Embed Size (px)
Citation preview
Arch Dermatol Res (2008) 300:365–370
DOI 10.1007/s00403-008-0861-2ORIGINAL PAPER
Haplotypic classiWcation of dystrophic epidermolysis bullosa in Tunisian consanguineous families: implication for diagnosis
Houyem Ouragini · Faïka Cherif · Wafa Daoud · Selma Kassar · Chérine Charfeddine · Ahmed Rebaï · Samir Boubaker · Amel Ben Osman-Dhahri · Sonia Abdelhak
Received: 30 July 2007 / Revised: 5 March 2008 / Accepted: 29 April 2008 / Published online: 22 May 2008© Springer-Verlag 2008
Abstract Dystrophic epidermolysis bullosa (DEB) is arare genodermatosis caused by mutations in the type VIIcollagen gene COL7A1. Clinical diagnosis of DEBshould be conWrmed by histopathological and electronmicroscopy analysis, which is not always accessible. Wereport here a genetic investigation of DEB consanguine-ous families in Tunisia. A total of 23 EB families weregenotyped with 5 microsatellite markers overlapping theCOL7A1 gene. Among these families, 19 presented withthe dystrophic form of EB, 9 were diagnosed by histopa-thological examination, 2 had the simplex form, 1 had ajunctional EB, and 1 was aVected by an unclassiWed form
of EB. The informativeness of the markers was studiedand allowed us to select three markers for genetic testingof DEB in Tunisian families at risk. Haplotype analysisand homozygosity by descent suggest that all familiesclassiWed clinically as having DEB and the patient whopresented with an unclassiWed form of EB are likelylinked to the COL7A1 gene, and showed evidence forexclusion for the simplex and junctional cases. ForCOL7A1 linked families, two main haplotypes wereshared by eight families. For all the other cases, haplo-typic heterogeneity was observed, thus suggesting amutational heterogeneity among Tunisian DEB families.The genetic results matched with the ultrastructuralanalysis in all the DEB families and with the clinicalexamination in 94.7% of all studied DEB families. Thisstudy is to our knowledge the Wrst genetic investigationof DEB in the Maghrebian population. We propose aselection of informative markers and show the impor-tance of haplotype analysis as a relatively easy and costand time eVective method for carrier screening and pre-natal diagnosis of DEB in consanguineous families atrisk.
Keywords Dystrophic epidermolysis bullosa · Haplotypic classiWcation · Genetic counselling · Homozygosity by descent · Northern African population
AbbreviationsDEB Dystrophic epidermolysis bullosaEB Epidermolysis bullosaBMZ Basement membrane zoneEBS Epidermolysis bullosa simplexJEB Junctional epidermolysis bullosaAF Anchoring WbrilsHS-RDEB Hallopeau-Siemens type of recessive dystro-
phic epidermolysis bullosa
Electronic supplementary material The online version of this article (doi:10.1007/s00403-008-0861-2) contains supplementary material, which is available to authorized users.
H. Ouragini · F. Cherif · C. Charfeddine · S. Abdelhak (&)Molecular Investigation of Genetic Orphan Diseases, Research Unit (MIGOD), Institut Pasteur de Tunis, BP 74, 13 Place Pasteur, 1002 Tunis, Tunisiae-mail: [email protected]
F. Cherif · W. Daoud · A. Ben Osman-DhahriService de Dermatologie, Hôpital La Rabta de Tunis, Tunis, Tunisia
S. Kassar · S. BoubakerService d’Anatomo-Pathologie, Institut Pasteur de Tunis, Tunis, Tunisia
S. KassarStudy of Hereditary Keratinization Disorders, Research Unit, Hôpital La Rabta de Tunis, Tunis, Tunisia
A. RebaïService de Bioinformatique, Centre de Biotechnologie de Sfax, Sfax, Tunisia
123

366 Arch Dermatol Res (2008) 300:365–370
nHS-RDEB non Hallopeau-Siemens type of recessivedystrophic epidermolysis bullosa
RDEB Recessive dystrophic epidermolysis bullosa
Introduction
Epidermolysis bullosa (EB) is a heterogeneous group ofhereditary mechanobullous disorders characterized by tissueseparation within the cutaneous basement membrane zone(BMZ) resulting in blistering and scarring of the skin andmucous membrane [13]. EB is classiWed into four major sub-groups on the basis of the level of cleavage within the BMZ,as demonstrated by diagnostic transmission electron micros-copy or immunohistochemical epitope mapping [13, 27]: (1)in the simplex form (EBS), tissue separation results from thefragility of the basal keratinocytes due to mutations in KRT5and KRT14 genes [14]; (2) the hemidesmosal form shows tis-sue cleavage at the level of hemidesmosomes, and the muta-tions reside in four diVerent genes: PLEC1, COL17A1,ITGB4 and ITGA6 [27]; (3) in the junctional form of EB(JEB), tissue separation occurs within the dermal–epidermalbasement membrane, and the mutations reside in LAMA3,LAMB3 et LAMC2 genes [27]; (4) in the dystrophic form(DEB), the blisters occur beneath the lamina densa, at thelevel of the anchoring Wbrils (AF), which are morphologi-cally altered, reduced in number or entirely absent in thesevere forms of DEB [28]. On the basis of the inheritancepattern and clinical manifestations, DEB is classiWed intothree major subtypes: one dominant (DDEB) and two reces-sive forms (the Hallopeau-Siemens type (HS-RDEB), themost severe form of recessive DEB (RDEB), and the nonHallopeau-Siemens type (nHS-RDEB) [13, 19]). Since AFare composed predominantly of type VII collagen [28], bothdominant and recessive DEB are caused by mutations in thetype VII collagen gene, COL7A1. This gene consists of 118exons spanning 32 Kb at chromosomal location 3p21.1 and itencodes a 9 Kb mRNA [7]. Over 200 various mutations havebeen, so far, reported, most are private, but few recurrentmutations have been described [8, 17, 21]. Screening formutations in patients with recessive form of DEB is thereforetime-consuming, labor-intensive and expensive [29].
According to the National Epidermolysis Bullosa Registry,the prevalence of EB is estimated to be 59/1,000,000 amongwhom 5% are aVected by the dystrophic form [12]. In Tuni-sia, the prevalence of EB is 115/1,000,000, and approximately46% of the EB patients present the dystrophic form, amongwhom 90% present the recessive form, while in the worldonly 5% have DEB (Faika CHERIF, unpublished data).
In the present study, we carried out a genetic investiga-tion of DEB Tunisian families and assessed the use of hap-lotype analysis and homozygosity by descent as a diagnosistool in consanguineous families.
Patients and methods
Patients
This study was carried out in 23 EB Tunisian families, codi-Wed EB-A to EB-W, with at least one aVected child. Charac-teristics of the studied families are summarized in Table 1.A total of 29 patients aVected by the recessive form of EB,as assessed by their genealogical trees, were investigated: 24DEB patients (19 families), 2 EBS (2 families) and 2 JEB (1family). One patient (family EB-V) aVected by an unclassi-Wed form of EB was also included in the present study.
All patients were diagnosed on the basis of clinical fea-tures of each EB subtype. For nine families, the diagnosisof DEB was conWrmed by ultrastructural examination of askin biopsy in at least one aVected member. This examina-tion revealed a dermo-epidermal separation beneath thelamina densa with electronic microscopy and AF absenceor marked reduction of AF.
Genotyping and haplotype analysis
After obtaining informed consent, blood samples were col-lected from each patient and relatives. Genomic DNA wasextracted by standard phenol-chlorophorm procedures [23]and used as a template for polymerase chain reaction (PCR)ampliWcation.
Genotyping for all available family members were deter-mined as described previously [3] using Wve microsatellitemarkers spanning a 5 Mb interval that overlaps the DEBinterval (cen-D3S1568, D3S3629, (COL7A1), D3S643,D3S1478, D3S3582-tel). The sex-averaged genetic dis-tance between the Xanking markers D3S3582 and D3S1568was 4.1 cM, according to the latest version of the Genethonmap [9].
Statistical analyses
Informativeness of markers
Within every family, a marker was considered as informa-tive, if at least one of the two parents is heterozygous forthe tested marker [25].
Linkage analysis
We performed multipoint nonparametric linkage analysisusing MERLIN [1]. The frequency of the disease is estimatedto be 0.0001, assuming a fully penetrant autosomal recessivemode of inheritance and equal frequencies for the markers.
A single locus and a multilocus FBAT tests were alsoperformed in order to identify a possible founder eVect inDEB Tunisian families using a recessive model [16].
123
Arch Dermatol Res (2008) 300:365–370 367
Results
Informativeness of the markers
A total of 29 patients were subtyped with Wve diVerentpolymorphic markers linked to the COL7A1 gene. All the23 studied families were informative for at least threemarkers (pedigrees and genotypes are provided in the sup-plementary data). Markers D3S1478 and the nearest markerto COL7A1 gene, D3S643, were the most informativemarkers in the studied DEB families, since they were fullyinformative in up to 80%, followed by D3S1568 which wasfully informative in 76.5% of the families. D3S3582 and
D3S3629 were the least informative markers, as they werefully informative in less than 45% of the tested families(see Tables 1, 2 in the supplementary data, ESM).
Haplotype analysis
For each family, the most likely haplotype was con-structed with visual inspection and using MERLIN. Hap-lotype analysis and homozygosity by descent providedevidence for linkage to the COL7A1 locus for all thepatients classiWed clinically as having DEB (24 patients)and for exclusion of EBS and JEB patients. For the DEBpatients, 21 were homozygous and 3 heterozygous
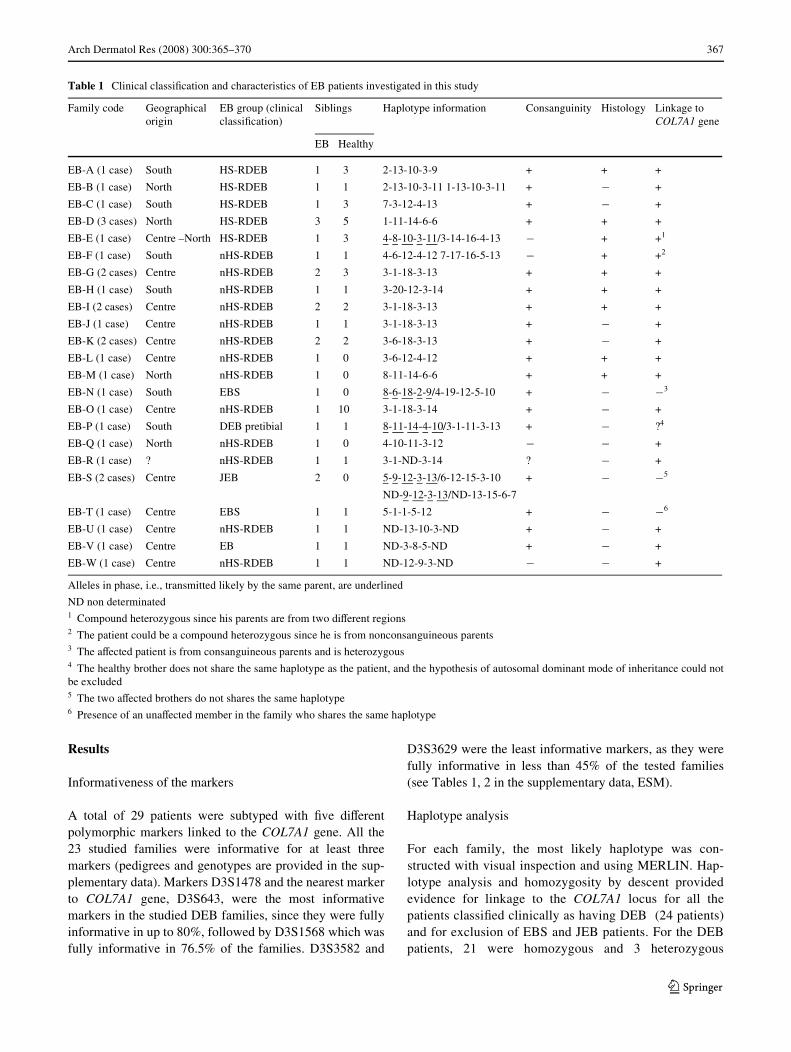
Table 1 Clinical classiWcation and characteristics of EB patients investigated in this study
Alleles in phase, i.e., transmitted likely by the same parent, are underlined
ND non determinated1 Compound heterozygous since his parents are from two diVerent regions2 The patient could be a compound heterozygous since he is from nonconsanguineous parents3 The aVected patient is from consanguineous parents and is heterozygous4 The healthy brother does not share the same haplotype as the patient, and the hypothesis of autosomal dominant mode of inheritance could notbe excluded5 The two aVected brothers do not shares the same haplotype6 Presence of an unaVected member in the family who shares the same haplotype
Family code Geographical origin
EB group (clinical classiWcation)
Siblings Haplotype information Consanguinity Histology Linkage to COL7A1 gene
EB Healthy
EB-A (1 case) South HS-RDEB 1 3 2-13-10-3-9 + + +
EB-B (1 case) North HS-RDEB 1 1 2-13-10-3-11 1-13-10-3-11 + ¡ +
EB-C (1 case) South HS-RDEB 1 3 7-3-12-4-13 + ¡ +
EB-D (3 cases) North HS-RDEB 3 5 1-11-14-6-6 + + +
EB-E (1 case) Centre –North HS-RDEB 1 3 4-8-10-3-11/3-14-16-4-13 ¡ + +1
EB-F (1 case) South nHS-RDEB 1 1 4-6-12-4-12 7-17-16-5-13 ¡ + +2
EB-G (2 cases) Centre nHS-RDEB 2 3 3-1-18-3-13 + + +
EB-H (1 case) South nHS-RDEB 1 1 3-20-12-3-14 + + +
EB-I (2 cases) Centre nHS-RDEB 2 2 3-1-18-3-13 + + +
EB-J (1 case) Centre nHS-RDEB 1 1 3-1-18-3-13 + ¡ +
EB-K (2 cases) Centre nHS-RDEB 2 2 3-6-18-3-13 + ¡ +
EB-L (1 case) Centre nHS-RDEB 1 0 3-6-12-4-12 + + +
EB-M (1 case) North nHS-RDEB 1 0 8-11-14-6-6 + + +
EB-N (1 case) South EBS 1 0 8-6-18-2-9/4-19-12-5-10 + ¡ ¡3
EB-O (1 case) Centre nHS-RDEB 1 10 3-1-18-3-14 + ¡ +
EB-P (1 case) South DEB pretibial 1 1 8-11-14-4-10/3-1-11-3-13 + ¡ ?4
EB-Q (1 case) North nHS-RDEB 1 0 4-10-11-3-12 ¡ ¡ +
EB-R (1 case) ? nHS-RDEB 1 1 3-1-ND-3-14 ? ¡ +
EB-S (2 cases) Centre JEB 2 0 5-9-12-3-13/6-12-15-3-10 + ¡ ¡5
ND-9-12-3-13/ND-13-15-6-7
EB-T (1 case) Centre EBS 1 1 5-1-1-5-12 + ¡ ¡6
EB-U (1 case) Centre nHS-RDEB 1 1 ND-13-10-3-ND + ¡ +
EB-V (1 case) Centre EB 1 1 ND-3-8-5-ND + ¡ +
EB-W (1 case) Centre nHS-RDEB 1 1 ND-12-9-3-ND ¡ ¡ +
123
368 Arch Dermatol Res (2008) 300:365–370
(Table 1) for the markers overlapping the COL7A1 generegion.
Linkage analysis
Multipoint parametric LOD scores were calculated for allfamilies between the COL7A1 gene and the Wve markerstested. SigniWcant LOD scores were obtained for all mark-ers, except the marker D3S1568, with a maximum multi-point LOD and HLOD scores of 5.019 and 5.020,respectively, at marker D3S3582 (Table 2). All HLODscores were above statistical signiWcance with the smallestvalue of 2.704 at marker D3S1568, which presents 40% ofheterogeneity due to a recombination in the family EB-I.Evidence of linkage for the informative families EB-D, EB-G, EB-I, EB-J, EB-K and EB-L was detected. The familyEB-S, who presented the junctional form of EB, gave nega-tive LOD scores in this region and provided evidence forexclusion from the COL7A1 region.
In order to identify a possible founder eVect in TunisianDEB families, haplotypes were analyzed in the familieslikely linked to the COL7A1 gene. Two common haplo-types were identiWed, 3-1-18-3-13 and 1-11-14-6-6, whichare shared by 25% (9 patients) and 8% (4 patients) of thefamilies, respectively. The most frequent haplotype ismainly found among families originating from CentralTunisia and presenting the non Hallopeau-Siemens form ofRDEB; and the second one is found among families origi-nating from northeastern regions (Table 1). These resultswere conWrmed by FBAT tests (Table 3). The other fami-lies shared partially these haplotype or presented a diVerenthaplotype. Alltogether, seven diVerent haplotypes wereidentiWed. These results show haplotypic heterogeneityamong Tunisian DEB families, thus suggesting a muta-tional heterogeneity.
Correlation of genetic and histopathologic examination
The genetic results matched with the ultrastructural analy-sis in all the studied families for whom the diagnosis ofDEB was conWrmed by electron microscopy examination.Indeed, the patients were homozygous for the tested mark-
ers overlapping the COL7A1 gene region and did not sharethe same disease haplotype as the available healthy mem-bers in each family. This was also the case for nine familiesclinically typed as being dystrophic and for whom the ultra-structural diagnosis was not made (families EB-B, EB-C,EB-J, EB-K, EB-O, EB-Q, EB-R, EB-U and EB-W), andfor the patient EB-V for whom it was not possible to deter-mine clinically the form of EB. This result suggests that theCOL7A1 gene is likely responsible for EB in these families,thus conWrming that these patients have a dystrophic form(Table 1).
Three DEB patients were heterozygous. For the patientsEB-E and EB-F, the diagnosis of DEB was conWrmed byelectron microscopy examination and they were from nonconsanguineous parents, suggesting that they corresponded tocompound heterozygous. For the consanguineous patient EB-P, he did not share the same haplotype as his unaVectedbrother. Either he was a compound heterozygous or as he wasaVected by the pretibial form of DEB, his parents wereunaVected thus he probably had a dominant de novo mutation.
For the other patients, clinically showing EBS and JEBforms, haplotype analysis showed evidence for exclusion toCOL7A1. Indeed, EBS patient EB-N is heterozygous forthe Wve tested markers and EBS family EB-T present oneaVected and one unaVected children who share the samehomozygous haplotype. The JEB family EB-S includes twoaVected children who are heterozygous and do not share thesame haplotype. Multipoint analysis conWrms exclusion ofthe region for the families EB-S and EB-T; EB-N was not-informative.
Discussion
DEB is a relatively rare skin disorder; nevertheless, morethan 200 pathogenic mutations have been described [26]. In
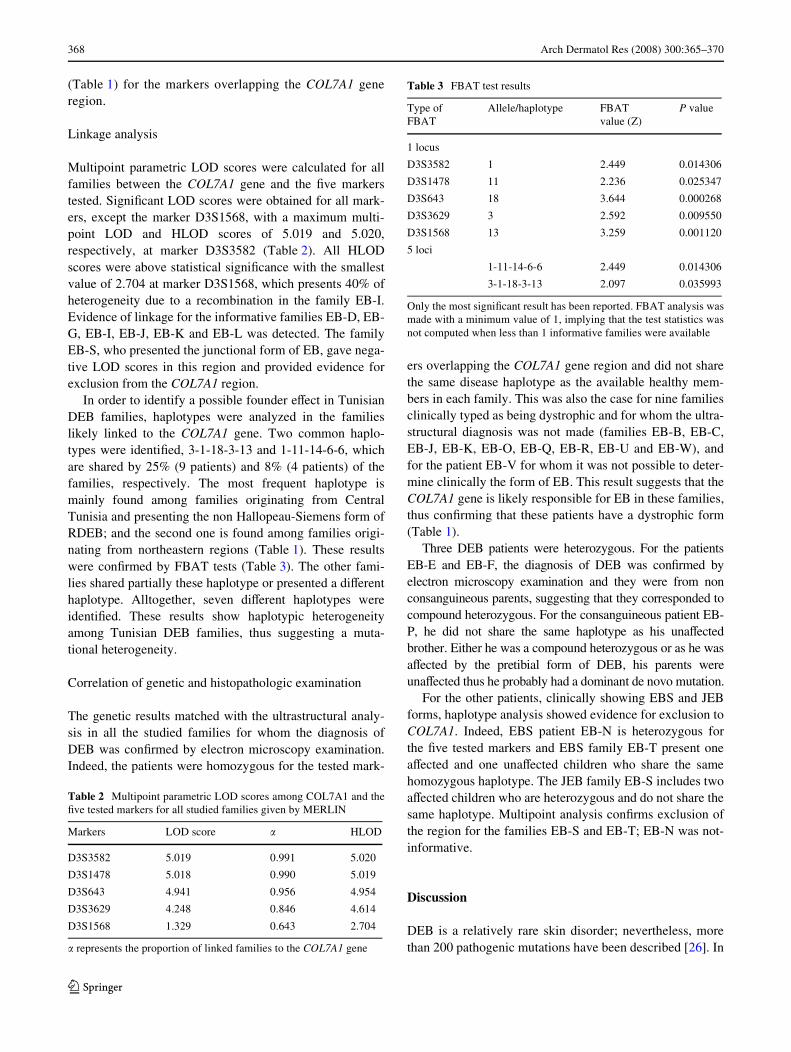
Table 2 Multipoint parametric LOD scores among COL7A1 and theWve tested markers for all studied families given by MERLIN
� represents the proportion of linked families to the COL7A1 gene
Markers LOD score � HLOD
D3S3582 5.019 0.991 5.020
D3S1478 5.018 0.990 5.019
D3S643 4.941 0.956 4.954
D3S3629 4.248 0.846 4.614
D3S1568 1.329 0.643 2.704
Table 3 FBAT test results
Only the most signiWcant result has been reported. FBAT analysis wasmade with a minimum value of 1, implying that the test statistics wasnot computed when less than 1 informative families were available
Type of FBAT
Allele/haplotype FBAT value (Z)
P value
1 locus
D3S3582 1 2.449 0.014306
D3S1478 11 2.236 0.025347
D3S643 18 3.644 0.000268
D3S3629 3 2.592 0.009550
D3S1568 13 3.259 0.001120
5 loci
1-11-14-6-6 2.449 0.014306
3-1-18-3-13 2.097 0.035993
123

Arch Dermatol Res (2008) 300:365–370 369
Tunisia, the prevalence of the recessive form of DEB is rel-atively high. This could be explained by a high rate of con-sanguineous marriages, which is estimated to be 33% [22].
We report here a genetic investigation of EB in the Tuni-sian population. This is to our knowledge the Wrst study inthe Maghrebian population. A total of 23 EB familiesincluding 29 aVected children were investigated with link-age analysis and homozygosity by descent using Wve mark-ers Xanking the COL7A1 region.
In a Wrst step, we evaluated the informativeness of thetested markers. Taking into consideration this informative-ness and distance of the tested markers, we propose the useof D3S1478, D3S643 and D3S3629 markers to identifyDEB carriers in North African families at risk.
Homozygosity by descent and haplotype analysisshowed that all the families classiWed clinically to haveDEB are likely linked to the COL7A1 locus. In spite of theautosomal recessive mode of inheritance of the disorderand consanguinity of the parents, three cases were hetero-zygous. This could be explained by an autosomal dominantmode of inheritance of the disease. The patients could becompound heterozygous, or could bear a neomutation thatbehaves dominantly as described previously [15, 17].
Alltogether, our study showed that seven homozygoushaplotypes segregated in the studied families. This suggeststhat at least seven diVerent mutations in COL7A1 geneoccurred in the Tunisian DEB patients. This hypothesis isfurther supported by previous data on mutational heteroge-neity of several Mendelian diseases aVecting the Tunisianpopulation [2, 3, 5, 6]. Among these haplotypes, two werecommon to diVerent families, thus suggesting the occur-rence of a founder eVect for DEB in northern and centralTunisia, with speciWc mutations segregating within eachhaplotype.
Among the DEB patients for whom the diagnosis wasconWrmed by electron microscopy examination, the geneticresults matched with the ultrastructural analysis in 94.7%of the studied families. In order to assess eYcacy of homo-zygosity by descent, four cases of EB, classiWed two clini-cally as EBS and two as JEB, provided evidence forexclusion from the COL7A1 locus. The family EB-Tshowed the importance of genotyping of the healthy sib-ling, thus improving the informativity of the family. OneunclassiWed case (patient EB-V) was genotyped to deter-mine the type of EB. Homozygosity by descent suggestedthat he was likely aVected by the DEB form.
Haplotypic classiWcation provides an eYcient pre-screening tool before mutation analysis, thus reducing thecost of sequencing of a relatively large gene [18]. We andothers have shown that homozygosity mapping is a power-ful tool for a rapid classiWcation of genetically heteroge-neous diseases [4, 10, 11]. Two recent studies demonstratedthat homozygosity by descent may serve as a useful tool in
the molecular diagnosis of JEB or congenital recessive ich-tyosis in consanguineous families [18, 20]. Our results sug-gest that this could be extended to other genodermatoses.
Since there is no cure or eVective treatment for DEB[24], prevention of the disease is important and stronglydepends on carrier-status information. We propose here theuse of haplotype analysis and homozygosity by descent as atool for diagnosis conWrmation of DEB in consanguineousfamilies when microscopic methods and a sequencing plat-form are not available. Furthermore, due to life-threateningcomplications and signiWcant long-term morbidity associ-ated with the severe, mutilating form of HS-RDEB, haplo-type analysis provides a cost-eVective and considerablyfaster method for carrier detection and prenatal diagnosis inat-risk consanguineous informative families.
Acknowledgments We wish to thank the patients and their familymembers for their cooperation in this study. The authors thank SoniaCHAKROUN and Nabil BEL HADJ HAMIDA for their technical con-tribution to the present work. This work was supported by the TunisianMinistry of Higher Education, ScientiWc and Technological Research.
References
1. Abecasis GR, Cherny SS, Cookson WO, Cardon LR (2002) Mer-lin-rapid analysis of dense genetic maps using sparse gene Xowtrees. Nat Genet 30:97–101
2. Ben Arab S, Hmani M, Denoyelle F, Boulila-Elgaied A, Charde-noux S, Hachicha S, Petit C, Ayadi H (2000) Mutations of GJB2in three geographic isolates from northern Tunisia: evidence forgenetic heterogeneity within isolates. Clin Genet 57:439–443
3. Bouchlaka C, Abdelhak S, Amouri A, Ben Abid H, Hadiji S,Frikha M, Ben Othman T, Amri F, Ayadi H, Hachicha M, RebaiA, Saad A, Dellagi K, Tunisian Fanconi Anemia Study Group(2003) Fanconi anemia in Tunisia: high prevalence of group Aand identiWcation of new FANCA mutations. J Hum Genet48:352–361
4. Bouchlaka C, Maktouf C, Mahjoub B, Ayadi A, Sfar MT, SioudM, Gueddich N, Belhadjali Z, Rebai A, Abdelhak S, Dellagi K(2007) Genetic heterogeneity of megaloblastic anaemia type 1 inTunisian patients. J Hum Genet 52:262–270
5. Chaabani H, Ben Arab S, Chebbi K (1995) Genetic heterogeneitystudy of non-syndromic autosomal recessive sensorineural deaf-ness within the Tunisian population. Ann Genet 38:158–161
6. Charfeddine C, Mokni M, Ben Mousli R, Elkares R, Bouchlaka C,Boubaker S, Ghedamsi S, Baccouche D, Ben Osman A, Dellagi K,Abdelhak S (2003) A novel missense mutation in the gene encod-ing SLURP-1 in patients with Mal de Meleda from northern Tuni-sia. Br J Dermatol 149:1108–1115
7. Christiano AM, HoVman GG, Chung-Honet LC, Lee S, Cheng W,Uitto J, Greenspan DS (1994) Structural organisation of the humantype VII collagen gene (COL7A1) composed of more exons thanany previously characterized gene. Genomics 21:169–179
8. Das BB, Sahoo S (2004) Dystrophic epidermolysis bullosa. J Per-inatol 24:41–47
9. Dib C, Faure S, Fizames C, Samson D, Drouot N, Vignal A, Mi-llasseau P, Marc S, Hazan J, Seboun E, Lathrop M, Gyapay G,Morissette J, Weissenbach J (1996) A comprehensive genetic mapof the human genome based on 5,264 microsatellites. Nature380:152–154
123
370 Arch Dermatol Res (2008) 300:365–370
10. El Kares R, Barbouche MR, Elloumi-Zghal H, Bejaoui M, ChemliJ, Mellouli F, Tebib N, Abdelmoula MS, Boukthir S, Fitouri Z,M’Rad S, Bouslama K, Touiri H, Abdelhak S, Dellagi MK (2006)Genetic and mutational heterogeneity of autosomal recessivechronic granulomatous disease in Tunisia. J Hum Genet 51:887–895
11. Elloumi-Zghal H, Barbouche MR, Chemli J, Bejaoui M, Harbi A,Snoussi N, Abdelhak S, Dellagi K (2002) Clinical and genetic het-erogeneity of inherited autosomal recessive susceptibility to dis-seminated Mycobacterium bovis bacille calmette-guerin infection.J Infect Dis 15:1468–1475
12. Fine J-D, Jhonson L, Suchindran C, Moshell A, Gedde-Dahl T(1999) The epidemiology of inherited epidermolysis bullosa: Wnd-ings within American, Canadian and European study populations.In: Fine J-D, Bauer EA, McGuire J, Moshell A (eds) Epidermoly-sis Bullosa Clinical, Epidemiologic, and Laboratory Advances andthe Findings of the National Epidermolysis Bullosa Registry. TheJohns Hopkins University Press, Baltimore, pp 101–113
13. Fine JD, Eady RA, Bauer EA, Briggaman RA, Bruckner-Tuder-man L, Christiano A, Heagerty A, Hintner H, Jonkman MF, McG-rath J, McGuire J, Moshell A, Shimizu H, Tadini G, Uitto J (2000)Revised classiWcation system for inherited epidermolysis bullosa:report of the second international consensus meeting on diagnosisand classiWcation of epidermolysis bullosa. J Am Acad Dermatol42:1051–1066
14. Fuchs EV (1999) The molecular biology of epidermolysis bullosasimplex. In: Fine JD, Bauer EA, McGuire J, Moshell A (eds)Epidermolysis Bullosa Clinical, Epidemiologic, and LaboratoryAdvances and the Findings of the National Epidermolysis BullosaRegistry. The Johns Hopkins University Press, Baltimore, pp 280–299
15. Gardella R, Zoppi N, Zambruno G, Barlati S, Colombi M (2002)DiVerent phenotypes in recessive dystrophic epidermolysis bull-osa patients sharing the same mutation in compound heterozygos-ity with two novel mutations in the type VII collagen gene. Br JDermatol 147:450–457
16. Horvath S, Xin Xu X, Laird NM (2001) The family based associ-ation test method: strategies for studying general genotype-pheno-type associations. Eur J Hum Gen 9:301–306
17. Kon A, Pulkkinen L, Ishida-Yamamoto A, Hashimoto I, Uitto J(1998) Novel COL7A1 mutations in dystrophic forms of epider-molysis bullosa. J Invest Dermatol 111:534–537
18. Lugassy J, Hennis HC, Indelman M, Khamaysi Z, Bergman R,Sprecher E (2007) Rapid detection of homozygous mutations incongenital recessive ichtyosis. Arch Dermatol Res 300:81–85
19. Mitsuashi Y, Hashimoto I (2003) Genetic abnormalities and clini-cal classiWcation of epidermolysis bullosa. Arch Dermatol Res295:S29–S33
20. Mizrachi-Koren M, Shemer S, Morgan M, Indelman M, KhamaysiZ, Petronius D, Bitterman-Deutsch O, Hennies HC, Bergman R,Sprecher E (2006) Homozygosity mapping as a screening tool forthe molecular diagnosis of hereditary skin diseases in consanguin-eous populations. J Am Acad Dermatol 55:393–401
21. Murata T, Masunaga T, Ishiko A, Shimizu H, Nishikawa T (2004)DiVerences in recurrent COL7A1 mutations in dystrophic epider-molysis bullosa: ethnic-speciWc and worldwide recurrent muta-tions. Arch Dermatol Res 295:442–447
22. Riou S, El Younsi C, Chaabouni H (1989) Consanguinity in thepopulation of northern Tunisia. Tunis Med 67:167–172
23. Sambrook J, Fritsh EF, Maniatis T (1989) Molecular cloning: alaboratory manual. Cold Spring Laboratory Press, Cold springHarbor
24. Tamai K, Hashimoto I, Hanada K, Ikeda S, Imamura S, Ogawa H,Japanese Study Group for Rare Intractable Skin Diseases (2003)Japanese guidelines for diagnosis and treatment of junctional anddystrophic epidermolysis bullosa. Arch Dermatol Res 295:S24–S28
25. Torrelo A, Valverde E, Zambrano A (1998) Informativeness ofpolymorphic markers for prenatal diagnosis of recessive dystro-phic epidermolysis bullosa in Spanish families at risk. J DermatolSci 17:233–238
26. Uitto J, Richard G (2004) Progress in Epidermolysis Bullosa: ge-netic classiWcation and clinical implications. Am J Med 131:61–74
27. Varki R, Sadowski S, Pfendner E, Uitto J (2006) Epidermolysisbullosa I. Molecular genetics of the junctional and hemidesmoso-mal variants. J Med Genet 43:641–652
28. Varki R, Sadowski S, Uitto J, Pfendner E (2007) Epidermolysisbullosa II. Type VII collagen mutations and phenotype-genotypecorrelations in the dystrophic subtypes. J Med Genet 44:181–192
29. Whittock NV, Ashton GH, Mohammedi R, Mellerio JE, MathewCG, Abbs SJ, Eady RA, McGrath JA (1999) Comparative muta-tion detection screening of the type VII collagen gene (COL7A1)using the protein truncation test, Xuorescent chemical cleavage ofmismatch, and conformation sensitive gel electrophoresis. J InvestDermatol 113:673–686
123















![Bonding and Electronic Structure in Consanguineous and Conjugal Iron and Rhenium sp Carbon Chain Complexes [MC 4 M‘] n + : Computational Analyses of the Effect of the Metal](https://img.dokumen.tips/doc/110x75/635d872fa3fa66b45c0e7134/bonding-and-electronic-structure-in-consanguineous-and-conjugal-iron-and-rhenium.jpg)













