Embed Size (px)
Citation preview
L L L K 0 neric ozon 5 .
1
Beverly E. Tilton U. S. Environmental Protection Agency
Research Triande Park, NC 27711
Ozone is an allotrope of oxygen that occurs naturally in the planetary bound- ary layer. At excessive levels, ozone has been demonstrated to induce per- turbations in a number of biological systems and to produce oxidative deg- radation in certain nonbiological mate- rials. It has also been imolicated as a contributor, to varying degrees and un- der specified atmospheric conditions, to the chemical and physical processes in ambient air that produce such particu- late- and aerosol-related phenomena as acidic precipitation and deposition, at- mospheric visibility reduction, and cli- mate modification.
Ozone is a “criteria” pollutant, regu- lated under Sections 108 and 109 of the
effect on public health and welfare . . .the presence of which in the ambi- ent air results from numerous or di- verse mobile or stationary sources.” In contrast, a hazardous air pollutant is de- fined in the CAA to mean “an air pollu- tant to which no ambient air quality standard is applicable and which in the judgment of the Administrator may cause, or contribute to, an increase in mortality or an increase in serious irre- versible, or incapacitating reversible, illness’’ (I). Thus, it will be helpful to keep in mind that ozone is a criteria pollutant.
Major health e5ects Ozone is a highly reactive gas and a It Clean Air Act (CAA) (1). A criteria cal strong systems oxidant. are Its heterogeneous, reactions in biologi- that is,
pollutant is defined in the CAA as an gas-liquid reactions, since biological air pollutant that in the judgment of the systems are aqueous systems. In heter- Administrator of EPA “has an adverse ogeneous reactions, ozone has been
f
This M i l e not subject to US. Copyright. Published 1-9 American Chemical Society Environ. Sci. Technol.. Voi. 23, No. 3, 1989 257

shown to react rapidly, but selectively, with many organic compounds. It re- acts with alkanes at room temperature, for example, but is about 400,ooO times more reactive toward alkenes than tw ward alkanes (2). Not unexpectedly, then, ozone reacts rapidly with bioorganic compounds containing dou- ble bonds, such as unsaturated fatty ac- ids (2,3), many of which are function- ally and structurally essential. Ozone will also react with sultlydryl and amino groups, which are found in en- zymes and other essential proteins (4).
Its reactivity toward biologically im- portant chemical moieties results in rapid reactions between ozone and the cells, fluids, and tissues that line the respiratory tract, since ozone enters the body via the respiratory tract. lkio ma- jor categories of effects of ozone on the respiratory tract have been identified: (1) alterations, usually impairment, in the mechanical functions of the lung,
to more rapid and more shallow breath- ing; limitation of the “depth” or size of the deepest breath an individual can take; and an increase in reactivity of the respiratory tract to inhaled stimulants or irritants. These changes have been measured by classical clinical spirome- try, a noninvasive procedure. (Spiro- meters measure the volume of air moved in and out of the lungs.)
The most commonly used spiromet- ric measure of ozone-induced lung function changes is the forced expir- atory volume at 1 s (FEV1.O). In this maneuver, an individual rakes the deep- est breath possible and then forcibly ex- hales, to the maximum extent possible, into the mouthpiece of the spirometer. The volume of expired air is measured at 1 s (FEVI.0) after start of exhalation and at the end of maximum exhalation. Reducing the “depth” of maximum in- halation obviously decreases the maxi- mum expired volume (forced vital ca-
The significance of ozone-induced lung function changes and respiratory symptoms seen in controlled
exposures is controversial
often accompanieu uy respiratory symptoms; and (2) structural injury or functional impairment of specific types of cells in the respiratory tract. The two categories will be discussed in the above sequence, with emphasis placed on the findings of controlled-exposure studies of human subjecs. (As used in this article, “effect” refers to any mea- surable change induced by ozone and should not be construed to mean “ad- verse’’ health effect, the definition of which is a major issue in the current review by EPA of the primary, health- based National Ambient Air Quality Standard, NAAQS).
Effects on pulmonary function Ozone has been shown to produce
respiratory symptoms and short-term, transient changes in lung function in human volunteers exposed under con- trolled conditions in environmental chambers. It is clearly a respiratory ir- ritant: symptoms can include coughing, shortness of breath, nose and throat ir- ritation, and discomfort or even pain on breathing deeply. Symptoms are usually rated by the individuals being studied, according to nonuniform numerical scales devised by investigators. The lung function changes seen include a shift in spontaneous breathing patterns
258 Environ. Sci. Technol.. Vol. 23. No, 3. 1989
pacity, r v c ) . i t as0 reduces FEVI.0 because the flow rate of expired air de- creases as volume decreases. Both FEV1.O and FVC give information about impairment of lung volumes; FEVl.0 also gives information about changes in flow rates; and the FVC/ FEV1.0 ratio gives information about impairment of flow rates resulting from increased flow resistance of the air- ways. Though ozone induces changes both in lung volumes and air flow, its main effect at even the highest ozone concentrations seen in ambient air in this country is to reduce the inspiratory capacity of the lung; that is, ozone lim- its the ability to take a deep breath.
The significance of ozone-induced lung function changes and respiratory symptoms seen in controlled exposures is controversial. Here it is sufficient to point out several major concerns. First, if the ability to rake a deep breath is sufficiently impaired, or if symptoms are severe enough, or if both of these conditions are present, ozone expo- sures may interfere with normal activi- ties. The second concern is that the symptoms and lung function changes induced hy ozone may be indices of more serious changes, not measurable hy noninvasive techniques, that could be occurring in the respiratory tract at
the cellular or tissue level. A nagging concern among a number of health s i - entists is that the cellular and tissues changes seen in controlled-exposure animal studies may occur in humans and, if they do, could contribute to the development of chronic lung disease or could accelerate the loss of function that normally accompanies aging.
Certain concepts, as well as some ba- sic descriptions of commonly used ex- perimental protocols, are important for understanding some of the issues under discussion in the current review by EPA of the primary ozone standard. For ex- ample, it is important to know that the magnitude of the effects induced in peo- ple by ozone depends on inherent sensi- tivity to ozone, which varies widely among individuals, and on three expo- sure parameters: ozone concentration (C), volume of air breathed during ex- posure (ventilation, VE), and exposure duration 0. Specifically, the magni- tude of the effects depends on the dura- tion of the combined exercise periods within the total exposure period (TEX). because exercise is an especially “prominent” modifier of the effects of ozone (5). VE (expressed in liters per minute) is the product of breaths taken per minute and,the average volume of air per breath; VE increases as the level of physical exertion increases.
Consideration of the data from con- trolled studies done over the past dec- ade has led to preliminary reports, far from conclusive, that ozone-induced FEV1.O changes occur as an exponen- tial function of concentration (T and VE held constant) (6, 7). possibly as a non- linear function of ventilation (T and C held constant) (7, g), and possibly as a linear function of duration of exposure (C and VE held constant) (7, 9). An area of heightened interest at present and a fertile area for continued research is the issue of the respective conuibu- tions to observed lung function changes of C, VE, and especially T.
The curves in Figure 1 were derived from pooled data from studies of healthy young adult males exposed to ozone in environmental chambers for 2 h, with alternating 15-min periods of exercise and of rest, at various exercise levels and ozone concentrations (5, 8). Fitting the data to a quadratic model constrained at 100% lung function, measured as FEV1.O, Hazucha plotted percentage lung function decrements as a function of VE and ozone concentra- tion for each of four exercise categories (5, 8). The curves show clearly the po- tentiating effect of exercise on lung function impairment.
Reasons for the impact of exercise in determining the concentration of ozone at which measurable effects on lung function occur (the “effects level”)
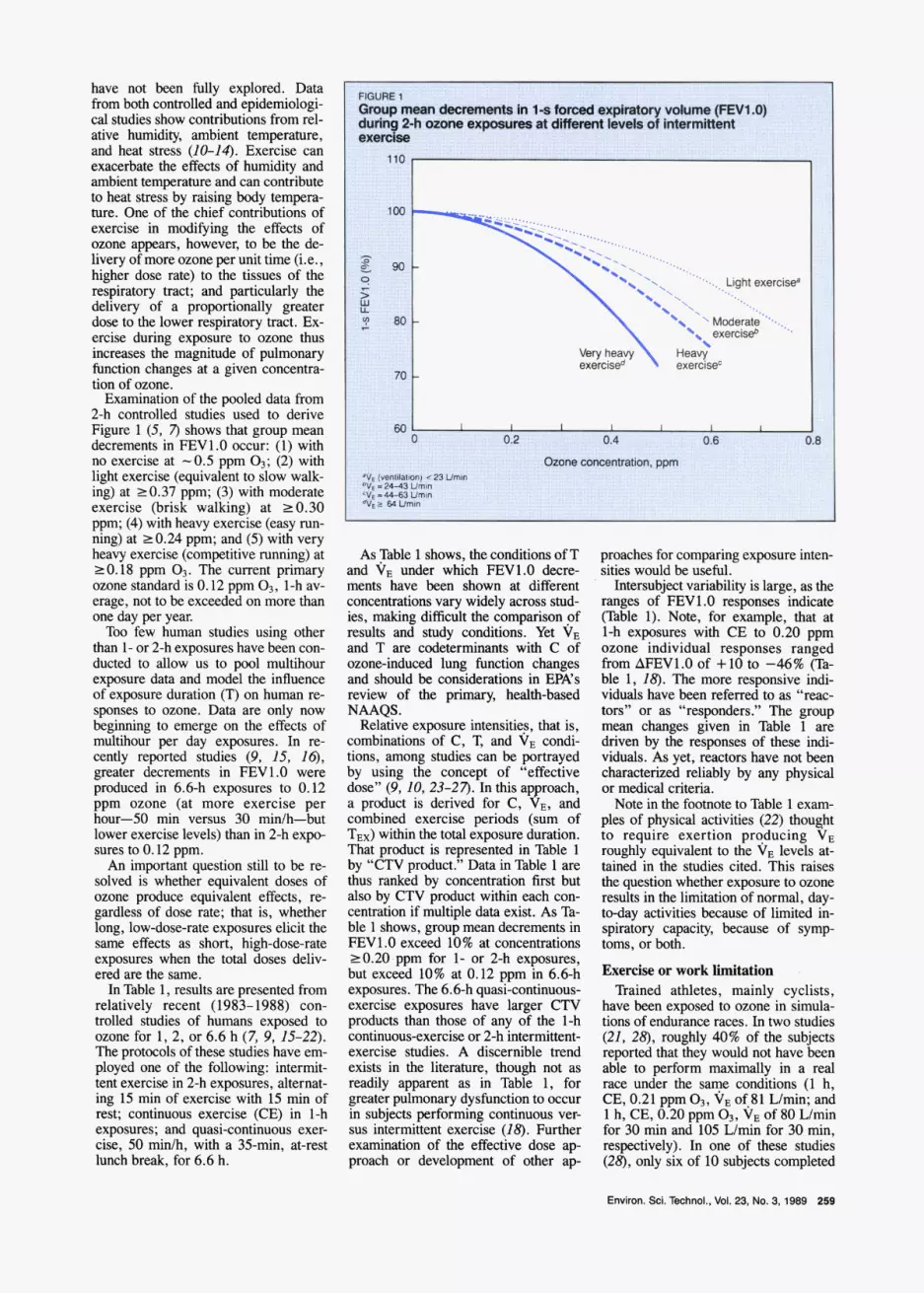
.IpJn*q3.-F from both contmUed.and gpidenuologi- cal stu&es show contributions from rel- ative humidw, ambient temDeratuIe, I ornrwrxpavr*Mi.rJI and heat stre& (10-14). Exeicise can exacerbate the effects of humidity and ambient temperature and can contribute to heat stress by raising body tempera- Nre. One of the chief conaibutions of exercise in modifying the effects of ozone B u m . however. to be the de- livery of more ozone per unit time (i.e., higher dose rate) to the tissues of the respiratory tract; and particularly the delivery of a proportionaUy greater dose to the lower respiratory tract. Ex- ercise during exposure to ozone thus increases the magnitude of pulmonary function changes at a given concentra- tion of m n e .
Examination of the pooled data from 2-h controlled studies used to derive Figure 1 (5, 7) shows that group mean decrements in FEVI.0 occur: (1) with no exercise at -0.5 ppm 03; (2) with light exercise (equivalent to slow walk- ing) at 20.37 ppm; (3) with moderate exercise (brisk walking) at 20.30 ppm; (4) with heavy exercise (easy run- ning) at 20.24 ppm; and (5 ) with very heavy exercise (competitive running) at 20.18 ppm 0,. The current primary ozone standard is 0.12 ppm O,, 1-h av- erage, not to be exceeded on more than one day per year. Too few human studies using other
than 1- or 2-h exposures have been con- ducted to allow us to pool multihour exposure data and model the influence of exposure duration (T) on human re- sponses to ozone. Data are only now beginning to emerge on the ef€ects of multihour per day exposures. In re- cently reported studies (9, 15, Z6), greater decrements in FEV1.O were produced in 6.6-h exposures to 0.12 ppm ozone (at more exercise per hour-50 min versus 30 min/h-but lower exercise levels) than in 2-h expo- sures to 0.12 ppm.
An important question still to be re- solved is whether equivalent doses of ozone produce equivalent effects, re- gardless of dose rate; that is, whether long, lowdose-rate exposures elicit the same effects as short, highdose-rate exposures when the total doses deliv- ered are the same.
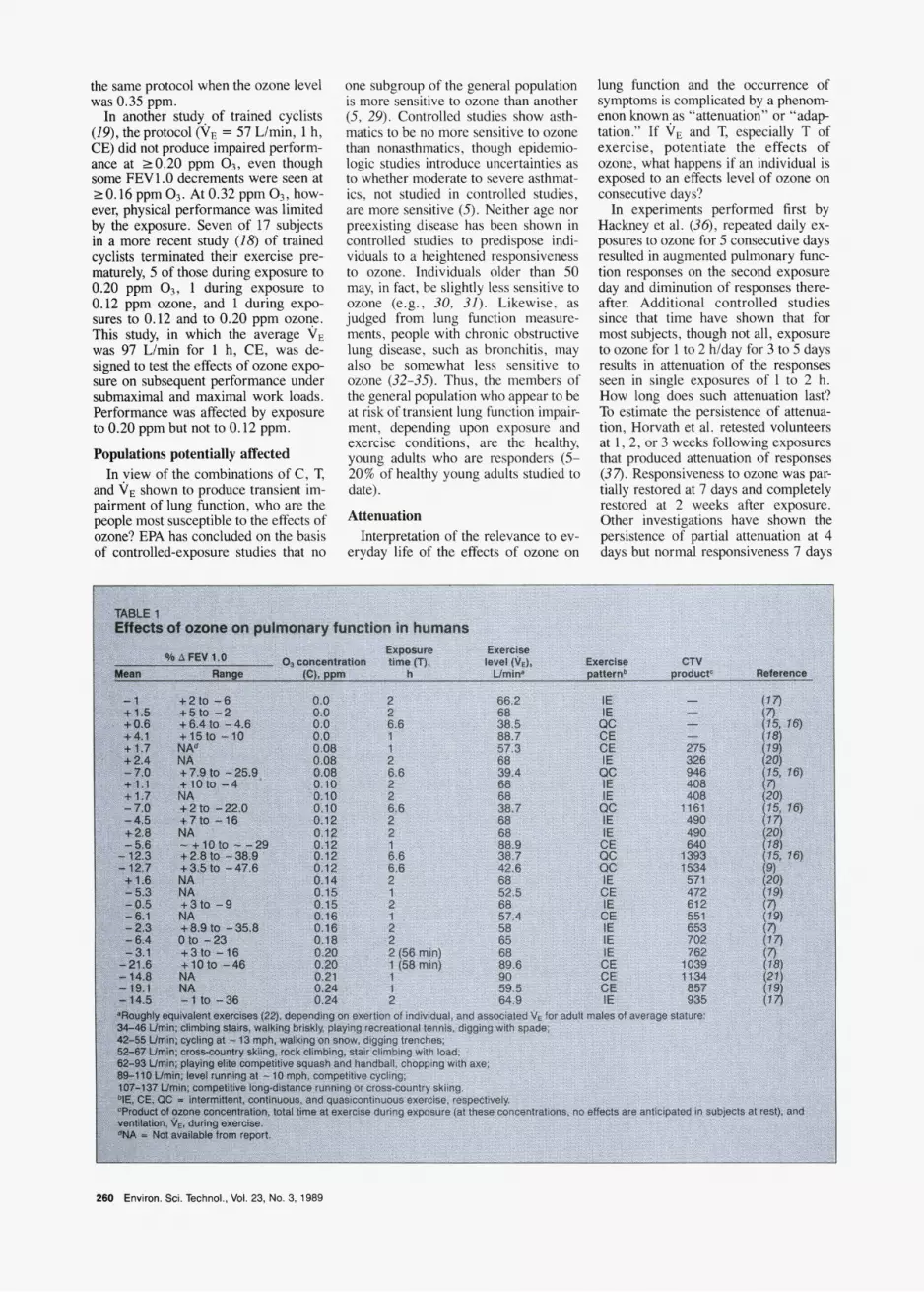
In Table 1, results are presented from relatively recent (1983-1988) con- trolled studies of humans exposed to ozone for 1, 2, or 6.6 h (7, 9, 15-22). The protocols of these studies have em- ployed one of the following: intermit- tent exercise in 2-h exposures, alternat- ing 15 min of exercise with 15 min of rest; continuous exercise (CE) in 1-h exposures; and quasi-continuous exer- cise, 50 min/h, with a 35-min, at-rest lunch break, for 6.6 h.
As ?le 1 shows, the conditions of T and VE under which FEVI.0 decre- ments have been shown at different concentrations vary widely across stud- ies, making difficult the comparison of results and study conditions. Yet VE and T are codeterminants with C of ozone-induced lung function changes and should be considerations in EFA’s review of the primary, health-based NAAQS.
Relative exposure intensitieg, that is, combinations of C, T, and VE condi- tions, among studies can be portrayed by using the concept of “effective dose” (9.10,23-27). In this ap roach, a product is derived for C, JE, and combined exercise pericds (sum of TEX) within the total exposure duration. That product is represented in Table 1 by “CTV product.” Data in Table 1 are thus ranked by concentration first but also by CTV product withii each con- centration if multiple data exist. As Ta- ble 1 shows, group mean decrements in FEVI.0 exceed 10% at concentrations 20.20 ppm for 1- or 2-h exposures, but exceed 10% at 0.12 ppm in 6.6-h exposures. The 6.6-h quasi-continuous- exercise exposures have larger CTV products than those of any of the 1-h continuousexercise or 2-h intermittent- exercise studies. A discernible trend exists in the literature, though not as readily apparent as in Table 1, for greater pulmonary dysfunction to occur in subjects performing continuous ver- sus intermittent exercise (18). Further examination of the effective dose a p proach or development of other a p
proaches for comparing exposure inten- sities would be usem.
Intersubject variability is large, as the ranges of FEVI.0 responses indicate (Table 1). Note, for example, that at 1-h exposures with CE to 0.20 ppm ozone individual responses ranged from AFEVI.0 of +10 to -46% (Ta- ble l, 18). The more responsive indi- viduals have been referred to as “reac- tors” or as “responders.” The group mean changes given in Table 1 are driven by the responses of these indi- viduals. As yet, reactors have not been characterized reliably by any physical or medical criteria.
Note in the footnote to Table 1 exam- ples of physical activities (22) thought to require exertion producing VE roughly equivalent to the VE levels at- tained in the studies cited. This raises the question whether exposure to ozone results in the limitation of normal, day- today activities because of limited in- spiratory capacity, because of symp toms, or both. EXeKise 01‘ Work limitation
Trained athletes, mainly cyclists, have been exposed to m n e in simula- tions of endurance races. In two studies (21, 28, roughly 40% of the subjects reported that they would not have been able to perform maximally in a real race under the saqe conditions (1 h, CE, 0.21 ppm 03, VE of.81 Urnin, and 1 h, CE, 0.20 ppm a, VE of 80 Wmin for 30 min and 105 Wmin for 30 min, respectively). In one of these studies (28), only six of 10 subjects completed
Envimn. *I. Technol.. Vol. 23, No. 3, IS89 259
the same protocol when the ozone level was 0.35 ppm.
In another sNdy. of trained cyclists (19), the protocol (VE = 57 Limin, 1 h, CE) did not produce impaired perform- ance at 20.20 ppm O,, even though some FEV1.O decrements were seen at 20.16ppm0,. At0.32ppm03, how- ever, physical performance was limited by the exposure. Seven of 17 subjects in a more recent study (18) of trained cyclists terminated their exercise pre- maturely, 5 of those during exposure to 0.20 ppm 0,. 1 during exposure to 0.12 ppm ozone, and 1 during expo- sures to 0.12 and to 0.20 ppm ozone. This sNdy, in which the average VE was 97 Limin for 1 h, CE, was de- signed to test the effects of ozone expo- sure on subsequent performance under submaximal and maximal work loads. Performance was affected by exposure to 0.20 ppm but not to 0.12 ppm.
Populations potentially affected In yiew of the combinations of C, T,
and VE shown to produce transient im- pairment of lung function, who are the people most susceptible to the effects of ozone? EPA has concluded on the basis of controlled-exposure studies that no
one subgroup of the general population is more sensitive to ozone than another (5, 29). Controlled studies show asth- matics to be no more sensitive to ozone than nonasthmatics, though epidemio- logic studies introduce uncertainties as to whether moderate to severe asthmat- ics, not studied in controlled studies, are more sensitive (5). Neither age nor preexisting disease has been shown in controlled studies to predispose indi- viduals to a heightened responsiveness to ozone. Individuals older than 50 may, in fact, be slightly less sensitive to ozone (e.&, 30, 31). Likewise, as judged from lung function measure- ments, people with chronic obstructive lung disease, such as bronchitis, may also be somewhat less sensitive to ozone (32-35). Thus, the members of the general population who appear to be at risk of transient lung function impair- ment, depending upon exposure and exercise conditions, are the healthy, young adults who are responders (5- 20% of healthy young adults studied to date).
Attenuation Interpretation of the relevance to ev-
eryday life of the effects of ozone on
lung function and the Occurrence of symptoms is complicated by a phenom- enon knowqas “attenuation” or “adap tation.” If VE and T, especially T of exercise, potentiate the effects of ozone, what happens if an individual is exposed to an effects level of ozone on consecutive days?
In experiments performed first by Hackney et al. (36), repeated daily ex- posures to ozone for 5 consecutive days resulted in augmented pulmonary func- tion responses on the second exposure day and diminution of responses there- after. Additional controlled studies since that time have shown that for most subjects, though not all, exposure to ozone for 1 to 2 hiday for 3 to 5 days results in attenuation of the responses seen in single exposures of I to 2 h. How long does such attenuation last? To estimate the persistence of attenua- tion, HONath et al. retested volunteers at I , 2, or 3 weeks following exposures that produced attenuation of responses (37). Responsiveness to ozone was par- tially restored at 7 days and completely restored at 2 weeks after exposure. Other investigations have shown the persistence of partial attenuation at 4 days but normal responsiveness 7 days
260 Emiron. Sci. Technol.. MI. 23, No. 3,1989

after exposure (38, 39). The various human studies of attenu-
ation have yielded a number of general observations: lower level exposures do not attenuate responses to higher level exposures (40); in a few subjects, atten- uation-at least during the 5-day re- peated-exposure studies-does not oc- cur (38); the time required for attenuation may k related to the mag- nitude of the concentration and the maximum decrements in lung function that occurred (38); and attenuation ap- pears to be reversed quickly in the ab- sence of frequent exposures (5).
Thus, some investigators have ques- tioned whether attenuation has any practical significance in populations ex- posed to ozone as it occurs in ambient air. Addressing that question, Hackney and coworkers in California exposed human volunteers in early spring to 0.18 ppm ozone for 2 h, with intermit- tent exercise, and subsequently grouped them by their responses into “reactive” and “nonreactive” groups (41). Both groups were then tested the following fall, winter, and the next spring. Nonreactors showed little re- sponse and their responses showed no seasonal variation. Reactors showed at- tenuated responses in the fall, persist- ence of attenuation into the winter, but a return to their initial lung function re- sponses to ozone by the following spring.
Although while it lasts it relieves the individual of symptoms and functional effects that would annoy or discomfort, or would hinder normal activities, at- tenuation is viewed by some research- ers not as beneficial but as masking the Occurrence and possible progression of ozone-induced cellular- and tissue-level effects in the respiratory tract (e.g., 42). This concern is based on changes seen in experimental animals exposed to ozone. For example, the lungs of an- imals exposed for 7 successive days to ozone (0.5 ppm) showed cell and tissue changes interpreted as injury (43, 44). More recently, both pulmonary func- tion attenuation and correlative tissue responses have been studied in rats ex- posed for 5 days to 0.5 ppm 0, for 2.25 hiday, with intermittent spikes of C02 to stimulate breathing and simulate the breathing patterns of humans during exercise. Histological evaluation of groups of rats on respective days of ex- posure showed maximal tissue changes on the fifth day, even though functional attenuation had occurred by then (45).
Cellular and tissue effects What are the cellular and tissue
changes observed in experimental ani- mals exposed to ozone? Numerous ef- fects have k e n observed, but they may be categorized as (1) effects shown or
thought to produce transient decreases in resistance to infection and (2) effects shown or thought to produce structural changes in the gas-exchange region of the lung. A summary is presented in the box. Figure 2 shows the location in hu- mans of cells, tissues, and structures analogous to those mentioned in the box for animals. It should be empha- sized, however, that the actual occur- rence in humans of the effects de- scribed in the box, though strongly suspected, has not been demonstrated. The techniques required to demonstrate them are invasive.
Cilia, mucus, and alveolar mdcro- phages (see box) are all components of host-defense mechanisms that help rid the body of foreign particles, both bi- otic and abiotic. Mucus traps foreign particles, and the cilia of the epithelial cells lying under the mucus layer (Fig- ure 2a) help move mucus to the phar- ynx, where the mucus-entrapped parti-
I------ Cellular and tissue effects of
ozone in airway and lungs of experimental animalsa Effects demonstrated or thought to result in short-term decreases in re- sistance to infection
!a-Absent or shorter, abnormal apes; reduced or absent ciliary
cos-Altered rate of mucus se- n; delayed mucociliary clear-
lar macrophages-Reduced ty, numbers: reduced bacte I activity; reduced interferon
ts demonstrated or thought to in reversible or, in long-term es to high levels, potentially
e changes in centriacinar cells and in anatomical
of respiratory bronchioles
inar epithelium-Epithelial cell injury, followed by prc-
ion of type 2 cells; inflamma- y changes in respiratory bron- ioies (“respiratory bronchioli- ” which persist throughout ex-
re but at a reduced rate be- initial exposure; increased collagen in interalveolar or interstitium (i.e.. mild fi- ); structural changes in dis-
airways, that is, development respiratory bronchioles having ckened interalveolar septa and ckened bronchiolar walls.
cles can be coughed up or swallowed. Alveolar macrophages can engulf (phagocytize) particles and contain, de- toxify, transport them, or do all three, to prevent infection or injury in the lung.
Because ozone has been shown to af- fect several components of the host-de- fense system, decreased resistance to infection as a consequence of ozone ex- posure has been hypothesized. Ozone has, in fact, been shown to decrease the resistance of mice to bacterial infection (5, 4648) and to alter the response of mice to a viral influenza infection (though not to enhance viral replica- tion) (49). The possible effects of ozone on human host-defense mechanisms are also postulated but have not been demonstrated in the few studies con- ducted. For example, ozone has been shown not to alter the course of a rhinovirus infection (common cold) in human volunteers (50). The possible occurrence of ozone-induced effects on human host-defense mechanisms re- mains of concern, however (5,29).
The effects induced by ozone on the centriacinar region of the lung (Figure 2b) are of particular concern to health scientists since at least some of these effects are suspected to be harbingers of the induction and progression of chronic lung disease. n p e 1 cells are thin, flat epithelial cells that line the al- veoli of the acinus (Figure 2b). Type 2 epithelial cells are more cuboidal, and their proliferation after ozone-induced injury of p p e 1 cells results in the ex- posure of less surface area per cell to air, and the ozone in it, but also tends to thicken the epithelial membrane of the alveolus.
Increases in collagen content and the development of thickened septa be- tween alveoli and of thickened walls of the respiratory bronchioles (Figure 2b) are generally viewed as changes that could lead, depending upon length and level of exposure, to “stiffer” lungs. The accretion of localized collagen is considered to be a precursor of pulmo- nary fibrosis, a disease that can cause disability, if it is severe enough, by re- stricting lung volume and slowing the transfer of oxygen from air to blood. Inflammatory changes are suspected to correlate with ozone-induced structural changes in the airways, though such a linkage has not been clearly shown. Furthermore, the functional relevance of observed structural changes at low ozone exposures remains uncertain.
Further chronic studies (longer than 1 year) of animals at ambient and near- ambient concentrations of ozone are necessary to resolve uncertainties about long-term effects and the exposure in- tensities and patterns that produce them. Considerably more data are
Environ. Sci. Technol., Vol. 23. NO. 3. 1989 261

needed especially on the extent and pat- tern of recovery with time following subchronic and chronic exposures to ozone.
The use of animal toxicologic data in standard-setting is hindered at present by the need for (1) improvements in existing models for extrapolation of an- imal data to humans; (2) systematic sta- tistical modeliig of doseresponse rela- tionships for effects of concern within a given species and across species (ex- perimental protocols have differed widely); and (3) better understanding of C x T relationships for effects of con- cern.
In all species of experimental animals studied to date, morpbologic and struc- tural effects of ozone have been ob- served in the centriacinar region of the lung (5). Similar effects may reasona- bly be expected to occur in humans. Even if one assumes their occurrence in humans, however, the doses expected to elicit these effects are uncertain be- cause of anatomical, physiological, and biochemical differences among species.
With respect to the quantitative ex- trapolation of animal toxicologic data to humans, m n e dose delivered to the respective regions of the respiratory tract (dosimetry) and species sensitivity
262 Envimn. Sei. Technd., MI. 23, No. 3,1909
are important; and the similarities and differences in dosimetry and sensitivity between animals and humans must be quantified. F a ozone, mathematical dosimetry models of the lower respira- tory tract (51. 52) need to be coupled with data on nasopharyngeal removal. “Since nasopharyngeal removal of ozone to lessen the insult to lower respiratory tmct tissue, an as- sessment of species difference in this area is critical to interspecies compari- sons of dosimetry’’ (5). Recently, new empirical data have become available on the regional dosimetry of the rat ver- sus humans. These newer data, though still sparse, indicate that in humans more than 90% of an inhaled dose of mne is taken up in the total respira- tory tract (53); in rats, around 40% is taken up (54). Of the inspired dose, rats (at rest) take up only about 17% in the nasopharyngeal region (55); nasopha- ryngeal uptake in humans (at rest) is about 40% or higher (53). These newer data now make it possible to incorpo- rate human nasopharyngeal deposition data in existing dosimetry models.
Newer data give preliminary indica- tions that some effects in animals show a l inear progression with increased ex- posure duration but that others do not
(5s). The newer data also indicate that the pattern of exposure to ozone may influence the magnitude of the effects induced. For example, intermittent, cy- clical exposures of macaque monkeys (1 month of ozone alternating with 1 month of clean air over 18 months) a p pear to prcduce somewhat greater ef- fects than continuous ozone exposures (57). Further data are needed on the roles of exposure duration and expo- sure patterns in modifying ozone-in- duced effects in humans.
Once these newly emerging data have been published in the journal liter- ature, their potential relevance for standard-setting can be determined. They should add to our knowledge of regional dosimetry of ozone deposition in the respiratory tract and of C x T relationships. In turn, resolution of un- certainties in these areas will provide better tools, as well as impetus, for ex- amining systematically the dose-re- sponse relationships for biological end- points of concern in animals and for extrapolating those data to humans.
Until then, the statements made by EPA in its 1986 criteria document (5) remain valid “Understanding the rela- tionship between acute effects that fol- low exposure of humans or animals and

the effects that follow long-term expo- sures of humans or animals is crucial to the evaluation of the full array of possi- ble human health effects of oxidant pol- lutants. Most of the acute responses to ozone described in animals and humans tend to reNrn toward control (filtered air) values with time after the exposure ends. While effects of longer periods of exposure have been documented in lab- oratory animals . . . human beings have not undergone long-term expo- sures in laboratory studies because of ethical and logistical considerations. In fact, little is known about the long-term implications of acute damage or about the chronic effects in man of prolonged exposure to ozone."
Acknowledgment This article was reviewed for suit-
ability as a feature article by James A. Raub and Judith A. Graham, Environ- mental Criteria and Assessment Office, U.S. Environmental Protection Agency, Research Triangle Park, NC; Larry Folinsbee, Environmental Moni- toring and Services, Inc., Chapel Hill, NC; and Jack Hackney, Environmental Health Service, Rancho Los Amigos Hospital, Downey, CA. The author gratefully acknowledges the comments and suggestions offered by the review- ers. The information described in this article has been reviewed by the Office of Health and Environmental Assess- ment of the US. Environmental Pro- tection Agency and approved for publi- cation. Approval does not signify that the contents necessarily reflect the views and policies of the agency.
References (I) "Clean Air Act"; section 108. U.S .
Code. Vol. 42; section 7408. 1982. (2) Pryar. W. A.; Dooley, M. M.: Church,
D. F. In Biomedical Eflecrecrs ofozone and Phorochemicol Oxidants: S . D. Lee, M. G. Mustafa. M. A. Mehlman. Eds.: Princeton Scientific: Princeton. NJ. 1983.
(3) Menzel, D. B. In Fundamenrols of Ex- rropolorion Modeling of Inhaled Toxi- conrs: Ozone and Nirrogen Dioxide; F. 1. Miller. D. B. Menzel, Eds.; Hemisphere Publishing: Washington, DC. 1984.
(4) Mudd, J. B. et al. Amos. Environ. 1969, 3. 669-81.
( 5 ) Air Qualily Crireriofor Ozone and Orher Phorochemicol Oxidonis: U.S. Environ- mental Protection Agency. Environmen- tal Criteria and Assessment Office. U.S. Government Printing Office: Research Triangle Park, NC, 1986 EPA160018-841 OZOdF, eF, Vols. I V and V.
(6) Hazucha. M. 1.; Ph.D. Thesis, McGill University. Montreal. Canada. 1973.
(7) Kulle. T. I . et al.; Arne,: Rev Respi,: Dis. 1985, 132. 36-41.
(8) Hilzucha. M. J. J. Appl. Phy.yiol. 1987, 62, 1671-680,
(9) Folinsbee. L. J.; McDonnell, W. F.; Harstman, D. H . JAPCA. 1988.38, 28- 35.
( IO) Folinsbee, L.1 .; Silverman. F.; Shepard. R. I. J. Appl. Physiol.: Rap;,: Environ. Exercise Physiol. 1977, 42. 531-36.
(11) Folinsbee, L. I . et al . ; J. Appl. Physiol.:
Respir Environ. Exercise Physiol. 1977, 43,409-13. Gibbons, S. 1.; Adams, W. C. J. Appl. Physiol. 1984,57,450-56. Selwyn, B. I . et al. In Tronsocrions of APCA Specially Conference: ScienriJk Basis for OzondOxidonrs Srondords. Lee. S. D., Ed.; Air Pollution Control Association: Pittsburgh. PA, 1985, pp. 7x1-96 ... Spektor. D. M. et 81. Am. Rcv. Resp. Dis.
Horstman, D. H.; etal . In Proceedingsof 3rd lnrernationol U.S. -Dutch Sympo- sium: Almospherie Ozone Reseorch and Irr Polics Imolicarions. 1958: Elsevier
mnn.137.313-20.
Scientific: Amsterdam, in press. Horstman, D. H. et al. Pksented at the 81st Annual Meeting of the Air Pollution Control Association. Dallas. TX. 1988. (Paper no. 88-122.5). Air Pollutidn Con- troi Association: Pittsburgh. PA. 1988. McDannell. W. F. et al. 1. Appl. Physiol.: Respir Environ. Exercise Physiol. 1983, 54. 1345-352. Gong, H.. Jr. et al. Am. Rev. Respir. Dis. 1986, 134, 726-33. Awl. E. L. et al. JAPCA. 1984.34, 8M- "" "I.
Linn. W. S. et al. Toxicol. h d . Heolrh 1986.2.99-112. Folinsbee. L. J.; Bedi, J. E; Horvath, S. M. 1. Appl. Physiol.: Respi,: Environ.
Work Physiology: McGraw-Hill: New York. 1977. Fol insbee , L . 1.; S i l v e r m a n . F.; Shephard. R. I . J. Appl. Physiol. 1975, 38. 996-1001. Silverman. F. et al. J. Appl. Physiol. 1976.41. 859-64. Folinsbee. L. 1.; et 81. In Environmental SITPSS: Individual Humon Adoprarions: Folinsbee. L. J. et al.. Eds; Academic: New York. 1978. Colucci, A. V. In Biomedical Effecrs of Ozone and Phorochemicol Oxidanrs: Lee. S. D.; Mustafa, M. G.; Mehlman. M. A.. Fds. Princeton Scientific: Princeton. NJ. 1983. Adams. W. C.; Savin. W. M.; Chrism, A. E. J. Appl. Physiol. 1981,51,415-22. Adams, W. C.; Schelegle. E. S. J. Appl. Physiol. 1983.55, 805-12. Preliminary As~essmenr of Scienrijc and Technical Informorion. U.S. Environ- mental Protection Agency: Office of Air Quality Planning and Standards. OAQPS Draft Staff Paper. Research Triangle Park. NC, 1987. Drechsler-Parks, D. M.; Bedi. I . E ; Hor- vath, S. M. E q . Geronrol. 1987,22.91-
ercise Physiol. 1984.57. 984-88. F strand, P-0.; Rodahl. K. Textbook of
r " , .".. Reisenauer, C.S. et SI. JAPCA 1988. 38, 51-55. Konig, G. et al. Arbeirsmed. Soriolmed. Pmewnrivmed. 1980. 151, 261-263. Linn, W. S. et al. Am. Rev. Rapi,: Dis.
Solic. 1. I . ; Hazucha. M. I . ; Bromberg, P A. Am. Rev. Respir. Dis. 1982, 125.
1982,125, 658-63.
f.M.60 -_I- "I.
Kehrl, H. R. et al. Am. Rev. Respir Dis.
Hackney, J. D. et al. 1. Appl. Phyriol.: Respit Environ. Exercise Physiol. 1977, 43, 82-85. Horvalh. S. M.; Gliner. I . A,; Folinsbee. L. I . Am. Rev. Rmpi): Dis. 1981, 123. 496-99. Linn. W. S. et al. Am. Rev. Resp. Dis. 1982, 125.491-95. Kulle, T. J. et al. Environ. Res. 1984,34, 55-63. Gliner, I . A,; Horvath, S . M.; Folinsbee. L. J. Am. Rev. Respir: Dis. 1983, 127, 51-55.
1 9 ~ 5 , 1 3 1 , 719-24.
Hack&. J. D. et al. In Proceedings of 3rd Inrernorional. U.S. -Dutch Sympo- sium: Atmospheric Ozone Research and
Irs Policy Implications. 1988; Elsevier Scientific: Amsterdam. in press.
(42) Bromberg, I? A.; Hazucha. M. I. Am. R ~ V . R ~ S D ~ , : D ~ S . 1982.125.489.90.
(43) Schwark, L. W. et al.'Lab.'lnvesr. 1976, 74 5 f , . l U - . , - -_ . -.
(44) Bnrmmer. M.E.G.; Schwartz. L. W.: McQuillen, N. K. Scan Elecrron Mi-
(45) Tepper, 1. S. et al. The Physiologisr. crosc. 1977.2. 513-18.
iwi. m (x .. . . . - -, - -. (46) Coffin. D. L.; Gardner, D. E. Ann. Oc-
(47) Coffin. D. L. et SI. In Proceedings of3rd cup. Hyg. 1972, IS. 219-35.
Patterson AFB: D AMRL-TR-67-
(48) Graham. I . A. Health. 1987, i
(49) Selgrade, M.J. 7oxicol. 1988,
(50) Hcndersan. F. ' Dis. 1988. 137,
(51) Miller. E 1.: Mm
Nayton. OH; 1668, 200. pp. 71-80. et 81. J. Toxicol. Environ. ! I . 113-25. K.; et al. Fund. Applied 11. 169-80. W. et al. Am. Rev, Rap;,:
1124-28. e~31:l. D. B.; Cofin, D.L.
17. M-101. ricol. Appl. Phormo-
Environ. Res. I Y I M , (52) Miller, F. I. et al. To;
col. 1985. 79. 11-27 . .
1988,65393-400. (54) Gerrity. T. R.; Wicster, M. I . Presented
at the 80th Annual Meeting of the Air Pollution Control Association. New York. 1987. (Paper no. 87-99.3).
(55) Hatch. G . E.; et al. In Proceedings of3rd lnrernarionol U.S. -Durch Symposium: Almosoheric Ozone Rcseorch ond 11s Pol- icy I&nlicario"s. 1985: Elsevier Scien- tific: Amsterdam. in press.
(56) Costa, D. L. et al. In Proceedings of 3rd lnrernarional U.S. -Dutch Svmoorium:
~I r~~ ~
Armospheric Ozone Rmearch and Its Pol- icy Implications. 1988; Elsevier Scien- tific: Amsterdam. in press.
(57) Hyde. D. M. et al. In Proceedings of3rd Inumorionol U.S.-Durch Symposium: Armosphcrie Ozone Research and 113 Pol- icy Implicorions. 1958; Elsevier Scien- tific: Amsterdam. in press.
Beverly E. Tillan is a physical scienrisr in rhe Environmenral Criteria and Assessmenr Ofice, Ofice of Health and Environmental Assessment, U.S. EPA. Research Tiiangle Park, NC. She was project manager for EPA for development of the ozone-oxidants crireria document rhar will serve as rhe principal scienrifc basis of the nexr ozone ambienr air qualify srandards. She holds a B.S. degree from American Universify, with a double major in biology and chemis- fry. and has done graduare work in borh felds as well as in English lirerarure. A career governmenr employee, she worked previously as a physical scienrisr for fhe Deparrmenr of rhe Air Force and as a re- search chemisf for rhe Food and Drug Ad- minisrrarion.
Envimn. Sci. Technol.. Val. 23, No. 3, 1989 263





























