Embed Size (px)
Citation preview
Healing assessment of osseous defects of periapical lesions associated with failed endodontically treated teeth with use of freeze-dried bone allograft A. Yousef Saad, BDS, HDD, PhD,O and El-Said M. Abdellatief, BDS, MSD, PhD,b Cairo, Egypt
AL-AZHAR UNIVERSITY
Freeze-dried bone allograft (FDBA) has been used extensively in periodontal surgery and in the treatment of pocket osseous defects resulting from inflammatory periodontal disease. No other endodontic investigation has used this type of graft material in the treatment of bony resorptive defects of the periapical lesions associated with failed endodontic therapy. Therefore this study was conducted with the use of FDBA, to assess healing ability of osseous defects after removal of periapical lesions associated with failed endodontically treated teeth. In all patients periapical lesions were surgically removed with retrograde amalgam seal and the graft material was then carefully packed without pressure into the bony defect. The lesions were fixed in 10% neutral buffered formalin and prepared for histologic examination. Long-term recall demonstrated bone regeneration and Qood tolerance of allograft material by the periapical tissues. The periapical lesions were either periapical granulomas or apical periodontal cysts. We conclude that FDBA is a biocompatible material of osteogenic potential and can be used effectively in treating osseous defects of periapical lesions associated with failed endodontically treated teeth. (ORAL SURC ORAL MED ORAL PATHOL 1991;71:612-7)
I t hasbeen estimated that 60% to 75% of endodon- tic failures might be due to incomplete preparation and obturation with subsequent lack of a hermetic apical seal at the dentinocemental junction.le3 Inad- equate silver cones, perforations, overextension, peri- odontal involvement, vertical fractures, missed ca- nals, and anatomic variations are other reasons stated for endodontic failure.4 Furthermore, success rate may also be influenced by the technical skill of the practitioners and type of root canal-filling mate- rial.5-7 Transudate from the bloodstream is trapped in the improperly filled canal and subsequently degraded into toxic substances that slowly diffuse out of the pe- riapical tissue, causing its inflammation.8 In addition, pulp tissue that has not been adequately removed by canal instrumentation may break down into toxic products and leak through the inadequate foraminal
aEndcdontist and Lecturer, Oral Histology Department, Faculty of Dental Medicine. bLecturer, Oral Surgery Department, Faculty of Dental Medicine. 7/15/21192
612
seal into the periapical tissues to produce periapical inflammation. In addition, bacteria that have not been destroyed before filling may also enter the periapical tissues to produce infection, leading to acute or chronic inflammation.9 The presence of periapical ir- ritation may cause periapical pathosis, resulting in hyperemia and edema of the periodontal ligament with infiltration of chronic inflammatory cells and in- creased vascularity of the surrounding tissues.“’ This also may stimulate the epithelial rests in the vicinity of the apical foramen to proliferate, forming periapi- cal lesions.‘0-‘4 Treatment of such lesions may require surgical or nonsurgical intervention.
Freeze-dried bone allograft (FDBA) has been used in both experimental and clinical investigations. De- spite excellent results reported in the orthopedicI and neurosurgical literature,16 only incidental case re- ports and noncomparative series, including alveolar cleft grafting,” orthognathic surgery, ] * ridge aug- mentation,19 delayed fracture union treatment,20 treatment of large cyst,21 and reconstructive sur- gery,22 as well as preliminary reports,23 have been re-
FDBA and periapical lesions 6 13 Volume 7 1 Number 5
Table I. Age, sex, location, and signs and symptoms of cases
Case No. Age IN Sex Location
(tooth No.) Signs and symptoms
1 28 M 2 40 M 3 32 M 4 23 F 5 19 M 6 2.5 M 7 29 F 8 16 M 9 33 M
10 36 F
11 27 M
23 Acute infection with diffuse swelling 24, 25 Pain, swelling, and sinus tract 22 Pain with bone expansion 24 Swelling and tender to percussion 26 Persistent sinus 23 Uncontrolled discharge of pus 26 Pain and swelling 24, 25 Rapid-growth swelling and pain 23, 24 Rapid-growth swelling 23 Swelling and constant oozing from
canal space 26 Swelling and tender to percussion
ported. Recently, numerous studies have reported the use of FDBA in treatment of periodontal osseous defects24-26 and in some maxillofacial surgical pro- cedures.27, 28 These studies have revealed favorable results with minor complications. On the other hand, some investigations have stated several disadvantages of using such material, including possible antigenic- ity and potential for disease transfer from the cadaver to the recipient.29
The use of freeze-dried bone in endodontics is un- common. In only one study has the graft material been used to fill the apical 2 to 5 mm of monkey teeth after apices were mechanically opened. Teeth were then obturated with gutta-percha. The results have dem- onstrated that freeze-dried bone is a biocompatible material that can be used effectively as a substitute barrier against which gutta-percha can be condensed. Furthermore, apical organizational osseous healing has been seen, and some teeth had mineralized tissue resembling osteocementum occupying the canals30
The use of FDBA in endodontic surgery to fill the bony defect after removal of the periapical lesion as- sociated with failed endodontic therapy, and its influ- ence on the periapical tissues, have not been previ- ously reported. Therefore we decided to examine this aspect of the subject.
MATERIAL AND METHODS
Eleven patients were included in this study. In all cases the teeth had a history of previous root canal filling associated with pain; periapical lesion, with or without sinus tract; and the need for endodontic sur- gery. Surgery was decided on after conventional therapy failed to stop patient symptoms. Patient data, including age, sex, location of the lesion, and associ- ated signs and symptoms, were recorded. None of pa- tients had any known medical complications incom- patible with successful endodontic surgery, and none was taking regular medication. All patients received
broad-spectrum antibiotics (Flumox; 250 mg amoxi- cillin, 250 mg floxacillin capsules), 500 mg every 8 hours 1 day before and 4 days after surgery.
A full-thickness flap was carefully reflected. The incision lines of the flap did not overlie any bony de- fect, and the base of the flap was the widest point with no sharp comers. Periapical curettage was performed to remove the diseased tissues surrounding the apices of teeth, with or without apical resection of a portion of the root end with a varying degree of bevel, followed by retrograde zinc-free amalgam seal. The graft ma- terial (obtained from a local hospital bone bank) was mixed with sterile saline solution, then carefully packed without pressure into the defect. The flap was replaced to its original position, digital pressure was applied for few minutes, and the flap was carefully sutured with silk to ensure complete soft tissue cover- age of the graft site. All surgical procedures were achieved under complete aseptic conditions. The lesions were fixed in 10% neutral buffered formalin. Fixed tissue was dehydrated in a series of graded al- cohols and embedded in paraffin. Serial sections, 5 pm thick, were cut and stained with hematoxylin and eosin stain for light microscopic examination. Sutures were removed after 5 days postoperatively. All proce- dures were performed by the same operator and assistant. The cases were followed up with clinical and radiographic examination and were recalled at inter- vals of 1, 3, 6, and sometimes 9 months to assess the condition of the periapical area.
RESULTS
A total of 11 patients were included in this study. The age range was 16 to 40 years; eight were males and three were females. All surgery was performed on the mandible (anterior region). All teeth were endo- dontically involved with persistent pain, uncontrolled infection, and swelling, with or without sinus tract. All cases showed radiographic evidence of periapical pa-

614 Saad and Abdellatief ORAI SIJRG ORAL MED OKAL PATHOL. May 1991
Fig. 1. Photomicrograph showing periapical granuloma. Note delicate fibrillar stroma with intense chronic inflam- matory cell infiltration. (Hematoxylin-eosin stain; original magnification, X 160.)
Fig. 3. Case 2. Successful use of FDBA. A, After remova of periapical lesion and retrograde amalgam seal. B, Afte packing of FDBA into bony defect. Tooth 25 was extractel because of lack of bony support.
Fig. 2. Photomicrograph showing apical periodontal cyst. Note that thin stratified squamous epithelium (E) lines cyst cavity and is surrounded by connective tissue (N) that makes up cyst wall. Also observe presence of cholesterol slits (C). (Hematoxylin-eosin stain; original magnification, X63.)
thosis. The data regarding age, sex, location of the le- sion, and signs and symptoms of these cases are pre- sented in Table I. Furthermore, histopathologic ex- amination of the periapical tissue specimens of surgically treated cases demonstrated that six speci- mens (54.5%) were apical granulomas (Fig. l), whereas the remaining five specimens (45.5%) were apical periodontal cysts (Fig. 2).
Clinically, the allograft material used in this study was well tolerated by all patients. No noticeable im- munologic complication, graft rejection, or infection occurred. Radiographic evaluation after 1 month showed distinct outline separating the graft material from the surrounding host bone, which indicated si- multaneous resorption of the graft. This resorption was increased at the 3-month follow-up examination. However, between 6 and 9 months postoperatively the grafts could no longer be identified as separate enti-
ties. This indicated regeneration by new bone forma- tion and complete graft incorporation. Two patients were lost to follow-up. Figs. 3 and 4 demonstrate suc- cessful use of FDBA in treatment of osseous defects of periapical lesions associated with failed endodon- tically treated teeth.
DISCUSSION
Several investigators established that the root canal was an important source of toxic products and infec- tion that may spread to the periapical tissues,*, 9 causing irritation and destruction of these tissues and resulting in periapical lesion development.rO, ‘I This may be attributed to the lack of a hermetic apical seallm3 or to many other reasons,3% 4 as well as that most root canal tilling materials fail to obturate com- pletely the root canal system.6, ’ We found in the cur- rent study that the periapical lesions were apical granulomas (Fig. 1) and apical periodontal cysts (Fig. 2) similar to those described by many other inves- tigators.‘2-14 Generally, nonsurgical therapy should be attempted first. Only after a suitable observation period, if periapical healing fails to occur, should sur- gery be initiated. Conventional endodontic manage- ment was therefore attempted first to treat all patients included in this investigation. Treatment was consid-
Volume 71 Number 5
FDBA and periapical lesions 6 16
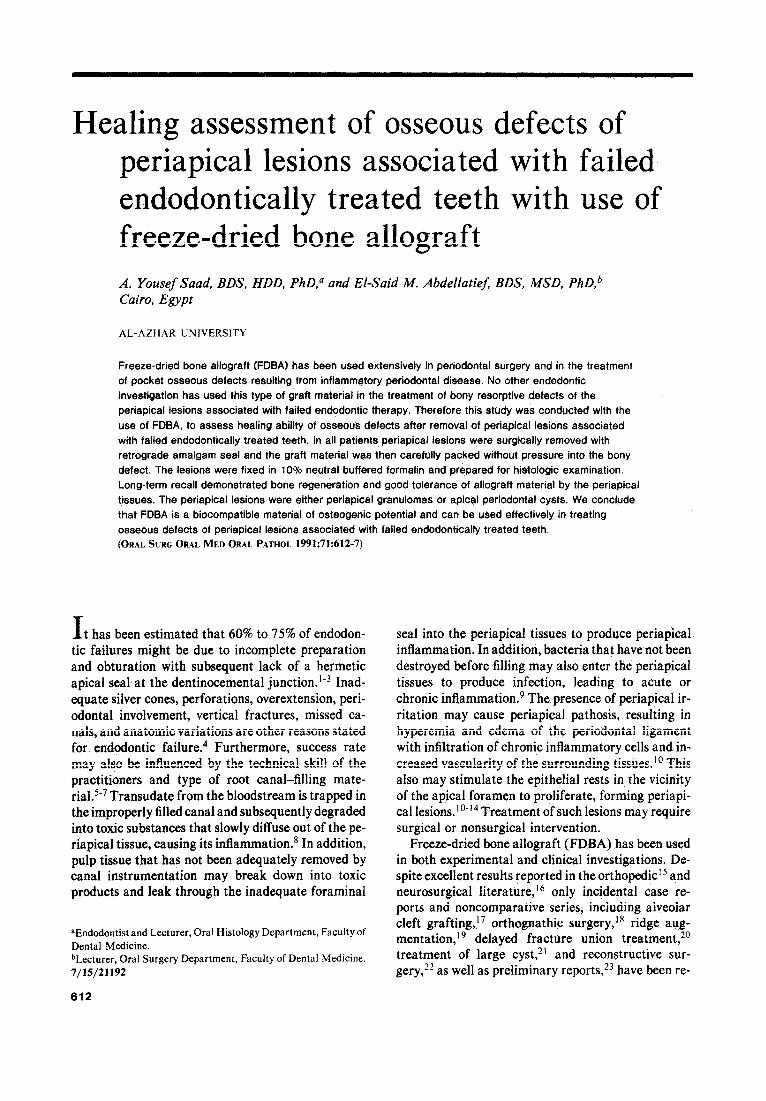
Fig. 4. Case 8. Patient had endodontic treatment 2 years earlier. A, Radiograph showing radiolucent area in relation to roots of teeth 24 and 25 (silver points could not be removed). B, After removal of periapical lesion, retrograde amalgam filling, and packing of FDBA. C, Postoperative radiograph after 3 months, show- ing resorption of graft material. D, After 6 months, healing almost complete.
ered to have failed, and the patient underwent sur- gery, when the infection was still not controlled, as evidenced by persistence of pain, sinus, discharge of pus, swelling, or constant oozing from the canal space, or when teeth were filled with silver points that could not be removed.
Our investigation was undertaken to provide pre- liminary observations on the effectiveness of a FDBA in treating bony resorptive defects associated with
failed endodontic therapy. No noticeable immuno- logic complication was observed. This finding was parallel to that reported by some investigators who have shown that freeze-drying of bone graft markedly reduces both the humoral and cell-mediated type of antigenicity compared with the response of fresh bone graft. 1 5, 23 Also, allogeneic freeze-dried bone is a bio- logically useful alternative to autogenous bone.23 Al- lard et a1.27 and Schallhorn2g stated that allografts

616 Saad and Abdellatief
have definite advantages over autografts. The al- lografts have good induction potential, are readily available and inexpensive, eliminate a second surgical procedure, and could reduce hospitalization time. In the present study, healing of osseous defects occurred in a period ranging from 6 to 9 months. Between 6 and 9 months postoperatively, the grafts could no longer be identified as separate entities. This indicated com- plete graft incorporation. Healing appeared to occur in two steps: phase of resorption and phase of bone replacement. In the resorption phase part of FDBA was resorped, whereas in replacement phase the remaining part of the graft material may act as a ma- trix for the ingrowth or as an area along which new host bone is deposited. This regeneration of bone grafts may be preceded by revascularization of the graft itself. Furthermore, placing the graft material in the osseous defect may induce host undifferentiated progenitor cells in the periapical area to differentiate into bone cells or to stimulate the already differenti- ated osteoblasts to form new bone. This means that FDBA is a graft material of osteogenic potential. Ad- ditionally, it is important that direct pressure on the grafts is avoided, because this may result in more rapid resorption and loss of volume.27T **
Our successful results comprise the first study on the usefulness of a FDBA in endodontic surgery. These findings have been confirmed by numerous fa- vorable results in human beings and animals, as reported in the orthopedic,15 neurosurgical,16 oral and maxillofacial,17~22~ 27, ** periodontal,24, 25 and endo- dontic30 literature, but in disagreement with the ear- lier study of Mellonig et al.,26 who concluded that such an allograft material was of questionable value. Moreover, two recent animal studies used the graft material in the treatment of bony defects surgically created in the calvaria of guinea pigs. The results demonstrated that decalcified FDBA is a graft mate- rial of high osteogenic potential and is superior than that of autogenous osseous coagulum, bone blend, and FDBA.3” 32 These findings suggest that demineral- ization of a bone graft would release the mineral that insulates the bone morphogenic protein and prevent its transmission from the bone matrix to proliferating mesenchymal cells. 23 In addition, multinucleated gi- ant cells were seen in association with freeze-dried bone. It has been hypothesized that these cells, presumably osteoclasts, may deplete the cell popula- tion surrounding an implant of potentially osteogenic cells. This may be a reason for the diminished osteo- genic potential of FDBA.33
Limitations to this study included lack of control subjects, no histologic evaluation, and inconsistent methods for estimating osseous regeneration. Finally, we emphasize that our results are preliminary and that a further controlled and histologic study with an
ORAL SLIRG ORAL MED ORAL PATH~I May 1991
animal model must be carried out. However, we be- lieve that our observations in this investigation should be reported now because they support the continued clinical use of FDBA in the treatment of osseous de- fects of the periapical lesions associated with failed endodontic therapy.
SUMMARY
Cases of failed endodontic therapy associated with periapical lesions and with the need of endodontic surgery were included in this investigation. After re- moval of periapical lesions and retrograde amalgam seal, FDBA was implanted into the osseous defects. Long-term recall revealed that healing occurred in a period ranging from 6 to 9 months. Healing appeared to occur in two steps: a phase of resorption followed by a phase of bone replacement. Results indicate that FDBA is a biocompatible material of osteogenic po- tential and can be used effectively in treating osseous defects of periapical lesions associated with failed en- dodontically treated teeth.
REFERENCES
1.
6.
I.
8.
9.
10.
II.
12.
13.
14.
15.
16.
lngle JI, Beveridge EE, Glick DH, Weichman JA, Abou-Rass M. Modern endcdontic therapy. In: Endodontics. 3rd ed. Phil- adelphia: Lea & Febiger, 1985:36. Nguyen NT. Obturation of the root canal system. In: Pathways of the pulp. 2nd ed. St Louis: CV Mosby, 1980:133-95. Crumo MC. Differential diagnosis in endodontic failure. Dent Clin North Am 1979;23:61?35. Schilder H. Filling root canal in three dimensions. Dent Clin North Am 1967;11:723-44. Heling B, Tamshe A. Evaluation of success of endodontically treated teeth. ORAL SURG ORAL MED ORAL PATHOL 1970; 30:533-6. Brayton SM, Davis SR, Goldman M. Gutta-percha root canal filling. ORAL SURG ORAL MED ORAL PATHOL 1973;25:226-31. Ainley JE. Fluorometric assay of the apical seal of root canal fillings. ORAL SURC ORAL MED ORAL PATHOL 1970;29:753- 62. Ingle JI, Luebke RG, Zidell JD, Walton RE, Taintor JF. Ob- turation of the radicular space. In: Endodontics. 3rd ed. Phil- adelphia: Lea & Febiger, 1985:223. Friedman CE, Pitts DL, Natkin E. Formaldehyde pastes. Dent Clin North Am 1979;23:705-I 5. Shafer WG, Hine MK, Levy BM. Diseases of the pulp and pe- riapical tissues. In: A textbook of oral pathology. 4th ed. Phil- adelphia: WB Saunders, 1983:487-93. Seltzer S, Soltanoff W, Bender IB. Epithelial proliferation in oeriaoical lesions. ORAL. SURG ORAL MED ORAL PATHOL. i969f27:I 11.21. Bhaskar SN. Periapical lesions-types, incidence, and clinical features. ORAL SURG ORAL MED ORAL PATHOL 1966;21:657- 71. Lalonde ER, Luebke RG. The frequency and distribution of periapical cysts and granulomas. ORAL SURG ORAL MED ORAL PATHOL 1968;25:861-8. Saad AY. Types, frequency and distribution of 382 periapical lesions associated with endodontic therapv. J Md State Dent ._ Assoc 1987;30:17-9. Friedlaender GE. Antigenicity of preserved allografts. Trans- plant Proc 1976;8:195-200. Malinin TI. Rosomoff HL, Sutton CH. Human cadaver fem- oral head homografts for anterior spine fusion. Surg Neurol 1977:7:249-51.

Volume 71 Number 5
FDBA and periapical lesions 617
17. Kraut RA. The use of allogeneic bone for alveolar cleft graft- ing. ORAL SURG ORAL MED ORAL PATHOL 1987;278-82.
18. Christian JM, Peterson LJ. Frozen femoral head allogeneic bone grafts for orthognathic surgery. J Oral Maxillofac Surg 1982;40:635-9.
19. Lekkas C, Wes BJ. Absolute augmentation of the extremely atrophic mandible. J Oral Maxillofac Surg 198 1;39:103-38.
20. Hovinga J, Wirds JJ, Lashley FO, Holaltcheff H, Lindwer J. Gestoorde fractuurgenezing van de mandibula. Ned Tijdschr Tandhk 1973;80:434-7.
2 I. Constantinides J, Zachariades N. Homogenous bone grafts to the mandible. J Oral Surg 1978;36:599-604.
22. Osbon DB, Feinberg SE, Finkelstein MW, Bumsted RM, Zeitler DL. Delayed mandibular reconstruction following re- moval of a mesenchymal chondrosarcoma. ORAL SURG ORAL MED ORAL PATHOS 1985;59:557-64.
23. Kellv JF. Friedlaender GE. Preurosthetic bone graft auemen- tat& with allogenic bone: a preliminary report. J OrarSurg 1977;35:268-75.
24. West TL, Brustein DD. Freeze-dried bone and coralline implants compared in the dog. J Periodontol 1985;56:348-51.
25. Pearson GE, Rosen S, Deporter DA. Preliminary observation on the usefulness of a decalcified, freeze-dried cancellous bone allograft material in periodontal surgery. J Periodontol 1981; 52:55-9.
26. Mellonig JT, Bowers GM, Bright R, Lawrence JJ. Clinical evaluation of freeze-dried bone allografts in periodontal os- seous defects. J Periodontol 1976;47:125-31.
27. Allard RHB, Lekkas C, Swart JGN. Autologous versus homologous bone grafting in osteotomies, secondary cleft re-
28.
29.
30.
31.
32.
33.
pairs, and ridge augmentations: a clinical study. ORAL SURC GRAL MED ORAL PATHOL 1987;64:269-74. Swart JGN. Allard RHB. Subaeriosteal onlav auementation of the mandible: a clinical and radiographic-sur;ey. J Oral Maxillofac Surg 1985;43: 183-7. Schallhorn RG. Present status of osseous grafting procedures. J Periodontol 1977;48:570-6. Rossmeisl R, Reader A, Melfi R, Marquard J. A study of freeze-dried (lyophilized) cortical bone used as an apical bar- rier in adult monkey teeth. J Endod 1982;8:219-26. Mellonig JT, Bowers GM, Bailey RC. Comparison of bone graft materials. Part I. New bone formation with autografts and allografts determined by strontium 85. J Periodontol 1981;52:291-6. Mellonig JT, Bowers GM, Cotton WR. Comparison of bone graft materials. Part II. New bone formation with autografts and allografts: a histological evaluation. J Periodontol 1981;52:297-302. Nade S. Osteogenesis after bone and bone marrow transplan- tation. II. The initial cellular events following transplantation of decalcified allografts of cancellous bone. Acta Orthop Stand 1977;48:572-7.
Reprint requests to: El-Said M. Abdellatief, BDS, MSD, PHD Oral Surgery Department Faculty of Dental Medicine Al-Azhar University Nasr City, Cairo, Egypt













![Assessment of bone microcirculation by contrast-enhanced ultrasound (CEUS) and [18F]-positron emission tomography/computed tomography in free osseous and osseocutaneus flaps for mandibular](https://img.dokumen.tips/doc/110x75/6347c3aff4145ce0ba026023/assessment-of-bone-microcirculation-by-contrast-enhanced-ultrasound-ceus-and-18f-positron.jpg)















