royal Society of Tropical Medicine and
Hygiene Ss, 44-47WHO.(tgys) Chemotherapy of Malaria an Resistance te
Antimalarial'. World Health Organisation Technical ReportSerifs ss9.
WHO (5994) Antimalarial Drug Policies: Data requirements,treatment of uncomplicated malaria. and management of
malaria in pregnancy. WHO /MAL/94.z two.
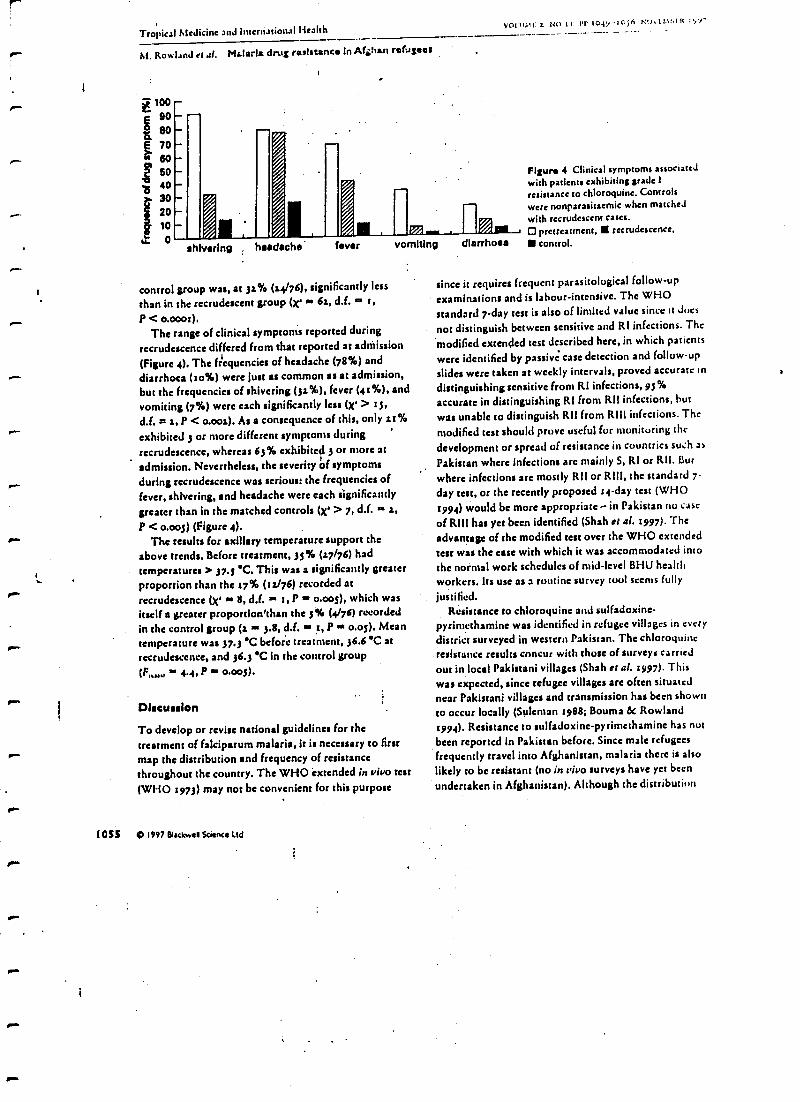
Tropical Medicine and International HealthVP1tt7.11i 2. N(11I Pr IOCI -'I0j(i NU.S.1.1::I11 lyy`
M. Rowland et a. Malaria drug resistance In Af ¡tran refugees
100E 90I 80
6706060
ó 40302010
u. 0shivering headache fever vomiting diarrhoea
control group was, at 31% (a4/76), significantly less
than in the recrudescent group (X' an 6s, d.f. m 1,
P < o.000t ).The range of clinical symptoms reported during
recrudescence differed from that reported at admission(Figure 4). The frequencies of headache (78%) anddiarrhoea (1o%) were just as common as at admission,but the frequencies of shivering (j: %), fever (41 %), andvomiting (7 %) were each significantly less (X- > rs,d.f. = s, P < o.00s). As a consequence of this, only 11%exhibited 3 or more different symptoms duringrecrudescence, whereas 63% exhibited 3 or more atadmission. Nevertheless, the severity óf symptomsduring recrudescence was serious: the frequencies offever, shivering, and headache were each significantlygreater than in the matched controls (X' > 7, d.f. a a,P < o.00s) (Figure 4).
The results for axillary temperature support theabove trends. Before treatment, 33% (17/76) hadtemperatures > 37.5' C. This was a significantly greaterproportion than the 17% (ís/76) recorded atrecrudescence (X' 8, d.f. - t, P - o.00s), which wasitself a greater proportion'than the 1% (4/76) recordedin the control group (a 3.8, d.f. 1, P o.os). Meantemperature was 37.3 'C before treatment, 36.6'C atrecrudescence, and 36.á'C in the control group
P' 0.00$).
Discussion
To develop or revise national guidelines for thetreatment of falciparum malaria, it is necessary to firstmap the distribution and frequency of resistancethroughout the country. The WHO 'extended in vivo test(WHO 1973) may not be convenient for this purpose
I OSI o 1997 Blackwell Science Ltd
Figure 4 Clinical symptoms associatedwith patients exhibiting grade 1
resistance to chloroquine. Controlswere nonparasitaemic when matchedwith recrudescent cases.O pretreatment, recrudescence,I control.
since it requires frequent parasitological follow -up
examinations and is labour- intensive. The WHOstandard 7 -day test is also of limited value since it dues
nor distinguish between sensitive and RI infections. Themodified extended test described here, in which patients
were identified by passive case detection and follow -upslides were taken at weekly intervals, proved accurate indistinguishing sensitive from Rl infections, 95°/,accurate in distinguishing RI from RI! infections, hurwas unable to distinguish Rl! from RIll infections. Themodified test should prove useful for monitoring thedevelopment or spread of resistance in countries such asPakistan where infections arc mainly S, RI or RI!. Butwhere infections are mostly RI! or RII1, the standard 7-day test, or the recently proposed 14 -day test (WHO1994) would be more appropriate - in Pakistan no case
of RIII has yet been identified (Shah et al. 1997). Theadvantage of the modified rest over the WHO extendedtest was the ease with which it was accommodated intothe normal work schedules of mid -level BHU healthworkers. Its use as a routine survey tool seems fullyjustified.
Resistance to chloroquine and sulfadoxine-pyrintethamine was identified in refugee villages in everydistrict surveyed in western Pakistan. The chloroquine
. resistance results concur with those of surveys carriedout in local Pakistani villages (Shah et al. 1997). Thiswas expected, since refugee villages are often situatednear Pakistani villages and transmission has been shownto occur locally (Suleman 1988; Bouma & Rowland1994). Resistance to sulfadoxine- pyrimethamine has nutbeen reported in Pakistan before. Since male refugeesfrequently travel into Afghanistan, malaria there is alsolikely to be resistant (no in vivo surveys have yet beenundertaken in Afghanistan). Although the distribution
I IIANSAI:I 14114S or I I119 Itl1YAl. S1n:I1? l'1' In' I Illtl'It:AI. AUSUII'INIS ANO IIt(;II?NI? (I'M')
An outbreak of cutaneous leisbmaniasis il) an Afghan refugee setllement ill north-
west Pakistan"
URGEN
Marls11,rirrrtitt7irnrr'tl'.111.11he.4,i9,11`rlsn»
On Ilnrry nullrf 1leaÁlt, Isl Vlr1hnJ, l'nklualhNrnlé/0,.1;.th,,lr
i/7ia/,rrnlAlr.hrinr, 1.ine7u0o1 1.1 5S1/I, UIC
Absu/set(:uoutt1)tss leishrrnrninsis (t:1.) tIii ut 1..eishmriria invoice: nppcnts to be nu'emet ging disease in pas Is of inn di.
cost AISIutnistntl anti math.wcst 1'nkistnn.'l'iurntgnrn, on Afghan refugee camp of 17 ycats' standing, in tl.c
disuiet of 1)1i, Nuttll West Pannier I'rsivince of l'nkistnn, expel ¡cocci] a mnjor uuthlenk of CL ii 1997 his
the fit st mine. As in t of the investigation, each section of the crimp was surveyed for CL. Around 311% of the
92110 iil,nbitams busc nctive Its' and n further I3%hnd:tents f earlier nttncks. According to iIitcrvicty
slotcrttcrtls, 99% of collier infc s Intl healed within die previous 2 years. 'roc unfit in the diagnosis,
sample o(cuucut C ;I,Icsi riss was examined pnrnsitnlugically. Arnnsligules wcr c dctcctnhle by tnicruscu).) .0
only )(I of Iesiarts. Ihowever. 411 of slide-negative cases producedpositive t:ullutes and sun re c:itcc
ncgnlfvr tu 111)111 tuicl usropy and (:opine vitre positive by VCR. Overall detection I ate was about 1107...1 hé
*n IIIy !'bliburm,rnt seigenli, n kr'tltvn vcclor of 1., nnpites, was CAW Ur'cd within the cnirt11, indicating Itical
Isnnamisainn. C :Lhms not heel' tcorn tcdliunt this linen of Pakistan before. Although the majority ors eftigccs
left Afglinnislnn 2 decade: came, astis-harder nutvement amen is cnnunun. ..111c Afghanistan capital, Kabul,
is etutcntly expesieneing a mnjur epidemic of Cl_; infected migrant carrion hunt Kabul arc piihably tl.c
soul cc if the Inuhlcak ii Fiiiini gai ii.
Keywords: (:ilmueons I,cishninninsis, l.ri,iun.urar nnpire, epidemiology, refugees,Afglra.iiiinu, I'nki,ia,, j 7.ltb it.io,t,
tnRente
Introduction( :nlnnesitin Icishuttiinsis ((:I.) doe tin Lei)lrtrinitin
í!.e1í1 ) nipicn nlgtenta Ili he nn emerging tiiscascin pen Is of smith-cuss Alj(hnnistnn and smith -west Pnki-
stan. ltcccit epidrvnlilogical dato Indicate Mat theAfghanistan capital, Kabul, is ex tetiencing n Inngµc ¡n-
enense in ( :h. (A. llryccsnn, \VI lop INI unpublishedAssignment seisms: 7iYariltrtrt njeutnorait( leiiluaosrintis inRabid, 4 -15 Ucccuthcr 1998; 1111wn'r er al., 1998).Itcfugce camps in ih -west l'ikisinii ate reportingcosec of C1. for the first time (United Nntitros t tigit(: 'ssiunrr for Refugees, UNI IC II, unpubllshédtypo's, l'IYR).
'I be 'l'inungoun refugee camp in the district of I)ir,sh -west Pakistan, is a settled r :airy of 17 yens x'
sounliog. Them nit' liver 91)00 teaideuls, .
rnslr It, *X111101, and nm slits Afghnilisuot. A few cnscsof CL Isnvc btc ell over ihr past few yen's. I low-ever. in 1097 -9R there wns a !nose outbreak, cnusiugMaim wiiltin Ilse ichigee ctnrluslushy nor1 ansang thehcnhli uthitities. Cl. nisi, tntw intents in nciµhbnuringI nkitltnni vilhl)trs.
Aa poll of slic invesligntirt11 of the rntllueak, the campwns conveyed fur Cl.. and to sample of lesions wascx 1 pniusiluliµicnlly 10 ctt,lirnt the dingnot'*.t :uufirnsnüun of this break is impost/nit in she plan-
' g of public health sitaiegics hu ill hi ills. camp nuit inslic Beni mien. It nisi iudicnies the iced (1)r vi((ilouCC fur
duvet sent discnses nssucinicd with 11upuhllinn nsovc-Dietn.
Methods'1 lees wes c 2main cnmpmtcma In this.:n,ly.Finn, the crimp was aus vcyed in Mny 1497 bvan tcnin of
resident eurntrnity Innllh two {Less ((:I I\Vs) Irniticd inthe use of sl[nctunedt: 1. a
ucstinmtnit es and Wens Mention oflesi uft I\Vs slotted in dinkiest' sections uf
the entity And arieX.IeII IIt11(achNlds nt sanclnnt, using nits itnrsiulf hunde as n tliner,tian pi tint Sissy luntschnldswest virtuell moil adults intervirwccl. I)run ou nll' csidems,the litouhcr it( ':,ricin( crtscs sil C;1., ihc nunshcr andtonsil' of lead nns, und nny Isistusy uf 1111111 (:I. wcsC
Amino' for coo rsp0ndrncc: Aim k IlnOlntal, I)is.ntr (:.pwti1mtd Vectur 1linlnRy Ilnil, I $.110111 Of tlttiene SMI1 t..pirnl Atr,Iitine, ICrtrytel Sire, I. I.p1 tVt :11? /II tll(;
lex I 1.1 (i) 171 i1í(1 r1t7i, r ulait ut u11vlu0rl(.r{Ishnn nt tilt
r \r,i.li' (1)t - i'I tue,
enllcued. The 1)y easince of lesions was examined. wherever plsüiltle.
Second, a diagnostic cnnfinnatiun of clinical CI, waswulcrtnken using 3 techniques: microscopy, l'nrasiicculture and polymcsnse chain icactiun (PC11). Families
of the original survey were selected using a random
unrulier Rencrntor nod Mc first 100 curi cases of (21.
were Invited to anent' Utc camp health ccntic fur
diagnostic validation.At tfrc time of the diagnostic study, a number of I,gl t-
traps were deployed in houses in the camp to idcnufylikely vectors of CI_
Owing to logistical problems, there wns n 7 -week gait
between the initial survey null the dingnnstic study Nun,.of the costs hail received trcnttnau as nil trcauncm waravnilnhlc of the time.
Twenty cases were abscm when called norm :Ind 5
refused to attend. These were rc)llncctl by the next 25
eases n g the randomly selected families.'roams were seen, their Icsiuns counted and urcasurctl,
nod the duration of disensc was noted. The undid:,min gin of die insist active-lot,. ins), ICI; ¡WI wns sliced ul.cnand n linens' token using n s- .,Ilse) 1 >lnde. Sincol s we t
fixed in methanol, stnincd avid Giensn, and examinedduring the evening. Those with negative slides wct c
invited In re-attend the [allowing day fur a repent srI (iIand culture sample, token front niitit ier slit -skin pr c-pnratlin. 'Twenty samples wort also t:.ken scout II ;tIIt
fur Inch li iln ibc slide -negative cases (G ttf which weft(mold to be slide -positive on tilt sitcom! cxnr.linanuo)All slides were examined by 2 experienced miles nsutltius.'171* microscopists cnch checked the findings of rite 1/111C1.
unnwnl c ,f the llrst result. 1
The samples for culture wcrc inoculated into 1)11111o.í'.
NNN mcilin, unnspor tell in ice I,1 the National III%riitileof Ilenith in Islamabad, and incubated nccniclii's in tlirmcdtudtif !;VANS of al. (1989). The solid phase if lltcNNN media eiosprised fresh, aseptically t:uIIceted.
cicllbrinnted rabbit binid, mixed with ng:u, Nn(I, gluciao, nntl ycmnmycisi. 'l'bm liquid phase cutnlprst.lIts'MI. I6'10 medium witty glinrilnine but tvitltuui sti.tllnnt Weal hinntc (Flow (-ihir mot ica town, moony),(Inned ihtough 02Z -Iisi' dispisnlilc liltcts to itt,.td '
bnctelinl contnminntlnn.lunr l'CR, snni11lta wcrc phiCCJ in 'no ),I- of 1.1)1
Rtuuiidinc thücynnnrc ((hi (;tJ) and Cl 25n1 I:1) I A,
ni tl sun cd at 4 "C: 'I shipped by air in tltc I Ave,
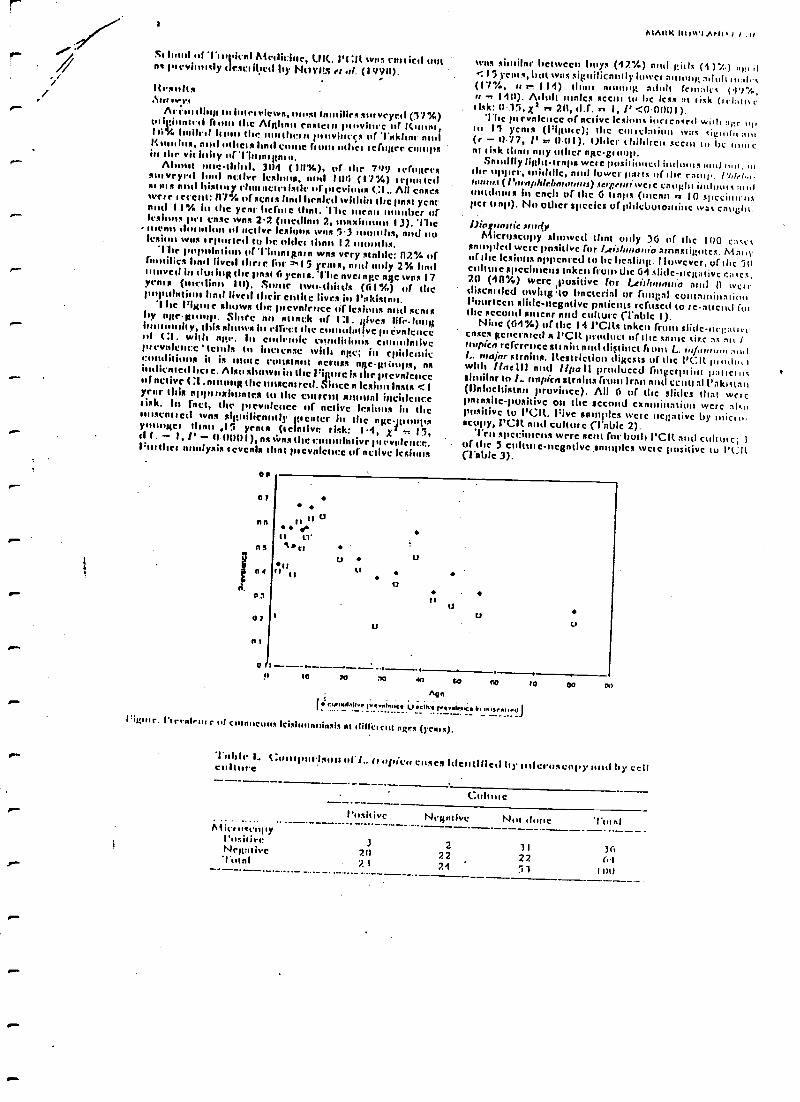
)
2
Sr Iotul ni Itolden! Medicine, UK. 14:It wits cultirtl outne Ive sly desci;hed by Ni,viIS et al. (19911).
it rinds.Asti Ives
Arcm ding tu inlet views, st f Iles surveyed (57 %)vit tinntrd from the Alplinn rnsscn pi¡wi ce or Cmnnr,Ii% Iiuilrrl Isom the mnnthr.is pmvi,,çc i mf riikhnr nodI. tors, nid olhets hnd c Gntn miles it:rn,ter campsill tow vicinity of'1"int:nitntn.Ahmnt nnethhd, 3114 (111%), rf die 799 fanner*
sniveled loud nt:ive Icsltn,s, nid I116 (17%) 'rpmiedsir urn nid history (luuncterisdt urprevinun (:1.. All caseswere 'event: ill% of scnis hnd headed within the pnst ycnrnntl I I % in itc ycnn tint. 'Clic utcnn number tiflexinns per t'ose wns 2.2 (mctIlnn 2, ntnxinnint 1 J). 'l'Iremom clurtni.n of uctive lesions wns 1.3 tmnrths, rind nulesion wns it-ported lu be older tlinn 12 intuition.The il I lar%tiott of1intnsRn*n was very slnbic: n23/4 offnmilics lend lived ihrie for I 5 years, nid only 2% bail(navel in dun ing the ions' ( yens s. l'hc nvci age age wits 1Vents (mellinn 111). Strate Iwo -(limos (6 I 4,) of IlleImpala(' hnd lived Ioder emotc Iives,hi l'altisini.1 he Phone sltuws tilt picvnlence tif lesions rind soon1/y note-group. Since nit smack of 1:1. ¡gives life. Icinginnntssty, Ibis nl n hi efrecl the c louve pi evidencesil t:1, witty n,tr. In endemic csmilidims c mauvepicvedcnee'tends In htetcnse with note; in epidemicr. I. it is 'mite cuttstnrrt across age- µsitups, nsütlicntetl here. Also shown in the 1 :üturc is the ptevnlcticco f nctive (:1.n g the mrscared. Since n Icsimn lasts <Iycnr Unis npptushsintes Its Ilse cmrrtl mutton! incidenceIink. In filet, the pi evidence of nctivc lesions in then isenis ed was siitnilicnntly pettier in the Pitt-pumpsy Rev tins 41.i yen's ((chive rink: 1 4, X z 15,d 1. - 1, l' - 11 (10111),ns icing the c !wive pievidence.:rushes aonlysis icvenls dint ptevnlcacc uractive Its'
00
n)
nn rt u11 LY'
ns 4rtns Iirlt
«a
u7
n
0 1
AIAIIK 11Utt11tN1, tl .11
was sitnilnr between buys (42%) and ,;it lc (i 37.0 it< I 5 Tents, but was siHuilicnniy lower .Salin,; .Stool( n,:,l c(17 %, n r. 114) (hart nntinlg adult fcloalccrr -> 1411). Mull males scan lu lic less :It I ick (i chi n rtlsk: O15, Xs n 211, tl.f, n 1, l' <0 0í111I ).
The pi evidence of fictive lesions inrrenacrt with :..r t.o,In I ycnis (l'iltutc); tile cots :I:uiun wit: cil:uilit:uu(r - 11.77, l' r. 0411). Older chiltlrcis scent lu Ix rt,mt:nt Iick toron nay other nitc- gtuult.
Snndlly li,tlit -traps wcrc positioned intlums und nut, inihr upper, middle, mid lower ports o( tltr mati l'1,Irh,,t (I'nrnphlrl,nrnuuri) weIe 011 011 intloot s :111.1
in cnch or the G (inns (mena yr. 10 cllccinlrnsper trnp). Nu oilier species of plilchutoutine was Cä116111
1.611.01fItailiC .Sfuri)'
Microscopy showed dint roily 3G ul' the Ií10 c:tcc.csnmilled were positive for /- eiihman,a amnstigiti cc. Mn ivof Ilse )ca' s nppcnrcd to he hcnlinit. l luwcvcr, of the 511culture specimens tnkcti (font the 64 slide-new' ivc tines,20 (4(1 %) wcrc punitive for /..eit /u,lnnia nod 11 witstliscnrtled owing to bnetcrial or rump) Cuntnmin :I innFourteen slide- rsegntivc pnticnts refused to rc -ment fusthe secund sticnr and culture (1-nblc I).
Nine (64%) of the 14 l'CILs taken from slide- n(, :n'i,cases gencrnictl s VCR lruducl or the snore sire at au Itrmpirn rcfcrricc sol min nuit d4titiC1 G ont L. in /,unuu,L. major stifling. Restriction digests of the l'CIt luutlu,swith !mete III and lipoII produced fnittcrprìnt )':saris csimilar to 1. nripitn slrnittn (mitt( lrnrt nntl cCntI n1 1'akictan(1)nlocltistnn province). All 6 of the slides that wctCpansite- positive on the second exnnlinaliun wcrc .Sienpositive to )'Cot. Five samples were nciptivc by nlicrn -scrpy, I'Clt nid culture (Friblc 2).
'ern specimens were sent for both VCR anti cols n c,or the 5 culture- megntive pimples wetc punitive to ('lilt(Table 3).
uu
u
u
u
n
uu
!r 10 w :10 40 rA r-0 i0 00 00Ago
Iiurn.dallrpvel..ucr Ua:lhrp b,...irnrJJt°il;mr. I'trrnlrm r 111 curnncuus Ieìslirrinninsis nt 111111:1 C111 ngrs (1cnra).
'Irrlrlt L ( ;urtilnuIsirn iii I., (err ¡idra cosca Itlettltlled hp ntlermtcnny tun ! by celiculture
h1 it't occupy(',tsitivcNr,t:tlivc'1'utnt
l'usitive Negutivc Nut 111111e
J 2 11 742t1 22 222/ 21 'ou
i- 1:t 1.I!1SIIAIANIASIS ItI AI't t11A01100'IItI!I!S IN PAINS I AN
Inicie 2. C. pm Ism% uf L. It *Wien tuses Iticnlillctl I,y microscopy ntttlpulyetscrise clouts renctlun
Positive
Nit toscegty-Positive (I
Negntive 9
Tanta 11
l'C:It
Negnlivc Not done ' i't'titi
'I'stifle 1. (: purista" uf I,. try oltir's roses identifiedby cell coitus e 1 partite' nse chitin "cotoso
VCR
Positive Nei/mire 'l'ntnl
Culticl'usidvr. 2 5
Nritntive .1 2. 5
Tulnl 5 5' 10
I lie menu doll nl{Itti tif ,license tuns alß1ilfivnii1ly longernntoiß twice neggnove tu nn)' tlingnuslic lest (0 immlbs,SI) -, 2 9) lion for cases positive In mty test (6.5 mouths.SI ) - 3 0) (Ninon-Whitey U -lest, r -t .7. 1, i'9 014). Shuilnly, the rlituucter of toc hugest lesion wnsgicnle' for cases negntivc to nny test (menu 3.1 cm,SI ) - 2.3) !lino kir cases positive to nny test (2.4 cut,SI)- I.5) (it -2n(,I'- +111139).
131arosslm"'1 he suivey uf'1Irungnun tao m hulitncs n lntgc wit-
luenk (ILO with 70w/, of tine papolntlun fist 1997
r- )I,,,, I,! 11.,s (nod(7 %)in the ycnr ta at' before !lint). lite reed! case1 oistutlrR, olio 1+opulnoon stnb{Ihy of l is catir nil the
lueseure of lite vector anudlly N. atriprmi (1(11.1.t(;í(KI!NUult :I( or oit., 1994, (991) halo-Ate dint the amhienkeutnnnted f wi(lii,i the cnteip.'i ite cliulcnl nppcat nitreof the lesions tuas culli isiu-ii with I_ tropic.' iofcelioo, nodt l.. mqi,,i kl.)NA tuns detected lit the lesions by I'C :11(NttY1111 et .11.. 19911) Intiirueiolt (lune 114e I :I. Is clue tuinl.,rn wlulch Is usually maim' ' nod tuluut.
(hits chilli' en suent ta be at osk thou any odic'n, e !rump nad men scent lento ni tick. l'clltnps older
10.` coihltcn nee leas disciplined 111 cnvclhl); u Itoiuß tic hutsortintet nights. Chott n ntc tcquh cd Ivy heels cunt c und("Notion Io geodes their modesty nt all limes, nod ose ofdim/dots (oie clothing for covering hic bend) is couunatteven nit night.
1. (:1. Ions not been repotted hotu tleis pact of l'nkisuiilirfote (11A11 et al 1997). 'I he uutbicnk luny hnvetestate -41 flac! n single {innduct{ur, ns the l'(:11 evidenceis of n shunte, I gr !:nos schirodcmc cline hi the 13unites canoduct) (NitYlts et nit., 1990). (I. bit i'nk(snm ducr lu i tny,ir.t c ly iccuts in Mohan in Mc suuthct n)'un/n, (IIIMNI!Y A I All, I!)H('), {i Ilnlurltisin,, innvirocetvhrie Mete wits u uuojm ry,ide he the cnitiutl (»ucotnn((cr toc en,Iot(unkc of IV 11 (MassionM h MAnlu,1991), nut) most It-edgily-In Arnrl, 1 <matte:it. (/tAll el 4.,
P. 1997) Aridity.¡ It t.;l, is cotinttoo in Afitlinoi-seoo; it is endemic to the s heist city oil I(nnduhnr, thewrstcon city of I Ice ni, nntl the ccrolt nit l's evinces of I(nlndnil I'ntvnn (U?.tAit el ni., 19611; NAI)IAI/ ItcsTAMI,1971; NAInM et al., 1979), but lins mil been reported
- limo the lue thee! nid rnslrtrl Alitiniti iitoutnccs boutwhich the mtijn,i(y tif1iitnignen fuunilics uciftinnlc.'I hesandre of the oullotwk is ptubnhly die cubital. Kabul.I liv thy is expeliricliK wino lins been described ns npiulutnrd epidemic of CI, (Amnon, .r n /.. 1992)ri,uvttly nllet'tltß !hail 5% ul lite I 2 hill' pupuh,-
t)55
311
50110
3664
10t1
)
(luit (A. ill yccsun, 1990; 1 I. Itcyb,o n, 1990, uninth-lishetl surveys). Asa result of ins,nbilitt nod civil w:t,Ihee is n tenant fluty of people, surate tuf them iufcitctl,between Knbul and refugee ennuis of l'nkistnil (I'Mniadco, unpublished report atilt. European (;uuunic.shpt: I.itri,R in exile; coping tnntegiet of Afghan rchigrrt,(997). Adult tonic tefugces me mobile in the scnich fortvutk (P. Mnrntlen, unpublished Ic)ro,l, 1997), nod horstflout 'l'iitnignrn would visit ICnbul or I'n, von whentavelling tu the sentent or then, Aft;hnn inuvincesTheir frequent absence front the crimp only cxpinin whythe inevalcncc of Cl. was lower in this pimp and whythey npprnr less nt risk.
'11te tlingiustic cad ChM (lent ;bed here wun,ltl srcn, rovnlitinle lite (findings of the initial survey. Although tl,cpitiful' dim of slide- positive cases wns very luw (36Y.), 20of the 42 slide- negntive cases scot for cult ui c wetcPositive (411 ). Ily exlrapulntion, it would be expectedotnt 49% of lite 64 slide- ncgnliec cases would) Iinvc beenpositive to culotte, rnising the role of positive diagnosis to76 %. This rote might hove been Iuii;hcr ltnd Mere outheel' n 7 -week delay between the initiai survey nod thedingnosiie study, d )j wlicli yelhnps 15% iii c :,setpuny hnve become neq nlive to pnrnsitulogicnl diaisnucisoin addition 1 of the felts token on 5 cutturc- ncl;ntitcdiscs were positive. If tipis is similnrly exit npulnlrrl, the1111C of pOnilive tlingmnis would hnve exceeded 00n/Crases ttegnlive ta nny of the proasitulogicul tests writ:likely tu be of longer durntion, ns successful ono nsitrttu-p,ical dingttosis uf CI. is knuwri to he inversely tciatcuI toIlle dunn{on of the dlscnse (llIIiiJty Ai íU1,1.31', 19113;AT,AI)Iti I et al., 1905).
I Tic occtutcncc of this huge ututocnk ui'Thum gntn "cruller mull Ions iurportma public hcnl,l,inoplicnliuns. Cl. may be railietl by ic(tigec.t hu t, nient
ieviuxly unnfrected by the discnne (11ÁU er ill., , 1997)l
u ill.,nny Ilnrc up with tinte wntning if veau,
snndllies ne {lissent, nul P. tr,,er,ui, tl,c vcclut of I.ia/,ica, is widespread in i'nItistnn (NA5111, 196.1; (lilrts,1967). Cnscs due to 1.. unpira may he pin sistUtt nod
: disfiguring, nod tlifficldt nod expensive to limo (A.Iltyccsao, unpuhlislicd irpmt, I99í1). Tito t is nain aliicklc of cuises tcpoited fool the tuent l'akis;nni pu(iuhi.tíoti (IJNI1( ;it, unpublished irpuii, 19911). l'iun,(rt nodeffective i ensures will be uci(uiictl tu prevent C:1, bun,becoming endemic hi the n'en.
Aghnnt.led(irmenusWc n,t atnlchil in Atntnfn Klont nnd I,(..lc 1(nhin, Iur Ut.
rrtkinseopl, I lnitteed tu Ilnhniwn rot Ilse t,tntitl)' detcctiui, nn.t1)r l'nye,.01 thrli,nn,nn, n hnsie henhh unii for :de? sing u. III III
I,renk. llhn Rr)butn nsJlaieti with the '1ìp:, in il it: tuive) I )r(;Ilve 1)nvles nn,l l'tufcxsur Anlhniy Ili ycrsnn kindly rtiunncnled nn ohe utnnuse,ipl. IlcnlihNcu tutciuntiuotl't M.Intia ni.tlItrishuou,intls I:nnn,1 l'nytrnnnuc it suplur,tcd hy ihr f.uro,rao (;uuunlsslnrt (1)(11 nod LCItO), tir Uni,c.l Nnii tu.I (: istioucr fur Itcfnaccs, anti Nu,wrytin,r (;Inu ctt A61
IlcfcrrnccsAthlbul, It. \V , ICuhcsiniiy, K. A. h I(ntiov.wd, M. A(1997)
Corwn Icishtnwuinais ln 1<nlud; ohtr,vs,iona not n'iuu-Inngcti cphlcoir,'. Annoto / lin¡ac.,t hirdoutr .u,d t4n,nuityt,sfi,lr,1-171.
Aznicl, 11., Snn,a1, A. A Aidcbnli, S. (1')115). Ilia,vlvgitnl
4 MAlll( IttItVl ANIt 1,1 ,11
tptcI111111 or cuisine, s ICith.lta111nt1t flue ID, 1.r.7hnmtr'nn,pien, 71at.11rlMltt n/ the 'loyal ,Snrlrlr rf 7 i.yornl Alrliertrnnd 1 hV't'rnr, 79.011-0.1n.
111....c7. 11.4. I. A Irtl, Ir. A. (I0116). Slams uf rutaneuntIrIslananlatla In l'ekla(an. IS,htsrnu J,nrn.nl n/ Altd,ce! Rttn,h, 2S, 1p1 Inn.
Ittnns, I). A,. (lodh ev. 1). ( t. h 1tnhnn., S. ( 1 nflV). linl..n..nin.lu: llnudhnah or, Isolnr.i.n, :hn,ncrrns.un.n nr..l c;rvnp.r.r,t.n
of I.r,itlr..tallln, livnns, 1). A. (cd' ). Stylizes hula:t INI ll'/\Znnhl Ilnnk/\VI IO ('1 Illt), pp. 1..2n,
Ilruiu, S., ttr)1tu.u, 11.. /Waned, It, h Ilutvi,u,tl. M. (19't11).Atthtul lc r.utnuetttt Ieithatnuinsit in 1(nitul, Afff{{ha.tl-slnu vrttlral t1lstllb/11Iat11 of taus in Nun intent Idncka.7i of the linynl Society n/ rupees' A(tdirìur and!hpp,rtt, 97, 271 274.
1(i116 kICeudflrk, It., 1(ilUekKendllek, M. h'Isnn, Y. (1994).Malunl le cutaneous Itishmmotinsis in ICnhul, Afghani-stan: the how luacrinlltllhy of ! hl.nnr ppnpatnsi iv l tih.
nnpirn. 7)nruecfinns nJ the Roya! .Sncittp o/ 7 inpicelAlydìei.0 nod IIY iene, RR, 252-251.
ICIIII.k I(endfltk,It., Itllliek-Kru.lrlrk, A4. hl'aun, Y. (1991).Antluul Ile cutaneous IOlthlllnldntls In ICnitul, AlRhnni-stan: lite high suseel.tibIliiy of Phlebotomist sirRn.ri tv lii,htomtits mitten. 71nnfnetìer.s of ,ht lloya/ Society o/ 7iupanlAlydirlut n.nl III i t g9, 47i.
twtvta, 11. j (13fi7). lyle )1ldehmutttbte tau,llllen uf KrrstPakistan (1)Ilnrtn: 1'0,0410614e). lhdlran o/ the 11 !t Alit.,r (Notion/ /homy) limo nmhigh 19. I-73.
Masstttnl, A1. Ñ A4ntli, S. M. (1991). C:unrnf atnws ofIriduuartlnds lu I'nkintan. In: (:.ttrnr lirn,h in 1.cishatatiaRrtnneh, Ilhadutl, A. N., Haw. A4, K., Srn, A. It. At 1Cu1.1f,
S. (cdittut). lndi: tìvoncil uf SLicntilic nnd InJnai,,..lItcscnrch11 IT. 231-2.1(i.
Na.11nt, A. rk Itoslanl, (1. S. (1074). Rlddeutiolugy o(Iclthn.nnlads In Kabul, AfRltnnistan. llrJlrnu / ehrIltnfdr (h' nnisnrien SI, 45-49.
Nndlnq A,, li., NnunhIn, M. K h Nn1h. A I( ( I 7 7'1)itl,IdanÌultRr nf cutaneous Irishntauinsit in A,a.nnt..n II
tithe (pc) le cutaneous Ieiitltllnttinsit. Milan, drdi l'n,hnlnr¡ic lixntqur. S. 461 -466.
Nntir, A. S. (1964). $sutlllies as a vcctnr nf hu.nsn tlncsac u.Pakistan. li,hium, Jr, 1 of Ilcnld., 14, 26- U.
Noyes, I1. A. Itcylntrn, 11., IlNiley, J. W. h Smith, Il (199(1) Anested l'(:Ìt based tchlsnticttte method for identifying I.nnnin kinein(dast u+btichde classes directly fron chnncstsamples and Its application to the tinily of the ehidcni.,i,rtof /itilutnerie tmpicn iu Pakistan. Jnu..rnl nf (,h.nrn/ AlnnA.ñlnRy, 36, 2877.2801.
Omar, A., Sabour, A., Said', S. & Set y, V. (196R). Cuunr.n.aIeltbntattlna4l fu Afghanistan. ilfghn,wrnn Jnu,tolHealth, 1, 1.-6.
Itnh, M. A., Itustan.nul, I.. A., Ilhunta, It. A, Ainhnu,od, At Ih Hanna, U. A. (1997). Cutnne teisluuatintis: itnrn,t.nrehnrneterisnlinn of I..fithu.nnin nupiert. Jnu.ttnl nf thc inón.n,.A(ndicel ilttocintin.., 47, 270-271,
Ritlley, 1). S. At Ridley, M. J. (19131).'Ilte evulut' f ilte IrIn eulaneots le)ahnlnuintis. Jot urtertl./l'nrhnln,V,, 141, n 1.9r.
lrrceit7ed !fr OpoGer 1998; reuiud IR Ue[rrrtfw 199,,accepted far publication 18 UeccmGrr 199R
a .. } .1% r . I .. 1t7t/
i
TRANSACTIONS OFTIIE ROYAL SOCIETY OFTROPICAL MIDICINR ANt) IIYGIENC (19971 yt, 252 -255
Transmission and control of vivax malaria in Afghan refugee settlements inPakistan
Mark Rowland', Sean Hewitt', Naeem Durranit, Naveeda Bano2 and RobertWirtz3 sllealtlrNet Interna-aortal, PO. Box 889, Peshawar, Pakistan; 2United Nations High Commission for Refugees, PD. Box 1163, Islamabad, 1 t,h,-
¡tan; 'Department of Entamvlogy, l%dslter Reed Army Institute or Medical Research, Ihfuhington, DC 10307 -5100, USA
AbstractRegular biting collections were conducted in 1993-1994 to investigate seasonal fluctuations in the abun-dance of anophdinea in Afghan refugee villages in north -western Pakistan. Enzyme- linkedimmunosorbent assays were used to test heads -plus- thoraces for the presence of malaria sporozoites.Anophelines giving positive results for Plasmodium vivax were captured in every month except January.Nine species were positive. Biting rates showed a marked increase in May, after the spring rains, and thusspring transmission of vivax malaria seems certain. However, transmission of vivax malaria reached itspeak only after the monsoon in July. To determine the optimal time to control vivax malaria by indoorspraying with residual insecticide, spray campaigns were conducted in either spring or summer in 14 ref-ugee villages. Villages sprayed in July 1994 showed a mean reduction in annual incidence of 62% (95%confidence interval (CII i 6 %) relative to the previous year, whereas villages sprayed in April 1994 showedonly a 15% reduction (95% CI ±32%). Parasite prevalence surveys conducted in April and October 199.1confirmed the greater efficacy of spray campaigns waged in July. The insecticide malathion proved as ef-fective as the pyrethroid lambdacyhalothrin, even though several species of anopheline were resistant to
malathion. .
Keywords: malaria, Ptasnnodiunt vivax, Anopheles spp., sporozolte rate, biting rate, control, malathion, latnbdacyha-
lothrin, refugees, Pakistan '.
IntroductionMalaria is a major health problem for Afghan refugees
in Pakistan ( ROWLAND et al., 1996). Transmission isseasonal, and the main method of control is indoorspraying with residual insecticide. '11,c annual spraycampaign starts in mid July, during the monsoon. Thisis the best time to control transmission of falciparummalaria, the first new cases of which are usuallyobserved in late August. If the campaign is delayed, anepidemic may ensue (unpublished observations). Al-though the campaign is directed primarily againstPlasmodium falciparum (see BOUMA et al., 1996), 70% ofmalaria in Afghan refugees is caused by P. vivax (seeROWLAND et al., 1994). Control of this species deserves
r-- greater attention, especially now that falciparum malariais being successfully curtailed (UNHCR, unpublishedreport). The first cases of vivax malaria appear muchearlier, in April. Sincep precision timing is critical to thesuccessful control of P. falciparum, it is conceivable thatan earlier spray campaign in villages where P. vivaxpredominates would be more effective in reducing P.vivax transmission. But first it needs to be shown thatthe early cases are due in part to new transmission andnot just to relapses from the previous year. Ther- occurrence in spring of anophelines naturally infectedwith P. vivax would justify an early spray round. Thefirst part of this paper describes the seasonal variation inanophelines and their sporozoite rates. The second partcompares the effect of spray campaigns waged in spring
r- or summer on the prevalence and incidence of vivaxmalaria in indicator villages.
MethodsEntomological surveys
During 1993 and 1994, seasonal fluctuations inanopheline densities in Azakhel refugee village in north-western Pakistan were monitored by means of monthlycollections from 4 trap nets, each baited with a single
r.. cow (HBwrIT et al., 1994). The sides of the nets wereraised 0.3 m above the ground to allow mosquitoes toenter. A two -man team at each site made collectionsfrom the inside of the net throughout the night. Afteridentification to species, these collections were proc-
.r. cued for enzyme -linked immunosorbent assay (RUSA).To minimize the risk of false positive results caused bycontamination of samples with bovine blood (SOM-BOON es a/., 1993), specimens were dried and then the
head- plus -thorax was separated from the abdomen ofeach mosquito. Although human catches would havebeen preferable, the cost of hiring enough staff to yieldthe numbers of nnophclines required for this studywould leave been prohibitive.
Enzyme- linked imnnatosorbent anayThe ELISA reagents were supplied by the Walter Reed
Army Institute for Medical Research, Washington, VC,USA. The heads -plus- thoraces of mosquitoes of knownspecies and collection site were tested in batches of 10for the presence of circutnsporozoite antigens (CSAs) ofP. vivax (variants 210 and 247) and P. falcipannn.Batches of laboratory- reared, uninfected Anophelesstephensi acted as negative controls.
Procedures were the same as those described byWIRTZ et al. (1987), with minor modifications. Thirtyminutes after the addition of peroxidasc substrate, ab-sorbance was measured at 414 nm with an II.lsA Platereader (Cambridge Life Sciences, Cambridge, UK). Atest well was considered positive if it gave a visible greencolour and an absorbance value greater than twice themean absorbance of the 5 negative controls.
Insecticide campaignsRefugee villages from 3 adjacent districts of the North
West Frontier Province in Pakistan participated in thestudy. Bight villages were randomly selected for spray -ing in April, and 6 villages for spraying in July (2 othervillages scheduled for spraying in July had to be exclud-ed owing to pesticide shortage). Five of the villages weresprayed with the pyrethroid lambdacyhalothrin at 30mg/m2 (Icon *M, 10% wettable powder; Zenecal and 9with the organophosphate malathion at 2 g/m (50%wettable powder; Cheminova). HealthNet Internationalmalaria inspectors conducted population censuses whilesupervising the spray teams. Insecticide coverage wassatisfactorily high (97% of the 23708 houses weresprayed). The quantities consumed (11000 kg ofmalathion and 600 kg of lambdacyhalothrin) were con-sistent between villages. Application rates in differentvillages ranged from 1.2 -1.4 houses /kg with m213011onand 13 -18 houses/kg with lambdacyhalothritt.
ClimateClimatic variables, recorded daily at the Pakistan Air
Force base in Peshawar, Pakistan, were cunsulidatcd
SuCali'l'Y A11'sETIN(i: Pl)S 1 ER PRESENTATIONS251
grandfathers; their age range was 22 -69 years. Nearly allmothers had attended antenatal clinics and most haddelivered within a health service facility. Virtually all hadnoticed the problem themselves before consultinghealth workers who, they felt, had not provided ade-quate information about their children's needs. Theyfound it difficult to attend physiotherapy or get equip-ment because of the distances and costs involved. Thereis no social welfare system and the education system isnot orientated to meet the needs of children with learn-ing difficulties.
Carers in the 'third world' are under particular strainat present as the structural programme is implemented.'lltcy are denied the information which could allowthen) to identify their children's needs and address themaccordingly. Can health promotion empower them for abetter quality of life, for both them and their depend-ents?
( :1111 kerosene oll lamps be used for personal pro-tection against mosquitoes?
H. V. Pates, J. E. Miller and J. D. Linea Deparimentof Medical Parasitology, London School of Hygiene andTropical Atedicint, Ktppel Street, London, WCIE 7H7;UK
111c effectiveness of a cheap and easy method ofhousehold protection against mosquitoes was investi-gated in Dar es Salaam, Tanzania. Two methods ofheating the volatile synthetic pyrethrold, transfluthrin,in kerosene oil lamps were investigated in 2 consecutivestudies by means of human landing catches in a LatinSquare design.
In Study 1, transfluthrin was incorporated into thekerosene in a lamp at a concentration of 0.1% as in aprevious study in India (SHARMA, V. P. et al., 1993: In-dian journal of Malariology, 30, 169 -176). This treat-ment reduced mean biting rates by 27%, which was notsignificantly different from the control. In another lamps 0.1% solution of transfluthrin in vegetable oil wasplaced in a specially designed 'crucible' held on a standjust above the flame. This produced a significant reduc-
lion in biting of 54 %. Mosquito coils reduced biting by38 %, significantly different from the control but notfrom the 'crucible' treatment.
In Study 2, transfluthrin dissolved in the kerosene wastested again at 0.1% and also at the higher concentra-tion of 1 %. The lauer gave a significantly greater de-crease in mean biting rates (44% vs. 15 %). The'crucible' treatment again gave the greatest reduction inmean biting rates (78%).(This poner shared the prize as the bet at the meeting. J
Primary health care: assessing progress in Nigeria
J. M. Udle Health Care Policy and Management,Heath Services Management Centre, University of Binning -ham, 40Egbaston Park Road, Birmingham, BIS 2RT, UK
Primary health care (PHC) in the last 3 decades hasemphasized the use of 2 models: 'selective' (SPHC) and'comprehensive' (CPIIC). Both models however tend
to share a weakness in terns of their capacity to incor-porate aspects of the local context of health care sys-tems.
The underlying objectives of PHC emphasize thegrowth and extension of basic health services and re-quire a cross -sectional approach bated on local commu-nities. This complexity adds to the difficulties ofimplementation.
This research offers an analytical framework of di-verse methods that can be used to evaluate whetherprogress has been achieved in the implementation of thePHC strategy. The method reflects a multi -disciplinarystake -up of the research endeavour, thereby creating a'triangulation' or ethnographical approach to the study
objectives.The research emphasizes the development of total
quality systems (MAXWELL, R. J., 1984: British Medicaljournal, 288, 1470-1472), within a more inclusive andlocally sensitive programme structure. It argues thatsuch systems enable rather than inhibit the developmentand delivery of adequate health care capable of address-ing local economic and social variables.
VIVAX MALARIA IN AFGIUAN REFUGEES
into monthly means for 1993 and 1994. Peshawar wasthe central of the 3 districts and its climate was repte-sentative.
Parluite prevalence surveysSurveys were conducted on schoolchildren from eachvillage in early April before the intervention and in Oc-
tober when cases of vivax malaria were most numerous.One school was selected from each village, and thickand thin blood films were prepared front all childrenpresent on the day, stained with Giemsa's stain and ex-amined at the HealthNet International reference labora-tory. Two hundred microscope fields were examinedbefore any slide was classified as negative. Children withparasitaemia were treated with chloroquine (25 mg/kgbody weight over 3 d).
Pusive case detectionEach village had a basic health unit where blood films
were taken and antimalarial drugs administered free ofcharge. Blood films were examined at district field labo-ratories by microscopists trained and monitored byHealthNet International. Monthly monitoring main-tained standards and kept the rate of incorrect diagnosesbelow 4%. The time between registration, slide exami-nation, and treatment was 2 d. Patients were given pre-sumptive treatment while awaiting the microscopyresult. Malaria patient records were extracted from theregisten for calculation of incidence rates. A special cf-.-fort was made to keep health unit services the same dur-ing 1993 and 1994, so as not to affect usage by thepopulation or confound the number of cases recordedannually.
P-Statistics
The effect of the Insecticide interventions ln April orJuly was examined separately for each village. Parasiteprevalence rates and incidence ratios were usually corn-
r
r
r
a rs
as
sa--)
o.--....C._ _ _ _.. _. .---I I w a w ! I a S O M
Months
A.
8
w 4 w I IMonths
Fig. 1. Relative numbers of anophellnes ('biting density')caught in 4 trap nets baited with cattle (A) in north -west Paki-stan and percentages containingcircumsporozolte antigen ('%positive'; B); shaded bars, ft vivax; open bars, P. fakiparuan.
200
160
100
60Io
Rainfall (mm), Humidity (s)
251
1993-94
Fig. 2. Climatic variables in Peshawar district, north -west Pa-kistan: temperature (C) (), humidity (), and rainfall(hatched bars).
Table 1. Sporozolte rates in host -seekinganophelines ln Afghan refugee villages in north-west Pakistan, as detected by head -and -thoraxELISA circumsporozolte antigen bioassay
SpeciesP, vivax
(%)P.Jakiparwu
(%)No.
testedA. maculatui 3.6 0 28A. pulcherimus 3.1 1.2 668A. nigerrimus 3.0 1.0 2975A. atephensi 2.2 0.7 15387A. colici, facies 1.9 1.1 2396A. subpsctus 1,7 0.5 5358A. superppictus 1.7 0.5 1513A. annularis 1.5 0.6 1554A. J/aviatìlis 1.4 1.4 1548
pared in the 2 sets of villages using the non -parametricWilcoxon rank sum test, since it was not certain whetherthe data for such small groups were normally distribut-ed. However, means and confidence intervals arc quot-ed when presenting the results, and this assumes thatthe data were normally distributed. The effect of differ-ent insecticides was assessed by means of two-way anal-ysis of variance.
ResultsAnophdine seasonal abundanceand circluuspuntzuite anti-gen positivity
During 1993 and 1994, 32427 anopltclines were cap -tured.and tested for the presence of sporozoites. Cap-ture rates were highest from July to October (Fig. I , A),during and after the monsoon rains (Fig. 2).Humiditywas also at its highest during those months (rig. 2), pro-ducing conditions highly suited to malaria transmission,as reflected in the sporozoite positivity rates of 2 -3% forP. vivax and c. 0.5% for P. falciparunt during that period(Fig. 1, B). The highest P. vivax positivity rates were ob-served during February and March (Fig. I, B), in mos-quitoes that were presumably overwintering. Capturerates were, however, st their lowest (Fig. I, A) duringthose relatively cold winter months (Fig. 2). Capturerates began to increase in May (Fig. I, A), after thespring rains and as the temperature increased (Fig. 2).Upto 4% of the trapped mosquitoes gave positive re-sults for P. vivax (Fig. 1, B). Although capture ratescontinued to increase from May to July, sporozoite ratesdecreased during that period (Fig. I); presumably mos-quito longevity had decreased owing to the high temper-ature and low humidity during the summer monthspreceding the monsoon (Fig. 2). Several sr !else gavepositive test results for P. vivax and P. falci, ... rt cir-cumaporozoite antigens (Table 1).
:51 MARK ROWLAND 6'T41.
Table 2. Parasite prevalence rates (age -adjusted) in Afghan refugee villages In north -west Pakistan, Apriland October 1994
Village
I.)arsantundDaghbananRadaberMichaniDallanDughesudJrluzaiilaghichaKotki 2KhazanaKotki I1'akkaghundNagumanC:hakdara
Spray No. examinedmonth April Oct.
JulyAprilJulyJulyJulyAprilJulyJulyAprilAprilAprilAprilAprilApril
210 204256 220121 167212 200220 253212 175242 226203 203212 221219 208211 219131 156300 207131 209
Mean (July villages) 201 209Mean (April villages) 209 202
13.911.79.21.52.31.0050.60.00.43.60.41.35.4
/? vivax rateDifference
April Oct. Oct. -April
'
2.1 -11.85.4 -6.33.8 -5.40.9 -0.62.0 -0.31.0 00.6 0.11.0 0.40.8 0.82.3 1.95.5 1.94.1 3.75.2 3.99.9 4.5
4.7 1.7 -2.93 0 4.3 1.3
1? fdIcipar
April Oct.
rateDifferenceOct. -April
2.1 1.2 -0-90.3 0 -0.33.0 1.8 -1.20 0 00.9 1.1 0.20 0.4 0.40 0.8 0.80 0 00.7 13 0.61.1 0 -1.10 , 0.4 0.40.9 0 -090.6 1.4 0.81.3 0 -1.31.0 0.8 -0.20.6 0.4 -0.2
'Age -adjusted prevalence rates were obtained by direct standardization; age- specific rates from each of the villages were applied to astandard population of all children surveyed in April and October. Villages are listed in order of increasing difference in the E vivaxi'ie%alcnce rate between April and October.
In.ld.n.. /1000 peyublian17
C
Incidence /1000 ppulalbr.
1 / M a M J J A f O N O J r M M J J A a O N 0 ) r M A M J J A 3 O N O J f M A1993 -94
Fig t. Munthly incidence of vivax (hatched bars) and falciparungroups of villages sprayed in either April (A) or July (II). Pooledrecords for the individual villages are shown inTable 3).
Illrecricids spray campaigns .
The differences in P. vivax prevalence rate betweenthe surveys in April and October are shown (in ascend-ing order) in Table 2. The distribution formed 2 dus-ters, with the villages sprayed in July showing areduction in mean prevalence of 2.95% (95% confi-dence interval (CI] ±4.6%) between the two surveysand those sprayed in April showing an increase in meanprevalence of 1.3% (95% CI ±3.4%) (P<0.05).
Incidence rates were calculated from health unitrecords for April -December in both 1993 and 1994(Table 3). The reduction in mean incidence between1993 and 1994 was 62 %±6% in the villages sprayed inJuly but only 15% ±32% in villages sprayed in April(110.05). There was no evidence that one or other in-secticide was better at controlling vivax malaria (P=0.9);lltalathiun reduced the incidence by 36134 %, lambda -cyhalothrin by 32132 %. The mean incidence of falci-parum malaria fell by 61% between 1993 and 1994 inthe July sprayed group but showed little change in theApril sprayed group; however, the difference was notsignificant (P>0.05).
Monthly incidence rates are shown in Fig. 3. Vivax .malaria normally reached a peak in September or Octo-ber. In the group of villages sprayed in July 1994, therewas a clear reduction in incidence in the subsequentmonths when compared to 1993. In the group sprayed
1993 -94(stippled bars) malaria in thedata from villages with the same season of spraying (incidence
in April 1994, the campaign had no obvious effect onthe seasonal increase in vivax incidence during the fol-lowing months.
DiscussionAnophelines were caught in trap nets in all months of
the year, and only in January was P. vivax circumsporo-zoite antigen not detected. Outdoor biting rates did notshow a notable increase until May but, since 4% of thesemosquitoes contained N vivax circumsporozoite anti-gen, the case fur spring transmission of P. vivax seemsirrefutable. The evidence certainly suggested that anearly spray round would be useful. April spray cam-paigns failed, however, to stem the seasonal increase invivax malaria, and thus many of the observed cases were .probably due to relapsed infections from the previousautumn (Fox & STRICKIAND, 1989). The campaignheld a few months later affirmed that the optimal timefor spraying is during the monsoon, when mosquitodensities and humidity are at their highest. Since a cam-paign held in July coincides with the needs for falci-parum control (ROWLAND et al., 1994), only a singicspray round is required to control both species of malar-ia, the operational management of malaria can be keptsimple, and costs can be kept low.
Although lambdacyhalothrin has longer residual ac-tivity than malathion and, at World Health Organiza-
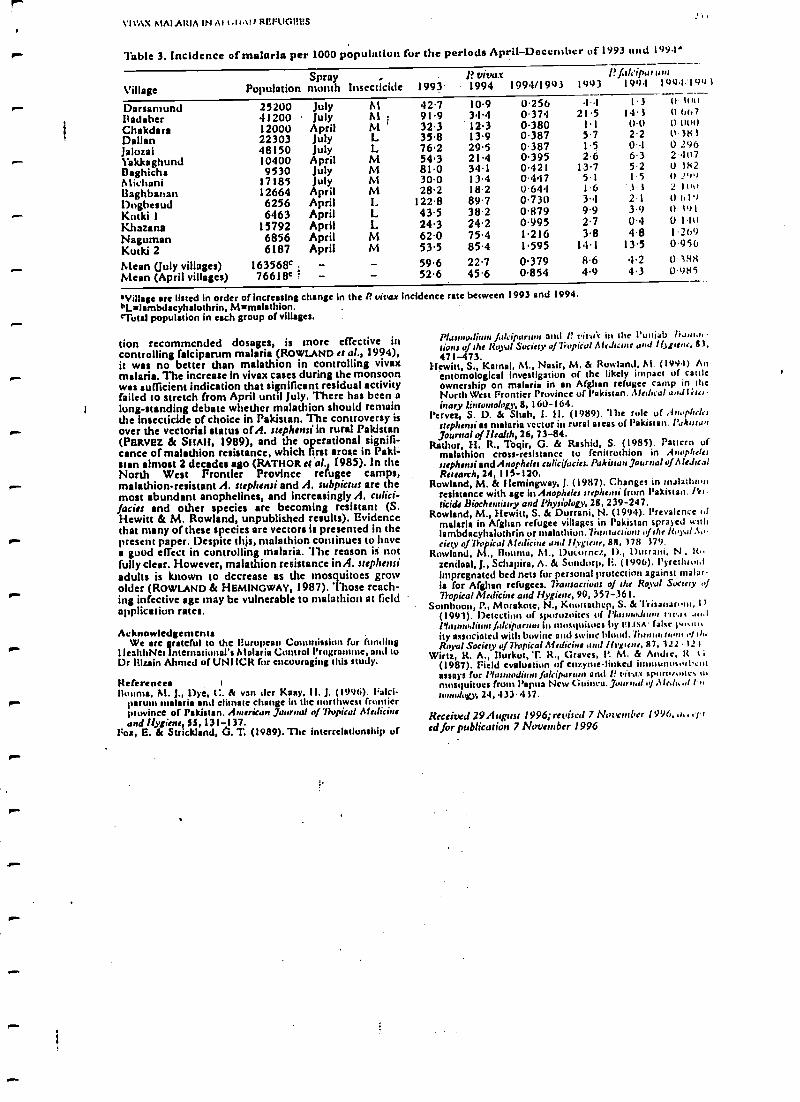
\I\AX MAI ARIA IN Al t.1tAt1 R1if°UCI3HS
Table 3. Incidence of malaria per 1000 population fur the periods April -December 01 1993 und 1994ä
SprayVillage Population month Insecticide 1993
DarsantundBritisherChakdaraDallanJalozaiYakkaghund©aghichaMichani13aghbananDogbesudKntki IKbazanaNagumanKutki 2Mean Uuly villages)Mean (April villages)
25200 July M41200 July ist
.12000 April M22303 July L48150 July L10400 April M9530 July M
17185 July M12664 April M6256 April L6463 April L
15792 April L6856 April M6187 April M
163568c . -76618c 1 - -
42.791.932.335.876.254.381.030.028.2
122.843.524.362.053.5
1? vitxs.r 1? f,tli ipururn1994 1994/1993 1993 1994 1094;1993
10.934.412.313.929.521.434.113.418.289.738.224.275.485.4
0.2560.3740.3800.3870.3870.3950.4210.4470.6440.7300.8790.9951.2161.595
1121.5
1.15.7152.6
13.75.1It
3.49.92.73.8
14.1
1.3I 1 3
t)t)2.20.16.3521.53 32- I3.90.44.8
13.5
59.6 22.7 0.379 8.6 4.252.6 45.6 0.854 4.9 4.3
0 titi)t) 667l) ll(ul11 38302962 t)17U 382(t !'r')2 looO h l'tU Or011u13690 956(l 3880.985
'Village are listed in order of increasing change in the f'vivax incidence rate between 1993 and 1994."Lulambdacyhalothrin, Mnmalsthion.°'Total population in each group of villages.
Lion recommended dosages, is more effective itscontrolling falciparum malaria ( ROWLAND et al., 1994),it was no better than malathion in controlling vivaxmalaria. The increase in vivax cases during the monsoonwas sufficient indication that siçnificant residual activityfailed to stretch from April until July. There has been along- standing debate whether tnalathion should remainthe insecticide of choice in Pakistan. The controversy is- over the vectorial status of A. stephensi in rural Pakistan(PERVEZ & SHAH, 1989), and the operational signifi-cance of malathion resistance, which first arose in Paki-stan almost 2 decades ago (RATHOR t; al. 1985). In theNorth West Frontier Province refugee camps,
P." malathion- resistant A. srephensi and A. subpictus are themost abundant anophelines, and increasingly A. culici-facies and other species are becoming resistant (S.Hewitt & M. Rowland, unpublished results). Evidencethat many of these species are vectors is presented in thepresent paper. Despite thjs, malathion continues to havea good effect in controlling malaria. 'Ilse reason is notfully clear. However, malathion resistance in A. srephensiadults is known to decrease as the mosquitoes growr older ( ROWLAND & HEMINGWAY, 1987). Those reach-ing infective age may be vulnerable to malathion at fieldapplication rates.
AcknowledgementsWe are grateful to the lIurupean Commission for funding
I IralthNet lineman onal's Malaria Control Programme, and tuDr lilzain Ahmed of UNI ICR for encouraging titis study.
ReferencesHouma, M. J., Dye, C. & van der Kany, II. J. (199(i). llalci-
paruus malaria and climate change in the northwest frontierprovince of Pakistan. American Journal of Tropical Alalicineund Hygiene, Ss, 131 -137.
Fox, E. & Strickland, 6. T. (1989). The interrelationship of
Plasmad f,,lapar and P t'irai in the I'unteb Is.int,l, -rims u the Royal Society of liupüu! A1eJrcote and !l)tune, 83,471 -473.
Hewitt, S., Kemal, M., Nasir, M. & Rowland, M. (199.1) Anentomological investigation of the likely impact of cattleownership on malaria in an Afghan refugee camp in theNorth West Frontier Province of Pakistan. Alnin.al and I }iounary Entomology, 8, 160 -164.
Pcrvez, S. D. & Shah, I. 11. (1989). "Ilse rule of Anophelesstephensi as malaria vector in rural areas of Pakistan. PakistanJournal of Health, 26, 73 -84.
Retina, H. R., Toqir, G. & Rashid, S. (1985). Pattern ofmalathion cross- resistance to fenitrothion in A,tophe /etstep/semi and Anopheles culicifocies. Pakistan Journal of AledrealResearch, 24, 115-120.
Rowland, M. & Hemingway, J. (1987). Changes in malatlutmresistance with age in Anopheles stephemi from Pakistan. Pet.acids Biochemistry and Physiology, 28, 239 -247.
Rowland, M., Hewitt, S. & Durrani, N. (1994). Prevalence tifmalaria in Afghan refugee villages in Pakistan sprayed tsnhlambdacyhaluthrin or malathion. Van:actio ns of the /loyal So-ciety of7h+pyical Medicine and 1lvgirnr, 88, 178 779.
Rowland, M., founts, M., Ducurncz, 1)., Durrani, N , It,.zendaal, J., Schapiro, A. & Sundorp, E. (1996). l'yrethrut,limpregnated bed nets for personal protection against malar-ia for Afghan refugees. Transactions of the Roval Sorte) ofTropical Medicine and Hygiene, 90, 357 -361.
Somhoon, P., Morakote, N., Koottathcp, S. &Trisauar.m,, t 1
(19933. Detection of sporuzuitcs of /timid,/ ttr.tt ...,.1Malmo& f.,lnparutrt in mosquitoes by 111.ISA- false t+,,u.ivy associated with bovine and swine MIA. Muria, t" ), .q,h.Royal Society of 7hrpical Medicine and Hygiene, R7, 122 -12
Wirtz, R. A., ilurkot, T R., Graves, P. M. & Amite, It t(1987). Field evaluation of enzyme- linked inusuun'' ,at'.ntassays fur Plannodiu,n falcrpartun and P turd.: spurur,ntt s u,mosquitoes from Papua New Guinea. Jocuna /.¡.51..h,,,í I ntonurloty, 24, 433-437.
Received 29 August 1 996; revised 7 November 1 996, ,t. , rlred for publication 7 Ntrve,nber 1996
1H 11:':11 1 lt 1NS a 11 1111: 1(0YA1. St)(:1197")' Ul°'17ìU1'lt'(1I. A11S1)1(:INIi ANI) HYGIENE (1997) 91, 256 262
The epidemiology of severe malaria in an area of low transmission in Thailand
tahristlner
Luxrnburhrrt.rs Ietutçular 1ticelh, Irnnçuls Nostenli=ui4, nmHal It, Saw ItuncetiaidNirhulnsJ SSitites.4 )SYukloAlaaiirlcsearrhLhni,AfaeSut,7silul;21rcultyuf7ürprra/Aledrure,Al,drJ,/I'nr t et WV. Nanyk,,k, 'J'huJ,neJ; IA li decira .Sans hraatirtres, Paris, Pittner; 4Cerrrre /rr 7fapieal AfeJkine, NhrJJiolJ I)cpar nnerul t auot.rl ,5ledicrne, John Radcliffe Iluspital, U.tjn'd, UK
AbstractThe predisposing factors, clinical presentation, and outcome of severe malaria in a Karen can tinunityliving on the western border of Thailand Were studied over a period of 2 years. This was an area of lowmalaria transmission (approximately one infection per person per year), where asymptomatic malaria isunusual. In a population of 4728 persons, who had good access to facilities for malaria diagnosis andtreatment, there were 2573 cases of vivax malaria, none of whom died, and there were 5776 cases offalciparum malaria, 303 (5 %) of whom had severe malaria and 11 (0.2 %) of whom died -a case fatalityrate of 1.9 per 1000 (95% confidence interval ICI) 1F0- 3.3).Tle risks of developing severe malaria anddying declined steadily with age. The clinical features of severe malaria differed between children andadults. Anaemia was more common in children under 5 years old than in older children and adults,whereas the incidence of cerebral involvement increased with age. Severe malaria was 3 times (95% Cl1.4 -02) more common in pregnant than in non- pregnant women, but was 4.2 times (95% CI 2.3 -7.9)less common in patients with mixed Plasumd falciparum and P. vivax infections than in those with Pfalciparum alone, suggesting that P. vivax may attentuate the severity of P falciparun malaria.
key words; ma(aria, ly,arnodiu: J,tcsparum, Pips him, vinn.r, epidemiulugy,'lhriluad
introductionThe clinical pattern and age distribution of severe ma-
laria varies with the intensity of transmission. In areag ofhigh and stable transmission, severe malaria is confinedmainly to the first 3 years of life and manifests predons-mantly as severe anaemia, whereas with lower and moreseasonal patterns of transmission the age distributionshifts upwards and cerebral malaria becomes the pre-dominant clinical manifestation of severe malaria(13RUCE- C1IWA1T, 1952; GREENWOOD et a1., 1987;Mut.VNEUX it al., 1989; BREWSTER & GREENWOOD,1 993; SNOW a al., 1993; MARS!' et al., 1995; WALLERrt ,r/ , 1995). At even lower levels of malaria transmis-sion, severe disease may occur at all ages (WIII'l't :,
I996). Syndromes which are relatively rare in child -hood, e.g., acute renal failure, pulmonary oedema, andsevere jaundice, are common manifestations of severemalaria in adults. In this epidemiological context preg-nant women are at particular risk of developing severemalaria, and have high maternal and fetal mortality ratest Nus 1 EN er al., 19910).
Among the Karen people in eastern Myanmar andwestern Thailand, multi -drug resistant falciparum ma-laria is the Most important medical problem, despite rel-antely low levels of transmission ( <1 infection perperson per year) (LUXEMBURGER el al., 1996). Sympto-matic and severe malaria are teen at all ages. Prospectivestudies of the clinical epidemiology of malaria in thiscontext (which is similar to that found in many parts ofeastern Asia) are difficult because populations are usu-ally 1. idcly dispersed in forested arcas and malaria trans-mission often varies considerably over short distancesIRt'5I NltI R(ì el di., 1990). We describe a prospectivestudy conducted in an unusually large population of dis-placed persons that aimed to quantify the clinical bur-den and to describe the age -specific clinical features ofse%cre malaria.
Airthuds'SnaJv me
The study site and the epidemiology of malaria in thisarea have been described previously (NOSTEN Cl al.,1 987; DOLAN a al., 1993; et al., LUXEMBURGER et al.,1996). In brief, Shoklo is a large camp for displaced per-sons of the Karen ethnic minority, situated in forested
Address for correspondence: Dr Christine Luxemburger,Shoklo Malaria Research Unit, P.U. Box 46, 63110 Mae Sot,'Ihailand; fax +66 55 532 637.
hills, 120 kin north of Mae Sot on the western harder ofThailand. Malaria occurs throughout the year with 2seasonal peaks, one at the beginning of the rainy season(May -July) and the other during winter (Novem-ber- January). Plasmodium vivax and multi -drug resist-ant P. falcipantw occur with approximately equalincidences, although the age distribution of the 2 infec-tions differs considerably. 1' malaria( is rare. A detailedprospective survey conducted in 1992 provided am esti-mated malaria incidence rate of 1.0 infection per personper year (95% confidence interval [CIJ 0.9- I I ): 47% ofthe cases were caused by P..falcipantrrr, either alone(37 %) or mixed with P. vivax (10 %). The estimatedmean pyrogenic density, or threshold parasitacmia atwhich symptoms occurred, was low and similar to thatreported previously in non- immune persons: an esti-mated 1460 parasites /ItL for P. falcipanrrrr and 181 /ill.for P. vivax. Most of the subjects (87 %) with malariaparasites detected during population surveys became ill,and this progression to symptoms was equally likely atall ages. The incidence of falciparum malaria increasedwith age and the majority of cases (92%) were diag-nosed in children over 5 years old and in adults, whereasthe incidence of vivax malaria decreased with age (Lux -IiAIIIU1tGER et al., 1996).
it lularia cwruvl programmeFollowing the ' l'hai national malaria control pro-
gramme strategy, early diagnosis and treatment havebeen established as time mains components of malariacontrol in Shoklo and similar camps. For 10 years theinhabitants have beets educated about malaria and ad-vised to attend the dispensaries run by Alidecins Sarahrontilres whenever they had fever. hour dispensaries,one hospital, and the dispensary of the research unitwere the only sources of antimalarial drugs in Sltuklucamp. All malaria cases were confirmed by microscopi-cal examination of a blood Min. Patients from the campwith severe malaria, or those referred from the sur-rounding area (estimated population about I000(1),were admitted to hospital in the 30 beds single ward ofthe in- patient department. Two medical assistants,working under the supervision of one physician, provid-ed continuous (24 h) medical cover.
As malaria in pregnancy is a major health problem its
this area, and falciparum malaria is associated with ma-ternal morbidity and mortality and with reduced birthweight, weekly antenatal clinics have been set up to de-tect and treat malaria infections before the developmentof symptoms (NOSTEN et al., 1991a). Approximately
r
I.j , ;
: I d I
f `
`5,,t,;T7AfiALlO OPTH OPTROPt'AL M1C1NB AHD HOi9r 8 f971 f- 172-153
jjt-Ì : -;}.::._,.¡ , ..
;
Transmission and Çó'nt'ról of Vivitx;it>ialaria in Afghan refugee settlements inPakistan
,. ,- .t =1.'r¡;> ,{ :
Maris Rowlaadl Sean Hawlt_ttf Naaem Durranil, Navecda Dental and Robert Wirtz) tflr.dltltNartionaf RQ Bar 889, ArsAawar, Petki tan; 2Unitsd Nation, High Commission for Relieves, PQ Dux 1263, !,),r,aba-1, 1tdurun; JDrparansru of Entomology, lt'bltsr Rsad el r,rry Institute for Medical RstesrnA, (Mu,Ahuyton, DC 20307- 51OU, USA
i,I ., AbstractRegular biting ncedens wire conducted in 1993 -1994 to investigate seasonal 11uctuations in the abun-dance of anopheiii cs in Afghan refugee villages in north -western Pakistan. Enzyme-linkedimmunosorbent ways Were rued to tae heads -plus- thoraces far the presence of malaria sporuwites.
t Anopheilaq giving poaldve results for Plasmodium vitax were captured in every month except January.f Nine specks were positive. Biting rates showed a marked increase in May, after the spruig rains, and thussapling traaimis.sion of vivax malaria seems certain. However transmission of vivax malarú re.t3ied iupeak only after the monsoon in July. To determine the optimal time to cunuol vivaz malaria by indoor
' :I ; spra with raldtial insecticide, spray campaigns were condtuteil is either spring or summer in 14 ref -Nixes a,ges.;V' sprayed in July 1994 showed a mean reduction in annual incidence of 62% (95%çonfiden = inscrvai [CI) ±6 %) relative to the previous year, whereas avilla sprayed in April 1994 showed
I Ì, ?nary a )5% reduction (95 %CI #32%). Parasite prevalence surveys conducted in April and October 1994.oanfrmçd die greater efficacy of spray campaigns waged in July,Thc insecticide malathion proved as cf-
; i çfeetive ss the pyrethrold larnladseyhalothrio,, aven though several specks of anophelinc were resistant to
rj r:i{ 1 t' lj1
'!;I l'¡( Wk. 0-11,
..I i
j1,
l'¡ ¡; I1 ' ;i:I`,, .
: mstirutPft}srvYiir nwrar, !!wS w9 twro:v ooptrd, a+slattsla4, tameaagrts., . ite rasa,
f ' ¡
:{;.. ,i) . l,
, l :,
;ky ; , , I ` i ; head-pt;-1Jedhyt[ `yr ataratei from the abdomen ofi i'j, ': , I i I.s , ;
Ia tii ' ttda iisjon health ' ' ' Af tefugees ' each a,¡oagtJliw,i,
*Owe!x mP1 r Ia,e
human catches would have(`1n' ..(RQw AND'a. i193ì6 . !rr.n rni too'is bccn pmdtiitb1¡,'the coat of hiring enough staff to yield
+ . ' the a for this scudt and train son i. lndoo etsopheltafa required ysp frith fgldual d ; The annul spray ' Would have pfo(,.ihidve.
' camptsign Own in mid f ruoers: tide die monsoon.' i : , ; ,
is the Ise* time to ooatrpl,;¢api godson of fálcpátsirn , Ens-yaw-144.d iupi't ososontsar auerymalaria,' feat new antes, ot;:,whkh art.-usually The RUM reagents were supplied by the Walter heedobserved is late August. If the cam is delayed, an Army Institytc for Medical Research, Wash,ngion, DC,epidemic 'may ensue (unPstsservadas). Al- USA. The heads-plus-thoraces ofnwsywwuofknu..nthough the casapaiga is -directed' p against species and collection site were tested to b.tJhc3 of 1u
' FKaratadi+ ass /alciporstm (sec SOU/AA A: rd., 199 ¡ 70% of for the preaecee of etreumsporozoite anus,:tss (C:SAs) ofmalaria In Afghan refugees is caused by P. viwsx (see P. vivax (variants 210 and 247) and P. J.tictparum.ROWLA D *sal., 1994). Control of this species deserve Batches !'oC; ¡laboratory-reared, tusirrfected An pheies
1trl i,uikcted as negative COAtrola.Freaks atteadetn, especially now that falctparum malariau being successfully curuiled (UNHÇR, unpublished . Proeedu;tes, were the saune u those dc,cnbcd byrepot: The first cases' of vivait malaria appear much .tilp 1.4 sg at, (1947), with minor modifications. 'fàu-ryearlier, iaAptii..Sinee precision timing is critical to the 1 minutes' after the addition of perozidase substrate, st»
sorbanee was measured at 414 nm with an EusA platereader (Cambridge Life Sciences, Cambridge, UK). Atest well was cop/Wend positive if it gave a visible greencolour and !P rb orbanee value greater than twice themet.n abeebante of the d negative controls.
sucs shill coo¢ol of P. f it is conceivable thatan 7. campaign Nbáe P. okraspintes 'would be mart affectjvç in reducing P.max rade; But fast í15geods ta be shown thattbo uses art due ln part too new Ftansnsisdon andnot 11161/ ..*D pFcyiów yeas
wi R'' .ofc3 naturally infectedjustify ad catty spray Sound. The
first ppaattst of toss paper describes; the seasonal variation intsnopbalts sad their spot+oaoite rates. The second part
: compere, táa'effect of spray+ ampaJ ras waged In springor sut;tmes on the prevelçpcf. and incdence of vivttx
inI)
indicator villages~
4t, 1 I ¡' ,! I
Dui* ;.1993: and 1994, seasonal fluctuations inanopbeline densities in Azakhcl refugee village in north-western Pakistan were monitored by means of monthlycollections from 4 trap nets, each baited with a singlecow (Haw= a a1., 1994). The sides of the nets wereraised 0.3 m above the ground to allow mosquitoes toenter. ;A two-man team at each site made collectionsfrom the inside of the net throughout the night. Afteridentification to species, these collections were proc-essed far ensyme- linked immunosotbent way (gUSA).To minimise the risk of false positive results caused bycontamination of samples with bovine blood (SOM-BOON et aL, 1993), specimens we* dried and then the
:1
r
t,
f I; i .; ;''; ;.
I.t ;
Inssçrs ' '
; . :
Rt4 geÇ P' Imes: 3 adjaccat diauicu of d c NocthoWest rond vim* in Pakistan pan.icipated in thestudy. Flight villages were randomly selected for spray-ing in April, and 6 villages for spraying in July (2 othervillages seheduk4 for spraying in July had to be exclud-ed owing to pesticide áhopage). Five of the villsgcs wentsprayed with táß pyrediroid iatnbdacyhaluthrin at 30mg/m2 10% wettable powder; Zeneca and 9with the orl;anophospbits malethion at 2 g/rn' (5Q%wettable powder; Cheminova). HealthNct interns mina!malaria inspectors conducted population censuses whitesupervising the spray teams. Insecticide coverage wassatisfactorily high (97% of the 23708 h aoua wucsprayed): The quantides consumed (1 1000 kg ofmalathion and 600 kg of lambdacyhalothrin) were con-sistent between villages. Application rates in differentvillages ranged from 1.21.4 houses/kg with malattuonand 13 -18 housca/kg with iambdacyltalutitrtn.
ClimateClimatic variable, recorded daily at the PAktstan r'ur
Force base in Peshawar, Pakistan, were consolida Lei,1;
I
'
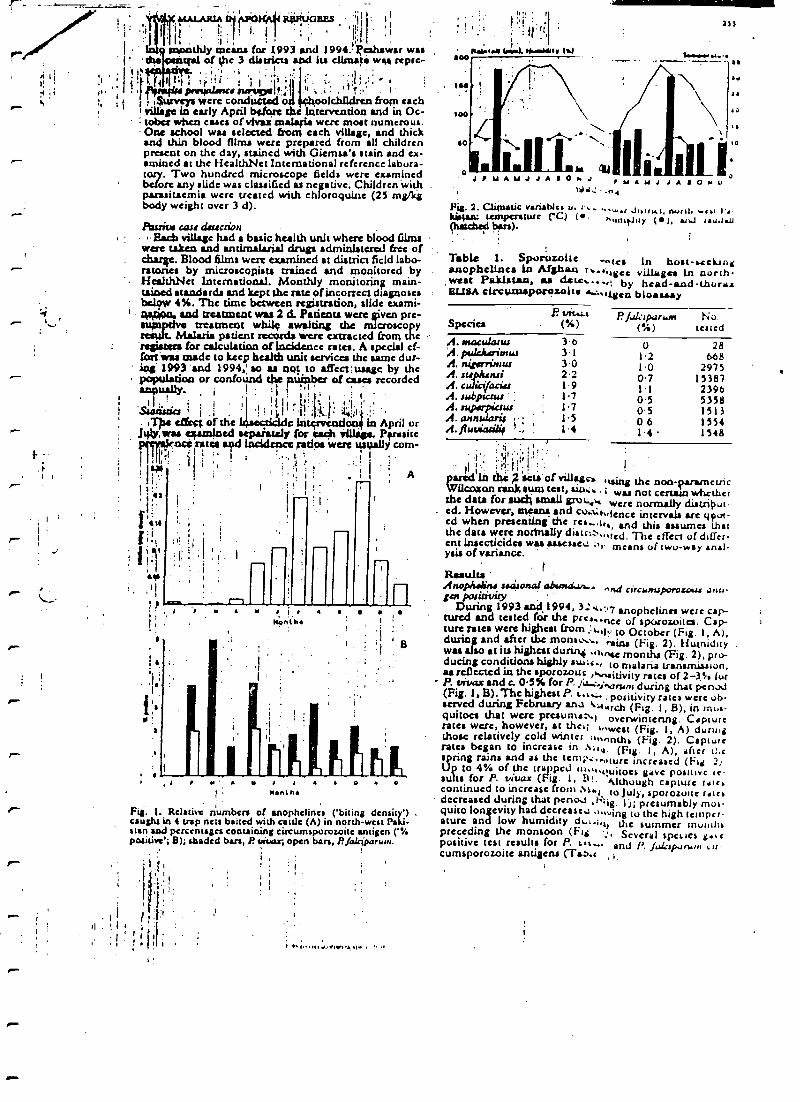
r-
1
.rP.6 1t011JaBBs ?¡; '
i ., , I.,
i
.
I Iasonthly means for 1993 and 1994.. Peshawar was' ' the . taral of the 3 districts and la climate wait tepee-
! I, licit. .. i ' i
i : ' ll l lit i ,..!ti 1. IiII } f(4I^RY...'^S lf.l I 1
11'f Ili I.
;, I i4uaveys were conducted o' oolchlldren from eachI ;Zags in early April before die ltitervention and in Oc-cobra when cases otvlvai malsyla were most numerous.One school was selected from each village, and thickand thin blood films were prepared from all childrenpresent on the day, stained with Giemsa's stain and ex-amined at the HealthNet International reference labura-taaryry. Two hundred microscope fields were examinedbefore any slide was classified as negative. Children with .
parasitaemia were treated with chloroquine (25 mg/kgbody weight over 3 d).
Passim cart dsucrionEarn village had a basic health unit where blood films
were taken and antimalarial drugs administered free ofchine. Blood films were examined at district field labo-ratories by microscopists trained and monitored byHealthNet International. Monthly monitoring main-tained standards and kept the rate of incorrect diagnosesbelow 4 %. The time between registration, slide exami-
' twijo i, and trutment was 2 d. Patienu were liven pre -sum treatment while awaiting the microscopy
Malaria patient records were extracted from therspsoas for calculation of incidence rates. A special cf-fort :wars made to keep health unit services the same dur-ing 1993 'and 1994,' so as not to affect :usage by thepopulation or confound the pumber of cases recorded
SurüricsI ¡ -l '.'. --1I}I I. i }:.: , ,
. ilia effect of the Inse ddc intervendoni in April or..141y, Was sJfarnlned aepaiately for each Village. Parasite
ptr, aknc! sates iu?d incidence ratios were usually corn -1 1, =' Ì I I " k : I
.., tI
i1 I Tti F
IáuIi1I
,1 ' i
assI I
P
A
IB
r i J
No iIl
Fig. 1. Relative numbers of anophelines ('biting density')caught in 4 trap nets baited with esule (A) in north -west Paki-stan and percentages containing circumsporowite antigen (%positive'; B); shaded bars, P *soar, open bars, P fafgparimi.
I
I I
. I i i.,p.nn.L.IW,y,i. .d
I .
r
:i!Si
tt.b.t.r I.J.nr g..rlMlr tolMoo
100
too
00
J/ Y A 1/ J J A a O n. .i I y1J1i .0e
711
.is
0A14 J J A a O M U
Fis. 2. Climatic variable. u. 1 t. W.r .luuK1, rwnl, r.a I .Batas: temperature re) ( , nwnt.luy (), aril i,,i.r.0(hatched ban).
Table 1. Sporozoltc ....ice In boat -settinganophellnes ln Afghan t._.;sgce villages ln north-west Pakistan, as dete.....t by head -and- churaa13113A eirctinssporesoite n:..t en bioassay
P. tJit..i.tSpecies (%)
A. ttisacsJlat.0 3eii. pJcJisn'rrtw 31A. rt{gartruw 3.0A. sophen.ri 2'2A. colici/aria 1.9A. rubpwrur 1'7A. srtppascc m 17A. annnujaris i 15A. ffuviasi8ie ., 1.4
I.:II 1i
7pared In t21t;{{.sets of village-, .yirsg the non- Qaraymctr ¡ccoxon tank sum test, sus. ;i . Ii was not eertair7 whetherthe data for staid; small grow+,q were normally diatribut-
. cd. However, means and co :;adence intervals are gpoc-ed when presentingthe res ».tr,, and this assumes thatthe data were normally distrt. ,,,red. The effect of differ-ent Insecticides was assessc.::.,. means ( two -way anal-ysis of variance. '
Results I
Artopha&ins siásonaf absrssd."-- circwruporosouJ anu-eea pos./awry
Durng 1993 and 1994, 3: v,ß7 anophelines were cap-tured and tested for the pres..nce of sporowites. Cap-ture rates were highest from }.,ly to October (Fig. 1, A),during and after the monsuv.,
Po-ntius (Fig. 2). Humidity
war also at its highest during -linear months (Fig. 2),dueing conditions highly since., to malaria transmission,as reflected in the sporozouc r*oat)vity rates of 2 -3% curP. vivax and e. 0.5% for P. Ivw .1 arum during that pcn.xl(Fig. 1, B). The highest P. art.:. positiviry rates were ob-served during February an:s arch (Fig. 1, B), in mus-quitocs that were presuntaN) overwintertng. Capturerates were, however, at thee; .,,west (Fig. 1, A) duringthose relatively cold winter :1,.,,nrhs (Fig. 2). Capturerates began to increase in Ni,v, (Fig. 1, A), after tl.cspring rains and as the temp :..,,cure increased (Fig 2)Up to 4% of the trapped iu...,ouitoes gave positive rcsuits for P. vivox (Fig. 1, B. Although capture rate,continued to increase from Nt.l loluly, sporoswtc ratsdecreased during that period ,1c: ¡ 1 ji presumably tuo,.quito longevity had decrease ..,, ¡rag to the high temper-ature and low humidity dt.t.i. the summer muiiilispreceding the monsoon (Fig Scvcral speucs g..cpositive test results for P. lit .- and P. falcipdMni tir-cumsporozoitc antigens (Tso.e
P f.Jkiparuirt No( %) tested
o 281.2 6681.0 29750.7 153871.1 23960.5 53580.5 15130 6 15541.4 1548
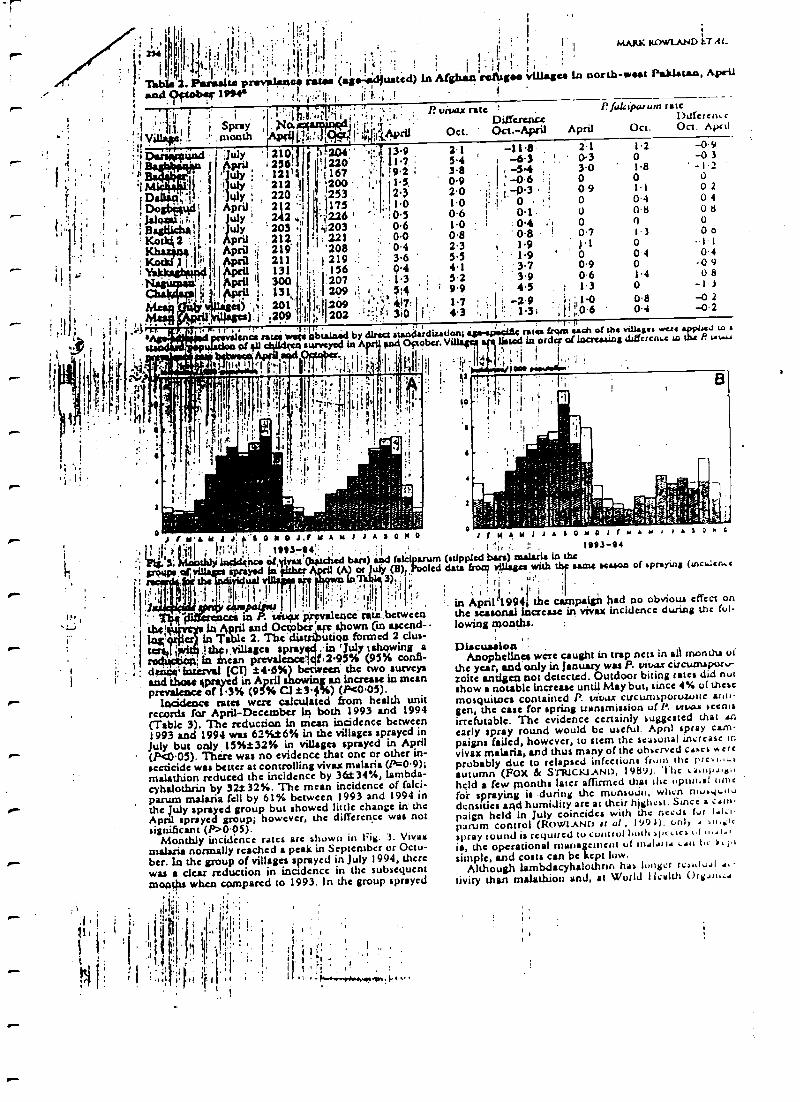
ff
r;.
: 1 I F i r -( .+ "
. , 1
l' ]1";
;I,i,.:+j,.,`,t,T.jl i,,,.p. r.. P.vicaxnte '
I i Spny '. Ia 1 .1Diffcrusu
.f V .naonth t{;:: i /-,r:l.'f(Aprii Oct. Oct.-Apri]'1:
i 1 üa'd . 1 ;July i 210 , 1 iZQ4' ' : 3G 7.1 -111.8
i °IDar
', _ ,+ ; 2s6!' j'l220' ';.. .
54'
, -63t2119 t 167 ' i9Z 38 S4 .
!## 219 ,1 '200 i' 14, 0.9 ! ; -0.6 ¡
;i DaWtq,1+
:July ; 220 ;I ?1233 . 123 20 ij ,,..-0.3 :
Doyd l I April; 212 "1 : 1173 ' ' :.1 1.0 1.0 ¡I ; 0
.;31119-104,,, '1 Lily ' 242 ,I ;226 ' 03 0.6 1 0.1 '
' , Ha8líklstl, 'j
u1y ' 203 /,' ;,1203 ' 0.6 1.0 : : 0.4
. ' Kode{ 2 : I 1 Apri! , . 212, I ; 221 , : 0.0 0.8 ' 0.8 (
2r131,11*''f' Apn7 .{ 219' I '208 0.4 2.3 1.9
: . April 211 11 1 219 .: ; 3.6.
; .
r,dd i 13t ii, 136 04 4.1 :'3.7i Tj I 300 I 207 ` .' 1 3 S 2 ' 3.9I 131 209 : 1 ,. 3,4
79.9 4.5
p) ,. 201 ., ,.' 109 ; 417. . 1 7 Z 9
MARK ROWLAND IT A1_
Pfalctparurn talc1)atfetenlc
April Oct. Oct. April
2.1 1.2 -0 9
' 03 0 -033.0 1r8 -12O 0 o0-9 0 2
04080
0.7 0 oJ.1 -1-10 04
-0 9U8
o -1 3
0.8 -0 204 -0-2
1l0 0.4O 080 0
t3004
0.9 00.6 14
rU11i' ;.09 11,4 ;.,202 ' 1'..a' 310 I j 43 .1.31 ;!!;06
I 11," , 4-o f - . 1 ..1( . T 11
enea ruq were obtained by direct ataaAudisadtsn; ans-apaeitl4 rates lr4m sach of she vJJaaaa were aptasJ e.
of ?u surveyed la Apt and Oftobu. V' listed in orda of increasing diHcrcnt:.c w t!u P. G.w+
Atx+t ! . .9 _ il '' ' ; ;
+/oa INhlasiw' I
'I
I,[:' :!:
tHI¡
11 t 1
o 1 I Ya Y J J r a 0 a 0 J.r Y A at J J A s O M 0
at {I i I11 : I 1993 -94' .'l loçldgisca cl,givaz Qtasdted ban) aJ fakiparum
tiprayed In fíthtF /1 (A) t July ($) Poolcdvipaa 1a Jaa+a 3):Í
1,1' II1ir:
1 , rr
ctx is P. sxvpx prevalence rits,bctwcenLh4ttfy a in ApP1 and Ocpobcs arc shown (an ascend-
in Table 2. The dis toga formed 2 dus-tom( ' (;villages spray to 'July t showing arodtcwpi Ia can prevalence 14.95% (95% confl-
i: i dttit' interval (al t46%) between the two surveys1 ' and those {prayed in April showirr an increase in mean
prevalence of .3% (95% Cl 13$ %) (P40.05).incidence rates were calculated from health unit
records for April- December In both 1993 and 1994(Table 3). The reduction in mean incidence between1993 and 1994 was 62%16% in the villages sprayed inJuly but only .15%t32% in villages sprayed in April(Pc0.05). There was no evidence that one or other in-secticide was better at controlling vivaz malaria (P=0.9);malathion reduced the incidence by 36t34 %, lambda -cyhalothrin by 32132%. The mean incidence of felci-parum malaria fell by 61% between 1993 and 1994 inthe July sprayed group but showed little change in theApnl sprayed group; however, the difference was notsignificant (P>0.05).
Monthly incidence rates arc shown in rig. 3. Vivaimalaria normally reached a peak in September or Octo-ber. In the group of villages sprayed in July 1994, therewas a dear reduction in inadence in the subsequentmonths when compared to 1993. In the group sprayed
;
i.
Ì i.r?! . - tv-- r+"w«At+. , .. .
r M M 1 1 . s o M o J r ,+ a, l a l
I '.i, :' 1993 -94(atippltd bars) malaria in thedata Prot? villages with tbp same season of &pnYina (tnca...en.e
1,1
'in April`199411 the campaign had no obvious effect onthe seasonal increase in vivax incidence during the ful-lowing months.
DlacusslouAnophelines were caught in trap nets inall months of
the year, acrd only in January was P. vivax circumspor '-zoite antigen not detected. Outdoor biting rates did notshow a notable increase until May but, since 4% of thesemosquitoes contained P. vivax circumsporusuite ar,u-gen, the case for spring transmission of P. vtl.a.a ccnieirrefutable. The evidence certainly suggested that .nearly spray round would be useful. Apnl spray cam-paigns failed, however, to stem the seasonal inrrcasc invivax malaria, and thus many of the observed cakes ...errprobably due to relapsed infections from the pre 1.,,.autumn (FOX & SrRICKLAND, 19891. 'I ht a41111).+1,0held a few months later affirmed that tilt optimal umcfor spraying is during the munsuúu, when nluay,wdensities and humidity are at their highest. Since a cam-paign held in July coincides with the ncods for t.1:1-parum control ( ROWLAND It a!, 199,1), only . eu ;lc
Spray toured is required to conuul both alcucathe operational management ut n,alatIi eau ti s.l1
simple, and costs can be kept low.Although lambdacyhalothnn has Ingrr rca,,lu.,I ..-
tivity than malathion and, at World Ilcalth ()meal..
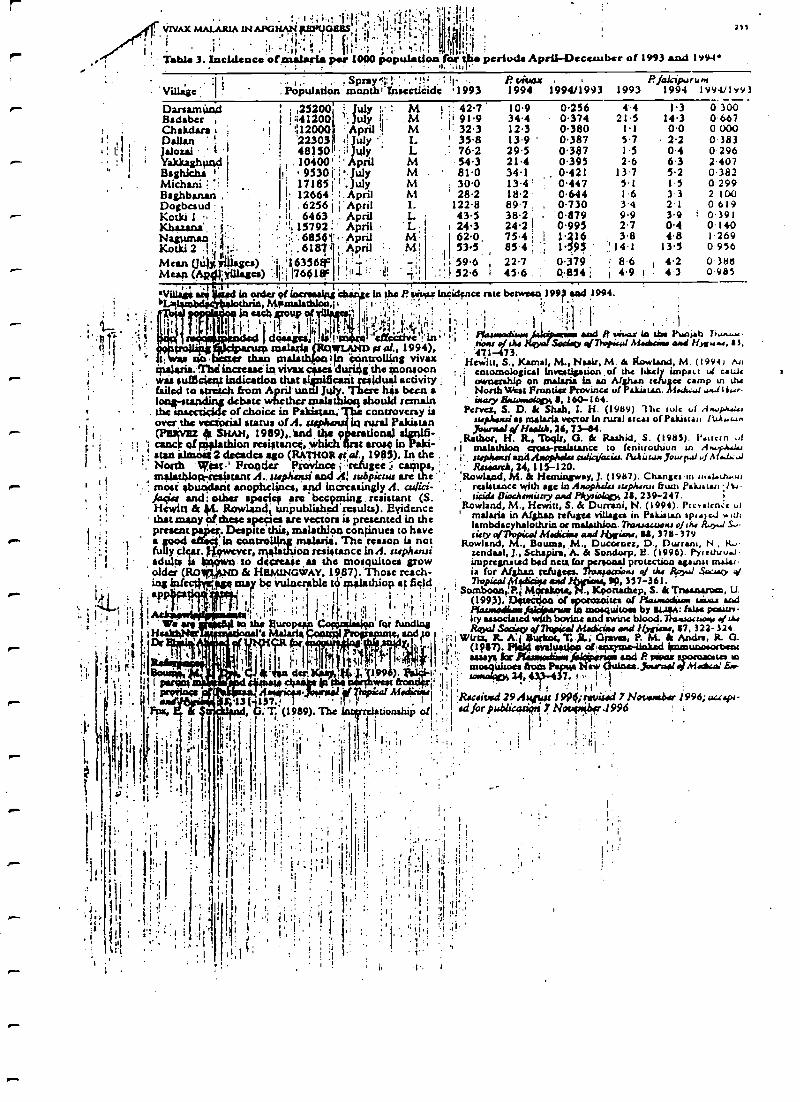
pm.
t j. ;vrvAx MA1J1RlA tN'AtGtlA1V tBñlJt788S , i i ! .;ì' i ;Í ,
,1:. ,I i',"i I ! 1V.;! ' ;:. , '. I,I.'
Table 3. Incidence olnaalaria per 1000 popuLtloa fR ulte periods Aprii-Deccaubcr of 1993 and 199.1t. .t,
2
,Sprayi:t .,1:VilLige :
Iç ' Population month! Tnaecticide '1993
R vivaz P./akrp.,rum1994 1994/1993 1993 1994 1994í1993.
Darsam(trtdBadaberChakdara t :
Dalian '
Jalozai .' '1
I
Baaghlcha IMichani ?Baghbanari ,
DogbcaudlKotki 1 ' 1
' ; ,25200' ;, July :. M 1 :: 42.7 10.9, 1 !;;41200 'July
iM i 91.9 34.4
I
:112000 ' April M 1 32.3 12.32303 t:')uly '; L ' 35.8 13.9 '
48)30 !; il July L ' 76.2 295. 10400 '' April M 54.3 21.4
I!: . 9530 ' I'July M' 81.0 34.117185 I .uly M : 30.0 13.4'
' 28.2 18.2122.8 89.7 . ,
' 43.5 38.2.I 24.3 242 I
1 12664 1. April M;I .6256
¡April I_
iI. 6463 .. April L.: i1 15792 ' April L
Nagytmañ : ': ' :'.. 685411"V April MKotki 2 ., ;.i . . ,' . 61874 ' M'
irlMean ()illy ',wages) 6336$°' 1 ; : ' 1 -'Meaft (Ap11;tfWages) 'j'¡76618F 1 1t1 i 1 ;':
,
ViUan 4.i
In osier of locreaairyglAl thrill MamalaMW/41 t
In each up ot't : ì t1t 1 j
.1.!( ''I 'lk 1.li I' , 41..krill:
gel, ! 18.!'d 94`l ` rya_ (RQWLAND rr 1994),
no beast than tnalaiiijo 1 n Controlling vivazmalaria. Mid increase' in vivaz cases during the monsoon
, i . wu sul5cien t Indication that flip ifcant residual activity ;failed to stretch from April until Jy}y There h*s been a
' 1 debate whether malt hioq should remaint the auuccdç ds of choice in Pakistan controversy is
over the vectorial status of A. in rural PakistanI ; (PStivliZ & SHAH, 1989),.1 nd, the 9 110041C I (*' rick of ptglathion resistance, which t erosC in -i I atan almost 2 decades ago (RATHOR Ital., 1985). In the
North West ' Frontier Province i refugee ;i camps,maladdo; reslztant A. rup/wui and Á; rubpicsua are the '
p- I ' 1 most abutidarit anophelinesa and incrcaaingiy A. cubes.-/near and; other specie f ire !becoming , resistant (S.
t Hewitt & 44. Rowland, unpublished results). Evidence:. ' that many cif these spetzea are vectors is presented in the
present Despite this, maluhloo continues to haves- i '' ì ' s good 'IA controlling alaria. The reason la not
fully clear. .tweyer, rt34Lthion rtsiatMCe Ind. stephuuiadults is to decrease u the mosquitoesgrowolder (RO & HEMINGWAY, 1987). Those reaút-ing intec*M fgq be vulnerable có'ralathiop at fiçld,
- , 1 sPp 4!g' t ; , ' ; IIII
I '
1;I ii. t' :r j! 1 !,,1,. 1; 1, ! ;t
. , ' We sec 1ó1bá sumps* C09;618411 fvi funding11 1 . 'a Malaria Cogan* c, wad jo
$otairr}, .1
.4 áa 1996). !,
'r
. k/rap ,}wpt . ,Ii
r.- . b1) i .
I pry içe1,(x,"37,,';r, ¡-'r"af
M.4tutel:
G.T. (1989). The lottouttion
11 ¡¡ . is
li ; -1.1 :1
0.256 4 4 1.3 0 3000.374 21.5 143 06670.380 11 0.0 0 0000.387 57 2.2 03830.3$7 1.5 0.4 02960.395 2.6 6.3 2.4070421 13.7 5.2 03820.447 5-1 1.5 02990.644 1 6 3 3 2 1000.730 3.4 21 06190.879 9.9 3.9 ` 0 3910.995 2.7 04 0.140
1I62
0, . 75 4; ;
1.4263.8 4.8 1.269
535 8S 4 ; 195 ,' !4 1 13 S 0 956
, 59.6 22.7 0379 8.6 I 42 0 31itl:' 152.6 I 45.6 . . 0.854 ;
;4.9 i 4 3 0 985
e ln the P. visses Incidçnce rate bctwoan,1993 and 1994.
;I:I. :y.
' ra of X4YV0 9I1d Aladsrv Dorf NXu+r, 13,471-473.
Hewitt, S., Kama!, M., Hoak, M. at i(owland, M. (1994 ) Anentomological investigation of the likely impat u[ atJc
I ownership on malaria In an Afghan tch+iioe camp ,o tiu; North West Ponder Province uf Pakistan. M.tk..J
mar>. 6wr.wtafogx 8, 160-164.Pcrvcz, S. D. á Shah, I. H. (1989) 17,c cols t.( A,..,.r,.t..
apAa,csi as malaria vector in rural arca, of Pakista, /itAt.un,arwalg/HeaW, lg, 73-84.
Robot, H. R,'Ibglt, G. 8c Rashid, S. (1985). l'.ticrn l
I malathloA erou-rsalatanee to feniuothiun tn A.N.4sI'. rtepAatsi and droop/Wm uJici/acia,. A,Jtù t.u. )oto rt.I l A ..e..,r
Raiarrh, 24, 115-120.'Rowland, M. á Hemingway', J. (1987). Changetn ,n,t.tlu 4t
resistance with age In Awophc4, ,upkaw &um Paktut l t, -acid. Ll¡ocha,wùtry and Plkyrioltpy, 28, 239-247.
Rowland, M., Hewitt, S. á Durrani, N. (1994). Prc..lcn:c' malaria in Afghan refugee villages in Pakistan sp(i)c..! with
lambdacyhalothrin at rnalarhlaw. 7)a,uausow, al rk.cia0 of7i,pcd Madiciae awdl{tow, ai, 378-379
Rowland, M., Bourns, M., Dueocoez, D., Durran,, N ,zendul, I., Seha ira, A. á Sontiorp, 1?. (1996). Pyretiu...iimpregnated bed neta for personal protection against ataiaria for Afghan refugees. 71ow}ocriow. q/ cka iiajul Sa+cp. a7hpical fiiiaìt¡a and !Q, 357-361.
! Somboan,,P.d Mgrakotq, i'f., Kpottuhep, S. a{ Trirastuvm, U.(1993). Dfctloa of aippott000zpglles of Piaawtaditott t:..aa and
faiieiry with bovine and swinetbloodThw,ocuo+t .Rq3nl Sa,ifOr q/7ktpicad Madüwa and Nygiawe, 87,322-324
ï iI Wirts. R A,i Btitkot. T, F.; G;avss, P. M. á Amin, R Q.
(1987). I+k14 evaluation Qf;eoupma-unk.d ymmuooaoccsnti.; ' aassy4 for lKfrtitotrw and P. tuiaaa e,pouao+tw io
. . mosquitoes ikons P,apt3a.7bvr+al d M.ócd 6.totwaritp 34, ¢3,1-4 7. 1 ,, I ' .
1 ! !;'
I
I
o urd 29AY¢;
1996;I pablicariQrt7 Ñ7t bF9b
1!
ausp(-
I.
and R tiara: la the Puni4 7'w..+.-
,-
-
TRANSACTION:. " sOCIETY Ct uL MEDICINE AND HYGIENE (1997) 91, 152 -255
Transmission and control of vivax malaria in Afghan refugee settlements inPakistan
Mark Rowlands, Sean aeem Durranil, Naviceda Bano2 and Robert Wirtz, 1HeahhNet Interna-tional RO. Box 889, Peshawar, Pakistan; 2United Nations High Co, nnission for Refugees, PO. Box 1263, Islamabad, l'ak,-stan; JDepartment of Esstomology, l9bIter Recd Army Instituter Medical Rauarclt, U%:hingtun, DC 20307 -5100, USA
AbstractRegular biting collections were conducted in 1993 -1994 to investigate seasonal fluctuations in the abun-dance of anophelines in Afghan refugee villages in north- weitern Pakistan. Enzyme -linkedimmunosorbent assays were used to test heads -plus- thoraces for the presence of malaria sporozoites.Anophelines giving positive results foi Plasmacl' vivax were captured in every month except January.Nine species were positive. Biting rates showed a marked increase in May, after the spring rains, and thusspring transmission of vivax malaria seems certain. However, transmission of vivax malaria reached itspeak only after the monsoon in July. To determine the optimal time to control vivax malaria by indoorspraying with residual insecticide, spray campaigns were conducted in either spring or summer in 14 ref-ugee villages. Villages sprayed in July 1994 showed a mean reduction in annual incidence of 62% (95%confidence interval (CI) i 6%) relative to the previous year, whereas villages sprayed in April 1994 showedonly a 15% reduction (95% Cl 132 %). Parasite prevalence surveys conducted in April and October 1994confirmed the greater efficacy of spray campaigns waged in July.The insecticide malathion proved as ef-fective as the pyrcthroid lambdacyhalothrin, even though several species of anopheline were resistant tomalathion.
Keywords: malaria, Plasmodium vivax, Anopheles app., spisrozoite rate, biting rate, control, malathion, lambdacyha-lothrin, refugees, Pakistan
IntroductionMalaria is a major health problem for Afghan refugees
in Pakistan (ROWLAND et al., 1996).. Transmission isseasonal, and the main method of control is indoorspraying with residual insecticide. The annual spraycampaign starts in mid July, during the monsoon. Thisis the best time to control transmission of falciparum=lade, the first new cases of which are usuallyobserved in late August. If the campaign is delayed, anepidemic may ensue (unpublished observations). Al-though the campaign is directed primarily againstPlasmodium faleipanttt (see BOUMA et al., 1996), 70% ofmalaria in Afghan refugees is caused by P. vivax (secROWLAND tt al., 1994). Control of this species deservesgreater attention, especially now that falcipntum malariais being successfully curtailed (UNHCR, unpublishedreport). The first cases of vivax malaria, appear muchearlier, in April. Since precision timing is critical to thesuccessful control ofP. Pale pannst, itis conceivable thatan earlier spray campaign in villages where P. vivaxpredominates would be more effective in reducing P.vivax transmission. But first it needs to be shown thatthe early cases are due in pan to new transmission andnot just to relapses from the previous year. Theoccurrence in spring of anophelines naturally infectedwith P. vivax would justify an early spray round. Thefirst part of this paper describes the seasonal variation inanophelines and their sporozoite rates. The second partcompares the effect of spray campaigns waged in springor summer on the prevalence and incidence of vivaxmalaria in indicator villages.
MethodsEntomological surveys
During 1993 and 1994, seasonal fluctuations inanopheline densities in Azakhel refugee village in north-western Pakistan were monitored by means of monthlycollections from 4 trap nets, each baited with a singlecow (HEWITT a al., 1994). The sides of the nets wereraised 0.3 m above the ground to allow mosquitoes toenter. A two -man team at each site made collectionsfrom the inside of the net throughout the night. Afteridentification to species, these collections were proc-essed for enzyme -linked immunosorbent assay (ELISA).To minimize the risk of false positive results caused bycontamination of samples with bovine blood (Som.BOON et al., 1993), specimens acre dried and then the
head -plus -thorax was separated from the abdomen ofeach mosquito. Although human catches would havebeen preferable, the cost of hiring enough staff to yieldthe numbers of anophelincs required for this studywould have been prohibitive.
Gnayins- linked immunosorbent assayThe ELISA reagents were supplied by the Walter Recd
Army Institute for Medical Research, Washington, DC,USA, The heads -plus- thoraces of mosquitoes of knownspecies and collection site were tested in batches of 1 Ufor the presence of circumsporozoitc antigens (CSAs) ofP. vivax (variants 210 and 247) and P. falcipanun.Batches of laboratory- reared, uninfected Anophelesnephetasi acted as negative controls.
Procedures were the sume as those described byWIRTZ et al. (1987), with minor modifications. 'shirtyminutes after the addition of peroxidasc substrate, ab-sorbance was measured at 414 mn with an ELISA !iliacreader (Cambridge life Sciences, Cambridge, UK). Atest well was considered positive if it gave a visible greencolour and an absorbance value greater than twice themean absorbance of the 5 negative controls.
Insecticide campaignsRefugee villages from 3 adjacent districts of the North
West Frontier Province in Pakistan participated in thestudy. Eight villages were randomly selected for spray-ing in April, and 6 villages for spraying in July (2 othervillages scheduled for spraying in July had to be exclud-ed owing to pesticide shortage). Five of the villages weresprayed with the pyrethroid lambdacylalothrin at 10mg/m2 (Icon ", 10% wettable powder; Zencca) and 9with the organophosphate malathion at 2 g/m2 (50%wettable powder; Cheminova). HealthNct Internationalmalaria inspectors conducted population censuses whilesupervising the spray teams. Insecticide coverage wassatisfactorily high (97% of the 23708 houses weresprayed). The quantities consumed (1 1000 kg ofmalathion and 600 kg of lambdacyhalothrin) were can -sistentbetween villages. Application rates in differentvillages ranged from 1.2 -1.4 houses/kg with malathionand 13 -18 houses/kg with lambdacyhalothrin.
ClimateClimatic variables, recorded daily at the Pakistan Air
Force base in Peshawar, Pakistan, were consolidated
SOCIETY MEETING; POSTER PRESENTATIONS 251
grandfathers; their age range was 22 -69 years. Nearly allmothers had attended antenatal, clinics and most haddelivered within a health service facility. Virtually all hadnoticed the problem themselves before consultinghealth workers who, they felt, had not provided ade-quate information about their children's needs. Theyfound it difficult to attend physiotherapy or get equip-ment because of the distances and costs involved. Thereis no social welfare system and the education 'system isnot orientated to meet the needs of children with learn-ing difficulties.
Carers in the 'third world' are under panicular strainat present as the structural programme is implemented.They are denied the information which could allowthem to identify their children's needs and address themaccordingly. Can health promotion empower them for abetter quality of life, for both them and their depend-ents?
Can kerosene oil lamps be used for personal pro-tection against mosquitoes?
11.N'. Pates, J. E. Miller and J. D. Lines Departmentof ,ticdical Parasitology, London School of Hygiene andTropical Medicine, Ksppsl Street, London, WCIE 7H7',UK
The effectiveness of a cheap and easy method ofhousehold protection against mosquitoes was investi-gated in Dar es Salaam, Tanzania. Two methods ofheating the volatile synthetic pyrethroid, transfluthrin,in kerosene oil lamps were investigated in 2 consecutivestudies by means of human landing catches in a LatinSquare design.
In Study I, transfluthrin was incorporated into thekennene in a lamp at a concentration of 0.1% as in aprevious study in India (SIIARMA, V. P. a ai., 1993: In-dian Journal of Malariology, 30, 169 -176). This treat-ment reduced mean biting rates by 27%, which was notsignificantly different from the control. In another lampa 0.1% solution of transfluthrin in vegetable oil wasplrreJ in a specially designed 'crucible' held on a standJust above the flame. This produced a significant'redtic-
lion in biting of 54 %. Mosquito coils reduced biting by38 %, significantly different from the control but notfrom the 'crucible' treatment,
In Study 2, transfluthrin dissolved in the kerosene wastested again at 0I% and also at the higher concentra-tion of 1%. The latter gave a significantly greater de-crease in mean bitin4 rates (44% vs. 15%). The'crucible' treatment again gave the greatest reduction inmean biting rates (78%).(This poster shared the prize as the best at the meeting.(
Primary health care: assessing progress in Nigeria
J. M. Udie Health Care Policy and Management,Heath Services Management Cesare, University of Binsring-hant, 40 Egbaston Park Road, Birmingham, BLS 2lí'7; (. K
Primary health care (PHC) in the last 3 decades hasemphasized the use of 2 models: 'selective' (SPHC) and'comprehensive' (CPHC). Both models however tendto share a weakness in terms of their capacity to incor-porate aspects of the local context of health care sys-tems.
The underlying objectives of PHC emphasize thegrowth and extension of basic health services and re-quire a cross -sectional approach based on local commu-nities. This complexity adds to the difficulties ofimplementation.
This research offers an analytical framework of di-verse methods that can be used to evaluate whetherprogress has been achieved in the implementation of thePHC strategy. The method reflects a multi- disciplinarymake -up oft the research endeavour, thereby creating a'triangulation' or ethnographical approach to the studyobjectives.
The research emphasizes the development of totalquality systems (MAXWELL, R. J., 1984: British MedicalJournal, 288, 1470 -1472), within a more inclusive andlocally sensitive programme structure. It argues thatsuch systems enable rather than inhibit the developmentand delivery of adequate health care capable of address-ing lucal economic and social variables.
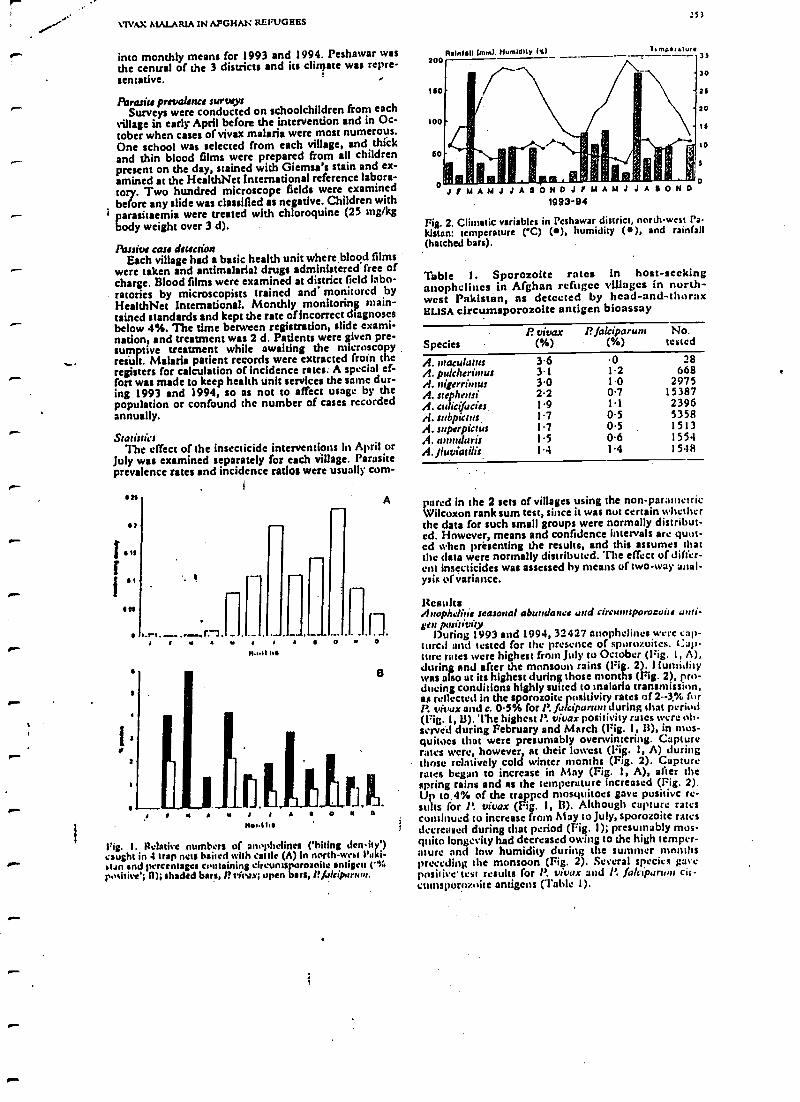
rMAX ASALARIA IN AFGHAN REFUGEES
into monthly means for 1993 and 1994. Peshawar wasthe central of the 3 districts and its climate was repre-sentative. '
Parasite prevalence surveysSurveys were conducted on schoolchildren from each
village in early April before the intervention and in Oc-tober when cases of vivax malaria were most numerous.One school was selected from each village, and thickand thin blood films were prepared from all childrenpresent on the day, stained with Giemsa's stain and ex-amined at the HealthNet International reference labora-tory. Two hundred microscope fields were examinedbefore any slide was classified as negadve. Children with
' parasitaemia were treated with chloroquine (25 mg/kgbody weight over 3 d).
Passive can detectionEach village had a basic health unit whereblood films
were taken and antimalarial drugs administered free ofcharge. Blood films were examined at district field labo-ratories by microscopists trained and monitored byHealthNet International. Monthly monitoring main-tained standards and kept the rate of incorrect diagnosesbelow 4%. The time between registration, slide exami-nation, and treatment was 2 d. Patients were given pre -sumptive treatment while awaking the microscopyresult. Malaria patient records were extracted (min theregisters for calculation of incidence rates. A special ef-fort was made to keep health unit services the seine dur-ing 1993 and 1994, so as not to affect usage by thepopulation or confound the number of cases recordedannually.
StatisticsThe effect of the insecticide interventions in April or
July was examined separately for each village. Parasiteprevalence rates and incidence ratios were usually corn-
0 -
111
fr 16l
6s
t
s
-.-a.
A
Fig. 1. Relative numbers of an.y+helines ('kiting density')caught in 4 trap nets baited with cattle (A) in north -west Paki-stan and percentages containing circunls oroaoite antigen (.%positive; ll); shaded bars, f? vitvx; open bus, f' /alciparlu,r.
200
1110
loo
60
Rainfall imml. Humldllr 1%)
:53
1, moil :ur33
30
26
20
is
so
.,.., .., .
o J f M A M J J A a 0 H 0 J r M A M J J A a 0 N 0 0
1993 -94
Fig. 2. Climatic variables in Peshawar district, north -west Pa.kistan: temperature (C) (a), humidity (), and rainfall(hatched bars).
Table 1. Sporozoite rates in host -seekinganophcliucs in Afghan refugee villages in north-west Pakistan, as detected by head -and -thoraxI L1SA circusnsporozoite antigen bioassay
SpeciesI? vivax
(%)1? falciparunt
( %)No.
tested
A. rrtaculauu 3.6 0 28A. pulcherinrut 3.1 1.2 668A. rtigerriutus 3.0 1.0 2975A. steplreusi 2.2 0.7 15387A. urliquciu 1.9 1.1 2396A. subparts 1.7 0.5 5358A. sttperpictus 1.7 0.5 1513A. annular": 1.5 0.6 1554A. /luviatilis 1.4 1.4 15.18
pored in the 2 sets of villages using the non -parametricWilcoxon rank sum test, since it was nut certain whetherthe data for such small groups were normally distribut-ed. However, means and confidence intervals are qum-cd when prbsenting the results, and this assumes thatthe data were normally distributed. The effect of differ-ent insecticides was assessed by means of two -way anal-ysis of variance.
ResultsAuophelirie seasonal abundance and circuuuporocuife urui-ten positivity
During 1993 and 1994, 32427 anophcliucs were cap-tured and tested for the presence of spurozoites. Cap-ture rates were highest (rain July to October (Pig. I, A),during and after the monsoon rains (Fig. 2 . Humiditywas also at its highest during those months (Trig. 2), pro-ducing conditions highly suited to malaria transmission,as reflected in the sporozoite positivity rates of 2 --3.% (.rl'. vivax and c. 0.5% for P. falcipunuu during that period(frig. 1, II). The highest l'. vivax positivity rates were ldh-scrvéd during February and March (Fig. 1, li), in mos-quitoes that were presumably overwintering. Capturerates were, however, at their lowest (Fig. 1, A) duringthose relatively cold winter months (Fig. 2). Capturerates began to increase in May (Fig. 1, A), after thespring rains and as the temperature increased (Fig. 2).Up to 4% of the trapped mosquitoes gave positive re-sults for P. vivax (Fig. I, 13). Although capture ratescontinued to increase from May to July, sporozoite ratesdecreased during that period (Fig. 1); presumably mos-quito longevity had decreased owing to the high temper-ature and low humidity during the summer monthspreceding the monsoon (Fig. 2). Several species gavepositive' test results for P. vivax and P. falcipartun cit-cumspornz..ite antigens (Table I).
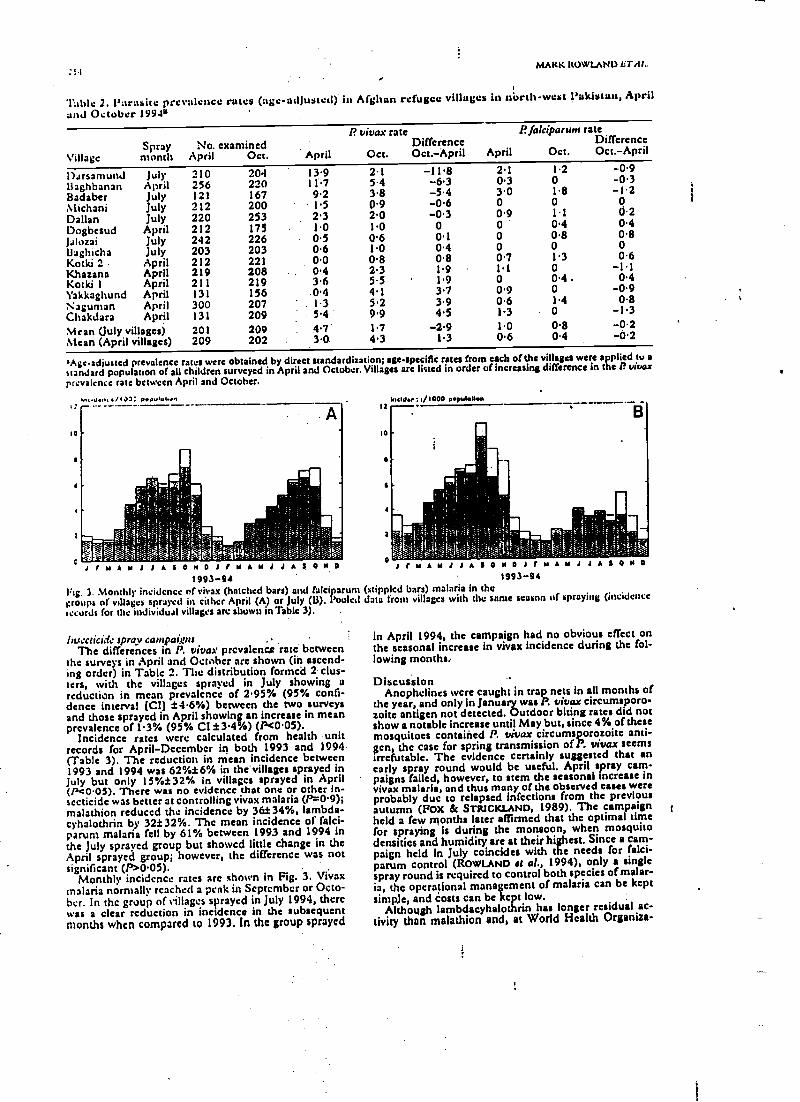
MARK ROWLAND l:TAM..
Taisle 2. Parasite prevalence rules (age-adjusted). in Afghan refugee villages in north -west !'akistun, Apriland October 1990
VillageSpraymonth
No. examinedApril Oct. April
P. vivax rate
Oct.DifferenceOct.-April April
PJalciparunt rateDifference
Oct. Oct. -April
1)arsanund Jul. 210 204 13.9 2.1 -11.8 2.1 1.2 -0.9
Baghbanan April 256 220 11.7 5.4 -6.3 0.3 0 -0.3
Badaber July 121 167 9.2 3.8 -5.4 3.0 l8 -12Michani July 212 200 1.5 09 -0.6 0 0 0
Dallan July 220 253 2.3 2.0 -0.3 0.9 1.1 0.2
Dogbesud April 212 175 1.0 10 0 0 ' 0.4 0.4
Jalozai July 242 226 0.5 0.6 0.1 0 0.8 0.8
i3aghicha July 203 203 0.6 1.0 0.4 0 0 0
Kotki 2 April 212 221 0.0 0.8 0.8 0.7 13 0.6
Khazana April 219 208 0.4 2.3 1.9 1.1 0 -11Kotki 1 April 211 219 3.6 55 1.9 0 0.4 . 0.4
l'akkagltund April 131 156 0.4 4.1 3.7 0.9 0 -0.9
Naguntan April 300 207 1.3 5.2 3.9 0.6 1.4 0.8
Chakdara April 131 209 5.4 ' 9.9 4.5 l3 0 -13Mean (July villages) 201 209 4.7 1.7 -2.9 1.0 0.8 -0.2Mean (April villages) 209 202 3.0. 4.3 1.3 0.6 0.4 -0.2
'Age-adjusted prevalence rates were obtained by direct standardization; age-specific rates from each of the villages were applied to astandard population of all children surveyed in April and October. Villages are listed in order of increasing difference in the P. vivaz
prevalence rate between April and October.
M<d.../IaJ: ppulul.rn
J I V A M A A A A A A A A A A A A A A A1993 -94
Fig. 3. Monthly incidence of vivax (hatched bars) and fakiparumgroups of villages sprayed in tither April (A) or July (li). Pooledtocards for the individual villages are shown in Table 3). .
Iluecticidc spray cantpait,'niThe differences in P. vivax prevalence rate between
the surveys in April and October are shown (in ascend-ing order) in Table 2. The distribution formed 2 dus-ters, with the villages sprayed in July showing areduction in mean prevalence of 2.95% (95% confi-dence interval (CI) t4.6 %) between the two surveysand those sprayed in April showing an increase in meanprevalence of 1.3% (95% CI t 3.4%) (P<0.05).
Incidence rates were calculated from health unitrecords for April -December in both 1993 and 1994(Table 3). The reduction in mean incidence between1993 and 1994 was 62 %t6% in the'villages sprayed inJuly but only 15 %i32% in villages sprayed in April(Pe0.05). There was no evidence that one or other In-secticide was better at controlling vivax malaria (Pr-0.9);malathion reduced the incidence by 3fet34 %, lambda -cyhalothrin by 32 #32 %. The mean incidence of falci-parum malaria fell by 61% between 1993 and 1994 inthe July sprayed group but showed little change in theApril sprayed group; however, the difference was notsignificant (P>0.05).
Monthly incidence rates arc shown in Fig. 3. Vivaxmalaria normally reached a peak in September or Octo-ber. In the group of villages sprayed in July 1994, therewas a clear reduction in incidence in the subsequentmonths when compared to 1993. In the group sprayed
Mltld : 0000 population
M A M J J A f 0 M 0 J r M1993-94
(stippled bars) malaria in thedata from villages with the same season of spraying (incidence
in April 1994, the campaign had no obvious effect onthe seasonal increase in vivax incidence during the fol-lowing months,
DiscussionAnophelines were caught in trap nets in all months of
the year, and only in January was P. vivaz circumsporo-zoite antigen not detected. Outdoor biting rates did notshow a notable increase until May but, since 4% of thesemosquitoes contained P. vivaz circumsporozoite anti -gen, the case for spring transmission ofP. vivaz seemsirrefutable. The evidence certainly suggested that anearly spray round would be useful. April spray cam-paigns failed, however, to stem the seasonal increase invivax malaria, and thus many of the observed cases wereprobably due to relapsed infections from the previousautumn (FOX & STRICKLAND, 1989). The campaignheld a few months later affirmed that the optimal timefor spraying is during the monsoon, when mosquitodensities and humidity are at their highest. Since a cam-paign held in July coincides with the needs for falci-parum control (ROWLAND et al., 1994), only a singlespray round is required to control both species of malar-ia, the operational management of malaria can be keptsimple, and costs can be kept low.
Although lambdacyhalothrin has longer residual ac-tivity than malathion and, at World Health Organiza-
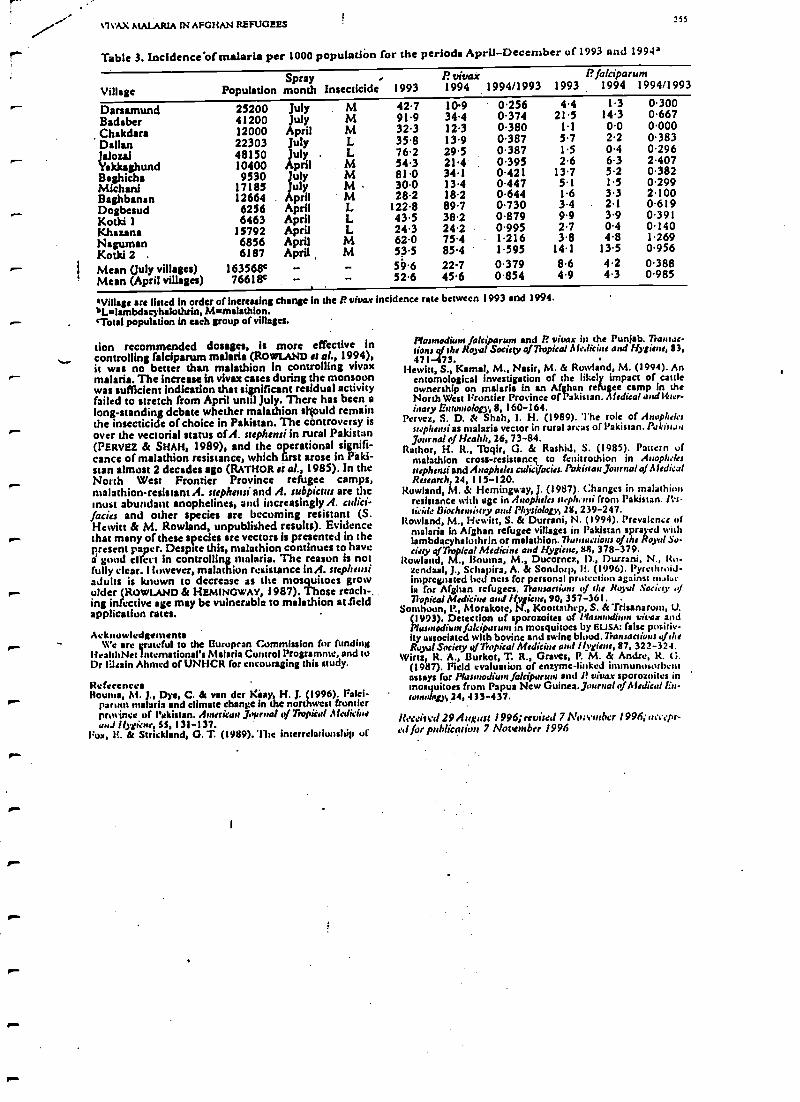
.-
%WAX MALARIA it AFGHAN REFUGEES
Table 3. Incldence of malaria per 1000 populatlòn for the periods April- December of 1993 and 1994'
255
VillageSpray
Population month Insecticide 1993R vivax1994 1994/1993
P. falciparum1993. 1994 1994/1993
Darsamund 25200 July M 42.7 109 0.256 4.4 1.3 0.300
Badaber 41200 July M 91.9 34.4 0.374 21 5 14.3 0.667
Chakdara 12000 April M 32.3 12.3 0.380 1 1 0.0 0.000
Dalian 22303 July L 358 13.9 0.387 5.7 2.2 0.383
Jaloui 48150 July L 76.2 29.5 0.387 1.5 0.4 0.296
Yakkaghund 10400 April M 54.3 214 0.395 2.6 6.3 2.407
Baghicha 9530 my M 81.0 34.1 0.421 13.7 5.2 0.382
Michani 17185 my M 30.0 13.4 0.447 5.1 1.5 0.299
Baghbanan 12664 pril M 28.2 18.2 0.644 1.6 3.3 2.100
Dogbesud 6256 April L 122.8 89.7 0.730 3.4 2.1 0.619
Kotki 1 6463 April L 43.5 38.2 0.879 9.9 3.9 0.391
Khazana 15792 April L 24.3 24.2 0.995 2.7 0.4 0.140
Nagurnan 6856 April M 62.0 75.4 1.216 3.8 4.8 1.269
Kotki 2 . 6187 April M 53.5 85.4 1.595 14.1 13.5 0.956
Mean (July villages) 163568c 59 6 22.7 0379 8.6 4.2 0.388
Mean (April villages) 76618e 52.6 45.6 0.854 4.9 4.3 0.985
'Village are listed in order of increasing change in the r vivax incidence rate between 1993 and 1994.bLnlambdacyhalothria, M =malathion.'Total population in each group of villages.
lion recommended dosages, is more effective incontrolling falciparum malaria (ROWLAND et al., 1994),it was no better than malathion in controlling vivaxmalaria. The increase in vivax cases during the monsoonwas sufficient indication that significant residual activityfailed to stretch from April until July. There has been along -standing debate whether malathion s)vrould remainthe insecticide of choice in Pakistan. The controversy isover the vectorial status of A. siephenri in rural Pakistan(PERVEZ & SHAH, 1989), and the operational signifi-cance of malathion resistance, which first arose in Paki-stan almost 2 decades ago (RATHOR et al., 1985). In theNorth West Frontier Province refugee camps,malathion- resistant A. riephemi and A. subpiattl arc themost abundant anophelines, and increasingly A. aid-facia and other species are becoming resistant (S.Hewitt & M. Rowland, unpublished results). Evidencethat many of these species are vectors is presented in the¡iresent paper. Despite this, malathion continues to havea goad effect in controlling malaria. The reason is notfully clear. l luwever, malathion resistance MA. rrephensiadults is known to decrease as the mosquitoes growolder (ROWLAND & HEMINGWAY, 1987). Those reach-.ing infective age may be vulnerable to malathion Wieldapplication rates.
AcknowledgementsWe arc grateful to the European Commission for funding
IiealthNet International's Malaria Control Programme, and tuDr levain Ahmed of UNHCR for encouraging this study.
Reference,Houma, M. J., Dye, C. & van der ki+ay, H. I. (1996). Falci-
parum malaria and climate change in the northwest frontierprovince of Pakistan. American journal u, /7iopical Medicineand Ilygt'enr, SS, 131 -137.
Pox, 1i. & Strickland, G. T. (1989). lise interrelationship of
Plasmodium falciparum and P. vivax in the Punjab. Transac-tions gqfJthe Royal Society q/7hspica! AleJicine and Hygiene, 83,471-473.
Hewitt, S. Kemal, M., Nasir, M. & Rowland, M. (1994). Anentomological investigation of the likely impact of cattleownership on malaria in an Afghan refugee camp in theNorth West Frontier Province of Pakistan. Aledical andl1ter-inary Entomology, 8, 160 -164.
I'ervez, S. D. & Shah, I. H. (1989). The role of /loop/irkss ephessi as malaria vector in rural areas of l'akistan. Paki a.,journal of Health, 26, 73 -84.
Rathor, H. R., Toqir, G. & Rashid, S. (1985). Pattern ofmalathion cross- resistancç to fenitrothion in Anopheles
stephouiand Anopheles csdicjfacies. Pakistan journal of AledicalResearch, 24, 115 -120.
Rowland, M. & Hemingway, J. (1987). Changes in malathionresistance with age in Anopheles mephemdi from Pakistan. !S,.ricide Biochemistry and Physiology, 28, 239 -247.
Rowland, M., Hewitt, S. & Durrani, N. (1994). Prevalence ofmalaria in Afghan refugee villages in Pakistan sprayed withlambdacyhalothrin or malathion.?iannic:ions of ;he Row! So-ciety of Tropical Medicine and Hygiene, 88,378-379.
Rowland, M., Houma, M., Ducorncz, I)., Durrani, N., It.,.zcndaal, J., Schapira, A. & Sondorp, H. (1996). Pyrcthroid-impregnated bed nets for personal prutcc ' against molaris for Afghan refugees. Trainee ' ,/ the Royal Society of7iopieal Medicine and gv use, 90, 357 -361.
Somlwun, P., Morakotc, N., Koottathrp, S. & Trisanaran, U.1993). Detection of sporozoites of Plasmodium vitrai andusmodiumfalciparum in mosquitoes by ELISA: false positiv-
ity associated with bovine and swine blood. 7la,uacsiom oldieRoyal Society of7Yopical Msdici,re and !ltgie,se, 87, 322 -324.
Wirtz, R. A., Burkett, T. R., Graves, P. M. & Andre, R. Q.(1987). Field evaluation of enzyme -linked intmunosutbeutassays for Plasmodium la/ciparum, sud P vivax sporozoites inmosquitoes from Papua New Guinea. journal of Alediu,l En-tomology, 24, 433 -437.
/leceinvl 29 August st 1996; revised 7 Noi.esmhcr 1996; accept-ed for publication 7 November 1996
TRANSACTIONS OFTHL' ROYAL SOCIETY OFTROPICAL ML'1)iCIND AND HYGIENE (1997) 91, 256 -262
The epidemiology of severe malaria in an area of low transmission in Thailand
Christine Luxembur er1,2,3 Françoise Ricci3, François Nostent'2'4, Dominique Ralmond3, Saw Hathetiand Nicholas J. White12.4 IShoklo Malaria Research Unit, Mas Sot Thailand;2Faculty of7lrpical Medicine, MakidolUniversity, Baa ;kok, Thailand; 3i14idecins Sans Frontières, Paris, France; 'Centre for Tropical Medicine, Nitf eld Departmentt'í Clinical John Radcliffe Hospital, Oxford, UK
AbstractThe predisposing factors, clinical presentation, and outcome of severe malaria in a Karen communityliving on the western border of Thailand were studied over a period of 2 years. This was an area Of lowmalaria transmission (approximately one infection per person per year), where asymptomatic malaria isunusual. In a population of 4728 persons, who had good access to facilities for malaria diugnosis andtreatment, there were 2573 cases of vivax malaria, none of whom died, and there were 5776 cases offalciparum malaria, 303 (5 %) of whom had severe malaria and 11 (0.2%) of whom died -a case fatalityrate of 1.9 per 1000 (95% confidence interval CI) 1.0 -3.3). The risks of developing severe malaria anddying declined steadily with age. The clinical features of severe malaria differed between Children andadults. Anaemia was more common in children under 5 years old than in older children and adults,whereas the incidence of cerebral involvement increased with age. Severe malaria was 3 times (95% CI1.4 -6.2) more common in pregnant than in non -pregnant women, but was 4.2 times (95% Cl 2.3 -7.9)less common in patients with mixed Plasmodium faktparunl and l' vivax infections than in those with Efalciparum alone, suggesting that I? vivax may attentuate the severity of P. fakiparuut malaria.
Keywords: malaria, Plasmodium falciparum, flavored vivax, epldemlology,Thailand
IntroductionThe clinical pattern and age distribution of severe ma-
laria varies with the intensity of transmission. In areas ofhigh and stable transmission, severe malaria is confinedmainly to the first 3 years of life and manifests predom-inantly as severe anaemia, whereas with lower and moreseasonal patterns of transmission the age distributionshifts upwards and cerebral malaria becomes the pre-dominant clinical manifestation of scvcrc malaria(BRUCE- CHWATT, 1952; GREENWOOD et al., 1987;11OLYNEUX et al., 1989; BREWSTER Ö. GREENWOOD,1993; SNOW et al., 1993; MARSH et al., 1995; WALLERa al., 1995). At even lower levels of malaria transmis-sion, severe disease may occur at all ages (W111Tl!,1996). Syndromes which arc relatively rare in child-hood, e.g., acute renal failure, pulmonary oedema, andsevere jaundice, are common manifestations of severemalaria in adults. In this epidemiological context preg-nant women are at particular risk of developing severemalaria, and have high maternal and fetal mortality rates(NosTEN et al., 1991a).
Among the Karen people in eastern Myanmar andwestern Thailand, multi -drug resistant falciparum ma-laria is the most important medical problem, despite rel-atively low levels of transmission ( <1 infection perperson per year) (LUXEMDURGER et al., 1996). Sympto-matic and severe malaria are seen at all ages. Prospectivestudies of the clinical epidemiology of malaria in thiscontext (which is similar to that found in many parts ofeastern Asia) are difficult because populations are usu-ally widely dispersed in forested areas.and malaria trans-mission often varies considerably over short distances(RoseN8ERG et al., 1990). We describe a prospectivestudy conducted in an unusually large population of dis-placed persons that aimed to quantify the clinical bur-den and to describe the age- specife clinical features ofsevere malaria.
MethodsStudy sua
Tlu study site and the epidemiology of malaria in thisarea have been described previously (NOSTEN et al.,1987; DOLAN et al., 1993; et al., LUXLMDURGER cl al.,1996). In brief, Shoklo is a large camp for displaced per-sons of the Karen ethnic minority, situated in forested
Address for correspondence: Dr CI ' 'ne Luxemburger,Shoklo Hilmi., Research Unit, P.O. Mix 46, 63110 Mae Sot,Thailand; fax +66 55 532 637.
hills, 120 km north of Mai Sqt on the western border ofThailand. Malaria occurs throughout the year with 2seasonal peaks, one at the beginning of the rainy season(Ma July) and the other during winter (Novem-ber-January). Plasmodium vivax and multi -drug resist-ant P. falciparut occur with approximately equalincidences, although the age distribution of the 2 infec-tions differs considerably. P. usalanac is rare. A detailedprospective survey conducted in 1992 provided an esti-mated malaria incidence rate of 1.0 infection per personper year (95% confidence interval (CI) 0.9 -1.1): 47% ofthe cases were caused by P. falciparum, either alone(37 %) or mixed with P. vivax (10 %). The estimatedmean pyrogenic density, or threshold parasitaecnia atwhich symptoms occurred, was low and similar to thatreported previously in non- immune persons: an esti-mated 1460 parasites/1iL. for P. falciparum and 181/ALfor P. vivax. Most of the subjects (87 %) with malariaparasites detected during population surveys became ill,and this progression to symptoms was equally likely atall ages. The incidence of falciparum malaria increasedwith age and the majority of cases (92%) were diag-nosed In children over 5 years old and in adults, whereasthe incidence of vivax malaria decreased with age (Lux.EMBURGUR st al., 1996).
Malaria control programmeeFollowing the Thai national malaria control pro-
gramme strategy, early diagnosis and treatment havebeen established as the main components of malariacontrol in Shoklo and similar camps. For 10 years theinhabitants have been educated about malaria and ad-vised to attend the dispensaries run by Mt.lrrn,,r SansFrontirires whenever they had fever. Four dispensaries,one hospital, and the dispensary of the research unitwere the only sources of antimalarial drugs in Shoklocamp. All malaria cues were confirmed by microscopi-cal examination of a blood film. Patients from the campwith severe malaria, or those referred from the sur-rounding area (estimated population ahem I(1000),were admitted to hospital in the 30 beds su.,;i. ward ofthe in- patient department. Two medical assistants,
,working under the supervision of one physician. provid-cd continuous (24 h) medical cover.
As malaria in pregnancy is a major health problem inthis arca, and falciparum malaria is associated with ma-ternal morbidity and mortality and with reduced birthweight, weekly antenatal clinics have been set up to de-tact and treat malaria infections before the developmentof symptoms (NOSTEN et al., 1991a). Approximately
a-
/111.
TRANSACTIONS OF THE Kt)YAf. SOCIETY t)l''IRt)l'ICAI. NUiDICINE AND Itl'G,ENii t1996190. Cl)ItittiSPoNttiNl:li
Correspondence
O come, let us wallow in glorious mud'"I read with interest the report of failure of passive zoo -
prophylaxis in Pakistan and the association between cat-tle ownership and higher malaria prevalence (Bouma &Rowland, 1995: Transactions, 89, 351). However, thechief vectors of malaria in Pakistan, Anopheles' culicifacies
' and A. stephensi, feed primarily on water buffaloes andare highly attracted by them, being easily collected atresting sites in or near buffalo huts (Reisen & Boreham,1982: Journal of Medical Entomology, 19, 98). In a pre-vious report we noted that a switch from primary.buffalofeeding to feeding on humans occurred at the time ofyear when plentiful surface mud made it possible forbuffaloes to wallow in mud holes and cover their hides,including the preferred mosquito biting sites (under-belly, teats, ankles), with a thick layer of dry, caked mud(Halm & Mahmood, 1983: Proceedings of the Third1CAAC Conference, 2S October 1983, Las Magus, Nevada(ISSN 0733- 6373j, abstract no 172). The theory was ad-vanced that this feeding switch from water buffaloes tohumans was very probably, triggered by the inability, tofind biteable buffaloes during the malaria transmissionseason, when mud coating of the buffaloes makes themunavailable to feeding anophelines. It was suggested thatwashing the buffaloes to maintain them free of mud atthat time of year, or otherwise preventing them frommud -coating themselves, might result in reduced ma-laria transmission.
Thus, the association between cattle (buffalo) owner -ship and higher malaria prevalence is not surprising;buffaloes are part of the vector bioecological system inPakistan and owning buffaloes results in higher vectordensity in the immediate environment. It is still likely,however, that intervention which could prevent seasonalmud -coating would result in reduced transmission, andthis deserves a controlled field test. Zooprophylaxis maywell play a useful role if the buffalo mud factor is recog-nized and addressed, even though an effect on transmis-sion and incidence may be demonstrable sooner andmore easily than an effect on prevalence, which is ofcourse determined by prior infections. An effect of buf-falo washing on malaria prevalence would require alonger period of follow -up to detect.
David R. Nalin- Clinical ResearchMerck Research LaboratoriesP.D. Box 1, BL 3-4West PointPA 19486, USA
.-
10 June 1996
'O come, let us wallow..'. A replyMuddying the waters, or turning zooprophylaxis fromfailure to success
The standard practice of bathing water buffalo inmuddy pools may conceivably form a mud coating
.- which acts as a partial barrier to mosquito biting. Unfor-tunately, Afghan refugees in our study area keep only
j cattle and not water buffalo. and cattle 'do not requireregular bathing during the hot summers. Local Paki-stanis keep both cattle and buffalo, but our observationsare that the mud layer is imperfect and mosquitoes havelittle trouble in feeding. in fact, cattle and buffalo are re-markably inept at deterring biting, unlike .humans, orgoats and shee_p which can 'flex' their hairy skins. Hence
.r- cattle and buffalo arc largely responsible for amplifying
pm.
'This phrase is derived from a song popularized by the late M.Flanders and U. Swann in the UK several decades ago (editor).
7f-
mosquito populations. A mud harrier might, in the shortterm, deflect mosquitoes on to humans and increase ma-laria transmission but, in the medium term, mosquitodensities and malaria should decrease because of the dif-ficulty mosquitoes have in obtaining blood. Thus wepredict the opposite: 'clean' cattle and bultalu amplifymosquito populations and increase malaria, muddy cat-tle and buffalo might conceivably reduce mosquitopopulations and reduce malaria. But a more realistic so-lution than mud, at least for Afghans, might be treat theskins of their cattle with an insecticide that is safe formammals. Permethrin, applied in this way, does controlanophelines for a while (McLaughlin et al., 1989: Jour,.,,!
of the American Mosquito Corurr+l Association, 5, 60), and apilot project currently under way in the North -WestFrontier Province indicates major reductions in mus-quito and tick densities, and in malaria incidence, plusthe added benefit of healthier cattle whose extra produc-tivity in milk and meat outweighs insecticide costs. Thisexciting new malaria control strategy is potentiallymuch more cost- effective and sustainable than the housespraying traditional to the area.
Mark RowlandSean Hewitt
Merino BoumaHealth Net InternationalP.O. Box 889PeshawarPakistan 16,ßuly 19%
When injections are not necessaryIn developing countries the use and overuse of syr-
ingea and needles is a major health hazard, especially forchildren. Lack of money, electricity cuts, poor trainingand disbelief in 'germs' have led to tolerance of unsterileinjections even in hospitals. In the libala virus epidemicin Zaire in 1976, hospitals were epidemic amplifiers: 71of 103 primary cases were caused by unsterile injectionsin Yambuku mission hospital. The risk of Ehola virusinfection from a single injection was greater than 90' :..
(Garrett, 1994: The Coming Plague. New York: Farrar,Straus & Giroux ').
As well as working towards sterile injections, the veryuse of injections must be discouraged. Practice can hechanged. Only a decade ago, under the threat of 111Vand AIDS, doctors in Africa were able to halve thenumber of blood transfusions to children immediately.All injections must be sterile and their number reduced.The health services must set un example for those in pri-vate practice.
Recent studies question the assumption that intra-muscular injection delivers a drug more effectively. In-tramuscular injection for malaria is the most likely treat-ment when vomiting prevents oral treatment. However,oral treatment of unconscious children with chloroquineby nasogastric tube is cheaper and spares the child therisk of poliomyelitis, injection abscesses, hepatitis, etc.(Neequaye et al., 1991: Transactions, 85, 718). Treatmentby rectum with Quinimax'" or quinine has been success-ful in Sierra Leone (Westman et al., 1994: Transactions,88, 446), Madagascar (Baronnes et al., 1993; ,llhdectik.d'Afrique Noire, 40, 401), Niger (Barennes cn al., 1995:Transactions, 89, 418) and Mali, Cameroun, Chic d'fvuireand Burkina Faso (Il. Barennes, personal cotnntunica-lion).
There must be more studies of rectal delivery anddrugs formulated for this route, especially for children
'Address fett correspondence: 1)r I1. V. Wyatt, e u I I1011hri4Terrace, Leeds, L515 711G, UK; fax +44 (U) 11 3 242 2042.
See p.719 for a review of this hook, published in UK by Vi-rago Press (1995).
I
t;t)µkL'SPt)N1NiNt:1:
«ith diarrhoea. Drug companies must be made aware ofthe dangers of intramuscular injections and must marketless dangerous products.
The use of the syringe in logos related to health mat-ters should be banned. Every health unit must keep anlow,. non abscess book to record who injected what andu here. Medical directors must review their hospitalpractices. Doctors must refuse injections except whenabsolutely necessary, DPT immunizations for example.
Injections damage your health: is that injection reallynecessary?
S: h,wl of Healthcare StudierC'nrcverriis of Leeds18 Blenheim Terrace1.4edr, LS2 9HD, UK 12 ,July 1996
H. V. Wyatt'
The ParaSight " -F testIn the abstract by Y. Dowthwaite et al. (1996: Trantrac-
ham, 90, 211), the writers expressed the opinion that
thick blood films remain the best method for diagnosingmalaria.
We agree that under good laboratory conditions, thismay in general be correct. However, the finding that S of52 Plasmodium vivax infections had HRP -2 antigen intheir serum seems to require consideration. The pres-ence of HRP -2, due to a P. falciparum infection unde-tected by thick blood film examination, would require arevised antimalarial drug schedule. Administration ofchloroquine, standard for P. vivax infection, could leadto possible complications, especially in the context of theworld -wide spread of chloroquine- resistant P. falci-parunt. We recommend that laboratories using standardthick blood film examination should use ParaSight' " -Ftechnique with all patients havin4 P. vivaxparasitaemia,thus allowing an informed decision about treatment ifHRP -2 should also be present.
Malaria Centre Region 2ChiangmaiThailand 50200
T. BanchongaksornW. Rooney
15 July 1996
1
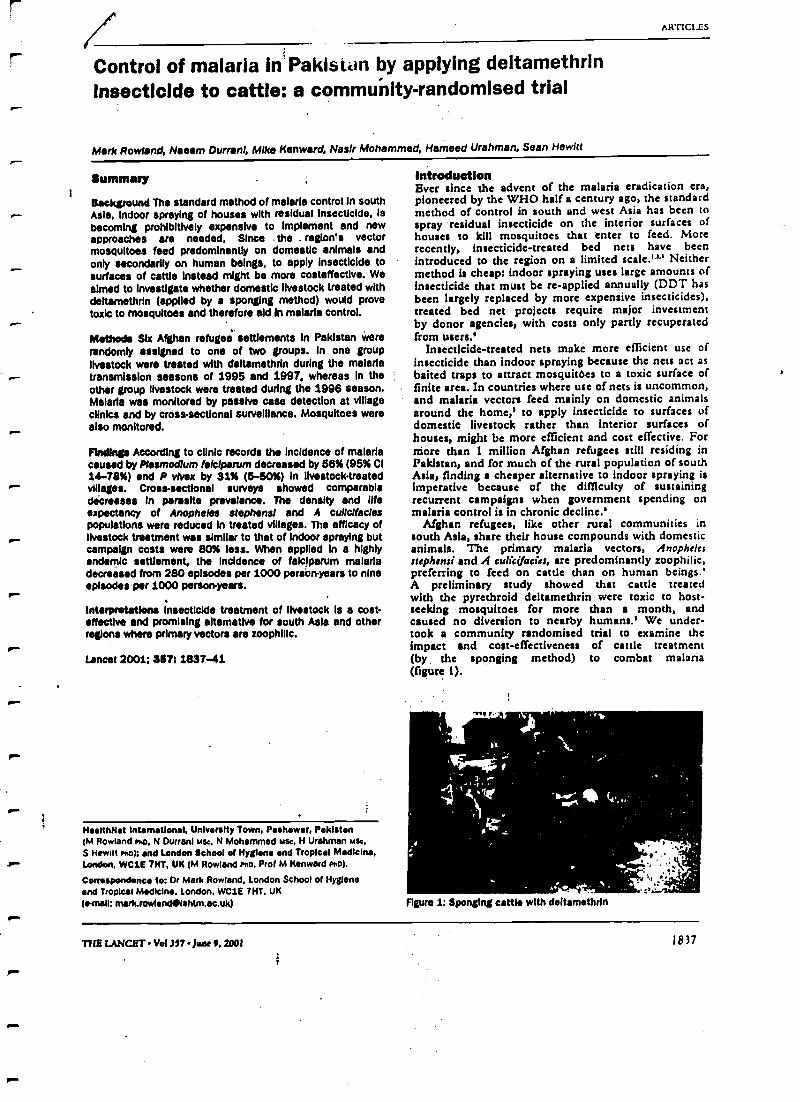
r
)
,
ARTICLES
Control of malaria in Pakistan by applying deltamethrinInsecticide to cattle: a community- randomised trial
Mark Rowland, Naeem Durrani, Mike Kenward, Naslr Mohammed, Hameed Urahman, Sean Hewitt
Summary
Background The standard method of malaria control In southAsia, Indoor spraying of houses with residual Insecticide, Isbecoming prohibitively expensive to Implement and newapproaches are needed. Since .the .region's vectormosquitoes feed predominantly on domestic animals andonly secondarily on human beings, to apply Insecticide tosurfaces of cattle Instead might be more costeffective. Weaimed to investigate whether domestic livestock treated withdeltamethrin (applied by a sponging method) would provetoxic to mosquitoes and therefore aid In malaria control.
Met ads Slx Afghan refugee settlements In Pakistan wererandomly assigned to one of two groups. In one grouplivestock were treated with deltamethrin during the malariatransmission seasons of 1995 and 1997, whereas In theother group livestock were treated during the 1996 season.Malaria was monitored by passive case detection at villageclinics and by cross -sectional surveillance. Mosquitoes werealso monitored.
Findings According to clinic records the Incidence of malariacaused by Plasmodium falclparum decreased by 58% (95% CI14 -78 %) end P Wax by 31% (5 -80%) In livestock treated
^- villages. Cross-sectional surveys showed comparabledécreasea In parasite prevalence. The density and lifeexpectancy of Anopheles Stephens, and A cullcifaclespopulations were reduced in treated villages. The efficacy oflivestock treatment was similar to that of indoor spraying butcampaign costs were 80% less. When applied In a highlyendemic settlement, the Incidence of faiciparum malariadecreased from 280 episodes per 1000 person-years to nineepisodes per 1000 person- years.
r^
rn
Interpretations Insecticide treatment of livestock is a cost -effective and promising alternative for south Asia and otherregions where primary vectors are zoophillc.
Lancet 2001; 337: 1837-41
HeatthNet international, University Town, Peshawar, PakistanlM Rowland no. N Durrani use, N Mohammed use, H Urahman Mae,S Hewitt no); and London School of Hygiene and Tropical Medicine,. London. WC1E THT, UK (M Rowland rno, Prof M Kenward no/.
Correspondence to: Or Mark Rowland, London School of Hygieneand Tropical Medicine. London. WC1E ?HT, UK(e -mail: mark.rowlandeishtm.ac.uk)
r
IntroductionEver since the advent of the malaria eradication era,pioneered by the WHO half a century ago, the standardmethod of control in south and west Asia has been tospray residual insecticide on the interior surfaces ofhouses to kill mosquitoes that enter to feed. Morerecently, insecticide- treated bed nets have beenintroduced to the region on a limited scale.'''' Neithermethod is cheap: indoor spraying uses large amounts ofinsecticide that must be re- applied annually (DDT hasbeen largely replaced by more expensive insecticides),treated bed net projects require major investmentby donor agencies, with costs only partly recuperatedfrom users.'
Insecticide -treated nets make more efficient use ofinsecticide than indoor spraying because the nets act asbaited traps to attract mosquitoes to a toxic surface offinite area. In countries where use of nets is uncommon,and malaria vectors feed mainly on domestic animalsaround the home,' to apply insecticide to surfaces ofdomestic livestock rather than interior surfaces ofhouses, might be more efficient and cost effective. Formore than 1 million Afghan refugees still residing inPakistan, and for much of the rural population of southAsia, finding a cheaper alternative to indoor spraying isimperative because of the difficulty of sustainingrecurrent campaigns when government spending onmalaria control is in chronic decline.'
Afghan refugees, like other rural communities insouth Asia, share their house compounds with domesticanimals. The primary malaria vectors, Anophelesstephsnsi and A cu 41c:cies, are predominantly zoophilic,preferring to feed on cattle than on human beings.'A preliminary study showed that cattle treatedwith the pyrethroid deltamethrin were toxic to host -seeking mosquitoes for more than a month, andcaused no diversion to nearby humans.' We under-took a community randomised trial to examine theimpact and cost -effectiveness of cattle treatment(by. the sponging method) to combat malaria(figure 1).
Tir
Figure 1: Sponging cattle with deltamethrin
THE LANCET vol 357 .June 9. 2001 1837
F411f v un........-
ARTICLES
MethodsStudy area and health servicesThe six refugee settlements that participated in the trial
were located in Hangu valley, a malaria endemic area of
the northwest frontier province of Pakistan. The villages
here were established 15 years ago; populations ranged
from 5900 to 25 000 people and are stable. Family
compounds are built from mud and stone in the style
typical of rural communities in Pakistan and Afghanistan.
Domestic animals are kept within the boundary walls of
compounds at night. Mosquito breeding sites.include river
margins and rice fields. Primary health services are
provided by the International Relief Committee (IRC), an
American non-governmental organisation. Each village has
a basic health unit staffed with a medical officer
and microscopy technician. Quality control of the
microscopy indicated that the accuracy of diagnosis is
around 98%. Diagnosis and treatment are provided for
free, so the clinics' services are well used. Chloroquine was
the first -line therapy, sulfadoxine- pyrimethamine (20:1),
the second line therapy. The trial ran from 1995 -97.
Study designThe design was a three -period crossover trial: The size of
the study was constrained by the number ofeligible villages
available. Only villages whose Annual Parasite Index
(incidence per year) had fallen below the threshold for
indoor spraying were included in the study by permission
of the United Nations High Commissioner for Refugees
(UNHCR). In these villages malaria incidence had fallen
to its lowest level for 5 years as a result of recurrent indoor
spraying campaigns. This was an appropriate moment to
assess a new control method. If inidal results wereencouraging, the trial would continue to a third year
endpoint.The six recruited villages were randomly divided into two
groups of three. One group was scheduled for treatment in
year 1 (1995) and year 3, whereas the other group was
scheduled for treatment in year 2. Livestock surveys were
carried out in each village. We recruited veterinarians to
give information to refugees about ectoparasite control and
animal health rind to collect data on ectoparasite infestation
rates. The key health messages to refugees were: insecticide
treatment is safe and effective and needs to be repeated
every 4-6 weeks; and all livestock (cattle, goats) must be
created and kept under shelter whenever possible.
We recruited the insecticide -treatment teams from the
refugee population. Livestock owners were encouraged to
treat their own animals under supervision. Insecticide
solution (concentration 0.075 g deltamethrin per L) was
applied with sponges and rubber gloves. The application
rate was 30 mg deltamethrin per m' (K- Qthrine 2.5%
suspension concentrate, Aventis, Frankfurt, Germany)
when animal hair was saturated. Because 90% of
mosquitoes feed below the mid -line of cattle,'
undersurfaces and legs were given special attention. Three
rounds of sponging were done between mid-July and mid -
October (6 week intervals between rounds). After
reviewing the early results, the technique was tested in a
highly endemic village (Adizai), near Peshawar, in 1997.
Malaria transmission in this waterlogged camp was
highest in northwest frontier province.
Epidemiological monitoringThe team carried out cross -sectional surveys every year in
October, the month that Plasmodium falciparum
transmission reaches a peak. We expected a parasite
prevalence of 8 -12% on the basis of previous surveys, and
estimated that a sample of 1000 individuals per village
would give 80% power to detect a 40% reduction inprevalence. 80 households per village were randomly
selected and blood smears were taken from all household
members present on the day. Individuals whose blood
samples contained malaria parasites were created with
chloroquine. Records of malaria cases were compiled
from the register of the basic health unit laboratories
between 1994 and 1997.
Entomological monitoring' Monthly space -spray collections were undertaken in 30
sentinel rooms in each village in years 1 and 2. Female
mosquitoes were identified to species and counted. To
show changes in mosquito survival rate, mosquitos were
collected from untreated cattle in each village each month
and the parous "rates determined; all anopheline species
were sampled in year i and known vector species in year 2.
Weight changes and milk yield in tick-infested cattle
We selected 30 mature tick- infested cattle at random from
each village in years 2 and 3, and weighed them in a mobili'
cattle -crush balance on days 0, 60, and 120 of the spongnnt
campaign. About 100 lactating cows were selected at
random from each village in year 2, and milk yields
measured on days 0 and 60 of the sponging campaign.
Relative costsWe kept records of the number oflivestock treated in year
3 (1997), the amount of insecticide consumed, sr
expenditure on labour, supervision, and consumables. T
make a comparison with the costs of indoor residual
spraying, records of consumption and expenditure from s
spray campaign in the same three villages in 1992 wt
obtained from the IRC, and costs convened to thequivalent value in 1997.
Statistical analysesThe two primary responses were counts of incidence t i
prevalence. The design was' three -period crossover M.h
an additional run-in bageline measurement for incidence.'
In terms of more familiar crossover concepts, villages -d
years can be translated to individuals and treats uperiods, respectively. We used a Poisson log -linear m. _el
for rates, in which village effects were assumed to be
fixed.' The model parameters and associated standard
errors were estimated with maximum likelihood met ds
with adjustment for overdispersion. The chosen n lei
showed no lack of fit for either response when compared
with a saturated means model. The model for the
expected counts (incidence and prevalence) ca bf
expressed as follows: let I,, and N,,, be the incidenc fnt
size of the k" village (k =1, 2, 3) in sequence i (1 =1, 2), if
period j (j =0, I, 2, 3 for incidence and j =1, 2, 3. fo
prevalence). Then, if 411 is the expected, or average, du
of 1,,, log, (4),) =tog, (N,') +V " +tr, for an untreated lap
and,, log, (43,,) =log, (N,,,) +V, +ar, +r for a treated villag
where V,, and w, arc village and year effects, respective
(r,=0), and t is the treatment effect. On the origin: ;ca
this can be expressed in terms of the expected int. en
rate, for an untreated village:
Est-=
and for a treated village:
Na
si"r, r
For analysis of mosquito -resting densities the rcuuct
in log density for the treatment year compared with
1838
THE LANCET Vol 357 June 9, : .
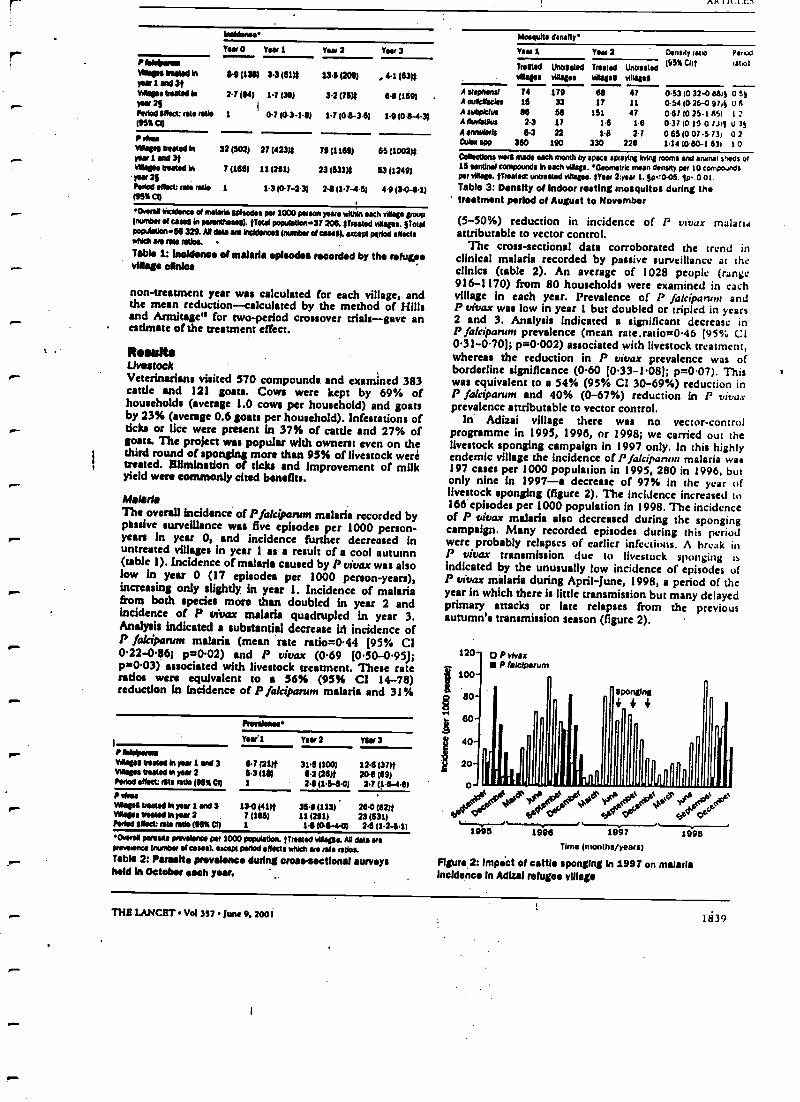
AK I Il.1.IJ
wM )wearVass avow' Nyew 1 sal 3tWages treated hsoar 2Shood offset: rate ratio195% CI)
I rhea%Won Posted Npar 1 end 3tvsleges Peeled inMu 26Ported effect rate ratio95%CI)
haldeereYear 0 Yew 1 Year 2 Year 3
6.0 (1301 3.3151)$ 13.0 (209) 4.1 (634
2.7164) 1.7 (39) 3.3 (754 6.8 (159)
1 O.7 103 -1.6) 1.7(0.8 -3.6) 1.9 (0 9-4.3)
32 (502)
7 (165)
21 N231í 75 (1109)
11 (251) 23(631)$
1 1.3 (07 -2.3) 2.6(1.7 -4.6)
65(1002)$
53 (1249)
4.9 (3.0 -6.1)
OvefM Incidents of melons episodes POI 1000 person yews wIUuIn each village groupplumber of avis In parentheses). Odd populton 37 200. Masted vinages. Patelpoprdstlen56 329. A0 data are Waldenses plumber of caws). except period affectswhich are Nu ratios.
Table i: incidence of malaria episodes recorded by the refugeeMeg. clinica
non -treatment year was calculated for each village, andthe mean reduction-calculated by the method of Hillsand Armitage" for two -period crossover trials -gave anestimate of the treatment effect.
ResultsLivestockVeterinarians visited 570 compounds and examined 383cattle and 121 goats. Cows were kept by 69% ofhouseholds (average 1.0 cows per household) and goatsby 23% (average 0.6 goats per household). Infestations ofticks or lice were present in 37% of cattle and 27% ofgoats. The project was popular with owners: even on thethird round of sponging more than 95% of livestock weretreated. Elimination of ticks and improvement of milkyield were commonly cited benefits.
MalariaThe overall incidence of Pfalcipanrm malaria recorded bypassive surveillance was five episodes per 1000 person -years in year 0, and incidence further decreased inuntreated villages in year 1 as a result of a cool autumn(table 1). Incidence of malaria caused by P vivax was alsolow in year 0 (17 episodes per 1000 person- years),increasing only slightly, in year 1. Incidence of malariafrom both species more than doubled in year 2 andincidence of P vivax malaria quadrupled in year 3.Analysis indicated a substantial decrease in incidence ofP fakiparum malaria (mean rate ratio =0.44 (95% CI0.22 -0.86; p =0.02) and P vivax (0.69 (0.50 -095);p =0.03) associated with livestock treatment. These raterados were equivalent to a 56% (95% CI 14-78)reduction in incidence of P falciparum malaria and 31%
Prevalent**
)IYvan 1 Year 2 Year 3
Aao*eowYAW* Vested In duer 1 and 3 0 7 (2111. 31.5 )100) 12.0 (37)fMagas vested h year 2 5.3 (18) 0.2 (201f 20.0 (69)Peros edict: rate and (95% CI) 1 241(1.5 -5.01 2.7 í16 -4eíP ra.eMagos treated h year 1 sM 3 13.0 (41)t 36.0 (1131 284 (82)treleva mata In yaw 2 711061 11 (251) 23 65311Pedal effect: rosa taso (as% CI) 1 141(01-40 2.5 (1.2-6.1I
'event parewte prevabnoe pw 1000 popdston. emoted swages. All data erepreveenee puarrber at cues). except period effects which em rate ratios.Table 2: parasite prevalence during cross-sectional surveysheld In October loch year.
Mesquite deadly'
Year 1 Year 2 Density uro Plimcl
bested WHIMS Tortes Untratad 1101S C111 fit*:
suasses visages villages bilases
A ttepMnd 74 179 60 47 05310 32-0 8815 0 55A dusclPCks 15 33 17 11 0.541026-0 974 v 6Asubpletus tlb 50 151 47 0671025-1651 I:AdbvNlAue 2.3 17 16 1 6 0-371019-0 rllt u 3yAarautab 6.3 22 16 27 0651007-573i 07WM spp 360 190 330 226 1.141080-1 631 1 0
CoWdlons were made each month by space swaying wing rooms and annul sheds ter15 sentinel compounds in each village. 'Geometric mean density per 10 compo.rMspet villa.. /boated: untreated biaepa. (Yew 2:yaw 1.50'005. 10.0 atTable 3: Density of Indoor resting mosquitos during thetreatment period of August to November
(5 -50%) reduction in incidence of P vivax malariaattributable to vector control.
The cross- sectional data corroborated the trend inclinical malaria recorded by passive surveillance at theclinics (table 2). An average of 1028 people. (range916 -1170) from 80 households were examined in eachvillage In each year. Prevalence of P falciparunr andP vivax was low in year 1 but doubled or tripled in years2 and 3. Analysis indicated a significant decrease inP faleipanan prevalence (mean rate.ratio =0.46 (95% Cl031 -0.70); p= 0.002) associated with livestock treatment,whereas the reduction in P vivax prevalence was ofborderline significance (0.60 (0.33 -1081; p= 0.07). Thiswas equivalent to a 54% (95% CI 30 -69 %) reduction inP falciparum and 40% (0 -67 %) reduction in P vivaxprevalence attributable to vector control.
In' Adizai village there was no vector -controlprogramme in 1995, 1996, or 1998; we carried out thelivestock sponging campaign in 1997 only. In this highlyendemic village the incidence of l'Jalcipanun malaria was197 cases per 1000 population in 1995, 280 in 1996, butonly nine in 1997 -a decrease of 97% in the year oflivestock sponging (figure 2). The incidence increased to166 episodes per 1000 population in 1998. The incidenceof P vivax malaria also decreased during the spongingcampaign. Many recorded episodes during this periodwere probably relapses of earlier infections. A break inP vivax transmission due to livestock sponging isindicated by the unusually low incidence of episodes ofP vivax malaria during April June, 1998, a period of theyear in which there is little transmission but many delayedprimary attacks or late relapses from the previousautumn's transmission season (figure 2).
120- O P vlvaxP lalclparum
WO-
80-
80-
40-
20- I
r
sponging4_i +
fi
r
o- ---- - --- -
#9 (# ,la 6"1995 1996 1997 1998
Time (months /years)
Figure 2; Impact of resale sponging in 1997 on malariaIncidence In AdIZal refugee village
TH8 LANCET Vol 357 June 9.2O0Í1 1339
ARTICLES
Entomology.4 rreplheari was 50% less abundant in year 2 than in
year t and A eulic(facidt was 40% less abundant inyear 2 than In year 1 (table 3). In both years, A stephensi
was 47% kss abundant (p=0.02) and A eulejadar was
10% less abundant (p =0.04) in treated villages than in
untreated villages. I'uruus rates in A rrepbuui were 27%
kss (95% CI 13 -39%; p= 0.0005) and in A 'culic¡facitr
were 22% less (1 -38 %; p=0.045) in treated villages,indicating lower survivorship associated with livestock
sponging (table 4).
Weight gain in cattleUntreated groups of cattle showed little change in mean
weight (hybrid breed weighed 202 -198 kg; local breed
weighed 147 -146 kg), whereas treated groups showed
significant weight gain (hybrid breed weighed 223 -241
kg; local breed weighed 147 -184 kg) during the 4 months
of the campaign. The net gain associated with treatment
was 22 kg (95% CI 17 -36 kg) in 66 hybrid cattle(p =0.003) and 20 kg (7 -33 kg) In 72 of the local breed
(p =0.004), Tick infestations cleared within 3 days of
treatment.
Milk yield in cowsThe mean milk yield in untreated hybrid cattle fell by
11% during the transmission season (from 1.85 LISD -007) to 1.64 L (0.07)) but remained at a constant
level in treated hybrid (mean 1.91 L10.10)); the net gain
associated with treatment was 0.2 L per day (n =248 (95%
L1 002 -0.39); p= 0.03). The local breed produced only
112 L per day on average, and there was no significant
change in yield associated with treatment.
Relative costThree cattle- sponging rounds cost US$0.07 per personprotected; more than 70% of the total expenditure wasspent on labour (table 5). Indoor residual spraying cost
five times as much (30.34 per person protected) in the
same group of villages; about 90% of the total expenditure
was spent on insecticide. If the 257 hybrid cattle
estimated to be tick infested at the beginning of the
campaign in 1997 each produced an extra 0.2 L of milk
per day, an extra 6000 L worth $3000 would be produced
during the 4 months of the programme, enough to cover
all insecticide and labour costs.
DiscussionSustained enthusiasm from the community is not
something normally associated with malaria- control
campaigns. The popularity of the project probably had
less to do with the health benefit to the community than
with the veterinary and economic benefits to individual
resew ratesae rake
Ttaatad wle8es UtaresW wsk{ei
Tse 1A uepnaul 0711103) 0.85146) 064
A CWC/atos 0.82(11) 1.00(14) 0.82
A wopkta 063 (68) 0.91(32) ' 0.70t
A rnaWkhN 073173) .0.97 (87) 0.715)
A anlwlpw 0.73 (37) 040130) . 0.91
Yoh 2A srepnfnJh 0.511302) 037 (196) 0.721
A cuaGat4s 0.581276) 0.494184) 0.85
A annWwls 060 (56) 0.44 125) 038
Prow rails ere proportions. with number dowsed In pwwNMsos.
7natse :urweston. fp .201.
Table 4: Parous fetes of mosquitoes in treated and untreated
groups of villages during the campaign period
tntaneaIoacaw sponging (Mow ussylsg
reputation ntivrred37 206 39 543
NunYer et Moroi (% ueasd) " 33f4
Nwmb.r a snkok looted 1% Inaad)ChileGoatsShoop
InsecU.lde won
Quantity mug
Iua01k1ü'out
30f8199115481961855 187)
3438(931
Deaem.Wla MrpWwur
361. 303011
756 11998
Cost of sup.Mekn (number a run d.ys) 8101153) 2861541
Coot of Iakw (numbera mea days). 1133 (1081 1203 (4321
Tell eat (u % of blow *1)4.5 sub). 2699120%1 12 484 (100%1
USS. As costs won) lo§ustad to USI reps h 1997.
Table 5: Comparison of costs of three rounds of cattle
sponging In 1997 with one round of Indoor residual spraying In
1992
households. The improvement in livestock health and
productivity after ectoparashe control was fully evident to
the villagers.There was no repon of toxic reaction in any treated
animal. Deltamethrin is commonly used on cattle for
controlling ticks tend tsetse flies,"." and the small amountspenetrating the skin are rapidly metabolised and not
thought to be a hazard to consumers."Although incidence of malaria was never high at any
stage of the trial, the crossover design showed a significant
reduction In incidence attributable to livestock sponging.
When the technique was applied in a village with high
levels of malaria, the technique proved more effective
against A fakipanon malaria than either indoor residual
spraying, insectidde-treated nets, or insecticide- treated
blankets used in earlier trials.'" Because a village's
livestock can be sponged in third of the time needed to
!spray the houses (with a labour force of similar size), the
technique should prove useful in epidemic control.
Malaria control is best met by quick intensive
campaigns in which all animals are treated. Ad hoc
treatments by individual families will have little effect on
malaria transmission because untreated cattle in the
vicinity, will sustain mosquito populations and prolong
survivorship. Cattle sponging should therefore be
promoted at the community level rather than at the
household level, but household benefits should beemphasised to improve overall compliance.
Cattle sponging is particularly useful when vectors are
both zoophilie and exophilic, such as the ries growing
areas of northern Afghanistan where A pukher.imur and
A nigsrrimtu predominate," and against A aquasalir in
South America, A minims(' in southeast Asia, and
A rine uis in China." Sponging would not be useful in
regions where vectors are strongly anthrophilic, such as
equatorial Africa (A cambiae) or forested pan: ofsoutheast Asia (A dims). Where A%alciparum has been re-
established:or u the limit of ha range, such as the Central
Asian Republics," malaria might be easier, cheaper, and
quicker to control through livestock sponging than
through indoor residual spraying or attempting cultural
conversion to insecticide-treated nets.Selection of pyrethroid resistance is a potential concern,
but selection pressure from livestock sponging should not
be any stronger than from the present strategy of residual
spraying of cattle sheds and houses with pyrethroid.'
Resistance monitoring should be included in an)
recurrent control programme. Livestock sponging could
however, select for anthropophily, assuming that genetic
1840
TH11 LANC9T Vol 357 June 9 2 ( $ l
ARTICLES
r-. variability for host preference exists. Areas in whichrepeated campaigns take place should be monitored forchanges in human blood index or host choice.
We believe that livestock sponging is a new way tocontrol malaria where vectors are zoophilic and feed
' predominantly on cattle; the technology h simple and canbe safely implemented by the community. . Werecommend livestock sponging as a substitute for indocsrspraying wherever malaria transmission due to zoophilicmosquitoes h risk to public health.
ContributorsM Rowland was principal investigator, secured the funding. designed thestudy, and analysed the data. N Dunned managed the pandtologlcal datacollection and reference laboratory. N Mohammed and H Urabmansupervised project knplemenadon and dte entomological and veterinarydan coUeedon. M Kanward designed the statistical models and did theepidemiological analysis. S Hewitt managed the project from 1995 -96,and analysed the data. All Itwesdgaton contributed to dte wtidng ash,.- papes.
AcknowledgmentsWe thank the International Rescue Committee and TUa Khan for supportand coopendooa Stayed Agha and Mahboob JabsU, Rost* Shier foradditional stadstkal advice, and Chris Curds, Diamdd Campbell-Lendrum, and Richard Reithnnger for comments on the paper. HealthNetIntemadorad'a Malaria Control Programme is supported by the EuropeanCommission (D01), tin United Nations High Commissioner forRefugees. and the WHO. The study received additional *ding fromHealthNet International, the Department for Intemadonal Development
.- *Me e UK, and the Oates Poundadon.
OM.
.
r-
-r-
aaNis as .
1 Rowland M. Hewitt S, Durrani N, Sack P, Houma M. Sendory E.SwtainebWty of pytethtold -impregnated bednen for malaria control InAfghan cammuoála. Butt World Haabll Organ 1997; 7$,23-29.
2 Zaim M, Ohioans! Mgr Nwri M. Bdriadao GH, Natcghpour M.Cyfruthein Impregnated bednen In a malaria control program inOhassnghand, Inn. Ant Man CnuAssot 1998;141421 -30.
r
3 Wars SP, Webber RH, Lines J. Jaffar S, UraJley DJ. Malaria control.bedncts or spraying? Spray versus treated nets using deltamethrin -acommunity randomized trial In India. Truro Roy Soc Trop .%1.J Hyg
1999; 931 456 -$7.4 Chavesse DC, Reed C, AttaweU K. Insecticide veered net projects: a
handbook for manegen, 1999. London and Liverpool: MalariaConsortium, 1999.
5 Reisen WK, Boreham PPL Estimates of malaria vectoriel capacity forAnopheles ealk((oeies and An step/send in rural Punjab province.Pakistan. J Med Es,rorol 1982; 19, 98 -101.
6 Shah I, Rowland M, Mehmood P, et al. Chloroquine resistance inPùWatan and the upsurge of fdciparum malaria in Pakistani andAfghan refugee populations. Annals Trop Mad Parasiwl 1997;11 591 -602.
7 Hewitt S. Rowland M. Control of zoophilic malaria vectors byapplying pyrethroid insecticides to cattle. Trop Med Intermit IBM 1999;41 481 -86.
8 Jones B, Kenward MG. Design and analysis of cross -over trials.London: Chapman & Hall, 1989.
p McCuliagh P, Neider JA. Generalized linear models. London:Chapman & Hall, 1989.
10 Hills M, Armitage P. The two -period crossover trial. Dr J ClinPf4annataJ 1989; 8. 7-20.
1 I Permit RO, Lemche J, Chlzyuka HGB, et al. Effect of sick control unlivewei5ht gain of cattle In central Zambia. Med Mit Eneouol 1989; 3,313-20.
12 Okello Ocean J, Helnonen R, Ssekltto VM, et al. Control of fiesin Uganda by dipping cattle In deltamethrin. Trop Animal Filth Product1994; 261 21 -27.
13 WHO. Deltamethrin. Environmental health criteria, 1997. Geneva:WHO, 1998.
14 Rowland M, Dunant N, Hewitt S, et al. PrekheUuin treated cheddarsand top -sheen: appropriate technology for protection against malariain Afghanistan and other complex emergencies. Trans Roy Soc TropMed Hyg 1999193' 465 -72.
15 Buck AA, Anderson RI, Kawara K, et al. Health end disease in ruralAfghanistan. Baltimore: York Press, 1972.
16 Service MW. Agricultural development and arthropod -borne dis .
a review. Ravise da Salle Palatka 1991; 258 165-78.17 Pitt S, Pearcy BE, Stevens RH, Sharipov A, Saarov K, Banatvala N.
War In Tajikisten and re- emergence of Pfannodium /akiparun,. Lancet1998; 3521 1279.
THE LANCET Vol 357 Jinn 9, 2001 1841
EARLY REPORT
{-Early report I
Efficacy and safety of lnfilximab monotherapy for plaque-type
psoriasis: a randomised trial
tl Chaudharl, P Romano, L D Mulcahy, L T Dooley, D G Baker, A B Gottlieb
Summary
Background Currently available treatments for moderate to
severe psoriasis are either incompletely effective In some
patients, or are associated with toxic effects. Since tumour
necrosis factor a (TNFa) Is thought to have a role In the
pathogenesis of psoriasis. we did a double -blind, randomised
trial to assess the clinical benefit and safety of (nfliximab -a
monoclonal antibody against TNFa.
Methods 33 patients with moderate to severe plaque
psoriasis were randomly assigned intravenous placebo
(n -11). Infliximab 5 mg/kg (ni11), or infliximab 10 mg/kg
(n =11) at weeks O, 2, and 6. Patients were assessed at
week 10 for the primary endpoint (score on the physician's
global assessment !PGA)). Analysis was by intention to treat.
Findings Of the 33 patients enrolled, three dropped out. Nine
of 11 (82%) patients in the infliximab 5 mg/kg group were
responders (good, excellent, or clear rating on PGA),
compared with two of 11 (18%) In the placebo group
(difference 64% (95% C( 20 -891, p =0.0089), and ten of 11
(91%) patients In the infliximab 10 mg/kg group were
responders (difference from placebo 73% (30 -94j,
p=0.0019). The median time to response was 4 weeks for
patients In both Infliximab groups. There were no serious
adverse events, and infliximab was well tolerated.
Interpretation in this controlled trial, patients receiving the
anti -TNFa agent infliximab as monotherapy experienced a
high degree of clinical benefit and rapid time to response In
the treatment of moderate to severe plaque psoriasis
compared with patients who received plaçebo. These
findings suggest that TNFa has a pivotal role in the
pathogenesis of psoriasis,
Lancet 2001; 367: 1842 -47
Clinical Raoesrch Canter,UMDN1Robert Wood Johnson Medical
School, 51 French Street, Now Brunswick, NJ eatlo1-0Cie, USA
(u ChouChart MO,P Romano es. Prof A 8 Gottlieb MO); and Centocor
Inc, Malvern, PA, USA (L D Mulcahy. L T Dooley owe, D G Baker a)
Con mpondence to: Prot Alice s Gottlieb
(emaU: gonllablaumdn).sdu)
IntroductionPsoriasis is a psychologically and physically disabling
diocese that affects 1 -3% of the US and Iiuropean
population;' about 25% of patients have moderate to severe
disease. The costs and other financial implications of caring
for padents with psoriasis can result in lower quality of life
for patients with more severe psoriasis' Treatments
approved by the US Food and DrugAdministration for this
class of patients include ciclosporin, methotrexate,
acitretin, ultraviolet B (UVB), and ultraviolet A with
psoralen (PUVA).Ciclospotin is the most effective of these
treatments, but exposure to this drug can result in toxic
effects such as hypertension and irreversible renal
insufficiency.' Methotrexate can take 4-8 weeks to produce
significant improvement,and there is a risk of toxic effects
on the liver and bone marrow. Acitretin alone is only partly
effective and rarely clears the disease.Additionally, it causes
substantial mucocutaneoustoxic effects and is a teratogen,
as is methotrexate. UVB and PUVA require an intensive
treatment regimen (about three times per week for many
months), . thereby reducing patients' compliance.
Additionally, PUVA has been associated with skin cancers
including malignant melanoma. Overall, the treatments
available for moderately to severely active psoriasis arc
either incompletely effective in some patients or are
associated with serious toxic effects.' There is therefore a
need for highly efficacious treatments that are safe to use in
a long -term regimen.The two major pathological lesions seen in psoriasis
are epidermal hyperproliferation with abnormal
differentiation, and inflammatory infiltration in the
epidermis and dermis. These processes are mainly driven
by activated T cells or antigen-presenting cells, which
release various chemokines and cytokines that signal the
keratinocyte to hyperproliferate, and which ultimately leads
to abnormal differentiation!' These signalling molecules
include tumobr necrosis factor is (TNF -a), interieukin 6,
interlcukin 8, granulocyte macrophage colony stimulating
factor, and interferon gamma. The cytokine TNF-a in
particular is believed to have a major role in this process:
increased concentrationshave been detected in p oriatic
skin lesions." TNF-a, via activation of nuclear factor KB
(NFKB), .induces synthesis of numerous cytokines,
including. interleukin 8, Interieukin 6, and colony -
stimuladng factors. Also, TNP. i potentially contributes to
the accumulation of inflammatory cells seen in epidermis
and dermis by inducing expression of intracellular adhesion
molecule (ICAM) -1 on endothelial cells and
keratinocytes." TNF-a therefore has a potential role in J
both of the major pathological lesions In psoriasis'
Consequently, blockade of TNF-a activity should, in
theory, reduce inflammation and keratinocyte proliferation
and differentiationabnormalities in psoriasis.
Infíximab is a chimeric monoclonal antibody that has
high specificity, affinity, and avidity for TNF-u " and is
currently approved in the USA and Europe for the
treatmént . of rheumatoid arthritis and Crohn's disease.
1842
Thu LANCtïr Vol 357 June 9, 2061
i
r
-
0".
1
Bulletin of Entotrtologicnl Research (1997) 87, 455 -459
The effect of bednets on unprotectedpeople: open -air studies in an
Afghan refugee, village
S. Hewitt, E. Ford, H. Urhaman, N. Muhammadand M. Rowland
HealthNet International, 4,, Karakal Lane, PO Box 889, University Town,
Peshawar, North West Frontier Province, Pakistan
Abstract
The possibility that mosquitoes are diverted from protected people sleeping
outdoors in a bednet to an unprotected person immediately adjacent was
investigated during field trials conducted in an Afghan refugee village. The
presence of an untreated bednet covering three people sleeping adjacent to the
subject did not cause a significant rise in the biting rate on that subject. At the
dose rates studied, biting rates in the presence of an Imperator" treated bednet
fell slightly (although not significantly). K- Othrine' treated bednets had no
discernible effect on biting rates. Similar studies conducted within giant net
traps showed that the Imperator treated bednet,' and to a lesser extent theK- Othrine' treated bednet, did repel mosquitoes. Within these net traps, biting
on the unprotected subject decreased considerably in the presence of theImperator' treated bednets (P<0.05 for both culicines and Anopheles shphensi
Liston in the presence of the Imperator' treated bednet). The net traps held in
volatile components from the treated bednets in much the same way as the
walls of a well ventilated room. We conclude that while sleeping next to a treated
bednet may be of considerable benefit inside, where one sleeps in relation to
a bednet outside is of little importance. Further studies revealed that for
each mosquito species, insecticide induced mortality was highest when the
bednet contained the preferred host of that species. This suggests that selection
for pyrethroid resistance by bednets may be relatively slow to develop in
areas where the primary vector's of malaria are zoophilic.
Introduction
Over the last four years HealthNet International (HNI)has been responsible for coordinating the sale of some200,000 'famitysized' Insecticide Impregnated bednets(covering about 600,000 people) in refugee communities inPakistan and in settlements' in the eastern provinces ofAfghanistan. In order to promote the concept of bednetsfor malaria control over as wide an area as possible andso as to deter reselling, HealthNet International has In thepast restricted the number of bednets sold to eath family.The possibility that mosquitoes (Diptera: Culicidae) arebeing diverted from bednet users to unprotected people
sleeping nearby (Lines et rte., 1987) is however a matter ofconcern; restricted sales could result in increased biting onmore vulnerable groups such as children (Curtis ei u!.,
1989).The inhabitants of rural Afghanistan generally sleep
outside during the warmer months when malariatransmission is at its height. For this reason these trial)were conducted in the open air. The investigationwas designed to measure both the degree of divereiuncaused by treated and untreated bednets and also theentomological impact of these bednets in terms of theirrepellent and killing effects. The trials took place in thesummer of 1994.
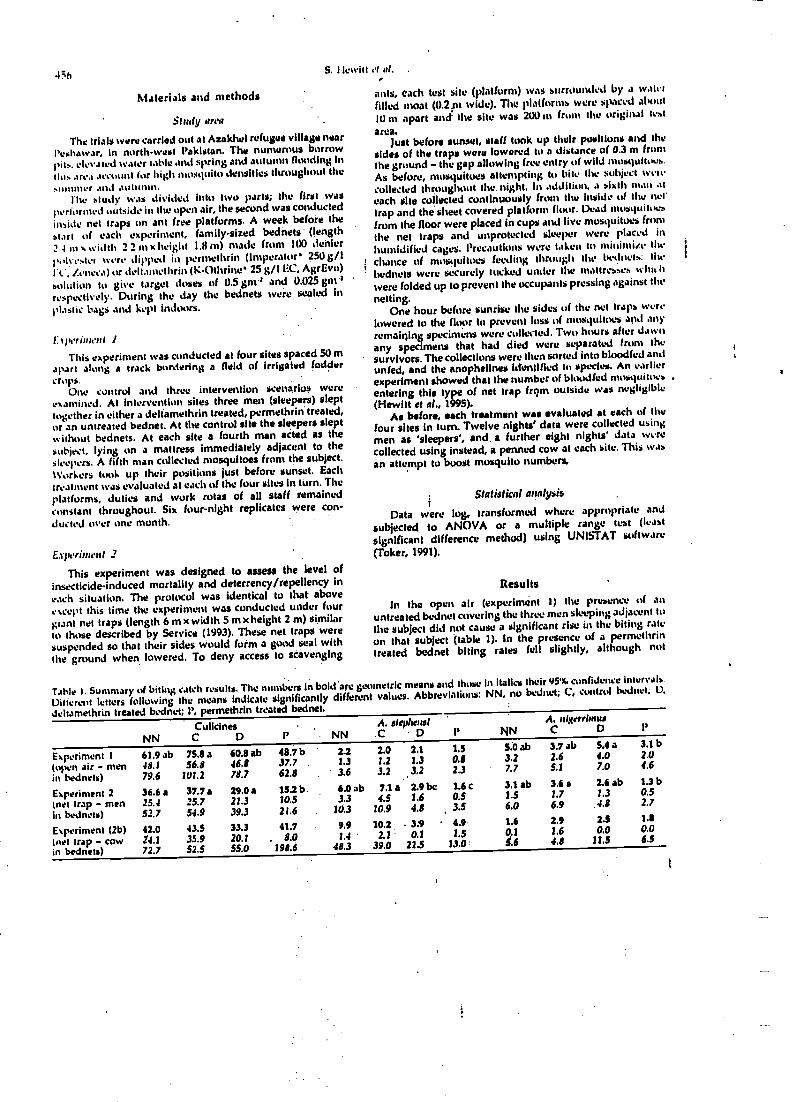
456S. Hewitt et al. .
Materials and methods
Study area
The trials were carried out at Azakhel refugee village nearPeshawar. in north -west Pakistan. The numerous borrowpits. elevated water table and spring and autumn flooding Intile, area account for high mosquito densities throughout thesummer and autumn. .
Ih study was divided into two parts; the first wasperforated outside in the open air, the second was conductedinside net traps on ant free platforms. A week before the
start of each experiment, family -sized bednets (length
2 4 in width 2.2 m x height 1.8 m) made from 100 denierpolyester were dipped in permethrin (Imperator 250 g/IFt.., /_meta) or tiehamethrin (K t)thrine 25 g/I EC, AgrEvo)solution to give target doses of 0.5 got'' and 0.025 gm'respectively. During the day the bednets were sealed inplastic bags and kept indoors.
I: t per iutruf
This experiment was conducted at four sites spaced 50 mapart along a track bordering a field of irrigated foddercrops.
One cuntrul and three intervention scenarios wereexamined. At intervention sites three men (sleepers) slepttogether in either a delfamethrin treated, permethrin treated,or an untreated bednet. At the control site the sleepers sleptwithout bednets. At each site a fourth man acted as thesubject, lying on a mattress immediately adjacent to thesleepers. A fifth man collected mosquitoes from the subject.1Vorkers tool. up their positions just before sunset.. Each
treatment was evaluated at each of the four sites In turn. Theplatforms, duties and work rotas of all staff remainedconstant throughout. Six four -night replicates were con-ducted over one month.
Ex ierinanf .2
This experiment was designed to assess the level ofinsecticide- induced mortality and deterrency/repellency ineach situation. The protocol was identical to that aboveexcept this time the experiment was conducted under fourgiant net traps (length 6 m x width 5 m x height 2 m) similarto those described by Service (1993). These net traps weresuspended so that their sides would form a good seal withthe ground when lowered. To deny access to scavenging
anis, each test site (platform) was surrounded by a waterfilled moat (0.2m wide). The platforms were spaced about
10 nt apart and the site was 200 m f the original test
area.Just before sunset, stall took up their positions and the
sides of the traps were lowered to a distance of 0.3 m fromthe ground - the gap allowing free entry of wild mosquitoes.As before, mosquitoes attempting to bite the subject werecollected throughout the. night. In addition, a sixth man at
each site cujiected continuously from the inside of the nut'trap and the sheet covered platform flour. Dead nosquittxafrom the floor were placed in cups and live mosquitoes fromthe net traps and unprotected sleeper were placed in
humidified cages. Precautions were taken to mininüe thechance of mosquitoes feeding 11 gh the bednets: thebednets were securely lucked under the mattress.attresses whit It
were folded up to prevent the occupants pressing against the
netting.One hour before sunrise the sides of the net traps were
lowered to the floor to prevent loss of mosquitoes and anyremaining specimens were collected. Two hours alter dawnany specimens that had died were separated from thesurvivors. The collections were then sorted into bloodfed andunfed, and the anophelhws identified to species. An earlierexperiment showed that the number of bloodied mosquitoesentering this type of net trap frqm outside w4s negligible(Hewitt et al., 1995).
As before, each treatment was evaluated at each of thefour sites in turn. Twelve nights' data were collected using
men as 'sleepers', and, a further eight nights' data werecollected using instead, a penned cow at each site. This was
an attempt to boost mosquito numbers,
Statistical analysisi
Data were log, transformed where appropriate and
subjected to ANOVA or a multiple range lest (least
significant difference method) using UNISTAT software(Toker, 1991).
Results
In the open air (experiment 1) the presence of anuntreated bednet covering the three men sleeping adjacent to
the subject did not cause a significant rise in the biting rateon that subject (table 1). In the presence of a permethrintreated bednet biting rates fell slightly, although not
Table 1. Summary of biting catch results The bers in bold' are geometric means and those in Italics their 95% confidence intervals.
Dilterent letters following the means indicate significantly different values. Abbreviai' NN, no bednet; C, control bednet; U,
dvitamethrin treated bednet; P, permethrin treated bednet.
NNCulicinesC D P NN
A. stephatsf.0 D 1' INN
A. u{serrlumtsC D I'
Experiment I 61.9 ab 75.8 a 60.8 ab 48.7 b 2.2 2.0 2.1 1.5 5:0 ab 3.7 ab 5.4 a 3.1 b
(open air - men 48.1 56.8 46.8 .37.7 1.3 1.2 1.3 0.8 3.2 2.6 4.0 2.0
in bednets) 79.6 101.2 78.7 62.8 3.6 3.2 3.2 2.3 7.7 5.1 7.0 4.6
Experiment 2 36.6 a 37.7 a 29.0 a 15.2b. 6.0 ab 7.1a 2.9bc 1.6c 3.1 ab 3.6 a 2.6 ab 1.3 b
(net trap - men 25.4 25.7 21.3 10.5 3.3 4.5 1.6 0.5 1.5 1.7 1.3 0.5
in bednets) 52.7 54.9 39.3 21.6 . 10.3 10.9 4.8 3.5 6.0 6.9 4.8 2.7
Experiment (2b) 42.0 43.5 33.3 41.7 9.9 10.2 3:9 4.9 1.6 2.9 2.5 1.8
(net trap - cow T4.1 35.9 20.1 . 8.0 1.4 2.1 0.1 1.5 0.1 1.6 0.0 0.0
in bednets) 72.7 52.5 55.0 198.6 .48.3 39.0 21.5 13.0 S:6 4.8 11.S 6.5
(
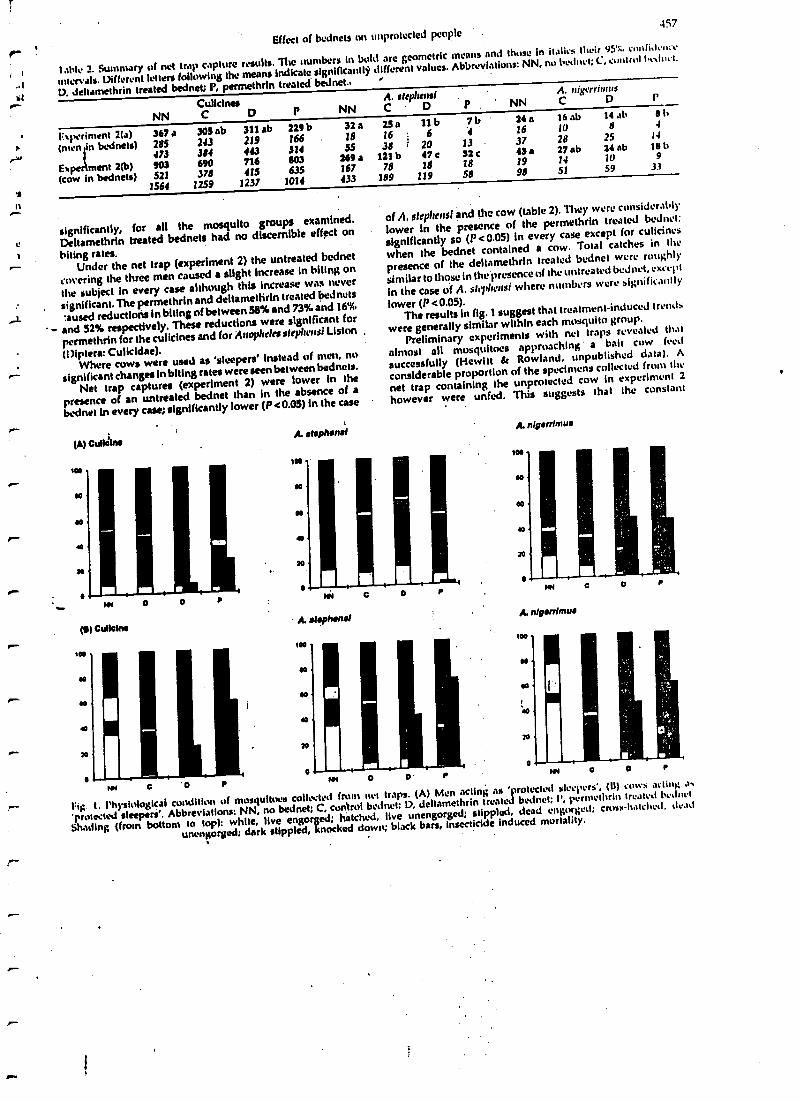
Effect of bednets on unprotected people457
lalde 2. Sununary of net trap capture results. The numbers in bold are geometric means and those in italic'. their 95% cunfidçn,r
intervals. Different letters following the means Indicate significantly different values.Abbreviations: NN, no bednet; C, control le.lnet.
D, deltamethrin treated bednet; P, permethrin treated' bednet.,
NNCulicinesC D
FN)xrimrnt 2(a)(men 'n Ixdnets)
367 a285
305 ab243
473 384
Ex pe 2(b)min 903 690
(cow bednets) 521 378
A. strylrorsfA. rtiacriums
P NN C D P. NN C D p
311 ab 229 b 32 a
219 166 . 18
143 314 5S
716 803 269 a
415 635 167
1564 1259 1237 1014 433
25a 11 b lb16 ; 6 4
38 r 20 13
121b 47c 32c78 18 .18
189 119 58
24a 16ab 14 ab Bi
16 10 8 f
37 28 25 14
43a 27ab 24ab Is I,
19 14 10 9
98 51 59 33
O
significantly, for all the mosquito groups examined.
t: Deitamethrin heated bednets had no discernible effect on
biting rates.r Under the net trap (experiment 2) the untreated bednet
covering the three men caused a slight increase in biting on
the subject in every case although this Increase was never
significant. The permethrinand deitamethrin treated bednets
r t :aused reduction in biting of between 58% and 73% and 16%
- and 52% respectively. These reductions were significant for
permethrin for the culicines and for Anopheles stepheusf Liston
( Diptera: Culicidae).Where cows were used as 'sleepers' instead of men, no
r- significant changes in biting rates were seen between bednets.
Net trap captures (experiment 2) were tower in the
presence of an untreated bednet than in the absence of a
bednet In every case; significantly lower (P <0.05) in the case
r
t
r
r
r
C '0 r
of A. stepltensf and the cow (table 2). They were considerably
lower in the presence of the permethrin treated bednet:
significantly so (P <0.05) in every case except for culicines
when the bednet contained a cow. Total catches in the
presence of the deltamethrin treated bednet were roughly
similar to those in the presence of the untreated bednet, except
in the case of A. slepherlsfwhere numbers were significantly
lower (P <0.05).The results in fig. 1 suggest that treatment -induced trend.
were generally similar within each mosquito group.
Preliminary experiments with net traps revealed that
almost all mosquitoes approaching' a bait cow feed
successfully (Hewitt & Rowland, unpublished data). A
considerable proportion of the specimens collected from the
net trap containing the unprotected cow in experiment 2
however were unfed. This suggests that the constant
NN O 0 r tit
r Fit; I. Physiological condition of mosquitoes collected from net traps. (A) Men acting as 'protected sleepers', (II) cows acting a.
'protected sleepers'. Abbreviations: NN, no bednet; C, control bednet; D, deltamethrin treated bednet; l', pernrthrin treated bcanvi
Shading (from bottom to top): white, live engorged; hatched, live unengorged; stippled, dead engorged; cross-hatched, dead
unengorged; dark stippled, knocked down; black bars, insecticide induced mortality.
o
458S. I lewitt el nf.
collecting from the inside of the net trap removed manymosquitoes before they had a chance to reach the bait; it is
well documented that many species of mosquito rest onvegetation and other convenient surfaces such as net traps
immediately prior to biting a host (Colless, 1959; Monrhouse
& 1Vharton, 19b5). The high proportion of unfed mosquitoescaptured in each net trap is probably therefore an artefact of
the esperintental design and this should be taken into
account when interpreting fig. 1.
A comparison of the bar representing the 'no -net control'
iNN) for each mosquito group in the man baited bednetswith the corresponding bar for each group in the cow baited
bednet), illustrates the relative ease with which mosquitoes
teed on cattle. Single (actor ANOVA revealed that these
dittere aces were highly significant for all the mosquitogroups: A, st.hlu'usi, P =0.001 (F4041, 16.91); A. ufgerrumus
Giles, P0.001 (Rob =19.87); culicines, P0.002(F,, ,.,. 26.20).
The dark bars (fig. I) represent the level of insecticide-
induced mortality (Abbott's correction) found in each net
trap containing a treated bednet. Mortality rates were
considerably higher when the treated bednet, were baited
with cows than when they were baited with men for both A.
aleyl,ensi (P= 0.015, Foss =6.70) and for culicines (P =0.014,
F, = 6.81). For A. ttilarrmms mortality rates were sirnilarfn
the presence of cows and Wren.
Discussion
The first experiment was designed to measure directly
any diversion of mosquitoes front people sleeping In bednets
to unprotected people in the vicinity. Even in the rather
extreme acumen) examined, where one unprotected person
was sleeping immediately adjacent to three people in a
bednet, there was little evidence of diversion. There was nosignificant increase in biting in the presence of the untreated
hednet (although numbers of biting culiclnes were up by 20%
overall) and no significant decrease in the presence of either
of the pyrethroíds tested (although in the presence of the .
permethrin treated bednet, biting rates fell for all the
mosquito groups examined). These findings are supported
by the results of recent clinical studies in the region which
showed that unprotected people sleeping outside in the saine
ctnnpound as bednet users were no Tess likely to contract
malaria than those sleeping in compounds without bednet
users (Rowland et al., 1996).The reductions in biting rates in the presence of treated
bednets seen in the net trap experiments suggest that the net
trap was holding in volatile repellent components from the
insecticides or their formulations (Lindsay el al., 1991);
indeed, when the bednets were freshly dipped a strong smell
was apparent on entering the net trap. One would expect this
eltect to be even more pronounced inside huts.We conclude that while it may be beneficial to sleep !next
to a treated bednet when inside, where one sleeps in relation
to a bednet outside is of little importance.The efficiency of net traps varies greatly between
mosquito groups: experiments in which single,. pre -dawncollections were made showed that the technique captured
85'., of culicines but only 11% of A. stephensl (Hewitt et al.,
1495). On the basis of these findings, one can assume that the
allnight Batches performed during this current investigationresulted in the capture of virtually all the culicines thatentered the trap.
Wheti men were used as sleepers, culicine net trap catches
were 17'%. lower In the presence of an untreated bednet than
when there was no bednet (P > 0.0S). This reduction can be
attributed to the diminished attractiveness of the bednet-
covered bait. The permethrin treated bednet caused anadditional 25% reduction in the culicine net trap catchsuggesting that mosquitoes are deterred (tom entering the
net trap; again probably a response to formulation volatile).
The deltamethrin treated bednet did not cause any reduction
in the size of the culicine catch. For culicines at cow-baited
bednets there were no clear differences between treatments;
the powerful stimuli coming from the' cow presumably
overcame all other influences.Despite the inefficiency of net traps for anophcline
capture, the technique did reveal similar trends to Ilium: seen
with culicines. When men were used as sleepers thepermethrin treated bednet caused a 72% reduction in the Si se
of the A. step/teas( catch compared with the untreated bednet,
while deltamethrin caused a 56% reduction.Hut trials in Tanzania revealed similar reductions in catch
size with untreated bednets (Lines el af., 1987). There are !wives*.
possible explanations: bednets may physically restrict the'eee
odour plume or (and), by preventing mosquitoes from
feeding, they may prevent tie release of aggregation
pheromones. Recent studies, conducted by Alekseev,
Rasnitsyn and Vitilin, and by Ahmadi and McClelland.
demonstrated an 'invitational effect' whereby female
mosquitoes (Aedes commonis (De Geer) and A. sierre tsis
(Ludlow)) are attracted to a host in proportion to the
numbers of females already feeding on that host (referred to
in Service, 1993). Either way, theoretically this effect should
result in increased biting un unprotected people sleeping
further afield. In Pakistan however, vectors are zoophilie.and
livestock Is abundant and It therefore seems unlikely that this
type of diversion would havea significant impact on malaria
incidence.For A. $teplunsl, insecticide-induced mortality was very
much higher when bednets contained a cow than whenthey contained men. In contrast, for A. nlgerrfutus insecti-cide-induced mortality was similar in both cases. A.
stepltensi tins a marked preference for cattle, while A.
afgerriunts (which prefers la , feed on goats) dotes not show
any strong preference for cattle over men (Hewitt &
Rowland, unpublished data). These results suggest tha'the.community impact of an impregnated bednet intcrven.y,
thin will depend on the host preferences of the target
mosquito and the availability of alternative hosts: while
treated bednets may have a marked Impact on parity rates
of anthropophilic vectors such as A. gaudriue Giles they are
unlikely to have much impact on highly zimuphilie vector
species such as A. stepheusl. This implies that selection for
pyrethroid resistance by bednets would be much lower
where Ow vectors are zoophilie. In such ' regions
pyrethroid impregnated bednets probably therefore offer a
longer term malaria control option and set particular
caution should ; be exercised regarding the use u(
pyrethrolds for wall spraying.
Acknowledgements
HealthNet international's Malaria Control Progranune
for displaced Afghans is funded by the European Commis-
sion. We should like to thank M. Farhan and M. Kamai for
all their hard work in the field.
r lu taitedra..,:.nents:tv m.thly
IC 11011
e--1+
ir"a
tclineseen
v thefit size
catch'e tealt th%).
from¡alios%seer,land.orale
11 .1 Illeer 'ad Ill
r i trilldPing
c andr ,i thisn 'aria
it %crtat when
a`t'Nr-a
.howk t &
thanit ven-se argotIs ...bileri ates'-t arcIa lMhlrct...n for1. leer
,Ulpr .,t .1
.11... ui.0r ar
e A.
r.
K oneli.u Ilot
Effect of bcdncts on
References
Cotisas, D.H. (1959) Notas on the cullcine mosquitoes ofSingapore VI. - observations on catches made with baitedand unbaited trap-nets. Annuls Of Trapilvl Medicine and
Parasitologylogy S3, 25I-258.Curtis, C.F., Lines, J.D., Carnevale, P., Robert, V., Boudin, C.,
llalna, JM., Pazert, L, Galin, P., Richard, A., Mouchet, J.,
Chariwood, J.D., Craves, P.M., Ilossain, M.i., Kurihara,T., Ichimorl, K., Li, Z., Lu, B., Major', G., Sabalinelll, G.,Coluzzi, M., Njunwa, KJ., Wilkes, T.J., Snow, R.W. dcLindsay, S.W. (1991) Impregnated bednets and curtainsagainst malaria mosquitoes. Chapter 2 In Curtis, C.F. (Ed.)
Control of disease vectors lit the community. London, WolfePublishing Ltd.
Ilewitt, S., Rowland, M., Muhammad, N., Kamal, M. & Kemp,E. (1995) Pyrethroid- sprayed tents for malaria control: anentomological evaluation in Pakistan. Medical and Veteri-nary Entomology 9, 344 -352.
Lindsay, S.W., Adlamah, J.H., Miller, J.E. & Armstrong, J.R.M.(1991) Pyrethroid- treated bednet effects on mosquitoes of
unprotected peuple
the A,,,oets gnnlhiae complex in Ihc Gambia I. I.' I,, if
Veterinary Entomology 5, 477 -4í13.Lines, J.D., Myamba, J. Jr Curtis, C.F. (19H7) Fxperiu,rnl.11 I,,,t
trials of permethrin- Impregnated nets and eweagainst malaria vectors in Tanzania. Me11it'dl arid t'etrrur.0 i
Entomology 1, 37 -51.Moorhouse, D.E. & Wharton, 11.11. (19'S) SI (OIL'S un 1.1.0.,4 i,
vectors of malaria: ntclhothi of trapping and lrb?tn .111.'n,
on biting cycicx. Jnurmnl of Wheal i:mhmnnit {i y 1, jr0
Rowland, M., Bouma, M., Ducornez, D., Duranni. N.,
Rozendaal, J., Schaplra, A. & Sondorp, E. (1990)
Pyrethrold Impregnated bednets for personal prutvctwitfrom malaria for Afghan refugees. Transactions of ¡A. R.,.tlSiwlety of Tropical Mrlliein'. .ul.l 11,ysicn'. 90, 357-361.
Service, M.W. (1993) Mosquito wo/ogy, /is Is1stulplius moth .t. `n, l
c.11Y. 988 pp. Barking, Essex, Elsevier Science l'ubli.ha1sToker, M.A. (1991) lfui.r.rl strdislü,d ),.tek.;se. London, Ún1.1,,1
(Accepted 16 February 1997)t, CAD INTERNAI'IONAI., I997
Supplements end Special Issues
The Bulletin of Entonwlogical Re:anrch aims to publish special issues andsupplements which conçentrate on a particular topic. These fulfil the dualfunctions of contributing to the existing knowledge and providing anoverview of the subject area.
All supplements and special issues will be supplied to subscribers as part of theirannual volme. Apply to either the Editor -in- Chief or Publishing Editor forfurther details or to suggest topics of interest. '
Dr G M TatchellEditor -In- Chief, Bulletin of Entomological Research, International Instituteof Entomology, 56 Queen's Gate, London SW7 5JR, UKFax no.: +44 (0)171 .938 930911 -mail address: BCROcabt.org
David NicholsonPublishing Editor, Bulletin of Entomological &war lr, CAB INTERNATIONAL,Wallingford, Oxon OX10 UM, , UKTelephone: +44 (0)1491 832111 Fax No.: +44 (0)1491 82609013-mair d.nicholsoncabi.org
Do you need fast, friendly access to the latest scientific Information as abasis for practical pest management? From January 1997 this
Information will be available on CD -ROM.
Coverage:1000 major posts and (heirnatural enemies, many ofglobal importance
Specific emphasis on South-East Asia and Pacific
Covers arthropods,pathogens, weeds,nematodes and vertebrates,including quarantine pests.
150 crops of the world
150 countries of the world
Detailed, Illustrateddata, written byspecialists, providing:
Taxonomy & Nomenclature,Hosts, GeographicalDistribution, Biology,Detection & Iden(ilication,Movement & Dispersal,Pest Significance, Control,Phytosanilary Measures
Illustrations, Includingsymptoms, pests, pathogensand weeds
Global and regionaldistribution maps
Other features include:A bibliographic database ofprore than 50,000 referenceson pest management
Illustrated diagnostic keys
CROPS ..,,
g,. >z t `rmcar:xsNNIrr;r
PESTS .,,.
MINIM .wLV.r..., .r. T.^!--v. ... . ...__.._:on.. .{"jü'{,'It,2Srr'cjil"(': Y
NATURAL ENEMIES .... ..,,.... ..,.. uunr 1hlr2Ca aro . , ..,.. . : ; _á,ati!Trf;/++..T'Rd,.T
2.4
.+.'.' dY r,
AND MUCH, MUCH MORE ....
05)CAB INTERNATIONAL
Geographicalcoverage:
A uniquely comprehensiveglobal compilation. OutlineInformation on pests,diseases and weeds of theworld and their naturalenemies, with synonyms,host range, and geographicrange (mapped).
Selectdd agricultural andpost management data for allcountries of the world.
Detailed Information for SEAsia (Brunel, Cambodia,Indonesia, Laos, Malaysia,Myanmar, Philippines,Singapore, Thailand,Vietnam) and Includingsouthern China and theSouth Pacific
Trial disc available freeA fully interactive Windows
version on CO-ROM withselected dala is available for trial
with no obligation to purchase
For your free trial contact:CAB INTERNATIONAL, Wallingford,
OXON, OX10 80E, UKTel: +44 (0)1491 832111Fax: +44 (0)1491 826090
E-mail: publishing Ocabi.orgor CAB INTERNATIONAL,
198 Madison Avenue, New York,NY 10016, USA
Tel: +11212) 726. 6490Fax: +1 (212) 686 7993
Emall. cablnaoacabtorg
r
e-
/--
Sustainability of pyrethroid-impregnated bednets
for malaria contròi.in'Afghan communities*
M. Rowland,' S. Hewitt,' N. Durrani,3 P. Saieh,4 M. Bourne,' & E. Sondorpe
Between 1992 and 1995 a ,series of studies was undertaken to assess the long -term suitability of pyrethroid-
impregnated bednets (PIBs) formalaria control in Afghan refugee communities In two villages in North -West
Frontier Province, Pakistan. During 1992, 86% of bednet owners volunteered to have their bednets re-
impregnated, and a further 15% of families purchased nets at two -thirds of cost price. From 1992 onwards,
27% of the villagers returned to Afghanistan, and annual house spraying campaigns were introduced to
protect those still resident but sleeping without bednets. Within 3 years, these campaigns, together with
P/Bs, reduced the annual Incidence of malaria by 87%, from 597 to 78 cases per 1000 population.
ertheless, 65% of resident families continued to re-Impregnate their nets annually with permethrin. To
'triton whether PIBs were still being used and were still protective, In view of these reduced transmission
rates, we carried out a case control study in 1994 on febrile or otherwise symptomatic patients presenting
at village health centres. Comparison of the slide -positivity rates of PIS users and those without bednets
showed that regular usage reduced the odds of contracting falciparum and vivax malaria to 0.22 (95%
confidence Interval (Cl): 0.09-0.55) and 0.31 (95% Cl: 0.19- 0.51), respectively. There was no evidence of
a sex- or age -bias in bednet use or in protective effect. The results Indicate that a community -based P1B
programme is an appropriate malaria control measure in areas where management or security problems
make traditional house -spraying campaigns Impossible.A relevant finding for those Involved In the monitoring of bednet dlstribuliori projects. is that the local
coverage of bednets and the local Impact on malaria, even when Introduced to remote areas, can be
estimated very cheaply by health centre microscopists who simply catalogue blood film diagnoses according
to patients' bednet use practices.
introductionField trials in ninny countries have demonstratedthat use of pyrethroid-impregnated bednets (l'II3s) is
effective for preventing malaria (1). Even in coun-tries where there is no great tradition of bednet use,
carefully conducted field triads, where appropriate'ention is paid to health education before and dur-
L..á implementation, generally show that recipientsuse the nets with enthusiasm and to good effect. Oner such trial was conducted in Afghan refugee cantps in1991; the incidence of clinical parasilaemic episodeswas reduced by 53% in an intervention group whose
previous use of nets was only 2% (2). Nevertheless, at
number of questions remain on whether use of Pins
From: tieanhNet International, P.O. Bos 11011, University Town,
Peshawar. North West Frontier Province. Pakistan. Requests lot
reprints should be sent to Or Rowland at this address.
' Coordinator. Malaria Control Programme.
Vector Control Manager..- Parasitologist and Laboratory Manager.
Bednet Project Manager.Formerly: Coordinator. Malaria Control Programme.
Director.T Reprint No. 0700
8uarbn of the Weld Health Orpanrrarion. 1997. TS (t): 23 -29
n+- .
is a sustainable soulegy for malaria control: Will
recipients continue to use their nets in the lung term
in the absence of further encouragement? Will re-
cipients actively participate in the re- impregnation
process and thereby help to reduce recurrent im-
plementation costs? Will neighbours buy bednets for
themselves? Will the reduction in malaria he sus-tained? Will people continue to use nets if a second
method of control - house spraying, for example -
is conducted simultaneously?This article describes a number of follow -up
studies in she Afghan trial villages that attempt toanswer such questions.
Methods.Distribution, re- Impregnation andsale of bednets
The two trial villages,l3aghiclut and Kagan, are situ-
ated in Mardan district. North -West Frontier Prov-ince, Pakistan. Extended faultily groups of Afghanrefugees live in houses constructed from mud andlocated within high -walled compounds. The underly-
ing water table is higher than normal for the district.
(I World Health Ow. arerahon 199723
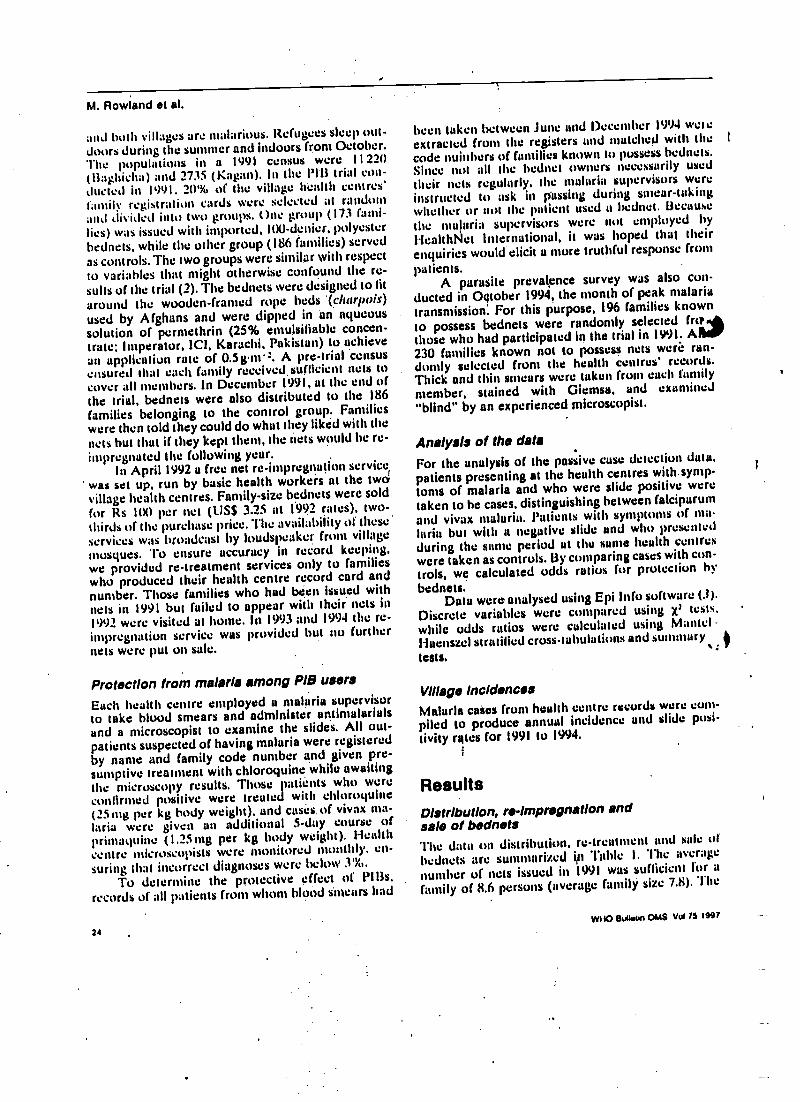
M. Rowland et al.
and both villages are ntalarious. Refugees sleep out-doors during the summer and indoors from October.The populations in a 1991 census were 11220(tlaghicha) and 2735 (Kagan). In the PCB trial con -ducted in 1991, 20'lí, of the village health centres'family registration cards were selected at randomand divided into two groups. One group (I73 fami-lies) was issued with imported, 100-denier, polyesterbednets, while the other group (186 families) servedas controls. The two groups were similar with respectto variables that might otherwise confound the re-sults of the trial (2). The bednets were designed to litaround the wooden -framed rope beds (charpois)used by Afghans and were dipped in un aqueoussolution of pernethrin (25% emulsifiable concen-trale; Imperator, 1C1, Karachi, Pakistan) to achievean application rote of 0.5g11'2. A pre -trial censusensured that each family received.suftleient nets tocover all members. In December 1991, at the end ofthe trial, bednets were also distributed to the 186families belonging to the control group. Familieswere then told they could do what they liked with thenets but that if they kept them, the nets would be re-impregnated the following year.
In April 1992 a free net re- impregnation service' was set up, run by basic health workers at the twávillage health centres. Family -size bednets were sold
for Rs 100 per net (LISS 3.25 at 1.992 rates), two -
thirds of the purchase price. "1'he availability of theseservices was broadcast by loudspeaker from villagemosques. To ensure accuracy in record keeping,we provided re- treatment services only to familieswho produced their health centre record card andnumber. Those families who had been issued withnets in 1991 but failed to appear with their nests in1992 were visited at home. In 1993 and 1994 the re-impregnation service was provided but no furthernets were put on sale.
Protection from malaria among P/B users
Each health centre employed a malaria supervisorto take blood smears and administer antimalarialsand a microscopist to examine the slides. All out-patients suspected of having malaria were registeredby name and family code number and given pre-sumptive treatment with chloroquine while awaitingthe microscopy results. Those patients who wereconfirmed positive were treated with chloroqulne(25 mg per kg body weight). and cases. of vivax ma-!aria were given an additional 5 -day course ofprincatluine (I.2S mg per kg body weight). Healthcentre microscopists were monitored monthly. en-suring that incorrect diagnoses were below 3 %.
To determine the protective effect of Pills,records of all patients from whom blood sincars had
24
been taken between June and December 1994 woeextracted from the registers and matched with the t
code nuiuhers of families known to possess hednets.Since not all the bednet owners necessarily usedtheir nets regularly, the malaria supervisors wereinstructed to ask in passing during smear- takingwhether or not the patient used u hedmet. Because
the malaria supervisors were not employed byHealthlsiet International, it was hoped that theirenquiries would elicit u more truthful response from
patients.A parasite prevalence survey was also con-
ducted in Oßlober 1994, the month of peak malariatransmission: For this purpose, 196 families knownto possess bednets were randomly selected frothose who had participated in the trial in 1991. A230 families known not to possess nets wera ran-domly selected from the health centres' records.Thick and thin smears were taken from each familymember, stained with Giemsa, and examined"blind" by an experienced microscopist.
Analysis of the dataFor the analysis of the passive case detection data.patients presenting at the health centres with.symp-toms of malaria and who were slide positive weretaken to he cases, distinguishing between falciparumand vivax malaria. Patients with symptoms of ma-laria hut with a negative slide and who presentedduring the same period at the sume health centreswere taken as controls. By comparing cases with con-trols, we calculated odds ratios for protection bybednets.
Data were analysed using Epí Info software (.1).Discrete variables were compared using x' tests.while odds ratios were calculated using Mantel -Huenszcl stratified cross -tabulations and summary
lests. e ;
Village incidencesMalaria cases from health centre records were cunt -
piled to produce annual incidence and slide posi-tivity rates for 1991 to 1994.
ResultsDistribution, re- Impregnation andsale of bednetsThe datum on distribution, re-treatment und sale of
bednets are summarized ion 'fable I. The averagenumber of nets issued in 1991 was sufficient l'or u
family of 8.6 persons (average family size 7.8). The
w110 sullrGn OMS Vol 7s 1957
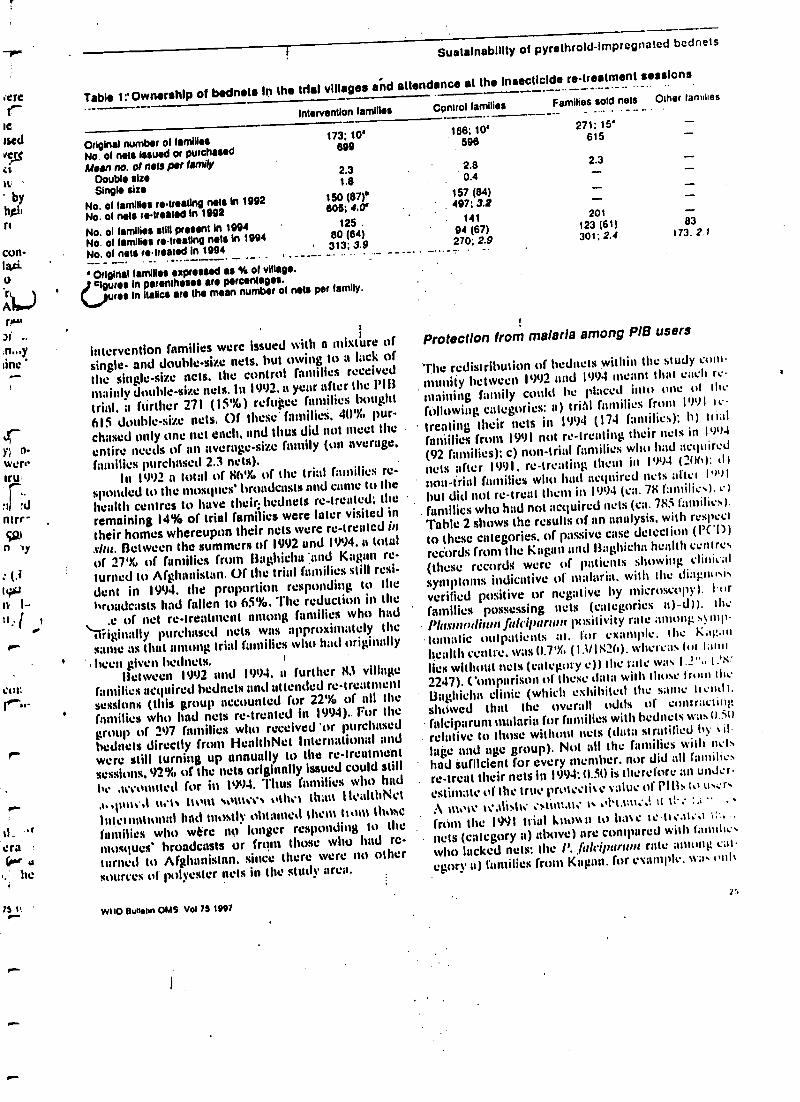
-10,"`
;ere
Ie
¡sedvat
tu
byharla
n
con-tari.o
A bly*"r!t'ar ,.
n...yaine '
17y; l'-wen.aru
!ci
ntrr-S1n tiy
i4+¡n i-tt, f 1rrcolt
r
75 It
Sustalnabllity of pyrelhrold-imprcçnatod bednels
Table 1 "Ownership of bednets In the trial villages and attendance at the Insecticide re- treatment sessions
Intervention families Cpntrol families Families sold nets Other families
83í73;2.r
Original number of familiesNo at nets Issued or purchasedMein W. 01 nets per tamij'
Doubts sizeSingle size
No. of families retreating nets In 1992No. of nets retreated In 1992
No. 01 families still present In 1994
No. of families retreating nets In 1994
No. of nets retreated in 1994
173; 10'699
2.31.0
150 (87)'606; 4.0'
125 .80 (84)
' 313: 3.9
186; 10'596
2.80.4
157 (84)497; 3.2
14194 (67)270; 2.9
271: 15'615
2.3
201123 (61)301; 2.4
Original tamales expressed u S of village.Nam in parenthesis are percentages.
urea In italics are the mean number of nets per family.
intervention families were issued with a mixture of
single- and double -size nets, but owing to a lack of
the single -size nets. the control families received
mainly double -size nets. in 1992. a year after the í'I13
trial. a flirther 271 (15'Xt) refugee families bought
615 double -size nets. Of these families. 40% pur-
chased only one net each. and thus did not meet the
entire needs of an average-size family (on average.families purchased 2.3 nets).
In 1992 a total of üt'i1 of the trial families re-sponded to the mosques' broadcasts and came to the
health centres to have their; bednets re- treated: theremaining 14% of trial families were later visited in
their homes whereupon their nets were re- treated in
situ. Between the summers of 1992 and 1994. a total
of 279L of fatuities from liagtlicita and Kagan re-turned to Afghanistan. Of the trial families still resi-
dent in 1994, the proportion responding to thel'raadcasts had fallen to 65%. The reduction in the
.e of net re- treatment among families who hadoriginally purchased nets was approximately thesame as that among trial families who had originally
been given bednets.Between 1992 and 1994. a further 83 village
families acquired bednets and attended re-treatmentsessions (this group accounted for 22'yu of all thefamilies who had nets re- treated in 1994).. For thegroup of 297 families who received or purchasedbednets directly from HealthNet International andwere still turning up annually to the re- treatmentsessions. 92% of the nets originally Issued could stillhr .counted for in 1994. Thus fatuities who had
'h.(utat.,l nets horn souses ttlht'% than 1lealthl\el
lntelnnttttmtl had mostly obtained them titian those
families who wbrc no longer responding to the
masques' broadcasts or front those who had re-turned to Afghanistan. since there were no other
sources of polyester nets in the study area.
WHO aun.m OMS. Vol 79 1997
Protection from malaria among PIB users
The redistribution of bednets within the study com-
munity between 1992 and 11)94 meant that each re-
maining fancily could he placed into one of the
following categories: a) trii11 families fruttt 1991 Ic-
treating their nets in 1994 (174 families): h) vialfnniities from 1991 not re-treating their nets in 19')4
(92 families): c) non-trial families who had acquired
nets after 1991, re-treating them in I')94 (21)(1): tai
non -trial families who had acquired nets after l's)Ibut did not re -treat them in 1994 (ca. 78 f'amttilies): e)
families who had not acquired nets (ca. 785 families).
Table 2 shows the results of an analysis. with respect
to these categories, of passive case detection (PC I))
records from the Kagan and 13aghicha health centres
(these records; were of patients showing clinical
symptoms indicative of malaria. with the diagnosis
verified positive or negative by microscopy). forfamilies possessing nets (categories a) -d)). the
Plasnarrrlium falcilraraur positivity rate antong SVntp-
lontaatic outpatients at. for example, the Kagan
health centre. was 0.7'X. (I3/I1t2(1), whereas It I;nllies wilh0111 nets (category e)) the rate was I.' ".. t.'ti(
2247). Comparison of these data with those trout IlanI3aghietta clinic (which exhihitecl the same tient11.
showed that the overall odds of contractingfalciparum malaria for families with bednets was 0.31)
relative to those without nets (data stratified hy ail.
Inge and age group). Not all the families with netshad Sufficient for every member. nor did all families
re -treat their nets in 1994: 0.5t1 is therefore an under.
estinatt.' of the true proteetiv e value of Pillsll. to
111.`11' realist): :stint.tt t'..tl`l.lttt;; it tf .
front the 1991 trial knout) to hate ie ¡1:.11;.1 t; ...
nets (category a) above) are compared with families
who lacked nets: the N.. fuh'ilittrrun rate among cat-
egory a) families front Kagan. for example. 1e :a, on),
25
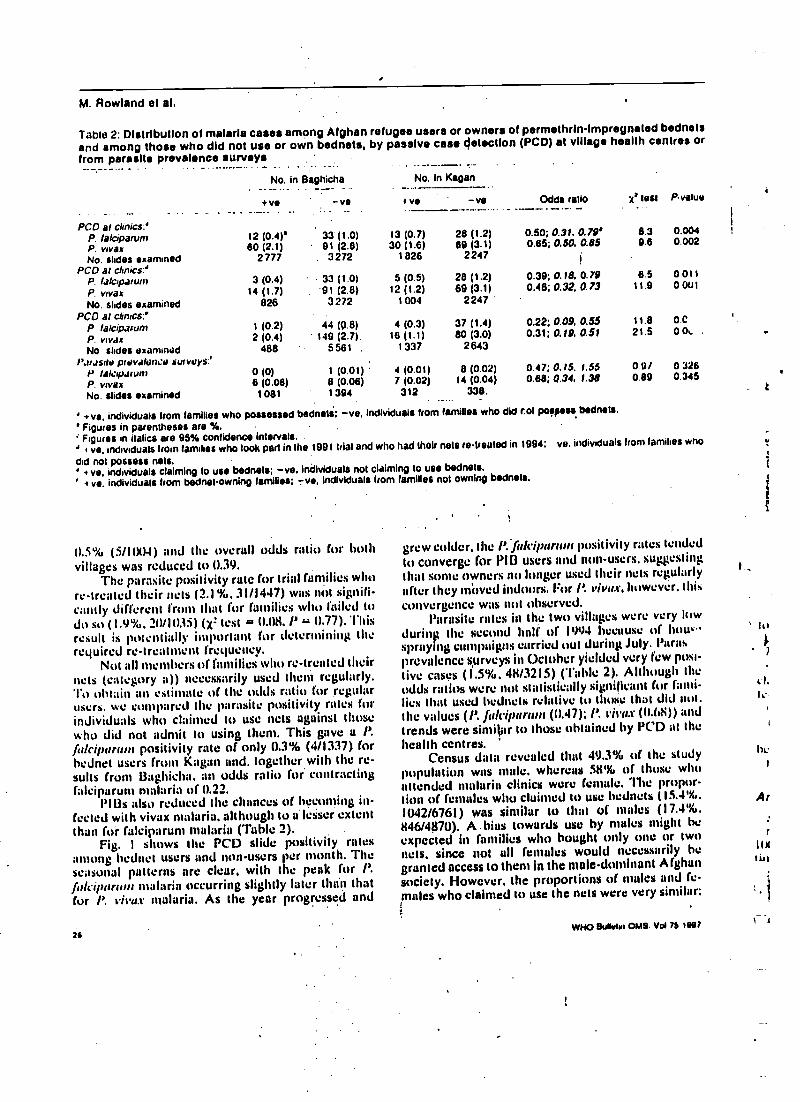
M. Rowland el al.
Table 2: Distribution of malaria cases among Afghan refugee users or owners of permelhrin- Impregnated bednetsand among those who did not use or own bednets, by passive case detection (PCD) at village health centres orfrom parasite prevalence surveys
PCO at clinics:'
No. in Baghicha
+ve -ve
No. In Kagan
Odds rati ;t' lest Pvalue+ ve -ve
P. lalciparum 12 (0.4)' 33 (1.0) 13 (0.7) 28 (1.2) 0.50; 0.31. 0.79' 8.3 0.004
P. max 60 (2.1) 91 (2.8) 30 (1.6) 89 (3.1) 0.85; 0.50, 0.85 9.8 0.002
No. slides examrned 2777 . 3272 1 826 2247PCO at chnics:'
P. lalcrpatunt 3 (0.4) 33 (1.0) 5 (0.5) 28 (1.2) 0.39; 0.18, 0.79 6.5 0 011
P. vrvax 14 (1.7) . 91 (2.8) 12 (1.2) 69 (3.1) 0.40; 0.32 0.73 11.9 0.001
No. slides examined 826 3272 1004 2247
PCO at cunres:'P lalcrpawnt 1 (0.2) 44 (0.8) 4 (0.3) 37 (1.4) 0.22; 0.09, 0.55 11.8 D.0
P. vrvdx 2 (0.4) 149 (2.7). 16 (1.1) 80 (3.0) 0.31; 0.19. 0.51 21.5 00i. .
No slides examined 488 5561 . 1337 2643
P,1rJSNtl prevalence surveys.'Y laldrpdrunt 0 (0) 1 (0.01) 4 (0.01) 8 (0.02) 0.47; 0.15. 1.55 0.9/ 0 326
P. vrvax 6 (0.08) 8 (0.06) 7 (0.02) 14 (0.04) 0.68; 0.34, 1.38 0.89 0.345
No. slides examined 1081 1394 312 338. t
' eve. individuals from families who possessed bednets; -ve, Individuals from families who did rot po }pess bednets.
' Figures in parentheses are %.Figures in italics are 95% confidence intervals.
' I ve. individuals from families who took part in the 1991 trial and who had their nets retreated in 1994: ve. individuals Iron tamales who
did not possess nets.I ve, individuals claiming to use bednets; -ve. Individuals not claiming to use bednets.
' + vs, individuals from bednetowning Iamibes; -ve, Individuals 'tom families not owning bednets.
01.5% /p (S /1004) and the overall odds ratio for bothvillages was reduced to 0.39.
The parasite positivity rate for trial families whore- treated their nets (2.1%. 31/1447) was not signifi-cantly different from that for families who failed todu so (1.9%. 20/103i) (X= test = 0.1)8. P - 0.77). Thisresult is potentially important for determining therequired re-treatment frequency.
Not all members of families who re- treated theirnets (category a)) necessarily used them regularly.To uhlaitt an estimate of the odds ratio for regularusers. we compared the parasite positivity rates forindividuals who claimed to use nets against thosewho did not admit to using them. This gave a P.falci/7arum positivity rate of only 0.3% (4/1337) forbednet users from Kagan and. together with the re-sults from 13aghicha. an odds ratio for contractingfalciparunt malaria of 0.22.
Pills also reduced the chances of be:conting in-fected with vivax malaria. although lu u lesser extentthan for falciparum malaria (Table 2).
Fig. 1 shows the PCD slide positivity ratesamong bednet users and non -users per month. Theseasonal patterns are clear, with the peak for P.fr,/riparson malaria occurring slightly later thain thatFor P. vivax malaria. As the year progressed and
24
grew colder. the P.f ticiparuur positivity rates tendedto converge for PIO users and non -users, suggestingthat sonic owners no longer used their nets regularlyafter they mitved indoors. For P. vit'u.r, however. 1111%
convergence was not observed.Parasite rotes in the two villages were very low
durinit the second half of 1994 because of how..spraying campaigns curried out during July. Parasprevalence surveys in October yielded very few posi-tive cases ( 1.5%. 411 /3215) ('fable 2). Although theodds ratios were not statistically significant for fami-lies that used bednets relative to those that did not.the values (l'. fuleiparulli (0.47); P. vii'ux (0.68)) and
trends were similaar to those obtained by PCD at the
health centres.Census data revealed that 49.3% of the study
population was male. whereas 58% of those whoattended malaria clinics were female. The propor-tion of females who claimed to use bednets (15.4 %.1(42/6761) was similar to that of males (17.4 %.
I{46/4870). A. bias towards use by males might beexpected in families who bought only one or Iwonets. since not all females would necessarily hegranted access to theni in the male -dominant Afghansociety. However, the proportions of stales and fe-males who claimed to use the nets were very similar:
t
WHO 8 ilvh.r OMS. Vol 76 real
lu
rI.Ir,
i,c
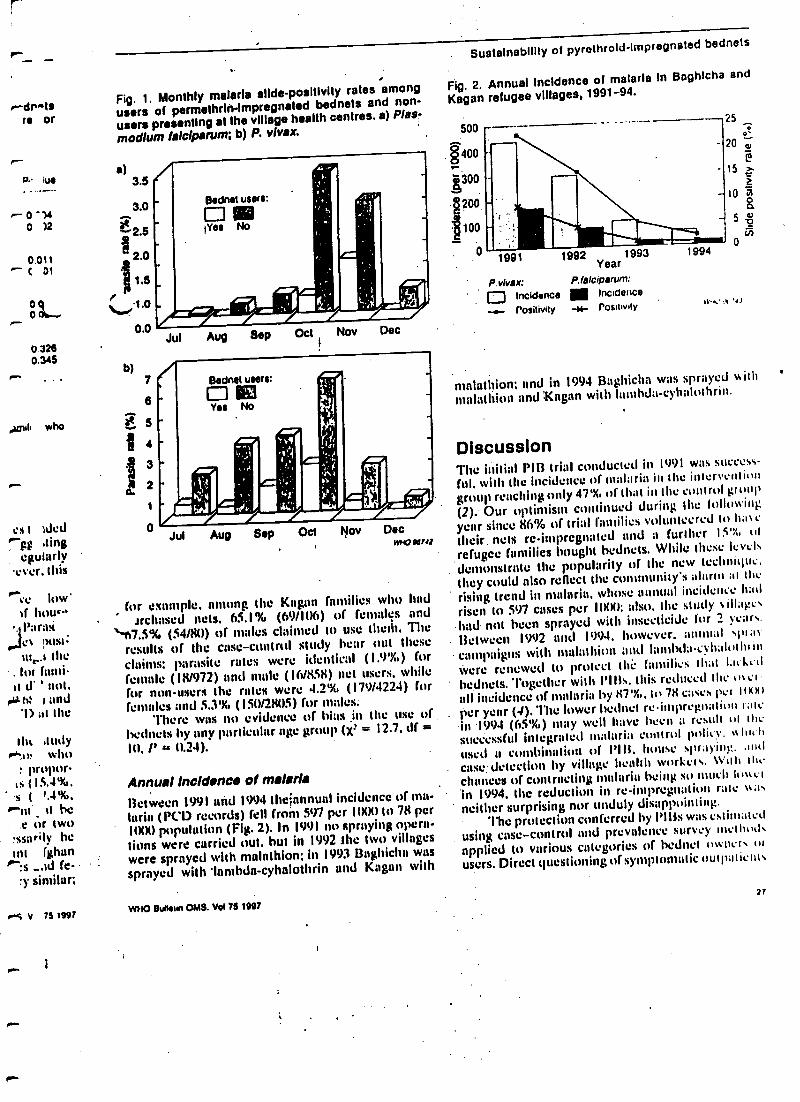
rdrstsTO or
p-
p.' hie
0-K0 )2
0.011C 01
0o qor...
032s0.345
Arbil who
es 1 tded0-Fg ,ting
egtularly'ever, this
'e low'of how.'l'lra%ea nest=ni ,.l the
. for farni-it d' ' not.
,F h: and'1) at the
BR antsy-^.u, who
prupor-is (13.4%,
.s ( +.4 %,
'tn _ It he.e or two
!ssarily hegrit fg ;hen
p" :s ...id (e-ry similar;
rS v 75 ,997
Fig. 1. Monthly matarla slide -positivity rates among
users of permethrin- Impregnated bednets and non-
users presenting at the village health centres. a) Plas-
modium lalclparum; b) P. vivax.
a)3.5
3.0
2.5
2.0
0.0
b)7
6
S
ji
Jul Aug 8ep Oct Nov Dec
Jul Aug Sep Oct Nov DecWHO WO
for example. among the Kagan families who hadirchased nets. 65.1% (69/11)6) of females and
'-t7.5% (54/80) of males claimed to use thetit, Theresults of the case -control study hear out theseclaims: parasite rates were identical (1.9'X,) forfemale (18/972) and male (16/858) net users. whilefor nun -users the rates were 4.2'X, (179/4224) forfemales and 5.3'X% (1511/28115) for males:
'l'here was no evidence of bias in the use ofbednets by any particular age group (X= = 12.7, df =
lu, l' ss 0.24).
Annual incidence el malariaBetween 1991 and 1994 theiannual incidence of ma-
laria (PCD records) fell from 597 per ((KK) to 78 per100) population (Fig. 2). In 1991 no spraying opera-tions were carried out. hut in 1992 The two villages
were sprayed with matathion; in 1993 Baghicha wassprayed with 'lambda-cyhaiothrin and Kagan with
Sustalnabllity of pyrothrold- Impregnated bednets
Fig. 2. Annual Incidence of matarla In Baghicha and
Kagan refugee villages, 1991 -94.
500
§400
,1̀ 300
g200
1100
01991 1992 1993
Year
P.vivax: P.fa/ciparwn:
EJ Incidence IIII Incidence
-..- Positivity -M- Positivity
20
1994
5
o
malathion; and in 1994 Baghicha was sprayed with
matathion and Kagan with lanihda- cyhalothrin.
DiscussionThe initial PIn trial conducted in 1991 was success
fui. with the incidence of malaria in the intervention
group reaching only 47'X, of that in the control group
(2). Our optimism continued during the following;
year since 86% of trial families volunteered to base
their. nets re-impregnated and a further I5'i, ofrefugee families bought hcdnets. While these levels
demonstrate the popularity of the new technitic.they could also reflect the community's alarm at the
rising trend in nutltria, whose annual incidence hadrisen to 597 cases per I(KKI: also. the study %M ag e.
had not been sprayed with insecticide for 2 years.Between 1992 and 1994. however, annual spt.ivcampaigns with matathion and lanlhdacvhaluthl iii
Were renewed to protect the families that lack cdbednets. Together with Pills. this reduced the met
all incidence of malaria by 87'%,, to 7N cases per itself
per year (4). The lower bednet re-impregnation rate-in I91)4 (65'X.) may well have been a result of tlcsuccessful integrated malaria control policy. %%hu h
Wed a etnlhination of 19 B. house spraying. andCase; detection by village health workers. 1ti grh die
chances of contracting malaria being so much loaact
in 1994, the reduction in re- impregnation rate was
neither surprising nor unduly disappointing.The protection conferred by flits was estimated
using case -control and prevalence survey umetho,a1s
applied to various categories of bednet owners ofusers. Direct questioning of symptomatic outpat ient.
WHO Bulletin OMS. Vol 75 1997
?>'
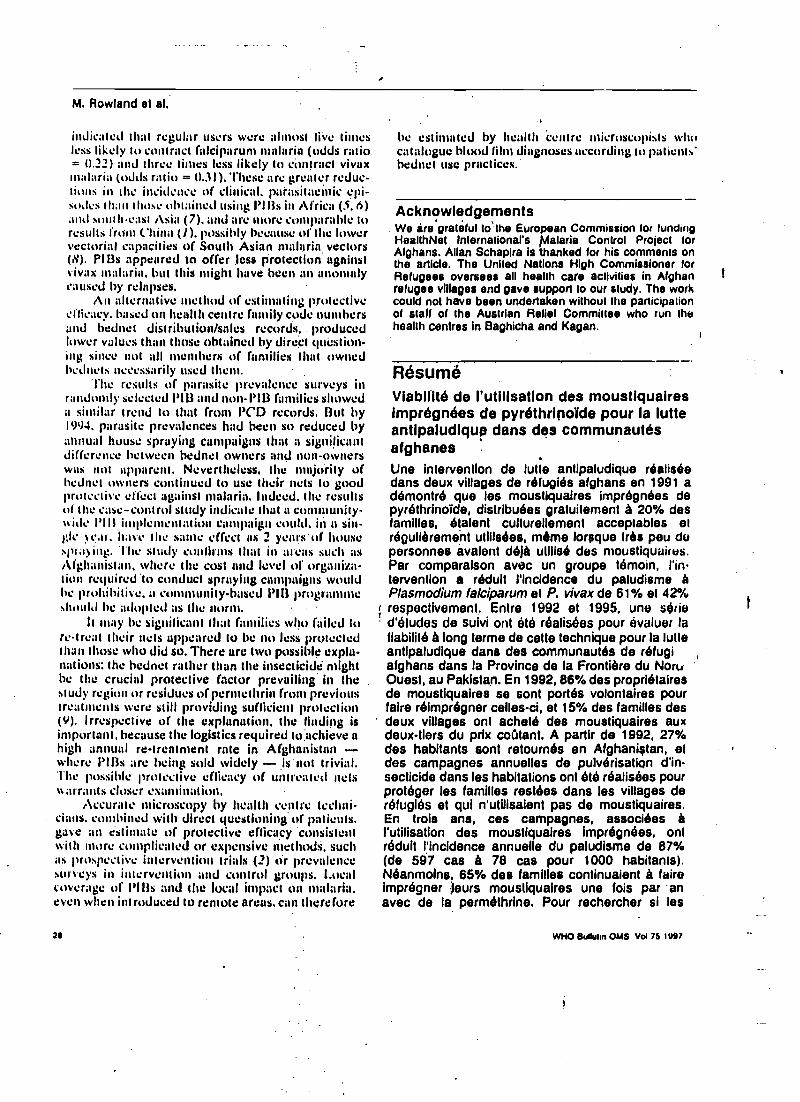
M. Rowland et al.
inJicatet that regular users were almost live limesless likely to contract falciparum malaria (odds ratio= 0.22) and three times less likely to contract vivaxmalaria (odds ratio = 0.31). These are greater redue,Lions in the incidence of clinical. parasitacinic epi-suJc% than those obtained using PI I3s in Africa (5.6)and south-east Asia (7). and are more comparable toresults from China (i). possibly because ol'the lowervectorial capacities of South Asian nu laria vectors(8). PlBs appeared to offer less protection ugninstvivax malaria, but this Wright have been an anon mycaused by relapses.
An alternative method of estimating Protectivecfticacy. based on health centre family code numbersand hednet distribution /sales records, . producedlower values than those obtained by direct question-ing since nut all members of families that ownedhcdncts necessarily used them.
The results of parasite prevalence surveys inrandomly selected P1U and non -Pl13 families showeda similar trend to that from PCD records. But by1994. parasite prevalences had been so reduced by:nunual house spraying campaigns that a significantdifference between hednet owners and non- ownerswas not apparent. Nevertheless, the majority ofhednet owners continued to use their nets to goodprotective effect against malaria. Indeed. the resultsof the case -control study indicate that a cummunity-ttide PlIt implementation campaign coula. in a sin-gle ear, have the saute effect as 2 ycars'of housesltra)ilg. The study confirms that in areas such asAfghanistan. where the cost and level of organiza-lion required conduct spraying campaigns wouldhe prohibitive. a community -based Pl13 programmeshould he adopted as the norm.
It may he significant thai families who failed tore -treat their nets appeared to he no less protectedthan those who did so. There are two possible expla-nations: the hednet rather than the insecticide mighthe the crucial protective factor prevailing in the .
study region or residues of permethrin front previoustreatments were still providing sufficient protection(9). Irrespective of the explanation, the landing isimportant, because the logistics required to:achieve ahigh annual re- treatment rate in Afghanistan -whcre PIBs are being sold widely - is 'not trivial.The possible protective efficacy of untreated netsarrants closer examination.
Accurate microscopy by hcallh centre techni-cians. combined with direct questioning of patients.gave an estimate of protective efficacy 'consistentwith more complicated or expensive methods, suchas prospective intervention trials (2) tir prevalencesurveys in intervention and control groups. Localcoverage Of l'113s and the local impact on malaria.even when introduced to remote areas, can therefore
21
he estimated by health centre microscopists whocatalogue blood lilnm diagnoses according to patients'hednet use practices.
AcknowledgementsWe are grateful to the European Commission for fundingHealthNet International's Malaria Control Project forAfghans. Allan Schapira is thanked for his comments onthe article. The United Nations High Commissioner forRefugees oversees all health care activities in Afghanrefugee villages and gave support to our study. The workcould not have been undertaken without the participationof staff of the Austrian Relief Committee who run thehealth centres in Baghicha and Kagan.
RésuméViabilité de l'utilisation des moustiquairesImprégnées de pyréthrinoïde pour la lutteantlpaludiqup dans des communautésafghanesUne intervention de lutte antipaludique réaliséedans deux villages de réfugiés afghans en 1991 adémontré que les moustiquaires imprégnées depyréthrinoide, distribuées gratuitement à 20% desfamilles, étaient culturellement acceptables elrégulièrement utilisées, mémo lorsque très peu dupersonnes avalent déjà utilisé des moustiquaires.Par comparaison avec un groupe témoin, l'in-tervention a réduit l'incidence du paludisme àPlasmodium falciparum et P. vivez de 61% et 42%respectivement. Entre 1992 et 1995, une serie
` d'études de suivi ont été réalisées pour évaluer lafiabilité à long terme de cette technique pour la lutteantipaludique dans des communautés de réfugiafghans dans la Province de la Frontière du Non,Ouest, au Pakistan. En 1992, 86% des propriétairesde moustiquaires se sont portés volontaires pourfaire réimprégner celles -ci, et 15% des familles desdeux villages ont acheté des moustiquaires auxdeux -tiers du prix coûtant. A partir de 1992, 27%des habitants sont retournés en Afghanistan, etdes campagnes annuelles de pulvérisation d'in-secticide dans les habitations ont été réalisées pourprotéger les familles restées dans les villages deréfugiés et qui n'utilisaient pas de moustiquaires.En trois ans, ces campagnes, associées àl'utilisation des moustiquaires imprégnées, ontréduit l'incidence annuelle du paludisme de 87%(de 597 cas à 78 cas pour 1000 habitants).Néanmoins, 65% des familles continuaient à faireimprégner leurs moustiquaires une lois par .anavec de la perméthrine. Pour rechercher si les
WHO Sullptm OMS Vol 75 1997
1
.la- uhe)).l ts'
r lendingai,,ct for)u ontc for
Aignanile woif.tir ton
the
luáiresa7 telE_
r sée1 ,a1 anées de
dus1t utti u deIretu sin es.
4+0 l'ir1-
d- 3 342%
rh) SullelVOL !I Li
UI ulte!I_.uglt
du "lorc,-pw mes0. . ¡Jouimues dessire aux39` ?7%
an. etlion d'in:ee aourIIr > de.lr, 'aires.)ciéAs àee: ont. 87%
L1 tains).;nt ' fairesoc ante .. les
moustiquaires étaient encore utilisées et con-servaient leur efficacité protectrice avec tin taux detransmission aussi réduit, nous avons effectué uneélude cas -témoins en 1994 sur les malades fébriles
ou présentant d'autres symptômes vus dans les
centres de santé des villages. Une comparaisonde la positivité des lames chez les utilisateurs etnon -utilisateurs de moustiquaires a montré quel'utilisation régulière de celles -ci réduisait le risquerelatif de contracter un paludisme à (alciparum à 5.
0,22 (intervalle de confiance à 95%: 0,09 -0,55 etun paludisme à vivax à 0,31 (IC 95 %: 0,19- 0,51).Aucun biais lié au sexe ou à l'äge n'est apparudans l'utilisation des moustiquaires ni dans l'effetrotecteur. Ces résultats indiquent qu'un pro-
...dramme communautaire d'utilisation des mousti- 6.
quaires imprégnées est une mesure appropriéede lutte antipatudique dans les régions où desproblèmes de gestion ou de sécurité rendentimpossibles les campagnes traditionnelles de pul-vérisation dans les habitations, et que la couverturede ces programmes el la protection qu'ils confèrentpeuvent ètre évaluées de façon simple et exactepar un microscopiste de poste sanitaire.
3.
4.
References1. Curtis CF. Control of disease vectors.in the commu-
nity. London, Wolfe Publishing, 1901.2. Rowland M el al. Pyiethroid- impregnatud bud nuts for
self protection (rom malaria in Afghan refugees. Trans-
7.
8.
9.
Sustatnabillty of pyrethroidirnpregnaled bednels
actions of the Royal Society of Tropical Mudicrnu andHygiene, 1996, 90: 357 -361.Dean AG el al. Epi Info, version 5: a word processing.database, and statistics propret!) for erpideruologyStone Mountain, GA, USU Inc, 1990.Rowland M, Hewtll S, Durraní N. Malaria prevalencesurveys in refugee camps sprayed with malathion andlambdacyhalolhrin. Transactions of the Royal Societyof Tropical Medicine and Hygiene. 1994. 88: 378-
379.Alonso PL et al. A malaria control trial using
insecticide -treated :bed nets and targeted citerne -
prophylaxis in a rural area of The Gambia. West Africa
6; The Impact of the intervention on mortality andmorbidity (rom malaria. Transactions of are RoyalSociety of Tropical Medicine and Hygiene. 1993.
87(suppl. 2): 37 -44.Beach RF et al. Effectiveness of permethnn
impregnated bed nets and curtains for malaria curd!°+
In a holoondumic area of western Kenya. An nc,utjournal of tropical medicino and hygiene, 1993. 49
290 -300.Luxemburger C et at. Permethrinimpregnated badnets for the prevention of malaria in schoolchildren oitthe Thai -Burmese border. Transactions of the RoyatSociety of Tropical Medicine and Hygiene. 1994, 88
155 -159.Reisen WK, 8orehem FL. Estimates of malaria
vectorial capacity for Anopheles culicilacies and Astephens! in rural Punjab province, Pakistan. Journalof rpedical entomology, 1982, 19: 98 -103.
Miller JE et al. Village trial of bed nets impregnaledwith wash -resistant permelhrin comparud with °tlhug
pyrelhroid formulations. Medical and vutenniry utilemoiety, 1995, 9: 43 -49.
., , gyl: WHO Lhdhu..i OMS Vol 75 1997
29
,--
Annals cif Tropical Medicine and l'arasitulegy, Vol. 90, No. 3, 337-344 (1999
Self -protection from malaria vectorsin Pakistan: an evaluation of popularexisting methods and appropriatenew techniques in Afghan refugeecommunities .
lii S. E. 11I:1V1T'l', M. FARIIAN, H. URIIAhIAN, N. MUIIAMMAI),M. KAMM. AND ht. W. RO\V1.ANI)lltuhhNrt International, P.O. But 889, lhtirersis:y 7utrit, Peshawar, North
West Frontier Province, Pakistan .
Receives! 25 July 1995, Revised 25 January 19%, Accepted 29 January 19tJG
Experimental huts were used to measure the impact of several techniques for self -protection from malaria
vectors in Pakistan. An electric fan, pyrethrum coils, untreated curtains, pyrethrumd- vaporizing nests
and permethrin- impregnated curtains reduced the total catches of blood -fed Anopheles stephensi by 27'!ú,
34%, 47 %, 56'ií, and 65':í,, respectively. The most marked effect of all the interventions was in reducing
the numbers of mosquitoes entering the huts, although all the techniques, except for die untreated cortain,
also reduced the proportion of mosquitoes inside the hut which fed. Although the trends seen were simi-
lar for both anopheline (all .In. stephenst) and culicine mosquitoes, they were more pronounced in the
culicines.Social surveys were conducted on current self-protection practices. The social and economic constraints
associated with each of the various techniques arc discussed. All the strategics were shown to offer a degree
of protection and their use should be encouraged. Impregnated curtains seem especially promising.Pyrethroid- impregnated bedncts have been widely promoted in eastern Afghanistan since 1991 and have oho;
advantage of providing protection when people sleep outside during the summer. 1 Iowever, surveys show
that some owner stop using their nets in late autumn, despite the continued risk of malaria. People should
be encouraged to use their bedncts as impregnated curtains rather than putting them into storage.
L.- Over the last 3 years HcalthNct International(UNI) has bccn responsible for co- ordinatingthe sale of 150 000 insecticide -impregnatedbedncts (covering approximately 400 000
people) in refugee communities in Pakistanand in settlements in the eastern provinces ofAfghanistan. This programme is expandingbut still only covers a small section of thepopulation. It was therefore decided to assessthe efficacy of various alternative means ofself - protection for use either in the absence ofnets or in conjunction with them. Althoughthe techniques evaluated here have been as-sessed before in different countries (Smithet al., 1972; Charlwuod and Jolley, 1984; I3irlcyet al., 1987; Lines et al., 1987; Majori et al.,
0(U14-4983/96/030337+08 St1.(10/(1
1987; Sexton et u!., 1990; Curtis a al., I991a,6), not all have been compared simultaneously,besides which regional differences in housingconstruction and vector species warranted aseparate study in Pakistan.
MATCRIAI.S ANI) METI iOUS
SurveyA survey was conducted by male and l'crtt;tlebasic -health workers in refugee communitiesnear Peshawar (North West lronticr Province,Pakistán) to gather information on practicesrelated to self -protection from mosquitoes.Only villages that had never been targeted for
.(t) 1.996 I.,vt:rpaol SchlNd or Ir1111ic1t Jlcaicinc
338 I 1 E\\'1'I"1' Er . 11..
bednet sales were visited. The interviewsstarted with open questions about the methodsof protection used (e.g. Do you protect your-.self from mosquito bites? How ?). These werefollowed by more direct questions (e.g. Du youuse fans ?). interviews were held simultane-ously, but in separate parts of each compound,with senior males and their wives. Any dis-crepancies between man and wife in the
answers tu leading questions were queried bythe health workers at the end of the formalinterview, after comparing the two sets ofanswers.
Trials'I'he trials wcrc carried out at Azakhel refugee
camp near Peshawar. The numerous borrowpits, elevated water table and spring andautumn flooding in this area account for rela-tively high mosquito densities in the camp,%%
hich had a population of about 20 000 at the
time of the study.
EXP RI\IENTAI. IIUT DESIGN
The trials were conducted in six experimentalhuts, each measuring, internally, 3.5 m Tong,3.5 nt wide and 2.3 nt high. 'l'hey were built intraditional style, with 0.7 -m -thick walls of mudand flat roofs made of reeds plastered an topwith a 0.2 -m layer of mud. Each hut had fourwindows (05 m X ll 5 m), one in the centre ofeach wall, and a single, tight -fitting door. Thehuts were arranged, 5 m from one another, intwo parallel rows of three, running from eastto west within the mud walls of a large com-pound. To try and prevent scavenging antsentering the huts, each concrete-based hutwas surrounded by a 0.2 -m -wide, water -filledmoat. To detect the presence of ants inside -the
huts, five dead mosquitoes were placed .at afixed site in each corner every night; none ofthese baits was taken.
NNt)hY)CC)l.Five interventions were chosen for this inves-tigation, one being used in each of five hutsand one hut being left without any interven-tion, as a control. In hut 1, an electric ceilingtan was run at high speed. In but 2, a single
pyrethrum coil (Peacock llranday, made inChina) was lit at sunset (this generally burntout about 1 h before sunrise and was notreplaced). A pyrethroid- impregnated tablet(Coopex6; Roussel Ucht °, in which esbiothrin.vas the active ingredient, was heated on acommercial electric vaporizer until dawn inhut 3. The south- and north -Facing windowsin each of the two remaining experimentalhuts were covered with the locally popular,.vide -mesh (i.e. holes 50.9 mm in diameter),polyester /cotton, lace curtains. i'he curtains inhut 4 were untrtated but those in hut 5 hadbeen dipped in. permcthrin solution (2S'ßí,
effective concentration) to give a dose of0.5 g /m2.
Exit traps were fixed to the cast- and west -
facing windows of each hut, the two otherwindows in each being left open. One manentered each hut just before sunset. lo serve asbait, sleeping on a traditional string bed (rhar-
pois) with a thin cotton mattress and wrappinghimself in a cloth blanket (chaddar) so that only
his face was exposed. At sunrise, the bait men
.left their huts and entomologists emptied theexit traps, collected any dead or knocked -downMosquitoes front the sheet -covered floors andthen performed a pyrcthroid space -spray (us-
ing 'l'ipTex6 containing 0.23% tetramethrinand 0.09tßí) . Fcnothrin; Vcti,l;a) to collect
any remaining resting specimens. Pyrcthroidspace- sprays were used in preference to handcapture because of their ease and accuracy.The low control mortality found throughoutthe course of this trial indicates that the re-sidual effect of the .pyrcthroid was negligible.
The litct that .the control mortality remained
fairly constant throughout indicates that sig-nificant residues did not buildup over time.
The rotation of the interventions ensured that
any carry -over effect applied equally to each,and the analysis of the data (using Abbot'scorrection) also takes any such effect intoconsideration. 'l'hc mosquitoes collected weresegregated into broad categories (exit -trap/hut, dead /alive, blood -fed /unfed) and anyanophclincs were Identified to species. .
Preliminary trials were carried out using
cows as bait, to determine the origin of blood -fed mosquitoes collected front huts. In three of
SELF-PRO"l'I:C'l'ION FROM MALARIA vl'.Cl'ORS IN PAKISTAN 339
the huts, cows were kept enclosed in Iargd,untreated bcdncts to prevent mosquito feed-ing, while in the other three the cows were leftunprotected. As pyrethroid space -spray collec-tions performed in the huts with protectedcows yielded only occasional bloodl'ed mos-quitoes, all blood -fed specimens in later trialswere assumed to have fed off the bait withinthe hut in which they were collected.
The self -protection trial ran for 36 workingnights between late April and early June 1994.A preliminary study confirmed that the attrac-tiveness of different men to mosquitoes and thefeeding success achieved on each could varyconsiderably. Therefore, in order to minimizeexperimental error, each man was allocated ahut at the start of the trial and the inter-ventions were rotated in a clockwise directioneach night. In order to minimize the impact ofpossible residual effects of certain interven-tions on the results of other ticatmcnts, thenumber of places moved by any particularinten'ention was decided by the throw of a die.In addition, fans were left on throughout theday in all the huts. As the electricity supply inthe study area was unreliable, a small, portablegenerator was used to provide cover duringpower cuts.
All field staff were given chloroquine andproguanil as prophylaxis.
Statistical AnalysisThe numbers of mosquitoes were loge trans-formed and subjected to analysis of varianceand multiple range tests (least significantdifference method) using urvtst'A'r software('Poker, 1991). The eRect of density-dependent feeding success was adjusted bylogistic regression.
RESULTS
SurveyInterviews were held with male heads andwives of 359 families (sec Table). In responseto open questioning about whether or not theyused any method of personal protection againstmosquitoes, 63% of male heads gave a posi-tive answer. The commonest method cited
TABLEPositivi rap. owes to open and leading questions about
personal protection methods
No. and (''u) r,spuitding posititelp tu:
. Irrion taken.Open
question
l.eadrn4question
NoneChaddarFan .
IlednetCoil
134 (37)172 (48)100 (28)
8 (2)7 (2)
350 (97)239 (67)
23 (6)65 (18)
was enshrouding in a chusldar. Overall, 28".,of families said they used lists, only 4 "mentioned use of bcdnets or coils.
Positive responses to leading questionsabout specific methods of protection usedtended to he more common than when upenquestioning was employed. "l'his was partlybecause .certain self -protection methods, suchas the use of chaddars and fans, have otherprimary uses. For example, more than twicethe number of male heads claimed to use fanswhcn asked directly than when simply askedwhich self -protection methods they used (67 "(corroborated by wives) y. 28 %í,j, 959, usingthem indoors and 77% using them outdoors.Answers to leading questions indicated that18'Sí, used coils and, of these, IO(Y li used themindoors and 44')b used them outdoors. Ofthose using coils, 16% used at least 10 /weekand 19% used 6 -10 /week.
TrialDuring the course of the trial, 2925 anuphe-lines . (all min. siepheasi) and IO 494 culicineswere collected. Compared with the catchesin the control, the electric fan, pyrethrumcoils, untreated curtains, vaporizing mats andpertnethrin- impregnated curtains reducedthe total- numbers of blood -fed AL s1ephensicaught by 27%, 36%, 47%, 56'yí and 6599),respectively (normalized data). 'l'hc corre-sponding values for the culicines were gener-ally, higher, at 74'X, 7796, 38 %, 699, and80 "(, respectively (Fig. I).
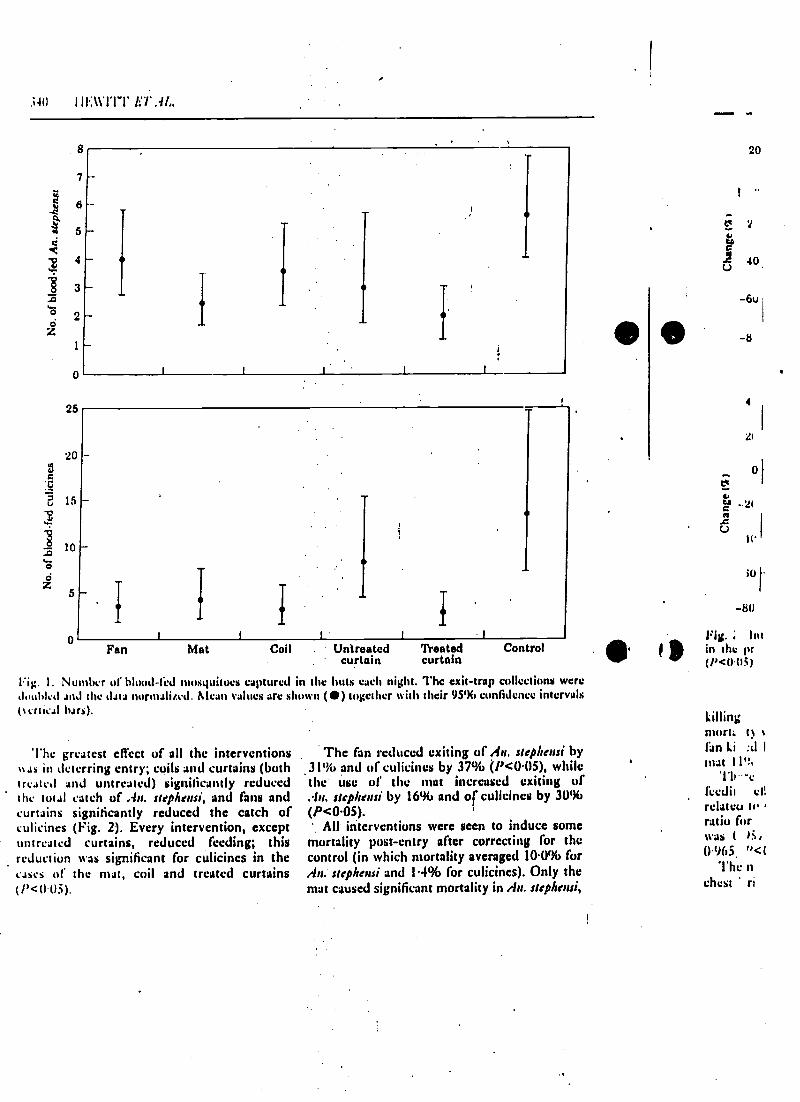
.;aU I il:11'I'I"l' LÍ',IL,
7
6
2
0
Fan Mat Coil . Untreated Treatedcurtain curtain
Control
Fig. 1. Number of blood -fed mosquitoes captured in the huts each night. The exit -trap collections weredoubled and the data normalized. Mean values are shown () together with their 9596 confidence intervals(tertieal bars).
The greatest effect of all the interventions%%as in deterring entry; coils and curtains (bothtreated and untreated) significantly reducedthe tot.tl catch of An. stephensi, and fans andcurtains significantly reduced the catch ofculicines (Fig. 2). Every intervention, exceptuntreated curtains, reduced feeding; thisreduction ttas significant for culicines in thecases of the mat, coil and treated curtains
The fan reduced exiting of An. stephensi by.31% and of culicines by 37% (P <0.05), whilethe use of the mat increased exiting of.la. stephensi by 16% and of culicines by 30%(P <0.05). '
All interventions were seen to induce somemortality post -entry after correcting for thecontrol (in which mortality averaged 10.0% forAn. stephensi and 141% for culicines). Only themat caused significant mortality in An. stephensi,
a
20
-6u
4
Yt
Of
-2(
1l' 1
i1
-80
; lotin the pr(p<Q(,i)
killingmort. t
fan Li :d I
mat1lt -c
ledit tali
relatcu to,ratio forwas ( á,0.965 " <(
The nchest ' ri
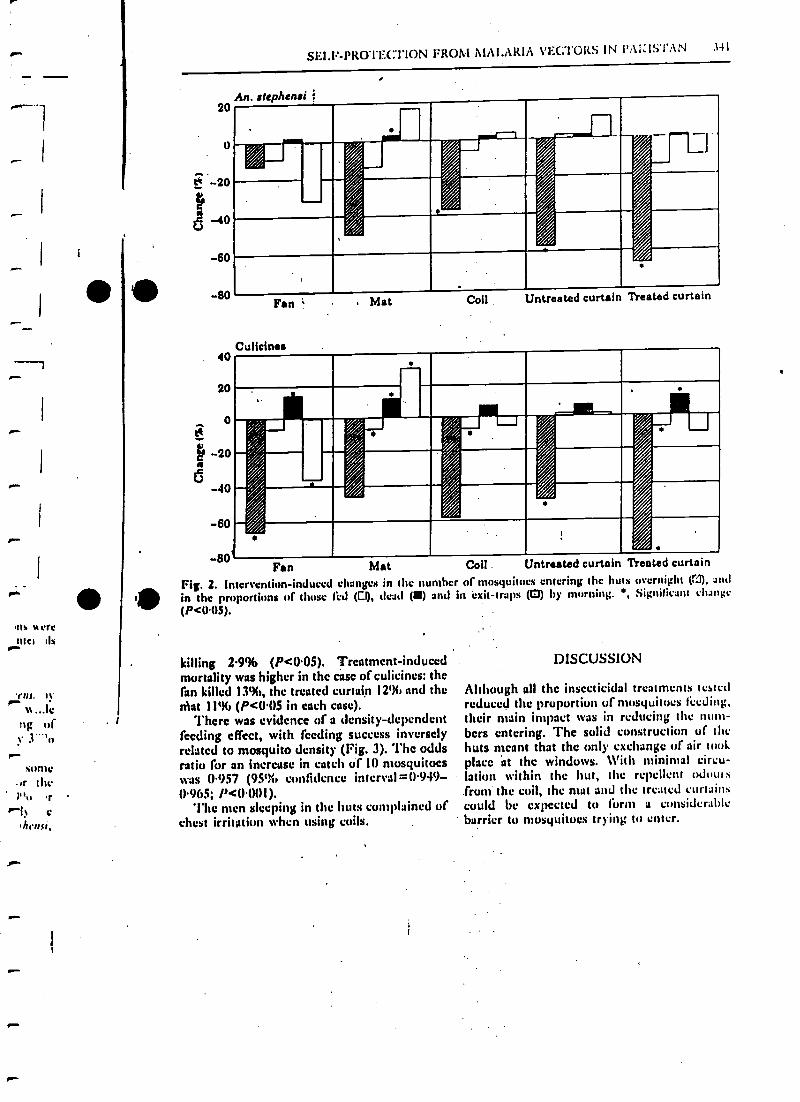
r-
pa-
pw.
us w rrcMel ils
%rng of
some,r thc
' tr
R^I} ehrnsr,
'SELF-PROTECTION FROM 1IAt.ARIA YEC"l'OitS IN t'a1.:IS'1':1N .14 I
20
0
20
-40
60
80
40
20
o
p 20i; 40
60
-ao'Fan
,.,.
,
////%/%
*j j///i r
,
Fan
Culicinea
Mat Coil Untreated curtain Treated curtain
e
M
Fig. 2. Intervention- induced changesin the proportions of those tad (Es,(P<0.05).
at CoII . Untreated curtain Treated curtainin the number of mosquitoes entering the huts overnight (I°l), and
tlead (W) asul in exit -traps (0) by morning. , Significant change
killing 2-9% (P <0.05). Treatment- inducedmortality was higher in the case of culicines: thefan killed 13h(í, the treated curtain 12% and theMat 11% (P <U05 in each case).
I There was evidence of a density -dependentfeeding effect, with feeding success inverselyrelated to mosquito density (Fig. 3). The oddsratio for an increase in catch of 10 mosquitoeswas 0.957 (95t;í confidence interval- 0.949 -0.965; P <0001).
'Ihe men sleeping in the buts complained ofchest irritation when using coils.
DISCUSSION
Although all the insecticidal treatments testedreduced the proportion of mosquitoes feeding,their main impact was in reducing the num-bers entering. The solid construction of thehuts meant that the only exchange of air wokplace at the windows. With minimal circu-lation within the hut, the repellent Winn s
from the coil, the mat and the treated curtainscould be expected to form a considerable
' barrier to mosquitoes trying to enter.
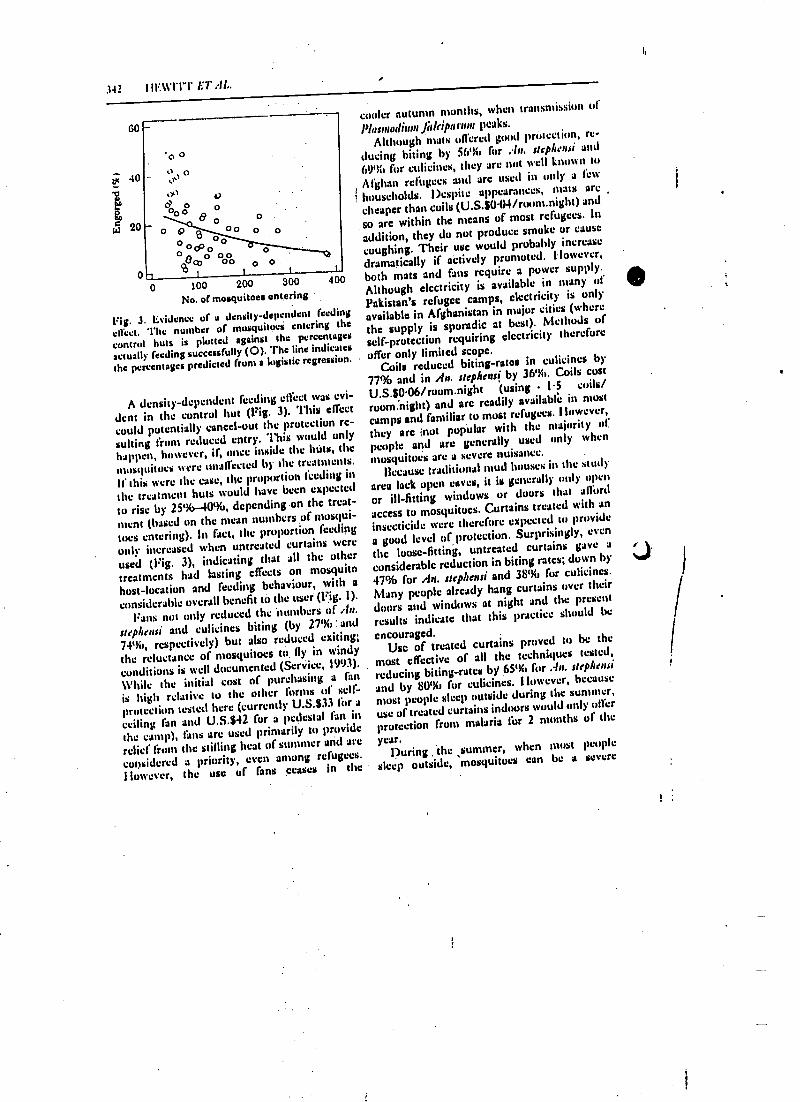
342 I il':wi'l-T LT ;fl..
60
; 40
pj 20
0-t
p 0o,.)
.r)d0 00o
o o o
o0 0
0 100 200 300
No. of mosquitoes entering
Fig. J. Evidence of a density -dependent feeding
effect. The number of mosquitoes entering the
control huts is plotted against the percentages
actually feeding successfully (0). 'The line indicates
the percentages predicted from a logistic regression.
400
A density -dependentfeeding effect was evi-
dent in the control but (Fig. 3). This effect
could potentially cancel -out the protection re-
sulting from reduced entry. This would only
happen, however, if, once inside the htits, the
mosquitoes were unaffected by the treatments.
if this were the case, the proportion feeding in
the treatment huts would have been expected
to rise by 25%-40%, depending on the treat-
ment (based on the mean numbers of mosqui-
toes entering). In fact, the proportion Iccding
only increased when untreated curtains were
used (Fig. 3), indicating that all the other
treatments had lasting effects on mosquito
host -location and feeding behaviour, with a
considerable overall benefit tit the user (Fig. l).
Fans not only reduced the 'numbers of .In.
ssepheusi and culicines biting (by 27íY, ; and
74th,, respectively) but also reduced exiting;
the reluctance of mosquitoes to. fly in windy
conditions is well documented (Service, 1993).
While the initial cost of purchasing a fan
is high relative to the other forms of self-
protection tested here (currently U.S.833 for a
ceiling fan and U.S.842 for a pedestal fan inthe camp), fans are used primarily to provide
relief from the stifling heat of summer and are
considered a priority, even among refugees.
However, the use of fans ceases in the
cooler autumn months, when transmission of
Plasmodium Ji,ls'iparwn peaks.
Although mats offered good protection, re-
ducing biting by 5670 for .' /n. st phe,rsi and
69% for cuticines, they are not well known u,
Afghan refugees and are used in only a few
T huuschotds. Despite appearances, mats are
cheaper than coils (U.S.$0.04 /room.night) and
so are within the means of most refugees. In
addition, they do not produce smoke or cause
coughing. Their use would probably increasedramatically if actively promoted. However,
both mats and fans require a power supply.
Although electricity is available in many of
Pakistan's refugee camps, electricity is only
available in Afghanistan in major cities (where
the supply is sporadic at best). Methods of
self- protection requiring electricity therefore
offer only limited scope.Coils reduced biting -ratas in culicincs by
77% and in An. stepheusi by 36 %. Coils cost
U.S.$0.06 /room.night (using l'S coils/
room:night) and are readily available in must
camps and familiar to most refugees. However,
they arc ;not popular with the majority of
people and are generally used only when
mosquitoes are a severe nuisance.
Because traditional mud houses in the sooty
area lack upen eaves, it is generally only open
or ill- fitting windows or doors that afford
access to mosquitoes. Curtains treated with an
insecticide were therefore expected to provide
a good level of protection. Surprisingly, even
the loose -fitting, untreated curtains gave a
considerable reduction in biting rates; down by
47% for An. stephensi and 38% for culicincs.
Many people already hang curtains over their
doors and windows at night and the present
results indicate that this practice should be
encouraged.Use of treated curtains proved to be the
most effective of all the techniques tested,
reducing biting -rates by 65% for .1n. ssephesi
and by 80'3ít for culicincs. Ilnwevcr, because
most people sleep outside during the summer,
use of treated curtains indoors would only offer
protection from malaria fur 2 mouths of the
year.During the ,summer, when most people
sleep outside,mosquitoes can be u severe
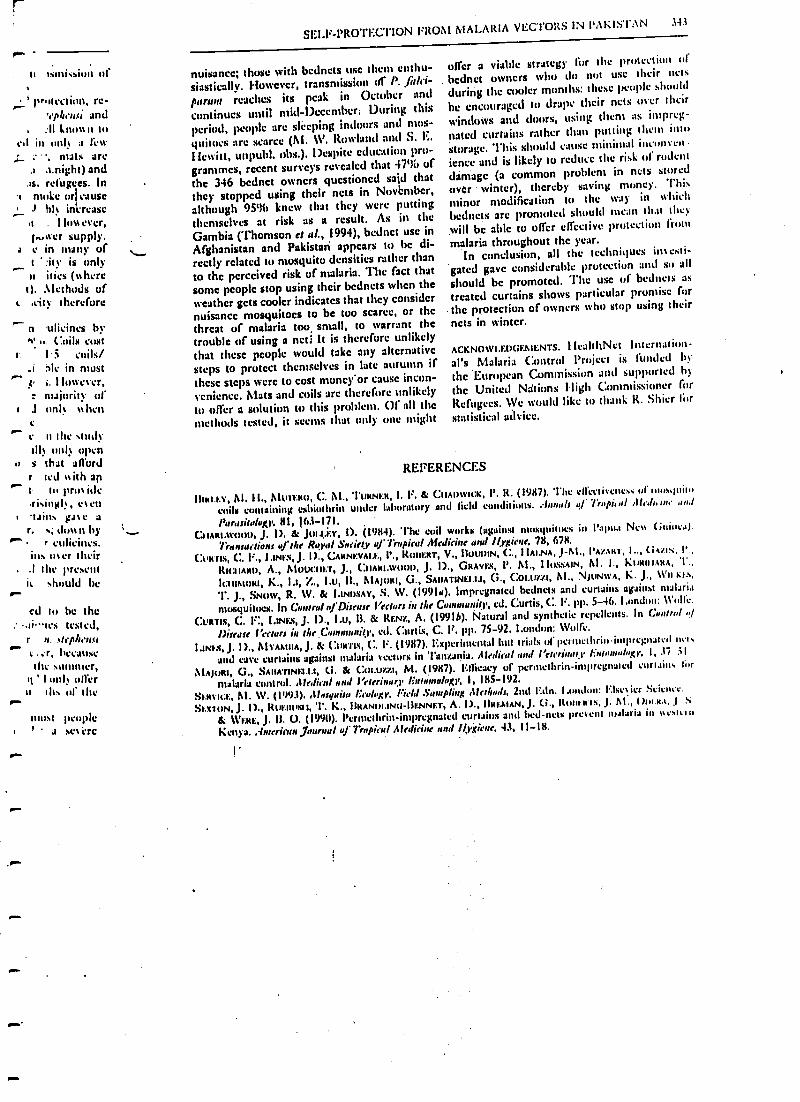
ti Isntissiun of
i-- protection, re-'eph,lti and
, :II lnu%%n atcd in only a few
nuts aree.night) and
.as. refugees. Ino mule orjeause
i hf inirrase.1 . I IO%%cycr,
i..,aer supply.c in many uft ' rit ) is only
^ )1 itics inhereI). .1letht)tls uf
t .city therefore
n .ulicines hvh' . Coils cost
c 1.5 coils/_i àlc in must1, I lowcver,: majority of
1 J unI% % %hen
r n the tinilyill) mil) open
u s that affordr fed ttith ant lu pro%iderising!), e%en-tains Foc ar, ,. don n by
r eulicincs.ins u%er their.1 the present
W should bercd to be the
.,ives tested,r n.lhrple2uc;r, heeauscihr summer,
q ' i only offern the of the
IIIU\t people1 ' - a sl't i.'re
SELF-PROTECTION FROM A4ALARiA VECTORS IN PAKISTAN 343
nuisance; those with bednets use them enthu-siastically. However, transmission of P. ,1rtlei-
paraal reaches its peak in October andcontinues until mid -December: During thisperiod, people are steeping indoors and mos-
quitoes are scarce (Al. W. Rowland and S. E.
i fcwitt, Unpubl. ohs.). Despite education pro-grammes, recent surveys revealed that 4796 of
the 346 bcdnct owners questioned said thatthey stopped using their nets in Novbnlltcr,although 951)1) knew that they were putting
themselves at risk as a result. As in the
Gambia (Thomson et al., 1994), bednct use inAfghanistan and Pakistan appears to be di-reedy related to mosquito densities rather than
to the perceived risk of malaria. The fact thatsome people stop using their bednets when theweather gets cooler indicates that they considernuisance mosquitoes to be too scarce, or thethreat of malaria too small, to warrant the
trouble of using a nets It is therefore unlikelythat these people would take any alternative
steps to protect themselves in late autumn ifthese steps were to cost moncy'or cause incon-venience. Mats and coils are therefore unlikely
to offer a solution to this problem. Of all themethods tested, it scenes that only one might
offer a viable strategy for the (rutcctiun ofbednet owners who do not use their nets
during the cooler months: these people should
he encouraged to drape their nets over their
windows and doors, using them as impreg-
nated curtains rather than putting them intostorage. This should cause minimal intunvenknee and is likely to reduce the risk of rodent
dámage (a common problem in nets storedover winter), thereby saving money. Thisminor modification to the way in %vhicit
bednets are promoted should mean that die)
will be able to offer effective protection frommalaria throughout the year.
In conclusion, all the techniques investi-
gated gave considerable protection and so all
should be promoted. The use of bednets astreated curtains shows particular promise forthe protection of Owners who stop using theirnets in winter.
ACKNOWLEDGEMENTS. I IcùhltNet Internation-
al's Malaria Control Project is funded bythe European Commission and supported by
the United Nations High Commissioner forRefugees. We would like to thank R. Shier for
statistical advice.
REFERENCES
IhNl.r.y, 111. 11., AlUTt:NI), C. Al., 'Mama, I. F. & C:uAnwNa, P. R. (1987). The effectiveness ul' 1nus,luilu
coils containing esliuthrin under Laboratory und field conditions. Annals q/' Ï usl ,tL,G, we and
l'uasitaloxr, 81, 163-171.C..11AN1.woon, J. I), & JoLI.r:Y, I). (1984). The coil works (against ntusyuilncs in Papua Net% Guinea).
Transactions ufthe Royal Surielp af Tropical Medicine and Hygiene, 78, 678.
(:t'N1ls, (:. F., I.INt.V, J. I)., C:ANNt:vAl.t:, I'., ROIIERT, V., BOUDIN, C., I IAI.NA, J-M., l'A/.ANT, I.., (i%11:, 1'.,
RIl:11ANU, A., Aluut:Ilt:T, J., (:IIANI.t%Onn, J. I)., GNAYI:\, P. AI., I h1.tiSAIN, Al. I., 11t1N111.%NA, 1 .,
It:l I1Mt1RI, K., I.1, %:., i.u, IL, AIA)I114I, (,ì., SAIIATINEI.I.I, G., COt.Ue.%I, AI., NJUNWA, K. J., Wll Kt .s,
T. J., SNOW, R. W. & 1.INUSAY, S. W. (1991u). Impregnated hednets and curtains against malaria
mosquitoes. in Control lfDisease Vectors in the Caaaulity, cd. Curtis, C. F. pp. 5-46. London: 1l'6lle.
CVRTIS, C. l':; LINES, J. D., Lu, B. & REN%, A. (19918). Natural and synthetic repellents. !n C,,,In1
!)fiero? ) irGrr in !hr C.:mtumuilt', col. Curtis, C. F. pp. 75-92. London: 1Vulfe.
Lusts, J. I)., AlYAA111A, J. & (atR1IS, (:. F. (1987). Experimental hut trials uf penucthrin-impregnatcd mt.
and cave curtains against malaria vectors in Tanzania. Alydiral aui i'rterilarl latwauluCl, I, 37 31
MAJuRI, G., SAUATINt:LI.I, Ci. & Col.uzzl, M.'(1987). Gliicacy uf perutelhrin-imprcgnalcd curtains formalaria control. AfedieIl and Veterinary 1:'ntnnsulaJ;y, I, 185-192.
S).Ny10E, Al. W. (1993). Mosquito lirolnky, Field Sampling Methods, 2nd Erin. London: 1?luier Science.
St:XION, J. f )., RUEIIIsII, 1'. K., iINANn1.IN1J-RENNt7r, A. I)., IINEAIAN, J. C., itU1tL.NTR, J. Al., ( )Ua.N.1, ,J 1
i.i WERE, J. I1. O. (19911). l'erntethrin-impregnateti curtains and bed-nets prevent malaria in %se.,cln
Kenya. .{meriraaJaurnal of 7r1pi1al Atedieine and llygfrne, 43, 11-I8.
344 I I1:11'ITC ET .-IL.
SMuru, A., I Iuns(N, J. E. & 1sox:n, S., (1972). Trials with pyrethrum mosquito coils against Anopheles
xamhiae Giles, Alansunia unifi,nnii Theo and Cular faligaus Wied. entering vermulatrap huts.P..yralhruin Purl, I1, III-11S.
Tt1OAMYON, M. C., WALE- ssANORO, U., UENNEI"r, S., CGONNOR, S. J., LANOEROC, P., JAWAIIA, M., TODD, .1.
& GREENwuqu, lt. M. (1994). Al:daria prevalence is inverselyrrelated to vector density in The Gambia;West Africa. /ra,,daiun, sf she' Rrpvd &stiely of Trapita! Making, anal / /Ixieue, 88, 638 -643.
'l'mi.lt, M. :1. (1991). i/uislal Slalülical Package, London; Unislat.
1
TRANSACTIONS OF THE ROYAL SOCI4TY OFTROPICAI. MEDICINIU AND I tYCI ENE (IS96) 90.357 -3ó I
Pyrethroid- impregnated bed ,nets for personal protection against malaria for
Afghan refugees
3'7
Mark Rowlands Menno Boumas, Dominique Ducornexi, Naeem. Durranii, Jan Rozcndaal2, Allan Schapiras and
Egbert Sondorpl 1NeahhNet ¡nIentatianal, P.O. Box 889, University Town, Peshawar, Pakistan; 1World Health
Organization, 1211 Geneva 27, Switzerland
AbstractA field trial of permethrin -impregnated bed nets (PIBs) was conducted in 2 Afghan refugee villages in
Pakistan. Nets were issued to only 10% of families (10 1398 people); this simulated a situation in which bed
nets are gradually adopted by villagers in Afghanistan. A further 10% lacking bed nets were selected as con-
trols from the same villages. An initial survey showed that 86% of household heads were aware that malaria
was transmitted by mosquito bites but only 2% had used bed nets before. Trial families were encouraged to
attend the village health centres if they fell ill, Microscopy records showed that, between July and Decem-
ber 1991, 22.4% of the control group became infected with Plasmodium vivax and 13.0% contracted P. falci-
rum while in the intervention group only 9.9% contracted P. vivax (relative risk 0.58, confidence interval
ICI) 95% 0.49 -0.68) and only 3.8% contracted P./alciparum (relative risk 0.39, 95% Cl 0.29 -0.53). A single
treatment of the nets with permethrin at 0.5g/m remained protective throughout the 6 months' transmis-
sion season. 73% of families claimed to use their nets every night; members of families who claimed to use
nets less regularly showed an incidence similar to that of the control group. There was no sex or age differ-
ence in net use or protective efficacy. Headlouse infestation rates were reduced in PIB users. Few nets were
washed, given away or sold. The prospect for PIBs as personal protection appears good, despite peoples
lack of previous experience.
Keywords: malaria, Plasmodium falciparun, Plasmodium vivax, headlice, permethrin -impregnated,bed nets
IntroductionOwing to 15 years of war, an estimated 3 million
Afghans have lived as refugees in Pakistan. The majorityare settled in hacha (undeveloped) villages, often on mar-
linalland with abundant mosquito breeding sites. Ma-
aria became a major health problem in the late 1980s
(SULEI11AN, 1988). The problem was transferred to Af-ghanistan by the cross- border movements of infectedrefugees, and then amplified locally as a consequence ofthe breakdown in pre-war national health and malariacontrol structures.
Within the refugee villages in Pakistan, malaria trans-mission has been brought under control by indoorspraying of residual insecticide, with the United NationsHigh Commission for Refugees taking reslfonsibility forthe annual campaigns (ROWLAND a al., 1984). Althoughspray campaigns were also routine in many parts of Af-ghanistan before the war, the organization and co-ordi-nation required to renew them on a substantial scale arcimpossible under existing conditions. But even if thesituation in Afghanistan were politically and economi-cally stable, it may not be wise to resurrect certain pre-war control practices. In many developing countries, forexample, large-scale spray campaigns are increasinglyseen as draining national health budgets, too dependentupon the vagaries of international aid supply, lacking incommunity involvement, and unsustainable (WHO,1993). By contrast, pyrethroíd impregnated bed nets(PIBs) offer a means of control that encourages self reli-ance and community participation, and requires less re-current expenditure on insecticide. In war -torn Afghani-stan, PIBs seem the best option available to those whodesire personal protection against malaria. The problem,however, is the lack of a tradition of bed net usage in apeople noted for their conservatism. Before embarkingupon a campaign of PIB distribution and sales, it is de-sirable to conduct a smaller field trial to investigate cul-torsi acceptability and efficacy.
This paper describes a field trial conducted in 2 Af-ghan refugee camps in Pakistan. Refugee camps werepreferred because of their comparative security and ac-cessibility. Since any PIB project in Afghanistan couldexpect to achieve only limited coverage initially, the trialattemptedattepted to simulate that b laving bed nets issued ioonly 10'aó of fatuities. Control groups were selected frontthe same villages. Use of PIBs by 10% was not expected
*Author for correspondence.
to affect transmission in the rest of the community.
MethodsStudy area and population
The 2 trial villages, Ba hicha and Kagan, tverc situ-ated in Mardan district, North-West Frontier Province,Pakistan. Their populations in 1991, the year of the trial,were 11 220 and 2735 respectively. All houses were builtfrom mud, in open courtyards surrounded by high pe-rimeter walls -a style typical of villages in Pakistan andAfghanistan. Water-filled borrow pits and rice fieldsprovided abundant mosquito breeding sites. 'The vectorsincluded Anopheles culcifacier, A. stephesui, A. nigemnntsand A. soh icnu, among others. Culicines were a Inafolnuisance. The incidence of Plasmodium vivax and P. fal-ciparum malaria had increased in recent years. Each vil-lage had a health centre providing free medical services.
Study design and procedure:Refugee families were selected by choosing at random
20% of the health centres' registration cards. The sched-ule of the 9 months' trial is summarized in Table I.
To gain the communities' confidence and compliance,respected basic health workers from I3aghicha and Ka-gan were recruited to conduct the field work. Six fieldteams were formed, each comprised of I female and I
male interviewer and 2 mule assistants. The teams weregiven tuition about malaria and training in interviewtechniques. At this stage the teams were not informedabout our plans to issue bed nets since we wanted themto conduct an unbiased survey of the villagers' existingpersonal protection practices and sleeping arrangementsso that the number of nets needed could be accuratelycalculated.
Each team visited 32 households. The head mule and
his wife were interviewed simultaneously in differentparts of the house. The 2 completed questionnaires wereimmediately compared and any large discrepancies :!ac-ried on the spot with those interviewed. During theseine visit a blood film and hacniatocrit capillary ts.hewere prepared from each family member.
Trial families were randomly divided into interven-tion and control groups. At mass meetings of the inter-vention group males, insecticide dipping procedures andnet erection methods were denwmanned. The group- requested not to wash the nets during the malaria seasonand to keep the nets out of direct sunlight. To discour-age selling of nets, heads were told the nets were un loan.
tss
l'ahlc 1. Schedule of the pyrcthroid-impregnated bed net trial
MARK ROWLAND E7'.U..
Dates' ActivityS S 91 -10 /5,91 Selection of families and trainjng of community health workers.
17,5:91-o/6/91 Pre- intervention census, KA1' , and parasite prevalence surveys.
s 6 91- 10/6,91 Muss meetings with family heads and village elders.
11 6 91- 29,oi91 Issue of bed nets and treatment with insecticide.
17 91- o/7r91 First headlouse survey.13,7,91-11/12/91 Passive case detection at the health centres, and entomological surveys.
1,9,91-20/9/91 Further health education about use of pyrethroid- impregnated bed nets as personal protection.
12/12,91-20/1/92 lost-intervention KAP and parasite prevalence surveys.
3/2,92 -9/2/92 Second headlouse survey.
'Dates are shown as day /month/year.Knowledge- attitude- practice.
During the control group meetings, heads were told .their nets would arrive in December, but would be givenaway tree in return for co-operation.
The teams then revisited the homes of the interven-tion group, impregnated the nets in full view of familyfemales, fitted support poles to charpoiz (wooden framedrope beds), and gave instruction to females on net care.Children were then examined for headlouse infestationat the health centres.
To encourage trial families to use the health centres, itwas arranged that they should get malaria diagnosis andtreatment within 24 h. HealthNet International de-ployed its own experienced microscopists at the centresfor the duration of the project. All suspected malaria pa-tients were given presumptive treatment with chloro-'iuiuc while awaiting the tnicroscopist's verdict. Patientsconfirmed as infected were treated with 25 mg chluroquine per kg body weight over 3 d. P. falciparum chloro-quine treatment failures were re- treated with either chlo-roquine or Fansidar4)
Two months after bed net distribution, the teams re -'visited the trial families to give further encouragement.
From acid - December, the teams conducted post- inter-%entinn parasite prevalence, hsematocrit and know-ledge- attitude- practice (KA!') surveys. Ito encouragehonest responses to questions about the regularity withwhich individual family members used their nets, thoseinterviewed were told in advance that families couldnow retain all the nets regardless of previous habits.Children were again examined for headlice, and control .families issued with new nets.
BrJ net and inucticideThe bed nets (from SiamDutch, Thailand) were made
from 100 denier knitted, green polyester fibre. Greenwas the most popular colour-partly because of its Is-lamic associations -and had the advantage of not ent-I+hasizing dirt or dust. Two sizes were issued: single nets
(I UU ctrl wide, 180 cm lung, 150 cm high) which fittedaround one charpoi, and family nets (220 cm wide, 180cut lung, ISO cm high) which fitted around 2. For theminority who slept un the ground, nets were suspendedIrom ceilings or between 4 upright poles held in mud -tilled ghee cans.
Bed nets were individually dipped in an aqueousemulsion of permethrin (prepared from Imperator. 25%emulsifiable concentrate; Zeneca Public Health) to givean average application rute of 0.5 g/m . Nets were driedin the shade and coded with water-soluble ink. Alto-gether, 310 single- sizeneta and 398 family -size nets wereissued. .
Statistical analysisData were analysed using Epi -Info (DEAN es al., 1990)
and Unistat software ('OK1iR, 1991). Discrete variables%sere compared by x= tests or by calculating the relativerisk using .'tantçl- ilaenszel stratified cross tabulationsand summary X tests. Normally distributed variables
were compared by analysis of variance.
Table 1. Admission variables and characteristics of the studypopulations In May -June 1991
Study groups
lied net Control
House compoundsBaghieha villageKagan village
FamiliesPersons enrolledFemalesAge' (years)
FemalesMales
Proportion of group membersWith malaria in 1990 21%Using health centres in' 1990 87%
Pre-interventionParasite prevalenceP. falctparumA vivax
Haematocrit'Emotes
liacinatocrit <30.0%eFemalesMales
IleadIouse infestations.'GirlsBoys
.._. .. .
74
173139849.6%
23186139449-4%
18(16) 19(17)20(18) 19(17)
24%92%
2.3 (23 /1117) 2.6(30/1145)10.2(114/1117) 11.5(132/1145)
393(47) 39.1(4.9)41.1 íS 7) 40.6 (S8)
3 l (11/384)3.1 (16/524)
66(60/91)37 (43/1171)
3.1(23/603)3.0(16/532)
42(22/52)27 (16/39)
Mean (standard deviation In parentheses).!Percentage (number infected/number examined in patcuthescs).
e1'crcentsge (number <30%/total number examined in parenthe-
ses).
ResultsCharacteristics of the study groups
According to the pre -intervention survey, 28% offamilies originated from the northern province of Kun-duz and 64% from the eastern provinces of Kunar, Nan -garbar and Paktya in Afghanistan. Further populationcharacteristics are summarized in Table 2; 44% of thevillagers were less than IO years old and hence had beenborn in the refugee villages. The average number of peo-
ple per house was 14.3. 89% slept on charpois and 11%
slept on the ground; 50% shared single charpais withother persons. Only 7% of adult females and 25% ofadult males had received formal education.
When male headi were asked about the causes of ma-
laria, 86% '(307/358) stated mosquito bites, 3% saiddrains or standing water, and 1196 did not knows 63%said they tried to protect themselves against mosquitobites; 48% used a cbaddar (religious wrap) as s protectiveblanket; 28% used electric fans to ward off mosquitoes,2% used mosquito coils, and 2% used bed nets.
Admission variables in the PIB und control groupsIn all, 2792 people and 192 households were enrolled.
The admission variables were consistent in the interven-
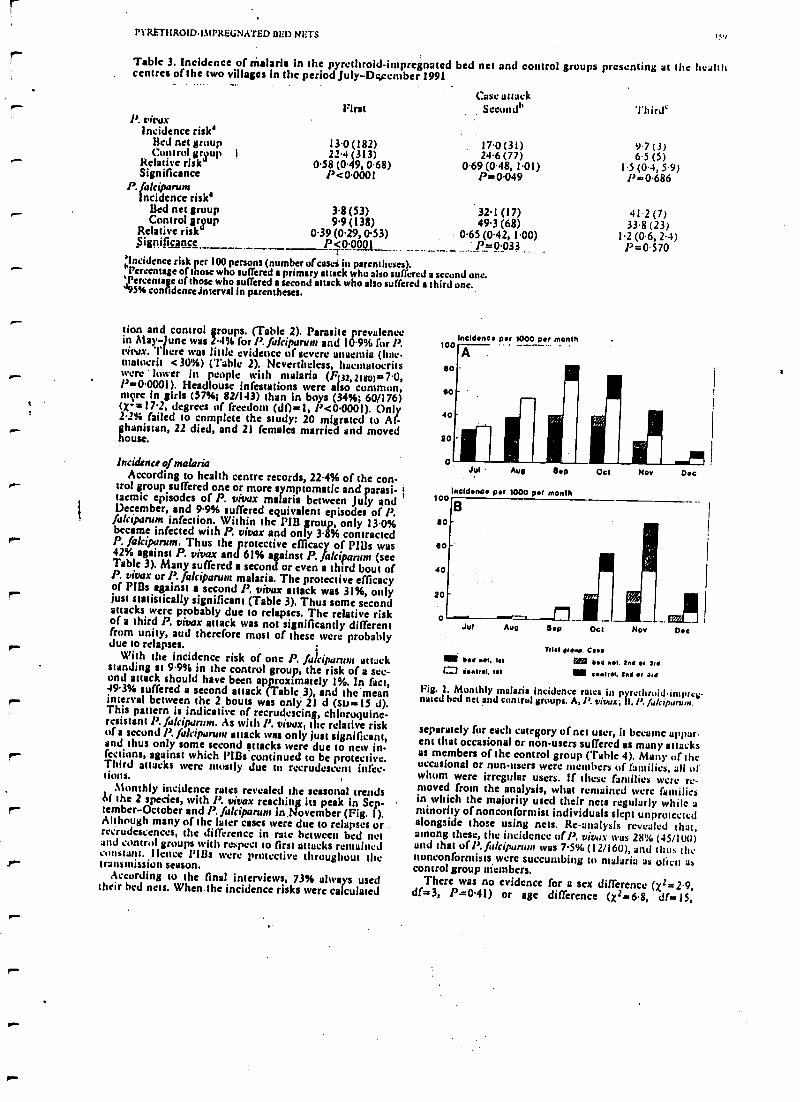
PYRETIIRO1DI1tPREGNATED BED NETS Ic4
Table 3. Incidence of malaria in the pyrethroid- impregnated bed net and control groups presenting at the Iwahttcentres of the two villages in the period July -December 1991
P. vivaxIncidence risk'
Ned net groupControl group
Relative riskSignificance
P. fakiparumIncidence risk'
lied net groupControl group
Relative riskSignificance
First
13.0 (182)22.4 (313)
0.58 (0.49, 0.68)P<0.0001
Cass attackSeconds,
17.0(31)24.6 (77)
0.69 (048, 1.01)P=0.049
3.8 (53) 32.1 (17)9.9 (138) 49.3 (68)
0.39 (0.29, 0.53) 0.65 (0.42, 1.00)P5, 0.0001 ` P=0.033 ..
'Incidence risk per 100 persons (number of casci in parentheses)."Percentage of those who suffered a primary attack who also suffered a second one.',Percentage of those who suffered a second attack who also suffered a third one.J95% conlidencelntervalin parentheses.
lion and control groups. (Table 2). Parasite prevalencein May-June was 2.4% for P. fakiparuul and 10.9% for P.vitas. There was little evidence of severe anaemia (hoe-matalcrit <30%) (Table 2). Nevertheless, huentatocritswere lower in people with malaria (F32,2180) =7'0,P =0.0001). Headlouse infestations were also common,more in girls (57%; 82/143) than in boys (34 %; 60/176).(X- =17.2, degrees of freedom (dfs1, P <0.0001). Only2.2% failed to complete the study: 20 migrated to Af-ghanistan, 22 died, and 21 females married and movedhouse.
Incidence of malariaAccording to health centre records, 22.4% of the con-y- trol group suffered one or more symptomatic and parasi-
tacmic episodes of P. vivax malaria between July andDecember, and 9.9% suffered equivalent episodes of P
fakiparum infection. Within the PIB group, only 13.0%became infected with P. vivax and only 3.8% contractedP. fakiparum. Thus the protective efficacy of PI13s was42% against P. vivax and 61% against P. fakiparum (seeTable 3). Many suffered a second or even a third bout ofP. vivax or P. fakiparum malaria. The protective efficacyof Pills against a second A vivax attack was 31 %, onlyjust statistically significant (Table 3). Thus some secondattacks were probably due to relapses. The relative riskof a third P. vivax attack was not significantly differentfrom unity, and therefore most of these were probablydue to relapses.
With the incidence risk of one P. fa %ipanuu attackstanding at 9.9% in the control group, the risk of a sec-ond attack should have been approximately 1%. In fact,49.3% suffered a second attack (Table 3), and the 'meanr interval between the 2 bouts was only 21 d (Soso l5 d).This pattern is indicative of recrudescing, chlioroquine-resistant P. fakiparum. As with A vivax, the relative riskof a second P. fakiparum attack was only just significant,and thus only some second attacks were due to new in-fections, against which Plßa continued to be protective.Third attacks were mostly due to recrudescent itkc-tions.
Monthly incidence rates revealed the seasonal trendsM the 2 species, with l'. vivax reaching its peak in Sep-t.- tember- October and P. fakiparunl in ,November(Fig. 1).Although many of the later cases were due to relapses orrecrudescences, the difference in rate between bed netand control groups with respect to first attacks remainedconstant. Ilene,: fills were protective throughout ther- transmission season.
According to the final interviews, 73% always usedtheir bed nets. When the incidence risks were calculated
Incidence per 1000 pot month
A .
Third`
9.7 (3)6.5 (5)
1.5(04,S9)l'=0.686
41.2 (7)33.8 (23)
1.2 (0.6, 24)P=0.570
Jul Aug Sop
noldnop ptr 1000 pet monthloo
so
so
40
so
o o ..=_.__lJul Aug adp
ttl p.l not. 01t Montml.1.1
Oct Now
Mal reap. eccebed Ml tad sr Ord
tal control. Sad e, art
Ode
Fig. 1. Monthly malaria incidence rates in pyrethroidimpre`mated bed net and control groups. A, P. vilwx; ti, /'. fulcipurvm.
separately for each category of net user, it became appar-ent that occasional or non-users suffered as many attacksas members of the control group (Table 4). Many of theoccasional or non -users were members of families, all ofwhom were irregular users. If these families were re-moved from the analysis, what remained were familiesin which the majority used their nets regularly while aminority of nonconformist individuals slept unprotectedalongside those using nets. Re- analysis revealed that,among these, the incidence of P. vivax was 28"/% (45/lull)and that ufl'. %ukipurlurr was 7.5%(12/160), and thus thenonconformists were succumbing to malaria as Wien ascontrol group members.
There was no evidence for a sex difference (X2 =2.9,df =3, P =0.41) or age difference (X2 =6.8, df =15,
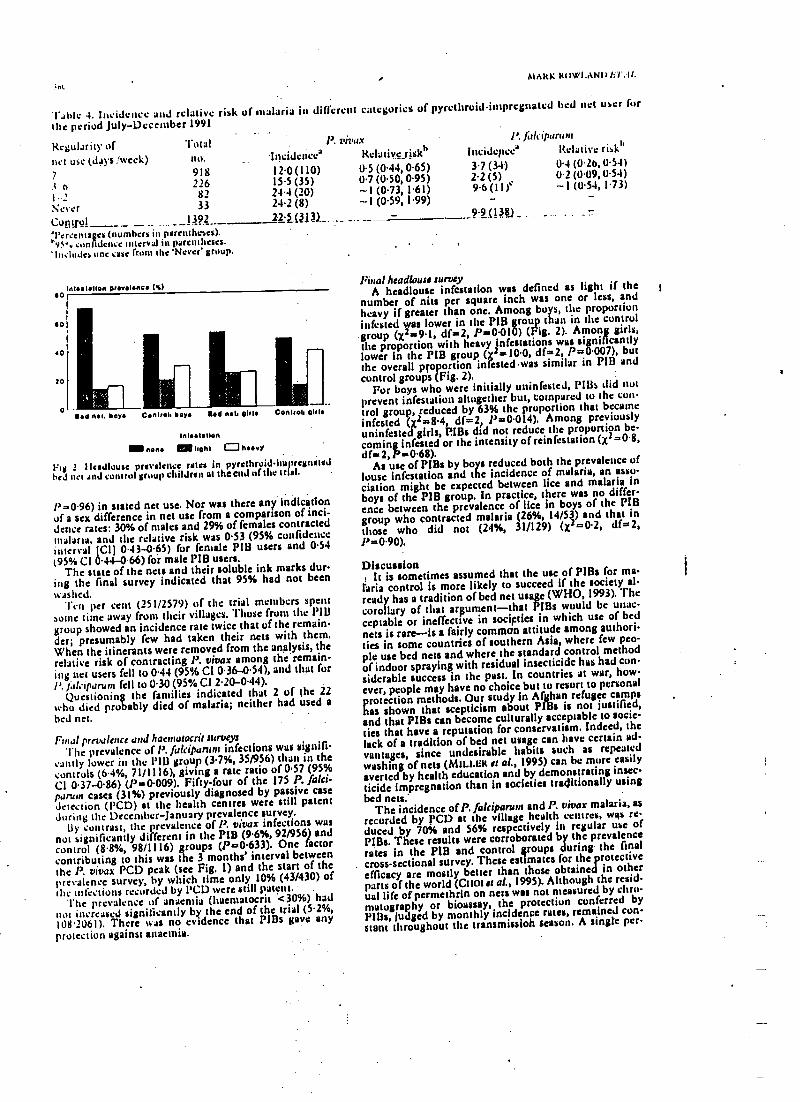
MARK ROWLAND lér':Ir.
Table 4. Incidence and relative ri$k of malaria in different categories of pyrcthruid -impregnated bed
the period July -December 1991
net user for
Regularity ofnet use (days /week)
'totalnu.
P. vivax
incidence Relative risk)'
P. /irlciparum
Incidepce Relative riskl'
7 918 12.0(110) 05 (0.44, 0.65) 3.7 (34) 04 (0.26, 054)
i e 726 15.5 (35) 07 (050, 0.95) 2.2 (5) 02 (0U9, 054)
I 2 82 24.4 (20) -1 (0.73, 1.61) 9.6(11)` -1 (0.54, 1.73)
Never 33 24.2 (8) -1 (0.59, 1.99) - -
Control 1392 22.5 (3_3) 9.9 (13111)
'Percentages (numbers in parentheses).v vw confidence interval in parentheses.
'Includes une case from the 'Never' group.
Woo lotion ProwUne (%)
140 nos, boy Control. boyo Bob non alrlb
Inlo=t$IIOn
MN none mg oohs (J heavy
1'Ig 2 )Icadlouse prevalence rates in pyrcthruid -iin rregnatcdbed net and control group children at the end attic. trial.
l' =0.96) in stated net use. Nor was there and indicationof a sex difference in net use from a comparison of inci-dence rates: 30% of males and 29% of females contractedmalaria, and the relative risk was 0.53 (95% confidenceinterval (CI) 0.43 -0.65) for female PIB users and 0.54(95% Cl 0.44-0.66) for male PIB usera.
The state of the nets and their soluble ink marks dur-ing the final survey indicated that 95% had not beenwashed.
"fen per cent (251/2579) of the trial members spentWine time away from their villages. Those from the l'IBgroup showed an incidence rate twice that of the remain-der; presumably few had taken their nets with them.When the itinerants were removed from the analysis, therelative risk of contracting P. vivax among the remain-ing net users fell to 0.44 (95% CI 0.36 -0.54), and that forl'. Jab Iparunr fell to 0.30 (95% CI 2.20- 0.44).
Questioning the families indicated that 2 of the 22who died probably died of malaria; neither had used abed net.
Final prevalence and hannatocrir surveysThe prevalence of P. fakiparunt infections was signifi-
cantly lower in the l'IB group (3.7 %, 35/956) than in thecontrols (6.4 %, 71/1116), giving a rate ratio of 0.57 (95%CI 0.37 -0.86) (P =0.009). Fifty -four of the 175 P. falci-parurn cases (31%) previously diagnosed by passive casedetection (PCD) at the health centres were still patentDuring the December- January prevalence survey.
By contrast, the prevalence of P. vivax infections wasnot significantly different in the PIB (9.6 %, 92/956) andcontrol (8.8%, 98/1116) groups (P =0.633). One factorcontributing to this was the 3 months' interval betweenthe P. vivax PCD peak (see Fig. 1) and the start of theprevalence survey, by which time only 10% (43/430) ofOle infections recorded by PCD were still patent.
The prevalence of anaemia (haematocrit <30%) hadnot increased significantly by the end of the trial (5.2 %,108'2061). There was no evidence that PIBs gave anyprotection against anaemia.
Final headlouse surveyA headlouse infestation was defined as light if the
number of nits per square inch was one or less, andheavy if greater than one. Among boys, the proportioninfested was lower in the PIB group than in the controlgroup (x2 =9.1, df =2, P=0.010) (Fig. 2). Among girls,the proportion with heavy infestations was significantlylower in the PIB group (x4=10.0, df =2, P =0.007), butthe overall proportion infested -was similar in PIB andcontrol groups (Fig. 2).
For boys who were initially uninfected, Pills did nutprevent infestation altogether but, compared to the con-trol group, reduced by 63% the proportion that becameinfested (X2==8.4, df =2, P =0.014). Among previouslyuninfected girls, l'IBs did not reduce the proportion be-coming infested or the intensity of reinfestation (x2 =0.8,
df =2, Pa 0.68).As use of PIBs by boys reduced both the prevalence of
louse infestation and the incidence of malaria, an asso-ciation might be expected between lice and malaria inboys of the PIB group. In practice, there was no differ-ence between the prevalence of lice in boys of the PIBgroup who contracted malaria (26 %, 14/53) and that inthose who did not (24%, 31/129) (x2=0.2, df=2,Pa0.90).
DiscussionI
It is sometimes assumed that the use of PIBa for m-ilitia control is more likely to succeed if the society al-ready has a tradition of bed net usage (WHO, 1993). Thecorollary of that argument -that PIBs would be unac-ceptable or ineffective in societies in which use of bednets is rare -is a fairly common attitude among authori-ties in some countries of southern Asia, where few peo-ple use bed nets and where the standard control methodof indoor spraying with residual insecticide has had con-siderable success in the past. In countries at war, how-ever, people may have no choice but to resort to personalprotection methods. Our study in Afghan refugee campshas shown that scepticism about PIBa is not justified,and that PIBN can become culturally acceptable to socie-ties that have a reputation for conservatism. Indeed, thelack of a tradition of bed net usage can have certain ad-
vantages, since undesirable habits such as repeatedwashing of nets (MILLER et al., 1995) can be more easily
averted by health education and by demonstrating insec-ticide impregnation than in societies traditionally usingbed nets.
The incidence of P fakiparum and P. vivar malaria, asrecorded by )'CD at the village health centres, wys re-duced by 70% and 56% respectively in regular use ofPIBs. These results were corroborated by the prevalencerates in the PIB and control roups during the final
cross-sectional survey. These estimates for the protectiveefficacy are mostly better than those obtained in otherparts of the world (Coot es al., 1995). Although the resit'.uul life of permethrin on nets was not measured by chro-matography or bioassay, the protection conferred byPIlls, judged by monthly incidence rates, remained con -
stant throughout the transmission season. A single per-
l'l'KtiTI t Kt)11) I.1f 1'Klit ;NATE» nu» NEI
methrin treatment in April -May each year would there-
fore be sufficient in this region. The high recurrencerate of P. falcil,,tntrn infections was due to chloroquincresistance; a survey in viva in I3rghit:hu in December ofthe same year revealed that 6S%I of ruses were K1 resis-tant, and 2% were resistant at the K11 level (M. Rowland
& 1. Shah, unpublished observations). Several otherfindings in this study augur well for PI Bs in Afghancommunities: the absence of a sex or age difference inPIB users or in the protective efficacy of the nets, thelow net -washing rate, the facts that few nets were givenaway or sold and that most used their nets every nightand the high level of awareness about the causes, controland treatment of malaria.
As in Africa (LINDSAY et al., 1989), headlouse infesta-tion rates were significantly lower in P113 users, espe-cially among boys. Direct contact between hair and in-secticide would be less in girls because they usually weartheir hair long, braided, and covered. During the plan-ning period of the trial, we hoped that headlouse infesta-tion rates would serve as an objective indicator of l'iUuse If the intervention had a disappointing Impact onmalaria. We found, however, that considerable trustcould be placed In what people said, since those peoplewho claimed to use their nets irregularly or pot ut all had
a malaria incidence rate equal to that of the controlgroup. Some people who claimed to use their nets everynight did develop malaria. This indication that evenregular users of PIBs may sometimes contract malaria issupported by the lack of association between the preva-lence of headlouse infestation and the prevalence of ma-laria in boys of the PIB group. Infection with malariamay occur before going to bed, since some anophelinesfeed around dusk (RIUSIiN & ASLAMKIIAN, 1978) andmost people prefer to go to bed after. it gets dark. ThusPIBs will not be fully protective, and certainly not for ir-regular users. In contrast to some entomological studies(LINES et aL, 1987; HEWITT et al, in press), we foundthat use of PIBs by some family members gave no pro-tection to others sleeping nearby without l'18a.
AcknowledgementsWe are grateful to the European Union (EU) and Mddecins
sans Frontières- Holland for funding the project. Drs Willy De-meyer of the EU and Oahu Swai and Naveeda Rano of theUnited Nations High Commission for Refugees gave encour-agement and support. The project could not have been under-
pt.
taken without the attive t1,ll:dl.11a1io11 of Ott: ,\liti1.111 )(tiltlCommittee, 1)r Zeman' ln particular, und their ceritll
stuff.
ReferencesChoi, II. W., fireman, J. G.,'l'eutsch, S. Ai., Litt, S., iIightut+cr.
A. W. & Sexton, J. I). (1995).The effectiveness 14 fend u u1e
impregnated bed nets in reducing tunes of nirlarir fuit, u.1,
a meta-analysis of published results. .-Internaa ,1 tar»Ji rlTropical ,SfeJicine and Hygiene, 52,377-382.
Deane A. G., Dean, J. A., Burton, A. H., & Dicker, R. C. t 19'>ti 1
Ept- Info, version S: a word processing, database. and maman,, pro-
gram for epidentiology. Stone Mountain, Georgia: USD Inc.
Hewitt, S. L-., Rowland, M., Ford, E. Pathan, M., Urhrsnru, I I
Nasir, M. & Kemal, At. (in press). 1'rutcetian tifmusgtntl, 1101
nets used outdoors ta persons sleeping nrarhy uühuut boni
nets. Bulletin of Entomological Research.Lindsay, S. W., Snow, R. W., Armstrong, J. K. M. & tiri il
wood, B. M. (1989). Permethrin- impregnated bedncls reJiinuisance arthropods in Gambian houses. Medical unJ I',tvnn-cry Entomologpy, 3, 337 -383.
Lines, J. D., Myainba, J. & Curtis, C. F. (1987). Expcnntelorlhut trials of permethrinim sregnased new ana ern. .1nir,1,against malaria vectors in Tanzania. AieJnral ana I'.ren »un
Entomology, 1,37-51.Miller, J. E., Lindsay, S. W. Armstrong Schellenberg, J It \l
Adiamah, J., *gars, M. & Curtis, C. 1 : :. (1995). Village trial ofbed nets impregnated with washresistunt permetllrui ..nupared with other pyrethruid formulations. Medical ana
nary Entomology, 9, 43-49.Reisen, W. K. & Aslamkhan, M. (1978). Biting rhythm, ul
some lakistan mosquitoes. Bulletin of Entomological Res :a,,li,
68, 313 -330.Rowland, M., Hewitt, S. & 1)urrani, N. (1994). Prevakn.e of
malaria in Afghan villages ill Pakistan sprayed with
lambdacyhaluthrin or malathion. Transactions oldie Royal .Vo-
clety of Tropical Medicine und Hygiene, 88, 378 -379.
Suleman, M. (1988). Malaria in Afghan refugees in l'rkit.ulTransactions of the Royal Sociay of Tropical Medicine and Ht.
giene, 82, 44-47.Toker, M. A. (1991). Unistai Statistical Package, version J.S. 1.0 n
don: Unisaat.WHO (1993). implementation of the Global Malaria Cumul Strut-
ev¡y. Report of a ir71O Study Group un the implementation .4 MeGlobal fluet ofAcNun fur Malaria Control /99.) 2001) t
World Health Organization, Tccluiieul Report Sentis, st
839.
ao
Received 15 January 1996; revised 5 March 1996; accepted
for publication 27 March 1996
TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND j1YGIENE (1996)90,362-265
Who misses out with school -based health programmes' A study of
schistosomiasis control in Egypt
M. H. Huseint, M. Talaat2, M. K. El- Sayed3, A. El- Badawle and D. B. Evans 'Department of Public Health, Faculty
g¡ . fedicirte, Cairo University, Cairo, Egypt; ?Department of Counity and Social Medicine, Theodor Bilhars Research
Institute, P.O. Box 30, Imbaba, Egypt; 5Clinicalmm
Epidemiology Unit, Faculty of Medicine, Sues Canal University, Ismailia,
EZPI;; eDeparrnunt of Comniuniy Medicine, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 1UNDP /World
Bank /If/HO Special Programme for Research and Training in Tropical Distases (TDR), World Health Organization, 12!!
Geneva 27, Switzerland
AbstractThere has been a recent revival of interest in school -based health programmes in developing countries as a
means of reducing the morbidity observed in school -aged children, of improving their physical growth and
cognitive development, and ofcontrolling transmission of disease in the community at large. This study
used data collected from a large epidemiological survey of schistosomiaals In Egypt to examine what pro-
portion of infected children missed treatment from an established national school-based schistosomiasis
control programme simply because they did not attend school. It showed that children who were not en-
rolled in school had a higher prevalence of infection and were more intensely infected than children who
attended school. At the extreme, over 80% of infected girls in one part ofEgypt could not be treated by the
existing school programme because they did not attend school. If these trends are similar in other countries
where school -bas programmes are being developed, school -based delivery may exacerbate existing in-
equalities in society and ways of expanding services to children who do not attend school regularly need to
be explored. .
Keywords: Schistosomiasis,Sckistaoma mamma, Schiuosóma haematobium, control, children, Egypt
IntroductionThe recent upsurge in interest in improving the
health of school -aged children in the developing worldderives from a number of sources (BUNDYj 1990;
I.wAMBO et al, 1992; WARREN, 1993; BUNDY & GUYATT,
1995). The prevalence and/or intensity of infection inschool -aged children is higher than in the adult popula-tion for a number of parasitic infections, particularlyhelminihs, and treatment can lead to immediate healthimprovements (WHO, 1993; EVANS & GUYATT, 1995).For example, treatment of Schistosmna tnansoni can re-vere the appearance of Symmer's fibrosis In children'(HoMEtDA It al. 1988, 1991), while treatment of hook-worm can raise haemoglobin levels in anaemic children(CROAIPTON & STEPHENSON, 1990). Treating helminthinfections can also lead to long -term benefits in the formof improved rates of physical growth and improvementsin some indicators of cognitive function ( STEPHENsON,1987; STEPHENSON et a!, 1989; NottEs et all 1992)which, due to the consistently positive correlation ob-served between adult wage rates and both education andanthropometric measures, should provide children frompoor areas with a better chance to escape from poverty(BE:IIR. %tAN, 1993; WARREN et al., 1993; EVANS &(-uiATrT, 1995).
In seeking to develop interventions aimed at school-aged children, groups such as the Partnership for ChildDevelopment (BUNDY, 1990) have focused on deliverythrough schools because of their relatively wide distribu-tion and the ease of making contact with the children(WARREN et al., 1993; BUNDY & GUYATT, 1995). However, the ability of school based interventions to makean impact in terms of public health depends on anumber of factors, including rates of school enrolmentand attendance, variations in rates of attendance overthe year, infection rates in enrolled and non-enrolledchildren, and provider and patient compliance with theintervention protocol. Low rates of attendance, for ex-ample, may well mean that the overall impact of,an in-tervention on public health is relatively small. In addi-tion, school -based interventions may even exacerbateexisting inequalities if children attending school andbenefiting from the intervention are from a higher socio-economic group, are more likely to be male, and are less
Addrets for correspondence: Dr Mahe Talast, Department ofCommunity and Social Medicine, Theodor Silhars Research In-stitute, P.O. Box 30, Imbaba, Egypt.
likely to be infected than children who do not attend school
regularly-This aper reports a study of an established school -
based achistosomiasis control programme in Egypt. Itsobjectives were to estimate the percentage of school en-
rolment in the 2 different ileographical areas in Egypt(Lower and Upper Egypt), to tdentil' the proportion of in-
fected children who were likely to miss treatment deliveredthrough the school system, and to establish whether thechildren who missed treatment were more likely to beheavily infected than children who were treated.
Materials and MethodsThe school -based programme in Egypt forms ppart of*
successful national control strategy (ABDEL- WAHAB,
1982; WEBBE & BL HAK, 1990; EL KHOBY at al, 1991).Control currently involves the identification and treat-ment of infected individuals by (i) screening people who
attend rural health units whit symptoms routed to achistosomiasis (passive returns); (h) active monthly exami-nation of 10% of the rural population on a rotating basisto ensure that the entire popWation is examined eachyear; and (iii) screening school children twice yearly
(EL -KHOBY & WEBBE, 1992). In each case only peoplewho show ova in a single stool or urine sample aretreated with praziquantel.
In the school -based programme, students identified asinfected are followed one month after treatment to en-sure cure. Although rata of school attendance in Egyptare relatively high and the school -based treatment pro-
gramme has been working well, and although there is
some information available on the performance of thescreening tests (TALAAT & EVANS, in press), no previouswork has been undertaken to identify the proportion ofinfected children who are not reached by the pro-gramme.
Data were taken from one of the largest and most re-cent surveys pf schistosomiasis in Egypt, EPI 1,2,3
(Epidemiology 1, 2, 3). Its purpose was to establish base-line data which would enable changes in the patterns ofschistosomiasis infection to be monitored over time in 9governorates in Lower and Upper Egypt. Five governo-rates (Kafr El- Shei4th, Gharbia, Qalyubia, Menofia andIsmailia) were in Lower Egypt where S. rnanwni is theprevailing s cies. The remaining 4 (Fayoum Minya,Assiut and Qena) were in Upper Egypt, where S. haenta-
tobittm predominates.
OM.
r^
.tleelical and Veterinarv En e luge (1995) 9, 344 --352
Pyrethroid- sprayed tents for malaria control:
an entomological evaluation in Pakistan
SEAN HEWITT, MARK ROWLAND, NASIR MUHAMMAD,MUHAMMAD KAMAL and ELIZABETH KEMP* MedccinsSansFrontier-es -
I lulLeneI /I lcalthNet International, University Town) Peshawar, North West Frontier Province. Pakistan, and
!-uadon School of Ilygiene and Tropical Medicine, U.K.
Introduction
Abstract. Field trials were undertaken in the North West Frontier Province or
Pakistan to determine the effects of pyrethroid- sprayed tents on feeding success.
mortality and biting -rates of wild mosquitoes attracted to bait cows confined
within the tents. Under natural conditions, endophagic mosquitoes rested only
briefly iri untreated tents during the night, followed by complete exodus at dawn..
In tents sprayed on the interior surface with permcthrin 0.5mg/m2 or with
delt :uitethrin 0.(13 g /n12 the biting rate of Anopheles srepluvr.ri was 'rc'luee'el
by about 4(1 %; delerrency against culicines and 'other anophelincs was Hitch
less. Mortulity -rotes of bloodied mosquitoes from the treated tents were 7i'Y,.
An.sleplscnsi, 65% An.subpicius but only 10% of culicines.
.Outer 11y- sheets prolonged the effective life of the treatment; bioassays on the
sprayed inner -sheets showed that insecticidal efficacy remained high for over
year, whereas on tents without fly- sheets permcthrin residual efficacy declined
rapidly 20 -40 weeks post treatment. It is concluded that tent- spraying wish
fast -acting photostuble residuul pyrethroid insecticide would probably provide
effective protection against malaria transmission for the inhabitants of tents in
any part of the world where the vector mosquitoes are endophilic and suseepl ihlc
to pyrethroids.
Key words. Anopheles culicifacies, An.sleplrensi, An.swbpicru.l', culicine mos-
quitoes, permcthrin, deltamethrin, pyrethroid insecticide, tents, pyrethroid-
sprayed tents, malaria control, Afghan refugees, Pakistan.
9- In 1991 there were 3.2 million Afghan refugees living in
Pakistan, concentrated in approximately 351) camps in
Baluchistan and the Non!) West Frontier Province (NWFP)..Despite the provision of health care through a network of
.- basic health units, diseases such as malaria remain major
health problems. For example 130,000 cases of malaria
(27% Plasmodium jakiparun :) were reported in 1991
amongst refugees in NWFP..- The majority of refugees have been living in Pakistan
for about lu years and. during this time, most haveconstructed mud houses. For these people. house-spraying
Correspondence: Mr S. E. Hewitt, MSF NcalthNct. Karakul
t.cutr. l'.U. Itos 8449. University Town.. Peshawar. N.1V.F.P..
Pakistan.
344
with residual insecticide - usually ntalathion 50%. %et..
table powder formulation - has been applied regularly hn
malaria control. A substantial minority of refugees Ituee
ever are nomadic, living in tents and migrating seasonal')between low altitude areas of the Punjab and the cool.,
hill regions of Waziristan in NWFP. Prior to 1990, rnalan.,
control for this community had hecn neglected, owing to
the unsuitability of insecticidal wettable powder as a r.sidual treatment for tents.
Efforts to control malaria by spraying tents with D1)1'.dieldrin ory -BHC were mude in Iran ( Mutuhur, 1974), nut
.gave disappointing results because of the poor adhesion ulwettable powder to canvas. Liquid formulations of photo
stable pyrethroid insecticide should be suitable fur treating
tents. as they adhere well to various fabrics, have long-
lasting residual efficacy as insecticides and Fan withstand
weathering or washing (Miller, 1191), 1995: Schreck, 1991:
Erruunrlugicrrl eralrralion of pyrcdtruir!-spruyrri rents in Pak Alan 115
I leal et al.. 1995). Therefore. following favourable reports
on the use of pyrcthroid- impregnated bcdnets for protec-
tion against malaria (Curtis et al.. 1989; Alonso et al..
1991) staff of the United Nations High Commission for
Refugees (UNHCR) sprayed 61NX) of the Waziristan tents
with aqueous emulsion of the pyrcthroid permcthrin. A
malariolugical assessment of the impact followed. (Parvez .
& Bourne. 1991) without entomological evaluation. Ethics I
and politics required all tents of the community to betreated, so comparison with an untreated control group
was not possible. In tented refugee children front onedistrict, where the spray programme had been strictly
supervised, the fold/reruns rate fell from 44 to 18 perthousand during the post -spray year whereas, in local
Pakistani children whose mud -brick homes had not beensprayed, it rose from 12 to 39 per thousand during the
same period.Many Afghan refugees return to a tent -dwelling life-
style after repatriation. Elsewhere, mïllioits of refugees or
victims of natural disasters have to usó tents, often In
malarious areas. if the UNHCR and aid agencies are to
continue to provide tents for these people, further evalu-
ation of pyrcthroid treatment is necessary before nudism
control policy can be decided. This paper describes a series
of investigations designed to assess the impact of sprayed
tents on malaria vector behaviour (feeding success, deter -
rency. repellency and mortality) and yield data, similar to
that from experimental hut studies of insecticide treatments
1(Smith & Webley, 1969; Curtis et al.. 1992). r
Material and Methods
Study urea. Field experiments were carried out at Azakhel
refugcc camp. near Peshawar In NWFP, during Augustand September 1992. As is the case with most refugeesettlements in Pakistan, Azakhcl is situated in a marginal
cone, un the banks of the Kabul River. The camp wasestablished in 1981 und, ut the time of our investigation,
had a population of 25.001. The numerous wet borrow
pits and elevated water table, with spring and autumnflooding account for high mosquito densities throughout
the summer and autumn. Transmission of malaria in NWFP
is seasonal. mainly between April and December. l'.riru.r
cases leak in September and October, l'.Jidriparunr in
November.Treat .rites and procedures. To avoid the threat of inter-
ruption from seasonal flooding, three raised platforms of
gravel. covered with stud plaster, were constructed above
the upper flooti level e. 1dm apart in a large mud -walled
compound. Each platform (6 x 5 n» had a central wooden -
frame cow pen (2 x 1 m), designed to keep the huit cow
secure without hindering host -seeking mosquitoes. and
was surrounded by a water -filled channel to deny access to
scavenging ants. As o precaution to detect ants. a shallow
paper dish holding 20 dead mosquitoes was placid on each
platform.and checked periodically to sec if any had been
removed, but none were. Support poles were erectci at
the four corners of each platform for attachment of rec-
tangulur trap nets, similar to thee: den-filmed I+y Sm. am ice
(1976).For each experiment, a tent was erected over the vow
pen on each platform. Doors of the tern were tied open
constantly. -as is customary in Pakistan during summer.
The ridge -pole tents consisted of a double sheet of
customs (30 nt' surface area: 3.5 rot wide..1.ltnt Tong. 2.1 nr
high) with a canvas outer 11y -sheet waterproofed %srth
paraffin wax and aluminium sulphate. Over each tent, a
trap net (made of 1(X) denier white polyester mosquito
netting, 2.5 nt high) was hung front the support pules.
Preliminary counts of mosquitoes attracted to vanuus
types of host revealed that cows and gouts were both
considerably more attractive than men. Per kilogram 110,1).-
weight the relative attractiveness of gouts:cows:men foranophetlnes was 9:6:1. No significant differences were
detected in the mosquito species attracted to each host.
Cows, being more attractive than men and less troublesome
than large numbers of goats, were chosen us the huit
animals for these trials. The same cows were used in their
respective pens throughout. To facilitate the collection of
dead -and knocked -down mosquitoes. white sheets +sere
spread over the mud- plastered platfrirnt floors.An hour before sunset a cow was tethered in the pen
within each tent and the sides of the trap nets werelowered around thin', leaving a gap of 0.3m from the
ground to allow entry of naturally host -seeking mosquitoes.
One hour before sunrise the nets were closed and the dead
and knocked -down mosquitoes were collected from the
platform floors. Live mosquitoes were then collected from
the trap nets and tents. All specimens were taken to the
laboratory for identification. Mosquito females collected
Irons all three tents were classified as cuticines or anuphe-
lines. the latter were identilicd to species..usted aceurdmg
to their abdominal condition (unfed or blood -IedI and
counted. To ensure consistency. the same ettonarlogrst
(S.H.) undertook all mosquito identifications. Each tent
was evaluated at camels of the three sites. over three conse-
cutive nights, using a Latin square design over treatments.
platforms and nights.Statistical analysis. For each type of mosquito. the
proportions of blood -fed females alive (bit) or deadknocked-down (hfD) and of unreel females alive (till t or
dead/knocked flown (till)) were Alt( SIN .r:uasiurnaed
and then subjected to analysis of variance IANt t\';\ 1
using UNISTA'l' ('Poker, 1191). Numbers al ruuyutoccollected were LOG' 1 transformed ;and then subjected t..
ANOVA as above.Experiment 1. i)ixtrirnrdurn uf'rnruuiulhrrs r,,nni rrri,,,1
untreated tents. in order to assess mosquito preferences for
resting on different ports of the tent. collections +scar
made from each section (Table I) of tents I and 2. and
from their trop nets, every 31s during three conseeuti +e
nights. To investigate the down exodus of mosquitoes. tent
3 was left uncovered until 30 min before the first light ofdawn, when the net sides were dropped and %seit:hted
down to the platform in order to prevent nur.squiuoesescaping. Mosquitoes resting on the inner surface ut the
net were then collected so that, by Iltmia below first
34h Sean !lrp'ill e't enl.+
light. the mosquitoes remaining within were only those
resting on the tent or on the ground. From first light, net
collections were made every 10min until no more mos-
quitoes could he found within the net.Experiment 2. Effects of pyrrlbruid treaters gents on trios-
1114u0 sun irul after blood-feeding: 'open net' trial. Inner
surfaces of the eutton inner tents were treated with py-
rcthroid insecticide applied by compression sprayer (Hudson
\-pert'), one week before the experiment started. One
tent was sprayed with permethrin (lmpertitor' 25% EC,
from 'Leneea). another with dcltamethrin ('K-Othrine'
2.5% EC, from Roussel- Uclaf), to give target doses of
t).5 g/m2 and 0.03 g/m2 respectively. The third tent was left
unsprayed for comparison. Mosquitoes were collected and
data interpreted according to the general procedures de-
scribed above.li.e perhneru .f. Effect ofpyreihruidtrealed tents on mos-
quito biting rates. The same three tents were used as for
Experiment 2: one treated with permcthrin 0,5 g/m2, one
treated with deltamcthrin 0.03 g/m2 and the. third tentuntreated. The same general evaluation procedures wcrc
followed and, in addition, all-night biting catches weremade from each of the cows. In euch tent, mosquitoes
biting the tethered cow were collected by one collector
from 19.00 until 24.(1(1 hours, and by another collector
from 24.(X) until 05.0X) hours. To minimize' any effects of
personal variation. individual collectors worked the sume
shifts at the same sites throughout the experiment, while
tents rotated between sites.Experiment 4. Effects ofpyrethroid treated tenis um cap-
tive mosquito, feeding and survival rates: 'closed net' trial.
Tents, nets and cOW$ were set up on each platform, as
before, but this time the sides of the. nuts were lowered and
scaled to the ground. At dusk, large numbers of wild -
caught unfed female mosquitoes were released into each
closed trap net and left there overnight. 'chose muslluitte$
had been collected nearby froni the outside of threeUntreated hedn'ets, each baited with a cow, during the
previous night. During the intervening day they were held
in uncrowded cages in u cool, dark room and were provided
with food of sugar solution on cotton -wool pads. Humidity
was kept high by wrapping the mesh cages in damp towels
and plastic sheeting. Half an hour before sunrise, mos-
quitoes were collected from the sheets, tents and nets,
then taken to the laboratory for identification. Each tent
was evaluated twice at each site.Experiment 5. Effects of weathering on the residual effi-
cacy of pyrethruid treatments. From the date of spraying in
August 1912 the tents used in these trials were left erected
to weather in the open air until August 1993. Additional
canvas tents (similar to the outer -fly of the double sheet
tents) were also sprayed with the sante target dosages of
lx rmethriu 11.5 Wm- and dcltaniethrin (1.03 g/m2 and left to
Ne.filter outdoors.Every it weeks. two 0.2 nr samples were cut from the
treated sheet of each tent and used fin contact bioassays
(.311 min exposure) of laboratory-reared females of Anopheles
eh'p /u'nsi (I)lull -ti strain). Unfortunately the single -sheet
tent that had been sprayed with deltamethrin was stolen
50011 utter the trial begun, su no hioussay data for this
permutation were obtained.
ResultsExperiment 1. Distribution of mosqui toes resting in
untreated tents (Table I)
Totals of 1619 culicines and 790 anophelines were col-
lected resting in untreated tents, of which 664 wereAatipltele:r stephensi and 800 were ui,i.calicifucies. Smaller
numbers of four other anophcline species collected have
been excluded front the analysis. Of the tent- resting nusquitoes, all the culicines, 98% of An.steplensi and 96% of
An.culicifacies were bloodied, showing that host -seeking
mosquitoes settled on the tent only briefly -if at all -before
feeding, whereas they rest on the inner surfaces of tents
for some time after feeding. The proportions collected
from the tent were 74% of An.culicifacies and 45% of
An.steplensl, with the remainder caught in the net trap.
Apparently An.culicifacies lusts for longer, or possibly es-
capes front the trap net more efficiently, than An.stcpheusi.Anophelines preferred the itpex, while culicines preferred
the wall panels of the tent. However, relatively few (4% )
culicines were collected on the tent, since they mostly
rested on the ground beneath the cow after blood-feeding.
and the majority (96%) were found in the net trap, showing
that they exited from the tent soon after (ceding.
Trap net-collections curried out at If)ntin intervals from
first light revealed a pre -down exodus of mosquitoes front
the tents, mostly 20 -30min before sunrise. By 10 min
after sunrise all had left (Table 2).
'the results demonstrate the relatively short resting time
of unophelines in tents. As so few mosquitoes occurred on
the fly -sheet or outer surface of the Inner tent, it wasdecided that treatment would involve spraying only the
Inner. surface of the inner sheet of the tents.
Experiment 2: 'open net' trial. Mortality -rates of blood -fed
mosquitoes from treated tenus (Fig. IA; Table 3)
2778 culicines and 876 anophelines were collected. in-
cluding 116 An.stephennsi, 618 Ai.subpictus and five other
anopheline species in smaller numbers. The deltamcthrin-
sprayed tent caused higher mortality than the permcthrin
sprayed tent, overall, but this difference was significant
only for Atr.subpictus (P <0.05, Student -Newman-Kuck
multiple range test).Proportions of bloodied mosquitoes killed by the treatct:
tents wore about 75% of An.stepheui, 65% of Au.suhpieta+
but only 109ó of culicines (Table 3).
Experiment .3: 'biting net' trial. Mosquito biting rates tin
cows in treated tents (Fig. 2)
Totals 'of 2716 culicines and 1929 anophelines were
collected; including 285 An.stephrnsi, 1536 An..rubpirtl
ti
r
Entomological evaluation ofpyraliroidsprayed ¡e,us in Pakistan
Table 1. Mosquito collections from five sections of tent interior surface andfrom net traps over the tents: pooled data
from three nights of collection In two untreated tent's.
Tern section
Culidncs An.stephutsl
Total .t /m2 Total
An.colirijprles
2/m1 Total .t lint
Inside Inner sheetApexSloping roof panelVertical wall panel
Inter-sheet spaceOuter side of Ay sheet
No. resting In tentNo. In trap net
Total
6'21
2306
56 .(4 %)1230 (96 %)
1286 (70 %)
2.52.25.8O
0.3.
.73
99.3508
216 (45%)268 (SS%)
484 (26%)
30.410.4
8.11
O
0.4
11 4.6
26 2.7
6 1.5
u It2 11..1
45 (74'X.)IO (26%)
61 (4%)
Table 2. Dawn exodus of mosquitoes from an untreated tent (pooled data from three
nights). The trap net Over the tent was pre-cleared of mosquitoes by first light. Mosquitoes
trapped after leaving the tent were then collected from the net at 10min intervals ( denotes
time If sunrise).
Minutes afterlint light
No. of mosquitoes caught in trop net:
Culicincs An.srephensl An.culkljacies Total
10 220 98 12 330 (62%)
r 20 93 54 5 I32 (29'%.)
30 l8 25 1 44 (8%)
40 o 2 ti 2 (0.4%)
50 2 I 1 4 (0.73%)
60 0 tl 0 0
532
FN.Table 3. Mortality-rates of blood-fed mosquitoes from the 'dosed'and 'open net' wtllcctiuns (percentages
corrected for control mortality using Abbott's formula). Experiment 2; t Experiment 4.
r Pcrmethrin Dcltamcthritt
xDead'
Confidenceinterval
xDead
ConfidenceInterval
r Culidltcx Closed nets 59.4 31-88 68.8 32-146
Open net 9.3 -I-211 11.4 4 ._'7
An.stephensi ('hosed stet' 88.3 811-97 ' 95.3 lei -102
Open net 71.3 35- ION 81.7 79 -85
0.111= An.sahpirrus Closed blet' 88.9 74 -114 94.1 84 -114
Open net 56.0 37-75 77.7 511 - 105
eand six other anopheline species in smaller numbers.
Comparing the numbers of blood-fed females collectedin the treated tent with those collected in the untreatedcontrol tent gives an estimate of the deterrent (i.e: feeding
prevented) effects of the tent treatments (Fig. 2). In bothIx nuethrin and deltamelhrin tents there was a significant40l'0 reduction in the nuniber of :loi.xtuplansi biting
347
(Fm 19.037, df 2. P <U.05). Detcrrcncy of culicines was
also. upparent, but not significant. whereas effects onAn.snbplents were unclear. There was no indication illmosquito repellency (i.e. resting in the tent pre%cntctI
after blood feeding) caused by contact with either pyrethroi,l (Fig. 2).
Zti\ Sean Hewitt et al.
cullclnes (n :2778) An. stephensi ( n =116) An. subpic/us ( n e 618)
A
8
culicines (n i4154)
4e118ee111'
100%
7 {
0
t0
0%
eonrrol OuleelA'
An. s/ephensi (n =648)
eIlemelM
nvnrelll' dellemelM
eln r.:3 IUD Llell.. MNsn.
00%
711
e0
26%
0
eOnlrol perwelK
An. sybpic/us In: 570)
elleweM'
elrel yIewelll' eelle,eein
Flg. 1. I'11)aiological condition of mosquitoes collected from net traps over three tents: untreated control: perncnhrin treated.
dcltamelhrin treated. (A) Wild mosquitoes from 'open net' trial (Experiment 2), (8) captive mosquitoes from 'closed net' trial
(E NrimenI d). Abbreviations: uf, unfcd: hf. blood -fed; D, dead /knocked-down; L. live.
1.1rr/, net efficiency. With the untreated tent, numbers of u d +e.,mosquitoes caught actually biting versus those caught
III Ifed in the 'open net' trial (Experiment '2) give u if E is the constant ratio of escaped mosquitoes (e ) to
ne.l urc of the relative efficiency of the trap net as a captured mosquitoes (d ), then:
c.gaun' technique.Itloo,lied mosquitoes were always found resting in the
'' ° E(do)
act .1t d.nln in Ii .P' rinenl 3. slowing that the. catching thus, from equation (I):
efficiency of the. collectors was less than 100'%, since u = d + E(d ) (2)
blood-fed mosquitoes rarely entered the net after feeding
outside. To calculate the capture efficiency of the net, a For the biting collections, if b a number caught feeding
formula was derived which takes catching efficiency of on the bait, at a number attracted to the bait, and
collectors into account. .
d,, ss number collected from the net at dawn, then:
For the 'open net' experiments. if a number attracted ar, r b + dr, + E(dr,) (3)
to ilie bait. d a number collected from the net of dawn,
and c = number escaping from the net. then: If a and al, are nssutiied to he the some. which is
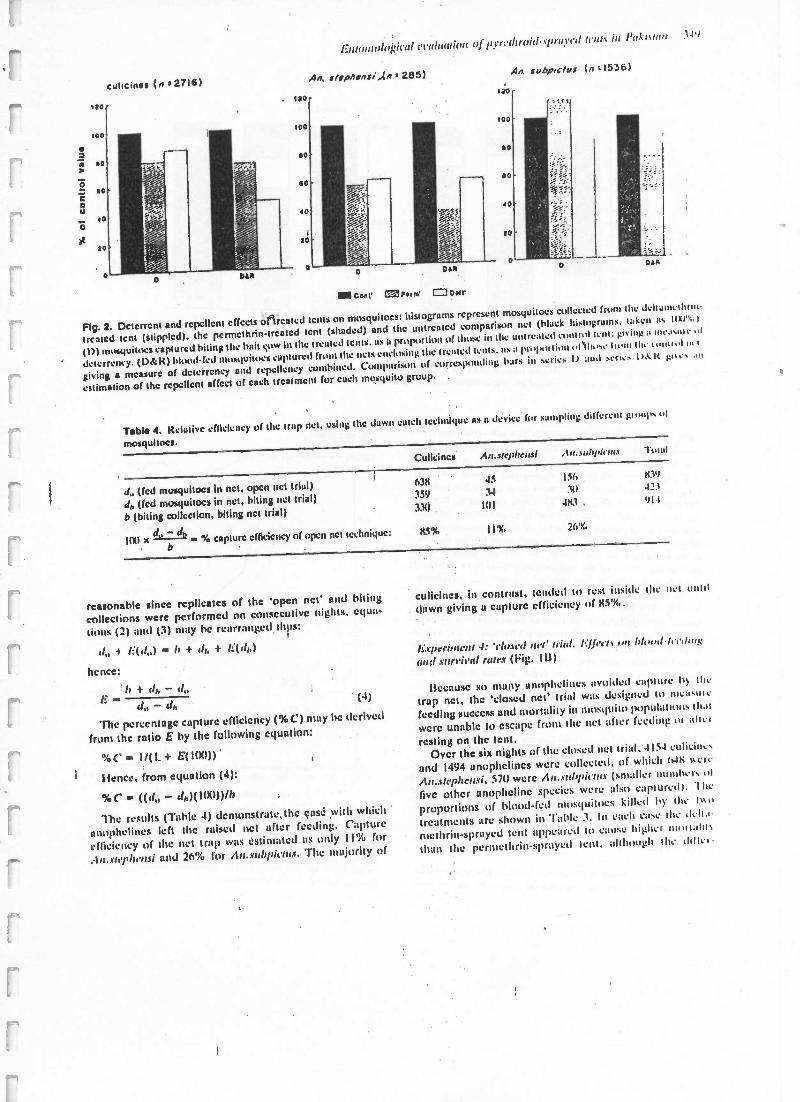
cullcinss (n s 2716)
Enlontuln¡;irul evaluationnjpwwlltruid,%prutv'd berm in l'al :')
An. s/ipASnsl.(n 285) An. subp,c/us (n,. 1536)
IN Con1' =Perm' 0 Do11'
o DAR
Flg. 2. Deterrent and repellent effects of treated tents on mosquitoes: histograms representmosquitoes collected from the dcltunmctllrnl-
treated tent (stippled). the permcthrin- treated tent (shaded) and the untreated comparison net (black histograms. taken as IXI ., )
(I)) mosquitoes captured biting the bait c.uw in the treated tents. ns a proportion of those in the untreated contiol tent: giving a nlc.lanc
deterrency. (D :R) blood-fed mosquitoes captured from the nets enclosing the trenled tents. as a pnq>,ulion of Uue 11nun the rmaw! n. I
giving s measure of dctcrrcncy and repellency combined.Comparison of curreslx,nding bars in Sol iex I) and .cnc. I). I< go... .u,
estimation of the repellent affect of each treatment fur each mosquito group.
Table 4. Kelutivc efficiency of the trap net. using the dawn catch technique as a device for sampling iiilfcrent group, ,.1
mosquitoes.
Culicinca An.srephc ai ,In..o,hpirm.% Tutu)
J (fed mosquitoes In net, open net trial) 638 45 156 83')
J,, (fcd mosquitoes in net, biting net trial) 359 34 311 421
b (biting collection, biting nct trial)
d, -dr
33()
85%
1111
11%
483.
26'%,
91.1
1101 x % capture cffkien cy of open net technique:
reasonable since replicates of the 'open net' and bitingcollections were performed on consecutive nights. equa-
tions (2) and (3) may he rearranged tips:
d 4 li(d + rh, + G(th,)
hence:
C d - d,,h+rh,-d
(4)
The percentage capture efficiency ( %C) may he derived
front the ratio E by the following equation:
%C - .1 /(1 4- E(I(1(1))
!fence. from equation (4):
%C - ((rl - dn)(100)) /b
The results (Table 4) demonstrate, the case with which
anuphclines left the raised net after feeding. Capture
efficiency of the net trap was estimated as only I I'%. for
:1,,..Ih'phensi and 26% for /1,r.subpit'lux. The majority of
culicinea, In contrast, tended to rest inside the act until
dawn giving u capture efficiency of 85'%..
Experiment 4: 'c/used net' niai. 1:111.4 .1% nn Him& lerdu,.0
and survival rates (Fig. Ill)
Ifecause so many linophelines avoided capture by the
trap net, the 'closed net' trial was designed to nnc:l.u,c
feeding success and mortality in mosquito population. 111.11
were unable to escape front the net after feeding on .11111
resting on the tent.Over the six nights of the closed net trial. 4154 culicine,
and 1494 unophelincs were collected, of which 648 %melt
iln.sltpllensi, 571) were A,t.subpirlas (smaller numbers of
five other anophcline species were also captured). 'I he
proportions of blood -fed mosquitoes killed by the t%n
treatments are shown in Table 3. In each case the delta
methrin- sprnycd tent appeared to cause highcl mintaht%
than the pertnethrin-sprayed tent, although the 1111111
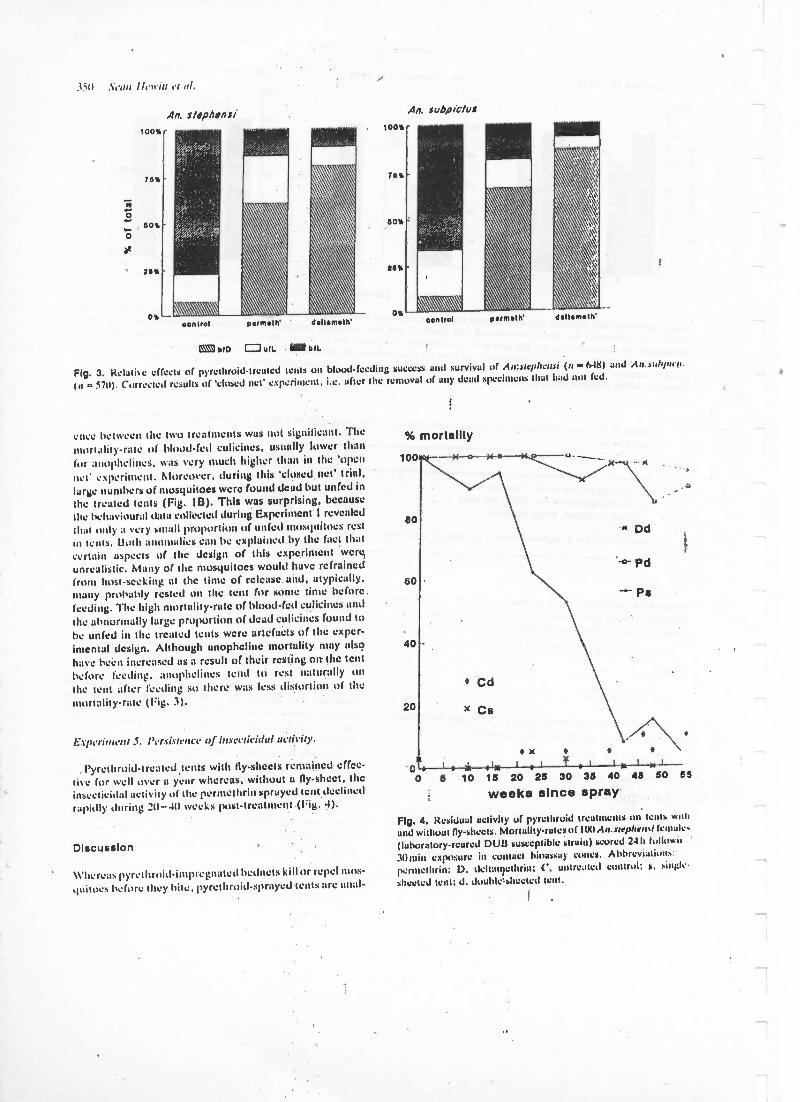
1311 .1.4'u11 llrn'i!! I'I al.
100%
76%
60%
' 26%
0%
An. s/spAsnsi
control ddumNh'
® CIO uIL DIL
An. subpic/us
oonlrol primula ddlamHh'
Ag. 3. Relatile effects of pyrclhroid- treated tents on blood -feeding success and survival of An:alrphcnai (n a 648) and A,,.auhpuu.
In = 5711). Corrected results of 'closed net' experiment. i.e. after the removal of any dead specimens that had not fed.
cncc between the two treatments was not significant. Themoil alit yrate of blood -fed culicincs, usually lower thanfor :Inollhclincs, was very much higher than in the 'opennet' experiment. Moreover, during this 'closed net' trial,large numbers of mosquitoes were found dead but unfed inthe treated tents (Fig. I13). This was surprising, because
the behavioural data collected during Experiment' I revealed
that only a very small proportion of (infect mosquitoes restIll tents. Both :monm:lies can be explained by the fact thatcertain aspects of the design of this experiment were,unrealistic. Many of the mosquitoes would have refrainedfrom host -seeking at the time of release. and, atypically,many probably rested on the tent for some time before.feeding. The high mortality -rate of blood -fed eulicines and
the abnormally large proportion of dead culicines found tohe unfed in the treated tents were artefacts of the exper-imental design. Although unophcline mortality may also
have been increased as a result of their resting on the tent
before feeding. anophelines tend to rest naturally onthe tent alter feeding so there was less distortion of themortality -rate (Fig. 3).
G.rprrilnrlu S. Persistence of insecticidal activity.
.
l'yrethroid- treated, tents with fly -sheets remained effec-live for well over a year whereas, without a fly -sheet, theinsecticidal activity of the permethrin sprayed tent declinedrapidly during 20 -411 weeks post -treatment (Fig. d).
Discussion
Whereas pyre throid-impregnated bedncts kill or repel 11105-
'luitocs before they bite, pyrcthroidsprayed tents are anal-
% mortality
10 15 20 25 30 35 40 45 50 55
weeks since spray
Fig. 4. Residual activity of pyrethroid treatments on Lento wail
and without fly- sbects. Mortality -rates of 100An.areplrrnal (crnalrs
(laboratory-reared DUO susceptible strain) scored 241k Iuiluwil
30min exposure ill CuntuCI bioassay cones. Abbreviations:permclhrin: D. dcllan'ethrin: C. untreated control; s. siuglc
sheeted tent: J. double= sheeted tent.
r
r
i--
r
r
r
P-
Or'
r
Entomological evaluation ojpyredroid-spruyed rents in l'uki.,turr 351
ogous to sprayed houses for killing freshly blood -feelendophagic female mosquitoes which rest punt- prundiallyon treated interior surfaces. In our study area of PakistanNWFP. Anopheles females were found to be very vulnerableto residual pyrethroid treatment inside tents because, aftertaking a bloodmeal, they tended to rest within the tentuntil first light. Culicines were less vulnerable because theyrested on the tent only briefly. if at all. and tended to exitimmediately after feeding or to rest on the ground withinthe tent until leaving at dawn. The dawn exodus of mosqui-toes from tents was complete, presumably due to photo -phobia. since it preceded the daytime rise in temperature.Fast- acting photostable pyrethroids, such as permethrinand delta- methrin, with their long residual efficacy, arc themost appropriate insecticides for killing mosquitoes duringtheir brief rest in treated tents.
The parallel with house -spraying Implies that tent sprayingshould have the same aim: community protection from .malaria, for which compliance from householders andgood spray coverage are esential. As a method of self -protection against mosquitoes and malaria in NWFP, treatedtents arc less effective than impregnated bedncts becauseinhabitants prefer to keep the door flaps open in the warmsummer months. Malaria transmission in Pakistan continuesinto the autumn when tent flaps are more likely to be closedfor warmth at night, giving better protection against endo-pliilic mosquitoes.
The methodology for evaluating Insecticidal house treat-ment is well established (Fontaine. 1983: Pant, 1988).Experimental huts fitted with veranda air window trapsfacilitate observations on various responses, such us mor-tality, deterrence, repellency and inhibited feeding ofmosquitoes (Smith & Weblcy, 1969). Entomological evalu-ation of sprayed tents is more problematic because pointsof entry and exit are numerous and because ¿raps cannotbe lilted readily. We hoped that the giant net traps used tocover the tents in our experiments would overcome theseproblems and allow mosquitoes to enter freely while trap-ping these that attempted to leave. Tree types of exper-timental design were devised to nensure the spectrum ofpossible responses.
The 'closed net experiment gave accurate mortalityestimates because mosquitoes were unable to escape fromthe site after contacting the bait or tent. Its stain limitationwas the disproportionate killing of mired mosquitoes aftertheir release within the net.
The 'open net' experiment required no human inter-ference and measurements were made on freely -entering.naturally host -seeking mosquitoes. It was particularly suc-cessful for culicines since the majority were trapped by theart. The estimate of e. 111% cullcine mortality is thereforeconsidered accurate. The 'open net' gave a,distorted viewof anopheline mortality because 75 -9(1% escaped afterfeeding.
lilting collections (Experiment 3) in sprayed and un-sprayed tents gave the best estimate of deterrence: approxi-mately 2(1% of eulicines and 40% of An.stepltensi weredeterred from biting in the pyrethroid- treated tents. but
luhpi,tits was apparently not affected, Evidence for
deterrence was also apparent in the 'open net' (I ?sperintent2). where the proportion of ruffed An..yrepluvo and cull.cines resting on the net trap was considerably larger in thecase of pyrethroid treated tents than the untreated tent.Perhaps the deterred mosquitoes found it difficult to resistthe attractive stintuli emanating from the cow and hencerested in the vicinity of the lent. i.e. in the trap net.because there was little or nu evidence of repellency 1,0m-feeding.
Of the anophelines that escaped front the 'open net siteafter feeding (89% of An.stephensi and 74% of Are.srohpìc-
lrrs), the important question is: how many had acquired alethal dose of insecticide? The most optimistic model isprovided by the 'closed net' experiment. showing mortality-rates of 88 -95%, whereas the 'open nct' experiment gaveestimates of 56 -82% mortality. The most pessimistic modelassumes that all mosquitoes which escaped from the opennet would have survived, implying mortality -rates of onlyiS -20% (or An.scthpictis and 8% or 9% forun..rte /rherrv.probably gross under -estimates, judging by the high pro-portion found on the tent versus the net (Experiment I).
Comparing the two pyrcthroids used for treatment ortents, deltamcthrin killed a slightly greater proportion ulall mosquito species than pernethrin. I (owever. toxicity isa function of dosage and. in our experiments, pernietluinwas applied at the rate of 0.5g /m= used operationallyfor bedncts (Alonso et al., 1991: Miller, 19')5) whereasdcitnmcthrin was sprayed at (1.03 g /n2, twice the rate of0.015 g/m2 recommended for bedncts (Dartigues. I'Ix71.Permethrin has the advantage of being less irritant to theskin than deltamethrin. un important factor when sprayingin the close confines of a tent. Ileal et al. (1993) recentlyreported that tents treated with oil -based I X formulationof permcthrin applied at e. I gai /m= gave significant pro-tection against pest Aeries in Canadian woodland It at
least 6 weeks. To avoid the smell. lire hazard and oilinessof this formulation. they recununended the use of aqueouspyrethroid for tent treatment, such as we employed inPakistan. Perniethrin's stain disadvantage is its relatiocltshorter residual life, although This should nut he a sei waslimitation when tents have fly- sheets. lt culti he concludedthat where large tented settlements, in ntuhrious districtssuch as NWI:P. are sprayed with either pernuthrin ordcitamellirin there will be a resultant nductiun in ni alai ua
transmission, us from residual house -spraying in this situa-tion (Rowland et al.. 1995). A strategy of tent -sprayingwould probably be effective against malaria in any part ofthe world where the vectors are enduphilic and susceptihkto pyrctliroids.
Acknowledgments
We thank the field staff of MSI' IleuiU;Net fur aH thenhard work. This research was supported by Medecins SansFrontiï`res Midland) und the European Union.
1i2 Sean Hewitt et al.
References
Aloms.r. I'.1... Lindsay. S.W'.. Armstrong. J.R.M.. Conch, M.,11111. A.lì.. Da%id. PII., Fcgan. G., dc Francisco. A.. hull,A.J.. Sheraton. l'.C'.. Chain. K. & Greenwood. LI.M. (1991)
the etfeet of insecticide-treated bedncis on mortality of Gambian
:hddr.a. Lancet. 317, 14')') -1502.Curt s. C. F.. Lines. J.D.. Carnevale, P., Herbert. V.. e1 il. (1989)
Impregnated hetbtes and curtains against ntahtrin inosquitocsAmara/ uium Technology for Vector Control (cd. by. C. F.Curtis). pp. 5 -116. CRC Press, Boca Raton, Florida.
t ln Os. ('.F.. Myamba; J. & Wilkes, T.J. (1992) Various pyrcthroids
mn hednels mid ,curtai s. ,llemarias Jo Institua, ()stealdo Cruz.
$7. Suppl. III. 363 -370.t).tnigues. V. (1987) Use of Oeltamet!rbr In the Control .of
Malaria. Roussel 11claf. Division Agrovcl, Paris.loniaine. R.E. (1983) lin use of residual insecticides for thi:
onool of adult mosquitoes. Integrated .Mosquito Control Meth-
odologies. Vol. I. Experience and c laments front cwrvenrionul chemical control (ed. by M. Laird and J. W. Miles). pp.
4') -81. Academic Press. London.ilea(. J.D.. Surgconcr. G.A. & Lindsay. L.R. (19 95) Permettais
as a tent treatment for protection against field papulutiuns of
mu.sy ' s. Journal of the American Most/ ' Control
Association. 11. 99 -11)2. .
Miller. J.E. (1990) Laboratory and field studies of insecticideimpregnated fibres for nrusrintint control. Ph.D. thcsis..Loudnn
School of I lygicsi :and Tropical Medicine.hillier. J.E., tindsay, S.W.. Armstrong Sehellenikrg. J,. Adiutuah
1 J.iw.r.r. .l' Curtis. C.F. (1995) Village trial of Iicdneis
impregnáted with wash-resistant pcnmctluut' comparedwith other pyrctltroid formulations. Medical arid Veterinary
Entomology, 9, 43 -49.Molubar, M. (1974) Malaria and nomadic tribes of southern Iran.
Cahiers (J.R.S.1O.M., Serie d'Entomologie Alerlicale et JrParashologie, 12, 175 -178.
Pant, C.P. (1988) Malaria va:etor control: imagoeiding. Malaria
P r i n c i p l e s and Practice o f Malurialudy, Vol. 1 (ed. lay W. I I
Wcrnsdorfcr and I. McGregpr). pp. 1173 -1212. ChurchillLivingstone, Edinburgh.
Pervcs, S.D. & Bouma, M.J. (1991) Pcrmcthrin application totents of Afghan refugees In NWF'P of Pakistan. Anmra! Retard,National Irutiims of Aluluriu Research and !ruining, LaMar.Pakistan, pp. 76 -99.
Rowland, M., Dewitt, S. & Martini. N. (1995) Prevalence of
malaria in Afghan refugee villages in Pakistan sprayed with
lanabdacyhaluthrin or malatlion. Transactions of the RuralSociety Of Tropical Medicine and Hygiene, 88, 178 -379.
Schrock, C.L. (1991) Permcthrio und diutclltyl phthalate as Ivor
fabric treatments against 4edesargypt!. Journal of the .t Mel 14
Mosquito Control Association, 7, 533 -536.Service, M.W. (1976) Mosquito Ecology: livid Sampling Alethud..
Applied Science Publishers. London.Smith. A. & Webluy, D.J. (1969) A vcrandahtrup but for
studying the house- frcquunlíng'habits of squito s and forassessing insecticides. III The effect of DD'f' un behaviour and
motatity. I irllethr of Entomological Research. 59. 33 -46.
Tokeir, M.A. (1991) Unistii Statistical Package. Unistil. London.
Accepted 17 June. revised December 199.1
1
1
Ta ....0 lams to mu kor.u. SIR u.n-,r, 'fauru.u. Murals' .e:u lhracsu:t1995) 89, 351-353
Failure of passive zooprophylaxis ;cattle ownership in Pakistan is associatedwith a higher prevalence of malaria
351
Menno Boumas and Mark Rowland1' tMídicins sans Frontières, P.O. Box 10014, 100! EA Amsterdam, The
\'eth,rlanJs;11lcahhNet International, P.O. Box 889, Peshawar, Pakistan
AbstractTo examine the possibility that domestic cattle kept In house courtyards might protect occupants againstmalaria through zooprophylaxis, parasite prevalence surveys were conducted of schoolchildren in Pakistaniand Afghan refugee villages and analysed according to whether each child's family kept cattle. Parasite pre-valence (15.2%) was significantly greater among children of families which kept cattle than among thosewhich did not (9.5 %). Comparison of prevalence between different villages revealed a positive correlationbetween parasite rates and the proportion of families owning cattle. The latter finding supports the predic-tion of the Sota Mogi theoretical model that domestic animals can enhance rather than reduce malaria trans-mission when vectors are zoophilic, the infection rate low, and the human:cattle ratio high. All theseconditions applied in the study area.
Keywords: malaria, prevalence, zooprophylaxis, effect of cattle, Pakistan
IntroductionZooprophylaxis has been defined by the World Health
Organization (WHO, 1982) as 'the use of wild or domes-tic animals, which are not the reservoir hosts of a givendisease, to divert the blood-seeking mosquito vectorsfrom the human hosts of that disease . It may he active orpassive. Active zooprophylaxis is a reduction in malariaor human-biting resulting from the deliberate deploy-ment of domestic animals os a barrier between mosquitobreeding sites and human settlements (WHO, 1991).Passive zooprophylaxis is the serendipitous reduction inmalaria purported to occur when cattle density increaseswithin a community (sec, e.g., Swi LLIiNGRIiIIIiL & L)liBucK, 1938; GIGLtou, 1963).
In Pakistan, a higher incidence of malaria is recordedat health centres for Afghan refugees than at centres serv-ing local Pakistanis. The difference was initially attribut-able to Afghans having been less exposed!to malaria andtherefore less immune during the first ears after their.arrival in Pakistan (SULEMAN, 1988). Ii has also beensuggested that, because refugee families possess fewerlivestock than Pakistani local residents (ENGLtstt, 1989),they are less able to benefit from any zooprophylactic ef-fect of cattle (ZULETA, 1989).
Conditions in Pakistan seem, at first sight, highly con-ducive to successful passive zooprophylaxis. The majormalaria vectors are highly zoophilic, and Afghans andlocal residents prefer to keep their cattle close to their liv-ing quarters. However, a mathematical model developedby SoTA & Moct (1989) has exposed problems with thetheory: simulations predict that introduction of cattle canlead to increased vector densities, increased human bit-ing rates, and greater malaria transmission. Appropriatedeployment of cattle away from human dwellings may becrucial to the success of zooprophylaxis (SCItuL'tz,1989).
This paper reports cattle ownership and malaria parasite prevalence surveys conducted in refugee and localvillages to the North -West Frontier province (NWFP).ofPakistan. It examines the relationship between cattle andmalaria at the household and village levels, and assesseswhether household cattle lessen or exacerbate the malariaproblem.
Materials and MethodsRural Pakistanis and Afghan refugees live in houses
made from mud, surrounded by an open courtyard andhigh perimeter wall. Both communities keep domesticanimals (cattle, water buffaloes, goats etc.) in courtyardsand sheds usually within 10 m of the living quarters.People sleep in the courtyards during summer, movingindoors from October onwards. Sources of mosquitobreeding include borrow pits, river margins and rice pad-
Author for correspondence and offprint requests.
dies, and the fauna includes Anopheles culictfacies, .4. ste.phensi and .4. subpictus among others. Transmission ofPlasmodium vivax and P. falcipurum occurs betweenApril and December and reaches a peak in October /No-vember.
The study areas wcrc 3 refugee and 4 local villagessituated along a 24 km valley in Kohat district, N11',Pakistan, and a pair of neighbouring refugee and localvillages in Mohmand, a tribal area 100 km north ofKohat. Health services were provided by the United Na-tions High Commission for Refugees and the Govern-ment Department of Health, both of which conduct vec-tor control campaigns louse spraying with malathion t inJuly each year. According to spray reports, house cover-age ranged from 82 to 100% and all study villages weresprayed.
Parasite prevalence surveys were conducted in villageschools in October 1989 in Mohmand, and in November1989 and November 1990 in Kohat. Schoolchildren wereaged 4-15 years; 90% were boys. Thick and thin bloodfilms were prepared from virtually all children present anthe day of examination, stained with Giemsa's stain andexamined at the Médecins sans Frontieres reference lab-oratory. One hundred microscope fields of each filmwere examined before reporting a slide as negative. l'ara-sitaemic children were given supervised treatment withchloroquinc (25 mg /kg body weight in divided doses over3 d), whether symptomatic or not. During blood collec-tion each child was asked in private by the survey teamwith the schoolteacher presiding -whether his or herfamily kept cattle (cows or water buffaloes) within thehouse compound.
ResultParasite prevalence in households with or without cattle
'parasite prevalence was correlated with age, increasingfrom 10.2% at 4 years to 18.1% at 15 years. All furthercomparisons were therefore conducted on ageadiustcdprevalence rates using the method of direct stand-ardization (the standard population was produced fromthe total of all the surveys).
In Kohat the prevalence rate in the Afghan comttttmitywas similar to that in the Pakistanis, whereas in Moltmend prevalence was siggnilic:onl greater in Afghan.(xt =18.9, degrees of freedom [d.f.j =2, l t) (NMI(Table). Prevalence also showed geographical variation
ee the data for 1989 in the Table), with P. /alcuparurnpredominant in Kohat and P. vivax predominant inMohmand. Prevalence also varied between years, par-ticularly that of P. falci arum which, in Kohut. w:Ishigher in 1990 than in 1989. Thus in order to evolualcthe relationship between cattle and parasite prevalence.and avoid the potentially confounding variation betweencommunities, localities and years, it was necessary toexamine each of the 6 subsets of data separately, age.
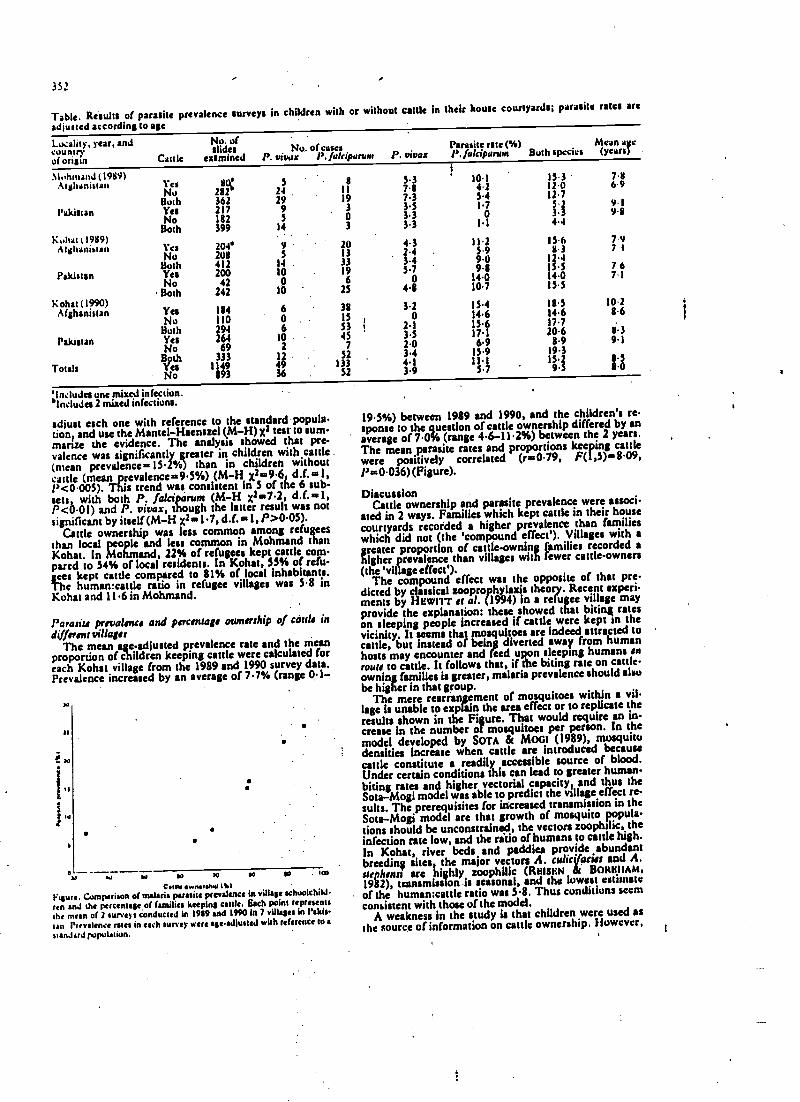
352
Table. Results of parasite prevalence surveys in children with or without cattle in their house counyardsi parasite rates are
adjusted according to age
Locality, year, andcountryof origin
.%tultnland (1989)Afghanistan
Pakistan
Kuhar ,1989)Afghanistan
Pakistan
Kohat (1990)Afghanistan
Pakistan
Totals
No. ofslides Nu. or cases
Cattle examined P. viva:: P. fakipartonParasite rate (%) Mean age
P. vivas P. fulciparwn Both species (years)
YesNoBothYesNoBoth
Yes
BothYesNoBoth
Yes
BBothYcsNo
BothYesNo
292362217182399 14
24299S
204'
4ÌÌ200
42242
184
26469
333
1893
91.4 .
10 190 6
10 23
lÌ1930
7.87.33.53.3
3 3.3
201333
60
lÓ2
12
36
Ss i
752
1S1
4.32.43.45.7
04.8
3.20
3.32.03.4
3.9
10.14.2S41.7
01.1
15.99.09.8
14.010.7
15.414.613.617.16.9
15.915.7
15.312.012.7523.34.4
7.86 "9
9.19.8
15.6 7 98.3 7 t
12.415.5 7 614.0 7.113.3
18.5 10.214.6 8.617.720.6 1138.9 9.1
19.3
19 3 .Ó
'Includes one mixed infection.°Includes 2 mired infections.
adjust each one with reference to the standard popula-tion, and use the Mantel- Haenszel (M -H) x3 test to summane the evidence. The analysts showed that pre.valence was significantly greater in children with cattle .(mean prevalence ..I52%) than in children withoutcattle (mean prevalence L.9.5%) (M -H x2m9.6 d.f. =1,P <0.005). This trend was consistent in S of the 6 sub-sets, with both P. /alciparum (M -H x27.2, d.f. ..1,P <0.01) and P. viva(, though the latter result was notsignificant by itself (M -H X2 -1 7, d.f. -1, P >0.05).
Cattle ownership was less common among refugeesthan local people and less common in Mohmand thanKohat. In Mohmand, 22% of refugees kept cattle com.pared to 54% of local residents. In Kohat, SS% of refu-
Thgees
kept cattle compared to 81% of local Inhabitants.e human:cattle ratio in refugee villages was 5.8 in
Kohat and 11.6 in Mohmand.
Parasite prevalence and percentage ownership of caul. in
different villagesThe mean age-adjusted prevalence rate and the mean
proportion of children keeping cattle were calculated foreach Kohat village from the 1989 and 1990 survey data.Prevalence increased by an average of 7.7% (range 0.1-
.
aa
a
oat so W a ra ea to too
Cott4.wMI.hte MIt'tare. Comparison of malaria parasite prevalence in village schoolchild.
ren and the percentage of families keeping cattle. Each point representsthe mein of 2 surveys conducted in 1989 and 1990 In 7 villages in Pakis.
tan Prevalence rates in each survey were sgeadjussed with reference to s
standard population.
19.5 %) between 1989 and 1990, and the children's re.sponse to the question of cattle ownership differed by anaverage of 7.0% (range 4.6-114%) between the 2 years.The mean parasite rates and proportions keeping cattlewere positively correlated (r -0.79, F(1,5) -8.09,P =0.036) (Figure).
DiscussionCattle ownership and parasite prevalence were associ-
ated in 2 ways. Families which kept cattle in their housecourtyards recorded a higher prevalence than familieswhich did not (the 'compound effect'). Villages with a
hgreaterproportion of cattleownin families recorded a
igher prevalence than villages with fewer cattle-owners(the 'village effect').
The compound effect was the opposite of that pre-dicted by classical zoopro hylaxis theory. Recent experi-ments by HEWIrI of al. (1994) in a refugee village mayprovide the explanation: these showed that biting rateson sleeping people increased if cattle were kept to thevicinity. It seems that mosquitoes are indeed attracted tocattle, but Instead of being diverted away from humanhosts may encounter and feed upon sleeping humans enrouts to cattle. It follows that, if the biting rate on cattle -owning families is greater, malaria prevalence should alsobe higher in that group.
The mere rearrangement of mosquitoes within a vil.lage Is unable to explain the area effect or to replicate theresults shown in the Figure. That would require an in-crease in the number of mosquitoes per person. In themodel developed by SOTA & Mort (1989), mosquitodensities Increase when cattle are introduced becausecattle constitute a readily accessible source of blood.Under certain conditions this can lead to greater human.biting rates and higher vectorial capacity, and thus theSota -Mogi model was able to predict the village effect re-
sults. The prerequisites for increased transmission in theSota-Mogi model are that growth of mosquito popula-tions should be unconstrained, the vectors zoophtltc, theinfection rate low, and the ratio of humans to cattle high.
In Kohat, river beds and paddies provide abundant
breeding si
i
tes, the major vectors A. colic acies and A.orphan s are highly zoophilie (RMSKN BQNHIIAM,1982), transmission is seasonal, and the lowest estimateof the human:cattle ratio was 5.8. Thus conditions seemconsistent with those of the model.
A weakness in the study is that children were used asthe source of information on cattle ownership. However,
1
pm.
v-
v-
v-
r
pom
allmt
r
the method of direct inquiry, presided over by theschoolteachers, may not be so unreliable, since the pro-portion of children claiming cattle ownership differed byonly 7% between the 2 years. Moreover, any inaccuracywould tend to bias against the observed results.
Apart from cattle, we were unable to identify any fac-tor that might L e responsible for the observed effects.The low incidence of malaria in urban areas, forexample, though correlated with low cattle densities, isprobably caused by breeding site scarcity and less -effi-cient vector species (REISEN & MILBY, 1986). Kohat,however, is uniformly rural with small scattered villages.Wealth and cattle arc also associated, but one would ex-pect wealthier, presumably better -educated, cattle-owners to record a lower rather than higher prevalence asa result of self- medication with antimalarial drugs.
Our original assumption that malaria was more com-mon in refugees received no support from the results ofthe Kuhat prevalence surveys. In this district some refu-gee villages had just as many cattle as Pakistani villagesand the prevalence rates reflected percentage cattleownership rather than local or refugee status. However,in the poorer, more and tribal areas of Mohmand, Pakis-tanis recorded a lower prevalence than refugees despiteowning more cattle. Breeding sites around the Pakistanivillage were scarce, and may have limited any expansion:of the mosquito population, a prerequisite of the villageeffect.
Current livestock management practices in Pakistanappear to exacerbate the malaria problem. According tothe Sota -Mogi model, cattle would reduce the mosquitohuman -biting rate only if very large numbers were Intro-duced. In Pakistan that seems unlikely, for economicreasons. A change in livestock management, so thatcattle were kept between village and breeding site, mightprove zooprophylactic (WHO 1991). But such a practicewould probably be unacceptable -- cattle are too valuableto be kept outside the compound -and would require al-most total community participation to be effective. Cur-rent investigations into insecticide dipià and insecticide -impregnated ear tags for cattle may offer some solutions.
AcknowledgementsWe thank field staff of the AtSF/UNHCR malaria reference
laboratory for conducting the microscopy. For comments andvaluable suggestions we ttank C. Curtis, C. Dye, S. l lewitt, J.Rozcndsal, A. Schapira, Il. J. van der Keay, and 2 anonymous
353
referees. Funding of the project was provided by the liurupcanUnion and AIS:4lulland.
ReferencesEnglish, R. (1989). The economic impact of Afghan refugee settle-
ment on the tribal agencies of northwest Pakistan. Geneva: TSSMission Report, UNHCR Technical Report Service
Glglioll, G. (1963). Ecological change as a factor in renewed ,eta!aria transmission in an eradication area. A localized outbreakof Anopheles aquasalis transmitted malaria on the Domararariver estuary, British Guyana. Bulletin of the World health Or-ganisation, 29,131-145.
Hewitt, S., Kemal, M., Nasir, M. & Rowland, M. (1994) Anentomological investigation of the likely impact of cattleownership un malaria in an Afghan refugee camp in the Nur titWest Frontier Province of Pakistan. Medical and VeterinaryEntomology 8,160 -164.
Reisen, W. K. & Bonham, F. L. (1982). Estimates of malariavectorial capacity for Ahopheits culicifacies and A. uephensi inrural Punish province, Pakistan. Journal of Medical Entomo-logy, 19,98-103.
Reisen, W. K. & Milby, M. M. (1986). Population dynanua utsome Pakistan mosquitoes: changes in adult relative abun-dance over time and space. Annals of Tropical Medicine andParasitolov , 80, 53-68.
Schultz, G. W. (1989). Animal influence on man -biting rates ata malarious site in Palawan, Philippines. South Eau .4s'anJournal of T ro'ieal Medicine and Public Health, 20.49-53.
Sots, T. & Mogi, M. (1989). Effectiveness of ztwpruphylaai+ utmalaria control: a theoretical enquiry, with a model for mn..quito populations with two blood meal hosts..tlydical and V , -
terinary Entomolo , 3,337-345. -
Suleman, M. (1988). Malaria in Afghan refugees in Pakistan.Transactions of the Royal Society of Tropical Medicine und 1lv-giene, 82,44-47.
Swcllengrebel, N. H. & de Duck, A. (1938). Malaria in TheNetherlands. Amsterdam: Scheiterns & Holkema.
WHO (1982). Manual on environmental management for mosquitocontrol, with special emphasis on malaria veston. Geneva: WorldHealth Organization, mimeographed document no. 66.
WHO (1991). Joint WHO /FAO /UNEP Panel of Experts on En-vironmenial Management for Vector Control (PE EM): Repport onMe Ninth (1989) and Tenth (1990) Meetings. Geneva: Wi,il JHealth Organization.
Zulueta, J. de (1989). Malaria among Afghan refuses in Paku-ran. Geneva: United Nations High Commission for Refugees,mimeographed document.
Received 29 October 1993; revised 8 December 1994,accepted for publication 8 December 1994
Continued from page 346
l)verbusch, D. (1992). Neurocysticercukis. An introductionwith special emphasis on new developments in pharmaeutherapy. Schei :erische Medicinischs Wochettschnft, 122,893 -898.
Pawlowski, Z. S. (1990). Cestode infections. In: Tropical andCìeographical Medicine, .2nd edition Warren, K. S. &Mah,noud, A. P. (editors). New Murk, London, Paris:McGraw-Hill, pp. 490 -504.
Raishrkhar, V. )loran. R. P., Prakash, G. S. & Chandy, M. J.t199.1). Differentiating sulitaty small cysticcrcus granulomasand tuberculumas in patients with epilepsy. Clinical andcomputerized tomographie criteria. Journal of Neurosurgery,78,402-407.
Schantz, P. M. & Gottstcin, B. (1986). In: hnmuuodiagnosis ofParasitic Disease, Walls, K. W. & Shantz, P. M. (editors).Orlando, Florida: Academic l'ress, pp. 69 -107.
l skayanagui, D. M. & Jardin, E. (1992). Therapy for ,tettrucystisercosis. Comparison between albcndazule and praziquan-tel. ArrMevs of Neurology, 49, 290 -294.
Tsang, V. C. V. & Wilson, M. (1995). Taenia sulium cysticcrcosts: an under -recognized but serious public health prob.fern. Parasitology Today. 11,124 -125.
Vasconcelos, D., Cruz -Segura, II., Maicus- Gumez, II. 4Alanis, G. Z. (1987). Selective indications fur the use of liraziquantel in treatment of brain cysticercosis. Journal of m'eut.ology, Neurosurgey, and Psychiatry, SO, 383 -388.
Webbe, G. (1986). Cestode infections of man In: Glientotherapvof Parasitic Diseases, Campbell, W. C. & Rew, R. S. (edi-tors). New York & London: Plenum Press, pp. 457 -177.
Webbe, G. (1994). Human cysticercosis: parasitology, patho-logy, clinical manifestations and available treatment. Pita..macolugy and Therapeutics, 64,175-200.
Wen, H. 8r Craig, P. S. (1994). Ìmmunoglobulin G subclass responses to human cystic and alveolar echinococcusis. Amen-canJTournal of Tropical Atedirine and hygiene, SI.741 -748.
' Wen, fH., Zou, P.. F., Yang, W. -G., Lu, J., Wang, Y. -11..Zang, J.lt., New, R. R. C. & Craig, P. S. (1994). Altnndazule chemotherapy fur human cystic and alveolar echin,w,Kcosts in north -western China. Transaction' of the RoyalSociety of Tropical Medicine and Hygiene, 88,340-343.
Worthington, M. & Horowitz, H. (1987). Gase11.1986: cgs.ticercosis. New England Journal of Medicine, 316,693-694.
r
I of 1111. Rut.u. Sot u. 1Y ut .I.11N4CAl. Atl:11N'iN11 AND IIY UM.. 11995) 89, 334-958
Recruitment to a trial of tuberculosis preventive therapy from a voluntary HIV
testing centre in Lusaka: relevance to implementation
Peter Godfrey- Faussett1j2, Rachel Baggafey21, Alwyn Mwingal2, Maria Howl a, John Porter2, Nka.idu 1 -uu4,
Michael Kellys, Roland MsiskaS and Keith McAdam2 IDepartsrsent of Medicine, University Teaching Hospital, Lusaka,
Zambia; 2Department of Clinical Sciences, London School of Hygiene and Tropical Medicine, London, UK; 3Kara
Counselling and Training Trust, Lusaka, Zambia; 4Departnsent of Pathology and Microbiology, University Teaching Hospital,
l.usaka, Zambia; SNational ,t/OS and Tuberculosis Programme,; Ministry of Heahh, Lusaka, Zambia
AbstractTo determine the number of clients attending for voluntary human immunodeficiency virus (HIV) testing
who are able to enter a trial of preventive therapy for tuberculosis, and the factors that determine who re-
ceives therapy, we studied 475 consecutive people attending for an HIV test at Lusaka's first voluntary HIV
testing centre and the preventive therapy study clinic at the University Teaching Hospital Lusaka, Zambia.
Semi -structured interviews were conducted by counsellors and collated with recruitment data from the trial.
Two hundred and twenty -five people were seropositive, of whom 201 returned to collect their results; 77
(38 %) of these (16% of the total number screened) entered the trial. Reasons for not entering the trial in-
cluded exclusion by trial protocol (30), including 18 who had active tuberculosis; psychological adjustment
to a positive result (27); death (6); worries about confidentiality (3); the experimental nature of the trial (12);
attitudes of staff in the hospital (5); and cost of transport (7). Targeting preventive therapy at those who are
already choosing to be tested for HIV seems appropriate and may be cost -effective. Although visiting a hos-
pital may deter some people, the prevalence of active tuberculosis among this group emphasized the import-
ance of arranging adequate screening facilities.
Keywords: tuberculosis, human Immunodeficiency virus, drug trial recruitment, Zambia
IntroductionThe incidence of tuberculosis among people infected
with both Mycobacterium tuberculosis and human immu-nodeficiency virus (HIV) is between 3% and 8% per year(SELWYN et al., 1989; BRAUN et al., 1991), with reactiva-tion of latent infection as an important mechanism. Insub - Saharan Africa, where both infections are prevalent,tuberculosis control programmes are already over-stretched. In Zambia, most of the adult population areinfected with Af. tuberculosis (see DUNCAN et al., 1995)and the prevalence of HIV infection among women at-tending antenatal clinics in periurban Lusaka is 33%.(Zambian Ministry of Health unpublished figures, 1992;n.976). The incidence of tuberculosis has risen (ruinaround 100 /100 000 in 1984 to over 300/100 000 in 1993tAtinistry of Health figures), and in 1989 73% of patientsreceiving antituberculous therapy were seroposiuve forHIV (ELLtorr et al., 1993). Preventive therapy with aone -year course of isoniazid reduced the incidence oftuberculosis over the subsequent 5 years in people withIII' infection in Haiti (PAPE et al., 1993) and prelimi-nary results using a 6 months' regimen in Zambia weresimilar (WADH WAN et al., 1991). Since 1992, a trial of 2different preventive therapy regimens has been runningin Lusaka (MWINGA etal., 1993). .
Possible strategies for using such treatment on a largerscale need to consider how to find people who ire in-fected with HIV. The cost of screening people for HIVantibodies, specifically to offer them tuberculosis preven-tive therapy, is likely to be prohibitive but will dependon the prevalence of HIV in the community targeted andon the number of people who cannot receive therapy forwhatever reason. However, if voluntary HIV testingcentres become established for reasons other than tuber-culosis control, it may be feasible to offer preventive.therapy to those found to be seropositive.
Since 1985, when the HIV antibody test was firstlicensed, the demand for counselling and testing hassteadily increased. In the USA, where testing has beencarried out since 1985, more than 2 000 000 tests werecarried out in public funded sites in 1991 (CDC, 1992).Counselling and testing have been used to help peopleassess their risks, to encourage or reinforce behaviourchange, to refer infected individuals to clinical care, and
.Address for correspondence: Dr Peter Godfrey-Faussett, ZAM-
SARI Project, Department of Medicine, University TeachingI1ospital, P.O. Box S0110, Lusaka, Zambia.
to start antiviral or preventive therapy when needed.Some longitudinal studies of homosexual men havefound that those who are seropositive show greater re-ductions in risky behaviour than those who are not (HIG.
GINS e/ al. 1991).In sub -Saharan Africa, where HIV infection is preval-
ent and medical resources are scarce, the role of counsel-ling and testing is less obvious (COLEBUNDERS &NDUMett 1993). Demand few such services exists, andbetween June 1991 and October 1992 the AIDS Informa-tion Centre in Kampala, Uganda, tested more than30 000 people (Attu et al., 1995). Studies in Africa havealso demonstrated changes in sexual behaviour thatwould be expected to reduce transmission of HIV(ALLEN et al., 1992). There may also be other benefits topeople who receive counselling such as en increase in'coping' mechanisms. Antiviral therapy is tau expensivefor general use in Africa, but preventive therapy againsttuberculosis might not only, be more cost -effective thantreating tuberculosis when it develops but may also re-duce transmission of M. tuberculosis in the communityand prolong the life of dually infected individuals.
The first voluntary HIV counselling and testing centrein Zambia was established by the Kara- 'LAMBAR'l' projectto meet a perceived demand, to help with coping and todetermine whether behaviour was being altered (BAGGALEEY et al., 1993). Whatever the result people are encour-aged to avoid risky behaviour, in order to reduce trans-mission or to remain uninfected. People found to be1-11V-seropositive are also encouraged to enter the
preventive therapy trial.We have looked at the number of clients entering the
trial and the reasons for failure so w du, in order to ex-plore the likely constraints on widespread implementa-tion of preventive therapy for tuberculosis.
MethodsThe study was conducted at the Kara- ZAMBART Vol.
untary HIV Counselling and Testing Project and at theUniversity Teaching Hospital (UTH) in Lusaka, Zam-bia.
z.A.tIB4Nt tuberculosis preventive therapy trialThis trial is a collaborative project between the De-
Zpartmentof Medicine at UTH, the Ministry of Health in
ambia and the London School of Hygiene and TropicalMedicine, comparing the efficacy of Preventive therapyagainst tuberculosis with 6 months intermittent iso-
1
1
r
p
rm.
P."
Ta.\4l.U'1NoNS ut IIII. KuY.U. Society tIF Taura:al, Amu Ilrou;NH (199S) 89, 3SI-353
Failure of passive zooprophylaxis: cattle ownership in Pakistan is associated
with a higher prevalence of malaria'
351
Menno Boumai and Mark Rowland2 t11 /t?dicitts sans Frontières, P.O. Box 10014, 1001 EA Amsterdam, The
Netherlands; tllealthNet lntsntational, P.O. Box 889, Peshawar, Pakistan
AbstractTo examine the possibility that domestic cattle kept in house courtyards might protect occupants against
malaria through zooprophylaxis, parasite prevalence surveys were conducted of schoolchildren to Pakistani
and Afghan refugee villages and analysed according to whether each child's family kept cattle. Parasite pre-
valence (1S2%) was si nificantly greater among children of families which kept cattle than among those
which did not (9 -S%). Comparison of prevalence between different villages revealed a positive correlation
between parasite rates and the proportion of families owning cattle. The latter finding supports the predic-
tion of the Sota -Mogi theoretical model that domestic animals can enhance rather than reduce malaria trans-
mission when vectors are zoophilic, the infection rate low, and the human:cattle ratio high. All these
conditions applied in the study area.
Keywords: malaria, prevalence, zooprophylaxis, effect of cattle, Pakistan
IntroductionZooprophylaxis has been defined by the World Health
Organization (WHO, 1982) as 'the use of wild or domes-tic animals, which are not the reservoir hosts of a givendisease, to divert the blood -seeking mosquito vectors
from the human hosts of that disease'. It may be active orpassive. Active zooprophylaxis is a reduction in malariaor human -biting resulting from the deliberate deploy-ment of domeauc animals as a barrier between. mosquitobreeding sites and human settlements (WHO, 1991).Passive zooprophylaxis is the serendipitous reduction inmalaria purported to occur when cattle density increaseswithin a community (see, e.g., SwELt.ENGKEui L & DEBUCK, 1938; GIGLIOLI, 1963).
In Pakistan, a higher incidence of malaria is recordedat health centres for Afghan refugees than at centres serv-ing local Pakistanis. The difference was initially attribut-able to Afghans having been less exposed to malaria and
therefore less immune during the first years after theirarrival in Pakistan (SULEMAN, 1988). It has also beensuggested that because refugee families possess fewerlivestock than Pakistani local residents (BNGLtatt, 1989),they are kss able to benefit from any zooprophylactic ef-fect delude (ZULETA, 1989).
Conditions in Pakistan seem, at first sight, highly con-ducive to successful passive zooprophylaxis. The majormalaria vectors are highly zoophilie, and Afghans andlocal residents prefer to keep their cattle close to their lili-ing quarters. However, a mathematical model developed
by SOTA & Moat (1989) has exposed problems with thetheory: simulations predict that introduction of cattle canlead to increased vector densities, increased human bit-íng rates, and greater malaria transmission. Appropriatedeployment of cattle away from human dwellings may be
=dal to the success of zooprophylaxis (SCHULTZ,1989).
This paper reports cattle ownership and malaria para-site prevalence surveys conducted in refugee and localvillages in the North-West Frontier province (NWFP) ofPakistan. It examines the relationship between cattle andmalaria at the household and village.levels, and assesseswhether household cattle lessen or exbcerbate the malariaproblem.
Materials and Methodsp- Rural Pakistanis and Afghan refugees live in houses
made from mud, surrounded by an open courtyard andhigh perimeter wall. Both communities keep domesticanimals (cattle, water buffaloes, goats etc.) in courtyardsand sheds usually within 10 m of the living quarters.People sleep in the courtyards during summer, movingindoors from October onwards. Sources of mosquitobreeding include borrow pits, river margins and rice pad.
'Author for correspondence and offprint requests,
(
dies, and the fauna includes Anopheles culicifucies, A. ste-pphensi and A. subpictus among others. Transmission ofPlasmodium vivax and P. falciparum occurs betweenApril and December and reaches a peak in October/No-vember.
The study areas were 3 refugee and 4 local villagessituated along a 24 km valley in Kohat district, NWFP,Pakistani and a pair of neighbouring refugee and localvillages in Mohmand, a tribal area 100 km north ofKohat. Health services were provided by the United Na-tions High Commission for Refugees and the Govern-ment Department of Health, both of which conduct vec-tor control campaigns (house spraying with malathion) inJuly each year. According to spray reports, house cuver-
age ranged from 82 to 100% and all study villages weresprayed.
Parasite prevalence surveys were conducted in villageschools in October 1989 in Mohmand, and in November1989 and November 1990 in Kohat. Schoolchildren wereaged 4-15 years; 90% were boys. Thick and thin bloodfilms were prepared from virtually all children present onthe day of examination, stained with Giemsa's stain andexamined at the Medecins sans Frontières reference lab -orptory. One hundred microscope fields of each filmwere examined before reporting a slide as negative. l'ara-sitaemic children were given supervised treatment withchloroquine (25 mg /kg body weight in divided doses over
3 d), whether symptomatic or not. During blood collec-tion each child was asked in private by the survey tcatn --with the schoolteacher presiding -whether his or herfamily kept cattle (cows or water buffaloes) within thehouse compound.
ResultsParasite prevalence in households with or without cattle
Parasite prevalence was correlated with age, increasingfrom 10-2% at 4 years to 18.1% at 15 years. All furthercomparisons were therefore conducted on age-ad¡ustedprevalence rates using the method of direct stand-ardization (the standard population was produced fromthe total of all the surveys).
In Kohat the prevalence rate in the Afghan communitywas similar to that in the Pakistanis, whereas in Moh-mand prevalence was significantly raater in Afghans(i '.18.9, degrees of freedom ld.1.)=2, l'- tí0001)
pable). Prevalence also showed geographical V:111.111111(ice the data for 1989 in the Table), with 1'. pal um
predominant in Kohat and P. vivax predominant ulMohmand. Prevalence also varied between years, par -ticularly that of P. falciparum which, in Kohat, washigher in 1990 than in 1989. Thus in order to evaluatethe relationship between cattle and parasite prevalence,and avoid the potentially confounding variation betweencommunities localities and years, it was necessary toexamine each of the 6 subsets of data separately, age-
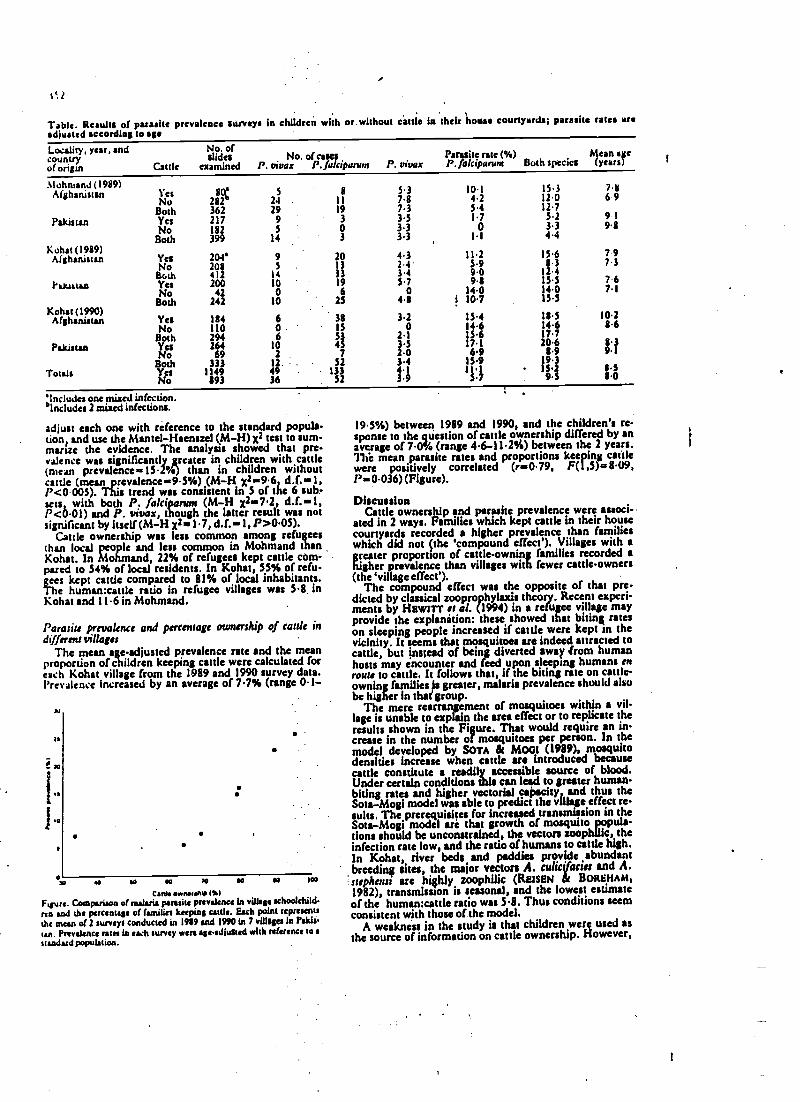
tSt
Table. Results of parasite prevalence surveys in children with or without cattle In their house courtyards; parasite ratea areadjusted according to age
Totals
Locality, year, and No. ofcountry slides No. of casesof origin Cattle examined P. vivax P. falcipanun
.ltuhntsnd (1989)Afghanistan
Pakistan
Kohat (1989)Afghanistan
Pakistan
Kohat (1990)Afghanistan
Pakistan
Yes 8(k: 5 8 5.3 10.1
No 282 24 11 7.8 4.2Both 362 29 19 7.3 54Yes 217 9 3 3.5 1.7
No 182 5 0 3.3 0
Both 399 14 3 3.3 1.1
Yes 204' 9 20 4.3 11.2No 208 S 13 2.4. 5.9Both 4)2 14 33 3.4 9.0Yes 200 10 19 5.7 9.8No 42 0 6 0 14.0
Both 242 10 25 4.8 1 10.7
Yes 184 6 38 3.2 15.4No 110 0: 15 o 14.6Both 294 6 53 2.1 13.6Yes 264 10 45 3.5 17.1No 69 2 7 2.0 6.9Both 333 12 . . 52 3.4 15.9Yes 1149 49 133 4.1 11.1
No 893 36 52 3.9 5.7
Parasite rate (%)P. vivax P. falcipanun Both species
7.811.012.7
5.23.34.4
15.68 3
12.4
14.015.5
18514.617.72063.9
1s9s.223
19S
'Includes one mixed infection.°Includes 2 mixed infections.
adjust each one with reference to the standard papule-clone and use the Mantel- Haenszel (M -H) z2 test to sum-marise the evidence. The analysis showed that pre-valence was significantlyy reater in children with cattle(mean prevalence- 15.2%) than in children withoutcattle (mean prevalence -9.5 %) (M -H I. 9.6 d.f. =l,P<0.005). This trend was consistent in 5 of the 6 sub-sets, with both P. jalciparunt (M -H x2 =7.2, d.f. =1,P <0.01) and P. vivar, though the latter result was notsignificant by itself (M -H x2a1.7, d.f. =1, P >0.05).
Cattle ownership was less common among refugeesthan local people and less common in Mohmand thanKohat. In Mohmand, 22% of refugees kept cattle com-pared to 54% of local residents. In Kohat, 55% of refu-gees kept cattle compared to 81% of local inhabitants.The human:cattle ratio in refugee villages was 5.8. inKohat and 11.6 in Mohmand.
Parasite prevalence and percentage ownership of cattle indifferent villages
The mean age-adjusted prevalence rate and the meanproportion of children keeping cattle were calculated foreach Kohat village from the 1989 and 1990 survey data.l'revrlence increased by an average of 7.7% (range 0.1-
r,
ii .,aiI .a
io a to so so a a lea
Canty aw0111 MIFigure. Comparison of autstia parasite prevalence in village schoolchild-ren and the percentage of (unites keeping cattle. Each point representsthe mean of 2 surveys conducted in 1989 and 1990 in 7 villages In raids.tan. Prevalence rata in each survey were ageadiuled with reference to astandard population.
Mean age(years)
6 9
9 19.8
7 97.3
7.1
10.286
9.1
t0
19.5%) between 1989 and 1990, and the children's re-sponse to the question of cattle ownership differed by anaverage of 7.0% (range 44- 11.2%) between the 2 years.The mean parasite rates and proportions keeping cattle
Pere 036 (ivelye).correlated(r -0.79, F(1,5).58.09,
DiscussionCattle ownership and parasite prevalence were associ-
ated in 2 ways. Families which kept cattle in their housecourtyards recorded a higher prevalence than familieswhich did not (the 'compound effect'). Villages with agreater proportion of cattle-owning families recorded ahigher prevalence than villages with fewer cattle-owners(the 'village effect').
The compound effect was the opposite of that pre-dicted by classical zooprophylaxis theory. Recent experi-ments by Hewerr et al. (1994) in a refugee village mayprovide the explanation: these showed that biting rateson sleeping people increased if cattle were kept in thevicinity. It seems that mosquitoes are indeed attracted tocattle, but instead of being diverted away from humanhosts may encounter and feed upon sleeping humans enroute to cattle. It follows that, if the biting rate on cattle -owning families is greater, malaria prevalence should alsobe higher in that' group.
The mere rearrangement of mosquitoes within a vil-lage is unable to explain the area effect or to replicate theresults shown in the Figure. That would require an in-crease in the number of mosquitoes per person. In themodel developed by Sou & MOGI (1989), mosquitodensities Increase when cattle are introduced becausecattle constitute a readily accessible source of blood.Under certain conditions this can i to greater human -biting rates and higher vectorial capacity, and thus theSota -Mogi model was able to predict the village effect re-sults. The prerequisites for increased transmission in theSota-Mogi model are that growth of mosquito popula-dons should be unconstrained, the vectors zoophWc, theinfection rate low, and the ratio of humans to cattle high.In Kohat, river beds and paddies provide abundant
breeding sites, the major vectors A. culisifactes and A.ste haul are highly zoophilie (RElsEN & BOREHAM,1982), transmission is seasonal, and the lowest estimateof the human:cattle ratio was 5.8. Thus conditions seemconsistent with those of the model.
A weakness in the study is that children were used asthe source of information on cattle ownership. However,
1
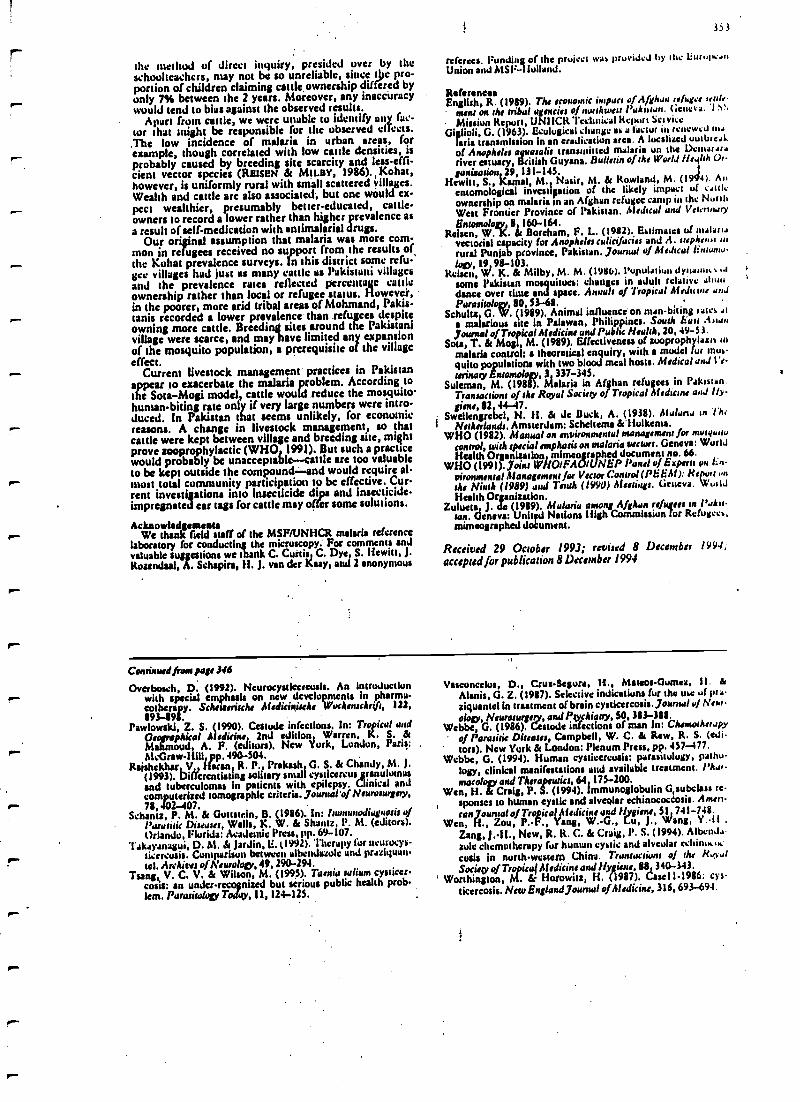
the method of direct inquiry, presided over by theschoolteachers, may not be so unreliable, since t c pro-portion of children claiming cattle, ownership differed byonly 7% between the 2 years. Moreover, any inaccuracywould tend to bias against the observed results.
Apart from cattle, we were unable to identify any fac-tor that aright be responsible for the observed clTccts.The low incidence of malaria in urban areas, forexample, though correlated with low cattle densities, isprobably caused by breeding site scarcity and Tess -effi-cient vector species (REISEN & MILBY, 1986). Kohat,however, is uniformly rural with small scattered villages.Wealth and cattle are also associated, but one would ex-pect wealthier, presumably better- educated, cattle -owners to record a lower rather than higher prevalence asa result of self -medication with antimalarial drugs.
Our original assumption that malaria was more com-mon in refugees received no support from the results ofthe Kobat prevalence surveys. In this district some refugee villages had just as many cattle us Pakistani villagesand the prevalence rates reflected percentage cattleownership rather than local or refugee status. However,in the poorer, more arid tribal areas gtMohmand, Pakis-tanis recorded a lower prevalence than refu ees despiteowning more cattle. Breeding sites around the Pakistanivillage were scarce, and may have limited any expansionut the mosquito population, a prerequisite of the villageeffect.
Current livestock management practices in Pakistanappear to exacerbate the malaria problem. According tothe Sota -Mogi model, cattle would reduce the mosquitohuman- biting rate only if very large numbers were intro-duced. In Pakistan that seems unlikely, for economicreasons. A change in livestock management, so thatcattle were kept between village and breeding site, mightprove sooprophylactic (WHO 1991). But such a practicewould probably be unacceptable -- cattle arc too valuableto be kept outside the compound -and would require al-most total community participation to be effective. Cur-rent investigations into insecticide dips and Insecticide -impregnated ear tags for cattle may offer some solutions.
AcknowledgementsWe thank field staff of the MSF/UNHCR malaria reference
laboratory for conducting the microscopy. For comments andvaluable suggestions we thank C. Curtis C. Dye S. Hewitt, J.Rosenthal, A. Schapirs, H. J. van der hazy, and 2 anonymous
353
referees. Funding of the pruiect was pruviJcJ by the 1iurop..s.Union and MSF- 1Iulland.
Reference.English, R. (1989). The economic impact of Afghan refugee tente.
ment on the tribal agencies of northwest Puht an. (,encra. I S'
Mission Report, UNI ICR Technical Report Sel viceGiglioli, G. (1963). Ecological change ss a factor in rentewcJ 1114
!aria transmission in an eradication area. A localised uutbrral:of Anopheles ayuarolis transmitted malaria on the lianariver estuary, British Guyana. Bulletin of the World 11s.41th Or
ganisation 29,131-145. t
Hewitt. S., Kemal, M. Nash, M. & Rowland, M. (1944). Auentomological investigation of the likely impact of .soleownership on malaria in an Afghan refugee camp in the NorthWest Frontier Province of Pakistan. Mcdnca! und Vercnu,uy
Entomology, 160 -164.Reisen, W. K. St Boreham, F. L. (1982). Estimates of nularta
vectorial capacity for Anopheles culicifacier and A. :tapirs/Jig aurural Punjab province, Pakistan. Poona! of Medical lirtnunww
logy, 19,98-1(13.RehmRei Vil. K. & Milby, M. M. (1986). Population dyuanu.+ ..1
some Pakistan mosquitoes: changes in adult relative abusedance over tinte and space. Aaiah of Tropical Aluitctits and
Parasitology, 80,53-68.Schultz G. W. (1989). Animal influence on Haan -biting raies Al
a malicious sate in Palawan, Philippines. South hart .43tanjournal of Tropical Medicine und Public Health, 20,49-53.
Sots, T. & Mogl M. (1989). Effectiveness of zuoprophyiaxu tomalaria control: a theoretical enquiry, with a model fur 'nusquito populations with two blood meal hosts. Medical and Ve-
terinary Entomology, 3 337 -345.Soloman, M. (1988). Malaria in Afghan refugees in Pakistan.
Transactions of Ms Royal Society of Tropical Medic's and Fly -giene, 82 44 -17.
Swetlengrebel, N. H. & dc Duck, A. (1938). Ala/ana an The
Netherlands. Amsterdam: Scheltema &'liulkensa.WHO (1982). Manual on environmental management for mosytatta
control, with special emphasis on malaria wctws. Geneva: WorldHealth Organisation, mimeographed document no. 66.
WHO (1991). joint WHOIFAOI(1NEP Panel of Experts on tinvironmental Management for Vector Control (PEEN): R/wrt nMe Ninth (1989) and Tenth (1990) Meetings. Grucva. WuiIdHealth Organization.
Zulueta J. de (1989). Malaria among Afghan refugees in Pakis-tan. Geneva: Unit Nations High Commission for Refugees,mimeographed doCument.
Received 29 October 1993; revised 8 December 1994,accepted for publication 8 December 1994
Coronad front paje M6
Overbosch, D. (1992). Neurucysticcrcusts. An Introductionwith special emphasis on new developments in pharmaeotherepy. Scheueiche Medicigische Wahenschrtft, 122,
893 -898.Pawlowski, Z. S. (1990). Cestode infections. In: Tropical and
Geographical Medicine 2nd edition Warren, K. S. &Mahmoud A. F. (editor). New !lurk, London, Paris:McGraw-1E11, pp. 490.404.
RaishekMr V. Harar R. P., Prakash G. S. & Chandy, M. J.(1993). Differentiating solitary small cysticercus ranuluasand tuberculomas in patients with epilepsy. CltnClinical andcomputerised tomographie criteria. jounwl'o /Neurosurgery,78,402 -407.
Schantz, P. M. & Gottstrin, B. (1986). In: lmnanodiagnosisofParasitic Diseuses, Walls, K. W. & Shantz, I'. M. (editors).Orlando. Florida: Academic Press, pp. 69 -107.
l'.kayanagui, D. M. & Jardin, li. t1992). Therapy for ncurocys-ticercusis. Comparison between albenJazole und praziyuan-tel. Archives of Neurology, 49, 290-294.
Tsang, V. C. V. & Wilson, M. (1995). Taenia talcum cysticer-cosis: an under-recognized but serious public health prob.lem. Parasiwloly Today, 11,124-125.
Veseoneelus, D., Crus -Segura, H., Mateos- Gumea, II. dManic, G. Z. (1987). Selective indications fur the use of peaziquantel in treatment of brain cysticercosis. journal of New.olopy, Neurosurgery, and Psychiatry, 50,3113-381.
Webbe, G. (1986). Cestode infections of man In: Chemotherapyof Parasitic Diseases, Campbell, W. C. Is Raw, R. S. (edi.
' tors). New York & London: Plenum Press, pp. 457 -477.Wcbbc, G. (1994). Human cysticcrcusis: parasitology, patho-
logy, clinical manifestations and available treatment. l'ha,.macology and Therapeutics, 64 175 -200.
Wen, H. 6e Craig, P. S. (1994). immunoglobulin G, subclass re-sponses to human cystic and alveolar echinococeosís. Amin-ton journal of Tropical Medicine and Hygiene, SI 741 -748.
Wen, ., Zou, P. -F., Yang, W. -G., Lu, J., ang, Y..11 ,
Zang, 3. -11., New, R. K. C. & Craig, l'. S. (1994). AlbenJ.-iule chemotherapy fur human cystic and alveolar rchiniktkcasts in north-western China. Transaction, of the !tarotSaiey of Tropica( Medicine and Hygiene, 88 340 -343.
Worthington, M. tir Horowitz, H. (1987). Casell1986; c >'sticercosis. New England journal of Medicine, 316,693-694.
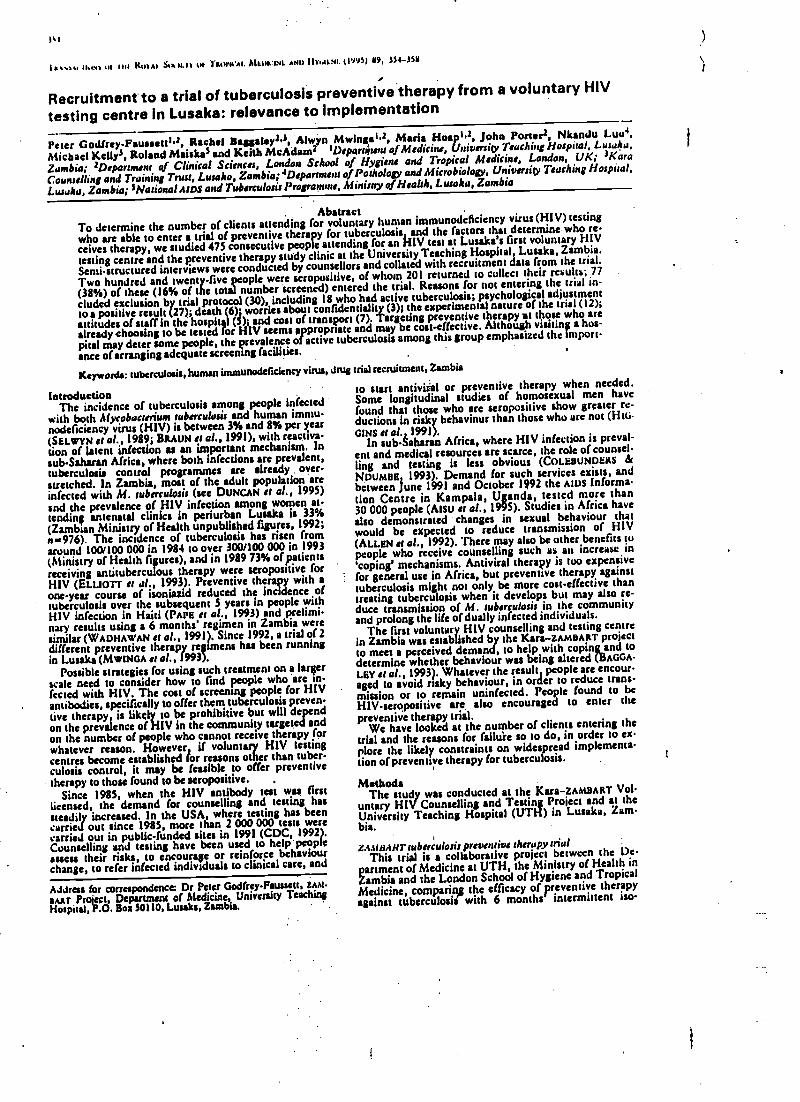
1%1
iYvom Il.wa uI IM Kl11Al. Small IM rMN'N'A1. MLIIp:INL AND I11'..11.NI. (199S) 59, 334-395
Recruitment to a trial of tuberculosis preventive therapy from a voluntary HIV
testing centre in Lusaka: relevance to implementation
Peter Godfrey- Fsusssttta, Rachel Baggsley=J, Alwyn Mwinga la, Maria Hoopla, John Porter=, Nkandu Luu +,
Michael Ketly3, Roland Middies and Keith McAdams t Departirtent of Medicine, University Tracking Hospital, Lusaka,
Zambia; 2Dppartment of Clinical Sciences, London School of Hygiene and Tropical Medicine, London, UK; 3Kara
Counselling and Training Trust, Lusaka, Zambia; +Department of Pathology andMicrobiology, University Teaching Hospital.
Ltuaka, Zambia; 'National AIDS and Tuberculosis Programme, Ministry of Hsahh, Lusaka, Zambia
AbstractTo determine the number of clients attending for voluntary human immunodeficiency virus (H1V) testing
who are able to enter a trial of preventive therapy for tuberculosis and the factors that determine who re-
ceives therapy, we studied 475 consecutivepeople attending for an HIV test at Lusaka's first voluntary HIV
testing centre and the preventive therapy study clinic at the University Teaching Hospital Lusaka, Zambia.
Semi-structured interviews were conducted by counsellors and collated with recruitment data from the trial.
Two hundred and twenty -five people were seropositive, of whom 201 returned to collect their results; 77
(38 %) of these (16% of the total number screened) entered the trial. Reasons for not entering the trial w-
cluded exclusion by trial protocol (30), including 18 who had active tuberculosis; psychological adjustment
to a positive result (27); death (6) worries about confidentiality (3); the experimental nature of the trial (12);
attitudes of staff in the hospital (5) and coat of transport (7). Targeting preventive therapy at those who are
already choosing to be tested for HIV seems appropriate and may be cost -effective. Although visiting a hos-
pital may deter some people, the prevalence of active tuberculosis among this group emphasized the import-
ance of arranging adequate screening facilities.
Keywords: tuberculosis, human immunodeficiency virus, drug trial recruitment, Zambia
IntroductionThe incidence of tuberculosis among people infected
with both Mycobacterium tuberculosis and human immu-nodeficiency virus (HIV) is between 3% and 8% per year(SELWYN a al., 1989; BRAUN et al., 1991), with reactiva-tion of latent infection u an important mechanism. Insub -Saharan Africa, where both infections are prevalent,tuberculosis control programmes are already over-stretched. In Zambia, most of the adult population areinfected with M. tuberculosis (see DUNGAN et al., 1995)and the prevalence of 111V infection among women at-tending antenatal clinics in periurban Lusaka is 33%(Zambian
7. The incidence of uberculosisunpublished figures,
frromaround 100/100 000 in 1984 to over 300/100 000 in 1993(Ministry of Health figures), and in 1989 73% of patientsreceiving antituberculous therapy were seropositive forHIV (ELLtorr e, al., 1993). Preventive therapy with aone -year course of isoniazid reduced the incidence oftuberculosis over the subsequent S years in people withHIV infection in Haiti (PAPE et al., 1993) and prelimi-nary results using a 6 months' regimen in Zambia weresimilar (WADHAWAN et al., 1991). Since 1992, a trial of 2different preventive therapy regimens has been runningin Lusaka (MWtGA et x1.,1993).
Possible strategies for using such treatment on a largerscale need to consider how to find people who 'are in-fected with HIV. The cost of screening people for HIVantibodies, specifically to offer them tuberculosis preven-tive therapy is likely to be prohibitive but will depend
on the prevalence of HIV In the community targeted andon the number of people who cannot receive therapy forwhatever reason. However if voluntary HIV testingcentres become established for reasons other than tuber-culosis control, h may be feasible to offer preventivetherapy to those found to be seropositive. .
Since 1985, when the HIV antibody test was firstlicensed, the demand for counselling and testing hassteadily increased. In the USA, where testing has beencarried out since 1985, more than 2 000 000 tests werecarried out in public- funded sites in 1991 (CDC, 1992).Counselling and testing have been used to heip'peopicassess their risks, to encourage or reinforce behaviourchange, to refer infected individuals to clinical care, and
Address for correspondence: Dr Peter Godfrey-Faussett, ZAP i-
sAar Protect, Department of Medicine, University TeachingHospital, P.O. Sox 50110, Lusaka, Zambia.
to start antiviM1 or preventive therapy when needed.Some longitudinal studies of homosexual men havefound that those who are seropositive show greater re-ductions in risky behaviour than those who are not (Hui,GINS st al. 1991).
In sub-Saharan Africa, where HIV infection is preval-ent and medical resources are scarce, the role of counsel-ling and testing is less obvious (CoLEBUNDEKS &NDUMBE 1993). Demand for such services exists, andbetween June 1991 and October 1992 the AIDS Informa-tion Centre in Kampala, Uganda, tested more than30 000 people (Also et al., 1995). Studies in Africa havealso demonstrated changes in sexual behaviour thatwould be expected to reduce transmission of HIV(ALLEN et al., 1992). There may also be other benefits topeople who receive counselling such as an increase in'coping' mechanisms. Antiviral therapy is too expensivefor general use in Africa, but preventive therapy againsttuberculosis might not only, be more cost -effective thantreating tuberculosis when it develops but may also re-duce transmission of M. tuberculosis in the communityand prolong the life of dually infected individuals.
The first voluntary HIV counselling and testing centrein Zambia was established by the Kara- zAmaART projectto meet a perceived demand, to help with coping and todetermine whether behaviour was being altered (BAGGALEY et al., 1993). Whatever the result people are encour-aged to avoid risky behaviour, in order to reduce trans-mission or to remain uninfected. People found to beHIV- seropositive are also encouraged to enter the
preventive therapy trial.We have looked at the number of clients entering the
trial and the reasons for failure so to do, in order to ex-¡lore the likely constraints on widespread implementa-tion of preventive therapy for tuberculosis.
MethodsThe study was conducted at the Kara -ZAMBART Vo1-
untery HIV Counselling and Testing Project and at theUniversity Teaching Hospital (UTH) in Lusaka, Zam-bia.
z.t.st &Alts tuberculosis preventive therapy trialThis trial is a collaborative project between the De-
partment of Medicine at UTH, the Ministry of Health inZambia and the London School of Hygiene and TropicalMedicine, comparing the efficacy of Preventive therapyagainst tuberculosis with 6 months intermittent no-
t
AG-distal and Vow y lier ugy ( I994) 8. 1(0-164
An entomological investigation of the likely impact ofcattle ownership on malaria in an Afghan refugee campin the North West Frontier Province of Pakistan
SEAN HEWITT. MUHAMMAD KAMAL, NASIR MUHAMMAD andMARK It O W L A N D htsu: I IcaltliNet, University Town, Peshawar, N. W.1 .P., Viski+t aaa
Abstract. Field trials were undertaken to determine the effect of dose proximityof humans to iivcsitck an the human biting rates exhibited by various anophetu.csThe results indicate that proximity to cattle and to goals increases the subject's
chances of being bitten by anophelines. Maul- biting by Anopheles.rrephovt.0 I uby 38% (8 -68% CI) in the presence of a caw, and by á) %, (l( -84% (1) in thepresence of two goals. Oilier species exhibited similar ticnds. These finding+explain the results of an earlier trial which .revenled that malaria 1lrevalcnLewas higher amongst families that kept cattle than those that did nut.
The endings are discussed its relation to existing information regarding thehost preferences of local unuphclines and classic them ics regattlilig zutipruphyIaxasOur findings suggest that animals are only likely to have a worthwhile pro-phylactic affect when Ilse vector is zoophilic, and there only when the animals at
deployed to form a barrier between that vector and man. lap situations wheredeployment of livestock to form a zoobarrier is impractical. the livestock should
be located as far from 01011 03 po'ssible.
Key words. Anopheline, host preferences, malaria, zooprophylaxis, Pakistan.
Introduction
The subject of zuoprophylaxis. extensively reviewed byService (1590). has been defined by the World !learntOrganization (1982) as 'the use of wild or domestic als.
which arc not the reservoir hosts of a given disease to
divert the binudseeking who vectors f 11c huutan
hints of that disease'.Over the last century there has been considerable
speculation on the prophylactic effect of domestic aninwls.'1 here have been a number of early reports f Europeand the former U.S.S.R. of reduced prevalence of malariaresulting front the active deployment of cattle and pigsto form barriers between breeding sites and human settle-ments (Urumpt. 1945). There have also been rei s ofinstances where the introduction of livestock has appar-ently reduced the prevalence of disease. For example. thereduction in malaria that occurred in Europe and theUnited States curlier this century has been attributed
Currespundcncc: Mr S. E. 1lcwitt. MSF IlcaltbNet. 19 Chinas*Road. l'.U. Dux ött9. Uuivcrsity Town. l'cshawar. N.W.h.f..Pakistan.
part
partly to the increase in livestock numbers (OruccChwatt1982).
Correspondingly. there have bccn at:Ciuf115 u( inn r e.isctlprevalence ofm alatia due 10 dill iimisheillivesuick dcn,aii +
Failing zuoplophylmxis as a result of agricultural alt.hailizrt' (and resultant livestock depletion) tluria'h rlc'(ìtcut Itevul ' ' has been put forward as a piohallccantor: of increased malaria. Om: such it :mph, was Icptuac.tby Cìigliuli (1963) in the Dements Estuary region IllGuyana. After residual applications of t)I)T brought ahouathe successful control of the anlhiupiphugic, rmtsoplailvector Anopheles durliugi (tool, malaria was elleciitel)eradicated in the 1950s. Then. in the curly 1960s. u shift inagricultural practices towards crop production Ira as .a
dramatic decrease in livestock numbers. '.'here followed anumiber of malaria outbreaks which were attributed to .ichange in the (ceding habit of ilnapllrles ayua;alis Corr y:because of the livestock tielicit this mosquito species,which had originally been zuuphilic, switched to fi eihnpon 111811.
Conversely. a few instances have been cited %liegecattle have apparently_ becas responsible fur an increase orthe prevalence of digease. For example, in Indonesia.
Kiuutwm(141pl I Supaliu (1'186) showed that the prevulenediof malaria was (higher in villages where enclosed cattlesheds were situated close to human dwellings than Invillages where open cattle sheds were located smite distance(tarn people's bedrooms.
Although there arc numerous anecdotal references toloop"ophylaxis, to date no case -control studies have beenreported and the majority of entomological investigationsperformed have been unconvincing. Musl of the con-clusions drawn in the reports referred to above ara based,at least to some extent, on conjecture and arc vulnerableto et iticiss's. For instance, in the Ciuyumus example, otherfactors such us the return of malaria- infected itinerantworkers from gold fields and diansond mines in the Interiormay have contributed ansidcrnhty to the malaria outbreaksin the 1960s (Service. 199(1). '
'Mc vutious examples referred to above illustrate thecomplexity of interactions between livestock and malariaprevalence. Numerous (actors must be involved in deter-mining the impact of livestock on malaria transmission inany particular area.
The basis fur the Investigation reported in this paper wasa recent epidemiological study conducted by Houma &Rowland (1994) in the North West Frontier Province ofPakistan. During that study, two probable affects of cattleun malaria prevalence were observed.
Firstly. a strong correlation between increased prevalenceof malaria in villages and increased cattic:man ratio wasfound. Houma & Rowland (1994) postulated that thisphenomenon, which they called the 'area effect', was ducto high vector densities which resulted from. the easilyavailable bluudmeals afforded by cattle, The possibility ofp ctforniing a definitive study, which would dctcrlitinc theexact role of cattle in this respect, seems unlikely. Theexplanation suggested by Houma St Rowland (1994) is,however, corroborated by the mathematical predictions ofSota ,ls Migi (1992) who modelled the epidcmiologiw(impact of changing host numbers where u two -host vectorwas reslwmsiblu for (suslarla transmission. .
'Ilse second finding of Houma & Rowland's study wasMat malaria prevalence was also signnificuntly raised amongstmembers of families owning cattle. These families werewidely dispersed throughout large, crowded settlementssad. other than their relative prusperily,surveys revealedno discernihie cultural or behavioural differences betweenthem and families that did nut own cattle. In contrast tothe correlation found between increased cattle :nrarn ratioand increased malaria, this evidence strongly suggested isdirect link between cluse proximity of cattle, raised man-biting rates and increased malaria prevalence. Bourne &Rowland (1994) called this phenoneson the *compoundeffect' and postulated that the cattle were quite simplyattracting large numbers of mosquitoes,uitces, a proportion ofwhich on their approach were diverting. their attention toleed on humans nearby.
Analysis revealed that there was no link between thetwo effects, hence the compound effect could not be used
to explain the area effect.During small -sale trials conducted in tile -Philippines,
Import of curie ownership on stahoia IfiI
Schultz (1989) showed that the presence of two Initialunear a house (one positioned each side) coasideialslyincreased the lilting rate on the occupants of the huusc.'Phis study could have been used to corroborate the findingsof Houma & Rowland (1994) except that. surprisingly.when the Sane protocol was performed outside lIscie
was a decrease in roan -biting in the prescucc of buffalo.Presumably, when fhc collectors were outside. the buffalowere somehow acting as u zoobarrier whereas, when theteam was Inside, this affect was absent.
In this paper we report the findings of a series ut trialsdesigned to investigate the compound effect lully,assessing the impact of livestock within the family tannpouiulon the entomological Inoculation rate in that compound.
Materials and Methods
Slgdy area. Field experiments were carried out at
Azakhcl refugee camp, near Peshawar, in the North WestFrontier Province of .Pakistan. As with must refugeesettlements in Pakistan. Azakhcl is situated in a marginalzone on the banks of. the Kabul River. The camp wasestablished in 19111 and had a pupulirtiun of 25.100 at thetime of this study.
Strict laws of purdah exist and extended families livein high -walled compounds constructed of mud in the
traditional Afghan style. Most families own une or twogoats and many also keep cattle. For security reasons these
animals are iovaliuWy kept inside the family compound alnight. People commonly sleep in close proximity to thenlivestock, particularly between June and October whcn itis customary to sleep outside.
'Ilse numerous borrow pits. elevated water table withspring and autunni flooding account for the high mosquitodensities throughout the summer and autumn. 'l'raos.mission of malaria,Fs seasonal, mainly between April andDecember. l'. s'ivr.r peaks in September and Oetubetl'.fulc/porism in November. I)uring the year of themonthly incidence of vivar varied between 1.3% ;sod5.0%, wills falciparunt nut surpassing 1% (Dewitt 4Rowland, unpublished data).
Mammal. Three similar derelict compounds. appruxt.'timely 31X)ns apart, were selected as test sites, with tineeehelle ogiel and one assistant allocated to each fur theduration of the trials.
At two of the test compounds, livestock (one cow or taugoals) were tethered Ens from the men art the atrt¡ol eachnight. The third compound, acting as the cuatrul, was tellfree of livestock. 'Ilse number of animals tool their distanceh the collectors gave u realistic rcpreseutalion ul alteehUei uu hi the eunqounds of livestock uwnets al night.
The protocol was designed to minimize the a((edt nit
direction of approach of mosquitoes. At each lest she.livestock were moved 90' at quarterly intervals 'loutishIlse night, In a clockwise direction around the collectiontenon. in order to take account of the fact that peak bitingoccurs during the first 3 h after sunset, the starting positionof the livestock relative to Mc men was changed by -r 90'
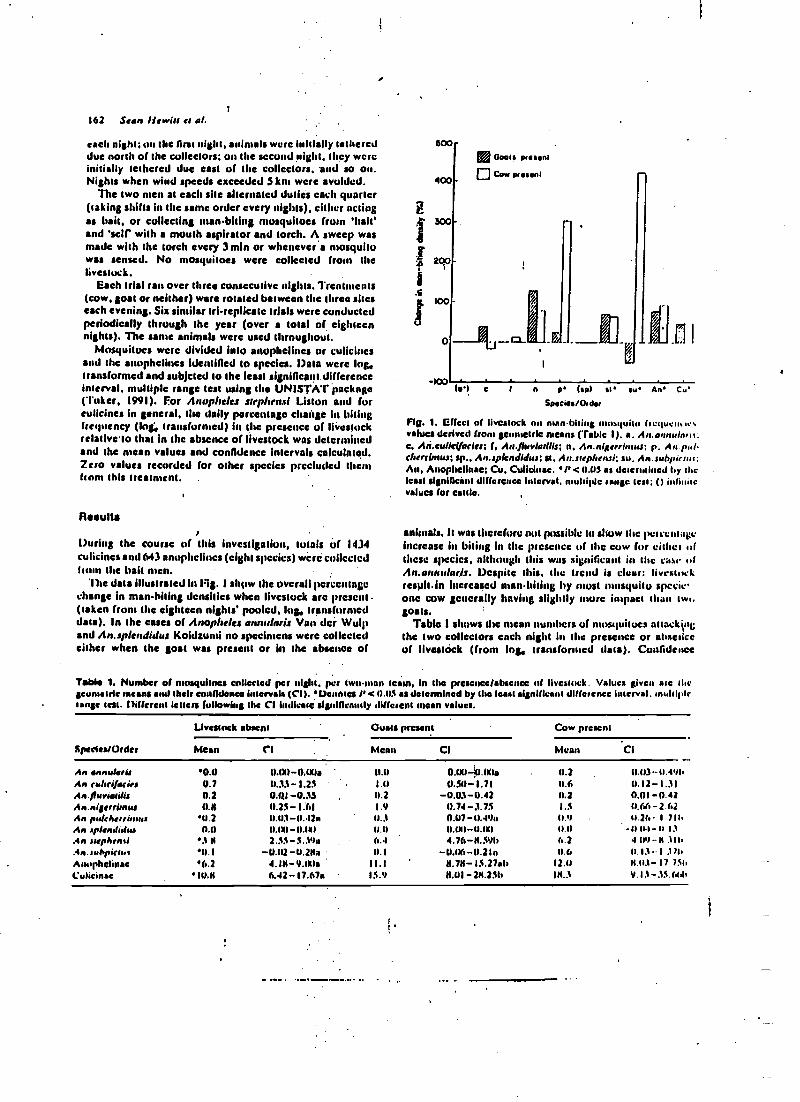
162 Sean Hewitt es al.
each night; on the Orst night. animals were Initially tethereddue north of the collectors; on the second night. they wereinitially tethered due east of the collectors. and so on.Nights when wind speeds exceeded 5 km were avoided.
The two men at each she alternated duties each quarter(taking shifts in the Bare order every nights), either actingas bait, or collecting reran -biting mosquitoes from 'bah'and 'self' with a mouth aspirator and torch. A sweep wasmade with the torch every 3min or whenever's mosquitowas sensed. No mosquitoes were collected from thelivestock.
Each trial ran over three consecutive nights. Treatments(cow, goat or neither) were rotated between the three siteseach evening. Six similar tri- replicate trials were conductedperiodically through the year (over a total of eighteennights). The sanie animals were used throughout.
Mosquitoes were divided into anopliclincs or cuiicincsand the anophelines identified to species. Data were log,Transformed and subjcted to the least significant differenceinterval. multiple range test using she UNISTAT*package('l'/ker, 1991). For Anopheles step!srnsl Liston and foreulicines in general the daily percentage chaisge In bitingfrequency (Ing, Transformed) in the presence of livestockrelativeto that In the absence of livestock was determinedand the mean values and confidence Intervals calculated.Zero values recorded for other species precluded thanhorn this treatment. .
Results
During the course of this investigation, totals of 1434culicines and 643 anophelines (eight species) wire collectedI the bait awn.
The data illustrated In Fig. I show the overall percentagechange in man-biting densities when livestock arc present(Taken from the eighteen nights' pooled, log, transformeddata). In the cases of Anopheles annrrlaris Van der Wulpand An.splendidus Koidaursi no specimens were collectedeither when the goat was present or in the absence of
É
.i
d
600
400
5170
200
100
-100
Goals passent
Cow passion!
_CC I n o bud st su An c,.
Species/Older
FIE. 1. affect of livestock on nsanbitiug nul%quit(' llcqu.u.,r.values derived from go Iris means (Table 1), a. A,,.annuln.+i:C. Ati.eullel(adw; f. An./luvladlls; n. An.nl errbnus; p, An paltherrinsur; sp.. An.splardidus; sl. An.srephensi; su. An. JUhpirnu;M, Anoplicllnac; Cu. Cullcinac. 'I' <11.1)5 as deter nsilicd by Weleast significant difference Interval. multiple range lest; O iu1'values for cattle.
animals. It was scrcfurc nul possible lo show the percentageincrease in biting in the presence of the cow for either ofthese species, alihnugh this was significant in the case ulAn.aruurlarls. Despite this. the trend is clear: livestockresilhin Increased man -biting by most mosquito specie'one cow generally having slightly mure impact tissu twt.goals.
Table I shows the mean numbers of mosquitoes attack4rigthe two collectors encls night lis the presence or absenceof Iivestóek (from log, transformed dala). Confidence
Table 1. Number of mosquitoes collected per night. per two-man scam, in the presence /absence of livestock. Values given are sluegcometrie means and their confidence Intervals (CI ). Denetea Pc 0.11$ as determined by she least significant difference interval. multiplerange less. Different letters following the CI indicate significantly different mean values.
Species/Order
Livestock absent Ouais present Cow present
Mean CI Moan CI Mean CI
An annuhlrL 0.0 I1.011-00Ia 11.11 0.1X14.l10a 11.2.
0.03.-0.491iAn fYllfifKieJ 0.7 11.33-1.25 I .11 11.511-1.71 11.6 11.12-1.31An./fuviarilia 0.2 0.i41-0.33 0.2 -0.03-0.42 0.2 0,01-0.42An.nistrrimtu 11.11 11.25-1.61 1.9 0.74-3.75 1.5 0.66-2.41An, pu/eharimru 11.2 11.113-0.42n 11..1 0.117-0.49u 0.9 11.26 I 711.
An ,pitndi.luJ 0.0 0.011-0.01 0.0 11.1X)-11.1X1 11.11 -1111.1-1r 13.4n Juphrnli .1$ 2.55-S.31a 6.4 4.76 -IL S9b 6.2 4.114-N .116.4n. suópieua 11.1 -11.112 -11.2113 11.1 -11.116-11.216 11.6 0.13-1 .111.Arruphtanae '6.2 4.1$-9.IXla 11.1 11.7$-15.27ab 12.11 11.11.1- 17 131.
C ulicinae 10.X 6.42-17.67a 15.4 $.01- 214.256 Ili..l 9.13-.15.aá.
intervals arc large, but this can be attributed in part tothe variation lis catches between ailes and nights. Thedifferences in these means were, nevertheless,'signifieúntin many cases. '
For Ar.stephert.r1 the nightly man- biting rate increasedby 38% (8 -68% CI) and by 30% (16 -84% CI) in thepresence of a cow and Iwo gouts respectively. For culicinesin general, the rase !ncrcascd by 29% (0-58% Cl) and20% (2 -42% CI) respectively.
Discussion
Information gathered during this investigation supportsthe 'compciund effect' as proposed by Bounsa & Rowland(1994). It is evident that the practice of keeping livestock,particularly cattle, within fancily compounds, as. is the
noon in refugee camps locally, considerably increasesthe occupants' chances of being bitten by a range ofanophelines and hence of contracting malaria.
As mentioned by Emma & Rowland (1994), recom-mendation that animals be kept outside compounds wouldbe unatcccptable locally as security of livestock is a primaryconcern. Alternative strategies such as treating cattle withinsecticides (either using impregnated cartags or liquidapplications) may offer a solution to the malaria problemand should be examined. However, pyrethroldbnpscgnatedbedncts are likely to afford better protection and thebenefits are mare obvious. lm both Pakistan and Afghanis.Ian, where impregnated bedncts arc now being promotedby a number of non -specialist relief agencies, this methodof scl(prolectlon is rapidly growing in popularity. Familiesowning livestock. being relatively wealthy, are likely topurchase more nets and be better protected than (smillesthat do not own cattle.
These findings raise number of questions regardingthe host preferences of local anophelines and about theimportance of host preferences as a factor Influencing theeffectiveness of zooprophylsctic measures generally.
Despite reports that Mt.stephesui, Asi.nigerrlauu Giles,An.annu/arls, An.pukherrimus Theobald and An.subpicsuiGrassi arc essentially zoophilie species (Reiser' & ßorelcans,1979), our results show that all were diverted frosts caillato man. suggesting a degree of opportunism in their (cedinghabits. Therefore h scents likely that. In other regions .also. even 'highly zoophilie' species encountering peopleon their approach to cattle will ha diverted and Iced ona human. If this is the case, then the positioning ofprophylactic cattle will be of the utmost importance.
Host preferences are difficult to quantify. Data derivedfrom analysis of the bloodmeals of resting mosquito col-lections are generally biased by the nature of (he collectionsitu; the vast majority of specimens collected from buildingswill have fed upon the occupants of Ihose buildings. Also,animal sheds normally offer more suitable resting sitestitan human dwellings; mosquitoes having fed in the latteroften rest elsewhere. . . .
lit the United States, Iless St Hayes (1970) used forageratios to assess the relative potentials of s number of
Impact of route ownership on malaria 163
domestic animals for zuoprophylaxis against mosquito
vectors of encephalitis. This method, whereby the numberunditypc of available hosts are taken into cotsidcra ionwhen analysing the bloodmeals of resting collections
(Hess, 1984), is, however. prone to similar bias, particularly
in builiup areas.A mare useful measure of host preferences. in any given
arca. may be obtained by examining the relative abundanceof specks feeding on certain hosts using the baited nettechnique described b Service (1976). Earlier investigallons of this nature,
byout by I lewitt it Rowland
(unpublished data) in Azakhel camp, revealed relative
anthropapltily increasing its the order At.atnuluri.,Au.suóplctus. 4,i.ste%)herui. An.nigcrrinas and An.culitt.jacks Giles. whereas Reisen & liorcham (1982) reportedAu.culicifacies as having a lower human blood index than
Anjtephensl. Taking this into account and examining she
dale illustrated in Fig. 1, it scents that the more zoophilie a
species the greater the increase in man-biting rate when
near livestock. Antltrop oplcilic species, which may wellbe the primary disease vectors, appear to be relativelyunaffected by the presence of livestock. This would sug-gest thus the increased prevalence of malaria seen incompounds with cattle, as demonstrated by Houma atRowland (1994). was probably caused by a zoophilic vector.
In conclusion, our findings show that sleeping close tocattle or goats al slight considerably increases the chances
bf a human being bitten by zoophilie anophelines such asAn.stepheasl, whereas it appeals it) have little allcct onmore anthropuphilic species such as An.rulicifut tri.Careful deployment of cattle to form a barrier betweenmosquito breeding sites and nsan probably does( have aprophylactic effect, st least In the case of suoishilic vectors.However, simply 'keeping livestock' is likely to be counter-productive; where it Is impractical to set up a soobarrier,livestock should be kept as fur from man as possible.Those advocating the use of livestock for prophylaxisshould in future stress the Importance of positioning.Zooprophylaxis would be batter defined as 'the deploymentof animals, which arc not reservoir hosts of a given disc scto divert the blood -seeking mosquito vectors from thehuman )loses of that disease'.
Acknowledgments
We thank MSIt field staff for all their hard work. Thisresearch was funded by the EEC and supported by MSI,.I Tolland /i lealthNct.
References
boums, M. Si Rowland, M. (1994) failure of passive zouprupl,tl-axis: carde uwuersitip increases the prevalence of malaria u,Afghan refugee and Pakistani coninsuuitks in she Nutt!' WestFrontier i'rovince of Pakistan. Trauactimu of sloe Royal Suret,of Tropical Alouette sod hygiene, (under review).
1 .Stan Hewitt to al.
II,u.e(l,watt. L.J. (1982) Essential Ataiarialogy. 2nd cala. WilliamIIeinemann Medical Hooks. Landon.
lltun.pt, E. (1143) Zawaprophylasie du paludisme. Annear de1.sastralogit. 20. (3 -q. 191 -21*.
l:iAholi. O. (1963) Estiduglrul clwnges as a factor ht renewedmalaria ttumsnsission in 111$ eradication area. A localised out-bleak of A.ayoaauhs.i,Ws, iihied malaria on the Demeraraover estuary. Uritisls (Iuyane. ln the fifteenth year of Adarlingiand malaria eradieatlun. Militate of the World Maids. Organiterian. U. 131 -143. . .
Ilcu. A.O. (1914) Ecological management of malaria vectors.ils /kris of the Societvfur Vector Kcalagy, t, (1), 23 -26.
I Its %. A.O. SC Ilayes..K.O. (19711) Relative potentials of domesticanimals for zagwupdsylaais against mosquito vectors of ewe-.phallus. Amer1san Jaunal of Tropical Medicine and llygiene.If. 327 -334.
KUalwotdoyu. S. ik Sultanas (1986) Zooprophylasls n a usefultool fur control of A.arooitas transmitted malaria in centralJava. Indonesia. Journal of Conwtrl.akabk Disease. IV, 911 -94.
Rcisen. W.K. L Wareham. P.F.L. (1979) Hoot selection patternsof some Pakistan mosquitoes. America.' Journal of TropicalMedicine and Hygiene. 3$. 406 -421.
Reiser, W.K. A Bonham. P.F.L. (1952) Estimates of malaria
vectorial atrocity (oc Aadici furies und A.srephensi in ruralPunjab Pruvórcc, Pakistan. Journal of Medical Emonrul.,xv. !v.qí).98 -1113.
Service. M.W. (1976) Maur ira Ecology: Field Suosplu,g Meth.mts.Applied Science Publishers. London.
Service. M.W. (1990) Livestock management and disease vectorcontrol. Report of tha Tenth Meeting of the fled of 1:over .m1 Environmental Manuga111eid i for Vector Cuutr..l.CWSt91.1 I, 37 -6V.
Schultz. O.W. (198V) Aninsa' influence on 111W1.1 g Web ut ansulurlous site in Palawan. l'bilipincs. 5uurh Eau( Asian !minim!of Tropical bir.lirhst and Public Walsh, 20..19 -33.
Sum. T. á Mugi. M. (1992) Effectiveness of uw.pruphylasis inmalaria control: a theoretical inquiry. wills a model for no squibspopulations wills two bloudmeal I . Medical and VeterinaryEntomology. 3. 337 -343.
'raker, M.A. (1991) Whim Staiiuical Package. Unistal. LondonW.I1.0. (1982) 'Manual un cnviruasscnlal management for
mosquito COMM! wills special esupllusis ns (alto vectors.W.II.O. Offset Publication Nu. 66. Geneva, 28)pp.
Accepted 26 August 1993
Prohibition of DDTRecommendation by the Division of Health and Environment,Pan American, Health Organization, Washington DC 20037 -2897, U.S.A.
Included in The Pesticide handbook (IUCU, 1986).'The PATIO (1993) review of Pesticides and health In theAmericas included eansidcratión of pesticides' utilized formalaria vector control and, Inter alla, recommended that:'National Governments, with support from the Inter;national Agencies and International Non OovernailelttolOrganisations, should prohibit the use of pesticidesthat are:
Included in the Preliminary List of Producle Detrimentaltu health and the Ens'trom,iesil, International Regiiterof Potentially Toxic C.henmical Substances (DAO /UNLP.1991); .
Included in the United Nations Consolidated Listof Products whose Consumption and /or Sale- harebeen /banned, IVithr/rawvs, .Severely Restricted, or. NutApproved by Gorensnnents (UN. 1992):
Restricted by the Environmental Protection Agency inthe U.S.A.;
Included hi the Dirty Dotes' of Ilse Intprnatiuuul ¡'esta.tide Action Network (PAN, 1993):
VDT is Included In' all live of these categories.
Rd.rencis
FAO /UNEP (1991) Repon of the Mooting of Esperts un PriorInformed Consent (PIC). June 1991. Food and AgricultureOrganization/United Nattons Environment Programme.
loCU (1986) The Pesticide i1asdborsk: Profiles fur Action. 2ndcdn.lIntcrnadonal Organisation of Consumers!Uniolu. Penang.Malaysia. I
PATIO (1993) Pesticides and Small. in the Americas. Envious'(rental Series No. 12. 109pp. Division of I lealth and Emilia'.mend, Pan American health Organization. Wuild IlealthOrganization. Washington O.C.
PAN (1993) Dormira of she Diny Paten. Pesticide Action Net-work. North America Regional Center. San Francisco.
UN (1992) C i.nsulldaset( Lim of Products -whose t u..surmpnrulun./for Safe havé been /banned. Withdrawn. &welch R. uuwdor Not A/y.rured by Guternment,.4th can. United NationsMineral Assembly. New York.
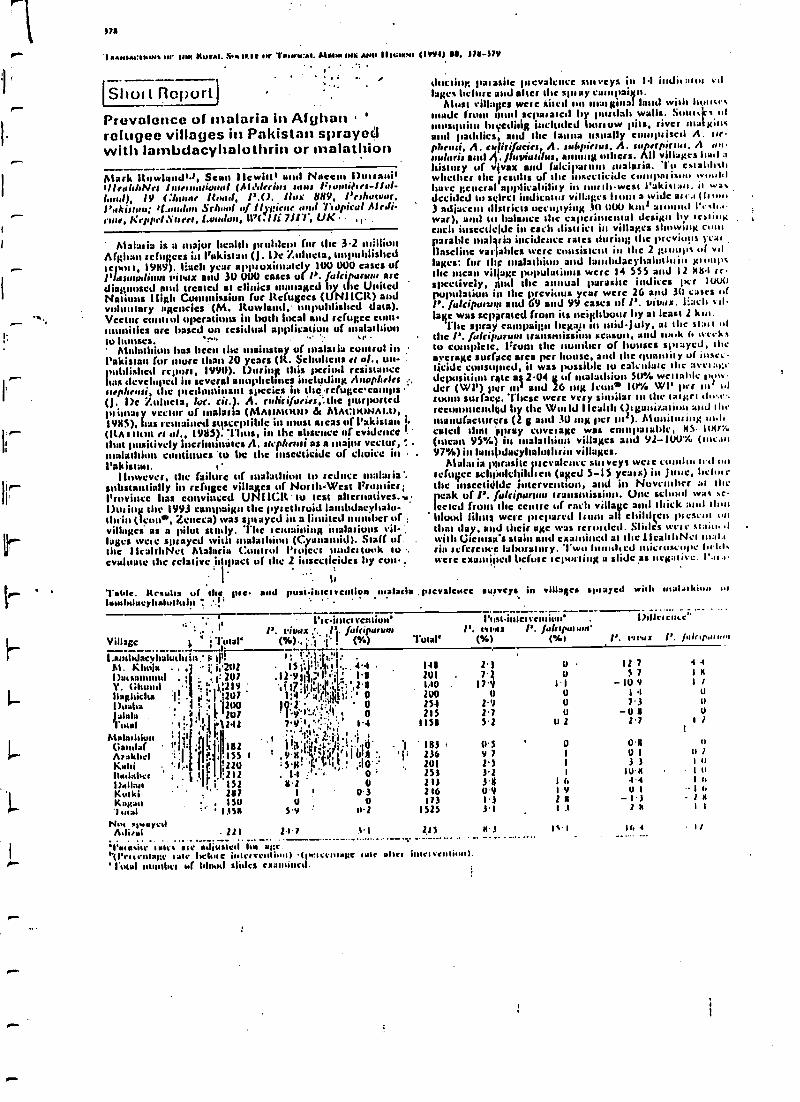
)7a
I aAN1A1:IM,Nt n/' 1111! KUTAr. 5. 1K111 .n' r..M44:A1. M1111.INlt AIM IIII:IK!/1 (19114) aa. 171479
l
. ..
S4)UI l)orl,Prevalence of malaria in Afghan '
refugee villages in Pakistan sprayedwith lambdacyhalolhrin or malathion
Atark ltarwlonJ'2, Sean Ilewittt and Noeen I)urranil'lleuhhNrt Isirnsiariunul (Al.'drrilrs sums 7:uuri?1ro-I1al-laud), IV f:/ flood, !'.O. Max 889, Peshawar,Pakistan; If- Ion Srl l of IIJgirre and %iopicul Ale11i-ruae, K eloped l'aret, l.un.luu, /li 7111', UK ,
Mat :nia is a major Iseallls problem for the 3.2 millionAfghan refugees in Pakistan (J 1)t Zulueta, unpublished:epos i, 19119). Bach year arms uxionately 100 000 casts ofPlasmodium tvtv,x and 30 WM cases of N. /alcippars nt. arediagnosed and treated at clinics ,managed by the UnitedNations I1igh Commission fur Refugees (UM Wit) andvoluntary agencies (M. Rowland, unpublished data).Vector conitrI operations in both local and refugee com-munities arc based un residual application of mlaladhiunSol ttttt sea. r'
Madathlun has been the mainstay of attains la cumul in('akisian for more than 20 years (R. Scbtrlicns es al., unpublished rcpurd, 1990). During this per1041 rc$ auIamce
box developed in I annplsclttlea including Anophelesstepheusi, the pteduutinaut 1111eeies in the refugcccamps(J. 1)e %Muera, loc. cir). A. ttdiràfucies,`.aIc purportedpii aasyy vector of malaria (MAIIMtuns & MACIKNAII1,19/15), Iras unstained susceptible in most as cas of Pakistan i.(KA I !lull es al., 1911S). 'Thus, in the absence of evidence 1.
ghat positively incriminates A. ugahnsi as a major vector, .malatl continues 'to be Ilse insecticide of choice in .
l'akisian.I Inwevcr, the failure of :naiad ' to seduce 'malaria *.
substantially in refugee villages of Nandi-West I7rusuicr;Province has convinced UNIICIt tu test alternatives. ,Dui ing the 1993 campaign the pyres 'avoid landdacylalu-thiin (Icon*, Zencca) was sitnaycd in a lisniicd ber of ,villages' as a pilot study. '1Ilc scamaining Mains isms villuges wets: sprayed with malatl ' (Claim nid). Staff uf.the 1IvaltIsNet Malaria C rail Ps meet lei took io .
evaluate the relative ishpact of the 2 iasecricidcs by C011..
I b
l'aide. Results of the pre. and pusii.letventivn Malaria . prevalencelua/btlmeyh*tullnhn t'
ducting parasite prevalcnce sinvcys in 14 indi1:1(1.5 :l!age% before and alter the shay campaign.
Alusl villa'pcs were 'theft tlsi Maignal land wish I i.sstade fiutu prod aellaralc41 by purdah walls. S all
mosquito hi editig included borrow pits, river aualxist%and paddies, and Ille lauua usually c prised A. ase-pheusi. A. cufitifJ.scier, A. sulrpirrus, A. superpicsur. A un,rularis and 4. Jfuviatsius, a g Misers. All villages hail ahistory of vivax and falcilrar malaria. Tip establa%lawhether the 'exults of the msccaicidc c/silparisms .vtaalalhave general applicability in norahwest I'aki%,ars, is wa.decided tu %elrt.l indit. muar vill./p;es It a wide al .1 ( I
3 adirccnt dlstricls occupying 31) 00) kn2 around I'ela.awar), and to balance the cape tinacnlal design by aria ogeach inseclieidc in each district in villages showing coolparable mal ria incidence rases during; the previous pcalVaseline variables troc consistent it the 2 +;rump% of valsages: for the Inalattaim, and lanrbdacylaluthain 10omsusthe mean village popish, x were 14 555 asid 12 0114 re-spectively, And the annual parasite indices 1Kr 11)00population nn flac prcviuus year were 26 and 30 casts ofP. fultipurvpa and 69 and 99 cases of J'. vivos. Each sallapis was notated from its neighbour by at (cast 2 kraa.
floe spray campaign Iegap n midJuly, at the slit a ofthe P. falcipyr transmission season, and souk fa weekstu complete, Drum the number of houses spaayed, theaverage surface area per 1 , and the qua y of inset.Nolde consumed, it was possible to calculus; slag aven :y;rdcp osi,ium rate alt 04 g of sitalathiou 50% we' iauseder (WI') Pair un asad 26 sang icon* I(ri. WI' per sial ofroom surface. These were very similar su the tsarltra alo.e.tecunuacadyd by Ille WoaId IIcaltll Osganiitauiuu and slat.manufacturers (2 g and 30 mg per sa2). Musiitmaiog iscaned thaw 'spray coves age was comparable, MS. Itxrf(mean 9S%) ín maim! ' villages and 92 -100% (meal97%) in Iassandacyhaloi brin villages.
Anal ;nia parasite incealesice sus vcys were condos ,ell nnscftagcc sdhtiolchildsen (aged 5-IS yeas s) ín Jmue, helmrIlse uucctidldc intervention, and in November :al thepeak of P. ful(ipunuu transmission. Oise school was se.lccted frutti she centre of each viIlab'e and thick and slam,blood films were psglared Isom all childicar present u11Mai day, and their agc was 'moiled. Slides serre sa;list 1
with Caen'sa's slain and esanli,etl at the IIcalalaNei naal aria arrerenp lalxpratury. 'Iwu 1 hid microscope ticks..were exrnsived berm e tquisling a slide as ncgalivc. 1',1.1
surveys in valla4c sprayed with loal..sl ur
al'leitnClyelliull'
! P. r iaax ; 1'. JultipurunrVillage 1 ` fatal' (S{.); ' (%)
l.amladacyhaludrtin,' 1: Ip! s: !:!.):t"4At. Khuia . i; ¡,2112 15 ¡: ,
ha.,. 41
1)als. 1.; p: 2U7 ,1191 ,''I. 'ill. illV. GI 1 :'' 1:119 'si 1Ì:11:1Ir,".s',2'Yllap;hicha ! "' I
1 0'1.'t,t:Ji,lit . '
ÓI)oaba '.:11200 I ;;,alala . , ).1 t tlll I'Y I i. 11. 4 Q
lutal 'i i'.'1212 79;',",. '' 14N iAtalasbiusi : 1'1 ' 1 ' . !l'''' i':i) ' '
Caudal' 1'ii ¡ 1a2 , 4!3!'4i'1`7i.! :silt). :Arakhtl 'I yI.I 155 1 y g;,yy,))
>J ¡1, 4' j blrjKNIII '.i:..
!'120 5g' 'M' 11. ,:ia' '
uaJ,ahrr ' . 1 212 . 1I .'. 0 ;ua,uan i' I. 152 112 uKoski ' 1717 1 ' 03Kagan 15U U O
lutal 1350 SY ' 11I
l'hslinlcarcnsiuu'P. arils P. JuhlpnrNrn
Total' (%) (.LI
I)il lei rime'
P. r'rrvrs N. J.Jrap.uunl
141 21 u 12 7101 7.2 u 5-7140 17.4 1.1 -I0v
. 21)0 0 0 1 1254 21 l) 73115 1.7 u -0 a
Ilsa 32 0 2 2.7
183'136
iss
716173
1525
Nut splayedAdisui .Ill 2.1.7 1.1 725
1'u,asise palet me *situated Isst- matt.al Pelt ela,agt liar bd...e inter veuli,n, (pas senuge une slier inlets' rural Iota of blond slides examined.
1.
0SY72S3.11
09
3.1
0
I6I9la
1 .1
4 41 It
r7u1)
U11
113 1%'1 16 4 I/
.-
sitaeurfe children were Itivrn supervised treadmill withchInt.K usuc (23 rag /kg burly wcighl iu divided ilusrs Derr
'., ! rl), whrelrer symptrunulir nr veut. Habitat aunsidrrariunsdid not allow inclusion of art untreated C 4444g) i,enup ofvillages. I luwever, by chauve a single village (Arlizai) didreola.n unsprayed and this was AM veyed in June and Nuvendee:. Revisse of variation in urscrtdarrrc in (retainanuses between she 2 surveys, il wets uccessar y in adjustparasite ptevislence rates according tu age by taking thetotal of else June and Nuvemhcr iu Vcys as the standard.The average ages of children in the Inch il ' and lame-
¡(. barylialolluin groups WIIC %Nampa' aide, nevcrIhrless (9.1and 9.6 years ces ccilvely),
The impact ofinsecticide h,itervrIliin was deter iii ired
5
separately for each villa e and fur cads pas mite: Novell.-
:. ber pscvaleuce of malaria was subtiacted boats the June
sa prevalence and the ehlecl of the two different iusrc-deities analysed using the MunnWttsey f/ Iesl, "fie re
P1.stilling values for P. fish ipu , presented in the Tableio descending older of difference, revealed 1 chlstetswith the majority of snalatltinnspetty'ed villages sl ing
.i; an increase in prevalence after insert/ention and lambda-
¡. cyhalothrin villages showing either a redues' or no
, change in prevalence (I' "O(It117). Overall, the agcat1justed I', aki anror prevalence tare increased from6.7111183 (IJ Z%) to 376/11183 (1.3%) in the malarbianpoop and decreased born 32.7/2400 (1.4%) eu 4.111.11$)
(t1 2%) in the lauslidaryyhaloduis group. In she single sow
sprayed millage l'. /Oh /poem prevalence Increased to agreater extent than Ile any of Ilse molar' lit,rs or Iambastey
hahothriu villages. While lambdacyhalolhrr appeared tobe Wrote efficacious than maluthiun in redwing P. lead-menu" infection sates, ils eleet un 1'. virus prevalence
was nut significantly dilferenl hobs drat of utalathiou(l'- O.23). be the malarhiuu vülugcA the overall P. vivatprevalence rate dci:rcased from 170/1883 (5.9%) to89/28V (3.1%) after illcrvenliun aria in Ire lantbdac hula
losluiet villages it decreased liant 191/241X) (7.9%) to
12612400(54%).Owing ro low rainfall, Owe' was less malaria trans
nsissiin in 1993 than In previous years, and only 59 1'.
r; e i
(
Alinouticomeritj
fulriparum cases were identified io Neevemleer. Neves dic-iest (he distribution of Ihese cases, mainly within the teafashion group of villages ant) iu the unsprayed villuy;c,'mimesis 11;a1 lauehdacybalntbrin was IS heeler preventiveagent. There are 2 possible s xplunasious' l:unbdacyh:do.Ihrin's hunger residual life (S. M. Atpnlu .4 Ii. (harm's, tinpullished reparl, 19'111) uwy'huvc estrudr.I its eltecsiw.nessilunger.lido the transmission scasuu or, if il. siepILLS o s'çglycuf 1'. fiekilureuni, ¿Heil resisuutcc o mulud,ion
. 'Issigl,j; )otieq ;,rtduccd 1 se; )ieirtuc'y.ul this insccsiskhc. flycontrllsty'neilhcr yv:ts found to be very clfcc
I live ld prcvcnliiI /', t'irax, lour wile uuc brtcr1111111 the other. )'his may ;;Ife because l'. viva i u:urs-
.; uIstlioip its well under ssnayla( the those of the spray inter
IM
vcstl'' if And was seasonally d.!ehis,init during the Nuve.mber'iliti'cy (IIc ss:nsnu>ilii II Isf bud:uitt iu Pakistan liasbec11 described by FOX' ¿c tit ltll :KI.ANi , 1989). The P.
. I fafrijIlnuu icsults (uslify a ¡Mire detailed epidemiological
1 evaluoliun of Inmhducylsaluthrin and exiensiurs of its userelative so nnlashiten, pnrticululy in areas where I'. huh I.
panes is the inure prevalent species.
Acknowlesaenrent'('his prolecr was funded ley flee liurulran IJuinn.
i. inns.(. n -e.o
Reference.Ikea, H. h SnIckhnd, (1. T. (19119). '1 Ise intro 44.6'11.8111d'. ul
i 'lnINA. loste alrip eeune and P. siu'a he nee Pouliot,. I
none re/ die Ravel Society sf 7'la¡uul Al Mel me u.J Ilvenr.u,
83,471-473.MahnlnNMl, P. h Macdonald. M. b. (19ß5). kealugy al u.al:Hia
Irsosnlsslon and vccuuial capacity of Aanpheles rah /.uus
P. species A In rand l'isusis e, Pakisurt, Ashman ,7a,n,.,1 .1
'Alydirol Riccardi 24 95 -106. '
Raskin., iI. It., Togir, t. h Ilashld, S: (19KS). I'atsci a of mina.
thhin eroureslesauce sn Irniuushhuu in Anopheles ssrpl.r.ni
and Anopheles euliiiforits. /'i, iuun.7 oaf u/ Alydind Itr-
' starch, 24, 113 -120.is
. n .s'i ',Nrreivet/ 20 !)trember 1993; etuised 14 hehsunly 199.1.
.accepted feir psiblkuiiun IS Minch 1994
t,e ,. i¿
I 1 .I:
,.11. . ; .
; . e
' . r.'e I .. ..n'Ad*, n
Robert Cochrane Irund for Leprosy
The fund, in memory of the great lepro)ngist Robert Cdchraue, is administered by the Royal Society of
Tropical Medicine and I hygiene. It is to be used to finance up to three travel fellowships cads year to a
maximum value of 01000 each.
The )'und will support (raye) for .
"Leprosy workers who hic d au obtain practical training Ili field work or lu research
haperiareed Ieprlugists to provide practical clinical train(ng in a developing cutntry
'fbere is no restriction on dite country of origin or destination providing Ilse about requirements are mei.
Application forests are available from the Society and completed forms muss be received by she Society as
least six nu)utbs ahead of else proposed trip. Ali applications 111141be sponsored by a suilablc representative
of the applicant's employer or study.ccntre, and agreed by the host organization. A two -page"gum on she
travel/study should he submitted within one tumult of the recipient's return, to: The I honorary Secretaries,
Royal Society of Tropical Medicine and )hygiene, Manson house, 26 Portland !'lace, London 'W IN 4I :Y,UK.
'111ANSAl:I IIINS 111' 1111; IlillA1. NI/(:Ili l'S'lll° 'l lilllI(:A(. /.1Ii1111 INIi AND IIY(:II:NI:
lilll I UII IAI. IIIlAa11
It I: 118,kais. tlImo. Now 1: 1'. It. l:. Wtn 11 Ism. \c:.1; 11, A. lia.alllim. I,,ta.':1. IL l: Alauun ION. (Iboo At. loto iU; Il II. IIcL..-... 1, A l'.Ib.ula;/i I:.I:N,k¡II. II. C.r.nd.:A. M l:.nlrllo; 1). A. 11: 1lusta 11. Al. Ihk,tIIIA. J. 11811;1:. J. Lemke; S. 11. l.urea; l'. A. Nu'ual1;U. l'aarue; K. J.
IINI.a..lbr1; M. 1:. AI. Iturda,ali M. W. SterfaYi K. 1'. titunutki P. A. ss'iunsudsy
/:J.hr J. R. llektl .lí./i,..n,.rilu,.w.u: l:a,..lint S. "Is
J J..w..d I'IMr: Atana.n ( Ism t. /Is Fos dated ('lac. WIN 111Y tlK. 'l'dtpl : 1171 VW lil1. 1aa: 071 11h If47
'Chaim nan .d elm llwcd
.VULa1Ml: ilJl
CONTENTS
Nu. 1
I.YAI/INt: Alt 1 t:I.i;Niger-
Mato, A. l')., Okrkc, E. N. and 1laniy:uu, (:.CI ' lini P. 1.. A'new' pas iodic: I Inlet: ' (:astllNl (lual tliKCasrs on the Jus plateau, Nil;erwith (.Ye%sputd e.pvvaraerals . . . 369 ia . . . . . . . 413
tiu um: 1Y Aim: I1Nt: !A1adlebo, "l'., L.IndljNnl, U. and Ilcariksrra,
Meeting ut St Alu en Unwind Atclisal Sellout,T.-Il. II4111 incidence ul oesophagus and sunnathcancers in the Dale highlands ul south Ethiopia . . 41S
Londuu, lU Juuuarr lYY4: 1 unlcr prescsitaliuts 372l)IAt:NUSIS
1'uw.Ir. 111íA1.111 ANI) C:uN7aU1 Pelmets, lt. and Marliab, N. 'I'. 911(.:* and thickRowland, M., Hewitt, S. and 1/tor/asid, N. blood lilsits for 'sodas in tlhi¢nosis Icr lividl'ISValencc of lnulatiu in Afghan tellgqce villages in conditions .. . . . . , . . 416Pak isual splayed with lanlbdacylnaluiintl, urmaloll ' . . .. . , . ... J78 1 rcmji, '/,.; AUcjas, ). N. und shift, C. J.
a l.ubüralury dit1J(nusis uf ulalaliu by village hllnChad I,aj.I),'l'hccuntrl/ufCldevyuinyue¡us, woo hers using the rapid manual !'uruSiKhlil1Jrtut,rr bleeding in wink: tanks using expanded ' test . . .. .. . . . 41iI1nIystylsms beads in situate; is .. '38U l'rue, l'., Ilailey. J. 1V., Uuua, l'., l.:weissierc,Ii1vnPAitULill:Y ' C. end Godfrey, 1). G. /1 culopaeisosi nf pul:lsito-IlinAa, F. N., Mon sit, S. S., Rots, t). A., As thus, .
' Ia11ical mlcihl)tls fur the diagnosis ul J;amhian
I'. and An)'ectcy, Al. ll. l'uti('ras uf sltalutiu tlypalluSalllia5is in an al 1:a al how endemicity inbidity and omit talky .in cilildscn im nurthcril i
tote d'IYUire . . . . Ilylihanu ..i . ! .. .,1:' :.;;:3>;I,' G Ng,, T. 1:.. and Ku, lt. C. Sesodiaf(nusis of/clout ieu, S. M. Il., Uliveira Il. M., Maeksir,i(':;. " ..1 rysllccreosis: a ccificily uf dilfrrcot unugcns uodS., (:osta, It. At., Sweet, J., Iuachnesilo, lt. '1 ., ':a' . ;', cosyneIinkcdnuntlnusull)cnt assuys . . . 411
I tar, K. 1:., I'cnauodes, M. Z., Jernigan, I. end l :', .t ,, Matta, G., 'l'rupc, J 1'., Legros, 1:, ItuKicr, C.Peas IAMB R. D. Ate us bait aatl)scak uf vlsccsul.;., '"'' und UupLuuicr, J. Al. A cungpalativc study ofIcishnuatinsis hl Nand, lltuzil'c ' .. ... . ' .. ' 386,
.
Ilvice nlcthlNll u JcieclluJ uf Iloraelrar truridur,rc inl)aviss, C. R., t.1: ('ucu.las A. (:an:tics, J,¡'' 'h': ; L will rullcnls li, Scnegul . . . 123I.cult, 1:., Alvin es, 1:., Atone, j.,'1'ulcnliuu, 1:.,; :, l;' ', ' I11ann, A1. S., I laçais, M. 1(., Asiah, At. A. II tot,l;uocsa, Q., l'ykc, S, und L)ye, (:. The lall and:. ..1; ' A., Ilerdhan, P. K., 'Sack, It. Ii. and Allies I. M.Iiss Ill Andean cut:111(tleln (eisbsn:utiasis: 11a11siC1111.'''''' . J. SJet:ilicit)' of ("ilall'Ia Ses ccnnAl test dui inn animpact of Ihc UIYI`campaign in l'ctu .. :.. + .389 epidemic of chulcsaliku intense duc to Ndniu,,:Cassai 1.. Santsis(:unnes C:. l'cutlunJ( 1:. ' r ' . r lulerur 0139 synunynt 111ngal . 41f
1 . , , r .; S.p : .
Ucdct, J. 1'. and Abrunclles, 1'. IIIV-(.tirl rain:,;;,, '' "1r : '!'ti' ("LINI(:At. S'l'L11111i5 AND l'A7'IItl1.I/UYcu-inlcctimu in 1 nitugul:,isulatiun uf l.eishpulnid;,i ' \
ut/ural A1UN2I . . ..'. ' I I ' ' ' i';','e. 3Q1 , ' : NVattanaguon, Y., Scivilar;eit, S., Laoarccsuwau,li P '.; ' S. suul 11'hite, N. J. Convulsions .in childhood .IsuacIlcu/uu. J . 1.., Lewis. L.: I'., Ong, C. S. L.. :' it
. naalaria : . . I 426and Nolseu, A1. F. A second cunnsittsitity uulhl cak' i.....'....., ,. ''of watcrboluc giardiasis in (:amuda asid swlulugiçal .
Armslrung Schcllcnbclg, J il. At. (:lrcuword-investigalitu of patients ,li: i . . . 1 , i ::, i,á'JS,., '.: lL Mi (iumc7., P. , Alcuvndca., C. autl Aluusn, 1 .
(:udariura, It., t4ucwtra, A., Cuutcr 11''. ' :' 1.. Uresrnal (:lriatit)n ill,butly isnynraunc ofI , . ¡ (idotbiau childsen . . I . . . , . . . 429
Ituxcics, A1. T. and ArasiRu, C. I l'l'L.V-1 nl'ct: 1 iljIinn and lltp topical spastic parapat ois in lisnicruidut';:;. Ilashinl, F. A., Ali, M. N. Sani, At., lilIlussan,I'tovin(c tog ?cuador , Il ;(. ..1.1o1.. . :, 3g') . A. A4., (ihuIlla, II. 1V., 41 Sali, S. and lit 11ag, 1.
i . 1 1 A. An uutlrrak of acute kulaarar in a adirVeo le, P., Sl.aata, l'., 1)csrcuntaus, l'., uicug, II:r''' uibe in vestern Sudan: Natures of Om disease in aA.. 1)iaw, tJ., 1(angs A. !slicing, M. Suwi S,'! " plcviuusiy numinmuuti: Jllpulatiun . . 411Talla. I., Ssunvlck, It. 1:.', Gryaecls, 11. anti(:ap1.si, A. l'sclimiitcav xt(Idy ul' minary scllisnl-,'..'p '. Illeiag, '1'. '1'h1:'cllcct sil' IaiJcled che IhlclalyI, 'asi.a isi a village isi itlr deli a id Ille: Sencgai ilçr.,5.
, uljaim;I al':Iti;lsi5 NII the IICi1;h1 of (Ilildstn in iutaltt.n.io, ScntJ:u1 . I. .
.a 1,4401" , 1 n1Fauucar . . 43J
Ahocda, J., ('tllItllan, At. &nana, A., Asiako,'`.,ti(II'" Ilaini, N. nud licsiuln'.ZVKltuli' d rluicfA,uls1:., l::ov;llhu. 4. AI., Itullingosi, I.). and Soullt.,,;'Via .1:i eclued KCapnsi's aulc 1 io Ieeo Alica;l,alct
and ('iincil.exI at attune.sllcptlIfeuf tau 'dt16 experience at the Juhanrtcshurg General I hospital
(198U-1990) ' I 1fltaatoo, It. N., Mon Ross. O. Si C., ;iodide, At. P. ,,mot Illataicr, W. A. Scoop' evident eul Il'I'1..V I ist ' Sehwart It:, Jenks, N. '1 . anal Shlinl I). Il.claaatit: iliscuss ism itvttx i/1 Jamaica , ... ,410 l')phuid Iepatilia us. Iypb'id lever and acute viaal
Al:eaon, l'. Il., I(r1ly P. J., Nilasut, I. and :laepalilis 4l7
11'udsliosil, 'I'. Appal cm absence uf Lyme Ion aeliosis in Xitltlydnvs . . .. .. . . .. . 411 I:,.......J .....r..r..a ,....
... ' a.. a II to 1011 01 Al' 'e .
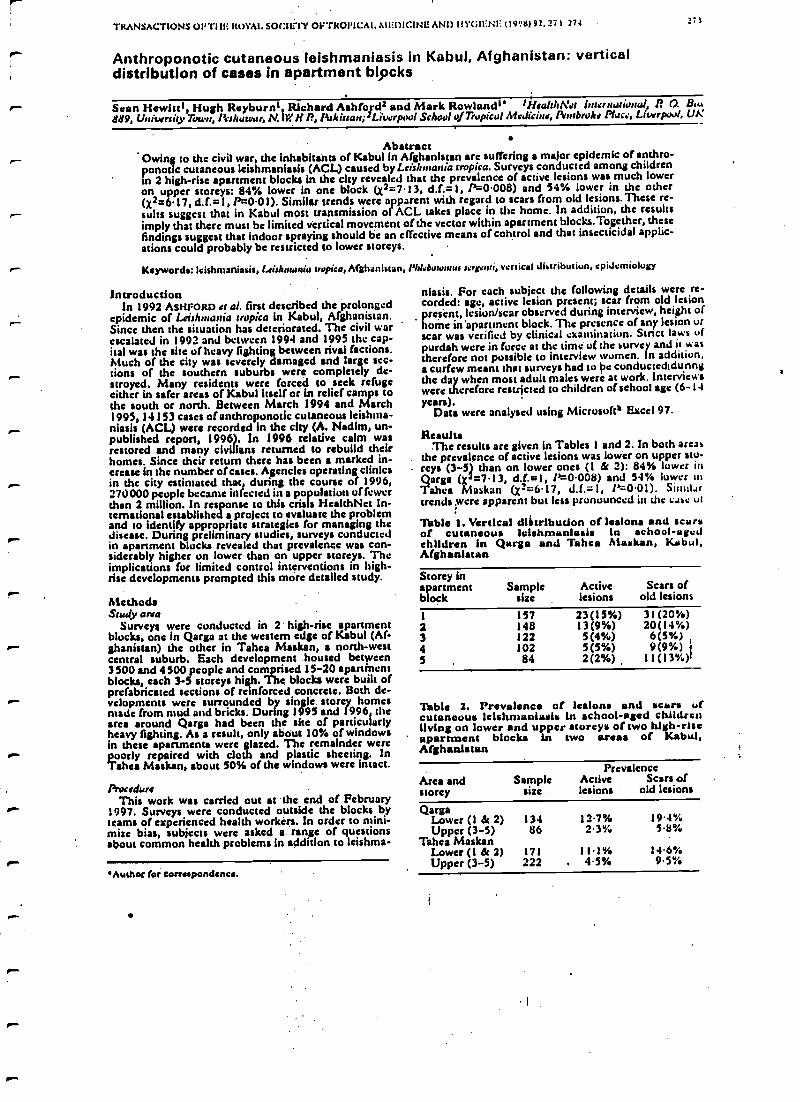
TRANSACTIONS OFT' ils ROYAL SOCIETY OI'TKOI9CAt. MEDICINE AND IIYUII :N1: (19.!6) 92, 27 S 271
Anthroponotic cutaneous leishmaniasis in Kabul, Afghanistan: verticaldistribution of cases in apartment blocks
27)
Sean Hewitt', Hugh Rayburn', Richard Ashford2 and Mark Rowlands' tffeal:Wet huarnutiunal, 1? O. B«.889, University Town, lìslwwur, N. IV P', litkixaa; 2Liverpul School of Tropical Medicine, Pembroke Place, Liverpool, UK
AbstractOwing to the civil war, the inhabitants of Kabul in Afghanistan are suffering a major epidemic otanthro-ponolic cutaneous leishmaniasis (ACL) caused by Leishnatia tropica. Surveysconducted among childrenin 2 high-rise apartment blocks in the city revealed that the prevalence of active lesions was much loweron upper storeys: 84% lower in one block Q2 =7.13, d.f. =l, P=0.008) and 54% lower in the other(x2 =6.17, d.f. =1, P=0.01). Similar trends were apparent with regard to scars from old lesions. These re-sults suggest that in Kabul most transmission of ACL takes place in the home. In addition, the resultsimply that there must be limited vertical movement of the vector within apartment blocks.Together, thesefindings suggest that indoor spraying should be an effective means of control and that insecticidal applic-ations could probably be restricted to lower storeys.
Keywords: leishmaniasis, lsirhnunia tropica, Afghanistan, Plú.bmutus serr.nti, vertical distribution, epidemiology
Introduction '
In 1992 ASHFORD a al. first described the prolongedepidemic of Leirhntauia tropica in Kabul, Afghanistan.Since then the situation has deteriorated. The civil warescalated in 1992 and between 1994 and 1995 the cap-ital was the site of heavy fighting between rival factions.Much of the city was severely damaged and large see-
r." Lions of the southern suburbs were completely de-stroyed. Many residents were forced to seek refugeeither in safer areas of Kabul itself or in relief camps tothe south or north. Between March 1994 and March1995, 14153 cases of anthroponotic cutaneous leishnia-niasis (ACL) were recorded in the city (A. Nadim, un-published report, 1996). In 1996 relative calm wasrestored and many civilians returned to rebuild theirhomes. Since their return there has been a marked in-crease in the number of cases. Agencies operating clinicsin the city estimated that during the course of 1996,270000 people became infected in a population of fewerthan 2 million. In response to this crisis HealthNct In-ternational established a project to evaluate the problemand to identity appropriate strategies for managing the
r- disease. During preliminary studies, surveys conductedin apartment blocks revealed that prevalence was con-siderably higher on lower than on upper storeys. Theimplications for limited control interventions in high -rise developments prompted this more detailed study.
A"'MethodsStudy area
Surveys were conducted in 2 high -rise apartmentblocks, one in Qarga at the western edge of Kabul (Af-ghanistan) the other in Tahea Maskan, a north -westcentral suburb. Each development housed between3500 and 4500 people and comprised 15 -20 apanincntblocks, each 3 -5 storeys high. The blocks were built ofprefabricated sections of reinforced concrete. Both de-
.-- velopments were surrounded by single storey homesmade from mud and bricks. During 1995 and 1996, thearea around Qarga had been the site of particularlyheavy fighting. As a result, only about 10% of windowsin these apartments were glazed. The remainder werepoorly repaired with cloth and plastic sheeting. InTahea Maskan, about 50% of the windows were intact.
ProcedureThis work was carried out at the end of February
1997. Surveys were conducted outside the blocks byteams of experienced health workers. In order to mini-mize bias, subjects were asked a range of questionsabout common health problems in addition to leishma-
Author for eorrespondenea.
niasis. For each subject the following details were re-corded: age, active lesion present; scar from old lesionpresent, lesion/scar observed during interview, height ofhome in 'apartment block. The presence of any lesion urscar was verified by clinical examination. Stnct laws ofpurdah were in force at the time of the surer y and it seastherefore not possible to interview women. In addition,a curfew meant that surveys had to be conductedidunngthe day when most adult males were at work. Interviewswere therefore restricted to children of school agc (6 -14years).
Data were analysed using Microsoft' Excel 97.
ResultsThe results are given in Tables l and 2. In both area
the prevalence of active lesions was lower on upper sto-reys (3 -51 than on lower ones (1 & 2): 84% lower inQarga (X 7.13, d.f.=1, P =0.008) and 54% lower inTahea Maskan (X2 =6.17, d.f. =l, P=0.01). Sitnil.,rtrends were apparent but less pronounced in the case, ul
Table 1. Vertical dl &trlbution of lesions and scarsof cutaneous lelahmanlasls In school -agedchildren in Qarga and Tahea Alaskan, Kabul,Afghanistan
Storey inapartment Sample Active Scars ofblock size lesions old lesions
1 157 23 (15%) 31 (20%)2 148 13(9%) 20(14%)3 122 5(4%) 6(5%)4 102 5(5%) 9(9%) '
5 , 84 2(2%) Il(13%)
Table 2. Prevalence of lesions and scars ofcutaneous leisltnsanlash. In school -aged childrenliving on lower and upper storeys of two high-riseapartment blocks in two areas of Kabul,Afghanistan
Area andstorey
Samplesize
PrevalenceActive Scars oflesions old lesions
QargaLower (1 & 2) 134 12.7% 19.4%Upper (3 -5) 86 2.3% 58s/
Tahea MaskanLower (1 & 2) 171 11.194 146°/sUpper (3 -5) 222 . 4.5% 9.5%
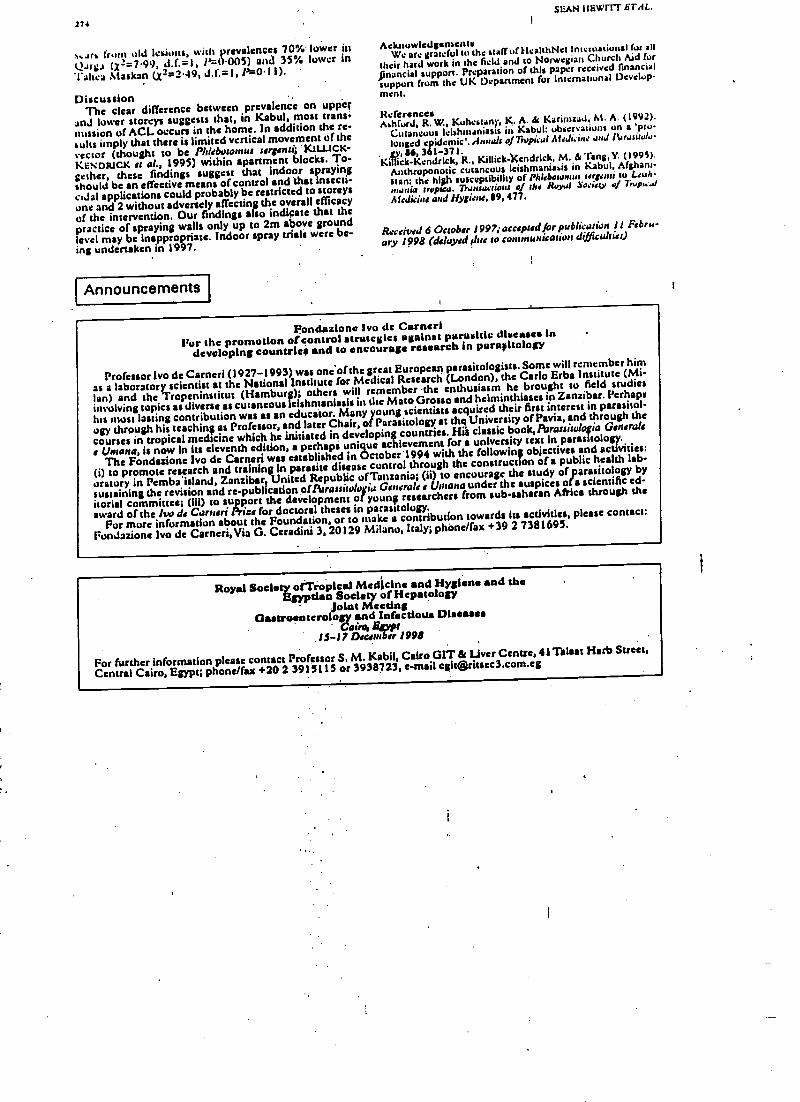
:74
a:an from old lesions, with prevalence, 70% lower in(.l.trgs (X= =7.99, d.f.=1, P=0.005) and 35% lower in'l'ahea Alaskan (x= =2.49, d.f.=1, I'= 0.11).
DiscussionThe clear difference between prevalence on upper
and lower storeys suggests that, in Kabul, most trans.mission of ACL occurs in the home. In addition the re-sults imply that there is limited vertical movement of thevector (thought to be PIJtbutosnus sergenti; .KtWCK-KENDRICK er 019 1995) within apartment blocks. To-gether, these findings suggest that indoor sprayingshould be an effective means ofcontrol and that insecti-cidal applications could probably be restricted to storeysone and 2 without adversely affecting the overall efficacy
of the intervention, Our findings also indicate that thepractice of spraying walls only up to 2m above groundlevel may be inappropriate. Indoor spray trials were be-ing undertaken in 1997.
Announcements
SEAN I I EVPITf !iTAL.
AcknowledgementsWe are grateful tu the staff of HcalthNet international for all
their hard work in the field and to Norwegian Church Aid for
financial support. Preparation of this paper received financialsupport from the UK Department for International Develop-
ment.
ReferencesAshford, R. W., Kuhestanl, K. A. & Karimzad. M. A. (1992).
Cutaneous Ieishmaniasts in Kabul: observations on a 'pro-
longed cpidcmie. dnnah o/Tropieai AfeJi. i,te und 1 Lrwilulo-
. sy, 86, 361 -371.Killick- Kendrick, R., Killick-)Çndrick, M. ä Tang, Y. (1995).
Anthroponotic cutaneous Ieishmanissis in Kabul, Afghani-stan: the high susceptibility of Phleboronrus lagoon to Leuh-?l&mia trrpua. 7linsactio,B of the Royal Sociay of Trop,:.dA1Jicine and Hysieno,119, 477.
Received 6 October 1997; acceptedfor pubIi anion 11 Febru-
ary 1998 (delayed Flue to con.nwnicarion d, ficultier)
Fondazione No de CarneriFor the promotion of control strategies against parasitic diseases in
developing countries and to encourage research in paragitology
Professor No de Carneri (1927 -1993) was one of the great European parasitologists. Some will remember him
as a laboratory scientist at the National Institute for Medical Research (London), the Carlo Erba Institute (Mi-
lan) and the Tropeninstitut (Hamburg); others will remember the enthusiasm he brought to field studies
involving topica as diverse as cutaneous lelahmaniasis in the Mato Grosso and helminthiases in Zanzibar. Perhaps
his most lasting contribution was as an educator. Many young scientists acquired their first interest in parasitol-
ogy through his teaching as Professor, and later Chair, of Parasitology at the University of Pavia, and through the
courses in tropical medicine which he initiated in developing countries. Hi's classic book,Parassírulofia Generals
t Untanet, is now in hs eleventh edition, a perhaps unique achievement for a university text in parasitology.
The Fondazione No de Cernai was eitablished in October 1994 with the following objectives and activities:
(i) to promote research and training in parasite disease control through the construction of a public health lab-
oratory in Pemba"island, Zanzibar United Republic ofTanzania; (ii) to encourage the study of parasitology by
sustaining the revision and re-publication ofParassiwlogia Generals a Umana under the auspices offa scientific ed-
itorial committee; (iii) to support the development of young researchers from sub- asharan Africa through the
award of the Iw de Carneri Phut for doctoral theses in parasitology.For more information about the Foundation, or to make a contribution towards its acdvitics, please contact:
Fondazione No de Carneri, Via G. Ceradini 3, 20129 Milano, Italy; phòne/fax +39 2 7381695.
Royal Society o[Ts opical Medicine and Hygiene and theEgyptian Society of Hepatology
joint MeetingGastroenterology and Infectious Diseases
Cairo, EgyptIS -17 Dmanbsr 1998
For further information please contact Professor S. M. Kabil, Cairo (HT & Liver Centre, 41 Talaat Herb Street,
Central Cairo, Egypt; phone/fax +20 2 39151 15 or 3938723, e -mail c([email protected]
1
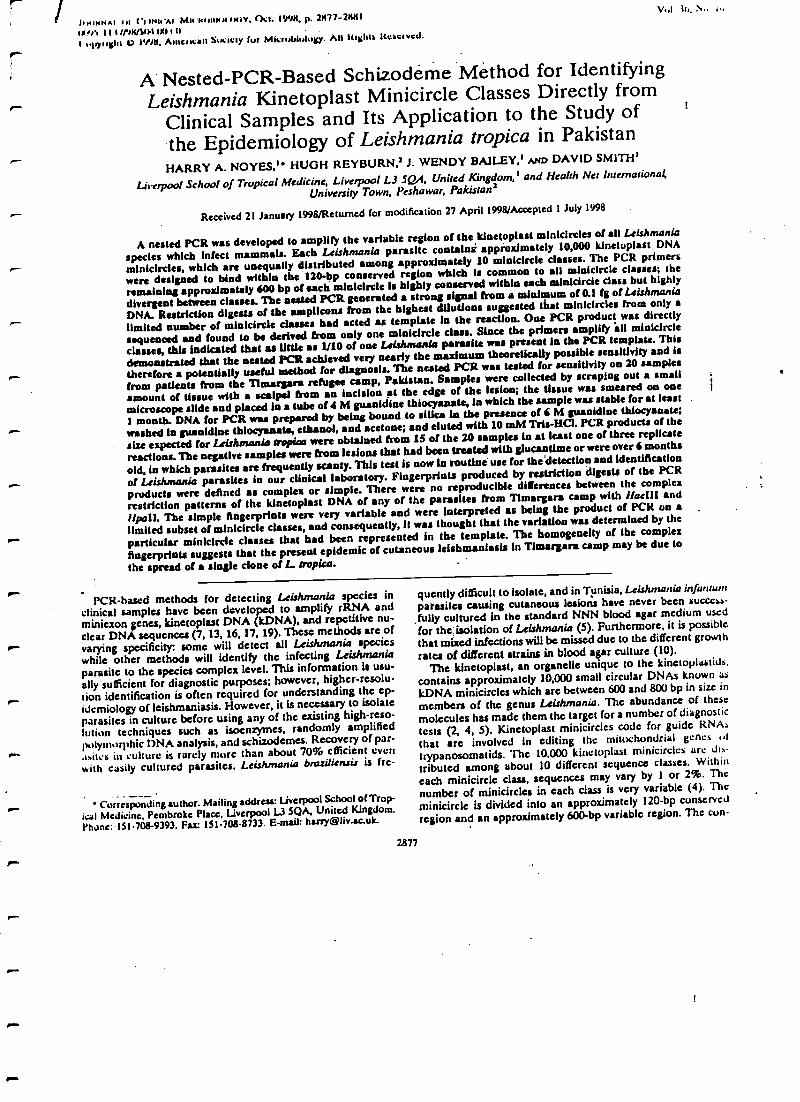
r-
,1111
--
r
1..11KNA1 ul t'I u+irAl MwUKUKlulrxiv, lkl. NN!$, p. 2$77-2/011
I/N1 II l //7$/31}1 1J0 I tl .
nlryuahl O I'M, A1nelK:an Sucicly fur Miaubtulugy. All Itlahta Itcae/ved.
WI II., N.. ,,
A Nested -PCR-Based Schizoderne Mèthod for IdentifyingLeishmania Kinetoplast Minicireie Classes Directly from
Clinical Samples and Its Application to the Study of
the Epidemiology of Leishmania tropica in PakistanHARRY A. NOYES," HUGH REYBURN,2 J. WENDY BAILEY,' AND DAVID SMITH'
Liverpool School of Tropical Medicine, Liverpool L3 SQ.A, United Kingdom,' and Health Net Intemationa4
University Town, Peshawar, Pakistan2
Received 21 January 1998/Returned for modification 27 April 1998/Accepted I July 1998
A nested PCR was developed to amplify the variable region of the kinetoplast minicircles of all Lelshmania
species which infect mammals. Each Leishmania parasite contains' approximately 10,000 kinetoplast DNA
minicircles, which are unequally distributed among approximately 10 minicircle classes. The PCR primers
were designed to bind wtthia the 120-bp conserved region which Is common to all minicircle classes; the
remaining approximately 600 bp of each minicircle is highly conserved within each minicircle class but highly
divergent between classes. The nested PCR generated a strong signal from a minimum of 0.1 fg of Leishmania
DNA. Restriction digests of the amplicons from the highest dilutions suggested that miniclrcles from only a
limited number of minicircle clauses bad acted as template in the reaction. One PCR product was directly
sequenced and found to be derived from only one minicircle class. Sines the primers amplify all minicircle
classes, this indicated that as little as 1110 of one Leishmania parasite was present In the PCR template. This
demonstrated that the nested PCR achieved very nearly the maximum theoretically possible sensitivity and is
therefore a potentially useful soetbod for diagnosis. The nested PCR was tested for sensitivity oa 20 samples
from patients from the Timargara refugee camp, Pakistan. Samples were collected by scraping out a small
amount of tissue with a scalpel from an incision it the edge of the lesion; the tissue was smeared on one
microscope slide and placed in a tube of4 M guanidine tbloganate, la which the sample was stable for at least
1 month. DNA for PCR was prepared by being bound to silica in the presence of 6 M guanidine thlocyanate;
washed In guanidine thloganate, ethanol, and acetone; and eluted with 10 mid Tris -IICI. PCR products of the
size expected for Leishmania tropics were obtained from 15 of the 20 samples in at least one of three replicate
reactions. The negative samples were from lesions that had been treated with glucantlme or were over 6 months
old, in which parasites are frequently scanty. This test is now to routine use for the detection and identification
of Leishmania parasites to our clinical laboratory. Fingerprints produced by restriction digests of the PCR
products were defined as complex or simple. There were no reproducible differences between the complex
restriction patterns of the kinetoplast DNA of any of the parasites from Timargara camp with Mull! and
!!pall. The simple fingerprints were very variable and were interpreted as being the product of PCR on a
limited subset of minicircle classes, and consequently, it was thought that the variation was determined by the
particular minicircle classes that had been represented In the template. The homogeneity of the complex
fingerprints suggests that the present epidemic of cutaneous leishmanlasis in Timargara camp may be due to
the spread of a single clone of L. tropica. .
PCR -hascd methods for detecting Leishmania species inclinical samples have been developed to amplify rRNA andminiexon genes, kinetoplast DNA (kDNA), and repetitive nu-clear DNA sequences (7, 13, 16, 17, 19). These methods are ofvarying specificity: some will detect all Leishmania specieswhile other methods will identify the infecting Leishmaniaparasite to the species complex level. This information is usu-ally sufficient for diagnostic purposes; however, higher-resolu-tion identification is often required for understanding the ep-idemiology of leishmaniasis. However, it is necessary to isolateparasites in culture before using any of the existing high -reso-lution techniques such as isoenrymes, randomly amplifiedpolymorphic DNA analysis, and schizodemes. Recovery of par-
r` .rates in culture is rarely more than about 70% efficient evenwith easily cultured parasites. Leishmania brasiliensis is fre-
Corresponding author. Mailing address: Liverpool School of Trop-
ical Medicine. Pembroke Place, Liverpool l3 SQA. United Kingdom.Phone: 151.708 -9393. Fax 151. 708.8733. E -mail: [email protected].
2.877
quently difficult to isolate, and in Tunisia, Leis unania injanlumparasites causing cutaneous lesions have never been success-fully cultured in the standard NNN blood agar medium usedfor the :isolation of Leishmania (5). Furthermore, it is possiblethat mixed infections will be missed duc to the different growthrates of different strains in blood agar culture (10).
The kinetoplast, an organelle unique to the kinetoplastida,contains approximately 10,000 small circular DNAs known askDNA minicircles which are between 600 and 800 bp in size in
members of the genus Leishmania. The abundance of thesemolecules has made them the target for a number of diagnostictests (2, 4, 5). Kinctoplast minicircles code for guide RNAsthat are involved in editing the mittxhondrial genes it
trypanosomalids. The 10.000 kinetoplast minicircles are dutributed among about 10 different sequence classes. Withineach minicircie class, sequences may vary by 1 or 2%. Thenumber of minicircles in each class is very variable (4). Theminicircle is divided into an approximately 120 -bp conserved
region and an approximately 600 -bp variable region. The con-
:::78 NUl'ES f:T Al..
served region contains shorter blocks that arc conservedIh ,11100 t the genus Leishmania and in some other tryp;uu)-sonl.tÚds as well. These conserved sequence blocks are idealLogrts tits )'l'I: printers which can amplify all known lUi-nicirelc classes from all Leishmmaia species. The high copynumber of the Le-is/mum/a minicircics makes then) an idylltarget for diagnostic tests. The heterogeneity of the variablelegion has been exploited to discriminate between strains ofthe saner species. Digestion of the kinctuplast DNA \with ic-sto'coon enzymes yields fingerprint patterns that vary cunsid-ci.Ihly within each Leishmania species. Populations that aredefined by shared fingerprint patterns are known as
schizodemes. and the technique is known as schizudeme anal -
vsis Schizodewe analysis has been widely used in the NewN'(í1(1 lei the Classilieation of Ltis'hauuriu and 7))y,urtsrsunar
rnr:a. The fingerprint patterns themselves provide one of themost specific ways available to identify Leishmania strains (I,9). kDNA for schizodeme analysis has usually been preparedby differential centrifugation of total DNA from cultured par-
- asites, although it has been shown that kDNA can also beprepared by PCR amplification of purified parasite DNA (3,15). A nested- PCR -based schizudeme method that permitsboth very sensitive detection and high- resoluticin identificationof Leishmania parasites directly from clinical samples is pre-
sented here.
htATERIALS AND METHODS
Clinical samples. DNA was prepared from clinical samples collected during apre%aience survey in the Timargara refugee camp. The Timargara refugee camp,In Du in northwest Pakistan. is a settled camp of IS years' standing. There areabout IU.000 residents, nosily refugees from the Kabul area of Afghanistan.Small numbers of cases of cutaneous kishmaniasis have been observed sinceIy.% In 1997. it mote outbreak occurred. with up to 2(IG' of the population ofthe coup being affected Lesvos consistent with euiane Icishnt ;uti;uis werecleaned with MLIII and wale' aiwl swabbed with ethanol. Samples were laden byusing a sterile scalpel to make an incision in the binder of the lesion. and a smallamount of material wits scraped out. The sample with divided between one thinsmear on a microscope side and an Eppendo rf tube containing 5(i pl of 4 Mguanidine thioeyanate (GuSCN) -0.25 M EDTA. Microscope slides were stainedwith Gients.i stain for direct deter of parasites: GuSCN lysates were storedat 4Y our 1 niomh ,,mil shipment to the United Kingd at ambient temper-Auer; (ur PCR analysis.
Preparation of DNA samples. Template DNA was extracted front aliquots of50.250. and IOU ill of the GuSCN lysate. Briefly. the sample was bound todiatomaceous earth (Sigma) in the presence of 6 M GuSCN. washed with ethanol
t and acetone. and clued with 50 pl of IO mM Tris.HCI (pH 8.4) (6). Onemicroliter of template was used in the firstround PCR. DNA was both preparedfrom all 211 samples and amplified by PCR at least three times. Each replicatehatch was prepared independently front previous hatches with fresh sets ofreagents. One set of replicates was prepared in a separate laboratory that had notprcuausly been used for Lris/rnianiu work. DNA of reference -strains was pre-pared by standard method (1 I ).
NeuedPCR conditions. External primers CSB2XF (C /GA/GTA/GCAGAAACYTC'C'CG1'TCA) and CSLI IXIt (Ai I I I ICG /CGA/iTTT /CGCAGAACG)mete designed by identilyittg suitable regptns around conserved sequence blocks
I and 2 in an alignment of DNA sequences front Leis/meanies guyane . Leiste.
penir . L. luu :,broom. I.. info . and Leislunani,, uupica. The primers were designed to be external to printers 13Z (ACTGGGGGTTGGTGTAAAATAG) (19). which is homologous to conserved sequence block 3 (iS). andLift (TCGCAGAACGCCCCT) (15), which is complementary tit conserved sequence block I. The conserved sequence Nock I is too small for two independentprimers. and consequently. the lU .V bases of CSUI XR are the some as the IU 5'bases of LiR. Firstraund PCR mixtures contained 2.11 mM MgCl2. 200 )LM
deosynucleostde triphasphales. 211 niM (NH.),SO.. 75 niM TrisHCI (plI V.0).0111x, Tween. 114 U of Red Hut Tay (Advanced Bioteehnulogles. Lentherleud.United Kingdom). and 411 ng each of primers CSB2XF and CSUIXR in ü finalsolumc of 20 pl The c -cling card. . were WC for 300 s. followed by 30 cyclesit v4(' our 311 s. SiC for MI a. and 72C for 911 s in u Techne Prugcne Merino.cycler One nucrnliler of a 9:I dilution in water of the first -round product wasused as template too the second ruunid in a total volume of 30 pl under the same
c Maui. ls those lull the hnsl round. except with primers LiR and I3Z. 1h ice.- ,un''ohters of the secondround PCR product was loaded unto a i', agonise gel
to confirm amplification. Positive samples were digested by the addition of I Uof reorichon enzyme. 15 pl of restriction enzyme buffer. and 14 pl of wafer to1:5 pl of PCR product and incubation for Ili h. The restriction digests were
1766.
1033-
653-317
29$-
FIG. I. Agarrua: (1.5 %) gel of products of the nested PCR un varuus .pss nof trypunr»umutid (lunes I tu 17) and the PCR with primers for the huu,..i /.sgene (lane IS). Lane M. lioehringer Mannheim molecular weight mar co .. t VI
lane 1. L. unruzunr MHOM /BI(/73/t. V7H: lame 2. 1. guiv.+r.ri Ml h+l.l our75/M4147: lane 3. 1.eisl w / vim MI IOM /NI /H7 /I S94 lari i I ..i ....
conierei MCAV /lilt /45 /LHH: lane S. L urr.wun., MN Y( /11//6.1/61' I..... .Leislunania inju ) M110M /11N /H7 /HN29. eau. 7. 1.MHOM/iNMIVIP'l'1; lane 8. L. tropic:I MI-10M /IR /H9/AR D22. lane 9, t. i,,.p ,
MHOM /PK/97/37\13; lane IU, L. rrrujur MHOM/El'N5 /FV I (570bp). lanemajor MHOM/ET /XX/LV3U3: lane 12, E. mu,uervxeii MCHO/CWn2 /LvuM.Av
lane 13. L rarenro/uc RTAR/DZ/39/i'urV1;LV414. lane 14. blood .ample :,1lected from patient in Guatemala. positive with 7: cn.zispeclhc primers (Ai tan.
15. T. Inni MHOM /BR/7A/SilviuXIlk lane 16. 7. Moca rhwleslr+rsr MIi(IM.11(.XX/WB25;G; lane 17. negative control: lane IH, primers for p5.1 hum. ,,, ben:..,,
clinical sample 1 front Pakistan (MHOM /l'N')7/I2131). Numhers at Icil
size in base pairs.
CI IN hilt 11, .lu, .1
M 1 2 3 4 5 6 7'8 9 101112131415161718
separated on u 1.5% I:1 Nualeve ;d as .gel to visuahtr the ..nu..,u. u.
patterns. Samples were tested for the presence of amplifiable hum .,,, rely\ .:n.primers for catin x of the single-copy hu,uun pt.l rumor suppress, n gs us Ih9LEB, TTGGGAGTAGATGGAGCCT. unit Il/9RE. AG1'GTTAGA(' 1 (.(. \ AACTiT) (12). These primers generate a 443.hp product and were used ,,ode.
same conditions as those for the nested PCR.DNA sequencing. DNA for sequencing was prepared by the uesicd l'( It 11..
firstround product was rcamplified with printers LUR and Ill in a hital ...Item,
of I(10 pl. Printers and den aynucleuside (liphuspbates were winos cd u., ..i. , he.
spin eulunnl (lib ;u ntacia). the DNA was precipitated with et moil .a. I i,,,
sample was submitted for cycle sequencing with printers LIR and 1.1Z1Z ur..w \IIIPrism Model 377 cycle sequencer.
Nucleotide sequence accession number. Nucleotide sequence dal...c ¡hothis paper have been submitted to the ( ieullank database wall the .l oa y.,. ...AF032997.
RESULTS
Specificity of PCR. The nested primer set was tested ion'DNA from a panel of Leishmania species and was found togenerate a single major product from representatives of allmajor species complexes of Leishmania that are inleetn.e to
humans:(Fig. 1). No product was detected from DNA utTrypanosome bnlcei rhodesiensc or from the lizard Lershmu,niui
parasite Leishmania larenlulae. kDNA from Enderive / minnlonlerogeii, a closely related parasite of sloths, was amplifiedA product of 300 bp was amplified from 10 pg of purihcd /cruzi DNA but not from n clinical sample from a 7 uIl_r-infected patient (Fig. I. lanes 14 and 15). L. iropice genctatc:Li
the largest Leishmania species PCR product (750 hp) andcould be distinguished with care from L. injunfunl (680 bp) and
more easily from Leishmanie major (560 hp). It was Oleicfoiepossible to identify the Old World human-infective Lershn,uswicomplexes on the basis of size alune. The New World biazlliensis complex could not he distinguished from Leis/ 1 auauu
ntexicana on the basis of size. although the smaller Lersluu,m,aanlazonensis product was readily identifiable. The E. aunae,u-geii product (780 hp) was slightly larger than the other t`t:wWorld Leishnuulia species products.
Sensltivlty of PCR. Decimal dilutions Itunr 5(0 pg to I a): ul
L. infanwnf MHOM/TN/80 /II'TI total DNA p.1 ' were anlpl :-
fied by the nested PCR and digested with HaeIll to determinethe limit of detection and the effect of concentration on fin-
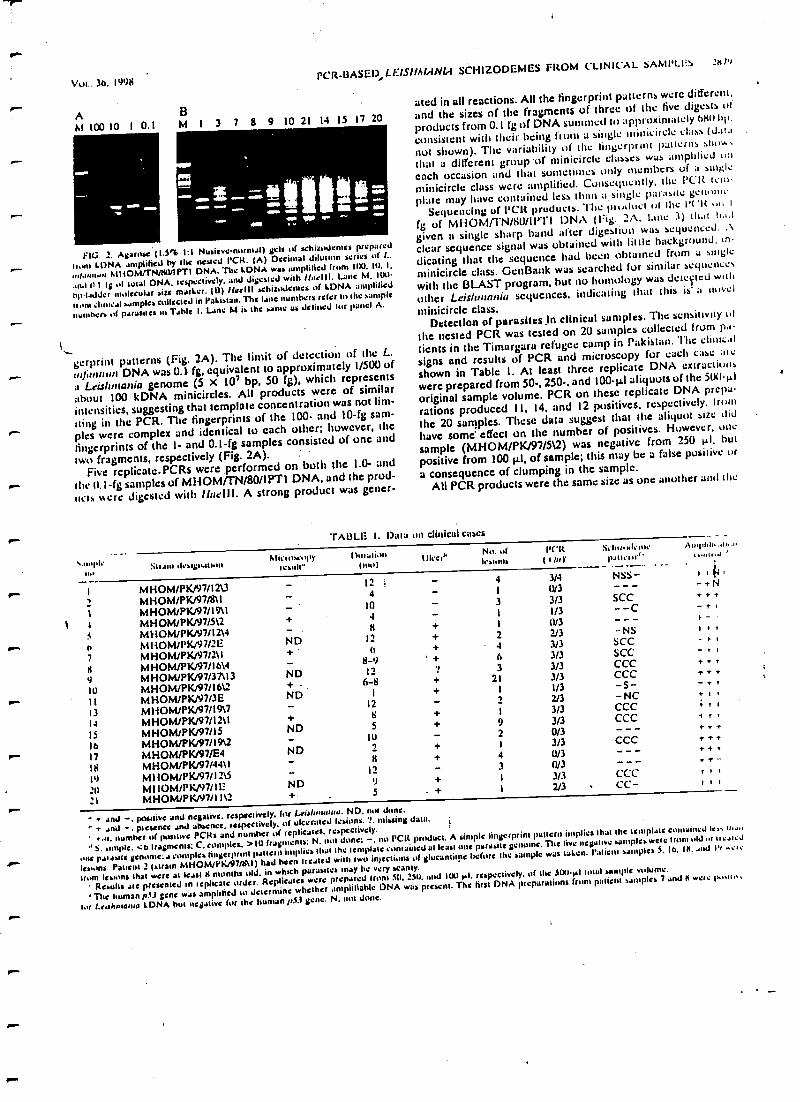
VUI.. 36.1998
rPCR-14ASG1) Ll:-lS!lMeINI.1
SCHIZODEMES FROM CLINICAL SAMPLES 2tt)1
A BAt 100 10 1 0.1 M 1 3 7 8 9 10 21 14 15 17 20
--
FIG. 2. Avulse (1.5% 1:1 Nusievc.mxmal) gels of schizotfentes preparedf atom IDNA amplified by the tested VCR. (A) Decimal dilution :cries of l..
MNOM/rNI WIPTI DNA. Tiw LONA was amplified from 1D0, I0, I.
.std Il t I` .d total DNA. tcspectivcly, and digested with /Ideal. Lane M, 100
bpt.idJcr molecular size mailer. (U) lluelli achiztxkincs of kDNA amplified
noon tuu:al samples collected in Pakistan. The lane numbers refer to the sample
numbers of parasites ul Table I. Lane M is the same as donned kir panel A.
gerprint patterns (Fig. 2A). The limit of detection of the L.
,n /i)nn,nr DNA was 0.1 fg, equivalent to approximately 1/500 of
a Leis/fn(ania genome (5 x l0' bp, 50 fg), which represents
about 100 kDNA minicircies. All products were of similar
intensities, suggesting that template concentration was not lim-
iting in the PCR. The fingerprints of the 100- and IO -fg sane-
r pies were complex and identical to each other; however, the
fingerprints of the t and 0.1 -fg samples consisted of one and
two fragments, respectively (Fig. 2A).Five rcplicatc.PCRs were performed on both the 1.0- and
the 0.1-fg samples of MHOM/'TN /80/1PT1 DNA, and the prod-
ucts were digested with Bari!. A strong product was gener-
ated in all reactions. All the fingerprint patterns were different,
and the sizes of the fragments of three of the five digests of
products from 0.1 fg of DNA sununwd to approximately 6811 his.
consistent with their being from a Singh; minicircle class (data
not shown). The variability of the fingerprint patterns shows
that a different group or minicircle classes was amplified on
each occasion and that sometimes only members of a single
minicircle class were amplified. Consequently, the l'CJR tem-
plate may have contained Tess than a single parasite geia aiii
Sequencing of l'CR products. The product sit kite l'('R u I
fg of MHOMTTN /80/1PTI DNA (Fig. 2A. lane 3) That Ia.l,l
given a single sharp band after digestion was sequenced. A
clear sequence signal was obtained with little background, an
dicating that the sequence had been obtained from a single
minicircle class. Genl3ank was searched fur similar icyucncc,
with the BLAST program, but no homology was dews:led with
other Lcisltutnnia sequences,indicating that this is' a novci
minicircle class.Detection of parasites in clinical samples. The sensitivity of
the nested PCR was tested on 20 samples collected from pa-
tients in the Timargara refugee camp in Pakistan. The cliiticat
signs and results of PCR and microscopy for each case ate
shown in Table I. At least three replicate DNA extractions
were prepared from 50 -, 250 -, and 100 -µ1 aliquots of the 500-µl
original sample volume. PCR on these replicate DNA prepa-rations produced 11, 14, and 12 positives, respectively. trout
the 20 samples. These data suggest that the aliquot size did
have some' effect on the number of positives. However, one
sample (MHOM /PK/97/512) was negative from 250 AI. but
positive from 100 µl, of sample; this may be a False positive or
a consequence of clumping in the sample.All PCR products were the same size as one another and the
TADLL I. Data un dinlcul crocs
S.utyttotu 5uaw Jsigo:uto
MitYtrxopyteanit"
I)utali.ulIMO)
tlket~Hai. oflestons
PC'R( thaY
So. dxi. Ii iii'panetti''
Awplib, ..w.0
MHOM/PK/97/121312 : - 4 3/4 NSS - tt114,
MHOM/PK/97/8\14 - 1 IU3
MHOM/PK/97/I9\I10 - 3 3/3 SCC
*+N
1 t MHOMlPKN7/512 + 4 - I 1/3 --C - r l
j MHOM/PK/97112148 + t (1/3 --- r-
n MHOM/PK197/2E ND 12 + 2 2/3 -NS / t ,
7 MHOMIPKN7121I(a + 4 3/3 SCC - r I
M HOM/PK/97/1 ól48-'I ` + 6 3/3 SCC - i
9 MHOM/PK/97/37\13 ND 12 7 3 3/3 CCC + + r
IU MHOM/PK/97/l6\2 + 6-8 + 21 3/3 CCC + + +
Il MHOM/PKN7/3E ND 1+ 1
1/3 -S- - + I
13 M HO M/PK/97/ 19\712 - 2 2/3 -NC +It
l4 MHOM/PK/97/1211 + 8 + I 3/3 CCC : r i
15 M H OM/PK/97/15 ND 5 + 9 3/3 CCC + r '
16 MHOM/PK/97/19\2IU - 2 0/3 - - - r++
17 MHOM/PK191/E4 ND 2 + I 3/3 CCC + + +
18 MHOM/PK/97/44 \ I 8 + 4 0/3 - - - ++r
1') M11OM/PK/97/12\512 - 3 0/3 --- ++ -
20_1
MI IOM/PK/97/ I 1:MHOM/PK/97/I 1\2
ND+
4S
++
1
1
3/32/3
CCCCC-
r I i
1 t t
* and -, Positive and negative. respectively. for Lciahmwuu. ND, not dune.
' + aria -. presence and absence, tespectivety, u( ulcerated lesions. ",.'Musing dale.
.,n. number of positive PCBs and number of replicates, respectively.
S. simple, <o Iragments: C, complex. > IO fragments: N. not done: -.110 rat product. A simplefingerprint pattern implies that the let:Ti le conlaincd I..' in.n
one psi aim{ yenonle: a colllptesfingerprint pUlleln ii11pliea that the lenlplate contained al least one parasite genuine. The live negative samples were from ola of a c.I.J
lesions. Patient 2 twain MHOM/PKi97n111)had been treated wish Iwo injections of glucantime before the sample was taken. Patient samples 5. in, lit..tnJ l', ..ele
Iran lesions that were at least s months old. in which parasites may IN very scanty.
Result& arc presented to Ieplicate order.Replicates were prepared from MI. 250. anal KM Isl, respectively, of Me 3011.µl total sample volume.
' The human p03 gene was amplified to determine whetheramplifiable DNA was present. The fim DNA preparations from patient aanlplea 7 and It were
104 Leishntama LDNA but oeptive fiat Mc human p5.I gene. N, not done.
2680 NOYES ET AL
same size as an L. rropica reference strain, MHO/MR/89/ARD22 (14) (Fig. I, lanes 8 and 9); identification was con-
firmed by the similarity of the schizodeme pattern of all the
clinical isolates to that of MHOMAR/89 /ARD22 (data not
shown). DNA was prepared from aliquots of each of the 20
patient samples at least three times. Of the 61 DNA prepara-
tions, 38 were positive and 23 were negative for Leishmania
kDNA by the nested PCR (Table 1). Six of the reactions that
were negative for Leishmania kDNA were also negative for the
human pS3 gene, suggesting that some of the Leishmania neg-
atives may be false negatives (Table 1). Five of the eight reac-
tions which were negative for human DNA were performed on
DNA prepared from only 50 IA of the total sample volume of
500 µl; 50 µl is clearly not sufficient, since this sample volume
also gave the lowest number of Leishmania-positive reactions
(11 of 20). Negative controls were negative in all experiments.
Sehlaodeme analysis of clinical samples. The 11 positive
samples from the first set of replicates were digested with
Hae111 to prepare DNA fingerprints. Seven of the samples had
comptez fingerprint patterns containing 11 to 12 well-resolved
fragments (Fig. 2B; Table 1). Nine of the 12 fragments in the
complex fingerprints were present in all samples. A further two
or three fragments from a repertoire of four fragments were
also present. These variable fragments were not always repro-
ducible in replicate reactions from the same patient sample
(Fig. 2B). In contrast, the fingerprints prepared from the L.
infunrtun MHOM1IN/80/1PTI DNA dilutions were reproduc-
ible (Fig. 2A). The four remaining clinical samples each had
unique but simpler fingerprints, three of which had only four
fragments each (Fig. 2B; Table 1). The simple fingerprints
suggest that the nested PCR could detect a fraction of the
1)NA released from a single parasite.
DISCUSSION
Sensitivity of the bested PCR. The nested PCR detected
extremely small amounts of L. infantum kDNA (0.1 fg), which
was shown by sequencing to be derived sometimes from indi-
vidual minicircle classes. Since the primers are expected to be
able to amplify all minicircles present in the template, this
implies that only members of one minicircle class were present
in the template. This would be the case if there was only one
minicircle present in the PCR template; alternatively, sonic
minicircle classes might be preferentially amplified or the
classes might be nonrandomlydistributed throughout the sant-
pie from which the template was taken.It is unlikely that only single minicircles were present in the
template, given the higher-than -expected number of restriction
patterns, which were consistent with a single minicircle class,
and the absence of negatives that would be expected as a
corollary of frequent single minicircles. Preferential amplifica-
tion of some minicircle classes might occur if the extensive
secondary structure found in minicircles reduced the efficiency
of amplification of some minicircle classes more than that of
uttieni. Nunrandom distribution of minicircles among classes
might occur if groups of concatenated minicircles were from
the saute class.The nested PCB for detection of Leishmania In clinical sam-
ples. Fifteen patient samples from the Timargara camp were
positive in at least one of three replicate DNA preparations.
The five patient samples from the Timargara camp that were
negative in all three replicates were also negative by micros-
copy and were from lesions that had been treated or were over
7 months old, in which parasites are frequently very scanty
(Table 1). Therefore, these negatives may reflect either a real
absence of parasites from the small quantity of material col-
J. (:urv. Mu mama
lected by the smears or a lack of sensitivity in the test. Singe
there is no "gold standard" for detecting Leishmania parasites.
it is not possible to distinguish between these two reasons for
negative PCRs. Since 6 of the 23 Lcishrnania-negative DNA
preparations were also negative for the 03 single -copy human
gene, some of the negative reactions may have been the Lull-
sequence of low concentrations of patient material, inefficient
DNA extraction, or the presence of inhibitors. However, 2 of
the 38 Leishmania- postttve DNA preparations were negative
with the p53 human gene primen; the Leishmania product in
these cases gave simple fingerprint patterns (Fig. 1A, lanes 7
and 8) consistent with very low concentrations of target kDNA
The nested PCR can evidently detect at least some of the
10,000 Leishmania kDNA minicircles, even when a single -
round PCR cannot detect a single -copy human gene from the
patient sample. This confirms the extreme sensitivity of the
nested PCR and suggests that the samples that were positive by
the pS3 human gene primers and negative by the Leishrna,ua
primers really did not contain any Leishmania kDNA. This test
is now in routine use forthe diagnosis and typing of Icishman-
iasis in our clinical laboratory in Liverpool, United Kingdom.
Single -round PCR on the 120 -bp conserved region of Leu /,
mania minicircles is between 1 and 3 orders of magnitude more
sensitive than single -round PCR on the approximately 700 -hp
variable region which was used in this study (2, 19). Single -
round PCR on the conserved region may therefore be more
suitable for diagnosis in areas where it is not necessary to
identify the infecting species; however, it is less suitable for
epidemiological studies, since it is not possible to use the
product for high -resolution studies by schizodeme analysis.
The clinical appearance of the patients in the Timargara
camp from which samples were taken was very variable, as
were the number and duration of lesions (Table 1). Given the
variability of the pathtílogy and the similarity of the parasites,
the outcome of infection with L. rropica in Pakistan may lie
more dependent on the host response to infection than un the
particular strain of parasite involved.The complex fingerprint patterns prepared from the ct,n,ca1
samples were not fully reproducible on replicate DNA prepa-
rations from the same clinical sample. In contrast, the finger-
prints prepared from the L. injantum MHOM/TN /b0/1111.1
DNA dilutions werereproducible (Fig. M), as were tinge:-
prints prepared by digestion of products of single -round PCR
on phenol-chloroform- extracted DNA from cultured parasites
(15). 1f this fingerprinting method is to be used in epidcnurr
logical studies, at least three replicates from each isolate wi,uld
be necessary to confirm that the fragments included its the
analysis were reproducible.The simple fingerprint patterns were an artifact caused by
operating at the extreme limits of detection and should tic
excluded from any analysis of populations. Therefore, pr-
vided that caution is exercised in interpreting the fingerprint
patterns, the nested PCR followed by schizodeme analysis pro-
vides the fastest, most specific, and most sensitive method for
identifying Leishmania parasite strains available to date and
has considerable potential for epidemiological studies.
L. injantunn strains from around the Mcditerraneau .lie
highly variable by schizodeme analysis, and 21 distinct btr,ut
have been identified among five zymodemcs (i). in cuntr.r.,t,
there were no reproducibledifferences between the L. limo,a
strains from the Timargara camp in Pakistan with Haelt l and
Hpall, and these parasites therefore all belong to the same
schizodeme. An L. rropica strain (MHOM/PK 195/05) isolated
in another part of Pakistan 2 years previously was distinguished
from the samples collected in the Timargara camp by the
different mobility ofsingle fragments in both HMI! and Jipo I I
r
r-
.ih. 1998 PCR-11AJId1) LF'ISI/AIANLI SCIIIZODIsMItS FROM C'I.INIC'AI. SAh1Il.it1 :a+t
digests (data not shown). The homogeneous fingerprints of thesdntples from the Timargara camp are consistent with a recentepidemic spread of a single parasite clone. This is consistentwith the significant increase in prevalence of cutaneous leish-maniasis in the Timargara camp. However, further studies ofthe variability of L. tropics schizodemes will be required beforefirm conclusions can be reached about the utility of thismethod for the study of L. tropica epidemiology. There ap-pears to have been a large increase in cutaneous leishmaniasisin Kabul since 1992, and significant outbreaks occurred in partsof eastern Afghanistan and in refugee camps in northwestPakistan in 1997 for the first time (18a). The PCR -basedschizodeme technique has considerable potential for elucidat-ing the association between human migration and the spreadof cutaneous leishmaniasis in the region. Since the PCR prim-ers described here have amplified kDNA from all human -infective Leishmania species tested, this method should provevaluable as Well in other areas where Leishmania is endemic.
ACKNOWLEDGMENTS
The apparatus used in this study was purchased out of funds donatedQueen Marys Roehampton Trust, Wallington, . Surrey, United.glom, which is gratefully acknowledged.
The p5.i gene primers were kindly donated by T. Liioglou, RoyCastle Lung Cancer Research Institute, Liverpool, United Kingdom.
REFERENCESI Aageltct, M. C. M. Gramteda, and L Grades'. 1989. Study on genetic
p.,iyrndrphi.nt of Leàsfunario in/cottons through the analysis of restriciionenzyme digestion patterns of kinetoplast DNA. Parasitology 99:301 -309.
.. Aaktoed, D. A-, M. loua, M hubs, J. C. Miranda, 1. Sherlock, C. Eulalie,U. Lopes, O. Fernandes, W. Degzsre, R. H. latter, Jr., R. Baden, and J. R.David. 1995. Comparison of the polymerase chain reaction and serology forthe detection of canine annul kúh1machui. Am. J. Trop. Med. Hyg.53:251 -25s.
1. Aras, H, A. M. Guanine, N. Sand Nelms, C. M. Morel, and L Simpson.19th. Schnodeme analysis of Tryptusomena alai stocks from South and('cntral America by analysis of PCR- amplified minicircle variable regionuqucnea. Mol. Diodhem. Paruitol. 42:175 -187.
4. amidst, D. C. 1987. DNA diagnosis of human leishmaniasis. Parasitol. Today3:177 -184.
5. ses- lsauU, R., D. F. Solna P. D. Ready, A. Ayadl, M. Grsmlt<la. A. Ben-Osman, and M. S. ben- Racbld. 1992. Sporadic cutaneous Icishinaniasis inwith Tunisia: identification of the causative agent as Leishmanía Wantonsby the iase of a diagnostic dcosyribonucleic acid probe. Trans. R. Soc. Trop.Med. Hyg. 84:506 -510.
6. Doom, It., C. J. A. Sol. M. M. M. Sallmans, C. L Juen, Y. M. L. Mrnhruuvan D111ea, and J. van der Hourd... 1990. Rapid and pic meth..J I...purification of nucleic acids. J. Clin. Microbial. 28:495 -503
7, Delgado, O., P. Guevara, S. Silva, E. Belfort. and J. L *famines. pre.Follow -up of a human accidental infection by Lriihm.,nia (Viann.aiJis using conventional immunological techniques and pulymcra.c rhnmicaction. Am. J. Trop. Med. Ilyg. 55:267 -272.
8. Dorn, P. L, S. Selgean, and M. Guillet. 1997. Simplified mcehuJ for pi, .civilian and polymerase chain reaction amplification of 7ryp.nuww.w . ru..DNA in human blood. Mem. Inst. Oswald., Cruz 92:235-255.
9. Conceives, A. M., N. S. Nehme, and C. M. Morel. 19M. Trypan....,in.t.Jcharacterisation by schirademe analysis, p. 95 -109. In C M. Muicl (ed t.Genes and antigens of parasites, 2nd ed. Fundaçao Oawaldu C'rur. kw d.Janeiro. Brazil.
10. Ibrablm, M. E, A. J. Smyth, M. H. All, D. C. Barker, and A. Kharaaml. 19-stThe polymerase chain reaction can reveal the occurrence of naturally muesinfections with Leiehnania parasites. Acts Trop. 57:327 -332.
I I. Kelly, J. M. 1993. Isolation of DNA and RNA from LruIwnanw, p 123-111In l: E. Hyde (ed.). Protocols in molecular parasitology. vol. 21. 1iun,.n.Pretia. Totowa, N.J.
12. Uloglou, T, A. G. M. Seholed, D. A. Spaadidlos, E. U. Vaughan, A. S. Jun...and J. K. Field. 1997. p53 mutations in squamous ceU carcinoma of the he.dand neck predominate in a subgroup of former and présent smulcrs nublow frequency of genetic instability. Cancer 9C4.57:4070-4074.
13. Meredith, S. B. O., B. E. Zipatra, G. J. Schoen*, C. C. M. !Gruen. G. J. J. M.van Eys, K. U. Schaefer, A. M. El -H , and P. G. Dwyer. 1993 Lk. cl-op/none and application of the polymer chain reaction for the de c.ionand identification of Lebhnwnla parasites in clinical material. Arch In.iPasteur Tunis 70.419 -431.
14. Morarsdlu, H, H. Noya, and R. Malagas. 1996. LeuMan.a and Saura.,kishmarda: the use of random amplified polymorphic DNA for the went.fication of parasites from yertebrates and invertebrates. Esp. Parasnul 83:150 -154.
15. Noyes. III M. Change, C. Ponce, B. Punt-t, and R. Malay-es 1997 l.eu/v.wnia chassai: genotypically similar parasites from Honduras saure la oh to lacoral and cutaneous leishmaniasis in humans. Exp. Paruitol. 65:204-273
16. (Ilse, Z. M A. Mlles, and S. M. Wilson. 1995. Detection of parasites ut ihrLei:Io na:lie donownl complex by a polymerase chain reaction -solution bybridization enzyme -linked immunoassay (PCR- SHELA). Parasitology 110269-275.
17. Ramos, A., D. A. Maslow, O. Fernandes, U. A. Campbell, and L Stoy.ou.1996. Detection and identification of human pathogenic f.euhman ..J7ìylwrwruna species by hybridization of PCR -amplified minìrunExp. Paruitol. 82:242 -250.
18. Ray, U. S. 1989. Conserved sequence blocks in kinctoplaat min.uicte,diverse species of trypanosomes. Mol. Cell. Uiol >.1365 -1367
IBa.Reyban, H., and M. Rowland. Unpubli.hcd ubacrv.iwru.19. Rodgers, M. It, S. J. Popper. and U. F. Wirth. 1990. Amphlw..t..n .i
kinetoplast DNA as a tool in the detection and diagnosis of Lei's/sum." LipParaitol. 71:267 -275.
r
Van
J.71,14t.AI. OF CLINICAL htIt.Nl)UIOLrR)Y, O11. 1998, p, 2877-7.181
a103 I137NBriW.00.0lupynght O 1998. American Society for Micrahilllugy. All Rights Reserved.
Vol, )rl. No In
A Nested-PCR -Based Schizodeme Method for Identifying
Leishmania Kinetoplast 'Minicircle Classes Directly from
Clinical Samples and Its Application to the Study of
the Epidemiology of Leishmania tropica in Pakistan
HARRY A. NOYES." HUGH REYBURN,2 J. WENDY BAILEY,' AND DAVID SMITH'
Liverpool School of Tropical Medicine, Liverpool L3 SCI. United Kingdom,' and Health Net international,
University Town, Peshawar, Pakistan'
Received 21 January 1998/Returned for modification 27 April I998/Accepted I July 1998
A nested PCR was developed to amplify the variable region of the kinetoplast minicircles of all Leishmania
species which infect mammals. Each Leishmania parasite contains approximately 10,000 kinetoplast DNA
rinicircles, which are unequally distributed amongapproximately 10 minicircle classes- The PCR primers
were designed to bind within the 120-bp conserved region which is common to all minicircle classes; the
remaining approximately 600 bp of each minicircle is highly conserved within each minicircle class but highly
divergent between classes. The nested PCR generated a strong signal from a ritinimumt of 0.1 fg of Leishmania
DNA. Restriction digests of the ampllcons from the highest dilutions suggested that minicircles from only
limited number of minicircle classes had acted as template in the reaction. One PCR product was directly
sequenced and found to be derived from only one minicircle class. Since the primers amplify all minicircle
classes, this indicated that as little as 1/10 of one Leishmaniaparasite was present In the PCR template. This
dernorutrsted that the nested PCR achieved very nearly the maximum theoretically possible sensitivity and is
therefore a potentially useful method for diagnosis. The nested PCR was tented for sensitivity on 20 samples
from patients from the Timargara refugee camp, Pakistan. Samples were collected by scraping out s small
amount of tissue with a scalpel from an incision at the edge of the lesion; the tissue was smeared on one
microscope slide and placed in a tube of 4 M guanidine thiocyanate, in which the sample was stable for at least
1 month. DNA for PCR was prepared by being bound to silica In the presence of 6 M guanidine thfucyanate;
washed in guanidine lhlocyanate, ethanol, and acetone; and eluted with 10 mM Tris-11CI. PCR products of the
size expected for Leishmania tropica were obtained from IS of the 20 samples In at least one of three replicate
reactions. The negative samples were from lesions that had been treated swills glucaatitne or were over 6 months
old. in which parasites arefrequeotly scanty. This test is now in routine use for the detection and identification
Of Leishmania parasites in our clinical laboratory. Fingerprints produced by restriction digests of the PCR
products were defined as complex or simple. There were no reproducible differences between the complex
restriction patterns of the kinetoplast DNA of any of the parasites from Timargara camp with Haelll and
1lpaH. The simple fingerprints were very variable and were interpreted as being the product of PCR on a
limited subset of minicircle classes, and consequently, It was thought that the variation was determined by the
particular minicircle classes that had been represented in the template. The homogeneity of the complex
fingerprints suggests that the present epidemic of cutaneous leishmaniasis in Timargara camp may be due to
the spread of a single clone of L. tropica.
PCR -based methods for detecting Lu#unanw species in
clinical samples have been developed to amplify rRNA and
ntinìexon genes, kinetoplast DNA (kDNA), and repetitive nu-
clear DNA sequences (7, 13. 16, 17, 19). These methods are of
r- Varying specificity: some will detect all Leishmania species
while other methods will identify the infecting Leishmania
parasite to the species complex level. This information Is usu-
ally sufficient for diagnostic purposes; however, higherresolu-
r, lion identification is often required for understanding the ep-
idemiology of leishmaniasis. However, it is necessary In isolate
parasites in culture before using any of the existing high -reso-
lution techniques such as isoenzymcs, randomly amplified
polymorphic DNA analysis. and schizodemcs. Recovery of par -
.rsites in culture is rarely snore than about 70% efficient even
with easily cultured parasites. Leishmaniabrasilieruis is fre-
.r- Coo responding author. Mailing address: Livetp ool School of Trop-
It'll Medicine. Pembroke Place, Liverpool U 5QA. United Kingdom.
)'hune: I51. 708.9393. Pas: ISI- 708.8733. E-mail: [email protected].
2877
quently difficult to isolate, and in Tunisia. Leis /vnania infunru ti
parasites causing cutaneous lesions have never been success-
fully cultured in the standard NNN blood agar medium used
for.the isolation of Leiahmania (5). Furthermore, it is possible
that mixed infections will be missed due to the different growth
rates of different strains in blood agar culture (I0).
The kinetoplast, anorganelle unique to the kinetuplastlds,
contains approximately 10,000 small circular DNAs known as
IcDNA minicircles which arebetween 600 and 8Q0 bp in size in
members of the genus Leishmania. The abundance of these
molecules has made them the target for a number of diagnostic
tests (2, 4, 5). Kinetopiast minicircles code for guide RNA\s
that are involved in editing the mitochondria) genes .if
trypanosomatids. The 10,000 kinetoplast ntinictrcles are dis-
tributed among about 10 different sequence classes. Withal
each minicircle class, sequences may vary by I or 2%. The
number of minicircles in each class is very variable 14) The
minicircle is divided into an approximately 120.bp unscrve.l
region and nn approximately 600 -bp variable regius. "I he iul
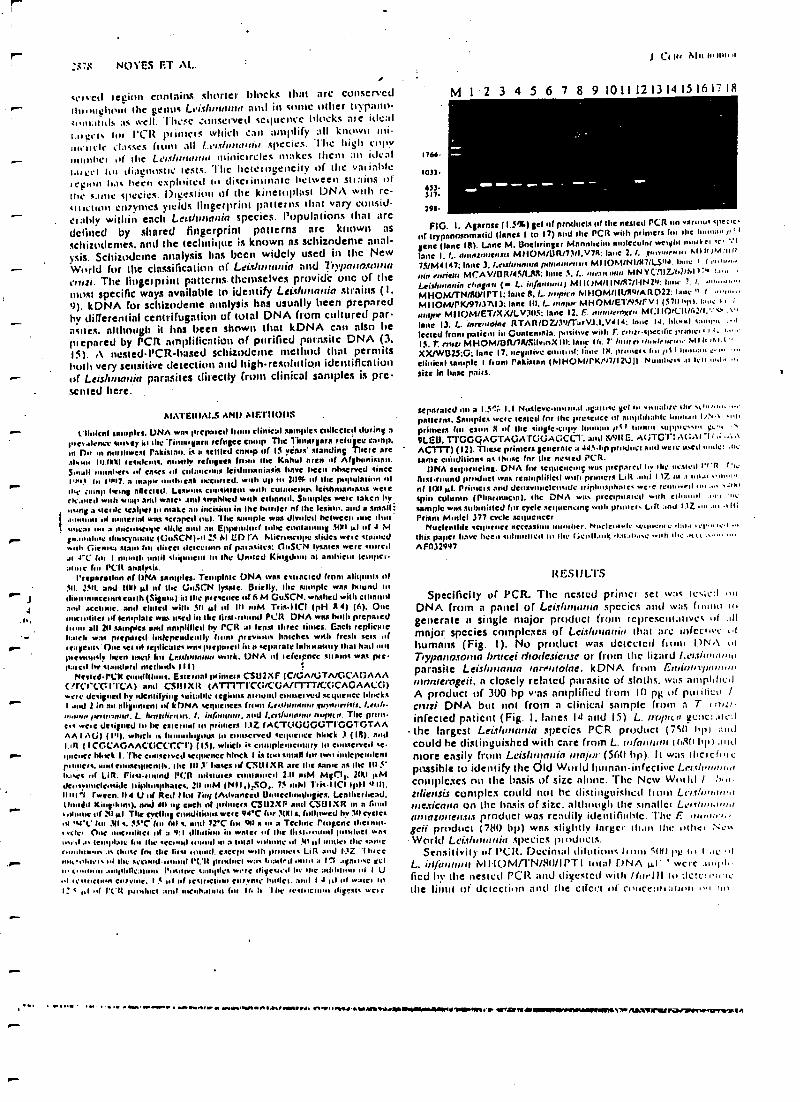
:i7$ NU1"f:S FT AL.
trlvctl legion contains shorter blocks that arc conservedr tbloughonl the genus Lei :fhnuutto anti in sortie outer tn'pano-:..utauJs as well. These ,unscrved sequence blocks ate ideall.0 gets foie l'CR plin els which can amplify all known ¡ni-
iintIc atsses (tuns all L1t.c /urtw,ti.t species. lhe high copyuonlll(I of the Lets/if/soma nlinicircles makes them In ideal¡meet lot diagnostic tests. The heterogeneity of the variableICpaut h.1s been exploited lu discriminate between sitains ofthe smile species. Digestion of the kinetoplasl I)NA with rc-tult:uun ci7vnleS yields fingerprint patterns that vary cunsid-claldy within each Ler.tlU,mnin species. Populations that arc
defined by shared fingerprint patterns are known ns
schizodemes, and the technique is known as schizodeme anal-ysis. Schizudcme analysis lias been widely used in the NewWorld for the classification of Lei.çiu,mnia and 7iV/)nnosOmn
cr1rzi. The Iingelplint patterns. themselves provide one of themost specific ways available to identify Leine main strains (I.t)). kDNA for schizodeme analysis has usually been preparedby differential centrifugation of total DNA from cultured par -asites. although it has been shown that kDNA can also be
pi epared by PCR amplification of purified parasite DNA (3.15). r\ nested-PCR-based schizodenle method that permitsbutt very sensitive detection and high -resolution identificationof Leishrnnuin parasites directly from clinical samples is pre-sented here.
r
r ,J
r-
r
r
JtIITERIAIS AND sMF.riIODs
Clinical samples. UNA was prepaled I clinical samples canceled touring atoo es dente misty in the Timugari refugee comp The limn /gain «hgee camp.m Dir m mnd,wesl Pakistan. is a stilled camp of 15 years' standing Titre are.dwan, II1JW) residents. mostly sefuples fowls Me cabin area et( Afghanistan.Small monl.era n( cases .d cminwenus !eiahutnniasis have been rthstrvCd tinCeLail In 1'$17. a maw, oulhoenk iscuned, with up u+ 2U?G of the psgWlnlinn itthe :amp Leong affected. Lesanns cnnsiutill WW1 culaieou, leishmamass weltcic.silet1 with snap amt wale, and awnhhed with ethnnul. Samples wcre taken by
.using :t sterile scalpel In ,,take an ineinhtdt in the border of she lesion. and a small:
1 in uuatnal WM scraped tom. The simlple wns divided helwcen 1111C IbntI su,ca0 to a micrutt..pe slide nod an Eppe,hlurf hd +e cunhunlog 31111 uI n( 4 M
g,.amdelc ihucylu, uI . IGI,SCN) -o 25 M ED rA Microscope slides welt stained»rah (lie now slam In1 direct detection of pa,asiles: 011504 Iysales were oaredal t "C In, 1 31110111 until ship,usenl Is+ the Unwed Kilted at ambient Iempcu
fns I'Clt analysis.Preparation et DNA samples. Template DNA was estrncied from aliqunls n(
Sd. 25n. and 11111 pi of the GuSCN lysate. Brielly, the sample was IM1und u1dbionuactinw earth (Sigma) in the presence of 6 M CuSCN. washed with ethanolaunt .ketone. and thned will 511 Al of to iiM Tris -iICI IpH R.4) (h). Oncunctltl11Cl u( lenlplalt wax used ill the first 1 Pelt DNA was hods ¡impaledt all 211 samples and amplified by root al lens) !Mee limes. Each replicatebeetle war pupated independently Mono previous Larches with fresh sets i(teapots floe set III repIICnICa wow prepped inn 'epirnIe hula t' ntm had nut(neenn.dr been wed for Lesthern work. DNA of left'rpnce sUarnt wits pre.p:ucui by tlalwlard nlclhtwh 11 I)
Neared -1CK toadllli,s. Eslernnl r"imss CSU2XF IC/GA /GTA/GCAGAAAC,rCeCCITTCA) anti C3IIIXR (ATT1TICc;/C Afr1TT/C:GCAGAACO)woe designed by,denli(ying suitable legions ;tomtit' cun.etvcd sequence blocksI and 2 in an nlignmenl of k DNA sequences (runs Lrs.dunmu.r,tu}stnr,id.g l.ertle
"ovum etenunnna. L. iarnedirisrt. I. he( , and Lilt /uinul, nrrintn. The primcis wc,e designed h, 111 estenud lu primers 11Z (ACT(ICGGOTIGGTGTAAAA J AG) (1'I), which is hunuduguus to tunserved sequence hock 3 ( Ili). and1. ,11 ( 1CGCAGAACC;CCCCT) (151. which is c plentenl :nv In eonsc,vcd sequc,KC hbrk 1. TLt clmse,ved sequence block 1 is tai an1,111$1w Iwo iodepeudcnlroomers. mod ennaegllends. the In 5' bates of C :SLIIXR are 11e same as the III 5'bases out Li R. Firs..ruund l'cn mhlures ennlanted 2.11 HIM MgClt. 2(111 OMdc.su+,dc.Itidt niphuapluges. 2(1111M (NI i.).S0. 7$ HIM Tull I ICI IpH 4JIi,Idol'( fermi. 1) 4 U wf Red Ilul Fag ¡Advanced Uiolecbnsdu,`i(s. Leallrerltcad.0m8160 King.kwn), nnu. ell no tuck 01 primers CS112XF and CSUIXR n1 n fund'olu,l.0 if 2iI al The cycling conditions were 94C fin 3181 n. (uauwed by 3f1 Cycleset %t' duo .1(1 a. NtC tu, All I. end 72C fm CIO s n1 a Teehne Progene theur lei One ,K, olilel u( a 4:1 'lib ttinn is wntCl .d 111e fi u..aonl ii,hh,CI wns..sill a Iemlwalc lot Ile acr,.ntl I in a 1u131 vii it 10;61 untkt 11e samernmdenes as thaw (nu the tiro ri tund. except with punnets Lift and I,'Z fh,ccaut,nlnrn ul thy st 1,1 1 rt.'lt pinluel was leaded rude is 111 agau.se gelu v.iem ...nptirtculnuu Pisu eve samples were digest: d In ,tut attihnn it I UI auinun ea7luue. 1 5 1.1 of iesu,dioo tnrvnle WdiH.:mil 1 .1 it or w :suet laI: t nl nl t'('ti pnaluct :nil incubation hit Ir. It 7Le reab,tluu+ Olen. weir
1 CI 114 111wnu,n
M i 2 3 4 5 6 7 8 9 101112131415161?1R
1766.
1033.
633317.
296.
FiG. 1. Aprnse (1.5%) geI n( prnducls of the nested PCR urn varu,,,sspencof trypnnnsmmatid (lanes 1 to 17) mid the PCR with primers fen the huuu :m I,' 1
gene (lane 18). Lane M. Uothringer Mannheim molecular cttl n,:,rl r, ac' :'IInne I, L. dmntmnen.us MHOM /UR 173 /I.V7R :lane 2. 1. ensuurnu. .i I If 3M ;t i It
75/M4147; Irrte 3. 1.tulrmnrun nementrrnsrs how o I eel
ein nuìtrrr MCA V /UR /45NJts: Inne 5. /.. neon nie,, MN YC.'li7.'tulrhl t 7 i.,,,, :.
Lelr/unmrin chnjnri (- L. «if I MID 0.4/1 Iwo. !. I. '..,...u.,..
MHOM(rN/RIYIPTI: Inne g. L. sonnen Mi1OM /IR/Ru!AR022; lane I loll..
MIIOM/PK/97I37113:Inne II).l.. Moil)" MHOM /ETNHFV I (57116). lam: I I i
mar, MIIUM /ET /XX /LV,II) :lane 12.L.,,urnrtenteu M( :iIo,cIt162r1.`,cs.vlane 13. L. inreerolne RTAR/OL39fTarVJ.1.V4 It; laue IJ, blond tame., .Ileered front patient in Cuntemnta. positive with T. cnrtr.gxcdic prime., i.:.1$. T. outs MHOM /U R/7R/SilvmX lit: Inn 14. 7' /mitre A,.drhrmv MI It ,st.IXX/wB25 ;G: lane 17. negative mallet: lane IN. pnnlc,a Int pt a I mo ...
clinical sample I (runt Pnk(srnn (MHOht /rKr'r7 /12U(I Nunthc,a al feu nab _'n
sine In boote pairs.
separated of a L5 ; 1.1 Nusievcnuamal avulse gel lo ynuahre the slams.,patients. Samples west: tested for the prise ice it anydd.alde human IU.N rahprimers fill cum S of the single copy 1 an ,u .t Latin aapp,l ae. et'. .
9LEU. TracQAGTAGATGG,At: ;cc1'. and $/VILE. A( ;TGrt A( ;AI I i .:.tACiTr) (12). These primers /entrap a JJS.I+p product and welt used mom:: M.same coiudilinns as "hose fnr the nested PCR.
DNA ',pivoting. DNA for sequencing was prepaled I.v ,he nested I'' i r uRico -round pioduci wax renmplilicd »ih primers Llit aid 117_ ut ., In,.0 ..u.um
of OW pI. Primtein nod denevIWCICIudt triphuspl,a(C .C'e rerun. " "d n., .u..J,aIspin column (Pilannucm). Use DNA was prec,p.lnlcd wuh ellumul ,t... mesample was submitted for cycle sequencing with pruners Lin and I .Z .n..u. ...II;Prism Model 377 cycle sequencer
NuelemIde errrue.tee aecessinn aunt her. Nucle. sale .c,lu.eut n -tau., , u t a .' I 'this paper have been %Mutinied II/ Iht (;enit.u,lç .iataita.c .rah ,ht .,t t... .. eo
AFn32997.
RESULTS
Specificity of PCR. The nested prinlci set was tes;ea to
DNA from a panel of Leislurrnrrin species and was fnunu Iragenerate a single major product from rcprescutanves if ailmajor species complexes of Lei.rluunrtid that are infecint 1.1humans (Fig. I). No product was detected fcuru 1)N.\ ofTrypiicoroiva brucei 1 /r0(leSferISe or from the lizard Ltv.ciintime,parasite Leishmantn inrerttolne. kDNA from Ereduntyeuumnnterogeii, a closely related parasite of sloths. was amplifiedA product of 300 hp was amplified from If/ pl; of pulMet' lcoal DNA but not from a clinical sample from i Tinfected patient (Fig. I. lanes 14 and 15) L. tropic° gcnc :.dialthe largest Lei.tlumutin species PCR product (750) hp) andcould he distinguished with care from L. ut(nnuun t(u8(1 bpi ,oldmore easily from LeisIinartin rnnjor (S6O bp). It was tllcichiepossible to identify the Old World hutnailinfective Lerçheanl,,,complexes no the basis of size alune. The Ncw Wot Idzilierlsis complex could not he distinguished bum Lu'içiu,arw.rmericmta on the basis of size. although the smaller Ltuc/r,i,trdmmnzemerr.tr.t product was readily identiftahtc. The E.geii product (780 bp) was slightly larger than the other Nis.World Lei.tbnu ,.id species pl,,ducts.
Sensitivity of felt. Decimal dilutions (ins Stlit Ise ter I ..e .IL. id%annrrn VIII0fvI/1 "N /Sid /IPTI total f)NA ill were ...sit,fled by the nested PCR and dip:stetl with /lur'lll co elite: u.1
the ilillil of detection and the effect of cuultceallannll on fin
.. w.. .«. et41,iNIa\rMfvYIan1O1MYMw./r7,saNfb'lrraaMorMarNYevMtMlr.rreenal7yrY.f7a'lafhlrs+tyv+Rrs'Men
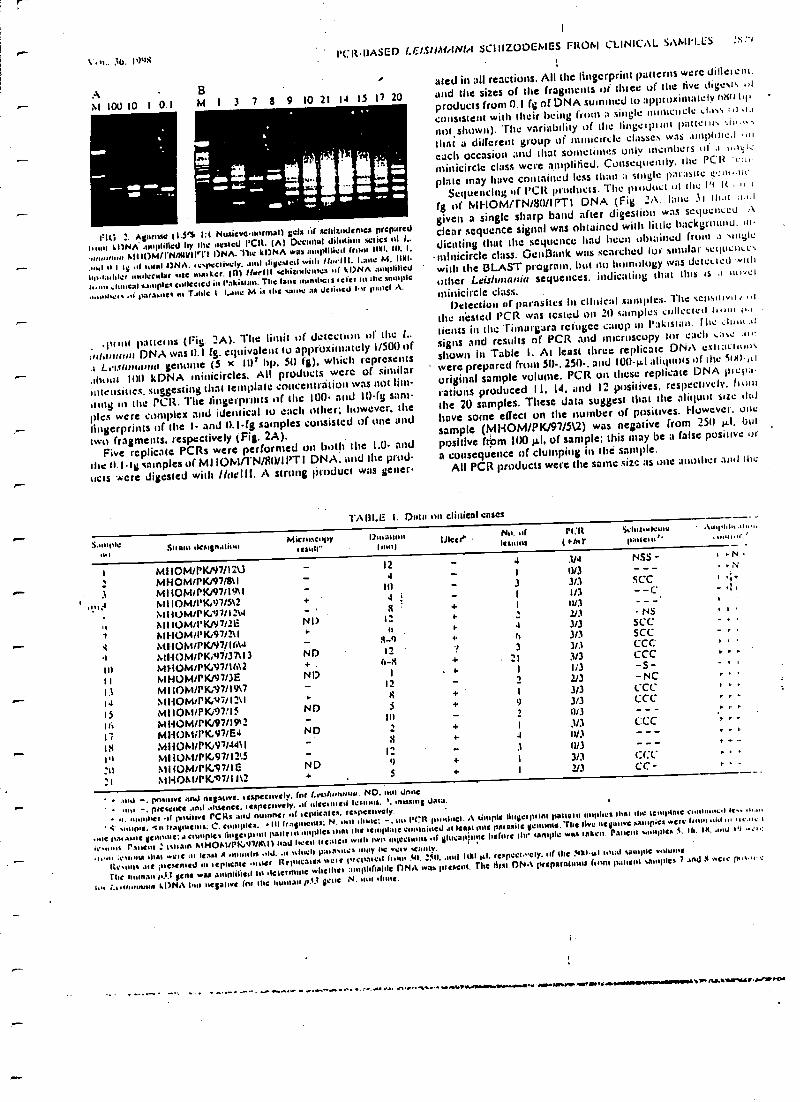
Vitt.. 36. I9a1PCRIIASED LEIS/GN/INLI
SCIIIZODEh1ES FItOhI CLINICAL SAMPLES
AM 100 10 I 0 1 M 1 3 7 8 9 10 21 14 15 17 20
tar
_Oft AMNI +
as
_a
rit; 2. Agar's.: 11.3% 1:1 Nuieverulrmal) Vets al' sellitndonlü prepared
1,51n7 11)NÁ ,.1111,111í0J hy 11e 1es10d VOL (A) Decimal dilution c.aics 171 L.
n¡ A(I IgM/PN/WVIIvt-I DNA.kUNA wus :nuplilieU (nu.1 IltlI, In. 1.
-- ..nt at I ly ..( 10101 1)NA. 1ey.eclively, .md diVesled with Moll I. I.a11e M. 11111-
I.n.laJder lecular sae mat km'. (nl Hnrlll aLit.nlcnns sil kDNA amplified
t..,u. auucal sm.ples conected in Pakistan. The lane mindsets ,eíer to Mc sample
parasite. in T.1hlc 1 Ling M as the 10.11¢ as Jdine.l 1n pnnel A.
splint paltteltts (Fig. 2A), The limit of detection of the L.
ult.nnn+n DNA was 0.1 (g. equivalent to approximately I/500 of
L.1.lhnhrtlut genullte (5 X IUr hp. 50 (g), which represents
Aunts $ 111) kDNA minicircles. All products were u( similar
intensities. suggesting that template concentration was not lim-
ning in the 1Cß. The fingerprints of the 100 and 10 -fg sam-
ples were .:untpICX and identical Io cacti other; huwevel the
fingerprints of the I- and 11.1-(g samples consisted of one and
two fragments. respectively (Fig. 2A).Five replicate PCRs were performed on both the 1.0. and
the t). IIg samples of MI1OM/rN /RIUIPTI DNA. and the prod-
ucts 4.-ere digested with /laelll. A Strong Product was gelier
:'1
ated in all reactions. All the fingerprint patterns were dille'cm.
and the sizes of the fragments of duce of the five digests
products from 0.1 fg of DNA summed to approximately win hi, .
consistent with their being tl'Uin a single InIIlICIICte ..Lass 1I i.,
not shown). The variability of the lingeiplint p:ltteln, ,i1 .,that a dilfere ìt group of ininicircte classes was InlpliI e.J . i
cacti Occasion and that Sometimes only members u( .t
nlinicircle class were amplified. Consequently. the PCR ran'
plate may have contained less than a single p:uaSUe t.twuSequencing of 1'CR prtidu4ts. The pi udurl ul the 1'r R
fg of MFIOM /rN /SU/IPTI DNA (Fig. 2A. lane 31 th.tl
given a single sharp band after digestion was scquenccu :\
clear sequence signal was obtained with little hackgtounti, uI
cheating that the sequence had been obtained front I \ulyle
minicircle class. Ga:11t3futk was searched ¡uf ;molar \t:c(ucii c,
with the BLAST program. but nn homology was detctacd 'nh
other Leisltinania sequences. indicating that this Is .1 nvct
minicircle class.Detection or parasilcs Iii Clinical samples. The scnsuwn...I
the itCStet1 PCR was tested on 21) samples cullCcitii
(tents in the rimargara refugee camp In Pakistan. The Jinn .,l
signs and results of ('CR and microscopy for each Lase at.
shown in Table I. At least three replicate DN,t e(iiacuuu\
were prepared from SI) -. 2511 -, and I00 -Al aliquuls of Ule í0111.1
original sample volume. PCR on these replicate DNA pit:l1ü
rations produced I1. 14. and 122 positives. respectively. flung
the 20 samples. These data suggest that the aliquot size did
have some effect on the number of positives. However. one
sample (MHOM /PK/97/5\2) was negative from 250 µl, but
positive frpm 100 µt, of sample; this may be a false positive or
a consequence of clumping in the sample.All PCR products were the same size as one another and the
1.A131E 1. Dala 1117 clinical eases
S1ny.le11.
Stiano destinationMieruscopy
testae't)nraltun
1 1
tllcer^Nu. nf Nitleu uns ( ró.r
SdUulen,e1111110111
' .\n,p1,I...1ronu,'
1 MII0M/rK/47/I2U_ MHOM/PK/97/8\I
MIIOM/rK/97/1SnIMI IOM/I'lCr97/5\2MIit)M/rK,1)7/12\4tsll IOM/rKJN7/?LMHOM/l'K;97/2\I
^ MII0M/PK/97/I6\4M110M/P1C,A17í3713
In M1.1OM/rIG97/14\2II hIHOM/rKP)7/3EI3 MIIOhurK.v7n9\714 J1HOMrPK.v7/121115 MI IOM/PKi97/15Iri dIHOM/rK,97/19a217 M1-10M/PK.97/E4
^ tlt HHOM/PICW97/4411l'1 MIIOhUPtC.97/12:5as N1I(OM/rK,91/IE21 aHOMUrKA7/1I\2
.1,7
s1
Nu
ND+
NI)
rND
N- D
NDa
12
In
8I:
t)
s
4 3/4
1 0/33 3/31 1/3I 1u3
'<34 3/3h 3/33 3/3
21 3/3t t/32 2J3
I 3/3tl 3/32 1113
I 3/34 11/3
3 0/3
) 3/3I 2/3
NS5 -
SC- C
- -C
-NSSCCSCCCCCCCC-5--NCt.CCCCC
C:CC
(.(:CCC -
- N
1 s
and -, pn.nive and repave. respccto-cl'. for Leo& an.n.a. ND. Jane
mu -, prearnce and Assents,. respectively, of filet! Mgt) lestons. ', missing data.
,r her of 1 yt rCRs and numnts of ecplicalc%. respectively.
' 4- .,n.pie. In Payments; C, comptes,III frarmentt; N. nul ,lane: -. nn VCR p..nlise1. A simple lli t i pi inn patlarn implies that the le mpinrt CnnUiumd 1e.. ,i
.,ti 1,a,.silt r :, C l i plc Iinte.p,m patinas implies Mal the template contained at Iman sae pal asile yenalne..rhs Itve nel(uuve sampKl were (run.,1.1 ,,, u...1c ,
Pautot : tannin A/NO7.U1'197/01111nad liec.1 hóued wont rua uyceumrs n( lucan,11ue bone 1111 temple wtu lnken. rausnr uunpks i. Ira. IX. mid IV ..,,.
1,.111 .C.15.111/0 dud .etc :u Ita11 Si months .14. ,.1 abash pat 3%11101 nuy 1,e vety scanty.
Remits .tit ;uesenled m i ephCatc .utter It epiìcates Net C Irepal cd (loin 311. 011, .out NMt µl, respeciwely. of the 41YI.u& 1m:d sample 'nome .
rile n.1man /.33 Vent was amnlilieiI ht ,kltnmoe whethct :nop1diah1C DNA was proem. rite arse ONt preparaunns (rom patient .amples 7 and X .e.c 1>'.,n c
I,.. L. 1.1)N.\ 1.111 ne$al.ve fnr the human 1,(t ycue N. sut ,tient.
w..-..woo .rw to. - r.J. y. . ,,,-.-.J n i.1 ..rwYf.Vlr.wiYYrw1Y'u11M\I'.Ni.tAYMNPYrMiYT/1R1111Viì/SW
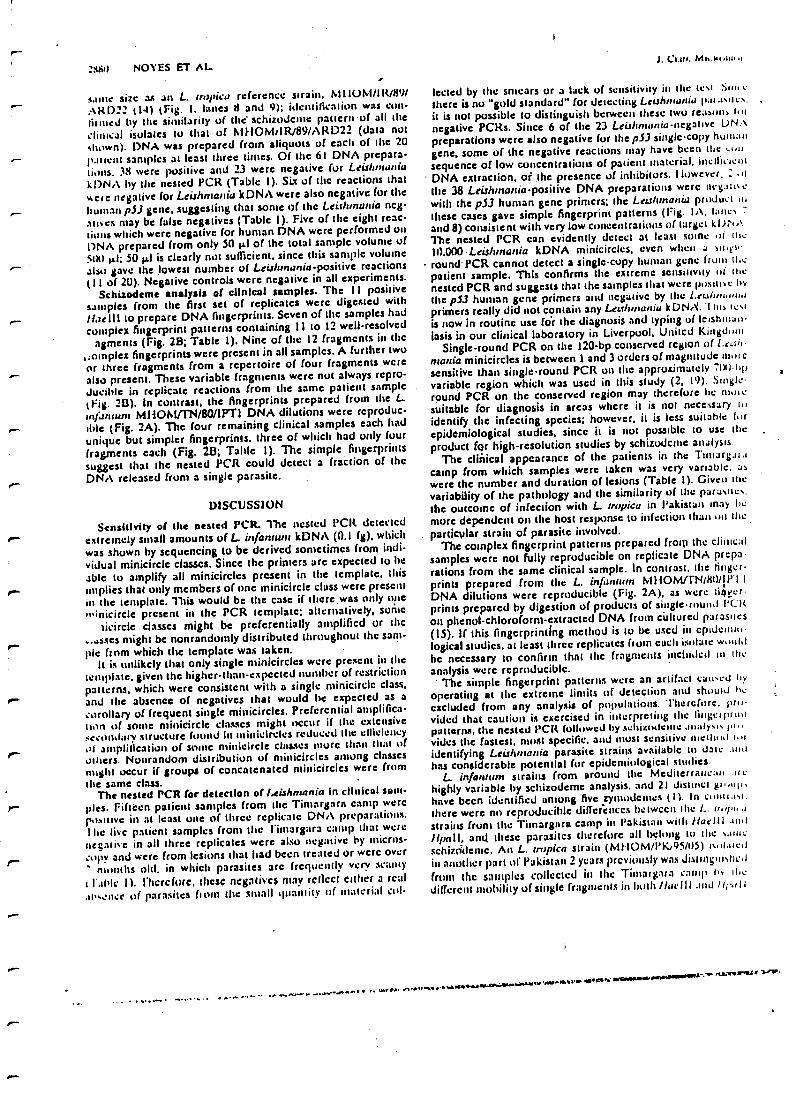
r-:41 NOYES ET AL
same size a.c an L.. tropica reference strain, MI IOM /111/89/AKD22 (14) ¡Fig. 1, lanes 8 and 9); identification was cun-iirmed by the similarity of the schizodeme pattern of all theclinical isolates to that of MUOM,IR/89/AKD22 (data notshown). DNA was prepared from aliquots of each of the 20raticnt samples at least three times. Of the 61 DNA prepara-tions. 38 were positive and 23 were negative for Leishmwniak!)NA by the nested PCR (Table 1). Six of the reactions thatMete negative for Leishmania kDNA were also negative for thehuman pSJ gene. suggesting that sonie of the Leishmania neg.oases may be false negatives (Table J ). Five of the eight reac-tions which were negative for human DNA were performed onI)NA prepared from only 50 p.I of the total sample volume of3tt0 ILL .50 µl is clearly not sufficient, since this sample volumealso gave the lowest number of Leisltrnania-positive reactions( l I of 2U). Negative controls were negative in all experiments.
Schizodeme analysis of clinical samples. The 11 positivesamples from the first set of replicates were digested with
r- N,rtlll to prepare DNA fingerprints. Seven of the samples hadcomplex fingerprint patterns containing 11 to 12 well -resolved
agments (Fig. 28; Table 1). Nine of the 12 fragments in the,:oinplex fingerprints were present in all samples. A further twoor three fragments from a repertoire of four fragments werealso present. These variable fragments were not always repro -
ducible in replicate reactions from the same patient sample(Fig. 213). In contrast, the fingerprints prepared from the L..in/;rmunt MHOMI N /80iiPT1 DNA dilutions were reproduc-
.- title (Fig. 2A). The four remaining clinical samples each hadunique but simpler fingerprints, three of which had only fourfragments each (Fig. 2B; Table I). The simple fingerprintssuggest that the nested PCR could detect a fraction of theDNA released from a single parasite.
DISCUSSION
Sensitivity of the nested PCR The nested PCR detectedextremely small amounts of L. infantunt kDNA (0.1 fg), whichwas shown by sequencing to be derived sometimes from indi-vidual minicircle classes. Since the primers are expected to he
able to amplify all minicircles present in the template, thisr implies that only members of one minicircle class were presentin the template. This would be the case if there was only oneesinicircle present in the PCR template; alternatively, sonic
cicircle classes might be preferentially amplified or the
..asses might be nonrandotnly distributed throughout the sam-pie from which the template was taken.
It is unlikely that only single minicircles were present in thetemplate. given the higher -than- expected number of restrictionpatterns, which were consistent with a single minicircle class,
r and the absence of negatives that would be expected as acorollary of frequent single minicircles. Preferential amplifica-thin of some minicircle classes might occur if the extensivesecondary structure f d in minicircles reduced the ellicicneyIli amplification of sortie minicircle classes more than that ofothers. Nonrandom distribution of minicircles among classes
might occur if groups of concatenated minicircles were fmmthe same class.
The nested PCR for detection of ¡.eishmania in clinical sam-ples. Fifteen patient samples from the Timargara camp werepositive in at least one of three replicate DNA preparations.the live patient samples from the 1 ïniargara camp that werenegative in all three replicates were also negative by micros-copy and were from lesions that had been treated or were over
months old. in which parasites arc frequently very scanty
c 1..119c 11. Flicrc(orc. these negatives may reflect either a real.1t'senee of parasites hoot the small quantity of material col-
J. C:.a,. MI. Mt III..1
Iected by the smears ur a lack of sensitivity in the test Sur. e
there is nu "gold standard" for detecting Leis/mania lt:,t.,s,tcs.it is not possible to distinguish between these two rcasons Iut
negative PCRs. Since 6 of the 23 Leis/Imo/Oa-negative DNApreparations were also negative for the pSJ single -copy human
gene, some of the negative reactions may have been the .,.0sequence of low concentrations of patient material, inefficientDNA extraction, of the presence of inhibitors. However, _ .11
the 38 Leishmania- positive DNA preparations were negatne
with the pSJ human gene primers; the Letrltrnania product in
these cases gave simple fingerprint patterns (Fig. IA, lanesand 8) consistent with very low concentrations of target kDNAThe nested PCR can evidently detect at least some ui the10.000Leishmania kDNA minicircles, even when a sinewroundPCR cannot detect a single -copy human gene frutti floepatient sample. This confirms the extreme sensitivity lit thenested PCR and suggests that the samples that were positive by
the p53 human gene primers and negative by the Leo/imam.,primers really did not contain any Le rhnianiu kDNA. 1 his testis now in routine use (or the diagnosis and typing of lc,shnta,t-iasis in our clinical laboratory in Liverpool, United Kingdom
Single -round PCR on the 120 -bp conserved region of Leo/t-ine/tie minicircles is between I and 3 orders of magnitude mot csensitive than single -round PCR on the approximately ':01)-hpvariable region which was used in this study (2, 19). S,ngleround PCR on the conserved region may therefore he molesuitable for diagnosis in areas where it is not necessary t.,identify the infecting species; however, it is less suitable furepidemiological studies, since it is not possible to use theproduct fqr high -resolution studies by schizodeme analysts.
The ctiiiical appearance of the patients in the Tintarbaracamp from which samples were taken was very variable. aswere the number and duration of lesions (Table 1). Given thevariability of the pathology and the similarity of the parasites.
the outcome of infection with L.:rr pica in i'akista, may bemore dependent on the host response to infection than on the
. particular strain of parasite involved.The complex fingerprint patterns prepared from the clinical
samples were not fully reproducible on replicate DNA prcparations from the same clinical sample. in contrast. tite fingerprints prepared from the L. infannun M)IOMITN /8U /IP 1 I
DNA dilutions were reproducible (Pig. 2A), as were tigverprints prepared by digestion of products of single -rerun! PClt
on phenol -chloroform- extracted DNA (ruin cultured parasites(15). If this fingerprinting method is to be used in cptderruulogical studies, at least three replicates from each imitate w ut,i
be necessary to confitm that the fragments included in theanalysis were reproducible.
The simple fingerprint patterns were an artifact caused byoperating at the extreme limits of detection and should heexcluded from any analysis of populations. Therefore. pr,vided that caution is exercised in interpreting the Iingetl,r,uipatterns, the nested PCR followed by scltizoslenie analysts 1.,.vides the fastest. most specific. and must sensitive ntetltutl t. 1
identifying Leishmania parasite strains available to date .111,1
has considerable potential for epidemiological studies.
L. infamum strains (mm around the Mediterranean suehighly variable by schizodeme analysis. and 21 distinct gr.,uthave been identified among five zynwdcines ( I). In emits ast.
there were no reproducible differences hetween the L. rn. ¡,, .,
strains front the Tirnargrtra camp in Pakistan with liarlil and/!pall, and these parasites therefore all belong to the sameschiztidente. An L. rropica strain (MI- IOM /PK,95 /1/5) ,c.,litc.lin another (tart of Pakistan 2 years previously was Jisling,s411front the samples Collected in the Tiniaiptara camp, its Abe
different !nubility Of single fragments in both /laelli and Ili siI l
. .. .. ..... , .... . ... 1 1. 0 ,. ..r.. e..uw.....s111..u110.w:11...w.rd . Y.: ,YiMMU4/IIMMi,wa.f .<ax.s1L r 1-07P,
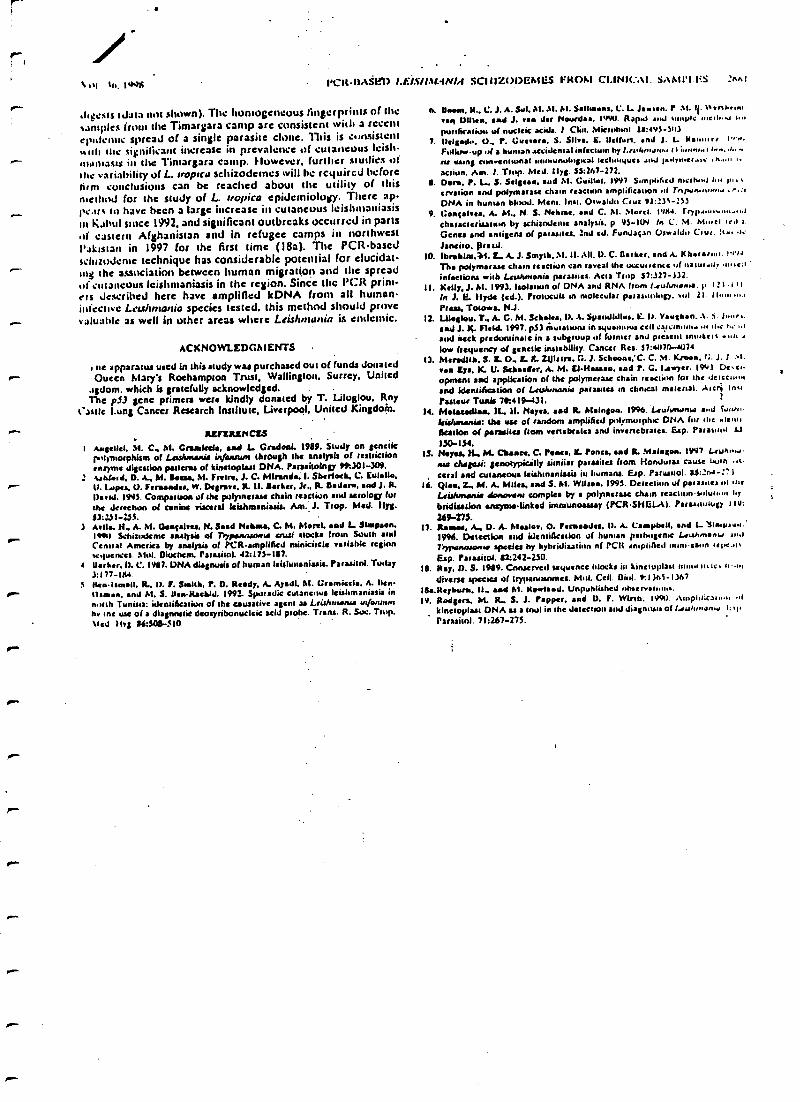
N Its, 1U.J( l4l'R-13ASY.'17 f.J:/.T/l.tf.-IN/il SClll-L()DGAfL'S I:R()A1 CI.INIt;Al. SA N11'1 :nn!
digests tibia not shown). The homogeneous fingerprints of thesamples from the Timargara camp are consistent with a recentepidemic spread of a single parasite clone. This is consistentwash the significant increase in prevalence of cutaneous Icisl-
.- mdntasts in the Timargara camp. However. further studies ofthe variability of L. tropica schizodemcs will he required beforefirm conclusions can be reached about the utility of thismethod for the study of L. tropics epidemiology. There :sp.p:.l1% to have been a large increase in cutaneous Icishniauiasissil h.Ibul since 1992, and significant outbreaks occurred in parts.t( eastern Afghanistan and in refugee camps in northwestl'rklstan in 1997 for the first time (18a). The PCR -basedschuuJcme technique has considerable potential for elucidarIn the association between human migration and the spreadof :utareuus Icishnwniasis in the region. Since the l'Clt prim-ers described here have amplified ICONA from all human-infective Leohntatlia species tested. this method should provevaluable as well in other areas where Leislutlunia is endemic.
ACKNOWLEDGMENTS
rte apparatus used in this study was purchased out of funds donated.- Oueen Marys Roehampton Trust, Wallington. Surrey. United.tgdom. which is gratefully acknowledged.The p53 gene primers were kindly donated by T. Liloglou, Roy
Castle Lung Cancer Research Institute, Liverpool, United Kingdom.
REFERENCES
I Aegeed, M. C. M. Craakda, and L Grades!. 1989. Study on geneticI.Hymorphism of LeiUtimonie infatvtun through the analysis of restrictionenryene digestion pasterns of kinetoplaat DNA. Paradtolop 99:301 -309.
: tinfoil. D. A., M. Bona. M. Frvin, J. C. Miranda. I. Sherlock. C. Eulalie,r- tt. lapes, O. Feraaades. W. Degrare. R.11. hiker. Jr., R. Radar., end J. R.
DaW. 1995. Comparison of the pulpncram chain reaction and serolop furthe detection of canine 'filet ral laishrnsaiuis. Am. i. Trop. Med. Ilyg.53:231 -23S.
3 Mlle. H.. A. M. Oearahu, N. Said Nelune, C. M. Morel. sad L Stapaon.lave, Schizudeme analysis of Trypevtrwsase ouri stocks from South amiCentral America by analysis of PCR- amplilted minicircle variable regionsequences. Mol. Diuehc n Palmitnl. 42:173 -187
4 Darker. D. C. 1987. DNA diagnosis of human leisltesaniania. Parssitnl. Today3:177-184lien.ismsil. R.. D. F. Stelth. P. D. Reedy. A. AyedI. M. Crsmicela, A. hen.r donee. end M. S. ilea- Rachid. 1992. Sporadic cutaneous Ieishmanissis innorth Tunisia: identification of the causative agent as Lcithrnanra infannu rby the use of a diagnostic deo yribonucleic acid prole. Trans. R. Suc. Trop.%Icd )Itg 84:308- -4I0, .
I"
r
r
h. Beam. R.. C. J. A. Sul. AI. Al. M. Salles nias. C. L. Jansen, P Al. Il. N enl.nmveal D11ke. lad J. time der Hourds.. IvSK,. Raper and on. ..11[111. NJ t,..
purification of nucleic acids. 1 Clin. MKnnhsnl 13:4v3 -)0)7. Delgado. 0.. P. C . S. Silva. E. Udfurt. end J. L. krns., t' N.
Fslk'..up.d a human accidenial irdectum by l.nd..nr.ur i I iunn..t t..., d.. ,au using aM.entrunal rn.a.unuh.p, al lcCl.rutqucs .uJ Iwdyu.cr.o,: ,n.....action. Am. 1. Toil,. Med. Ilyg. SS:267 -272,
I. Dort. P. L-. S. Silicon. sud M. Ouillai. 1997 S.mpliócd mciMalerviion and polymerise chain reaction amplificationDNA in human blood. Mcm. Init. Oswaldn Cruz 91::31 -233
9. Gentility's. A. M., N. S. Nebae. slid C. M. Morel. 19)w.characterisaoun by schisnaleme analysis. p 93 -IV/ In C. M. M...cl ied I.Genes and antigens of pariades. Ind ed. Fundagao Oswald. ., Cru..:t...t.Janeiro. prazd.
ID. lbrobla. 744. L. A. J. Smyth. M. H. All. D. C. Darker. and A. Khersaa,. 1.0)4The polymaraae chain reaction can I the uccunence wf nawr.u. nu,cainfections with Leidnmenie parasites. Acta Flop 37:327 -132.
IL Kelly. J. hl. 1993. laolatiun of DNA and RNA from 1.eulurunu. p i 21.1 r I
to 1. E. Hyde (ed.). Protocou in molecular parassuih,p. 01 21 II .......Press. Totowa, N.1.
12. LUoglou. T.. A. C. M. Schooes. D. A. Spamildlus. k. D. Vsuahan..1. i. J.......sad .1. 1(. field 1997. pS7 Mutations in syuamous colt esicon.uor .0 lice r....1and neck predominate in a subgroup of former and present 'motel%low ftequary of genetic instability. Canar Res. 37:44170 -W74
13. Meredith. S. L O. L L 21Jlrlra. G. J. Schools: C. C. M. Kroon. 1 :, J. J >t.
rab Eye. IL U. Schaeffer, A. M. FJ.H . sad P. C. Lawyer. 19'41 Dc,e.opmenl and application of the polymerase chain reaction for the lcicci...nand identihotion of Letawnanit parasita in clinical material. Arct>; In.r
Pasteur Tuais 70:419-431. t
14.MaIneadlaa, IL. H. Noyes. and L hlaingoa. 19%. Leulurwnw a..4 Sr...feishasenia: t e use of random amplified p.ilymuiph.c DNA fur rice .tenu6eatlon o( parasites room vertebrates and invenebratcs. Esp. Para utni ai
130-139.IS. Hayes, H.. M. Ouse., C. Pewee. IL Ponca. and R. Maloioa. 1997 L euim-.
nia ehagasi: genotypically simiiar parasites (torn Honduras taux tsar? , +
, <eral and cucarieous kishmaniuia in humans. Esp. Parasuol. SS::n4 -2')16. Qlw. Z., M. A. Mlles. and S. M. Wilson. 1993. Detection ut parasites nt .1.c
4irhnsanle sfonoveni awake by a polymerise chain reacuuns.duu..n t.ybridiaatlas etisyate.linked immunoassay (PCRSHGLA). Pararrtutup glu:269 -273.
17. Resew. A., D. A. Mails., O. Perused'''. 1). A. Campbell. end L vSlw.y,uu.'1996. Detection and identification of human pathogenic Lcuh.n.nW ,u,lT.)ponaeo..ie species by hybridization of PCit rnrpliAe l nnnics..n rei.c..r.Eip. Parasitol. 82:242 -250.
18. Ray. D. S. 1989. Conserved) sequence flocks hr kinetuplaat Hann nth:. t...,diverse species of trypanosomes. Mill. Cell. Biol. 9:11h5-11h7
lita.Reyburs. IL. mad M. Rowleed. Unpublished.Mervu.nua.19. Rodgers. M. L. S. J. Popper. ead D. F. Wirth. 1990. Ainpht:caI..." .l
kinesoplest DNA as a triol in the detection and diagnosis of I.aulrnwn... 1: y,
P a r as i tol . 71:267-275.
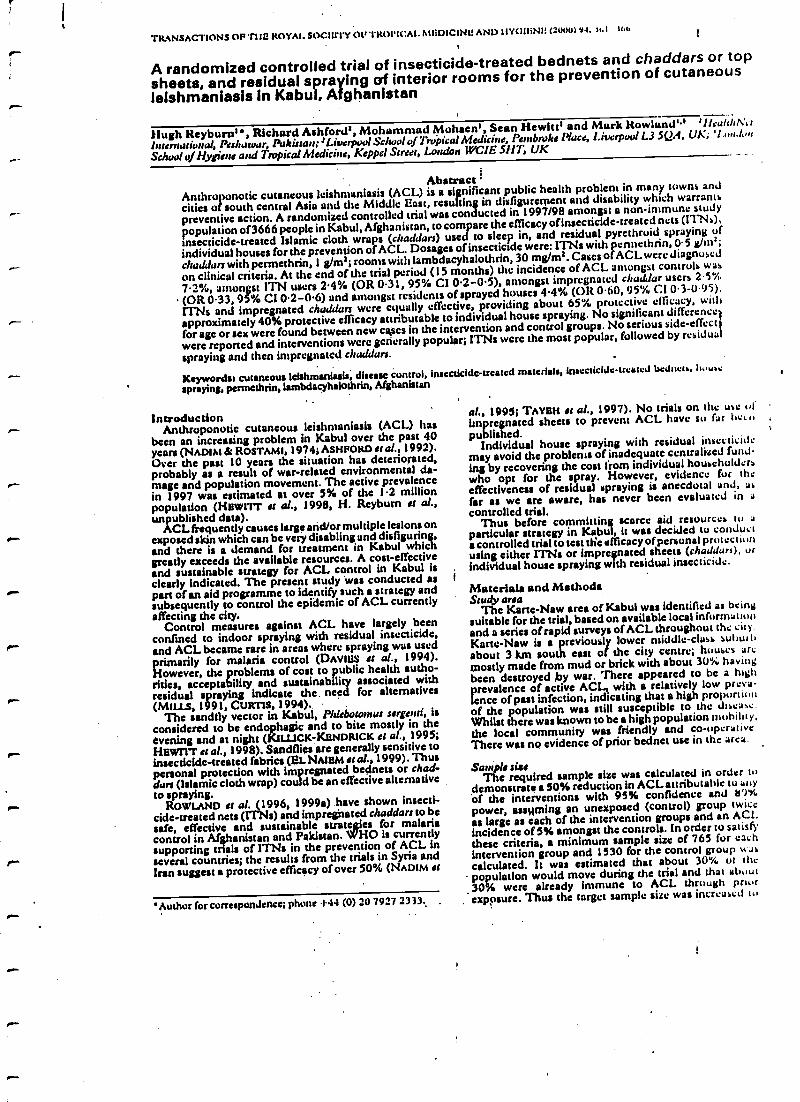
TRANSACTIONS OF TIIU ROYAL SOCIUTY Ot +TRt)tICAL.MUDICINU AND IIYCi IiNI: (200u) 94. fol I.
A randomized controlled trial of insecticide -treated bednets and chaddars or topsheets, and residual spraying of interior rooms for the prevention of cutaneouslelshmaniasis In Kabul, Afghanistan
Hugh Reyburni , Richard Ashford',Mohammad Mohsen', Sean Hewitt' and Mark Rowland" 'llealtlhN,v
International, Peshawar, Pakistan:: Liverpool School of tropical Medicine, Pembroke Pace, Liverpool L3 SSA, UK;
School of Hygiene and Tropical Medicine, Keppel Street, London WCIE SAIT, UK
AbstractAnthroponotic cutaneous lcishmaniusis (ACL) is a significant public health problem in many towns and
cities of south central Asia and the Middle Last, resulting in disfigurement and disability which warrants
preventive action. A randomized controlled trial was conducted in 1997/98 amongst a non- immune study
population of3666 people in Kabul, Afghanistan, to compare the efficacy ofinsecticidc- treated nets (ITNs),
insecticide- treated Islamic cloth wraps (chaddars) used to sleep in, and residual pyrethruid spraying of
individual houses for the prevention of ACL. Dosages of insecticide were: ITNs with pennethrin, 0.5 g/1n';
chaddar with permcthrin, l g/m3; rooms with lambdacyhalothrin, 30 mg/m2. Cases of ACL were diagnosed
on clinical criteria. At the end date trial period (15 months) the incidence of ACL amongst controls was
7.2 %, amongst ITN users 2.4% (OR 0.31, 95% CI 0.2 -0.5), amongst impregnated chuddar users 2.5%
(OR 0.33, 95% CI 0.2 -0.6) and amongst residents of sprayed houses 4.4% (OR 0.60, 95% CI 0.3- 0.95).
ITNs and impregnated chaddars were equally effective, providing about 65% protective efficacy, with
approximately 40% protective efficacy attributable to individual house spraying. No significant difference
for age or sex were found between new cases in the intervention and control groups. No serious side -effect
were reported and interventions were generally popular; ITNs were the most popular, followed by residua
spraying and then impregnated chaddars.
Keywordst cutaneous leishmaniasis, disease control, insecticide -treated materials, insecticide -treated bcduwn, twine
spraying, permethrin, lambdacyhalothrin, Afghanistan
IntroducdonAnthroponotic cutaneous leishn)aniasis (ACL) has
been an increasing problem in Kabul over the past 40years (NADIM & ROSTAMI) 1974; ASHPORD et al., 1992).Over the past 10 years the situation has deteriorated,probably as a result of war -related environmental da-mage and population movement. The active prevalencein 1997 was estimated at over 5% of the 1.2 millionpopulation (Hawn at al., 1998, H. Reyburn sr aL,unpublished data).
ACL frequently causes large and/or multiple lesions onexposed skin which can be very disabling and disfiguring,and there is a demand for treatment in Kabul whichgreatly exceeds the available resources. A cost-effectiveand sustainable strategy for ACL control in Kabul isclearly indicated. The present study was conducted aspart of an aid programme to identify such a strategy andsubsequently to control the epidemic of ACL currentlyaffecting the city.
Control measures against ACL have largely beenconfined to indoor spraying with residual insecticide,and ACL became rare in areas where spraying was usedprimarily for malaria control (DAMES a al., 1994).However, the problems of cost to public health autho-rities, acceptability and sustainability associated withresidual spraying indicate the . need for alternatives(MILLS, 1991, CURTIS, 1994)..
The sandlly vector in Kabul, Pblsbotomus sergenti, isconsidered to be endophagic and to bite mostly in theevening and at night (KILLICK- KSNDlttcK st al., 1995;Hawn st al., 1998). Sandflies are generally sensitive toinsecticide- treated fabrics (El. NAMEM st aL, 1999). Thuspersonal protection with impregnated bednets or chad-dars (Islamic cloth wrap) could be an effective alternativeto spraying.
ROWLAND et al. (1996, 1999e) have shown insecti-cide- treated nets (ITNs) and impregnated chaddars to besafe, effective and sustainable strategics for malariacontrol in Afghanistan and Pakistan. WHO is currentlysupporting trials of ITNs in the prevention of ACL inseveral countries; the results from the trials in Syria andIan suggest a protective efficacy of over 50% (NADIM st
'Author for correspondence; phone +44 (0) 20 7927 2333.. ,
al., 1995; TAYBH es al., 1997). No trials on the use ofimpregnated sheets to prevent ACL have su far he,,published.
Individual house spraying with residual insecticidemay avoid the problems of inadequate centralized fund-ing by recovering the cost from individual householderswho opt for the spray. However, evidence fur theeffectiveness of residual spraying is anecdotal and, asfar as we are aware, has never been evaluated in a
controlled trial.Thus before committing scarce aid resources to a
particular strategy in Kabul, it was decided to conducta controlled trial to test tie eficacyofpersonal pnItcctit Inusing either ITNs or impregnated sheets (Madams), urindividual house spraying with residual insecticide.
Materials and MethodsStudy area
The Karte -Naw area of Kabul was identified as beingsuitable for the trial, based on available local informatlutfand a series of rapid surveys of ACL throughout the city.Kane -New is a previously lower middle -class suhw itabout 3 km south east of the city centre; houses arcmostly made from mud or brick with about 30% havingbeen destroyed Eby war. 'There appeared to be a highprevalence of active ACL, with a relatively low preva-lence of past infection, indicating that a high proportionof the population was still susceptible to the disease.Whilst there was known to be a high population nfuhíht y,the local community was friendly and co- operativeThere was no evidence of prior bednct use in the area.
SconNt sizeThe required sample size was calculated in order to
demonstrate a 50% reduction in ACL attributable to tut),of the interventions with 95% confidence and 8')`Y..power, assuming an unexposed (control) group twiceas large as each of the intervention groups and an ACL.incidence of 5% amongst the controls. In order to satisfythese criteria, a minimum sample size of 765 for eachintervention group and 1530 for the control group Hascalculated. It was estimated that about 30% ut thepopulation would move during the trial and that about30% were already immune to ACL through priorexpç)sure. Thus the target sample site was increased to
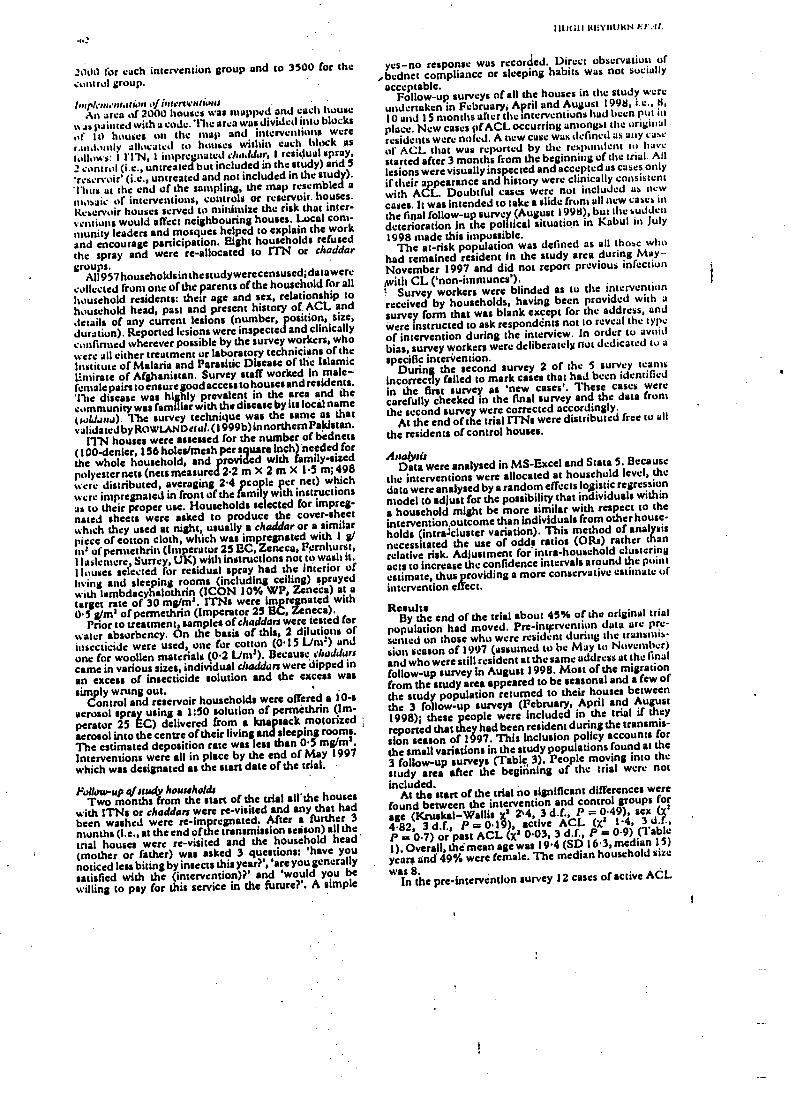
.:111)(ill klillllJ}tN l:l':ll.
2t100 for each intervention group and co 3500 for thecontrol group.
lnspl:nientationaJintery tAn area of 2000 houses was mapped and each house
'% as painted with a code. The area was divided into blocksof I t) houses on the map and interventions werer (nd ly allocated to I es within each block us'allows: I l'l'N, I impregnated chaehlasr, I residue! spray,2 control (i.e., untreated but included in the study) and 5'reservoir' (i.e., untreated and not included in the study).'thus at the end of the sampling, the map resembled amosaic of interventions, controls or reservoir. houses.Reservoir houses served to minimize the risk that inter-ventions would affect neighbouring houses. Local com-munity leaders and mosques helped to explain the workand encourage participation. Eight households refusedthe spray and were re- allocated to ITN or chaddargroups.
All 957 households in thestudywerecensuscd;data were
collected from one of the parents of the household for allhousehold residents: their age and sex, relationship tohousehold head, past and present history of ACL anddetails of any current lesions (number, position, size,duration). Reponed lesions were inspected and clinicallyconferred wherever possible by the survey workers, whowere all either treatment or laboratory technicians of theInstitute of Malaria and Parasitic Disease of the IslamicIlmirate of Afghanistan. Survey staff worked in male -female pairs to ensure good access to houses and residents.the disease was highly prevalent in the area and thecommunity was familiar with the disease by its local name(sahhi,su). The survey technique was the same as thatvalidated by RttwtANDstul. (1999b) innorthemPaklstan.
ITN houses were assessed for the number of bednets(100- denier, 156 holes/mesh per square inch) needed forthe whole household, and provided with family -sizedpolyester nets (nets measured 2.2 m X 2 m X 1.5 m; 498were distributed, averaging 2.4 people per net) whichwere impregnated in front of the family with instructionsas to their proper use Households selected for impreg-nated sheets were asked to produce the cover -sheetwhich they used at night, usually a chaddar or a similarpiece of cotton cloth, which was impregnated with 1 g/m' of petmethrin (Imperator 25 EC, Zencca, Fernhurst,11aslemere, Surrey, UK) with instructions not to wash it.Houses selected for residual spray had the interior ofliving and sleeping rooms (including ceiling) sprayedwith lsmbdacyhalothrin (ICON 10% WP, Zcneca) at atarget rate of 30 mg/ma. ITNs were impregnated with0.5 g/m1 of permed-inn (Imperator 25 EC, Zeneca).
Prior to treatment, samples of cheddars were tested forwater absorbency. On the basis of this, 2 dilutions ofinsecticide were used, one for cotton (0.15 Lim') andone for woollen materials (0.2 LAW). Because cheddarscame in various sizes, individual chaddars were dipped inan excess of insecticide solution and the excess wassimply wrung out.
Control and reservoir households were offered a 10 -saerosol spray using a 1 :50 solution of perméthrin (Im-pesetor 25 EC) delivered from a knapsack motorizedaerosol into the centre of their living and sleeping rooms.The estimated deposition rate was less than 0.5 mg/m'.Interventions were all in place by the end of May 1997which was designated as the start date of the trial.
Follow -up ((study householdsTwo months from the start of the trial all* the houses
with ITNs or chaddars were re- visited and any that hadbeen washed were re-impregnated. After a further 3months (i.e., at the end other transmissionseason) all thetrial houses were re- visited and the household head(mother or father) was asked 3 questions: 'have younoticed less biting by insects this year?','are you generallysatisfied with the (intervention) ?' and 'would you bewilling to pay for this service in the future ?'. A simple
yes -no response was recorded. Direct obse vutiou of,bednet compliance or steeping habits was not socially
acceptable.Follow -up surveys of all the houses in the study were
undertaken in February, April and August 1998, i.e., 8,10 and 15 months after the interventions had been put inplace. New cases pfACL occurring amongst the originalresidents were noted. A new case was defined as any cast'of ACL that was reported by the respondent to havestarted after 3 months from the beginning of the trial. Alllesions were visually inspected and accepted as cases only
if their appearance and history were clinically consistentwith ACL. Doubtful cases were not included as newcases. It was intended to take a slide froni all new cases inthe final follow -up survey (August 1998), but the suddendeterioration in the political situation in Kabul in July1998 made this impossible.
The at -risk population was defined as all those whohad remained resident in the study area during May- -November 1997 and did not report previous infectionwith CL ('non- inununes').
Survey workers were blinded as to the interventionreceived by households, having been provided with asurvey form that was blank except for the address, andwere instructed to ask respondénts not to reveal the typeof intervention during the interview. In order to avoidbias, survey workers were deliberately not dedicated to a
specific intervention.During the second survey 2 of the 5 survey teams
incorrectly failed to mark cases that had been identifiedin the first survey as 'new cases'. These cases werecarefully checked in the final survey and the data fromthe second survey were corrected accordingly.
At the end of the trial ITNs were distributed free to allthe residents of control houses.
AnalysisData were analysed in MS -Excel and Stata 5. Because
the interventions were allocated at household level, thedata were analysed by a random effects logistic regressionmodel tb adjust for the possibility that individuals withina household might be more similar with respect to theintervention.outcome than individuals from other house-holds (íntrajcluster variation). This method of analysisnecessitated the use of odds ratios (ORs) rather thanrelative risk. Adjustment for intra- household clusteringacts to increase the confidence intervals around the pointestimate, thus providing a more conservative estimate ofintervention effect.
ResultsBy the end of the trial about 45% of the original trial
population had moved. Pre -intervention data are pre-sented on those who were resident during the transmis-sion season of 1997 (assumed to be May to November)and who were still resident at the saine address at the finalfollow -up survey in August 1998. Most of the migrationfrom the study area appeared to be seasonal and a few of
the study population returned to their houses betweenthe 3 follow -up surveys (February, April and August1998); these people were included in the trial if theyreponed that they had been resident during the transmis-sion season of 1997. This Inclusion policy accounts forthe small variations in the study populations found at the3 follow -up surveys (Table, 3). People moving into thestudy area after the beginning of the trial were notincluded.
At the start of the trial no significant differences werefound between the intervention and control groups forage (Kruskal- Wallis xs 2`4, 3 d.f., P = 0.49), sex (x2
4-82 3 d.f., P = 0.19), active ACL (X3 1.4, 3P = 0.7) or past ACL (x' 0.03, 3 d.f., P a: 0.9) (Table1). Overall, the mean age was 19.4 (SD 16.3, median 15)
years and 49% were female. The median household size
was 8.In the pre -intervention survey 12 cases of active ACL
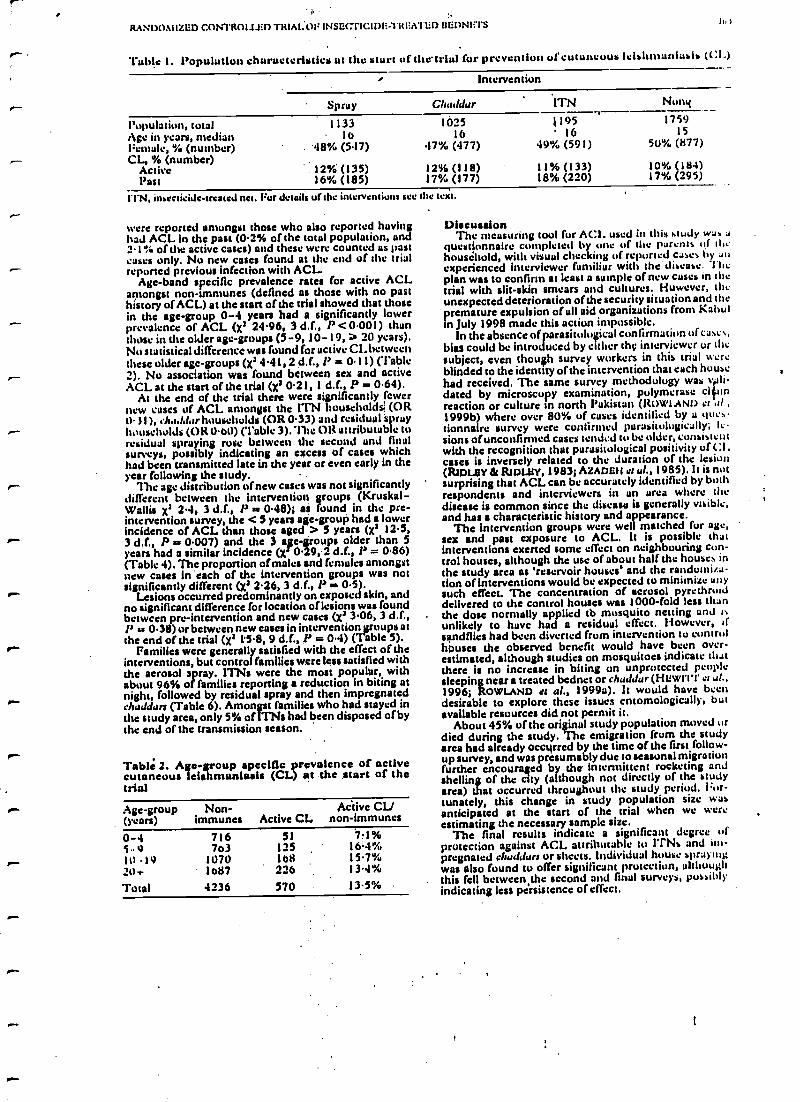
I,
RANDOMIZED C.ONTROl11Ep TRIAI.OF INSECTICIDE-TREATED I11iDNt l'S III
Table 1. Population characteristics ut the start uf thctriul for prevention uf cutancuus leishn,unfuaia (Cl.)
g Intervention
Spray Clualdar ITN Nonq
Population, totalAge in years, median
1133I6
102516
119516
175915
Female, (number) 48% (517) 47% (477) 49% (591) 50% (877)CL, % (number)
Active 12% (135) 12% (I 18) 11% (133) 10% (184)Past 16% (185) 17% (177) 18% (220) 17% (295)
fl'N, insecticide- treated net. Fur details of the interventions see the text.
were reported amongst those who also reported havinghad ACL in the past (0.2% of the total population, and2.1% of the active cases) and these were counted as pasteases only. No new cases found at the end of the trialreponed previous infection with ACL.
Age -band specific prevalence rates for active ACLamongst non -immunes (defined as those with no pasthistory of ACL) st the start of the trial showed that thosein the age -group 0 -4 years had a significantly lowerprevalence of ACL (X2 24.96, 3 d.f., P < 0.001) thanthose in the older age -groups (5 -9, 10 -19, > 20 years).No statistical difference was found for active CL betweenthese older age -groups (x24.41, 2 d.f., 1' = 0.11) (Table2). No association was found between sex and activeACL at the start of the trial (x2 0.21, 1 d.f., P = 0.64).
At the end of the trial there were significantly fewernew cases of ACL amongst the ITN huuschola (ORO. I I ), ehadd r households (OR 0.33) and residual sprayhouseholds (OR 0.00) (Table 3).'11íe OR attributable toresidual spraying rose between the second and finalsurveys, possibly indicating an excess of cases whichhad been transmitted late in the year or even early in theyear following the study.
The age distribution of new cases was not significantlydifferent between the intervention groups (Kruskal-Wallis x2 2.4, 3 d.f., P v 0.48)1 ai found in the pre -intervention survey, the < 5 years age -group had a lowerincidence of ACL than those aged > 5 years (x2 12.5,. 3 d.f., P a 0.007) and the 3 age- groups older than Syears had a similar incidence (xl 0.29, 2 d.f., P = 0.86)(Table 4). The proportion of males and females amongstnew cases in each of the intervention groups was notsignificantly different (x2 2.26, 3 d.f., P - 0.5).
Lesions occurred predominantly on exposed skin, andno significant difference for location of lesions was foundbetween pre -intervention and new cases (x2 3.06, 3 d.f.,l' u 0.38) or between new cases in interventionroups at
.- the end of the trial (X2 1.5.8, 9 d.f., P = 0.4) (7 able 5).Families were generally satisfied with the effect of the
interventions, but control families were less satisfied withthe aerosol spray. 1TNs were the most popular, withabout 96% of families reporting s reduction in biting at
r` night, followed by residual spray and then impregnatedehaJdars (Table 6). Amongst families who had stayed inthe study area, only 5% 01 1TNM had been disposed of bythe end of the transmission season.
r-Table 2. Age-group specific prevalence of activecutaneous leishmunlasls (CL) at the start of thetrial
Age -group(years)
Non-immunes Active CL
Active CL/non -immunes
0 -4 716 51 7?1%59 763 125 l6'4"/aIll -19 1070 168 15.7%20* 1687 2:6 13.i%
Total 4236 570 13.5%
DiscussionThe measuring tool for ACt. used in this 'study was a
questionnaire completed by one of the parents of Mehousehold, with visual checking of reported canes by auexperienced interviewer familiar with the disease. Theplan was to confirm st least a sample of new cases in thetrial with slit -skin smears and cultures. However, theunexpected deterioration of the security situation and thepremature expulsion of all aid organizations from Kabulin July 1998 made this action impossible.
In the absence of parasitological confirmation of cases,bias could be introduced by either the interviewer ur thesubject, even though survey workers in this trial wereblinded to the identity of the intervention that each househad received. The same survey methodology was vali-dated by microscopy examination, pulymerase clittnreaction or culture in north Pakistan (ROWLAND et .11 ,1999b) where over 80% of casesidentified by a titles-tionnaire survey were confirmed purasituloutcally; le-sions of unconfirmed cases tended to be older, consistentwith the recognition that parasitological positivity of Cl.cases is inversely related to the duration of the lesion(RIDLSY& RIDLBY, 1983; A2ADGIt et al., 1985). It is notsurprising that ACL can be accurately identified by bothrespondents and interviewers in an area where thedisease is common since the disease is generally visible,and has a characteristic history and appearance.
The intervention groups were well matched for age,sex and past exposure to ACL. It is possible thatinterventions exerted some effect on neighbouring con-trol houses, although the use of about half the houses inthe study area as 'reservoir houses' and the randomiza-tion of interventions would be expected to minimize anysuch effect. The concentration of aerosol pyruthroiddelivered to the control houses was 1000 -fold less thanthe dose normally applied tb mosquito netting and i+unlikely to have had a residual effect. However, ifsandflies had been diverted from intervention to controlNausea the observed benefit would have been over-estimated, although studies on mosquitoes indicate thatthere is no increase in biting on unprotected peoplesleeping near a treated bednet or chaddur (He wttt' et al.,1996; ROWLAND et al., 1999a). It would have beendesirable to explore these issues entomologically, butavailable resources did not permit it.
About 45% of the original study population moved ordied during the study. The emigration from the studyarea had already occurred by the time of the first follow -up survey, and was presumably due to seasonal migrationfurther encouraged by the intermittent rocketing andshelling of the city (although not directly of the studyarca) that occurred throughout the study period. For-tunately, this change in study population size wasanticipated at the start of the trial when we wereestimating the necessary sample size.
The final results indicate a significant degree .dprotection against ACL attributable to ITNa and im-pregnated ehaddars or sheets. Individual house sprayingwas also found to offer significant prutection, althoughthis fell between the second and final surveys, possiblyindicating less persistence of effect.
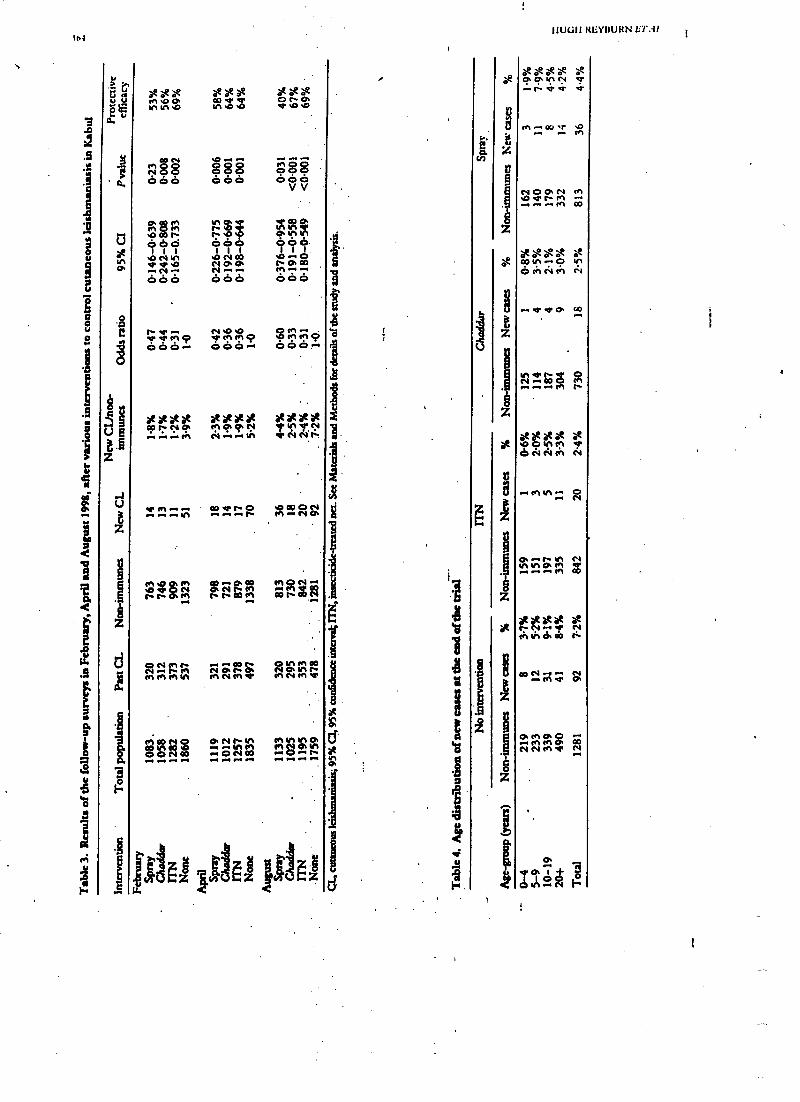
In4
>
ú ú
N
Ú
O
V
z
.z
d0.
.
1^
.
zie at atV1 Y1 .O V1M V' Ó
Ñ O S 888 Ó O SÓÓÓ ÓÓO Ov
V
momt-
vs.4O Oo. Ñ
óóó óóó óóó.
srsr.NO ÑON.CT 0.0.000. -.N... N..... M......
ÓÓÓ 666 ÓÓÓ
f V N .O .O
II"), rMçe6ÓÓ
MM .-.
Ne M Q666M r
xxÑOx.. 0x/10x.XÑax**
---m 0V .Q
M1 I0' Ñ Ñ IR
^^ ODtFt.O.-.N .......-.r
Ñ.N+tiM Ñ ',RP IMMMN MNMd' M
MD0Ñ0N01OON11A MNVIO..+ .+ N M1 M O. N
O O N 00 .. O N 00 -. .-. 1 .I... .. ... .+ .-. ... .4 0
AtIghlw d
:Y
C
Ñ
.
Z
e
0
z
1
V
.z
IIUCìIi RItYßURN llT.il..
1111 ,oCT CT 0104 V'
-.t`d'V V'
^C4 C3 CT C4d' t- M1M
.+..M 00
eee e òe0301 .. O 01
0;1 CV CV
Ñr. íö.. .. .. t`
exx xMD N M V'ó N 0V t+1 N
Ñ
O. .. r N N4.1 41°:íñ
o
Ñ ÑdlNdao
co rc cs, sr á
CT.. el 0¡1 00 CONNMv N
..r
to-
R{vDOdU'LIsD CONTROLLED 'FILIAL OF INSLCTICID[ TRIEA7'131) Ut91)NLrtS )os
Table S. Location of cutunuous lulshinutslasla Italians at the 'tart and end ofthe Intervendon trial
HeadUpper limbLower limbTrunkTotalLesions/case
Pre -Intervention cases
498487
'26827
12801.25
% New cases
39%38%21%
2%100%
85 40%73 34%48 22%
8 4%214 100%
1.29
%
Table 6. User survey of different interventions (family heads), October 1997
Spray Chaddar ITN % Control %
Generally satisfied 182 .'97% 163 84% 191 100% 73 23%
Willing to pay next year 103 55% 84 43% 140 73% 15 5%
Less biting at night 178 95% 145 75% 184 96% 73 23%
Total responden 188 194 191 318
That ITNs and chaddars were found to be equallyeffective was unexpected since ITNs provide both aphysical as well as chemical barrier to sandfly bites.Possible explanations are that chaddars are traditionallyfamiliar and generally easier to use and they might havebeen used as a wrap whilst sitting around earlier in theevening. Although sleeping outdoors in Kabul does notappear to be common, those who slept outdoors mayhave found it easier to continue to use the chaddar thanthe bednet. Sandflics may be very sensitive to therepellent effect of pcnnctltrin, and an itispregnatedsleeping sheet may be sufficient to repel them even frontparts of the body that are not directly covered.
No age- or sex -related differences in protective efficacywere associated with any of the interventions. This wasalso the case when permethrin- treated nets were evalu-ated against malaria (ROWLAND et al., 1996) althoughpermethrin- treated chaddars were found to be moreprotective against malaria in children than adults (Row/-LAND st al., 1999b).
Lesions at both the beginning and the end of the trialpredominantly affected exposed skinith both sexesand all ages equally affected. Le PONT r el al. (1989) havedescribed this pattern as characteristic of infra- domicilli-ary transmission, which is supported in this study by thefact that preventive strategies focused at the householdlevel have been associated with a significant reduction inincidence.
In addition to offering good prospects of localsustain=ability, LTNs and impregnated chaddars have the advan-tage of being portable, an important consideration forsuch a mobile population. Impregnated chaddars andITNs each have advantages and disadvantages. The useof impregnated chaddan avoids the initial cost of pur-chasing an ITN and they may also be more likely to beused in the evening or when sleeping outside. However,chaddars are more likely to be washed and thus mayrequire re- impregnation 2 or 3 times per year. ITNs mayprovide more protection against nuisance biting (ROW-LAND st al., 1999a). From the brief survey of usersatisfaction in this study, ITNs were the most popular,followed by residual spray and then impregnated chart:.Jan. It seems that the choice between ITNs and im-pregnated chaddars as protection against ACL should bea matter for consumer preference. .
At the present time, in the absence of a suitablevaccine, personal protection is an effective and sustain-able means of preventing and controlling ACL. We feel
that the results of this trial justify the more widespreaduse oral* and impregnated sheets in preventing ACL.
AcknowledgementsHcalthNet International's Leishinaniasis Control l'nk-
Cramme is supported by Norwegian Church Aid, the liurope.iiiommission (ECHO), WHODP/Wii Special Programme
for Research and Training in Tropical Diseases (project no.960662), the Department for International Development (UK),and HesithNet International. None of these donors acceptsresponsibili for the information provided or views unto:tacd.We thank (live Davies, (tuna Canwiru, and Abdur !tab torcomments on data analysis. We thank also the lostittnc ulMalaria and Parasitic Disease, Islamic timbale of Afghanistan,for their cooperation and implementation of the field work.
ReferencesAshford, R. Kohestany, K. & Karimaad, M. (1992). Cutaneous
Ieishmanlasls in Kabul: observations on a prolonged epi-demic. Annals of 7iopicaf Medicine and Parasisolosy, $6,
361 -371.Audeh, B., Samad, A. & Ardehali S. (1985). Hi.iolugical
spectrum of cutaneous leishmanluis due to L.lshnsaniatropics,. Trauactions of she Royal Society of Tropical Medicineand Hygiene, 79, 631 -636.
Curtis, C. F. (1994). Approaches to vector control: new andtrusted. 4. Appropriate technology for vector control: irn jpregnated bednets, polystyrene beads and Ily traps. 'spina: -siau of the Royal Society of Tropical Medicine and Hygiene, UV,144 -146.
Davies, C. R. Llanos- Cuentas A., Canales, J., 1. 0n, Li.,Alvaro, E., Mon e, j., Tolentino, 13', Gomero, Q., l'yke, S.& Dye, C. (1994). The fall and rise of Andean cutaneouslelslunaniesls: transient impact of the DDT campaign in Peru.Transactions of the Royal Society of Topical Multiage andHygiene, 88, 388 -393.
81 Minn, D. A., Blnahas, A. M. & Aboud, M. A. (1999).Prot.cdve efficacy of lambdacyhaluthrin- ímpre$nsted bed-nets against Phl.bowmw oriental& the vector of visceralkbhmanluls In Sudan. Medical and Veterinary $atoniolosy,13 310 -314.
Hewitt, S., Parhan, M., Whitman, H., Muhammad, N., Kemal,M. & Rowland, M. W. (1996). Self protection from malariavectors in Pakistan: an evaluation of popularexisting methodsand appropriate new techniques in Afghan refugee commu-ables. Annals of Tropical Medicine and Parasitology, 90,337 -344.
Hewitt, S., Reybum, H., Ashford, R. & Rowland, M. (19911)..Anthroponotic cutaneous lcishmaniasis in Kabul, Afghani-stan: vertical distribution of cases in apartment blocks.Transactions of the Royal Society of Tropical AfeJiesne wu.lHygiene, 92, 2773 -279.
Killick- Kendrick, R., Killick- Kendrick, M. & Tung, Y. (1995).
too
Anihrop.ulotic Cutaneous Ieislnliaiiiasis in Kabul, Afghani-the high susceptibility of Phleboro tergenti w Leish-
WNW frt,pwa. Traivaefiwn of the Rawl Society ./ Tropic's/.11e.heine and Hygiene, 89, 477.
Le Pont, F.. Mouchet, J., Desjcux, P., Torres Espcjo, J. &Richard, A. (1989). Bpide logic de la leishmaniose tegu-mentaire en Bolivie. Annals Je la S.ciird Belge Js Alldecinelñ.pie.ik, 69, 297 -312.
Aille, A. (1991). The economics of malaria control. In: Ala /aria.Waiting for the Vaccine. Target', G. A. T. (editor). Chichester:Wiley at Sons, pp. 141 -10
\.iJim, A. & Rostami G. S. (1974). Epidemiology of cutaneousleishmaniasis in Kabul. Afghanistan. Bulletin of the WorldHealth lhguli:arm, SI, 4S -49.
\.1.11111. A., Malahar, A1., Iloushntund, B., Keyghohaai. K. &Atl.nonlan. M. R. (1995). Evaluation of pyrethroid impregnatedNJ-aeu for control of aurluoponotic cutaneous lsirlunaniatfr in134111, Islamic Republic of Iran, Genova: World Health Organiza-tion. WHO/LEISH/95.37.
Ridley, D. S. & Ridley, M. J. (1983). The evolution of the lesionin cutaneous leishmaniasis..7ountul o /Pathology, 141, 83 -96.
Rowland, M., Boums, M., Ducomcs, D. Durrani, N., Rosen-J4111, J., Schapiro, A. & Sundorp, H. (1996). Pyrethroid
11U611 RtsYiIUKN é7'.11..
impregnated bed nets for personal protection against maim i.ofor Afghan refugees. Truusactiutuofdu Royal Soetetyof l'ropie.ilMedicine and Hygiene, 90, 357 -361.
Rowland, M., Durrani, N., Hewitt, S., Mohammed, N.,Bouma, M., Cameira, 1., Rosenthal, J. St Schapiro, A.(1999a). Pemetluin- treated cheddars and top- sheets: appro-priate technology fur protection against malaria in Afghani-stan and other complex emergencies. Transact liuu of the RoyalSoddy of Tropical Medicine and Hygiene, 93, 465-472.
Rowland, M.. Munir, A., Durrani, N., Noyes. li. & Ieyburit, 11.(1999b). An outbreak of cutaneous Ieishnianiesis in anAfghan refugee settlement in north -west Pakistan. Transac-tions of the Royal Society of Tropical Medicine aml Hygiene, 93,133 -136.
'l'uyeh. A., Jaluuk, L. & Al Khiaini, A. M. (1997). AI ent.tneo,nleis/unaniasis control uiol sui,. pyreihn,i.- impregnated Leaflet, invillager near 4kppppoa. Syria. Geneva: World IIealth Urgant .ilion. WHO/LEISH/97.4L
Received 13 September 1999; revised 8 l:ebrtiraiy 2000,ttcccptwil for publication I I Febnrary 2000
IAnnouncements
ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENEThe Transactions
'l1te' Transactions of the Royal Sucicry of Trollied:.rupied:I Medicine and Hygiene is issued bi- monthly (six parts peryear) and
publishes not only papers presented at Society meetings and symposia but also papers and correspondencesubmitted by Fellows and non -Fellows from all over the world on every aspectof tropical medicine and iuternutiuuuIhealth. Supplements on specialist topics are published from time to time.
The annual subscription payable by Fellows 15 .460.00 which becomes due in advance on the first of April eachyear. Subscriptions may be taken out for a period of five years at five times the current fee. Applications forFellowship must he made on the correct form, obtainable fmin the address below. 'Mere is a reduced subscription of42'3.00 for bona /i.b' students which is limited to three years.
The Transactions may he purchased by those other than Fellows of the Society, at 424.00 per issue; 0185.00 pervolume (hard copy plus Cl)); 4140.00 per volume (hard copy or CD). It hdispatched by accelcruted surface mall(air freight) at no extra charge. A licence to network the Cl) costs 450.00.Further information and application forms fur NI- Subscription orders from libraries andlawship can be obtained from: nun- Fellows should be sent to:
The Honorary SecretariesRoyal Society of Tropical Medicine and HygieneManson House26 Portland PlaceLondon, W 1 B lEY, UKTelephone +44 (0)20 7580 2127Fax +44 (0)20 7436 1389e -mail [email protected]
Royal Society of Tropical Medicine and HygieneSubscription DepartmentRobquest Ltd, Triumvirate HouseMilibank RoadKingsnorth, AshfordKent, TN23 3JD, UKTelephone +44 (0)1233 611299Fax +44 (0)1233 639423e -mail Rquest ®robquest.demon.co.uk
ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENEManson and Chalmers Medals, 2001
The Manson Medal is awarded triennially. It is the Sock ty'sl'highest markof distinction, and shall be made to theperson whose contribution to any branch of tropical medicine or hygiene is considered by Council to merit thehunstur moat. .
The Chalmers Medal is awarded each year in recognition of research contributing to the knowledge of tropicalmedicine or tropical hygiene. Only persons of 45 years or under on 1 June of the year of the award shall be eligible.
Nondnations may be made by any Fellow of the Society, on forms available from Manson House. Completed(onus should be sent to the Honorary Secretaries by 1 September 2000. For full details please refer to the Yearbook.
1 KANSAC. PIONS 01,1111; ROYAL. SoCI1('IT 01,1 1101'IC:M. A1111)ICINI: AND I1l't ;l1EÑI: (?ton) 94, )a 1 Ina
A randomized controlled trial of insecticide -treated bednets and chaddars or topsheets, and residual spraying of interior rooms for the prevention of cutaneousleishmaniasis in Kabul,. Afghanistan
Ilugh Reyburt", Richard Ashford', Mohammad Multsen', Senn IIcwitt' and Mark Rowland" 'llr,tlrh.\'rrinternational. Peshawar, Pakistan; 'l.ivrtp,url School tf Ïr,rpü,dAledicinc, Pembroke /Yace, 1ivarpuull..7 S,)/I, UK; '/. t...,,tic/root a/ lftXiene dud '!'trpieal Afedieine, Kelrpel Street, 1. luta Ir/C16 511 1; UK
AbstractAnthrcpi nutic cutaneous Ieislintaniasis (AC!.) is a significant public health problem in many towns andcities of south central Asia and'the Middle Hast, resulting in disfigurement and disability which warrantspreventive action. A ranidomized.controlled trial was conducted in 1997/98 amongst a non- immune studypopulation of 3666 people in Kabul, Afghanistan, to compare the efficacy of insecticide- treated nets (I'INs),insecticide- treated Islamic cloth wraps (chaddars) used to sleep in, and residual pyrethroid spraying ofindividual houses for the prevention of ACL, Dosages of insecticide were: ITNs with permethrin, 0.5 g/m';chaddars with permethrin, I g/ms; rooms with lamtbdacyltalothrin, 30 tang /m'. Cases ofACL. were diagnosedon clinical criteria. At the end of the trial period (1.5 months) the incidence of ACL. amongst controls was7.2%, amongst l'I'N users 2.4% (OR 0.31, 95% CI 0.2 -0.5), amongst impregnated chaddar users 2.5%(OR 0.33, 95% 010.2 -0.6) and amongst residents of sprayed houses 4.4% (OR 0.60, 95% CI 0.3- 0.95).I I Ns and impregnated chaddars were equally effective, providing about 65% protective efficacy, withapproximately 40% protective efficacy attributable to individual house spraying. No significant differencesfor age or sex were found between new cases in the intervention and coma)! groups. No serious side -effectswere reported and interventions were generally popular; ITNs were the most popular, followed by residualspraying and then impregnated chaddars.
Ksywordss cutaneous leishmeniasis, disease control, insecticide -treated materials, insecticide -treated hednets, housespraying, permethrin, Iambdscyhalothrin, Afghanistan
introductionAnthropanotic cutaneous leishmaniasis (ACL) lias
been an increasing problem in Kabul over the past 40years (NADIM & ROSTAMI, 1974; ASHFORD st al., 1992).Over the past 10 years the situation has deteriorated,probably as a result of war -related environmental da-mage and population movement. 'file active prevalencein 1997 was estimated at over 5%.äf the 1.2 millionpopulation (I !MITI' et al., 1998, 11. Rayburn et al.,unpublished data).
ACL frequently causes large and /or multiple lesions onexposed skin which can he very disabling and disfiguring,and there is a demand for treatment in Kabul whichgreatly exceeds the available resourcea., A cost-effectiveand sustainable strategy fw. ACL.. control in Kabul isclearly indicated. The present study was conducted aspart of an aid programme io identify such a strategy andsubsequently to control the epidemic of ACL currentlyaffecting the city.
Control measures against ACL have largely beenconfined to indoor spraying with residual insecticide,and ACI. became rare in areas where spraying was usedprimarily for malaria control (DAVIItS sr al., 1994).However, the problems of cost to public health autho-rities, acceptability and sustainabtlity associated withresidual spraying indicate the need for alternatives(MILLS, 1991, CURTIS, 1994).
'l1e santifly vector in Kabul, l'lileboiomtar urgenti, isconsidered to be endophagic and to bite mostly in theevening and at night (IUt.LICK- KIINDRICK st el., 1995;I i nwrIT st al., 1998). SandOies are generally sensitive toinsecticide -treated fabrica (RI. NMIIM et el., 1999). Thuspersonal protection with impregnated bednets or chad-el.tn (Islamic cloth wrap) could be an effective alternativeto spraying.
ROWLAND a ai. (1996, 1999a) have shown insecti-cide- treated nets (11Ns) and impregnated chaddars to hesafe, effective and sustainable strategies for malariacontrol in Afghanistan and Pakistan. WI I0 is currentlysupporting trials of ITNs in the prevention of ACL inseveral countries; the results from the trials in Syria andIris suggest a protective efficacy of over 50% (NAIUM et
'Author for correspondence; phone 14.1 (0) 21179272 113.
al., 1995 ;'l'AYlitt et al., 1997). No trials on the use ofimpregnated sheets to prevent ACL have su fat beenpublished.
Individual house spraying with residual inse ticidcmay avoid the problems of inadequate centralizedfund-ing by recovering the cost from individual householderswho opt for the spray. However, evidence for theeffectiveness of residual spraying is anecdotal and, asfar as we are aware, has never been evaluated in a
controlled trial.Thus before committing scarce aid resources to a
particular strategy in Kabul, it was decided to cott.dutta controlled trial to test the efficacy of personal protectionusing either l'l'Ns or impregnated sheets (chin/Jars), orindividual house spraying wills residual insecticide.
Materials and MethodsStudy area
The Karte -Naw area of Kabul was identified as beingsuitable for the trial, based on available local informationand a series of rapid surveys of ACL throughout the city.Karte -New is a previously lower middle -class suburbabout 3 km south east of the city centre; houses aremostly made from mud or brick with about 30% havingbeen destroyed by war. There appeared to be a highprevalence of active ACL, with a relatively low preva-
fhence of past infection, indicating that high proportionof the population was still susceptible to the disease.Whilst there was known to be a high population mobility,the local community was friendly and co- operative.'!'here was no evidence of prior bednet use in the area.
Sample sireThe required sample slay was calculated in order to
demonstrate a 50% reduction its ACL. attributable to anyof the interventions with 95% confidence and li0%power, assuming; an unexposed (control) group twiceas large as each of the intervention roups and an ACLIncidence of 5% amongst the controls. In order to satisfythese criteria, a minimum sample size of 765 for eachintervention group and 1530 for the control group wascalculated. It was estimated that about 30% of thepopulation would move during the trial and that about30% were already immune to ACL. through priorexposure. Thus the target sample size was increased to
1e:tUGII RßYOURN ET AI..
2000 for each intervention group and to 3500 for thecontrol group.
Inipientenfa/ion of at:envnninlsAn area of 2000 houses was mapped and each house
was painted with a code. The area wasdivided into blocksof 10 1 ses on the map and interventions wereramfontly allocated to I sea within each block asfollows: I ITN, I impregnated chaddar, I residual spray,2 control (i.e., untreated hut included in the study) and 5'reservoir' (i.e., untreated and not included in the study).'thus at the end of the sampling, the map resembled amosaic of interventions, controls or reservoir houses.Reservoir houses served to minimize the risk that inter-ventions would affect neighbouring houses. Local com-munity leaders and mosques helped to explain the workand encourage participation. Eight households refusedthe spray and were re- allocated to ITN or chaddargroups.
AI1957 householdsintheatudywerecensused ;datawerecollected from one of the parents of the household for allhousehold residents: their age and sex, relationship tohousehold head, past and present history of ACL anddetails of any current lesions (number, position, size,duration). Reported lesions were inspected and clinicallyconfirmed wherever possible by the survey workers, whowere all either treatment or laboratory technicians of theInstitute of Malaria and Parasitic Disease of the IslamicEmirate of Afghanistan. Survey staff worked in male-female pairs to ensure good access tohousel and residenti.'Me disease was highly prevalent in the area and thecommunity was familiar with the disease by its local name(r,'ldana). the survey technique was the same as thatvalida icd by Rt)Wl ANI f anal. ( i 999b) in northern Pakistan.
l'l'N houses were assessed for the number of bednets(100- denier, 156 holes/mesh per square inch) needed forthe whole household, and provided with family -sizedpolyester nets (nets measured 2.2 m X 2 m X 1.5 m; 498were distributed, averaging 2.4 people per net) which%vere ion iregnated in front of the family with instructionsas to their proper use. I louseholds selected for impreg-nated sheets were asked to produce the coversheetwhich they used at night, usually a chaddar or a similarpiece of cotton cloth, which was impregnated with I g/mt of permethrin (Imperator 25 EC, Zeneca, Fernhurst,I laslemere, Surrey, UK) with instructions not to wash it.I louses selected for residual spray had the interior ofto ing and sleeping rooms (including ceiling) sprayedwith lambdacyhalothrin (ICON 10% WP, Zeneca) at atarget rate of 30 mg/m'. ITN, were impregnated with0.5 gin' of permethrin (Imperator 25 EC, Zeneca).
Prior to treatment, samples of chaddar were tested for%oter absorbency. On the basis of this, 2 dilutions ofinsecticide were used, one for cotton (0.1i Lint') andonefor woollen materials (0.2 Um'). Because chaddarscame in various sizes, individual chaddars were dipped inan excess of insecticide solution and the excess wassimply wrung out.
Control and reservoir households were offered a 10 -saerosol spray using a 1:50 solution of perniethrin (Im-perator 25 RC) delivered from a knapsack motorizedaerosol into the centre of their living and sleeping rooms.'rhe estimated deposition rate was less than 0.5 mg/m'.interventions were all in place by the end of May 1997which was designated as the start date of the trial.
Follow-up of may householdsTwo months front the start of the trial Al the houses
with l'rNs or ehaddars were re- visited and any that hadbeen washed were re- impregnated. After a further 3
months (i.e., at the end of the transmission season) all theIIial houses were re- visited and the household head
t Cher or tinker) was asked 3 .questions: 'have younoticed less biting by insects this year ?', 'are you generallysatisfied with the (intervention) ?' and 'would you bewilling to pay for this service in the future ?'. A simple
yes -no response was recorded. Direct observation ofbednet compliance or sleeping habits was nut socially
acceptable.Follow -up surveys of all the houses in the study were
undertaken in February, April and August 1998, i.e., H.I0 and 15 months after the interventions had been put illlplace. New cases of ACI. occurring amongst the originalresidents were noted. A new case was defined as any caseof ACL that was reported by the rest dent to havestarted after 3 months from the beg' ' g oldie trial. Alllesions were visually inspected and accepted as cases onlyif their appearance and history were clinically consistentwith ACL. Doubtful cases were not included as newcasts. It was intended to take a slide from all new cases inthe final follow -up survey (August 1998), but the suddendeterioration in the political situation in Kabul in July1998 made this impossible.
The at -risk population was defined as all those whohad remained resident in the study area during May -November 1997 and did not report previous infectionwith CL ('non- inmunes').
Survey workers were blinded as to the interventionreceived by households, having been provided with asurvey form that was blank except for the address, andwere instructed to ask respondents not to reveal the typeof intervention during the interview. in order to avoidbias, survey workers were deliberately not dedicated to aspecific intervention.
During the second survey 2 of the 5 survey scamsincorrectly failed to mark cases that had been identifiedin the first survey as 'new cases'. These cases werecarefully checked in the final survey and the data fromthe second survey were corrected accordingly.
At the end of the trial l'INs were distributed free to allthe residents of control houses.
Ana(yiirData were analysed in MS -Rxcel and Stata 5. Because
the interventions were allocated at household level, thedata were analysed by a random effects logistic regressionmodel to adjust for the possibility that individuals withina household might be more similar with respect to theintervention outcome than individuals from other house-holds (intra- cluster variation). This method of analysisnecessitated the use of odds ratios (ORs) rather thanrelative risk. Adjustment for infra- household clusteringacts to increase the confidence intervals around the puiotestimate, thus providing a snore conservative estimate ofintervention effect.
Resultsfix the end of tine trial about 45%.oí the original trial
population had moved. Pre -intervention data are pre -sented on those who were resident during the transmis-sion season of 1997 (assumed to he May to November)and who were still resident at the same address at the finalfollow -up survey in August 1998. Most of the migrationfrom the study area appeared to be seasonal and a few ofthe study population returned to their houses betweenthe 3 follow -up surveys (February, April and August1998)i these people were included in the trial if theyreported that they had been resident during the transmis-sion season of 1997. This inclusion policy accounts forthe small variations in the study populations found at the3 follow -up surveys (Table 3). People moving into thestudy area after the beginning of the trial were notincluded.
At the start of the trial no significant differences werefound between the intervention and control groups forage (Kruskal- Wallis ) 2.4, 3 d.f., P = 0.49), sex (x'4.82, 3 d.f., P = 0.19), active ACL (x' 1.4, 3 d.f.,N = 0.7) or past ACI. Q. 0.03, 3 ti.f., P = (1.9) ('!'ableI ). Overall, the mean age was 19.4 (SI) 16' 3, median 15)years and 49% were female. 'rite median household sirewas 8.
In the pre -intervention survey 12 cases of active ACL
)
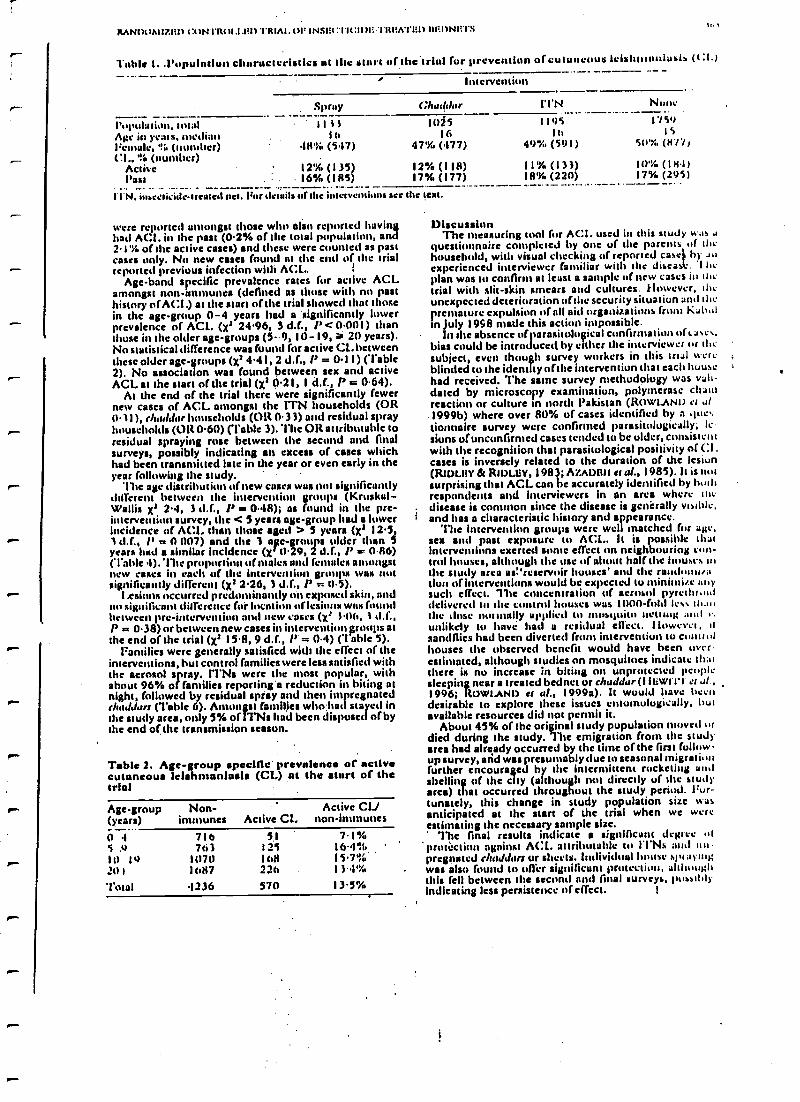
RANpt1AUL1L11 t:c1N1Rt11.1.111) TRIAI. uF INSI:cï l'K:11li'I'ItMA'l'1a) 11M1)Nlil'S1,
Table 1..l'opulntluii clumsscst:eli es nt the Yttirt of the 'trial for prevention of cutaneous leisht111111iusIs (CI.)
Intervention
Spray Churllur ITN None
t'ot'al: ' , total I t ì l Ifli5 1 195 1 759
Alec in years, median lo 16 10 15
Female, '!6 (number) 48% (547) 47% (477) 49% (5e) I) 5U'%, 0177i
Cl., Is (number)Active 12% (1 35) 12% (I 1 8) 11% (I 3 3) 10% (16.1)Past . : . 16% (185) 17% (177) 1830 (220) 17% (295)
-11'N. insecticide-treated net. 1'ur details or the interventions see the text. - -- _ - -- _ - -- '+
were reported amongst those who also ref ed havingbad ACI. in the past (0.2% of the total population, and2.1% of the active cases) and these were counted as pastcases only. No new cases found at the end of the trialreported previous infection with ACL.
Age -band specific prevalence rates for active ACLamongst non -immune& (defined as those with no pasthistory of ACI.) at the start of the trial showed that thosein the age -group 0 -4 years had a 'significantly lowerprevalence of ACE. (Xr 24.96, 3 d.f., P < 0.001) thanthose in the older age -groups (5 -9, 10 -19, 20 years).No statistical difference was found for active CL. betweenthese older age -groups (xi 4.4 I, 2 d.f., P = 0.1 I) (Table2). No association was found between sex and activeACL at the start of the trial (X1 0.21, I d.t., P = 0.64).
At the end of the trial there were significantly fewernew cases of ACL amongst the ITN households (OR0.11), r/addarhouseholds (OR 0.33) and residual sprayhouseholds (OR 0.60) (l'able 3). The OR attributable toresidual spraying rose between the second and finalsurveys, possibly indicating an excess of cases whichhad been transmitted late in the year or even early in theyear following the study. '
'lite age distribution anew eases was not significantlydifferent between the intervention groups (Kruskul-Wallis X' 2.4, 3 d.f., /' is 0.48); as found in the prc-interveulit)n survey, the < 5 years age -group had a lowerincidence of A(:L than those aged > 5 years (Xt 12.5,1 d.f., l' 01)07) and the 3 a'e- groups older than 5years had a similar Incidence (X 11.29, 2 'If., /' w 0.86)('!'able .1). 'Ile proportion of males and females amongstnew cases in cacti of the hlterventiun groups was notsignificantly different (Xt 2.26, 3 d.f., P 710.5).
I . osions occurred predominantly on exposed skin, andno significant difference for location oflesions was foundbetween pre -intervene and new cases (X° 1.06, 1 d.f.,P = 0.38) or between new cases in intervention Froups atthe end of the trial (X3 15.8, 9 d.f., /' = 0.4) (1 able 5).
Families were generally satisfied with the effect of theinterventions, hut control families were less satisfied withthe aerosol spray. ITN& were the most popular, withabout 96% of families reporting 'a reduction in biting atnight, followed by residual spray and that impregnatedrhaJJars (Table 6). Amongst families who had stayed inthe study area, only 5% of I Ns had been disposed of bythe end of the transmission season.
Table 2. Age -group specific prevalence of activecutaneous Ieishmanlasis (CL) nt the start of thetrial
Age-group(years)
Non-immunes Active CL
Active CIJnon-immunes
0I...5 )10 1020 I
Total
716763
1071)1687
1236
5112511,8226
570
7.1%16.4°S,15.7%131%13.5"/0
DiscussionThe measuring tool for ACL. used its this study was a
questionnaire completed by one of the parents of thehousehold, with visual checking of reported easel h) anexperienced interviewer familiar with the dìseas . I ticplan was to confirm at least o sample of new cases in thetrial with slit -skin smears and cultures. However, theunexpected deterioration of the security situation and thepremature expulsion of all aid organizations from Kah,tlIn July 1958 made this action impossible.
In the absence of parasitological cunfirntatiun of t ases,bias could be introduces( by either the interviewer nr tltcsubject, even thoufli survey workers in this trial wcrcblinded to the identity of the intervention that each househad received. The saine survey methodology was vali-dated by microscopy examination, polymerase chainreaction or culture In north Pakistan (RowL ANI) er al1999b) where over 80% of cases identified by a .Luc,tionnaire survey were confirmed parasitolugically; Icstuns of unconfirmed cases tended to be older, consistentwith the recognition that parasitological positivity of CI.cases is inversely related to the duration of the lesion(RwwLIIY & RIDLLY, 1983; MAIMS' er al., 1985). It is notsurprising that ACL can he accurately identified by hull,respondents and interviewers in an area where ritedisease is common since the disease is generally visible,
f and has a characteristic history and appearance.The Intervention groups were well matched for age,
sex and past exposure to ACL.. It is possible thatinterventions exerted some effect on neighbouring controt houses, although the use of al half the houses u1the study area as,'reservoir houses' and the ruutluntu.atiun of interventions would be expected to minimize :illysuch effect. 71te concentration of aerosol pyrethrumdelivered to Ilse control houses was 1000-fold less th.wthe dose Ilu11111111y applied lu tltimitiitt isettu¡g :uul t.unlikely to have had is residual effect. Iluwevet, itsandfiies had been diverted from intervention to controlhouses the observed benefit would have been nvtr-estintated, although studies on mosquitoes indicate thatthere is no increase in biting on unprotected peoplesteeping near a treated bednet or cbuddar (I Iliwtrr er1996; ROWtJ,NI) a al., 1999a). It would have beendesirable to explore these issues entomologically, butavailable resources did not permit it.
About 45% of the original study population moved II(
died during the study. The emigration from the studyarea had already occurred by the time of the first follow-up survey, and was presumably due to seasonal migraiionfurther encouraged by the intermittent rocketing andshelling of the city (although nut directly of Ale studyarea) that occurred throughout the study period. Fur -tunately, this change in study population size wasanticipated at the start of the trial when we wereestimating the necessary sample size.
The final results indicate significant degree illprotcction against A([. attributable to l'l'Ns and onpregtulted rltuddarr or sheets. Individual house splayingwas also found to allcr significant protection, oftltuuphthis fell between the second and final surveys, possiblyindicating less persistence of effect. I
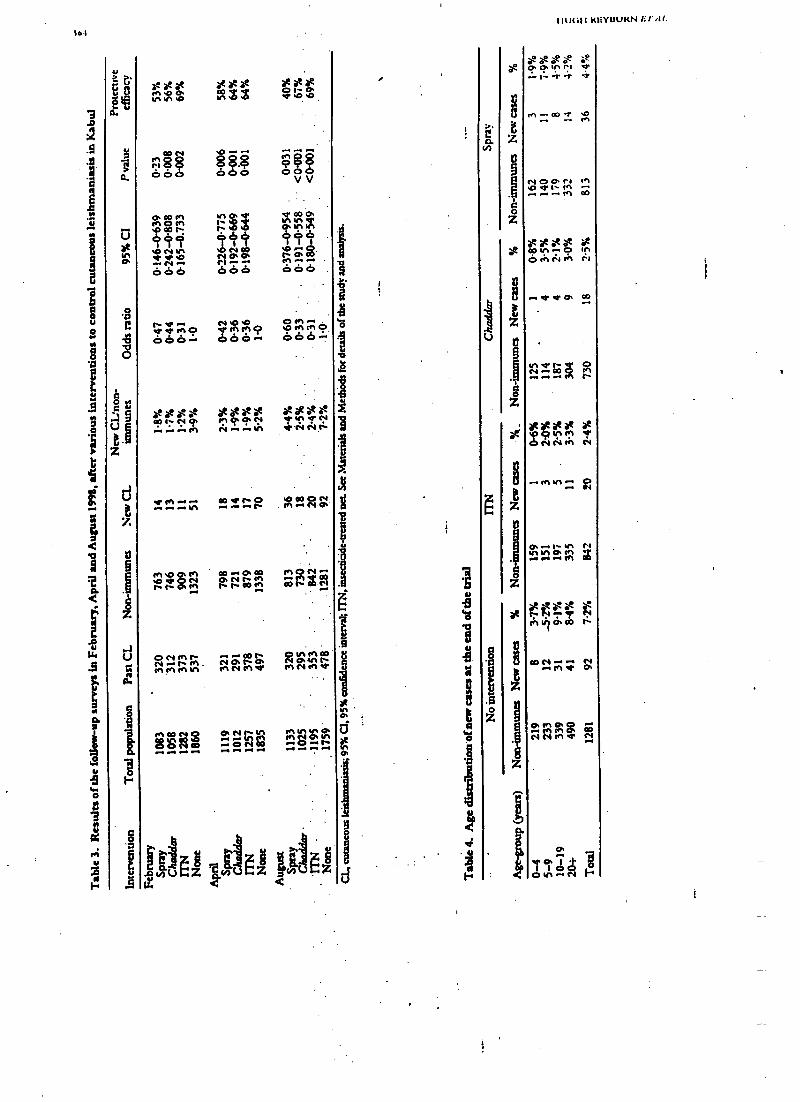
1eI
V
aka}. V
a
o
43
de
ava
ó
5
In In .O
e at atIn33
00N O.
ae OatV 0 .O
a88 s$ o$
t oo« N0 áív
f t4 I ó f ói0
dóó c6ó óóó
den0000- VNi100 60%+
0000 0000áoh N0. O";":4.... .... . tf1 Ñ
.. ON«...
......H1
GOMMO000 -
OD.. V'.. I's O 'O {q O Nr . N1.NO
pl OD .. 0. 00N O t'enON
ONIf1PeNnMInÑ
EIRE
...00tiNO.hO.InNN1V
o... r. .r ti .. .... -r .r
enON-+ôo"tiX.gR
OlnMOoNOan1P1NN1vs.
N O. ñ.r ... .. ...
Z
a°
ae
at
I I l)(:I l KIiYüUHN /if i11.
ó°é ó ó éEO. O.In rt wt.
- I- f T `:f'
on, ... 00 ..Y.
NOOrl WIOVI- mrr-r...e.1 co
xacXa= at00UN-0 InÓ eh e11 .:, e`I
+v'rO. CO
Ñ 00 M.w-r-.HM1111 I
*fogV'
N N tK1 N
.-.N1h.. Ñ
O. M1.N.}}
... IN. .Pr Iry m
at at ÑPI VIO 03 N
CO N.. M V N.. O.
Ch plCh Q301
N N In Is C4
ae.aÓIÁN
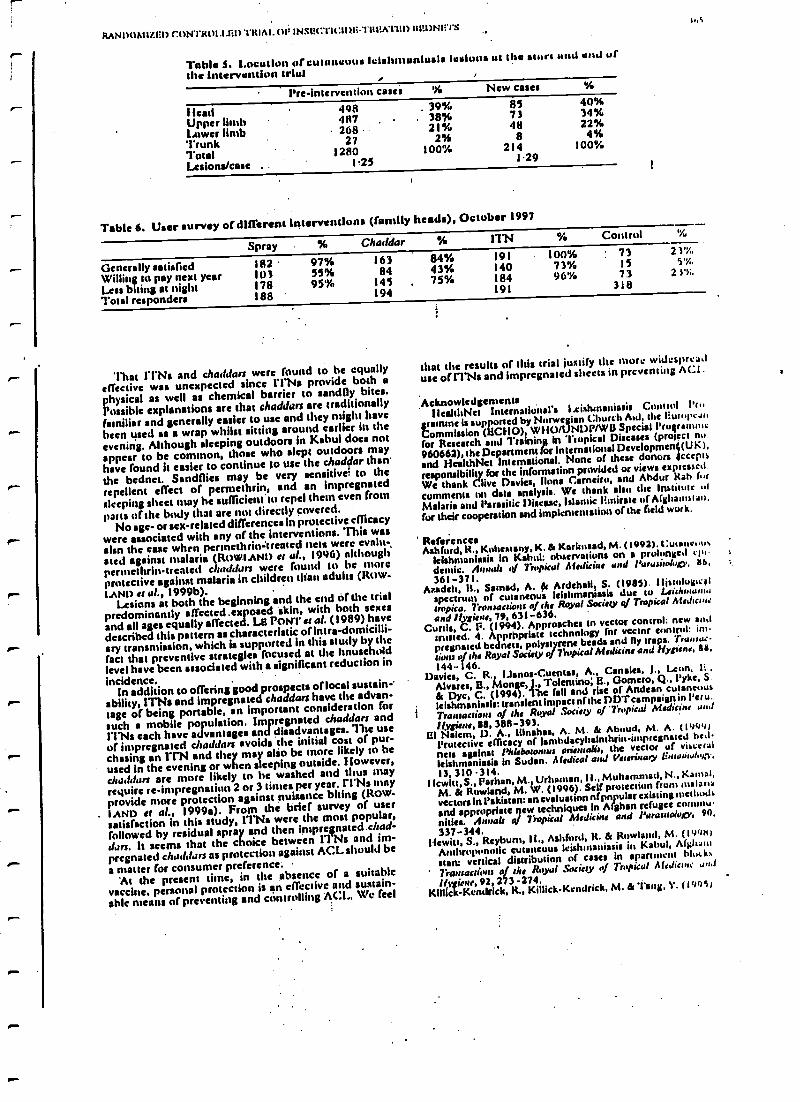
RANI)UMI'LGl) C:hNTR01.1.11l)'l'ItIAI. Ol' INSI?(:'l'It:ll)R= l'Itl?KI'I:D lt1:UN1'.IS
Table S. Location of cutaneous' Iclshmunlusls lesions ut the stunt and end of
the intervention trial . ,
Pre- intervention cases 96 New cases KL
Ilead 498 39% 85,40 3fo
Upper limb 487 . . 38% 73 3496
Lower limb 268 21% 48 22%
Trunk 27 2% 8 4%
' Cotai 1280 100/, 214 100%
Lesions/case 1.25 1.29
Table 6. User survey of different Interventions (family heads), October 1997
Spray % Chaddar 96 ITN % Control
Generally satisfied 182 97% 163 84% 191 10096 73 21%
Willing to pay next year 103 55% 84 43% 140 73% 15 5'%,
Less biting at night 178 95% 145 , 75% 184 96% 73 21%.
Total responders 188 194 191 318
That ITN: and chaddars were found to be equallyeffective was unexpected since l'l'Na provide both aphysical as well as chemical barrier to aandfly bites.Possible explanations are that chaddars are traditionallyFamiliar and generally easier to use and they might have
been used as a wrap whilst sitting around earlier in the
evening. Although sleeping outdoors in Kabul does notappear to be common, those who slept outdoors mayhave found h easier to continue to use the chadflar than
the bednet. Sonnies may be very sensitive= to the
repellent effect of permethrin, and an impregnatedsleeping sheet may he aufftcient to repel them even from
parts of the body that are not directly covered.No age- or sex -related differences in protective efficacy
were associated with any of the Interventions. This wasalso the we when pennethristtreated nets were evnht-
sted against malaria (ROWIANI) et al., 1996) althougliperntethrin- treated char/dun were found to be moreprotective against malaria in children than adults (Row-LAND et at, 1999b).
Lesions at both the beginning and the end cif the trialpredominantly affected .exposed skin, with both sexesand all ages equally affected. LE PONT et al. (1989) havedescribed this pattern as characteristic of intra-domicilli-sry transmission, which is supported in this study by the
fact that preventive strategies focused at the household
level have been associatedwith a significant reduction in
incidence.In addition to offering good prospects of loco! sustain-
ability, ITNs and impregnated chaddars have the advan-
tage of being portable, an important consideration forsuch a mobile population. Impregnated chaddars andl'l'Ns each have advantages and disadvantages. 'h is use
of impregnated chaddars avoids the initial cost of pur-chasing an ITN and they may alto be more likely to heused in the evening or when sleeping outside. However,chaddars are more likely to he washed and thus mayrequire re- impregnation 2 or 3 times per year. l'l'Ns mayprovide more protection against nuisance biting (ROW -
LAND et al., 1999a). From the brief survey of usersatisfaction in this study, 11Ns were the most popular,
followed by residual spray and then impreçnated.chad-dirn. It seems that the choice between 11 Ns and im-pregnated chaddars as protection against ACL should be
a matter for consumer preference.At the present hone, in the absence of a suitable
vaccine, personal protection is an effective and sustain-able means of preventing and controlling ACL. We feel
that the results of this trial justify the more widespreaduse of ITN: and impregnated sheets in preventing ACI .
AcknowledgementslleallhNei International's 1.cishmanissis Cumrol l'n.
gramme is supported by Norwegian Church Aid, the liurupeau
Commission (ECHO) WHO/ NOP/WI) Special Programme
for Research and Training in "Tropical Diseases (prow( nu.
960662), the Department for"T
r International Developmen U K ),
and HealthNet international. None of these donors accepts
responsibility for the information provided or views expressed.
We thank Clive Davies, Ilona C,arneiro, and Abdur Rah fur
comments on data analysis. We thank also the Institute ul
Malaria and Parasitic Disease, Islamic Emirate of Afghanistan,
fur their cooperation and implementation of the field work.
ReferencesAshford, R., Kuhestany, K. & Karitnsad, M. (1992). C:utancuu.
leishmaniasis in Kabul: observations on a prolonged epndemie. Annals q( T ntpical Medicinee and Parasitology, IU
361 -371.Munich, IL, Sarad, A. & Ardehsli, S. (1985). Histological
spectrum of cutaneous leishmaniasis due to Leis/warn.,invite. Transactions of the Royal Society of Tropical Medicineand Hygiene, 79, 631 -636.
Curtis, C. P. (1994). Approaches to vector control: new ao,i
t ed. 4. Apprhpriate technology for vector control: im.militated beddneth polystyrene beads and fly traps. Traiuuc-
uuns of the Royal Satiety of Tropical Medicine and Hygiene, es.
144-146.Davies, C. R., IJanos- Cuentas, A., Canales, J Leon. I:..
Alvares, IL , Monge, )) Tolentino; E., Gomero, Q., Tyke, S.
& Dye, C. (199. 1te tall and rise of Andean cutaneousleishmaniasis: transient impact of the DDT campaign in l'eru.
Transactions of the Royal .Society o ¡ 'Tropical Medicine and
hygiene, as', 388 -393.El Naiem, D. A., Mochas, A. M. & Aboud, M. A. (1')99)
Protective efficacy of lambdacyhalnthrininspregnaied he.lnets against Phlebotomus orientali,, the vector of visceral
leishmaniasis in Sudan. Medical and Veunne y l ntimintn1,i .
13, 310 -314.!!twin, S., Pathan, M. Urhausan, l 1., Muhammad, N., Kamm,
M. 8e Rowland, M. 1/. (1996). Self protection from malaria
vectors in Pakistan: an evaluation of popular existing nietiuuds
and appropriate ew techniques in Afghan refugee commu-
nities. Annals of Tropical Medicine and Parasitology, 90,
337 -344.Hewitt, S., Rayburn, It., Ashford, R. & Rowland, M. (l'0'1N)
Anthropunotic cutaneous leishmaniasis in Kabul, A(I;luui
start: vertical distribution of cases in apartment hlutk%
' Transactions of du Royal Sociey Of Tropical Medicine am!
HMRRicn,.92,273 -274.Klllick- Kendrick, R., Killick- Kendrick, M. & Tang, Y. (19951
Muhro; ' cutaneous leishmaniasis in Kabul, Afghani-stan: the high susceptibility of l'Ideboo,s rergentonn to l.ei,h-hnu,, nptca. Transaction, of the Royal Society of TropicalMedicine till., /hgi.ne, 89, 477.
Le Pont , F., Mouchet, J., Desjeux, I'.. Torres )?spejn, .J. &Richard, A. (1989). Epideminln7Qie de la leishmanini<e tegu-nxnuire en Ilulivie..lnnals .ie la Srcüsi Belge de Midecine7ñincale, 69, 267 112.
XI lls. A. (1961). 'Die cc Ica nfmalaria control. ln: Malaria,H.. g¡/or the I accine,'l'argets, G. A. 'I'. (editor). Chichester:Wiley & Sons, pp. 141-168.
Nadirn, A. & Rostami G. S. (1974): Epidemiology ofeutaneousleishmaniasis in Kabul, Afghanistan. Bulletin of she WorldHealth Organisation, SI, 45 -49.
Nadint, A., Mochar, M., I loushmand, II., Keyghobadi, K. &Allot (titian. M. R. (1995). litwlatiti(tn of pyrethntid impregnatedtt dnen /or toutoul of anthnT noose cutaneous leishn,an,asi, inDam. /s/amic Republic of Iran. Geneva: World Health Organisa -110w. WH0/1.EISH/95.37.
Ridley. D. S. & (tidley, M. J. (1983). 'Do evolution of the lesionin cutaneous leishmaniasis. journal of Pathology, 141, 83 -9.6.
Rowland. M.. Rhuma. M., Duc tuoea, D.. t)urrani, N., Rona-dial. J., Schapiro, A. & Sondorp, IL (1996). ('yrethroid.
HUtal l KUYUUtW ET Al.
impregnated bed nets (or personal protection against malariafor Afghan refugees. Transactions of the Royal Society of TropicalAledicute.and Hygiene 90, 357 -161.
Rowland, M., I)urrani, N., Ilcwim. S.. Mohamincd, N.,Boums, M., Carneiro, I , Rrtzentlaal, J. & Schapiro, A.(1999*). I'ermethrin- treated chaddars and top- sheets: appro-priate technology for protection against malaria in Afghani-stan and other complex emergencies. 7'runsu,,,;ws o f roeSociety o T n plcal Medicine and Hygiene. 93, 46 172.
Rowland, M Munir, A., Durrani, N., Noyes, 11. & Reyburtt, IAn outbreak of cutaneous leishmaniasis in an
Afghan refugee seulement In north -west Pakistan. T rauue-lio s of the Royal Society of Tropical Medicine and Hygiene, 93,133.-136.
'l'aych, A., Jalouk, 1.. & AI Khismi, A. M. (1997). A coton rois,leislunoniasis control vial pyre hruidin,preguuted bedneu utvillages near Aleppo, Syria. Geneva: World Hcrlth Organiza-tion. WIIO /LIIISIÌ /97.41
Received 13 September 1999; revised 8 Febntury 2000;accepted for publication 11 February 2000
Announcements
ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENEThe Transactions
The Transaction t of the Royal Society of Tropical Medicine and Hygiene Is issued bi- monthly (six pans per year) andpublishes not only papers presented at Society meetings and iymposis but also papers and correspondencesubmitted by Bellows and non - Fellows from.all over the world on every aspect of tropical medicine and internationalhealth. Supplements on specialist topics are published from time to time.
The annual subscription payable by Fellows Is £60.00 which becomes due in advance on the first of April eachyear. Subscriptions may be taken out for a period of five years at five times the current fee. Applications forFellowship must be made on the correct form, obtainable front the address below. There is a reduced subscription of425.00 for bons fide students which is limited to three years.
The Transactions may be purchased by those. other than Fellows of the Society, at £24.00 per Issue; £185.00 pervolume (hard copy plus (.D); £ I40.00 per volume (hard copy or CD). It is dispatched by accelerated surface mail(air freight) at no extra charge. A licence to network the CD costs £50.00.Further information and application (onus for Fel- Subscription orders from libraries andlowship can be obtained from: non- Fellows should be sent to:
'lise Honorary SecretariesRoyal Society ofTropical Medicine and Hygiene:Manson !louse26 Portland PlaceLondon, W113 1 LW, UKTelephone ) 44 (0)20 7580 2127Fax 1.44 (0)20 7436 1389e -mail mail(1Jrstmh.org
Royal Society ofTropical Medicine and HygieneSubscription DepartmentRnbquest Ltd, 3 riutnvirate HouseMilibank RoadKinganorth, AshfordKent, TN23 3JD, UKTelephone +44 (0)1233 611299Fax +44 (0)1233 639423e -mail Rquest ®robquest.demon.co.uk
ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENEManson and Chalmers Medals, 2001
The Manson Medal is awarded triennially. It.lathe Society's highest mark ofdistinction, and shall be made to theperson whose contribution to any branch of tropical medicine or hygiene is considered by Council to merit thehonour most. .
The Chalmers Medal is awarded each year in recognition of research contributing to the knowledge of tropicalmedicine ter tropical hygiene. Only persona of 45 years or under on I June of the year of the award shall be eligible.
Nominations may he trade by any renown( the Society, on forms available from Manson House. Completedforms should he sent to the Honorary Secretaries by 1 September 2000. Por full details please refer to the Yearbook.
TRANSACTIONS OP THE ROYAL SUCIIr IY UI°TROPICAL AItiDICINE AND I IYr7IliNl's (21101)) 94, Jul Sub
A randomized controlled trial of insecticide- treated bednets and chaddars or topsheets, and residual sprayingpf interior rooms for the prevention of cutaneousleishmanlasis ln Kabul, Afghanistan ;
Hugh Rayburn' , Richard Ashford', Muhantmnd Mohsen', Sean Hewitt' and Murk Ituwlund'' ' l /c Rh.`:. ,1ettn,atiaual, Peshawar, Pakistan; 'Liverpool School of Tropical Medicine, Pembroke /fare. Liverpool 1. i Still, f 1f;. ' I ,.,,.t..,School of Hygisns and 7epieal Msdicins, Keppel Strest, London I fICIC Sí17; UK
AbstractAnthroponotic cutaneous leishmanlasis (ACL) is, a significant public health problem in many towns andcities of south central Asia and the Middle East, resulting in disfigurement and disability winch warrant,preventive action. A randomized controlled trial was conducted in 1997/98 amongst a non- iInn)une studypopulation of 3666 people in Kabul, Afghanistan, to compare the efficacy of insecticide -treated 'lets (1'1'N s) ,insecticide -treated Islamic cloth wraps (cheddars) used to sleep in, and residual pyrethroid sprayingindividual houses for the prevention)of ACL. Dosages of insecticide were: ITNs with permethrin, 0.5 k/1112,cheddars with permethrin, l g/m'; rooms with lambdacyhalothrin, 30 mg/m3. Cases of ACL were diag ose.lon clinical criteria. At the end of the trial period (15 months) the incidence of ACL amongst controls was7.2 %, amongst ITN users 2.4% (OR 0.31, 95% CI 0.2 -0.5), amongst impregnated cheddar uscls 2 5'y;.(OR 0.33 95% CI 0.2 -0.6) and amongst residents of sprayed houses 4.4% (OR 0.60, 95% CI 0.3- (1.95 ).r I-N. and impregnated cheddars were equally effective, providing about 65% protective efficacy, o itl)approximately 40% protective efficacy attributable to individual house spraying. No significant differencesfor age or sex were fóund between new cases in the intervendcn and control groups. No serious side- act. uwere reported and interventions were generally popular; ITNs were the most popular, followed by residualspraying and then impregnated cheddars.
Kaywordst cutaneous leislrmaniesis, disease control, insecticide -treated materials. insecticide -treated licitness. L,..cspraying, perntethrin, lantbdacyhalothrin, Afghanistan
IntroductionAnthroponotic cutaneous leishmaniasis (ACL) has
been an increasing problem in Kabul over the past 40years (NADIM dt ROSTAMI, 1974; ASHFORD et all 1992).Over the past 10 years the situation has deteriorated,probably as a result of war -related environmental da-mage and population movement. The active prevalencein 1997 was estimated at over 5% of the I.2 millionpopulation (HEW= st al., 1998, H. Reyburn st a {.,unpublished data).
ACL frequently causes large and/or multiple lesions onexposed skin which can be very disabling and disfiguring,and there is a demand for treatment in Kabul whichgreatly exceeds the available resources. A cost -effectiveand sustainable strategy for ACL control in Kabul isclearly indicated. 7be present study was conducted aspart of an aid programme to identify such a strategy andsubsequently to control the epidemic of ACL currentlyaffecting the city.
Control measures against ACL have largely beenconfined to indoor spraying with residual insecticide,and ACL became rare in areas where spraying was usedprimarily for malaria control (DAVIES et al., 1994).However, the problems of cost to public health autho-rides, acceptability and sustainabiliry associated withresidual spraying indicate the need for alternatives(MiU.S, 1991, CURTIS, 1994).
The satiny vector in Kabul, Phlsbotomus urgsnti, isconsidered to be endophagic and to bite mostly in theevening and at night (KILLICK- KENDRICK st al., 1995;HMV= et al., 1998). Sandtlies are generally sensitive toinsecticide- treated fabrics (ELNAIEM etai.,1999). Thuspersonal protection with impregnated bednets or ched-dars (Islamic cloth wrap) could be an effective alternativeto spraying.
ROWLAND et al. (1996; 1999a) have shown insecti-cide- treated nets (ITNs) and impregnated cheddars to besafe, effective and sustainable strategies for malariacontrol in Afghanistan and Pakistan. WHO is currentlysupporting trials of ITN. in the prevention of ACL inseveral countries; the resulta from the trials in Syria andIran suggest a protective efficacy of over 50% (NADIM et
'Author for correspondence; phone +44 (0) 20 7927 2333.
al., 1995; TAYBH st al., 1997). No trials un the use ofimpregnated sheets to prevent ACE. have su tar t.ecnpublished.
Individual house spraying with residual insecuculcmay avoid the problems of inadequate centralized fund-ing by recovering the cost from individual householderswho opt for the spray. However, evidence fur citeeffectiveness of residual spraying is anecdotal undl, :.s
far as we are aware, has never been evaluated) incontrolled trial.
Thus before committing scarce aid resuutLcs t., .,
particular strategy in Kabul, it was decided to c,ut,ht. ta controlled trial to test the efficacy of personal prat ctusing either l'I'Ns or impregnated sheets Io ha. l,I,,.)...,individual house spraying with residual inset. t 1,1c
Materials and Method,'Stu area
The Kartb -Naw area of Kabul was identified as heist,;suitable for the trial, based on available local inforntartortand a series of rapid surveys of ACL throughout the sit )Karte -Naw is a previously lower middle -class suhut I.about 3ktn south eau of the city centre; houses atemostly made from mud or brick with about 30% havingbeen destroyed by war. There appeared to he a highprevalence of active ACL, with a relatively low preva-lence of past infection, indicating that a high proportionof the population was still susceptible to the thseaseWhilst there was known to be a high population tnubilit y,the local community was friendly and co- operativeThere was no evidence of prior bednet use in the area
Sample sissThe required sample size was calculated its order t..
demonstrate a 50% reduction in ACL attributable to anyof the interventions with 95% confidence and kit.power, assuming an unexposed (control) group twi:eas large as each of the intervention groups and an AC1.
i incidence of 5% amongst the controls. In order w satisfythese criteria, a minlnlum sample size of 765 for ca.ltintervention group and 1530 for the control group Hascalculated. It was estimated that about 30% of thepopulation would move during the triai and that about30% were already immune to ACL: through priorexposure. Thus the target sample size was increased to
bIIIUt:tt REVUE-MN li'l'.al
2000 for each intervention group and to 3500 for thecontrol group.
Implementation of interventionsAn area of 2000 houses was mapped and each house
was painted with a code. The area was divided into blocksof 10 houses on the map and interventions wererandomly allocated to houses within each 'block asfollows: I ITN, l impregnated cheddar, 1 residual spray,2 t.untrol (i.e., untreated but included in the study) and 5'reservoir' (i.e., untreated and not included in the study).'Dios at the end of the sampling, the snap resembled amosaic of interventions, controls or reservoir houses.Reservoir houses served to minimize the risk that Inter -ventions would affect neighbouring houses. Local com-munity leaders and mosques helped to explain the workand encourage participation. Eight households refusedthe spray and were re- allocated to ITN Or cheddargroups.
Al 957householdsinthestudywerecensused ;dstawere: collected from one of the parents of the household for allhousehold residents: their age and sex, relationship tohousehold head, past and present history of ACL anddetails of any current lesions (number, position, size,duration). Reported lesions were inspected and clinicallyconfirmed wherever possible by the surveyworkers, whowere all either treatment orlaboratory technicians of theInstitute of Malaria and Parasitic Disease of the IslamicEmirate of Afghanistan. Survey staff worked in male -female pairs to ensure good access to houses and residents.
The disease was highly prevalent in the .area and thecommunity was fanuliar with the disease by its local naine
(widens!). The survey technique was the same as thatvalidated by ROwtANO eral. (1999b) in northern Pakistan.
ITN houses were assessed for the number of bednet:(100-denier, 156 holes/mesh per square inch) needed forthe whole household, and provided with family -sizedpolyesternets (nets measured 2.2 in X 2 in X 1.5 m; 498were distributed, averaging 2.4 eopple per net) whichwere impregnated in front of the family with instructionsas to their proper use. Households selected for itnpreg-nated sheets were asked to produce the cover -sheetwhich they used at night, usually a cheddar or a similarpiece of cotton cloth, which was impregnated with 1 g/m' of permcthrin (Imperator 25 EC, Zeneca, Fernhtrst,Hasiemere, Surrey, UK) with instructions not to wash it.
Houses selected for residual spray had the interior ofliving and sleeping rooms (including ceiling) sprayedwith lambdacyhslothrin (ICON 10% WP, Zeneca) at atarget rate of 30 mg/ms. ITN: were impregnated with0.5 Wm' of permethrin ( Imperator 25 EC, Zeneca).
Prior to treatment, samples of cheddars were tested forwater absorbency. On the basis of this, .2 dilutions ofinsecticide were used, one for cotton (0.15 Um') andone for woollen materials (0.2 Um3). Because cheddarscame in various sizes, individual chaddars were dipped inan excess of insecticide solution and the excess wassimply wrung out.
Control and reservoir households were offered a 10 -s
aerosol spray using a 1:50 solution of permethrin (Im-perator 25 EC) delivered from a knapsack motorizedaerosol into the centre of their living and sleeping rooms.The estimated deposition rate was less than 0.5 mg/m'.Interventions were all in place by the end of May 1997which was designated as the start date of the trial.
Follow -up of study householdsTwo months front the start of the trial all the houses
with ITN: or cheddars were re-visited and any that hadbeen washed were re- Impregnated. After further 3months (i.e., at the end of the transmission Season) all thetrial houses were re- visited and the household head(mother or father) was asked 3 questions: 'have younoticed less biting by insects thisyear?', 'are you generallysatisfied with the (intervention)?' and 'would you bewilling to pay for this service in the future ?'. A simple
yes -no response was recorded. Direct observation of
bednet compliance or sleeping habits was not socially
acceptable.Follow -up surveys of all the houses in the study were
undertaken in February, April and August 1998, i.e., 8,
10 and 15 months after the interventions had been put inplace. New cases of ACL occurring amongst the uriginulresidents were noted. A new case was defined as any case
of ACL that was reported by the respondent to havestarted after 3 months from the beginning of the trial. Alllesions were visually inspected and accepted as cases only
if their appearance and history were clinically consistentwith ACL. Doubtful cases were not included as new
cases. It was Intended to take a slide from all new cases in
the final follow -up survey (August 1998), but the suddendeterioration in the political situation in Kabul in July1998 made this impossible.
The st -risk population was defined as alt those whohad remained resident in the study area during MayNovember 1997 and did not report previous infectionwith CL ('non -immunes').
Survey workers were blinded as to the interventionreceived by households, having been provided with asurvey form that was blank except Tor the address, and
were instructed to ask respondents not to reveal the typeof intervention during the interview. In order to avoidbias, survey workers were deliberately not dedicated to a
specific Intervention.During the second survey 2 of the 5 survey teams
incorrectly failed to mark cases that had been identifiedin the first survey as 'new cases'. These cases werecarefully checked in the final survey and the data from
the second survey were corrected accordingly.At the end of the trial ITNs were distributed free to all
the residents of control houses.
AnalysisData were analysed ill MS-Excel and State 5. Because
the interventions were allocated at household level, the
data were analysed by a random effects logistic regressionmodel to adjust for the possibility that individuals within
a household might be more similar with respect to the
intervention outcome than individuals from other house-
holds (intro- cluster venation). 'Dais method of analysisnecessitated the use of odds ratios (ORs) rather thanrelative risk. Adjustment for intra- household clusteringacts to increase the confidence intervals around the point
estimate, thus providing a more conservative estimate of
intervention effect. .
ResultsBy the end of the trial about 45% of the original trial
population had shoved. Pre- intervention duca arc pre-sensed on those who were resident during the transmis-sion season of 1997 (assumed to be May to November)and who were still resident at the same address at the fmal
follow -up sursky in August 1998. Most of the migrationfrom the study area appeared to be seasonal and a few of
the study population returned to their houses betweenthe 3 follow -up surveys (February, April and August1998); these people were included in the trial if theyreported that they had been resident during the transmis-sion season of 1997. This inclusion policy accounts for
,
the small variations in the study populations found at the
3 follow -up surveys (Table 3). People moving into the
study area after the beginning of the trial were notincluded. .
At the start of the trial no significant differences werefound between the intervention and control groups for
age. (Kruskal- Wallin x' 2.4, 3 d.f., P m 0.49), sex (X'
4.82, 3 d.f., P =s 0.19), active ACL (x' 1.4, 3 di.,P = 0.7) or past ACL (X' 0.03, 3 d.f., P = 0.9) (Table1). Overall, the mean age was 19.4 (SD 16.3, median 15 )
years and 4Wi were female.'1lw median household size
was 8.In the pre- intervention survey 12 cases of active ACL
RANI)UAtI-LIED CONTROLLED ()I, IN3li(:'l'I(:IL)Ii-'l'IrIEA'r1E1) I11E1)N1:1'S
' Table 1. Population characteristics at the start of the trial for prevention ofcut;u,euua leiyhn, :,uiu +i+ (( 1.)
intervention '
Nola.Spray (aaulddr 11N
l'opale ' , total 1135 11125 1195 !!9VAge in }vars, median 16 16 In 15
Dentale, ",L (number) tIt'i (5.17) .17. , (177) I9'i (591) SU';b (x77)CL, !ó (number)
r` Active 12'Y, (1 35) 12% (118) 11% (133) 10% (18.1)!vast 16% (185) 17% (177) 18% (220) 17'%. (295)
FIN, inscctieide- treated net. Fur details of the intcrventiuns see the text.
were reported amongst those who also reported havinghad ACL in the past (0.2% of the total population, and2.1% of the active cases) and these were counted as pastcases only. No new cases found at the end of the trialreported previous infection with ACL.
Age -band specific prevalence rates for active ACLamongst non -immunes (defined as those with no pasthistory of ACL) at the start of the trial showed that thosein the age -group 0 -4 years had a significantly lowerprevalence of ACL (x' 24.96, 3 d.f., l' < 0.001) thanthose in the older age -groups (5-9, 10 .19, P, 20 years).No statistical difference was found for active CI . betweenthese older age -groups (x' 4.41, 2 d:f., 1' = 0.11) (Table2). No association was found between sex and activer ACL at the start of the trial (x' 0.21, 1 d.f., P = 064).
At the end of the trial there were significantly fewernew cases of ACL amongst the l'l'N households (OR(1.31), chaddtrhouseholds (OR 0.33) and residual sprayhouseholds (OR 0.6(1) ('('able 3). The OR attributable toresidual spraying rose between the second and finalsurveys, possibly indicating an excess of cases whichhad been transmitted late in the year or even early in theyear following the study.
The age distribution anew cases was not significantlyr different between the intervention groups (Kruskal-\ \'allis x' 2 1, 3 d.f., 1' - 018); as found in the pre -intervention survey, the < 5 years age -group had a lowerincidence of ACL than those aged > 5 years (x' 12.5,
P"'" 3 d.f., Pad 0.007) and the 3 age-groups older than 5years had a similar incidence (x 0.29, 2 d.f., P = 0.86)(Table 4). 'Ilse proportion of tales and females amongstnew cases in each of the intervention groups was notsignificantly different (x' 2.26, 3 d.f., 1' = 0.5).- Lesions occurred predominantly on exposed skin, andno significant difference for location of lesions was foundbetween pre -intervention and new cases (x' 3.06, 3 d.f.,P = 0.38) or between new cases in intervention groups atthe end of the trial (x' 15.8, 9 d.f., P = 0.4) (Table 5).
r- Families were generally satisfied with the effect of theinterventions, but control families were less satisfied withthe aerosol spray. 11 -Ns were the most popular, withabout 96% of families reporting a reduction in biting atnight, followed by residual spray and then impregnatedchadd,)n ('Fable 6). Amongst families who had stayed inthe study area, only 5% of l-l'Ns hail been disposed al)),the end of the transmission season.
r
r'ruble 2. Aye -group specific prevalence of activecutaneous lelshuuutlusis (Cl.) ut the *hurt of thetrial i
Age -group ' Non- Active CU(years) immunes Active CL non- immunes
0 -45 -910 -1920 fTotal
716 51 7.1%763 125 16.4%
1070 168 15.7%1687 226 13.4%
4236 570 . 13.5%
1
DiscussionThe measuring tool for ACL used in this study sous
questionnaire completed by one of the parents of thehousehold, with visual checking of reported cases by ;unexperienced interviewer familiar with the disease. 'I Iseplan was to confirm at least u sample anew cases in sirtrial with slit -skin smears and cultures. however, theunexpected deterioration of the security situation and thepremature expulsion of all aid organizations from Kabulin July 1998 made this action impossible.
In the absence ofparasitological confirmation ofca +c .,bias could be introduced by either the interviewer in Ilnsubject, even though survey wurkes in tiro vial tk, nblinded to the identity of the intervention that eat. I1had received. The saine survey methudulogy was voltdated by microscopy examination, polymera.e thawreaction or culture in north l'ukistan (Ittox't AND cr ,
1999b) where over 8U' %, of cases identified by a tine+tiot)naire survey were conliruted parasit tlogically; Ic
skins ofunconfirmed cases tended to be uldet, cunustcntwith the recognition that parasitological positivity al ( :I.cases is inversely related to the duration of the lesion(RIDLIEY & RIDL.EY, 1983; A'LAUlili x101., 1985). It is outsurprising that ACL can be accurately identified by bk,tl,respondents and interviewers in an area white thedisease is common since the disease is generally vc.,l,I.,and has a characteristic history and appeurame.
'The intervention groups were well matched for ago,sex and past exposure to AC1.. It is possible ulna,interventions exerted some effect on neighbouring i antrol houses, although the use of ;liana half the house u,the study area as *reservoir houses' and the raadunui.,lion of interventions would be expected to minimise ai I.such effect. The concentration of aerosol pyrethruuldelivered to the control houses was 1000 -fold less thanthe dose normally applied to mosquito netting andunlikely to have had a residual effect. However, ifsandflies had been diverted (ruin intervention to cunualhouses the observed benefit would have been ayes -estimated, although studies on mosquitoes indicatethere is no increase in biting un unprotected peolklcsleeping near a treated bednet ur chad,Iar (I itt\r'rlI et ul ,1996; ROWL#ND cr al., 1999a). It would have livendesirable to explore these issues entomologically, butavailable resources did not permit it.
About 45 %, of the original study population nn,vckl k.,died during the study. The emigra (rum the silk!)area had already occurred by the time ul'the first fallakeup survey, and was presumably due to seasonal uugrafurther encouraged by the intermittent rocketing u,klshelling of the city (although not ditetty of the stjk.l)urea) that occurred througl t the study I' nil 1 ku
tunately, this change in study population sirs w.,,anticipated at the start of the trial when we wereestimating the necessary sample size.
The final results indicate u significant degree , fprotection against AC1. attributable to ITNs and im-pregnated chaddarr or sheets. individual house sprayingwas also found to offer significant protection, althoughthis fell between the second and final surveys, possiblyindicating leas persistence of effect.
304
á
à etn %O ITtnNO
aD N
Ñ 00óóó
O O OOD -t .1*N o .o
O$S664>
O Y p\o Coaoo
Ó O ÓoVV
sr. CO CTCT o0 vl
V wñ r ' átNntnóóc óóó .óóó
x ÓÑIA tÓN010 W..ÓN C4 CA á00O
000 000 O.00/
o
ebÓ
d
to
.1O
í
' 3
S
g r Ir10V.4 4D OMtnO
ÓóÓ.+ ÓÓÓ-+ ÓÓC^'
at at at at at\at1 atpE\pEOO N1ttT N NV'N... . .r iÁ V
0:r .. I( ' V' lV N t
vl . ..h ~ 1+1ÑP
bON OO.+0.00 N10.NVTr
tPtOtM tiÑ0^Oí1 OOÑOOÑ.N ..t ..1
ONt+1h 001-. CD a0
fN/1N1f~t1Ñ IHÑt1 , tt1ÑGwV'
In CO
ÓÓN00ilme di.
.Ch+N1tsAM
.+ONOO'.. ...r .. .r
01 N WI Oh
Ó ñ.
1zz xutY. c 4
ti
U
1
6o`
ú
z
.
èE
z
.Óz
HUM! IUi, llUlttl !í l:1I
-o -o .o .o`oç o` o O O`tTl7.VIfl 7-1-T-r r
tn - w -r otn
ro G o r 1 .nO rt 1- t- t . Cl.,
at at ¡E at attANr.Q It1
644, q:1441' f l
CP. -ru+It,1 IG, O
ó C at 't1. vi f1
tn M+ ti. co I-
°Ó=.Itna á
ChtviGPná 00
N N tt1 V' ^
c.aa 1 t 0ÓNÑ i"
1
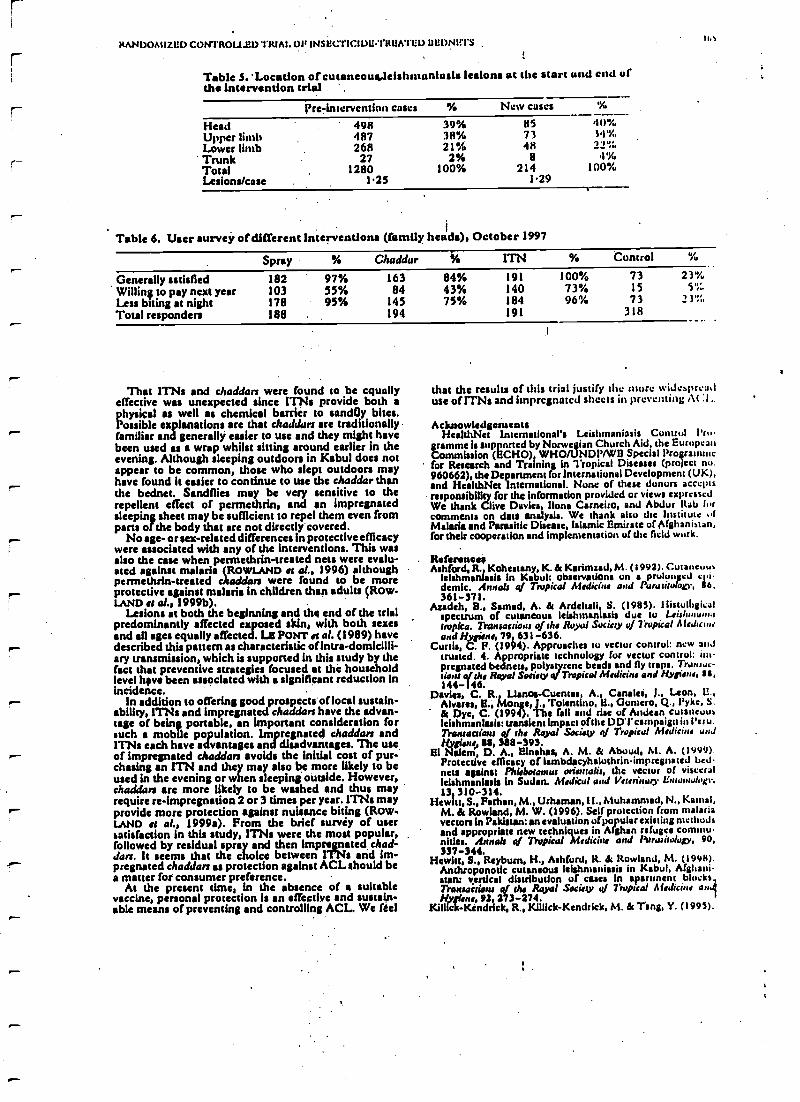
RANDOMIZED CONTROLLED TRIAL Olt INSECTICIDE- TREATED uutiNL'TS
Table S. ' Location of cutaneousyleishmanlasis lesions at the start und cad ofthe Intervendon trial . .
l' re-Jntervcrstion cases % New cases
HeadUpper limbLower limbTrunkTotalLesions/case
498487268
271280
1'25
39%38%21%2%
100%
857348
8214
1.29
40'%,;4'%.2_r;
4'%,100%
Table 6. User survey of different interventions (family heads), October 1997
Spray % Cheddar ßi6 ITN % Control
Generally satisfied 182 97% 163 84% 191 100% 73 23'%,
Willin; to pay next year 103 55% 84 43% 140 73% 15 5'hLess biting at night 178 95% 145 75% 184 96% 73 ? )"t.
Total responden 188 194 191 318
rThat 1TNs and cheddars were found to be equally
effective was unexpected since ITN: provide both aphysical as well as chemical barrier to sandßy bite,.Possible explanations are that cheddars are traditionallyr familiar and generally easier to use and they might havebeen used as a wrap whilst sitting around earlier in theevening. Although sleeping outdoors in Kabul does notappear to be common, those who slept outdoors mayhave found it easier to continue to use the cheddar thanthe bednet. Sandflies may be very sensitive to therepellent effect of permethrin, and an impregnatedsleeping sheet may be sufficient to repel them even fromparts of the body that are not directly covered.
No age- or sex -related differences In protective efficacywere associated with any of the interventions. This wasalso the case when permethrin- treated nets were evalu-ated against malaria (ROWLAND et al., 1996) althoughpermethrin- treated cheddars were found to be more
r- protective against malaria in children than adults (ROW-LAND et af., 1999b). .
Lesions at both the beginning and the end of the trialpredominantly affected exposed skin, with both sexesand all ages equally affected. LE PONT et al. (1989) havedescribed this pattern as characteristic of infra- domicilli-ary transmission, which is supported in this study by thefact that preventive strategies focused at the householdlevel h(tve been associated with a significant reduction inincidence.
In addition to offering good rospects of local sustain -ability, 1TNs and impregnated cheddars have the advan-tage of being portable, an important consideration forsuch a mobile population. Impregnated cheddars andITNs each have advantages and disadvantages. The use
r- of impregnated cheddars avoids the initial cost of pur-chasing an ITN and they may also be more likely to beused in the evening or when sleeping outside. However,cheddars are more likely to be washed and thus mayrequire re- impregnation 2 or 3 times per year. 1TNs mayprovide more protection against nuisance biting (Row.LAND et al., 1999a). From the brief survéy of usersatisfaction in this study, ITN, were the most popular,followed by residual spray and then impregnated ched-dars. It seems that the choice between ITN5 and im-pregnated cheddars as protection against ACL should bea matter for consumer preference.
M the present time, in the absence of a suitablevaccine, personal protection is an effective and sustain-able means of preventing and controlling ACL We feel
that the results of this trial justify the more widespreaduse of ITN: and impregnated sheets in preventing At :1..
AcknowledgeusentsHealthNet International's Leishmaniasis Cuntrul Pro-
gramme is supported by Norwegian Church Aid, the EuropeanCommission (ECHO) WHO/UNDP/WB Special Proeranuocfor Research and Training in Tropical Diseases (pro ect no.960662), the Department for International Development (UK),and HealthNet International. None of these donors acccpisresponsibiliry for the information provided or views expressedWe thank Clive Davies, Ilona Carneiro, and Abdur !tab forcomments on data analysis. We thank also the Institute ofMalaria and Parasitic Disease, Islamic Emirate of Afghanistan,for their cooperation and implementation of the field work.
Reference jAshford, R Kohestany, K. & Karimzad, M. ( I 992). Cut ancuu,
Idshmanlaais in Kabul: observations on a prolonged c .iiedem. Annals of Tropical Medicine and Purasisoloov, 56,
361 -371.Azadeh, li., Samad, A. & Ardehali S. (1985). Ilistulhgieal
spectrum of cutaneous leishmantasis due tu l tit /uuu +u.,tropiea. Transactions of the Royal Society of Tropical Medicinearid pane, 79, 631 -636.
Curtis. P. (1994). Approaches tu vector control: new andtrusted. 4. Appropriate technology for vector control: im-pregnated bednets, polysryrene beads and fly traps. Tranure-riosu q/ the Royal Society 4/ Tropical Medicine and Hygiene, 55,144 -146.
Davis,, C. R., Llanos -Cuentas, A.. Canalca, J., Leon, U.,varAlo, Mons,)) , Tolentino. I3., Gomm, Q., Pyke, S.
& Dye, C. (1994). The fall and rise of Andean cutaneousleishmanlasis: transient Impact of the DUI' campaign in Peru.7Yonsactioru of the Royal Society of Tropical Medicine andHygiene, 88, 388 -393.
El Nalem, D. A., Elnahas, A. M. & Aboud, M. A. (1999).Protective efficacy of lambdacyhalothrin- impregnated bednets against Phlebotomist onerttalis, the vector of visceralleishmaniasls in Sudan. Medical and Veterinary li, assiol' h,13 310 -314.
Hewitt, S., Ferhan, M., Urhaman, II.. Muhammad, N., Kemal,M. & Rowland, M. W. (1996). Self protection from malariavectors in Pakistan: an evaluation of popular existing methodsand appropriate new techniques in Afghan refugee communulles. Annals of 7iapical Medicine and Parasitology, 90,337 -344.
Hewitt, S., Reybum, H., Ashford, R. & Rowland, M. (199$).Anthroponotie cutaneous lelshmaniasi, in Kabul, Afghani-stan: vertical distribution of cases in apartment blocks,Transactions of the Royal Society of Tropical Medicine analHygiene, 92, 273 -274.
Killick- Kendrick, R., Killick- Kendrick, M. & Tang, Y. (1995).
100
Amino' tic cutaneous leishnnaniasis in Kabul, Afghani-stan: the high susceptibility of Phkboromru sergenii to Leish-uania trollied. Trank:etiam of she Royal Society ,y Tropical.t l(Jicine asid Hygiene, 89, 477.
Le Pont, F., Mouchet, J., Desjeux, P., Torres lisp *Íu, J. &Richard, A. (1989). Epidemiolugie de la Icishonaninse tegu-menraire in Bolivie. Annale de Its Susilll Belie de Alidecine7 ivpicaI s 69, 297-312.
Mills, A. (1991). 'Du economics of malaria control. In: Atalari,,,Waiting for the Vaccine, Tsrgett, G. A. T. (editor). Chichester:Wiley & Sons, pp. 141 -168.
Na,tim, A. & Rostami G. S. (1974). Epidemiology of cutaneousIeishmaniasis in Kabul, Afghanistan. Dalkon of the WoddHealth Or anisanoti, SI, 45 -49.
Nadim, A., Atotabar, M., Iloushmand, U., Keyghubadi K. &Allatonian, M. R. (1995). Evaluation of pyrerhnid impregnatedled -nets for cannot of anlhrapouark cutaneous lsishonamasia inn
Rani, Islamic Reppublico/lrats. Genera: IVoddHealth Organisa-tion. WHO/1BISH195.37.
Ridley, D. S. & Ridley, M. J. (1983). The evolution of the lesionin cutaneous leishmaniasis. jaunted 0/Pathology, 141, 83 -96.
Rowland, M., Houma, M. Ducomes, D., Durrani, N., Rosetn-daal, J., Schapira, A. St Sondurp, B. (1996). Pyreihrold-
1IUt il I ItItYlIU14N El Al
impregnated bcd nets for personal protection against magnaifor Afghan refugees. Transactions st/ the Royal Society n/7 apicalMedicare and 0giene, 90, 357 361.
Rowland, M., Durrani, N., Hewitt, S., Mohammed, N..Douma, M., Carncirtr, i., Rosemlaat, J. & Schapira, A.
(1999e). Pernnu(luin- treated chaJdan and sup -sheets: apprisMate technology for protection against malaria in Afghani-stan and other complex emergencies. 7' limn u / the ltnralSucks o Tropical Medicine and Hygiene, 93, 465-472.
Rowland, M., Munir, A., Distend, N., Noyes, 11. & Hcyburrn, 11(1999b). An outbreak of cutaneous leishnnalniasis in unAfghan refugee settlement In north -west Pakistan. To/mac-11.1)118 of the Royal Society r{f Tiapieal Medicine and Hygiene, e, 93,133 -136.
Tayeh, A., jaluuk, L. & M ¡Chianti, A. M. (1997). .1 in.leishntaniasis control trial using pyre: d- impregnated he,luen wvillages near Aleppo, Syria. Geneva: World I leulth Organürdon. WHO /LBISIH /97.41
Received 13 September 1999; revised 8 Pcbnrar,' 2000;accepted for publications 11 Febntay 2000
Announcements
ROYAL SOCIETY OF TROPICAL MEDICINE AND )HYGIENEThe Transactions
The Transactions of the Royal Socís(y of Tlvpical Medicine and Hygiene h issued bi- monthly (six puns per year) andpublishes not only papers presented at Society meetings and symposia but also papers and correspondencesubmitted by Fellows and non -Fellows from all over the world on every aspectof tropical medicine and internationalhealth. Supplements on specialist topics are published from time to time.
The annual subscription payable by Fellows is £60.00 which becomes due in advance on the first of April eachyear. Subscriptions may be taken out for a period of five years at five times the current fee. Applications furFellowship must be made on the correct form, obtainable from the address below. There ii a reduced subscription of£25.00 for bona fins students which is limited to three years. .
The Transactions may be purchased by those other than Fellows of the Society, at £24.00 per issue; £185.00 pervolume (hard copy plus CD); £140.00 per volume (hard copy or CD). It is dispatched by accelerated surface mail(air freight) at no extra charge. A licence to network the CD costs 450.00.Further information and application forms for Feu- Subscription orders from libraries andIowship can be obtained from: non -Fellows should be sent to;
The Honorary SecretariesRoyal Society of Tropical Medicine and HygieneManson House26 Portland PlaceLondon, WI 8 I EY, UKTelephone +44 (0)20 7580 2127Fax +44 (0)20'7436 1389e -mail mailerstmlt.org
Royal Society of Tropical Medicine and HygieneSubscription DepartmentRobquest Ltd, Triumvirate rouseMillbank RoadKinganorth, AshfordKent, TN23 3JD, UKTelephone +44 (0)1233 611299Fax 1.44 (0)1233 639423c -mill RqucslGNrobyucsl.dcsn .cu.uk
ROYAL SOCIETY OP TROPICAL MEDICINE AND HYGIENEMatson and Chalmers Medals, 2001
The Manson Medal is awarded triennially. It is the Society's highest mark of distinction, and shall be made to theperson whose contribution to any branch of tropical medicine or hygiene is considered by Council to merit the
honour most.
The Chalmers Medal is awarded each tear in recognition of research contributing to the knowledge of tropicalmedicine or tropical hygiene. Only persons of 45 years or under on 1 June of the year of the award shall be eligible.
Nominations may be made by any Fellow of the Society, on forms available fromManson House. Completedforms should be sent to the Honorary Secretaries by 1 September'2000. For full details please refer to the Yearbook.





























