Embed Size (px)
Citation preview

doi: 10.2522/ptj.20090303Originally published online April 15, 2010
2010; 90:860-879.PHYS THER. Maher, Jane Latimer and James H. McAuleyLuciana G. Macedo, Rob J.E.M. Smeets, Christopher G.Nonspecific Low Back Pain: A Systematic ReviewGraded Activity and Graded Exposure for Persistent
http://ptjournal.apta.org/content/90/6/860found online at: The online version of this article, along with updated information and services, can be
Collections
Therapeutic Exercise Systematic Reviews/Meta-analyses
Patient/Client-Related Instruction Pain
Injuries and Conditions: Low Back Fear-Avoidance
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Graded Activity and Graded Exposurefor Persistent NonspecificLow Back Pain: A Systematic ReviewLuciana G. Macedo, Rob J.E.M. Smeets, Christopher G. Maher, Jane Latimer,James H. McAuley
Background. Graded activity and graded exposure are increasingly being used inthe management of persistent low back pain; however, their effectiveness remainspoorly understood.
Purpose. The aim of this study was to systematically review randomized con-trolled trials that evaluated the effectiveness of graded activity or graded exposure forpersistent (�6 weeks in duration or recurrent) low back pain.
Data Sources. Trials were electronically searched and rated for quality by use ofthe PEDro scale (values of 0–10).
Study Selection. Randomized controlled trials of graded activity or gradedexposure that included pain, disability, global perceived effect, or work statusoutcomes were included in the study.
Data Extraction. Outcomes were converted to a scale from 0 to 100. Trials werepooled with software used for preparing and maintaining Cochrane reviews. Resultsare presented as weighted mean differences with 95% confidence intervals.
Data Synthesis. Fifteen trials with 1,654 patients were included. The trials hada median quality score of 6 (range�3–9). Pooled effects from 6 trials comparinggraded activity with a minimal intervention or no treatment favored graded activity,with 4 contrasts being statistically significant: mean values (95% confidence intervals)for pain in the short term, pain in the intermediate term, disability in the short term,and disability in the intermediate term were �6.2 (�9.4 to �3.0), �5.5 (�9.9 to�1.0), �6.5 (�10.1 to �3.0), and �3.9 (�7.4 to �0.4), respectively. None of thepooled effects from 6 trials comparing graded activity with another form of exercise,from 4 trials comparing graded activity with graded exposure, and from 2 trialscomparing graded exposure with a waiting list were statistically significant.
Limitations. Limitations of this review include the low quality of the studies,primarily those that evaluated graded exposure; the use of various types of outomemeasures; and differences in the implementation of the interventions, adding to theheterogeneity of the studies.
Conclusions. The available evidence suggests that graded activity in the shortterm and intermediate term is slightly more effective than a minimal intervention butnot more effective than other forms of exercise for persistent low back pain. Thelimited evidence suggests that graded exposure is as effective as minimal treatmentor graded activity for persistent low back pain.
L.G. Macedo, MSc, is a PhD can-didate at The George Institute forInternational Health, University ofSydney, PO Box M201, MissendenRd, Camperdown, New SouthWales 2050, Australia. Address allcorrespondence to Ms Macedo at:[email protected].
R.J.E.M. Smeets, MD, PhD, is Pro-fessor, Adelante Zorggroep, Hoens-broek, the Netherlands, andDepartment of Rehabilitation Med-icine, School of Public Health andPrimary Care, Maastricht University,Maastricht, the Netherlands.
C.G. Maher, PhD, is Director,Musculoskeletal Division, TheGeorge Institute for InternationalHealth, University of Sydney.
J. Latimer, PhD, is Associate Pro-fessor, The George Institute for In-ternational Health, University ofSydney.
J.H. McAuley, PhD, is ResearchManager, The George Institute forInternational Health, University ofSydney.
[Macedo LG, Smeets RJEM, MaherCG, et al. Graded activity andgraded exposure for persistentnonspecific low back pain: a sys-tematic review. Phys Ther. 2010;90:860–879.]
© 2010 American Physical TherapyAssociation
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
860 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Many patients with low backpain (LBP) have concernsthat are inadequately ex-
plained with a traditional biomedicalmodel. Contemporary approacheshave recognized the multifactorialetiology of LBP and the necessity toadopt a biopsychosocial modelwhen dealing with the condition.Cognitive behavioral models pro-pose that pain-related fear, kinesio-phobia, and unhelpful beliefs aboutback pain may be primary factorsleading to increased pain and a de-creased level of activity or function-ing.1,2 It has been suggested thatthese factors not only may representpsychosocial barriers to recovery butalso may contribute to important bi-ological changes, such as disuse anddeconditioning after an injury.3
Graded activity and graded exposureare interventions commonly used inthe management of persistent LBP.These treatments incorporate behav-ioral and cognitive approaches toimprove activity tolerance. The pri-mary difference between these inter-ventions is that, with graded expo-sure, patients are asked to create ahierarchy of feared activities. The ex-posure starts with the least fearedactivity, and the therapist helps thepatient appraise the exposure and itsconsequences and then address ir-rational and counterproductive be-liefs, leading to reductions in theanxiety associated with the activity.Once the negative associations are ex-tinguished, activities associated withhigher levels of anxiety are addressedin the same way. With graded activity,operant conditioning principles areused to reinforce healthy behaviors.The program focuses on functionalactivities and progresses in a time-contingent manner regardless ofpain to achieve functional goals andincreased activity. Principles of quo-tas, pacing, and self-reinforcementare key features of the program. Al-though both treatments have beenendorsed in clinical guidelines for
the management of persistent LBP,4,5
the effectiveness of the 2 treatmentshas not been well established.
Although no systematic review ofgraded activity or graded exposurehas been published, a Cochrane sys-tematic review of cognitive and be-havioral interventions for chronicLBP has been completed. The reviewconcluded that combined cognitivetherapy/respondent therapy and pro-gressive relaxation alone are effec-tive treatment modalities for short-term pain reduction in patients withchronic LBP but that there are nosignificant differences between thedifferent forms of behavioral inter-ventions.6 Because most of the stud-ies included in that review involvedonly psychological interventions,with minimal or no exercise compo-nent, the effectiveness of graded ac-tivity or graded exposure cannot beestablished from that review.
Therefore, the purpose of the presentstudy was to systematically review ran-domized controlled trials that evalu-ated the effectiveness of graded activ-ity and graded exposure interventionsfor the treatment of persistent (�6weeks in duration or recurrent) non-specific LBP at short-, intermediate-,and long-term follow-up evaluations.The outcomes of interest were pain,disability, global perceived effect, andreturn to work.
MethodData Sources and SearchesA computerized electronic search wasperformed to identify relevant arti-cles. The search was conducted onMEDLINE (1950 to February 2009),CINAHL (1982 to February 2009),PsychINFO (1806 to February 2009),PEDro (to February 2009), andEMBASE (1988 to February 2009). Keywords relating to the domains of ran-domized controlled trials and backpain were used, as recommended bythe Cochrane Back Review Group.7
Terms for graded activity and graded
exposure were included in the searchby use of MeSH (Medical Subject Head-ings of the National Library of Medi-cine) terms and specific guidelines foreach database (Appendix). Subjectsubheadings and word truncationsspecific for each database were used.There was no language restriction.
One reviewer screened the searchresults for potentially eligible stud-ies, and 2 reviewers independentlyreviewed the screened articles foreligibility. A third independent re-viewer resolved any disagreementabout the inclusion of trials. Authorswere contacted when more informa-tion about a trial was needed to al-low the inclusion of that trial. Manyauthors were contacted for addi-tional information related to inclusioncriteria.8–16 From the latter studies, weincluded 5 trials11,12,14–16 and ex-cluded 4 trials (2 authors confirmedthat their trials were not eligible,8,10
and we did not receive a responsefrom 2 authors). Staal et al16 pro-vided data for the subset of partici-pants who met the inclusion criteriafor this review (ie, excluding partic-ipants with acute pain).
Researchers who published relevantarticles were contacted to help iden-tify gray literature and articles inpress. Citation tracking was per-formed by use of the database Webof Science on ISI Web of Knowl-edge,* and a manual search of thereference lists of previous reviews
* Thomson Reuters, Level 3, 100 Harris St,Pyrmont, New South Wales 2009 Australia.
Available WithThis Article atptjournal.apta.org
• The Bottom Line Podcast
• Audio Abstracts Podcast
This article was published ahead ofprint on April 15, 2010, atptjournal.apta.org.
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 861 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

and eligible trials also was per-formed. The International ClinicalTrials Registry platform from theWorld Health Organization and theCochrane Centre Register of Con-trolled Trials also were searchedwith terms for LBP, graded activity,and graded exposure.
Study SelectionStudies were eligible for inclusionwhen they were randomized con-trolled trials or quasi-randomizedcontrolled trials comparing gradedactivity or graded exposure to pla-cebo, no treatment, or another ac-tive treatment or when graded activ-ity or graded exposure was added asa supplement to other interventions.The reviewers followed a researchprotocol that was developed beforethe beginning of the review processand that included a checklist for in-clusion criteria.
Trials were considered to have eval-uated graded activity when the treat-ment included the following 3features:
• The treatment involved principlesof operant conditioning, such as re-inforcement of healthy behaviors.
• Treatment goals were functionalactivities.
• The program included a baselineand then incremented activities in atime-contingent manner regardlessof pain.
Additionally, trials in which treat-ments were described as graded ac-tivity and in which various hand-books2,17 were cited were deemedeligible.
Trials were considered to have eval-uated graded exposure when thetreatment included the following 4features:
• Feared activities were identified.• A hierarchy of feared activities was
created.• Exposure started with the least
feared activity.• The therapist assisted the patient in
appraising the exposure to fearedactivities and its consequences. Thetherapist addressed irrational be-
liefs, counterproductive beliefs, orboth.
Additionally, trials in which treat-ments were described as graded ex-posure and in which various hand-books18,19 were cited were deemedeligible.
Randomized or quasi-randomizedcontrolled trials were included whenthey explicitly reported that a crite-rion for entry was nonspecific LBP(with or without leg pain) with aduration of at least 6 weeks (non-acute LBP) or recurrent LBP. Therewas no age or sex restriction. Trialswere included when one of the fol-lowing outcome measures was re-ported: pain, disability, quality oflife, perceived effect, return to work,or recurrence.
Data Extraction andQuality AssessmentThe methodological quality of thetrials was assessed by use of thePEDro scale (values of 0–10), withscores extracted from the PEDrodatabase.20 Assessment of the qualityof trials in the PEDro database wasperformed by 2 trained independentraters, and disagreements were re-solved by a third rater. Methodolog-ical quality was not an inclusioncriterion.
Two independent reviewers ex-tracted data from the included stud-ies by using a standardized data ex-traction form. Mean scores, standarddeviations, and sample sizes were ex-tracted from the studies. When thisinformation was not provided in thetrial, the values were calculated orestimated by use of methods recom-mended in the Cochrane Handbookfor Systematic Reviews of Interven-tions.21 When there was insufficientinformation about outcomes to al-low data analysis, the authors of theincluded studies were contacted.All11,16,22–25 but one26 of the authors
The Bottom Line
What do we already know about this topic?
Graded activity and graded exposure differ from traditional exercisebecause these interventions incorporate psychological principles intoactivity prescription. It remains unclear whether either of these interven-tions is effective.
What new information does this study offer?
This review established that graded activity, but not graded exposure, isan effective treatment for persistent low back pain, although the effectsize is small. There is no evidence that either is superior to a traditionalexercise program for persistent low back pain.
If you’re a patient, what might these findings meanfor you?
Exercise is an effective treatment for persistent low back pain but thetype of exercise does not seem particularly important.
Graded Activity and Graded Exposure for Low Back Pain
862 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

who were contacted to provide trialdata responded to our queries.
Means, standard deviations, and sam-ple sizes were extracted for short-term (less than 3 months after ran-domization), intermediate-term (atleast 3 months but less than 12months after randomization), andlong-term (12 months or more after
randomization) follow-up evalua-tions. When multiple time points fellwithin the same category, the onethat was closer to the end of treat-ment for the short term, closer to 6months for the intermediate term,and closer to 12 months for the longterm was used. These references fortime points were based on guide-lines from the Cochrane Back Re-
view Group.7 Scores for pain, disabil-ity, and global perceived effect wereconverted to a scale from 0 to 100.When more than 1 outcome measurewas used to assess pain, disability,and work status, the outcome mea-sure described as the primary out-come measure for the trial was in-cluded in this review.
Database searches : February 2009 PsychINFO: 183
CINAHL: 89 EMBASE: 2,161
MEDLINE: 1,545 PEDro: 868
Hand search: 4 Total after removing duplicates: 3,971
74 potentially eligible after assessing titlesand abstracts
Web of Science search 3 potentially eligible
15 original studies included in review (18 articles)
Reasons for exclusion:
33 did not use graded activity or graded exposure,8–10,28–57
6 included patients without nonspecific low back pain,58–63
3 included patients with acute low back pain,64–66 14 were not RCTs,67–80 8 were secondary analyses of another trial,81–88 and 1 used graded activity for both treatment groups89
83 potentially eligible
Indicated by experts 6 potentially eligible
Figure 1.Flow chart of systematic review inclusion and exclusion. RCTs�randomized controlled trials.
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 863 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Data Synthesis and AnalysisResults were pooled when trialswere considered sufficiently homo-geneous with respect to participantcharacteristics, interventions, and out-comes. I2 was calculated by use ofRevMan 527 to assess statistical het-erogeneity. I2 describes the percent-age of the variability in effect estimatesthat is due to heterogeneity ratherthan sampling error (chance). A valuegreater than 50% may be consideredsubstantial heterogeneity.21 When tri-als were statistically homogeneous(I2�50%), pooled effects (weightedmean differences) were calculated byuse of a fixed-effects model. When tri-als were statistically heterogeneous(I2�50%), estimates of pooled effects(weighted mean differences) were ob-tained by use of a random-effectsmodel.21
ResultsStudy SelectionThe initial electronic database searchresulted in a total of 3,971 articlesafter the removal of duplicates. Ofthese, 74 articles were selected aspotentially eligible on the basis oftheir title and abstract. Through aWeb of Science search of these arti-cles, 3 other potentially eligible arti-cles were identified. A total of 77potentially eligible articles were con-sidered for inclusion; only 14 werefound to be eligible for inclusion inthis review (Fig. 1). Twenty-four ex-perts were contacted to provide in-formation about gray literature andarticles that we may have missed. Wereceived 12 responses suggesting 6potentially eligible studies; only 1 ofthese was included in this review.Therefore, we included a total of 15original studies with results pre-sented in 18 different articles.
The International Clinical Trials Reg-istry platform contained 8 random-ized controlled trials that were po-tentially eligible for inclusion. Ofthose, 3 were already included in ourstudy,22,26,90 3 were still recruiting
patients, and 2 were not eligible be-cause patients with acute back painwere included.
Methodological QualityThe methodological quality assess-ment with the PEDro scale revealed amedian score of 6 (range�3–9).Masking of the therapist was not in-cluded in any of the trials, as ex-pected in studies of activity prescrip-tion, and masking of patients wasincluded in only 1 trial.23 Point esti-mates and between-group compari-sons were present in 14 of 15 trials,12 of 15 trials had comparability atbaseline, and 10 of 15 trials had con-cealed allocation, intention to treat,and adequate follow-up evaluations.
Study CharacteristicsFourteen of the randomized con-trolled trials included in this reviewcompared graded activity or gradedexposure with another treatment orwith no treatment (Tabs. 1 and 2).One trial with a factorial design (2 �2) was also included; the first factorwas graded activity, the second fac-tor was advice, and each factor had 2levels (active versus sham).23
In 7 trials, graded activity was com-pared with a minimal intervention(usual care, waiting list, sham exer-cise, advice to stay active, or care by ageneral practitioner).12,16,22,23,26,86,92
In 6 trials, graded activity was com-pared with another form of exercise(motor control, high-intensity backschool, general physical therapy ex-ercises, active physical treatment, orphysical therapy according to guide-lines).11,14,15,22,25,26 In 4 trials, gradedactivity was compared with gradedexposure,12,90,91,94 and in 2 trials,graded exposure was comparedwith a waiting list.12,94
Graded Activity Versusa Minimal InterventionSeven trials with a total of 920 pa-tients compared graded activity witha minimal intervention.12,16,22,23,26,86,92
The methodological quality of thesetrials ranged from 4 to 9. Data forpooling were available for pain anddisability in the short, intermediate,and long terms and for perceived ef-fect in the short term. Data werepooled by use of a fixed-effectsmodel for all outcomes except painand disability in the long term andperceived effect in the short term,for which a random-effects modelwas used.
The pooled results favored gradedactivity for both pain and disability atshort- and medium-term follow-upevaluations, but the effects weresmall; for example, for pain in theshort term, the weighted mean dif-ference on a scale from 0 to 100was �6.2 points (95% confidence in-terval [CI]��9.4 to �3.0). For bothpain and disability at long-termfollow-up evaluations, the effectswere close to zero and not signifi-cant; for example, for pain the valuewas �0.1 (95% CI��10.4 to 10.2)(Fig. 2).
Results for return to work were pre-sented by 3 studies.26,92,95 The re-sults of 1 trial, that of Lindstrom etal,92 were expressed in likelihood ra-tios and showed that return to workwas faster for patients in the graded-activity group than for patients in thecontrol group. The median numberof days to return to work for thegraded-activity group was 35 days;that for the control group was 61days. Heymans et al26 used survivalanalysis to show that there were nosignificant differences between treat-ment groups at short-term follow-upevaluations (hazard ratio�1.0; 95%CI�0.8 to 1.4). The median numberof days of sick leave for the graded-activity group was 85; that for theusual-care group was 75. In contrast,the results of a survival analysisconducted by Streenstra et al95
showed a significantly earlier returnto work for the usual-care group(hazard ratio�0.52; 95% CI�0.32 to
Graded Activity and Graded Exposure for Low Back Pain
864 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Table 1.Details of Included Randomized Controlled Trials (RCTs)a
TrialParticipant Characteristics, Sample Size
(N), and Duration of ComplaintInterventions and
Study Design
Outcomes (Measures)and Time Points Included
in This ReviewPEDroScore
Critchley et al (2007)11 Recruited from referrals by specialist or primarycare practitioners to hospital’s physical therapydepartment
Age: �18 yMain exclusions: prior spinal surgery,
hematologic disease, and physical therapy inthe preceding 6 mo
N�143Duration: �12 wk
Graded activity vs motorcontrol vs manual therapy� home exercises (RCT)
Pain (VAS)Disability (RMDQ-24)Quality of life (EuroQol
Questionnaire)6- and 12-mo follow-up
evaluations
7
de Jong et al (2005)91 Referred for outpatient behavioral rehabilitationand reporting substantial fear of movement
Age: 18–65 yMain exclusions: pregnancy and
psychopathologyN�6Duration: �6 mo
Graded activity � educationvs graded exposure �education (crossoverstudy)
Disability (RMDQ-24)Crossover in short term only,
with 6- or 8-wk follow-upevaluations
3
Heymans et al (2006)26 Patients who visited their occupationalphysicians
Age: 18–65 yMain exclusions: specific pathologies,
pregnancy, and legal conflicts at workN�299Duration: �7 wk (at least 1 mo of pain and
3 wk of sick leave)
Graded activity (high-intensity back school) �usual care vs low-intensityback school (one thirdeducation, two thirdsexercise) � usual care vsusual care (RCT)
Pain (VAS)Disability (RMDQ-24)Global perceived effect (0–5)Sick leave (d) and return to
work (d)3- and 6-mo follow-up
evaluations
8
Leeuw et al (2008)90 Recruited by physicians and from advertisementsAge: 18–65 yMore than 3 points on the RMDQ-24More than 33 points on the Tampa Scale for
KinesiophobiaN�85Duration: �3 mo
Graded activity vs gradedexposure (RCT)
Pain (McGill VAS)Disability (QBPDS and PSFS)Posttreatment, 6-mo, and
12-mo follow-up evaluations
6
Lindstrom and colleagues(1992)92,93
Workers in industrial (“blue-collar”) jobs, on sickleave for 6 wk due to any low back paindiagnosis and not on sick leave for 12 wkbefore the current leave
Main exclusions: specific pathologies, surgery,and psychiatric diagnosis
N�103Duration: �8 wk of sick leave
Graded activity vs waitinglist (RCT)
Return to work (d), sick leave(d), and % of workersreturning to work
12-mo follow-up evaluations
5
Linton et al (2008)94 Recruited from primary care facilities andadvertisements in local newspaper
More than 35 points on the Tampa Scale forKinesiophobia
Age: 18–60 yN�46Duration: �3 mo
Graded exposure � usualcare vs waiting list �usual care (RCT)
Pain intensity (from Orebro)Disability (QBPDS)Posttreatment follow-up
evaluations
4
Nicholas et al (1991)15 Referred to a pain clinicAge: 20–60 yMain exclusion: no compensation claim within
12 moN�62Duration: �6 mo
Cognitive treatment vsbehavioral treatment(graded activity) vscognitive treatment �relaxation vs behavioraltreatment � relaxation vsattention controlcondition vs physicaltherapy only (RCT)
Pain rating chart5-wk, 6-mo, and 12-mo
follow-up evaluations
4
Nicholas et al (1992)14 Referred from a pain clinic and by specialist andgeneral medical practitioners
Age: 20–60 yMain exclusion: compensation claim due for
settlement within 12 moN�20Duration: �6 mo
Cognitive behavioraltreatment � physicaltherapy (graded activity)vs physical therapy �attention controlcondition (RCT)
Pain rating chart5-wk and 6-mo follow-up
evaluations
6
(Continued)
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 865 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Table 1.Continued
TrialParticipant Characteristics, Sample Size
(N), and Duration of ComplaintInterventions and
Study Design
Outcomes (Measures)and Time Points Included
in This ReviewPEDroScore
Pengel et al (2007)23 Recruited by health care professionals and fromhospital waiting lists
Age: 18–80 yMain exclusions: spinal surgery, specific
pathologies, and contraindications to exerciseN�260Duration: �6 wk but �12 wk
Graded activity � advice vssham exercises � advicevs graded activity � shamadvice vs sham gradedactivity � sham exercises(RCT factorial design)
Pain (VAS)Disability (PSFS)Global perceived effect
(�5 to 5)6-wk, 4-mo, and 12-mo
follow-up evaluations
9
Smeets et al (2006)22
Smeets et al (2008)24Recruited by general practitioners and medical
specialistsAge: 18–65 yMore than 3 points on the RMDQ-24Ability to walk at least 100 mMain exclusions: specific pathologies,
comorbidities, and clear treatment preferenceN�227Duration: �3 mo
Graded activity � problemsolving vs active physicaltreatment vs gradedactivity � problemsolving � active physicaltreatment vs waiting list(RCT)
Pain (McGill VAS)Disability (RMDQ-24)Global perceived effect
(1–7)10-wk, 6-mo, and 12-mo
follow-up evaluations
8
Staal et al (2004)16
Hlobil et al (2005)98Workers employed by a major Dutch airlineMain exclusions: signs of nerve root compression
and cardiovascular problemsN�88Duration: �6 wk (for patients included in this
review)
Graded activity vs usual care(RCT)
Pain (VAS)Disability (RMDQ-24)Absence from work (d)3-mo, 6-mo, and 12-mo
follow-up evaluations
8
Steenstra et al (2006)95
Anema et al (2007)96Recruited by occupational physiciansPatients in return-to-work program at 2–6 wk of
sick leaveAge: 18–65 yMain exclusions: specific low back pain,
cardiovascular and psychiatriccontraindications, pregnancy, and sick leavegranted for low back pain �1 mo
N�112Duration: �8 wk of sick leave
Graded activity vs usual care(advice to stay active �care by generalpractitioners) (RCT)
Pain (VAS)Disability (RMDQ-24)Sick leave (d) and return to
work (d)3-mo, 6-mo, and 12-mo
follow-up evaluations
7
van der Roer et al (2008)25 Age: 18–65 yNew episode of nonspecific back painInability to resume daily activities in the last 3 wkN�114Duration: �12 wk
Graded activity vs guidelines(physical therapyaccording to clinicalguidelines) (RCT)
Pain (numerical rating scale)Disability (RMDQ-24)Global perceived effect
(0–6)6-wk, 6-mo, and 12-mo
follow-up evaluations
7
Vlaeyen et al (2002)97 Referred for outpatient behavioral rehabilitationand reporting substantial fear of movement
Age: 18–65 yMain exclusions: pregnancy and
psychopathologyN�6Duration: �6 mo
Graded activity vs gradedexposure (crossoverstudy)
Pain (VAS)Disability (RMDQ-24)Crossover with 12-wk and 12-
mo follow-up evaluations
4
Woods and Asmundson (2008)12 Recruited from newspapers, e-mailadvertisements, and posters
Age: 19–65 yMore than 38 points on the Tampa Scale for
KinesiophobiaMain exclusions: pending medical investigations
and back surgeryN�83Duration: �6 mo
Graded activity vs gradedexposure vs waiting list(RCT)
Pain Disability IndexMcGill Pain Questionnaire
(short form)4-wk follow-up evaluations
5
a VAS�visual analog scale, RMDQ-24�24-Item Roland-Morris Disability Questionnaire, QBPDS�Quebec Back Pain Disability Scale, PSFS�Patient-Specific FunctionalScale, Orebro�Orebro Musculoskeletal Pain Questionnaire.
Graded Activity and Graded Exposure for Low Back Pain
866 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Table 2.Details of Graded-Activity (GA) and Graded-Exposure (GE) Interventions
Study
Duration ofGA and
GE Interventions
Expertise of theCaregiver and
Integrity Check Home Program
Plans forFutureRelapse Adherence
Critchley et al (2007)11 Maximum of 9 sessionsof 90 min
Physical therapists whohad at least 2 y ofclinical experienceand who agreed totreat according tothe trial protocolwere provided brieftraining. Thehospitals had theirown commoninternal teachingprogram for theleaders of thegraded-activityprogram; otherwise,there was no furthertraining. Adherenceto the protocol wasassessed by recordingtreatments fromphysical therapynotes after treatmentallocation wasrevealed.
Not stated Not stated Participants reported difficultyattending classes twice/wk
de Jong et al (2005)91 Graded activity for32 h over 8 wk andgraded exposure for24 h over 6 wk
Not stated Not stated Not stated Not stated
Heymans et al (2006)26 16 sessions of 1 h over8 wk
Supervised physicaltherapist
Home exercises were givenduring the treatmentperiod
Not stated Patients attended an averageof 13 sessions; 70% ofworkers completed alltreatments, and 10%received no treatment
Leeuw et al (2008)90 Graded activity in 26sessions of 1-htreatments startingtwice/wk and gradedexposure in 16sessions of 1-htreatments startingtwice/wk
Physical therapists withat least 6 mo ofexperience weretrained in bothtreatments andreceived a manualwith guidelines fordealing withproblems. Therapistsattended collectivesupervision sessions 3times/y. Asophisticated methodfor judgingadherence totreatment andcontamination wasused. Thirty randomsamples from 265recorded sessionswere judged.
Most practice of exercisesoccurred at home, andprogress was evaluatedat sessions; homeexercises were givenonly for the graded-activity group
Not stated 29% of patients receivinggraded exposure and 33%of patients receiving gradedactivity did not finish thetreatments
Lindstrom et al (1992)92 3 d/wk until return towork
Physical therapist No home exercises Not stated Not stated
Linton et al (2008)94 13–15 individualsessions of behavioraltherapy and 8–10sessions of exposurein vivo
Therapy was performedby psychologists whowere trained byVlaeyen et al97 andalso received supportfrom a physicaltherapist. A writtentreatment manualwas developed forthe study.
Sessions ended with homeassignment thatincorporatedmovements intoactivities of daily living athome and work
Not stated Not stated
(Continued)
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 867 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Table 2.Continued
Study
Duration ofGA and
GE Interventions
Expertise of theCaregiver and
Integrity Check Home Program
Plans forFutureRelapse Adherence
Nicholas et al (1991)15 One 2-h session andone 1.5-h session/wkfor 5 wk (only 5sessions werecognitive behavioraltherapy)
Therapy was performed bya clinical psychologistwith 5 y of experienceand registered physicaltherapists under thesupervision of a seniorphysical therapist. Twomasked ratersindependently andcorrectly identified 6audiotapes randomlyselected from cognitivebehavioral, behavioral,and attention controlconditions, providingevidence that thecontent of eachcondition was consistentwith the treatmentprotocol.
Patients were verballypraised by thepsychologist forpracticing physicaltherapy exercises eachweek
Not stated Not stated
Nicholas et al (1992)14 One 2-h session andone 1.5-h session/wkfor 5 wk
One hour of the firstsession each week wasconducted by a physicaltherapist, and the otherhour was conducted bya psychologist who had5 y of experience sincecompleting clinicalqualifications. A physicaltherapist under thesupervision of a seniorphysical therapistconducted the secondsession each week.
Patients were encouragedby physical therapists topractice exercises athome, but no check onthe practice was madeand no specificreinforcement forperforming exercises wasprovided by physicaltherapists
Not stated Not stated
Pengel et al (2007)23 12 sessions over 6 wk:3 times/wk in weeks1 and 2, twice/wk inweeks 3 and 4, andonce/wk in weeks 5and 6; participantsalso attended 3sessions of advice
Registered physicaltherapists receivedtraining from anexperienced clinicalpsychologist. Aninvestigator recordedand assessed a sampletreatment session andvisited each treatmentsite regularly to monitordelivery.
Individualized hometreatment was regularlyreviewed, and patientswere encouraged tocontinue after the end ofthe treatment period
Not stated Means of 9.4 (SD�3.2)sessions of exercises and 2.9(SD�1.1) sessions of advice
Smeets et al (2006)22
Smeets et al (2008)2418 sessions over 10 wk,
changing from3 sessions/wk to1 session/wk, for atotal of 11.5 h oftreatment
All therapists receivedextensive training beforethe start of the trialand refresher courses.Social workers andpsychologists had atleast 5 y of experience.
Home assignment wasgiven to allow patientsto practice skills in theirdaily lives
Not stated Means of 14.3 sessions(maximum�20) for thecognitive behavioral therapygroup and 11.9 sessions(maximum�19) for thecombination group
Staal et al (2004)16
Hlobil et al (2005)981-h exercise session
twice/wk until returnto work or amaximum of 3 mo
Three therapists providedtreatment according toa protocol. Therapistswere trained before thestudy in three 2-hsessions and practicedpatient-therapistinteractions. Sessionsbefore and after thestudy were audiotapedand analyzed forcontent.
Not stated Not stated Not stated
(Continued)
Graded Activity and Graded Exposure for Low Back Pain
868 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

0.86). The median number of days toreturn to work was 139 days for thegraded-activity group and 111 daysfor the usual-care group.
Graded Activity VersusOther Forms of ExerciseSix trials (597 patients) with a meth-odological quality ranging from 4 to8 compared graded activity withother forms of exercise.11,14,15,22,25,26
Data for pooling were available forpain, disability, and perceived effectin the short, intermediate, and longterm. Data were pooled by use of afixed-effects model for all outcomesexcept perceived effect in the short
and intermediate term, for which arandom-effects model was used.Pooled results revealed no statisti-cally significant differences betweengraded activity and other forms ofexercise for pain, disability, or globalperceived effect at each time point(Fig. 3).
A hazard ratio for the difference indays to return to work was calcu-lated by Heymans et al26; the resultsrevealed no significant differencesbetween treatment groups (hazardratio�1.4; 95% CI�1.0 to 1.9). Themedian number of days of sick leavewas 85 days for the graded-activity
group and 68 days for the exercisegroup.
Graded Exposure VersusGraded ActivityTwo low-quality trials (PEDro scoresof 3 and 4), with 6 patients each,compared graded activity withgraded exposure.91,97 Both studieshad a crossover design, making itmore difficult to reach any conclu-sion about the results because noevaluation of carryover effects wasperformed. Another 2 studies12,90
had information that allowed pool-ing for pain and disability in the shortterm. These 2 trials had PEDro scores
Table 2.Continued
Study
Duration ofGA and
GE Interventions
Expertise of theCaregiver and
Integrity Check Home Program
Plans forFutureRelapse Adherence
Steenstra et al (2006)95
Anema et al (2007)9626 sessions of 1 h
(twice/wk) over13 wk or until returnto work
Physical therapists(47 in 16 centers)were trained by thephysical therapistparticipating in thestudy of Staal et al.77
A protocol was usedto standardize theintervention. Physicaltherapists had a 2-hfeedback sessionevery 3 mo.
Not stated Not stated 35% of patients did notadhere to the treatment;average frequency was 14.1sessions
van der Roer et al(2008)25
10 individual sessionsand 20 groupsessions
Physical therapistsattended 2 intensive6-h workshops andwere trainedaccording to thestudy protocol. Studyforms were used toassess therapistadherence to thestudy protocol; 18%of patients did notreceive adequatetreatment.
Not stated Not stated Not stated
Vlaeyen et al (2002)97 3 wk of treatment Not stated Patients were given 1 wkto practice new skills inhome situations after theend of the 3-wktreatment
Not stated Not stated
Woods and Asmundson(2008)12
Eight 45-min sessionsconducted on twice-weekly basis over4 wk
Graded activity wasconducted by aregistered physicaltherapist, and gradedexposure wasconducted by aclinical psychologistgraduate studenttrained in thetherapy andsupervised by aregistered doctoral-level psychologist.
Not stated Not stated Not stated
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 869 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Figure 2.Forest plot of results of randomized controlled trials comparing graded activity with a control (minimal intervention). Values representeffect sizes (weighted mean differences) and 95% confidence intervals. The pooled effect sizes were calculated by use of afixed-effects model for all outcomes except pain and disability in the long term and perceived effect in the short term, for which arandom-effects model was used.
Graded Activity and Graded Exposure for Low Back Pain
870 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Figure 3.Forest plot of results of randomized controlled trials comparing graded activity with other forms of exercise. Values represent effectsizes (weighted mean differences) and 95% confidence intervals. The pooled effect sizes were calculated by use of a fixed-effectsmodel for all outcomes except perceived effect in the short and intermediate term, for which a random-effects model was used.
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 871 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

of 5 and 6 and included 146 patients.The results of the pooled analysisrevealed no statistically significantdifferences between treatmentgroups for pain and disability in theshort term (Fig. 4).
Graded Exposure Versus aMinimal InterventionTwo trials (104 patients) (PEDroscores of 4 and 5) compared gradedexposure with a minimal interven-tion (waiting list or usual care).12,94
Data for pooling were available forpain and disability in the short term.Pooled results revealed no statisti-cally significant differences betweentreatment groups for pain in theshort term (weighted mean differ-
ence on a scale of 0–100��3.7points [95% CI��12.3 to 4.9]) anddisability in the short term (weightedmean difference on a scale of0–100��3.5 points [95% CI��19.4 to 12.3]) (Fig. 5). No datawere available for quality of life orrecurrence for any of thecomparisons.
DiscussionIn this systematic review, we com-pared the effects of graded activityversus a minimal intervention,graded activity versus other forms ofexercise, graded activity versusgraded exposure, and graded expo-sure versus a minimal interventionfor patients with persistent LBP.
Only 4 of the pooled effect sizeswere statistically significant. Thesestatistically significant results favoredgraded activity over a minimal inter-vention for pain and disability atshort- and intermediate-term follow-upevaluations. However, the effectsizes were small, approximately 7points on a 100-point scale; this find-ing may indicate that they are notclinically meaningful.
Among the studies in which gradedactivity was compared with a mini-mal intervention, 2 trials had coun-terintuitive results: The minimal in-tervention provided better outcomesthan graded activity.12,95 The studyof Woods and Asmundson12 poten-
Figure 4.Forest plot of results of randomized controlled trials comparing graded activity with graded exposure. Values represent effect sizes(weighted mean differences) and 95% confidence intervals. The pooled effect sizes were calculated by use of a fixed-effects model.
Figure 5.Forest plot of results of randomized controlled trials comparing graded exposure with a control (waiting list or usual care). Valuesrepresent effect sizes (weighted mean differences) and 95% confidence intervals. The pooled effect sizes were calculated by use ofa fixed-effects model for pain and a random-effects model for disability.
Graded Activity and Graded Exposure for Low Back Pain
872 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

tially provided biased estimates oftreatment effects because of a lack ofmasking, failure to conceal alloca-tion, and a loss to follow-up of ap-proximately 50%. In contrast, thestudy of Steenstra et al95 seemed tobe well conducted, and we are un-able to explain why the results forpain and disability in the long termfavored a minimal intervention overgraded activity.
The results of the 3 trials that mea-sured return to work after gradedactivity versus a minimal interven-tion were conflicting. In 1 of these 3trials,92 graded activity provided afaster return to work than a minimalintervention. In the second trial,26
there were no significant differencesbetween treatment groups. In thethird study,95 a minimal interventionprovided a faster return to work thangraded activity. The authors of thelast study suggested that the longerdelay in return to work for patientsin the graded-activity group was at-tributable to a delay in the beginningof the treatment for this group. De-spite the possible bias present inthese studies, the results regardingreturn to work are inconclusive, andfurther research is needed.
The results for comparisons ofgraded activity with other forms ofexercise are in accordance with therecommendations of most clinicalguidelines, which suggest that noform of exercise is more effectivethan another.99 However, Smeets etal84 did find that graded activity wasmore cost-effective than active phys-ical treatment (exercises), drawingattention to the need for more cost-effectiveness studies.
In many cases, the interventionswere implemented by trained physi-cal therapists. Although adherenceto the treatment protocols was as-sessed in 6 of the 15 studies, no re-sults of this assessment were pro-vided; therefore, it remains unclear
whether the interventions wereproperly administered. Additionally,it is uncertain whether 2 or 3 ses-sions of training provided the clini-cians with sufficient skills to effec-tively implement the treatmentprotocols. There is some evidencethat trained physical therapists lackthe skills required to effectively im-plement a psychologically basedintervention.100
One important feature of both treat-ments considered in this review isinclusion of a plan for managing re-lapses. This strategy not only helpspatients deal with anxiety and fearabout a flare-up but also may assist inmaintaining the long-term effects ofthe intervention. Although none ofthe studies mentioned the use of thisstrategy, it is not clear whether itwas omitted from the intervention orsimply was not reported.
There are some limitations to theconclusions of this review. These in-clude the low quality of the studies,primarily those evaluating graded ex-posure, the use of various types ofoutcomes, and differences in the im-plementation of the interventions.The small number of trials testinggraded exposure is also an importantlimitation of this review. Some au-thors92,97 suggested that graded ex-posure may have larger effects thangraded activity because the formerintervention more specifically tar-gets a patient’s fears; however, thesmall number of trials included inthis review for this comparison doesnot allow a reliable conclusion to bedrawn. Future research should focuson the conduct of higher-quality trialsevaluating issues such as return towork and compensation and the con-duct of cost-effectiveness studies. Ad-ditionally, trials including patientsidentified as having greater fear behav-iors should be carried out becausethese patients may respond better toboth graded activity and graded expo-sure interventions.97
ConclusionThe results of this systematic reviewsuggest that graded activity is slightlymore effective than a minimal inter-vention but not more effective thanother forms of exercise for pain, dis-ability, and global perceived effect inthe short and intermediate terms forpatients with persistent nonspecificLBP. The results also suggest thatgraded exposure is no more effectivethan a minimal intervention orgraded activity. Because of the poorreporting in many of the studies, itoften was unclear precisely how theinterventions were implemented.Additionally, the smaller number andlower quality of graded-exposure tri-als limits the conclusions that can bedrawn regarding this intervention.
Ms Macedo, Dr Smeets, Dr Maher, and DrLatimer provided concept/idea/research de-sign. All authors provided writing and datacollection. Ms Macedo and Dr Smeets pro-vided data analysis. Ms Macedo providedproject management. Dr Smeets, Dr Maher,and Dr Latimer provided facilities/equipment.Dr Smeets provided institutional liaisons. DrSmeets, Dr Maher, Dr Latimer, and DrMcAuley provided consultation (includingreview of manuscript before submission).The authors of this systematic review thankthe authors of the retrieved trials who pro-vided additional information or data fromtheir trials.
Ms Macedo holds a PhD scholarship jointlyfunded by the University of Sydney and theAustralian Government. Dr Maher’s researchfellowship is funded by Australia’s NationalHealth and Medical Research Council, andDr Latimer’s research fellowship is funded bythe Australian Research Council.
The results of this study were presented atthe Australian Physiotherapy AssociationConference; October 1–5, 2009; Sydney,Australia.
This article was submitted September 14,2009, and was accepted January 24, 2010.
DOI: 10.2522/ptj.20090303
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 873 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

References1 Vlaeyen J, Linton S. Pain-related fear and
its consequences in chronic musculo-skeletal pain. In: Linton S, ed. New Ave-nues for the Prevention of Chronic Mus-culoskeletal Pain and Disability, PainResearch and Clinical Management.Amsterdam, the Netherlands: Elsevier;2002:83–103.
2 Fordyce WE. Behavioral Methods forChronic Pain and Illness. St Louis, MO:Mosby; 1976.
3 Asmundson GJG, Norton PJ, Norton GR.Beyond pain: the role of fear and avoid-ance in chronicity. Clin Psychol Rev.1999;19:97–119.
4 Rossignol M, Arsenault B, Dionne C, et al.Clinic on Low-Back Pain in Interdisci-plinary Practice (CLIP) Guidelines.Montreal, Quebec, Canada: Direction deSante Publique, Agence de la Sante et desServices Sociaux de Montreal; 2007.
5 Airaksinen O, Brox JI, Cedraschi C, et al.European guidelines for the managementof chronic nonspecific low back pain.Eur Spine J. 2006;15(suppl 2):S192–S300.
6 Ostelo RW, van Tulder MW, Vlaeyen JW,et al. Behavioural treatment for chroniclow-back pain. Cochrane Database SystRev. 2005;1:CD002014.
7 Bombardier C, Van Tulder M, Pennick V,et al; Cochrane Back Group. About theCochrane Collaboration (Cochrane Re-view Groups [CRGs]). 2008, issue 3.
8 Johnson RE, Jones GT, Wiles NJ, et al.Active exercise, education, and cognitivebehavioral therapy for persistent dis-abling low back pain: a randomized con-trolled trial [with consumer summary].Spine. 2007;32:1578–1585.
9 Turner JA. Comparison of group progressive-relaxation training and cognitive-behavioralgroup therapy for chronic low back pain.J Consult Clin Psychol. 1982;50:757–765.
10 von Korff M, Balderson BH, Saunders K,et al. A trial of an activating interventionfor chronic back pain in primary care andphysical therapy settings. Pain. 2005;113:323–330.
11 Critchley DJ, Ratcliffe J, Noonan S, et al.Effectiveness and cost-effectiveness ofthree types of physiotherapy used to re-duce chronic low back pain disability: apragmatic randomized trial with economicevaluation. Spine. 2007;32:1474–1481.
12 Woods MP, Asmundson GJG. Evaluatingthe efficacy of graded in vivo exposurefor the treatment of fear in patients withchronic back pain: a randomized con-trolled clinical trial. Pain. 2008;136:271–280.
13 Turner JA, Clancy S, McQuade KJ, et al.Effectiveness of behavioral therapy forchronic low back pain: a componentanalysis. J Consult Clin Psychol. 1990;58:573–579.
14 Nicholas MK, Wilson PH, Goyen J. Com-parison of cognitive-behavioral grouptreatment and an alternative non-psychological treatment for chronic lowback pain. Pain. 1992;48:339–347.
15 Nicholas MK, Wilson PH, Goyen J.Operant-behavioural and cognitive-behavioural treatment for chronic lowback pain. Behav Res Ther. 1991;29:225–238.
16 Staal JB, Hlobil H, Twisk JW, et al. Gradedactivity for low back pain in occupationalhealth care: a randomized, controlled tri-al. Ann Intern Med. 2004;140:77–84.
17 Sanders SH. Operant conditioning withchronic pain: back to basics. In: GatchelRJ, Turk DC, eds. Psychological Ap-proaches to Pain Management: A Prac-titioner’s Handbook. New York, NY:The Guilford Press; 1996:112–130.
18 Vlaeyen JWS, de Jong J, Sieben JM, et al.Graded exposure in vivo for pain-relatedfear. In: Turk DC, Gatchel RJ, eds. Psy-chological Approaches to Pain Manage-ment: A Practitioner’s Handbook. 2nded. New York, NY: The Guilford Press;2002:210–233.
19 Vlaeyen JWS, de Jong J, Leeuw M, et al.Fear reduction in chronic pain: gradedexposure in vivo with behavioural exper-iments. In: Asmundson GJ, Vlaeyen JWS,Crombez G, eds. Understanding andTreating Fear of Pain. New York, NY:Oxford University Press; 2004:313–343.
20 Sherrington C, Herbert RD, Maher CG,et al. PEDro: a database of randomizedtrials and systematic reviews in physio-therapy. Man Ther. 2000;5:223–226.
21 Higgins JPT, Green S, editors. CochraneHandbook for Systematic Reviews of In-terventions 4.2.6 [updated September2006]. In: The Cochrane Library, Issue 4,2006. Chichester, UK: John Wiley &Sons, Ltd.
22 Smeets RJEM, Vlaeyen JWS, Hidding A,et al. Active rehabilitation for chroniclow back pain: cognitive-behavioral,physical, or both? First direct post-treatment results from a randomized con-trolled trial. BMC Musculoskelet Disord.2006;7:5.
23 Pengel LHM, Refshauge KM, Maher CG,et al. Physiotherapist-directed exercise,advice, or both for subacute low backpain: a randomized trial. Ann InternMed. 2007;146:787–796.
24 Smeets RJEM, Vlaeyen JWS, Hidding A,et al. Chronic low back pain: physicaltraining, graded activity with problemsolving training, or both? The one-yearpost-treatment results of a randomizedcontrolled trial. Pain. 2008;134:263–276.
25 van der Roer N, van Tulder M, BarendseJ, et al. Intensive group training protocolversus guideline physiotherapy for pa-tients with chronic low back pain: a ran-domised controlled trial. Eur Spine J.2008;17:1193–1200.
26 Heymans MW, de Vet HC, Bongers PM,et al. The effectiveness of high-intensityversus low-intensity back schools in an oc-cupational setting: a pragmatic randomizedcontrolled trial. Spine. 2006;31:1075–1082.
27 Review Manager (RevMan) [computerprogram]. Version 5.0. Copenhagen,Denmark: The Nordic Cochrane Centre,The Cochrane Collaboration, 2008.
28 Menzel NN, Robinson ME. Back pain indirect patient care providers: early inter-vention with cognitive behavioral ther-apy. Pain Manag Nurs. 2006;7:53–63.
29 Alaranta H, Rytokoski U, Rissanen A,et al. Intensive physical and psychosocialtraining program for patients withchronic low back pain: a controlled clin-ical trial. Spine. 1994;19:1339–1349.
30 Bendix T, Bendix A, Labriola M, et al.Functional restoration versus outpatientphysical training in chronic low backpain: a randomized comparative study.Spine. 2000;25:2494–2500.
31 Fairbank J, Frost H, Wilson-MacDonald J,et al. Randomised controlled trial to com-pare surgical stabilisation of the lumbarspine with an intensive rehabilitationprogramme for patients with chroniclow back pain: the MRC Spine Stabilisa-tion Trial. BMJ. 2005;330:1233–1239.
32 Gohner W, Schlicht W. Preventingchronic back pain: evaluation of a theory-based cognitive-behavioural training pro-gramme for patients with subacute backpain. Patient Educ Couns. 2006;64:87–95.
33 Harkapaa K, Jarvikoski A, Mellin G, et al.Health locus of control beliefs and psy-chological distress as predictors for treat-ment outcome in low-back pain patients:results of a 3-month follow-up of a con-trolled intervention study. Pain. 1991;46:35–41.
34 Jellema P, Van Der Roer N, Van DerWindt DAWM, et al. Low back pain ingeneral practice: cost-effectiveness of aminimal psychosocial intervention ver-sus usual care. Eur Spine J. 2007;16:1812–1821.
35 Magnussen L, Rognsvag T, Tveito TH,et al. Effect of a brief cognitive trainingprogramme in patients with long-lastingback pain evaluated as unfit for surgery.J Health Psychol. 2005;10:233–243.
36 Jousset N, Fanello S, Bontoux L, et al.Effects of functional restoration versus 3hours per week physical therapy: a ran-domized controlled study. Spine. 2004;29:487–493.
37 Keller A, Brox JI, Gunderson R, et al.Trunk muscle strength, cross-sectionalarea, and density in patients with chroniclow back pain randomized to lumbar fu-sion or cognitive intervention and exer-cises. Spine. 2003;29:3–8.
38 Jensen IB, Bergstrom G, Ljungquist T,et al. A 3-year follow-up of a multidisci-plinary rehabilitation programme forback and neck pain. Pain. 2005;115:273–283.
39 Jensen IB, Bergstrom G, Ljungquist T,et al. A randomized controlled compo-nent analysis of a behavioral medicinerehabilitation program for chronic spinalpain: are the effects dependent on gen-der? Pain. 2001;91:65–78.
Graded Activity and Graded Exposure for Low Back Pain
874 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

40 Moore JE, Von Korff M, Cherkin D, et al.A randomized trial of a cognitive-behavioral program for enhancing backpain self care in a primary care setting.Pain. 2000;88:145–153.
41 Newton-John TR, Spence SH, Schotte D.Cognitive-behavioural therapy versusEMG biofeedback in the treatment ofchronic low back pain. Behav Res Ther.1995;33:691–697.
42 Pfingsten M, Leibing E, Harter W, et al.Fear-avoidance behavior and anticipationof pain in patients with chronic low backpain: a randomized controlled study.Pain Med. 2001;2:259–266.
43 Rasmussen-Barr E, Ang B, Arvidsson I,et al. Graded exercise for recurrent low-back pain: a randomized, controlled trialwith 6-, 12-, and 36-month follow-ups.Spine. 2009;34:221–228.
44 Schweikert B, Jacobi E, Seitz R, et al. Ef-fectiveness and cost-effectiveness of add-ing a cognitive behavioral treatment tothe rehabilitation of chronic low backpain. J Rheumatol. 2006;33:2519–2526.
45 Storheim K, Brox JI, Holm I, et al. Inten-sive group training versus cognitive inter-vention in sub-acute low back pain:short-term results of a single-blind ran-domized controlled trial. J Rehabil Med.2003;35:132–140.
46 Strong J. Incorporating cognitive-behavioral therapy with occupational ther-apy: a comparative study with patientswith low back pain. J Occup Rehabil.1998;8:61–71.
47 Turner JA, Jensen MP. Efficacy of cogni-tive therapy for chronic low back pain.Pain. 1993;52:169–177.
48 Jellema P, van der Windt DA, van derHorst HE, et al. Should treatment of (sub)acute low back pain be aimed at psycho-social prognostic factors? Cluster ran-domised clinical trial in general practice.BMJ. 2005;331:84.
49 Heinrich RL, Cohen MJ, Naliboff BD,et al. Comparing physical and behaviortherapy for chronic low back pain onphysical abilities, psychological distress,and patients’ perceptions. J Behav Med.1985;8:61–78.
50 Haldorsen EMH, Kronholm K, Skouen JS,et al. Predictors for outcome of a multi-modal cognitive behavioural treatmentprogram for low back pain patients: a12-month follow-up study. Eur J Pain.1998;2:293–307.
51 Bendix AF, Bendix T, Vaegter K, et al. Multi-disciplinary intensive treatment forchronic low back pain: a randomized, pro-spective study. Cleve Clin J Med. 1996;63:62–69.
52 Basler HD, Jakle C, Kroner-Herwig B. In-corporation of cognitive-behavioral treat-ment into the medical care of chroniclow back patients: a controlled random-ized study in German pain treatment cen-ters. Patient Educ Couns. 1997;31:113–124.
53 Basler H-D, Rehfisch HP. Follow-up re-sults of a cognitive-behavioural treatmentfor chronic pain in a primary care setting.Psychol Health. 1990;4:293–304.
54 Turner JA, Clancy S. Comparison of op-erant behavioral and cognitive-behavioralgroup treatment for chronic low backpain. J Consult Clin Psychol. 1988;56:261–266.
55 Cohen MJ, Heinrich RL, Naliboff BD,et al. Group outpatient physical and be-havioral therapy for chronic low backpain. J Clin Psychol. 1983;39:326–333.
56 Keller S, Ehrhardt-Schmelzer S, Herda C,et al. Multidisciplinary rehabilitation forchronic back pain in an outpatient set-ting: a controlled randomized trial. Eur JPain. 1997;1:279–292.
57 Klaber Moffet J, Torgerson D, Bell-Syer S,et al. Randomised controlled trial of ex-ercise for low back pain: clinical out-comes, costs and preferences. BMJ.1999;319:279–283.
58 Lindell O, Johansson SE, Strender LE.Subacute and chronic, non-specific backand neck pain: cognitive-behavioural re-habilitation versus primary care—a ran-domized controlled trial. BMC Musculo-skelet Disord. 2008;9:172.
59 Marhold C, Linton SJ, Melin L. Acognitive-behavioral return-to-work pro-gram: effects on pain patients with a his-tory of long-term versus short-term sickleave. Pain. 2001;91:155–163.
60 Linton SJ, Andersson T. Can chronic dis-ability be prevented? A randomized trialof a cognitive-behavior intervention andtwo forms of information for patientswith spinal pain. Spine. 2000;25:2825–2831.
61 Linton SJ, Nordin E. A 5-year follow-up eval-uation of the health and economic conse-quences of an early cognitive behavioralintervention for back pain: a randomized,controlled trial. Spine. 2006;31:853–858.
62 Lofvander MB. Cognitive-behavioural treat-ment of chronic pain in primary care: athree-year follow-up. Eur J Gen Pract.2002;8:151–158.
63 Bliokas VV, Cartmill TK, Nagy BJ. Does sys-tematic graded exposure in vivo enhanceoutcomes in multidisciplinary chronic painmanagement groups? Clin J Pain. 2007;23:361–374.
64 George SZ, Fritz JM, Bialosky JE, et al.The effect of a fear-avoidance-basedphysical therapy intervention for pa-tients with acute low back pain: resultsof a randomized clinical trial. Spine.2003;28:2551–2560.
65 George SZ, Zeppieri G Jr, Cere AL, et al.A randomized trial of behavioral physicaltherapy interventions for acute and sub-acute low back pain (NCT00373867).Pain. 2008;140:145–157.
66 Hay EM, Mullis R, Lewis M, et al. Com-parison of physical treatments versus abrief pain-management programme forback pain in primary care: a randomisedclinical trial in physiotherapy practice.Lancet. 2005;365:2024–2030.
67 Lambeek LC, Anema JR, van Royen BJ,et al. Multidisciplinary outpatient careprogram for patients with chronic lowback pain: design of a randomized con-trolled trial and cost-effectiveness study.BMC Public Health. 2007;7:254.
68 Boersma K, Linton S, Overmeer T, et al.Lowering fear-avoidance and enhancingfunction through exposure in vivo: amultiple baseline study across six pa-tients with back pain. Pain. 2004;108:8–16.
69 Kole-Snijders AM, Vlaeyen JW, GoossensME, et al. Chronic low-back pain: whatdoes cognitive coping skills training addto operant behavioral treatment? Resultsof a randomized clinical trial. J ConsultClin Psychol. 1999;67:931–944.
70 Linton SJ, Overmeer T, Janson M, et al.Graded in vivo exposure treatment forfear-avoidance pain patients with func-tional disability: a case study. Cogn Be-hav Ther. 2002;31:49–58.
71 Vlaeyen JWS, Haazen IWCJ, SchuermanJA, et al. Behavioural rehabilitation ofchronic low back pain: comparison of anoperant treatment, an operant-cognitivetreatment and an operant-respondenttreatment. Br J Clin Psychol. 1995;34:95–118.
72 Jensen IB, Nygren A, Lundin A.Cognitive-behavioural treatment forworkers with chronic spinal pain: amatched and controlled cohort study inSweden. Occup Environ Med. 1994;51:145–151.
73 Kernan T, Rainville J. Observed out-comes associated with a quota-based ex-ercise approach on measures of kinesio-phobia in patients with chronic low backpain. J Orthop Sports Phys Ther. 2007;37:679–687.
74 Klinger R, Nutzinger D, Geissner E, et al.Follow-up results of an in patient behav-ioral pain treatment program. Zeitschriftfur Klinische Psychologie. 1999;28:267–272.
75 Laborde JM. Cognitive-behavioral tech-niques in the treatment of chronic lowback pain: preliminary results. J SouthOrthop Assoc. 1998;7:81–85.
76 Nielson WR, Weir R. Biopsychosocial ap-proaches to the treatment of chronicpain. Clin J Pain. 2001;17:S114–S127.
77 Rose MJ, Reilly JP, Pennie B, et al.Chronic low back pain rehabilitation pro-grams: a study of the optimum durationof treatment and a comparison of groupand individual therapy. Spine. 1997;22:2246–2253.
78 Van den Hout JHC, Vlaeyen JWS, Kole-Snijders AMJ, et al. Graded activity andproblem solving therapy in sub-acutenon-specific low back pain. Physiother-apy. 1998;84:167.
79 Woby SR, Watson PJ, Roach NK, Ur-mston M. Are changes in fear-avoidancebeliefs, catastrophizing, and appraisals ofcontrol, predictive of changes in chroniclow back pain and disability? Eur J Pain.2004;8:201–210.
80 Vlaeyen JWS, de Jong JR, Onghena P,et al. Can pain related fear be reduced?The application of cognitive-behaviouralexposure in vivo. Pain Res Manag. 2002;7:144–153.
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 875 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

81 Goossens ME, Rutten-van Molken MP,Kole-Snijders AM, et al. Health economicassessment of behavioural rehabilitationin chronic low back pain: a randomisedclinical trial. Health Econ. 1998;7:39–51.
82 George SZ, Fritz JM, Childs JD. Investiga-tion of elevated fear-avoidance beliefs forpatients with low back pain: a secondaryanalysis involving patients enrolled inphysical therapy clinical trials. J OrthopSports Phys Ther. 2008;38:50–58.
83 Goossens MEJB, Vlaeyen JWS, Hidding A,et al. Treatment expectancy affects theoutcome of cognitive-behavioral inter-ventions in chronic pain. Clin J Pain.2005;21:18–26.
84 Smeets RJ, Severens JL, Beelen S, et al.More is not always better: cost-effectiveness analysis of combined, singlebehavioral and single physical rehabilita-tion programs for chronic low back pain.Eur J Pain. 2009;13:71–81.
85 Smeets RJ, Vlaeyen JW, Kester AD, Knott-nerus JA. Reduction of pain catastrophiz-ing mediates the outcome of both phys-ical and cognitive-behavioral treatmentin chronic low back pain. J Pain. 2006;7:261–271.
86 Steenstra IA, Anema JR, Bongers PM,et al. A workplace intervention, gradedactivity, or both to prevent long-termsick leave for subacute back pain? A ran-domized controlled study. NederlandsTijdschrift Voor Fysiotherapie. 2007;117:207–215.
87 Hlobil H, Uegaki K, Staal JB, et al. Sub-stantial sick-leave costs savings due to agraded activity intervention for workerswith non-specific sub-acute low backpain. Eur Spine J. 2007;16:919–924.
88 Staal JB, Hlobil H, Koke AJA, et al. Gradedactivity for workers with low back pain:who benefits most and how does itwork? Arthritis Rheum. 2008;59:642–649.
89 Van den Hout JHC, Vlaeyen JWS, HeutsPHTG, et al. Secondary prevention ofwork-related disability in nonspecific lowback pain: does problem-solving therapyhelp? A randomized clinical trial. Clin JPain. 2003;19:87–96.
90 Leeuw M, Goossens MEJB, van BreukelenGJP, et al. Exposure in vivo versus oper-ant graded activity in chronic low backpain patients: results of a randomizedcontrolled trial. Pain. 2008;138:192–207.
91 de Jong JR, Vlaeyen JWS, Onghena P,et al. Fear of movement/(re)injury inchronic low back pain: education or ex-posure in vivo as mediator to fear reduc-tion? Clin J Pain. 2005;21:9–17; discus-sion 69–72.
92 Lindstrom I, Ohlund C, Eek C, et al. Mobil-ity, strength, and fitness after a graded ac-tivity program for patients with subacutelow back pain: a randomized prospectiveclinical study with a behavioural therapyapproach. Spine. 1992;17:641–652.
93 Lindstrom I, Ohlund C, Eek C, et al. Theeffect of graded activity on patients withsubacute low back pain: a randomizedprospective clinical study with anoperant-conditioning behavioral ap-proach. Phys Ther. 1992;72:279–293.
94 Linton SJ, Boersma K, Jansson M, et al. Arandomized controlled trial of exposurein vivo for patients with spinal pain re-porting fear of work-related activities.Eur J Pain. 2008;12:722–730.
95 Steenstra IA, Anema JR, Bongers PM,et al. The effectiveness of graded activityfor low back pain in occupational health-care. Occup Environ Med. 2006;63:718–725.
96 Anema JR, Steenstra IA, Bongers PM,et al. Multidisciplinary rehabilitation forsubacute low back pain: graded activity orworkplace intervention or both? A ran-domized controlled trial. Spine. 2007;32:291–298.
97 Vlaeyen JWS, de Jong J, Geilen M, et al.The treatment of fear of movement/(re)injury in chronic low back pain: fur-ther evidence on the effectiveness of ex-posure in vivo. Clin J Pain. 2002;18:251–261.
98 Hlobil H, Staal JB, Twisk J, et al. The ef-fects of a graded activity intervention forlow back pain in occupational health onsick leave, functional status and pain: 12-month results of a randomized controlledtrial. J Occup Rehabil. 2005;15:569–580.
99 Koes BW, van Tulder MW, Ostelo R, et al.Clinical guidelines for the managementof low back pain in primary care: an in-ternational comparison. Spine. 2001;26:2504–2513.
100 van der Windt D, Hay E, Jellema P, et al.Psychosocial interventions for low backpain in primary care: lessons learnedfrom recent trials. Spine. 2008;33:81–89.
Graded Activity and Graded Exposure for Low Back Pain
876 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Appendix.Search Strategies
MEDLINE1. randomized controlled trial/2. controlled clinical trial/3. randomized controlled trials.mp.4. random allocation/5. random allocation.mp.6. double-blind method/7. single-blind method/8. exp clinical trial/9. (clinic$ adj25 trial$).tw.10. ((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.11. placebos/12. placebo$.tw.13. random$.tw.14. research design/15. (latin adj square).tw.16. comparative study/17. exp evaluation studies/18. follow-up studies/19. (control$ or prospective$ or volunteer$).tw.20. cross-over studies/21. or/1–2022. animal/not human/23. 21 not 2224. low back pain/25. low back pain.mp.26. backache.mp.27. lumbago.mp.28. sciatica/29. sciatica.mp.30. back pain/31. or/24–3032. 23 and 3133. graded activity.mp.34. graded exposure.mp.35. behavioral therapy.mp.36. behavior therapy/37. cognitive therapy/38. psychology/39. cognitive.mp.40. gradual exercises.mp.41. function.mp.42. physical therapy modalities/43. or/33–4244. 32 and 43
PsychINFO1. randomized controlled trial$.mp2. random allocation.mp.3. exp clinical trials/4. (clinic$ adj25 trial$).tw.5. ((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.
(Continued)
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 877 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

Appendix.Continued
6. placebo$.tw.7. random$.tw.8. research design/9. (latin adj square).tw.10. (control$ or prospective$ or volunteer$).tw.11. or/1–1012. low back pain.mp13. backache.mp14. lumbago.mp15. sciatica.mp16. back pain/17. or/12–1618. graded activity.mp19. graded exposure.mp20. behavioral therapy.mp21. behavior therapy/22. cognitive therapy/23. cognitive.mp.24. psychology/25. function.mp26. or/18–2527. 11 and 17 and 26
EMBASE1. randomized controlled trial/2. exp controlled clinical trial/3. randomized controlled trial$.mp4. exp randomization/5. random allocation.mp.6. double-blind procedure/7. single-blind procedure/8. clinical trial/9. (clinic$ adj25 trial$).tw.10. ((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.11. exp placebo/12. placebo$.mp.13. random$.mp14. research design.mp15. exp comparative study/16. exp evaluation/17. exp follow-up/18. (control$ or prospective$ or volunteer$).tw.19. crossover procedure/20. or/1–1921. animal/not human/22. 20 not 2123. exp low back pain/24. low back pain.mp25. exp backache/26. lumbago.mp27. sciatica.mp28. or/23–27
(Continued)
Graded Activity and Graded Exposure for Low Back Pain
878 f Physical Therapy Volume 90 Number 6 June 2010 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from
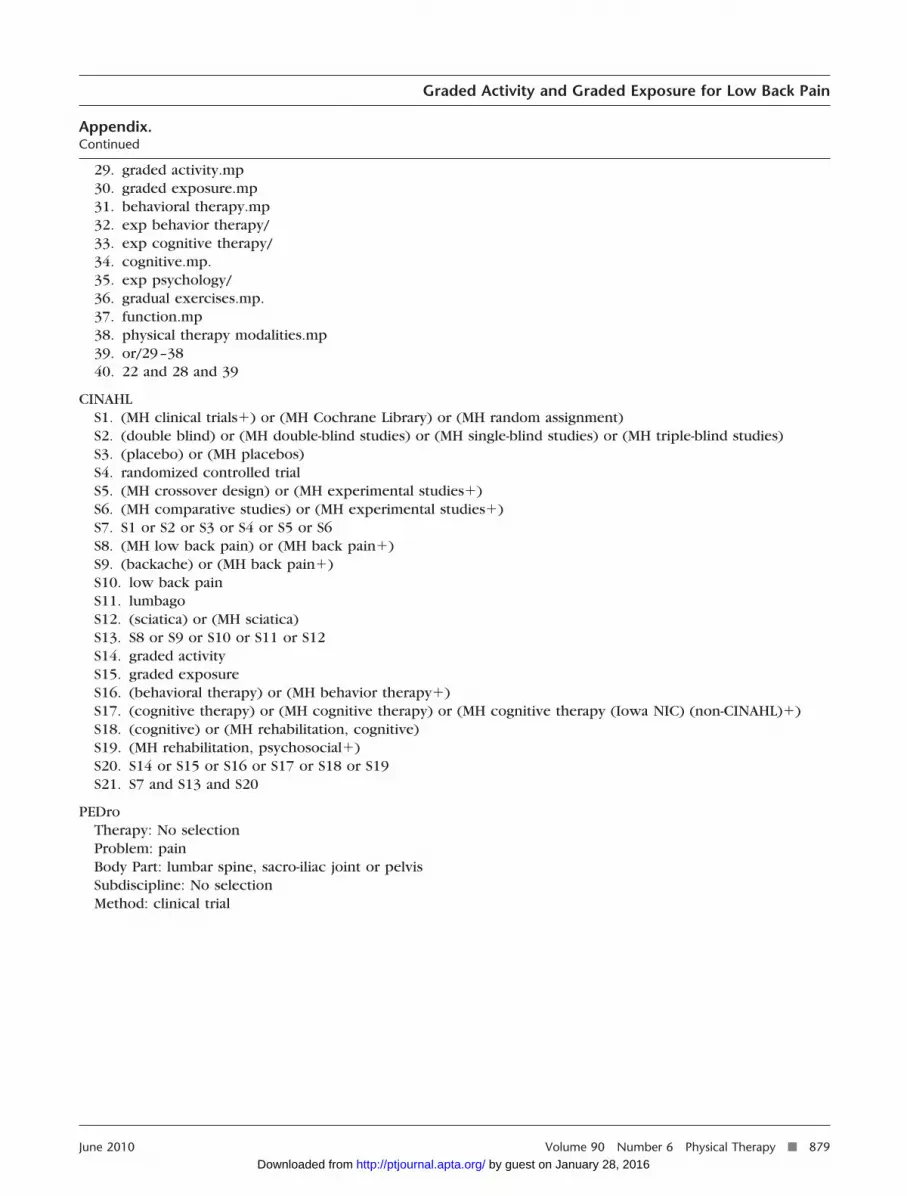
Appendix.Continued
29. graded activity.mp30. graded exposure.mp31. behavioral therapy.mp32. exp behavior therapy/33. exp cognitive therapy/34. cognitive.mp.35. exp psychology/36. gradual exercises.mp.37. function.mp38. physical therapy modalities.mp39. or/29–3840. 22 and 28 and 39
CINAHLS1. (MH clinical trials�) or (MH Cochrane Library) or (MH random assignment)S2. (double blind) or (MH double-blind studies) or (MH single-blind studies) or (MH triple-blind studies)S3. (placebo) or (MH placebos)S4. randomized controlled trialS5. (MH crossover design) or (MH experimental studies�)S6. (MH comparative studies) or (MH experimental studies�)S7. S1 or S2 or S3 or S4 or S5 or S6S8. (MH low back pain) or (MH back pain�)S9. (backache) or (MH back pain�)S10. low back painS11. lumbagoS12. (sciatica) or (MH sciatica)S13. S8 or S9 or S10 or S11 or S12S14. graded activityS15. graded exposureS16. (behavioral therapy) or (MH behavior therapy�)S17. (cognitive therapy) or (MH cognitive therapy) or (MH cognitive therapy (Iowa NIC) (non-CINAHL)�)S18. (cognitive) or (MH rehabilitation, cognitive)S19. (MH rehabilitation, psychosocial�)S20. S14 or S15 or S16 or S17 or S18 or S19S21. S7 and S13 and S20
PEDroTherapy: No selectionProblem: painBody Part: lumbar spine, sacro-iliac joint or pelvisSubdiscipline: No selectionMethod: clinical trial
Graded Activity and Graded Exposure for Low Back Pain
June 2010 Volume 90 Number 6 Physical Therapy f 879 by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from

doi: 10.2522/ptj.20090303Originally published online April 15, 2010
2010; 90:860-879.PHYS THER. Maher, Jane Latimer and James H. McAuleyLuciana G. Macedo, Rob J.E.M. Smeets, Christopher G.Nonspecific Low Back Pain: A Systematic ReviewGraded Activity and Graded Exposure for Persistent
References
http://ptjournal.apta.org/content/90/6/860#BIBLfor free at: This article cites 91 articles, 10 of which you can access
Cited by
http://ptjournal.apta.org/content/90/6/860#otherarticles
This article has been cited by 7 HighWire-hosted articles:
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on January 28, 2016http://ptjournal.apta.org/Downloaded from





























