Embed Size (px)
Citation preview

Dental.EliteCME.com Page i
What are the requirements for license renewal?Licenses Expire CE Hours Required Mandatory Courses
Every two years on the last day of your birth month.
50(No more than 25 hours can be completed
through home-study. Eight units shall be the maximum continuing education credits granted
in one day.)
2 hours of California Infection Control
2 hours of California Dental Practice Act
How do I complete this course and receive my certificate of completion? On-Line Submission: Go to Dental.EliteCME.com and follow the prompts. You will be able to print your certificate immediately upon completion of the course.
Fax Submission: Fax to (386) 673-3563, be sure to include your credit card information. All completions will be processed within 2 business days of receipt and certificates e-mailed to the e-mail address provided.*
Mail Submission: Use the envelope provided or mail to Elite, PO Box 37, Ormond Beach, FL 32175. All completions will be processed and certificates issued within 10 business days from the date it is mailed.*
*Please note - providing a valid e-mail address is the quickest and most efficient way to receive your certificates when submitting via fax, e-mail or mail.
Submissions without a valid e-mail address will be mailed to the address provided at registration.
How much will it cost?Cost of Courses
Course Title CE Hours PriceCalifornia Dental Practice Act - Mandatory 2 $12.00Guidelines for Infection Control in Dental Health Care Settings - Mandatory 4 $24.00Health Information Technology: The Future is Now 7 $42.00Medical Emergencies in the Dental Office 4 $24.00Peri-Implantitis: Basics and Beyond 2 $12.00Professional Care and Patient Maintenance of Implant-Supported Dentures 2 $12.00Updates on Laser Therapy in Dentistry and Integration in the Dental Office 4 $24.00
25-HOUR COURSE BOOK PACKAGE SAVE $51.00 Save money and purchase all 25 hours. Complete up to 8 maximum hours per day until all your hours allowed through home-study are completed.
25 $99.00
Are you a California board-approved provider?Elite is a continuing education registered provider, Provider No. RP4737.
Are my credit hours reported to the California board?No, the Dental Board of California requires licensees to certify at the time of renewal that he/she has complied with the continuing education requirement. The board performs audits at which time proof of continuing education must be provided.
Is my information secure?Yes! Our website is secured by Thawte, we use SSL encryption, and we never share your information with third-parties.
What if I still have questions? What are your business hours?No problem, we have several options for you to choose from! Online at Dental.EliteCME.com you will see our robust FAQ section that answers many of your questions, simply click FAQ in the upper right hand corner, Email us at [email protected] or call us toll free at 1-866-344-0972, Monday - Friday 9:00 am - 6:00 pm, EST.
Important information for licenseesAlways check your state’s board website to determine the number of hours required for renewal, and the amount that may be completed through home-study. Also, make sure that you notify the board of any changes of address. It is important that your most current address is on file.
Dental Board of California Contact Information
Dental Board of California2005 Evergreen Street, Suite 1550Sacramento, CA 95815Phone: (877) 729-7789 | Fax: (916) 263-2140Website: http://www.dbc.ca.gov/
Frequently Asked Questions

Page ii Dental.EliteCME.com
Table of ContentsCE for California Dental Professionals
CHAPTER 1: CALIFORNIA DENTAL PRACTICE ACT - MandatoryBoard-Approved Course No. 02-4737-17100 Page 1
The California Dental Practice Act is the section of the Business and Professions Code (1600-1976) that contains the laws that regulate the dental profession. California law requires that every dental professional has a thorough understanding of these laws, along with Title 16, California Code of Regulations, Division 10, Dental Board of California (Chapter 1, General Provisions Applicable to All Licensees) and other related California statutes. This is why it is a mandatory requirement for all dental health care professionals to have a minimum of two continuing education hours on the Dental Practice Act each biennium.
California Dental Practice Act Final Exam Page 24
CHAPTER 2: GUIDELINES FOR INFECTION CONTROL IN DENTAL HEALTH CARE SETTINGS - Mandatory Board-Approved Course No. 04-4737-17200 (Course meets Dental Board of California’s requirements for 2 units of CE, remaining hours go to Category 1) Page 25
The purpose of this course is to provide dental health care professionals (who are at risk everyday) with a solid understanding of infection control practices. By taking sterilization precautions, developing a written plan for the key elements of an infection control process, maintaining the necessary records, evaluating the plan on a routine basis and making changes to keep the processes up-to-date, the goal of minimizing the risk of disease transmission in the dental office can be met.
Guidelines for Infection Control in Dental Health Care Settings Final Exam Page 47
CHAPTER 3: HEALTH INFORMATION TECHNOLOGY: THE FUTURE IS NOW - Course No. 07-4737-17300 Page 48
Health information is generated with each and every patient encounter and the management of this information has changed enormously in the past century. What was previously documented in paper charts or microfiche and stored away in a locked room can now be recorded and stored solely on computers. Constant changes in technology require healthcare professionals to remain diligent in managing this protected information appropriately.
Health Information Technology: The Future is Now Final Exam Page 70
©2018: All Rights Reserved. Materials may not be reproduced without the expressed written permission or consent of Elite Professional Education, LLC. The materials presented in this course are meant to provide the consumer with general information on the topics covered. The information provided was prepared by professionals with practical knowledge in the areas covered. It is not meant to provide medical, legal or professional advice. Elite Professional Education, LLC recommends that you consult a medical, legal or professional services expert licensed in your state. Elite Professional Education, LLC has made all reasonable efforts to ensure that all content provided in this course is accurate and up to date at the time of printing, but does not represent or warrant that it will apply to your situation or circumstances and assumes no liability from reliance on these materials.
What if I Still Have Questions?No problem, we have several options for you to choose from! Online at Dental.EliteCME.com you will see our robust FAQ section that answers many of your questions. Simply click FAQ in the upper right hand corner or Email us at [email protected] or call us toll free at 1-866-344-0972, Monday - Friday 9:00 am - 6:00 pm, EST.
Visit Dental.EliteCME.com to view our entire course library and get your CE today!
PLUS...Lowest Price Guaranteed
Serving Professionals Since 1999
$6 per credit hour
EliteContinuing Education

Dental.EliteCME.com Page iii
Table of ContentsCE for California Dental Professionals
CHAPTER 4: MEDICAL EMERGENCIES IN THE DENTAL OFFICECourse No. 04-4737-17301 Page 71
In this course, we will discuss common emergencies that one might encounter when interacting with dental patients, as well as steps that should be taken to ensure that all of the bases are covered, including responsibilities, safety measures, and accident prevention.
Medical Emergencies in the Dental Office Final Exam Page 84
CHAPTER 5: PERI-IMPLANTITIS: BASICS AND BEYOND Course No. 02-4737-17302 Page 85
Dental implants have seen a big boom in the field of dentistry and have emerged as a new vista in the arena of full mouth rehabilitations. This course will explore the histology of peri-implant tissue in detail, classification, risk factors, microbiology, etiopathogenesis, and management of peri-implantitis.
Peri-Implantitis: Basics and Beyond Final Exam Page 92
CHAPTER 6: PROFESSIONAL CARE AND PATIENT MAINTENANCE OF IMPLANT- SUPPORTED DENTURES - Course No. 02-4737-17303 Page 93
Because of the types of implant-supported dentures used in patient care, dental professionals and patients should understand the methods, techniques, and oral hygiene aids that are most appropriate for maintaining the various types of prostheses.
Professional Care and Patient Maintenance of Implant-Supported Dentures Final Exam Page 99
CHAPTER 7: UPDATES ON LASER THERAPY IN DENTISTRY AND INTEGRATION IN THE DENTAL OFFICE - Course No. 04-4737-17304 Page 100
This course will review the latest developments in dental laser application and will provide evidence for its multitude of benefits in general dentistry. It will discuss the practical application and integration of lasers in dental offices. The science behind lasers, and the types of lasers available in the market and their specific dental applications, will also be reviewed.
Updates on Laser Therapy in Dentistry and Integration in the Dental Office Final Exam Page 114
Student Final Examination Answer Sheet Page 116
Course Evaluation Page 117
Page 1 Dental.EliteCME.com
Chapter 1: California Dental Practice Act
2 CE Hours - Mandatory
By: Elite Staff
Learning objectives � Summarize the California Dental Practice Act. � Define dentistry as determined by Dental Code 1625. � List the duties of dental assistants. � List the duties of dental hygienists according to the Dental
Hygiene Committee, sections 1900-1976. � Describe the utilization and scope of practice for auxiliaries and
dentists.
� List the acts in violation of the Dental Practice Code. � Learn the regulations regarding controlled substances in the
Business and Professions Code 4076, 4170 and 4172. � Review the process and requirements of renewing a license. � Explain the mandatory reporter obligations set forth in the Child
Abuse and Neglect Reporting Act and the Elder Abuse and Dependent Civil Protection Act.
IntroductionThe California Dental Practice Act is the section of the Business and Professions Code (1600-1976) that contains the laws regulating the dental profession. California law requires that every dental professional have a thorough understanding of these laws, along with Title 16, California Code of Regulations, Division 10, Dental
Board of California (Chapter 1, General Provisions Applicable to All Licensees) and other related California statutes. This is why it is a mandatory requirement for all dental health care professionals to have a minimum of two continuing education hours on the Dental Practice Act each biennium.
The governing agencies and their roles (Summary 1601.1 – 1603a)The Department of Consumer Affairs, a department within the California Business, Consumer Services, and Housing Agency, regulates private business and professions that have an impact on public health, safety and welfare. They set the minimum qualifications and levels of competency for licensed persons to provide effective public services. The department issues licenses in more than 100 business and 200 professional categories. It also licenses, registers or certifies practitioners, investigates complaints and disciplines violators. This department conducts periodic checks of licensees, registrants or otherwise certified persons to make sure they are complying with the Business and Professions Code 101.6. This department, in conjunction with the board and the Joint Committee on Boards, Commissions and Consumer Protection, shall review the scope of practice for dental auxiliaries.
The Dental Board of California was formerly known as the Board of Dental Examiners of California. The Dental Board is the main authority of dentistry in the state of California. The California Dental Board includes eight practicing dentists, five public members, one registered dental hygienist and one registered dental assistant. Of the
eight practicing dentists, one must be a member of a faculty of any California dental college, and one must be a dentist practicing in a nonprofit community clinic.
The governor of California is responsible for appointing three of the public members of the board, the dental assistant member, the dental hygienist member, and the eight licensed dentist members of the board. The Senate Rules Committee and the speaker of the Assembly each appoint a public member. Their initial appointments occupies the first and second public member seats as vacancies occur. All of the members of the board, excluding the public members, must have been active professionals in California for at least five years preceding their date of appointment. The public members cannot be licensees under this division or of any board referred to in Sections 1000 and 3600, and no more than one member of the board can be a member of the faculty of a dental or medical college or have a financial interest in any such college in the state of California.
Any member of the Board of Dental Examiners who has served two full terms is not eligible for reappointment to the board.
Role of the board (Summary 1601.1 – 1621)Protection of the public shall be the highest priority for the Dental Board of California in exercising its licensing, regulatory and disciplinary functions.
The board shall carry out the purposes and enforce the provisions of this chapter. It shall examine all applicants for a license to practice dentistry according to the provisions of this chapter and shall issue licenses to practice dentistry in this state to applicants who successfully pass the examination of the board and otherwise comply with the provisions of this chapter. The board shall collect and apply all fees as directed by this chapter.
The board may inspect the books, records and premises of any dentist licensed under this chapter in response to a complaint that a licensee has violated any law or regulation that constitutes grounds for disciplinary action by the board, and may employ inspectors for this purpose. A licensee’s failure to allow an inspection or any part thereof shall be grounds for suspension or revocation of the license in accordance with Section 1670.
The board shall keep a record of the names of all persons to whom licenses have been granted by it to practice dentistry, and such other records as may be necessary to show plainly all of its acts and proceedings.

Dental.EliteCME.com Page 2
The board may adopt reasonably necessary rules not inconsistent with the provisions of this chapter concerning:
● The holding of meetings. ● The holding of examinations. ● The manner of issuance and reissuance of licenses.
● The establishment of standards for the approval of dental colleges. ● Prescribing subjects in which applicants are to be examined. ● The administration and enforcement of this chapter.
Such rules shall be adopted, amended or repealed in accordance with the provisions of the Administrative Procedure Act.
Define dentistryThe California Dental Code Section 1625 defines dentistry as follows:“Dentistry” is the diagnosis or treatment, by surgery or other method, of diseases and lesions and the correction of malpositions of the human teeth, alveolar process, gums, jaws, or associated structures; and such diagnosis or treatment may include all necessary related procedures as well as the use of drugs, anesthetic agents, and physical evaluation. Without limiting the foregoing, a person practices dentistry within the meaning of this chapter who does any one or more of the following:a. By card, circular, pamphlet, newspaper or in any other way
advertises himself or represents himself to be a dentist. b. Performs, or offers to perform, an operation or diagnosis of any
kind, or treats diseases or lesions of the human teeth, alveolar
process, gums, jaws or associated structures, or corrects malposed positions thereof.
c. In any way indicates that he will perform by himself or his agents or servants any operation upon the human teeth, alveolar process, gums, jaws, or associated structures, or in any way indicates that he will construct, alter, repair, or sell any bridge, crown, denture or other prosthetic appliance or orthodontic appliance.
d. Makes, or offers to make, an examination of, with the intent to perform or cause to be performed any operation on the human teeth, alveolar process, gums, jaws, or associated structures.
e. Manages or conducts as manager, proprietor, conductor, lessor, or otherwise, a place where dental operations are performed.
Ownership/management of a dental practice 1625.1 – Any of the following entities may employ licensees and dental assistants and charge for the professional services they render, and shall not be deemed to be practicing dentistry within the meaning of Section 1625. The entity must not interfere with, control or otherwise direct the professional judgment of a licensee or dental assistant acting within his or her scope of practice:
● A primary care clinic that is licensed pursuant to subdivision (a) of Section 1204 of the Health and Safety Code.
● A primary care clinic that is exempt from licensure pursuant to subdivision (b), (c), or (h) of Section 1206 of the Health and Safety Code.
● A clinic owned or operated by a public hospital or health system. ● A clinic owned and operated by a hospital that maintains the
primary contract with a county government to fill the county’s role under Section 17000 of the Welfare and Institutions Code.
1625.2 – If the entity is owned or managed by a tax-exempt nonprofit organization and supported and maintained in whole or in substantial part by donations, bequests, gifts, grants, government funds, or contributions, that may be in the form of money, goods or services, of a place where dental operations are performed, shall not be construed to be the unlicensed practice of dentistry, as long as all of the following apply:
● The entity obtains the board’s approval to offer dental services pursuant to regulations adopted by the board.
● The entity does nothing to interfere with, control or otherwise direct the professional judgment of or provision of dental services by a licensee or dental assistant acting within his or her scope of practice as defined in this chapter.
● The licensees and dental assistants of the entity providing services are in compliance with all applicable provisions of this chapter.
● The entity is otherwise in compliance with this chapter and all other applicable provisions of state and federal law.
This section does not apply to any of the following entities: ● A primary care clinic that is licensed pursuant to subdivision (a) of
Section 1204 of the Health and Safety Code. ● A primary care clinic that is exempt from licensure pursuant to
subdivision (b), (c), or (h) of Section 1206 of the Health and Safety Code.
● A clinic owned or operated by a public hospital or health system. ● A clinic owned and operated by a hospital that maintains the
primary contract with a county government to fill the county’s role under Section 17000 of the Welfare and Institutions Code.
Death of an owner1625.3 – Notwithstanding any other provision of law, upon the incapacity or death of a dentist, if the requirements of Section 1625.4 are met, any of the following persons may employ licensees and dental assistants and charge for the professional services they render for a period not to exceed 12 months from the date of the dentist’s death or incapacity without being deemed to be practicing dentistry within the meaning of Section 1625:
● The legal guardian, conservator or authorized representative of an incapacitated dentist.
● The executor or administrator of the estate of a dentist who is deceased.
● The named trustee or successor trustee of a trust or subtrust that owns assets consisting only of the incapacitated or deceased dentist’s dental practice and that was established solely for the purpose of disposition of the dental practice upon the dentist’s incapacity or death.
● The management shall not interfere with, control or otherwise direct the professional judgment of a licensee or dental assistant acting within his or her scope of practice as defined in this chapter.
1625.4 – Where the dental practice of an incapacitated or deceased dentist is a sole proprietorship or where an incapacitated or deceased dentist is the sole shareholder of a professional dental corporation, a person identified in subdivision (a) of Section 1625.3 may enter into a contract with one or more dentists licensed in the state to continue the operations of the incapacitated or deceased dentist’s dental practice for a period of no more than 12 months from the date of death or incapacity, or until the practice is sold or otherwise disposed of, whichever occurs first, if all of the following conditions are met:
● The person identified in subdivision (a) of Section 1625.3 delivers to the board a notification of death or incapacity that includes all of the following information:
● The name and license number of the deceased or incapacitated dentist.
○ The name and address of the dental practice.

Page 3 Dental.EliteCME.com
○ If the dentist is deceased, the name, address, and tax identification number of the estate or trust.
○ The name and license number of each dentist who will operate the dental practice.
○ A statement that the information provided is true and correct, and that the person identified in subdivision (a) of Section 1625.3 understands that any interference by the person or by his or her assignee with the contracting dentist’s or dentists’ practice of dentistry or professional judgment is grounds for immediate termination of the operations of the dental practice without a hearing. The statement shall also provide that if the person required to make this notification willfully states as true any material fact that he or she knows to be false, he or she shall be subject to a civil penalty of up to ten thousand dollars ($10,000) in an action brought by any public prosecutor. A civil penalty imposed under this subparagraph shall be enforced as a civil judgment.
● The dentist or dentists who will operate the practice shall be licensed by the board and that license shall be current, valid, and shall not be suspended, restricted, or otherwise the subject of discipline.
● Within 30 days after the death or incapacity of a dentist, the person identified in subdivision (a) of Section 1625.3 or the contracting dentist or dentists shall send notification of the death or incapacity by mail to the last known address of each current patient of record with an explanation of how copies of the patient’s records may be obtained. This notice may also contain any other relevant information concerning the continuation of the dental practice. The failure to comply with the notification requirement within the 30-day period shall be grounds for terminating the operation of the dental practice under subdivision (b). The contracting dentist or dentists shall obtain a form signed by the patient, or the patient’s guardian or legal representative, that releases the patient’s confidential dental records to the contracting dentist or dentists prior to use of those records.
○ The board may order the termination of the operations of a dental practice operating pursuant to this section if the board determines that the practice is operating in violation of this section. The board shall provide written notification at the address provided pursuant to subparagraph (B) of paragraph (1) of subdivision (a). If the board does not receive a written appeal of the determination that the practice is operating in violation of this section within 10 days of receipt of the notice, the determination to terminate the operations of the dental practice shall take effect immediately. If an appeal is received in a timely manner by the board, the executive officer of the board, or his or her designee, shall conduct an informal hearing. The decision of the executive officer or his or her designee shall be mailed to the practice no later than 10 days after the informal hearing, is the final decision in the matter, and is not subject to appeal under the Administrative Procedure Act (Chapter 5 (commencing with Section 11500) of Part 1 of Division 3 of Title 2 of the Government Code).
○ Notwithstanding subdivision (b), if the board finds evidence that the person identified in subdivision (a) of Section 1625.3, or his or her assignee, has interfered with the practice or
professional judgment of the contracting dentist or dentists or otherwise finds evidence that a violation of this section constitutes an immediate threat to the public health, safety, or welfare, the board may immediately order the termination of the operations of the dental practice without an informal hearing.
○ A notice of an order of immediate termination of the dental practice without an informal hearing, as referenced in subdivision (b), shall be served by certified mail on the person identified in subdivision (a) of Section 1625.3 at the address provided pursuant to subparagraph (B) or (C) of paragraph (1) of subdivision (a), as appropriate, and on the contracting dentist or dentists at the address of the dental practice provided pursuant to subparagraph (B) of paragraph (1) of subdivision (a).
○ A person receiving notice of an order of immediate termination pursuant to subdivision (d) may petition the board within 30 days of the date of service of the notice for an informal hearing before the executive officer or his or her designee, which shall take place within 30 days of the filing of the petition.
○ A notice of the decision of the executive officer or his or her designee following an informal hearing held pursuant to subdivision (b) shall be served by certified mail on the person identified in subdivision (a) of Section 1625.3 at the address provided pursuant to subparagraph (B) or (C) of paragraph (1) of subdivision (a), as appropriate, and on the contracting dentist or dentists at the address of the dental practice provided pursuant to subparagraph (B) of paragraph (1) of subdivision (a).
○ The board may require the submission to the board of any additional information necessary for the administration of this section.
1625.5 – The following written notification shall be included with or as part of all application forms required for a license to practice or to renew a license:
“Effective January 1, 2008, certain nondentists may, upon your death or incapacity, contract with another licensed dentist or dentists to continue your dental practice for a period not exceeding 12 months if certain conditions are met. Sections 1625.3 and 1625.4 of the Business and Professions Code permit the legal guardian or conservator or authorized representative of an incapacitated dentist, the executor or administrator of the estate of a deceased dentist, or the named trustee or successor trustee of a trust or subtrust who meets certain requirements, to contract with a licensed dentist or dentists to continue the incapacitated or deceased dentist’s dental practice for a period not to exceed 12 months from the date of death or incapacity if the practice meets specified criteria and if certain other conditions are met, including providing a specific notification to the Dental Board of California. You and your estate planner should become familiar with these requirements and the notification process. Please contact the Dental Board of California for additional information.”
1626.2. – A dentist licensed under this chapter is a licentiate for purposes of paragraph (2) of subdivision (a) of Section 805, and thus is a health care practitioner subject to the provisions of Section 2290.5 pursuant to subdivision (b) of that section.
Acupuncture1626.5. – A licensed dentist, or group of dentists, or dental corporation shall not share in any fee charged by a person for performing acupuncture or receive anything of value from or on behalf of such acupuncturist for any referral or diagnosis.
A licensed dentist shall not employ more than one person to perform acupuncture services, and a group of dentists or a dental corporation shall not employ more than one person to perform acupuncture services for every 20 dentists in such a group or corporation.

Dental.EliteCME.com Page 4
Expiration of license1627. – The license of any dentist, existing at the time of the passage of this chapter, shall continue in force until it expires or is forfeited in the manner provided by this chapter.
Liability during emergencies1627.5. – No person licensed under this chapter, who in good faith renders emergency care at the scene of an emergency occurring outside the place of that person’s practice, or who, upon the request of another person so licensed, renders emergency care to a person for a complication arising from prior care of another person so licensed, shall be liable for any civil damages as a result of any acts or omissions by that person in rendering the emergency care.
A person licensed under this chapter, who voluntarily and without compensation or expectation of compensation, and consistent with the dental education and emergency training that he or she has received, provides emergency medical care to a person during a state of emergency declared pursuant to a proclamation issued pursuant to Section 8588, 8625, or 8630 of the Government Code or a declaration of health emergency issued pursuant to Section 101080 of the Health and Safety Code shall not be liable in negligence for any personal injury, wrongful death, or property damage caused by the licensee’s good faith but negligent act or omission. This subdivision shall not provide immunity or limit the immunity provided for acts or omissions of gross negligence or willful misconduct.
Notwithstanding any other provision of law, for the duration of a declared state of emergency, pursuant to a proclamation of emergency issued pursuant to Section 8625 of the Government Code, the board may suspend compliance with any provision of this chapter or regulation adopted thereunder that would adversely affect a licensee’s ability to provide emergency services.
Definitions Section 1627.7 “Dentist” means a person licensed as a dentist pursuant to this chapter.
“Emergency situation occurring in a hospital” means a situation occurring in a hospital, whether or not it occurs in an emergency room, requiring immediate services for alleviation of severe pain or immediate diagnosis and treatment of unforeseeable dental conditions, which, if not immediately diagnosed and treated, would lead to serious disability or death.
“Hospital” means a licensed general acute care hospital as defined in subdivision (a) of Section 1250 of the Health and Safety Code.
“Emergency situation occurring in the dentist’s office” means a situation occurring in an office, other than a hospital, used by the dentist for the examination or treatment of patients, requiring immediate services for alleviation of severe pain, or immediate diagnosis and treatment of unforeseeable dental conditions, which, if not immediately diagnosed and treated, would lead to serious disability or death.
1627.7. – A dentist shall not be liable for damages for injury or death caused in an emergency situation occurring in the dentist’s office or in a hospital on account of a failure to inform a patient of the possible consequences of a dental procedure where the failure to inform is caused by any of the following:
● The patient was unconscious. ● The dental procedure was undertaken without the consent of
the patient because the dentist reasonably believed that a dental procedure should be undertaken immediately and that there was insufficient time to fully inform the patient.
● A dental procedure was performed on a person legally incapable of giving consent, and the dentist reasonably believed that a dental procedure should be undertaken immediately and that there was insufficient time to obtain the informed consent of a person authorized to give such consent for the patient.
This section is applicable only to actions for damages for injuries or death arising because of a dentist’s failure to inform, and not to actions for such damages arising because of a dentist’s negligence in rendering or failing to render treatment.
Utilization and scope of practice for auxiliaries and dentistsThe Dental Board of California encourages the full utilization of dental auxiliaries in order to meet the needs of the state’s citizens. The Legislature further intends that the dental auxiliaries constitute a career ladder as stated in B&P 1740. The role of the dental auxiliary is very important in a dental office, and the legislature has taken action to provide for several different specialties of dental auxiliaries. The law allows the advancement of persons to higher levels of licensure with additional training. The Dental Board of California in its Committee on Dental Auxiliaries governs these classes.
The specialties are: ● Registered dental assistant (RDA). ● Registered dental assistant extended functions (RDAEF). ● Registered dental hygienist (RDH). ● Registered dental hygienist extended functions (RDHEF). ● Registered dental hygienist alternative practice (RDHAP).
Two specialties were added January 1, 2010, for which existing RDAs may apply:
● Orthodontic assistant (OA). ● Dental sedation assistant (DSA).
RDAs will be allowed to continue to perform the overlapping OA duties that they are currently allowed to perform without seeking an OA permit (placing ligature ties and archwires, removing orthodontic bands, and removing excess cement from tooth surfaces with a hand instrument), and RDAs applying for an OA permit will not be required to complete further training in such duties.
An RDA may apply for an OA permit or a DSA permit or both, by completing the applicable board-approved course and passing a written examination.

Page 5 Dental.EliteCME.com
Utilization of auxiliaries: Business and Professions Code 17401740. – Legislative intent. It is the intention of the Legislature by enactment of this article to permit the full utilization of dental auxiliaries in order to meet the dental care needs of all the state’s citizens. The Legislature further intends that the classifications of dental auxiliaries established pursuant to this article constitute a career ladder, permitting the continual advancement of persons to successively higher levels of licensure with additional training, and without repeating training for skills already acquired. The Legislature further intends that the Board of Dental Examiners of the State of California and its Committee on Dental Auxiliaries, in implementing this article, give specific consideration to the recommendations of the Advisory Committee on Utilization and Education of Dental Auxiliaries, established pursuant to Chapter 645 of the Statutes of 1972, and contained in its report to the Legislature dated March 20, 1973.
California Title 16, Section 1068. Posting of Dental Auxiliary Duties.
All dentists utilizing the services of dental auxiliaries shall post a notice in a common area of the office which delineates duties and functions deemed by the board as delegable within stipulated settings and/or circumstances.
Such notice shall be readily accessible to all individuals under supervision of the dentist.
1742. – There is hereby created a Dental Assisting Council of the Dental Board of California, which shall consider all matters relating to dental assistants in this state, on its own initiative or upon the request of the board, and make appropriate recommendations to the board and the standing committees of the board, including, but not limited to, the following areas:
● Requirements for dental assistant examination, licensure, permitting, and renewal.
● Standards and criteria for approval of dental assisting educational programs, courses, and continuing education.
● Allowable dental assistant duties, settings, and supervision levels.
● Appropriate standards of conduct and enforcement for dental assistants.
● Requirements regarding infection control.
The members of the council shall be appointed by the board and shall include the registered dental assistant member of the board, another member of the board, and five registered dental assistants, representing as broad a range of dental assisting experience and education as possible, who meet the requirements of paragraph (2).
The board shall consider, in its appointments of the five registered dental assistant members, recommendations submitted by any incorporated, nonprofit professional society, association, or entity whose membership is comprised of registered dental assistants within the state. Two of those members shall be employed as faculty members of a registered dental assisting educational program approved by the board, and shall have been so employed for at least the prior five years. Three of those members, which shall include one registered dental assistant in extended functions, shall be employed clinically in private dental practice or public safety net or dental health care clinics. All five of those members shall have possessed a current and active registered dental assistant or registered dental assistant in extended functions license for at least the prior five years, and shall not be employed by a current member of the board.
No council appointee shall have served previously on the dental assisting forum or have any financial interest in any registered dental assistant school. All final candidate qualifications and applications for board-appointed council members shall be made available in the published board materials with final candidate selection conducted during the normal business of the board during public meetings.
A vacancy occurring during a term shall be filled by appointment by the board for the unexpired term, according to the criteria applicable to the vacancy within 90 days after it occurs.
Each member shall comply with conflict of interest requirements that apply to board members.
The council shall meet in conjunction with other board committees, and at other times as deemed necessary.
Each member shall serve for a term of four years, except that, of the initial appointments of the nonboard members, one of the members shall serve a term of one year, one member shall serve a term of two years, two members shall serve a term of three years, and one member shall serve a term of four years, as determined by the board.
Recommendations by the council pursuant to this section shall be approved, modified, or rejected by the board within 120 days of submission of the recommendation to the board. If the board rejects or significantly modifies the intent or scope of the recommendation, the council may request that the board provide its reasons in writing for rejecting or significantly modifying the recommendation, which shall be provided by the board within 30 days of the request.
The council shall select a chair who shall establish the agendas of the council and shall serve as the council’s liaison to the board, including the reporting of the council’s recommendations to the board.
Board responsibilities 1743. – The board shall have the following duties and authority related to applications:
● Shall review and evaluate all applications for licensure in all dental assisting categories to ascertain whether a candidate meets the appropriate licensing requirements specified by statute and board regulations.
● Shall maintain application records, cashier application fees and perform any other ministerial tasks as are incidental to the application process.
● May delegate any or all of the functions in this subdivision to its staff.
● Shall issue dental assistant licenses in all cases, except where there is a question as to a licensing requirement.
○ The board shall develop or cause to be developed and administer examinations. The board shall set pass points for all dental assisting licensing examinations.
○ The board shall be responsible for all aspects of the license renewal process, which shall be accomplished in accordance with this chapter and board regulations. The board may delegate any or all of its functions under this subdivision to its staff.
1747. – The procedure on all matters relating to the denial, suspension, or revocation of licenses granted under this article shall be governed by the provisions of Chapter 5 (commencing with Section 11500) of Part 1 of Division 3 of Title 2 of the Government Code.
1749.1. – In addition to any other examination required by this article, the board may require applicants for licensure under this article to successfully complete an examination in California law and ethics.
1750.1 – A dental assistant may perform the following duties under the general supervision of a supervising licensed dentist:1. Extra-oral duties or procedures specified by the supervising
licensed dentist, provided that these duties or procedures meet

Dental.EliteCME.com Page 6
the definition of a basic supportive procedure specified in Section 1750.
2. Operate dental radiography equipment for the purpose of oral radiography if the dental assistant has complied with the requirements of Section 1656.
3. Perform intraoral and extraoral photography.
A dental assistant may perform the following duties under the direct supervision of a supervising licensed dentist:1. Apply nonaerosol and noncaustic topical agents.2. Apply topical fluoride.3. Take intraoral impressions for all nonprosthodontic appliances.4. Take facebow transfers and bite registrations.5. Place and remove rubber dams or other isolation devices.6. Place, wedge, and remove matrices for restorative procedures.7. Remove post-extraction dressings after inspection of the surgical
site by the supervising licensed dentist.8. Perform measurements for the purposes of orthodontic treatment.9. Cure restorative or orthodontic materials in operative site with a
light-curing device.10. Examine orthodontic appliances.11. Place and remove orthodontic separators.12. Remove ligature ties and archwires.13. After adjustment by the dentist, examine and seat removable
orthodontic appliances and deliver care instructions to the patient.
14. Remove periodontal dressings.15. Remove sutures after inspection of the site by the dentist.16. Place patient monitoring sensors.17. Monitor patient sedation, limited to reading and transmitting
information from the monitor display during the intraoperative phase of surgery for electrocardiogram waveform, carbon dioxide and end tidal carbon dioxide concentrations, respiratory cycle data, continuous noninvasive blood pressure data, or pulse arterial oxygen saturation measurements, for the purpose of interpretation and evaluation by a supervising licensed dentist who shall be at the patient’s chairside during this procedure.
18. Assist in the administration of nitrous oxide when used for analgesia or sedation. A dental assistant shall not start the administration of the gases and shall not adjust the flow of the gases unless instructed to do so by the supervising licensed dentist who shall be present at the patient’s chairside during the implementation of these instructions. This paragraph shall not be construed to prevent any person from taking appropriate action in the event of a medical emergency.
When operating in a school-based setting or a public health program created or administered by a federal, state, county or local governmental entity pursuant to Sections 104762 and 104830 of the Health Safety Code, a dental assistant may apply topical fluoride under the general direction of a licensed dentist or physician.
Under the supervision of a registered dental hygienist in alternative practice, a dental assistant may perform intraoral retraction and suctioning.
The board may specify additional allowable duties by regulation.
The duties of a dental assistant or a dental assistant holding a permit in orthodontic assisting or in dental sedation do not include any of the following procedures unless specifically allowed by law:1. Diagnosis and comprehensive treatment planning.2. Placing, finishing, or removing permanent restorations.3. Surgery or cutting on hard and soft tissue including, but not limited
to, the removal of teeth and the cutting and suturing of soft tissue.4. Prescribing medication.5. Starting or adjusting local or general anesthesia or oral or
parenteral conscious sedation, except for the administration of nitrous oxide and oxygen, whether administered alone or in combination with each other and except as otherwise provided by law.
The duties of a dental assistant are defined in subdivision (a) of Section 1750 and do not include any duty or procedure that only an orthodontic assistant permit holder, dental sedation assistant permit holder, registered dental assistant, registered dental assistant in extended functions, registered dental hygienist, or registered dental hygienist in alternative practice is allowed to perform.
Assistants 1750.2 – Orthodontic assistants a. On and after January 1, 2010, the board may issue an orthodontic
assistant permit to a person who files a completed application including a fee and provides evidence, satisfactory to the board, of all of the following eligibility requirements:1. Completion of at least 12 months of work experience as a
dental assistant.2. Successful completion of a board-approved course in the
Dental Practice Act and a board-approved course in infection control.
3. Successful completion of a course in basic life support offered by an instructor approved by the American Red Cross or the American Heart Association, or any other course approved by the board as equivalent.
4. Successful completion of a board-approved orthodontic assistant course, which may commence after the completion of six months of work experience as a dental assistant.
5. Passage of a written examination administered by the board after completion of all of the other requirements of this subdivision. The written examination shall encompass the knowledge, skills and abilities necessary to competently perform the duties specified in Section 1750.3.
b. A person who holds an orthodontic assistant permit pursuant to this section shall be subject to the same continuing education requirements for registered dental assistants as established by the board pursuant to Section 1645 and the renewal requirements of Article 6 (commencing with Section 1715).
1750.3 – A person holding an orthodontic assistant permit pursuant to Section 1750.2 may perform the following duties under the direct supervision of a licensed dentist:a. All duties that a dental assistant is allowed to perform.b. Prepare teeth for bonding, and select, preposition, and cure
orthodontic brackets after their position has been approved by the supervising licensed dentist.
c. Remove only orthodontic brackets and attachments with removal of the bonding material by the supervising licensed dentist.
d. Size, fit, and cement orthodontic bands.e. Remove orthodontic bands and remove excess cement from
supragingival surfaces of teeth with a hand instrument.f. Place and ligate archwires.g. Remove excess cement with an ultrasonic scaler from supragingival
surfaces of teeth undergoing orthodontic treatment.h. Any additional duties that the board may prescribe by regulation.
1750.4 – Dental sedation assistants a. On and after January 1, 2010, the board may issue a dental
sedation assistant permit to a person who files a completed application including a fee and provides evidence, satisfactory to the board, of all of the following eligibility requirements:1. Completion of at least 12 months of work experience as a
dental assistant.2. Successful completion of a board-approved course in the
Dental Practice Act and a board-approved, course in infection control.

Page 7 Dental.EliteCME.com
3. Successful completion of a course in basic life support offered by an instructor approved by the American Red Cross or the American Heart Association, or any other course approved by the board as equivalent.
4. Successful completion of a board-approved dental sedation assistant course, which may commence after the completion of six months of work experience as a dental assistant.
5. Passage of a written examination administered by the board after completion of all of the other requirements of this subdivision. The written examination shall encompass the knowledge, skills and abilities necessary to competently perform the duties specified in Section 1750.5.
b. A person who holds a permit pursuant to this section shall be subject to the continuing education requirements established by the board pursuant to Section 1645 and the renewal requirements of Article 6 (commencing with Section 1715).
1750.5 – A person holding a dental sedation assistant permit pursuant to Section 1750.4 may perform the following duties under the direct supervision of a licensed dentist or other licensed health care professional authorized to administer conscious sedation or general anesthesia in the dental office:a. All duties that a dental assistant is allowed to perform.b. Monitor patients undergoing conscious sedation or general
anesthesia utilizing data from noninvasive instrumentation such as pulse oximeters, electrocardiograms, capnography, blood pressure, pulse, and respiration rate monitoring devices. Evaluation of the condition of a sedated patient shall remain the responsibility of the dentist or other licensed health care professional authorized
to administer conscious sedation or general anesthesia, who shall be at the patient’s chairside while conscious sedation or general anesthesia is being administered.
c. Drug identification and draw, limited to identification of appropriate medications, ampule and vial preparation, and withdrawing drugs of correct amount as verified by the supervising licensed dentist.
d. Add drugs, medications, and fluids to intravenous lines using a syringe, provided that a supervising licensed dentist is present at the patient’s chairside, limited to determining patency of intravenous line, selection of injection port, syringe insertion into injection port, occlusion of intravenous line and blood aspiration, line release and injection of drugs for appropriate time interval. The exception to this duty is that the initial dose of a drug or medication shall be administered by the supervising licensed dentist.
e. Removal of intravenous lines.f. Any additional duties that the board may prescribe by regulation.g. The duties listed in subdivisions (b) to (e), inclusive, may not be
performed in any setting other than a dental office or dental clinic.
1751 – At least once every seven years, the board shall review the allowable duties for dental assistants, registered dental assistants, registered dental assistants in extended functions, dental sedation assistant permit holders, and orthodontic assistant permit holders, the supervision level for these categories, and the settings under which these duties may be performed, and shall update the regulations as necessary to keep them current with the state of the dental practice.
Section 1067. – Definitions.As used in this subchapter: “Dental auxiliary” means a person who may perform dental supportive procedures authorized by the provisions of these regulations under the specified supervision of a licensed dentist.
“Dental assistant” means an unlicensed person who may perform basic supportive dental procedures specified by these regulations under the supervision of a licensed dentist.
“Registered dental assistant” or “RDA” means a licensed person who may perform all procedures authorized by the provisions of these regulations and in addition may perform all functions which may be performed by a dental assistant under the designated supervision of a licensed dentist.
“Registered dental hygienist” or “RDH” means a licensed person who may perform all procedures authorized by the provisions of these regulations and in addition may perform all functions which may be performed by a dental assistant and registered dental assistant, under the designated supervision of a licensed dentist.
“Registered dental assistant in extended functions” or “RDAEF” means a person licensed as a registered dental assistant who has completed post-licensure clinical and didactic training approved by the board and satisfactorily performed on an examination designated by the board for registered dental assistant in extended function applicants.
“Registered dental hygienist in extended functions” or “RDHEF” means a person licensed as a registered dental hygienist who has completed post-licensure clinical and didactic training approved by the board and satisfactorily performed on an examination designated
by the board for registered dental hygienist in extended functions applicants.
“Oral prophylaxis” means the preventive dental procedures including complete removal of explorer-detectable calculus, soft deposits, plaque, stains, and the smoothing of unattached tooth surfaces. The objective of this treatment shall be creation of an environment in which hard and soft tissues can be maintained in good health by the patient.
“Coronal polishing” means a procedure limited to the removal of plaque and stain from exposed tooth surfaces, utilizing an appropriate rotary instrument with rubber cup or brush and a polishing agent.
“Satisfactory educational qualification” means theory, laboratory and/or clinical experience approved by the board.
“Basic supportive dental procedures” means fundamental duties or functions which may be performed by an unlicensed dental assistant under the supervision of a licensed dentist because of their technically elementary characteristics, complete reversibility and inability to precipitate potentially hazardous conditions for the patient being treated.
“Root planing” means the process of instrumentation by which the unattached surfaces of the root are made smooth by the removal of calculus and/or cementum.
“Periodontal soft tissue curettage” means the closed removal of tissue lining the periodontal pocket, not involving the reflection of a flap.
“Gingival” means pertaining to the gingivae, the mucous membrane with the supporting fibrous tissue.

Dental.EliteCME.com Page 8
1752.4 – A registered dental assistant may perform all of the following duties:1. All duties that a dental assistant is allowed to perform.2. Mouth-mirror inspections of the oral cavity, to include charting of
obvious lesions, existing restorations, and missing teeth.3. Apply and activate bleaching agents using a nonlaser light-curing
device.4. Use of automated caries detection devices and materials to gather
information for diagnosis by the dentist.5. Obtain intraoral images for computer-aided design (CAD), milled
restorations.6. Pulp vitality testing and recording of findings.7. Place bases, liners, and bonding agents.8. Chemically prepare teeth for bonding.9. Place, adjust, and finish direct provisional restorations.10. Fabricate, adjust, cement, and remove indirect provisional
restorations, including stainless steel crowns when used as a provisional restoration.
11. Place post-extraction dressings after inspection of the surgical site by the supervising licensed dentist.
12. Place periodontal dressings.13. Dry endodontically treated canals using absorbent paper points.14. Adjust dentures extra-orally.15. Remove excess cement from surfaces of teeth with a hand
instrument.16. Polish coronal surfaces of the teeth.17. Place ligature ties and archwires.18. Remove orthodontic bands.19. All duties that the board may prescribe by regulation.
A registered dental assistant may only perform the following additional duties if he or she has completed a board-approved registered dental assistant educational program in those duties, or he or she has provided evidence, satisfactory to the board, of having completed a board-approved course in those duties.1. Remove excess cement with an ultrasonic scaler from supragingival
surfaces of teeth undergoing orthodontic treatment.2. The allowable duties of an orthodontic assistant permit holder
as specified in Section 1750.3. A registered dental assistant shall
not be required to complete further instruction in the duties of placing ligature ties and archwires, removing orthodontic bands, and removing excess cement from tooth surfaces with a hand instrument.
3. The allowable duties of a dental sedation assistant permit holder as specified in Section 1750.5.
4. The application of pit and fissure sealants.
Except as provided in Section 1777, the supervising licensed dentist shall be responsible for determining whether each authorized procedure performed by a registered dental assistant should be performed under general or direct supervision.
1753.7 – A licensed dentist may simultaneously utilize in his or her practice no more than three registered dental assistants in extended functions or registered dental hygienists in extended functions licensed pursuant to Section 1753 or 1918.
1765. – No person other than a licensed dental hygienist or a licensed dentist may engage in the practice of dental hygiene or perform dental hygiene procedures on patients, including, but not limited to, supragingival and subgingival scaling, dental hygiene assessment, and treatment planning, except for the following persons:a. A student enrolled in a dental or a dental hygiene school who is
performing procedures as part of the regular curriculum of that program under the supervision of the faculty of that program.
b. A dental assistant, registered dental assistant, or registered dental assistant in extended functions acting in accordance with the provisions of this chapter.
c. A registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions licensed in another jurisdiction performing a clinical demonstration for educational purposes.
1771. – Any person, other than a person who has been issued a license or permit by the board, who holds himself or herself out as a registered dental assistant, orthodontic assistant permit holder, dental sedation assistant permit holder, or registered dental assistant in extended functions, or uses any other term indicating or implying he or she is licensed or permitted by the board as such, is guilty of a misdemeanor.
DEnTAL CORPORATIOnSA dental corporation is a corporation that is authorized to render professional services, as defined in Sections 13401 and 13401.5 of the Corporations Code, if that corporation, its shareholders, officers, directors and employees rendering professional services who are dentists, physicians and surgeons, dental assistants, registered dental assistants, registered dental assistants in extended functions, registered dental hygienists, registered dental hygienists in extended functions, or registered dental hygienists in alternative practice are in compliance with the Moscone-Knox Professional Corporation Act (Part 4 (commencing with Section 13400) of Division 3 of Title 1
of the Corporations Code), this article, and other statutes, rules, and regulations applicable to a dental corporation and the conduct of its affairs. Subject to all applicable statutes, rules and regulations, a dental corporation is entitled to practice dentistry. With respect to a dental corporation, the governmental agency referred to in the Moscone-Knox Professional Corporation Act is the Dental Board of California. A dental corporation shall provide adequate security by insurance or otherwise for claims against it by its patients arising out of the rendering of professional services.
new regulations – Dental Hygiene Committee (1900 – 1966.6)1901-1905: The Dental Hygiene Committee is appointed by the governor; it consists of nine members. Of the nine members, one shall be a practicing general or public health dentist who holds a current license in California, and four members shall be registered dental hygienists, who hold current licenses in California. One of the four shall be licensed either in alternative practice or in extended functions, one shall be a dental hygiene educator, and two shall be registered dental hygienists. No public member shall have been licensed under this chapter within five years of the date of his or her appointment or have any current financial interest in a dental-related business.
Each member shall serve a four-year term, and no member shall serve for more than two consecutive terms.
The committee shall perform the following functions:1. Evaluate all registered dental hygienist, registered dental hygienist
in alternative practice, and registered dental hygienist in extended functions educational programs that apply for approval and grant or deny approval of those applications in accordance with regulations adopted by the committee. Any such educational programs approved by the dental board on or before June 30, 2009, shall be deemed approved by the committee. Any dental hygiene program accredited and in good standing by the Commission on Dental Accreditation shall be approved.
2. Withdraw or revoke its prior approval of a registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions educational
Page 9 Dental.EliteCME.com
program in accordance with regulations adopted by the committee. The committee may withdraw or revoke a dental hygiene program approval if the Commission on Dental Accreditation has indicated an intent to withdraw approval or has withdrawn approval.
3. Review and evaluate all registered dental hygienist, registered dental hygienist in alternative practice, and registered dental hygienist in extended functions applications for licensure to ascertain whether the applicant meets the appropriate licensing requirements specified by statute and regulations, maintain application records, cashier application fees, issue and renew licenses, and perform any other tasks that are incidental to the application and licensure processes.
4. Determine the appropriate type of license examination consistent with the provisions of this article, and develop or cause to be developed and administer examinations in accordance with regulations adopted by the committee.
5. Determine the amount of fees assessed under this article, not to exceed the actual cost.
6. Determine and enforce the continuing education requirements specified in this article, specifically Section 1936.1.
7. Deny, suspend, or revoke a license under this article, or otherwise enforce the provisions of this article. Any such proceedings shall be conducted in accordance with Chapter 5 (commencing with Section 11500) of Part 1 of Division 3 of Title 2 of the Government Code, and the committee shall have all of the powers granted therein.
8. Make recommendations to the dental board regarding dental hygiene scope of practice issues.
9. Adopt, amend, and revoke rules and regulations to implement the provisions of this article, including the amount of required supervision by a registered dental hygienist, a registered dental hygienist in alternative practice, or a registered dental hygienist in extended functions of a registered dental assistant.
The committee may employ employees and examiners that it deems necessary to carry out its functions and responsibilities under this article.
Definitions1902. – For purposes of this course, the following definitions apply:“Committee” means the Dental Hygiene Committee of California.
“Dental board” means the Dental Board of California.
“Direct supervision” means the supervision of dental procedures based on instructions given by a licensed dentist who is required to be physically present in the treatment facility during the performance of those procedures.
“General supervision” means the supervision of dental procedures based on instructions given by a licensed dentist who is not required to
be physically present in the treatment facility during the performance of those procedures.
“Oral prophylaxis” means preventive and therapeutic dental procedures that include bacterial debridements with complete removal, supra and subgingivally, of calculus, soft deposits, plaque, and stains, and the smoothing of tooth surfaces. The objective of this treatment is to create an environment in which the patient can maintain healthy hard and soft tissues.
Registered dental hygienist duties1907. – The following functions may be performed by a registered dental hygienist, in addition to those authorized pursuant to Sections 1908 to 1914, inclusive:a. All functions that may be performed by a registered dental
assistant.b. All persons holding a license as a registered dental hygienist,
registered dental hygienist in alternative practice, or registered dental hygienist in extended functions as of December 31, 2005, are authorized to perform the duties of a registered dental assistant specified in this chapter. All persons issued a license as a registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions on or after January 1, 2006, shall qualify for and receive a registered dental assistant license prior to performance of the duties of a registered dental assistant specified in this chapter.
1908. a. The practice of dental hygiene includes dental hygiene assessment
and development, planning, and implementation of a dental hygiene care plan. It also includes oral health education, counseling, and health screenings.
b. The practice of dental hygiene does not include any of the following procedures:1. Diagnosis and comprehensive treatment planning.2. Placing, condensing, carving, or removal of permanent
restorations.3. Surgery or cutting on hard and soft tissue including, but not
limited to, the removal of teeth and the cutting and suturing of soft tissue.
4. Prescribing medication.5. Administering local or general anesthesia or oral or parenteral
conscious sedation, except for the administration of nitrous oxide and oxygen, whether administered alone or in
combination with each other, or local anesthesia pursuant to Section 1909.
1909. – A registered dental hygienist is authorized to perform the following procedures under direct supervision of a licensed dentist, after submitting to the committee evidence of satisfactory completion of a course of instruction, approved by the committee, in the procedures:a. Soft-tissue curettage.b. Administration of local anesthesia.c. Administration of nitrous oxide and oxygen, whether administered
alone or in combination with each other.
1910. – A registered dental hygienist is authorized to perform the following procedures under general supervision:a. Preventive and therapeutic interventions, including oral
prophylaxis, scaling, and root planing.b. Application of topical, therapeutic, and subgingival agents used for
the control of caries and periodontal disease.c. The taking of impressions for bleaching trays and application and
activation of agents with nonlaser, light-curing devices.d. The taking of impressions for bleaching trays and placements of
in-office, tooth-whitening devices.
1911.a. A registered dental hygienist may provide, without supervision,
educational services, oral health training programs, and oral health screenings.
b. A registered dental hygienist shall refer any screened patients with possible oral abnormalities to a dentist for a comprehensive examination, diagnosis, and treatment plan.
c. In any public health program created by federal, state, or local law or administered by a federal, state, county, or local governmental entity, a registered dental hygienist may provide, without supervision, dental hygiene preventive services in addition to

Dental.EliteCME.com Page 10
oral screenings, including, but not limited to, the application of fluorides and pit and fissure sealants. A registered dental hygienist employed as described in this subdivision may submit, or allow to be submitted, any insurance or third-party claims for patient services performed as authorized in this article.
1912. – Any procedure performed or service provided by a registered dental hygienist that does not specifically require direct supervision shall require general supervision, so long as it does not give rise to a situation in the dentist’s office requiring immediate services for alleviation of severe pain, or immediate diagnosis and treatment of unforeseeable dental conditions that, if not immediately diagnosed and treated, would lead to serious disability or death.
1913. – Unless otherwise specified in this chapter, a registered dental hygienist may perform any procedure or provide any service within the scope of his or her practice in any setting, so long as the procedure is performed or the service is provided under the appropriate level of supervision required by this article.
1914. – A registered dental hygienist may use any material or device approved for use in the performance of a service or procedure within his or her scope of practice under the appropriate level of supervision, if he or she has the appropriate education and training required to use the material or device.
1915. – No person other than a registered dental hygienist, registered dental hygienist in alternative functions, or registered dental hygienist in extended functions or a licensed dentist may engage in the practice
of dental hygiene or perform dental hygiene procedures on patients, including, but not limited to, supragingival and subgingival scaling, dental hygiene assessment, and treatment planning, except for the following persons:a. A student enrolled in a dental or a dental hygiene school who is
performing procedures as part of the regular curriculum of that program under the supervision of the faculty of that program.
b. A dental assistant acting in accordance with the rules of the dental board in performing the following procedures:1. Applying nonaerosol and noncaustic topical agents.2. Applying topical fluoride.3. Taking impressions for bleaching trays.
c. A registered dental assistant acting in accordance with the rules of the dental board in performing the following procedures:1. Polishing the coronal surfaces of teeth.2. Applying bleaching agents.3. Activating bleaching agents with a nonlaser light-curing
device.4. Applying pit and fissure sealant.
d. A registered dental assistant in extended functions acting in accordance with the rules of the dental board in applying pit and fissure sealants.
e. A registered dental hygienist, registered dental hygienist in alternative practice or registered dental hygienist in extended functions licensed in another jurisdiction, performing a clinical demonstration for educational purposes.
Registered dental hygienist in extended functions duties1921. – In addition to any other duties or functions authorized by law, a registered dental hygienist in extended functions or a registered dental hygienist in alternative practice may perform any of the duties or functions authorized to be performed by a registered dental hygienist.
1925. – A registered dental hygienist in alternative practice may practice, pursuant to subdivision (a) of Section 1907, subdivision (a) of Section 1908, and subdivisions (a) and (b) of Section 1910, as an employee of a dentist or of another registered dental hygienist in alternative practice, as an independent contractor, as a sole proprietor of an alternative dental hygiene practice, as an employee of a primary
care clinic or specialty clinic that is licensed pursuant to Section 1204 of the Health and Safety Code, as an employee of a primary care clinic exempt from licensure pursuant to subdivision (c) of Section 1206 of the Health and Safety Code, as an employee of a clinic owned or operated by a public hospital or health system, or as an employee of a clinic owned and operated by a hospital that maintains the primary contract with a county government to fill the county’s role under Section 17000 of the Welfare and Institutions Code, or as an employee of a professional corporation under the Moscone-Knox Professional Corporation Act (commencing with Section 13400) of Part 4 of Division 3 of Title 1 of the Corporations Code.
Registered dental hygienist in alternative practice duties1926. – A registered dental hygienist in alternative practice may perform the duties authorized pursuant to subdivision (a) of Section 1907, subdivision (a) of Section 1908, and subdivisions (a) and (b) of Section 1910 in the following settings:a. Residences of the homebound.b. Schools.c. Residential facilities and other institutions.d. Dental health professional shortage areas, as certified by the Office
of Statewide Health Planning and Development in accordance with existing office guidelines.
1927. – A registered dental hygienist in alternative practice shall not do any of the following:a. Infer, purport, advertise, or imply that he or she is in any way
able to provide dental services or make any type of dental health diagnosis beyond evaluating a patient’s dental hygiene status, providing a dental hygiene treatment plan, and providing the associated dental hygiene services.
b. Hire a registered dental hygienist to provide direct patient services other than a registered dental hygienist in alternative practice.
1928. – A registered dental hygienist in alternative practice may submit or allow to be submitted any insurance or third-party claims for patient services performed as authorized pursuant to this article.
1929. a. A registered dental hygienist in alternative practice may hire other
registered dental hygienists in alternative practice to assist in his or her practice.
b. A registered dental hygienist in alternative practice may hire and supervise dental assistants performing intraoral retraction and suctioning.
1930. – A registered dental hygienist in alternative practice shall provide to the committee documentation of an existing relationship with at least one dentist for referral, consultation, and emergency services.
1931. – A dental hygienist in alternative practice may provide services to a patient without obtaining written verification that the patient has been examined by a dentist or physician and surgeon licensed to practice in this state.
If the dental hygienist in alternative practice provides services to a patient 18 months or more after the first date that he or she provides services to a patient, he or she shall obtain written verification that the patient has been examined by a dentist or physician and surgeon licensed to practice in this state. The verification shall include a prescription for dental hygiene services as described in subdivision (b).

Page 11 Dental.EliteCME.com
A registered dental hygienist in alternative practice may provide dental hygiene services for a patient who presents to the registered dental hygienist in alternative practice a written prescription for dental hygiene services issued by a dentist or physician and surgeon licensed to practice in this state. The prescription shall be valid for a time period based on the dentist’s or physician and surgeon’s professional judgment, but not to exceed two years from the date it was issued.
The committee may seek to obtain an injunction against any registered dental hygienist in alternative practice who provides services pursuant to this section, if the committee has reasonable cause to believe that the services are being provided to a patient who has not received a prescription for those services from a dentist or physician and surgeon licensed to practice in this state. Performing services pursuant to this section without obtaining a prescription in accordance with subdivision (b) shall constitute unprofessional conduct on the part of the registered dental hygienist in alternative practice, and reason for the committee to revoke or suspend the license of the registered dental hygienist in alternative practice, pursuant to Section 1947.
1933. – A licensee shall be issued a substitute license upon request and payment of the required fee. The request shall be accompanied by an affidavit or declaration containing satisfactory evidence of the loss or destruction of the license certificate.
1934. – A licensee who changes his or her address of record shall notify the committee within 30 days of the change. A licensee who changes his or her legal name shall provide the committee with documentation of the change within 10 days.
1935. – If not renewed, a license issued under the provisions of this article, unless specifically excepted, expires at 12 midnight on the last day of the month of the legal birth date of the licensee during the second year of a two-year term. To renew an unexpired license, the licensee shall, before the time at which the license would otherwise expire, apply for renewal on a form prescribed by the committee and pay the renewal fee prescribed by this article.
1936. – Except as otherwise provided in this article, an expired license may be renewed at any time within five years after its expiration by filing an application for renewal on a form prescribed by the committee and payment of all accrued renewal and delinquency fees. If the license is renewed after its expiration, the licensee, as a condition precedent of renewal, shall also pay the delinquency fee prescribed by this article. Renewal under this section shall be effective on the date on which the application is filed, on the date on which the renewal fee is paid, or on the date on which the delinquency fee, if any, is paid, whichever last occurs. If so renewed, the license shall continue in effect until the expiration date provided in Section 1935 that next occurs after the effective date of the renewal.
1936.1. – If the committee determines that the public health and safety would be served by requiring all holders of licenses under this article to continue their education after receiving a license, the committee may require, as a condition of license renewal, that licensees submit assurances satisfactory to the committee that they will, during the succeeding two-year period, inform themselves of the developments in the practice of dental hygiene occurring since the original issuance of their licenses by pursuing one or more courses of study satisfactory to the committee, or by other means deemed equivalent by the committee. The committee shall adopt, amend and revoke regulations providing for the suspension of the licenses at the end of the two-year period until compliance with the assurances provided for in this section is accomplished.
The committee may also, as a condition of license renewal, require licensees to successfully complete a portion of the required continuing education hours in specific areas adopted in regulations by the committee. The committee may prescribe this mandatory coursework within the general areas of patient care, health and safety, and law and ethics. The mandatory coursework prescribed by the committee
shall not exceed seven and one-half hours per renewal period. Any mandatory coursework required by the committee shall be credited toward the continuing education requirements established by the committee pursuant to subdivision (a).
The providers of courses referred to in this section shall be approved by the committee. Providers approved by the dental board shall be deemed approved by the committee.
1937. – A suspended license is subject to expiration and shall be renewed as provided in this article. The renewal does not entitle the licensee, while the license remains suspended and until it is reinstated, to engage in the licensed activity or in any other activity or conduct in violation of the order or judgment by which the license was suspended.
1938. – A revoked license is subject to expiration as provided in this article. A revoked license may not be renewed. If it is reinstated after its expiration, the licensee, as a condition precedent to its reinstatement, shall pay a reinstatement fee in an amount equal to the renewal fee in effect on the last regular renewal date before the date on which it is reinstated and the delinquency fee, if any, accrued at the time of its revocation.
1939. – A license that is not renewed within five years after its expiration may not be renewed, restored, reinstated or reissued. The holder of the license may apply for and obtain a new license upon meeting all of the requirements of a new applicant prescribed in this article.
1940. a. A licensee who desires an inactive license shall submit an
application to the committee on a form provided by the committee.b. In order to restore an inactive license to active status, the licensee
shall submit an application to the committee on a form provided by the committee, accompanied by evidence that the licensee has completed the required number of hours of approved continuing education in compliance with this article within the last two years preceding the date of the application.
c. The holder of an inactive license shall continue to pay to the committee the required biennial renewal fee.
d. Within 30 days of receiving a request either to restore an inactive license or to inactivate a license, the committee shall inform the applicant in writing whether the application is complete and accepted for filing or is deficient and, if so, the specific information required to complete the application.
1941.a. The committee shall grant or renew approval of only those
educational programs for a registered dental hygienist, a registered dental hygienist in alternative practice, or a registered dental hygienist in extended functions that continuously maintain a high quality standard of instruction and, where appropriate, meet the minimum standards set by the Commission on Dental Accreditation of the American Dental Association or an equivalent body, as determined by the committee.
b. A new educational program for registered dental hygienists shall submit a feasibility study demonstrating a need for a new educational program and shall apply for approval from the committee prior to seeking approval for initial accreditation from the Commission on Dental Accreditation of the American Dental Association or an equivalent body, as determined by the committee. The committee may approve, provisionally approve, or deny approval of any such new educational program.
c. For purposes of this section, a new educational program for registered dental hygienists means a program provided by a college or institution of higher education that is accredited by a regional accrediting agency recognized by the United States Department of Education and that has as its primary purpose providing college level courses leading to an associate or higher degree, that is either affiliated with or conducted by a dental school

Dental.EliteCME.com Page 12
approved by the dental board, or that is accredited to offer college level or college parallel programs by the Commission on Dental Accreditation of the American Dental Association or an equivalent body, as determined by the committee.
1944. a. The committee shall establish by resolution the amount of the
fees that relate to the licensing of a registered dental hygienist, a registered dental hygienist in alternative practice, and a registered dental hygienist in extended functions. The fees established by board resolution in effect on June 30, 2009, as they relate to the licensure of registered dental hygienists, registered dental hygienists in alternative practice, and registered dental hygienists in extended functions, shall remain in effect until modified by the committee. The fees are subject to the following limitations:1. The application fee for an original license and the fee for
issuance of an original license shall not exceed two hundred fifty dollars ($250).
2. The fee for examination for licensure as a registered dental hygienist shall not exceed the actual cost of the examination.
3. The fee for examination for licensure as a registered dental hygienist in extended functions shall not exceed the actual cost of the examination.
4. The fee for examination for licensure as a registered dental hygienist in alternative practice shall not exceed the actual cost of administering the examination.
5. The biennial renewal fee shall not exceed one hundred sixty dollars ($160).
6. The delinquency fee shall not exceed one-half of the renewal fee. Any delinquent license may be restored only upon payment of all fees, including the delinquency fee, and compliance with all other applicable requirements of this article.
7. The fee for issuance of a duplicate license to replace one that is lost or destroyed, or in the event of a name change, shall not exceed twenty-five dollars ($25) or one-half of the renewal fee, whichever is greater.
8. The fee for certification of licensure shall not exceed one-half of the renewal fee.
9. The fee for each curriculum review and site evaluation for educational programs for dental hygienists who are not accredited by a committee-approved agency shall not exceed two thousand one hundred dollars ($2,100).
10. The fee for each review or approval of course requirements for licensure or procedures that require additional training shall not exceed seven hundred fifty dollars ($750).
11. The initial application and biennial fee for a provider of continuing education shall not exceed five hundred dollars ($500).
12. The amount of fees payable in connection with permits issued under Section 1962 is as follows:A. The initial permit fee is an amount equal to the renewal
fee for the applicant’s license to practice dental hygiene in effect on the last regular renewal date before the date on which the permit is issued.
B. If the permit will expire less than one year after its issuance, then the initial permit fee is an amount equal to 50 percent of the renewal fee in effect on the last regular renewal date before the date on which the permit is issued.
b. The renewal and delinquency fees shall be fixed by the committee by resolution at not more than the current amount of the renewal fee for a license to practice under this article nor less than five dollars ($5).
c. Fees fixed by the committee by resolution pursuant to this section shall not be subject to the approval of the Office of Administrative Law.
d. Fees collected pursuant to this section shall be collected by the committee and deposited into the State Dental Hygiene Fund, which is hereby created. All money in this fund shall, upon appropriation by the Legislature in the annual Budget Act, be used to implement the provisions of this article.
e. No fees or charges other than those listed in this section shall be levied by the committee in connection with the licensure of registered dental hygienists, registered dental hygienists in alternative practice, or registered dental hygienists in extended functions.
f. The fee for registration of an extramural dental facility shall not exceed two hundred fifty dollars ($250).
g. The fee for registration of a mobile dental hygiene unit shall not exceed one hundred fifty dollars ($150).
h. The biennial renewal fee for a mobile dental hygiene unit shall not exceed two hundred fifty dollars ($250).
i. The fee for an additional office permit shall not exceed two hundred fifty dollars ($250).
j. The biennial renewal fee for an additional office as described in Section 1926.4 shall not exceed two hundred fifty dollars ($250).
k. The initial application and biennial special permit fee is an amount equal to the biennial renewal fee specified in paragraph (6) of subdivision (a).
l. The fees in this section shall not exceed an amount sufficient to cover the reasonable regulatory cost of carrying out the provisions of this article.
Cause for suspension or revoked licenses for hygienists1947. – A license issued under this article and a license issued under this chapter to a registered dental hygienist, to a registered dental hygienist in alternative practice, or to a registered dental hygienist in extended functions may be revoked or suspended by the committee for any reason specified in this article for the suspension or revocation of a license to practice dental hygiene.
1949. – A licensee may have his or her license revoked or suspended,or may be reprimanded or placed on probation by the committee for unprofessional conduct, incompetence, gross negligence, repeated acts of negligence in his or her profession, receiving a license by mistake, or for any other cause applicable to the licentiate provided in this article. The proceedings under this article shall be conducted in accordance with Chapter 5 (commencing with Section 11500) of Part 1 of Division 3 of Title 2 of the Government Code, and the committee shall have all the powers granted therein.
1950.a. A licensee may have his or her license revoked or suspended, or
may be reprimanded or placed on probation by the committee, for conviction of a crime substantially related to the licensee’s qualifications, functions, or duties. The record of conviction or a copy certified by the clerk of the court or by the judge in whose court the conviction occurred shall be conclusive evidence of conviction.
b. The committee shall undertake proceedings under this section upon the receipt of a certified copy of the record of conviction. A plea or verdict of guilty or a conviction following a plea of nolo contendere made to a charge of a felony or of any misdemeanor substantially related to the licensee’s qualifications, functions, or duties is deemed to be a conviction within the meaning of this section.
c. The committee may order a license suspended or revoked, or may decline to issue a license, when any of the following occur:1. The time for appeal has elapsed.

Page 13 Dental.EliteCME.com
2. The judgment of conviction has been affirmed on appeal.3. An order granting probation is made suspending the imposition
of sentence, irrespective of a subsequent order under any provision of the Penal Code, including, but not limited to,
Section 1203.4 of the Penal Code, allowing a person to withdraw his or her plea of guilty and to enter a plea of not guilty, or setting aside the verdict of guilty, or dismissing the accusation, information, or indictment.
Section 1950.5: Unprofessional conduct by dentists and dental hygienists California laws that define unprofessional conduct by dentists and dental hygienists are generally identical, although some rules of conduct are specific to each. Here are the general statutory definitions of unprofessional conduct for all dental professionals.
Unprofessional conduct by a person licensed under California code is defined as, but is not limited to, any one of the following:
● The obtaining of any fee by fraud or misrepresentation. ● The aiding or abetting of any unlicensed person to practice
dentistry or dental hygiene. ● The aiding or abetting of a licensed person to practice dentistry or
dental hygiene unlawfully. ● The committing of any act or acts of sexual abuse, misconduct or
relations with a patient that are substantially related to the practice of dental hygiene.
● The use of any false, assumed, or fictitious name, either as an individual, firm, corporation, or otherwise, or any name other than the name under which he or she is licensed to practice, in advertising or in any other manner indicating that he or she is practicing or will practice dentistry, except that name as is specified in a valid permit issued pursuant to Section 1962.
● The practice of accepting or receiving any commission or the rebating in any form or manner of fees for professional services, radiograms, prescriptions, or other services or articles supplied to patients.
● The making use by the licensee or any agent of the licensee of any advertising statements of a character tending to deceive or mislead the public.
● The advertising of either professional superiority or the advertising of performance of professional services in a superior manner. This subdivision shall not prohibit advertising permitted by subdivision (h) of Section 651.
● The employing or the making use of solicitors. ● Advertising in violation of Section 651. ● Advertising to guarantee any dental hygiene service, or to perform
any dental hygiene procedure painlessly. This subdivision shall not prohibit advertising permitted by Section 651.
● The violation of any of the provisions of this division. ● The permitting of any person to operate dental radiographic
equipment who has not met the requirements of Section 1656. ● The clearly excessive administering of drugs or treatment,
or the clearly excessive use of treatment procedures, or the clearly excessive use of treatment facilities, as determined by the customary practice and standards of the dental hygiene profession. Any person who violates this subdivision is guilty of a misdemeanor and shall be punished by a fine of not less than $100 or more than $600, or by imprisonment for a term of not less than 60 days or more than 180 days, or by both a fine and imprisonment.
● The use of threats or harassment against any patient or licensee for providing evidence in any possible or actual disciplinary action, or
other legal action; or the discharge of an employee primarily based on the employee’s attempt to comply with the provisions of this chapter or to aid in the compliance.
● Suspension or revocation of a license issued, or discipline imposed, by another state or territory on grounds that would be the basis of discipline in this state.
● The alteration of a patient’s record with intent to deceive. ● Unsanitary or unsafe office conditions, as determined by
the customary practice and standards of the dental hygiene profession.
● The abandonment of the patient by the licensee, without written notice to the patient that treatment is to be discontinued and before the patient has ample opportunity to secure the services of another registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions and provided the health of the patient is not jeopardized.
● The willful misrepresentation of facts relating to a disciplinary action to the patients of a disciplined licensee.
● Use of fraud in the procurement of any license issued pursuant to this article.
● Any action or conduct that would have warranted the denial of the license.
● The aiding or abetting of a registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions to practice dental hygiene in a negligent or incompetent manner.
● The failure to report to the committee in writing within seven days any of the following:
○ The death of his or her patient during the performance of any dental hygiene procedure.
○ The discovery of the death of a patient whose death is related to a dental hygiene procedure performed by him or her.
○ Except for a scheduled hospitalization, the removal to a hospital or emergency center for medical treatment for a period exceeding 24 hours of any patient as a result of dental or dental hygiene treatment. Upon receipt of a report pursuant to this subdivision, the committee may conduct an inspection of the dental hygiene practice office if the committee finds that it is necessary.
○ A registered dental hygienist, registered dental hygienist in alternative practice or registered dental hygienist in extended functions shall report to the committee all deaths occurring in his or her practice with a copy sent to the dental board if the death occurred while working as an employee in a dental office. A dentist shall report to the dental board all deaths occurring in his or her practice with a copy sent to the committee if the death was the result of treatment by a registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions.
Other acts deemed unprofessional for dentists ● Participating in or operating any group advertising and referral
services that are in violation of Section 650.2. ● The failure to use a fail-safe machine with an appropriate exhaust
system in the administration of nitrous oxide. The board shall, by regulation, define what constitutes a fail-safe machine.
● Engaging in the practice of dentistry with an expired license.
● Except for good cause, the knowing failure to protect patients by failing to follow infection control guidelines of the board.
● The utilization by a licensed dentist of any person to perform the functions of any registered dental assistant, registered dental assistant in extended functions, dental sedation assistant permit holder, orthodontic assistant permit holder, registered dental hygienist, registered dental hygienist in alternative practice, or

Dental.EliteCME.com Page 14
registered dental hygienist in extended functions who, at the time of initial employment, does not possess a current, valid license or permit to perform those functions.
● The prescribing, dispensing or furnishing of dangerous drugs or devices, as defined in Section 4022, in violation of Section 2242.1.
● Having more than one patient undergoing conscious sedation or general anesthesia on an outpatient basis at any given time unless each patient is being continuously monitored on a one-to-one ratio while sedated by either the dentist or another licensed health professional authorized by law to administer conscious sedation or general anesthesia.
● Failing to have patients recovering from conscious sedation or general anesthesia closely monitored by licensed health professionals experienced in the care and resuscitation of patients recovering from conscious sedation or general anesthesia. If one licensed professional is responsible for the recovery care of more
than one patient at a time, all of the patients shall be physically in the same room to allow continuous visual contact with all patients and the patient to recovery staff ratio should not exceed three to one.
● Failing to have patients who are undergoing conscious sedation continuously monitored during the dental procedure with a pulse oximeter or similar or superior monitoring equipment required by the board.
● Having dental office personnel who are not certified in basic cardiac life support (CPR) and recertified biennially directly involved with the care of patients undergoing conscious sedation.
● Failing to obtain the written informed consent of a patient prior to administering general anesthesia or conscious sedation. In the case of a minor, the consent shall be obtained from the child’s parent or guardian.
Controlled substances and dental professionalsIt is unprofessional conduct for a person licensed under the code to do any of the following:
● Obtain or possess in violation of law, or except as directed by a licensed physician and surgeon, dentist, or podiatrist, a controlled substance, as defined in Division 10 (commencing with Section 11000) of the Health and Safety Code, or any dangerous drug as defined in Section 4022.
● Use a controlled substance, as defined in Division 10 (commencing with Section 11000) of the Health and Safety Code, or a dangerous drug as defined in Section 4022, or alcoholic beverages or other intoxicating substances, to an extent or in a manner dangerous or injurious to himself or herself, to any person, or the public to the extent that the use impairs the licensee’s ability to conduct with safety to the public the practice authorized by his or her license.
● Be convicted of a charge of violating any federal statute or rules, or any statute or rule of this state, regulating controlled substances, as defined by California codes, or be convicted of more than one
misdemeanor, or any felony, involving the use or consumption of alcohol or drugs, if the conviction is substantially related to the practice authorized by his or her license. The record of conviction or a copy certified by the clerk of the court or by the judge in whose court the conviction is had, shall be conclusive evidence of a violation of this section. A plea or verdict of guilty or a conviction following a plea of nolo contendere is deemed to be a conviction within the meaning of this section; the committee may order the license suspended or revoked, or may decline to issue a license, when the time for appeal has elapsed or the judgment of conviction has been affirmed on appeal, or when an order granting probation is made suspending imposition of sentence, irrespective of a subsequent order under any provision of the Penal Code, including, but not limited to, Section 1203.4 of the Penal Code, allowing a person to withdraw his or her plea of guilty and to enter a plea of not guilty, or setting aside the verdict of guilty, or dismissing the accusation, information, or indictment.
Dental recordsDentists and registered hygienists who perform a service on a patient in a dental office shall identify themselves in the patient record by signing their name or identification number and initials next to the service performed, and shall date those treatment entries in the record. A repeated violation of this section constitutes unprofessional conduct. Any person licensed under these laws who owns, operates or manages a dental office shall ensure compliance with this requirement.
A licensee who fails or refuses to comply with a request for a patient’s dental hygiene records that is accompanied by that patient’s written authorization for release of the records to the committee, within 15 days of receiving the request and authorization, shall pay to the committee a civil penalty of $250 per day for each day that the documents have not been produced after the 15th day, up to a maximum of $5,000 unless the licensee is unable to provide the documents within this time period for good cause.
A licensee who fails or refuses to comply with a court order, issued in the enforcement of a subpoena, mandating the release of records to the board shall pay to the board a civil penalty of $1,000 per day for each day that the documents have not been produced after the date by which the court order requires the documents to be produced, unless it is determined that the order is unlawful or invalid. Any statute of limitations applicable to the filing of an accusation by the board shall be tolled during the period the licensee is out of compliance with the court order and during any related appeals.
Any licensee who fails or refuses to comply with a court order, issued in the enforcement of a subpoena, mandating the release of records to the board is guilty of a misdemeanor punishable by a fine payable
to the board not to exceed $5,000. The fine shall be added to the licensee’s renewal fee if it is not paid by the next succeeding renewal date. Any statute of limitations applicable to the filing of an accusation by the board shall be tolled during the period the licensee is out of compliance with the court order and during any related appeals.
A health care facility that fails or refuses to comply with a court order, issued in the enforcement of a subpoena, mandating the release of patient records to the board, that is accompanied by a notice citing this section and describing the penalties for failure to comply with this section, shall pay to the board a civil penalty of up to $1,000 per day for each day that the documents have not been produced, up to $10,000, after the date by which the court order requires the documents to be produced, unless it is determined that the order is unlawful or invalid. Any statute of limitations applicable to the filing of an accusation by the board against a licensee shall be tolled during the period the health care facility is out of compliance with the court order and during any related appeals.
● Any health care facility that fails or refuses to comply with a court order, issued in the enforcement of a subpoena, mandating the release of records to the board is guilty of a misdemeanor punishable by a fine payable to the board not to exceed $5,000. Any statute of limitations applicable to the filing of an accusation by the board against a licensee shall be tolled during the period the health care facility is out of compliance with the court order and during any related appeals.
Multiple acts by a licensee in violation of subdivision (b) shall be punishable by a fine not to exceed $5,000 or by imprisonment in a county jail not exceeding six months, or by both that fine and

Page 15 Dental.EliteCME.com
imprisonment. Multiple acts by a health care facility in violation of subdivision (b) shall be punishable by a fine not to exceed $5,000 and shall be reported to the State Department of Health Services and shall be considered as grounds for disciplinary action with respect to licensure, including suspension or revocation of the license or certificate.
A failure or refusal to comply with a court order, issued in the enforcement of a subpoena, mandating the release of records to the
board constitutes unprofessional conduct and is grounds for suspension or revocation of his or her license.
For the purposes of this section, a “health care facility” means a clinic or health care facility licensed or exempt from licensure pursuant to Division 2 (commencing with Section 1200) of the Health and Safety Code.
Section 1954: Scope of practice for dental hygienistsa. It is unprofessional conduct for a person licensed under this article
to perform, or hold himself or herself out as able to perform, professional services beyond the scope of his or her license and field of competence, as established by his or her education, experience, and training. This includes, but is not limited to, using an instrument or device in a manner that is not in accordance
with the customary standards and practices of the dental hygiene profession.
b. This section shall not apply to research conducted by accredited dental schools or dental hygiene schools, or to research conducted pursuant to an investigational device exemption issued by the United States Food and Drug Administration.
Section 1956: Unnecessary treatmentIt is unprofessional conduct for a person licensed under California code to require, either directly or through an office policy, or knowingly permit the delivery of dental hygiene care that discourages
necessary treatment, or permits clearly excessive, incompetent, unnecessary, or grossly negligent treatment, or repeated negligent acts, as determined by the standard of practice in the community.
Section 1951: Disciplinary actions for dental hygienists The committee may discipline a licensee by placing him or her on probation under various terms and conditions that may include, but are not limited to, the following:
● Requiring the licensee to obtain additional training or pass an examination upon completion of training, or both. The examination may be a written or oral examination, or both, and may be a practical or clinical examination, or both, at the option of the committee.
● Requiring the licensee to submit to a complete diagnostic examination by one or more physicians appointed by the committee, if warranted by the physical or mental condition of the licensee. If the committee requires the licensee to submit to an examination, the committee shall receive and consider any other report of a complete diagnostic examination given by one or more physicians of the licensee’s choice.
● Restricting or limiting the extent, scope or type of practice of the licensee.
● Requiring restitution of fees to the licensee’s patients or payers of services, unless restitution has already been made.
● Providing the option of alternative community service in lieu of all or part of a period of suspension in cases other than violations relating to quality of care.
1957. – Suspension of license for hygienists:a. A person whose license has been revoked or suspended, who
has been placed on probation, or whose license was surrendered pursuant to a stipulated settlement as a condition to avoid a disciplinary administrative hearing, may petition the committee for reinstatement or modification of the penalty, including modification or termination of probation, after a period of not less than the following minimum periods have elapsed from the effective date of the decision ordering disciplinary action:1. At least three years for reinstatement of a license revoked
for unprofessional conduct or surrendered pursuant to a stipulated settlement as a condition to avoid an administrative disciplinary hearing.
2. At least two years for early termination, or modification of a condition, of a probation of three years or more.
3. At least one year for modification of a condition, or reinstatement of a license revoked for mental or physical illness, or termination, or modification of a condition, of a probation of less than three years.
b. The petition shall state any fact required by the committee.c. The petition may be heard by the committee, or the committee
may assign the petition to an administrative law judge designated in Section 11371 of the Government Code.
d. In considering reinstatement or modification or penalty, the committee or the administrative law judge hearing the petition may consider the following:1. All activities of the petitioner since the disciplinary action was
taken.2. The offense for which the petitioner was disciplined.3. The petitioner’s activities during the time the license,
certificate or permit was in good standing.4. The petitioner’s rehabilitative efforts, general reputation for
truth, and professional ability.e. The hearing may be continued from time to time as the committee
or the administrative law judge as designated in Section 11371 of the Government Code finds necessary.
f. The committee or the administrative law judge may impose necessary terms and conditions on the licentiate in reinstating a license, certificate or permit or modifying a penalty.
g. A petition shall not be considered while the petitioner is under sentence for any criminal offense, including any period during which the petitioner is on court-imposed probation or parole.
h. A petition shall not be considered while there is an accusation or petition to revoke probation pending against the person.
i. The committee may deny without a hearing or argument any petition filed pursuant to this section within a period of two years from the effective date of the prior decision following a hearing under this section. Nothing in this section shall be deemed to alter Sections 822 and 823.

Dental.EliteCME.com Page 16
Section 1958: Violations and penalties for hygienistsA person, company or association is guilty of a misdemeanor, and upon conviction, shall be punished by imprisonment in a county jail not less than 10 days nor more than one year, or by a fine of not less than $100 nor more than $1,500, or by both that fine and imprisonment, who does any of the following:a. Assumes the title of “registered dental hygienist,” “registered dental
hygienist in alternative practice,” or “registered dental hygienist in extended functions” or appends the letters “R.D.H.,” “R.D.H.A.P.,” or “R.D.H.E.F.” to his or her name without having had the right to assume the title conferred upon him or her through licensure.
b. Assumes any title, or appends any letters to his or her name, with the intent to represent falsely that he or she has received a dental hygiene degree or a license under this article.
c. Engages in the practice of dental hygiene without causing to be displayed in a conspicuous place in his or her office his or her license under this article to practice dental hygiene.
d. Within 10 days after demand is made by the executive officer of the committee, fails to furnish to the committee the name and address of all persons practicing or assisting in the practice of dental hygiene in the office of the person, company, or association, at any time within 60 days prior to the demand, together with a sworn statement showing under and by what license or authority this person, company, or association and any employees are or have been practicing or assisting in the practice of dental hygiene. This sworn statement shall not be used in any prosecution under this section.
e. Is under the influence of alcohol or a controlled substance while engaged in the practice of dental hygiene in actual attendance on patients to an extent that impairs his or her ability to conduct the practice of dental hygiene with safety to patients and the public.
Section 1960: Other misdemeanorsFor the first offense, a person is guilty of a misdemeanor and shall be punishable by a fine of not less than $200 nor more than $3,000, or by imprisonment in a county jail for not to exceed six months, or by both that fine and imprisonment, and for the second or a subsequent offense is guilty of a felony and upon conviction thereof shall be punished by a fine of not less than $2,000 nor more than $6,000, or by imprisonment in the state prison, or by both that fine and imprisonment, who does any of the following:
● Sells or barters or offers to sell or barter a dental hygiene degree or transcript or a license issued under, or purporting to be issued under, laws regulating licensure of registered dental hygienists, registered dental hygienists in alternative practice, or registered dental hygienists in extended functions.
● Sells or offers to sell or barter any dental degree or license or transcript made or purporting to be made pursuant to the laws regulating the license and registration of dentists.
● Purchases or procures by barter a diploma, license, or transcript with intent that it shall be used as evidence of the holder’s qualification to practice dentistry or dental hygiene, or in fraud of the laws regulating the practice of dentistry and dental hygiene.
● With fraudulent intent, makes, attempts to make, counterfeits, or materially alters any such diploma, certificate or transcript.
● Uses, or attempts or causes to be used, any diploma, certificate, or transcript that has been purchased, fraudulently issued, counterfeited, or materially altered or in order to procure licensure
as a registered dental hygienist, registered dental hygienist in alternative practice, or registered dental hygienist in extended functions; or as a license to practice dentistry or to procure registration as a dentist.
● In an affidavit required of an applicant for an examination or license under this article, willfully makes a false statement in a material regard.
● Practices dentistry or dental hygiene or offers to practice dentistry or dental hygiene, as defined in the code, either without a license, or when his or her license has been revoked or suspended.
● Under any false, assumed or fictitious name, either as an individual, firm, corporation or otherwise, or any name other than the name under which he or she is licensed, practices, advertises, or in any other manner indicates that he or she practices or will practice dentistry or dental hygiene, except a name specified in a valid permit issued pursuant to Section 1962.
A person who willfully, under circumstances that cause risk of bodily harm, serious physical or mental illness, or death, practices, attempts to practice, advertises, or holds himself or herself out as practicing dental hygiene without having at the time of so doing a valid, unrevoked, and unsuspended license as provided in this chapter, is guilty of a crime, punishable by imprisonment in a county jail for up to one year. The remedy provided in this section shall not preclude any other remedy provided by law.
Alternative and group practices by hygienistsAn association, partnership, corporation or group of three or more registered dental hygienists in alternative practice engaging in practice under a name that would otherwise be in violation of the laws may practice under that name if the association, partnership, corporation or group holds an unexpired, unsuspended and unrevoked permit issued by the committee. An individual registered dental hygienist in alternative practice or a pair of registered dental hygienists in alternative practice who practice dental hygiene under a name that would otherwise violate Section 1960 may practice under that name if the licensees hold a valid permit issued by the committee under this section.
The committee shall issue a written permit authorizing the holder to use a name specified in the permit in connection with the holder’s practice if the committee finds all of the following:1. The applicant or applicants are duly licensed registered dental
hygienists in alternative practice.2. The place where the applicant or applicants practice is owned or
leased by the applicant or applicants, and the practice conducted at the place is wholly owned and entirely controlled by the applicant
or applicants and is an approved area or practice setting pursuant to Section 1926.
3. The name under which the applicant or applicants propose to operate contains at least one of the following designations: “dental hygiene group,” “dental hygiene practice,” or “dental hygiene office,” contains the family name of one or more of the past, present, or prospective associates, partners, shareholders, or members of the group, and is in conformity with Section 651 and not in violation of subdivisions (i) and (l) of Section 1950.5.
4. All licensed persons practicing at the location designated in the application hold valid licenses and no charges of unprofessional conduct are pending against any person practicing at that location.
A permit issued under this section shall expire and become invalid unless renewed in the manner provided for in this article for the renewal of certificates issued under this article. A permit issued under this section may be revoked or suspended if the committee finds that any requirement for original issuance of a permit is no longer being fulfilled by the permit holder. Proceedings for revocation or suspension shall be governed by the Administrative Procedure Act.

Page 17 Dental.EliteCME.com
If charges of unprofessional conduct are filed against the holder of a permit issued under this section, or a member of an association, partnership, group, or corporation to whom a permit has been issued under this section, proceedings shall not be commenced for revocation or suspension of the permit until a final determination of the charges of unprofessional conduct, unless the charges have resulted in revocation or suspension of a license.
The committee may prefer a complaint for violation of any part of this article before any court of competent jurisdiction and may, by its officers, counsel and agents, assist in presenting the law or facts at the trial. The district attorney of each county in this state shall prosecute all violations of this article in their respective counties in which the violations occur.
In addition to the other proceedings provided for in this article, on application of the committee, the superior court of any county shall issue an injunction to restrain an unlicensed person from conducting the practice of dental hygiene, as defined in this article.
If a person has engaged in or is about to engage in an act that constitutes an offense against this chapter, the superior court of any county, on application of 10 or more persons holding licenses to practice dental hygiene issued under this article, may issue an injunction or other appropriate order restraining that conduct. Proceedings under this section shall be governed by Chapter 3 (commencing with Section 525) of Title 7 of Part 2 of the Code of Civil Procedure.
Section 1966: Rehabilitation and diversion program a. It is the intent of the Legislature that the committee seek ways and
means to identify and rehabilitate licensees whose competency may be impaired due to abuse of dangerous drugs or alcohol, so that licensees so afflicted may be treated and returned to the practice of dental hygiene in a manner that will not endanger the public health and safety. It is also the intent of the Legislature that the committee establish a diversion program as a voluntary alternative approach to traditional disciplinary actions.
b. One or more diversion evaluation committees shall be established by the committee. The committee shall establish criteria for the selection of each diversion evaluation committee. Each member of a diversion evaluation committee shall receive per diem and expenses as provided in Section 103.
1966.1. a. The committee shall establish criteria for the acceptance, denial, or
termination of licensees in a diversion program. Unless ordered by the committee as a condition of a licensee’s disciplinary probation, only those licensees who have voluntarily requested diversion treatment and supervision by a diversion evaluation committee shall participate in a diversion program.
b. A licensee who is not the subject of a current investigation may self-refer to the diversion program on a confidential basis, except as provided in subdivision (f).
c. A licensee under current investigation by the committee may also request entry into a diversion program by contacting the committee. The committee may refer the licensee requesting participation in the program to a diversion evaluation committee for evaluation of eligibility. Prior to authorizing a licensee to enter into the diversion program, the committee may require the licensee, while under current investigation for any violations of this article or other violations, to execute a statement of understanding that states that the licensee understands that his or her violations of this article or other statutes, that would otherwise be the basis for discipline, may still be investigated and the subject of disciplinary action.
d. If the reasons for a current investigation of a licensee are based primarily on the self-administration of any controlled substance or dangerous drugs or alcohol under Section 1951, or the illegal possession, prescription, or nonviolent procurement of any controlled substance or dangerous drugs for self-administration that does not involve actual, direct harm to the public, the committee shall close the investigation without further action if the licensee is accepted into the committee’s diversion program and successfully completes the requirements of the program. If the licensee withdraws or is terminated from the program by a diversion evaluation committee, the investigation shall be reopened and disciplinary action imposed, if warranted, as determined by the committee.
e. Neither acceptance nor participation in the diversion program shall preclude the committee from investigating or continuing
to investigate, or taking disciplinary action or continuing to take disciplinary action against, any licensee for any unprofessional conduct committed before, during or after participation in the diversion program.
f. All licensees shall sign an agreement of understanding that the withdrawal or termination from the diversion program at a time when a diversion evaluation committee determines the licensee presents a threat to the public’s health and safety shall result in the utilization by the committee of diversion treatment records in disciplinary or criminal proceedings.
g. Any licensee terminated from the diversion program for failure to comply with program requirements is subject to disciplinary action by the committee for acts committed before, during, and after participation in the diversion program. A licensee who has been under investigation by the committee and has been terminated from the diversion program by a diversion evaluation committee shall be reported by the diversion evaluation committee to the committee.
1966.2. – Each diversion evaluation committee shall have the following duties and responsibilities:a. To evaluate those licensees who request to participate in the
diversion program according to the guidelines prescribed by the committee and to consider the recommendations of any licensees designated by the committee to serve as consultants on the admission of the licensee to the diversion program.
b. To review and designate those treatment facilities to which licensees in a diversion program may be referred.
c. To receive and review information concerning a licensee participating in the program.
d. To consider in the case of each licensee participating in a program whether he or she may safely continue or resume the practice of dental hygiene.
e. To perform other related duties as the committee may by regulation require.
1966.3. – Notwithstanding the provisions of Article 9 (commencing with Section 11120) of Chapter 1 of Part 1 of Division 3 of Title 2 of the Government Code, relating to public meetings, a diversion evaluation committee may convene in closed session to consider reports pertaining to any licentiate requesting or participating in a diversion program. A diversion evaluation committee shall only convene in closed session to the extent that it is necessary to protect the privacy of a licensee.
1966.4. – Each licensee who requests participation in a diversion program shall agree to cooperate with the treatment program designed by a diversion evaluation committee and to bear all costs related to the program, unless the cost is waived by the committee. Any failure to comply with the provisions of a treatment program may result in termination of the licensee’s participation in a program.
1966.5.a. After a diversion evaluation committee, in its discretion, has
determined that a licensee has been rehabilitated and the diversion

Dental.EliteCME.com Page 18
program is completed, the diversion evaluation committee shall purge and destroy all records pertaining to the licensee’s participation in the diversion program.
b. Except as authorized by subdivision (f) of Section 1966.1, all committee and diversion evaluation committee records and records of proceedings pertaining to the treatment of a licensee in a program shall be kept confidential and are not subject to discovery or subpoena.
1966.6. – The committee shall provide for the representation of any person making reports to a diversion evaluation committee or the committee under this article in any action for defamation for reports or information given to the diversion evaluation committee or the committee regarding a licensee’s participation in the diversion program.
Acts in violation of the Dental Practice Code The California Business and Professions Code Section 108, and 125.9, gives each of the respective department boards the authority to issue citations and fines after conducting investigation of violations of laws under their jurisdiction as follows:
● Each of the boards comprising the department exists as a separate unit, and has the functions of setting standards, holding meetings, and setting dates thereof, preparing and conducting examinations, passing upon applicants, conducting investigations of violations of laws under its jurisdiction, issuing citations and holding hearings for the revocation of licenses, and the imposing of penalties following those hearings, insofar as these powers are given by statute to each respective board.
● Failure of a licensee to pay a fine within 30 days of the date of assessment, unless the citation is being appealed, may result in disciplinary action being taken by the board, bureau, or commission. Where a citation is not contested and a fine is not paid, the full amount of the assessed fine shall be added to the fee for renewal of the license. A license shall not be renewed without payment of the renewal fee and fine.
The system may contain the following provisions: ● A citation may be issued without the assessment of an
administrative fine.
● Assessment of administrative fines may be limited to only particular violations of the applicable licensing act.
● Notwithstanding any other provision of law, if a fine is paid to satisfy an assessment based on the finding of a violation, payment of the fine shall be represented as satisfactory resolution of the matter for purposes of public disclosure.
● Administrative fines collected pursuant to this section shall be deposited in the special fund of the particular board, bureau or commission.
1611.5. – The board may inspect the books, records and premises of any dentist licensed under this chapter in response to a complaint that a licensee has violated any law or regulation that constitutes grounds for disciplinary action by the board, and may employ inspectors for this purpose. A licensee’s failure to allow an inspection or any part thereof shall be grounds for suspension or revocation of the license in accordance with Section 1670.
Legal, valid, unexpired license1626. – It is unlawful for any person to engage in the practice of dentistry in the state, either privately or as an employee of a governmental agency or political subdivision, unless the person has a valid, unexpired license or special permit from the board.
Scope of practiceIn addition to other acts constituting unprofessional conduct under this chapter, it is unprofessional conduct for a person licensed under this chapter to perform, or hold himself or herself out as able to perform, professional services beyond the scope of his or her license and field or fields of competence as established by his or her education, experience, training, or any combination thereof. This includes, but is not limited to, the use of any instrument or device in a manner that is
not in accordance with the customary standards and practices of the dental profession.
This section shall not apply to research conducted by accredited dental schools or colleges, or to research conducted pursuant to an investigational device exemption issued by the United States Food and Drug Administration.
More on unprofessional conduct1684.5. - In addition to other acts constituting unprofessional conduct listed above, it is unprofessional conduct for any dentist to perform or allow to be performed any treatment on a patient who is not a patient of record of that dentist. A dentist may, however, after conducting a preliminary oral examination, require or permit any dental auxiliary to perform procedures necessary for diagnostic purposes, provided that the procedures are permitted under the auxiliary’s authorized scope of practice. Additionally, a dentist may require or permit a dental auxiliary to perform all of the following duties prior to any examination of the patient by the dentist, provided that the duties are authorized for the particular classification of dental auxiliary pursuant to Article 7 (commencing with Section 1740):1. Expose emergency radiographs upon direction of the dentist.2. If the dental auxiliary is a registered dental assistant in extended
functions, a registered dental hygienist, or a registered dental hygienist in alternative practice, determine and perform radiographs for the specific purpose of aiding a dentist in completing a comprehensive diagnosis and treatment plan for a patient using telehealth, as defined by Section 2290.5, for the purpose of communication with the supervising dentist pursuant to Sections 1753.55, 1910.5, and 1926.05. A dentist is not required to review patient records or make a diagnosis using telehealth.
3. Perform extra-oral duties or functions specified by the dentist.4. Perform mouth-mirror inspections of the oral cavity, to include
charting of obvious lesions, malocclusions, existing restorations, and missing teeth.
For purposes of this section, “patient of record” refers to a patient who has been examined, has had a medical and dental history completed and evaluated, and has had oral conditions diagnosed and a written plan developed by the licensed dentist.
For purposes of this section, if dental treatment is provided to a patient by a registered dental assistant in extended functions, a registered dental hygienist, or a registered dental hygienist in alternative practice pursuant to the diagnosis and treatment plan authorized by a supervising dentist, at a location other than the dentist’s practice location, it is the responsibility of the authorizing dentist that the patient or the patient’s representative receive written notification that the care was provided at the direction of the authorizing dentist and that the notification include the authorizing dentist’s name, practice location address, and telephone number. This provision shall not require patient notification for dental hygiene preventive services provided in public health programs as specified and authorized in

Page 19 Dental.EliteCME.com
Section 1911, or for dental hygiene care when provided as specified and authorized in Section 1926.
A dentist shall not concurrently supervise more than a total of five registered dental assistants in extended functions, registered dental hygienists, or registered dental hygienists in alternative practice providing services pursuant to Sections 1753.55, 1910.5, and 1926.05.
This section shall not apply to dentists providing examinations on a temporary basis outside of a dental office in settings including, but not limited to, health fairs and school screenings. It also shall not apply to fluoride mouth rinse or supplement programs administered in a school or preschool setting.
Revoked or suspended licenses1686. – A person whose license, certificate, or permit has been revoked or suspended, who has been placed on probation, or whose license, certificate, or permit was surrendered pursuant to a stipulated settlement as a condition to avoid a disciplinary administrative hearing, may petition the board for reinstatement or modification of penalty, including modification or termination of probation, after a period of not less than the following minimum periods have elapsed from the effective date of the decision ordering disciplinary action:a. At least three years for reinstatement of a license revoked for
unprofessional conduct or surrendered pursuant to a stipulated settlement as a condition to avoid an administrative disciplinary hearing.
b. At least two years for early termination, or modification of a condition, of a probation of three years or more.
c. At least one year for modification of a condition, or reinstatement of a license revoked for mental or physical illness, or termination, or modification of a condition, of a probation of less than three years. The petition shall state any fact required by the board.
The petition may be heard by the board, or the board may assign the petition to an administrative law judge designated in Section 11371 of the Government Code. In considering reinstatement or modification or penalty, the board or the administrative law judge hearing the petition may consider:
1. All activities of the petitioner since the disciplinary action was taken.
2. The offense for which the petitioner was disciplined.3. The petitioner’s activities during the time the license,
certificate or permit was in good standing. 4. The petitioner’s rehabilitative efforts, general reputation for
truth, and professional ability. The hearing may be continued from time to time as the board or the administrative law judge as designated in Section 11371 of the Government Code finds necessary. The board or the administrative law judge may impose necessary terms and conditions on the licentiate in reinstating a license, certificate or permit or modifying a penalty.
Criminal offensesNo petition under this section shall be considered while the petitioner is under sentence for any criminal offense, including any period during which the petitioner is on court-imposed probation or parole. No petition shall be considered while there is an accusation or petition to revoke probation pending against the person. The board may deny
without a hearing or argument any petition filed pursuant to this section within a period of two years from the effective date of the prior decision following a hearing under this section. Nothing in this section shall be deemed to alter Sections 822 and 823.
Registered sex offenders1687 - a. Notwithstanding any other provision of law, with regard to an
individual who is required to register as a sex offender pursuant to Section 290 of the Penal Code, or the equivalent in another state or territory, under military law, or under federal law, the board shall be subject to the following requirements:1. The board shall deny an application by the individual for
licensure pursuant to this chapter.2. If the individual is licensed under this chapter, the board shall
revoke the license of the individual. 3. The board shall not stay the revocation and place the license
on probation.4. The board shall not reinstate or reissue the individual’s
licensure under this chapter. The board shall not issue a stay of license denial and place the license on probation.
b. This section shall not apply to any of the following:1. An individual who has been relieved under Section 290.5 of
the Penal Code of his or her duty to register as a sex offender,
or whose duty to register has otherwise been formally terminated under California law or the law of the jurisdiction that requires his or her registration as a sex offender.
2. An individual who is required to register as a sex offender pursuant to Section 290 of the Penal Code solely because of a misdemeanor conviction under Section 314 of the Penal Code. However, nothing in this paragraph shall prohibit the board from exercising its discretion to discipline a licensee under other provisions of state law based upon the licensee’s conviction under Section 314 of the Penal Code.
3. Any administrative adjudication proceeding under Chapter 5 (commencing with Section 11500) of Part 1 of Division 3 of Title 2 of the Government Code that is fully adjudicated prior to January 1, 2008. A petition for reinstatement of a revoked or surrendered license shall be considered a new proceeding for purposes of this paragraph, and the prohibition against reinstating a license to an individual who is required to register as a sex offender shall be applicable.
Practicing without a valid license, expired or suspended licenses1700. – Any person, company, or association is guilty of a misdemeanor, and upon conviction thereof shall be punished by imprisonment in the county jail not less than 10 days nor more than one year, or by a fine of not less than one hundred dollars ($100) nor more than one thousand five hundred dollars ($1,500), or by both fine and imprisonment, who:a. Assumes the degree of “doctor of dental surgery,” “doctor of
dental science,” or “doctor of dental medicine” or appends the letters “D.D.S.,” or “D.D.Sc.” or “D.M.D.” to his or her name
without having had the right to assume the title conferred upon him or her by diploma from a recognized dental college or school legally empowered to confer the same.
b. Assumes any title, or appends any letters to his or her name, with the intent to represent falsely that he or she has received a dental degree or license.
c. Engages in the practice of dentistry without causing to be displayed in a conspicuous place in his or her office the name of each and every person employed there in the practice of dentistry.

Dental.EliteCME.com Page 20
d. Within 10 days after demand is made by the executive officer of the board, fails to furnish to the board the name and address of all persons practicing or assisting in the practice of dentistry in the office of the person, company, or association, at any time within 60 days prior to the demand, together with a sworn statement showing under and by what license or authority this person, company, or association and any employees are or have been practicing dentistry. This sworn statement shall not be used in any prosecution under this section.
e. Is under the influence of alcohol or a controlled substance while engaged in the practice of dentistry in actual attendance on patients to an extent that impairs his or her ability to conduct the practice of dentistry with safety to patients and the public.
1701.5. – Any association or partnership or corporation or group of three or more dentists, engaging in practice under any name that would otherwise be in violation of Section 1701 may practice under this name if, and only if, the association, partnership, corporation or group holds an outstanding, unexpired, unsuspended and unrevoked permit issued by the board under this section. On and after July 1, 1995, any individual dentist or pair of dentists engaging in the practice of dentistry under any name that would otherwise be in violation of Section 1701 may practice under that name if and only if the dentist or pair of dentists hold an outstanding, unexpired, unsuspended, and unrevoked permit issued by the board under this section. The board shall issue written permits authorizing the holder to use a name specified in the permit in connection with the holder’s practice if, and only if, the board finds to its satisfaction that:a. The applicant or applicants are duly licensed dentists.b. The place or establishment, or the portion thereof, where the
applicant or applicants practice, is owned or leased by the
applicant or applicants, and the practice conducted at the place or establishment, or portion thereof, is wholly owned and entirely controlled by the applicant or applicants.
c. The name that the applicant or applicants propose to operate contains at least one of the following designations: “dental group,” “dental practice,” or “dental office” and contains the family name of one or more of the past, present, or prospective associates, partners, shareholders, or members of the group, and is in conformity with Section 651 and subdivisions (i) and (l) of Section 1680.
d. All licensed persons practicing at the location designated in the application hold valid and outstanding licenses and that no charges of unprofessional conduct are pending against any persons practicing at that location.
Permits issued under this section by the board shall expire and become invalid unless renewed at the times and in the manner provided for the renewal of certificates issued under this chapter. Any permits issued under this section may be revoked or suspended at any time that the board finds that any one of the requirements for original issuance of a permit is no longer being fulfilled by the holder to whom the permit was issued. Proceedings for revocation or suspension shall be governed by the Administrative Procedure Act. In the event charges of unprofessional conduct are filed against the holder of a permit issued under this section, or a member of an association or partnership or a member of a group or corporation to whom a permit has been issued under this section, proceedings shall not be commenced for revocation or suspension of the permit until final determination of the charges of unprofessional conduct and unless the charges have resulted in revocation or suspension of license.
Dispensing controlled substances Prescribers (which under California law includes people with licenses to practice dentistry) who dispense controlled substances must comply with the requirements of Business and Profession Code Sections 4076, 4170, 4172:
Dispensing controlled substancesAlways store controlled substances in a locked cabinet or drawer.1. Maintain a log. 2. Prior to dispensing, offer to give a written prescription to the
patient that the patient may elect to have filled by you, the dentist, or by any pharmacy. You must provide the patient with a written disclosure that the patient has a choice between obtaining the prescription from you, the dentist, or obtaining the prescription at a pharmacy of the patient’s choice.
3. When dispensing controlled substances to a patient, you must: ○ Label the container with the prescriber’s name, patient’s
name, drug name, strength, date of issue, dosage, quantity, directions for use, and expiration date.
○ Inform the patient orally or in writing of possible side effects of the drug.
A dentist with a current DEA registration may dispense to a patient under his or her care a Schedule II controlled substance in an amount not to exceed a 72-hour supply in accordance with normal use.
4170. a. No prescriber shall dispense drugs or dangerous devices to patients
in his or her office or place of practice unless all of the following conditions are met:
1. The dangerous drugs or dangerous devices are dispensed to the prescriber’s own patient, and the drugs or dangerous devices are not furnished by a nurse or physician attendant.
2. The dangerous drugs or dangerous devices are necessary in the treatment of the condition for which the prescriber is attending the patient.
3. The prescriber does not keep a pharmacy, open shop, or drugstore, advertised or otherwise, for the retailing of dangerous drugs, dangerous devices or poisons.
4. The prescriber fulfills all of the labeling requirements imposed upon pharmacists by Section 4076, all of the recordkeeping requirements of this chapter, and all of the packaging requirements of good pharmaceutical practice, including the use of childproof containers.
5. The prescriber does not use a dispensing device unless he or she personally owns the device and the contents of the device, and personally dispenses the dangerous drugs or dangerous devices to the patient packaged, labeled, and recorded in accordance with paragraph (4).
6. The prescriber, prior to dispensing, offers to give a written prescription to the patient that the patient may elect to have filled by the prescriber or by any pharmacy.
7. The prescriber provides the patient with written disclosure that the patient has a choice between obtaining the prescription from the dispensing prescriber or obtaining the prescription at a pharmacy of the patient’s choice.

Page 21 Dental.EliteCME.com
Renewal of license1715. – Licenses issued under the provisions of this chapter, unless specifically excepted, expire at 12 midnight on the legal birth date of a licentiate of the board during the second year of a two-year term if not renewed.
The board shall establish procedures for the administration of the birth date renewal program, including, but not limited to, the establishment of a pro rata formula for the payment of fees by licentiates affected by the implementation of such program and the establishment of a system of staggered license expiration dates such that a relatively equal number of licenses expire annually.
1715.1. – The provisions of Sections 1715, 1716, 1717, 1718, 1718.1, 1718.2, and 1718.3 shall also apply to and govern the expiration, renewal, restoration, reinstatement, and reissuance of permission to conduct an additional place of practice.
1715.5. – Dental specialtiesa. A licensee shall, upon his or her initial licensure and any
subsequent application for renewal, report the completion of any advanced educational program accredited by the Committee on Dental Accreditation in a dental specialty recognized by the American Dental Association.
b. The licensee shall also report, upon his or her initial licensure and any subsequent application for renewal, the practice or employment status of the licensee, designated as one of the following:1. Full-time practice or employment in a dental practice of
32 hours per week or more in California. This reporting requirement shall also apply to a dental auxiliary licensee.
2. Full-time practice or employment in a dental practice outside of California.
3. Part-time practice or employment in a dental practice for less than 32 hours per week in California.
4. Dental administrative employment that does not include direct patient care, as may further be defined by the board.
5. Retired.6. Other practice or employment status, as may be further defined
by the board.c. Information collected pursuant to subdivision (b) shall be posted
on the Internet website of the board or the Committee on Dental Auxiliaries (COMDA), as appropriate.
d. (1) A licensee may report, in his or her application for renewal, and the board shall collect, information regarding the licensee’s cultural background and foreign language proficiency. (2) Information collected pursuant to this subdivision shall be aggregated on an annual basis, based on categories utilized by the board in the collection of the data, into both statewide totals and ZIP Code of primary practice or employment location totals. (3) Aggregated information under this subdivision shall be compiled annually, and reported on the Internet Web site of the board on or before July 1 of each year.
1716. – Nothing contained in this chapter shall exempt from the payment of the renewal fee any person authorized to practice dentistry in the state of California, and every person practicing dentistry in this state shall pay the renewal fee irrespective of the time when he was licensed or first had the right to lawfully practice dentistry in this state or elsewhere.
Retired or disabled dentists1716.1. a. Notwithstanding Section 1716, the board may, by regulation,
reduce the renewal fee for a licensee who has practiced dentistry for 20 years or more in this state, has reached the age of retirement under the federal Social Security Act (42 U.S.C. Sec. 301 et seq.), and customarily provides his or her services free of charge to any person, organization, or agency. In the event that charges are made, these charges shall be nominal. In no event shall the aggregate of these charges in any single calendar year be in an amount that would render the licensee ineligible for full Social Security benefits. The board shall not reduce the renewal fee under this section to an amount less than one-half of the regular renewal fee.
b. Notwithstanding Section 1716, any licensee who demonstrates to the satisfaction of the board that he or she is unable to practice dentistry due to a disability, may request a waiver of 50 percent of the renewal fee. The granting of a waiver shall be at the discretion of the board, and the board may terminate the waiver at any time. A licensee to whom the board has granted a waiver pursuant to this subdivision shall not engage in the practice of dentistry unless and until the licensee pays the current renewal fee in full and establishes to the satisfaction of the board, on a form prescribed by the board and signed under penalty of perjury, that the licensee’s disability either no longer exists or no longer affects his or her ability to safely practice dentistry.
Dental license renewal1717. – To renew an unexpired license, the licensee shall, before the time at which the license would otherwise expire, apply for renewal on a form prescribed by the board and pay the renewal fee prescribed by this chapter. The receipt of the executive officer shall be indispensable evidence that payment has been made.
1718. – Except as otherwise provided in this chapter, an expired license may be renewed at any time within five years after its expiration on filing of application for renewal on a form prescribed by the board, and payment of all accrued renewal and delinquency fees. If the license is renewed more than 30 days after its expiration, the licensee, as a condition precedent to renewal, shall also pay the delinquency fee prescribed by this chapter. Renewal under this section shall be effective on the date on which the application is filed, on the date on which the renewal fee is paid, or on the date on which the delinquency fee, if any, is paid, whichever last occurs. If so renewed, the license shall continue in effect through the expiration date provided in Section 1715 which next occurs after the effective date of the renewal, when it shall expire if it is not again renewed.
1718.1. – A suspended license is subject to expiration and shall be renewed as provided in this article, but such renewal does not entitle the licensee, while the license remains suspended and until it is reinstated, to engage in the licensed activity, or in any other activity or conduct in violation of the order or judgment by which the license was suspended.
1718.2.– A revoked license is subject to expiration as provided in this article, but it may not be renewed. If it is reinstated after its expiration, the licensee, as a condition precedent to its reinstatement, shall pay a reinstatement fee in an amount equal to the renewal fee in effect on the last regular renewal date before the date on which it is reinstated, plus the delinquency fee, if any, accrued at the time of its revocation.
1718.3. – After five years a license which is not renewed within five years, after its expiration may not be renewed, restored, reinstated or reissued, but the holder of the license may apply for and obtain a new license if certain requirements are satisfied.

Dental.EliteCME.com Page 22
1017. – Continuing education units required for renewal of license.a. As a condition of renewal, all licensees are required to complete
continuing education as follows:1. Two units of continuing education in infection control specific
to California regulations as defined in section 1016(b)(1)(A).2. Two units of continuing education in the California Dental
Practice Act and its related regulations as defined in section 1016(b)(1)(B).
3. A maximum of four units of a course in basic life support as specified in section 1016(b)(1)(C).
b. Mandatory continuing education units count toward the total units required to renew a license or permit; however, failure to complete the mandatory courses will result in non-renewal of a license or permit. Any continuing education units accumulated before April 8, 2010, that meet the requirements in effect on the date the units were accumulated will be accepted by the board for license or permit renewals taking place on or after April 8, 2010.
c. All licensees shall accumulate the continuing education units equal to the number of units indicated below during the biennial license or permit renewal period assigned by the board on each license or permit. All licensees shall verify to the board that he or she who has been issued a license or permit to practice for a period less than two years shall begin accumulating continuing education A in his or her application for renewal, and the board or COMDA, As appropriate shall collect information licensee may report credits within the next biennial renewal period occurring after the issuance of a new license or permit to practice.1. Dentists: 50 units.2. Registered dental hygienists: 25 units.3. Registered dental assistants: 25 units.4. Dental sedation assistant permit holders: 25 units.5. Orthodontic assistant permit holders: 25 units.6. Registered dental hygienists in extended functions: 25 units.7. Registered dental assistants in extended functions: 25 units.8. Registered dental hygienists in alternative practice: 35 units.
d. Each dentist licensee who holds a general anesthesia permit shall complete, as a condition of permit renewal, continuing education requirements pursuant to Section 1646.5 of the Business and Professions Code at least once every two years, and either (1) an advanced cardiac life support course which is approved by the American Heart Association and which includes an examination on the materials presented in the course or (2) any other advanced cardiac life support course which is identical in all respects, except for the omission of materials that relate solely to hospital emergencies or neonatology, to the course entitled “2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care” published by the American Heart Association December 13, 2005, which is incorporated herein by reference.
e. Each dentist licensee who holds a conscious sedation permit shall complete at least once every two years a minimum of 15 total units of coursework related to the administration of conscious sedation and to medical emergencies, as a condition of permit renewal, in continuing education requirements pursuant to Section 1647.5 of the of the Business and Professions Code. Refusal to execute the required assurance shall result in non-renewal of the permit.
f. Each dentist licensee who holds an oral conscious sedation permit for minors, as a condition of permit renewal, shall complete at least once every two years a minimum of 7 total units of coursework related to the subject area in continuing education requirements pursuant to Section 1647.13 of the Business and Professions Code.
g. Each dentist licensee who holds an oral conscious sedation permit for adults, as a condition of permit renewal, shall complete at least once every two years a minimum of 7 total units of coursework related to the subject area in continuing education requirements
pursuant to Section 1647.21 of the of the Business and Professions Code.
h. Notwithstanding any other provisions of this code, tape-recorded courses, home-study materials, video courses and computer courses are considered correspondence courses, and will be accepted for credit up to, but not exceeding, 50 percent of the licensee’s total required units.
i. In the event that a portion of a licensee’s units have been obtained through non-live instruction, as described in Section (h) above, all remaining units shall be obtained through live interactive course study with the option to obtain 100 percent of the total required units by way of interactive instruction courses. Such courses are defined as live lecture, live telephone conferencing, live video conferencing, live workshop demonstration, or live classroom study.
j. Licensees who participate in the following activities shall be issued continuing education credit for up to 20 percent of their total continuing education unit requirements for license renewal:1. Participation in any Dental Board of California or Western
Regional Examination Board (WREB) administered examination including attendance at calibration training, examiner orientation sessions, and examinations.
2. Participation in any site visit or evaluation relating to issuance and maintenance of a general anesthesia, conscious sedation or oral conscious sedation permit.
3. Participation in any calibration training and site evaluation training session relating to general anesthesia, conscious sedation or oral conscious sedation permits.
4. Participation in any site visit or evaluation of an approved dental auxiliary program or dental auxiliary course.
k. The board shall issue to participants in the activities listed in subdivision (j) a certificate that contains the date, time, location, authorizing signature, 11-digit course registration number, and number of units conferred for each activity consistent with all certificate requirements herein required for the purposes of records retention and auditing.
l. The license or permit of any person who fails to accumulate the continuing education units set forth in this section or to assure the board that he or she will accumulate such units, shall not be renewed until such time as the licensee complies with those requirements.
m. A licensee who has not practiced in California for more than one year because the licensee is disabled need not comply with the continuing education requirements of this article during the renewal period within which such disability falls. Such licensee shall certify in writing that he or she is eligible for waiver of the continuing education requirements. A licensee who ceases to be eligible for such waiver shall notify the board of such and shall comply with the continuing education requirements for subsequent renewal periods.
n. A licensee shall retain, for a period of three renewal periods, the certificates of course completion issued to him or her at the time he or she attended a continuing education course and shall forward such certifications to the board only upon request by the board for audit purposes. A licensee who fails to retain a certification shall contact the provider and obtain a duplicate certification.
o. Any licensee who furnishes false or misleading information to the board regarding his or her continuing education units may be subject to disciplinary action. The board may audit a licensee continuing education records as it deems necessary to ensure that the continuing education requirements are met.
p. A licensee who also holds a special permit for general anesthesia, conscious sedation, oral conscious sedation of a minor or of an adult, may apply the continuing education units required in the specific subject areas to their dental license renewal requirements.
q. A registered dental assistant or registered dental assistant in extended functions who holds a permit as an orthodontic assistant

Page 23 Dental.EliteCME.com
or a dental sedation assistant shall not be required to complete additional continuing education requirements beyond that which is required for licensure renewal in order to renew either permit.
r. Pertaining to licensees holding more than one license or permit, the license or permit that requires the largest number of continuing education units for renewal shall equal the licensee’s full renewal requirement. Dual licensure, or licensure with permit, shall not require duplication of continuing education requirements.
s. Current and active licensees enrolled in a full-time educational program in the field of dentistry, including dental school program, residency program, postdoctoral specialty program, dental hygiene school program, dental hygiene in alternative practice program, or registered dental assisting in extended functions program approved by the board or the ADA Commission on Dental Accreditation shall be granted continuing education credits for completed
curriculum during that renewal period. In the event of audit, licensees shall be required to present school transcripts to the board as evidence of enrollment and course completion.
t. Current and active dental sedation assistant and orthodontic assistant permit holders enrolled in a full-time dental hygiene school program, dental assisting program, or registered dental assisting in extended functions program approved by the board or the ADA Commission on Dental Accreditation shall be granted continuing education credits for completed curriculum during that renewal period. In the event of audit, assisting permit holders shall be required to present school transcripts to the committee or board as evidence of enrollment and course completion.
Note: Authority cited: Sections 1614 and 1645, Business and Professions Code. Reference: Sections 1645, 1646.5 and 1647.5, Business and Professions Code.
Mandatory reporting obligationsChild Abuse and Neglect Reporting Act, California Penal Code Section 11164-11174.4, and the Elder Abuse and Dependent Adult Civil Protection Act.In the state of California, Penal Code Section 11164-11174.4 is known as the Child Abuse and Neglect Reporting Act. In this act, “child” means a person under the age of 18 years. The intent and purpose of the act is to protect children from abuse and neglect. In any investigation of suspected child abuse or neglect, all persons participating in the investigation of the case shall consider the needs of the child victim and shall do whatever is necessary to prevent psychological harm to the child victim.
California law requires certain statutorily defined categories of persons (“mandated reporters”), including dental care professionals, to report to appropriate authorities the known or reasonably suspected abuse or neglect of a child, elder, or dependent adult. California law provides immunity from liability for a mandated reporter who complies with his or her reporting obligations, and also provides a more limited immunity for non-mandated reporters who notify authorities of suspected child, elder or dependent adult abuse or neglect. A mandated reporter who fails to report a known or reasonably suspected incident of child, elder, or dependent adult abuse or neglect may be subject to criminal fines and penalties.
Except as otherwise provided by law, a mandated reporter must report to appropriate authorities when told by an elder or dependent adult that he or she has experienced behavior, including an act or omission, that constitutes abuse or neglect, including physical abuse, abandonment, isolation, or financial abuse. A mandated reporter also must report an injury that indicates possible abuse of an elder, dependent adult or child or if they have personally treated a patient with injuries from an apparent assault.
All health care providers, including dentists, hygienists and assistants, should familiarize themselves with the statutory definitions of the terms “abuse” and “neglect,” and the procedures for reporting incidents to appropriate authorities. A summary of several of the key statutory definitions is provided below.
Reports of suspected child abuse or neglect or abuse to an elder should be made by mandated reporters to any police department or sheriff’s department – not including a school district police or security department – county probation department if designated by the county to receive mandated reports, or the county welfare department. Any of those agencies shall accept a report of suspect child abuse or neglect or abuse to an elder for any jurisdiction. The agency can immediately refer the case by telephone, fax or electronic transmission to an agency with proper jurisdiction.
Reports of suspected abuse should contain the name, business address and telephone number of the mandated reporter, and the capacity that makes the person a mandated reporter; the child or elder person’s name and address, present location and where applicable, school, grade and class; the names, address and telephone numbers of the child’s parents or guardians or caregivers; the information that gave rise to the reasonable suspicion of abuse or neglect and the source or sources of that information; and any information about the person or persons who might have abused or neglected the child/elder. The mandated reporter shall make a report even if some of this information is not known or is uncertain to him or her.
The identity of all persons who report an incident under this act is kept confidential and disclosed only among agencies receiving or investigating the situation.
Failure of a health professional to file a required report is a misdemeanor, punishable by a fine of up to $1,000, or confinement in the county jail for up to six months, or both.
DefinitionsAbuse: Intentionally or recklessly causing or attempting to cause bodily injury or causing reasonable apprehension of imminent serious bodily injury to himself, herself or another.
Abuse of an elder or a dependent adult means: Physical abuse, neglect, financial abuse, abandonment, isolation or other treatment with resulting physical harm or pain or mental suffering, or the deprivation by a care custodian of goods or services that are necessary to avoid physical harm or mental suffering.
Child abuse or neglect: includes sexual abuse, sexual exploitation, other physical or emotional abuse, severe or general neglect of the child’s needs (food, clothing, shelter, medical care, and willful cruelty or unjustifiable punishment of a child).
Dependent adult: Any person between the ages of 18 and 64 years residing in California, who has physical or mental limitations that restrict his or her ability to carry out normal activities or to protect his or her rights including, but not limited to, persons who have physical or developmental disabilities or whose physical or mental abilities have diminished because of age. It includes all such persons admitted to a 24-hour health facility.
Elder: Any person residing in California who is 65 years of age or older.

Dental.EliteCME.com Page 24
Neglect of an elder or dependent adult: The negligent failure of any person having the care or custody of an elder or a dependent adult to exercise that degree of care that a reasonable person in a like position would exercise. Neglect includes, but is not limited to:
● Failure to assist in personal hygiene, or in the provision of food, clothing or shelter.
● Failure to provide medical care for physical and mental health needs.
● Failure to protect from health and safety hazards. ● Failure to prevent malnutrition.
Reasonable suspicion: An objectively reasonable suspicion that a person would entertain, based upon facts that could cause a reasonable person in a like position, drawing when appropriate upon his or her training and experience, to suspect abuse or neglect.
SummaryThis is only a few of the laws that the dental professionals in California must adhere to in order to maintain their licenses and to continue to offer their services every day. Remember, these laws change regularly and will continue to do so - just as your profession
does. Continuing education will help you to stay on top of the new regulations, the modern equipment, and the health and safety hazards that you need to be aware of to protect you and your patients.
CALIfORnIA DEnTAL PRACTICE ACT
final Examination QuestionsSelect the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116,
or for faster service complete your test online at Dental.EliteCME.com.
1. The Dental Board is the main authority of dentistry in the state of California.a. True. b. False.
2. At least once every three years, the board shall review the allowable duties of dental assistants and registered dental assistants.a. True. b. False.
3. A professional corporation in the state of California falls under the Moscone-Knox Professional Corporation Act and is regulated by the Dental Hygiene Committee.a. True. b. False.
4. The practice of dental hygiene does not include diagnosis and comprehensive treatment planning.a. True. b. False.
5. A registered dental hygienist in alternative practice may perform duties of a registered dental hygienist in residences of the homebound.a. True. b. False.
6. It is unprofessional conduct for any dentist performing dental procedures to have more than one patient undergoing conscious sedation or general anesthesia on an outpatient basis at any given time unless each patient is being continuously monitored on a one-to-one ratio while sedated by either the dentist or another licensed health professional authorized by law to administer conscious sedation or general anesthesia.a. True. b. False.
7. A licensee must comply with a request for the dental records of a patient if the request is accompanied by written authorization from the patient, and failure to do so within 15 days can result in a fine of up to $250 dollars per day.a. True. b. False.
8. Any licensed dentist may dispense to a patient under his or her care a Schedule II controlled substance in an amount up to a 96-hour supply in accordance with normal use.a. True. b. False.
9. Under California law, each dentist licensee who holds a conscious sedation permit shall complete a minimum of 10 total units of coursework related to the administration of conscious sedation and to medical emergencies every two years.a. True. b. False.
10. Failure of a health professional to file a required report of suspected abuse is a misdemeanor, punishable by a fine of up to $1,000, or confinement in the county jail for up to six months, or both.a. True. b. False.
DCA02PAE18

Page 25 Dental.EliteCME.com
Chapter 2: Guidelines for Infection Control in Dental Health Care Settings
4 CE Hours - Mandatory
By: Elite Staff
Learning objectives � Establish the process of educating and protecting dental health care
personnel. � Explain the prevention of transmission of blood-borne pathogens. � Discuss the concerns of hand hygiene. � Identify protection against spatter by use of personal protective
equipment. � Learn how to avoid the risk of contact dermatitis and latex
hypersensitivity.
� Emphasize the importance of sterilization and disinfection of patient-care items.
� List the special considerations that should be taken with dental handpieces, waterlines, water quality, biofilm, radiology, oral surgical procedures and dental laboratories.
� Review Section 1005 California Minimum Standards for Infection Control.
IntroductionInfection control and health care epidemiology is the discipline concerned with preventing the spread of infections within the health care setting. As such, it is a practical (rather than an academic) subdiscipline of epidemiology. It is an essential (though often under recognized and under supported) part of the infrastructure of health care. Infection control and hospital epidemiology are akin to public health practice, practiced within the confines of a particular health care delivery system rather than directed at society as a whole.
Infection control concerns itself both with prevention (hand hygiene/hand-washing, cleaning/disinfection/ sterilization, vaccination, surveillance) and with investigation and management of a demonstrated or suspected spread of infection within a particular health care setting (e.g., outbreak investigation). It is on this basis that the common title being adopted within health care is “infection prevention and control.”
This course consolidates recommendations for preventing and controlling infectious diseases and managing personnel health and safety concerns related to infection control in dental settings. It:
● Updates and revises previous CDC recommendations regarding infection control in dental settings.
● Incorporates relevant infection control measures from other CDC guidelines.
● Discusses concerns not addressed in previous recommendations for dentistry. These updates and additional topics include:
○ Application of standard precautions rather than universal precautions.
○ Work restrictions for health care personnel (HCP) infected with or occupationally exposed to infectious diseases.
○ Management of occupational exposures to blood-borne pathogens, including post-exposure prophylaxis (PEP) for work exposures to hepatitis B virus (HBV), hepatitis C virus (HCV); and human immunodeficiency virus (HIV).
○ Selection and use of devices with features designed to prevent sharps injury.
○ Hand-hygiene products and surgical hand antisepsis. ○ Contact dermatitis and latex hypersensitivity. ○ Sterilization of unwrapped instruments. ○ Dental water-quality concerns (e.g., dental unit waterline
biofilms; delivery of water of acceptable biological quality for
patient care; usefulness of flushing waterlines; use of sterile irrigating solutions).
○ Oral surgical procedures; handling of community boil water advisories.
○ Dental radiology. ○ Aseptic technique for parenteral medications. ○ Preprocedural mouth rinsing for patients. ○ Oral surgical procedures. ○ Laser/electrosurgery plumes. ○ Tuberculosis (TB). ○ Creutzfeldt-Jakob disease (CJD) and other prion-related
diseases. ○ Infection control program evaluation. ○ Research considerations.
These guidelines were developed by CDC staff members in collaboration with other authorities on infection control. Draft documents were reviewed by other federal agencies and professional organizations from the fields of dental health care, public health and hospital epidemiology and infection control. A Federal Register notice elicited public comments that were considered in the decision-making process. Existing guidelines and published research pertinent to dental infection control principles and practices were reviewed. Wherever possible, recommendations are based on data from well-designed scientific studies. However, only a limited number of studies have characterized risk factors and the effectiveness of prevention measures for infections associated with dental health care practices.
Some infection control practices routinely used by health care practitioners cannot be rigorously examined for ethical or logistical reasons. In the absence of scientific evidence for such practices, certain recommendations are based on strong theoretical rationale, suggestive evidence or opinions of respected authorities based on clinical experience, descriptive studies or committee reports. In addition, some recommendations are derived from federal regulations. No recommendations are offered for practices for which insufficient scientific evidence or lack of consensus supporting their effectiveness exists.

Dental.EliteCME.com Page 26
BackgroundIn the United States, an estimated 9 million persons work in health care professions, including approximately 168,000 dentists, 112,000 registered dental hygienists, 218,000 dental assistants and 53,000 dental laboratory technicians. In this report, dental health care personnel (DHCP) refers to all paid and unpaid personnel in the dental health care setting who might be occupationally exposed to infectious materials, including body substances and contaminated supplies, equipment, environmental surfaces, water, or air. Dental health care personnel includes dentists, dental hygienists, dental assistants, dental laboratory technicians (in-office and commercial), students and trainees, contractual personnel and other persons not directly involved in patient care but potentially exposed to infectious agents (e.g., administrative, clerical, housekeeping, maintenance or volunteer personnel).
Recommendations in this report are designed to prevent or reduce potential for disease transmission from patient to dental health care personnel, from dental workers to patient, and from patient to patient. Although these guidelines focus mainly on outpatient, ambulatory dental health care settings, the recommended infection control practices are applicable to all settings in which dental treatment is provided. Dental patients and workers can be exposed to pathogenic microorganisms including cytomegalovirus (CMV), HBV, HCV, herpes simplex virus types 1 and 2, HIV, Mycobacterium tuberculosis, staphylococci, streptococci and other viruses and bacteria that colonize or infect the oral cavity and respiratory tract. These organisms can be transmitted in dental settings through:
● Direct contact with blood, oral fluids or other patient materials. ● Indirect contact with contaminated objects (e.g., instruments,
equipment or environmental surfaces). ● Contact of conjunctival, nasal or oral mucosa with droplets (e.g.,
spatter) containing microorganisms generated from an infected person and propelled a short distance (e.g., by coughing, sneezing or talking).
● Inhalation of airborne microorganisms that can remain suspended in the air for long periods.
Infection through any of these routes requires that all of the following conditions be present:
● A pathogenic organism of sufficient virulence and in adequate numbers to cause disease.
● A reservoir or source that allows the pathogen to survive and multiply (e.g., blood).
● A mode of transmission from the source to the host. ● A portal of entry through which the pathogen can enter the host. ● A susceptible host (i.e., one who is not immune).
Occurrence of these events provides the chain of infection. Effective infection control strategies prevent disease transmission by interrupting one or more links in the chain.
Previous CDC recommendations regarding infection control for dentistry focused primarily on the risk of transmission of blood-borne pathogens among dental care personnel and patients and use of universal precautions to reduce that risk. Universal precautions were based on the concept that all blood and body fluids that might be contaminated with blood should be treated as infectious because patients with blood-borne infections can be asymptomatic or unaware they are infected. Preventive practices used to reduce blood exposures, particularly percutaneous exposures, include:
● Careful handling of sharp instruments. ● Use of rubber dams to minimize blood spattering. ● Hand washing. ● Use of protective barriers (e.g., gloves, masks, protective eyewear
and gowns).
The relevance of universal precautions to other aspects of disease transmission was recognized, and in 1996, CDC expanded the concept and changed the term to standard precautions. Standard precautions
integrate and expand the elements of universal precautions into a standard of care designed to protect health care personnel and patients from pathogens that can be spread by blood or any other body fluid, excretion or secretion.
Standard precautions apply to contact with: ● Blood. ● All body fluids, secretions and excretions (except sweat),
regardless of whether they contain blood. ● Nonintact skin. ● Mucous membranes.
Saliva has always been considered a potentially infectious material in dental infection control; thus, no operational difference exists in clinical dental practice between universal precautions and standard precautions.
In addition to standard precautions, other measures (e.g., expanded or transmission-based precautions) might be necessary to prevent potential spread of certain diseases (e.g., TB, influenza and varicella) that are transmitted through airborne, droplet or contact transmission (e.g., sneezing, coughing and contact with skin). When acutely ill with these diseases, patients do not usually seek routine dental outpatient care. Nonetheless, a general understanding of precautions for diseases transmitted by all routes is critical because:
● Some dental health workers are hospital-based or work part-time in hospital settings.
● Patients infected with these diseases might seek urgent treatment at outpatient dental offices.
● Dental workers might become infected with these diseases.
Necessary transmission-based precautions might include patient placement (e.g., isolation), adequate room ventilation, respiratory protection (e.g., N-95 masks) for workers, or postponement of nonemergency dental procedures.
Dental health care personnel should be familiar also with the hierarchy of controls that categorizes and prioritizes prevention strategies. For blood-borne pathogens, engineering controls that eliminate or isolate the hazard (e.g., puncture-resistant sharps containers or needle retraction devices) are the primary strategies for protecting dental workers and patients. Where engineering controls are not available or appropriate, work-practice controls that result in safer behaviors (e.g., one-hand needle recapping or not using fingers for cheek retraction while using sharp instruments or suturing), and use of personal protective equipment (PPE) (e.g., protective eyewear, gloves and mask) can prevent exposure. In addition, administrative controls (e.g., policies, procedures and enforcement measures targeted at reducing the risk of exposure to infectious persons) are a priority for certain pathogens (e.g., M. tuberculosis), particularly those spread by airborne or droplet routes.
Dental practices should develop a written infection control program to prevent or reduce the risk of disease transmission. Such a program should include establishment and implementation of policies, procedures and practices (in conjunction with selection and use of technologies and products) to prevent work-related injuries and illnesses among dental care workers as well as health care-associated infections among patients. The program should embody principles of infection control and occupational health, reflect current science and adhere to relevant federal, state and local regulations and statutes. An infection control coordinator (e.g., dentist or other dental health worker) knowledgeable or willing to be trained should be assigned responsibility for coordinating the program. The effectiveness of the infection control program should be evaluated on a day-to-day basis and over time to help ensure that policies, procedures and practices are useful, efficient, and successful.

Page 27 Dental.EliteCME.com
Although the infection control coordinator remains responsible for overall management of the program, creating and maintaining a safe work environment ultimately requires the commitment and accountability of all dental workers. This course is designed to provide guidance to workers for preventing disease transmission in dental health care settings, for promoting a safe working environment and for assisting dental practices in developing and implementing infection control programs. These programs should be followed in addition to practices and procedures for worker protection required by the Occupational Safety and Health Administration’s (OSHA)
standards for occupational exposure to blood-borne pathogens, including instituting controls to protect employees from exposure to blood or other potentially infectious materials (OPIM), and requiring implementation of a written exposure-control plan, annual employee training, HBV vaccinations and post-exposure follow-up. Interpretations and enforcement procedures are available to help dental workers apply this OSHA standard in practice. Also, manufacturers’ Material Safety Data Sheets (MSDS) should be consulted regarding correct procedures for handling or working with hazardous chemicals.
CALIfORnIA SECTIOn 1005: MInIMUM STAnDARDS fOR InfECTIOn COnTROL
Definitions of terms used in this section“Standard precautions” are a group of infection prevention practices that apply to all patients, regardless of suspected or confirmed infection status, in any setting in which healthcare is delivered. These include: hand hygiene, use of gloves, gown, mask, eye protection, or face shield, depending on the anticipated exposure, and safe handling of sharps. Standard precautions shall be used for care of all patients regardless of their diagnoses or personal infectious status.
“Critical items” confer a high risk for infection if they are contaminated with any microorganism. These include all instruments, devices, and other items used to penetrate soft tissue or bone.
“Semi-critical items” are instruments, devices and other items that are not used to penetrate soft tissue or bone, but contact oral mucous membranes, non-intact skin or other potentially infectious materials (OPIM).
“Non-critical items” are instruments, devices, equipment, and surfaces that come in contact with soil, debris, saliva, blood, OPIM and intact skin, but not oral mucous membranes.
“Low-level disinfection” is the least effective disinfection process. It kills some bacteria, some viruses and fungi, but does not kill bacterial spores or mycobacterium tuberculosis var bovis, a laboratory test organism used to classify the strength of disinfectant chemicals.
“Intermediate-level disinfection” kills mycobacterium tuberculosis var bovis indicating that many human pathogens are also killed. This process does not necessarily kill spores.
“High-level disinfection” kills some, but not necessarily all bacterial spores. This process kills mycobacterium tuberculosis var bovis, bacteria, fungi, and viruses.
“Germicide” is a chemical agent that can be used to disinfect items and surfaces based on the level of contamination.
“Sterilization” is a validated process used to render a product free of all forms of viable microorganisms.
“Cleaning” is the removal of visible soil (e.g., organic and inorganic material) debris and OPIM from objects and surfaces and shall be accomplished manually or mechanically using water with detergents or enzymatic products.
“Personal Protective Equipment” (PPE) is specialized clothing or equipment worn or used for protection against a hazard. PPE items may include, but are not limited to, gloves, masks, respiratory devices,
protective eyewear and protective attire which are intended to prevent exposure to blood, body fluids, OPIM, and chemicals used for infection control. General work attire such as uniforms, scrubs, pants and shirts, are not considered to be PPE.
“Other Potentially Infectious Materials” (OPIM) means any one of the following:A. Human body fluids such as saliva in dental procedures and
any body fluid that is visibly contaminated with blood, and all body fluids in situations where it is difficult or impossible to differentiate between body fluids.
B. Any unfixed tissue or organ (other than intact skin) from a human (living or dead).
C. Any of the following, if known or reasonably likely to contain or be infected with human immunodeficiency virus (HIV), hepatitis B virus (HBV), or hepatitis C virus (HCV):1. Cell, tissue, or organ cultures from humans or experimental
animals;2. Blood, organs, or other tissues from experimental animals; or
culture medium or other solutions.
“Dental Healthcare Personnel” (DHCP), are all paid and non-paid personnel in the dental healthcare setting who might be occupationally exposed to infectious materials, including body substances and contaminated supplies, equipment, environmental surfaces, water, or air. DHCP includes dentists, dental hygienists, dental assistants, dental laboratory technicians (in-office and commercial), students and trainees, contractual personnel, and other persons not directly involved in patient care but potentially exposed to infectious agents (e.g., administrative, clerical, housekeeping, maintenance, or volunteer personnel).
All DHCP shall comply with infection control precautions and enforce the following minimum precautions to protect patients and DHCP and to minimize the transmission of pathogens in health care settings as mandated by the California Division of Occupational Safety and Health (Cal/OSHA).1. Standard precautions shall be practiced in the care of all patients.2. A written protocol shall be developed, maintained, and periodically
updated for proper instrument processing, operatory cleanliness, and management of injuries. The protocol shall be made available to all DHCP at the dental office.
3. A copy of this regulation shall be conspicuously posted in each dental office.
Personal protective equipmentAll DHCP shall wear surgical facemasks in combination with either chin length plastic face shields or protective eyewear whenever there is potential for aerosol spray, splashing or spattering of the following: droplet nuclei, blood, chemical or germicidal agents or OPIM. Chemical-resistant utility gloves and appropriate, task specific PPE shall be worn when handling hazardous chemicals. After each patient treatment, masks shall be changed and disposed. After each
patient treatment, face shields and protective eyewear shall be cleaned, disinfected, or disposed.
Protective attire shall be worn for disinfection, sterilization, and housekeeping procedures involving the use of germicides or handling contaminated items. All DHCP shall wear reusable or disposable protective attire whenever there is a potential for aerosol spray, splashing or spattering of blood, OPIM, or chemicals and germicidal

Dental.EliteCME.com Page 28
agents. Protective attire must be changed daily or between patients if they should become moist or visibly soiled. All PPE used during patient care shall be removed when leaving laboratories or areas
of patient care activities. Reusable gowns shall be laundered in accordance with Cal/OSHA Bloodborne Pathogens Standards (Title 8, Cal. Code Regs., section 5193.)
Hand hygieneAll DHCP shall thoroughly wash their hands with soap and water at the start and end of each workday. DHCP shall wash contaminated or visibly soiled hands with soap and water and put on new gloves before treating each patient. If hands are not visibly soiled or contaminated an alcohol based hand rub may be used as an alternative to soap and water. Hands shall be thoroughly dried before donning gloves in order to prevent promotion of bacterial growth and washed again
immediately after glove removal. A DHCP shall refrain from providing direct patient care if hand conditions are present that may render DHCP or patients more susceptible to opportunistic infection or exposure.
All DHCP who have exudative lesions or weeping dermatitis of the hand shall refrain from all direct patient care and from handling patient care equipment until the condition resolves.
Gloves(8) Medical exam gloves shall be worn whenever there is contact with mucous membranes, blood, OPIM, and during all pre-clinical, clinical, post-clinical, and laboratory procedures. When processing contaminated sharp instruments, needles, and devices, DHCP shall wear heavy-duty utility gloves to prevent puncture wounds. Gloves
must be discarded when torn or punctured, upon completion of treatment, and before leaving laboratories or areas of patient care activities. All DHCP shall perform hand hygiene procedures before donning gloves and after removing and discarding gloves. Gloves shall not be washed before or after use.
needle and sharps safetyNeedles shall be recapped only by using the scoop technique or a protective device. Needles shall not be bent or broken for the purpose of disposal. Disposable needles, syringes, scalpel blades, or other
sharp items and instruments shall be placed into sharps containers for disposal as close as possible to the point of use according to all applicable local, state, and federal regulations.
Sterilization and disinfectionAll germicides must be used in accordance with intended use and label instructions.Cleaning must precede any disinfection or sterilization process. Products used to clean items or surfaces prior to disinfection procedures shall be used according to all label instructions. Critical instruments, items and devices shall be discarded or pre-cleaned, packaged or wrapped and sterilized after each use. Methods of sterilization shall include steam under pressure (autoclaving), chemical vapor, and dry heat. If a critical item is heat-sensitive, it shall, at minimum, be processed with high-level disinfection and packaged or wrapped upon completion of the disinfection process. These instruments, items, and devices, shall remain sealed and stored in a manner so as to prevent contamination, and shall be labeled with the date of sterilization and the specific sterilizer used if more than one sterilizer is utilized in the facility.
Semi-critical instruments, items, and devices shall be pre-cleaned, packaged or wrapped and sterilized after each use. Methods of sterilization include steam under pressure (autoclaving), chemical vapor and dry heat. If a semi-critical item is heat sensitive, it shall, at minimum, be processed with high level disinfection and packaged or wrapped upon completion of the disinfection process. These packages or containers shall remain sealed and shall be stored in a manner so as to prevent contamination, and shall be labeled with the date of
sterilization and the specific sterilizer used if more than one sterilizer is utilized in the facility.
Non-critical surfaces and patient care items shall be cleaned and disinfected with a California Environmental Protection Agency (Cal/EPA)-registered hospital disinfectant (low-level disinfectant) labeled effective against HBV and HIV. When the item is visibly contaminated with blood or OPIM, a Cal/EPA-registered hospital intermediate-level disinfectant with a tuberculocidal claim shall be used.
All high-speed dental hand pieces, low-speed hand pieces, rotary components and dental unit attachments such as reusable air/water syringe tips and ultrasonic scaler tips, shall be packaged, labeled and heat-sterilized in a manner consistent with the same sterilization practices as a semi-critical item.
Single use disposable items such as prophylaxis angles, prophylaxis cups and brushes, tips for high-speed evacuators, saliva ejectors, air/water syringe tips, and gloves shall be used for one patient only and discarded.
Proper functioning of the sterilization cycle of all sterilization devices shall be verified at least weekly through the use of a biological indicator (such as a spore test). Test results shall be documented and maintained for 12 months.
IrrigationSterile coolants/irrigants shall be used for surgical procedures involving soft tissue or bone. Sterile coolants/irrigants must be delivered using a sterile delivery system.
facilitiesIf non-critical items or surfaces likely to be contaminated are manufactured in a manner preventing cleaning and disinfection, they shall be protected with disposable impervious barriers. Disposable barriers shall be changed when visibly soiled or damaged and between patients.
Clean and disinfect all clinical contact surfaces that are not protected by impervious barriers using a California Environmental Protection
Agency (Cal/EPA) registered, hospital grade low- to intermediate-level germicide after each patient. The low-level disinfectants used shall be labeled effective against HBV and HIV. Use disinfectants in accordance with the manufacturer’s instructions. Clean all housekeeping surfaces (e.g. floors, walls, sinks) with a detergent and water or a Cal/EPA registered, hospital grade disinfectant. Products used to clean items or surfaces prior to disinfection procedures shall

Page 29 Dental.EliteCME.com
be clearly labeled and DHCP shall follow all material safety data sheet (MSDS) handling and storage instructions.
Dental unit water lines shall be anti-retractive. At the beginning of each workday, dental unit lines and devices shall be purged with air or flushed with water for at least two (2) minutes prior to attaching
handpieces, scalers, air water syringe tips, or other devices. The dental unit lines and devices shall be flushed between each patient for a minimum of twenty (20) seconds.
Contaminated solid waste shall be disposed of according to applicable local, state, and federal environmental standards.
Lab areasSplash shields and equipment guards shall be used on dental laboratory lathes. Fresh pumice and a sterilized or new rag-wheel shall be used for each patient. Devices used to polish, trim, or adjust contaminated intraoral devices shall be disinfected or sterilized, properly packaged or wrapped and labeled with the date and the specific sterilizer used if more than one sterilizer is utilized in the facility. If packaging is compromised, the instruments shall be recleaned, packaged in new wrap, and sterilized again. Sterilized items will be stored in a manner so as to prevent contamination.
All intraoral items such as impressions, bite registrations, prosthetic and orthodontic appliances shall be cleaned and disinfected with an intermediate-level disinfectant before manipulation in the laboratory and before placement in the patient’s mouth. Such items shall be thoroughly rinsed prior to placement in the patient’s mouth.
The Dental Board of California and Dental Hygiene Committee of California shall review this regulation annually and establish a consensus.
REVIEW Of SCIEnCE RELATED TO DEnTAL InfECTIOn COnTROL
Personnel health elements of an infection control programA protective health component for dental health care personnel is an integral part of a dental practice infection control program. The objectives are to educate workers about the principles of infection control, identify work-related infection risks, institute preventive measures and ensure prompt exposure management and medical follow-up. Coordination between the dental practice’s infection control coordinator and other qualified health care professionals is necessary to provide dental workers with appropriate services. Dental programs in institutional settings, (e.g., hospitals, health centers and educational institutions) can coordinate with departments that provide personnel health services.
However, the majority of dental practices are in ambulatory, private settings that do not have licensed medical staff and facilities to provide complete on-site health service programs. In such settings, the infection control coordinator should establish programs that arrange for site-specific infection control services from external health care facilities and providers before workers are placed at risk for exposure. Referral arrangements can be made with qualified health care professionals in an occupational health program of a hospital, with educational institutions or with health care facilities that offer personnel health services.
Education and trainingPersonnel are more likely to comply with an infection control program and exposure control plan if they understand its rationale. Clearly written policies, procedures and guidelines can help ensure consistency, efficiency and effective coordination of activities. Personnel subject to occupational exposure should receive infection control training on initial assignment, when new tasks or procedures affect their occupational exposure, and at a minimum, annually. Education and training should be appropriate to the assigned duties of specific workers (e.g., techniques to prevent cross-contamination or instrument sterilization). For dental workers who perform tasks or procedures likely to result in occupational exposure to infectious agents, training should include:
● A description of their exposure risks.
● Review of prevention strategies and infection control policies and procedures.
● Discussion regarding how to manage work-related illness and injuries, including post-exposure prophylaxis.
● Review of work restrictions for an exposure or infection.
Inclusion of dental workers with minimal exposure risks (e.g., administrative employees) in education and training programs might enhance facility-wide understanding of infection control principles and the importance of the program. Educational materials should be appropriate in content and vocabulary for each person’s educational level, literacy and language, as well as be consistent with existing federal, state and local regulations.
Immunization programsDental workers are at risk for exposure to, and possible infection with, infectious organisms. Immunizations substantially reduce both the number of workers susceptible to these diseases and the potential for disease transmission to other workers and patients. Thus, immunizations are an essential part of prevention and infection control programs for dental health care personnel, and a comprehensive immunization policy should be implemented for all dental health care facilities. The Advisory Committee on Immunization Practices (ACIP) provides national guidelines for immunization of health care personnel, which includes dental workers.
Dental practice immunization policies should incorporate current state and federal regulations as well as recommendations from the U.S. Public Health Service and professional organizations.
On the basis of documented health care-associated transmission, health care workers are considered to be at substantial risk for acquiring
or transmitting hepatitis B, influenza, measles, mumps, rubella and varicella. All of these diseases are vaccine-preventable. ACIP recommends that all health care personnel be vaccinated or have documented immunity to these diseases. ACIP does not recommend routine immunization of workers against TB (i.e., inoculation with bacille Calmette-Guérin vaccine) or hepatitis A. No vaccine exists for HCV. ACIP guidelines also provide recommendations regarding immunization of workers with special conditions (e.g., pregnancy, HIV infection or diabetes).
Immunization of workers before they are placed at risk for exposure remains the most efficient and effective use of vaccines in health care settings. Some educational institutions and infection control programs provide immunization schedules for students and workers. OSHA requires that employers make hepatitis B vaccination available to all employees who have potential contact with blood or OPIM. Employers

Dental.EliteCME.com Page 30
are also required to follow CDC recommendations for vaccinations, evaluation and follow-up procedures. Nonpatient care staff (e.g., administrative or housekeeping) might be included, depending on their potential risk of coming into contact with blood or OPIM.
Employers are also required to ensure that employees who decline to accept hepatitis B vaccination sign an appropriate declination
statement. Dental workers unable or unwilling to be vaccinated as required or recommended should be educated regarding their exposure risks, infection control policies and procedures for the facility, and the management of work-related illness and work restrictions (if appropriate) for exposed or infected workers.
Exposure prevention and post-exposure managementAvoiding exposure to blood and OPIM, as well as protection by immunization, remain primary strategies for reducing occupationally acquired infections, but occupational exposures can still occur. A combination of standard precautions, engineering, work practice and administrative controls is the best means to minimize occupational exposures. Written policies and procedures to facilitate prompt reporting, evaluation, counseling, treatment and medical follow-up of all occupational exposures should be available to all dental health care personnel. Written policies and procedures should be consistent with
federal, state and local requirements addressing education and training, post-exposure management and exposure reporting.
Dental health personnel who have contact with patients can also be exposed to persons with infectious TB, and should have a baseline tuberculin skin test (TST), preferably by using a two-step test at the beginning of employment. Thus, if an unprotected occupational exposure occurs, TST conversions can be distinguished from positive TST results caused by previous exposures. The facility’s level of TB risk will determine the need for routine follow-up TSTs.
Medical conditions, work-related illness and work restrictionsDental workers are responsible for monitoring their own health status. Those who have acute or chronic medical conditions that render them susceptible to opportunistic infection should discuss with their personal physicians or other qualified authority whether the condition might affect their ability to safely perform their duties.
However, under certain circumstances, health care facility managers might need to exclude dental health personnel from work or patient contact to prevent further transmission of infection. Decisions concerning work restrictions are based on the mode of transmission and the period of infectivity of the disease (Table 1). Exclusion policies should:
● Be written. ● Include a statement of authority that defines who can exclude
dental workers (e.g., personal physicians). ● Be clearly communicated through education and training.
Policies should also encourage workers to report illnesses or exposures without jeopardizing wages, benefits or job status. With increasing concerns regarding blood-borne pathogens and introduction of
universal precautions, use of latex gloves among health care workers has increased markedly. Increased use of these gloves has been accompanied by increased reports of allergic reactions to natural rubber latex among workers and patients, as well as increased reports of irritant and allergic contact dermatitis from frequent and repeated use of hand-hygiene products, exposure to chemicals and glove use.
Dental health workers should be familiar with the signs and symptoms of latex sensitivity. A physician should evaluate workers exhibiting symptoms of latex allergy, because further exposure could result in a serious allergic reaction. A diagnosis is made through medical history, physical examination and diagnostic tests. Procedures should be in place for minimizing latex-related health problems among DHCP and patients while protecting them from infectious materials. These procedures should include:
● Reducing exposures to latex-containing materials by using appropriate work practices.
● Training and educating dental workers on monitoring symptoms. ● Substituting nonlatex products where appropriate.
Maintenance of records, data management and confidentiality The health status of dental workers can be monitored by maintaining records of work-related medical evaluations, screening tests, immunizations, exposures and post-exposure management. Such records must be kept in accordance with all applicable state and federal laws. Examples of laws that might apply include the Privacy Rule of the Health Insurance Portability and Accountability Act (HIPAA) of 1996, 45 CFR 160 and 164, and the OSHA Occupational Exposure to Blood-borne Pathogens; Final Rule 29 CFR 1910. 1030(h)(1)(i–iv). The HIPAA Privacy Rule applies to covered entities, including certain defined health providers, health care clearinghouses and health plans. OSHA requires employers to ensure that certain information contained in employee medical records is:
● Kept confidential. ● Not disclosed or reported without the employee’s express written
consent to any person within or outside the workplace except as required by the OSHA standard.
● Maintained by the employer for at least the duration of employment plus 30 years.
Dental practices that coordinate their infection control program with off-site providers might consult OSHA’s blood-borne pathogen standard and employee access to medical and exposure records standard, as well as other applicable local, state and federal laws, to determine a location for storing health records.
Preventing transmission of blood-borne pathogensAlthough transmission of blood-borne pathogens (e.g., HBV, HCV and HIV) in dental health care settings can have serious consequences, such transmission is rare. Exposure to infected blood can result in transmission from patient to dental workers, from workers to patients, and from one patient to another. The opportunity for transmission is greatest from patients to dental workers, who frequently encounter patient blood and blood-contaminated saliva during dental procedures. Since 1992, no HIV transmission from dental care personnel to patients has been reported, and the last HBV transmission from dental workers to patients was reported in 1987. HCV transmission from
workers to patients has not been reported. The majority of dental care workers infected with a blood-borne virus do not pose a risk to patients because they do not perform activities meeting the necessary conditions for transmission. For workers to pose a risk for blood-borne virus transmission to patients, the worker must:
● Be viremic, i.e., have infectious virus circulating in the bloodstream.
● Be injured or have a condition (e.g., weeping dermatitis) that allows direct exposure to their blood or other infectious body fluids.

Page 31 Dental.EliteCME.com
● Enable their blood or infectious body fluid to gain direct access to a patient’s wound, traumatized tissue, mucous membranes or similar portal of entry. Although an infected worker might be viremic, unless the second and third conditions are also met, transmission cannot occur.
The risk of occupational exposure to blood-borne viruses is largely determined by their prevalence in the patient population and the
nature and frequency of contact with blood and body fluids through percutaneous or permucosal routes of exposure. The risk of infection after exposure to a blood-borne virus is influenced by inoculum size, route of exposure and susceptibility of the exposed health care personnel. The majority of attention has been placed on the blood-borne pathogens HBV, HCV and HIV, and these pathogens present different levels of risk to dental care workers.
Hepatitis B virusHBV is a well-recognized occupational risk for health care workers. HBV is transmitted by percutaneous or mucosal exposure to blood or body fluids of a person with either acute or chronic HBV infection. Persons infected with HBV can transmit the virus for as long as they are HBsAg-positive. The risk of HBV transmission is highly related to the HBeAg status of the source person. In studies of health care personnel who sustained injuries from needles contaminated with blood containing HBV, the risk of developing clinical hepatitis if the blood was positive for both HBsAg and HBeAg was 22 percent to 31 percent; the risk of developing serologic evidence of HBV infection was 37–62 percent. By comparison, the risk of developing clinical hepatitis from a needle contaminated with HBsAg-positive, HBeAg-negative blood was 1-6 percent, and the risk of developing serologic evidence of HBV infection, 23-37 percent.
Blood contains the greatest proportion of HBV infectious particle titers of all body fluids and is the most critical vehicle of transmission in the health care setting. HBsAg is also found in multiple other body fluids, including breast milk, bile, cerebrospinal fluid, feces, nasopharyngeal washings, saliva, semen, sweat and synovial fluid. However, the majority of body fluids are not efficient vehicles for transmission because they contain low quantities of infectious HBV, despite the presence of HBsAg. The concentration of HBsAg in body fluids can be 100-1,000 times greater than the concentration of infectious HBV particles.
Although percutaneous injuries are among the most efficient modes of HBV transmission, these exposures probably account for only a minority of HBV infections among health care workers. In multiple investigations of nosocomial hepatitis B outbreaks, the majority of infected health care workers could not recall an overt percutaneous injury, although in certain studies, approximately one-third of infected workers recalled caring for a patient who was HBsAg-positive. In addition, HBV has been demonstrated to survive in dried blood at room temperature on environmental surfaces for one week. Thus, HBV infections that occur in workers with no history of nonoccupational exposure or occupational percutaneous injury might have resulted from direct or indirect blood or body fluid exposures that inoculated HBV into cutaneous scratches, abrasions, burns, other lesions or on mucosal surfaces. The potential for HBV transmission through contact with environmental surfaces has been demonstrated in investigations of HBV outbreaks among patients and health care personnel in hemodialysis units.
Since the early 1980s, occupational infections among health workers have declined because of vaccine use and adherence to universal precautions. Among U. S. dentists, more than 90 percent have been vaccinated, and serologic evidence of past HBV infection decreased from prevaccine levels of 14 percent in 1972, to approximately 9 percent in 1992. During 1993–2001, levels remained relatively unchanged. Infection rates can be expected to decline further as vaccination rates remain high among young dentists and as older dentists with lower vaccination rates and higher rates of infection retire.
Although the potential for transmission of blood-borne infections from dental care workers to patients is considered limited, precise risks have not been quantified by carefully designed epidemiologic studies. Reports published during 1970-1987 describe nine clusters in which
patients were thought to be infected with HBV through treatment by an infected dental worker. However, transmission of HBV from dentist to patient has not been reported since 1987, possibly reflecting such factors as:
● Adoption of universal precautions. ● Routine glove use. ● Increased levels of immunity as a result of hepatitis B vaccination
of dental care workers. ● Implementation of the 1991 OSHA blood-borne pathogen
standard. ● Incomplete ascertainment and reporting.
Standard precautions are strategies used to reduce the risk of infection from exposure to blood, all body fluids and secretions (except sweat), non-intact skin and mucous membranes.
Only one case of patient-to-patient transmission of HBV in the dental setting has been documented (CDC, unpublished data, 2003). In this case, appropriate office infection control procedures were being followed, and the exact mechanism of transmission was undetermined.
Because of the high risk of HBV infection to health care and dental workers who perform tasks that might involve contact with blood, blood-contaminated body substances, other body fluids or sharps, such workers should be vaccinated. Vaccination can protect both dental care workers and patients from HBV infection and, whenever possible, should be completed when dentists or other dental staff are in training and before they have contact with blood.
Prevaccination serological testing for previous infection is not indicated, although it can be cost-effective where prevalence of infection is expected to be high in a group of potential vacinees (e.g., persons who have emigrated from areas with high rates of HBV infection). Dental workers should be tested for anti-HBs 1-2 months after completion of the three-dose vaccination series. Those who do not develop an adequate antibody response (i.e., anti-HBs less than 10 mIU/mL) to the primary vaccine series should complete a second three-dose vaccine series or be evaluated to determine if they are HBsAg-positive. Revaccinated persons should be retested for anti-HBs at the completion of the second vaccine series. Approximately half of nonresponders to the primary series will respond to a second three-dose series. If no antibody response occurs after the second series, testing for HBsAg should be performed.
Persons who prove to be HBsAg-positive should be counseled regarding how to prevent HBV transmission to others and regarding the need for medical evaluation. Nonresponders to vaccination who are HBsAg-negative should be considered susceptible to HBV infection and should be counseled regarding precautions to prevent HBV infection and the need to obtain HBIG prophylaxis for any known or probable parenteral exposure to HBsAg-positive blood.
Vaccine-induced antibodies decline gradually over time, and 60 percent of persons who initially respond to vaccination will lose detectable antibodies over 12 years. Even so, immunity continues to prevent clinical disease or detectable viral infection. Booster doses of vaccine and periodic serologic testing to monitor antibody concentrations after completion of the vaccine series are not necessary for vaccine responders.

Dental.EliteCME.com Page 32
Hepatitis D virus An estimated 4 percent of persons with acute HBV infection are also infected with hepatitis delta virus (HDV). Discovered in 1977, HDV is a defective blood-borne virus requiring the presence of HBV to replicate. Patients co-infected with HBV and HDV have substantially
higher mortality rates than those infected with HBV alone. Because HDV infection is dependent on HBV for replication, immunization to prevent HBV infection, through either pre- or post-exposure prophylaxis, can also prevent HDV infection.
Hepatitis C virusHepatitis C virus appears not to be transmitted efficiently through occupational exposures to blood. Follow-up studies of HCP exposed to HCV-infected blood through percutaneous or other sharps injuries have determined a low incidence of seroconversion (mean: 1.8 percent; range, 0 percent-7 percent). One study determined transmission occurred from hollow-bore needles but not other sharps. Although these studies have not documented seroconversion associated with mucous membrane or nonintact skin exposure, at least two cases of HCV transmission from a blood splash to the conjunctiva and one case of simultaneous transmission of HCV and HIV after nonintact skin exposure have been reported.
Data are insufficient to estimate the occupational risk of HCV infection among health care workers, but the majority of studies indicate the prevalence of HCV infection among dentists, surgeons and hospital-based workers is similar to that among the general population, approximately 1-2 percent. In a study that evaluated risk factors for infection, a history of unintentional needlesticks was the only occupational risk factor independently associated with HCV infection. No studies of transmission from HCV-infected dental workers to patients have been reported, and the risk for such transmission appears limited. Multiple reports have been published describing transmission from HCV-infected surgeons, which apparently occurred during performance of invasive procedures; the overall risk for infection averaged 0.17 percent.
Human immunodeficiency virusIn the United States, the risk of HIV transmission in dental settings is extremely low. As of December 2001, a total of 57 cases of HIV seroconversion had been documented among health care workers, but none among dental care workers, after occupational exposure to a known HIV-infected source. Transmission of HIV to six patients of a single dentist with AIDS has been reported, but the mode of transmission could not be determined. As of Sept. 30, 1993, CDC had information regarding test results of more than 22,000 patients of 63 HIV-infected health care workers, including 33 dentists or dental students. No additional cases of transmission were documented.
Prospective studies worldwide indicate the average risk of HIV infection after a single percutaneous exposure to HIV-infected blood is 0.3 percent (range: 0.2-0.5 percent). After an exposure of mucous membranes in the eye, nose or mouth, the risk is approximately 0.1 percent. The precise risk of transmission after skin exposure remains
unknown, but is believed to be even smaller than that for mucous membrane exposure.
Certain factors affect the risk of HIV transmission after an occupational exposure. Laboratory studies have determined that if needles that pass through latex gloves are solid rather than hollow-bore, or are of small gauge (e.g., anesthetic needles commonly used in dentistry), they transfer less blood. In a retrospective case-control study of health care personnel, an increased risk for HIV infection was associated with exposure to a relatively large volume of blood, as indicated by a deep injury with a device that was visibly contaminated with the patient’s blood, or a procedure that involved a needle placed in a vein or artery. The risk was also increased if the exposure was to blood from patients with terminal illnesses, possibly reflecting the higher titer of HIV in late-stage AIDS.
Exposure prevention methodsAvoiding occupational exposures to blood is the primary way to prevent transmission of HBV, HCV and HIV, to workers in health care settings. Exposures occur through percutaneous injury (e.g., a needlestick or cut with a sharp object), as well as through contact between potentially infectious blood, tissues or other body fluids and mucous membranes of the eye, nose, mouth or nonintact skin (e.g., exposed skin that is chapped, abraded or shows signs of dermatitis).
Observational studies and surveys indicate that percutaneous injuries among general dentists and oral surgeons occur less frequently than among general and orthopedic surgeons and have decreased in frequency since the mid-1980s. This decline has been attributed to safer work practices, safer instrumentation or design, and continued dental care workers education. Percutaneous injuries among DHCP usually:
● Occur outside the patient’s mouth, thereby posing less risk for recontact with patient tissues.
● Involve limited amounts of blood. ● Are caused by burs, syringe needles, laboratory knives and other
sharp instruments.
Injuries among oral surgeons might occur more frequently during fracture reductions using wires. Experience, as measured by years in practice, does not appear to affect the risk of injury among general dentists or oral surgeons.
The majority of exposures in dentistry are preventable, and methods to reduce the risk of blood contacts have included use of standard precautions, use of devices with features engineered to prevent sharp injuries and modifications of work practices. These approaches might have contributed to the decrease in percutaneous injuries among dentists during recent years. However, needlesticks and other blood contacts continue to occur, which is a concern because percutaneous injuries pose the greatest risk of transmission.
Standard precautions include use of personal protective equipment (e.g., gloves, masks, protective eyewear or face shield, and gowns) intended to prevent skin and mucous membrane exposures. Other protective equipment (e.g., finger guards while suturing) might also reduce injuries during dental procedures.
Engineering controls are the primary method to reduce exposures to blood and OPIM from sharp instruments and needles. These controls are frequently technology-based and often incorporate safer designs of instruments and devices (e.g., self-sheathing anesthetic needles and dental units designed to shield burs in handpieces) to reduce percutaneous injuries.
Work-practice controls establish practices to protect dental workers whose responsibilities include handling, using, assembling or processing sharp devices (e.g., needles, scalers, laboratory utility knives, burs, explorers and endodontic files) or sharps disposal

Page 33 Dental.EliteCME.com
containers. Work-practice controls can include removing burs before disassembling the handpiece from the dental unit, restricting use of fingers in tissue retraction or palpation during suturing and administration of anesthesia and minimizing potentially uncontrolled movements of such instruments as scalers or laboratory knives.
As indicated, needles are a substantial source of percutaneous injury in dental practice, and engineering and work-practice controls for needle handling are of particular importance. In 2001, revisions to OSHA’s blood-borne pathogens standard as mandated by the Needlestick Safety and Prevention Act of 2000 became effective. These revisions clarify the need for employers to consider safer needle devices as they become available and to involve employees directly responsible for patient care (e.g., dentists, hygienists and dental assistants) in identifying and choosing such devices. Safer versions of sharp devices used in hospital settings have become available (e.g., blunt suture needles, phlebotomy devices and butterfly needles), and their impact on reducing injuries has been documented. Aspirating anesthetic syringes that incorporate safety features have been developed for dental procedures, but the low injury rates in dentistry limit assessment of their effect on reducing injuries among dental care workers.
Work-practice controls for needles and other sharps include placing used disposable syringes and needles, scalpel blades and other sharp items in appropriate puncture-resistant containers located as close as
feasible to where the items were used. In addition, used needles should never be recapped or otherwise manipulated by using both hands or any other technique that involves directing the point of a needle toward any part of the body. A one-handed scoop technique, a mechanical device designed for holding the needle cap to facilitate one-handed recapping, or an engineered sharps injury protection device (e.g., needles with resheathing mechanisms) should be employed for recapping needles between uses and before disposal. Dental care workers should never bend or break needles before disposal because this practice requires unnecessary manipulation. Before attempting to remove needles from nondisposable aspirating syringes, they should recap them to prevent injuries. For procedures involving multiple injections with a single needle, the practitioner should recap the needle between injections by using a one-handed technique or use a device with a needle-resheathing mechanism. Passing a syringe with an unsheathed needle should be avoided because of the potential for injury.
Additional information for developing a safety program and for identifying and evaluating safer dental devices is available at:
● http://www.cdc.gov/OralHealth/infectioncontrol/ forms.htm (forms for screening and evaluating safer dental devices).
● http://www.cdc.gov/niosh/topics/bbp (state legislation on needlestick safety).
Post-exposure management and prophylaxisPost-exposure management is an integral component of a complete program to prevent infection after an occupational exposure to blood. During dental procedures, saliva is predictably contaminated with blood. Even when blood is not visible, it can still be present in limited quantities and therefore is considered a potentially infectious material by OSHA. A qualified health care professional should evaluate any occupational exposure incident to blood or OPIM, including saliva, regardless of whether blood is visible, in dental settings.
Dental practices and laboratories should establish written, comprehensive programs that include hepatitis B vaccination and post-exposure management protocols that:
● Describe the types of contact with blood or OPIM that can place dental care workers at risk for infection.
● Describe procedures for promptly reporting and evaluating such exposures.
● Identify a health care professional who is qualified to provide counseling and perform all medical evaluations and procedures in accordance with current recommendations of the U. S. Public Health Service (PHS), including prophylaxis with chemotherapeutic drugs when indicated.
Dental workers, including students, who might reasonably be considered at risk for occupational exposure to blood or OPIM should be taught strategies to prevent contact with blood or OPIM and the principles of post-exposure management, including prophylaxis options, as part of their job orientation and training. Educational programs for dental workers and students should emphasize reporting all exposures to blood or OPIM as soon as possible, because certain interventions have to be initiated promptly to be effective.
Policies should be consistent with the practices and procedures for worker protection required by OSHA and with current Public Health Service recommendations for managing occupational exposures to blood.
After an occupational blood exposure, first aid should be administered as necessary. Puncture wounds and other injuries to the skin should be washed with soap and water; mucous membranes should be flushed with water. No evidence exists that using antiseptics for wound care or expressing fluid by squeezing the wound further reduces the risk of blood-borne pathogen transmission; however, use of antiseptics is not contraindicated. The application of caustic agents (e.g., bleach)
or the injection of antiseptics or disinfectants into the wound is not recommended. Exposed workers should immediately report the exposure to the infection control coordinator or other designated person, who should initiate referral to the qualified health care professional and complete necessary reports.
Because multiple factors contribute to the risk of infection after an occupational exposure to blood, the following information should be included in the exposure report, recorded in the exposed person’s confidential medical record and provided to the qualified health care professional:
● Date and time of exposure. ● Details of the procedure being performed, including where and
how the exposure occurred and whether the exposure involved a sharp device, the type and brand of device, and how and when during its handling the exposure occurred.
● Details of the exposure, including its severity and the type and amount of fluid or material.
○ For a percutaneous injury, severity might be measured by the depth of the wound, gauge of the needle and whether fluid was injected.
○ For a skin or mucous membrane exposure, the estimated volume of material, duration of contact and the condition of the skin (e.g., chapped, abraded or intact) should be noted.
○ Details regarding whether the source material was known to contain HIV or other blood-borne pathogens.
○ If the source was infected with HIV, the stage of disease, history of antiretroviral therapy and viral load, if known.
● Details regarding the exposed person (e.g., hepatitis B vaccination and vaccine-response status).
● Details regarding counseling, post-exposure management and follow-up.
Each occupational exposure should be evaluated individually for its potential to transmit HBV, HCV and HIV, based on the following:
● The type and amount of body substance involved. ● The type of exposure (e.g., percutaneous injury, mucous membrane
or nonintact skin exposure, or bites resulting in blood exposure to either person involved).
● The infection status of the source. ● The susceptibility of the exposed person.

Dental.EliteCME.com Page 34
All of these factors should be considered in assessing the risk for infection and the need for further follow-up (e.g. post-exposure prophylaxis, or PEP).
During 1990-1998, the Public Health Service published guidelines for PEP and other management of health care worker exposures to HBV, HCV or HIV. In 2001, these recommendations were updated and consolidated into one set of Public Health Service guidelines.
The new guidelines reflect the availability of new anti-retroviral agents, new information regarding the use and safety of HIV PEP, and considerations regarding employing HIV prophylaxis when resistance of the source patient’s virus to anti-retroviral agents is known or suspected. In addition, the 2001 guidelines provide guidance to clinicians and exposed workers regarding when to consider HIV prophylaxis and recommendations for treatment regimens.
Hand hygieneHand hygiene (e.g., hand-washing, hand antisepsis or surgical-hand antisepsis) substantially reduces potential pathogens on the hands and is considered the single most critical measure for reducing the risk of transmitting organisms to patients and health care personnel. Hospital-based studies have demonstrated that noncompliance with hand hygiene practices is associated with health care-associated infections and the spread of multiresistant organisms. Noncompliance also has been a major contributor to outbreaks. The prevalence of health care-associated infections decreases as adherence of health care workers to recommended hand hygiene measures improves.
The microbial flora of the skin, first described in 1938, consist of transient and resident microorganisms. Transient flora, which colonize the superficial layers of the skin, are easier to remove by routine hand-washing. They are often acquired by workers during direct contact with patients or contaminated environmental surfaces; these organisms are most frequently associated with health care-associated infections. Resident flora attached to deeper layers of the skin are more resistant to removal and less likely to be associated with such infections.
The preferred method for hand hygiene depends on the type of procedure, the degree of contamination and the desired persistence of antimicrobial action on the skin. For routine dental examinations and nonsurgical procedures, hand-washing and hand antisepsis is achieved by using either a plain or antimicrobial soap and water. If the hands are not visibly soiled, an alcohol-based hand rub is adequate.
The purpose of surgical hand antisepsis is to eliminate transient flora and reduce resident flora for the duration of a procedure to prevent introduction of organisms in the operative wound, if gloves become punctured or torn. Skin bacteria can rapidly multiply under surgical gloves if hands are washed with soap that is not antimicrobial. Thus, an antimicrobial soap or alcohol hand rub with persistent activity should be used before surgical procedures.
Agents used for surgical hand antisepsis should substantially reduce microorganisms on intact skin, contain a nonirritating antimicrobial preparation, have a broad spectrum of activity, be fast-acting and have a persistent effect. Persistence (i.e., extended antimicrobial activity that prevents or inhibits survival of microorganisms after the product is applied) is critical because microorganisms can colonize on hands in the moist environment underneath gloves.
Alcohol hand rubs are rapidly germicidal when applied to the skin, but should include such antiseptics as chlorhexidine, quaternary ammonium compounds, octenidine or triclosan to achieve persistent activity. Factors that can influence the effectiveness of the surgical hand antisepsis in addition to the choice of antiseptic agent include duration and technique of scrubbing, as well as condition of the hands, and techniques used for drying and gloving. CDC’s 2002 guideline on hand hygiene in health care settings provides more complete information.
Selection of antiseptic agentsSelecting the most appropriate antiseptic agent for hand hygiene requires consideration of multiple factors. Essential performance characteristics of a product (e.g., the spectrum and persistence of activity and whether or not the agent is fast acting) should be determined before selecting a product. Delivery system, cost per use, reliable vendor support and supply are also considerations. Because worker acceptance is a major factor regarding compliance with recommended hand hygiene protocols, considering their needs is
critical and should include possible chemical allergies, skin integrity after repeated use, compatibility with lotions used and offensive agent ingredients (e.g., scent). Discussing specific preparations or ingredients used for hand antisepsis is beyond the scope of this report. Health care workers should choose from commercially available health care worker hand washes when selecting agents for hand antisepsis or surgical hand antisepsis.
Storage and dispensing of hand-care productsHand-washing products, including plain (i.e., non-antimicrobial) soap and antiseptic products, can become contaminated or support the growth of microorganisms. Liquid products should be stored in closed containers and dispensed from either disposable containers
or containers that are washed and dried thoroughly before refilling. Soap should not be added to a partially empty dispenser, because this practice of topping off might lead to bacterial contamination. Store and dispense products according to manufacturers’ directions.
LotionsThe primary defense against infection and transmission of pathogens is healthy, unbroken skin. Frequent hand-washing with soaps and antiseptic agents can cause chronic irritant contact dermatitis among workers. Damage to the skin changes skin flora, resulting in more frequent colonization by staphylococci and gram-negative bacteria. The potential of detergents to cause skin irritation varies considerably, but can be reduced by adding emollients. Lotions are often recommended to ease the dryness resulting from frequent
hand-washing and to prevent dermatitis from glove use. However, petroleum-based lotion formulations can weaken latex gloves and increase permeability. For that reason, lotions that contain petroleum or other oil emollients should only be used at the end of the work day. Dental practitioners should obtain information from lotion manufacturers regarding interaction between lotions, gloves, dental materials and antimicrobial products.
Fingernails and artificial nailsAlthough the relationship between fingernail length and wound infection is unknown, keeping nails short is considered key because
the majority of flora on the hands are found under and around the fingernails. Fingernails should be short enough to allow dental workers

Page 35 Dental.EliteCME.com
to thoroughly clean underneath them and prevent glove tears. Sharp nail edges or broken nails are also likely to increase glove failure. Long artificial or natural nails can make donning gloves more difficult and can cause gloves to tear more readily.
Hand carriage of gram-negative organisms has been determined to be greater among wearers of artificial nails than among nonwearers, both
before and after hand-washing. In addition, artificial fingernails or extenders have been epidemiologically implicated in multiple outbreaks involving fungal and bacterial infections in hospital intensive-care units and operating rooms. Freshly applied nail polish on natural nails does not increase the microbial load from periungual skin if fingernails are short; however, chipped nail polish can harbor added bacteria.
JewelryStudies have demonstrated that skin underneath rings is more heavily colonized than comparable areas of skin on fingers without rings. In a study of intensive-care nurses, multivariable analysis determined rings were the only substantial risk factor for carriage of gram-negative bacilli and Staphylococcus aureus, and the concentration of organisms correlated with the number of rings worn. However, two other studies demonstrated that mean bacterial colony counts on hands after hand-washing were similar among persons wearing rings and those
not wearing rings. Whether wearing rings increases the likelihood of transmitting a pathogen is unknown; further studies are needed to establish whether rings result in higher transmission of pathogens in health care settings. However, rings and decorative nail jewelry can make donning gloves more difficult and cause gloves to tear more readily. Thus, jewelry should not interfere with glove use (e.g., impair ability to wear the correct-sized glove or alter glove integrity).
Personal protective equipmentPPE is designed to protect the skin and the mucous membranes of the eyes, nose and mouth of dental care workers from exposure to blood or OPIM. Use of rotary dental and surgical instruments (e.g., handpieces or ultrasonic scalers) and air-water syringes creates a visible spray that contains primarily large particle droplets of water, saliva, blood, microorganisms and other debris. This spatter travels only a short distance and settles out quickly, landing on the floor, nearby operatory surfaces, dental care workers or the patient. The spray also might
contain certain aerosols (i.e., particles of respirable size, less than 10 μm). Aerosols can remain airborne for extended periods and can be inhaled. However, they should not be confused with the large-particle spatter that makes up the bulk of the spray from handpieces and ultrasonic scalers. Appropriate work practices, including use of dental dams and high-velocity air evacuation, should minimize dissemination of droplets, spatter and aerosols.
Protective clothingProtective clothing and equipment (e.g., gowns, lab coats, gloves, masks and protective eyewear or face shield) should be worn to prevent contamination of street clothing and to protect the skin of dental workers from exposures to blood and body substances. Uniforms/scrubs are not considered personal protective equipment when anticipating spatter of blood or body fluids. OSHA blood-borne pathogens standard requires sleeves to be long enough to protect the forearms when the gown is
worn as personal protective equipment (i.e., when spatter and spray of blood, saliva or OPIM to the forearms is anticipated). Dental personnel should change protective clothing when it becomes visibly soiled and as soon as feasible if penetrated by blood or other potentially infectious fluids. All protective clothing should be removed before leaving the work area.
Gloves and glovingDHCP wear gloves to prevent contamination of their hands when touching mucous membranes, blood, saliva or OPIM, and also to reduce the likelihood that microorganisms present on the workers’ hands will be transmitted to patients during surgical or other patient-care procedures. Medical gloves, both patient examination and surgeon’s gloves, are manufactured as single-use disposable items that should be used for only one patient, then discarded. Gloves should be changed between patients and when torn or punctured.
Wearing gloves does not eliminate the need for hand-washing. Hand hygiene should be performed immediately before donning gloves. Gloves can have small, unapparent defects or can be torn during use, and hands can become contaminated during glove removal. These circumstances increase the risk of operative wound contamination and exposure of the worker’s hands to microorganisms from
patients. FDA regulates the medical glove industry, which includes gloves marketed as sterile surgeon’s and sterile or nonsterile patient examination gloves. General-purpose utility gloves are also used in dental health care settings but are not regulated by FDA because they are not promoted for medical use. More rigorous standards are applied to surgeon’s gloves than to examination gloves. FDA has identified acceptable quality levels (e.g., maximum defects allowed) for glove manufacturers, but even intact gloves eventually fail with exposure to mechanical (e.g., sharps, fingernails or jewelry) and chemical (e.g., dimethy-acrylates) hazards and over time. These variables can be controlled, ultimately optimizing glove performance, by:
● Maintaining short fingernails. ● Minimizing or eliminating hand jewelry. ● Using engineering and work-practice controls to avoid injuries
with sharps.
Sterile surgeon’s gloves and double-gloving during oral surgical procedures Certain limited studies have determined no difference in postoperative infection rates after routine tooth extractions when surgeons wore either sterile or nonsterile gloves. However, wearing sterile surgeon’s gloves during surgical procedures is supported by a strong theoretical rationale. Sterile gloves minimize transmission of microorganisms from the hands of surgical dental care personnel to patients and prevent contamination of the hands of the workers with the patient’s blood and body fluids. In addition, sterile surgeon’s gloves are more
rigorously regulated by FDA and therefore, might provide an increased level of protection for the provider if exposure to blood is likely.
Although the effectiveness of wearing two pairs of gloves in preventing disease transmission has not been demonstrated, the majority of studies among health care workers have demonstrated a lower frequency of inner glove perforation and visible blood on the surgeon’s hands when double gloves are worn. In one study evaluating double gloves during oral surgical and dental hygiene procedures, the perforation of outer latex gloves was greater during longer procedures

Dental.EliteCME.com Page 36
(i.e., more than 45 minutes), with the highest rate (10 percent) of perforation occurring during oral surgery procedures. Based on these studies, double-gloving might provide additional protection from occupational blood contact. Double-gloving does not appear
to substantially reduce either manual dexterity or tactile sensitivity. Additional protection might also be provided by specialty products (e.g., orthopedic surgical gloves and glove liners).
Contact dermatitis and latex hypersensitivityOccupationally related contact dermatitis can develop from frequent and repeated use of hand hygiene products, exposure to chemicals, and glove use. Contact dermatitis is classified as either irritant or allergic. Irritant contact dermatitis is common, nonallergic and develops as dry, itchy, irritated areas on the skin around the area of contact. By comparison, allergic contact dermatitis (type IV hypersensitivity) can result from exposure to accelerators and other chemicals used in the manufacture of rubber gloves (e.g., natural rubber latex, nitrile and neoprene), as well as from other chemicals found in the dental practice setting (e.g., methacrylates and glutaraldehyde). Allergic contact dermatitis often manifests as a rash beginning hours after contact and, similar to irritant dermatitis, is usually confined to the area of contact.
Latex allergy (type I hypersensitivity to latex proteins) can be a more serious systemic allergic reaction, usually beginning within minutes of exposure, but sometimes occurring hours later and producing varied symptoms. More common reactions include runny nose, sneezing, itchy eyes, scratchy throat, hives and itchy, burning skin sensations. More severe symptoms include asthma marked by difficult breathing, coughing spells and wheezing; cardiovascular and gastrointestinal ailments; and in rare cases, anaphylaxis and death. The American Dental Association (ADA) began investigating the prevalence of type I latex hypersensitivity among dental care personnel at the ADA annual meeting in 1994. In 1994 and 1995, approximately 2,000 dentists, hygienists and assistants volunteered for skin-prick testing. Data demonstrated that 6.2 percent of those tested were positive for type I latex hypersensitivity. Data from the subsequent five years of this ongoing cross-sectional study indicated a decline in prevalence from 8.5 percent to 4.3 percent. This downward trend is similar to that reported by other studies and might be related to use of latex gloves with lower allergen content.
Natural rubber latex proteins responsible for latex allergy are attached to glove powder. When powdered latex gloves are worn, more latex protein reaches the skin. In addition, when powdered latex gloves are donned or removed, latex protein/powder particles become aerosolized and can be inhaled, contacting mucous membranes. As a result, allergic patients and dental workers can experience cutaneous, respiratory and conjunctival symptoms related to latex protein exposure. Dental care workers can become sensitized to latex protein with repeated exposure. Work areas where only powder-free, low-allergen latex gloves are used demonstrate low or undetectable amounts of latex allergy-causing proteins and fewer symptoms among workers related to natural rubber latex allergy. Because of the role of glove powder in exposure to latex protein, NIOSH recommends that if latex gloves are
chosen, workers should be provided with reduced protein, powder-free gloves. Nonlatex (e.g., nitrile or vinyl) powder-free and low-protein gloves are also available. Although rare, potentially life-threatening anaphylactic reactions to latex can occur, and dental practices should be appropriately equipped and have procedures in place to respond to such emergencies.
Dental care personnel and dental patients with latex allergy should not have direct contact with latex-containing materials and should be in a latex-safe environment with all latex-containing products removed from their vicinity. Dental patients with histories of latex allergy can be at risk from dental products (e.g., prophylaxis cups, rubber dams, orthodontic elastics and medication vials). Any latex-containing devices that cannot be removed from the treatment environment should be adequately covered or isolated. Persons might also be allergic to chemicals used in the manufacture of natural rubber latex and synthetic rubber gloves, as well as metals, plastics or other materials used in dental care.
Taking thorough health histories for both patients and dental workers, followed by avoidance of contact with potential allergens, can minimize the possibility of adverse reactions. Certain common predisposing conditions for latex allergy include previous history of allergies, a history of spina bifida, urogenital anomalies or allergies to avocados, kiwis, nuts or bananas. The following precautions should be considered to ensure safe treatment for patients who have possible or documented latex allergy:
● Be aware that latent allergens in the ambient air can cause respiratory or anaphylactic symptoms among persons with latex hypersensitivity. Patients with latex allergy can be scheduled for the first appointment of the day to minimize their inadvertent exposure to airborne latex particles.
● Communicate with other dental workers regarding patients with latex allergy (e.g., by oral instructions, written protocols and posted signage) to prevent them from bringing latex-containing materials into the treatment area.
● Frequently clean all working areas contaminated with latex powder or dust.
● Have emergency treatment kits with latex-free products available at all times.
● If latex-related complications occur during or after a procedure, manage the reaction and seek emergency assistance as indicated. Follow current medical emergency response recommendations for management of anaphylaxis.
Sterilization and disinfection of patient-care itemsPatient-care items (dental instruments, devices and equipment) are categorized as critical, semicritical or noncritical, depending on the potential risk for infection associated with their intended use (Table 1). Critical items used to penetrate soft tissue or bone have the greatest risk of transmitting infection and should be sterilized by heat. Semicritical items touch mucous membranes or nonintact skin and have a lower risk of transmission; because the majority of semicritical items in dentistry are heat-tolerant, they also should be sterilized by using heat. If a semicritical item is heat-sensitive, it should, at a minimum, be processed with high-level disinfection.
Noncritical patient-care items pose the least risk of transmission of infection, contacting only intact skin, which can serve as an effective
barrier to microorganisms. In the majority of cases, cleaning, or if visibly soiled, cleaning followed by disinfection with an EPA-registered hospital disinfectant is adequate. When the item is visibly contaminated with blood or OPIM, an EPA-registered hospital disinfectant with a tuberculocidal claim (i.e., intermediate-level disinfectant) should be used. Cleaning or disinfection of certain noncritical patient-care items can be difficult or damage the surfaces; therefore, use of disposable barrier protection of these surfaces might be a preferred alternative.
FDA-cleared sterilant/high-level disinfectants and EPA registered disinfectants must have clear label claims for intended use, and manufacturer instructions for use must be followed.
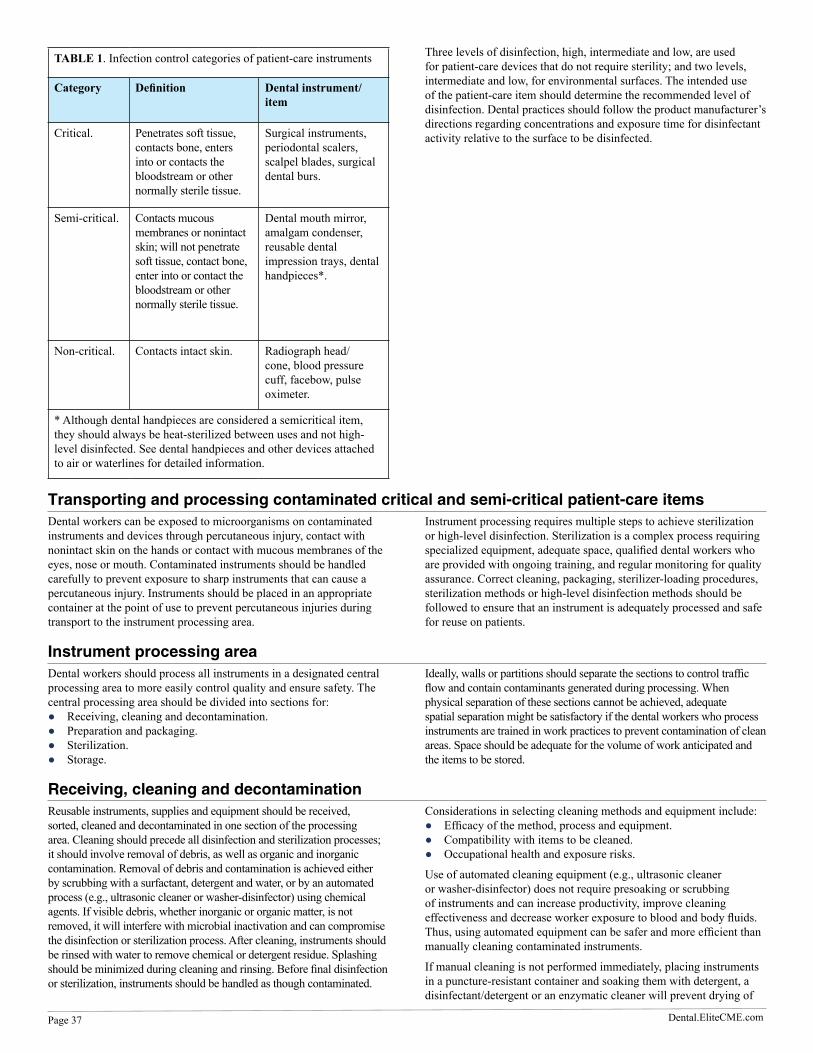
Page 37 Dental.EliteCME.com
TABLE 1. Infection control categories of patient-care instruments
Category Definition Dental instrument/item
Critical. Penetrates soft tissue, contacts bone, enters into or contacts the bloodstream or other normally sterile tissue.
Surgical instruments, periodontal scalers, scalpel blades, surgical dental burs.
Semi-critical. Contacts mucous membranes or nonintact skin; will not penetrate soft tissue, contact bone, enter into or contact the bloodstream or other normally sterile tissue.
Dental mouth mirror, amalgam condenser, reusable dental impression trays, dental handpieces*.
Non-critical. Contacts intact skin. Radiograph head/cone, blood pressure cuff, facebow, pulse oximeter.
* Although dental handpieces are considered a semicritical item, they should always be heat-sterilized between uses and not high-level disinfected. See dental handpieces and other devices attached to air or waterlines for detailed information.
Three levels of disinfection, high, intermediate and low, are used for patient-care devices that do not require sterility; and two levels, intermediate and low, for environmental surfaces. The intended use of the patient-care item should determine the recommended level of disinfection. Dental practices should follow the product manufacturer’s directions regarding concentrations and exposure time for disinfectant activity relative to the surface to be disinfected.
Transporting and processing contaminated critical and semi-critical patient-care itemsDental workers can be exposed to microorganisms on contaminated instruments and devices through percutaneous injury, contact with nonintact skin on the hands or contact with mucous membranes of the eyes, nose or mouth. Contaminated instruments should be handled carefully to prevent exposure to sharp instruments that can cause a percutaneous injury. Instruments should be placed in an appropriate container at the point of use to prevent percutaneous injuries during transport to the instrument processing area.
Instrument processing requires multiple steps to achieve sterilization or high-level disinfection. Sterilization is a complex process requiring specialized equipment, adequate space, qualified dental workers who are provided with ongoing training, and regular monitoring for quality assurance. Correct cleaning, packaging, sterilizer-loading procedures, sterilization methods or high-level disinfection methods should be followed to ensure that an instrument is adequately processed and safe for reuse on patients.
Instrument processing areaDental workers should process all instruments in a designated central processing area to more easily control quality and ensure safety. The central processing area should be divided into sections for:
● Receiving, cleaning and decontamination. ● Preparation and packaging. ● Sterilization. ● Storage.
Ideally, walls or partitions should separate the sections to control traffic flow and contain contaminants generated during processing. When physical separation of these sections cannot be achieved, adequate spatial separation might be satisfactory if the dental workers who process instruments are trained in work practices to prevent contamination of clean areas. Space should be adequate for the volume of work anticipated and the items to be stored.
Receiving, cleaning and decontaminationReusable instruments, supplies and equipment should be received, sorted, cleaned and decontaminated in one section of the processing area. Cleaning should precede all disinfection and sterilization processes; it should involve removal of debris, as well as organic and inorganic contamination. Removal of debris and contamination is achieved either by scrubbing with a surfactant, detergent and water, or by an automated process (e.g., ultrasonic cleaner or washer-disinfector) using chemical agents. If visible debris, whether inorganic or organic matter, is not removed, it will interfere with microbial inactivation and can compromise the disinfection or sterilization process. After cleaning, instruments should be rinsed with water to remove chemical or detergent residue. Splashing should be minimized during cleaning and rinsing. Before final disinfection or sterilization, instruments should be handled as though contaminated.
Considerations in selecting cleaning methods and equipment include: ● Efficacy of the method, process and equipment. ● Compatibility with items to be cleaned. ● Occupational health and exposure risks.
Use of automated cleaning equipment (e.g., ultrasonic cleaner or washer-disinfector) does not require presoaking or scrubbing of instruments and can increase productivity, improve cleaning effectiveness and decrease worker exposure to blood and body fluids. Thus, using automated equipment can be safer and more efficient than manually cleaning contaminated instruments.
If manual cleaning is not performed immediately, placing instruments in a puncture-resistant container and soaking them with detergent, a disinfectant/detergent or an enzymatic cleaner will prevent drying of

Dental.EliteCME.com Page 38
patient material and make cleaning easier and less time-consuming. Use of a liquid chemical sterilant/high-level disinfectant (e.g., glutaraldehyde) as a holding solution is not recommended.
Using work-practice controls (e.g., a long-handled brush) to keep the scrubbing hand away from sharp instruments is recommended. To avoid injury from sharp instruments, workers should wear puncture-resistant, heavy-duty utility gloves when handling or manually
cleaning contaminated instruments and devices. Employees should not reach into trays or containers holding sharp instruments that cannot be seen (e.g., sinks filled with soapy water in which sharp instruments have been placed). Work-practice controls should include use of a strainer-type basket to hold instruments and forceps to remove the items. Because splashing is likely to occur, a mask, protective eyewear or face shield, and gown or jacket should be worn.
Preparation and packagingIn another section of the processing area, cleaned instruments and other dental supplies should be inspected, assembled into sets or trays, and wrapped, packaged or placed into container systems for sterilization. Hinged instruments should be processed open and unlocked. An internal chemical indicator should be placed in every package. In addition, an external chemical indicator (e.g., chemical indicator tape) should be used when the internal indicator cannot be seen from outside the package. For unwrapped loads, at a minimum, an internal chemical indicator should be placed in the tray or cassette with items to be sterilized (see Sterilization of unwrapped instruments). Dental practices should refer to the manufacturer’s instructions
regarding use and correct placement of chemical indicators (see Sterilization monitoring). Critical and semicritical instruments that will be stored should be wrapped or placed in containers (e.g., cassettes or organizing trays) designed to maintain sterility during storage.
Packaging materials (e.g., wraps or container systems) allow penetration of the sterilization agent and maintain sterility of the processed item after sterilization. Materials for maintaining sterility of instruments during transport and storage include wrapped perforated instrument cassettes, peel pouches of plastic or paper and sterilization wraps (woven and nonwoven). Packaging materials should be designed for the type of sterilization process being used.
SterilizationThe sterilization section of the processing area should include the sterilizers and related supplies, with adequate space for loading, unloading and cool down. The area can also include incubators for analyzing spore tests and enclosed storage for sterile items and disposable (single-use) items. Manufacturer and local building code specifications will determine placement and room ventilation requirements.
Sterilization procedures – Heat-tolerant dental instruments usually are sterilized by:
● Steam under pressure (autoclaving). ● Dry heat. ● Unsaturated chemical vapor.
All sterilization should be performed by using medical sterilization equipment cleared by FDA. The sterilization times, temperatures and other operating parameters recommended by the manufacturer of the equipment used, as well as instructions for correct use of containers, wraps and chemical or biological indicators, should always be followed.
Items to be sterilized should be arranged to permit free circulation of the sterilizing agent (e.g., steam, chemical vapor or dry heat); manufacturer’s instructions for loading the sterilizer should be followed. Instrument packs should be allowed to dry inside the sterilizer chamber before removing and handling. Packs should not be touched until they are cool and dry because hot packs act as wicks, absorbing moisture, and hence, bacteria from hands. The ability of equipment to attain physical parameters required to achieve sterilization should be monitored by mechanical, chemical and biological indicators. Sterilizers vary in their types of indicators and their ability to provide readings on the mechanical or physical parameters of the sterilization process (e.g., time, temperature and pressure). Consult with the sterilizer manufacturer regarding selection and use of indicators.
Steam sterilization – Among sterilization methods, steam sterilization, which is dependable and economical, is the most widely used for wrapped and unwrapped critical and semicritical items that are not sensitive to heat and moisture. Steam sterilization requires exposure of each item to direct steam contact at a required temperature and pressure for a specified time needed to kill microorganisms. Two basic types of steam sterilizers are the gravity displacement and the high-speed prevacuum sterilizer.
The majority of tabletop sterilizers used in a dental practice are gravity displacement sterilizers, although prevacuum sterilizers are becoming more widely available. In gravity displacement sterilizers, steam is admitted through steam lines, a steam generator or self-generation of steam within the chamber.
Unsaturated air is forced out of the chamber through a vent in the chamber wall. Trapping of air is a concern when using saturated steam under gravity displacement; errors in packaging items or overloading the sterilizer chamber can result in cool air pockets and items not being sterilized.
Prevacuum sterilizers are fitted with a pump to create a vacuum in the chamber and ensure air removal from the sterilizing chamber before the chamber is pressurized with steam. Relative to gravity displacement, this procedure allows faster and more positive steam penetration throughout the entire load. Prevacuum sterilizers should be tested periodically for adequate air removal, as recommended by the manufacturer. Air not removed from the chamber will interfere with steam contact. If a sterilizer fails the air removal test, it should not be used until inspected by sterilizer maintenance personnel and it passes the test. Manufacturer’s instructions, with specific details regarding operation and user maintenance information, should be followed.
Unsaturated chemical-vapor sterilization – Unsaturated chemical-vapor sterilization involves heating a chemical solution of primarily alcohol with 0.23 percent formaldehyde in a closed pressurized chamber. Unsaturated chemical vapor sterilization of carbon steel instruments (e.g., dental burs) causes less corrosion than steam sterilization because of the low level of water present during the cycle. Instruments should be dry before sterilizing. State and local authorities should be consulted for hazardous waste disposal requirements for the sterilizing solution.
Dry-heat sterilization – Dry heat is used to sterilize materials that might be damaged by moist heat (e.g., burs and certain orthodontic instruments). Although dry heat has the advantages of low operating cost and being noncorrosive, it is a prolonged process and the high temperatures required are not suitable for certain patient-care items and devices. Dry-heat sterilizers used in dentistry include static-air and forced-air types:
● The static-air type is commonly called an oven-type sterilizer. Heating coils in the bottom or sides of the unit cause hot air to rise inside the chamber through natural convection.

Page 39 Dental.EliteCME.com
● The forced-air type is also known as a rapid heat-transfer sterilizer. Heated air is circulated throughout the chamber at a high velocity, permitting more rapid transfer of energy from the air to the instruments, thereby reducing the time needed for sterilization.
Sterilization of unwrapped instruments – An unwrapped cycle (sometimes called flash sterilization) is a method for sterilizing unwrapped patient-care items for immediate use. The time required for unwrapped sterilization cycles depends on the type of sterilizer and the type of item (i.e., porous or nonporous) to be sterilized. The unwrapped cycle in tabletop sterilizers is preprogrammed by the manufacturer to a specific time and temperature setting and can include a drying phase at the end to produce a dry instrument with much of the heat dissipated. If the drying phase requirements are unclear, the operation manual or manufacturer of the sterilizer should be consulted. If the unwrapped sterilization cycle in a steam sterilizer does not include a drying phase or has only a minimal drying phase, items retrieved from the sterilizer will be hot and wet, making aseptic transport to the point of use more difficult. For dry-heat and chemical-vapor sterilizers, a drying phase is not required.
Unwrapped sterilization should be used only under certain conditions: ● Thorough cleaning and drying of instruments precedes the
unwrapped sterilization cycle. ● Mechanical monitors are checked and chemical indicators used for
each cycle. ● Care is taken to avoid thermal injury to dental care personnel or
patients. ● Items are transported aseptically to the point of use to maintain
sterility.
Because all implantable devices should be quarantined after sterilization until the results of biological monitoring are known, unwrapped or flash sterilization of implantable items is not recommended.
Critical instruments sterilized unwrapped should be transferred immediately by using aseptic technique, from the sterilizer to the actual point of use. Critical instruments should not be stored unwrapped. Semicritical instruments that are sterilized unwrapped on a tray or in a container system should be used immediately or within a short time. When sterile items are open to the air, they will eventually become contaminated. Storage, even temporary, of unwrapped semicritical instruments is discouraged because it permits exposure to dust, airborne organisms and other unnecessary contamination before use on a patient. A carefully written protocol for minimizing the risk of contaminating unwrapped instruments should be prepared and followed.
Other sterilization methods – Heat-sensitive critical and semicritical instruments and devices can be sterilized by immersing them in liquid chemical germicides registered by FDA as sterilants. When using a liquid chemical germicide for sterilization, certain post-sterilization procedures are essential. Items need to be:
● Rinsed with sterile water after removal to remove toxic or irritating residues.
● Handled using sterile gloves and dried with sterile towels. ● Delivered to the point of use in an aseptic manner.
If an instrument is stored before use, the instrument should not be considered sterile and should be sterilized again just before use. In addition, the sterilization process with liquid chemical sterilants cannot be verified with biological indicators.
Because of these limitations and because liquid chemical sterilants can require approximately 12 hours of complete immersion, they are almost never used to sterilize instruments. Rather, these chemicals are more often used for high-level disinfection. Shorter immersion times (12-90 minutes) are used to achieve high-level disinfection of semicritical instruments or items. These powerful, sporicidal chemicals (e.g., glutaraldehyde, peracetic acid and hydrogen peroxide) are highly toxic. Manufacturer instructions (e.g., regarding dilution, immersion
time and temperature) and safety precautions for using chemical sterilants/high-level disinfectants must be followed precisely.
These chemicals should not be used for applications other than those indicated in their label instructions. Misapplications include use as an environmental surface disinfectant or instrument-holding solution.
When using appropriate precautions (e.g., closed containers to limit vapor release, chemically resistant gloves and aprons, goggles and face shields), glutaraldehyde-based products can be used without tissue irritation or adverse health effects. However, dermatologic, eye irritation, respiratory effects and skin sensitization have been reported. Because of their lack of chemical resistance to glutaraldehydes, medical gloves are not an effective barrier. Other factors might apply (e.g., room exhaust ventilation or 10 air exchanges/hour) to ensure workers’ safety. For all of these reasons, using heat-sensitive semicritical items that must be processed with liquid chemical germicides is discouraged; heat-tolerant or disposable alternatives are available for the majority of such items.
Low-temperature sterilization with ethylene oxide gas (ETO) has been used extensively in larger health care facilities. Its primary advantage is the ability to sterilize heat- and moisture-sensitive patient-care items with reduced deleterious effects. However, extended sterilization times of 10-48 hours and potential hazards to patients and workers requiring stringent health and safety requirements make this method impractical for private-practice settings. Handpieces cannot be effectively sterilized with this method because of decreased penetration of ETO gas flow through a small lumen.
Other types of low-temperature sterilization (e.g., hydrogen peroxide gas plasma) exist but are not yet practical for dental offices. Bead sterilizers have been used in dentistry to sterilize small metallic instruments (e.g., endodontic files). FDA has determined that a risk of infection exists with these devices because of their potential failure to sterilize dental instruments and has required their commercial distribution cease unless the manufacturer files a premarket approval application. If a bead sterilizer is employed, DHCP assume the risk of employing a dental device FDA has deemed neither safe nor effective.
Sterilization monitoring – Monitoring of sterilization procedures should include a combination of process parameters, including mechanical, chemical and biological. These parameters evaluate both the sterilizing conditions and the procedure’s effectiveness.
Mechanical techniques for monitoring sterilization include assessing cycle time, temperature and pressure by observing the gauges or displays on the sterilizer and noting these parameters for each load. Some tabletop sterilizers have recording devices that print out these parameters. Correct readings do not ensure sterilization, but incorrect readings can be the first indication of a problem with the sterilization cycle.
Chemical indicators, internal and external, use sensitive chemicals to assess physical conditions (e.g., time and temperature) during the sterilization process. Although chemical indicators do not prove sterilization has been achieved, they allow detection of certain equipment malfunctions, and they can help identify procedural errors. External indicators applied to the outside of a package (e.g., chemical indicator tape or special markings) change color rapidly when a specific parameter is reached, and they verify that the package has been exposed to the sterilization process. Internal chemical indicators should be used inside each package to ensure the sterilizing agent has penetrated the packaging material and actually reached the instruments inside. A single-parameter internal chemical indicator provides information regarding only one sterilization parameter (e.g., time or temperature). Multiparameter internal chemical indicators are designed to react to more than two parameters (e.g., time and temperature; or time, temperature and the presence of steam) and can provide a more reliable indication that sterilization conditions have been

Dental.EliteCME.com Page 40
met. Multiparameter internal indicators are available only for steam sterilizers (i.e., autoclaves).
Because chemical indicator test results are received when the sterilization cycle is complete, they can provide an early indication of a problem and where in the process the problem might exist. If either mechanical indicators or internal or external chemical indicators indicate inadequate processing, items in the load should not be used until reprocessed.
Biological indicators (BIs) (i.e., spore tests) are the most accepted method for monitoring the sterilization process because they assess it directly by killing known highly resistant microorganisms (e.g., Geobacillus or Bacillus species), rather than merely testing the physical and chemical conditions necessary for sterilization. Because spores used in BIs are more resistant and present in greater numbers than the common microbial contaminants found on patient-care equipment, an inactivated BI indicates other potential pathogens in the load have been killed.
Correct functioning of sterilization cycles should be verified for each sterilizer by the periodic use (at least weekly) of BIs. Every load containing implantable devices should be monitored with such indicators, and the items quarantined until BI results are known. However, in an emergency, placing implantable items in quarantine until spore tests are known to be negative might be impossible.
Manufacturer’s directions should determine the placement and location of BI in the sterilizer. A control BI, from the same lot as the test indicator and not processed through the sterilizer, should be incubated with the test BI; the control BI should yield positive results for bacterial growth.
In-office biological monitoring is available; mail-in sterilization monitoring services (e.g., from private companies or dental schools) can also be used to test both the BI and the control. Although some dental care personnel have expressed concern that delays caused by mailing specimens might cause false negatives, studies have determined that mail delays have no substantial effect on final test results.
Procedures to follow in the event of a positive spore test have been developed. If the mechanical (e.g., time, temperature and pressure) and chemical (i.e., internal or external) indicators demonstrate that the sterilizer is functioning correctly, a single positive spore test probably does not indicate sterilizer malfunction. Items other than implantable devices do not necessarily need to be recalled; however, the spore test should be repeated immediately after correctly loading the sterilizer and using the same cycle that produced the failure. The sterilizer
should be removed from service, and all records reviewed of chemical and mechanical monitoring since the last negative BI test.
Also, sterilizer operating procedures should be reviewed, including packaging, loading and spore testing, with all persons who work with the sterilizer to determine whether operator error could be responsible. Overloading, failure to provide adequate package separation and incorrect or excessive packaging material are all common reasons for a positive BI in the absence of mechanical failure of the sterilizer unit. A second monitored sterilizer in the office can be used, or a loaner from a sales or repair company obtained, to minimize office disruption while waiting for the repeat BI.
If the repeat test is negative and chemical and mechanical monitoring indicates adequate processing, the sterilizer can be put back into service. If the repeat BI test is positive, and packaging, loading and operating procedures have been confirmed as performing correctly, the sterilizer should remain out of service until it has been inspected, repaired and rechallenged with BI tests in three consecutive empty chamber sterilization cycles. When possible, items from suspect loads dating back to the last negative BI should be recalled, rewrapped and resterilized.
A more conservative approach has been recommended in which any positive spore test is assumed to represent sterilizer malfunction and requires that all materials processed in that sterilizer, dating from the sterilization cycle having the last negative biologic indicator to the next cycle indicating satisfactory biologic indicator results, should be considered nonsterile and retrieved, if possible, and reprocessed or held in quarantine until the results of the repeat BI are known. This approach is considered conservative because the margin of safety in steam sterilization is sufficient enough that infection risk associated with items in a load indicating spore growth is minimal, particularly if the item was properly cleaned and the temperature was achieved (e.g., as demonstrated by acceptable chemical indicator or temperature chart). Published studies are not available that document disease transmission through a nonretrieved surgical instrument after a steam sterilization cycle with a positive biological indicator. This more conservative approach should always be used for sterilization methods other than steam (e.g., dry heat, unsaturated chemical vapor, ETO or hydrogen peroxide gas plasma).
Results of biological monitoring should be recorded and sterilization monitoring records (i.e., mechanical, chemical and biological) retained long enough to comply with state and local regulations. Such records are a component of an overall dental infection control program (see program evaluation).
Storage of sterilized items and clean dental suppliesThe storage area should contain enclosed storage for sterile items and disposable (single-use) items. Storage practices for wrapped sterilized instruments can be either date- or event-related. Packages containing sterile supplies should be inspected before use to verify barrier integrity and dryness.
Although some health care facilities continue to date every sterilized package and use shelf-life practices, other facilities have switched to event-related practices. This approach recognizes that the product should remain sterile indefinitely unless an event causes it to become contaminated (e.g., torn or wet packaging). Even for event-related
packaging, minimally, the date of sterilization should be placed on the package, and if multiple sterilizers are used in the facility, the sterilizer used should be indicated on the outside of the packaging material to facilitate the retrieval of processed items in the event of a sterilization failure. If packaging is compromised, the instruments should be recleaned, packaged in new wrap and sterilized again.
Clean supplies and instruments should be stored in closed or covered cabinets, if possible. Dental supplies and instruments should not be stored under sinks or in other locations where they might become wet.
Environmental infection controlIn the dental operatory, environmental surfaces (i.e., a surface or equipment that does not contact patients directly) can become contaminated during patient care. Certain surfaces, especially ones touched frequently (e.g., light handles, unit switches and drawer knobs) can serve as reservoirs of microbial contamination, although they have not been associated directly with transmission of infection
to either dental workers or patients. Transfer of microorganisms from contaminated environmental surfaces to patients occurs primarily through dental care personnel hand contact. When these surfaces are touched, microbial agents can be transferred to instruments, other environmental surfaces or to the nose, mouth or eyes of workers or patients. Although hand hygiene is key to minimizing this transferal,

Page 41 Dental.EliteCME.com
barrier protection or cleaning and disinfecting of environmental surfaces also protects against health care-associated infections.
Environmental surfaces can be divided into clinical contact surfaces and housekeeping surfaces. Because housekeeping surfaces (e.g., floors, walls and sinks) have limited risk of disease transmission, they can be decontaminated with less rigorous methods than those used on dental patient-care items and clinical contact surfaces. Strategies for cleaning and disinfecting surfaces in patient-care areas should consider the following:
● Potential for direct patient contact. ● Degree and frequency of hand contact. ● Potential contamination of the surface with body substances
or environmental sources of microorganisms (e.g., soil, dust or water).
Cleaning is the necessary first step of any disinfection process. Cleaning is a form of decontamination that renders the environmental surface safe by removing organic matter, salts and visible soils, all of which interfere with microbial inactivation. The physical action of scrubbing with detergents and surfactants and rinsing with water removes substantial numbers of microorganisms. If a surface is not cleaned first, the success of the disinfection process can be compromised. Removal of all visible blood and inorganic and organic matter can be as critical as the germicidal activity of the disinfecting agent. When a surface cannot be cleaned adequately, it should be protected with barriers.
Clinical contact surfacesClinical contact surfaces can be directly contaminated from patient materials by direct spray or spatter generated either during dental procedures or by contact with dental care personnel’s gloved hands. These surfaces can subsequently contaminate other instruments, devices, hands or gloves. Examples of such surfaces include:
● Light handles. ● Switches. ● Dental radiograph equipment. ● Dental chair-side computers. ● Reusable containers of dental materials. ● Drawer handles. ● Faucet handles. ● Countertops. ● Pens. ● Telephones. ● Doorknobs.
Barrier protection of surfaces and equipment can prevent contamination of clinical contact surfaces, but is particularly effective for those that are difficult to clean. Barriers include clear plastic wrap, bags, sheets, tubing and plastic-backed paper or other materials impervious to moisture. Because such coverings can become contaminated, they should be removed and discarded between patients while dental workers are still gloved. After removing the barrier, examine the surface to make sure it did not become soiled inadvertently. The surface needs to be cleaned and disinfected only
if contamination is evident. Otherwise, after removing gloves and performing hand hygiene, dental workers should place clean barriers on these surfaces before the next patient. If barriers are not used, surfaces should be cleaned and disinfected between patients by using an EPA-registered hospital disinfectant with an HIV, HBV claim (i.e., low-level disinfectant) or a tuberculocidal claim (i.e., intermediate-level disinfectant). Intermediate-level disinfectant should be used when the surface is visibly contaminated with blood or OPIM. Also, general cleaning and disinfection are recommended for clinical contact surfaces, dental unit surfaces and countertops at the end of daily work activities and are required if surfaces have become contaminated since their last cleaning. To facilitate daily cleaning, treatment areas should be kept free of unnecessary equipment and supplies.
Manufacturers of dental devices and equipment should provide information regarding material compatibility with liquid chemical germicides, whether equipment can be safely immersed for cleaning, and how it should be decontaminated if service is required. Because of the risks associated with exposure to chemical disinfectants and contaminated surfaces, dental workers who perform environmental cleaning and disinfection should wear gloves and other protective equipment to prevent occupational exposure to infectious agents and hazardous chemicals. Chemical- and puncture-resistant utility gloves offer more protection than patient examination gloves when using hazardous chemicals.
Housekeeping surfacesEvidence does not support that housekeeping surfaces (e.g., floors, walls and sinks) pose a risk for disease transmission in dental health care settings. Actual physical removal of microorganisms and soil by wiping or scrubbing is probably as critical, if not more so, than any antimicrobial effect provided by the agent used. The majority of housekeeping surfaces need to be cleaned only with a detergent and water or an EPA-registered hospital disinfectant/detergent, depending on the nature of the surface and the type and degree of contamination. Schedules and methods vary according to the area (e.g., dental operatory, laboratory, bathrooms or reception rooms), surface and amount and type of contamination.
Floors should be cleaned regularly, and spills should be cleaned up promptly. An EPA-registered hospital disinfectant/detergent designed for general housekeeping purposes should be used in patient-care areas if uncertainty exists regarding the nature of the soil on the surface (e.g., blood or body fluid contamination versus routine dust or dirt). Unless contamination is reasonably anticipated or apparent, cleaning or disinfecting walls, window drapes and other vertical surfaces is unnecessary. However, when housekeeping surfaces are visibly contaminated by blood or OPIM, prompt removal and surface
disinfection is appropriate infection control practice and required by OSHA.
Part of the cleaning strategy is to minimize contamination of cleaning solutions and cleaning tools (e.g., mop heads or cleaning cloths). Mops and cloths should be cleaned after use and allowed to dry before re-use, or single-use, disposable mop heads and cloths should be used to avoid spreading contamination.
Cost, safety, product-surface compatibility and acceptability by housekeepers can be key criteria for selecting a cleaning agent or an EPA-registered hospital disinfectant/detergent. Protective equipment used during cleaning and housekeeping procedures should be appropriate to the task.
Another reservoir for microorganisms can be solutions of detergents or disinfectants, especially if prepared in dirty containers, stored for long periods of time or prepared incorrectly. Manufacturers’ instructions for preparation and use should be followed. Making fresh cleaning solution each day, discarding any remaining solution and allowing the container to dry will minimize bacterial contamination. Preferred cleaning methods produce minimal mists and aerosols or dispersion of dust in patient care areas.

Dental.EliteCME.com Page 42
Cleaning and disinfection strategies for blood spillsThe majority of blood contamination events in dentistry result from spatter during dental procedures using rotary or ultrasonic instrumentation. Although no evidence supports that HBV, HCV or HIV has been transmitted from a housekeeping surface, prompt removal and surface disinfection of an area contaminated by either blood or OPIM are appropriate infection control practices and required by OSHA.
Strategies for decontaminating spills of blood and other body fluids differ by setting and volume of the spill. Blood spills on either clinical contact or housekeeping surfaces should be contained and managed as quickly as possible to reduce the risk of contact by patients and workers. The person assigned to clean the spill should wear gloves and
other protective equipment as needed. Visible organic material should be removed with absorbent material (e.g., disposable paper towels discarded in a leak-proof, appropriately labeled container). Nonporous surfaces should be cleaned and then decontaminated with either an EPA-registered hospital disinfectant effective against HBV and HIV or an EPA-registered hospital disinfectant with a tuberculocidal claim (i.e., intermediate-level disinfectant). If sodium hypochlorite is chosen, an EPA-registered sodium hypochlorite product is preferred. However, if such products are unavailable, a 1:100 dilution of sodium hypochlorite (e.g., approximately ¼ cup of 5.25 percent household chlorine bleach to 1 gallon of water) is an inexpensive and effective disinfecting agent.
Carpeting and cloth furnishingsCarpeting is more difficult to clean than nonporous hard surface flooring, and it cannot be reliably disinfected, especially after spills of blood and body substances. Studies have documented the presence of diverse microbial populations, primarily bacteria and fungi, in carpeting. Cloth furnishings pose similar contamination risks in areas
of direct patient care and places where contaminated materials are managed (e.g., dental operatory, laboratory, or instrument processing areas). For these reasons, use of carpeted flooring and fabric-upholstered furnishings in these areas should be avoided.
nonregulated and regulated medical wasteStudies have compared microbial load and diversity of microorganisms in residential waste with waste from multiple health care settings. General waste from hospitals or other health care facilities (e.g., dental practices or clinical/research laboratories) is no more infective than residential waste. The majority of soiled items in dental offices are general medical waste, and thus can be disposed of with ordinary waste. Examples include used gloves, masks, gowns, lightly soiled gauze or cotton rolls, and environmental barriers (e.g., plastic sheets or bags) used to cover equipment during treatment.
Although any item that has had contact with blood, exudates or secretions might be infective, treating all such waste as infective is neither necessary nor practical. Infectious waste that carries a substantial risk of causing infection during handling and disposal is regulated medical waste. A complete definition of regulated waste is included in OSHA’s blood-borne pathogens standard. Regulated medical waste is only a limited subset of waste: 9-15 percent of total waste in hospitals and 1-2 percent of total waste in dental offices.
Regulated medical waste requires special storage, handling, neutralization and disposal and is covered by federal, state and local
rules and regulations. Examples of regulated waste found in dental-practice settings are solid waste soaked or saturated with blood or saliva (e.g., gauze saturated with blood after surgery), extracted teeth, surgically removed hard and soft tissues, and contaminated sharp items (e.g., needles, scalpel blades and wires). Regulated medical waste requires careful containment for treatment or disposal. A single leak-resistant biohazard bag is usually adequate for containment of nonsharp regulated medical waste, provided the bag is sturdy and the waste can be discarded without contaminating the bag’s exterior. Exterior contamination or puncturing of the bag requires placement in a second biohazard bag. All bags should be securely closed for disposal. Puncture-resistant containers with a biohazard label, located at the point of use (i.e., sharps containers), are used as containment for scalpel blades, needles, syringes and unused sterile sharps.
Dental health care facilities should dispose of medical waste regularly to avoid accumulation. Any facility generating regulated medical waste should have a plan for its management that complies with federal, state and local regulations to ensure health and environmental safety.
Discharging blood or other body fluids to sanitary sewers or septic tanksAll containers with blood or saliva (e.g., suctioned fluids) can be inactivated in accordance with state-approved treatment technologies, or the contents can be carefully poured down a utility sink, drain or toilet. Appropriate protective equipment (e.g., gloves, gown, mask and protective eyewear) should be worn when performing this task. No evidence exists that blood-borne diseases have been transmitted from contact with raw or treated sewage. Multiple blood-borne pathogens,
particularly viruses, are not stable in the environment for long periods, and the discharge of limited quantities of blood and other body fluids into the sanitary sewer is considered a safe method for disposing of these waste materials. State and local regulations vary and dictate whether blood or other body fluids require pretreatment or if they can be discharged into the sanitary sewer and in what volume.
Dental unit waterlines, biofilm, and water qualityStudies have demonstrated that dental unit waterlines (i.e., narrow-bore plastic tubing that carries water to the high-speed handpiece, air/water syringe and ultrasonic scaler) can become colonized with microorganisms, including bacteria, fungi and protozoa. Protected by a polysaccharide slime layer known as a glycocalyx, these microorganisms colonize and replicate on the interior surfaces of the waterline tubing and form a biofilm, which serves as a reservoir that can amplify the number of free-floating (i.e., planktonic)
microorganisms in water used for dental treatment. Although oral flora and human pathogens (e.g., Pseudomonas aeruginosa, Legionella species, and nontuberculous Mycobacterium species), have been isolated from dental water systems, the majority of organisms recovered from dental waterlines are common heterotrophic water bacteria. These exhibit limited pathogenic potential for immuno-competent persons.

Page 43 Dental.EliteCME.com
Dental unit water qualityResearch has demonstrated that microbial counts can reach 200,000 colony-forming units (CFU)/mL within five days after installation of new dental unit waterlines, and levels of microbial contamination 106 CFU/mL of dental unit water have been documented. These counts can occur because dental unit waterline factors (e.g., system design, flow rates and materials) promote both bacterial growth and development of biofilm.
Although no epidemiologic evidence indicates a public health problem, the presence of substantial numbers of pathogens in dental unit waterlines generates concern. Exposing patients or dental workers to water of uncertain microbiological quality, despite the lack of documented adverse health effects, is inconsistent with accepted infection control principles. Thus, in 1995, ADA addressed the dental water concern by asking manufacturers to provide equipment with
the ability to deliver treatment water with less than 200 CFU/mL of unfiltered output from waterlines. This threshold was based on the quality assurance standard established for dialysate fluid, to ensure that fluid delivery systems in hemodialysis units have not been colonized by indigenous waterborne organisms.
Standards also exist for safe drinking water quality as established by EPA, the American Public Health Association (APHA) and the American Water Works Association (AWWA); they have set limits for heterotrophic bacteria of less than 500 CFU/mL of drinking water. Thus, the number of bacteria in water used as a coolant/irrigant for nonsurgical dental procedures should be as low as reasonably achievable and, at a minimum, less than 500 CFU/mL, the regulatory standard for safe drinking water established by EPA and APHA/AWWA.
SPECIAL COnSIDERATIOnS
Dental handpieces and other devices attached to air and waterlinesMultiple semicritical dental devices that touch mucous membranes are attached to the air or waterlines of the dental unit. Among these devices are high- and low-speed handpieces, prophylaxis angles, ultrasonic and sonic scaling tips, air abrasion devices and air and water syringe tips. Although no epidemiologic evidence implicates these instruments in disease transmission, studies of high-speed handpieces using dye expulsion have confirmed the potential for retracting oral fluids into internal compartments of the device. This determination indicates that retained patient material can be expelled intraorally during subsequent uses. Studies using laboratory models also indicate the possibility for retention of viral DNA and viable virus inside both high-speed handpieces and prophylaxis angles. The potential for contamination of the internal surfaces of other devices (e.g., low-speed handpieces and ultrasonic scalers), has not been studied, but restricted physical access limits their cleaning. Accordingly, any dental device connected to the dental air/water system that enters the patient’s mouth should be run to discharge water, air or a combination for a minimum of 20-30 seconds after each patient. This procedure is intended to help physically flush out patient material that might have entered the turbine and air and waterlines.
Heat methods can sterilize dental handpieces and other intraoral devices attached to air or waterlines. For processing any dental device that can be removed from the dental unit air or waterlines, neither surface disinfection nor immersion in chemical germicides is an acceptable method. Ethylene oxide gas cannot adequately sterilize internal components of handpieces. In clinical evaluations of high-speed handpieces, cleaning and lubrication were the most critical factors in determining performance and durability. Manufacturer’s instructions for cleaning, lubrication and sterilization should be followed closely to ensure both the effectiveness of the process and the longevity of handpieces.
Some components of dental instruments are permanently attached to dental unit waterlines, and although they do not enter the patient’s oral cavity, they are likely to become contaminated with oral fluids during treatment procedures. Such components (e.g., handles or dental unit attachments of saliva ejectors, high-speed air evacuators and air/water syringes) should be covered with impervious barriers that are changed after each use. If the item becomes visibly contaminated during use, dental care personnel should clean and disinfect with an EPA-registered hospital disinfectant (intermediate-level) before use on the next patient.
Saliva ejectorsBackflow from low-volume saliva ejectors occurs when the pressure in the patient’s mouth is less than that in the evacuator. Studies have reported that backflow in low-volume suction lines can occur, and microorganisms can be present in the lines retracted into the patient’s mouth when a seal around the saliva ejector is created (e.g., by a patient closing their lips around the tip of the ejector, creating a partial vacuum). This backflow can be a potential source of cross-contamination; occurrence is variable because the quality of the seal formed varies between patients.
Furthermore, studies have demonstrated that gravity pulls fluid back toward the patient’s mouth whenever a length of the suction tubing holding the tip is positioned above the patient’s mouth, or during simultaneous use of other evacuation (high-volume) equipment. Although no adverse health effects associated with the saliva ejector have been reported, practitioners should be aware that in certain situations, backflow could occur when using a saliva ejector.
Dental radiologyWhen taking radiographs, the potential to cross-contaminate equipment and environmental surfaces with blood or saliva is high if aseptic technique is not practiced. Gloves should be worn when taking radiographs and handling contaminated film packets. Other protective equipment (e.g., mask, protective eyewear and gowns) should be used if spattering of blood or other body fluids is likely. Heat-tolerant versions of intraoral radiograph accessories are available, and these semicritical items (e.g., film-holding and positioning devices) should be heat-sterilized before patient use.
After exposure of the radiograph and before glove removal, the film should be dried with disposable gauze or a paper towel to remove
blood or excess saliva and placed in a container (e.g., disposable cup) for transport to the developing area. Alternatively, if FDA-cleared film barrier pouches are used, the film packets should be carefully removed from the pouch to avoid contamination of the outside film packet and placed in the clean container for transport to the developing area. Various methods have been recommended for aseptic transport of exposed films to the developing area, and for removing the outer film packet before exposing and developing the film. Other information regarding dental radiography infection control is available.

Dental.EliteCME.com Page 44
Oral surgical proceduresThe oral cavity is colonized with numerous microorganisms. Oral surgical procedures present an opportunity for entry of microorganisms (i.e., exogenous and endogenous) into the vascular system and other normally sterile areas of the oral cavity (e.g., bone or subcutaneous tissue); therefore, an increased potential exists for localized or systemic infection. Oral surgical procedures involve the incision, excision or reflection of tissue that exposes the normally sterile areas
of the oral cavity. Examples include biopsy, periodontal surgery, apical surgery, implant surgery and surgical extractions of teeth (e.g., removal of erupted or nonerupted tooth requiring elevation of mucoperiosteal flap, removal of bone or section of tooth, and suturing if needed) (see “Hand hygiene, PPE, single-use or disposable devices,” and “Dental unit water quality”).
Handling of biopsy specimensTo protect persons handling and transporting biopsy specimens, each specimen must be placed in a sturdy, leak-proof container with a secure lid for transportation. Care should be taken when collecting the specimen to avoid contaminating the outside of the container. If
the outside of the container becomes visibly contaminated, it should be cleaned and disinfected or placed in an impervious bag. The container must be labeled with the biohazard symbol during storage, transport, shipment and disposal.
Handling of extracted teeth disposalExtracted teeth that are being discarded are subject to the containerization and labeling provisions outlined by OSHA’s blood-borne pathogens standard. OSHA considers extracted teeth to be potentially infectious material that should be disposed in medical waste containers. Extracted teeth sent to a dental laboratory for shade or size comparisons should be cleaned, surface-disinfected with an EPA-registered hospital disinfectant with intermediate-level activity (i.e., tuberculocidal claim), and transported in a manner consistent
with OSHA regulations. However, extracted teeth can be returned to patients on request, at which time provisions of the standard no longer apply. Extracted teeth containing dental amalgam should not be placed in a medical waste container that uses incineration for final disposal. Commercial metal recycling companies also might accept extracted teeth with metal restorations, including amalgam. State and local regulations should be consulted regarding disposal of the amalgam.
M. tuberculosisPatients infected with M. tuberculosis occasionally seek urgent dental treatment at outpatient dental settings. Understanding the pathogenesis of the development of TB will help dental care workers determine how to manage such patients.
M. tuberculosis is a bacterium carried in airborne infective droplet nuclei that can be generated when persons with pulmonary or laryngeal TB sneeze, cough, speak or sing. These small particles (1–5 μm) can stay suspended in the air for hours. Infection occurs when a susceptible person inhales droplet nuclei containing M. tuberculosis, which then travel to the alveoli of the lungs. Usually within two to 12 weeks after initial infection with M. tuberculosis, immune response prevents further spread of the TB bacteria, although they can remain
alive in the lungs for years, a condition termed latent TB infection. Persons with latent TB infection usually exhibit a reactive tuberculin skin test (TST), have no symptoms of active disease and are not infectious. However, they can develop active disease later in life if they do not receive treatment for their latent infection.
Any dental worker with a persistent cough (i.e., lasting more than three weeks), especially in the presence of other signs or symptoms compatible with active TB (e.g., weight loss, night sweats, fatigue, bloody sputum, anorexia or fever), should be evaluated promptly. The person should not return to the workplace until a diagnosis of TB has been excluded or he or she is on therapy and has been determined noninfectious by a physician.
Creutzfeldt-Jakob disease and other prion diseasesCreutzfeldt-Jakob disease (CJD) belongs to a group of rapidly progressive, invariably fatal, degenerative neurological disorders, transmissible spongiform encephalopathies (TSEs) that affect both humans and animals and are thought to be caused by infection with an unusual pathogen called a prion. Prions are isoforms of a normal protein, capable of self-propagation although they lack nucleic acid. Prion diseases have an incubation period of years and are usually fatal within one year of diagnosis. Among humans, TSEs include CJD,
Gerstmann-Straussler-Scheinker syndrome, fatal familial insomnia, kuru and variant CJD (vCJD). Occurring in sporadic, familial and acquired (i.e., iatrogenic) forms, CJD has an annual incidence in the United States and other countries of approximately one case per million population. In approximately 85 percent of affected patients, CJD occurs as a sporadic disease with no recognizable pattern of transmission. A smaller proportion of patients (5-15 percent) experience familial CJD because of inherited mutations of the prion protein gene.
Program evaluationThe goal of a dental infection control program is to provide a safe working environment that will reduce the risk of health care-associated infections among patients and occupational exposures among workers. Medical errors are caused by faulty systems, processes and conditions that lead persons to make mistakes or fail to prevent errors being made by others. Effective program evaluation is a systematic way to ensure procedures are useful, feasible, ethical and accurate. Program evaluation is an essential organizational practice; however, such evaluation is not practiced consistently across program areas, nor is it sufficiently well-integrated into the day-to-day management of the majority of programs.
A successful infection control program depends on developing standard operating procedures, evaluating practices, routinely documenting adverse outcomes (e.g., occupational exposures to blood) and work-related illnesses in dental workers, and monitoring health care-associated infections in patients. Strategies and tools to evaluate the infection control program can include periodic observational assessments, checklists to document procedures and routine review of occupational exposures to blood-borne pathogens. Evaluation offers an opportunity to improve the effectiveness of both the infection control program and dental practice protocols. If deficiencies or problems in the implementation of infection control procedures are identified, further evaluation is needed to eliminate the problems. Examples of infection control program evaluation activities are provided on (Table 2).

Page 45 Dental.EliteCME.com
TABLE 2. Examples of methods for evaluating infection control programs
Program element Evaluation activity
Appropriate immunization of dental health care personnel (DHCP).
Conduct annual review of personnel records to ensure up-to-date immunizations.
Assessment of occupational exposures to infectious agents.
Report occupational exposures to infectious agents. Document the steps that occurred around the exposure and plan how such exposure can be prevented in the future.
Comprehensive postexposure management plan and medical follow-up program after occupational exposures to infectious agents.
Ensure the postexposure management plan is clear, complete, and available at all times to all DHCP. All staff should understand the plan, which should include toll-free phone numbers for access to additional information.
Adherence to hand hygiene before and after patient care.
Observe and document circumstances of appropriate or inappropriate handwashing. Review findings in a staff meeting.
Proper use of personal protective equipment to prevent occupational exposures to infectious agents.
Observe and document the use of barrier precautions and careful handling of sharps. Review findings in a staff meeting.
Routine and appropriate sterilization of instruments using a biologic monitoring system.
Monitor paper log of steam cycle and temperature strip with each sterilization load, and examine results of weekly biologic monitoring. Take appropriate action when failure of sterilization process is noted.
Evaluation and implementation of safer medical devices.
Conduct an annual review of the exposure control plan and consider new developments in safer medical devices.
Compliance of water in routine dental procedures with current U.S. Environmental Protection Agency drinking water standards (fewer than 500 CFU of heterotrophic water bacteria).
Monitor dental water quality as recommended by the equipment manufacturer, using commercial self-contained test kits, or commercial water-testing laboratories.
Proper handling and disposal of medical waste.
Observe the safe disposal of regulated and nonregulated medical waste and take preventive measures if hazardous situations occur.
Health care–associated infections.
Assess the unscheduled return of patients after procedures and evaluate them for an infectious process. A trend might require formal evaluation.
Infection control research considerationsAlthough the number of published studies concerning dental infection control has increased in recent years, questions regarding infection control practices and their effectiveness remain unanswered. Multiple concerns were identified by the working group for this report, as well as by others during the public comment period. This list is not
exhaustive and does not represent a CDC research agenda, but rather is an effort to identify certain concerns, stimulate discussion, and provide direction for determining future action by clinical, basic science and epidemiologic investigators, as well as health and professional organizations, clinicians and policy makers.
Education and promotion ● Design strategies to communicate, to the public and providers, the
risk of disease transmission in dentistry. ● Promote use of protocols for recommended postexposure
management and follow-up.
● Educate and train dental health care personnel (DHCP) to screen and evaluate safer dental devices by using tested design and performance criteria.
Laboratory-based research ● Develop animal models to determine the risk of transmitting
organisms through inhalation of contaminated aerosols (e.g., influenza) produced from rotary dental instruments.
● Conduct studies to determine the effectiveness of gloves (i.e., material compatibility and duration of use).
● Develop devices with passive safety features to prevent percutaneous injuries.
● Study the effect of alcohol-based hand-hygiene products on retention of latex proteins and other dental allergens (e.g., methyl methacrylate, glutaraldehyde, thiurams) on the hands of workers after latex glove use.
● Investigate the applicability of other types of sterilization procedures (e.g., hydrogen peroxide gas plasma) in dentistry. Encourage manufacturers to determine optimal methods and
frequency for testing dental-unit waterlines and maintaining dental-unit water-quality standards.
● Determine the potential for internal contamination of low-speed handpieces, including the motor, and other devices connected to dental air and water supplies, as well as more efficient ways to clean, lubricate, and sterilize handpieces and other devices attached to air or waterlines.
● Investigate the infectivity of oral tissues in Creutzfeldt-Jakob disease (CJD) or variant CJD patients.
● Determine the most effective methods to disinfect dental impression materials.
● Investigate the viability of pathogenic organisms on dental materials (e.g., impression materials, acrylic resin, or gypsum materials) and dental laboratory equipment.

Dental.EliteCME.com Page 46
● Determine the most effective methods for sterilization or disinfection of digital radiology equipment.
● Evaluate the effects of repetitive reprocessing cycles on burs and endodontic files.
● Investigate the potential infectivity of vapors generated from the various lasers used for oral procedures.
Clinical and population-based epidemiologic research and development ● Continue to characterize the epidemiology of blood contacts,
particularly percutaneous injuries, and the effectiveness of prevention measures.
● Further assess the effectiveness of double gloving in preventing blood contact during routine and surgical dental procedures.
● Continue to assess the stress placed on gloves during dental procedures and the potential for developing defects during different procedures.
● Develop methods for evaluating the effectiveness and cost effectiveness of infection control interventions.
● Determine how infection control guidelines affect the knowledge, attitudes, and practices of dental workers.
Selected definitionsAlcohol-based hand rub – An alcohol-containing preparation designed for reducing the number of viable microorganisms on the hands.
Antiseptic – A germicide used on skin or living tissue for the purpose of inhibiting or destroying microorganisms (e.g., alcohols, chlorhexidine, chlorine, hexachlorophene, iodine, chloroxylenol [PCMX], quaternary ammonium compounds, and triclosan).
Bead sterilizer – A device using glass beads 1.2–1.5 mm diameter and temperatures 217ºC–232ºC for brief exposures (e.g., 45 seconds) to inactivate microorganisms. (This term is actually a misnomer because it has not been cleared by the Food and Drug Administration [FDA] as a sterilizer.)
Bioburden – Microbiological load (i.e., number of viable organisms in or on an object or surface) or organic material on a surface or object before decontamination, or sterilization. Also known as bioload or microbial load.
Colony-forming unit (CFU) – The minimum number (i.e., tens of millions) of separable cells on the surface of or in semisolid agar medium that give rise to a visible colony of progeny. CFUs can consist of pairs, chains, clusters, or as single cells and are often expressed as colony-forming units per milliliter (CFUs/mL).
DHCP – Dental health care personnel/professionals (DHCP) include dentists, dental hygienists, dental assistants, dental laboratory technicians (in-office and commercial), students and trainees, contractual personnel, and other persons not directly involved in patient care but potentially exposed to infectious agents (e.g., administrative, clerical, housekeeping, maintenance, or volunteer personnel). Working in a dental health care facility.
Dental treatment water – Nonsterile water used during dental treatment, including irrigation of nonsurgical operative sites and cooling of high-speed rotary and ultrasonic instruments.
Droplet nuclei – Particles <5 μm in diameter formed by dehydration of airborne droplets containing microorganisms that can remain suspended in the air for long periods of time.
Endotoxin – The lipopolysaccharide of gram-negative bacteria, the toxic character of which resides in the lipid protein. Endotoxins can produce pyrogenic reactions in persons exposed to their bacterial component.
HCP – Health care personnel/professionals include doctors, nurses, radiologist, laboratory technicians, pharmacists, assistants, (in-office and commercial), students and trainees, contractual personnel, and other persons not directly involved in patient care but potentially exposed to infectious agents (e.g., administrative, clerical, housekeeping, maintenance, or volunteer personnel) working in a health care facility.
HCW – Health care worker includes anyone working in a health care facility of any kind whenever there is potential contact for spattering of blood or OPIM.
Hepatitis B immune globulin (HBIG) – Product used for prophylaxis against HBV infection. HBIG is prepared from plasma containing high titers of hepatitis B surface antibody (anti-HBs) and provides protection for 3–6 mos.
Hepatitis B surface antigen (HBsAg) – Serologic marker on the surface of HBV detected in high levels during acute or chronic hepatitis. The body normally produces antibodies to surface antigen as a normal immune response to infection.
Hepatitis B e-antigen (HBeAg) – Secreted product of the nucleocapsid gene of HBV found in serum during acute and chronic HBV infection. Its presence indicates that the virus is replicating and serves as a marker of increased infectivity.
Hepatitis B surface antibody (anti-HBs) – Protective antibody against HBsAg. Presence in the blood can indicate past infection with, and immunity to, HBV, or immune response from hepatitis B vaccine.
Heterotrophic bacteria – Those bacteria requiring an organic carbon source for growth (i.e., deriving energy and carbon from organic compounds).
Iatrogenic – Induced inadvertently by HCP, medical (including dental) treatment, or diagnostic procedures. Used particularly in reference to an infectious disease or other complication of treatment.
Nosocomial – Infection acquired in a hospital as a result of medical care.
OPIM – Other potentially infectious materials. OPIM is an OSHA term that refers to: 1.) Body fluids including semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pleural fluid, pericardial fluid, peritoneal fluid, amniotic fluid, saliva in dental procedures; any body fluid visibly contaminated with blood; and all body fluids in situations where differentiating between body fluids is difficult or impossible; 2.) Any unfixed tissue or organ (other than intact skin) from a human (living or dead); and 3.) HIV-containing cell or tissue cultures, organ cultures; HIV- or HBV-containing culture medium or other solutions; and blood, organs, or other tissues from experimental animals infected with HIV or HBV.
Prion – Protein particle lacking nucleic acid that has been implicated as the cause of certain neurodegenerative diseases (e.g., scrapie, CJD, and bovine spongiform encephalopathy [BSE]).
Retraction – Entry of oral fluids and microorganisms into waterlines through negative water pressure.
Seroconversion – The change of a serological test from negative to positive indicating the development of antibodies in response to infection or immunization.

Page 47 Dental.EliteCME.com
Sterile – Free from all living microorganisms; usually described as a probability (e.g., the probability of a surviving microorganism being 1 in 1 million).
Sterilization – Use of a physical or chemical procedure to destroy all microorganisms including substantial numbers of resistant bacterial spores.
ConclusionDental health care professionals are at risk everyday, but here we have seen many infection control practices a dentist, his staff and his patients can take to reduce those risks By taking the sterilization precautions, developing a written plan for the key elements of
an infection control process, maintaining the necessary records, evaluating the plan on a routine basis and making changes to keep the processes up-to-date, the goal of minimizing the risk of disease transmission in the dental office can be met.
References � CDC. Guidelines for Infection Control in Dental Health care Setings-2003. MMWR
Dec 19, 2003/Vol. 52/ No. RR-17. � Provisions Applicable To All Licensees, Article 1. Section 1005. Minimum Standards
for Infection Control.
GUIDELInES fOR InfECTIOn COnTROL In DEnTAL HEALTH CARE SETTInGS
final Examination QuestionsSelect the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116,
or for faster service complete your test online at Dental.EliteCME.com.
1. Avoiding exposure to blood and OPIM as well as protection by immunization remain primary strategies for reducing occupationally acquired infections, but occupational exposures can still occur. a. True. b. False.
2. Standard precautions are strategies used to reduce the risk of infection from exposure to blood, all body fluids and secretions (except sweat), non-intact skin and mucous membranes.a. True. b. False.
3. There is evidence that shows using antiseptics for wound care or expressing fluid by squeezing the wound further reduces the risk of blood-borne pathogen transmission.a. True. b. False.
4. Dental devices that are connected to the dental water system and that enter the patient’s mouth (e.g., handpieces, ultrasonic scalers or air/water syringes) should be operated to discharge water and air for a minimum of 5-10 seconds after each patient.a. True. b. False.
5. Sterilization is the use of a chemical procedure to destroy all microorganisms, including substantial numbers of resistant bacterial spores.a. True. b. False.
DCA04ICE18

Chapter 3: Health Information Technology: The future is now
7 CE Hours
By: Staff Writer
Learning objectivesAfter completion of this course, healthcare professionals will be able to:
� Explain the purpose of the HITECH Act. � Compare and contrast the characteristics of electronic health
records vs electronic medical records. � Discuss the benefits of electronic health records for patient care
outcomes. � Describe how electronic health records can decrease medical
errors and improve efficiency in healthcare practices. � Explain the criteria for meaningful use of electronic health records. � Describe the process for certifying electronic health record systems. � List the steps for implementing an electronic health record system. � Discuss the implications of the HIPAA Security Rule for health
information technology. � List the administrative, technical, and physical safeguards required
by the HIPAA Security Rule to protect patient information.
� Describe the ten cybersecurity practices recommended by the Office of the National Coordinator for Health Information Technology to protect patient information.
� List e-prescribing system requirements. � Explain the significance of regulations issued by the DEA’s
interim final rule on the use of e-prescribing systems to prescribe controlled substances.
� Describe the functional standards used to guide the nationwide use of immunization information systems.
� Explain the role of the NASPER Act in the implementation and improvement of prescription drug monitoring programs.
� Explain the Institute of Medicine’s operational guidelines for telehealth services.
IntroductionHealth information is generated with each and every patient encounter, and the management of this information has changed enormously in the past century. What was previously documented in paper charts or microfiche and stored away in a locked room can now be recorded and stored solely on computers. Constant changes in technology require healthcare professionals to remain diligent in managing this protected information appropriately.
Health information technology (health IT or HIT) refers to the technology used to store, manage, or share health information. Managing health information through technology can be challenging, due to the sensitivity of the data and a lack of uniformity among computer systems. Improving the efficiency of storing and accessing health information through technology has been a priority since the turn of the century and remains a priority today.
The potential advantages of an efficient health information technology system are substantial. Online system information management, such as the use of shared computerized patient records to facilitate communication among doctors, patients, and other members of the patient’s healthcare team, can positively affect patient care and treatment outcomes. Health IT also gives patients the opportunity to take a more active role in their healthcare.
This course provides an overview of health information technology systems. Because state laws vary in their regulation and enforcement, individuals using health information technology must ensure their activities are in compliance with all applicable local, state, and federal laws.
History Records of patient health conditions and treatments were not routinely maintained until the 1920s. By this time, many healthcare providers realized documentation of patient treatment helped them provide better care. Patient’s health records became increasingly common as providers learned their beneficial effects on healthcare safety and quality. Physicians found the patient record provided a more comprehensive picture of the patient’s condition, in a more efficient manner than simple notes or discussion.
Not all medical records were equally useful. Many healthcare personnel did not know the principles of good recordkeeping. In 1928, the American College of Surgeons (AMC) established a standardized medical recordkeeping procedure, for health information management in the form of paper records. The AMC also established the American Association of Record Librarians, now known as the American Health Information Management Association (AHIMA), a professional organization dedicated to improving medical recordkeeping systems.
Medical records were printed on paper from the 1920s until the 1990s. As early as the 1960s and 1970s, several universities partnered with hospitals to explore the use of computers to house medical records. These experiments were confined to a small number of facilities, however, due to the prohibitive price of computers, which limited use until the early 1990s. At this time, it became common to store master patient lists on computerized systems, providing services such as computerized check-in procedures in hospitals.
Computerized records gained popularity in the 1990s. Many different hospital departments developed applications for the technology, but a number of factors limited the utility of electronic records at that time. While laboratory and radiology test results were stored electronically, the data was not linked in any way to other patient information or previous lab results. Additionally, information could not be shared by different departments. In 2000, this limitation in the healthcare computer system was identified as a possible reason for an increase in medical errors, emphasizing the need for change.
Dental.EliteCME.com Page 48

President George W. Bush emphasized the importance of electronic medical records in his State of the Union address, in January 2004, explaining, “By computerizing health records, we can avoid dangerous medical mistakes, reduce costs, and improve care”. He established the Office of the National Coordinator for Health Information Technology (ONCHIT or ONC), the “principal federal entity charged with coordination of nationwide efforts to implement and use the most advanced health information technology and the electronic exchange of health information”. The ONC is housed within the Department of Health and Human Services (HHS) and is dedicated to supporting the adoption of health information technology and the promotion of nationwide health information exchange to improve health care.
In 2009, under the Obama Administration, the Senate passed the American Recovery and Reinvestment Act (ARRA), earmarking more than $19 billion to increase the use of electronic health records, specified in a section of the ARRA called the Health Information Technology for Economic and Clinical Health Act, or the HITECH Act. It was created with the objective of improving the delivery
of healthcare through increased investment in health information technology.
Funds from this act were allocated to: ● Support the infrastructure of the ONC. ● Create incentives for providers who become meaningful users of
electronic health record systems. ● Implement health IT within the Indian Health Service ● Research the effects of health IT on health outcomes. ● Support the secure exchange of health information.
The HITECH Act authorized the Office of the National Coordinator to adopt health information technology standards and create two committees, the HIT Policy Committee and the HIT Standards Committee, to assist the National Coordinator for Health Information Technology in making informed decisions.
This legislation provided incentives to adopt the technology, both through financial means and the creation of Regional Extension Centers (REC) to support healthcare providers establishing their own electronic health record systems. The legislation established a deadline of 2014 to implement a national electronic health record system.
Terminology Electronic health recordIn the simplest definition, an electronic health record (EHR) is a computerized version of the paper charts previously used to track a patient’s health care. They are real-time records of a patient’s medical condition that bring information from current and past providers, clinics in schools or workplaces, laboratories, pharmacies, radiology clinics, and emergency departments, together in one streamlined record for optimal patient care. The key identifying feature of electronic health records is that they can be created, managed, and shared by healthcare providers across multiple healthcare organizations or systems. This means the patient has one record accessible and transferrable to all his or her various providers across different organizations, locations, and state lines.
Electronic medical record (EMR)The electronic medical record contains the computerized records of the patient’s medical chart from a single practice or facility, including laboratory, radiology, and pharmacy records from that provider. EMR benefit patients who meet all their healthcare needs from providers in one practice, but they do not follow patients to different facilities. It is generally difficult to transfer electronic medical record information to another facility; if information must be transferred, it may need to be printed and mailed to other members of the patient’s care team.
InteroperabilityInteroperability is the capability of multiple systems to exchange information and be able to use the information that was exchanged. Electronic medical records must not only communicate information from one source to another, they must be able to read and use the information imported from another system. Since different information management systems may not be designed to communicate with one
another, the Office of the National Coordinator (ONC) for Health Information Technology sets nationwide standards and guidelines for electronic health records, to improve communication among computer systems and ensure efficient and seamless management, utilization, and transfer of medical data.
Personal health record (PHR)The personal health record (PHR) is similar to the electronic health record (ECR), except the information is controlled by the patient instead of the medical provider. Some healthcare facilities and insurance companies have systems that allow patients to monitor, review, and access services through the facility’s software or an online system. These systems (sometimes known as “health portals”) help patients manage information such as prescription and over-the-counter medications, history of immunizations and allergies, lab results, and emergency contact numbers. Some of these programs even have applications (apps) that can be used in conjunction with smartphones to track sleeping patterns or exercise routines. Some facilities are capable of linking an individual’s PHR and EMR, if both are housed within the same system, but this technology was not widespread at the time of this writing.
Electronic prescribingElectronic prescribing allows providers to send prescriptions directly into a pharmacy’s computer system, instead of by phone, fax, or handwritten order, which might need deciphering by pharmacy staff. While an electronic order, like any prescription, must be verified by a pharmacist, it provides more protection than other types of prescriptions against data entry and interpretive errors, safeguarding patient care. While this system is not completely foolproof, simplifying the prescribing process helps decrease error potential and saves both the patient and pharmacy precious time.
ELECTROnIC HEALTH RECORDS (EHR)Why should healthcare providers adopt EHR?Interdisciplinary teamwork is a critical tool in patient healthcare management, as the ability to share information with other members of a patient’s healthcare team effects the safety and quality of patient care.
Healthcare professionals who use electronic health records recognize the relationship between comprehensive medical records and an improved ability to make sound clinical decisions . ECR allow healthcare providers to:
● Access complete, up-to-date, and accurate patient’s health information, regardless of the care setting.
● Provide care more quickly in a crisis, due to increased availability of allergy, medical, and medication histories in one, easy-to-access system.
● Improve coordination of care in patients with multiple chronic medical conditions.
● Share information with patients, families, and caregivers, and empower patients to take a more decisive role in their healthcare.
● Recognize potentially serious drug interactions before they affect the patient.
● Verify that medications and dosages are accurate and appropriate. ● Improve preventive care and decrease the necessity of risky
procedures.
Page 49 Dental.EliteCME.com

Research showing EHR benefitsA recent study conducted by the National Center for Health Statistics (NCHS) showed over 70% of all physicians who purchased an electronic health record system would purchase it again, and half of all physicians who did not have a system in place planned to purchase one within a year.
Nearly twenty years ago, the Department of Veterans Affairs (DVA) established one of the first computerized health IT systems. Since that time, EHR have been associated with improvements in quality of care, significant financial savings, and even increased patient satisfaction. The VA further improved health outcomes and healthcare efficiency by adding capabilities to HER, including bar code technology and computerized ordering for electronic imaging, medications, and laboratory tests, all of which streamline patient management and reduce the risk of medical error.
Research conducted over a ten-year period at the VA by the Center for IT Leadership (CITL) studied the VA’s investment in information technology (IT) and its costs and benefits to the organization. The study concluded the VA spent nearly $4 billion on health information technology, but saved more than $7 billion due to improvements in safety, healthcare quality, and patient satisfaction. The study found over 86% of savings were related to a reduction in unnecessary duplicate testing and decreased incidence of medical errors. The remaining 14 percent savings were associated with a reduction in operating costs and workload.
This study also explored the EHR system’s potential to improve the use of clinical guidelines for treating chronic illnesses. Research focused on the treatment of diabetes (an illness that affects approximately 25% of patients in the VA health system) among VA patients versus those in the private sector. VA patients with diabetes were found to have better cholesterol levels, better glucose testing compliance, and retinal exams conducted at more appropriate intervals as compared to Medicare patients. The study found the DVA preventive treatment of diabetic patients averaged a score 15% higher on average than that of diabetic patients in the private sector.
Improvements in convenience and quality of healthcareEHC have the potential to improve the convenience and quality of healthcare, which are important to patients and healthcare providers alike. Healthcare professionals are likely to see all the following changes in healthcare quality and convenience with an electronic health record system:
● Simplified access to patient records from both inpatient and remote locations.
● Improved decision-making support with the use of system-integrated alerts and reminders.
● Tools to improve performance and report information in real time. ● Improvements in documentation, billing, and coding procedures. ● Efficient transfer of EHR and other data from external healthcare
facilities, laboratories, and disease registries. ● Safer prescribing practices.
Patients are likely to see the following improvements in the quality and convenience of their care:
● Less time spent filling out forms. ● More accurate and reliable information at the point of care. ● Electronic prescriptions that can be sent directly to the pharmacy. ● Online portals used by patients to access personal healthcare
information, such as lab results, and communicate with healthcare providers.
● Electronic referrals for faster and easier access to specialists.
A study conducted in Indianapolis showed emergency healthcare professionals also benefit from access to EHR. Having information about a patient’s allergies, current and former medications, and medical history simplified care, especially for uncooperative or unconscious patients, those with frequent emergencies, and those unable to provide medical histories. Providing the most complete
medical history possible at the point of care was shown to contribute to higher quality care, leading to better patient outcomes. EHR enable providers to be more informed and efficient decision makers throughout patient care.
Patient participation through PHR Ideally, patients and healthcare providers work together to make the best decisions for the patient’s care. PHR support this strategy, as they make collaboration and communication between the patient and provider more convenient and efficient, enabling patients to be better informed and take more active roles in their healthcare decisions. Patients and their family members can use the information in their PHR to keep track of, lab test results, and medications, and any other personal healthcare information desired by the patient.
A patient’s PHR is a simplified version of the EHR, accessed through the EHR system or externally used as a mode of communication between the provider and patient. The personal health record can be used by patients to services such as paying bills or scheduling appointments with the provider using an online system. Messaging systems, such as texting or email, are typically integrated into the system to ease communication and ensure it is sufficiently frequent that providers identify potentially health issues as possible. PHR also provide important discharge information and medical instructions for patients following appointments and hospital stays.
Patients able to access an electronic record showing and/or explaining the results of a health exam are more likely to discuss the information with their provider, particularly if the provider takes an opportunity to review the information with the patient and provide additional information about their care. Providers can send information to patients about past and future appointments, directions for follow-up care, taking prescription medication, proper wound care, or any other instructions for patient care, even referral to online resources for relevant medical information.
There are two main types of PHR: ● Stand alone PHR require patients to fill in health information
forms relying on their own records or memory, then store the information digitally .
● Connected or tethered PHR are those linked a provider’s or insurance company’s EHR. This type of health record allows patients to log on to their records and view information, such as lab test results.
Improvements in diagnosis and safety for patientsEHR systems are poised to improve patient outcomes by enabling providers to diagnose medical conditions more accurately. Prescribers surveyed in 2012 reported that electronic health records were available at the point of healthcare for 94% of prescribers, with 88% of EHR users reporting clinical benefits from the system, and 75% concluding EHR improved the delivery of patient care.
EHR enhance a provider’s ability to accurately and efficiently diagnose patients’ ailments because systems can consolidate, organize, and present the information in a useful, easily interpreted manner more likely to bring meaningful information to the provider’s attention. EHR help providers reduce errors by:
● Maintaining a record of the patient’s current medication list, as well as allergies to medications, and automatically checking for drug interactions or contraindications when the prescriber adds new medications.
● Allowing providers in the emergency department to gather information on a patient’s medications, allergies, and medical conditions in a timely fashion, which is especially helpful if the patient is uncooperative or unconscious.
● Alerting the provider to potential safety issues before they become serious problems.
● Helping identify the source of problems when they occur, simplifying problem resolution.
Liability issues can also be resolved more easily with use of an electronic health record. When information is contained in a single
Dental.EliteCME.com Page 50

electronic file, outsiders can more easily review a case to determine the order of events and whether the provider’s decision-making process is grounded in evidence-based practices. Informed Consent and other
patient-provider agreements can be stored in the EHR, and provided upon request of legal personnel.
Improving patient health outcomesEHR can improve patient health outcomes because the electronic data within each record can be sorted and analyzed to provide a more complete picture of an individual’s health status, or compare and contrast characteristics within and among groups. Looking at patient with specific characteristics (such as those who share the same medical condition, or are taking the same medication) as a group can help providers evaluate their patients’ quality of care and decide the best course of treatment for each individual. For example, providers can look at all of their patients with asthma who are taking Budesonide (Pulmicort), assess the beneficial and detrimental effects of the medication for each individual, and use this growing patient database to determine the most effective treatments and the direction for future patient care.
Several studies have assessed the benefits of EHR on patient outcomes. In 2010, a survey conducted to examine attitudes toward EHR found patients were highly satisfied with practices in which doctors implemented EHR-assisted services. The primary perceived benefit to patients, according to 92 percent of respondents, was streamlining the prescription-filling process, with 76% considering the e-prescribing process easier, and 90% reporting that when e-prescribing was used, only rarely was a prescription not already filled when they went to the pharmacy to pick up their order. Patients also reported a 63% reduction in medication errors. Providers in the study expressed satisfaction with the EHR system, reporting it decreased the number of calls to their medical offices after hours.
Quality of healthcare often improves with the implementation of electronic health records. A 2013 study conducted to assess the effects
of an EHR system within community-based clinics in the New York State Hudson Valley found providers using EHR showed increased numbers of screenings for diabetes (A1C testing), chlamydia, breast cancer, and colorectal cancer. The higher screening rates gave providers the ability to identify and treat potential health concerns earlier than might otherwise have been possible.
Research in Philadelphia examined the care of children with asthma to determine whether integrating clinical decision support programs into health records might improve adherence to the national guidelines for asthma treatment in children. Providers across twelve primary care pediatric offices used either passive clinical decision support methods, or active pop-up alerts to assist them in making clinical decisions for children with persistent asthma. Several areas showed significant improvements in both intervention groups: Use of maintenance asthma medication increased by 6% overall; asthma care plan usage increased by 14%, and patient spirometry results (e.g., pulmonary function testing) also showed improvement. Findings provide good evidence that the integration of active clinical decision support programs into electronic health records can promote greater adherence to national guidelines for the treatment of chronic illnesses.
A similar study examining the effects of an electronic health record system at Fletcher Allen Health Care Medical Center in Vermont showed a 60 percent reduction in reports of near-miss medication events, and a 20 percent increase in the completion of daily fall assessments, used for the purpose of preventing prolonged hospital visits due to falls; both changes translated into safer and improved medical care.
Improving care coordinationManaging chronic medical conditions often requires the efforts of a team of healthcare providers who help the patient maintain optimal health. Primary care providers, nurses, pharmacists, specialists, and other mental and physical care practitioners making up the healthcare team, tend to be more attuned to aspects of the patient’s health that fall within their specific area of care. While some providers may have overlapping information about a patient’s history or condition, without a single system for collecting all of the information on a single patient in one place, and a plan of care that coordinates communication among team members, treatment becomes segmented, to the patient’s possible detriment.
EHR implementation facilitates coordination of care and the sharing of patient information among providers, resulting in improved treatment care and outcomes. For example, a master medication and allergy list can be
updated by any of the patient’s providers, to ensure records contain current accurate patient information. Computer programs are chosen and adapted to the needs of each specific healthcare environment to allow the greatest ease in transition to the system, data entry, and searching procedures. The system can be programmed to notify other team members if the patient was in the hospital or emergency room, or any other issues or events calling for “checking in” or medical follow-up.
Shared information and communication improve the coordination of care, which can decrease the risk of medical errors and prevent unnecessary testing and medical procedures. Every member of the patient’s medical team can access and review the patient’s history of medical conditions, procedures, tests, and medications, resulting in higher quality care and better health outcomes for patients.
Efficient practicesIn addition to improving patient care, EHR increase efficiency in the following ways:
● Integrated scheduling systems connect appointments to claims, automatic coding systems, and progress notes.
● Shortcuts, such as improved search functions and chart management functions, that save time.
● Improved communication among providers, insurance plans, and laboratories.
● Providing links to the patient’s health plan in the patient record, enabling providers to choose treatments that provide the best insurance coverage up front.
● Simplified ordering systems for lab and imaging studies. ● Links to public health registries, adverse event reporting systems,
and communicable disease databases. ● Streamlining the billing process, allowing providers and their staff
to spend less time filling out forms and handling billing requests. ● Streamlining the process of ordering tests and procedures,
reducing potential for duplication.
● Improved documentation of clinical events, such as eliminating the need for traditional medical transcription, or “pulling” patient charts, as well as additional factors that reduce lag times and increase billing accuracy.
Seventy-nine percent of healthcare providers who implemented an EHR system reported a more efficient working environment , according to a recent survey, with 82% of all respondents saving time with an e-prescribing system, and 75% of all respondents receiving lab results more quickly.
Cost savings for health care practicesAlthough installing an EHR system comes with an initial investment of time and money, the financial benefits associated with its implementation can be significant and far-reaching, as the benefits of optimal patient care extend beyond the patient to networks of family members, friends, healthcare providers, and beyond.
Page 51 Dental.EliteCME.com

EHR systems bring immediate and direct cost savings associated with automating labor-intensive procedures such as transcription, pulling, storing, and re-filing charts, or any other time-consuming tasks previously recorded on paper. Savings are also attributable to improved accuracy in billing, which enables medical centers to obtain reimbursement from insurance companies more quickly and easily. Initial costs and resulting savings for hospitals implementing electronic health record systems vary based on their size.
Large hospitals can experience savings of $37 to $59 million over a 5-year period, before collecting incentive payments.
A study conducted in 2006 assessed the costs and benefits of several aspects of HIT systems to determine their value in various healthcare settings. The study reviewed available literature focusing on pediatric care. Findings from review and analysis of 256 cases electronic medical record use, decision support, and computerized order entry in the outpatient and inpatient setting showed substantial savings from EHR implementation. Benefits outweighed the cost of investment, with a financial break-even point ranging from three to thirteen years. The study concludes HIT has the potential to dramatically alter the delivery of healthcare, creating a safer, more effective, and more efficient environment, but its widespread use is limited by a lack of knowledge regarding the types of HIT that provide the most cost-effective results.
Incentive programs for electronic health record implementationIn 2009, the American Recovery and Reinvestment Act (ARRA) earmarked money for the Centers for Medicare & Medicaid Services (CMS) to provide up to $27 billion for incentive payments to eligible professionals, hospitals, and other facilities adopting, implementing, or upgrading certified electronic health record systems, and demonstrating their meaningful use. Eligible healthcare professionals can qualify for incentive payments of up to $44,000 through Medicare, or $63,750 through Medicaid, and eligible hospitals can qualify for incentive payments of $2 million or more. These incentives are provided to offset the high costs of implementing this technology, to improve the value, reliability, and quality in the nation’s health records.
The program established two separate incentive payment systems, one through Medicare and one through Medicaid. The Medicare incentive payment system is regulated by the federal government, and requires proof of meaningful use of a certified electronic health record system in the first year to receive incentive payments. The Medicaid incentive payment system functions on the state level, with payments issued
for implementing, upgrading, or adopting a certified electronic health record system in the first year of participation.
In order to qualify for the Medicare incentive payment system, the system must demonstrate meaningful use. This means that certified electronic health record technology is used for:
● Improving quality, safety, and efficiency of healthcare. ● Reducing treatment and service disparities. ● Engaging patients and family in patient care. ● Improving coordination of care. ● Maintaining privacy and security of patient health information.
The positive effects of EHR systems are demonstrated by improved: ● Clinical outcomes. ● Population health outcomes. ● Transparency of healthcare. ● Efficiency of healthcare. ● Patient empowerment. ● Research data on health systems.
Regional extension centersBecause small practices that provide essential preventive care and are not electronically linked to larger hospitals and healthcare systems are more likely to lack the resources needed to implement HIT, the Office of the National Coordinator founded 62 Regional Extension Centers (REC). REC are support and resource centers located throughout the country staffed with experts to assist healthcare providers develop HIT systems to improve patient care.
Transition to an EHR system, and ensuring adherence to incentive regulations can be challenging; REC experts can provide advice to healthcare facilities and providers, or assist with an entire EHR implementation process, from choosing an EHR system through development of meaningful use. Healthcare providers and facilities seeking funds are strongly encouraged to work with their local REC to ensure they understand the criteria for demonstrating meaningful use of EHR, as multiple specific objectives must be met to qualify for incentive payments.
Regional Extension Centers are financially supported by the providers they assist, collecting one-third of the incentive payment that each provider earns. This fee structure ensures REC are financially able to continue supporting providers through HIT. REC personnel can assist providers with project management, health IT training and education, selecting an EHR vendor, financial consultations, incorporating health IT into workflow, security and privacy issues, connecting with state and federal health information exchanges, and continued technical assistance after implementation. Support is geared to the needs of each individual practice, and is provided after implementation as well.
Of the more than 147,000 healthcare providers enrolled with REC as of July 2013, over 124,000 providers have implemented EHR systems. Of those providers implementing EHR, more than 70,000 (56 percent) demonstrated meaningful use of their system. Regional Extension Centers were initially designed to assist primary care providers (PCP),
who showed a national rate of REC enrollment of 41 percent as of July 2013, with 51% of those PCP located in rural areas.
Certification of EHR systemsThe process for certifying electronic health record technology was established by the Office of the National Coordinator for Health Information Technology. In 2011, ONCHIT introduced an HIT certification program for certifying EHR technologies, to ensure they follow established standards and achieve meaningful use.
The Health and Human Services (HHS) Secretary is responsible for the development of specific rules for testing and certifying EHR systems, and standards and certification criteria are updated on a regular basis.
Certifying EHR systems assures providers and healthcare facilities that the software they plan to purchase is capable of meeting meaningful use requirements and other objectives established by the CMS. System certification also assures providers and patients that the information in electronic systems is secure and interoperable.
The certification process starts with vendors creating EHR systems that meet the HHS Secretary’s defined standards and criteria. After system development, Accredited Testing Laboratories (ATLs) test the product and evaluate it according to HHS-defined standards and criteria. Upon successful completion, the Office of the National Coordinator-Authorized Certification Bodies (ONC-ACB) certifies that the EHR meet the necessary standards and criteria. After certification, the product qualifies for inclusion on the Office of the National Coordinator’s List of Certified Health IT Products.
The National Voluntary Laboratory Accreditation Program (NVLAP), administered by the National Institute of Standards and Technology (NIST), accredits testing facilities, develops testing requirements and tools, and produces test cases to support ONCHIT certification programs by ensuring electronic health record systems are compliant with meaningful use requirements.
Dental.EliteCME.com Page 52

IMPLEMEnTInG An ELECTROnIC HEALTH RECORD SySTEMImplementing an electronic health record system in a small medical practice is one of the most complicated and resource-intensive projects that any establishment can undertake. It requires a significant investment in financial and human resources, as well as time and patience. Despite advances in technology, complications along the way are inevitable. Medical facilities interested in EHR should contact an expert at the REC for technical and logistical support, especially if implementing large-scale computer software systems, as they can provide invaluable expertise throughout the entire process.
The following steps can be used in conjunction with Regional Extension Center support to guide providers through the EHR implementation process.
Step one: Assessment of current practicesThe first step in implementing an electronic health record system is assessing whether the facility is ready to change from a paper recordkeeping system to a computerized one, or upgrade an existing electronic system to one that meets certification requirements. To make this determination, management should evaluate the extent to which the facility’s practice goals are being met, if an EHR system is affordable for the practice, and the time transitional time required until the staff and systems can effectively utilize the new technology.
A thorough assessment of the current practice of recordkeeping is necessary to determine what processes are working well, and what need improvement. The assessment should include the following questions, recommended by HealthIT.gov, to assist the organization in evaluating its level of productivity and efficiency:
● Are administrative processes organized, efficient, and fully documented?
● Are clinical workflows efficient, clearly designed, and understood by all staff?
● Are data collection and reporting processes established and documented?
● Are staff members computer literate and comfortable with information technology?
● Does the practice have access to secure high-speed Internet connectivity?
● Does the practice have access to financial capital required to purchase new or additional hardware?
● Are there clinical priorities or other needs that should be addressed first?
● Does the practice have specialty-specific requirements?”
The assessment should help management envision the future of the practice, including how implementation of the EHR system will affect providers and staff members, and change the quality of care experienced by patients.
Goals for guiding program implementation should be established once an organization decides to install an electronic health record system. Goals should be meaningful to the practice setting, relevant to clinical and financial goals, or the workplace environment. Using the “SMART” system for setting goals helps ensure they are reasonable and attainable. “SMART” goals are: Specific, Measurable, Attainable, Relevant, and bound by Time. This last factor means goals must be reassessed frequently to ensure decisions are based on current, accurate information to achieve the established goals as quickly and efficiently as possible.
During the assessment phase, the organization should establish a team to lead the EHR implementation process. Individuals in the organization advocating conversion to an electronic system may be candidates for this position as they can help guide staff members through the transition, but should only be selected if they are can manage other responsibilities of the position as well. The assessment should provide the implementation team with a clear understanding of the process for implementing an ERH system, including specific steps necessary to complete the program.
Step two: Create a planAn EHR implementation plan can assist team leaders in identifying tasks necessary for system setup and in what order those tasks must be completed, and stimulates discussion of the plan among team members. The team must decide which elements and processes from the old system will transfer to the new, which will no longer be used, and what new practices will replace them. This allows the implementation team to determine the characteristics of the new working environment and prioritize various plan tasks.
An implementation plan should include the following steps: ● Analyze current workflow and assess the strengths and weaknesses
of the current recordkeeping system. ● Determine how the EHR system can address the facility’s
weaknesses and improve workflow and efficiency. ● Create a backup plan to address possible contingencies and
complications that can arise when implementing the EHR system. ● Plan the transition from paper or an uncertified electronic
recordkeeping system to a certified system, including how and when each phase will proceed, and the name of the people managing the process.
● Discuss what data, such as demographic or scheduling information, will need to transfer to the new system.
● Determine and document exactly how information will transfer from the old recordkeeping system to the certified EHR system, including which data elements will need manual entry, and if scanning paper records will be necessary.
● Discuss potential obstacles to transferring information, such as risks to the privacy of patient health information, and develop a plan for handling these issues.
Step three: Selecting a certified electronic health record systemChoosing a specific electronic health record system is one of the most important decisions in the implementation process, and people disagree about the optimum time to take this step. It is best when a practice has sufficient time to identify its healthcare goals before trying to choose an EHR system that will achieve those goals.
REC produced the following list of considerations to help providers identify deficits and strengths when comparing EHR software options:
● Assess products from several different companies/vendors, and determine whether the system in question will help the practice accomplish the goals determined in Step 1. Discuss the practice’s goals with the vendors, and discuss how these goals can be addressed to achieve meaningful use. A list of vendors that sell certified EHR systems is available here: http://oncchpl.force.com/ehrcert?q=CHPL.
● Clarify and confirm costs associated with purchasing and implementing the electronic health record system, including software, hardware, maintenance, upgrades, different interfaces for various departments, connecting to the health information exchange, customized report creation, potential legal fees, and any costs related to establishing or guaranteeing meaningful use.
● Discuss what level and type of support the provider can expect from the vender during implementation, such as the availability and scheduling of support sessions, or the educational credentials and experience of the person who will be training staff on the new system, as well as options for extended or ongoing support from the company after installation.
● Discuss the process of moving information from the previous recordkeeping system to the new one, who will be responsible for each task, and costs associated with this phase of the process.
● Clarify how information will be stored, including the location and format of the files (e.g., using a server housed on location in the medical office or offsite; web-based or text format), and assess risks related to privacy of patient information stored in this manner.
Page 53 Dental.EliteCME.com

● Determine the ability of the prospective EHR system to integrate other, more current software or databases, such as public health registries, scheduling systems, or billing software, that will need to be installed or used after the system is in place.
● Discuss a primary and backup plan for information storage that ensure privacy and security.
● Examine and assess the factors used to determine when incentives have been earned, and how to manage payments.
● Evaluate the reputation of the software vendor to determine if there are any characteristics that might negatively affect their product in regard to its use or implementation, future maintenance, or support of the product.
Vendors can help providers decide if the product will meet the provider’s needs by conducting a product demonstration, or providing a list of previous customers who have successfully implemented a similar EHR system. REC can be consulted about any questions or issues that arise in selection of an EHR vendor.
Step four: Implement the electronic health record system and train personnelThe actual implementation of the electronic record system includes the physical installation of software and hardware, and pilot testing in sections of the facility to anticipate and address potential problems before system-wide installation. The implementation plan developed in step two guides this phase.
This step also involves the physical movement of health information from the old to the new system using data migration software or manual data entry, if necessary. Personnel must maintain the privacy and security of patient health information throughout the implementation process. Security software should be programmed to scan the system regularly to identify and address potential vulnerabilities before they become security breaches.
Step five: Ensure the EHR system achieves meaningful useSince the CMS has an incentive program for organizations that demonstrate meaningful use of their certified electronic health record systems, the implementation process should confirm the system qualifies for meaningful use, as defined by CMS. Their primary criteria for assessing meaningful use are the extent to which they enable the practice to:
● Improve healthcare quality, safety, and efficiency. ● Engage patients and families in healthcare decisions. ● Improve healthcare coordination. ● Improve public health due to a decrease in communication wait
times that therefore allow healthcare providers to address issues more quickly.
● Ensure privacy and security of personal health information.
Each of these criteria is associated with its own set of requirements that affect a provider’s eligibility for incentive payments. For example, “Improving healthcare quality, safety, and efficiency,” is demonstrated by ensuring there is a medication list for each patient, and, “Improving Public Health,” requires immunizations are submitted to national immunization registries. REC and system vendors can provide indispensable assistance in meeting meaningful use criteria.
Step six: Continue to improve qualityAfter implementation, the electronic health record system requires review and testing to ensure the facility’s goals have been met and determine areas for improvement. During this step, team leaders should assess the need for additional training, adjustments in staffing , whether the technology is appropriate for the facility, and if it is functioning as it should. Since the actual implementation process may diverge greatly from that described in the initial plan, the facility should assess to how well the final product meets the provider’s needs, and what changes, if any, are required to fulfill the EHR originally outlined in the plan. Measures of healthcare quality should be reassessed at regular intervals to ensure the system continues to meet facility objectives and expectations.
PRIVACy AnD SECURITyMajor changes in health information technology, such as greater use of electronic health information, have created an increased need for information security. Information security is the protection of information from unapproved use, access, disclosure, or modification. The information’s integrity, availability, and confidentiality, as defined below, must be maintained at all times:
● Integrity: Health information must not be modified or destroyed by unauthorized personnel.
● Availability: Health information must be accessible by authorized personnel when necessary.
● Confidentiality: Health information must not be disclosed to unauthorized personnel or systems.
Federal law protects health records and ensures confidentiality of personal health information. Creating awareness of these regulations can help create an understanding of the importance of supporting the security of this information. Maintaining the privacy and security electronically stored personal information is crucial to building the trust in patients necessary to appreciate the benefits of electronic health records.
Health Insurance Portability and Accountability Act of 1996The Health Insurance Portability and Accountability Act of 1996 (HIPAA) established legal standards for the use and disclosure of
patient health information. HIPAA requires healthcare professionals acknowledge the basic privacy rights of all patients, and explain those rights to patients. It ensures the confidentiality of protected health information (PHI), requires the use of the minimum amount of PHI necessary, and gives patients the right to see who has accessed their PHI. It also requires that all healthcare professionals who have access to PHI receive formal training on HIPAA.
HIPAA establishes that healthcare workers have a professional responsibility to protect a patient’s PHI. It applies to all covered entities, defined as any person or group who provides healthcare services to a patient, bills for healthcare services, or receives payment for healthcare services. Examples of PHI include:
● Name, address, and other demographic information. ● Date of birth. ● Social Security Number. ● Payment history. ● Account, license, and record numbers. ● Prescription and medical history. ● Email address. ● Device identifiers, such as IP addresses. ● Genetic information.
HIPAA Security RuleThe HIPAA Security Rule established national standards to ensure protection of electronically communicated health information. Electronically transmitted health information must use HIPAA-compliant channels of communication and secure storage to protect patient records from unauthorized access.
The Security Standards for the Protection of Electronic Protected Health Information (SSPEPHI), known as the HIPAA Security Rule (HSR or Security Rule), focuses on the application of HIPAA to electronic protected health information (e-PHI). Since the increased use of electronic health records increases the risk of disclosing patient information, the HIPAA Security Rule was created to protect
Dental.EliteCME.com Page 54

patient information in this format while encouraging the use of new technology to enhance patient care. While the HSR designates the requirements to ensure e-PHI protection, the Office for Civil Rights (OCR) within the Department of Health and Human Services (DHHS) is responsible for enforcement of the HIPAA Security Rule.
The HIPAA Security Rule specifies the administrative, technical, and physical security procedures that anyone who transmits health information in an electronic format must use to ensure e-PHI confidentiality. Under this Security Rule, covered entities must:
● Ensure the confidentiality, integrity, and availability of all e-PHI they create, receive, maintain, or transmit.
● Identify and protect against reasonably anticipated threats to the security or integrity of data.
● Identify and protect against reasonably anticipated impermissible uses or disclosures of data.
● Ensure employee compliance.
The Security Rule is designed to be flexible, since covered entities range from single provider practices to large healthcare systems, and
the needs of each organization can differ greatly. Instead of requiring a specific security strategy for all providers, the Security Rule mandates that covered entities implement security measures appropriate for their size and complexity, technical infrastructure, and financial capability, and minimize potential risk to e-PHI. Security measures must be reviewed periodically to ensure e-PHI is protected on a continuing basis and able to integrate changes in technology.
Under the Security Rule, covered entities must complete a risk analysis as a part of security management. A risk analysis should include:
● Evaluating potential risks and their effects on e-PHI. ● Implementing security measures to ensure risks discovered during
analysis are resolved. ● Documenting existing security measures and the rationale for
choosing them. ● Using appropriate and reasonable security measures at all times.
Risk analyses should be ongoing, to ensure security issues are detected and resolved promptly, and assess the strength of existing security measures.
Safeguarding electronically stored health information The HIPAA Security Rule imposes a number of required physical and technical safeguards for electronically stored health information stored electronically that must be incorporated into an organization’s administrative policies and procedures for information storage. Physical safeguards are security elements such as barriers in offices and hospitals that can prevent unauthorized personnel from accessing patient information stored on computer systems. Technical safeguards are security features such as passwords; both are critical in protecting the privacy of electronic information.
The HIPAA Security Rule requires the following administrative safeguards to ensure the protection of e-PHI:
● Designating a security officer to ensure security policies and procedures are appropriately established and implemented.
● Developing strategies that ensure e-PHI access is limited to authorized users accessing only e-PHI appropriate to the user’s role.
● Ensuring personnel who access e-PHI are authorized and supervised appropriately, trained in security policies and procedures, and disciplined for violations of security policies and procedures.
● Evaluating security policies and procedures at regular intervals to ensure they meet the HIPAA Security Rule conditions.
The HIPAA Security Rule requires the following physical safeguards to ensure the protection of e-PHI:
● Ensuring physical entry to facilities where e-PHI is accessed is limited to authorized individuals only, by use of locked offices and security guards when necessary.
● Implementing policies and procedures that limit entry and specify proper use of workstations where e-PHI is accessed.
● Ensuring policies and procedures are in place concerning the removal, disposal, transfer, and re-use of electronic media.
The HIPAA Security Rule requires the following technical safeguards to ensure the protection of e-PHI:
● Installing firewalls and virus protection to protect information stored remotely.
● Using certified applications to store electronic health information. ● Requiring computer account authentication to verify that access is
given only to users granted the proper levels of access to systems that store electronic health information.
● Requiring passwords to access patient health information systems. ● Encrypting health information stored electronically. ● Auditing health information technology operations. ● Back up stored electronic health information on a regular basis using
a reliable backup system, such as a server or web-based storage.
Any unauthorized disclosure of health information that compromises the patient’s security or privacy is considered a breach. The Secretary of Health and Human Services must be notified of breaches that affect more than 500 people; if more than 500 people in one state or jurisdiction are affected, the media must be notified.
Covered entities aware of activities in possible violation of the Security Rule must take reasonable steps to ensure the violation is resolved. The Office of Civil Rights in the Department of Health and Human Services may conduct compliance investigations and reviews to ensure continuing protection of e-PHI.
Implementing privacy and security practicesWhen considering privacy and security safeguards in the healthcare setting, it is important to examine the facility’s existing health information technology practices. Knowing how the current technology serves clinical purposes, the physical locations where it is used in the facility, and how it is used, will provide information about the integrity, availability, and confidentiality needs of the practice. It can also contribute to decisions about possible situations in which health information can be disclosed, modified, used, or otherwise accessed by unauthorized personnel. Situations when information is accessed by unauthorized personnel are often unique to a particular facility, and can be due to technological, procedural, or personnel error.
CybersecuritySince patient information is often exchanged over the Internet, cybersecurity principles and practices are necessary to maintain the confidentiality of patient information. Cybersecurity is defined as:
“The protection of information and systems that connect to the Internet….including your personal information or any form of digital asset stored in your computer or in any digital memory device. It includes detection and response to a variety of cyber (online) attacks”.
Cybersecurity practices are required by the HIPAA Security Rule, and crucial to protecting patient information and a facility’s technological assets. They ensure the security of patient information in any context, including data that is not exchanged over an Internet connection, such as files saved on a physician’s compute.
The Office of the National Coordinator for Health Information Technology produced the following checklist of recommendations identifying the ten cybersecurity practices most critical to maintaining confidentiality of patient information.
Page 55 Dental.EliteCME.com

1. Using strong passwords that are changed regularly.Using a strong password to gain access to computer systems that store patient health information is a critical first barrier in preventing unauthorized users from accessing patient records. Passwords must be used to access operating systems in healthcare facilities. Computers should be programmed to require a password at log in, with no way to bypass this step. Using strong passwords may not prevent hackers from getting access to patient records, but can slow their progress, potentially preventing unauthorized access. Strong passwords can also be combined with physical safeguards to prevent intentional misuse, such as a staff member gaining unauthorized access to her ex-husband’s medical records.
A strong password is one that another person cannot guess easily, and does not have characteristics hackers can exploit through automatic systems. Strong passwords:
● Do not contain words found in the dictionary, even if the password slightly alters the word by substituting a letter with a punctuation mark or number.
● Do not contain any: ○ Information posted on a social media site. ○ Personal information easily obtained by another person, such
as birth date, Social Security Number, or address. ● Contain at least eight characters, including at least one number, one
special character, and a combination of upper and lower case letters.
Computer systems can be used to remind users to change their passwords on a regular basis. Frequently changed passwords decrease the risk of unauthorized users obtaining access to computer systems through stolen passwords. Because the strongest passwords contain many letters or digits and several different types of characters, people tend to write them down so they do not forget them. Employees should be discouraged from writing down passwords as reminders and encouraged to use computerized password recovery systems instead, or designate at least two staff members to resolve password issues.
Passwords can be combined with alternative authentication methods such as fingerprint scans or key card access, for increased security. These strategies, which greatly decrease the risk of unauthorized access, are typically used to protect highly targeted systems, such as those used to e-prescribe controlled substances.
2. Installing and using appropriate anti-virus software.Hackers commonly access computer systems through viruses, malware, or other mechanisms that can exploit weaknesses of the system. All computers and applications, no matter how up-to-date or technologically advanced, have vulnerabilities and design flaws that have the potential to be detected by hackers. Computer systems can also be attacked through external media such as flash drives, email, CD-ROM, and Internet downloads. Once hackers gain access to the computer system, they can take control of it, and destroy, alter, or steal data. Using anti-virus software that continuously and automatically updates, is well tested, with a proven reputation for securing confidential data, will provide the best protection against potential hackers.
If a virus infects a computer system, users may notice one or more of the following symptoms:
● The computer may not start normally (e.g., showing a blue screen at startup).
● The computer may crash repeatedly for no apparent reason. ● The Internet browser may open unwanted web pages on its own. ● It may seem that the anti-virus software is not functioning properly. ● Unwanted advertising may appear (“pop-up ads”), obscuring the
screen or interrupting the user’s task. ● The user may not be able to control the cursor.
Regularly updating anti-virus software is crucial to ensuring the software is effective. Anti-virus software can be programmed to remind users to update software, or update software automatically to ensure protection against the most recent viruses and malware.
3. Installing a firewall.Firewalls are required on all computer systems that store patient health information and connect to the Internet, to protect against attacks from external sources. A firewall acts as a barrier that prevents intruders from entering the computer system. Unlike anti-virus software, it does not find and remove viruses that have already gained access to the computer system.
Firewalls can take the form of software installed on the computer system, or hardware that added externally. Both systems monitor information attempting to enter the computer from the Internet, a local network, or other source, and allow only messages that meet pre-determined criteria to enter. Trained IT personnel should be responsible for configuring hardware firewalls, as setup can be complicated.
Some operating systems come with firewalls pre-installed to protect the computer system upon installation. It is also possible to purchase separate firewall software and many vendors of anti-virus software sell firewall technology as well. Firewalls are available in pre-configured formats with commonly used settings. Regardless of the type of firewall software, confirm availability of technical support and installation assistance for questions that arise along the way.
Large hospitals and healthcare systems using local area networks (LANs) should consider installing a hardware firewall. This type of firewall is a physical object that rests between the LAN and the Internet connection. A hardware firewall ensures that security settings are the same for everyone who uses the computer system within the network protected by the firewall, providing the higher level of security required by large healthcare systems. Hardware firewalls should be installed, configured, monitored, and maintained by an IT specialist.
4. Using technology to control access to protected health information. To further reduce the risk of unauthorized access to patient information, passwords can be combined with another identifying feature, usually a user name. Passwords constitute one-half of a user’s credentials; the user name is the other half.
Healthcare facilities can manage system use and users through an access control system, which determines who has the right to use the computer system, and their level of access. Access control systems are helpful in ensuring providers are compliant with the HIPAA Security Rule, and can be implemented through the operating system or a computer application. In all cases, access to protected health information should only be authorized on a need-to-know basis. Only those legitimately requiring access to patient information related on their professional role should be assigned a user name and password.
Many healthcare facilities manage who can access what information with an access control list. Permission is given according to specific filters; in role-based access control, an individual’s role in the facility determines his or her level of access. This system is configured so employees are only able to access the information they are authorized to have. An internal medicine specialist would be granted more access to patient files than a secretary in the oncology division of a hospital. Only extremely trustworthy individuals with administrative rights should have authorization to set user permissions. Permissions are set manually by adding each person and selecting what information he or she is allowed to access.
Access of protected health information by unauthorized users is a violation of HIPAA Privacy and Security Rules. Providers may be required to report unauthorized access to the Department of Health and Human Services and/or state agencies, depending on the severity of the breach.
5. Implementing controls to limit physical access to information systems. Preventing unauthorized access to e-PHI is only one part of a larger system for protecting patient information. Because the loss of electronic equipment is one of the most common ways patient health records are compromised, limiting physical storage and access to
Dental.EliteCME.com Page 56

computers and electronic equipment can increase PHI security. Any loss of personal data in electronic form, from storage media, such as flash drives or CDs, to laptops, tablets, and desktops can mean a serious breach of security.
Missing computer equipment containing patient information is always a cause for concern, as even the most protected data can be compromised despite the use of secure passwords, thorough access control, and adequate file permission standards. Unauthorized individuals have been able to remove hard drives, backup disks, and even servers from offices without detection. Limiting the possibility of equipment theft or loss by preventing physical access can greatly reduce the risk of lost or stolen personal health information.
Strategies for physically protecting patient information include using devices that can be secured to furniture or stored in locked rooms with keys held by trusted personnel, or alarm systems that notify management when equipment has been removed from its designated place. Servers containing patient health information should be located in locked areas accessible only by designated personnel, and stored away from potential environmental hazards such as water or fire damage.
6. Limiting network access to designated personnel.Wireless networks are used for Internet access in many office settings. Installation and implementation procedures must maintain confidentiality of patient information and compliance with federal law. Wireless router signals, for example, can be detected by neighboring buildings or facilities in the vicinity of the healthcare practice. To ensure data security, providers must confirm that devices brought into the office by outsiders or used in neighboring buildings cannot connect to the facility’s network. If patient information is transmitted over a wireless network, routers must be configured to operate in encrypted modes only, identify each device attempting to access the network, and permit system access only to qualifying devices.
Instant messaging (IM) systems are vulnerable to unauthorized access, expose the computer system to potential security threats ,and should not be installed on facility computers without thorough review of the possible consequences. Personnel should not be allowed to install software on healthcare facility computers without prior approval to prevent any installation that could pose a security threat.
7. Creating a plan to manage unexpected events. Unexpected natural or manmade events – from hurricanes and tornadoes to traffic accidents—can happen at any moment. The best way to minimize the impact of unexpected, adverse events is regularly creating backup files and implementing a pre-established recovery plan.
Regular data backup is crucial to preventing accidental data loss from unexpected events. Reliable data backup must be able to save and restore data accurately and efficiently. Various methods for data storage, such as external hard drives, CDs, or alternative servers are approved for use. Storage media requires regular testing to ensure it is functioning correctly, data is properly stored, and files can be reliably restored when necessary.
Regardless of the type of storage media used, backup data should be stored in a separate place, so it remains safe if an unexpected event deletes, damages, or alters the main system files. Storage media should be housed away from the main system, in a place resistant to environmental damage that is tested regularly to ensure adequate storage capabilities. Alternative servers should be located as far away from the main server as possible, to reduce the risk that data in both locations might be damaged by a single event. Information can also be stored in a web-based format, such as a “cloud” storage system, as long as it is as secure as the main system, and complies with HIPAA regulations for maintaining the confidentiality of patient information.
Providers must develop a detailed procedure for data recovery in the event of a disaster. Facility personnel should be familiar with emergency procedures for restoring information so they can know
how to provide copies of health records quickly in a crisis. In a large facility, this responsibility may fall to the IT department, but smaller practices with fewer employees may need to designate an individual who is not normally responsible for IT matters to manage back-up procedures and related tasks.
8. Enforcing proper maintenance of computer systems. New computers and software programs offer many options for configuring the system to users’ preferences. It can be difficult to determine which options are unnecessary or could potentially interfere with system security. Some simple tips to guide the configuration of a new piece of equipment or software include:
● Any software that does not contribute to running a medical practice, such as games and instant messaging, should not be installed on the computer system. If an application’s purpose is unknown, the electronic health record vendor or the local Regional Extension Center can provide information about its function.
● During installation, default options should not be accepted automatically. Each option should be selected with caution and a clear understanding of its function and risks. If choices are not understood, seek technical assistance.
● Discuss any potential security gaps in electronic health record software with the software vendor. Some companies maintain an open connection, or “back door,” for sending updates to the system that can become security threats. These “doors” should be well secured with a firewall, and monitored closely for unauthorized access.
● Remote file sharing and printing should be disabled to prevent unauthorized personnel from sharing or printing information.
Computer systems, like patients, need proper maintenance to continue working efficiently and effectively. Small preventive measures can make a big difference in maintaining the overall health of a computer system.
Installation of software updates should be performed on a regular basis to ensure adequate security. Updates are often sent through automatic downloads, but are also available through portable storage media. They are also available to patients, who may need them for their personal records or other needs. Updates often address recently discovered software vulnerabilities; using an automatic updating system that installs updates as they become available is the best way to prevent security breaches. Critical updates must be addressed immediately to ensure security is maintained.
Settings and data should be reviewed at periodic intervals to ensure information is not outdated. Usernames and passwords for former employees should be deactivated at the time of termination, and employees terminated involuntarily should have access removed before they receive their termination notice to ensure they cannot access patient information before leaving the position.
Information on hard drives can be recovered even after data has been “deleted,” so data stored on electronic equipment should be removed from the equipment before it is discarded. Only designated IT professionals with experience in removing patient information from hard drives should be assigned to this task.
Data files no longer in use should be electronically archived and stored securely, or completely removed from the computer system to guarantee the privacy of patient information. Unused software programs, such as trial versions and older versions of programs, should be completely uninstalled to reduce the possibility that vulnerabilities in these programs could be exploited to put patient information at risk.
Providers can use computer monitoring software to conduct desktop audits to keep employees from downloading programs they are not authorized to access. Software can be configured to delete downloaded programs, report downloads to management, or stop the process of downloading.
Page 57 Dental.EliteCME.com

9. Protecting mobile devices.Rapidly changing technology, evident in the increasingly commonplace use of tablets, smartphones, portable media storage, and laptops, means electronic health information is increasingly used on devices other than the standard desktop computer. Unfortunately, this raises the risk of security threats to patient information.
Because the portability of these devices makes them more vulnerable to theft or loss, their location should be monitored carefully. Portable devices are more likely than desktop computers to experience electromagnetic interference, which can corrupt or delete information from the device. The portability of mobile devices also increases the risk that information shown on the screen might be seen by others, as they are frequently used in public places.
Since portable devices are less likely to be equipped with access control and authentication measures, extra steps may be required to ensure these devices are secured against unauthorized access. Password protection and physical controls can prevent most unauthorized access, but portable devices that use wireless data transmission also require encryption of all wireless communication, especially data transmitted over public networks. Portable equipment that does not support encryption should not be used to store or transmit patient information.
Laptops and other portable devices should not be taken from secure areas unless absolutely necessary. If they must be removed, the hard drive should be encrypted to prevent security breaches. Employees who remove devices from secure areas assume responsibility for protecting patient information in their possession. Providers must delineate the circumstances under which it is appropriate to remove
portable devices from secure areas, and enforce these policies without exception.
10. Creating a security-friendly healthcare environment.Raising awareness of potential security threats and vulnerabilities in the healthcare environment is a critical factor in the success of a security system. The cybersecurity practices enumerated here are only effective if healthcare workers are willing to follow them. Administrative personnel must implement policies and procedures that enforce established safeguards, and require training on the consequences of inadequate data security for all employees who use patient health records in their work.
One of the challenges of creating a security-friendly culture in the healthcare environment is convincing personnel that they—not just “other people”—are vulnerable to electronic security breaches. In reality, these events are unexpected and can occur at any time, to anyone. The ten cybersecurity practices outlined here can reduce the incidence of security breaches, but are only effective when used consistently and properly by all employees. Data security should be tightly woven into daily practices so it becomes second nature to complete security tasks as directed.
Supporting a security-friendly culture requires personnel are educated and trained in security practices on a regular and ongoing basis. Team leaders and supervisors should take security responsibilities very seriously, and be especially vigilant about completing security tasks on time, as directed, to lead by example . Employees must understand that they have a serious and important responsibility, from their first day of employment to the last. Protecting patient health information should become second nature, like infection control practices.
E-PRESCRIBInGElectronic prescribing, also known as e-prescribing, is defined by the Medicare Part D prescription drug program as:
“…the transmission, using electronic media, of prescription or prescription-related information between a prescriber, dispenser, pharmacy benefit manager, or health plan, either directly or through an intermediary, including an e-prescribing network. E-prescribing includes, but is not limited to, two-way transmissions between the point of care and the dispenser”.
Using an e-prescribing system to prescribe prescription medications allows prescribers to transmit prescriptions directly to pharmacies, bypassing the need for pharmacy personnel to decipher handwritten prescriptions, a common source of medical error. E-prescribing systems are certified by the National Council for Prescription Drug Programs (NCPDP). This organization issues a list of industry standards to ensure e-prescribing systems are effective, safe, and efficient.
Beginning in 2013, Medicare began imposing penalties on physicians who did not utilize qualified e-prescribing programs. To meet the criteria for a qualified e-prescribing system, the program must be able to:
● Create a list of all active medications a patient is taking, incorporating information from prescription insurance plans if applicable.
● Choose medications, print paper copies of prescriptions, transmit prescriptions to pharmacies electronically, and conduct the following safety checks:
○ Automatic prompts to provide drug information on the prescribed product.
○ Warnings of potentially inaccurate dosing or route of administration.
○ Drug interaction warnings. ○ Allergy warnings.
● Provide information on less expensive therapeutic alternatives, if any are available.
● List information from the patient’s prescription insurance plan on formulary medications, identify which tier is associated with a particular medication for a given patient, provide eligibility information, and specify the authorization requirements necessary for prescribed medications.
Benefits of e-prescribing technologyElectronic prescribing is an important technological step forward in the effort to improve patient care. From the simplification of the prescribing process to improvements in the safety and efficacy of patient care, e-prescribing systems are powerful tools that have the potential to improve the practice of medicine. Qualified e-prescribing programs provide clinical decision support and simplified prescribing information to assist clinicians in prescribing safer and more cost-effective therapies to patients.
Improving patient care and safetyImproving the quality and safety of patient care is one of the most important benefits associated with regular use of e-prescribing technology. Growing numbers of people taking multiple prescription medications, and the increasing complexity of medical treatment and patient management link to the ever-growing risk of medication errors
and adverse events related to the processing of prescription orders. E-prescribing systems decrease the risk of errors related to illegible or miscommunicated prescriptions, as computerized prescriptions electronically sent to the pharmacy bypass the need for handwritten or verbal orders.
E-prescribing systems use warnings and alerts to notify the prescriber at the point of care about any potential errors before the prescription proceeds to the pharmacy. When prescribing a new medication, support systems within e-prescribing software have the ability to check if the medication is appropriate for the patient by analyzing data such as a patient’s medication list for potential drug interactions, allergy history and potential allergic reactions, contraindications, and dosage, all based on the patient’s individual characteristics and diagnosis. Prescribers can access the patient’s medication history at the point of
Dental.EliteCME.com Page 58

care as well, to verify information before prescribing new medications, reducing the risk of medication-related errors. E-prescribing software can integrate a important details about a pharmaceutical product or therapeutic practice into the system, to assist the physician in deciding on an appropriate medication.
Less time spent on the phone and at the fax machineIn 1999, before e-prescribing existed, a study conducted by the National Association of Chain Drug Stores concluded that pharmacies made more than 150 million phone calls to clarify prescriptions and review potential errors. E-prescribing reduces the amount of time that pharmacy and physician office staff spend on the phone or at the fax machine clarifying prescription orders and faxing prescriptions to the pharmacy. Savings in time and money for pharmacy and office staff can result in lower costs and greater convenience for the patient filling prescriptions.
Streamlining prescription filling Simplifying the process for filling prescriptions can improve patients’ adherence to treatment plans, as patients are more likely to fill a prescription if the process is not time-consuming, cumbersome, or difficult. Using an e-prescribing system to send prescriptions to a pharmacy simplifies the process, which can lower the number of unfilled prescriptions.
The process of renewing medications for chronic conditions can also affect patient compliance. Before e-prescribing software was available, a patient needing a prescription renewed by the doctor would require the pharmacy to generate and fax a refill request to the doctor. Once the doctor’s staff obtained authorization, the necessary information would be faxed to the pharmacy, and recorded manually in the patient’s chart. The more steps involved in this process, the more opportunities for error, such as requests falling through the cracks, due to failed faxes or loss of paperwork.
E-prescribing reduces the steps required to authorize refills; requests are sent, in electronic form, directly from the pharmacy to the doctor, enabling the prescriber to electronically authorize or deny the request
to refill a prescription, and send the order back to the pharmacy for processing, all through electronic communication. The information is automatically recorded in the patient’s chart. E-prescribing software simplifies the process of replying to refill requests as well, closing up some of the cracks that prescription requests can fall through.
Improved adherence to insurance formularies, resulting in cost savingsThe process of selecting medications authorized by the insurance company’s formulary is greatly simplified by e-prescribing software, which can link with the patients insurance plan information to confirm acceptance by the insurance company or check policies. When this information is available at the point of care, providers can see all the available medications and their prices, and select lower cost options, such use of generic medications and less expensive therapeutic alternatives.
Enhanced medication monitoring E-prescribing gives providers the ability to view a more complete picture of a patient’s medication history because it collects and consolidates data from multiple sources, including the patient’s other physicians and any pharmacies the patient uses. Having this information in one location enables the provider to evaluate the patient’s complete medication list and protect him or her from adverse effects due to drug interactions or contraindications, and any other potential risks.
E-prescribing software gives providers easy access to population-based medication and prescribing information, which can be very useful to communicate important information. If, for example, recent research studies suggest an increased incidence of adverse effects or medical error is related to a particular medication , providers prescribing the medication, and patients taking it, can be identified and notified quickly and easily through electronic records. Population-based data provides a more comprehensive picture of prescribing habits and allows providers to better assess treatment plans to improve patient care and outcomes.
Challenges to implementing e-prescribing programsAn e-prescribing program can create a more efficient healthcare environment and improve the quality of patient care, but only if a number of implementation challenges can be overcome. Adapting to change can be difficult, but most organizations find the long-term benefits of using health information technology far outweigh the short-term difficulties involved in the implementation process.
High cost of initial investment and balancing investment with returnsTransitioning to an e-prescribing system requires a significant financial investment in the initial stages of implementation . Installation typically requires the purchase of new software and/or hardware. Program costs vary based on whether its structure is integrated into the electronic health record system or exists as a stand alone program. Expenses involved in electronic prescribing include the costs of lost time and efficiency during the period of transition from the old to new system, and expenses associated with employing the Health IT personnel needed to:
● Install new equipment. ● Customize software. ● Secure patient health information throughout the transition. ● Train all personnel on the new system. ● Maintain and upgrade software and equipment.
Smaller practices with limited financial resources usually have a more difficult time balancing the cost of implementation with return on investment than large healthcare systems. Organizations concerned about an excessive financial burden should investigate what incentives are available from federal or state government to offset some of the costs of implementation.
Managing changeChange in the workplace can be difficult, especially in a busy healthcare environment. It is important not to underestimate the challenges involved in the transition to e-prescribing technology. Replacing established computer software with unfamiliar programs will temporarily decrease efficiency and create additional stress for employees. Staff members averse to new technologies may have a more difficult time adapting to the new system. Adequate prior training is essential to program success.
Managing the conversion properly from the beginning can greatly ease the transition period for everyone. Notifying staff members about the plan and providing a schedule for phasing in the new technology will help them plan ahead and prepare for challenges. Training staff members before the transition takes place will increase their level of familiarity and confidence and smooth system implementation.
Changing workflow proceduresAdapting the workflow to incorporate new systems can be challenging, especially when software is first introduced. It is common for productivity to decline during the first few weeks of new system use, as staff adapt to the new procedures for prescribing medications. E-prescribing software integrated into an electronic health record system appears to slow workflow less than stand alone software, but both can take some getting used to.
It is common for staff members to find their roles and responsibilities changing when new software is implemented. For example, the assistant who previously transferred information from copies of handwritten prescription orders into patient files can be assigned to
Page 59 Dental.EliteCME.com

other tasks, as the e-prescribing software automates this process. Automation can significantly increase efficiency in the medical practice, but adapting to new procedures takes time.
Selecting appropriate software Deciding on the best e-prescribing software for a medical practice can be a daunting task, especially for those who are not technologically savvy. Deciding how to get started, choose a vendor, negotiate prices, and implement the program is complicated, but support is available. E-prescribing and electronic health record systems can be set up at the same time; REC offer support to guide the provider through the entire process of selecting all software and implementing both systems.
Despite the improvements in technology that make electronic prescribing efficient and useful, some patients simply do not trust the use of this technology to transmit prescriptions to the pharmacy. Older patients or those who do not use computers, for example, may prefer paper copies of their prescriptions, and may feel more comfortable submitting prescriptions to the pharmacy on their own. While most patients find e-prescriptions more convenient, many others are uncertain about reliability, accuracy, or confidentiality of electronic data, and these patients’ attitudes must be respected.
How does e-prescribing work?There are several steps involved in the creation of a new prescription and the management of medication orders through an electronic prescribing system. The exact steps vary from system to system, but the general procedure, described here, is similar overall.
The first step in e-prescribing is signing onto the e-prescribing software system. Users typically must provide authentication through a username and password, digital certificate, or fingerprint scan, to ensure access is only granted to authorized personnel based on the user’s professional role and level of authorization for system use. For example, a doctor is granted authority to create new medication orders, while his assistant might only be able to view these orders.
The next step in creating an e-prescription is identifying the patient in the database. Many different types of identifying data, including date of birth, first and last name, phone number, or patient identification code can be used to identify and bring up a patient’s file, Offices often link their e-prescribing and scheduling software, so a list of the patients scheduled for a given day can be collected together to find them more easily.
Once the prescriber accesses the patient’s file, he or she can view the patient’s list of currently prescribed medications, see prescription details, and make changes to the prescription, such as discontinuing a medication, changing dosage, or revising instructions for use. The provider can also do any of the following:
● Update the patient’s medication list. ● Create a new prescription. ● Renew medications. ● Send prescriptions electronically to a patient’s chosen pharmacy. ● Reconcile the list of medication in the patient file with other
medication lists from other sources. ● Verify the accuracy of file contents with the patient.
To prescribe a new medication, the provider can search for a drug by name, or use the dropdown menu to find the appropriate medication filtered by treatment indication, the patient’s prescription insurance formulary, or lists of preferred medications. After the medication is chosen, many systems automatically generate standard directions for
dosage and duration of use that can be altered by the prescriber if necessary.
E-prescribing software is programmed to alert prescribers to potential dangers regarding the chosen medication. After a prescriber selects the medication dosage, directions, and quantity, he or she is alerted to any cautionary statements or warnings associated with the prescription before sending it to the pharmacy. This critical information includes potential drug interactions, drug-disease interactions, contraindications, and potential side effects.
If the provider chooses to prescribe the medication after reviewing these alerts, he or she will electronically sign the prescription to show authorization. Some software requires providers electronically sign prescriptions individually (one-at-a-time), while others allow providers to electronically sign all requested prescriptions at once. Electronic signatures require use of a password or other method of authentication to ensure only authorized individuals use the system. Electronically signed prescriptions can be sent to the patient’s pharmacy for processing. There are usually several options for transmitting prescriptions to the pharmacy, depending on the software. They can be sent by fax or electronically one-at-a-time or in batches. Prescribers can also print paper copies of prescriptions if requested by the patient or required by law.
Upon receiving the prescription, pharmacists review, process , and fill the prescription, then dispense it to the patient. Many types of pharmacy software pre-populate information from the prescription, meaning data fields on the computer form are automatically filled in, greatly speeding up the process and reducing transcription or data entry errors. Pharmacy technicians check each field to ensure all fields are filled in correctly, then submit the information to the patient’s prescription insurance for approval. Once the prescription is successfully submitted to the patient’s insurance, it is filled (often by a technician) and given to the pharmacist for a final review to identify the source of warnings and alerts, ensure the prescription and instructions for taking it are correct, and assess whether the prescription is appropriate for the patient. If it passes this final quality check, the medication can be sold to the patient or a representative.
Electric Prescriptions for Controlled Substances (EPCS)The use of e-prescribing systems for controlled substances is legal under federal law, but each state may issue its own restrictions or prohibitions on the practice. Because state laws require organizations implement specific workflow procedures for e-prescription of controlled substances, e-prescription system design must meet the prescriber’s needs and comply with state law.
The Drug Enforcement Administration’s (DEA) interim final rule on e-prescribing of controlled substances (EPCS), issued in 2010, authorizes physicians to e-prescribe controlled substances under federal law. This decision gave pharmacies and prescribers the opportunity to implement technological improvements in prescribing and filling controlled substance prescriptions, while maintaining an intact, secure system for dispensing commonly abused medications.
E-prescribing is appealing to those who dispense controlled substances because it reduces paperwork, and, at the same time, reduce the risk of prescription forgery.
As of July 2014, e-prescribing of controlled substances is available in 49 states (all but Montana), with the percent of pharmacies able to actually provide this service ranging from less than ten percent to over 50 percent, and climbing rapidly (In 2011, only 32 states allowed e-prescription of controlled substances). Forty-eight states allow the e-prescription of Schedule II to V controlled substances (all schedules); Kansas is the exception, limiting the e-prescription of controlled substances to Schedule III to V.
It is important for providers and pharmacy personnel to be aware of the current legal status of e-prescribing controlled substances,
Dental.EliteCME.com Page 60

and comply with both federal and state regulations. A list of states with their current e-prescribing status and procedures for controlled substances is available here: http://surescripts.com/products-and-services/medication-network-services/e-prescribing-of-controlled-substances.
The interim final rule issued by the DEA establishes mandatory minimum standards for e-prescribing controlled substances. These standards were developed to decrease the risk of drug diversion while allowing providers to prescribe controlled substances to patients as part of a medically approved treatment plan. The DEA maintains stringent requirements for physicians, e-prescribing software, e-prescribing networks, pharmacy software, pharmacies, and pharmacists involved in e-prescribing controlled substances.
PhysiciansPhysicians who prescribe controlled substances through e-prescribing systems must follow strict regulations issued by the DEA. Only prescribers who have the right to prescribe controlled substances under both the DEA and state law may electronically prescribe controlled substances. Prescribers must submit to identify proofing, a process to verify the prescriber’s identity, confirm state credentials to guarantee the provider is in good standing with the state medical board, and check their status with the DEA.
After the prescriber passes the identity-proofing process, he or she is issued a credential to e-prescribe controlled substances (EPCS) by the General Services Administration Office of Technology Strategy/Division of Identity Management. The credential requires two-factor authentication, a process requiring two of the following authentication methods:
● A piece of information the clinician knows, such as a password or challenge question.
● A piece of physical information from the clinician’s body, such as a fingerprint or iris scan.
● A hardware token, such as a physical card or other device possessed by the clinician that contains a password or cryptographic key that can be used only one time. Cryptographic keys are associated with a digital certificate and stored on a hard token. They are obtained from a certification organization authorized by the Federal Bridge Certification Authority.
The two-factor authentication procedure required to electronically sign and authorize electronic transmission of e-prescriptions is considered a legal signature. The complexity of this authentication method helps to decrease diversion of controlled substances. Physicians are responsible for protecting their authentication credentials, which must not be shared with anyone. They are also responsible for using only e-prescribing software certified by a third party, to maintain the security of e-prescriptions.
E-prescribing software requirements for providersCertification of e-prescribing software for prescribers through third-party audits is one of the requirements for meeting the DEA’s interim final rule. Uncertified software may not be used to transmit EPCS. To qualify for certification, e-prescribing software must meet the following requirements:
● It must not allow controlled substances to be e-prescribed unless the authorizing prescriber has provided two-factor authentication to sign the prescription.
● It must implement logical access controls to prevent unauthorized individuals from accessing the software and e-prescribing controlled substances.
● It must have the ability to associate DEA-registered providers with their unique DEA number.
● It must require entry of all data necessary in a controlled substance prescription, including the signing date of the prescription, the patient’s complete name and address, the name, strength, form and dosage of the medication, the prescribed quantity and directions, and the name, address and DEA number of the prescriber.
After the two-factor authentication process of electronically signing the prescription is complete, the e-prescribing software dates and time stamps the prescription, and a copy of the digitally signed prescription is archived to create a permanent record. The prescription is encrypted and sent to the pharmacy.
Once the process of electronically signing the prescription is complete, the e-prescribing software must date and time stamp the prescription.
The e-prescribing software verifies the prescriber’s identity using the software or prescriber’s “private key”, which is method used to prove the prescriber is who he or she say they are. If the prescriber’s private key is used, the software verifies the validity of the prescriber’s digital certificate. If the certificate is invalid, the prescription is invalidated and cannot be filled by the pharmacy. The software is required to provide the receiving pharmacy with an indication that the prescribing physician has electronically signed the prescription, but this requirement is waived if the prescriber uses his or her own private cryptographic key to sign the prescription because the pharmacy software can verify the prescriber’s digital certificate to confirm that the prescription was electronically signed by a valid prescriber.
E-prescribing software is required to recognize when electronic transmission of a controlled substance prescription has already been processed or printed, and prohibit generation of prescription duplicates. Prescriptions printed after they have already been filled must have a label stating “copy not for dispensing”. If an initial electronic transmission fails, requiring a prescription to be printed again, details of the failed transmission should be noted on the printed copy of the prescription.
Intermediary E-prescribing network requirementsIntermediary e-prescribing networks are responsible for transmitting e-prescriptions from prescribers to pharmacies, and are required to notify prescribers of any failed e-prescription transmissions. In the event of transmission failure, the intermediary is not permitted to alter or change the required components of the prescription (except to ensure that the pharmacy’s computer system can import and read the data correctly), or convert the e-prescription to an alternative transmission medium, such as a fax.
Pharmacy software requirementsIn order for pharmacists to process and dispense controlled substances prescribed through electronic mechanisms, their pharmacy software must be certified by a third party to ensure it meets the requirements enacted by the DEA’s interim final rule. If software is non-compliant with any aspect of DEA regulations, e-prescriptions for controlled substances may not be filled.
Additionally, pharmacies must implement logical access controls to ensure alterations and annotations to controlled substance e-prescriptions are only made as legally permitted by authorized personnel. If a pharmacist needs to make a notation on an electronically transmitted controlled substance prescription, the same annotation must be created and stored electronically. Verbal or paper prescriptions that were originally sent to a different pharmacy electronically, but were incomplete or failed, must be verified by the pharmacist to ensure they were not received or filled by the other pharmacy.
Third parties certifying pharmacy software to guarantee compliance with the DEA’s interim final rule require the following of pharmacy software:
● It must have the ability to read, import, store, and display information entered by the prescriber and necessary for a valid prescription.
● It must be able to validate the identity of providers who use private cryptographic keys to sign prescriptions.
● It must be able to verify the prescriber’s digital certificate to confirm the prescription was electronically signed by an authorized prescriber.
Page 61 Dental.EliteCME.com

● It must be able to show proof that a valid prescriber signed the prescription if the prescriber used a cryptographic key integrated into the prescribing software instead of a private key.
● It must able to store the prescriber’s complete DEA number and dispensing information, such as the name of the pharmacist who verified the prescription; digitally sign the prescription, and archive the digitally signed prescription.
● It must contain logical access controls to prevent unauthorized individuals from accessing controlled substance e-prescription records
● It must be back up records on a daily basis and store them for at least two years.
IMMUnIzATIOn InfORMATIOn SySTEMSImmunization information systems (IIS), also known as immunization registries (IR), are defined as “confidential, population-based, computerized databases that record all immunization doses administered by participating providers to persons residing within a given geopolitical area”.
Immunization information collected from various sources is consolidated into a single official immunization record for each patient that can be used in a range of healthcare environments. This record can be distributed to schools, camps, and other places requiring immunization histories. IIS can exchange information with healthcare providers who administer immunizations to ensure vaccines are
administered in a timely manner, consolidate records, and increase efficiency of immunization programs.
Widespread use of IIS aligns with the health improvement goals of Healthy People 2020, a program dedicated to improving a range of health indicators among Americans within a 10-year period. The plan contains several specific immunization objectives, with an overall goal of improving immunization rates to reduce, eliminate, or prevent the recurrence of a vaccine-preventable disease. Improving the ability of electronic records to collect immunization information and notify providers when immunizations are due can help close the gap between actual immunization rates and public health goals.
Benefits of immunization information systemsIIS benefit healthcare providers at the point of care in a variety of ways. A provider can review a patient’s electronic immunization record to determine if the patient is due for any vaccinations; it can generate reminders to alert providers and families when a patient is due for immunization or when a scheduled immunization has been missed; and can reduce the incidence of duplicate vaccination.
On a larger scale, the widespread use of IIS can benefit nearly every American. An electronic immunization record is an invaluable tool in the event of a disaster or the outbreak of a vaccine-preventable illness. The IIS gives public health officials the ability to identify vulnerable populations that could be targeted for immunization, to reduce their risk of disease and protect public health. IIS vaccination data can
also be monitored by public health officials to identify high-risk populations and allocate immunization resources appropriately.
Data from IIS are often used in research. In 2011, a study analyzed IIS immunization data for children in Minnesota, Georgia, and Connecticut, to assess the effects of a rotavirus vaccine in a case-control study. Researchers comparing the effectiveness of three doses of a rotavirus vaccine to no vaccine found the three-dose protocol 89-94% more effective in children eight months and older, and 86-92% more effective in children 24 months and older. Two rotavirus doses were found more effective than no dose in over 90% of children eight months and older. This research would not have been possible without IIS data.
Who can communicate with immunization information systems?IIS were created to provide a comprehensive electronic record of patient immunization data for the following entities:
● Healthcare providers and organizations value electronic immunization records because they provide easy access to immunization information needed for clinical purposes, and provide a way to easily submit data to complete vaccination histories.
● Insurance plans access immunization data to identify covered patients who have not been immunized, and encourage them to be vaccinated to reduce their risk of infection.
● Vital records systems that document births can be used as a basis for the creation of new patient files to ensure as many newborns as possible are included in the IIS, and as many as possible are vaccinated.
● Several public health programs rely on IIS data for public health activities including emergency and disaster response, including the Vaccines for Children program, Strategic National Stockpile, disease outbreak control and management, disease surveillance, immunization campaigns, epidemiology, and quality improvement.
● Regional Health Information Organizations (RHIO) that facilitates the exchange of health information among electronic health systems transmit immunization information to and from IIS.
● Other groups that access immunization information include schools needing student immunization data, and government programs for women, infants and children (WIC) that use IIS data to improve immunization rates for these groups.
Requirements for immunization information systemsBoth federal and state laws govern IIS operations. Some states only permit immunization data collected on children below a certain age, while other states permit collecting information for all ages. Some states enforce mandatory reporting of immunization information, while others provide patients the choice of opting out of IIS participation.
State law dictates who is authorized to access the IIS. While the federal HIPAA Privacy Rule establishes guidelines for protecting patient health information, states can issue more stringent laws to further protect the patient records. More information on state-specific laws can be found on the CDC’s website at http://www2a.cdc.gov/vaccines/iis/iissurvey/legislation-survey.asp.
On a federal level, the HIPAA Privacy and Security Rules help ensure the privacy and security of patient information stored in the immunization information systems. While IIS generally do not perform functions that would make them “covered entities” under the HIPAA rules, following the guidance of HIPAA can help providers ensure patient information remains private and secure.
Another federal law that affects the use of IIS is the Family Educational Rights and Privacy Act, also known as FERPA. This law, designed to protect the privacy of student education records, applies to schools receiving federal funding from the US Department of Education. FERPA grants certain rights to parents regarding control of their children’s educational records, including the requirement
Dental.EliteCME.com Page 62
that parents provide written permission to the school before any information from the child’s record, including vaccination history, is released.
Since IIS contain confidential patient data, they must be managed with the same care as other confidential records to guarantee security is maintained. The Centers for Disease Control and Prevention (CDC) require all IIS to retain a written policy that outlines the following:
● Parents of children receiving immunizations that will be recorded in IIS must receive notification explaining the existence and
purpose of the systems, what information is collected, and how the information can be used.
● IIS data must be used for its intended purpose, as described in this policy, and cannot be used to disadvantage the patient in any way.
● Information detailing who may access these systems, how information is disclosed, what constitutes a breach of confidentiality, and what penalties are associated with it.
● Parents must be given the option of choosing if their child’s immunization information will or will not be included in IIS.
● How long IIS data is maintained.
How do immunization information systems work?Many children enter the immunization information system at birth or have a file created for them by their health care provider at the patient’s first vaccination. Data can be entered into IIS by different agencies and individuals, including the patient’s healthcare provider, electronic health records, Medicaid claims, and other insurance or billing systems.
IIS patient records are composed of three main sections: ● General information. ● Current immunization status and forecasting. ● Patient’s immunization history.
The exact information contained in each section varies by state, but some general guidelines apply to collecting this information. The general information section enables providers to correctly identify the patient and provide the following contact information in case of an emergency:
● Patient name, mother’s maiden name, and any previous names or aliases used.
● Demographic information for the patient, including birth date, address, and gender.
● If the patient was born as part of a multiple birth, such as twins or triplets.
● Emergency contact information, such as the patient’s parents, spouse, or responsible caretaker.
The National Vaccine Advisory Committee (NVAC) provides a list of data elements such as demographic information, vaccine history, or
name and relationship of emergency contact, that should be included in each patient’s IIS file A full list of data elements required in IIS files can be found on the CDC’s website at http://www.cdc.gov/vaccines/programs/iis/func-stds-appxB.pdf.
The section for immunization status and forecasting assesses whether the patient is current, due, or overdue for vaccination. Forecast data is compiled from immunization schedules created by the Advisory Committee on Immunization Practices (ACIP). It compares the patient’s vaccination history and immunization schedule to determine what, if any, immunizations are required, and when.
Providers can access the patient’s immunization history for the following information regarding previous vaccinations:
● The dates vaccines were administered. ● The vaccine type or specific antigen administered. ● The manufacturer of the vaccine administered and the lot number
used. ● The site of injection. ● The injection method, such as intramuscular or subcutaneous. ● The dose. ● The name of the administering provider. ● The date on the Vaccine Information Statement (VIC) given to the
patient.
Providers not currently contributing to an IIS should contact their state’s immunization registry to enroll.
Progress of immunization information systemsIIS have existed since 1993, when their primary content was pediatric population data. Characteristics such as complex immunization schedules, and inconsistencies among immunization records maintained by multiple healthcare providers made vaccine tracking and scheduling for pediatric patients particularly complicated, necessitating a better recordkeeping and inventory management system. Additionally, public health organization such as the Vaccines for Children program specifically required this data.
There have been significant improvements in IIS since its inception. The CDC conducts an annual assessment of IIS efficiency and publishes the findings in the IIS Annual Report (IISAR). The 2012 IISAR showed 86% of children under 6 years of age participated in IIS, with child participation defined as receiving two or more immunizations documented in an IIS. In 2006, only 63 percent of children participated in IIS. The magnitude of this increase suggests the Healthy People 2020 objective of 95% participation by the year 2020 might be possible.
Although their historical focus was pediatric populations, improving adult participation in immunization information systems is also a high priority. The 2012 IISAR stated only 25% of American adults participate in IIS, with adult participation defined by documentation of one or more immunizations in adults equal to or greater than 19 years of age. Because adults commonly receive vaccinations from multiple providers, at multiple locations, including non-traditional settings such as pharmacies or retail clinics, they are likely to benefit from IIS participation, which can reduce the risk of duplicate vaccinations.
Adult participation in IIS can be challenging. Many jurisdictions do not make reporting to IIS mandatory for adults, and identifying and enrolling the multitudes of healthcare providers who provide vaccinations to adults can be daunting. Despite the difficulty, adult reporting rates to IIS improve every year, with system enhancements likely to increase participation for adults across the country.
Immunization information system functional standards for 2013-2017The Immunization Information Systems Support Branch of the Centers for Disease Control and Prevention’s National Center for Immunization and Respiratory Diseases has developed a set of standards to guide the framework for developing immunization information systems through 2017. These standards were created to
establish the requirements that all immunization information systems should be able to meet by the end of 2017.
The following goals and functional standards were developed to guide the nationwide use of immunization information systems. All immunization information systems must meet standards developed by
Page 63 Dental.EliteCME.com

the CDC to guide the growth of IIS in the near future. The following goals and functional standards are required by the end of 2017:
1. Support the delivery of immunization services at the point of care, regardless of the healthcare setting. Improving the quality of care in terms of immunization services means patients receive all vaccines necessary, based on current ACIP schedule recommendations for their age. To accomplish this goal, providers must be able to access IIS immunization data and clinical decision support programs at the point of care. Primary care providers have historically administered the vast majority of immunizations, but the responsibility is increasingly shared by new healthcare providing centers, such as drug stores or schools. This means healthcare providers in all care settings must have access to IIS to ensure safe and effective vaccine administration.
To comply with vaccine schedules, immunize the greatest number of individuals, and pursue the elimination of vaccine- preventable disease, the IIS must:
● Provide patient immunization records at the point of care. ● Automatically determine when vaccines are due, coming due,
or past due, according to current ACIP immunization schedules, and display this information for clinicians each time the patient’s immunization record is viewed.
● Identify patients who are due or past due for a vaccine. ● Create reminders for patients identified as overdue for a vaccine,
and provide other helpful tools to ensure these patients are immunized.
● Allow interoperability of data with other health information systems to increase vaccination rates.
● Receive information from other systems to add patient vaccination data to the immunization registry.
2. Support requirements for vaccinations purchased publicly, from state or federal immunization programs.Significant portions of pediatric vaccinations administered annually are purchased under Vaccines for Children, a federal program with monitoring and reporting requirements, such as documenting eligibility, maintaining vaccine inventory records, and tracking vaccines for patients receiving vaccines through the program.
IIS must have the following capabilities to meet public vaccine purchase program requirements:
● A software function able to track vaccine inventory and show accurate numbers of remaining stock as vaccines are used.
● Inventory functions that are interoperable with other health information technology systems, and sufficiently user friendly that individuals at various data entry access levels can use the system.
● Recording patient eligibility for publicly purchased vaccines at the time they are administered.
● Interoperability functions that allow IIS to communicate with national vaccine inventory, ordering, and distribution systems.
● Creating data management reports for publicly purchased vaccine programs.
3. Maintain the quality of patient immunization and demographic data and keep it current.To ensure patients receive the appropriate vaccines, based on age, but are not administered duplicate or unnecessary doses, IIS must give providers complete, up-to-date immunization data and demographic data to facilitate patient monitoring and follow up, when necessary. Accurate IIS information protects public health by reliably identifying who has and has not been vaccinated.
In order to maintain high quality data, the IIS must: ● Provide immunization and demographic data for a given
population.
● Evaluate existing and incoming demographic and immunization data to prevent, identify, and resolve duplicate and incomplete records.
● Store complete and comprehensive demographic and immunization data.
● Create records for newborns as soon as possible after birth. ● Record all immunization and demographic data within a
reasonable timeframe, after submission.
4. Ensure and maintain the privacy, security, integrity, and availability of patient health information.As the number of organizations using IIS increase, the risk to the privacy, security, integrity, and availability of an individual’s personal health records increases as well. IIS must comply with laws and standards for storing, using, and transferring sensitive patient information.
Patients and providers alike must be able to trust that patient data stored and used in immunization systems will remain private and secure.
To comply with laws and standards for the privacy, security, integrity, and availability of patient health information, IIS must:
● Maintain written privacy practices to protect all patients who have personal data stored in the immunization information system.
● Utilize access controls to prevent unauthorized users from accessing sensitive information.
● Operate on secure software and hardware systems that meet industry standards for security, encryption, and recovery, in the event of a disaster.
5. Allow all authorized personnel to access immunization information.Since a wide variety of users, including health and emergency care providers and public health agencies, require IIS access, access controls must allow entry to all authorized users, in accordance with state and federal laws. IIS must be able to:
● Provide access to all authorized users. ● Generate reports for authorized users, such as vaccine use and
population-based reports. ● Provide copies of immunization records to authorized individuals. ● Produce official immunization records for use by authorized
groups, such as schools, daycare facilities, and camps.
6. Encourage vaccine safety in healthcare settings.Supporting vaccine safety in the healthcare environment means vaccinated patients should be observed following vaccine administration in case of allergy or other adverse effects. When a particular lot of vaccine raises health concerns, patients who were vaccinated with it should be monitoring in case of ill effects, and may need re-immunization with a problem-free lot. Detailed IIS vaccine administration data is key to identifying vaccine recipients in order to conduct proper follow up.
Because reporting adverse events related to a specific vaccine is crucial to detecting risks or symptoms related to a particular vaccine lot, the National Vaccine Injury Compensation Program (NVICP) and the Vaccine Adverse Events Reporting System (VAERS) require reporting of vaccine-related adverse events. It is to all users’ advantage to maintain current, detailed IIS vaccine administration data as it greatly facilitates the adverse event reporting process. To encourage vaccine safety in the healthcare setting, IIS must:
● Provide data reports, in cases of vaccine recalls, identifying patients who received the vaccine.
● Facilitate simplified reporting and investigation of vaccine-related adverse events.
Dental.EliteCME.com Page 64

PRESCRIPTIOn DRUG MOnITORInG PROGRAMSThe National Alliance for Model State Drug Laws (NAMSDL) defines a prescription drug monitoring program (PDMP) as:
“…a statewide electronic database which collects designated data on substances dispensed in the state. The PDMP is housed by a specified statewide regulatory, administrative or law enforcement agency. The housing agency distributes data from the database to individuals who are authorized under state law to receive the information for purposes of their profession.”
PDMP facilitate the collection, reporting, and analysis of information for the prescribing, dispensing, and use of controlled substances, allowing authorized providers to check a patient’s history of treatment with controlled substances, before prescribing a new treatment plan.
Preventing prescription drug abuseThe illegal use of psychotherapeutic prescription medications in America over the past decade is a serious and growing concern. The Substance Abuse and Mental Health Services Administration’s (SAMHSA) 2005 National Survey on Drug Use and Health (NSDUH) reported these findings:
● An estimated 15.2 million persons aged 12 or older (6.2 percent of all people in that age group) used prescription-type psychotherapeutic drugs non-medically in the past 12 months.
● Almost 5 million young adults aged 18 to 25 (12.4 percent) used prescription pain relievers, such as OxyContin®, non-medically; and 1.7 percent of young adults met the criteria for dependence or abuse of prescription pain relievers for the past year.
● Drugs for non-medical users of prescription drugs were commonly provided free, “from a friend or relative”.
While the increase in prescription drug abuse is troubling, preventing or reducing availability is complicated by the importance of controlled substances in patient care. Unfortunately, legitimate prescriptions for controlled substances can supply nonmedical drug user. Federal and state programs try to combat nonmedical prescription drug use while ensuring patients with legitimate medical needs are able to obtain necessary medications.
Since many prescription drug abusers begin taking controlled substances provided by friends or family members, many federal strategies for preventing drug abuse and diversion attempt to reduce the quantity of controlled substances prescribed to the general public, to minimize the number ultimately used by someone other than the individual with a prescription.
The sale of prescription medications must be approved by the FDA. Only prescribers with valid DEA registration numbers, which verify the prescriber’s authority to use controlled substances in patient care, can issue prescriptions for controlled substances. Controlled substances may only be prescribed for legitimate medical purposes, by prescribers acting within their scope of professional practice, and may only be dispensed by pharmacies with valid DEA licensing.
States are responsible for regulating healthcare professionals who prescribe or dispense prescription controlled substances. Controlled substance prescribers must be actively licensed in the state where they practice, with current DEA registration, and maintain records in compliance with state and federal law. States have the authority to issue and revoke the license of a healthcare professional, if necessary.
Despite controls restricting the prescribing of controlled substances, rates of abuse and diversion continue to rise. In response, most states have developed PDMP to monitor the prescribing, dispensing, and use of controlled substances. (Prescription drug monitoring programs are regulated by state agencies, not the DEA.) PDMP regulations vary from state to state. For specific terms, such as who may access the PDMP and how compliance is enforced, refer to that state’s regulations.
Prescription drug monitoring programs operate on a state level. As of October 2013, 45 states had functional PDMPs, four states and Guam were still in the implementation phase, and Missouri and the District of Columbia did not yet have supporting legislation to establish a PDMP. Further information about each state’s PDMP status can be found at http://www.fsmb.org/pdf/GRPOL_pmp_overview_by_state.pdf.
History and legislation for prescription drug monitoring programsPrograms that monitor the dispensing of prescription medications have existed for more than 70 years. Ten states had some form of controlled substance monitoring program by the 1980s, but they were complex systems, different in every state, and commonly required duplicate or triplicate copies of prescription forms.
In 2002, Congress funded the Harold Rogers Prescription Drug Monitoring Program (HRPDMP), to assist law enforcement and regulatory agencies in improving data collection and analysis of controlled substance prescription patterns. The main focus of the program is helping states establish and improve controlled substance prescription monitoring programs. State PDMP received additional funding in 2005 when the NASPER Act authorized the Department of Health and Human Services to offer grants to states to establish and improve PDMP.
In addition to fostering state PDMP, the NASPER Act created a set of best practices to direct the development of state PDMs. The Act established the following requirements:
● Pharmacies and other dispensers of controlled substances must report all dispensing of controlled substances to the state in electronic format within 1 week. Exceptions to this rule include direct controlled substance administration to a patient, or for a quantity less than a 48-hour supply.
● Information reported to the PDMP for each prescription must include:
○ The dispenser’s DEA number. ○ The prescriber’s name and DEA number.
○ The name, address, and phone number of the prescribed user. ○ The national drug code (NDC) number, and quantity
dispensed. ○ The number of refills indicated by the prescriber. ○ Whether the prescription was a refill or new prescription. ○ The date the prescription was written and date it was
dispensed. ○ Any additional information required by state law.
● States must establish an electronic database containing specific controlled substance prescription information searchable by any field of data, with appropriate safeguards to ensure the information is accurate, complete, and secure.
● Information in the PDMP database may be disclosed to: ○ Practitioners who certify it will be used to provide medical or
pharmaceutical care, or evaluate a current patient’s treatment. ○ Local, state, and federal law enforcement agents or narcotics
control authorities, to facilitate investigations into the illegal diversion or misuse of schedule II-IV controlled substances, or assist with legal proceedings.
○ Other state PDMP with interoperability agreements. ○ Agents of the DHHS, DEA, and State Medicaid or Health
Departments who use the information to conduct research for their departments.
○ Members of the state agency responsible for establishing the state’s PDMP, to assist in its development.
These guidelines have been instrumental in the development of new PDMP, and improving PDMP in states with existing programs.
Page 65 Dental.EliteCME.com

Benefits of prescription drug monitoring programsPDMP are tools used to prevent prescription drug diversion, abuse, and addiction. They can provide numerous benefits, such as:
● Promoting the legitimate medical use of controlled substances. ● Identifying patients at risk of abusing or diverting controlled
substances for the purpose of preventing or deterring them. ● Facilitating intervention and treatment for patients addicted to
prescription medications. ● Allowing public health officials to collect information detailing
trends of prescription drug use and abuse. ● Increasing awareness and understanding of prescription drug use,
abuse, addiction, and diversion.
Goals of prescription drug monitoring programsWhile PDMP are diverse in operation, they share a number of common goals, such as providing informational and material resources to educate prescribers and pharmacists in best practices for prescribing controlled substances. PDMP protect the confidentiality of the data entered into their programs. Access is restricted to authorized health care professionals and other personnel. Unauthorized personnel are blocked from accessing protected patient health information.
Providers can access information on prescribing records to review and evaluate their own prescribing habits, and identify patients who may have forged prescriptions or obtained them illegally. PDMP can generate reports examining or analyzing prescribing trends in a specific geographic area, medical specialty, or drug class. PDMP reports increase public awareness of controlled substance diversion and abuse, and educate the public and healthcare professionals about the prevalence and signs of nonprescription drug use.
PDMP support public health initiatives by analyzing collected data to identify trends and address issues of over- and under-use of controlled substances. PDMP data inform educational programs and abuse prevention strategies, develop policies, laws, and regulations, and establish treatment guidelines. Initiatives can target specific healthcare providers, requiring, for example, all prescribers of fentanyl to take a course covering its potential risks and benefits.
A primary goal of PDMP is preventing diversion of controlled substances. PDMP can provide diversion information to law enforcement personnel earlier than any other information gathering or surveillance agency. PDMPs are able to identify healthcare providers who prescribe unusual quantities of controlled substances, pharmacists who consistently fill medications prematurely, patients who are filling multiple providers’ prescriptions for controlled substances, and patients attempting to forge prescriptions. Early interventions by PDMP provide the best opportunity to catch patients and providers who are attempting to divert controlled substances.
Prescription monitoring programs assist law enforcement agencies in identifying and investigating illegal activities surrounding the prescribing and use of controlled substances. PDMP facilitate this process by gathering and consolidating all relevant information easily and quickly. Previous data collection methods required labor-intensive searching through medical and prescription-dispensing records to identify prescribing irregularities. Current procedures increase the efficiency of legal investigations by minimizing the need for law enforcement personnel to intrude into the healthcare environment; police officers can access the electronic controlled substance record, if needed, instead of requiring providers and pharmacies to produce the information.
finally, how do prescription drug monitoring programs work?Each time a controlled substance prescription is filled, the dispensing agent is required to electronically report this information to the PDMP. Practitioners accessing the system must verify they are authorized PDMP users. To do so, the user is required to submit a completed application for approval by the state governing body responsible for regulating PDMP; some states require a notarized application.
After the application is approved, the healthcare provider must establish a user name and password (most systems require a two-step authentication process) to verify the user’s identity. In many cases, this requires obtaining a virtual token that is e-mailed to the user’s e-mail address on file, to ensure the authorized user receives the information. Users must not divulge the password, as this may constitute a security breach.
Once the user’s identity is validated, and he or she is authorized to access the system by entering a user name and password, the PDMP typically requires users to agree to the system’s terms and conditions of use each time they access the system. Once the user signifies agreement with PDMP terms and conditions, healthcare professionals can search patient files by name and birthdate, among other search terms that vary by state. The patient file contains a list of the controlled substances prescribed to the patient, which is critical to determining the appropriate use of controlled substances in the patient’s treatment plan.
PDMP store and utilize patient healthcare data, making them subject to regulation by federal HIPAA rules. Information may not be shared with unauthorized persons and may only be used to evaluate a current patient’s treatment plan or provide medical treatment.
Pharmacies are required to submit information to the PDMP regarding all controlled substances dispensed. Pharmacies may need to register with the PDMP before they can access the software or upload controlled substance data. Large chain pharmacies typically manage this process through their central offices, but independent or small chain pharmacies may need to register on their own. For each
controlled substance dispensed, pharmacies must submit demographic information for the pharmacy, patient, and prescriber, and specific dispensing information for each controlled substance sold. Information must be submitted in a secure format that protects patient health information.
Assessment of the National All Schedules Prescription Electronic Reporting ActIn 2005, the NASPER Act required the Center for Substance Abuse Treatment (CSAT) to conduct an assessment within 180 days of passing the Act, to determine if the use of PDMP had a “substantial negative impact on patients’ access to treatment”. The CSAT assessment was commissioned to investigate the impact of PDMP on patient care, but did not examine the effects of PDMP on drug abuse or diversion.
The 180 days allotted for the assessment was not enough time to conclusively determine how PDMP affect patient’s access to treatment with controlled substances. Findings provided some support for the conclusion that PDMP can negatively influence patient care but this effect was seen predominantly in PDMP requiring multiple copies of medications, using duplicate or triplicate forms, and PDMP that collect Schedule II prescription data but not from Schedule III-V.
Evaluation of the effectiveness of prescription drug monitoring programsA study conducted in 2006 assessed the indirect and direct effects of PDMP on the supply and abuse of prescription medications: An indirect effect would be a reduction in abuse rates due to a smaller supply of drugs resulting from PDMP functions, which may decrease the supply of prescription medications. A direct effect would be a formal assessment on drug abuse.
At the time of the study, 20 states had operational PDMP, and 23 states were in the implementation process. States participating in the study used one of two general types of PDMP: Reactive PDMP generate reports when an authorized user makes a specific request; and
Dental.EliteCME.com Page 66
proactive PDMP, which generate reports automatically if the system detects suspicious activities. Some PDMP in the study monitored only schedule II medications, while others monitored schedule II-V medications.
Due to complications posed by the lack of uniformity in DPMP, the study confined its scope to schedule II medications with the highest
abuse potential. Data show the use of PDMP reduce the public supply of schedule II medications, which, in turn, reduces the risk of abuse for these prescription drugs. The study also found that proactive PDMP may be even more effective at reducing the supply of prescription pain medications.
TELEHEALTHThe Health Resources and Services Administration (HRSA) defines telehealth as:
“…the use of electronic information and telecommunications technologies to support long-distance clinical health care, patient and professional health-related education, public health, and health administration. Technologies include videoconferencing, the Internet, store-and-forward imaging, streaming media, and terrestrial and wireless communications.”
The growing use of technology in healthcare services brings significant positive effects for many patients, such as those living in rural areas with limited access to medical care. The types of services offered by telehealth seem endless, ranging from monitoring a patient’s blood sugar from a remote facility, to sending an x-ray of a patient’s lungs from a rural clinic to a teaching hospital, to training and education programs for rural physicians. Another critical function of telecommunications technology in healthcare is providing clinicians with a reliable method of communicating with patients located a significant distance away.
Physicians can provide patients with the option of a virtual appointment (using videoconferencing equipment) or meeting in person, at the provider’s office. Virtual appointments have additional value for patients in rural or remote areas who need to see a specialist. Patients can relay their medical histories and current symptoms verbally, while cameras and other remote monitoring equipment convey diagnostic information. Remote monitoring equipment is available for many types of vital sign measurement, including blood pressure, heart rate, oxygen saturation, blood glucose, and Prothrombin Time and International Normalized Ratio (PT/INR). Radiologic imaging performed at a remote or small clinic can be sent to a larger facility for a radiologist to read.
Physicians working from remote locations can increase their knowledge of countless topics through telecommunications. They can also complete continuing education requirements over the Internet, as e-course modules, or through live teleconferences, and participate in grand rounds and meetings far from their location through web broadcasts.
Benefits of telehealthTelehealth technology gives:
● Providers the ability to virtually visit and treat rural patients located a significant distance away.
● Patients the possibility of receiving medical services without travelling a prohibitively long distance.
● Healthcare options to rural patients who would otherwise have no access to medical specialists.
Using telecommunications for patient interactions promotes patient-centered care by encouraging direct communication between the patient and provider, allowing patients more autonomy and responsibility for managing their own care, but retaining contact and input from their prescriber. These factors contribute to greater health literacy, adherence to prescription drug instructions, and positive changes in patients’ lifestyle behaviors.
Telehealth has the potential to save the healthcare system significant amounts of time and money. Some savings are related to the reduced
travel time, expenses, and costs associated with the time patients are away from work for appointments or treatment. The population most in need of telehealth technology, and its potential savings, are patients with chronic disease. The Institute of Medicine (IOM) reports that 100 million Americans annually are diagnosed with chronic diseases, accounting for approximately 75% of healthcare spending.
The use of telehealth technology to contact patients is more effective and productive for medical treatment purposes than a telephone conversation, and can take place more frequently and conveniently than a traditional visit to the doctor’s office, particularly for incapacitated patients. Remote monitoring of vital signs and objective measurements provided by telehealth technology enables providers to assess patient health status more expeditiously, which can lead to reductions in the need for hospitalization, readmission, and length of hospital stays, along with improved adherence to medication directions, and increased patient satisfaction.
Challenges of telehealth technologyThere are several challenges that slow widespread use of telemedicine. One of the most important is money. Many providers cite reimbursement as a major barrier, as Medicare has low fee-for-service reimbursement rates, and reimbursement is limited to certain geographic areas and medical conditions. Also, many small or rural practices may not have the funding to invest in telemedicine equipment.
Regulatory challenges are another factor limiting the use of telemedicine. Many multistate facilities that would benefit from the use of telemedicine choose not to participate due to the prohibitively complex regulations required to use the system, and unresolved issues for healthcare facilities and providers licensed in multiple jurisdictions. Medical practice regulations can also discourage use; many medical boards require prescribers to see their patient in person at least once before telemedicine services can be administered. Federal regulations
can also impose barriers through the Social Security Act, by limiting the types of providers permitted to participate in the telemedicine system.
Healthcare providers must be willing to learn and use telehealth services before it can establish itself in mainstream healthcare. Some healthcare providers resist adopting telehealth services due to concerns it will affect patient care; others believe that technology has not evolved enough to safely support telemedicine. While there is some evidence to indicate telehealth technology is effective in managing patient care, data on this topic is lacking or inadequate. Conducting sound comprehensive research studies focused on the effects of telehealth for patient care and cost savings could provide strong support for widespread telehealth use.
Page 67 Dental.EliteCME.com

Telehealth guidelinesIn May 2014, the IOM published a set of guidelines (Core Operational Guidelines for Telehealth Services Involving Provider-Patient Interaction, or Core Guidelines) advocating the use of telehealth technology. The IOM developed the following administrative guidelines to direct the development of organizational policies and procedures for telehealth services and provide fundamental standards for healthcare communications using telecommunications networks:
● Facilities must follow their standard operating procedures and administrative regulations when providing telehealth services.
● Facilities should conduct quality assurance and performance management evaluations on a regular basis to ensure compliance with regulatory, facility, and accreditation requirements.
● Facilities must ensure compliance with local, state, and federal law, in regard to clinical decision making, consent, and protection of patient health information.
● Facilities must develop methods and processes to notify patients and providers of their rights, and evaluate complaints that arise when providing healthcare services through telecommunications.
● Facilities must respect requests from patients for in-person care, whenever possible.
● Before beginning telehealth services, the healthcare provider must convey to the patient, orally or in writing, all the following information and expectations regarding the telehealth encounter including:
○ How confidentiality will be managed, and any potential risks associated with telecommunication.
○ An emergency plan agreed to by the provider and patient. ○ How patient information will be stored and documented. ○ How failures in technology will be addressed. ○ How care will be coordinated with other healthcare
professionals. ○ Follow-up protocol detailing the schedule and mode of contact
between the patient and caregiver between appointments. ○ Why telehealth services may be terminated, and circumstances
that could require in-person care. ● Facilities in collaborative partnerships with other facilities
and providers must be cognizant of legal requirements and responsibilities specified in shared agreements and contracts.
Healthcare professionals who participate in telehealth services must adhere to the following guidelines:
● Healthcare professionals must comply with regulations imposed by regulatory and licensing agencies in both the provider’s and patient’s location, throughout the course of patient care.
● Providers must be aware that the use of telehealth services constitutes a provider-patient relationship, meaning evidence-based care standards apply to these patients.
● Providers must be educated, trained, and licensed in their field to provide telehealth services.
● Workplaces providing telehealth services must be located in a locked area that is secure, private, and reasonably soundproof. The presence of any other people in the provider’s or patient’s room must be approved by both the provider and patient.
The Core Guidelines established the following clinical guidelines for the care of patients through telehealth services:
● Healthcare professionals must ensure professional and clinical guidelines and standards are upheld in telehealth service encounters.
● Providers must provide verification of their qualifications and licensure to the patient, as well as provide the patient with a means of verifying this information with a trusted outside source.
● Patients must provide proof of identification, including their full name, birth date, and contact information, before using telehealth services.
● Healthcare professionals and organizations must document patient and provider locations to comply with local laws and manage emergency situations.
● The facility and healthcare professional must communicate expectations for additional consultation between appointments and emergency care management to the patient.
● Healthcare professionals must be familiar with any technological devices used in patient care during telehealth sessions.
● Healthcare professionals should be aware of health resources near the patient’s location, and familiar with the patient’s health insurance information.
● Patients located far from any sites with clinical staff must select an emergency contact, and the healthcare professional must develop an appropriate emergency procedure, before telehealth will provide services.
● The healthcare professional must be familiar with options for providing the patient with additional medication, in case of acute changes in the patient’s status.
● Healthcare providers must be sensitive to cultural issues that can arise during the provision of services.
The IOM report established the following technical guidelines to protect patient medical data when using telehealth technologies:
● Use methods of communication that have adequate security and privacy features.
● Use high quality video and audio with up-to-date security and device management software to record and transmit data.
● A contingency plan must be in place in the event of a security breach or technological failure, and must be communicated to the patient prior to the first telehealth appointment.
● Equipment used during the telehealth session must be in good working order, able to safely support the patient’s diagnostic needs while complying with all applicable laws, regulations, and codes.
● Providers must establish infection control policies related to the use of telehealth equipment, and comply with all local, state, and federal laws.
● Ensure equipment is safe and effective through regular maintenance.
● Devices must meet FDA requirements for safe and effective devices.
● Bandwidths used for telehealth services must be at least 384 kbps, with a resolution of at least 640 x 480 at 30 frames/second, to ensure an adequate connection.
● Videoconferencing software must have systems in place to ensure data transmission is available during periods with unstable or changing connectivity.
● All methods of transmitting data must be secure and use standard encryption.
● Mobile devices should be used as little as possible, and patient information stored on any mobile device must safeguard access with a password or equivalent security feature.
● Multi-factor authentication and activity timeouts should be used whenever possible to prevent unauthorized access.
● Videoconferencing software may only keep one session open at a time, meaning the first session users must log out before a second session can open. Session logs must be secure and accessible only by authorized personnel.
● Patient health information cannot be stored or backed up on cloud services.
● Healthcare professionals should inform patients about any plans to record patient information, how the data will be stored and protected, and how the patient can safely store his or her own copies of medical records.
● Recordings of telehealth sessions must be encrypted, stored in a secured location, and accessible only to authorized users.
Dental.EliteCME.com Page 68

Telehealth at the Department of Veterans Affairs The DVA implemented telehealth services very early, in an attempt to reduce costs, improve quality, and increase access to care. It is considered a national leader in the technology, and can provide a range of telehealth services, including video conferencing, teleradiology, mobile health, and secure messaging.
In 2011, more than 150 DVA medical centers and 750 outpatient clinics provided healthcare services for more than 380,000 patients. Approximately 37% of these patients were located in rural areas, with about 3% located in highly rural areas. According to estimates by the DVA, approximately 480,000 patients, or 9% of their veteran population, are projected to receive telehealth services in 2012
Findings from a DVA study that assessed treatment outcomes for patients using telehealth services showed approximately 53% of clinical patients and 25% of mental health patients experienced fewer “bed days” requiring telehealth services. The study noted savings in travel costs of $34.45 per video consultation, and found 86% of patients in the study expressed satisfaction with home telehealth programs.
Many patients in the DVA’s telehealth program use mental health services. In 2011, more than 55,000 patients were treated using DVA telemental health services. A review of mental health programs at the DVA shows patients receiving telemental care between 2006-2010 experienced a 25% decrease in hospitalization rates.
COnCLUSIOnThe role of technology in healthcare has grown enormously in recent history, with computerized healthcare systems increasingly responsible for managing patient information and elements of care. Despite barriers, widespread use of health information technology is growing due to its potential to improve efficiency in storing and accessing health information, which, in turn, can significantly improve patient care and treatment outcomes.
Healthcare providers and patients rely on information technology to facilitate patient care and communication. Managing information using
computerized systems that communicate and transfer information with other systems (interoperability) can assist providers in improving preventive care and managing complex medical conditions, and enable patients to take a more active role in healthcare decisions.
Because state laws vary in their regulation and enforcement of health information technology, employees must ensure their activities are in compliance with all applicable local, state, and federal laws.
References � HealthIT.gov. Basics of Health IT. Accessed May 5, 2014 at http://healthit.gov/patients-families/
basics-health-it. � Bush, George W. State of the Union Address. January 20, 2004. Accessed May 7, 2014 at http://
stateoftheunionaddress.org/2004-george-w-bush. � HealthIT.gov. About ONC. Accessed July 14, 2014 at http://healthit.gov/newsroom/about-onc. � HealthIT.gov. HITECH Program and Advisory Committees. Accessed May 22, 2014 at http://www.
healthit.gov/policy-researchers-implementers/hitech-programs-advisory-committees. � Fleet D. Health Information Management (HIM) History: Past to Current Day. Rasmussen College.
2010:Dec. Accessed May 3, 2014 at http://www.rasmussen.edu/degrees/health-sciences/blog/health-information-management-history/.
� HealthIT.gov. Learn EHR Basics. Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/learn-ehr-basics.
� Jamoom E, Beatty P, Bercovitz A, et al. (2012) Physician adoption of electronic health record systems: United States, 2011. NCHS data brief, no 98. Hyattsville, MD: National Center for Health Statistics, cited in HealthIT.gov. What is an Electronic Medical Record (EMR)? Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/electronic-medical-records-emr.
� Byrne CM et al. The Value from Investments in Health Information Technology at the U.S. Department of Veterans Affairs. Health Affairs. April 2010. 29(4):629-638. Accessed May 17, 2014 at http://content.healthaffairs.org/content/29/4/629.full.
� Finnell and Overhage (2010), cited in HealthIT.gov. Why Adopt EHRs? Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/why-adopt-ehrs.
� HealthIT.gov. Health Care Quality and Convenience. Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/health-care-quality-convenience.
� Jamoom, E., Patel, V., King, J., & Furukawa, M. National perceptions of ehr adoption: Barriers, impacts, and federal policies. National conference on health statistics. 2012: August. Accessed May 12, 2014 at http://www.cdc.gov/nchs/ppt/nchs2012/SS-03_JAMOOM.pdf.
� HealthIT.gov. Improved Diagnostics and Outcomes. Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/improved-diagnostics-patient-outcomes.
� Duffy L, et. al. Effects of electronic prescribing on the clinical practice of a family medicine residency. Fam Med. 2010;42(5):358-63. Accessed May 12, 2014 at http://www.stfm.org/fmhub/fm2010/May/R.%20Lamar358.pdf.
� Kern, L. et al. Electronic Health Records and Ambulatory Quality of Care. J Gen Intern Med. Apr 2013; 28(4): 496–503. Accessed May 12, 2014 at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3599037/.
� Bell, L. et al. Electronic Health Record–Based Decision Support to Improve Asthma Care: A Cluster-Randomized Trial. Pediatrics. 2010 Apr;125(4):e770-7. Accessed May 12, 2014 at http://pediatrics.aappublications.org/content/125/4/e770.long.
� Bell, B, Thornton, K. From promise to reality achieving the value of an EHR. Healthcare Financial Management, 2011: 65(2), 51-56. Accessed May 12, 2014 at http://www.hfma.org/Content.aspx?id=2902.
� HealthIT.gov. Improved Care Coordination. Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/improved-care-coordination.
� HealthIT.gov. Medical Practice Efficiencies and Cost Savings. Accessed May 12, 2014 at http://www.healthit.gov/providers-professionals/medical-practice-efficiencies-cost-savings.
� Shekelle P, Morton S, Keeler E. Costs and Benefits of Health Information Technology. AHRQ Evidence Reports: Evidence Reports/Technology Assessments, No. 132. Rockville MD: Agency for Healthcare Research and Quality. 2006:Apr. Accessed May 3, 2014 at http://www.ncbi.nlm.nih.gov/books/NBK37988/.
� HealthIT.gov. EHR Incentives and Certification. Accessed June 6, 2014 at http://www.healthit.gov/providers-professionals/ehr-incentives-certification.
� HealthIT.gov. Meaningful Use Definition and Objectives. Accessed June 6, 2014 at http://www.healthit.gov/providers-professionals/meaningful-use-definition-objectives.
� HealthIT.gov. REC History. Accessed May 21, 2014 at http://www.healthit.gov//providers-professionals/rec-history.
� HealthIT.gov. Certification Programs and Policy. Accessed June 1, 2014 at http://www.healthit.gov/policy-researchers-implementers/about-certification.
� HealthIT.gov. How to Implement EHRs. Accessed May 3, 2014 at http://www.healthit.gov/providers-professionals/ehr-implementation-steps.
� HealthIT.gov. How to Implement EHRs – Step 1: Assess Your Practice Readiness. Accessed June 6, 2014 at http://www.healthit.gov/providers-professionals/ehr-implementation-steps/step-1-assess-your-practice-readiness.
� HealthIT.gov. Certified Health IT Product List. Accessed May 22, 2014 at http://oncchpl.force.com/ehrcert?q=CHPL.
� Abood R. Pharmacy Practice and the Law. Sudbury, MA: Jones and Bartlett Publishers. 2012. � US Department of Health and Human Services. Summary of the HIPAA Security Rule. Accessed
May 24, 2014 at http://www.hhs.gov/ocr/privacy/hipaa/understanding/srsummary.html. � The Office of the National Coordinator for Health Information Technology. Guide to Privacy and
Security of Health Information. Accessed May 24, 2014 at http://www.healthit.gov/sites/default/files/pdf/privacy/privacy-and-security-guide-chapter-4.pdf.
� HealthIT.gov. CyberSecurity. Accessed May 24, 2014 at http://www.healthit.gov/providers-professionals/cybersecurity.
� eHealth Initiative. A Clinician’s Guide to Electronic Prescribing. October 2008. Accessed May 25, 2014 at http://www.aaos.org/research/committee/evidence/eprescribing-guide.pdf.
� US Department of Health and Human Services Health Information Technology and Quality Improvement. What are some of the benefits of e-prescribing? Accessed May 25, 2014 at http://www.hrsa.gov/healthit/toolbox/HealthITAdoptiontoolbox/ElectronicPrescribing/benefitsepres.html.
� Surescripts. E-prescribing of Controlled Substances – Readiness by State. June 2014. Accessed June 1, 2014 at http://surescripts.com/products-and-services/medication-network-services/e-prescribing-of-controlled-substances.
� Figge, H. Technology Support for Pain Management: e-Prescribing Controlled Substances. US Pharm. 2013;8(6):HS6-HS9. Accessed May 3, 2014 at http://www.uspharmacist.com/content/t/health_information_technology/c/41437/.
� Centers for Disease Control and Prevention. About Immunization Information Systems. May 2012. Accessed May 25, 2014 at http://www.cdc.gov/vaccines/programs/iis/about.html.
� Healthy People 2020. Summary of Objectives. Accessed June 4, 2014 at http://www.healthypeople.gov/2020/topicsobjectives2020/pdfs/Immunization.pdf.
� Committee on Practice and Ambulatory Medicine. Immunization Information Systems. Pediatrics 2006;118;1293. Accessed June 1, 2014 at http://pediatrics.aappublications.org/content/118/3/1293.full.pdf.
� Cortese M, et al. Leveraging State Immunization Information Systems to Measure Effectiveness of Rotavirus Vaccine. Pediatrics. December 2011. 128:6;e1474-e1481. Accessed June 2, 2014 at http://pediatrics.aappublications.org/content/128/6/e1474.short.
� Arzt, N. Guide to Immunization-related Information Data Exchange. June 2008. Accessed June 4, 2014 at http://www.hln.com/assets/pdf/IZ-DataX-Guide.pdf.
� Centers for Disease Control and Prevention. Survey of State Immunization Information System Legislation. June 2013. Accessed June 7, 2014 at http://www2a.cdc.gov/vaccines/iis/iissurvey/legislation-survey.asp.
� Centers for Disease Control and Prevention. Immunization Information Systems. May 2012. Accessed June 7, 2014 at http://www2.cdc.gov/vaccines/ed/iis/IIS101_Transcript.doc.
� Centers for Disease Control and Prevention. Appendix B – IIS Core Data Elements. December 2012. Accessed June 4, 2014 at http://www.cdc.gov/vaccines/programs/iis/func-stds-appxB.pdf.
� Centers for Disease Control and Prevention. Progress in Immunization Information Systems – United States, 2012. Morbidity and Mortality Weekly Report (MMWR). December 13, 2013 / 62(49);1005-1008. Accessed June 1, 2014 at http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6249a4.htm.
� Centers for Disease Control and Prevention. Immunization Information System Functional Standards, 2013-2017. December 2012. Accessed June 1, 2014 at http://www.cdc.gov/vaccines/programs/iis/func-stds.pdf.
� Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services. National All Schedules Prescription Electronic Reporting Act of 2005: A Review of Implementation of Existing State Controlled Substance Monitoring Programs. 2005. Accessed June 4, 2014 at http://www.dpt.samhsa.gov/doc/NASPER%2009142007.doc.
� Federation of State Medical Boards. Prescription Drug Monitoring Program State by State Overview. October 2013. Accessed June 4, 2014 at http://www.fsmb.org/pdf/GRPOL_pmp_overview_by_state.pdf.
Page 69 Dental.EliteCME.com

� 109th Congress of the United States of America. National All Schedules Prescription Electronic Reporting Act of 2005. January 4, 2005. Accessed June 4, 2014 at https://www.govtrack.us/congress/bills/109/hr1132/text.
� Drug Enforcement Administration Office of Diversion Control. State Prescription Drug Monitoring Programs Questions and Answers. October 2011. Accessed May 25, 2014 at http://www.deadiversion.usdoj.gov/faq/rx_monitor.htm.
� Alliance of States with Prescription Monitoring Programs. The Goals of Prescription Monitoring. October 1999. Accessed June 5, 2014 at http://www.pdmpassist.org/pdf/Prescription_Monitoring_Goals.pdf.
� Alaska Board of Pharmacy Prescription Monitoring Program. Training Guide for Alaska Practitioners and Pharmacists. May 2013. Accessed June 5, 2014 at http://www.alaskapdmp.com/Files/AK%20PDMP_Training%20Guide%20for%20AK%20Practitioners%20and%20Pharmacists.pdf.
� Simeone R, Holland L. An Evaluation of Prescription Drug Monitoring Programs. September 2006. Accessed June 4, 2014 at http://www.simeoneassociates.com/simeone3.pdf.
� Health Resources and Services Administration. Telehealth. 2012. Accessed June 5, 2014 at http://www.hrsa.gov/ruralhealth/about/telehealth/.
� University of Missouri School of Medicine. Missouri Telehealth Network General Information. March 2014. Accessed June 5, 2014 at http://medicine.missouri.edu/telehealth/general.html.
� Institute of Medicine. The Role of Telehealth in an Evolving Health Care Environment. 2014. Accessed June 5, 2014 at http://books.nap.edu/openbook.php?record_id=13466&page=R1.
� American Telemedicine Association. Core Operational Guidelines for Telehealth Services Involving Provider-Patient Interactions. May 2014. Accessed June 5, 2014 at http://www.americantelemed.org/docs/default-source/standards/core-operational-guidelines-for-telehealth-services.pdf?sfvrsn=2.
HEALTH InfORMATIOn TECHnOLOGy: THE fUTURE IS nOWfinal Examination Questions
Select the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116, or for faster service complete your test online at Dental.EliteCME.com.
1. Health information technology is:a. A way to store, manage, or share health information.b. The capability of multiple systems to exchange information
and be able to use the information that was exchanged.c. The computerized records of a patient’s medical chart from a
single practice.d. The health record controlled by the patient instead of the
medical provider.
2. _________________ contain the computerized records of the patient’s medical chart from a single practice or facility.a. Electronic health records.b. Electronic medical records.c. Personal health records. d. Personal medical records.
3. The process for certifying electronic health record technology was established by: a. The Institute of Medicine.b. The Office of the National Coordinator for Health Information
Technology.c. The Centers for Medicare and Medicaid Services.d. The Centers for Disease Control and Prevention.
4. What is the first step in implementing an electronic health record system in a small medical practice?a. Creating a plan.b. Selecting a certified electronic health record system.c. Assessment of current practices.d. Implementing the electronic health record system and training
personnel.
5. Which of the following is a physical safeguard required by the HIPAA Security Rule to ensure the protection of e-PHI?a. Leaving doors to offices with computers that store PHI
unlocked after hours.b. Removing physical hard drive locks to disable noisy alarms.c. Implementing policies and procedures that limit access and
specify proper use of workstations where e-PHI is accessed. d. Giving the janitor the key to an office containing computers
with e-PHI.
6. If patient information is transmitted over a wireless network, routers must be configured to operate in ____________ modes only.a. Unsecured.b. Easy to access.c. Encrypted.d. Private.
7. _______________ is defined by the Medicare Part D prescription drug program as the transmission, using electronic media, of prescription or prescription-related information between a prescriber, dispenser, pharmacy benefit manager, or health plan.a. Electronic health record.b. Electronic prescribing.c. Immunization information system.d. Telehealth.
8. _________________ are responsible for transmitting the e-prescription from the prescribers to the pharmacies.a. Prescribers.b. Intermediary e-prescribing networks.c. Pharmacies.d. E-prescribing software.
9. ___________________are defined as confidential, population-based, computerized databases that record all immunization doses administered by participating providers to persons residing within a given geopolitical area.a. Electronic health records.b. Immunization information systems.c. Electronic medical records. d. Telehealth systems.
10. ________________ authorized the Department of Health and Human Services to offer grants to states to establish and improve prescription drug monitoring programs. a. The NASPER Act.b. The HIPAA Act.c. The Institute of Medicine.d. The Centers for Disease Control and Prevention.
DFL07ITE18
Dental.EliteCME.com Page 70

Page 71 Dental.EliteCME.com
Chapter 4: Medical Emergencies in the Dental Office
4 CE Hours
By: Elite Staff
Learning objectives � Identify medical emergencies that may occur in a dental practice. � Recognize symptoms of specific medical conditions. � Describe warning signs that can occur before a medical
emergency. � Identify situations that should cause a delay in dental care.
� Describe how to position a patient who is experiencing a medical emergency.
� Define an office emergency action plan. � List essential equipment and medications that should be kept in an
in-office emergency kit.
IntroductionMedical emergencies happen every day. They come unexpectedly and are something that health care providers never like to experience. As health care professionals, how dental team members manage emergencies in their offices is crucial.
Because most instances catch people off guard, preparing ahead of time for an emergency is important. An established plan of action, emergency kit and game plan can help the dental office operate at a higher level of efficiency and care for patients in need.
In this course, we will discuss common emergencies that one might encounter when interacting with dental patients as well as steps that should be taken to ensure that all of the bases are covered, including responsibilities, safety measures, and accident prevention. From the moment your patient begins having health troubles until the paramedics arrive, there is a crucial window of time where you as the health care provider are responsible for their care and well-being.
Common emergencies that occur in a dental practice settingThere is a wide range of emergencies that dental professionals have experienced in their offices. Falls, head trauma, foreign objects in the eye and physical accidents may occur. However, we will limit this course to cover medical emergencies that are related to underlying health conditions that predispose people to experiencing medical problems. By understanding the signs and symptoms of an emergency as it is occurring, a dental professional can identify the proper method of care, intervention, and if at all possible, prevention of the episode.
Identifying the warning signs of these medical related emergencies is essential. By being aware of precursors and risks that make patients susceptible to emergencies, you can refer them to medical services in a timely manner. Unfortunately, even with thorough patient screening, if you work in an office long enough, you will probably have a patient experience one or more of the following medical emergencies when you work in a practice setting.
Cardiovascular arrest and chest painChest pain, cardiac arrest or other forms of tightness in the chest are cause for alarm. While some forms of discomfort may be nothing other than something such as GERD or anxiety, chest pain can be a sign of a serious health condition.
The discomfort may not necessarily be a sharp, painful feeling, but the person may instead feel as if his or her chest is being squeezed or under pressure. Chest pain results from the artery becoming narrow, blocking oxygenated blood from chest muscles and the heart. Quick response to heart attack symptoms is important for the life of your patient, because it’s estimated that approximately half of all heart attack patients will die in the first hours after their attack.
Classic heart attack symptoms usually include: ● Chest pain or pressure. ● Shortness of breath. ● Pain or numbness through the arms, shoulders, jaw, neck, back or
upper abdomen. ● Nausea. ● Perspiration.
Women may suffer from atypical heart attack symptoms that are unlike classic symptoms of chest pain experienced by men. They may not have any chest pain at all. Because of the differences in symptoms, women may take longer to diagnose as having a heart attack. It is estimated that women have as long as a 15-minute delay in seeking care because of the differences in symptoms [1].
Heart attack symptoms in female patients can include [2]: ● Upper body discomfort in the neck, back, jaw and shoulders. ● Fatigue and weakness due to decreased oxygen flow. ● Sleep disturbances from a partially blocked airway. ● Nausea or indigestion because the stomach and heart are sharing
similar nerve supplies. ● Shortness of breath even during a period of rest because of
decreased heart pumping. ● Anxiety, rapid heartbeat and perspiration.
Patients who are experiencing chest pain should be allowed to rest in any position they find comfortable, which is usually sitting upright. Based on the patient’s health history, determine whether he or she has a history of heart problems. If the patient has never experienced this type of feeling before, then EMS should be notified so the person can be taken to the hospital.
Pain that isn’t severe or elevated blood pressure may be angina pectoris instead of a myocardial infarction. If the pain continues through the left side of the body, such as the arm, or blood pressure falls sharply below what the patient’s normal baseline value is, then the patient is likely experiencing a heart attack.
If the patient is experiencing a heart attack, you should contact EMS immediately. The patient may be given a single dose of aspirin, and then a dose of nitroglycerine from an emergency kit can be administered every five minutes. Some first-time nitroglycerine users may experience low

Dental.EliteCME.com Page 72
blood pressure, so placing them in a supine position can help them relax. The patient may also be placed on a 50:50 nitrous oxide and oxygen delivery [3].
An unconscious patient experiencing a cardiovascular attack may exhibit spontaneous breathing. Check the patient’s vital signs and initiate CPR if necessary until the paramedics arrive and take over the situation.
Loss of consciousness, fainting, syncopePatients may faint for any number of reasons, and that may be the cause of more than half of all dental office emergencies. Drug use, seizures, anxiety or low blood pressure may be the cause. A drop in blood sugar may also be to blame, and we will address that separately. Fainting can sometimes be caught before it happens by being attentive to patients’ behaviors and vital signs. They may first feel dizzy because of a drop in blood pressure.
If anxiety is the cause of syncope, patients may need to have nitrous oxide during their procedure to help them relax. Some patients also require an anti-anxiety medication before their visit to be comfortable. Be sure to explain anything that patients have questions about so they understand the procedure and are not left with any surprises. Keeping patients comfortable is of key importance.
In some cases, patients who get up too quickly after reclining can experience syncope. It is important that all dental patients sit upright
for a minute or two before excusing them from the chair. Help patients to get up slowly, and caution them to not jolt up quickly from a sitting position.
While some patients prefer to sit with their head dropped between their knees, this may cause them to hurt themselves if they actually do faint. Instead, place the patient in a supine position to help increase blood flow to the brain and leave the person in the position for several minutes.
Most people typically become alert within one minute after fainting. If not, then there is most likely a more serious underlying condition. Even after regaining consciousness, the patient should be left in the supine position before slowly being placed in an upright position. Reschedule the patient’s treatment for another day.
Diabetic syncope/hypoglycemiaDiabetic syncope can occur when a patient experiences a drop in blood sugar levels and there is not enough glucose in the bloodstream to support metabolic cell functions. Most hypoglycemia will only occur in Type 1 diabetics (insulin dependent), but it can also occur in Type II diabetics who are taking hypoglycemic medication.
Before fainting, people may experience dizziness and confusion. They also may complain of a headache or behave strangely. It is also possible that in rare circumstances, a hypoglycemic diabetic may experience stroke- or seizure-like symptoms. All diabetic patients should be asked what their blood sugar levels were at their previous daily reading before having dental treatment performed to avoid a glycemic event during dental treatment.
The American Diabetes Association suggests the following blood sugar targets for diabetic adults who are not pregnant [4]:
● A1C of 7 percent or eAG 145 mg/dl. ● 70-130 mg/dl before eating a meal. ● Less than 180 mg/dl one to two hours before the next meal.
Some diabetics take insulin to lower a high level of blood sugar, and must take food at the time of their injection. This prevents their blood sugar level from becoming too low. Below 80 mg/dl is when
hypoglycemia occurs, and a rapid drop can bring levels as low as 20-30 mg/dl.
If Type 1 diabetics gives themselves an insulin injection but do not eat afterward, they may experience hypoglycemia and have a fainting episode. If the patient is still conscious, place him or her in a comfortable position and give the person something to eat that contains sugar, such as juice, soda or cake icing.
If the patient is unconscious, he or she should be placed in a supine position and be given an injection to raise the blood sugar. If unconscious, EMS should also be notified. It is important to not place anything in an unconscious patient’s mouth because choking or aspiration may occur.
Place the person in a supine position and he or she should typically regain consciousness within 60 seconds. If the patient has not regained consciousness within this window of time, then there is likely a serious underlying condition. Begin initiating basic life support steps as necessary, checking the patient’s airway, breathing and blood circulation. If the patient has extremely elevated blood pressure, the person may be experiencing a cardiovascular attack instead of diabetic syncope.
To avoid diabetic emergencies in the office, it is best to schedule these patients first thing in the morning, after they have eaten a full meal.
Diabetic ketosisKetosis occurs in diabetics when there isn’t enough insulin to move their blood sugars into cells. Fats and protein are used instead, and the result is a buildup of waste in the blood. As a result, blood sugar levels increase over a period of time. Predispositions like cardiovascular disease may make even a controlled diabetic likely to suffer from a rise in blood sugar.
Symptoms include: ● Fruity-scented breath.
● Thirst. ● Increased urination. ● Red, warm skin. ● Dehydration.
Because of advanced dehydration, diabetic ketosis can raise blood sugar levels to 300 mg/dl or higher, at which point the patient would become unconscious. Should this occur, EMS must be notified and basic life support initiated as needed based on vital signs.
Allergic reactionsAllergic reactions are situations that dental professionals are familiar with because many patients experience allergies to latex gloves. A patient’s reaction to allergens can range from a mild irritation to a severe, life-threatening condition.
Symptoms of an allergic reaction may include: ● Hives. ● Rash. ● Itchiness. ● Swelling. ● Intestinal distress.

Page 73 Dental.EliteCME.com
● Trouble breathing. ● Redness of the skin.
● Anaphylaxis. ● Loss of consciousness.
Anaphylaxis and loss of consciousnessSevere allergic emergencies that result in anaphylaxis (constriction of the airway and reduction in air flow) can cause a patient to lose consciousness and go into distress from the lack of oxygen. Oxygen should be administered using a positive-pressure device such as a
bag-valve-mask. This is a life-threatening condition; if the patient is beginning to exhibit problems breathing, then EMS should be notified and the patient should be given epinephrine immediately.
Mild allergiesA mild allergic reaction that results in minor symptoms typically only calls for the patient to be made comfortable and the delivery of an antihistamine from the emergency drug kit. The patient should be
watched to ensure that more serious symptoms do not become evident, and that vital signs are appropriate.
Examples of allergensThere are several everyday allergens found in a dental office, some of which may not be obvious. Patients with severe dietary restrictions, such as abstaining from gluten, nuts and dairy, may be exposed during a typical visit.
Below is a list of some allergens and where they can be found in the office:
● Latex – Found in gloves and some equipment. Most people develop contact dermatitis at the area of their skin that was affected.
● Local anesthesia – While rare, some patients may experience a serious reaction that causes trouble breathing, irregular pulse, and syncope.
● Egg protein – Used for general anesthesia delivery. While nitrous oxide does not contain egg protein, it can cause a severe reaction in some patients because of a similarity in the molecular compound.
● Fruit flavoring – Found in topical anesthetic.
● Gluten – Contained in some polishing pastes, toothpastes. ● Nuts – Found in polishing pastes and brand-specific fluorides. ● Milk protein – An ingredient in polishing paste, Recaldent, some
gum, and toothpastes. ● Clove oil – Used to make eugenol, which is found in temporary
dental cements.
Quick response is important for patients experiencing a severe allergic reaction to something they are sensitive to. An antihistamine can be administered to help block milder symptoms. Patients experiencing severe reactions must be given a dose of epinephrine from the emergency kit, delivered in their thigh or upper arm. Epinephrine is extremely effective because it prevents further histamine release and helps reverse histamine-caused conditions.
EMS must be notified if the patient is experiencing a severe allergic reaction, and the patient should be placed on oxygen as you monitor vital signs.
RESPIRATORy DISTRESS
Asthma attackAll asthmatic patients should be asked about their asthma-related conditions and flare-ups:
● When was their last attack? ● What seems to bring attacks on? ● Do they use an emergency inhaler? If so, where is it located?
Asthma affects people of all ages and causes a response that tightens the airways. Aerosols in the treatment area or fear of dental treatment may trigger an attack in some people. With patients who use an inhaler, have them place it out for easy access during their appointment in case of an attack.
Symptoms of an asthma attack include coughing, wheezing and trouble breathing. Patients may also feel pressure in their chest and
begin to appear cyanotic. Should your patient begin to experience these symptoms during treatment, put the person into an upright position. Examine the airway to check for swelling or obstruction and record the patient’s vitals.
Conscious patients can administer their own drugs (usually albuterol) through their inhaler, and then be given oxygen. If they recover in a timely manner, treatment can be continued.
If the patient has persistent symptoms and requires a second dose of albuterol, then treatment should be delayed until another day. Should the patient become unconscious, a bronchodilator and epinephrine should be delivered while also activating EMS.
ObstructionFrom time to time, foreign objects, such as dental supplies, equipment, appliances or restorations, may find their way into the patient’s airway. If obstruction is partial, the patient will begin coughing, but if obstruction is complete, the patient can become cyanotic and clasp the hands across the throat, which is the universal sign for choking. If the patient is able to speak, then obstruction is only partial. A complete
blockage can lead to a life-threatening situation if the object is not removed.
If a patient begins to choke, remove all foreign objects from the person’s mouth immediately. Allow the patient to forcefully cough, which will hopefully open the airway. If the person is unable to cough or gasp, indicating a completely blocked airway, then abdominal thrusts should be performed.
How to perform abdominal thrustsThe best way to dislodge an object from a patient’s airway is to administer abdominal thrusts (also known as the Heimlich Maneuver.) This is done when the patient has a completely blocked airway,
which prevents them from talking, gasping or coughing and helps to forcefully remove the object.
● Stand behind the patient.

Dental.EliteCME.com Page 74
● Wrap your arms around the person, making a fist and placing your thumb just above the navel, and grasping the fist with your other hand.
● Slowly make forceful thrusts, moving inward and upward just under the rib cage.
● Repeat the thrusts until the foreign object is dislodged.
If the patient is unconscious … ● Contact EMS. ● Lay the patient flat on the floor. ● Open the airway using a head-tilt, chin-lift maneuver. ● Perform a finger sweep if the object can be seen.
○ Never perform a blind finger sweep because this can cause the object to become lodged deeper.
● Perform appropriate steps of CPR based on the patient’s oxygen flow and pulse.
HyperventilationSevere anxiety or fear of the dentist can trigger hyperventilation, an increased respiratory rate that can be difficult for the patient to control. During the rapid breaths, excessive levels of carbon dioxide are released. Symptoms such as tingling and numbness may occur, and the patient may become apprehensive. If breaths continue to remain uncontrolled, spasms or fainting may occur. Thankfully, hyperventilation-induced syncope will typically result in a normal respiratory rate and the patient can regain consciousness.
Hyperventilation is the only emergency seen in the dental office where oxygen delivery is contraindicated. A paper bag for breathing should be avoided because this can cause elevated carbon dioxide levels. Communicate with the patient so that the person is aware of his or her breathing speed, and then verbally coach the person into slower breaths, one at a time. Under no circumstances should you deliver oxygen to the patient.
SeizuresIf a patient experiences a seizure in your office, it is most likely that the person has a medical history of seizures or epilepsy [5]. It is highly unlikely that someone without a history of seizures will experience one while in your care, but you should be prepared nonetheless.
Seizures are caused by erratic electrical activity in the brain. These electrical signals can spread over the brain and stimulate areas that
control other things, such as muscle control. Some patients can tell when they are about to experience a seizure, which is called an “aura.” The aura usually involves strange smells, sounds, sensations or hallucinations and can give them a chance to prepare for the seizing event. After seizing, patients will typically be fatigued or confused.
Types of seizuresGeneralizedThese seizures affect both sides of the brain and result in unconsciousness. Types of generalized seizures include tonic-clonic, myoclonic, absence and atonic. Tonic-clonic (also known as grand mal) are the most common. Patients who experience this type of seizure should be placed in a supine position and given a head-tilt, chin-lift to open the airway.
PartialPartial seizures are localized to a specific portion of the brain. Consciousness may or may not be lost. They do not last long, but may spread and cause a generalized seizure [6].
Non-epilepticThese seizures may resemble an epileptic seizure in appearance and symptoms. While difficult to identify, they differ from epileptic seizures in that non-epileptic seizures are not caused by electrical changes in the brain.
Status epilepticusRarely, seizures occur for a prolonged duration. This type of seizure describes an ongoing, continuous seizure.
Seizing patients should have the immediate area freed of equipment or foreign objects that they could come into contact with and possibly harm themselves. Move everything back out of the way and do not restrain the patient. All instruments and supplies must be removed from the patient’s mouth to prevent aspiration or trauma. Do not attempt to prop the patient’s mouth open in any way or give rescue breaths.
If a relative or caregiver has accompanied the patient to the office, call the person into the treatment area to find out whether the seizure is typical. Most of the time it is only necessary to monitor the patient and have someone drive him or her home, but if the seizure is severe, it will be necessary to call EMS.
Drug overdoseAccidental overdose may occur from prescription, over-the-counter, or illegal drug use. The patient’s body weight and age must be kept in mind when administering medication as well as a history of drug sensitivities.
Some ethnicities of people may be more susceptible to reactions from specific drugs. For example, Ethiopian and some North African children may experience deadly reactions to the drug codeine [7]. It is important to understand unique sensitivities to particular drugs to which specific groups are susceptible.
Always administer intravascular medication very slowly. Review the patient’s health history, including allergies, current medications and any recreational drug use, to avoid an adverse reaction.
● IV injected sedation drugs – Should always be administered slowly. Begin with only the lowest amount of drug possible to avoid accidentally delivering too high of a dose to the patient.
● Block injections – Use only an aspirating syringe when delivering the medication.
● Lidocaine – May cause central nervous system toxicity and seizures. Toxicity, unconsciousness and respiratory failure may occur [8]. There is no antidote available for Lidocaine.
● Nitrous oxide – Nausea and vomiting are typical symptoms of an N2O overdose [9]. If nitrous levels are too high and oxygen deprivation occurs, patients may enter into a deep level of sedation and possibly death.
● General sedation – Problems related to sedation are typically associated with a drug overdose, especially when three or more medications are used [10].
● Illegal and prescription drugs – There are approximately 100 drug overdose deaths each day in the U.S. [11]

Page 75 Dental.EliteCME.com
If needed, antidote medication from your office emergency supply kit may be administered to a patient. Monitor the person’s vital signs and airway, and contact EMS if the patient does not improve.
Bleeding disorderBlood is something that dental professionals deal with each day. When significant blood loss occurs, it can quickly become an emergency situation. Patients who hemorrhage should be positioned upright to reduce blood flow to the head. Most of the time, firm pressure and care to the local area of bleeding will be enough to control the blood flow.
Severe bleeding may be caused by: ● The patient taking blood thinners close to the time of their
treatment. ● Aspirin use. ● Trauma to orofacial blood vessels during surgical procedures.
● Surgical procedures, such as sinus lifts, dental implants and extractions.
Patients who take blood thinners should have treatment needs addressed with their physician. Do not instruct the patient to discontinue medication on his or her own. The person’s medical care provider should make this decision.
If the bleeding is caused by a traumatic injury from a fall (caused by loss of consciousness or accident), quickly apply pressure to the area. It is not likely that bleeding will be severe enough to need a tourniquet in a dental setting, but should you find that it does, apply steady pressure while EMS is notified.
StrokeWhen the brain experiences a blockage in blood flow, strokes are the result. Known as a cerebrovascular accident, strokes typically occur in adults with high blood pressure or hardening of the arteries caused by a buildup of plaque within them. Blood clots also are a common cause of stroke, and when the episode occurs, the symptoms are visible almost immediately. Most of the time these episodes are short-lived, but it is possible that they will continue for a lengthy period. Smaller strokes (transient ischemic attacks) are a sign that a more severe attack may be on its way.
Symptoms of stroke include: ● Trouble walking. ● Problems talking or understanding what others are saying. ● Partial paralysis of the face, arm or leg. ● Difficulty seeing with one or both eyes. ● Headache [12].
Contact EMS immediately if you suspect your patient is experiencing a stroke. To determine whether that is happening, act F.A.S.T. [13]:F: Face
Ask the person to smile. Does one side of the face droop?A: Arms
Ask the person to raise both arms. Does one drift downward?S: Speech
Ask the person to repeat a simple phrase. Is the speech slurred or strange?
T: TimeIf you observe any of these signs, call 911 immediately.
Lay the patient on his or her side and remove all instruments or other objects from the person’s mouth to prevent aspiration. If necessary, you may utilize the suction to prevent the patient from inhaling material or large quantities of saliva and blood. It is very common for the patient to lose control of some muscles or facial control, so work to keep the person comfortable and calm while waiting for paramedics.
Patient positions and emergency stepsThe first priority when positioning patients is to ensure their safety and comfort. Whether this is by placing them on their back so that blood flow can quickly reach their head or by relocating surrounding equipment to preventing a seizing patient from incurring accidental trauma, it’s important to act quickly. The position of patients and the
environment that they are kept in will depend on what type of medical emergency is happening.
Ultimately, you should keep the patient in a safe and comfortable position until the person can be handed off to the care of emergency medical personnel when they arrive.
Supine positionUnconscious patients should be placed back into the supine position. This is the position in the treatment chair where the head is reclined, with the legs slightly elevated so they are higher than the head. Placing a patient in the supine position will support blood flow to vital organs in the upper body, such as the brain and heart. By supporting blood
flow to the brain, the supine position helps prevent possible oxygen deficiency.
In medical emergencies, the prime concern should be that there is enough blood flow and oxygen to the brain [14]. This prevents irreversible brain damage, heart failure and other problems related to the deficiency of oxygenated blood flow.
Upright positionSome patients need to be placed in an upright position for comfort and care for their emergency. Examples include a patient who is experiencing an asthma attack and needs to have albuterol
administered, or a patient who has asphyxiated something during their treatment.
It’s now the “emergency CAB”There are three essential steps that should be taken after ensuring the patient’s positioning and comfort. These are assessing and assisting the patient’s circulation, airway, and breathing.
Until 2010, most health care providers called a memory aid for these actions the Emergency ABC’s because the guidelines called for
the sequence to be airway, breathing and circulation assessments. However, that year, American Heart Association guidelines changed this basic life support sequence by placing circulation before airway or breathing checks. So the memory aid became known as “CAB” instead of “ABC.”

Dental.EliteCME.com Page 76
When faced with an emergency situation, perhaps you might remember these guidelines for the three key actions and what to do by creating your own memory aid – for example, you need an “emergency CAB” (as in a taxi) for this person.
By mentally working through the three steps, you can prevent an important step from being missed and thereby possibly risking the patient’s health. If you were familiar with the emergency ABCs, remember that circulation is now considered key, and the “C” step should be performed before airway or breathing is assessed.
CirculationThe first step in the emergency CAB is circulation. Patients’ pulses should be checked; for adults, you can check the pulse along the wrist or neck (alongside of the thyroid cartilage.) Use two fingers next to one another to palpate the areas along the radial, brachial or carotid arteries. A child’s pulse may be easier felt beneath the upper arm.
When checking patients’ pulses, not only do you want to see what their rate per minute is, you should also note whether the rate is regular or irregular, and the quality, that is, if it is weak or strong. A deep pulse may be found in someone with elevated blood pressure, while weaker pulses are found in someone suffering from hypotension.
Normal resting heart rates based on age are [17]: ● Newborns 0 to 1 month old: 70-190 beats per minute. ● Infants 1 to 11 months old: 80-160 beats per minute. ● Children 1 to 2 years old: 80-130 beats per minute. ● Children 3 to 4 years old: 80-120 beats per minute. ● Children 5 to 6 years old: 75-115 beats per minute. ● Children 7 to 9 years old: 70-110 beats per minute. ● Children 10 years and older, and adults (including seniors): 60-100
beats per minute. ● Well-trained athletes: 40-60 beats per minute.
A pulse rate that is too rapid is referred to as tachycardia. Bradychardia is a pulse rate that is too slow.
If you have checked the patient’s circulation for longer than 10 seconds and are unable to detect a pulse, then you should begin performing chest compressions as you were trained in CPR or basic life support training. Compression rates and ratios with rescue breathing continue to be revised almost on an annual basis based on
the most recent guidelines of the American Heart Association, so be sure to keep your guides current.
If chest compressions are necessary, it is important to use proper hand positioning is used so that the compressions will be effective. To find the point where pressure should be administered, draw an imaginary line between the patient’s nipples and locate the lower portion of the sternum directly in the middle. Stack one hand over the other and place the heel of the lower hand over the area of compression.
Your torso should be positioned so that your arms are directly downward, straight into the patient’s chest, not at an angle. Use the heel of your hand to press straight downward approximately two inches, being careful to come back up enough for the chest to completely recoil.
Repeat chest compressions at a rate of at least 100 compressions per minute [18]. For a child, aim to compress their chest by one-third to one-half the depth of the chest, also at a rate of 100 compressions per minute. The goal of the firm compressions is to simulate a pumping heart so that oxygenated blood can flow through the circulatory system, preventing death.
Compression to breath ratios used in adult CPR are 30:2, meaning that 30 compressions are given with a short pause to administer 2 rescue breaths. For children and infants, a 15:2 ratio is used.
Because it is easy for the person administering chest compressions to become fatigued, two-person CPR can be used. This allows one person to give chest compressions and the other to deliver rescue breaths, and then the pair can switch after several cycles. CPR should be continued until rescue paramedics arrive and instruct you to allow them to take over.
AirwayConscious patients are able to let you know if they are having trouble breathing. Patients who are choking typically know how to use the universal choking sign, which is having one hand clasped around the throat. If the patient can cough, speak and breathe, then there is not a complete airway obstruction.
However, if the patient is experiencing anaphylaxis from an allergic reaction, the person may have a compressed airway, preventing adequate oxygen intake. Patients who are choking will need to have an abdominal thrust performed to help dislodge a foreign object.
The Red Cross recommends first delivering five back blows with the heel of your hand, followed by five abdominal thrusts [15]. This is done by standing behind the patient, wrapping your arms around the person, putting the thumb side of your fist just above the belly button, grasping the other hand around it and thrusting inward quickly five times. On a pregnant or obese person, perform the same procedure, but locate your hands higher up, over the abdomen.
If a patient is experiencing any signs of obstruction, quickly remove any equipment or materials, such as bite blocks, cotton rolls or other instruments. A finger sweep should not be performed unless there is visible debris that the clinician can directly see. If debris is visible, then removal can be attempted.
Should a patient become unconscious, the dental professional must ensure that the person’s airway is open. The head-tilt, chin-lift that is used in CPR administration does this. It is extremely important to do this carefully to avoid damage to the spinal cord if accidental trauma has occurred during the situation.
To open the airway, the practitioner should position him- or herself immediately behind the patient’s head. Gently place the thumbs on the outside of the patient’s jaw and the remaining fingers underneath, softly guiding the mandible forward and up. This opens soft tissues in the back of the mouth so that the airway can operate without anatomical blockage.
BreathingAs soon as the airway has been opened, breathing should be checked. A normal respiratory rate for a healthy adult is 12-20 breaths per
minute [16]. Children tend to breath much faster until they reach adolescence.
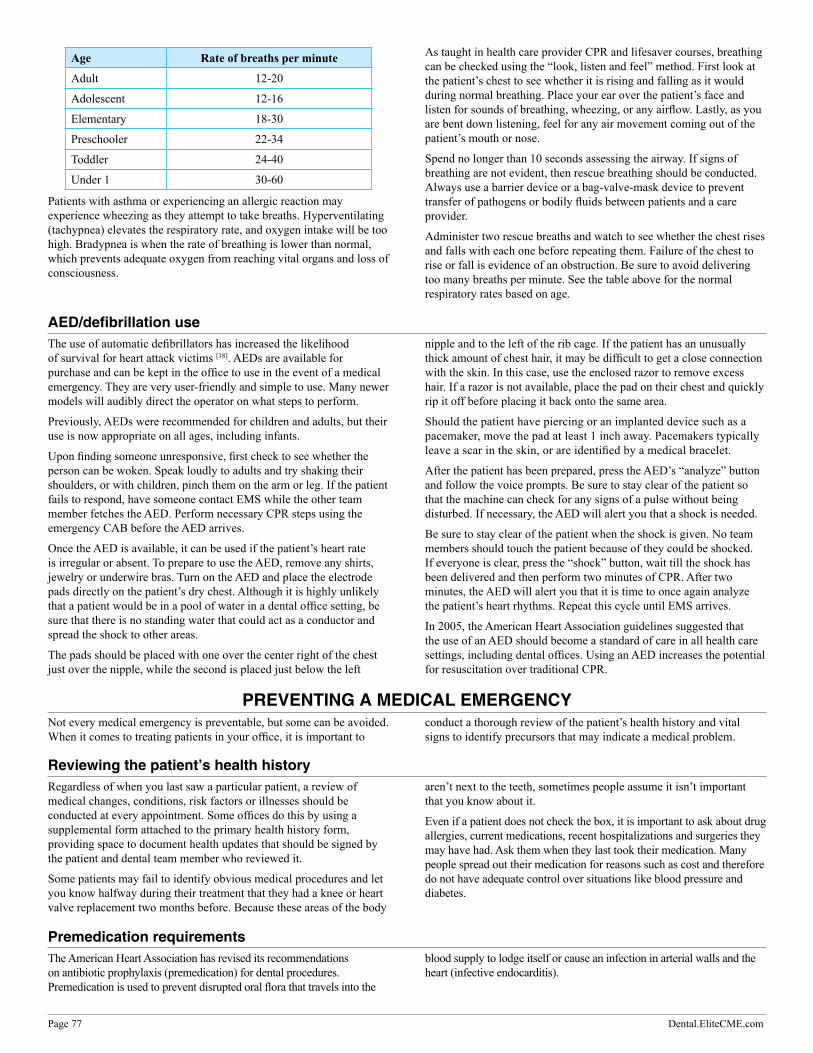
Page 77 Dental.EliteCME.com
Age Rate of breaths per minute
Adult 12-20
Adolescent 12-16
Elementary 18-30
Preschooler 22-34
Toddler 24-40
Under 1 30-60
Patients with asthma or experiencing an allergic reaction may experience wheezing as they attempt to take breaths. Hyperventilating (tachypnea) elevates the respiratory rate, and oxygen intake will be too high. Bradypnea is when the rate of breathing is lower than normal, which prevents adequate oxygen from reaching vital organs and loss of consciousness.
As taught in health care provider CPR and lifesaver courses, breathing can be checked using the “look, listen and feel” method. First look at the patient’s chest to see whether it is rising and falling as it would during normal breathing. Place your ear over the patient’s face and listen for sounds of breathing, wheezing, or any airflow. Lastly, as you are bent down listening, feel for any air movement coming out of the patient’s mouth or nose.
Spend no longer than 10 seconds assessing the airway. If signs of breathing are not evident, then rescue breathing should be conducted. Always use a barrier device or a bag-valve-mask device to prevent transfer of pathogens or bodily fluids between patients and a care provider.
Administer two rescue breaths and watch to see whether the chest rises and falls with each one before repeating them. Failure of the chest to rise or fall is evidence of an obstruction. Be sure to avoid delivering too many breaths per minute. See the table above for the normal respiratory rates based on age.
AED/defibrillation useThe use of automatic defibrillators has increased the likelihood of survival for heart attack victims [18]. AEDs are available for purchase and can be kept in the office to use in the event of a medical emergency. They are very user-friendly and simple to use. Many newer models will audibly direct the operator on what steps to perform.
Previously, AEDs were recommended for children and adults, but their use is now appropriate on all ages, including infants.
Upon finding someone unresponsive, first check to see whether the person can be woken. Speak loudly to adults and try shaking their shoulders, or with children, pinch them on the arm or leg. If the patient fails to respond, have someone contact EMS while the other team member fetches the AED. Perform necessary CPR steps using the emergency CAB before the AED arrives.
Once the AED is available, it can be used if the patient’s heart rate is irregular or absent. To prepare to use the AED, remove any shirts, jewelry or underwire bras. Turn on the AED and place the electrode pads directly on the patient’s dry chest. Although it is highly unlikely that a patient would be in a pool of water in a dental office setting, be sure that there is no standing water that could act as a conductor and spread the shock to other areas.
The pads should be placed with one over the center right of the chest just over the nipple, while the second is placed just below the left
nipple and to the left of the rib cage. If the patient has an unusually thick amount of chest hair, it may be difficult to get a close connection with the skin. In this case, use the enclosed razor to remove excess hair. If a razor is not available, place the pad on their chest and quickly rip it off before placing it back onto the same area.
Should the patient have piercing or an implanted device such as a pacemaker, move the pad at least 1 inch away. Pacemakers typically leave a scar in the skin, or are identified by a medical bracelet.
After the patient has been prepared, press the AED’s “analyze” button and follow the voice prompts. Be sure to stay clear of the patient so that the machine can check for any signs of a pulse without being disturbed. If necessary, the AED will alert you that a shock is needed.
Be sure to stay clear of the patient when the shock is given. No team members should touch the patient because of they could be shocked. If everyone is clear, press the “shock” button, wait till the shock has been delivered and then perform two minutes of CPR. After two minutes, the AED will alert you that it is time to once again analyze the patient’s heart rhythms. Repeat this cycle until EMS arrives.
In 2005, the American Heart Association guidelines suggested that the use of an AED should become a standard of care in all health care settings, including dental offices. Using an AED increases the potential for resuscitation over traditional CPR.
PREVEnTInG A MEDICAL EMERGEnCyNot every medical emergency is preventable, but some can be avoided. When it comes to treating patients in your office, it is important to
conduct a thorough review of the patient’s health history and vital signs to identify precursors that may indicate a medical problem.
Reviewing the patient’s health historyRegardless of when you last saw a particular patient, a review of medical changes, conditions, risk factors or illnesses should be conducted at every appointment. Some offices do this by using a supplemental form attached to the primary health history form, providing space to document health updates that should be signed by the patient and dental team member who reviewed it.
Some patients may fail to identify obvious medical procedures and let you know halfway during their treatment that they had a knee or heart valve replacement two months before. Because these areas of the body
aren’t next to the teeth, sometimes people assume it isn’t important that you know about it.
Even if a patient does not check the box, it is important to ask about drug allergies, current medications, recent hospitalizations and surgeries they may have had. Ask them when they last took their medication. Many people spread out their medication for reasons such as cost and therefore do not have adequate control over situations like blood pressure and diabetes.
Premedication requirementsThe American Heart Association has revised its recommendations on antibiotic prophylaxis (premedication) for dental procedures. Premedication is used to prevent disrupted oral flora that travels into the
blood supply to lodge itself or cause an infection in arterial walls and the heart (infective endocarditis).

Dental.EliteCME.com Page 78
According to the American Dental Association, the two types of patients that require premedication include people who:
● Are predisposed to infective endocarditis because of specific heart conditions.
● Have had joint replacement surgery and also found at risk for developing an infection near the prosthetic device.
It is recommended that people with the following conditions receive premedication if undergoing more invasive dental procedures:
● Artificial heart valves. ● History of IE. ● Heart transplant with a history of valve problems. ● Congenital heart problems that are unrepaired or have been
repaired and still have defects or prosthesis.
Recent science supports the idea that infective endocarditis is less likely to occur in dental patients than previously thought. In the past, patients were premedicated with antibiotics even during routine cleanings if they had a history of mitral valve prolapse, rheumatic heart disease, bicuspid valve disease, calcified aortic stenosis and congenital heart defects [19].
Although infective endocarditis should not result in an office emergency, it is worth mentioning because lack of prophylactic care during routine dental procedures can place your patient in a compromising health condition. The ADA suggests that, according to research, premedication may not actually prevent the patient’s susceptibility for IE, because regular daily habits such as flossing or brushing can expose the patient to the same conditions as preventive dental procedures.
Remind patients to take or bring their medicationsRemind patients who have a specific health condition that requires medications to bring them with them during your confirmation call. For instance, an asthmatic patient should be reminded to bring an inhaler to the appointment. Patients with a history of angina attacks
should also bring their nitroglycerin tablets with them. Remind all patients to take their medication as prescribed to ensure their safety during dental care.
Recording vital signsVital signs should be taken at each appointment. With routine vital sign documentation, abnormal readings that are not consistent with the patient’s history can easily be identified. If necessary, treatment can be deferred and medical referrals made.
The patient’s first visit will consist of a “baseline” reading, to which all future readings should be compared for consistency and health. Monitoring these signs at each visit can allow the dental professional to identify if a patient is at risk for a medical emergency.
Blood pressurePatients’ blood pressures should be recorded at every dental appointment, even if the patient was seen just the day before. Traditionally, blood pressure is taken using a standard blood pressure cuff and stethoscope, but many offices now prefer to use an electronic cuff. Unfortunately, with an electronic cuff, you may find some minor discrepancies in the readings and be unable to detect irregular heartbeats.
When taking patients’ blood pressure, have them sit upright with their legs uncrossed. Place the cuff on their right arm and ask them to not speak during the reading. This time can also be useful for monitoring their respiratory rate and quality of breaths as well as pulse. Be sure to use the proper-sized cuff; a cuff that is too loose, narrow or wide can result in a false reading.
If you are taking blood pressure using a stethoscope and traditional BP cuff, you should follow the following steps:
● Place the cuff approximately 1 inch above the bend on the inside of the elbow.
● Place the diaphragm of the stethoscope above the brachial artery, just below the BP cuff, and hold it in place.
● With the other hand, use the inflating bulb to begin filling the cuff. ● Continue filling the cuff 20-30mm of mercury past the point where
the patient’s pulse can no longer be heard or felt. ● Slowly release the air using the bulb valve until you hear the first
heartbeat in the stethoscope. This number on the dial is recorded as the systolic reading.
● Continue releasing air from the cuff until the sounds are no longer evident. The last sound is the diastolic reading.
● Release all remaining air from the cuff and remove it from the patient’s arm.
The American Heart Association has defined the following adult blood pressure categories:Category Systolic DiastolicNormal Under 120 and Under 80Hypertension 120-139 or 80-89High blood pressure, stage 1 140-159 or 90-99High blood pressure, stage 2 160 or over or 100 or overHypertensive crisis Over 180 or Over 110
In the event that blood pressure falls into the hypertensive crisis category, emergency care should be sought immediately. All patients whose blood pressure levels measure high enough to fall into stage 2 hypertension should have elective dental treatment delayed until after they receive medical care from their primary care physician [20].
Blood pressure guidelines for children vary greatly, based on age as well as height and weight percentiles, with healthy systolic ranges never exceeding a reading of 120. Even a slight elevation can be cause for alarm. For example, a 10-year-old female with a systolic reading of 134 and a 10-year-old male with a systolic reading of 135 would both be categorized as having stage 2 hypertension.
Patients who are anxious may experience higher blood pressure readings while they are at a dental office. If a reading is too elevated, the practitioner should wait five minutes and take a second reading. If the patient continues to have an elevated blood pressure, proper measures should be taken for the person’s dental care, and he or she should be referred to a medical provider. When in doubt, contact a patient’s doctor to determine whether the treatment can be completed.
Pulse and respiratory ratesRecord patients’ pulse after reviewing their health history. A good time to do this is immediately after recording their blood pressure. Use two fingers to palpate the wrist for at least 15 to 30 seconds. You can multiply the pulse by the appropriate amount of time needed for an average number of beats per minute. Document the quality of the pulse. Was it strong, weak, or normal? Regular or irregular?
Hold the area for 15 more seconds as you also monitor the respiratory rate. Many people will alter their breathing if they are consciously aware that someone is checking it. By taking the pulse and respiratory rates consecutively and without telling the patient, you can record their normal breath rate. Make a note of the quality of breaths. Are they slow, normal or fast? Normal, shallow or deep?

Page 79 Dental.EliteCME.com
Pulse oximeter usePulse oximetry use during sedation services can detect conditions such as hypoxemia when no other visible signs are present. They also effectively monitor oxygen levels in dental patients of all ages. This can prevent a low oxygen uptake and possible medical emergency that might not otherwise be detected during treatment.
Using a pulse oximeter is typically optional, depending on the type of sedation services being used, but choosing to invest in this type of equipment can protect both patients’ health and the doctor from facing liabilities.
TemperatureMost dental offices do not record patients’ temperatures on a routine basis. However, doing so can help identify whether they are experiencing any type of underlying viral or bacterial infection. Taking a patient’s temperature can be done conjunctively with recording their blood pressure, thus not adding any additional chair time to the scheduled appointment.
The average temperature for healthy individuals is 98.6 degrees Fahrenheit (37.5 degrees Centigrade). A low-grade fever at a temperature that exceeds 99.6 degrees Fahrenheit is a sign that the patient is battling some type of infection.
Health care providers typically record temperatures using a tympanic/temporal thermometer, ear canal thermometer, or an oral thermometer. If an oral thermometer is used, you will also need to have disposable covers. Temporal thermometers are easily cleaned, making them more convenient, and they give readings that are consistent with oral thermometers. Mercury oral thermometers are now considered unsafe for use because accidental breakage of the glass could expose patients to toxic mercury inside of the thermometer.
nitrous oxideWhen patients are using nitrous oxide, never leave them unattended!
There are several side effects that can occur very quickly when a patient is on nitrous oxide during a routine dental procedure. Nausea may cause vomiting and a risk for the patient to aspirate some of the debris.
If a patient has a history of vomiting during a procedure using N2O, be sure that the nitrous is being administered slowly, in low concentrations. Nausea is more likely if the patient did not have a meal or consumed too heavy of a meal.
An oxygen fail-safe alarm can alert the practitioner when oxygen supply levels are depleted, eliminating the risk of a patient emergency from overexposure to nitrous oxide.
Only a dentist can administer nitrous oxide. Other staff members, such as a hygienist or dental assistant, are only legally able to monitor the patient after the dentist has administered the drug. They can, however, lower the concentration of nitrous oxide during the appointment, placing the patient on a higher volume of oxygen.
Leaving the patient and stepping out of the room or becoming so distracted that the patient is being poorly monitored (or not monitored at all) can compromise the health of the patient, risking oversedation, loss of consciousness and physical harm.
Learn how to recognize an emergencyThe earlier a medical emergency is recognized, the more time the dental team has to respond, call for emergency medical care and begin addressing the patient’s immediate needs, such as performing basic life support.
Visible physical symptoms, such as sweating, paleness, fatigue, change in respiratory rate or vomiting, should be addressed as soon as they are
evident. Some symptoms, such as nausea, chest pain, elevated blood pressure or irregular pulse, may not be evident unless the patient is asked or special equipment is used. This is why vital signs should be recorded at the beginning of the appointment, and repeated within five minutes if the readings are irregular.
Make note of existing health conditionsIt is essential that patients’ health history is updated at every visit and checked for possible health conditions or allergies that the person has experienced in the past. If you know a patient had a heart attack 11 years ago, ask the person when was the last time he or she saw the cardiologist.
Perhaps the patient is an epileptic. When was the last seizure? How severe was it, and what kind of care is the person getting from a medical doctor? Make note of patients who are at risk for medical emergencies, because they will typically be more likely to experience one in your office than an overall healthy patient with no medical concerns.
All too often, dental practitioners fall into a repetitive habit of routine. Charts do not get checked, and patients are placed at an increased risk for problems, such as accidentally forgetting to use nitrile gloves on a patient who has a latex allergy.
HIPAA confidentiality restricts what type of information can be placed on the outside of a patient’s chart. It may be useful to put a sticker or red star on the outside of paper charts for patients who have significant allergies or medical conditions.
Electronic charting is very convenient, because most practice management software programs will send you a popup alert on medical conditions as soon as you open the patient’s file.
Consult with the patient’s physician and a drug reference bookWhen in doubt, ask for a medical clearance from patients’ primary care physician before beginning dental treatment. Notify the doctor if you record any abnormal vital signs, such as stage II hypertension, and get a confirmation from the doctor’s office on what treatment restrictions the patient has been placed on, if any.
Consult with a drug reference book to note medications and dosages the patient is taking and what they are being taken for. Certain medications have a contraindication for other medications, such as birth control pills or NSAIDs.

Dental.EliteCME.com Page 80
Check to see that patients have taken all of their medications for the day and are not spreading out the dosages for some reason. Inappropriate intake of medications can lead to resistance or ill management of their medical conditions.
Ask patients for a current list of medications and dosages at each appointment. Use the office’s physician’s drug reference handbook to note any new medications, side effects and dosages. Ask whether patients are taking any herbal medications or supplements.
Take actionAs soon as you realize a patient is experiencing an emergency, all treatment should be stopped. If the situation appears to be severe, then follow your office’s emergency action plan. We will discuss emergency
action plans in more detail a little further along in this course. Make the patient comfortable, record vital signs, call EMS, and enact basic life support if necessary.
EMERGEnCy kITDental offices should have an emergency medical kit that contains equipment to perform basic life support (BLS), emergency drugs and a defibrillator. All team members should know the location of this emergency kit and how to use all of the included equipment or medication should an emergency arise.
Because medications expire, it is important to routinely examine the emergency kit and document the contents as well as expiration dates. A log sheet can be part of the office’s monthly checklist, and the responsible staff member should check all of the contents each month to be sure there are no leaks, damaged materials, and an ample supply of emergency drugs.
Kits can be purchased from medical supply companies or can be compiled by your office in separate pieces. Your state dental board may require specific contents, so be sure to check and ensure that you comply with local safety regulations.
Hopefully, your office will never need to use the emergency medical kit. You can expect to have to discard expired, unused medication and supplies as you keep the contents up-to-date. It is very important that you do not keep old, expired drugs in your emergency kit. As drugs expire, they lose their effectiveness, and an emergency situation can become more complicated by not knowing what medical measures have been effective.
Most kits will fit nicely in a very large container, such as a tackle box. A list or chart of the contents should be inside the box and include their proper usage and dosages. Laminating the chart and keeping it in the top of the kit will ensure that it is not misplaced or overlooked when it is most needed. Some people also find it useful to tape it to the lid of the kit.
kit contentsAED/external defibrillator. This can be kept adjacent to the emergency kit location because most AEDs are large, bulky or may be mounted on the wall.
Oxygen delivery device to use during CPR. This may be a bag-mask-valve device, resuscitation pocket mask or other disposable CPR barrier. Barriers prevent practitioners from cross-contaminating bodily fluids between the patient and themselves, and valve-type devices increase the uptake of air by the patient.
A nasal cannula along with a portable E cylinder or a nitrous oxide nasal hood with 100 percent oxygen flow can provide a good source
of oxygen when the patient is conscious and positive pressure is not needed. Place the patient on minimum flow rate of 6 liters per minute. Oxygen is administered in almost every medical emergency other than hyperventilation.
Sphygmomanometer and stethoscope. Although these pieces of equipment should be used routinely in the dental office, having a spare in the emergency kit that is reserved only for medical emergencies will prevent the risk or not being able to locate the device during an emergency.
Essential emergency drugsEpinephrine – Perhaps the most important medication in your entire emergency kit, epinephrine is useful for emergencies with allergic reactions, respiratory distress and cardiovascular emergencies. This injectable drug is easily delivered through a preloaded syringe or pen-type device. Most people with severe food allergies will keep a device such as an EpiPen with them in the event of an exposure. Epinephrine should be given to asthmatic patients who do not respond to albuterol during an attack.
Diphenhydramine/histamine-blocker – Also for use with allergic reactions, histamine blockers may be preferred in patients with a milder reaction. Injectable antihistamines are for more serious reactions (such as when a patient is experiencing anaphylaxis); orally administered antihistamines are appropriate for mild allergic responses.
Sugar/glucose – This is for diabetic patients who are experiencing hypoglycemia from an insulin imbalance. This can be in the form of juice, cake icing or soda and should be given to a patient only if the person is conscious. A tube of icing can easily be kept in the
emergency box; something such as juice would need to be kept in a separate refrigerator.
Nitroglycerine – In the form of a spray or tablet, nitroglycerine is used on patients who are experiencing sharp chest pain and have a history of angina attacks. Patients who take nitroglycerine should bring their medication with them to their appointment, but people with undiagnosed conditions may experience symptoms of a heart attack and need to have nitroglycerine administered to them. The dosage can be given every five minutes with a total of three dosages. Most nitroglycerine has a shelf life of only three months after it has been opened.
Aspirin – A minimal, single dose of 162 mg aspirin should be given to heart attack victims. It can also be accompanied by nitroglycerine. Pills should be chewed and then swallowed by the patient.
Bronchodilator/Albuterol – This is used when asthmatic patients experience an asthma attack or exhibit symptoms of anaphylaxis. It is the first medicine of choice for patients who are experiencing bronchospasm.
Additional emergency medications and equipmentIn addition to essential medications, if dental offices desire, they may use other emergency medications. This can come in useful if the office
is rurally located and expects a longer response from EMS in the event 911 is called.

Page 81 Dental.EliteCME.com
Some of these drugs are optional, while others are required by state regulating authorities based on procedures performed in your office. For instance, if your office performs general anesthesia or sedative services, then you may be required to keep specific reversal drugs on hand for easy access should the patient become over-sedated.
Airway devices – If your dentist has advanced training in the use of devices such as a laryngoscope or endotracheal tube, these devices can come in useful.
Hydrocortisone – A corticosteroid, hydrocortisone used for suppressing anaphylaxis. Unfortunately, the drug has a slow onset, sometimes taking as long as an hour to become effective. This medication can also be used to manage an adrenal crisis.
Naloxone – This is used to reverse respiratory depression associated with opioids. When opioids are used for sedation, then naloxone is the drug of choice for emergencies because it is a specific opioid antagonist. Naloxone can also be used when there is an overdose of specific narcotics (Demerol, morphine) and help reverse any decreased consciousness associated with their use.
Flumazenil – This also is used for reversing respiratory sedation and used to counteract effects from benzodiazepine because it is a specific benzodiazepine antagonist. This medicine is also used for overdose
situations when other narcotics, such as Valium or Versed, have been used.
Benzodiazepine – In a water-soluble form, dentists can administer benzodiazepine (midazolam or lorazepam) intramuscularly to patients experiencing status epilepticus [21]. Traditionally, this drug is administered through venipuncture, so an alternative form should be used if making it part of your office’s emergency kit.
Glucagon – Injectable glucagon may be used in the event of a hypoglycemic emergency when sugar (glucose) cannot be given orally to a patient who is unconscious. It must be delivered intravenously and is not for intramuscular use.
Morphine – This is used to treat patients in pain during a heart attack. Use caution when administering this medication to the elderly. Most dental offices would need to deliver this intramuscularly, but intravenous is the method of delivery.
Ephedrine – For management of severe hypotension, ephedrine has similar effects as epinephrine. Ephedrine has a longer duration than epinephrine and can last up to 1.5 hours.
Atropine – Also for the management of hypotension, atropine is appropriate for use when bradycardia is also present.
Team preparednessFormal steps must be taken to properly train the office team members on how to respond to an emergency. Doing so not only protects patients, but also helps provide legal protection for doctors and their
practice when paper documentation shows training has been performed on a consistent basis.
Appropriate formal training of all staff membersComprehensive training in health care provider CPR and basic life support may be best achieved when the entire team trains together. Most health care provider CPR is typically active for two years and can be completed through Red Cross or American Heart Association certified providers. Doing this on a frequent basis will maintain all staff member’s certifications and ensure that the office is also fulfilling legal obligations. It also serves as a refresher to team members who already know how to practice life support. Proper documentation should be recorded in a central location.
No matter what a staff member’s role is in the office, all team members are obligated to receive basic life support and CPR training. Each person will play a key role in an emergency action plan and should serve as backup to team members who are not present or unable to perform emergency actions for some reason.
Formal training will enable staff members to perform one- or two-person CPR on both children and adults. The course will also include
instructions on the use of an AED and other emergency equipment used during CPR.
Separate office training should also prepare all team members to know: ● The location and contents of the emergency medical kit. ● How to administer drugs from the emergency kit if needed. ● How to use the emergency kit, such as bag-valve-mask equipment. ● How to properly record vital signs, such as pulse, blood pressure,
temperature and respiratory rates. ● The emergency action plan for the office. ● Where emergency oxygen equipment is located and how it is used. ● Which team members hold specific responsibilities in the action
plan. ● When to call paramedics or other emergency numbers, such as an
oral surgeon, local pharmacy and poison control. ● First aid, such as the care of bleeding, burns and falls.
Establish an office emergency action planPerhaps the most important part of managing medical emergencies in the dental office is your office emergency action plan. This plan should be provided in writing to all employees and reviewed on a routine basis so all parties understand their roles and responsibilities when responding to an emergency. A written team plan can prevent key areas from being overlooked and help the office respond quickly and appropriately based on the circumstances that are occurring.
● Have a code word or phrase.Using a code word or phrase can help alert all of the team members to the situation without startling other patients or people in the waiting room. The word or phrase should sound like something that wouldn’t worry anyone, but instantly connects with the team members. For example, the dentist does not have any sisters, but an emergency phrase could be “Tell Dr. Smith that his sister is calling.” Hearing this phrase will alert the doctor as well as the staff that there is an emergency and their attention is needed
immediately. Other words might sound silly but still be effective, such as “apple pie” or “sunburn.”
● Act quickly.The faster you respond to a medical emergency, the better. In instances where an AED needs to be used, it has been shown that every minute that passes before artificial defibrillation decreases the patient’s survival rate by as high as 10 percent. Good team communication and an emergency plan that has been enacted, practiced and known by all of the team members can help decrease response time to the patient’s needs.
● Have a play-by-play planned ahead.Written action plans for your emergency routine are essential. They ensure that the entire office knows emergency protocol, which member is responsible for what, and helps emergencies be addressed quicker. When you are preparing your emergency action plan, be sure to include these specific steps:
Dental.EliteCME.com Page 82
○ Recognize.Is your patient experiencing a medical emergency? What symptoms or signs cause you to believe that is happening? At what point should the team members alert the doctor or other staff that the emergency plan needs to be enacted? A vital communication step that is taught in health care provider CPR is having one team member point to another one and say “You dial 911.” This prevents the call from being delayed and mass confusion as a result of multiple people thinking that someone has already contacted EMS.
○ Communicate.What will your emergency phrase or keyword be? All team members need to stop whatever they are doing when they hear this phrase. The doctor will come to the area where the patient is located and alert the team members if it is appropriate to alert EMS in addition to already established emergency protocols. Everyone should know where emergency equipment is located and where a phone is to dial 911.
○ Act.While waiting for the response of your other team members, place the patient in the proper position, including administering oxygen, if appropriate. If the patient has brought medication along, such as an inhaler or nitroglycerine, locate and administer it immediately. All team members should then complete their assigned roles in the emergency action plan, which will be explained shortly. Contact EMS and alert it of the situation as well as any family members who have accompanied the patient to the appointment. If the medical emergency is one that the patient has experienced before, the family member’s input is essential.
One member should bring the emergency medical kit as well as an AED if available. Assess the patient’s vital signs and begin basic life support or CPR as necessary, providing backup to other team members when needed. Traditional CPR can be very strenuous to a health care provider, so two-man CPR is a good way to prevent fatigue.
Assign roles to specific staff members ● Team member No. 1.
○ Recognize whether the patient is experiencing an emergency. ○ If you suspect a possible emergency, use the code word or
phrase to alert the doctor and other staff. ○ Turn off all nitrous oxide and give the patient oxygen unless
the person is hyperventilating. ○ Administer the patient’s medicine if there is one available,
such as an inhaler. ○ Place the patient in the appropriate position, supine or upright,
depending on symptoms. Check vitals. ○ Ask the patient whether he or she is OK, using a loud voice.
If the patient appears unconscious, attempt to wake the person by shaking him or her firmly by the shoulders. Children can be pinched or slapped on the arm.
○ Inform team member No. 2 to dial 911 by looking at the person directly and saying, “You – call 911!”
○ Inform a team member to bring an emergency medical kit and AED.
○ Administer CPR and basic life support as needed until an emergency medical service team arrives.
● Team member No. 2. ○ Respond to team member No. 1’s alarm.
○ Determine along with team member No. 1 whether it is appropriate to contact EMS. If so, verbally confirm that you are going to call 911 and then go directly to the phone and dial 911. If possible, dial from a phone that is not at the reception desk. Be sure to include your office address and the situation you suspect the patient is experiencing. It can help to keep a business card taped to your phone or desk, because the confusion during an emergency could cause a lapse in memory for the office address.
○ Stay on the phone with 911 until EMS arrives. Relay any information to 911 that other team members present to you.
● Team member No. 3. ○ Respond to team member No. 1’s alarm by immediately
fetching the emergency medical kit and AED. Bring these supplies to the area where the patient is located.
○ Assist team member No. 1 in recording vitals. ○ Prepare AED, if necessary. ○ Prepare and administer emergency drugs as appropriate. ○ Practice two-rescuer CPR as appropriate until EMS arrives.
Switch periodically with team member No. 1 to prevent rescuer fatigue.
Practice makes perfectPractice your emergency plan on a regular basis. Twice per year may be adequate. Always have the entire team practice the plan together any time a new team member is added to the staff.
Allowing input and questions can allow for necessary alterations or clarification when needed so that all are confident in their role. When
you practice an emergency, have team members rotate roles and identify areas that may have been missed or done differently.
Being overly prepared by multiple mock situations can prevent confusion and improve the team member’s comfort level should an actual emergency take place. Panic by team members during an emergency does not help the patient.
Cross-trainIt is important that more than one person be trained for each rescuer role. In addition, a team member should be cross-trained so he or she can fulfill two or three different roles if needed. As a result, the office team can be more efficient and remind other members if a step is being missed.
Cross-training also is important when a specific team member is out or unavailable. This is yet another reason why all team members should be CPR certified, even if they are never in the actual treatment area with the patient.

Page 83 Dental.EliteCME.com
DOCUMEnTATIOn Of A PATIEnT EMERGEnCyDetailed record keeping is essential when a patient has experienced a medical emergency in your office. From the moment the emergency symptoms are observed to when the patient is transferred to EMS
personnel, each step of the way should be carefully outlined in your treatment notes.
Assess your team’s response Within a day or two of an emergency in the dental office, conduct a team assessment of the emergency action plan. In this assessment you should document all involved team members and their roles in the situation. Ask for the team’s input on each person’s roles in the care of the patient, allowing an opportunity to determine what changes may be needed if another medical emergency should arise.
Key points to evaluate should include: ● What signs pointed to an emergency? ● Who first recognized those signs? ● Did the patient’s health history indicate an increased likelihood to
experience a medical problem? ● What alerts put in place helped detect the emergency, such as notes
or electronic record warnings? ● Were there any signals that were missed that could have been
avoided? ● Were the patient’s vital signs recorded? Were they normal? ● What was the initial reaction to the situation by the involved team
members? ● Could other preventive steps have been taken that could have
avoided the emergency? ● Did the team follow the emergency action plan as roles were
assigned? ● Do these roles need to be altered? ● When was the emergency kit accessed and were the contents
appropriate for the situation? ● At what point was EMS notified, and how did you decide it was
time to call 911?
A team assessment is not an opportunity for judgment or badgering of other team members. It is a serious step that should be taken for the office to efficiently respond to any situations that may arise in the future.
Team members should be given a chance to assess the experience and provide input on ways to be more efficient in the future with their personal responsibilities.
Because dental care providers are licensed health care workers, there is some legal liability in the way they respond to medical emergencies.
All team members should have current health care provider CPR certification and know their roles in the office emergency plan. This plan should be reviewed on a regular basis, especially when new staff members join the office or job roles change.
Ultimately, all liability rests on the shoulders of the supervising dentist. However, licenses and certifications to other staff members, such as the hygienist and assistant, are also at risk, placing an added responsibility on those team members.
Emergency care that is reasonable and prudent is at the dentist’s discretion. All team members should know what the dentist’s plan of action involve, so the office can act as effectively and quickly as possible. Simply being ignorant of the law, responsibilities, or a lack of training are a liability for all dental professionals, no matter what their role. Until the emergency response team arrives, the sole responsibility of the patient’s condition lies under the supervision of the dental team.
Your patients and their families expect that you will provide expert medical care that ensures their safety and personal interests. While it can be a scary situation to help a patient during an emergency, remaining calm throughout the entire situation and thinking through the proper steps can help you make good choices that improve the safety of your patient.
Proper precautions should be taken to eliminate medical episodes while the patient is under your care. Up-to-date medical records, health history screenings and vital signs should be recorded at every single appointment. Neglecting to ask patients about medications they are taking, recording their blood pressure, pulse or documenting blood sugar levels can place both patients and dental team members in a dangerous situation.
The best way to prepare for a medical emergency is to make emergency training part of your annual continuing education for the entire office. Many times we remember essential parts of our responsibilities and emergency plan, but annual refreshers can bring to mind key components that are easy to forget.
Undergoing emergency training as a complete office is an effective way to make sure that all staff members are on the same page and understand the weight of their personal responsibilities.
References 1. Concannon, T.; Griffith, J.; Kent, D.; Normand, S,; Newhouse, J; Atkins, J.; Beshansky, J.; Selker,
H.; Elapsed time in emergency medical services for patients with cardiac complaints: are some patients at greater risk for delay?; American Heart Association; web version available 7/29/13 at http://circoutcomes.ahajournals.org/content/2/1/9.full
2. Dolgen, E.; 6 often-missed heart attack symptoms in women.; Huffington Post; Mar 6, 2013. 3. Homayounfar, SH.; Broomandi, SH.; Evaluation of entonox as an analgesic for relief of pain in
patients with acute myocardial infarction.; Iran Heart J2006;7(3):16-19. 4. Checking your blood glucose; American Diabetes Association; Jul 7, 2013. 5. Bryan, RB; Sullivan, SM; Management of dental patients with seizure disorders.; Dent Clin North
Am 2006;50 (4):607-623, vii. 6. Types of Seizures; Epilepsy foundation; Jul 24, 2013; www.epilepsyfoundation.org7. FDA drug safety communication: codeine use in certain children after tonsillectomy and/or
adenoidectomy may lead to rare, but life-threatening adverse events or death; Feb 20, 2013; www.fda.gov/drugs/drugsafety/ucm313631.htm
8. Sherry, J.; Child deaths from anesthesia; RDH Magazine; Vol 29. Issue 2. 9. Guideline on use of nitrous oxide for pediatric dental patients; Council on Clinical Affairs; 2013;
www.aapd.org/media/policies_guidelines/g_nitrous.pdf10. Cote, CJ; Karl, HW; Notterman, DA; Weinberg, JA, McCloskey, C.; Adverse sedation events in
pediatrics: analysis of medications used for sedation. Pediatrics; 2000 Oct;106(4):633-44.
11. CDC.; Vital Signs: overdoses of prescription opioid pain relievers – United States, 1999-2008; MMWR 2011;60:1-6
12. Mayo Clinic; Stroke symptoms; Jul 3, 2013.13. 13. National Stroke Association; Warning signs of a stroke.; Jul 25, 2013; www.stroke.org14. Basic management of medical emergencies: recognizing a patient’s distress.; J Am Dent Assoc.;
2010 May;141 Suppl 1:20S-4S.15. American Red Cross: Conscious choking.; http://www.redcross.org/flash/brr/English-html/
conscious-choking.asp.16. Hunger, J; Rawlings-Anderson, K.; Respiratory assessment.; Nursing Standard. Apr 15,2008;
22,41,41-43. 17. Pulse; Medline Plus; National Library of Medicine, National Inst. Of Health. http://www.nlm.nih.
gov/medlineplus/ency/article/003399.htm.18. American Heart Association; Guidelines for CPR and ECC 2010. 19. Wilson, W., Taubert, K., Gewitz, M.; et. al.; Prevention of infective endocarditis: guidelines from the
American heart Association…; JADA; Jan 2008;139,3S-24S. 20. Siegal, MA; Medical management guidelines for the provision of dental care.; MedEdPORTAL;
2012.

Dental.EliteCME.com Page 84
MEDICAL EMERGEnCIES In THE DEnTAL OffICE
final Examination QuestionsSelect the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116,
or for faster service complete your test online at Dental.EliteCME.com.
1. Which of the following symptoms is not a classic symptom of a heart attack? a. Pain through the arms, neck or back. b. Nausea.c. Perspiration. d. Vomiting.
2. Which of the following allergens is not usually found in polishing paste?a. Gluten. b. Fruit flavoring.c. Nuts.d. Milk protein.
3. Placing a patient in the supine position will:a. Help asphyxiation.b. Support blood flow to the brain.c. Make it easier to perform abdominal thrusts.d. Enable a cleared airway for CPR.
4. Which drug in the emergency medical kit is the most important medication to have on hand?a. Epinephrine.b. Glucose.c. Nitroglycerine.d. Albuterol.
5. What method should be used to alert team members that a medical emergency has occurred in the office?a. Yelling.b. Finding the nearest team member.c. Asking one to call 911.d. Using a code word or phrase.
DCA04EDE18

Chapter 5: Peri-Implantitis: Basics and Beyond
2 CE Hours
By: Dr. Madhumietha Arumugam, B.D.S., M.D.S.
Learning objectives � Define peri-implantitis and peri-implant mucositis. � Discuss the prevalence of peri-implantitis and peri-implant mucositis. � Outline the histology of peri-implant tissues. � List the grades of classification of peri-implantitis. � Identify the risk factors associated with peri-implantitis. � Explain etiopathogenesis of peri-implantitis. � Discuss the steps involved in obtaining the diagnosis of peri-
implantitis.
� Contrast differences between peri-implantitis and peri-implant mucositis.
� Describe the management strategies for peri-implantitis. � Explain Cumulative Interceptive Supportive Therapy for peri-
implantitis. � Summarize the clinical implications of peri-implantitis and the
importance of implant maintenance.
IntroductionDental implants have seen a big boom in the field of dentistry, and have emerged as a new vista in the arena of full mouth rehabilitations. It has been estimated that 2 million implants will be installed annually and this number is expected to rise in the coming years. Hence, the maintenance of the dental implants becomes an important matter of subject. Akin to the natural teeth, implants emerge through the oral mucosa and are susceptible to plaque formation and disease progression in the susceptible host [1, 2].
DefinitionsThe latest consensus about peri-implant diseases, reached in the seventh European Workshop on Periodontology has affirmed the definitions of peri-implantitis and peri-implant mucositis. Peri-implantitis was
defined as an inflammatory process affecting the tissues around an osseointegrated implant in function, resulting in loss of supporting bone. Peri-implant mucositis is defined as reversible inflammatory changes of the peri-implant soft tissues without any bone loss [3].
Prevalence of peri-implantitis and peri-implant mucositisThe sixth European workshop of periodontology on peri-implant diseases has stated that peri-implant mucositis occurs in about 80 percent of subjects (50 percent of sites) restored with implants, and peri-implantitis in between 28 percent and 56 percent of subjects (12–40 percent of sites) [4]. This course will explore in detail the histology of peri-implant tissues, classification, risk factors, microbiology, etiopathogenesis, and management of peri-implantitis.
Histology of peri-implant tissuesThe soft tissue surrounding healthy osseointegrated dental implants shares anatomic and functional features with the gingiva around teeth. The outer surface of the peri-implant mucosa is lined by a stratified keratinized oral epithelium that is continuous with a junctional epithelium attached to the titanium surface by a basal lamina and by hemi-desmosomes. The peri-implant epithelium is a keratinized, multi-layered squamous epithelium with four layers:
● Stratum basale with cylindrical or cubical mitotic active cells. ● Stratum spinosum. ● Stratum granulosum. ● Stratum corneum.
The junctional epithelium is separated from the alveolar bone by collagen-rich connective tissue, which is ~3 to 4mm. This forms a
‘biological barrier,’ and protects the zone of osseointegration from factors released from plaque and the oral cavity. The connective tissue can be divided into an inner zone and an outer zone.
The inner zone is 50-100 µm wide with collagen fibers aligned parallel to the implant surface. The outer zone consists of collagen fibers in various directions and is highly vascularized [5].
The biologic width of an implant can be defined as the distance from most coronal extension of the junctional epithelium to the alveolar bone. The average biologic width around an implant is ~3mm, consisting of 1.8mm of junctional epithelium and 1.05mm of connective tissue attachment [6]. Supracrestal implant surface with an apical coronal expansion of at least 3 mm is essential for the development of a stable biologic width.
Classification of peri-implantitisVarious authors have classified peri-implantitis for ease of communication and management. Some of the commonly used
classifications are listed below. Spiekermann (1995) has classified peri-implantitis into four classes such as follows [7]:
CLASS I Slight horizontal bone loss with minimal peri-implant defect.
CLASS II Moderate horizontal bone loss with isolated vertical defect.CLASS III Moderate horizontal/vertical bone loss with circular bony defects.
CLASS IV Advanced bone loss with broad, circumferential vertical defects as well as loss of buccal and/or palatal bony wall.
Schwarz et al. (2007) have classified the bone defects that occur in peri-implantitis [8]. They classified bone defects as: Class I –intra osseous bone defects.
Class II – supra alveolar bone defects. Generally, a combination of class I and class II defects is observed at one implant. Class I was further classified as:
Page 85 Dental.EliteCME.com
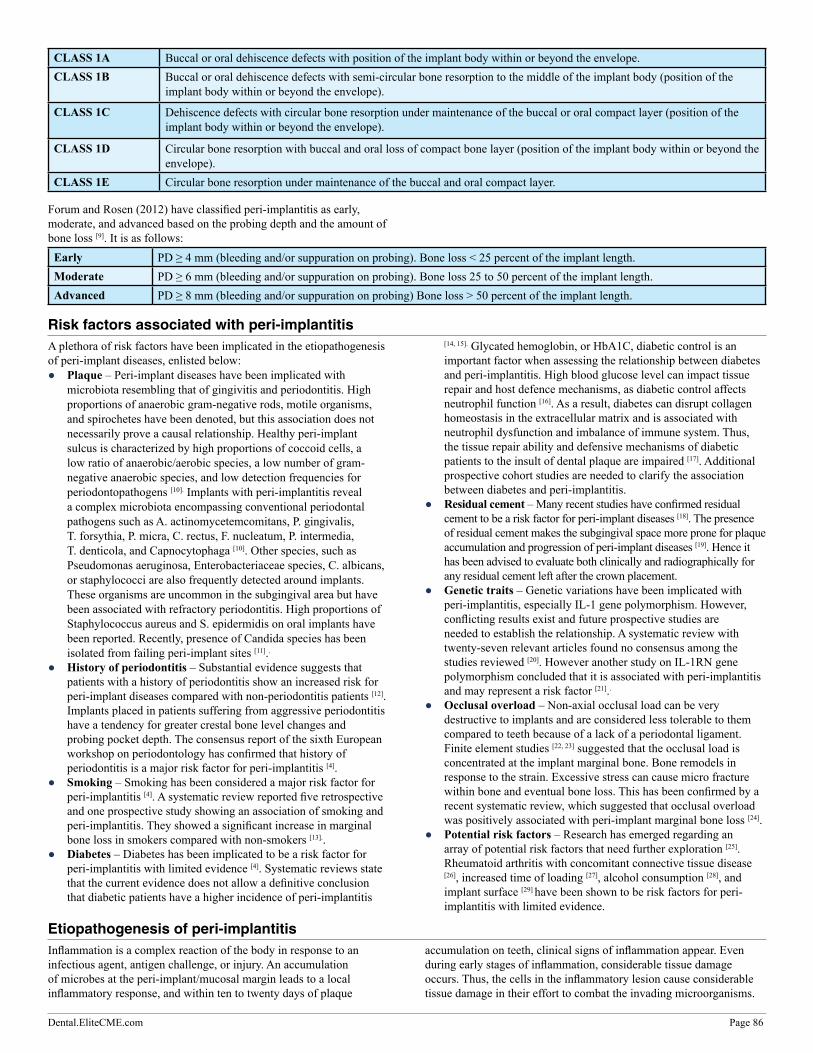
CLASS 1A Buccal or oral dehiscence defects with position of the implant body within or beyond the envelope.CLASS 1B Buccal or oral dehiscence defects with semi-circular bone resorption to the middle of the implant body (position of the
implant body within or beyond the envelope).
CLASS 1C Dehiscence defects with circular bone resorption under maintenance of the buccal or oral compact layer (position of the implant body within or beyond the envelope).
CLASS 1D Circular bone resorption with buccal and oral loss of compact bone layer (position of the implant body within or beyond the envelope).
CLASS 1E Circular bone resorption under maintenance of the buccal and oral compact layer.
Forum and Rosen (2012) have classified peri-implantitis as early, moderate, and advanced based on the probing depth and the amount of bone loss [9]. It is as follows:Early PD ≥ 4 mm (bleeding and/or suppuration on probing). Bone loss < 25 percent of the implant length.Moderate PD ≥ 6 mm (bleeding and/or suppuration on probing). Bone loss 25 to 50 percent of the implant length.Advanced PD ≥ 8 mm (bleeding and/or suppuration on probing) Bone loss > 50 percent of the implant length.
Risk factors associated with peri-implantitisA plethora of risk factors have been implicated in the etiopathogenesis of peri-implant diseases, enlisted below:
● Plaque – Peri-implant diseases have been implicated with microbiota resembling that of gingivitis and periodontitis. High proportions of anaerobic gram-negative rods, motile organisms, and spirochetes have been denoted, but this association does not necessarily prove a causal relationship. Healthy peri-implant sulcus is characterized by high proportions of coccoid cells, a low ratio of anaerobic/aerobic species, a low number of gram-negative anaerobic species, and low detection frequencies for periodontopathogens [10]. Implants with peri-implantitis reveal a complex microbiota encompassing conventional periodontal pathogens such as A. actinomycetemcomitans, P. gingivalis, T. forsythia, P. micra, C. rectus, F. nucleatum, P. intermedia, T. denticola, and Capnocytophaga [10]. Other species, such as Pseudomonas aeruginosa, Enterobacteriaceae species, C. albicans, or staphylococci are also frequently detected around implants. These organisms are uncommon in the subgingival area but have been associated with refractory periodontitis. High proportions of Staphylococcus aureus and S. epidermidis on oral implants have been reported. Recently, presence of Candida species has been isolated from failing peri-implant sites [11]..
● History of periodontitis – Substantial evidence suggests that patients with a history of periodontitis show an increased risk for peri-implant diseases compared with non-periodontitis patients [12]. Implants placed in patients suffering from aggressive periodontitis have a tendency for greater crestal bone level changes and probing pocket depth. The consensus report of the sixth European workshop on periodontology has confirmed that history of periodontitis is a major risk factor for peri-implantitis [4].
● Smoking – Smoking has been considered a major risk factor for peri-implantitis [4]. A systematic review reported five retrospective and one prospective study showing an association of smoking and peri-implantitis. They showed a significant increase in marginal bone loss in smokers compared with non-smokers [13]..
● Diabetes – Diabetes has been implicated to be a risk factor for peri-implantitis with limited evidence [4]. Systematic reviews state that the current evidence does not allow a definitive conclusion that diabetic patients have a higher incidence of peri-implantitis
[14, 15]. Glycated hemoglobin, or HbA1C, diabetic control is an important factor when assessing the relationship between diabetes and peri-implantitis. High blood glucose level can impact tissue repair and host defence mechanisms, as diabetic control affects neutrophil function [16]. As a result, diabetes can disrupt collagen homeostasis in the extracellular matrix and is associated with neutrophil dysfunction and imbalance of immune system. Thus, the tissue repair ability and defensive mechanisms of diabetic patients to the insult of dental plaque are impaired [17]. Additional prospective cohort studies are needed to clarify the association between diabetes and peri-implantitis.
● Residual cement – Many recent studies have confirmed residual cement to be a risk factor for peri-implant diseases [18]. The presence of residual cement makes the subgingival space more prone for plaque accumulation and progression of peri-implant diseases [19]. Hence it has been advised to evaluate both clinically and radiographically for any residual cement left after the crown placement.
● Genetic traits – Genetic variations have been implicated with peri-implantitis, especially IL-1 gene polymorphism. However, conflicting results exist and future prospective studies are needed to establish the relationship. A systematic review with twenty-seven relevant articles found no consensus among the studies reviewed [20]. However another study on IL-1RN gene polymorphism concluded that it is associated with peri-implantitis and may represent a risk factor [21]..
● Occlusal overload – Non-axial occlusal load can be very destructive to implants and are considered less tolerable to them compared to teeth because of a lack of a periodontal ligament. Finite element studies [22, 23] suggested that the occlusal load is concentrated at the implant marginal bone. Bone remodels in response to the strain. Excessive stress can cause micro fracture within bone and eventual bone loss. This has been confirmed by a recent systematic review, which suggested that occlusal overload was positively associated with peri-implant marginal bone loss [24].
● Potential risk factors – Research has emerged regarding an array of potential risk factors that need further exploration [25]. Rheumatoid arthritis with concomitant connective tissue disease [26], increased time of loading [27], alcohol consumption [28], and implant surface [29] have been shown to be risk factors for peri-implantitis with limited evidence.
Etiopathogenesis of peri-implantitisInflammation is a complex reaction of the body in response to an infectious agent, antigen challenge, or injury. An accumulation of microbes at the peri-implant/mucosal margin leads to a local inflammatory response, and within ten to twenty days of plaque
accumulation on teeth, clinical signs of inflammation appear. Even during early stages of inflammation, considerable tissue damage occurs. Thus, the cells in the inflammatory lesion cause considerable tissue damage in their effort to combat the invading microorganisms.
Dental.EliteCME.com Page 86

Accumulation of plaque in the gingival crevice aggravates the inflammatory reaction over time, and consequently, irreversible tissue destruction occurs. Degradation of connective tissue is followed by epithelial migration and bone resorption, which marks the borderline between gingivitis/mucositis and periodontitis/peri-implantitis [30].
Peri-implant disease goes through the following stages: 1. Early peri-implant mucositis, 2. Established peri-implant mucositis, 3. Advanced peri-implant mucositis, and finally 4. Peri-implantitis. Early peri-implant mucositis is characterized by changes caused by supragingival plaque bacteria that cause alterations in junctional epithelium and subepithelial connective tissue. Junctional epithelium shows lateral proliferation and is stimulated to produce IL-8. Histopathology shows increased polymorphonuclear leukocytes, macrophages, T lymphocytes, plasma cells and increased vessel permeability. Established peri-implant mucositis shows junctional epithelium with lateral and apical proliferation and formation of pocket epithelium with mild degeneration. Dense inflammatory infiltration further increases with increase in polymorphonuclear leukocytes, macrophages and lymphocytes. Macrophages release IL-1, IL-6, IL-8, IL-12, and TNF-α in response to bacterial LPS.
Advanced peri-implant mucositis shows ulcerated pocket epithelium with apical proliferation and subepithelial connective tissue degeneration. There is presence of micro or macro abscess formation. Macrophages start producing prostaglandins (PG), cytokines and matrix metalloproteinases (MMPs). TNF-α and IL-1 stimulate fibroblasts to produce MMPs and PG. TNF-α, IL-1, and PGs stimulate osteoclasts to initiate crestal bone resorption. It further progresses to peri-implantitis where progressive dense infiltration of cells in lateral and apical direction takes place. It has been noted that continued apical proliferation and ulceration of epithelium with loss of collagen proceeds to peri-implant bone resorption [10].
The increased susceptibility for bone loss around implants may relate to the absence of inserting collagen fibers into the implant, as is the case with a tooth. A self-limiting process exists in the tissues around natural teeth that results in a protective connective tissue capsule of the supracrestal gingival fibers of the tooth that separate the lesion from the alveolar bone in contrast to peri-implantitis. Such a self-limiting process does not occur in peri-implant tissues and the lesion usually extends to the bony crest, which is different than the periodontitis lesions [31]. Another distinct feature in studies on experimentally induced peri-implantitis was that following ligature removal, there was spontaneous continuous progression of the disease with additional bone loss. All implants appear to be susceptible to peri-implantitis [32, 33].
Diagnosis of peri-implantitisDiagnosis of peri-implantitis is essential in order to treat and maintain the dental implants. The sixth European workshop of periodontology on peri-implant diseases gave a consensus on the salient features to be considered for diagnosis of peri-implantitis [4]. They are as follows:
● Probing is essential for diagnosis of peri-implant diseases. ● Conventional probing using a light force (0.25 N) does not damage
the peri-implant tissues. ● Bleeding on probing indicates the presence of inflammation in the
peri-implant mucosa. ● Bleeding on probing may be used as a predictor for loss of
tissue support. ● An increase in probing depth over time is associated with the loss
of attachment and supporting bone. ● The probing depth, the presence of bleeding on probing and
suppuration should be assessed regularly for the diagnosis of peri-implant diseases.
● Radiographs are required to evaluate supporting bone levels around implants.
● Analysis of peri-implant crevicularfluid (PICF) is not a clinically useful diagnostic parameter for peri-implant disease.
The American Academy of Periodontology has devised the steps to be followed in its recent academy report on peri-implantitis [25].
Probing, bleeding, and suppuration: Dental professionals should probe the implant after the installation of the final restoration, with a force of 0.25N, parallel to the implant, and the probing depth should be measured from the base of the sulcus to the gingival crest. The level of the crestal soft tissue can be measured using a fixed reference point on the restoration and should be noted as the clinical attachment level or the relative attachment level. The extent of probe penetration is influenced by an array of factors such as probing force and angulation, probe tip diameter, roughness of the implant, inflammation of the periodontium and the firmness of the marginal tissues. Hence, careful evaluation of the probing depth is crucial. Plaque assessment and mucosal assessment can aid in evaluation of the peri-implant disease process. A change in the parameters is essential to determine the diagnosis.
Bleeding on gentle probing indicates soft tissue inflammation. Presence of exudation/suppuration indicates pathological changes that demand further investigation.
It has been noted that suppuration associated with intense infiltration containing polymorphonuclear leukocytes, B cells, macrophages, and plasma cells have been observed in sites taken from failed implants due to peri-implantitis [34]. Changes in the parameters of the attachment level lead to the next step in investigation to perform additional radiographic examinations.
Radiographic examination: Periapical radiographic examinations are considered essential to determine the diagnosis of peri-implantitis. Immediate post-implant placement periapical radiograph is considered as the baseline to which the subsequent radiographs are compared to establish the diagnosis. The periapical radiographs should be taken perpendicular to the implant body and ensured that the threads of the implant are clearly demarcated. Usually ~1.5mm bone loss one year after loading and ~0.2mm bone loss in the subsequent years is considered normal. Other radiographic examinations including cone beam computed tomography (CBCT) can be used to examine the location of progressing attachment loss. Consequently, digital image analysis has expanded into implantology to monitor peri-implant bone healing and gain or loss of alveolar bone density.
Implant mobility: Implant mobility is a finding associated with implant failure, as the presence of mobility usually coincides with complete loss of osseointegration. However, perceived implant mobility may relate to the restoration and/or abutment components that have loosened, which may or may not lead to crestal bone loss without loss of integration. A loose implant-supported prosthesis may contribute to the accumulation of plaque, which may lead to the development of peri-implant mucositis and/or peri-implantitis, and as such, this should be corrected. Primary implant stability is an important measure of osseointegration and many devices which make use of this principle can be used as a diagnostic tool for peri-implantitis. Periotest or Dental Fine Tester has been used in the past for the same; however, these methods have been criticized for their lack of resolution, poor sensitivity, and susceptibility to being influenced by the operator. Resonance frequency analysis (RFA) is a novel clinical, non-invasive quantitative assessment tool for determining the stability and presumed osseointegration of implants. This system utilizes a basic vibration theory and is applied to design a transducer that can be excited using a steady state and frequency waveform; its response is measured to determine the implant stiffness in the surrounding tissues [35].
Page 87 Dental.EliteCME.com

RFA values are represented by a quantitative unit called the implant stability quotient (ISQ) on a scale from 1 to 100 and are measured using the Osstell device. RFA values for successfully osseointegrated implants have been reported to be in the range of 57 to 82 ISQ with a mean of 69 ISQ after one year [36]; values under 50 ISQ should be seen as critical and should be evaluated further for peri-implantitis.
Secondary diagnostics: Besides these main criteria for diagnosis of peri-implantitis, various other factors have been used to study the disease process of peri-implantitis. These include bacterial culturing, inflammatory markers, and genetic diagnostics. Further studies are needed to establish relationship between these factors and peri-implantitis.
Differences between peri-implantitis and peri-implant mucositisIn order to effectively treat peri-implant diseases, dental professionals must determine the differences between peri-implantitis and peri-implant mucositis. The contrasting differences between peri-implantitis and peri-implant mucositis are listed below.
Peri-implant mucositis Peri-implantitis
Reversible + -
Plaque accumulation + +Bleeding on probing + +
Pain + (+)Pocket formation - +
Suppuration - +Swelling (+) +Redness + +
Bone resorption - +Implant mobility - (+)
Management of peri-implantitisA systematic review on treatment of peri-implantitis has confirmed that mechanical debridement combined with antiseptic/antibiotic therapy, the Er: YAG laser or regenerative techniques may be used for treating peri-implantitis [37]. There has been a plethora of strategies tried and tested for the management of peri-implantitis. They are detailed below.
Mechanical debridementLocal debridement of hyperplastic peri-implant tissues using hand or ultrasonic plastic instruments has been suggested to be one of the most important management strategies for peri-implantitis. The recommendation is to avoid metallic or hard instruments when touching the abutment/implant surface. This is to minimize surface damages and roughening, which can favor plaque adhesion, and has been based on several in vitro investigations and randomized controlled trials [38, 39, 40]. However, it should be noted that implant surfaces are abraded by toothbrush bristles as well and that roughening of the surface by different maintenance methods has not yet been shown to increase the amount of mineralized deposits on abutments or their adherence to implant surfaces.
Surface decontamination and conditioning A nonspecific decrease of the total bacterial load in the peri-implant pocket, together with a suppression of specific pathogens, may be enough to re-establish equilibrium between the peri-implant microbiota and the host defense. If perfect oral hygiene procedures can prevent massive recolonization of treated sites, implants may remain stable over prolonged periods after such therapy, even though the surfaces of the implants may not be biocompatible enough to allow a direct re-apposition of bone. Surface decontamination has been seen as an important technique for treatment of peri-implantitis. Studies have shown that titanium alloy implants can be decontaminated with citric acid, stannous fluoride, tetracycline-HCl, chlorhexidine gluconate, hydrogen peroxide, chloramine T, sterile water, plastic sonic scaler tip and air powder abrasive unit.
Various mechanical and chemical techniques have been proposed for cleaning infected implant surfaces. Low-speed rotary instruments can be used for removing the plasma-sprayed layer from rough surfaces. Additional application of chlorhexidine gel for five minutes on the mechanically cleaned implant surface has been recommended to provide topical disinfection.
Chlorhexidine rinsing also establishes adequate surface deconditioning. It has been suggested that infected surfaces of Hydroxyapatite-coated (HA) implants should be cleaned with citric acid (pH 1) for 30 seconds to one minute. Burnished hydrogen peroxide has not been found to be superior to saline in removing bacterial endotoxins. It has been proposed that an altered HA coating be removed or that titanium plasma-sprayed surfaces be cleaned with ultrasonic or air-powder abrasives [40]. Sonic scalers with plastic tips were found to be as effective as or more effective than burnished saline controls in removing endotoxins from implant surfaces. Randomized controlled studies have shown that air-powered abrasives can clean a rough implant surface of bacteria and organic materials [41]. However, it is not known whether air-powered abrasives can effectively clean narrow infrabony defects, as the contact profile angle may be too acute to deliver an effective spray to the implant surface. In addition, such an acute angle of the air-powered abrasive instrument may induce emboli in the bone marrow spaces. Indeed, several authors have advised against the risk of embolism induced by pressurized air when using air-powered abrasives.
Antimicrobial therapyTo improve the resistance to mechanical load, almost all implants today have a roughened surface in the area where osseointegration is supposed to occur. These surfaces can become contaminated by bacteria as a consequence of peri-implantitis. Mechanical debridement on such surfaces has a limited effect and can certainly not remove all bacteria. Adjunctive chemical agents have thus been recommended to enhance the treatment effect.
In case of suspected infectious complications and peri-implantitis, adjunctive subgingival irrigation of the pocket with 0.12% to 0.2% chlorhexidine two to time times per day for ten days to three weeks has been suggested as an efficient local disinfectant [41]. Chlorhexidine is believed to be the antimicrobial agent of choice.
However, its bactericidal effect in vivo at low concentrations (0.12 percent to 0.2 percent), coupled with crevicular fluid dilution and the apparent protective function of serum, may render chlorhexidine weakly bactericidal or even ineffective. Metronidazole has been found to be effective at the tested concentrations of 25 percent in gel form [40]. Local application of tetracycline fibers has also been proposed as an effective adjunctive treatment for failing implants. A randomized controlled trial proved that minocycline microspheres can be effectively used for treating for peri-implantitis [42]. If systemic antibiotic therapy is considered, it has been suggested that it be guided by bacterial culturing and sensitivity tests. However, it is unknown whether the results of such diagnostic tests would actually influence the course of the therapy.
Dental.EliteCME.com Page 88

Bacteria associated with failing implants have been found to be sensitive to the following antibiotics: penicillin G, amoxicillin, combination of amoxicillin and metronidazole, and amoxicillin-clavulanate, respectively. Bacteria around implants may form biofilms to protect themselves from the host. Dental plaque is a typical example of biofilm. Although biomaterial centered infections for implants placed in the maxillofacial region are rarely associated with conspicuous biofilms, such deposits have been shown to protect the embedded bacteria from antibiotic. In case of suppurative peri-implant infection, the use of specific systemic antibiotics against anaerobic microorganisms is generally recommended. In particular, it has been proposed that the administration of a combination of antibiotics such as amoxicillin and metronidazole, be employed for ten days. This protocol is derived directly from the treatment of refractory periodontitis and is specifically targeted against Actinobacillus actinomycetemcomitans. Systemic ornidazole (1000 mg for ten days) together with chlorhexidine subgingival irrigation can also be used for the treatment of failing implants. The possibility of using nonsteroidal anti-inflammatory drugs for inhibiting peri-implant bone loss in cases of peri-implantitis has been proposed. Even though preliminary animal results seem to be promising, such therapy may not be indicated for the treatment of an acute phase.
The effect of combination therapy, including systemic amoxicillin and metronidazole and local debridement, has also been suggested for peri-implantitis treatment. The combination of systemic antimicrobial therapy and mechanical debridement has shown to result in the resolution of the peri-implantitis lesion, resolution of recession of the marginal peri-implant mucosa, and a minor additional apical shift of the base of the bone defect.
Use of lasers for implant surface detoxificationVarious laser systems have been tried and tested for implant surface decontamination. It is known that photosensitization and soft lasers can eliminate bacteria from different implant surfaces (i.e., machined, sandblasted/acid-etched, flame-sprayed, and HA-coated) in one minute. The most widely used lasers for implant surface detoxification has been Er:YAG laser. Nd:YAG and Ho:YAG lasers are not suitable for use in decontamination of implant surfaces, irrespective of the power output. With the Er:YAG and CO2 laser, the power output must be limited so as to avoid surface damage. The GaAIAs laser seems to be safe as far as possible surface alterations are concerned. Various randomized control trials have been performed to compare mechanical debridement and Er:YAG laser for implant decontamination [43, 44]. These studies have shown no statistical differences between the probing attachment levels, probing pocket depths and recession levels between the methods, yet effective improvement in the parameters individually.
Occlusal therapyWhen centric or lateral premature contacts or interference have been detected, occlusal adjustment has been recommended. Dental professionals should evaluate the fit of the prosthesis and the abutment. When parafunctional activity is suspected, night-guard therapy has been
suggested. It has also been reported that if overload etiology is suspected, the clinician should remove the prosthesis with the hope of improving the situation. A systematic review by Carl Misch has shown a positive correlation between occlusal overload and peri-implant bone loss [45].
Surgical therapySurgical procedures for the treatment of complications and “failing” implants have been advocated by several authors, particularly after unsuccessful antimicrobial treatment and progressive marginal bone loss. Early perforations of the mucoperiosteum covering a submerged implant, often caused by decubital ulcers related to inadequate relief of the denture on the implant site, can be treated with excision of the bordering mucosa, full-flap coverage of the perforation, and adequate relief of the denture. For some implant systems, it is also possible to replace a standard cover screw with a smaller one. Hyperplastic mucositis refractory to increased oral hygiene procedures, in the absence of other treatable conditions (for example, loose implant components that can be tightened after local cleaning and sterilization of the abutment), is usually treated with gingivectomy procedures. Chronic fistulae originating from infected soft tissues entrapped at the abutment junction level have been treated by removing the abutment and interposed granulation tissue, cleaning the implant head, sterilizing the abutment, fitting a new silicon ring (when present), surgically excising the epithelialized sinus tract (not always necessary), and properly reseating the abutment. Surgical revision of failing implants aims mainly at cleaning the abutment/implant surfaces of bacteria through open flap debridement. Effective cleaning of the implant surface represents an important issue in the treatment of failing implants. In fact, cleaning rough implant surfaces is very difficult since bacteria are protected in micro irregularities or undercuts of the surface. For this reason, it seems wise to carry out any surgical intervention under antibiotic coverage to maximize the antibacterial effect. There is unanimous consensus that bacteria should be eliminated from the surfaces of failing implants. Further, there is a belief that if endotoxins or other contaminants are left, there cannot be biologic repair or re-osseointegration.
Resective and regenerative proceduresOnce the primary goal of surgical intervention of a bacteria-free implant surface has been achieved, it may be necessary for dental professionals to correct the anatomic conditions to improve plaque
control and eliminate the favorable environment for anaerobic bacteria such as deep pockets. This may be accomplished either with resective procedures such as bone resection and apically repositioned flaps or with regenerative procedures such as guided bone regeneration [GBR], autologous, or allogenic bone grafts.
Bone graftsNumerous bone graft materials have been used to aid in the reconstruction of bone defects. These range from allografts to xenografts and alloplasts.
Autogenous bone graftsThese bone grafts are considered to be the “gold standard,” since the graft is harvested from the donor itself. These grafts are osteoinductive.
Intraoral sources: ● Bone from extraction wounds. ● Edentulous ridges. ● Bone from within the jaw. ● Newly formed bone in wound. ● Bone removed from ostectomy and osteoplasty.
Extra oral sources: ● Iliac autografts.
Allografts: ● Decalcified freeze-dried bone allograft (DFDBA). ● It is thought to have osteoinductive effect because it releases
BMPs. Schwartz et al. reported that variations in the amount of bone formation induced by DFDBA may relate to the source and processing of bone.
Alloplasts: ● These grafts are synthetic and prepared from artificial sources.
Page 89 Dental.EliteCME.com

Guided tissue regeneration and guided bone regeneration in peri-implantitisThe concept of guided tissue regeneration is based on the principle of exclusion of fast growing epithelial and connective tissue cells paving the way for periodontal ligament cells osteoblasts, cementoblasts to regenerate new bone. Nyman et al. put forward the concept of guided tissue regeneration in 1982.
The decision-making process regarding the use of resective or regenerative procedures may be influenced by the degree and/or morphology of the peri-implant tissue destruction. If the amount of lost supporting bone is minimal, a resective approach may be preferable. If a major portion of the supporting bone has been resorbed, forming a craterlike defect with remaining wall structures, a regenerative technique has been recommended. Finally, if the destruction has reached the vents of a hollow-cylinder implant, or if the dental professional determines the remaining supporting bone is insufficient to withstand the usual loading conditions, the implant should be removed. After a flap is apically repositioned, it has been suggested that a surgical pack be used to secure the position of the flap. No studies have been published that substantiated such a procedure. Several randomized controlled trials have investigated the possibility of regenerating new supporting bone around failing implants using barriers (GBR) [46, 47]. Partial bone fill around failing implants using GBR alone or in combination with autogenous bone grafts or various types of allografts/alloplastic grafts have been reported [48, 49]. Despite different antibiotic regimens, barriers usually required premature removal because of infections. It has been shown that premature barrier exposure and removal is generally associated with poor clinical outcomes. Although some case reports have displayed a pronounced radiographic bone fill, such results should be viewed with caution, since unsuccessful reports can be found as well. Barriers are usually placed both in a completely submerged fashion or adapted to a permucosal abutment. Many differences in bone regeneration among different studies can be explained partly
by anatomic variations of the bony defects and by barrier infections and exposures. The combination of GBR and resorbable HA or freeze-dried bone has shown a statistically higher percentage of reosseointegration when compared to GBR alone [47]. Recombinant human bone morphogenetic protein-2 has been shown to have the potential to promote bone formation and reosseointegration in advanced peri-implantitis bony defects, although the amount of bone to implant contact in the reosseointegrated portion of bone was significantly lower than bone contact within the resident bone. It has been suggested that microbial leakage at the abutment-implant junction might influence the outcome of GBR. In addition to sterilization of the abutment, disinfection of the internal part of the implant has been advocated, but its effectiveness has not been proven. To improve the likelihood of bone regeneration, it has been recommended that the area be isolated from the oral cavity with full-flap coverage of the barrier. A long-term follow-up study has concluded that the use of regenerative procedures such as bone graft techniques with or without the use of barrier membranes has been reported with various degrees of success. Implants with peri-implant defects that are treated with GBR had similar survival rates and crestal bone levels compared with implants in native bone with survival rates of 96.1 percent [50]. However, it must be stressed that such techniques do not address disease resolution but rather merely attempt to fill the osseous defect. There are strong recommendations against using HA or allogenic freeze-dried bone to fill bone pockets around infected implant sites, warning of the potential consequences for the patient. In fact, biomaterial-centered infections may bear catastrophic consequences for the patient, such as acute localized suppurative osteomyelitis. Biomaterial-centered infections are extremely resistant to antibiotics and combined antibiotic/surgical therapy. Therefore, whenever a clinician feels uncertain with regard to the possibility of eliminating bacteria in an area of difficult access (i.e., vents of hollow implants, rough coatings, etc.), the solution of choice is implant removal.
Cumulative Interceptive Supportive Therapy for implants Lang et al. in 2004 gave a strategy for supportive maintenance plan for implant patients called Cumulative Interceptive Supportive Therapy (CIST). He modified and devised a concept called the AKUT concept, which is a concept of implant maintenance based on repeated
recall and assessment of plaque, bleeding, suppuration, pocket and radiological evidence of bone loss [51]. The CIST gave a clear-cut protocol for treatment of peri-implantitis depending on the probing depth and bone loss. It is as follows:
Stage Result Therapy
Pocket depth (PD) <3mm, no plaque or bleeding on probing.
No therapy.
A Pocket depth (PD) <3mm, plaque and/or bleeding on probing.
Mechanical debridement, scaling, and polishing, oral hygiene instructions.
B PD 4-5 mm, radiologicallyno bone loss or PD >5mm but no cratering.
Mechanical debridement, scaling & polishing, oral hygiene instructions, plus local anti-infective therapy 0.1 percent chlorhexidine twice daily for three to four weeks.
C PD >5 mm, radiologically bone loss <2mm.
Mechanical debridement, scaling, and polishing, oral hygiene instructions, microbial testing plus local and systemic anti-infective therapy.
D PD >5 mm, radiologically bone loss >2mm.
Mechanical debridement, scaling and polishing, oral hygiene instructions, microbial testing, local and systemic anti-infective therapy PLUS resective and regenerative surgery.
Another commonly accepted protocol given by Zitmann et al. referred to as systematic periodontitis therapy. The initial phase of the protocol consists of oral hygiene instructions with an adjunct of local and systemic anti-infective therapy as required. If non-surgical treatment fails, it has been recommended to treat further with open flap debridement and resective/ regenerative surgery [52].
Schmage et al. gave a protocol for peri-implantitis treatment that followed the concept of CIST-protocol but recommended mechanical and local disinfective treatments at stage A and B. He recommended interventions if probing depths exceeded 5 mm or are progressive, as well as if they occurred under any local inflammation signs [53]. Hence, following such protocols can aid in long-term treatment and maintenance of dental implants.
Dental.EliteCME.com Page 90

Clinical implications for the dentistAny dentist who deals with implants, either with its placement, prosthetics, or maintenance, should be well aware of the pathological process of peri-implantitis and should be well informed about its clinical implications in the day-to-day dental practice. The clinical implications of peri-implant diseases are summarized as follows [4]:
● The dentist should inform the patient that peri-implant tissues respond to plaque in the same way as the periodontal tissues, and hence in the absence of adequate plaque control, diseases may develop in the tissues around the implant.
● Poor oral hygiene and subsequent plaque accumulation leads to peri-implant diseases.
● Patients with history of periodontitis should be informed about their increased risk for peri-implantitis.
● Patients who smoke should be informed about their increased risk for developing peri-implantitis.
● Diabetic patients should be encouraged to maintain a normal range blood glucose level and should be made aware of their increased risk for developing peri-implantitis.
● Bleeding on probing should be considered as an objective sign for inflammation of peri-implant tissues and prolonged presence of which indicates increased risk for future bone loss and attachment loss.
● The clinician should be aware that suppuration and mobility are definite indicators of peri-implantitis.
● Mobility indicates complete loss of osseointegration and requires removal of the implant.
● Peri-implant probing and recording at annual intervals is essential to determine the course of the disease and to help establish the diagnosis.
● Baseline probing measurements should be recorded at the time of placement of implant super structure.
● Probing does not damage peri-implant tissues and at least one site per implant should be established to record the relative attachment levels.
● Baseline radiograph is considered mandatory and should be taken at the time of placement of implant super structure to determine the initial bone levels.
● When suspecting peri-implantitis, the clinician should take radiographs and confirm the bone loss to establish and confirm the diagnosis.
● Bacterial deposits must be removed in the treatment of peri-implant mucositis and peri-implantitis.
● The clinician should be aware that peri-implantitis is difficult to treat and the outcomes may not be predictable.
● Clinicians should consider non-surgical mechanical therapy for the treatment of peri-implantitis and if that does not resolve the lesion, adjunctive antimicrobials and access flap surgery are recommended.
● In order to restore the hard-tissue defect, reconstructive surgery may be considered.
ConclusionPrevention is better than cure. The implantologist must be aware of the importance of preventing peri–implantitis, should consider appropriate case selection, keep in mind the risk factors involved with the disease process, and make the patient aware of the importance of implant maintenance. Future research should focus on the various strategies for combatting peri-implantitis with larger samples to
generalize the results. Longitudinal studies on large subject samples must be performed in order to confirm that factors associated with peri-implant disease are indeed risk factors or indicators. Betterment in future clinical research will lead to the betterment of treatment and management strategies and hence a better clinical practice.
References1. Serino, G., & Ström, C. (2009). Peri‐implantitis in partially edentulous patients: association with
inadequate plaque control. Clinical Oral Implants Research, 20(2), 169-174.2. Ferreira, S. D., Silva, G. L., Cortelli, J. R., Costa, J. E., & Costa, F. O. (2006). Prevalence and risk
variables for peri‐implant disease in Brazilian subjects. Journal of Clinical Periodontology, 33(12), 929-935.
3. Lang NP, Berglundh T. (2011) on Behalf of Working Group 4 of the Seventh European Workshop on Periodontology: Periimplant diseases: where are we now? – Consensus of the Seventh European Workshop on Periodontology. Journal of clinical periodontology, 38 (s11), 178–181.
4. Lindhe, J., & Meyle, J. (2008). Peri‐implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. Journal of clinical periodontology,35(s8), 282-285.
5. Shioya, K., Sawada, T., Miake, Y., Inoue, S., & Yanagisawa, T. (2009). Ultrastructural study of tissues surrounding replanted teeth and dental implants. Clinical oral implants research, 20(3), 299-305.
6. Linkevicius, T., & Apse, P. (2008). Biologic width around implants. An evidence-based. Stomatologija, 10(1), 27-35.
7. Spiekermann, H. (1995). Implantology. Thieme.8. Schwarz, F., Herten, M., Sager, M., Bieling, K., Sculean, A., & Becker, J. (2007). Comparison of
naturally occurring and ligature induced peri-implantitis bone defects in humans and dogs. Clinical Oral Implants Research, 18(2), 161-170.
9. Froum, S. J., & Rosen, P. S. (2012). A proposed classification for peri-implantitis. International Journal of Periodontics and Restorative Dentistry, 32(5), 533.
10. Heitz‐Mayfield, L. J., & Lang, N. P. (2010). Comparative biology of chronic and aggressive periodontitis vs. peri‐implantitis. Periodontology 2000, 53(1), 167-181.
11. Karbach, J., Brunner, A., Pieter, D., Thal, S. C., & Al-Nawas, B. (2015). Case Control Study to Evaluate the Role of Candida, Staphylococcus and Enterococccus Species in Peri-implant Infections in Irradiated Patients after Tumour Surgery and Non-irradiated Patients. Oral Health Dental Management, 14(5), 306-312.
12. Renvert, S., & Persson, G. R. (2009). Periodontitis as a potential risk factor for peri‐implantitis. Journal of clinical periodontology, 36(s10), 9-14.
13. Heitz‐Mayfield, L. J. (2008). Peri‐implant diseases: diagnosis and risk indicators. Journal of clinical periodontology, 35(s8), 292-304.
14. Bornstein, M. M., Cionca, N., & Mombelli, A. (2009). Systemic conditions and treatments as risks for implant therapy. Int J Oral Maxillofac Implants,24(Suppl), 12-27.
15. Mombelli, A., & Cionca, N. (2006). Systemic diseases affecting osseointegration therapy. Clinical oral implants research, 17(S2), 97-103.
16. Salvi, G. E., Carollo‐Bittel, B., & Lang, N. P. (2008). Effects of diabetes mellitus on periodontal and peri‐implant conditions: update on associations and risks. Journal of clinical periodontology, 35(s8), 398-409.
17. Abiko, Y., & Selimovic, D. (2010). DIABETES. REVIEW. Bosnian Journal of Basic Medical Sciences, 10(3), 186-191.
18. Wilson Jr, T. G. (2009). The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. Journal of Periodontology, 80(9), 1388-1392.
19. Linkevicius, T., Puisys, A., Vindasiute, E., Linkeviciene, L., & Apse, P. (2013). Does residual cement around implant‐supported restorations cause peri‐implant disease? A retrospective case analysis. Clinical oral implants research, 24(11), 1179-1184.
20. Bormann, K. H., Stühmer, C., Z’Graggen, M., Kokemöller, H., Rücker, M., & Gellrich, N. C. (2009). IL-1 polymorphism and periimplantitis. A literature review. Schweizer Monatsschrift fur Zahnmedizin= Revue mensuelle suisse d’odonto-stomatologie= Rivista mensile svizzera di odontologia e stomatologia/SSO, 120(6), 510-520..
21. Laine, M. L., Leonhardt, Å., Roos‐Jansåker, A. M., Peña, A. S., Van Winkelhoff, A. J., Winkel, E. G., & Renvert, S. (2006). IL‐1RN gene polymorphism is associated with peri‐implantitis. Clinical Oral Implants Research, 17(4), 380-385.
22. Rungsiyakull, C., Rungsiyakull, P., Li, Q., Li, W., & Swain, M. (2010). Effects of occlusal inclination and loading on mandibular bone remodeling: a finite element study. The International journal of oral & maxillofacial implants, 26(3), 527-537.
23. Hudieb, M. I., Wakabayashi, N., & Kasugai, S. (2011). Magnitude and direction of mechanical stress at the osseointegrated interface of the microthread implant. Journal of periodontology, 82(7), 1061-1070.
24. Fu, J. H., Hsu, Y. T., & Wang, H. L. (2011). Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants.European journal of oral implantology, 5, S91-103.
25. Rosen, P., Clem, D., Cochran, D., Froum, S., McAllister, B., & Renvert, S. (2013). Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. Journal of periodontology, 84(4), 436-443.
26. Krennmair, G., Seemann, R., & Piehslinger, E. (2010). Dental implants in patients with rheumatoid arthritis: clinical outcome and peri‐implant findings.Journal of clinical periodontology, 37(10), 928-936.
27. Máximo, M. B., De Mendonça, A. C., Alves, J. F., Cortelli, S. C., Peruzzo, D. C., & Duarte, P. M. (2008). Peri-implant diseases may be associated with increased time loading and generalized periodontal bone loss: preliminary results. Journal of Oral Implantology, 34(5), 268-273.
28. Galindo‐Moreno, P., Fauri, M., Ávila‐Ortiz, G., Fernández‐Barbero, J. E., Cabrera‐León, A., & Sánchez‐Fernández, E. (2005). Influence of alcohol and tobacco habits on peri‐implant marginal bone loss: a prospective study.Clinical oral implants research, 16(5), 579-586.
29. Renvert, S., Polyzois, I., & Claffey, N. (2011). How do implant surface characteristics influence peri‐implant disease?. Journal of clinical periodontology, 38(s11), 214-222.
30. Klinge, B., Hultin, M., & Berglundh, T. (2005). Peri-implantitis. Dental Clinics of North America, 49(3), 661-676.
31. Berglundh, T., Zitzmann, N. U., & Donati, M. (2011). Are peri‐implantitis lesions different from periodontitis lesions? Journal of clinical periodontology, 38(s11), 188-202.
32. Albouy JP, Abrahamsson I, Persson LG, Berglundh T. (2008) Spontaneous progression of peri-implantitis at different types of implants. An experimental study in dogs. I: Clinical and radiographic observations. Clinical oral implants research, 19, 997-1002.
33. Albouy, J. P., Abrahamsson, I., Persson, L. G., & Berglundh, T. (2009). Spontaneous progression of ligatured induced peri‐implantitis at implants with different surface characteristics. An experimental study in dogs II: histological observations. Clinical oral implants research, 20(4), 366-371.
34. Salvi, G. E., & Lang, N. P. (2003). Diagnostic parameters for monitoring peri-implant conditions. The International journal of oral & maxillofacial implants,19, 116-127.
35. Valderrama, P., Oates, T. W., Jones, A. A., Simpson, J., Schoolfield, J. D., & Cochran, D. L. (2007). Evaluation of two different resonance frequency devices to detect implant stability: a clinical trial. Journal of periodontology,78(2), 262-272.
36. Cassetta, M., Ricci, L., Iezzi, G., Dell’Aquila, D., Piattelli, A., & Perrotti, V. (2012). Resonance frequency analysis of implants inserted with a simultaneous grafting procedure: a 5-year follow-up study in man. The International journal of periodontics & restorative dentistry, 32(5), 581-589.
37. Kotsovilis, S., Karoussis, I. K., Trianti, M., & Fourmousis, I. (2008). Therapy of peri‐implantitis: a systematic review. Journal of clinical periodontology,35(7), 621-629.
38. Renvert, S., Samuelsson, E., Lindahl, C., & Persson, G. (2009). Mechanical non‐surgical treatment of peri‐implantitis: a double‐blind randomized longitudinal clinical study. I: clinical results. Journal of clinical periodontology, 36(7), 604-609.
Page 91 Dental.EliteCME.com

39. Persson, G. R., Samuelsson, E., Lindahl, C., & Renvert, S. (2010). Mechanical non‐surgical treatment of peri‐implantitis: a single‐blinded randomized longitudinal clinical study. II. Microbiological results. Journal of clinical periodontology, 37(6), 563-573.
40. Karring, E. S., Stavropoulos, A., Ellegaard, B., & Karring, T. (2005). Treatment of peri‐implantitis by the Vector® system. Clinical Oral Implants Research, 16(3), 288-293.
41. Sahm, N., Becker, J., Santel, T., & Schwarz, F. (2011). Non‐surgical treatment of peri‐implantitis using an air‐abrasive device or mechanical debridement and local application of chlorhexidine: a prospective, randomized, controlled clinical study. Journal of clinical periodontology, 38(9), 872-878.
42. Renvert, S., Lessem, J., Dahlén, G., Renvert, H., & Lindahl, C. (2008). Mechanical and repeated antimicrobial therapy using a local drug delivery system in the treatment of peri-implantitis: a randomized clinical trial. Journal of periodontology, 79(5), 836-844.
43. Schwarz, F., Sculean, A., Rothamel, D., Schwenzer, K., Georg, T., & Becker, J. (2005). Clinical evaluation of an Er: YAG laser for nonsurgical treatment of peri‐implantitis: a pilot study. Clinical oral implants research,16(1), 44-52.
44. Schwarz, F., Bieling, K., Bonsmann, M., Latz, T., & Becker, J. (2006). Nonsurgical treatment of moderate and advanced periimplantitis lesions: a controlled clinical study. Clinical Oral Investigations, 10(4), 279-288.
45. Misch, C. E., Suzuki, J. B., Misch-Dietsh, F. M., & Bidez, M. W. (2005). A positive correlation between occlusal trauma and peri-implant bone loss: literature support. Implant dentistry, 14(2), 108-116.
46. Roos‐Jansåker, A. M., Renvert, H., Lindahl, C., & Renvert, S. (2007). Submerged healing following surgical treatment of peri‐implantitis: a case series. Journal of clinical periodontology, 34(8), 723-727.
47. Roos‐Jansåker, A. M., Renvert, H., Lindahl, C., & Renvert, S. (2007). Surgical treatment of peri‐implantitis using a bone substitute with or without a resorbable membrane: a prospective cohort study. Journal of clinical periodontology, 34(7), 625-632.
48. Schwarz, F., Sahm, N., Bieling, K., & Becker, J. (2009). Surgical regenerative treatment of peri‐implantitis lesions using a nanocrystalline hydroxyapatite or a natural bone mineral in combination with a collagen membrane: a four‐year clinical follow‐up report. Journal of clinical periodontology, 36(9), 807-814.
49. Schwarz, F., Bieling, K., Latz, T., Nuesry, E., & Becker, J. (2006). Healing of intrabony peri‐implantitis defects following application of a nanocrystalline hydroxyapatite (Ostim™) or a bovine‐derived xenograft (Bio‐Oss™) in combination with a collagen membrane (Bio‐Gide™). A case series. Journal of Clinical Periodontology, 33(7), 491-499.
50. Blanco, J., Alonso, A., & Sanz, M. (2005). Long‐term results and survival rate of implants treated with guided bone regeneration: a 5‐year case series prospective study. Clinical oral implants research, 16(3), 294-301.
51. Lang, N. P., Berglundh, T., HeitzMayfield, L. J., Pjetursson, B. E., Salvi, G. E., & Sanz, M. (2004). Consensus statements and recommended clinical procedures regarding implant survival and complications. International Journal of Oral and Maxillofacial Implants, 19(SUPPL.), 150-154.
52. Zitzmann, N. U., Walter, C., & Berglundh, T. (2006). Ätiologie, Diagnostik und Therapie der Periimplantitis–Eine Übersicht. Deutsche Zahnärztliche Zeitschrift, 61(12), 642-649.
53. Schmage, P. (2010). Befundorientiertes Behandlungskonzept bei periimplantären Infektionen. Parodontol, 21, 339-358.
PERI-IMPLAnTITIS: BASICS AnD BEyOnDfinal Examination Questions
Select the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116, or for faster service complete your test online at Dental.EliteCME.com.
1. Class II of Spikermann’s classification of peri-implantitis is characterized as what? a. Slight horizontal bone loss with minimal peri-implant defect. b. Moderate horizontal/vertical bone loss with circular bony
defects. c. Advanced bone loss with broad, circumferential vertical
defects as well as loss of buccal and/or palatal bony wall. d. Moderate horizontal bone loss with isolated vertical defect.
2. History of periodontitis cannot be considered as a risk factor for peri-implantitis.a. True. b. False.
3. Dental professionals should probe the implant after the installation of the final restoration, with a force of 0.25N. a. True. b. False.
4. Chlorhexidine is believed to be the antimicrobial agent of choice.a. True. b. False.
5. __________ is better than a cure. a. Health.b. Prevention. c. Surgery. d. Implantation.
DFL02PEE18
Dental.EliteCME.com Page 92

Chapter 6: Professional Care and Patient Maintenance of Implant-Supported Dentures
2 CE Hours
By: Sharon Boyd, RDH
Learning objectivesUpon completion of this course, the learner should be able to:
� Choose appropriate instruments during prophylactic and therapeutic care appointments.
� Evaluate the health of tissues surrounding dental implant abutments.
� Determine appropriate home care methods for patients that wear implant-supported prosthesis.
� Create a re-care plan that is appropriate to the implant patient’s needs.
� Identify appropriate oral hygiene aids in addition to traditional toothbrush and floss.
� Calculate instrumentation techniques to be used on implant patients receiving periodontal scaling and root planing.
� Adapt probing methods as necessary from traditional periodontal probing to altered pocket charting that is implant-specific.
� List types of implant-supported denture options used frequently in dentistry.
� Determine how frequently radiographs should be taken on a patient with a fixed implant prosthesis.
IntroductionApproximately 3 million Americans currently have dental implants, and another 500,000 are expected to get implants every year (1).Thus, dental hygienists and dentists are expected to understand how to properly manage their implant patients during preventive care appointments as well as provide proper education for home care purposes. If not, peri-implantitis may develop and impact the success of the implant prosthesis, resulting in premature failure.
Dental implant overdentures are removable prosthesis that are stabilized by dental implant systems. In most cases, the overdenture is supported by a ball or bar retention device and held into place using clips or locators attached to the removable denture. Ball retention systems involve individual implant abutments with locators placed into the denture, where the implants align and snap into place. Bar-retained overdentures include housings inside of the denture, which clip over the bars suspended between the dental implants.
Fixed dentures, otherwise known as non-removable, hybrid, or fixed detachable dentures are permanently anchored onto the jaw using a screw system. This permits the prosthesis to be removed if necessary by the dentist, but not the patient. Commonly known as “all-on-4 dentures,” these fixed dentures have gained a tremendous amount of popularity among modern dental patients as a convenient alternative to traditional removable dentures and overdentures.
Because of the types of implant-supported dentures used in patient care, dental professionals and patients should understand the methods, techniques, and oral hygiene aids that are most appropriate for maintaining the various types of prosthesis. Removable implant overdentures and fixed hybrid dentures are similar, but the care methods for the oral and gingival health of the patient vary.
Appointment optionsMaintenance of patients wearing implant-supported dentures is similar to managing patients that are periodontally compromised. However, the diagnostic process is much different (2). Managing patients with implant-supported dentures will depend on the current health of
gingival and peri-implant tissues in their mouths, as well as whether or not any teeth still exist in the opposite arch. Like patients with natural teeth, implant patients with fixed prostheses require regular preventive care to avoid peri-implantitis and other forms of implant risks.
Prophylaxis/maintenancePreventive care appointments are more maintenance than preventative. Initially, patients wearing an implant-supported denture should have maintenance appointments at least every 3 months after the prosthesis is placed. However, they may need to be seen as frequently as every month until adequate re-care and proper home oral hygiene habits are established.
The frequency of these visits allows the dental professional to evaluate any changes in the oral health of the patient, including possible complications or risks associated with the health of the dental implant. More frequent visits minimize the risk of failure for the implants supporting the denture (3). Visits should be frequent for the first year following the placement of the denture, but can then be more sporadic.
If the patient’s home care is appropriate, he or she may be placed on a 6-month recall schedule after a year. It is essential that no more than 6 months pass between preventive care appointments for at least the first 2 years after the implant placement.
It is recommended that only a fine grit polishing paste be used with selective polishing techniques, using a rubber cup around the implant to remove soft debris and stains. Tin-oxide can also be used, or the practitioner can purchase a polishing paste that is formulated for the specific use of implant polishing.
Prophy angles with rubber points may also be useful for selective polishing along harder-to-reach areas and between implants. Air polishing implants may be too abrasive, but it has been shown to be safe enough for maintenance of healthy implant patients.
Page 93 Dental.EliteCME.com

DebridementA full mouth debridement may be necessary when heavy plaque and calculus is in the patient’s mouth. This may be due to poor patient care or a lapse in prophylactic care appointments. If heavy calculus deposits extend over the implant prosthesis or in supra gingival areas of the implants, a debridement may be necessary before an exam can be completed.
During the debridement, it is important to note the health of the gingival tissue surrounding the implants. If exudate or suppuration is present, a peri-implant infection may be the cause.
A debridement is usually only necessary due to a lapse in care caused by a delay in preventive care (prophylactic) appointments or extremely poor oral hygiene.
Periodontal scaling and root planingIn most cases, scaling around an implant should be restricted to areas supragingivally or immediately surrounding a deposit. However, periodontal scaling and root planing (SCRP) may be needed when existing teeth are on the opposite arch, or if peri-implantitis impacts the areas surrounding the implants that are supporting the denture.
When implants are involved in an SCRP procedure, appropriate instrumentation is essential.
Plastic instruments are flexible, yet durable enough to remove both hard and soft deposits from implant surfaces (4). They can also be sharpened, if they are reinforced with graphite.
Do not use traditional ultrasonic instruments while cleaning implants, as this could damage the surface of the titanium. Instead, implement an implant-appropriate ultrasonic tip to use during the SCRP.
Recognizing implant failureDuring each appointment, whether it be preventive or therapeutic, each individual implant should be assessed for signs of failure. More often than not, this is noted by signs of bone loss over 1 mm during the first year after implant placement, or greater than 0.2 mm per year during subsequent years (5). Other symptoms to be aware of include:
● Implant mobility. ● Bleeding on probing.
● Presence of purulent exudate around the implant. ● Peri-implant radiolucency. ● A “dull” sound during percussion of the implant.
Implant patients that smoke or use tobacco products are more likely to experience prosthetic failure than healthy, non-smoking patients, but all individuals should have the integrity of their implants assessed to avoid potential complications.
Instrumentation selection and techniques Although scratching the surfaces of implants has not yet been shown to increase the risk of peri-implantitis, it should still be avoided; this is why air polishing is highly debated and not recommended for use on these patients (4).
There is also some concern that the titanium oxide surface layer could allow for corrosion of the implant if it is altered through instrumentation. Thus, selection of implant-specific instruments is important for each patient.
Inspection of the removable prosthesis during appointmentsFor removable overdentures, the prosthesis attachments should be inspected during each appointment. This includes O-rings, locators, and clips. Most O-rings and locators will need to be replaced annually, but clips only require replacement if they are damaged. Record the color of the attachment in the patient’s chart to monitor the integrity of the locators from visit to visit.
Ensure that the patient is removing their overdenture nightly to prevent infections throughout their mouth. Examine the denture to see that the patient is using appropriate home hygiene equipment including soaking the denture overnight in a cleansing solution, followed by brushing the soft debris away each morning.
Chemotherapeutic agentsSite-specific chlorhexidine irrigation can help the patient manage isolated areas of peri-implant inflammation. Patients may also need to be given a disposable oral irrigation device to use around specific areas, to limit staining caused by the antiseptic. Chlorhexidine, plant alkaloids, and phenolic agents have all been shown to produce only minimal alterations to implant surfaces (3).
Implementing chemotherapeutics early can be useful in slowing or reversing inflammation (3). These can include rinses such as peroxide, chlorhexidine, or locally applied medications such as Arrestin ® or PerioChip ®.
If chemotherapeutics are applied with a dispenser, the delivery method must use a non-metallic cannula with rounded tips to prevent tissue trauma or surface damage to the implant. Carefully insert the tip of the cannula into the implant sulcus without disturbing existing tissue attachment.
The use of micro-encapsulated minocycline or chlorhexidine gel can be used in peri-implantitis, and has been shown to reduce both pocket depths as well as bleeding on probing for up to one year after placement.(3). In chemotherapeutics that contain tetracycline-loaded fibers, the medication is slowly released over a 10-day period, lengthening the amount of time that medication is delivered to the peri-implant infection.
CurettesBecause dental implants are more likely to be affected by inflammation caused by plaque accumulation than natural teeth are, instrumentation selection and use is extremely important (3). Conventional scalers and curettes are capable of altering the surface of titanium dental implants by scratching the outer layer of the titanium. Thus, scalers and other types of instruments that are used to clean implants should be made of material that does not damage the implant or create small scratches that could harbor bacteria between appointments.
Scalers that are appropriate and safe to use for removing both soft and calcified buildup include those made from plastic, graphite, nylon, titanium or covered in a Teflon®coating.
Dental.EliteCME.com Page 94

These materials will not scratch, harm, or alter the titanium surface when used for instrumentation purposes.
Plastic scalers may leave some residue behind after cleaning around the dental implant. If the instrument tip is reinforced with graphite or gold, it can be sharpened (3). Unfortunately, gold scalers can easily be worn down or altered in shape when scaling rougher areas. This presents itself as a risk, as underlying metals may be exposed and thereby harm the implant being scaled. Resin scalers are also appropriate for use on implants.
Refrain from using stainless steel scalers, as they may alter the titanium implant in a way that increases their susceptibility to corrosion.
In fact, dissimilar metals like stainless steel can increase the number of gingival fibroblasts that are removed from the peri-implant area during
scaling, compared to using a titanium-alloy curette. This alters the retention of the implant by the peri-implant gingiva. Using a titanium or plastic scaler will help preserve the fibroblasts surrounding the implant.
In some cases, disposable scalers can also be used. However, the instrument should not be bulky enough to interfere with the gingiva in the peri-implant area surrounding the abutment. Select an appropriate curette that allows for adaptation within the sulcus surrounding the implant.
Some practitioners find that using titanium scalers is more effective in removing calcified deposits over plastic scalers, although plastic scalers can still be successfully and easily used for the removal of soft plaque biofilm.
Use of manual scalers Typically, calcified deposits are much easier to remove from smooth titanium implant surfaces than calculus attached to natural teeth.(2)
Because no microscopic textures or surface changes on the titanium implant exist, the calculus is far easier to manually sweep away. If the deposit is found to be tenacious and difficult to remove, a tartar softening product may be used to loosen the debris and make it easier to lift away.
Before scaling away calcified deposits, air-dry the visible buildup. This will usually make it easier to sweep the deposit away with the hand scaler using minimal effort. Use short working strokes and walk the scaler around accessible implant surfaces. Only light pressure is necessary (2).
Using scalers along the implant is similar to the method used for scaling natural teeth. Close the blade completely against the abutment before sliding it subgingivally below the deposit. When scaling around fixed implant prosthesis like an “All on 4” denture, instrument adaptation can prove to be more difficult. Scale what is accessible. Once properly positioned, open the scaler gently and make short working strokes appropriate to the needs of the implant root. Again, only light pressure is necessary, as the deposit should come off much easier than one on the surface of a natural tooth root.
In most cases, calculus is found supragingivally along dental implants, rather than subgingivally (3). In fact, most deposits can simply be removed with a prophy angle. Refrain from scaling subgingivally within the implant sulcus unless infection or deposits are present.
Ultrasonic scalersTraditional ultrasonic instruments can significantly alter the titanium surfaces of dental implants. Multiple scratches, grooves, and rough surfaces can be left in place following the use of a conventional ultrasonic scaler in these sites. These increased rough surfaces thereby harbor elevated levels of plaque biofilm, which creates a susceptible environment for future peri-implant infections, jeopardizing the retention and success of the implant prosthesis. Although very minor scratches can be polished away, large and significant damage caused by metal ultrasonic tips cannot.
Plastic ultrasonic tips prevent significant alteration to the titanium surface during scaling. Although plastic tips may create some changes in the implant surface, after the surfaces are polished there is usually no noticeable difference. Plastic ultrasonic tips are generally more effective in removing biofilm than manual plastic curettes.(1)
Using a carbon fiber, plastic, or plastic-coated ultrasonic allows dental practitioners to maintain smooth implant surfaces during prophylactic procedures (2). Metal ultrasonic or piezo tips may also be covered with plastic inserts for ultrasonic cleaning purposes. This prevents the need to buy additional instruments or change tips throughout the procedure.
Polishing methodsIt is not necessary to polish the exposed surfaces of titanium implant. However, polishing may be useful for removing excessive plaque or debris during the appointment. Use the rubber cup to deplaque prior to scaling, if preferred, as it is estimated that polishing alone will remove about 90% of all deposits over the implant surface.
If a rubber cup is used for polishing, refrain from using traditional gritty or abrasive polish. Instead, select tin oxide slurry, aluminum oxide or a nonabrasive polishing paste that is specifically for dental implant use. All polishing paste should be free of Acidulated Phosphate Fluoride. Generic toothpaste may also be used.(1) In cases where no polishing paste is needed, chlorhexidine may be used instead.
Usually, the manufacturer of the implant abutment will prepare it with a polished finish that is difficult to alter using a rubber cup prophy angle (3).
Light air polishing can be performed using glycerine powder. Air polishing may be preferred if leaving residual rubber particles is a concern following rubber cup polishing. Although more recent research supports air polishing safety, some dentists still consider air polishing to be contraindicated around all dental implants as this has been the train of thought for quite some time. Some studies show that air-abrasion is completely safe, while others suggest it may damage titanium surfaces or even lead to detached tissues in the peri-implant area.
Due to the conflicting research available, practitioners should verify with implant manufacturers whether or not air abrasives are appropriate for use around specific designs of implants used within their office.
Page 95 Dental.EliteCME.com

LasersThe use of lasers around implants for peri-implant infections is promising. Using lasers around implants may reduce the depth of peri-implant pockets, as well as bacterium levels (8). Unfortunately there are still many mixed studies regarding the success and safety of dental lasers
surrounding implant sites. Multiple appointments may be necessary for laser therapy before desirable results are achieved around the prosthesis (9).
Professional cleaning of the denture prosthesisIf deposits are present over the surface of a removable denture, place the denture into a zip-top bag filled with stain and tartar removal solution and place it into the ultrasonic machine according to manufacturer’s directions. After being thoroughly rinsed, scrub away any remaining deposits. Light ultrasonic instrumentation may also be used.
Avoid abrasive rubber cup polishing if possible, to prevent scratches in the surface of the overdenture. Polish abutment surfaces as appropriate before having the patient place the removable overdenture back into their mouth.
It is acceptable to work around fixed removable prosthesis without having them removed during the appointment. However, these prosthesis should be removed intermittently for inspection and thorough cleaning as the need arises.
In most cases, the fixed prosthesis will typically not be removed during re-care appointments unless complications exist. This means that it is vital for providers to be competent in working around the prosthesis during most prophylactic visits.
Periodontal probing around implant supported denturesProbing around implants requires some modification in the way the data is interpreted as well as recorded. For healthy teeth, probing depths of 3 mm or less are desirable. However, a dental implant can have healthy readings anywhere up to 5 mm. When dental implants have pockets deeper than 5 to 6 mm, they are more likely to fail. In fact, over 50% of failed implants have pocket deeper than 6 mm.
Implant experts agree that about 1 to 1.5 mm of bone loss occurs within the first year of placing the dental implant, and an additional 0.1 to 0.2 mm each year after. If the patient presents with bone loss amounts more than this average, it should catch the attention of his or her dental practitioner.
It is recommended that implants be probed within 3 months of placing the prosthesis, and every 3 to 5 months thereafter.(3) After probing depths have been stabilized for one year, it is recommended that only the buccal and lingual surfaces of implants be probed on a routine basis. This is also easier to manage when patients wear fixed denture prosthesis. Interproximal bone height should be observed with radiographs.(2) This allows for minimal disruption of the perimucosal seal with the periodontal probe.
Probing techniquesWhen probing along an implant, it is important to avoid insulting the perimucosal seal. Gently sweep the probe into the sulcus, but take note to avoid pressing the probe into the extreme deepest point of the pocket.
In addition to recording pocket depth, the appearance of the peri-implant tissues is also key to indicating a healthy environment. Tissues surrounding the implant should be keratinized, as a lack of keratinized tissues are more susceptible to peri-implantitis (8). The appearance of the tissues should be light pink, but firm. When the tissues are not keratinized enough, the area around the implant is more likely to be impacted by pathogenic microorganisms.
Probe material The probe of choice can be either metal or plastic. There have yet to be any studies that indicate damage to implant surfaces by traditional probes, but many sources still claim that a metal probe could potentially harm the peri-implant site or scratch the surface of the titanium. However, a plastic probe may be more effective in areas where contour is difficult to access with a rigid metal probe. Less force should be used than what is appropriate for probing natural teeth. Otherwise the gingival attachment could possibly be damaged. However, if signs of peri-implantitis like bleeding or purulent exudate are present, it is crucial that an accurate pocket depth is recorded.
Radiographs Diagnostic x-rays play an important role in monitoring the health of patients with dental implants—especially those that support fixed or removable denture prosthesis. The radiographic imaging allows dental providers to evaluate bone quality, including changes in the crestal bone height surrounding the implants. In fact, x-rays may be the single most important tool that is used to assess the success and heath of the supporting implants during a patient’s re-care.
Initially, vertical bitewings should be taken on a frequent basis—as often as every 6 to 8 months for new implant patients (3). Others suggest taking bitewings as frequently as every 3 months during the first year following implant installation. Peri-apical films can be used on the front teeth if preferred, but otherwise, vertical bitewings are adequate for routine use. As long as images of the crystal bone are included in the radiographs, either one will be acceptable. The key is to ensure that each one of the supporting implants is properly recorded during each series of films.
These images should be compared to the original radiographs that were taken immediately after the placement of the implants. This is
done so that crestal bone levels can be carefully measured in order to identify early or advanced bone loss.
Assuming that there are no unfavorable changes in bone height or quality after the first few visits, radiographs can be taken much less frequently during subsequent visits—in some cases, even as long as 3 years between each patient’s appointment.(3).
If the patient exhibits any evidence of bone loss greater than the accepted and expected range of 1 mm the first year following placement; or 0.2 mm during subsequent years; or has symptoms of peri-implantitis, then radiographs should be continually taken at least every 6 months during recall appointments until signs of the infection or bone loss cease.
Although radiographs are used to identify signs of bone loss around the implants, they should also be used to screen for other types of oral pathology such as:
● Lesions throughout the jaw. ● Foreign objects. ● Abnormal growths.
Dental.EliteCME.com Page 96

● Following traumatic events.
If cone beam computed tomography (CBCT) equipment is readily available, it can be utilized to more effectively measure cortical bone
thickness and quality around each implant. However, CBCT is not mandatory for routine maintenance of implant patients within a general care facility.
Patient home care methodsResearch shows that controlling plaque biofilm levels around dental implants is vital to maintain the health of the restoration.(4) It is just as important as caring for natural teeth. Because of this, it is extremely important that implant patients understand their role in the maintenance of their oral health as it relates to the success of their implants over the course of their life.
Unfortunately, many dental implant patients lack adequate oral hygiene habits, which is most likely a significant contributing factor as to why they are replacing missing teeth in the first place.
A complete overhaul on the patient’s oral hygiene habits may be necessary. Care providers should assume that the patient does not have the information or tools needed to begin immediate and adequate home hygiene. Thus, a rigorous oral hygiene educational plan should begin.
Alternately, patients who are overzealous about their oral hygiene methods may create tissue trauma around their implants by being too aggressive with their oral care techniques. Proper instruction on implant and denture care is essential to prevent failure of the fixed prosthesis due to tissue trauma or recession.
Oral hygiene assessmentIt is important for each implant patient to receive an individual oral hygiene evaluation, assessing his or her home care methods. Modifications or re-evaluations at subsequent appointments may be necessary. Have the patient stand in front of a mirror (or hold a hand mirror) while he or she shows you how to remove biofilm from the appliances using various types of oral hygiene aids.
During the oral hygiene assessment, patients should be instructed both visually and verbally on the cleaning methods appropriate around their new prosthesis. If the patient’s methods are inadequate, trade places with the patient, allowing him or her to watch in the mirror while you demonstrate how to properly access areas around the implants, fixed (or removable) prosthesis, as well as methods for oral hygiene aids such as floss threaders and proxa-brushes.
Using an intra-oral camera during prophylactic appointments or exams can improve the patient’s knowledge of what areas require additional care.
Identify areas of biofilm deposits, inflammation, and redness that exist due to inadequate oral care, followed by showing the patient the appropriate way to clean those areas. Record the image in the patient’s file, so that it can be compared to subsequent visits for patient educational purposes.
Assessment of removable implant prostheses Instruct the patient on how to evaluate the overdenture for signs of biofilm collection and wear. Removable overdentures should be cleaned with a separate denture brush and denture cleanser than those retained within the mouth permanently.
Once the patient removes the overdenture, inspect the prosthesis for any complications, such as broken or loose attachments on the denture or implant abutments. Attachments such as O-rings and locator caps can wear out, requiring them to be replaced fairly frequently to retain a snug fit. Most removable denture locators and O-rings need to be replaced once per year, and clips replaced only as necessary.(8)
ToothbrushesBoth manual and electric toothbrushes can be used for effective plaque removal around fixed dentures.(2). The key is to use the brush properly, along the margin of the gingiva to lift soft deposits from the implant surface. Both soft and extra soft brushes can safely be used to clean titanium implants without risk of surface damage. If the patient has limited dexterity, it is best to recommend the use of an electric toothbrush for oral hygiene.
A gentle toothbrush should be used twice each day along the fixed prosthesis or visible implants. Tufted brushes may be useful along bar
connectors. Whether the patient is using a traditional brush or a tufted brush, implant patients should follow the traditional Bass toothbrushing technique; tilting the bristles toward the gum lines at a 45-degree angle and applying only enough gentle pressure to produce light blanching of the tissues.
Although electric toothbrushes can be used, abrasive automatic toothbrushes may be too aggressive for healthy gum tissues. Recommend that your patients use a quality sonic or ultrasonic electric brush with soft or extra-soft bristles.
Interproximal cleaners and tufted brushesCleaning around the neck of the implant along the gingival margin can be carefully performed using oral hygiene devices such as an interdental brushes or floss. Various types of interdental cleaners may provide improved access and biofilm removal under fixed implant prosthetics such as an “All on 4” denture. The interproximal cleanser should be used both under the prosthesis, as well as around and under the peri-implant crevice (8).
End-tuft brushes may be too bulky for some fixed prosthesis, but can be used to remove larger pieces of food or plaque debris along the contour of fixed dentures. However, tapered brushes may be most appropriate for cleaning around cross bars under removable implant prosthetics.
If the brush has exposed metal surfaces, extreme care should be taken. Otherwise it may be possible to scratch the titanium abutment with the surface of the brush core.
Advise your patients to select interproximal brushes that are constructed from or coated with plastic to prevent implant damage or tissue trauma with a metal wire. Nylon brushes are also safe to use, as they will not cause scratching to either the implant or the implant prosthesis.
Interproximal brushes should be chosen based on the size and space around the embrasures. In addition to tufted brushes, some patients may also prefer foam tips or wooden picks for plaque removal.
Rubber-tipped stimulators can assist in maintaining healthy keratinized tissue along the implant retention bars or along a fixed denture. Healthy keratinized tissue promotes a healthy peri-mucosal implant seal. Patients should be educated on the proper way to use the rubber-tip stimulator, so as not to damage the gingiva with the pointed end. The goal is to place the stimulator horizontally along the gum tissue to massage the gingiva. Only light pressure is needed, producing mild blanching similar to that achieved during Bass method brushing.
Page 97 Dental.EliteCME.com

Oral irrigation/water flossingWater irrigation or “water flossing” has been found to be extremely successful in biofilm removal within the sulcus surrounding natural teeth as well as along the surfaces of dental implants. It is safe to use water flossers, at appropriate mild pressure levels, around dental implants and fixed full mouth prosthesis. However, the stream of water should be placed perpendicular to the implant prosthesis to avoid horizontal irrigation into the peri-implant seal, and thus possibly causing damage to the area.
In many cases, using an oral irrigator may be more effective for cleaning hard-to-reach areas around and underneath the fixed implant prosthesis. It may be the most effective way for patients to clean around their fixed dentures. Be sure that the water flosser has a non-metal tip in the likelihood that it could come into contact with the implant abutment, so that scratches can be avoided.
Although most people use oral irrigators only once a day, it is beneficial to have implant patients use the irrigation advice up to twice
daily. Especially in the case of patients that wear fixed “All-on-4” prosthesis.
When implant patients use chlorhexidine inside of their oral irrigation device, it can reduce bleeding by up to 87% compared to using a rubber-tip stimulator dipped in a stronger concentration of the same antimicrobial rinse. Not only that, but oral irrigators used with chlorhexidine are three times better at reducing gingivitis than if the patient were to simply rinse their mouths (8).
When patients use a bristle-tipped oral irrigation attachment, it can be up to 81% more effective at reducing bleeding around their dental implants, compared to just using floss, which is only about 33% effective (8). Thus, recommending an oral irrigator, along with a bristle-tipped irrigation attachment is highly recommended for implant patients with fixed prosthesis, such as “All-on-4” dentures.
Floss and floss threadersTraditional floss may be too difficult for patients to access areas around their implants, unless the implant prosthesis is removable. For fixed dentures, a floss threader can be used to guide traditional floss or dental tape underneath the prosthesis.
Tufted floss with a firm tip, such as “super floss” may make cleaning under a fixed implant prosthesis more efficient. This wider form of floss may be the method of choice in areas where larger spaces between implant retained prosthesis exist. However, some patients may find that it is too tight of a fit these wider variety of flosses under their fixed prosthesis.
In addition to flossing along the interproximal areas of the implant, the floss should also be wrapped or looped around the abutment using a “shoe shine” method for cleaning the lingual and facial surfaces more efficiently. Once the floss is passed under the prosthesis, loop it around the other side and back to the facial side of the implant. Then, cross the floss one side over the other to create a flush circle around the abutment. Gently tugging on each end of the floss will result in a “shoe
shine” flossing pattern around the individual implant. Release one end of the floss and then move along to the next implant site to repeat the process.
Both dental practitioners and patients are often hesitant to place floss subgingivally around implants. However, floss should extend subgingivally to the point where some resistance is felt, as when flossing around natural teeth (3). Healthy implant pockets tend to be deeper than healthy pockets around natural teeth, which means flossing methods are unlikely to impact the level of peri-implant attachment.
FluorideDo not allow patients to use any types of pumice or dentifrice that contains stannous fluoride, or acidulated phosphate fluoride over 3.0 (8). Some studies suggest that fluoride ions create unwanted surface changes on titanium materials, such as that used in dental implants. However, patients may continue using over the counter fluoridated toothpaste for their everyday home hygiene purposes.
DentifricePatients should avoid abrasive dentifrice such as baking soda and stain removing products, such as “smoker’s toothpaste.” Recommend a non-abrasive toothpaste. Fluoridated over the counter toothpaste is acceptable to use. Although there are concerns about fluoride etching titanium, the lower concentrations found in store bought dentrifice has not been shown to impact the surface integrity of implants.
One study simulated approximately 10 years of brushing with fluoridated dentrifice, and measured the levels of S. mutans adhesion to the titanium surfaces. The experiment showed that bacterial levels were the same on titanium surfaces brushed with fluoride as those where non-fluoride dentrifice were used (9).
Chemical agentsIf for any reason brushing or other mechanical hygiene steps are contraindicated, such as immediately following a surgery, advise the patient to use chlorhexidine instead of conventional toothpaste.
Antiseptics can also be placed on floss for delivery along the marginal gingiva surrounding the implant abutment. Or, have patients dip their interproximal brushes or other types of interdental cleansers into non-alcoholic antimicrobial mouth rinse before using them along the margin of their implants.
For patients that are susceptible to gingival inflammation, recommend placing the antimicrobial rinse onto a rubber-tip stimulator for application (8).
Antimicrobial rinses such as chlorhexidine gluconate or chlorine dioxide can also be diluted and placed into water irrigators for oral irrigation (8). Have patients dilute the chlorhexidine or other non-alcoholic mouth rinse into a 1:10 solution with tap water rather than using fully concentrated rinse inside of the irrigator.
If an area of gingiva appears to have peri-implant disease or gingivitis, recommend applying an antimicrobial rinse at least twice daily, for 3 to 6 weeks until the area can be re-evaluated.
Most of all, patients should avoid all mouth rinses that contain alcohol, or even whitening solutions. If an alcohol containing rinse is used, it may contribute to dry gingival around the implant site.
ConclusionManaging fixed and removable dental implant prosthesis is very important for dental professionals, as implant are now regarded to be the standard of care for future tooth replacement. As more patients choose
implants for their oral health needs, re-care appointments will consist of a higher percentage of implant patients wearing fixed or removable overdentures.
Dental.EliteCME.com Page 98

Both removable and fixed implant prosthesis are fairly easy to manage both in the dental office as well as at home. The key is to understand proper techniques, instruments, methods, and diagnostic approaches for implants compared to natural teeth.
Implant patients are not simply re-care patients. They also sometimes require debridements, or even scaling and root planing appointments. Utilizing appropriate chemotherapeutic agents and instrumentation techniques will ensure that implant sites are healthy and able to continue supporting the prosthesis for a longer period of time.
Most curettes, scalers, and ultrasonic instruments can be used, if they are made out of implant-friendly materials, such as plastic, titanium, or nylon. However, the majority of calculus deposits can be removed from implant surfaces simply by using a rubber cup polishing angle. Cleaning the actual denture prosthesis is very similar to the same methods used to clean traditional dentures.
Probing around the implants should reveal pockets no deeper than 5 to 6 mm. These deeper pocket readings are still considered acceptable around the implant, assuming no signs of inflammation or infection is present. Once probing depths are stabilized for one year, it is recommended that only the buccal and lingual surface areas be probed at concurrent appointments.
Radiographs are extremely useful in managing the support of fixed prosthesis. It is recommended that x-rays be taken every 6 to 8 months after implant placement until the alveolar levels have stabilized. Then, x-rays may be taken as infrequently as every 3 years.
Patient education on the care of fixed and removable dentures is vital to implant success. Many people are too aggressive with their implants, or carry over inadequate oral hygiene habits, which contributed to the initial tooth loss to begin with. A proper assessment and follow up of their oral hygiene habits is key. As well as educating the patient on which oral hygiene aids to select, and how to use them around their appliance. Tools such as water flossers or interproximal brushes can be both effective as well as simple to use. Be sure the patient refrains from using abrasive dentifrice or products that contain APF over 3.0. Traditional oral hygiene methods such as flossing or using a water flosser may need to be significantly altered in order to prevent trauma or irritation to the peri-implant site.
Managing a patient with fixed or removable implant prosthesis may present itself more challenging than a traditional dental patient, but the process can be extremely rewarding. Due to the high success rating that most implants are capable of, the dental professional plays an extremely large role in the outcome of their patients’ future oral health.
REfEREnCES1. Beck T. A periodontist’s protocols to avoid dental implant complications: Part 2 - establishing an
implant maintenance protocol. Perio-implant advisory. Retrieved online Oct 20, 2015 from http://www.perioimplantadvisory.com/articles/2014/05/a-periodontists-protocols-to-avoid-dental-implant-complications-part-2-establishing-an-implant-maintenance-protocol.html.
2. Wadsworth L. Common Threads: Care and Maintenance of Implants. Dentistry IQ. Retrieved online Oct 20, 2015 from http://www.dentistrytoday.com/articles-hygiene/8674-common-threads-care-and-maintenance-of-implants.
3. Gulati M, Govila V, Anand V, and Anand B. Implant Maintenance: A Clinical Update. International Scholarly Research Notices. 2014;(2014):Article ID 908534.
4. Todescan S, Lavigne S, Kelekis-Cholakis A. Guidance for the Maintenance Care of Dental Implants: Clinical Review. J Can Dent Assoc. 2012;27:c107.
5. Fehrenbach MJ, Weiner J. Saunders Review of Dental Hygiene. 2nd ed.
6. Mailoa J, Lin G, Chan H, MacEachern M, Wang H. Clinical Outcomes of Using Lasers for Peri-implantitis Surface Detoxification: A Systematic Review and Meta-analysis. J Periodontol. 2014 Sep;85(9):1194-202.
7. Ashnagar S, Nowzari H, Nokhbatolfoghahaei H, Yaghoub Zadeh B, Chiniforush N, Choukhachi Zadeh N. Laser Treatment of Peri-implantitis: A Literature Review. J Lasers Med Sci. 2014 Fall;5(4):153-62.
8. Wingrove S. Focus on Implant Home Care. RDH Magazine. Retrieved online Oct 20, 2015 from http://www.rdhmag.com/articles/print/volume-33/issue-9/features/focus-on-implant-home-care.html.
9. Fais L, Carmello J, Spolidorio D, Adabo G. Streptococcus Mutans Adhesion to Titanium after Brushing with Fluoride and Fluoride-free Toothpaste Simulating 10 Years of Use. Int J Oral Maxillofac Implants. 2013 Mar-Apr;28(2):463-9.
PROfESSIOnAL CARE AnD PATIEnT MAInTEnAnCE Of IMPLAnT-SUPPORTED DEnTURES
final Examination QuestionsSelect the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116,
or for faster service complete your test online at Dental.EliteCME.com.
1. During the first year following implant placement, no more than 2.0 mm in bone loss should occur. a. True.b. False.
2. Gold scalers can remove the number of gingival fibroblasts within the peri-implant area. a. True.b. False.
3. Nearly all dental implant patients have impeccable oral hygiene habits. a. True.b. False.
4. Non-alcoholic mouth rinses can be diluted into a 1:10 solution with tap water for use in irrigation devices. a. True.b. False.
5. No more than 6 months should lapse between preventive care appointments for implant patients for at least the first 2 years after the implant placement. a. True.b. False.
DCA02ISE18
Page 99 Dental.EliteCME.com

Dental.EliteCME.Com Page 100
Chapter 7: Updates on Laser Therapy in Dentistry and Integration in the Dental Office
4 CE Hours
By: Negar Jamshidi, B.Sc. (Hons1), B.DSc.
Learning objectives � Describe the basics of laser physics and the mechanism of laser action. � List five uses of laser therapy in orthodontics. � List the latest laser technologies available in dentistry, and give
one example of each application and the advantages compared to traditional modalities.
� Explain the main application of lasers in each stage of the implant process.
� Explain five main clinical applications of lasers in restorative dentistry.
� List three key applications of lasers in Prosthodontics, and describe parameters setting for each laser.
� List three lasers used in the diagnosis of caries as well as the limitations and treatments available for TMD.
� List the application of lasers in oral surgery. � Describe the practical application of lasers in periodontics. � List three main safety requirements of lasers. � Describe practical laser use in pediatric dentistry. � Discuss ways to integrate lasers into dental practice.
IntroductionIn the last decade alone, the research and application of laser therapy technology in general dentistry has expanded remarkably, heralding lasers as one of the most exciting advances in dental technology. This course will review the latest developments in dental laser application and provide evidence for its multitude of benefits in general dentistry, and also discuss the practical application and integration of lasers in dental offices. The science behind lasers, and the types of lasers available in the market and their specific dental applications will be reviewed. At
the end of this course, general dental practitioners will be armed with knowledge and understanding of how and when to apply laser therapy in management of oral diseases as adjunct to or instead of other traditional treatments. Clinicians will also learn to carefully approach laser application with adequate training and an understanding of the optimal parameters required to achieve specific treatments. It is envisioned that this technology will increase the ability to provide quality oral treatment, and in effect, increase the standard of patient care.
Basics of laser physics and mechanism of action“A splendid light has dawned on me...”- Albert Einstein
The concept of lasers was first proposed by Einstein in his 1917 paper on the theory of quantum radiation which postulated that light consists of photons with different wave energies which can produce amplified or stimulated particles of powerful light beams [1]. In fact, Einstein won the Noble Prize for describing the concept of radiation photoelectric amplification, not the theory of relativity! It took another 43 years for the first laser to be built by Theodore Maiman in California. The word LASER is an acronym for “Light Amplification by Stimulated Emission of Radiation” and was coined by Gordon Gould in 1957, an independent researcher considered one of the original fathers of laser [2].
Since its inception, laser has found numerous applications in the medical field and there are now growing practical uses for oral and dental-related treatment modalities. The amazing array of amplification mechanisms and the wavelength range of lasers are the drivers for these rapidly expanding dental applications. A laser produces energy in a coherent radiation of one wavelength, in either the infrared, the visible or the ultraviolet part of the electromagnetic spectrum. In effect, this means that laser light is a single colour (monochromatic) and each light wave is identical in physical properties (coherence). The principle mechanism of action of laser involves four main elements which are represented diagrammatically in Figure 1 [2]:1. Amplifier: An active medium composed of either gas, liquid or
solid molecules in a gas, that amplifies a passing light wave.2. Pumping source: An excitation system that allows the active
medium to turn into an amplifier for electromagnetic radiation.
3. Optical resonator: An optical cavity with excitable atoms that allows the pumping source to turn it into an oscillation resonator.
4. Output coupler: I.e. a mirror, that allows partial transmission of the stored radiation inside the optical cavity.
Figure 1. Schematic representation of laser mechanism
The light for dental laser systems is delivered through an optical fibre cable which is a hollow articulated arm [2]. The wavelength varies between 488nm-10,600nm. Lasers are classified according to the emission type (spontaneous or stimulated emission), output power, active medium (liquid, solid or gas state), target tissue (hard or soft tissue) and possible biological damage (Class I-IV) which will be discussed further below [3,4].
Update on laser technologies used in dentistryThe first laser designed for dental use was introduced in 1989 by an American dentist, Dr. Terry Myers, and was intended for commercial use on soft tissues only [4]. It was not until almost 18 years later when
laser application in dentistry began to gain acceptance [5-7]. These applications expanded into the surgical areas of periodontal therapy, implantology, and endodontics [7]. More recent advances into the 3-D

Page 101 Dental.EliteCME.Com
capability of lasers has allowed digital impressions using Computer-Assisted Design and Manufacturing (CAD/CAM) technology [8].
Currently there are more than 24 indications for clinical application of lasers in dentistry with mounting evidence of the benefits for treatment and patient well-being [9]. In this section, the different laser technologies, and their parameters and limitations will be discussed.
The lasers currently used in dentistry are argon, carbon dioxide, erbium (Nd: YAG and Er: YAG), diode, DIAGNOdent, DopplerFlowmetry, chromium (Er, Cr: YSGG), and Low-level Laser Therapy (LLLT). The names of the lasers reflect their active medium contents and states of suspension [7]. Optimal laser parameters depend on the target tissue, and involve power output, wavelength, exposure time, and energy quantity [6]. Some of the more common laser applications in dentistry include, but are not limited to, crown lengthening, caries detection, mid-line frenectomy, pain reduction and hypersensitivity treatment, gingevectomy, and removal of aphthous ulcers and soft tissue lesions (Table 1).
An argon laser produces light at the light wavelengths of 488nm blue, and 514nm blue-green in an active medium of argon gas with a high current of electrical charge. Due to its poor absorption by hard tissues, the risk of damage to enamel is negligible during soft tissue surgeries. The main uses of argon lasers are to control haemorrhage during gingival surgery, and to detect cracks or decay on tooth surfaces [7].
The carbon dioxide (CO2) laser is another laser which uses gas as active medium. They produce light at about 10,600 nm in the visible range and have very high water and hydroxyapatite absorbance properties compared to other dentistry laser systems [3]. The major advantage of carbon dioxide lasers is that they allow soft tissue surgery with ease and precision. The drawbacks are that the laser is not suitable for hard tissue use, and that it is technique-sensitive. During application the surrounding tooth structure requires protection [5].
Erbium lasers are the most frequently used lasers in dentistry. There are different types of erbium lasers including the Erbium-YAG (2,940
nm) and the Erbium-Chromium-YSGG (2,780 nm) which have active mediums of yttrium-aluminium-garnet and solid yttrium-scandium-garnet, respectively [10,11]. Due to their high hydroxyapatite and water absorbance properties, both of these lasers are excellent to use for caries and hard tissue removal [11]. The success rate of these lasers is also due to their minimal tissue penetration, and hence negligible thermal effects on pulp, as the soft tissue is removed [11]. Of note, there is no need for anaesthetics with an Er-YAG laser during caries removal. It has less vibration than a high speed drill, which is highly satisfying and comfortable for patients [9]. Recent studies have shown effective reduction of dentinal hypersensitivity using Er-YAG lasers with less thermal side effect than CO2 lasers [12,13]. The Er-YAG laser also has significant antimicrobial effects and is suitable for use in endodontic treatments. Similarly, the Er-Cr-YSGG laser has no thermal effect on pulp and results in excellent bonding properties [14].
Diode lasers’ active medium source of emission is a semi-solid semiconductor with varying wavelengths in the 800nm-980nm range. This laser can be safely used for soft tissue surgery including crown lengthening and frenectomy due to its poor absorption by the tooth structure [3].
The LLLT laser is applied via a light emitting diode (LED) to support tissue repair and healing, induce analgesic effects, and decrease inflammation. Current studies indicate that LLLT is useful in the treatment of a plethora of oral conditions and has applications in nearly every dental-related field. This versatility is due to the mode of LLLT action, as light is absorbed by cell mitochondria with no thermal effect on tissues [15].
Nd-YAG lasers are the first laser system used in dentistry with an active medium of YAG crystal doped with neodymium. It produces a wavelength at 1,064 nm which is absorbed only by hard tissue, and has great use in surgery and soft tissue removal [8]. They can also be used to remove some enamel caries and provide good homeostasis during surgery. The main disadvantage with these lasers is the depth of penetration, which results in a risk of damage to the pulp and possibly the underlying bone [8,9].
Table 1. Summary of current dental lasers in the market and their main clinical applicationsLaser type Wavelength Laser characteristics Indication and tissue depth Clinical use
Argon. 488nm, 514nm. Low water absorption. Soft tissue, 1mm. Gingevectomy.
CO2. 960nm, 10600nm. High water and hydroxyapatite absorption.
Soft tissue, 0.1mm. Oral surgery.
Diode. 800-980nm. Poor hard tissue absorption. Soft tissue, 0.1-0.3mm. Crown lengthening, frenectomy, diagnosis and disinfection.
Er-YAG. 1030nm. High water and hydroxyapatite absorption.
Soft and hard tissue, 5um. Remove dentinal, enamel/dentin cutting, hypersensitivity.
Potassium-titanyl-Phosphate.
532nm. Low water absorption. Soft tissue. Surgery and periodontal bleaching.
Low level lasers (LLL).
600-1000nm. Low water absorption. Soft tissue. Disinfection, treatment of recurrent aphthos ulcer and TMJ disorders.
Nd-YAG. 1030nm. High water and hydroxyapatite absorption.
Soft tissue, >1mm. Endodontics, disinfection, and selective caries removal.
Laser operationDental lasers either emit energy in a continuous wave or a free-running pulse. Both carbon dioxide and diode lasers emit energy in a continuous wave mode, which continues while the laser remains activated. The limitations of these lasers include associated thermal burn which is abated by using an electronic-controlled or gated-pulse laser. Laser systems that use Nd-YAG, Er-YAG, and Er,Cr-YSGG
operate on the free-running pulse mode, where true pulses of ten thousandths of a second originate from a flash lamp [9].
Laser-tissue interactionLaser-tissue interactions are dependent on the wavelength, laser mode of emission, and tissue characteristics [8,9]. The key factor for

Dental.EliteCME.Com Page 102
absorption of light in tissues is wavelength of the light. Generally, pigmented tissues tend to absorb more energy from shorter wavelengths in the 500-1000 nm range, such as the diode and Nd-YAG lasers. Tissues with higher water content and apatite crystals absorb energy better in the longer wavelength range (3000 nm-10,600 nm) which encompasses ER-YAG, Erbium and CO2 wavelengths [9]. Thus the depth of light absorption by target material is an indicator of the application of the laser: the CO2 laser depth of penetration is a maximum of 0.1mm which is capable of sealing blood vessels and achieving sufficient haemostasis [9]. However, while the Nd-YAG laser is capable of deeper (2-5mm) tissue penetration, the risk of damage to the surrounding tissue increases accordingly [9]. The energy absorbed from the light is converted to heat, which depending on tissue characteristics and the duration of light exposure, may alter the tissue structure and cause various effects such as carbonization, or in the case of hard tissues, recrystallization [7-9].
In summary, laser-tissue interactions depend on four properties of light energy and target tissues [16,17]:
● Absorption: Tissue characteristics such as pigmentation, and presence of chromophores (agents that absorb light) determine the amount of energy absorbed. Other factors include the laser emission mode and wavelength, the laser wavelength used, and the laser emission mode.
● Transmission: This effect depends on tissue optical characteristics and the laser wavelength used.
● Reflection: There are either specular (mirror-image) reflections or diffuse (different directions) reflections of the light from the target surface without any effect on the target.
● Scattering: The laser light enters the target tissue across multiple directions, reducing the effect of the laser energy.
Advantages and disadvantages of laser systemsThe advent of lasers in dentistry carries many benefits. One such benefit is the removal of a diseased or infected tooth structure while not affecting healthy tissues by using the selectivity of their higher water content. Recent studies have shown that lasers eliminate microfractures, and compared to high-speed handpieces, have a much lower thermal effect on the pulp [18]. Also there are reports of quicker healing of bone tissue after laser-surgical osseous tissue removal. Notably, it has been shown that lasers used to prepare enamel increase the bonding surface for composites [19].
One of the main advantages of utilizing a laser is the decreased microbial contamination risk in the operating field, especially during cavity preparation. Several studies show that laser post-operative healing is rapid and scar formation is diminished [18,20]. Additionally,
the use of lasers in children and pregnant women has been deemed safe and is practiced regularly.
The obvious limitation of lasers is their high outlay and ongoing costs; these costs include training, maintenance, and the time taken to implement laser protocols in the practice. In addition to each manufacturer’s in-house training, there are high end courses offered by the Academy of Laser Dentistry (ALD) that support dental teams in developing efficiency and skills. There are some limitations in the delivery system of lasers due to accessibility in the operating field. The removal speed of most lasers is slower than a high speed drill, but at the same time the damage to healthy tooth structures is minimal. Another drawback is that erbium lasers cannot interact with gold or porcelain materials [18]; although, they are advantageous when removing caries adjacent to these materials.
Table 2. Summary of key benefits and limitations of dental lasers in clinical applicationsKey benefits for laser application in dentistry Limitations of laser application in dentistry
Reduced risk of infection due to bactericidal action. Cost prohibitive in terms of the outlay, maintenance and supplies for the laser.
No scar formation and excellent wound healing. Lasers are wavelength specific with different properties.
Less requirements for anaesthetics and little to no pain or discomfort during and post operatively.
Insufficient clinical trials and standardization of protocols for use in RSTAPT.
Control of bleeding and achieving good hemostatic control. Implementation of safety measures for all involved in the operating field and ensuring that staff are supportive and follow safety regulations.
Excellent diagnostic tool especially for pulp vitality assessment. Continuing education and ongoing training required for the entire dental staff.
Laser applications in restorative dentistry The traditional procedures for tooth preparation for restorations use high or slow speed rotary handpieces which are uncomfortable to patients and more time consuming because of the requirement to administer local anesthetics. In restorative dentistry, lasers have a long history of overcoming these limitations, and they have found application in diagnostic and common operative applications such as caries detection, curing composite restorations, bleaching, cavity preparation and caries removal [18]. More recent key applications of lasers in restorative dentistry areas include using lasers as an adjunct to bonding composite restorations, in the removal of defective restorations, and for the treatment of dentin hypersensitivity [18, 21].
Caries assessment, diagnosis, and prevention Generally, the diagnosis of tooth decay or caries involves a visual clinical examination and the use of probes, complemented by bitewing radiographs. However, the conventional tools for decay detection are largely affected by the complexities of tooth morphology, accessibility
and visibility hampered by presence of plaque, and limitations of radiographs to interproximal tooth decay. Furthermore, development of quantitative methods in dentistry for the detection and monitoring of caries have enhanced the reliability of detecting earlier caries lesions, and allowed quantitative assessment of the progress of the lesion [22].
The introduction of caries detection technologies including laser fluorescence tools such as DIAGNOdent (Kavo), and LED fluorescence tools such as Spectra Caries Detection Aid System (SCDAS) and Sopro-Life, have vastly improved the early detection of carious lesions [23-25]. Recently, Rechmann et al. [26] compared these technologies and concluded that the sensitivity and specificity of all three systems allows them to be utilized as an efficient addition to monitor and diagnose early carious lesions.
The sensitivity and specificity, respectively, of the systems were found to be: DIAGNOdent, 87% and 66%; Sopro-Life daylight

Page 103 Dental.EliteCME.Com
mode, 95% and 55%, and fluorescence blue mode, 93% and 63%; and SCDA, 92% and 37% [26].
DIAGNOdent quantitatively measures presence of decay by photodiodes (655nm wavelength). It takes advantage of the differences in fluorescence emitted by healthy tissues and plaque metabolites. The digital values of fluorescence intensity ranges from zero to ninety-nine, and is represented as an audio signal reading as follows (Source: DIAGNOdent, KaVo, Biberac, Germany):
● 0-14: healthy occlusal surfaces. ● 15-20: enamel caries. ● >21: dentin caries.
There is no correlation between the depth of decay and the signal reading value [23,27]; however, the DIAGNOdent has been shown to be very effective as an adjunct to conventional clinical diagnostic methods, especially in early detection of occlusal caries [28].
The more recently introduced Sopro-Life (Sopro-Life, La Ciotat, France) laser has the extra benefit of magnification, and relies on visual assessment with the laser fluorescence device. The output of this system is largely influenced by the presence of calculus, plaque, prophylactic pastes, and therefore meticulous cleaning of the tooth surface before reading is essential. In addition, fluorosis or stained surfaces on teeth maybe give false positive score, so it is important that an adequate training session is undertaken before tooth examination to increase the sensitivity and specificity of the values [25]. The Spectra Caries Detection Aid System (SCDAS) utilizes fluorescence technology using light emitting diodes (LED) to project high energy light onto the tooth surface which results in plaque metabolites displaying as red and healthy enamel as green fluoresce [26].
Quantitative light-induced fluorescence (QLF, InspektorTM) lasers are the most widely reported diagnostic lasers shown to be more efficient at early caries detection. They have the added benefit of visual cues, and the ability to involve patients in treatment plan [29]. The principle mechanism involves enamel auto-fluorescence with the excitation of dentin using a blue light of 370 nm which allows detection of lesions as dark spots on a bright green background. An area with <5% fluorescence is considered a demineralized lesion. The QLF system demonstrates excellent reliability and reproducibility as well as sensitivity for early caries quantification [30]. Similarly, the Sopro-Life camera was developed as a potential diagnostic tool for early carious detection [24]. Furthermore, both of these latest technologies detect active lesions up to a depth of 500μm on the surface of demineralized tooth area [31,32].
One of the most useful diagnostic lasers in restorative dentistry is the Laser Doppler Flowmetry (LDF) which was developed to measure tooth vitality. Its mechanism of action is dependent on the vascular response of the pulp; red cells scatter light emitted from the LDF with a subsequent frequency shift processed as a signal [33].
The purpose of these caries detection tools is as an adjunct to visual assessment and to enhance the specificity and sensitivity of diagnoses in general. There are few clinical studies due to the lack of reference tests with most of the diagnostic tools. The exception is the QLF camera, the most widely reported tool, which has been shown to differentiate between caries and adjacent sound enamel accurately and consistently [34]. Therefore, laser fluorescence provides a quantitative and non-invasive method for the diagnosis of dental caries, and complements the conventional diagnostic methods.
Cavity preparation and caries preventionThe traditional preparation of a cavity first involves application of localized anaesthetic to eliminate patient discomfort during the procedure, followed by removal of carious tooth structures using rotary instruments. The drawback to this conventional method is the patient discomfort during the entire procedure, from the injection phase to the drilling noise and vibration stage, combined with the disadvantage of inevitably some healthy tooth structure removal during the process. The advent of lasers circumvents both of these
issues. With lasers, local anaesthesia is not required, and most lasers selectively remove infected hard tissue while leaving healthy tooth structure intact. The three most commonly used lasers are from the erbium family and include the ER-YAG (2940 nm), the Er, Cr-SGG (780 nm) and Er-YSGG (2790 nm). Each of these provide unique applications in tooth ablation [35]. Er-YAG lasers have been demonstrated to be more efficient at removing infected hard tissue than conventional handpieces, and they stimulate dentin formation and exert an antibacterial effect [36]. However, some studies have indicated a risk of thermal damage to the pulp as a main drawback, despite use of water spray during the procedure [37]. Several more recent studies have demonstrated that adjustments to the pulse repetition rate and the power intensity have diminished this thermal alteration to safe levels for the pulp [37-40]. Although the literature is inundated with inconsistent reports on the thermal effects of erbium lasers during cavity preparation, the emerging evidence on erbium lasers, especially long term dataset, support the clinical use of erbium lasers for tooth ablation [38]. The factors that contribute to these inconsistencies are due to different operator factors including laser parameters (e.g. power intensity), pulse length, light profile, and other parameters that ultimately affect the outcome of laser-tissue interaction. Further clinical research on erbium lasers will be required to cement the position of these lasers in dentistry, and to encourage more clinicians to utilize the technology.
Another laser with potential in caries removal is the specific CO2-laser system (short-pulsed), also shown to reduce enamel demineralization. The remarkable efficacy of caries removal by hard tissue ablation and cavity design precision has been demonstrated with the more recent application of Ultra Short Pulsed Laser (USPL) systems which also showed minimal side effects [41-43]. The mechanism of ablation of the Nd-YVO4-USPL (1064 nm, 8 picosecond duration) in a recent study was described as that of a multi-photon process, which is in contrast to the ER-YAG thermal-mechanism; each exhibited different tissue-laser interaction [41]. Thus, the USPL technology offers huge potential for clinical dentistry in efficient and selective caries removal by allowing for different laser parameter settings to the control ablation rate, hence minimizing the thermal side effects.
Use of laser in enamel remineralizationOne of the emerging benefits of lasers in restorative dentistry is their protection of the enamel surface from acid attack and demineralization [44-46]. This apparent acid resistance feature of lasers is of particular advantage in patients who have difficulty in maintaining an oral hygiene routine, high caries susceptibility, or rampant caries, and/or those under orthodontic treatment. Recent reports have shown an 87% reduction in the demineralization of enamel surface using specific Carbon dioxide (CO2) lasers with a wavelength of 9300-9600 nm and a short pulsed microsecond setting [47,48].
While the exact mechanism of enamel resistance to acid during laser exposure is not clear, there is accumulating evidence to suggest that the laser may introduce mechanical surface changes to the enamel crystals [49,50]. Other plausible mechanisms of action are discussed by Karandish et al. [46] in a recent review. Of note, several studies have established that a combination of fluoride application and laser exposure significantly reduces carious lesion depth and increases enamel acid resistance [45,51-53].
Laser application in management of dentin hypersensitivityOne of the key applications of lasers in restorative dentistry is in management of dentin hypersensitivity (DH). This condition is generally due to gingival recession, tooth wear and cracks as well as caries presence. Many lasers are capable of reducing DH and are essentially divided into two groups: (1) the low-power level lasers, such as Helium-Neon (He-Ne) and Gallium-ALuminumArsenide (GaAlAs or diode) lasers; and (2) the middle output power or high-level lasers such as CO2, Er-YAG and Er,Cr-YSGG and Nd-YAG lasers [21,54,55]. The low-power lasers such as the GaALA lasers

Dental.EliteCME.Com Page 104
(780, 830 or 900 nm) have been shown to lower pain levels and inflammation by suppressed nerve transmission [54], whereas irradiation with higher level lasers such as Nd-YAG and CO2 lasers results in thermal effects leading to complete obliteration of dentinal tubules [55].
A recent clinical study showed that a tooth brush with a built-in Low Level Laser was an effective alternative for treatment of DH [56]. This results were corroborated in another study which found that application of LLL therapy (685 nm) significantly reduced DH compared to a desensitizing agent containing 8% arginine-calcium carbonate [57]. The use of He-Ne Lasers has a varied efficacy of DH treatment ranging from 5-100%, and there is no consensus among studies to draw any conclusions regarding its application [21,54]. On the other hand, GaALAs lasers for the treatment of DH is well documented with at least a 50% rate of effectiveness [21].
The CO2 laser effectiveness in treatment of DH is reportedly in the 59.8%-100% range, but no analgesic effect has been noted [21, 55]. Similarly, the Nd-YAG laser mechanism of DH involves narrowing of dentinal tubules [58] as well as analgesic effect [59] despite mixed reports on its treatment effects in the 5-100% range [55]. In addition, the combination of Nd-YAG with topical fluoride has been shown to be quite effective at reducing dentin hypersensitivity [60].
The Er-YAG lasers have a range of treatment effectiveness in the range of 38%-47% , and are shown to enhance the bond strength of common desensitizing agents [61]. Furthermore, a recent systematic review of clinical research concluded that the ER-YAG efficacy in reducing DH was markedly higher than GaALA lasers [62].
In summary, the treatment of DH is essentially directed at inhibiting pulpal nerve response or limiting displacement of fluid within the dentin tubules. LLLT lasers such as He-Ne (630 nm) or GaAlA lasers (diode) limit pain stimulus transmission by increasing nerve cell function [55]. Both CO2 and Nd-YAG lasers (1064nm) are capable of stimulating secondary dentin production and sealing open tubules. There is also strong evidence indicating that combination of laser therapy and desensitizing agents is very effective in management of DH [63,64].
Use of lasers in direct pulp cappingOne of the most successful application of lasers in restorative dentistry is in direct pulp capping. For decades, conventional methods used calcium hydroxide-based materials to treat exposed vital pulp once hemostasis and bacterial decontamination had been achieved [65].
Lasers offer the unique opportunity of non-invasive, minimal treatment of vital exposed pulps with both great success and a proven track record [65]. CO2 laser exposure in direct pulp capping, compared to calcium hydroxide treatment, has been shown to have a clinical success rate of 89% after a 12 month follow-up [66]. Remarkably, Nd-YAG laser treatment of vital pulps in permanent teeth showed a greater than 90% survival rate after 54 months compared to teeth treated with the conventional calcium hydroxide direct pulp capping method [67]. More recent clinical studies using Er-YAG lasers in human molar teeth achieved a clinical success rate of 93% after two years of pulpotomy treatment [68]. Similarly, clinical evaluation, eight months after Er,Cr-YSGG laser treatment of vital pulps, indicated positive vitality results with no sign of inflammation in 89% of the cases studied [69]. More
recently, the diode lasers have also proven to be significantly effective in successful direct pulp capping with a long-term prognosis [70].
In a recent literature review on the “use of lasers for direct pulp capping”, Komabayashi et al. [65], summarizes and illustrates the step-by-step clinical procedures for direct pulp capping with lasers. Clinicians are encouraged to examine this extensive review before embarking on laser-assisted direct pulp capping for the first time. Currently, laser application for direct pulp capping has an incredible 90% success rate compared to the 60% rate for conventional methods. This is a promising future alternative to the current methods and should result in greater long-term success rates and increase the quality of patient care [66-71].
Other applications of lasers in restorative dentistryThe use of lasers in etching the enamel has been shown to be comparable to the conventional acid-etching method [71,72]. More recently, laser etching as an adjunct to the conventional acid-etch method has been shown to increase tooth-resin adhesion with a significantly higher bond strength compared to using acid-etch alone [74,75].
Another useful application of lasers is in removal or repair of defective restorations. Conventional methods using high speed handpieces have the disadvantage of removing healthy tooth structure which increases the risk of pulp exposure and undermines the mechanical strength of the treated tooth. The advent of USPL technology has largely overcome these limitations of traditional restoration removal, and are reportedly effective at removing restorative materials with minimal thermal effects [43]. Further clinical research is required on the thermal effects of laser exposure on pulp to confirm their long term effectiveness in restoration removal.
One of the most effective applications of lasers is in the management of recurrent aphthous ulcers (RAUs), which commonly affect up to 60% of the general population [76]. These lesions are often painful oral ulcers that are a result of exposed nerve endings. They are debilitating to the patient without any definitive cure. The challenge in management of RAUs is to find a resolution in minimal time without side effects or patient discomfort [76]. Lasers such as Low-Level Laser Therapy (LLLT) have been suggested as alternative treatment for management of these ulcers. Several reports have demonstrated significant alleviation of RAU symptoms upon application of LLLT. LLLT not only reduced pain but also completely resolved the ulcer in less than half the time [77,78]. Since the pathogenesis of RAUs have been thought to involve the immune system, a plausible mechanism for the LLLT action is the reduction of inflammatory biomarkers such as cytokines and interleukin expression [79].
In summary, lasers are a more efficient and attractive alternative to conventional dentistry and appears to be effective in a number of restorative treatments. However, the cost, together with the need for specialised training and ongoing maintenance issues, has hampered their widespread use among dental professional. Nevertheless, the long term benefits for clinicians include predictable successful treatment outcomes when correct parameters of laser application together with sufficient training are applied. The benefits for patient include comfort, reduced pain, and optimal treatment results.
Laser uses in bleaching As discussed earlier, the fundamental components of laser light that define its interaction with the target tissue include: the wavelength emitted by the laser; the density of power of the beam; and the operation of laser characteristics, such as a continuous versus pulsed delivery system. When the energy emission is low, laser-tissue interactions tend to be optical or a combination of optical effects, photochemical effects, or photo-biostimulation [80]. When the pulse energy is increased, photothermic interactions take over, leading to photoablation [81, 82], an undesirable effect in a bleaching gel [80]. Therefore, when bleaching, it is crucial to consider the level of light
absorption (and hence laser wavelength) required to achieve the desirable bleaching efficacy with minimal thermal effects. Of note, the effect of additives in the bleaching gel and their effect on the absorption range of photons must be considered when using lasers.
Bleaching gel can be heated using lasers or special electric heating devices to enhance bleaching efficiency, as the chemical reaction occurs faster at higher temperature [82]. In addition, peroxide penetrates dental structures much more efficiently with thermal expansion [80]. The

Page 105 Dental.EliteCME.Com
drawback is that heat can cause enamel dehydration and irreversible pulpal damage [80,81].
The process of the photo-oxidation (molecules in a triplet excited state becoming oxidized) effect leads to direct photo-bleaching, which is capable of penetrating tooth structure without absorption by water or hydroxyapatite. Lasers are more efficient at photo-bleaching due to their high density of light, and are effective at removing extrinsic stains [80,82]. Dental enamel can be stained with coffee, tea, wine and/or nicotine and these stains are traditionally removed using hydrogen peroxide bleaching. In some cases, these extrinsic stains can become embedded in the outer layer of the enamel which is then difficult to
remove with bleaching treatments. Near UV Laser heat has been shown to remove such extrinsic stains with added benefit of ablating the affected underlying enamel [83]. Intrinsic stains are normally removed with photochemical or photo-thermal bleaching methods. Argon diode and CO2 lasers have both been used in tooth bleaching. Furthermore, excellent results in bleaching has been shown using potassium– titanyl–phosphate (KTP) lasers (specific Nd-YAG lasers) that have a wavelength of 532nm which is visible in the green spectrum. Further studies confirmed the safety and validity of KTP lasers for tooth bleaching, and showed significantly more whitening results compared to diode lasers [84]. Noteworthy, photodynamic office bleaching using KTP laser produced improvement in tetracycline discoloration [85].
Laser uses in pediatric dentistryThe application of lasers in pediatric dentistry has been by far the most active and widest clinical use to date. Lasers offer an attractive alternative to conventional methods as a minimally invasion technology for dental treatment in children. Not only are lasers well-accepted by children and parents alike, but studies have also indicated enhanced cooperation of children during more arduous treatments such as pulp and surgical treatments [86,87]. The most common application of lasers in pediatric dentistry are for caries detection and prevention, tooth structure preparation for sealants or restorations, and pulpotomies as well as numerous soft tissue indications [87].
The American Academy of Pediatric Dentistry (AAPD) has set protocols for the dental specialist on the judicious use of lasers in pediatric dentistry [88]:
● “Recognizes the use of lasers as an alternative and complementary method of providing soft and hard tissue dental procedures for infants, children, adolescents, and persons with special health care needs.
● Advocates the dental professional receive additional didactic and experiential education and training on the use of lasers before applying this technology on pediatric dental patients.
● Encourages dental professionals to research, implement, and utilize the appropriate laser specific and optimal for the indicated procedure.
● Endorses use of protective eyewear specific for laser wavelengths during treatment for the dental team, patient, and observers.”
For diagnosis of caries, the most commonly used laser in pediatric dentistry is the DIAGNOdent laser (655 nm). This laser is effective for detection of occlusal caries in both deciduous and permanent teeth [87,89,90]. As described before, the degree of demineralization correlates with the emitted fluorescence and is quantified as the amount of decay present. The drawback is the lack of efficacy in detection of early enamel lesions; DIAGNOdent is more efficient at diagnosis of dentin occlusal caries. Argon lasers (488nm) address this shortcoming and have been successfully used as diagnostic tool in occlusal and interproximal caries detection; however, they are more efficient in detecting demineralization in primary rather than permanent teeth [91]. In addition, Argon lasers are a fantastic adjunct diagnostic tool during routine examinations to diagnose caries underneath fissure sealants [92].
There is some evidence for the application of argon lasers in enamel protection against caries. Especially when combined with topical application of fluoride, it has been shown to remarkably decrease the depth of carious lesions [44,93]. Another possible use of a laser system is for enameloplasty just before fissure sealant is applied; enamel becomes more acid resistant and bonding is enhanced as the laser complements the use of the acid-etch technique [89].
In pediatric dentistry, accumulating evidence on erbium lasers (Er-YAG and Er,Cr-YSGG) has demonstrated the efficacy of hard tissue ablation with minimal thermal effects [17,89,94]. This is in contrast to some of the research on erbium laser applications for adult teeth. This disparity could be either due to larger clinical samples on primary teeth, or possibly due to laser parameters more carefully set to reduce pulp effects in children. In either case, there is a great need for more
clinical studies to standardize use of erbium lasers for hard tissue ablation without thermal side effects. The reduced vibration and noise and the negligible need for local anaesthesia during cavity preparation has been reported with successful applications of Er-YAG lasers [95,96].
In particular, research has demonstrated effective anaesthesia with success rates of 50-75% using pulsed Nd-YAG (660nm) lasers during cavity preparation of primary molar teeth [97]. LLLT is also effective at reducing pain and swelling during eruption of primary or permanent teeth as well as in instances of soft tissue trauma [98].
Pulpotomies are very common treatment procedures in pediatric dentistry. The results of CO2 laser application for vital pulp therapy have shown a 98.1% clinical success rate of treatment after a two year follow-up [99]. Similarly, a recent study using diode lasers for pulpotomy treatment showed a 100% clinical success rate after a 12 month follow up [100].
Soft tissue application of lasers in pediatric dentistry include gingevectomies, removal of fibromas, gingival hyperplasias, mucoceles and aphthous ulcer treatments [87]. The main lasers for soft tissue surgery have been the argon, CO2, and diode lasers, and Nd-YAG laser systems, especially for coagulations, and decontamination of the soft tissues [90]. Specific Er-YAG lasers with shorter pulse lengths modified for soft tissue surgery have also been utilized. Furthermore, lasers can be used to treat traumatic injuries to dental tissues with ease, with minimal local anaesthetics and discomfort. Laser Doppler Flowmetry (LDF) is a reliable and accurate tool used in the assessment of pulp vitality and monitoring mobility of traumatized teeth for the long term [33]. Also, ER-YAG and Er,Cr-YSGG lasers can be used to seal dentinal tubules in traumatized teeth, leading to reduced dentin hypersensitivity [98]. Other applications of lasers for traumatized tissues include localized application of lasers for facial swelling, soft tissue trauma, and wounds to reduce associated discomfort and pain [9].
Laser use in pediatric dentistry is on the cusp of becoming the Gold Standard with ever increasing new applications, and refinement of the existing ones to address conventional disease with modern non-invasive technology. Therefore, it is vital for the dental practitioners and their dental teams to continuously familiarize and educate themselves on the accumulating clinical evidence and research on safety issues, effectiveness, multiple applications, and more importantly, the laser parameters used for specific dental applications to deliver optimal patient care.

Dental.EliteCME.Com Page 106
Table 3. Laser applications in pediatric dentistryBenefits Limitations
Hemostasis achieved during soft tissue surgery. Costly in terms of outlay, and the time to plan and implement laser system in dental office.
Selective laser-interaction with infected tissue. More than one laser may be needed for different soft and hard tissue applications requiring specific wavelengths.
Enhanced wound healing with reduced need for analgesics. Strict adherence to infection control by all dental team involved is paramount to avoid contaminated aerosols.
Bacterial decontamination and disinfection of the localized area. Safety protocols must be followed and individuals involved in the laser vicinity must wear laser specific eye protection.
Complementary tool to visual diagnosis for caries detection. Limited diagnostic tool to unrestored surfaces due to fluorescence of the restorative material.
Less post-operative discomfort & scarring following soft tissue surgery.
Laser use in periodonticsLasers have been advocated and increasingly used as an adjunct to conventional scale and root planning to overcome limitations with periodontal therapies such as non-accessible pockets and delayed healing following non-surgical periodontal therapy (NSPT). The main concern with lasers is that there is no accepted standardized protocol for their use in dental practice, potentiating the risk for adverse events affecting the hard tissue and patient compared to other traditional modalities. In addition, the wavelength of each laser setting is different and exerts a different effect on the soft and hard tissues, leading to difficulties in comparing lasers and therefore achieving repeatable results among studies. Overall, there are very few randomized clinical trials and a statistically low number of sample sizes published. A recent systemic review and meta-analysis on NSPT concluded that sufficient evidence only exists for the use of PDT diode lasers as beneficial for adjunctive NSPT [101]. However, lasers continue to be beneficial and are successfully used in other areas of periodontal therapy. Here several types of lasers used in periodontal disease treatment with the supportive evidence will be discussed.
The main lasers with periodontal clinical applications include the CO2, diode, and Er-YAG and Er,Cr-YSGG as well as Nd-YAG lasers [102]. The applications include: biostimulation; microbial decontamination of roots and implants; soft tissue surgery; and bone (osseous) surgery [102]. The mechanism of lasers, as mentioned before, are governed by penetration depth into the target tissue, absorption characteristics including wavelength, and target tissue characteristics. Both CO2 and erbium families have surface penetration, while the diode and Nd-YAG lasers penetrate the target tissue deeply, up to 2-3 millimetres, and suit procedures that require coagulation. In addition, the diode and Nd-YAG lasers are desirable for removal of gingival pigmentation due to their absorption by the tissue. Owing to their high absorption by water and hydroxyapatite, the erbium family lasers are more ideal for efficient bone removal than other lasers [102].
The benefits of lasers in periodontal treatment have been shown in their control of microbial infection, bacterial reduction [102], efficient removal of subgingival calculus [104], and improvement of periodontal regeneration in human with minimal damage to the surrounding tissues [104]. Accumulating evidence supports the effective use of laser therapy in conjunction with traditional treatment modalities to reduce active periodontal pathogens, rather than the use of SRP alone [104-106]. This combination therapy efficacy is mainly due to the complete removal of the infected sulcular epithelium resulting in improved connective tissue attachment [107]. A recent study further corroborated the adjunctive use of lasers by demonstrating significant improvement in periodontal disease and treating pocket depths of 4-6 mm [108].
Laser therapy has been also shown to accelerate the periodontal healing process and attachment [109]. The bio-stimulation effect of laser therapy has been clearly demonstrated in recent studies. Laser therapy
stimulates acceleration in cellular duplication process without any structural or functional changes of the target tissues.
Periodontal healingSeveral lines of evidence have demonstrated effective application of lasers in regeneration and healing of periodontal tissues [110,111]. The emerging evidence on laser applications in non-surgical periodontal therapy suggests the use of lasers as adjuncts to conventional mechanical treatments. Recent clinical studies using different wavelengths confirm that combination laser-mediated therapy is the most effective approach for optimal treatment outcomes [112-114]. The combined use of SRP and diode laser therapy has been shown to produce the best results in reducing clinical probing depths and attachment loss than laser application alone [112,115]. Similarly, SRP, in combination with an Er-YAG laser, treated sites showed significant improvement in reduction of probing depth and attachment level [114]. More recent studies have demonstrated comparable results of SRP in combination with KTP laser (modified Nd-YAG) therapy supported improvements in all periodontal clinical parameters [116-118]. The KTP laser has been previously shown to be safe to use on root surfaces with minimal thermal effect on vital pulp or periodontal ligament [119].
Soft tissue periodontal laser applicationOne of the many benefits of lasers in periodontal therapy is their application in soft tissue surgery. The very first laser reported to have surgical application was the Nd-YAG laser. It was found to efficiently control gingival bleeding and bacteraemia as well as reduce periodontal pockets [120]. In addition, the Nd-YAG was shown to be efficient at removal of epithelium pocket linings [121], which is effective in reduction of probing depths and gingival recession [122]. Both diode and Er-YAG lasers have also demonstrated positive effects in subgingival curettage with significantly improved periodontal parameters compared to manual instrumentation [123].
Laser application in bacterial reduction & root surface conditioning Laser applications in periodontal pocket and root surface decontamination are the most promising adjunct for periodontal conventional therapy due to their efficient bactericidal effect [9]. Originally, the Nd-YAG laser was found to reduce periodontal pathogens, and later diode laser (980 nm) applications, adjunct to ultrasonic scaling, showed a remarkably low prevalence of bacteraemia [124], suggesting a promising application in immunocompromised patients [102]. Furthermore, Er-YAG lasers (2940 nm) together with diode laser irradiation are proven effective in the removal of subgingival calculus without the risk of thermal damage to the vital tooth [125,126]. Similar studies corroborated these findings by using diode lasers to reduce periodontal pathogens in pockets without the need for antibiotic therapy [112].
The application of CO2 lasers in decontamination of root surfaces has been demonstrated by several clinical reports [127,102], provided that the

Page 107 Dental.EliteCME.Com
power setting and parameters stay within a safety range to prevent root damage [128]. A recently published report found that combined CO2
laser root conditioning with coronal flap advancement resulted in long-term tissue stability after 15 years [127].
Laser use in orthodontic treatmentLaser use in orthodontics, similar to other fields of dentistry, has seen rapid growth in diagnosis, imaging, bonding and surgical applications. The key diagnostic applications include caries detection, digital models, and laser scanning. Laser etching, bonding to porcelain and adhesive curing are other applications. The laser effect extends to bio-modulations such as tooth movement, growth modification, pain control, and retention or relapse [129].
Laser application in diagnosisIn orthodontics, three-dimensional laser scanning has multiple applications in diagnosis, growth changes assessment, and in clinical results after orthognathic surgery [129]. The advantages of this technology include auto-calibration and correction, ease of use, and lower costs. Applications include the ability to monitor facial soft tissue changes that occur with growth and following orthognathic surgery, and functional movements of facial muscles [129]. Diagnostic dental casts are prepared using 3-D computer-aided design (CAD) systems once the dental model is generated from 3-D graphic information using laser scanning. Digital models not only abolish the need for storage space, but also allow reliable, reproducible, and efficient assessment of arch form, tooth size and tooth-arch discrepancies [130]. Laser scanning is also beneficial for studies of craniofacial abnormalities, assessment of cleft lip and palate, and nasal reconstruction procedures. Data from a 3-D laser scanner can be transformed to produce orthodontic appliances, splints, electronic models, and surgical simulation models.
Laser Doppler Flowmetry (LDF), aside from its application in restorative dentistry, is a very useful non-invasive diagnostic tool in assessment of tooth vitality before and during orthodontic treatment. In addition, LDF can accurately monitor pulp responses to orthodontic forces generated by rapid maxillary expansion [131]. Other diagnostic technology includes DIAGNOdent and QFL lasers supporting conventional methods in early detection of incipient caries lesions around orthodontic brackets.
Lasers are great tools for etching to possibly improve resin bonding and also reduce caries incidence by producing enamel surface that is acid resistant. The mechanism of action is thought to be due to the heat effect of the laser resulting in an enamel roughness comparable to the acid-etching method [132]. There is no need for water and air application during laser etching, and more importantly, there is remineralization of the enamel surface reducing acid attack [129].
Laser application in bonding bracketsArgon lasers have been shown to not only reduce the frequency of bracket de-bonding, but also to induce orthodontic resin polymerization four times faster than conventional curing lights while maintaining a comparable bond strength. While a drawback with this laser as a curing light has been cost, this issue has been largely overcome with the advent of diode-pumped solid-state lasers [131]. Laser etching is also advantageous for bonding to porcelain as it
eliminates the use of hydrofluoric acid as well as the need to repolish the porcelain at the bracket de-bonding stage.
Lasers have the great advantage of decreasing operation time during the de-bonding stage and abolishing all the issues concerned with conventional ceramic de-bonding methods. The plausible mechanism of lasers during de-bonding is thermal mediated: initial laser heat softens the bonding agent, which results in the bracket sliding off the enamel [131].
Laser application in soft tissue surgeryThe other useful applications of lasers in orthodontics are in soft tissue surgery, such as gingival recontouring, frenectomy, fibrotomy, exposure of unerupted teeth, ablation of inflamed tissue and gingival hyperplasia [129,133-135]. The main lasers used for soft tissue application are the Nd-YAG lasers [131]. The thermal ablation of tissue via the absorption, melting, and vaporization process is thought to be the mechanism by which lasers exert effects. Indeed, laser soft tissue ablation is more advantageous than use of a scalpel in terms of accuracy and minimal tissue damage, control of bleeding, ability to sterilize the wound area. Lasers reduce the operative time, and provide less post-operative discomfort as well as minimal swelling [135-137].
Other applications of laser in orthodontic practiceThe most frequently used laser therapy in orthodontics is Low-Level Laser Therapy (LLLT), especially for pain relief. The plausible mechanism of the LLLT analgesic effect is its inhibitory action on pain fibres, which decreases action potentials and suppresses neurogenic inflammation [15]. Several reports have indicated that GaAlAs diode [138], Nd-YAG and CO2 laser therapy also exert analgesic effects, decreasing pain associated with orthodontic movement [139,140]. Therefore, analgesia-inducing lasers are beneficial in orthodontic treatment as they are non-invasive without causing any tissue-related side effects.
LLLT has also been shown to stimulate bone regeneration as well as mandible growth, possibly via stimulation of cellular proliferation and differentiation [15,141]. Similarly, GaAlAs diode lasers have been shown to accelerate bone regeneration during application of a rapid palatal expansion appliance [142]. Similarly, the combination of retainer and LLL therapy has been shown to reduce the retention period due to accelerating periodontal tissue remodelling.
LLLT has also been found to influence rate of tooth movement during orthodontic treatment phase in animal studies [15]. This could possibly be due to the increase of osteoclast formation, resulting in tooth movement, elevation of receptor activator of a nuclear factor kappa-B ligand in periodontal ligament, and possibly, stimulation of osteogenesis and bone formation on the traction side [129]. The implications of these research findings are significant for orthodontic treatment, and it is essential to be aware of optimizing the laser parameters to achieve positive treatment outcome. However, studies on the use of laser in tooth movement are controversial, and more research is required to determine the optimal laser parameters required to achieve tooth movement [15].
Laser applications in prosthodonticsThe advent of lasers in prosthodontic field has been very encouraging, leading to increasing laser-integration in specialist clinics. These technical applications are replacing most of the traditional treatment procedures [143]. Lasers have numerous applications, especially as adjunctive therapy to conventional methods, in prosthodontics with the more common uses including crown lengthening, soft tissue ablation, troughing and veneer removal [144]. While initially, soft tissue lasers were used, with the development of a wider range of wavelengths, hard tissue lasers took centre stage and are used in tooth preparation and bone ablation, among other applications.
The greatest impact of laser application in prosthodontics has been on aesthetic considerations and functional stability [143]. In fixed prosthodontics, soft laser applications such as cosmetic crown lengthening, management of gingival overgrowth and retraction during crown placement and impression taking, are very frequent. In patients with “gummy smile”, erbium lasers have allowed apical lifting of both soft and hard tissue to achieve an improved and favourable aesthetic result without the risk of damage to adjacent tissues or thermal effects [143]. Lasers used in crown lengthening are the CO2 and erbium lasers capable of removing bone without damaging the adjacent cementum

Dental.EliteCME.Com Page 108
[143]. Argon lasers are excellent for retraction and hemostasis of gingival tissue, allowing for accurate impression taking.
Lasers are also very effective at the removal of gingival overgrowth prior to re-cementation of a fixed prosthesis. In the aesthetic zone, lasers have the advantage of shaping soft tissue to fabricate ovate pontic for aesthetic improvement. Lasers result in efficient, predictable results with minimal discomfort and bleeding, which reduces operative time.
Gingival laser troughing is more efficient, and allows for better visibility of the margins than using retraction cords prior to impression taking. Diode lasers have been shown to be effective in tissue retraction instead of the cord, and show great results in accurate accessible margins for impression taking [143]. These lasers are also fantastic at recontouring gingiva and removing minor inflamed tissues without any thermal damage to the underlying tissues. There are times when porcelain veneers are required to be replaced and erbium lasers are able to predictably assist in efficient and safe removal of veneers with minimal harm to the underlying tooth structures [144]. Application of lasers in clearing tooth preparation margins by retraction of gingival tissue is highly desirable to produce distinct margins for impression, management of gingival overgrowth during temporization, and final prosthetic restoration placement.
Hard tissue lasers have wide applications in prosthodontics such as tooth preparation for crowns and veneers, caries and defective restoration removal, as well as the removal of failed or defective veneers, crowns or bridges [143]. Lasers such as Er-YAG and Er,Cr-YSGG have the advantage of removing veneers without any damage to the underlying tooth structure. The mechanism of laser involves the
beam passing through the porcelain and de-bonding it at the silane-resin interface [144].
The applications of hard and soft tissue lasers include ovate pontic site preparation, and crown fractures at the gingival margin level. The design of pontic is important as part of the final fixed prosthodontic restoration and is particularly critical in the anterior region. To create a natural look, ovate pontic design is sculpted as a depression in the soft tissue using lasers [143]. In the event that the biological width is violated, lasers with a hard tissue setting can remove minimal bone to allow for the 2mm gingiva between the bone and pontic [143]. The application of Er-YAG lasers in crown fractures have been shown to safely ablate bone and expose the fractured edge when crown fracture extends below the bone margin [145].
In addition to the above applications, lasers are capable of increasing surface roughness to improve bond strength of the fixed restoration and luting cement. Recently, a study showed the use of CO2 and Er-YAG lasers enhanced bond strength between the zirconia crown and cement [146]. Of note, laser scanning of casts is becoming increasingly popular among specialists for the creation and design of indirect restorations as it is efficient, cost effective in the long term, and more comfortable for the patient.
The multiple advantages of hard and soft tissue combination treatment with lasers have facilitated extensive applications, and increased the interest of dental practitioners in integrating the technology into dental offices. Not only do patients benefit from less chair time and comfortable treatment without the need for anaesthetics or sutures, but the dentist can deliver a predictable and successful outcome by using optimal laser parameters for the specific treatment application.
Laser application in dental implantologySoft tissue lasers such as CO2 and Argons have been shown to be beneficial in soft-tissue peri-implant recontouring, enhancing hemostasis, and decreasing post-operative discomfort and swelling as well as increasing wound healing [147]. Likewise, dental implantology benefits from hard tissue laser technologies such as Er-YAG and Er,Cr-YSGG lasers in the early osseointegration phase and in treatment of peri-implantitis [102]. Therefore, there are positive indications for both soft and hard tissue laser application in almost all phases of implant placement, including the post-implant healing stage which will be described below [102.147-149].
Implant dentistry and lasersLaser applications in implant dentistry includes: prior to and during all stages of implant placement; treatment of peri-implantitis; removal of peri-implant soft tissue; and disinfection of failed implants [147-150]. Both CO2 and Er,Cr-YSGG lasers have demonstrated effective decontamination of the implant surface and re-osseointegration in pre-clinical studies [151]. Of particular interest is the CO2 laser application on the implant surface which was shown recently to reduce the risk of overheating, a concern with implant surface melting when using lasers [152].
During the implant placement process, lasers have been shown to be beneficial in decontamination of the site and flap incision, removal of any granulation tissues, and levelling the bone for restoration placement [147-150]. Erbium lasers are capable of bacterial reduction in the implant site [153], removal of granulation tissue as well as disinfection of the extraction site without damaging the surrounding bone [147]. Lasers, in general, are excellent at hemostasis compared to scalpel blades and are able to reduce discomfort and swelling post-surgery. Traditionally, electrosurgical units are used for implant processes, however these units usually induce heat and have thermal damage compared [154] to lasers such as erbium which has water-cooling mechanisms and thereby reduces thermal damaging effect to surrounding bone [155]. In addition, erbium lasers ablate bone and have been shown to produce osteotomies with post-operative stability of implants at the two-month mark [156]. Diode laser applications have
been shown to encourage in hard tissue ablation, assist in coagulation as well as their soft tissue applications [157].
During implant placement, lasers have been indicated mainly in precise flap incision, creation of osteotomy, and guided tissue regeneration. The procedure for predictable bone generation for a deficient area follows four principles: wound closure to promote uneventful healing; vascularization of the healing area; space creation for bone; and wound stability for blood clot formation [158]. Research has shown that lasers such as Er-YAG irradiation appear to stimulate secretion of platelet-derived growth factors which promote bone repair and thus enhances healing of the osteotomy sites [159]. There are inconsistent studies on benefits of CO2 (9600nm) lasers in bone ablation. While they has been found to be safe when used for decontamination of implant sites [160], previous studies report a risk of thermal damage associated with use of CO2 lasers during irradiation, causing carbonization of the adjacent bone [161]. Therefore, erbium lasers with their water-cooling spray offer a safe and precise bone ablation tool without thermal damage during the initial implant placement [162]. Nevertheless, during the osteotomy process, just like using handpieces, clinicians must exercise caution to avoid thermal damage to the adjacent vascular structures when using lasers [147].
Once the fixture is in place, bone recontouring may be required to level the bone around the implant and allow for accurate impression as well as proper seating of the healing abutment, especially when the immediate implant placement technique is used. Here, the application of erbium lasers is ideal, as studies have found erbium lasers to be safe and posing no risk to the implant surface or causing thermal damage to the adjacent bone area [163]. Studies have shown erbium lasers to be precise in bone ablation for accurate placement of healing abutment. This prevents later discomfort and swelling associated with placement of final implant restoration [147,148, 163]. In addition, erbium lasers can be applied to minor soft tissue recontourings adjacent to the healing abutments. The clinical application of erbium lasers for both soft and

Page 109 Dental.EliteCME.Com
hard tissue ablations are described and demonstrated in detail by van As (2015) [148,149].
The renewed interest in diode lasers in more recent years has resulted in electrosurgical units being replaced in dental practices owing to diode laser reliability, convenience, affordability and ease of application with dental implants [147,148]. Diode lasers are very safe to use around metals and implants without causing damage to the structure of the metal. Laser application in other areas of implant dentistry include implant site preparation, ablation of excessive tissue during implant placement, and removal of overlay hard or soft tissue during the uncovering implant stage [147-149].
Another useful laser with an emergent application profile in most areas of dental implantology is the Low Level Laser with wavelengths in the 655-810 nm range [164,165]. These lasers are used for pain reduction and wound healing and exert their therapeutic effects at very low powers without any damage to the tissues [166,167]. Several studies have demonstrated that LLL therapy irradiation resulted in stimulation of osseointegration, increased bone mineralization, and healing in the early stages of implant placement as well as improvement in nerve regeneration [168-170].
Lasers also have applications in the implant uncovering stage. While studies have shown that diode lasers at low settings allow safe uncovering of implant fixtures [171], it has been suggested to use water spray intermittently to manage potential thermal effect on the surgical site [157]. Furthermore, diode lasers reduce the number of appointments due to them decreasing both the need for sutures and the post-operative healing period.
Soft tissue management during the healing phase of implant therapy is possible using diode, CO2 and erbium lasers. Studies have suggested Er,Cr-YSGG to be very effective in soft tissue surgery as it showed minimal thermal damage compared to diode or CO2 lasers [172,173]. Indeed, soft tissue recontouring can save time and effort in the difficult management of the final restoration process.
Peri-implantitis and lasersDespite the great long-term success of implant therapy in replacement of missing teeth in dentistry [174-176], there are increasing reports of implant failure either due to inflammation of the soft tissue (mucositis) or the bone (peri-implantitis). These conditions lead to chronic pain, infection, bone loss and eventual implant failure if untreated [174, 177,178]. A recent systematic review on peri-implant diseases found a significant incidence of both mucositis and peri-implantitis [178], potentially due to systemic disease (diabetes), smoking, improper implant placement, and/or poor oral hygiene [179].
It has been suggested to approach early peri-implantitis cases (probing depths of <5mm and bone loss of <2mm) using non-surgical treatment modalities [180]. The most challenging parts of peri-implantitis treatment are the decontamination of the implant surface, soft tissue ablation, and long-term maintenance of healthy tissues [181]. While mechanical decontamination methods combined with antibiotic therapy have been used, the side effects of surface damage to the implant and antibiotic resistance have been reported [182,183]. Lasers are reportedly very effective as an adjunct in the decontamination of implants. The most frequently applied lasers are the CO2, diode and erbium lasers simply because all have antibacterial effects, but also assist in removal of calculus as well as improving hemostasis [147]. Studies have shown the combination of traditional modalities with LLL therapy produces predictable results in dental implant decontamination. Recent studies have indicated that the effect of diode lasers (810 nm) at low power (LLLT) combined with conventional therapies is effective at decontaminating implant surfaces as well as in possible stimulation of collagen production [184,185]. Similarly, the CO2 and erbium lasers have been shown to be effective at elimination of bacteria from implant surfaces provided appropriate laser parameters are used [186].
There are cases where the bone loss around an implant is moderate-severe and a non-surgical option is not feasible. In such instances, whether to replace or save the existing implant should be carefully considered. Forum et al. developed a regenerative surgical approach for treatment of peri-implantitis with encouraging results of no implant loss after seven years of follow-up [187]. More recently, studies have demonstrated that the application of erbium lasers to effectively remove the contaminated layer with an optimal laser setting has potential application in surgical approach to peri-implantitis [188,189]. More clinical studies, especially long-term with multiple sessions of laser therapy, are required to establish the application and effectiveness of these lasers over conventional therapy in peri-implantitis treatment [190].
Despite limited published randomized clinical studies on lasers in dental implantology, there are emerging studies that describe widespread use in bacterial decontamination of extracted sockets for immediate implant placement, osseous remodelling and osseointegration, surgical flap raise, and uncovering submerged implants to preserve crestal bone [147]. The successful laser application in any dental procedure is dependent on adequate training and education on laser use, especially the application of correct parameters specific for the particular procedure as well as safety considerations [102, 147].
Laser application in oral surgeryThe clinical application of lasers in oral surgery includes treatment of oral mucosal lesions, oral cancers, and oral benign lesions. In oral surgery, the most commonly used lasers are the CO2, erbium family, diode and Nd-YAG. There have also been some applications of the LLLs in disinfection and wound healing reported [191]. Since most of the applications are very specialized and out of the scope of this course, only a brief outline of the broad oral surgery applications will be discussed here for the general dental practitioner.
The most common oral mucosal lesions are oral leucoplakia and lichen planus. Treatment of oral leucoplakia, a pre-malignant oral mucosa lesion, was demonstrated effectively and safely using CO2 laser therapy and photodynamic therapy in randomized clinical studies [192,193]. Oral lichen planus treatment with a diode laser was shown to be effective for relief of associated symptoms. In addition, the efficacy of ER-YAG lasers in reducing symptoms of oral lichen planus has been reported [194].
In oral cancer treatment, clinical studies have reported use of: Nd-YAG lasers for management of lip carcinoma lesions; a specific CO2 (trans-oral) laser for early glottis cancer treatment and soft palate tumours; and diode lasers for healing and reduction in post-operative
pain. The advantages of laser therapy include less treatment time, less costs compared to radio- or chemo- radiotherapy, and significantly less toxicity [195].
Application of lasers in removal of oral benign lesions includes the removal of mucoceles which are benign lesions of the minor salivary glands that most commonly occur in children on the lower lip. Application of erbium and CO2 lasers is demonstrated to effectively remove mucoceles with rapid wound healing and no scaring [86,196]. Other benign lesions are ranuals, which are traumatic sublingual mucus lesions; they have been reported to be removed by CO2 laser treatment safely with minimal recurrence [197].
Laser application in TMD managementThe most common cause of orofacial pain of non-dental origin is from the Temporomandibular Disorders (TMD) which occur at a prevalence of more than 85% of the population [198]. This dysfunction is a collection of clinical symptoms involving the temporomandibular joint and its associated structures [198]. It is a debilitating condition affecting sleep quality, mood and cognition function [199]. The treatment usually is multidisciplinary and includes a physiotherapist in addition

Dental.EliteCME.Com Page 110
to a general dental practitioner. Traditional modalities used to address treatment of TMD frequently involve medication, adjunctive occlusal splint, physiotherapy, electrotherapy, or manual therapy in combination or individually. The availability of Low Level Laser Therapy (LLLT) expanded the horizon of treatment options. LLLT has been shown to not only reduce pain, but also reduce any associated inflammation and swelling [198]. Its mechanism of action is possibly a result of light penetration in target tissue leading to stimulation and
release of many signalling pathways involved in analgesia, nerve excitability and increased blood circulation [15, 198,199]. Currently, there is no consensus on the benefits of LLL as therapy for TMD and the literature is saturated with conflicting reports that are not consistent in terms of parameters of the laser application. Further research and standardization of treatment parameters is required to clarify the emerging benefits of LLLT for TMD treatment.
Laser safety considerations The safety consideration of lasers is an important aspect of providing quality treatment in a safe and efficient manner. It is crucial to be aware of the correct operation of the laser equipment and provisions must made for the protection of the dental team, patient and operator. The standards set out by American National Standards Institute and Occupational Safety and Health Administration classifies lasers according to their associated risks into four categories [200]:
● Class I: Low-powered lasers. These are safe to view. ● Class IIa: Low-powered visible lasers. These do not cause damage
unless direct eye contact is made with the beam for >1000 seconds. ● Class II: Low-powered visible lasers. These are harmful when
viewed directly for <0.25 seconds. ● Class IIIa: Medium-powered lasers. These are harmful when
viewed directly for >0.25 seconds.
● Class IIIb: Medium-powered lasers. These are dangerous when viewed directly regardless of the length of time.
● Class IV: High-powered lasers that can cause damage to eyes and skin. Even a reflected or radiated beam is harmful. Appropriate safety measures required.
In summary, when visible or infrared radiation at wavelengths 400-1400nm are used, directly looking at the laser risks damage to the eyes. Therefore, all persons involved in the treatment room must wear the safety goggles normally supplied by the manufacturer. At all times, safety protocols associated with the particular laser machine must be followed. Protection of the skin is also required during laser operation at wavelength <400nm to avoid risk of tissue burning.
Integration of lasers in the dental practiceThe integration of lasers just like any other new technology and requires fundamental planning for training, financial outlay, and ongoing costs. This planning must also include marketing, including introduction of the concept to the existing clients of the practice. The investment of time in planning meticulously to address all aspects of laser addition to a dental office will assist in achieving a smooth transitional phase in the process of integration.
In choosing a laser, the clinical applications that are more commonly employed in the dental office should be considered, in addition to space. The indications for investing in a laser system include:
● New treatments offered: Addition of a laser may provide new opportunities for treatments to the patients which were not available previously. These include crown lengthening, gingevectomy or uncovering tooth for orthodontic bracket bonding.
● Simplified and efficient treatments: Subgingival retraction for implant or crown restorations with localised hemostasis resulting in an accurate impression in a timely and cost effective (i.e., less materials used) manner. Manageable soft tissue surgery with successful hemostasis and recontouring margins around decayed lesions. Disinfection of aphthous ulcers to reduce patient discomfort and save treatment time.
● External referrals reduced: Depending on the level of clinician experience and training, most procedures referred out can be
completed in-house. This is to the benefit of the dental office and the patient in terms of costs, time and efficiency. Suspicious lesions can be biopsied and send for pathology. Tissue contouring during orthodontic procedure can occur, common fibromas can be removed, and operculums over wisdom teeth can be removed for immediate relief.
● Efficiency in treatment procedures: Most lasers allow for excellent bleeding control and reduced use of anaesthetics, saving time to perform multiple treatment procedures. Restoration of few teeth in different quadrants that have cervical caries and require gingival recontouring can be completed efficiently and ultimately provide quality patient care.
The success of the integration process is largely dependent on the support and active involvement of the dental office team, from inception to implementation. The clinician is responsible for ensuring training opportunities are made available to all team members and involving the staff in experiencing laser effects first hand. Notably, most patients are not only grateful for additional treatment opportunities that add to their quality of care, but will also increase internal referrals to other patients who seek modern, cutting edge, and literally pain-free treatment.
ConclusionThe dental field is rapidly evolving and the advent of lasers offers more treatment options (Figure 2). Using lasers as an adjunct to specific procedures has not only imparted clinical benefits, but also increased patient comfort and ease. More and more patients are technology-savvy, and use online tools to educate themselves, looking for dental options that are technically advanced and offer a pain-free and comfortable dental experience. Dental practices can effectively integrate lasers as part of their routine dental procedures and offer lasers as an alternative or adjunct treatment for their patients. The most important part of the successful integration and practical use is the understanding of the essentials of laser application and safety requirements by clinicians and their dental teams.
There is comprehensive planning involved in integrating lasers including ongoing training, educating the dental team, and marketing and financial planning. Ultimately the economics, quality of dentistry on offer, patient comfort and financial rewards outweigh the initial time and costs spent for the inclusion of lasers into a dental office. This course highlighted the mechanism of laser actions, different types and typical application of lasers in dentistry with a focus on optimal laser parameters for positive treatment benefits as well as safety requirements and integration into dental offices. It also provided a comprehensive update on evidence-based laser applications in dentistry. The benefits of therapeutic effects of lasers are astounding and safe laser implementation should be considered in every dental office.

Page 111 Dental.EliteCME.Com
Restorative - Caries diagnosis & removal- Dentin hypersensi- tivity- Bleaching teeth- Direct pulp cap- Enamel etching
Periodontics &
Implantology- Eliminate periodontal pathogens- Remove diseased epithilum- Reduce pocket depths- Soft tissue surgery- Treat peri- implantitis
Orthodontics- Tooth movement- Bracket bonding-3D cast models- Pain relief soft tissue surgery- Growth modification
Pediatrics- Caries removal & diagnosis- Anesthesia - Pulpotomies- Pain control- Enamel ablation
Prosthodontic- Crown lengthening- Gingivecto- my- Soft tissue surgery- Hard tissue ablation- Veneer removal
Oral Surgery- Soft tissue surgery- Apthus ulcer treatment - Lichen planus removal
DENTAL LASERSFigure 2. Summary of common laser applications in general
dentistry practice
References1. Maiman, T.H. (1960). Stimulated optical radiation by ruby. Nature,187, 493-4.2. Coluzzi, D.J. (2004). Fundamentals of dental lasers: Science and instruments. Dent Clin North Am,
48,751-70.3. Lomke, MA. (2009). Clinical applications of dental lasers. Gen Dent, 57, 47-59.4. Myers, T. D., Myers, W. D, Stone, R. M. (1989). First soft tissue study utilising a pulsed Nd YAG
dental laser. Northwest Dent. 68, 14–17.5. Moritz, A. (2006) Cavity preparation. In: Moritz A, editor. Oral Laser Application. Berlin:
Quintessenz, 75-136.6. van As, G. (2004) Erbium lasers in dentistry. Dent Clin North Am, 48, 1017-59, viii.7. Gupta, S. and Kumar, S. (2011). Laser in dentistry. An Overview. Trends Biomater. Artif. Organs,
25(3), 119-123. 8. van Noort, R. (2012). The future of dental devices is digital. Dent Mater, 28(1), 3-12. doi: 10.1016/j.
dental.2011.10.0149. Koci E, Almas A. (2009). Laser application in dentistry: an evidence-based clinical decision-making
update. Pak Oral Dent J, 29(2):409-423.10. Hibst, R. (2002). Laser for caries removal and cavity preparation: State of the Art and Future
Directions. J Oral Laser Applications, 203–12.11. Nair, P.N., Baltensperger, M.M., Luder, H.U., Eyrich, G.K. (2003). Pulpal response to Er:YAG laser
drilling of dentine in healthy human third molars. Lasers Surg Med, 32(3):203-9.12. Belal, M. H., & Yassin, A. (2014). A comparative evaluation of CO2 and erbium-doped yttrium
aluminium garnet laser therapy in the management of dentin hypersensitivity and assessment of mineral content. J Periodontal Implant Sci, 44(5), 227-234. doi:10.5051/jpis.2014.44.5.227
13. Cakar, G., Kuru, B., Ipci, S. D., Aksoy, Z. M., Okar, I., & Yilmaz, S. (2008). Effect of Er:YAG and CO2 lasers with and without sodium fluoride gel on dentinal tubules: a scanning electron microscope examination. Photomed Laser Surg, 26(6), 565-571. doi:10.1089/pho.2007.2211
14. Coluzzi DJ. (2008). Fundamentals of laser in Dentistry: Basic Science, Tissue-Interaction and Instrumentation. J Laser Dent. 16 (Spec. Issue): 4-10
15. Carroll, J.D., Milward, M.R., Cooper, P.R., Hadis M, Palin W.M. (2014).Developments in low level light therapy (LLLT) for dentistry. Dent Mater. 30(5):465-75. doi: 10.1016/j.dental.2014.02.006.
16. Meire M., de Moor R. J. G. Lasers in endodontics: laser disinfection, an added value. ENDO.2007;1(3):159–172.
17. de Moor R. J. G., Delmé K. I. M. (2009). Laser-assisted cavity preparation and adhesion to erbium-lased tooth structure: part 1. Laser-assisted cavity preparation. The Journal of Adhesive Dentistry. ;11(6):427–438
18. Najeeb S, Khurshid Z, Zafar MS, Ajlal S. Applications of light amplification by stimulated emission of radiation (Lasers) for restorative dentistry. Med Princ Pract. (2015): 1-11.
19. Steiner-Oliveira, C., Rodrigues, L.K, Soares, L.E, Martin, A.A, Zezell, D.M, Nobre-dos-Santos M. (2006). Chemical, morphological and thermal effects of 10.6-microm CO2 laser on the inhibition of enamel demineralization. Dent Mater J. 25(3),455-62.
20. Sculean A, Schwarz F, Berakdar M, Windisch P, Arweiler NB, Romanos GE. (2004). Healing of intrabony defects following surgical treatment with or without an Er: YAG laser. J Clin Periodontol, 31, 604–8.
21. KimuraY, Wilder-SmithP, YonagaK, MatsumotoK. (2000). Treatment of dentine hypersensitivity by lasers: a review. J Clin Periodontol 10,715–721
22. ten Bosch JJ, Angmar-Månsson B. (2000). Characterization and validation of diagnostic methods. Monogr Oral Sci., 17,174-89.
23. Lussi A, Imwinkelried S, Pitts N, Longbottom C, Reich E. Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Research. 1999; 33:261–6
24. Markowitz K, Gutta A, Merdad HE, Guzy G, Rosivack G. In vitro study of the diagnostic performance of the Spectra Caries Detection Aid. J Clin Dent. 2015;26(1):17-22.
25. Zeitouny M, Feghali M, Nasr A, Abou-Samra P, Saleh N, Bourgeois D, Farge P. (2014). SOPROLIFE system: an accurate diagnostic enhancer. Scientific World Journal.;2014:924741.
26. Rechmann, P, Charland, D., Rechmann B.T, Featherstone, J.B. (2012). Performance of laser fluorescence devices and visual examination for the detection of occlusal caries in permanent molars. J. Biomed. Opt., 17(3), 036006
27. Nokhbatolfoghahaie, H., Alikhasi, M., Chiniforush, N., Khoei, F., Safavi, N., & Yaghoub Zadeh, B. (2013). Evaluation of Accuracy of DIAGNOdent in Diagnosis of Primary and Secondary Caries in Comparison to Conventional Methods. Journal of Lasers in Medical Sciences, 4(4), 159–167.
28. Kouchaji, C. (2012). Comparison between a laser fluorescence device and visual examination in the detection of occlusal caries in children. The Saudi Dental Journal, 24(3-4), 169–174.
29. Alammari MR, Smith PW, de Josselin de Jong E, Higham SM. (2013). Quantitative light-induced fluorescence (QLF): a tool for early occlusal dental caries detection and supporting decision making in vivo. J Dent.41(2):127-32.
30. Gomez, J. (2015). Detection and diagnosis of the early caries lesion. BMC Oral Health, 15(Suppl 1), S3. http://doi.org/10.1186/1472-6831-15-S1-S3
31. Van der Veen, M. H. (2015). Detecting Short-Term Changes in the Activity of Caries Lesions with the Aid of New Technologies. Current Oral Health Reports, 2(2), 102–109.
32. Gugnani, N., Pandit, I., Srivastava, N., Gupta, M., & Gugnani, S. (2011). Light induced fluorescence evaluation: A novel concept for caries diagnosis and excavation. Journal of Conservative Dentistry: JCD, 14(4), 418–422.
33. Vaghela DJ, Sinha AA. (2011). Pulse oximetry and laser Doppler flowmetry for diagnosis of pulpal vitality. Journal of Interdiscip Dentistry, 1, 14-21
34. Ellwood RP, Gomez J, Pretty I.A. (2012). Caries clinical trial methods for the assessment of oral care products in the 21st century. Adv Dent Res. 24:32–5.
35. Jingawar MM., Bajwa NK., & Pathak A, (2014). Minimal Intervention Dentistry – A New Frontier in Clinical Dentistry. Journal of Clinical and Diagnostic Research: JCDR, 8(7), ZE04–ZE08.
36. Tassery, H., Levallois, B., Terrer, E., Manton, D., Otsuki, M., Koubi, S., Gugnani, N., Panayotov, I., Jacquot, B., Cuisinier, F. and Rechmann, P. (2013), Use of new minimum intervention dentistry technologies in caries management. Australian Dental Journal, 58, 40–59
37. Alessandra M. (2008). Correa-Afonso, Jesus Djalma Pécora, and Regina G. Palma-Dibb. Photomedicine and Laser Surgery. 26(3), 221-225.
38. Buyukhatipoglu, I., & Secilmis, A. (2015). The use of Erbium: Yttrium-aluminum-garnet laser in cavity preparation and surface treatment: 3-year follow-up. European Journal of Dentistry, 9(2), 284–287. http://doi.org/10.4103/1305-7456.156843
39. Al-Batayneh OB, Seow WK, Walsh LJ. Assessment of Er:YAG laser for cavity preparation in primary and permanent teeth: a scanning electron microscopy and thermographic study. Pediatr Dent. 2014 May-Jun;36(3):90-4
40. Cvikl B, Lilaj B, Franz A, Degendorfer D, Moritz A. 2015Evaluation of the Morphological Characteristics of Laser-Irradiated Dentin. Photomed Laser Surg, 33(10),504-8.
41. Engelbach C, Dehn C, Bourauel C, Meister J, Frentzen M. Ablation of carious dental tissue using an ultrashort pulsed laser (USPL) system. Lasers Med Sci. 2015 Jul;30(5):1427-34.
42. Schelle F, Polz S, Haloui H, Braun A, Dehn C, Frentzen M, Meister J. Ultrashort pulsed laser (USPL) application in dentistry: basic investigations of ablation rates and thresholds on oral hard tissue and restorative materials. Lasers Med Sci. 2014 ;29(6):1775-83.
43. Bello-Silva MS, Wehner M, Eduardo CP, Lampert F, Poprawe R, Hermans M, Esteves-Oliveira, M. (2013). Precise ablation of dental hard tissues with ultra-short-pulsed lasers. Preliminary exploratory investigation on adequate laser parameters. Lasers Med Sci, 28(1):171-84. doi:10.1007/s10103-012-1107-2.
44. Rezaei,,Y., H., Bagheri, M., Esmaeilzadeh. (2011) Effect of laser irradiation on caries prevention. Journal of Lasers in Medical Sciences.,2(4):159–64.
45. Miresmaeili A, Farhadian N, Rezaei-soufi L, Saharkhizan M, Veisi M. 2014Effect of carbon dioxide laser irradiation on enamel surface microhardness around orthodontic brackets. Am J Orthod Dentofacial Orthop. Aug;146(2):161-5
46. Karandish, M. (2014). The Efficiency of Laser Application on the Enamel Surface: A Systematic Review. Journal of Lasers in Medical Sciences, 5(3), 108–114.
47. Alleman, D. S., & Magen, P. (2012). A systematic approach to deep caries removal end points: The peripheral seal concept in adhesive dentistry. Quintessence International, 43(3), 197-208
48. Rechmann P, Fried D, Le CQ, et al. (2011). Caries inhibition in vital teeth using 9.6-μm CO2-laser irradiation. J Biomed Opt, 16(7), 071405
49. Jorge AC, Cassoni A, de Freitas PM, Reis AF, Brugnera Junior A, Rodrigues JA. (2015). Influence of cavity preparation with Er,Cr:YSGG laser and restorative materials on in situ secondary caries development. Photomed Laser Surg 33(2), 98-103
50. Schmidlin PR, Dorig I, Lussi A, Roos M, Imfeld T 2007. CO2 laser-irradiation through topically applied fluoride increases acid resistance of demineralised human enamel in vitro. Oral health & preventive dentistry,5(3), 201–8.
51. Zezell D. M., Boari H. G., Ana P. A., Cde P. (2009). Eduardo, and Powell G. L., “Nd:YAG laser in caries prevention: a clinical trial,” Lasers Surg. Med. 41(1), 31–35.
52. Fekrazad R, Ebrahimpour L. (2014). Evaluation of acquired acid resistance of enamel surrounding orthodontic brackets irradiated by laser and fluoride application. Lasers Med Sci, 29(6):1793-8.
53. Rechmann P, Charland DA, Rechmann BMT, Le CQ, Featherstone JDB. (2010). In vivo occlusal caries prevention by pulsed-CO2 laser and fluoride varnish treatment. J Dent Res, 17:036006
54. Matsumoto K, Kimura Y. (2007). Laser therapy of dentin hypersensitivity. J Oral Laser Application.,7, 7–25.
55. Asnaashari, M., & Moeini, M. (2013). Effectiveness of lasers in the treatment of dentin hypersensitivity. Journal of Lasers in Medical Sciences, 4(1), 1–7.

Dental.EliteCME.Com Page 112
56. Ko Y, Park J, Kim C, Park J, Baek SH, Kook YA. (2014). Treatment of dentin hypersensitivity with a low-level laser-emitting toothbrush: double-blind randomised clinical trial of efficacy and safety. J Oral Rehabil,41(7),523-31. doi: 10.1111/joor.12170.
57. Bal Mehmet Vehbi, Keskiner İlker, Sezer Ufuk, Açıkel Cengizhan, and Saygun Işıl. (2015). Photomedicine and Laser Surgery, 33(4), 200-205.
58. Lan, W-H & Lui, H-C. (1996). Treatment of dentin hypersensitivity by Nd: YAG Laser. Journal of Clinical Laser Medicine & surgery, 14, 89-92.
59. Whitters, C. J., Hall, A., Creanor, S. L., Moseley, H., Gilmour, W. H., Strang, R., Saunders, W. P. & Orchardson, R. (1995) A clinical study of pulsed Nd:YAG laser induced pulpal analgesia. Journal of Dentistry, 23,145–150.
60. Kumar NG, Mehta DS. (2005). Short-term assessment of the Nd:YAG laser with and without sodium fluoride varnish in the treatment of dentin hypersensitivity--a clinical and scanning electron microscopy study. J Periodontol.,76(7),1140-7.
61. Omae, M., Inoue, M., Itota, T., et al. (2007). Effect of a desensitizing agent containing glutaraldehyde and HEMA on bond strength to Er:YAG laser-irradiated dentine. J Dent, 35, 398–402.
62. He S, Wang Y, Li X, Hu D. (2011). Effectiveness of laser therapy and topical desensitising agents in treating dentine hypersensitivity: a systematic review. J Oral Rehabil ,38, 348–358.
63. Lopes AO, de Paula EC, Aranha AC. (2015). Clinical evaluation of low-power laser and a desensitizing agent on dentin hypersensitivity. Lasers Med Sci, 30(2), 823-9. doi: 10.1007/s10103-013-1441-z.
64. Umberto R, Claudia R, Gaspare P, Gianluca, T. Alessandro del, V. (2012). Treatment of dentine hypersensitivity by diode laser: a clinical study. Int J Dent 2012:858950.
65. Komabayashi, T., Ebihara, A., Aoki, A. (2015). The use of lasers for direct pulp capping. J Oral Sci.,57(4),277-86. doi: 10.2334/josnusd.57.277.
66. Moritz, A., Schoop, U., Goharkhay, K., Sperr, W. (1998). Advantages of a pulsed CO2 laser in direct pulp capping: a long-term in vivo study. Lasers Surg Med 22, 288-293
67. Santucci, P.J. (1999). Dycal versus Nd:YAG laser and Vitrebond for direct pulp capping in permanent teeth. J Clin Laser Med Surg 17, 69-75.
68. Huth KC, Paschos E, Hajek-Al-Khatar N, Hollweck R, Crispin A, Hickel R et al. (2005) Effectiveness of 4 pulpotomy techniques--randomized controlled trial. J Dent Res 84, 1144-1148.
69. Blanken JW (2005) Direct pulp capping using an Er,Cr:YSGG laser. J Oral Laser Applic 5, 107-114.70. Yazdanfar I, Gutknecht N, Franzen R (2015) Effects of diode laser on direct pulp capping treatment:
a pilot study. Lasers Med Sci 30, 1237-124371. Jayawardena JA, Kato J, Moriya K, Takagi Y (2001) Pulpal response to exposure with Er:YAG laser.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 91, 222-229.72. Castro, F.L, Andrade MF, Hebling J, Lizarelli RF. (2012). Nd:YAG laser irradiation of etched/
unetched dentin through an uncured two-step etch-and-rinse adhesive and its effect on microtensile bond strength. J Adhes Dent.,14(2):137-45.
73. Karaman E, Yazici AR, Baseren M, Gorucu J. (2013). Comparison of acid versus laser etching on the clinical performance of a fissure sealant: 24-month results. Oper Dent., 38(2):151-8.
74. Jaberi Ansari, Z., Fekrazad, R, Feizi S, Younessian F, Kalhori KA, Gutknecht N. (2012) The effect of an Er,Cr:YSGG laser on the micro-shear bond strength of composite to the enamel and dentin of human permanent teeth. Lasers Med Sci., 27(4),761-5.
75. Sun, X., Ban, J., Sha, X., Wang, W., Jiao, Y., Wang, W., Yang, Y., Wei, J., Shen, L., Chen, J. (2015). Effect of Er,Cr:YSGG Laser at Different Output Powers on the Micromorphology and the Bond Property of Non-Carious Sclerotic Dentin to Resin Composites. PLoS One. ,10(11), e0142311
76. Vale, F. A., Moreira, M. S., Almeida, F. C. S. d., & Ramalho, K. M. (2015). Low-Level Laser Therapy in the Treatment of Recurrent Aphthous Ulcers: A Systematic Review. The Scientific World Journal, 7. doi:10.1155/2015/150412
77. Aggarwal, H., Singh, M. P., Nahar, P., Mathur, H., & Gv, S. (2014). Efficacy of low-level laser therapy in treatment of recurrent aphthous ulcers - a sham controlled, split mouth follow up study. J Clin Diagn Res, 8(2), 218-221. doi:10.7860/jcdr/2014/7639.4064
78. Albrektson, M., Hedstr¨om, L. and Bergh H. (2014). Recurrent aphthous stomatitis and pain management with low-level laser therapy: a randomized controlled trial. Oral Surg, Oral Med, Oral Path and Oral Rad,117, 590–594.
79. Safavi, S. M., Kazemi, B., Esmaeili, Fallah, M. A., Modarresi, A. and Mir, M. (2008). Effects of low-level He-Ne laser irradiation on the gene expression of IL-1𝛽, TNF-𝛽, IFN-𝛽, TGF-𝛽, bFGF,and PDGF in rat’s gingiva. Lasers in Medical Science, 23, 331–335.
80. De Moor RJ, Verheyen J, Diachuk A, Verheyen P, Meire MA, De Coster PJ, Keulemans F, De Bruyne M, Walsh LJ. (2015). Insight in the chemistry of laser-activated dental bleaching. Scientific World Journal.;2015:650492.
81. Luk K., Tam L., Hubert M. (2004). Effect of light energy on peroxide tooth bleaching. Journal of the American Dental Association, 135(2):194–201.
82. Buchalla W., Attin T. (2007). External bleaching therapy with activation by heat, light or laser—a systematic review. Dental Materials., 23(5):586–596
83. Schoenly, J.E., Seka, W., Rechmann P. (2010). Investigation into the optimum beam shape and fluence for selective ablation of dental calculus at lambda = 400 nm. Lasers Surg Med.,42(1), 51-61. doi: 10.1002/lsm.20884.
84. Zhang C, Wang X, Kinoshita JI, Zhao B, Toko T, Kimura Y,Matsumoto K (2007) Effects of KTP laser irradiation, diode laser, and LED on tooth bleaching: a comparative study. Photomed Laser Surg 25, 91–95
85. Kuzekanani, M, Walsh LJ (2009). Quantitative analysis of KTP laser photodynamic bleaching of tetracycline-discolored teeth. Photomed Laser Surg 27, 521–525
86. Boj, JR, Poirier C, Espasa E, Hernandez M, Espanya A. (2009). Lower lip mucocele treated with an erbium laser. Pediatr Dent.,31(3),249-252.
87. Nazemisalman, B, Farsadeghi M, Sokhansanj M. (2015). Types of Lasers and Their Applications in Pediatric Dentistry. J Lasers Med Sci.,6(3),96-101.
88. Policy on the use of lasers for pediatric dental patients, oral health policies, (2013). AAPD reference manual. 37(6):79–81.
89. Prathima, G. S., Bhadrashetty, D., Babu, S. B. U., & Disha, P. (2015). Microdentistry with Lasers. Journal of International Oral Health: JIOH, 7(9), 134–137
90. Olivi G, Genovese MD. (2011). Laser restorative dentistry in children and adolescents. Eur Arch Paediatr Dent,12 (2):68-78
91. Ando M, van Der Veen MH, Schemehron BR, Stookey GK. 2001Comparative study to quantify demineralized enamel in deciduous and permanent teeth using laser and light-induced fluorescence techniques. Caries Res., 35,464-470
92. Takamori K, Hokari N, Okumura Y, Watanabe S.(2001). Detection of occlusal caries under sealants by use of a laser fluorescence system. J Clin Laser Med Surg.,19, 267-271
93. Westerman GH, Hicks MJ, Flaitz CM, Ellis RW, Powell GL. (2004). Argon laser irradiation and fluoride treatment effects on caries-like enamel lesion formation in primary teeth: An in vitro study. Am J Dent.,17(4), 241–4.
94. Wigdor, H, Abt, E, Ashrafi, S, Walsh, JT., Jr 1993The effect of lasers on dental hard tissues. J Am Dent Assoc.,124(2):65–70.
95. Anic I, Miletic I, Krmek SJ, Borcic J, Pezelj-Ribaric S. (2009). Vibrations produced during erbium:yttrium-aluminum-garnet laser irradiation. Lasers Med Sci.,24(5),697-701.
96. Dommisch H, Peus K, Kneist S, Krause F, Braun A, Hedderich J, Jepsen S, Eberhard J. (2008) Fluorescence-controlled Er:YAG laser for caries removal in permanent teeth: a randomized clinical trial. Eur J Oral Sci. Apr,116(2),170-6.
97. Gutknecht N, Franzenb R, Vanweerschc L, Lampert F. (2005). Lasers in pediatric dentistry – A review. J Oral Laser Appl.,4(5):207–18.
98. Olivi G, Genovese MD, Caprioglio C. (2009). Evidence based dentistry on laser paediatric dentistry: review and outlook. Eur J Paediatr Dent.,10(1):29-40.
99. Olivi G, Genovese MD, Maturo P, Docimo R. (2007). Pulp capping: advantages of using laser technology. Eur J Paediatr Dent.,8(2),89-95.
100. Gupta, G., Rana, V., Srivastava, N., & Chandna, P. (2015). Laser Pulpotomy–An Effective Alternative to Conventional Techniques: A 12 Months Clinicoradiographic Study. International Journal of Clinical Pediatric Dentistry,8(1), 18–21.
101. Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N. (2015). Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc.,146(7), 508-24.
102. Romanos G. (2015). Current concepts in the use of lasers in periodontal and implantdentistry. J Indian Soc Periodontol.,19(5),490-4.
103. Moritz A, Schoop U, Goharkhay K, Schauer P, Doertbudak O, Wernisch J, Sperr W (1998). Treatment of periodontal pockets with a diode laser. Lasers Surg Med 22, 302–311.
104. Eberhard J., Ehlers H., Falk W., Acil Y., Albers H.K. & Jepsen S. (2003). Efficacy of subgingival calculus removal with Er:YAG laser compared to mechanical debridement: an in situ study. J Clin Peridontol.,30, 511-518.
105. Dukić W, Bago I, Aurer A, Roguljić M. (2013). Clinical effectiveness of diode laser therapy as an adjunct to non-surgical periodontal treatment: a randomized clinical study. J Periodontal. , 84(8), 1111-7.
106. Saglam, M., Kantarci, A., Dundar, N., Hakki, S.S. (2014). Clinical and biochemical effects of diode laser as an adjunct to nonsurgical treatment of chronic periodontitis: a randomized, controlled clinical trial. Lasers Med Sci., 29(1),37–46.
107. Neill, M.E, and Mellonig, J.T. (1997). Clinical efficacy of the Nd: YAG laser for combination periodontitis therapy. Pract Periodontics Aesthet Dent., 9(6 Suppl),1–5.
108. Lévesque L, Noël JM, Scott C. (2015). Controlling the temperature of bones using pulsed CO2 lasers: observations and mathematical modelling. Biomed Opt Express., 96(12), 4768-80.
109. Rossmann, J.A., Cobb, C.M. (1995). Lasers in periodontal therapy. Periodontol 2000., 9,150–64.110. Aoki A, Mizutani K, Schwarz F, Sculean A, Yukna RA, Takasaki AA, Romanos GE,Taniguchi Y,
Sasaki KM, Zeredo JL, Koshy G, Coluzzi DJ, White JM, Abiko Y, Ishikawa I, Izumi Y. (2015). Periodontal and peri-implant wound healing following laser therapy. Periodontol 2000,68(1), 217-69.
111. Kreisler M, Al Haj H, d’Hoedt B. (2005). Clinical efficacy of semiconductor laser application as an adjunct to conventional scaling and root planing. Lasers Surg Med., 37(5), 350–5.
112. Kamma JJ, Vasdekis VG, Romanos GE. (2009). The effect of diode laser (980 nm) treatment on aggressive periodontitis: evaluation of microbial and clinical parameters. Photomed Laser Surg., 27(1), 11–9.
113. Qadri T, Tunér J, Gustafsson A. (2015). Significance of scaling and root planing with and without adjunctive use of a water-cooled pulsed Nd:YAG laser for the treatment of periodontal inflammation. Lasers Med Sci., 30(2), 797-800.
114. Yilmaz S, Algan S, Gursoy H, Noyan U, Kuru BE, Kadir T. 2013 Evaluation of the clinical and antimicrobial effects of the Er:YAG laser or topical gaseous ozone as adjuncts to initial periodontal therapy. Photomed Laser Surg., 31(6), 293–298.
115. Roncati M, Gariffo A. (2014). Systematic review of the adjunctive use of diode and Nd:YAG lasers for nonsurgical periodontal instrumentation. Photomed Laser Surg.,32(4),186-97.
116. Dilsiz A, Sevinc S. (2014). KTP laser therapy as an adjunctive to scaling and root planing in treatment of chronic periodontitis. Acta Odontol Scand.,72(8):681-6
117. Dilsiz A, Canakci V, Aydin T. (2013). Clinical effects of potassium-titanyl-phosphate laser and photodynamic therapy on outcomes of treatment of chronic periodontitis:a randomized controlled clinical trial. J Periodontol., 84(3), 278-86.
118. Romeo U, Palaia G, Botti R, Leone V, Rocca JP, Polimeni A. (2010). Non-surgical periodontal therapy assisted by potassium-titanyl-phosphate laser: a pilot study. Lasers Med Sci., 25(6), 891-9.
119. Nammour S, Rocca JP, Keiani K, Balestra C, Snoeck T, Powell L, Van Reck J (2005). Pulpal and periodontal temperature rise during KTP laser use as a root planing complement in vitro. Photomed Laser Surg 23,10–14.
120. Romanos GE. (1994). Clinical applications of the Nd:YAG laser in oral soft tissue surgery and periodontology. J Clin Laser Med Surg. 12(2),103-8.
121. Gold SI, Vilardi MA. (1994). Pulsed laser beam effects on gingiva. J Clin Periodontol. ,21(6),391-6.122. Reddy S, Bhowmik N, Prasad MG, Kaul S, Rao V, Singh S. (2014). Evaluation of postsurgical
clinical outcomes with/without removal of pocket epithelium: A split mouth randomized trial. J Indian Soc Periodontol., 18, 749–59.
123. Lin J, Bi L, Wang L, Song Y, Ma W, Jensen S, Cao D. (2011). Gingival curettage study comparing a laser treatment to hand instruments. Lasers Med Sci., 26(1),7-11
124. Assaf M, Yilmaz S, Kuru B, Ipci SD, Noyun U, Kadir T. Effect of the diode laser on bacteremia associated with dental ultrasonic scaling: A clinical and microbiological study. Photomed Laser Surg.2007; 25:250–6.
125. Eberhard J, Ehlers H, Falk W, Açil Y, Albers HK, Jepsen S. (2003). Efficacy of subgingival calculus removal with Er: YAG laser compared to mechanica debridement: An in situ study. J Clin Periodontol.,30, 511–8.
126. Folwaczny M., Heym, R., Mehl, A., & Hickel, R. (2002). Subgingival calculus detection with fluorescence induced by 655nm InGaAsP diode laser radiation. J of Peridontol. ,73, 597-601.
127. Crespi R, Cappare P, Gherlone E, Romanos GE. (2011). Comparison of modified widman and coronally advanced flap surgery combined with Co2 laser root irradiation in periodontal therapy: A 15-year follow-up. Int J Periodontics Restorative Dent. 31,641–51.
128. Barone A, Covani U, Crespi R, Romanos GE. (2002). Root surface morphological changes after focused versus defocused CO2 laser irradiation: A scanning electron microscopy analysis. J Periodontol., 73, 370–3.
129. Milling Tania, S. D., Sathiasekar, C., Anison, J. J., & Samyukta Reddy, B. V. (2015). The extended tentacles of laser - From diagnosis to treatment in orthodontics: An overview. Journal of Pharmacy & Bioallied Sciences, 7(Suppl 2), S387–S392.
130. Motohashi, N., & Kuroda, T. (1999). A 3D computer-aided design system applied to diagnosis and treatment planning in orthodontics and orthognathic surgery. Eur J Orthod, 21(3), 263-274.
131. Nalcaci, R., Cokakoglu, S. (2013). Lasers in orthodontics. Eur J Dent, 7,119-25.132. Usümez S, Orhan M, Usümez A. (2002) Laser etching of enamel for direct bonding with an Er, Cr:
YSGG hydrokinetic laser system. Am J Orthod Dentofacial Orthop.,122, 649–56133. Fornaini C, Rocca JP, Bertrand MF, Merigo E, Nammour S, Vescovi P. (2007). Nd: YAG and diode
laser in the surgical management of soft tissues related to orthodontic treatment. Photomed Laser Surg., 25, 381-92.
134. Sarver DM. (2006) Use of the 810 nm diode laser: Soft tissue management and orthodontic applications of innovative technology. Pract Proced Aesthet Dent. ,18(Suppl), 7–13.
135. Sarver DM, Yanosky M. (2005). Principles of cosmetic dentistry in orthodontics: Part 2. Soft tissue laser technology and cosmetic gingival contouring. Am J Orthod Dentofacial Orthop. ,127,85–90.
136. Fornaini, C., Merigo, E., Vescovi, P., Lagori, G., & Rocca, J. (2013). Use of laser in orthodontics: applications and perspectives. Laser Ther, 22(2), 115-124. doi:10.3136/islsm.22.115
137. Harazaki M, Isshiki Y. (1997). Soft laser irradiation effects on pain reduction in orthodontic treatment. Bull Tokyo Dent Coll, 38, 291-5.

Page 113 Dental.EliteCME.Com
138. Turhani D, Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP. (2006). Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. Am J Orthod Dentofacial Orthop, 130,371-7.
139. Haytac MC, Ozcelik O. (2006). Evaluation of patient perceptions after frenectomy operations: A comparison of carbon dioxide laser and scalpel techniques. J Periodontol., 77,1815–9.
140. Fujiyama K, Deguchi T, Murakami T, Fujii A, Kushima K,Takano-Yamamoto T. (2008). Clinical effect of CO (2) laser in reducing pain in orthodontics. Angle Orthod,78, 299-303.
141. Angeletti P, Pereira MD, Gomes HC, Hino CT, Ferreira LM. 2010; Effect of low-level laser therapy (GaAlAs) on bone regeneration in midpalatal anterior suture after surgically assisted rapid maxillary expansion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 109: e38-46.
142. Saito S, Shimizu N. (1997). Stimulatory effects of low-power laser irradiation on bone regeneration in midpalatal suture during expansion in the rat. Am J Orthod Dentofacial Orthop,111, 525-32.
143. Nagaraj KR. (2012). Use of lasers in prosthodontics: a review. Int J Clin Dent ,5(1):91-112.144. Shajahan, P. A., Kumar, P. R., Hariprasad, A., Mathew, J., Shaji, A. P., & Ahammed, M. F. (2015).
Lasers: The Magic Wand in Esthetic Dentistry!! J Int Oral Health, 7(6), 119-121.145. Parker, S. (2007). Lasers and soft tissue: periodontal therapy. Br Dent J, 202(6), 309-315.
doi:10.1038/bdj.2007.224146. Ural Ç, Külünk T, Külünk Ş, Kurt M. (2010). The effect of laser treatment on bonding
between zirconia ceramic surface and resin cement. Acta Odontol Scand. 68(6):354-9. doi: 10.3109/00016357.
147. Romanos, G. E., Gupta, B., Yunker, M., Romanos, E. B., & Malmstrom, H. (2013). Lasers use in dental implantology. Implant Dent, 22(3), 282-288. doi: 10.1097/ID.0b013e3182885fcc
148. van As, G. A. (2015). Lasers in Implant Dentistry, Part I. Dent Today, 34(7), 134, 136-139. 149. van As, G. A. (2015). Lasers in Implant Dentistry, Part 2. Dent Today, 34(8), 94, 96-99. 150. Romanos GE, Gutknecht N, Dieter S, Schwarz F, Crespi R, Sculean A. (2009). Laser wavelengths
and oral implantology. Lasers Med Sci.,24, 961–70.151. Deppe H, Horch HH, Henke J, Donath K. (2001). Peri-implant care of ailing implants with the
carbon dioxide laser. Int J Oral Maxillofac Implants., 16, 659–67.152. Lévesque L, Noël JM, Scott C. Controlling the temperature of bones using pulsed CO2 lasers:
observations and mathematical modeling. (2015). Biomed Opt Express. 9, 6(12), 4768-80. doi: 10.1364/BOE.6.004768.
153. Kusek, E.R. (2011). Immediate implant placement into infected sites: bacterial studies of the Hydroacoustic effects of the YSGG laser. J Oral Implantol. 37,Spec No, 205-11. doi: 10.1563/AAID-JOI-D-10-00014
154. Sawabe M, Aoki A, Komaki M, Iwasaki K, Ogita M, Izumi Y. (2015). Gingival tissue healing following Er:YAG laser ablation compared to electrosurgery in rats. Lasers Med Sci., 30(2), 875-83.
155. Stübinger S, Landes C, Seitz O, Sader R. (2007). Er:YAG laser osteotomy for intraoral bone grafting procedures: a case series with a fiber-optic delivery system. J Periodontol., 78(12), 2389-94.
156. Schwarz F, Olivier W, Herten M, Sager M, Chaker A, Becker J. (2007). Influence of implant bed preparation using an Er:YAG laser on the osseointegration of titanium implants: a histomorphometrical study in dogs. J Oral Rehabil., 34(4), 273-81.
157. Romanos, G. E., Everts, H., & Nentwig, G. H. (2000). Effects of diode and Nd:YAG laser irradiation on titanium discs: a scanning electron microscope examination. J Periodontol, 71(5), 810-815. doi:10.1902/jop.2000.71.5.810
158. Wang, H.L., Boyapati, L. (2006). “PASS” principles for predictable bone regeneration. Implant Dent.,15:8-17.
159. Kesler, G., Shvero, D. K., Tov, Y. S., & Romanos, G. (2011). Platelet derived growth factor secretion and bone healing after Er:YAG laser bone irradiation. J Oral Implantol, 37 Spec No, 195-204. doi:10.1563/aaid-joi-d-09-00120.1
160. Stubinger, S., Henke, J., Donath, K., & Deppe, H. (2005). Bone regeneration after peri-implant care with the CO2 laser: a fluorescence microscopy study. Int J Oral Maxillofac Implants, 20(2), 203-210.
161. Kreisler M, Götz H, Duschner H. (2002). Effect of Nd:YAG, Ho:YAG, Er:YAG, CO2, and GaAIAs laser irradiation on surface properties of endosseous dental implants. Int J Oral Maxillofac Implants. ,17(2), 202-11.
162. Aoki, A., Mizutani, K., Takasaki, A. A., Sasaki, K. M., Nagai, S., Schwarz, F., Izumi, Y. (2008). Current status of clinical laser applications in periodontal therapy. Gen Dent, 56(7), 674-687; quiz 688-679, 767.
163. Stubinger, S. (2010). Advances in bone surgery: the Er:YAG laser in oral surgery and implant dentistry. Clin Cosmet Investig Dent, 2, 47-62.
164. Boldrini, C., de Almeida, J. M., Fernandes, L. A., Ribeiro, F. S., Garcia, V. G., Theodoro, L. H., & Pontes, A. E. (2013). Biomechanical effect of one session of low-level laser on the bone-titanium implant interface. Lasers Med Sci, 28(1), 349-352. doi:10.1007/s10103-012-1167-3
165. Naka, T., & Yokose, S. (2012). Application of laser-induced bone therapy by carbon dioxide laser irradiation in implant therapy. Int J Dent, 2012, 409496. doi:10.1155/2012/409496
166. Enwemeka, C. S., Parker, J. C., Dowdy, D. S., Harkness, E. E., Sanford, L. E., & Woodruff, L. D. (2004). The efficacy of low-power lasers in tissue repair and pain control: a meta-analysis study. Photomed Laser Surg, 22(4), 323-329. doi:10.1089/1549541041797841
167. Aoki, A., Mizutani, K., Schwarz, F., Sculean, A., Yukna, R. A., Takasaki, A. A., Izumi, Y. (2015). Periodontal and peri-implant wound healing following laser therapy. Periodontol 2000, 68(1), 217-269. doi:10.1111/prd.12080
168. de Oliveira, R. F., de Andrade Salgado, D. M., Trevelin, L. T., Lopes, R. M., da Cunha, S. R., Aranha, A. C., . . . de Freitas, P. M. (2015). Benefits of laser phototherapy on nerve repair. Lasers Med Sci, 30(4), 1395-1406. doi:10.1007/s10103-014-1531-6
169. Shen, C. C., Yang, Y. C., Huang, T. B., Chan, S. C., & Liu, B. S. (2013). Neural regeneration in a novel nerve conduit across a large gap of the transected sciatic nerve in rats with low-level laser phototherapy. J Biomed Mater Res A, 101(10), 2763-2777. doi:10.1002/jbm.a.34581
170. Khadra, M. (2005). The effect of low level laser irradiation on implant-tissue interaction. In vivo and in vitro studies. Swed Dent J Suppl (172), 1-63.
171. Yeh, S., Jain, K., & Andreana, S. (2005). Using a diode laser to uncover dental implants in second-stage surgery. Gen Dent, 53(6), 414-417.
172. Jin, J. Y., Lee, S. H., & Yoon, H. J. (2010). A comparative study of wound healing following incision with a scalpel, diode laser or Er,Cr:YSGG laser in guinea pig oral mucosa: A histological and immunohistochemical analysis. Acta Odontol Scand, 68(4), 232-238. doi:10.3109/00016357.2010.492356
173. Ryu, S. W., Lee, S. H., & Yoon, H. J. (2012). A comparative histological and immunohistochemical study of wound healing following incision with a scalpel, CO2 laser or Er,Cr:YSGG laser in the guinea pig oral mucosa. Acta Odontol Scand, 70(6), 448-454. doi:10.3109/00016357.2011.635598
174. Romanos, G. E., Gaertner, K., Aydin, E., & Nentwig, G. H. (2013). Long-term results after immediate loading of platform-switched implants in smokers versus non-smokers with full-arch restorations. Int J Oral Maxillofac Implants, 28(3), 841-845. doi:10.11607/jomi.3223
175. Romanos, G. E., Gupta, B., Yunker, M., Romanos, E. B., & Malmstrom, H. (2013). Lasers use in dental implantology. Implant Dent, 22(3), 282-288. doi: 10.1097/ID.0b013e3182885fcc
176. Javed, F., Al-Hezaimi, K., Al-Rasheed, A., Almas, K., & Romanos, G. E. (2010). Implant survival rate after oral cancer therapy: a review. Oral Oncol, 46(12), 854-859. doi: 10.1016/j.oraloncology.2010.10.004
177. Zitzmann, N. U., & Berglundh, T. (2008). Definition and prevalence of peri-implant diseases. J Clin Periodontol, 35(8 Suppl), 286-291. doi:10.1111/j.1600-051X.2008.01274.
178. Atieh, M. A., Alsabeeha, N. H., Faggion, C. M., Jr., & Duncan, W. J. (2013). The frequency of peri-implant diseases: a systematic review and meta-analysis. J Periodontol, 84(11), 1586-1598. doi:10.1902/jop.2012.120592
179. Smeets, R., Henningsen, A., Jung, O., Heiland, M., Hammacher, C., & Stein, J. M. (2014). Definition, etiology, prevention and treatment of peri-implantitis--a review. Head Face Med, 10, 34. doi:10.1186/1746-160x-10-34
180. Padial-Molina, M., Suarez, F., Rios, H. F., Galindo-Moreno, P., & Wang, H. L. (2014). Guidelines for the diagnosis and treatment of peri-implant diseases. Int J Periodontics Restorative Dent, 34(6), e102-111. doi:10.11607/prd.1994
181. Esposito, M., Grusovin, M. G., Coulthard, P., & Worthington, H. V. (2008). The efficacy of interventions to treat peri-implantitis: a Cochrane systematic review of randomised controlled clinical trials. Eur J Oral Implantol, 1(2), 111-125.
182. Louropoulou, A., Slot, D. E., & Van der Weijden, F. A. (2012). Titanium surface alterations following the use of different mechanical instruments: a systematic review. Clinical Oral Implants Research, 23(6), 643-658. doi:10.1111/j.1600-0501.2011.02208.
183. Mann, M., Parmar, D., Walmsley, A. D., & Lea, S. C. (2012). Effect of plastic-covered ultrasonic scalers on titanium implant surfaces. Clinical Oral Implants Research, 23(1), 76-82. doi:10.1111/j.1600-0501.2011.02186.
184. Roncati, M., Lauritano, D., Tagliabue, A., & Tettamanti, L. (2015). Nonsurgical periodontal management of iatrogenic peri-implantitis: A clinical report. J Biol Regul Homeost Agents, 29(3 Suppl 1), 164-169.
185. Roncati, M., Lucchese, A., & Carinci, F. (2013). Non-surgical treatment of peri-implantitis with the adjunctive use of an 810-nm diode laser. J Indian Soc Periodontol, 17(6), 812-815. doi:10.4103/0972-124x.124531
186. Tosun E, Tasar F, Strauss R, Kıvanc DG, Ungor C. (2012). Comparative evaluation of antimicrobial effects of Er:YAG, diode, and CO𝛽 lasers on titanium discs: an experimental study. J Oral Maxillofac Surg, 70(5), 1064-9. doi:10.1016/j.joms.2011.11.021.
187. Froum SJ, Froum SH, Rosen PS. (2012) Successful management of peri-implantitis with a regenerative approach: a consecutive series of 51 treated implants with 3- to 7.5- year follow-up. Int J Periodontics Restorative Dent, 32(1):11-20.
188. Yamamoto, A., and Tanabe, T. (2013). Treatment of peri-implantitis around TiUnite-surface implants using Er:YAG laser microexplosions. Int J Periodontics Restorative Dent. 33(1):21-30.
189. Natto ZS, Aladmawy M, Levi PA Jr, Wang H.L. (2015). Comparison of the efficacy of different types of lasers for the treatment of peri-implantitis: a systematic review. Int J Oral Maxillofac Implants, 30(2), 338-45. doi:10.11607/jomi.3846.
190. Ashnagar, S., Nowzari, H., Nokhbatolfoghahaei, H., Yaghoub Zadeh, B., Chiniforush, N., & Choukhachi Zadeh, N. (2014). Laser treatment of peri-implantitis: a literature review. J Lasers Med Sci, 5(4), 153-162.
191. Asnaashari M, Zadsirjan S. (2014). Application of Laser in Oral Surgery. J Lasers Med Sci, 5(3):97-107
192. Kawczyk-Krupka A, Waskowska J, Raczkowska-Siostrzonek A, Kosciarz-Grzesiok A, Kwiatek S, Straszak D, et al. (2012). Comparison of cryotherapy and photodynamic therapy in treatment of oral leukoplakia. Photodiagnosis Photodyn Ther,9(2):148-55.
193. Shafirstein G, Friedman A, Siegel E, Moreno M, Baumler W, Fan CY, et al. (2011). Using 5-aminolevulinic acid and pulsed dye laser for photodynamic treatment of oral leukoplakia. Arch Otolaryngol Head Neck Surg ,137(11):1117-23.
194. Fornaini C, Raybaud H, Augros C, Rocca JP. (2012) New clinical approach for use of Er:YAG laser in the surgical treatment of oral lichen planus: a report of two cases. Photomed Laser Surg, 30(4):234-8.
195. Luna-Ortiz K, Gomez-Pedraza A, Mosqueda-Taylor A. (2013). Soft palate preservation after tumor resection with transoral laser microsurgery. Med Oral Patol Oral Cir Bucal,18(3): e445-8.
196. Yague-Garcia J, Espana-Tost AJ, Berini-Aytes L, Gay-Escoda C.(2009). Treatment of oral mucocele-scalpel versus CO2 laser. Med Oral Patol Oral Cir Bucal.,14(9), e469-74.
197. Lai JB, Poon CY. (2009). Treatment of ranula using carbon dioxide laser--case series report. Int J Oral Maxillofac Surg 38(10):1107-11.
198. Maia ML, Bonjardim LR, Quintans J., de S, Ribeiro MA, Maia LG, Conti PC. (2012). Effect of low-level laser therapy on pain levels in patients with temporomandibular disorders: a systematic review. J Appl Oral Sci, 20(6), 594-602.
199. Herranz-Aparicio J, Vázquez-Delgado E, Arnabat-Domínguez J, España-Tost A, Gay-Escoda C. (2013). The use of low level laser therapy in the treatment of temporomandibular joint disorders. Review of the literature. Med Oral Patol Oral Cir Bucal., 18(4), e603-12.
200. Miserendino LJ, Pick RM, Blankenau RJ. (1995). Laser safety in dental practice. In: Miserendino LJ, Pick RM, editors. Lasers in Dentistry. Singapore:Quintessence Publishing Co, Inc., 85-103.

Dental.EliteCME.Com Page 114
Suggested reading list on dental lasersLaser safetyAmerican National Standard for Safe Use of Lasers in Health Care Facilities https://www.lia.org/PDF/Z136_3_s.pdf
Comprehensive overview of all lasers in dentistryKoci E, Almas A. Laser application in dentistry: an evidence-based clinical decision-making update. Pak Oral Dent J. 2009;29(2):409-423.
Orthodontics1. Milling Tania, S. D., Sathiasekar, C., Anison, J. J., & Samyukta
Reddy, B. V. (2015). The extended tentacles of laser - From diagnosis to treatment in orthodontics: An overview. Journal of Pharmacy & Bio allied Sciences, 7(Suppl 2), S387–S392.
2. Nalcaci R, Cokakoglu S. Lasers in orthodontics. Eur J Dent 2013; 7:119-25
Oral surgeryAsnaashari M, Zadsirjan S. Application of Laser in Oral Surgery. J Lasers Med Sci 2014;5(3):97-107
Restorative dentistry1. Najeeb S, Khurshid Z, Zafar MS, Ajlal S. Applications of Light
Amplification by Stimulated Emission of Radiation (Lasers) for Restorative Dentistry. Med Princ Pract. (2015): 1-11.
2. Tassery, H., Levallois, B., Terrer, E., Manton, D., Otsuki, M., Koubi, S., Gugnani, N., Panayotov, I., Jacquot, B., Cuisinier, F. and Rechmann, P. (2013), Use of new minimum intervention
dentistry technologies in caries management. Australian Dental Journal, 58: 40–59
Pediatric dentistry1. Prathima, G. S., Bhadrashetty, D., Babu, S. B. U., & Disha, P.
(2015). Microdentistry with Lasers. Journal of International Oral Health: JIOH, 7(9), 134–137.
2. Nazemisalman B, Farsadeghi M, Sokhansanj M. Types of Lasers and Their Applications in Pediatric Dentistry. J Lasers Med Sci. 2015;6(3):96-101.
PeriodonticsRomanos, G. (2015). Current concepts in the use of lasers in periodontal and implant dentistry. Journal of Indian Society of Periodontology, 19(5), 490–494.
Ulcers Vale FA, Moreira MS, de Almeida FC, Ramalho KM. (2015). Low-level laser therapy in the treatment of recurrent aphthous ulcers: a systematic review. Scientific World Journal. ; 2015:150412. doi: 10.1155/2015/150412.
TMDShaffer, S. M., Brismée, J.-M., Sizer, P. S., & Courtney, C. A. (2014). Temporomandibular disorders. Part 2: conservative management. The Journal of Manual & Manipulative Therapy, 22(1), 13–23. http://doi.org/10.1179/2042618613Y.0000000061
UPDATES On LASER THERAPy In DEnTISTRy AnD InTEGRATIOn In THE DEnTAL OffICE
final Examination QuestionsSelect the best answer for each question and mark your answers on the Final Examination Answer Sheet found on page 116,
or for faster service complete your test online at Dental.EliteCME.com.
1. Lasers produce a source of energy as a coherent radiation of one wavelength in the infrared, visible, or ultraviolet part of the electromagnetic spectrum. a. True. b. False.
2. The optimal parameters of lasers depend on the target tissue, and involve only the wavelength, exposure time, and energy quantity. a. True. b. False.
3. Laser-tissue interaction is dependent on the wavelength and mode of laser emission only.a. True. b. False.
4. ________ cannot interact with gold or porcelain material.a. Diode lasers. b. LLLT lasers. c. Erbium lasers. d. Nd-YAG lasers.
5. Strict adherence to ___________ by all dental team members in the vicinity of the laser is paramount to avoid contaminated aerosols.a. Rules. b. State guidelines.c. Ethical codes.d. Infection control.
DCA04LTE18

Page 115 Dental.EliteCME.com
What if I Still Have Questions?
No problem, we have several options for you to choose from! Online at Dental.EliteCME.com you will see our robust FAQ section that answers many of your questions, simply click FAQ in the upper right hand corner or Email us at [email protected] or call us toll free at 1-866-344-0972, Monday - Friday 9:00 am - 6:00 pm, EST.
$6 per credit hour
EliteContinuing Education
Three Easy Steps to Completing your License Renewal
Step 1: Complete your Elite continuing education courses:
9 Read the course materials and complete the final examination questions.
9 Complete the course evaluation. 9 Submit your final exam and course evaluation along with your payment to Elite online, by fax, or by mail.
Step 2: Receive your certificate of completion.
9 On-Line Submission: Go to Dental.EliteCME.com and follow the prompts. You will be able to print your certificate immediately upon completion of the course.
9 fax or E-mail Submission: Fax to (386) 673-3563, be sure to include your credit card information. All completions will be processed within 2 business days of receipt and certificates e-mailed to the e-mail address provided.*
9 Mail Submission: Use the envelope provided or mail to Elite, PO Box 37, Ormond Beach, FL 32175. All completions will be processed and certificates issued within 10 business days from the date it is mailed.*
*Please note - providing a valid e-mail address is the quickest and most efficient way to receive your certificates when submitting via fax, e-mail or mail.
Submissions without a valid e-mail address will be mailed to the address provided at registration.
Step 3: Once you have received your certificate of completion you can renew your license online at http://www.dbc.ca.gov/licensees/rda/renewals.shtml, or mail in your renewal. In order to avoid late fees, your CE and license renewal must be completed by the last day of your birth month.
Board Contact Information: Dental Board of California 2005 Evergreen Street, Suite 1550 Sacramento, California 95815 Phone: (877) 729-7789 | Fax: (916) 263-2140 Website: http://www.dbc.ca.gov/
2018 Continuing Education Course for California Dental Professionals
Customer Information

ELITE CE COURSE FOR CALIFORNIA DENTISTSQUESTIONS? CALL US TOLL FREE: 1-866-344-0972 FINAL EXAMINATION ANSWER SHEETPlease fill in all information below in CAPITAL LETTERS. Upon completion, please place this sheet in the envelope provided and mail. If paying by check or money order, please make payable to Elite. For faster service, specify your credit card information on this form in the space provided and fax to 1-386-673-3563. For even faster service, we offer the test online with instant grading and certificate issuance. Please visit Dental.EliteCME.com to complete your test on the web.
Please PRINT NEATLY in CAPITAL LETTERS in the areas below using black or blue pen only:FIRST NAME MI LAST NAME
STREET ADDRESS
Suite/Apt # CITY (do not abbreviate) STATE
ZIP CODE AREA CODE + TELEPHONE NUMBER DENTIST LICENSE NUMBER
- - D D S -
E-mail (Include to receive processing confirmation and instant certificate access)
PAYMENT METHODqCheck/Money Order made payable to Elite for full amount due qVisa/Mastercard/American Express/Discover Visa/Mastercard/American Express/Discover Card Expiration Date
/
Signature_____________________________________________________
Course Payment: You may complete the individual courses for the price listed below.
Final Exam Questions are located at the end of each chapter.Unanswered questions will be scored as incorrect.
CHAPTER PAYMENT Ch. 1 - California Dental Practice Act (Mandatory)
(2 CE Hours)
Exam p. 24Questions 1-10
Ch. 2 - Guidelines for Infection Control in Dental Health Care
Settings (Mandatory)(4 CE Hours- Course meets
board requirement for 2 CE units, remaining hours go to Category I)
Exam p. 47 Questions 1-5
Ch. 3 - Health Information Technology:
The Future is Now(7 CE Hours)
Exam p. 70 Questions 1-10
Ch. 4 - Medical Emergencies in the
Dental Office(4 CE Hours)
Exam p. 84Questions 1-5
1 - California Dental Practice Act (2 CE Hours)
q$12.00
2 - Guidelines for Infection Control in Dental Health Care Settings (4 CE Hours)
q$24.00
3 - Health Information Technology: The Future is Now (7 CE Hours)
q$42.00 A B1. m m2. m m3. m m4. m m5. m m6. m m7. m m8. m m9. m m10. m m
A B1. m m2. m m3. m m4. m m5. m m
A B C D1. m m m m2. m m m m3. m m m m4. m m m m5. m m m m6. m m m m7. m m m m8. m m m m9. m m m m10. m m m m
A B C D1. m m m m2. m m m m3. m m m m4. m m m m5. m m m m
4 - Medical Emergencies in the Dental Office(4 CE Hrs)
q$24.00
5 - Peri-Implantitis: Basics and Beyond(2 CE Hours) q$12.00
6 - Professional Care and Patient Maintenance of Implant-Supported Dentures (2 CE Hours)
q$12.00
Ch. 5 - Peri-Implantitis:Basics and Beyond
(2 CE Hours)
Exam p. 92Questions 1-5
Ch. 6 - Professional Care and Patient Maintenance of
Implant-Supported Dentures(2 CE Hours)
Exam p. 99Questions 1-5
Ch. 7 - Updates on Laser Therapy in Dentistry and Integration in the
Dental Office(4 CE Hours)
Exam p. 114Questions 1-5
7 - Updates on Laser Therapy in Dentistry and Integration in the Dental Office (4 CE Hours)
q$24.00
Purchase 25 hours and save money q$99.00
A B C D1. m m m m2. m m3. m m4. m m5. m m m m
A B1. m m2. m m3. m m4. m m5. m m
A B C D1. m m2. m m3. m m4. m m m m5. m m m m
TOTAL ENCLOSED $ .
FOR INTERNAL USE ONLY - PLEASE DO NOT MARK IN THIS AREADental.EliteCME.com 1-DCA02PAE18 2-DCA04ICE18 3-DCA07ITE18 4-DCA04EDE18 5-DCA02PEE18 6-DCA02ISE18 7-DCA04LTE18 Page 116

We value your opinion! Please take a minute to complete the course evaluation
so that we can better serve you in the future. Any comments would be greatly appreciated.
Fill in circles below numbers 0=Not likely at all, 5=Neutral and 10=Extremely likelyHow likely is it that you would recommend Elite .......................0 1 2 3 4 5 6 7 8 9 10
The course material was presented in a clear, conciseand well-organized format ..........................................................0 1 2 3 4 5 6 7 8 9 10
I would rate this course .................................................................0 1 2 3 4 5 6 7 8 9 10
The content of this course met my expectations ......................0 1 2 3 4 5 6 7 8 9 10
The material presented met the course’s stated objectives ........................................ Yes No
I found this course a good value for my money ............................................................. Yes No
Please list any recommendations that you may have for this course ___________________
___________________________________________________________________________________
Please list any course subjects you would like to see in the future ______________________
___________________________________________________________________________________
Comments _________________________________________________________________________
___________________________________________________________________________________
q I agree to allow Elite Continuing Education to use my above comments.
Did you remember: 1) To clearly print your name and address on the answer sheet? 2) To fill out your license number on the answer sheet? 3) To include your payment or credit card information? 4) A $25.00 fee will be added for all checks that are returned for insufficient funds.
Thank you for choosing Elite for your continuing education!
P.O. Box 37Ormond Beach, FL 32175-0037
Fax: 1-386-673-3563
EliteContinuing Education
ourse EvaluationC
Page 117 Dental.EliteCME.com





























