Embed Size (px)
Citation preview
GYNAECOLOGY20thEDITIONbyTenTeachers
Editedby
HelenBickerstaffMD,MRCOGSeniorLecturerinMedicalEducationKing’sCollegeLondonLondon,UKandHonoraryConsultantObstetricianandGynaecologistGuy’sandStThomas’NHSFoundationTrustLondon,UK
LouiseCKennyMBChB(Hons),MRCOG,PhDProfessorofObstetricsandGynaecologyUniversityCollegeCorkCork,IrelandandDirectorTheIrishCentreforFetalandNeonatalTranslationalResearch(INFANT)Cork,Ireland
www.medicalebookpdf.com
CRCPressTaylor&FrancisGroup6000BrokenSoundParkwayNW,Suite300BocaRaton,FL33487-2742
©2017byTaylor&FrancisGroup,LLCCRCPressisanimprintofTaylor&FrancisGroup,anInformabusiness
NoclaimtooriginalU.S.Governmentworks
Printedonacid-freepaper
InternationalStandardBookNumber-13:978-1-4987-4428-7(Pack–BookandEbook)InternationalStandardBookNumber-13:978-1-4987-4461-4(Paperback;restrictedterritorialavailability)
Thisbookcontainsinformationobtainedfromauthenticandhighlyregardedsources.Whileallreasonableeffortshavebeenmadetopublishreliabledataandinformation,neithertheauthor[s]northepublishercanacceptanylegalresponsibilityorliabilityforanyerrorsoromissionsthatmay bemade. The publishers wish tomake clear that any views or opinions expressed in this book by individual editors, authors orcontributorsarepersonaltothemanddonotnecessarilyreflecttheviews/opinionsofthepublishers.Theinformationorguidancecontainedinthisbookisintendedforusebymedical,scientificorhealth-careprofessionalsandisprovidedstrictlyasasupplementtothemedicalorotherprofessional’sownjudgement, theirknowledgeof thepatient’smedicalhistory,relevantmanufacturer’s instructionsandtheappropriatebestpracticeguidelines.Becauseoftherapidadvancesinmedicalscience,anyinformationoradviceondosages,proceduresordiagnosesshouldbeindependentlyverified.Thereaderisstronglyurgedtoconsulttherelevantnationaldrugformularyandthedrugcompanies’anddeviceormaterial manufacturers’ printed instructions, and their websites, before administering or utilizing any of the drugs, devices or materialsmentioned in this book. This book does not indicate whether a particular treatment is appropriate or suitable for a particular individual.Ultimately it is thesole responsibilityof themedicalprofessional tomakehisorherownprofessional judgements, soas toadviseand treatpatients appropriately. The authors and publishers have also attempted to trace the copyright holders of all material reproduced in thispublicationandapologizetocopyrightholdersifpermissiontopublishinthisformhasnotbeenobtained.Ifanycopyrightmaterialhasnotbeenacknowledgedpleasewriteandletusknowsowemayrectifyinanyfuturereprint.
ExceptaspermittedunderU.S.CopyrightLaw,nopartofthisbookmaybereprinted,reproduced,transmitted,orutilizedinanyformbyanyelectronic, mechanical, or other means, now known or hereafter invented, including photocopying, microfilming, and recording, or in anyinformationstorageorretrievalsystem,withoutwrittenpermissionfromthepublishers.
Forpermissiontophotocopyorusematerialelectronicallyfromthiswork,pleaseaccesswww.copyright.com(http://www.copyright.com/)orcontact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-profitorganizationthatprovideslicensesandregistrationforavarietyofusers.FororganizationsthathavebeengrantedaphotocopylicensebytheCCC,aseparatesystemofpaymenthasbeenarranged.
TrademarkNotice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification andexplanationwithoutintenttoinfringe.
VisittheTaylor&FrancisWebsiteathttp://www.taylorandfrancis.com
andtheCRCPressWebsiteathttp://www.crcpress.com
www.medicalebookpdf.com

DedicationThisbookisdedicatedtothefirstandbestteachersweeverhad:
MyDad,Frank(HB)MyMum,Elizabeth(LCK)
www.medicalebookpdf.com
Contents
PrefaceContributorsAbbreviationseResources
CHAPTER1ThedevelopmentandanatomyofthefemalesexualorgansandpelvisHelenBickerstaff
CHAPTER2Gynaecologicalhistory,examinationandinvestigationsHelenBickerstaff
CHAPTER3HormonalcontrolofthemenstrualcycleandhormonaldisordersHelenBickerstaff
CHAPTER4DisordersofmenstrualbleedingHelenBickerstaff
CHAPTER5ImplantationandearlypregnancyAndrewHorne
CHAPTER6ContraceptionandabortionSharonCameron
CHAPTER7SubfertilityStuartLavery
CHAPTER8ThemenopauseandpostreproductivehealthEdwardMorris
CHAPTER9GenitourinaryproblemsMargaretKingston
CHAPTER10UrogynaecologyandpelvicfloorproblemsDouglasTincello
CHAPTER11BenignconditionsoftheovaryandpelvisTJustinClark
CHAPTER12Benignconditionsoftheuterus,cervixandendometriumTJustinClark
www.medicalebookpdf.com
CHAPTER13Benignconditionsofthevulvaandvagina,psychosexualdisordersandfemalegenitalmutilationLeilaCGFrodsham
CHAPTER14MalignantdiseaseoftheovaryEmmaJCrosbie
CHAPTER15MalignantdiseaseoftheuterusEmmaJCrosbie
CHAPTER16PremalignantandmalignantdiseaseofthelowergenitaltractEmmaJCrosbie
CHAPTER17GynaecologicalsurgeryandtherapeuticsDouglasTincello
Index
www.medicalebookpdf.com

Preface
Gynaecology byTenTeacherswas first published in 1919 as ‘Diseases ofWomen’ and is one of theoldest,most respectedandaccessible textson thesubject.GynaecologybyTenTeachershas informedgenerationsofgynaecologists,andnowhasawideinternationalaudience.Thereisgreatresponsibilityinrevisingthislandmark20thedition,toensureitsaccessibilityandrelevancearemaintainedintothenextcentury.
The 20th edition has been almost entirely rewritten to reflect both changing undergraduatemedicalcurriculaandchangingdiagnosticandmanagementprotocolsingynaecology.The‘TenTeachers’areallinternationallyrenownedexpertsintheirfieldsandallactivelyinvolvedinthedeliveryofundergraduateand postgraduate teaching in the UK. This volume has been edited carefully to ensure consistency ofstructure,styleandlevelofdetail,incommonwiththoseofitssistertextObstetricsbyTenTeachers.Thebooks can therefore be used together or independently as required. New self assessment sections arepresentedconsistentlythroughout,withdetailedclinicalscenariosforeachsubjectinastructuresimilartothoseusedinmostmedicalschools.
The global status of women’s and girls’ sexual and reproductive health and rights is disturbing.Millions ofwomenhave no access to contraception, undergo female genitalmutilation and receive nogynaecologicalcare.Itisfitting,therefore,thatthe20thedition,publishedalmost100yearsafterthefirst,maintainsaglobalaspectthroughout.
The aim of the text now, as it was a century ago, is to prepare students for their undergraduateexaminations,andtocontinuetobeusefulafterwardsinpostgraduatestudiesandclinicalpractice.Itisatextthattheeditorsusedasstudents,whichinspiredustopracticeandteachinthespecialty,andwhichwestill enjoy readingbecause it isconciseyetcomprehensive.Wehope that inaddition to supportingmedical students throughout their studies, general practitioners, trainees and allied health careprofessionalswillfinditusefulintheirwork.
Ithasbeenaprivilegeandanhonourtobetheeditorsofthistextbookasitapproachesthisimportantmilestone;weechoacenturyofpreviouseditorsinhopingthatthisbookwillenthuseanewgenerationofdoctors tobecomegynaecologists andwork to improve thehealthand the safetyofwomen throughallreproductiveages.
HelenBickerstaffLouiseCKenny
www.medicalebookpdf.com

Contributors
HelenBickerstaffMD,MRCOG
SeniorLecturerinMedicalEducationKing’sCollegeLondonandHonoraryConsultantObstetricianandGynaecologistGuy’sandStThomas’NHSFoundationTrustLondon,UK
SharonCameronMD,MFSRH,FRCOG
ConsultantGynaecologistandClinicalLeadforSexualHealthServicesNHSLothianChalmersCentreEdinburgh,UK
TJustinClarkMBChB,MD(Hons),FRCOG
ConsultantGynaecologistBirminghamWomen’sHospitalandHonoraryProfessorinGynaecologyUniversityofBirminghamBirmingham,UK
EmmaJCrosbieBSc,MBChB,PhD,MRCOG
SeniorLecturerandHonoraryConsultantGynaecologicalOncologistUniversityofManchesterStMary’sHospitalManchester,UK
LeilaCGFrodsham,MBChB,MRCOG
ConsultantGynaecologistChairoftheInstituteofPsychosexualMedicine(2012–15)
AndrewHornePhD,FRCOGPersonalChairinGynaecologyandReproductiveSciencesHonoraryConsultantGynaecologistMRCCentreforReproductiveHealth
www.medicalebookpdf.com
UniversityofEdinburghEdinburgh,UK
MargaretKingstonBMBS,BMedSci,FRCP,DipGUM,DFSRHMSc
ConsultantPhysicianGenitourinaryMedicineandAssociateMedicalDirectorCentralManchesterFoundationTrustManchester,UK
StuartLaveryMBBCh,MSc,FRCOG
ConsultantGynaecologistDirectorIVFHammersmithandQueenCharlotte’sandChelseaHospitalandHonorarySeniorLecturerImperialCollegeLondonLondon,UK
EdwardMorrisMD,FRCOG
ConsultantGynaecologistNorfolkandNorwichUniversityHospitalNHSFoundationTrustNorwich,UKandVicePresident,ClinicalQualityRoyalCollegeofObstetriciansandGynaecologistsLondon,UK
DouglasGTincelloBSc,MBChB,MD,FRCOG,FHEA
ProfessorofUrogynaecologyDepartmentofHealthSciencesCollegeofMedicine,BiologicalSciencesandPsychologyUniversityofLeicesterLeicester,UK
www.medicalebookpdf.com
Abbreviations
AFC antralfolliclecountAFP α-fetoproteinAIDS acquiredimmunedeficiencysyndromeALO actimomyces-likeorganismAMH anti-MüllerianhormoneAPS antiphospholipidsyndromeART assistedreproductivetreatmentAUB abnormaluterinebleedingAUC areaunderthecurveAZF azoospermicfactor
BBV blood-bornevirusBEO bleedingofendometrialoriginBEP bleomycin,etoposideandcisplatinBMD bonemineraldensityBMI bodymassindexBNF BritishNationalFormularyBOT borderlineovariantumourBRCA breastovariancancersyndromeBSO bilateralsalpingo-oophorectomyBV bacterialvaginosis
CAH congenitaladrenalhyperplasiaCAIS completeandrogeninsensitivitysyndromeCBT cognitive-behaviouraltherapyCGIN cervicalglandularintraepithelialneoplasiaCHC combinedhormonalcontraceptionCIN cervicalintraepithelialneoplasiaCL corpusluteumCLIA chemiluminescenceimmunoassayCNS centralnervoussystemCOCP combinedoralcontraceptivepillCOX cyclooxygenase
www.medicalebookpdf.com
CPP chronicpelvicpainCRP C-reactiveproteinCT computedtomographyCu-IUD copperintrauterinedeviceCVD cardiovasculardisease
D&C dilatationandcurettageDHEA dehydroepiandrosteroneDHT dihydrotestosteroneDNA deoxyribonucleicacidDO detrusoroveractivityDSD disordersofsexualdevelopmentDUB dysfunctionaluterinebleeding
EB endometrialbiopsyEC emergencycontraceptionECG electrocardiographyEGF epidermalgrowthfactorEIA enzymeimmunoassayEP ectopicpregnancyEVA electricalvacuumaspiration
FAB fertilityawareness-basedmethodFBC fullbloodcountFGF fibroblastgrowthfactorFGM femalegenitalmutilationFH fetalheartbeatFIGO InternationalFederationofGynecologyandObstetricsFSH follicle-stimulatinghormone
GFR glomerularfiltrationrateGnRH gonadotrophin-releasinghormoneGP generalpractitionerGTA gynaecologyteachingassociateGTD gestationaltrophoblasticdisease
HAART highlyactiveretroviraltherapy(β)hCG (beta-)humanchorionicgonadotrophinHDL high-densitylipoproteinHFEA HumanFertilisationandEmbryoAuthorityHIV humanimmunodeficiencyvirus
www.medicalebookpdf.com
HMB heavymenstrualbleedingHNPCC hereditarynon-polyposiscolorectalcancerHPO hypothalamo–pituitary–ovarian(axis)HPV humanpapillomavirusHRT hormonereplacementtherapyHSG hysterosalpingographyHSIL high-gradesquamousintraepithelial(lesion)HSV herpessimplexvirusHVS highvaginalswabHyCoSy hysterocontrastsynography
ICSI intracytoplasmicsperminjectionIg immunoglobulinIGF insulin-likegrowthfactorIMB intermenstrualbleedingISD intrinsicsphincterdeficiencyIUD intrauterinedeviceIUI intrauterineinseminationIUS intrauterinereleasingsystemIVF in-vitrofertilization
LARC long-actingreversiblemethodsofcontraceptionLAVH laparoscopic-aidedvaginalhysterectomyLBC liquid-basedcytologyLDL low-densitylipoproteinLH luteinizinghormoneLLETZ largeloopexcisionoftransformationzoneLMP lastmenstrualperiodLMWH low-molecularweightheparinLNG-IUS levonorgestrelintrauterinesystemLOD laparoscopicovariandrilling
MAS minimalaccesssurgeryMBL meanbloodlossMDT multidisciplinaryteamMEC medicaleligibilitycriteriaMRI magneticresonanceimagingMRKH Mayer–Rokitansky–Kuster–HausersyndromeMSU midstreamurinesampleMTCT mother-to-childtransmissionMVA manualvacuumaspiration
www.medicalebookpdf.com
NAAT nucleicacidamplificationtest
NICE NationalInstituteforHealthandCareExcellenceNSAID non-steroidalanti-inflammatorydrug
OAB overactivebladderOCP oralcontraceptivepill17-OHP 17-hydroxyprogesteroneOHSS ovarianhyperstimulationsyndromeOI ovulationinductionOPH outpatienthysteroscopy
PAC preassessmentclinicPAF plateletactivatingfactorPCB postcoitalbleedingPCOS polycysticovarysyndromePCR polymerasechainreactionPG prostaglandinPGD preimplantationgeneticdiagnosisPGI prostacyclinPID pelvicinflammatorydiseasePMB postmenopausalbleedingPMS premenstrualsyndromePOCT pointofcaretestPOF prematureovarianfailurePOI prematureovarianinsufficiencyPOP progestogen-onlypillPPC primaryperitonealcarcinomaPPH postpartumhaemorrhagePUL pregnancyofunknownlocation
REM rapideyemovementRCOG RoyalCollegeofObstetriciansandGynaecologistsRMI RiskofMalignancyIndexRNA ribonucleicacidRPOC retainedproductsofconceptionRPR rapidplasmareaginRR relativerisk
SCJ squamocolumnarjunctionSERM selectiveoestrogenreceptormodulator
www.medicalebookpdf.com
SFA semenfluidanalysisSHBG sexhormone-bindingglobulin
SIS salineinstillationsonographySPRM selectiveprogesteronereceptormodulatorSSR surgicalspermretrievalSSRI selectiveserotonin-reuptakeinhibitorSTI sexually-transmittedinfectionSTIC seroustubalintraepithelialcarcinomaSTOP surgicalterminationofpregnancy
TAUSS transabdominalultrasoundscanTCRF transcervicalresectionoffibroidTED thromboembolicstockingTGF transforminggrowthfactorTLH totallaparoscopichysterectomyTOT transobturatortapeTPHA T.pallidumhaemagglutinationassayTPPA T.pallidumparticleassayTV TrichomonasvaginalisTVT tension-freevaginaltapeTVUSS transvaginalultrasoundscanTZ transformationzone
UAE umbilical/uterinearteryembolizationUPA ulipristalacetateUPT urinarypregnancytestUSS ultrasoundscan
VaIN vaginalintraepithelialneoplasiaVDRL VenerealDiseaseReferenceLaboratoryVEGF vascularendothelialgrowthfactorVIN vulvalintraepithelialneoplasiaVTE venousthromboembolism
WCC whitecellcountWHI Women’sHealthInitiativeWHO WorldHealthOrganization
www.medicalebookpdf.com
eResources
Chapter2 Gynaecologicalhistory,examinationandinvestigations
eResource2.1 Thegynaecologicalconsultationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv2.1.php
eResource2.2 Ultrasoundimagingingynaecologyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv2.2.php
Chapter3 Hormonalcontrolofthemenstrualcycleandhormonaldisorders
eResource3.1 Polycysticovarysyndrome(PCOS)http://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv3.1.php
eResource3.2 Premenstrualsyndrome(PMS)patientguidancehttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv3.2.php
Chapter4 Disordersofmenstrualbleeding
eResource4.1 Heavymenstrualbleeding(HMB)historyandexaminationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv4.1.php
eResource4.2 Endometrialablationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv4.2.php
Chapter5 Implantationandearlypregnancy
eResource5.1 Pregnancybetween5and12weeks’gestationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv5.1.php
eResource5.2 Ectopicpregnancyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv5.2.php
www.medicalebookpdf.com
Chapter6 Contraceptionandabortion
eResource6.1 Laparoscopicsterilizationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv6.1.php
Chapter7 Subfertility
eResource7.1 Tubalblockagehttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.1.php
eResource7.2 Normalandabnormalspermhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.2.php
eResource7.3 Eggcollectionusingtransvaginalultrasound(TVUSS)http://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.3.php
eResource7.4 Transvaginalultrasound(TVUSS)guidedembryotransferhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.4.php
eResource7.5 Embryobiopsyforpreimplantationgeneticdiagnosis(PGD)http://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.5.php
Chapter11 Benignconditionsoftheovaryandpelvis
eResource11.1 Ovariancystshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv11.1.php
eResource11.2 Transvaginalultrasound(TVUSS)ofthepelviswithendometriosishttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv11.2.php
Chapter12 Benignconditionsoftheuterus,cervixandendometrium
eResource12.1 Endometrialpolypshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv12.1.php
eResource12.2 Surgicaltreatmentoffibroidshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv12.2.php
Chapter14 Malignantdiseaseoftheovary
eResource14.1 Surgeryforepithelialovariancancerhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv14.1.php
www.medicalebookpdf.com
Chapter15 Malignantdiseaseoftheuterus
eResource15.1 Surgicaltreatmentofendometrialcancerhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv15.1.php
Chapter17 Gyaecologicalsurgeryandtherapeutics
eResource17.1 Laparoscopyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv17.1.php
Youcanaccesstheresources(videoclipsandstillimages)thatarereferencedaboveandindicatedinthetextwiththeicon byenteringtheURLsprovidedinthebrowserofyourchoice.
In addition, the videos and images from this book canbe accessedvia the companionwebsite thataccompanies this textbook www.routledge.com/cw/kenny where you will also find resources for thesistervolume,ObstetricsbyTenTeachers,20thEdition.Additionalvideoclipsandstillimageswillbeaddedtothislibraryovertime.
www.medicalebookpdf.com
CHAPTER1Thedevelopmentandanatomyofthefemale
sexualorgansandpelvis
HELENBICKERSTAFF
Sexualdifferentiationofthefetusanddevelopmentofsexualorgans
Femaleanatomy
Structuralproblemsofpelvicorgans
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthatsexualdifferentiationanddevelopmentbegininearlyembryoniclife.
•Understand theembryonicdevelopmentand theanatomyof theperineum, thevagina, cervixanduterus,theadnexaandovaryandthebladderandureters.
•Describethebloodsupplyandlymphaticsoftheperineumandpelvis.
•Understandtheinnervationoftheperineumandpelvis.
•Understandthevulnerabilityofcertainstructuresingynaecologicalsurgery.
•DescribethestructuralanomaliesresultingfromMülleriantractdisorders.
www.medicalebookpdf.com

SexualdifferentiationofthefetusanddevelopmentofsexualorgansThegonadalrudimentsappearas the‘genital ridge’overlying theembryonickidney in the intermediatemesodermduringthefourthweekofembryoniclife,andtheyremainsexuallyindifferentuntiltheseventh(Figure1.1).Theundifferentiatedgonadhasthepotentialtobecomeeitheratestisoranovary,andhenceis termed bipotential, and the chromosomal complement of the zygote determines whether the gonadbecomes a testis or anovary.Thedevelopmentof either the testis or ovary is an activegene-directedprocess.InthemaletheactivityoftheSRYgene(sex-determiningregionoftheYchromosome)causesthegonadtobegindevelopmentintoatestis.Inthepast,ovariandevelopmentwasconsidereda‘default’developmentduesolely to theabsenceofSRY,but in the last10yearsovarian-determininggeneshavealsobeenfoundthatactivelyleadtothedevelopmentofafemalegonad.
ThefetushastwosetsofstructurescalledtheMüllerian(orparamesonephric)ductsandWolffian(ormesonephric) ducts, which have the potential to develop into male or female internal and externalgenitaliarespectively.
DevelopmentofthemalesexualorgansAsthegonaddevelopsintoatestis, itdifferentiatesintotwocell types.TheSertolicellsproduceanti-Müllerian hormone (AMH) and the Leydig cells produce testosterone. AMH suppresses furtherdevelopmentoftheMüllerianductswhereastestosteronestimulatestheWolffianductstodevelopintothevas deferens, epididymis and seminal vesicles. In addition, in the external genital skin, testosterone isconverted by the enzyme 5-alpha-reductase into dihydrotestosterone (DHT). This acts to virilize theexternal genitalia. The genital tubercle becomes the penis and the labioscrotal folds fuse to form thescrotum.Theurogenitalfoldsfusealongtheventralsurfaceofthepenisandenclosetheurethrasothatitopensatthetipofthepenis.
www.medicalebookpdf.com
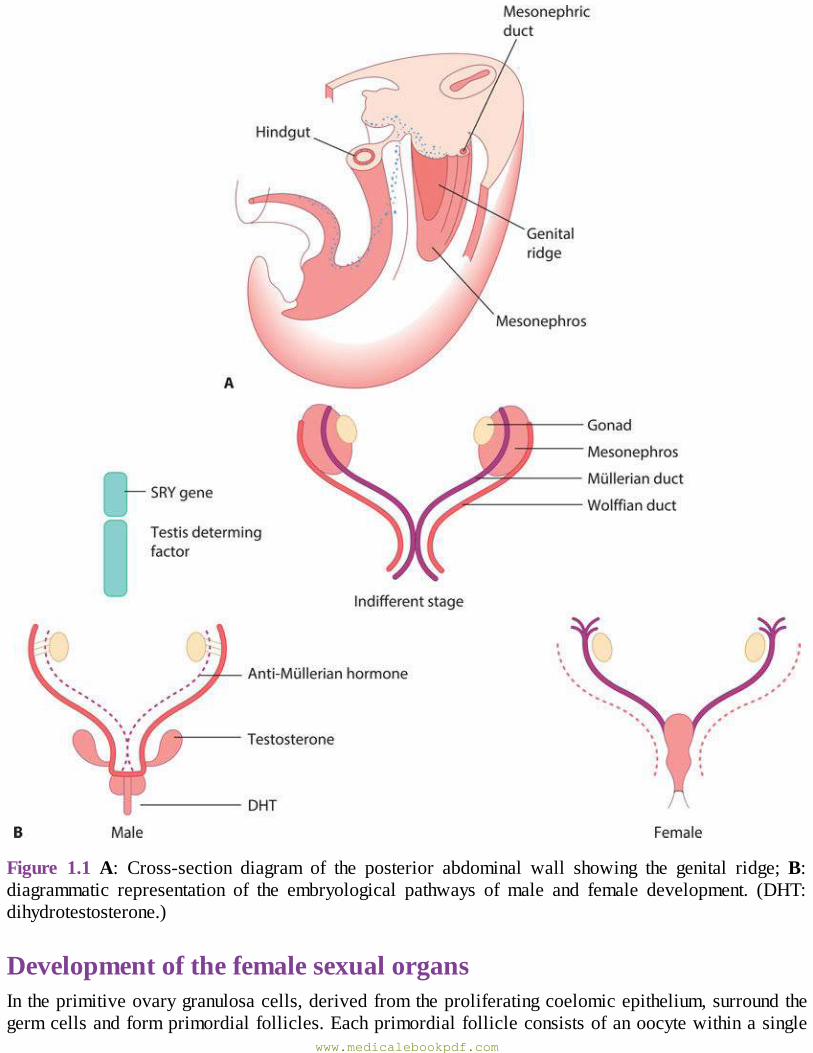
Figure 1.1A: Cross-section diagram of the posterior abdominal wall showing the genital ridge;B:diagrammatic representation of the embryological pathways of male and female development. (DHT:dihydrotestosterone.)
DevelopmentofthefemalesexualorgansIntheprimitiveovarygranulosacells,derivedfromtheproliferatingcoelomicepithelium,surroundthegermcellsandformprimordialfollicles.Eachprimordialfollicleconsistsofanoocytewithinasingle
www.medicalebookpdf.com
layer of granulosa cells. Theca cells develop from the proliferating coelomic epithelium and areseparated from the granulosa cells by a basal lamina.Themaximumnumber of primordial follicles isreached at 20 weeks’ gestation when there are six to sevenmillion primordial follicles present. Thenumbersofthesereducebyatresiaandatbirthonly1–2millionremain.Atresiacontinuesthroughoutlifeandbymenarcheonly300,000–400,000arepresent,andbymenopausenone.
The development of an oocyte within a primordial follicle is arrested at the prophase of its firstmeioticdivision.Itremainsinthatstateuntilitundergoesatresiaorentersthemeioticprocessprecedingovulation.
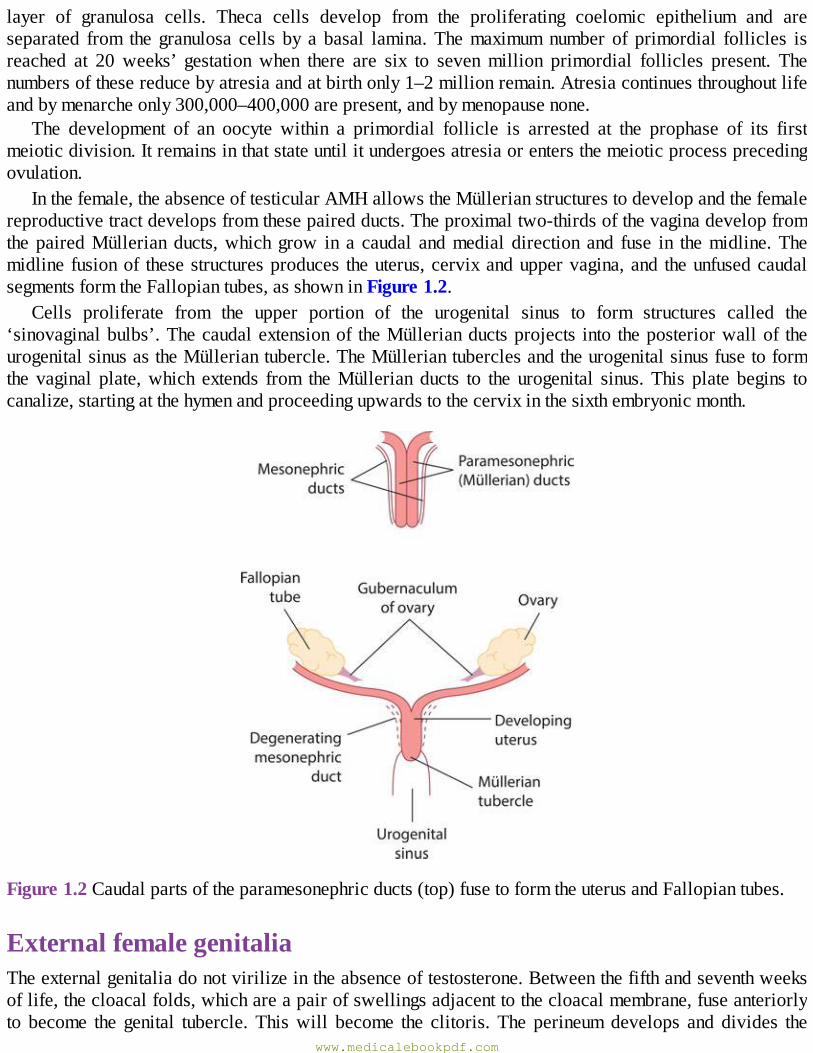
Inthefemale,theabsenceoftesticularAMHallowstheMüllerianstructurestodevelopandthefemalereproductivetractdevelopsfromthesepairedducts.Theproximaltwo-thirdsofthevaginadevelopfromthepairedMüllerianducts,whichgrow in a caudal andmedial direction and fuse in themidline.Themidline fusionof thesestructuresproduces theuterus,cervixanduppervagina,and theunfusedcaudalsegmentsformtheFallopiantubes,asshowninFigure1.2.
Cells proliferate from the upper portion of the urogenital sinus to form structures called the‘sinovaginalbulbs’.Thecaudalextensionof theMüllerianductsprojects into theposteriorwallof theurogenitalsinusastheMülleriantubercle.TheMülleriantuberclesandtheurogenitalsinusfusetoformthe vaginal plate,which extends from theMüllerian ducts to the urogenital sinus.This plate begins tocanalize,startingatthehymenandproceedingupwardstothecervixinthesixthembryonicmonth.
Figure1.2Caudalpartsoftheparamesonephricducts(top)fusetoformtheuterusandFallopiantubes.
ExternalfemalegenitaliaTheexternalgenitaliadonotvirilizeintheabsenceoftestosterone.Betweenthefifthandseventhweeksoflife,thecloacalfolds,whichareapairofswellingsadjacenttothecloacalmembrane,fuseanteriorlyto become the genital tubercle. Thiswill become the clitoris. The perineumdevelops and divides the
www.medicalebookpdf.com
cloacalmembraneintoananteriorurogenitalmembraneandaposterioranalmembrane.Thecloacalfoldsanteriorly are called the urethral folds,which form the labiaminora.Another pair of foldswithin thecloacalmembrane form the labioscrotal folds that eventually become the labiamajora.The urogenitalsinusbecomesthevestibuleofthevagina.Theexternalgenitaliaarerecognizablyfemalebytheendofthetwelfthembryonicweek.
KEYLEARNINGPOINTS•Theprimitivegonadisfirstevidentat5weeksofembryoniclifeandformsonthemedialaspectofthemesonephricridge.
•Theundifferentiatedgonadhasthepotentialtobecomeeitheratestisoranovary.• The paramesonephric duct, which later forms theMüllerian system, is the precursor of femalegenitaldevelopment.
•ThelowerendoftheMüllerianductsfuseinthemidlinetoformtheuterusanduppervagina.•MostoftheuppervaginaisofMüllerianorigin,whilethelowervaginaformsfromthesinovaginalbulbs.
• Primordial follicles contain an oocyte arrested in prophase surrounded by granulosa cellsseparatedbyabasementmembranefromLeydigcells.
•Themaximumnumberofprimordialfolliclesisreachedat20weeks’gestation.Thesereducebyatresiathroughoutchildhoodandadultlife.
Femaleanatomy
ExternalgenitaliaThe external genitalia are commonly called the vulva and include the mons pubis, labia majora andminora,thevaginalvestibule,theclitorisandthegreatervestibularglands.Themonspubisisafibro-fattypadcoveredbyhair-bearingskinthatcoversthebonypubicramus.
Thelabiamajoraaretwofoldsofskinwithunderlyingadiposetissuelyingeithersideofthevaginalopening.Theycontainsebaceousandsweatglandsandafewspecializedapocrineglands.Inthedeepestpartofeachlabiumisacoreoffattytissuecontinuouswiththatoftheinguinalcanalandthefibresoftheroundligament,whichterminatehere.
Thelabiaminoraaretwothinfoldsofskinthatliebetweenthelabiamajora.Thesevaryinsizeandmay protrude beyond the labiamajorwhere they are visible, butmay also be concealed by the labiamajora.Anteriorly, theydivide in two to form theprepuceand frenulumof theclitoris (clitoralhood).Posteriorly,theydividetoformafoldofskincalledthefourchetteatthebackofthevaginaintroitus.Theycontainsebaceousglands,buthavenoadipose tissue.Theyarenotwelldevelopedbeforepubertyandatrophy after themenopause. Both the labiaminora and labiamajora become engorged during sexualarousal.
The clitoris is an erectile structuremeasuring approximately0.5–3.5 cm in length.Thebodyof theclitoris is themainpartof thevisibleclitoris and ismadeupofpairedcolumnsoferectile tissueandvasculartissuecalledthe‘corporacavernosa’.Thesebecomethecruraatthebottomoftheclitorisand
www.medicalebookpdf.com
rundeeperandlaterally.Thevestibuleisthecleftbetweenthelabiaminora.Itcontainsopeningsoftheurethra, theBartholin’s glands and the vagina. The vagina is surrounded by two bulbs of erectile andvascular tissue that are extensive and almost completely cover the distal vaginal wall. These havetraditionallybeennamedthebulbof thevaginalvestibule,althoughrecentworkonbothdissectionandmagneticresonanceimaging(MRI)suggeststhattheymaybepartoftheclitorisandshouldberenamed‘clitoral bulbs’.Their function is unknownbut theyprobably add support to thedistal vaginalwall toenhanceitsrigidityduringpenetration.
TheBartholin’sglandsarebilateralandabout thesizeofapea.Theyopenviaa2cmduct intothevestibulebelowthehymenandcontributetolubricationduringintercourse.
The hymen is a thin covering ofmucousmembrane across the entrance to the vagina. It is usuallyperforated,whichallowsmenstruation.Thehymenisrupturedduringintercourseandanyremainingtagsarecalled‘carunculaemyrtiformes’.
Internalreproductiveorgans(Figure1.3)ThevaginaThevaginaisafibromuscularcanallinedwithstratifiedsquamousepitheliumthatleadsfromtheuterustothevulva.Itislongerintheposteriorwall(approximately9cm)thanintheanteriorwall(approximately7cm).Thevaginalwallsarenormallyinapposition,exceptatthevaultwheretheyareseparatedbythecervix.Thevaultofthevaginaisdividedintofourfornices:posterior,anteriorandtwolateral.
Themidvagina is a transverse slitwhile the lowervagina is anH-shape in transverse section.Thevaginalwallsarelinedwithtransversefolds.Thevaginahasnoglandsandiskeptmoistbysecretionsfromtheuterineandcervicalglandsandbytransudationfromitsepitheliallining.Theepitheliumisthickandrichinglycogen,whichincreasesinthepostovulatoryphaseofthecycle.However,beforepubertyand after the menopause, the vagina is devoid of glycogen due to the lack of oestrogen. Doderlein’sbacillus is a normal commensal of the vaginal flora and breaks down glycogen to form lactic acid,producing a pH of around 4.5. This has a protective role for the vagina in decreasing the growth ofpathogenicbacteria.
TheupperposteriorwallformstheanteriorperitonealreflectionofthepouchofDouglas.Themiddlethirdisseparatedfromtherectumbypelvicfasciaandthelowerthirdabutstheperinealbody.Anteriorly,thevaginaisindirectcontactwiththebaseofthebladder,whiletheurethrarunsdownthelowerhalfinthemidline to open into the vestibule. Itsmuscles fusewith the anterior vaginawall. Laterally, at thefornices, thevagina isrelated to thecardinal ligaments.Belowthisare the levatoranimusclesandtheischiorectalfossae.Thecardinalligamentsandtheuterosacralligaments,whichformposteriorlyfromtheparametrium,supporttheupperpartofthevagina.
www.medicalebookpdf.com
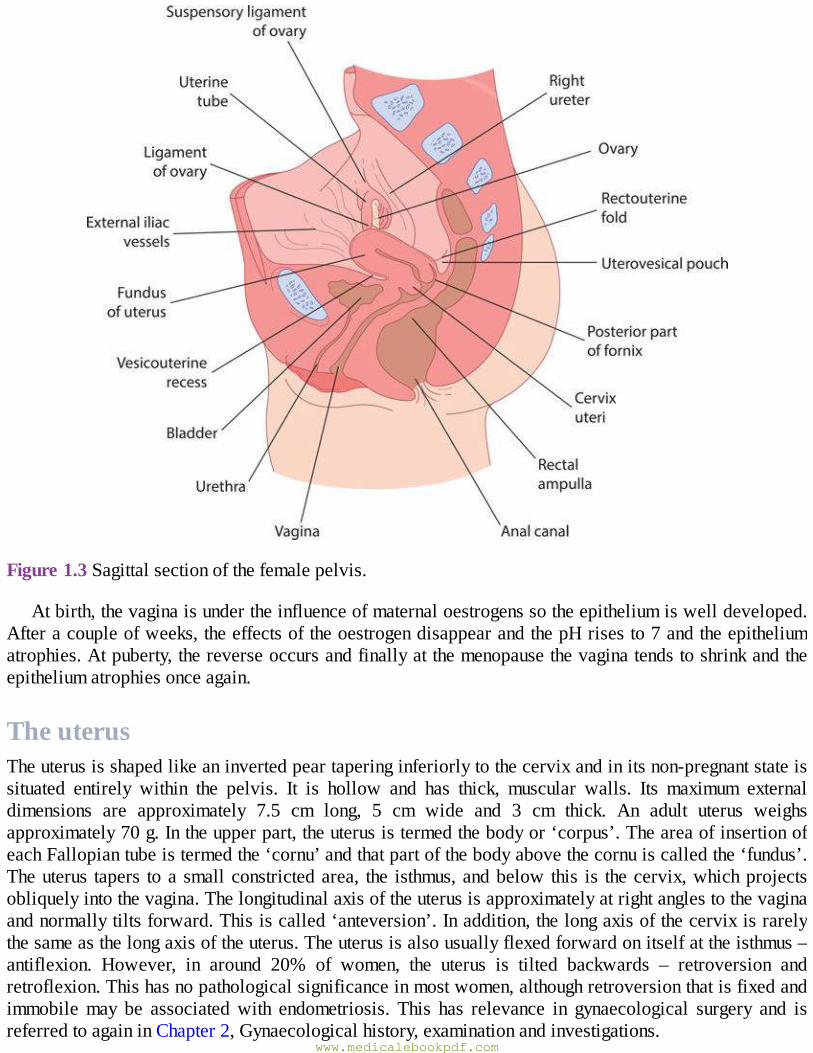
Figure1.3Sagittalsectionofthefemalepelvis.
Atbirth,thevaginaisundertheinfluenceofmaternaloestrogenssotheepitheliumiswelldeveloped.Afteracoupleofweeks,theeffectsoftheoestrogendisappearandthepHrisesto7andtheepitheliumatrophies.Atpuberty,thereverseoccursandfinallyatthemenopausethevaginatendstoshrinkandtheepitheliumatrophiesonceagain.
TheuterusTheuterusisshapedlikeaninvertedpeartaperinginferiorlytothecervixandinitsnon-pregnantstateissituated entirely within the pelvis. It is hollow and has thick, muscular walls. Its maximum externaldimensions are approximately 7.5 cm long, 5 cm wide and 3 cm thick. An adult uterus weighsapproximately70g.Intheupperpart,theuterusistermedthebodyor‘corpus’.TheareaofinsertionofeachFallopiantubeistermedthe‘cornu’andthatpartofthebodyabovethecornuiscalledthe‘fundus’.Theuterus tapers toasmallconstrictedarea, the isthmus,andbelow this is thecervix,whichprojectsobliquelyintothevagina.Thelongitudinalaxisoftheuterusisapproximatelyatrightanglestothevaginaandnormallytiltsforward.Thisiscalled‘anteversion’.Inaddition,thelongaxisofthecervixisrarelythesameasthelongaxisoftheuterus.Theuterusisalsousuallyflexedforwardonitselfattheisthmus–antiflexion. However, in around 20% of women, the uterus is tilted backwards – retroversion andretroflexion.Thishasnopathologicalsignificanceinmostwomen,althoughretroversionthatisfixedandimmobilemay be associatedwith endometriosis. This has relevance in gynaecological surgery and isreferredtoagaininChapter2,Gynaecologicalhistory,examinationandinvestigations.
www.medicalebookpdf.com
ThecavityoftheuterusistheshapeofaninvertedtriangleandwhensectionedcoronallytheFallopiantubes open at lateral angles The constriction at the isthmus where the corpus joins the cervix is theanatomical os. Seen microscopically, the site of the histological internal os is where the mucousmembraneoftheisthmusbecomesthatofthecervix.
The uterus consists of three layers: the outer serous layer (peritoneum), themiddlemuscular layer(myometrium)andtheinnermucouslayer(endometrium).Theperitoneumcoversthebodyoftheuterusandposteriorlyitcovers thesupravaginalpartof thecervix.Theperitoneumis intimatelyattachedtoasubserousfibrouslayer,exceptlaterallywhereitspreadsouttoformtheleavesofthebroadligament.
Themuscularmyometrium forms themain bulk of the uterus and ismade up of interlacing smoothmuscle fibres intermingling with areolar tissue, blood vessels, nerves and lymphatics. Externally, themuscle fibres are mostly longitudinal, but the thicker intermediate layer has interlacing longitudinal,obliqueandtransversefibres.Internally,theyaremainlylongitudinalandcircular.
Theinnerendometriallayerhastubularglandsthatdipintothemyometrium.Theendometriallayeriscoveredbyasinglelayerofcolumnarepithelium.Ciliatedpriortopuberty,thisepitheliumismostlylostdue to the effects of pregnancy andmenstruation. The endometrium undergoes cyclical changes duringmenstruation,asdescribedinChapter3,Hormonalcontrolofthemenstrualcycleandhormonaldisorders,andvariesinthickness.
ThecervixThecervixisnarrowerthanthebodyoftheuterusandisapproximately2.5cminlength.Lateraltothecervixliescellularconnectivetissuecalledtheparametrium.Theureterrunsabout1cmlaterallytothesupravaginal cervix within the parametrium. The posterior aspect of the cervix is covered by theperitoneumofthepouchofDouglas.
Theupperpartofthecervixmostlyconsistsofinvoluntarymuscle,whereasthelowerpartismainlyfibrous connective tissue. The mucous membrane of the cervical canal (endocervix) has anterior andposterior columns from which folds radiate out, the ‘arbour vitae’. It has numerous deep glandularfollicles thatsecreteclearalkalinemucus, themaincomponentofphysiologicalvaginaldischarge.Theepithelium of the endocervix is columnar and is also ciliated in its upper two-thirds. This changes tostratifiedsquamousepitheliumaroundtheregionoftheexternalosandthejunctionofthesetwotypesofepitheliumiscalledthe‘squamocolumnarjunction’.
AgechangestoanatomyThedisappearanceofmaternaloestrogensfromthecirculationafterbirthcausestheuterustodecreaseinlengthbyaroundone-thirdand inweightbyaroundone-half.Thecervix is then twice the lengthof theuterus.Duringchildhood,theuterusgrowsslowlyinlength,inparallelwithheightandage.Theaveragelongitudinaldiameterrangesfrom2.5cmattheageof2years,to3.5cmat10years.Aftertheonsetofpuberty,theanteroposteriorandtransversediametersoftheuterusstarttoincrease,leadingtoasharperrise in thevolumeof theuterus.The increase inuterinevolumecontinueswell aftermenarcheand theuterusreachesitsadultsizeandconfigurationbythelateteenageyears.Afterthemenopause,theuterusatrophies, themucosabecomesvery thin, theglandsalmostdisappearand thewallbecomes relativelylessmuscular.
TheFallopiantubeswww.medicalebookpdf.com
The Fallopian tube extends outwards from the uterine cornu to end near the ovary. At the abdominalostium,thetubeopensintotheperitonealcavity,whichisthereforeincommunicationwiththeexteriorofthebodyviatheuterusandthevagina.Thisisessentialtoallowthespermandeggtomeet.TheFallopiantubes convey the ovum from the ovary towards the uterus and promote oxygenation and nutrition forsperm,ovumandzygoteshouldfertilizationoccur.
TheFallopiantuberunsintheuppermarginofthebroadligament,knownasthemesosalpinx,whichenclosesthetubesothat it iscompletelycoveredwithperitoneum,exceptforanarrowstripalongthisinferioraspect.Eachtubeisabout10cmlongandisdescribedinfourparts:
•Theinterstitialportion.•Theisthmus.•Theampulla.•Theinfundibulumorfimbrialportion.
The interstitial portion lies within the wall of the uterus, while the isthmus is the narrow portionadjoiningtheuterus.Thispassesintothewidestandlongestportion,theampulla.This,inturn,terminatesin the extremity known as the ‘infundibulum’. The opening of the tube into the peritoneal cavity issurroundedbyfinger-likeprocesses,knownasfimbria,intowhichthemusclecoatdoesnotextend.Theinner surfaces of the fimbriae are covered by ciliated epithelium that is similar to the lining of theFallopian tube itself. One of these fimbriae is longer than the others and extends to, and partiallyembraces,theovary.Themuscularfibresofthewallofthetubearearrangedinaninnercircularandanouterlongitudinallayer.
Thetubalepitheliumformsanumberofbranchedfoldsorplicaethatrunlongitudinally;thelumenofthe ampulla is almost filledwith these folds. The folds have a cellular stroma, but at their bases theepitheliumisonlyseparatedfromthemusclebyaveryscantyamountofstroma.Thereisnosubmucosaand there arenoglands.Theepitheliumof theFallopian tubes contains two functioningcell types: theciliated cells, which act to produce constant current of fluid in the direction of the uterus, and thesecretorycells,whichcontribute to thevolumeof tubal fluid.Changesoccurunder the influenceof themenstrualcycle,butthereisnocellsheddingduringmenstruation.
TheovariesThesizeandappearanceoftheovariesdependsonbothageandstageofthemenstrualcycle.Inachild,theovariesaresmallstructuresapproximately1.5cmlong;however,theyincreasetoadultsizeinpubertydue to proliferation of stromal cells and commencingmaturation of the ovarian follicles. In the youngadult,theyarealmond-shapedandmeasureapproximately3cmlong,1.5cmwideand1cmthick.Afterthemenopause,noactivefolliclesarepresentand theovarybecomessmallerwithawrinkledsurface.Theovaryistheonlyintra-abdominalstructurenottobecoveredbyperitoneum.Eachovaryisattachedto the cornu of the uterus by the ovarian ligament and at the hilum to the broad ligament by themesovarium,whichcontainsitssupplyofnervesandbloodvessels.Laterally,eachovaryisattachedtothesuspensory ligamentof theovarywith foldsofperitoneumthatbecomescontinuouswith thatof theoverlyingpsoasmajor.
AnteriortotheovarieslietheFallopiantubes,thesuperiorportionofthebladderandtheuterovesicalpouch.Posteriortotheovaryliestheureterwhereitrunsdownwardsandforwardsinfrontoftheinternaliliacartery.
www.medicalebookpdf.com
StructureoftheovaryTheovaryhasacentralvascularmedullaconsistingof looseconnective tissuecontainingmanyelastinfibresandnon-striatedmusclecells.Ithasanouterthickercortex,denserthanthemedulla,consistingofnetworksof reticular fibres and fusiformcells, although there is no clear-cut demarcationbetween thetwo.Thesurfaceoftheovariesiscoveredbyasinglelayerofcuboidalcells, thegerminalepithelium.Beneath this isan ill-defined layerofcondensedconnective tissuecalled the‘tunicaalbuginea’,whichincreasesindensitywithage.Atbirth,numerousprimordialfolliclesarefound,mostlyinthecortex,butsome are found in themedulla.With puberty, some form eachmonth into the graafian follicles undergonadotrophiccontrol,toovulateandsubsequentlyformcorpusluteaandultimatelytheatreticfollicles,thecorporaalbicans.
Thebladder,urethraandureterThebladderThebladderwallismadeofinvoluntarymusclearrangedinaninnerlongitudinallayer,amiddlecircularlayerandanouterlongitudinallayer.Itislinedwithtransitionalepitheliumandhasanaveragecapacityof400ml.
Theuretersopenintothebaseofthebladderafterrunningmediallyforabout1cmthroughthebladderwall.Theurethra leaves thebladderbelow theuretericorifices.The triangulararea lyingbetween theuretericorificesandtheinternalmeatusoftheurethraisknownasthe‘trigone’.Attheinternalmeatus,themiddlelayerofmuscleformsanteriorandposteriorloopsroundtheneckofthebladder,somefibresoftheloopsbeingcontinuouswiththecircularmuscleoftheurethra.
The base of the bladder is adjacent to the cervix,with only a thin layer of tissue intervening. It isseparatedfromtheanteriorvaginalwallbelowbythepubocervicalfasciathatstretchesfromthepubistothecervix.
TheurethraThefemaleurethraisabout3.5cmlongandislinedwithtransitionalepithelium.Ithasaslightposteriorangulationat the junctionof its lowerandmiddle thirds.Thesmoothmuscleof itswall is arranged inouterlongitudinalandinnercircularlayers.Astheurethrapassesthroughthetwolayersoftheurogenitaldiaphragm,itisembracedbythestriatedfibresofthedeeptransverseperinealmuscle(alsoknownasthecompressorurethrae)andsomeofthestriatedfibresofthismuscleformaloopontheurethra.Betweenthemuscularcoatandtheepitheliumisaplexusofveins.Thereareanumberoftubularmucousglandsandinthelowerpartanumberofcryptsthatoccasionallybecomeinfected.Initsuppertwo-thirds, theurethraisseparatedfromthesymphysisbylooseconnectivetissue,butinitslowerthirditisattachedtothe pubic ramus on each side by strong bands of fibrous tissue called the ‘pubourethral tissue’.Posteriorly,itisfirmlyattachedinitslowertwo-thirdstotheanteriorvaginalwall.Thismeansthattheupperpartoftheurethraismobile,butthelowerpartisrelativelyfixed.
Medialfibresofthepubococcygeusofthelevatoranimusclesareinsertedintotheurethraandvaginalwall.Whentheycontract, theypull theanteriorvaginalwallandtheupperpartof theurethraforwardsforming an angle of about 100° between the posterior wall of the urethra and the bladder base. Onvoluntary voiding of urine, the base of the bladder and the upper part of the urethra descend and theposteriorangledisappearssothatthebaseofthebladderandtheposteriorwalloftheurethracometolieinastraightline.
www.medicalebookpdf.com
TheureterAstheuretercrossesthepelvicbrim,itliesinfrontofthebifurcationofthecommoniliacartery.Itrunsdownwards and forwards on the lateral wall of the pelvis to reach the pelvic floor and then passesinwardsandforwardsattached to theperitoneumof thebackof thebroad ligament topassbeneath theuterineartery.Itnextpassesforwardthroughafibroustunnel,theuretericcanal,intheupperpartofthecardinalligament.Finally,itrunsclosetothelateralvaginalfornixtoenterthetrigoneofthebladder.
Itsbloodsupplyisderivedfromsmallbranchesoftheovarianartery,fromasmallvesselarisingnearthe iliac bifurcation, from a branch of the uterine artery where it crosses beneath it and from smallbranchesofthevesicalartery.
Box1.1UretericdamageduringhysterectomyBecauseofitscloserelationshiptothecervix,thevaultofthevaginaandtheuterineartery,theuretermaybedamagedduringhysterectomy.Apartfrombeingcutortied,inradicalprocedures,theuretermayundergonecrosisbecauseofinterferencewithitsbloodsupply.Itmaybedisplacedbyscartissueorbyfibromyomataorcyststhataregrowingbetweenthelayersofthebroadligamentandmaysufferinjuryifitspositionisnotnoticedatsurgery.
TherectumThe rectum extends from the level of the third sacral vertebra to a point about 2.5 cm in front of thecoccyxwhere itpasses throughthepelvicfloor tobecomecontinuouswith theanalcanal. Itsdirectionfollows the curve of the sacrumand is about 11 cm in length.The front and sides are covered by theperitoneumoftherectovaginalpouch.Inthemiddlethirdonlythefrontiscoveredbyperitoneum.Inthelower third there is no peritoneal covering and the rectum is separated from the posteriorwall of thevagina by the rectovaginal fascial septum. Lateral to the rectum are the uterosacral ligaments, besidewhichrunsomeofthelymphaticsdrainingthecervixandvagina.
Thepelvicmuscles,ligamentsandfasciaThepelvicdiaphragm(Figure1.4)Thepelvicdiaphragmisformedbythelevatoranimuscles,whicharebroad,flatmusclesthefibresofwhich pass downwards and inwards. The two muscles, one on either side, constitute the pelvicdiaphragm.Themusclesarisebylinearoriginfromthefollowingpoints:
•Thelowerpartofthebodyoftheospubis.•Theinternalsurfaceoftheparietalpelvicfasciaalongthewhiteline.•Thepelvicsurfaceoftheischialspine.
www.medicalebookpdf.com
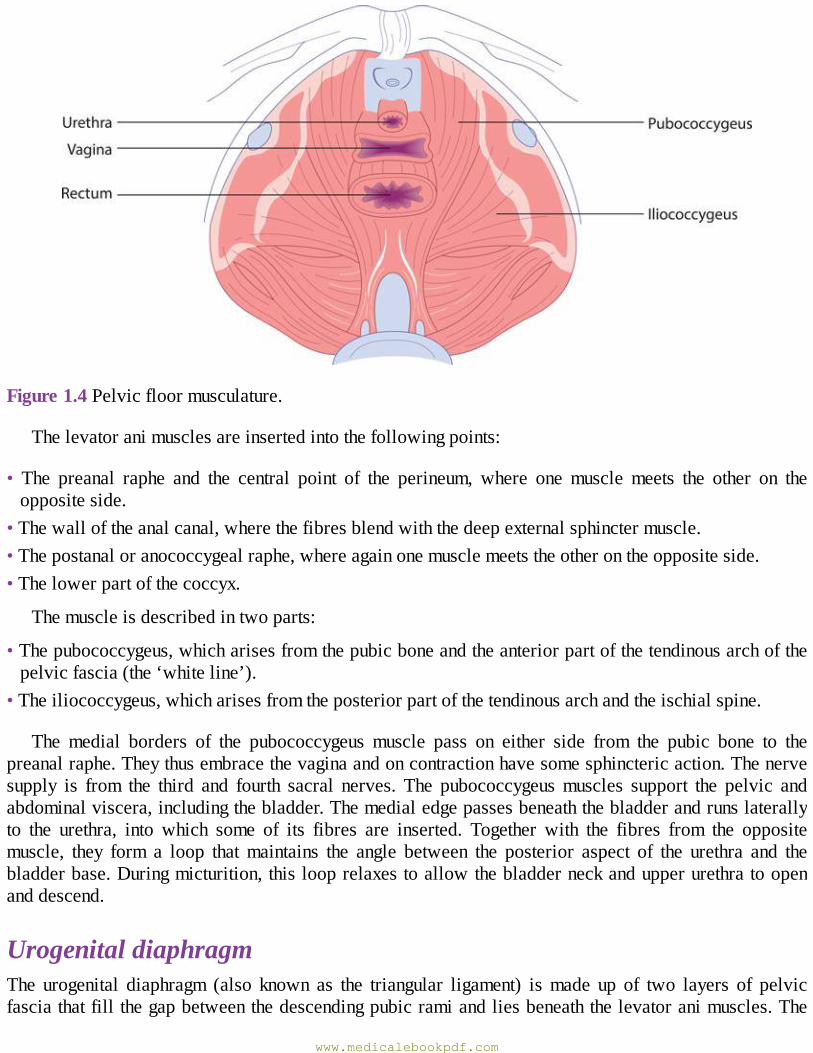
Figure1.4Pelvicfloormusculature.
Thelevatoranimusclesareinsertedintothefollowingpoints:
• The preanal raphe and the central point of the perineum, where one muscle meets the other on theoppositeside.
•Thewalloftheanalcanal,wherethefibresblendwiththedeepexternalsphinctermuscle.•Thepostanaloranococcygealraphe,whereagainonemusclemeetstheotherontheoppositeside.•Thelowerpartofthecoccyx.
Themuscleisdescribedintwoparts:
•Thepubococcygeus,whicharisesfromthepubicboneandtheanteriorpartofthetendinousarchofthepelvicfascia(the‘whiteline’).
•Theiliococcygeus,whicharisesfromtheposteriorpartofthetendinousarchandtheischialspine.
The medial borders of the pubococcygeus muscle pass on either side from the pubic bone to thepreanalraphe.Theythusembracethevaginaandoncontractionhavesomesphinctericaction.Thenervesupply is from the third and fourth sacral nerves. The pubococcygeusmuscles support the pelvic andabdominalviscera,includingthebladder.Themedialedgepassesbeneaththebladderandrunslaterallyto the urethra, into which some of its fibres are inserted. Together with the fibres from the oppositemuscle, they form a loop thatmaintains the angle between the posterior aspect of the urethra and thebladderbase.Duringmicturition,thislooprelaxestoallowthebladderneckandupperurethratoopenanddescend.
UrogenitaldiaphragmThe urogenital diaphragm (also known as the triangular ligament) ismade up of two layers of pelvicfasciathatfillthegapbetweenthedescendingpubicramiandliesbeneaththelevatoranimuscles.The
www.medicalebookpdf.com
deeptransverseperinealmuscles(compressorurethrae)liebetweenthetwolayersandthediaphragmispiercedbytheurethraandvagina.
TheperinealbodyThisisamassofmuscular tissuethat liesbetweentheanalcanalandthelowerthirdof thevagina.Itsapexisat thelowerendoftherectovaginalseptumatthepointwheretherectumandposteriorvaginalwallscomeintocontact.Itsbaseiscoveredwithskinandextendsfromthefourchettetotheanus.Itisthepointof insertionof the superficialperinealmuscles and isboundedaboveby the levator animuscleswheretheycomeintocontactinthemidlinebetweentheposteriorvaginalwallandtherectum.
ThepelvicperitoneumTheperitoneumisreflectedfromthelateralbordersoftheuterustoform,oneitherside,adoublefoldofperitoneum–thebroadligament.Despitethename,thisisnotaligamentbutaperitonealfoldanditdoesnotsupporttheuterus.TheFallopiantuberunsintheupperfreeedgeofthebroadligamentasfarasthepointatwhichthetubeopensintotheperitonealcavity.Thepartofthebroadligamentthatislateraltotheopeningiscalledthe‘infundibulopelvicfold’andinittheovarianvesselsandnervespassfromthesidewallofthepelvistoliebetweenthetwolayersofthebroadligament.Themesosalpinx,theportionofthebroadligament that liesabovetheovary, is layered;betweenits layersareseenanyWolffianremnantsthatmayremain.Belowtheovary,thebaseofthebroadligamentwidensoutandcontainsaconsiderableamountoflooseconnectivetissuecalledthe‘parametrium’.Theureterisattachedtotheposteriorleafofthebroadligamentatthispoint.
The ovary is attached to the posterior layer of the broad ligament by a short mesentry (themesovarium)throughwhichtheovarianvesselsandnervesenterthehilum.
Theovarianligamentandroundligament(Figure1.5A)Theovarianligament liesbeneaththeposterior layerof thebroadligamentandpassesfromthemedialpoleoftheovarytotheuterusjustbelowthepointofentryoftheFallopiantube.
Theroundligamentisthecontinuationofthesamestructureandrunsforwardsundertheanteriorleafofperitoneumtoentertheinguinalcanal,endinginthesubcutaneoustissueofthelabiummajor.
Thepelvicfasciaandpelviccellulartissue(Figure1.5B)Connectivetissuefillstheirregularspacesbetweenthevariouspelvicorgans.Muchofitisloosecellulartissue,butinsomeplacesitiscondensedtoformstrongligamentsthatcontainsomesmoothmusclefibresandwhichformthefascialsheathsthatenclosethevariousviscera.Thepelvicarteries,veins,lymphatics,nervesanduretersrunthroughit.Thecellulartissueiscontinuousabovewiththeextraperitonealtissueoftheabdominalwall,butbelowitiscutofffromtheischiorectalfossabythepelvicfasciaandthelevatoranimuscles.Thepelvic fasciamaybe regardedasa specializedpartof thisconnective tissueandhasparietalandvisceralcomponents.
Theparietalpelvicfascialinesthewallof thepelviccavitycoveringtheobturatorandpyramidalismuscles.Thethickenedtendinousarch(knownasthewhiteline)liesonthesidewallofthepelvis.Itishere that the levatoranimusclearisesand thecardinal ligamentgains its lateralattachment.Where the
www.medicalebookpdf.com
parietalpelvicfasciaencountersbone,asinthepubicregion,itblendswiththeperiosteum.Italsoformstheupperlayeroftheurogenitaldiaphragm.
Eachviscushasafascialsheaththatisdenseinthecaseofthevaginaandcervixandatthebaseofthebladder,butistenuousorabsentoverthebodyoftheuterusandthedomeofthebladder.Fromthepointofviewofthegynaecologist,certainpartsofthevisceralfasciaareimportant,asfollows:
•Thecardinal ligaments(transversecervical ligaments)provide theessentialsupportof theuterusandvaginal vault. These are two strong fan-shaped fibromuscular bands that pass from the cervix andvaginalvaulttothesidewallofthepelvisoneitherside.
•Theuterosacralligamentsrunfromthecervixandvaginalvaulttothesacrum.Intheerectposition,theyarealmostverticalindirectionandsupportthecervix.
•Thebladderissupportedlaterallybycondensationsofthevesicalpelvicfascia,oneeachside,andbyasheetofpubocervicalfascia,whichliesbeneathitanteriorly.
Thebloodsupply(Figure1.6)ArteriessupplyingthepelvicorgansBecausetheovarydevelopsontheposteriorabdominalwallandlatermigratesdownintothepelvis,itcarriesitsbloodsupplywithitdirectlyfromtheabdominalaorta.Theovarianarteryarisesfromtheaortajustbelowthe renalarteryandrunsdownwardson thesurfaceof thepsoasmuscle to thepelvicbrim,where it crosses in front of the ureter and then passes into the infundibulopelvic fold of the broadligament.The arterydivides intobranches that supply theovary and tube and then runon to reach theuterus,wheretheyanastamosewiththeterminalbranchesoftheuterineartery.
Theinternaliliac(hypogastic)arteryThisvesselisabout4cminlengthandbeginsatthebifurcationofthecommoniliacarteryinfrontofthesacroiliacjoint.Itsoondividesintoanteriorandposteriorbranches;thebranchesthatsupplythepelvicorgansareallfromtheanteriordivisionandareasfollows:
www.medicalebookpdf.com
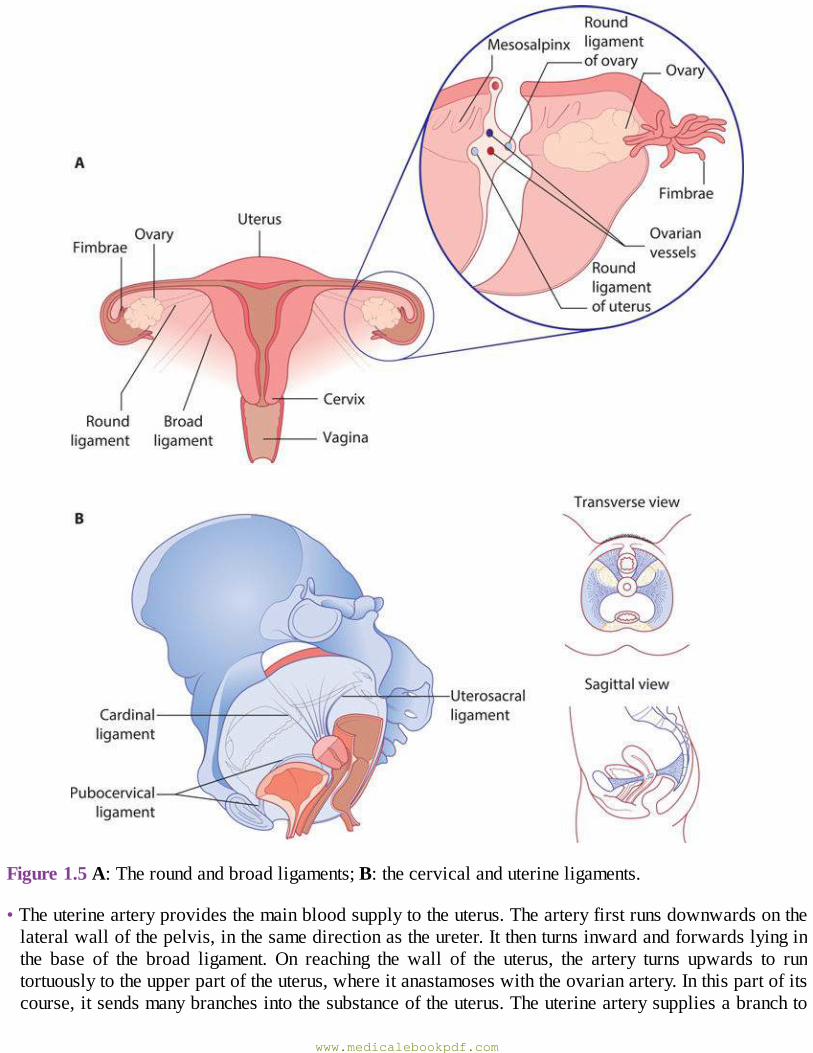
Figure1.5A:Theroundandbroadligaments;B:thecervicalanduterineligaments.
•Theuterinearteryprovidesthemainbloodsupplytotheuterus.Thearteryfirstrunsdownwardsonthelateralwallofthepelvis,inthesamedirectionastheureter.Itthenturnsinwardandforwardslyinginthe base of the broad ligament. On reaching the wall of the uterus, the artery turns upwards to runtortuouslytotheupperpartoftheuterus,whereitanastamoseswiththeovarianartery.Inthispartofitscourse,itsendsmanybranchesintothesubstanceoftheuterus.Theuterinearterysuppliesabranchto
www.medicalebookpdf.com
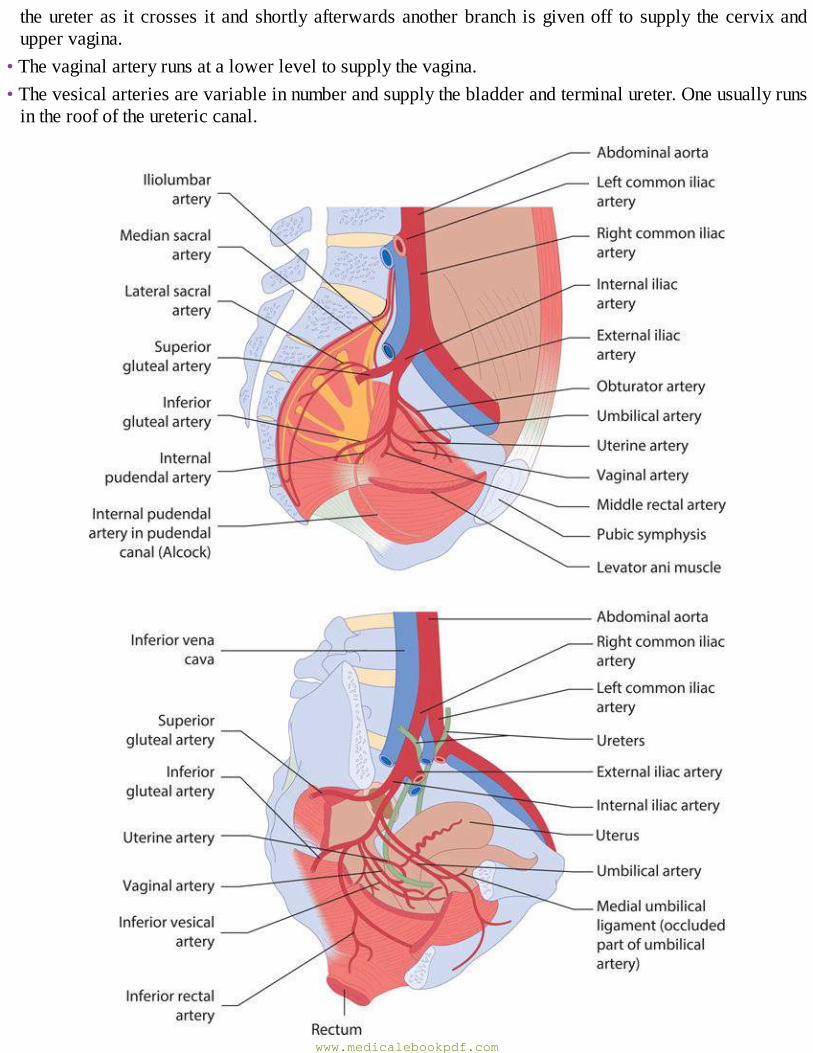
theureteras it crosses it andshortlyafterwardsanotherbranch isgivenoff to supply thecervixanduppervagina.
•Thevaginalarteryrunsatalowerleveltosupplythevagina.•Thevesicalarteriesarevariableinnumberandsupplythebladderandterminalureter.Oneusuallyrunsintheroofoftheuretericcanal.
www.medicalebookpdf.com
Figure1.6Bloodsupplyofthepelvisandperineum.
•Themiddlerectalarteryoftenarisesincommonwiththelowestvesicalartery.•Thepudendalartery leaves thepelviccavity throughthesciatic foramenand,afterwindingroundtheischialspine,enterstheischiorectalfossawhereitgivesofftheinferiorrectalartery.Itterminatesintheperinealandvulvalarteries,supplyingtheerectiletissueofthevestibularbulbsandclitoris.
ThesuperiorrectalarteryThisarteryisthecontinuationoftheinferiormesentericarteryanddescendsinthebaseofthemesocolon.Itdividesintotwobranchesthatrunoneithersideoftherectumandsupplynumerousbranchestoit.
ThepelvicveinsThe veins around the bladder, uterus, vagina and rectum form plexuses that intercommunicate freely.Venous drainage from the uterine, vaginal and vesical plexus is chiefly into the internal iliac veins.Venousdrainagefromtherectalplexus isvia thesuperiorrectalveins to the inferiormesentericveins,andthemiddleandinferiorrectalveinstotheinternalpudendalveinsandsototheiliacveins.
Theovarianveinsoneachsidebegininthepampiniformplexus,whichliesbetweenthelayersofthebroadligament.Atfirst,therearetwoveinsoneachsideaccompanyingthecorrespondingovarianartery.Higheruptheveinbecomessingle,withthatontherightendingintheinferiorvenacavaandthatontheleftintheleftrenalvein.
LymphaticsThepelviclymphatics(Figure1.7)Lymphdrainingfromall thelowerextremitiesandthevulvaandperinealregionsisallfilteredthroughtheinguinalandsuperficialfemoralnodesbeforecontinuingalongthedeeppathwaysonthesidewallofthepelvis.Onedeepchainpassesupwardslateraltothemajorbloodvessels,forminginturntheexternaliliac,commoniliacandpara-aorticgroupsofnodes.
www.medicalebookpdf.com

Figure1.7Lymphaticdrainageofthepelvisandperineum.
Medially,anotherchainofvesselspassesfromthedeepfemoralnodesthroughthefemoralcanaltotheobturatorandinternal iliacgroupsofnodes.Theselastnodesareinterspersedamongtheoriginsof thebranches of the internal iliac artery receiving lymph directly from the organs supplied by this artery,includingtheuppervagina,cervixandbodyoftheuterus.
Fromtheinternal iliacandcommoniliacnodes,afferentvesselspassupthepara-aorticchains,andfinallyalllymphaticdrainagefromthelegsandpelvisflowsintothelumbarlymphatictrunksandcisternachyliatthelevelofthesecondlumbarvertebra.Fromhere,allthelymphiscarriedbythethoracicductthroughthethoraxwithnointerveningnodestoemptyintothejunctionoftheleftsubclavianandinternaljugularveins.
Tumourcells thatpenetrateorbypass thepelvicandpara-aorticnodesarerapidlydisseminatedviathegreatveinsattherootoftheneck.
LymphaticdrainagefromthegenitaltractThelymphvesselfromindividualpartsofthegenitaltractdrainintothissystemofpelviclymphnodesinthefollowingmanner:
•Thevulva andperineummedial to the labiocrural skin folds contain superficial lymphatics that passupwards towards themonspubis, thencurve laterally to thesuperficialand inguinalnodes.Drainagefrom these is through the fossa ovalis into the deep femoral nodes.The largest of these, lying in theupperpartofthefemoralcanal,isknownasthenodeofCloquet.
www.medicalebookpdf.com
• The lymphatics of the lower third of the vagina follow the vulval drainage to the superficial lymphnodes, whereas those from the upper two-thirds pass upwards to join the lymphatic vessels of thecervix.
•Thelymphaticsofthecervixpasseitherlaterallyinthebaseofthebroadligamentorposteriorlyalongtheuterosacralligamentstoreachthesidewallofthepelvis.Mostofthevesselsdraintotheinternaliliacobturatorandexternal iliacnodes,butvesselsalsopassdirectly to thecommoniliacandlowerpara-aorticnodes.Radicalsurgeryforcarcinomaofthecervixshouldincluderemovalofallthesenodegroupsonbothsidesofthepelvis.
•Most of the lymphatic vessels of the body of the uterus join those of the cervix and therefore reachsimilar groups of nodes. A few vessels at the fundus follow the ovarian channels and there is aninconsistentpathwayalongtheroundligamenttotheinguinalnodes.
•TheovaryandFallopiantubehaveaplexusofvesselsthatdrainalongtheinfundibulopelvicfoldtothepara-aorticnodesonbothsidesofthemidline.Ontheleft,thesearefoundaroundtheleftrenalpedicle,whileontherighttheremayonlybeonenodeinterveningbeforethelymphflowsintothethoracicduct,thusaccountingfortherapidearlyspreadofmetastaticcarcinomatodistantsitessuchasthelungs.
•Thelymphaticdrainageofthebladderandupperurethraistotheiliacnodes,whilethoseofthelowerpartoftheurethrafollowthoseofthevulva.
•Lymphaticsfromtheloweranalcanaldraintothesuperficial inguinalnodesandtheremainderoftherectaldrainage followspararectalchannelsaccompanying thebloodvessels toboth the internal iliacnodes(middlerectalartery)andthepara-aorticnodesandtheoriginoftheinferiormesentericartery.
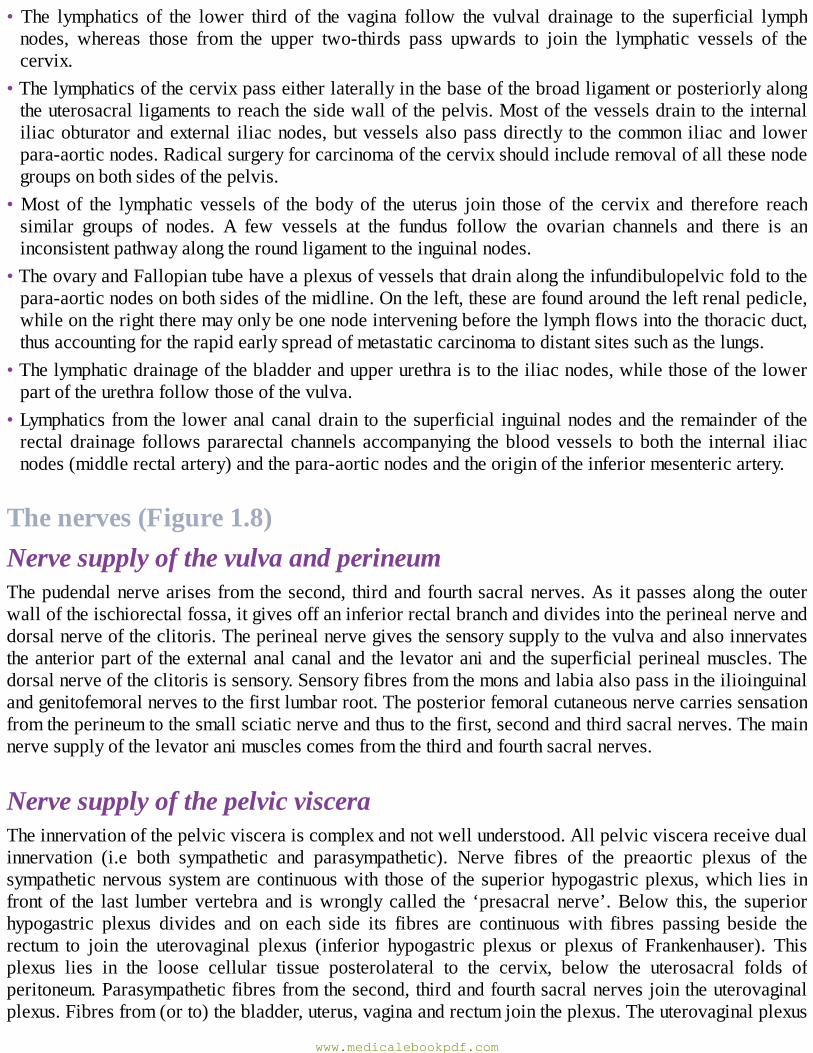
Thenerves(Figure1.8)NervesupplyofthevulvaandperineumThepudendalnervearisesfromthesecond, thirdandfourthsacralnerves.Asitpassesalongtheouterwalloftheischiorectalfossa,itgivesoffaninferiorrectalbranchanddividesintotheperinealnerveanddorsalnerveoftheclitoris.Theperinealnervegivesthesensorysupplytothevulvaandalsoinnervatestheanteriorpartoftheexternalanalcanalandthelevatoraniandthesuperficialperinealmuscles.Thedorsalnerveoftheclitorisissensory.Sensoryfibresfromthemonsandlabiaalsopassintheilioinguinalandgenitofemoralnervestothefirstlumbarroot.Theposteriorfemoralcutaneousnervecarriessensationfromtheperineumtothesmallsciaticnerveandthustothefirst,secondandthirdsacralnerves.Themainnervesupplyofthelevatoranimusclescomesfromthethirdandfourthsacralnerves.
NervesupplyofthepelvicvisceraTheinnervationofthepelvicvisceraiscomplexandnotwellunderstood.Allpelvicviscerareceivedualinnervation (i.e both sympathetic and parasympathetic). Nerve fibres of the preaortic plexus of thesympatheticnervoussystemarecontinuouswith thoseof thesuperiorhypogastricplexus,which lies infront of the last lumber vertebra and iswrongly called the ‘presacral nerve’.Below this, the superiorhypogastric plexus divides and on each side its fibres are continuous with fibres passing beside therectum to join the uterovaginal plexus (inferior hypogastric plexus or plexus of Frankenhauser). Thisplexus lies in the loose cellular tissue posterolateral to the cervix, below the uterosacral folds ofperitoneum.Parasympatheticfibresfromthesecond,thirdandfourthsacralnervesjointheuterovaginalplexus.Fibresfrom(orto)thebladder,uterus,vaginaandrectumjointheplexus.Theuterovaginalplexus
www.medicalebookpdf.com
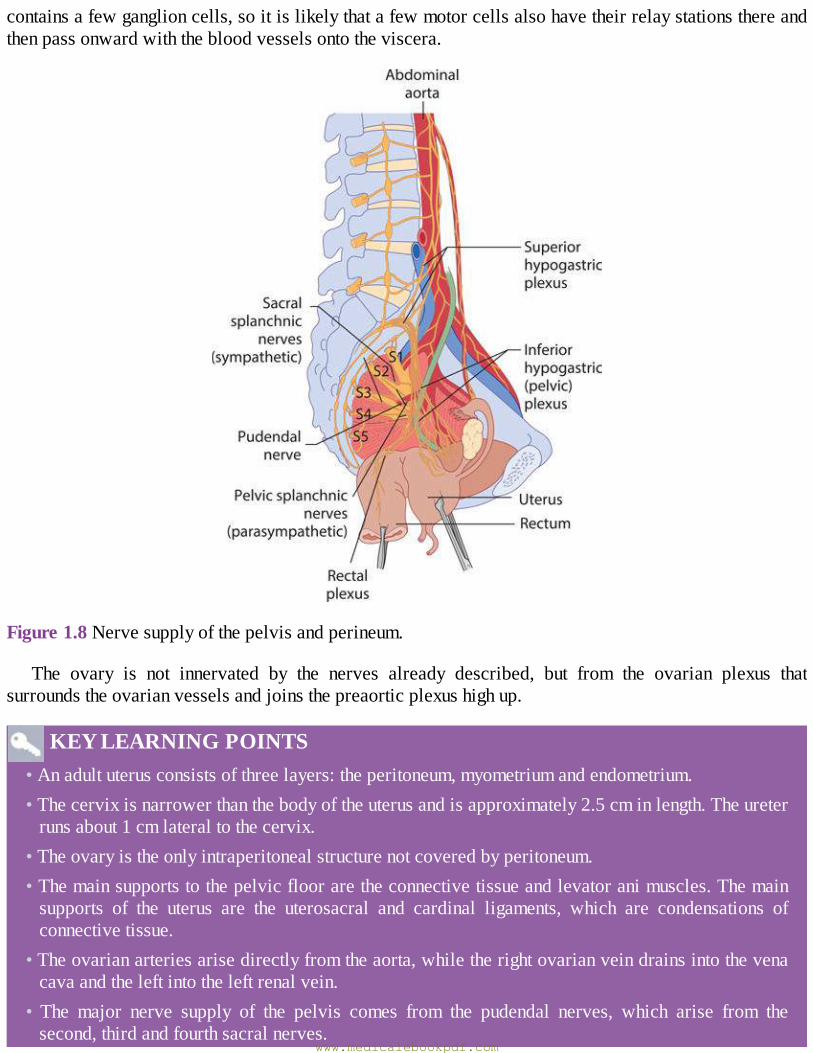
containsafewganglioncells,soitislikelythatafewmotorcellsalsohavetheirrelaystationsthereandthenpassonwardwiththebloodvesselsontotheviscera.
Figure1.8Nervesupplyofthepelvisandperineum.
The ovary is not innervated by the nerves already described, but from the ovarian plexus thatsurroundstheovarianvesselsandjoinsthepreaorticplexushighup.
KEYLEARNINGPOINTS•Anadultuterusconsistsofthreelayers:theperitoneum,myometriumandendometrium.•Thecervixisnarrowerthanthebodyoftheuterusandisapproximately2.5cminlength.Theureterrunsabout1cmlateraltothecervix.
•Theovaryistheonlyintraperitonealstructurenotcoveredbyperitoneum.•Themainsupportstothepelvicflooraretheconnectivetissueandlevatoranimuscles.Themainsupports of the uterus are the uterosacral and cardinal ligaments, which are condensations ofconnectivetissue.
•Theovarianarteriesarisedirectlyfromtheaorta,whiletherightovarianveindrainsintothevenacavaandtheleftintotheleftrenalvein.
• The major nerve supply of the pelvis comes from the pudendal nerves, which arise from thesecond,thirdandfourthsacralnerves.
www.medicalebookpdf.com

Structuralproblemsofpelvicorgans
MülleriananomaliesThese are common, occurring in up to 6% of the female population, and may be asymptomatic. Theaetiology is unknown, although associated renal anomalies are present in up to 30%. Severalclassifications are used that have relevance to the clinical management. Figure 1.9 represents theclassificationusedinEurope.
MüllerianobstructionFailure of complete canalization of the Müllerian structures can lead to menstrual obstruction. Theobstructionmost commonly occurs at the junction of the lower third of the vagina at the level of thehymen,althoughmoreproximalobstructioncanoccur.Presentationwithanimperforatehymenisusuallywithincreasingabdominalpaininagirlinearlyadolescence.Theretainedmenstrualbloodstretchesthevagina,causingahaematocolpus.Thiscancausealargepelvicmassandinadditioncanusuallybeseenasabulgingmembraneatthevaginalentrance.Treatmentissimplewithasurgicalincisionofthehymenanddrainageoftheretainedblood.
www.medicalebookpdf.com
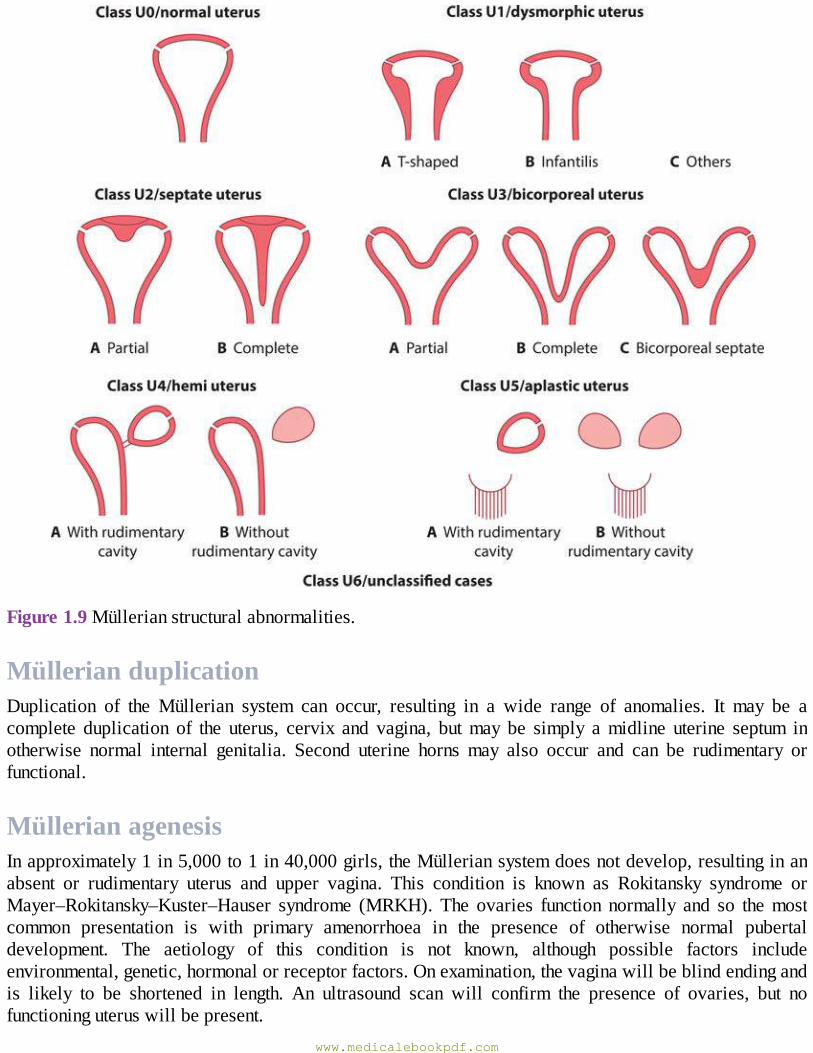
Figure1.9Müllerianstructuralabnormalities.
MüllerianduplicationDuplication of the Müllerian system can occur, resulting in a wide range of anomalies. It may be acomplete duplication of the uterus, cervix and vagina, butmay be simply amidline uterine septum inotherwise normal internal genitalia. Second uterine horns may also occur and can be rudimentary orfunctional.
MüllerianagenesisInapproximately1in5,000to1in40,000girls,theMülleriansystemdoesnotdevelop,resultinginanabsent or rudimentary uterus and upper vagina. This condition is known as Rokitansky syndrome orMayer–Rokitansky–Kuster–Hauser syndrome (MRKH). The ovaries function normally and so themostcommon presentation is with primary amenorrhoea in the presence of otherwise normal pubertaldevelopment. The aetiology of this condition is not known, although possible factors includeenvironmental,genetic,hormonalorreceptorfactors.Onexamination,thevaginawillbeblindendingandis likely to be shortened in length. An ultrasound scan will confirm the presence of ovaries, but nofunctioninguteruswillbepresent.
www.medicalebookpdf.com
Treatment options focus on psychological support and on the creation of a vagina comfortable forpenetrativeintercourse,asdiscussedinChapter3,Hormonalcontrolofthemenstrualcycleandhormonaldisorders. There is currently no treatment available to transplant a uterus in humans, although there isextensiveongoingresearchbeingundertakeninthisarea.WomenwithMRKHsyndromemayhavetheirowngeneticchildren,usingovumretrievalandassistedconceptiontechniques,andasurrogatemother.
VestigialstructuresVestigial remains of the mesonephric duct and tubules are always present in young children, but arevariablestructuresinadults.Theepoophoron,aseriesofparallelblindtubules,liesinthebroadligamentbetween the mesovarium and the Fallopian tube. The tubules run to the rudimentary duct of theepoophoron,whichrunsparalleltothelateralFallopiantube.Situatedinthebroadligamentbetweentheepoophoronandtheuterus,afewrudimentarytubulesareoccasionallyseen, theparoophoron.Inafewindividuals,thecaudalpartofthemesonephricductiswelldeveloped,runningalongsidetheuterustotheinternalos.ThisistheductofGartner.
FurtherreadingNetterFH(2011)AtlasOfHumanAnatomy.Philadelphia,PA:Saunders/Elsevier.SetchellM,HudsonCN(2013)Shaw’sTextbookOfOperativeGynaecology.NewDelhi:Elsevier.
Selfassessment
CASEHISTORY
A 15-year-old girl was seen in gynaecology clinic with her mother. She had not yet started herperiods.Shedescribedbreastdevelopmentatage12andpubichairdevelopment.Allher friendshadstartedtheirperiodsandshewonderedwhatwaswrong.
She also described abdominal pain that had started a couple of years ago. Initially she hadignoreditbutnowitwasinterferingwithsport.Itwasintermittentandonquestioningshewonderedifitwascomingaboutmonthly.Itwasacrampinglowerabdominalpain.
Shehadaboyfriendbutwasnotsexuallyactive.Medicallytherewerenoproblems,nopreviousoperationsandnoallergies.Sociallyshewasdoingwellatschool.
Onexaminationtherewasnormalbreastdevelopmentanddistributionofpubichair.Therewasahardswelling in the lowerabdomen thatwasquite tender.Onobservationof thegenitalia,ablueswellingatthelevelofthehymenwasseen.
AWhatisthemostlikelydiagnosis?BWhichinvestigations(s)shouldbeperformedandwhatisthedifferentialdiagnosis?
ANSWERSwww.medicalebookpdf.com
AThemost likely diagnosis is a haematocolpos from an imperforate hymen.Menstrual fluid hadbeencollectingabovethehymenasitcouldnotescape.Overtimethishaddistendedthevaginaandfilledtheuterinecavity.Thiswascausingtheswellingandthecyclicalpain.
BAnultrasoundshouldbeperformedtoconfirmthediagnosisandexcludeanyMüllerianstructuralalterations.Theimportantdifferential isobstructionduetoahorizontalvaginalplateatahigherlevel. In this case theultrasoundwouldnot showblood filling thevaginadown to the introitusbecausethesiteofanimperforateplateishigherinthevaginaandisduetoimperforateurogenitalsinus.Theadditionalfindingofthebluevaginalswellingalsopointstothehymenbeingthelevelofobstruction.
Thegirlwasadmittedfordaycasesurgery.Anincisionwasmadeinthehymenundergeneralanaesthetic. 700 ml of old blood was evacuated. She made a good recovery and her periodscommencedshortlyafterwards.
SBAQUESTIONS
1Whichofthefollowingstatementsistrueabouttheroundligament?Choosethesinglebestanswer.ATheroundligamentliesposteriortotheuterus.BTheroundligamentsupportsthefundusoftheuterus.CTheroundligamentisavestigialstructure.DTheroundligamentendsdistallyintheinguinalcanal.ETheroundligamentcontainstheneuromuscularbundlesupplyingtheovary.
ANSWER
DTheroundligamentliesanteriortotheuterus.Itdoesnotphysicallysupporttheuterusandisnotavestigialstructure.Itrunsfromthecornuoftheuterusfromtheanteriorleafofthebroadligament,to the inguinalcanal.Theroundligamentdoesnotcontain thevascularbundleof theovary; thisrunsinthemesovarian.
2WhichofthefollowingstatementsistrueabouttheFallopiantube?Choosethesinglebestanswer.ATheFallopiantubeis20cmlong.BTheFallopiantubehasaglandularsubmucosa.CTheFallopiantubeisindependentofhormonalinfluence.DTheFallopiantubeislinedbyciliatedepithelium.ETheFallopiantubeliesintheroundligament.
ANSWER
www.medicalebookpdf.com

DTheFallopian tube is about10cm long. It runs in theuppermarginof thebroad ligament.Theepitheliumisresponsivetohormonesandhastwotypesofcell:ciliatedandsecretorycells.Thereisnosubmucosanorglands.
www.medicalebookpdf.com
CHAPTER2Gynaecologicalhistory,examinationand
investigations
HELENBICKERSTAFF
History
Examination
Investigations
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Tounderstandthatadetailedandstructuredgynaecologicalhistoryisvitalformakingadiagnosis,andwillplacethepatient’ssymptomsinhersocialcontext.
•Tounderstand that thegynaecologicalexaminationwillbecustomizedby thehistory toelicit theappropriatesigns.
•Imagingingynaecologymayincludeultrasound,magneticresonanceimaging(MRI)andcomputedtomography(CT)scanning.
•Biochemical,haematologicalandmicrobiologicalinvestigationswillbeguidedbythehistoryandexaminationfindings.
www.medicalebookpdf.com
HistoryThe gynaecological consultation should ideally be held in a closed roomwith adequate facilities andprivacy. Some women will feel anxious or apprehensive about the forthcoming consultation, so it isimportantthatthestudentordoctorestablishesinitialrapportwiththepatientandputsthematease.Thepractitioner should introduce themselves by name and status, and should check the patient’s details.Ideally, there shouldbenomore thanoneother person in the room,but any student or attendingnurseshouldbeintroducedbynameandtheirrolebrieflyexplained.
Anumber ofwomen attendwith their partner, close familymember or friend. Provided the patientherselfconsentstothis,thereisnoreasontoexcludethemfromtheinitialconsultation,butthisshouldbelimited tooneperson. Insomeinstances, theadditionalpersonmayberequired tobeakeypartof theconsultation(i.e.ifthereisalanguageorcomprehensiondifficulty).However,anindependentinterpretershouldalwaysbeusedtoensurethepatient’sbestinterestsarebeingpresented.Atleastsomepartoftheconsultationorexaminationshouldbewiththewomanalone,toallowhertoansweranyspecificqueriesmoreopenly.
eResource2.1
Thegynaecologicalconsultationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv2.1.php
It is important to be aware of the different attitudes to women’s health issues in a religious andculturallydiversepopulation.Appropriaterespectandsensitivityshouldalwaysbeshown.
Enoughtimeshouldbeallowedfor thepatient toexpressherselfandthedoctor’smannershouldbeoneofinterestandunderstanding,whileguidingherwithappropriatequestioning.Ahistorythatistakenwith sensitivity will often encourage the patient to revealmore details thatmay be relevant to futuremanagement.While there arenumberof termsused ingynaecology (Box2.1), care should be taken toavoidmedicalizedlanguage,usinglaytermswherepossible.
Asettemplateshouldbeusedforhistorytaking,asthispreventstheomissionofimportantpointsandwill help direct the consultation (Box 2.2). Some clinics employ a template routinely to ensure allquestionsarecovered.
SocialhistorySensitiveenquiryshouldbemadeaboutthewoman’ssocialsituationincludingdetailsofheroccupation,whoshe liveswith,herhousingandwhetherornot she is inastable relationship.Ahistory regardingsmoking and alcohol intake should also be obtained. Any pertinent family or other relevant socialproblemsshouldbebrieflydiscussed.Ifadmissionandsurgeryarebeingcontemplateditisnecessarytoestablishwhatsupportthewomanhasathome,particularlyifsheiselderlyorfrail.
Box2.1Glossary
Menarche Startofmenstruation
www.medicalebookpdf.com
Lastmenstrualperiod(LMP)
Dateoflastmenstrualbleed
Amenorrhoea Absenceofbleedsformorethan6monthsinwomenofreproductiveage,seeChapter3,Hormonalcontrolofthemenstrualcycleandhormonaldisorders
Oligomenorrhoea Infrequentmenstrualbleedsmorethan35daysapart,seeChapter3,Hormonalcontrolofthemenstrualcycleandhormonaldisorders
Dysmenorrhoea Painfulmenstrualbleeding(primaryorsecondary)seeChapter4,Disordersofmenstrualbleeding
Menorrhagia Nowcalledheavymenstrualbleeding(HMB),seeChapter4,Disordersofmenstrualbleeding
Abnormaluterinebleeding(AUB)
Includespostcoitalbleeding(PCB)/intermenstrualbleeding(IMB),seeChapter4,Disordersofmenstrualbleeding
Dyspareunia Painfulintercourse,superficialordeep,seeChapter13,Benignconditionsofthevulvaandvagina,psychosexualdisordersandfemalegenitalmutilation
Incontinence Involuntarylossofurine,stress,urgeormixed,seeChapter10Urogynaecologyandpelvicfloorproblems
Prolapse Feelingofsomethingcomingdowninthevagina,seeChapter10,Urogynaecologyandpelvicfloorproblems
Box 2.2 Template for gynaecological history taking in suggestedorder
1General
Name,ageandoccupation.Abriefstatementofthegeneralnatureanddurationofthemaincomplaints(trytousethepatient’s
ownwordsratherthanmedicaltermsatthisstage).
2Historyofpresentingcomplaint
This section should focus on the presenting complaint (e.g. menstrual problems, pain, subfertility,urinaryincontinence,etc).
3Menstrualhistory
Thiswillbeexploredinallpatientsexceptmenopausalwomen:
•usualdurationofeachperiodandlengthoffullcycle(howmanydaysfromday1ofbleedtoday1ofnextbleed);
•firstdayoftheLMP;•patternofbleeding:regularorirregularandlengthofcycle;•amountofbloodloss:patientswillhavedifferentideasastowhatconstitutesa‘heavyperiod’.
www.medicalebookpdf.com
4Cervicalscreening
Thiswillbeexploredinallpatients:
•dateoflastsmear,itsoutcomeandanypreviousabnormalities,colposcopyortreatments.
5Sexualandcontraceptivehistory
•presentpartner(s),sexualorientation;•contraceptivemethodorneeds.
6Othergynaecologicalsymptoms
Abriefexplorationofthefollowingcomplaintsshouldfollow.Thedetailedquestionsrelatingtoeachcomplaintareexplainedinmoredetaillater:
•anyirregularbleeding?•anyHMB,IMB,PCB?•anypelvicpain?•anyproblemswithfertility?•anyproblemswithcontinence?•anydyspareuniaorsexualdifficulty?•anyvaginaldischarge?•menopausalhistoryanduseofHRT.
7Previousgynaecologicalhistory
Thissectionshouldincludeanypreviousgynaecologicaltreatmentsorsurgery.Previousobstetrichistory:
•numberofchildrenwithagesandbirthweights,modeofdeliveryandanycomplications;•numberofmiscarriagesandgestationatwhichtheyoccurred;•anyterminationsofpregnancywithrecordofgestationalageandanycomplications.
8Previousmedicalhistory
•anyseriousillnessesoroperationswithdates.
9Medicationandallergies
•allergies:includingtowhatandthereaction;•current/previousmedicationstried.
10Familyhistory
Significantautoimmunedisease,BRACrelatedcancersandthrombophilias.
www.medicalebookpdf.com
11Systemsenquiry
•appetite,weightloss,weightgain;•bowelfunction(ifurogynaecologicalcomplaint,moredetailmayberequired);•bladderfunction(ifurogynaecologicalcomplaint,moredetailmayberequired).
Box2.3HowtodetermineifthereisHMB•Isthebleedingmoreorlessthanusual?•Doyouusetampons,towelsorboth?•Howoftendoessoakedsanitarywearneedtobechanged?•Istherepresenceofclots?•Isthebleedingsoheavy(flooding)thatitspillsoveryourtowel/tamponandontoyourpants,clothesorbedding?
•Haveyouhadtotakeanytimeoffworkduetothisbleeding?•Doyoueverfindyouareconfinedtoyourhousewhenthebleedingisatitsworst?•Doyoufeeldizzyorshortofbreath,particularlyafteraperiod,orfindithardtoclimbstairs?•Doesitconstrainyourlifestyle?
Specificgynaecologicalproblemsrequiremorefocussedhistorytaking,andthequestionstobeaskedaredetailedbelow.
Abnormal uterine bleeding (AUB) (see Chapter 4, Disorders ofmenstrualbleeding)•Lengthoftimeofproblem.•Amountofbloodloss.•Relationshipsofbleeding to sexand tomenstrual cycle,or to the lastmenstrualbleed in thecaseofpostmenopausalbleeding(PMB).
•ForHMBtheobjectivemeasurementisdifficult,seeBox2.3.
Early pregnancy problems (see Chapter 5, Implantation and earlypregnancy)•DateofLMP,whetheritwasnormalandtheregularityofcycleareusedtoestablishlikelygestation.•Whethercontraceptionusedandwhetherthepatientplanstoproceedwithpregnancyifunintended.•Pregnancysymptoms.•Episodesofbleedingorpaininthispregnancy.•Whetherascanhasalreadybeenperformedtoestablishviabilityandsiteofthepregnancy.
www.medicalebookpdf.com
•Whether thereare riskfactors foranectopicpregnancy(sexually-transmitted infection[STI],delayedconception,previousectopics).
•Previoushistoryofmiscarriages,thegestationandtheirmanagement(surgical,medical,conservative).
Contraception and emergency contraception (EC) (see Chapter 6,Contraceptionandabortion)•LMP.•Exacttimingofunprotectedintercourse(s)ifrequiresEC.• Contraindications to oestrogen-based contraception (thromboembolism, obesity, smoking, age,migraineswithaura).
•Regularormultiplepartners.•Previoussexualhealthscreening.•Othermenstrualproblems(whichmaybeimprovedwithcertainformsofcontraception).
Fertility(seeChapter7,Subfertility)•Lengthoftimeinpresentrelationshipusingnocontraception.•Lengthoftime‘tryingforpregnancy’.•Previoustestsperformed,bothmaleandfemale.•PreviousSTIs.•Previousfertilitytreatmentsattempted.•Particularattentiontolengthandregularityofmenstrualcycle.•Evidenceofuterineproblems(HMB,scantyperiods,previoussurgery,abdominalfullness).•Evidenceofpolycysticovarysyndrome(oligomenorrhoea,hirsutism,excessweight,acne).• Evidence of endocrine problems such as thyroid symptoms (heat sensitivity,weight change, tremor),prolactinomas(galactorrhea,visualfielddisturbance,headaches).
Menopause (see Chapter 8, The menopause and postreproductivehealth)•Dateoflastperiod.•PMB.• Evidence of any menopausal symptoms (such as hot flushes, sleep disturbance, emotional orpsychologicaldifficulty,sexualdifficulty,vaginaldryness,bladdersymptoms).
•Anyhormone replacement therapy (HRT) takennoworpreviously and any specific cautions such asbreastcancer,thromboembolicevents,hypertension.
Urogynaecology (see Chapter 10, Urogynaecology and pelvic floorproblems)
www.medicalebookpdf.com
•Numberoftimespassingurineduringthedayandatnight.•Difficultyinpassingurine.•Uncontrolledpassageofurineoncoughingorstraining.•Urgentneedtopassurineandlossofurinewithurge.•Exacerbatingfactorssuchasalcohol,caffeine.•Extenttowhichaffectsgenerallifesuchasfluidrestrictingorplanningroutesaroundtoiletfacilities.•Incontinenceofflatusorfaeces.•Incontinenceduringsexualintercourse.•Feelingofsomethingcomingdowninvagina.•Riskfactorssuchasnumberofpregnanciesandvaginalandinstrumentalbirths.•Evidenceofabdominalmassessuchasfibroids.•MenopausalstatusandHRT.
Sexualhealth(seeChapter9,Genitourinarymedicine)•Presentsexualpartner,regularornotandotherpartners.•Vaginal/anal/oralsex.•Contraception.•Previouscontraceptionandsexualpartners.•Previoussexualhealthscreening.•PreviousSTIs.•Symptomsofvaginaldischarge,itscolourandodour.•Vaginalandperinealdiscomfortoritchingorlesions.
Pelvic pain (see Chapter 11, Benign conditions of the ovary andpelvis)•Siteofpain,itsnatureandseverity.• Anything that aggravates or relieves the pain – specifically enquire about temporal relationship tomenstrualcycleandintercourse.
•Doesthepainradiateanywhereorisitassociatedwithbowelorbladderfunction?•Istherepainhavingintercourseandisthisdeeporsuperficialandisthereassociatedsexualdysfunction(seeChapter13,Benignconditionsofthevulvaandvagina,psychosexualdisordersandfemalegenitalmutilation)?
SummaryThehistoryshouldbesummarizedinonetotwosentencesbeforeproceedingtotheexaminationtofocustheproblemandalerttheexaminertothesalientfeatures.
•Privacyandconfidentialityareessentialingynaecologicalhistorytaking.www.medicalebookpdf.com
•Itisimportanttoavoidmedicallanguage.•Thesymptomsexperiencedbythepatientandtherelevanceintheirlivesarebothimportant.•Asystematicandthoroughgynaecologicalhistoryshouldbeaskedateachconsultation.•Specificareasofthehistoryshouldthenbeexplored.
Box2.4SamplehistoryThis32-year-oldAfro-Caribbeanladyhaspresentedtogynaecologywithheavyregularperiods.Sheuses eight towels a day and floods at night. She has symptoms of anaemia. Her periods becameheavier3yearsago.Thereisnoabnormalpain.Shehasalsonotedabdominalfullnessandfrequencyofurineduringtheday.
Herlastsmeartestwas2yearsagoandwasnormal.Shehashadtwofulltermnormaldeliveries,her children are aged 6 and 10. She uses condomswith her regular partner for contraception. Shewouldlikemorechildreninafewyearstime.ShehashadnoSTIs.Shehashadnoprevioussurgeryandisfitandwell,takesnomedication,andhasnoallergies.
ExaminationImportantinformationaboutthepatientcanbeobtainedbywatchingthemwalkintotheexaminationroom.Poor mobility may affect decisions regarding surgery or future management. Any examination shouldalwaysbecarriedoutwiththepatient’sconsentandwithappropriateprivacyandsensitivity.Checkandexplainthatthedoorisclosed,checkthepatient’scomfort(e.g.isanelderlypatientcomfortablewithoutthe head being raised, is she warm enough) before proceeding. A female chaperone must be presentthroughouttheexamination.
It isgoodpractice toperformageneralexamination,whichshould includeexaminingthehandsandmucous membranes for evidence of anaemia. The supraclavicular area should be palpated for thepresenceofnodes,particularlyontheleftsidewhereincasesofabdominalmalignancyonemightpalpatethe enlarged Virchow’s node (this is also known as Troissier’s sign). The thyroid gland should bepalpated.Thebreastsshouldbeexaminedaspartoftheexaminationifindicatedbythehistoryorpelvicexamination; this isparticularly relevant if there isasuspectedovarianmass,as theremaybeabreasttumourwithsecondariesintheovariesknownasKrukenburgtumours.Inaddition,apleuraleffusionmaybeelicitedasaconsequenceofabdominalascites.
Bloodpressureandbodymassindex(BMI)shouldberecordedasthiswillberelevanttomedicalandsurgicalmanagement.
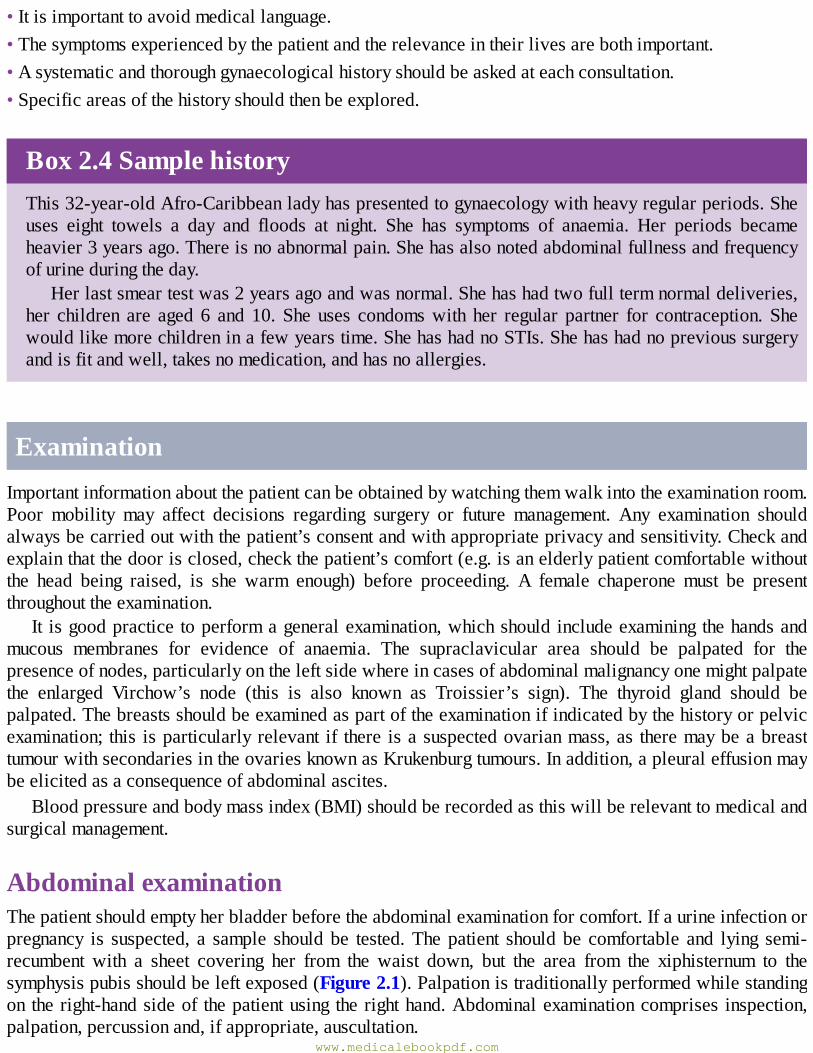
AbdominalexaminationThepatientshouldemptyherbladderbeforetheabdominalexaminationforcomfort.Ifaurineinfectionorpregnancy is suspected, a sample shouldbe tested.Thepatient shouldbe comfortable and lying semi-recumbent with a sheet covering her from the waist down, but the area from the xiphisternum to thesymphysispubisshouldbeleftexposed(Figure2.1).Palpationistraditionallyperformedwhilestandingontheright-handsideof thepatientusing therighthand.Abdominalexaminationcomprises inspection,palpation,percussionand,ifappropriate,auscultation.
www.medicalebookpdf.com
InspectionThecontouroftheabdomenshouldbeinspectedandnoted.Theremaybeanobviousdistensionormass.Thepresenceofsurgicalscars,dilatedveinsorstriaegravidarum(stretchmarks)shouldbenoted.ItisimportantspecificallytoexaminetheumbilicusforlaparoscopyscarsandjustabovethesymphysispubisforPfannenstielscars(usedforcaesareansection,hysterectomy,etc).Thepatientshouldbeaskedtoraiseherheadorcoughandanyherniasordivaricationoftherectusmuscleswillbeevident.
PalpationFirst,ifthepatienthasanyabdominalpainsheshouldbeaskedtopointtothesite–theareashouldnotbeexamined until the end of palpation. Palpation is performed examining the left lower quadrant andproceedinginatotaloffourstepstotherightlowerquadrantoftheabdomen.Palpationshouldincludeexaminationformasses,theliver,spleenandkidneys.Ifamassispresentbutonecanpalpatebelowit,thenitismorelikelytobeanabdominalmassratherthanapelvicmass.Itisimportanttorememberthatone of the characteristics of a pelvicmass is that it arises from the pelvis, hence one cannot palpatebelowit.Ifthepatienthaspain,herabdomenshouldbepalpatedgentlyandtheexaminershouldlookforsigns of peritonism (i.e. guarding and rebound tenderness). The patient should also be examined foringuinalherniasandlymphnodes.
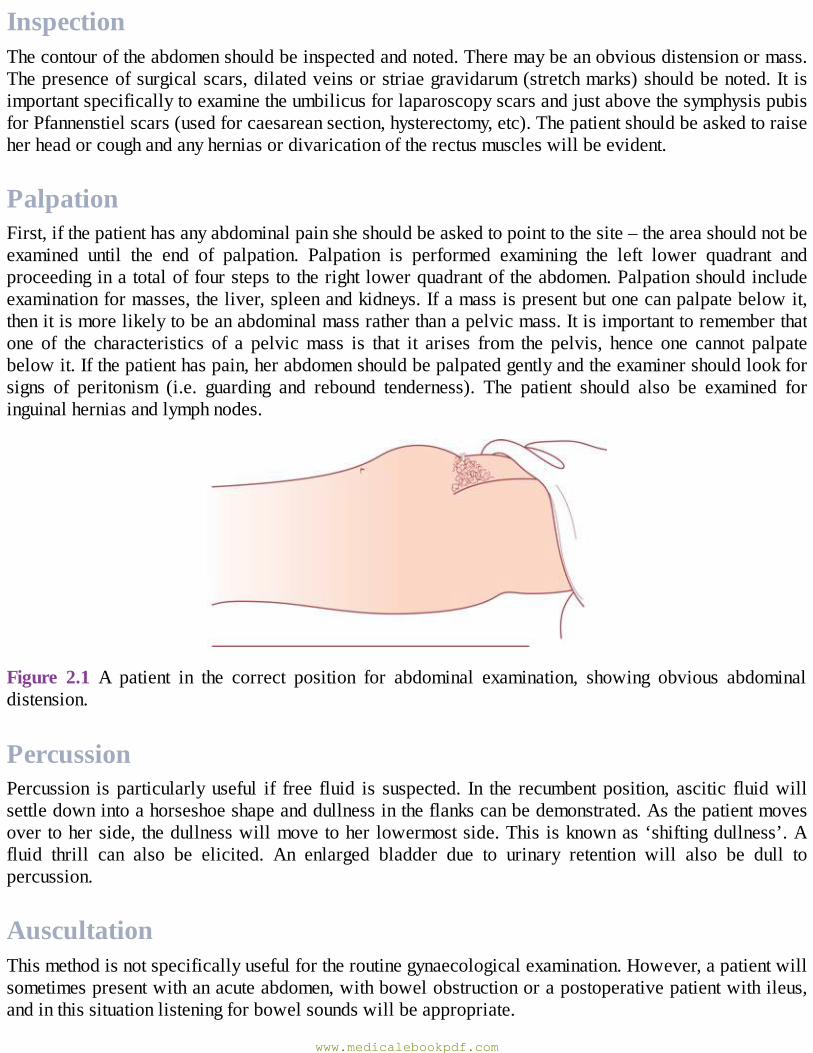
Figure 2.1 A patient in the correct position for abdominal examination, showing obvious abdominaldistension.
PercussionPercussion is particularlyuseful if free fluid is suspected. In the recumbentposition, ascitic fluidwillsettledownintoahorseshoeshapeanddullnessintheflankscanbedemonstrated.Asthepatientmovesovertoherside, thedullnesswillmovetoher lowermostside.Thisisknownas‘shiftingdullness’.Afluid thrill can also be elicited. An enlarged bladder due to urinary retention will also be dull topercussion.
AuscultationThismethodisnotspecificallyusefulfortheroutinegynaecologicalexamination.However,apatientwillsometimespresentwithanacuteabdomen,withbowelobstructionorapostoperativepatientwithileus,andinthissituationlisteningforbowelsoundswillbeappropriate.
www.medicalebookpdf.com

PelvicexaminationBeforeproceedingtoavaginalexamination,thepatient’sverbalconsentshouldbeobtainedandafemalechaperoneshouldbepresentforanyintimateexamination.Itisgoodpractice(andcommoninmostUKmedical schools) for a student to havewritten consent. This ismandatory if the patientwill be underanaestheticfortheexamination.Non-sterileglovescanbeusedfortheexaminationunlessthepatientispregnant, in which case sterile gloves should be worn. There are three components to the pelvicexamination.
InspectionTheexternalgenitaliaandsurroundingskin,includingtheperianalarea,arefirstinspectedunderagoodlightwiththepatientinthedorsalposition,thehipsflexedandabductedandkneesflexed(Figure2.2).Thepatientisaskedtocoughorbeardowntoenablesignsofaprolapseorstressincontinence.Abnormalsignssuchasskindiscolouration,lumps,scarsfrompreviousepisiotomy,deficientperineumorprolapse(seeChapter10,Urogynaecologyandpelvicfloorproblems)arenoted.Femalegenitalmutilation(FGM)(seeChapter13,Benignconditionsof thevulvaandvagina,psychosexualdisordersandfemalegenitalmutilation)shouldbedescribed.
SpeculumAsterilespeculumisaninstrumentthatisinsertedintothevaginatoobtainaclearerviewofpartofthevagina or pelvic organs. There are two principal types in widespread use. The first is a bivalve orCusco’sspeculum(Figure2.3A),whichholds back the anterior andposteriorwalls of thevagina andallowsvisualizationof thecervixwhenopenedout (Figure2.3B). Ithasa retaining screw that canbetightenedtoallowthespeculumtostayinplacewhileaprocedureorsampleistakenfromthecervix(e.g.smear or swab).ASim’s speculum (Figure2.4A)may also be used for examination of prolapse as itallowsinspectionofthevaginalwalls.Itisusedintheleftlateralposition(Figure2.4B).Thechoiceofspeculumwilldependonthepatient’spresentingproblem.
Excessivelubricationshouldbeavoidedandifasmearisbeingtaken,lubricationwithanythingotherthanwatershouldbeavoidedasitmayinterferewiththeanalysis.Microbiologyswabsaretakenfromthevaginalfornices.Endocervicalswabsforchlamydiaaretakenfromtheendocervicalcanal(seeChapter9,Genitourinaryproblems).
www.medicalebookpdf.com
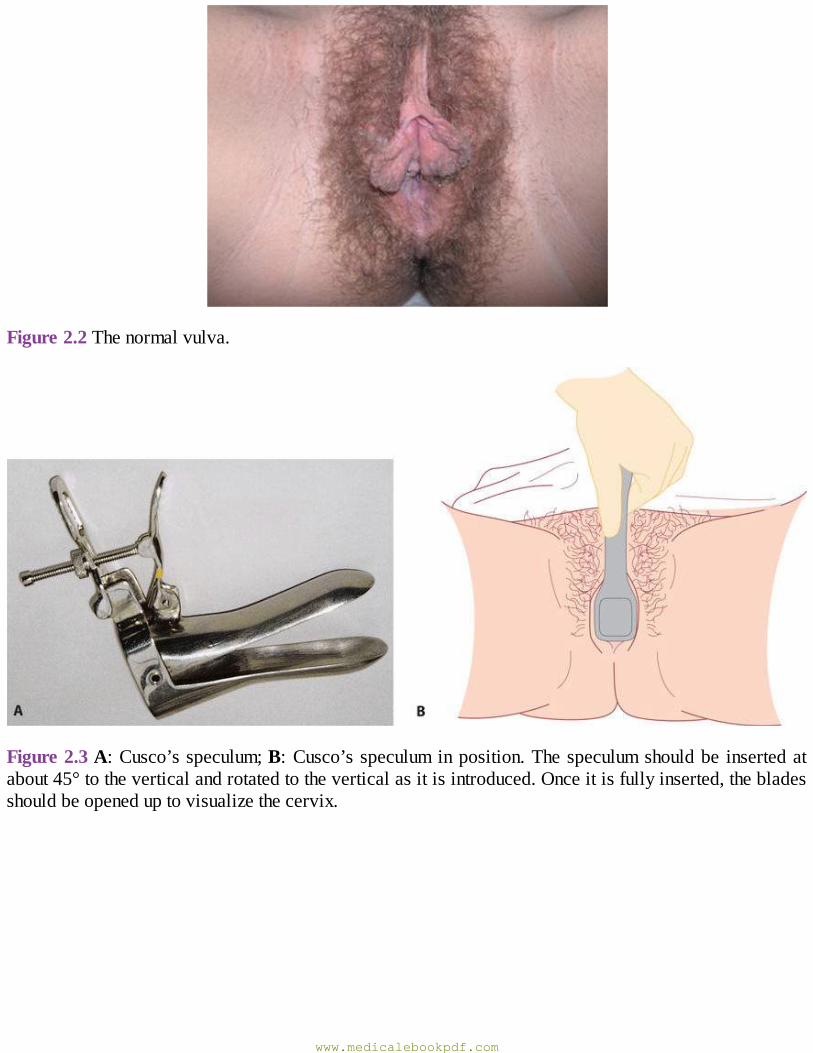
Figure2.2Thenormalvulva.
Figure2.3A:Cusco’sspeculum;B:Cusco’sspeculuminposition.Thespeculumshouldbe insertedatabout45°totheverticalandrotatedtotheverticalasitisintroduced.Onceitisfullyinserted,thebladesshouldbeopeneduptovisualizethecervix.
www.medicalebookpdf.com
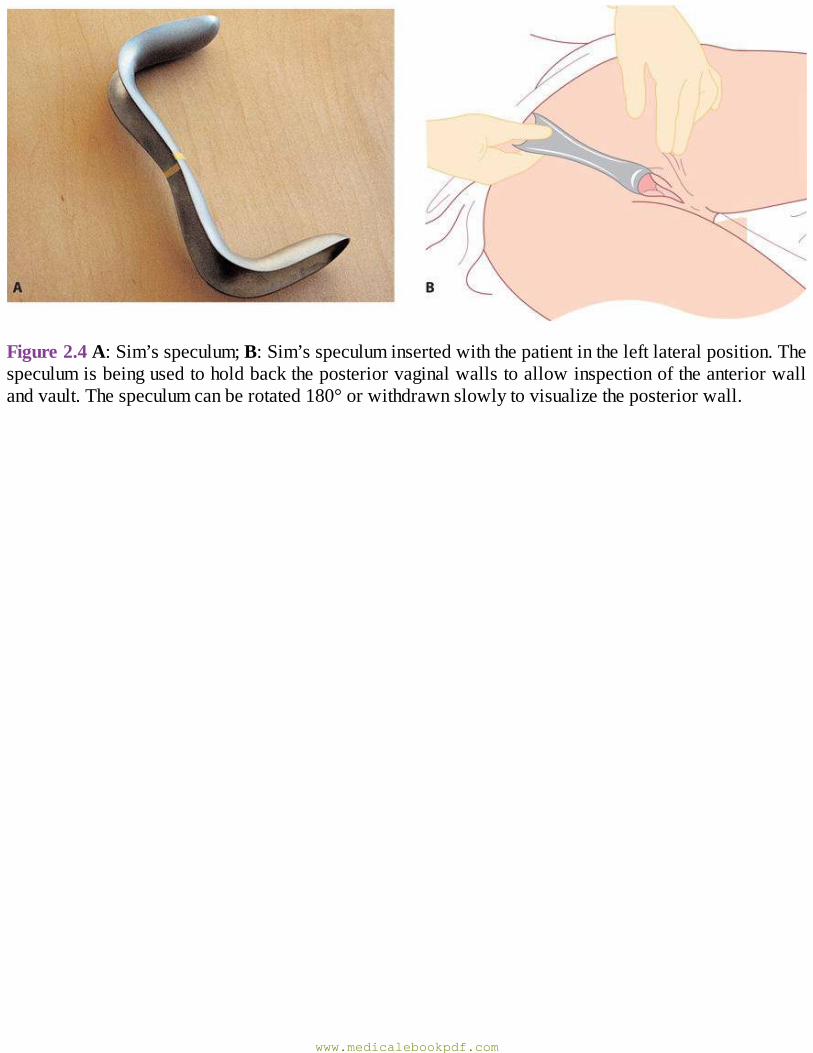
Figure2.4A:Sim’sspeculum;B:Sim’sspeculuminsertedwiththepatientintheleftlateralposition.Thespeculumisbeingusedtoholdbacktheposteriorvaginalwallstoallowinspectionoftheanteriorwallandvault.Thespeculumcanberotated180°orwithdrawnslowlytovisualizetheposteriorwall.
www.medicalebookpdf.com
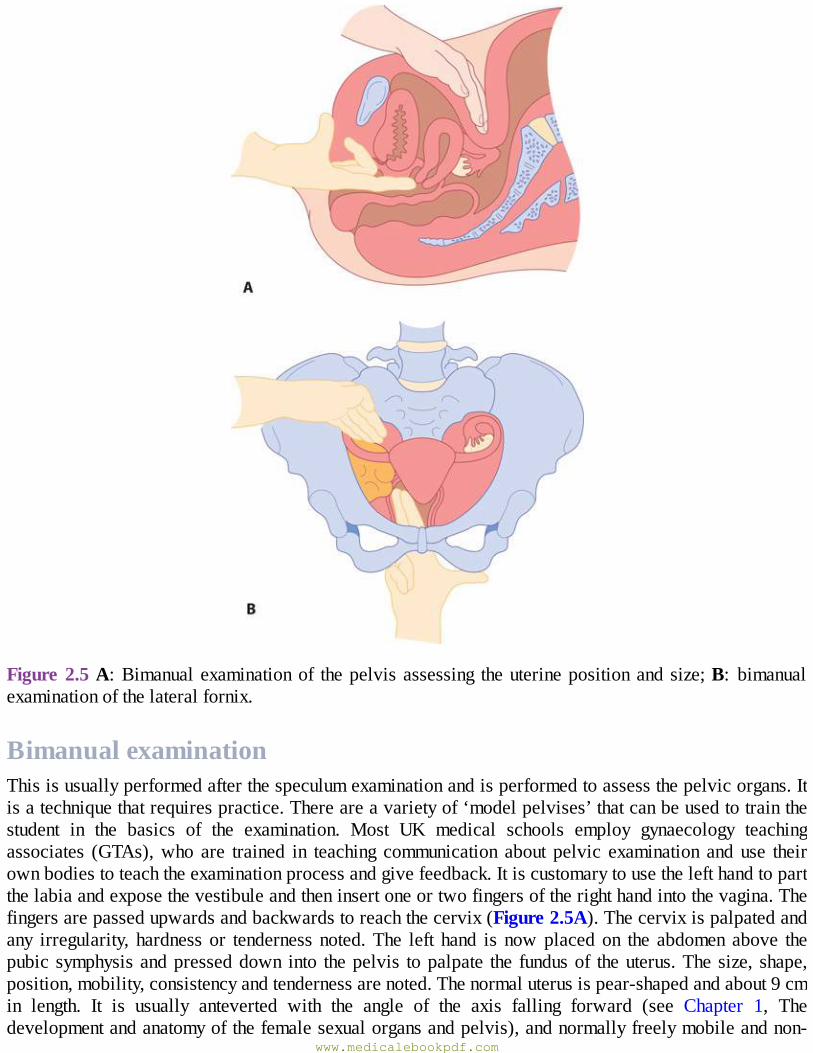
Figure2.5A:Bimanualexaminationof thepelvisassessing theuterinepositionandsize;B: bimanualexaminationofthelateralfornix.
BimanualexaminationThisisusuallyperformedafterthespeculumexaminationandisperformedtoassessthepelvicorgans.Itisatechniquethatrequirespractice.Thereareavarietyof‘modelpelvises’thatcanbeusedtotrainthestudent in the basics of the examination. Most UK medical schools employ gynaecology teachingassociates (GTAs),who are trained in teaching communication about pelvic examination and use theirownbodiestoteachtheexaminationprocessandgivefeedback.Itiscustomarytousethelefthandtopartthelabiaandexposethevestibuleandtheninsertoneortwofingersoftherighthandintothevagina.Thefingersarepassedupwardsandbackwardstoreachthecervix(Figure2.5A).Thecervixispalpatedandany irregularity, hardness or tenderness noted.The left hand is nowplacedon the abdomen above thepubic symphysisandpresseddown into thepelvis topalpate the fundusof theuterus.Thesize, shape,position,mobility,consistencyandtendernessarenoted.Thenormaluterusispear-shapedandabout9cmin length. It is usually anteverted with the angle of the axis falling forward (see Chapter 1, Thedevelopmentandanatomyofthefemalesexualorgansandpelvis),andnormallyfreelymobileandnon-
www.medicalebookpdf.com
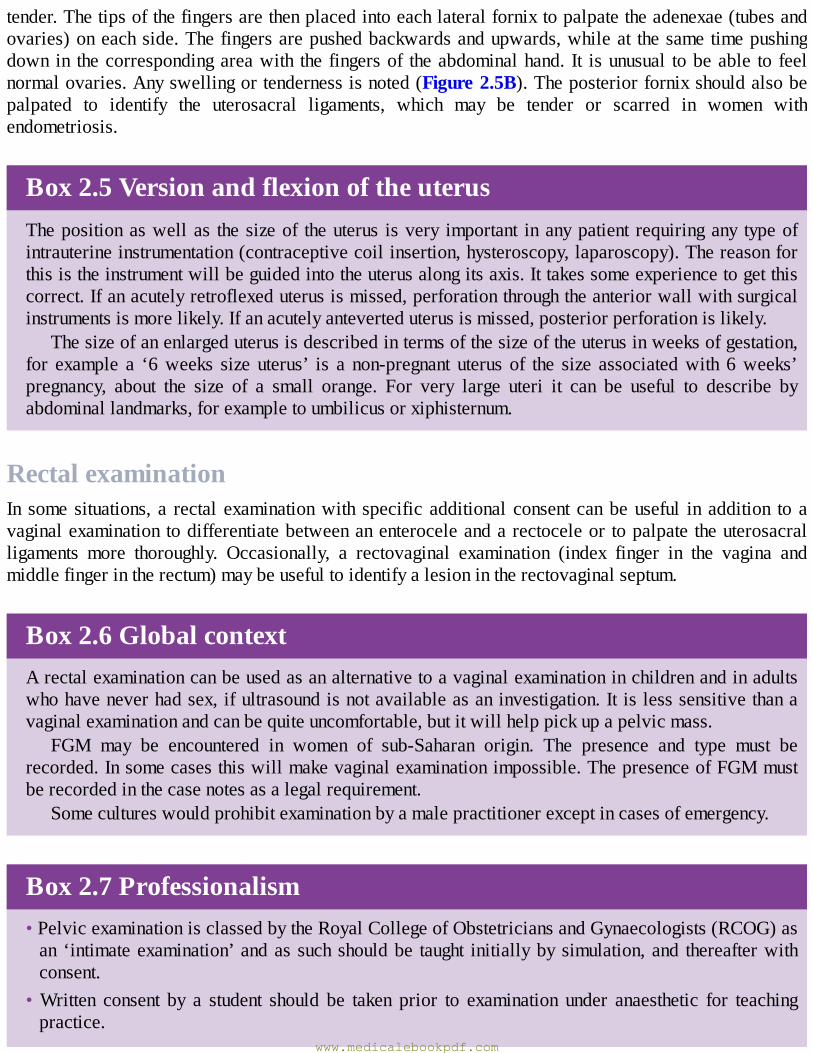
tender.Thetipsofthefingersarethenplacedintoeachlateralfornixtopalpatetheadenexae(tubesandovaries)oneachside.Thefingersarepushedbackwardsandupwards,whileat thesametimepushingdown in thecorrespondingareawith the fingersof theabdominalhand. It isunusual tobeable to feelnormalovaries.Anyswellingortendernessisnoted(Figure2.5B).Theposteriorfornixshouldalsobepalpated to identify the uterosacral ligaments, which may be tender or scarred in women withendometriosis.
Box2.5VersionandflexionoftheuterusThepositionaswellas thesizeof theuterus isvery important inanypatient requiringany typeofintrauterineinstrumentation(contraceptivecoilinsertion,hysteroscopy,laparoscopy).Thereasonforthisistheinstrumentwillbeguidedintotheuterusalongitsaxis.Ittakessomeexperiencetogetthiscorrect.Ifanacutelyretroflexeduterusismissed,perforationthroughtheanteriorwallwithsurgicalinstrumentsismorelikely.Ifanacutelyanteverteduterusismissed,posteriorperforationislikely.
Thesizeofanenlargeduterusisdescribedintermsofthesizeoftheuterusinweeksofgestation,for example a ‘6weeks size uterus’ is a non-pregnant uterus of the size associatedwith 6weeks’pregnancy, about the size of a small orange. For very large uteri it can be useful to describe byabdominallandmarks,forexampletoumbilicusorxiphisternum.
RectalexaminationIn somesituations, a rectal examinationwith specific additional consent canbeuseful in addition toavaginalexaminationtodifferentiatebetweenanenteroceleandarectoceleor topalpatetheuterosacralligaments more thoroughly. Occasionally, a rectovaginal examination (index finger in the vagina andmiddlefingerintherectum)maybeusefultoidentifyalesionintherectovaginalseptum.
Box2.6GlobalcontextArectalexaminationcanbeusedasanalternativetoavaginalexaminationinchildrenandinadultswhohaveneverhadsex,ifultrasoundisnotavailableasaninvestigation.Itislesssensitivethanavaginalexaminationandcanbequiteuncomfortable,butitwillhelppickupapelvicmass.
FGM may be encountered in women of sub-Saharan origin. The presence and type must berecorded.Insomecasesthiswillmakevaginalexaminationimpossible.ThepresenceofFGMmustberecordedinthecasenotesasalegalrequirement.
Somecultureswouldprohibitexaminationbyamalepractitionerexceptincasesofemergency.
Box2.7Professionalism•PelvicexaminationisclassedbytheRoyalCollegeofObstetriciansandGynaecologists(RCOG)asan ‘intimateexamination’andas suchshouldbe taught initiallybysimulation,and thereafterwithconsent.
•Written consent by a student should be taken prior to examination under anaesthetic for teachingpractice.
www.medicalebookpdf.com
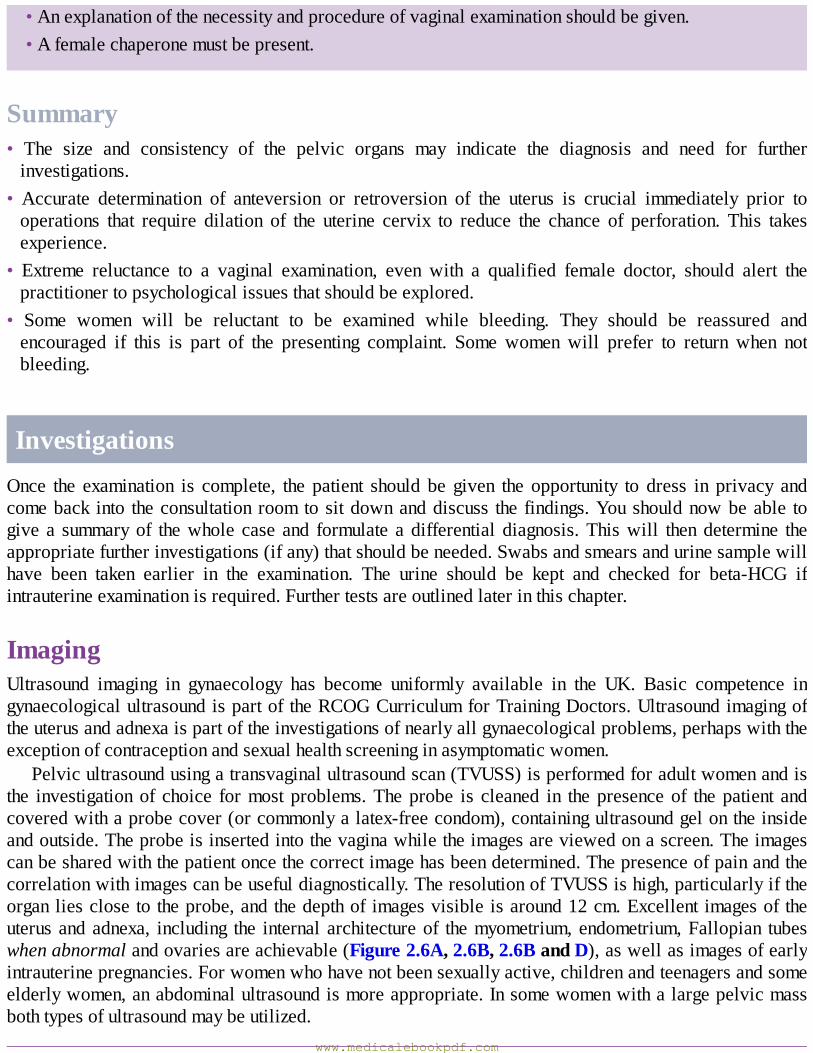
•Anexplanationofthenecessityandprocedureofvaginalexaminationshouldbegiven.•Afemalechaperonemustbepresent.
Summary• The size and consistency of the pelvic organs may indicate the diagnosis and need for furtherinvestigations.
• Accurate determination of anteversion or retroversion of the uterus is crucial immediately prior tooperations that require dilation of the uterine cervix to reduce the chance of perforation. This takesexperience.
• Extreme reluctance to a vaginal examination, even with a qualified female doctor, should alert thepractitionertopsychologicalissuesthatshouldbeexplored.
• Some women will be reluctant to be examined while bleeding. They should be reassured andencouraged if this is part of the presenting complaint. Some women will prefer to return when notbleeding.
InvestigationsOnce the examination is complete, the patient should be given the opportunity to dress in privacy andcomeback into theconsultation roomtositdownanddiscuss the findings.Youshouldnowbeable togivea summaryof thewhole case and formulate a differential diagnosis.Thiswill thendetermine theappropriatefurtherinvestigations(ifany)thatshouldbeneeded.Swabsandsmearsandurinesamplewillhave been taken earlier in the examination. The urine should be kept and checked for beta-HCG ifintrauterineexaminationisrequired.Furthertestsareoutlinedlaterinthischapter.
ImagingUltrasound imaging in gynaecology has become uniformly available in the UK. Basic competence ingynaecologicalultrasoundispartoftheRCOGCurriculumforTrainingDoctors.Ultrasoundimagingoftheuterusandadnexaispartoftheinvestigationsofnearlyallgynaecologicalproblems,perhapswiththeexceptionofcontraceptionandsexualhealthscreeninginasymptomaticwomen.
Pelvicultrasoundusingatransvaginalultrasoundscan(TVUSS)isperformedforadultwomenandisthe investigationof choice formostproblems.Theprobe is cleaned in thepresenceof thepatient andcoveredwithaprobecover(orcommonlyalatex-freecondom),containingultrasoundgelontheinsideandoutside.Theprobeisinsertedintothevaginawhiletheimagesareviewedonascreen.Theimagescanbesharedwiththepatientoncethecorrectimagehasbeendetermined.Thepresenceofpainandthecorrelationwithimagescanbeusefuldiagnostically.TheresolutionofTVUSSishigh,particularlyiftheorganliesclosetotheprobe,andthedepthofimagesvisibleisaround12cm.Excellentimagesoftheuterusandadnexa, including the internal architectureof themyometrium,endometrium,Fallopian tubeswhenabnormalandovariesareachievable(Figure2.6A,2.6B,2.6BandD),aswellasimagesofearlyintrauterinepregnancies.Forwomenwhohavenotbeensexuallyactive,childrenandteenagersandsomeelderlywomen,anabdominalultrasoundismoreappropriate.Insomewomenwithalargepelvicmassbothtypesofultrasoundmaybeutilized.
www.medicalebookpdf.com
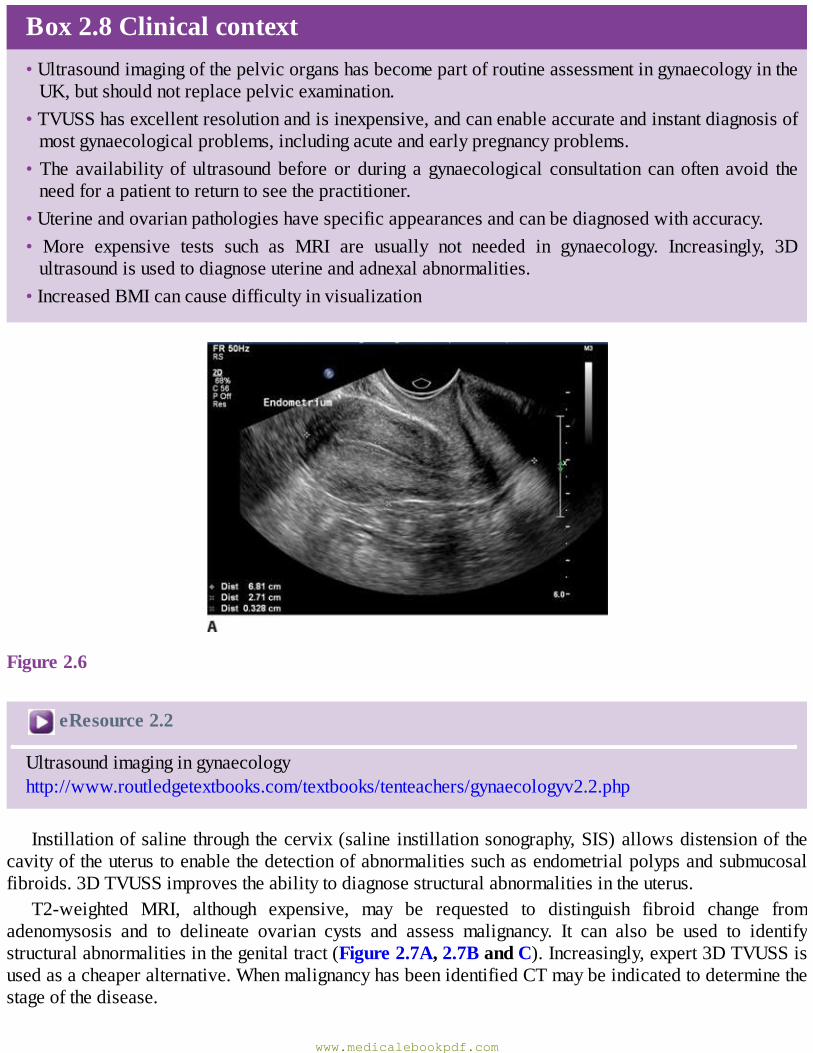
Box2.8Clinicalcontext•UltrasoundimagingofthepelvicorganshasbecomepartofroutineassessmentingynaecologyintheUK,butshouldnotreplacepelvicexamination.
•TVUSShasexcellentresolutionandisinexpensive,andcanenableaccurateandinstantdiagnosisofmostgynaecologicalproblems,includingacuteandearlypregnancyproblems.
•The availability of ultrasoundbefore or during a gynaecological consultation canoften avoid theneedforapatienttoreturntoseethepractitioner.
•Uterineandovarianpathologieshavespecificappearancesandcanbediagnosedwithaccuracy.• More expensive tests such as MRI are usually not needed in gynaecology. Increasingly, 3Dultrasoundisusedtodiagnoseuterineandadnexalabnormalities.
•IncreasedBMIcancausedifficultyinvisualization
Figure2.6
eResource2.2
Ultrasoundimagingingynaecologyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv2.2.php
Instillationofsaline throughthecervix(saline instillationsonography,SIS)allowsdistensionof thecavityoftheuterustoenablethedetectionofabnormalitiessuchasendometrialpolypsandsubmucosalfibroids.3DTVUSSimprovestheabilitytodiagnosestructuralabnormalitiesintheuterus.
T2-weighted MRI, although expensive, may be requested to distinguish fibroid change fromadenomysosis and to delineate ovarian cysts and assess malignancy. It can also be used to identifystructuralabnormalitiesinthegenitaltract(Figure2.7A,2.7BandC).Increasingly,expert3DTVUSSisusedasacheaperalternative.WhenmalignancyhasbeenidentifiedCTmaybeindicatedtodeterminethestageofthedisease.
www.medicalebookpdf.com
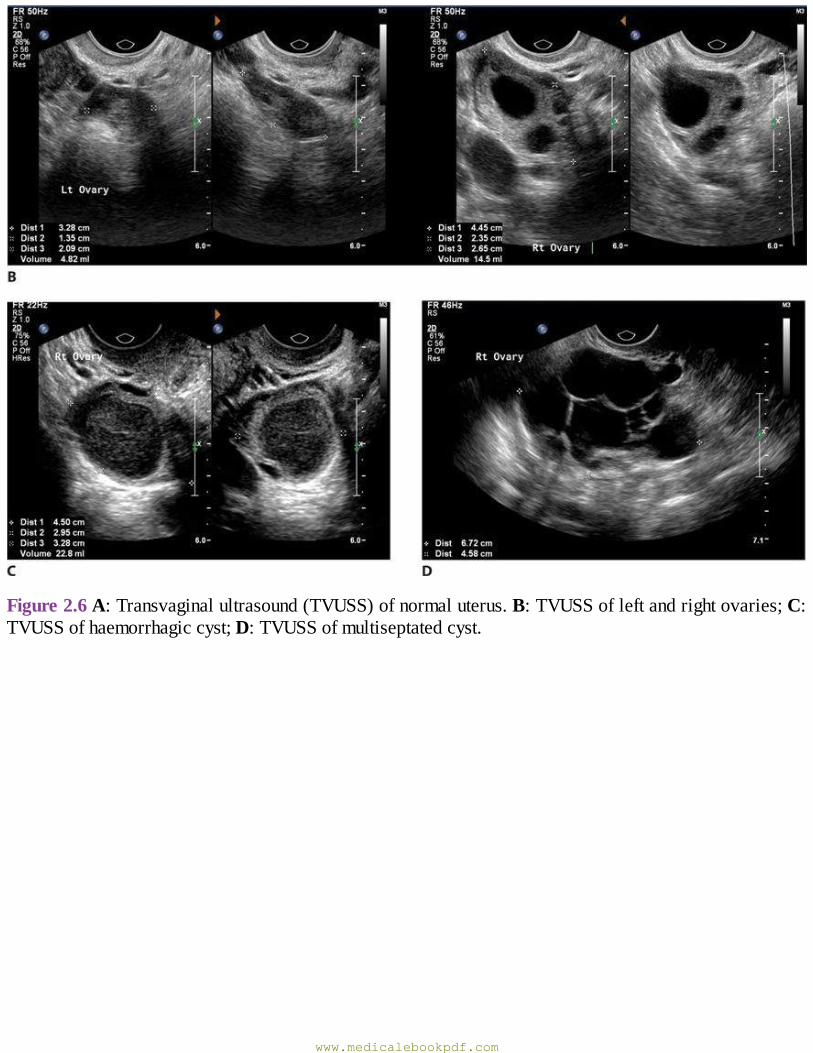
Figure2.6A:Transvaginalultrasound(TVUSS)ofnormaluterus.B:TVUSSofleftandrightovaries;C:TVUSSofhaemorrhagiccyst;D:TVUSSofmultiseptatedcyst.
www.medicalebookpdf.com
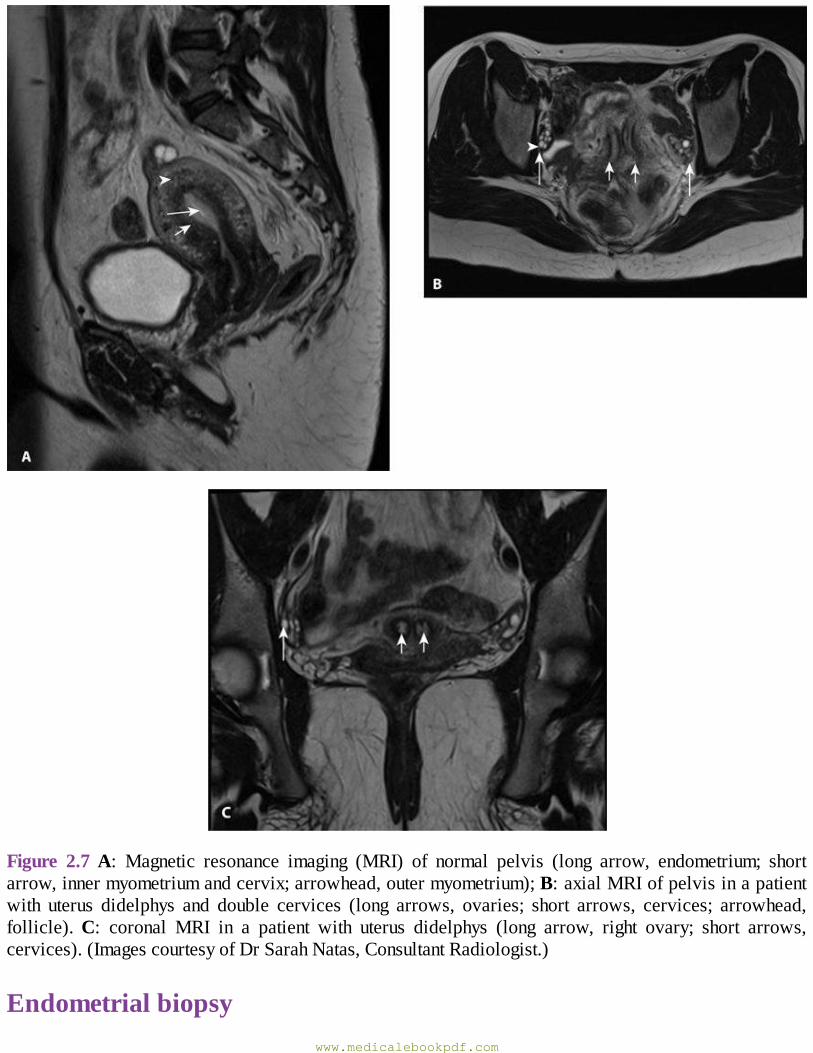
Figure 2.7A: Magnetic resonance imaging (MRI) of normal pelvis (long arrow, endometrium; shortarrow,innermyometriumandcervix;arrowhead,outermyometrium);B:axialMRIofpelvisinapatientwith uterus didelphys and double cervices (long arrows, ovaries; short arrows, cervices; arrowhead,follicle).C: coronal MRI in a patient with uterus didelphys (long arrow, right ovary; short arrows,cervices).(ImagescourtesyofDrSarahNatas,ConsultantRadiologist.)
Endometrialbiopsywww.medicalebookpdf.com
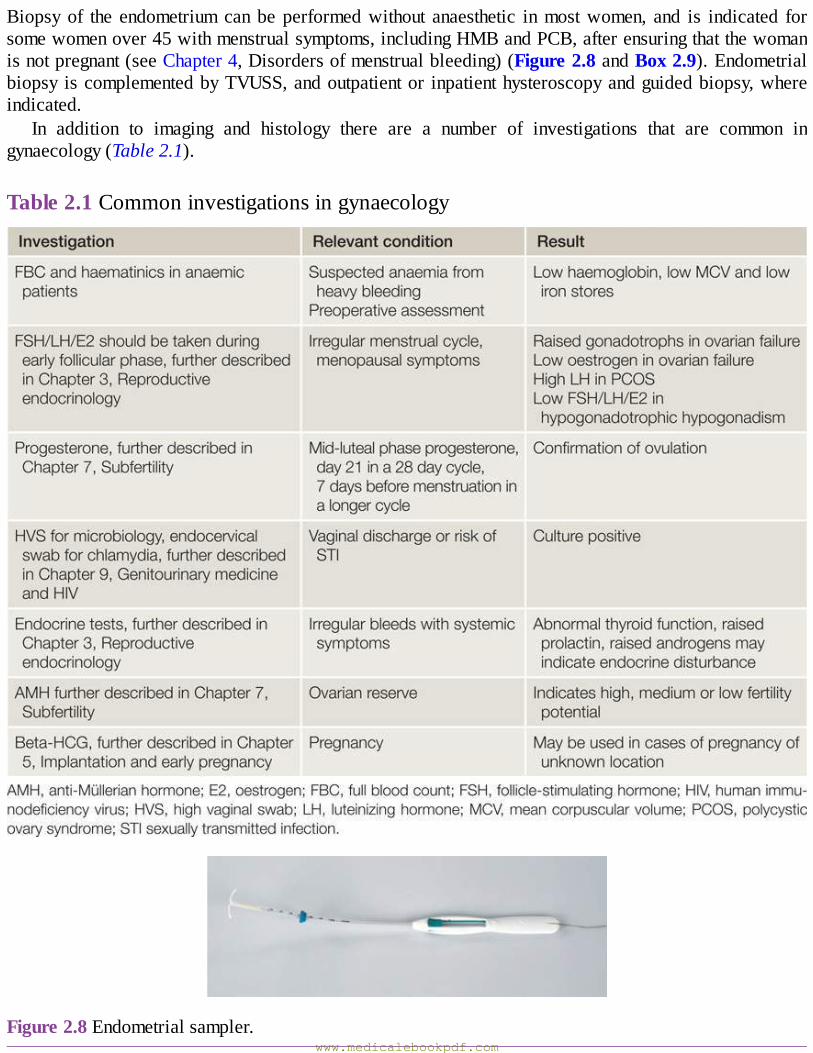
Biopsyof the endometriumcanbe performedwithout anaesthetic inmostwomen, and is indicated forsomewomenover45withmenstrualsymptoms,includingHMBandPCB,afterensuringthatthewomanisnotpregnant(seeChapter4,Disordersofmenstrualbleeding)(Figure2.8andBox2.9).Endometrialbiopsy iscomplementedbyTVUSS,andoutpatientor inpatienthysteroscopyandguidedbiopsy,whereindicated.
In addition to imaging and histology there are a number of investigations that are common ingynaecology(Table2.1).
Table2.1Commoninvestigationsingynaecology
Figure2.8Endometrialsampler.www.medicalebookpdf.com
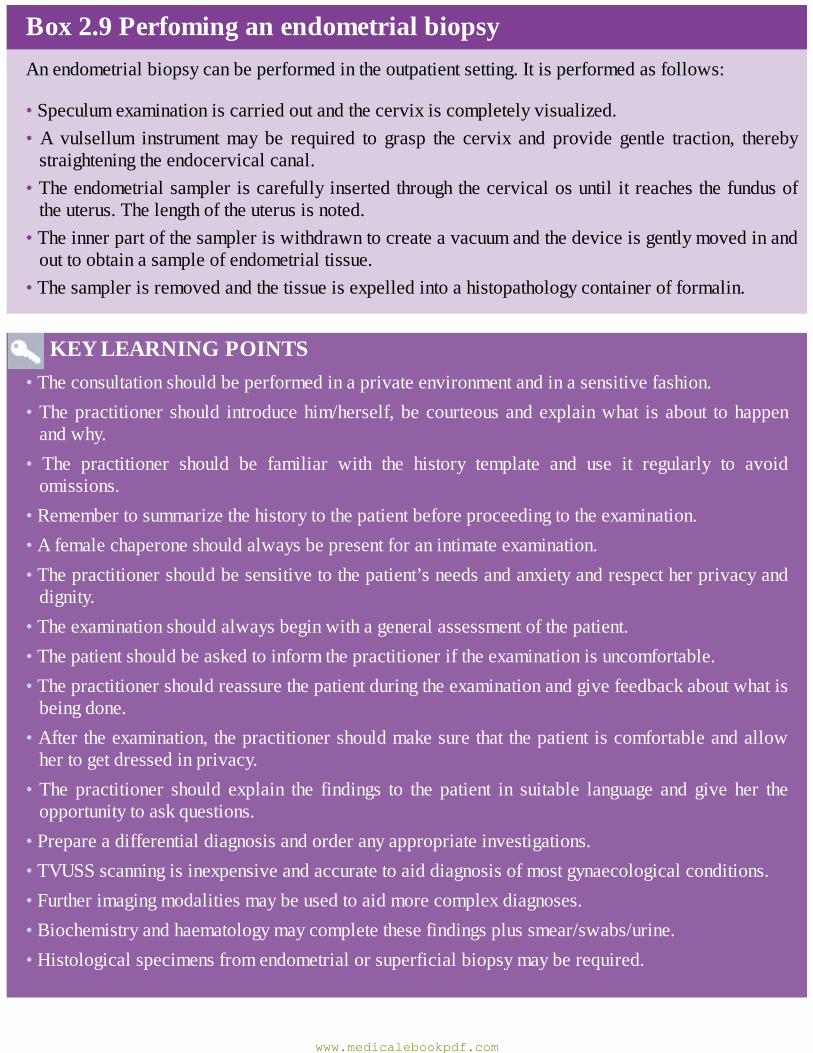
Box2.9PerfominganendometrialbiopsyAnendometrialbiopsycanbeperformedintheoutpatientsetting.Itisperformedasfollows:
•Speculumexaminationiscarriedoutandthecervixiscompletelyvisualized.•A vulsellum instrumentmay be required to grasp the cervix and provide gentle traction, therebystraighteningtheendocervicalcanal.
•Theendometrialsampleriscarefullyinsertedthroughthecervicalosuntilitreachesthefundusoftheuterus.Thelengthoftheuterusisnoted.
•Theinnerpartofthesampleriswithdrawntocreateavacuumandthedeviceisgentlymovedinandouttoobtainasampleofendometrialtissue.
•Thesamplerisremovedandthetissueisexpelledintoahistopathologycontainerofformalin.
KEYLEARNINGPOINTS•Theconsultationshouldbeperformedinaprivateenvironmentandinasensitivefashion.•Thepractitioner should introducehim/herself,becourteousandexplainwhat isabout tohappenandwhy.
• The practitioner should be familiar with the history template and use it regularly to avoidomissions.
•Remembertosummarizethehistorytothepatientbeforeproceedingtotheexamination.•Afemalechaperoneshouldalwaysbepresentforanintimateexamination.•Thepractitionershouldbesensitivetothepatient’sneedsandanxietyandrespectherprivacyanddignity.
•Theexaminationshouldalwaysbeginwithageneralassessmentofthepatient.•Thepatientshouldbeaskedtoinformthepractitioneriftheexaminationisuncomfortable.•Thepractitionershouldreassurethepatientduringtheexaminationandgivefeedbackaboutwhatisbeingdone.
•Aftertheexamination,thepractitionershouldmakesurethatthepatientiscomfortableandallowhertogetdressedinprivacy.
•The practitioner should explain the findings to the patient in suitable language and give her theopportunitytoaskquestions.
•Prepareadifferentialdiagnosisandorderanyappropriateinvestigations.•TVUSSscanningisinexpensiveandaccuratetoaiddiagnosisofmostgynaecologicalconditions.•Furtherimagingmodalitiesmaybeusedtoaidmorecomplexdiagnoses.•Biochemistryandhaematologymaycompletethesefindingsplussmear/swabs/urine.•Histologicalspecimensfromendometrialorsuperficialbiopsymayberequired.
www.medicalebookpdf.com
FurtherreadingRCOGTraininginUltrasound.https://www.rcog.org.uk/en/careers-training.
Selfassessment
CASEHISTORY
A32-year-oldAfro-Caribbeanteacherhascometoclinictoseeyou.Shehashadincreasinglyheavyperiodsoverthelast18months.HerperiodsareregularandthereisnoIMBorPCB,bleedingisfor5daysevery28days.Onthesecondandthirddayofbleedingsheusestamponsandtowelstogether,whichgetsoakedinbloodwithin1hour.Inclassesshehashadtorunoutwhenshehadflooding,andpassedclotsabout4cminsize.Thisisreallyembarrassingwiththeschoolchildrenandshehastakentowearingnappiesjustincase.Sheisavoidingclassroomteachingwhileshehasaperiodbutcannotexplainwhytohermaleheadteacher.Whenherperiodfinishesshefeels‘washedout’andgetsshortofbreathexercisingeasily.Shehasnottriedanytreatmentsofar.
She has never been pregnant and hoped to get pregnant soon after hermarriage last year, butnothinghashappenedinthelast8months.ShehasneverhadanSTI,isinheronlyandstablesexualrelationshipandhasnoabnormalvaginaldischarge,andhersmearshavealwaysbeennormal, thelastwas2yearsago.
Onquestioningsheadmitstofeelingfullintheabdomenwhensheliesonherstomach.Thereisnopainassuchandsexisnotpainful.Shehasneverhadsurgery,hasahealthylifestyle,doesnotsmokeordrinkmuchalcoholandhasnomedicalconditions.Thereisnofamilyhistoryofillnesses.Sheisnotallergictoanyprescribedmedicines.
Onexaminationtheabdomenisdistendedbyahardmassrisingfromthepelvisandcominghalfwaybetween thepubicsymphysisandumbilicus. It isnot tender.Cuscoespeculumshowsthat thecervixisnormal.Bimanualexaminationrevealstheanteverteduterustobeenlargedtothesizeofagrapefruit(about12weeks’sizeforapregnantuterus).
AWhataretheimportantpartsofthehistory?BWhichinvestigationsshouldbecommenced?CWhattreatmentwouldyousuggest?
ANSWERS
AImportantpartsofthehistoryhereareaclearhistoryofmenstrualdisturbanceandthetimescaleover which it occurred. There are three issues: the heavy embarrassing periods, the likelysymptomsofanaemiaandthedesiretogetpregnantsofarwithoutsuccess.Thehealthylifestyleandlackofprevioussurgeryareimportantincasesurgeryisrequired.Lackofdrugallergiesisveryimportanttoknowformedications.
BInvestigationsshouldinclude:
www.medicalebookpdf.com
Full blood count to exclude anaemia.Without a personal or family history of thyroid disease,biochemicalthyroidfunctionisnotindicated.Asthecycleisregularnootherhormonaltestsareindicatedatthisstage.
Transvaginalultrasoundscan.Thescanshowsthattheuterusisenlargedwithfibroids.Therearethree fibroids of which the largest is 6 cm × 8 cm at the fundus. There is a 2 cm × 2.5 cmsubmucosalfibroidintheuterinecavity.
SmearorswabsarenotrequiredastherearenosymptomsofdischargeorIMBandlastsmearisnormal.
CTreatmentsshouldbediscussedwiththepatientasdescribedinlaterchapters.Thispatientwillbenefitfromatranscervicalresectionofhersubmucosalfibroid,whichisprobablycausingbothherheavymenstrualbleedingandalsohersubfertility.
SBAQUESTION
1 A 32-year-old woman has come to the gynaecology clinic complaining of heavy menstrualbleeding.Onexaminationtheuterusisantevertedandbulky.Whatisthebestimagingmodalitytofurtherinvestigatehersymptoms?Choosethesinglebestanswer.AAbdominalultrasoundscan.BCT.CHysterosalpingogram(HSG).DMRI.ETVUSS.
ANSWER
ETVUSSprovidesexcellentresolution, is inexpensiveandallowsimmediatediagnosisofuterineandadnexalpathology.
www.medicalebookpdf.com
CHAPTER3Hormonalcontrolofthemenstrualcycleand
hormonaldisorders
HELENBICKERSTAFF
Introduction
Physiologyofthemenstrualcycle
Pubertyandsecondarysexualdevelopment
Disordersofsexualdevelopment
Disordersofmenstrualregularity
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Describethefeaturesofthenormalmenstrualcycleandtheovarianandendometrialchangesthataccompanythem.
•Describethenormalchangesofpubertyandthesecondarysexualdifferentiationthataccompaniesit.
•Understandtheclassificationandcausesofabnormalpubertyanddisordersofsexualdevelopment(DSD).
• Describe the causes and investigation of primary and secondary amenorrhoea andoligomenorrhoea.
www.medicalebookpdf.com

•Understandtheepidemiologyandeffectsofpolycysticovarysyndrome(PCOS),itsdiagnosisandmanagement.
•Describethecommoneffectsandmanagementofpremenstrualsyndrome(PMS).
•Describeprematurecessationofperiods.
IntroductionThischapterconsidershormonalcontrolofthemenstrualcycleandtheabnormalitiesthatmayaffectthephysiological initiation,regulationandcessationofthecycle.Abnormalitiesofuterinebleedingarethesubjectofthenextchapter.
PhysiologyofthemenstrualcycleTheexternalmanifestationofanormalmenstrualcycleisthepresenceofregularvaginalbleeding.Thisoccursasaresultofthesheddingoftheendometrialliningfollowingfailureoffertilizationoftheoocyteorfailureofimplantation.Thecycledependsonchangesoccurringafterpubertywithintheovariesandfluctuationinovarianhormonelevels,whicharethemselvescontrolledbythepituitaryandhypothalamuswithin thehypothalamo–pituitary–ovarianaxis (HPO). InsituationsofDSDorhormonalabnormalities,menstruationmaynotbegin.
ThehypothalamusThe hypothalamus in the forebrain secretes the peptide hormone gonadotrophin-releasing hormone(GnRH),whichinturncontrolspituitaryhormonesecretion.GnRHmustbereleasedinapulsatilefashiontostimulatepituitarysecretionofluteinizinghormone(LH)andfollicle-stimulatinghormone(FSH).
ThepituitaryglandGnRHstimulationofthebasophilcellsintheanteriorpituitaryglandcausessynthesisandreleaseofthegonadotrophichormonesFSHandLH.Thisprocess ismodulatedby theovarian sex steroidhormonesoestrogenandprogesterone.LowlevelsofoestrogenhaveaninhibitoryeffectonLHproduction(negativefeedback), whereas high levels of oestrogen will increase LH production (positive feedback). ThemechanismofactionforthepositivefeedbackeffectofoestrogeninvolvesanincreaseinGnRHreceptorconcentrations, while the mechanism of the negative feedback effect is uncertain. The high levels ofcirculatingoestrogeninthelatefollicularphaseoftheovaryactviathepositive-feedbackmechanismtogenerateaperiovulatoryLHsurgefromthepituitary.
Theclinicalrelevanceofthesemechanismsisseenintheuseofthecombinedoralcontraceptivepill,which artificially creates a constant serum oestrogen level in the negative-feedback range, inducing acorrespondinglylowlevelofgonadotrophinhormonerelease.
Unlikeoestrogen,lowlevelsofprogesteronehaveapositive-feedbackeffectonpituitaryLHandFSHsecretion(asseenimmediatelypriortoovulation)andcontributetotheLHandFSHsurge.Highlevelsof
www.medicalebookpdf.com
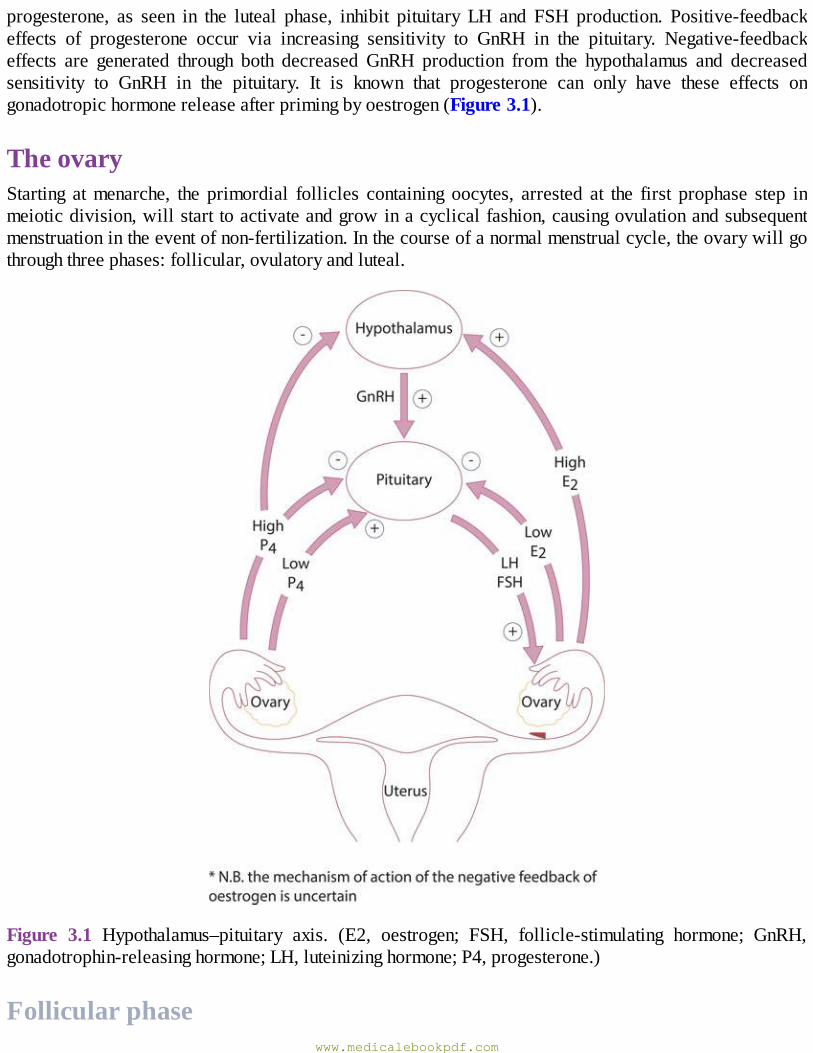
progesterone, as seen in the luteal phase, inhibit pituitary LH and FSH production. Positive-feedbackeffects of progesterone occur via increasing sensitivity to GnRH in the pituitary. Negative-feedbackeffects are generated through both decreased GnRH production from the hypothalamus and decreasedsensitivity to GnRH in the pituitary. It is known that progesterone can only have these effects ongonadotropichormonereleaseafterprimingbyoestrogen(Figure3.1).
TheovaryStarting atmenarche, the primordial follicles containing oocytes, arrested at the first prophase step inmeioticdivision,willstarttoactivateandgrowinacyclicalfashion,causingovulationandsubsequentmenstruationintheeventofnon-fertilization.Inthecourseofanormalmenstrualcycle,theovarywillgothroughthreephases:follicular,ovulatoryandluteal.
Figure 3.1 Hypothalamus–pituitary axis. (E2, oestrogen; FSH, follicle-stimulating hormone; GnRH,gonadotrophin-releasinghormone;LH,luteinizinghormone;P4,progesterone.)
Follicularphasewww.medicalebookpdf.com

Theinitialstagesoffolliculardevelopmentareindependentofhormonestimulation.However,folliculardevelopmentwillfailatthepreantralstage,andfollicularatresiawillensueifpituitaryhormonesLHandFSHareabsent.
FSH levels rise in the first days of themenstrual cycle,when oestrogen, progesterone and inhibinlevels are low. This stimulates a cohort of small antral follicles on the ovaries to grow.Within thefollicles,therearetwocelltypesthatareinvolvedintheprocessingofsteroids,includingoestrogenandprogesterone.These are the theca and the granulosa cells,which respond toLH andFSH stimulation,respectively.LHstimulatesproductionofandrogensfromcholesterolwithinthecacells.Theseandrogensareconvertedintooestrogensbytheprocessofaromatization ingranulosacells,under the influenceofFSH.
Asthefolliclesgrowandoestrogensecretionincreases,thereisnegativefeedbackonthepituitarytodecrease FSH secretion. This assists in the selection of one follicle to continue in its developmenttowardsovulation–thedominantfollicle.Intheovary,thefolliclethathasthemostefficientaromataseactivityandhighestconcentrationofFSH-inducedLHreceptorswillbethemostlikelytosurviveasFSHlevelsdrop,whilesmallerfollicleswillundergoatresia.
There are other autocrine and paracrine mediators playing a role in the follicular phase of themenstrualcycle.Theseincludeinhibinandactivin.Inhibinissecretedbythegranulosacellswithintheovaries. It participates in feedback to the pituitary to down-regulateFSH release, and also appears toenhanceongoingandrogensynthesis.Activinisstructurallysimilartoinhibin,buthasanoppositeaction.Itisproducedingranulosacellsandinthepituitary,andactstoincreaseFSHbindingonthefollicles.
Insulin-likegrowthfactors(IGF-I,IGF-II)actasparacrineregulators.Circulatinglevelsdonotchangeduringthemenstrualcycle,butfollicularfluidlevels increasetowardsovulation,withthehighest levelfoundinthedominantfollicle.
Kisspeptinsareproteins thathavemorerecentlybeenfoundtoplayarole inregulationof theHPOaxis,viathemediationofthemetabolichormoneleptin’seffectonthehypothalamus.Leptinisthoughttobekey in the relationshipbetweenenergyproduction,weightand reproductivehealth.Mutations in thekisspeptinreceptor,gpr-54,areassociatedwithdelayedorabsentpuberty,probablyduetoareductioninleptin-linkedtriggersforgonadotrophinrelease.
OvulationBytheendofthefollicularphase,whichlastsanaverageof14days,thedominantfolliclehasgrowntoapproximately20mmindiameter.As thefolliclematures,FSHinducesLHreceptorson thegranulosacells to compensate for lower FSH levels and prepare for the signal for ovulation. Production ofoestrogen increases until it reaches the necessary threshold to exert a positive feedback effort on thehypothalamusandpituitarytocausetheLHsurge.Thisoccursover24–36hours,duringwhichtimetheLH-inducedluteinizationofgranulosacellsinthedominantfolliclecausesprogesteronetobeproduced,addingfurthertothepositivefeedbackforLHsecretionandcausingasmallperiovulatoryriseinFSH.Androgens, synthesized in the thecacells, also risearound the timeofovulation, and this is thought tohaveanimportantroleinstimulatinglibido,ensuringthatsexualactivityislikelytooccuratthetimeofgreatestfertility.
TheLHsurgeisoneofthebestpredictorsofimminentovulation,andthisisthehormonedetectedinurine by most over-the-counter ‘ovulation predictor’ tests. The LH surge has another function instimulatingtheresumptionofmeiosisintheoocytejustpriortoitsrelease.Thephysicalovulationoftheoocyte occurs after breakdown of the follicularwall takes place under the influence of LH, FSH andproteolyticenzymes,suchasplasminogenactivatorsandprostaglandins(PGs).Studieshaveshownthat
www.medicalebookpdf.com
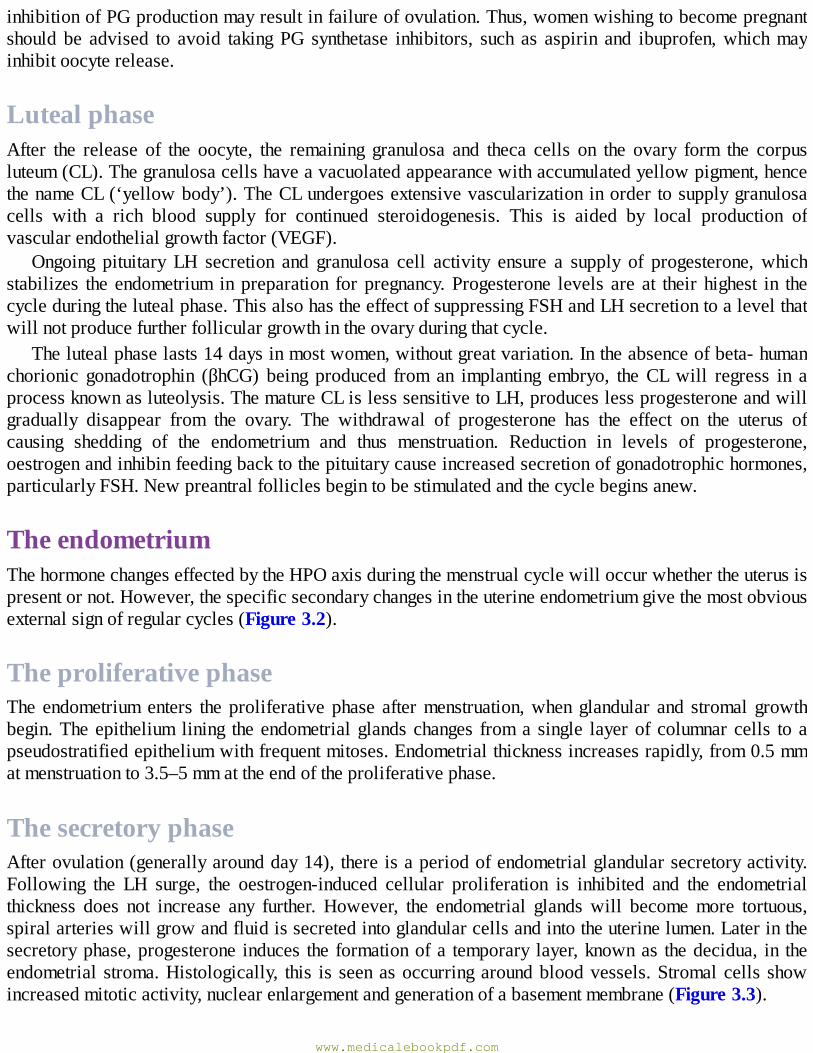
inhibitionofPGproductionmayresultinfailureofovulation.Thus,womenwishingtobecomepregnantshould be advised to avoid takingPG synthetase inhibitors, such as aspirin and ibuprofen,whichmayinhibitoocyterelease.
LutealphaseAfter the release of the oocyte, the remaining granulosa and theca cells on the ovary form the corpusluteum(CL).Thegranulosacellshaveavacuolatedappearancewithaccumulatedyellowpigment,hencethenameCL(‘yellowbody’).TheCLundergoesextensivevascularizationinordertosupplygranulosacells with a rich blood supply for continued steroidogenesis. This is aided by local production ofvascularendothelialgrowthfactor(VEGF).
Ongoing pituitary LH secretion and granulosa cell activity ensure a supply of progesterone,whichstabilizes the endometrium inpreparation forpregnancy.Progesterone levels are at their highest in thecycleduringthelutealphase.ThisalsohastheeffectofsuppressingFSHandLHsecretiontoalevelthatwillnotproducefurtherfolliculargrowthintheovaryduringthatcycle.
Thelutealphaselasts14daysinmostwomen,withoutgreatvariation.Intheabsenceofbeta-humanchorionic gonadotrophin (βhCG) being produced from an implanting embryo, theCLwill regress in aprocessknownasluteolysis.ThematureCLislesssensitivetoLH,produceslessprogesteroneandwillgradually disappear from the ovary. The withdrawal of progesterone has the effect on the uterus ofcausing shedding of the endometrium and thus menstruation. Reduction in levels of progesterone,oestrogenandinhibinfeedingbacktothepituitarycauseincreasedsecretionofgonadotrophichormones,particularlyFSH.Newpreantralfolliclesbegintobestimulatedandthecyclebeginsanew.
TheendometriumThehormonechangeseffectedbytheHPOaxisduringthemenstrualcyclewilloccurwhethertheuterusispresentornot.However,thespecificsecondarychangesintheuterineendometriumgivethemostobviousexternalsignofregularcycles(Figure3.2).
TheproliferativephaseThe endometriumenters theproliferativephase aftermenstruation,whenglandular and stromal growthbegin.Theepithelium lining theendometrialglandschanges froma single layerofcolumnarcells toapseudostratifiedepitheliumwithfrequentmitoses.Endometrialthicknessincreasesrapidly,from0.5mmatmenstruationto3.5–5mmattheendoftheproliferativephase.
ThesecretoryphaseAfterovulation(generallyaroundday14),thereisaperiodofendometrialglandularsecretoryactivity.Following the LH surge, the oestrogen-induced cellular proliferation is inhibited and the endometrialthickness does not increase any further. However, the endometrial glandswill becomemore tortuous,spiralarterieswillgrowandfluidissecretedintoglandularcellsandintotheuterinelumen.Laterinthesecretoryphase,progesterone induces the formationofa temporary layer,knownas thedecidua, in theendometrial stroma.Histologically, this is seenasoccurringaroundbloodvessels.Stromalcells showincreasedmitoticactivity,nuclearenlargementandgenerationofabasementmembrane(Figure3.3).
www.medicalebookpdf.com
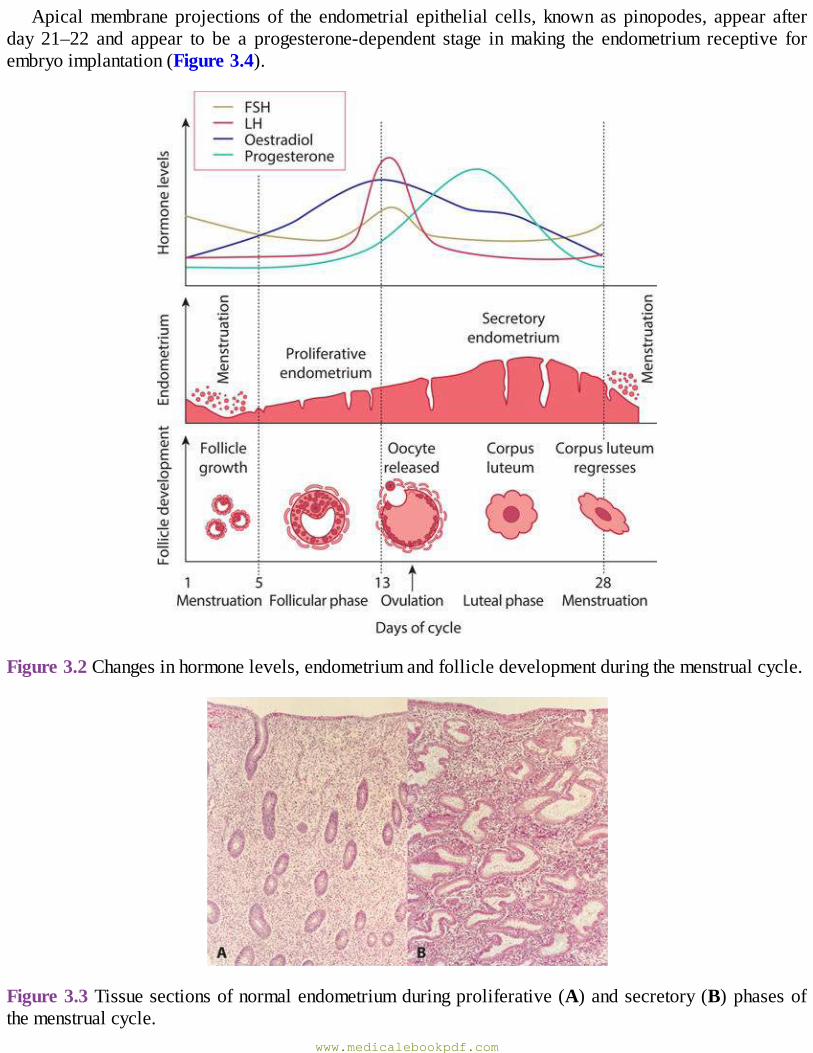
Apicalmembraneprojectionsof the endometrial epithelial cells, knownaspinopodes, appear afterday 21–22 and appear to be a progesterone-dependent stage inmaking the endometrium receptive forembryoimplantation(Figure3.4).
Figure3.2Changesinhormonelevels,endometriumandfollicledevelopmentduringthemenstrualcycle.
Figure3.3Tissuesectionsofnormalendometriumduringproliferative(A)andsecretory(B)phasesofthemenstrualcycle.
www.medicalebookpdf.com
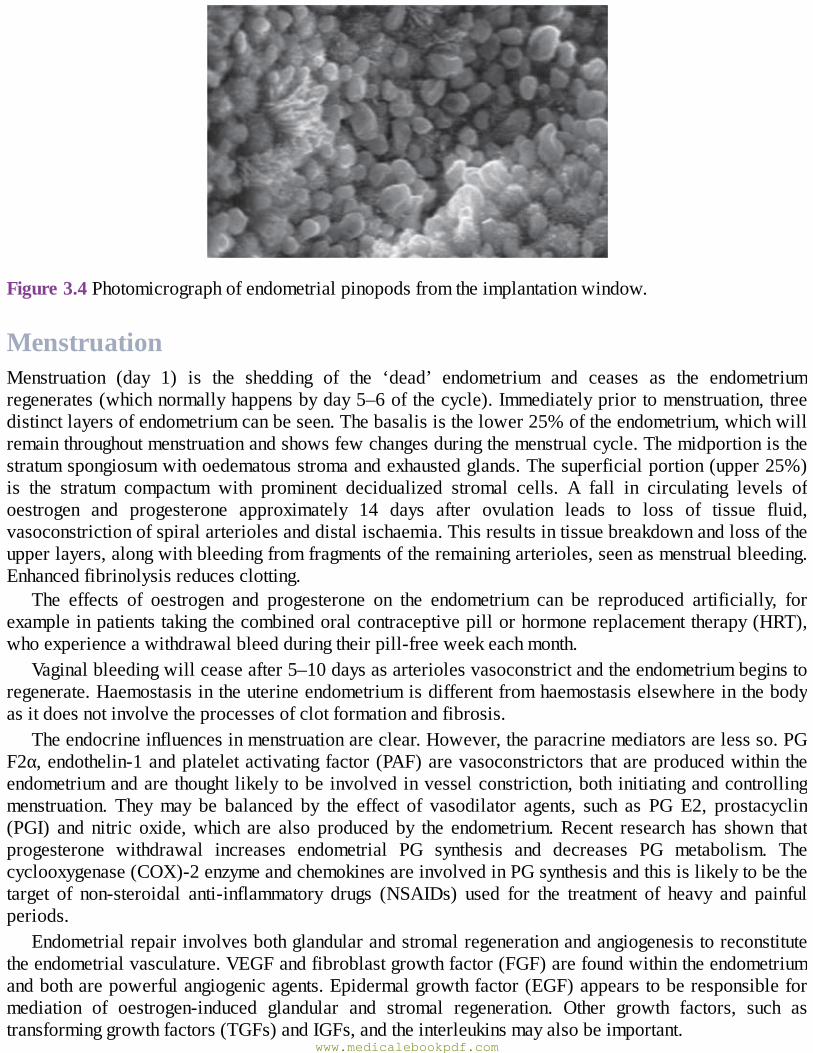
Figure3.4Photomicrographofendometrialpinopodsfromtheimplantationwindow.
MenstruationMenstruation (day 1) is the shedding of the ‘dead’ endometrium and ceases as the endometriumregenerates(whichnormallyhappensbyday5–6ofthecycle).Immediatelypriortomenstruation,threedistinctlayersofendometriumcanbeseen.Thebasalisisthelower25%oftheendometrium,whichwillremainthroughoutmenstruationandshowsfewchangesduringthemenstrualcycle.Themidportionisthestratumspongiosumwithoedematousstromaandexhaustedglands.Thesuperficialportion(upper25%)is the stratum compactum with prominent decidualized stromal cells. A fall in circulating levels ofoestrogen and progesterone approximately 14 days after ovulation leads to loss of tissue fluid,vasoconstrictionofspiralarteriolesanddistalischaemia.Thisresultsintissuebreakdownandlossoftheupperlayers,alongwithbleedingfromfragmentsoftheremainingarterioles,seenasmenstrualbleeding.Enhancedfibrinolysisreducesclotting.
The effects of oestrogen and progesterone on the endometrium can be reproduced artificially, forexampleinpatientstakingthecombinedoralcontraceptivepillorhormonereplacementtherapy(HRT),whoexperienceawithdrawalbleedduringtheirpill-freeweekeachmonth.
Vaginalbleedingwillceaseafter5–10daysasarteriolesvasoconstrictandtheendometriumbeginstoregenerate.Haemostasisintheuterineendometriumisdifferentfromhaemostasiselsewhereinthebodyasitdoesnotinvolvetheprocessesofclotformationandfibrosis.
Theendocrineinfluencesinmenstruationareclear.However,theparacrinemediatorsarelessso.PGF2α,endothelin-1andplateletactivatingfactor(PAF)arevasoconstrictors thatareproducedwithintheendometriumandarethought likelytobeinvolvedinvesselconstriction,bothinitiatingandcontrollingmenstruation. Theymay be balanced by the effect of vasodilator agents, such as PG E2, prostacyclin(PGI) and nitric oxide,which are also produced by the endometrium.Recent research has shown thatprogesterone withdrawal increases endometrial PG synthesis and decreases PG metabolism. Thecyclooxygenase(COX)-2enzymeandchemokinesareinvolvedinPGsynthesisandthisislikelytobethetarget of non-steroidal anti-inflammatory drugs (NSAIDs) used for the treatment of heavy and painfulperiods.
Endometrialrepairinvolvesbothglandularandstromalregenerationandangiogenesistoreconstitutetheendometrialvasculature.VEGFandfibroblastgrowthfactor(FGF)arefoundwithintheendometriumandbotharepowerfulangiogenicagents.Epidermalgrowthfactor(EGF)appearstoberesponsibleformediation of oestrogen-induced glandular and stromal regeneration. Other growth factors, such astransforminggrowthfactors(TGFs)andIGFs,andtheinterleukinsmayalsobeimportant.
www.medicalebookpdf.com
Pubertyandsecondarysexualdevelopment
NormalpubertyPubertyistheprocessofreproductiveandsexualdevelopmentandmaturationthatchangesachildintoanadult.Duringchildhood, theHPOaxis is suppressed and levels ofGnRH,FSHandLHare very low.Fromtheageof8–9yearsGnRHissecretedinpulsationsofincreasingamplitudeandfrequency.Theseare initially sleep-related, but as puberty progresses, these extend throughout the day. This stimulatessecretion of FSH and LH by the pituitary glands, which in turn triggers follicular growth andsteroidogenesisintheovary.Theoestrogenproducedbytheovarytheninitiatesthephysicalchangesofpuberty.Theexactmechanismdetermining theonsetofpuberty isstillunknown,but it is influencedbymany factors including race, heredity, bodyweight and exercise.Leptinplays a permissive role in theonsetofpuberty.
Thephysicalchangesoccurringinpubertyarebreastdevelopment(thelarche),pubicandaxillaryhairgrowth(adrenarche),growthspurtandonsetofmenstruation(menarche).
Thefirstphysicalsignsofpubertyarebreastbuddingandthisoccurs2–3yearsbeforemenarche.Theappearanceofpubichairisdependentonthesecretionofadrenalandrogensandisusuallyafterthelarche.In addition to increasing levels of adrenal and gonadal hormones, growth hormone secretion alsoincreases, leading toapubertalgrowthspurt.Themeanageofmenarche is12.8yearsand itmay takeover 3 years before the menstrual cycle establishes a regular pattern. Initial cycles are usuallyanovulatoryandcanbeunpredictableandirregular.Theabsenceofmenstruationiscalledamenorrhoeaandmaybeprimaryorsecondary(seeBox3.2,page41).PubertaldevelopmentwasdescribedbyTannerandthestagesofbreastandpubichairdevelopmentareoftenreferredtoasTannerstages1–5(Figure3.5).
PrecociouspubertyThisisdefinedastheonsetofpubertybeforetheageof8inagirlor9inaboy.Itisclassifiedaseithercentral or peripheral. Central precocious puberty is gonadotrophin dependent. The aetiology is oftenunknown,althoughupto25%areduetocentralnervoussystem(CNS)malformationsorbraintumours.Peripheralprecociouspuberty,which isgonadotrophin independent, isalwayspathologicalandcanbecausedbyoestrogensecretion,suchasexogenousingestionorahormone-producingtumour.
DelayedpubertyWhentherearenosignsofsecondarysexualcharacteristicsbytheageof14yearsthisistermeddelayedpuberty. It is due to either a central defect (hypogonadotrophic hypogonadism) or a failure of gonadalfunction(hypergonadotrophichypogonadism),whicharedescribedbelow.
www.medicalebookpdf.com
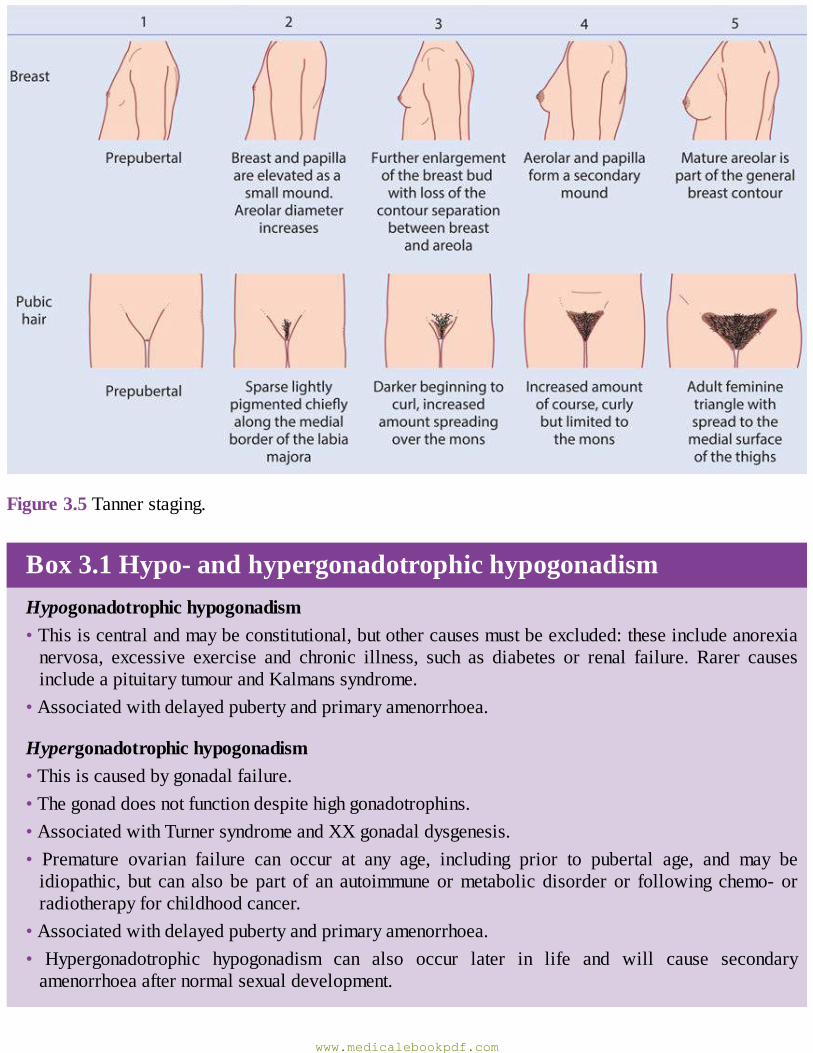
Figure3.5Tannerstaging.
Box3.1Hypo-andhypergonadotrophichypogonadismHypogonadotrophichypogonadism•Thisiscentralandmaybeconstitutional,butothercausesmustbeexcluded:theseincludeanorexianervosa, excessive exercise and chronic illness, such as diabetes or renal failure. Rarer causesincludeapituitarytumourandKalmanssyndrome.
•Associatedwithdelayedpubertyandprimaryamenorrhoea.
Hypergonadotrophichypogonadism•Thisiscausedbygonadalfailure.•Thegonaddoesnotfunctiondespitehighgonadotrophins.•AssociatedwithTurnersyndromeandXXgonadaldysgenesis.• Premature ovarian failure can occur at any age, including prior to pubertal age, and may beidiopathic, but can also be part of an autoimmuneormetabolic disorder or following chemo- orradiotherapyforchildhoodcancer.
•Associatedwithdelayedpubertyandprimaryamenorrhoea.• Hypergonadotrophic hypogonadism can also occur later in life and will cause secondaryamenorrhoeaafternormalsexualdevelopment.
www.medicalebookpdf.com
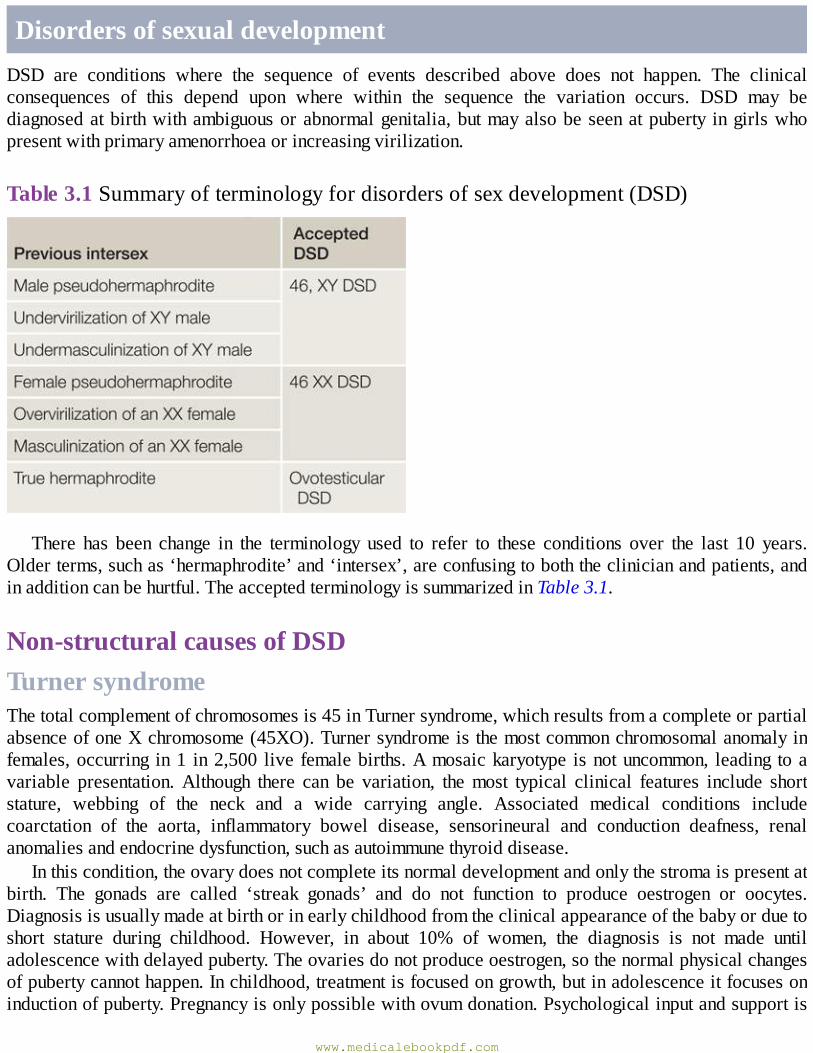
DisordersofsexualdevelopmentDSD are conditions where the sequence of events described above does not happen. The clinicalconsequences of this depend upon where within the sequence the variation occurs. DSD may bediagnosedatbirthwithambiguousorabnormalgenitalia,butmayalsobeseenatpuberty ingirlswhopresentwithprimaryamenorrhoeaorincreasingvirilization.
Table3.1Summaryofterminologyfordisordersofsexdevelopment(DSD)
There has been change in the terminology used to refer to these conditions over the last 10 years.Olderterms,suchas‘hermaphrodite’and‘intersex’,areconfusingtoboththeclinicianandpatients,andinadditioncanbehurtful.TheacceptedterminologyissummarizedinTable3.1.
Non-structuralcausesofDSDTurnersyndromeThetotalcomplementofchromosomesis45inTurnersyndrome,whichresultsfromacompleteorpartialabsenceofoneXchromosome(45XO).Turnersyndromeisthemostcommonchromosomalanomalyinfemales,occurring in1 in2,500 live femalebirths.Amosaickaryotype isnotuncommon, leading toavariable presentation.Although there can be variation, themost typical clinical features include shortstature, webbing of the neck and a wide carrying angle. Associated medical conditions includecoarctation of the aorta, inflammatory bowel disease, sensorineural and conduction deafness, renalanomaliesandendocrinedysfunction,suchasautoimmunethyroiddisease.
Inthiscondition,theovarydoesnotcompleteitsnormaldevelopmentandonlythestromaispresentatbirth. The gonads are called ‘streak gonads’ and do not function to produce oestrogen or oocytes.Diagnosisisusuallymadeatbirthorinearlychildhoodfromtheclinicalappearanceofthebabyorduetoshort stature during childhood. However, in about 10% of women, the diagnosis is not made untiladolescencewithdelayedpuberty.Theovariesdonotproduceoestrogen,sothenormalphysicalchangesofpubertycannothappen.Inchildhood,treatmentisfocusedongrowth,butinadolescenceitfocusesoninductionofpuberty.Pregnancyisonlypossiblewithovumdonation.Psychologicalinputandsupportis
www.medicalebookpdf.com
important.Ingirlswithmosaicismtheclinicalpicturecanvaryandnormalpubertyandmenstruationcanoccur,withearlycessationofperiods.
46XYgonadaldysgenesisInthissituation,thegonadsdonotdevelopintoatestis,despitethepresenceofanXYkaryotype.Inabout15%ofcases,thisisduetoamutationintheSRYgeneontheYchromosome,butinmostcasesthecauseisunknown.Incompletegonadaldysgenesis(Swyersyndrome),thegonadremainsasastreakgonadanddoes not produce any hormones. In the absence of anti-Müllerian hormone (AMH), the Müllerianstructuresdonot regress and theuterus, vagina andFallopian tubesdevelopnormally.The absenceoftestosteronemeans the fetus does not virilize.The baby is phenotypically female, although has anXYchromosome.Thegonadsdonotfunctionandpresentationisusuallyatadolescencewithdelayedpuberty.Thedysgeneticgonadhasahighmalignancyriskandshouldberemovedwhenthediagnosisismade.Thisis usually performed laparoscopically. Pubertymust be induced with oestrogen and pregnancies havebeen reported with a donor oocyte. Full disclosure of the diagnosis including the XY karytoype isessential,althoughthiscanbedevastatingandspecializedpsychologicalinputiscrucial.
Mixedgonadal dysgenesis is amore complex condition.The karyotypemaybe 46XX, butXX/XYmosaicismispresentinupto20%.Inthissituation,bothfunctioningovarianandtesticulartissuecanbepresentandifso,thisconditionisknownasovotesticularDSD.Theanatomicalfindingsvarydependingonthefunctionofthegonads.Forexample,ifthetestisisfunctional,thenthebabywillvirilizeandhaveambiguous or normal male genitalia. The Müllerian structures are usually absent on the side of thefunctioningtestis,butaunicornuateuterusmaybepresentifthereisanovaryorstreakgonad.
46XYDSDThemost common cause of 46XYDSD, complete androgen insensitivity syndrome (CAIS), occurs inindividuals where virilization of the external genitalia does not occur, due to a partial or completeinabilityoftheandrogenreceptortorespondtoandrogenstimulation.InthefetuswithCAIS,testesformnormallyduetotheactionoftheSRYgene.Attheappropriatetime,thesetestessecreteAMH,leadingtothe regression of theMüllerian ducts.Hence,CAISwomen do not have a uterus.Testosterone is alsoproducedattheappropriatetime;however,duetotheinabilityoftheandrogenreceptortorespond,theexternalgenitaliadonotvirilizeandinsteadundergofemaledevelopment.Thebabyisbornwithnormalfemaleexternalgenitalia, anabsentuterusand testes that are found somewhere in their lineofdescentthroughtheabdomenfromthepelvistotheinguinalcanal.Presentationisusuallyatpubertywithprimaryamenorrhoea,althoughifthetestesareintheinguinalcanaltheycancauseaherniainayoungergirl.Oncethediagnosisismade,initialmanagementispsychologicalwithfulldisclosureoftheXYkaryotypeandtheinformationthatthepatientwillbeinfertile.
Gonadectomyisrecommendedbecauseofthesmalllong-termriskoftesticularmalignancy,althoughthiscanbedeferreduntilafterpuberty.Oncethegonadsareremoved,long-termHRTwillberequired.Thevaginaisusuallyshortenedandtreatmentwillberequiredtocreateavaginasuitableforpenetrativeintercourse. Vaginal dilation is the most effective method of improving vaginal length and entails theinsertion of vaginal moulds of gradually increasing length and width for at least 30 minutes a day.Surgical vaginal reconstruction operations are reserved for thosewomen that have not responded to adilationtreatmentprogramme.
In cases of partial androgen insensitivity, the androgen receptor can respond to some extent withlimitedvirilization.Thechildisusuallydiagnosedatbirthwithambiguousgenitalia.
www.medicalebookpdf.com
5-Alpha-reductasedeficiencyInthiscondition,thefetushasanXYkarytypeandnormalfunctioningtestesthatproducebothtestosteroneandAMH.However, thefetus isunable toconvert testosteronetodihydrotestosteronein theperipheraltissuesandsocannotvirilizenormally.Presentationisusuallywithambiguousgenitaliaatbirth,butcanalsobewithincreasingvirilizationatpubertyofafemalechild,duetothelargeincrease incirculatingtestosteronewiththeonsetofpuberty.IntheWesternworld,thechildisusuallyassignedtoafemalesexofrearing,buttherehavebeendescriptionsofafewcommunitieswheretransitionfromafemaletomalegenderatpubertyisaccepted.
46XXDSDThemostcommoncauseof46XXDSD,congenitaladrenalhyperplasia(CAH),leadstovirilizationofafemale fetus. It is due to an enzymedeficiency in the corticosteroidproductionpathway in the adrenalgland, with over 90% being a deficiency in 21-hydroxylase, which converts progesterone todeoxycorticosterone and 17-hydroxyprogesterone (17-OHP) to deoxycortisol. The reduced levels ofcortisolbeingproduceddrivethenegative-feedbackloop,resultinginhyperplasiaoftheadrenalglands.This leads to an excess of androgen precursors and then to elevated testosterone production. Raisedandrogenlevelsinafemalefetuswillleadtovirilizationoftheexternalgenitalia.Theclitorisisenlargedandthelabiaarefusedandscrotal inappearance.Theuppervaginajoins theurethraandopensasonecommonchannelonto theperineum. In addition, two-thirdsof childrenwith21-hydroxylaseCAHwillhavea‘salt-losing’variety,whichalsoaffectstheabilitytoproducealdosterone.Thisrepresentsalife-threateningsituation, and thosechildrenwhoare salt-losingoftenbecomedangerouslyunwellwithinafew days of birth. Affected individuals require life-long steroid replacement, such as hydrocortisone,alongwithfludrocortisoneforsaltlosers.Oncetheinfantiswellandstabilizedontheirsteroidregime,surgical treatment of thegenitalia is considered.Traditionally, all female infantswithCAHunderwentfeminizing genital surgerywithin the first year of life. Thismanagement is now controversial as adultpatientswithCAHareverydissatisfiedwiththeoutcomeoftheirsurgeryandarguethatsurgeryshouldhavebeendeferreduntil theywereoldenough tohaveachoice.Surgerycertainly leaves scarringandmayreducesexualsensitivity,but thealternativeof leaving thegenitaliavirilized throughoutchildhoodcanbedifficultforparentstoconsider.Atpresent,casesaremanagedindividuallybyamultidisciplinaryteam(MDT)involvingsurgeons,endocrinologistsandpsychologists.
Disordersofmenstrualregularity
AmenorrhoeaandoligomenorrhoeaAmenorrhoea is defined as the absence of menstruation for more than 6 months in the absence ofpregnancyinawomanoffertileage,andoligomenorrhoeaisdefinedasirregularperiodsatintervalsofmorethan35days,withonly4–9periodsayear.Thecausesmaybehypothalamic,pituitary,ovarianorendometrial,andbothamenorrhoeaandoligomenorrhoeamaybeprimaryorsecondary.
Box3.2Amenorrhoea•Primaryamenorrhoeaiswhengirlsfailtomenstruateby16yearsofage.
www.medicalebookpdf.com
•Secondaryamenorrhoea isabsenceofmenstruation formore than6months inanormal femaleofreproductiveagethatisnotduetopregnancy,lactationorthemenopause.
HypothalamicdisordersHypothalamicdisorderswillgiverisetohypogonadotrophichypogonadism,withthefollowingcauses:
•Excessiveexercise,weightlossandstress.•Hypothalamiclesions(craniopharyngioma,glioma),whichcancompresshypothalamictissueorblockdopamine.
•Headinjuries.• Kallman’s syndrome (X-linked recessive condition resulting in deficiency in GnRH causingunderdevelopedgenitalia).
• Systemic disorders including sarcoidosis, tuberculosis resulting in an infiltrative process in thehypothalamo-hypophysealregion.
•Drugs:progestogens,HRTordopamineantagonists.
PituitarydisordersPituitarydisorderswillalsogiverisetohypogonadotrophichypogonadism,withthefollowingcauses:
•Adenomas,ofwhichprolactinomaismostcommon.• Pituitary necrosis (e.g. Sheehan’s syndrome, due to prolonged hypotension followingmajor obstetrichaemorrhage).
•Iatrogenicdamage(surgeryorradiotherapy).•Congenitalfailureofpituitarydevelopment.
OvariandisordersAnovulationisoftenduetopolycysticovarysyndrome(PCOS),describedbelow.Ovarianfailureisthecauseofhypergonadotrophichypogonadism.Prematureovarianfailure(POF)isdefinedascessationofperiods before 40 years of age and is described in Chapter 8, The menopause and postreproductivehealth.
EndometrialdisordersPrimaryamenorrhoeamayresultfromMülleriandefectsinthegenitaltractincludinganabsentuterus,oroutflowtractabnormalities,leadingtoahaematocolpos.Secondaryamenorrhoeamayresultfromscarringof the endometrium called Asherman syndrome and is described further in Chapter 4, Disorders ofmenstrualbleeding.
Findingsfromthehistoryshouldguidetheexamination(Table3.2).Ageneralinspectionofthepatientshouldbecarriedout toassessbodymass index (BMI), secondarysexualcharacteristics (hairgrowth,breast development using Tanner scores) and signs of endocrine abnormalities (hirsutism, acne,abdominalstriae,moonface,skinchanges).Ifthehistoryissuggestiveofapituitarylesion,anassessment
www.medicalebookpdf.com
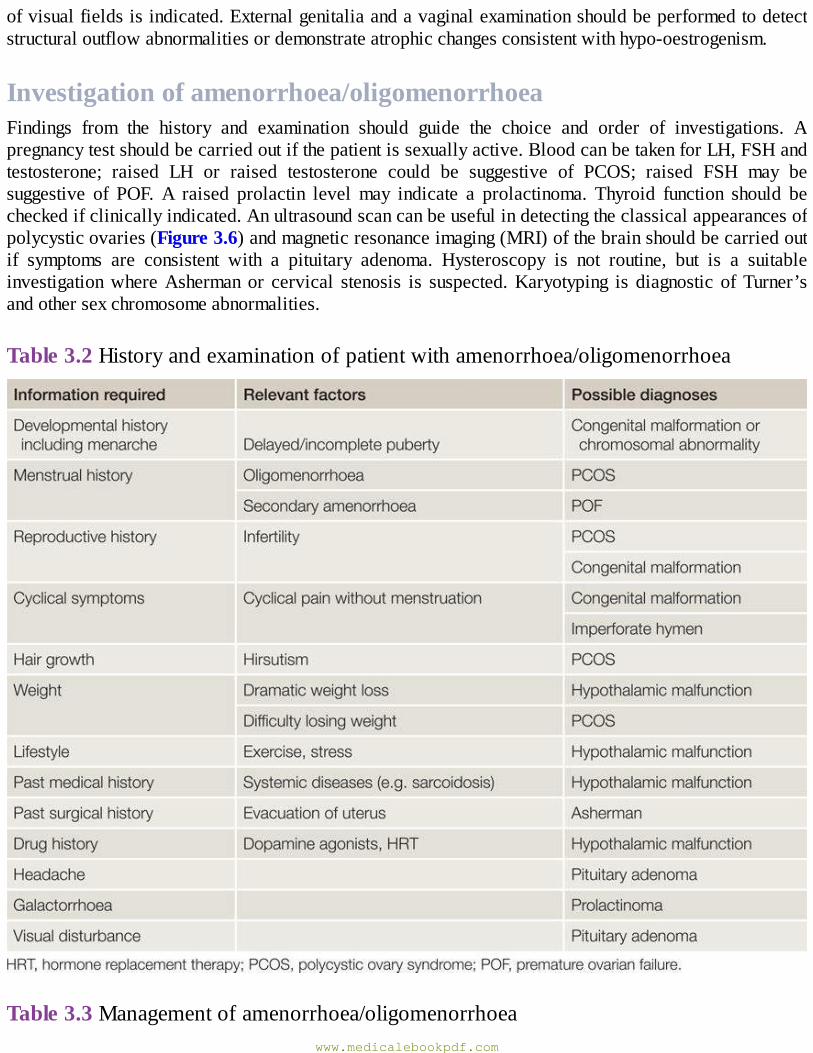
ofvisualfieldsisindicated.Externalgenitaliaandavaginalexaminationshouldbeperformedtodetectstructuraloutflowabnormalitiesordemonstrateatrophicchangesconsistentwithhypo-oestrogenism.
Investigationofamenorrhoea/oligomenorrhoeaFindings from the history and examination should guide the choice and order of investigations. Apregnancytestshouldbecarriedoutifthepatientissexuallyactive.BloodcanbetakenforLH,FSHandtestosterone; raised LH or raised testosterone could be suggestive of PCOS; raised FSH may besuggestive of POF. A raised prolactin level may indicate a prolactinoma. Thyroid function should becheckedifclinicallyindicated.Anultrasoundscancanbeusefulindetectingtheclassicalappearancesofpolycysticovaries(Figure3.6)andmagneticresonanceimaging(MRI)ofthebrainshouldbecarriedoutif symptoms are consistent with a pituitary adenoma. Hysteroscopy is not routine, but is a suitableinvestigationwhereAshermanor cervical stenosis is suspected.Karyotyping is diagnostic ofTurner’sandothersexchromosomeabnormalities.
Table3.2Historyandexaminationofpatientwithamenorrhoea/oligomenorrhoea
Table3.3Managementofamenorrhoea/oligomenorrhoeawww.medicalebookpdf.com
Themanagementofamenorrhoea/oligomenorrhoeaisoutlinedinTable3.3.Morespecificdescriptionsofmanagementaredetailedinthechaptersindicated.
PolycysticovarysyndromePCOS is a syndromeof ovarian dysfunction alongwith the cardinal features of hyperandrogenismandpolycysticovarymorphology(Figure3.6).Theprevalenceofpolycystic ovaries seenonultrasound isaround25%ofallwomenbut isnotalwaysassociatedwith the full syndrome.Clinicalmanifestationsincludemenstrualirregularities,signsofandrogenexcess(e.g.hirsutismandacne)andobesity.Elevatedserum LH levels, biochemical evidence of hyperandrogenism and raised insulin resistance are alsocommonfeatures.
PCOS is associatedwith an increased risk of type 2 diabetes and cardiovascular events. It affectsaround5–10%ofwomenofreproductiveage.TheaetiologyofPCOSisnotcompletelyclear,althoughthefrequentfamilialtrendpointstoageneticcause.
Clinicalfeatures•Oligomenorrhoea/amenorrhoeainupto75%ofpatients,predominantlyrelatedtochronicanovulation.•Hirsutism.•Subfertilityinupto75%ofwomen.
eResource3.1www.medicalebookpdf.com
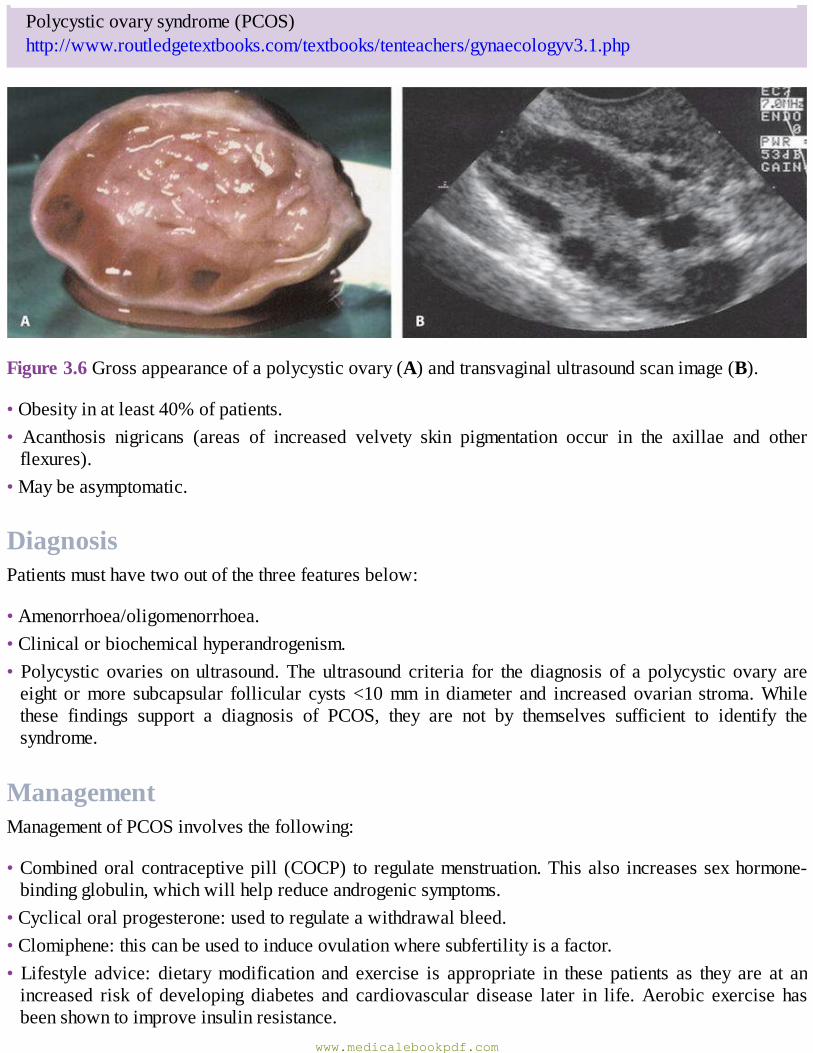
Polycysticovarysyndrome(PCOS)http://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv3.1.php
Figure3.6Grossappearanceofapolycysticovary(A)andtransvaginalultrasoundscanimage(B).
•Obesityinatleast40%ofpatients.• Acanthosis nigricans (areas of increased velvety skin pigmentation occur in the axillae and otherflexures).
•Maybeasymptomatic.
DiagnosisPatientsmusthavetwooutofthethreefeaturesbelow:
•Amenorrhoea/oligomenorrhoea.•Clinicalorbiochemicalhyperandrogenism.• Polycystic ovaries on ultrasound.The ultrasound criteria for the diagnosis of a polycystic ovary areeight ormore subcapsular follicular cysts <10mm in diameter and increased ovarian stroma.Whilethese findings support a diagnosis of PCOS, they are not by themselves sufficient to identify thesyndrome.
ManagementManagementofPCOSinvolvesthefollowing:
•Combinedoralcontraceptivepill (COCP) toregulatemenstruation.Thisalso increasessexhormone-bindingglobulin,whichwillhelpreduceandrogenicsymptoms.
•Cyclicaloralprogesterone:usedtoregulateawithdrawalbleed.•Clomiphene:thiscanbeusedtoinduceovulationwheresubfertilityisafactor.• Lifestyle advice: dietarymodification and exercise is appropriate in these patients as they are at anincreased risk of developing diabetes and cardiovascular disease later in life.Aerobic exercise hasbeenshowntoimproveinsulinresistance.
www.medicalebookpdf.com
•Weightreduction.• Ovarian drilling, a laparoscopic procedure to destroy some of the ovarian stroma that may promptovulatorycycles.
•Treatmentofhirsutism/androgenicsymptoms:•eflornithinecream(Vaniqua™)appliedtopically;•cyproteroneacetate (anantiandrogencontained in theDianette™contraceptivepill, sometimesusedalone);
• metformin: this is beneficial in a subset of patients with PCOS, those with hyperinsulinaemia andcardiovascular risk factors. It improves parameters of insulin resistance, hyperandrogenaemia,anovulation and acne in PCOS, and may aid weight loss. It is less effective than clomiphene forovulationinductionanddoesnotimprovepregnancyoutcome;
•GnRHanalogueswith low-doseHRT: this regimeshouldbereservedforwomen intolerantofothertherapies;
•surgicaltreatments(e.g.laserorelectrolysis).
PremenstrualsyndromePremenstrual syndrome (PMS) is the occurrence of cyclical somatic, psychological and emotionalsymptoms that occur in the luteal (premenstrual) phase of themenstrual cycle and resolve by the timemenstruationceases.Premenstrualsymptomsoccurinalmostallwomenofreproductiveage.In3–60%symptomsaresevere,causingdisruptiontoeverydaylife,inparticularinterpersonalrelationships.
AetiologyThepreciseaetiologyofPMSisunknown,butcyclicalovarianactivityandtheeffectsofoestradiolandprogesteroneoncertainneurotransmitters,includingserotonin,appeartoplayarole.
HistoryandexaminationThepatientislikelytocomplainofsomeorallofthefollowing:bloatingcyclicalweightgain,mastalgia,abdominal cramps, fatigue, headache, depression, irritability. The cyclical nature of PMS is thecornerstoneofthediagnosis.Asymptomchart,tobefilledinbythepatientprospectively,mayhelp.
ManagementThemanagementofPMSisdepictedinFigure3.7.
eResource3.2
PMSpatientguidancehttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv3.2.php
www.medicalebookpdf.com
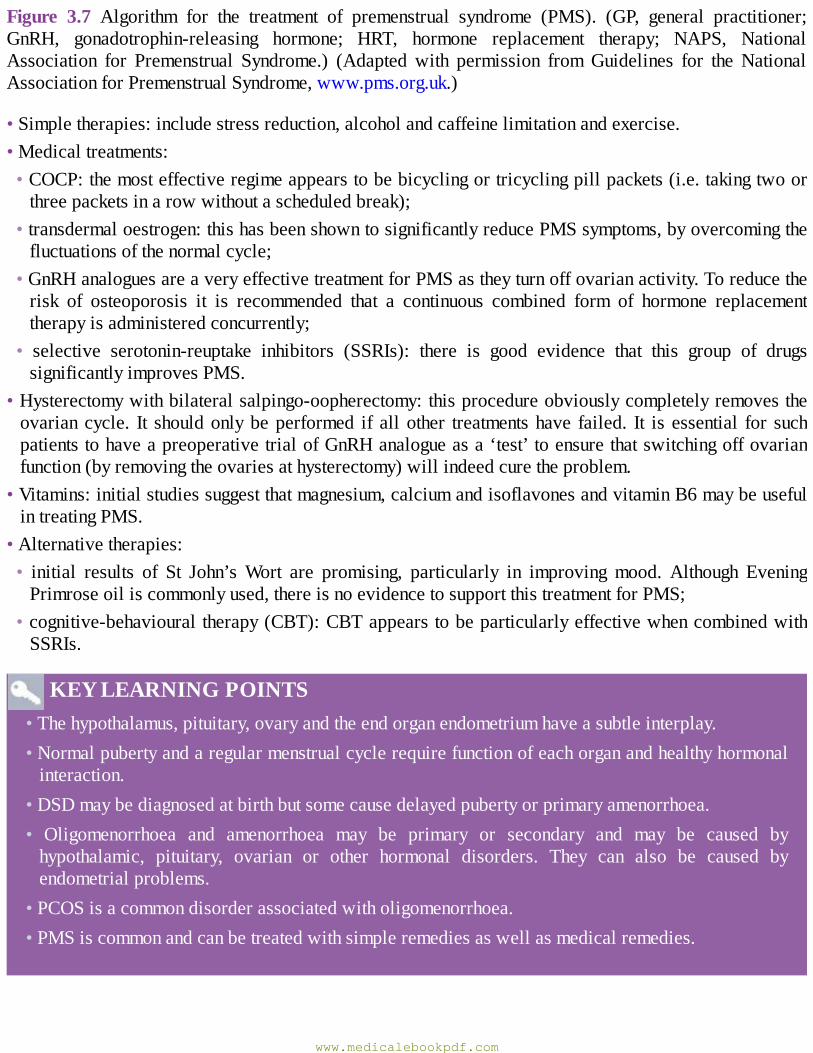
Figure 3.7 Algorithm for the treatment of premenstrual syndrome (PMS). (GP, general practitioner;GnRH, gonadotrophin-releasing hormone; HRT, hormone replacement therapy; NAPS, NationalAssociation for Premenstrual Syndrome.) (Adapted with permission fromGuidelines for the NationalAssociationforPremenstrualSyndrome,www.pms.org.uk.)
•Simpletherapies:includestressreduction,alcoholandcaffeinelimitationandexercise.•Medicaltreatments:•COCP:themosteffectiveregimeappearstobebicyclingortricyclingpillpackets(i.e.takingtwoorthreepacketsinarowwithoutascheduledbreak);
•transdermaloestrogen:thishasbeenshowntosignificantlyreducePMSsymptoms,byovercomingthefluctuationsofthenormalcycle;
•GnRHanaloguesareaveryeffectivetreatmentforPMSastheyturnoffovarianactivity.Toreducetherisk of osteoporosis it is recommended that a continuous combined form of hormone replacementtherapyisadministeredconcurrently;
• selective serotonin-reuptake inhibitors (SSRIs): there is good evidence that this group of drugssignificantlyimprovesPMS.
•Hysterectomywithbilateralsalpingo-oopherectomy:thisprocedureobviouslycompletelyremovestheovariancycle. It shouldonlybeperformed if allother treatmentshave failed. It is essential for suchpatientstohaveapreoperativetrialofGnRHanalogueasa‘test’toensurethatswitchingoffovarianfunction(byremovingtheovariesathysterectomy)willindeedcuretheproblem.
•Vitamins:initialstudiessuggestthatmagnesium,calciumandisoflavonesandvitaminB6maybeusefulintreatingPMS.
•Alternativetherapies:• initial results of St John’sWort are promising, particularly in improving mood. Although EveningPrimroseoiliscommonlyused,thereisnoevidencetosupportthistreatmentforPMS;
•cognitive-behaviouraltherapy(CBT):CBTappearstobeparticularlyeffectivewhencombinedwithSSRIs.
KEYLEARNINGPOINTS•Thehypothalamus,pituitary,ovaryandtheendorganendometriumhaveasubtleinterplay.•Normalpubertyandaregularmenstrualcyclerequirefunctionofeachorganandhealthyhormonalinteraction.
•DSDmaybediagnosedatbirthbutsomecausedelayedpubertyorprimaryamenorrhoea.• Oligomenorrhoea and amenorrhoea may be primary or secondary and may be caused byhypothalamic, pituitary, ovarian or other hormonal disorders. They can also be caused byendometrialproblems.
•PCOSisacommondisorderassociatedwitholigomenorrhoea.•PMSiscommonandcanbetreatedwithsimpleremediesaswellasmedicalremedies.
www.medicalebookpdf.com
FurtherreadingBalen AH, Conway GS, Homburg R, Legro RS (2005). Polycystic Ovary Syndrome: A Guide toClinicalManagement.London,NewYork:Taylor&Francis.
Hughes IA,HoukC,AhmedSF,LeePA;LWPESConsensusGroup;ESPEConsensusGroup (2006).Consensusstatementonmanagementofintersexdisorders.ArchDisChild91(7):554–63.
National Association for Premenstrual Syndrome.http://www.pms.org.uk/assets/files/guidelinesfinal60210.pdf.
Selfassessment
CASEHISTORY
A22-year-oldwomanapproachedherGPcomplainingof irregularperiodsandexcess facialhairandspots.Shehadincreasedherweightby5kginthelastyear.Examinationwasnotremarkable,butherBMIwasraisedat30.
AWhatadditionalfeaturesofthehistorywouldyouseek?BOutlinetheinvestigationsandmanagement.
ANSWERS
A In the history it would be important to know the number of periods in the last year, asoligomenorrhoeaisariskfactorforendometrialhypertrophy.Althoughsheisonly22,itwouldbeimportanttoknowherplansforfuturechildren,asmanywomenwillhavereadaboutpolycysticovariesontheinternetandbeconcernedabouttheinfertilityrisk.Askwhethershehasapartneratthemoment andwhether she is sexually active.Askabout contraindications to thepill, as evenwithoutinvestigationthepossibilityofPCOSshouldhaveoccurredtoyoubecauseitisthemostcommon cause of anvolution and strongly associated with obesity. You find that she has nocontraindicationstothepill,hasapartnerandissexuallyactiveusingcondomsbutdoesnotwantchildrenyet.
BYourecommendatransvaginalultrasoundscan(TVUSS).This reveals that theovaries are enlargedwithmore than10prenatal follicleson each side
with a dense stroma. The combination of this and the clinical signs are sufficient to make adiagnosisofPCOS,andyoudonotneedtoperformfurtherbloodtestsatthispoint.
The first-linemedical treatmentwould be the oral contraceptive pill.Thiswill regulate herbleeds. It will also help reduce facial hair growth by elevating sex hormone-binding globulin(SHBG),hencereducingfreetestosterone.However,themostimportanttreatmentistoreduceherweight and increase her aerobic exercise, as a reduction in weight will promote spontaneousovulation.
www.medicalebookpdf.com
SBAQUESTIONS
1Menstruationisthesheddingofthedeadendometrium.Whichofthefollowingfactsarecorrect?Choosethesinglebestanswer.ADuringmenstruationthestratumbasalisisshed.BDuringmenstruationthestratumcompactumisshed.CDuringmenstruationfibrinolysisisenhanced.DEndometrialregenerationbeginsafterovulation.EVasodilationofthespiralarteriolesprecedesmenstruation.
ANSWER
BPriortomenstruationvasoconstrictionofthespiralarteriolesoccurscausingischaemia.Thestratumbasalisremainswhilethecompactumisshed.Fibrinolysisisenhancedtoprevent
clotting;haemostasisisnotthesameaselsewhereisthebody.Endometrialregenerationbeginsasthebleedends.
2 With regards polycystic ovary syndrome (PCOS), which of the following statements is true?Choosethesinglebestanswer.APCOSisanunusualcauseofanovulation.BUltrasonicevidenceofpolycysticovariesispresentin50%ofallwomen.CPCOSisassociatedwithobesityin10%ofwomen.DPCOSisassociatedwithacanthosisnigricans.EThediagnosisofPCOScanonlybemadewithbiochemicalevidenceofhyperandrogenism.
ANSWER
DPCOSisthemostcommoncauseofanovolution.Basedonultrasoundalone,PCOS-typeovariesareseenin25%ofwomen,someofwhomarenotsymptomatic.Morethan40%ofwomenwithPCOSareoverweight,andPCOSisassociatedwithacanthosisnigricansmediatedbyhighinsulin.Women must have two of three diagnostic criteria: ultrasonic evidence of PCOS, clinical orbiochemicalhyperandrogenism,chronicanovulation.
www.medicalebookpdf.com
CHAPTER4Disordersofmenstrualbleeding
HELENBICKERSTAFF
Introduction
Heavymenstrualbleeding
Dysmenorrhoea
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthesymptomsandaetiologyofabnormaluterinebleeding(AUB).
•DescribetheterminologyofAUB.
•Understandthesymptoms,investigationandmanagementofheavymenstrualbleeding(HMB).
•AppreciatetheimpactofHMBonabilitytofunction.
•Understandthecausesandinvestigationofdysmenorrhoea.
•Understandtheactionofmedicationusedformenorrhagiaanddysmenorrhoea.
Introductionwww.medicalebookpdf.com
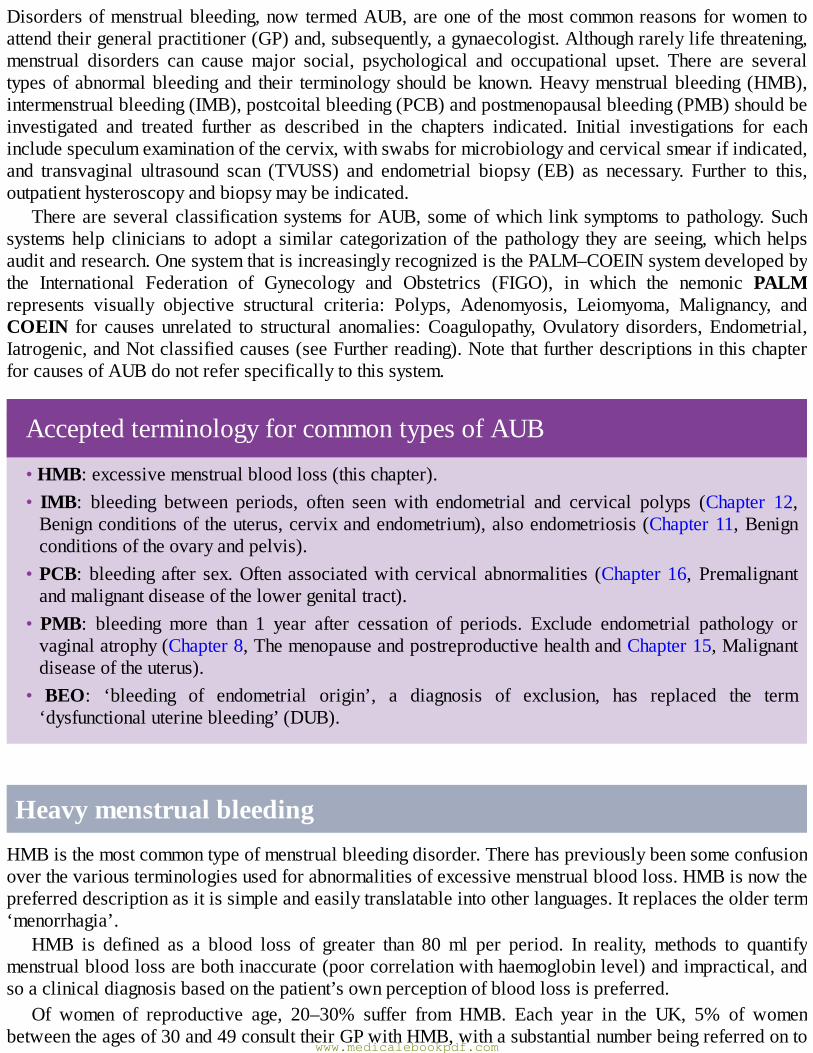
Disordersofmenstrualbleeding,nowtermedAUB,areoneof themostcommonreasonsforwomentoattendtheirgeneralpractitioner(GP)and,subsequently,agynaecologist.Althoughrarelylifethreatening,menstrual disorders can cause major social, psychological and occupational upset. There are severaltypesofabnormalbleedingand their terminologyshouldbeknown.Heavymenstrualbleeding (HMB),intermenstrualbleeding(IMB),postcoitalbleeding(PCB)andpostmenopausalbleeding(PMB)shouldbeinvestigated and treated further as described in the chapters indicated. Initial investigations for eachincludespeculumexaminationofthecervix,withswabsformicrobiologyandcervicalsmearifindicated,and transvaginal ultrasound scan (TVUSS) and endometrial biopsy (EB) as necessary. Further to this,outpatienthysteroscopyandbiopsymaybeindicated.
ThereareseveralclassificationsystemsforAUB,someofwhich linksymptoms topathology.Suchsystemshelp clinicians to adopt a similar categorizationof thepathology they are seeing,whichhelpsauditandresearch.OnesystemthatisincreasinglyrecognizedisthePALM–COEINsystemdevelopedbythe International Federation of Gynecology and Obstetrics (FIGO), in which the nemonic PALMrepresents visually objective structural criteria: Polyps, Adenomyosis, Leiomyoma, Malignancy, andCOEIN for causes unrelated to structural anomalies:Coagulopathy,Ovulatory disorders,Endometrial,Iatrogenic,andNotclassifiedcauses(seeFurtherreading).NotethatfurtherdescriptionsinthischapterforcausesofAUBdonotreferspecificallytothissystem.
AcceptedterminologyforcommontypesofAUB
•HMB:excessivemenstrualbloodloss(thischapter).• IMB: bleeding between periods, often seen with endometrial and cervical polyps (Chapter 12,Benignconditionsoftheuterus,cervixandendometrium),alsoendometriosis(Chapter11,Benignconditionsoftheovaryandpelvis).
•PCB: bleedingafter sex.Oftenassociatedwithcervical abnormalities (Chapter16, Premalignantandmalignantdiseaseofthelowergenitaltract).
•PMB: bleeding more than 1 year after cessation of periods. Exclude endometrial pathology orvaginalatrophy(Chapter8,ThemenopauseandpostreproductivehealthandChapter15,Malignantdiseaseoftheuterus).
• BEO: ‘bleeding of endometrial origin’, a diagnosis of exclusion, has replaced the term‘dysfunctionaluterinebleeding’(DUB).
HeavymenstrualbleedingHMBisthemostcommontypeofmenstrualbleedingdisorder.Therehaspreviouslybeensomeconfusionoverthevariousterminologiesusedforabnormalitiesofexcessivemenstrualbloodloss.HMBisnowthepreferreddescriptionasitissimpleandeasilytranslatableintootherlanguages.Itreplacestheolderterm‘menorrhagia’.
HMB is defined as a blood loss of greater than 80ml per period. In reality, methods to quantifymenstrualbloodlossarebothinaccurate(poorcorrelationwithhaemoglobinlevel)andimpractical,andsoaclinicaldiagnosisbasedonthepatient’sownperceptionofbloodlossispreferred.
Of women of reproductive age, 20–30% suffer from HMB. Each year in the UK, 5% of womenbetweentheagesof30and49consulttheirGPwithHMB,withasubstantialnumberbeingreferredonto
www.medicalebookpdf.com
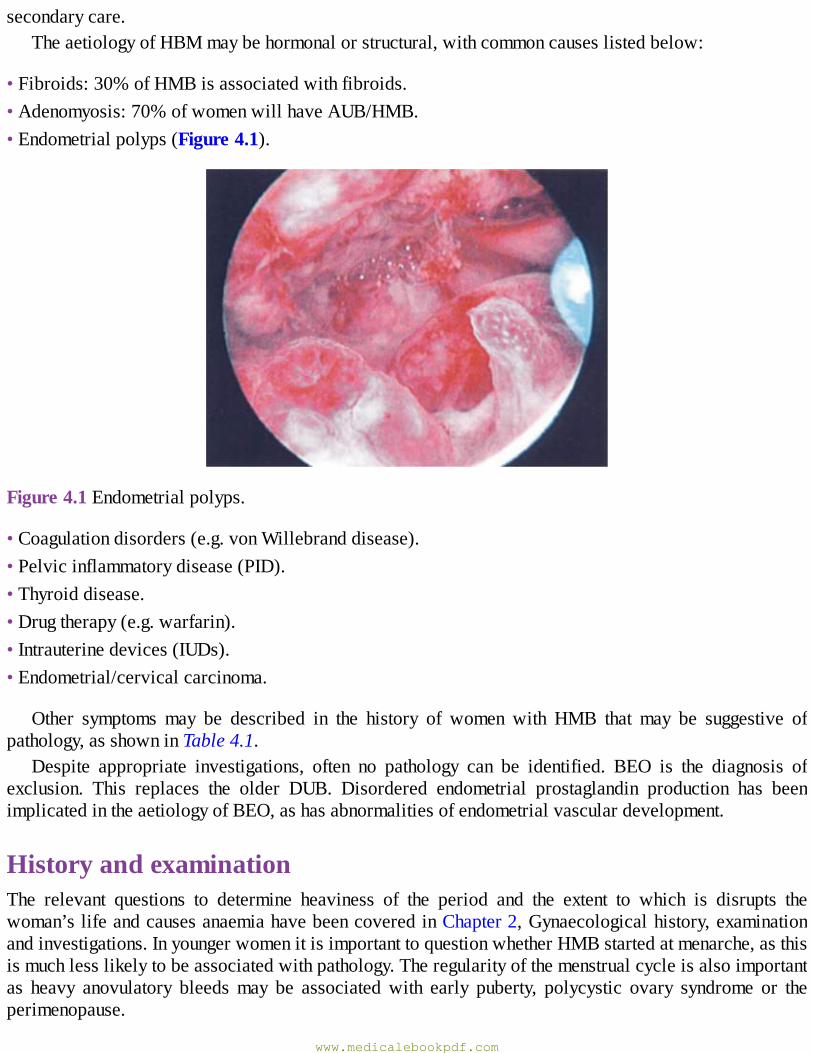
secondarycare.TheaetiologyofHBMmaybehormonalorstructural,withcommoncauseslistedbelow:
•Fibroids:30%ofHMBisassociatedwithfibroids.•Adenomyosis:70%ofwomenwillhaveAUB/HMB.•Endometrialpolyps(Figure4.1).
Figure4.1Endometrialpolyps.
•Coagulationdisorders(e.g.vonWillebranddisease).•Pelvicinflammatorydisease(PID).•Thyroiddisease.•Drugtherapy(e.g.warfarin).•Intrauterinedevices(IUDs).•Endometrial/cervicalcarcinoma.
Other symptoms may be described in the history of women with HMB that may be suggestive ofpathology,asshowninTable4.1.
Despite appropriate investigations, often no pathology can be identified. BEO is the diagnosis ofexclusion. This replaces the older DUB. Disordered endometrial prostaglandin production has beenimplicatedintheaetiologyofBEO,ashasabnormalitiesofendometrialvasculardevelopment.
HistoryandexaminationThe relevant questions to determine heaviness of the period and the extent to which is disrupts thewoman’slifeandcausesanaemiahavebeencoveredinChapter2,Gynaecologicalhistory,examinationandinvestigations.InyoungerwomenitisimportanttoquestionwhetherHMBstartedatmenarche,asthisismuchlesslikelytobeassociatedwithpathology.Theregularityofthemenstrualcycleisalsoimportantas heavy anovulatory bleedsmay be associatedwith early puberty, polycystic ovary syndrome or theperimenopause.
www.medicalebookpdf.com
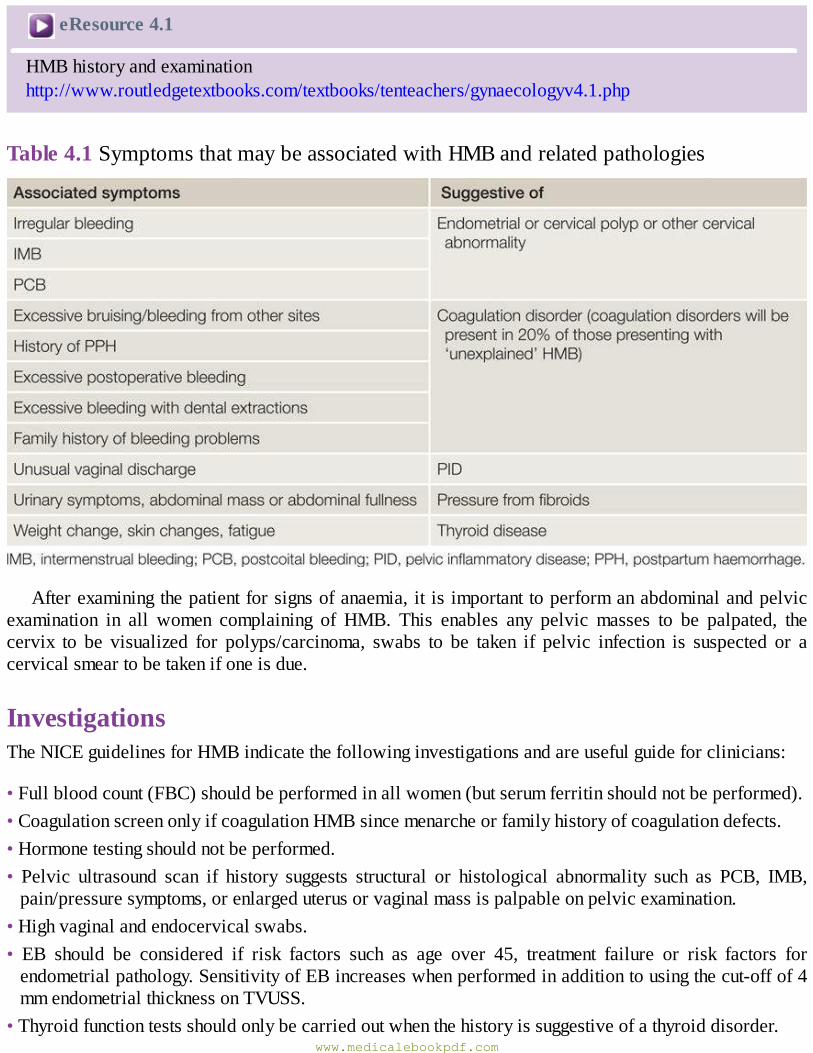
eResource4.1
HMBhistoryandexaminationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv4.1.php
Table4.1SymptomsthatmaybeassociatedwithHMBandrelatedpathologies
Afterexaminingthepatientforsignsofanaemia,it isimportanttoperformanabdominalandpelvicexamination in all women complaining of HMB. This enables any pelvic masses to be palpated, thecervix to be visualized for polyps/carcinoma, swabs to be taken if pelvic infection is suspected or acervicalsmeartobetakenifoneisdue.
InvestigationsTheNICEguidelinesforHMBindicatethefollowinginvestigationsandareusefulguideforclinicians:
•Fullbloodcount(FBC)shouldbeperformedinallwomen(butserumferritinshouldnotbeperformed).•CoagulationscreenonlyifcoagulationHMBsincemenarcheorfamilyhistoryofcoagulationdefects.•Hormonetestingshouldnotbeperformed.• Pelvic ultrasound scan if history suggests structural or histological abnormality such as PCB, IMB,pain/pressuresymptoms,orenlargeduterusorvaginalmassispalpableonpelvicexamination.
•Highvaginalandendocervicalswabs.• EB should be considered if risk factors such as age over 45, treatment failure or risk factors forendometrialpathology.SensitivityofEBincreaseswhenperformedinadditiontousingthecut-offof4mmendometrialthicknessonTVUSS.
•Thyroidfunctiontestsshouldonlybecarriedoutwhenthehistoryissuggestiveofathyroiddisorder.www.medicalebookpdf.com
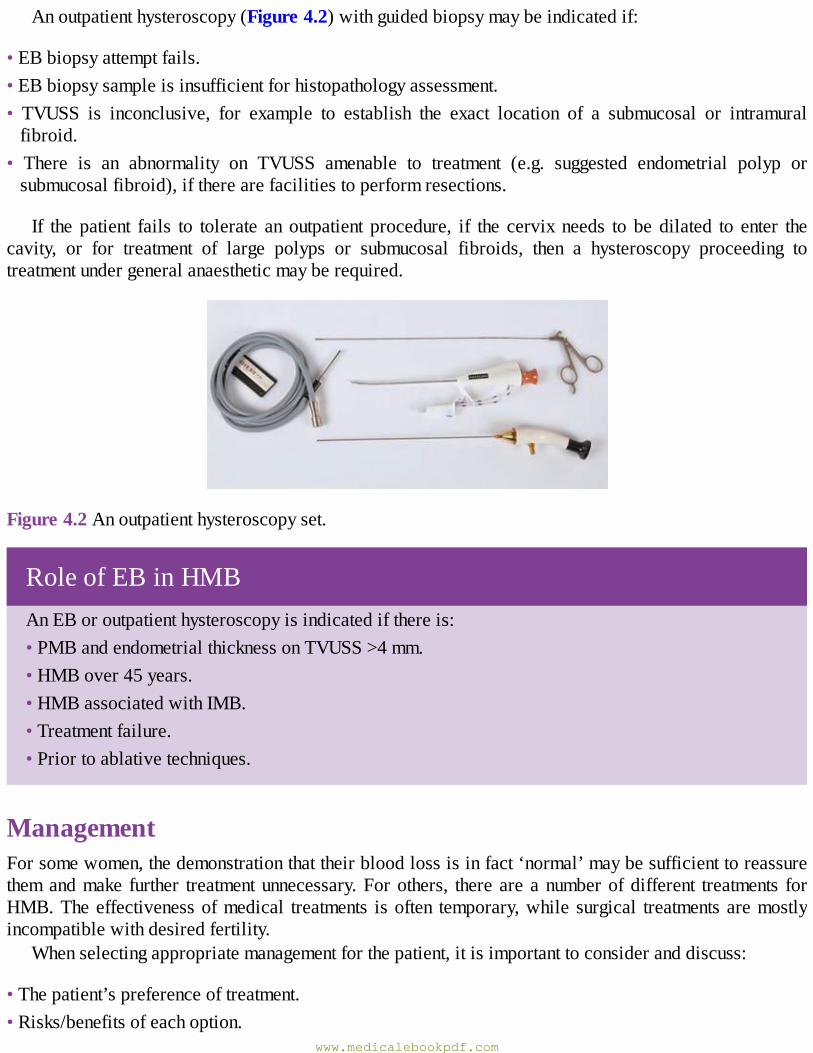
Anoutpatienthysteroscopy(Figure4.2)withguidedbiopsymaybeindicatedif:
•EBbiopsyattemptfails.•EBbiopsysampleisinsufficientforhistopathologyassessment.• TVUSS is inconclusive, for example to establish the exact location of a submucosal or intramuralfibroid.
• There is an abnormality on TVUSS amenable to treatment (e.g. suggested endometrial polyp orsubmucosalfibroid),iftherearefacilitiestoperformresections.
If the patient fails to tolerate an outpatient procedure, if the cervix needs to be dilated to enter thecavity, or for treatment of large polyps or submucosal fibroids, then a hysteroscopy proceeding totreatmentundergeneralanaestheticmayberequired.
Figure4.2Anoutpatienthysteroscopyset.
RoleofEBinHMBAnEBoroutpatienthysteroscopyisindicatedifthereis:•PMBandendometrialthicknessonTVUSS>4mm.•HMBover45years.•HMBassociatedwithIMB.•Treatmentfailure.•Priortoablativetechniques.
ManagementForsomewomen,thedemonstrationthattheirbloodlossisinfact‘normal’maybesufficienttoreassurethemandmake further treatmentunnecessary.Forothers, thereareanumberofdifferent treatments forHMB.Theeffectivenessofmedical treatments isoften temporary,while surgical treatmentsaremostlyincompatiblewithdesiredfertility.
Whenselectingappropriatemanagementforthepatient,itisimportanttoconsideranddiscuss:
•Thepatient’spreferenceoftreatment.•Risks/benefitsofeachoption.
www.medicalebookpdf.com
•Contraceptiverequirements:•familycomplete?•currentcontraception?•Pastmedicalhistory:•anycontraindicationstomedicaltherapiesforHMB?•suitabilityforananaesthetic.•Previoussurgicalhistoryonuterus.
ManagementofHMB
•LNG-IUS.•Transexmicacid/mefenamicacidorcombinedoralcontraceptivepill(COCP).•Progestogens.•Endometrialablation.•Hysterectomyorumbilicalarteryembolization(UAE)forfibroids.
MedicalInitialmanagementofHMBin theabsenceofstructuralorhistologicalabnormalityshouldbemedical.TheNationalInstituteforHealthandCareExcellence(NICE)guidelines(seeFurtherreading)suggestthefollowingorder:
•Levonorgestrelintrauterinesystem(LNG-IUS,Mirena™),providedlong-termuseofatleast12monthsisexpected.LNG-IUS,Mirena™(as furtherdescribed inChapter6,Contraceptionandabortion)hasrevolutionizedthetreatmentofHMB.Meanreductionsinmeanbloodloss(MBL)ofaround95%areachieved by 1 year after LNG-IUS insertion. It provides a highly effective alternative to surgicaltreatment, with few side-effects. Indeed, the Royal College of Obstetricians and Gynaecologists(RCOG) has suggested that the LNG-IUS should be considered in the majority of women as analternativetosurgicaltreatment.Itisobviouslynotsuitableforwomenwishingtoconceive.
•Tranexamicacid,anantifibrinolyticthatreducesbloodlossby50%andistakenduringmenstruation,ormefenamic acid, which inhibits prostaglandin synthesis and reduces blood loss by 30%, or COCP,whichwillinduceslightlylighterperiods.
•Norethisterone,taken15mgdailyinacyclicalpatternfromday6today26ofthemenstrualcycle.• Gonadotrophin-releasing hormone (GnRH) agonists: these drugs act on the pituitary to stop theproductionofoestrogen,whichresultsinamenorrhoea.Theseareonlyusedintheshorttermduetotheresultinghypo-oestrogenicstatethatpredisposestoosteoporosis.Theymaybeusedpreoperativelytoshrink fibroids or cause endometrial suppression to enhance visualization at hysteroscopy. In severeHMBtheycanallow thepatient theopportunity to improve theirhaemoglobinbyprovidinga respitefrombleeding.
Surgicalwww.medicalebookpdf.com

Details of surgical interventions including preoperative assessment, consent and complications arecoveredinChapter17,Gynaecologicalsurgeryandtherapeutics.
Surgicaltreatmentisnormallyrestrictedtowomenforwhommedicaltreatmentshavefailedorwherethere are associated symptoms such as pressure symptoms from fibroids or prolapse. WomencontemplatingsurgicaltreatmentforHMBmustbecertainthattheirfamilyiscomplete.Whilethiscaveatisobviousforwomencontemplatinghysterectomy,inwhichtheuteruswillberemoved,italsoappliestowomen contemplating endometrial ablation. Therefore, women wishing to preserve their fertility forfuture attempts at childbearing should be advised to usemedicalmethods of treatment. The risks of apregnancyafteranablationproceduretheoreticallyincludeprematurityandmorbidlyadherentplacenta.
EndometrialablationAllendometrialdestructiveproceduresemploytheprinciplethatablationoftheendometrialliningoftheuterustosufficientdepthpreventsregenerationoftheendometrium.Ablationissuitableforwomenwithauterusnobiggerthan10weeks’sizeandwithfibroidslessthan3cm.
The first-generation techniques including transcervical resection of the endometriumwith electricaldiathermy or rollerball ablation have largely been replaced by newer second-generation techniquesincluding:
•Impedancecontrolledendometrialablation(Novosure™).•Thermaluterineballoontherapy.•Microwaveablation(Microsulis™)(Figure4.3).
As a general rule, all women undergoing endometrial ablation should have access to a second-generationtechnique.Aftertreatment,40%willbecomeamenorrhoeic,40%willhavemarkedlyreducedmenstrual lossand20%willhavenodifferenceintheirbleeding.Someauthoritieshavesuggestedthatendometrial ablation is so successful that all women with HMB should be encouraged to consider itbefore opting for hysterectomy.While there aremerits to this argument, somewomen, after informeddiscussion, will still prefer hysterectomy and they should therefore be considered for this procedureinstead.
Figure4.3Microwaveablation(Microsulis™).
eResource4.2
Endometrialablationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv4.2.php
www.medicalebookpdf.com
UmbilicalarteryembolizationUAEistreatmentusefulforHMBassociatedwithfibroids,asdiscussedinChapter12,Benignconditionsoftheuterus,cervixandendometrium.
MyomectomyThismaybeasensibleoptionorwomenwithHMBsecondarytolargefibroidswithpressuresymptomswhowishtoconceive(andareatanagewherethisisrealistic).
TranscervicalresectionoffibroidAsdescribed inChapter12,Benignconditionsof theuterus, cervix andendometriumandChapter 17,Gynaecologicalsurgeryandtherapeutics, transcervical resectionofa largesubmucosalfibroid(TCRF)mayreduceHMBandisappropriateinwomenwishingtoconceive.
HysterectomyAhysterectomyisthesurgicalremovaloftheuterusasdescribedinChapter17,Gynaecologicalsurgeryandtherapeutics.Itcanbeavoidedinsomewomenbymedicalandablationprocedures.However,itcanbe necessary to control HMB in women who have not responded. It may be a first-line treatment inwomenwhohaveHMBassociatedwithlargefibroidswhoalsohavepressuresymptoms,orwhohaveasmalleruterusandassociateduterineprolapse.
AcuteHMBNot infrequentlywomenare admitted tohospitalwithAUB.They require stabilization, examination toexclude cervical abnormalities and pelvicmasses,medication to arrest bleeding and correct anaemia,investigationanddischargewithalong-termplantoavoidfurtheradmissions.
ManagementofacuteHMB
•Admit.•Pelvicexamination.•FBC,coagulopathyscreen,biochemistry.•Intravenousaccessandresuscitationortransfusionasrequired.•TranexamicacidoralorIV.•TVUSS.•High-doseprogestogenstoarrestbleeding.•ConsidersuppressionwithGnRHorulipristolacetateinthemediumterm.•Longer-termplanwhenadiagnosishasbeenmade.
www.medicalebookpdf.com
DysmenorrhoeaDysmenorrhoea is defined as painful menstruation. It is experienced by 45–95% of women ofreproductive age. Primary dysmenorrhoea describes painful periods since onset of menarche and isunlikely tobeassociatedwithpathology.There is someevidence to support the assertion thatprimarydysmenorrhoeaimprovesafterchildbirth,anditalsoappearstodeclinewithincreasingage.Secondarydysmenorrhoeadescribespainful periods that havedevelopedover time andusuallyhave a secondarycause.
AetiologyofsecondarydysmenorrhoeaAetiologyincludes:
•Endometriosisandadenomyosis(Chapter11,Benignconditionsoftheovaryandpelvis).•Pelvicinflammatorydisease(Chapter9,Genitourinaryproblems).•Cervicalstenosisandhaematometra(rarely).
HistoryandexaminationPatientswillhavedifferentideasastowhatconstitutesapainfulperiod.Forsomepatientsreassurancethatthepainmaybenormalforherwillhelp.Forotherstheabilitytoalterthemenstrualcycletoavoidhavingaperiodduringkeyevents,forexampleschoolexaminationsorholidays,willbehelpful.
Toascertaintheactualseverityofthepain,thefollowingquestionsmaybeuseful:
•Doyouneedtotakepainkillersforthispain?Whichtabletshelp?•Haveyouneededtotakeanytimeoffwork/schoolduetothepain?
Some primary dysmenorrhoea is associatedwith flushing and nausea, whichmay be prostaglandinrelated. It is important to distinguish betweenmenstrual pain that precedes the period (a vital clue inendometriosis)andpainthatonlyoccurswithbleeding.Otherimportantcluesabouttheaetiologyincludepainthatoccurswithpassageofclots,inwhichcasemedicationtoreduceflowmaybeeffective.
SecondarydysmenorrhoeamaybeassociatedwithdyspareuniaorAUB,whichmaypoint towardsapathologicaldiagnosis.
An abdominal and pelvic examination should be performed (excepting adolescents). Certain signsassociatedwithendometriosis includeapelvicmass(ifanendometriomaispresent),a fixeduterus(ifadhesionsarepresent)andendometrioticnodules(palpableinthepouchofDouglasorontheuterosacralligaments).Anenlargeduterusmaybefoundwithfibroids.AbnormaldischargeandtendernessmaybeseenwithPID.
‘Red flags’ in the expression of dymenorrhoea lead the clinician to suspect serious pathology andincludeanabnormalcervixonexamination,persistentPCBorIMB,whichmayindicateendometrialorcervicalpathology,orapelvicmassthatisnotobviouslytheuterus.
Investigations•Highvaginalandendocervicalswabs.
www.medicalebookpdf.com
• TVUSS scan may be useful to detect endometriomas or appearances suggestive of adenomyosis(enlargeduteruswithheterogeneoustexture)ortoimageanenlargeduterus.
•Diagnosticlaparoscopy:performedtoinvestigatesecondarydysmenorrhoea:•whenthehistoryissuggestiveofendometriosis;•whenswabsandultrasoundscanarenormal,yetsymptomspersist;•whenthepatientwantsadefinitediagnosisorwantsreassurancethattheirpelvisisnormal.
Discussionaboutlaparoscopyshouldincluderisksandthepossibilitythatthisinvestigationmayshownoobviouscausesfortheirsymptoms.
If features in the history suggest cervical stenosis, ultrasound-guided hysteroscopy can be used toinvestigate further. However, this condition is an infrequent cause of dysmenorrhoea, and thisinvestigation should not be routine. Laparoscopy for primary dysmenorrhoea should not usually beperformed.
Management• Non-steroidal anti-inflammatory drugs (NSAIDs): effective in a large proportion of women. Someexamplesarenaproxen,ibuprofenandmefenamicacid.
• Hormonal contraceptives: COCP is widely used but, surprisingly, a recent review of randomizedcontrolled trials provides little evidence supporting this treatment as being effective for primarydysmenorrhoea. Progestogens, either oral (desogestrol) or parenteral (medroxyprogesterone,etonogestrel)maybeusefultocauseanovulationandamenorrhoea.
•LNG-IUS: there is evidence that this isbeneficial fordysmenorrhoeaand indeedcanbeaneffectivetreatmentforunderlyingcauses,suchasendometriosisandadenomyosis.Itisoftenusedasafirst-linetreatmentbeforelaparoscopy.
• Lifestyle changes: there is some evidence to suggest that a low fat, vegetarian diet may improvedysmenorrhoea.Therearesuggestionsthatexercisemayimprovesymptomsbyimprovingbloodflowtothepelvis.
•Heat:althoughthismayseemaratherold-fashionedmethodforhelpingdysmenorrhoea,thereisstrongevidencetoproveitsbenefit.ItappearstobeaseffectiveasNSAIDs.
•GnRHanalogues: this isnota first-line treatmentnoranoption forprolongedmanagementdue to theresultinghypo-oestrogenicstate.Thesearebestusedtomanagesymptomsifawaitinghysterectomyorasa formofassessmentas to thebenefitsofhysterectomy. If thepaindoesnot settlewith theGnRHanalogue,itisunlikelytoberesolvedbyhysterectomy.
•Surgery: signsor symptomsofpathology suchas endometriosismaywarrant surgical laparoscopy toperformadhesiolysisortreatmentofendometriosis/drainageofendometriomas.
KEYLEARNINGPOINTS•HMBisoneofthemostfrequentcausesforconsultationinprimarycareandreferraltosecondarycare.
•HMGmaybeassociatedwithsymptomsthatmayindicatepathology,suchasfibroids.•MedicaltreatmentofHMBwithLNG-IUS,NSAIDsorotherhormonaltreatmentsisfirstline.
www.medicalebookpdf.com
•Women should have access to second-generation ablation techniques, which should be offeredbeforehysterectomyforHMB.
•Womenwithassociatedpathologysuchasfibroidsorprolapsemayoptforhysterectomy.•Primarydysmenorrhoeaisrarelypathological.•SecondarydysmenorrhoeamaybeassociatedwithpathologysuchasendometriosisorPID.•First-linetreatmentofdysmenorrhoeaismedicalwithNSAIDs,COCPorprogestogens.• Women with secondary dysmenorrhoea and signs or symptoms of other pathology may needlaparoscopy.
FurtherreadingMunro MG, Critchley HOD, Broder MS, Fraser IS, for the FIGO Working Group on MenstrualDisorders (2011). FIGO classification system (PALM-COEIN) for causes of abnormal uterinebleedinginnongravidwomenofreproductiveage.IntJGynaecolObstet113(1):3–13.
National Institute for Health and Care Excellence. Heavy menstrual bleeding: assessment andmanagement.https://www.nice.org.uk/guidance/cg44ICEguideline.
Selfassessment
CLINICALHISTORY
A28-year-oldwomanhaspresentedtoherGPwithHMBof2years’duration.Shealsocomplainedof some dysmenorrhoea that was getting worse. On examination there is tenderness over theuterosacralligaments.
AWhatadditionalfeaturesofthehistoryareimportant?BWhataretheinitialinvestigations?CWhatisyourmanagementplan?
ANSWERS
AWhentakingthehistoryitisimportanttodeterminehowmuchthewoman’speriodsareinterferingwithherdailylife.Therelationshipofthepaintotheperiodsisparticularlyimportant.Herplansfor children will influence your choice of treatment, as will any previous treatments and drugallergiesorcontraindications.
Shetellsyouthatsheisneedinganalgesiaandfrequentsanitarychanges.Sheisworkingasanurse,andisfindingsomeshiftsdifficultandhastakensomesickdays.Thepainisworsebefore
www.medicalebookpdf.com
theperiodratherthanwiththemenstrualbleed.Additionally,shehasbeenwantingtoconceiveforthelastyear.
B Appropriate investigations include FBC, TVUSS, high vaginal swab (HVS) and endocervicalswab.
CTreatmentoptionsarelimitedbythedesiretoconceive.Itisappropriatetoofferlaparoscopytodiagnose/treatendometriosis.Itmaybeappropriatetoperformtubalinsufflationatthesametimeastherehasbeenaslightdelayinconception.
SBAQUESTIONS
1A47-year-oldwomanpresentstoherGPwithsymptomsofHMBwithfloodingandclots.Sheisotherwisewell.Examinationrevealsanon-tenderuterus that isnotenlarged.AFBChasshownsignsofreducedhaemoglobin.
WhatinvestigationisindicatednextaccordingtorecentNICEguidelines?Choosethesinglebestanswer.
AThyroidfunctiontests.BHormonalprofile.CSerumferritin.DOutpatienthysteroscopy.EEB.
ANSWER
EThyroid function is not indicated unless there are symptoms compatiblewith abnormal thyroidfunction. Likewise, a hormonal profile is not likely to yield useful results in the absence ofsymptoms. Serum ferritin will not add useful information to the FBC showing anaemia, whichindicates theneed for iron replacement anyway.ATVUSS isnotnecessaryunless theuterus isenlarged, as itwill not alter treatment (although in factwill often be ordered pragmatically topresentadiagnosissuchasadenomysosistothepatients).
Inwomenover theageof45EB is indicatedasa smallpercentagewillhaveanunderlyingmalignancyorendometrialhyperplasia.
2A32-year-oldwomanpresents toherGPwithregularHMB.Shehas twochildrenanddoesnotwantmoreatpresent.Sheismedicallywellandhasnoallergies.Onexaminationshehasanormalsizeduterusthatisnottender.
Whatisthefirst-linetreatmentforHMBaccordingtorecentNICEguidelines?Choosethesinglebestanswer.
AEndometrialablation.BTheoralcontraceptivepill.
www.medicalebookpdf.com
CTheoralcontraceptivepillusedbacktoback.DNorthisterone.ELNG-IUS.
ANSWER
EInwomenwhodonotwishtoconceive,theLNG-IUSisrecommendedasafirst-linetreatmentforHMB. Endometrial ablation can be considered as a permanent solution inwomenwhere othertreatmentshavefailed.Northisteroneusedregularlyondays6–26ofthecycleislikelytoimprovesymptoms but the side-effect profile is worse. The oral contraceptive pill may slightly reducebloodflow.
www.medicalebookpdf.com
CHAPTER5Implantationandearlypregnancy
ANDREWHORNE
Implantationandtheestablishmentofpregnancy
Otherearlypregnancyproblems
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthesocialandemotionalcontextofearlypregnancyloss.
•Understandwhyahighsuspicionofpregnancy isneeded inallwomenof reproductiveagewithsymptoms.
• Obtain a detailed knowledge of the clinical presentation and management of miscarriage andectopicpregnancy.
•Obtainanawarenessoflesscommonearlypregnancyconditions,includingrecurrentmiscarriage,gestationaltrophoblasticdiseaseandhyperemesisgravidarum.
Implantationandtheestablishmentofpregnancy
www.medicalebookpdf.com
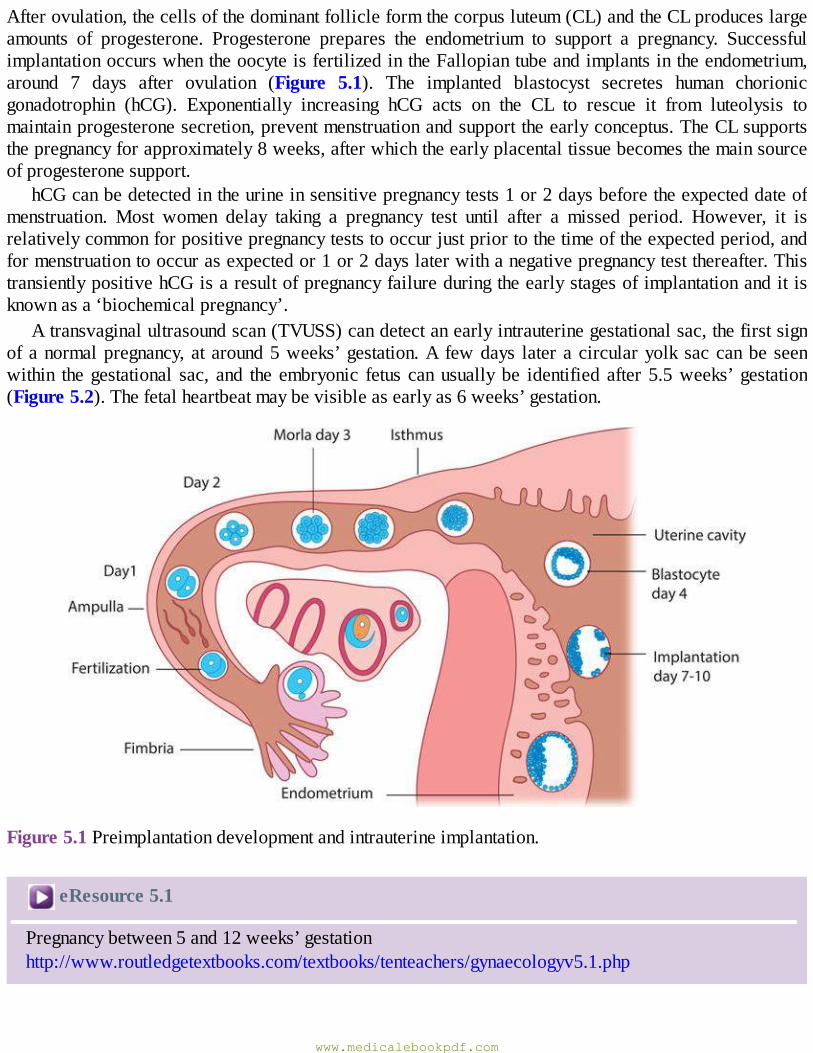
Afterovulation,thecellsofthedominantfollicleformthecorpusluteum(CL)andtheCLproduceslargeamounts of progesterone. Progesterone prepares the endometrium to support a pregnancy. SuccessfulimplantationoccurswhentheoocyteisfertilizedintheFallopiantubeandimplantsintheendometrium,around 7 days after ovulation (Figure 5.1). The implanted blastocyst secretes human chorionicgonadotrophin (hCG). Exponentially increasing hCG acts on the CL to rescue it from luteolysis tomaintainprogesteronesecretion,preventmenstruationandsupporttheearlyconceptus.TheCLsupportsthepregnancyforapproximately8weeks,afterwhichtheearlyplacentaltissuebecomesthemainsourceofprogesteronesupport.
hCGcanbedetectedintheurineinsensitivepregnancytests1or2daysbeforetheexpecteddateofmenstruation. Most women delay taking a pregnancy test until after a missed period. However, it isrelativelycommonforpositivepregnancyteststooccurjustpriortothetimeoftheexpectedperiod,andformenstruationtooccurasexpectedor1or2dayslaterwithanegativepregnancytestthereafter.ThistransientlypositivehCGisaresultofpregnancyfailureduringtheearlystagesofimplantationanditisknownasa‘biochemicalpregnancy’.
Atransvaginalultrasoundscan(TVUSS)candetectanearlyintrauterinegestationalsac,thefirstsignofanormalpregnancy,ataround5weeks’gestation.A fewdays lateracircularyolksaccanbeseenwithin thegestational sac, and the embryonic fetus canusuallybe identified after 5.5weeks’gestation(Figure5.2).Thefetalheartbeatmaybevisibleasearlyas6weeks’gestation.
Figure5.1Preimplantationdevelopmentandintrauterineimplantation.
eResource5.1
Pregnancybetween5and12weeks’gestationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv5.1.php
www.medicalebookpdf.com
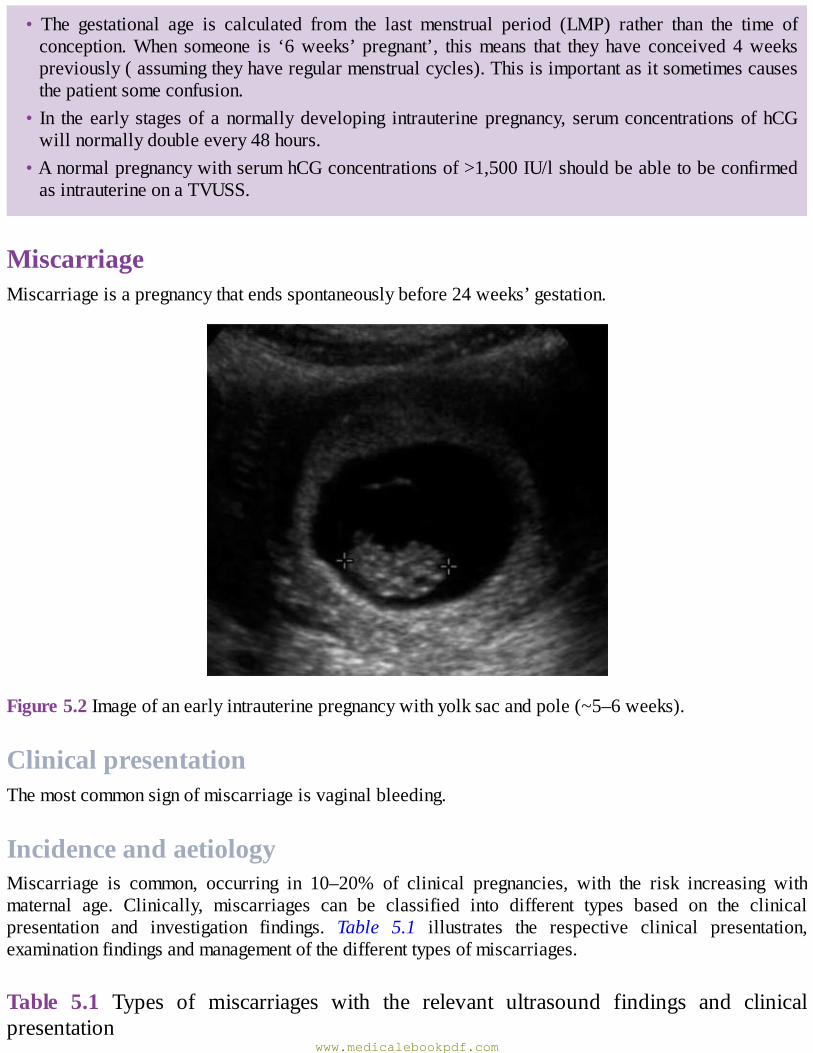
• The gestational age is calculated from the last menstrual period (LMP) rather than the time ofconception.When someone is ‘6weeks’ pregnant’, thismeans that they have conceived4weekspreviously(assumingtheyhaveregularmenstrualcycles).Thisisimportantasitsometimescausesthepatientsomeconfusion.
• In the early stagesof anormallydeveloping intrauterinepregnancy, serumconcentrationsofhCGwillnormallydoubleevery48hours.
•AnormalpregnancywithserumhCGconcentrationsof>1,500IU/lshouldbeabletobeconfirmedasintrauterineonaTVUSS.
MiscarriageMiscarriageisapregnancythatendsspontaneouslybefore24weeks’gestation.
Figure5.2Imageofanearlyintrauterinepregnancywithyolksacandpole(~5–6weeks).
ClinicalpresentationThemostcommonsignofmiscarriageisvaginalbleeding.
IncidenceandaetiologyMiscarriage is common, occurring in 10–20% of clinical pregnancies, with the risk increasing withmaternal age. Clinically, miscarriages can be classified into different types based on the clinicalpresentation and investigation findings. Table 5.1 illustrates the respective clinical presentation,examinationfindingsandmanagementofthedifferenttypesofmiscarriages.
Table 5.1 Types of miscarriages with the relevant ultrasound findings and clinicalpresentation
www.medicalebookpdf.com
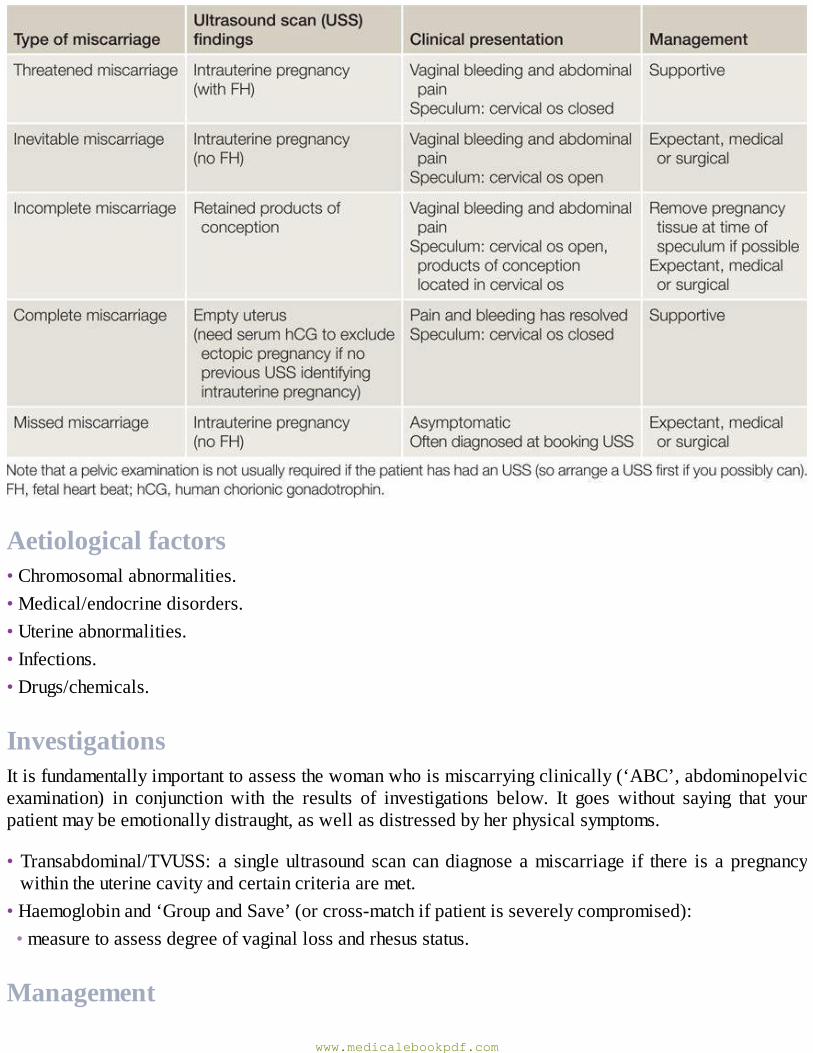
Aetiologicalfactors•Chromosomalabnormalities.•Medical/endocrinedisorders.•Uterineabnormalities.•Infections.•Drugs/chemicals.
InvestigationsItisfundamentallyimportanttoassessthewomanwhoismiscarryingclinically(‘ABC’,abdominopelvicexamination) in conjunction with the results of investigations below. It goes without saying that yourpatientmaybeemotionallydistraught,aswellasdistressedbyherphysicalsymptoms.
•Transabdominal/TVUSS: a singleultrasound scan candiagnose amiscarriage if there is a pregnancywithintheuterinecavityandcertaincriteriaaremet.
•Haemoglobinand‘GroupandSave’(orcross-matchifpatientisseverelycompromised):•measuretoassessdegreeofvaginallossandrhesusstatus.
Management
www.medicalebookpdf.com
Amiscarriagecanbemanagedusinganexpectant(natural),medicalorasurgicalapproach,dependingonclinicalpresentationandpatientchoice.
ExpectantmanagementExpectantmanagementallows for theavoidanceof surgery.Aftera spontaneousmiscarriagewhere thepainandbleedingresolve,arepeatultrasoundscanisnotrequiredtoconfirmcompletion.Womenmaybeadvised to take a urinary pregnancy test after 3weeks and attend if it is positive.Women undergoingexpectantmanagementmayrequireunplannedsurgeryiftheystarttobleedheavily.
MedicalmanagementMedical treatment is increasinglyused inanoutpatient setting toallowwomen tomiscarryathome. Itinvolves the administration of a single, or repeated, vaginal or sublingual dose of the prostaglandinEanaloguemisoprostol. Some centres use pretreatmentwith the progesterone antagonistmifepristone (ifover9weeks’gestation).Theside-effectsincludepain,vomitinganddiarrhoea,andwomenareroutinelyprovidedwithpain relief andantiemetics.Aswith expectantmanagement, there is noneed for routinescan follow-up, although a post-treatment pregnancy test is recommended.Women undergoingmedicalmanagementofmiscarriageneedtounderstandthattheymayneedsurgicaltreatmentifmedicaltreatmentfails(10%failurerate)oriftheybleedheavily.
SurgicalmanagementSurgical management of miscarriage is preferred if there is persistent excessive bleeding orhaemodynamic instability,or ifwomenfavour thisoption. Itcanbedonebymanualvacuumaspirationunderlocalanaestheticinanoutpatientclinicsettingifthewomanisnotcompromised.Morecommonlyitisdoneasadaycaseintheatreundergeneralanaesthesia.Vaginalorsublingualmisoprostolisfrequentlyusedtoripenthecervixtofacilitatecervicaldilatationforsuctioncuretteinsertionandreducetheriskoftraumaandhaemorrhage.However,surgicalevacuationhasitsdrawbacksincludingriskssuchasuterineperforation, postoperative pelvic infection and cervical trauma and subsequent cervical incompetence(seeChapter17,Gynaecologicalsurgeryandtherapeutics).
CounsellingMiscarriagecanbeaverydistressingexperienceandthepsychologicalimpact,senseofbereavementandfeelingsofdepressionandanxietyshouldnotbeunderestimated.Patientswhohavesufferedmiscarriagesshouldbecounselledtoensurethattheyunderstandthatmostmiscarriagesarenon-recurrentandthattheyarenottoblamefortheirloss.
RecurrentmiscarriageRecurrentmiscarriageisdefinedasthelossofthreeormoreconsecutivepregnanciesanditaffects1%ofcouples.Riskfactorsforrecurrentmiscarriageincludebothadvancingmaternalandpaternalage,obesity,balanced chromosomal translocations, uterine structural anomalies and antiphospholipid syndrome(APS).Investigationofrecurrentmiscarriageshouldinvolvetestingforantiphospholipidantibodiesandimagingof theuterus.Productsofconceptioninsubsequentmiscarriagesshouldbesentforcytogeneticanalysis and, where testing reports an unbalanced structural chromosomal abnormality, parental
www.medicalebookpdf.com
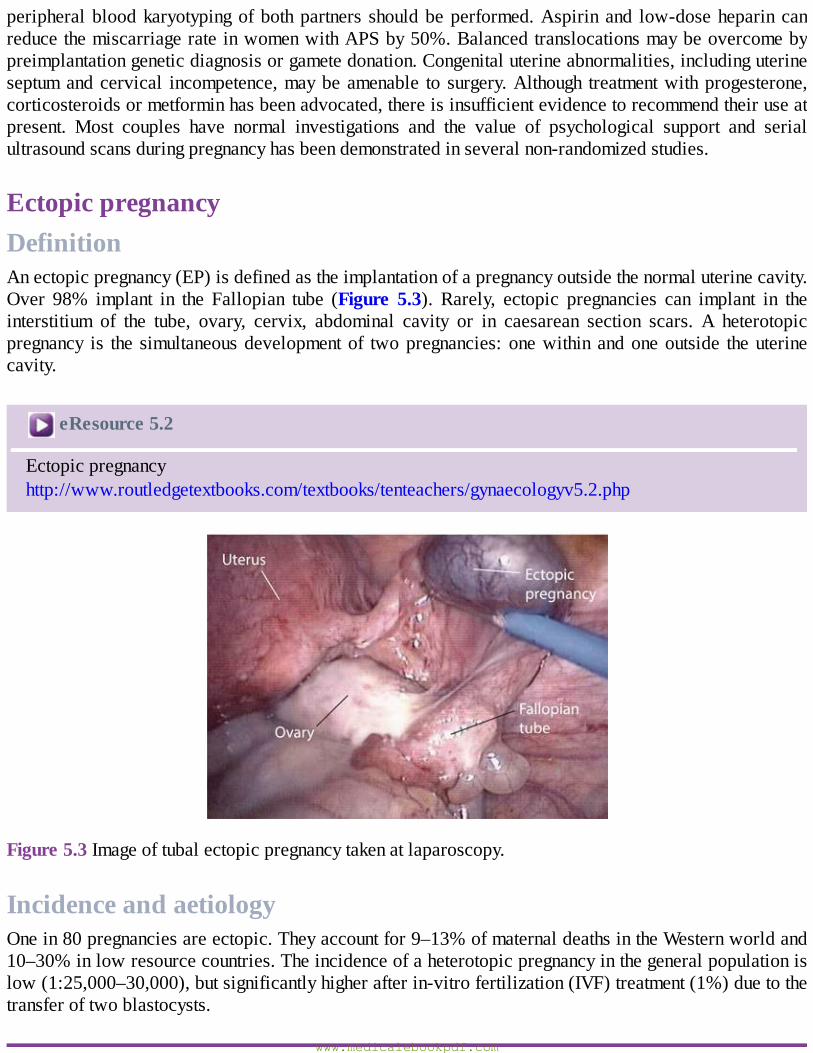
peripheralbloodkaryotypingofbothpartners shouldbeperformed.Aspirinand low-doseheparincanreducethemiscarriagerateinwomenwithAPSby50%.Balancedtranslocationsmaybeovercomebypreimplantationgeneticdiagnosisorgametedonation.Congenitaluterineabnormalities,includinguterineseptumandcervical incompetence,maybeamenable to surgery.Although treatmentwithprogesterone,corticosteroidsormetforminhasbeenadvocated,thereisinsufficientevidencetorecommendtheiruseatpresent. Most couples have normal investigations and the value of psychological support and serialultrasoundscansduringpregnancyhasbeendemonstratedinseveralnon-randomizedstudies.
EctopicpregnancyDefinitionAnectopicpregnancy(EP)isdefinedastheimplantationofapregnancyoutsidethenormaluterinecavity.Over 98% implant in the Fallopian tube (Figure 5.3). Rarely, ectopic pregnancies can implant in theinterstitium of the tube, ovary, cervix, abdominal cavity or in caesarean section scars. A heterotopicpregnancy is the simultaneousdevelopmentof twopregnancies:onewithinandoneoutside theuterinecavity.
eResource5.2
Ectopicpregnancyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv5.2.php
Figure5.3Imageoftubalectopicpregnancytakenatlaparoscopy.
IncidenceandaetiologyOnein80pregnanciesareectopic.Theyaccountfor9–13%ofmaternaldeathsintheWesternworldand10–30%inlowresourcecountries.Theincidenceofaheterotopicpregnancyinthegeneralpopulationislow(1:25,000–30,000),butsignificantlyhigherafterin-vitrofertilization(IVF)treatment(1%)duetothetransferoftwoblastocysts.
www.medicalebookpdf.com
Aetiologicalfactorsforectopicpregnancy
• Fallopian tube damage due to pelvic infection (e.g. Chlamydia/Gonorrhoea), previous ectopicpregnancyandprevioustubalsurgery.
•FunctionalalterationsintheFallopiantubeduetosmokingandincreasedmaternalage.• Additional risk factors include previous abdominal surgery (e.g. appendicectomy, caesareansection), subfertility, IVF, useof intrauterine contraceptivedevices, endometriosis, conceptiononoralcontraceptive/morningafterpill.
ClinicalpresentationThemajority of patientswith anEPpresentwith a subacute clinical picture of abdominal pain and/orvaginal bleeding in early pregnancy. Rarely, patients present very acutely with rupture of the EP andmassive intraperitoneal bleeding. The free blood in the peritoneal cavity can cause diaphragmaticirritationandshouldertippain.ThediagnosisofrupturedEPisusuallyclearastheypresentwithsignsofanacuteabdomenandhypovolaemicshockwithapositivePT.Itis,however,importanttobeawarethatitiscommonforwomentoexperiencebleedingorabdominalpainwithaviableintrauterinepregnancy.
InvestigationsThe followingareuseful investigations for thediagnosisofEP.Nonetheless, again, it is fundamentallyimportanttoassessthewomanclinically(‘ABC’,abdominopelvicexamination)inconjunctionwiththeresultsofinvestigationstomanagethepatient.
•TVUSS:identificationofanintrauterinepregnancy(intrauterinegestationsac,yolksac+/−fetalpole)onTVUSSeffectivelyexcludes thepossibilityofanEPinmostpatientsexcept in thosepatientswithrareheterotopicpregnancy.ATVUSSshowinganemptyuteruswithanadnexalmasshasasensitivityof90%andspecificityof95%inthediagnosisofEP.ThepresenceofmoderatetosignificantfreefluidduringTVUSSissuggestiveofarupturedEP.
•SerumhCG:theserumhCGlevelalmostdoublesevery48hoursinanormallydevelopingintrauterinepregnancy. In patientswith EP, the rise of hCG is often suboptimal.However, hCG levels can varywidely in individuals and thus consecutive measurements 48 hours apart are often required forcomparisonpurposes.
•Haemoglobinand‘GroupandSave’(orcross-matchifpatientisseverelycompromised):•measuretoassessdegreeofintra-abdominalbleedingandrhesusstatus.
Pregnancyofunknownlocation
• In up to 40% of women with an EP the diagnosis is not made on first attendance and they arelabelledashavinga‘pregnancyofunknownlocation’(PUL).
•APULisaworkingdiagnosisdefinedasanemptyuteruswithnoevidenceofanadnexalmassonTVUSS(inapatientwithapositivepregnancytest).
www.medicalebookpdf.com
•Themainstayof investigationofaPULisconsecutivemeasurementofserumhCGconcentrations.AnendometrialbiopsycanoccasionallybehelpfulwhenhCG levelsare static.AllPULmustbeinvestigatedtodeterminethelocationofthepregnancy.
ManagementAn EP can be managed using an expectant, medical or a surgical approach, depending on clinicalpresentationandpatientchoice.
ExpectantmanagementExpectantmanagement isbasedon theassumption that a significantproportionof allEPswill resolvewithout any treatment. This option is suitable for patients who are haemodynamically stable andasymptomatic (and remain so). The patient requires serial hCG measurements until levels areundetectable.
MedicalmanagementIntramuscularmethotrexate is a treatment option for patientswithminimal symptoms, an adnexalmass<40mmindiameterandacurrentserumhCGconcentrationunder3,000IU/l.Methotrexateisafolicacidantagonistthatinhibitsdeoxyribonucleicacid(DNA)synthesis,particularlyaffectingtrophoblasticcells.Thedoseofmethotrexateiscalculatedbasedonthepatient’sbodysurfaceareaandis50mg/m2.Aftermethotrexate treatment serum hCG is usually routinely measured on days 4, 7 and 11, then weeklythereafteruntilundetectable(levelsneedtofallby15%betweenday4and7,andcontinuetofallwithtreatment).Medicaltreatmentshouldthereforeonlybeofferediffacilitiesarepresentforregularfollow-up visits. The few contraindications to medical treatment include: (1) chronic liver, renal orhaematological disorder; (2) active infection; (3) immunodeficiency; and (4) breastfeeding. There arealsoknownside-effects suchas stomatitis, conjunctivitis,gastrointestinalupsetandphotosensitive skinreaction,andabouttwo-thirdsofpatientswillsufferfromnon-specificabdominalpain.Itisimportanttoadvisewomen toavoid sexual intercourseduring treatmentand toavoidconceiving for3monthsaftermethotrexatetreatmentbecauseoftheriskofteratogenicity.It isalsoimportanttoadvisethemtoavoidalcoholandprolongedexposuretosunlightduringtreatment.
SurgicalmanagementThe standard surgical treatment approach is laparoscopy (Figure 5.3). Laparotomy is reserved forseverelycompromisedpatientsorwhere therearenoendoscopic facilities.Theoperationofchoice isremovaloftheFallopiantubeandtheEPwithin(salpingectomy),orinsomecasesasmallopeningcanbemade over the site of theEP and theEP extracted via this opening (salpingostomy). Salpingostomy isrecommended only if the contralateral tube is absent or visibly damaged, and it is associated with ahigherrateofsubsequentEP.Pregnancyratessubsequentlyremainhighifthecontralateraltubeisnormalbecausetheoocytecanbepickedupbytheipsilateralorcontralateraltube.
Anti-Dadministrationwww.medicalebookpdf.com
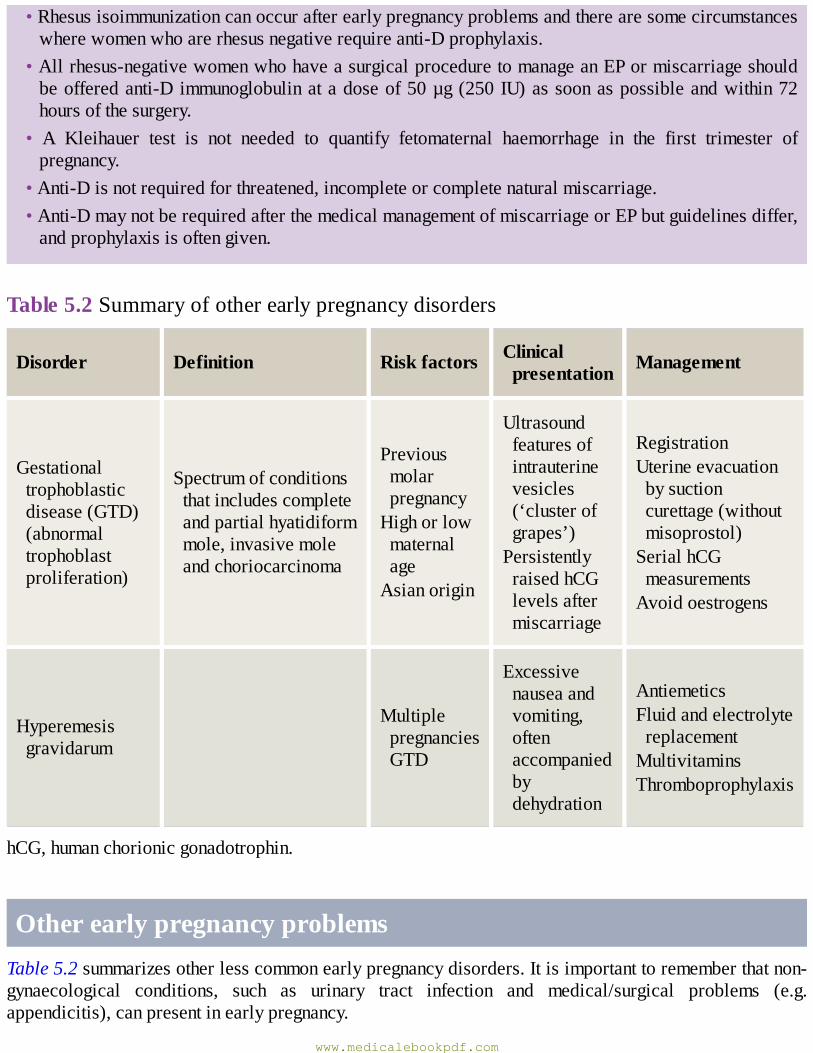
•Rhesusisoimmunizationcanoccurafterearlypregnancyproblemsandtherearesomecircumstanceswherewomenwhoarerhesusnegativerequireanti-Dprophylaxis.
•Allrhesus-negativewomenwhohaveasurgicalproceduretomanageanEPormiscarriageshouldbeofferedanti-Dimmunoglobulinatadoseof50µg(250IU)assoonaspossibleandwithin72hoursofthesurgery.
• A Kleihauer test is not needed to quantify fetomaternal haemorrhage in the first trimester ofpregnancy.
•Anti-Disnotrequiredforthreatened,incompleteorcompletenaturalmiscarriage.•Anti-DmaynotberequiredafterthemedicalmanagementofmiscarriageorEPbutguidelinesdiffer,andprophylaxisisoftengiven.
Table5.2Summaryofotherearlypregnancydisorders
Disorder Definition Riskfactors Clinicalpresentation Management
Gestationaltrophoblasticdisease(GTD)(abnormaltrophoblastproliferation)
Spectrumofconditionsthatincludescompleteandpartialhyatidiformmole,invasivemoleandchoriocarcinoma
PreviousmolarpregnancyHighorlowmaternalageAsianorigin
Ultrasoundfeaturesofintrauterinevesicles(‘clusterofgrapes’)PersistentlyraisedhCGlevelsaftermiscarriage
RegistrationUterineevacuationbysuctioncurettage(withoutmisoprostol)SerialhCGmeasurementsAvoidoestrogens
Hyperemesisgravidarum
MultiplepregnanciesGTD
Excessivenauseaandvomiting,oftenaccompaniedbydehydration
AntiemeticsFluidandelectrolytereplacementMultivitaminsThromboprophylaxis
hCG,humanchorionicgonadotrophin.
OtherearlypregnancyproblemsTable5.2summarizesotherlesscommonearlypregnancydisorders.Itisimportanttorememberthatnon-gynaecological conditions, such as urinary tract infection and medical/surgical problems (e.g.appendicitis),canpresentinearlypregnancy.
www.medicalebookpdf.com
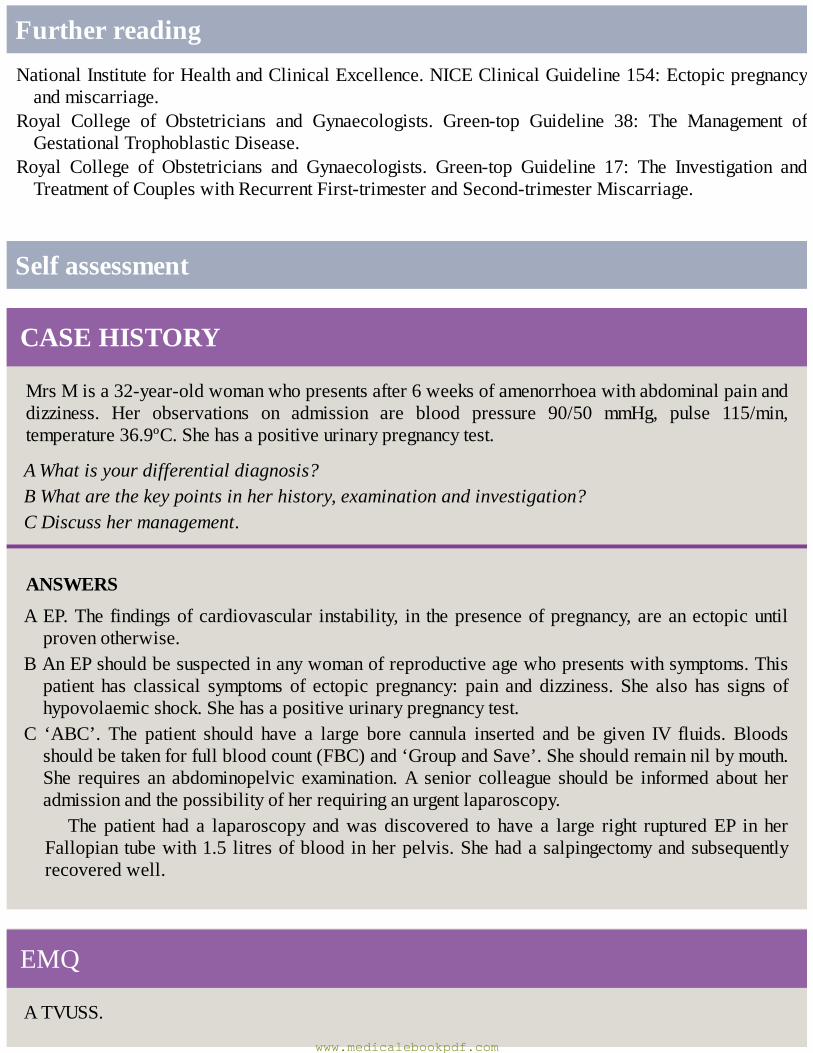
FurtherreadingNationalInstituteforHealthandClinicalExcellence.NICEClinicalGuideline154:Ectopicpregnancyandmiscarriage.
Royal College of Obstetricians and Gynaecologists. Green-top Guideline 38: The Management ofGestationalTrophoblasticDisease.
Royal College of Obstetricians and Gynaecologists. Green-top Guideline 17: The Investigation andTreatmentofCoupleswithRecurrentFirst-trimesterandSecond-trimesterMiscarriage.
Selfassessment
CASEHISTORY
MrsMisa32-year-oldwomanwhopresentsafter6weeksofamenorrhoeawithabdominalpainanddizziness. Her observations on admission are blood pressure 90/50 mmHg, pulse 115/min,temperature36.9ºC.Shehasapositiveurinarypregnancytest.
AWhatisyourdifferentialdiagnosis?BWhatarethekeypointsinherhistory,examinationandinvestigation?CDiscusshermanagement.
ANSWERS
AEP.Thefindingsofcardiovascular instability, in thepresenceofpregnancy,areanectopicuntilprovenotherwise.
BAnEPshouldbesuspectedinanywomanofreproductiveagewhopresentswithsymptoms.Thispatient has classical symptoms of ectopic pregnancy: pain and dizziness. She also has signs ofhypovolaemicshock.Shehasapositiveurinarypregnancytest.
C ‘ABC’. The patient should have a large bore cannula inserted and be given IV fluids. Bloodsshouldbetakenforfullbloodcount(FBC)and‘GroupandSave’.Sheshouldremainnilbymouth.She requires an abdominopelvic examination.A senior colleague shouldbe informed about heradmissionandthepossibilityofherrequiringanurgentlaparoscopy.
The patient had a laparoscopy andwas discovered to have a large right rupturedEP in herFallopiantubewith1.5litresofbloodinherpelvis.Shehadasalpingectomyandsubsequentlyrecoveredwell.
EMQ
ATVUSS.
www.medicalebookpdf.com
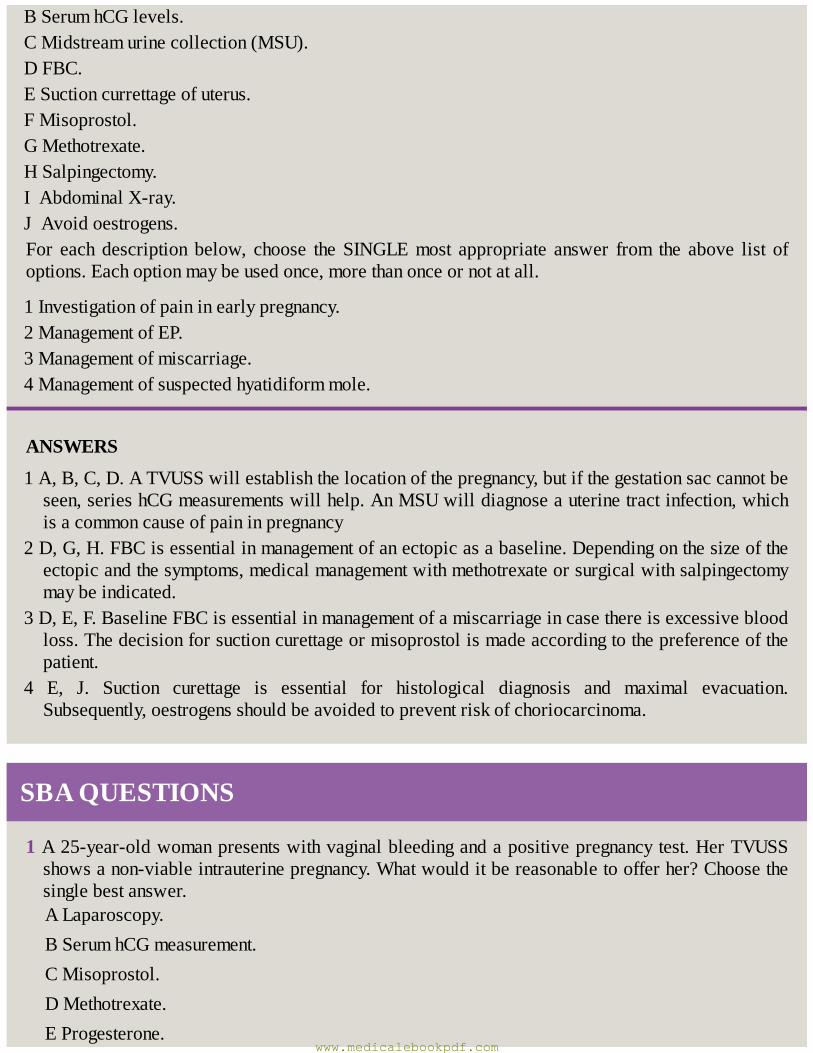
BSerumhCGlevels.CMidstreamurinecollection(MSU).DFBC.ESuctioncurrettageofuterus.FMisoprostol.GMethotrexate.HSalpingectomy.IAbdominalX-ray.JAvoidoestrogens.For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
1Investigationofpaininearlypregnancy.2ManagementofEP.3Managementofmiscarriage.4Managementofsuspectedhyatidiformmole.
ANSWERS
1A,B,C,D.ATVUSSwillestablishthelocationofthepregnancy,butifthegestationsaccannotbeseen,serieshCGmeasurementswillhelp.AnMSUwilldiagnoseauterinetractinfection,whichisacommoncauseofpaininpregnancy
2D,G,H.FBCisessentialinmanagementofanectopicasabaseline.Dependingonthesizeoftheectopicandthesymptoms,medicalmanagementwithmethotrexateorsurgicalwithsalpingectomymaybeindicated.
3D,E,F.BaselineFBCisessentialinmanagementofamiscarriageincasethereisexcessivebloodloss.Thedecisionforsuctioncurettageormisoprostolismadeaccordingtothepreferenceofthepatient.
4 E, J. Suction curettage is essential for histological diagnosis and maximal evacuation.Subsequently,oestrogensshouldbeavoidedtopreventriskofchoriocarcinoma.
SBAQUESTIONS
1A25-year-oldwomanpresentswithvaginalbleedingandapositivepregnancytest.HerTVUSSshowsanon-viableintrauterinepregnancy.Whatwoulditbereasonabletoofferher?Choosethesinglebestanswer.ALaparoscopy.BSerumhCGmeasurement.CMisoprostol.DMethotrexate.EProgesterone.
www.medicalebookpdf.com
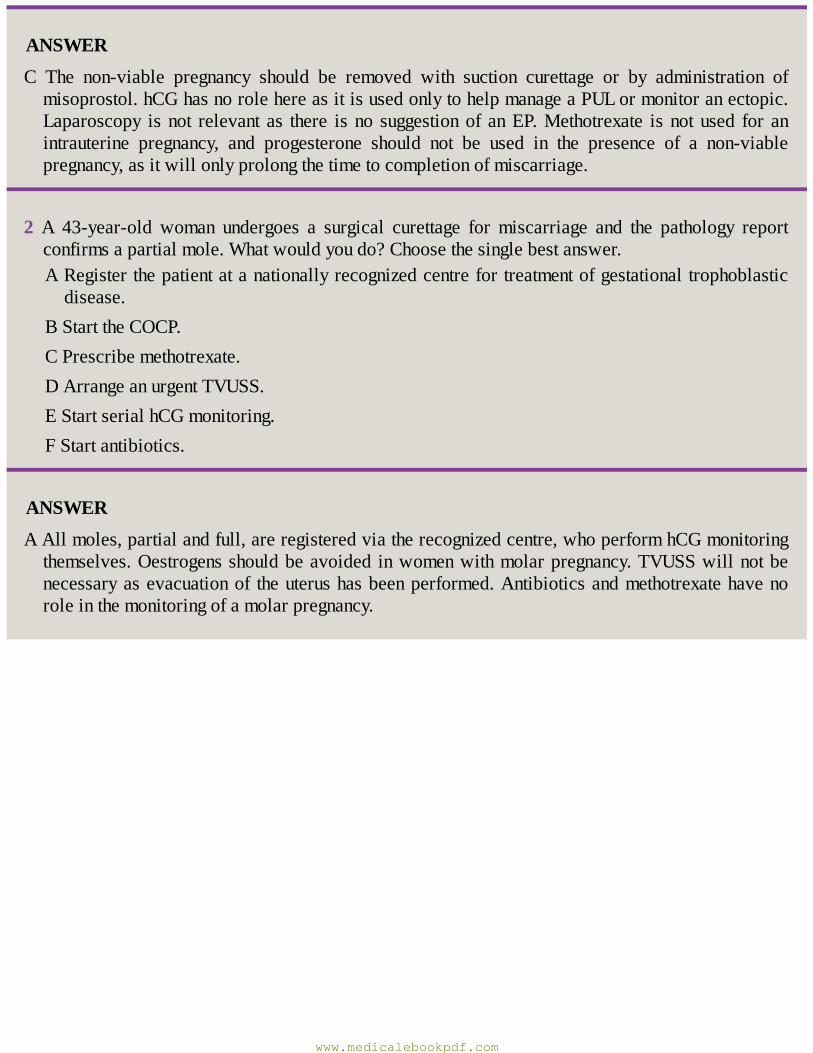
ANSWER
C The non-viable pregnancy should be removed with suction curettage or by administration ofmisoprostol.hCGhasnorolehereasitisusedonlytohelpmanageaPULormonitoranectopic.Laparoscopy isnot relevant as there isno suggestionof anEP.Methotrexate isnotused for anintrauterine pregnancy, and progesterone should not be used in the presence of a non-viablepregnancy,asitwillonlyprolongthetimetocompletionofmiscarriage.
2 A 43-year-old woman undergoes a surgical curettage for miscarriage and the pathology reportconfirmsapartialmole.Whatwouldyoudo?Choosethesinglebestanswer.ARegisterthepatientatanationallyrecognizedcentrefortreatmentofgestationaltrophoblasticdisease.
BStarttheCOCP.CPrescribemethotrexate.DArrangeanurgentTVUSS.EStartserialhCGmonitoring.FStartantibiotics.
ANSWER
AAllmoles,partialandfull,areregisteredviatherecognizedcentre,whoperformhCGmonitoringthemselves.Oestrogensshouldbeavoided inwomenwithmolarpregnancy.TVUSSwillnotbenecessaryasevacuationof theuterushasbeenperformed.Antibioticsandmethotrexatehavenoroleinthemonitoringofamolarpregnancy.
www.medicalebookpdf.com
CHAPTER6Contraceptionandabortion
SHARONCAMERON
Introduction
Contraceptivetargetsinthefemalereproductivetract
Methodsofcontraception
Abortion
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthemechanismofactionofcurrentcontraceptivemethods.
•Describefactorsthataffectcontraceptiveeffectiveness.
•Understandthenon-contraceptivebenefitsofmethods.
•Remembertheuseofmedicaleligibilitycriteriaforcontraception.
•Understandthemechanismofactionofmodernmedicalmethodsofabortion.
•Describecommoncomplicationsofabortion.
•Understandtheimportanceofpostabortalcontraception.
www.medicalebookpdf.com
IntroductionCorrect and consistent use of effective methods of contraception can prevent most unintendedpregnancies.Abortion isamajorconsequenceofunintendedpregnancy,and inmany low-andmiddle-incomecountriesthatrestrictabortion,abortionsareoftenperformedunderunsafeconditionsandresultin women dying or suffering serious injuries. Unintended pregnancies can also lead to delayed or noantenatalcare,whichcanposehealthriskstobothmothersandinfants.It isestimatedthat thereare22million unsafe abortions each year, approximately 47,000 deaths from unsafe abortion and 5 millionwomensufferinjury/disabilityfromunsafeabortion.Thesearepreventablethroughcontraceptionand,asaback-up,accesstosafeabortion.
Globalunmetneedforcontraception
•Over200millionwomenworldwidewouldliketoavoidapregnancy,butarenotusinganeffectivemethodofcontraception.Thisisduetoalackofsupplies,culturalandpoliticalbarriersandpoorqualityofservices.
•Estimated22millionunsafeabortionseachyear.•Approximately47,000deathsfromunsafeabortion.•5millionwomensufferinjury/disabilityfromunsafeabortion.
ContraceptivetargetsinthefemalereproductivetractInordertopreventpregnancy,contraceptivemethodscouldbedevelopedtotargetoneoranumberofkeyreproductiveprocessesorsitesinthemaleorfemalereproductivetract.Noneoftheexistingmethodsofcontraceptionare100%effectiveatpreventingpregnancy.Theeffectivenessofamethoddependsonbothmechanismofactionandcorrectandconsistentuse.Compliancedependsonacceptabilityofthemethodto theuserand tolerabilitywithanyuntowardeffects that theyexperiencerelated touseof themethod.Even inhigh-incomecountriessuchas theUK,wherecontraception is freeandarangeofmethodsarereadilyavailable,unintendedpregnancyratesremainhigh.Manywomenwhopresentwithanunintendedpregnancyhaveusedamethod,butitisusuallyamethodofloweffectiveness(e.g.condom)oramethodthathasbeenusedincorrectlyorinconsistently(e.g.missedoralcontraceptivepills).Uptakeofexistingmethodsislimitedbytheiracceptabilitytowomenandformanymethodsdiscontinuationratesarehigh.
Awoman’schoiceofcontraceptionisjustaslikelytobebaseduponinformationfrommedia,friendsandfamily,asfromahealthcareprofessional.Themosteffectivemethodsofcontraceptionarethelong-acting reversiblemethodsof contraception (LARC)–or socalled ‘fit and forgetmethods’ suchas thecopperintrauterinedevice(Cu-IUD),levonorgestrelintrauterinesystem(LNG-IUS)andprogestogen-onlyimplant. Unfortunately, myths and misconceptions amongst both women and health care professionalssurrounding use of LARC, are major factors that limit their uptake. Education, dispelling myths andpromoting the significant non-contraceptive benefits of LARC methods could improve uptake andcontinuation,andhavethepotentialtopreventmanymoreunintendedpregnanciesformorewomen.
www.medicalebookpdf.com
MechanismofactionThecurrentavailablemethodsofcontraceptionworkinthefollowingways:
• Prevent ovulation: this is the mechanism of action of the following methods: combined hormonalmethods (pill, patch and vaginal ring), progestogen-only injectables, progestogen-only implant(Nexplanon®),oralemergencycontraception,lactationalamenorrhoea.
•Preventspermreachingtheoocyte:femalesterilizationandmalesterilization(vasectomy).•Preventanembryoimplantingintheuterus:thisisamechanismofactionoftheCu-IUDandLNG-IUS.•Allowspermintothevaginabutpoisonthem:mechanismofactionofspermicides.•Allowspermintothevaginabutblockfurtherpassage:mechanismofactionofdiaphragmandcap.Alsooneofthemechanismsofactionofprogestogens.
•Preventspermenteringthevagina:•maleandfemalecondoms;•avoidsexduringthefertiletimeofthecycle;•fertilityawareness-basedmethods(FAB).
EfficacyandeffectivenessTheefficacyofamethoddependsonitsmechanismofaction.However,real-lifeeffectivenessdependsoncomplianceandcontinuationwiththemethod.Complianceisinfluencedbytherouteofadministration;somemethodsareeasiertousethanothers.Continuationwithamethoddependsontheacceptabilitytotheuser.Themost effectivemethod for awoman (or couple), therefore, is amethod thatwill beusedcorrectlyandconsistently.
Failureratesduringperfectuseshowhoweffectivemethodscanbe,whereperfectuseisdefinedasfollowingthedirectionsforuse.Failureratesduringtypicaluseshowhoweffectivethedifferentmethodsareduringactualuse(includinginconsistentorincorrectuse).Table6.1showsestimatesoftheprobabilitiesofpregnancyduringthefirstyearoftypicaluseofeach
method (based upon data from the USA). For some methods, such as implants and intrauterinecontraceptives,theefficacyishighandproperandconsistentuseisnearlyguaranteedonceinserted,thatextremelylowpregnancyratesarefoundinallstudies.Forothermethods,suchastheoralcontraceptivepillandprogestogen-onlyinjectable,efficacyishigh,buttheycanpotentiallybemisused(e.g.forgettingtotakepillsorfailuretogetrepeatinjections).Characteristicsoftheuserthatdetermineriskofpregnancyincludecompliance,age(reducingfertilityinlate30s)andfrequencyofintercourse.
Table 6.1 Percentage ofwomen experiencing an unintended pregnancywithin the firstyearofusewithtypicaluseandperfectuse
www.medicalebookpdf.com
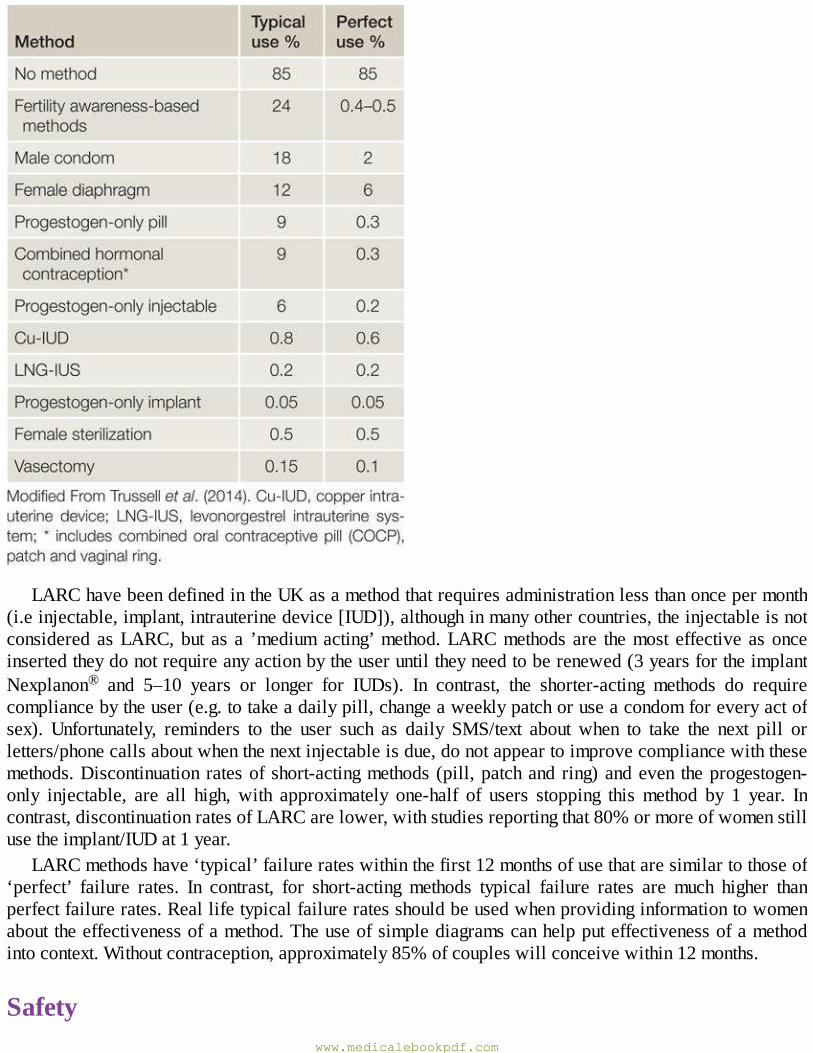
LARChavebeendefinedintheUKasamethodthatrequiresadministrationlessthanoncepermonth(i.einjectable,implant,intrauterinedevice[IUD]),althoughinmanyothercountries,theinjectableisnotconsideredasLARC,but as a ’mediumacting’method.LARCmethods are themost effective asonceinsertedtheydonotrequireanyactionbytheuseruntiltheyneedtoberenewed(3yearsfortheimplantNexplanon® and 5–10 years or longer for IUDs). In contrast, the shorter-acting methods do requirecompliancebytheuser(e.g.totakeadailypill,changeaweeklypatchoruseacondomforeveryactofsex). Unfortunately, reminders to the user such as daily SMS/text about when to take the next pill orletters/phonecallsaboutwhenthenextinjectableisdue,donotappeartoimprovecompliancewiththesemethods.Discontinuation ratesofshort-actingmethods (pill,patchandring)andeven theprogestogen-only injectable, are all high, with approximately one-half of users stopping thismethod by 1 year. Incontrast,discontinuationratesofLARCarelower,withstudiesreportingthat80%ormoreofwomenstillusetheimplant/IUDat1year.
LARCmethodshave‘typical’failurerateswithinthefirst12monthsofusethataresimilartothoseof‘perfect’ failure rates. In contrast, for short-acting methods typical failure rates are much higher thanperfectfailurerates.Reallifetypicalfailureratesshouldbeusedwhenprovidinginformationtowomenabouttheeffectivenessofamethod.Theuseofsimplediagramscanhelpputeffectivenessofamethodintocontext.Withoutcontraception,approximately85%ofcoupleswillconceivewithin12months.
Safetywww.medicalebookpdf.com
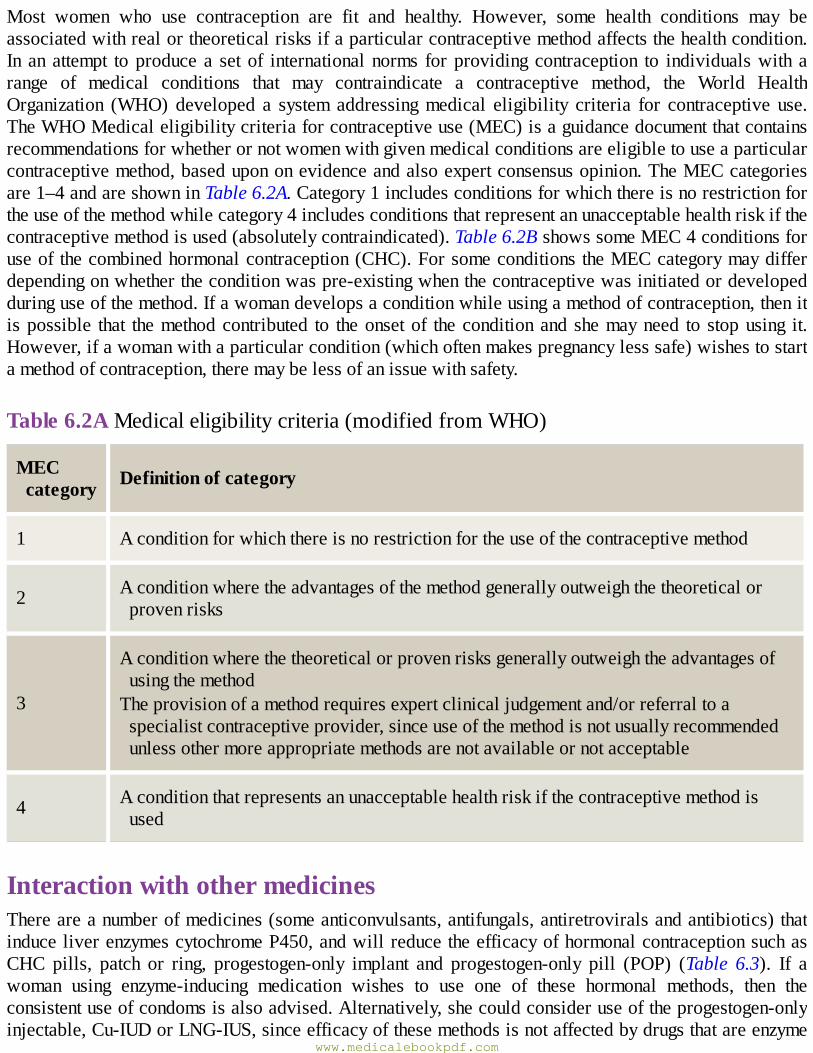
Most women who use contraception are fit and healthy. However, some health conditions may beassociatedwithrealortheoreticalrisksifaparticularcontraceptivemethodaffectsthehealthcondition.In an attempt toproducea setof internationalnorms forprovidingcontraception to individualswith arange of medical conditions that may contraindicate a contraceptive method, the World HealthOrganization (WHO) developed a system addressingmedical eligibility criteria for contraceptive use.TheWHOMedicaleligibilitycriteriaforcontraceptiveuse(MEC)isaguidancedocumentthatcontainsrecommendationsforwhetherornotwomenwithgivenmedicalconditionsareeligibletouseaparticularcontraceptivemethod,basedupononevidenceandalsoexpertconsensusopinion.TheMECcategoriesare1–4andareshowninTable6.2A.Category1includesconditionsforwhichthereisnorestrictionfortheuseofthemethodwhilecategory4includesconditionsthatrepresentanunacceptablehealthriskifthecontraceptivemethodisused(absolutelycontraindicated).Table6.2BshowssomeMEC4conditionsforuseof thecombinedhormonalcontraception(CHC).ForsomeconditionstheMECcategorymaydifferdependingonwhethertheconditionwaspre-existingwhenthecontraceptivewasinitiatedordevelopedduringuseofthemethod.Ifawomandevelopsaconditionwhileusingamethodofcontraception,thenitispossible that themethodcontributed to theonsetof theconditionandshemayneed to stopusing it.However,ifawomanwithaparticularcondition(whichoftenmakespregnancylesssafe)wishestostartamethodofcontraception,theremaybelessofanissuewithsafety.
Table6.2AMedicaleligibilitycriteria(modifiedfromWHO)
MECcategory Definitionofcategory
1 Aconditionforwhichthereisnorestrictionfortheuseofthecontraceptivemethod
2 Aconditionwheretheadvantagesofthemethodgenerallyoutweighthetheoreticalorprovenrisks
3
AconditionwherethetheoreticalorprovenrisksgenerallyoutweightheadvantagesofusingthemethodTheprovisionofamethodrequiresexpertclinicaljudgementand/orreferraltoaspecialistcontraceptiveprovider,sinceuseofthemethodisnotusuallyrecommendedunlessothermoreappropriatemethodsarenotavailableornotacceptable
4 Aconditionthatrepresentsanunacceptablehealthriskifthecontraceptivemethodisused
InteractionwithothermedicinesThereareanumberofmedicines(someanticonvulsants,antifungals,antiretroviralsandantibiotics)thatinduceliverenzymescytochromeP450,andwillreducetheefficacyofhormonalcontraceptionsuchasCHC pills, patch or ring, progestogen-only implant and progestogen-only pill (POP) (Table 6.3). If awoman using enzyme-inducing medication wishes to use one of these hormonal methods, then theconsistentuseofcondomsisalsoadvised.Alternatively,shecouldconsideruseoftheprogestogen-onlyinjectable,Cu-IUDorLNG-IUS,sinceefficacyofthesemethodsisnotaffectedbydrugsthatareenzyme
www.medicalebookpdf.com
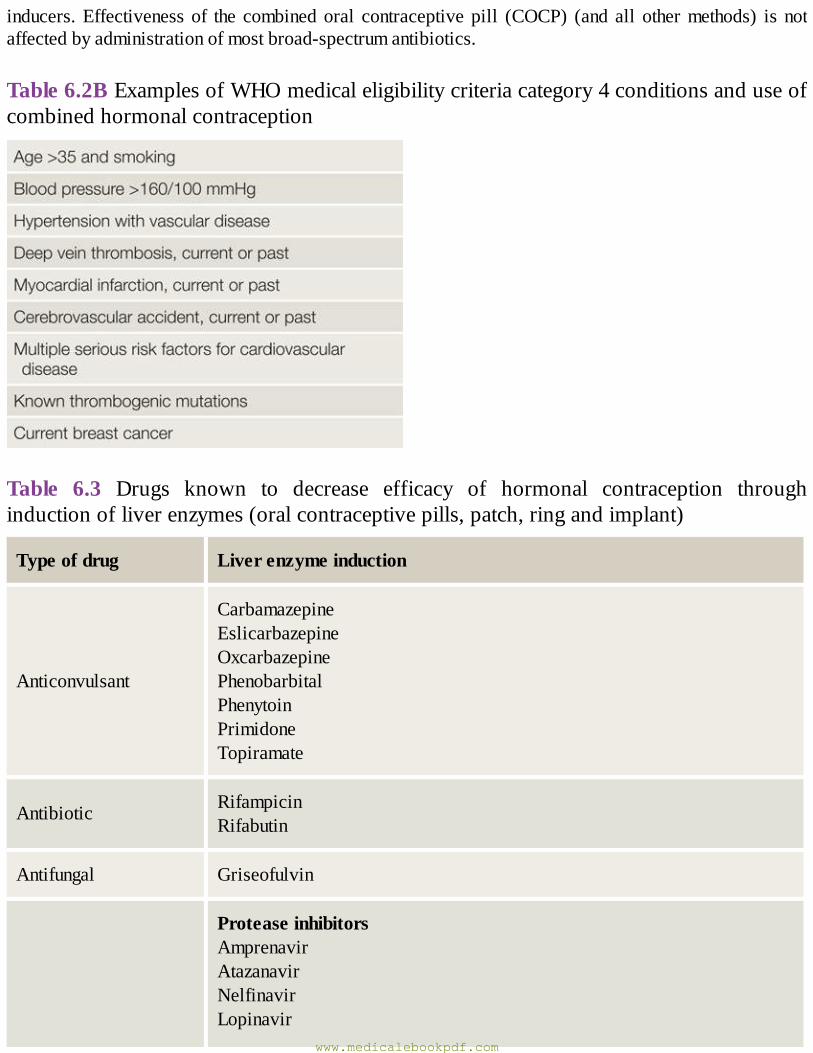
inducers.Effectivenessof the combinedoral contraceptivepill (COCP) (and all othermethods) is notaffectedbyadministrationofmostbroad-spectrumantibiotics.
Table6.2BExamplesofWHOmedicaleligibilitycriteriacategory4conditionsanduseofcombinedhormonalcontraception
Table 6.3 Drugs known to decrease efficacy of hormonal contraception throughinductionofliverenzymes(oralcontraceptivepills,patch,ringandimplant)
Typeofdrug Liverenzymeinduction
Anticonvulsant
CarbamazepineEslicarbazepineOxcarbazepinePhenobarbitalPhenytoinPrimidoneTopiramate
Antibiotic RifampicinRifabutin
Antifungal Griseofulvin
ProteaseinhibitorsAmprenavirAtazanavirNelfinavirLopinavir
www.medicalebookpdf.com
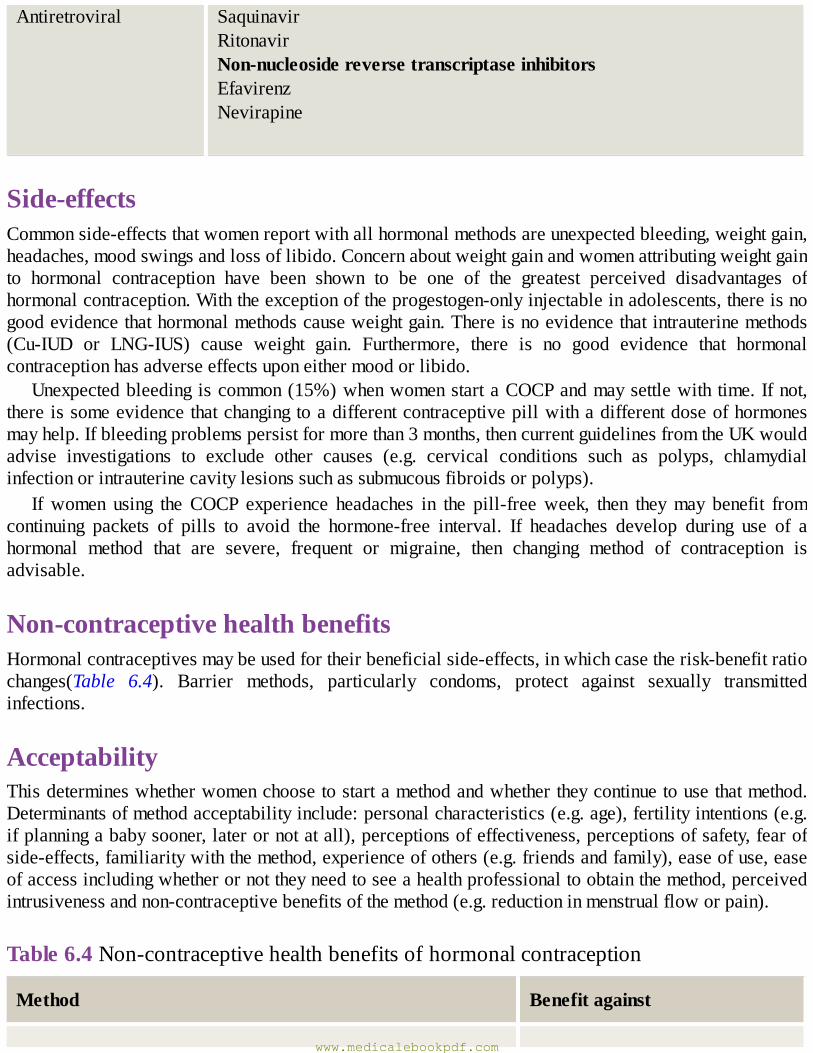
Antiretroviral SaquinavirRitonavirNon-nucleosidereversetranscriptaseinhibitorsEfavirenzNevirapine
Side-effectsCommonside-effectsthatwomenreportwithallhormonalmethodsareunexpectedbleeding,weightgain,headaches,moodswingsandlossoflibido.Concernaboutweightgainandwomenattributingweightgainto hormonal contraception have been shown to be one of the greatest perceived disadvantages ofhormonalcontraception.Withtheexceptionoftheprogestogen-onlyinjectableinadolescents,thereisnogoodevidencethathormonalmethodscauseweightgain.Thereisnoevidencethatintrauterinemethods(Cu-IUD or LNG-IUS) cause weight gain. Furthermore, there is no good evidence that hormonalcontraceptionhasadverseeffectsuponeithermoodorlibido.
Unexpectedbleedingiscommon(15%)whenwomenstartaCOCPandmaysettlewith time.Ifnot,thereissomeevidencethatchangingtoadifferentcontraceptivepillwithadifferentdoseofhormonesmayhelp.Ifbleedingproblemspersistformorethan3months,thencurrentguidelinesfromtheUKwouldadvise investigations to exclude other causes (e.g. cervical conditions such as polyps, chlamydialinfectionorintrauterinecavitylesionssuchassubmucousfibroidsorpolyps).
If women using the COCP experience headaches in the pill-freeweek, then theymay benefit fromcontinuing packets of pills to avoid the hormone-free interval. If headaches develop during use of ahormonal method that are severe, frequent or migraine, then changing method of contraception isadvisable.
Non-contraceptivehealthbenefitsHormonalcontraceptivesmaybeusedfortheirbeneficialside-effects,inwhichcasetherisk-benefitratiochanges(Table 6.4). Barrier methods, particularly condoms, protect against sexually transmittedinfections.
AcceptabilityThisdetermineswhetherwomenchoosetostartamethodandwhethertheycontinuetousethatmethod.Determinantsofmethodacceptabilityinclude:personalcharacteristics(e.g.age),fertilityintentions(e.g.ifplanningababysooner,laterornotatall),perceptionsofeffectiveness,perceptionsofsafety,fearofside-effects,familiaritywiththemethod,experienceofothers(e.g.friendsandfamily),easeofuse,easeofaccessincludingwhetherornottheyneedtoseeahealthprofessionaltoobtainthemethod,perceivedintrusivenessandnon-contraceptivebenefitsofthemethod(e.g.reductioninmenstrualfloworpain).
Table6.4Non-contraceptivehealthbenefitsofhormonalcontraception
Method Benefitagainst
www.medicalebookpdf.com
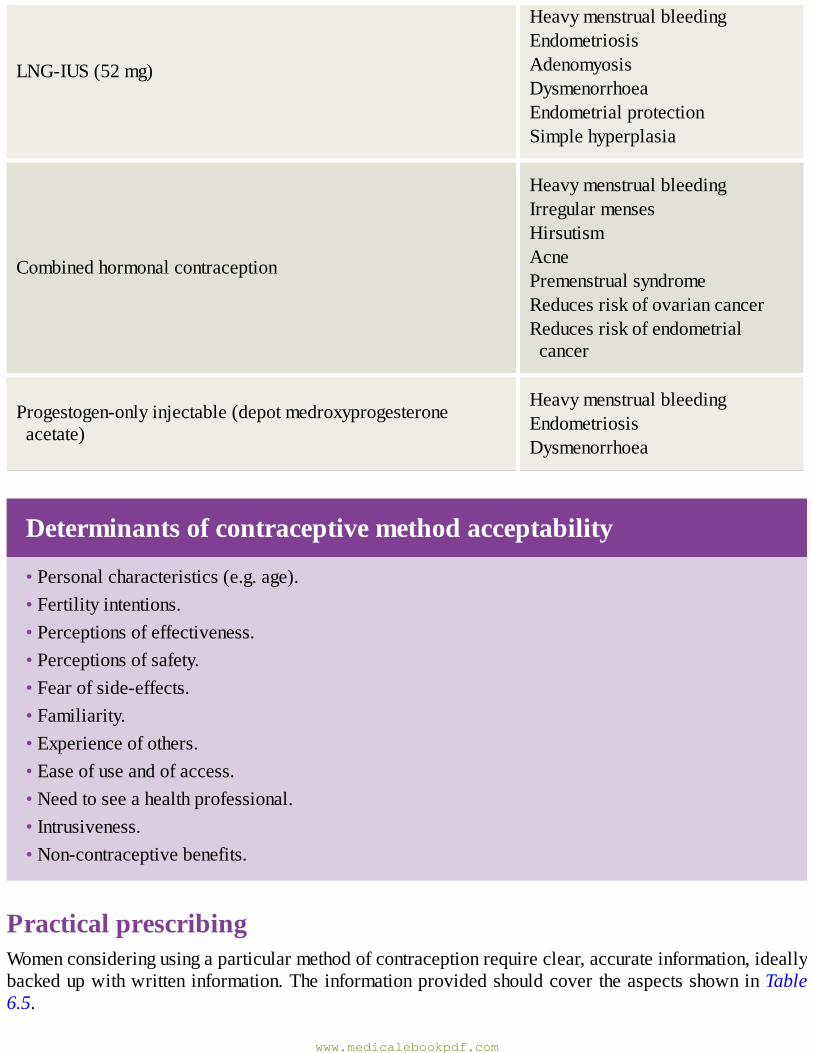
LNG-IUS(52mg)
HeavymenstrualbleedingEndometriosisAdenomyosisDysmenorrhoeaEndometrialprotectionSimplehyperplasia
Combinedhormonalcontraception
HeavymenstrualbleedingIrregularmensesHirsutismAcnePremenstrualsyndromeReducesriskofovariancancerReducesriskofendometrialcancer
Progestogen-onlyinjectable(depotmedroxyprogesteroneacetate)
HeavymenstrualbleedingEndometriosisDysmenorrhoea
Determinantsofcontraceptivemethodacceptability
•Personalcharacteristics(e.g.age).•Fertilityintentions.•Perceptionsofeffectiveness.•Perceptionsofsafety.•Fearofside-effects.•Familiarity.•Experienceofothers.•Easeofuseandofaccess.•Needtoseeahealthprofessional.•Intrusiveness.•Non-contraceptivebenefits.
PracticalprescribingWomenconsideringusingaparticularmethodofcontraceptionrequireclear,accurateinformation,ideallybackedupwithwritteninformation.TheinformationprovidedshouldcovertheaspectsshowninTable6.5.
www.medicalebookpdf.com
Table6.5Whatawomanneedstoknowbeforestartingamethodofcontraception
•Howtousethemethod(pill,patchorring)andwhattodowhenmisused(e.g.missedpill)
•Typicalfailurerates
•Commonside-effects
•Healthbenefits
•Fertilityreturnonstopping
•Whensherequiresreview
Methodsofcontraception
CombinedhormonalcontraceptionCHCmethodscontaintwohormones:anoestrogenandaprogestogen.Theyareavailableasoralpills,atransdermalpatchandasavaginalring.Theyaresimilarintermsofeffectiveness,safetyandside-effects.Thesemethodsallworkbyinhibitionofovulationvianegativefeedbackofoestrogenandprogestogenonthepituitary,withsuppressionoffollicle-stimulatinghormone(FSH)andluteinizinghormone(LH).
PillsMostofthecommonlyusedCOCPsare‘lowdose’andcontainethinyloestradiolinadoseof15–35µg(Figure 6.1). Some newer pills contain oestradiol valerate or oestradiol hemihydrate, which is moresimilarinstructuretothe‘naturallyoccurring’oestradiol,butconfersnootherprovenbenefits.
Most‘traditional’preparationscontain21pillsfollowedbya7-daypill-freeinterval(or7placebotabletsinplaceofa7-daypill-freeinterval).Somepreparationscontain24daysofpillswithashorterpill-free interval.Preparationsarecommonlymonophasic (i.e. samedoseofhormones throughout),butsome are phasic (dose varies). There is no advantage of phasic preparations over monophasicpreparations.Althoughtraditional21daysonand7daysoffusuallyresultsinawithdrawalbleedduringthe pill-free interval, there is no reason why women cannot take the pill continuously. Women withdysmenorrhoeaorheadachesduringthepill-freeinterval,areoftenadvisedtodosotoavoidrecurrenceof symptoms during the hormone-free interval by tricycling (taking three packets without any break).Tailoredpill use is alsooften recommended.This iswherewomencontinue to take thepill until theywanttostartableedingepisode.Theythenhavethepill-freeintervalatthistime.
Theprogestogensthatareusedincurrentlyavailablepillsareoftenreferredtoassecond-generation(levonorgestrel, norethisterone), third-generation (gestodene desogestrel) and fourth-generationprogestogens (drospirenone and dienogest). Newer (third-and fourth-generation) progestogens were
www.medicalebookpdf.com
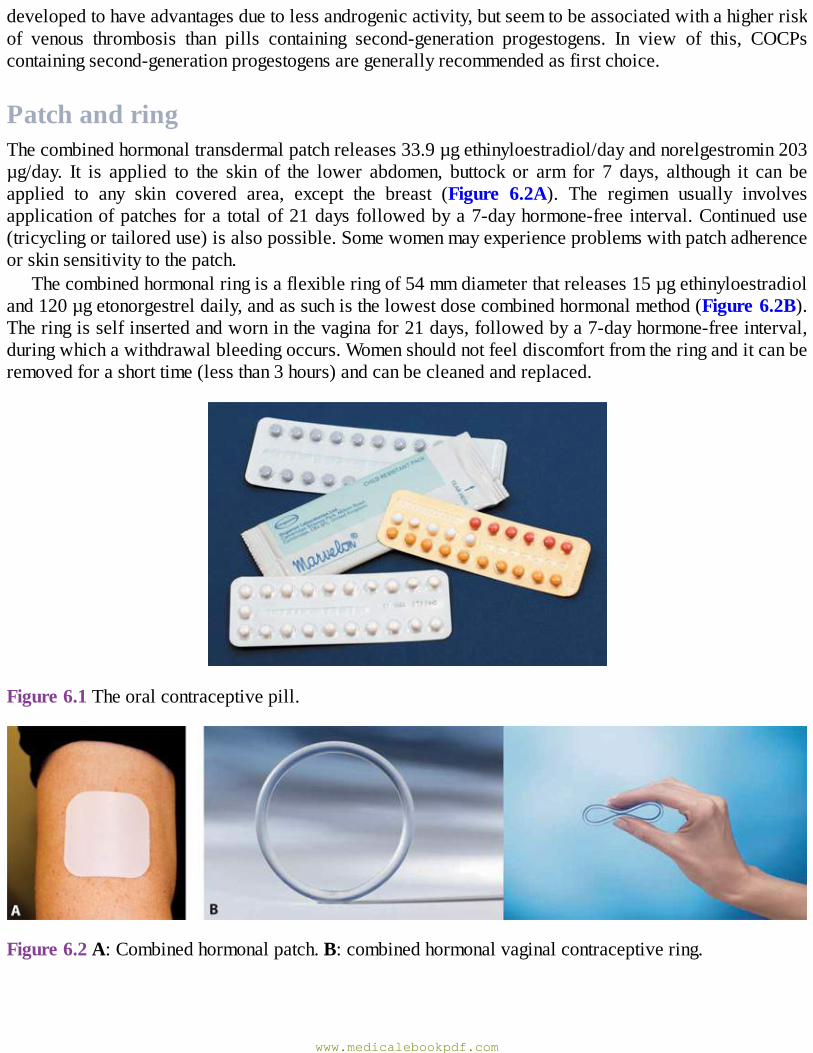
developedtohaveadvantagesduetolessandrogenicactivity,butseemtobeassociatedwithahigherriskof venous thrombosis than pills containing second-generation progestogens. In view of this, COCPscontainingsecond-generationprogestogensaregenerallyrecommendedasfirstchoice.
PatchandringThecombinedhormonaltransdermalpatchreleases33.9µgethinyloestradiol/dayandnorelgestromin203µg/day. It is applied to the skin of the lower abdomen, buttock or arm for 7 days, although it can beapplied to any skin covered area, except the breast (Figure 6.2A). The regimen usually involvesapplicationofpatchesfora totalof21daysfollowedbya7-dayhormone-free interval.Continueduse(tricyclingortailoreduse)isalsopossible.Somewomenmayexperienceproblemswithpatchadherenceorskinsensitivitytothepatch.
Thecombinedhormonalringisaflexibleringof54mmdiameterthatreleases15µgethinyloestradioland120µgetonorgestreldaily,andassuchisthelowestdosecombinedhormonalmethod(Figure6.2B).Theringisselfinsertedandworninthevaginafor21days,followedbya7-dayhormone-freeinterval,duringwhichawithdrawalbleedingoccurs.Womenshouldnotfeeldiscomfortfromtheringanditcanberemovedforashorttime(lessthan3hours)andcanbecleanedandreplaced.
Figure6.1Theoralcontraceptivepill.
Figure6.2A:Combinedhormonalpatch.B:combinedhormonalvaginalcontraceptivering.
www.medicalebookpdf.com
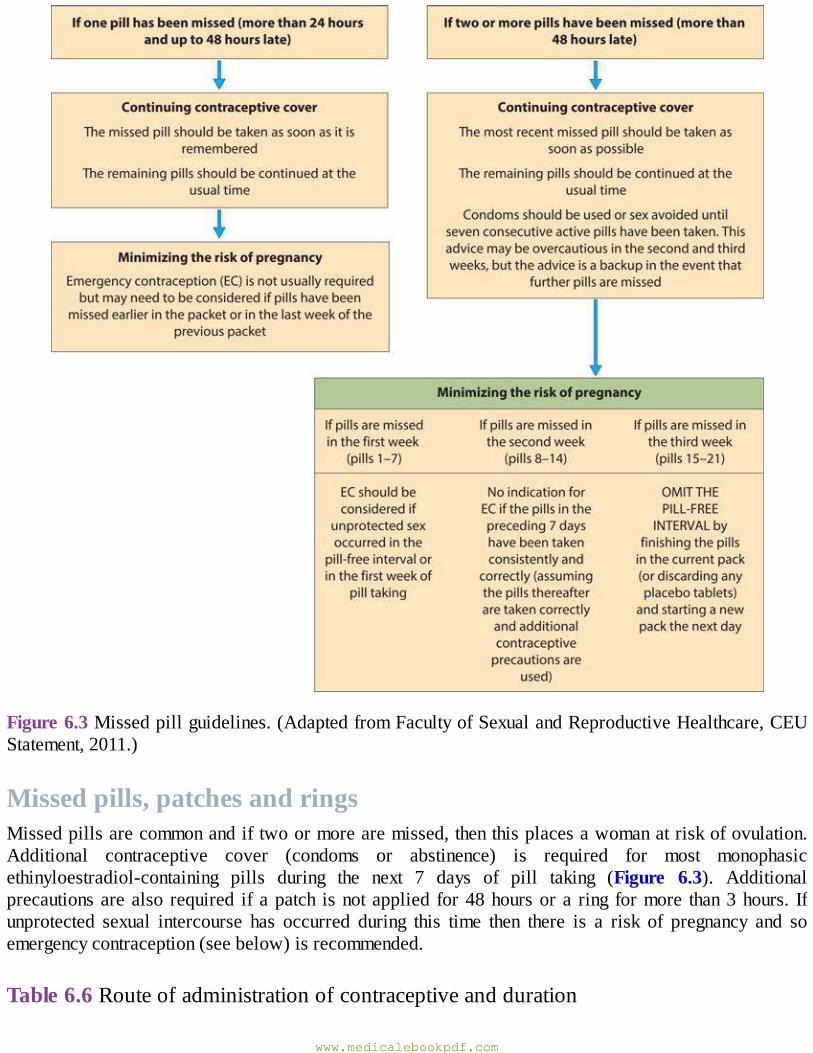
Figure6.3Missedpillguidelines.(AdaptedfromFacultyofSexualandReproductiveHealthcare,CEUStatement,2011.)
Missedpills,patchesandringsMissedpillsarecommonandiftwoormorearemissed,thenthisplacesawomanatriskofovulation.Additional contraceptive cover (condoms or abstinence) is required for most monophasicethinyloestradiol-containing pills during the next 7 days of pill taking (Figure 6.3). Additionalprecautionsarealso required ifapatch isnotapplied for48hoursora ring formore than3hours. Ifunprotected sexual intercourse has occurred during this time then there is a risk of pregnancy and soemergencycontraception(seebelow)isrecommended.
Table6.6Routeofadministrationofcontraceptiveandduration
www.medicalebookpdf.com
LengthofactionThelengthofactionhasaninfluenceontheacceptabilityandefficacyandisshowninTable6.6.
SafetyofCHCCancer
CancerrisksamongusersofCOCPs
•A12%reductionintheriskofanycancer.•Reducedriskofcolorectalcancer.•Reducedriskofendometrialcancer.•Reducedriskofovariancancer.•Increasedriskofbreastcancerduringuse(decreasesonstoppingandsimilarrisktoneverusedby10yearsafterstopping).
• Increased risk of cervical cancer (but early changes detected by cervical cytology and humanpapillomavirus[HPV]vaccination).
LargeobservationalstudieshaveshownthatwomenwhoarecurrentoreverusersofCOCPshavea12%reductionintheirriskofdeathfromanycancer.Everuseoforalcontraceptionhasbeenassociatedwitha46%reducedriskofovariancancercomparedtoneveruse,andwith10yearsuseofCOCPthereisahalvingoftheriskofovariancancer.Thisprotectionisalsoevidentforwomenwithafamilyhistoryof breast cancer (whomay be particularly at risk of ovarian cancer). In the same studies, the risk ofendometrial cancer was almost halved amongst women who had ever used the contraceptive pill
www.medicalebookpdf.com
comparedtoneverusers.Reductionin theriskofcoloncancerwasalsoobserved.Thereasonfor thisreductioninriskofcancerswithcontraceptivepilluseisnotknown.Protectionagainstovariancancercouldbeduetothesuppressionoffollicularrupturefromthesurfaceoftheovaryeachmonth.Protectionagainst endometrial cancer could be due to the progestogen content of the pill, which opposes themitogeniceffectsofoestrogenontheendometrium.
Thisprotectionagainstovarianandendometrialcancerseemstopersistformorethan15yearsafterstoppingthepill.
Most(butnotall)observationalstudieshavereportedanincreaseintheriskofbreastcanceramongstcurrent users of the COCPs.Ameta-analysis of observational studies of breast cancer inwomen andhormonal contraception suggests that current users of COCPs have an increased risk of breast cancerwhiletakingthepill,butthatsoonafterdiscontinuingthisriskdiminishes,sothattheirrisk10yearsafterstoppingisthesameasawomenwhoneverusedthepill.Ithasbeensuggestedthatstartingtousethepillmayacceleratetheappearanceofbreastcancerinsusceptiblewomen.Alternatively,womenusingthepillmighthave their tumoursdiagnosedearlier, although it isdifficult toexplainwhya tendency toearlierdiagnosiswouldpersistforyearsafterstopping.Nevertheless,abiologicaleffectofCHConthebreastremainsapossibility.
ObservationalstudieshavealsoreportedanincreaseintheriskofcervicalcanceramongstusersofCOCPs.Whilethismaybeduetoconfoundingfactorssuchasusersbeinglesslikelytousecondoms(thatprotectagainstHPV),abiologicalassociationcannotbeexcluded.However,womencanbe reassuredthatparticipatinginacervicalscreeningprogrammecandetectprecancerouscellsthatcanbeeffectivelytreated. Having HPV vaccination (against oncogenic HPV subtypes 16 and 18) before sexual activitycommences,usingcondomsandnotsmokingalsoreducestheriskofcervicalcancer.
VenousthromboembolismandarterialdiseaseCHC (pill, patch and ring) increases the tendency to thrombosis in both the venous and arterialcirculation.Theadverseeffectonvenousthrombosisisrelatedtothedoseofoestrogenandappearslesswith combined pills containing second-generation progestogens compared to those containing third- orfourth-generation progestogens. However, whichever progestogen is used, the absolute risk of venousthromboembolism (VTE) is very small and much less than that associated with pregnancy (see boxhighlightedbelow).
RiskofVTEinusersandnon-usersofCHC
•5per10,000innon-pregnantnonusers.•10per10,0000COCPusers.•29–400per10,0000inpregnant/postpartum.
The riskofVTE is greatest during the first year of use, possiblydue to theunmaskingof inheritedthrombophilias. Screening for known thrombophilias is not cost effective, butwomen should be askedabout a personal and family history of VTE if considering using this method, as these arecontraindications tousingaCHCmethod.WomenwhoareusingCHCandmaking long-distance travel(>3 h of immobility) should take appropriate exercise on the journey and considerwearing graduatedcompressionsocks.
www.medicalebookpdf.com
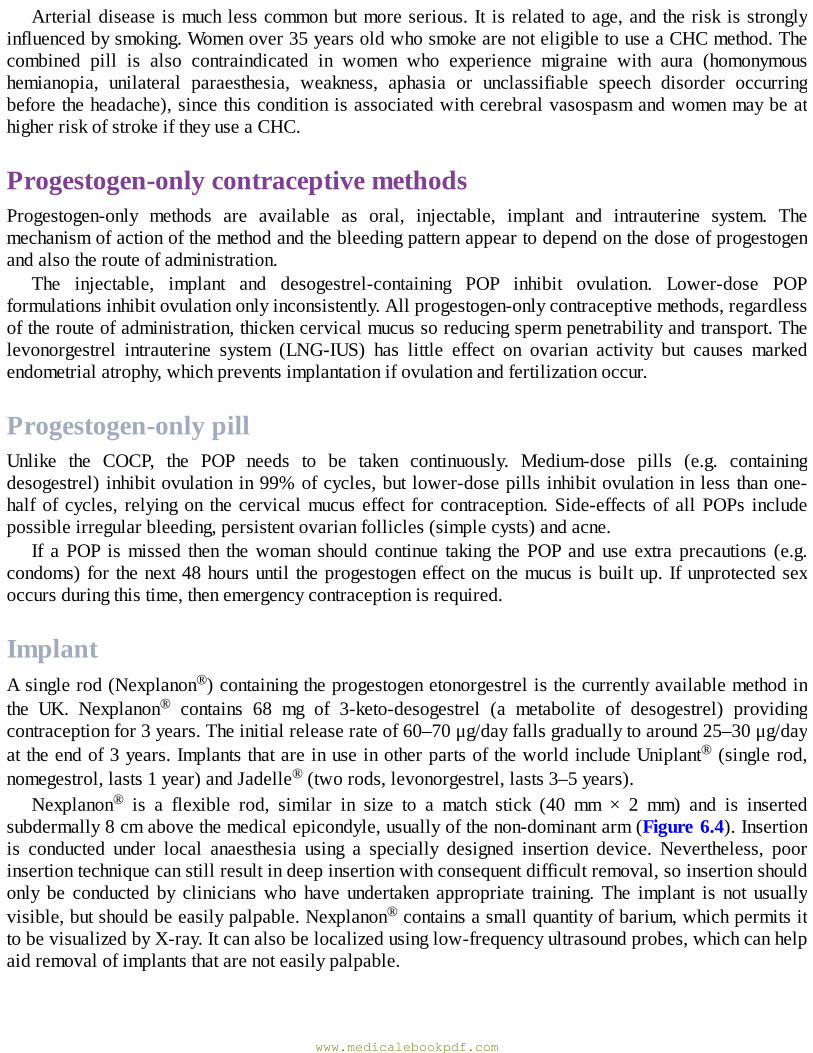
Arterialdisease ismuchlesscommonbutmoreserious. It is related toage,and therisk isstronglyinfluencedbysmoking.Womenover35yearsoldwhosmokearenoteligibletouseaCHCmethod.Thecombined pill is also contraindicated in women who experience migraine with aura (homonymoushemianopia, unilateral paraesthesia, weakness, aphasia or unclassifiable speech disorder occurringbeforetheheadache),sincethisconditionisassociatedwithcerebralvasospasmandwomenmaybeathigherriskofstrokeiftheyuseaCHC.
Progestogen-onlycontraceptivemethodsProgestogen-only methods are available as oral, injectable, implant and intrauterine system. Themechanismofactionofthemethodandthebleedingpatternappeartodependonthedoseofprogestogenandalsotherouteofadministration.
The injectable, implant and desogestrel-containing POP inhibit ovulation. Lower-dose POPformulationsinhibitovulationonlyinconsistently.Allprogestogen-onlycontraceptivemethods,regardlessoftherouteofadministration,thickencervicalmucussoreducingspermpenetrabilityandtransport.Thelevonorgestrel intrauterine system (LNG-IUS) has little effect on ovarian activity but causes markedendometrialatrophy,whichpreventsimplantationifovulationandfertilizationoccur.
Progestogen-onlypillUnlike the COCP, the POP needs to be taken continuously. Medium-dose pills (e.g. containingdesogestrel) inhibitovulationin99%ofcycles,but lower-dosepills inhibitovulationinless thanone-halfof cycles, relyingon the cervicalmucus effect for contraception.Side-effectsof allPOPs includepossibleirregularbleeding,persistentovarianfollicles(simplecysts)andacne.
If a POP ismissed then thewoman should continue taking the POP and use extra precautions (e.g.condoms)for thenext48hoursuntil theprogestogeneffecton themucus isbuiltup. Ifunprotectedsexoccursduringthistime,thenemergencycontraceptionisrequired.
ImplantAsinglerod(Nexplanon®)containingtheprogestogenetonorgestrelisthecurrentlyavailablemethodinthe UK. Nexplanon® contains 68 mg of 3-keto-desogestrel (a metabolite of desogestrel) providingcontraceptionfor3years.Theinitialreleaserateof60–70μg/dayfallsgraduallytoaround25–30μg/dayattheendof3years.ImplantsthatareinuseinotherpartsoftheworldincludeUniplant® (single rod,nomegestrol,lasts1year)andJadelle®(tworods,levonorgestrel,lasts3–5years).
Nexplanon® is a flexible rod, similar in size to a match stick (40 mm × 2 mm) and is insertedsubdermally8cmabovethemedicalepicondyle,usuallyofthenon-dominantarm(Figure6.4).Insertionis conducted under local anaesthesia using a specially designed insertion device. Nevertheless, poorinsertiontechniquecanstillresultindeepinsertionwithconsequentdifficultremoval,soinsertionshouldonly be conducted by clinicianswho have undertaken appropriate training. The implant is not usuallyvisible,butshouldbeeasilypalpable.Nexplanon®containsasmallquantityofbarium,whichpermitsittobevisualizedbyX-ray.Itcanalsobelocalizedusinglow-frequencyultrasoundprobes,whichcanhelpaidremovalofimplantsthatarenoteasilypalpable.
www.medicalebookpdf.com
Figure6.4Nexplanon.
Onceinserted,thereisnoneedforanyroutinefollow-upuntilthedeviceisdueforreplacementortheuserwishes it removed.Nexplanon® releasesasteady lowdoseofprogestogen(similar to levelsofaPOP).Afterremoval,serumlevelsofetonorgestrellevelsareundetectablewithin1week,andfertilityisrestoredimmediatelyafterremoval.
Progestogen-onlyinjectableThe most commonly used injectable worldwide is a depot injection of medroxyprogesterone acetate,which can be administered intramuscularly (buttock, upper arm, lower abdomen) as the formulationDepoprovera® (150mg)orsubcutaneouslyas themicronizedlower-doseformulationofSayanapress®(104mg).Bothintramuscularandsubcutaneouspreparationshavesimilarfeatures:samemodeofaction(inhibition of ovulation), same efficacy, similar injection interval (every 12–14 weeks) and similarbleeding pattern (over 50% amenorrhoea rates at 1 year). Since subcutaneous injections are easier togive, this preparation offers the possibility of training users to self administer, and also increases therangeofhealthcareprofessionalswhocangivetheinjection(e.g.trainedpharmacists).Thiscanincreaseaccesstothismethodforwomen,andmayincreaseitsacceptability(Figure6.5).
Theinjectableistheonlyhormonalmethodthatmaydelayreturnoffertilityafterdiscontinuation.Insomecasesitmaytakeupto1yearafterthelastinjectionforovulationtoreturn.Thereisnopermanentimpairmentof fertilitybut thisdelaymakes the injectable an inappropriatemethod forwomenwishingshort-termcontraception.
Figure6.5Sayana®-presssingle-dosecontainer.
Boththeintramuscularandsubcutaneouspreparationmaycauseweightgaininaminorityofwomenandlossofbonemineraldensity(BMD)(5%lossofBMDatlumbarspine)inthefirstfewyearsofuse.
www.medicalebookpdf.com
However, women should be advised that BMD loss seems to plateau, has not been associated withosteoporoticfracturesandappearstobereversibleonstopping.
Therehavebeenconcernsoverstudiesfromcountriesofhighhumanimmunodeficiencyvirus(HIV)prevalence (such as sub-SaharanAfrica) that have reported increased transmission and acquisition ofHIVamongstusersofDepoprovera®,comparedtousersofotherhormonalmethods.However,usersoftheinjectablearelesslikelytousecondomsthatprotectagainstHIV,andsoatpresent,theexpertopinionof theWHOis that the injectablecanbesafelyused inwomen livingwithHIVorathighriskofHIV.Condomuse in addition to the injectable should also be encouraged to protect against transmissionoracquisitionofHIV.
Progestogen-releasingintrauterinesystemThecurrentlyavailableintrauterinesystemsreleasetheprogestogenlevonorgestrelintotheuterus.TherearetwoLNG-IUSthatareavailableinEuropeandtheUSA.The52mgLNG-IUS(Mirena®)(Chapter4,Disordersofmenstrualbleeding,Figure4.3)islicensedfor5yearsforcontraceptiveuse(butifinsertedinwomen45yearsorolder,maybeusedforcontraceptionuntilthemenopause)andthe13.5mgLNG-IUS(knownasJaydess®inEuropeandSkyla®intheUSA)islicensedfor3yearsforcontraceptiveuse.The13.5mgLNG-IUShas a slightlynarrower insertiondeviceand it has a shorter frame,whichmaymakeinsertioneasierinyoungornulliparouswomen.The13.5mgLNG-IUSalsohasasilverbandattheproximalend,whichhelpsdistinguishitfromthe52mgLNG-IUSonultrasound.
The LNG-IUS works by exerting a potent hormonal effect on the endometrium, which preventsendometrialproliferationandimplantation.Itsprogestogeniceffectonthickeningthecervicalmucusalsoimpedesentryofsperm.
The LNG-IUS does not prevent ovulation. In the first fewmonths of use,manywomen experienceunpredictablebleeding.Womenshouldbeadvisedthatthisusuallyimproveswithtimeandmanywomenwill eventually have lighter or absent periods. Provision of quality information about side-effects inadvanceof fittingaLNG-IUS is important to reduceunnecessarydiscontinuation rates.Reported side-effectsoftheLNG-IUSincludeacne,breasttenderness,mooddisturbanceandheadaches.
Themostnotablenon-contraceptivebenefitofthe52mgLNG-IUSisthatofreducingHMB(reducedby90%at 12months). It ismore effective thanoral treatments, such asnorethisterone, theCOCPandtranexamicacid,atreducingmenstrualblood(seeChapter4,Disordersofmenstrualbleeding).Itisalsoeffectivefortreatingdysmenorrhoea,painassociatedwithendometriosisandadenomyosisandprotectingtheendometriumagainsthyperplasia.
Intrauterinecontraceptives(Cu-IUD,LNG-IUS)
•Last3–10years(ormore)dependingontype,woman’sageatinsertion.•Failureratelessthan1in100.•Preventfertilization.•Impaircervicalmucus.•Inhibitimplantation.
www.medicalebookpdf.com
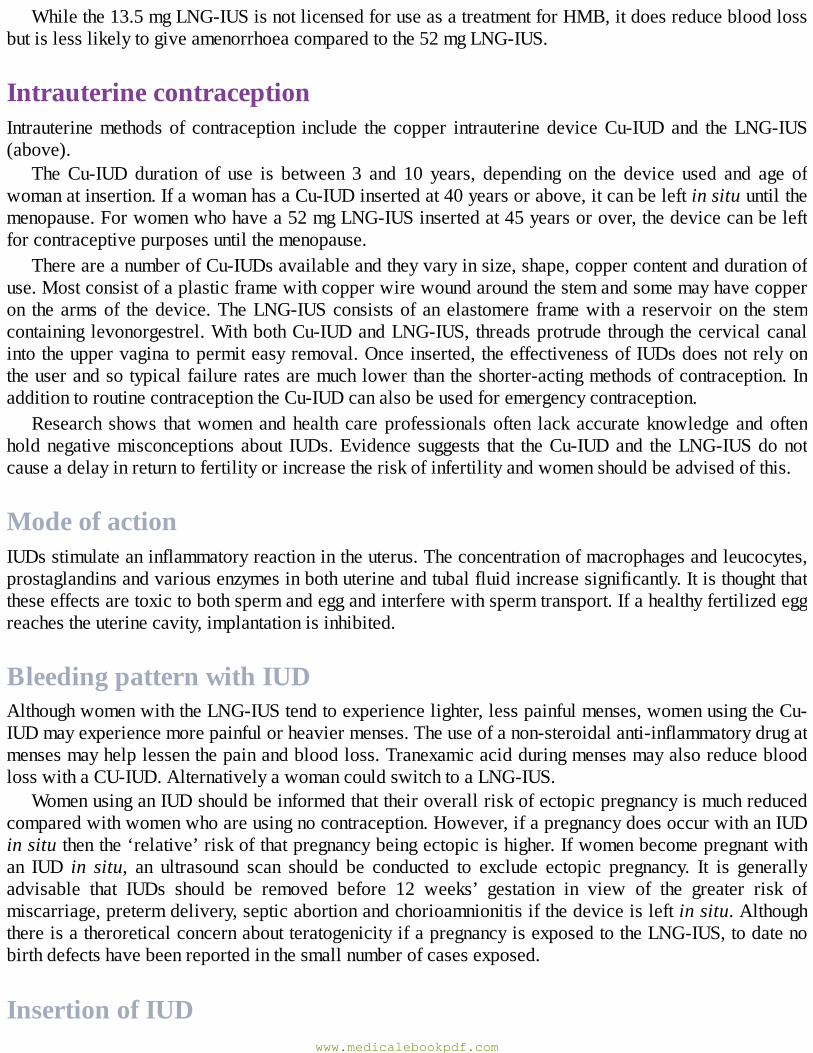
Whilethe13.5mgLNG-IUSisnotlicensedforuseasatreatmentforHMB,itdoesreducebloodlossbutislesslikelytogiveamenorrhoeacomparedtothe52mgLNG-IUS.
IntrauterinecontraceptionIntrauterinemethodsof contraception include the copper intrauterinedeviceCu-IUDand theLNG-IUS(above).
TheCu-IUD duration of use is between 3 and 10 years, depending on the device used and age ofwomanatinsertion.IfawomanhasaCu-IUDinsertedat40yearsorabove,itcanbeleftinsituuntilthemenopause.Forwomenwhohavea52mgLNG-IUSinsertedat45yearsorover,thedevicecanbeleftforcontraceptivepurposesuntilthemenopause.
ThereareanumberofCu-IUDsavailableandtheyvaryinsize,shape,coppercontentanddurationofuse.Mostconsistofaplasticframewithcopperwirewoundaroundthestemandsomemayhavecopperon thearmsof thedevice.TheLNG-IUSconsistsofanelastomere framewitha reservoiron the stemcontaininglevonorgestrel.WithbothCu-IUDandLNG-IUS, threadsprotrudethroughthecervicalcanalintotheuppervaginatopermiteasyremoval.Onceinserted,theeffectivenessofIUDsdoesnotrelyontheuserandsotypicalfailureratesaremuchlowerthantheshorter-actingmethodsofcontraception.InadditiontoroutinecontraceptiontheCu-IUDcanalsobeusedforemergencycontraception.
Research shows thatwomenandhealth careprofessionalsoften lack accurateknowledgeandoftenholdnegativemisconceptionsabout IUDs.Evidence suggests that theCu-IUDand theLNG-IUSdonotcauseadelayinreturntofertilityorincreasetheriskofinfertilityandwomenshouldbeadvisedofthis.
ModeofactionIUDsstimulateaninflammatoryreactionintheuterus.Theconcentrationofmacrophagesandleucocytes,prostaglandinsandvariousenzymesinbothuterineandtubalfluidincreasesignificantly.Itisthoughtthattheseeffectsaretoxictobothspermandeggandinterferewithspermtransport.Ifahealthyfertilizedeggreachestheuterinecavity,implantationisinhibited.
BleedingpatternwithIUDAlthoughwomenwiththeLNG-IUStendtoexperiencelighter,lesspainfulmenses,womenusingtheCu-IUDmayexperiencemorepainfulorheaviermenses.Theuseofanon-steroidalanti-inflammatorydrugatmensesmayhelplessenthepainandbloodloss.TranexamicacidduringmensesmayalsoreducebloodlosswithaCU-IUD.AlternativelyawomancouldswitchtoaLNG-IUS.
WomenusinganIUDshouldbeinformedthattheiroverallriskofectopicpregnancyismuchreducedcomparedwithwomenwhoareusingnocontraception.However,ifapregnancydoesoccurwithanIUDinsituthenthe‘relative’riskofthatpregnancybeingectopicishigher.Ifwomenbecomepregnantwithan IUD in situ, an ultrasound scan should be conducted to exclude ectopic pregnancy. It is generallyadvisable that IUDs should be removed before 12 weeks’ gestation in view of the greater risk ofmiscarriage,pretermdelivery,septicabortionandchorioamnionitisifthedeviceisleftinsitu.AlthoughthereisatheroreticalconcernaboutteratogenicityifapregnancyisexposedtotheLNG-IUS,todatenobirthdefectshavebeenreportedinthesmallnumberofcasesexposed.
InsertionofIUDwww.medicalebookpdf.com

An IUD can be fitted at any point in the cycle provided there is no risk of pregnancy. Insertion isassociatedwiththefollowingrisks:
•Perforation.Uterineperforationwith insertionof an IUD is rare: approximately1 in1,000.Factorsassociatedwithanincreasedriskofperforationincluderelativeinexperienceofclinician,breastfeedingand being less than 6months postpartum. Usually the woman presents with ‘missing threads’ and ahistoryofseverepainfollowinginsertion.Anultrasoundof theuterusconfirmsnoIUDisseenin theuterus and an abdominalX-ray shows an IUD.Laparoscopic retrieval of the device from the pelvis(oftenattachedtoomentum)ispossibleinmostcases,butlaparotomymayrarelyberequiredtoremovetheIUD.
•Expulsion.1in20IUDdeviceswillbeexpelledinthefirst3monthsafterinsertion.Afterthis,theriskof expulsion diminishes. Given that some expulsions are not always obvious to women, IUD usersshould be advised to perform regular self checks for the presence of threads in the upper vagina toensurethedeviceisstillpresent.
•Infection.Theoverallriskofpelvicinfectioninthefirst3weeksfollowinginsertionofanIUDislow(1in100).Thereafter,theriskofinfectionisthesameaswomennotusingcontraception.Inmostcases,theIUDcanbeleftinsituandantibiotictherapycommenced.IftheIUDisremovedthentheclinicianshould provide oral emergency contraception if required (i.e. due to recent unprotected sex).Actimomyces-likeorganisms(ALOs)arecommonlyidentifiedoncervicalsmearsinwomenwithandwithoutanIUD.TheroleofALOsininfectioninIUDusersisnotclear.IfawomanwithanIUDhasALOsbuthasnosymptomsofinfection,thentheIUDcanbeleftinsitu.However,ifALOsarepresentandawomanwithanIUDhassymptomsofinfection,thenthedeviceshouldberemovedandpenicillin-basedantibioticsgiven.Inaddition,womenwithsymptomsofpelvicinfectionwithanIUDshouldbetestedforsexually-transmittedinfections(STIs).Inordertominimizeriskofpelvicinfection,screeningwomenatriskofSTIsbeforeinsertionisadvised.Prophylacticantibiotics(atleasttocoverchlamydia)canbegiventowomenathighriskofinfectionifinsertionneedstobedonebeforeresultsoftestsareknown(e.g.Cu-IUDinsertionforemergencycontraception).
•‘Missing’threads.‘Missing’threadsmayindicatepregnancy,expulsionorperforation.However,itisoftenthecasethatthethreadsaremerelysittinginthecervicalcanaloruterus.Apregnancytestshouldbe performed and emergency contraception/alternative contraception provided until the IUD can beconfirmedtobeinsitu,eitherbyvisualizationofthethreadsonspeculumexaminationoranultrasoundconfirmingpresenceoftheIUDwithintheuterus.
BarriercontraceptionCondomsMalecondomsare cheapandwidely available.Theyprotect againstSTIs includingHIV.Theyare theonlyreversiblemalemethod.Typicalfailureratesareintheregionof24%sincetheyrelyontheusertoputitonitcorrectly,beforepenetrationandbeforeeveryactofsex.Thefemalecondomisalubricatedpolyurethanecondomthatisinsertedintothevagina.ItalsoprotectsagainstSTIs(Figure6.6).
www.medicalebookpdf.com

Figure6.6A:Femalecondom;B:malecondom.
DiaphragmandcapThesearelatexornon-latexdevicesthatareinsertedintothevaginatopreventpassageofspermtothecervix(Figure6.7).Theycanbeinsertedinadvanceofsex.Capsfitoverthecervixwhereasdiaphragmsformahammockbetweenthepost-fornixandthesymphysispubis.Capsanddiaphragmsareoftenusedinconjunctionwithaspermicide.Disadvantagesarethatwomenneedtobetaughthowtoinsertandremovethedeviceandtypicalfailureratesintheregionof18%arereported.Insomewomentheirusemaybeassociatedwithincreasedvaginaldischargeandurinarytractinfections.
SpermicidesSpermicide alone is not recommended for prevention of pregnancy as it is of low effectiveness.Nonoxynol9(N-9)isaspermicidalproductsoldasagel,cream,foam,spongeorpessaryforusewithdiaphragmsorcaps.Somedatahavesuggested that frequentuseofN-9might increase the riskofHIVtransmission.ItisthereforenolongerrecommendedforwomenwhoareathighriskofHIVinfection.
www.medicalebookpdf.com
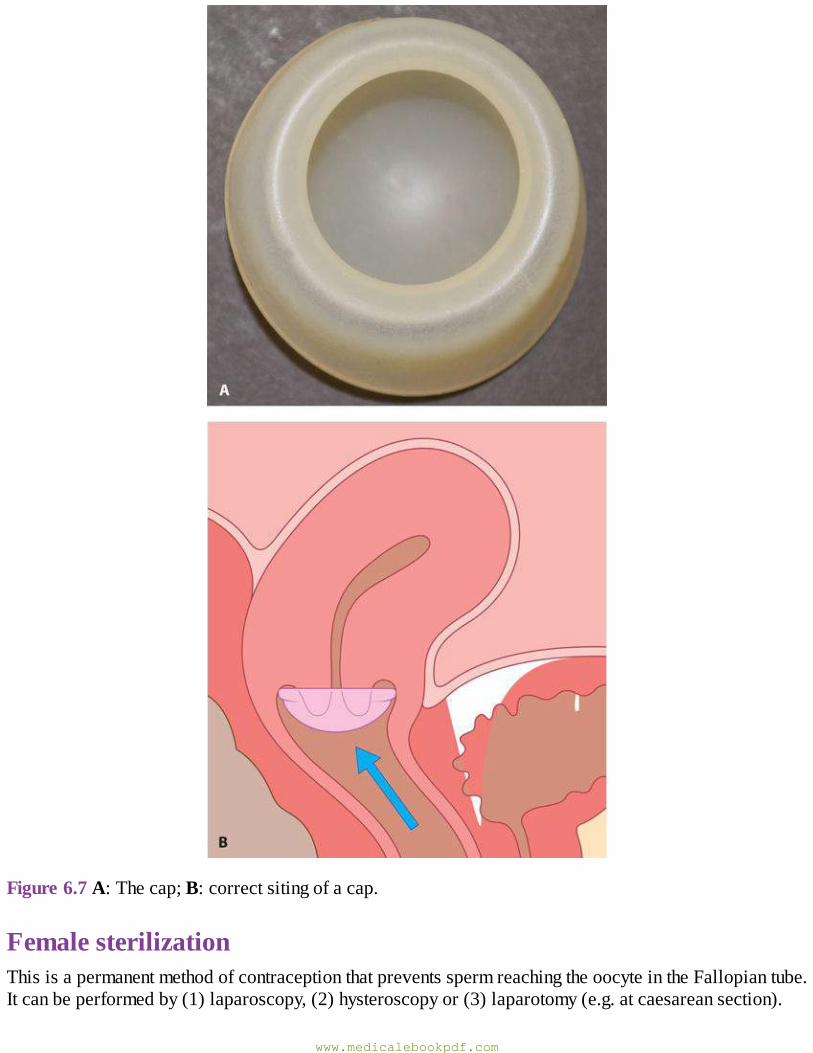
Figure6.7A:Thecap;B:correctsitingofacap.
FemalesterilizationThisisapermanentmethodofcontraceptionthatpreventsspermreachingtheoocyteintheFallopiantube.Itcanbeperformedby(1)laparoscopy,(2)hysteroscopyor(3)laparotomy(e.g.atcaesareansection).
www.medicalebookpdf.com
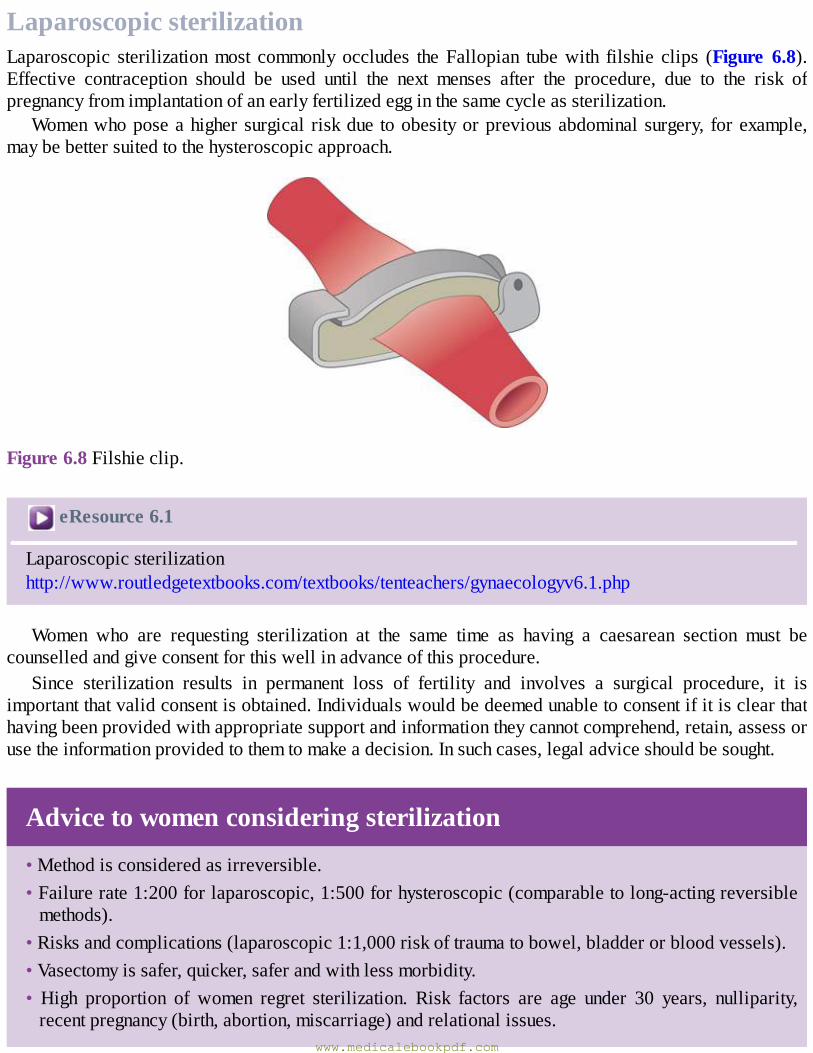
LaparoscopicsterilizationLaparoscopic sterilizationmost commonly occludes theFallopian tubewith filshie clips (Figure 6.8).Effective contraception should be used until the next menses after the procedure, due to the risk ofpregnancyfromimplantationofanearlyfertilizedegginthesamecycleassterilization.
Womenwhoposeahighersurgical riskdue toobesityorpreviousabdominalsurgery, forexample,maybebettersuitedtothehysteroscopicapproach.
Figure6.8Filshieclip.
eResource6.1
Laparoscopicsterilizationhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv6.1.php
Women who are requesting sterilization at the same time as having a caesarean section must becounselledandgiveconsentforthiswellinadvanceofthisprocedure.
Since sterilization results in permanent loss of fertility and involves a surgical procedure, it isimportantthatvalidconsentisobtained.Individualswouldbedeemedunabletoconsentifitisclearthathavingbeenprovidedwithappropriatesupportandinformationtheycannotcomprehend,retain,assessorusetheinformationprovidedtothemtomakeadecision.Insuchcases,legaladviceshouldbesought.
Advicetowomenconsideringsterilization
•Methodisconsideredasirreversible.•Failurerate1:200forlaparoscopic,1:500forhysteroscopic(comparabletolong-actingreversiblemethods).
•Risksandcomplications(laparoscopic1:1,000riskoftraumatobowel,bladderorbloodvessels).•Vasectomyissafer,quicker,saferandwithlessmorbidity.• High proportion of women regret sterilization. Risk factors are age under 30 years, nulliparity,recentpregnancy(birth,abortion,miscarriage)andrelationalissues.
www.medicalebookpdf.com
•DoesnotprotectagainstSTIs.•Effectivecontraceptionisrequireduntilthemenstrualperiodfollowinglaparoscopicprocedureor3monthsfollowinghysteroscopicprocedure.
•Pregnancy following female sterilization is rarebut if it doesoccur there is an increased riskofectopic.
•Reversal of sterilization is a highly-skilledprocedure to obtain tubal reanastomosis. It cannot beperformed after hysteroscopic sterilization, and if it is successfully conducted after laparoscopicsterilization,thenitisassociatedwithanincreasedriskofectopicpregnancy.
HysteroscopicsterilizationThishastheadvantagethat itcanbeperformedasanoutpatientprocedurewithoutgeneralanaesthesia.Microinserts (Essure®),which are expanding springs (of 2mmdiameter and4 cm in length)madeoftitanium, steel andnickel-containingDacron fibres, are inserted into the tubalostiavia ahysteroscope(Figure6.9).TheseinducefibrosiswithinthecornualsectionofeachFallopiantubeoverthefollowing3months. Contraception is required during the 3 months and can only be discontinued once correctplacementoftheinsertsareconfirmedbyX-rayimagingorultrasound.
VasectomyThisisthetechniqueofinterruptingthevasdeferenstoprovidepermanentocclusion.Theso-called‘noscalpel’vasectomyinvolvesapuncturewoundintheskinofthescrotumunderlocalanaesthesiatoaccessandthendivideandoccludethevasusingcautery(Figure6.10).
Thereisasmallriskofascrotalhaematomaandinfectionwiththeprocedure.Postvasectomysemenanalysis should be conducted at 12 weeks to confirm the absence of spermatozoa in the ejaculate.Alternativecontraceptionshouldbeuseduntilazoospermiaisconfirmed.Thefailurerateissignificantlylessthanfemalesterilizationatapproximately1in2,000.
www.medicalebookpdf.com
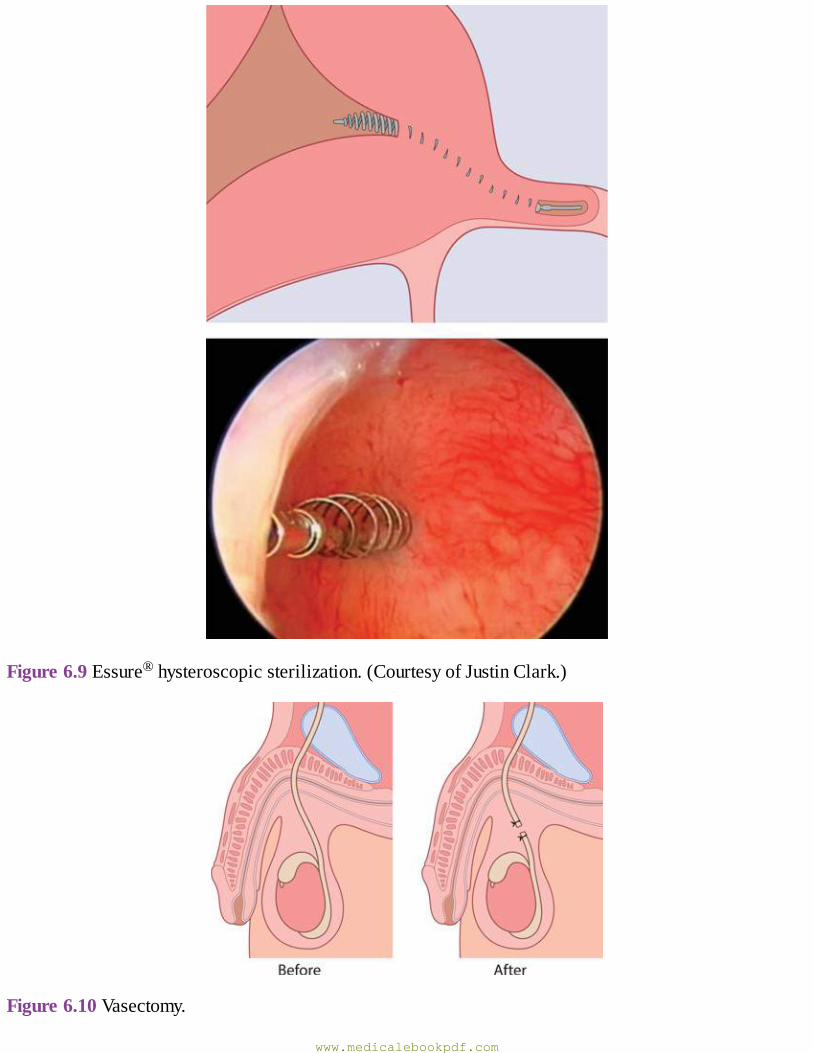
Figure6.9Essure®hysteroscopicsterilization.(CourtesyofJustinClark.)
Figure6.10Vasectomy.
www.medicalebookpdf.com
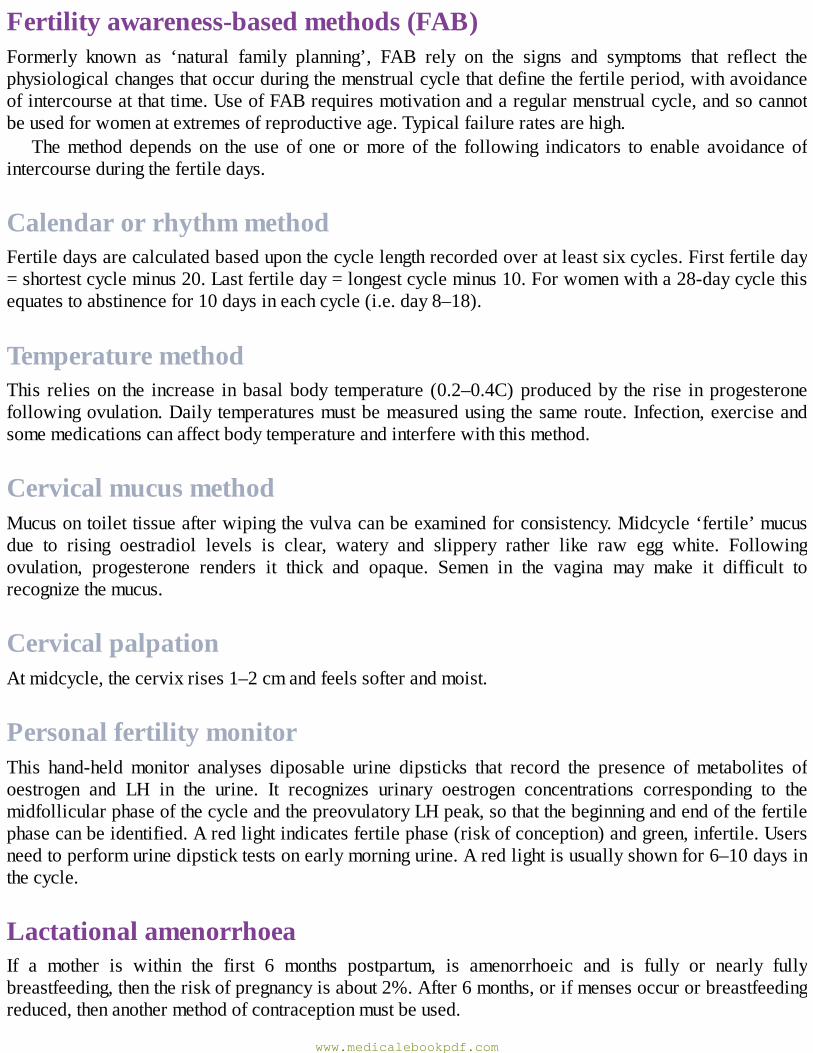
Fertilityawareness-basedmethods(FAB)Formerly known as ‘natural family planning’, FAB rely on the signs and symptoms that reflect thephysiologicalchangesthatoccurduringthemenstrualcyclethatdefinethefertileperiod,withavoidanceofintercourseatthattime.UseofFABrequiresmotivationandaregularmenstrualcycle,andsocannotbeusedforwomenatextremesofreproductiveage.Typicalfailureratesarehigh.
Themethod depends on the use of one ormore of the following indicators to enable avoidance ofintercourseduringthefertiledays.
CalendarorrhythmmethodFertiledaysarecalculatedbaseduponthecyclelengthrecordedoveratleastsixcycles.Firstfertileday=shortestcycleminus20.Lastfertileday=longestcycleminus10.Forwomenwitha28-daycyclethisequatestoabstinencefor10daysineachcycle(i.e.day8–18).
TemperaturemethodThis relieson the increase inbasalbody temperature (0.2–0.4C)producedby the rise inprogesteronefollowingovulation.Dailytemperaturesmustbemeasuredusingthesameroute.Infection,exerciseandsomemedicationscanaffectbodytemperatureandinterferewiththismethod.
CervicalmucusmethodMucusontoilettissueafterwipingthevulvacanbeexaminedforconsistency.Midcycle‘fertile’mucusdue to rising oestradiol levels is clear, watery and slippery rather like raw egg white. Followingovulation, progesterone renders it thick and opaque. Semen in the vagina may make it difficult torecognizethemucus.
CervicalpalpationAtmidcycle,thecervixrises1–2cmandfeelssofterandmoist.
PersonalfertilitymonitorThis hand-held monitor analyses diposable urine dipsticks that record the presence of metabolites ofoestrogen and LH in the urine. It recognizes urinary oestrogen concentrations corresponding to themidfollicularphaseofthecycleandthepreovulatoryLHpeak,sothatthebeginningandendofthefertilephasecanbeidentified.Aredlightindicatesfertilephase(riskofconception)andgreen,infertile.Usersneedtoperformurinedipsticktestsonearlymorningurine.Aredlightisusuallyshownfor6–10daysinthecycle.
LactationalamenorrhoeaIf a mother is within the first 6 months postpartum, is amenorrhoeic and is fully or nearly fullybreastfeeding,thentheriskofpregnancyisabout2%.After6months,orifmensesoccurorbreastfeedingreduced,thenanothermethodofcontraceptionmustbeused.
www.medicalebookpdf.com
EmergencycontraceptionAllwomendeserveasecondchancetopreventanunintendedpregnancy.
TheCu-IUDisthemosteffectivemethodofemergencycontraception(EC)available(failurerate1in1,000) and should ideally be offered as first choice to women.When used for EC, its effect on theendometriumisthoughttopreventimplantationiffertilizationhasoccurred.TheCu-IUDcanberemovedoncepregnancyhasbeenexcludedorcanbeleftinplaceforongoingcontraception.Sincetheblastocystwillimplantbetween6and10daysafterfertilization,anemergencyCu-IUDcanbeinsertedupto5daysaftertheunprotectedsexor5daysafterpredictedovulation(i.e.ina28-daycycle,predictedovulationday14plus5days= insertup today19forEC) inorder toavoiddisruptingan implantedpregnancy.There is no evidence that the LNG-IUS is effective as EC and should therefore not be used for thispurpose.
The two oral methods of EC that are licensed for use are levonorgestrel (LNG 1.5 mg) and theprogesteronereceptormodulatorulipristalacetate(30mg).LNGappearseffectiveupto96hoursafterunprotectedsexandulipristalacetateforupto120hours.Bothmethodsworkbydelayingovulation,sothatanyspermpresentinthereproductivetractwillhavelosttheabilitytofertilizetheoocyteonceitiseventuallyreleased.OralECismuchlesseffectivethantheCu-IUDforECandisestimatedtopreventonlytwo-thirdsofpregnancies.OralECismuchlesseffectivethanregularcontraception.Womenshouldbe encouraged to start an effective method of contraception immediately after EC, to protect againstpregnancyfromfurtheractsofintercourse.
Emergencycontraception
•ThemosteffectivemethodofECisanIUD(about99%effective).•AnIUDcanbeinsertedupto5daysafterovulationforEC.•Ulipristalacetate(UPA)orlevonorgestrel(LNG)areavailableasoralmethodsofEC.•UPAcanbegivenwithin120hoursofunprotectedintercourse.•LNGcanbeusedwithin96hoursofunprotectedintercourse.•EffectiveongoingcontraceptionshouldbestartedafterEC.
OpportunitiestoprovidecontraceptionThereareimportantopportunitiestodiscussandprovideeffectivecontraceptionwhenwomenpresenttogynaecologyclinics(Table6.7).Theseincludepresentationtoageneralgynaecologyclinic,presentationsfor EC, presentation to request an induced abortion and also antenatally or after childbirth. Theantenatal/postpartumperiodisaparticularlyimportantopportunitysince95%ofpostpartumwomenwantto avoidpregnancy in thenext12months, and inwomenwhoarenot fullybreastfeeding, fertilitymayreturn at 1 month postpartum. In addition, closely-spaced pregnancies increase the risks of pretermdelivery,lowbirthweightandsmallforgestationalagebabies.Theriskofchildmortalityishighestforvery short birth topregnancy intervals (<12months). It is estimated that 30%ofmaternal and10%ofchilddeathsworldwidecouldbepreventedifcouplesspacepregnanciesmorethan2yearsapart.
Table6.7Opportunitiestoprovidecontraceptionwww.medicalebookpdf.com
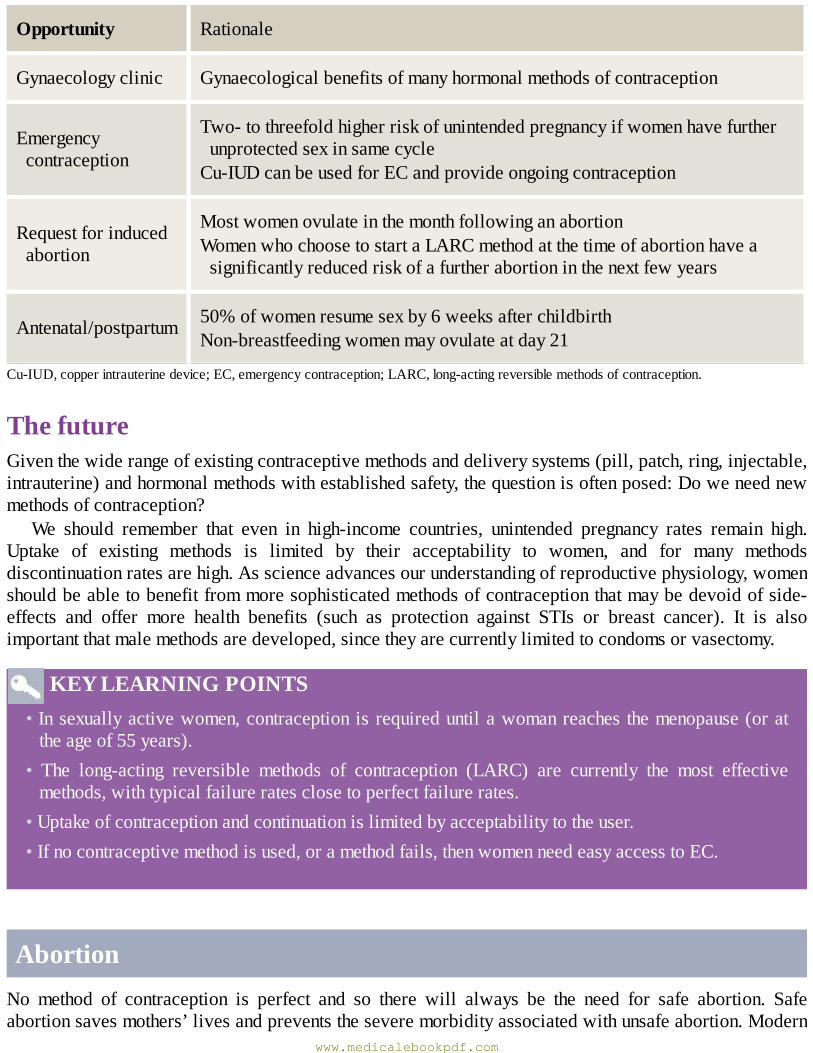
Opportunity Rationale
Gynaecologyclinic Gynaecologicalbenefitsofmanyhormonalmethodsofcontraception
Emergencycontraception
Two-tothreefoldhigherriskofunintendedpregnancyifwomenhavefurtherunprotectedsexinsamecycleCu-IUDcanbeusedforECandprovideongoingcontraception
Requestforinducedabortion
MostwomenovulateinthemonthfollowinganabortionWomenwhochoosetostartaLARCmethodatthetimeofabortionhaveasignificantlyreducedriskofafurtherabortioninthenextfewyears
Antenatal/postpartum 50%ofwomenresumesexby6weeksafterchildbirthNon-breastfeedingwomenmayovulateatday21
Cu-IUD,copperintrauterinedevice;EC,emergencycontraception;LARC,long-actingreversiblemethodsofcontraception.
ThefutureGiventhewiderangeofexistingcontraceptivemethodsanddeliverysystems(pill,patch,ring,injectable,intrauterine)andhormonalmethodswithestablishedsafety,thequestionisoftenposed:Doweneednewmethodsofcontraception?
We should remember that even in high-income countries, unintended pregnancy rates remain high.Uptake of existing methods is limited by their acceptability to women, and for many methodsdiscontinuationratesarehigh.Asscienceadvancesourunderstandingofreproductivephysiology,womenshouldbeabletobenefitfrommoresophisticatedmethodsofcontraceptionthatmaybedevoidofside-effects and offer more health benefits (such as protection against STIs or breast cancer). It is alsoimportantthatmalemethodsaredeveloped,sincetheyarecurrentlylimitedtocondomsorvasectomy.
KEYLEARNINGPOINTS•Insexuallyactivewomen,contraceptionisrequireduntilawomanreaches themenopause(orattheageof55years).
• The long-acting reversible methods of contraception (LARC) are currently the most effectivemethods,withtypicalfailureratesclosetoperfectfailurerates.
•Uptakeofcontraceptionandcontinuationislimitedbyacceptabilitytotheuser.•Ifnocontraceptivemethodisused,oramethodfails,thenwomenneedeasyaccesstoEC.
AbortionNo method of contraception is perfect and so there will always be the need for safe abortion. Safeabortionsavesmothers’livesandpreventstheseveremorbidityassociatedwithunsafeabortion.Modern
www.medicalebookpdf.com
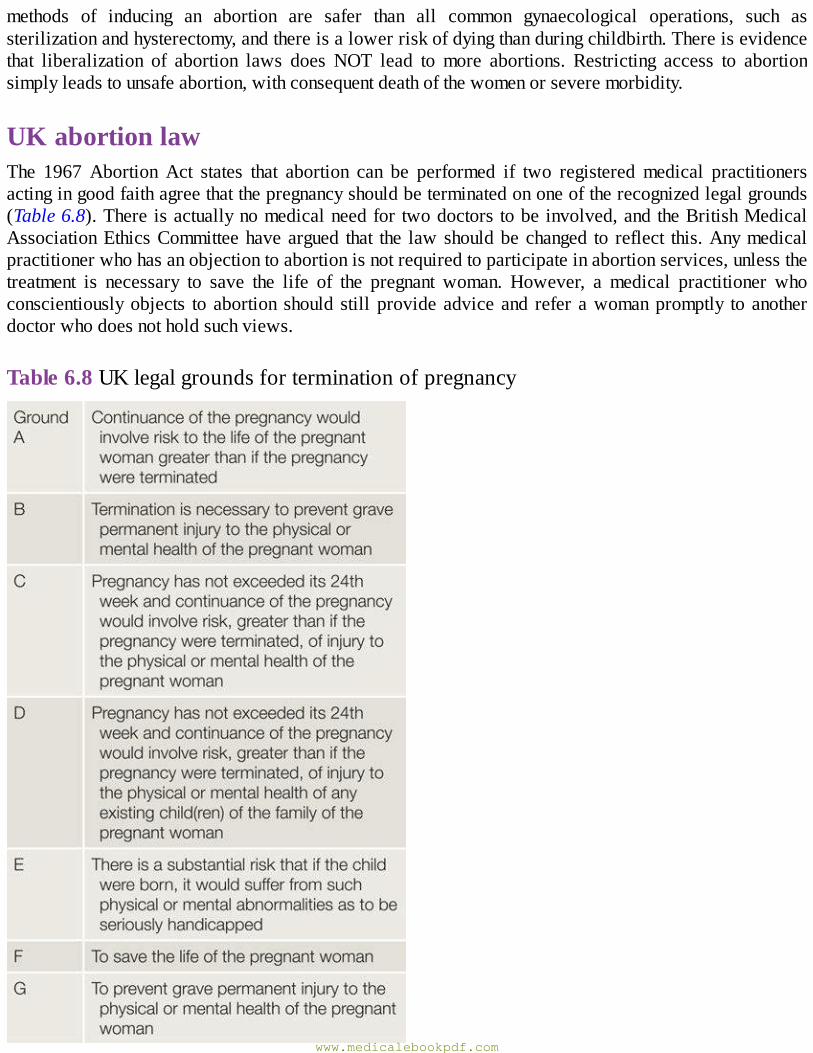
methods of inducing an abortion are safer than all common gynaecological operations, such assterilizationandhysterectomy,andthereisalowerriskofdyingthanduringchildbirth.Thereisevidencethat liberalization of abortion laws does NOT lead to more abortions. Restricting access to abortionsimplyleadstounsafeabortion,withconsequentdeathofthewomenorseveremorbidity.
UKabortionlawThe 1967 Abortion Act states that abortion can be performed if two registeredmedical practitionersactingingoodfaithagreethatthepregnancyshouldbeterminatedononeoftherecognizedlegalgrounds(Table6.8).Thereisactuallynomedicalneedfor twodoctors tobeinvolved,andtheBritishMedicalAssociationEthicsCommitteehaveargued that the lawshouldbechanged to reflect this.Anymedicalpractitionerwhohasanobjectiontoabortionisnotrequiredtoparticipateinabortionservices,unlessthetreatment is necessary to save the life of the pregnant woman. However, a medical practitioner whoconscientiouslyobjects toabortion should stillprovideadviceand refer awomanpromptly toanotherdoctorwhodoesnotholdsuchviews.
Table6.8UKlegalgroundsforterminationofpregnancy
www.medicalebookpdf.com
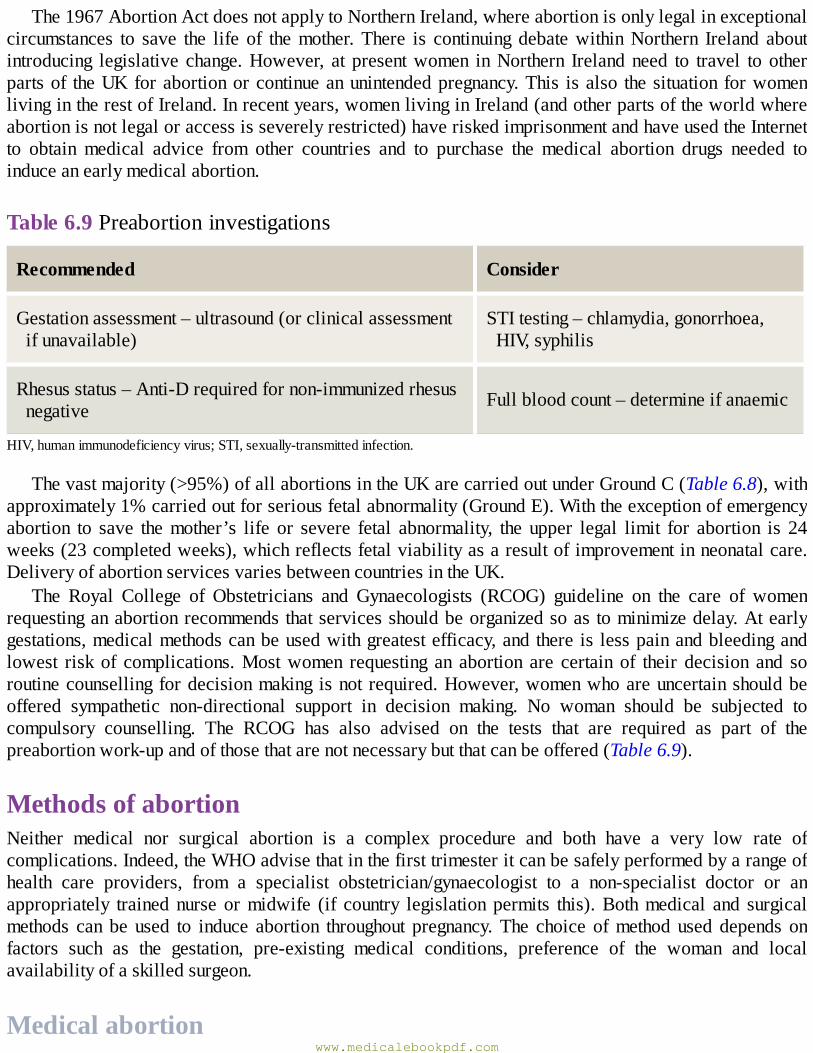
The1967AbortionActdoesnotapplytoNorthernIreland,whereabortionisonlylegalinexceptionalcircumstances to save the life of themother.There is continuing debatewithinNorthern Ireland aboutintroducing legislative change.However, at presentwomen inNorthern Irelandneed to travel to otherpartsof theUKforabortionorcontinueanunintendedpregnancy.This isalso thesituation forwomenlivingintherestofIreland.Inrecentyears,womenlivinginIreland(andotherpartsoftheworldwhereabortionisnotlegaloraccessisseverelyrestricted)haveriskedimprisonmentandhaveusedtheInternetto obtain medical advice from other countries and to purchase the medical abortion drugs needed toinduceanearlymedicalabortion.
Table6.9Preabortioninvestigations
Recommended Consider
Gestationassessment–ultrasound(orclinicalassessmentifunavailable)
STItesting–chlamydia,gonorrhoea,HIV,syphilis
Rhesusstatus–Anti-Drequiredfornon-immunizedrhesusnegative Fullbloodcount–determineifanaemic
HIV,humanimmunodeficiencyvirus;STI,sexually-transmittedinfection.
Thevastmajority(>95%)ofallabortionsintheUKarecarriedoutunderGroundC(Table6.8),withapproximately1%carriedoutforseriousfetalabnormality(GroundE).Withtheexceptionofemergencyabortion to save themother’s life or severe fetal abnormality, the upper legal limit for abortion is 24weeks(23completedweeks),whichreflectsfetalviabilityasaresultofimprovementinneonatalcare.DeliveryofabortionservicesvariesbetweencountriesintheUK.
The Royal College of Obstetricians and Gynaecologists (RCOG) guideline on the care of womenrequestinganabortionrecommendsthatservicesshouldbeorganizedsoas tominimizedelay.Atearlygestations,medicalmethodscanbeusedwithgreatestefficacy,andthere is lesspainandbleedingandlowest risk of complications.Mostwomen requesting an abortion are certain of their decision and soroutinecounsellingfordecisionmaking isnot required.However,womenwhoareuncertainshouldbeoffered sympathetic non-directional support in decision making. No woman should be subjected tocompulsory counselling. The RCOG has also advised on the tests that are required as part of thepreabortionwork-upandofthosethatarenotnecessarybutthatcanbeoffered(Table6.9).
MethodsofabortionNeither medical nor surgical abortion is a complex procedure and both have a very low rate ofcomplications.Indeed,theWHOadvisethatinthefirsttrimesteritcanbesafelyperformedbyarangeofhealth care providers, from a specialist obstetrician/gynaecologist to a non-specialist doctor or anappropriately trained nurse ormidwife (if country legislation permits this).Bothmedical and surgicalmethods can be used to induce abortion throughout pregnancy.The choice ofmethod used depends onfactors such as the gestation, pre-existing medical conditions, preference of the woman and localavailabilityofaskilledsurgeon.
Medicalabortionwww.medicalebookpdf.com
ThemajorityofwomenundergoingabortionintheUK(asinothercountrieswheremedicalmethodsareavailable)choosetohaveabortionperformedmedically.Thisinvolvesthecombinationofmifepristone(aprogesteronereceptormodulator)followedbyaprostaglandinanalogue,misoprostol.
Progesterone is necessary to maintain uterine quiescence, so administration of mifepristone (oral)bringsaboutanincreaseinuterinecontractility.Italsosensitizestheuterustoexogenousprostaglandins.Thispermitslowerdosesofmisoprostoltobeusedtobringaboutexpulsion.Theeffectofmifepristoneismaximalat48hourssothatifmisoprostolisadministeredatanintervalof24–48hourslater,thenthereisanincreaseincrampingpain,bleedingandexpulsionofthefetusthroughtheslightlydilatedcervix.Inthefirst9weeksofpregnancy,womencansafelyself-administer thesemedicationsathome(if thecountrylegislation permits) and expel the pregnancy at home. Simple oral analgesia (e.g. ibuprofen,dihydrocodeine) is usually sufficient to provide pain relief.Women can be advised that at 9 weeks’gestationtheywillbleedforonaverage2weeksfollowingthemedicalabortion.
After9weeks’gestation, thesamecombinationofmifepristoneandmisoprostol isused,except thatthe regimen requires repeated doses of misoprostol to be administered every 3 hours until expulsionoccurs.After9weeks’gestation,thediscomfort, increasedbleedingandpassageofalargerfetusmeanthatwomenaremanaged inaclinicalsetting. In thesecondtrimester, theaverage induction toabortiontime(fromfirstdoseofmisoprostoltoexpulsion)is7hours.
After 21 completed weeks (i.e. 21 weeks and 6 days) the RCOG recommends that for womenundergoingmedical abortion, feticide should be used to eliminate the possibility of the aborted fetusdisplayinganysignsoflife.Thisisusuallyconductedbyintracardiacinjectionofpotassiumchlorideoranintrafetalor intramniotic injectionofdigoxin.Theneuralpathwaysnecessarytoexperiencepainarenotfullydevelopedinthefetusuntilafter24weeks.
SurgicalmethodsVacuumaspirationVacuumaspirationisthemethodthatshouldbeusedtoconductasurgicalterminationofpregnancyupto14weeks.Theprocedureinvolvesgentlydilatingthecervixwithgraduateddilators(usuallytothesizeinmmthattheuterusisinweeks’gestation)andthenevacuatingthecavitywithgentlesuction.Thisusuallytakes less than 10 minutes to perform. Sharp curettage should never be performed (increased risk ofperforation and intrauterine adhesions). Vacuum aspiration can be performed either using a manualhandheldaspirator(manualvacuumaspiration,MVA)orusingelectricalvacuumaspiration(EVA).ThereislittletochoosebetweenMVAandEVA.TheMVAmaybemorepracticalandportableforuseintheoutpatientsetting.TheEVAgivesamoreconstantsuction.
Surgicalterminationcanbeperformedundereitherlocalorgeneralanaesthesia.Localanaesthesiainthe first trimester is preferred as it minimizes any small risk of anaesthestic drugs. It is important toconsiderpretreatmentofthecervixwithmisoprostolforallwomenundergoingsurgicalabortion.Theuseofmisoprostolhasbeenshowntobringaboutcervicaldilationandsomakesinstrumentalcervicaleasierandminimizestheriskofincompleteabortion.Asaminimum,pretreatmentshouldalwaysbeusedafter12weeks’gestationorinwomeninwhomcervicaldilationmaybeanticipatedtobemoredifficult(e.g.nulliparous,adolescent,previouscervicalsurgery).Theoptimalregimenforcervicalpretreatmentis400µgmisoprostolgivensublingually1hourpriortothesurgicalprocedure.
Itisrecommendedthatprophylacticantibioticsshouldbegiven(periabortal)withsurgicalabortion,since this has been shown to significantly reduce the risk of postabortal infection following this
www.medicalebookpdf.com
procedure.Prophylacticantibiotics arenot considerednecessary followingmedical abortion, since theoverallincidenceofpostabortalinfectionisloweraftermedicalthanaftersurgicalabortion.
DilationandevacuationAfter 14 weeks, the surgical technique of choice is dilation and evacuation. In skilled hands, thisprocedure has a low complication rate and is highly acceptable towomen. It iswidely used inNorthAmerica, but is less common in Europe. It is necessary to achieve good cervical dilation before theprocedure (up to 20 mm) in order to remove larger fetal parts. This is achieved using one or acombination of either osmotic dilators (hygroscopic sticks placed in the cervix several hourspreprocedurethatabsorbfluidfromsurroundingtissues,causingthemtoswellandbringaboutcervicaldilation), ormisoprostol (vaginal or sublingual) ormifepristone (oral). At surgery, the cervix is thenfurther dilated using graduated dilators and the contents of the uterus removed by a combination ofaspirationandextractionoffetaltissueusingappropriateinstruments;ultrasoundisperformedtoconfirmcompleteevacuation.
SequelaeofabortionBothmedicalandsurgicalabortionaresafewithalowincidenceofcomplications.Complicationswhentheydooccur include failure to end the pregnancy (ongoingpregnancy), incomplete abortion requiringevacuation, infection and haemorrhage. In the absence of a serious complication (such as operativecomplicationorsevereinfection),thereisnoimpactonfuturereductivepotential.Thereisnoassociationwith future infertility or ectopic pregnancy.While several studies have suggested an increased risk ofpretermdeliveryfollowingabortion,findingsofrecentstudieshavesuggestedthatmodernmedicalandsurgicalmethodsofinducingabortionarenotassociatedwiththisrisk.
There is no association with breast cancer. There is no adverse effect on mental health, althoughwomenwithanexistinghistoryofmentalhealthareatincreasedriskofexacerbationpostabortion,astheyarepostpartum.Womenforwhomthepregnancywasoriginally intended,womenwhoareunsupported,women who are ambivalent about the decision to terminate or who belong to a group that feels thatabortion is morally wrong, are at higher risk of ongoing distress or regret following the procedure.Womenshouldbegiveninformationonhowtoseekhelpundersuchcircumstances.
Follow-upafterabortionThere is nomedical need for a follow-up after an uncomplicated abortion. Rather, women should beprovidedwithgoodverbalandwrittenadviceaboutsignsandsymptomsthatmightindicatetheneedtoseek medical attention, together with access to a 24-hour emergency care. Women should also beprovidedwith theirchosenmethodofongoingcontraceptionat the timeof theabortionprocedure.Forwomen who have had an early medical abortion at home, there should be an effective method ofconfirmingsuccessoftheabortion.Thiscouldbeascheduledultrasound(toexcludeongoingpregnancy)oraself-performedurinepregnancytestathomeincombinationwith/withouta telephonecallfromtheprovider to determine the result of the pregnancy test and confirm that the woman has had expecteddurationofbleedingandthatsymptomsofpregnancyhavedisappeared.
Postabortalcontraceptionwww.medicalebookpdf.com
Mostwomenovulate in the firstmonth after the abortion, andmore thanone-half ofwomenwill haveresumed sex by 2 weeks postabortion. Effective contraception should therefore be commencedimmediatelyifwomenwanttoavoidanotherunintendedpregnancy.
There is evidence thatwomenwho choose to use themost effectiveLARCpostabortion (and starttheseimmediatelyaftertheabortion)haveasignificantlyreducedriskofhavingasubsequentunintendedpregnancy, compared towomenchoosingothermethods.Therehasbeenmucheffort in recentyears inensuringabortionservicesprovidehigh-qualityinformationaboutcontraceptionandareabletoprovideallmethodsatthetimeofdischargefollowingtheprocedure(includingprovisionofLARC).Allmethods(including hormonal and intrauterine) can be safely commenced at the time of abortion. Intrauterinemethodscanbeinsertedatthetimeofsurgicalabortion,andfollowingexpulsionofthefetusatmedicalabortion.
FurtherreadingFaculty of Sexual and Reproductive Healthcare, Clinical Effectiveness Unit Guideline (2015).Problematicbleedingwithhormonalcontraception.www.fsrh.org.
Trussell J (2014). Contraceptive efficacy.Glob Libr Womens Med [last accessed 06.05.14], ISSN:1756-2228, http://dx.doi.org/10.3843/GLOWM10375. This chapter was last updated,http://www.glowm.com/section_view/item/374;2014.
World Health Organization (2015). Medical Eligibility Criteria for Contraceptive Use, 5th edn.Geneva:WHO;www.WHO.org.
Selfassessment
CASEHISTORY
A44-year-oldwomanrequestssterilizationasshedoesnotwantanymorechildren.Shehasthreechildren. Her partner will not consider a vasectomy. She has regular but heavy menses. She iscurrentlyusingnomethodofcontraception.Shesmokesandsuffersfrommigraine.
AWhatarethekeypointstocoverinthecounsellingonsterilization?BWhatalternativemethodsofcontraceptionmightbeappropriateforthiswoman?CWhatmethodsofcontraceptionisshenotmedicallyeligiblefor?
ANSWERS
AImportantpointstocoverarethatsterilizationshouldbeconsideredasirreversible,thatithasafailure rate of approx 1:200 and that it is a surgical procedure with associated risks andcomplications. It is no more effective than long-acting reversible methods. Also, pregnancyfollowingfemalesterilizationisrarebutifitdoesoccurthereisanincreasedriskofectopic,andreversalofsterilization isahighly-skilledprocedure toobtain tubal reanastomosis. Itcannotbe
www.medicalebookpdf.com
performedafterhysteroscopicsterilizationand if it issuccessfullyconductedafter laparoscopicsterilization,thenitisassociatedwithanincreasedriskofectopicpregnancy.
B The LNG-IUS provides comparable contraceptive effectiveness, and also has the non-contraceptivebenefit of reducedmenstrual blood loss.Otherprogestogen-onlymethods such asPOPor implantmayalsobeappropriate,but irregularbleeding iscommonandPOPhashighertypicalfailurerates.Theinjectablecouldalsobeconsidered.
CCHCiscontraindicatedsincethewomanisasmokerwhoisover35yearsandalsohasmigraine.TheCu-IUDisnotidealsincethismayexacerbatetheexistingheavymenses.
EMQ
Characteristicsofcontraceptivemethods
AUPA.BProgestogen-onlyinjectable.CCOCP.DCu-IUD.ELNG-IUS.FProgestogen-onlyimplant.GLactationalamenorrhoea.HDiaphragm.For each description below choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
1Whichisthemosteffectiveemergencycontraceptiveavailable?2Candelayreturntofertilityondiscontinuation.3Isassociatedwithtypicalfailureratesof12per100inthefirst12months.4Mainmodeofactionispreventionoffertilization.
ANSWERS
1DCu-IUD.Butmustbeusedwithin5daysofpredictedovulation.2BProgestogen-onlyinjectable.Irregularbleedingandinvolutioncanpersistforseveralmonths.3CCOCP.ThisfigureshouldbeknownastheCOCPisfrequentlyprescribedandpatientsneedto
knowtheriskoffailure.4DCu-IUD.Throughtheeffectofspermicideaswellasthickenedcervicalmucus.
SBAQUESTIONS
www.medicalebookpdf.com
1 A 19-year-old woman who previously had a medical abortion attends a clinic requestingcontraception.Sheisoverweightandhasacnebuthasnoothermedicalhistoryofnote.Hermotherhadadeepveinthrombosis(DVT)afterchildbirth.Whichofthefollowingisnotasuitablemethodforher?Choosethesinglebestanswer.
ADepoprovera.BPOP.CCHCpatch.DLNG-IUS.EProgestogen-onlyimplant.
ANSWER
CThefamilyhistoryofDVTinafirst-degreerelativeisacontraindicationtoallCHCmethods.
2A29-year-old femalepresents requesting contraception.She is known tohavepolycystic ovarysyndromeandstruggleswithacneandhirsutism.Shewouldliketohaveababyin12monthstime.Shehasnoothermedicalconditionsandisfitandhealthy.Whatwouldbethebestcontraceptiveoptionforher?Choosethesinglebestanswer.
AIUD.BProgestogen-onlyimplant.CCOCP.DProgestogen-onlyinjectable.EIUS.
ANSWER
CCOCPwillprovidenon-contraceptivebenefitforacneandhirsutismbecauseitcausesanincreaseinsexhormone-bindingglobulin(SHBG),whichreducesfreetestosterone.Thereisnodelayofreturntofertility.
TheotherchoiceswouldprovidegoodcontraceptionbutnoimprovementinPCOSsymptoms.
www.medicalebookpdf.com
CHAPTER7Subfertility
STUARTLAVERY
Introduction
Naturalconception
Causesofsubfertility
Historyandexamination
Investigations
Management
Fertilitypreservation
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthedefinitionandcausesofsubfertility.
•Describetheconceptofovarianreserve.
•Understandthehistory,examinationandinvestigationsrelevanttosubfertility.
•Understandtheprovisionandregulationoffertilitytreatment.
•Explaintheprocessesandproceduresinvolvedinassistedreproductivetreatment(ART).
•UnderstandtheoutcomesandsuccessratesofART.www.medicalebookpdf.com
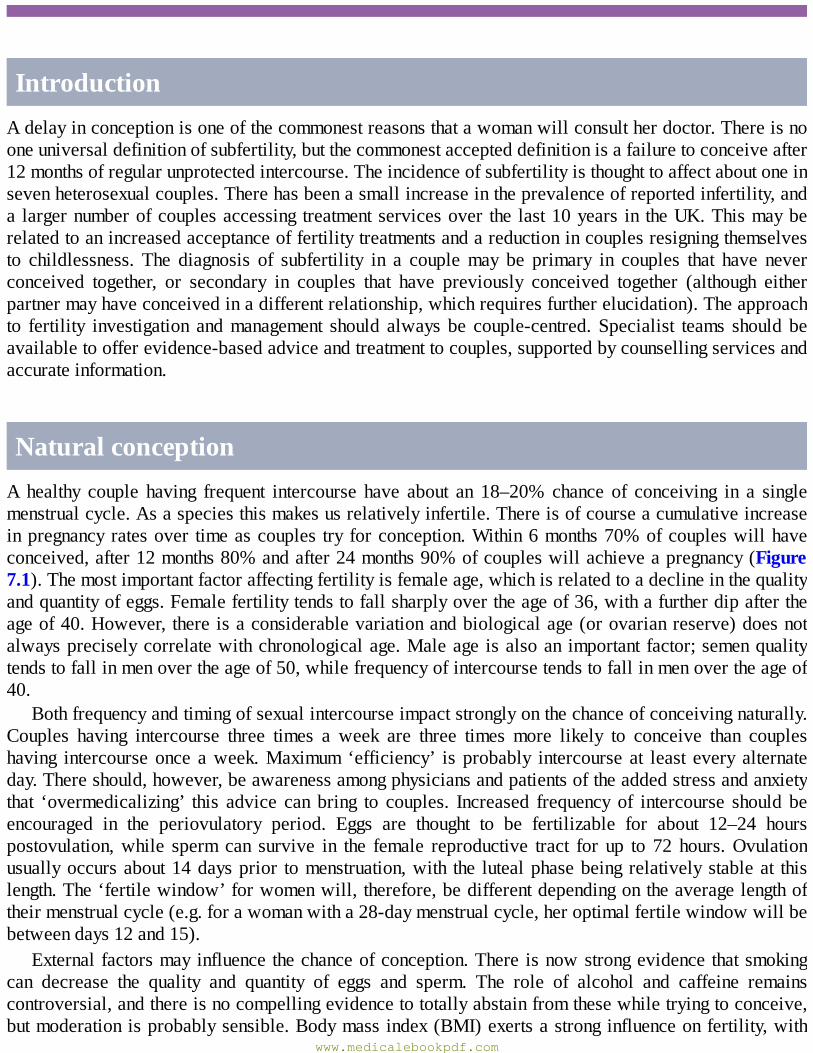
IntroductionAdelayinconceptionisoneofthecommonestreasonsthatawomanwillconsultherdoctor.Thereisnooneuniversaldefinitionofsubfertility,butthecommonestaccepteddefinitionisafailuretoconceiveafter12monthsofregularunprotectedintercourse.Theincidenceofsubfertilityisthoughttoaffectaboutoneinsevenheterosexualcouples.Therehasbeenasmallincreaseintheprevalenceofreportedinfertility,anda largernumberofcouplesaccessing treatmentservicesover the last10years in theUK.Thismayberelatedtoanincreasedacceptanceoffertilitytreatmentsandareductionincouplesresigningthemselvesto childlessness. The diagnosis of subfertility in a couplemay be primary in couples that have neverconceived together, or secondary in couples that have previously conceived together (although eitherpartnermayhaveconceivedinadifferentrelationship,whichrequiresfurtherelucidation).Theapproachto fertility investigation andmanagement should always be couple-centred. Specialist teams should beavailabletoofferevidence-basedadviceandtreatmenttocouples,supportedbycounsellingservicesandaccurateinformation.
NaturalconceptionAhealthy couple having frequent intercourse have about an 18–20% chance of conceiving in a singlemenstrualcycle.Asaspeciesthismakesusrelativelyinfertile.Thereisofcourseacumulativeincreaseinpregnancyratesover timeascouples try forconception.Within6months70%ofcoupleswillhaveconceived,after12months80%andafter24months90%ofcoupleswillachieveapregnancy(Figure7.1).Themostimportantfactoraffectingfertilityisfemaleage,whichisrelatedtoadeclineinthequalityandquantityofeggs.Femalefertilitytendstofallsharplyovertheageof36,withafurtherdipaftertheageof40.However, thereisaconsiderablevariationandbiologicalage(orovarianreserve)doesnotalwayspreciselycorrelatewithchronologicalage.Maleage isalsoan important factor;semenqualitytendstofallinmenovertheageof50,whilefrequencyofintercoursetendstofallinmenovertheageof40.
Bothfrequencyandtimingofsexualintercourseimpactstronglyonthechanceofconceivingnaturally.Couples having intercourse three times a week are three times more likely to conceive than coupleshaving intercourse once aweek.Maximum ‘efficiency’ is probably intercourse at least every alternateday.Thereshould,however,beawarenessamongphysiciansandpatientsoftheaddedstressandanxietythat ‘overmedicalizing’ this advice can bring to couples. Increased frequency of intercourse should beencouraged in the periovulatory period. Eggs are thought to be fertilizable for about 12–24 hourspostovulation,while sperm can survive in the female reproductive tract for up to 72 hours.Ovulationusuallyoccursabout14daysprior tomenstruation,with the lutealphasebeing relativelystableat thislength.The‘fertilewindow’forwomenwill, therefore,bedifferentdependingontheaveragelengthoftheirmenstrualcycle(e.g.forawomanwitha28-daymenstrualcycle,heroptimalfertilewindowwillbebetweendays12and15).
Externalfactorsmayinfluencethechanceofconception.There isnowstrongevidencethatsmokingcan decrease the quality and quantity of eggs and sperm. The role of alcohol and caffeine remainscontroversial,andthereisnocompellingevidencetototallyabstainfromthesewhiletryingtoconceive,butmoderationisprobablysensible.Bodymassindex(BMI)exertsastronginfluenceonfertility,with
www.medicalebookpdf.com
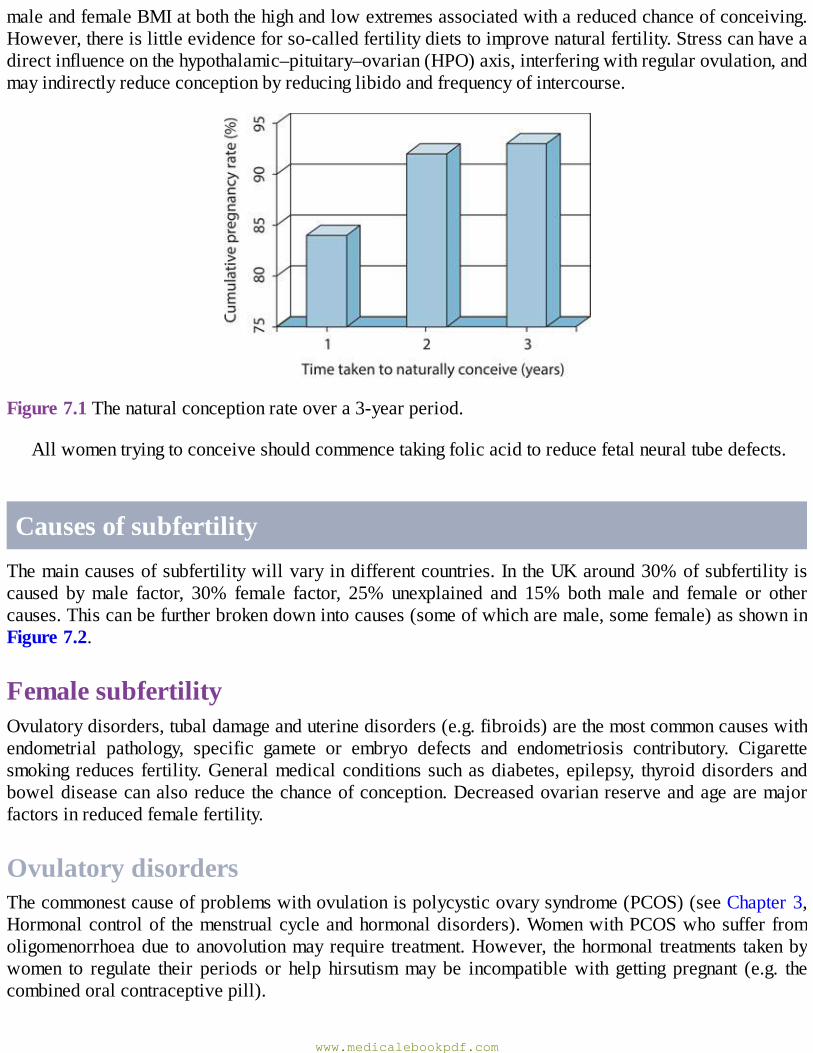
maleandfemaleBMIatboththehighandlowextremesassociatedwithareducedchanceofconceiving.However,thereislittleevidenceforso-calledfertilitydietstoimprovenaturalfertility.Stresscanhaveadirectinfluenceonthehypothalamic–pituitary–ovarian(HPO)axis,interferingwithregularovulation,andmayindirectlyreduceconceptionbyreducinglibidoandfrequencyofintercourse.
Figure7.1Thenaturalconceptionrateovera3-yearperiod.
Allwomentryingtoconceiveshouldcommencetakingfolicacidtoreducefetalneuraltubedefects.
CausesofsubfertilityThemaincausesofsubfertilitywillvaryindifferentcountries.IntheUKaround30%ofsubfertilityiscaused bymale factor, 30% female factor, 25% unexplained and 15% bothmale and female or othercauses.Thiscanbefurtherbrokendownintocauses(someofwhicharemale,somefemale)asshowninFigure7.2.
FemalesubfertilityOvulatorydisorders,tubaldamageanduterinedisorders(e.g.fibroids)arethemostcommoncauseswithendometrial pathology, specific gamete or embryo defects and endometriosis contributory. Cigarettesmoking reduces fertility.Generalmedicalconditionssuchasdiabetes,epilepsy, thyroiddisordersandboweldiseasecanalsoreducethechanceofconception.Decreasedovarianreserveandagearemajorfactorsinreducedfemalefertility.
OvulatorydisordersThecommonestcauseofproblemswithovulationispolycysticovarysyndrome(PCOS)(seeChapter3,Hormonalcontrolof themenstrualcycleandhormonaldisorders).WomenwithPCOSwhosuffer fromoligomenorrhoeadue toanovolutionmayrequire treatment.However, thehormonal treatments takenbywomen to regulate their periods or help hirsutismmay be incompatiblewith getting pregnant (e.g. thecombinedoralcontraceptivepill).
www.medicalebookpdf.com
Hypothalamic disorders (e.g. hypothalamic hypogonadism), pituitary disease (e.g.hyperprolactinaemia) and endocrine abnormalities (thyroid disease) are less common causes due toanovulation.
Figure7.2Causesofsubfertility.
TubalproblemsTubal blockage is usually associated with inflammatory processes in the pelvis such as pelvicinflammatorydisease(PID)orendometriosis.Chlamydialinfectionsinparticularcanproducesignificantdegrees of tubal damage, often resulting in a hydrosalpinx – a blocked Fallopian tube, often with athickenedwall,flattenedepithelialmucosaandperitubaladhesions.
Previouspelvicorabdominalsurgerycanresultinpostoperativescartissueoradhesionsthatcanalsocompromise tubal patency and function. The Fallopian tube is not a passive conduit – normal tubalfunctionrequiresbothpatencyandahealthyanatomyandphysiologyforgameteandembryotransport.
eResource7.1
Tubalblockagehttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.1.php
UterineproblemsUterine factors such as fibroids can interferewith fertility, but their impact depends on their size andlocation.Thereisgoodevidencethatsubmucosalfibroidshaveadirectimpactonembryoimplantationandintramuralfibroidsmayreducefertilityiftheyarelarge(>5cm).Subserosalfibroidshaveverylittleimpact if present in isolation.Endometrial polyps can reduce the chanceof implantation, although thistendsnot tobeabsolute.Endometrialscarring(Asherman’ssyndrome)fromsurgeryor infectioncanbeassociatedwithlighterperiodsandasignificantlyreducedchanceofconception.
www.medicalebookpdf.com
MalefactorCompromisedspermnumberorqualityisanimportantcontributortosubfertility.Thereissomeevidencethat sperm counts are falling, and there are various theories that try to explain this, includingenvironmental and dietary issues. Spermatogonial cells that produce the sperm can be damaged byinflammation (orchitis) or the epididymis that stores mature sperm can also be damaged. Certainiatrogenicinfluencessuchaspelvicradiotherapyorsurgeryforundescendedortortedtestescanreducespermproductionordamageorblock themalereproductive tract.Medicalconditionssuchasdiabetesand certain occupations involving contactwith chemicals or radiation are associatedwithmale factorsubfertility.Occasionally,spermproductionmaybenormalbutthereareerectiledifficultiesorproblemswithejaculation.
Genetic causes ofmale factor infertility include aneuploidy of sex chromosomes (KlinefelterXXYmostcommonly)orstructuralabnormalitiesoftheautosomes,suchasinversions,deletionsorbalancedtranslocations. Microdeletions of the azoospermic factor (AZF) regions of the Y chromosome areassociatedwithlowspermcountsandmotility.
eResource7.2
Normalandabnormalspermhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.2.php
Table 7.1 Key points to cover in history and examination of patients presenting withsubfertility
www.medicalebookpdf.com
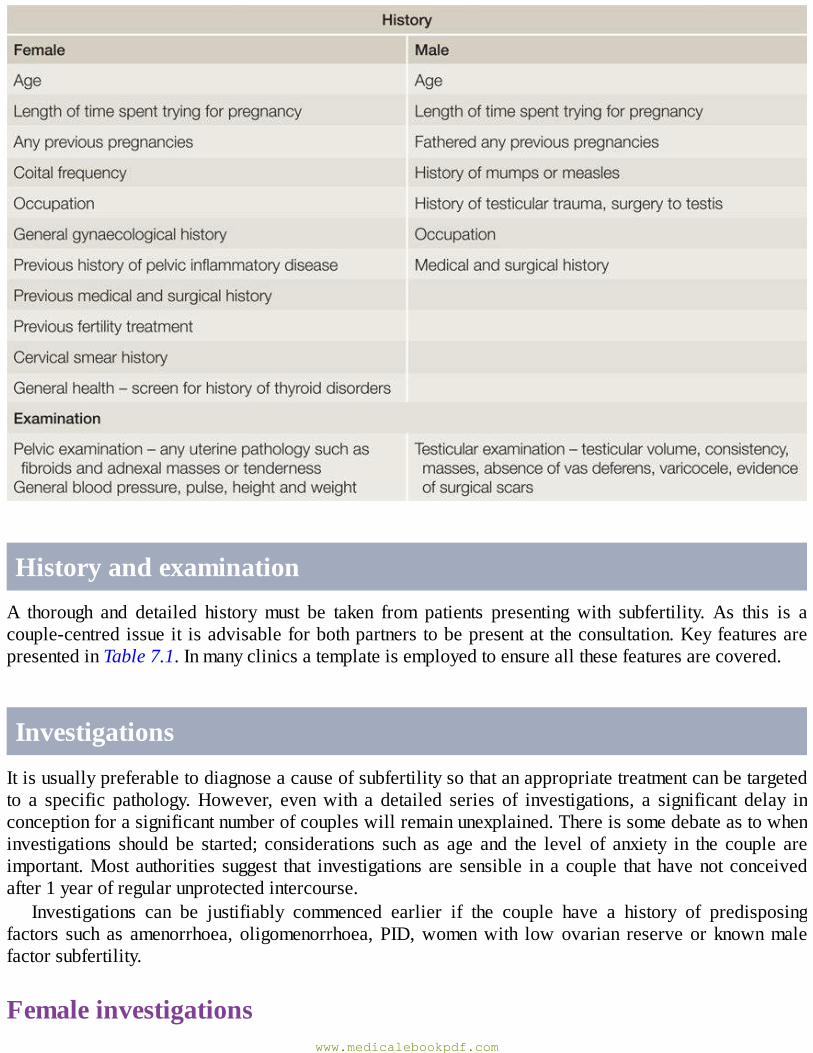
HistoryandexaminationA thorough and detailed history must be taken from patients presenting with subfertility. As this is acouple-centredissueit isadvisableforbothpartnerstobepresentat theconsultation.KeyfeaturesarepresentedinTable7.1.Inmanyclinicsatemplateisemployedtoensureallthesefeaturesarecovered.
InvestigationsItisusuallypreferabletodiagnoseacauseofsubfertilitysothatanappropriatetreatmentcanbetargetedto a specific pathology.However, evenwith a detailed series of investigations, a significant delay inconceptionforasignificantnumberofcoupleswillremainunexplained.Thereissomedebateastowheninvestigations should be started; considerations such as age and the level of anxiety in the couple areimportant.Most authorities suggest that investigationsare sensible inacouple thathavenot conceivedafter1yearofregularunprotectedintercourse.
Investigations can be justifiably commenced earlier if the couple have a history of predisposingfactors such as amenorrhoea, oligomenorrhoea, PID,womenwith lowovarian reserve or knownmalefactorsubfertility.
Femaleinvestigationswww.medicalebookpdf.com
Bloodhormoneprofile. Inawomanwitha regularmenstrual cycle this should includeearly follicularphase follicular-stimulating hormone (FSH), oestradiol and luteinizing hormone (LH). Anti-Müllerianhormone(AMH)(seebelow)isprovingparticularlyhelpfulintheassessmentofovarianreserveandisindependentofthemenstrualcycle,whichispractical.Amidlutealprogesteronemeasurementshouldbetaken toconfirmovulation. Inwomenwithan irregularmenstrualcycle, thyroid function,prolactin andtestosteronecanalsoproveuseful.
Chlamydiatestingshouldbeofferedpriortoanyuterineinstrumentation.IfARTistobeoffered,viralscreeningforhumanimmunodeficiencyvirus(HIV)andhepatitisBandCshouldbeoffered.
Transvaginal ultrasound (TVUSS) should be performedwhere possible. This provides an accurateassessmentofpelvicanatomy,includinguterinesizeandshape,thepresenceofanyfibroids,ovariansize,position andmorphology,with antral follicle count (AFC) an important parameter of ovarian reserve.Pathologysuchashydrosalpingesandendometrioticcystscanbedetected,andaccesstotheovariesforARTcanbeassessed.Tubalpotencytestingmaybenecessaryasdescribedbelow.
Measurementofovarianreserve
•Female reproductivepotential isdirectlyproportionate to the remainingnumberofoocytes in theovaries,whichiscalledovarianreserve.
•Ovarianreservedeclinesaftertheageof35inanaveragehealthywoman,oratanearlierageduetogeneticpredisposition,surgeryorfollowingexposuretotoxins,suchaschemotherapy.
•TheovarianreservecanhelptopredicttheresponsetoovarianstimulationinART.•TheAFCseenonTVUSSisagoodindicatorofovarianreserve(<4predictinglowresponse,>16highresponse).
•AMH is produced in the granulosa cells of ovarian follicles anddoes not change in response togonadotrophinsduringthemenstrualcycle.Asaresult,itcanbemeasuredandcomparedfromanypointinthecycleand,atpresent,isthemostsuccessfulbiochemicalmarker.
•NeitherAMHnorAFCareperfectindicatorsandmostclinicsutilizebothtoassessovarianreserve.
TubalassessmentTubal patency and an assessment of the uterine cavity are traditionally investigated byhysterosalpingography (HSG) using X-ray, hysterocontrast synography (HyCoSy) using ultrasound or,morerecently,3Dhysterocontrastsynography(Figure7.3).Thereissomeevidencethatpatientsdeemedathighriskofpelvicpathologycouldbenefit fromamore invasive laparoscopyandhysteroscopyasadualdiagnosticandpotentiallytherapeuticprocedure.Itiscrucialtorememberthattubalpatencyisnotequivalenttotubalfunction.Currently,thereisasyetnoeffectivetesttocheckfortubalfunction.
www.medicalebookpdf.com
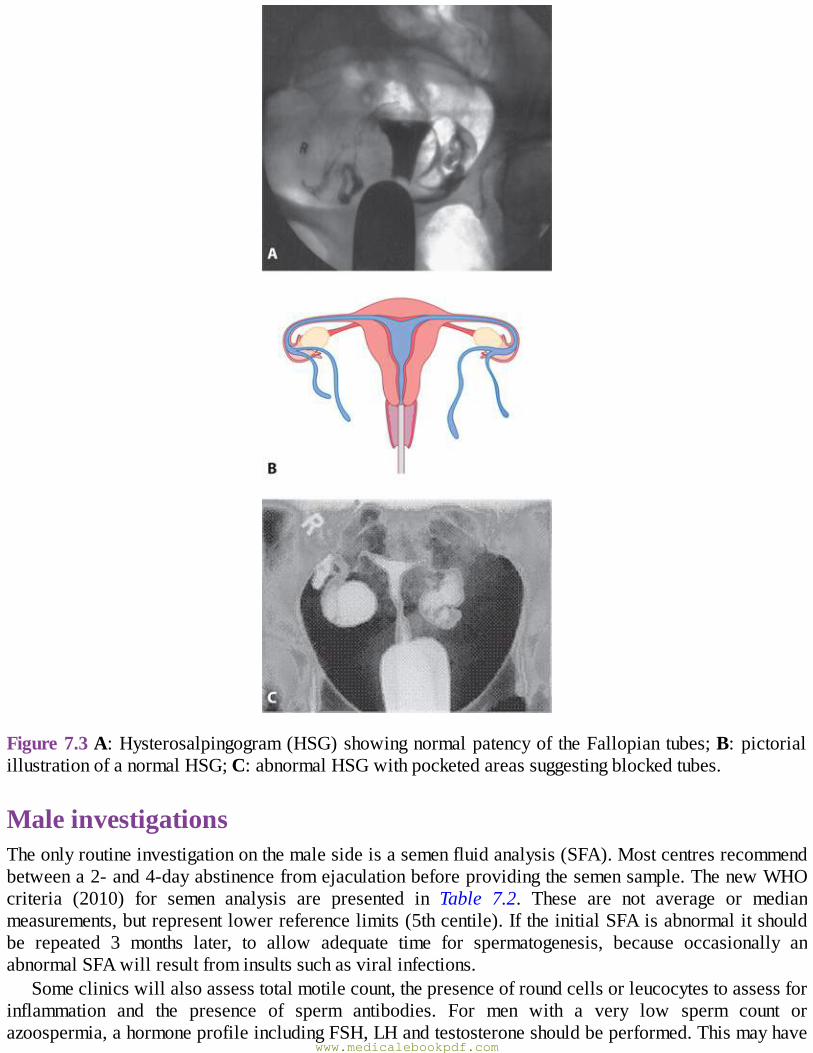
Figure7.3A:Hysterosalpingogram(HSG)showingnormalpatencyoftheFallopiantubes;B:pictorialillustrationofanormalHSG;C:abnormalHSGwithpocketedareassuggestingblockedtubes.
MaleinvestigationsTheonlyroutineinvestigationonthemalesideisasemenfluidanalysis(SFA).Mostcentresrecommendbetweena2-and4-dayabstinencefromejaculationbeforeprovidingthesemensample.ThenewWHOcriteria (2010) for semen analysis are presented in Table 7.2. These are not average or medianmeasurements,butrepresentlowerreferencelimits(5thcentile).IftheinitialSFAisabnormalitshouldbe repeated 3 months later, to allow adequate time for spermatogenesis, because occasionally anabnormalSFAwillresultfrominsultssuchasviralinfections.
Someclinicswillalsoassesstotalmotilecount,thepresenceofroundcellsorleucocytestoassessforinflammation and the presence of sperm antibodies. For men with a very low sperm count orazoospermia,ahormoneprofileincludingFSH,LHandtestosteroneshouldbeperformed.Thismayhave
www.medicalebookpdf.com
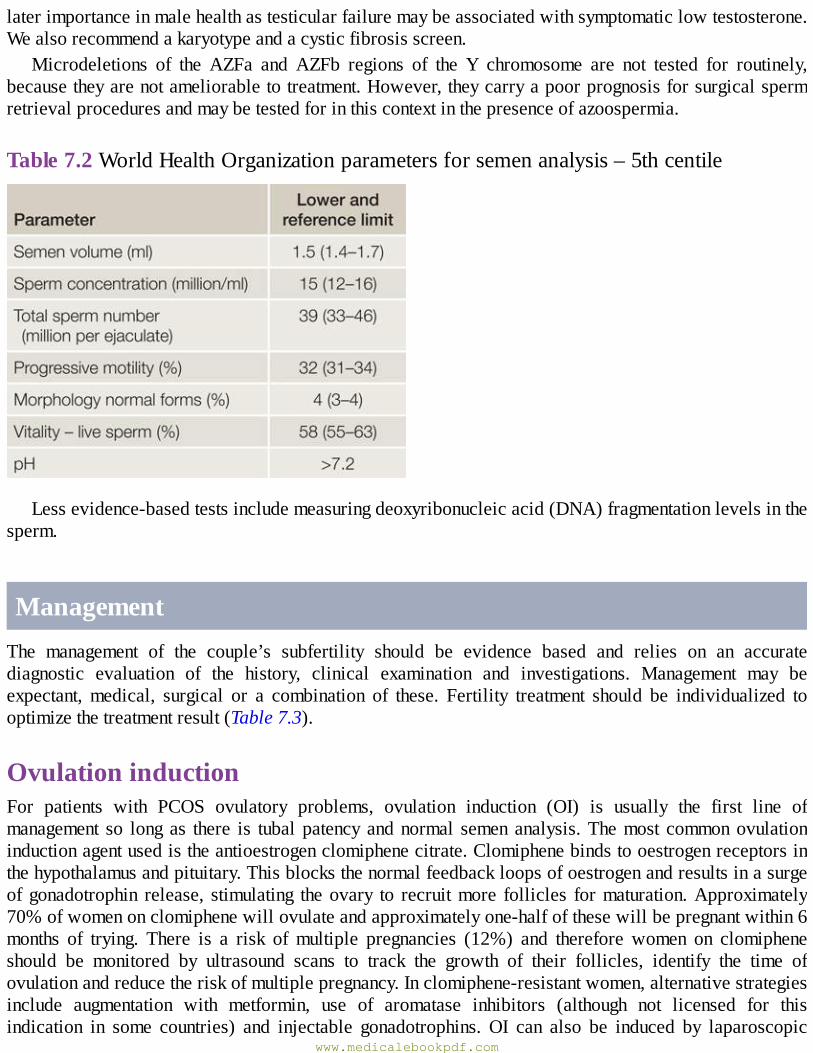
laterimportanceinmalehealthastesticularfailuremaybeassociatedwithsymptomaticlowtestosterone.Wealsorecommendakaryotypeandacysticfibrosisscreen.
Microdeletions of the AZFa and AZFb regions of the Y chromosome are not tested for routinely,becausetheyarenotameliorabletotreatment.However,theycarryapoorprognosisforsurgicalspermretrievalproceduresandmaybetestedforinthiscontextinthepresenceofazoospermia.
Table7.2WorldHealthOrganizationparametersforsemenanalysis–5thcentile
Lessevidence-basedtestsincludemeasuringdeoxyribonucleicacid(DNA)fragmentationlevelsinthesperm.
ManagementThe management of the couple’s subfertility should be evidence based and relies on an accuratediagnostic evaluation of the history, clinical examination and investigations. Management may beexpectant,medical, surgical or a combination of these. Fertility treatment should be individualized tooptimizethetreatmentresult(Table7.3).
OvulationinductionFor patients with PCOS ovulatory problems, ovulation induction (OI) is usually the first line ofmanagement so longas there is tubalpatencyandnormal semenanalysis.Themost commonovulationinductionagentusedistheantioestrogenclomiphenecitrate.Clomiphenebindstooestrogenreceptorsinthehypothalamusandpituitary.Thisblocksthenormalfeedbackloopsofoestrogenandresultsinasurgeofgonadotrophin release, stimulating theovary to recruitmore follicles formaturation.Approximately70%ofwomenonclomiphenewillovulateandapproximatelyone-halfofthesewillbepregnantwithin6months of trying. There is a risk ofmultiple pregnancies (12%) and therefore women on clomipheneshould be monitored by ultrasound scans to track the growth of their follicles, identify the time ofovulationandreducetheriskofmultiplepregnancy.Inclomiphene-resistantwomen,alternativestrategiesinclude augmentation with metformin, use of aromatase inhibitors (although not licensed for thisindication in some countries) and injectable gonadotrophins. OI can also be induced by laparoscopic
www.medicalebookpdf.com
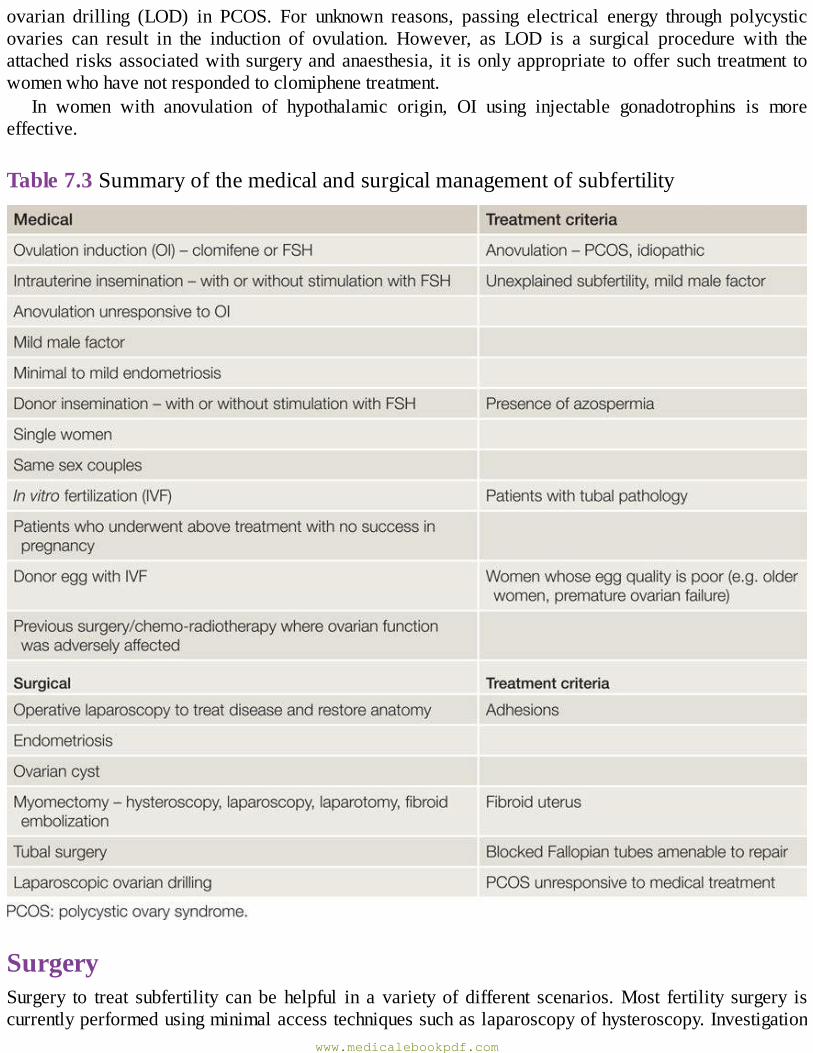
ovarian drilling (LOD) in PCOS. For unknown reasons, passing electrical energy through polycysticovaries can result in the induction of ovulation. However, as LOD is a surgical procedure with theattached risksassociatedwith surgeryandanaesthesia, it isonlyappropriate tooffer such treatment towomenwhohavenotrespondedtoclomiphenetreatment.
In women with anovulation of hypothalamic origin, OI using injectable gonadotrophins is moreeffective.
Table7.3Summaryofthemedicalandsurgicalmanagementofsubfertility
SurgerySurgery to treat subfertility can be helpful in a variety of different scenarios.Most fertility surgery iscurrentlyperformedusingminimalaccesstechniquessuchaslaparoscopyofhysteroscopy.Investigation
www.medicalebookpdf.com
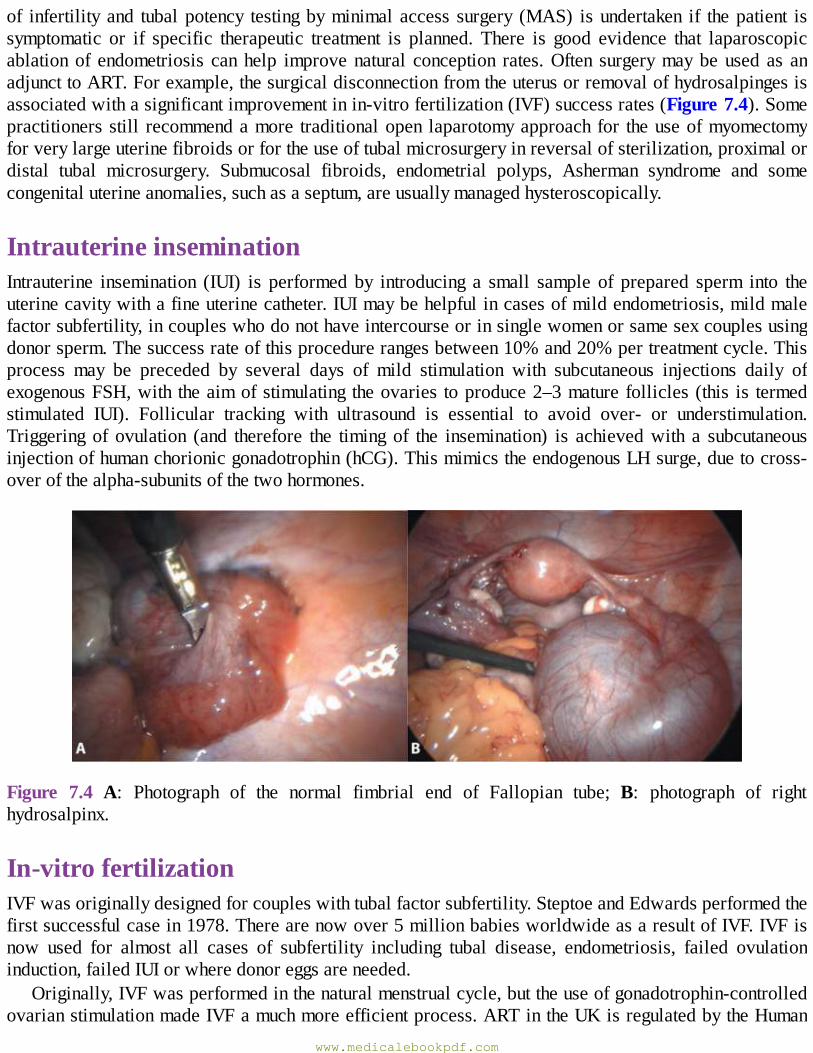
of infertility and tubalpotency testingbyminimal access surgery (MAS) isundertaken if thepatient issymptomatic or if specific therapeutic treatment is planned. There is good evidence that laparoscopicablationof endometriosis canhelp improvenatural conception rates.Often surgerymaybeused as anadjuncttoART.Forexample,thesurgicaldisconnectionfromtheuterusorremovalofhydrosalpingesisassociatedwithasignificantimprovementinin-vitrofertilization(IVF)successrates(Figure7.4).Somepractitionersstill recommendamore traditionalopen laparotomyapproachfor theuseofmyomectomyforverylargeuterinefibroidsorfortheuseoftubalmicrosurgeryinreversalofsterilization,proximalordistal tubal microsurgery. Submucosal fibroids, endometrial polyps, Asherman syndrome and somecongenitaluterineanomalies,suchasaseptum,areusuallymanagedhysteroscopically.
IntrauterineinseminationIntrauterine insemination (IUI) is performed by introducing a small sample of prepared sperm into theuterinecavitywithafineuterinecatheter.IUImaybehelpfulincasesofmildendometriosis,mildmalefactorsubfertility,incoupleswhodonothaveintercourseorinsinglewomenorsamesexcouplesusingdonorsperm.Thesuccessrateofthisprocedurerangesbetween10%and20%pertreatmentcycle.Thisprocess may be preceded by several days of mild stimulation with subcutaneous injections daily ofexogenousFSH,with theaimofstimulating theovaries toproduce2–3maturefollicles(this is termedstimulated IUI). Follicular tracking with ultrasound is essential to avoid over- or understimulation.Triggering of ovulation (and therefore the timing of the insemination) is achievedwith a subcutaneousinjectionofhumanchorionicgonadotrophin(hCG).ThismimicstheendogenousLHsurge,duetocross-overofthealpha-subunitsofthetwohormones.
Figure 7.4 A: Photograph of the normal fimbrial end of Fallopian tube; B: photograph of righthydrosalpinx.
In-vitrofertilizationIVFwasoriginallydesignedforcoupleswithtubalfactorsubfertility.SteptoeandEdwardsperformedthefirstsuccessfulcasein1978.Therearenowover5millionbabiesworldwideasaresultofIVF.IVFisnow used for almost all cases of subfertility including tubal disease, endometriosis, failed ovulationinduction,failedIUIorwheredonoreggsareneeded.
Originally,IVFwasperformedinthenaturalmenstrualcycle,buttheuseofgonadotrophin-controlledovarianstimulationmadeIVFamuchmoreefficientprocess.ARTintheUKisregulatedbytheHuman
www.medicalebookpdf.com
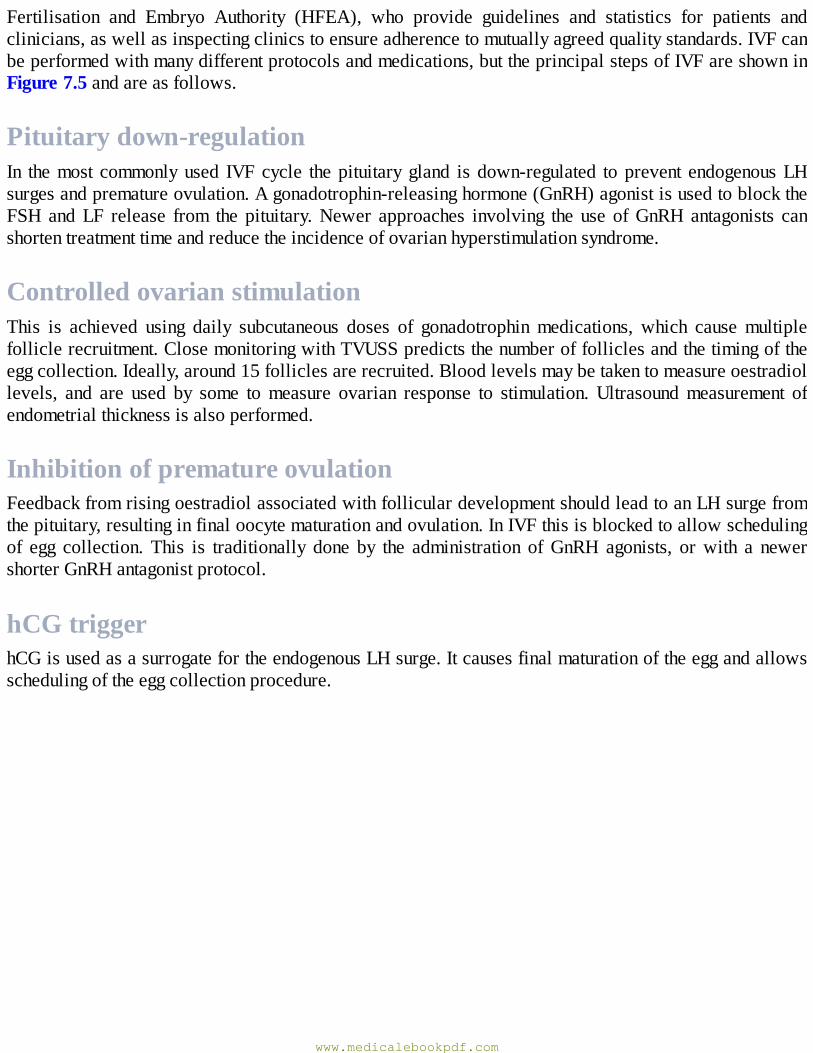
Fertilisation and Embryo Authority (HFEA), who provide guidelines and statistics for patients andclinicians,aswellasinspectingclinicstoensureadherencetomutuallyagreedqualitystandards.IVFcanbeperformedwithmanydifferentprotocolsandmedications,buttheprincipalstepsofIVFareshowninFigure7.5andareasfollows.
Pituitarydown-regulationIn themost commonlyused IVFcycle thepituitarygland isdown-regulated toprevent endogenousLHsurgesandprematureovulation.Agonadotrophin-releasinghormone(GnRH)agonistisusedtoblocktheFSH andLF release from the pituitary.Newer approaches involving the use ofGnRHantagonists canshortentreatmenttimeandreducetheincidenceofovarianhyperstimulationsyndrome.
ControlledovarianstimulationThis is achieved using daily subcutaneous doses of gonadotrophinmedications, which causemultiplefolliclerecruitment.ClosemonitoringwithTVUSSpredictsthenumberoffolliclesandthetimingoftheeggcollection.Ideally,around15folliclesarerecruited.Bloodlevelsmaybetakentomeasureoestradiollevels, and are used by some tomeasure ovarian response to stimulation.Ultrasoundmeasurement ofendometrialthicknessisalsoperformed.
InhibitionofprematureovulationFeedbackfromrisingoestradiolassociatedwithfolliculardevelopmentshouldleadtoanLHsurgefromthepituitary,resultinginfinaloocytematurationandovulation.InIVFthisisblockedtoallowschedulingof egg collection. This is traditionally done by the administration ofGnRH agonists, orwith a newershorterGnRHantagonistprotocol.
hCGtriggerhCGisusedasasurrogatefortheendogenousLHsurge.Itcausesfinalmaturationoftheeggandallowsschedulingoftheeggcollectionprocedure.
www.medicalebookpdf.com
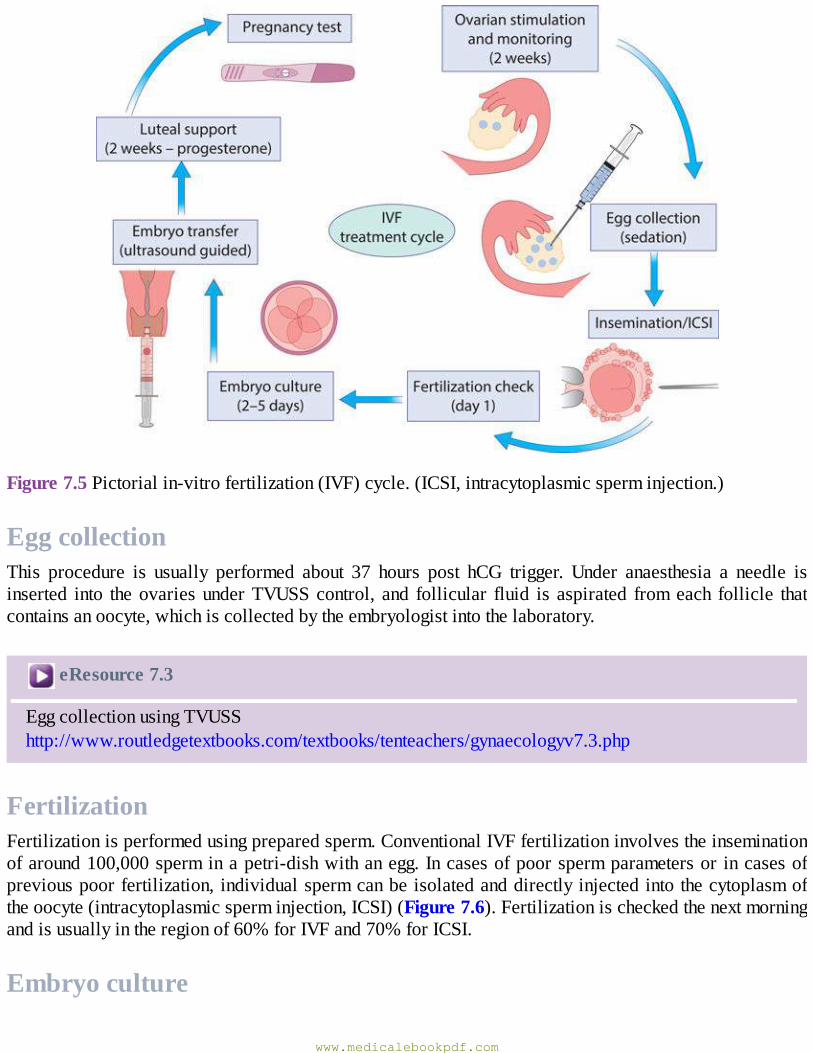
Figure7.5Pictorialin-vitrofertilization(IVF)cycle.(ICSI,intracytoplasmicsperminjection.)
EggcollectionThis procedure is usually performed about 37 hours post hCG trigger. Under anaesthesia a needle isinserted into theovariesunderTVUSScontrol, and follicular fluid is aspirated fromeach follicle thatcontainsanoocyte,whichiscollectedbytheembryologistintothelaboratory.
eResource7.3
EggcollectionusingTVUSShttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.3.php
FertilizationFertilizationisperformedusingpreparedsperm.ConventionalIVFfertilizationinvolvestheinseminationofaround100,000sperminapetri-dishwithanegg.Incasesofpoorspermparametersor incasesofpreviouspoorfertilization,individualspermcanbeisolatedanddirectlyinjectedintothecytoplasmoftheoocyte(intracytoplasmicsperminjection,ICSI)(Figure7.6).Fertilizationischeckedthenextmorningandisusuallyintheregionof60%forIVFand70%forICSI.
Embryoculture
www.medicalebookpdf.com
Embryos are incubated under strict conditions of temperature, pH, humidity and oxygen concentration.Theymaybetransferredbackintotheuterusafter2,3or5daysofdevelopment.Embryosreachingtheblastocyst stage onday5 of development usually exhibit the best chance of implantation.Avariety ofdifferentprotocolsareavailableforembryoselection, includingamorphologicalandamorpho-kineticassessment.
Figure7.6Intracytoplasmicsperminjection.
EmbryotransferEmbryosaretransferredintotheuterususingasoftplasticcatheter.Thechoiceofhowmanyembryostotransfer is thedecisionof the couple followingexpertmedical and embryological advice; thismay beconstrained by local regulatory or funding parameters. Embryo transfer is usually performed undertransabdominalultrasoundcontroltoensurecorrectplacementoftheembryos.IntheUKandEuropethereare recommendations regarding the transfer of single embryos to reduce the incidence of multiplepregnanciesandtheirassociatedrisks.
eResource7.4
TVUSS-guidedembryotransferhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.4.php
EmbryocryopreservationSpareembryosofgoodqualitymaybecryopreservedforfutureuse.Vitrificationtechniquesnowallowforsuccessratesfromfrozenembryostoapproximatesuccessratesinfreshtreatmentcycles.Thismakesthetransferoffreshsingleembryoswiththevitrificationofspareembryosmoreappealingtocouples.
LutealphasesupportTheuseofgonadotrophinagonistsorantagoniststopreventaprematureLHsurgewillleadtoareductionin the ability of the corpus luteum to produce progesterone. Patients are therefore supplemented withprogesteronefollowingtheeggcollection.Thereisnoconsensusontheidealdose,routeordurationofprogesteronesupplementation.Apregnancytestisperformedaround14daysafterembryotransfer.
www.medicalebookpdf.com
ARTsuccessratesIVFsuccessratesareexquisitelysensitivetofemaleage.Inyoungpatientsundertheageof35successratescanbeashighas40–45%fromasinglecycle,while inwomenover theageof40 theywill fallbelow15%.UndergoingIVFdoesnotprecludethepatientfromthenormalcomplicationsofpregnancy,such as miscarriage or ectopic pregnancies. The most significant risk of IVF treatment is ovarianhyperstimulationsyndrome(OHSS),occurringin1–3%ofcases.PatientswithsevereOHSSpresentwithascites,enlargedmultifollicularovaries,pulmonaryoedemaandcoagulopathy.Thesepatientsneedtobeadmitted tohospital andmanagedunder strict protocolsunder the careof specialist teams.Theuseoflow-dose stimulation, ultrasoundmonitoring,GnRH antagonist protocols,GnRH agonist triggers and amoreliberalfreezingpolicyhavesignificantlyreducedtheincidenceofthisveryseriouscondition.
DonorgametesDonorspermcanbeusedtotreatpatientswherethemalepartnerisazoospermicorinthecaseofsinglewomenorfemalesamesexcouples.BothIUIandIVFtreatmentsarepossible.Donoreggsmaybeusedifthe femalehasundergoneearlymenopauseor if IVF treatmentshavebeenunsuccessful andassociatedwithareducedovarianreserveand loweggnumberandquality.Gametedonationrequirescarefulandthoroughcounsellingandmostcountrieshavelegislationtoregulateitsuse.
SurgicalspermretrievalWhere the sperm quality or quantity is low but sperm are present, ICSI is required to help achieve apregnancy. However, in the absence of naturally ejaculated sperm (termed azoospermia – whichmayrelate to blockage of the vas deferens or testicular problems), patients may undergo surgical spermretrieval(SSR).SSRcanbeperformedundersedationorgeneralanaesthesia.Afineneedleisinsertedintotheepididymisorthetesticulartissuetoobtainspermortesticulartissuewithsperm,respectively.The retrieved spermcan thenbecryopreservedor injected into theoocyte aspartof a fresh IVF/ICSIcycle.
PreimplantationgeneticdiagnosisCoupleswhocarryageneticdisease (butwhoare fertile)maychoose touse IVFandpreimplantationgeneticdiagnosis(PGD)toavoidanaffectedpregnancy.Thesepatientsmaypreviouslyhavehadaffectedchildrenorterminationsforanaffectedfetus.IVFwillcreatemultipleembryos.Theseembryoscanthenbegeneticallytestedfortherelevantdisease,bytheremovalofseveralcellsattheblastocyststagethataretestedandtakentoreflectthegenotypeoftheremainingembryo.Onlyembryosfreeofthediseasearetransferredintotheuterus.PGDhasnowbeenusedworldwideformostmonogenicdiseases,aswellasfor translocations. The use of PGD for social sex selection is illegal in the UK but availablecontroversiallyinmanyothercountries.
There is a large attrition rate in PGD treatment from the number of eggs to embryos to unaffectedembryos available for transfer. In some cycles noneof the embryoswill beunaffected andno embryotransferwillresult.Successrates thereforereflect this,andvaryaccordingtotheinheritancepatternofthedisorder.
eResource7.5www.medicalebookpdf.com
EmbryobiopsyforPGDhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv7.5.php
Similargeneticanalysisofembryoshasbeenused todetectchromosomalaneuploidy inembryos inpatientshavingIVFtreatment,inanattempttoselecttheembryoswiththegreatestimplantationpotentialandreducethetimetoapregnancy.Thisremainscontroversialandsubjecttoresearchtrials.
FertilitypreservationPatients may face treatments such as chemotherapy, radiotherapy or surgery that could significantlydamage their gonads and reduce their reproductive potential. For many years men have been able to‘bank’spermaheadofthesetreatments.CouplescannowundergorapidIVFproceduresandcryopreserveembryosforuselateronwhenhealthisregained.
KEYLEARNINGPOINTS•Acarefulhistory,appropriateclinicalexamination,correctinvestigationandadviceonevidence-based treatmentsunderpin successful fertility treatment.Theapproach shouldalwaysbecouple-centredwithcounsellingwhennecessary.
•Thecoupleshouldbegiveninformationonthechancesofconceivingnaturallyandhowtooptimizethis.Thisshouldincludetheimpactofadvancingageandadviceonlifestyleissuesrelatingtodiet,smoking,weightandalcoholconsumption.
•Ovarianreservedecreasessignificantlywithage,withthegradientincreasingovertheageof36andagainat40.
• Fertility treatment is a combination of expectant, surgical and medical treatments that arecomplementarytoeachother.
•Treatmentsshouldbetailoredtoanindividualcouple’sneeds,andcanincludeovulationinduction,surgery,IUIandIVF.
•FertilitypreservationandPGDarenewandeffectivetreatmentoptionsforselectedpatientgroups.
Recentadvances invitrificationhavenowalsoallowedyoung,healthy,singlewomen togo throughIVFandfreezetheiroocytes.
There is very promising evidence, and some successful reports of live births, on the role oflaparoscopicovariancortexcollectionandcryopreservation.Tissuecouldbeauto-transplantedbackintothepatient’spelvisoncehealthisregained.
FurtherreadingHumanFertilisationandEmbryologyAuthority.www.hfea.gov.uk.
www.medicalebookpdf.com
National Institute forClinical Excellence. Fertility assessment and treatment for peoplewith fertilityproblems.Clinicalguidelines(CG11)https://www.nice.org.uk/guidance/cg156.
VanVoorlisBJ(2007).Clinicalpractice.Invitrofertilisation.NewEnglJMed356:379–86.
Selfassessment
CLINICALHISTORY
A36-year-oldwoman, Jane, andher 39-year-oldpartner,David, have come to the fertility clinicaftertryingforababyfor3years.ThereferralletternotesthatJanehasirregularperiodsandDavidhadaherniarepairasachild.Neitherhaveanychildren.AWhatimportantpartsofthehistorymustyouask?BWhatinvestigationswillyourequest?CWhattreatmentwilltheyneed?
ANSWERS
AInthefertilityclinicageneralgynaecologicalhistorymustfirstbeobtained,andthenmorespecificquestionswill follow.Youmustdeterminehow longexactly theyhavebeenhaving unprotectedintercourseandwhat‘irregularperiods’meansbyenquiringaboutfrequencyofbleeds,lengthofbleeds, any other abnormal uterine bleeding. Irregular periods must prompt questions abouthirsutism, weight and acne, as these will support the diagnosis of PCOS, a common cause ofanovulation.Youmustaskforhowlongtheirregularbleedshavehappened,asyoumaybemindfulofadiagnosisofdecreasingovarianreserve,acausethatmaybeassociatedwithhotsweats.Donot forget toaskabout smear testsandSTIs.Confirm that Janehasneverbeenpregnantbefore,including miscarriages and ectopic pregnancies. Also check that none of David’s previouspartnershavebecomepregnant.
Ask about frequency of intercourse and any problems with intercourse, because fertilityproblemsarestronglyassociatedwithpsychosexualproblems,bothfemaleandmale.Onthemalesideyouneedtoaskmoreabouttheherniarepair:wasitonesideorboth,andatwhatage?
You find that Jane has always had irregular periods exceptwhen shewas on theOCP. Sheusuallyhasaperiodevery2–3monthsandtheyvaryfromveryheavytonormal.Shehasstruggledwithandrogenicsymptoms,exceptwhenontheOCP.Shemanagestokeepherweightdownwithdifficulty,andkeepsherBMIbelow30withacombinationofdietandexercise.
David had a unilateral uncomplicated hernia repair aged 4 years. He had a sperm countmeasured about 2 years ago by the GP, which was ‘borderline’, so they felt it was worthcontinuingtotrynaturallyforawhile.Intercourseiseveryfewdays;theynolongertrytoworkoutwhenovulationhasoccurred.
BTheinvestigationsrequiredareahormoneprofileforJane,aTVUSStolookforPCOSandotherabnormalitiesandSFAforDavid.Tubaltestingatthispointisnotindicated.
www.medicalebookpdf.com
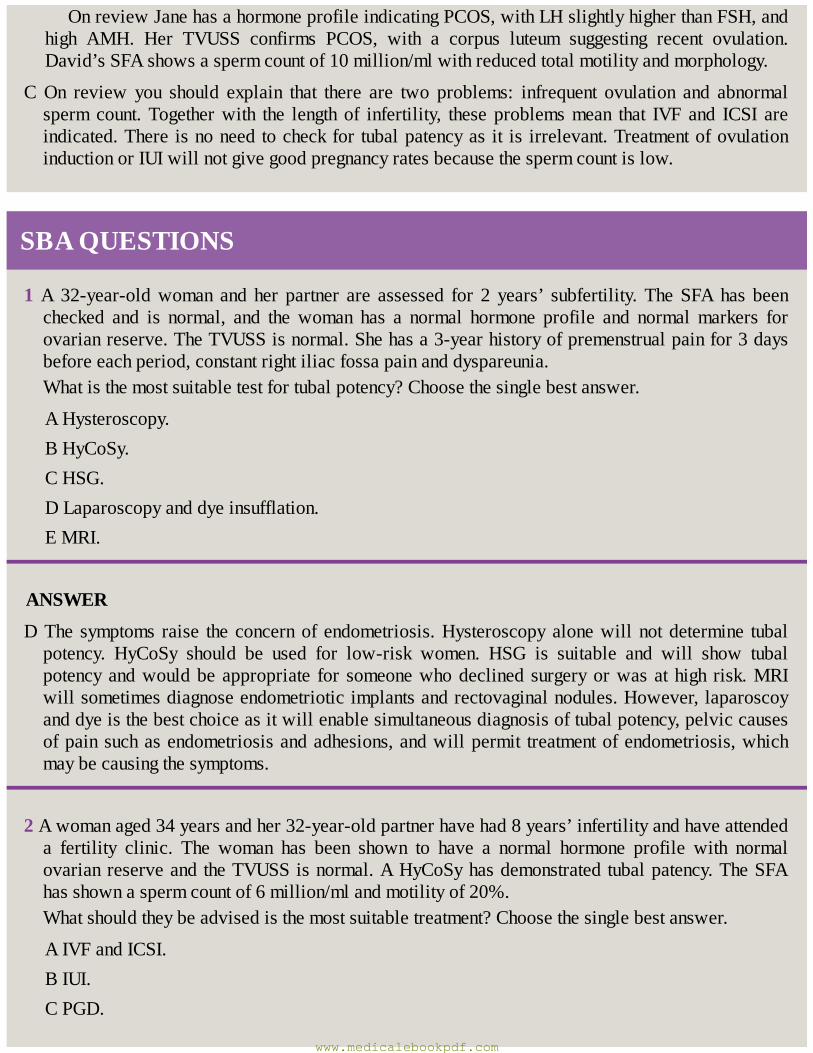
OnreviewJanehasahormoneprofileindicatingPCOS,withLHslightlyhigherthanFSH,andhigh AMH. Her TVUSS confirms PCOS, with a corpus luteum suggesting recent ovulation.David’sSFAshowsaspermcountof10million/mlwithreducedtotalmotilityandmorphology.
COn review you should explain that there are two problems: infrequent ovulation and abnormalspermcount.Togetherwith the length of infertility, these problemsmean that IVF and ICSI areindicated.There isnoneedtocheckfor tubalpatencyas it is irrelevant.TreatmentofovulationinductionorIUIwillnotgivegoodpregnancyratesbecausethespermcountislow.
SBAQUESTIONS
1A 32-year-oldwoman and her partner are assessed for 2 years’ subfertility.TheSFAhas beenchecked and is normal, and the woman has a normal hormone profile and normalmarkers forovarianreserve.TheTVUSSisnormal.Shehasa3-yearhistoryofpremenstrualpainfor3daysbeforeeachperiod,constantrightiliacfossapainanddyspareunia.Whatisthemostsuitabletestfortubalpotency?Choosethesinglebestanswer.
AHysteroscopy.BHyCoSy.CHSG.DLaparoscopyanddyeinsufflation.EMRI.
ANSWER
DThe symptoms raise theconcernof endometriosis.Hysteroscopyalonewillnotdetermine tubalpotency. HyCoSy should be used for low-risk women. HSG is suitable and will show tubalpotencyandwouldbeappropriate for someonewhodeclined surgeryorwasathigh risk.MRIwillsometimesdiagnoseendometrioticimplantsandrectovaginalnodules.However,laparoscoyanddyeisthebestchoiceasitwillenablesimultaneousdiagnosisoftubalpotency,pelviccausesofpainsuchasendometriosisandadhesions,andwillpermit treatmentofendometriosis,whichmaybecausingthesymptoms.
2Awomanaged34yearsandher32-year-oldpartnerhavehad8years’infertilityandhaveattendeda fertility clinic. The woman has been shown to have a normal hormone profile with normalovarianreserveandtheTVUSSisnormal.AHyCoSyhasdemonstratedtubalpatency.TheSFAhasshownaspermcountof6million/mlandmotilityof20%.Whatshouldtheybeadvisedisthemostsuitabletreatment?Choosethesinglebestanswer.
AIVFandICSI.BIUI.CPGD.
www.medicalebookpdf.com

DOvulationinduction.EIVFalone.
ANSWER
AThespermcountandmotilityisverylowandIUIwillhaveverylowpregnancyrates.InIVFalonethe fertilization rate of eggs will be low, resulting in few embryos to transfer, hence a lowpregnancyrate.Ovulation induction isnotasuitable treatmentas there isnoovulationproblem.PGDisnotrequiredunlessthereisadiagnosedinheritablegeneticdisease.Ifthespermcountwasbelow1million/ml,furthermalegenetictestingforsexchromosomeabnormalitiesandbalancedtranslocationswouldbeindicated.Absenceofonevasdeferenswouldindicatetheneedforcysticfibrosistesting.IVFandICSIwillgivegoodfertilizationratesandagoodchanceofpregnancyforthiscouple.
www.medicalebookpdf.com
CHAPTER8Themenopauseandpostreproductivehealth
EDWARDMORRIS
Definitions
Physiologicalmenopause
Non-physiologicalmenopause
Postmenopausalreproductivehealth
Assessmentofthemenopausalwoman
Hormonalreplacementtherapy
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Knowthedefinitionofmenopause.
•Understandphysiologicalandnon-physiologicalmenopause.
•Understandtheeffectofmenopauseonwomen.
•Understandthemodifiableandnon-modifiableaspectsofmenopausalhealth.
•Explainthemainformsoftreatmentofthemenopause.
•Know the side-effects and the relative and absolute contraindications of hormonal replacementtherapy(HRT).
www.medicalebookpdf.com
•Describethebenefitsofhormonalandnon-hormonalHRT.
DefinitionsThemenopauseisdefinedasthewoman’sfinalmenstrualperiodandtheacceptedconfirmationofthisismade retrospectively after 1 year of amenorrhoea.The cause of themenopause is cessationof regularovarianfunction.Thereisgreatheterogeneityintheexperiencesofdifferentwomenastheygothroughthemenopausal transition and several descriptive phrases exist, which can cause confusion amongstpractitionersandwomenalike.
Descriptivetermsformenopause
•Menopause:thelastmenstrualperiod(LMP).•Perimenopause:timeoflifefromtheonsetofovariandysfunctionuntil1yearafterthelastperiodandthediagnosisofmenopauseismade.Thistimeisalsoknownastheclimacteric.
• Postmenopause: all women who have been 1 year since their last period are deemedpostmenopausal.
•The‘change’:acolloquialdescriptionofperimenopauseandpostmenopause.
Physiologicalmenopause
TimingofthemenopauseTheaverageageofthemenopauseworldwidehasnotchangedfordecades(Figure8.1) remainingatamedianageofbetween51and52years,with95%ofwomenattainingmenopausebetweentheageof45and55years.Menopauseoccurringoutsidetheseagesisrelativelyrareandprematureovarianfailureisdiscussedlater.
EndocrinechangesCurrentunderstandingisthatmenopauseoccursatthetimeofthedepletionofoocytesfromtheovaryandisirreversible.Groundbreakingandyettobewidelyacceptedresearchchallengesthisassumption,withthefindingofoogonialstemcellsfromprimordialfolliclesintheovary.Thismightradicallyaffectourunderstandingofthemenopauseandoffertheremotepossibilityofbeingabletoinfluencethetimingofmenopause.
Unsurprisingly, the endocrinology is not as simple as the ovaries just running out of eggs and thecapacity toproducehormones at aparticular age.Asdiscussed inChapter3,Hormonal control of themenstrualcycleandhormonaldisorders,reproductivefunctionismaintainedbyasubtleinterplayofthehypothalamicproductionofgonadotrophin-releasinghormone(GnRH),thepituitaryhormonesluteinizinghormone (LH) and follicle-stimulatinghormone (FSH), the ovarianpeptide hormone inhibinB and the
www.medicalebookpdf.com
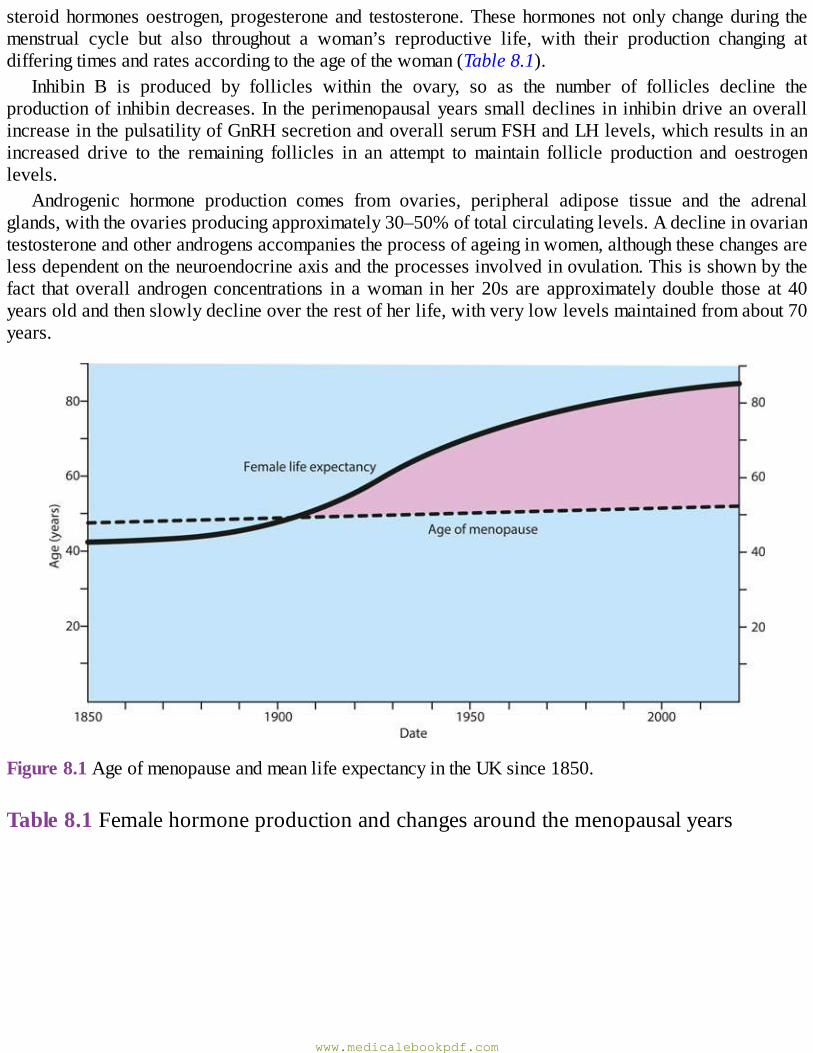
steroidhormonesoestrogen,progesteroneand testosterone.Thesehormonesnotonlychangeduring themenstrual cycle but also throughout a woman’s reproductive life, with their production changing atdifferingtimesandratesaccordingtotheageofthewoman(Table8.1).
Inhibin B is produced by follicles within the ovary, so as the number of follicles decline theproductionof inhibindecreases.In theperimenopausalyearssmalldeclines in inhibindriveanoverallincreaseinthepulsatilityofGnRHsecretionandoverallserumFSHandLHlevels,whichresultsinanincreased drive to the remaining follicles in an attempt to maintain follicle production and oestrogenlevels.
Androgenic hormone production comes from ovaries, peripheral adipose tissue and the adrenalglands,withtheovariesproducingapproximately30–50%oftotalcirculatinglevels.Adeclineinovariantestosteroneandotherandrogensaccompaniestheprocessofageinginwomen,althoughthesechangesarelessdependentontheneuroendocrineaxisandtheprocessesinvolvedinovulation.Thisisshownbythefact that overall androgen concentrations in awoman in her 20s are approximatelydouble those at 40yearsoldandthenslowlydeclineovertherestofherlife,withverylowlevelsmaintainedfromabout70years.
Figure8.1AgeofmenopauseandmeanlifeexpectancyintheUKsince1850.
Table8.1Femalehormoneproductionandchangesaroundthemenopausalyears
www.medicalebookpdf.com
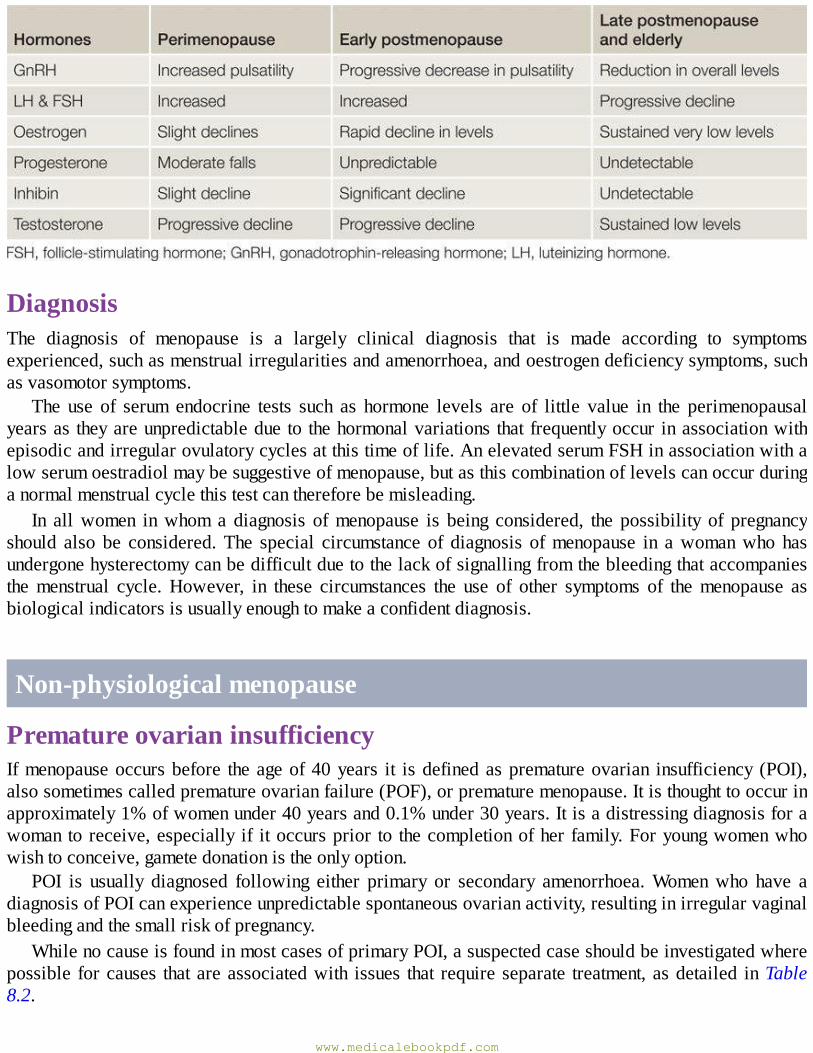
DiagnosisThe diagnosis of menopause is a largely clinical diagnosis that is made according to symptomsexperienced,suchasmenstrualirregularitiesandamenorrhoea,andoestrogendeficiencysymptoms,suchasvasomotorsymptoms.
The use of serum endocrine tests such as hormone levels are of little value in the perimenopausalyearsas theyareunpredictabledueto thehormonalvariations thatfrequentlyoccur inassociationwithepisodicandirregularovulatorycyclesatthistimeoflife.AnelevatedserumFSHinassociationwithalowserumoestradiolmaybesuggestiveofmenopause,butasthiscombinationoflevelscanoccurduringanormalmenstrualcyclethistestcanthereforebemisleading.
In allwomen inwhom a diagnosis ofmenopause is being considered, the possibility of pregnancyshould also be considered.The special circumstance of diagnosis ofmenopause in awomanwho hasundergonehysterectomycanbedifficultduetothelackofsignallingfromthebleedingthataccompaniesthemenstrual cycle.However, in these circumstances the use of other symptoms of themenopause asbiologicalindicatorsisusuallyenoughtomakeaconfidentdiagnosis.
Non-physiologicalmenopause
PrematureovarianinsufficiencyIfmenopauseoccursbefore theageof40years it isdefinedasprematureovarian insufficiency (POI),alsosometimescalledprematureovarianfailure(POF),orprematuremenopause.Itisthoughttooccurinapproximately1%ofwomenunder40yearsand0.1%under30years.Itisadistressingdiagnosisforawomantoreceive,especially if itoccursprior to thecompletionofher family.Foryoungwomenwhowishtoconceive,gametedonationistheonlyoption.
POI is usually diagnosed following either primary or secondary amenorrhoea.Womenwho have adiagnosisofPOIcanexperienceunpredictablespontaneousovarianactivity,resultinginirregularvaginalbleedingandthesmallriskofpregnancy.
WhilenocauseisfoundinmostcasesofprimaryPOI,asuspectedcaseshouldbeinvestigatedwherepossible forcauses thatareassociatedwith issues that require separate treatment,asdetailed inTable8.2.
www.medicalebookpdf.com
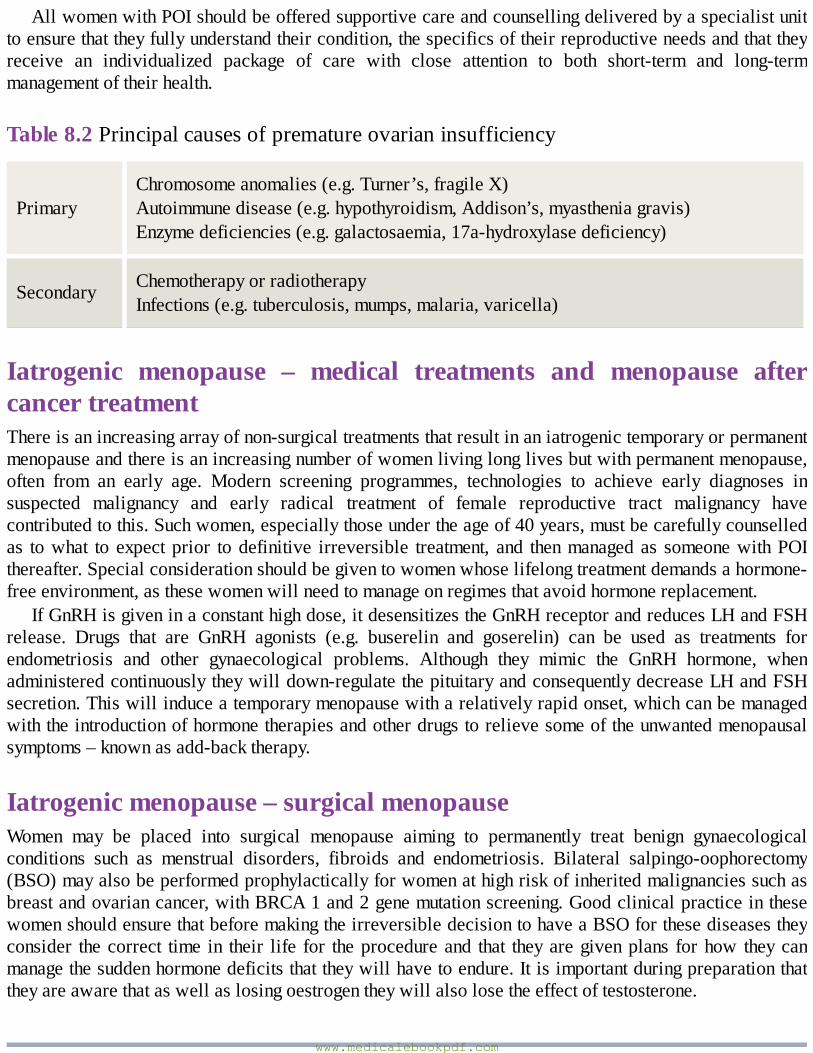
AllwomenwithPOIshouldbeofferedsupportivecareandcounsellingdeliveredbyaspecialistunittoensurethattheyfullyunderstandtheircondition,thespecificsoftheirreproductiveneedsandthattheyreceive an individualized package of care with close attention to both short-term and long-termmanagementoftheirhealth.
Table8.2Principalcausesofprematureovarianinsufficiency
PrimaryChromosomeanomalies(e.g.Turner’s,fragileX)Autoimmunedisease(e.g.hypothyroidism,Addison’s,myastheniagravis)Enzymedeficiencies(e.g.galactosaemia,17a-hydroxylasedeficiency)
Secondary ChemotherapyorradiotherapyInfections(e.g.tuberculosis,mumps,malaria,varicella)
Iatrogenic menopause – medical treatments and menopause aftercancertreatmentThereisanincreasingarrayofnon-surgicaltreatmentsthatresultinaniatrogenictemporaryorpermanentmenopauseandthereisanincreasingnumberofwomenlivinglonglivesbutwithpermanentmenopause,often from an early age. Modern screening programmes, technologies to achieve early diagnoses insuspected malignancy and early radical treatment of female reproductive tract malignancy havecontributedtothis.Suchwomen,especiallythoseundertheageof40years,mustbecarefullycounselledas towhat to expectprior todefinitive irreversible treatment, and thenmanagedas someonewithPOIthereafter.Specialconsiderationshouldbegiventowomenwhoselifelongtreatmentdemandsahormone-freeenvironment,asthesewomenwillneedtomanageonregimesthatavoidhormonereplacement.
IfGnRHisgiveninaconstanthighdose,itdesensitizestheGnRHreceptorandreducesLHandFSHrelease. Drugs that are GnRH agonists (e.g. buserelin and goserelin) can be used as treatments forendometriosis and other gynaecological problems. Although they mimic the GnRH hormone, whenadministeredcontinuouslytheywilldown-regulatethepituitaryandconsequentlydecreaseLHandFSHsecretion.Thiswillinduceatemporarymenopausewitharelativelyrapidonset,whichcanbemanagedwiththeintroductionofhormonetherapiesandotherdrugstorelievesomeoftheunwantedmenopausalsymptoms–knownasadd-backtherapy.
Iatrogenicmenopause–surgicalmenopauseWomen may be placed into surgical menopause aiming to permanently treat benign gynaecologicalconditions such as menstrual disorders, fibroids and endometriosis. Bilateral salpingo-oophorectomy(BSO)mayalsobeperformedprophylacticallyforwomenathighriskofinheritedmalignanciessuchasbreastandovariancancer,withBRCA1and2genemutationscreening.GoodclinicalpracticeinthesewomenshouldensurethatbeforemakingtheirreversibledecisiontohaveaBSOforthesediseasestheyconsider thecorrect time in their life for theprocedureand that theyaregivenplans forhow theycanmanagethesuddenhormonedeficitsthattheywillhavetoendure.Itisimportantduringpreparationthattheyareawarethataswellaslosingoestrogentheywillalsolosetheeffectoftestosterone.
www.medicalebookpdf.com
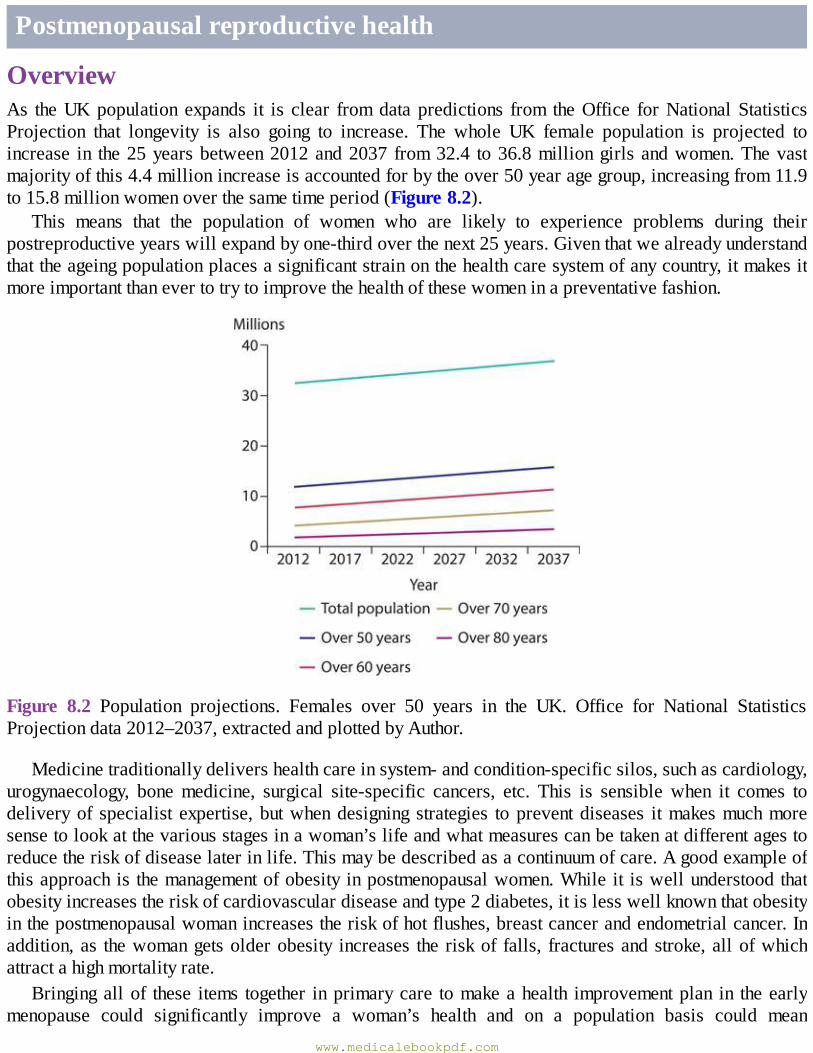
Postmenopausalreproductivehealth
OverviewAs theUKpopulation expands it is clear fromdatapredictions from theOffice forNationalStatisticsProjection that longevity is also going to increase. The whole UK female population is projected toincrease in the25yearsbetween2012and2037 from32.4 to36.8milliongirlsandwomen.Thevastmajorityofthis4.4millionincreaseisaccountedforbytheover50yearagegroup,increasingfrom11.9to15.8millionwomenoverthesametimeperiod(Figure8.2).
This means that the population of women who are likely to experience problems during theirpostreproductiveyearswillexpandbyone-thirdoverthenext25years.Giventhatwealreadyunderstandthattheageingpopulationplacesasignificantstrainonthehealthcaresystemofanycountry,itmakesitmoreimportantthanevertotrytoimprovethehealthofthesewomeninapreventativefashion.
Figure 8.2 Population projections. Females over 50 years in the UK. Office for National StatisticsProjectiondata2012–2037,extractedandplottedbyAuthor.
Medicinetraditionallydelivershealthcareinsystem-andcondition-specificsilos,suchascardiology,urogynaecology, bonemedicine, surgical site-specific cancers, etc. This is sensible when it comes todeliveryof specialist expertise,butwhendesigning strategies topreventdiseases itmakesmuchmoresensetolookatthevariousstagesinawoman’slifeandwhatmeasurescanbetakenatdifferentagestoreducetheriskofdiseaselaterinlife.Thismaybedescribedasacontinuumofcare.Agoodexampleofthisapproachis themanagementofobesityinpostmenopausalwomen.While it iswellunderstoodthatobesityincreasestheriskofcardiovasculardiseaseandtype2diabetes,itislesswellknownthatobesityinthepostmenopausalwomanincreasestheriskofhotflushes,breastcancerandendometrialcancer.Inaddition,as thewomangetsolderobesity increases the riskof falls, fracturesandstroke,allofwhichattractahighmortalityrate.
Bringingallof these items together inprimarycare tomakeahealth improvementplan in theearlymenopause could significantly improve a woman’s health and on a population basis could mean
www.medicalebookpdf.com
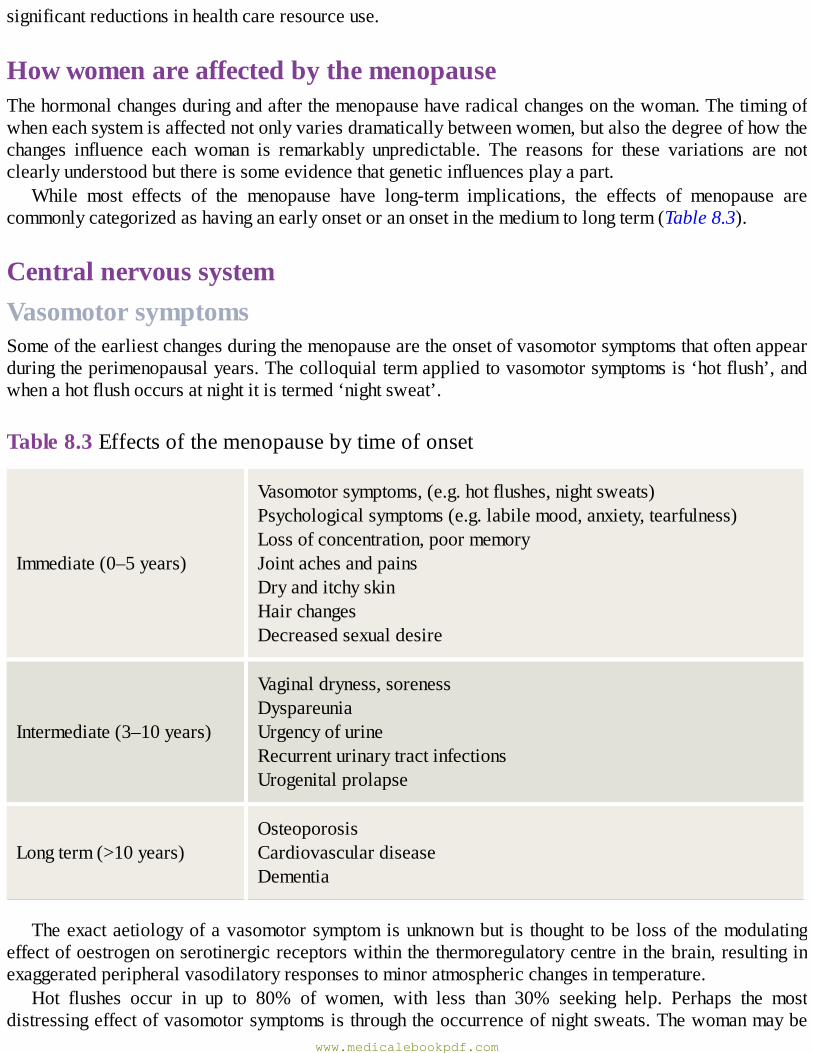
significantreductionsinhealthcareresourceuse.
HowwomenareaffectedbythemenopauseThehormonalchangesduringandafterthemenopausehaveradicalchangesonthewoman.Thetimingofwheneachsystemisaffectednotonlyvariesdramaticallybetweenwomen,butalsothedegreeofhowthechanges influence each woman is remarkably unpredictable. The reasons for these variations are notclearlyunderstoodbutthereissomeevidencethatgeneticinfluencesplayapart.
While most effects of the menopause have long-term implications, the effects of menopause arecommonlycategorizedashavinganearlyonsetoranonsetinthemediumtolongterm(Table8.3).
CentralnervoussystemVasomotorsymptomsSomeoftheearliestchangesduringthemenopausearetheonsetofvasomotorsymptomsthatoftenappearduringtheperimenopausalyears.Thecolloquialtermappliedtovasomotorsymptomsis‘hotflush’,andwhenahotflushoccursatnightitistermed‘nightsweat’.
Table8.3Effectsofthemenopausebytimeofonset
Immediate(0–5years)
Vasomotorsymptoms,(e.g.hotflushes,nightsweats)Psychologicalsymptoms(e.g.labilemood,anxiety,tearfulness)Lossofconcentration,poormemoryJointachesandpainsDryanditchyskinHairchangesDecreasedsexualdesire
Intermediate(3–10years)
Vaginaldryness,sorenessDyspareuniaUrgencyofurineRecurrenturinarytractinfectionsUrogenitalprolapse
Longterm(>10years)OsteoporosisCardiovasculardiseaseDementia
Theexactaetiologyofavasomotorsymptomisunknownbut is thought tobe lossof themodulatingeffectofoestrogenonserotinergicreceptorswithinthethermoregulatorycentreinthebrain,resultinginexaggeratedperipheralvasodilatoryresponsestominoratmosphericchangesintemperature.
Hot flushes occur in up to 80% of women, with less than 30% seeking help. Perhaps the mostdistressingeffectofvasomotorsymptomsisthroughtheoccurrenceofnightsweats.Thewomanmaybe
www.medicalebookpdf.com
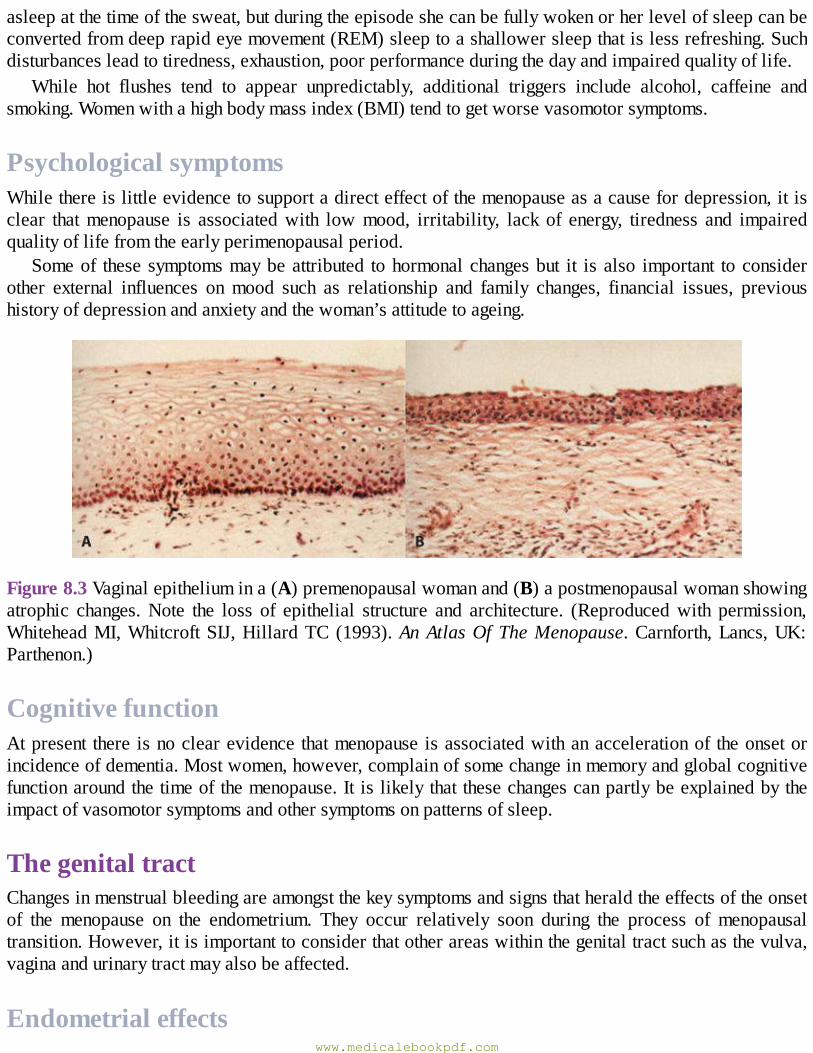
asleepatthetimeofthesweat,butduringtheepisodeshecanbefullywokenorherlevelofsleepcanbeconvertedfromdeeprapideyemovement(REM)sleeptoashallowersleepthatislessrefreshing.Suchdisturbancesleadtotiredness,exhaustion,poorperformanceduringthedayandimpairedqualityoflife.
While hot flushes tend to appear unpredictably, additional triggers include alcohol, caffeine andsmoking.Womenwithahighbodymassindex(BMI)tendtogetworsevasomotorsymptoms.
PsychologicalsymptomsWhilethereislittleevidencetosupportadirecteffectofthemenopauseasacausefordepression,itisclear thatmenopause is associatedwith lowmood, irritability, lack of energy, tiredness and impairedqualityoflifefromtheearlyperimenopausalperiod.
Someof these symptomsmaybeattributed tohormonalchangesbut it isalso important toconsiderother external influences onmood such as relationship and family changes, financial issues, previoushistoryofdepressionandanxietyandthewoman’sattitudetoageing.
Figure8.3Vaginalepitheliumina(A)premenopausalwomanand(B)apostmenopausalwomanshowingatrophic changes.Note the loss of epithelial structure and architecture. (Reproducedwith permission,WhiteheadMI,WhitcroftSIJ,HillardTC (1993).AnAtlasOfTheMenopause.Carnforth,Lancs,UK:Parthenon.)
CognitivefunctionAtpresent there isnoclearevidence thatmenopause isassociatedwithanaccelerationof theonsetorincidenceofdementia.Mostwomen,however,complainofsomechangeinmemoryandglobalcognitivefunctionaroundthetimeofthemenopause.It islikelythatthesechangescanpartlybeexplainedbytheimpactofvasomotorsymptomsandothersymptomsonpatternsofsleep.
ThegenitaltractChangesinmenstrualbleedingareamongstthekeysymptomsandsignsthatheraldtheeffectsoftheonsetof the menopause on the endometrium. They occur relatively soon during the process of menopausaltransition.However,itisimportanttoconsiderthatotherareaswithinthegenitaltractsuchasthevulva,vaginaandurinarytractmayalsobeaffected.
Endometrialeffectswww.medicalebookpdf.com
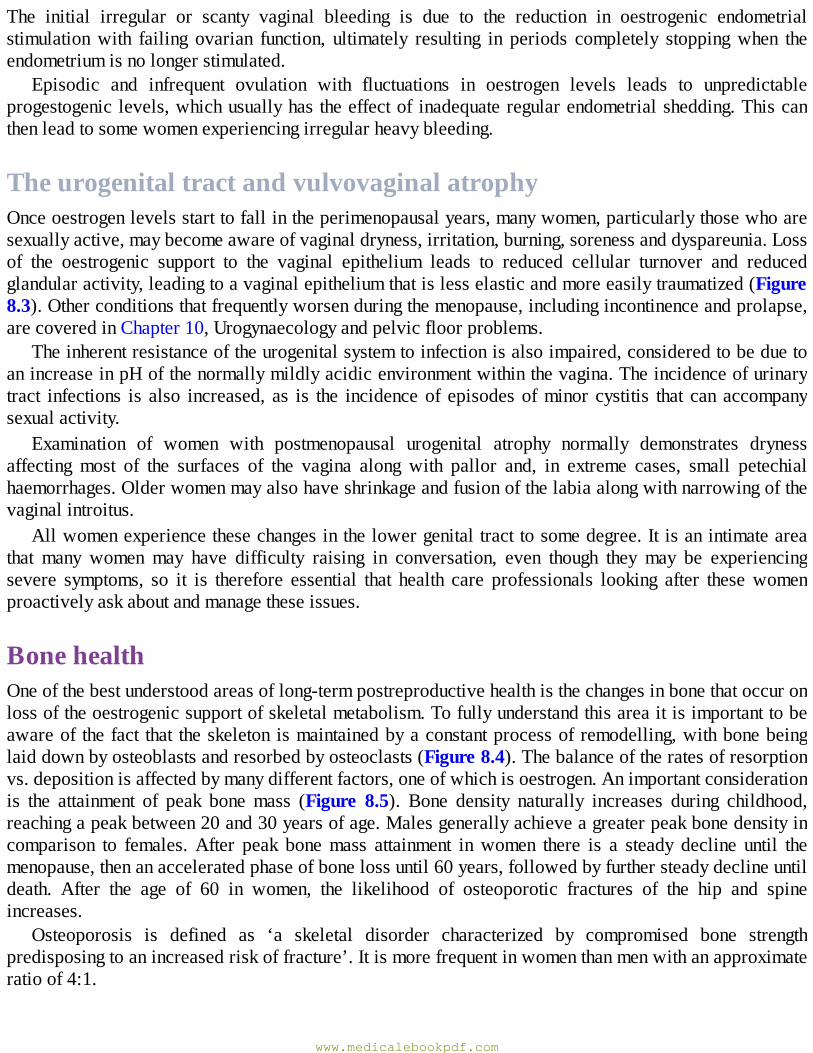
The initial irregular or scanty vaginal bleeding is due to the reduction in oestrogenic endometrialstimulationwith failing ovarian function, ultimately resulting in periods completely stoppingwhen theendometriumisnolongerstimulated.
Episodic and infrequent ovulation with fluctuations in oestrogen levels leads to unpredictableprogestogeniclevels,whichusuallyhastheeffectof inadequateregularendometrialshedding.Thiscanthenleadtosomewomenexperiencingirregularheavybleeding.
TheurogenitaltractandvulvovaginalatrophyOnceoestrogenlevelsstarttofallintheperimenopausalyears,manywomen,particularlythosewhoaresexuallyactive,maybecomeawareofvaginaldryness,irritation,burning,sorenessanddyspareunia.Lossof the oestrogenic support to the vaginal epithelium leads to reduced cellular turnover and reducedglandularactivity,leadingtoavaginalepitheliumthatislesselasticandmoreeasilytraumatized(Figure8.3).Otherconditionsthatfrequentlyworsenduringthemenopause,includingincontinenceandprolapse,arecoveredinChapter10,Urogynaecologyandpelvicfloorproblems.
Theinherentresistanceoftheurogenitalsystemtoinfectionisalsoimpaired,consideredtobeduetoanincreaseinpHofthenormallymildlyacidicenvironmentwithinthevagina.Theincidenceofurinarytract infections is also increased, as is the incidenceof episodesofminor cystitis that can accompanysexualactivity.
Examination of women with postmenopausal urogenital atrophy normally demonstrates drynessaffecting most of the surfaces of the vagina along with pallor and, in extreme cases, small petechialhaemorrhages.Olderwomenmayalsohaveshrinkageandfusionofthelabiaalongwithnarrowingofthevaginalintroitus.
Allwomenexperiencethesechangesinthelowergenitaltracttosomedegree.Itisanintimateareathat many women may have difficulty raising in conversation, even though they may be experiencingsevere symptoms, so it is therefore essential that health care professionals looking after thesewomenproactivelyaskaboutandmanagetheseissues.
BonehealthOneofthebestunderstoodareasoflong-termpostreproductivehealthisthechangesinbonethatoccuronlossoftheoestrogenicsupportofskeletalmetabolism.Tofullyunderstandthisareaitisimportanttobeawareof thefact that theskeleton ismaintainedbyaconstantprocessof remodelling,withbonebeinglaiddownbyosteoblastsandresorbedbyosteoclasts(Figure8.4).Thebalanceoftheratesofresorptionvs.depositionisaffectedbymanydifferentfactors,oneofwhichisoestrogen.Animportantconsiderationis the attainment of peak bonemass (Figure 8.5). Bone density naturally increases during childhood,reachingapeakbetween20and30yearsofage.Malesgenerallyachieveagreaterpeakbonedensityincomparison to females.After peak bonemass attainment inwomen there is a steady decline until themenopause,thenanacceleratedphaseofbonelossuntil60years,followedbyfurthersteadydeclineuntildeath. After the age of 60 in women, the likelihood of osteoporotic fractures of the hip and spineincreases.
Osteoporosis is defined as ‘a skeletal disorder characterized by compromised bone strengthpredisposingtoanincreasedriskoffracture’.Itismorefrequentinwomenthanmenwithanapproximateratioof4:1.
www.medicalebookpdf.com
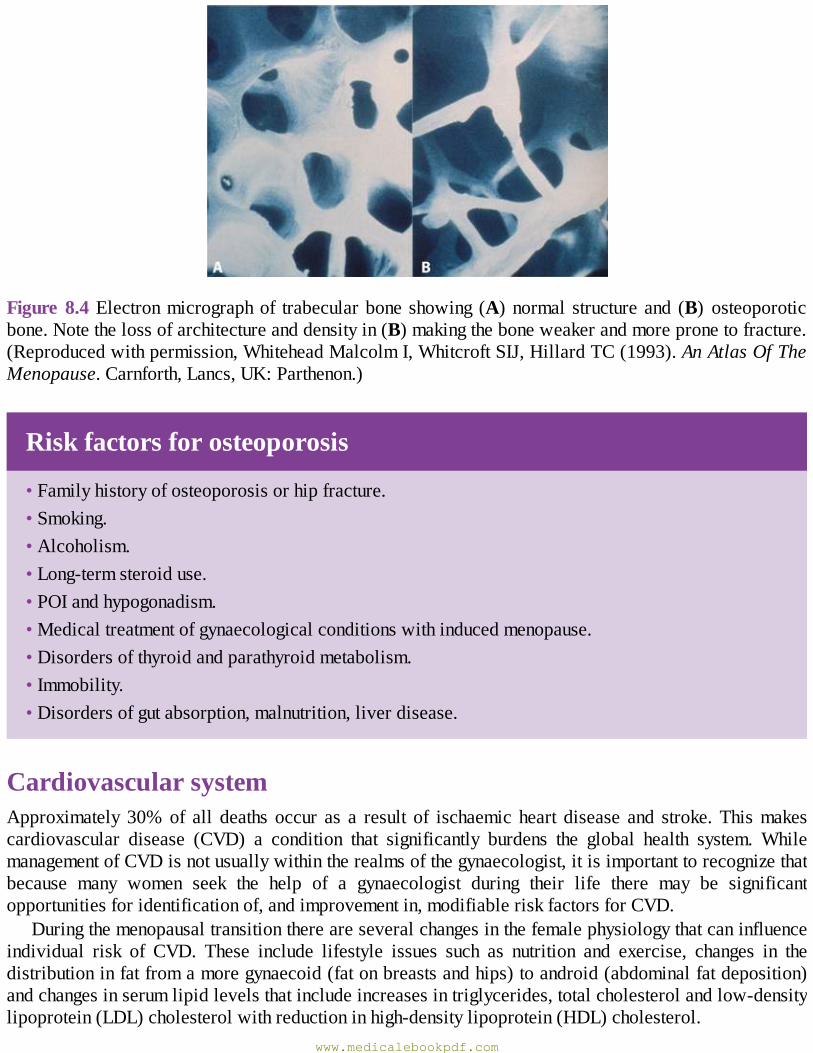
Figure8.4Electronmicrographof trabecularboneshowing (A)normal structureand (B) osteoporoticbone.Notethelossofarchitectureanddensityin(B)makingtheboneweakerandmorepronetofracture.(Reproducedwithpermission,WhiteheadMalcolmI,WhitcroftSIJ,HillardTC(1993).AnAtlasOfTheMenopause.Carnforth,Lancs,UK:Parthenon.)
Riskfactorsforosteoporosis
•Familyhistoryofosteoporosisorhipfracture.•Smoking.•Alcoholism.•Long-termsteroiduse.•POIandhypogonadism.•Medicaltreatmentofgynaecologicalconditionswithinducedmenopause.•Disordersofthyroidandparathyroidmetabolism.•Immobility.•Disordersofgutabsorption,malnutrition,liverdisease.
CardiovascularsystemApproximately 30%of all deaths occur as a result of ischaemic heart disease and stroke.Thismakescardiovascular disease (CVD) a condition that significantly burdens the global health system. WhilemanagementofCVDisnotusuallywithintherealmsofthegynaecologist,itisimportanttorecognizethatbecause many women seek the help of a gynaecologist during their life there may be significantopportunitiesforidentificationof,andimprovementin,modifiableriskfactorsforCVD.
Duringthemenopausaltransitionthereareseveralchangesinthefemalephysiologythatcaninfluenceindividual risk of CVD. These include lifestyle issues such as nutrition and exercise, changes in thedistributioninfatfromamoregynaecoid(fatonbreastsandhips)toandroid(abdominalfatdeposition)andchangesinserumlipidlevelsthatincludeincreasesintriglycerides,totalcholesterolandlow-densitylipoprotein(LDL)cholesterolwithreductioninhigh-densitylipoprotein(HDL)cholesterol.
www.medicalebookpdf.com
Oestrogen also has a supportive effect on the vesselwall that favours vasodilatation and preventsatherogenesis;effectsthatarereducedafterthemenopause.
Figure8.5Theprincipalstagesof theboneremodellingcyclerepresenteddiagrammatically(left)withcorresponding lightmicrographsof iliac crest biopsies (right).A: Resorption by osteoclasts (OC);B:reversalwithdisappearanceofOC;C:OCformationwiththedepositionofosteoidbyosteoblasts(OB);D:mineralizationoftheosteoid;E:completionofthecyclewithboneliningcellsonthesurface(LC).(Light micrographs reproduced with permission, Dempster DW [1992]. Disorders of the Bone andMineralMetabolism.NewYork:RavenPress.)
www.medicalebookpdf.com
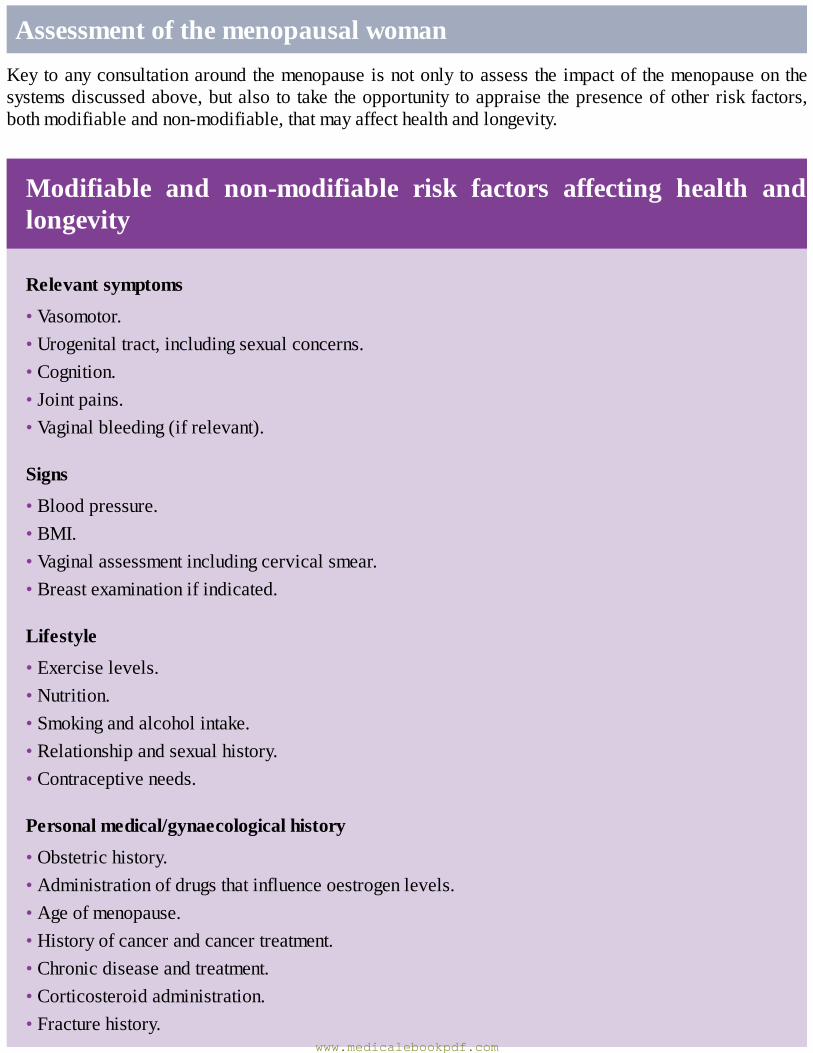
AssessmentofthemenopausalwomanKeytoanyconsultationaroundthemenopauseisnotonlytoassesstheimpactof themenopauseonthesystemsdiscussedabove,butalsototaketheopportunitytoappraisethepresenceofotherriskfactors,bothmodifiableandnon-modifiable,thatmayaffecthealthandlongevity.
Modifiable and non-modifiable risk factors affecting health andlongevity
Relevantsymptoms
•Vasomotor.•Urogenitaltract,includingsexualconcerns.•Cognition.•Jointpains.•Vaginalbleeding(ifrelevant).
Signs
•Bloodpressure.•BMI.•Vaginalassessmentincludingcervicalsmear.•Breastexaminationifindicated.
Lifestyle
•Exerciselevels.•Nutrition.•Smokingandalcoholintake.•Relationshipandsexualhistory.•Contraceptiveneeds.
Personalmedical/gynaecologicalhistory
•Obstetrichistory.•Administrationofdrugsthatinfluenceoestrogenlevels.•Ageofmenopause.•Historyofcancerandcancertreatment.•Chronicdiseaseandtreatment.•Corticosteroidadministration.•Fracturehistory.
www.medicalebookpdf.com
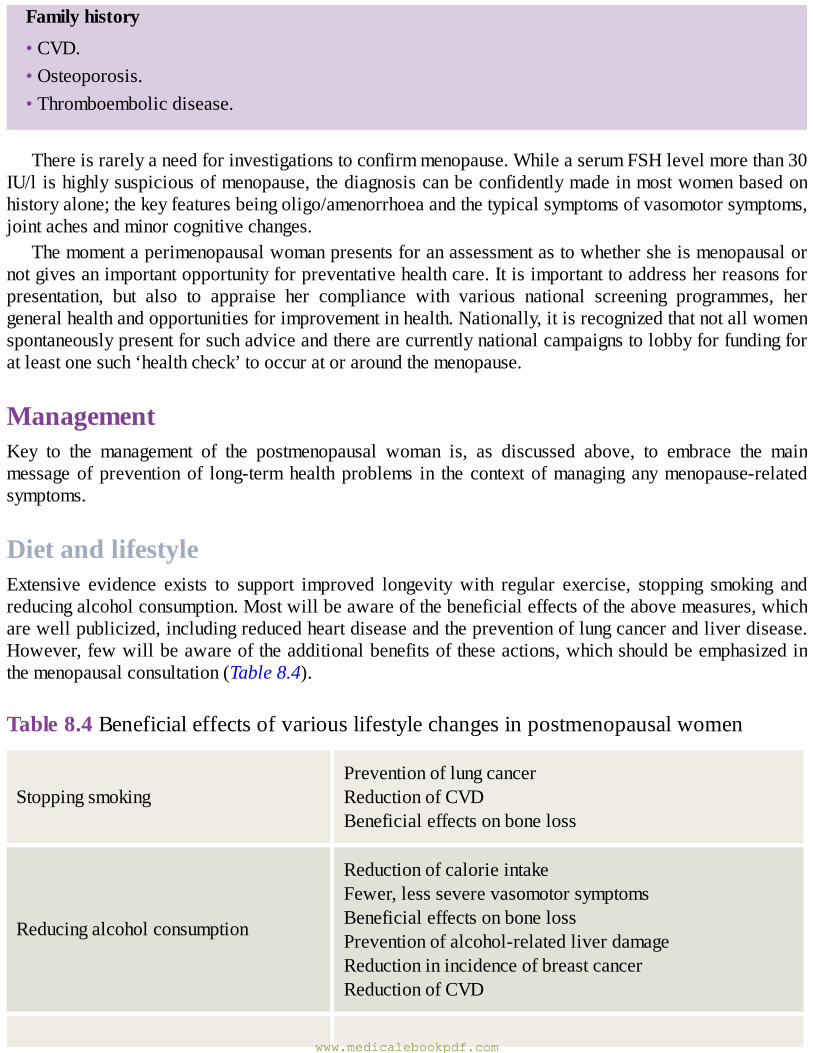
Familyhistory
•CVD.•Osteoporosis.•Thromboembolicdisease.
Thereisrarelyaneedforinvestigationstoconfirmmenopause.WhileaserumFSHlevelmorethan30IU/lishighlysuspiciousofmenopause,thediagnosiscanbeconfidentlymadeinmostwomenbasedonhistoryalone;thekeyfeaturesbeingoligo/amenorrhoeaandthetypicalsymptomsofvasomotorsymptoms,jointachesandminorcognitivechanges.
Themomentaperimenopausalwomanpresentsforanassessmentastowhethersheismenopausalornotgivesanimportantopportunityforpreventativehealthcare.Itisimportanttoaddressherreasonsforpresentation, but also to appraise her compliance with various national screening programmes, hergeneralhealthandopportunitiesforimprovementinhealth.Nationally,itisrecognizedthatnotallwomenspontaneouslypresentforsuchadviceandtherearecurrentlynationalcampaignstolobbyforfundingforatleastonesuch‘healthcheck’tooccuratoraroundthemenopause.
ManagementKey to the management of the postmenopausal woman is, as discussed above, to embrace the mainmessageof preventionof long-termhealthproblems in the context ofmanaging anymenopause-relatedsymptoms.
DietandlifestyleExtensive evidence exists to support improved longevitywith regular exercise, stopping smoking andreducingalcoholconsumption.Mostwillbeawareofthebeneficialeffectsoftheabovemeasures,whicharewellpublicized,includingreducedheartdiseaseandthepreventionoflungcancerandliverdisease.However,fewwillbeawareoftheadditionalbenefitsoftheseactions,whichshouldbeemphasizedinthemenopausalconsultation(Table8.4).
Table8.4Beneficialeffectsofvariouslifestylechangesinpostmenopausalwomen
StoppingsmokingPreventionoflungcancerReductionofCVDBeneficialeffectsonboneloss
Reducingalcoholconsumption
ReductionofcalorieintakeFewer,lessseverevasomotorsymptomsBeneficialeffectsonbonelossPreventionofalcohol-relatedliverdamageReductioninincidenceofbreastcancerReductionofCVD
www.medicalebookpdf.com
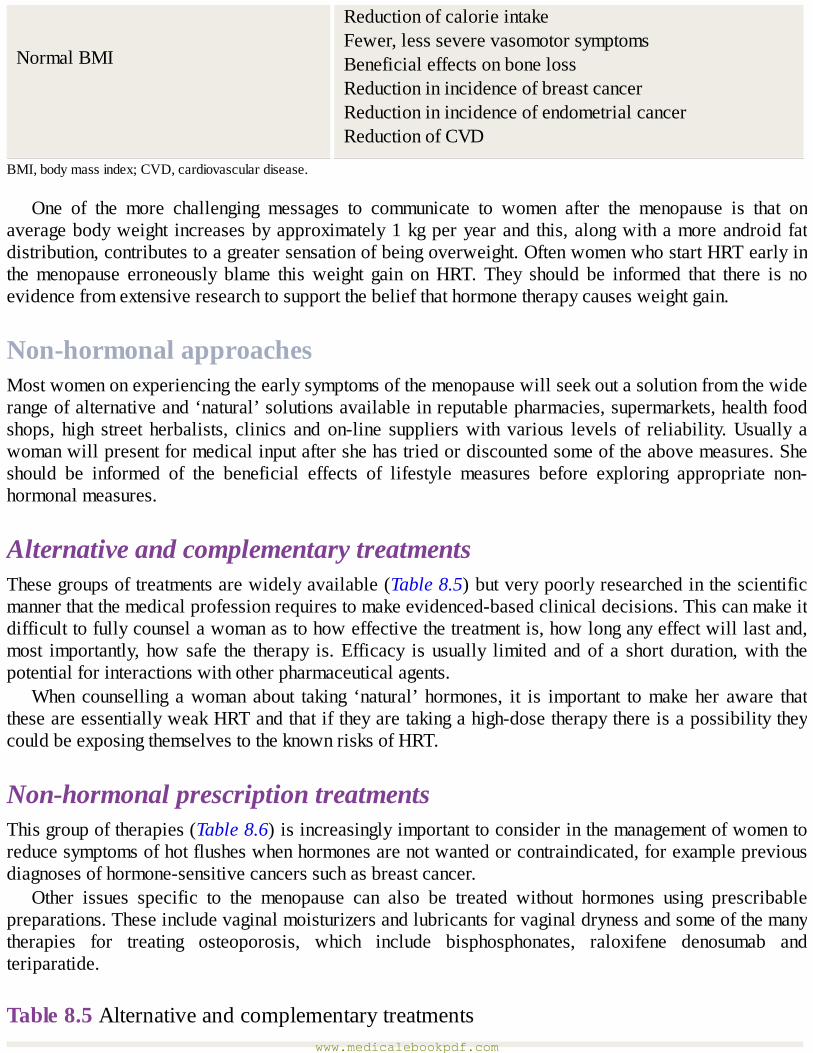
NormalBMI
ReductionofcalorieintakeFewer,lessseverevasomotorsymptomsBeneficialeffectsonbonelossReductioninincidenceofbreastcancerReductioninincidenceofendometrialcancerReductionofCVD
BMI,bodymassindex;CVD,cardiovasculardisease.
One of the more challenging messages to communicate to women after the menopause is that onaveragebodyweight increasesbyapproximately1kgperyearand this,alongwithamoreandroidfatdistribution,contributestoagreatersensationofbeingoverweight.OftenwomenwhostartHRTearlyinthemenopause erroneously blame thisweight gain onHRT. They should be informed that there is noevidencefromextensiveresearchtosupportthebeliefthathormonetherapycausesweightgain.
Non-hormonalapproachesMostwomenonexperiencingtheearlysymptomsofthemenopausewillseekoutasolutionfromthewiderangeofalternativeand‘natural’solutionsavailableinreputablepharmacies,supermarkets,healthfoodshops, high street herbalists, clinics and on-line supplierswith various levels of reliability.Usually awomanwillpresentformedicalinputaftershehastriedordiscountedsomeoftheabovemeasures.Sheshould be informed of the beneficial effects of lifestyle measures before exploring appropriate non-hormonalmeasures.
AlternativeandcomplementarytreatmentsThesegroupsoftreatmentsarewidelyavailable(Table8.5)butverypoorlyresearchedinthescientificmannerthatthemedicalprofessionrequirestomakeevidenced-basedclinicaldecisions.Thiscanmakeitdifficulttofullycounselawomanastohoweffectivethetreatmentis,howlonganyeffectwilllastand,most importantly, how safe the therapy is.Efficacy is usually limited andof a short duration,with thepotentialforinteractionswithotherpharmaceuticalagents.
When counselling awoman about taking ‘natural’ hormones, it is important tomakeher aware thattheseareessentiallyweakHRTandthatiftheyaretakingahigh-dosetherapythereisapossibilitytheycouldbeexposingthemselvestotheknownrisksofHRT.
Non-hormonalprescriptiontreatmentsThisgroupoftherapies(Table8.6)isincreasinglyimportanttoconsiderinthemanagementofwomentoreducesymptomsofhotflusheswhenhormonesarenotwantedorcontraindicated,forexamplepreviousdiagnosesofhormone-sensitivecancerssuchasbreastcancer.
Other issues specific to the menopause can also be treated without hormones using prescribablepreparations.Theseincludevaginalmoisturizersandlubricantsforvaginaldrynessandsomeofthemanytherapies for treating osteoporosis, which include bisphosphonates, raloxifene denosumab andteriparatide.
Table8.5Alternativeandcomplementarytreatmentswww.medicalebookpdf.com

Complementarydrug-freetherapies(deliveredbyapractitioner)
AcupunctureReflexologyMagnetismReikiHypnotism
Herbal/naturalpreparations(designedtobeingested)
Blackcohosh(Actaearacemosa)Dongquai(Angelicasinensis)Eveningprimroseoil(Oenotherabiennis)Gingko(Gingkobiloba)Ginseng(Panaxginseng)Kavakava(Pipermethysticum)StJohn’swort(Hypericumperforatum)
‘Natural’hormones(designedtobeingestedorappliedtotheskin)
PhytoestrogenssuchasisoflavonesandredcloverNaturalprogesteronegelDehydroepiandrosterone(DHEA)
Table8.6Non-hormonaltreatmentsforvasomotorsymptoms
Alpha-adrenergicagonists Clonidine
Beta-blockers Propanolol
Modulatorsofcentralneurotransmission
VenlafaxineFluoxetineParoxetineCitalopramGabapentin
HormonalreplacementtherapyHRT has been themainstay of the treatment ofmenopausal symptoms for decades. Its use has alwaysattracted controversy, initially in its promotion as adrugwith rejuvenating abilities, and thenduring aperiodwhere long-term benefits on osteoporosis andCVD prevention from large cohort studieswereappearing. In2002a large randomized trialhighlighteda seriesofpotential risks fromHRTuse.Thisattracted so much media attention that many women either stopped treatment themselves or theirprescribersstoppedprescribing.
www.medicalebookpdf.com
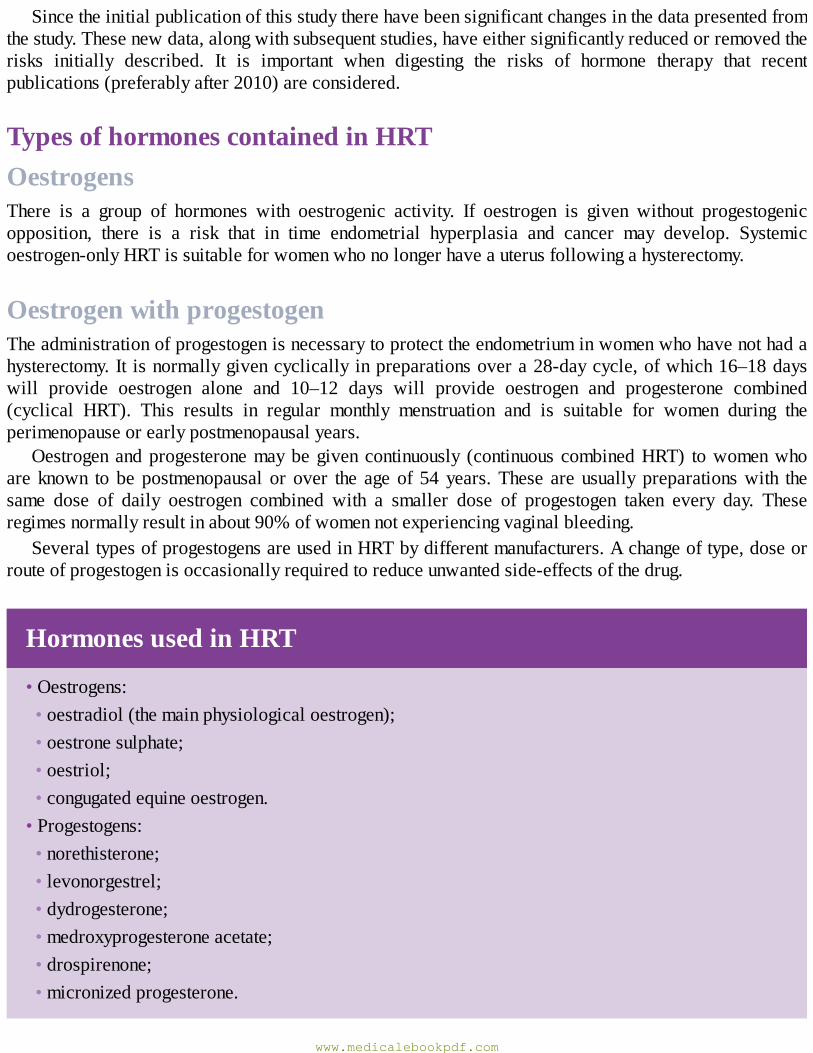
Sincetheinitialpublicationofthisstudytherehavebeensignificantchangesinthedatapresentedfromthestudy.Thesenewdata,alongwithsubsequentstudies,haveeithersignificantlyreducedorremovedtherisks initially described. It is important when digesting the risks of hormone therapy that recentpublications(preferablyafter2010)areconsidered.
TypesofhormonescontainedinHRTOestrogensThere is a group of hormones with oestrogenic activity. If oestrogen is given without progestogenicopposition, there is a risk that in time endometrial hyperplasia and cancer may develop. Systemicoestrogen-onlyHRTissuitableforwomenwhonolongerhaveauterusfollowingahysterectomy.
OestrogenwithprogestogenTheadministrationofprogestogenisnecessarytoprotecttheendometriuminwomenwhohavenothadahysterectomy.It isnormallygivencyclicallyinpreparationsovera28-daycycle,ofwhich16–18dayswill provide oestrogen alone and 10–12 days will provide oestrogen and progesterone combined(cyclical HRT). This results in regular monthly menstruation and is suitable for women during theperimenopauseorearlypostmenopausalyears.
Oestrogenandprogesteronemaybegivencontinuously (continuouscombinedHRT) towomenwhoare known to be postmenopausal or over the ageof 54years.These are usually preparationswith thesame dose of daily oestrogen combined with a smaller dose of progestogen taken every day. Theseregimesnormallyresultinabout90%ofwomennotexperiencingvaginalbleeding.
SeveraltypesofprogestogensareusedinHRTbydifferentmanufacturers.Achangeoftype,doseorrouteofprogestogenisoccasionallyrequiredtoreduceunwantedside-effectsofthedrug.
HormonesusedinHRT
•Oestrogens:•oestradiol(themainphysiologicaloestrogen);•oestronesulphate;•oestriol;•congugatedequineoestrogen.•Progestogens:•norethisterone;•levonorgestrel;•dydrogesterone;•medroxyprogesteroneacetate;•drospirenone;•micronizedprogesterone.
www.medicalebookpdf.com
TestosteroneTestosterone has traditionally been given towomenwith disorders of sexual desire and energy levelswhohavefailedtorespondtonormalHRT.Thesebeneficialeffectsoftestosteronearewelldocumented;however,fewlong-termstudiesintotheadverseeffectsoftestosteroneexist.
Overthepastyearsmanufacturershavestoppedmakingtestosteronedrugsforwomentothepointthattheonlyavailablepreparationsavailablenowarethoselicensedforuseinmen.Thisusuallymeansthattestosteroneneedstobeinstigatedunderthecareofadoctorwithspecialistmenopauseknowledge.
RoutesofhormonetherapyadministrationThetwomainroutesofHRTdeliveryareoralandtransdermal.Theoralrouteisnormallyadailytabletthatcontains theappropriatemixofoestrogenandprogestogen,dependingon thepreparation.Theoralrouteisconvenientandcheapbutdoesinfluencelipidmetabolismandthecoagulationsystemthroughitseffectsontheliverduringfirst-passmetabolism.
Thetransdermalroute,eithergivenaspatchesappliedtotheskinonthetrunkorasmeasuredamountsofgel,isalsoeffective,withtheadvantageofdeliveryofoestradioldirectlyintothecirculation,avoidingtheabovepotentiallyadverseeffectsontheliverandthecoagulationsystem.Oestradiolisalsoavailableas small vaginal tablets and a vaginal ring, and oestriol as measured dose vaginal creams that areimportantinthemanagementoflowergenitaltractsymptoms.
Progestogen in the form of levonorgestrelmay be administered as an intrauterine releasing system(IUS),Mirena®.This devicenot onlyprovides contraception and control of troublesomebleeding, butalso provides endometrial protection for up to 5 years (see Chapter 17, Gynaecological surgery andtherapeutics).
BeneficialeffectsofhormonetherapyVasomotorsymptomsTheprincipalreasonfortakingHRTisvasomotorsymptomimprovement.Wellover90%ofwomennoteasignificant improvementwithin6weeks,withreductions infrequencyandseverityofhot flushesandnightsweatsandconsequentimprovementsinsleepanddaytimeenergylevelsaswellasconcentration.
TheskeletonThe protective effects of HRT on the skeleton include prevention of bone loss and the prevention ofosteoporotic fracturesof thehipandspine.TheuseofHRT is strongly recommended forwomenafterPOFas they are at amuchgreater riskof osteoporosis.Most postmenopausalwomen should considerHRTasameanstopreventboneloss,especiallyiftheyrequireHRTforothersymptomatology.
KeybenefitsofHRT
•Symptomsimproved:•vasomotorsymptoms;•sleeppatterns;
www.medicalebookpdf.com
•performanceduringtheday.•Preventionofosteoporosis:•increasedbonemineraldensity;•reducedincidenceoffragilityfractures.•Lowergenitaltract:•dryness;•soreness;•dyspareunia;•CVD:preventativeeffectifstartedearlyinmenopause.
ThelowergenitaltractBothsystemicandlocallyadministeredHRThavesignificantbeneficialeffectsonthelowergenitaltract.There is good evidence that its administration improves vulvovaginal dryness, irritation, soreness anddyspareunia. There is also an improvement in symptoms of cystitis and occasionally dysuria. Localhormonetherapyisunlikelytocureprolapsebutmayimprovesomeofthesymptomsofprolapse.ThereisnoevidencethatlocalHRTimprovesincontinence.ManywomenconsideringlocalHRTaredissuadedfromitsuseduetoconcernsaboutthepublishedrisks.Theycanoftenbereassuredthatweretheytousethe form of local hormone therapy as a 10 µg twice weekly dose vaginal tablet, theywould only beadministeringapproximatelytheequivalentofa1mgoraltabletoverawholeyear.
ThecardiovascularsystemThecardiovascularbenefitsofHRTwere firstdemonstrated in largeobservationalcohort studies.Theprincipal benefitswere reduction in ischaemic heart disease and overallmortality.However the largerandomizedWomen’sHealth Initiative (WHI) study demonstrated reductions in survival fromCVD inwomen takingHRT. This study has beenwidely criticized due to the overweight and generally olderpopulationstudied,apopulationprobablyatgreaterriskofCVD.Thecurrentunderstandingisthatthereis a ‘window of opportunity’ in the perimenopausal or early postmenopausal years during which theadministration of HRTmay reduce the morbidity andmortality from CVD by prevention of atheromaformation.
WhilethepreventionofCVDisnotcurrentlyalicensedindicationforHRT,thedataaresufficienttoincludeadiscussionwithwomenthattheyshouldconsiderthesebenefits.
ThecolonWhiletheWHIstudydemonstratedaclearbenefitofHRTontheincidenceandmortalityofcoloncancer,theuseofHRTtopreventthismalignancyisnotindicated.
Prescribingandside-effectsofhormonetherapyPriortoprescribingHRTitisimportanttoweighuptheindications,proposedbenefitsandpotentialrisksforeachpatient individually.Forexample,hormone therapymaybecontraindicated inapatientwithapriorhistoryofbreastcancerorthromboembolicdisease.
www.medicalebookpdf.com
Ingeneral,side-effectswithHRTarefewandminor.ItisthereforeimportantbeforestartingHRTtoensurethatthewomanhasnocontraindicationstoHRTandtoensurethatshehashadnoseriouseffectsinthepastwhenonthecontraceptivepill,suchasvenousthrombosisormigrainewithaura.
Contraindicationsandpotentialside-effects
•Absolutecontraindications:•suspectedpregnancy;•breastcancer;•endometrialcancer;•activeliverdisease;•uncontrolledhypertension;•knowncurrentvenousthromboembolism(VTE);•knownthrombophilia(e.g.FactorVleiden);•otosclerosis.•Relativecontraindications:•uninvestigatedabnormalbleeding;•largeuterinefibroids;•pasthistoryofbenignbreastdisease;•unconfirmedpersonalhistoryorastrongfamilyhistoryofVTE;•chronicstableliverdisease;•migrainewithaura.•Side-effectsassociatedwithoestrogen:•breasttendernessorswelling;•nausea;•legcramps;•headaches.•Side-effectsassociatedwithprogestogen:•fluidretention;•breasttenderness;•headaches;•moodswings;•depression;•acne.
Most side-effects can be managed with a change in dose of oestrogen or a change in type ofprogestogen.Somepatientscanalsobenefit fromaswitchofroute.ManywomenfindtheIUSausefuldeviceasitdeliversmuchlessprogestogenintothecirculation,thusreducingprogestogenicside-effects.
www.medicalebookpdf.com
ThedurationforwhichawomanshouldtakeHRTisfrequentlydebated.Thereislittleclearevidencetosupporthowlong,butitisrecommendedthatthereshouldbenoexactmaximumageatwhichawomanshouldstopHRT,ratheremployingregularassessmentofthewomanandherneedsalongwithreviewofthetypeanddoseofHRTsheistaking.
RisksofhormonetherapyThe risks attributed toHRT have attractedmuchmedia attention.At present, due to a combination ofreanalysisof thedata,newstudiesandabetterunderstandingof thecommunicationofrisk,manymorewomenareconsideringHRTinthemanagementoftheirmenopause.
CancerBreastcanceriswithoutdoubtthecancerthatattractsmostconcernfrompatientsandmostattentionfromtheworld’smedia.The studiesperformed still donot fully informpatientsof the additional risks theyexposethemselvestobyusingHRT.Usefulfigurestoquotearethatthebackgroundriskofbreastcancerin the 50–59year age group is 22.5 per 1,000women for 7.5 years use ofHRTand theremaybe anadditional2–6cancerswithcombinedHRTuse,whichreducesafterstoppingHRT.ItisimportanttobeawarethatrecentdatawithoestradiolHRTsuggestthatmortalityfrombreastcancerisnotincreasedandthat certain types of HRTmay promote the growth of pre-existing malignant cells rather than initiatetumours.
Endometrial cancer and ovarian cancer are not considered significant risks with HRT use.Endometrialmalignancyriskislargelyeliminatedifwomenaregivenprogestogens.IncidenceofovariancancerhasnotbeenshowntosignificantlyincreasewithHRTuse.
CardiovasculardiseaseandstrokeAs discussed above,most of the effects ofHRT on the cardiovascular systemwhen given to youngerwomenarebeneficial.However,whengiven toolderwomen theeffectsmaybecomedeleterious.ThedegreetowhichthishappensisunclearbutislikelytobehigherinwomentakingcombinedHRT.
Stroke incidencehasa similar ageeffect,with the increased incidencegreater in theolderwoman.The effect is small and is only on the incidence of ischaemic stroke, thought to be an increase of anadditional2womenper10,000womenperyearwhenonHRT.
VenousthromboembolismTheinfluenceofHRTontheclottingsystemissimilartothatoftheoralcontraceptive.ThebackgroundincidenceofallVTEinwomenover50islow(approximately15–20per10,000)andHRTdoublesthisrisk.ThereisevidencetosuggestthattransdermalHRT,throughitsavoidanceofeffectsontheliver,maynothavesuchagreateffectonVTEincidence.
KEYLEARNINGPOINTS•Themenopauseisakeytimeinthelifeofawoman.•Thephysiologicalchangesthatoccurhavesignificanteffectsonthewomanasawhole,affectingnumerousbodysystems.
www.medicalebookpdf.com

• Care ofwomen during the postreproductive years should bemanaged in a holistic fashion thataddresses lifestyle and general health issues first. Using such an approach can address manyelementsofhealth,improvinglongevityandqualityoflife.
•HRT exists in a variety of forms and is effective in improvingmenopausal symptoms and bonemineraldensity.
•ThepotentialuseofHRTinpreventionofdisease,whileconsideringthesmalladditionalrisksitsuseattracts,meansthatoverthecomingyearsitmaybecomeacost-effectivemeansofimprovingthelivesoftheexpandingnumbersoftheglobalpopulationofmenopausalwomen.
FurtherreadingLobo RA1, Davis SR, De Villiers TJ, et al. (2014). Prevention of diseases after menopause.Climacteric17(5):540–56.
Panay N, Hamoda H, Arya R, SavvasM; BritishMenopause Society andWomen’s Health Concern(2013). The 2013 British Menopause Society & Women’s Health Concern recommendations onhormonereplacementtherapy.MenopauseInt19(2):59–68.
ReesM,StevensonJ,HopeS,RozenbergS,PalaciosS (2009).Managementof theMenopause, 5thEdition.London:RoyalSocietyofMedicinePressandBritishMenopauseSocietyPublications.
Selfassessment
CASEHISTORY
MrsAisa36-year-oldwoman.Shehashadonechilddeliverednormally6yearspreviouslyafterabriefperiodof subfertility.Followingdeliveryof thatchildshehad4yearsof infrequentperiodsandoverthelast2yearsshehasbeenamenorrhoeicandhashaddifficultysleeping,oftenwakingupfeelinghot.AWhatisthelikelydiagnosis?BHowwouldthediagnosisbeconfirmed?CFollowing diagnosisMrsA askswhat the immediate and long-term issues are and how theymightbemanaged.Outlinethekeyissues.
ANSWERS
APOI.BAcombinationof theclinicalpictureandserumFSHlevelsareusuallyadequate toconfirmthediagnosis.OnreceiptofoneelevatedFSHlevel it is recommended thata repeat testnosoonerthan6weeksafterthefirstisperformedtoconfirmthediagnosis.
www.medicalebookpdf.com
COneofthefirstissuesondiagnosisofPOIistoinformMrsAthatthereisstillanappreciableriskofunpredictableovulationandassuchhercontraceptiveneedsshouldbediscussed.The issueofboneprotectionshouldbeexplained toher.Withherprolongedentry intoPOIshecouldhaveosteoporosisorosteopaenia.ConsiderationofbonedensitometryandmanagementwithHRTorbisphosphonatesshouldbeconsidered.
ThebenefitsofHRTshouldbeexplainedtoher.Itisoftenhelpfultohighlightthatbecauseshehaslostherendogenousoestrogenatanearlyageincomparisontoherpeers,ifsheweretotakeHRTshewouldnotbeexposingherselftoanyappreciableexcessrisksfromHRTuntiltheageofapproximately51.
SBAQUESTIONS
1A68-year-oldwomanpresentswithrecurrentepisodesofpostmenopausalbleeding.Thevolumeof blood loss is only very small amounts of spotting that often, but not exclusively, followintercourse. Her previous gynaecological history is unremarkable, with a lifetime of normalcervical smears. She is not on any drugs, including HRT. Pelvic ultrasound and endometrialbiopsyarenormal.Vaginalexaminationdemonstratesvaginaldryness,smallpetechiaeandlossofrugae.Whatisthemostappropriatenextstepinhermanagement?Choosethesinglebestanswer.
AOutpatienthysteroscopicassessmentoftheendometrium.BTransdermalcontinuouscombinedHRT.CWater-basedvaginallubricants.DOestrogen-containingvaginalpessaries.EFlexiblecystourethroscopy.
ANSWER
D The normal ultrasound and endometrium indicate that there is no concern about endometrialpathologyincludingmalignancy.Therefore,outpatienthysteroscopyorexaminationofthebladderwith flexible cystourethroscopy is unnecessary. Vaginal lubricants are useful for painfulintercoursebutlocaloestrogenwillinduceareturnofthevaginatopremenopausalflexibilityandlubrication.Transdermaloestrogentherapyisnotnecessaryunlesstherearesystemicsymptomsofhypoestrogenism.
2Withregardtothehormonechangesthataccompanythemenopause,whichofthefollowingistrue?Choosethesinglebestanswer.AAsovarianfunctionfails,serumFSHlevelsincrease.B12monthsaftertheLMPserumlevelsoftestosteroneareclosetozero.CSecretionofGnRHfromthehypothalamusincreasessignificantlyinthelatemenopausetodriveovarianactivity.
www.medicalebookpdf.com
DProgesteronelevelsareundetectableintheperimenopause.E High levels of peripherally-produced oestrogens reduce the frequency and severity of hotflushesinobesewomen.
ANSWER
AFSHrisesinresponsetoincreasingpulsatilityofGnRH,itselfrespondingtofallinginhibinasthefolliclesbecomedepletedintheperiomenopause.Subsequently,thereisaprogressivedeclineinGnRHpulsatilityandGnRHlevelsoverallfall.
Only 30–50%of testosterone production is ovarian, and levels fall slowly aftermenopausebecauseitsproductionismainlyindependentoftheneuroendocrineaxis.Althoughadiposetissueproducesoestrogen, it is an insulator interferingwithheatdissipation;hot flushesareworse inobesewomen.
Thereisaonlyaslowdeclineinprogesteroneduringtheperimenopause,andsolevelsremaindetectable.
www.medicalebookpdf.com
CHAPTER9Genitourinaryproblems
MARGARETKINGSTON
Introduction
Takingasexualhistory
TestingforSTIsandassociatedconditions
Humanimmunodeficiencyvirus
Conclusion
Furtherreading
Selfassessment
LEARNINGOUTCOMES•Understandtheimportanceofsexuallytransmittedinfections(STIs)ingynaecology.
•Describethetesting,diagnosisandtransmissionofcommonSTIsandblood-borneviruses(BBVs).
•Understandthatsupportisneededforpatientstoenablethemtoundertakescreening.
•Appreciatethathumanimmunodeficiencyvirus(HIV)haschangedfromlifelimitingintoachronic,manageablecondition.
•Learnhowtotakeasexualhistory.
•UnderstandthediagnosisofandscreeningforHIV.
•DescribethecarefortheHIV-positivemotherandchild.
www.medicalebookpdf.com

IntroductionAnunderstandingofSTIsandtheircomplicationsiscruciallyimportantingynaecologicalpractice.Thesubject is frequentlymisunderstoodand the impactonaffectedwomen, theirpartnersandat times theirchildrenmay be considerable. STIs are often asymptomatic, but can still be transmitted to others andcause significantproblemsat the timeof infectionor in the future; for example, humanpapillomavirus(HPV)infectionandcervicalcancer.STIsdisproportionatelyaffectyoungerpeople,butincreasinglytheyareidentifiedinolderpeople,inwhomthediagnosisisoftennotconsideredandsocanbemissed.STIsoftencoexistandwhenoneisfound,screeningforothersisrequired.
TestsforSTIshavehugelyimprovedinrecentyears,withtheadventofhighlysensitiveandaccuratemolecular tests that are very easy to use and can detect several infections on a single swab or urinesample.Inaddition,serologicaltestsforBBVsandsyphilishavealsoincreasedinaccuracy,andcanbeperformed sooner after possible exposure than in thepast.Womenareoftendiagnosed firstwhen theyhaveyoungfamiliesandtheyattendforreproductivehealthcareandareofferedscreening.Theyrequiresupporttoinformpresent(andwherenecessary)previouspartners,sotheycanalsoreceivetestingandtreatmentfortheirownhealthtopreventreinfectionand/oron-goingtransmissionwithinthecommunity.Childrenmay also require testing and treatment if they have been exposed during pregnancy, birth orbreastfeeding. This aspect of managing STIs can be very challenging but is crucially important. Theconsultationmay lead to a consideration of safeguarding ofwomen and girlswhomay be exposed tosexualordomesticviolence, abuse, coercionor exploitation,whichmayonlybecomeapparent in thiscontext.
The treatment andmanagementofHIV infectionhasbeen transformed, and thediseasehas changedfrom life limiting into a chronic manageable condition. In addition, effective treatment also preventstransmission to sexual partners and children. The treatments are simpler with less toxicity and thewidespread availability of cheaper, generic medicines has resulted in therapies that are acceptable,affordableandmanageable,requiringlessmonitoringthanbefore.
Unfortunately, STIs and HIV remain stigmatizing conditions for many women, who find informingpartnersorsharingnewsofanydiagnosiswithfriendsorfamilyverydifficult.Consequentlytheycanfeelisolatedandmayneedadditionalsupportfromtheirhealthcareprofessionals.RespectingandmaintainingpatientconfidentialityisvitalwhenmanagingwomenwithanSTIorHIVdiagnosis.
TakingasexualhistoryThisisthefirststeptoidentifyingandtreatingSTIs.Itallowsthehealthcareprofessionaltoquantifyrisk,decidewhichtestsarerequiredandwhethertheyneedtoberepeatedlater,andgatherinformationneededfortreatment.Inaddition,itprovidesanopportunityforpatientstoexpressconcernsandaskquestions.Raising the issue of STIsmay be unexpected and it is important to start by ensuring privacy and thenexplainingwhy the subject isbeingbroached, toaskpermission toproceedand to reassure thepatientabout confidentiality. Important points to cover are summarized in Table 9.1. Abuse, exploitation orcoercion can happen to anyone, but younger women and sexually active children especially so, andscreeningquestionsforthisarealsoincludedinTable9.1.
www.medicalebookpdf.com
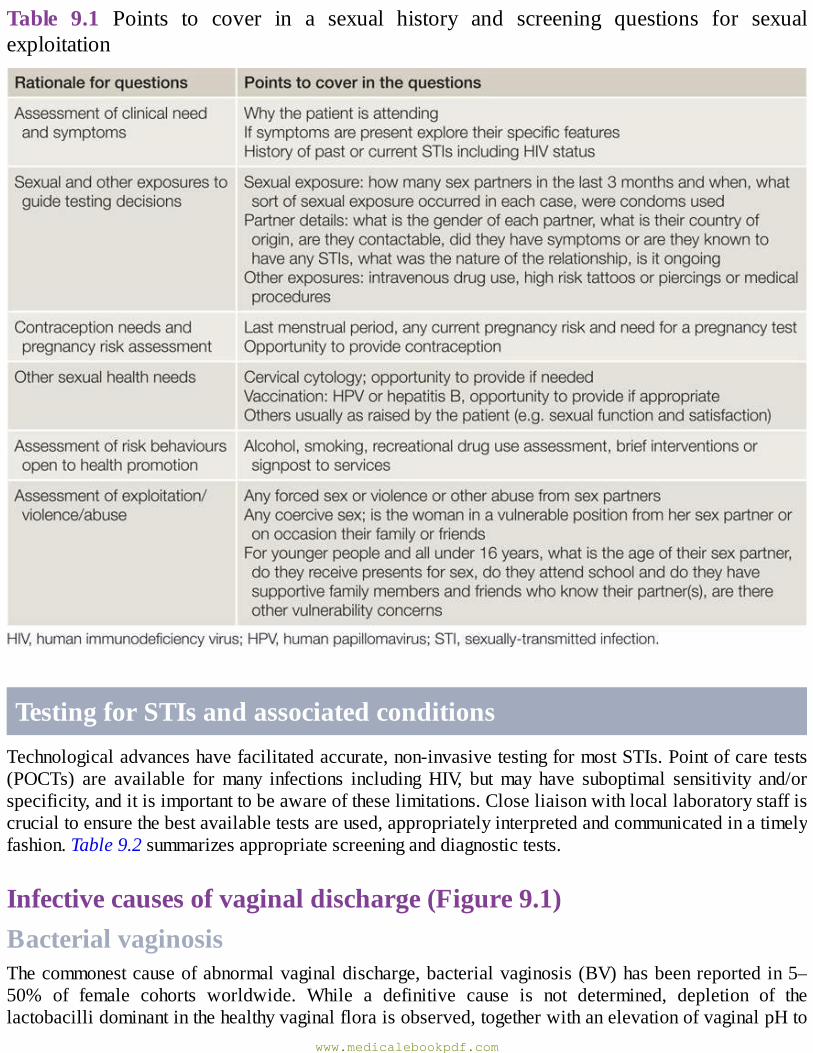
Table 9.1 Points to cover in a sexual history and screening questions for sexualexploitation
TestingforSTIsandassociatedconditionsTechnologicaladvanceshavefacilitatedaccurate,non-invasivetestingformostSTIs.Pointofcaretests(POCTs) are available formany infections includingHIV, butmay have suboptimal sensitivity and/orspecificity,anditisimportanttobeawareoftheselimitations.Closeliaisonwithlocallaboratorystaffiscrucialtoensurethebestavailabletestsareused,appropriatelyinterpretedandcommunicatedinatimelyfashion.Table9.2summarizesappropriatescreeninganddiagnostictests.
Infectivecausesofvaginaldischarge(Figure9.1)BacterialvaginosisThecommonestcauseofabnormalvaginaldischarge,bacterialvaginosis(BV)hasbeenreportedin5–50% of female cohorts worldwide. While a definitive cause is not determined, depletion of thelactobacillidominantinthehealthyvaginalfloraisobserved,togetherwithanelevationofvaginalpHto
www.medicalebookpdf.com
above4.5.Theexistenceof avaginal epithelialbiofilmconsistingofGardnerellavaginalis and otherspecies has been more recently described. Other risk factors include douching, black race, smoking,havinganewsexualpartnerandreceivingoralsex.
Symptomsincludeanoffensivevaginaldischargethatisoftenreportedashavinga‘fishy’malodour,andonexaminationahomogenousoff-whitevaginaldischargewithahighpHisobserved.DiagnosisismadebyevaluatingaGramstainofthevaginaldischargeusingavalidatedmethod,suchastheHay-IsonorNugentcriteria,or,lessfrequentlyinmodernpractice,byusingAmselscriteria(3of4arerequired:homogenous discharge, high pH, ‘clue cells’ on microscopy and a fishy odour when 10% potassiumhydroxideisaddedtoasampleofdischarge).BVisassociatedwithanumberofpathologiesincludingpelvic inflammatory disease (PID), posthysterectomy vaginal cuff cellulitis and, in pregnancy, pretermbirth and rupture ofmembranes andmiscarriage.An increased risk ofHIV acquisition is observed inwomenatriskwithBV.
Oral or intravaginal treatments with metronidazole or clindamycin are indicated in women withsymptomsorthoseinwhomitisdiagnosedandelectfortreatment–especiallypriortogynaecologicalsurgical procedures. Women with BV should be advised that vaginal douching or excessive genitalwashingshouldbeavoided.
Table9.2TestsforSTIsandrelatedconditionsinwomen
www.medicalebookpdf.com
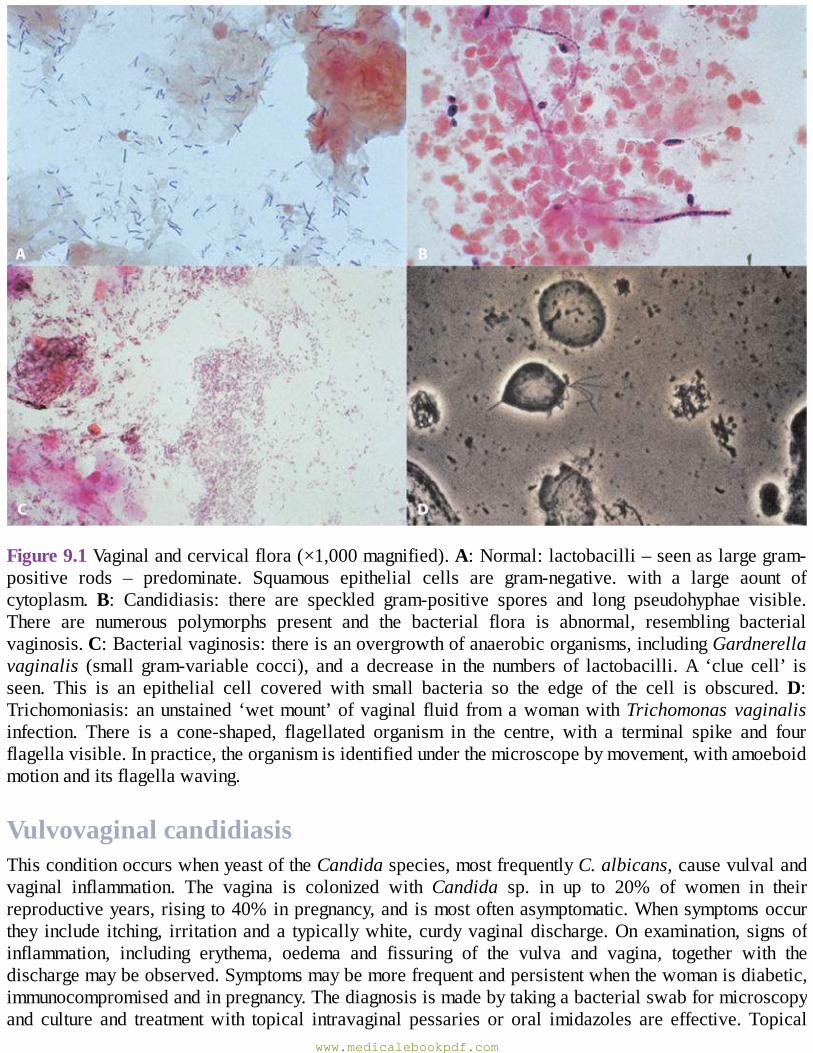
Figure9.1Vaginalandcervicalflora(×1,000magnified).A:Normal:lactobacilli–seenaslargegram-positive rods – predominate. Squamous epithelial cells are gram-negative. with a large aount ofcytoplasm.B: Candidiasis: there are speckled gram-positive spores and long pseudohyphae visible.There are numerous polymorphs present and the bacterial flora is abnormal, resembling bacterialvaginosis.C:Bacterialvaginosis:thereisanovergrowthofanaerobicorganisms,includingGardnerellavaginalis (small gram-variable cocci), and a decrease in the numbers of lactobacilli.A ‘clue cell’ isseen. This is an epithelial cell covered with small bacteria so the edge of the cell is obscured.D:Trichomoniasis: anunstained ‘wetmount’ ofvaginal fluid fromawomanwithTrichomonas vaginalisinfection. There is a cone-shaped, flagellated organism in the centre, with a terminal spike and fourflagellavisible.Inpractice,theorganismisidentifiedunderthemicroscopebymovement,withamoeboidmotionanditsflagellawaving.
VulvovaginalcandidiasisThisconditionoccurswhenyeastoftheCandidaspecies,mostfrequentlyC.albicans,causevulvalandvaginal inflammation. The vagina is colonized with Candida sp. in up to 20% of women in theirreproductiveyears,risingto40%inpregnancy,andismostoftenasymptomatic.Whensymptomsoccurthey include itching, irritationanda typicallywhite, curdyvaginaldischarge.Onexamination, signsofinflammation, including erythema, oedema and fissuring of the vulva and vagina, together with thedischargemaybeobserved.Symptomsmaybemorefrequentandpersistentwhenthewomanisdiabetic,immunocompromisedandinpregnancy.Thediagnosisismadebytakingabacterialswabformicroscopyand culture and treatmentwith topical intravaginal pessaries or oral imidazoles are effective. Topical
www.medicalebookpdf.com
vulvalantifungalsandtheuseofaqueouscreamasanemollientandcleansingagentprovidesymptomaticrelief.ThisisnotanSTIandpartnerswithoutsymptomsdonotrequiretreatment.
TrichomoniasisVaginal and urethral infection with the flagellate protozoan Trichomonas vaginalis (TV) results insymptomsofvaginaldischargewithavariableappearanceandsymptomsand/orsignsofvulvovaginitis.Asymptomaticinfectionisobservedinupto50%ofwomenandmostoftheirmalesexualpartners.TVissexuallytransmittedandsimultaneoustreatmentofcurrentandrecentsexualpartnersisrequired.Thereissomeevidenceofanassociationwithpregnancyoutcome:pretermbirth, lowbirthweightandmaternalpostpartumsepsis,althoughfurtherresearchisrequired.Testingisindicatedinsymptomaticwomen,andthegold standard is anucleic acid amplification test (NAAT)preferablyon avaginalor endocervicalswaboronurine,withsensitivitiesandspecificitiesreachingover95%,dependingonthespecimenandthetest.SomeNAATsalsodetectNeisseriagonorrhoeaandChlamydiatrachomatisonthesamesample;for these the optimal test is a vulvovaginal swab.Microscopy and culture of a sample of the vaginaldischarge and POCT using different techniques are also used but are limited by reduced sensitivity.Treatmentiswithasystemicmetronidazoleregime.
CervicitisandpelvicinflammatorydiseaseGonorrhoea(Figure9.2)Thiscondition iscausedby infectionwith thebacteriaNeisseriagonorrhoea. Infectionoccurs throughsexualcontactandsimultaneoustreatmentofcurrentandrecentsexualpartnersisrequired.Endocervicalinfection is asymptomatic in up to 50% of cases, with altered vaginal discharge the most commonsymptomandlowerabdominalpain inup to25%.Rectal infectionoccurs throughtransmucosalspreadand receptiveanal sex, andpharyngeal infection through receptiveoral sex; the latter isnearlyalwaysasymptomatic.Examinationisoftennormal,althoughcervicitiswithorwithoutamucopurulentdischargemay be seen. Ascending infection may result in PID and, rarely, haematogenous spread can causedisseminatedgonococcalinfectionwithapurpuricnon-blanchingrashand/oranarthralgiaorarthritisthatistypicallymonoarticularinaweight-bearingjoint.Ophthalmicinfectionoccursduetoinoculationfrominfectedgenitalsecretions,andneonatal infectionoccurswhenthemotherhasendocervical infectionatthetimeofdelivery.
www.medicalebookpdf.com
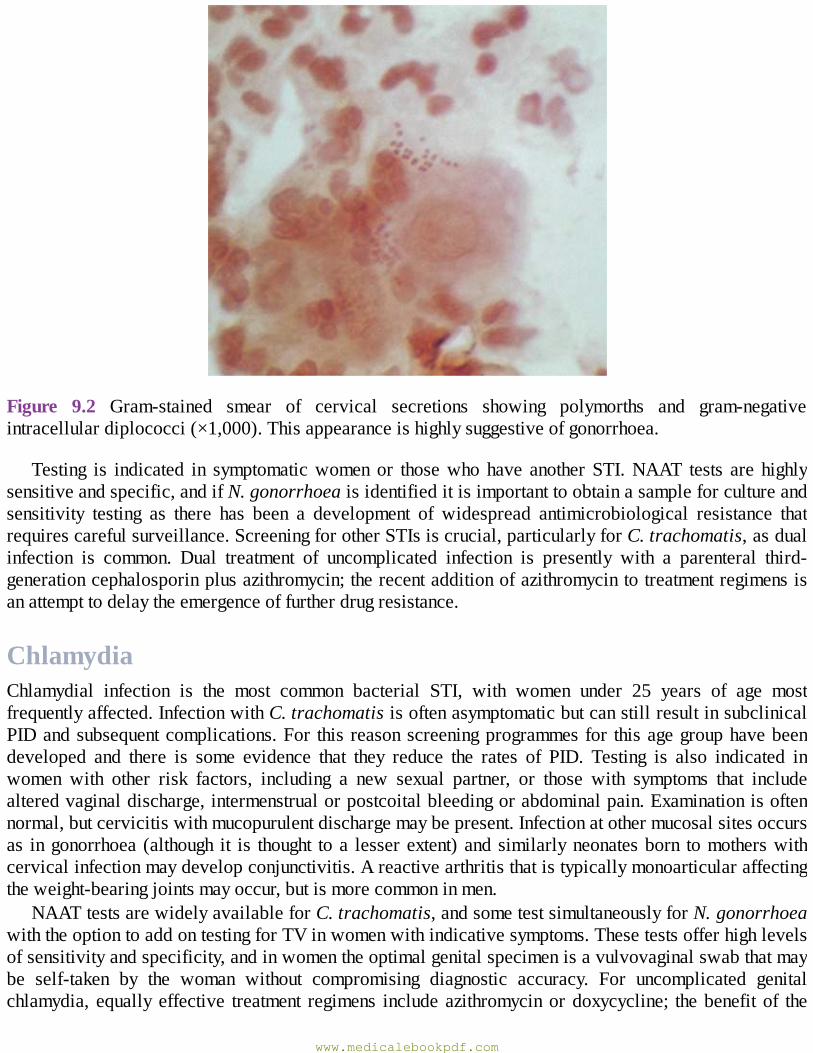
Figure 9.2 Gram-stained smear of cervical secretions showing polymorths and gram-negativeintracellulardiplococci(×1,000).Thisappearanceishighlysuggestiveofgonorrhoea.
Testing is indicated in symptomaticwomenor thosewhohave anotherSTI.NAAT tests are highlysensitiveandspecific,andifN.gonorrhoeaisidentifieditisimportanttoobtainasampleforcultureandsensitivity testing as there has been a development of widespread antimicrobiological resistance thatrequirescarefulsurveillance.ScreeningforotherSTIsiscrucial,particularlyforC.trachomatis,asdualinfection is common. Dual treatment of uncomplicated infection is presently with a parenteral third-generationcephalosporinplusazithromycin;therecentadditionofazithromycintotreatmentregimensisanattempttodelaytheemergenceoffurtherdrugresistance.
ChlamydiaChlamydial infection is the most common bacterial STI, with women under 25 years of age mostfrequentlyaffected.InfectionwithC.trachomatisisoftenasymptomaticbutcanstillresultinsubclinicalPIDandsubsequentcomplications.For this reasonscreeningprogrammesfor thisagegrouphavebeendeveloped and there is some evidence that they reduce the rates of PID. Testing is also indicated inwomen with other risk factors, including a new sexual partner, or those with symptoms that includealteredvaginaldischarge,intermenstrualorpostcoitalbleedingorabdominalpain.Examinationisoftennormal,butcervicitiswithmucopurulentdischargemaybepresent.Infectionatothermucosalsitesoccursas ingonorrhoea (although it is thought toa lesserextent)andsimilarlyneonatesborn tomotherswithcervicalinfectionmaydevelopconjunctivitis.Areactivearthritisthatistypicallymonoarticularaffectingtheweight-bearingjointsmayoccur,butismorecommoninmen.
NAATtestsarewidelyavailableforC.trachomatis,andsometestsimultaneouslyforN.gonorrhoeawiththeoptiontoaddontestingforTVinwomenwithindicativesymptoms.Thesetestsofferhighlevelsofsensitivityandspecificity,andinwomentheoptimalgenitalspecimenisavulvovaginalswabthatmaybe self-taken by the woman without compromising diagnostic accuracy. For uncomplicated genitalchlamydia, equally effective treatment regimens includeazithromycinordoxycycline; thebenefitof the
www.medicalebookpdf.com
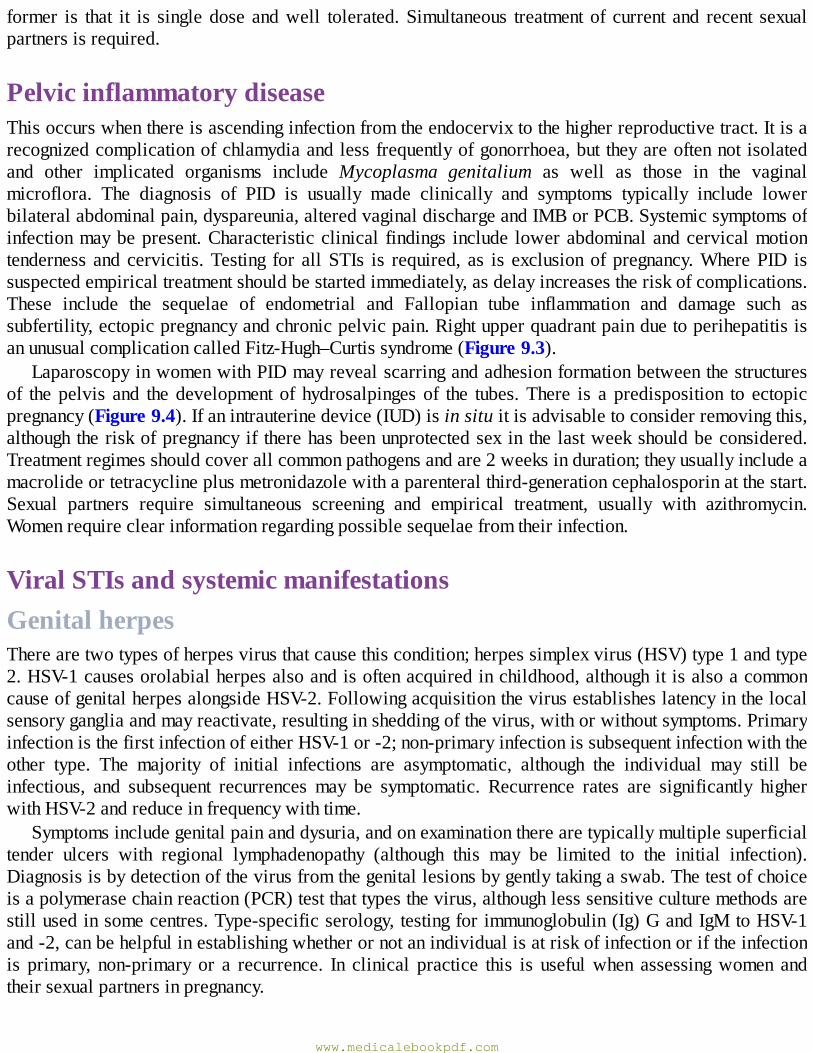
former is that it is singledose andwell tolerated.Simultaneous treatmentof current and recent sexualpartnersisrequired.
PelvicinflammatorydiseaseThisoccurswhenthereisascendinginfectionfromtheendocervixtothehigherreproductivetract.Itisarecognizedcomplicationofchlamydiaandlessfrequentlyofgonorrhoea,but theyareoftennot isolatedand other implicated organisms include Mycoplasma genitalium as well as those in the vaginalmicroflora. The diagnosis of PID is usually made clinically and symptoms typically include lowerbilateralabdominalpain,dyspareunia,alteredvaginaldischargeandIMBorPCB.Systemicsymptomsofinfectionmaybepresent.Characteristicclinical findings include lowerabdominalandcervicalmotiontenderness andcervicitis.Testing for allSTIs is required, as is exclusionofpregnancy.WherePID issuspectedempiricaltreatmentshouldbestartedimmediately,asdelayincreasestheriskofcomplications.These include the sequelae of endometrial and Fallopian tube inflammation and damage such assubfertility,ectopicpregnancyandchronicpelvicpain.RightupperquadrantpainduetoperihepatitisisanunusualcomplicationcalledFitz-Hugh–Curtissyndrome(Figure9.3).
LaparoscopyinwomenwithPIDmayrevealscarringandadhesionformationbetweenthestructuresof thepelvis and thedevelopment of hydrosalpingesof the tubes.There is a predisposition to ectopicpregnancy(Figure9.4).Ifanintrauterinedevice(IUD)isinsituitisadvisabletoconsiderremovingthis,althoughtheriskofpregnancy if therehasbeenunprotectedsex in the lastweekshouldbeconsidered.Treatmentregimesshouldcoverallcommonpathogensandare2weeksinduration;theyusuallyincludeamacrolideortetracyclineplusmetronidazolewithaparenteralthird-generationcephalosporinatthestart.Sexual partners require simultaneous screening and empirical treatment, usually with azithromycin.Womenrequireclearinformationregardingpossiblesequelaefromtheirinfection.
ViralSTIsandsystemicmanifestationsGenitalherpesTherearetwotypesofherpesvirusthatcausethiscondition;herpessimplexvirus(HSV)type1andtype2.HSV-1causesorolabialherpesalsoandisoftenacquiredinchildhood,althoughitisalsoacommoncauseofgenitalherpesalongsideHSV-2.Followingacquisitionthevirusestablisheslatencyinthelocalsensorygangliaandmayreactivate,resultinginsheddingofthevirus,withorwithoutsymptoms.PrimaryinfectionisthefirstinfectionofeitherHSV-1or-2;non-primaryinfectionissubsequentinfectionwiththeother type. The majority of initial infections are asymptomatic, although the individual may still beinfectious, and subsequent recurrences may be symptomatic. Recurrence rates are significantly higherwithHSV-2andreduceinfrequencywithtime.
Symptomsincludegenitalpainanddysuria,andonexaminationtherearetypicallymultiplesuperficialtender ulcers with regional lymphadenopathy (although this may be limited to the initial infection).Diagnosisisbydetectionofthevirusfromthegenitallesionsbygentlytakingaswab.Thetestofchoiceisapolymerasechainreaction(PCR)testthattypesthevirus,althoughlesssensitiveculturemethodsarestillusedinsomecentres.Type-specificserology,testingforimmunoglobulin(Ig)GandIgMtoHSV-1and-2,canbehelpfulinestablishingwhetherornotanindividualisatriskofinfectionoriftheinfectionis primary, non-primary or a recurrence. In clinical practice this is usefulwhen assessingwomen andtheirsexualpartnersinpregnancy.
www.medicalebookpdf.com
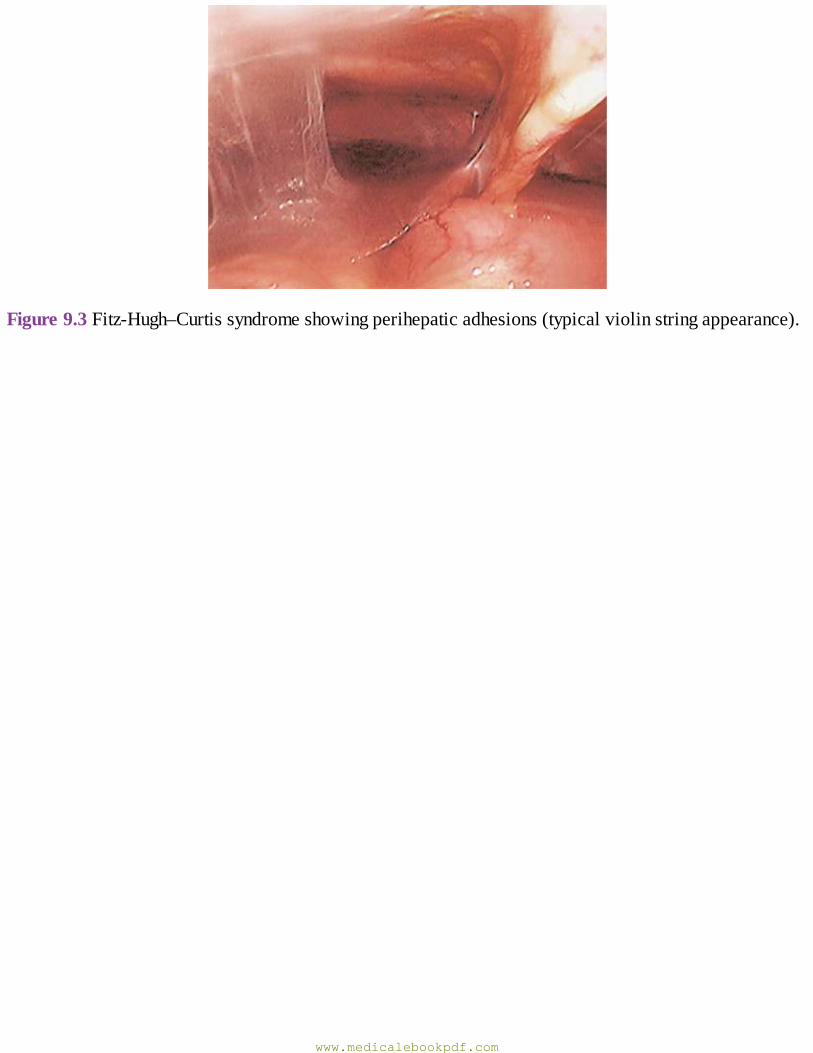
Figure9.3Fitz-Hugh–Curtissyndromeshowingperihepaticadhesions(typicalviolinstringappearance).
www.medicalebookpdf.com

Figure9.4A:PeritubaladhesionsoftheleftFallopiantube;B:ectopicpregnancywithinhydrosalpinx;C: left Fallopian tube hydrosalpinx;D: large hydrosalpinx of the left Fallopian tube with a smallerhydrosalpinxontherightside.
Neonatalherpesisadevastatinginfectionwithamortalityrateofupto30%andconsequentlifelongneurologicalmorbidityinupto70%.Itismostoftenacquiredduringdeliveryifthemotherhasprimaryornon-primaryinitialinfectionwithinthethirdtrimesterandespeciallythelast6weeks,whenreportedneonatal infection rates are as high as 41%. IgG to the virus in the serum crosses the placenta andprovidesneonatalprotectionfrominfection,andtheriskofneonatalherpeswhenthemotherhaslesionsof recurrent infection present at delivery is less than 3%. For this reason the recommendedmode ofdelivery for women with first-acquisition genital herpes in the third trimester is prelabour caesareansection,andinthosewithprovenrecurrentlesions,vaginaldeliverymaybeanticipatedifotherobstetricfactorsallow.
Treatmentofthesymptomsofgenitalherpesisacourseofaciclovir,whichisverysafeandeffective,includinginpregnancy,orarelatedcompound(suchasvalaciclovir).Thesemedicinesaremosteffectivewhen given as soon as possible after symptoms develop, and episodic and suppressive regimens areeffectiveinmanagingsymptomsfromrepeatedrecurrences.Informationforpatients,includingthelifelongnature of the infection, asymptomatic shedding and therefore risk to sexual partners and the need fordisclosure, the effectiveness of condoms (up to 50%) and antivirals in limiting transmission, areimportant.
GenitalwartsThesearebenignepithelialtumourscausedbyHPVinfection.Thereareover100genotypesofHPVandtypes6and11causeover90%ofgenitalwarts.InfectionwithHPVinthegenitalepitheliumviasexualtransmission isextremelycommon,with thevastmajorityofcasesbeingsubclinical. Infectionwith theoncogenicgenotypesincludingtypes16and18isalsothroughsex,butthesecauseanogenitaldysplasiaand cancer, not warts. HPV vaccination is available as a bivalent (against types 16 and 18) orquadrivalent(types6,11,16and18)vaccine,andincohortswherethelatterhasbeenintroduced(suchasingirlsinAustralia),adramaticdropinthecasesofgenitalwartshasbeenobserved.
Diagnosisisbyclinicalexaminationandtreatmentsincludeablativetherapiessuchasapplicationofliquid nitrogen or surgical techniques or patient-applied topical therapies, including podophyllotoxin-containingpreparationsorthelocalimmunemodulatorimiquimod.Asthesearebenignlesionstreatmentisoptional.Whengenitalwartsarepresentinpregnancytreatmentislimitedtoablativeoptions.Rarely,wartsmaybecomeverylargeandobstructthebirthcanal,necessitatingcaesareandelivery.Veryrarelythe neonate can develop respiratory papillomatosis, but the risk is extremely small and the benefit ofcaesareandelivery inpreventing thisunproven.Screening forotherSTIs is requiredand screening forcervicalcancerisasusual.
SyphilisSyphilis is caused by infection with the bacterium Treponema pallidum subspecies pallidum, whichoccursthroughdirectcontactwithsecretionsfromaninfectivelesionorviatransplacentalpassageofthebacteriaduringpregnancy.This infection ismultisystemandhasmanyclinical features thatmaymimicotherconditions.Untreateditcanrelapseandremitandlatecomplicationscanpresentmanyyearsafterthe original infection. Infectivity declines with time and treatment with penicillin-based regimens are
www.medicalebookpdf.com
curative,althoughreinfectionmayoccur.ThoselivinginAfricanandAsiancountriesandEasternEuropearemoreoftenaffected,andinthelasttwodecadestherehavebeenresurgencesofinfectionobservedinhomosexualmeninWesterncountries.
The infection isclassifiedascongenitaloracquired,andeachof theseas lateorearly. Inacquiredearly syphilis the initialmanifestation is the ‘chancre’,whichdevelopsat the siteofexposure.This isusuallyasingle,genitallesionbutisincreasinglyseenatothersitessuchastheoralcavityandmaybemultiple.Typicallythelesionispainless,induratedandexudesserousfluidcontainingT.pallidum,andthereisregionallymphadenopathy.Thisresolveswithinafewweeksandfollowingthisasthebacteriadisseminate a plethora of variable clinical symptoms and signs may be apparent. These include awidespreaderythematousrashtypicallyincludingthepalmsandsolesandthatcanresultinalopecia,oralandgenitalmucouslesionsandraisedlesions,usuallyintheanogenitalarea,termed‘condylomatalata’.
Complications include neurological involvement, resulting inmeningitis, an eighth nerve palsy andconsequent deafness or tinnitus and ophthalmic involvement, most often uveitis. This stage alsospontaneously resolves as the host immune response is effective in controlling the infection, althoughrelapsemayoccurforupto2years, theacceptedtimelimitofearlyinfection,andapproximatelytwo-thirdsofinfectedindividualssuffernofurtherilleffects.
Latecomplicationsinclude:
•Gummatouslesions:granulomatous,locallydestructivelesionstypicallyaffectingskinandbone.• Cardiovascular involvement: usually affecting the ascending aorta, resulting in aortic valveincompetence.
• Neurological involvement: classified as meningovascular disease, tabes dorsalis and a progressivedementingillness,generalparesis.
CongenitalinfectionalsoconsistsofmanysymptomsandsignsthataresummarizedinTable9.3.Theriskiest time for congenital infection is when syphilis is acquired either very soon before or duringpregnancy.Screeningforsyphilisinpregnancyiswellestablished,allowingeffectivetreatmentofmostwomen,althoughinfectionmayoccurinpregnancyafterthis.
Diagnosis isbyserologyand/ordirectlydetectingT.pallidum in infectious lesions,usuallybydarkfield microscopy or, more recently, by PCR testing, although availability of this is limited. Non-treponemal serological tests include the rapid plasma reagin (RPR) and Venereal Disease ReferenceLaboratory(VDRL),whichdemonstraterisingtitresduringacute,activeinfectionthatdropwithtimeandfollowing treatment, and socanbeused tomonitor treatment.Theymaybenegative inearly infection,falselypositiveinotherphysiological(suchaspregnancy)ordisease(includingseveralrheumatologicalconditions) states, and so require confirmation by non-treponemal tests such as enzyme orchemiluminescence immunoassays (EIA/CLIA) or T. pallidum particle or haemagglutination assays(TPPA/TPHA). These treponemal tests may also be negative in the very early stages of disease, andshouldberepeatedifnegative4–6weekslaterifthisissuspected.Serologicaltestsforsyphilismaybepositive for life,although reinfection results in thenon-treponemal titre rising rapidly.Different testingalgorithmsareappliedaccordingtolocallyavailabletestsandexpertiseisrequiredtogetherwithafullclinicalhistorytointerprettheirresultsadequately.Treatmentiscurativeandinvolvesdepotpreparationsofpenicillin;differentregimesfordifferingstagesofinfectionarethetreatmentofchoice.Simultaneoustreatmentofcurrentsexualpartnersisrequired,certainlyinearlydisease.Whenthetimeofinfectionisnotknown,tracingandtestingofpreviouspartners,andwhereapplicablechildren,isrequired.
www.medicalebookpdf.com
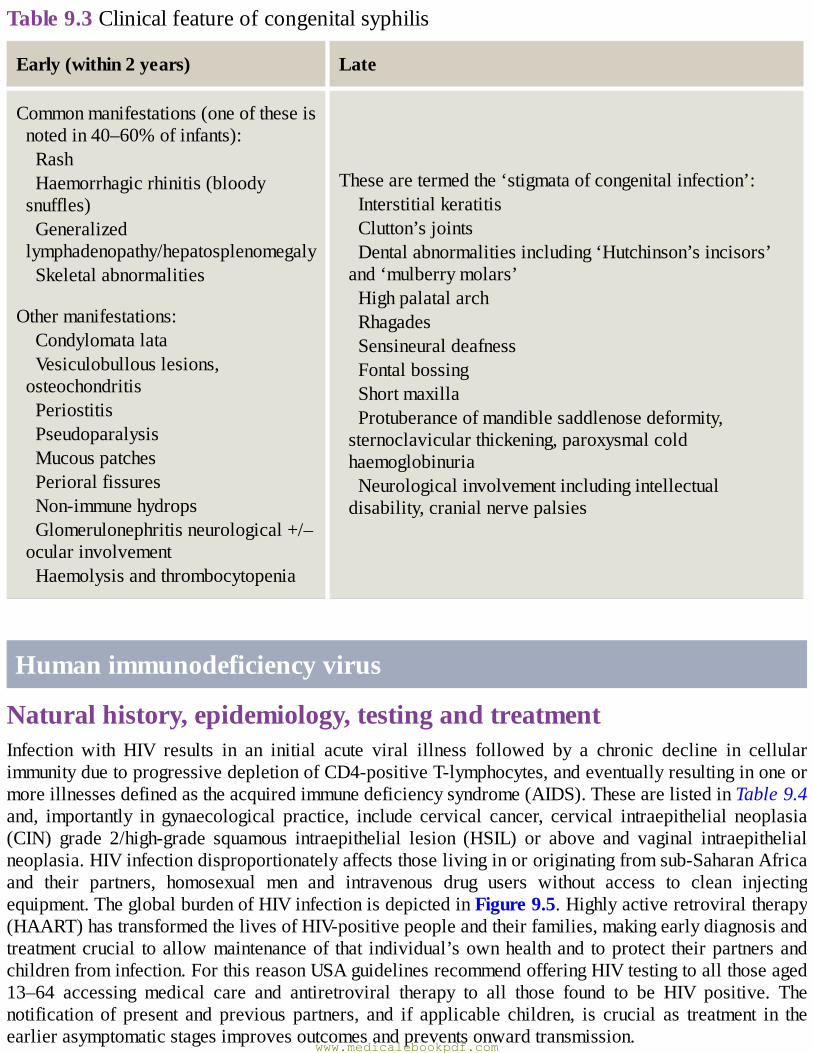
Table9.3Clinicalfeatureofcongenitalsyphilis
Early(within2years) Late
Commonmanifestations(oneoftheseisnotedin40–60%ofinfants):RashHaemorrhagicrhinitis(bloodysnuffles)Generalizedlymphadenopathy/hepatosplenomegalySkeletalabnormalities
Othermanifestations:CondylomatalataVesiculobullouslesions,osteochondritisPeriostitisPseudoparalysisMucouspatchesPerioralfissuresNon-immunehydropsGlomerulonephritisneurological+/–ocularinvolvementHaemolysisandthrombocytopenia
Thesearetermedthe‘stigmataofcongenitalinfection’:InterstitialkeratitisClutton’sjointsDentalabnormalitiesincluding‘Hutchinson’sincisors’and‘mulberrymolars’HighpalatalarchRhagadesSensineuraldeafnessFontalbossingShortmaxillaProtuberanceofmandiblesaddlenosedeformity,sternoclavicularthickening,paroxysmalcoldhaemoglobinuriaNeurologicalinvolvementincludingintellectualdisability,cranialnervepalsies
Humanimmunodeficiencyvirus
Naturalhistory,epidemiology,testingandtreatmentInfection with HIV results in an initial acute viral illness followed by a chronic decline in cellularimmunityduetoprogressivedepletionofCD4-positiveT-lymphocytes,andeventuallyresultinginoneormoreillnessesdefinedastheacquiredimmunedeficiencysyndrome(AIDS).ThesearelistedinTable9.4and, importantly in gynaecological practice, include cervical cancer, cervical intraepithelial neoplasia(CIN) grade 2/high-grade squamous intraepithelial lesion (HSIL) or above and vaginal intraepithelialneoplasia.HIVinfectiondisproportionatelyaffectsthoselivinginororiginatingfromsub-SaharanAfricaand their partners, homosexual men and intravenous drug users without access to clean injectingequipment.TheglobalburdenofHIVinfectionisdepictedinFigure9.5.Highlyactiveretroviraltherapy(HAART)hastransformedthelivesofHIV-positivepeopleandtheirfamilies,makingearlydiagnosisandtreatmentcrucial toallowmaintenanceof that individual’sownhealthand toprotect theirpartnersandchildrenfrominfection.ForthisreasonUSAguidelinesrecommendofferingHIVtestingtoallthoseaged13–64 accessing medical care and antiretroviral therapy to all those found to be HIV positive. Thenotification of present and previous partners, and if applicable children, is crucial as treatment in theearlierasymptomaticstagesimprovesoutcomesandpreventsonwardtransmission.
www.medicalebookpdf.com
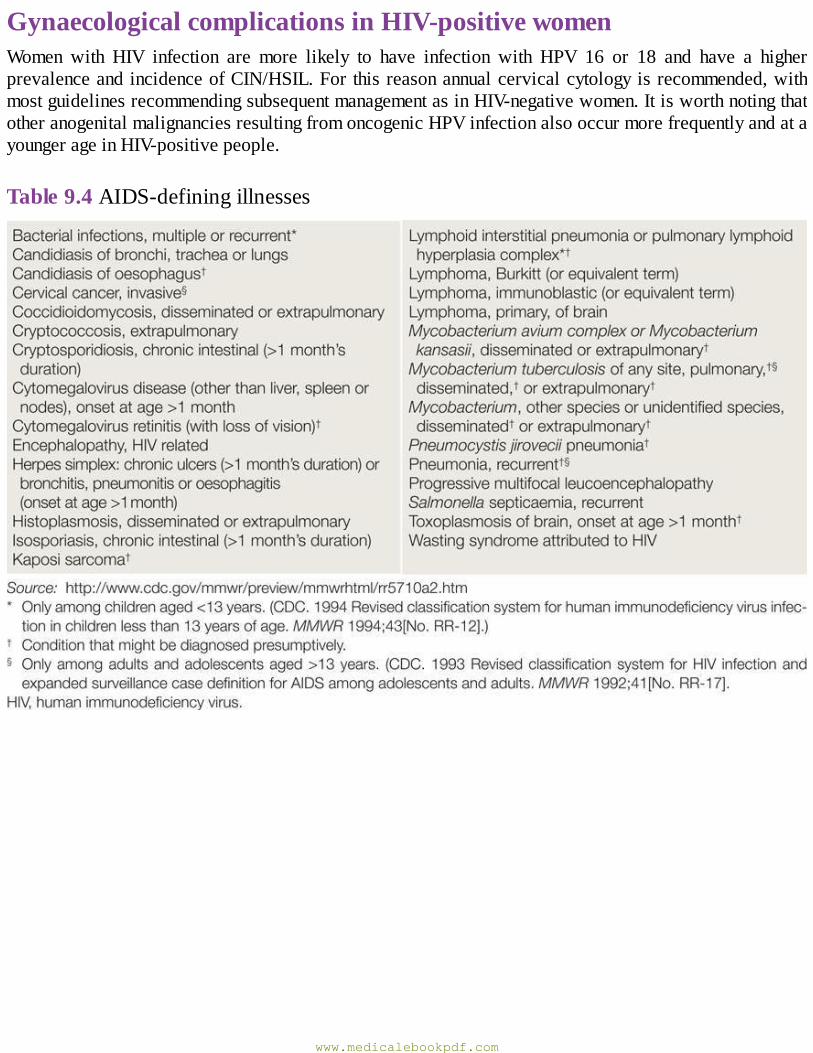
GynaecologicalcomplicationsinHIV-positivewomenWomen with HIV infection are more likely to have infection with HPV 16 or 18 and have a higherprevalenceandincidenceofCIN/HSIL.Forthisreasonannualcervicalcytologyisrecommended,withmostguidelinesrecommendingsubsequentmanagementasinHIV-negativewomen.ItisworthnotingthatotheranogenitalmalignanciesresultingfromoncogenicHPVinfectionalsooccurmorefrequentlyandatayoungerageinHIV-positivepeople.
Table9.4AIDS-definingillnesses
www.medicalebookpdf.com
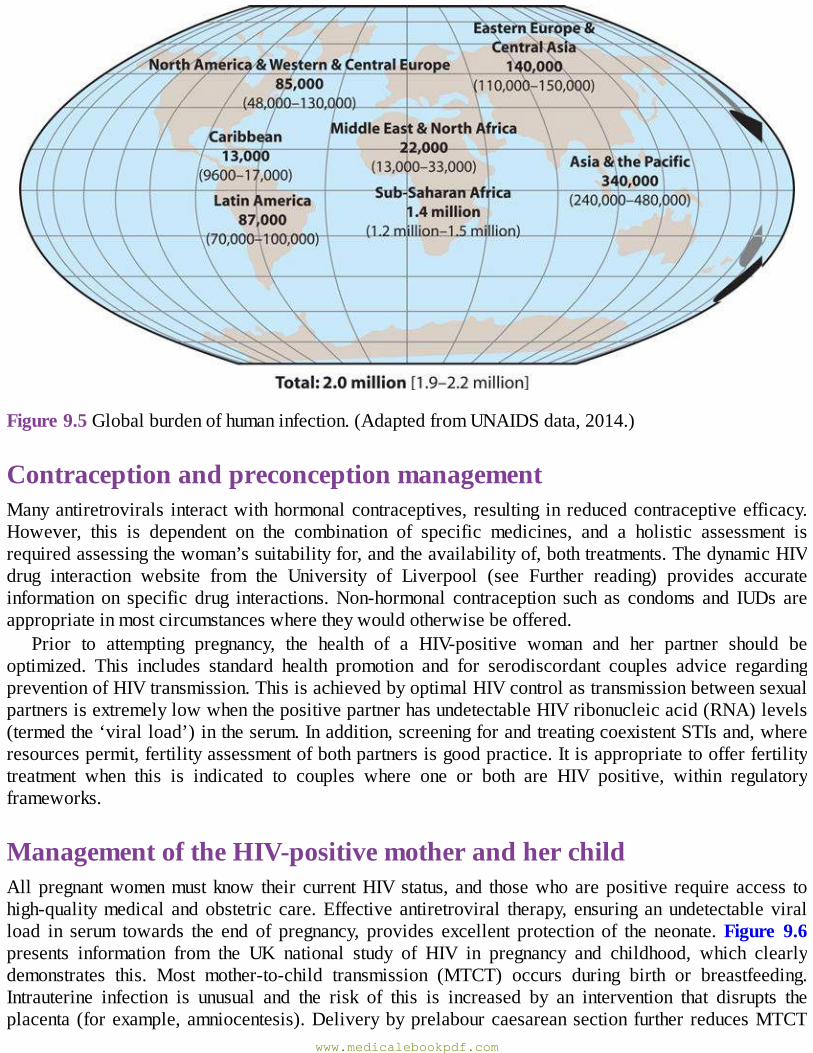
Figure9.5Globalburdenofhumaninfection.(AdaptedfromUNAIDSdata,2014.)
ContraceptionandpreconceptionmanagementManyantiretrovirals interactwithhormonalcontraceptives, resulting in reducedcontraceptiveefficacy.However, this is dependent on the combination of specific medicines, and a holistic assessment isrequiredassessingthewoman’ssuitabilityfor,andtheavailabilityof,bothtreatments.ThedynamicHIVdrug interaction website from the University of Liverpool (see Further reading) provides accurateinformation on specific drug interactions.Non-hormonal contraception such as condoms and IUDs areappropriateinmostcircumstanceswheretheywouldotherwisebeoffered.
Prior to attempting pregnancy, the health of a HIV-positive woman and her partner should beoptimized. This includes standard health promotion and for serodiscordant couples advice regardingpreventionofHIVtransmission.ThisisachievedbyoptimalHIVcontrolastransmissionbetweensexualpartnersisextremelylowwhenthepositivepartnerhasundetectableHIVribonucleicacid(RNA)levels(termedthe‘viralload’)intheserum.Inaddition,screeningforandtreatingcoexistentSTIsand,whereresourcespermit,fertilityassessmentofbothpartnersisgoodpractice.Itisappropriatetoofferfertilitytreatment when this is indicated to couples where one or both are HIV positive, within regulatoryframeworks.
ManagementoftheHIV-positivemotherandherchildAllpregnantwomenmustknow their currentHIVstatus, and thosewhoarepositive require access tohigh-qualitymedical andobstetric care.Effective antiretroviral therapy, ensuring anundetectable viralload in serum towards the end of pregnancy, provides excellent protection of the neonate.Figure 9.6presents information from the UK national study of HIV in pregnancy and childhood, which clearlydemonstrates this. Most mother-to-child transmission (MTCT) occurs during birth or breastfeeding.Intrauterine infection is unusual and the risk of this is increased by an intervention that disrupts theplacenta (forexample,amniocentesis).Deliverybyprelabourcaesareansection further reducesMTCT
www.medicalebookpdf.com
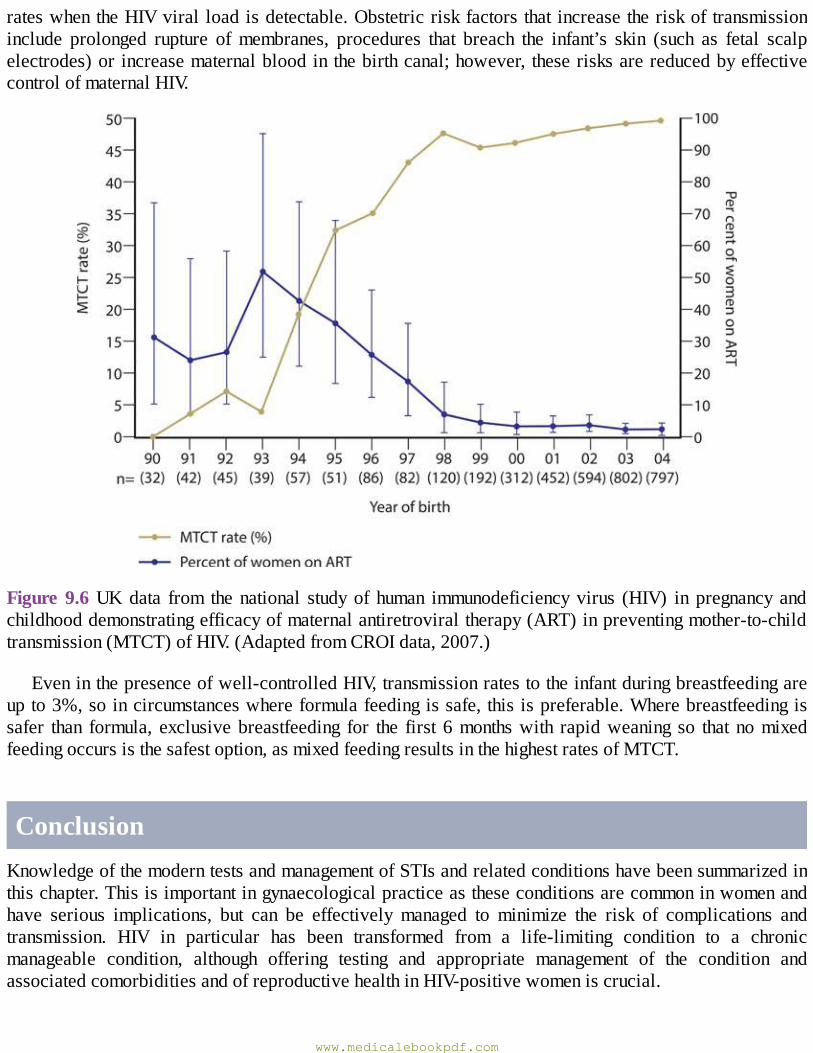
rateswhentheHIVviral loadisdetectable.Obstetricriskfactorsthat increasetheriskoftransmissioninclude prolonged rupture ofmembranes, procedures that breach the infant’s skin (such as fetal scalpelectrodes)orincreasematernalbloodinthebirthcanal;however, theserisksarereducedbyeffectivecontrolofmaternalHIV.
Figure9.6UKdata from thenational studyof human immunodeficiencyvirus (HIV) in pregnancy andchildhooddemonstratingefficacyofmaternalantiretroviraltherapy(ART)inpreventingmother-to-childtransmission(MTCT)ofHIV.(AdaptedfromCROIdata,2007.)
Eveninthepresenceofwell-controlledHIV,transmissionratestotheinfantduringbreastfeedingareupto3%,soincircumstanceswhereformulafeedingissafe,thisispreferable.Wherebreastfeedingissafer than formula, exclusivebreastfeeding for the first 6monthswith rapidweaning so that nomixedfeedingoccursisthesafestoption,asmixedfeedingresultsinthehighestratesofMTCT.
ConclusionKnowledgeofthemoderntestsandmanagementofSTIsandrelatedconditionshavebeensummarizedinthischapter.Thisisimportantingynaecologicalpracticeastheseconditionsarecommoninwomenandhave serious implications, but can be effectively managed to minimize the risk of complications andtransmission. HIV in particular has been transformed from a life-limiting condition to a chronicmanageable condition, although offering testing and appropriate management of the condition andassociatedcomorbiditiesandofreproductivehealthinHIV-positivewomeniscrucial.
www.medicalebookpdf.com
FurtherreadingTheBritishAssociationforSexualHealth&HIV:http://www.bashh.org/BASHH/Guidelines/Guidelines/BASHH/Guidelines/Guidelines.aspx.TheBritishHIVAssociation:http://www.bhiva.org/guidelines.aspx.TheCentresforDiseaseControlandPreventionCDC:http://www.cdc.gov/std/tg2015/.TheInternationalUnionagainstSTIs:http://iusti.org/sti-information/guidelines/default.htm.UnitedStatesHIVtreatmentguidelines:https://aidsinfo.nih.gov/guidelinesSpotting the signs of child sexual exploitation: http://www.bashh.org/documents/Spotting-the-signs-A%20national%20proforma%20Apr2014.pdf.
TheUniversityofLiverpoolHIVDruginteractionswebsite:http://www.hiv-druginteractions.org/.
Selfassessment
CASEHISTORY
A 29-year-oldwoman presents to the emergency gynaecology unitwith a 5-day history of lowerabdominalandpelvicpain thathasgotprogressivelyworseover the last24hours.Shealsofeelsgenerallyunwellwithchillsandrigors.Shehashadseveralpartnersinrecentmonthsandwasfoundto have chlamydia a fewweeks ago. She is not surewhether she completed thewhole course oftreatmentanddidnotgobacktogettested.Shedoesnotuseanyformofcontraceptionandhashadunprotectedintercourserecently.
Onexamination,shelooksunwell.Shehasaraisedtemperatureat38°Candistachycardic.Sheis very tender on abdominal examination with guarding. On speculum examination, the cervixappearsinflamedwithaprofusemucopurulentdischarge.Ahighvaginalswab,endocervicalswabandaurethral swabare taken.Onpelvic examination there ismarkedcervical tenderness.She isalsogenerally tender topalpate throughout thepelvisand isunable to tolerate theexamination.Apregnancytestisnegative.
AWhatisthediagnosis?BWhattestsarerequired?CWhatisthemanagement?
ANSWERS
ATheclinicaldiagnosisissuggestiveofacutePIDwithpelvicperitonitis.B Vulvovaginal, high vaginal and cervical swabs (as available depending on your localmicrobiology service) are taken, aswell as amidstreamurine sample, full bloodcount andC-reactiveprotein(CRP).Apelvicultrasoundshowsthepossibilityofanadnexalmasswithsomefreefluidinthepelvis.
www.medicalebookpdf.com
CShe is admitted and startedwith intravenous antibiotics (ceftriaxone+metronidazole) and oraldoxycycline.Sheisalsosupportedwithintravenousfluids,analgesicsandregularparacetamol.
She continues to be unwellwith a raised temperature even after 48 hours of antibiotics. Thus, adecisionistakentoperformalaparoscopy.Usuallyconservativemanagementispreferred,butwhenitisunsuccessfulafter24–48hourslaparoscopyisindicated.Attheoperation,sheisfoundtohavea7-cm enlarged tubo-ovarian abscess and marked inflammation of the uterus and other tube. Theabscess is drained and the patient markedly improves after the surgery. She is found to havechlamydiaontheendocervicalswabwithanaerobesonthehighvaginalswab.Sheimprovesoverthecourseofafewdaysandistreatedwithoralantibioticsfor2weeks.Sheiscounselledregardingtheimplicationsoftheinfectionandisencouragedtocontactherpresentandpreviouspartnersfortesting,ofwhomone testedpositiveforchlamydiaandwassubsequently treated. In thefutureshewouldrequirereferraltofertilityservicesearlyifshefailedtoconceive.Anearlyscaninpregnancyisindicatedtoconfirmintrauterinepregnancy,astheriskofanectopicpregnancyisincreased.
SBAQUESTIONS
1A32-year-oldwomanpresentsatthecommunityreproductiveclinicwithalteredvaginaldischargeand mild abdominal pain. On examination there is a profuse mucopurulant discharge from aninflamedcervix.
Whatistheappropriatemanagement?Choosethesinglebestanswer.
ATreatwithcephalosporinforapresumedgonorrhoealinfection.BPerformNAATtesting,treatpresumptivelywithwide-spectrumantibiotic.CTreatwithpenicillinandtestforotherSTIs.DTreatwithcephalosporinandazithromycinandperformNAATtestingifunresponsive.E Perform NAAT testing and culture and sensitivity, test for other STIs and treat withcephalosporinandazithromycin.
ANSWER
EThelikelydiagnosisisGCandacceptedmanagementistotestforotherSTIsasdualinfectioniscommon.NAATtestingforchlamydia,gonorrhoeaordualinfectionisperformedbutcultureandsensitivitiesarealsoperformed,asincreasinglythereisresistantinfection.Meanwhiletreatmentiscommencedwithcephalosporinsandazithromycin,and,ofcourse,contacttracingasforallsuchvisits.Ifbimanualexaminationdemonstratescervicalmotionandadnexaltenderness,then2weeksofdoxycyclineandmetronidazoleshouldalsobegiven.
2Whichofthefollowinginfectionscanbediagnosedonwetmountmicroscopy?Choosethesinglebestanswer.ACandidiasis.
www.medicalebookpdf.com

BGonorrhoea.CTrichomoniasis.DSyphilis.EBV.
ANSWER
BEachofthesepathogens/infectionshavespecificfeaturesonmicroscopy,butsomeonlyonGramstain. Candida has pseudo-hyphae, Neisseria gonorrhoeae is a gram-negative intracellulardiplococcus,syphilisiscausedbyaspirochaetebacteriumthatisvisibleondarklightmicroscopyand BV is associated with Clue cells. Trichomoniasis is caused by a flagellate protozoan,Trichomonasvaginalisvisibleonasimplewetmountedswab.
www.medicalebookpdf.com
CHAPTER10Urogynaecologyandpelvicfloorproblems
DOUGLASTINCELLO
Urinarysymptomterminology
Relevantfunctionalanatomy
Clinicalassessmentofincontinence
Treatmentforincontinence
Prolapse
Clinicalassessmentofprolapse
Treatmentforprolapse
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandtheanatomyofsupportingligamentsandfasciaofthefemalepelvicorgans.
•Understandthemechanismofcontinenceinwomen,andhowdisordersofthisleadtosymptoms.
• Appreciate the relationships between anatomical prolapse and functional symptoms, includingurinary,bowelandsexualdysfunction.
•Learnhowtoassessthepatientwithincontinenceorprolapsebymeansofhistory,examinationandrelevantinvestigations.
•Understandtheprinciplesofurodynamictesting.www.medicalebookpdf.com
•Understand theprinciplesof treatmentofprolapse and incontinenceandbeable todescribe theeffectiveness of each treatment, together with an understanding of potential side-effects andcomplications.
UrinarysymptomterminologyUrinarysymptomscanbedividedintothoserelatingtourinestorageandthoserelatingtovoiding.Thesymptomof stress incontinence (leakingwithcough, straining, exercise, etc)maybe isolated,butmostpatients present with mixed incontinence, which is where stress incontinence occurs with frequency,urgencyandurgeincontinence.Thecombinationoffrequency,urgencyand/orurgeincontinenceisgiventhe term overactive bladder (OAB). Voiding symptoms are uncommon in women who have not hadpreviouscontinencesurgery.
Urinestoragesymptoms•Frequency:patientconsidershe/shevoidstoooftenbyday.•Nocturia:wakingatnightoneormoretimestovoid.•Urgency:asuddencompellingdesiretopassurine,whichisdifficulttodefer.•Urgeincontinence:involuntaryleakageaccompaniedbyorimmediatelyprecededbyurgency.•Stressincontinence:involuntaryleakageoneffort,exertion,sneezingorcoughing.•Nocturnalenuresis:thelossofurineoccurringduringsleep.
Urinevoidingsymptoms
•Slowstream:perceptionofreducedurineflow.•Splittingorspraying:wherethestreamorurineisnotasingleflow.•Intermittentstream:urineflowthatstopsandstarts.•Hesitancy:difficultyininitiatingmicturitionresultinginadelayintheonsetofvoiding.•Terminaldribble: aprolonged finalpartofmicturition,when the flowhas slowed toa trickleordribble.
RelevantfunctionalanatomyInhealth thebladder stores, and thenvoids,urine.This isknownas themicturitioncycle.Mostof thetime,thedetrusormuscleofthebladderisrelaxedallowingstorageofincreasingurinevolumeswithnoincreaseinpressure.Asbladdercapacityisreached,sensorysignalsfromstretchreceptorsinthebladderwall send the sensation of bladder filling. The sphinctermechanism is closed.As an adult, voluntarydelay of micturition until socially convenient is achieved by cortical inhibition of the spinal voidingreflexarc.Beforevoidingbegins,thisinhibitionisremovedandthepelvicfloorandurethralsphincters
www.medicalebookpdf.com
relaxinacoordinatedfashion,toallowdetrusorcontractionandbladderemptying.Thedetrusormuscleisinnervatedbymuscariniccholinergicnervesoftheparasympatheticnervoussystem(causingdetrusormuscle contraction), and the urethral sphincter by noradrenergic neurons of the sympathetic nervoussystem (sphincter contraction) and somatic fibres (voluntary contraction and relaxation) from thepudendalnerves.
Inwomen theurethral sphinctermechanism isa functional system that includes the internal (smoothmuscle) and external (striatedmuscle) sphincters, themuscles of thepelvic floor and thepubourethralligament supporting the urethra within the abdominal cavity. Increases in abdominal pressure aretransmitted equally to the bladder and bladder neck (Figure10.1A). In the premenopausalwoman theurethralepitheliumhasarichbloodsupplyandcontributestocontinencebyactingasaseal.
StressincontinenceIn isolation, the symptom of stress incontinence is a reasonably good predictor of the presence of anincompetenturethralsphincter.Urethralsphincterweaknessinmostcasesisduetohypermobility,wherethepelvicfloorandligamentscannotretaintheurethrainpositionanditfallsthroughtheurogenitalhiatusduringincreasesinabdominalpressure,leadingtolossofpressuretransmissiontotheurethraandhenceleakageofurine(Figure10.1B).
Intrinsicsphincterdeficiency(ISD)islesscommonandoccurswhereurethralclosurepressureislowwithoutanyurethralmobility.ISDisduetoweaknessofthesphinctermusclesandlossofthecushioningsealeffectintheurethra.
Urethral sphincterweakness is associated stronglywith a history of vaginal childbirth and variousrelatedriskfactors,andwithsomenon-obstetricfactors.Obstetricriskfactorsactbyacombinationeffectof stretching/damage to the pudendal nerves and overstretching, or even avulsion, of the pelvic floormusclesfromtheirinsertionsonthepelvicsidewall.Directmuscledamageresultsinlossofpelvicfloorsupportandhenceurethralhypermobility.Pudendalnervedamagecausesbothweakeningof thepelvicfloormusclesandurethralsphincter.Itisnowpossibletoidentifylevatormuscledefectsinsymptomaticwomen by means of magnetic resonance imaging or transperineal/transvaginal ultrasound. Most riskfactorsmaynotbemodifiable(withexceptionsnotedbyasterisksbelow).
Riskfactorsforstressurinaryincontinence
•Multiparity(particularlyvaginalbirths).•Forcepsdelivery*.•Perinealtrauma.•Longlabour*.•Epiduralanalgesia.•Birthweight>4kg.•Increasingage.•Postmenopause.• Obesity studies have shown that significant weight loss among obesewomen is associatedwithmajorimprovementsinurinaryleakagesymptoms.
•Connectivetissuedisease.www.medicalebookpdf.com
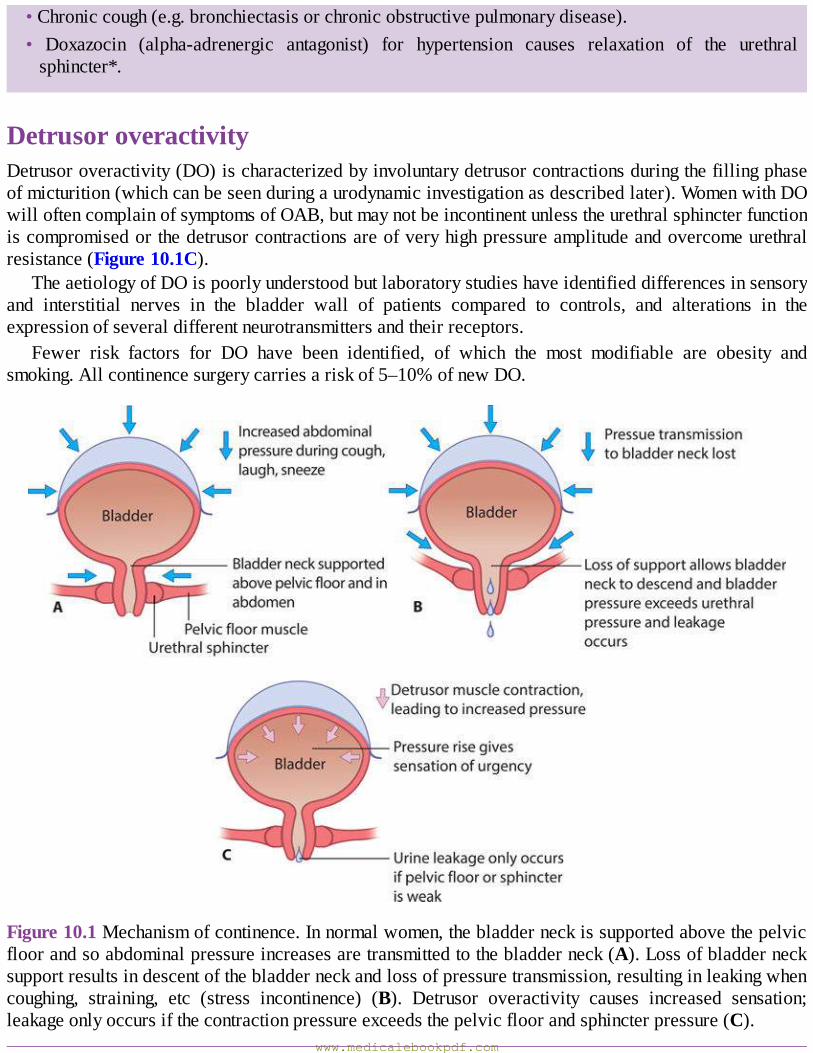
•Chroniccough(e.g.bronchiectasisorchronicobstructivepulmonarydisease).• Doxazocin (alpha-adrenergic antagonist) for hypertension causes relaxation of the urethralsphincter*.
DetrusoroveractivityDetrusoroveractivity(DO)ischaracterizedbyinvoluntarydetrusorcontractionsduringthefillingphaseofmicturition(whichcanbeseenduringaurodynamicinvestigationasdescribedlater).WomenwithDOwilloftencomplainofsymptomsofOAB,butmaynotbeincontinentunlesstheurethralsphincterfunctioniscompromisedorthedetrusorcontractionsareofveryhighpressureamplitudeandovercomeurethralresistance(Figure10.1C).
TheaetiologyofDOispoorlyunderstoodbutlaboratorystudieshaveidentifieddifferencesinsensoryand interstitial nerves in the bladder wall of patients compared to controls, and alterations in theexpressionofseveraldifferentneurotransmittersandtheirreceptors.
Fewer risk factors for DO have been identified, of which the most modifiable are obesity andsmoking.Allcontinencesurgerycarriesariskof5–10%ofnewDO.
Figure10.1Mechanismofcontinence.Innormalwomen,thebladderneckissupportedabovethepelvicfloorandsoabdominalpressureincreasesaretransmittedtothebladderneck(A).Lossofbladdernecksupportresultsindescentofthebladderneckandlossofpressuretransmission,resultinginleakingwhencoughing, straining, etc (stress incontinence) (B). Detrusor overactivity causes increased sensation;leakageonlyoccursifthecontractionpressureexceedsthepelvicfloorandsphincterpressure(C).
www.medicalebookpdf.com
Riskfactorsfordetrusoroveractivity
•Childhoodbedwetting.•Obesity.•Smoking.•Previoushysterectomy.•Previouscontinencesurgery.
ClinicalassessmentofincontinenceA detailed history should be taken to elicit the patient’s presenting symptoms, to identifywhether thepatient has only stress incontinence symptoms, only OAB symptoms or mixed symptoms. If there aremixedsymptoms,anassessmentshouldbemadeastowhichpredominate.Itisusefultorecordmeasuresof severity, including: the number of episodes per day of frequency, urgency and leakage; whethercontinencepadsareneeded,andifsohowmanyandwhatsize;whetherthepatientneedstochangeherunderclothes or outer clothes because of leakage; and what behaviour changes have been employed.Commonly,womenwill have reduced their fluid intake andmay limit their social activities to placeswheretheyalreadyknowaboutthepositionandcleanlinessoftoiletfacilities.Associatedsymptomsofprolapse (see later), faecal incontinence symptoms (whichpatients rarelyoffer spontaneously)andanysexual difficulties should be sought, as well as a detailed medical history to identify potentialpredisposing factors and to identify any ongoing medical or surgical conditions that may impact ontreatment (including comorbidities that may increase the risk of anaesthesia, or present cautions orcontraindicationstodrugtherapy).Remembertobealertfor‘redflag’signssuggestingmalignancysuchashaematuria,rectalbleedingorsignificantpain.
Physicalexaminationshould includegeneralexaminationandanabdominalandpelvicexamination.Abdominalexaminationwillidentifyanysurgicalscars,evidenceofobesityandthepresenceorabsenceofanypelvicmass thatmaybea factor inurinary frequency.Thepresenceofa large fibroiduterusorovariancystfillingthepelvisisanuncommonfinding,butwillcauseurinaryfrequencybyoccupyingthespaceinthepelviswherethefullbladderwouldnormallylie.Insuchcases,surgicalremovalofthemasswillbeindicatedandshouldimprovetheurinarysymptoms.Pelvicexaminationoftheincontinentwomanideallyshouldbedoneinthelithotomypositionusingaright-angledSimsspeculum(seeFigure2.4) toassesseachvaginalwalladequatelyforassociatedprolapse(seelater).VisibleleakageduringcoughingorValsalvamanoeuvreshouldbesought,andanassessmentofthepatient’sabilitytocontractandholdthecontractionofherpelvicfloormusclesisessential.
Allpatientsshouldbeaskedtoprovideafreshmidstreamspecimenofurinetoexcludeovertinfectionorasymptomaticbacteriuria.Additionalsimpleinvestigationsincludeapatientbladderdiary(for3daysisusuallyadequate) to record theamount, typeand frequencyofdrinks takenand to record the timing,frequencyandvolumeofvoids(Figure10.2).Thiscanbeausefulexerciseforthepatientherselftotakenoteofexactlywhatsheisdrinkingandhervoidinghabits.Thebladderdiarywillalsoallowthepatienttorecordleakageepisodesandurgency.Manyclinicianswillalsoaskpatientstocompleteoneofarangeofdisease-specificqualityoflifeinstrumentstoassesstheimpactofthepatient’sproblemandthiscanberepeated after treatment to allow collection of outcomes,which is extremely useful for the purpose of
www.medicalebookpdf.com

serviceauditandforindividualclinicianappraisalandrevalidation.Itispossibletoobtainanobjectivemeasureofurineleakbyconductingapadtest.Thisisaninvestigationwherethepatientwearsoneormorepreweighedsanitarypadsforavariable lengthof time(between1hour inclinicand24hoursathome) while performing specific provocation tests (e.g. hand washing, climbing stairs, coughing) oractivitiesofdailyliving.Thechangeinweight(g)isameasureoftheamountofurinelost(ml).Onlythe24-hourhomepadtesthasbeenshowntobereliableandreproducible,andpadtestshavebecomemuchlesscommonlydoneinthelast5–10years.
Apelvicand/orrenaltractultrasoundmaybeindicatediftherearesymptomsofpelvicpain,clinicalsuspicionofapelvicmass,haematuria,bladderpainorrecurrenturinarytractinfection.Forpatientswithmixedsymptoms,orthosewithrecurrentproblemsafterprevioustreatment,itisgoodpracticetodiscussmanagementplanswithinamultidisciplinaryteam(MDT)meeting,includingagynaecologist,urologist,continence nurse, physiotherapist and possibly a medicine for the elderly consultant. Within the UK,currentguidancetobestpractice is thatallwomen(evenprimarycases)shouldbediscussedinsuchameetingbeforeinitiatingsurgicaltreatmentofanytype.
www.medicalebookpdf.com
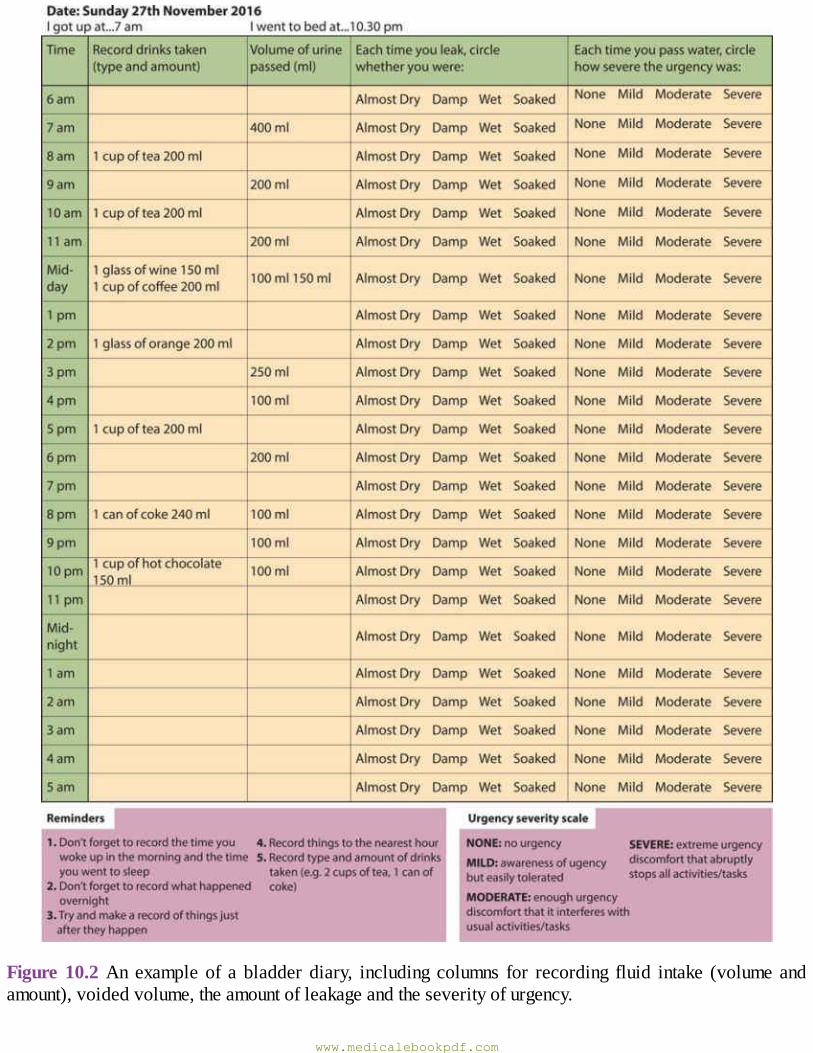
Figure10.2An exampleof a bladder diary, including columns for recording fluid intake (volume andamount),voidedvolume,theamountofleakageandtheseverityofurgency.
www.medicalebookpdf.com
KEYLEARNINGPOINTS•Stress incontinence is typically a result of aweakurethral sphincter, often as a consequence ofchildbirth.
•DOcausesurgency,frequencyandnocturia,butnotallpatientswillhaveleakage.•Historyshouldincludedirectquestionsaboutfaecalleakageorleakageduringsexualintercourse.•Clinical examination should exclude pelvicmasses (e.g. fibroid uterus) and assess the patient’sabilitytocontractherpelvicfloormusclesandthestrengthofthatcontraction.
• Women with pain, haematuria or recurrent infections should have the renal tract investigatedradiologicallyandbycystoscopy.
Treatmentforincontinence
ConservativetreatmentandtheroleofurodynamicassessmentFor many years, most gynaecologists and urologists would perform urodynamic investigation on allwomen before initiating treatment. However, it has become clear that urodynamic testing has anappreciable false-negative rate, carries a small risk of urinary tract infection and does not reliablyidentify women at risk of complications after surgery or those who are likely to benefit from drugtreatment. Ithasalsobecomeapparent thatapackageofconservative treatmentwilldeliversignificantsymptombenefit forwomenwithstress incontinence,OABandmixed incontinence, irrespectiveof theunderlyingurodynamicfindings(Figure10.3).
www.medicalebookpdf.com
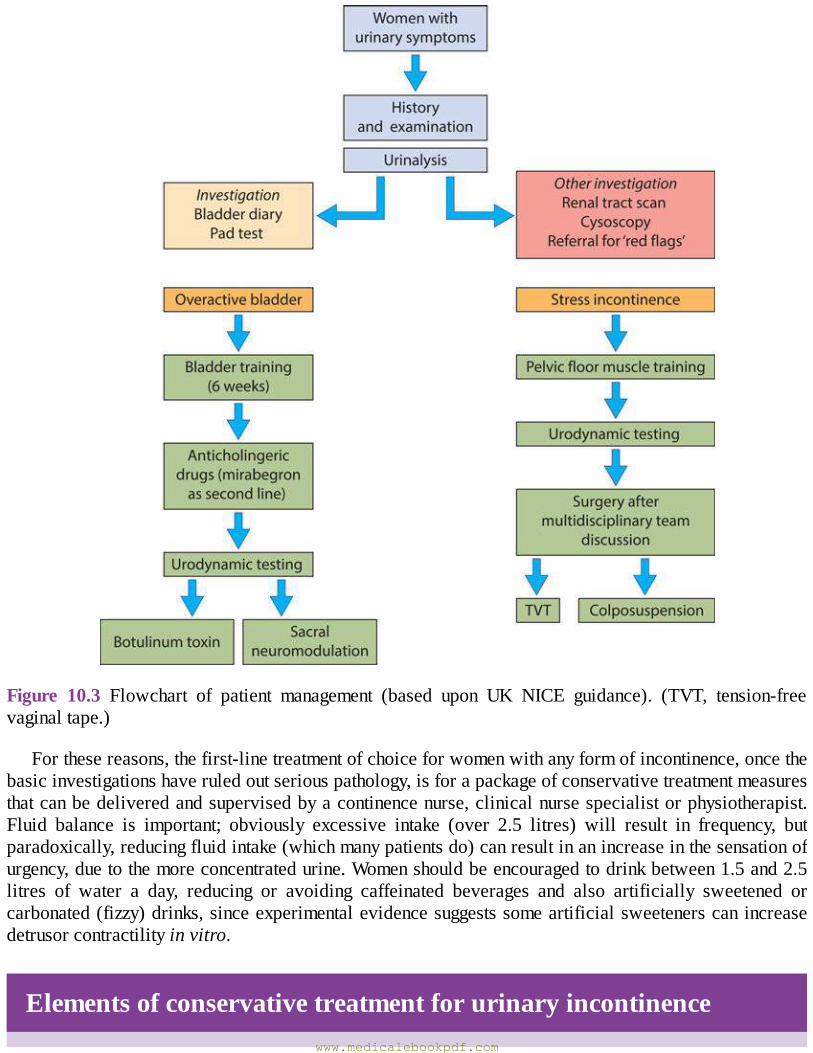
Figure 10.3 Flowchart of patient management (based upon UK NICE guidance). (TVT, tension-freevaginaltape.)
Forthesereasons,thefirst-linetreatmentofchoiceforwomenwithanyformofincontinence,oncethebasicinvestigationshaveruledoutseriouspathology,isforapackageofconservativetreatmentmeasuresthatcanbedeliveredandsupervisedbyacontinencenurse,clinicalnursespecialistorphysiotherapist.Fluid balance is important; obviously excessive intake (over 2.5 litres) will result in frequency, butparadoxically,reducingfluidintake(whichmanypatientsdo)canresultinanincreaseinthesensationofurgency,duetothemoreconcentratedurine.Womenshouldbeencouragedtodrinkbetween1.5and2.5litres of water a day, reducing or avoiding caffeinated beverages and also artificially sweetened orcarbonated(fizzy)drinks,sinceexperimentalevidencesuggestssomeartificialsweetenerscanincreasedetrusorcontractilityinvitro.
Elementsofconservativetreatmentforurinaryincontinencewww.medicalebookpdf.com

•Adviceaboutfluidbalance.•Reductionofcaffeineintake.•Bladderretraining.•Pelvicfloormuscleexercise.
PelvicfloormuscleexerciseInparallelwith fluidmanagement,mostwomenare taught ‘pelvic floorexercises’where theycontracttheir pelvic floor muscles by direct coaching while being examined vaginally to ensure correctidentificationof the levatormuscle complex.Without confirmationbydirect examination,only40%ofwomen will be able to correctly initiate a contraction of the pelvic floor. Individualized exerciseprogrammes are devised for each patient, to increase both the number of contractions that can beperformedconsecutivelyandalsotoincreasethedurationof‘hold’ofeachcontraction.Thistwo-prongedapproachisimportanttobuildbothstrengthandenduranceofthemuscle,bothofwhichareessentialtoimprovecontinencefunction.Successfuladherencetoaprogrammeofpelvicfloorexercisescanleadtocure in over 50% of women and improvement in 75% or more. The major barrier to success is thewoman’swillingnesstoperseverewiththeexercisesoveraperiodofseveralweeks,inordertoachievemaximum benefit, but the most obvious advantage is that a course of exercise carries no risk ofcomplications!PelvicfloorexercisesworkforbothstressincontinenceandOAB.Inthelattercase,itislikelythatthebenefitisfromimprovingmusclestrengthtogivewomentheconfidencetoresisttheurgewithoutfearofleakage,andalsobypelvicfloorcontractionhavingareflexinhibitionactionondetrusormusclecontraction.
BladderretrainingForwomenwithOABormixed incontinence,pelvic floormuscle training iscombinedwitha formofbladderdrillorbladderretraining.Bladderdrill involvesre-educating thepatient (andherbladder) toincrease the intervalbetweenvoids, tore-establishnormalfrequency.FormanywomenwithOAB, theurgencyandassociatedleakage(orfearofleakage)leadsthemtoestablishapatternofvoidingwhenevertheyareawareofbladderfillingsensations.Anawarenessofbladderfillingisanormalphysiologicalsignalthatoccursonceormorethanonceasthebladderfills,butbeforefullbladdercapacityisreached.Bladderretraining(inconjunctionwithpelvicfloormuscletraining)includesteachingthewomanaboutnormalbladdersensation,therateofurineproduction(usually1–2ml/min)andnormalbladdercapacity(350–500ml),andthenencouraginghertopracticedelayingvoidingforseveralminutesbeyondwhenshewouldnormallyvoid.Itisusualdotothisinastepwisefashion,topushbackvoidingin5or10minutesteps,ratherthantryingtoholdforawholehour.Bladderretrainingcanbeverysuccessfulinreducingfrequencyandurgency,butlikepelvicfloorexercises,itrequiresperseveranceanddeterminationonthepartofthepatient.
It is important tocounselwomenaboutthebenefitsofweightloss,for thosewhoareoverweightorobese.Obesityisassociatedwithincreasedriskandseverityofstressincontinence,duetotheincreaseinabdominal pressure, but it is also associated with increased severity of OAB. Several studies havedemonstratedthatweightlossleadstoimprovementinbothstressincontinenceandOAB,andcanresultincure.
Urodynamictestingwww.medicalebookpdf.com
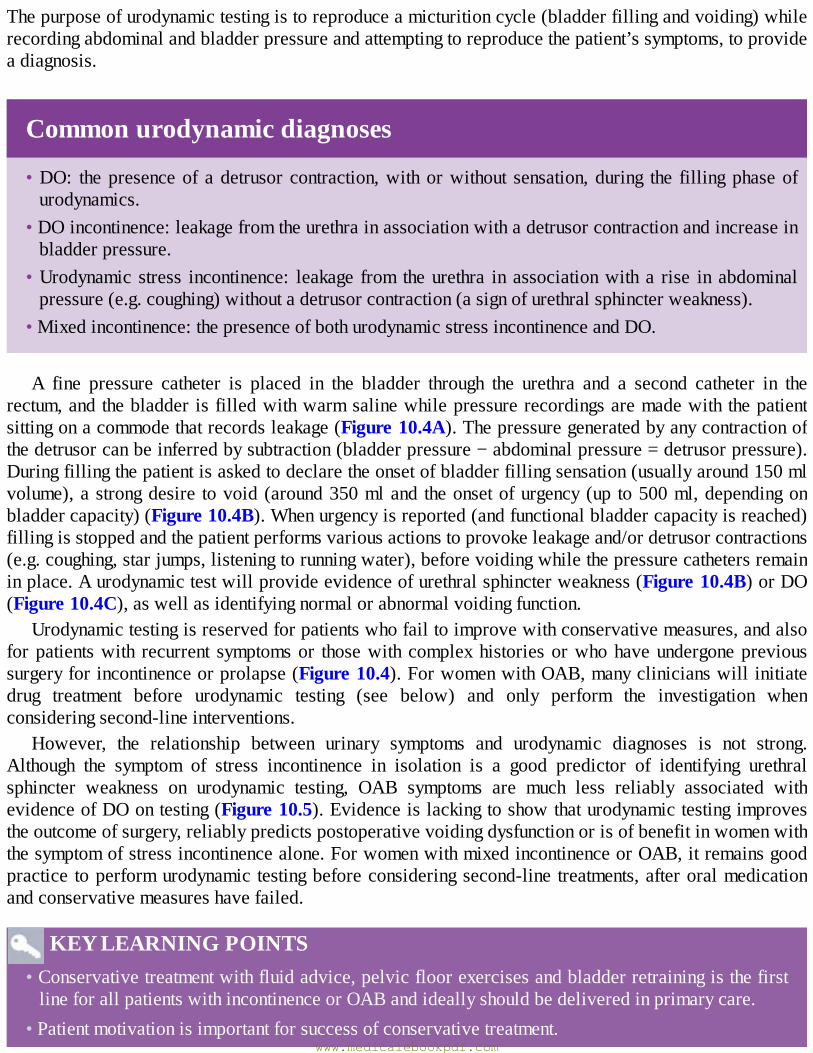
Thepurposeofurodynamictestingistoreproduceamicturitioncycle(bladderfillingandvoiding)whilerecordingabdominalandbladderpressureandattemptingtoreproducethepatient’ssymptoms,toprovideadiagnosis.
Commonurodynamicdiagnoses
•DO: thepresenceof adetrusor contraction,withorwithout sensation,during the fillingphaseofurodynamics.
•DOincontinence:leakagefromtheurethrainassociationwithadetrusorcontractionandincreaseinbladderpressure.
•Urodynamic stress incontinence: leakage from theurethra inassociationwitha rise inabdominalpressure(e.g.coughing)withoutadetrusorcontraction(asignofurethralsphincterweakness).
•Mixedincontinence:thepresenceofbothurodynamicstressincontinenceandDO.
A fine pressure catheter is placed in the bladder through the urethra and a second catheter in therectum,andthebladderisfilledwithwarmsalinewhilepressurerecordingsaremadewiththepatientsittingonacommodethatrecordsleakage(Figure10.4A).Thepressuregeneratedbyanycontractionofthedetrusorcanbeinferredbysubtraction(bladderpressure−abdominalpressure=detrusorpressure).Duringfillingthepatientisaskedtodeclaretheonsetofbladderfillingsensation(usuallyaround150mlvolume),astrongdesire tovoid(around350mland theonsetofurgency(up to500ml,dependingonbladdercapacity)(Figure10.4B).Whenurgencyisreported(andfunctionalbladdercapacityisreached)fillingisstoppedandthepatientperformsvariousactionstoprovokeleakageand/ordetrusorcontractions(e.g.coughing,starjumps,listeningtorunningwater),beforevoidingwhilethepressurecathetersremaininplace.Aurodynamictestwillprovideevidenceofurethralsphincterweakness(Figure10.4B)orDO(Figure10.4C),aswellasidentifyingnormalorabnormalvoidingfunction.
Urodynamictestingisreservedforpatientswhofailtoimprovewithconservativemeasures,andalsoforpatientswith recurrent symptomsor thosewithcomplexhistoriesorwhohaveundergoneprevioussurgeryforincontinenceorprolapse(Figure10.4).ForwomenwithOAB,manyclinicianswillinitiatedrug treatment before urodynamic testing (see below) and only perform the investigation whenconsideringsecond-lineinterventions.
However, the relationship between urinary symptoms and urodynamic diagnoses is not strong.Although the symptom of stress incontinence in isolation is a good predictor of identifying urethralsphincter weakness on urodynamic testing, OAB symptoms are much less reliably associated withevidenceofDOontesting(Figure10.5).Evidenceislackingtoshowthaturodynamictestingimprovestheoutcomeofsurgery,reliablypredictspostoperativevoidingdysfunctionorisofbenefitinwomenwiththesymptomofstressincontinencealone.ForwomenwithmixedincontinenceorOAB,itremainsgoodpractice toperformurodynamic testingbeforeconsideringsecond-line treatments,afteroralmedicationandconservativemeasureshavefailed.
KEYLEARNINGPOINTS•Conservativetreatmentwithfluidadvice,pelvicfloorexercisesandbladderretrainingisthefirstlineforallpatientswithincontinenceorOABandideallyshouldbedeliveredinprimarycare.
•Patientmotivationisimportantforsuccessofconservativetreatment.www.medicalebookpdf.com
•Urodynamic investigation is not always necessary before commencing drug treatment or beforesurgeryinwomencomplainingonlyofstressincontinence.
• A urodynamic assessment should be done for women who fail to respond to anticholinergicmedicationorinwomenwithmixedsymptomsforwhomsurgeryisbeingconsidered.
MedicaltreatmentMedicaltreatmentsforurinaryincontinenceareprimarilyaimedattreatmentofOABsymptomsandDO.Becausetheparasympatheticnervesstimulatethedetrusormuscletocontract,anticholinergicmedicationshave been the mainstay of medical treatment for many years. There is a wide range of differentcompoundsandpreparationsavailable.Themainsiteofactionofanticholinergicdrugsisthemotorend-plateof theneuromuscular junction,where theyantagonizetheactionofacetylcholineat themuscarinicreceptorsandinhibitdetrusorcontraction.Inthelast5years,ithasbecomeapparentthatacetylcholineisalsoanimportantneurotransmitterintheafferent,sensorypathwaysinthebladderandthusthedrugsalsohaveadirecteffectinreducingtheperceivedsensationsofbladderfillingbyinhibitingreceptor-mediatedafferentsignals.
www.medicalebookpdf.com
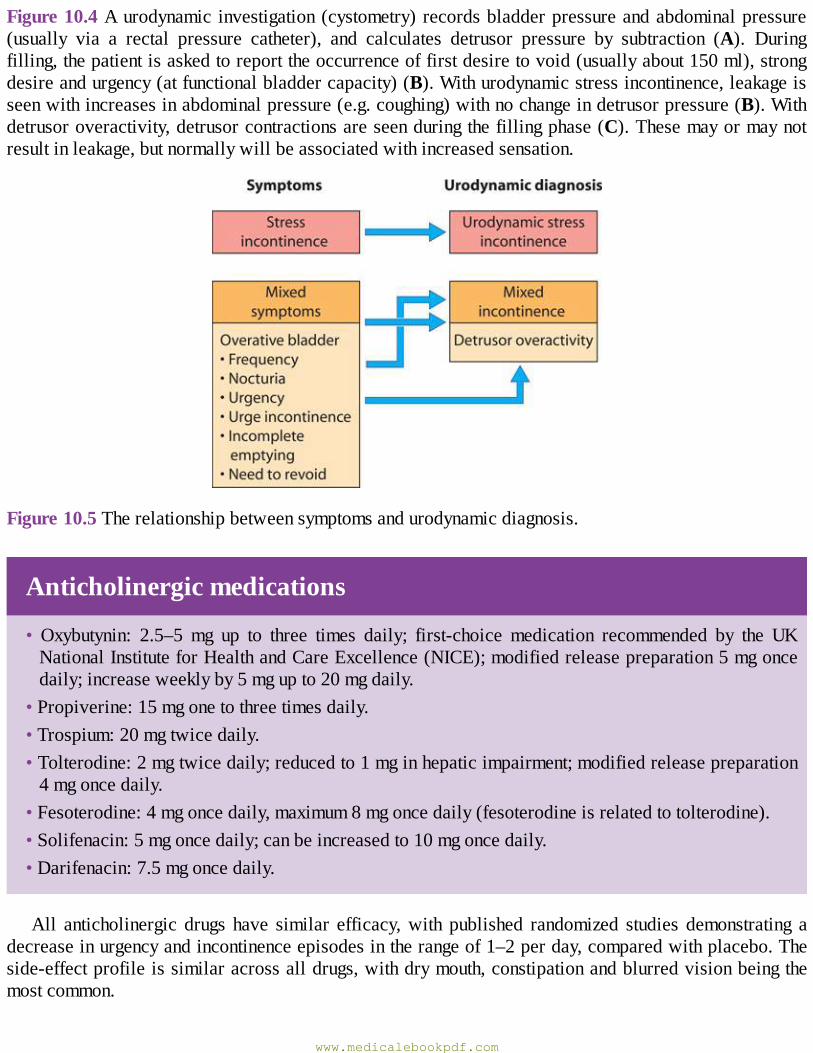
Figure10.4Aurodynamic investigation(cystometry)recordsbladderpressureandabdominalpressure(usually via a rectal pressure catheter), and calculates detrusor pressure by subtraction (A). Duringfilling,thepatientisaskedtoreporttheoccurrenceoffirstdesiretovoid(usuallyabout150ml),strongdesireandurgency(atfunctionalbladdercapacity)(B).Withurodynamicstressincontinence,leakageisseenwithincreasesinabdominalpressure(e.g.coughing)withnochangeindetrusorpressure(B).Withdetrusoroveractivity,detrusorcontractionsareseenduringthefillingphase(C).Thesemayormaynotresultinleakage,butnormallywillbeassociatedwithincreasedsensation.
Figure10.5Therelationshipbetweensymptomsandurodynamicdiagnosis.
Anticholinergicmedications
• Oxybutynin: 2.5–5 mg up to three times daily; first-choice medication recommended by the UKNationalInstituteforHealthandCareExcellence(NICE);modifiedreleasepreparation5mgoncedaily;increaseweeklyby5mgupto20mgdaily.
•Propiverine:15mgonetothreetimesdaily.•Trospium:20mgtwicedaily.•Tolterodine:2mgtwicedaily;reducedto1mginhepaticimpairment;modifiedreleasepreparation4mgoncedaily.
•Fesoterodine:4mgoncedaily,maximum8mgoncedaily(fesoterodineisrelatedtotolterodine).•Solifenacin:5mgoncedaily;canbeincreasedto10mgoncedaily.•Darifenacin:7.5mgoncedaily.
All anticholinergic drugs have similar efficacy,with published randomized studies demonstrating adecreaseinurgencyandincontinenceepisodesintherangeof1–2perday,comparedwithplacebo.Theside-effectprofileissimilaracrossalldrugs,withdrymouth,constipationandblurredvisionbeingthemostcommon.
www.medicalebookpdf.com
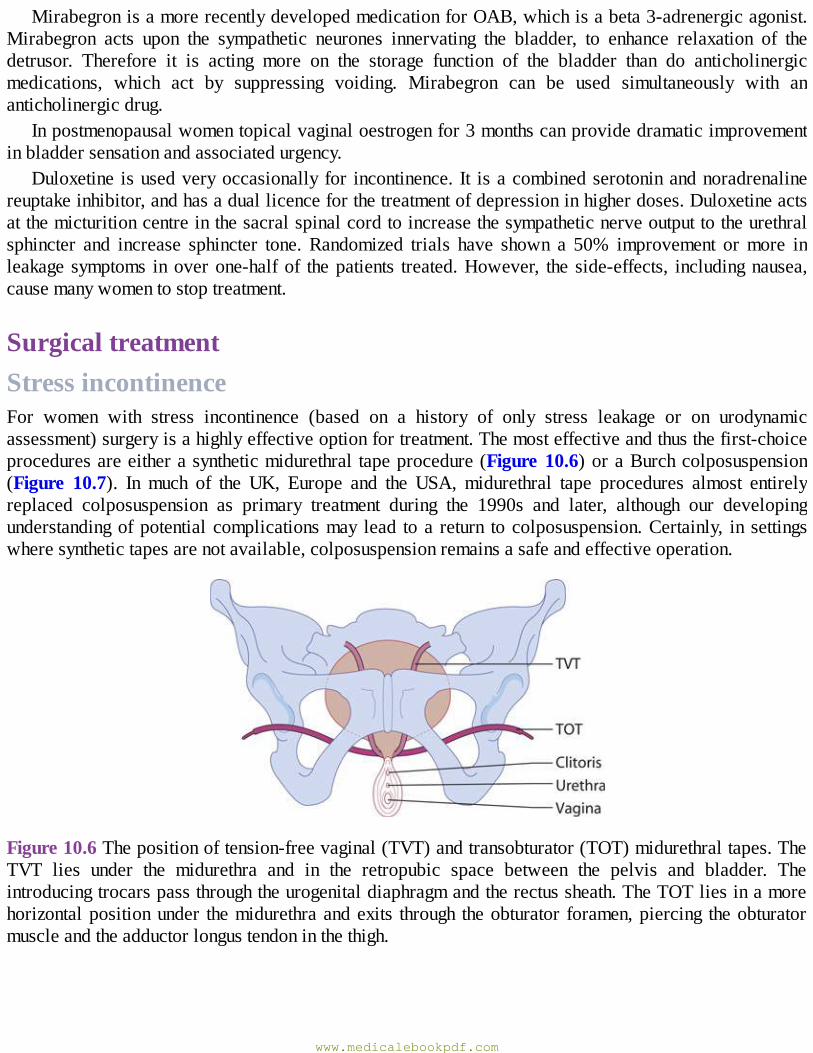
MirabegronisamorerecentlydevelopedmedicationforOAB,whichisabeta3-adrenergicagonist.Mirabegron acts upon the sympathetic neurones innervating the bladder, to enhance relaxation of thedetrusor. Therefore it is acting more on the storage function of the bladder than do anticholinergicmedications, which act by suppressing voiding. Mirabegron can be used simultaneously with ananticholinergicdrug.
Inpostmenopausalwomentopicalvaginaloestrogenfor3monthscanprovidedramaticimprovementinbladdersensationandassociatedurgency.
Duloxetine isusedveryoccasionally for incontinence. It isacombinedserotoninandnoradrenalinereuptakeinhibitor,andhasaduallicenceforthetreatmentofdepressioninhigherdoses.Duloxetineactsatthemicturitioncentreinthesacralspinalcordtoincreasethesympatheticnerveoutputtotheurethralsphincter and increase sphincter tone. Randomized trials have shown a 50% improvement ormore inleakagesymptoms inoverone-halfof thepatients treated.However, the side-effects, includingnausea,causemanywomentostoptreatment.
SurgicaltreatmentStressincontinenceFor women with stress incontinence (based on a history of only stress leakage or on urodynamicassessment)surgeryisahighlyeffectiveoptionfortreatment.Themosteffectiveandthusthefirst-choiceproceduresareeitherasyntheticmidurethral tapeprocedure(Figure10.6)oraBurchcolposuspension(Figure 10.7). In much of the UK, Europe and the USA, midurethral tape procedures almost entirelyreplaced colposuspension as primary treatment during the 1990s and later, although our developingunderstandingofpotentialcomplicationsmay lead toa return tocolposuspension.Certainly, in settingswheresynthetictapesarenotavailable,colposuspensionremainsasafeandeffectiveoperation.
Figure10.6Thepositionoftension-freevaginal(TVT)andtransobturator(TOT)midurethraltapes.TheTVT lies under the midurethra and in the retropubic space between the pelvis and bladder. Theintroducingtrocarspassthroughtheurogenitaldiaphragmandtherectussheath.TheTOTliesinamorehorizontalpositionunder themidurethraandexits through theobturator foramen,piercing theobturatormuscleandtheadductorlongustendoninthethigh.
www.medicalebookpdf.com
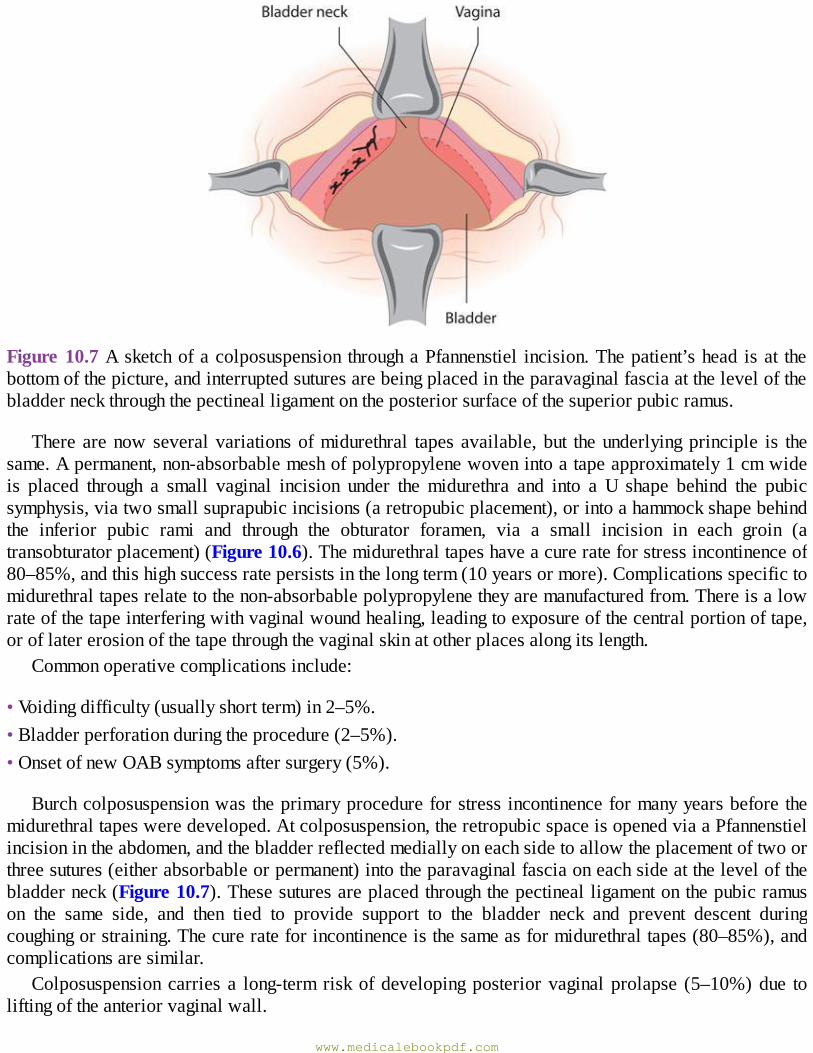
Figure10.7Asketchofacolposuspension throughaPfannenstiel incision.Thepatient’shead isat thebottomofthepicture,andinterruptedsuturesarebeingplacedintheparavaginalfasciaatthelevelofthebladderneckthroughthepectinealligamentontheposteriorsurfaceofthesuperiorpubicramus.
Therearenowseveralvariationsofmidurethral tapesavailable,but theunderlyingprinciple is thesame.Apermanent,non-absorbablemeshofpolypropylenewovenintoatapeapproximately1cmwideis placed through a small vaginal incision under themidurethra and into a U shape behind the pubicsymphysis,viatwosmallsuprapubicincisions(aretropubicplacement),orintoahammockshapebehindthe inferior pubic rami and through the obturator foramen, via a small incision in each groin (atransobturatorplacement)(Figure10.6).Themidurethraltapeshaveacurerateforstressincontinenceof80–85%,andthishighsuccessratepersistsinthelongterm(10yearsormore).Complicationsspecifictomidurethraltapesrelatetothenon-absorbablepolypropylenetheyaremanufacturedfrom.Thereisalowrateofthetapeinterferingwithvaginalwoundhealing,leadingtoexposureofthecentralportionoftape,oroflatererosionofthetapethroughthevaginalskinatotherplacesalongitslength.
Commonoperativecomplicationsinclude:
•Voidingdifficulty(usuallyshortterm)in2–5%.•Bladderperforationduringtheprocedure(2–5%).•OnsetofnewOABsymptomsaftersurgery(5%).
Burchcolposuspensionwastheprimaryprocedureforstressincontinenceformanyyearsbeforethemidurethraltapesweredeveloped.Atcolposuspension,theretropubicspaceisopenedviaaPfannenstielincisionintheabdomen,andthebladderreflectedmediallyoneachsidetoallowtheplacementoftwoorthreesutures(eitherabsorbableorpermanent)intotheparavaginalfasciaoneachsideatthelevelofthebladderneck(Figure10.7).Thesesuturesareplacedthroughthepectinealligamentonthepubicramuson the same side, and then tied to provide support to the bladder neck and prevent descent duringcoughingorstraining.Thecurerateforincontinenceisthesameasformidurethraltapes(80–85%),andcomplicationsaresimilar.
Colposuspensioncarries a long-term riskofdevelopingposteriorvaginalprolapse (5–10%)due toliftingoftheanteriorvaginalwall.
www.medicalebookpdf.com
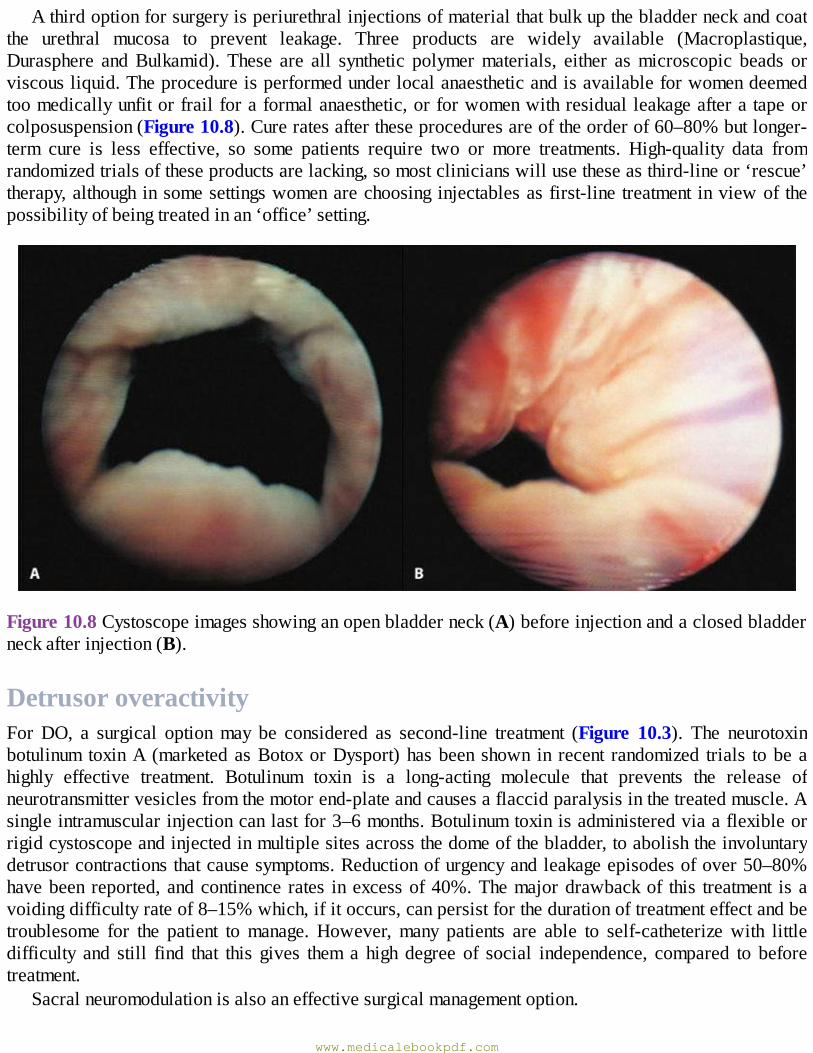
Athirdoptionforsurgeryisperiurethralinjectionsofmaterialthatbulkupthebladderneckandcoatthe urethral mucosa to prevent leakage. Three products are widely available (Macroplastique,Durasphere andBulkamid). These are all synthetic polymermaterials, either asmicroscopic beads orviscousliquid.Theprocedureisperformedunderlocalanaestheticandisavailableforwomendeemedtoomedicallyunfitorfrailforaformalanaesthetic,orforwomenwithresidualleakageafteratapeorcolposuspension(Figure10.8).Cureratesaftertheseproceduresareoftheorderof60–80%butlonger-term cure is less effective, so some patients require two or more treatments. High-quality data fromrandomizedtrialsoftheseproductsarelacking,somostclinicianswillusetheseasthird-lineor‘rescue’therapy,althoughinsomesettingswomenarechoosinginjectablesasfirst-line treatment inviewof thepossibilityofbeingtreatedinan‘office’setting.
Figure10.8Cystoscopeimagesshowinganopenbladderneck(A)beforeinjectionandaclosedbladderneckafterinjection(B).
DetrusoroveractivityForDO, a surgical optionmay be considered as second-line treatment (Figure 10.3). The neurotoxinbotulinum toxinA (marketedasBotoxorDysport)hasbeenshown in recent randomized trials tobeahighly effective treatment. Botulinum toxin is a long-acting molecule that prevents the release ofneurotransmittervesiclesfromthemotorend-plateandcausesaflaccidparalysisinthetreatedmuscle.Asingleintramuscularinjectioncanlastfor3–6months.Botulinumtoxinisadministeredviaaflexibleorrigidcystoscopeandinjectedinmultiplesitesacrossthedomeofthebladder,toabolishtheinvoluntarydetrusorcontractionsthatcausesymptoms.Reductionofurgencyandleakageepisodesofover50–80%havebeen reported,andcontinence rates inexcessof40%.Themajordrawbackof this treatment isavoidingdifficultyrateof8–15%which,ifitoccurs,canpersistforthedurationoftreatmenteffectandbetroublesome for the patient tomanage. However,many patients are able to self-catheterizewith littledifficulty and still find that this gives them a high degree of social independence, compared to beforetreatment.
Sacralneuromodulationisalsoaneffectivesurgicalmanagementoption.
www.medicalebookpdf.com
KEYLEARNINGPOINTS•Surgeryforstressincontinenceishighlyeffectivewithcureratesof85%orhigher.• Midurethral tapes and colposuspension are equally effective, but tape surgery is more cost-effectiveduetotheshorthospitalstayandrapidreturntonormalactivities.
• Patients should be warned of the risk of voiding dysfunction, bladder injury and new OABsymptomsaftersurgery.
•Mesh-related complications are uncommon aftermidurethral tape surgery but can be difficult totreat;patientsshouldbefullyinformedoftherisks,andofthepotentialforfurthersurgerytodealwiththesecomplications.
• Botulinum toxin and sacral neuromodulation are highly effective second-line treatments fordetrusoroveractivity.
Prolapse
SymptomsfrompelvicorganprolapsePelvicorganprolapsecancausesymptomsdirectlyduetotheprolapsedorganorindirectlyduetoorgandysfunction secondary to displacement from the anatomical position. Proplase symptoms include asensationofvaginalbulge,heavinessoravisibleprotrusionatorbeyondtheintroitus.Patientsmayalsodescribelowerabdominalorbackpain,oradraggingdiscomfortrelievedbylyingorsitting.
Indirectsymptomswilldependonwhichotherorgansare involved in theprolapsebutmay includedifficulty in voiding urine or emptying the bowel (termed obstructive defaecation), and sensations ofincompleteemptyingofbladderorrectum.Patientsmayhavetosupportorreducetheprolapsewiththeirfingers to be able to void or evacuate stool completely (termed digitation, distinct from manualevacuationoftherectum).Urinaryorfaecalincontinencemayalsobepresent.Itisimportanttoaskaboutsexual activity, even in theolderpatient, and to enquire aboutdifficulty achievingpenetration, painordiscomfort during intercourse and loss of sensation and difficulty achieving orgasm due to vaginal orintroitallaxity.
Patientsmayexperiencevaginalbleedingfromaprolapse that isexternalandbecomesulceratedorabraded,butinwomenwithauterus,onemustremembertoexcludeendometrialcarcinomabybiopsyandultrasound.
Risk factors predisposing to prolapse are very much similar to those predisposing to stressincontinence.Research has shown the pudendal nerves to be damaged after childbirth,with increasednerve conduction times, and ultrasound studies of the pelvic anatomy of women with prolapse havedemonstrated thinningor avulsionof thepuborectalismuscle from its insertionon thepubic ramus,oneitheroneorbothsidesinahighproportionofcases.
RelevantanatomyUterovaginal prolapse is caused by failure of the interaction between the levator animuscles and theligaments and fascia that support thepelvicorgans.For adetaileddescriptionof the relationships andfunction of these structures, see the review byWei&De Lancey in Further reading. The levator ani
www.medicalebookpdf.com
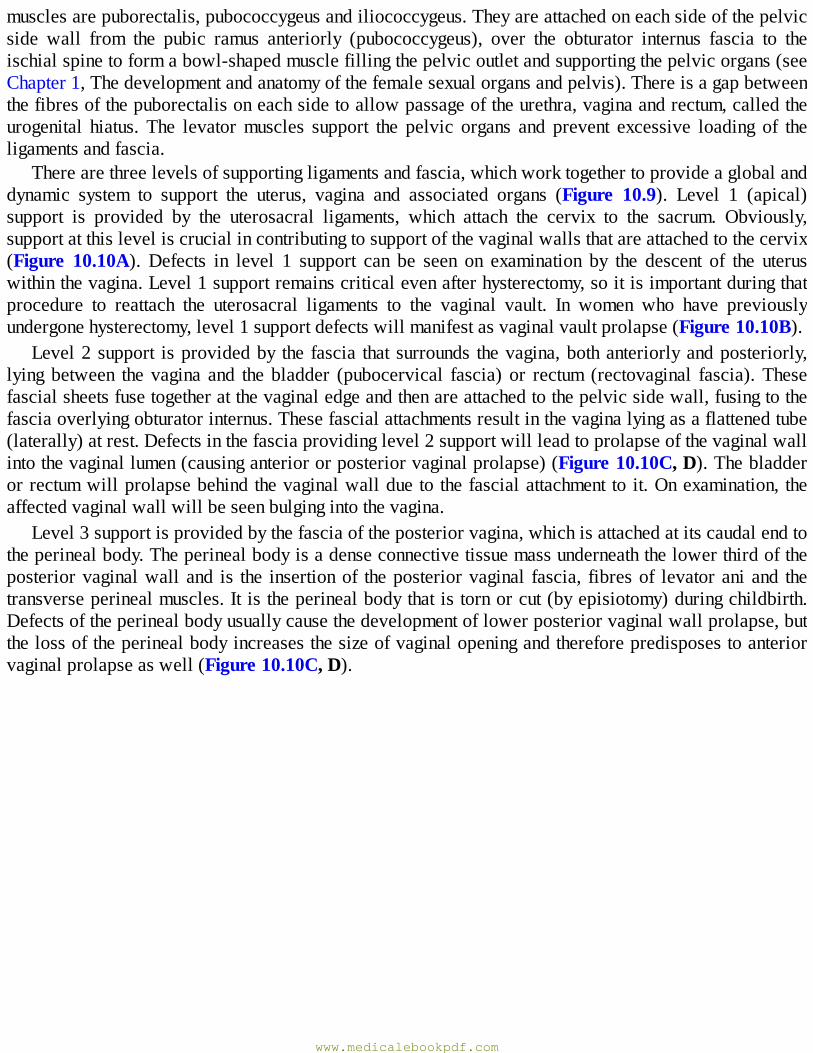
musclesarepuborectalis,pubococcygeusandiliococcygeus.Theyareattachedoneachsideofthepelvicside wall from the pubic ramus anteriorly (pubococcygeus), over the obturator internus fascia to theischialspinetoformabowl-shapedmusclefillingthepelvicoutletandsupportingthepelvicorgans(seeChapter1,Thedevelopmentandanatomyofthefemalesexualorgansandpelvis).Thereisagapbetweenthefibresofthepuborectalisoneachsidetoallowpassageoftheurethra,vaginaandrectum,calledtheurogenital hiatus. The levatormuscles support the pelvic organs and prevent excessive loading of theligamentsandfascia.
Therearethreelevelsofsupportingligamentsandfascia,whichworktogethertoprovideaglobalanddynamic system to support the uterus, vagina and associated organs (Figure 10.9). Level 1 (apical)support is provided by the uterosacral ligaments, which attach the cervix to the sacrum. Obviously,supportatthisleveliscrucialincontributingtosupportofthevaginalwallsthatareattachedtothecervix(Figure 10.10A). Defects in level 1 support can be seen on examination by the descent of the uteruswithinthevagina.Level1supportremainscriticalevenafterhysterectomy,soitisimportantduringthatprocedure to reattach the uterosacral ligaments to the vaginal vault. In women who have previouslyundergonehysterectomy,level1supportdefectswillmanifestasvaginalvaultprolapse(Figure10.10B).
Level2support isprovidedby the fascia thatsurrounds thevagina,bothanteriorlyandposteriorly,lyingbetween the vagina and the bladder (pubocervical fascia) or rectum (rectovaginal fascia).Thesefascialsheetsfusetogetheratthevaginaledgeandthenareattachedtothepelvicsidewall,fusingtothefasciaoverlyingobturatorinternus.Thesefascialattachmentsresultinthevaginalyingasaflattenedtube(laterally)atrest.Defectsinthefasciaprovidinglevel2supportwillleadtoprolapseofthevaginalwallintothevaginallumen(causinganteriororposteriorvaginalprolapse)(Figure10.10C,D).Thebladderorrectumwillprolapsebehindthevaginalwallduetothefascialattachmenttoit.Onexamination, theaffectedvaginalwallwillbeseenbulgingintothevagina.
Level3supportisprovidedbythefasciaoftheposteriorvagina,whichisattachedatitscaudalendtotheperinealbody.Theperinealbodyisadenseconnectivetissuemassunderneaththelowerthirdoftheposteriorvaginalwalland is the insertionof theposteriorvaginal fascia, fibresof levatoraniand thetransverseperinealmuscles.Itistheperinealbodythatistornorcut(byepisiotomy)duringchildbirth.Defectsoftheperinealbodyusuallycausethedevelopmentoflowerposteriorvaginalwallprolapse,butthelossoftheperinealbodyincreasesthesizeofvaginalopeningandthereforepredisposestoanteriorvaginalprolapseaswell(Figure10.10C,D).
www.medicalebookpdf.com
Figure 10.9 Fascial supports of the pelvic organs. Level 1 support is provided by the uterosacralligaments,suspendingtheuterusandattachedvaginalvault.Level2(midvagina)supportisprovidedbythefascialyingbetweenthevaginaandthebladderorrectumthatfuseslaterallyandrunstoattachonthepelvicsidewall.Level3supportisprovidedbytheperinealbody,whichhastheposteriorvaginalfasciafusedtoitsuppersurface.
KEYLEARNINGPOINTS• The levator ani muscles (puborectalis, pubococcygeus and iliococcygeus) support the pelvicorgansandrelieveexcessivepressurefromtheligamentsandfascia.
•Theuterosacralligamentsprovideessentialapicalsupport(level1support).•Vaginalfasciasupportsthevagina(level2support).•Theperinealbodyisveryimportantinsupportingthelowervagina(level3support).•Allthestructuresprovideadynamicandintegratedsupporttothepelvicorgans.
ClinicalassessmentofprolapseThehistoryshouldelicitthepresentingsymptom(s)andseverity,andincludequestionstoascertainifthepatient has any coexisting urinary, faecal or sexual symptoms as discussed above for the incontinent
www.medicalebookpdf.com

patient.Oneshouldbesensitivetotheemotionalaspectoftheproblem,butspecificquestionsshouldbeaskedaboutsexualdiscomfortanddifficultyachievingorgasm.Forwomenwhoarenotsexuallyactive,itshouldbediscussedwhetherthisisduetotheprolapsesymptomsorotherpersonalorsocialissues(e.g.healthof thepartner).For somewomen, intercourse isavoidedbecauseofanxietiesorembarrassmentovertheappearanceofthegenitaliaandalossofperceivedattractiveness.
Clinical examination should ideally be done in the lithotomy position with a Sims speculum (seeChapter2,Gynaecologicalhistory,examinationandinvestigations,Figure2.4).Thisallowsretractionoftheanteriorandposteriorvaginalwallinturn,toallowfullassessmentofthedegreeofprolapseandtoassess howmuch descent of the cervix and uterus is present. Prolapse is described in three stages ofdescent,andnoteshouldbemadeofwhetheritoccursatpatientstrainingoratrestandwhethertractionhasbeenapplied:
www.medicalebookpdf.com
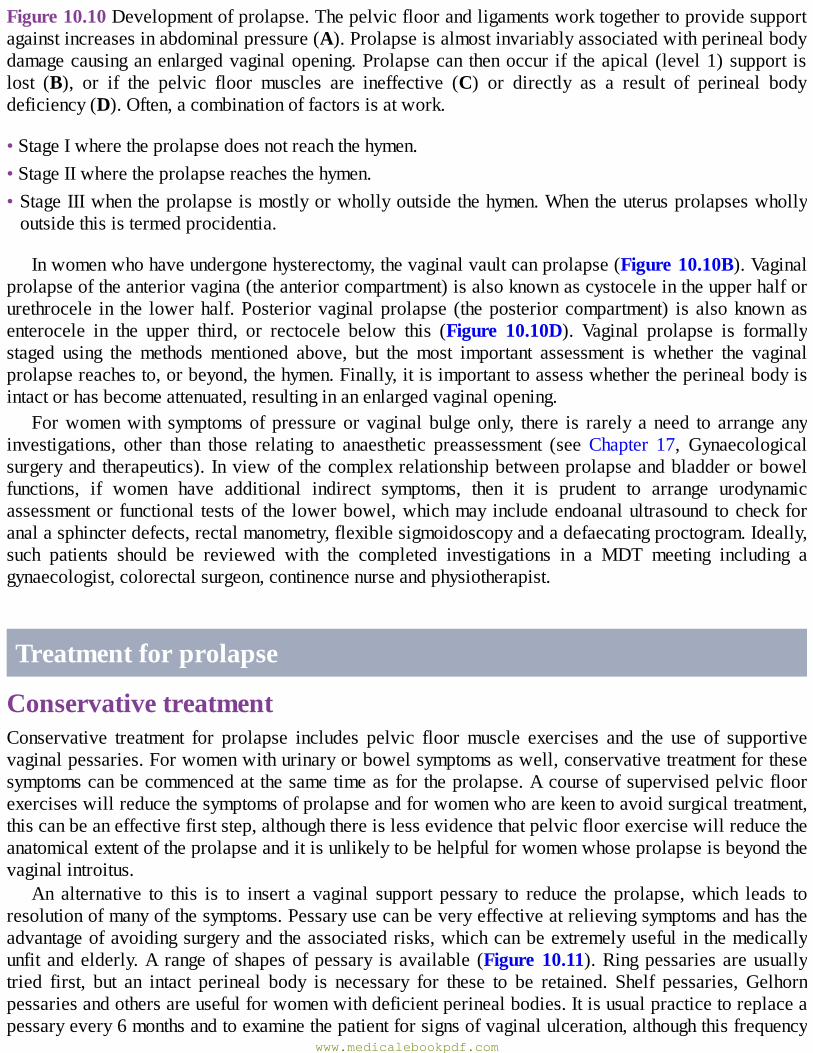
Figure10.10Developmentofprolapse.Thepelvicfloorandligamentsworktogethertoprovidesupportagainstincreasesinabdominalpressure(A).Prolapseisalmostinvariablyassociatedwithperinealbodydamagecausinganenlargedvaginalopening.Prolapsecan thenoccur if theapical (level1)support islost (B), or if the pelvic floor muscles are ineffective (C) or directly as a result of perineal bodydeficiency(D).Often,acombinationoffactorsisatwork.
•StageIwheretheprolapsedoesnotreachthehymen.•StageIIwheretheprolapsereachesthehymen.•StageIIIwhentheprolapseismostlyorwhollyoutsidethehymen.Whentheuterusprolapseswhollyoutsidethisistermedprocidentia.
Inwomenwhohaveundergonehysterectomy,thevaginalvaultcanprolapse(Figure10.10B).Vaginalprolapseoftheanteriorvagina(theanteriorcompartment)isalsoknownascystoceleintheupperhalforurethrocele in the lowerhalf.Posteriorvaginalprolapse (theposteriorcompartment) is alsoknownasenterocele in the upper third, or rectocele below this (Figure 10.10D). Vaginal prolapse is formallystaged using the methods mentioned above, but the most important assessment is whether the vaginalprolapsereachesto,orbeyond,thehymen.Finally,itisimportanttoassesswhethertheperinealbodyisintactorhasbecomeattenuated,resultinginanenlargedvaginalopening.
Forwomenwith symptomsofpressureorvaginalbulgeonly, there is rarely aneed to arrange anyinvestigations, other than those relating to anaesthetic preassessment (see Chapter 17, Gynaecologicalsurgeryand therapeutics). Inviewof thecomplexrelationshipbetweenprolapseandbladderorbowelfunctions, if women have additional indirect symptoms, then it is prudent to arrange urodynamicassessmentor functional testsof the lowerbowel,whichmayincludeendoanalultrasoundtocheckforanalasphincterdefects,rectalmanometry,flexiblesigmoidoscopyandadefaecatingproctogram.Ideally,such patients should be reviewed with the completed investigations in a MDT meeting including agynaecologist,colorectalsurgeon,continencenurseandphysiotherapist.
Treatmentforprolapse
ConservativetreatmentConservative treatment for prolapse includes pelvic floormuscle exercises and the use of supportivevaginalpessaries.Forwomenwithurinaryorbowelsymptomsaswell,conservativetreatmentforthesesymptomscanbecommencedat thesametimeasfortheprolapse.Acourseofsupervisedpelvicfloorexerciseswillreducethesymptomsofprolapseandforwomenwhoarekeentoavoidsurgicaltreatment,thiscanbeaneffectivefirststep,althoughthereislessevidencethatpelvicfloorexercisewillreducetheanatomicalextentoftheprolapseanditisunlikelytobehelpfulforwomenwhoseprolapseisbeyondthevaginalintroitus.
An alternative to this is to insert a vaginal support pessary to reduce the prolapse,which leads toresolutionofmanyofthesymptoms.Pessaryusecanbeveryeffectiveatrelievingsymptomsandhastheadvantageofavoidingsurgeryandtheassociatedrisks,whichcanbeextremelyuseful in themedicallyunfitandelderly.A rangeof shapesofpessary isavailable (Figure10.11).Ringpessariesareusuallytried first, but an intact perineal body is necessary for these to be retained. Shelf pessaries, Gelhornpessariesandothersareusefulforwomenwithdeficientperinealbodies.Itisusualpracticetoreplaceapessaryevery6monthsandtoexaminethepatientforsignsofvaginalulceration,althoughthisfrequency
www.medicalebookpdf.com
istraditionalandnotbasedonanyevidence.Complicationsareuncommonandusuallyminor(bleeding,discharge),althoughrarelythepessarycanbecomeincarcerated,requiringgeneralanaesthesiatoremove,andrarecasesofrectovaginalorvesicovaginalfistulaformationhavebeenreported.Sexualintercourseremains theoretically possiblewith awell-placed ring pessary, but not with the others, sowould notgenerallybesuitableforwomenwhoaresexuallyactive.Motivatedpatientscanbetaughttoinsertandremovetheirownpessariesiftheydowishtoremainsexuallyactive.
Figure10.11Vaginalsupportpessaries.
SurgeryforpelvicorganprolapseSurgicaltreatmentforprolapseiscommon,andcanbeofferedifconservativetreatmentshavefailedorifthe patient chooses surgery from the outset. There are a wide range of specific procedures that aredescribedfurtherinChapter17,Gynaecologicalsurgeryandtherapeutics.Theprocedurechosendependsonwhichcompartmentisaffected,whetherthewomanwishestoretainheruterusandwhetherthevaginalor abdominal route of surgery is chosen. The essential principles of prolapse surgery apply for allprocedures.Prolapsesurgeryisperformedthroughthevaginatorestoretheligamentoustissuesupportstotheapex,anteriorandposteriorvagina(anteriorrepair,posteriorrepair)andrepairoftheperinealbody.Thevaginalroutecanalsobeusedforposthysterectomyvaultprolapse,attachingthevaginalvaulttotheright sacrospinous ligamentwith non-absorbable or slowly absorbable sutures, but here an abdominalapproachtoperformasacrocolpopexyisanoptionthatwillprovideexcellent,durablelong-termcure.TherelativemeritsofabdominalcomparedtovaginalsurgeryandtheusualrecoverytimesarediscussedinChapter17,Gynaecologicalsurgeryandtherapeutics.Inthelast3–5years,therehasbeenanincreasingnumberofwomenwishingtoavoidhysterectomyduringprolapsesurgery,sobothsacrospinousfixationandsacrocolpopexycanbeperformedbyattachingameshorsuturestothecervixratherthanthevaginalvault.
Principlesofprolapsesurgery
•Remove/reducethevaginalbulge.•Restoretheligament/tissuesupportstotheapex,anteriorandposteriorvagina.•Replaceassociatedorgansintheircorrectpositions.
www.medicalebookpdf.com
•Retainsufficientvaginallengthandwidthtoallowintercourse.•Restoretheperinealbody.•Correctorpreventurinaryincontinence.•Correctorpreventfaecalincontinence.•Correctobstructeddefaecation.
Vaginalrepairusingmeshimprovestheanatomicaloutcomeandreducestheriskofrecurrentprolapse.However, the available long-term data do not demonstrate a difference in symptom relief betweenstandardrepairandmeshrepair.Meshrepaircarriestheriskoflatererosionandneedforremoval,whichis challenging surgery. Therefore, many surgeons will only consider mesh repair for women withrecurrentvaginalprolapse, andonlyproceedafter careful and full counsellingof thewomanabout therelativebenefitsandpotentialrisksofsurgery.
KEYLEARNINGPOINTS•Uterovaginalprolapsecausestroublesomesymptomsbutisnotlifethreatening.•Acourseofpelvicfloorexercisescanreducesymptomsandmayreduceprolapseprogressioninwomenwithmild/moderateprolapse.
•Vaginalpessariesareausefulconservativetreatmentbutdonotsuitallwomen.•Surgeryforprolapseiseffective,buthasarecurrencerateofabout5%.•Itisnotessentialtoperformhysterectomyforprolapse.•Meshrepairsforprolapsegiveabetteranatomicalcure,butthereisnoconvincingevidencethatsymptomreliefisdifferentfromstandardsurgery.
•Meshcomplicationsarecommonandcanbeextremelydifficulttomanage.
FurtherreadingDmochowskiRR,Blaivas JM,GormleyEA, etal. (2010).Update ofAUAguideline on the surgicalmanagementoffemalestressurinaryincontinence.JUrol183:1906–14.
Smith A, Bevan D, Douglas HR, James D (2013). Management of urinary incontinence in women:summaryofupdatedNICEguidance.BMJ347:f5170.doi:10.1136/bmj.f5170.:f5170.
Wei JT,De Lancey JO (2004). Functional anatomy of the pelvic floor and lower urinary tract.ClinObstetGynecol47:3–17.
Selfassessment
CASEHISTORYwww.medicalebookpdf.com
A 47-year-old patient, who is a lawyer, presents to clinic with symptoms of leaking urine oncoughing,sneezingandexercise,andwhenshehastheurgetopassurine.ADescribetheimportantpartsofthehistorytobetaken.BDescribetheinvestigationsrequired.CDescribethebesttreatment.
ANSWERS
ATake a standard gynaecological history first, noting any severemenstrual symptoms (in case ahysterectomyshouldbeconsidered),AUBormenopause.Notenumber andmodeofdeliveries.Noteanyabdominalsurgery.Whentakingthehistoryhaveamindtoboththeeffectonthepatient’slifeandindicationsfor,oragainst,medicalorsurgicaltreatment.
Nextadetailedurogynecologicalhistoryisrequiredasdiscussedinthischapter.
The patient reveals on direct questions that she has no menstrual problems, has had threevaginal deliveries and no abdominal surgery. She is fit and not overweight and exercisesregularly.Shedrinksanormalvolumeoffluids,hasafewcaffeinateddrinksperday.Sheavoidsredwineasitmakesherbladderworse.
Shenotesleakageonexercise,coughingandsneezingandonintercourse.Sheisgettingsomeburningonpassingurineinthelastfewweeks.Shehasanurgetopassurinewhenherbladderisnot very full, and the urge is very strong.She leaks urinewhen this happens.Shepasses urineabouteighttimesadayandonceatnight.
Onexaminationshehasadeficientperineum,amoderatecystoceleandminimalrectocele.Shehaspoorpelvictone.
BAmidstreamurinesample(MSU)shouldbe takenas thesymptomsarequitenew.Urodynamicsarenotthefirstlineoftreatmentbecausetheirrelationtodetruserinstabilityisnotgood.
CThe first-line ofmanagement is supervised pelvic floor exercises. If theMSU shows infectionantibioticsshouldbeprescribed.
EMQ
AUrodynamicassessment.BUrgentflexiblecystoscopy.CRenaltractultrasound.DInsertionofmidurethraltape.EImmediatereleaseoyxbutynin.FTopicaloestrogen.GOralantibiotics.HBotulinumtoxininjection.IDuloxetine.
www.medicalebookpdf.com
For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
1Immediatemanagementofa73-year-oldwomanwithfrequency,urgencyandhaematuria.2 Management of a 38-year-old woman with symptoms of only stress incontinence who hascompletedacourseofpelvicfloorexerciseswithoutimprovement.
3 Should be performed after failed conservative and/or medical management before second-linetreatmentsforincontinence.
4First-linedrugtreatmentforOAB.
ANSWERS
1BBecauseofthehaematuria,cystoscopyisrequiredtoexcludeamalignancy.2D It is reasonable to insert a midurethral tape without further investigations in this situation,
becausetherearenosymptomsofmixedincontinence.3AUrodynamicassessmentwillexcludeapictureofmixedincontinence,whichisnecessarybefore
moreinvasivetreatment.4EImmediatereleaseoxybutyninwilleffectivelytreatoveractivebladdersymptomsandnofurther
investigationsarerequiredbeforetreatment.
SBAQUESTIONS
1A45yearoldwomanattendsoutpatientscomplainingofa3-yearhistoryofstress incontinence,urgencyandurgeincontinence.Sheleaksurineaboutfourtimesaday,hastowearsanitarypadsallthetimeandrarelytravelsduetotheurgencyandneedtopassurine8or9timesduringtheday.ExaminationrevealshertobeofnormalBMI,withaweakpelvicfloormusclestrength.Whatwouldbetherecommendedfirstlineofmanagement?Choosethesinglebestanswer.
ACommencethepatientonanoralanticholinergicmedicationfor8weeks.BArrangeurodynamicassessmenttodefinetheunderlyingcauseofherproblems.CArrangea6–8weekcourseofsupervisedpelvicfloorexercisesandbladderretraining.DAdmitthepatientforacystoscopy.ETesttheurineforinfectionandtreatwithantibiotics.
ANSWER
CPelvicfloorstrengtheningexerciseswillimproveupto50%ofstressincontinenceproblemsandmay avoid the need to treat urge incontinence with anticholinergics. Urodynamics are notnecessarybefore first-line treatment.Althoughaurinary tract infectionmustbeexcludedbeforeinvestigationsortreatment,itisnotafirst-lineinvestigationanddoesnotfitwiththesymptomsorsigns.Nobladderabnormalityisexpectedheretonecessitateacystoscopy.
www.medicalebookpdf.com
2A73-year-oldwomanattendsclinicwithalargeprolapse.Sheunderwentabdominalhysterectomyattheageof42forheavyperiods,andlaterrequiredasecondlaparotomyforalargeleft-sidedovariancyst,whichwascomplicatedbydenseabdominaladhesions.Shehasnoothersignificanthistory.Onexaminationshehasavaginalvaultprolapsethatextendsbeyondtheintroitusandalsohasaverydeficientperineumwithalargevaginalopening.Sheismarriedandwishestobeabletoresumeintercourse.Whatisthebestoptionfortreatmentforthispatient?Choosethesinglebestanswer.
AInsertionofavaginalpessary.BColpocleisis.CAbdominalsacrocolpopexy.DVaginalrepairwithsacrospinousfixation.EAntero-posteriorrepair.
ANSWER
DAbdominalsurgerymustbeavoidedinthiswomanbecauseoftheadhesions.Avaginalpessarywillnothelpher to resume intercourse.Repairof thevaginalwallswillnothelpherdeficientperineumorvaultprolapse.Colpocleisisistheclosureofthevagina,performedinolderwomenwhodonotwishtohaveintercourse,toeffectivelytreatprolapse.
www.medicalebookpdf.com
CHAPTER11Benignconditionsoftheovaryandpelvis
TJUSTINCLARK
Benigndiseasesoftheovary
Endometriosis
Chronicpelvicpain
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Describethetypesofbenignovariancysts,theirsymptoms,diagnosisandtreatment.
•Describethepresentationandmanagementofacutepelvicpain.
•Understand thepathologyof endometriosis and recognize its involvement in chronicpelvicpainandsubfertility.
•Understandhowtodiagnoseandtreatendometriosis.
•Listpotentialcausesforchronicpelvicpain(CPP).
•AppreciatethemultifactorialnatureofCPPandpotentialmanagementoptions.
Benigndiseasesoftheovarywww.medicalebookpdf.com
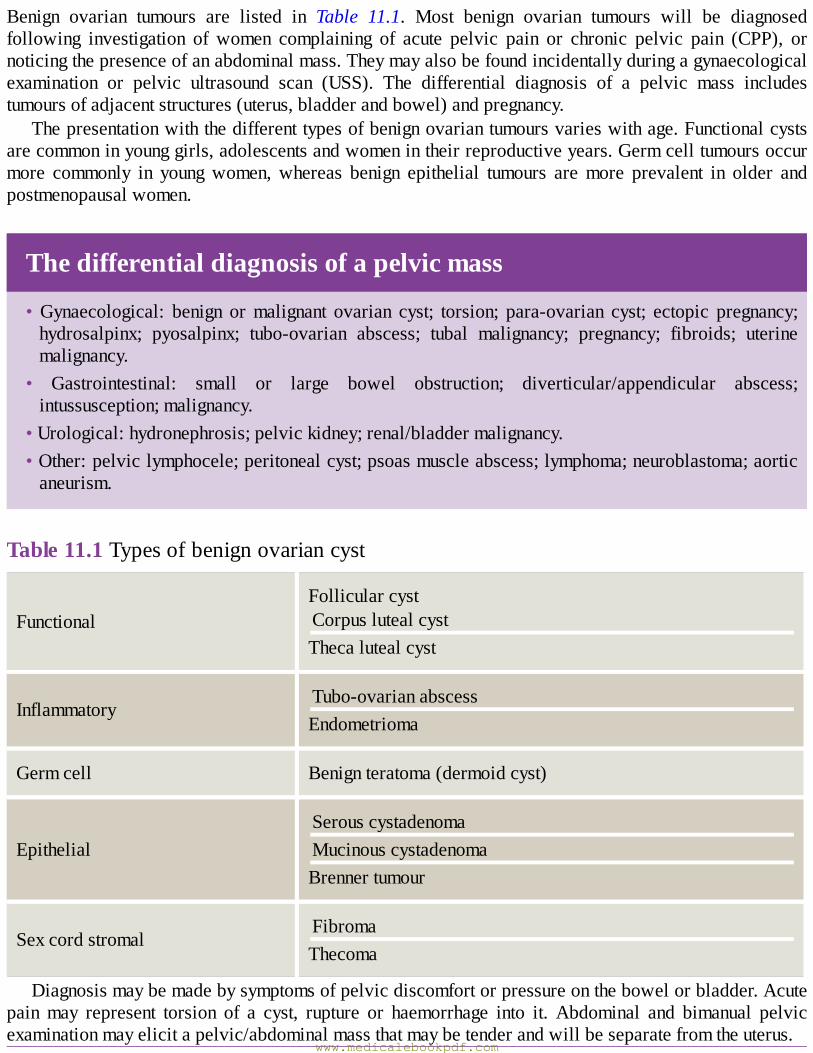
Benign ovarian tumours are listed in Table 11.1. Most benign ovarian tumours will be diagnosedfollowing investigation of women complaining of acute pelvic pain or chronic pelvic pain (CPP), ornoticingthepresenceofanabdominalmass.Theymayalsobefoundincidentallyduringagynaecologicalexamination or pelvic ultrasound scan (USS). The differential diagnosis of a pelvic mass includestumoursofadjacentstructures(uterus,bladderandbowel)andpregnancy.
Thepresentationwiththedifferenttypesofbenignovariantumoursvarieswithage.Functionalcystsarecommoninyounggirls,adolescentsandwomenintheirreproductiveyears.Germcelltumoursoccurmore commonly in youngwomen,whereas benign epithelial tumours aremore prevalent in older andpostmenopausalwomen.
Thedifferentialdiagnosisofapelvicmass
•Gynaecological: benign ormalignant ovarian cyst; torsion; para-ovarian cyst; ectopic pregnancy;hydrosalpinx; pyosalpinx; tubo-ovarian abscess; tubal malignancy; pregnancy; fibroids; uterinemalignancy.
• Gastrointestinal: small or large bowel obstruction; diverticular/appendicular abscess;intussusception;malignancy.
•Urological:hydronephrosis;pelvickidney;renal/bladdermalignancy.•Other:pelviclymphocele;peritonealcyst;psoasmuscleabscess;lymphoma;neuroblastoma;aorticaneurism.
Table11.1Typesofbenignovariancyst
FunctionalFollicularcystCorpuslutealcystThecalutealcyst
InflammatoryTubo-ovarianabscessEndometrioma
Germcell Benignteratoma(dermoidcyst)
EpithelialSerouscystadenomaMucinouscystadenomaBrennertumour
SexcordstromalFibromaThecoma
Diagnosismaybemadebysymptomsofpelvicdiscomfortorpressureonthebowelorbladder.Acutepainmay represent torsion of a cyst, rupture or haemorrhage into it. Abdominal and bimanual pelvicexaminationmayelicitapelvic/abdominalmassthatmaybetenderandwillbeseparatefromtheuterus.
www.medicalebookpdf.com
Ovariantorsion
•Torsionofanovaryreferstoasituationwherethereisrotationofthevascularpediclesupplyingtheovary,whichcompressesandcutsitsbloodsupply.Torsionismorelikelywithenlargementoftheovaryasisseeninthepresenceofanovariancyst.Upto15%ofdermoidcystspresentacutelywithtorsion.
•Presentingsymptomsareusuallyacuteonsetof lowerabdominalpainassociatedwithnauseaandvomiting.PelvicUSSwithDopplermeasurementofbloodflowmaybeusefulinthediagnosis,toconfirmthepresenceofacystandcommentonbloodflowtotheovary.Torsionofanormalovaryisveryunlikely.
•Emergency surgical treatment to untwist the ovary and its attached pedicle is required to restoreblood flow, and the ovarian cyst should then be removed. However, if this complication is notrecognized within a few hours of presentation, infarction and gangrene may result, necessitatingremovalofthenecroticovary.Decisionmakingtooperateshouldbebasedonclinicalfindings,withtransvaginalultrasoundscan(TVUSS)support.
The first-line investigation for womenwith a suspected pelvic mass or pelvic pain is an USS. ATVUSShasbetterresolutionforpelvicmasses.Atransabdominalultrasoundscan(TAUSS)isindicatedinwomenwhohaveneverbeensexuallyactive,orincombinationswithaTVUSSwherelargeovarianmassesextendingbeyondthepelvisandintotheabdomenarepresent.Additionalimagingwithcomputedtomography (CT) scanningormagnetic resonance imaging (MRI) can further characterize thenatureofovariancysts,especiallywheretheyarethoughttobepotentiallymalignant.Serologicaltumourmarkersshouldalsobe taken tohelpdetermine the typeofovariancystanddifferentiatebetweenabenignandmalignantneoplasm(Table11.2andChapter14,Malignantdiseaseoftheovary).Apregnancytestshouldbeperformedtoexcludepregnancy.Inflammatorymarkers,suchasC-reactiveprotein(CRP)andwhitecell count (WCC), are important if the differential diagnosis includes appendicitis or a tubo-ovarianabscess.
Table11.2Tumourmarkersusedintheinvestigationandfollow-upofovariancysts
www.medicalebookpdf.com
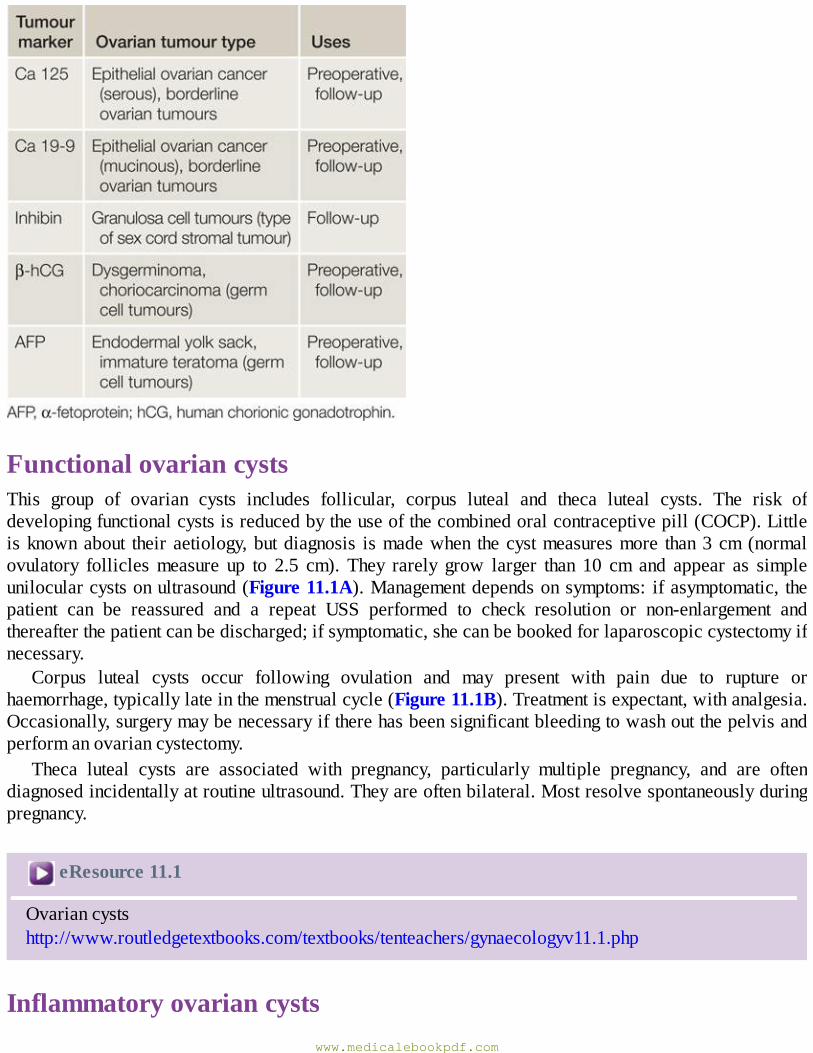
FunctionalovariancystsThis group of ovarian cysts includes follicular, corpus luteal and theca luteal cysts. The risk ofdevelopingfunctionalcystsisreducedbytheuseofthecombinedoralcontraceptivepill(COCP).Littleisknownabout their aetiology,butdiagnosis ismadewhen thecystmeasuresmore than3cm(normalovulatory folliclesmeasure up to 2.5 cm). They rarely grow larger than 10 cm and appear as simpleunilocularcystsonultrasound(Figure11.1A).Managementdependsonsymptoms: ifasymptomatic, thepatient can be reassured and a repeat USS performed to check resolution or non-enlargement andthereafterthepatientcanbedischarged;ifsymptomatic,shecanbebookedforlaparoscopiccystectomyifnecessary.
Corpus luteal cysts occur following ovulation and may present with pain due to rupture orhaemorrhage,typicallylateinthemenstrualcycle(Figure11.1B).Treatmentisexpectant,withanalgesia.Occasionally,surgerymaybenecessaryiftherehasbeensignificantbleedingtowashoutthepelvisandperformanovariancystectomy.
Theca luteal cysts are associated with pregnancy, particularly multiple pregnancy, and are oftendiagnosedincidentallyatroutineultrasound.Theyareoftenbilateral.Mostresolvespontaneouslyduringpregnancy.
eResource11.1
Ovariancystshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv11.1.php
Inflammatoryovariancystswww.medicalebookpdf.com
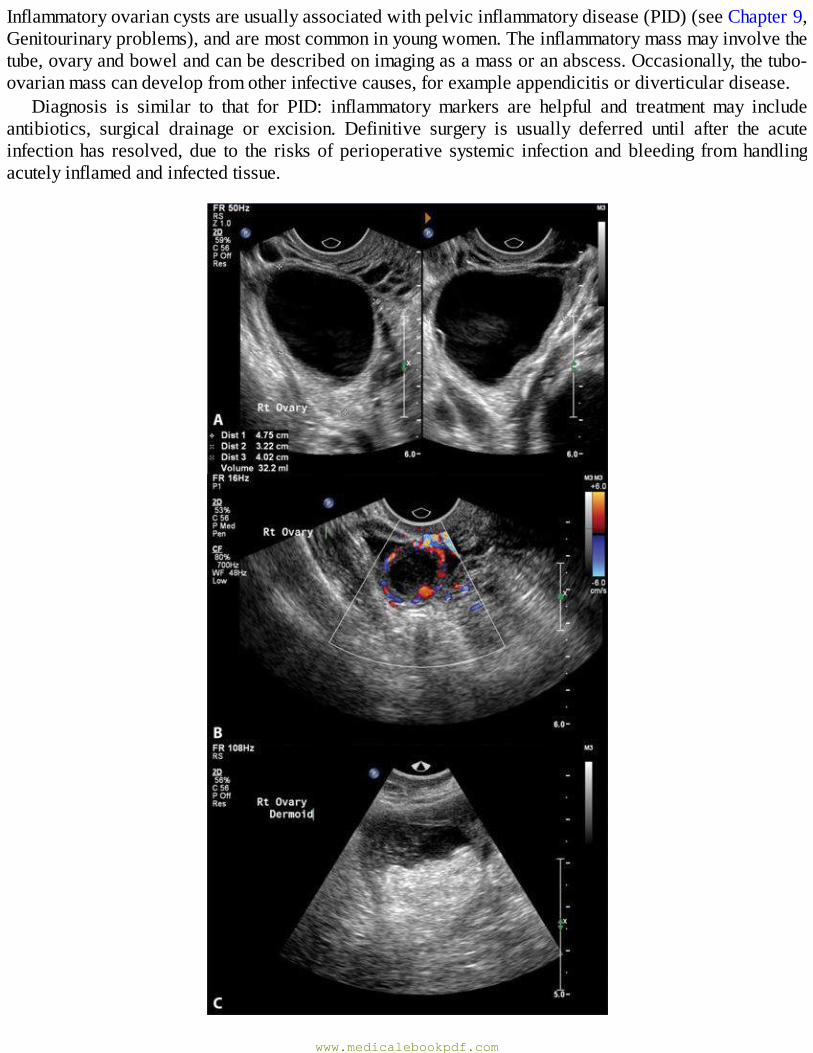
Inflammatoryovariancystsareusuallyassociatedwithpelvicinflammatorydisease(PID)(seeChapter9,Genitourinaryproblems),andaremostcommoninyoungwomen.Theinflammatorymassmayinvolvethetube,ovaryandbowelandcanbedescribedonimagingasamassoranabscess.Occasionally,thetubo-ovarianmasscandevelopfromotherinfectivecauses,forexampleappendicitisordiverticulardisease.
Diagnosis is similar to that for PID: inflammatory markers are helpful and treatment may includeantibiotics, surgical drainage or excision. Definitive surgery is usually deferred until after the acuteinfectionhas resolved,due to the risksofperioperative systemic infectionandbleeding fromhandlingacutelyinflamedandinfectedtissue.
www.medicalebookpdf.com
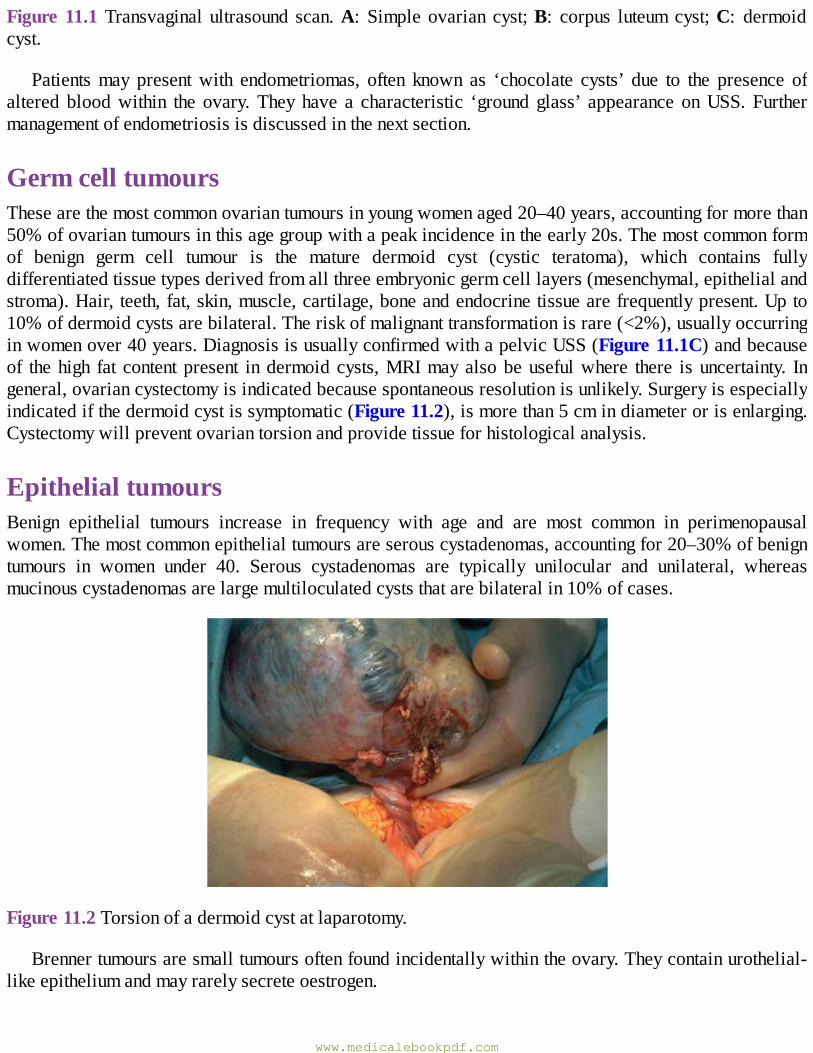
Figure11.1Transvaginal ultrasound scan.A: Simpleovarian cyst;B: corpus luteumcyst;C: dermoidcyst.
Patientsmay presentwith endometriomas, often known as ‘chocolate cysts’ due to the presence ofaltered bloodwithin the ovary.They have a characteristic ‘ground glass’ appearance onUSS. Furthermanagementofendometriosisisdiscussedinthenextsection.
GermcelltumoursThesearethemostcommonovariantumoursinyoungwomenaged20–40years,accountingformorethan50%ofovariantumoursinthisagegroupwithapeakincidenceintheearly20s.Themostcommonformof benign germ cell tumour is the mature dermoid cyst (cystic teratoma), which contains fullydifferentiatedtissuetypesderivedfromallthreeembryonicgermcelllayers(mesenchymal,epithelialandstroma).Hair, teeth,fat,skin,muscle,cartilage,boneandendocrinetissuearefrequentlypresent.Upto10%ofdermoidcystsarebilateral.Theriskofmalignanttransformationisrare(<2%),usuallyoccurringinwomenover40years.DiagnosisisusuallyconfirmedwithapelvicUSS(Figure11.1C)andbecauseof thehigh fat contentpresent indermoidcysts,MRImayalsobeusefulwhere there isuncertainty. Ingeneral,ovariancystectomyisindicatedbecausespontaneousresolutionisunlikely.Surgeryisespeciallyindicatedifthedermoidcystissymptomatic(Figure11.2),ismorethan5cmindiameterorisenlarging.Cystectomywillpreventovariantorsionandprovidetissueforhistologicalanalysis.
EpithelialtumoursBenign epithelial tumours increase in frequency with age and are most common in perimenopausalwomen.Themostcommonepithelialtumoursareserouscystadenomas,accountingfor20–30%ofbenigntumours in women under 40. Serous cystadenomas are typically unilocular and unilateral, whereasmucinouscystadenomasarelargemultiloculatedcyststhatarebilateralin10%ofcases.
Figure11.2Torsionofadermoidcystatlaparotomy.
Brennertumoursaresmalltumoursoftenfoundincidentallywithintheovary.Theycontainurothelial-likeepitheliumandmayrarelysecreteoestrogen.
www.medicalebookpdf.com
SexcordstromaltumoursOvarian fibromas are the most common sex cord stromal tumours. They are solid ovarian tumourscomposedofstromalcells.Theypresentinolderwomen,oftenwithtorsionduetotheheavinessoftheovary. Occasionally, patients may present withMeig syndrome (pleural effusion, ascites and ovarianfibroma).Followingremovaloftheovarianfibroma,thepleuraleffusionwillusuallyresolve.
Thecomas are benign oestrogen-secreting tumours. They often present after the menopause withmanifestationsof excessoestrogenproduction,usuallypostmenopausalbleeding.Althoughbenign, theymayinduceanendometrialcarcinoma.
OtherovariancystsOthernon-ovariancystscanoccasionallypresentasovariantumours.FimbrialcystsandparatubalcystsoriginatefromtheadjacentFallopiantubeandbroadligament.TheuncommonembryologicallyderivedparaovariancystsofMorganiarelargecollectionsofgrape-likecystsderivedfromtheparaoopheron.
EndometriosisEndometriosisisacommonconditionthatisdefinedasendometrialtissuelyingoutsidetheuterinecavity.It is usually foundwithin the pelvis, being commonly located on the peritoneum lining the pelvic sidewalls, pouchofDouglas, uterosacral ligaments andbladder.This ‘ectopic’ endometrial-like tissue caninducefibrosisandbefoundinfiltratingintodeepertissuesuchastherectovaginalseptumandbladder.Whenendometrialtissueisimplantedintotheovaryanendometriomaforms.Thiscystmaybelargeandcontainsold,alteredbloodthathasathickbrownappearance,andforthisreasonisfrequentlyreferredtoas a ‘chocolate cyst’. Less commonly, endometriotic deposits can be found in other sites such asumbilicus,abdominalscarsandthepleuralcavity.
Endometriotictissuerespondstocyclicalhormonalchangesandthereforeundergoescyclicalbleedingand local inflammatory reactions. These regularly repeated episodes of bleeding and healing lead tofibrosisandadhesion formationbetweenpelvicorgans,causingpainand infertility. Inextremecasesa‘frozenpelvis’results,whereextensiveadhesionstether thepelvicorgansandobliteratenormalpelvicanatomy.
Adenomyosisisauterineconditionoftenseenwithendometriosis,whereislandsofendometrialtissuearefounddeepwithintheunderlyingmyometrium(seeChapter12,Benignconditionsoftheuterus,cervixandendometrium).
IncidenceEndometriosisoccursinapproximately5–10%ofwomenofreproductiveage.Itisfoundinatleastone-thirdofwomenundergoingadiagnosticlaparoscopyforpelvicpainorinfertility.Itisaconditionthatisoestrogendependentandthereforeitresolvesafterthemenopauseorwhentreatmentisdirectedtowardsinducingapseudomenopause.
Aetiology
www.medicalebookpdf.com
Theaetiologyofendometriosisisunknownalthoughthereareseveraltheories.Thereisunlikelytobeasingletheorythatexplainsitsaetiology,butthetwomostcommonlyacceptedtheoriesare:
•Sampson’simplantationtheory:menstrualbloodcanbeseenwithinthepelvisduringlaparoscopyatthetime of menses. Sampson’s implantation theory postulates that it is this retrograde menstrualregurgitationofviableendometrialglandsandtissuealongpatentFallopiantubes,andthatsubsequentimplantation on the pelvic peritoneal surface causes endometriosis. Using animal/primate modelsendometriosis has been induced with menstrual blood. Implantation of endometrium within humansurgicalscarsaftercaesareansectionorperinealrepairfollowingdeliverylendssupporttothistheory.
• Meyer’s ‘coelomic metaplasia’ theory: coelomic epithelium transformation describes thededifferentiationofperitonealcellsliningtheMüllerianductbacktotheirprimitiveorigin,whichthentransform into endometrial cells. This transformation into endometrial cellsmay be due to hormonalstimuliorinflammatoryirritation.
GeneticandimmunologicalfactorsIthasbeensuggestedthatgeneticandimmunologicalfactorsmayalterthesusceptibilityofawomanandallowhertodevelopendometriosis.Thereappearstobeanincreasedincidenceinfirst-degreerelativesofpatientswiththedisorderandracialdifferences,withincreasedincidenceamongorientalwomenandalowprevalenceinwomenofAfro-Caribbeanorigin.
VascularandlymphaticspreadVascularandlymphaticembolizationtodistantsiteshasbeendemonstratedandexplainstherarefindingsofendometriosisinsitesoutsidetheperitonealcavity,suchasthelung.
ClinicalfeaturesClassical clinical features are severe cyclical non-colickypelvic pain restricted to around the timeofmenstruation,sometimesassociatedwithheavymenstrual loss.Symptomsmaybeginafewdaysbeforemenses starts until the end of menses. However, women often also complain of chronic non-cyclicalpelvicpainandseverefatigue.Itiswellrecognizedthatthereisalackofcorrelationbetweentheextentofthediseaseandtheintensityofsymptoms.
Pelvic pain presenting with colicky pain throughout the menstrual cycle may be associated withirritablebowelsyndromesymptoms.Deeppainwithintercourse(deepdyspareunia)andondefaecation(dyschezia)arekeyindicatorsofthepresenceofendometriosisdeepwithinthepouchofDouglas.
Endometriosis in distant sites can cause local symptoms, for example cyclical epistaxiswith nasalpassagedepositsandcyclicalrectalbleedingwithboweldeposits(Table11.3).
DiagnosisPhysicalexaminationTheaccuracyofclinicalexaminationindiagnosingendometriosisislimitedandsotheconditionshouldbe suspected even if the vaginal examination is normal. Positive examination findings indicative ofendometriosis include thickening or nodularity of the uterosacral ligaments, tenderness in the pouch of
www.medicalebookpdf.com
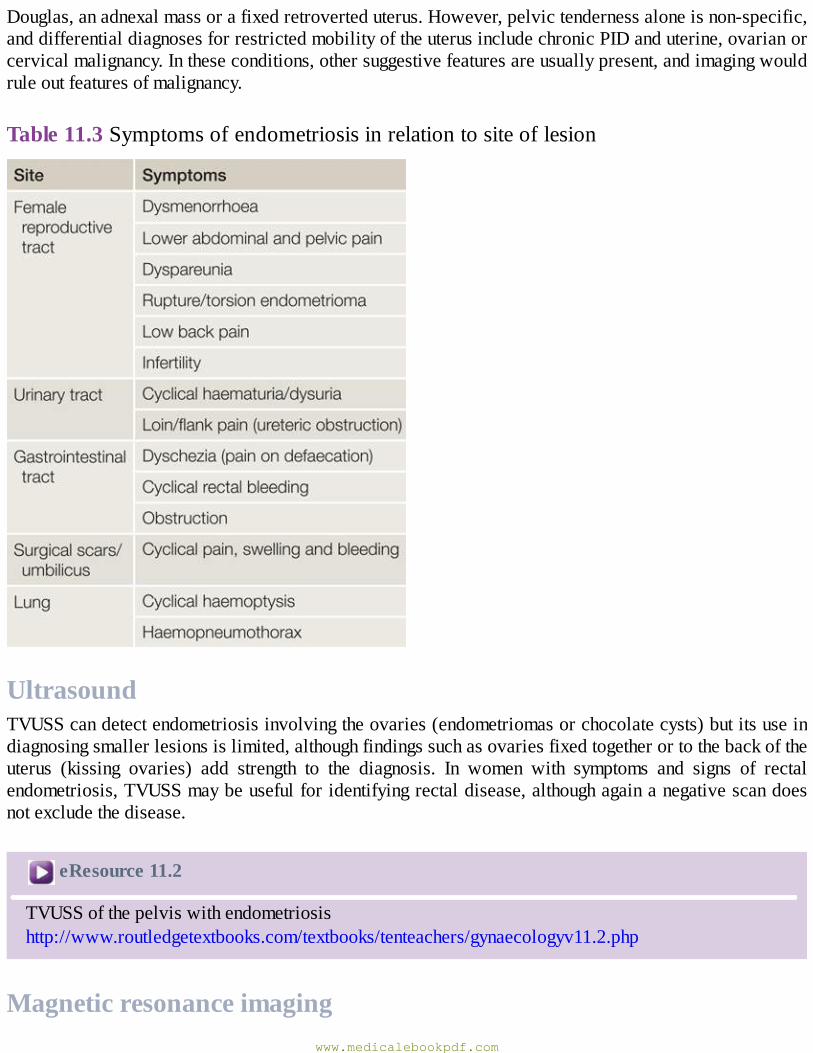
Douglas,anadnexalmassorafixedretroverteduterus.However,pelvictendernessaloneisnon-specific,anddifferentialdiagnosesforrestrictedmobilityoftheuterusincludechronicPIDanduterine,ovarianorcervicalmalignancy.Intheseconditions,othersuggestivefeaturesareusuallypresent,andimagingwouldruleoutfeaturesofmalignancy.
Table11.3Symptomsofendometriosisinrelationtositeoflesion
UltrasoundTVUSScandetectendometriosisinvolvingtheovaries(endometriomasorchocolatecysts)butitsuseindiagnosingsmallerlesionsislimited,althoughfindingssuchasovariesfixedtogetherortothebackoftheuterus (kissing ovaries) add strength to the diagnosis. In women with symptoms and signs of rectalendometriosis,TVUSSmaybeusefulforidentifyingrectaldisease,althoughagainanegativescandoesnotexcludethedisease.
eResource11.2
TVUSSofthepelviswithendometriosishttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv11.2.php
Magneticresonanceimagingwww.medicalebookpdf.com

MRIcandetectlesions>5mminsize,particularlyindeeptissues,forexampletherectovaginalseptum.Thiscanallowcarefulpresurgicalplanningindifficultcases.
LaparoscopyAlthough laparoscopy remains the traditionalmethod for diagnosis, it is based on the accuracy of thevisual diagnosis of endometriotic lesions, which is dependent on the experience of the surgeon. Theendometrioticlesionscanbered,puckered,black‘matchstick’orappearwhiteandfibrous(Figure11.3).The advantage of laparoscopy is that it allows lesions to be biopsied for histological confirmation ofdiagnosisand it affordsconcurrent surgicaldiathermyand/orexcisionof theendometriotic lesionsandalsostagingofthedisease.ThepatencyoftheFallopiantubescanalsobechecked.
www.medicalebookpdf.com
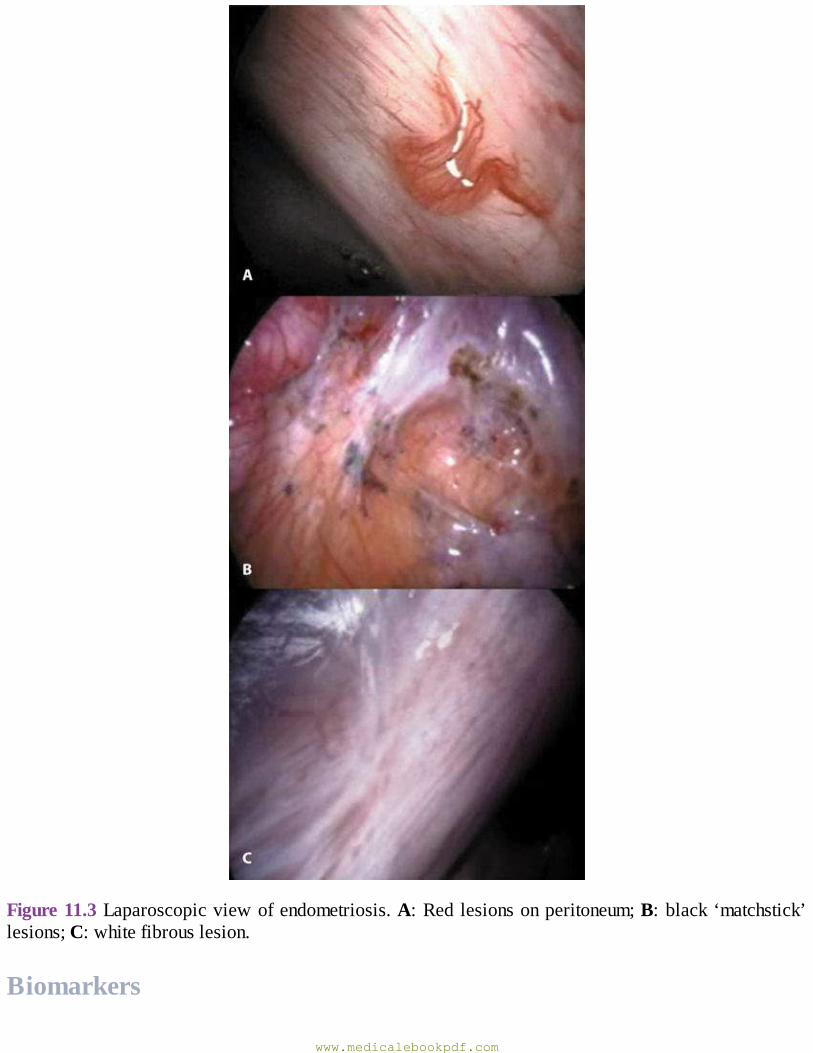
Figure11.3Laparoscopicviewofendometriosis.A:Redlesionsonperitoneum;B:black‘matchstick’lesions;C:whitefibrouslesion.
Biomarkers
www.medicalebookpdf.com
Therehasbeenrecentinterestinthediagnosisofendometriosisusingimmunologicalbiomarkers,suchasCA125, inplasma,urineor serum.However, todate thesenon-invasivediagnosticapproachesare tooinaccurateforuseinclinicalpractice.
EndometriosisandinfertilityIt is estimated that between 30% and 40% of patients with endometriosis complain of difficulty inconceiving. Inmany patients, there is amultifactorial pathogenesis to this subfertility (see Chapter 7,Subfertility).Itisuncertainifandwhyminimalendometrioticdepositsmightrenderapatientsubfertile.However, in the more severe stages of endometriosis, there is commonly anatomical distortion, withperiadnexal adhesions and destruction of ovarian tissue when endometriomas develop. A number ofpossible and variablemechanisms have been postulated to connectmild endometriosiswith infertility(Table11.4).
Fromthebalanceofavailableevidence,medicaltreatmentofendometriosisdoesnotimprovefertilityandshouldnotbegiventopatientswishingtoconceive.However,surgicalablation/excisionofminimaland mild endometriosis does improve fertility chances. It is uncertain whether surgical treatment ofendometriomasincreasespontaneousorin-vitrofertilization(IVF)pregnancyrates,astheremovaloftheendometriomas must be balanced against damage to ovarian tissue. The consensus from fertilityspecialistsatpresentistoleaveendometriomasalonepriortoIVFunlesstheyaresymptomaticorreduceaccessforeggcollection.
ManagementAnalgesics and hormonal ovarian suppression can be effective for treating cyclical and non-cyclicalpelvicpainassociatedwithendometriosis.Medicaltreatmentofpresumedendometriosiscanbestartedifthe clinical examination and TVUSS are normal, without the need for more invasive laparoscopy.However, if no symptom relief is obtained after 3–6 months of treatment, a laparoscopy should beconsidered.Patientswithendometriosisareoftendifficulttotreat,notonlyfromaphysicalpointofview,but also often because of associated psychological issues associated with their pain. Long-termtherapeutic strategies should be formulated where possible. Coexisting additional diseases such asirritable bowel syndrome and constipation (present in up to 80% of cases) should also be treated toimprove overall success rates. Endometriosis is known to recur throughout reproductive life and it isimpossible to guarantee complete cure. Treatment should therefore be tailored for the individualaccording to her age, symptoms, extent of the disease and her desire to have children. In a significantproportionofpatientsthereislittleprogressionofthediseaseovertime,andthismaybereassuring.Dueto the variation in presentation it has been shown that there is a significant delay to diagnosis, withresearch indicating around 6 years on average, and some patients will be relieved by a positivelaparoscopythatvalidatestheirsymptoms.
Table11.4Infertilityandendometriosis–possiblemechanisms
www.medicalebookpdf.com
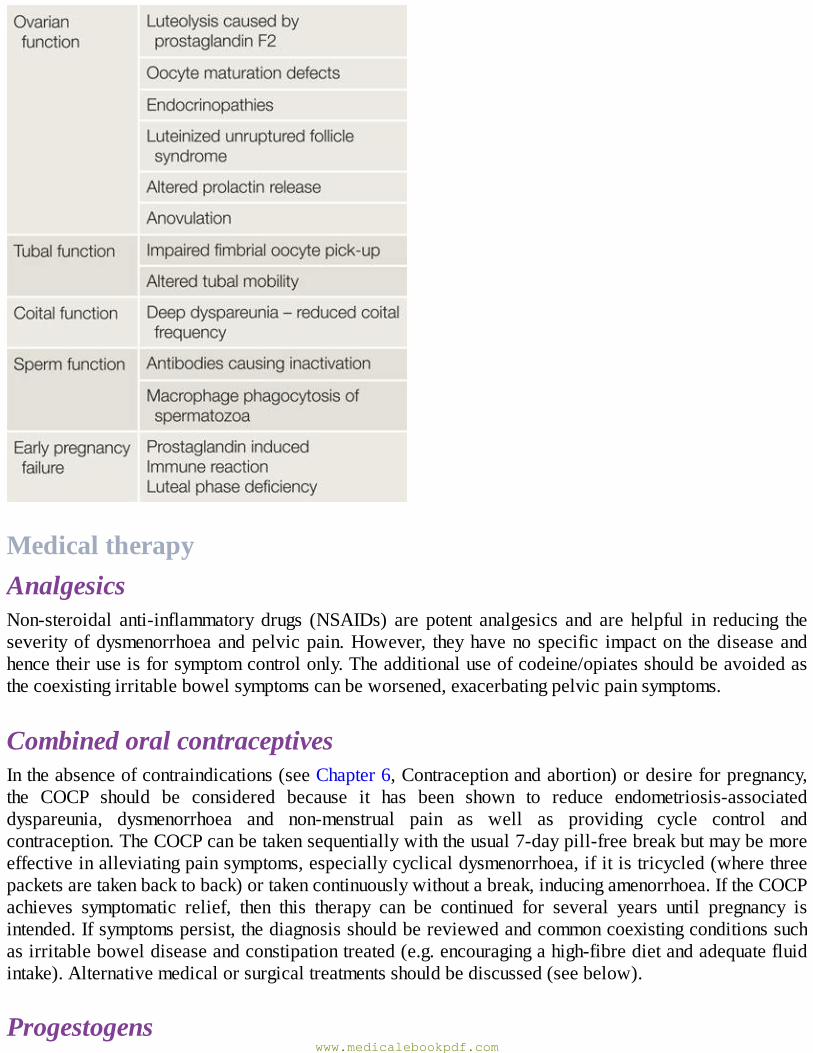
MedicaltherapyAnalgesicsNon-steroidal anti-inflammatory drugs (NSAIDs) are potent analgesics and are helpful in reducing theseverityofdysmenorrhoeaandpelvicpain.However, theyhaveno specific impacton thediseaseandhencetheiruseisforsymptomcontrolonly.Theadditionaluseofcodeine/opiatesshouldbeavoidedasthecoexistingirritablebowelsymptomscanbeworsened,exacerbatingpelvicpainsymptoms.
CombinedoralcontraceptivesIntheabsenceofcontraindications(seeChapter6,Contraceptionandabortion)ordesireforpregnancy,the COCP should be considered because it has been shown to reduce endometriosis-associateddyspareunia, dysmenorrhoea and non-menstrual pain as well as providing cycle control andcontraception.TheCOCPcanbetakensequentiallywiththeusual7-daypill-freebreakbutmaybemoreeffectiveinalleviatingpainsymptoms,especiallycyclicaldysmenorrhoea,ifitistricycled(wherethreepacketsaretakenbacktoback)ortakencontinuouslywithoutabreak,inducingamenorrhoea.IftheCOCPachieves symptomatic relief, then this therapy can be continued for several years until pregnancy isintended.Ifsymptomspersist,thediagnosisshouldbereviewedandcommoncoexistingconditionssuchasirritableboweldiseaseandconstipationtreated(e.g.encouragingahigh-fibredietandadequatefluidintake).Alternativemedicalorsurgicaltreatmentsshouldbediscussed(seebelow).
Progestogenswww.medicalebookpdf.com
In those where there are risk factors for the use of a COCP, progestogens should be used to induceamenorrhoea. The long-acting reversible contraceptives (LARCs), depot-medroxyprogesterone acetateand the levonorgestrel intrauterine system(LNG-IUS) (Mirena®)areparticularlyuseful inprovidingalong-termtherapeuticeffectparticularlyaftersurgicaltreatment.Theeffectisprobablyrelatedto100%compliancewithtreatment.
Gonadotrophin-releasinghormoneagonistsGonadotrophin-releasinghormoneagonists(GnRH-a)areeffectiveinrelievingtheseverityandsymptomsofendometriosis.GnRHhasbeendiscussedinChapter4,Disordersofmenstrualbleeding.Despitetheirside-effects, the drugs are well tolerated by some and they have become established agents in thediagnosis(ifCPPisofagynaecologicalorigin[e.g.endometriosis],thensymptomswillbeeradicated)andtreatmentofendometriosis.Theyareavailableasmultiple,daily-administeredintranasalspraysbutareusuallyadministeredasslow-releasedepotformulations,eachlastingfor1monthormore.Long-termuseover6monthsisprecludedbecausedrug-inducedosteoporosisresultsTherecurrenceofsymptomsoncessationoftherapyisusuallyrapid.
OtherhormonalagentsIn thepast, theovariansuppressiveagentsdanazolandgestrinonewereused togoodeffect,butarenolongerappropriateasnewertreatmenthavebecomeavailable,notablyLNG-IUS.Theyhadanumberofandrogenicside-effects,suchasweightgain,greasyskinandacneaswellascausingalterationsinlipidprofilesandliverfunctionandpotentialdeepeningofthevoice.
There has been some interest in a newer class of drug called aromatase inhibitors that inhibit theaction of the enzyme aromatase, which converts androgens into oestrogens and is over expressed inendometriotictissue.Furtherresearchisongoingfortheiruseinrefractorycases.
SurgicaltreatmentFertility-sparingsurgeryMostsurgeryforendometriosiscanbeachievedlaparoscopically.Symptomaticendometrioticchocolatecysts should not just be drained but the inner cyst lining should be excised to reduce the risk ofrecurrence;however, thiswillbeassociatedwithdamagetofunctionalovariantissue.Therefore,whendrainageisperformedasanadjuncttofertilitytreatment,drainageonlymaybeconsidered.Depositsofsuperficialperitonealendometriosiscanbeeasilyablatedorexcisedduringlaparoscopyusingdiathermyorlaserenergy.
Specialistsurgeryisneededtotreatendometriosiswherethediseasehascausedextensiveadhesionsdistortingnormalpelvicanatomyorinvolvedotherorganssuchastherectum,largebowelorbladder,orwhen there are rectovaginal nodules of disease.Recurrent risks following conservative surgery are ashighas30%and thereforeconcurrent long-termmedical therapy isoftennecessaryandstarted straightaftersurgery.
HysterectomyandoophorectomyHysterectomywith removal of the ovaries and all visible endometriosis lesions should be consideredonlyinwomenwhohavecompletedtheirfamilyandfailedtorespondtomoreconservativetreatments.
www.medicalebookpdf.com
Women should be informed that hysterectomy will not necessarily cure the symptoms or the disease.Oestrogen-onlyhormonereplacementtherapy(HRT)canbestartedimmediatelyfollowingsurgeryoncethepatientismobile,butsomesurgeonsprefertodefercommencingHRTforupto6monthstopreventactivationofanyresidualdisease.Combined(oestrogenandprogestogen)HRTcanalsobeconsideredasasuppressivetreatment,wherereactivationofneworresidualdiseaseissuspected.
ChronicpelvicpainCPPisadebilitatingsymptomamongwomen,whichhasamajorimpactonhealth-relatedqualityoflife,work productivity and health care utilization. The Royal College ofObstetricians andGynaecologists(RCOG)hasdefinedCPPas‘intermittentorconstantpaininthelowerabdomenorpelvisofawomanofatleast6monthsinduration,notoccurringexclusivelywithmenstruation(dysmenorrhoea)orintercourseandnotassociatedwithpregnancy’.
IncidenceCPPpresentsinprimarycareasfrequentlyasmigraine,asthmaorlowbackpainandaccountsfor20%ofalloutpatient appointments ingynaecological secondarycare.Estimatesofprevalencevarywidelybutarethoughttobebetween10%and20%.
AetiologyThepotentialcausesofCPPinwomenarelistedinTable11.5.Incontrasttoacutepelvicpain,thereisoftenmorethanoneunderlyingcausecontributingtoCPP.Theexperienceofpainisaffectedbyphysical,psychologicalandsocialfactors.
Table11.5Causesofchronicpelvicpaininwomen
www.medicalebookpdf.com
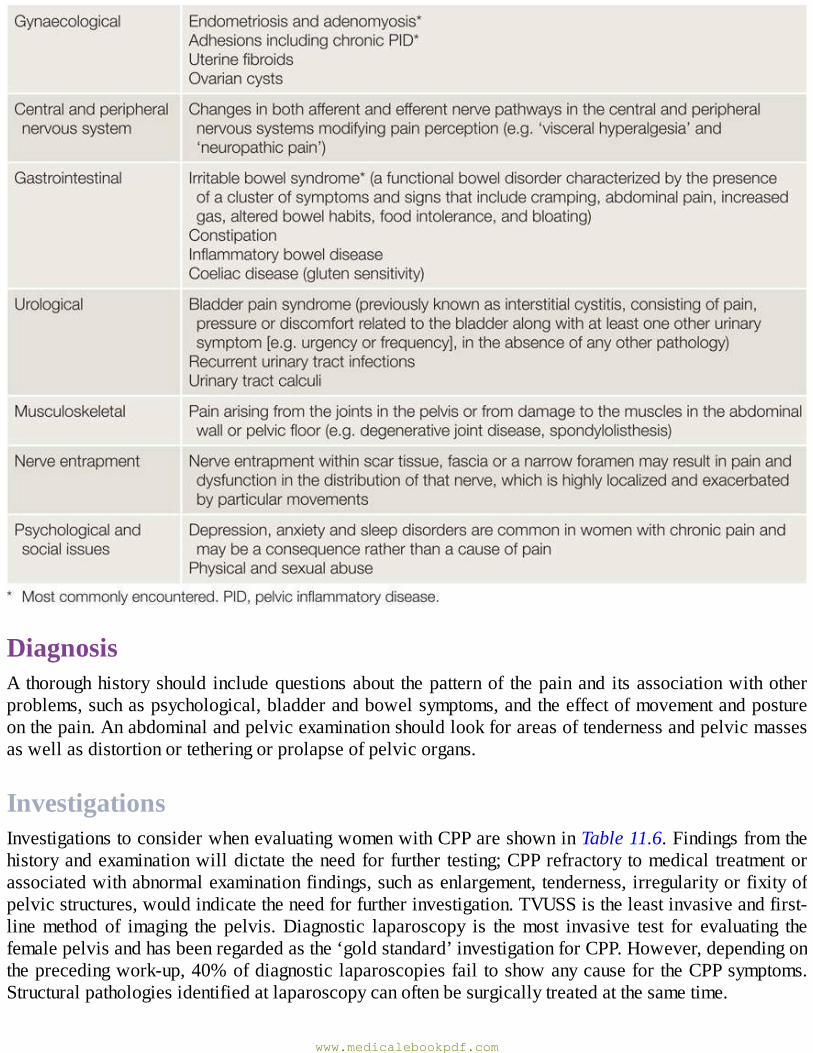
DiagnosisAthoroughhistoryshould includequestionsabout thepatternof thepainand itsassociationwithotherproblems,suchaspsychological,bladderandbowelsymptoms,andtheeffectofmovementandpostureonthepain.Anabdominalandpelvicexaminationshouldlookforareasoftendernessandpelvicmassesaswellasdistortionortetheringorprolapseofpelvicorgans.
InvestigationsInvestigationstoconsiderwhenevaluatingwomenwithCPPareshowninTable11.6.Findingsfromthehistoryandexaminationwilldictate theneedforfurther testing;CPPrefractorytomedical treatmentorassociatedwithabnormalexaminationfindings,suchasenlargement,tenderness,irregularityorfixityofpelvicstructures,wouldindicatetheneedforfurtherinvestigation.TVUSSistheleastinvasiveandfirst-linemethod of imaging the pelvis.Diagnostic laparoscopy is themost invasive test for evaluating thefemalepelvisandhasbeenregardedasthe‘goldstandard’investigationforCPP.However,dependingontheprecedingwork-up,40%ofdiagnosticlaparoscopiesfail toshowanycausefortheCPPsymptoms.Structuralpathologiesidentifiedatlaparoscopycanoftenbesurgicallytreatedatthesametime.
www.medicalebookpdf.com
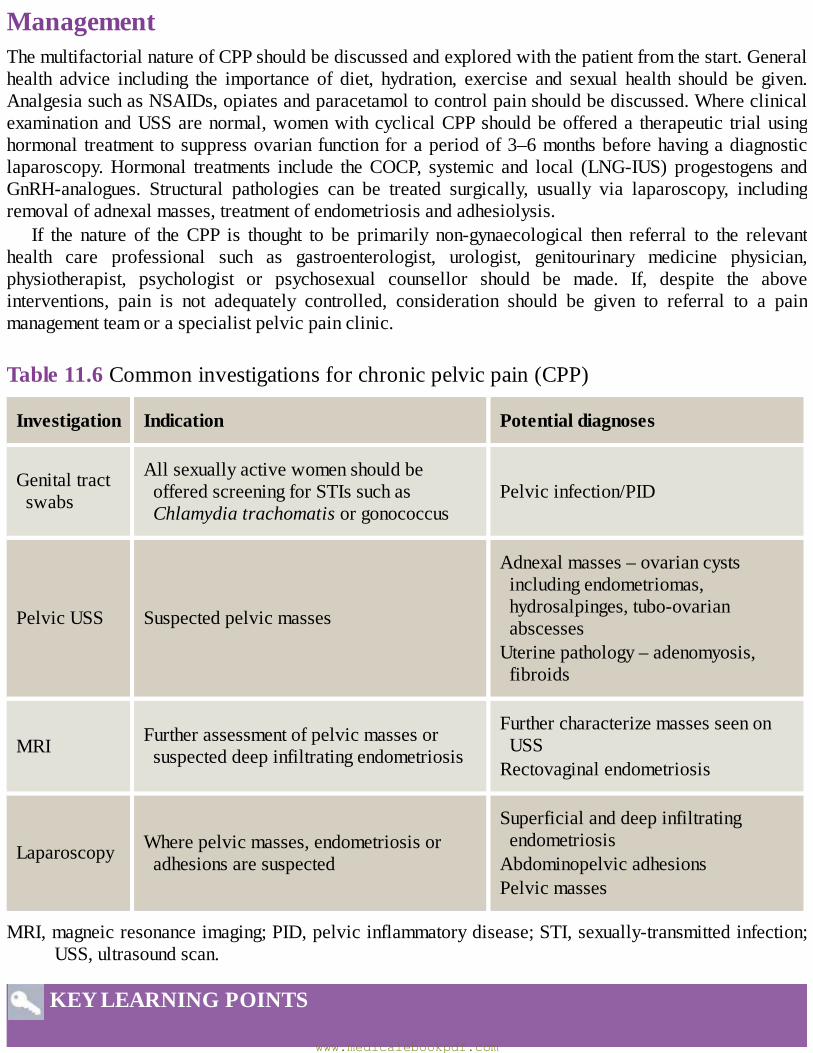
ManagementThemultifactorialnatureofCPPshouldbediscussedandexploredwiththepatientfromthestart.Generalhealth advice including the importance of diet, hydration, exercise and sexual health should be given.AnalgesiasuchasNSAIDs,opiatesandparacetamoltocontrolpainshouldbediscussed.WhereclinicalexaminationandUSSarenormal,womenwithcyclicalCPPshouldbeoffereda therapeutic trialusinghormonal treatment tosuppressovarianfunctionforaperiodof3–6monthsbeforehavingadiagnosticlaparoscopy.Hormonal treatments include theCOCP, systemic and local (LNG-IUS) progestogens andGnRH-analogues. Structural pathologies can be treated surgically, usually via laparoscopy, includingremovalofadnexalmasses,treatmentofendometriosisandadhesiolysis.
If the nature of theCPP is thought to be primarily non-gynaecological then referral to the relevanthealth care professional such as gastroenterologist, urologist, genitourinary medicine physician,physiotherapist, psychologist or psychosexual counsellor should be made. If, despite the aboveinterventions, pain is not adequately controlled, consideration should be given to referral to a painmanagementteamoraspecialistpelvicpainclinic.
Table11.6Commoninvestigationsforchronicpelvicpain(CPP)
Investigation Indication Potentialdiagnoses
Genitaltractswabs
AllsexuallyactivewomenshouldbeofferedscreeningforSTIssuchasChlamydiatrachomatisorgonococcus
Pelvicinfection/PID
PelvicUSS Suspectedpelvicmasses
Adnexalmasses–ovariancystsincludingendometriomas,hydrosalpinges,tubo-ovarianabscessesUterinepathology–adenomyosis,fibroids
MRI Furtherassessmentofpelvicmassesorsuspecteddeepinfiltratingendometriosis
FurthercharacterizemassesseenonUSSRectovaginalendometriosis
Laparoscopy Wherepelvicmasses,endometriosisoradhesionsaresuspected
SuperficialanddeepinfiltratingendometriosisAbdominopelvicadhesionsPelvicmasses
MRI,magneicresonanceimaging;PID,pelvicinflammatorydisease;STI,sexually-transmittedinfection;USS,ultrasoundscan.
KEYLEARNINGPOINTS
www.medicalebookpdf.com

•Commonlyencounteredbenignovariantumoursincludefunctionalcysts,teratomas(dermoidcysts)andendometriomas.
•Ovariancystscanbeasymptomaticorpresentwithpainorasanabdominalmass.Acutepainmayarisebecauseofanovariancyst‘accident’suchashaemorrhage,ruptureortorsion.
•TVUSSistheprimarytestusedtodiagnosedifferenttypesofovariancyst.AlongwiththeCA125serological tumour marker, ultrasound can be used to help differentiate between benign andmalignantovariantumours.
• Treatment is based on the symptoms, size and type of cyst. Ovarian cystectomy or evenoophorectomymayberequiredandthisisusuallyundertakenusingalaparoscopicapproach.
•Endometriosisrefers to thefindingofendometrialglandsandstromaoutsideof theuterusandisoneofthecommonestconditionsseeningynaecology,affecting5–10%ofwomenofreproductiveage.
• Endometriosis usually presents with cyclical non-colicky pelvic pain around the time ofmenstruation,and issometimesassociatedwithheavymenstrual loss.However,affectedwomenmayalsocomplainofchronicnon-cyclicalpelvicpain,dyspareunia,dyscheziaandseverefatigue.
•Endometriosisisassociatedwithtubalandovariandamageandtheformationofadhesionsandcancompromisefertility.
•MedicaltreatmentofendometriosisinvolvessuppressingoestrogenlevelstoinduceamenorrhoeausingtheCOCP,progestogensorGnRHagonists.
• Conservative laparoscopic surgical treatment of endometriosis involves excising or ablatingvisible lesions. More radical excisional laparoscopic surgery may be required for deeplyinfiltrating endometriosis involving the bowel and rectovaginal septum. Total hysterectomy andbilateralsalpingo-oophorectomyisoftenundertakenforrefractorysymptoms.
• CPP is usuallymultifactorial involving physical, psychological and social factors.Managementshould be directed at the underlying causes and include general health advice, analgesics,hormonal therapies and surgery. Multidisciplinary pelvic pain clinics are necessary to managesevere,refractorycases.
FurtherreadingDunselmanGA,VermeulenN,BeckerC,etal.(2014).ESHREguideline:managementofwomenwithendometriosis.HumReprod29(3):400–12.doi:10.1093/humrep/det457.
NHS Clinical Knowledge Summaries on Endometriosis. Available from:www.cks.nhs.uk/endometriosis.April2015.
RCOGGreen-topGuidelineNo. 34:Ovarian cysts in postmenopausalwomen.RCOG 2010 [on linesource:https://www.rcog.org.uk/globalassets/documents/guidelines/gtg34ovariancysts.pdf].
RCOGGreen-topGuidelineNo.41:The initialmanagementof chronicpelvicpain.RCOG2012 [onlinesourcehttps://www.rcog.org.uk/globalassets/documents/guidelines/gtg_41.pdf].
RCOG Green-top Guideline No. 62: Management of suspected ovarian masses in premenopausalwomen. RCOG 2011 [on line source:https://www.rcog.org.uk/globalassets/documents/guidelines/gtg_62.pdf].
www.medicalebookpdf.com
Selfassessment
CASEHISTORY
A26-year-old lawstudentpresentswitha2-yearhistoryofCPP.Sheadmits toapoordietbut isotherwisefitandhealthy.Shecontractedgenitalchlamydialinfectionfromapreviousrelationship3years ago, but is currently in a new and stable relationship. A urinary pregnancy test has beenperformedandtheresultisnegative.
AWhatquestionswouldyouaskaboutthepresentingcomplaint?BWhatfeaturesofthehistorywouldsuggestagynaecologicalcauseforthepain?CWhat features fromabimanualpelvicexaminationwouldsuggestagynaecologicalcause forthepain?
DListlikelygynaecologicalcausesofCPP.EListlikelynon-gynaecologicalcausesofCPP.FSuggestdiagnostictestsyouwouldperform.GHowmightyoumanagethispatient?
ANSWERS
AEstablish the nature of the pain, such as using ‘SOCRATES’ – Site,Onset (e.g. relationship tochlamydial infection), Character, Radiation (gynaecological pain may be bilateral and into theback, groins and vagina), Associations, Time course (especially relationship to the menstrualcycle),Exacerbating/relievingfactors(e.g.sexualintercourse,voidinganddefaecation),Severity(e.g.effectonactivitiesofdailyliving,useofanalgesics,etc).
BOnsetorexacerbationinrelationtothemenstrualcyclealongwithdeepdyspareuniaissuggestiveofagynaecologicaloriginforthepain,althoughCPPisoftenmultifactorial.
C Presence of a pelvic mass may suggest the presence of an adnexal mass (e.g. ovarian cyst,hydrosalpinx)orenlargeduterus(e.g.fibroids,adenomyosis).Tenderness,fixed,immobilepelvicorgans (suggestive of adhesions secondary to endometriosis or infection) and nodularity of theuterosacralligaments(indicativeofdeepinfiltratingendometriosis)areotherfeaturestoassess.
DChronicPIDcausingadhesionsand/orachronictubo-ovarianabscessshouldbeconsideredgiventhehistoryofasexuallytransmittedinfection.Endometriosisiscommoninwomenofreproductiveageandusuallypresents in thesecondor thirddecade.Anovariancyst should formpartof thedifferentialdiagnosis.
EGastrointestinalcausessuchasirritablebowelsyndromeorconstipationinlightofherpoordiet.Anegativepregnancytestexcludesanectopicpregnancy.Genitourinaryproblemssuchasbladderpainsyndrome,musculoskeletalcauses,neuropathicpainandpsychologicalcontributorsshouldbeevaluateddependingonthehistoryandexamination.
FGenital tract swabsandamidstreamurine specimen (if thereare symptoms).First-line imagingshouldbe a pelvicUSS inorder to identifyuterine and adnexalmasses.Laparoscopy todetect
www.medicalebookpdf.com
adhesions and endometriosis if the pain is resistant tomedical treatment or the gynaecologicalexaminationisabnormal.
GThisdependson the cause.Generalhealth advice, analgesics andhormonal treatments (e.g. theCOCP,systemicandlocal[LNG-IUS])tosuppressovulationforatleast3–6monthsassumingalikely gynaecological origin for the chronic pain and the absence of an adnexalmass requiringsurgical removal. Laparoscopic surgery should be considered in the presence of adhesions(adhesiolysis), endometriosis (excision or ablation of endometriotic deposits) or adnexalpathology(removalofadnexalmasses[e.g.ovariancystectomy]).
EMQ
AEndometriosis.BAdenomyosis.CBladderpainsyndrome.DIrritablebowelsyndrome.EConstipation.FDepression.GNerveentrapment.HTortedovariancyst.IEndometrioma.JDermoidcyst(benignteratoma).KFunctionalovariancyst.LTube–ovarianabscess.For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
1 A recently divorced 36-year-old woman presents with 6 months of generalized pelvic pain,insomnia,fatigue,constipationandheadaches.Onfurtherquestioningsheadmitstobeinganxiousandtearful.
2Aparous,30-year-oldwomancomplainsofincreasinglyheavymenstrualperiodsthatarepainfulthroughouttheir5dayduration.Sheispainfreefortherestofthemonth.Onexaminationshehasanenlarged‘bulky’uterus.
3 A 22-year-old woman presents with a history of CPP and dyspareunia. She has a history ofchlamydial infection when she was 19 years old. On vaginal examination a tender mass ispalpableandpelvicUSSconfirmsthepresenceofbilateralcomplexadnexalmasses.
4A24-year-oldwomanpresentswithlong-standingpelvicpain.Herperiodsarepainfulforthefirstdaybutareregularandlight.Shehasoccasionalpainwithsexualintercourse.Sheadmitstobeingananxiouspersonandweightconscious,exercisingdaily.Sheopensherbowelsonalternatedaysandsometimeshasloosestoolsaswellasfeelingbloated,especiallypriortoherperiod.
5 A 38-year-old woman complains of pelvic pain for the last 5 years. The pain can be worsecyclicallybutshehasnotnotedadefinitepatterntoit.Shehasbeentreatedforrecurrenturinarytract infections byher general practitioner (GP) because of pain andpressure on voidingurine
www.medicalebookpdf.com
alongwithurgencyandfrequency.However,manyoftheseinfectionshavenotbeenconfirmedonmicrobiologicalexaminationofmidstreamurinespecimens (MSUs).A laparoscopy3yearsagowasnormal.
ANSWERS
1FThegeneralizedsomaticsymptomsofdepressionareclearhere,andabdominalpainiscommonin this scenario. If the pain persisted after the emotional problems had passed then furtherinvestigationswould be indicated. Investigations at this pointmay increase anxiety, unless ofcoursetherewereclearclinicalfindings.
2BThe key symptom here is painwith the bleed that persists throughout the period. Thismakesendometriosis unlikely, as this is associated with premenstrual pain as a rule. Tubo-ovarianpathologywouldnotcausecyclicalmenstrualpain.
3L Pelvic inflammaory disease can cause the tubes to be obstructed and swell to causehydrosalpinges. Subsequently, infection can turn the tubes into abscesses that can envelop theovary, a tubo-ovarian abscess. This may be bilateral. The inflammation surrounding this cancausea ‘frozenpelvis’,where thepelvicorgansbecomestuck togetherand immobile,causingpain.Thedifferentialdiagnosiswouldbeendometriosis,butthehistoryandtheTVUSSfindingsmake this unlikely. TVUSS with severe endometriosis would show the presence of ovarianendometriomas,butusuallythetubeswouldnotbeinvolved.
4DThenormalperiods(painonday1beingacommonandnon-pathologicalcomplaint),andlackofsymptomsinthepelvisspecifically,makesagynaecologicalcauseforpainunlikely.Patientsarefrequentlyseentoexcludeagynaecologicalcauseofpain,becauseitcanbedifficulttopinpointthe site of pain. The alteration in the bowel habit and the bloating is the key to diagnosingirritablebowel. Irritablebowel isoftenworsepremenstruallybecause theprogesteroneof thelutealphasecausesarelaxationofthesmoothmuscleinbowel.
5CThe symptoms point to the bladder as the site of pain. It is useful that theGP has performedMSUstoexcluderecurrenturinarytractinfections.Occasionallythereisaspotofendometriosiscausingbladderpain,butthelaparoscopy3yearspreviouslyexcludesthis.
SBAQUESTIONS
1A25-year-oldparouswomanisadmittedtohospitalwithacuteleft-sided,colickypain.Shehasnoabnormalvaginaldischargenorurinaryorbowelsymptoms.Sheisapyrexialandtachycardic.Onexaminationher abdomen is soft, not distendedandnon-tender.Shehasnotmissed amenstrualperiodandherurinarypregnancytestisnegative.Sherequiresmorphineforpainrelief.Which diagnostic test would you consider first-line in this situation? Choose the single bestanswer.
ASerumβhCG.
BMRI.
CCTscan.
DTransabdominal+transvaginalpelvicUSS.www.medicalebookpdf.com
ELaparoscopy.
ANSWER
D The clinical assessment of this woman suggests that she has considerable pain necessitatingnarcoticanalgesiabutdoesnothaveanacute surgical abdomen.Thus immediate surgery in theform of laparoscopy or laparotomy is not indicated. In the absence of genitourinary orgastrointestinal symptomsor a temperature or significant abdominal tenderness on examination,infection and/or peritonitis is unlikely. An ovarian cystic accident is the most likelygynaecologicaldiagnosis.Of the radiological imaging tests listed,pelvicUSS is the safest andmost readily available and provides excellent images of adnexal cystic masses. An earlypregnancycomplicationsuchasanectopicpregnancyisimprobablegiventhatshehasnotmissedaperiodandtheurinarypregnancytest(UPT)isnegative;aUPThashighsensitivityandsoserumquantificationofβhCGlevelsisunnecessary.
2A32-year-oldwomanhasapelvicTVUSSaspartofinvestigationsforprimarysubfertility.Thescanshowsbilateral5cm‘kissing’ovariancystsinthepouchofDouglas,bothofwhichcontaindiffuse, low-level echoes giving a solid ‘ground-glass’ appearance. She reports severedysmenorrhoeaanddyspareunia.Whattypeofovariancystsarethesemostlikelytobe?Choosethesinglebestanswer.
AHaemorrhagicfunctionalovariancysts.
BDermoidcysts.
CEndometriomas.
DTubo-ovarianabscesses.
ESerouscystadenomas.
ANSWER
CThe age of thiswoman and her history of subfertility and cyclical pain are consistentwith thepresenceofendometriosis(‘chocolatecysts’).Furthermore, thecloseproximityofbothovaries,known as ‘kissing ovaries’, is caused by adhesions, which is considered a sign of pelvicendometriosis andwould cause painwith sexual intercourse. The description on ultrasound ofhomogenous, low-level ‘echoes’ represents old altered blood are also characteristic ofendometriomas.However, thesolidappearancecouldalsoreflectahaemorrhagiccyst,dermoidcyst or chronic tubo-ovarian abscess. A tubo-ovarian abscess can also be associated withsubfertilityanddyspareuniaalthoughnottypicallycyclicalpain.Theothercystslistedareusuallyasymptomaticorpresentwithnon-cyclicalpelvicpain.Serouscystadenomasarerarelybilateral,usuallyasymptomaticunlesslarge(>10cm)andclearwithoutsolidcomponents.
www.medicalebookpdf.com
CHAPTER12Benignconditionsoftheuterus,cervixand
endometrium
TJUSTINCLARK
Benigncervicalsurfacelesions
Benignendometriallesions
Benignlesionsofthemyometrium
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Describethecommonbenignconditionsthataffecttheuterusaccordingtotheirtissueoforigin:thecervix,theendometriumandthemyometrium.
• Understand the presenting symptoms and examination findings associated with benign uterinepathology.
•Describethecommontestsusedtoevaluatetheuterusandendometrialcavity.
•Explaintheavailabletreatmentoptionsforuterinefibroidsandadenomyosisandtherationaleforselection.
Uterinecervixwww.medicalebookpdf.com
Thecervix is the cylindrical lower extremityof theuterus and consistsmainlyof collagen fibres.Thevaginal part of the cervix, called the ectocervix, is lined by thick non-keratinized stratified squamousepitheliumandhasapinkappearance.Theexternalosisvisibleinthecentreoftheectocervixasadarkcircularorslit-likeareaandistheopeningtotheendocervicalcanal,whichislinedbysimplecolumnarepithelium. There is a clear demarcation of this transformation between the two types of epithelium,called the ‘squamocolumnar junction’.This anatomical junction fluctuates under hormonal influence asdescribedfurther inChapters1,Thedevelopmentandanatomyof the femalesexualorgansandpelvis,andChapter16,Premalignantandmalignantdiseaseofthelowergenitaltract.Benignlesionscanoccuronthesurfaceorstructureofthecervix.
Benigncervicalsurfacelesions
CervicalectropionInwomenofreproductiveagethecolumnarepitheliumisvisibleontheectocervixasacircular,redareasurrounding theexternalcervicalos (Figure12.1A).This isanormal findingandshouldnotbecalled‘cervicalerosion’becausethiserroneouslyimpliesitisanulcer.Anectropioncommonlydevelopsundertheinfluenceofthe‘threePs’:puberty,pillandpregnancy.Thefragile,glandularcolumnarepitheliumofalargecervicalectropionmaypredisposetointermenstrualandpostcoitalbleeding(IMB,PCB).Somewomenmaypresentwithanexcessive,clear,odourlessmucus-typedischarge.Toreduce theectropionandassociatedsymptomswomenshouldbechangedfromoestrogen-basedhormonalcontraceptives.Theother option is cervical ablation where the visible glandular producing columnar cells are ablated,usuallywithcryocautery,asanoutpatient.Priortotreatmentend,cervicalandlowergenitaltractswabsare taken to exclude chlamydia and other sexually-transmitted infections and normal cervical cytologyshouldbe confirmed to exclude cervical premalignancyandmalignancy (seeChapter16, Premalignantandmalignantdiseaseofthelowergenitaltract).
NabothianfolliclesSometimes the columnar glands within the transformation zone become sealed over, forming small,mucus-filled cysts visible on the ectocervix. These are termed ‘nabothian follicles’ and are of nopathologicalsignificance.Notreatmentisusuallyrequiredalthoughextremelylargeonescanbedrainedusingalarge-boreneedle(Figure12.1B).
CervicalpolypsCervicalpolypsarebenigntumoursarisingfromtheendocervicalepitheliumandmaybeseenassmooth,reddish protrusions. They are usually asymptomatic, being identified incidentally during a routinecervicalsmear,butaswithacervicalectropiontheycancausevaginaldischarge,IMBandPCB.Theyareeasilyremovedbyavulsionwithpolypforcepsasanoutpatient.
CervicalstenosisCervicalstenosisreferstopathologicalnarrowingoftheendocervicalcanalandisusuallyaniatrogenicphenomenon caused by a surgical event.Treatment of premalignant disease of the cervix using a cone
www.medicalebookpdf.com

biopsyor loopdiathermycancausecervicalstenosis,ascanendometrialablationaffectingtheos.Theensuing trappedblood in the uterus (haematometra) causes cyclical dysmenorrhoeawith no associatedmenstrual bleeding.Treatment is by surgical dilatationof the cervixunderultrasoundor hysteroscopicguidance.
Benignendometriallesions
EndometrialpolypsEndometrialpolypsarefocalendometrialoutgrowthscontainingavariableamountofglands,stromaandbloodvessels,whichinfluencetheirmacroscopicappearance.Endometrialpolypsmaybeasymptomaticbut can cause abnormal uterine bleeding (AUB) (heavy menstrual bleeding [HMB], IMB andpostmenopausalbleeding[PMB])andadverselyimpactonfertility.Theyarecommonandestimatedtobepresent in around10–20%ofwomenwithAUBand10%ofwomenwith subfertility.Risk factors forendometrialpolypdevelopmentincludeobesity,latemenopause,theuseofthepartialoestrogenagonisttamoxifenandpossiblytheuseofhormonereplacementtherapy(HRT).Mostpolypsdonotappeartobesubjecttothenormalcellularmechanismsthatregulatetheendometrium.Consequently,theyarerelativelyinsensitivetocyclicalhormonalchanges,leadingthemtopersistandcauseunscheduledvaginalbleeding.Endometrial polyps contain hyperplastic foci in 10–25% of symptomatic cases and 1% is franklymalignant.The riskofpolypsharbouring seriousendometrialdisease is increasedafter themenopauseandwiththeuseoftamoxifen.Endometrialpolypsmaybepedunculatedorsessile,singleormultipleandvaryinsize(0.5–4cm).
www.medicalebookpdf.com
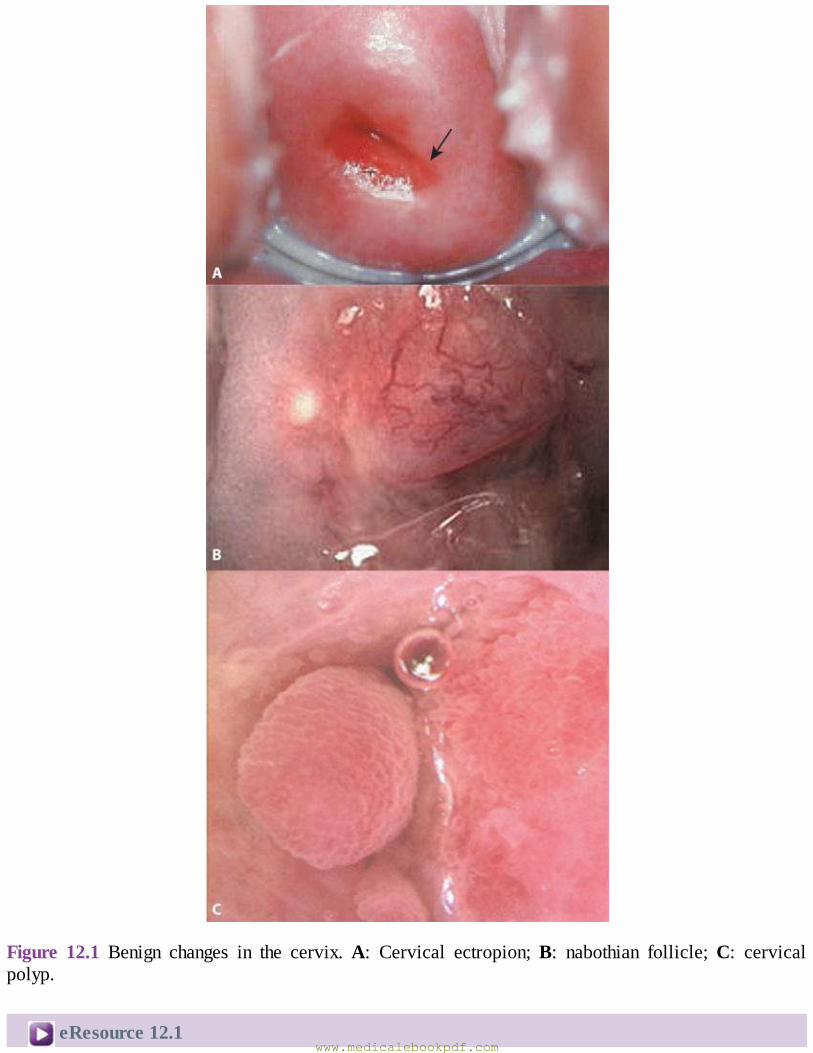
Figure 12.1 Benign changes in the cervix.A: Cervical ectropion;B: nabothian follicle;C: cervicalpolyp.
eResource12.1www.medicalebookpdf.com
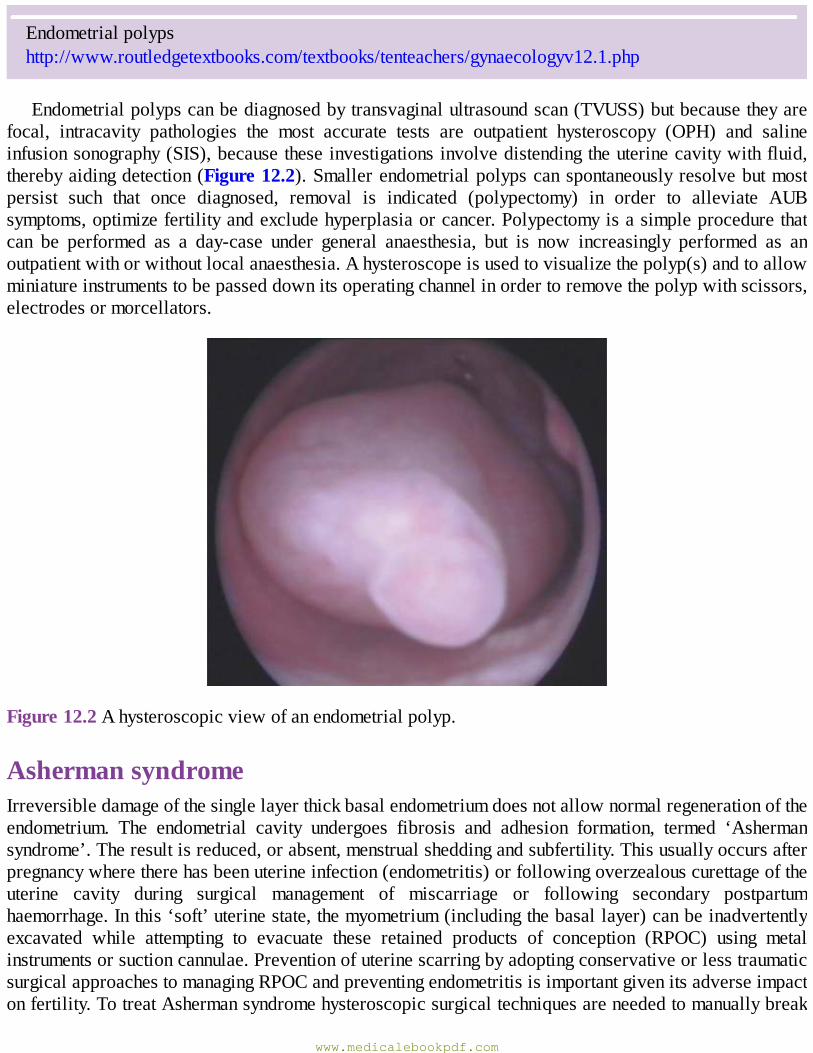
Endometrialpolypshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv12.1.php
Endometrialpolypscanbediagnosedbytransvaginalultrasoundscan(TVUSS)butbecausetheyarefocal, intracavity pathologies the most accurate tests are outpatient hysteroscopy (OPH) and salineinfusionsonography(SIS),becausetheseinvestigationsinvolvedistendingtheuterinecavitywithfluid,therebyaidingdetection(Figure12.2).Smallerendometrialpolypscanspontaneouslyresolvebutmostpersist such that once diagnosed, removal is indicated (polypectomy) in order to alleviate AUBsymptoms,optimizefertilityandexcludehyperplasiaorcancer.Polypectomyisasimpleprocedurethatcan be performed as a day-case under general anaesthesia, but is now increasingly performed as anoutpatientwithorwithoutlocalanaesthesia.Ahysteroscopeisusedtovisualizethepolyp(s)andtoallowminiatureinstrumentstobepasseddownitsoperatingchannelinordertoremovethepolypwithscissors,electrodesormorcellators.
Figure12.2Ahysteroscopicviewofanendometrialpolyp.
AshermansyndromeIrreversibledamageofthesinglelayerthickbasalendometriumdoesnotallownormalregenerationoftheendometrium. The endometrial cavity undergoes fibrosis and adhesion formation, termed ‘Ashermansyndrome’.Theresultisreduced,orabsent,menstrualsheddingandsubfertility.Thisusuallyoccursafterpregnancywheretherehasbeenuterineinfection(endometritis)orfollowingoverzealouscurettageoftheuterine cavity during surgical management of miscarriage or following secondary postpartumhaemorrhage.Inthis‘soft’uterinestate,themyometrium(includingthebasallayer)canbeinadvertentlyexcavated while attempting to evacuate these retained products of conception (RPOC) using metalinstrumentsorsuctioncannulae.PreventionofuterinescarringbyadoptingconservativeorlesstraumaticsurgicalapproachestomanagingRPOCandpreventingendometritisisimportantgivenitsadverseimpactonfertility.TotreatAshermansyndromehysteroscopicsurgicaltechniquesareneededtomanuallybreak
www.medicalebookpdf.com
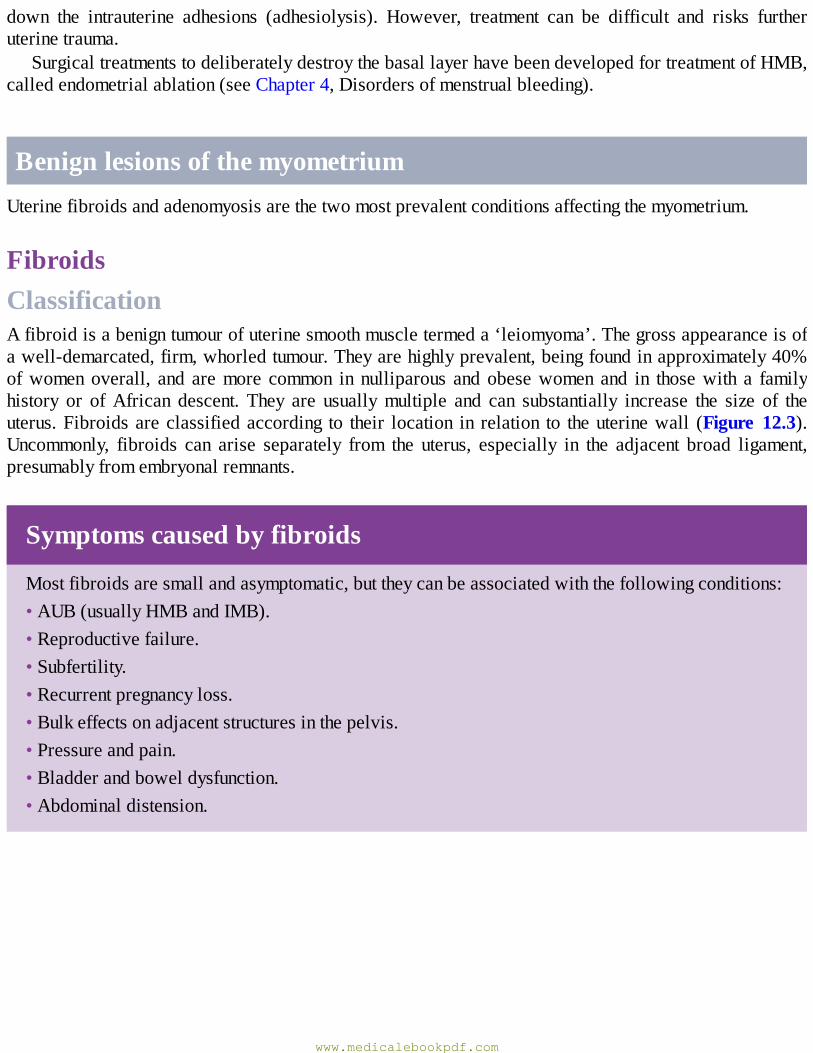
down the intrauterine adhesions (adhesiolysis). However, treatment can be difficult and risks furtheruterinetrauma.
SurgicaltreatmentstodeliberatelydestroythebasallayerhavebeendevelopedfortreatmentofHMB,calledendometrialablation(seeChapter4,Disordersofmenstrualbleeding).
BenignlesionsofthemyometriumUterinefibroidsandadenomyosisarethetwomostprevalentconditionsaffectingthemyometrium.
FibroidsClassificationAfibroidisabenigntumourofuterinesmoothmuscletermeda‘leiomyoma’.Thegrossappearanceisofawell-demarcated,firm,whorledtumour.Theyarehighlyprevalent,beingfoundinapproximately40%ofwomenoverall, and aremore common in nulliparous and obesewomen and in thosewith a familyhistory or ofAfrican descent. They are usuallymultiple and can substantially increase the size of theuterus.Fibroidsareclassifiedaccording to their location in relation to theuterinewall (Figure 12.3).Uncommonly, fibroids can arise separately from the uterus, especially in the adjacent broad ligament,presumablyfromembryonalremnants.
Symptomscausedbyfibroids
Mostfibroidsaresmallandasymptomatic,buttheycanbeassociatedwiththefollowingconditions:•AUB(usuallyHMBandIMB).•Reproductivefailure.•Subfertility.•Recurrentpregnancyloss.•Bulkeffectsonadjacentstructuresinthepelvis.•Pressureandpain.•Bladderandboweldysfunction.•Abdominaldistension.
www.medicalebookpdf.com
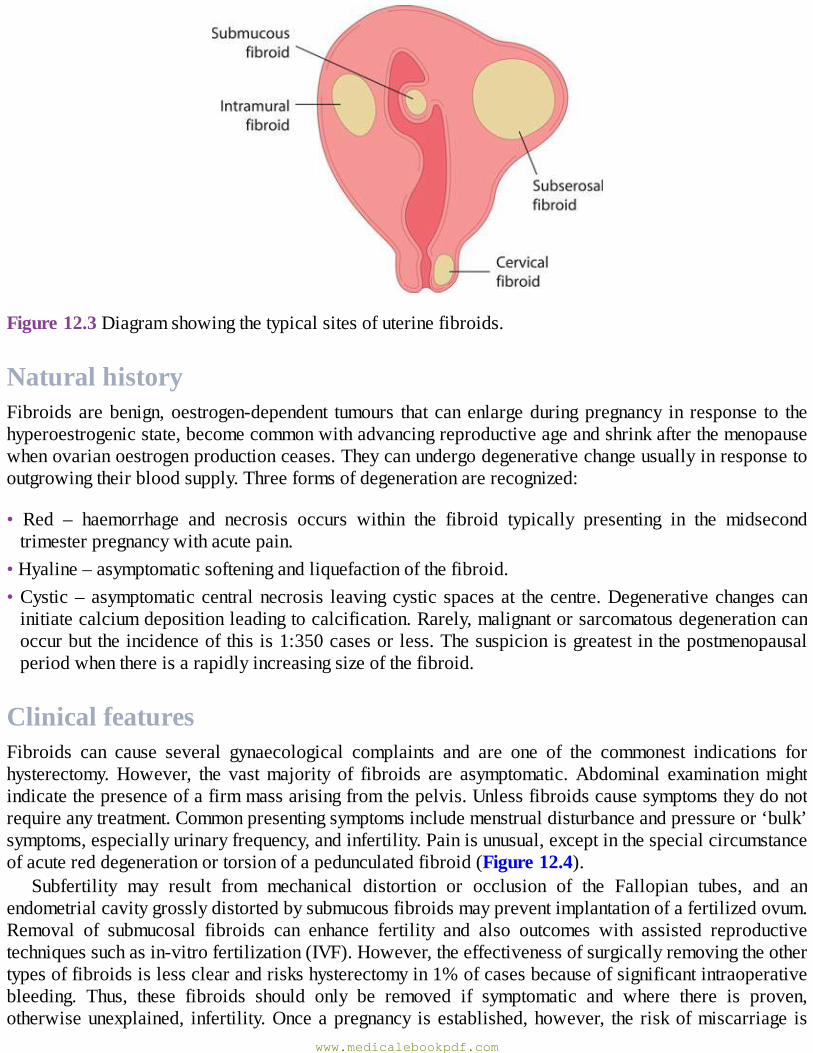
Figure12.3Diagramshowingthetypicalsitesofuterinefibroids.
NaturalhistoryFibroidsarebenign,oestrogen-dependent tumours that canenlargeduringpregnancy in response to thehyperoestrogenicstate,becomecommonwithadvancingreproductiveageandshrinkafterthemenopausewhenovarianoestrogenproductionceases.Theycanundergodegenerativechangeusuallyinresponsetooutgrowingtheirbloodsupply.Threeformsofdegenerationarerecognized:
• Red – haemorrhage and necrosis occurs within the fibroid typically presenting in the midsecondtrimesterpregnancywithacutepain.
•Hyaline–asymptomaticsofteningandliquefactionofthefibroid.•Cystic–asymptomaticcentralnecrosis leavingcystic spacesat thecentre.Degenerativechangescaninitiatecalciumdepositionleadingtocalcification.Rarely,malignantorsarcomatousdegenerationcanoccurbuttheincidenceofthisis1:350casesorless.Thesuspicionisgreatestinthepostmenopausalperiodwhenthereisarapidlyincreasingsizeofthefibroid.
ClinicalfeaturesFibroids can cause several gynaecological complaints and are one of the commonest indications forhysterectomy.However, the vastmajority of fibroids are asymptomatic.Abdominal examinationmightindicatethepresenceofafirmmassarisingfromthepelvis.Unlessfibroidscausesymptomstheydonotrequireanytreatment.Commonpresentingsymptomsincludemenstrualdisturbanceandpressureor‘bulk’symptoms,especiallyurinaryfrequency,andinfertility.Painisunusual,exceptinthespecialcircumstanceofacutereddegenerationortorsionofapedunculatedfibroid(Figure12.4).
Subfertility may result from mechanical distortion or occlusion of the Fallopian tubes, and anendometrialcavitygrosslydistortedbysubmucousfibroidsmaypreventimplantationofafertilizedovum.Removal of submucosal fibroids can enhance fertility and also outcomes with assisted reproductivetechniquessuchasin-vitrofertilization(IVF).However,theeffectivenessofsurgicallyremovingtheothertypesoffibroidsislessclearandriskshysterectomyin1%ofcasesbecauseofsignificantintraoperativebleeding. Thus, these fibroids should only be removed if symptomatic and where there is proven,otherwiseunexplained, infertility.Onceapregnancy isestablished,however, the riskofmiscarriage is
www.medicalebookpdf.com
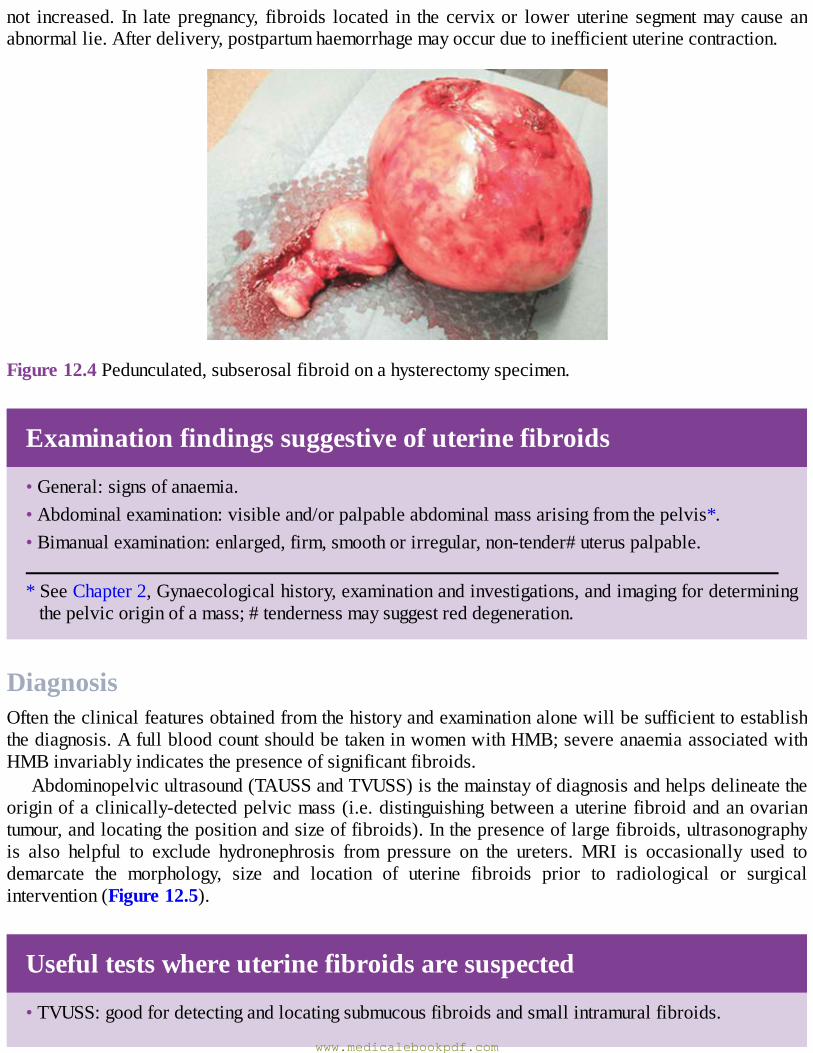
not increased. In latepregnancy, fibroids located in the cervixor loweruterine segmentmaycause anabnormallie.Afterdelivery,postpartumhaemorrhagemayoccurduetoinefficientuterinecontraction.
Figure12.4Pedunculated,subserosalfibroidonahysterectomyspecimen.
Examinationfindingssuggestiveofuterinefibroids
•General:signsofanaemia.•Abdominalexamination:visibleand/orpalpableabdominalmassarisingfromthepelvis*.•Bimanualexamination:enlarged,firm,smoothorirregular,non-tender#uteruspalpable.
*SeeChapter2,Gynaecologicalhistory,examinationandinvestigations,andimagingfordeterminingthepelvicoriginofamass;#tendernessmaysuggestreddegeneration.
DiagnosisOftentheclinicalfeaturesobtainedfromthehistoryandexaminationalonewillbesufficienttoestablishthediagnosis.AfullbloodcountshouldbetakeninwomenwithHMB;severeanaemiaassociatedwithHMBinvariablyindicatesthepresenceofsignificantfibroids.
Abdominopelvicultrasound(TAUSSandTVUSS)isthemainstayofdiagnosisandhelpsdelineatetheoriginofaclinically-detectedpelvicmass(i.e.distinguishingbetweenauterinefibroidandanovariantumour,andlocatingthepositionandsizeoffibroids).Inthepresenceoflargefibroids,ultrasonographyis also helpful to exclude hydronephrosis from pressure on the ureters. MRI is occasionally used todemarcate the morphology, size and location of uterine fibroids prior to radiological or surgicalintervention(Figure12.5).
Usefultestswhereuterinefibroidsaresuspected
•TVUSS:goodfordetectingandlocatingsubmucousfibroidsandsmallintramuralfibroids.
www.medicalebookpdf.com
• Transabdominal ultrasound scan (TAUSS): good for detecting larger intramural and subserosalfibroidsandexcludinghydronephrosissecondarytopressurefromfibroidsobstructingtheureters.
•SIS:goodfordetectingandlocatingsubmucosalfibroidsandendometrialpolyps.•Hysteroscopy:•goodfordetectingsubmucosalfibroidsandendometrialpolyps;•goodforplanningsubsequenthysteroscopicsurgicaltreatment;•surgicalhysteroscopycanremovepolyps,adhesionsandsubmucosalfibroids.•Magneticresonanceimaging(MRI):•goodfordescribingthemorphologyandlocationoffibroids;•indicatedpriortouterinearteryembolizationandtomonitortreatmentresponse.
TreatmentoffibroidsMedicaltreatmentConservative management is appropriate where asymptomatic fibroids are detected incidentally. Themaintypesofmedical treatmentforHMB(seeChapter4,Disordersofmenstrualbleeding)namely thelevonorgestrel intrauterine system (LNG-IUS), tranexamicacid,mefenamicacidand thecombinedoralcontraceptivepill(COCP)tendtobeineffectiveinthepresenceofasubmucousfibroidoranenlargeduterus that is palpable abdominally (>12 weeks size). The only effective medical treatment is to useinjectable gonadotrophin-releasing hormone (GnRH) agonists, which induce a menopausal state byshuttingdownovarianoestradiol production.However,GnRH treatment is not toleratedby allwomenbecauseofseveremenopausalsymptoms.Morerecently, theselectiveprogesteronereceptormodulator(SPRM)ulipristalacetatehasbeenshowntobeaseffectiveasGnRHagonistsinreducingfibroidvolumeandalleviatingHMBsymptoms,althoughitisnotyetwidelyacceptedintoclinicalpractice.Inadditiontobeinganoraltablet,thisSPRMdoesnotinduceamenopausalstateandassociatedsymptoms.However,neitherGnRHnorSPRMrepresentaviablelong-termtreatmentoption.Moreover,whenovarianfunctionreturns,thefibroidsregrowtotheirpreviousdimensions.
www.medicalebookpdf.com
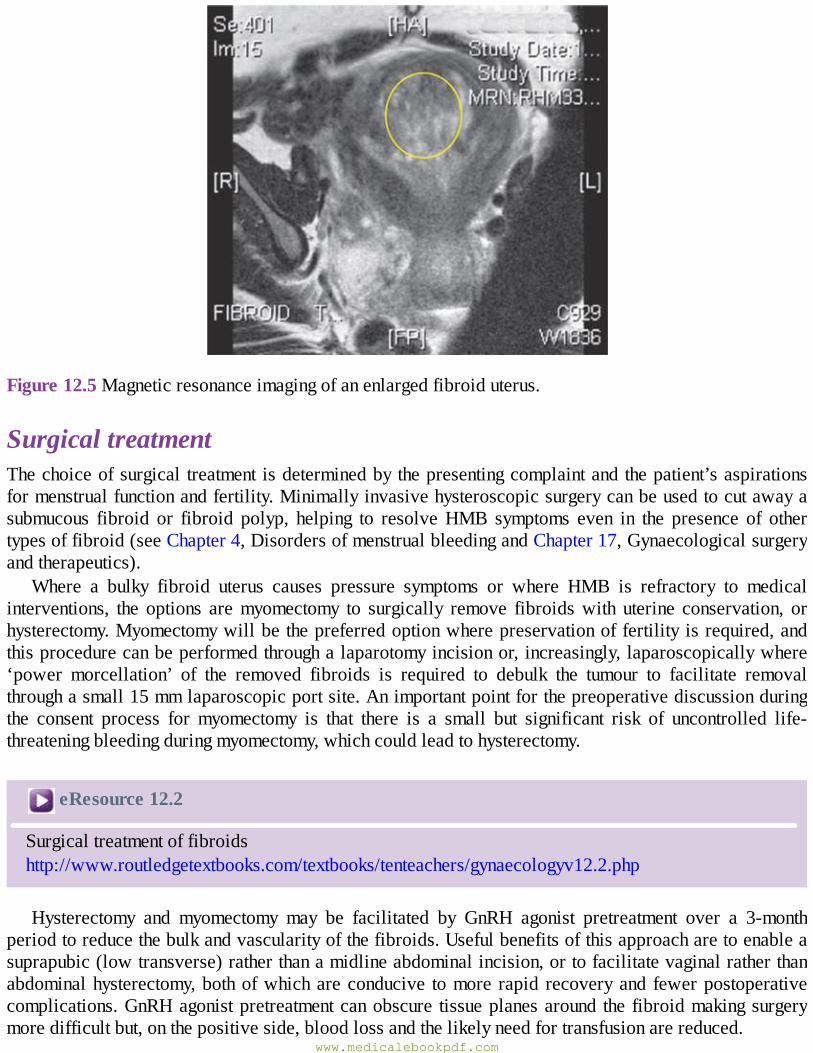
Figure12.5Magneticresonanceimagingofanenlargedfibroiduterus.
SurgicaltreatmentThechoiceofsurgical treatmentisdeterminedbythepresentingcomplaintandthepatient’saspirationsformenstrualfunctionandfertility.Minimallyinvasivehysteroscopicsurgerycanbeusedtocutawayasubmucous fibroid or fibroid polyp, helping to resolveHMB symptoms even in the presence of othertypesoffibroid(seeChapter4,DisordersofmenstrualbleedingandChapter17,Gynaecologicalsurgeryandtherapeutics).
Where a bulky fibroid uterus causes pressure symptoms or where HMB is refractory to medicalinterventions, the options aremyomectomy to surgically remove fibroidswith uterine conservation, orhysterectomy.Myomectomywillbethepreferredoptionwherepreservationoffertilityisrequired,andthisprocedurecanbeperformedthroughalaparotomyincisionor,increasingly,laparoscopicallywhere‘power morcellation’ of the removed fibroids is required to debulk the tumour to facilitate removalthroughasmall15mmlaparoscopicportsite.Animportantpointforthepreoperativediscussionduringthe consent process for myomectomy is that there is a small but significant risk of uncontrolled life-threateningbleedingduringmyomectomy,whichcouldleadtohysterectomy.
eResource12.2
Surgicaltreatmentoffibroidshttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv12.2.php
Hysterectomy and myomectomy may be facilitated by GnRH agonist pretreatment over a 3-monthperiodtoreducethebulkandvascularityofthefibroids.Usefulbenefitsofthisapproacharetoenableasuprapubic(lowtransverse)ratherthanamidlineabdominalincision,ortofacilitatevaginalratherthanabdominalhysterectomy,bothofwhichareconducive tomore rapid recoveryand fewerpostoperativecomplications.GnRHagonistpretreatmentcanobscure tissueplanesaround the fibroidmakingsurgerymoredifficultbut,onthepositiveside,bloodlossandthelikelyneedfortransfusionarereduced.
www.medicalebookpdf.com
RadiologicalUterine artery embolization (UAE) is a technique performedby interventional radiologists. It involvesembolizationofbothuterinearteriesunderradiologicalguidance.Asmallincisionismadeinthegroinunderlocalanaesthesiaandacannulaplacedintothefemoralarteryandguidedintotheuterinearteries.Embolizationparticlesaretheninjected,reducingthebloodsupplytotheuterus,whichinducesinfarctionanddegenerationoffibroidssuchthattheoverallreductioninfibroidvolumeisaround50%.FollowingUAE,patientsusuallyrequireadmissionovernightbecauseofpainfollowingarterialocclusion,requiringopiateanalgesia.Complicationsincludefever,infection,fibroidexpulsionandpotentialovarianfailure.
WomenwishingtoretaintheirfertilityshouldbecounselledcarefullybeforeundergoingUAEastheeffects on subsequent reproductive function are uncertain. Pregnancies have been reported in theliterature,butconcerns remainoverprematureovarian failureandeffectson theendometrium thatmayleadtoabnormalplacentation.Theprocedureisequivalenttomyomectomyforalleviatingfibroid-relatedHMB and pressure symptoms. However, one-third of women subsequently require further medical,radiological or surgical intervention within 5 years of UAE. Thus, when counselling women abouttreatment options for symptomatic fibroids it is important to balance the less invasive nature ofUAEcomparedwithsurgicalmyomectomyagainstthemuchhigherlikelihoodofneedingfurthertreatments.
AdenomyosisTheendometriumisusuallywelldemarcatedfromtheunderlyingmyometrium.Adenomyosisisadisorderinwhichendometrialglandsandstromaarefounddeepwithinthemyometrium.Adenomyosiscanonlybedefinitivelydiagnosedfollowinghistopathologicalexaminationofahysterectomyspecimen,where it isidentified in 40% of uteri from a general female population of reproductive age. This ectopicendometriumisresponsive tocyclicalhormonalchanges that result inbleedingwithin themyometrium,leading to increasingly severe secondarydysmenorrhoea (pain throughoutmenses), uterine enlargementandHMB.
Relative advantages and disadvantages of treatments forsymptomaticuterinefibroids
Medical
•Tranexamicacid/non-steroidalanti-inflammatorydrugs[NSAIDs]/COCP/LNG-IUS(Mirena®):allare simple and fertility sparing (although COCP/LNG-IUS are contraceptive) and avoid moreinvasiveinterventions,buttheyaregenerallylesseffectiveinthepresenceofsubmucosalfibroidsorauterus>12weekssizewhereanenlargeduterinecavitycanbeexpected.
•COCP:containsoestrogen,whichmayincreasethegrowthofoestrogen-dependentfibroids.• LNG-IUS: increased likelihood of expulsion if cavity is enlarged or distorted by submucosalfibroids.
•GnRH-agonists:reducefibroidvolumepriortosurgerybutinduceatemporaryoestrogendeficient‘menopausal’stateprecludinglong-termuse.
•Ulipristalacetate(SPRM):oralmedicationand,aswithGnRH-agonists,itreducesfibroidvolumepriortosurgery,butmoredataaboutsafetywithlong-termuseareneeded.
www.medicalebookpdf.com
Surgical
•Hysteroscopicmyomectomy:minimally invasive, day-caseprocedure for submucous fibroids thatavoidssurgical incisionsandiseffectiveinresolvingHMBandimprovingfertility.Willnot treatothertypesoffibroid.
• Myomectomy: fertility sparing and will treat HMB and bulk symptoms. Usually requires alaparotomy,butalessinvasivelaparoscopicapproachispossiblewithsmallerandfewerfibroids.Associated with intraoperative bleeding from vascular fibroids, a 1% risk of unplannedhysterectomyandpostoperativeintra-abdominaladhesions.
• Hysterectomy: indicated for women with no future fertility desires.May be achieved vaginally,laparoscopicallyorviaopensurgerydependingon thesizeof theuterus.Definitive,guaranteeingamenorrhoeabutasinvasiveasmyomectomy.
Radiological
•Uterinearteryembolization:minimallyinvasive,avoidsgeneralanaesthesiaandsurgery.Althoughfertility sparing there are concerns over effect on subsequent reproductive function. Equivalentpatientsatisfactioncomparedwithmyomectomybuttheneedforfurthertreatmentsmuchhigher.
• Novel radiological treatments are currently being explored to destroy fibroids through thermalablation. These include MRI-guided transcutaneous focussed ultrasound and transcervicalintrauterine ultrasound-guided radiofrequency ablation. However, the effectiveness and safety ofthese interventions need further study before they can be considered for use in routine clinicalpractice.
Women with adenomyosis are usually multiparous and diagnosed in their late 30s or early 40s.Examination may reveal a bulky and sometimes tender ‘boggy’ uterus, particularly if examinedperimenstrually.Ultrasoundexaminationoftheuterusmaybehelpfulfordiagnosiswhenadenomyosisisparticularly localized, showing haemorrhage-filled, distended endometrial glands. Sometimes thismaygiveanirregularnodulardevelopmentwithintheuterus,verysimilartothatofuterinefibroids.MRIisthe investigation of choice although expensive, as it provides excellent images of the myometrium,endometriumandareasofadenomyosis(Figure12.6).
www.medicalebookpdf.com
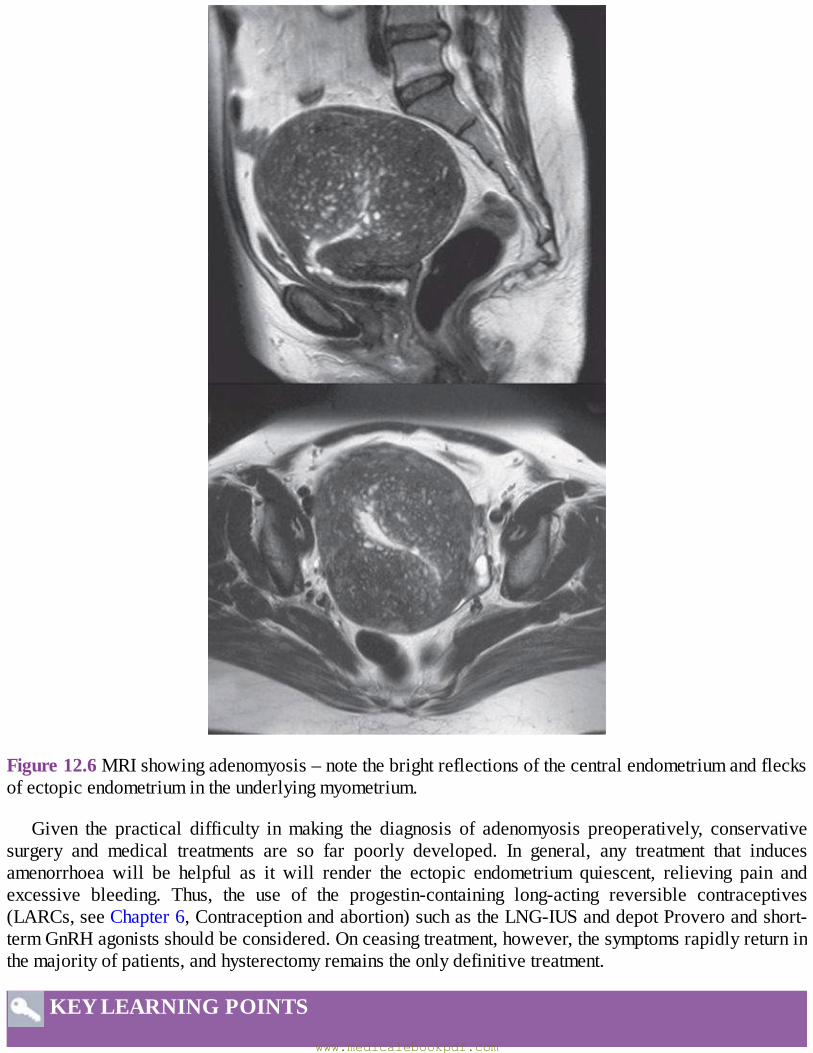
Figure12.6MRIshowingadenomyosis–notethebrightreflectionsofthecentralendometriumandflecksofectopicendometriumintheunderlyingmyometrium.
Given the practical difficulty inmaking the diagnosis of adenomyosis preoperatively, conservativesurgery and medical treatments are so far poorly developed. In general, any treatment that inducesamenorrhoea will be helpful as it will render the ectopic endometrium quiescent, relieving pain andexcessive bleeding. Thus, the use of the progestin-containing long-acting reversible contraceptives(LARCs,seeChapter6,Contraceptionandabortion)suchastheLNG-IUSanddepotProveroandshort-termGnRHagonistsshouldbeconsidered.Onceasingtreatment,however,thesymptomsrapidlyreturninthemajorityofpatients,andhysterectomyremainstheonlydefinitivetreatment.
KEYLEARNINGPOINTS
www.medicalebookpdf.com

•A cervical ectropion is a normal finding in women of reproductive age and is usually due tohormonalinfluence–thethreePs:puberty,pillandpregnancy.
•TeststoevaluatetheuterusincludeTVUSS,SIS,MRI,hysteroscopyandendometrialbiopsy.•Endometrialpolypsarecommon,usuallybenignfocallesionsarisingfromtheendometrium.TheycancauseabnormalpatternsofuterinebleedingincludingHMB,IMBandPMB.
• Surgical removal of endometrial polyps, known as polypectomy, is a simple procedure usuallyperformedunderdirectvisionwiththeaidofahysteroscopeasanoutpatientorday-case.
•Fibroids(leiomyomas)arecommon,oestrogen-dependent,benigntumoursofthemyometriumandare estimated to be present in about 40% of women over 30 years of age. Fibroids undergoshrinkageafterthemenopause.Malignantchangetoleiomyosarcomasoccursin1:350fibroidsandisusuallyassociatedwithrapidfibroidgrowthandAUBinapostmenopausalwomen.
• Fibroids are classified according to their relationship to the uterine wall, being described assubmucosalorintramuralandsubserosal.Fibroidscanbedetectedonabdominaland/orbimanualpelvicexaminationasanenlargedpelvicmassofuterineorigin.
• Fibroids can cause HMB and pressure ‘bulk’-related abdominal symptoms and in some casessubfertility.However, thevastmajorityof fibroids are asymptomatic.Treatment is indicated forsymptomatic fibroids. Surgical or radiological intervention is often required because medicaltreatmentsaregenerallylesseffective.
•Surgicalremovaloffibroidsistermedmyomectomy.Submucousfibroidsprotrudeintotheuterinecavityandsocanberemovedusinghysteroscopictechniques.Intramuralandsubserosalfibroidsareremovedviaalaparotomyincisionorlaparoscopicallydependingontheirsize, locationandnumber.
•Adenomyosis is a disorder in which endometrial glands and stroma are found deepwithin themyometrium, which can cause dysmenorrhoea, HMB and uterine enlargement. The mechanismwherebyfibroidsaffectfertilityisunclear.
•Medical treatments suchas theLNG-IUS (Mirena®) that can induceamenorrhoeawill alleviatesymptomsassociatedwithadenomyosis.Hysterectomyremainstheonlydefinitivetreatment.
FurtherreadingAmerican Association of Gynecologic Laparoscopists (2012). AAGL practice report: practiceguidelinesforthediagnosisandmanagementofendometrialpolyps.JMinimInvasiveGynecol19:3–10.
Garcia L, Isaacson K (2011). Adenomyosis: review of the literature. J Minim Invasive Gynecol18:428–37.
Gupta JK, Sinha A, Lumsden MA, Hickey M (2014). Uterine artery embolization for symptomaticuterinefibroids.CochraneDatabaseSystRev12:CD005073.
MunroMG,CritchleyHOD,FraserIS(2012).TheFIGOsystemsfornomenclatureandclassificationofcausesofabnormaluterinebleedinginthereproductiveyears:whoneedsthem?AmJObstetGynecol207:259–65.
www.medicalebookpdf.com
OwenC,ArmstrongAY (2015).Clinicalmanagement of leiomyoma.ObstetGynecolClinNorthAm42:67–85.
Selfassessment
CASEHISTORY
A34-year-oldwomanpresentswithincreasinglyheavymenstrualperiodsandanabdominalmass.She is known to have uterine fibroids. She is due to getmarried nextmonth and plans to start afamily soon. Several hormonal and non-hormonalmedical treatments prescribed by her GP havefailedinthepast5years.
AWhatquestionswouldyouaskinordertofurtherexplorethepresentingcomplaint?BWhatexaminationwouldyouperformandwhatdiagnostictestswouldyouperformorrequest?CWhatmedicaltreatmentswouldyouconsiderandexplainwhy?DWhatsurgicalorradiologicaltreatmentswouldyouconsiderandexplainwhy?EDoyouthinkshemaybeworriedaboutanythinginrelationtoherpresentingcomplaint?
ANSWERS
AAssessthenatureandseverityofthemenstrualbleeding(e.g.thechronicityofthesymptoms,theduration,regularityandamount[e.g.‘flooding’throughsanitaryprotection]ofmenstruallossandthe adverse impact on health-related quality of life [e.g. impact onwork, social and emotionalrelationships,physicalandsexualfunctioning]).EstablishwhetherthereisanyIMBorPCBthatmay indicate cervical pathology. Enquire about dysmenorrhoea and whether this is primary,spasmodicandshortlivedattheonsetofmensesorsecondarylastingthroughouttheperiod,whichmaysuggestothergynaecologicalpathologyespeciallyifthereisassociatedchronicpelvicpain.Informationrelatingtothepelvicmassshouldbeobtained(e.g.whenwasitfirstnoticedandhow,isitenlargingand/orcausingbulk,pressuresymptomsandhowwereuterinefibroidsdiagnosed?).Fertilityplans/desiresshouldbeestablishedfromtheoutsetinadditiontopast‘failed’treatmentsasthisinformationwillinfluencesuitablemanagementoptions.
Gastrointestinalcausessuchasirritablebowelsyndromeorconstipationshouldbeconsideredinlightofherpoordiet.Anegativepregnancytestexcludesanectopicpregnancy.Genitourinaryproblems such as bladder pain syndrome, musculoskeletal causes, neuropathic pain andpsychologicalcontributorsshouldbeevaluateddependingonthehistoryandexamination.
BAgynaecologicalexaminationshouldbeundertakentobettercharacterizethenatureandoriginofthe mass; the size, regularity, mobility and tenderness of the mass should be determined.InvestigationstoconsiderincludeapelvicUSSandpossiblyaMRIscanifthefibroidsarelarge,rapidlyenlargingormorphologicallyabnormalonultrasound.Anendometrialbiopsyisgenerallyunnecessary in women under 45 years of age unless they have risk factors for endometrialhyperplasia (e.g.erraticcycles,obesity,polycysticovaries).Anoutpatienthysteroscopymaybeindicatedifsubmucosalfibroidsaresuspectedorseenonradiologicalimaging.
www.medicalebookpdf.com
CAssheplanstostartafamilysoon,contraceptivehormonaltreatmentsshouldbeavoidedalthoughmaybeusedintheshortterm.TranexamicacidandNSAIDsaregoodoptionsalthoughitislikelythesehavealreadybeentried,giventhelong-standinghistory.HMBinthepresenceofsubstantialuterinefibroidsaremoreresistanttomedicaltreatmentsandsosurgeryshouldbeconsidered.
D In this instance it should be fertility conserving so hysterectomy and endometrial ablation arecontraindicated. Myomectomy can be performed but as there is a small risk of emergencyhysterectomybecauseofsevere intraoperativebleeding, thisshouldprobablybeavoidedunlessshe is unable to conceive within a year of trying. In contrast, hysteroscopic myomectomy isindicated if submucosal fibroids are detected as the operation isminimally invasive, can treatHMB and can optimize subsequent fertility. UAE is another option, although the impact onsubsequentreproductivefunctionremainsunclear.
EShemaybeworriedabouttheeffectoffibroidsonherfertilityandsubsequentpregnancyinviewofherforthcomingmarriage.Shemayalsobeworriedaboutthepossibilityofcancerouschangeifshefeelstheuterinemasshasincreasedinsize.
EMQ
AEndometrialbiopsy(EB).BSIS.COutpatienthysteroscopy(OPH).DTVUSS.ETAUSS.FMRI.GGenitaltractswabs.HLaparoscopy.IComputedtomography(CT)scan.JCervicalsmear.KColposcopy+/−cervicalbiopsy.LHysterosalpingogram(HSG).
For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
1An obese, diabetic 49-year-oldwoman presentingwith erratic, heavy and prolongedmenstrualbleeding.
2A 32-year-oldwomanwith IMB, subfertility and a suspected 2 cm endometrial polyp seen onpelvicUSS.
3A22-year-oldvirginwithHMBandapelvicmasspalpatedonabdominalexamination.4Anobese44-year-oldwomanwithregular,heavyandpainfulmenstrualbleedingandsomePCB.Examination of the genital tract appears normal and she has a normal and up-to-date cervicalsmearhistory.
www.medicalebookpdf.com
5A32-year-oldwomanwithahistoryofamenorrhoeaandsecondarysubfertilitysinceapostpartumdilatationandcurettage(D&C)forRPOC2yearsago.
6A44-year-oldwomanconsideringaUAEfora34weekssizedfibroiduterus.
ANSWERS
1AThiswomanisathighriskforendometrialcarcinoma.AsperHMBguidelinesandinviewofrisk, EB is indicated. Other tests such as cervical smear, swabs and TVUSS may also benecessarylater,dependingonthehistory.
2CTheIMBis likelytobedueto thepolyp,whichmayalsobeaffectingimplantation.OPHwillafforddirectvisionandresection.SISisnotnecessaryasthepolyphasbeenvisualizedalready,HSGisalsounnecessaryatthispoint.
3EVisualizationoftheuterusisnecessarybutTVUSSisnotsuitableassheisavirgin,andanywaythe mass is large. No further imaging such as CT or MRI is indicated yet, and would beunnecessarily expensive and invasive. Operative procedures are not indicated here, nor aresmears,swabsorcolposcopy.
4D Further examination of the cervix is unnecessary given her normal smear history. TVUSS isrequired to image the uterus and the cervical structure. Swabs may prove necessary later,depending on history. More expensive and invasive imaging such as MRI and CT areunnecessary.
5CThehistoryindicatesanendometrialcausefor theamenorrhoea.AlthoughaTVUSSmayshowscarringasabrightlineintheendometriumandSISmayshowanoccludedendometrium,OPHwillaffordtheopportunitytotreatanyscarringbyresection.Itisthereforethemostefficientnextstep.
6FPrior toUAEaMRI is essential to identify the size andexact locationof the fibroids, and toensurethattheUAEispossible.TVUSSwillalsoshowverygoodidentificationofthefibroids,butMRIisabetterimagingmodalitytoreviewspecificfibroidsatalaterdate.
SBAQUESTIONS
1 A parous 35-year-old woman complains of cyclical heavy and painful menstrual bleeding. Onexaminationsheisfoundtohaveanenlarged,‘boggy’uterusandaTVUSSsuggeststhepossibilityofadenomyosis.Shehascompletedherfamilyandcurrentlyreliesoncondomsforcontraception.She smokes 10 cigarettes per day but is otherwise fit and well. Which treatment would youconsidermostappropriate?Choosethesinglebestanswer.ALNG-IUS(Mirena®).BCOCP.CHysterectomyDGnRHanalogues.EEndometrialablation.
ANSWER
www.medicalebookpdf.com

AAlthoughadenomyosis canonlybedefinitivelydiagnosed followinghistological examinationofthe uterus after hysterectomy, the history, examination and scan findings are suggestive of thisbenign condition of the uterus. As she has completed her family a hysterectomy could beconsidered, but this should not be considered a first-line treatment given its greater potentialmorbidity.Any treatment that induces amenorrhoeawill behelpful as itwill render the ectopicendometrium quiescent, relieving symptoms of pain and excessive bleeding. Local progestogentreatment using the LNG-IUS can induce amenorrhoea and also provide more effectivecontraception so seems the best option. GnRH analogues are not a long-term treatment andendometrial ablation is primarily a treatment forHMBof endometrial origin in the absence ofotherpathology.
2 Submucous fibroids are not associated with which of the following presentations? Choose thesinglebestanswer.AIMB.BSubfertility.CPregnancyloss.DHMB.EPressureandpain.
ANSWER
ESubmucousfibroidsaremostcommonlydiagnosedwheninvestigatingabnormaluterinebleedingorsubfertility.Pressureandpainisnotafeatureofuterinefibroidsconfinedtotheuterinecavityunlesssubmucousfibroidscoexistwithother intramuraland/orsubserosal fibroids, leading toasubstantiallyenlargeduterus.
www.medicalebookpdf.com
CHAPTER13Benignconditionsofthevulvaandvagina,psychosexualdisordersandfemalegenital
mutilation
LEILACGFRODSHAM
Anatomyandhistology
Vulvaloverview
Assessment
Psychosexualmedicine
Howtoapproachconsultations
Femalegenitalmutilation
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Describethepresentationandmanagementofcommonbenignconditionsofthevulvaandvagina.
•Describethecausesofsuperficialanddeepdyspareunia.
•Understandtheimpactofvulvalandvaginalconditionsonsexualfunction.
•Understandthedefinitionofpsychosexualdisorders.www.medicalebookpdf.com

•Describethediagnosis,impactandmanagementofpsychosexualdisorders.
AnatomyandhistologyThevulva is the termusedtodescribe theexternalfemalegenitalia– thesexualorgans. It includes thelabiamajoraandminor,clitorisandfourchette.Thevulvalvestibuleisdefinedanatomicallyastheareabetween the lower end of the vaginal canal at the hymenal ring and the labia minora. The differentanatomical areas of the external genitalia have different histological characteristics and embryologicalorigins.Boththelabiaminoraandmajoraarecoveredwithkeratinized,pigmented,squamousepithelium.The labiamajora are two large folds of adipose tissue covered by skin containing hair follicles andsebaceousandsweatglands.Incontrast,thelabiaminoraaredevoidofadiposetissueandhairfollicles,but contain sebaceous follicles. The normal vulval vestibule is covered with non-keratinized, non-pigmentedsquamousepitheliumandisdevoidofskinadnexa.Withinthevulvalvestibulearetheductsoftheminor vestibular glands, the periurethral glands of Skene, the urethralmeatus and the ducts of theBartholin’sglands.TheBartholin’sglands(majorvestibularglands)arethemajorglandsofthevestibuleandliedeepwithintheperineum.Boththemajorandtheminorvestibularglandscontainmucus-secretingaciniwithductslinedbytransitionalepithelium.TheductsoftheBartholin’sglandsexitattheintroitusjustabovethefourchetteatapproximatelyfiveandseveno’clockontheperineum,andthoseoftheminorvestibular glands are distributed throughout the vulval vestibule. The vagina and vulva are commonlyknownasthelowergenital tractwiththevaginaleadingtotheuppergenital tract(uterus,cervix, tubesand ovaries). The vagina has is a tubular structure but has anterior and posterior walls that lie inopposition.
Vulvalskinhasdifferentphysiologicalpropertieswhencomparedtootherregionsofthebodysuchastheforearm.Transepidermalwaterlossistwicetheamountinvulvalskincomparedtoforearmskin.Thissuggests that thestratumcorneum,theprotectivelayerofvulvalskin,functionspoorlyasaskinbarrierwhencomparedtootherskinareasandmayexplainwhyvulvalskinismorepronetoirritancy.
VulvaloverviewBenignvulvalconditionshaveafarrangingimpactonwomen’shealthandlifestylesandyetthereareadearthofcliniciansabletoprovideaholisticapproachtocare.Approximately20%ofwomenwillhavevulval symptoms such as itching, skin changes or pain at any time. Effective management of vulvaldiseases incorporates skills in dermatology, oncology, infectious diseases and psychosexualmedicine.Current training in these areas for gynaecologists are scanty and sowomen are at best seen in vulvalclinicswithamultidisciplinaryteam(MDT)approach.Atworst, theymaybepassedbetweenprimary,secondaryandtertiarycarefeelingincreasinglyfrustratedanddisgruntledthatnooneseemstounderstandor be able to help them. In turn, this canmake the speciality less appealing to clinicians. The recentsurvey, Tomorrow’s Specialist, by the Royal College of Obstetricians and Gynaecologists (RCOG)suggests that women expect psychosexual, dermatological and surgical skills from their gynaecologistand,whilethischapterdoesnotaimtocoveralltheseareasindetail,itishopedtogiveanoverviewinthemanagementofthesecasesinorderthatasolecliniciancanmanagethemajorityofcasesthemselves.
www.medicalebookpdf.com
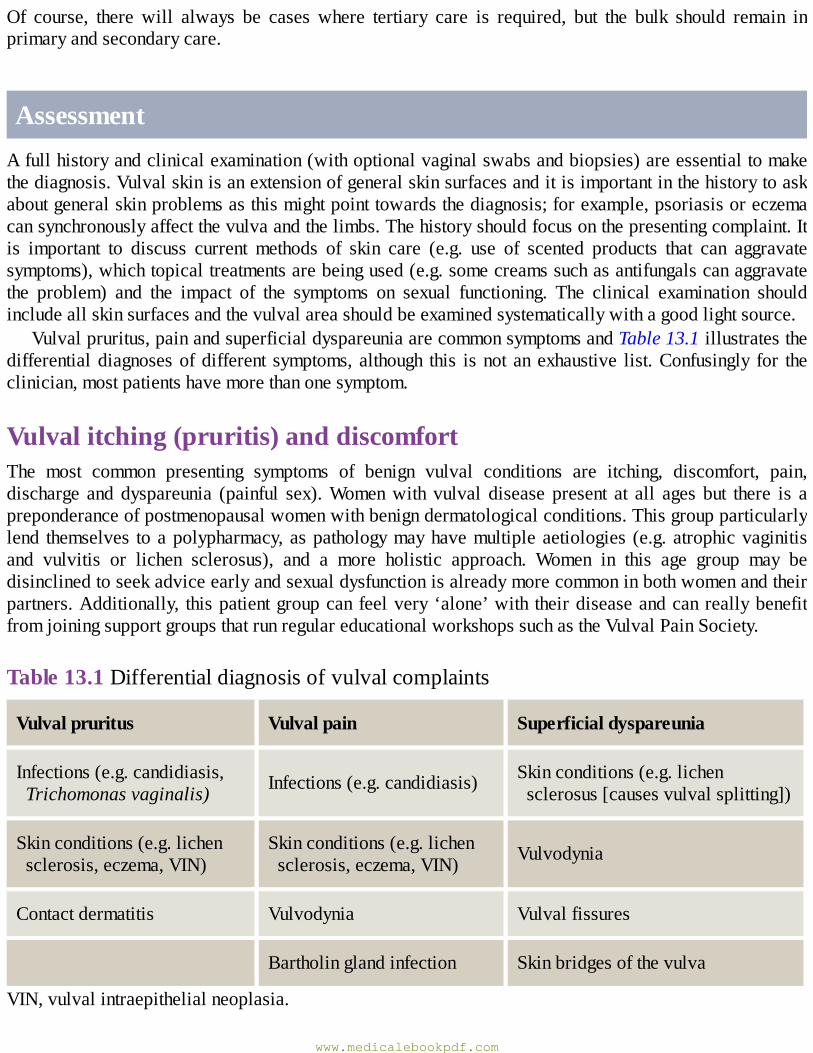
Of course, there will always be cases where tertiary care is required, but the bulk should remain inprimaryandsecondarycare.
AssessmentAfullhistoryandclinicalexamination(withoptionalvaginalswabsandbiopsies)areessentialtomakethediagnosis.Vulvalskinisanextensionofgeneralskinsurfacesanditisimportantinthehistorytoaskaboutgeneralskinproblemsasthismightpointtowardsthediagnosis;forexample,psoriasisoreczemacansynchronouslyaffectthevulvaandthelimbs.Thehistoryshouldfocusonthepresentingcomplaint.Itis important to discuss current methods of skin care (e.g. use of scented products that can aggravatesymptoms),whichtopicaltreatmentsarebeingused(e.g.somecreamssuchasantifungalscanaggravatethe problem) and the impact of the symptoms on sexual functioning. The clinical examination shouldincludeallskinsurfacesandthevulvalareashouldbeexaminedsystematicallywithagoodlightsource.
Vulvalpruritus,painandsuperficialdyspareuniaarecommonsymptomsandTable13.1illustratesthedifferentialdiagnosesofdifferent symptoms,although this isnotanexhaustive list.Confusingly for theclinician,mostpatientshavemorethanonesymptom.
Vulvalitching(pruritis)anddiscomfortThe most common presenting symptoms of benign vulval conditions are itching, discomfort, pain,discharge and dyspareunia (painful sex).Womenwith vulval disease present at all ages but there is apreponderanceofpostmenopausalwomenwithbenigndermatologicalconditions.Thisgroupparticularlylend themselves toapolypharmacy,aspathologymayhavemultipleaetiologies (e.g.atrophicvaginitisand vulvitis or lichen sclerosus), and a more holistic approach. Women in this age group may bedisinclinedtoseekadviceearlyandsexualdysfunctionisalreadymorecommoninbothwomenandtheirpartners.Additionally, thispatientgroupcanfeelvery‘alone’with theirdiseaseandcanreallybenefitfromjoiningsupportgroupsthatrunregulareducationalworkshopssuchastheVulvalPainSociety.
Table13.1Differentialdiagnosisofvulvalcomplaints
Vulvalpruritus Vulvalpain Superficialdyspareunia
Infections(e.g.candidiasis,Trichomonasvaginalis) Infections(e.g.candidiasis) Skinconditions(e.g.lichen
sclerosus[causesvulvalsplitting])
Skinconditions(e.g.lichensclerosis,eczema,VIN)
Skinconditions(e.g.lichensclerosis,eczema,VIN) Vulvodynia
Contactdermatitis Vulvodynia Vulvalfissures
Bartholinglandinfection Skinbridgesofthevulva
VIN,vulvalintraepithelialneoplasia.
www.medicalebookpdf.com
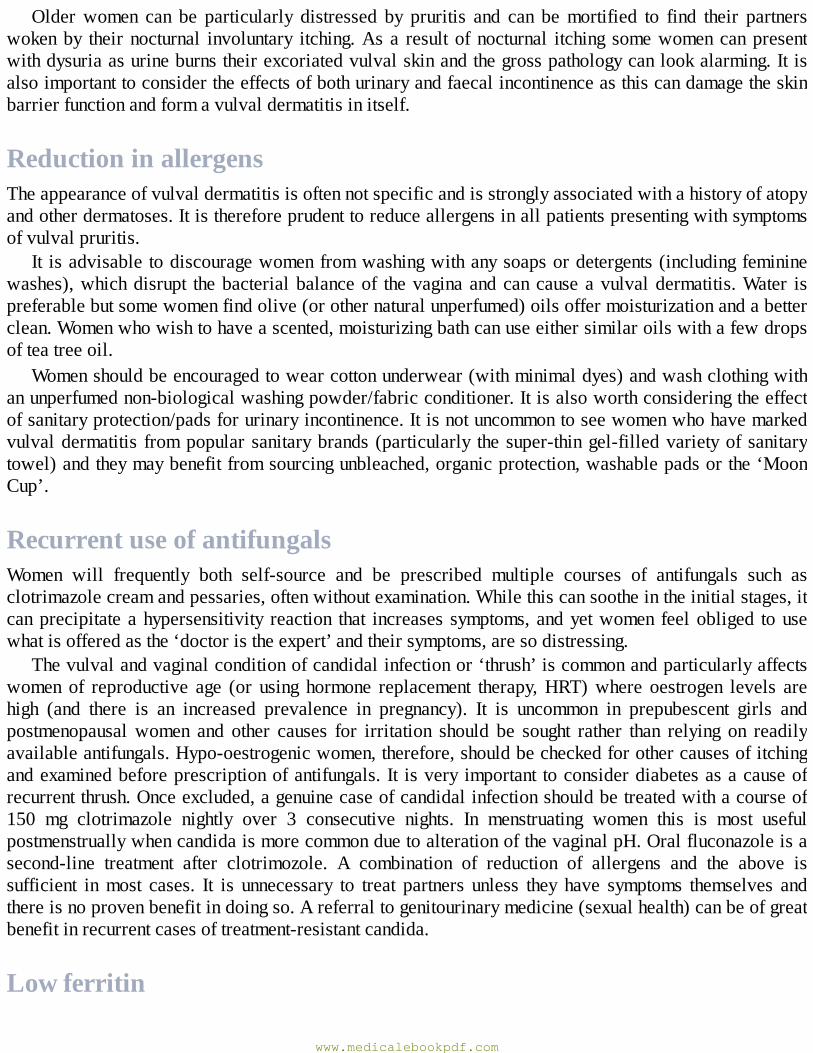
Olderwomen can be particularly distressed by pruritis and can bemortified to find their partnerswokenby theirnocturnal involuntary itching.Asa resultofnocturnal itching somewomencanpresentwithdysuriaasurineburnstheirexcoriatedvulvalskinandthegrosspathologycanlookalarming.Itisalsoimportanttoconsidertheeffectsofbothurinaryandfaecalincontinenceasthiscandamagetheskinbarrierfunctionandformavulvaldermatitisinitself.
ReductioninallergensTheappearanceofvulvaldermatitisisoftennotspecificandisstronglyassociatedwithahistoryofatopyandotherdermatoses.Itisthereforeprudenttoreduceallergensinallpatientspresentingwithsymptomsofvulvalpruritis.
It isadvisable todiscouragewomenfromwashingwithanysoapsordetergents(includingfemininewashes),whichdisrupt thebacterialbalanceof thevaginaandcancauseavulvaldermatitis.Water ispreferablebutsomewomenfindolive(orothernaturalunperfumed)oilsoffermoisturizationandabetterclean.Womenwhowishtohaveascented,moisturizingbathcanuseeithersimilaroilswithafewdropsofteatreeoil.
Womenshouldbeencouragedtowearcottonunderwear(withminimaldyes)andwashclothingwithanunperfumednon-biologicalwashingpowder/fabricconditioner.Itisalsoworthconsideringtheeffectofsanitaryprotection/padsforurinaryincontinence.Itisnotuncommontoseewomenwhohavemarkedvulvaldermatitis frompopular sanitarybrands (particularly thesuper-thingel-filledvarietyof sanitarytowel)andtheymaybenefitfromsourcingunbleached,organicprotection,washablepadsorthe‘MoonCup’.
RecurrentuseofantifungalsWomen will frequently both self-source and be prescribed multiple courses of antifungals such asclotrimazolecreamandpessaries,oftenwithoutexamination.Whilethiscansootheintheinitialstages,itcanprecipitateahypersensitivity reaction that increases symptoms, andyetwomen feelobliged tousewhatisofferedasthe‘doctoristheexpert’andtheirsymptoms,aresodistressing.
Thevulvalandvaginalconditionofcandidalinfectionor‘thrush’iscommonandparticularlyaffectswomen of reproductive age (or using hormone replacement therapy,HRT)where oestrogen levels arehigh (and there is an increased prevalence in pregnancy). It is uncommon in prepubescent girls andpostmenopausalwomen and other causes for irritation should be sought rather than relying on readilyavailableantifungals.Hypo-oestrogenicwomen,therefore,shouldbecheckedforothercausesofitchingandexaminedbeforeprescriptionofantifungals. It isvery important toconsiderdiabetesasacauseofrecurrentthrush.Onceexcluded,agenuinecaseofcandidalinfectionshouldbetreatedwithacourseof150 mg clotrimazole nightly over 3 consecutive nights. In menstruating women this is most usefulpostmenstruallywhencandidaismorecommonduetoalterationofthevaginalpH.Oralfluconazoleisasecond-line treatment after clotrimozole. A combination of reduction of allergens and the above issufficient inmost cases. It is unnecessary to treat partners unless they have symptoms themselves andthereisnoprovenbenefitindoingso.Areferraltogenitourinarymedicine(sexualhealth)canbeofgreatbenefitinrecurrentcasesoftreatment-resistantcandida.
Lowferritin
www.medicalebookpdf.com
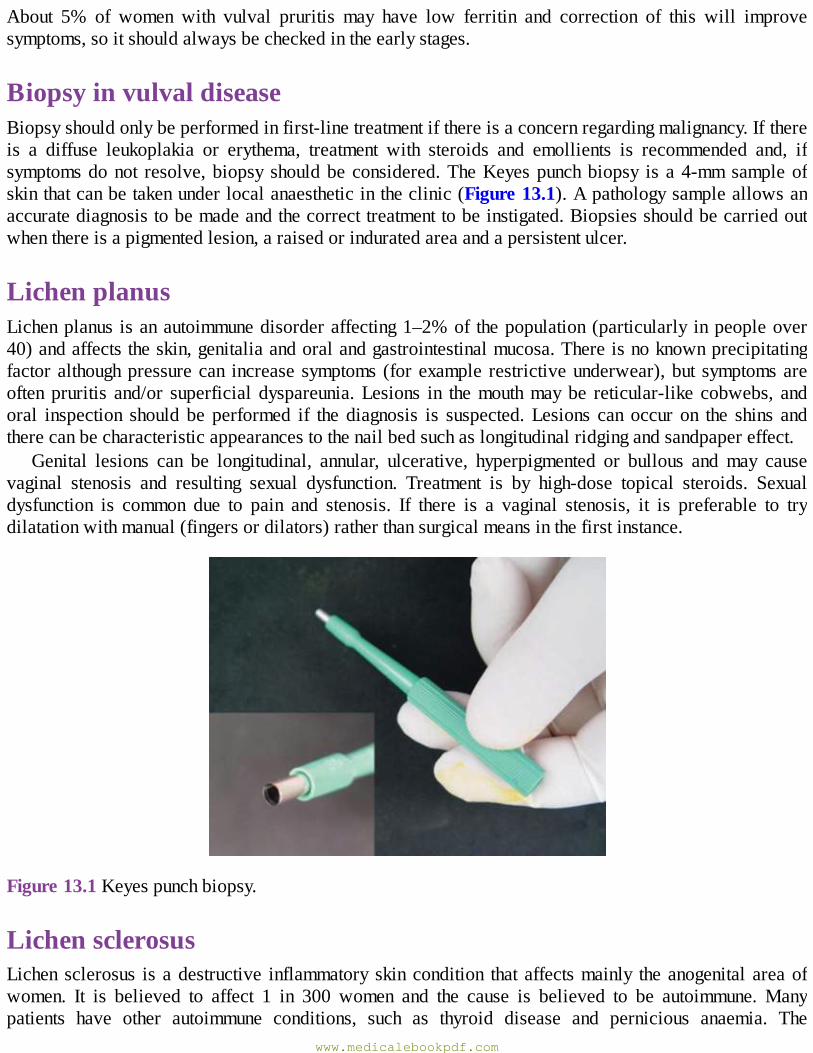
About 5% of women with vulval pruritis may have low ferritin and correction of this will improvesymptoms,soitshouldalwaysbecheckedintheearlystages.
BiopsyinvulvaldiseaseBiopsyshouldonlybeperformedinfirst-linetreatmentifthereisaconcernregardingmalignancy.Ifthereis a diffuse leukoplakia or erythema, treatment with steroids and emollients is recommended and, ifsymptomsdonot resolve,biopsy shouldbeconsidered.TheKeyespunchbiopsy is a4-mmsampleofskinthatcanbetakenunderlocalanaestheticintheclinic(Figure13.1).Apathologysampleallowsanaccuratediagnosistobemadeandthecorrecttreatmenttobeinstigated.Biopsiesshouldbecarriedoutwhenthereisapigmentedlesion,araisedorinduratedareaandapersistentulcer.
LichenplanusLichenplanus isanautoimmunedisorderaffecting1–2%of thepopulation(particularly inpeopleover40)andaffectstheskin,genitaliaandoralandgastrointestinalmucosa.Thereisnoknownprecipitatingfactoralthoughpressurecan increasesymptoms (forexample restrictiveunderwear),but symptomsareoftenpruritis and/or superficial dyspareunia.Lesions in themouthmaybe reticular-like cobwebs, andoral inspection should be performed if the diagnosis is suspected.Lesions can occur on the shins andtherecanbecharacteristicappearancestothenailbedsuchaslongitudinalridgingandsandpapereffect.
Genital lesions can be longitudinal, annular, ulcerative, hyperpigmented or bullous and may causevaginal stenosis and resulting sexual dysfunction. Treatment is by high-dose topical steroids. Sexualdysfunction is common due to pain and stenosis. If there is a vaginal stenosis, it is preferable to trydilatationwithmanual(fingersordilators)ratherthansurgicalmeansinthefirstinstance.
Figure13.1Keyespunchbiopsy.
LichensclerosusLichen sclerosus is adestructive inflammatory skincondition that affectsmainly theanogenital areaofwomen. It is believed to affect 1 in 300 women and the cause is believed to be autoimmune.Manypatients have other autoimmune conditions, such as thyroid disease and pernicious anaemia. The
www.medicalebookpdf.com

destructivenatureoftheconditionisduetounderlyinginflammationinthesubdermallayersoftheskin,which results in hyalinization of the skin. This leads to a fragility and white ‘parchment paper’appearance of the skin and loss of vulval anatomy. The condition can involve the foreskin ofmen toproduce a phimosis. Lichen sclerosus is evident elsewhere on the body in 15%of patients. Themainsymptoms on the vulva are itching and subsequent soreness of the vulva, usually due to scratching.Abiopsy can confirm the diagnosis and treatment is a combination of good skin care and strong steroidointmentssuchas thosecontainingclobetasol.Lichensclerosus isassociatedwithvulvalcancer,but isnot a cause.Manywomenwith vulval cancer have lichen sclerosis at the time of diagnosis and it isestimatedthatthereisalowriskofcancerdevelopinginawomenwithlichensclerosus(around3–5%).
Lichensclerosuscharacteristicallypresentsina‘figureof8’patternaroundthevulvaandanus.Thereis frequently hypopigmentation, loss of anatomy, vaginal stenosis and cracking (particularly in theposterior fourchette) but appearances can be subtle in early-stage disease (Figure 13.2). Treatment ofboth lichen planus and sclerosus is by high-dose topical steroids (clobetasol proprionate), applying apea-sizedamountdailyfor1month,alternatedaysforthesecondmonthandtwiceaweekforthethirdmonth.Ifthereisnotcompleteresolutionofsymptoms,biopsyisindicated.Womenshouldbeadvisedtoseek advice if the lesions become raised or resistant to treatment. Once the course of treatment iscompleted,thesteroidcreamcanbeusedbywomenasandwhenrequired.
VulvalcystsBartholin’s cysts,Skeneglandcysts andmucous inclusioncysts canaffect thevulval area andcause alumpwithorwithoutvulvaldiscomfort.Iftheydonotcausethepatientanyproblem,theycanbeeithermonitoredorexcised.ABartholin’scystisthemostcommontypeofcystanddevelopsintheregionoftheBartholin’sgland(Figure13.3).TheBartholin’sglandhasalongductwhich,whenblocked,causesfluidtobuildupandeventually formsacyst. It isnotuncommon for thesecysts toget infectedandcauseaBartholin’sabscessthatusuallypresentsacutelyandmayrequireincisionanddrainage.Marsupializationof the cyst is the termusedwhen the internal aspectof the cyst is sutured to theoutsideof the cyst tocreate a window so that the cyst does not reform.Marsupialization of Bartholin’s cysts is usually anelectiveprocedureundergeneralorspinalanaesthesia.Outpatientdrainageisalsopossible,sometimesfollowedbytheinsertionofatinycatheterintotheincision,whichremainsinplaceforseveralweekstomaintainitspatency.
www.medicalebookpdf.com
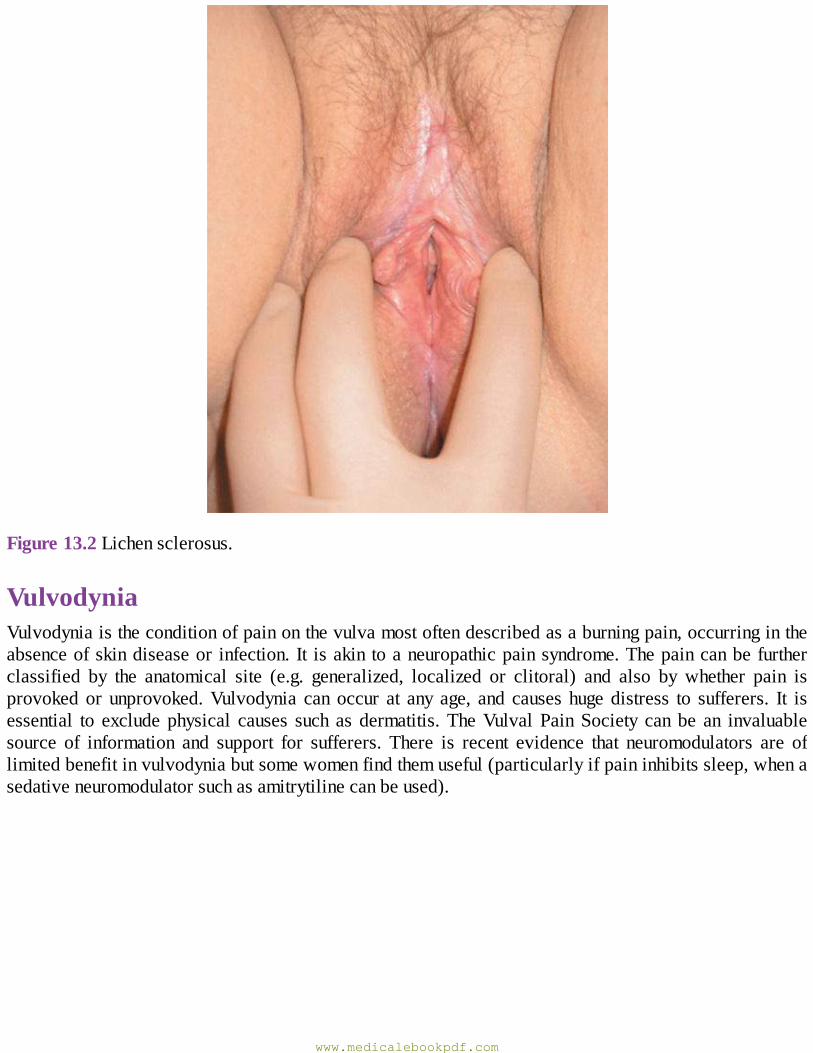
Figure13.2Lichensclerosus.
VulvodyniaVulvodyniaistheconditionofpainonthevulvamostoftendescribedasaburningpain,occurringintheabsenceofskindiseaseor infection.It isakin toaneuropathicpainsyndrome.Thepaincanbefurtherclassified by the anatomical site (e.g. generalized, localized or clitoral) and also by whether pain isprovokedor unprovoked.Vulvodynia can occur at any age, and causes hugedistress to sufferers. It isessential to exclude physical causes such as dermatitis.TheVulval PainSociety can be an invaluablesource of information and support for sufferers. There is recent evidence that neuromodulators are oflimitedbenefitinvulvodyniabutsomewomenfindthemuseful(particularlyifpaininhibitssleep,whenasedativeneuromodulatorsuchasamitrytilinecanbeused).
www.medicalebookpdf.com
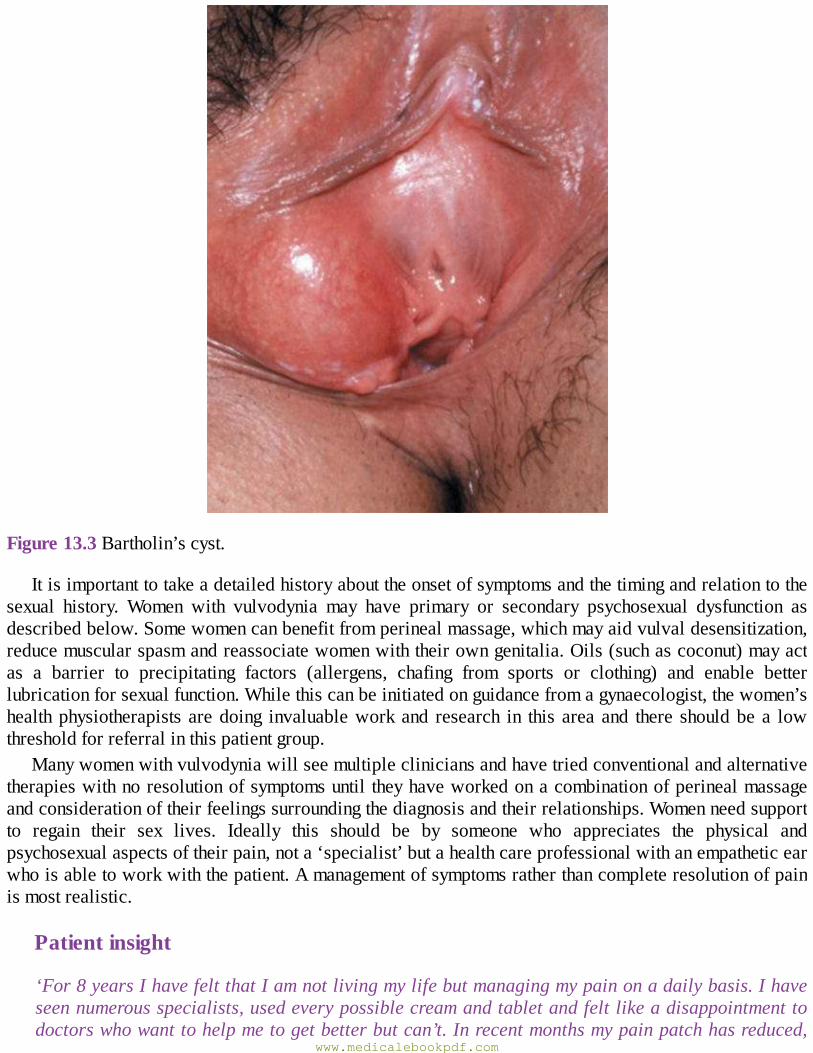
Figure13.3Bartholin’scyst.
Itisimportanttotakeadetailedhistoryabouttheonsetofsymptomsandthetimingandrelationtothesexual history. Women with vulvodynia may have primary or secondary psychosexual dysfunction asdescribedbelow.Somewomencanbenefitfromperinealmassage,whichmayaidvulvaldesensitization,reducemuscularspasmandreassociatewomenwiththeirowngenitalia.Oils(suchascoconut)mayactas a barrier to precipitating factors (allergens, chafing from sports or clothing) and enable betterlubricationforsexualfunction.Whilethiscanbeinitiatedonguidancefromagynaecologist,thewomen’shealthphysiotherapists aredoing invaluableworkand research in this area and there shouldbe a lowthresholdforreferralinthispatientgroup.
Manywomenwithvulvodyniawillseemultiplecliniciansandhavetriedconventionalandalternativetherapieswithnoresolutionofsymptomsuntil theyhaveworkedonacombinationofperinealmassageandconsiderationoftheirfeelingssurroundingthediagnosisandtheirrelationships.Womenneedsupportto regain their sex lives. Ideally this should be by someone who appreciates the physical andpsychosexualaspectsoftheirpain,nota‘specialist’butahealthcareprofessionalwithanempatheticearwhoisabletoworkwiththepatient.Amanagementofsymptomsratherthancompleteresolutionofpainismostrealistic.
Patientinsight
‘For8yearsIhavefeltthatIamnotlivingmylifebutmanagingmypainonadailybasis.Ihaveseennumerousspecialists,usedeverypossiblecreamandtabletandfeltlikeadisappointmenttodoctorswhowanttohelpmetogetbetterbutcan’t.Inrecentmonthsmypainpatchhasreduced,
www.medicalebookpdf.com
mysexlifeimprovedandIcanseethatoneday,likeabutterfly,itwilljustflyaway’.Vulvodyniasufferer.
DyspareuniaDyspareunia is defined as pain during sexual intercourse. Dyspareunia may be associated with manygynaecologicalproblemsand isdescribedas superficial ordeep, the latter sometimes associatedwithpathology such as endometriosis or pelvic inflammatory disease (PID). On many occasions, despiteappropriateinvestigations,nocausecanbefoundandpsychologicalsupportshouldbeoffered.
Dyspareunia
•Definition:painduringoraftersexualintercourse,whichcanbeclassifiedassuperficialaffectingthevagina,clitorisorlabia,ordeepwithpainexperiencedwithinthepelvis.
• Epidemiology: the estimated prevalence is between 10% and 20%, although this may be anunderestimate as many women may not present. Risk factors include female genital mutilation(FGM),suspectedPIDandendometriosis,peri/postmenopausalstatus,depressionoranxietystatesandhistoryofsexualassault.
•Clinicalevaluation:• the clinical history should explore the nature and onset of pain, the relationship to intercourse,associatedchronicpelvicpainsymptoms,reproductiveandpastmedicalhistory.Apyschosexualhistoryshouldbeconsideredespeciallyforsuperficialdyspareunia;
•abdominalandpelvicexaminationshouldlookforlowergenital tractlesions(e.g.skindisorder,scarring,anatomicalabnormality),vaginismus(involuntarycontractionofvaginalmusclesduringvaginalexamination),areasoftendernesswithintheloweranduppergenitaltractandevidenceofpelvicdisease(masses,tenderness,fixityoforgans).
•Investigations:•superficialdyspareunia:considerabiopsyoflowergenitaltractlesionsandswabs;•deepdyspareunia:considertransvaginalultrasoundscan(TVUSS),swabsandlaparoscopy.•Treatment:•superficialdyspareunia:treatanyidentifiablecause;•deepdyspareunia:treatasforchronicpelvicpain.
PsychosexualmedicinePsychosexualproblemsmaybeprimaryorsecondary.
Psychosexualdysfunction
www.medicalebookpdf.com
•Primarypsychosexualdysfunctiondescribessexualdifficultieswheretheremaybepsychosomaticpain.
•Secondarypsychosexualdysfunctiondescribessexualdifficultiesresultingfrompainoremotionalissues.
HowtoapproachconsultationsVulvaldisordersareinvariablylinkedwithfemale(andoccasionallysecondarymale)sexualdysfunction.Whether primary or secondary, and regardless of the aetiology, it is important to explore this in theconsultation.
TheInstituteofPsychosexualMedicineusestheLOFTImodeltoaidwithconsultation.
TheLOFTImodel
Listening
• Open questions and periods of silence allow the patient to divulge and elaborate on essentialinformation.
•Whatistheirtone/styleoflanguage?•Whatis/isnotsaid?Howandwhen?
Observing
•Patternsofbehaviour(e.g.frequentcancellations/avoidanceofappointments).•Urgency,demeanour,styleofdressandmannerisms.•Referrallettersfromthegeneralpractitioner(GP)maybedetailedandpressurized,emphasizingtheurgencyofthereferral(anexampleoftransference,theunconsciousredirectionoffeelingsfromthepatienttotheGP).
Feelings
•Beawareoffeelingsintheroom.•Howdoesthepatientmakeyoufeel?•Feelingsarousedinanydoctorbythepatient’slanguage,behaviourandtheattitudeofthedoctortothepatientareseenaspossibleevidenceofthepatient’sownlessthanconsciousfeelings.
Thinking
•Notewhatsortofdoctoryouarebeingintheconsultation–aparent?Teacher?•Whyisthepatientpresentingnow?Howdidthepatientcometohavetheconsultation/whatistheirmotivation?
•Notehowyoufeelbeforeandaftertheconsultation.www.medicalebookpdf.com
Interpreting
•Assess the overall picture – is the patient displaying certain types of behaviour or attitude as adefencemechanismorameansofhidinganxietyorfearsuchastearsoranger?
•Defencemechanismsincluderegression,dissociation,introjection,sublimationordenial.•Whatdoyounoticefromgenitalexamination?Isthereavoidance(i.e.patientsmenstruatingateveryappointmentoralwayshavingdifficultieswithsmears)?
Vaginismusandnon-consummationVaginismus cases are often some of the most challenging for both gynaecologists and psychosexualtherapists.Vaginismuscan lead tonon-consummationandallgynaecologistsshouldappreciate thehugeimpactofsuchsexualdysfunctionontheirpatients’relationshipsandlives.
Thereisoftenapressureoftime(fertilityorrelationshipissues),inadditiontothepatientsconcernsaboutaphysicalanomaly, thatmaylead thegynaecologist toaphysical interventionsuchasaFenton’sprocedure. While this may satisfy a short-term desire for a patient to widen what appears to be animpossibly small hole, it very rarely succeeds in providing an answer to non-consummation and theunderlyingvaginismusthatwilldefeatthepartnerfrompenetration.
Patientinsight
‘PleasewillyoujustdrivesomethingthroughtheblockagewhilstI’masleepsomyhusbandcangetinthere?’Patientwithnon-consummation.
Traditionally, both doctors and sex therapists have used vaginal dilators to enable the woman to‘overcomeherblockage’buttheyoftenbecomeveryadeptatsatisfyingthedoctoringoingupthesizesbut, anecdotally, rarely translate this into sexual activity. Although frequently prescribed, the use ofdilatorshasnoprovenbenefitandtheevidenceinfavouroftheiruseremainsanecdotal,withoutevidenceofefficacyifthereisnophysicalpathology.Moreresearchisneededinthisarea.
Patientinsight
‘Hegavemevaginaldilators,butwhenIusedthemitfeltlikeanextensiononthedoctorsfingersandgotmenoclosertohavingsexwithmyhusband’.Vaginismuspatient.
Practitioners undertaking psychosexual training will begin to recognize the transference of thepartner’sfeelingsontothemselvesandadrivetoopenthevaginaandachievepenetrationthatmayexhibititselfsubconsciouslyasafrustrationandirritationwiththepatient.Additionally,theymayfeelinhibitedfrom examining women with vaginismus and willingly accept the ‘everlasting period’ as a means ofavoidingexaminationasaresultofthepatient’sfearofthevaginaandthusexamination.Inaddition,thismayfurtherleadtoatemptationtoprovideanexaminationunderanaesthesiaandmanualdilation,whichmaypositivelyreinforcethepatient’sperceptionofaphysicalissuethatmighteventuallyleadtofurtherunnecessarysurgery.
Womenwithvaginismusmaymakethemostprogresswithaprofessionalwhoisabletoaddressthephysicalconcernsbypsychological‘flooding’(forexamplepayingcloseattentiontowordingandaction).Insteadof responding to ‘toosmall’byusing thesmall speculumand therebypositively reinforcing the
www.medicalebookpdf.com
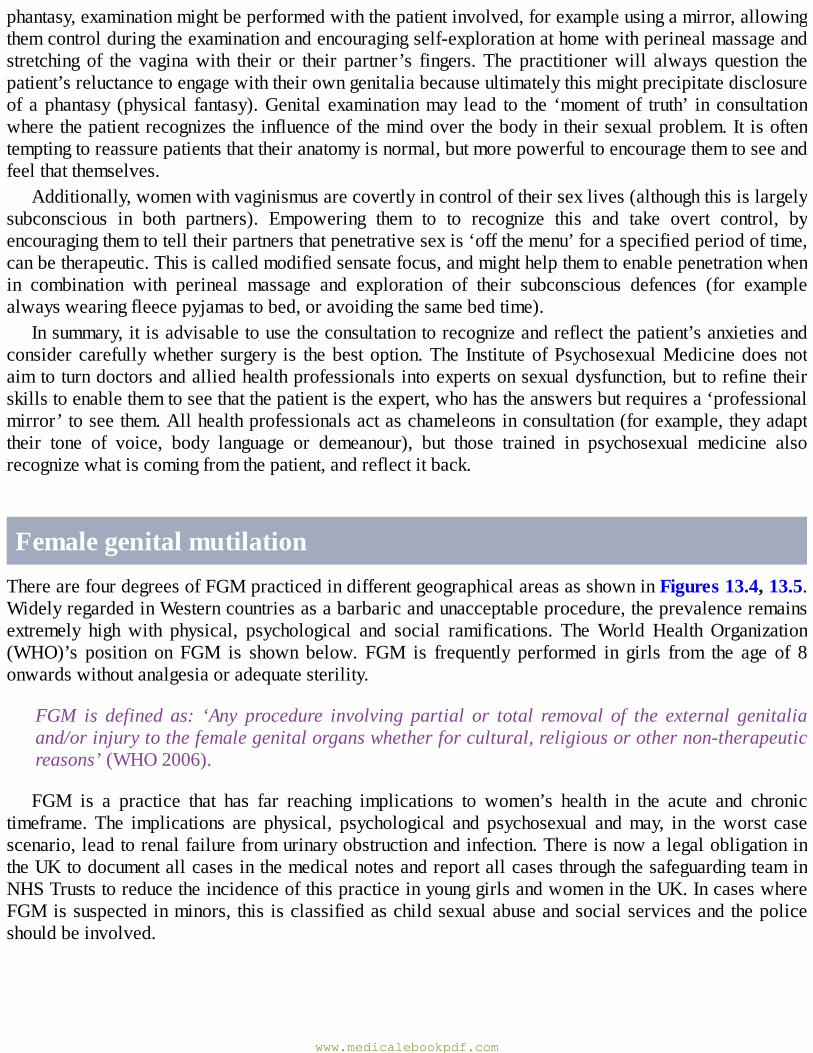
phantasy,examinationmightbeperformedwiththepatientinvolved,forexampleusingamirror,allowingthemcontrolduringtheexaminationandencouragingself-explorationathomewithperinealmassageandstretching of the vaginawith their or their partner’s fingers.The practitionerwill always question thepatient’sreluctancetoengagewiththeirowngenitaliabecauseultimatelythismightprecipitatedisclosureof aphantasy (physical fantasy).Genital examinationmay lead to the ‘momentof truth’ in consultationwherethepatientrecognizestheinfluenceofthemindoverthebodyintheirsexualproblem.It isoftentemptingtoreassurepatientsthattheiranatomyisnormal,butmorepowerfultoencouragethemtoseeandfeelthatthemselves.
Additionally,womenwithvaginismusarecovertlyincontroloftheirsexlives(althoughthisislargelysubconscious in both partners). Empowering them to to recognize this and take overt control, byencouragingthemtotelltheirpartnersthatpenetrativesexis‘offthemenu’foraspecifiedperiodoftime,canbetherapeutic.Thisiscalledmodifiedsensatefocus,andmighthelpthemtoenablepenetrationwhenin combination with perineal massage and exploration of their subconscious defences (for examplealwayswearingfleecepyjamastobed,oravoidingthesamebedtime).
Insummary,itisadvisabletousetheconsultationtorecognizeandreflectthepatient’sanxietiesandconsider carefullywhether surgery is thebestoption.The InstituteofPsychosexualMedicinedoesnotaimtoturndoctorsandalliedhealthprofessionalsintoexpertsonsexualdysfunction,buttorefinetheirskillstoenablethemtoseethatthepatientistheexpert,whohastheanswersbutrequiresa‘professionalmirror’toseethem.Allhealthprofessionalsactaschameleonsinconsultation(forexample,theyadapttheir tone of voice, body language or demeanour), but those trained in psychosexual medicine alsorecognizewhatiscomingfromthepatient,andreflectitback.
FemalegenitalmutilationTherearefourdegreesofFGMpracticedindifferentgeographicalareasasshowninFigures13.4,13.5.WidelyregardedinWesterncountriesasabarbaricandunacceptableprocedure,theprevalenceremainsextremely high with physical, psychological and social ramifications. TheWorld Health Organization(WHO)’s position on FGM is shown below. FGM is frequently performed in girls from the age of 8onwardswithoutanalgesiaoradequatesterility.
FGM is defined as: ‘Any procedure involving partial or total removal of the external genitaliaand/orinjurytothefemalegenitalorganswhetherforcultural,religiousorothernon-therapeuticreasons’(WHO2006).
FGM is a practice that has far reaching implications to women’s health in the acute and chronictimeframe. The implications are physical, psychological and psychosexual andmay, in theworst casescenario,leadtorenalfailurefromurinaryobstructionandinfection.ThereisnowalegalobligationintheUKtodocumentallcasesinthemedicalnotesandreportallcasesthroughthesafeguardingteaminNHSTruststoreducetheincidenceofthispracticeinyounggirlsandwomenintheUK.IncaseswhereFGMissuspectedinminors, this isclassifiedaschildsexualabuseandsocialservicesandthepoliceshouldbeinvolved.
www.medicalebookpdf.com
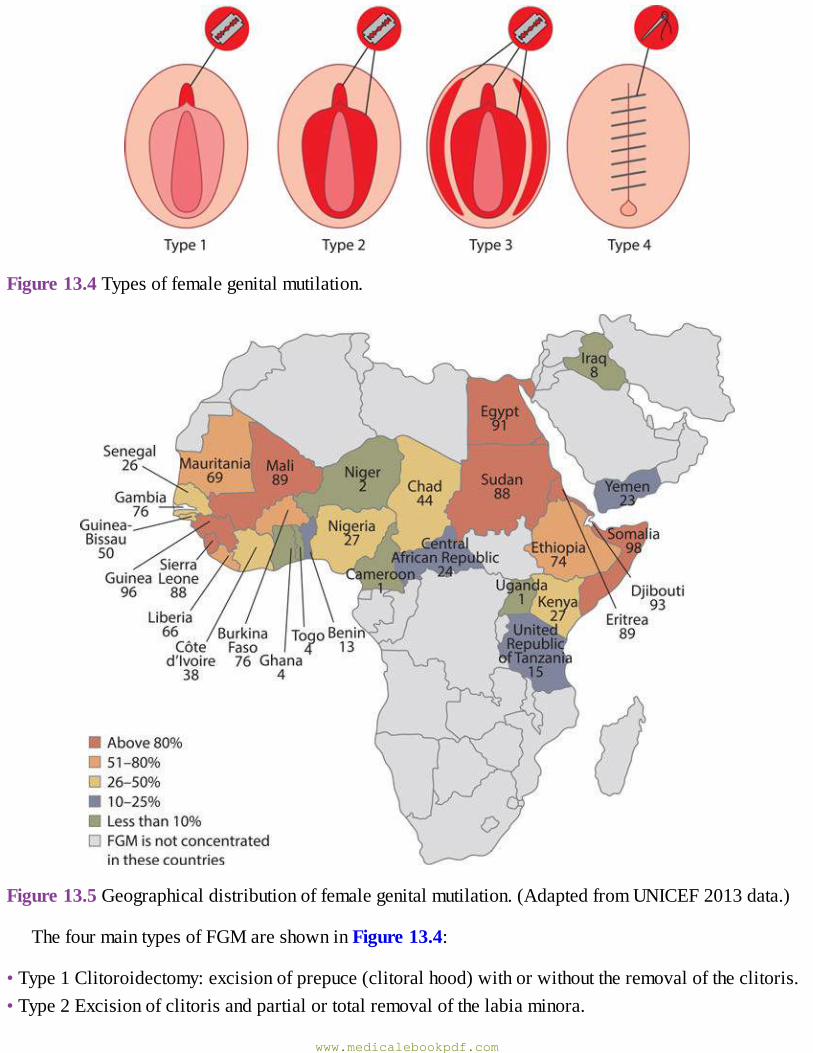
Figure13.4Typesoffemalegenitalmutilation.
Figure13.5Geographicaldistributionoffemalegenitalmutilation.(AdaptedfromUNICEF2013data.)
ThefourmaintypesofFGMareshowninFigure13.4:
•Type1Clitoroidectomy:excisionofprepuce(clitoralhood)withorwithouttheremovaloftheclitoris.•Type2Excisionofclitorisandpartialortotalremovalofthelabiaminora.
www.medicalebookpdf.com
• Type 3 Excision of part or all of the external genitalia and stitching/narrowing of the vagina –infundibulation.
•Type4Piercingtheclitoris,cauterization,cuttingthevagina,insertingcorrosivesubstances.Thisalsoincludesanyplasticsurgeryproceduresdoneasanadult.
There is often an extremely fine line between cosmetic surgery on the vulva and FGM and thegynaecologist must seek advice before considering such procedures. Prevalence of requests forlabioplastyprocedureshave risendramatically in recentyears (possibly as a result of accessibility ofpornographyand‘photoshopping’on theweb)andmanyhealthcareprovidershavewithdrawnfundingforsuchproceduresontheNHS.Thishas,inturn,increasedprivatepracticeinthisarea,whichmayofferless vigorous support for the emotionally vulnerable patient. Pre- and postsurgery patients are nowattending NHS psychosexual medicine clinics for help with sexual dysfunction either related to bodydysmorphiaorside-effectsofsurgery.Ausefultoolforwomentouseis‘TheGreatWallofVagina’,byJamieMcCartney, aBritish artistwhohas takenhundredsof plaster casts of vulvas.Women are oftenpleasantlysurprisedtoseehow‘normal’theirvulvaisafterlookingatthis.
It is difficult for UK gynaecologists to appreciate the cultural context of FGM, particularly whenworkinginareaswhereitisinfrequentlyseen.Thenovel‘PossessingtheSecretofJoy’byAliceWalkeris an essential read for gynaecologists interested in the impact of FGM on women and the culturalinfluencesbehindthepractice.ThemaincharacterchoosesFGMafterpubertytofeelmore‘intunewithherculture’andeloquentlydescribestheemotionalandphysicalimpactofherdecision.
Theobstetricianmustbealert to formaplan for suchpatients in labouranddelivery inhospital isadvisedwith a clear planof care detailed. It is not fully knownwhether labour is obstructed in thesewomenfromtheevidencetodate,butiscertainlyapossibilityinType3FGM.DependingonthetypeofFGM, it may be necessary to perform midline episiotomy for safe delivery. However, what is farpreferableistoenquireearlyinthepregnancyandrefertoaspecialistcentrefordeinfundibulation.Itisillegaltoresuture(whichmanywomenrequest)anFGM.
Reversalofinfundibulation(deinfundibulation)Ideallywomenshouldbe identifiedpreconceptuallyandsent toaspecialistcentrebutcanbemanagedantenatally.Itshouldberarethatwomenaremanagedonthelabourward,asallwomenfelttobeatriskshouldbe identifiedby theirbookingmidwivesand, if this is thecase,a seniorobstetricianshouldbepresent.
Deinfundibulation should be performed with adequate analgesia to avoid flashbacks to the FGMprocedure(localanaestheticcanbeusedbutmaydistortanatomy).Theincisionshouldbemadealongthevulvalincisionscarandtheurethraidentifiedbeforesurgerycommencestoreducedamage.Allwomenshould have prior urinary infection screening and given appropriate antibiotic therapy, as bladderobstructionandurinaryinfectionratesarehigh.Afineabsorbablesutureshouldbeusedandprophylacticantibioticsconsidered.
It should not be assumed that both sexual dysfunction and emotional distress is resolved bydeinfundibulationandspecialistcentreswillbeablemoreadequately toaccessspecialistservicesandsupportgroupsforaffectedwomen.
KEYLEARNINGPOINTS
www.medicalebookpdf.com
•Womenwithvulvaldiseaseoftenpresent latewithextensiveanddebilitatingdisease thataffectstheirdailylivesandintimaterelationships.
•Vulvaldiseasemaycausepruritisandgoodskincareandsteroidtreatmentmayhelp.•Biopsymayaiddiagnosisandexcludemalignancy.•Dyspareuniaisdescribedasdeeporsuperficial.•Patientswithpsychosexualdisordersareoftenfrustratedandangryandsomayfeel ‘difficult’ tomanage,butprovideanopportunity touse the skills thatallgynaecologistspossess inaholisticmannertohelpthemimprovesymptoms,livewiththeirdiseaseandachieveasatisfactorysexuallife.
• FGM is frequently performed on girls worldwide, and it is essential to recognize and offerdeinfundibulation.
FurtherreadingBritishAssociation for SexualHealth andHIVUKNationalGuideline on theManagement ofVulvalConditions2014.
McEwanI(2007).OnChesilBeach.JonathanCape.Royal College of Gynaecologists and Obstetricians. Female Genital Mutilation and its Management(Green-topGuidelineNo.53)2015.
SkrineR,MontfordH.PsychosexualMedicine:AnIntroduction,2ndEdition.HodderArnold,2001.WalkerA(1992).PossessingtheSecretofJoy.HarcourtBraceJovanovich.
Usefulwebsites:TheInstituteofPsychosexualMedicinewww.ipm.org.ukCollegeofSexualandRelationshipTherapieswww.cosrt.co.ukwww.csp.org.uk
Selfassessment
CASEHISTORY
A25-year-oldwomanhasbeen seenbyher communitymidwifeanddisclosedprevious ‘cutting’.Themidwifehasurgentlyreferredhertoyourantenatalclinic.Sheisnow28weekspregnant.Whatarethenextstepsthatyoushouldtake?
www.medicalebookpdf.com
ANSWERS
Initial examination is helpful to determine the degree of FGM (1–4) as this will affect themanagement initially and of labour. The safe guarding teammust be aware, and it essential thatdocumentation,datedandtimed,ispresentinthenotes.Thesearelegalrequirements.Ensurethatatranslatorisavailableifnecessaryforallvisits.DependingonthetypeofFGM,midlineepisiotomyinlabourmaybenecessary.Earlydeinfundibulationispreferable.Suturingpostdeliveryshouldbeperformedbyaseniorobstetrician.IntheUKitisillegaltoperformrestorationoftheFGM,evenonrequest.
SBAQUESTIONS
1 A 36-year-old obese woman presents with recurrent thrush, increased thirst and frequency ofurination.Whattestisessentialinthiscase?Choosethesinglebestanswer.ASerumferritin.BHighvaginalswab.CVulvalbiopsy.DFastingbloodglucose.ESkinprickallergytesting.
ANSWER
DThereisaassociationofdiabetesandrecurrentcandida,duetotheincreasedserumglucose.Thispatienthassymptomsofdiabetesaswellasriskfactor.
2A30-year-oldwomanpresentswithherpartnerunabletoconsummatehermarriage.Sheasksyoutoassistherinachievingpenetrativepenilesex.Whatshouldbeyourfirststep?Choosethesinglebestanswer.
APrescribedilatorsandadvisehertowatchtheinstructionfilm.BBookexaminationanddilationundergeneralanaesthetic.CBookherforaFenton’sprocedureundergeneralanaesthetic.DArrangeBotoxinjectionstotheperinealmusculature.EPerformexaminationandencourageflooding.
ANSWER
E Invasive investigations or treatments are unhelpful and can be damaging.Vaginal dilators havebeen shown to have little benefit in this circumstance. Psychosexualmanagement ismuchmoreeffectiveforthiscouple.
www.medicalebookpdf.com
CHAPTER14Malignantdiseaseoftheovary
EMMAJCROSBIE
Introduction
Ovariancancers
Epithelialtumours
Primaryperitonealcarcinoma
Sexcordstromaltumours
Germcelltumours
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Learnhowmalignantdiseaseoftheovary,Fallopiantubeandperitoneumpresents.
•Learnhowovariancancerisinvestigatedandstaged.
•Learnhowovariancancerismanaged.
Introductionwww.medicalebookpdf.com
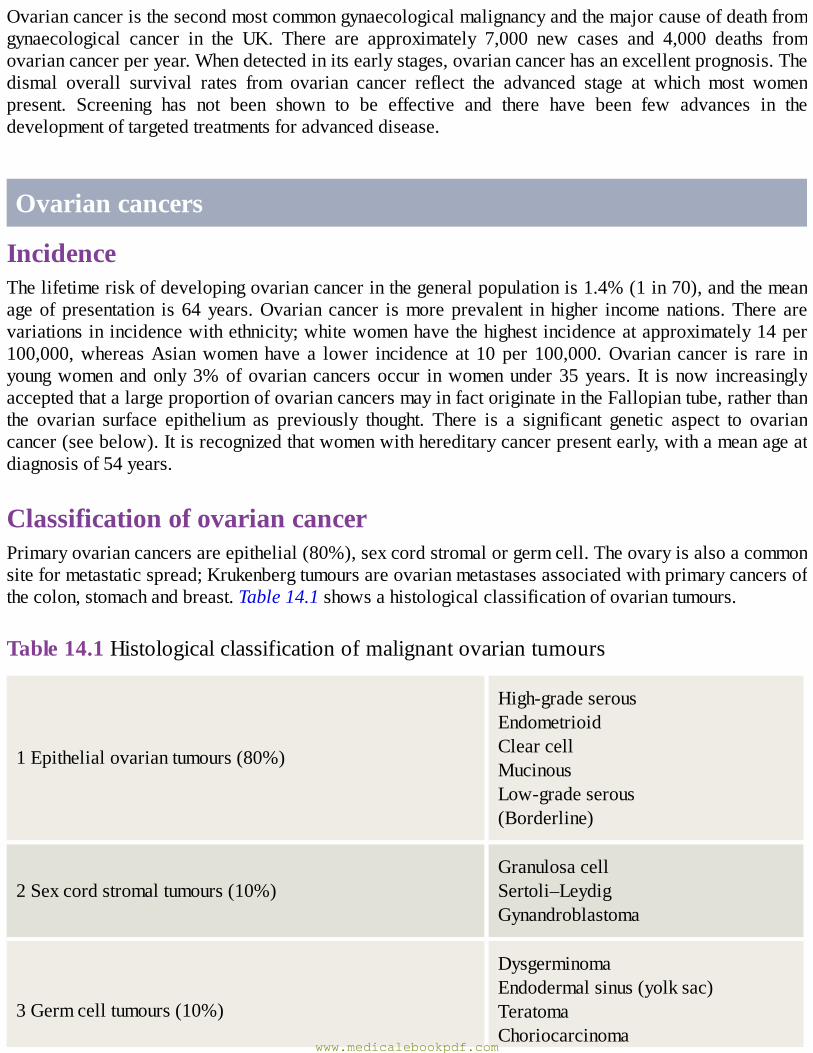
Ovariancanceristhesecondmostcommongynaecologicalmalignancyandthemajorcauseofdeathfromgynaecological cancer in the UK. There are approximately 7,000 new cases and 4,000 deaths fromovariancancerperyear.Whendetectedinitsearlystages,ovariancancerhasanexcellentprognosis.Thedismal overall survival rates from ovarian cancer reflect the advanced stage at which most womenpresent. Screening has not been shown to be effective and there have been few advances in thedevelopmentoftargetedtreatmentsforadvanceddisease.
Ovariancancers
IncidenceThelifetimeriskofdevelopingovariancancerinthegeneralpopulationis1.4%(1in70),andthemeanageofpresentation is 64years.Ovarian cancer ismoreprevalent inhigher incomenations.There arevariationsinincidencewithethnicity;whitewomenhavethehighestincidenceatapproximately14per100,000,whereasAsianwomenhave a lower incidence at 10 per 100,000.Ovarian cancer is rare inyoungwomenandonly3%ofovarian cancersoccur inwomenunder35years. It is now increasinglyacceptedthatalargeproportionofovariancancersmayinfactoriginateintheFallopiantube,ratherthanthe ovarian surface epithelium as previously thought. There is a significant genetic aspect to ovariancancer(seebelow).Itisrecognizedthatwomenwithhereditarycancerpresentearly,withameanageatdiagnosisof54years.
ClassificationofovariancancerPrimaryovariancancersareepithelial(80%),sexcordstromalorgermcell.Theovaryisalsoacommonsiteformetastaticspread;Krukenbergtumoursareovarianmetastasesassociatedwithprimarycancersofthecolon,stomachandbreast.Table14.1showsahistologicalclassificationofovariantumours.
Table14.1Histologicalclassificationofmalignantovariantumours
1Epithelialovariantumours(80%)
High-gradeserousEndometrioidClearcellMucinousLow-gradeserous(Borderline)
2Sexcordstromaltumours(10%)GranulosacellSertoli–LeydigGynandroblastoma
3Germcelltumours(10%)
DysgerminomaEndodermalsinus(yolksac)TeratomaChoriocarcinoma
www.medicalebookpdf.com

Mixed
4Metastatic(includingKrukenbergtumours)
EpithelialtumoursEpithelialtumoursoftheovarycanbebenign,malignantorborderline.Approximately10%ofepithelialtumoursareclassifiedasborderlineovariantumours(BOTs).Thesetumoursarewelldifferentiated,withsome features of malignancy (nuclear pleomorphism, cellular atypia) but do not invade the basementmembrane.BOTsspreadtootherabdominopelvicstructures(peritoneum,omentum)butdonotoftenrecurfollowinginitialsurgery.ThemajorityofBOTsareseroustumours.MucinousBOTsmayactuallyarisefrom appendiceal carcinomas of low malignant potential and can be associated with pseudomyxomaperitoneii.
High-gradeserouscarcinomasaccountforaround75%ofallepithelialovariancancers;mucinousandendometrioid tumoursare lesscommon,accounting for10%, followedbyclearcellcarcinomas.High-grade serous tumours are characterized histologically by concentric rings of calcification, known as‘psammoma bodies’.Mucinous carcinomas are generally largemultiloculated tumours associatedwithpseudomyxoma peritoneii. Endometrioid carcinomas are similar in histological appearance toendometrial cancer, are associated with endometriosis in approximately 10% of cases and also asynchronous separate endometrial cancer in 10–15%. They tend to be well differentiated and areassociatedwithabettersurvivalthanhigh-gradeserouscarcinomas.Clearcellcarcinomascanalsoarisefromendometriosisandarecharacterizedhistologicallybyclearcells,muchlikerenalcancer.
AetiologyandriskfactorsEpithelial ovarian cancers include a heterogeneous group of tumours of different histological subtypesandaetiologiesthataffecttheovary,Fallopiantubeandperitoneum.
High-gradepelvicserouscarcinomasBecausemosthigh-gradepelvicserouscarcinomaspresentwithadvanceddisease involving theovary,Fallopian tubeandperitoneal surfaces, it isoften impossible toestablish theanatomical siteoforigin.Assigningprimary tumoursite isof littleclinical relevanceanywaysince thebehaviour,prognosisandtreatment of these tumours are identical. Thus the term high-grade pelvic serous carcinoma has beencoined to incorporate all high-grade serous tumours arising from the ovary, Fallopian tube and/orperitoneum. Data from women with BRCAmutations who have undergone risk-reducing prophylacticbilateralsalpingo-oophorectomy(BSO)suggestaFallopiantubalprecursorlesionforhigh-gradepelvicserous tumours.Theseprecursorsarecalledserous tubal intraepithelialcarcinoma(STIC) lesions,andtheyarecharacterizedbymutationsinp53insecretorycellsofthedistalFallopiantube.Asmanyas30%of high-grade pelvic serous cancers haveBRCAmutations,which has implications for themajority ofwomenwhopresentwithapparentlysporadicdisease.
www.medicalebookpdf.com
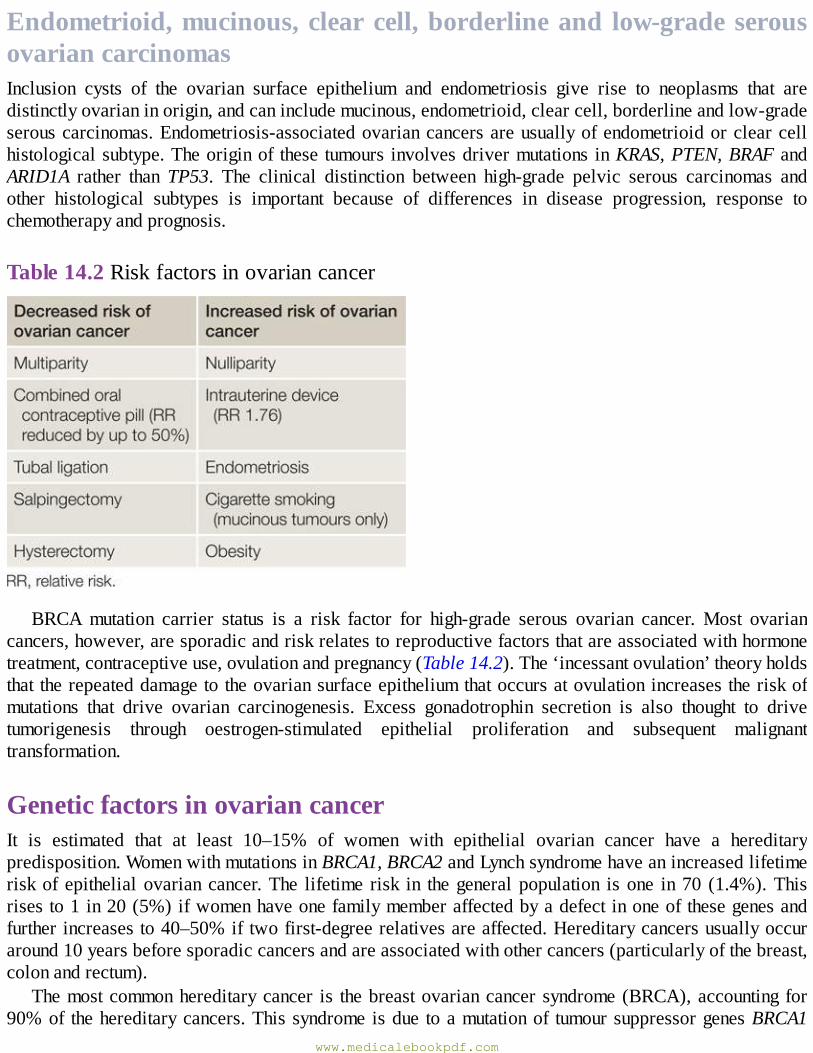
Endometrioid,mucinous,clearcell,borderlineand low-gradeserousovariancarcinomasInclusion cysts of the ovarian surface epithelium and endometriosis give rise to neoplasms that aredistinctlyovarianinorigin,andcanincludemucinous,endometrioid,clearcell,borderlineandlow-gradeserouscarcinomas.Endometriosis-associatedovariancancersareusuallyofendometrioidorclearcellhistologicalsubtype.Theoriginof these tumours involvesdrivermutations inKRAS,PTEN,BRAFandARID1A rather than TP53. The clinical distinction between high-grade pelvic serous carcinomas andother histological subtypes is important because of differences in disease progression, response tochemotherapyandprognosis.
Table14.2Riskfactorsinovariancancer
BRCAmutation carrier status is a risk factor for high-grade serous ovarian cancer. Most ovariancancers,however,aresporadicandriskrelatestoreproductivefactorsthatareassociatedwithhormonetreatment,contraceptiveuse,ovulationandpregnancy(Table14.2).The‘incessantovulation’theoryholdsthat therepeateddamagetotheovariansurfaceepitheliumthatoccursatovulationincreasestheriskofmutations that drive ovarian carcinogenesis. Excess gonadotrophin secretion is also thought to drivetumorigenesis through oestrogen-stimulated epithelial proliferation and subsequent malignanttransformation.
GeneticfactorsinovariancancerIt is estimated that at least 10–15% of women with epithelial ovarian cancer have a hereditarypredisposition.WomenwithmutationsinBRCA1,BRCA2andLynchsyndromehaveanincreasedlifetimeriskof epithelialovariancancer.The lifetime risk in thegeneralpopulation isone in70 (1.4%).Thisrisesto1in20(5%)ifwomenhaveonefamilymemberaffectedbyadefectinoneofthesegenesandfurtherincreasesto40–50%iftwofirst-degreerelativesareaffected.Hereditarycancersusuallyoccuraround10yearsbeforesporadiccancersandareassociatedwithothercancers(particularlyofthebreast,colonandrectum).
Themostcommonhereditarycancer is thebreastovariancancer syndrome(BRCA),accounting for90%of thehereditarycancers.Thissyndrome isdue toamutationof tumoursuppressorgenesBRCA1
www.medicalebookpdf.com
(80%)andBRCA2(15%).Lynchsyndromeishereditarynon-polyposiscolorectalcancer(HNPCC)andis associated with endometrial cancer and a 10% lifetime risk of ovarian cancer. Hereditary ovariancancers tend to be adenocarcinomas, present in later stages with the exception of Lynch-associatedtumours,andrecentevidencesupportsimprovedsurvival,probablyduetoabetterresponsetoplatinumchemotherapy.
PreventingovariancancerWomenwho test positive for aBRCAmutation areoffered risk-reducingprophylacticBSOwhen theyhave completed their families. This can usually be performed laparoscopically. Prophylactic surgeryreducestheriskofovariancancer(by90%)andpremenopausalbreastcancer(by50%),althoughitdoesnoteliminatetheriskofprimaryperitonealcancer.Itisimportanttocarryoutrisk-reducingsurgerypriorto the age-related surge in ovarian cancer observed in BRCAmutation carriers, which is younger inBRCA1 (mid30s) thanBRCA2patients (early40s).Anothersuggestionfor riskreductionbuildson thetheorythatBRCA-associatedovariancancersactuallyoriginateintheFallopiantube;henceperformingbilateral salpingectomywith delayed oophorectomy in the 30s and early 40smay offset themorbidityassociatedwithasurgicalmenopauseinyoungwomenwhilereducingtheriskofcancer.Thisstrategyhasyet to be subjected to rigorous testing and its efficacy is unknown. Recent data indicate that theopportunistic removal of the Fallopian tubes during hysterectomy for benign indications also reducesovarian cancer risk inwomen at average lifetime risk of ovarian cancer.Other procedures associatedwith ovarian cancer risk reduction include tubal ligation (sterilization) and hysterectomywith ovarianconservation. Chemoprevention using the combined oral contraceptive pill (COCP) reduces ovariancancerriskbyupto50%inbothBRCAmutationcarriersandwomenataverageriskofovariancancer.
ScreeningScreeningusing transvaginalultrasoundscan(TVUSS)andCA125measurementhasnotbeenshowntoimprovesurvival inwomenwitha familialpredisposition toovariancancer.This isbecause thehigh-gradeseroustumoursthatareassociatedwithBRCAmutationcarrierstatusdeveloprapidlyandmostareat an advanced stage before they can be picked up by screening. The role of screening forwomen ofaverage lifetime risk of ovarian cancer remains unclear; further results from the population-basedUKCTOCSrandomizedcontrolledtrialareawaited,asthe2015initialdatawereequivocal.
ClinicalfeaturesMostwomenwithovariancancerhavesymptoms;however, thesesymptomsarenon-specificandoftenvague.Thedifficultywithclinicaldiagnosisisthemainreasonthatpatientswithovariancancerpresentwithlatestagedisease(66%presentwithstage3diseaseorgreater),andthishasadramaticeffectonsurvival.Themostcommonsymptomsare:
•Increasedabdominalgirth/bloating.•Persistentpelvicandabdominalpain.•Difficultyeatingandfeelingfullquickly.
Othersymptomssuchaschangeinbowelhabit,urinarysymptoms,backache,irregularbleedingandfatigueoccurfrequentlyandanywomenwithpersistenceofthesesymptomsshouldbeassessedbytheir
www.medicalebookpdf.com
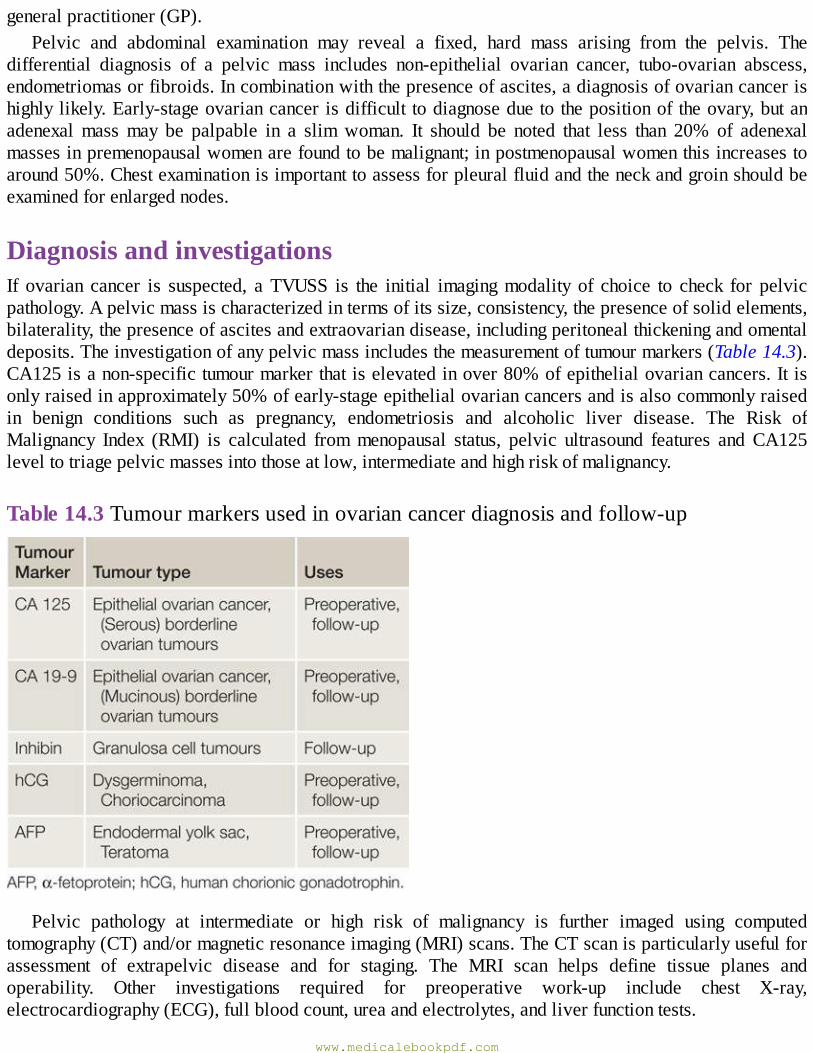
generalpractitioner(GP).Pelvic and abdominal examination may reveal a fixed, hard mass arising from the pelvis. The
differential diagnosis of a pelvic mass includes non-epithelial ovarian cancer, tubo-ovarian abscess,endometriomasorfibroids.Incombinationwiththepresenceofascites,adiagnosisofovariancancerishighlylikely.Early-stageovariancancerisdifficult todiagnoseduetothepositionoftheovary,butanadenexalmassmay be palpable in a slimwoman. It should be noted that less than 20% of adenexalmassesinpremenopausalwomenarefoundtobemalignant;inpostmenopausalwomenthisincreasestoaround50%.Chestexaminationisimportanttoassessforpleuralfluidandtheneckandgroinshouldbeexaminedforenlargednodes.
DiagnosisandinvestigationsIf ovarian cancer is suspected, aTVUSS is the initial imagingmodality of choice to check for pelvicpathology.Apelvicmassischaracterizedintermsofitssize,consistency,thepresenceofsolidelements,bilaterality,thepresenceofascitesandextraovariandisease,includingperitonealthickeningandomentaldeposits.Theinvestigationofanypelvicmassincludesthemeasurementoftumourmarkers(Table14.3).CA125isanon-specifictumourmarkerthatiselevatedinover80%ofepithelialovariancancers.Itisonlyraisedinapproximately50%ofearly-stageepithelialovariancancersandisalsocommonlyraisedin benign conditions such as pregnancy, endometriosis and alcoholic liver disease. The Risk ofMalignancy Index (RMI) is calculated frommenopausal status, pelvic ultrasound features and CA125leveltotriagepelvicmassesintothoseatlow,intermediateandhighriskofmalignancy.
Table14.3Tumourmarkersusedinovariancancerdiagnosisandfollow-up
Pelvic pathology at intermediate or high risk of malignancy is further imaged using computedtomography(CT)and/ormagneticresonanceimaging(MRI)scans.TheCTscanisparticularlyusefulforassessment of extrapelvic disease and for staging. The MRI scan helps define tissue planes andoperability. Other investigations required for preoperative work-up include chest X-ray,electrocardiography(ECG),fullbloodcount,ureaandelectrolytes,andliverfunctiontests.
www.medicalebookpdf.com
Ifthepatientpresentswithgrossascitesorpleuraleffusion,paracentesisorpleuralaspirationmayberequired for symptom relief and/or diagnosis. A sample of the fluid removed is sent for cytologicalassessment. If thediagnosis isuncertainor ifprimarychemotherapy isbeingconsidered (foradvanceddisease,orinpatientsnotfittoundergosurgery),abiopsyisneededbeforetreatmentcanbegiven.Thisisperformedlaparoscopicallyorradiologically(ultrasoundorCT-guidedbiopsy).Usuallytheomentumisagoodsiteforbiopsy.
StagingOvarian cancer staging is based on clinicopathological assessment and, like other gynaecocolocialcancers, uses the FIGO staging system (Table 14.4). Overall, 25% of patients present with stage 1disease,10%stage2,50%stage3and15%stage4disease.Metastatic spread isbydirect spread toperitoneumandotherorgansandbylymphaticspreadtopelvicandpara-aorticnodes.Ahighpercentageofwomenwithadvanceddiseasehaveevidenceofperitonealdiseaseonthediaphragmaticperitoneum(Figure14.1).Womenwithearlyovariancancer (stages1and2)haveup to20%metastaticspread tolymphnodesandthisrisesto60%inadvanceddisease(stages3and4).
Table 14.4 International Federation of Gynecology and Obstetrics (FIGO) staging ofovariancancer
www.medicalebookpdf.com
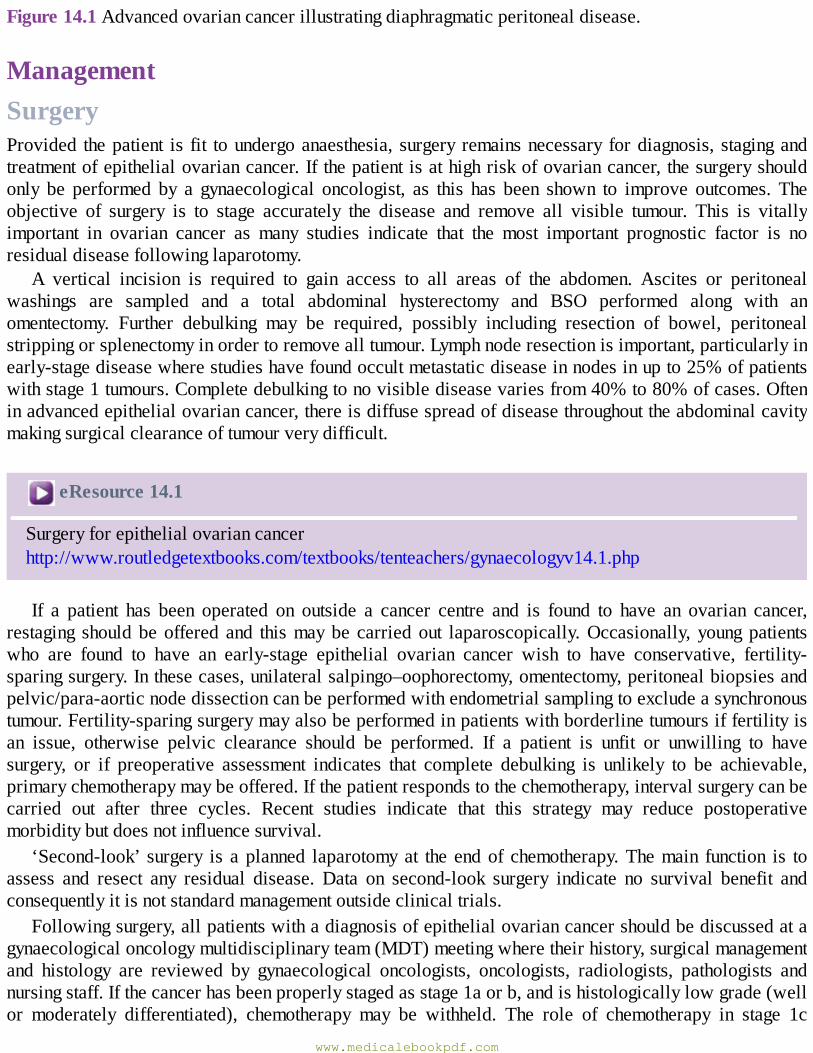
Figure14.1Advancedovariancancerillustratingdiaphragmaticperitonealdisease.
ManagementSurgeryProvided thepatient is fit toundergoanaesthesia, surgery remainsnecessary fordiagnosis, stagingandtreatmentofepithelialovariancancer.Ifthepatientisathighriskofovariancancer,thesurgeryshouldonly be performed by a gynaecological oncologist, as this has been shown to improve outcomes. Theobjective of surgery is to stage accurately the disease and remove all visible tumour. This is vitallyimportant in ovarian cancer as many studies indicate that the most important prognostic factor is noresidualdiseasefollowinglaparotomy.
A vertical incision is required to gain access to all areas of the abdomen. Ascites or peritonealwashings are sampled and a total abdominal hysterectomy and BSO performed along with anomentectomy. Further debulking may be required, possibly including resection of bowel, peritonealstrippingorsplenectomyinordertoremovealltumour.Lymphnoderesectionisimportant,particularlyinearly-stagediseasewherestudieshavefoundoccultmetastaticdiseaseinnodesinupto25%ofpatientswithstage1tumours.Completedebulkingtonovisiblediseasevariesfrom40%to80%ofcases.Ofteninadvancedepithelialovariancancer,thereisdiffusespreadofdiseasethroughouttheabdominalcavitymakingsurgicalclearanceoftumourverydifficult.
eResource14.1
Surgeryforepithelialovariancancerhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv14.1.php
If a patient has been operated on outside a cancer centre and is found to have an ovarian cancer,restaging shouldbeoffered and thismaybe carriedout laparoscopically.Occasionally, youngpatientswho are found to have an early-stage epithelial ovarian cancer wish to have conservative, fertility-sparingsurgery.Inthesecases,unilateralsalpingo–oophorectomy,omentectomy,peritonealbiopsiesandpelvic/para-aorticnodedissectioncanbeperformedwithendometrialsamplingtoexcludeasynchronoustumour.Fertility-sparingsurgerymayalsobeperformedinpatientswithborderlinetumoursiffertilityisan issue, otherwise pelvic clearance should be performed. If a patient is unfit or unwilling to havesurgery, or if preoperative assessment indicates that complete debulking is unlikely to be achievable,primarychemotherapymaybeoffered.Ifthepatientrespondstothechemotherapy,intervalsurgerycanbecarried out after three cycles. Recent studies indicate that this strategy may reduce postoperativemorbiditybutdoesnotinfluencesurvival.
‘Second-look’ surgery is aplanned laparotomyat the endof chemotherapy.Themain function is toassess and resect any residual disease. Data on second-look surgery indicate no survival benefit andconsequentlyitisnotstandardmanagementoutsideclinicaltrials.
Followingsurgery,allpatientswithadiagnosisofepithelialovariancancershouldbediscussedatagynaecologicaloncologymultidisciplinaryteam(MDT)meetingwheretheirhistory,surgicalmanagementand histology are reviewed by gynaecological oncologists, oncologists, radiologists, pathologists andnursingstaff.Ifthecancerhasbeenproperlystagedasstage1aorb,andishistologicallylowgrade(wellor moderately differentiated), chemotherapy may be withheld. The role of chemotherapy in stage 1c
www.medicalebookpdf.com
diseaseisuncertain,butinpracticemostpatientswillbeofferedpostoperativechemotherapyaswithallotherstagesofepithelialovariancancer.
Surgicalmanagementofovariancancer
• Surgery combined with platinum-based chemotherapy is the mainstay of treatment for advancedovariancancer.
•The aimof surgery is complete or optimal cytoreduction (where<1 cmof residualmacroscopicdiseaseisleftbehind).
•Tumourdepositsonthebowel,spleen,peritonealsurfacesanddiaphragmareusuallyamenabletoresection,whilediseaseinvolvingtheportahepatisandbowelmesenteryarenot.
• ‘Supraradical ovarian cancer surgery’ is appropriate in previously well, fit women withdisseminated disease if complete cytoreduction is achievable; it is associatedwith perioperativemorbidityandmortalityandwomenmustbecarefullycounselled.
•Threecyclesofneoadjuvantchemotherapyfollowedbyintervaldebulkingsurgeryisnotinferiortoupfrontsurgeryandhasbeenshowntobeassociatedwithlessmorbidity.
ChemotherapyChemotherapy can be given as primary treatment, as an adjunct following surgery or for relapse ofdisease.Itcanbeusedtoprolongclinicalremissionandsurvivalorforpalliation.First-linetreatmentisusuallyacombinationofaplatinumcompoundwithpaclitaxel.Mostregimesaregivenonanoutpatientbasis,3weeksapartforsixcycles.
Platinumcompoundsarethemosteffectivechemotherapeuticagentsinovariancancer.Theyareheavymetal agents that cause cross linkage of deoxyribonucleic acid (DNA) strands, thus arresting cellreplication.Carboplatinisnowthemainplatinumcompoundusedasitislessrenaltoxicandcauseslessnauseathancisplatin,butisequallyaseffective.Thedoseofcarboplatiniscalculatedaccordingtotheglomerularfiltrationrate(GFR)usingtheareaunderthecurve(AUC).
PaclitaxolisderivedfromthebarkofthePacificyewandworksbycausingmicrotubulardamagetothecell.Thispreventsreplicationandcelldivision.Pre-emptivesteroidsaregivenduetohigh-sensitivityreactions; side-effects of peripheral neuropathy, neutropenia and myalgia are common and dosedependent.Paclitaxolcausestotallossofallbodyhair,irrespectiveofdose.
Bevacizumab, a monoclonal antibody against vascular endothelial growth factor (VEGF), inhibitsangiogenesis. It has been shown to be clinically effective at improving recurrence free and overallsurvival when given in combinationwith carboplatin and paclitaxel in advanced ovarian cancer. Theside-effectprofileofthisdrugincludeshypertension,delayedwoundhealing,gastrointestinalperforationand arterial thromboembolic events. This drug is not routinely prescribed as first-line treatment foradvanced ovarian cancer on theNHS due to cost issues; however, it is available for the treatment ofrecurrentdisease.
Following completion of chemotherapy, patients have a further CT scan to assess response totreatment.Thisscancanbeusedforcomparisoninthefutureifthereisclinicalorbiochemicalevidenceofrecurrence.
www.medicalebookpdf.com
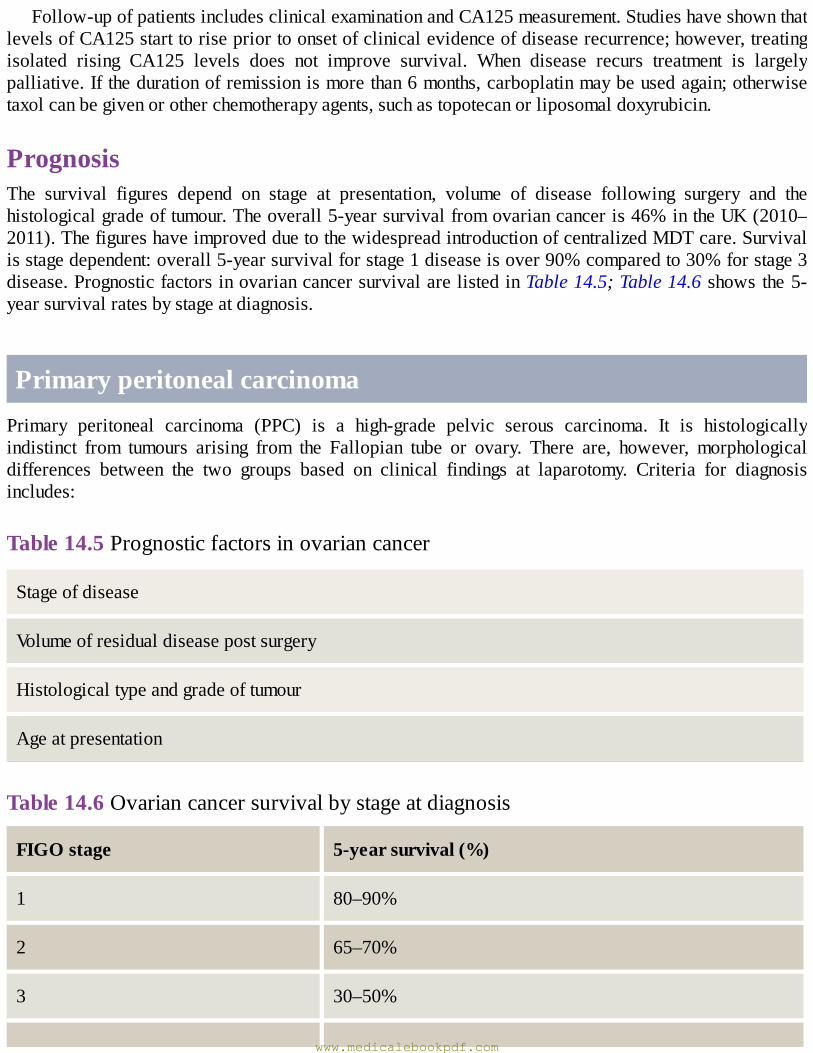
Follow-upofpatientsincludesclinicalexaminationandCA125measurement.StudieshaveshownthatlevelsofCA125starttorisepriortoonsetofclinicalevidenceofdiseaserecurrence;however,treatingisolated rising CA125 levels does not improve survival. When disease recurs treatment is largelypalliative.Ifthedurationofremissionismorethan6months,carboplatinmaybeusedagain;otherwisetaxolcanbegivenorotherchemotherapyagents,suchastopotecanorliposomaldoxyrubicin.
PrognosisThe survival figures depend on stage at presentation, volume of disease following surgery and thehistologicalgradeoftumour.Theoverall5-yearsurvivalfromovariancanceris46%intheUK(2010–2011).ThefigureshaveimprovedduetothewidespreadintroductionofcentralizedMDTcare.Survivalisstagedependent:overall5-yearsurvivalforstage1diseaseisover90%comparedto30%forstage3disease.PrognosticfactorsinovariancancersurvivalarelistedinTable14.5;Table14.6 shows the5-yearsurvivalratesbystageatdiagnosis.
PrimaryperitonealcarcinomaPrimary peritoneal carcinoma (PPC) is a high-grade pelvic serous carcinoma. It is histologicallyindistinct from tumours arising from the Fallopian tube or ovary. There are, however, morphologicaldifferences between the two groups based on clinical findings at laparotomy. Criteria for diagnosisincludes:
Table14.5Prognosticfactorsinovariancancer
Stageofdisease
Volumeofresidualdiseasepostsurgery
Histologicaltypeandgradeoftumour
Ageatpresentation
Table14.6Ovariancancersurvivalbystageatdiagnosis
FIGOstage 5-yearsurvival(%)
1 80–90%
2 65–70%
3 30–50%
www.medicalebookpdf.com
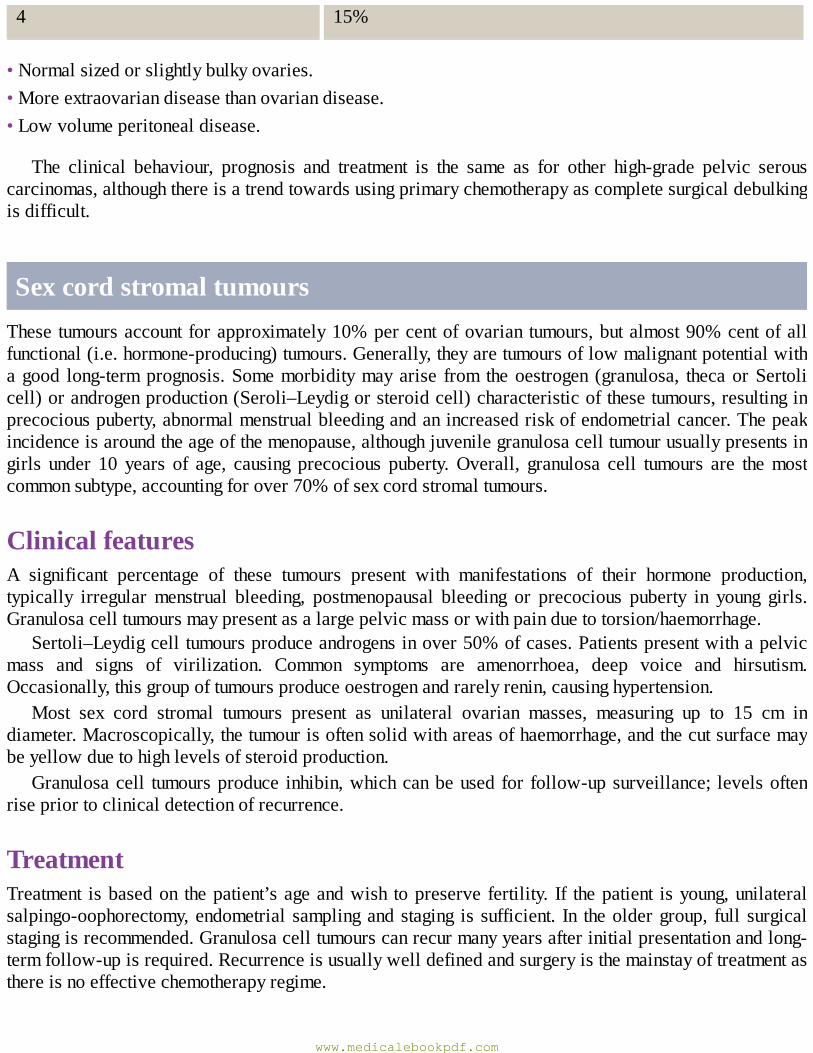
4 15%
•Normalsizedorslightlybulkyovaries.•Moreextraovariandiseasethanovariandisease.•Lowvolumeperitonealdisease.
The clinical behaviour, prognosis and treatment is the same as for other high-grade pelvic serouscarcinomas,althoughthereisatrendtowardsusingprimarychemotherapyascompletesurgicaldebulkingisdifficult.
SexcordstromaltumoursThese tumoursaccountforapproximately10%percentofovarian tumours,butalmost90%centofallfunctional(i.e.hormone-producing)tumours.Generally,theyaretumoursoflowmalignantpotentialwithagood long-termprognosis.Somemorbiditymayarise from theoestrogen (granulosa, thecaorSertolicell)orandrogenproduction(Seroli–Leydigorsteroidcell)characteristicofthesetumours,resultinginprecociouspuberty,abnormalmenstrualbleedingandanincreasedriskofendometrialcancer.Thepeakincidenceisaroundtheageofthemenopause,althoughjuvenilegranulosacelltumourusuallypresentsingirls under 10 years of age, causing precocious puberty.Overall, granulosa cell tumours are themostcommonsubtype,accountingforover70%ofsexcordstromaltumours.
ClinicalfeaturesA significant percentage of these tumours present with manifestations of their hormone production,typically irregularmenstrual bleeding, postmenopausal bleeding or precocious puberty in young girls.Granulosacelltumoursmaypresentasalargepelvicmassorwithpainduetotorsion/haemorrhage.
Sertoli–Leydigcelltumoursproduceandrogensinover50%ofcases.Patientspresentwithapelvicmass and signs of virilization. Common symptoms are amenorrhoea, deep voice and hirsutism.Occasionally,thisgroupoftumoursproduceoestrogenandrarelyrenin,causinghypertension.
Most sex cord stromal tumours present as unilateral ovarian masses, measuring up to 15 cm indiameter.Macroscopically,thetumourisoftensolidwithareasofhaemorrhage,andthecutsurfacemaybeyellowduetohighlevelsofsteroidproduction.
Granulosacell tumoursproduce inhibin,whichcanbeused for follow-upsurveillance; levelsoftenrisepriortoclinicaldetectionofrecurrence.
TreatmentTreatment isbasedon thepatient’sageandwish topreserve fertility. If thepatient isyoung,unilateralsalpingo-oophorectomy,endometrial samplingandstaging is sufficient. In theoldergroup, full surgicalstagingisrecommended.Granulosacelltumourscanrecurmanyyearsafterinitialpresentationandlong-termfollow-upisrequired.Recurrenceisusuallywelldefinedandsurgeryisthemainstayoftreatmentasthereisnoeffectivechemotherapyregime.
www.medicalebookpdf.com
GermcelltumoursMalignant germ cell tumours occur mainly in young women and account for approximately 10% ofovariantumours.Theyarederivedfromprimordialgermcellswithintheovaryandbecauseofthismaycontainanycell type.Theemphasisofmanagement isbasedmainlyon fertility-preservingsurgeryandchemotherapy.
The most common presenting symptom is a pelvic mass; 10% present acutely with torsion orhaemorrhageandduetotheageincidence,somepresentduringpregnancy.Seventypercentofgermcelltumoursarestage1;spreadisbylymphaticsorbloodborne.
Dysgerminomas account for 50%of all germcell tumours.They are bilateral in 20%of cases andoccasionallysecretehumanchorionicgonadotrophin(hCG).
Endodermal sinusyolk sac tumours are the secondmost commongermcell tumours, accounting for15%of the total.They are rarelybilateral and secreteα-fetoprotein (AFP).Theypresentwith a largesolidmassthatoftencausesacutesymptomswithtorsionorrupture.Spreadofendodermalsinustumoursisalateeventandisusuallytothelungs.
Immature teratomas account for 15–20% of malignant germ cell tumours and about 1% of allteratomas.Theyareclassifiedasmatureorimmaturedependingonthegradingofneuraltissuepresent.Aboutone-thirdofteratomassecreteAFP.Occasionally,therecanbemalignanttransformationofacelltype within a mature teratoma. The most common cell type to transform is the epithelium, usuallysquamouscellcarcinoma.
Non-gestational choriocarcinomas are very rare, usually presenting in young girls with irregularbleedingandveryhighlevelsofhCG.
ClinicalfeaturesGermcelltumoursshouldbesuspectedifayoungwomanpresentswithalargesolidovarianmassthatisrapidly growing. Tumour markers as detailed in Table 14.3 are measured preoperatively as this mayinfluence the need for postoperative chemotherapy.MRI is helpful to assess morphology, particularlywithin teratomas. CT scaning of the abdomen allows assessment of the liver and lymph nodes. AllpatientsshouldhaveachestX-raytoexcludepulmonarymetastases.
TreatmentSurgeryistailoredtosuitthepatient.Asmostwomenpresentingwithmalignantgermcelltumoursareofreproductiveage,fertility-sparingtreatmentmaybepreferred.Anexploratorylaparotomyisperformedtoremovethetumourandassesscontralateralspreadtotheotherovary(20%indysgerminoma).Ifthereisacyst present on theother ovary, this shouldbe removed.Careful inspectionof the abdominal cavity isrequiredwithperitonealbiopsiesandsamplingofanyenlargedpelvicorpara-aorticnodesperformed.Ifmetastatic disease is found, it should be debulked at surgery. Intraoperative frozen sections may berequiredtoassessnodalstatus.
Postoperative chemotherapy depends on stage of disease. Stage 1 dysgerminomas and low-gradeteratomasaretreatedbysurgeryaloneandthe5-yearsurvivalisinexcessof90%.Fortheremainderoftumoursandforpatientswithdiseaseoutsidetheovary,chemotherapyisgiven.Themostcommonregimeused is a combinationofbleomycin, etoposide andcisplatin (BEP), given as a courseof three to four
www.medicalebookpdf.com
treatments,3weeksapart.Thisregimegiveslong-termcureratesofover90%andalsopreservesfertilityifrequired.
If the patient has recurrent disease, 90%will usually present in the first year following diagnosis;salvagechemotherapyhasverygoodsuccessrates.
KEYLEARNINGPOINTS•Ovariancancertendstopresentlate,withadvanceddiseasebecausesymptomsarenon-specific.•ScreeninghasnotproveneffectiveusingtumourmarkersorTVUSS.• Treatment is based on removing all tumour surgically, combined with platinum-basedchemotherapy.
• Prognosis is stage dependent: stage 1 disease has a 80–90% 5-year survival, whereas stage 3diseasehasa30%5-yearsurvival.
• Sex cord stromal tumours usually present with endocrine effects due to excess secretion ofoestrogenorandrogens.
•Germcelltumoursaffectyoungwomenandareoftencuredbyfertility-preservingsurgery.
FurtherreadingBarakat RR, Bevers MW, Gershenson DM, Hoskins WJ (eds) (2002). Handbook of GynecologicOncology,2ndedn.London:Dunitz.
ChitratharaK,RajaramS,MaheswariA (eds) (2009).OvarianCancer, Contemporary andCurrentManagement.Delhi:Jaypee.
Jacobs IJ, Menon U, Ryan A, et al. (2016). Ovarian cancer screening and mortality in the UKCollaborativeTrialofOvarianCancerScreening(UKCTOCS):arandomisedcontrolledtrial.Lancet387(10022):945–56.ErratumLancet2016;387(10022):944.
Selfassessment
CASEHISTORY
MrsLisa62-year-oldwomanwhopresentstothegynaecologyclinicwithnon-specificabdominalpain,achangeinbowelhabitandbloating.HerGParrangedapelvicultrasoundscan,whichfoundbilateralcomplexsolid/cysticpelvicmasses,largevolumeascitesandomentalcaking.
AWhatisthemostlikelydiagnosis?BWhatarethekeypointsintheexaminationandinvestigation?
MrsLisfoundtohavestage3high-gradeserousovariancancer.
www.medicalebookpdf.com
CHowwouldyoumanageher?
ANSWERS
AThesymptomsassociatedwithovariancancerarenon-specificanddoctorsmustmaintainahighindex of suspicion when faced with persistent symptoms of bloating, irritable bowel andabdominal pain. The scan report shows features suggestive of advanced ovarian cancer(solid/cysticpelvicmasses,ascitesandextraovariandisease).
BPelvicexaminationmayrevealhard,fixedpelvicmassesandfreefluidintheabdomen(ascites)isdemonstratedbyshiftingdullnessand/orafluidthrill.InvestigationsincludeserumCA125levels.IfthetumoursecretesCA125,thiscanbeusedasanon-invasivetesttomonitortreatmentresponseandsubsequentlyscreenforrecurrentdisease.ACTscanisneededtostagethediseaseandplantreatment.Ifthereisapleuraleffusion,thisisgenerallytappedandasamplesentforcytologicalassessment.Sometimesthereisverylargevolumeascitesanddrainingthiscanimprovesymptomsintheshorttermaswellasfacilitatingomentalbiopsy,whichismoredifficultwhenthereisalotoffluidaround.
CTreatment formostwomenwithadvancedovariancancer isdeterminedfollowingdiscussionatthe gynaecological oncology MDT meeting. If Mrs L is fit for surgery and preoperativeinvestigationssuggestthatcompletetumourdebulkingisachievable,upfrontsurgeryfollowedbysix cycles of adjuvant carboplatin and paclitaxel chemotherapy is generally preferred. Surgeryinvolves a midline laparotomy, total hysterectomy (removal of uterus and cervix) and BOS(removal of both Fallopian tubes and ovaries), omentectomy, pelvic lymphadenectomy anddebulking of any extraovarian tumour deposits. Sometimes surgery is avoided in the primarysetting because the disease is not completely resectable, and in this scenario, three cycles ofneoadjuvantchemotherapyaregivenandarestagingCTscanperformedtodecidewhethersurgerynowislikelytoremovealltumourdeposits.Ifsurgerytakesplace,thepatientreceivesafurtherthreecyclesofchemotherapyafterwards.
EMQ
AHigh-gradepelvicserouscarcinoma.BMucinousBOT.CEndometrioidovariancancer.DImmatureteratoma.EDysgerminoma.FGranulosacelltumour.GChoriocarcinomaoftheovary.HSertoli–Leydigovariantumour.IDermoidcyst.JKrukenbergtumour.
For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.
www.medicalebookpdf.com
1AssociatedwithSTIClesionsintheFallopiantube.2CommonlyassociatedwithBRCAmutationcarrierstatus.3Maypresentwithamenorrhoea,deepvoice,hirsutismandacne.4Mayprovokeprecociouspubertyinyounggirls.5Associatedwithendometriosis.6Secretesinhibin.7Associatedwithappendicealtumoursandpseudomyxomaperitoneii.8Maycontainhair,teeth,bone,cartilageandsebum.9Metastaticovariantumourfromcolorectalorbreastprimary.
ANSWERS
1A The term high-grade pelvic serous carcinoma has been coined to incorporate all high-gradeserous tumours arising from the ovary, Fallopian tube and/or peritoneum.Theremay be tubalprecursors,whicharecalledseroustubalintraepithelialcarcinoma(STIC)lesions,andtheyarecharacterizedbymutationsinp53insecretorycellsofthedistalFallopiantube.
2AAsmanyas30%ofhigh-gradepelvicserouscancershaveBRCAmutations.3HSertoli—Leydigcelltumoursproduceandrogensinover50%ofcases.Patientspresentwitha
pelvicmassandsignsofvirilization.4FGranulosacell tumours frequentlysecreteoestrogen.Partof thework-upofgirlspresenting in
this way would be to exclude oestrogen-secreting tumours. Granulosa cell tumours may alsopresentasalargepelvicmassorwithpainduetotorsion/haemorrhage.
5CEndometriosis-associatedovariancancersareusuallyofendometrioidorclearcellhistologicalsubtype.
6FGranulosa cell tumoursproduce inhibin,whichcanbeused for follow-up surveillance; levelsoftenrisepriortoclinicaldetectionofrecurrence.
7BMucinousBOTsmayactuallyarisefromtheappendicealcarcinomasoflowmalignantpotentialandcanbeassociatedwithpseudomyxomaperitoneii.
8I Dermoids are classically associated with tissue such as hair and teeth, and a TVUSS can bediagnostic.Theyareusuallybenign.
9J The ovary is also a common site for metastatic spread; Krukenberg tumours are ovarianmetastasesassociatedwithprimarycancersofthecolon,stomachandbreast.
SBAQUESTIONS
1A34-year-oldwomanattends thegynaecologydepartmentbecause shehas testedpositive for aBRCA1mutation. Shewishes to lower her risk of ovarian cancer asmuch as possible. She isotherwisefitandwellwithnopastmedicalhistoryofnote.Hercervicalsmearsareuptodateandnormal.Whatsurgerywouldyourecommend?Choosethesinglebestanswer.
ABilateraloophorectomy.
www.medicalebookpdf.com
BBilateralsalpingectomywithdelayedoophorectomy.CBSO.DSubtotalhysterectomyandBSO.ETotalhysterectomyandBSO.
ANSWER
CUnlessthereareconvincingreasonsforhysterectomyaswell,removingbothFallopiantubesandovaries is the best way to reduce the risk of ovarian cancer (90%) and premenopausal breastcancer(50%).Thedownsideisthesurgicalmenopausethatwillensue,butthiscanbeeffectivelymanagedwithcontinuouscombinedhormonereplacementtherapy(HRT).Thereislittleevidenceto suggest that this is harmful to cancer risk if there is nopersonal historyof breast cancer (inwhichcase,allformsofHRTareavoided).
2 A 58-year-oldwoman presentswith a large pelviabdominalmass extending to the level of thexiphisternum. Ithasaheterogeneousappearanceonscanwithsolidandcysticcomponents.Therestofthepelvisandabdomenappearsnormalandthereisnofreefluid.TheCA125levelis430units.Sheisasymptomatic.Howwouldyoumanagethispatient?Choosethesinglebestanswer.
ALaparoscopicovariancystectomy.BLaparotomy,totalabdominalhysterectomy,BSO,pelvicandpara-aorticlymphnodesampling,omentectomyanddebulkingoftumourdeposits.
CRepeatscanandCA125in3monthstocheckforintervalchange.DSixcyclesofneoadjuvantcarboplatinandpaclitaxel-basedchemotherapyfollowedbyrestagingCTscanat3months.
EUltrasound-guidedtranscutaneousaspirationofovariancystfluidandcytologicalassessment.
ANSWER
BThispatienthasahighriskofmalignancyindex(RMI)andthereforeshouldundergoafullstaginglaparotomy and complete debulking. If the ovarian mass is the only abnormal finding atlaparotomy, intraoperative frozen sections can be used to direct further surgical effort, sincepelvicandpara-aorticlymphadenectomyisnotrequiredifthecystisbenign.Aspirationofthecystisavoidedwhenmalignancy is suspected, toprevent ‘seeding’malignantcells in theperitonealcavity.
www.medicalebookpdf.com
CHAPTER15Malignantdiseaseoftheuterus
EMMAJCROSBIE
Introduction
Endometrialcancer
Sarcomasoftheuterus
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Describetheclassificationofuterinemalignancy.
•Learnhowmalignantdiseaseoftheuteruspresents.
•Describewhichinvestigationsareneededforwomenwithsuspectedendometrialcancer.
•Know the International Federation ofGynecology andObstetrics (FIGO) staging of endometrialcancer.
•Understandhowendometrialcancerismanaged.
Introduction
www.medicalebookpdf.com
Uterinecancerreferstotumoursthatarisefromtheuterinecorpus(bodyoftheuterus).Byfarthemostcommon are endometrial tumours that originate from the lining of the uterine cavity (endometrium).Tumoursarisingfromthemyometrium(sarcomas)arerare.
Endometrialcancer
IncidenceEndometrial cancer is themost commongynaecologicalmalignancy affectingUKwomenwith an age-related incidence of 95 per 100,000 women. The life-time risk of developing endometrial cancer isapproximately 1 in 46. Themean age of diagnosis is 62 years, although cancers can be diagnosed inwomen throughout their reproductive life.Approximately25%ofendometrialcancersoccurbefore themenopause.
Theincidenceofendometrialcancerhasrisensteadilyoverthepast20yearsasaconsequenceoftheageingpopulation, the trendawayfromhysterectomyforbenigngynaecologicaldiseaseand theobesityepidemic.
ClassificationEndometrialcancerusuallyarisesfromtheglandularcomponentoftheendometriumandstromaltumoursare exceedingly rare. Endometrial cancers are classified as type 1 or type 2, depending on theirhistologicalsubtype(Figure15.1)andaregraded1–3,with3beinghighgrade(mostlyabnormalcells).Type1tumoursareendometrioidadenocarcinomasthatareoestrogendrivenandarisefromabackgroundofendometrialhyperplasia.Type2tumoursincludehigh-gradeserousandclearcellhistologicalsubtypesandarisefromanatrophicendometrium.
Figure 15.1 Histological comparison of endometrial adenocarcinoma (A) with endometrial serouscarcinoma(B).
AetiologyTheriskfactorsfortype1endometrialcancerarewellestablished(Table15.1).Mostofthesereflectanincreased life-timeexposure tooestrogen.Oestrogencausesendometrial cells toproliferatewhen it isunopposedbyprogesterone.Therefore,hyperoestrogenicstates increaseendometrialcancer risk,while
www.medicalebookpdf.com
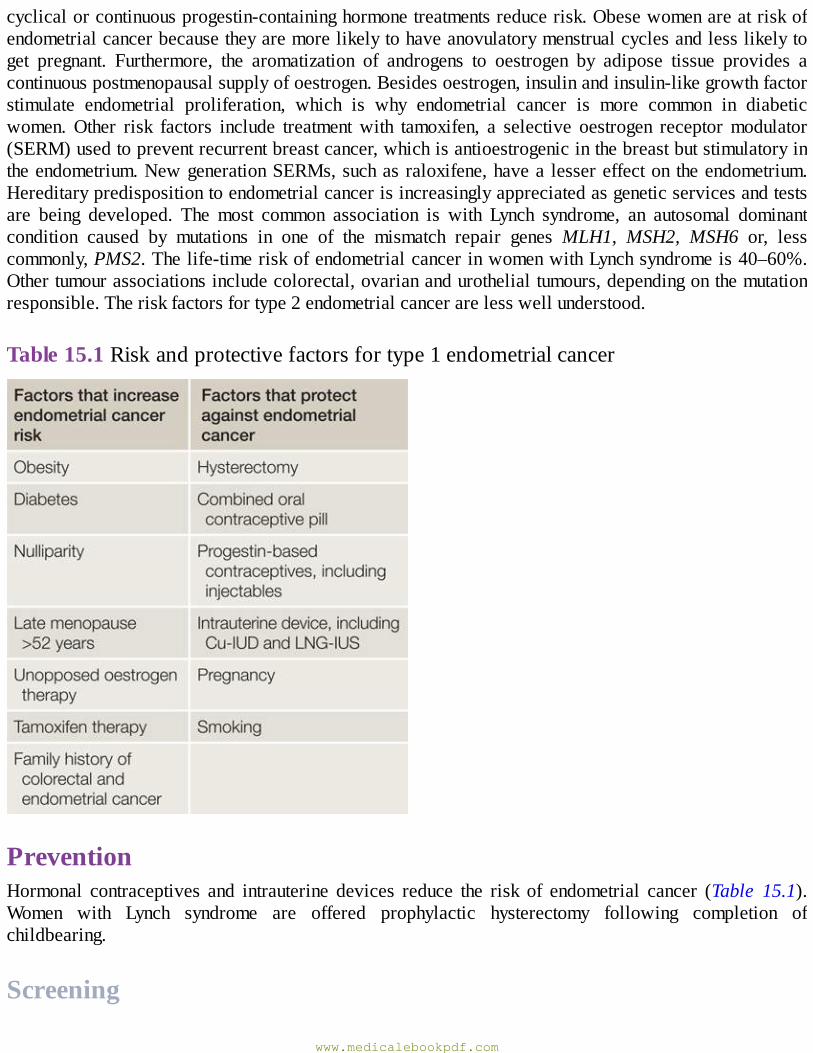
cyclicalorcontinuousprogestin-containinghormonetreatmentsreducerisk.Obesewomenareatriskofendometrialcancerbecausetheyaremorelikelytohaveanovulatorymenstrualcyclesandlesslikelytoget pregnant. Furthermore, the aromatization of androgens to oestrogen by adipose tissue provides acontinuouspostmenopausalsupplyofoestrogen.Besidesoestrogen,insulinandinsulin-likegrowthfactorstimulate endometrial proliferation, which is why endometrial cancer is more common in diabeticwomen.Other risk factors include treatmentwith tamoxifen, a selective oestrogen receptormodulator(SERM)usedtopreventrecurrentbreastcancer,whichisantioestrogenicinthebreastbutstimulatoryintheendometrium.NewgenerationSERMs,suchasraloxifene,havea lessereffecton theendometrium.Hereditarypredispositiontoendometrialcancerisincreasinglyappreciatedasgeneticservicesandtestsare being developed. The most common association is with Lynch syndrome, an autosomal dominantcondition caused by mutations in one of the mismatch repair genes MLH1, MSH2, MSH6 or, lesscommonly,PMS2.Thelife-timeriskofendometrialcancerinwomenwithLynchsyndromeis40–60%.Othertumourassociationsincludecolorectal,ovarianandurothelialtumours,dependingonthemutationresponsible.Theriskfactorsfortype2endometrialcancerarelesswellunderstood.
Table15.1Riskandprotectivefactorsfortype1endometrialcancer
PreventionHormonal contraceptives and intrauterine devices reduce the risk of endometrial cancer (Table 15.1).Women with Lynch syndrome are offered prophylactic hysterectomy following completion ofchildbearing.
Screening
www.medicalebookpdf.com
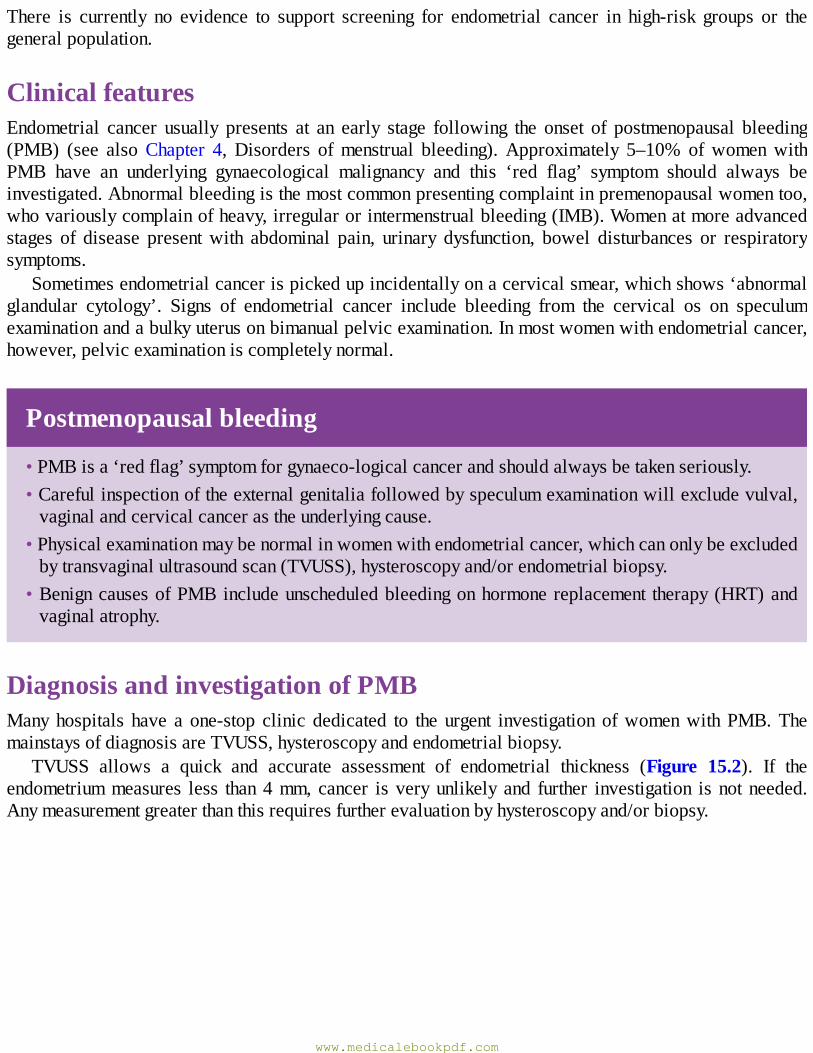
There is currently no evidence to support screening for endometrial cancer in high-risk groups or thegeneralpopulation.
ClinicalfeaturesEndometrial cancer usually presents at an early stage following the onset of postmenopausal bleeding(PMB) (see alsoChapter 4,Disorders ofmenstrual bleeding).Approximately 5–10% ofwomenwithPMB have an underlying gynaecological malignancy and this ‘red flag’ symptom should always beinvestigated.Abnormalbleedingisthemostcommonpresentingcomplaintinpremenopausalwomentoo,whovariouslycomplainofheavy,irregularorintermenstrualbleeding(IMB).Womenatmoreadvancedstages of disease presentwith abdominal pain, urinary dysfunction, bowel disturbances or respiratorysymptoms.
Sometimesendometrialcancerispickedupincidentallyonacervicalsmear,whichshows‘abnormalglandular cytology’. Signs of endometrial cancer include bleeding from the cervical os on speculumexaminationandabulkyuterusonbimanualpelvicexamination.Inmostwomenwithendometrialcancer,however,pelvicexaminationiscompletelynormal.
Postmenopausalbleeding
•PMBisa‘redflag’symptomforgynaeco-logicalcancerandshouldalwaysbetakenseriously.•Carefulinspectionoftheexternalgenitaliafollowedbyspeculumexaminationwillexcludevulval,vaginalandcervicalcancerastheunderlyingcause.
•Physicalexaminationmaybenormalinwomenwithendometrialcancer,whichcanonlybeexcludedbytransvaginalultrasoundscan(TVUSS),hysteroscopyand/orendometrialbiopsy.
•BenigncausesofPMBincludeunscheduledbleedingonhormonereplacement therapy(HRT)andvaginalatrophy.
DiagnosisandinvestigationofPMBManyhospitals have a one-stop clinic dedicated to the urgent investigation ofwomenwithPMB.ThemainstaysofdiagnosisareTVUSS,hysteroscopyandendometrialbiopsy.
TVUSS allows a quick and accurate assessment of endometrial thickness (Figure 15.2). If theendometriummeasures less than4mm, cancer isveryunlikely and further investigation is notneeded.Anymeasurementgreaterthanthisrequiresfurtherevaluationbyhysteroscopyand/orbiopsy.
www.medicalebookpdf.com
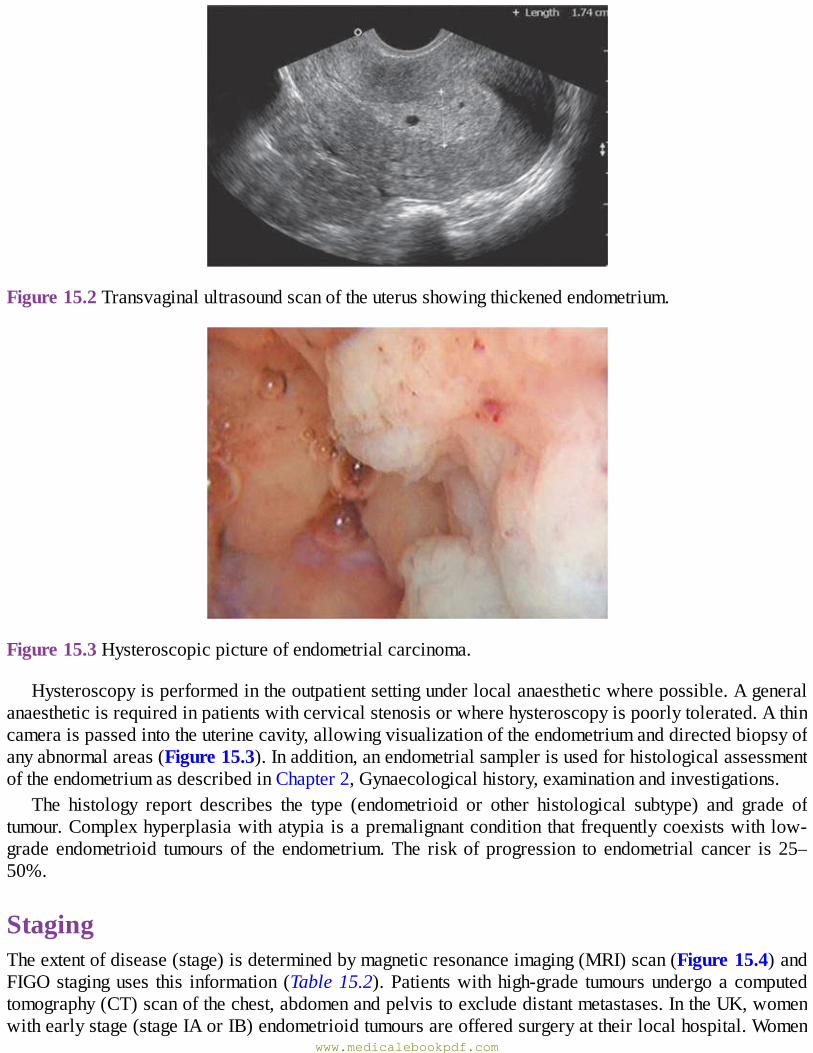
Figure15.2Transvaginalultrasoundscanoftheuterusshowingthickenedendometrium.
Figure15.3Hysteroscopicpictureofendometrialcarcinoma.
Hysteroscopyisperformedintheoutpatientsettingunderlocalanaestheticwherepossible.Ageneralanaestheticisrequiredinpatientswithcervicalstenosisorwherehysteroscopyispoorlytolerated.Athincameraispassedintotheuterinecavity,allowingvisualizationoftheendometriumanddirectedbiopsyofanyabnormalareas(Figure15.3).Inaddition,anendometrialsamplerisusedforhistologicalassessmentoftheendometriumasdescribedinChapter2,Gynaecologicalhistory,examinationandinvestigations.
The histology report describes the type (endometrioid or other histological subtype) and grade oftumour.Complexhyperplasiawithatypia isapremalignantconditionthatfrequentlycoexistswith low-grade endometrioid tumours of the endometrium.The riskof progression to endometrial cancer is 25–50%.
StagingTheextentofdisease(stage)isdeterminedbymagneticresonanceimaging(MRI)scan(Figure15.4)andFIGOstaginguses this information (Table15.2).Patientswithhigh-grade tumoursundergoacomputedtomography(CT)scanofthechest,abdomenandpelvistoexcludedistantmetastases.IntheUK,womenwithearlystage(stageIAorIB)endometrioidtumoursareofferedsurgeryattheirlocalhospital.Women
www.medicalebookpdf.com
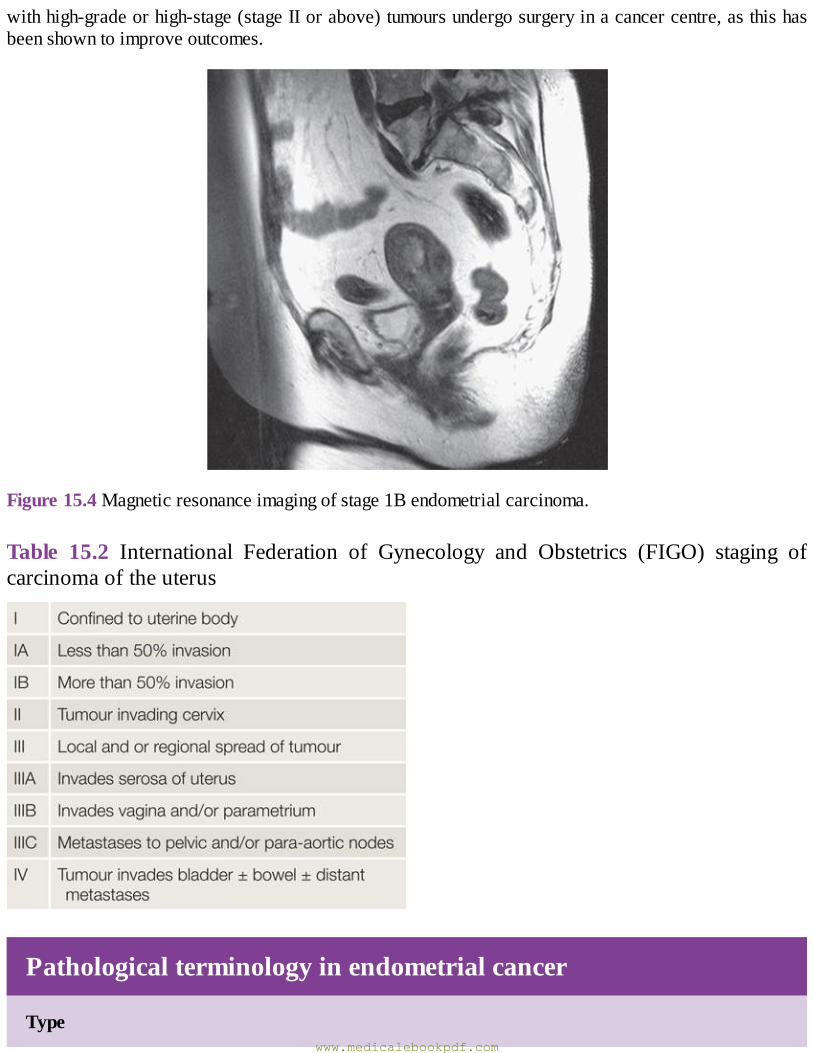
withhigh-gradeorhigh-stage(stageIIorabove)tumoursundergosurgeryinacancercentre,asthishasbeenshowntoimproveoutcomes.
Figure15.4Magneticresonanceimagingofstage1Bendometrialcarcinoma.
Table 15.2 International Federation of Gynecology and Obstetrics (FIGO) staging ofcarcinomaoftheuterus
Pathologicalterminologyinendometrialcancer
Typewww.medicalebookpdf.com
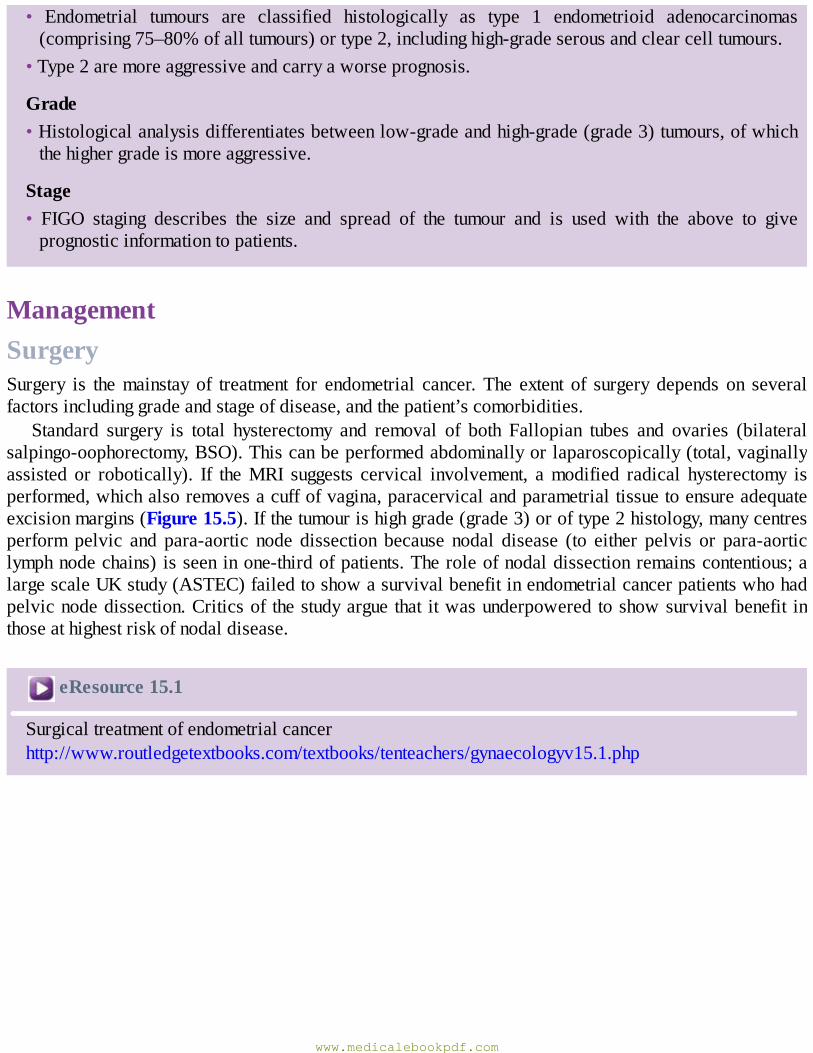
• Endometrial tumours are classified histologically as type 1 endometrioid adenocarcinomas(comprising75–80%ofalltumours)ortype2,includinghigh-gradeserousandclearcelltumours.
•Type2aremoreaggressiveandcarryaworseprognosis.
Grade•Histologicalanalysisdifferentiatesbetweenlow-gradeandhigh-grade(grade3)tumours,ofwhichthehighergradeismoreaggressive.
Stage• FIGO staging describes the size and spread of the tumour and is used with the above to giveprognosticinformationtopatients.
ManagementSurgerySurgery is themainstay of treatment for endometrial cancer. The extent of surgery depends on severalfactorsincludinggradeandstageofdisease,andthepatient’scomorbidities.
Standard surgery is total hysterectomy and removal of both Fallopian tubes and ovaries (bilateralsalpingo-oophorectomy,BSO).Thiscanbeperformedabdominallyorlaparoscopically(total,vaginallyassisted or robotically). If theMRI suggests cervical involvement, amodified radical hysterectomy isperformed,whichalsoremovesacuffofvagina,paracervicalandparametrialtissuetoensureadequateexcisionmargins(Figure15.5).Ifthetumourishighgrade(grade3)oroftype2histology,manycentresperform pelvic and para-aortic node dissection because nodal disease (to either pelvis or para-aorticlymphnodechains)isseeninone-thirdofpatients.Theroleofnodaldissectionremainscontentious;alargescaleUKstudy(ASTEC)failedtoshowasurvivalbenefitinendometrialcancerpatientswhohadpelvicnodedissection.Criticsof thestudyarguethat itwasunderpoweredtoshowsurvivalbenefit inthoseathighestriskofnodaldisease.
eResource15.1
Surgicaltreatmentofendometrialcancerhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv15.1.php
www.medicalebookpdf.com
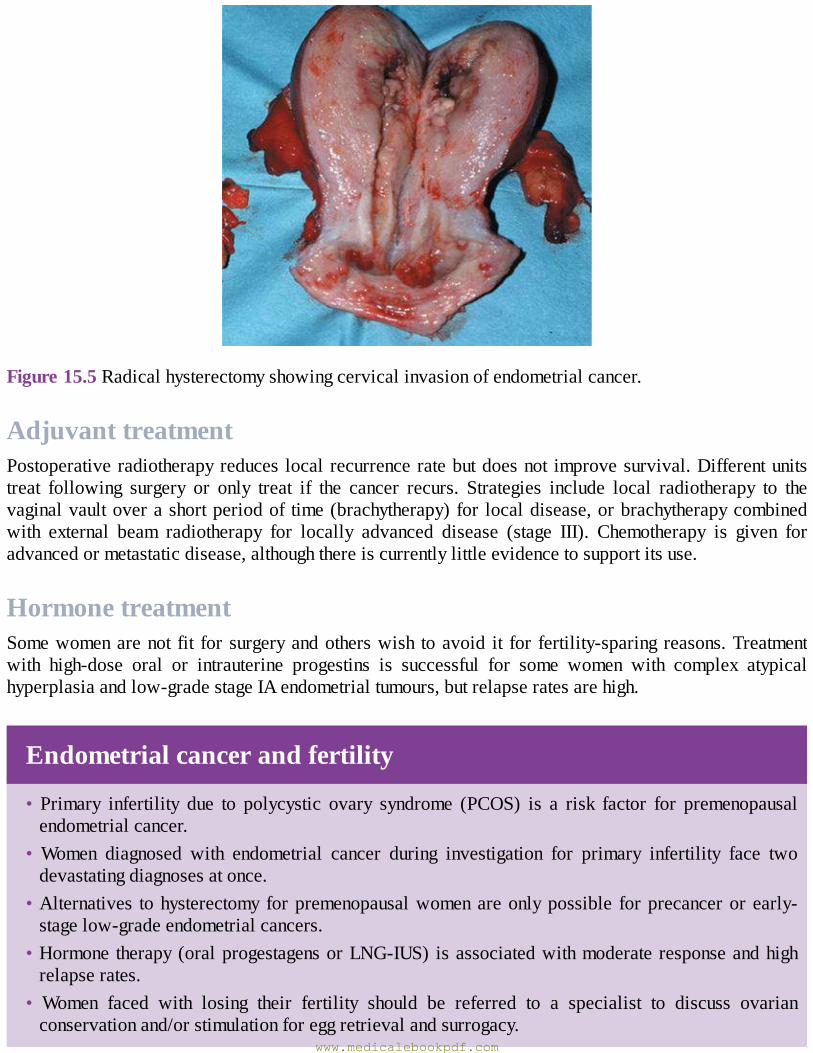
Figure15.5Radicalhysterectomyshowingcervicalinvasionofendometrialcancer.
AdjuvanttreatmentPostoperativeradiotherapyreduces local recurrenceratebutdoesnot improvesurvival.Differentunitstreat following surgery or only treat if the cancer recurs. Strategies include local radiotherapy to thevaginalvaultoverashortperiodof time(brachytherapy)for localdisease,orbrachytherapycombinedwith external beam radiotherapy for locally advanced disease (stage III). Chemotherapy is given foradvancedormetastaticdisease,althoughthereiscurrentlylittleevidencetosupportitsuse.
HormonetreatmentSomewomenarenot fit forsurgeryandotherswish toavoid it for fertility-sparing reasons.Treatmentwith high-dose oral or intrauterine progestins is successful for some women with complex atypicalhyperplasiaandlow-gradestageIAendometrialtumours,butrelapseratesarehigh.
Endometrialcancerandfertility
• Primary infertility due to polycystic ovary syndrome (PCOS) is a risk factor for premenopausalendometrialcancer.
• Women diagnosed with endometrial cancer during investigation for primary infertility face twodevastatingdiagnosesatonce.
•Alternatives tohysterectomy forpremenopausalwomenareonlypossible forprecancerorearly-stagelow-gradeendometrialcancers.
•Hormone therapy(oralprogestagensorLNG-IUS) isassociatedwithmoderate responseandhighrelapserates.
• Women faced with losing their fertility should be referred to a specialist to discuss ovarianconservationand/orstimulationforeggretrievalandsurrogacy.
www.medicalebookpdf.com
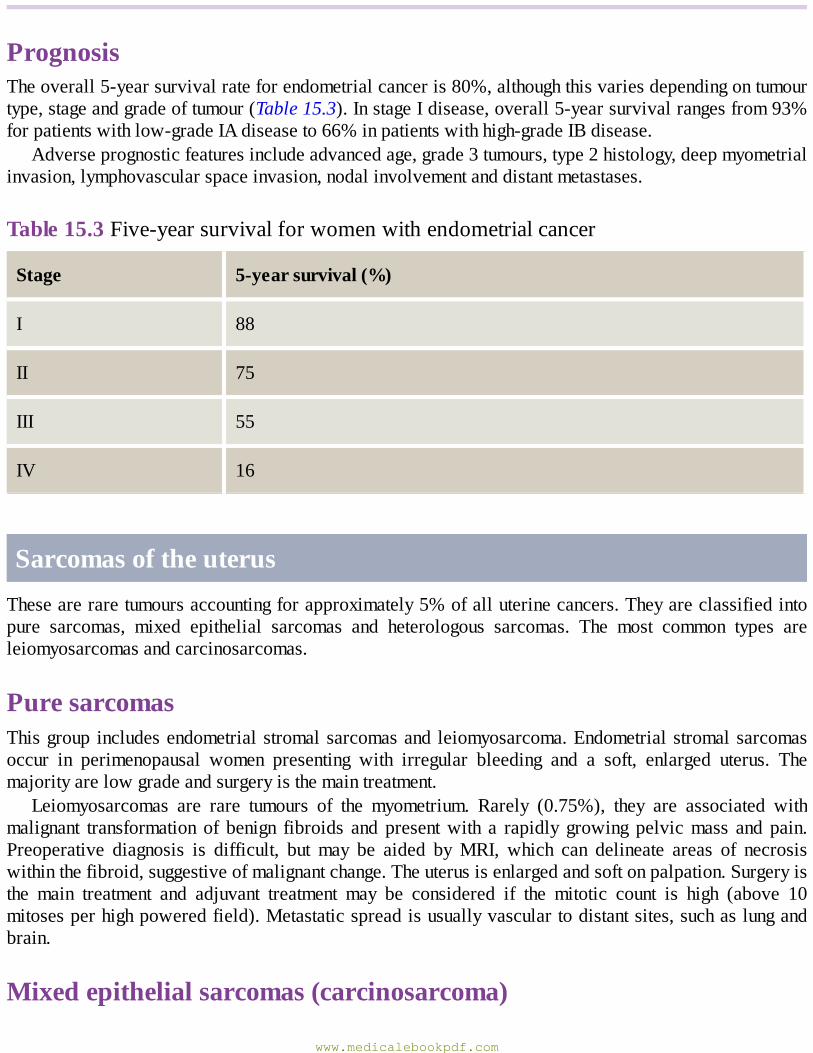
PrognosisTheoverall5-yearsurvivalrateforendometrialcanceris80%,althoughthisvariesdependingontumourtype,stageandgradeoftumour(Table15.3).InstageIdisease,overall5-yearsurvivalrangesfrom93%forpatientswithlow-gradeIAdiseaseto66%inpatientswithhigh-gradeIBdisease.
Adverseprognosticfeaturesincludeadvancedage,grade3tumours,type2histology,deepmyometrialinvasion,lymphovascularspaceinvasion,nodalinvolvementanddistantmetastases.
Table15.3Five-yearsurvivalforwomenwithendometrialcancer
Stage 5-yearsurvival(%)
I 88
II 75
III 55
IV 16
SarcomasoftheuterusTheseareraretumoursaccountingforapproximately5%ofalluterinecancers.Theyareclassifiedintopure sarcomas, mixed epithelial sarcomas and heterologous sarcomas. The most common types areleiomyosarcomasandcarcinosarcomas.
PuresarcomasThisgroup includesendometrialstromalsarcomasand leiomyosarcoma.Endometrialstromalsarcomasoccur in perimenopausal women presenting with irregular bleeding and a soft, enlarged uterus. Themajorityarelowgradeandsurgeryisthemaintreatment.
Leiomyosarcomas are rare tumours of the myometrium. Rarely (0.75%), they are associated withmalignant transformation of benign fibroids and presentwith a rapidly growing pelvicmass and pain.Preoperative diagnosis is difficult, but may be aided byMRI, which can delineate areas of necrosiswithinthefibroid,suggestiveofmalignantchange.Theuterusisenlargedandsoftonpalpation.Surgeryisthe main treatment and adjuvant treatment may be considered if the mitotic count is high (above 10mitosesperhighpoweredfield).Metastaticspreadisusuallyvasculartodistantsites,suchaslungandbrain.
Mixedepithelialsarcomas(carcinosarcoma)
www.medicalebookpdf.com
This group of tumours, formerly known as malignant mixed Müllerian tumours, contain bothcarcinomatous and sarcomatous elements. The carcinomatous component is usually glandular and thesarcomatous component is homologous (endometrial, stromal and/or smooth muscle) or heterologous(tissues not normally found in the uterus, including bone, cartilage and skeletalmuscle). Themajoritypresent after themenopause and sometimes there is a history of previous pelvic irradiation. There isusually a history of PMB and a fleshy mass is often seen protruding from the cervix along with anenlargedsoftuterus.Treatmentissurgeryfollowedbypostoperativeradiotherapy.The5-yearsurvivalis73%ifconfinedtotheuterus,butonly25%ifthetumourhasspreadoutsidetheuterus.
HeterologoussarcomasThisraregroupoftumoursconsistsofsarcomatoustissuenotusuallyfoundintheuterus,suchasstriatedmuscle,boneorcartilage.Themostcommonisrhabdomyosarcoma,whichmaypresentinchildrenasagrape-like mass protruding from the cervix with a watery discharge. Histology reveals primitiverhabdomyoblasts.Recurrenceratesarehighwithdistantmetastases.
KEYLEARNINGPOINTS•Endometrialcanceristhemostcommongynaeco-logicalmalignancy.•ThemajorityofcancerspresentwithstageIdiseaseandtheoverall5-yearsurvivalis80%.•Type2andhigh-gradetumourshavetheworstprognosis.•Obesityandotherhyperoestrogenicstatesplayamajoraetiologicalrole.• The majority of patients present with PMB; however, 25% of cases occur in premenopausalwomen.
•5–10%ofwomenwithPMBwillhaveanunderlyinggynaecologicalmalignancy.•Endometrialbiopsy±hysteroscopyisthegoldstandardfordiagnosis,whileMRIdefinestheextentofdisease.
•TotalhysterectomyandBSOisthetreatmentofchoiceformostpatients.
FurtherreadingMacKintoshML,Crosbie EJ (2013).Obesity-driven endometrial cancer: isweight loss the answer?BJOG120:791–4.
Morice P, Leary A, Creutzberg C, Abu-Rustum N, Darai E (2015). Endometrial cancer. Lancet387:1094–108.
Selfassessment
CASEHISTORYwww.medicalebookpdf.com

MrsPisa65-year-oldwomanwhopresentstothegynaecologyclinicwithPMB.Sheisobeseandsuffers from type2diabetes.Shehasnochildren,hasnever takenHRTanddoesnot smoke.Hercervicalsmearshavealwaysbeennormal.AWhatisthemostlikelydiagnosis?BWhatarethekeypointsintheexaminationandinvestigation?MrsPisfoundtohaveagrade1stage1Aendometrioidadenocarcinoma.CHowwouldyoumanageher?
ANSWERS
APMBisaredflagsymptomforgynaecologicalcancer.Cancersoftheendometrium,cervix,vaginaand vulva all present with abnormal bleeding.Mrs P’smedical history and risk factor profilemakeendometrialcancerthemostlikelydiagnosis.
BMrs P has several risk factors for endometrial cancer, including obesity, type 2 diabetes andnulliparity. A normal, up-to-date cervical smear history makes cancer of the cervix extremelyunlikely.Cancersofthevulva,vaginaandcervixshouldbeexcludedbycarefulinspection.Bloodcomingfromthecervicalosindicatesuterinebleeding.Bimanualpelvicexaminationmayfindabulkyuterusorpelvicmass,althoughanormalexaminationdoesnotexcludeendometrialcancer.
CTreatmentformostwomenwithendometrialcancerinvolvestotalhysterectomy(removalofuterusand cervix) and BSO (removal of both Fallopian tubes and ovaries). It is important to assessfitness for anaesthetic as many women with endometrial cancer have comorbidities, includingobesity, type 2 diabetes, hypertension, cardiovascular disease, sleep apnoea andpoormobility,that limit their ability to tolerate general anaesthesia. Laparoscopic surgery is now standard ofcare for women with endometrial cancer but this may be difficult to achieve in women withmorbid obesity who cannot tolerate the prolonged head-down tilt required or where previousabdominal surgery has resulted in adhesions and scarring.Allwomenwith endometrial cancershould be discussed at the central gynaecological oncology multidisciplinary team (MDT)meeting.Womenwith low-gradeearly-stagediseasemayundergosurgery in their localhospitalwhile high-risk cases are referred centrally for care. All women are offered support fromgynaecological oncology clinical nurse specialists orMacmillan nurses, who provide a singlepointofcontactforcontinuityofcareaswellaswritteninformation,contactphonenumbersandemotionalsupport.
EMQ
ASimplehyperplasiaoftheendometrium.BComplexhyperplasiaoftheendometriumwithatypia.CEndometrioidadenocarcinomaoftheendometrium.DSerousuterinecarcinoma.EClearcellcarcinomaoftheuterus.FCarcinosarcomaoftheuterus.GLeiomyosarcomaoftheuterus.HEndometrialstromalsarcoma.
www.medicalebookpdf.com
IRhabdomyosarcoma.
For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.1Mostcommonuterinemalignancy.2Raretumourofmyometrium.3Rareuterinetumourderivedfromskeletalmuscle.4Precursorlesionofendometrioidadenocarcinomaoftheendometrium.
ANSWERS
1C75–80%ofendometrialtumoursaretype1,whichareendometrioidadenocarcinomas.Therestaretype2,includinghigh-gradeserousandclearcellhistologicalsubtype.
2G Leiomyosarcomas are rare tumours of the myometrium. Carcinosarcomas contain bothcarcinomatousandsarcomatouselements.
3I This rare tumour may be diagnosed in children; it is a heterologous sarcoma as it containssarcomatoustissuenotusuallylocatedintheuterus.
4BThetype1endometroidadenocarcinomasarehormonedependentanddevelopfromhyperplasiaoftheendometrium.Incontrast,type2tumoursmaydevelopfromanatrophicendometrium.
SBAQUESTIONS
1 A 54-year-old woman attends the gynaecology department with PMB. A TVUSSmeasures herendometrial thickness as 8 mm. An endometrial biopsy shows moderately differentiatedadenocarcinomacells.Whatisthemostappropriatestaginginvestigation?Choosethesinglebestanswer.
AChestX-ray.BCTscanofherthorax,abdomenandpelvis.CHysteroscopy.DMRIscanofherpelvis.ETransabdominalultrasoundscan.
ANSWER
DMRIisusedtodeterminetheextentofthetumourforstaging.Itispossibletotellhowfarthroughthemyometriumthetumourhasspread,sosurgerycanthenbeplanned.Nootherimagingmodalitywillgivethisinformationaccurately.AnultrasoundscanistoosubjectiveandaCTscandoesnothaveidealenhancementoftissuetypes.
2 A fit 72-year-old woman has an MRI after an endometrial biopsy shows endometrioidadenocarcinoma of the endometrium. Staging from the MRI is stage II. What management is
www.medicalebookpdf.com

indicated?Choosethesinglebestanswer.ACarboplatin-basedchemotherapy.BTotalabdominalhysterectomywithbilateralsalpingo-oophrectomy.CExternalbeamradiationtherapytothepelvis.DModifiedradicalhysterectomy.EBrachytherapy.
ANSWER
DIf theMRIsuggestscervical involvement,amodified radicalhysterectomy isperformed,whichalso removes a cuff of vagina, paracervical and parametrial tissue to ensure adequate excisionmargins.Simplehysterectomywouldhaveahighrelapserate.Chemotherapyorbrachytherapyisnotindicated.However,inveryelderlyunfitforsurgerywomen,theseoptionscouldbeexplored.Externalbeamradiotherapywouldalsonotbeafirst-linetreatmentandthereisnoevidencethatitwouldpreventprogressionofthetumour.
www.medicalebookpdf.com
CHAPTER16Premalignantandmalignantdiseaseofthe
lowergenitaltract
EMMAJCROSBIE
Introduction
Premalignantdiseaseofthecervix
Malignantdiseaseofthecervix
Malignantdiseaseofthevagina
Malignantdiseaseofthevulva
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Understandthepathogenesisoflowergenitaltractmalignancy.
• Understand primary prevention of cervical cancer through human papillomavirus (HPV)vaccinationandcervicalscreening.
•Understand thediagnosis, InternationalFederationofGynecologyandObstetrics (FIGO) stagingandmanagementofpremalignantandmalignantdiseaseofthelowergenitaltract,includingcervix,vaginaandvulva.
www.medicalebookpdf.com
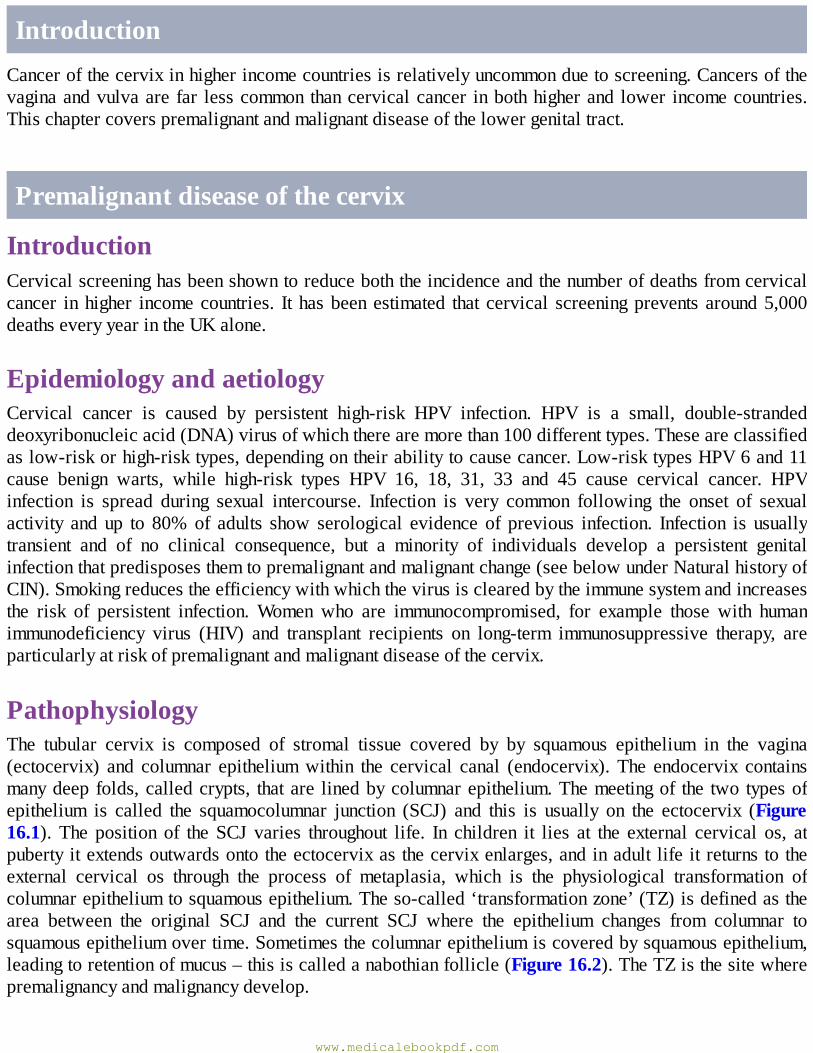
IntroductionCancerofthecervixinhigherincomecountriesisrelativelyuncommonduetoscreening.Cancersofthevaginaandvulvaare far lesscommonthancervicalcancer inbothhigherand lower incomecountries.Thischaptercoverspremalignantandmalignantdiseaseofthelowergenitaltract.
Premalignantdiseaseofthecervix
IntroductionCervicalscreeninghasbeenshowntoreduceboththeincidenceandthenumberofdeathsfromcervicalcancer inhigher incomecountries. It hasbeenestimated that cervical screeningprevents around5,000deathseveryyearintheUKalone.
EpidemiologyandaetiologyCervical cancer is caused by persistent high-risk HPV infection. HPV is a small, double-strandeddeoxyribonucleicacid(DNA)virusofwhichtherearemorethan100differenttypes.Theseareclassifiedaslow-riskorhigh-risktypes,dependingontheirabilitytocausecancer.Low-risktypesHPV6and11cause benign warts, while high-risk types HPV 16, 18, 31, 33 and 45 cause cervical cancer. HPVinfection is spread during sexual intercourse. Infection is very common following the onset of sexualactivity and up to 80%of adults show serological evidence of previous infection. Infection is usuallytransient and of no clinical consequence, but a minority of individuals develop a persistent genitalinfectionthatpredisposesthemtopremalignantandmalignantchange(seebelowunderNaturalhistoryofCIN).Smokingreducestheefficiencywithwhichthevirusisclearedbytheimmunesystemandincreasesthe risk of persistent infection.Women who are immunocompromised, for example those with humanimmunodeficiency virus (HIV) and transplant recipients on long-term immunosuppressive therapy, areparticularlyatriskofpremalignantandmalignantdiseaseofthecervix.
PathophysiologyThe tubular cervix is composed of stromal tissue covered by by squamous epithelium in the vagina(ectocervix) and columnar epitheliumwithin the cervical canal (endocervix). The endocervix containsmanydeepfolds,calledcrypts, thatare linedbycolumnarepithelium.Themeetingof the two typesofepithelium is called the squamocolumnar junction (SCJ) and this is usually on the ectocervix (Figure16.1). The position of the SCJ varies throughout life. In children it lies at the external cervical os, atpubertyitextendsoutwardsontotheectocervixasthecervixenlarges,andinadult lifeitreturnstotheexternal cervical os through the process of metaplasia, which is the physiological transformation ofcolumnarepitheliumtosquamousepithelium.Theso-called‘transformationzone’(TZ)isdefinedasthearea between the original SCJ and the current SCJ where the epithelium changes from columnar tosquamousepitheliumovertime.Sometimesthecolumnarepitheliumiscoveredbysquamousepithelium,leadingtoretentionofmucus–thisiscalledanabothianfollicle(Figure16.2).TheTZisthesitewherepremalignancyandmalignancydevelop.
www.medicalebookpdf.com
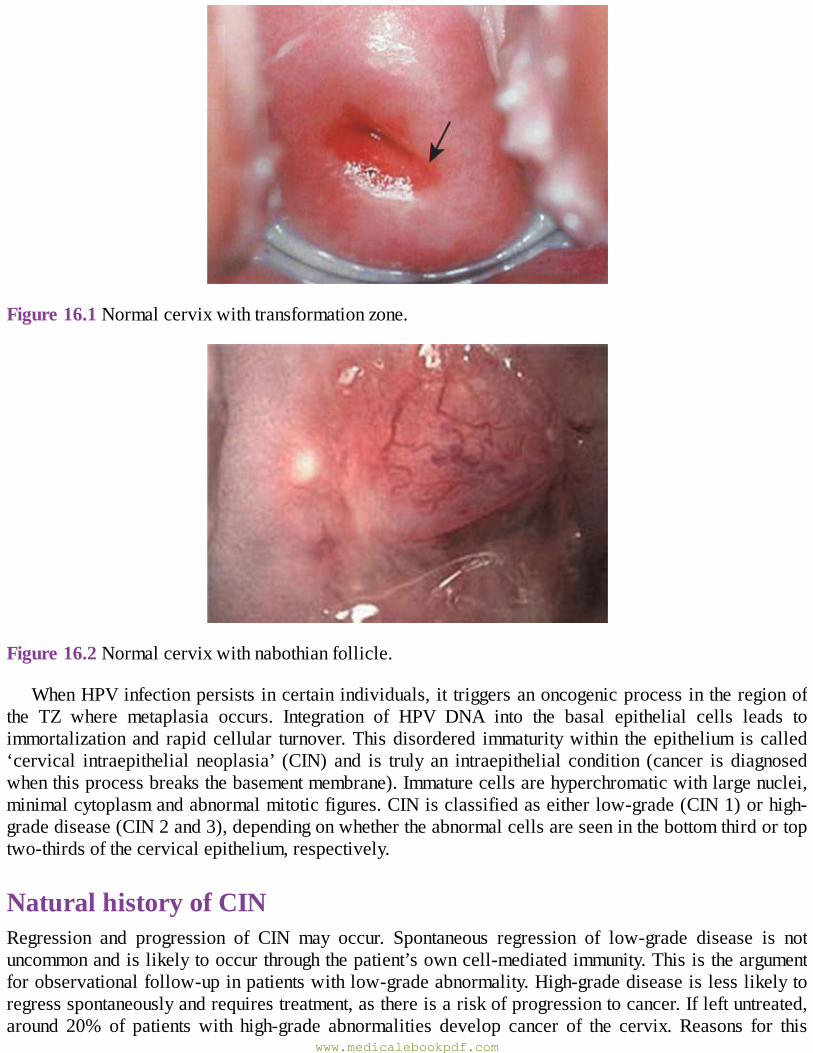
Figure16.1Normalcervixwithtransformationzone.
Figure16.2Normalcervixwithnabothianfollicle.
WhenHPVinfectionpersistsincertainindividuals,it triggersanoncogenicprocessintheregionofthe TZ where metaplasia occurs. Integration of HPV DNA into the basal epithelial cells leads toimmortalizationand rapidcellular turnover.Thisdisordered immaturitywithin theepithelium iscalled‘cervical intraepithelial neoplasia’ (CIN) and is truly an intraepithelial condition (cancer is diagnosedwhenthisprocessbreaksthebasementmembrane).Immaturecellsarehyperchromaticwithlargenuclei,minimalcytoplasmandabnormalmitoticfigures.CINisclassifiedaseitherlow-grade(CIN1)orhigh-gradedisease(CIN2and3),dependingonwhethertheabnormalcellsareseeninthebottomthirdortoptwo-thirdsofthecervicalepithelium,respectively.
NaturalhistoryofCINRegression and progression of CIN may occur. Spontaneous regression of low-grade disease is notuncommonandislikelytooccurthroughthepatient’sowncell-mediatedimmunity.Thisistheargumentforobservationalfollow-upinpatientswithlow-gradeabnormality.High-gradediseaseislesslikelytoregressspontaneouslyandrequirestreatment,asthereisariskofprogressiontocancer.Ifleftuntreated,around 20% of patients with high-grade abnormalities develop cancer of the cervix. Reasons for this
www.medicalebookpdf.com
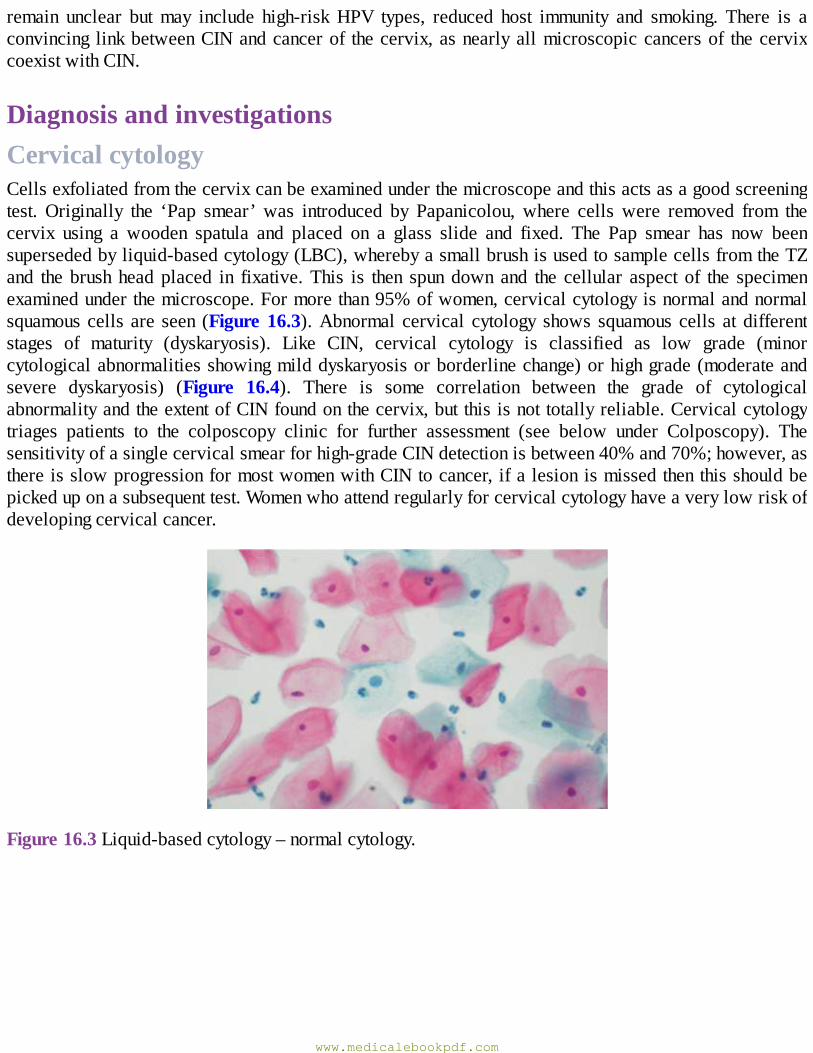
remain unclear butmay include high-riskHPV types, reduced host immunity and smoking. There is aconvincing linkbetweenCINandcancerof thecervix,asnearlyallmicroscopiccancersof thecervixcoexistwithCIN.
DiagnosisandinvestigationsCervicalcytologyCellsexfoliatedfromthecervixcanbeexaminedunderthemicroscopeandthisactsasagoodscreeningtest. Originally the ‘Pap smear’ was introduced by Papanicolou, where cells were removed from thecervix using a wooden spatula and placed on a glass slide and fixed. The Pap smear has now beensupersededbyliquid-basedcytology(LBC),wherebyasmallbrushisusedtosamplecellsfromtheTZand the brushheadplaced in fixative.This is then spundown and the cellular aspect of the specimenexaminedunderthemicroscope.Formorethan95%ofwomen,cervicalcytologyisnormalandnormalsquamouscells are seen (Figure16.3).Abnormal cervical cytology shows squamous cells at differentstages of maturity (dyskaryosis). Like CIN, cervical cytology is classified as low grade (minorcytologicalabnormalitiesshowingmilddyskaryosisorborderlinechange)orhighgrade(moderateandsevere dyskaryosis) (Figure 16.4). There is some correlation between the grade of cytologicalabnormalityandtheextentofCINfoundonthecervix,butthisisnottotallyreliable.Cervicalcytologytriages patients to the colposcopy clinic for further assessment (see below under Colposcopy). Thesensitivityofasinglecervicalsmearforhigh-gradeCINdetectionisbetween40%and70%;however,asthereisslowprogressionformostwomenwithCINtocancer,ifalesionismissedthenthisshouldbepickeduponasubsequenttest.Womenwhoattendregularlyforcervicalcytologyhaveaverylowriskofdevelopingcervicalcancer.
Figure16.3Liquid-basedcytology–normalcytology.
www.medicalebookpdf.com
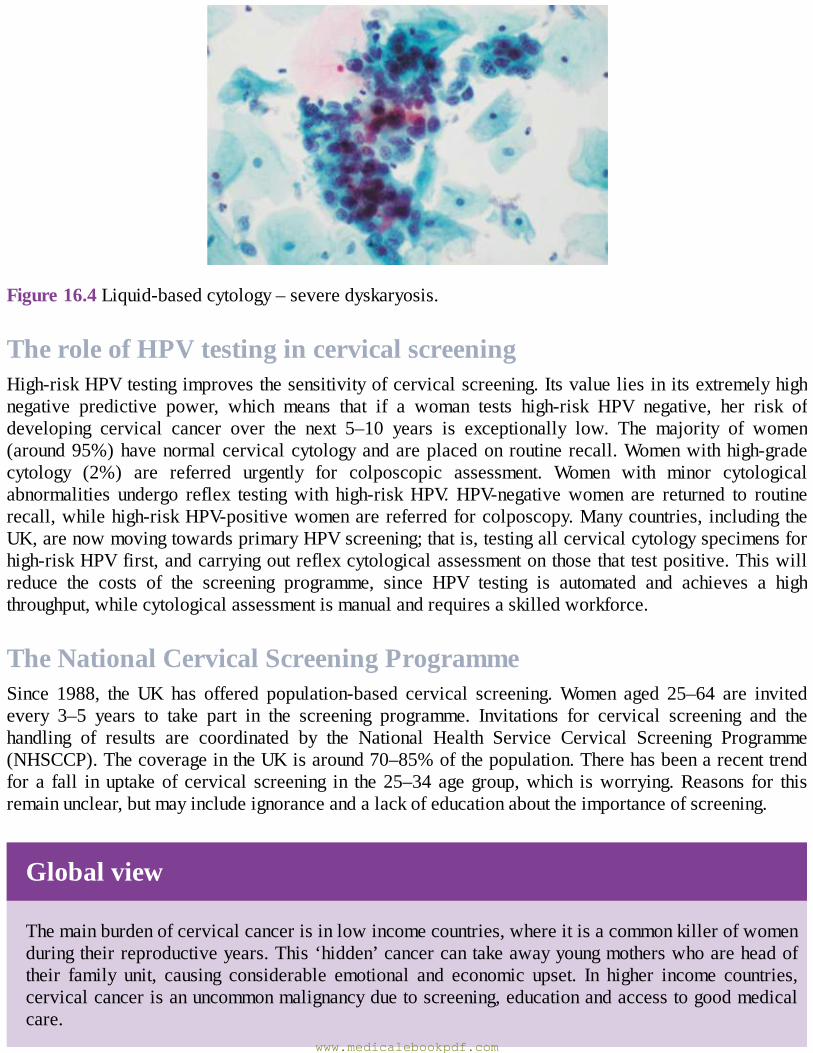
Figure16.4Liquid-basedcytology–severedyskaryosis.
TheroleofHPVtestingincervicalscreeningHigh-riskHPVtestingimprovesthesensitivityofcervicalscreening.Itsvalueliesinitsextremelyhighnegative predictive power, which means that if a woman tests high-risk HPV negative, her risk ofdeveloping cervical cancer over the next 5–10 years is exceptionally low. The majority of women(around95%)havenormalcervicalcytologyandareplacedonroutine recall.Womenwithhigh-gradecytology (2%) are referred urgently for colposcopic assessment. Women with minor cytologicalabnormalities undergo reflex testingwith high-riskHPV.HPV-negativewomen are returned to routinerecall,whilehigh-riskHPV-positivewomenarereferredforcolposcopy.Manycountries, includingtheUK,arenowmovingtowardsprimaryHPVscreening;thatis,testingallcervicalcytologyspecimensforhigh-riskHPVfirst,andcarryingoutreflexcytologicalassessmentonthosethattestpositive.Thiswillreduce the costs of the screening programme, since HPV testing is automated and achieves a highthroughput,whilecytologicalassessmentismanualandrequiresaskilledworkforce.
TheNationalCervicalScreeningProgrammeSince 1988, the UK has offered population-based cervical screening.Women aged 25–64 are invitedevery 3–5 years to take part in the screening programme. Invitations for cervical screening and thehandling of results are coordinated by the National Health Service Cervical Screening Programme(NHSCCP).ThecoverageintheUKisaround70–85%ofthepopulation.Therehasbeenarecenttrendfor a fall inuptakeof cervical screening in the25–34agegroup,which isworrying.Reasons for thisremainunclear,butmayincludeignoranceandalackofeducationabouttheimportanceofscreening.
Globalview
Themainburdenofcervicalcancerisinlowincomecountries,whereitisacommonkillerofwomenduringtheirreproductiveyears.This‘hidden’cancercantakeawayyoungmotherswhoareheadoftheir family unit, causing considerable emotional and economic upset. In higher income countries,cervicalcancerisanuncommonmalignancyduetoscreening,educationandaccesstogoodmedicalcare.
www.medicalebookpdf.com
ColposcopyColposcopyistheexaminationofthemagnifiedcervixusingalightsource(Figure16.5). It isusedforbothdiagnosisandtreatment.Thewomanundressesandplacesherlegsinthesemi-lithotomyposition.Aspeculumisplacedinthevaginaandthecervixexaminedwithalightsource,undermagnification(5–20-fold).Theapplicationofaceticacidandiodinesolutionshighlightsabnormalareasofthecervixthatcanbebiopsied.Aceticacidcausesnucleoproteinswithincellstocoagulatetemporarily;therefore,areasofincreasedcellturnover,includingCIN,appearwhite(Figure16.6).AreasofCINlackintracytoplasmicglycogenandfailtostainbrownwheniodineisapplied.CINisapreneoplasticprocessandtheprocessofangiogenesis(newbloodvessel formation) isapparent inCINwhenviewedthroughthecolposcope(Figure16.7). IfCIN ispresent, thecolposcopistdetermineswhether theappearancesare loworhighgrade.Thelattercanbetreatedinthecliniconthesamevisit(knownas‘seeandtreat’);theformercanbemonitoredwithasubsequentcolposcopyandcytology6monthslater.Abiopsyusuallyhelpsmakethedecision if unsure (‘select and treat’).All doctors and nurses carrying out colposcopy are required toundergo a period of training and examination to ensure high quality and standards of care aremet. Inaddition, each colposcopy service undergoes a rigorous external quality assurance assessment every 5yearstoensurehighstandards.
www.medicalebookpdf.com
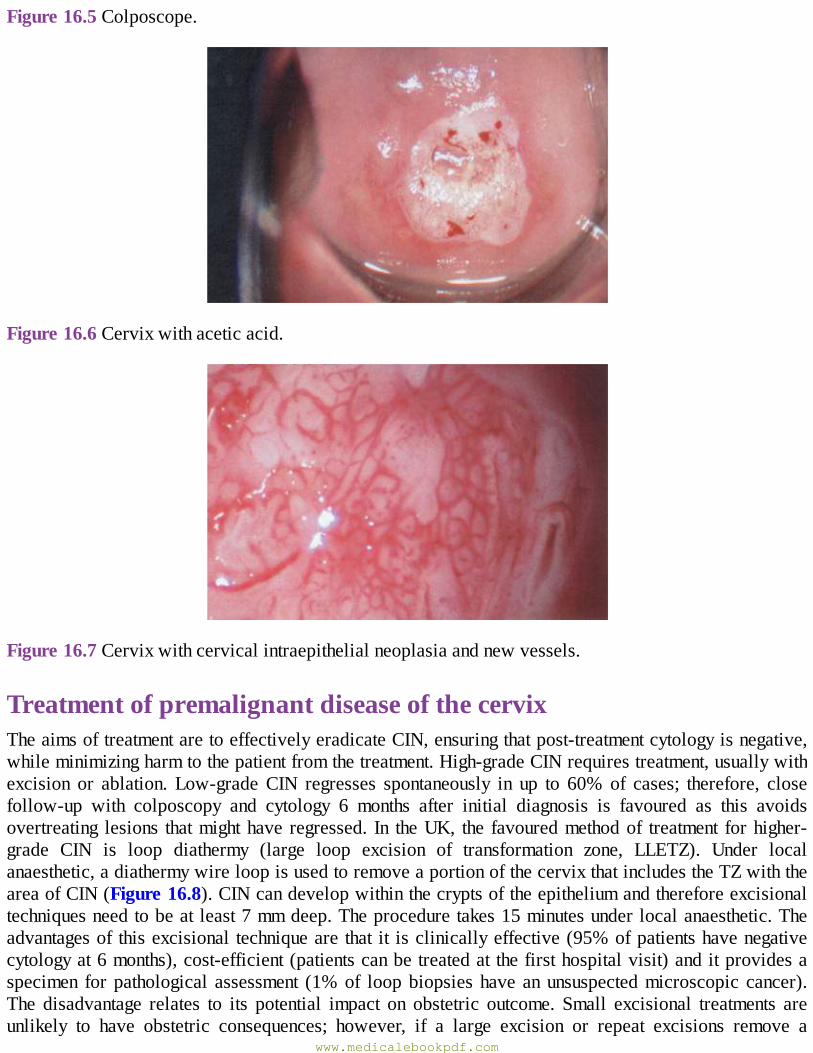
Figure16.5Colposcope.
Figure16.6Cervixwithaceticacid.
Figure16.7Cervixwithcervicalintraepithelialneoplasiaandnewvessels.
TreatmentofpremalignantdiseaseofthecervixTheaimsoftreatmentaretoeffectivelyeradicateCIN,ensuringthatpost-treatmentcytologyisnegative,whileminimizingharmtothepatientfromthetreatment.High-gradeCINrequirestreatment,usuallywithexcision or ablation. Low-gradeCIN regresses spontaneously in up to 60% of cases; therefore, closefollow-up with colposcopy and cytology 6 months after initial diagnosis is favoured as this avoidsovertreating lesions thatmighthave regressed. In theUK, the favouredmethodof treatment forhigher-grade CIN is loop diathermy (large loop excision of transformation zone, LLETZ). Under localanaesthetic,adiathermywireloopisusedtoremoveaportionofthecervixthatincludestheTZwiththeareaofCIN(Figure16.8).CINcandevelopwithinthecryptsoftheepitheliumandthereforeexcisionaltechniquesneedtobeatleast7mmdeep.Theproceduretakes15minutesunderlocalanaesthetic.Theadvantagesof thisexcisional techniqueare that it isclinicallyeffective(95%ofpatientshavenegativecytologyat6months),cost-efficient(patientscanbetreatedatthefirsthospitalvisit)anditprovidesaspecimen forpathological assessment (1%of loopbiopsieshave anunsuspectedmicroscopic cancer).The disadvantage relates to its potential impact on obstetric outcome. Small excisional treatments areunlikely to have obstetric consequences; however, if a large excision or repeat excisions remove a
www.medicalebookpdf.com
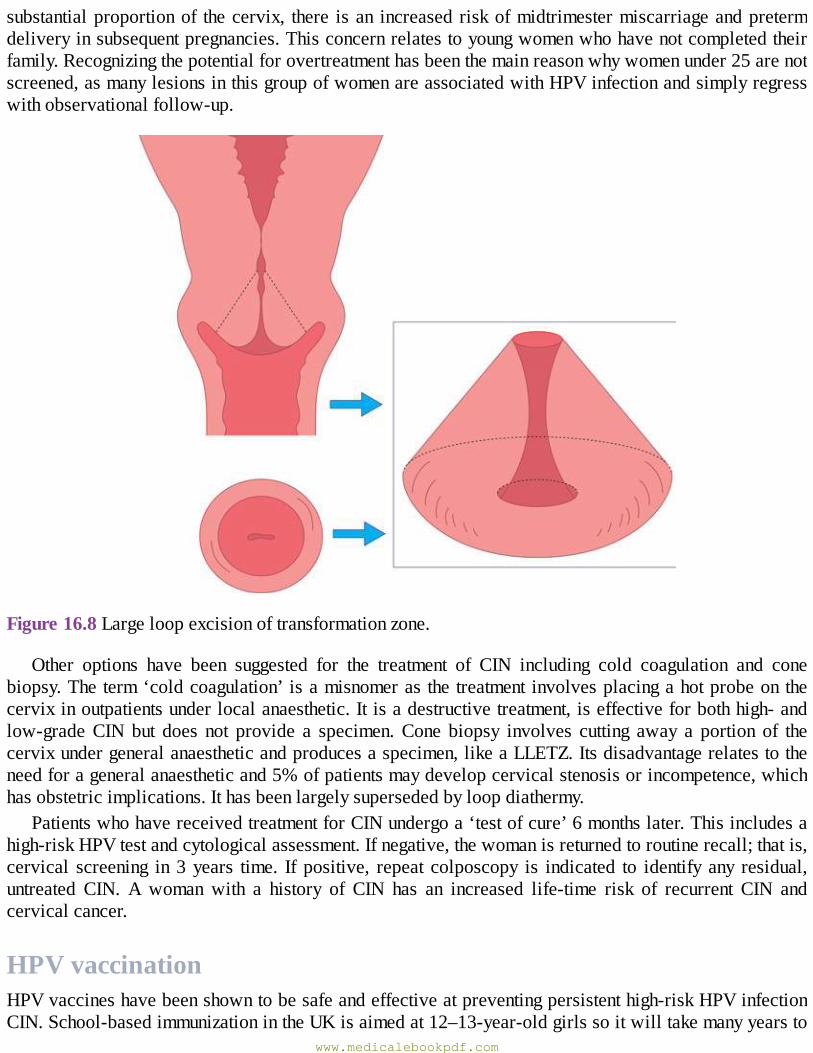
substantialproportionof thecervix, there isan increased riskofmidtrimestermiscarriageandpretermdeliveryinsubsequentpregnancies.Thisconcernrelatestoyoungwomenwhohavenotcompletedtheirfamily.Recognizingthepotentialforovertreatmenthasbeenthemainreasonwhywomenunder25arenotscreened,asmanylesionsinthisgroupofwomenareassociatedwithHPVinfectionandsimplyregresswithobservationalfollow-up.
Figure16.8Largeloopexcisionoftransformationzone.
Other options have been suggested for the treatment of CIN including cold coagulation and conebiopsy.Theterm‘coldcoagulation’ isamisnomeras thetreatment involvesplacingahotprobeonthecervixinoutpatientsunderlocalanaesthetic.Itisadestructivetreatment,iseffectiveforbothhigh-andlow-gradeCIN but does not provide a specimen.Cone biopsy involves cutting away a portion of thecervixundergeneralanaestheticandproducesaspecimen,likeaLLETZ.Itsdisadvantagerelatestotheneedforageneralanaestheticand5%ofpatientsmaydevelopcervicalstenosisorincompetence,whichhasobstetricimplications.Ithasbeenlargelysupersededbyloopdiathermy.
PatientswhohavereceivedtreatmentforCINundergoa‘testofcure’6monthslater.Thisincludesahigh-riskHPVtestandcytologicalassessment.Ifnegative,thewomanisreturnedtoroutinerecall;thatis,cervical screening in3years time. If positive, repeat colposcopy is indicated to identify any residual,untreated CIN. A woman with a history of CIN has an increased life-time risk of recurrent CIN andcervicalcancer.
HPVvaccinationHPVvaccineshavebeenshowntobesafeandeffectiveatpreventingpersistenthigh-riskHPVinfectionCIN.School-basedimmunizationintheUKisaimedat12–13-year-oldgirlssoitwilltakemanyyearsto
www.medicalebookpdf.com
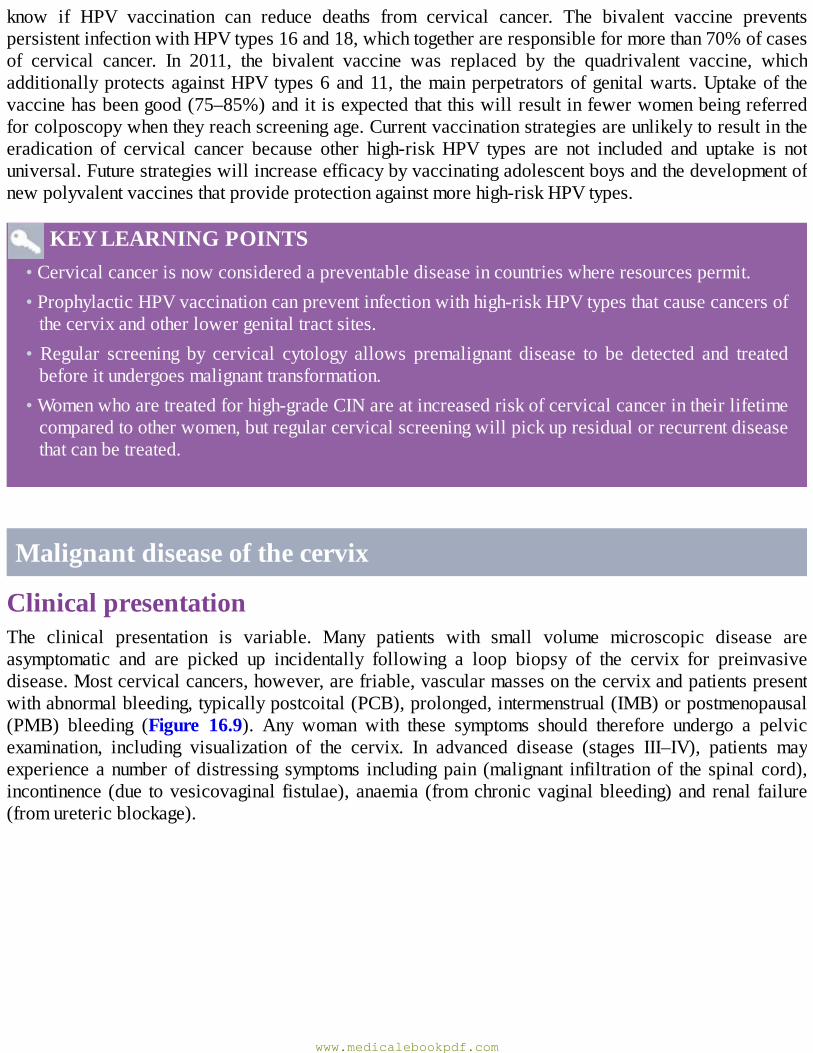
know if HPV vaccination can reduce deaths from cervical cancer. The bivalent vaccine preventspersistentinfectionwithHPVtypes16and18,whichtogetherareresponsibleformorethan70%ofcasesof cervical cancer. In 2011, the bivalent vaccine was replaced by the quadrivalent vaccine, whichadditionallyprotectsagainstHPVtypes6and11, themainperpetratorsofgenitalwarts.Uptakeof thevaccinehasbeengood(75–85%)anditisexpectedthatthiswillresultinfewerwomenbeingreferredforcolposcopywhentheyreachscreeningage.Currentvaccinationstrategiesareunlikelytoresultintheeradication of cervical cancer because other high-risk HPV types are not included and uptake is notuniversal.Futurestrategieswillincreaseefficacybyvaccinatingadolescentboysandthedevelopmentofnewpolyvalentvaccinesthatprovideprotectionagainstmorehigh-riskHPVtypes.
KEYLEARNINGPOINTS•Cervicalcancerisnowconsideredapreventablediseaseincountrieswhereresourcespermit.•ProphylacticHPVvaccinationcanpreventinfectionwithhigh-riskHPVtypesthatcausecancersofthecervixandotherlowergenitaltractsites.
• Regular screening by cervical cytology allows premalignant disease to be detected and treatedbeforeitundergoesmalignanttransformation.
•Womenwhoaretreatedforhigh-gradeCINareatincreasedriskofcervicalcancerintheirlifetimecomparedtootherwomen,butregularcervicalscreeningwillpickupresidualorrecurrentdiseasethatcanbetreated.
Malignantdiseaseofthecervix
ClinicalpresentationThe clinical presentation is variable. Many patients with small volume microscopic disease areasymptomatic and are picked up incidentally following a loop biopsy of the cervix for preinvasivedisease.Mostcervicalcancers,however,arefriable,vascularmassesonthecervixandpatientspresentwithabnormalbleeding,typicallypostcoital(PCB),prolonged,intermenstrual(IMB)orpostmenopausal(PMB) bleeding (Figure 16.9). Any woman with these symptoms should therefore undergo a pelvicexamination, including visualization of the cervix. In advanced disease (stages III–IV), patients mayexperienceanumberofdistressing symptoms includingpain (malignant infiltrationof the spinal cord),incontinence (due tovesicovaginal fistulae),anaemia (fromchronicvaginalbleeding)and renal failure(fromuretericblockage).
www.medicalebookpdf.com
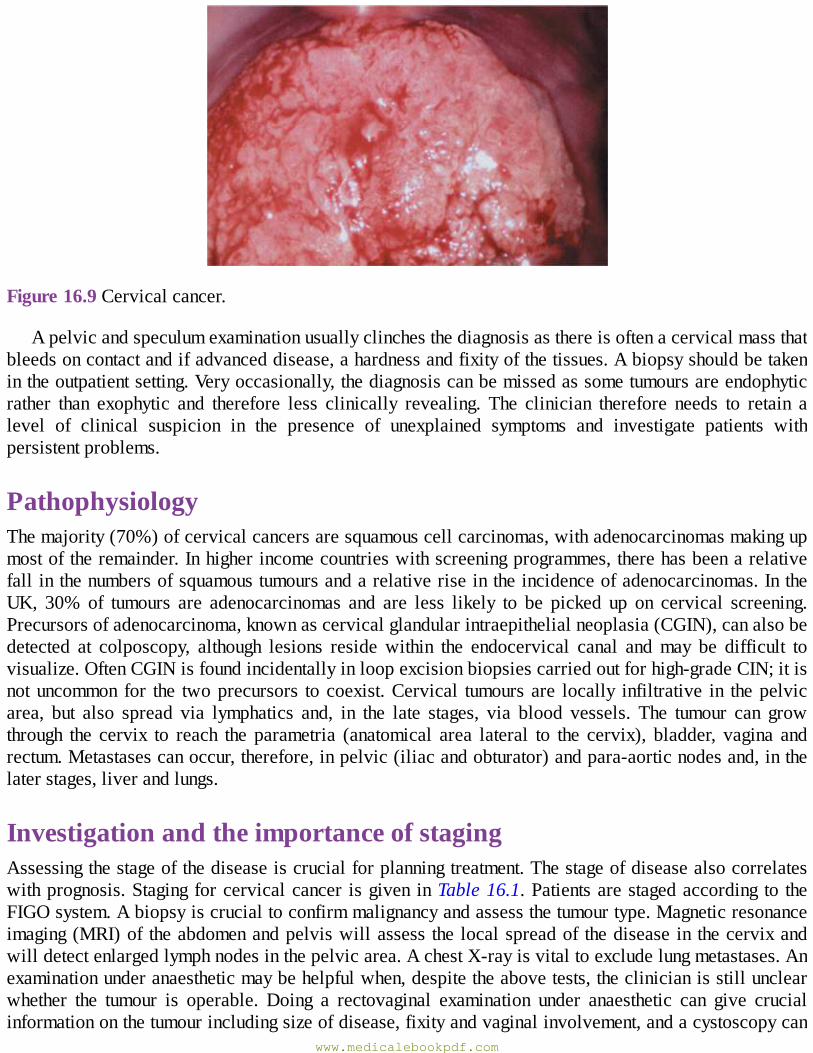
Figure16.9Cervicalcancer.
Apelvicandspeculumexaminationusuallyclinchesthediagnosisasthereisoftenacervicalmassthatbleedsoncontactandifadvanceddisease,ahardnessandfixityofthetissues.Abiopsyshouldbetakenintheoutpatientsetting.Veryoccasionally,thediagnosiscanbemissedassometumoursareendophyticrather than exophytic and therefore less clinically revealing. The clinician therefore needs to retain alevel of clinical suspicion in the presence of unexplained symptoms and investigate patients withpersistentproblems.
PathophysiologyThemajority(70%)ofcervicalcancersaresquamouscellcarcinomas,withadenocarcinomasmakingupmostoftheremainder.Inhigherincomecountrieswithscreeningprogrammes,therehasbeenarelativefallinthenumbersofsquamoustumoursandarelativeriseintheincidenceofadenocarcinomas.IntheUK, 30% of tumours are adenocarcinomas and are less likely to be picked up on cervical screening.Precursorsofadenocarcinoma,knownascervicalglandularintraepithelialneoplasia(CGIN),canalsobedetected at colposcopy, although lesions reside within the endocervical canal andmay be difficult tovisualize.OftenCGINisfoundincidentallyinloopexcisionbiopsiescarriedoutforhigh-gradeCIN;itisnotuncommon for the twoprecursors tocoexist.Cervical tumoursare locally infiltrative in thepelvicarea, but also spread via lymphatics and, in the late stages, via blood vessels. The tumour can growthrough the cervix to reach the parametria (anatomical area lateral to the cervix), bladder, vagina andrectum.Metastasescanoccur,therefore,inpelvic(iliacandobturator)andpara-aorticnodesand,inthelaterstages,liverandlungs.
InvestigationandtheimportanceofstagingAssessingthestageofthediseaseiscrucialforplanningtreatment.Thestageofdiseasealsocorrelateswithprognosis.Stagingforcervicalcancer isgiven inTable16.1.Patientsarestagedaccording to theFIGOsystem.Abiopsyiscrucialtoconfirmmalignancyandassessthetumourtype.Magneticresonanceimaging(MRI)of theabdomenandpelviswillassess the localspreadof thedisease in thecervixandwilldetectenlargedlymphnodesinthepelvicarea.AchestX-rayisvitaltoexcludelungmetastases.Anexaminationunderanaestheticmaybehelpfulwhen,despitetheabovetests,theclinicianisstillunclearwhether the tumour is operable. Doing a rectovaginal examination under anaesthetic can give crucialinformationonthetumourincludingsizeofdisease,fixityandvaginalinvolvement,andacystoscopycan
www.medicalebookpdf.com
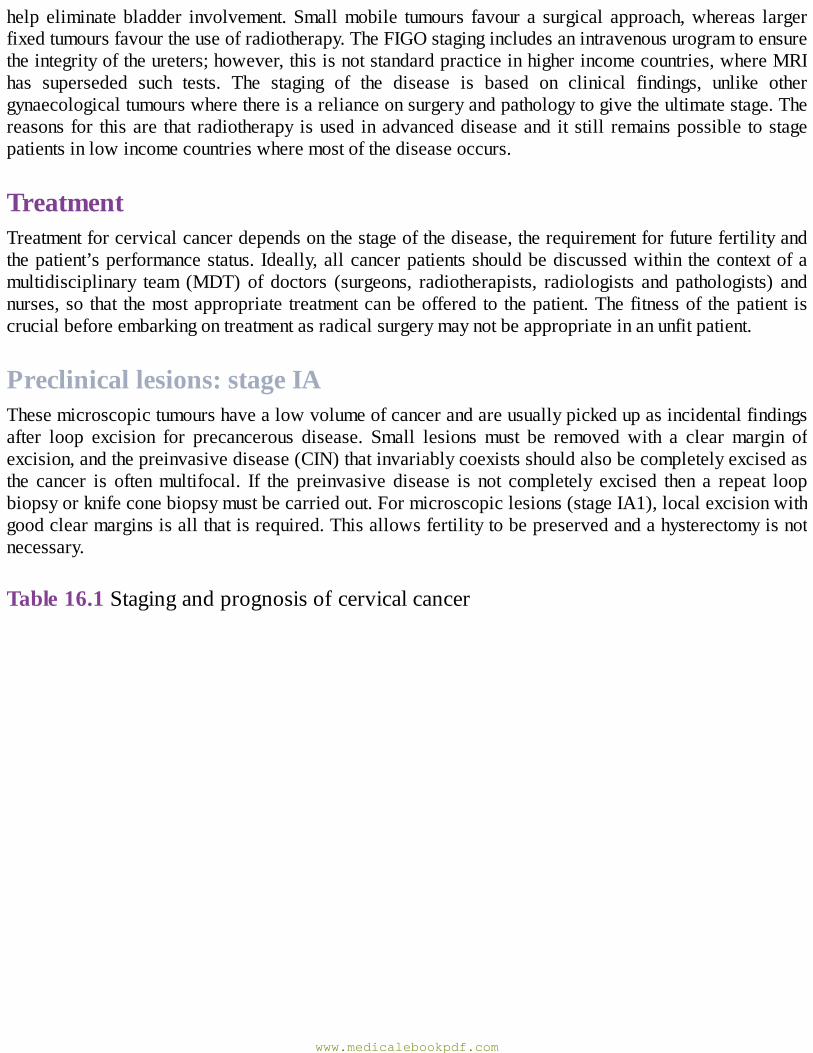
help eliminatebladder involvement.Smallmobile tumours favour a surgical approach,whereas largerfixedtumoursfavourtheuseofradiotherapy.TheFIGOstagingincludesanintravenousurogramtoensuretheintegrityoftheureters;however,thisisnotstandardpracticeinhigherincomecountries,whereMRIhas superseded such tests. The staging of the disease is based on clinical findings, unlike othergynaecologicaltumourswherethereisarelianceonsurgeryandpathologytogivetheultimatestage.Thereasonsfor thisare that radiotherapy isused inadvanceddiseaseand it still remainspossible tostagepatientsinlowincomecountrieswheremostofthediseaseoccurs.
TreatmentTreatmentforcervicalcancerdependsonthestageofthedisease,therequirementforfuturefertilityandthepatient’sperformancestatus.Ideally,allcancerpatientsshouldbediscussedwithin thecontextofamultidisciplinary team (MDT) of doctors (surgeons, radiotherapists, radiologists and pathologists) andnurses,so that themostappropriate treatmentcanbeoffered to thepatient.Thefitnessof thepatient iscrucialbeforeembarkingontreatmentasradicalsurgerymaynotbeappropriateinanunfitpatient.
Preclinicallesions:stageIAThesemicroscopictumourshavealowvolumeofcancerandareusuallypickedupasincidentalfindingsafter loop excision for precancerous disease. Small lesions must be removed with a clear margin ofexcision,andthepreinvasivedisease(CIN)thatinvariablycoexistsshouldalsobecompletelyexcisedasthe cancer is oftenmultifocal. If the preinvasive disease is not completely excised then a repeat loopbiopsyorknifeconebiopsymustbecarriedout.Formicroscopiclesions(stageIA1),localexcisionwithgoodclearmarginsisallthatisrequired.Thisallowsfertilitytobepreservedandahysterectomyisnotnecessary.
Table16.1Stagingandprognosisofcervicalcancer
www.medicalebookpdf.com
Clinicalinvasivecervicalcarcinoma:stagesIB–IVThetumourvolumesaremuchgreaterinpatientswithstage1Bdiseaseandthereforefertility-preservingtreatment for thisgroupofpatients ismorechallenging.When smallvolumedisease is confined to thecervix(stageIB1),radicalhysterectomyandbilateralpelvicnodedissection(Wertheim’shysterectomy)is standard of care. For young women who have not completed their families, radical trachelectomy(surgicalremovalof thecervixandupperpartof thevagina)andbilateralpelvicnodedissectionisanalternative(seeChapter17,Gynaecologicalsurgeryandtherapeutics).
ItisimportanttorememberthatinearlystageIBdisease,pelvicradiotherapyhassimilarsuccessratestosurgeryandthereforethistreatmentisconsideredinwomenwhoaretoooverweightforradicalsurgeryorwhoareanaestheticallyunfit.
When the disease is beyond the cervix (stages II–IV disease), radiotherapy (with or withoutchemotherapy)becomestheoptimal treatment.Surgeryin isolationisproblematicascomplicationscanoccur(severehaemorrhage)andalsoachievingclearanceofthetumourisunlikely.Incompleteexcisionofcancerbysurgeryrequiresadjuvantpostoperativeradiotherapyandthecombinedtreatmentscanleadtohighcomplicationrates.Asanoncologicalruleitisnotwisetocutthroughcancer.
www.medicalebookpdf.com

SurgeryThe standard surgicaloperation for stage IB tumours is a radicalhysterectomyandpelvic lymphnodedissection.This involves removal of the cervix, upper third of the vagina, uterus and the paracervicaltissue.Pelviclymphnoderemovalincludestheobturator,internalandexternaliliacnodes.Theovariesinpremenopausalwomencanbe spared.There ishighermorbiditywith thisprocedureover the standardtotalabdominalhysterectomy.Bladderdysfunction(atony),sexualdysfunction(duetovaginalshortening)andlymphoedema(duetoremovalof thepelvic lymphnodes)arenotuncommon.Anatonicbladder isfrequentintheimmediatepostoperativeperiodduetoneuronaldamagefromthesurgery,andintermittentself-catheterizationmayberequireduntilthebladdertonereturns.
Lymphoedema isvariable and isdescribedbypatients as awooden,heavy feeling to the legswithswellingandreducedmobility.Managementincludeslegelevation,goodskincare(e.g.avoidshaving),massage and occasionally compression stockings. Despite these potential problems, surgery is thepreferred treatment as thecure rate ishigh,ovarian tissuecanbepreservedand thepatient avoids thecomplicationsofradiotherapy(seebelow).
KEYLEARNINGPOINTS•Cervicalcanceraffectsyoungwomenwhomaynothavecompletedtheirfamilies.•Manycervical tumours arepickedupwhen theyaremicroscopicorvery smallvolume,makingfertility-sparingtreatmentapossibility.
•Conebiopsyorradicaltrachelectomywithbilateralpelviclymphadenectomyallowspreservationoftheovariesanduterus,permittingpregnancyinthefuture.
•Thelong-termcurerateofradicaltrachelectomyislesswellestablishedthanradical(Wertheim’s)hysterectomy.
RadiotherapyTheaimofradiotherapyistodeliveralethaldoseofradiationtothetumourandminimizedamagetothesurrounding tissues.Treatment isoverseenbya radiotherapist and team.Treatment isdelivered in twoways:externalbeamradiotherapy(asteletherapy)andinternalradiotherapy(brachytherapy).Inexternalbeamradiotherapy,thesourceoftheradiationisfromamachinecalledalinearaccelerator,andradiationisdeliveredtothepelvisadistancefromthepatient(Figure16.10).Thedoseofradiotherapyiscarefullycalculatedaccordingtothepatientandthetumour,andisusuallyadministeredas45Gyintotal.Thisisgiveninseveraltreatmentsor‘fractions’asanoutpatientover4weeks.Althoughthistreatmentisgivendaily, the timeof each fraction is nomore than10minutes.Brachytherapy is a radiotherapy techniquewheretheradiationisdeliveredinternallytothepatient.Thesourceoftheradiationisusuallyseleniumandpatientsgenerallyhavetoundergoanexaminationunderanaesthetictoinserttherodsintotheuterus.These rods are then attached to the radiotherapy source; the patient receives this internal treatment inisolationtoprotectthestaff.Brachytherapydeliversahighdoseofradiationtothetumoursourceanditsharmfuleffectsonthebladderandbowelareminimizedasitseffectsaretargetedonly5mmfromtherod.
Patientsfrequentlysufferlethargywithtreatmentandmayexperiencebothbowelandbladderurgency,which is due to the initial inflammatory effects of the radiation. Skin erythema-like sunburn is notuncommon after external beam radiotherapy. Symptomatic treatment is usually required, such as anti-inflammatorycreamsforskin.Around5%ofpatientsexperienceaseriousside-effectthatmightinterrupt
www.medicalebookpdf.com
treatment, forexamplebowelperforation.Therearemany long-termcomplicationsof radiotherapy thataffectonlyaminorityofpatientsbutdohaveasignificantimpactonpatients’qualityoflife.The initialinflammatory process is replaced by fibrosis in the long term.Vaginal stenosis can cause sexual pain,bladderdamagecanleadtocystitis-likesymptoms,haematuriaandboweldamageleadtomalabsorptionand mucous diarrhoea. None of these complications can be managed easily. Patients who arepremenopausalwillundergoaradiotherapy-inducedmenopauseastheovariesareverysensitivetosmalldosesofirradiation.
Figure16.10Linearaccelerator.
Chemotherapy (cisplatin) is ideally given in conjunctionwith the radiotherapy, as this combinationincreasescureratesmorethanwhenradiotherapyisusedinisolation.Itprobablyworksbyenhancingtheeffectsofradiotherapyandmightalsoaddressmicrometastasesthatareoutsidetheradiotherapyfield.
PalliativetreatmentWhenitisnotpossibletooffercurativetreatment,palliationofsymptomsbecomesimportantandearlyinvolvementofthepalliativecareteamisessentialforsymptomcontrol.Thediseasecanbehiddenfromfamily and friends even in the late stages of the disease; patients may be experiencing a number ofsymptomsfromlocalinfiltrationofthepelvisbythecancer.Malignantpain,rectoand/orvesicovaginalfistulaeandbleedingmayoccur.Distantspreadisoftenaverylatestageofthedisease.Radiotherapymaybeconsideredwithapalliativeintent;forexample,aone-offtreatmentmaybeusedforsymptomaticbonemetastases.
Malignantdiseaseofthevagina
EpidemiologyandaetiologyVaginalcancerisrare,accountingforjust1–2%ofgynaecologicalmalignancies.Themajorityofvaginaltumoursarisefrommetastaticspreadfromtheendometriumandcervix.Primarycancersofthevaginaareusuallysquamouscellcarcinomas,althoughclearcelladenocarcinomasandmalignantmelanomasoccur
www.medicalebookpdf.com
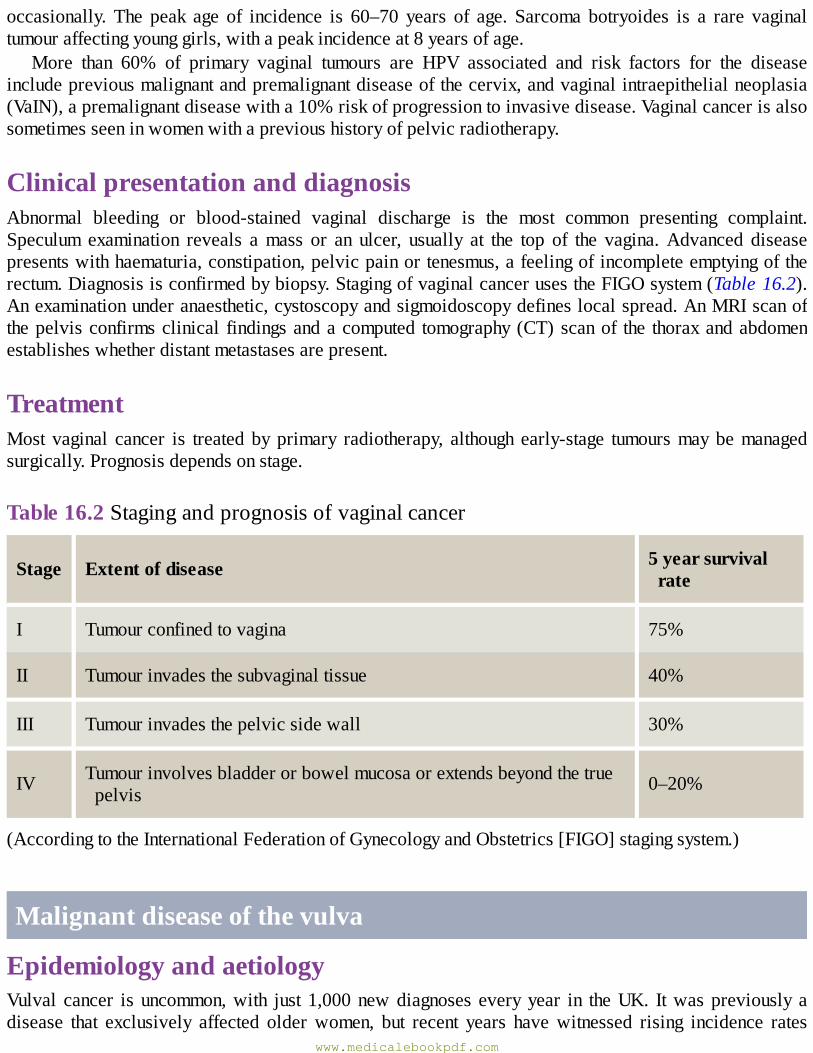
occasionally. The peak age of incidence is 60–70 years of age. Sarcoma botryoides is a rare vaginaltumouraffectingyounggirls,withapeakincidenceat8yearsofage.
More than 60% of primary vaginal tumours are HPV associated and risk factors for the diseaseincludepreviousmalignantandpremalignantdiseaseofthecervix,andvaginalintraepithelialneoplasia(VaIN),apremalignantdiseasewitha10%riskofprogressiontoinvasivedisease.Vaginalcancerisalsosometimesseeninwomenwithaprevioushistoryofpelvicradiotherapy.
ClinicalpresentationanddiagnosisAbnormal bleeding or blood-stained vaginal discharge is the most common presenting complaint.Speculum examination reveals amass or an ulcer, usually at the top of the vagina.Advanced diseasepresentswithhaematuria,constipation,pelvicpainortenesmus,afeelingofincompleteemptyingoftherectum.Diagnosisisconfirmedbybiopsy.StagingofvaginalcancerusestheFIGOsystem(Table16.2).Anexaminationunderanaesthetic,cystoscopyandsigmoidoscopydefineslocalspread.AnMRIscanofthepelvisconfirmsclinical findingsandacomputed tomography(CT)scanof the thoraxandabdomenestablisheswhetherdistantmetastasesarepresent.
TreatmentMost vaginal cancer is treated byprimary radiotherapy, although early-stage tumoursmaybemanagedsurgically.Prognosisdependsonstage.
Table16.2Stagingandprognosisofvaginalcancer
Stage Extentofdisease 5yearsurvivalrate
I Tumourconfinedtovagina 75%
II Tumourinvadesthesubvaginaltissue 40%
III Tumourinvadesthepelvicsidewall 30%
IV Tumourinvolvesbladderorbowelmucosaorextendsbeyondthetruepelvis 0–20%
(AccordingtotheInternationalFederationofGynecologyandObstetrics[FIGO]stagingsystem.)
Malignantdiseaseofthevulva
EpidemiologyandaetiologyVulval cancer is uncommon,with just 1,000newdiagnoses everyyear in theUK. Itwaspreviously adisease that exclusively affected olderwomen, but recent years havewitnessed rising incidence rates
www.medicalebookpdf.com
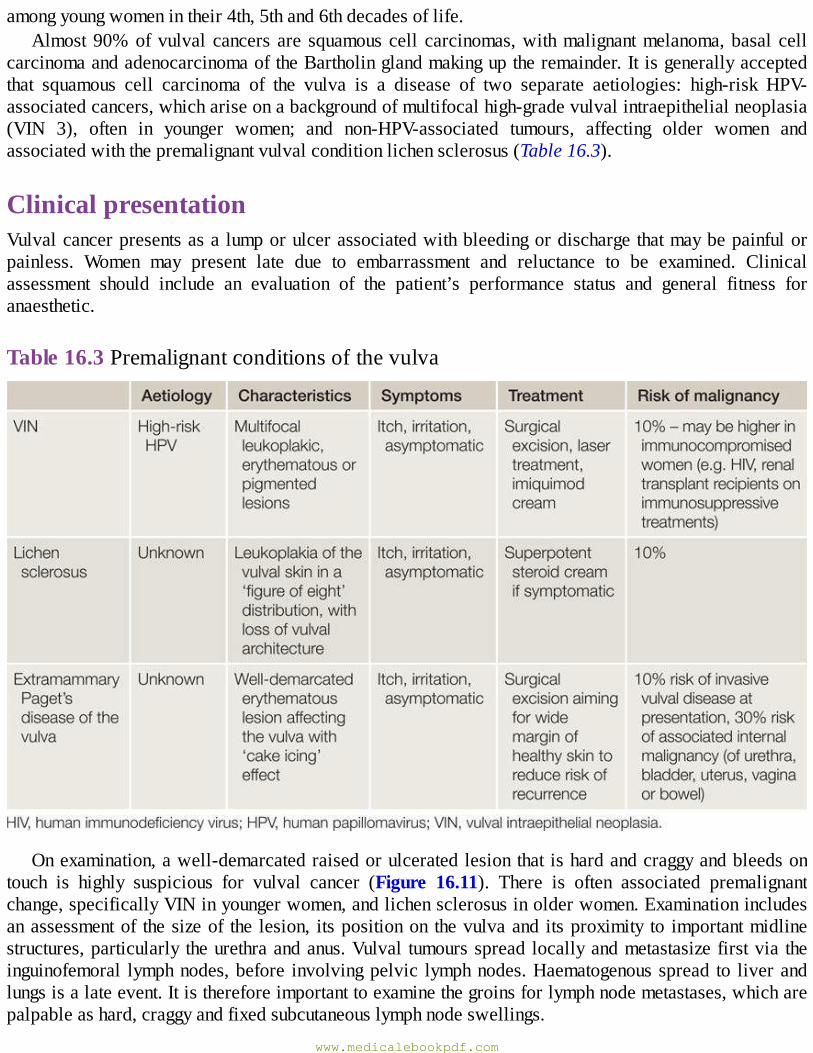
amongyoungwomenintheir4th,5thand6thdecadesoflife.Almost90%ofvulval cancers are squamouscell carcinomas,withmalignantmelanoma,basal cell
carcinomaandadenocarcinomaoftheBartholinglandmakinguptheremainder.Itisgenerallyacceptedthat squamous cell carcinoma of the vulva is a disease of two separate aetiologies: high-risk HPV-associatedcancers,whichariseonabackgroundofmultifocalhigh-gradevulvalintraepithelialneoplasia(VIN 3), often in younger women; and non-HPV-associated tumours, affecting older women andassociatedwiththepremalignantvulvalconditionlichensclerosus(Table16.3).
ClinicalpresentationVulvalcancerpresentsasalumporulcerassociatedwithbleedingordischargethatmaybepainfulorpainless. Women may present late due to embarrassment and reluctance to be examined. Clinicalassessment should include an evaluation of the patient’s performance status and general fitness foranaesthetic.
Table16.3Premalignantconditionsofthevulva
Onexamination,awell-demarcatedraisedorulceratedlesionthatishardandcraggyandbleedsontouch is highly suspicious for vulval cancer (Figure 16.11). There is often associated premalignantchange,specificallyVINinyoungerwomen,andlichensclerosusinolderwomen.Examinationincludesanassessmentof thesizeof the lesion, itspositionon thevulvaand itsproximity to importantmidlinestructures,particularly theurethraandanus.Vulval tumoursspread locallyandmetastasizefirstvia theinguinofemoral lymphnodes,before involvingpelvic lymphnodes.Haematogenousspread to liverandlungsisalateevent.Itisthereforeimportanttoexaminethegroinsforlymphnodemetastases,whicharepalpableashard,craggyandfixedsubcutaneouslymphnodeswellings.
www.medicalebookpdf.com
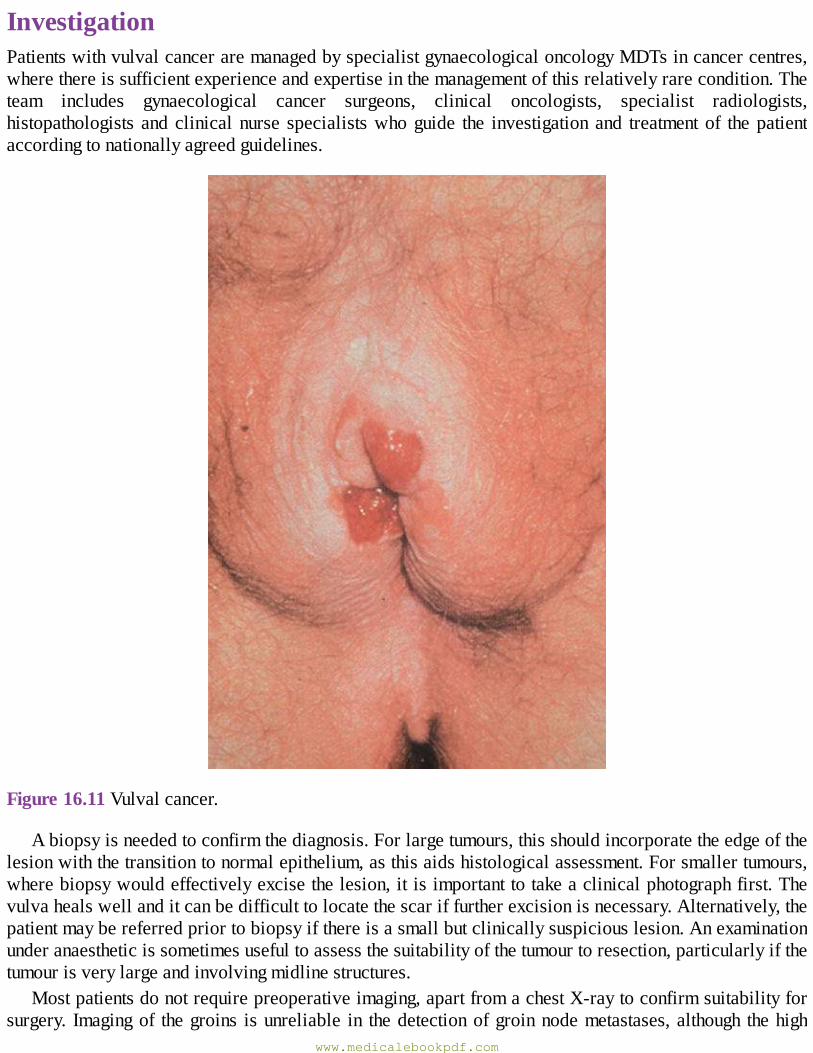
InvestigationPatientswithvulvalcanceraremanagedbyspecialistgynaecologicaloncologyMDTsincancercentres,wherethereissufficientexperienceandexpertiseinthemanagementofthisrelativelyrarecondition.Theteam includes gynaecological cancer surgeons, clinical oncologists, specialist radiologists,histopathologists andclinicalnurse specialistswhoguide the investigation and treatmentof thepatientaccordingtonationallyagreedguidelines.
Figure16.11Vulvalcancer.
Abiopsyisneededtoconfirmthediagnosis.Forlargetumours,thisshouldincorporatetheedgeofthelesionwiththetransitiontonormalepithelium,asthisaidshistologicalassessment.Forsmallertumours,wherebiopsywouldeffectivelyexcisethelesion,itisimportanttotakeaclinicalphotographfirst.Thevulvahealswellanditcanbedifficulttolocatethescariffurtherexcisionisnecessary.Alternatively,thepatientmaybereferredpriortobiopsyifthereisasmallbutclinicallysuspiciouslesion.Anexaminationunderanaestheticissometimesusefultoassessthesuitabilityofthetumourtoresection,particularlyifthetumourisverylargeandinvolvingmidlinestructures.
Mostpatientsdonotrequirepreoperativeimaging,apartfromachestX-raytoconfirmsuitabilityforsurgery. Imagingof thegroins isunreliable in thedetectionofgroinnodemetastases,although thehigh
www.medicalebookpdf.com
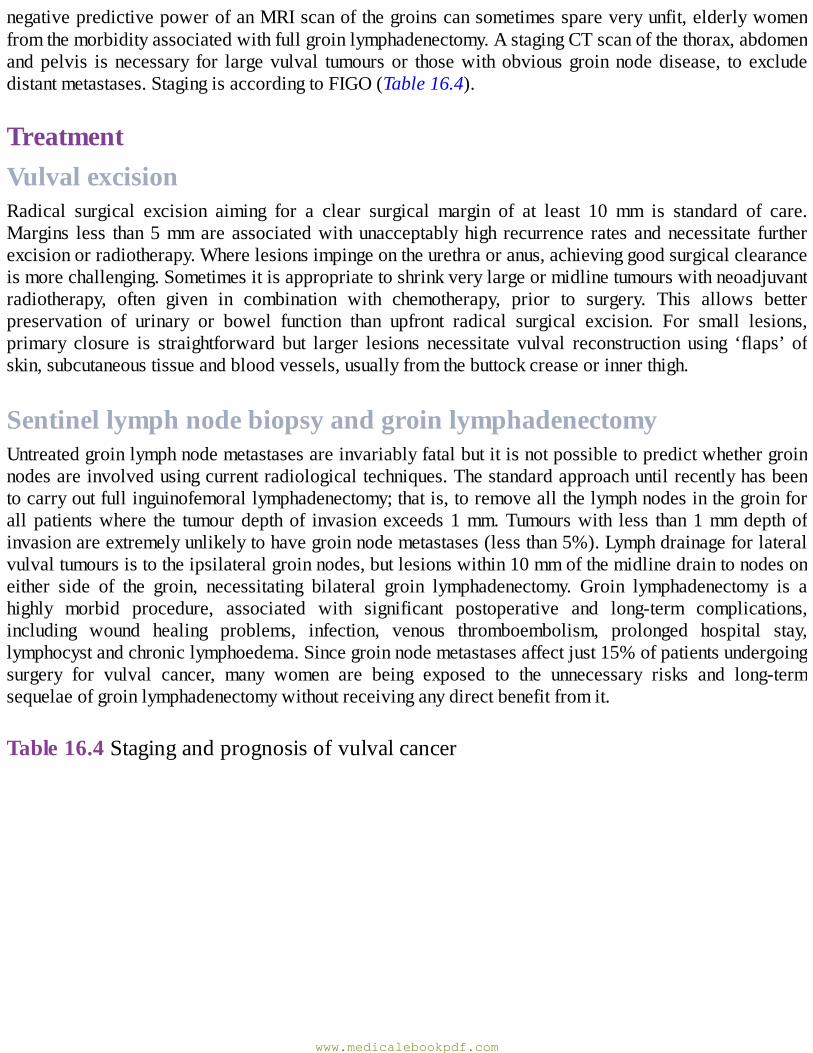
negativepredictivepowerofanMRIscanofthegroinscansometimesspareveryunfit,elderlywomenfromthemorbidityassociatedwithfullgroinlymphadenectomy.AstagingCTscanofthethorax,abdomenandpelvis isnecessary for largevulval tumoursor thosewithobviousgroinnodedisease, to excludedistantmetastases.StagingisaccordingtoFIGO(Table16.4).
TreatmentVulvalexcisionRadical surgical excision aiming for a clear surgical margin of at least 10 mm is standard of care.Margins less than5mmare associatedwithunacceptablyhigh recurrence rates andnecessitate furtherexcisionorradiotherapy.Wherelesionsimpingeontheurethraoranus,achievinggoodsurgicalclearanceismorechallenging.Sometimesitisappropriatetoshrinkverylargeormidlinetumourswithneoadjuvantradiotherapy, often given in combination with chemotherapy, prior to surgery. This allows betterpreservation of urinary or bowel function than upfront radical surgical excision. For small lesions,primary closure is straightforward but larger lesions necessitate vulval reconstruction using ‘flaps’ ofskin,subcutaneoustissueandbloodvessels,usuallyfromthebuttockcreaseorinnerthigh.
SentinellymphnodebiopsyandgroinlymphadenectomyUntreatedgroinlymphnodemetastasesareinvariablyfatalbutitisnotpossibletopredictwhethergroinnodesareinvolvedusingcurrentradiologicaltechniques.Thestandardapproachuntilrecentlyhasbeentocarryoutfullinguinofemorallymphadenectomy;thatis,toremoveallthelymphnodesinthegroinforall patientswhere the tumourdepthof invasionexceeds1mm.Tumourswith less than1mmdepthofinvasionareextremelyunlikelytohavegroinnodemetastases(lessthan5%).Lymphdrainageforlateralvulvaltumoursistotheipsilateralgroinnodes,butlesionswithin10mmofthemidlinedraintonodesoneither side of the groin, necessitating bilateral groin lymphadenectomy. Groin lymphadenectomy is ahighly morbid procedure, associated with significant postoperative and long-term complications,including wound healing problems, infection, venous thromboembolism, prolonged hospital stay,lymphocystandchroniclymphoedema.Sincegroinnodemetastasesaffectjust15%ofpatientsundergoingsurgery for vulval cancer, many women are being exposed to the unnecessary risks and long-termsequelaeofgroinlymphadenectomywithoutreceivinganydirectbenefitfromit.
Table16.4Stagingandprognosisofvulvalcancer
www.medicalebookpdf.com
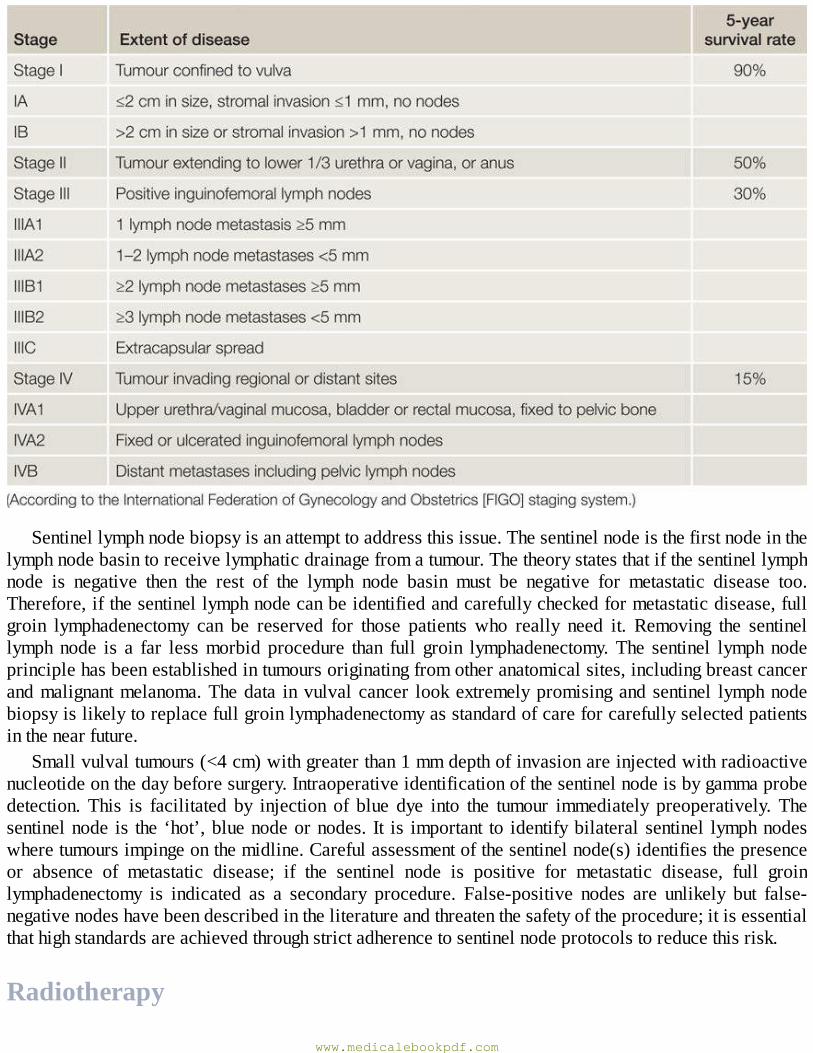
Sentinellymphnodebiopsyisanattempttoaddressthisissue.Thesentinelnodeisthefirstnodeinthelymphnodebasintoreceivelymphaticdrainagefromatumour.Thetheorystatesthatifthesentinellymphnode is negative then the rest of the lymph node basin must be negative for metastatic disease too.Therefore,ifthesentinellymphnodecanbeidentifiedandcarefullycheckedformetastaticdisease,fullgroin lymphadenectomy can be reserved for those patients who really need it. Removing the sentinellymphnode is a far lessmorbid procedure than full groin lymphadenectomy.The sentinel lymph nodeprinciplehasbeenestablishedintumoursoriginatingfromotheranatomicalsites,includingbreastcancerandmalignantmelanoma.Thedata invulvalcancer lookextremelypromisingandsentinel lymphnodebiopsyislikelytoreplacefullgroinlymphadenectomyasstandardofcareforcarefullyselectedpatientsinthenearfuture.
Smallvulvaltumours(<4cm)withgreaterthan1mmdepthofinvasionareinjectedwithradioactivenucleotideonthedaybeforesurgery.Intraoperativeidentificationofthesentinelnodeisbygammaprobedetection. This is facilitated by injection of blue dye into the tumour immediately preoperatively. Thesentinelnode is the ‘hot’,bluenodeornodes. It is important to identifybilateral sentinel lymphnodeswheretumoursimpingeonthemidline.Carefulassessmentofthesentinelnode(s)identifiesthepresenceor absence of metastatic disease; if the sentinel node is positive for metastatic disease, full groinlymphadenectomy is indicated as a secondary procedure. False-positive nodes are unlikely but false-negativenodeshavebeendescribedintheliteratureandthreatenthesafetyoftheprocedure;itisessentialthathighstandardsareachievedthroughstrictadherencetosentinelnodeprotocolstoreducethisrisk.
Radiotherapy
www.medicalebookpdf.com
Adjuvantradiotherapy,givenaftersurgerywithcurativeintent,isindicatedwhenvulvalexcisionmarginsarecloseorinvolvedorinthepresenceoftwoormoregroinnodemetastases.Adjuvantradiotherapyisgiven to reduce the risk of recurrence. Neoadjuvant radiotherapy, given before surgery to shrink thetumourandrenderitoperable, isusedforverylargevulval tumours,particularlythosethat involvetheurethraoranusandwhereadequatesurgicaleffortwouldhavefunctionalurinaryorbowelimplications.Occasionally,radicalradiotherapyisgiveninsteadofsurgeryinwomenwhoarenotfitforananaestheticdue to severe medical comorbidities (see previous section). Chemoradiotherapy is associated withimproved cure rates compared to radiotherapy alone. Treatment of recurrent disease and palliativetreatmentfollowsthesameprinciplesasforcervicalmalignancydiscussedintheprevioussection
KEYLEARNINGPOINTS•Cervical cancer is adisease commonlyaffectingwomen in low incomecountries.Mostwomenneverseeahealthprofessionalintheirlifeanddiefromtheirdiseaseintheircommunity.
• Population-based cervical screening of adult women has prevented 70% of cases of cervicalcancer developing in theUK.HPV vaccination of children in schools is likely to reduce ratesfurther,butthiswilltakemanyyearstoshowbenefit.
•Allpatientswithabnormalbleedingshouldundergospeculumandpelvicexaminationstoexcludemalignantdisease.
• Early-stage malignant disease of the lower genital tract is treated by surgical excision. Theprincipleofsurgeryinthiscontextistoremoveallthetumourwithadequatesurgicalmargins.
•Fertility-sparing treatment ispossible inearly-stagecervical tumours inyoungwomenwhohavenotcompletedtheirfamilies.
•Mostlowergenitaltracttumoursareradiosensitive,butsurgeryispreferredasfirst-linetreatmentduetoalowertoxicityprofile.
• Chemotherapy is used alongside radiotherapy to improve response rates and in the setting ofmetastaticdisease.
FurtherreadingCrosbie EJ, Brabin L (2010). Cervical cancer: problem solved? Vaccinating girls against humanpapillomavirus.BJOG117:137–42.
Crosbie EJ, Einstein MH, Franceschi S, Kitchener HC (2013). Human papillomavirus and cervicalcancer.Lancet382:889–99.
KitchenerHC,DentonK, SoldanK,CrosbieEJ (2013).Developing role ofHPV in cervical cancerprevention.BMJ347:f4781.
Selfassessment
www.medicalebookpdf.com
CASEHISTORY
MrsSisan88-year-oldwomanwhopresentstothegynaecologyclinicwithavulval lump.Ithasbeenbleedingintermittently.Itisverysoreandsheisfindingitdifficulttositdown.Sheisfrailandlivesinshelteredaccommodation.AWhatisthemostlikelydiagnosis?BWhatarethekeypointsintheexaminationandinvestigation?MrsS is found tohavea6cmvulval tumour involving theclitoris, right labiummajorumand theintroitalmargin.Itextendstoafewmillimetresawayfromtheexternalurethralmeatus.HerstagingCTscanexcludesdistantmetastases.CHowwouldyoumanageher?
ANSWERS
AAnewvulvallumpinanelderlywomanisvulvalcanceruntilprovenotherwise.ItisnotunusualforelderlywomentoputoffconsultingtheirGPbecauseofembarrassmentandreluctancetobeexamined.
BItisimportanttoinspectthevulva,notingthesizeofthelesion,itspositiononthevulvaanditsproximity to theurethra andanus.Abiopsy in theoutpatient settingwill expeditediagnosisbutmaybedifficult if thelesionisexquisitelytender,as thehistorysuggests.Anexaminationunderanaesthetic including biopsy may be necessary. Assessment of the groins is important sinceenlarged,hard,fixednodalmassesmaynotberesectable.Ifdistantmetastasesaresuspected,aCTscanofthethorax,abdomenandpelvisisimportantfortreatmentplanning.
C It is important to establish up frontwhat treatment the patientwants andwhether she is fit forgeneralanaestheticandthemorbidityofradicalvulvalcancersurgery.Fromanoncologicalpointof view, the best treatment is radical vulval excisionwith flap reconstruction of the vulva andbilateral groin lymphadenectomy. This may be followed by adjuvant radiotherapy if surgicalmargins are close or two or more groin nodes are positive. If proximity of the tumour to theurethra prohibits good surgical clearance without rendering Mrs S incontinent, it may beappropriate to consider neoadjuvant (chemo)radiotherapy to shrink the tumour prior to surgery.Radicalvulvalsurgeryandplacementofapermanentsuprapubiccatheterisanotheroption.IfMrsSisnotfitordoesnotwishtohavesurgery,radicalradiotherapywith/withoutchemotherapyisthetreatmentofchoice.AlldecisionsaremadefollowingfullconsultationwiththepatientandherfamilyandafterdiscussionwiththespecialistgynaecologicaloncologyMDT.
EMQ
ACryotherapy.BDirectedpunchbiopsy.CHigh-riskHPVtest.DLLETZ.EReferralforcolposcopy.
www.medicalebookpdf.com
FRepeatcervicalcytologyin3months.GRepeatcervicalcytologyin6months.HRepeatcervicalcytologyin3years.ITestofcure.
For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.Whatistheappropriatefollow-upfor:1Inadequatecervicalcytology.2Milddyskaryosis.3CIN2ondirectedpunchbiopsy.4Negativetestofcure.
ANSWERS
1FThesensitivityofasinglecervicalsmearforhigh-gradeCINdetectionisbetween40and70%;however,asthereisslowprogressionformostwomenwithCINtocancer,ifalesionismissedthen this should be picked up on a subsequent test.Womenwho attend regularly for cervicalcytologyhaveaverylowriskofdevelopingcervicalcancer.
2CWomenwithminor cytological abnormalities undergo reflex testingwithhigh-riskHPV.HPV-negativewomenarereturnedtoroutinerecall,whilehigh-riskHPV-positivewomenarereferredforcolposcopy.Womenwithhigh-gradeabnormalitiesarereferreddirecttocolposcopy.
3DLLETZisintendedtobecurativetoremovetheareaofabnormalitywithmargins.4H Patients who have received treatment for CIN undergo a ‘test of cure’ 6 months later. This
includesahigh-riskHPVtestandcytologicalassessment.Ifnegative,thewomanisreturnedtoroutine recall; that is, cervical screening in 3 years time. If positive, repeat colposcopy isindicated to identify any residual, untreated CIN. A woman with a history of CIN has anincreasedlifetimeriskofrecurrentCINandcervicalcancer.
SBAQUESTIONS
1A48-year-oldwomanattends thegynaecologydepartmentwithprolongedvaginalbleeding.Herlastcervicalsmearwas8yearspreviously.Aspeculumexaminationrevealsasuspicious-lookingcervixthatbleedsoncontact.Whatisthemostappropriateinitialinvestigation?Choosethesinglebestanswer.
ACervicalbiopsy.BLLETZ.CHysteroscopy.DMRIscanofherpelvis.ETransabdominalultrasoundscan.
www.medicalebookpdf.com
ANSWER
ACervical biopsy is required to make a histological diagnosis first, before imaging to stage orsurgicaltreatment.
2A32-year-oldwomanisdiagnosedwitha3cmstageIB1squamouscellcarcinomaofthecervix.Sheisdevastatedbecausesheandherpartnerwouldliketostartafamily.Whatfertility-sparingtreatmentwouldyourecommend?Choosethesinglebestanswer.
AColdknifeconebiopsy.BLLETZ.CRadicalhysterectomywithbilateralpelviclymphadenectomy.DRadicalradiotherapywithcisplatinchemotherapy.ERadicaltrachelectomywithbilateralpelviclymphadenectomy.
ANSWER
E IB1 lesions are greater than 4 cm in size but confined to the cervix.Radical hysterectomy andbilateral pelvic node dissection (Wertheim’s hysterectomy) is the standard of care. However,radicaltrachelectomywithbilateralpelviclymphadenectomyallowspreservationoftheovariesanduterus,permittingpregnancyinthefuture.
www.medicalebookpdf.com
CHAPTER17Gynaecologicalsurgeryandtherapeutics
DOUGLASTINCELLO
Gynaecologicalsurgery
Commongynaecologicalprocedures
Therapeutics
Furtherreading
Selfassessment
LEARNINGOBJECTIVES•Revisethekeypointsofsurgicalanatomyappliedtogynaecology.
• Understand the relative risks and benefits of abdominal and vaginal hysterectomy as well aslaparoscopichysterectomy.
•Understandtheadvantagesandprinciplesofminimalaccesssurgery.
•Understandtheadvantagesanddisadvantagesofcommonincisions.
•Understandthepurposeofcarefulpreassessmentandpostoperativecare.
•Beawareofhowtominimizesurgicalriskduringandimmediatelyaftersurgery.
•Recognizetheimportanceoffullyinformedconsent.
•Beawareofthecommongynaecologicalproceduresandtheirrisks.
•Describethecommonhormonalandnon-hormonaldrugsusedingynaecology,andunderstandtheprinciplesofsafeprescribing.
www.medicalebookpdf.com

Gynaecologicalsurgery
IntroductionInthischapter,theprinciplesofgoodsurgicalpracticeastheyrelatetogynaecologywillbediscussed.Variousproceduresthathavebeendiscussedinotherchaptersareexaminedinmoredetailhere,asaretherapeutics.FormoredetaileddescriptionsseeFurtherreading.
Gynaecologyisasurgicalspecialty;beforeobstetricsandgynaecologywasrecognizedasaspecialityinitsownright,mostgynaecologicalprocedureswereperformedbysurgeons.
KeysurgicalanatomyAnatomyhasbeendiscussedinChapter1,TheDevelopmentandanatomyofthefemalesexualorgansandpelvis.Athoroughknowledgeofpelvicanatomyisessentialforsafesurgicalpractice.Themajorvesselssupplyingtheuterusandadnexaearetheovarianvessels(arisingintheabdomenfromtheaortaandrenalartery), which enter the pelvis over the sacroiliac joints in the infundibulopelvic ligament (a fold ofperitoneum), and the uterine vessels. The uterine arteries are branches from the posterior trunk of theinternaliliacarteryandrunmediallyinthebaseofthebroadligamenttoturnupwardsandcoursealongthelateralborderoftheuterusoneachside.Atthebaseofthebroadligament,theuterinearteryruns1cmaboveand1cmlateraltotheureter,whereitisatriskofinjuryifcareisnottaken.Thisismuchmorelikely if there is scarring in the pelvis from endometriosis, or if the anatomy is distorted by anygynaecologicalcancersorovariancysts.
Theureterrunsfromthekidneyoverthepsoasmuscleinlinewiththelateralprocessesofthelumbarvertebraeandentersthepelvisoverthesacroiliacjoint.Itrunsintheposteriorleafofthebroadligamentto the level of the ischial spine,where it turns inwards and forwards to enter thebladder. Inorder tosafely dissect the uterine arteries away from the ureter, the bladder is reflected downwards at anabdominalhysterectomyorupwardsatavaginalhysterectomy.Thebladderisemptiedbeforeopenandlaparoscopic surgery to protect it from injury. The bladder is intimately associated with the anteriorvaginalwallandthefrontoftheuterinecervixandisthmus.Thevesicouterinefoldofperitoneummustbeopenedtoallowthebladdertobereflectedbeforeclampingtheuterinearteriesduringhysterectomy.Itisfor thesereasons thatbladderandureteric injuriesmayoccurduringgynaecologicalsurgery.If there isany doubt as to the position of the ureter, the broad ligament can be opened by dividing the roundligament,andtheuretercanalwaysbeenseenonthereflectedperitoneum.
The sigmoid colon runs along the left side wall of the abdomen and pelvis and becomesretroperitonealmidway along its passage through the pelvis. In a healthy pelvis the rectum falls awaywhentheuterusislifted,toallowclearidentificationoftherectumandposteriorvaginainthepouchofDouglas.Scarring(particularlyfromendometriosis)canobliteratethepouchofDouglasandincreasetherisk of rectal injury considerably.Also, after hysterectomy, the anatomical planes between vagina andrectumarelesseasilyseenandsorectalinjurycanoccuratthetimeofsacrocolpopexy.
ForadiscussionoftheanatomyoftheligamentsandfascialsupportsrelevanttoprolapseseeChapters1, The Development and anatomy of the female sexual organs and pelvis, and Chapter 10,Urogynaecologyandpelvicfloorproblems.
www.medicalebookpdf.com
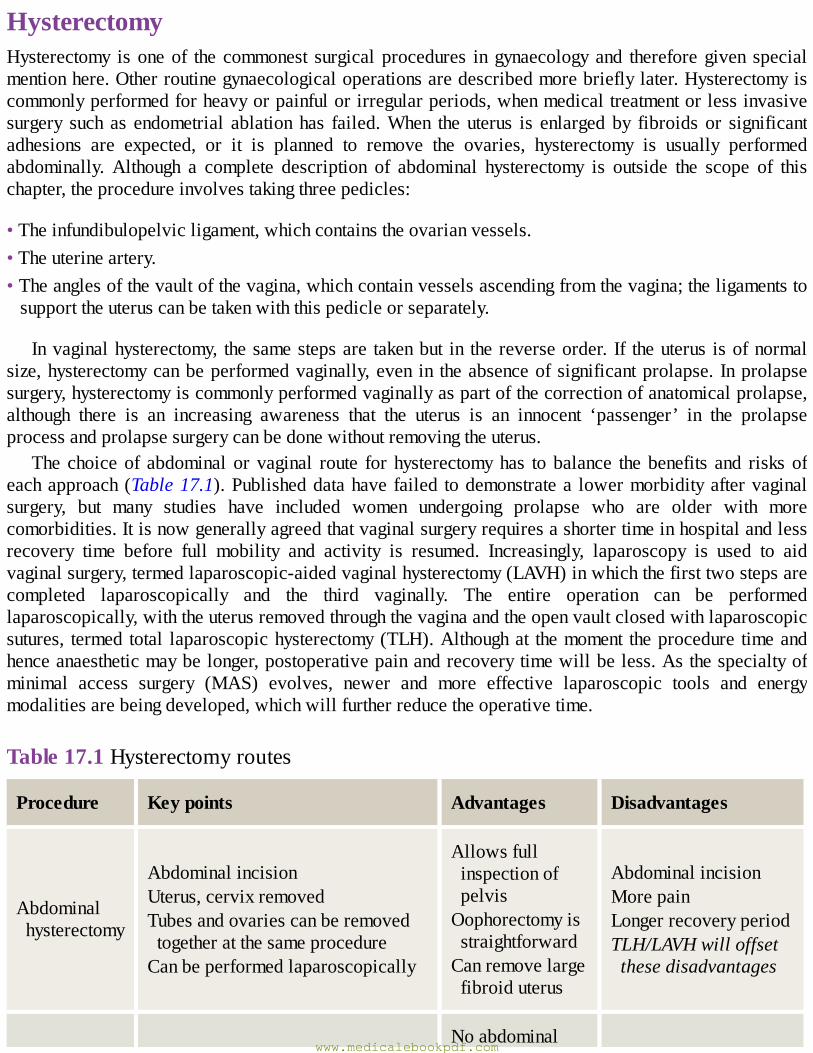
HysterectomyHysterectomy isoneof the commonest surgicalprocedures ingynaecologyand thereforegiven specialmentionhere.Otherroutinegynaecologicaloperationsaredescribedmorebrieflylater.Hysterectomyiscommonlyperformedforheavyorpainfulorirregularperiods,whenmedicaltreatmentorlessinvasivesurgery such as endometrial ablationhas failed.When the uterus is enlargedby fibroids or significantadhesions are expected, or it is planned to remove the ovaries, hysterectomy is usually performedabdominally. Although a complete description of abdominal hysterectomy is outside the scope of thischapter,theprocedureinvolvestakingthreepedicles:
•Theinfundibulopelvicligament,whichcontainstheovarianvessels.•Theuterineartery.•Theanglesofthevaultofthevagina,whichcontainvesselsascendingfromthevagina;theligamentstosupporttheuteruscanbetakenwiththispedicleorseparately.
Invaginalhysterectomy, thesamestepsare takenbut in thereverseorder. If theuterus isofnormalsize,hysterectomycanbeperformedvaginally,even in theabsenceofsignificantprolapse. Inprolapsesurgery,hysterectomyiscommonlyperformedvaginallyaspartofthecorrectionofanatomicalprolapse,although there is an increasing awareness that the uterus is an innocent ‘passenger’ in the prolapseprocessandprolapsesurgerycanbedonewithoutremovingtheuterus.
The choiceof abdominal or vaginal route for hysterectomyhas tobalance thebenefits and risksofeachapproach(Table17.1).Publisheddatahavefailed todemonstratea lowermorbidityaftervaginalsurgery, but many studies have included women undergoing prolapse who are older with morecomorbidities.Itisnowgenerallyagreedthatvaginalsurgeryrequiresashortertimeinhospitalandlessrecovery time before full mobility and activity is resumed. Increasingly, laparoscopy is used to aidvaginalsurgery,termedlaparoscopic-aidedvaginalhysterectomy(LAVH)inwhichthefirsttwostepsarecompleted laparoscopically and the third vaginally. The entire operation can be performedlaparoscopically,withtheuterusremovedthroughthevaginaandtheopenvaultclosedwithlaparoscopicsutures, termed total laparoscopichysterectomy(TLH).Althoughat themoment theprocedure timeandhenceanaestheticmaybelonger,postoperativepainandrecoverytimewillbeless.Asthespecialtyofminimal access surgery (MAS) evolves, newer and more effective laparoscopic tools and energymodalitiesarebeingdeveloped,whichwillfurtherreducetheoperativetime.
Table17.1Hysterectomyroutes
Procedure Keypoints Advantages Disadvantages
Abdominalhysterectomy
AbdominalincisionUterus,cervixremovedTubesandovariescanberemovedtogetheratthesameprocedureCanbeperformedlaparoscopically
AllowsfullinspectionofpelvisOophorectomyisstraightforwardCanremovelargefibroiduterus
AbdominalincisionMorepainLongerrecoveryperiodTLH/LAVHwilloffsetthesedisadvantages
Noabdominalwww.medicalebookpdf.com
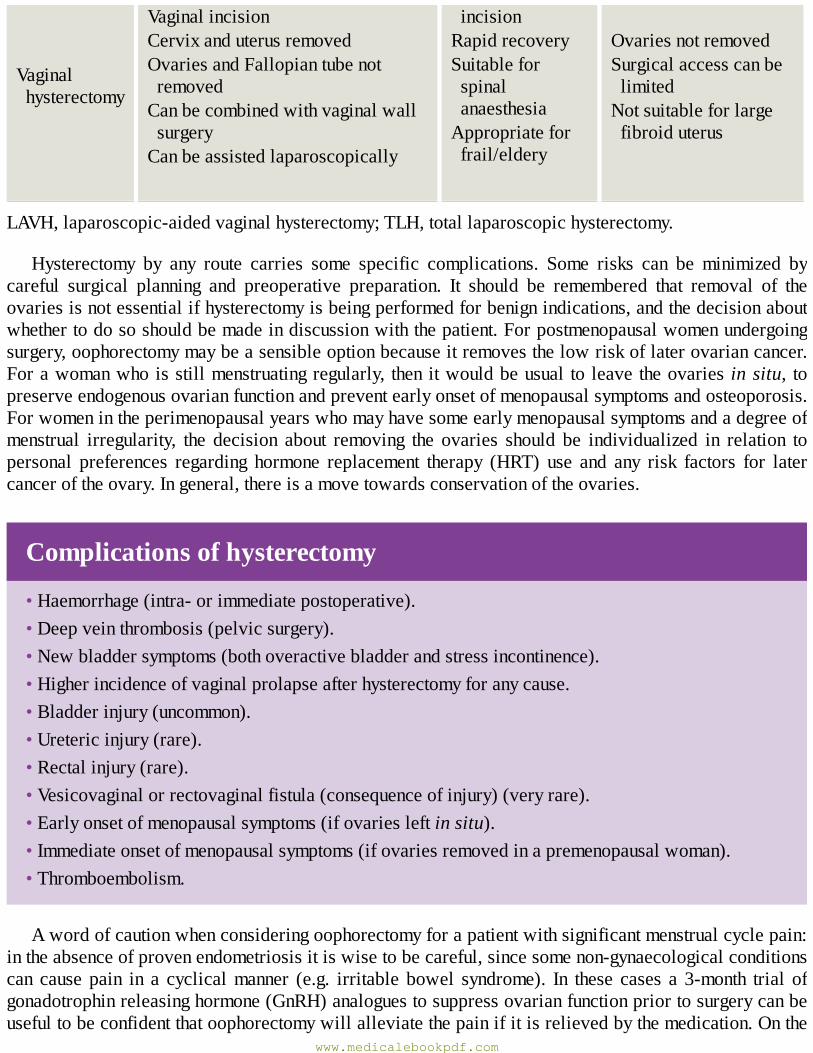
Vaginalhysterectomy
VaginalincisionCervixanduterusremovedOvariesandFallopiantubenotremovedCanbecombinedwithvaginalwallsurgeryCanbeassistedlaparoscopically
incisionRapidrecoverySuitableforspinalanaesthesiaAppropriateforfrail/eldery
OvariesnotremovedSurgicalaccesscanbelimitedNotsuitableforlargefibroiduterus
LAVH,laparoscopic-aidedvaginalhysterectomy;TLH,totallaparoscopichysterectomy.
Hysterectomy by any route carries some specific complications. Some risks can be minimized bycareful surgical planning and preoperative preparation. It should be remembered that removal of theovariesisnotessentialifhysterectomyisbeingperformedforbenignindications,andthedecisionaboutwhethertodososhouldbemadeindiscussionwiththepatient.Forpostmenopausalwomenundergoingsurgery,oophorectomymaybeasensibleoptionbecauseitremovesthelowriskoflaterovariancancer.Forawomanwhoisstillmenstruatingregularly, thenitwouldbeusual to leavetheovaries insitu, topreserveendogenousovarianfunctionandpreventearlyonsetofmenopausalsymptomsandosteoporosis.Forwomenintheperimenopausalyearswhomayhavesomeearlymenopausalsymptomsandadegreeofmenstrual irregularity, the decision about removing the ovaries should be individualized in relation topersonal preferences regarding hormone replacement therapy (HRT) use and any risk factors for latercanceroftheovary.Ingeneral,thereisamovetowardsconservationoftheovaries.
Complicationsofhysterectomy
•Haemorrhage(intra-orimmediatepostoperative).•Deepveinthrombosis(pelvicsurgery).•Newbladdersymptoms(bothoveractivebladderandstressincontinence).•Higherincidenceofvaginalprolapseafterhysterectomyforanycause.•Bladderinjury(uncommon).•Uretericinjury(rare).•Rectalinjury(rare).•Vesicovaginalorrectovaginalfistula(consequenceofinjury)(veryrare).•Earlyonsetofmenopausalsymptoms(ifovariesleftinsitu).•Immediateonsetofmenopausalsymptoms(ifovariesremovedinapremenopausalwoman).•Thromboembolism.
Awordofcautionwhenconsideringoophorectomyforapatientwithsignificantmenstrualcyclepain:intheabsenceofprovenendometriosisitiswisetobecareful,sincesomenon-gynaecologicalconditionscan cause pain in a cyclicalmanner (e.g. irritable bowel syndrome). In these cases a 3-month trial ofgonadotrophinreleasinghormone(GnRH)analoguestosuppressovarianfunctionpriortosurgerycanbeusefultobeconfidentthatoophorectomywillalleviatethepainifitisrelievedbythemedication.Onthe
www.medicalebookpdf.com

other hand, if one is sure the pain is related to the ovaries, then performing hysterectomy withoutoophorectomycanleaveapatientwithongoingpain,andlateroophorectomycanbetechnicallydifficult,withadhesionsandwiththeovaryadherenttothepelvicsidewallandureter.
Exceptions to the principle of ovarian conservation in young patients would be a woman withsignificantanddebilitatingpremenstrualsyndromewhereoophorectomywouldalleviatethis,orawomanwithsevereendometriosis,whereoophorectomyisnecessarytoachieveacure.Oophorectomyinyoungwomen will usually require immediate recourse to systemic HRT, which is not always withoutcomplications(seeChapter8,TheMenopauseandpostreproductivehealth).
KEYLEARNINGPOINTS•Thebladderanduretersarecloselyrelatedtotheuterus,cervixanduterinevesselsandareatriskofinjuryduringhysterectomy.
•Abdominalhysterectomyhasalongerrecoverytimethanvaginalhysterectomybutmakesremovaloflargefibroidsandovarieseasier.
•Hysterectomybyanyrouteincreasestheriskofnewurinaryandprolapsesymptoms.•Oophorectomyisnotmandatoryatthetimeofhysterectomy.• The decision whether to remove the ovaries should consider the patient’s age, presence ofmenopausalsymptoms,painandtheindividualriskoflaterovariancancer.
PreassessmentInmodernmedical practice, patients are admitted for as short a time as is practical and safe for thepatient.As a result, thepresurgicalpreparationofpatients innowoftenperformed in apreassessmentclinic(PAC)upto2weeksbeforethedateofsurgery.Atpreassessmentaclinicalreviewisundertaken,usuallybya juniordoctororspecialistnurse, toconfirmthepatient’smedicalconditionisstillpresentand to identify any new or existingmedical comorbidities that may affect the risks of anaesthesia orincrease the risk of intra- and postoperative complications. All patients will have a full blood count(FBC) and blood group and serum save (or a full cross-match in advance if significant bleeding isanticipated), and patients over the age of 50 or thereabouts, plus those with known cardiac, renal orrespiratory problems, will also have serum biochemistry measured (urea, electrolytes, renal function,hepatic function), a chest X-ray and electrocardiography (ECG) performed. These results will beavailableforthesurgeonandanaesthetistinadvanceofthesurgery.
The PAC is a valuable opportunity to arrange additional investigations andmake specific surgicalplans forhigh-riskpatients.For instance,patientswithsignificantcardiac failureor severe respiratorydiseasemayrequireechocardiographyorlungfunctiontest.Patientswithknowncoagulationdisorders,orthose taking long-term anticoagulants such as warfarin, can be reviewed by the haematologist and adetailed bridging plan prepared.Many hospitals support their PACswith consultant anaesthetistswhoprovideexpertreviewofhigh-riskpatientsevenbeforethedecisionforsurgeryhasbeenmade,andwhocan make detailed plans for the care of the very high-risk patient, including the provision of a highdependencyorintensivecarebedintheimmediatepostoperativeperiod.
TheriskofthromboembolismisbestassessedatthePACsothatplanscanbemadeforpostoperativethromboprophylaxis.Thecombinedoralcontraceptivepill(COCP)shouldbestopped4weekspriortosurgery and alternative contraception used. HRT should also be stopped, although there is some
www.medicalebookpdf.com
disagreementabout this.Coveringwomenwithlow-molecularweightheparin(LMWH)evenforminorsurgerywouldbeanoptionifHRTiscontinued.Allwomenmustbemobilizedearlyaftersurgery,andgivingwomentheexpectationthatthiswillbethecaseisuseful.Allwomenaregiventhromboembolicstockings(TEDS)andkepthydrated.LMWHisgivenaccordingtostandardriskassessment.
Thromboprophylaxisinsurgery
•Lowrisk:surgerylessthan30minwithoutriskfactors.•Moderaterisk:•useTEDSandLMWH;• surgery more than 30 min, high body mass index (BMI), varicose veins, sepsis, immobility,comorbidity.
•Highrisk:•useTEDSandLMWHfor5daysoruntilmobile;•cancer,prolongedsurgery,previousthromboembolicevent,thrombophiliaor>3ofmoderateriskfactors.
PACsarealsoanopportunityforthepatienttodiscussanyremainingconcernsorquestionsshemayhaveaboutherimpendingsurgery,anditisconsideredgoodpracticetousepreassessmentappointmentsasanopportunitytoobtainwrittenconsentfromthepatientatatimeslightlydistantfromtheanxietiesofthedayofsurgery(seebelow).
SurgicalpracticeanddecisionmakingSafesurgicalpracticeandcarefuldecisionmakingbeginsintheoutpatientclinic.Withtheexceptionofcancer, most gynaecology conditions we treat affect quality of life and are not life-threatening. It isimportant, therefore, toworkwith thepatient toensure thatallavailableconservativeandnon-medicalinterventionshavebeen triedor at least discussedbefore considering surgery.Although in themodernworldanaesthesiaandsurgeryaresafe,anysurgicalproceduredoescarryrisksandcomplications,someofwhichcanrarelybelife-threateningorcausesignificantphysicalmorbidity.Itisoneofthedutiesofaprofessional toensure thathisorherpatientsaremadeawareofall the issues.Manypatients seem toconsidersurgerytobetheonlyinterventionthatwillmakealastingdifferenceandcanbeoveroptimisticaboutthelikelyoutcome.Thebestwaytoavoidsurgicalcomplicationsandmishapsisnottooperate!
Havingmadethedecisiontoperformanoperation,onemustbecarefultoconsiderthealternatives,toarrive at the best operation for that patient with that condition. Abdominal surgery requires longerrecoverythanvaginalsurgery,andinvolveslongerincisionsusually,whilelaparoscopicsurgeryrequiresapatienttoendurealongeranaesthetic(often)whileinasteepTrendelenburgposition(headdown).So,for instance, one might decide to avoid an abdominal approach on a very frail elderly patient withcomorbidities in favour of a laparoscopic or vaginal approach. One might decide to avoid complexlaparoscopicsurgeryinamorbidlyobesewoman,oronemightdecideagainstbilateraloophorectomyinapatientknowntohavehadseveralpreviouslaparotomies,extensiveendometriosisandintra-abdominaladhesions. In complex cases, it is often prudent to seek the viewsof colleagues, either in an informaldiscussionormorerecentlyintheformatofmultidisciplinaryteam(MDT)meetingsasbestpractice.At
www.medicalebookpdf.com
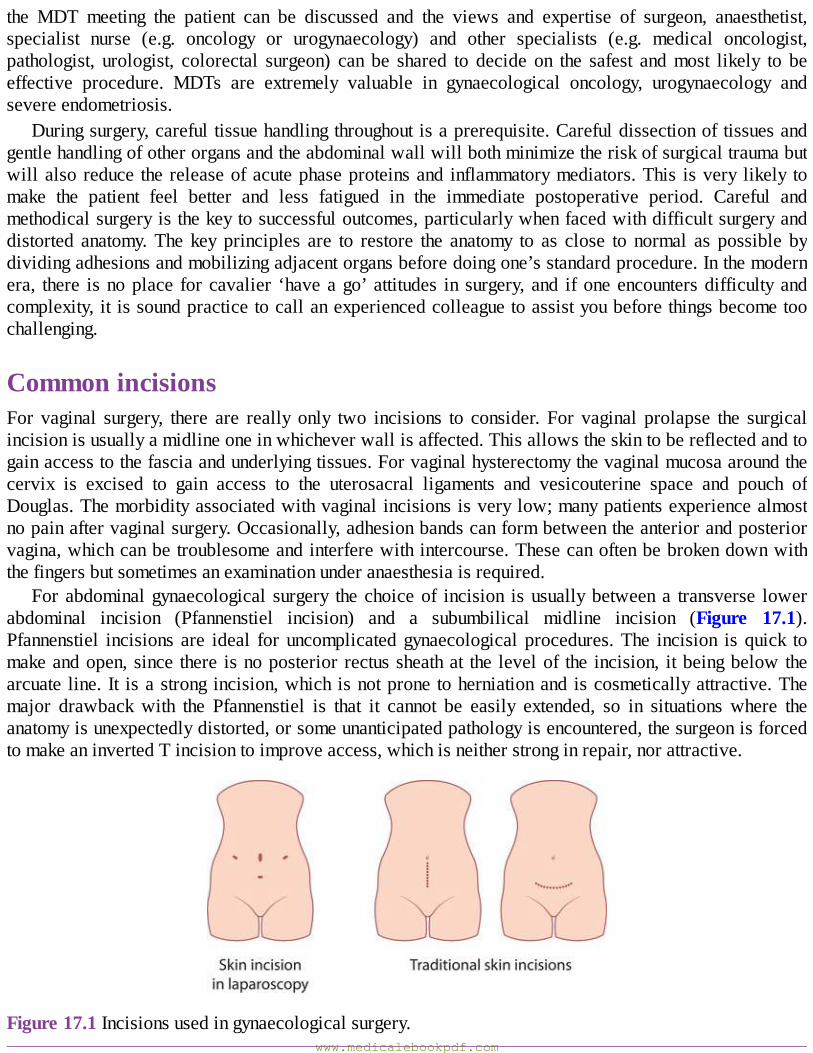
the MDT meeting the patient can be discussed and the views and expertise of surgeon, anaesthetist,specialist nurse (e.g. oncology or urogynaecology) and other specialists (e.g. medical oncologist,pathologist, urologist, colorectal surgeon) can be shared to decide on the safest andmost likely to beeffective procedure. MDTs are extremely valuable in gynaecological oncology, urogynaecology andsevereendometriosis.
Duringsurgery,carefultissuehandlingthroughoutisaprerequisite.Carefuldissectionoftissuesandgentlehandlingofotherorgansandtheabdominalwallwillbothminimizetheriskofsurgicaltraumabutwillalsoreduce thereleaseofacutephaseproteinsand inflammatorymediators.This isvery likely tomake the patient feel better and less fatigued in the immediate postoperative period. Careful andmethodicalsurgeryisthekeytosuccessfuloutcomes,particularlywhenfacedwithdifficultsurgeryanddistorted anatomy.The key principles are to restore the anatomy to as close to normal as possible bydividingadhesionsandmobilizingadjacentorgansbeforedoingone’sstandardprocedure.Inthemodernera, there isnoplace forcavalier ‘haveago’attitudes in surgery,and ifoneencountersdifficultyandcomplexity,itissoundpracticetocallanexperiencedcolleaguetoassistyoubeforethingsbecometoochallenging.
CommonincisionsFor vaginal surgery, there are really only two incisions to consider. For vaginal prolapse the surgicalincisionisusuallyamidlineoneinwhicheverwallisaffected.Thisallowstheskintobereflectedandtogainaccesstothefasciaandunderlyingtissues.Forvaginalhysterectomythevaginalmucosaaroundthecervix is excised to gain access to the uterosacral ligaments and vesicouterine space and pouch ofDouglas.Themorbidityassociatedwithvaginalincisionsisverylow;manypatientsexperiencealmostnopainaftervaginalsurgery.Occasionally,adhesionbandscanformbetweentheanteriorandposteriorvagina,whichcanbetroublesomeandinterferewithintercourse.Thesecanoftenbebrokendownwiththefingersbutsometimesanexaminationunderanaesthesiaisrequired.
Forabdominalgynaecological surgery thechoiceof incision isusuallybetweena transverse lowerabdominal incision (Pfannenstiel incision) and a subumbilical midline incision (Figure 17.1).Pfannenstiel incisions are ideal foruncomplicatedgynaecological procedures.The incision is quick tomakeandopen,since there isnoposterior rectussheathat the levelof the incision, itbeingbelowthearcuate line. It isastrong incision,which isnotprone toherniationand iscosmeticallyattractive.Themajor drawback with the Pfannenstiel is that it cannot be easily extended, so in situations where theanatomyisunexpectedlydistorted,orsomeunanticipatedpathologyisencountered,thesurgeonisforcedtomakeaninvertedTincisiontoimproveaccess,whichisneitherstronginrepair,norattractive.
Figure17.1Incisionsusedingynaecologicalsurgery.www.medicalebookpdf.com
Pfannenstielincision
•Transversely,twofingerbreadthsabovethepubicsymphysis.•Strongwhenrepairedwithlowriskofherniationordehiscence.•Notverypainful(limitedtooneortwodermatomes).•Cosmeticallyattractive(lowerthanthe‘underwearline’).•Cannotbeeasilyextendedormadelarger.•Surgicalaccesslimitedtopelvicorgans.
Midlineincision
•Verticallyfrompubicsymphysisuptoumbilicus.•Lessstrong;pronetoherniationordehiscence.•Morepainful(involvesseveraldermatomes).•Cosmeticallyunattractive.•Caneasilybeextendaroundumbilicusuptothexiphisternum.•Givesexcellentsurgicalaccess.
A midline (or paramedian) incision is often favoured by oncologists, and also when significantsurgical difficulty is anticipated (e.g. from adhesions, large fibroids or ovarian cysts). Although lessstrong thanaPfannenstiel incision, themajor advantageof themidline incision is that is caneasilybeextendedtoprovideexcellentsurgicalaccess.Alargeincisionwillofcoursecausemorepostoperativepain,whichcanincreasetheriskofrespiratoryinfectionbylimitingbreathingandcoughingefforts.Theauthor recommends a vertical incision in emergency caseswhen the exact underlying diagnosis is notentirelyclear(e.g.apelvicmassinapyrexialpatient)toallowflexibilityofaccessshouldthefindingsbeunexpected.
Laparoscopic surgery holds several advantages over open abdominal surgery. Laparoscopic entrywoundsareusually less than1cm in lengthand thuscausemuch lesspostoperativepain thananopenwound.The risk of herniation is very low.The lack of pain and extensive externalwoundsmean thatpatientsbecomemobileaftersurgeryveryquicklyandmostlaparoscopicprocedures(evenhysterectomy)allow for hospital discharge within 24–48 hours. The laparoscopic approach allows for enhancedvisibilityforsomepelvicprocedures,especiallythosedeepinthepelvis,suchasexcisionofinfiltratingendometriosis or performing the mesh attachment at a laparoscopic sacrocolpopexy. Although theoperating time may be longer than with open surgery, the more rapid discharge from hospital makeslaparoscopic surgerymore cost-effective in general, although there are limited data suggesting it alsoleadstobettersurgicaloutcomes.
KEYLEARNINGPOINTS•Surgicalpreassessmentisanimportantpartofpatientcareandallowspersonalizedplansofcaretobemadeforthosewithcomorbidities.
www.medicalebookpdf.com
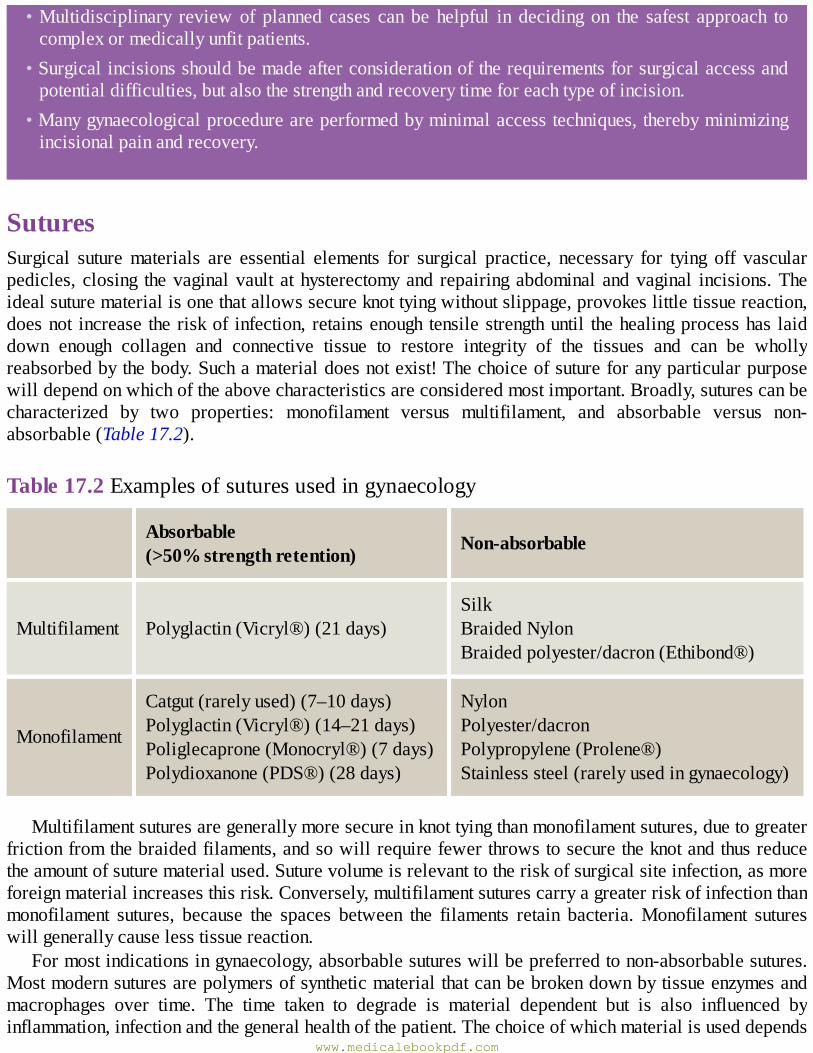
•Multidisciplinary review of planned cases can be helpful in deciding on the safest approach tocomplexormedicallyunfitpatients.
•Surgicalincisionsshouldbemadeafterconsiderationoftherequirementsforsurgicalaccessandpotentialdifficulties,butalsothestrengthandrecoverytimeforeachtypeofincision.
•Manygynaecologicalprocedureareperformedbyminimalaccesstechniques,therebyminimizingincisionalpainandrecovery.
SuturesSurgical suturematerials are essential elements for surgical practice, necessary for tying off vascularpedicles, closing thevaginalvault athysterectomyand repairingabdominal andvaginal incisions.Theidealsuturematerialisonethatallowssecureknottyingwithoutslippage,provokeslittletissuereaction,doesnot increase theriskof infection, retainsenough tensilestrengthuntil thehealingprocesshas laiddown enough collagen and connective tissue to restore integrity of the tissues and can be whollyreabsorbedbythebody.Suchamaterialdoesnotexist!Thechoiceofsutureforanyparticularpurposewilldependonwhichoftheabovecharacteristicsareconsideredmostimportant.Broadly,suturescanbecharacterized by two properties: monofilament versus multifilament, and absorbable versus non-absorbable(Table17.2).
Table17.2Examplesofsuturesusedingynaecology
Absorbable(>50%strengthretention) Non-absorbable
Multifilament Polyglactin(Vicryl®)(21days)SilkBraidedNylonBraidedpolyester/dacron(Ethibond®)
Monofilament
Catgut(rarelyused)(7–10days)Polyglactin(Vicryl®)(14–21days)Poliglecaprone(Monocryl®)(7days)Polydioxanone(PDS®)(28days)
NylonPolyester/dacronPolypropylene(Prolene®)Stainlesssteel(rarelyusedingynaecology)
Multifilamentsuturesaregenerallymoresecureinknottyingthanmonofilamentsutures,duetogreaterfrictionfromthebraidedfilaments,andsowillrequirefewerthrowstosecuretheknotandthusreducetheamountofsuturematerialused.Suturevolumeisrelevanttotheriskofsurgicalsiteinfection,asmoreforeignmaterialincreasesthisrisk.Conversely,multifilamentsuturescarryagreaterriskofinfectionthanmonofilament sutures, because the spaces between the filaments retain bacteria.Monofilament sutureswillgenerallycauselesstissuereaction.
Formostindicationsingynaecology,absorbablesutureswillbepreferredtonon-absorbablesutures.Mostmodernsuturesarepolymersofsyntheticmaterialthatcanbebrokendownbytissueenzymesandmacrophages over time. The time taken to degrade is material dependent but is also influenced byinflammation,infectionandthegeneralhealthofthepatient.Thechoiceofwhichmaterialisuseddepends
www.medicalebookpdf.com
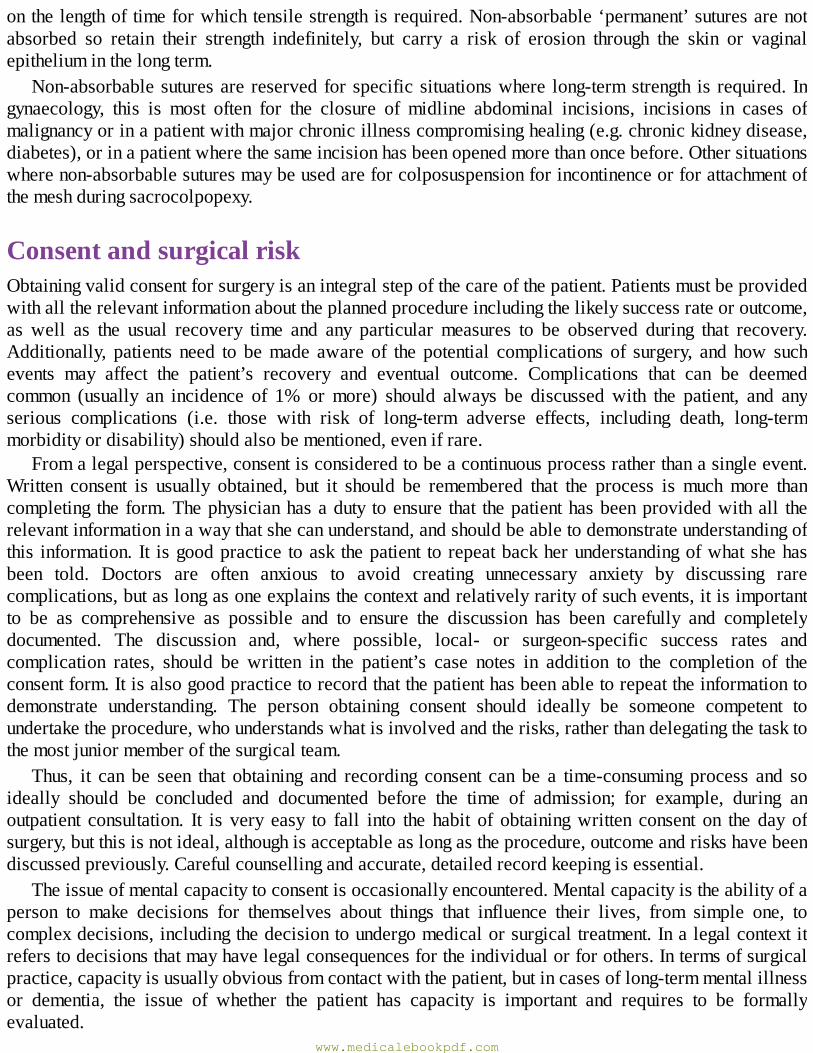
onthelengthoftimeforwhichtensilestrengthisrequired.Non-absorbable‘permanent’suturesarenotabsorbed so retain their strength indefinitely, but carry a risk of erosion through the skin or vaginalepitheliuminthelongterm.
Non-absorbablesuturesare reservedforspecificsituationswhere long-termstrength is required. Ingynaecology, this is most often for the closure of midline abdominal incisions, incisions in cases ofmalignancyorinapatientwithmajorchronicillnesscompromisinghealing(e.g.chronickidneydisease,diabetes),orinapatientwherethesameincisionhasbeenopenedmorethanoncebefore.Othersituationswherenon-absorbablesuturesmaybeusedareforcolposuspensionforincontinenceorforattachmentofthemeshduringsacrocolpopexy.
ConsentandsurgicalriskObtainingvalidconsentforsurgeryisanintegralstepofthecareofthepatient.Patientsmustbeprovidedwithalltherelevantinformationabouttheplannedprocedureincludingthelikelysuccessrateoroutcome,as well as the usual recovery time and any particular measures to be observed during that recovery.Additionally, patients need to bemade aware of the potential complications of surgery, and how suchevents may affect the patient’s recovery and eventual outcome. Complications that can be deemedcommon (usually an incidence of 1% ormore) should always be discussedwith the patient, and anyserious complications (i.e. those with risk of long-term adverse effects, including death, long-termmorbidityordisability)shouldalsobementioned,evenifrare.
Fromalegalperspective,consentisconsideredtobeacontinuousprocessratherthanasingleevent.Written consent is usually obtained, but it should be remembered that the process is muchmore thancompleting the form.Thephysicianhasaduty toensure that thepatienthasbeenprovidedwithall therelevantinformationinawaythatshecanunderstand,andshouldbeabletodemonstrateunderstandingofthis information. It isgoodpractice toask thepatient to repeatbackherunderstandingofwhatshehasbeen told. Doctors are often anxious to avoid creating unnecessary anxiety by discussing rarecomplications,butaslongasoneexplainsthecontextandrelativelyrarityofsuchevents,itisimportantto be as comprehensive as possible and to ensure the discussion has been carefully and completelydocumented. The discussion and, where possible, local- or surgeon-specific success rates andcomplication rates, should be written in the patient’s case notes in addition to the completion of theconsentform.Itisalsogoodpracticetorecordthatthepatienthasbeenabletorepeattheinformationtodemonstrate understanding. The person obtaining consent should ideally be someone competent toundertaketheprocedure,whounderstandswhatisinvolvedandtherisks,ratherthandelegatingthetasktothemostjuniormemberofthesurgicalteam.
Thus, it can be seen that obtaining and recording consent can be a time-consuming process and soideally should be concluded and documented before the time of admission; for example, during anoutpatient consultation. It is very easy to fall into the habit of obtainingwritten consent on the day ofsurgery,butthisisnotideal,althoughisacceptableaslongastheprocedure,outcomeandriskshavebeendiscussedpreviously.Carefulcounsellingandaccurate,detailedrecordkeepingisessential.
Theissueofmentalcapacitytoconsentisoccasionallyencountered.Mentalcapacityistheabilityofaperson to make decisions for themselves about things that influence their lives, from simple one, tocomplexdecisions,includingthedecisiontoundergomedicalorsurgicaltreatment.Inalegalcontextitreferstodecisionsthatmayhavelegalconsequencesfortheindividualorforothers.Intermsofsurgicalpractice,capacityisusuallyobviousfromcontactwiththepatient,butincasesoflong-termmentalillnessor dementia, the issue of whether the patient has capacity is important and requires to be formallyevaluated.
www.medicalebookpdf.com

Froma legalperspective,aperson lackscapacitywhenat the timeofdecisionmakingheorshe isunabletomakeorcommunicatethatdecisionduetoan‘impairmentof,oradisturbanceinthefunctionofthemindorbrain’.Assessingcapacityhastwostages:firstly,isthereanimpairmentordisturbancetothemindorbrain;andsecondly,isthissufficienttorenderthepersonunabletomakethisdecision.Itshouldberememberedthatcapacityis taskandtimespecific.Thus,apersonwithdementia,forexample,mayhave capacity for simple decisions (e.g. to have a cupof tea), but not for a complexdecision, or thatcapacitymightvaryfromdaytoday.
Thekey issue forhealthprofessionals is to ensure that capacityhasbeenassessed.Legally, havingcapacityisdistinctfromthenatureof thedecisionmade,and individualswithcapacitymaywellmakedecisionsthatothersregardasrash,foolishordangerous.However,ifcapacitycanbedemonstrated,theindividual can make whatever decision they wish! Where capacity is in doubt, the responsibility toascertaincapacitylieswiththehealthcareprofessional,andsometimesitmaybenecessarytoseektheopinionofmorethanonepractitioner.Manyhospitalshaveaformalprocesswhereapanelwillmakethedecision.Wherecapacityisabsentorunclear,clinicaldecisionshavetobemadeonthebasisofwhatisin the patient’s best interests. This can be difficult to establish andwill often require discussionwithfamily members or friends who can advise on what the patient would usually wish or any previousexpressionsorviewsmadewhenthepatienthadcapacity.Anindividualwillbeprotectedbylawwhenmakingaclinicaldecisionwheretheyhave‘reasonablebelief’thatthepersonlacksconsentandthatthecourseofactionisintheperson’sbestinterest.Thisislimitedbycertainthings,includinganyadvancedecision by the individual (e.g. a ‘livingwill’), or by a legal judgement. Inmany cases, the issue ofcapacity is easy to determine, but sometimes it can be difficult, and identifying the patient’s ‘bestinterests’canalsobedifficult.Ifindoubt,cliniciansshouldseekadvicefromtheiremployer’slegalteam.Occasionally,decisionsoncareneedtobemadebycourtruling.
On thedayof surgery, the surgicalMDTmustwork together to ensure that theanaesthetic, surgicalprocedureandrecoveryoccursefficientlyandwithoutcomplicationsoradverseevents.Communicationwithintheteamisofparamountimportanceandwilloftenbeginbeforethedayofsurgerywithdiscussionbetweenthesurgeonandanaesthetistregardingissuesidentifiedatpreassessment.
TheWorldHealthOrganization(WHO)hasdevelopedasafesurgerychecklist that isrecommendedforuseforallsurgicalactivities.Itisawrittenchecklistdevelopedtominimizesurgicaladverseevents.Worldwide the crude mortality rate after surgery is between 0.5% and 5% and postoperativecomplicationsoccurinupto25%ofcases.Inhigherincomecountries,nearlyhalfofadverseeventsinhospitalrelatetosurgicalcare,one-halfofwhichareconsideredtohavebeenavoidable.Thechecklistisavalidatedand tested tool toreduce theserisks,which includesspecific tasksbefore,duringandaftersurgerytoensurethewholeteamisawareofissuesrelatingtothespecificcaseabouttobeperformed(Figure17.2).Itincludeselementstoensureanaesthesiasafety,identificationofthecorrectsurgicalsiteand confirmation of the procedure planned, discussion of any specific or non-standard elements to theprocedureandattentiontocarefulpostoperativecareintheimmediaterecoveryperiod.
KEYLEARNINGPOINTS•Consentforsurgeryisacontinuousprocess,andshouldbefullydocumented.• Where possible, local figures for cure and complications should be given to the patient andincludedinthewrittennotesrecorded.
•Mentalcapacityisrequiredtogiveconsent.• Assessing mental capacity where doubt exists is a formal process and must be carefullydocumented.Formallegaladvicemaybenecessary.
www.medicalebookpdf.com

•Wherecapacityislacking,treatmentdecisionscanonlybemadeiftheycanbeshowntobeinthepatient’sbestinterests.
PostoperativecareandrecoveryThe first 48–72 hours after surgery are when the patient is most at risk of immediate surgicalcomplications.Nursingandmedicalcareisfocussedonidentifyingearlysignsofsepsis,andthesourceof any infection, haemorrhage or thromboembolic disease. The patient will have regular (usually 4hourly)observationsoftemperature,pulseandbloodpressureinthefirst24hourstoidentifytheclinicalsignsofinfectionorhypovolaemiccollapse.Mostpatientswillbegivenintravenousfluidsforthefirst12–24hoursaftersurgeryuntiltheycanresumeeatinganddrinking,butthetimingofresumptionoforalintake will vary depending on the length of surgery, whether the abdominal cavity was opened andwhethertherewereanyintraoperativecomplicationsthatmightrequiredelayedoralfeeding.
Thepostoperativewardroundisadaily(ortwicedaily)opportunitytoreviewthepatient’sprogress.Thepatientshouldbeaskedaboutthepresenceandsiteofanypain,particularlypainthatismorethanonewouldexpect froma recent surgicalwoundorwhich is inadifferent site.Thepulse, temperatureandbloodpressureshouldbechecked,andsignsofconjunctivalpallororathreadypulseshouldbesought,asyoungpatientsmayoftencompensateforbloodlosswithminimalchangesinpulserateorbloodpressureat first. For all cases of either abdominal or vaginal surgery, the abdomen should be palpated forlocalizedtenderness(suggestingahaematomaorfocusofinfection),peritonismordistension,andbowelsounds should be checked (for return of peristalsis and exclude obstruction or ileus). The abdominalwoundshouldbecheckedforinflammation,bruisingordischarge.Ifdrainsarepresent,theseshouldbechecked. If there are any concerns about bleeding or infection after vaginal surgery, a gentle pelvicexamination is appropriate to exclude a haematoma or collection. Routine blood sampling forhaemoglobinconcentrationcanbedoneonthesecondpostoperativeday,andureaandelectrolyteswillneedtobecheckedforthosepatientswhoremainonintravenousfluids.
www.medicalebookpdf.com
Figure17.2WHOsurgicalsafetychecklist.(AdaptedfromWHO,2009.)
Generallypatientsshouldbeencouragedtomobilizeassoonaspossibleandoral intakeresumedatthe earliest opportunity. Single-dose antibiotic prophylaxis is usually give intraoperatively for allgynaecologicalsurgery,butoneshouldbemindfulofavoidingempiricalprescriptionofantibioticsinthepostoperativeperiod.Itiscommontoseealow-gradepyrexiainthefirst12–24hoursasamanifestationof the release of acute phase proteins, particularly interleukin-1, and this will usually settle withoutintervention.Persistentpyrexia,orpyrexiaabove39°C,shouldbetreated.Afterclinicalexaminationtoexclude obviouswound infection or chest infection, a screen should be undertaken bymeans of urineculture, vaginal swabs andblood cultures before commencing antibiotics in all patients, to ensure thatappropriate antibiotic sensitivities can be checked. Where the focus of infection is identified orsuspected, liaison with microbiology will ensure appropriate choice of antibiotic based on localresistance patterns, and this is evenmore important when no source of infection has been identified.Rememberthatintravenouscannulaeorcentrallinescanoftenbethesourceofinfection.
Wounddressingsshouldberemovedby48–72hoursaftersurgeryandabdominalwoundsuturesareusually removed on day 5 for Pfannenstiel incisions or day 7–10 for midline incisions.Thromboprophylaxiscommencesonthedayofsurgeryuntildischarge,intheformofTEDsandLMWH.In patients with gynaecological malignancy, this will often be continued for longer. There is growingevidencethattheriskwindowforthromboemobolicdiseasecanlastforupto6weeks,somanycliniciansrecommendtheirpatientscontinuetowearantiembolicstockingsforthatlengthoftime.Thepostoperativereviewislastlyagoodopportunitytodebriefthepatientabouthersurgeryandtoaddressanyremainingconcernsaboutwoundcareandrecoveryafterdischarge,resumptionofnormalactivityandintercourse,
www.medicalebookpdf.com
and the need or not forHRT.Usually 6weeks is recommended before resumption of full activity andintercourseaftermajorsurgery,basedonthetimerequiredforscartissuetoregainfullstrength,butthereislittleevidencesupportingthisrecommendation.Forlessmajorsurgeryagradualresumptionofactivityfromabout4weeksisacceptable.
CommongynaecologicalproceduresFulldetailsofeachprocedurearebeyondthescopeofthisbook,butabriefsummaryofthemostcommonprocedures,indicationsandcomplicationsarepresentedinTable17.3.
Hysteroscopy(Figures17.3,17.4)Hysteroscopyinvolvespassingasmall-diametertelescope,eitherflexibleorrigid,throughthecervixtodirectlyinspecttheuterinecavity.Excellentimagescanbeobtained.Aflexiblehysteroscopemaybeusedintheoutpatientsetting.Rigidinstrumentsemploycirculatingfluidsandthereforecanbeusedtovisualizetheuterinecavityevenifthewomanisbleeding.
IndicationsAnyabnormalbleedingfromtheuteruscanbeinvestigatedbyhysteroscopy,including:
•Postmenopausalbleeding.•Irregularmenstruation,intermenstrualbleedingandpostcoitalbleeding.•Persistentheavymenstrualbleeding.
Table17.3Commongynaecologicalsurgeries
www.medicalebookpdf.com
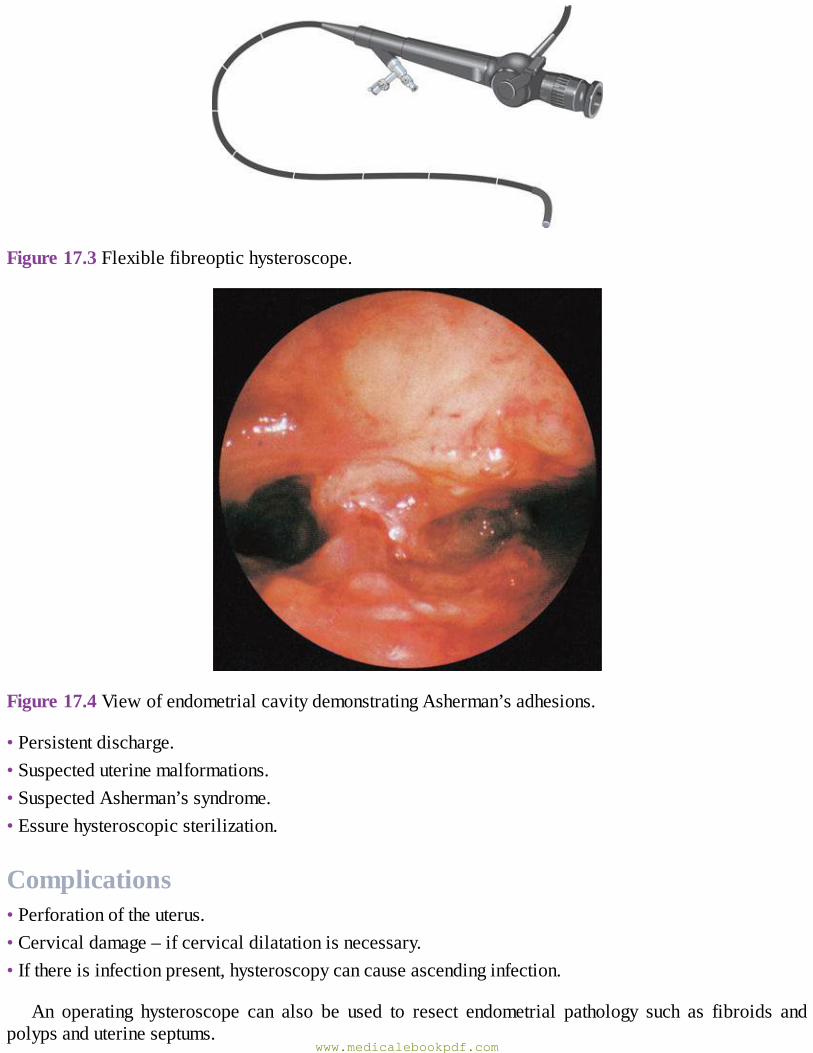
Figure17.3Flexiblefibreoptichysteroscope.
Figure17.4ViewofendometrialcavitydemonstratingAsherman’sadhesions.
•Persistentdischarge.•Suspecteduterinemalformations.•SuspectedAsherman’ssyndrome.•Essurehysteroscopicsterilization.
Complications•Perforationoftheuterus.•Cervicaldamage–ifcervicaldilatationisnecessary.•Ifthereisinfectionpresent,hysteroscopycancauseascendinginfection.
An operating hysteroscope can also be used to resect endometrial pathology such as fibroids andpolypsanduterineseptums.
www.medicalebookpdf.com

Laparoscopy(Figures17.5,6and17.7)Laparoscopyallowsvisualizationof theperitonealcavity.This involves insertionofaneedlecalledaVeressneedle intoa suitablepuncturepoint in theumbilicus.Thisallows insufflationof theperitonealcavitywithcarbondioxidesothatalargerinstrumentcanbeinserted.Themajorityofinstrumentsusedfor diagnostic laparoscopy are 5 mm in diameter, and 10 mm instruments are used for operativelaparoscopy.Morerecently,a2mmlaparoscopehasbecomeavailable.
Indications•Suspectedectopicpregnancy.•Ovariancystaccidentandacutepelvicpain.•Undiagnosedpelvicpain.•Tubalpatencytesting.•Sterilization.
Operative laparoscopy can be used to perform ovarian cystectomy or oophorectomy and to treatendometriosis with cautery or laser. As discussed above, more extensive laparoscopic work is nowperformedforhysterectomy,lymphnodebiopsy,omentectomyandmyomectomy.
ComplicationsComplicationsareuncommon,butincludedamagetoanyoftheintra-abdominalstructures,suchasbowelandmajorbloodvessels.Thebladderisalwaysemptiedpriortotheproceduretoavoidbladderinjury.Incisionalherniahasbeenreported.
eResource17.1
Laparoscopyhttp://www.routledgetextbooks.com/textbooks/tenteachers/gynaecologyv17.1.php
Cystoscopy(Figures17.8,17.9)Cystoscopyinvolvespassingasmall-diametertelescope,eitherflexibleorrigid,throughtheurethraintothebladder.Excellent imagesofboth thesestructurescanbeobtained.Acystoscopewithanoperativechannelcanbeusedtobiopsyanyabnormality,performbladderneckinjection,retrievestonesandresectbladdertumours.
www.medicalebookpdf.com
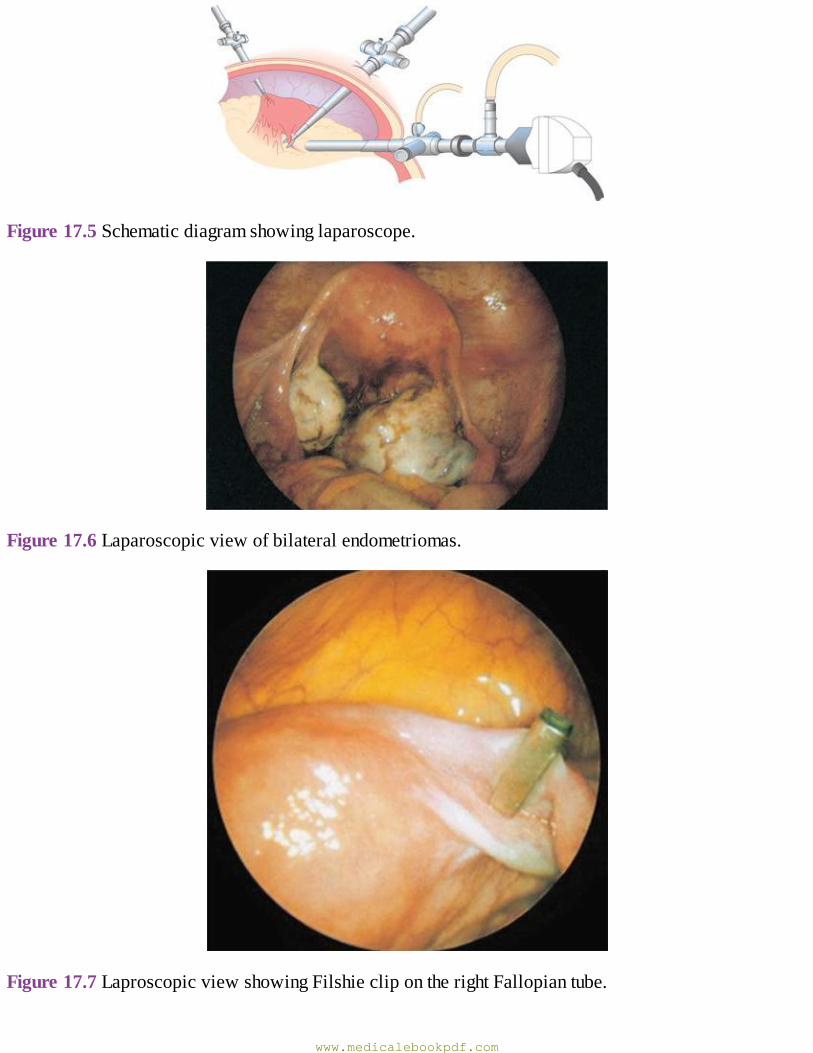
Figure17.5Schematicdiagramshowinglaparoscope.
Figure17.6Laparoscopicviewofbilateralendometriomas.
Figure17.7LaproscopicviewshowingFilshieclipontherightFallopiantube.
www.medicalebookpdf.com
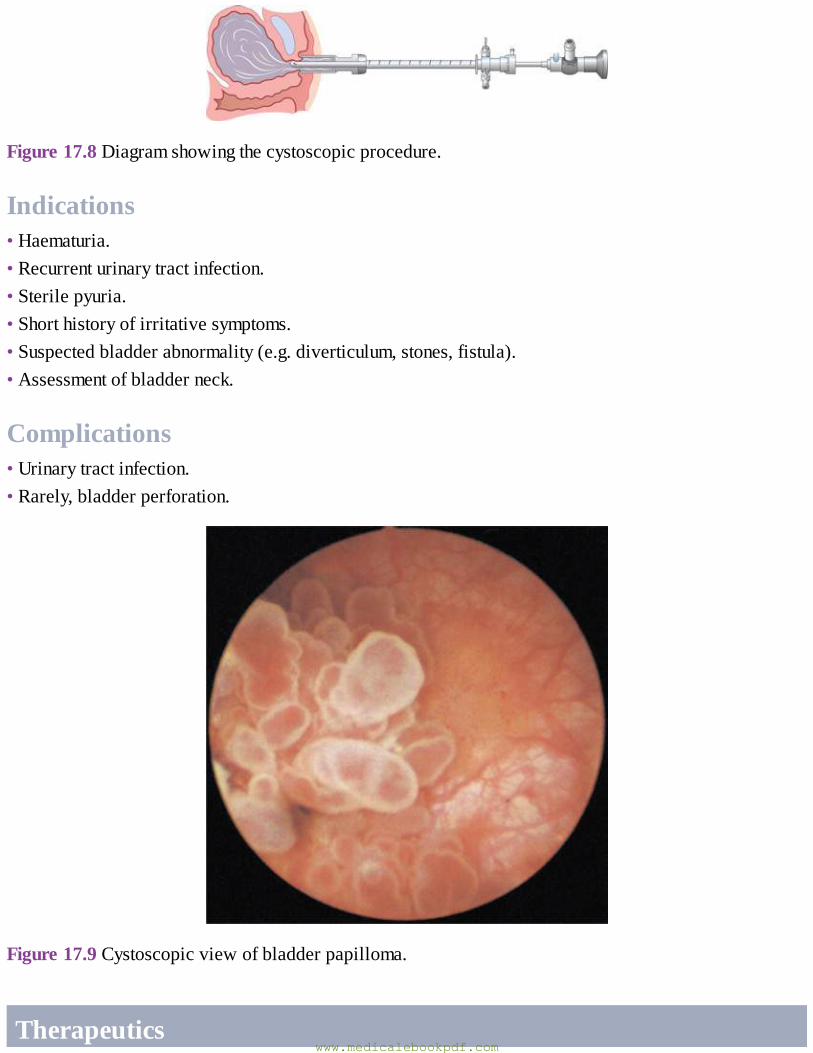
Figure17.8Diagramshowingthecystoscopicprocedure.
Indications•Haematuria.•Recurrenturinarytractinfection.•Sterilepyuria.•Shorthistoryofirritativesymptoms.•Suspectedbladderabnormality(e.g.diverticulum,stones,fistula).•Assessmentofbladderneck.
Complications•Urinarytractinfection.•Rarely,bladderperforation.
Figure17.9Cystoscopicviewofbladderpapilloma.
Therapeuticswww.medicalebookpdf.com
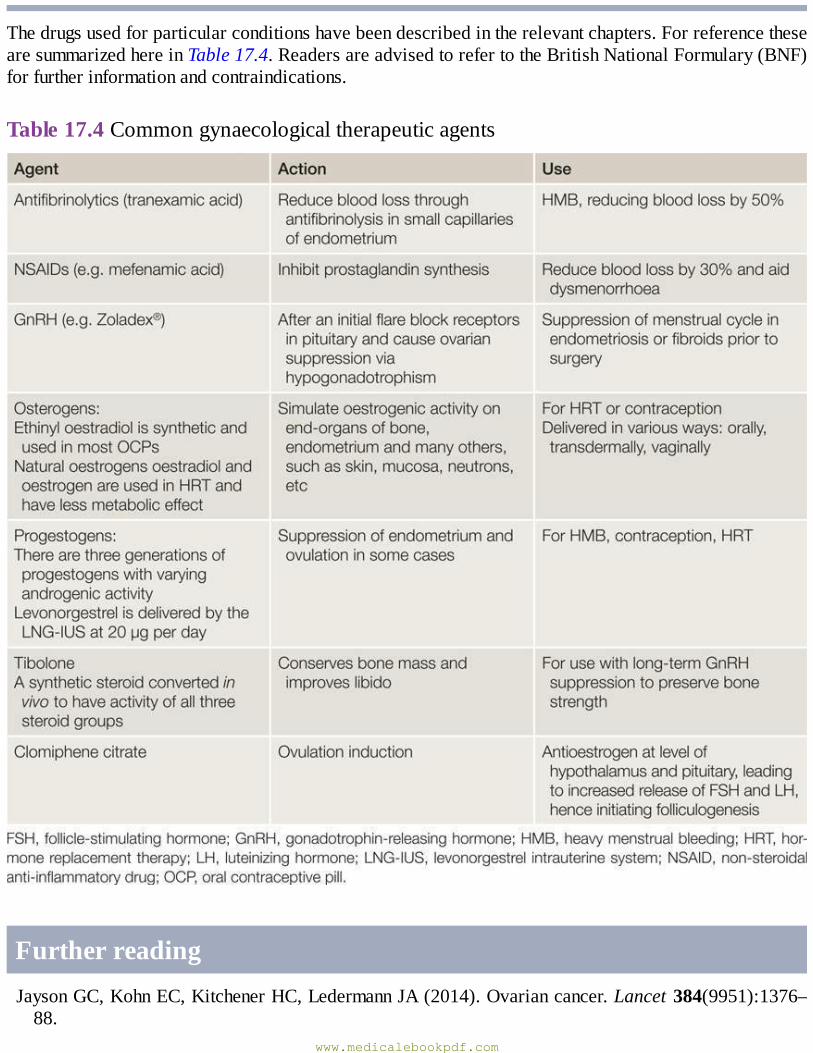
Thedrugsusedforparticularconditionshavebeendescribedintherelevantchapters.ForreferencethesearesummarizedhereinTable17.4.ReadersareadvisedtorefertotheBritishNationalFormulary(BNF)forfurtherinformationandcontraindications.
Table17.4Commongynaecologicaltherapeuticagents
FurtherreadingJaysonGC,KohnEC,KitchenerHC,LedermannJA(2014).Ovariancancer.Lancet384(9951):1376–88.
www.medicalebookpdf.com
Mental capacity advice from the BritishMedical Association: http://bma.org.uk/practical-support-at-work/ethics/mental-capacity.
BritishNationalFormularyhttp://www.bnf.org.The UK Mental Capacity Act: http://www.mentalhealth.org.uk/help-information/mental-health-a-z/M/mental-capacity-act-2005/.
RCOGGuidetoConsenthttps://www.rcog.org.uk/guidelines.WHOSafeSurgeryChecklistwebsite:http://www.who.int/patientsafety/safesurgery/en/.
Selfassessment
CASEHISTORY
A34-year-oldwoman has been seen in clinicwith severe dysmenorrhoea and pelvic pain and apossible diagnosis of endometriosis. Shewould also like to become pregnant.An ultrasound hasshown a normal uterus and ‘kissing ovaries’, with a 6-cm endometrioma on the right ovary. Shewouldliketoundergoalaparoscopyfordiagnosisandtreatment.AWhatadditionalpointsinthehistoryshouldbesought?BWhatpreoperativechecksandtestsshouldbemadeforthiswoman?CWhatconsentprocessshouldtakeplace?
ANSWERS
AThegynaecologicalhistory shouldcover lengthof symptoms, severity, interferencewithnormalfunction and her expectations of surgery. In particular, symptoms of dyschexia are important toassesslikelihoodofrectovaginalnodes.
Thelengthoftimetryingforapregnancy,treatmentstriedandpartner’sfertilityassessmentarevitalhere,astheymayaffectadecisiontotreattubalorovariandisease.Thebalanceoffertilityissuesandsymptomatologyarecrucialinsurgeryforendometriosis(forexample,ifsheisaboutto undergo in-vitro fertilization, then minimal intervention is advised beyond draining largeendometriomasiftheywillaffecteggcollection).
As in all surgery pastmedical history is important, as is previous surgery on the abdomen,whichmaymakelaparoscopicsurgerymorehazardous.
Thewomanrevealsthatshehasnotyettriedforapregnancybuthasjustcomeoffthepillandisawaitingaperiod.Shehasbeentricyclingthisfor2yearssinceendometriosiswassuspectedfrom symptoms. Initially she felt better but her pain is returning. She has developed newabdominalswellingoverthelastyear,andattributesthistotheendometrioma.Shedoesnothavedyspareuniaordyschexia.Atthemomenthersymptomsareofgreatestimportance.
Sherevealsthatshehasasthma,althoughsherarelytakesaninhaler.However,shewasoncehospitalizedaftercontractingthe‘flu,requiringnebulizers.
BSherequiresreferralforanaestheticassessmentforherasthma.SherequiresaFBCandgroupandsaveforsurgery.Apregnancytestisveryimportant,andshemustusecontraceptioninthecyclein
www.medicalebookpdf.com
whichhersurgerywillfall.C Initial informed consentwill cover the procedure and the risks of surgery.Written informationshould be given. Common complications are written down (or printed) on the consent formincludingperforationofuterus,damagetobladder,bowelorviscera,procedurestorepairdamageandlaparotomy.
Itisgoodpracticetorecorddetailsoftheconsultationthatarecovered,whichshouldincludeinsertionofalevonorgestrelintrauterinesystem(LNG-IUS)(butnotappropriateifshewishestoconceive), complications that are more likely with endometriosis and the extent of procedureplanned.Forexample,itisusefultorecordthatadiscussionhastakenplacethatifthepelvisisfrozenandinoperable,theprocedurewillendwithoutfulltreatmentoftheendometriosis.Inthissituation a referral to the nearest endometriosis centre should bemade,where elective surgerywithageneralsurgeonmightbeplanned.
On the day of procedure confirmation of consent will be completed, and further questionsanswered.
EMQ
AInternaliliacartery.BUterus.CFallopiantube.DUterineartery.EOvaries.FPudendalartery.GAorta.HOvarianartery.ICervix.For each description below, choose the SINGLEmost appropriate answer from the above list ofoptions.Eachoptionmaybeusedonce,morethanonceornotatall.1Containedintheinfundibulopelvicligament.2Theoriginoftheuterineartery.3Shouldalwaysberemovedathysterectomytocureendometriosis.4Theureterisatsurgicalriskwhereitrunsclosetothisstructure.
ANSWERS
1HTheovarianvesselsarisefromtheaorta justbelowtherenalartery.At the levelof thepelvicbrimtheovarianvesselscrossinfrontoftheureterandpassintotheinfundibular-pelvicfoldofthebroadligament.
2ATheuterinearteryoriginatesfromtheanteriorbranchoftheinternaliliac,asdotheothervesselssupplyingthepelvis.
www.medicalebookpdf.com
3EWhenhysterectomyandpelvicclearanceisperformedtoproviderelieffromendometriosis,itisadvisable to remove the ovaries. Not doing so may allow continued hormonal cycling andrecurrenceofpelvicendometriosis.Furthersurgery to remove theovaries laterwouldbehighrisk,duetothepresenceofadhesionsaroundtheovariesthattendtosealtothepelvicsidewall.
4DTheureteriscloselyrelatedtotheuterinearteryatthelevelofthecervix.Duringahysterectomythebladderiscarefullydissectedawayfromtheuterusandpusheddown,sothattheuretersarealsomovedoutof theway.Theureter isvisualizedorpalpated toensure it isoutof thewaybeforeclampingisappliedtotheuterinearterypedicle.
SBAQUESTIONS
1 A 38-year-old woman underwent total abdominal hysterectomy for heavy menstrual bleedingyesterday,withovarianconservation.Onyourmorningwardroundyoufindthatsheispale,withabloodpressureof110/68mmHgandapulseof88.Her temperature is36.8ºC.Herabdomenissoft,butthereisconsiderabletendernessintheleftlowerquadrant.Herurineoutputsincesurgeryhasbeen350ml.Thenursecaringforthepatientreportsthatthepatientwasverydizzyandlightheaded,andvomitedwhenshewastakenoutofbedthatmorning.Whichofthefollowingstatementsdescribesthemostappropriatemanagement?Choosethesinglebestanswer.
A Ensure the patient has adequate analgesia and prescribe extra intravenous fluids and anantiemetic.
BTakeaurinesampleandcommenceintravenousantibiotics.CArrangeanurgentFBCandaskforreviewbyyourconsultant.D Explain that the patient does not require hormone replacement therapy and review her thatafternoon.
ANSWER
C The signs of paleness, tachycardia and dizziness suggest blood loss. Blood pressure is oftenmaintainedinhealthywomen.Thesiteofapossibleintra-abdominalbleedistheleftside.Alwayskeepyourconsultantinformed.FBCwillconfirmifthereisbloodlossasexpected,thenfurtherimagingwillidentifythesizeofthecollection.Subsequently,herclinicalstatusandserialbloodpicture will identify further management. The FBC will identify whether blood transfusion isneeded, butmeanwhile intravenous crystalloid should be given tomaintain blood pressure andurineoutput.Thesiteofthebleedingisoftenthevaginalangle.
2 A 56-year-old woman with endometrial cancer diagnosed on outpatient biopsy attends herpreassessment appointment for her planned laparoscopic hysterectomy and bilateral salpingo-oophorectomy.Shehashypertension,hyperlipidaemia,ischaemicheartdiseaseandaBMIof39.Shesmokes25cigarettesday.Whichofthefollowingstatementsisnotcorrect?Choosethesinglebestanswer.
www.medicalebookpdf.com
AShewillrequireahigh-dependencyanaestheticbedtobeavailableaftersurgery.BEarlymobilizationandantiembolicstockingswillbesufficientthromboprophylaxis.CYouwillarrangeachestX-ray,ECG,ureaandelectrolytes.DSheshouldbecounselledaboutthepossibleneedforlaparotomyaspartofhersurgicalconsentprocess.
ANSWER
BSheisathighriskforthromboemboliceventsandwillrequirelow-molecularweightheparinforaminimumofherinpatientstayandpossiblyfor6weeks.
www.medicalebookpdf.com
Index
Note:Pagenumbersinitalicrefertotablesorboxes;thoseinboldrefertofigures
abdominalexamination24abnormaluterinebleeding(AUB)21,21,31–2,49
acute53–4,54heavy(HMB)21,50–3,56–7postmenopausal(PMB)50,207–8,207terminology49,50
abortion69,69,85–8,90AbortionAct(1967)85–6actinomyces-likeorganisms(ALOs)80adenomyosis50,159,167,175–6,179adhesions
endometrium42,43,93,166,171,242Fallopiantubes93,126,127
ageingpopulation108–9AIDS-definingillnesses130alcohol925-alpha-reductasedeficiency40–1α-fetoprotein(AFP)156,196,200alternativeandcomplementarytherapies114,114amenorrhoea41–3,41,84,179analcanal14anatomy
female4–14surgical229–30,246
androgeninsensitivity40androgens35,106,107anovulation42,48anti-Dimmunoglobulin64anti-Müllerianhormone(AMH)1–2,40,94,95antibioticprophylaxis239anticholinergicmedications144anticonvulsants72antifibrinolytics52,175,244
www.medicalebookpdf.com
antifungals72,183antiphospholipidsyndrome(APS)62antiretroviraltherapy(ART)72,129,131,131aromataseinhibitors162arterialdisease,andoralcontraceptiveuse77arteries,pelvicorgans10–11Ashermansyndrome42,43,171,242
bacterialvaginosis(BV)123–4,123,133barriercontraception80–1Bartholin’scysts184–5,185Bartholin’sglands4,181bilateralsalpingo-oophorectomy(BSO)108,195,203bimanualexamination26–7,26bladder7,10,14
anatomy230cystoscopy242–3,243retraining141urinestorage136
bladderdiary138,139bladderneck,injection145,146bladderpainsyndrome163,167blastocyst59,60bleeding
surgical246–7seealsoabnormaluterinebleeding
bodymassindex(BMI)92,113bonehealth,postmenopausal111,112botulinumtoxin146brachytherapy209,221BRCAmutations194,195,202,203breastcancerrisk76,76,117breastdevelopment38,38breastovariancancersyndrome195breastfeeding,HIVtransmission132Brennertumours158broadligament6,8,9–10,11Burchcolposuspension144,145
Ca19-9156,196Ca125156,196,196,199,201cancerrisk
HRT117oralcontraceptives76,76
www.medicalebookpdf.com
candidiasis123,124,124,183,191carcinosarcomas210cardiovasculardisease(CVD)111,116,117–18casehistories
abnormaluterinebleeding31–2chronicpelvicpain165–6dysmenorrhoea56ectopicpregnancy65endometrialcancer210–11endometriosis,surgery245femalegenitalmutilation191imperforatehymen16–17infertility102ovariancancer201–2PCOS46,47,48pelvicinflammatorydisease132–3prematureovarianfailure118sterilization89urinaryincontinence152uterinefibroids177–8vulvaltumour226–7
cervicalcancer76,213–18clinicalpresentation218–22diagnosis215–16,217globalburden216pathophysiology219prevention213,215–16,218treatment219–22,228
cervicalcytology215,227cervicalectropion169–70,170,176cervicalglandularintraepithelialneoplasia(CGIN)219cervicalintraepithelialneoplasia(CIN)129,130,214–15
treatment217–18,217,227cervicalpolyps170,170cervicalscreening215–16cervicalstenosis170cervix
anatomy6,13,169biopsy216,218,219,220,228,241
chancre128chemotherapy198–9,222childbirth,injuryduring136,147children121–3,122
www.medicalebookpdf.com
chlamydiainfection123,125–6choriocarcinomas,non-gestational200chronicpelvicpain(CPP)23,163–6,163clearcellcarcinomas194–5clitoris3,4clomiphenecitrate96,244‘cluecells’123,124cognitivefunction,post-menopause110colpocleisis153colporrhaphy240colposcopy216,217colposuspension144,145,240combinedhormonalcontraception(CHC)37,73,74–7
endometriosis162interactions72safetyandcontraindications71–2,72,76,77,89,90side-effects73
completeandrogeninsensitivitysyndrome(CAIS)40conception,naturalrates91condoms80,81congenitaladrenalhyperplasia(CAH)41consent236–7,245contraception22,55
efficacy70–1,71emergency84,84,90followingabortion88,90globalunmetneed69andHIV131interactions72,72,131long-actingreversiblemethods(LARC)70,71mechanismsofaction70medicaleligibilitycriteria71–2,72methods74–84,89–90non-contraceptivehealthbenefits73,90opportunitiestoprovide84–5,85safetyandside-effects71–3,72,76–7,76,89,90
contraceptivecap81,81copperintrauterinedevice(Cu-IUD)79–80,79,84,90corpuslutealcyst157corpusluteum(CL)35–6,36,59cystoscopy242–3,243
danazol162www.medicalebookpdf.com
deinfundibulation190dementia110depression167dermoidcyst157,158,158,203detrusormuscle136detrusoroveractivity(DO)137,137,138
diagnosis142,143treatment146
diabetesmellitus191,206,210–11diaphragm(contraceptive)81,81diet113disordersofsexualdevelopment(DSD)39–41druginteractions72,72,131duloxetine144dysgerminomas200,202dysmenorrhoea54–5,56,245dyspareunia182,186
ectopicpregnancy62–4,65,126,127embryos
implantation36,37,59–60,60preimplantationgeneticdiagnosis100–1transfertechnologies99–100
endodermalsinusyolksactumours200endometrialbiopsy(EB)30–1,51,52,56,179endometrialcancer117,205–11
aetiology206,206classification205,206,211clinicalfeatures207diagnosisandstaging207–8,208,212incidence205managementandprognosis208–9,209,247prevention206,206
endometrialpolyps50,50,93,170–1,171,176,179endometrioidadenocarcinomas205,208,211,212endometriomas(‘chocolatecysts’)157,158,160,162,168,243endometriosis93,102,158–63,165
aetiology159associatedovariancancers194–5,203clinicalfeatures159diagnosis159–61incidence159andinfertility161,161
www.medicalebookpdf.com
management161–3,245–6endometrium6,36–7,36,37
ablation53,53hyperplasia205,207–8,211scarring42,43,93,171,242
ethinyloestradiol244etonorgestrel77externalgenitalia
anatomyanddevelopment3,4,181examination25,25
Fallopiantubes6–7,17blockage93,97,98,126,127cysts158ectopicpregnancy62,62,64occlusion81–2,243patencyassessment95,95,96,102–3
femalegenitalmutilation(FGM)188–91,189ferritinlevels183fertility
awareness83–4preservation101seealsosubfertility
fetaldevelopment1–3fibroids28,32,50,138,172–8
classification172,180clinicalfeatures172–3,172,177–8,180diagnosis173,173andfertility93,97treatment53,173–5,178,179,241
fibromas,ovarian158FIGOstaging
cervicalcancer219,220endometrialcancer208ovariantumours197,199vaginalcancer222vulvalcancer225
Filshieclips81,82,243Fitz-High–Curtissyndrome126,126follicle-stimulatinghormone(FSH)34–6,34,36,38,106,107,113,119
Gardnerellavaginalis123,124geneticdiagnosis,preimplantation100–1germcelltumours155–6,158,194,200–1
www.medicalebookpdf.com
gestationalage60gestationaltrophoblasticdisease(GTD)64,67gestrinone162gonadaldysgenesis40gonadotrophin-releasinghormone(GnRH)34,34,38,106,107,119gonadotrophin-releasinghormone(GnRH)agonists52,55,98,108,162,173–4,175,232,244gonorrhoea123,125,125,133granulosacelltumours200,203
heavymenstrualbleeding(HMB)21,50–3,56–7hepatitisBandC123herbaltreatments114hereditarynon-polyposiscolorectalcancer(HNPCC)195herpessimplexvirus(HSV),types1and2126–7heterotopicpregnancy62,63history
gynaecological19–23sexual122–3,122
hormonereplacementtherapy(HRT)37,114–18hotflushes109,114,114,116,119humanchorionicgonadotrophin(hCG)59,60,63,64,98–9,156,196HumanFertilisationandEmbryoAuthority(HFEA)98humanimmunodeficiencyvirus(HIV)122,123,129–32,214
globalburden129,130humanpapillomavirus(HPV)127–8,213–14,222
testing215,227vaccines218
hydatidiformmole64,67hydrosalpinx93,97,98,126,127hymen4
imperforate15–17hyperemesisgravidarum64hyperprolactinaemia43,43hypo-andhypergonadism38–9,39,41–2hypothalamus33,34,41hysterectomy230–2
complications8,231–2,231,246–7endometriosis162–3,245–6fibroids174,175menstrualdisorders46,53oophorectomy231–2,246radicalincervicalcancer220,221,228radicalinendometrialcancer208–9,209,212
www.medicalebookpdf.com
routes230–1,231vaginalprolapse,after150
hysterocontrastsynography(HyCoSy)95,102hysterosalpingogram(HSG)95,95,102hysteroscopy51,51,239,240,242
endometrialcarcinoma207–8,207endometrialpolyp171,171fibroids173sterilization82,83
implantation36,37,59–60,60in-vitrofertilization(IVF)98–101,99incisions234,234inhibin106,107,156,196,200intracytoplasmicsperminjection(ICSI)99,103intrauterinecontraceptives78–80,79,84,90
copperdevice(Cu-IUD)79–80,79,84,90progestogen-releasing52,54,56,78–9,84,116,173,175,179,244
intrauterineinsemination(IUI)97–8intrinsicsphincterdeficiency(ISD)136investigations,commongynaecological30irritablebowelsyndrome161,163,167
Kallman’ssyndrome41‘kissingovaries’160,168Krukenbergtumours23,193–4,203
labiamajora/minora3,4,181laparoscopy234–5,241,242,243
endometriosis160–1,160ovariandrilling96,97
largeloopexcisionoftransformationzone(LLETZ)217,217,227,241leiomyomas,seefibroidsleiomyosarcomas210,211levatoranimuscles5,8,9,9,14,147levonorgestrelintrauterinesystem(LNG-IUS)52,54,56,78–9,79,84,116,173,175,179,244lichenplanus184lichensclerosus184,185,223lifestylechanges55,113,113linearaccelerator221,221LOFTImodel187low-molecularweightheparin232luteinizinghormone(LH)34,34,35–6,38,98,106,107lymphadenectomy,groin224–5
www.medicalebookpdf.com
lymphatics13–14,13lymphoedema221Lynchsyndrome195,206
magneticresonanceimaging(MRI)28,29,30adenomyosis176,176endometrialcancer208,208,212endometriosis160fibroids173,174ovariantumours196
malefertility93,96malesexualdevelopment1–2Mayer–Rokitansky–Kuster–Hausersyndrome16Meigsyndrome158menarche34,38menopause5,6,7
assessmentandmanagement22,107,112–14,113definitions105,105genitaltractchanges110–11,110,119iatrogenic108impactof109–11,112non-physiological107–8physiological106–7,119
menstrualcycle,physiology33–7,36menstrualobstruction15–17menstruation37,47–8seealsoabnormaluterinebleeding(AUB);premenstrualsyndrome(PMS)
metformin44methotrexate64Meyer’s‘coelomicmetaplasia’theory159microscopy,STIs123,124,133midstreamspecimenofurine(MSU)138,152midurethraltapeprocedures144,145,153,240mifepristone61–2,87mirabegron144miscarriage60–2,61,241misoprostol61–2,87mucinouscarcinomas194–5,203Mülleriandefects15–16,42Müllerianstructures3,3myomectomy53,174,175,177,178,241myometrium6
nabothianfollicles170,170,214www.medicalebookpdf.com
neonatalherpes127nerveentrapment163nerves,pelvic14,14,147non-consummation187–8,191non-steroidalanti-inflammatorydrugs(NSAIDs)37,161–2,175,244norethisterone52,57nucleicacidamplificationtest(NAAT)123,125,126,133
obesity109,141,195,206,211oestrogen
physiological34,34contraceptives74,244HRT115–16,119,144,244inmenopause107
oligomenorrhoea41–3oophorectomy
endometriosis162–3inhysterectomy231–2,246
oralcontraceptivepill74–7osteoporosis111,111,112ovarianartery10ovariancancers117
aetiologyandriskfactors194–5,195borderline(BOTs)194–5,203classification193–4,194clinicalfeatures196diagnosis196–7,196germcelltumours155–6,158,194,200–1incidence193managementandprognosis197–9,198,199,201–2andoralcontraceptiveuse76prevention195–6sexcordstromaltumours158,194,199–200,202
ovariancysts156,157,165,168ovariandrilling96,97ovarianfollicles2–3,34–5ovarianhyperstimulationsyndrome(OHSS)100ovarianinsufficiency,premature(POI)42,107–8,118ovarianligament10,11ovarianreserve95,101ovaries
anatomy7,10,11benigndiseases155–8
www.medicalebookpdf.com
physiology34–6stimulation98suppression162,244torsion156
overactivebladder(OAB)135,141ovulation35
induction96,97,244inhibitionofpremature98
oxybutynin144,153
paclitaxol198–9padtest138Paget’sdisease,vulva223palliativetherapy,cervicalcancer222pelvicdiaphragm8–9,9pelvicexamination24–7,26pelvicfascia10,11,147,148pelvicfloormuscles136,147–8,149
exercises141,150,153pelvicinflammatorydisease(PID)125–6,132–3,157,167pelvicmass,differentialdiagnosis155pelvicpain23,163–6,163pelvicperitoneum9–10perinealbody9,147,149Pfannenstielincision234,234pituitarygland34,34
disorders41–2down-regulation98,108
platinumcompounds198,222polycysticovarysyndrome(PCOS)42,43–4,46,47,48,90,209
fertility92,102ovulationinduction96,97
postmenopausalbleeding(PMB)50,207–8,207postoperativecare/recovery237,239pouchofDouglas4,6,230preassessmentclinic232–3,247pregnancy
ectopic62–4,65,126,127establishment59–60,60history21–2andHIV131–2,131molar64,67non-viable66
www.medicalebookpdf.com
pregnancyofunknownlocation63prematureovarianinsufficiency(POI)42,107–8,118premenstrualsyndrome(PMS)44–6,232primaryperitonealcarcinoma(PPC)199professionalism27progesterone34,36,36,107,119progestogen-onlycontraceptives77–9,162progestogens115,115,244prolapse146–51,153
surgery151,151,234,240propiverine144prostaglandins(PGs)35psammomabodies194pseudomyxomaperitoneii194psychologicalissues
afterabortion88menopause109–10pelvicpain163,167
psychosexualproblems186–8,186puberty5,6,7,37–9pubichair38,38puborectalis147pudendalarteries12,12pudendalnerve14,147
radiotherapy209,220,221–2,226rectalarteries12,12rectalartery,superior12rectalexamination27,27rectum8retainedproductsofconception(RPOC)171,241rhabdomyosarcoma210,211rhesusisoimmunization64RiskofMalignancyIndex(RMI)196,203roundligament10,11,17RoyalCollegeofObstetriciansandGynaecologists(RCOG)86
safesurgerychecklist237,238Sampson’simplantationtheory159sarcomabotryoides222sarcomas,uterus209–10semenfluidanalysis(SFA)96,96,102sentinellymphnodebiopsy224–5serouscarcinoma194,199,202
www.medicalebookpdf.com
serouscystadenomas158Sertoli–Leydigcelltumours199–200,202sexcordstromaltumours158,194,199–200,202sexualabuse/exploitation122–3,122sexualdevelopment1–3
disorders39–41secondary37–9
sexualhistory122–3,122sexually-transmittedinfections(STIs)
causingvaginaldischarge123–5,124cervicitisandpelvicinflammatorydisease125–6testing121–2,123,123viral126–8seealsonamedinfections
sigmoidcolon230smoking89,92,195,206,214socialhistory20–1speculum25,25,26sperm
donor100intracytoplasmicinjection(ICSI)99,103quality/number93,96,96surgicalretrieval100
spermicides81squamouscellcarcinoma
cervix219,222,228vulva223
sterilization,female81–2,82,83,84strokerisk118subfertility91
causes92–4,96andendometriosis161,161historyandexamination22,94,94,101–2investigations94–6management96–101
surgerycervicalcancer220,221consent236–7decision-making233endometrialcancer208–9endometriosis162–3,245ovariantumours197–8,198,200–1,202postoperativecare237,239
www.medicalebookpdf.com
postoperativecomplications231–2,231,246–7preassessment232–3,247prolapse151,151,234,240subfertility97urinaryincontinence144–6,240uterinefibroids174,241
sutures235–6,235syphilis123,128–9,129,133
tamoxifen206Tannerstaging38,38teratomas200testosterone2,106,107,115,119thecalutealcysts157thecomas158therapeuticagents244thromboprophylaxis232,233,239,247tibolone244trachelectomy,radical220,228tranexamicacid52,175,244transvaginalultrasoundscan(TVUSS)28,29,32,156,157,160Treponemapallidumsubsp.pallidum128trichomoniasis123,124–5,124,133Troissier’ssign23tubo-ovarianabscess132–3,156,167tumourmarkers156,161,196,196Turnersyndrome39–40
ulipristalacetate175ultrasound28,28,29,32
ectopicpregnancy63endometrialthickness207,207fibroids173miscarriage61pelvicmass/pain156,157pregnancy59–60,60subfertility95transvaginal,seetransvaginalultrasoundscan
ureters7,8,8,230urethra7–8urethralsphincter136,142,143urinaryincontinence152–3
aetiology136–7assessment138–40,139
www.medicalebookpdf.com
detrusoroveractivity136,137,138,146stress136,137,144–6,153terminology135,136treatment140–6,240
urinarytract,anatomy7–8urodynamictesting140,141–2,143urogenitalatrophy110–11urogenitaldiaphragm(triangularligament)9uterinearteries8,11,12,229–30,246uterinearteryembolization(UAE)52,53,174–5,175,179uterinebleeding,seeabnormaluterinebleedinguterosacralligaments10uterus
agechanges6anatomy5–6,11,12,13–14anomalies15–16fibroids,seefibroidssarcomas209–10suctioncurettage62,66versionandflexion27
vacuumaspiration87–8vagina
anatomy4–5,5,181–2flora124malignantdisease222,222prolapse146–51,153,234repair(colporrhaphy)240
vaginalartery11,12vaginaldilators187–8vaginalintraepithelialneoplasia(VaIN)22vaginalsupportpessaries150vaginismus187–8,191vasectomy82–3,83vasomotorsymptoms,menopause109,114,114,116veins,pelvic12–13venousthromboembolism(VTE)
andHRT118andoralcontraceptiveuse77,77,90prevention232,233,239,247
vestigialstructures16vulva181–2
biopsy183–4,184www.medicalebookpdf.com
cysts184–5examination25,182lichenplanus184lichensclerosus184,185,223malignantdisease184,223–7pain(vulvodynia)182,185–6pruritus182–3,182
vulvalintraepithelialneoplasia(VIN)223,223vulvovaginalatrophy110–11
warts,genital127–8weightgain,postmenopausal109,114Wertheim’shysterectomy220,221,228Wolffianducts2WorldHealthOrganization(WHO)71,72,96,237,238wounddressings239
www.medicalebookpdf.com