Embed Size (px)
Citation preview

EVALUATION ON IMPLEMENTATION OF NHIF BENEFIT
PACKAGE IN THE SELECTED ACCREDITED HEALTH
FACILITIES IN ILALA MUNICIPALITY
By
Rodney M. A Chiduo
A Dissertation submitted to the School of Public Administration and Management
in Partial Fulfillment of the Requirement for the Award of Degree in Master of
Science in Health Monitoring and Evaluation( MSc-HME) of Mzumbe University.
2017
i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for acceptance by
Mzumbe University, a dissertation entitled; “Evaluation on Implementation of NHIF
Benefit Package in the Selected Accredited Health Facilities in Ilala Municipality” I
recommend it be accepted in partial fulfillment of the requirements for the award of the
Degree in Masters of Science in Health Monitoring and Evaluation.
_______________________________
Major Supervisor
We have examined this Dissertation and recommended it for acceptance
...................................................................
Internal Examiner
……………………………………………
External Examiner
Accepted for the Board of School of Public Administration and Management
……………………………………………………….
DEAN, SCHOOL OF PUBLIC ADMINISTRATION AND MANAGEMENT
ii
DECLARATION
I, Rodney M. A Chiduo, declare that this is my own original work and that it has not
been and will not be presented to any other university for a similar or any other degree
award.
Signature: ____________________________
Date: ________________________________
iii
COPYRIGHT
©
This dissertation is a copyright material protected under the Berne Convention, the
Copyright Act 1999 and other international and national enactments in that behalf or an
intellectual property. It may not be reproduced by any means in full or in part, except for
short extracts in fair dealings, for research or private study, critical scholarly review or
discourse with an acknowledgment with written permission of Mzumbe University on
behalf of the author.
iv
ACKNOWLEDGEMENTS
The successful accomplishment of this report is a result and support i received from
many dignities and individuals; however it is not possible to mention them all. I
therefore take the opportunity just to mention few of them.
Most importantly, I would like to thank God for my good health that granted an
opportunity to write this Dissertation. I could not have been able to complete my
Dissertation without much support and assistance of my supervisor, co- workers, friends,
my family and my beloved wife.
I offer my sincere most appreciation to my supervisor Dr Wilhelm Mafuru of Mzumbe
University, He worked diligently in making productive criticisms, ideas, and corrections
from research proposal development to final stage of report write up. His intellectual
skills, comments, guidance, assurances, close supervision and patience are relatively
remarkable towards successful completion of my Research.
I take this great opportunity also to thank my beloved wife Salome Irene for her
patience, prayers, support and encouragement throughout the good and difficult times
during my period of study; really without her support my studies would have been
difficult.
I also convey my special thanks to my lovely beautiful daughters Karen Nenelwa and
Samantha Wanyenda for tolerantly bearing with me and showed resilience during my
prolonged absence throughout a period in University when they needed me most. Your
patience and understanding will never be forgotten and may God bless you all
abundantly.
I would also like to extend my thanks to my brothers, Sydney Rehoboam and Geoffrey
Sehewa; and my sisters Sarah Naomi and Wendo Oripa together with their families for
their moral support, guidance and encouragement during the period of my studies. Also I
thank you my cousin brother Winston Godfrey and Sister Dr Maria Mgulambwa.
v
To all of you I say, “Kwimageni”, in Kaguru language meaning thank you very much!
I also wish to extend my heartfelt gratitude and appreciation to the School of Public
Administration, Department of Health System Management for accepting me to join this
program. Also to all of my lectures of MSc in HMnE for the year 2015-2017 for
imparting me the knowledge and support during the entire period of my study. Each
subject taught was very important for my career and it equipped me with more
knowledge and needed skills of writing this dissertation, my fellow postgraduate
students of Master of Science in Health Monitoring and Evaluation Cohort 3 for their
contributions, teamwork, sharing of ideas and support throughout the entire period of 3
semesters during the time of course work.
I am highly thankful to my employer National Health Insurance Fund (NHIF) especially
Ag Director General in particular for the permission to undertake this course.
I also wish to thank all people from Amana Hospital, Muhimbili National referral
Hospital, Regency Medical Centre and all other health facility staff, Members, NHIF
staff and research assistants that consented to participate in this study, without whom,
this work would not have been possible.
vi
DEDICATION
This work is dedicated to my parents; my adorable late father Dr Aaron D Chiduo and
my beloved mother Mrs Ahilai Chiduo for their unconditional love, spiritual guidance
and the way they raise me, it‘s because they worked tireless hard to build my personality
and ability to be who i am today. Their trust made me to have confidence and courage to
achieve this level of education.
I also dedicated this dissertation to my beautiful lovely wife Salome and our beautiful
daughters Karen and Samantha;
May the Almighty God grant all of them a peaceful everlasting life!
I can do all things in him who strengthens me (Philippians 4:13).
vii
LIST OF ABBREVIATIONS AND ACRONYMS
ADDO Accredited Dispensing Drug Outlets
CHAG) Christian Health Association of Ghana
CT- Scan Computerized Tomography Scan
CPA Complementary Package of Activities
HCWs Health Care Workers
ILO International labor Organization
MoHCDGEC Ministry of Health Community development, Gender,
Elderly and Children
MRI Magnetic Resonance Image
NEMLIT National Essential Medicine List of Tanzania
NHIF National Health Insurance Fund
NHIS National Health Insurance Scheme
SHI Social Health Insurance
SHIS Social Health Insurance Scheme
WHO World Health Organization
HSSP IV Health sector strategic plan IV
URT United Republic of Tanzania
CHT Community Health Fund
NIC National Insurance Corporation
NHIA National Health Insurance Authority
G-DGR Ghana – Diagnosis related Group
FFS Fee – for – Services
ZHAC Zambia Health Accreditation Council
USAID United States Agency for International Development
COHSASA Council for Heath Services Accreditation of Southern
Africa
PBF Performance Based Financing
ISO International Organization for Standardization
EAC East African Community
viii
ABSTRACT
The National Health Insurance Fund (NHIF) was established under the National Health
Insurance Act No. 8 of 1999 as contributory Social Health Insurance Scheme.
Social Health Insurance Scheme is a health scheme insurance which is provided by the
governments to its employee. Tanzania presented social health insurance by creation of
the National Health Insurance Fund (NHIF) in 1999 with the objective of improving the
quality and accessibility of health services to Government employees. NHIF facilitates
admission of health care services to its beneficiaries through a network of accredited
health facilities nationwide. This study evaluated implementation of NHIF benefit
package in selected accredited health facilities, challenges encountered and
improvement measures.
The study was conducted in Dar es salaam, Ilala Municipal whereby a facility based
Case studies of both quantitative and qualitative nature was carried. A total of 300
beneficiaries, 10 NHIF staff from Ilala office and respondents from 10 selected
accredited health facilities participated in the study. The study population comprised of
both male and female respondents aged 21 to 60 years with the education level from
secondary to university and above, (80%) had a working experience of more than five
years. Quantitative data were processed and analyzed by using Microsoft excel and
Statistical Package for Social Sciences (SPSS) software while Atlas ti. Software was
used to analyze Qualitative data. Over half of the respondents (over 50%) agreed that
NHIF objectives were achieved and there are several items within the benefit package
that can be accessed by the beneficiaries from accredited health facilities. Besides, a
number of challenges were reported to have been encountered by the accredited health
facilities in the process of implementing the NHIF service provision as per benefit
package. For example, 60 % mentioned lack of modern diagnostic equipment‘s, 80%
mentioned Medicine out of stock, 90% mentioned delayed reimbursement of funds from
NHIF, 17% Unrealistic prices for some items within the package, 15%.Services not in
the package, 90% shortage of staff and lack of space.
From these findings, the following recommendation can be drawn; more effort is still
needed to address the challenges encountered by accredited health facilities and increase
awareness on benefit Package. Government set a policy to establish regulatory authority
to govern price of services in Health sector, timely claims reimbursement. However,
measures are needed to be taken to strengthen and improve services within the facilities;
take measure to address the issues of unrealistic prices on some of the services and
include the services that are not in the current package but much needed by beneficiaries
and final recommendation is to increase budget in Health Sector.
ix
TABLE OF CONTENTS
CERTIFICATION .............................................................................................................. i
DECLARATION .............................................................................................................. ii
COPYRIGHT ................................................................................................................... iii
ACKNOWLEDGEMENTS .............................................................................................. iv
DEDICATION .................................................................................................................. vi
LIST OF ABBREVIATIONS AND ACRONYMS ........................................................ vii
ABSTRACT ................................................................................................................... viii
LIST OF TABLES ........................................................................................................... xv
LIST OF FIGURES AND PICTURES ........................................................................... xvi
LIST OF APPENDICES ............................................................................................... xvii
CHAPTER ONE .............................................................................................................. 1
INTRODUCTION ............................................................................................................ 1
1.1 Background .................................................................................................................. 1
1.1.1 General Overview ..................................................................................................... 1
1.1.2 NHIF Accreditation Overview .................................................................................. 3
1.2 Description of Program to be evaluated under NHIF Tanzania ................................... 4
1.2.1 Expected Program effects/objectives ........................................................................ 4
1.2.2 Expected program effect/ objectives ......................................................................... 4
1.3 Major Strategies Intended Strategies /activities for improvement of services onto
facilities .............................................................................................................................. 5
1.3.1 Program Activities and Resources: .......................................................................... 5
1.3.2 Major strategies ......................................................................................................... 5
1.3.3 Program activities...................................................................................................... 5
1.4 Program Logic Model .................................................................................................. 6
1.5 Stakeholders Analysis .................................................................................................. 8
1.6 Statement of the problem ........................................................................................... 10
1.7 Objective of the Study .............................................................................................. 12
1.7.1 Main Objectives ...................................................................................................... 12
x
1.7.2 Specific Objectives.................................................................................................. 12
1.8 Research Questions .................................................................................................... 13
1.9 Significance of the Research ...................................................................................... 13
1.10 Scope of the study ................................................................................................... 15
1.11 Limitation of the study ............................................................................................. 15
1.12 Organization of the thesis/ dissertation .................................................................... 16
1.13 Definitions of key terms .......................................................................................... 17
CHAPTER TWO ........................................................................................................... 19
LITERATURE REVIEW .............................................................................................. 19
2.1 Introduction ................................................................................................................ 19
2.2 Theoretical Literature Review.................................................................................... 19
2.2.1 Program evaluation ................................................................................................. 19
2.2.2 Formative evaluation ............................................................................................... 20
2.2.3 Process/implementation evaluation ......................................................................... 21
2.2.4 Outcome Based Evaluation ..................................................................................... 21
2.2.5 Economic Evaluation .............................................................................................. 21
2.2.6 Impact evaluation ................................................................................................... 22
2.3 Accreditation of Health facilities ............................................................................... 22
2.3.1 Accreditation of health facilities in the implementation of NHIF scheme in Ilala . 22
2.3.2 Accreditation of health facilities under NHIF schemes in other countries ............. 23
2.4 Study Overview .......................................................................................................... 30
2.5 The concept of Health Insurance................................................................................ 32
2.5.1 Health Insurance Scheme ........................................................................................ 33
2.6 Types of health insurance........................................................................................... 33
2.6.1 Social health insurance ............................................................................................ 33
2.6.2 Private health insurance .......................................................................................... 33
2.6.3 Community based insurance ................................................................................... 34
2.7 Health Sector Reforms in Tanzania ........................................................................... 34
2.8 Health care financing in Tanzania.............................................................................. 34
xi
2.9 Health Insurance System in Tanzania ........................................................................ 35
2.10 National Health Insurance Fund............................................................................... 35
2.10.1 The Basic Functions of NHIF ............................................................................... 36
2.11 The Fund governance ............................................................................................... 36
2.12 Empirical Literature Review .................................................................................... 37
2.12.1 National Health Insurance as a Global Phenomenon ............................................ 37
2.12.2 The National Health Insurance in Germany.......................................................... 37
2.12.3 The National Health Insurance Scheme in Japan .................................................. 38
2.12.4 The National Health Insurance Scheme in Netherlands ....................................... 40
2.12.5 The National Health Insurance Scheme in Switzerland ........................................ 41
2.12.6 The National Health Insurance Scheme in Uganda .............................................. 43
2.12.7The National Health Insurance Scheme in Costa Rica .......................................... 43
2.12.8 The National Health Insurance Scheme in Estonia ............................................... 46
2.12.9 The National Health Insurance Scheme in Netherlands ....................................... 48
2.12.10 The National Health Insurance Scheme in Chile ................................................ 50
2.13 Conceptual framework of the evaluation ................................................................. 59
CHAPTER THREE ....................................................................................................... 61
RESEARCH METHODOLOGY ................................................................................. 61
3.1 Introduction ................................................................................................................ 61
3.1.1 Evaluation design .................................................................................................... 61
3.1.2 Evaluation Approach ............................................................................................... 62
3.1.3 Evaluation period .................................................................................................... 62
3.2 Description of the Study area ..................................................................................... 62
3.3 Target population ....................................................................................................... 63
3.4 Source Population and Study Population ................................................................... 64
3.5 Units of analysis ......................................................................................................... 64
3.6 Variables and their measurements ............................................................................. 64
3.6.1 Indicators and Variables .......................................................................................... 64
3.6.1.1Variables ............................................................................................................... 64

xii
3.6.1.2 Dependent variable............................................................................................... 64
3.6.1.3 Independent variables........................................................................................... 64
3.7 Sample Size and sampling technique. ........................................................................ 65
3.8 Sampling technique .................................................................................................... 66
3.9 Approaches to the Study ............................................................................................ 67
3.10 Inclusion criteria....................................................................................................... 67
3.11 Exclusion criteria ..................................................................................................... 68
3.12 Data Collection......................................................................................................... 68
3.12.1 Data collection Process ......................................................................................... 68
3.13 Development of data collection tools ....................................................................... 68
3.13.1 Questionnaire ........................................................................................................ 68
3.13.2 Interview Guide ..................................................................................................... 69
3.13.3 Observation ........................................................................................................... 69
3.14 Validity and Reliability issues ................................................................................. 70
3.14.1 Validity .................................................................................................................. 70
3.14.2 Reliability .............................................................................................................. 70
3.15 Data management and analysis ................................................................................ 71
3.15.1 Data entry .............................................................................................................. 71
3.15.2 Data cleaning ......................................................................................................... 71
3.15.3 Data analysis ......................................................................................................... 71
3.15.4 Ethical Issues ......................................................................................................... 71
3.15.5 Possible limitations of evaluation ......................................................................... 72
CHAPTER FOUR .......................................................................................................... 73
PRESENTATION OF THE FINDINGS ...................................................................... 73
4.1 Introduction ................................................................................................................ 73
4.2 Demographic Characteristics of respondents ............................................................. 73
4.2.1 Education distribution of health workers ................................................................ 74
4.2.2 Level of health facility ............................................................................................ 75
4.2.3 Work experiences .................................................................................................... 76

xiii
4.3 NHIF Benefit Package ............................................................................................... 78
4.3.1 Excluded benefits .................................................................................................... 80
4.4 The contents of NHIF Benefit Package are comprehensive to suit for beneficiaries
needs ................................................................................................................................. 81
4.4.1 NHIF benefit packages as identified by NHIF members ........................................ 81
4.4.2 NHIF Benefit Package comprehensive suit for beneficiaries needs ....................... 82
4.5 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages .................................................................... 88
4.5.1 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages as findings from health facilities ............... 88
4.5.2 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages as findings from NHIF staff ...................... 91
4.6 Compliance of the selected accredited health facilities with the accreditation criteria
.......................................................................................................................................... 93
4.7 Challenges encountered by the selected health facilities while implementing NHIF
benefit package................................................................................................................. 95
4.8 Other Benefits Packages as implemented in other Countries .................................... 97
CHAPTER FIVE .......................................................................................................... 101
DISCUSSION OF THE FINDINGS ........................................................................... 101
5.1 Introduction .............................................................................................................. 101
5.2 Contents of NHIF Benefit Package are comprehensive to suit for beneficiaries needs
........................................................................................................................................ 101
5.3 Views and perception of the beneficiaries on the NHIF benefit packages provided as
to whether they have comprehensive coverage in terms of quality ............................... 103
5.4 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages .................................................................. 104
5.5 Extent to which the selected accredited health facilities comply with the
accreditation criteria ....................................................................................................... 106
xiv
5.6 Challenges encountered by the selected health facilities while implementing NHIF
benefit package............................................................................................................... 107
CHAPTER SIX ............................................................................................................ 111
SUMMARY, CONCLUSION AND RECCOMENDATION ................................... 111
6.1 Introduction .............................................................................................................. 111
6.2 Conclusion ............................................................................................................... 111
6.3 Recommendation and policy implication................................................................. 114
6.4 Recommendation...................................................................................................... 115
6.5 Areas for further studies ........................................................................................... 115
REFERENCES ............................................................................................................. 117
APPENDICES .............................................................................................................. 120
xv
LIST OF TABLES
Table 1.1: Stakeholders Matrix ......................................................................................... 9
Table 3.1: Population of the study ................................................................................... 63
Table 3.2: Variables and their measurements.................................................................. 65
Table 4.1: Level of health facility ................................................................................... 76
Table 4.2: Demographic Characteristics of the Respondents .......................................... 78
Table 4.3: NHIF packages and their correspondence frequencies and percentages........ 82
Table 4.5: Views and perception of the beneficiaries on the NHIF benefit packages
provided as to whether they have comprehensive coverage in terms of quality
........................................................................................................................ 87
Table 4.6: Status and capabilities of the selected accredited health facilities in fulfilling
the requirements of the NHIF Benefit Packages ............................................ 90
Table 4.7: Status and capabilities of the selected accredited health facilities in fulfilling
the requirements of the NHIF Benefit Packages as findings from NHIF staff
........................................................................................................................ 92
Table 4.8: Extent to which the selected accredited health facilities comply with the
accreditation criteria ....................................................................................... 94
Table 4.9: Challenges encountered by the selected health facilities while implementing
NHIF benefit package .................................................................................... 95

xvi
LIST OF FIGURES AND PICTURES
Figure 1.1: Program Logic Model at facility level............................................................ 7
Figure 2.1: The Conceptual framework of the study ...................................................... 60
Figure 4.1: Age distribution of NHIF staff, NHI members and Health providers .......... 74
Figure 4.2: Education distributions of respondents ........................................................ 75
Figure 4.3: Work experiences for Respondents (NHIF members, Providers) ................ 77
xvii
LIST OF APPENDICES
Appendix I: Dodoso kwa Wanachama/Wanufaika kwa Huduma za Matibabu ya Mfuko
wa Taifa wa Bima ya Afya............................................................................................. 120
Appendix II: Dodoso kwa Wafanyakazi wa kituo vya Afya ........................................ 125
Appendix III: Dodoso kwa Wafanyakazi Wa Mfuko Wa Taifa Wa Bima Ya Afya .... 129
Appendix IV: Questionnaire for NHIF Members ......................................................... 134
Appendix V: Questionnaire for Accredited Health Provider ........................................ 141
Appendix VI: Questionnaire for NHIF Staff ................................................................ 148
Appendix VII: Interview Guide to Health Providers .................................................... 153
Appendix VIII: Interview Guide for NHIF Members .................................................. 155
Appendix IX: Interview Guide for NHIF Staff ............................................................. 157
1
CHAPTER ONE
INTRODUCTION
1.1 Background
1.1.1 General Overview
Social health insurance schemes are generally understood as health insurance schemes
provided by Governments to its citizens, especially to low and middle income
populations. Recently, apart from governments, several non-government organizations at
the community level provide social Health insurance in developing countries (Churchill,
2006). Social health insurance pools both the health risks of its members, on the one
hand, and the contributions of enterprises, households and government, on the other
hand, and is generally organized by governments (Carrin and James, 2002). Most social
health insurance schemes combine different sources of funds, government often
contributing on behalf of people who cannot afford to pay themselves (WHO 2004).
Social health insurance differs from ‗tax based financing‘ which typically entitles all
citizens (and sometimes residents) to services thereby giving universal coverage.
However, social health insurance entitlement is linked to a contribution made by, or on
behalf of, specific individuals in the population (WHO 2004).The prime objectives of
social health insurance are: To provide health care that avoids large out of pocket
expenditure, Increase appropriate utilization of health services and improved health
status. (ILO, 2008).
The first broad system of Social Health Insurance was created by the Government of
Germany under Chancellor Bismarck between 1883 and 1889, following introduction of
Social Health Insurance Scheme in Germany and Latin America, there was considerable
interest in exploring the potential of Social Health Insurance to increase access to health
services and affordability of health care in Africa. SHI is seen as one of the health
financing approaches with a strong potential to share risks across population groups and
time. As membership is mandatory, it avoids many of the problems of adverse selection
2
which smaller, voluntary health insurance schemes face. A number of African countries
are currently experimenting with different approaches, including Nigeria, Rwanda,
Kenya, Tanzania and Ghana. (Wagstaff, 2009)
The National Health Insurance Fund (NHIF) was established under the National Health
Insurance Act No. 8 of 1999 as contributory Social Health Insurance Scheme. The
operation commenced in 2001 whereby it covered only civil servants. Later in 2002 The
Fund expanded its operation and amendments were done to cover entire public service
employees. From 2001 several amendments has been done to expand membership
coverage and ensure that every Tanzanian who is formal and informal sector, employed
and non-employed can join NHIF. The National Health Insurance Scheme is based on
internationally accepted insurance principles and provides a wide range of health
insurance benefits to the NHIF beneficiaries. Contributions of members are a major
source of Finance of the scheme. The scheme maintains a risk pooling Fund account into
which such contributions and other incomes are deposited. Out of this Account, the
scheme makes reimbursement of Medical costs to Accredited Medical providers in
respect of medical services provided to Beneficiaries. The Scheme covers six people in
the family who are principal member, spouse, children and parents. Currently NHIF has
693,063 principal members with total number of 3,727,709 beneficiaries as per III
Strategic Plan 2015-2020.
The Fund covers all Public Servants, Employees of private companies, Councilors,
members of public force, Immigration, prisons, fire and rescue brigade, informal sector,
groups, individual members, Higher learning students, retired members of the Fund and
other categories of groups. While the Law to establish the NHIF was enacted in 1999,
NHIF commenced its operations on 1st July 2001 and beneficiaries started to access
medical services from 1st October 2001
3
The NHIF is in use of a fee for service payment mechanism and not capitation system to
reimburse payments to the accredited health service providers because demand and
supply sides in the health sector are at disequilibrium. NHIF face the challenge of
customer satisfaction to the services provided by accredited service providers since there
are so many complaints from beneficiaries concerning dissatisfaction of services
received.
NHIF does not provide health care services directly in the sense of ownership of health
facilities; rather, it facilitates access to such services through a network of accredited
health facilities. Accredited Health facilities are classified as government, Faith Based
Organizations, NGO and Private Health facilities (NHIF, 2015).The position of
accredited health facilities stood at 6, 371 by June, 2015. Out of total accredited health
facilities, 4,837 (76%) are Government facilities, 580 (9%) are Faith Based
Organizations facilities and 954 (15%) are Private facilities. NHIF Strategic plan (2015-
2020)
1.1.2 NHIF Accreditation Overview
The Fund envisions to becoming the leading Health Insurance Scheme of choice in the
Sub-Saharan region in terms of sustainability and quality of services and is dedicated to
providing support to its beneficiaries to access health services through a wide network of
accredited quality health facilities throughout Tanzania. (http://www.nhif.or.tz)
The National Health Insurance Fund as a fund will be contracting with hospitals, health
centers, and potentially pharmacies. It will need to accredit all these types of facilities
that seek to be reimbursed for services to NHIF members so that the member can have
wide choice to choose the facility that will fulfill the needs. The requirements for
accreditation are spelled out in Section 20 of NHIF act.
4
1.2 Description of Program to be evaluated under NHIF Tanzania
1.2.1 Expected Program effects/objectives
NHIF has the following objectives:
i. To avail necessary guidelines as per NHIF standards to every accredited health
facility, by the end of 2015.
ii. To improve accessibility and quality of services to beneficiaries and service
providers by June, 2020;
iii. Increase accreditation of health facilities from current average of 80% to 95% by
2015
iv. Increase number of health facilities submitting e-claims from 245 to 306 by June
2020;
v. To increase reimbursement rate from 60% to 90% in each health facilities from
year 2010 to 2015.
vi. To train 10,000 health professionals (clinic(clinicians) on NHIF matters at the end
of 2015. (vi) To conduct supervision at accredited health facilities at least 2 times
in hospitals and at least once in health centre and dispensaries per year from the
year 2010 to 2015. (vii)To increase membership coverage from the current level of
26% to 50% by June, 2020.
vii. To increase contributions collection from the current annual average growth rate of
12% to 15% by June, 2020;
1.2.2 Expected program effect/ objectives
Increase accessibility and quality of services based on the benefit package to
beneficiaries and providers.
The Fund recognizes 50% of the available bedded dispensaries;

5
1.3 Major Strategies Intended Strategies /activities for improvement of services
onto facilities
1.3.1 Program Activities and Resources:
i. Undertake strategic accreditation of health facilities;
ii. Improve quality assurance functions (reimbursement rate, supportive supervision,
health facility surveillance, claims processing audit and pre-accreditation
inspection);
iii. Institute periodical review of benefits package to improve benefit package;
iv. Enhance service providers‘ education;
v. Enhance funding of activities related to health services improvement; iefacilities
for Medical Equipment Loans and Facility Improvement loan.
vi. To support health services delivery at Public Regional referral Hospitals.
1.3.2 Major strategies
(i) Early reimbursement to the accredited health facilities (ii) Training health workers in
accredited health facilities in adherence to NHIF standards (iii) Feedback to the
accredited health facilities by providing payment advice letter that allows an assessment
of performance for the health facilities (iv) Distribution of guidelines, benefit package,
price list, and disease code to every accredited health facility. (v) Ensure quality of
services to members as per NHIF benefits package.
1.3.3 Program activities
NHIF major activities of NHIF are: (i) To register members and employers and issue
identity cards to beneficiaries; (ii) To accredit and inspect health service providers and
avail a broader network of health facilities for improving access to health services in the
country (iii) To undertake quality assurance processes of the claims from accredited
facilities; (iv) To collect monthly contributions from employers; (v) To provide health
insurance education to the public with the aim of marketing it and enhance public
relations.
6
1.4 Program Logic Model
A logic model is a visual conceptualization of how the elements of a program are
connected together (Mtei, 2012).The theoretical model below shows how different
inputs that are necessary to be introduced into the program so that the activities/ process
can be carried out for the expected/ intended outputs .it also depicts the important
component of the activities and how it is related to its either short term or long term
outcomes as well as the impact brought by successful program implementation
.
7
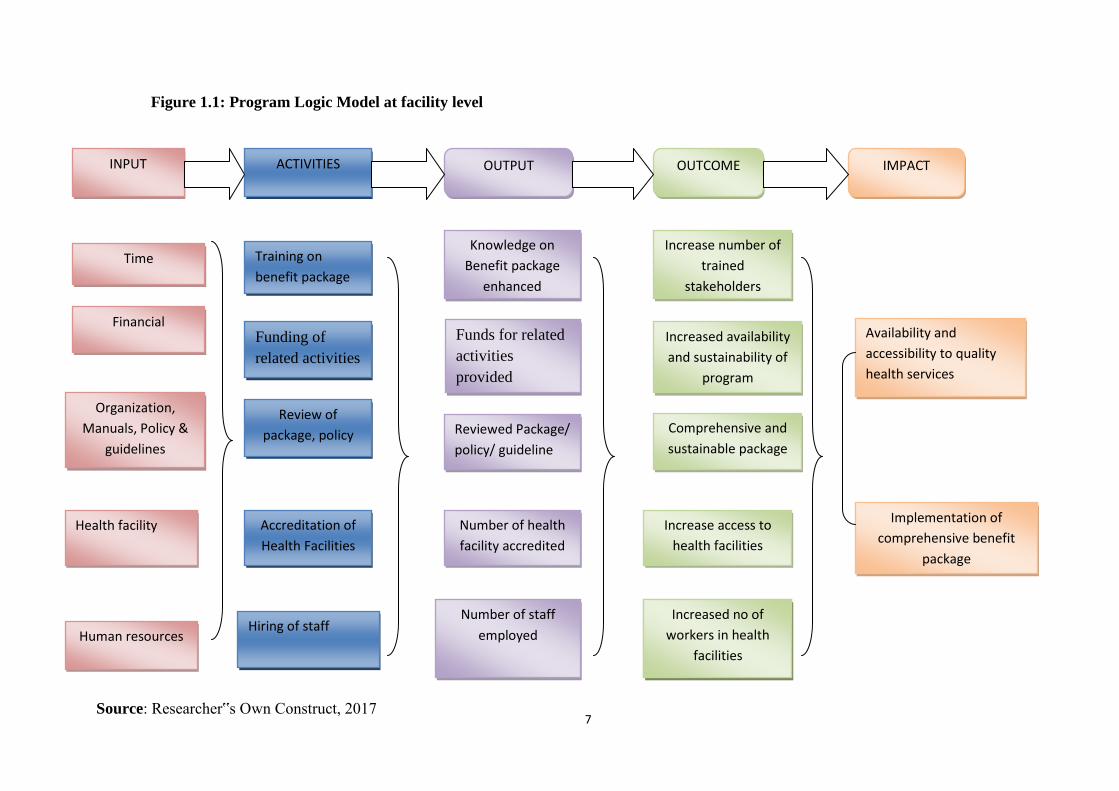
Figure 1.1: Program Logic Model at facility level
ACTIVITIES OUTPUT OUTCOME IMPACT INPUT
Time
Financial
Organization,
Manuals, Policy &
guidelines
Training on
benefit package
Knowledge on
Benefit package
enhanced
Increase number of
trained
stakeholders
Availability and
accessibility to quality
health services
Funding of
related activities
Funds for related
activities
provided
Increased availability
and sustainability of
program
Implementation of
comprehensive benefit
package
Review of
package, policy Reviewed Package/
policy/ guideline
Comprehensive and
sustainable package
Health facility
Accreditation of
Health Facilities
Number of health
facility accredited
Increase access to
health facilities
accredited
Human resources Hiring of staff
Number of staff
employed
Health provider
Satisfaction
Increased no of
workers in health
facilities
Source: Researcher‟s Own Construct, 2017

8
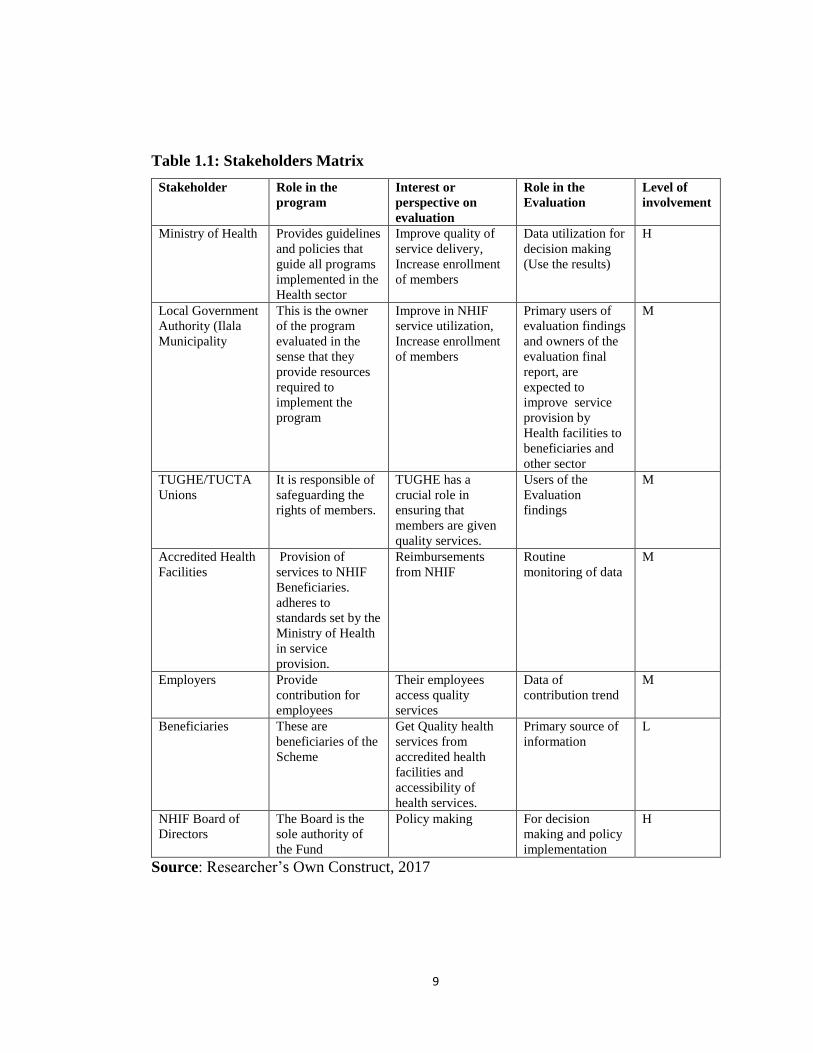
1.5 Stakeholders Analysis
Stakeholders are individuals, groups, or organizations having significant interest in how
well a program functions, they are decision making authority, funders, personnel, health
providers, clients or intended beneficiaries (Mtei, 2012).Stakeholders to be involved in
this evaluation are Ministry of Health Community development, Gender, Elderly and
Children, Ilala municipal, accredited facilities, Trade Unions, NHIF staff, Members /
beneficiaries, Employers and Media.
Their involvement is as described in the table 1.1 below.
9
Table 1.1: Stakeholders Matrix
Stakeholder Role in the
program
Interest or
perspective on
evaluation
Role in the
Evaluation
Level of
involvement
Ministry of Health Provides guidelines
and policies that
guide all programs
implemented in the
Health sector
Improve quality of
service delivery,
Increase enrollment
of members
Data utilization for
decision making
(Use the results)
H
Local Government
Authority (Ilala
Municipality
This is the owner
of the program
evaluated in the
sense that they
provide resources
required to
implement the
program
Improve in NHIF
service utilization,
Increase enrollment
of members
Primary users of
evaluation findings
and owners of the
evaluation final
report, are
expected to
improve service
provision by
Health facilities to
beneficiaries and
other sector
M
TUGHE/TUCTA
Unions
It is responsible of
safeguarding the
rights of members.
TUGHE has a
crucial role in
ensuring that
members are given
quality services.
Users of the
Evaluation
findings
M
Accredited Health
Facilities
Provision of
services to NHIF
Beneficiaries.
adheres to
standards set by the
Ministry of Health
in service
provision.
Reimbursements
from NHIF
Routine
monitoring of data
M
Employers Provide
contribution for
employees
Their employees
access quality
services
Data of
contribution trend
M
Beneficiaries These are
beneficiaries of the
Scheme
Get Quality health
services from
accredited health
facilities and
accessibility of
health services.
Primary source of
information
L
NHIF Board of
Directors
The Board is the
sole authority of
the Fund
Policy making For decision
making and policy
implementation
H
Source: Researcher‘s Own Construct, 2017
10
1.6 Statement of the problem
Social health insurance scheme is a new industry in Tanzania and in most of developing
countries. Since its beginning, NHIF has been facing multiple challenges such as
resistance from members and shortage of medicine and medical consumables at
accredited health facilities. Since 2001, NHIF has made an intensive effort to become
insurance schemes that provide a comprehensive insurance coverage to its beneficiaries
(URT, 2013).
According to NHIF (2015) statistics it shows that there has been increased number of
accredited health facilities that met the criteria and the set MoH standards for Health
facilities hence expecting improvement of services offered to its beneficiaries in the
context of quality health care. As mentioned above 6,371 Health facilities are accredited
by the fund countrywide and offer services, among them 97 facilities are in Ilala
Municipal of which 8 are of National referral status, 1 Regional Referral Hospital, 3
District level Hospitals, 8 Health centers, 39 Dispensaries, 33 Pharmacies, 1 ADDO
shop and 2 Special clinics. This is according to quality assurance report of 2015/2016.
With these statistics, no one can doubt on the Fund‘s performance. The main purpose of
NHIF is to make sure that member of the fund access better health services which are up
to date and timely (Austin, 2010). The Scheme purposely accredit the private health
facilities so as to increase the ease reach to the services by its members as well as giving
them assurance of getting even the services which are not available in the government
hospitals.
Despite the fact that, the Fund strives to expand its services in every corner in Tanzania,
still members of the Scheme raise claims of not getting some services from the health
facilities though listed in the benefits package. Complaints such as Low quality of health
care services (HR for health, equipment, Lack of medicines, customer care and
infrastructures, Lack of Laboratory services), inconvenience of accessing health services
(the expectation of NHIF beneficiaries is to get health services in one stop center)
11
inadequate accredited facilities, delay in reimbursement of claims to health facilities and
negative attitude of health workers at the accredited health facilities. (NHIF, 2010).
According to the study conducted in Ilala Municipal based on facility inspection report
and Quality assurance report for 2015/2016, It was observed that availability of properly
working diagnostic tools like MRI and CT Scan machines were a big problem in
Muhimbili National Hospital, Muhimbili Orthopedic Institute, Ocean Road Hospital and
Amana Hospital respectively.
There was overcrowding of patients at MNH wards due to constrained capacity,
especially bedding capacity compared to the number of inpatient to the Hospital, also
Some of the cases received at MNH could have been attended at lower facilities, this is
attributed to lack of such services at most regional/ District hospitals.
There were Limited number of Oncologist as compared to the number of patients
attending the facility at Ocean Rd Hospital, Medicine out of stock were a big problem to
all Public Hospitals in Ilala Municipality
It was observed in Amana Hospital that, among other things there were lack of some
specialized services eg orthopedic clinics and inadequate space especially in pediatric
wards.
Not much of the Researches have been done in Evaluation of the implementation of
benefit package here in Tanzania but there has been series of effort done by NHIF to
address issues and concerns raised by various stakeholders on the challenges both those
that are within NHIF scope and that are not within the organization scope In the course
of implementation of new benefit package and its price list.According to CMIS (2016)
paid Claims by ownership report, annual report on the expenditures of claim unit
especially on fund that have been used as reimbursement to service providers,
approximately 161,660,306,340/= Tanzanian Shillings were spent by the fund
beneficiaries to reimburse accredited facilities during the financial year 2015/2016. In
addition, the NHIF new 5yrs strategic plan report of 2015-2020 indicates that a total of
12
TZS 25,154.06 million were paid to service providers in 2009/10 and it increased to TZS
157,472.92 million in June, 2015. In the perspectives of the NHIF, this tremendous
increase of payment to medical providers is one of the threats to the financial stability of
the fund but with this alarming increase of payment but still with raised concerns from
stakeholders this might be suggesting there is more than what is known concerning the
way the package is implemented, the quality of service provided versus how much those
providers claims. Therefore, this study aims to evaluate Implementation of NHIF Benefit
Package in the Selected Accredited Health Facilities in Ilala Municipality as point of
references of which about 36.9 % of reimbursements made was done to Medical
Providers from Ilala Municipal.
It is important to ask our self, why despite of all the Fund‘s efforts to achieve its goals
but still there are complaints from beneficiaries on poor or at other facilities the services
provided are not as stipulated by the package and at some cases beneficiaries do not get
the services they are supposed to access.
[
1.7 Objective of the Study
1.7.1 Main Objectives
The main objectives of this study is to evaluate the implementation of NHIF Benefit
Package in the selected accredited health facilities in Ilala municipality, Dar es salaam-
Tanzania.
1.7.2 Specific Objectives
This study was guided by the following specific objective
1. To identify and evaluate whether the contents of NHIF Benefit Package are
comprehensive to suit for beneficiaries needs.
2. To evaluate the views and perceptions of the beneficiaries on the NHIF benefits
package as to whether they have comprehensive coverage in terms of quality.
3. To evaluate the status and capabilities of the selected accredited health facilities
in fulfilling the requirements of the NHIF Benefit Package.
13
4. To evaluate the extent to which the selected accredited health facilities comply
with the accreditation criteria as provided for by MoHCDGEC standard
guidelines and NHIF accredited checklist.
5. To determine and evaluate the challenges encountered by the selected health
facilities while implementing NHIF benefit package.
1.8 Research Questions
The evaluation study will be guided by the following research questions:-
1. Are the contents of NHIF Benefit Package comprehensive to suit for
beneficiaries needs?
2. What are the views and perceptions of the beneficiaries on the NHIF benefits
package as to whether they have comprehensive coverage in terms of quality?
3. What are the status and capabilities of the selected accredited health facilities
fulfilled as per the requirements of the NHIF Benefit Package?
4. To what extent are the selected accredited health facilities comply with the
accreditation criteria as provided for by MoHCDGEC standard guidelines and
NHIF accredited
5. What are the challenges encountered by the selected health facilities while
implementing NHIF benefit package
1.9 Significance of the Research
Evaluating the implementation of NHIF benefit package in the accredited health
facilities in Ilala municipality will provide necessary information on program
achievement.
The evaluation will also generate information‘s which will be used as an inputs to
inform policy makers and NHIF/ stakeholders for making evidence based decisions in
the designing, planning and implementing benefit packages, different manuals and other
guidelines.

14
Moreover the findings of this study can be used to facilitate improvement of services
provided by NHIF to her members
The Study is equally important to find out issues related to improved facilities
accessibility, improve the availability of drugs, and facilitate service improvement
especially in accredited Health facilities in Ilala Municipal.
This research will come out with information of major causes of the existing gaps in
NHIF operational activities especially accreditation and claims management systems, it
will also provide information/suggest ways which will help NHIF management to fill up
the existing gaps as well as to assist the NHIF to develop a plan of action on
improvement of services through accredited facilities to beneficiaries.
Ministry of Health can use the findings from this study to improve policy and/or
strategies designed to improve quality of services provided by the accredited health
facilities by NHIF and other insurance schemes in the Country.
Similarly, Information gathered through the evaluation will provide an opportunity to
ensure a number of modern imaging equipment as well as other important diagnostic
equipment‘s from the level of District, Regional Referral, Zonal Regional Hospitals as
well as National Hospital are provided.
Despite the fact that NHIF bridge the gap between health facilities and Beneficiaries by
allowing fund to amends at some point of time its package and regulations so that NHIF
Beneficiaries receive health quality care services, not much is known with respect to
achievement of implemented package in Ilala Municipal since the program has not yet
thoroughly evaluated hence the need for this evaluation study. Therefore, this study will
evaluate the implementation of nhif benefit package in the selected accredited health
facilities in ilala municipality. It will provide an answer to how and to what extent
implementation of benefit Package and service provision has been achieved in Ilala
District particularly for the period of 2014-2016.
15
This Research is designed to meet Evaluators partial fulfillment for master‘s degree in
Health Monitoring and Evaluation at Mzumbe University in Tanzania. Lastly, this
evaluation is for academic purpose the results will assist the principle evaluator to attain
his master‘s degree in health monitoring and evaluation and add value on the evaluation
documents [
1.10 Scope of the study
This study focuses on knowing how NHIF benefit package is implemented in accredited
health facilities by selecting few accredited health facilities. Specifically the study aims
at evaluating the implementation of the package when giving medical services to
beneficiaries in the facilities and the perception of those beneficiaries and medical
providers on this package. Nevertheless not all facilities that are treating NHIF
members or hospitals dealing with patients will be involved in this study. Therefore this
study employed descriptive case design whereas ten hospitals were selected from Ilala
Municipal in Dar es Salaam Region which is in the northern most of 5 District in Dar es
Salaam, its total surface area is 531 km square, administratively with 5 divisions, 27
wards, 114 streets, 14 villages and 14 hamlets (DMC Profile, 2011). The Municipal has
a population of 1,220,611 people (among them 624,683 are females and 595,928 are
Males with an average household size of 4.0 (Population and Housing Census, 2012).
According to Ilala Municipal health facility Inventory Data base, Ilala has 145 Health
facilities.
1.11 Limitation of the study
Due to wide coverage of Ilala municipal council and the shorter period of data
collection, to cover the whole areas of 531 km squares to disseminate the questionnaire
in all the health facilities accredited and collect them in time was very difficult. The
researcher also faced the problem of transport movement especially when heavy traffic
jams were involved.
16
Basically the extent of area to cover, finance and time constraints were the main reasons
successfully meet the expenses and deadline of submission of this research was also the
challenges of this study.
Another limitation of study was the evaluation design that was used, since it was a cross
sectional study with the case study of selected facilities in Ilala Municipal, the findings
cannot be generalized to all institutions especially those in remote areas because it
covers only Ten health facilities. However, the fact that it cannot be replicable to other
setting doesn‘t affect importance of undertaking the evaluation since it has potential
implication in becoming a base for further big studies on the same subject in future.
1.12 Organization of the thesis/ dissertation
This study was well organized and arranged into six chapters which have been explained
below:
The first chapter presented the introduction of the study which is problem setting,
statement of the problem; research objectives as well as research questions. Also the
chapter further covered significance of the study, scope of the study, limitation of the
study and lastly it ended with an organization of the study.
The second chapter written as chapter two mostly covered literature review related to the
study providing the reflective of the theoretical literature review, analysis of empirical
literature as well as conceptual framework of the study.
Also, Chapter three explains the research methodology which was used in conducting
the study. Additionally it provides research design, research approach, study population,
units of analysis, variables and their measurements, sampling sizes, technique and
procedures, sources of data, data collection methods and tools used, data analysis plan
and the issue of ethical consideration is well covered.
Chapter four presents results of the findings obtained from the study based on evaluation
objectives
17
In Chapter five, the discussion of the findings is covered in detailed.
Whereas in Chapter six, the summary of the findings of the study concerning evaluation
of implementation of NHIF benefit package in selected accredited health facilities,
conclusion made from those findings, recommendation for policy implication that also
include limitations of the study and areas for further research have been presented.
1.13 Definitions of key terms
1. Provider Requirements: Providers are required to provide quality health services
to entitled beneficiaries in accordance with the Standard Treatment Guidelines,
benefits package and adhering to the Fund‘s price schedule which forms part of
the attachments to a contractual agreement, while also observing Standard
Facility Guidelines set by the Ministry of Health and Social Welfare, and
Standard Treatment Guidelines as provided by the various professional
authorities
2. Accreditation: Is the process of assessing health institutions against a commonly
accepted set of standards
3. Accredited Health Facilities are Health Facilities that has signed a contract with
NHIF to provide services to its beneficiaries. Accredited health facility is a
facility which is registered by the ministry responsible for health matters and
thereafter approved by the Fund to render medical services to NHIF beneficiaries
in accordance with set down rules and procedures. The facility can be Hospital,
Health center, dispensary, clinic, medicines outlet, health post, nursing and
maternity home and diagnostic Centre
4. NHIF Beneficiaries: Is the general term which includes a contributing member,
spouse and up to four dependents that are legally identified.
5. NHIF Member: A principal member who contributing to the Fund.
6. Fund: Refers to the National Health Insurance Fund Tanzania.
7. Providers: Providers are defined in the Act as institutions such as hospitals,
health centers, dispensaries, and pharmacies. Pharmacies are only to be
18
accredited to receive payment by NHIF if the dispensaries, health centers, or
hospitals do not have available the essential drugs and medicines needed by
NHIF patients, thus Health providers are People who provide health care services
to consumers/NHIF
8. Benefit package these are medical services which are approved by Board of
Directors to be provided to Fund‘s beneficiaries.
19
CHAPTER TWO
LITERATURE REVIEW
2.1 Introduction
This chapter will cover theoretical, empirical review of literatures as well as the
conceptual framework of the study so as to identify and evaluate the gaps in service
provision by the NHIF accredited health facilities. The implementation of the NHIF like
any other similar insurance schemes, have been described by principles and bases of
social unity and risks sharing. The NHIF Scheme has a prearranged package of benefits
and does not cover anything not stipulated in the benefit package.
Contributions are gathered in a specific account, self-regulating from the Government
budget, The Scheme is compulsory in nature in that the membership coverage is
stipulated in the NHIF Act No.9 of 1999.
There is cross subsidization among members of the Scheme such that the healthier assist
the sick and the members earning high income subsidize those with low income etc. The
Scheme is financed through payroll contributions that are collected from employees and
employers on monthly basis. NHIF Third Five years Strategic plan (2015- 2020).
2.2 Theoretical Literature Review
2.2.1 Program evaluation
According to (Staff 1995 -2012).Evaluation is a systematic determination of a subject's
merit, worth and significance, using criteria governed by a set of standards. It can assist
an organization, program, project or any other intervention or initiative to assess any
aim, realizable concept/proposal, or any alternative, to help in decision-making; or to
ascertain the degree of achievement or value in regard to the aim and objectives and
results of any such action that has been completed. Within the evaluation process,
general performance of the program is analyzed using set indicators of the work plan
20
Cheryl Poth, Mary Kay Lamarche, Alvin Yapp, Erin Sulla, and Cairine Chisamore also
published Toward a Definition of Evaluation Within the Canadian Context: Who Knew
This Would Be So Difficult? in the Canadian Journal of Program Evaluation, vol. 29,
no. 3.)
Evaluation is the systematic assessment of the design, implementation or results of
an initiative for the purposes of learning or decision-making, according to (UNEG,
2005)
An evaluation is methodical, providing information that is realistic, reliable, and useful
to enable the incorporation of lessons learned into decision-making process of users and
funders (OECD, 2010).
Evaluation is based on empirical evidence and typically on social research methods, thus
on the process of collecting and synthesizing evidence (Rossi Lipsey and Freeman,
2004). In all definitions, evaluations should be as systematic and impartial as possible.
Evaluations usually focuses on effectiveness, significance and impact, therefore it can be
undertaken by programme managers, supervisors, funders, external evaluators and
beneficiaries (Mtei, 2012).
Based on CDC report there are several types of evaluations that can be conducted. Some
of them include the following
2.2.2 Formative evaluation
Ensures that a program or program activity is feasible, appropriate, and acceptable
before it is fully implemented. It is usually conducted when a new program or activity is
being developed or when an existing one is being adapted or modified. Basically,
formative Evaluation focuses on evaluability Assessment and/or Needs Assessment
During the development of a new program, can also being used to do a study when an
existing program is being modified or is being used in a new setting or with a new
population Therefore, this design of evaluation assists the organization to further
develop a successful process and either take out or reconfigure unsuccessful goals.

21
2.2.3 Process/implementation evaluation
Determines whether program activities have been implemented as intended. Process
Evaluation determines whether program activities have been implemented as intended
and resulted in certain outputs. You may conduct process evaluation at times throughout
the life of your program and start by reviewing the activities and output components of
the logic model (i.e., the left side). Results of a process evaluation will strengthen your
ability to report on your program and use information to improve future activities. It
allows you to track program information related to Who, What, When and Where
questions: thus this type of evaluation is conducted either as soon as program
implementation begins or when it is used during operation of an existing program this
design of evaluation examines operations of the program and identifies strength,
weakness and areas that need improvement.
2.2.4 Outcome Based Evaluation
Is the evaluation which takes place to assess what occurred in the program and whether
the program objectives has been achieved (Bultman et al, 2012). It is used to assess the
outcome of the stated short-term, intermediate and long term program objectives
(Bultman et al, 2012).Therefore, this design should be conducted when the program is
matured enough to produce the intended outcome.
Outcome/effectiveness evaluation measures program effects in the target population by
assessing the progress in the outcomes or outcome objectives that the program is to
achieve, it measures program effects in the target population by assessing the progress in
the outcomes that the program is to address. To design an outcome evaluation, begin
with a review of the outcome components of your logic model (i.e., the right side).
2.2.5 Economic Evaluation
This type of evaluation mainly focuses on the Cost Analysis, Cost-Effectiveess
Evaluation, Cost-Benefit Analysis, Cost-Utility Analysis, it is either done at the
beginning of a program or during the operation of an existing program.

22
2.2.6 Impact evaluation
Assesses program effectiveness in achieving its ultimate goals. This type of evaluation
is done during the operation of an existing program mainly at appropriate intervals.or at
the end of a program. It is important to note the usefulness of conducting process
evaluation while you are implementing outcome evaluation. If the outcome evaluation
shows that the program did not produce the expected results, it may be due to program
implementation issues. Therefore, it is recommended that if you conduct outcome
evaluation, you also implement process evaluation.
http://www.cdc.gov/std/program/ProgEvaluation.pdf....13;50 date 29/6/2017
Program Operations Guidelines for STD Prevention manual on program evaluation
2.3 Accreditation of Health facilities
Accreditation is usually a voluntary process in which an accrediting body, usually non-
governmental, assesses and certifies that an institution meets the quality standards
adopted by the accreditation body. Facilities that receive a acceptable score are
accredited, usually for a period of three years. Accreditation programs typically adopt
standards that are considered optimum yet achievable to encourage continual quality
improvement. Health insurance plans often require health facility certification as a
condition for approved provider status.(GJMEDPH 2014; Vol. 3, issue 2).
2.3.1 Accreditation of health facilities in the implementation of NHIF scheme in
Ilala
NHIF beneficiaries can access health services through a wide network of accredited
health facilities in Tanzania. The Fund‘s recognized health facilities among others
include Public health facilities, Private health facilities and Faith Based Organization
(FBO‘s) which are geographically spread all over the country. (NHIF, 2010)
23
According to section 9 of the National Health Insurance Fund Act, Cap 395 R.E. 2002,
the authority to award accreditation to health care provider is entrusted into the Fund‘s
Board of Directors.
According to the NHIF Claims Manual (2014) and NHIF Quality Assurance Manual
(2014) the system of accessing health services is an organizational arrangement required
when a beneficiary needs to access medical services under the Scheme at Fund‘s
accredited facilities. For health facilities categorized either as National Referral
hospital, Regional hospitals, District hospitals, Health Centers, Dispensaries,
Pharmacies, ADDO Shops to be accredited they have to satisfy the Basic Accreditation
Criteria.
2.3.2 Accreditation of health facilities under NHIF schemes in other countries
According to the Ghana National Health Insurance Scheme (NHIS 2010), in order to
provide the elementary package of services, NHIS covers both public and private health
care providers at all levels of the health system, subject to their accreditation by the
NHIA. As of December 2009, 966 private, 1,368 public and 163 CHAG providers were
enrolled in NHIS. At present all public facilities have been given a temporary
accreditation and 800 private providers (many of them pharmacies and ‗chemical
shops‘) have been accredited by the NHIA.
In order to provide the basic package of services, the NHIS covers both public and
private health care providers at all levels of the health system, subject to their
accreditation by the NHIA. At present all public and Christian Health Association of
Ghana (CHAG) facilities (about 4000) have been given a temporary accreditation and
1551 private providers including (hospitals and clinics, maternity homes, pharmacies,
licensed chemical shops and diagnostic facilities) have been accredited to provide
service and to make the service more easily available to beneficiaries (NHIA, 2009).
Claims are made by service providers and then give in to the district schemes for
payment using the Ghana-Diagnosis Related Group (G-DRG) rates for services and Fee-
24
For-Service (FFS) for medicines. Discussions are ongoing to design, pilot and evaluate a
per person (capitation) provider payment system for primary care under the National
Health Insurance Scheme aimed at improving; cost control, control cost increase by
sharing risk between schemes, providers and subscribers, and improving efficiency
through more balanced use of health resources (NHIA, 2010).
In Kenya, National Hospital Insurance Fund contracts with about 600 health
facilities that are managed by both the public and private sector throughout Kenya‘s 8
provinces. About 150 of these facilities are state-run, while the remaining hospitals are
managed by private and mission organizations. Individuals who are members of NHIF
are able to use their benefits at any of the hospitals associated with NHIF regardless of
locations. Kenya National Hospital Insurance Fund (NHIF), 2010.
Evidence base for accreditation systems in sub-Saharan Africa Literature assessing
the effectiveness of accreditation systems in develop countries has been mixed .In
contrast, a small number of studies inspecting the effectiveness of health facility
accreditation systems in sub-Saharan Africa have shown the possible for significant
improvements in facility performance This difference could be a result of health
facilities in developed countries typically participating in multiple internal and
external quality assurance processes. In contrast, quality assurance and even simple
clinical supervision systems in sub -Saharan Africa are generally weak due to budgetary
and human resource shortages.
Thus, the relative absence of rigorous quality assurance systems in sub Saharan Africa
may allow national accreditation systems to have a more observable effect. National
Hospital Insurance Fund contracts with about 600 health facilities that are managed by
both the public and private sector throughout Kenya‘s 8 provinces. About 150 of these
facilities are state-run, while the remaining hospitals are managed by private and mission
organizations. Individuals who are members of NHIF are able to access their benefits at
any of the hospitals affiliated with NHIF regardless of locations.

25
Zambia established a hospital accreditation program known as the Zambian Health
Accreditation Council (ZHAC). ZHAC was established in 1997 with funding from
USAID and was administered by a council with representation from government
agencies and health professional associations. A 2005 study randomized hospitals into
participating and control groups and the average score for each group was in comparison
following an intervention period. The average acceptable score for participating
hospitals was 48%, compared to 38% for non-participating hospitals two other studies
inspecting the ZHAC system identified a number of weaknesses, including that ZHAC
had no national Secretariat, no separate funding, and no legal mandate. In addition,
turnout at ZHAC council meetings was poor. The studies warned ZHAC needed a long-
term financing plan to replace USAID funding which proved prophetic as ZHAC was
suspended following the end of USAID funding.
The Council for Health Service Accreditation of Southern Africa (COHSASA) is a
free, non-profit accrediting body based in South Africa. More than 500 health facilities,
mostly found in South Africa, have joined in COHSASA‘ programs. An unpublished
study from 2003 evaluated the result of participating in the COHSASA accreditation
process on hospitals in KwaZulu Natal Province, South Africa. In this study, hospitals
were randomized into participating and control groups, and average obedience scores for
each group were compared before and after the interference period. The study found the
average compliance score for the participating hospitals improved from 48% to 78%,
while the average score for non- participating hospitals remained still at 43%.
Rwanda- Linking Quality Assessments with Financial Incentives Instead of creating a
traditional accreditation system, Rwanda formed a Performance Based Financing (PBF)
scheme whereby facilities underwent quarterly external quality assessments and the
results were used to set payment rates. A 2009 study examined the effect of the
Performance Based Financing system as per Articles on Rwanda‘s public sector health
centers.www.gjmedph.org Vol.3, No. 2 2014. The study found facility quality scores at
the beginning of the PBF phase ranged between 10% and 55%. However, after
26
participating in the PBF system, all participating health centers attained constant quality
scores between 80% and 95%. In Rwanda, hospitals and health center were planned to
undergo quality assessments once per quarter by a team of peer reviewers District
supervisors employed by the Ministry of Health assessed health centers. Hospitals were
assessed by a team of peer reviewers from a similarly situated hospital. The study
authors concluded that participating in the process led to ―huge improvements on quality
of health care services. The study authors also speculated that strengthening other
components of the health system, such as data collection, monitoring, and combined
supervision, may have contributed more to the observed quality improvements than the
financial motivations. Focus countries were selected because each country had applied a
national accreditation system. Between July 10, 2009 and August 10, 2009, interviews
were conducted in three focus countries (Uganda, Kenya, and Tanzania). Important
informant interviews were conducted with a total of 27 participants (Kenya: 9; Uganda:
9; Tanzania: 9) who had personal knowledge regarding accreditation systems in our
focus countries. Ministry of health officials, representatives of private hospital
associations, and hospital administrators were interviewed in each country. Health
insurance fund administrators, representatives of regional multilaterals, physician and
nurse supervisors were also interviewed.
Ethics review board from the following institutions approved this study: University of
Washington (USA), Muhimbili University of Health and Allied Sciences (Tanzania),
National Council for Science and Technology (Kenya), and Makerere University
(Uganda). A questionnaire was used as an interview guide and an audio recording device
was used for the majority of interviews. In addition to, important policies, reports,
manuals, guidelines, and other documents connecting to accreditation systems in the
region were collected. A restriction of the study was actual facility assessment scores
from our focus countries were not able to be collected or conduct a cost-effectiveness
analysis.
27
The Tanzania Ministry of Health established the quality standards used by the NHIF.
These standards included both input standards (e.g. staff, equipment, and laboratory) and
process standards (e.g. establishing an internal quality assurance program). The NHIF
was financed primarily through monthly payments from the fund‘s members and
appeared fiscally solvent. However, the NHIF Act that created the fund limited the
amount the NHIF could spend on administrative costs to 15%. This cap reportedly
limited the ability of the NHIF to effectively administer the fund, including conducting
accreditation and quality assessment activities. (Health Care Financing in Tanzania
2005 Fact Sheet No. 2. Dar es Salaam.
However at that time, the Tanzania Ministry of Health was developing an accreditation
system separate from the one used by NHIF. However, it was uncertain how this
Ministry of Health based accreditation program would act together with the NHIF‘s
accreditation activities
In Kenya, the National Hospital Insurance Fund (NHIF) used a hospital accreditation
system. The NHIF was a public health insurance scheme with approximately 15 million
beneficiaries, covering almost one-third of Kenya‘s population. Hospitals were supposed
to participate in the NHIF‘ accreditation system to receive NHIF refund.
As of 2009, the NHIF had accredited more than 400 hospitals. Private, faith-based, and
public hospitals were entitled for accreditation. Private hospitals were required to
undertake an initial assessment to obtain accreditation. However, public hospitals were
automatically accredited. Following accreditation, all participating facilities were
planned to undergo external quality assessments every three months and a full
accreditation assessment every two years.
28
The NHIF accreditation activities were mostly financed by NHIF member premium
payments, and, therefore the program was self-funded. The NHIF employed two cadres
of full time quality assessment officers to conduct and perform quality assessments.
NHIF surveyors were stationed at more than twenty NHIF field offices across Kenya.
In addition to perform and conducting assessments, NHIF staff also conducted trainings
at NHIF accredited hospitals concerning the development of internal quality
improvement committees. The NHIF assessed compliance with the Kenya Health
Standards, which consisted of input, practice and outcome standards. Input standards
covered areas such as: staff, facility, supplies, equipment, and transport. Process
standards assessed compliance with Ministry treatment guidelines, referral systems,
financial management, and internal quality improvement systems. Outcome standards
assessed patient, staff, and community member satisfaction rates.
A hospital‘s assessment score considerably affected its NHIF refund rates. Hospital
administrators we interviewed noted that the potential for an increase in NHIF refund
rates was a strong motivation to improve standard compliance, but the links between
how a specific improvement in assessment scores would increase return rates was not
clear. This may be due to the fact that the NHIF‘s. Board of Management retained the
ultimate authority to set reimbursement rates for specific hospitals. One interviewee
noted that refund rates for public hospitals were kept comparatively similar to avoid
creating large differences between public facilities.
Tanzania Similar to Kenya, Tanzania‘s National Health Insurance Fund (NHIF)
Operated a health facility accreditation system. Tanzania‘s NHIF remained a public
health insurance fund with a benefit package that included both inpatient and outpatient
services. As a result, all levels of health facilities, including health centers, dispensaries,
and pharmacies, were entitled for accreditation. Health facilities were required to
participate in the NHIF‘s accreditation program to receive reimbursements.
29
Private and faith-based health facilities were required to undergo an initial accreditation
survey and regular assessments thereafter. However, as in Kenya, all public health
facilities in Tanzania were automatically accredited. Tanzania‘s NHIF did not adjust
reimbursement rates based assessment scores. NHIF employees, known as Regional
Supervisors, steered accreditation surveys and quality assessments.
Uganda launched a health facility accreditation system in 2000 that was known as the
Yellow Star Program. The goal of Yellow Star was to ―improve and maintain quality of
services through a system of accreditation and appreciation. Yellow Star was
demonstrated on similar efforts in Egypt, Brazil, and West Africa. Yellow Star was
administered by the Uganda Ministry of Health, but was principally financed by USAID.
All hospitals, including private and faith-based hospitals, were required to participate if
their district opted into the program. Yellow Star evaluated health facilities using a set of
35 Basic Standards for Quality Health Care Services, which had more than 100 sub-
standards. The standards contained input and process standards covering areas including:
infrastructure, equipment management systems, infection control and prevention, and
communication skills. As the name indicates, these standards were set at a primary
level, similar to facility licensure standards (e.g., access to a reliable supply of clean and
safe water).
Two international health facility accreditation programs, the International Organization
for Standardization (ISO) and COHSASA were active in our focus countries. A small
number of large hospitals in Kenya had acquired or were looking for ISO 9000
certification. At least one major hospital in Rwanda was looking for accreditation
through COHSASA. A number of government officials and hospital administrators
interviewed noted that international accreditation processes were perceived positively in
the area. However, they also reported that fees from these international organizations
were likely cost prohibitive for most hospitals in the region. The East African
Community (EAC) was also in the process of designing a regional hospital accreditation
system. Under the proposed EAC program, a regional body would develop unchanging
30
quality standards, but each country would be responsible for assessing compliance with
the EAC standards.
It was so unclear which national organizations would be responsible for conducting the
on-site assessments; however, national medical councils were one of the choice of being
considered. Jeffrey Lane et el (2014) The Emergence of Hospital Accreditation
Programs in East Africa: Lessons from Uganda, Kenya, and Tanzania
2.4 Study Overview
Social Health Insurance Scheme is a health insurance which is provided by
governments to its employees (Churchill, 2006). This type of insurance maintains a risk
pooling fund account into which contributions and other incomes from different sources
are deposited. Out of this account; the scheme makes reimbursement of medical
expenses to accredited health facilities in respect of medical services provided to
beneficiaries (Carrin and James, 2002). The main objectives of Social Health Insurance
are: ―To provide health care that avoids large out of pocket expenditure, to raise
appropriate use of health services and to improve health status‖ (ILO, 2008). .It is a
system of national social security and health insurance introduced into the nineteenth
century by German empire under then Chancellor Bismarck. This system is a legally
compulsory system for the majority or the whole population to get health insurance with
a designated (statutory) third-party payer through non-risk related contributions which
are kept separate from taxes or any other legally mandated payments‖ (Saltman, R. B.
2004).
Social Health Insurance systems are in general characterized by independent or quasi-
independent insurance funds, a reliance on mandatory set aside payroll contributions
(usually from individuals and employers) and a clear link between these contributions
and the right to a well-defined package of health benefits (Gottre & Schieber, 2006).
Social health insurance mandates by law the enrolment for both those in the workplace

31
and those outside it; various levels of subsidies and supports for the population from
different socio-economic levels are also provided.
The first Social Health Insurance Scheme was established and introduced by the
Government of Germany between 1883 and 1889 (Wagstaff, 2009). The beneficiaries
and/or members of the scheme access health services through accredited public and
private facilities whereby the accredited health facilities are being reimbursed by the
insurance structure (Wagstaff, 2009). The scheme set the standards which all accredited
health facilities must adhere to in order for their claims to be reimbursed, otherwise
failure to do so, it may resulted into rejections or adjustment of the claims (Churchill,
2006).
The insurance scheme of Germany was very successful, therefore it was a good example
to other countries; by 1930s Social Health Insurance had spread to Latin America, the
United States and Canada (Wagstaff, 2009). After the end of the Second World War,
Social Health Insurance was introduced in many countries in Africa, Asia and the
Caribbean area (Wagstaff, 2009).Previously it was been established in more than 60
countries in the world,out of those, Twenty-seven have reached universal coverage
through social health insurance (Carrin & James, 2004). Social health insurance is
particularly widespread among OECD countries, but is also in use in developing
countries, mainly in Latin America (Argentina, Bolivia, Brazil, Chile, Colombia, Costa
Rica, the Dominican Republic, Ecuador, Peru, Uruguay, República, Bolivariana de
Venezuela, and others) and to a lesser extent in other parts of the world (Algeria,
Kenya, Lebanon, and Tunisia).
To date, many low and middle-income countries have instituted, or are considering
starting, social health insurance systems (Bosnia and Herzegovina, China, Croatia,
Estonia, Ghana, Hungary, Indonesia, the Kyrgyz Republic, Macedonia, Moldova,
Morocco, Nigeria, the Philippines, Poland, the Russian Federation, Serbia, Slovenia,
Tanzania, and Vietnam).Very often, policy makers view social health insurance as an

32
effective way to raise additional resources for health and as a means for decreasing the
financing burden of health care coverage (Carrin, 2002).
There is also a strong presumption that individuals may be more willing to be taxed (pay
payroll taxes) if there is a specific individual entitlement that accompanies the tax (a
benefit tax). In some cases, especially in countries that experienced communist rule,
social health. Insurance provides an opportunity to reduce the role of the state or to build
democratic and participatory institutions (as in China, Estonia, and Hungary). Finally,
countries that used to have National Health Service systems or ―Beveridgean‖ systems
may experiment with social health insurance as a way to improve the efficiency of the
health care system by ―outsourcing‖ health insurance coverage (as in Jamaica, Kenya,
and Malaysia). In order to measure the impact of social health insurance, one seeks to
determine whether there is greater access to health care and a reduction in out-of-pocket
expenditure. The welfare impact of social health insurance should be judged in terms of
some measure of utilization of health care for treatment, take-up of preventive care,
avoidance of large one-off expenditures and improvement in health through being able
to receive adequate care (Wagstaff, 2010 Currently a number of African countries are
implementing Social Health Insurance Scheme with different approach.
2.5 The concept of Health Insurance
Health Insurance is a plan designed to pay costs associated with health care. Health
insurance plans pays bills from physicians, hospitals and other providers of medical
services. By doing so, health insurance protects people from financial hardship caused
by large or unexpected medical bills (Nielsen, 2000) Health insurance is emerging as the
most preferred form of health financing mechanism in situations where private out-of-
pocket expenditures on health are significantly high and cost recovery strategies affect
the access to health care (Gilson 1998).
33
2.5.1 Health Insurance Scheme
Health insurance can be defined as a way to distribute the financial risk associated with
the variation of individuals ‗health care expenditures by pooling costs over time through
pre-payment and over people by risk pooling (OECD, 2004). Tanzania is in the process
to meet the commitment under the Millennium Development Goal and the Abuja
Declaration of extending health services to the citizens. The main objective is to cover
45% of population with sufficient Health Insurance by the year 2015 (Health Sector
Strategy Plan 2009 -2015).
2.6 Types of health insurance
There are three major types of health insurance which include: Social Health Insurance;
Private Health Insurance and Community Based Health Insurance (NHIF, 2013).
2.6.1 Social health insurance
Social health insurance is a mechanism of health financing to enables the burden of cost
of health services to be spread on a time to the people who share costs and risks. It is a
system of national social security and health insurance introduced into the 19th century
by German empire under then Chancellor Bismarck. This system is a legally mandatory
system for the majority or the whole population to obtain health insurance with a
designated (statutory) third-party payer through non-risk related contributions which are
kept separate from taxes or other legally mandated payments‖ (Saltman, R. B. 2004).
The main feature of this type of social insurance is that, it is compulsory and mostly
limited to those with salary stable wage earning employment, normally referred in
Tanzania as National Health Insurance (Ibrahim, 2001)
2.6.2 Private health insurance
Private health insurance - that normally covers groups or individuals through a third
party payer institution operating in the private sector.(Ibrahim, 2001). The key
difference here is that those premiums are set at a level that provides a profit to a third
part and provider institution.
34
2.6.3 Community based insurance
Community Health insurance - generally voluntary and does not cover the full cost of
health care, contributions are collected when cash incomes are highest and this help to
guarantee that the contributors have ongoing access to health care.(Ibrahim, 2001).
2.7 Health Sector Reforms in Tanzania
In the early 1990s, the Tanzania government adopted new social and economic
development policies characterized by the structural adjustment program, and internal
changes in the health sector. These changes are referred as health sector reforms. In
implementation of the Health sector reforms, the government redefined its role to be
more focused on policy formulation and to increase support to the role of the private
sector development. Along with these changes, the government started to look at
alternative sources of health financing such as cost-sharing in public facilities, pre-
payment systems and insurance arrangements. This led to the emergence of The
National Health Insurance Fund, Community Health Fund and Cost sharing programs.
2.8 Health care financing in Tanzania
The government of Tanzania adopted health sector reform strategy in 1995 particularly
on health care financing which is the first step in introducing user fees in public
hospitals. Several other alternatives of funding option were explored of which
government introduced two new major ones in line with the principle of social security
in health sector (MoH) budget speech, 2003). Firstly, the National Health Insurance
Fund (NHIF), a compulsory health insurance scheme for formal sector employees, and
secondly, the voluntary Community Health Fund (CHF) which aimed to cover the
informal sector. In additional to the government programs, there are ranges of private
health insurance initiatives (Tanzania NHA, 2001). These are either in form of micro,
local communities and provider-based health financing projects. The country was
pushed to opt for such financing mechanisms according to the general trend of economic
policies towards increasing the role of private sectors.
35
2.9 Health Insurance System in Tanzania
Social Health Insurance is still a new industry in Tanzania if compared to other
countries. According to NHIF report of 2013, it is still at an infantry stage. The
provision of health services up to1990s was free to all citizens and was financed by the
government (NHIF 2013). However, the National Insurance Corporation (NIC) was
providing, the voluntary Health Insurance cover. Very few people, especially
businessmen and few people with fair income managed to buy such premiums (NHIF,
2013). In the light of these factors, the government made reforms on the health sector
which initiated insurance schemes in the country (NHIF, 2013), this health sector
reforms also involved privatization of health services in 1993, which then went hand in
hand with privatization of insurance in the country (Risha, 2002). In 1997 the National
Insurance Company established a health insurance scheme known as Medicare for its
members (Risha, 2002). In 1998 Igunga Community Health Fund (ICHF) was
established by the government in Tabora (Risha, 2002). In 1999 NHIF was established
by the government for formal sector employees and CHF was established by
parliamentary law no 8 in 2001 for informal sector (NHIF, 2013).
2.10 National Health Insurance Fund
The National Health Insurance Fund is a social health insurance scheme in Tanzania;
It was established by the Act number 8 of 1999 of Parliament (NHIF, 2013).The
establishment of this fund was the outcome of 1990 -1992 study on long term options for
financing health services in Tanzania. Operations of this scheme started on 1st July 2001
by members and their respective employers starting to contribute and beneficiaries
started to access medical services from 1st October 2001 (NHIF, 2013). The scheme
maintains a risk pooling fund account into which such contributions and other incomes
are deposited, Out of this account, the scheme makes reimbursement for medical costs to
accredited health facilities in respect of medical services provided to beneficiaries
(NHIF, 2013).The contribution are made by both employees and their employers making
a total of 6% which done directly from employees‗ payroll. Under equity perspective,
36
social health insurance (mandatory) is progressive. The contributions are proportional
related to the income of the beneficiaries. These beneficiaries receive the same benefit
packages. Financial burden fall under those who are formally employed .In addition,
SHI create two tier systems that result into one system funded by mandatory health
insurance for those with specified income and they can purchase comprehensive health
services. Efficiently, the scheme has defined benefit package (outpatients and
hospitalization services). The members are free to access services at any accredited
health faculty of their choice. The fund accredited all government facilities, few private
pharmacies and some few faith based organizations. The scheme provides quick and
quality of services to its members to promote technical efficiency. The costs of
administrative are high. National Health Insurance Fund revenue is reliable as the
contributions are directly deducted from payroll.
2.10.1 The Basic Functions of NHIF
National Health Insurance Fund has been created with the view of providing members of
the public services with the health insurance coverage. The functions are; to collect
monthly contributions and process providers‗ claims, to register members and issue
identity cards, undertake the process of quality assurance, to provide health assurance
education to the public and enhance public relations, to account for the funds so
collected and invested to accredit and inspect health givers and broaden accessibility to
health particularly in rural areas of the country and investigate fund so collected order to
earn income, inspect employers to check compliance and carry out an actuarial
assessment and evaluation.
2.11 The Fund governance
The administration and management of the fund is governed by ten members of the
Board of Directors. The Board is composed of 10 members from key stakeholders of
health sector namely Association of Private Hospitals, Ministry of Health, community
development, Gender, Elderly and Children (MoHCDGEC), Trade Unions, the
Treasury, the ICT‗s representative, Employers and Experts within the field of health
37
Insurance and Economics. The NHIF‗s Board is appointed by the Minister responsible
for health .The day to day activities are carried out under the supervision of the Director
General who is the Chief Executive and Secretary to the Board. In additional to the Head
Office, the fund engineers its operations through a decentralized process using
established zone offices to facilitate service to and communication with members, care
providers and other stakeholders.
2.12 Empirical Literature Review
2.12.1 National Health Insurance as a Global Phenomenon
National health care is a wide concept that has been applied in numerous ways. The
common denominator for all such program is some form of government action aimed at
extending access to health care as extensively as possible. Most countries implement
health care through legislation, regulation and taxation from those involved. Legislation
and regulation direct in the matter on what care must be provided, to whom and on what
basis. Usually some costs are borne by the patient at the time of consumption but the
greater part of expenses come from a combination of compulsory insurance and tax
revenues. Some programs are paid for completely out of tax revenues. In some cases,
government involvement also includes directly handling the health care system, but
many countries use mixed private public private systems to deliver health services.
2.12.2 The National Health Insurance in Germany
Statutory health insurance (SHI) was believed to covers about 85 percent of the
population of Germany. Around 10 percent of the population is covered by private
health insurance, with civil servants and the self-employed being the biggest groups. The
rest of the groups (e.g., soldiers, policemen, and others) are covered under special
regimes. Undocumented immigrants are covered by social security in case of illness.
Since 2009, health insurance has been compulsory for all citizens and permanent
residents living in Germany, either in the statutory or the private health insurance
scheme (Thomson, S. & Reed, S. J.2011). SHI scheme covers preventive services,
inpatient and outpatient hospital care services, physician services, mental ill health care,
38
dental and oral care, prescription drugs, medical aids, rehabilitation and physiotherapy,
hospice care, and sick leave compensation. SHI preventive services scheme include
regular dental check-ups, well-child check-ups, basic immunizations service, check-ups
for chronic diseases, and cancer screening at certain ages. All prescription drugs,
including newly licensed ones, are covered unless clearly excluded by law (applies to
so-called way of life drugs) or following evaluation.
The various levels of government have virtually no role in the straight delivery of health
care services. However, states own the huge majority of university hospitals and
municipalities play a big role in public health activities and own around half of hospital
beds. A large degree of regulation is given to the self-governing corporatist bodies of
both the sickness funds and the provider associations. The most important body is the
Federal Joint Committee (G-BA), which was created in 2004.
2.12.3 The National Health Insurance Scheme in Japan
Japan as a country operates a widespread social health insurance system with more than
3,500 insurers. Employees and their families (60 percent of the population) are
obligatory as per requirement of the law to enroll in the health insurance offered through
their employers, and the remaining 40 percent (unemployed, self-employed, and retired)
are covered through plans administered by their local municipality or zone. All plans
cover the same legal benefit package. Individuals cannot choose their plans. Those who
avoid enrolling must pay back up to two years of premiums when they re-enter the
system (although public assistance will help to cover them if they are unable to pay this
fee). Permanent residents and long-term visitors who are either living or visiting Japan
are also required to obtain coverage; undocumented immigrants are not covered. The
statutory national benefit package in this country covers hospital care, ambulatory care,
and approved prescription drugs, and covers most dental care; it does not cover
spectacles. Since 2000, long-term care has been covered under its own insurance system,
administered by local governments. A number of preventive measures are publicly
provided to those aged 40 and older, including screening, health education, and
39
counseling. Mental health care is also covered under the statutory benefit package
(Thomson, S. & Reed, S. J.2011).
In Japan, prime and specialist care are not held apart as distinct disciplines, as they are in
other countries of the world; rather, specialists generally operate in community-based
clinics, provide many primary care functions, and can be easily accessed and available
without referral. Very few clinics have a official scheduling system; rather, patients wait
in the waiting room until they can be seen. Outpatient visits are normally very short, yet
common—in 2009, physician visits per year (13.9 per capita) were more than twice as
frequent as the OECD median (6.2) and three times as frequent as in the U.S. (3.9).
Practically all clinics used to dispense medication (which doctors can provide directly to
patients), but only a minority do so now. Clinics are mostly physician-led, with nurses
playing less of a role in caring for patients than in some other countries, such as the U.S.
Outpatient care is also delivered at hospitals. After-hours care is usually delivered by on-
call physicians; there are few emergency departments in Japan. Hospital-based
physicians are paid fixed salaries.
The health care system has to be evaluated based on its effectiveness, efficiency, and
equity on its operational. There are three elements of effectiveness of care: accessibility
and availability of care, quality of care, and integration. Integration means that the
system functions well in guaranteeing that a patient receives care in facilities that are
appropriate for the seriousness of the disease (Fukawa, T. 2002). In other words, it
means there is a good referral system. Evaluating Japan based on these determinants, we
find that the accessibility and availability of the health care system is excellent; its
quality is not known because there is no official data easily available on this aspect or a
system that monitors and ensures the quality of medical care; and integration is poor/
below standard because there is no clear referral system (Gunji, 1994).
40
2.12.4 The National Health Insurance Scheme in Netherlands
The National Health Insurance Scheme (NHIS) is funded primarily by contributions
from members based on income. For the Formal Sector Social Health Insurance Program
contributions are premiums that make up 15% of an individual‗s basic salary, with the
employer contributing 10% while the employee pays 5% for coverage of themselves,
their spouse, and up to 4 children. An employer may negotiate with an HMO for
coverage of additional supplementary benefits and pay the extra contributions required.
Participants in the Informal Sector Program are expected to make a monthly contribution
based on the benefits package of their choice as well as other factors. The poor, elderly,
veterans, and disabled are exempted from paying membership premiums.
Since January 1, 2006, all residents of the Netherlands, as well as nonresidents who pay
Dutch income tax, are required to purchase health insurance coverage, except those with
conscientious objections and active members of the armed forces. Coverage is statutory
under the Health Insurance Act (Zorgverzekeringswet, or ZVW), but is provided by
private health insurers and regulated under private law. In 2009, roughly 152,000
persons (1% of the Dutch population) were uninsured. That figure has remained stable
since 2007.
Approximately 50 percent of the uninsured are in their twenties or thirties. In addition to
those who should be insured but are not, there is a category of the uninsured who failed
to pay their premium for at least six months (so-called defaulters). Insurers are legally
required to provide a standard benefit package (per the Health Insurance Act) covering
the following: medical care, including care provided by general practitioners (GPs),
hospitals, specialists, and midwives; hospitalization; dental care (up to the age of 18;
coverage after age 18 is confined to specialist dental care and dentures); medical aids
and devices; pharmaceutical care; maternity care; ambulance and patient transport
services; paramedical care (limited physiotherapy/remedial therapy, speech therapy,
occupational therapy, and dietary advice); ambulatory mental care (primary care
psychologist, eight sessions); and outpatient and inpatient mental care for the first year.
41
Insurers may decide by whom and how this care is delivered, giving the insured a choice
of policies based on quality and costs (Thomson, S. & Reed, S. J. 2011).
At the health system level, quality of care is ensured through legislation governing
professional performance, quality in health care institutions, patient rights, and health
technologies.
2.12.5 The National Health Insurance Scheme in Switzerland
Coverage is universal, with residents mandated under the 1996 Health Insurance Law to
purchase statutory health insurance (SHI) from competing insurers. There are virtually
no uninsured residents. Every individual is required to take out an insurance policy
within three months of arrival in the country, which is then applied retroactively to the
date of arrival.
The SHI benefits package covers most general practitioner (GP) and specialist services,
as well as an extensive list of pharmaceuticals, physiotherapy (if commissioned by a
physician), and some preventive measures. It also covers outpatient and inpatient out-of-
canton services in case of medical need, even though many residents purchase voluntary
health insurance (VHI) for nationwide coverage of inpatient care (Cantons are like
states, in that they are sovereign in all matters that are not specifically designated the
responsibility of the Swiss Confederation by the federal constitution. Each canton and
demi-canton has its own constitution and a comprehensive body of legislation stemming
from its constitution.) Starting in 2012, the SHI benefits package will also include
certain forms of complementary medicine (Thomson, S. & Reed, S. J.2011).
The SHI benefits package also covers mental illnesses on the condition that certified
physicians provide treatment. Services from nonmedical professionals (e.g.
psychotherapy by psychologists) are only covered when prescribed by a qualified
specialist. If this is not the case, these services must be covered by VHI or paid for out-
of-pocket by patients. SHI covers the costs of selected vaccinations, selected general
health examinations, and early detection of disease among certain risk groups and for
42
certain diseases (e.g., one mammogram a year if a woman has a family history of breast
cancer). Once again, additional services have to be paid for by patients themselves
unless they have VHI to cover these costs.
Two-thirds of the costs of long-term inpatient care (nursing homes and institutions for
disabled and chronically ill persons) are funded by contributions from private
households (out-of-pocket and cost sharing). SHI funds only 15 percent of such services
(nursing care), with the rest paid for by state subsidies and disability insurance.
For long-term outpatient care (called Spitex in Switzerland), SHI also covers the cost of
home nursing care; this makes up roughly a third of Spitex‗s total expenditure. The other
two-thirds, devoted mainly to support and household services, are paid for by customers
and via state subsidies. Dental care is largely excluded from the SHI benefits package.
More than 90 percent of all expenditure on dental treatment is paid for by households.
Residents generally have free choice of GPs and access without a referral to specialists
in private practice (unless enrolled with a gate-keeping managed care plan). Outpatient
care tends to be physician-cantered with nurses playing a relatively small role. The
majority of private medical practices in Switzerland only have one practicing medical
doctor. Apart from some managed care plans, where physician groups are paid on a
capitation basis, ambulatory physicians are paid according to a national fee-for-service
scale. Here the corresponding cost rate values are negotiated between insurers and
providers or their organizations at the cantonal level. Hospital-based physicians are
normally paid a salary. Fee-for-service remuneration is possible for the treatment of
privately insured patients.
The Federal Law on Health Insurance (KVG) of 1996 brought about a fundamental
change in the health system. The law introduced regulated competition among health
insurers and among service providers to achieve a series of key objectives such as
containing costs; guaranteeing high-quality, comprehensive health care; and establishing
greater solidarity among the insured. While scientific analyses and public perception
43
have been particularly critical of competition‗s ability to cut or control health care costs,
the other objectives are generally regarded as having been successfully achieved.
A system of risk equalization is designed to encourage insurers to compete on cost and
quality rather than via risk selection, employing the power of market forces to improve
efficiency. However, observers generally acknowledge that risk selection is widespread
under the current risk equalization formula, which only considers canton, age, and
gender. As previously mentioned, in 2012 the formula will be refined to include hospital
and nursing home stays of more than three days in the previous year. This should bolster
insurers‗ incentives to improve efficiency.
2.12.6 The National Health Insurance Scheme in Uganda
As per (CHMI website), a study (2008) by WHO revealed that Ugandans spend 22
percent of their earnings on health care, and six percent of the poorest who have the
highest number of health bills have to sell their assets to meet medical bills. The
National Social Health Insurance Scheme was expected to take off in July 2007, but was
tabled before the Parliament of Uganda in March 2009. The National Health Insurance
Fund failed to make it to through the parliament because of resistance from employers,
trade unions and worker representatives. They were skeptical about the government‗s
ability to guarantee efficient service delivery given the poor state of health facilities in
the country. Despite the fact of the above case studies, Savedoff, W. D. &Gottret,
P.(2008) potray the other case studies based on governance of the scheme as follows
2.12.7The National Health Insurance Scheme in Costa Rica
Costa Rica as a country implements very well in two of the five dimensions, namely
Consistency and stability and Stakeholder participation. With regard to the aspect of
Consistency and stability, the objectives of the health insurance system have remained
unchanged since the formation of the system in 1941. The Constitutive Law (Ley
Constitutive) of the Costa Rica Social Security System (CCSS) has been basically the
same since its declaration in 1943, with only few amendments, and the main components
44
of the MHI system remained unchanged. For example, the package of benefits stayed
practically the same and changed only when the Constitutional Court forced the Costa
Rica Social Security System (CCSS) to include particular treatments (such as AIDS
antiretroviral) as part of the benefits. The fundamental legislation for the basic drugs list
dates from 1989, and is another example of the steadiness of the system.
Consistency and stability is also seem to be marked at the management level—since the
year 1974 only two executive presidents did not complete their term, one because of
death and the other because on involvement of a corruption scandal. In relations of
Stakeholder participation, the board of directors—which is the main body for regulatory
oversight and institutional governance—is a three-way body with representatives from
employees, employers, and government? Within each group from that three way body
the range of key stakeholders, including medical doctors is sufficient and diverse.
However, some experts felt that, despite the equilibrium of powers in the board of
directors, clients were underrepresented in their participation.
The weakest dimensions were Supervision and regulation and Comprehensible decision-
making structures. The low rating for Supervision and regulation is determined, in part,
by the evidence that, in spite of clear legal competencies to sanction individuals and
organizations that fail to comply with their responsibilities as supposed to be, such
approvals are rare in practice. Situations covered by the legislation are either out-of-date
or lack specificity, and associated agreements are not clear and objective. Furthermore,
most of the supervisory regulations are applied ex post, with little provision for
preventing such problems in the first place. In cases where agreements are clearly
defined, the penalty is inadequate. For instance, those who skip and avoid their
responsibility to make social security contributions, if caught and punished, are assessed
fines of US$350 irrespective of the size of the unpaid debt. Also, even if the sanction is
correctly specified, administrative problems and processes tend to make difficulties the
work of the institutions.
45
Other features of Supervision and regulation have related weaknesses. For example,
when you look at the financial management rules with respect to reserves clearly
allocate responsibility to the board of directors. Nevertheless, the law is unclear with
respect to how these reserves should be managed and what kinds of investments are
allowed. For ―ongoing supervision and monitoring,‖ the Costa Rica Social Security
System has in a way formed specific departments for on-site and off-site inspections,
such as the Procurement Department and the Medical Management Department.
Nevertheless, the capacity to effectively carry out inspections is restricted by the amount
of resources allocated to these activities, by the weak scope of responsibilities and
powers as they have been defined by law, and by the low priority given to inspection
activities by the Costa Rica Social Security System. In conclusion, financial information
is provided to the public through Web sites, but both financial and clinical data and
information generally lag by a year or more.
Concerning the dimension of Coherent decision-making structures, the Costa Rica
Social Security System (CCSS) has the power to change contribution rates, instrument
new health plans, and redefine the package of benefits and essential drugs. In fact,
according to experts, the board of directors of the CCSS has been given such power that
its 29 regulations have the similar effect as an Act approved by Congress. In other
arguments, the board of director‗s is not tied to most regulations that affect the
performance of other similar autonomous institutions. Despite these wide-ranging
decision-making powers, the CCSS in general lacks routine risk assessment and
management strategies in their operation manual. It has no everlasting program or
capacity to analyze and manage risk, although it tracks the progress of revenues and
expenses and has a department of Actuarial Studies and Economic Planning.
Relative to the other dimensions, Transparency and information performance is average.
The code of ethics for CCSS personnel adopted by the CCSS board in1999 attempted to
establish standards of conduct. However, the code has failed to prevent some major
scandals in the areas of, for example, purchase of medical services at overstated prices,

46
procurement of medicines, medical consumables and other equipment, provision of set
apart and tailor made training courses and medical research, building of hospitals, and
management of the CCSS pensions system. There are limited provisions to address
conflicts of interest and check the power of the decision-making president and board of
directors. These issues became especially apparent in 2004 when almostUS$9 million
from a Finnish loan was used for bribes and other illegal payments.
2.12.8 The National Health Insurance Scheme in Estonia
Estonia‘s mandatory health insurance (MHI) system appears to be well governed and
performs well to very good on all five magnitudes. It performed best with regard to
Consistency and stability, receiving the maximum score due to the ongoing commitment
to its original objectives and basic values and principles. While the creation of the
current health insurance system in 1992 was a very essential change, the system since
then has not been changed significantly. For example, the contribution rate has remained
at 13 percent since it began, and there have been only minor changes in entitlement
rules. Legislative changes have largely focused on developing the system further.
Likewise, ups and downs in political power have not unduly influenced important
characteristics of the health insurance system
Stakeholder participation performed nearly as well. Stakeholders and other key persons
are represented in the governing bodies of the Estonian Health Insurance Fund (EHIF) in
ways that appear fairly effective. The highest body of the EHIF is the tripartite
supervisory board with 15 members: five representatives chosen by the government, five
by employers, and five by beneficiaries. Although provider representatives are not
clearly included in the EHIF‗s supervisory board, they play an important role indecision-
making because all questions related to the benefits package and contra conditions are
negotiated with provider associations. Providers‘ involvement and participation is
important to the EHIF and development is measured by provider satisfaction surveys,
which currently are piloted every year. In 2006 the general satisfaction with partnership

47
with the EHIF was quite high—76 percent of contracting partners considered it very
good or perceived in good manner.
Supervision and regulation is one of the a little weaker areas, largely because
agreements and corrective actions are not generally applied in real practice, despite rules
allowing for them. For this reason, it is difficult to assess the quality of corrective
actions, the capacity for implementation of these sanctions and actions, and whether they
would require be publicized or otherwise publicly discussed. Estonia scores well for
Transparency and information for several reasons. Financial management rules for the
EHIF are quite clear and the system has good structures for supervision and monitoring.
Moreover, financial performance of the EHIF is monitored to see if they are as they are
supposed to be quarterly by the supervisory board. In addition to financial information,
quarterly reports are meant to include an overview of EHIF performance in terms of
strategic objectives and yearly action plans. All quarterly reports are publicized on the
EHIF‗s Web page and those who have no access to the Internet can get this Information
on request in hard copy or any other means. (Beneficiaries and other users also have the
right to get more comprehensive information on themselves from the EHIF‗s database,
for example, treatment costs.)
The EHIF‗s annual report is more comprehensive and audited by an external auditor; it
is also public, and has gained the best public reporting award for four consecutive years.
(Thomson, S. & Reed, S. J.2011).
48
However, there is room for improvement on Transparency and information because
consumer protection is comparatively weak. Currently there is no single patient/insured
protection legislation other than the Law of Obligations, which regulates all contractual
relationships. According to insured satisfaction surveys (annual population-based
surveys), recipients ‗awareness of their rights, obligations and of changes in health
insurance system (benefits, copayments, etc.) is relatively limited. Also, receivers have
the right to put their complaints to the EHIF, but procedures are not established or clear.
If the EHIF receives a complaint and no agreement is reached, then the complaint goes
directly to an administrative court according to general procedures. However, the
number of court cases is restricted and this is uncommon.
A Coherent decision-making structure is another important dimension for Estonia.
Given the impact of different decision-making bodies, the creation of separate financial
reserve accounts is potentially useful. The financial reserve fund of the EHIF is
accessible to the supervisory board for covering normal commercial risks and
management difficulties associated with managing the EHIF. The additional backup can
be released only by the government and is meant to cover the costs of government
decisions affecting EHIF finances. In addition, the union of health insurance entities
may make operational performance more effective, particularly for lesser populations.
Estonia appears to have considerably reduced administrative costs by consolidating 22
regional insurers into a solo fund covering the country‗s entire population of 1.3 million.
2.12.9 The National Health Insurance Scheme in Netherlands
Governance of MHI in the Netherlands is rated quite high. It scored well in most of the
governance dimensions. The score was highest for Consistency and stability, followed
by Supervision and regulation. Although the institutional and legal framework of MHI
legislation was substantially reformed in 2006, the broad objectives and instruments of
legislation for the MHI system have remained substantially the same since the 1960s
(even though less fundamental changes did occur, such as the extension of the

49
population covered and the benefits package). MHI has remained unaffected by political
changes
With regard to Supervision and regulation, rules on compliance and sanctions are clearly
defined in legal texts and the Supervisory Board for Health Care Insurance has imposed
corrective actions (mainly financial). All regulatory agents publish annual reports with
information on cases of rule violation and subsequent actions. For Transparency and
information, the Netherlands performs less well because disclosure rules regarding
business activities, ownership, and finances were not in place until recently. A new
disclosure arrangement states that each health insurer (or provider) must annually
publish information on the salary of its chief executive. Frequent efforts are made to
measure the performance of health insurers and provider organizations, and to disclose
information to the general public through the Internet. In addition to formal information
requirements, a number of social factors, including citizen groups and the press, play a
role in reporting information, such as the salaries of chief executives of sickness funds,
as they do for other publicans semi-public institutions. The Netherlands also has
consumer protection regulations related to consumer information, responsibilities,
grievance procedures, and appeal mechanisms. However the complaints and appeals
mechanisms are relatively weak and rarely used. An ombudsman exists, and the insured
have the right to appeal decisions made by their sickness fund to this officer.
Stakeholder participation was good. In the past, representatives of employers, unions,
provider, and insurers sat on the semi-public independent agencies that regulate the
sector. However, recent reform of these bodies has put an end to this ―representative
model.‖ At present, their boards consist of independent experts, appointed by the
minister of health. Reporting to the board are usually various working groups.
Stakeholders often have representatives in these working groups and such representation
is generally effective. Also, there is a tradition in the Netherlands of decision-making by
consensus and shared responsibility.
50
Thus, for example, the minister of health is expected to negotiate with interest groups
when problems arise, rather than acting unilaterally.
Regarding Coherent decision-making structures, improvements in efficiency may not be
achieved, despite the existence of multiple competing health insurers, if fundamental
pricing and service decisions are imposed by the government. The Netherlands‗ recent
health reform seeks to structure competition so that health insurers will suffer financially
for poor management but not for insuring a disproportionately high-risk population. The
government has the authority to regulate the benefits package but there is flexibility by
insurers to complement packages. The supervisory authority is independent and
periodically assesses the risk borne by insurers.
2.12.10 The National Health Insurance Scheme in Chile
The assessment of Chile‗s mandatory health insurance (MHI) governance performance
included both, National Health Insurance Fund (Fondo Nacional de Salud-FONASA)
and the private health insurers; Health insurance funds (instituciones de
saludprovisional-ISAPREs). Although the two kinds of insurers are quite different, they
both operate within the context of a single MHI system.
Therefore, the assessment for each dimension was made on the basis of information for
both types of insurers, and a combined rating was then given. Generally the ISAPREs
are regulated much more comprehensively than FONASA. Consequently the overall
results are more variable than in the other three countries. The divergence between the
two systems can be illustrated with Supervision and regulation, in regard to rules on
compliance, enforcement, and sanctions. The Superintendence of Health
(Superintendence de Salud-SIS) has no power to sanction the public insurer, FONASA,
if it fails to meet its obligations; the SIS has the right to audit FONASA‗s activities, but
not to directly impose sanctions; there is no information regarding corrective actions
based on clear and objective criteria for FONASA that are publicly disclosed; and
finally, no rule violations have been documented in the case of FONASA.
51
In contrast, SIS has substantial authority to impose sanctions on the ISAPREs—specific
regulations govern their oversight and imposition; sanctions take the form of legislative
investigations against the institution involved; the new laws allow SIS to impose
financial sanctions on ISAPREs; the SIS Web site publishes he sanctions imposed on
private insurers, as well as the cause of the sanction and the fee levied; and finally, SIS
publishes the sanctions imposed against ISAPREs on its Web page and in other media.
Chile‗s MHI governance system performs very well in terms of Consistency and
stability. For FONASA and the ISAPREs, the system‗s basic objectives have remained
the same. Fundamental characteristics of the MHI system, including the minimum
benefits package, contribution requirements, and basic institutional requirements for
operators, are defined in different laws. The current system was established in 1981, and
legislators have since sought to improve it: in 2004 are form process was initiated,
including new laws and new rights that apply to all beneficiaries, regardless of the
insurance system, but changes have largely related to expanding the rights and benefits
of the insured.
The Transparency and information dimension was good, although objectives of the
system are not always clearly defined and easily understood by beneficiaries. For
example, a SIS opinion survey shows that just over 20 percent of beneficiaries feel that
they have enough information, 60 percent feel that they have little information, and the
rest feel that they have none. The differences between FONASA and ISAPREs in this
regard are small. The legal framework is adequate given the local context, even though
key players and beneficiaries did not help establish the framework. Consumer complaint
mechanisms exist for both ISAPREs and FONASA, but only the private system has a
culture of consumer complaint. The regulatory agency periodically publishes data
regarding the nature and rates of complaints for each of the ISAPREs, usually in the
form of a ranked list. No complaints data are available for FONASA.
52
For other MHI governance dimensions there is also room for improvement, especially
Stakeholder participation, which is very weak. FONASA‗s stakeholders do not have
direct representation in the institution‗s supervision. Since FONASA reports directly to
the government, through the Ministry of Health, no representatives from unions,
employers, beneficiaries, or providers meet in an oversight body. FONASA does have
14 user committees (participatory bodies of patient associations and beneficiaries), but
these are advisory and have no power to impose or vote on decisions. Similarly, the SIS
is a technical body appointed by the government and has no representatives from unions,
employers, beneficiaries, or providers. ISAPRE boards of directors are generally chosen
by shareholders, leaving beneficiaries, employees, and providers without explicit
representation.
Coherent decision making structures are the weakest dimension in the case of Chile. The
ISAPREs have, over time, been able to risk-select the insured population, forcing the
transfer of higher risk to the realm of FONASA. Recent changes in regulations imposed
explicit health guarantees (garantías explícitas de salud- GES) on all health insurers, but
it is uncertain that this change will affect existing risk selection.
Ghana National Health Insurance Scheme (NHIS) was established under the National
Health Insurance Act of 2003 and is based on District-wide Mutual Health Insurance
Schemes (DMHIS) which operate in all districts in the country (Slavea et al, 2009).
At the end of 2008, 61% of the population of Ghana was covered by the NHIS (Slaves et
al 2009). In 2009 an evaluation was conducted to evaluate the effects of NHIS to service
provider and beneficiaries of the scheme, data was collected using closed and open
ended questionnaires. The evaluation findings was that; there was delays in insurance
cards to beneficiaries, lack of motivation of DMHIS staff, lack of understanding of the
need for health insurance by community members and delays in the reimbursement
accredited health facilities (Slaves et al 2009). The authors argued that delays in
reimbursement soured relationship among service providers in the district, who in some
cases threatened to stop accepting insurance patients. The study concluded that NHIS
53
faced challenges which require Ghana Government to use the findings of the study to
improve the performance of NHIS by making necessary reforms. However authors
didn‘t point out the factors which contributed to mentioned challenges especially the
delays in the reimbursement process, therefore this evaluation will look in the same
scenario as Ghana but specifically on service provision in accredited health facilities
The District Mutual, Private Mutual and Private Commercial Schemes are regulated by
the National Health Insurance Council (NHIC) to provide Health services to the
community. The National Health Insurance Policy was set up to allow everybody to
make contributions into a fund so that in the event of illness contributors could be
supported by the fund to receive affordable healthcare. The NHIS covered all 138
districts, Municipal and Sub-Metro contributions. The contributors are grouped
according to the levels of Income; there is a specific premium that ought to be paid. This
was done since the socio-income condition scheme contributors is not the same and the
contributions was to be affordable for all to ensure that nobody is forced to remain in
Cash and Carry System.
The above contributions are after 13 months, after the time is over the contributor will
renew the contract and continue to enjoy the national health services provided. Workers
in formal sector join the District Wide Health Insurance Scheme through the enacted law
on Health Insurance. The law makes it mandatory for 2.5% of workers social security
contributions to be put into the National Health fund to be subsequently disbursed to the
district mutual health Insurance Scheme as their contributions to the schemes. Children
under 18 years of formal sector workers will also be exempted from paying any
contributions provided workers spouses in the informal sector. The package covered
about 95% of diseases in Ghana including Malaria, Asthma, Diabetes, Diarrhea, Hearing
aids, Dentures, Beautification, Supply of Aids drugs and treatment of chronic reveal
failure.

54
The effort of re-designed National Health Insurance System was adopted in 2006; seek
to establish a realistic health financing system that has capacity of meeting health system
of improved health status of Nigerians, financial protection of citizens against cost of
illness, fair financing of health services and responsiveness to the citizen‗s expectations.
The National Health Insurance Scheme (NHIS) is the body responsible for regulation of
the system and the different health insurance schemes. The Governing Board of the
National Health Insurance Scheme is the National Health Insurance Council (NHIC).
NHIC works to regulate the scheme (including setting standards, determining
contribution rates, providing technical support, etc), license HMOs and providers, train
health care providers, and manage the National Health Insurance Fund (NHIF).
Patients are allowed to choose their primary provider from the list of accredited
facilities, which includes both public and private providers. The provider network is
used for access and secondary referrals, which acts to control costs and maintain
viability of the system. Provider payment mechanisms are primarily determined by the
National Health Insurance System (NHIS) Governing Council.
The National Health Insurance Scheme (NHIS) is funded primarily by contributions
from members based on income. For the Formal Sector Social Health Insurance Program
contributions are premiums that make up 15% of an individual‗s basic salary, with the
employer contributing 10% while the employee pays 5% for coverage of themselves,
their spouse, and up to 4 children.
An employer may 24 negotiate with an HMO for coverage of additional supplementary
benefits and pay the extra contributions required. Participants in the Informal Sector
Program are expected to make a monthly contribution based on the benefits package of
their choice as well as other factors. The poor, elderly, veterans, and disabled are
exempted from paying membership premiums. Health insurance is obtained either
through private insurers or the National Health Insurance Scheme (NHIS). About 5
million people are enrolled in the 3 NHIS Programs, which represents just about 3% of
55
the population. In the Formal Sector Program, employees in the formal sector who pay
premiums are covered, in addition to their spouse and up to 4 dependents. Companies
that employ more than 10 workers are responsible for enrollment of their employees
The benefits package for the National Health Insurance Scheme for workers in the
formal sector is pre-determined and includes: Out-patient care, including necessary
consumables prescribed drugs, pharmaceutical care and diagnostic tests on the National
Essential Drugs List and Diagnostic Test Lists, maternity care for up to 4 live births for
every insured contributor, Preventive care, including immunization, health education,
family planning, antenatal and post-natal care ,consultation with specialists with a
referral ,hospital in-patient care in a standard ward for a 15 cumulative days per year,
eye examination and care, excluding the provision of spectacles and contact lenses, a
range of prostheses (limited to artificial limbs produced in Nigeria) and preventive
dental care and pain relief (including consultation, dental health education, amalgam
filling, and simple extraction).
Patients are allowed to choose their primary provider from the list of accredited
facilities, which includes both public and private providers. The provider network is
used for access and secondary referrals, which acts to control costs and maintain
viability of the system. Provider payment mechanisms are primarily determined by the
National Health Insurance System (NHIS) Governing Council
As revealed by the (Kenya website), the National Hospital Insurance Fund is a State
Parastatal that was established in 1966 as a department under the Ministry of Health.
The original Act of Parliament that set up this Fund in 1966 has over the years been
reviewed to accommodate the changing healthcare needs of the Kenyan population,
employment and restructuring in the health sector. Currently the National Hospital
Insurance Fund Act No 9 of 1998 governs the scheme

56
The transformation of National Hospital Insurance Fund from a department of the
Ministry of Health to a state of corporation was aimed at improving effectiveness and
efficiency. The Fund's core mandate is to provide medical insurance cover to all its
members and their declared dependants (spouse and children). The National Hospital
Insurance Fund membership is open to all Kenyans. Each of these branches offers all
National Hospital Insurance Fund services including payment of benefits to hospitals or
members or employers. Smaller satellite offices and service points in district hospitals
also serve these branches.
National Hospital Insurance Fund operations have been computerized and decentralized,
enhancing efficiency in settling claims and effective management of membership
database. The Fund also increased its service accessibility through the current networked
23 fully-fledged branches, 7 satellite offices and service points at most district hospitals
countrywide. The branches function independently to offer services similar to any other
office across the country.
As revealed by the (Kenya website), the National Hospital Insurance Fund is a State
Parastatal that was established in 1966 as a department under the Ministry of Health.
The original Act of Parliament that set up this Fund in 1966 has over the years been
reviewed to accommodate the changing healthcare needs of the Kenyan population,
employment and restructuring in the health sector. Currently the National Hospital
Insurance Fund Act No 9 of 1998 governs the scheme
In 2008 Mohammed et al, conducted an evaluation of NHIS in Zaria estate in Nigeria to
determine the satisfaction of enrollees regarding the health service provision under a
health insurance scheme and the factors which influence the satisfaction. Mohammed et
al (2008) showed that extent of employment, salary income, hospital visits and duration
of enrolment to some extent influenced satisfaction. Similarly, in 2012 Onyedibe et al
conducted a study to evaluate the level of enrolment of member to NHIS, the results of
the report showed that the enrolment was very poor, authors pointed out that, thpoor
57
enrolment was mainly contributed by dissatisfaction of health services offered to NHIS
beneficiaries. The authors concluded that the quality of the services was the most
important factor which influenced the enrolment of members to any insurance scheme;
therefore the Nigerian Government should use the evaluation findings to improve the
services in order to increase the enrolment. However, author‘s didn‘t point out anything
concerning the performance of the scheme in compliance with the accredited health
facilities, therefore this evaluation will evaluate the insurance scheme in Tanzania but
specifically on accredited health facilities.
According to Obonyo 1996, the Kenya National Health Insurance Fund (NHIF) has been
successful in implementing the scheme since 1966 to date, whereby the coverage is 25%
for the whole nation‟s population. The reason for their success is that they have set a fee
for services which is reasonable; hence health providers are able to provide high quality
health services (Obonyo, 1996.) Beneficiaries are satisfied with the services and are
fully utilizing them and have attracted even those who are not compulsorily liable to join
the scheme, such as self-employed people and part-time workers who have joined the
scheme as voluntary members (Obonyo,1996). The second reason for Kenya‟s NHIF
success is that it has the fund‟s inspectorate unit, which inspects health providers
regularly; they inspect their quality of services and grade the providers according to
score, they inspect drugs and medical equipment availability and grade the facilities
based on compliance with the guidelines and standards. Thus, the author (Obonyo, 1996)
presented utilization of health insurance in Kenya and the factors that influence the
utilization and how the insurance inspects and grades the health providers. The author
concluded that inspection to the health providers is the key for improving the quality of
NHIF services. This evaluation will look on the same scenario but specifically for NHIF
accredited health facilities in the context of Tanzania.
In 2016, Joseph Githinji, in his work published The Road to UHC in Kenya: Inside
NHIF Reforms, the author talked about the way in recent years, the country has
undergone significant health reforms, implemented largely by the National Hospital
58
Insurance Fund (NHIF), Kenya‘s primary provider of health insurance with a mandate to
provide all Kenyans with quality and affordable health services. In this interview, Mr.
Githinji discusses the strengths and weaknesses of the NHIF, as well as the passage of
new guidelines that expands coverage to outpatient services and increases the annual
premium for the first time since the launch of the scheme. Yes, there have been several
reforms. This includes the introduction of contracts with healthcare providers, which
mandate that all patients receive high-quality health care. Other reforms include: internal
staff restructuring to ensure optimal employee performance; and increase of
contributions so as to increase the depth of the benefit package as more funding will be
available, how NHIF will work with different stakeholders in this case private and
public facilities in the implementations of the services within the expanded coverage of
the package, talked about the approximated 1600 facilities that members can access
across the country; the services that are available and expected impact those reforms will
produce. Findings on this study will be used as an example to evaluate the
implementation of benefit package specifically by NHIF accredited health facilities in
the context of Tanzania.
In 2012 Musau et al conducted an evaluation on the health system of Tanzania,
specifically the National Health Insurance Fund. Data was collected using closed and
open ended questionnaires to NHIF beneficiaries and health workers in the accredited
health facilities. Authors pointed out that despite the significant effort in developing
insurance options; only13% of the population in Tanzania is currently covered by health
insurances (7.3%covered by NHIF). The study findings showed that there was low
member enrolment which was contributed by the health facilities staff attitudes in
treating NHIF patients, weaknesses of the public facilities financially thus affects the
services in terms of quality and availability. The authors concluded that difficult
reimbursement procedures done by NHIF is one of the factor which led to poor services
on accredited health facilities, therefore the Government under MOHSW needs to
review them in order to improve the performance of the facilities.

59
Therefore, this evaluation will specifically evaluate on service provision as in benefit
package is implemented in accredited health facilities.
2.13 Conceptual framework of the evaluation
The conceptual framework for this study assumes that NHIF implemented Benefit
Package in Accredited health facilities (as a dependent variable) is determined by the
following
(Independent variables): Compliance with NHIF/MoH standards and Accreditation
guidelines, Knowledge and involvement of Stakeholders on NHIF Benefit Package,
Accreditation of health facilities, Periodic review of package, claims reimbursement,
adherence to Standard treatment guidelines/ other treatment protocols. Health sector
Policy, Guideline and legal framework, Knowledge and trainings on the package, Health
facility network and accessibility, Staffing and personnel,
Thus, this conceptual framework which diagrammatically shows the whole picture of
the study, gives the boundaries the research is grounded to study about the effectiveness
of the NHIF, see figure 2.1 below
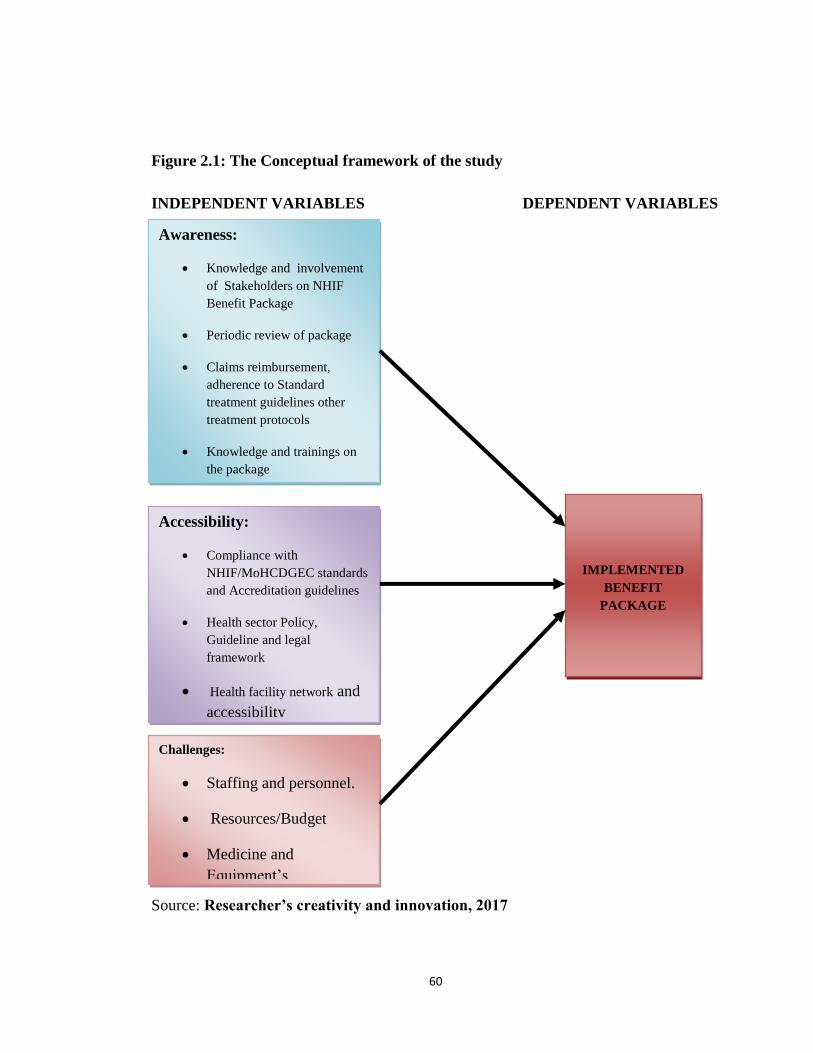
60
Figure 2.1: The Conceptual framework of the study
INDEPENDENT VARIABLES DEPENDENT VARIABLES
Source: Researcher’s creativity and innovation, 2017
IMPLEMENTED
BENEFIT
PACKAGE
Awareness:
Knowledge and involvement
of Stakeholders on NHIF
Benefit Package
Periodic review of package
Claims reimbursement,
adherence to Standard
treatment guidelines other
treatment protocols
Knowledge and trainings on
the package
Health facility network and
accessibility
Accessibility:
Compliance with
NHIF/MoHCDGEC standards
and Accreditation guidelines
Health sector Policy,
Guideline and legal
framework
Health facility network and
accessibility
Challenges:
Staffing and personnel.
Resources/Budget
Medicine and
Equipment‘s

61
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Introduction
This chapter explains the methods and techniques that were used in the process of data
collection, types of data collected as well as techniques that were used in data analysis. It
Describes the sampling technique/ procedure and states the main instruments that were
used in data collection from the field.
3.1.1 Evaluation design
An evaluation design is the arrangement of conditions for collection and analysis of data
in a manner that aims to combine relevance to the research purpose with economy
procedure (Kothari, 2010).
It is a conceptual structure within which research is conducted. The research design
constitutes the plan for the collection, measurement and analysis of data. Therefore, a
descriptive case study design was used in this Research. This type of design will lead to
identify wider situation of the problem as slight or no vital information was available in
the study area. This design was chosen in order to provide a general explanation of the
topic under study. In addition, this study design mainly focused to gather information
from respondents who by the virtue of their health status and involvement contributed
sufficiently to provide data for this study. This seemed to be necessary in order to serve
the triangulation purposes. Case study may involve both qualitative and quantitative
research methods and so for the purpose of this study facility based various case studies
was carried out to evaluate implementation of NHIF Benefit Package in accredited
health facilities.

62
3.1.2 Evaluation Approach
According to Patton (2012), formative evaluation is carried out in order to understand
what is going on with the implementation of the program, to find ways and make
recommendations on improving the program outcome. A formative evaluation was
conducted to assess the ongoing NHIF activities in order to provide information that
could be used for improvement
[
3.1.3 Evaluation period
The design of this evaluation study began in February, 2016 by developing evaluation
proposal. Data collection was done starting from mid of March 2017 – end of May 2017,
followed by data analysis and report writing that was completed in June 2017. Prior to
data collection, a proposal which highlighted the backgrounds, problem statement,
objectives, evaluation questions and rationale for conducting an evaluation study was
shared to Stakeholders for comments and inputs.
3.2 Description of the Study area
This evaluation study was conducted in Ilala Municipality in Dar es Salaam Region.
Ilala is the northern most of 5 District in Dar es Salaam, its total surface area is 531 km
square, administratively and it has 5 divisions, 27 wards, 114 streets, 14 villages and 14
hamlets (DMC Profile, 2011). The Municipal is among the 5 districts of Dar es Salaam
region, the district has a population of 1,220,611 people (among them 624,683 are
females and 595,928 are Males with an average household size of 4.0 (Population and
Housing Census, 2012)
According to Ilala Municipal health facility Inventory Data base, Ilala has 145 Health
facilities, among them, 96 Health facilities has been accredited by NHIF in Ilala
Municipal. 8 are of National referral status, 1 Regional Referral Hospital, 3 District level
Hospitals, 8 Health centers, 39 Dispensaries, 33 Pharmacies, 1 ADDO shop and 2
Special clinics. This is according to quality assurance report of 2015/2016.
63
Rationale for conducting this evaluation in Ilala is that, this Municipal is the only one in
the country with 8 Hospitals of the status of National referral status, also the facilities
with important specialties services like Oncology( Ocean Road Cancer Institute),
Orthopedics ( Muhimbili Orthopedic Institute), Invasive Cardiac services provision (
JakayaKikwete Cardiac Institute), Muhimbili National Hospital), Regency Medical
Centre, Shree Hindu Mandal Hospital and Pharmacies that supply immunosuppressant
and immunostimulants medicines ( for treatment of cancers) and orthopedics appliances
as well as implants services just to mention the few, with assumption that facilities
available in this municipal serves for beneficiaries from all over the country, has
sophisticated equipment‘s for diagnosis and with Facilities using Modern high
technology services. Based from various reports, it has been noted that accredited
facilities available in Ilala Municipality accounts for 36 % of all claims reimbursements
paid to accredited Health facilities all over the country for the financial year 2015/2016.
3.3 Target population
The target population of this study was beneficiaries of the NHIF, Staff from the
Accredited Health facilities and Staff of NHIF. The target population of the study was
divided into three main groups. The first group is NHIF Staff; the second group is
Health care providers, (hospitals and pharmacies) and the last group NHIF members.
The total number of NHIF Staff interviewed from Quality and Claims department
respectively is 10, the NHIF beneficiaries were 300 and 10 health care providers all in
Ilala Municipality.
Table 3.1: Population of the study
S/No Participant category Total Population Sample size Sample percentage
1 NHIF Staff( Quality
assurance & claims
Ilala office
20 10 50%
2 NHIF Beneficiaries 300
3 Health Facilities 96 10 10.4%
Total
Source: (NHIF, Ilala Quality Assurance Report 2016)
64
3.4 Source Population and Study Population
Accredited health facilities that ranges from Hospitals, Health centers, Dispensaries,
Pharmacies, Specialized Clinics, Diagnostic centers and ADDO Shops found in Ilala
Municipal are the Source Population in this particular study while Study population for
this study are members of NHIF who are treated in Ilala Municipal council, health
workers from the selected government and private owned hospitals health centers and
Dispensaries, pharmacy etc,
3.5 Units of analysis
For the purpose of this assessment, the unit of analysis involved 300 NHIF beneficiaries
accessing services in Ilala Health facilities, 10 respondents from ten selected health
facilities in Ilala Municipal and 10 NHIF staff working in Quality assurance department.
3.6 Variables and their measurements
3.6.1 Indicators and Variables
3.6.1.1Variables
A variable is a characteristic of a person, object or phenomenon which can take on
different values. These may be in the form of numbers (e.g., age) or non-numerical
characteristics (e.g., sex). (Corlien, A; Pathmanathan, M; Brownlee, A 1991).
3.6.1.2 Dependent variable
Dependent variable in this study is the implemented NHIF Benefit Packages.
3.6.1.3 Independent variables
Health sector Policy, Guideline and legal framework – Independent Variable
Knowledge and trainings on the package - Independent Variable
Health facility network and accessibility - Independent Variable
Staffing and personnel - Independent Variable.
Contents/Items within Benefit Package - Independent Variable
Accreditation guideline and requirements-Independent Variable
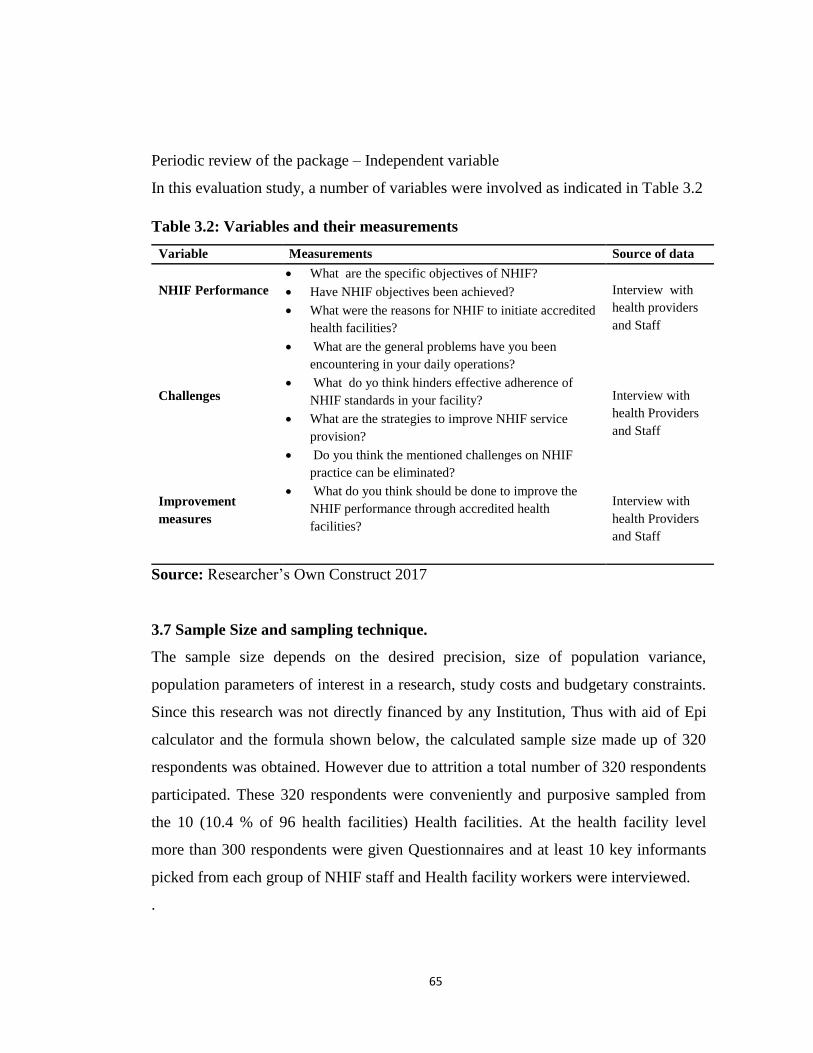
65
Periodic review of the package – Independent variable
In this evaluation study, a number of variables were involved as indicated in Table 3.2
Table 3.2: Variables and their measurements
Variable Measurements Source of data
NHIF Performance
What are the specific objectives of NHIF?
Have NHIF objectives been achieved?
What were the reasons for NHIF to initiate accredited
health facilities?
What are the general problems have you been
encountering in your daily operations?
What do yo think hinders effective adherence of
NHIF standards in your facility?
What are the strategies to improve NHIF service
provision?
Do you think the mentioned challenges on NHIF
practice can be eliminated?
What do you think should be done to improve the
NHIF performance through accredited health
facilities?
Interview with
health providers
and Staff
Challenges
Interview with
health Providers
and Staff
Improvement
measures
Interview with
health Providers
and Staff
Source: Researcher‘s Own Construct 2017
3.7 Sample Size and sampling technique.
The sample size depends on the desired precision, size of population variance,
population parameters of interest in a research, study costs and budgetary constraints.
Since this research was not directly financed by any Institution, Thus with aid of Epi
calculator and the formula shown below, the calculated sample size made up of 320
respondents was obtained. However due to attrition a total number of 320 respondents
participated. These 320 respondents were conveniently and purposive sampled from
the 10 (10.4 % of 96 health facilities) Health facilities. At the health facility level
more than 300 respondents were given Questionnaires and at least 10 key informants
picked from each group of NHIF staff and Health facility workers were interviewed.
.

66
It is important during calculating for Sample size to know the situation (in terms of
means or proportion), and the conditions, then we need to ask our self what Variables do
i use and how are these Variables going to be Measured.
Sample size is a function of three factors – the acceptable significance level, power of
the study, and magnitude of the difference (expected effect size), underlying event rate
in the population and standard deviation in the population.( Devane et al (2004)
Based on the fact that my study was meant to cover for the population of above 10,000,
the sample size for this study was calculated by using the formula: -
According to Naing et al. (2006), formula for sample size stated as follows;
N=(z/d)² (p) (1-p) , where
N= sample size
z = the standard score corresponding to a given confidence level;
d = the proportion of sampling error; and
p = estimated proportion or incidence of cases.
By definition, for a 90% confidence level, z = 1.65; for 95%, z = 1.96 and for 99%, it is
2.58. Traditionally, an acceptable error level is up to plus or minus (ten % points).
3.8 Sampling technique
Both Probability as well as non-Probability sampling methods was used in this study.
Stratified Random sampling was used to select respondents by diving them into 3
groups, ie Health Care Workers, Beneficiaries and NHIF staffs whereas Purposive
sampling was applied especially for the respondents whose selection was based on the
experience or knowledge on the subject in hand. It means i selected respondents by
virtue of their position and involvements in the implementation of Benefit package such
as Health facility in charge, Beneficiaries who receives Medical services in accredited
67
health facilities, other Health care workers and NHIF staffs who directly deals with
Claims and Quality assurance issues. Convenient random sampling was used to select
beneficiaries where by any member or dependents available in health facilities were
approached and once agree to participate were included in the evaluation
While probability sampling gave equal chance of being selected to every member in the
population, non-probability sampling is a biased technique so as to decide who to be
included or excluded in the sample.
3.9 Approaches to the Study
Due to the nature of the Study, both qualitative and quantitative approaches were used.
The study adopts qualitative approaches because is concerned with subjective on the
views and perceptions of the beneficiaries on the NHIF benefits package on its
comprehensiveness and the way it is implemented and also determine the challenges that
occurs during the implementation of the package and how those challenges were solved
within NHIF and Health providers, this will help the researcher in knowing if the content
is comprehensive to give good quality of service provided and also provide the answers
to the organization .Quantitative type was used with simple measures in terms of
percentages from the responses to know the status and capabilities of the health facilities
as well as to know in what percent the accredited facilities comply with the accreditation
criteria.
3.10 Inclusion criteria
In this Research, the inclusion criteria were beneficiaries of NHIF who receives
treatment in accredited Healthcare facilities in Ilala Municipality, Health Care Workers/
facilities in charge who agreed to participate and comprehensibly articulate their views
and NHIF staff working in Ilala Regional office. Their inclusion criteria in the study
based on their knowledge, participation and involvement on the topic under the study.
68
3.11 Exclusion criteria
Those respondents who were not willing to participate in the study based on any reasons
or other care workers and NHIF staffs that are not working or found in Ilala municipality
were not included in the study.
3.12 Data Collection
3.12.1 Data collection Process
Collection of data in this study was based on two types of data, primary and secondary
data. Primary data collected directly from responded through questionnaires, interview
guide and observation. The process cater for both Qualitative and Quantitative Data
Secondary data were mainly collected through documentations from various NHIF
reports and from Medical provider‘s office records. Also another means was in a form of
documentary review whereby the researcher reviewed the available information from
published and unpublished materials relevant to the research topic. Various relevant
documents such as Medical provider reports, NHIF reports, Ministry of Health‘s
policies, treatment protocols and accreditation guidelines related to the subject were
consulted.
Ethical issues associated with carrying out the research were adhered and observed in all
process of data collection
3.13 Development of data collection tools
Data collection tools used in this study included Questionnaire, an in-depth interview
guide and observation checklist for both Nhif Members, Medical providers and Nhif
staff
3.13.1 Questionnaire
Questionnaires were used to collect data from the study participants. Structured
questionnaires with both open-ended and closed-end questions were developed. The
questionnaires were developed in English and then translated into Swahili language. The

69
essence of translation intended to make sure that all respondents would feel free to
respond in the language they are comfortable with. For the correctness of the translation,
the researcher asked linguist expert to translate those questionnaires.
Semi-structured questionnaire was used to collect data. Semi-structured questionnaire
had both open-ended and closed-ended questions that were used to obtain information
from the study participants. The reason for using questionnaire was that respondents had
a complete freedom of response that best fit their situation. Most of the respondent opted
to fill the questionnaires which were administered either by the researcher or research
assistants. About 350 Questionnaires were distributed to the respondent‘s altogether.
3.13.2 Interview Guide
10 respondents were identified and requested to answer some questions through in-depth
interview guide. The researcher and research assistants noted down the answers given in
the questionnaire recorded. The aim was to gather additional data and information that
were collected, the structured interview, subjecting every informant in a sample was
made also with probing questions was applied so as to achieve high reliability of the
information gathered. This proved to be very effective and also of great value as the
additional information was so important in the process of interpreting the results.
3.13.3 Observation
This method was applied so as to provide additional information about actual behavior
of the health care workers while giving services to beneficiaries and the current
infrastructural status of health facilities. Since the researcher visited the study areas,
direct observations was also done to allow the researcher to put behavior in context and
to back up the information gathered by the researcher from the respondents during
interviews and filling of questionnaire, this method helped in knowing the real picture
on how HCWs provides medical services to NHIF Members and also the status of health
facilities in terms of infrastructures and by doing so the researcher could as well knew
on the quality of services provided.

70
3.14 Validity and Reliability issues
This section explain the extent to which the study findings and data collected are
accurate and shows good consistency of the information gathered and the findings
obtained. Also it explains as to what extent the results obtained was obtained through
comprehensive systematic approach.
3.14.1 Validity
According Kothari (C.R, 2010) Validity refers to the extent to which the measurement
captures the intended information from the subject. To ensure validity researcher
Purposive sampling was applied especially for the respondents whose selection was
based on the experience or knowledge on the subject in hand. Also the technique of
asking the same question to more than one respondent so as to see the consistency of the
answers was used. At the same time, questionnaires were distributed in large number to
respondents assuming that if some may not return the number respondent will remain
sufficient.
3.14.2 Reliability
Reliability is the ability degree of using research tools and procedures to produce same
results on repeated measures on the subject. This enables replication of research
procedures by other independent researchers (Tashakkori and Teddlie 2010).
To ensure consistency and reliability of the answers, data collection tools based on study
questions that reflects objectives of the study were developed by researcher. To
determine the validity and reliability of data, data collection tools ie Questionnaire and
interview guide were pre-tested before the actual field data collection. The aim of the
pre-testing was to verify if questionnaire was able to capture the desired information.
The pre-testing was done in 2 different Hospitals 1 Public and the other Private owned
Facilities of the status of Regional referral level. 20 respondents were given
questionnaires to fill whereby feedback from the respondents was used to rectify the
questionnaires so that they meet the desired standards, then both tools were translated
into Swahili language for easy administration during field works.
71
3.15 Data management and analysis
3.15.1 Data entry
Quantitative Data obtained were collected by questionnaire then by using the client exit
interview the data were cleaned, coded & entered to Microsoft excel 2007 computer
software.
3.15.2 Data cleaning
Collected data were cleaned before were processed and all data that were found not to be
completed or accurate were left out.
3.15.3 Data analysis
Data analysis is the examination of collected data in the field and making a deduction
and inference .Data that were collected by using both quantitative and qualitative
methods were processed and analyzed by using Statistical Package for Social Sciences
(SPSS) Software and ATLAS -ti. At this stage the data collected from complete filled
and clean questionnaires and other data collection tools were summarized, coded and
those data which seems to be irrelevant or all the questionnaire with inconsistency filling
were removed/ rejected by means of data cleaning/winnowing (Patton, 2002). Data were
checked for accuracy and completeness before analysis.
The findings are presented by frequency table, graphs, charts and two by two tables
depending nature of data. Basically, data were coded, examined, compared and
categorized based on the evaluation questions and comparison has been done to find
differences, similarities and meaning.
3.15.4 Ethical Issues
This evaluation study was conducted after the approval of the ethical committee of
Mzumbe University post graduate and research studies office. Permission was obtained
from the Ag Director General of NHIF, the Director of Ilala municipal council and other
leaders from respective health facilities to allow the study to be conducted.
72
All study participants were informed about the purpose of the study and verbal informed
consent was obtained from them prior to any evaluation activities. Confidentiality was
assured to the participants that their information provided will only be used for the
purposes of this evaluation and not otherwise. No such information shall be disclosed to
unintended audiences but will only be limited to researcher and supervisors from
Mzumbe University.
Privacy was maintained during data collection to give the participants the freedom to
express themselves without external or internal interferences. Data collections tools ie
(the electronic materials and paper based database) that were used were carefully stored
in manner that wouldn‘t allow any unauthorized persons to access.
3.15.5 Possible limitations of evaluation
Health professionals might have changed their previous behavior once they knew that
they are observed during data collection using observation method. The use of local
language (Swahili) to some respondents, may have led to misunderstanding or
misinterpretation of the important of the set questions and therefore lead to inaccurate
results.
Since the evaluation design for this particular study is case study the result cannot be
generalized to all health facilities. Basing on the fact that this study was not directly
financed by any institute, I decided to conduct the study in Ilala Municipal only the only
District in Tanzania with about 9 Hospitals of the status of National Referral or
equivalent and 2 Regional level status Hospitals and 12 specialized clinics; otherwise the
multi stage sampling used in this study could have involved several districts. Therefore
the study findings will not be the representative of the phenomenon in the country
73
CHAPTER FOUR
PRESENTATION OF THE FINDINGS
4.1 Introduction
This chapter presents results of the findings obtained from the study based on evaluation
objectives. It includes Analysis and interpretation of evaluating the implementation of
national health insurance fund (NHIF) benefit package in the selected accredited health
facilities in Ilala municipality. Furthermore, this chapter puts into consideration the
demographic information of the some of the category of respondents, eg It shows their
characteristics on Age, Sex, Education level and Work experience.
4.2 Demographic Characteristics of respondents
This study comprised of 52 % female and 48 % male respondents from the sample of
300 interviewed beneficiaries who were available in different accredited Health facilities
in Ilala municipal council during the period of this study, the evaluator considered sex
categories in order to get opinion from both sexes. The findings revealed that the
minimum age of respondents was 21yrs and maximum age 61yrs whereby Age group
participated included that age group between 21-30, 31-40, 41-50, 51-60 and 61 and
above. Their correspondence percentages are presented in figure 4.1. As it is presented
in figure 4.1 41.3% NHIF members and 40% health facilities staff were in the age group
between31-40. However there was no NHIF staff or health provider in the age group
between 51- 60 while 8.7% members of NHIF were in that age group(61 and above).
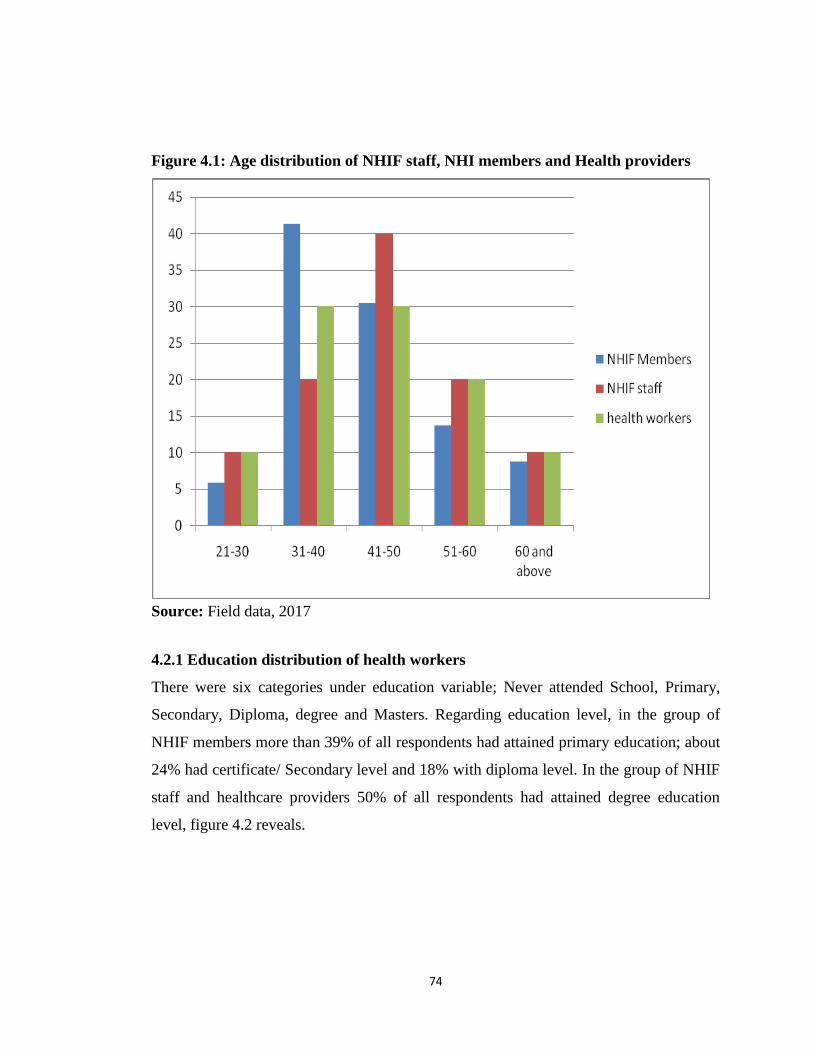
74
Figure 4.1: Age distribution of NHIF staff, NHI members and Health providers
Source: Field data, 2017
4.2.1 Education distribution of health workers
There were six categories under education variable; Never attended School, Primary,
Secondary, Diploma, degree and Masters. Regarding education level, in the group of
NHIF members more than 39% of all respondents had attained primary education; about
24% had certificate/ Secondary level and 18% with diploma level. In the group of NHIF
staff and healthcare providers 50% of all respondents had attained degree education
level, figure 4.2 reveals.
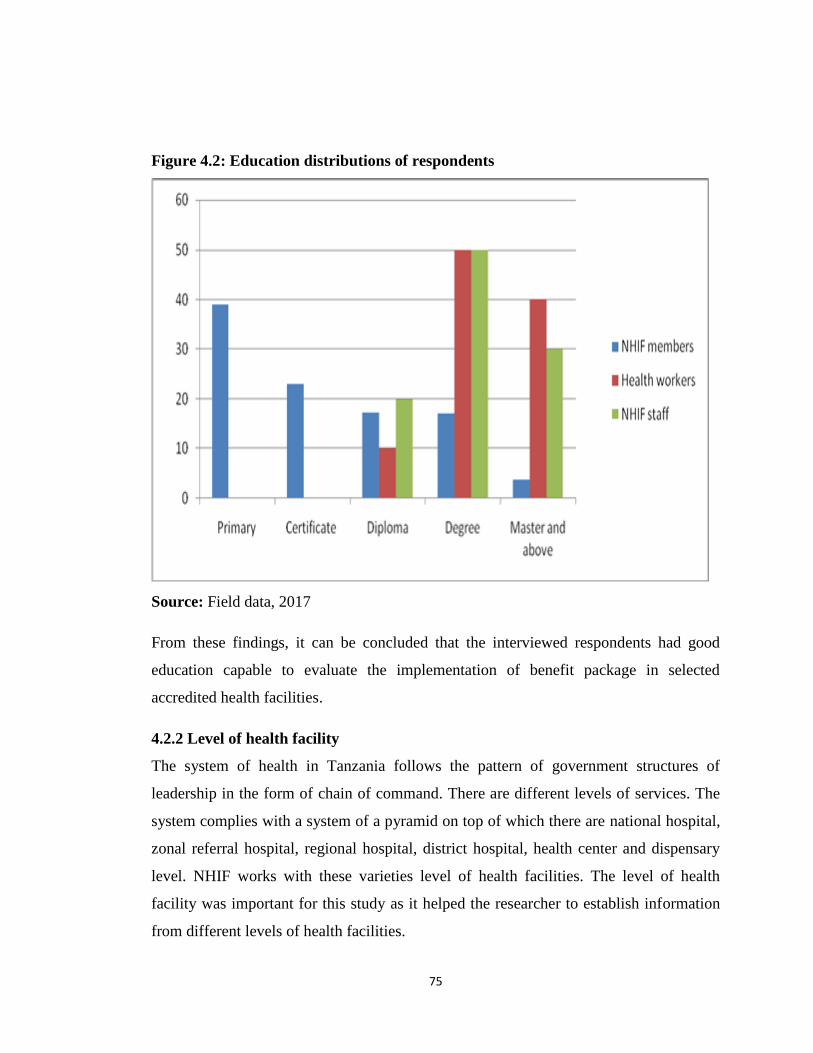
75
Figure 4.2: Education distributions of respondents
Source: Field data, 2017
From these findings, it can be concluded that the interviewed respondents had good
education capable to evaluate the implementation of benefit package in selected
accredited health facilities.
4.2.2 Level of health facility
The system of health in Tanzania follows the pattern of government structures of
leadership in the form of chain of command. There are different levels of services. The
system complies with a system of a pyramid on top of which there are national hospital,
zonal referral hospital, regional hospital, district hospital, health center and dispensary
level. NHIF works with these varieties level of health facilities. The level of health
facility was important for this study as it helped the researcher to establish information
from different levels of health facilities.
76
The study involved 10 different health facilities being: 3 Dispensaries, 2 health centers,
2 District level hospital, 1 Regional level hospital, 1 zonal referral hospital and 1
National referral Hospital. Basing on the findings it can be said that, Dispensary was the
least level and National referral Hospital and zonal referral Hospital which also
contained majority of respondents were the top level. See table 4.1 below
Table 4.1: Level of health facility
Level of health facility Frequency
Dispensary 3
Health center 2
District hospital 2 Health Facilities
TOHS,
CARDINAL RUGAMBWA HOSP
Regional hospital 1 Health Facility
AMANA HOSPITAL
Zonal referral hospital 1 Health Facility
REGENCY MEDICAL CENTRE
National Refferal Hospital 1Health Facility
MNH
Source: Field data, 2017
4.2.3 Work experiences
The work experiences of the study varied between > 5 years and <five years. With
regard to the working experience of the respondents, the findings revealed that (80%) of
the selected respondents had a working experience of working with NHIF and/or its
accredited Health facilities of more than five years while 20% of the respondents had the
working experiences between 0-5 years. Figure 4.3 shows working experiences. Also in
the group of health providers more respondents (80%) had the working experiences of
more than five years of age.
77
Figure 4.3: Work experiences for Respondents (NHIF members, Providers)
Respondents
5 >
5 <
Source: Field data, 2017
It can be concluded that the combinations of the respondent‘s education and working
experiences was very important in this study. This was justifiable to produce
respondents with enough knowledge and experience with NHIF benefit package.
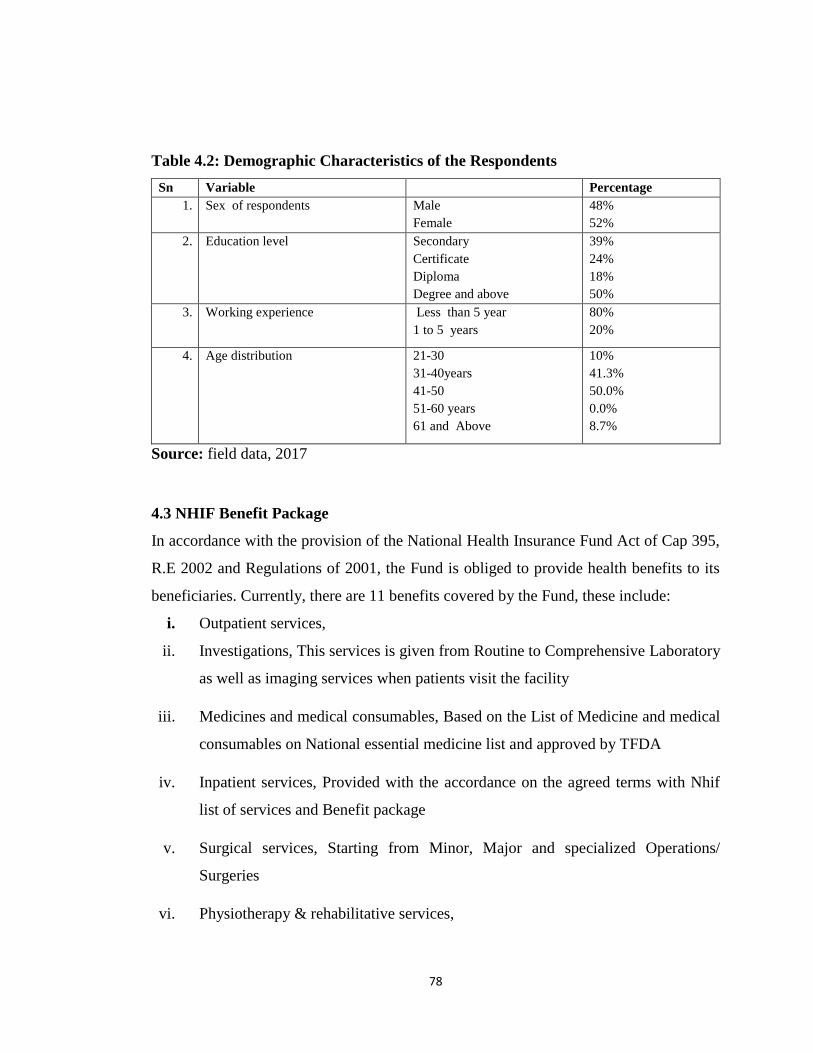
78
Table 4.2: Demographic Characteristics of the Respondents
Sn Variable Percentage
1. Sex of respondents Male
Female
48%
52%
2. Education level Secondary
Certificate
Diploma
Degree and above
39%
24%
18%
50%
3. Working experience Less than 5 year
1 to 5 years
80%
20%
4. Age distribution 21-30
31-40years
41-50
51-60 years
61 and Above
10%
41.3%
50.0%
0.0%
8.7%
Source: field data, 2017
4.3 NHIF Benefit Package
In accordance with the provision of the National Health Insurance Fund Act of Cap 395,
R.E 2002 and Regulations of 2001, the Fund is obliged to provide health benefits to its
beneficiaries. Currently, there are 11 benefits covered by the Fund, these include:
i. Outpatient services,
ii. Investigations, This services is given from Routine to Comprehensive Laboratory
as well as imaging services when patients visit the facility
iii. Medicines and medical consumables, Based on the List of Medicine and medical
consumables on National essential medicine list and approved by TFDA
iv. Inpatient services, Provided with the accordance on the agreed terms with Nhif
list of services and Benefit package
v. Surgical services, Starting from Minor, Major and specialized Operations/
Surgeries
vi. Physiotherapy & rehabilitative services,
79
vii. Ophthalmological services,
viii. Optical services, This are given only to Principle member after completion of the
set procedures
ix. Medical / Orthopedic appliances, This are given to Member after the approval
being provided the authorized NHIF staff based of the recommendation of the
Specialist
x. Dental and Oral Health services,
xi. Retirees‘ health benefit. These are given to those members with their spouse after
they have retired form services
The providers issue medicines based on the NEML and additional list drawn by NHIF in
regard to the regulation of using generic formulations, adherence to the mutually agreed
NHIF MEDICINES price list schedule. The schedule is prepared after taking into
account macroeconomic changes such as price index (inflation) and any other relevant
economic indicators. Diagnostic tests are carried out when a patient visits a health
facility. Surgical services include Minor, Major and specialized surgical services
performed from the health centers to the referral level.
Inpatient care services are provided in accordance with the agreed NHIF inpatient care
fee schedule at health facility levels allowed for admissions it should be noted that
Package contents are subject to review in accordance with changing technological
recommendations in disease Management modalities, and art of the day diagnostic,
medical innovations inventions, and professional recommendations. (Quality Assurance
Manual, 2012)
Note: Some of the above services have to be approved before accessing service.
80
Services that require prior fund approval
The list includes the following services:
CT – Scan (with or without contrast), MRI , Dialysis services, Anti – cancer Medicines,
and Immunosuppressant and Immunostimulants, Intraocular Coherence Tomography
(IOCT) , Complex Implants , Few selected medicines , EMG needle ,Medical and
orthopedic appliance.
4.3.1 Excluded benefits
NHIF has been enhancing the Benefits Package for its beneficiaries from time to time
depending on the capability of the Fund as determined by Actuarial studies. However,
there are some services which are not covered by the Fund which are generally grouped
into 4 major types: i. Services covered by the Government through special programs ii.
Services that are a breach of Government Laws iii. Services that are covered by other
Ministries and Government organs iv. Services that are a luxury (e.g. cosmetic
procedures)
Services that are not enlisted in the NHIF benefits package are therefore the
responsibility of the Government, employer or the patient. They are stipulated in the
National Health Insurance Fund Act of Cap 395, R.E 2002- Section 17, as amended by
Act no. 25 of 2002.
These include:
i. All diseases covered by National vertical Programs such as Vaccinations, ARV
medicines, TB and Leprosy ii. Cosmeticsurger yiii. Prosthetics organs such as limbs, and
artificial teeth iv. Travel costs to and from referral facilities and subsistence allowances
while treated outside working station v. Disease outbreaks and calamities VI.
Compensation for partial or total incapacitation which is covered under the Scheme. vii.
Any medicines and procedures not included in the Fund‘s price schedule viii. Medical
treatment outside Tanzania ix. Mortuary and burial services x. Wheel chairs and
tricycles xi. Transport costs to and from a health facility
81
The NHIF operates in an environment that is governed by, various national sectorial
policies and guidelines including the National Health Policy/NHP (2007), Primary
Health Care Development Programs (PHCDP/MMAM) 2007-2017, Big Results Now-
Health (BRN-H), Standard Treatment Guidelines and NEMLIT and Health Sector
Strategic Plan (HSSP IV). These policies and guidelines provide strategic direction of
the health sector in the Country. During the life span of this Strategic Plan, NHIF will
strive to operate within the provisions of these policies, plans and guidelines
The NHIF Act section 30 (j) empowers the Board of Directors to review and make some
improvements to the benefit package, including views of the rates used to reimburse the
health care providers.
4.4 The contents of NHIF Benefit Package are comprehensive to suit for
beneficiaries needs
In identifying and evaluating whether the contents of NHIF Benefit Package are
comprehensive to suit for beneficiaries needs the researcher collected information from
300 NHIF members. The aim for this objective was to establish whether NHIF members
are aware on the NHIF benefit packages and whether the identified packages fit their
needs. The respondents were required to mention NHIF benefit packages they are aware
of, also they were required to agree, disagree strongly agree and strongly disagree on
different packages to whether they fits to their needs. The details of the findings are
presented below;
4.4.1 NHIF benefit packages as identified by NHIF members
The findings showed that NHIF members were able to evaluate NHF benefit packages as
shown in table 4.2 below. The NHIF packages mentioned were outpatient services
Investigations, medicines and consumables, Inpatient services, medical/orthopedic
appliances, dental and oral health services and surgical services. However other NHIF
benefit packages were not mentioned by NHIF members, the services which were not
mentioned are Physiotherapy and rehabilitative services, ophthalmological services,
optical services, retiree‘s health service. One of the Respondents explained, “I am only
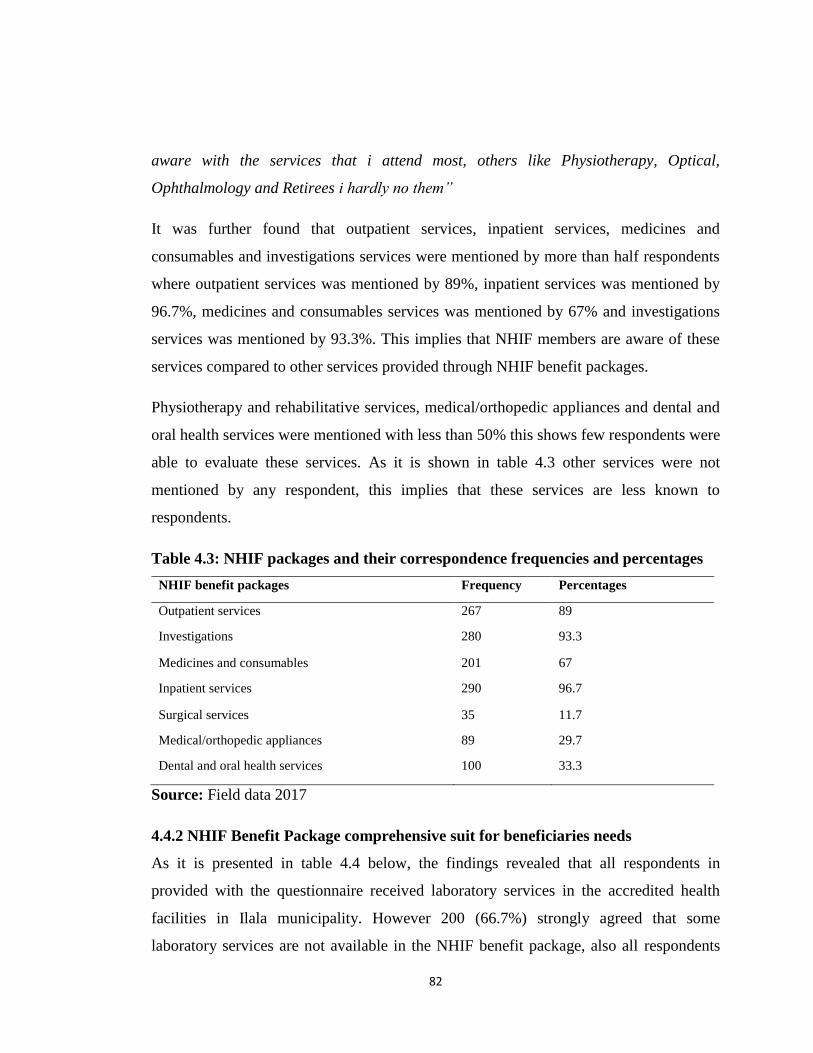
82
aware with the services that i attend most, others like Physiotherapy, Optical,
Ophthalmology and Retirees i hardly no them”
It was further found that outpatient services, inpatient services, medicines and
consumables and investigations services were mentioned by more than half respondents
where outpatient services was mentioned by 89%, inpatient services was mentioned by
96.7%, medicines and consumables services was mentioned by 67% and investigations
services was mentioned by 93.3%. This implies that NHIF members are aware of these
services compared to other services provided through NHIF benefit packages.
Physiotherapy and rehabilitative services, medical/orthopedic appliances and dental and
oral health services were mentioned with less than 50% this shows few respondents were
able to evaluate these services. As it is shown in table 4.3 other services were not
mentioned by any respondent, this implies that these services are less known to
respondents.
Table 4.3: NHIF packages and their correspondence frequencies and percentages
NHIF benefit packages Frequency Percentages
Outpatient services 267 89
Investigations 280 93.3
Medicines and consumables 201 67
Inpatient services 290 96.7
Surgical services 35 11.7
Medical/orthopedic appliances 89 29.7
Dental and oral health services 100 33.3
Source: Field data 2017
4.4.2 NHIF Benefit Package comprehensive suit for beneficiaries needs
As it is presented in table 4.4 below, the findings revealed that all respondents in
provided with the questionnaire received laboratory services in the accredited health
facilities in Ilala municipality. However 200 (66.7%) strongly agreed that some
laboratory services are not available in the NHIF benefit package, also all respondents
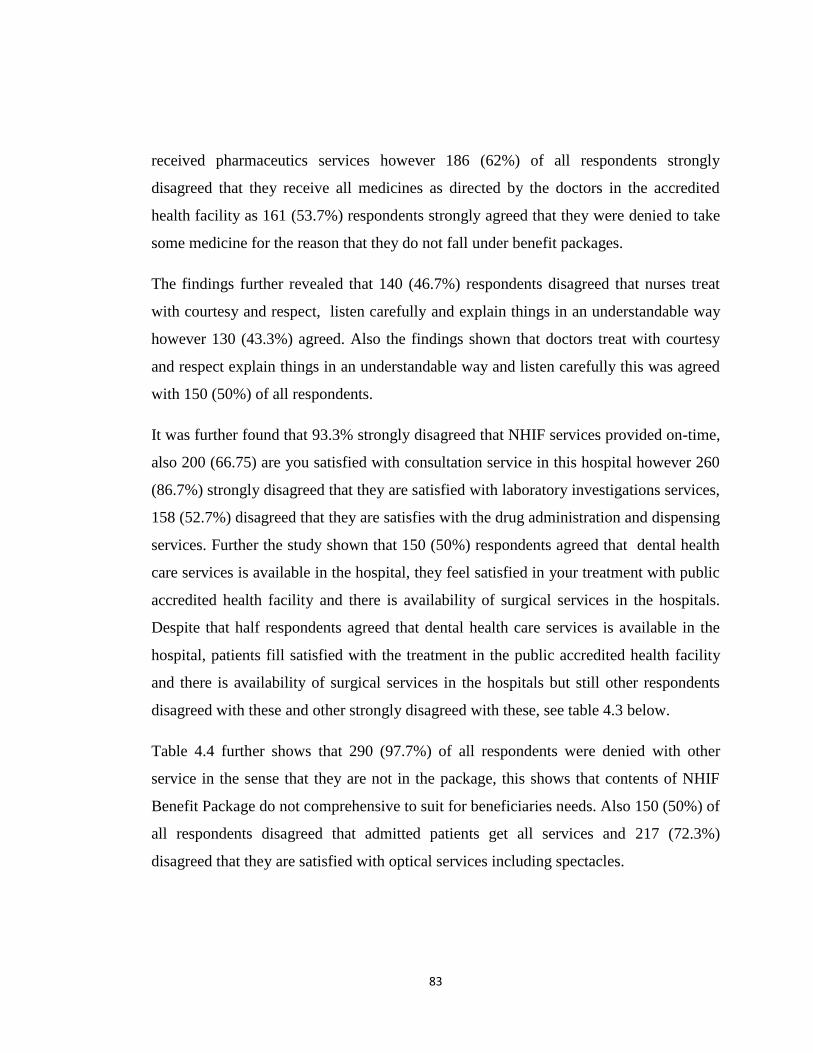
83
received pharmaceutics services however 186 (62%) of all respondents strongly
disagreed that they receive all medicines as directed by the doctors in the accredited
health facility as 161 (53.7%) respondents strongly agreed that they were denied to take
some medicine for the reason that they do not fall under benefit packages.
The findings further revealed that 140 (46.7%) respondents disagreed that nurses treat
with courtesy and respect, listen carefully and explain things in an understandable way
however 130 (43.3%) agreed. Also the findings shown that doctors treat with courtesy
and respect explain things in an understandable way and listen carefully this was agreed
with 150 (50%) of all respondents.
It was further found that 93.3% strongly disagreed that NHIF services provided on-time,
also 200 (66.75) are you satisfied with consultation service in this hospital however 260
(86.7%) strongly disagreed that they are satisfied with laboratory investigations services,
158 (52.7%) disagreed that they are satisfies with the drug administration and dispensing
services. Further the study shown that 150 (50%) respondents agreed that dental health
care services is available in the hospital, they feel satisfied in your treatment with public
accredited health facility and there is availability of surgical services in the hospitals.
Despite that half respondents agreed that dental health care services is available in the
hospital, patients fill satisfied with the treatment in the public accredited health facility
and there is availability of surgical services in the hospitals but still other respondents
disagreed with these and other strongly disagreed with these, see table 4.3 below.
Table 4.4 further shows that 290 (97.7%) of all respondents were denied with other
service in the sense that they are not in the package, this shows that contents of NHIF
Benefit Package do not comprehensive to suit for beneficiaries needs. Also 150 (50%) of
all respondents disagreed that admitted patients get all services and 217 (72.3%)
disagreed that they are satisfied with optical services including spectacles.

84
As it is presented above it seems that there are services required by NHIF members
which are not in the NHIF benefit packages, also despite that many services have been
mentioned as NHIF benefit packages but NHIF members are denied to take some
medicines and laboratory investigations being told that , those services are not in the
NHIF benefit packages, this could be due to the nature of the health facility as according
to NHIF guidelines each health level have specific services to offer to patients and other
services are offered by the higher health facility. Responder no 70 narrated,
“…Sometimes we are even denied to access some of the service by health workers and
we are told that that service is not in the package!”
85
Table 4.4: NHIF Benefit Package comprehensive suit for beneficiaries needs
Variables Strongly
agree
Agree Disagree Strongly
disagree
Receive laboratory services in the
accredited health facility
300 (100%)
Some laboratory services are not
available in the NHIF benefit package
200 (66.7%) 50 (16.7%) 37 (12.3%) 13 (4.3%)
Receive pharmaceutics services 300 (100%)
Receive all medicines as directed by
the doctors in the accredited health
facility
19 (6.3%) 14 (4.7%) 81 (27%) 186 (62%)
Denied to take some medicine for the
reason that they do not fall under
benefit package
161 (53.7%)
9 (3%) 120 (40%) 10 (3.3%)
Public Health Facilities provides
individual oriented attention to NHIF
beneficiaries.
60 (20%) 40 (13.3%) 129 (43%) 71 (23.7%)
Nurses treat with courtesy and respect,
listen carefully
and explain things in an
understandable way
10 (3.3%) 130 (43.3%) 140 (46.7%) 20 (6.7%)
Doctors treat with courtesy and
respect, explain things in an
understandable way and listen
carefully
20 (6.7%) 150 (50%) 130 (43.3%)
NHIF service provided on-time 20 (6.7%) 280 (93.3%)
Are you satisfied with consultation
service in this hospital
100 (33.3%) 200 (66.7%)
Satisfied with laboratory
investigations services
260 (86.7%) 40 (13.3%)
Satisfies with the drug administration
and dispensing services
42 (14%) 158 (52.7%) 30 (10%) 70 (23.3%)
Dental health care services available
in this hospital
20 (6.7%) 150 (50%) 130 (43.3%)
Feel satisfied in your treatment with
public accredited health facility
10 (3.3%) 150 (50%) 140 (46.7%)
Surgical services are available 100 (33.3%) 150 (50%) 50 (16.7%)
Satisfied with optical services
including spectacles services
33 (11%) 20 (6.7%) 217 (72.3%) 30 (10%)
Admitted patients get all services 75 (25%) 75 (25%) 150 (50%)
Patients receive all physiotherapy and
rehabilitative services
20 (6.7%) 171 (57%) 100 (33.3%) 9 (3%)
Denied other service in the sense that
they are not in the package
10 (3.3%) 290 (96.7%)
Source: Field data 2017
86
Evaluate the views and perception of the beneficiaries on the NHIF benefit packages
provided as to whether they have comprehensive coverage in terms of quality
In evaluating the views and perception of the beneficiaries on the NHIF benefit packages
provided as to whether they have comprehensive coverage in terms of quality the
researcher used a questionnaire to collect information from NHIF members
(beneficiaries). The aim for this objective is to evaluate whether the benefit packages
provided in different accredited hospitals in Ilala municipality have comprehensive
coverage in terms of quality. The details of the responses are provided in table 4.4.
As it is provided in table 4.5, the findings revealed that public Health Facilities provides
individual oriented attention to NHIF beneficiaries, this was agreed by 233 (77.7%) of
all respondents, however 180 (60%) strongly disagreed that NHIF service are provided
on-time. It was further agreed by 204 (68%) that cconsultation services is provided by
doctors and patients are satisfied, however 200 (66.7%) disagreed that laboratory
services are clear and provided on time. The findings further agreed that drug
administration and dispensing services are provided to all patients.
More than half respondents 168 (89.3%) strongly disagreed that there is availability of
medicine in the hospitals and 290 (96.7%) strongly disagreed that there are enough
doctors to provide services to all patients. The findings further agreed that dental health
care services is available in this hospital and patients feel satisfied in your treatment with
public accredited health facility this was agreed by 201 (67%) and 207 (69%)
respectively.
Patients disagreed that Health service provider able to provide quality healthcare NHIF
clients, dental and oral health are available and provided with high quality and patients
satisfy with eyes treatments in the hospital the correspondence frequency and
percentages found were 159 (53%), 160 (53.3%) and 129 (43%)‘ respectively, it was
further strongly disagreed that beds for impatient services are good, clean and of high
quality, however 2014 respondents agreed that surgical services are provided to all
required patients.
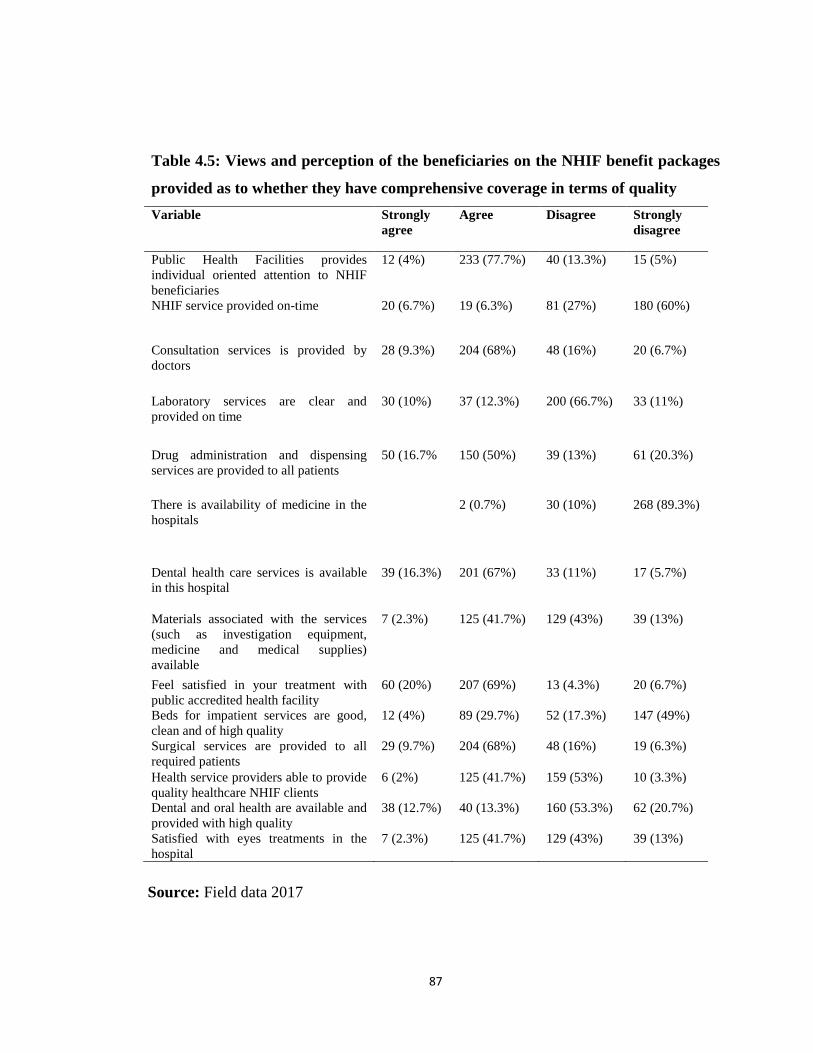
87
Table 4.5: Views and perception of the beneficiaries on the NHIF benefit packages
provided as to whether they have comprehensive coverage in terms of quality
Variable Strongly
agree
Agree Disagree Strongly
disagree
Public Health Facilities provides
individual oriented attention to NHIF
beneficiaries
12 (4%) 233 (77.7%) 40 (13.3%) 15 (5%)
NHIF service provided on-time 20 (6.7%) 19 (6.3%) 81 (27%) 180 (60%)
Consultation services is provided by
doctors
28 (9.3%) 204 (68%) 48 (16%) 20 (6.7%)
Laboratory services are clear and
provided on time
30 (10%) 37 (12.3%) 200 (66.7%) 33 (11%)
Drug administration and dispensing
services are provided to all patients
50 (16.7% 150 (50%) 39 (13%) 61 (20.3%)
There is availability of medicine in the
hospitals
2 (0.7%) 30 (10%) 268 (89.3%)
Dental health care services is available
in this hospital
39 (16.3%) 201 (67%) 33 (11%) 17 (5.7%)
Materials associated with the services
(such as investigation equipment,
medicine and medical supplies)
available
7 (2.3%) 125 (41.7%) 129 (43%) 39 (13%)
Feel satisfied in your treatment with
public accredited health facility
60 (20%) 207 (69%) 13 (4.3%) 20 (6.7%)
Beds for impatient services are good,
clean and of high quality
12 (4%) 89 (29.7%) 52 (17.3%) 147 (49%)
Surgical services are provided to all
required patients
29 (9.7%) 204 (68%) 48 (16%) 19 (6.3%)
Health service providers able to provide
quality healthcare NHIF clients
6 (2%) 125 (41.7%) 159 (53%) 10 (3.3%)
Dental and oral health are available and
provided with high quality
38 (12.7%) 40 (13.3%) 160 (53.3%) 62 (20.7%)
Satisfied with eyes treatments in the
hospital
7 (2.3%) 125 (41.7%) 129 (43%) 39 (13%)
Source: Field data 2017

88
4.5 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages
In evaluating the status and capabilities of the selected accredited health facilities in
fulfilling the requirements of the NHIF Benefit Packages, the questionnaire was
provided to NHIF staff and NHIF accredited health care providers. The aim for this
objective was to measure whether accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages. The questionnaire was distributed to 10
respondents.
4.5.1 Status and capabilities of the selected accredited health facilities in fulfilling
the requirements of the NHIF Benefit Packages as findings from health facilities
The findings revealed that all accredited health care facilities were given the Benefit
Package and the price list before they started giving services. It was strongly disagreed
that accredited health facilities were trained on Benefit Package on how it should be
implemented, also it was strongly disagreed that staff have knowledge about the rights
and benefits of the NHIF members, respondents further strongly disagreed that facility
has adequate workers as per staff establishment (IKAMA) requirement of its level,
respondents further disagreed that all the services as stipulated in the package are
provided and there is sufficient diagnostic equipment in the health facilities the
corresponding frequencies and percentages were 6 (60%), 5 (50%), 6 (60%), 8 (80%)
and 5 (50%) respectively. See table 4.6 below.
The findings further revealed that more than half respondents as shown in table 4.4
below strongly agreed that health facilities have adequate stock of laboratory reagents,
qualified and experienced laboratory staff, conduct surgical services, serve the NHIF
members at your facility on-time without delaying compared to non-NHIF members and
serve the NHIF members with the entire contracted benefits package at your facility
their corresponding percentages were 7 (70%), 10 (100%), 10 (100%), 10 (100%) and
10 (100%) respectively.

89
However 5 (50%) are able to implement ophthalmology services as stipulated in the
NHIF and price list and 10 (100%) are able to implement diagnostic equipment services
like Xray, CT Scan, MRI as stipulated in NHIF benefit package and price list.
It was further disagreed that there is separate window/ area that used to save only NHIF
beneficiaries, also 5 (50%) strongly disagreed that there is an adequate stock of
Medicine and medical consumable as stipulated in NHIF price list. See table 4.6
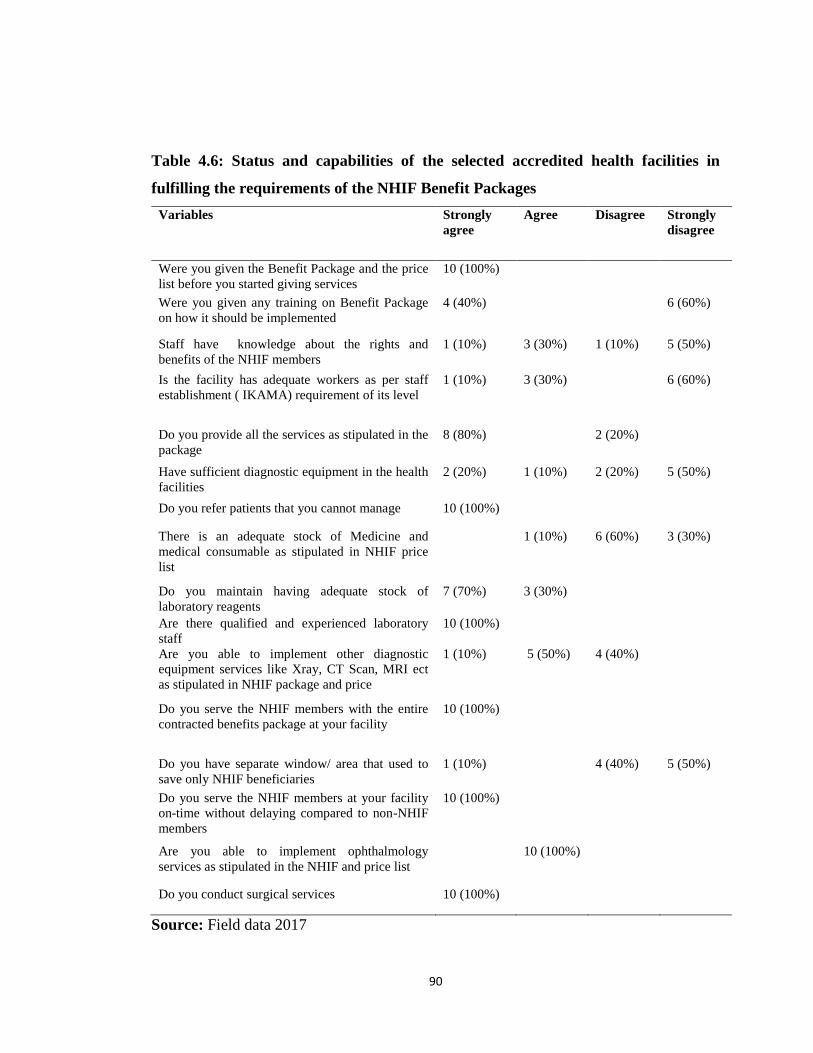
90
Table 4.6: Status and capabilities of the selected accredited health facilities in
fulfilling the requirements of the NHIF Benefit Packages
Variables Strongly
agree
Agree Disagree Strongly
disagree
Were you given the Benefit Package and the price
list before you started giving services
10 (100%)
Were you given any training on Benefit Package
on how it should be implemented
4 (40%) 6 (60%)
Staff have knowledge about the rights and
benefits of the NHIF members
1 (10%) 3 (30%) 1 (10%) 5 (50%)
Is the facility has adequate workers as per staff
establishment ( IKAMA) requirement of its level
1 (10%) 3 (30%) 6 (60%)
Do you provide all the services as stipulated in the
package
8 (80%) 2 (20%)
Have sufficient diagnostic equipment in the health
facilities
2 (20%) 1 (10%) 2 (20%) 5 (50%)
Do you refer patients that you cannot manage 10 (100%)
There is an adequate stock of Medicine and
medical consumable as stipulated in NHIF price
list
1 (10%) 6 (60%) 3 (30%)
Do you maintain having adequate stock of
laboratory reagents
7 (70%) 3 (30%)
Are there qualified and experienced laboratory
staff
10 (100%)
Are you able to implement other diagnostic
equipment services like Xray, CT Scan, MRI ect
as stipulated in NHIF package and price
1 (10%) 5 (50%) 4 (40%)
Do you serve the NHIF members with the entire
contracted benefits package at your facility
10 (100%)
Do you have separate window/ area that used to
save only NHIF beneficiaries
1 (10%) 4 (40%) 5 (50%)
Do you serve the NHIF members at your facility
on-time without delaying compared to non-NHIF
members
10 (100%)
Are you able to implement ophthalmology
services as stipulated in the NHIF and price list
10 (100%)
Do you conduct surgical services 10 (100%)
Source: Field data 2017
91
4.5.2 Status and capabilities of the selected accredited health facilities in fulfilling
the requirements of the NHIF Benefit Packages as findings from NHIF staff
In evaluating the status and capabilities of the selected accredited health facilities in
fulfilling the requirements of the NHIF Benefit Packages, questionnaire were provided
to NHIF staff in order to see whether the accredited health facilities are capable in
fulfilling the requirements of NHIF benefits packages. The findings are detailed
presented below;
The findings shown that 6 (60%) Health facilities have enough workers as per approved
staff establishment requirement of its level; also it was disagreed with 6 (60%)
respondents that different health facilities provide all services as stipulated in the
package. The same information was communicated by the NHIF staff as one of the staff
members stated that:
ooooh workers shortage in the accredited health facility is becoming a serious
problem, it is unfortunately that many accredited health facility insufficient
workers as per approved staff establishment, also accredited health facility do
not provide all services as stipulated in the package. This could be resulted by
competent and sufficient health workers or insufficient tools.
Despite that the same question was asked to the accredited health facility and they
agreed that they have sufficient workers but NHIF staff stated that the accredited lower
level facilities in public sectors, private and faith based organization do not have
sufficient number of staff in almost all cadres.
The findings further revealed that more than half of the respondents 8 (80%) health
providers fulfill all requirements before they are accredited also 10 (100%) strongly
agreed that during accreditations do you provide NHIF compliance rules to the services
provision, SOP, other claim forms and the contract terms.
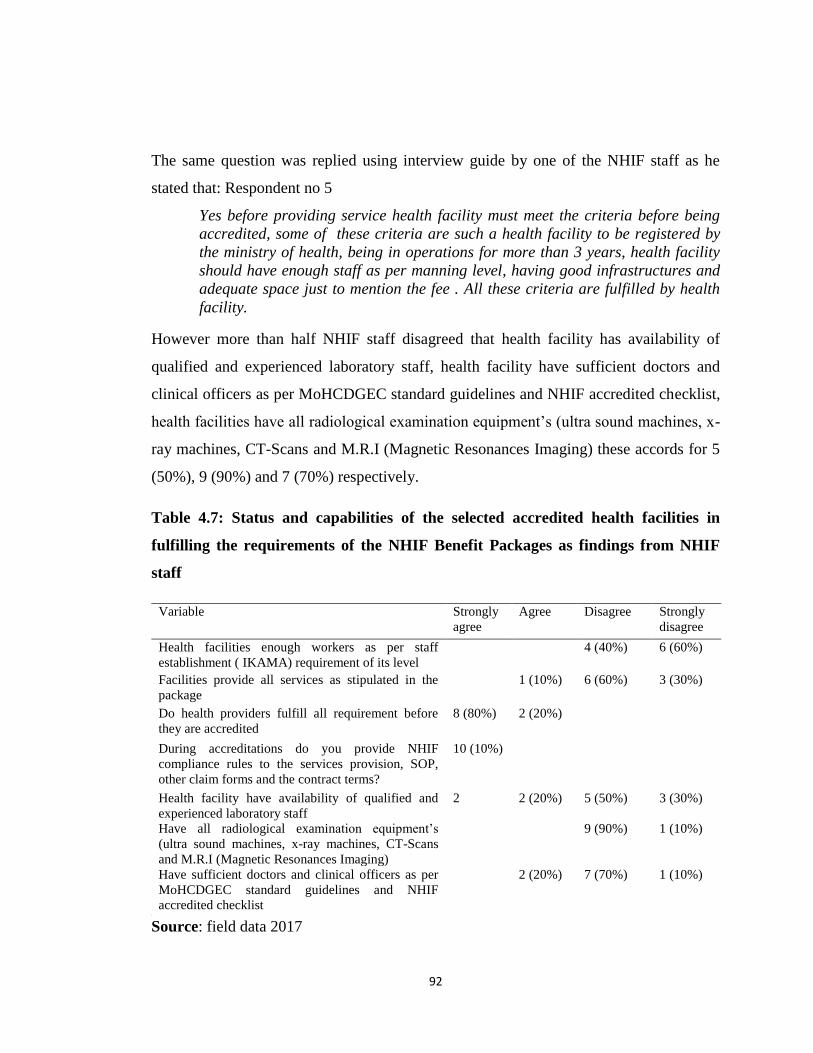
92
The same question was replied using interview guide by one of the NHIF staff as he
stated that: Respondent no 5
Yes before providing service health facility must meet the criteria before being
accredited, some of these criteria are such a health facility to be registered by
the ministry of health, being in operations for more than 3 years, health facility
should have enough staff as per manning level, having good infrastructures and
adequate space just to mention the fee . All these criteria are fulfilled by health
facility.
However more than half NHIF staff disagreed that health facility has availability of
qualified and experienced laboratory staff, health facility have sufficient doctors and
clinical officers as per MoHCDGEC standard guidelines and NHIF accredited checklist,
health facilities have all radiological examination equipment‘s (ultra sound machines, x-
ray machines, CT-Scans and M.R.I (Magnetic Resonances Imaging) these accords for 5
(50%), 9 (90%) and 7 (70%) respectively.
Table 4.7: Status and capabilities of the selected accredited health facilities in
fulfilling the requirements of the NHIF Benefit Packages as findings from NHIF
staff
[
Source: field data 2017
Variable Strongly
agree
Agree Disagree Strongly
disagree
Health facilities enough workers as per staff
establishment ( IKAMA) requirement of its level
4 (40%) 6 (60%)
Facilities provide all services as stipulated in the
package
1 (10%) 6 (60%) 3 (30%)
Do health providers fulfill all requirement before
they are accredited
8 (80%) 2 (20%)
During accreditations do you provide NHIF
compliance rules to the services provision, SOP,
other claim forms and the contract terms?
10 (10%)
Health facility have availability of qualified and
experienced laboratory staff
2 2 (20%) 5 (50%) 3 (30%)
Have all radiological examination equipment‘s
(ultra sound machines, x-ray machines, CT-Scans
and M.R.I (Magnetic Resonances Imaging)
9 (90%) 1 (10%)
Have sufficient doctors and clinical officers as per
MoHCDGEC standard guidelines and NHIF
accredited checklist
2 (20%) 7 (70%) 1 (10%)
93
4.6 Compliance of the selected accredited health facilities with the accreditation
criteria
In evaluating the extent to which the selected accredited health facilities comply with the
accreditation criteria as provided for by MoHCDGEC standard guidelines and NHIF
accredited checklist, the questionnaire was used to collect information from 10
accredited health facilities, the aim was to establish whether the health facilities comply
with MoHCDGEC standard guidelines and NHIF accredited checklist. The findings are
presented in chapter 4.8 below.
The findings revealed that more respondents strongly agreed that they started providing
service in more than three years ago, health facilities were registered with the Ministry
of Health and Social Welfare (MoHCDGEC) and they had the original registration
certificate. The findings further shown that they have e Practicing Registration/License
of practitioners and they were accredited by NHIF to provide service for its members,
they also had accreditation numbers. Also the findings revealed that the facilities were
inspected before being accredited, they had reliable source of electricity energy and they
were given a copy of contract immediately after being signed by both parties. See table
4.8 below.
The findings further disagreed that there are clean and well painted walls, with washable
paint on the inside, also floors are even and easy to clean with antiseptics, they also they
disagreed that rooms are well ventilated allowing adequate natural light, it was strongly
disagreed that health facilities have sufficient doctors and clinical officers as per
MoHCDGEC standard guidelines and NHIF accredited checklist. See table 4.8 below.
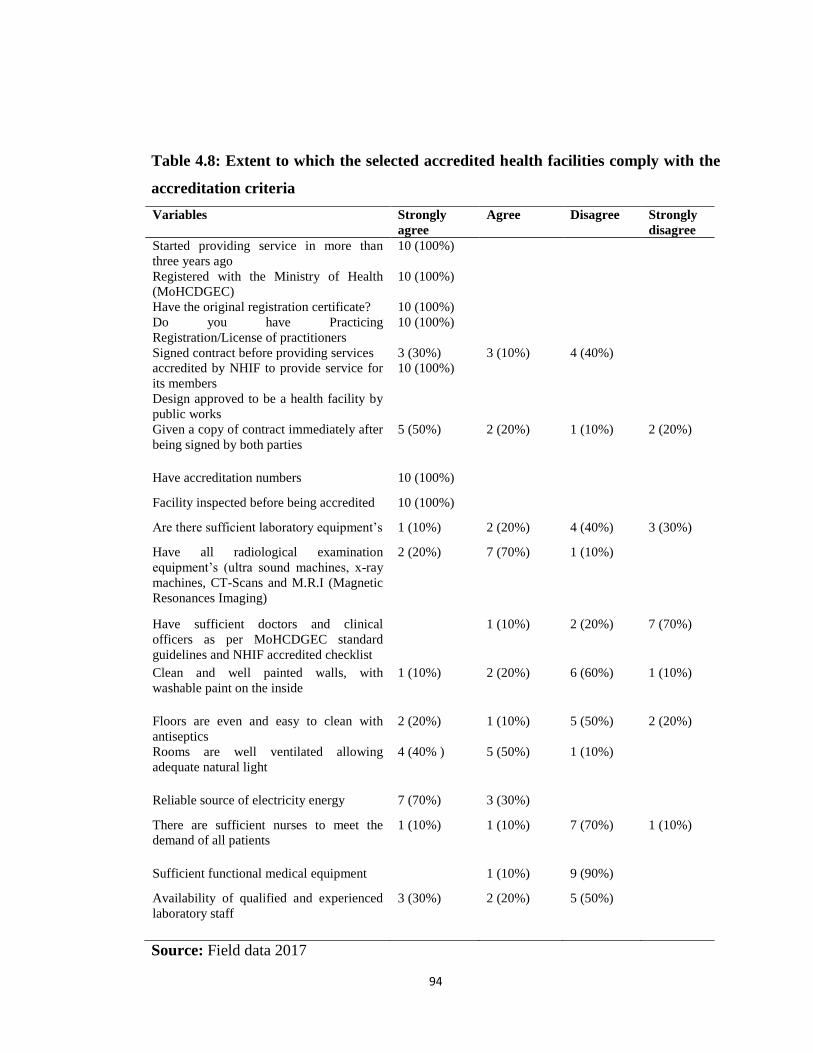
94
Table 4.8: Extent to which the selected accredited health facilities comply with the
accreditation criteria
Variables Strongly
agree
Agree Disagree Strongly
disagree
Started providing service in more than
three years ago
10 (100%)
Registered with the Ministry of Health
(MoHCDGEC)
10 (100%)
Have the original registration certificate? 10 (100%)
Do you have Practicing
Registration/License of practitioners
10 (100%)
Signed contract before providing services 3 (30%) 3 (10%) 4 (40%)
accredited by NHIF to provide service for
its members
10 (100%)
Design approved to be a health facility by
public works
Given a copy of contract immediately after
being signed by both parties
5 (50%) 2 (20%) 1 (10%) 2 (20%)
Have accreditation numbers 10 (100%)
Facility inspected before being accredited 10 (100%)
Are there sufficient laboratory equipment‘s 1 (10%) 2 (20%) 4 (40%) 3 (30%)
Have all radiological examination
equipment‘s (ultra sound machines, x-ray
machines, CT-Scans and M.R.I (Magnetic
Resonances Imaging)
2 (20%) 7 (70%) 1 (10%)
Have sufficient doctors and clinical
officers as per MoHCDGEC standard
guidelines and NHIF accredited checklist
1 (10%) 2 (20%) 7 (70%)
Clean and well painted walls, with
washable paint on the inside
1 (10%) 2 (20%) 6 (60%) 1 (10%)
Floors are even and easy to clean with
antiseptics
2 (20%) 1 (10%) 5 (50%) 2 (20%)
Rooms are well ventilated allowing
adequate natural light
4 (40% ) 5 (50%) 1 (10%)
Reliable source of electricity energy 7 (70%) 3 (30%)
There are sufficient nurses to meet the
demand of all patients
1 (10%) 1 (10%) 7 (70%) 1 (10%)
Sufficient functional medical equipment 1 (10%) 9 (90%)
Availability of qualified and experienced
laboratory staff
3 (30%) 2 (20%) 5 (50%)
Source: Field data 2017
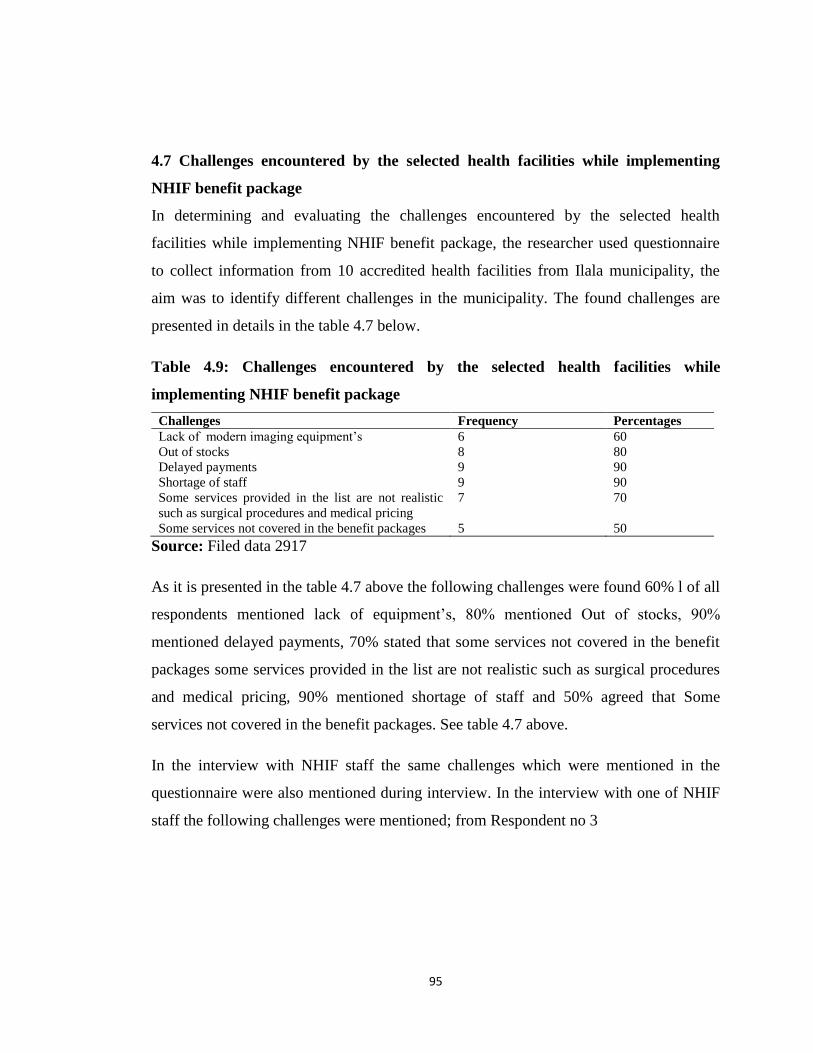
95
4.7 Challenges encountered by the selected health facilities while implementing
NHIF benefit package
In determining and evaluating the challenges encountered by the selected health
facilities while implementing NHIF benefit package, the researcher used questionnaire
to collect information from 10 accredited health facilities from Ilala municipality, the
aim was to identify different challenges in the municipality. The found challenges are
presented in details in the table 4.7 below.
Table 4.9: Challenges encountered by the selected health facilities while
implementing NHIF benefit package
Challenges Frequency Percentages
Lack of modern imaging equipment‘s 6 60
Out of stocks 8 80
Delayed payments 9 90
Shortage of staff 9 90
Some services provided in the list are not realistic
such as surgical procedures and medical pricing
7 70
Some services not covered in the benefit packages 5 50
Source: Filed data 2917
As it is presented in the table 4.7 above the following challenges were found 60% l of all
respondents mentioned lack of equipment‘s, 80% mentioned Out of stocks, 90%
mentioned delayed payments, 70% stated that some services not covered in the benefit
packages some services provided in the list are not realistic such as surgical procedures
and medical pricing, 90% mentioned shortage of staff and 50% agreed that Some
services not covered in the benefit packages. See table 4.7 above.
In the interview with NHIF staff the same challenges which were mentioned in the
questionnaire were also mentioned during interview. In the interview with one of NHIF
staff the following challenges were mentioned; from Respondent no 3
96
Most of the health facilities lack diagnostic equipment services like X-ray, CT
Scan, MRI reason behind lacking these equipment could be due to the financial
capability in some of the health facilities, availability of competent and sufficient
health workers in the health facilities and the level of the health facilities.
Regarding the stated above it can be noted that lack of modern diagnostic equipment is
one of the major challenges facing Health facilities.
Also in the interview with one of the Health provider (R number 10) it was noted that:
.delay in the payment from NHIF leads to most of the hospitals in Ilala
municipality experiences Medicine Out of Stock as some of the health facilities
especially FBO and Private Health facilities uses the % of reimbursement from
NHIF in order to purchase medicine and other medical consumables
Also in the interview it was noted that services provided in the list are not realistic with
the price list of NHIF such services are like surgical procedures and medical pricing, it
was found that these services are provided with high price while the price provided by
NHIF is small this might be causing some of the health facilities fail to provide these
service since they see as a loss to them.
One of the respondent (Respondent 1) explained;
This guys from NHIF is as if they don’t realize the price they are using to refund
for the service we give their clients is not realist, if you look at some of the
surgical procedures, prices for some of the medicines you will see, it is very low
compared to the actual market price..........How could you imagine to run the
services in this way!
Also other respondents narrate;“……. Sometimes it takes more than 1 hour or so to
access for medical service in this facility, they have shortage of staff but the providers
they don’t accept to take this challenge positively and hire more staff’

97
Besides the Findings presented above, this Chapter also narrates on other information
based on Benefit Packages of other countries.
4.8 Other Benefits Packages as implemented in other Countries
The National Health Insurance Scheme (NHIS) of Ghana was established under Act 650
of 2003 by the Government of Ghana to provide basic healthcare services to persons
resident in the country through mutual and private health insurance schemes. The
District Mutual, Private Mutual and Private Commercial Schemes are regulated by the
National Health Insurance Authority (NHIA).
Types of Benefits Comprehensive
The basic benefits package is fairly extensive and purports to cover 95% of all health
problems reported in Ghanaian health care facilities, though there is a noticeable
emphasis on female reproductive health. Expensive, highly specialized care such as
dialysis and organ transplants are not covered by the NHIS. ARVs for the treatment of
HIV/AIDS are also not covered as these drugs are supplied by a separate government
program.
The health services covered by the NHIS are laid out in the minimum basic benefits
package. The list also delineates prescribed medicines. Benefits for maternity care
include antenatal care, caesarean sections, and postnatal care for up to six months after
birth. Treatment for breast and cervical cancer are included in the package, although
Services that are included in Benefit Package includes i) Outpatient services ii) Inpatient
services iii) Oral health iv) Maternity care v) Emergencies as ofMedical emergencies,
Surgical emergencies, Pediatric emergencies, Obstetric and gynecological emergencies,
Road traffic accident.
98
Exclusions list
Appliance and prostheses including optical aids, heart aids, orthopedic aids, dentures,
etc. Cosmetic surgeries and aesthetic treatment, HIV retroviral drugs, Assisted
reproduction (e.g., artificial insemination) and gynecological hormone replacement
therapy, Echocardiography, Photography and angiography, Dialysis for chronic renal
failure, Organ transplantation, All drugs not listed on the NHIS list, Heart and brain
surgery other than those resulting from accidents, Cancer treatment other than breast and
cervical, Mortuary services, Diagnosis and treatment abroad, Medical examinations for
purposes other than treatment in accredited health facilities, VIP ward accommodation.
National Hospital Insurance Fund - Kenya
National Hospital Insurance Fund is a State Parastatal that was established in 1966 as a
department under the Ministry of Health. The original NHIF Act of Parliament that set
up this Fund in 1966 has over the years been reviewed to accommodate the changing
healthcare needs of the Kenyan population, employment and restructuring in the health
sector. Currently an NHIF Act No 9 of 1998 governs the Fund. The transformation of
NHIF from a department of the Ministry of Health to a state of corporation was aimed at
improving effectiveness and efficiency. The Fund‘s core mandate is to provide medical
insurance cover to all its members and their declared dependents (spouse and
children).National Hospital Insurance Fund (NHIF) | Health in Kenya
https://softkenya.com/health/national-hospital-insurance-fund-nhif
Under Civil Servant schemes, Benefit Package under NHIF Kenya includes;
i) Inpatient cover ii) Outpatient cover
All necessary outpatient medical treatment and services provided by or on the order of a
clinical to the member when admitted to an NHIF Accredited Hospital offering services
under levels as defined by the Kenya Essential Package for Health (KEPH).The
outpatient cover shall include but is not limited to:

99
i) Consultation, ii) Laboratory investigations, iii) Drug administration and dispensing,
iv) Dental health care services, v) Radiological examination, vi)Nursing and midwifery
services, vii) Minor surgical services, viii) Physiotherapy services, ix) Optical care, x)
Occupational therapy services xi) Referral for specialized services, xii) Any other
benefit as approved by the NHIF Board of management
iii) Maternity cover and reproductive health
The benefits package in Rwanda - Mutuelles de Sante
The benefits package in Rwanda has two primary parts: the Minimum Package of
Activities (MPA) and the Complementary Package of Activities (CPA). The MPA
covers all services and drugs provided at the health centers including pre- and post-natal
care, vaccinations, family planning, minor surgical operations, and essential and generic
drugs. All individuals in Rwanda with health insurance are entitled to comprehensive,
subsidized preventative care through the MPA. The CPA covers a limited number of
services at the district hospitals, including the cost of hospitalization, caesarian
operations, minor and major surgical operations, medical imaging, and all diseases
afflicting children ages 0 to 5 years. As of 2006, the CPA benefits package was extended
to cover select services in national hospitals. In order to receive these benefits,
individuals must be referred from the health centers to district or national level hospitals.
Mutuelle members are entitled to comprehensive benefits for primary care, secondary
care, and tertiary care provided through public or private non-profit contracted facilities.
The scheme provides basic services such as family planning, pre-natal care,
consultations, basic laboratory examinations, generic drugs, and hospital treatment. All
medications from hospitals are also included in the benefits.
For those covered under RAMA, benefits include all the major preventative services in
addition to all curative services and pharmaceuticals. The benefits package for MMI is
the same as RAMA, with the addition of prostheses coverage added under MMI.

100
Excluded are contact lenses and braces as well as cosmetic surgery for purely aesthetic
reasons. RAMA and MMI have signed contracts with all public health centers and
reference hospitals, as well as 16 private institutions. MMI has the added advantage of
using military hospitals, thus, individuals covered under these plans are able to access
health care benefits at almost all health centers in Rwanda.

101
CHAPTER FIVE
DISCUSSION OF THE FINDINGS
5.1 Introduction
5.2 Contents of NHIF Benefit Package are comprehensive to suit for beneficiaries
needs
As it is presented in chapter four it was found that NHIF members were able to identify
NHIF benefit packages, among of the identified benefit packages were outpatient
services Investigations, medicines and consumables, Inpatient services,
medical/orthopedic appliances, dental and oral health services and surgical services.
However other NHIF benefit packages were not identified by NHIF members, the
services which were not mentioned are Physiotherapy and rehabilitative services,
ophthalmological services, optical services, retiree‘s health service.
Despite that these services were not mentioned by NHIF members but they are within
the NHIF benefit packages, failure to mention these services could be due to the reason
that few people accessed them; another reason is that the services are provided in some
of the health facilities while in other health facilities they are not provided.
Despite that different benefit packages were identified but other services were
mentioned by more than half respondents compared to other benefit packages. The
services which were identified with more than half respondents were outpatient services,
inpatient services, medicines and consumables and investigations services while
Physiotherapy and rehabilitative services, medical/orthopedic appliances and dental and
oral health services were mentioned with less than 50% of all respondents. It seems that
the benefit packages mentioned by more respondents are used more by different patients
compared to the ones mentioned by few respondents.
102
As it is presented in chapter four the findings revealed that most benefit packages
provided by NHIF do not fit the beneficiaries need, few packages fits the beneficiaries
need, this was due to the reason that NHIF members disagreed and strongly disagreed
that they receive all services as they are denied to take some services in the sense that
the services are not within NHIF benefit packages.
The findings revealed that respondents strongly agreed that some laboratory services are
not available in the NHIF benefit package, they also strongly disagreed that they receive
all medicines as directed by the doctors in the accredited health facility as 161 (53.7%)
respondents strongly agreed that they were denied to take some medicine for the reason
that they do not fall under benefit packages. It was further strongly disagreed that NHIF
services provided on-time, also 260 (86.7%) strongly disagreed that they are satisfied
with all laboratory investigations services while 158 (52.7%) disagreed that they are
satisfies with the drug administration and dispensing services, despite the availability of
surgical services but still other respondents disagreed that they receive the services, as
they are told to pay for the services.
The reason as to why NHIF members do not receive all the services are provided in the
benefit packages could be due to the level of the health facility since according to the
NHIF guidelines each level of the health facility have specific services to offer and other
services are to be provided by the higher levels, apart from this factor, it seems some
services within the NHIF benefit packages including medicines, laboratory services and
surgical services are either not provided to a certain level of health facility or are not
within the contents of the mentioned package since most respondents were denied to
access some medicine for the reason that the services are not within the packages.
The findings corresponds to the findings by Kumburu (2015) who conducted the study
on national health insurance fund (NHIF) in Tanzania as a tool for improving universal
coverage and accessibility to health care services: case from Dar es salaam –Tanzania.
103
The study found that some of the NHIF benefits and packages services which are
supposed to be provided to NHIF members are not provided.
Despite that the above discussed services seemed not fit beneficiaries need but
consultation service in this hospital and drug administration and dispensing services fit
beneficiaries needs since the respondents agreed that they receive the services and they
are satisfied with the services.
5.3 Views and perception of the beneficiaries on the NHIF benefit packages
provided as to whether they have comprehensive coverage in terms of quality
As it is provided in chapter four it was found that more respondents disagreed that
laboratory services are clear and provided on time also it was strongly disagreed that
there is availability of all required medicine in the hospitals and enough doctors to
provide services to all patients. It was further strongly disagreed that beds for impatient
services are good, clean and of high quality, it was further strongly disagreed that dental
and oral health are available and provided with high quality and patients satisfy with
eyes treatments in the hospital and that Health service provider able to provide quality
healthcare NHIF clients.
Regarding the above statement it can be said that laboratory services, pharmaceutical
services, dental and oral services, impatient services, surgical services and availability
health service providers in the accredited health facilities they have no comprehensive
coverage in terms of quality. However cconsultation services, drug administration and
dispensing services are provided to all patients has comprehensive coverage in terms of
quality.
The reason as to why laboratory services, pharmaceutical services, dental and oral
services, impatient services, surgical services and availability health service providersdo
not have comparatively coverage in terms of quality, this could be due to the reason that
most respondents were denied the services in the sense that they are not within the
packages however this could be due the level of the health facility since.
104
Also some of the health facilities experiences Out of Stock as they have no all
medicines to offer to the patients, the patients are told to buy some of the medicine in the
private pharmacies.
5.4 Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Packages
As it is presented in chapter four part 4.5 it was strongly disagreed that accredited health
facilities were trained on Benefit Package implementation, also it was strongly disagreed
that staff have knowledge about the rights and benefits of the NHIF members,
respondents further strongly disagreed that facility has adequate workers as per staff
establishment requirement of its level, respondents further disagreed that all the services
as stipulated in the package are provided, it was also disagreed that there is sufficient
diagnostic equipment in the health facilities. This implies that most of the health
facilities are less capable in fulfilling the requirements of the NHIF Benefit Packages.
This is due to the reasons that most of the accredited health facilities were not trained on
how to use guidelines provided by NHIF, lack of training among doctors and nurses in
different accredited hospitals could be one of the reasons for poor services provided in
the accredited hospitals, lack of training also led to low knowledge among nurses and
doctors in the accredited health facilities. Inadequate workers as per staff establishment
and lack of separate window for NHIF staff in most of the health facilities in Ilala
municipality could be one of the reasons for patients to take long time waiting for the
services in the accredited health facilities.
Insufficient diagnostic equipment in the accredited health facilities led most of the health
facilities fail to implement diagnostic equipment services like Xray, CT Scan, MRI as
stipulated in NHIF package and price list, also inadequate stock of Medicine and
medical consumable as stipulated in NHIF price list challenged the capabilities of health
facilities in the selected accredited health facilities in fulfilling the requirements of the
NHIF Benefit Packages.
105
Regarding the above statements it can be said that most of the health facilities fulfills the
requirements of the NHIF Benefit Packages but not 1005% in some areas. The
incapability in the health facility could be caused by delay in the payment from NHIF to
the health facilities, budget constraints and shortage of staff
The findings further revealed that more than half respondents as shown in table 4.5
above strongly agreed that health facilities have adequate stock of laboratory reagents,
qualified and experienced laboratory staff, conduct surgical services, serve the NHIF
members at your facility on-time without delaying compared to non-NHIF members and
serve the NHIF members with the entire contracted benefits package at your facility and
different in price between the service provided and the price set by NHIF, also the
incapability is caused by the level of the health facilities since each level of the health
facility have specific services to offer as per NHIF guidelines.
As it is presented in chapter four the findings from NHIF staff in evaluating the status
and capabilities of the selected accredited health facilities in fulfilling the requirements
of the NHIF Benefit Packages revealed that Health facilities have no enough workers as
per staff establishment requirement of its level, also it was disagreed with 6 (60%)
respondents that different health facilities provide all services as stipulated in the
package. It was further disagreed by more than half NHIF staff that health facility has
availability of qualified and experienced laboratory staff, sufficient doctors and clinical
officers as per MoHCDGEC standard guidelines and NHIF accredited checklist, also it
was disagreed that health facilities have no all radiological examination equipment‘s
(ultra sound machines, x-ray machines, CT-Scans and M.R.I (Magnetic Resonances
Imaging).This implies that most of the health facilities have low status and capabilities
in fulfilling the requirements of the NHIF Benefit Packages
Despite of the incapacity shown by the accredited health facilities in providing NHIF
benefit packages, the health facilities were able to provide the benefit packages are they
provided some laboratory services, consultation services, minor surgical services and
106
pharmaceutical services, dispensing services ophthalmology services as stipulated in the
NHIF and price list. This shows that they can provide particular services basing on the
level of their health facilities.
5.5 Extent to which the selected accredited health facilities comply with the
accreditation criteria
As it is provided in chapter four in evaluating the extent to which the selected accredited
health facilities comply with the accreditation criteria as provided for by MoHCDGEC
standard guidelines and NHIF accredited checklist, the questionnaire was used to collect
information from 10 accredited health facilities, the aim was to establish whether the
health facilities comply with MoHCDGEC standard guidelines and NHIF accredited
checklist. The findings are presented in table 4.6 above.
The findings revealed that more respondents strongly agreed that they started providing
service in more than three years ago, health facilities were registered with the Ministry
of Health Community development, gender, elderly and children (MoHCDGEC) and
they had the original registration certificate. The findings further shown that they have
Practicing Registration/License of practitioners and they were accredited by NHIF to
provide service for its members, they also had accreditation numbers. Also the findings
revealed that the facilities were inspected before being accredited, they had reliable
source of electricity energy and they were given a copy of contract immediately after
being signed. This implies that the accredited health facilities complied with the
accreditation criteria‘s
However it was disagreed that there are clean and well painted walls, with washable
paint on the inside, also floors are even and easy to clean with antiseptics, they also they
disagreed that rooms are well ventilated allowing adequate natural light, it was strongly
disagreed that many health facilities have sufficient doctors and clinical officers as per
MoHCDGEC standard guidelines and NHIF accredited checklist.
107
5.6 Challenges encountered by the selected health facilities while implementing
NHIF benefit package
In determining and evaluating the challenges encountered by the selected health
facilities while implementing NHIF benefit package, the researcher used questionnaire
to collect information from 10 accredited health facilities from Ilala municipality, the
aim was to identify different challenges in the municipality. The found challenges are
presented in details in the table 4.7 above in chapter 4.
As it is presented in chapter four challenges mentioned were lack of equipment‘s, Out of
stocks, delayed payments, some services not covered in the benefit packages some
services provided in the list are not realistic such as surgical procedures and medical
pricing and shortage of staff.
Lack of modern diagnostic equipment’s
Most of the health facilities lacked diagnostic equipment services like X-ray, CT Scan,
MRI reason behind lacking these equipment could be due to the financial capability in
some of the health facilities. Also some of the facilities were observed to have this
modern diagnostic equipment‘s but could be not in operational due to either not working
or do not have the competent or sufficient health workers in their health facilities at
different level of the health facilities that could operate this equipment‘s. These tools
require competent and trained staff to operate them.
These factors were seen as might be one of the major factors for lack of operating the
services in the facilities, another reason that could be a cause of the facilities not to have
modern diagnostic equipment‘s that was seen as a challenge was due to the delay in
payment from NHIF, since most of the private facilities among other funds depended in
these fund to pay the incentives for their health workers and also increase their source of
income that helped them to buy for the equipment‘s.

108
Medicine Out of stock
Most of the hospitals in Ilala municipality experience medicine Out of Stock in most of
the times this might be due to the delay in the payment from NHIF or Out of Stock
might be caused by the bureaucratic/ prolonged procurement procedures from MSD,
especially public facilities that procure most of their medicine and medical consumables
from.
Delayed payments/ claims reimbursements
Most health facilities stated that they provide services to the health workers however
they are not paid back by NHIF on time, this might be caused by the quality checking
and verification processes conducted by NHIF officers as before payment NHIF official
are suppose to pass through all claim forms and prove beyond reasonable doubt that the
patients received services in the particular health facility, the process takes a some time
hence delay in the payment.
The findings corresponds to the findings by Kumburu (2015) who conducted the study
on national health insurance fund (NHIF) in Tanzania as a tool for improving universal
coverage and accessibility to health care services: case from Dar es salaam –Tanzania.
the findings revealed that the reimbursement of NHIF bills to health care providers take
long time contrary to NHIF reimbursement policy (within 60 working days)from when
complains were tabled. This implies that there is a delay in the payments of fund from
NHIF to accredited hospitals.
Also in the study by Ntundu (2015) it was found that 36.3% of the respondents
mentioned short of active inspection and monitoring to ensure appropriate and timely
reimbursement of funds from NHIF is one of the factor for delay payment. In addition,
20% of the respondents recommended that stakeholders to be involved in decision
making is one of the strategies to improve the NHIF service provision.

109
Further in the study by Msaki (2013) it was found that late of payments from the fund to
medical providers, lack of knowledge to members, missing items of some of the medical
services, poor quality of services, and improper facility inspection and supervision were
among the major challenges facing NHIF.
[
Unrealistic price
It was found that some of the services provided in the list are not realistic with the price
list of NHIF, such services are like surgical procedures and medical pricing, it was found
that these services are provided with high price while the price provided by NHIF is low,
this might cause some of the health facilities fail to provide these service in good quality
or not to provide them at all since they see as a loss to them. This reason goes together
with another reason that the contents of the package missing some of the important
services that are provided by health facilities but are not in the package
Shortage of Staff as per staff establishment in different Health facilities.
It was observed that most of the Health facilities especially public health facilities are
facing shortage of staff in almost all cadres, this could have been caused by either
financial constraints or unavailable competent staff who can work on specialized areas
within the facility.
Poor laboratory services
As it was observed in the study that about 200 (66.7%) of the respondents strongly
agreed that some of the laboratory services are either not available in the NHIF benefit
package or are available but are not provided in good quality, this factor could
jeopardize the provision of health services as per requirements benefit package.
110
Lack of proper training to stakeholders.
This was observed to be one of the challenges facing providers as well as beneficiaries
during the implementation of the benefit package, This was seen in 60% of the
respondents who were asked whether were they given any training on benefit package
on how it should be implemented and 50% of the respondents who were asked whether
staff have knowledge about the rights and benefit of the NHIF members
.
111
CHAPTER SIX
SUMMARY, CONCLUSION AND RECCOMENDATION
6.1 Introduction
This chapter will brief presents the summary of the findings of the study concerning
evaluation of implementation of NHIF benefit package in selected accredited health
facilities, Challenges encountered by accredited facilities and measures to address those
challenges, conclusion made, recommendation for policy implication and areas for
further research.
6.2 Conclusion
This study aimed at evaluating the implementation of national health insurance fund
(NHIF) benefit package in the selected accredited health facilities in Ilala municipality.
The main objectives of this study is to evaluate the implementation of NHIF Benefit
Package in the selected accredited health facilities in Ilala municipality, Dar es salaam-
Tanzania, specific objectives were to identify and evaluate whether the contents of NHIF
Benefit Package are comprehensive to suit for beneficiaries needs, to evaluate the views
and the perceptions of beneficiaries on the NHIF benefits package provided as to
whether they have a comprehensive coverage in terms of quality, to evaluate the status
and capabilities of the selected accredited health facilities in fulfilling the requirements
of the NHIF Benefit Package, to evaluate the extent to which the selected accredited
health facilities comply with the accreditation criteria as provided for by MoHCDGEC
standard guidelines and NHIF accredited checklist and to determine and evaluate the
challenges encountered by the selected health facilities while implementing NHIF
benefit package.
112
In relation to the first specific objective of the study, it was observed that most NHIF
members identified different contents of NHIF benefit packages which were outpatient
services Investigations, medicines and consumables, Inpatient services,
medical/orthopedic appliances, dental and oral health services and surgical services.
However other items within the contents of NHIF benefit packages were not identified
by other NHIF members, the services which were not mentioned are Physiotherapy and
rehabilitative services, ophthalmological services, optical services and retiree‘s health
service. Based on the findings, it can be concluded that though not all of the contents
within the benefit package were identified, but what i can say is that most of the benefit
packages provided by NHIF do fit the beneficiaries needs, and those few items within
the packages that were not mentioned is not that they do not fit the beneficiaries need,
but the fact that they are not frequently utilizes by beneficiaries makes them uncommon.
It is agreed that, sensitization needs to be increased for those items within the benefit
packages which were not identified by some of the beneficiaries and also strengthens
those that are well known as frequently accessed.
Regarding the second specific objective of the study, evaluating the views and the
perceptions of beneficiaries on the NHIF benefits package provided as to whether they
have a comprehensive coverage in terms of quality, the findings revealed that laboratory
services pharmaceutical services, beds for inpatient services, dental and oral health
services and optical services do not have comprehensive coverage in terms of quality
since not all health facilities especially those facility level of Health Centre and
dispensaries provide limited services of the above mentioned services or if they provide,
the quality provided is not of the best especially in the public facilities.
113
The study further revealed that there was lack of training among staff health facilities,
also there was lack of knowledge about the rights and benefits of the NHIF members,
there were inadequate workers as per staff establishment (IKAMA) requirement in the
health facilities, and there was insufficient modern diagnostic equipment in the health
facilities. This implies that most of the health facilities are not fully capable in fulfilling
the requirements of the NHIF Benefit Packages.
The findings revealed that most selected accredited health facilities comply with the
accreditation criteria since they started providing service in more than three years, they
were registered with the Ministry of Health (MoH), they had the original registration
certificate. The findings further shown that they have Practicing Registration/License of
practitioners and they were accredited by NHIF to provide service for its members, they
also had accreditation numbers. Also the findings revealed that the facilities were
inspected before being accredited, they had reliable source of electricity energy and they
were given a copy of contract immediately after being signed. This implies that the
accredited health facilities complied with the accreditation criteria‘s.
Concerning the specific objective that was meant to determine and evaluate the
challenges encountered by the selected health facilities while implementing NHIF
benefit package.
The challenges found were lack of modern diagnostic equipment‘s, Medicine out of
stock, poor laboratory services, delayed payments; some services not covered in the
benefit packages, lack of/ inadequate training of health facility staffs, some services
provided in the list are not realistic such as surgical procedures and medical pricing and
shortage of staff, low of community awareness and knowledge concerning benefit
package issues versus right and obligation of beneficiaries, shortage of space to some of
the wards in health facilities.
114
6.3 Recommendation and policy implication
Policy implications
There is a special need for the government through MOHCDGEC to prepare a new
policy which will see the establishment of price regulatory authority that set rationalize
prices and will deal with issues concerning of prices for different items in medical
services. Currently there has been and outcry and complaints from many medical
providers and other stakeholders in health sector who are either in formal, informal,
government, NGO, FBO or private sectors that involves Prices dissatisfaction. The
policy to change could be one of the solutions to minimize the complaints from
providers all over the country would reduce financial hardship on ordinary citizen.
The government through MOHCDGEC and local government authorities should set
enough budgets to attain its goal of ensuring the provision of quality health services with
adequate number of qualified staff and availability of all modern diagnostic equipment‘s
and laboratory services especially in public health facilities. This will ensure easy
accessibility and good quality of services to health services among community members
at large.
The information contained in this evaluation is intended to create opportunities for
multi-sectorial dialogue, to enhance collaborative planning efforts, and ultimately to
facilitate partnerships that will lead to an improved health systems, will sought to
provide a roadmap for optimizing health sector inputs within the context of the overall
health systems and continue to support the government through NHIF in enhancing
quality health service provision to the population of Tanzania which has achieved much
in this area, basically due to the support from stakeholders from both public and private
sectors. This has been possible due to good policies toward public-private collaboration.
115
6.4 Recommendation
Government of Tanzania through the Ministry of Health should formulate Body to
regulate medical prices in the country, so as to harmonize medical services across
facility levels and ensuring that prices of items in the Benefit Package reflect the
prevailing median market prices.
NHIF should maintain current price until costing, actuarial evaluation and market survey
is done
Medical services which are not covered by the Fund but have been proposed by health
care providers and/ or Members for inclusion, to wait for further actuarial assessment
and valuation; though the NHIF Management through its Benefit Package Committee
take note in addressing issues raised.
NHIF Board of Directors and Management should engage few but important
stakeholders during the designing stage of the package especially policy makers, users
and implementers of the package.
Ongoing program on sensitization meetings and training to staff from health facilities
and members conducted on awareness and knowledge concerning benefit package issues
versus right and obligation of beneficiaries should be emphasized.
Government and other Medical providers should strengthen their facilities so that the
problem of lack of modern diagnostic equipment‘s, Medicine out of stock, poor
laboratory services, shortage of space to some of the wards in health facilities and
shortage of staff comes to an end.
6.5 Areas for further studies
This evaluation study was not exhaustive since it was only confined in Dar and covered
few respondents in selected Hospitals due to financial limitations, specificity and time
frame.

116
Similar studies that will involve a reasonable number of hospitals, NHIF members and
staff working all over the country for generalization of the results for the whole
Tanzania would be beneficial.
In this regard, further evaluation could be considered to the following areas:
Financial contribution of the members against reality of service provided by
accredited health facilities from Dispensaries to the National level.
The impact of the current Benefit package towards universal health coverage for
members
The sustainability of accredited health facilities who are the main implementers
of the package
117
REFERENCES
Agar Brugiavini, Ca‘ Foscari, University of Venice, Noemi Pace, Ca‘ Foscari,
University of Veni, (2010)
Arnab Acharyaet al (2007), Do Social health insurance schemes in developing country
settings improve health outcomes and reduce the impoverishing effect of
healthcare payments for the poorest people?
Bultman, J., Kanywanyi, J. L., Maarifa, H. & Mtei, G. (2012). Tanzania Health
Insurance Regulatory Framework Review. Ministry of Health and Social
welfare and Social Security Regulatory Authority.
C.R Kothari, (2010), research methodology, 2nd
Revised Edition methods and
techniques, Social health insurance Report: Key factors affecting the
transition towards universal coverage
Carrin, G. and James, C. (2002). Reaching universal coverage via social health
insurance.
City Profile (2004) Dar es Salaam City Profile, United Republic of Tanzania Profile
CMIS (2016) ,Claims Management Information System
(Churchill, 2006). Churchill, C. (2006). An Investigation into the determinants of
Customer satisfaction. Journal of Marketing Research, Vol.19:491-504
Devane et al (2004) Extending Health Insurance: Effects Of the National Health
Insurance scheme in Ghana, (Population and Housing Census, 2012),
Fukawa, T. (2002) .Public Health Insurance in Japan. World Bank Institute, pp. 1- 23
Glanz, K. et. al. (2002).Health Behavior and Health Education: Theory, Research, and
Practice. San Francisco, pp 2-33
Gunji, A. (1994). ―The Vision of the Health Care System in Japan‖ in Bulletin of the
Institute of Public Health 43(3),pp. 254–262
118
Harris, B., Macha, J., Meheus, F. and Mcintyre, D. (2012). Equity in Financing and use
of health care in Ghana, South Africa, and Tanzania: Implications for
paths to universal coverage. Lancet, 380, 126-33.
http://www.cdc.gov/std/program/ProgEvaluation.pdf....13;50 date 29/6/2017
http;// www.nhif.or.tz.
Jeffrey Lane et el (2014) The Emergence of Hospital Accreditation Programs in East
Africa: Lessons from Uganda, Kenya, and Tanzania International Labor
Organization. (2008). Protecting the poor.
Kolstad, J. R. and Lindkvist, I. (2013). Pro-social preferences and self-selection into the
public health sector: evidence from an economic experiment. Health
Policy Plan, 28, 320-7.
Mills, A., Ataguba, J. E., Akazili, J., Borghi, J., Garshong, B., Makawia, S., Mtei, G.,
Mtei, G. (2012). Who pays and who benefits from health care? An assessment of Equity
in health care financing and benefit distribution in Tanzania. Health
Policy and Planning, 2012. 27(suppl 1): p. i23-i34.
Mukhwana Eugine Sundays et al (2015) Strategies to Enhance Utilization of National
Hospital Insurance Fund Scheme Medical Cover by Informal Sector
Populations in Kakamega County, Kenya
Naing et al. (2006) Practical Issues in Calculating the Sample Size for Prevalence
Studies NHIF benefit Package, 2012
National health Insurance Fund Act no 8 of 1999.
National Health Insurance Fund of Uganda,( 2012). http;//www.chmi.ug.visited on 2016
National Health Insurance Fund, Actuarial and Statistical Bulletin, June 2015
National Health Insurance Fund, Corporate Plan, 2010.
National Health Policy of Tanzania. (2007).
National Hospital Insurance Fund of Kenya, (2012). http;//www.nhif.go.ke/. visited on 2016
NHIF Third Five Years Strategic Plan,2015/16 – 2019/20 (TFYSP).
119
Nielsen, R.B. & Mayer, R.N. (2000). Why do people buy cancer insurance?
Anexploratory study advancing the Customer Interest: A journal of
Law,policy and research.
Obonyo, A. (1996). National Hospital Insurance Fund in Kenya, Paper presented to the
National Health Insurance Workshop. CEDHA Arusha.1996.
Obonyo, A. (1996). National Hospital Insurance Fund in Kenya, Paper presented to the
National Health Insurance Workshop. CEDHA Arusha.1996.
OECD (2004). Principles of Corporate Governance. Paris, pp. 1-105 Population and
Housing Census (2012).
Saltman, R. B. (2004). ―Social Health Insurance in Perspective: The Challenge of
Sustaining Stability.‖ In R. B. Saltman, R. Busse, and J. Figueras, (eds),
Social Health Insurance Systems in Western Europe. European
Observatory on Health Systems and Policies. Berkshire, U.K.: Open
University Press, pp. 33-67
Savedoff, W. D. &Gottret, P.(2008) potray the other case studies based on governance
of the schem
Thomson, S. & Reed, S. J. (2011).International Profiles of Health Care Systems. The
Commonwealth Fund, pp. 6-111 (Wagstaff, 2009). – Social health
Insurance reexamined
www.nhif.or.tz Tanzania National Health Insurance Fund web site.
120
APPENDICES
APPENDIX: I
DODOSO KWA WANACHAMA/WANUFAIKA KWA HUDUMA ZA
MATIBABU YA MFUKO WA TAIFA WA BIMA YA AFYA
Dodoso hili limetayarishwa na mwanafunzi wa Shahada ya uzamili katika Chuo kikuu
cha Mzumbe Morogoro. Lengo la dodoso ni kukusanya taarifa kutoka kwa wanachama
/wanufaika wa Mfuko wa Taifa wa Bima ya Afya (MTABA) ambaZo zitaniwezesha
kuandika ripoti ya utafiti wangu kwa madhumuni ya kitaaluma.
Kwa heshima fahamu kwamba taarifa zote zitakazotolewa kupitia dodoso hili
hazitatumika tofauti isipokuwa kwa kusudio nililolitaja hapo juu. Atakaejibu dodoso hili
atatakiwa kujibu maswali kutokana na mtazamo na matarajio yake kutegemea na
kiwango cha uelewa wake juu ya mambo ya Mfuko wa Taifa wa Bima ya Afya kwa
ujumla.
Taarifa itakayotolewa itachukuliwa kama ni siri mno na hakuna sehemu ya taarifa
itakayotumika vinginevyo bila idhini na mamlaka ya aliyejaza dodoso.Natanguliza
shukurani kwa ushirikiano wako na uwazi.
Nambari ya Dodoso: ……………………… Tarehe ya usaili:
…………………………..Wilaya ………………………… Jina la kituo………………
121
UTAMBULISHO:
Weka alama ya pata panapohusika.
WASIFU WAKO:
(a) Umri miaka: [15 – 25] [26- 35] [36 – 45] [46 na zaidi]
( b) Jinsia ke/ me
(c) Hali ya ndoa: [Nina ndoa] [Sina ndoa] [Nimeachana na mwenza] [Mjane]
(d) Kiwango cha Elimu:[ Ya msingi] [Ya sekondari] [Ya Stashahada] [Shahada] [Elimu/
Shahada ya juu] [Sijasoma]
(e) Huwa unapata huduma za Matibabu kama;-
i) Mwanachama mchangiaji
ii)Mwenza
iii)Mtegemezi
1. Je unaufahamu Mfuko wa Taifa wa Bima ya Afya?
Ndiyo ( ) Hapana ( )
2. Kama ndiyo elezea Unafahamu nini kuhusu Mfuko wa Taifa wa Bima ya Afya?
……………………………………………………………………………………………
……………………………………………………………………………………………
……………………………………………………………………………………………
122
3. Je unafahamu mafao ya matibabu yanayotolewa na Mfuko wa Taifa wa Bima ya
Afya?
Ndio ( ) Hapana ( )
Kama ndio;
4. Unafahamu mafao ya aina ngapi? ………
5. Yataje mafao unayoyafahamu
……………………………………………………………………………………………
……………………………………………………………………………………………
……………………………………………………………………………………………
……………………………………………………………………………………………
Swali Kubali Kataa Kubali kwa
Kusisitiza
Kataa kwa
kusisitiza
Ulipata huduma ya maabara katika
hospitali iliyopitishwa
Baadhi ya huduma za maabara
hazipatikani kwa njia ya kadi ya
bima ya afya
Ulipata huduma za dawa
Ulipata huduma dawa zote katika
hospitali kama iliyoelekezwa na
daktari
Nilizuiliwa kuchukua baadhi ya
dawa kwa sababu kuwa dawa hizo
haziko chini ya mfuko wa bima ya
afya
Je wafanyakazi wa hospitali za
serikali zinazo tumia bima
wanakusaidia kupata huduma?
Je wafanyakazi katika hospitali za
binafsi zinazotumia bima ya afya
wanakusaidia kupata huduma pindi
123
ufikapo hospitalini?
Unaridhishwa na Kitita cha mafao
ya matibabu kinachotolewa na
NHIF?
Huduma za bima kwa wanufaika
hutolewa kwa wakati
Huduma za afya kwa wanufaika
zina matokeo chanya
Kuna huduma yoyote uliyoambiwa
kulipia au kuongezea fedha ambayo
haiku katika mfuko wa bima
Unaridhika na mashauri unayopewa
na daktari katika hospitali
Unaridhika na vipimo vya maabara
vinavyotolewa
Unaridhika na huduma ya dawa
inayotolewa
Huduma za meno hupatikana katika
hospitali hii na zinaridhisha
Naridhika na huduma zinazotolewa
katika hospitali hii
Huduma za upasuaji zinapatikana
katika hospitali hii
Huduma za macho na miwani
hutolewa katika hospitali hii na
zinaridhisha
Wagonjwa waliolazwa hupata
huduma zote
Patients receive all physiotherapy
and rehabilitative services
Kuna huduma ulizozuiliwa kupata
ukaambiwa haziko katika mfuko wa
bima
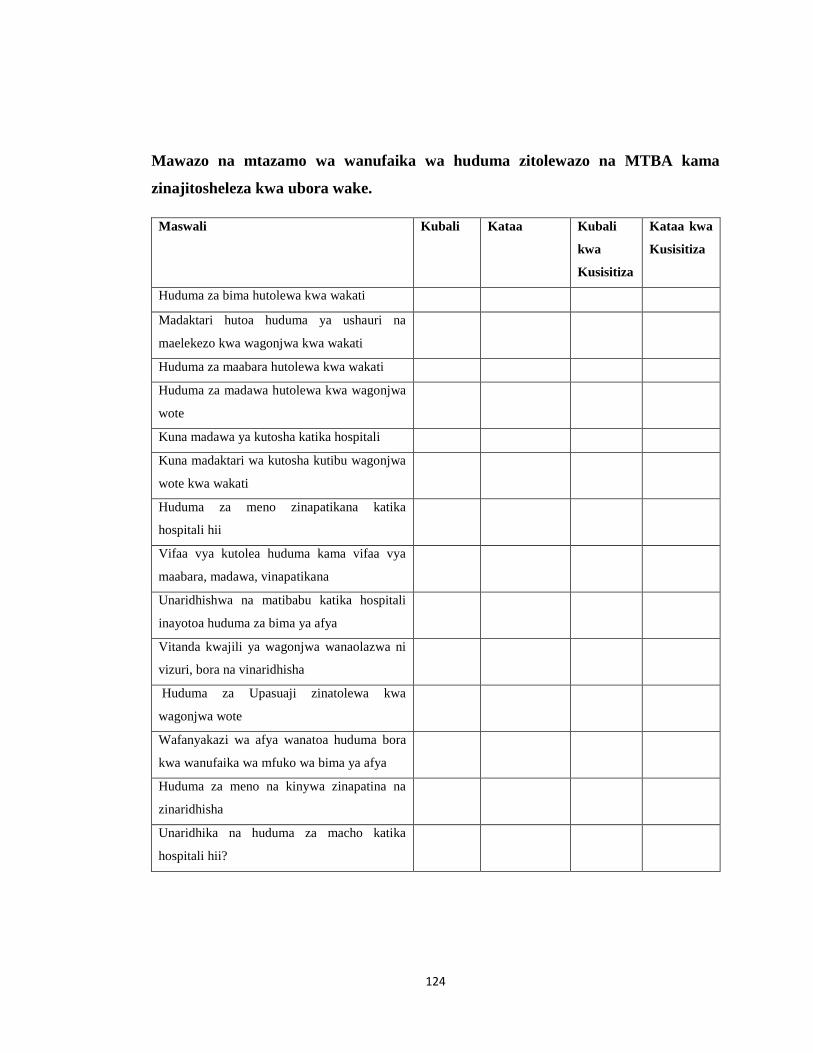
124
Mawazo na mtazamo wa wanufaika wa huduma zitolewazo na MTBA kama
zinajitosheleza kwa ubora wake.
Maswali Kubali Kataa Kubali
kwa
Kusisitiza
Kataa kwa
Kusisitiza
Huduma za bima hutolewa kwa wakati
Madaktari hutoa huduma ya ushauri na
maelekezo kwa wagonjwa kwa wakati
Huduma za maabara hutolewa kwa wakati
Huduma za madawa hutolewa kwa wagonjwa
wote
Kuna madawa ya kutosha katika hospitali
Kuna madaktari wa kutosha kutibu wagonjwa
wote kwa wakati
Huduma za meno zinapatikana katika
hospitali hii
Vifaa vya kutolea huduma kama vifaa vya
maabara, madawa, vinapatikana
Unaridhishwa na matibabu katika hospitali
inayotoa huduma za bima ya afya
Vitanda kwajili ya wagonjwa wanaolazwa ni
vizuri, bora na vinaridhisha
Huduma za Upasuaji zinatolewa kwa
wagonjwa wote
Wafanyakazi wa afya wanatoa huduma bora
kwa wanufaika wa mfuko wa bima ya afya
Huduma za meno na kinywa zinapatina na
zinaridhisha
Unaridhika na huduma za macho katika
hospitali hii?

125
APPENDIX: II
DODOSO KWA WAFANYAKAZI WA KITUO VYA AFYA
Dodoso hili limetayarishwa na mwanafunzi wa Shahada ya uzamili katika Chuo kikuu
cha Mzumbe Morogoro. Lengo la dodoso ni kukusanya taarifa kutoka kwa wanachama
/wanufaika wa Mfuko wa Taifa wa Bima ya Afya (MTABA) ambaZo zitaniwezesha
kuandika ripoti ya utafiti wangu kwa madhumuni ya kitaaluma.
Kwa heshima fahamu kwamba taarifa zote zitakazotolewa kupitia dodoso hili
hazitatumika tofauti isipokuwa kwa kusudio nililolitaja hapo juu. Atakaejibu dodoso hili
atatakiwa kujibu maswali kutokana na mtazamo na matarajio yake kutegemea na
kiwango cha uelewa wake juu ya mambo ya Mfuko wa Taifa wa Bima ya Afya kwa
ujumla.
Taarifa itakayotolewa itachukuliwa kama ni siri mno na hakuna sehemu ya taarifa
itakayotumika vinginevyo bila idhini na mamlaka ya aliyejaza dodoso.Natanguliza
shukurani kwa ushirikiano wako na uwazi.
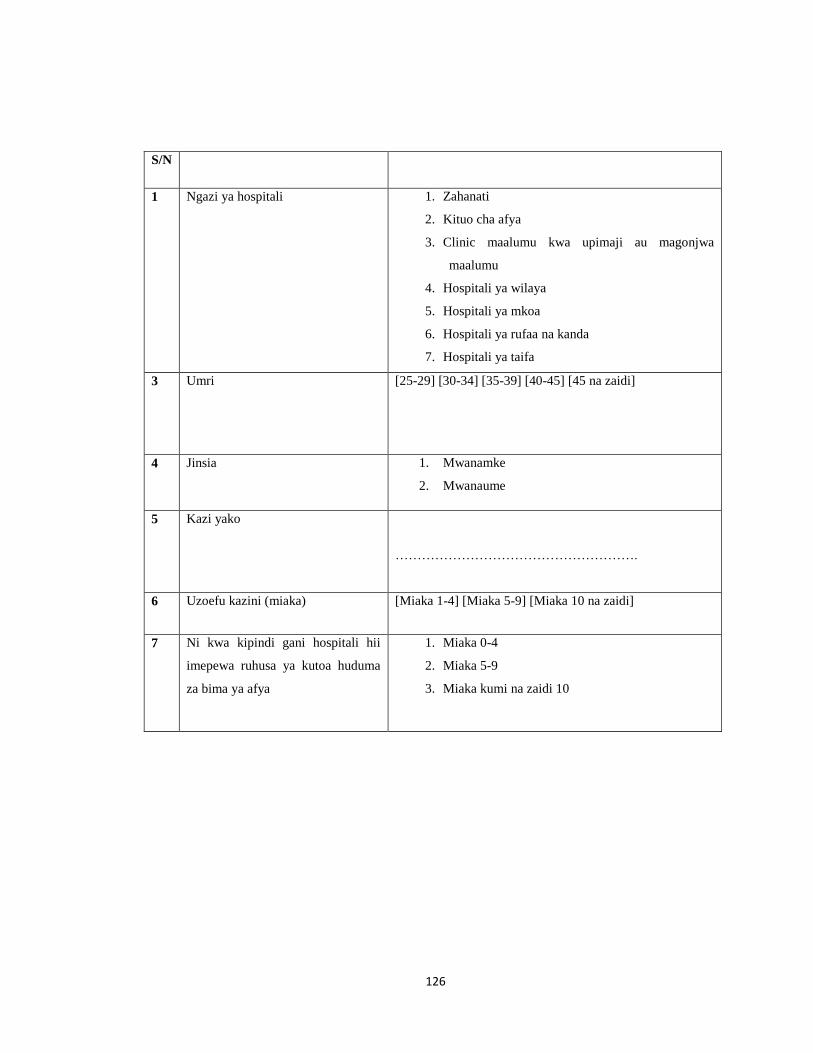
126
S/N
1 Ngazi ya hospitali 1. Zahanati
2. Kituo cha afya
3. Clinic maalumu kwa upimaji au magonjwa
maalumu
4. Hospitali ya wilaya
5. Hospitali ya mkoa
6. Hospitali ya rufaa na kanda
7. Hospitali ya taifa
3 Umri [25-29] [30-34] [35-39] [40-45] [45 na zaidi]
4 Jinsia 1. Mwanamke
2. Mwanaume
5 Kazi yako
……………………………………………….
6 Uzoefu kazini (miaka) [Miaka 1-4] [Miaka 5-9] [Miaka 10 na zaidi]
7 Ni kwa kipindi gani hospitali hii
imepewa ruhusa ya kutoa huduma
za bima ya afya
1. Miaka 0-4
2. Miaka 5-9
3. Miaka kumi na zaidi 10
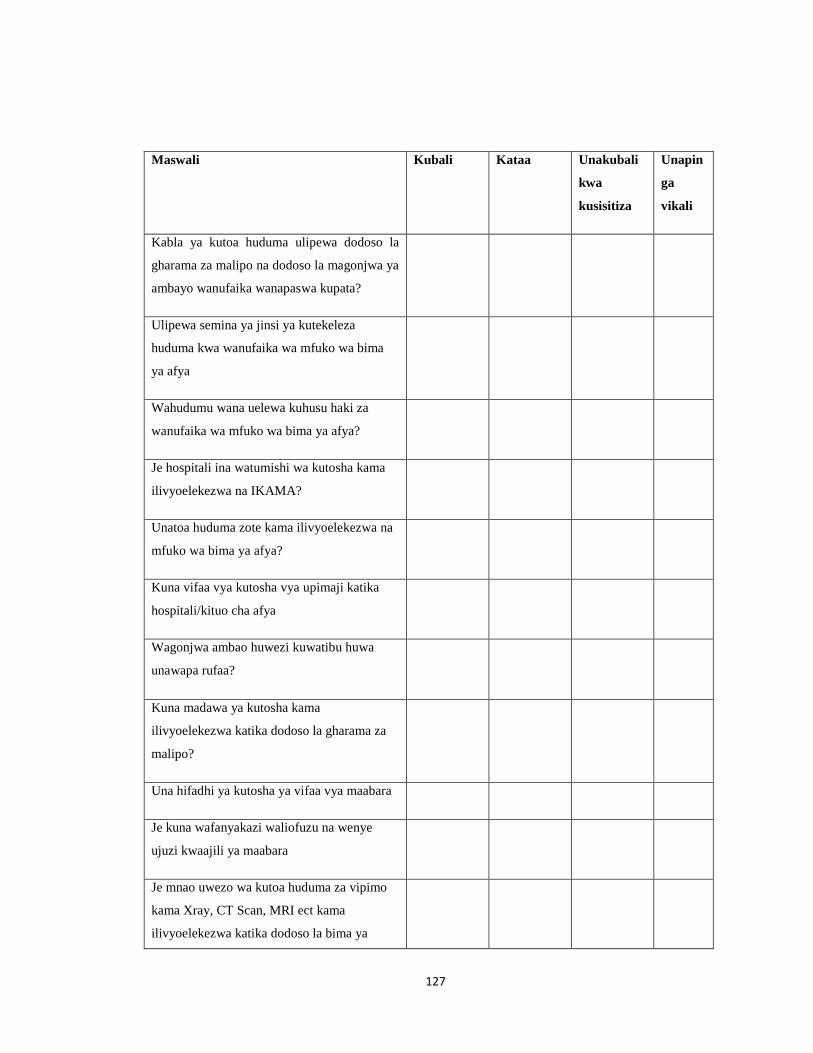
127
Maswali Kubali Kataa Unakubali
kwa
kusisitiza
Unapin
ga
vikali
Kabla ya kutoa huduma ulipewa dodoso la
gharama za malipo na dodoso la magonjwa ya
ambayo wanufaika wanapaswa kupata?
Ulipewa semina ya jinsi ya kutekeleza
huduma kwa wanufaika wa mfuko wa bima
ya afya
Wahudumu wana uelewa kuhusu haki za
wanufaika wa mfuko wa bima ya afya?
Je hospitali ina watumishi wa kutosha kama
ilivyoelekezwa na IKAMA?
Unatoa huduma zote kama ilivyoelekezwa na
mfuko wa bima ya afya?
Kuna vifaa vya kutosha vya upimaji katika
hospitali/kituo cha afya
Wagonjwa ambao huwezi kuwatibu huwa
unawapa rufaa?
Kuna madawa ya kutosha kama
ilivyoelekezwa katika dodoso la gharama za
malipo?
Una hifadhi ya kutosha ya vifaa vya maabara
Je kuna wafanyakazi waliofuzu na wenye
ujuzi kwaajili ya maabara
Je mnao uwezo wa kutoa huduma za vipimo
kama Xray, CT Scan, MRI ect kama
ilivyoelekezwa katika dodoso la bima ya
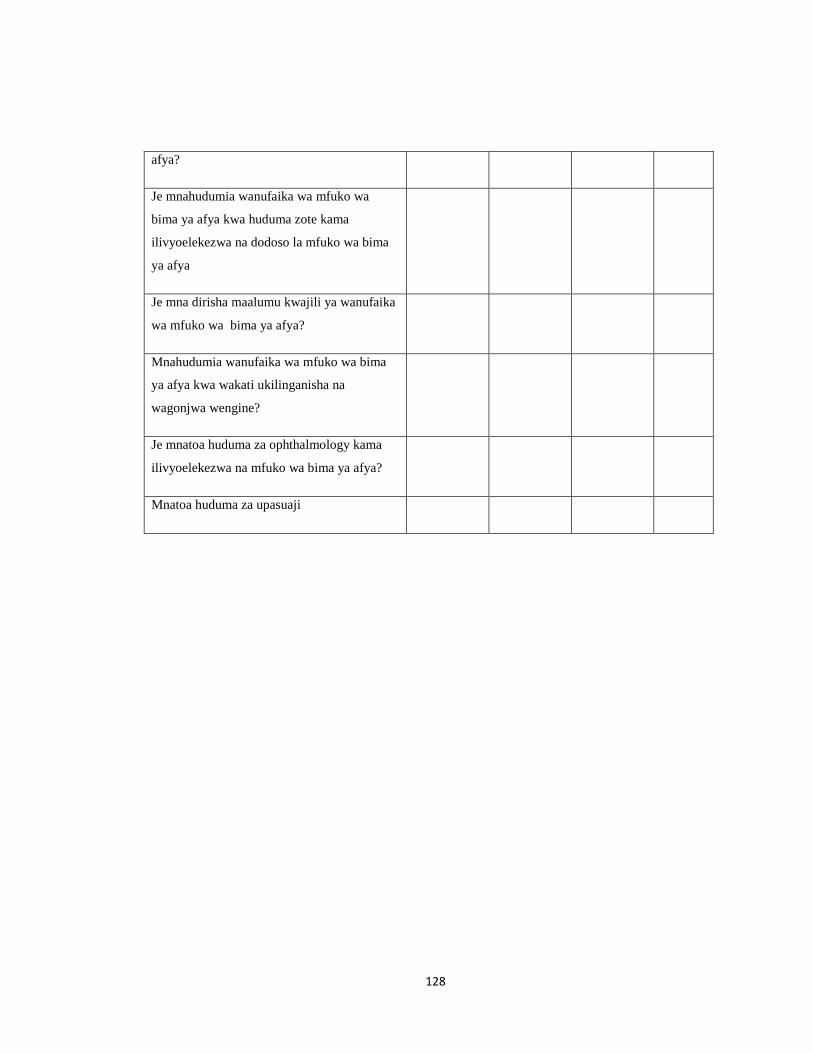
128
afya?
Je mnahudumia wanufaika wa mfuko wa
bima ya afya kwa huduma zote kama
ilivyoelekezwa na dodoso la mfuko wa bima
ya afya
Je mna dirisha maalumu kwajili ya wanufaika
wa mfuko wa bima ya afya?
Mnahudumia wanufaika wa mfuko wa bima
ya afya kwa wakati ukilinganisha na
wagonjwa wengine?
Je mnatoa huduma za ophthalmology kama
ilivyoelekezwa na mfuko wa bima ya afya?
Mnatoa huduma za upasuaji
129
APPENDIX: III
DODOSO KWA WAFANYAKAZI WA MFUKO WA TAIFA WA BIMA YA
AFYA
Dodoso hili limetayarishwa na mwanafunzi wa Shahada ya uzamili katika Chuo kikuu
cha Mzumbe Morogoro. Lengo la dodoso ni kukusanya taarifa kutoka kwa wanachama
/wanufaika wa Mfuko wa Taifa wa Bima ya Afya (MTABA) ambazo zitaniwezesha
kuandika ripoti ya utafiti wangu kwa madhumuni ya kitaaluma.
Kwa heshima fahamu kwamba taarifa zote zitakazotolewa kupitia dodoso hili
hazitatumika tofauti isipokuwa kwa kusudio nililolitaja hapo juu. Atakaejibu dodoso hili
atatakiwa kujibu maswali kutokana na mtazamo na matarajio yake kutegemea na
kiwango cha uelewa wake juu ya mambo ya Mfuko wa Taifa wa Bima ya Afya kwa
ujumla.
Taarifa itakayotolewa itachukuliwa kama ni siri mno na hakuna sehemu ya taarifa
itakayotumika vinginevyo bila idhini na mamlaka ya aliyejaza dodoso.
Natanguliza shukurani kwa ushirikiano wako na uwazi.
Nambari ya Dodoso: ……………………… Tarehe ya usaili:
…………………………..Wilaya…………………………Jina la kituo………………
130
UTAMBULISHO:
Weka alama ya pata panapohusika.
WASIFU WAKO:
(a) Umri miaka: [15 – 25] [26- 35] [36 – 45] [46 na zaidi]
( b) Jinsia ke/ me
(c) Hali ya ndoa: [Nina ndoa] [Sina ndoa] [Nimeachana na mwenza] [Mjane]
(d) Kiwango cha Elimu; [Ya sekondari] [Ya Stashahada] [Shahada] [Elimu/ Shahada ya
juu] [Sijasoma]
(e) Huwa unapata huduma za Matibabu kama;-
i) Mwanachama mchangiaji
ii)Mwenza
iii)Mtegemezi
1. Je unaufahamu Mfuko wa Taifa wa Bima ya Afya?
Ndiyo ( ) Hapana ( )
2. Kama ndiyo elezea Unafahamu nini kuhusu Mfuko wa Taifa wa Bima ya Afya?
……………………………………………………………………………………………
…………………………………………………………………………………….………
……………………………………………………………………………………………
131
3. Je unafahamu mafao ya matibabu yanayotolewa na Mfuko wa Taifa wa Bima ya
Afya?
Ndio ( ) Hapana ( )
Kama ndio;
4. Unafahamu mafao ya aina ngapi? ………
5. Yataje mafao unayoyafahamu
……………………………………………………………………………………………
……………………………………………………………………………………………
……………………………………………………………………………………………
……………………………………………………………………………………………
Maswali Kubali Kataa Unakubali kwa
kusisitiza
Unapinga
vikali
Hospitali zina wafanyakazi wa kutosha
kama ilivyoelekezwa na IKAMA
Hospitali hutoa huduma zote kama
ilivyoelekezwa na madodoso ya mfuko
wa bima ya afya
Je hospitali zinatekeleza taratibu zote
kabla ya kuruhusiwa kutoa huduma
Wakati wa kuruhusu je mlitoa vifaa
vinavyohitajika kama NHIF compliance
rules to the services provision, SOP, other
claim forms and the contract terms?
Hospitali ina wafanyakazi wa kutosha
katika maabara
Hospitali zina vifaa vyote vya upimaji
kama (ultra sound machines, x-ray
machines, CT-Scans and M.R.I (Magnetic
132
Kiwango ambacho Vituo vya kutoa huduma vilivyosajiliwa na MTBA
zinakubaliana na vigezo vya usajili.
Maswali Unakubali Kataa Kataa kwa
kusisitiza
Unakubali
kwa kusisitiza
Kituo kilianza kutoa huduma za matibabu
miaka mitatu iliyopita
Kituo kimesajiliwa na wizara ya afya
(MoH)
Kituo kimesajiliwa na kuna cheti cha
ruhusa ya kutoa huduma
Kuna kibali cha kutolea huduma
Ulisaini mkataba kabla ya kutoa huduma
Ulikubaliwa kutoa huduma
Baaada ya kusaini kuruhusiwa kutoa
huduma za bima ya afya makataba wa
utoaji huduma kwa wakati
Kuna namba ya kutolea huduma
Ukaguzi ulifanyika katika kituo hiki kabla
ya kuruhusiwa kutoa huduma
Kuna vifaa vya maabara vya kutosha
Kuna vifaa vya upimaji vya kama (ultra
sound machines, x-ray machines, CT-
Scans and M.R.I (Magnetic Resonances
Imaging)
Kuna madaktari wa kutosha
Ukuta umepakwa rangi inayowezesha
kusafisha
Sakafu ni nzuri na inawea kusafishika
Resonances Imaging)
Kuna madaktari wa kutosha kama
ilivyoelekezwa katika MoHCDGEC
133
kirahisi
Vyumba ni vikubwa vyenye madirisha
makubwa yatoshayo kuingiza mwanga
Kuna umeme wa wenye nguvu na usio
katika katika
Kuna manesi wa kutosha kwaajili ya
wafanyakazi wote
Kuna vifaa tiba vya kutosha
Kuna wafanyakazi wa kutosha na wenye
ujuzi kwajili ya maabara
134
APPENDIX: IV
QUESTIONNAIRE FOR NHIF MEMBERS
MZUMBE UNIVERSITY SCHOOL OF PUBLIC ADMINISTRATION AND
MANAGEMENT
MASTERS OF SCIENCE IN HEALTH MONITORING AND EVALUATION
(MScHME)
Schedule for the NHIF member
Title of the study: ―EVALUATION ON IMPLEMENTATION OF NHIF BENEFIT
PACKAGE IN THE SELECTED ACCREDITED HEALTH FACILITIES IN ILALA
MUNICIPALITY
I, Rodney Chiduo, conduct this study for academic purposes only. The purpose of this
study is to evaluate the implementation of NHIF Benefit Package in the selected
accredited health facilities in Ilala municipality,
You are among the NHIF members who enjoy the benefits package of the National
Health Insurance Fund. I therefore kindly request you to respond to the following
questions to the best of your knowledge. I promise and assure you that all the answers
will remain confidential and will only be used for the purpose of this study.
Thank you in advance for your cooperation.

135
Questionnaire no………
Ward……….…………
Cycle at any at any appropriate number in each Question
A BACKGROUND INFORMANTION
S/N QUESTIONS CODED RESPONSES
1 Age years [Below 14] [15-25] [26-35] [36-45] [46 and above]
2 Sex: 1. Female
2. Male
3 Marital status 1. Single
2. Married
3. Divorced
4. widow/widower
4 Education Level 1. Never attended school
2. Primary
3. Secondary
4. Diploma
5. Degree
6. Masters and above
5 Do you access Medical services as 1 Principal/ Contributing member
2 Spouse
3 Dependent
6 For how long have you been a
member/ Beneficiary of NHIF?
(Year)
[Below1yr][1-4yrs][5-9yrs][10-15yrs] [Above 15yrs]
7 Do you have NHIF membership
card?
0. No
1. Yes
8 Are you aware about the existing
NHIF benefit package?
National health insurance fund‘s
benefit consists of 11 benefits
covered by the Fund, these include:
i. Outpatient services,

136
ii. Investigations,
iii. Medicines and medical
consumables,
iv. Inpatient services,
v. Surgical services,
vi. Physiotherapy &
rehabilitative services,
vii. Ophthalmological services,
viii. Optical services,
ix. Medical / Orthopedic
appliances,
x. Dental and Oral Health
services,
xi. Retirees‘ health benefit.
0. No
1. Yes
I. If YES how did you hear about it
II. If NO have you tried to find any
information about NHIF benefit
package from NHIF office/ website?
……………………………………………………..
0. No
1. Yes
9 During the last 6 Months have you
ever used one of the benefits
package provided by NHIF
i. If YES what was that services
0. No
1.Yes
…………………………………………………….
…………………………………………………….
10 Were you given that service on-
time?
If NO, why not given on-time
1. No
2. Yes
………………………………………………………
………………………………………………………
Contents of NHIF Benefit Package are comprehensive to suit for beneficiaries needs
1 How do you rate performance of
Accredited facilities regarding
provision of services as per NHIF
1. Good
2. Bad
3. Satisfactory
137
benefit Package
2 Have ever been denied your right to
a particular benefit at the health
facility?
0. No
1. Yes
3 If yes mention the service you was
denied
……………………………………………….
……………………………………………….
………………………………………………..
4 What was the level of that facility 1. Hospital
2. Health Centers
3. Dispensary
4. Pharmacy
5. Specialized clinic
5 Have you ever required any service
which you were told that it is not in
the package?
0. No
1. Yes
6 If Yes what was that Service?
…………………………………………….
…………………………………………….
…………………………………………….
7 Do you visit laboratory services? 0. No
1. Yes
8 How do you rate the performance of
Laboratory services in accredited
facilities
1.Good
2. Not Good
3. Satisfying
4. Very Good
9 Is there any laboratory service you
needed and you were informed that
it is not within NHIF benefit
0. No
1. Yes
138
package? If Yes what was that Laboratory
service…………………………………………
…………………………………………….
10 Do you receive pharmaceutics
services
0. No
1. Yes
11 If yes do you get all medicine as
directed by the Doctor?
0. No
1. Yes
12 How do you rate the performance of
Pharmaceutical services in
accredited facilities
1.Good
2. Not Good
3. Satisfactory
4 Very Good
13 Have you ever seek for any
medicine and you were told that the
medicine do not fall under benefit
package?
0. No
1. Yes
14 If yes what was the name/s of that
medicine
………………………………………..
………………………………………..
15 Have you ever been referred to any
pharmacy because of the drug Out
of stock at the facility
0. No
1. Yes
16 When you are attending referred
Pharmacy as an NHIF beneficiary,
How were you treated?
1.Good
2. Not Good
3. Satisfactory
4 Very Good
17 Do you easily get the Medicines
prescribed?
0. No
1. Yes
2. Always
3. Not Always
4. Sometimes
18 Are staffs in public accredited
health facility willing to help you?
0. No
1. Yes
2. Always
3. Not Always
4. Sometimes
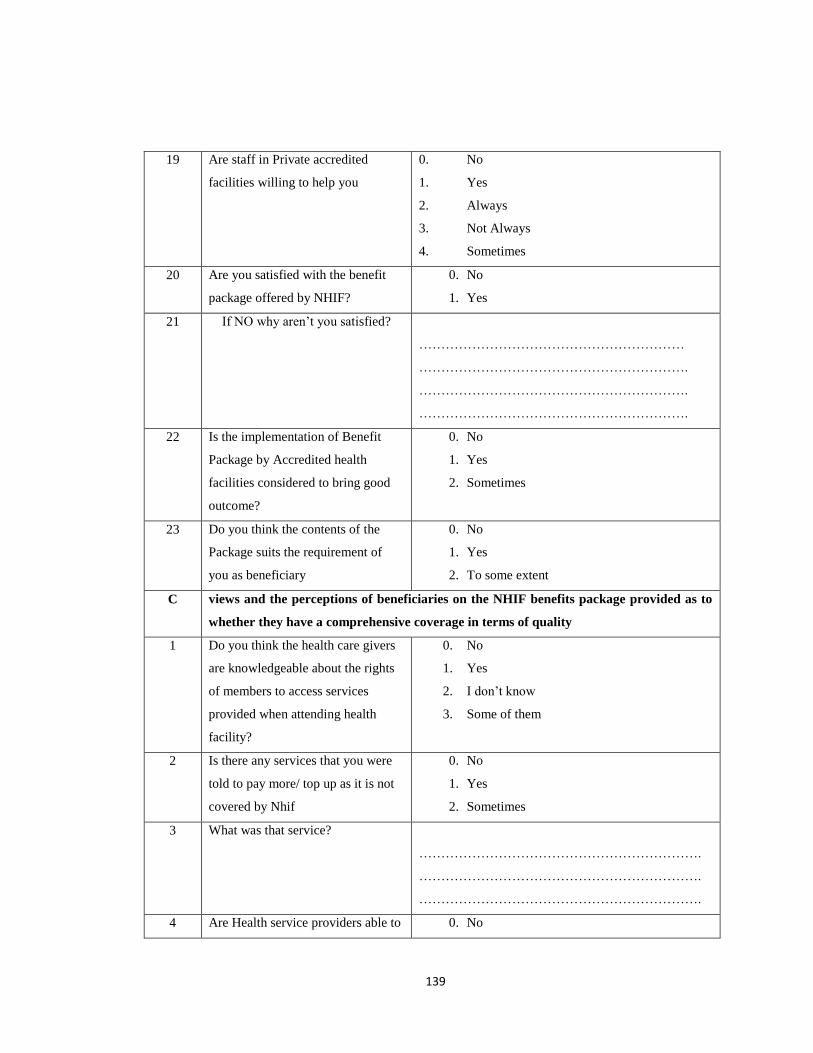
139
19 Are staff in Private accredited
facilities willing to help you
0. No
1. Yes
2. Always
3. Not Always
4. Sometimes
20 Are you satisfied with the benefit
package offered by NHIF?
0. No
1. Yes
21 If NO why aren‘t you satisfied?
……………………………………………………
…………………………………………………….
…………………………………………………….
…………………………………………………….
22 Is the implementation of Benefit
Package by Accredited health
facilities considered to bring good
outcome?
0. No
1. Yes
2. Sometimes
23 Do you think the contents of the
Package suits the requirement of
you as beneficiary
0. No
1. Yes
2. To some extent
C views and the perceptions of beneficiaries on the NHIF benefits package provided as to
whether they have a comprehensive coverage in terms of quality
1 Do you think the health care givers
are knowledgeable about the rights
of members to access services
provided when attending health
facility?
0. No
1. Yes
2. I don‘t know
3. Some of them
2 Is there any services that you were
told to pay more/ top up as it is not
covered by Nhif
0. No
1. Yes
2. Sometimes
3 What was that service?
……………………………………………………….
……………………………………………………….
……………………………………………………….
4 Are Health service providers able to 0. No
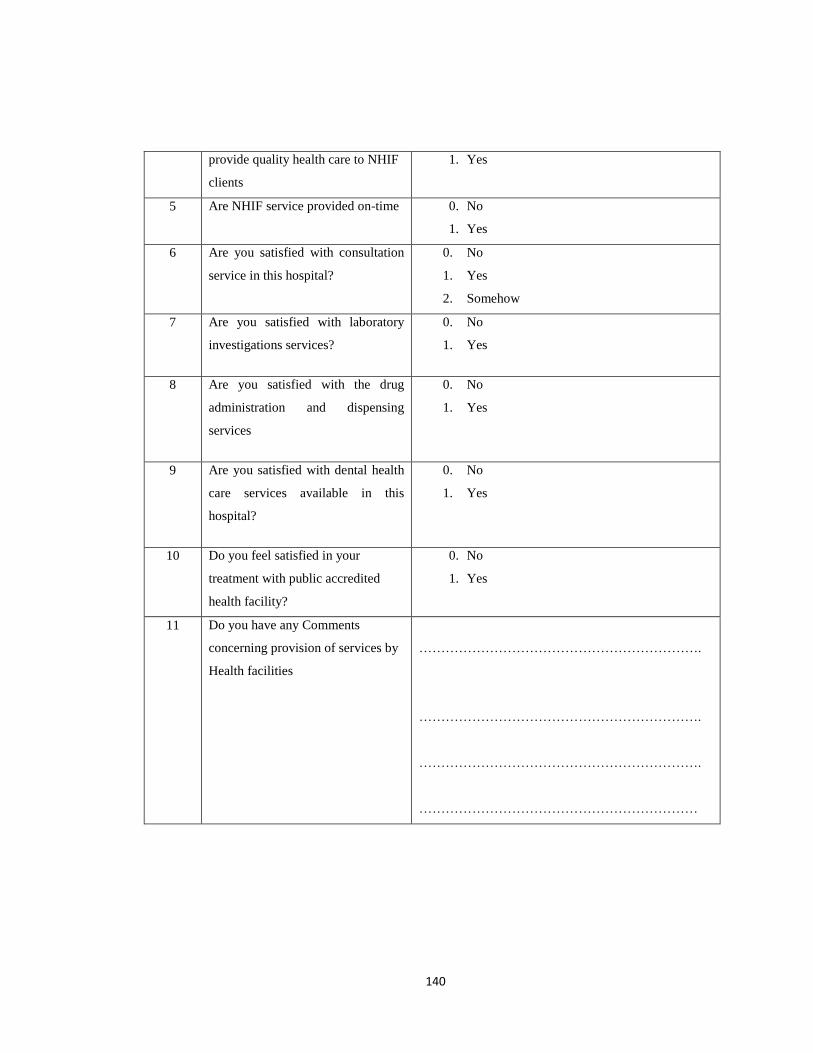
140
provide quality health care to NHIF
clients
1. Yes
5 Are NHIF service provided on-time 0. No
1. Yes
6 Are you satisfied with consultation
service in this hospital?
0. No
1. Yes
2. Somehow
7 Are you satisfied with laboratory
investigations services?
0. No
1. Yes
8 Are you satisfied with the drug
administration and dispensing
services
0. No
1. Yes
9 Are you satisfied with dental health
care services available in this
hospital?
0. No
1. Yes
10 Do you feel satisfied in your
treatment with public accredited
health facility?
0. No
1. Yes
11 Do you have any Comments
concerning provision of services by
Health facilities
……………………………………………………….
……………………………………………………….
……………………………………………………….
………………………………………………………
141
APPENDIX: V
QUESTIONNAIRE FOR ACCREDITED HEALTH PROVIDER
MZUMBE UNIVERSITY SCHOOL OF PUBLIC ADMINISTRATION AND
MANAGEMENT
MASTERS OF SCIENCE IN HEALTH MONITORING AND EVALUATION
(MScHME)
Schedule for the NHIF accredited Health care provider
Title of the study: ―EVALUATION ON IMPLEMENTATION OF NHIF BENEFIT
PACKAGE IN THE SELECTED ACCREDITED HEALTH FACILITIES IN ILALA
MUNICIPALITY
I, Rodney Chiduo, a Masters student from Mzumbe University, conducting this
evaluation as part of requirements of the University award of master‘s degree, conduct
this study for academic purposes only. The purpose of this study is to evaluate the
implementation of NHIF Benefit Package in the selected accredited health facilities.
You are among the NHIF accredited health care provider who enjoys the contract of the
National Health Insurance Fund. I therefore kindly request you to respond to the
following questions to the best of your knowledge. I promise and assure you that all the
answers will remain confidential and will only be used for the purpose of this study. I
value your contribution towards the success of my study.
THANKING YOU IN ADVANCE FOR YOUR COOPERATION!

142
Cycle on the answer that is appropriate!
S/N
1 Health facility level 8. Dispensary
9. Health center
10. Specialized clinic/ Diagnostic center
11. District hospital
12. Regional hospital
13. Zonal Referral hospital
14. National hospital
2 Location of the facility
..................................................................
3 Age in Years [25-29] [30-34] [35-39] [40-45] [45 and Above]
4 Sex of the respondent 3. Male
4. Female
5 Position of Respondent
……………………………………………….
6 Work experience [1-4Yrs] [5-9 Yrs] [10Yrs and above]
7 For how long is your facility accredited
by NHIF to provide service for its
members?
4. 0-4years
5. 5-9 years
6. 10 years and above
B Status and capabilities of the selected accredited health facilities in fulfilling the
requirements of the NHIF Benefit Package
8 Do you know the NHIF benefit Package? 0. No
1. Yes
9 Were you given the Benefit Package and
the price list before you started giving
services
0. No
1. Yes
10 Were you given any training on Benefit
Package on how it should be
implemented?
0. No
1. Yes
11 Do you think the trainings are sufficient
to support your work during
implementation of the Package?
0. No
1. Yes
12 Does all of your staff at the facility have
knowledge about the rights NHIF
beneficiaries when they serve them?
0. No
1. Yes
2. Some
13 Is the facility has adequate workers as per
staff establishment ( IKAMA) required
for its level as per Ministry of Health
facility standard
0. No
1. Yes
2. Other comment……………………………
……………………………………………………….
14 Do you provide all the services as
stipulated in NHIF benefit package?
0. No
1. Yes
2. Not all
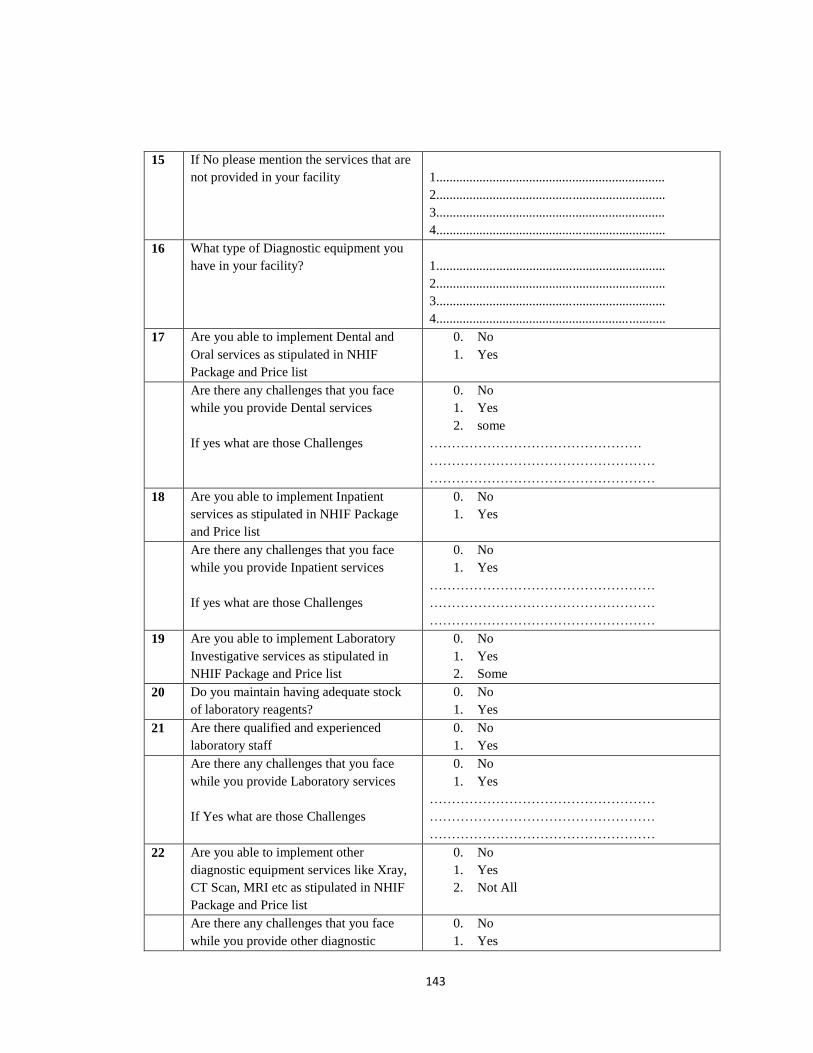
143
15 If No please mention the services that are
not provided in your facility
1.....................................................................
2.....................................................................
3.....................................................................
4.....................................................................
16 What type of Diagnostic equipment you
have in your facility?
1.....................................................................
2.....................................................................
3.....................................................................
4.....................................................................
17 Are you able to implement Dental and
Oral services as stipulated in NHIF
Package and Price list
0. No
1. Yes
Are there any challenges that you face
while you provide Dental services
If yes what are those Challenges
0. No
1. Yes
2. some
…………………………………………
……………………………………………
……………………………………………
18 Are you able to implement Inpatient
services as stipulated in NHIF Package
and Price list
0. No
1. Yes
Are there any challenges that you face
while you provide Inpatient services
If yes what are those Challenges
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
19 Are you able to implement Laboratory
Investigative services as stipulated in
NHIF Package and Price list
0. No
1. Yes
2. Some
20 Do you maintain having adequate stock
of laboratory reagents?
0. No
1. Yes
21 Are there qualified and experienced
laboratory staff
0. No
1. Yes
Are there any challenges that you face
while you provide Laboratory services
If Yes what are those Challenges
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
22 Are you able to implement other
diagnostic equipment services like Xray,
CT Scan, MRI etc as stipulated in NHIF
Package and Price list
0. No
1. Yes
2. Not All
Are there any challenges that you face
while you provide other diagnostic
0. No
1. Yes
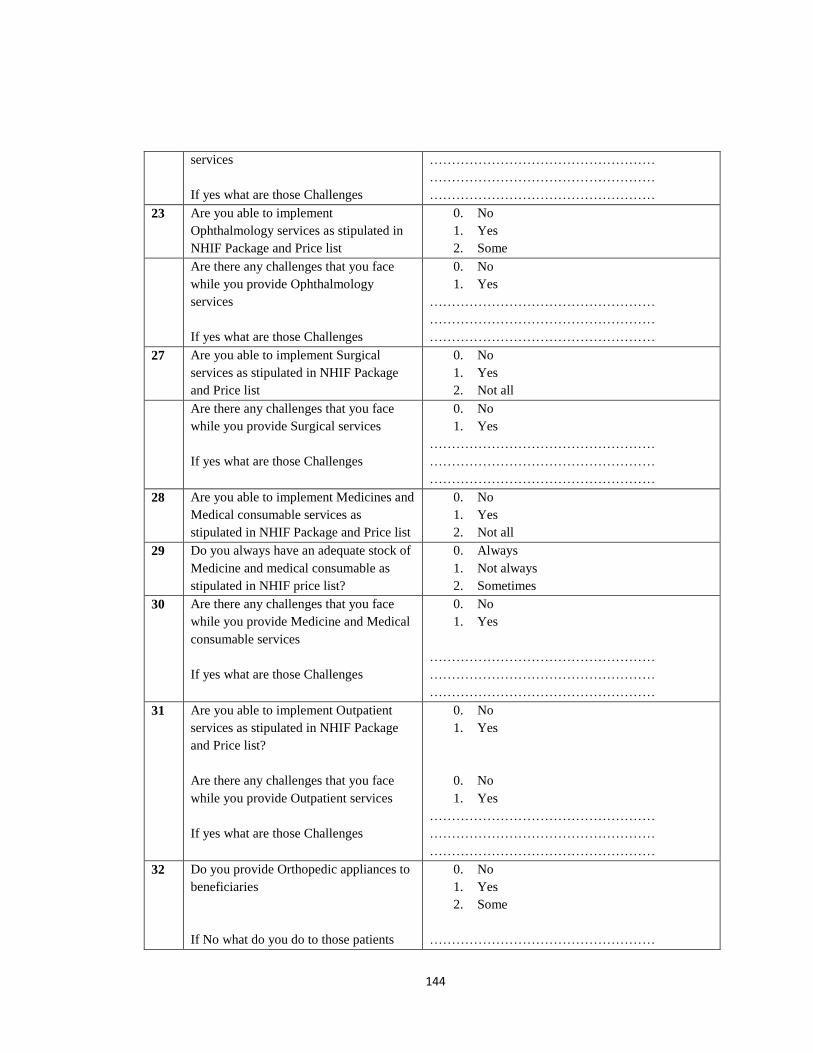
144
services
If yes what are those Challenges
……………………………………………
……………………………………………
……………………………………………
23 Are you able to implement
Ophthalmology services as stipulated in
NHIF Package and Price list
0. No
1. Yes
2. Some
Are there any challenges that you face
while you provide Ophthalmology
services
If yes what are those Challenges
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
27 Are you able to implement Surgical
services as stipulated in NHIF Package
and Price list
0. No
1. Yes
2. Not all
Are there any challenges that you face
while you provide Surgical services
If yes what are those Challenges
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
28 Are you able to implement Medicines and
Medical consumable services as
stipulated in NHIF Package and Price list
0. No
1. Yes
2. Not all
29 Do you always have an adequate stock of
Medicine and medical consumable as
stipulated in NHIF price list?
0. Always
1. Not always
2. Sometimes
30 Are there any challenges that you face
while you provide Medicine and Medical
consumable services
If yes what are those Challenges
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
31 Are you able to implement Outpatient
services as stipulated in NHIF Package
and Price list?
Are there any challenges that you face
while you provide Outpatient services
If yes what are those Challenges
0. No
1. Yes
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
32 Do you provide Orthopedic appliances to
beneficiaries
If No what do you do to those patients
0. No
1. Yes
2. Some
……………………………………………
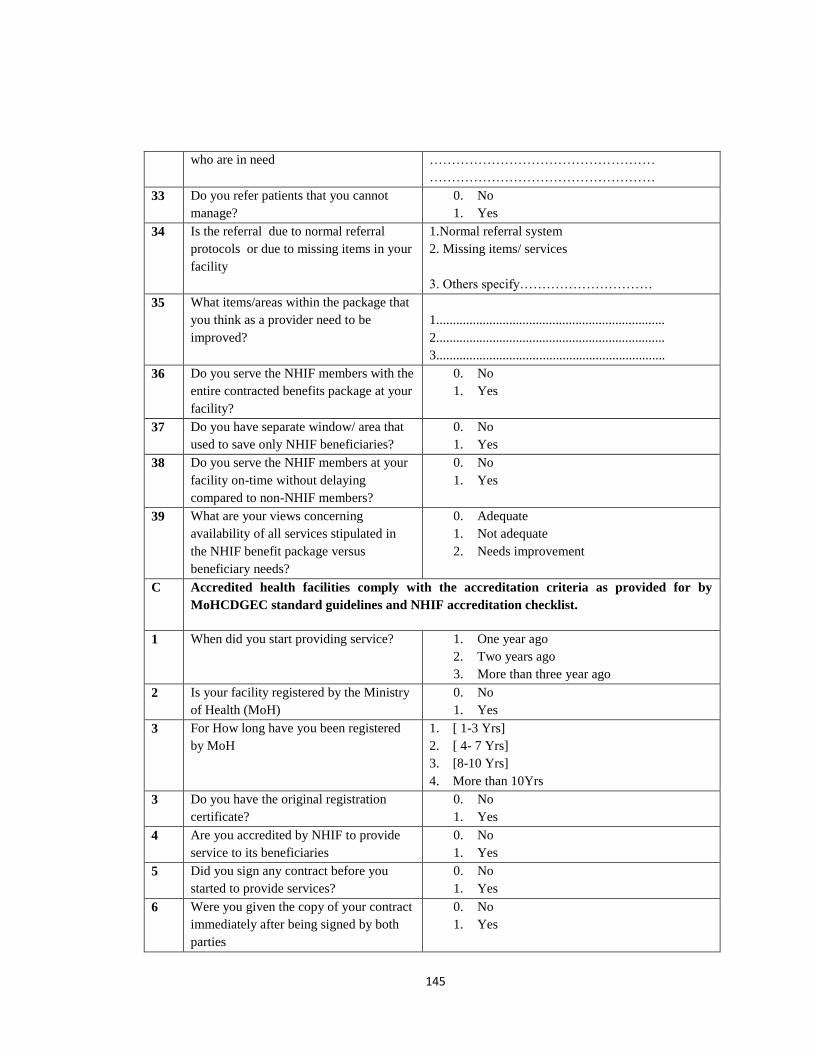
145
who are in need ……………………………………………
……………………………………………
33 Do you refer patients that you cannot
manage?
0. No
1. Yes
34 Is the referral due to normal referral
protocols or due to missing items in your
facility
1.Normal referral system
2. Missing items/ services
3. Others specify…………………………
35 What items/areas within the package that
you think as a provider need to be
improved?
1.....................................................................
2.....................................................................
3.....................................................................
36 Do you serve the NHIF members with the
entire contracted benefits package at your
facility?
0. No
1. Yes
37 Do you have separate window/ area that
used to save only NHIF beneficiaries?
0. No
1. Yes
38 Do you serve the NHIF members at your
facility on-time without delaying
compared to non-NHIF members?
0. No
1. Yes
39 What are your views concerning
availability of all services stipulated in
the NHIF benefit package versus
beneficiary needs?
0. Adequate
1. Not adequate
2. Needs improvement
C Accredited health facilities comply with the accreditation criteria as provided for by
MoHCDGEC standard guidelines and NHIF accreditation checklist.
1 When did you start providing service? 1. One year ago
2. Two years ago
3. More than three year ago
2 Is your facility registered by the Ministry
of Health (MoH)
0. No
1. Yes
3 For How long have you been registered
by MoH
1. [ 1-3 Yrs]
2. [ 4- 7 Yrs]
3. [8-10 Yrs]
4. More than 10Yrs
3 Do you have the original registration
certificate?
0. No
1. Yes
4 Are you accredited by NHIF to provide
service to its beneficiaries
0. No
1. Yes
5 Did you sign any contract before you
started to provide services?
0. No
1. Yes
6 Were you given the copy of your contract
immediately after being signed by both
parties
0. No
1. Yes
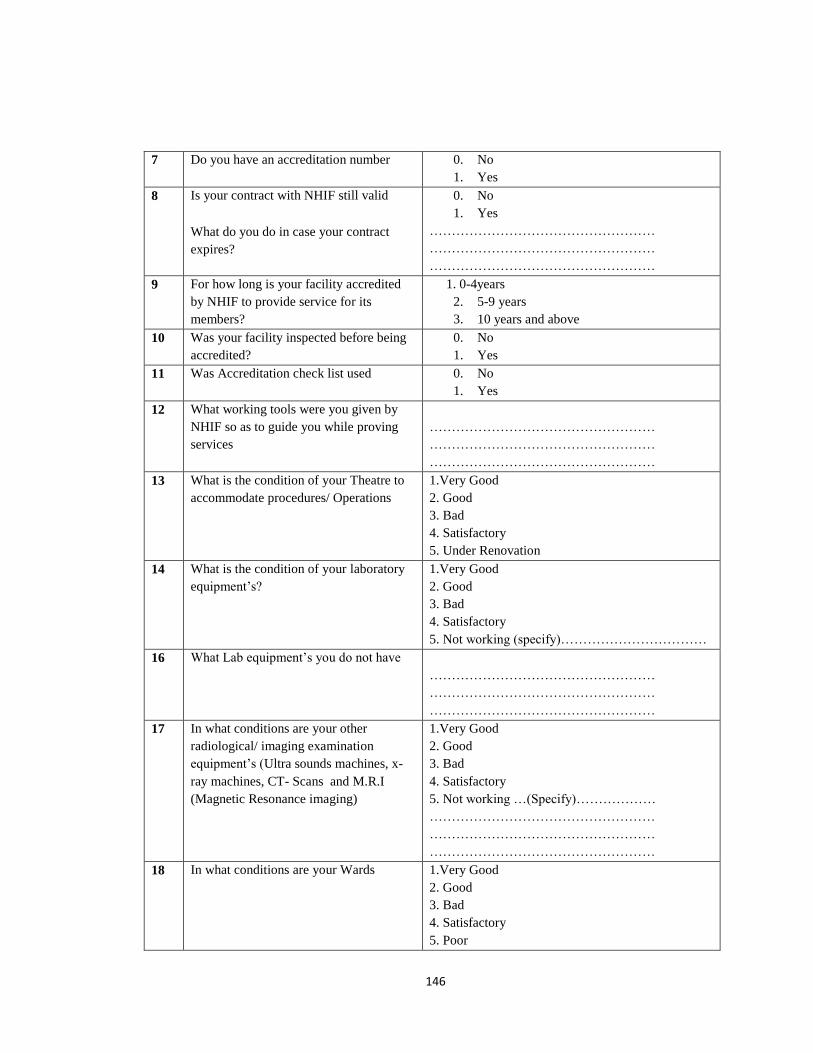
146
7 Do you have an accreditation number 0. No
1. Yes
8 Is your contract with NHIF still valid
What do you do in case your contract
expires?
0. No
1. Yes
……………………………………………
……………………………………………
……………………………………………
9 For how long is your facility accredited
by NHIF to provide service for its
members?
1. 0-4years
2. 5-9 years
3. 10 years and above
10 Was your facility inspected before being
accredited?
0. No
1. Yes
11 Was Accreditation check list used 0. No
1. Yes
12 What working tools were you given by
NHIF so as to guide you while proving
services
……………………………………………
……………………………………………
……………………………………………
13 What is the condition of your Theatre to
accommodate procedures/ Operations
1.Very Good
2. Good
3. Bad
4. Satisfactory
5. Under Renovation
14 What is the condition of your laboratory
equipment‘s?
1.Very Good
2. Good
3. Bad
4. Satisfactory
5. Not working (specify)……………………………
16 What Lab equipment‘s you do not have
……………………………………………
……………………………………………
……………………………………………
17 In what conditions are your other
radiological/ imaging examination
equipment‘s (Ultra sounds machines, x-
ray machines, CT- Scans and M.R.I
(Magnetic Resonance imaging)
1.Very Good
2. Good
3. Bad
4. Satisfactory
5. Not working …(Specify)………………
……………………………………………
……………………………………………
……………………………………………
18 In what conditions are your Wards
1.Very Good
2. Good
3. Bad
4. Satisfactory
5. Poor
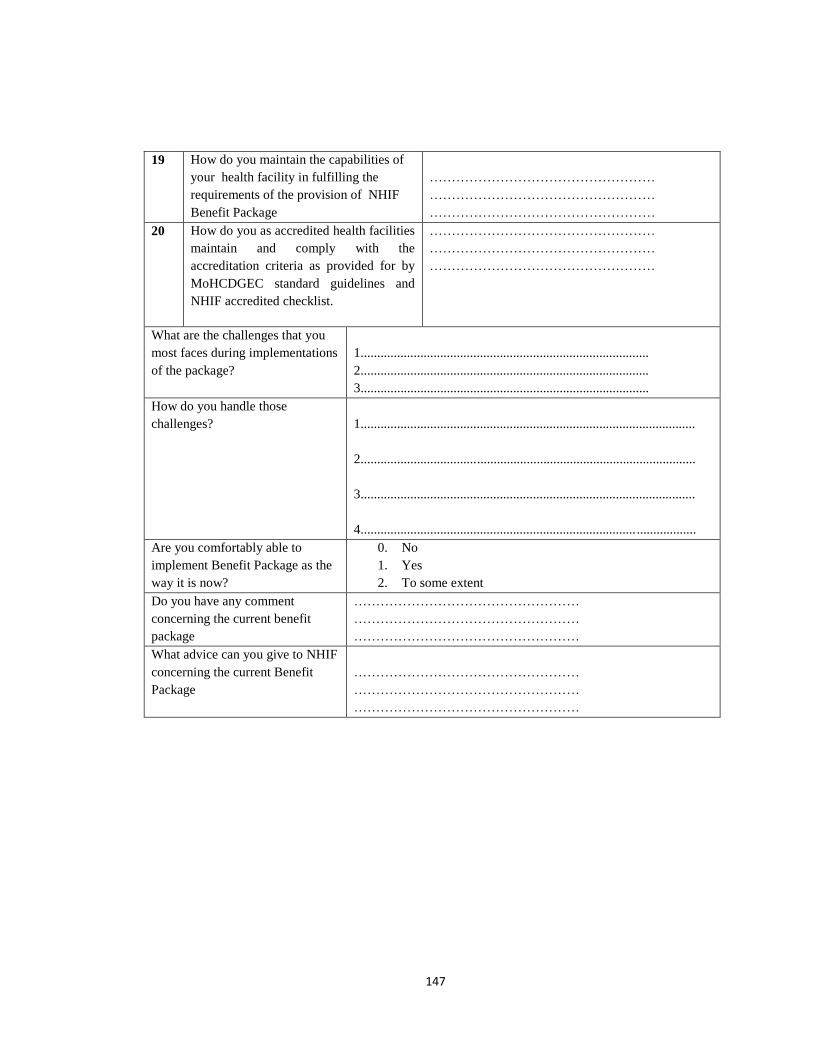
147
19 How do you maintain the capabilities of
your health facility in fulfilling the
requirements of the provision of NHIF
Benefit Package
……………………………………………
……………………………………………
……………………………………………
20 How do you as accredited health facilities
maintain and comply with the
accreditation criteria as provided for by
MoHCDGEC standard guidelines and
NHIF accredited checklist.
……………………………………………
……………………………………………
……………………………………………
What are the challenges that you
most faces during implementations
of the package?
1.......................................................................................
2.......................................................................................
3.......................................................................................
How do you handle those
challenges?
1.....................................................................................................
2.....................................................................................................
3.....................................................................................................
4................................................................................... ..................
Are you comfortably able to
implement Benefit Package as the
way it is now?
0. No
1. Yes
2. To some extent
Do you have any comment
concerning the current benefit
package
……………………………………………
……………………………………………
……………………………………………
What advice can you give to NHIF
concerning the current Benefit
Package
……………………………………………
……………………………………………
……………………………………………
148
APPENDIX: VI
QUESTIONNAIRE FOR NHIF STAFF
MZUMBE UNIVERSITY SCHOOL OF PUBLIC ADMINISTRATION AND
MANAGEMENT
MASTERS OF SCIENCE IN HEALTH MONITORING AND EVALUATION
(MScHME)
Schedule for the NHIF staff
Title of the study: ―EVALUATION ON IMPLEMENTATION OF NHIF BENEFIT
PACKAGE IN THE ACCREDITED HEALTH FACILITIES IN ILALA
MUNICIPALITY
I, Rodney Chiduo, conduct this study for academic purposes only. The purpose of this
study is to evaluate the implementation of NHIF Benefit Package in the accredited
health facilities in Ilala municipality leading to its efficiency in service provision to
beneficiaries. You are among the NHIF staff who is an employee of the National Health
Insurance Fund. I therefore kindly request you to respond to the following questions to
the best of your knowledge. I promise and assure you that all the answers will remain
confidential and will only be used for the purpose of this study.
THANKING YOU IN ADVANCE FOR YOUR COOPERATION!

149
Cycle on the appropriate answer
S/N Age years [15-25] [26-35] [36-45] [46 and above]
1 Sex: 1. Female
2. Male
2 Marital status 1. Single
2. Married
3. Divorced
4. widow/widower
3 Education Level 1. Never attended school
2. Primary
3. Secondary
4. Diploma
5. Degree
6. Masters and above
4 Work experiences (years) 1. <5 years
2. > 5years
5 Department
6 Are you aware of NHIF benefit package 0. No
1. Yes
7 Do you know how NHIF Beneficiaries
benefit with this package
0. No
1. Yes
8 Do you enter contract with the health
care providers?
0. No
1. Yes
9 Do you provide Benefit Package and
the price list to Health providers before
they started giving services
0. No
1. Yes
10 During accreditations do you provide
NHIF compliance rules to the services
provision, SOP, other claim forms and
the contract terms?
0. No
1. Yes
If No why? …………………………………………………
…………………………………………………
………………………
11 Are there Basic Accreditation Criteria
that Health provider needs to meet
before being accredited?
0. No
1. Yes
If No why? …………………………………………………
…………………………………………………
…………
If Yes what are those criteria
……………………………………
……………………………………
……………………………………
……………………………………
12 Do you use any tools when assessing
the status of the facility
0. No
1. Yes
If Yes what tools do you use

150
……………………………………
……………………………………
……………………………………
If No what do you normally use …………………………………………………
…………………………………………………
…………
13 Are the health facilities aware on the
requirements that are needed to be met
before being accredited?
0. No
1. Yes
2. Not all
14 Do you conduct trainings to support on
NHIF benefit package?
0. No
1. Yes
15 In your own view do you think health
facility have sufficient knowledge on
Benefit package?
0. No
1. Yes
2. Not all
16 Are the facilities have enough workers
as per staff establishment ( IKAMA)
requirement of its level
0. No
1. Yes
2. Some
17 If no which facilities do most faces
shortage of staff
Specify if in Public , Private,
FBO/NGO………………
1.Dispensaries
2.Health Centers
3.Districct Hospitals
4.Regional Hospitals
5.Zonal Referral Hospitals
6.Nationa Hospital
7.Specialized Clinics
8. Diagnostic centers
18 Do you think the facilities provide all
services as stipulated in the package?
0. No
1. Yes
If no why? …………………………………………
…………………………………………
…………………………………………
……………………………………
19 Do health providers fulfill all
requirement before they are accredited
0. No
1. Yes
2. Not all
If no in what scenario are health
providers accredited even though they
did not met all the requirements
…………………………………………
…………………………………………
…………………………………………
…………………………………….
20 Do you conduct inspection to the health
facilities to check about their
compliance to NHIF terms and
regulations
0. No
1. Yes
21 How do you evaluate the capabilities of
the selected accredited health facilities
in fulfilling the requirements of the
NHIF Benefit Package?
…………………………………………
…………………………………………
…………………………………………
22 How do you as NHIF staff evaluate the
extent to which the selected accredited
…………………………………………
151
health facilities comply with the
accreditation criteria as provided for by
MoHCDGEC standard guidelines and
NHIF accredited checklist.
…………………………………………
…………………………………………
23 What mechanism do you have for
receiving individual member‗s
complaints or information
…………………………………………
…………………………………………
…………………………………………
24 Are all NHIF staff knowledgeable
about the members ‗benefits package,
NHIF legal frameworks, rules and
procedures of the scheme as well as the
compliance policy
0. No
1. Yes
2. Not all
If no Why? …………………………………………………
…………………………………………………
…………………………
25 Are NHIF member‘s complaints and
problems solved on time?
0. No
1. Yes
2. Some
26 If no Why do NHIF staff not process
and solve the problems of its member‘s
on-time?
1......................................................
2.....................................................
3....................................................
4....................................................
27 Do you control and check for the
compliance of the accredited health care
providers in serving well the benefits
package to your members
0. No
1. Yes
28 In your views, is the Fund stable
financially to cover for the entire
benefits package and other management
operations for at least ten years to
come?
0. No
1. Yes
2. To some extent
29 Do you know if there are requirements
and set standards by NHIF that needs to
be fulfilled Health facility before being
accredited?
0. No
1. Yes
If yes mention the areas
………………………………………
…………………………………………
…………………………………………
30 How do you rate the performance of
Private Hospitals in providing services
as stipulated in benefit package
1 Good
2 Not Good
3 Satisfying
4 Very Good
31 What are the challenges that you face
while dealing with accredited Private
Hospitals
…………………………………………
…………………………………………
…………………………………………
32 How do you rate the performance of
Public Hospitals in providing services
as stipulated in benefit package
1 Good
2 Not Good
3 Satisfying
4 Very Good

152
32 What are the challenges that you face
while dealing with accredited Public
Hospitals
…………………………………………
…………………………………………
…………………………………………
33 How do you rate the performance of
FBO/NGO Hospitals in providing
services as stipulated in benefit
package
1 Good
2 Not Good
3 Satisfying
4 Very Good
34 What are the challenges that you face
while dealing with accredited
FBO/NGO Hospitals
35 Do you think that all the stakeholders
where consulted during the process of
creating the package
0. No
1. Yes
2. Not all
36 If no what areas do you think needs to
be added/ improved and why
…………………………………………
…………………………………………
…………………………………………
37 What challenges are encountered by
NHIF staff when dealing with selected
health facilities during implementation
of NHIF benefit package
…………………………………………
…………………………………………
…………………………………………
38 Do you think the current package is
comprehensive enough to meet
Beneficiaries needs
0. No
1. Yes
2. To some extent
If no what items do you suggest should
be added to improve
…………………………………………
…………………………………………
…………………………………………
153
APPENDIX: VII
INTERVIEW GUIDE TO HEALTH PROVIDERS
How are you?
My Name is Rodney Chiduo, I am a student of MSc in Health Monitoring and
Evaluation from Mzumbe University. My study tries to evaluate Implementation of
NHIF Benefit Package in the selected accredited Health facility. In order to accomplish this
task i would like to ask you some questions concerning this study. I expect my interview to take
about 10 minutes. I will ask you questions concerning NHIF and the Benefit Package in general,
feel free to respond to my questions, In case of any question or doubt that makes you feel
uncomfortable don‘t hesitate to tell me and we can skip over that question or stop the interview
any time you want, I will appreciate for your participation.
Are you willing and ready to participate?
Part A: Demographic Information
Name of Health Facility………………………………………………………….
Qualification/ Position…………………………………………………................
Date of interview…………………………………………………………………
Q1: For how long have you been in this facility?
Q2: What do you understand about NHIF?
Probe; What can you say about NHIF benefit Package
Q3: How do you find the implementation of the package in your facility?
Probe (In case there are challenges how do you handle/ overcome them?)
154
Part B: Specific Objectives
To determine and evaluate the challenges encountered by the selected health
facilities while implementing NHIF benefit package.
QN1: How is provision of medical Services as stipulated in the package in your facilities
QN 2: How do you see the implementation of Nhif Benefit Package program?
QN 3: How does the Benefit Package help on the provision of Quality in accredited
health facilities?
QN 4: What challenges do you face on implementing the program?
Probe; How do you handle those challenges?
QN 5. In your day to day experience what can you say on beneficiaries‘ attitude towards
Benefit Package?
Probe; How do you always respond to those attitudes?
QN 7; What are your recommendation for improving the programme?
QN 8; What advice do you have for NHIF Management concerning the existing benefit
Package
WIND UP QUESTIONS:
Qn: Do you have anything to share on what we have talked?
Qn; How do you feel to be interviewed?
May I take this opportunity to thank you for giving me your valuable time to answer all
the questions I asked you, if I will need more clarification of any issue we talked today I
will call you. Have a good day, once again thank you.
155
APPENDIX: VIII
INTERVIEW GUIDE FOR NHIF MEMBERS
How are you?
My Name is Rodney Chiduo, I am a student of MSc in Health Monitoring and
Evaluation from Mzumbe University. My study tries to evaluate Implementation of
NHIF Benefit Package in the selected accredited Health facility. In order to
accomplish this task i would like to ask you some questions concerning this study. I
expect my interview to take about 10 minutes. I will ask you questions concerning NHIF
and the Benefit Package in general, feel free to respond to my questions, In case of any
question or doubt that makes you feel uncomfortable don‘t hesitate to tell me and we can skip
over that question or stop the interview any time you want, I will appreciate for your
participation.
Are you ready to participate?
Specific Objectives
To evaluate the views and perceptions of the beneficiaries on the NHIF benefits
package as to whether they have comprehensive coverage in terms of quality.
Q1: For how long have you been a beneficiary of NHIF
Q2: What do you understand about NHIF?
Q3: Tell me how much you know about NHIF Benefit Package.
Q4: What are you views concerning the services provided as per requirements of Benefit
Package?
Q5: How do you explain on the coverage of the Package if are Comprehensive to give quality
service needed.
Probe; Do you think there are some areas to improve/ strengthen?
Q6: What are the challenges that you face most while accessing the service?
Probe: Are there any services that you were refused to access?
And what are the reasons they give?
How did you handle that situation?
156
QN 7: What is your perception on the current Benefit Package?
Probe: Can you explain in what way do you think if it their coverage satisfy/ does not
satisfy on your needs
WIND UP QUESTIONS:
I: Do you have anything to share on what we have talked?
I: How do you feel to be interviewed?
Thank you for your cooperation
157
APPENDIX: IX
INTERVIEW GUIDE FOR NHIF STAFF
How are you?
My Name is Rodney Chiduo, I am a student of MSc in Health Monitoring and Evaluation from
Mzumbe University. My study tries to evaluate Implementation of NHIF Benefit Package in
the selected accredited Health facility. In order to accomplish this task i would like to ask you
some questions concerning this study. I expect my interview to take about 10 minutes. I will ask
you questions concerning NHIF and the Benefit Package in general, feel free to respond to my
questions, In case of any question or doubt that makes you feel uncomfortable don‘t hesitate to
tell me and we can skip over that question or stop the interview any time you want, I will
appreciate for your participation.
QN: Are you ready to participate?
Specific Objective
To evaluate the extent to which the selected accredited health facilities comply with
the accreditation criteria as provided for by MoHCDGEC standard guidelines and
NHIF accredited checklist
QN 1:For how long have you been working in this Department
QN 2: How do you accredit Health facilities
QN 3: How long can it take for the application to be approved by the Fund?
QN 4: How do you make sure that the accredited health facilities comply with the
accreditation criteria as provided for by MoHCDGEC standard guidelines and NHIF
accredited checklist.
QN 5: What is your view about the accreditation procedures?
QN 6: In what way do you see how has the program achieved so far?
QN 7: How do you monitor the progress of the program?
158
Probe: How often,
Any challenges that you come across while you monitor the facility
Qn 8: What do you think could be the strategies used in designing, creating and
implementing the Benefit Package?
WIND UP QUESTIONS:
QN ; Do you have anything to share on what we have talked?
Qn; How do you feel to be interviewed?
May I take this opportunity to thank you for giving me your valuable time to answer all
the questions I asked you, if I will need more clarification of any issue we talked today I
will call you. Have a good day, once again thank you.
Thank you for your cooperation





























