Embed Size (px)
Citation preview
Effective Management of Primary Health Center (PHC)
Set Up through Panchayati Raj Institution Members
(Model Project for Haryana) Final Report
VARDAAN CONSULTANTS, Baroda (Gujarat) December 2005
PRI
NGOPHC/SC
A B
X
C

© Copy Rights: Vardaan Consultants, Baroda & PFI, New Delhi, Dec 2005 Circulation: Restricted to Professionals only First Draft: Nov 2005 Final Report: Dec 2005 Author: Harshit Sinha Disclaimer: - This study was conducted with the support of Population Foundation of India, New Delhi. Hence no part of the findings and results may be referred or reproduced (or disclosed or reprinted or utilized in any form) other than the funding agency (Population Foundation of India, New Delhi) and other supporting agency (Government of India). The inference and options expressed in the report are not the opinion of funding agency or any central or state authorities of India.
Effective Management of Primary Health Center (PHC) Set Up through Panchayati Raj Institution Members
(Model Project for Haryana)
Harshit Sinha
VARDAAN CONSULTANTS, Baroda (Gujarat) CONTACT AT
Website: www.vardaan.org Email: [email protected]
December 2005
This Report is dedicated to the Father of Nation
Mahatma Gandhi
The Founder of the Panchayati Raj System in the modern democratic set up of our country
Vardaan Consultants, Baroda i
Acknowledgement
Developing a sustainable model for the effective management of public health institution in rural area is a mammoth and challenging task. Vardaan Consultants is very grateful to Shri. A.R. Nanda (Executive Director, PFI, New Delhi), who provided us the opportunity to implement our innovative idea for the effective management of PHC through PRI members. Fruitful discussions with him were of immensely useful to develop new ideas. We are also very thankful to all member of governing board of PFI who approved our idea. I also take this opportunity to thank Dr. B.P. Thaigarjan; Dr .A. A. Jayachandren and Dr. A. J. Francis Zavier for designing baseline survey and improving quality of data during the course of discussions and also in their field visits. Our TRIO Management model would have not being completed without the support of the voluntary organization, S.M.S. Foundation, Gurgoan. They had played a crucial and significant role in carrying out the objective of the project and much of the burden of field work and its supervision. We are very grateful to Shri Jay Seghal Executive Director for the support and useful discussion. We are grateful to Dr. Archana Mandal and Ms. Lalima Shrivastava for their untiring efforts in coordination and integration of the team and resources. Our special thanks to all Senior PIT (Mrs. Sushila Bala; Mrs. Urmila Gupta, Mrs. Raziya, Mrs. Kamlesh; Mr. Jan Mohammad and Mr. Zaffar Hussein) members, field officers, and grassroot level volunteers (Mr. Sunil Kumar; Khalil Ahmed, and Mr. Rajuddin) for their valuable contribution in making smooth execution of the project We also would like to thankful to public health officials and staff, without, the success of current project would have not been possible. We are grateful Dr .D.V. Sharan, Civil Surgeon, Gurgaon district, Dr .M.G. Sharma, and Dr. Sucha Singh, Senior Medical Officer, Ferozpur Jhirkha, Dr .Gajender Singh Medical Officer of Nagina PHC, Dr .Rajendra Prasad, Dr. Kamlesh Singh and Dr. Anil Mathur of Mendikheda hospital and Mrs. Usha Mathur from Nagina PHC and all PHC and SC staff for understanding and executing the project concept. Our sincere thanks to Mrs. Falguni Patel and Mrs. Praveena Mistry for data coding and Mr. Rajani Patel for data analysis and other tabulation work. Mrs Bhavan Patwa, Mr. Preeti Parwani and Ms. Neha Chauhan provided proficient word processing and other assistance work.
Dr. Monika Sinha Proprietor, Vardaan Consultants,
Baroda
Vardaan Consultants, Baroda ii
Preface
Changing the public health scenario in the rural areas of India is a challenging task because of the many constraints associated with it. The PRI system of our country is considered to be the back bone of federal democratic system where, at the bottom every gram panchayat had power of governance in the matter of planning, budgeting, and distribution of resources’ equally. Moreover, the Tenth Plan has prioritized reorganization and restructuring of the existing health care infrastructure at primary, secondary and tertiary levels through a decentralized process with the existing structure of the panchayati raj system so that, the rural communities get the desired level of health services and improve our country health index. We have made an attempt for effective management of PHCs through panchayati raj institutions members by involving PHC staff and NGO volunteers as equal partners. The TRIO management model was pilot tested without any compulsion in very informal way and was found to be effective in the management of any public health institutions. I hope that policy makers and programme managers will use the TRIO management model under the rural health mission with proper structural integration and assigning mandatory roles and responsibilities in the PRI system and public health administration for better transparency and community participation.
Harshit Sinha Expert Consultants
Vardaan Consultants, Baroda iii
Index
No. Topics Page No
Acknowledgemen t…………………………………………………………..ii Preface……....................................................................................................iii List of Box……………………………………………………………….…..v List of Tables………………………………………………………………...v List of figures ………………………………………………………………..v Acronyms and Abbreviations ………………………………………………vi Executive Summary………………………………………………………..vii Chapter One: INTRODUCTION
1.1 Rationale 02 1.2 Historical Journey PRI systems to current challenges………………………03 1.3 Decentralization Policy and its importance in Health Sector………………..06 1.4 Literature Review……………………………………………………………10
Chapter Two: DESCRIPTIONS OF THE PROJECT
2.1 Description of the Project Area……………………………………………..19 2.2 Objectives and Study Design………………………………………………..20 2.3 Project Strategy……………………………………………………………...22 2.4 Limitation of Study………………………………………………………….24
Chapter Three: LEARNING EXPEREINCE
3.1 Understanding Partners……………………………………………………..25 3.2 Exploring Ground Realities…………………………………………………29 3.3 Developing Collaborative Action Plan……………………………………...33 3.4 Interest and Participation……………………………………………………34 3.5 Resource Mobilization………………………………………………………36 3.6 Up scaling Public Health Services………………………………………......39 3.7 Status of Women and Gender Equalities ……………………………………41 3.8 Review and Follow up Mechanism…………………………………….…....44 3.9 Short coming in the system……………………………………………....….45 Chapter Four CONCEPTUALIZING THE MODEL……………………47
Chapter Five CONCLUSIONS AND RECOMMENDATION…….……51
References......................................................................................................54
Vardaan Consultants, Baroda iv
Boxes No. Topics Page No
1. Important Features of Panchayati Raj System………………………03 2. PRI roles under NRHM of GOI……………………………………..05 3. Different Commission and Committees for PRI system……………08 4. Role model of Kerala in decentralization process in health………...11 5. People Campaign for Decentralized Planning in Kerela……………12 6. Health achievement Status of West Bengal…………………………13 7. Miles stone of Andhra Pradesh’s decentralization………………….14 8. Miles Stone of Madhya Pradesh’s decentralization………………...15 9. Recommendation of Karnataka task force for popularizing PRI……16 system 10. Miles stone of Haryana’s Panchayati Raj system…………………..19 11. Planned Intervention for execution for the project…………………..23 12. Individual PRI efforts in Promoting Public health Services…………36 13. Improving public health infrastructure……………………………....38 14. Promoting Public – Private Participations…………………………...40 15. Strategy for distributing IEC material …………………………….…40 16. Usage of contraceptives……………………………………………...43
Tables No. Topics Page No
2.1 Number of Panchayats in all blocks of Gurgaon district…………...20 2.2 Sample classification with criteria adopted………………………...22 3.1 Problems identified by PRI and NGO volunteers…………………..32 3.2 Details of Action plan …………………………………..……33 3.3 Details of PRI participation in health programme…………………..35 3.4 Option for resources mobilization…………………………………..37 3.5 Details of up-scaling of public health services……………………...39 3.6 Overlapping health issues among PRI, NGO ………………….……49 and Public Health Staff
Diagram No. Topics Page No
1. Vein Diagram………………………………………..………………….48
Vardaan Consultants, Baroda v
Acronyms and Abbreviations AFR Agenda for Reforms ANM Auxiliary Nurse Midwife ASHA Accredited Social Health Activist BDO Block Development Officer BPL Below Poverty Line CBO Community Based Organization CHC Community Health Center CHWS Community health worker schemes DRDA District Rural Development Agency DOTS Direct Observed therapy short term GDP Gross Domestic Product GOI Government of India GP Gram Panchayat GVS Gram Vikas Samiti IMF Infant Mortality Rate ICPD International Conference of Population and Development IEC Information Education and Communication JY Janmangal Yojana JSR Jan Swasthya Rakshak MMR Maternal Mortality Rate NCMP National Common Minimum Programme NGO Non Government Organization NRHM National Rural Health Mission PHC Primary Health Center PRI Panchayati Raj Institutions PFI Population Foundation of India PCI Per Capita Income PWD Public Work Department RCH Reproductive and Child Health RNTCP Revised National Tuberculosis Control Program SC Sub Center SHG Self Help Group SJSGY Swastha Jeevan Sewa Guarantee Yojana SMO Senior Medical Officer SMSF S.M. Seghal Foundation SMY Swastha Mangal Yojana TP Taluka Panchayat TBA Traditional Birth Attendants VC Vardaan Consultants VHC Village Health Committee WB World Bank
Vardaan Consultants, Baroda vi
Executive Summary
Panchayati raj in India is one of the largest "transformational experiments" The father of Nation, Mahatma Gandhi played a significant role in integrating it into the three-tier panchayati raj system to ensure people’s participation in the great task of rural reconstruction. Panchayats have been the backbone of Indian Villages since the beginning of the recorded history. The transformation and decentralization process must begin at the bottom and every village ought to be a republic with the panchayat having powers. Decentralization of the health sector is one of the policy reforms discussed in the Agenda for Reforms (AFR) of the World Bank (1987). AFR discusses decentralization in the context of the structural adjustment program and the squeeze on government expenditure. Assertions in favour of democratic decentralization are often founded upon the notion that democratization and empowerment of local political bodies will create institutions that are more accountable to local citizens and also appropriate to local needs.
The challenge of providing affordable, available, accessible, acceptable and appropriate healthcare to over a billion people of India is daunting. The problems are many: limited resources, poor governance, skewed manpower, inadequate infrastructure, lack of accountability, misdirected investments, mounting hospital costs, monumental corruption, ignorance, and illiteracy. Hence to overcome such problems, it is essential to make the local government (such as panchayats) to be stronger. The local government’s freedom to adapt to local conditions and access needs must be balanced with the health sector. In addition, decentralizing policy needs to be done along with functional coordinating mechanisms. This brings strength to local bodies that are responsive to and address the local needs.
For the first time in India a TRIO management model has been designed and pilot tested in a backward area for effective management of primary healthcare centre in the Mewat block of Gurgaon district in Haryana. We have given more importance for developing the process and system to integrate PRI members, PHC staff, and NGO volunteers for effective management of public health institutions.
Bringing three partners working together is itself a challenging task. None of village panchayat can work at individual level for the effective management of public health institutions without the support of PHC staff and NGO volunteers. There many overlapping health issues that has to be resolved with trio combination for the resident community. Not all, but countable number of PRI members have proved it that working in team combination could promote more community participation. The NGO or civil society had played an important and significant role in coordination and integration of the team and resources.
Overall the pilot experience suggests that the “TRIO” management model could be very effective if it is integrated in the PRI system with structural integration and define the mandatory roles and responsibilities at various levels of the PRI system and public administration. More weightage to community participation and a decentralize process could provide better result for public health programmes if “TRIO” model is incorporated the basic healthcare service delivery system in the forth coming National Rural Health Mission Programme.
Vardaan Consultants, Baroda vii
Chapter 1: Introduction India’s achievements in the field of health have been less than satisfactory and the burden of disease among the Indian population remains high. High incidence of maternal and infant mortality and morbidity (excluding some states) and reemergence of infectious diseases (T.B; HIV/AIDS; malaria etc) indicate considerable inadequacies in the quality and reach of healthcare services. This has largely affected the human developmental indicators of the country. Many of these illnesses and deaths can be prevented and/or treated cost-effectively with primary healthcare services provided by the public health system. This relies on the quality of services in the social development sector related to health services, infrastructure, and management. Constraints related to health services are at various levels – allocation of resources, planning, and coordination between the implementing agencies and also with quality of services. In the context of providing desired healthcare services, the important question is about the reach, accessibility, and affordability of these services to the population in rural areas.
In India an extensive infrastructure of public health system has been provided by the government but yet, it is inadequate in terms of coverage of population, especially in rural areas, and grossly underutilized because of the dismal quality of health services. In most public health centres which provide primary healthcare services, drugs and equipments are missing or in short supply, there is shortage of staff and the system is characterized by endemic absenteeism on the part of medical personnel owing to lack of oversight and control (Mavalankar 1988). This is because from the date of its inception the Indian family welfare and health programmes are being vertically polarized at all levels of the health functionaries. Healthcare delivery systems in India are divided into two, viz., government and private such that the private sector is confined only to the urban areas. The country as such is run by the government health care system which provides services in the remote villages. Public health investment on health is very low and is stagnant at less than one per cent of the GDP (Bajpai and Goyal 2004). The nation displays wide range of spectrum in the expenditure pattern. States like Kerala, Punjab, and Tamil Nadu recorded double the per capita public health spending of Bihar and Madhya Pradesh.
The Tenth Plan has prioritized reorganization and restructuring of existing health care infrastructure at primary, secondary and tertiary levels through a decentralized process with the existing structure of the panchayati raj system so that the resident population especially the rural communities get the desired level of health services and improves the country’s health index. Here an attempt has been made to develop a model for the effective management of public health institutions through panchayati raj institutions members (PRIs) in Gurgaon district of Haryana.
The report is divided into five sections. Chapter one describes the rationale with the historical journey of the PRI system to the current challenges about decentralization policy and its importance in health sector. The second chapter describes the Haryana panchayati raj System, study design, project strategy and its limitations. Chapter three describes the experience of the intervention and its sustainability in the current
Vardaan Consultants, Baroda, Gujarat, INDIA
1

settings. Based on the current experience section four describes the sustainable model for PRIs – PHCs-NGOs interface consistent with the spirit and provisions of the 73rd Constitutional Amendment Act. The last Chapter presents findings; lessons learnt with recommendations and policy implications of the study.
1.1 Rationale:
The Tenth Plan has prioritized reorganization and restructuring of the existing healthcare infrastructure at primary, secondary and tertiary levels so that it has the capacity to render healthcare services to the population residing in well defined geographical areas and has appropriate referral linkages with each other. Besides, the ICPD agenda gave much impetus to provide quality-client centered services and sustain it for the rural communities. It is necessary to assess the quality in healthcare delivery systems to provide substantial support to improve the working condition and functioning of the health system.
The quality of services at the primary health centre has always been compared with the demographic achievements made in various family planning programmes. The need for providing quality service to the clients was never felt, because of the ignorance of the clients and also negligence on the part of service providers. Besides, poor surveillance and lack of accountability restricted the service providers to provide quality services at the primary level. It is only after the ICPD Cairo conference, (1994) that all countries including India endorsed a Plan of Action for quality improvement. It recommends continuing efforts to satisfy unmet need, through improvement in the quality of reproductive health services and IEC through counselling and interpersonal communication.
In India, the experience in family planning services shows serious shortcomings in quality of care that characterize the Indian health programme in such areas that restricted choice of contraceptive method, limited information provided to clients, poor technical standards and low levels of follow-up and continuity of care. Earlier studies (Mavalankar and Sharma, 1999; Townsend and Khan 1999) have shown that the concept of quality was restricted to particular clinical activities. However some studies linked quality with total institution from which the health services are imparted to the community. On the other hand some studies related quality with service providers and some with user or client perspective. No studies have been conducted as described in the framework of quality (Bruce1990).
Institutional infrastructure, human resources, availability of material, technical know- how, perspective of both service providers and clients and related administrative problem that directly affects the quality of services have not been taken in totality or viewed simultaneously. Many tangible benefits could not be analysed by viewing “quality” by one perspective. Thus there is an urgent need to devise a strategy that looks/narrates the “quality health care” from all perspectives as mentioned above. It should also emphasize on sustainable strategy to mobilize Panchayati Raj Institutions to sustain and provide quality of health services through PHC system as observed in the State of West Bengal and Kerala.
Vardaan Consultants, Baroda, Gujarat, INDIA
2
1.2 Historical Journey - PRI systems to Current Challenges:
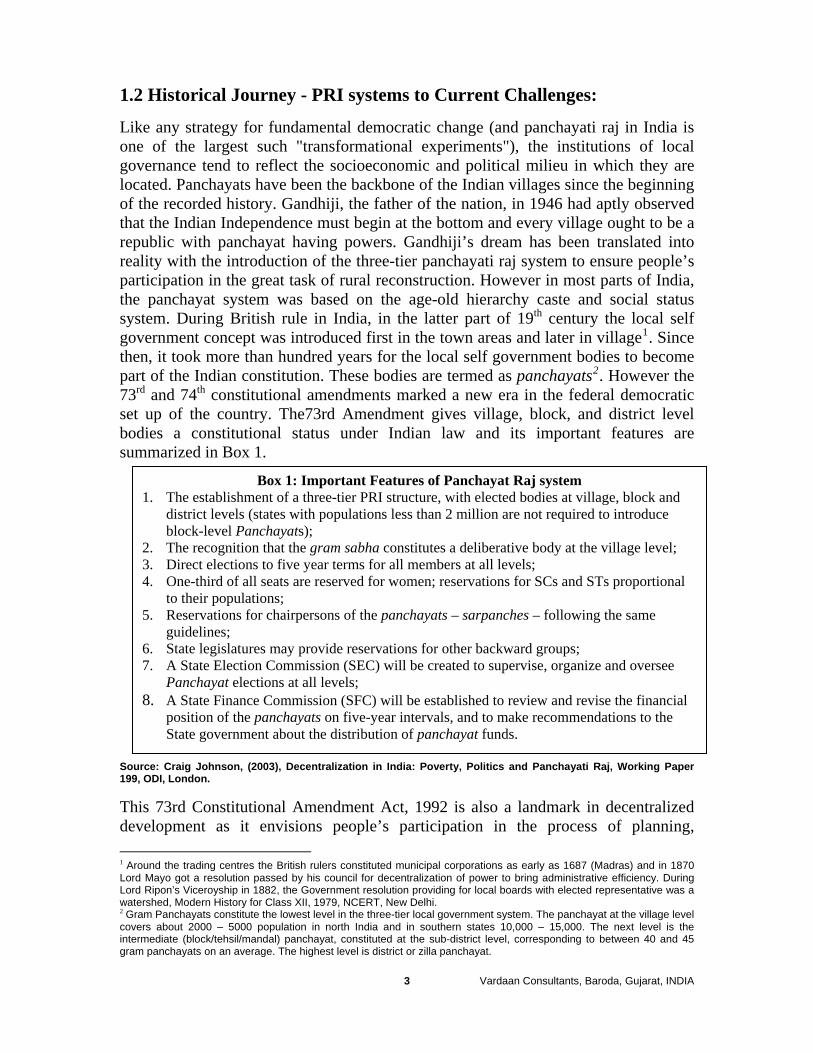
Like any strategy for fundamental democratic change (and panchayati raj in India is one of the largest such "transformational experiments"), the institutions of local governance tend to reflect the socioeconomic and political milieu in which they are located. Panchayats have been the backbone of the Indian villages since the beginning of the recorded history. Gandhiji, the father of the nation, in 1946 had aptly observed that the Indian Independence must begin at the bottom and every village ought to be a republic with panchayat having powers. Gandhiji’s dream has been translated into reality with the introduction of the three-tier panchayati raj system to ensure people’s participation in the great task of rural reconstruction. However in most parts of India, the panchayat system was based on the age-old hierarchy caste and social status system. During British rule in India, in the latter part of 19th century the local self government concept was introduced first in the town areas and later in village1. Since then, it took more than hundred years for the local self government bodies to become part of the Indian constitution. These bodies are termed as panchayats2. However the 73rd and 74th constitutional amendments marked a new era in the federal democratic set up of the country. The73rd Amendment gives village, block, and district level bodies a constitutional status under Indian law and its important features are summarized in Box 1.
Box 1: Important Features of Panchayat Raj system 1. The establishment of a three-tier PRI structure, with elected bodies at village, block and
district levels (states with populations less than 2 million are not required to introduce block-level Panchayats);
2. The recognition that the gram sabha constitutes a deliberative body at the village level; 3. Direct elections to five year terms for all members at all levels; 4. One-third of all seats are reserved for women; reservations for SCs and STs proportional
to their populations; 5. Reservations for chairpersons of the panchayats – sarpanches – following the same
guidelines; 6. State legislatures may provide reservations for other backward groups; 7. A State Election Commission (SEC) will be created to supervise, organize and oversee
Panchayat elections at all levels; 8. A State Finance Commission (SFC) will be established to review and revise the financial
position of the panchayats on five-year intervals, and to make recommendations to the State government about the distribution of panchayat funds.
Source: Craig Johnson, (2003), Decentralization in India: Poverty, Politics and Panchayati Raj, Working Paper 199, ODI, London.
This 73rd Constitutional Amendment Act, 1992 is also a landmark in decentralized development as it envisions people’s participation in the process of planning, 1 Around the trading centres the British rulers constituted municipal corporations as early as 1687 (Madras) and in 1870 Lord Mayo got a resolution passed by his council for decentralization of power to bring administrative efficiency. During Lord Ripon’s Viceroyship in 1882, the Government resolution providing for local boards with elected representative was a watershed, Modern History for Class XII, 1979, NCERT, New Delhi. 2 Gram Panchayats constitute the lowest level in the three-tier local government system. The panchayat at the village level covers about 2000 – 5000 population in north India and in southern states 10,000 – 15,000. The next level is the intermediate (block/tehsil/mandal) panchayat, constituted at the sub-district level, corresponding to between 40 and 45 gram panchayats on an average. The highest level is district or zilla panchayat.
Vardaan Consultants, Baroda, Gujarat, INDIA
3

decision-making, implementation, and delivery. These constitutional provisions provide for devolution of powers and responsibilities to different tiers of PRIs with respect to preparation of plans and programmes for economic development and social justice and their implementation in relation to 29 subjects listed in the eleventh schedule.
Consistent with the spirit of the provisions, the central ministries / departments and state governments are expected to confer necessary executive powers and administrative authority along with control over functionaries in their jurisdiction dealing with subjects allotted to them and devolves financial resources to the concerned level of PRIs to enable them to discharge their responsibilities effectively and efficiently. In the decade since the 73rd Amendment Act was added to the statue book. PRIs have started functioning and are in their second elective tenure in many states. The process of empowering PRIs has followed a varied pattern across States showing the poor status of integration the PRI system with other developmental programmes (PRI Report 2001).
It has been observed that concerned ministries / departments have yet to integrate the PRIs in planning and implementation of programmes which essentially fall in their jurisdiction. The centrally sponsored / central sector schemes of central ministries continue to be implemented departmentally or through parallel delivery arrangements such as the users’ associations, programme specific committees / agencies, self-help/beneficiary groups, mahila sangh or through NGOs, virtually by passing PRIs. The situation is worse in respect of internationally funded projects which have set up separately structures for decision making and monitoring at various levels. PRIs do not really figure in this strategy of implementation and in fact there is not even a conceptual recognition that essentially NGOs are operating in areas and subjects which belong to the PRIs and therefore they should work in tandem with them.
In the health sector, the situation is more or less similar. After the International Conference on Population and Development (ICPD) in Cairo (1994), a historical conceptual shift had taken place that viewed population programmes with a broader concern for sexual and reproductive health. One can also say that the ICPD conference revealed a shift from a top-down, target-based approach to a need-based, client-centered, demand driven approach. Such a conceptual shift brought our national health and family welfare programmes from the segregated approach to that of integrated approach under reproductive and child health (RCH) services for future. Taking account of involvement of PRIs in family welfare programmes, there are immense differences between states in the involvement of PRIs in the family welfare programme. States like Kerala have embarked on decentralized planning and monitoring programmes utilizing PRIs and have provided power and finances to PRIs. Rajasthan, Andhra Pradesh, Madhya Pradesh, and Karnataka have implemented their own models for the involvement of PRIs in the health sector. In other states (including Haryana), involvement is mainly in planning and monitoring without devolution of power and finances. In some states, PRIs have not yet started
Vardaan Consultants, Baroda, Gujarat, INDIA
4
participating in the programme. There is a need to continuously review the situation and initiate appropriate interventions (PC Report 2002-07).
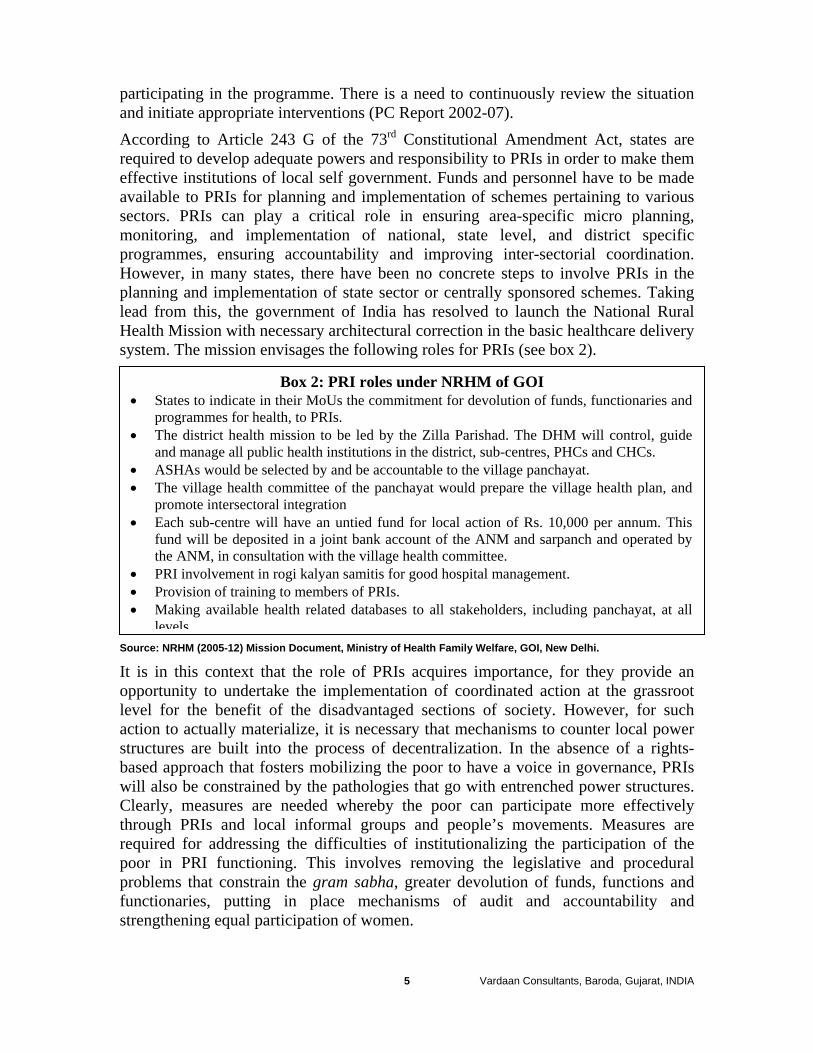
According to Article 243 G of the 73rd Constitutional Amendment Act, states are required to develop adequate powers and responsibility to PRIs in order to make them effective institutions of local self government. Funds and personnel have to be made available to PRIs for planning and implementation of schemes pertaining to various sectors. PRIs can play a critical role in ensuring area-specific micro planning, monitoring, and implementation of national, state level, and district specific programmes, ensuring accountability and improving inter-sectorial coordination. However, in many states, there have been no concrete steps to involve PRIs in the planning and implementation of state sector or centrally sponsored schemes. Taking lead from this, the government of India has resolved to launch the National Rural Health Mission with necessary architectural correction in the basic healthcare delivery system. The mission envisages the following roles for PRIs (see box 2).
Box 2: PRI roles under NRHM of GOI • States to indicate in their MoUs the commitment for devolution of funds, functionaries and
programmes for health, to PRIs. • The district health mission to be led by the Zilla Parishad. The DHM will control, guide
and manage all public health institutions in the district, sub-centres, PHCs and CHCs. • ASHAs would be selected by and be accountable to the village panchayat. • The village health committee of the panchayat would prepare the village health plan, and
promote intersectoral integration • Each sub-centre will have an untied fund for local action of Rs. 10,000 per annum. This
fund will be deposited in a joint bank account of the ANM and sarpanch and operated by the ANM, in consultation with the village health committee.
• PRI involvement in rogi kalyan samitis for good hospital management. • Provision of training to members of PRIs. • Making available health related databases to all stakeholders, including panchayat, at all
levelsSource: NRHM (2005-12) Mission Document, Ministry of Health Family Welfare, GOI, New Delhi.
It is in this context that the role of PRIs acquires importance, for they provide an opportunity to undertake the implementation of coordinated action at the grassroot level for the benefit of the disadvantaged sections of society. However, for such action to actually materialize, it is necessary that mechanisms to counter local power structures are built into the process of decentralization. In the absence of a rights-based approach that fosters mobilizing the poor to have a voice in governance, PRIs will also be constrained by the pathologies that go with entrenched power structures. Clearly, measures are needed whereby the poor can participate more effectively through PRIs and local informal groups and people’s movements. Measures are required for addressing the difficulties of institutionalizing the participation of the poor in PRI functioning. This involves removing the legislative and procedural problems that constrain the gram sabha, greater devolution of funds, functions and functionaries, putting in place mechanisms of audit and accountability and strengthening equal participation of women.
Vardaan Consultants, Baroda, Gujarat, INDIA
5

Taking account of these agenda it becomes necessary to develop a sustainable model that would be implemented through PRIs and ensure effective PRIs - NGO interface consistent with the spirit and provisions of the 73rd Constitutional Amendment Act by involving diversified developmental schemes of various ministries3 that in some or the other way are linked with each other. In this study, efforts are made to develop a sustainable model keeping the health sector in focus to ensure effective management of PHC through PRI-NGO interface within a block having village as unit.
1.3 Decentralization Policy and its importance in Health Sector:
Decentralization of the health sector is one of the policy reforms discussed in the Agenda for Reforms (AFR) of the World Bank published in 1987. AFR discusses decentralization in the context of Structural Adjustment Programme and the squeeze on government expenditure. The specific circumstance was the difficulty of attracting private health practitioners to low income rural areas and the role of government health care services in such areas. Decentralization means granting greater financial, and management autonomy to local units of the system. It gives local units greater responsibility for planning and budgeting, for collecting user charges and for determining how collected funds will be spent.
Before elaborating more on decentralization policy and its importance in the health sector, the term decentralization can be defined as a political process whereby administrative authority, public resources, and responsibilities are transferred from central government agencies to lower-level organs of government or to non-governmental bodies, such as community-based organizations (CBOs), ‘third party’ non-governmental organizations (NGOs), or private sector actors (Crook and Manor, 19986-7; Rondinelli et al., 1989; Meenakshisundaram, 1999). Thus conceptually, it is very important to understand distinction between deconcentration4, devolution5, delegation6, and privatization7 as part of decentralization policy. Assertions in favour of democratic decentralization are often founded upon the notion that democratization and empowerment of local political bodies will create institutions that are more accountable to local citizens and more appropriate to local needs.
India, of course, is not alone in this process. Decentralization has emerged as a dominant trend in world politics. In 1998, the World Bank estimated that all but 12 of the 75 developing and transitional countries with populations greater than 5 million had embarked on a process of political devolution (cited in Crook and Manor, 1998: 1). At the heart of this transformation are a number of complex yet inter-related themes. One is an ideological shift, in which the legitimacy of central State-led 3 Rural Development, Health & Family Welfare, Social Justice and Empowerment, Women and Child Development, Environment and Forests, Agriculture, Irrigation, and Education 4 in which political, administrative and fiscal responsibilities are transferred to lower units within central line ministries or agencies (cited in Craig Johnson, 2003), 5 in which sub-national units of government are either created or strengthened in terms of political, administrative and fiscal power (cited in Craig Johnson, 2003), 6 in which responsibilities are transferred to organizations that are ‘outside the regular bureaucratic structure and are only indirectly controlled by the central government,’ (cited in Craig Johnson, 2003), 7 in which all responsibility for government functions is transferred to non-governmental organizations (NGOs) or private enterprises independent of government (cited in Craig Johnson, 2003),
Vardaan Consultants, Baroda, Gujarat, INDIA
6
development has been challenged on the grounds that it produces systems of governance that undermine national economic performance and effective public policy (Gore, 2000; Johnson and Start, 2001). A second is a (remarkably widespread) political agenda, which asserts that decentralization of public administration and introduction of locally elected bodies will produce systems of governance that are better able to meet the needs of poor and politically marginal groups in society. A third and related theme suggests that democratic decentralization is a political strategy that national elites have used to maintain legitimacy and control in the face of political disintegration (Johnson, 2003).
In India, decentralization is an old concept. Traditionally there were Panchayati Raj Institutions. Village committees called gram panchayat were incharge of affairs of the village. Decentralization was the logical way to govern when communication was slow. During British ruler power became centralized in the hands of the master and the whole system became defunct. Since independence in 1947, the concept of decentralization has been discussed and practiced for many decades in some form or the other, although the decentralization may have been informally practiced rather than formally recognized. Many committees have recommended decentralization of governance, especially in rural areas, to give it a more formal structure and legal validity. In the post independence period many committees namely Balwantrai Mehta Committee (1957), Ashok Mehta Committee (1978), and Sakaria Commission (1988) strongly argued for people’s participation through the panchayati raj at village level.
Box 3 gives of some information of the various commission and committees that have inspired contemporary thinking about Panchayati Raj in India. Perhaps the most important among these – particularly since independence – were the B. Mehta Commission of 1957, the Asoka Mehta Commission of 1978, and the G.V.K. Rao Committee of 1985.
Box 3: Different commission and Committees for PRI System 1882 The Resolution on Local Self-Government. 1907 The Royal Commission on Decentralization. 1948 Constitutional debates between Gandhi and Ambedkar on Gram Swaraj, ‘self-rule’. 1957 Balwantrai Mehta Commission – an early attempt to implement the Panchayat
Structure at district and block (Samithi) levels. 1963 K. Santhanam Committee – recommended limited revenue raising powers for Panchayats and the
establishment of State Panchayati Raj Finance Corporations. 1978 Asoka Mehta Committee – appointed to address the weaknesses of PRIs, concluded that a resistant
bureaucracy, lack of political will, ambiguity about the role of PRIs, and élite capture had undermined previous attempts at decentralization, recommending that the District serve as the administrative unit in the PRI structure. Based on these recommendations, Karnataka, Andhra Pradesh and West Bengal passed new legislation to strengthen PRIs.
1985 G.V.K. Rao Committee – appointed to address weaknesses of PRIs, recommended that the block development office (BDO) should assume broad powers for planning, implementing and monitoring rural development programmes. 1986 L.M. Singvhi Committee – recommended that local self-government should be constitutionally enshrined, and that the Gram Sabha (the village assembly) should be the base of decentralized democracy in India. 1993 The 73 rd Amendment to the Indian Constitution – PRIs at district, block and village levels are granted
Constitutional status. The Gram Sabha is recognized as a formal democratic body at the village level. The 74 th Amendment, granting Constitutional status to municipal bodies, is passed soon after.
1996 The Adivasi Act – Powers of self-government are extended to tribal communities living in ‘Fifth Schedule’ areas
Source: Craig Johnson, (2003), Decentralization in India: Poverty, Politics and Panchayati Raj, Working Paper 199, ODI, London.
Vardaan Consultants, Baroda, Gujarat, INDIA
7
An enduring issue features in all of these assessments is the notion that the Panchayats have been weakened or undermined on three fronts: First the States that are unwilling to devolve substantive power Second, a resistant bureaucracy and third, the power of ‘local elites.’ These are the reason for making decentralization less success in the all developmental sector programmes including health. In addition, community participation was poorly conceptualized and operationalised: in the governance of the health sector as well as technical intervention, the specific contribution to health system outcomes was undermined.
The challenge of providing affordable, available, accessible, acceptable and appropriate healthcare to over a billion people of India is daunting. The problems are many: limited resources, poor governance, skewed manpower, inadequate infrastructure, lack of accountability, misdirected investments, mounting hospital costs, monumental corruption, ignorance, and illiteracy. To overcome such problems, it is essential to make the local government (such as panchayats) stronger. Local governments freedom to adapt to local conditions and access needs must be balanced with the health sector. In addition, decentralizing policy needs to be done along with functional coordinating mechanisms. This brings about and strengthening local power that are responsive to and address the local needs.
This has become essential because the National Health Policy 2002 – (NHP) set the goal of increasing public health expenditure from 0.9 per cent of GDP to 2 per cent of GDP by 2010. This calls for enhancement of states’ health expenditure from 5.5 per cent of total budget to 8 per cent by 2010; and union expenditure from 1.3 per cent of total budget to about 7 pre cent – almost six-fold increase. The National Common Minimum Programme 2004 (NCMP) has set the target of raising public spending on healthcare to at least 2-3 percent of GDP by 2009, with focus on primary health care.
Thus it seems that financing decentralized healthcare is very crucial and the significant gap between the central government and the local governments must not be overlooked, as this would cause equity problems and compromise the health sectors ability to provide equitable and quality health care under decentralizations. On the other hand, capacity building and its constraints are as important as decentralizing efforts. The need to train staff in their new role is a mammoth task and transfer of qualified staff and for them to adapt to local conditions should be addressed with careful scrutiny.
Complex linkages between different services require more planning and careful introduction of organizational roles and organizational structures. As in the case of most of the states of India, the integrated decentralized district health concept which took years to formulate and sustain collapsed when performance and coordination of its operation was taken into consideration at the grassroot level. In spite of the proper three tier structure of the panchayati raj system, no proper accountability and linkages were created and hence effective management of public health institutions did not take place in the desired manner, in most parts of the country, the public health system had collapsed.
Vardaan Consultants, Baroda, Gujarat, INDIA
8
One of the important issues of decentralization policy is related to the participation because decentralization and participation in some or the other has symbiotic relation ship. In order to decentralize the local government, participation is necessary to respond to local needs and information flow between Citizens and the local government and state should exist. Decentralizing could also enhance opportunities for participation of communities by empowering and resource provision. Participation could be a means or end for a successful decentralizations process. Community participation is a pre-condition for broad decision making and decentralizing. However, lack of participatory mechanisms could not evolve decentralizations in order to create responsiveness and demand. The process by which stakeholders participate with legitimate interest to share control over developments, decision, and resources which affect them, becomes imperative.
One should not forget that participation comprises community involvement at the inception and throughout the project or programme cycle. Participation is the means or the ends of development and decentralization, participation empowers mobilizes people as actors and overseers of their own development. A well designed participatory approach would resolve any conflict of interest it can also be a ground for negotiation for benefits to accrue to all sections of society. It also increases accountability thereby reducing supervision costs.
How can the panchayat play a major role in the health of a community can be seen in the recommendations of a recent report of the Task force of Panchayati Raj Institutions (PRI Report 2000). After massive effort and decades of providing basic health care and building up of impressive and huge infrastructure the programmes are unable to reach those who need it most, and the needs are not addressed appropriately. Lack of a system or a mechanism where people rights were informed and the right to demand and monitor services available to them are absent. Right to health services in terms of adequacy, quality, and accessibility that is the entitlement of community needs and assurance needs to be asserted by communities and this is possible by empowerment of communities.
It has been observed that community participation would improve community’s perception and need for better health practices in areas such as sanitation, water supply, nutrition, and well-being. This raises the need for training and orientation. This is because, community participation methods could act as catalysts to aid this process for robustness and efficiency and effective need based sustainable health interventions could be considered as positive steps towards decentralization in the health sector.
Thus we have seen that local level planning for people-centred development is an important component of the panchayati raj system. This aspect, however, has not received as much attention as some of the other aspects of panchayati raj. There is a need to strengthen panchayats to undertake participatory local planning and budgeting. This is because it provides support to them in resource identification and mobilization, local budgeting and plan formulation but also in promoting participation of gram sabha, participatory monitoring, and evaluation of plans and social audit.
Vardaan Consultants, Baroda, Gujarat, INDIA
9
1.4 Literature Review
India has a long history of experimenting with decentralization. However the concept role and structure of decentralization with different players have changed over a period of time. Brief review of experience will be incomplete without some reference to the reality in different states. This is a subject that has been extensively studied by many, in particular the Institute of Social Science, the National Institute of Rural Development and the Institute of Social Studies Trust. However looking the variation that exists among the states and region where government has been relatively supportive to the interest of Panchayati Raj, we have confined to the role of PRI in context of healthcare and decentralization associated with it. The role of women in this context has been discussed separately in the latte part of the report.
1.4a Kerala experience: Kerala is in the forefront and a role model of decentralization (refer Box 4) of power following the 73rd and 74th Constitutional Amendments. In spite of the economic backwardness, Kerala has made remarkable achievements in health almost comparable to that of even developed countries. The widely accepted health indicators like crude death rate, infant mortality rate and life expectancy evidence are this.
Box 4: Role model of Kerala in Decentralization process in health The World Health Organization was advocating Community Involvement in Health (CIH) as a prerequisite for solving the health problems of the developing countries (Community Involvement in Health Development: Challenging Health Services-Report of a WHO Study Group WHO Geneva – 1991). WHO study group reports says that “A critical step will be the decentralization of health services and the corresponding strengthening of the local health services that will serve as the basis for CIH” and further “Structural changes in health systems will be necessary to support the CIH process. These changes include: decentralization of planning, management, and budgeting.”
Toning up of the healthcare system in the state and making it capable of taking on the burden of provision of equitable, efficient, and good quality healthcare needs concerted action from the political parties, social movements, and professional organizations. These objectives can be realized only through an administrative and financial decentralization of the health services department, while ensuring community involvement in formulating and implementing healthcare programmes and reforms. The panchayati raj now provides the possibility for the people to demand the resources to operate a health service in which the people themselves will play the dominant role and of which they will be the chief beneficiaries. The people can be mobilized to improve not only curative care but even more so in health education as well as in the prevention and control of diseases that originate in their environment. This system involves the entire community and especially women in identifying their health problems (Ekbal, 2000). However, the problem of benefit spillover is quite serious with regard to secondary health care services accessed from the taluka head quarters hospitals, which have been brought under the municipal councils. The problem arises from the
Vardaan Consultants, Baroda, Gujarat, INDIA
10
concentration of hospital beds in municipal towns. The system of "matching transfers" might address the problem of benefit spillover but it will introduce a new problem owing to inequality in the distribution of hospital beds across the talukas of the state (Narayana and Krup, 2000). Overall, the administration of the primary health centres, community health centres and the taluka and district hospitals have been already handed over to the local bodies. Thus today in Kerala, the possibilities that have been opened up with the financial and administrative decentralisation of the health sector and the people’s campaign for decentralized planning are as shown in Box 5. Source: B. Ekbal, (2000) Decentralize Planning and Health Sector in Kerela, Issue Paper at People Health Assembly
Box 5: People Campaign for Decentralized planning in Kerala 1. The control of infectious diseases and even the prevention, early detection, and management
of the life style diseases can be achieved only by strengthening the primary and secondary level healthcare facilities. With the local bodies in control, this can be achieved with better community involvement.
2. Once the primary and secondary healthcare facilities are improved through the local bodies, the tertiary care centers like the medical colleges can entirely concentrate on medical education, research, and tertiary healthcare.
3. The problem of resource constraint in the health sector can be solved with a more need-based reallocation of resources and generating local resources through community participation.
4. A better relationship between health workers, people’s representatives, and the people at large can be accomplished.
5. Once the public health system is reinforced, the poor people who cannot afford private health services will be benefited and social equity in health care will be re- established.
6. There are provisions in the Panchayat Raj Act which can be invoked for the social control of the private sector.
One of the key findings of the PRI taskforce was that central ministries also take up internationally funded projects. All such projects are implemented through bureaucratic functionaries and do not involve panchayati raj institutions even though the subjects they deal with fall in the domain of panchayats. What is true of the central government is also more or less true of the state governments barring a few states which have taken some steps to transfer power and resources to the PRIs. However, even these states feel handicapped in involvement of PRIs in execution of centrally sponsored schemes as the guidelines concerning them are drawn by the concerned central ministries which they have no authority to change. Even states like Kerala feel handicapped with regard to central schemes since the guidelines for implementation are drawn by the concerned agency of central government.
1.4b West Bengal experience: The experience of West Bengal under the panchayat system stands in sharp contrast with that of other states and, together with land reform, it has been credited for playing an important role in the impressive economic turnaround of the state since the mid 1980s. West Bengal is the first and the only major state to have had timely panchayat elections on a party basis regularly every five years since 1978. However, despite its pioneering status in terms of reforms of the panchayat system, West Bengal lags behind several other states in terms of
Vardaan Consultants, Baroda, Gujarat, INDIA
11

devolution of power, finances and functions to the panchayat. Also, the extent of people’s participation in the planning process is significantly less compared to that in Kerala (Ghatak and Ghatak 2002).
There is much to admire in the achievements of West Bengal as a pioneering model of participatory government. It has enjoyed by far the longest and most stable existence among similar experiments carried out in other Indian states, including of Kerala. This is because of the village council officials have to give an account of their performance and reply to charges of non-performance or other acts of impropriety and even corruption to the voters in the village constituency meetings. This in itself is a major development. It stands in sharp contrast with other Indian states, or even the situation in West Bengal a few years ago.
Until very recently the people in the state of West Bengal, like most other states in India, did not have as much access to information about development programmes and availability of funds for their own areas as they have today. The only control they had was the ability to vote elected officials out of power every five years. With the introduction of the system of mandatory village constituency meetings the people now have access to the accounts of expenditure, are able to question elected officials for the use of public funds and implementation of public projects, participate in deciding the kind of programmes that should be undertaken in their villages and who should get priority for specific programmes (Ghatak and Ghatak 1999). However there is no direct evaluation of the impact of public health through PRI: therefore we have to rely on health indicators mentioned in NSS and NFHS. Box 6 shows that that the achievements of the West Bengal government in the area of public health through PRI participation are substantial.
Box 6: Health achievement Status of West Bengal 1. West Bengal had the second lowest crude death rate in 1999 (7.1, the lowest being 6.4 for
Kerala) among all States in India. 2. In 1999, West Bengal had the third lowest birth rate among all states of India. 3. Life expectancy at birth is about 72 years in West Bengal, which is next only to Kerala
and Maharashtra. 4. Among all states, the public health system in West Bengal covers the largest proportion
of the population (about 70 per cent). 5. As regards infant mortality rate (48.7%), it stands tenth in position after Kerala, HP,
Manipur, Mizoram Maharashtra, Delhi, Sikkim, Nagaland, and Goa.
1.4c Andhra Pradesh Experience: The south Indian State of Andhra Pradesh has received a lot of attention, because of its is economic reform programmes in the 1990s. A new type of dynamic leadership had made decentralization as an essential part of the programme to make government institutions more efficient and responsive. The state is therefore determined to strengthen its administration through responsible management by PRIs and community organizations. Here local empowerment is already emphasized in the 73rd and 74th Constitutional Amendments. Attempts have been made to reduce the power of the district collector with the Gram Panchayat Amendment Act in 1976. Thus the non – elected bureaucracy is an enduring theme in Andhra Pradesh’s decentralization process (refer Box 7).
Vardaan Consultants, Baroda, Gujarat, INDIA
12
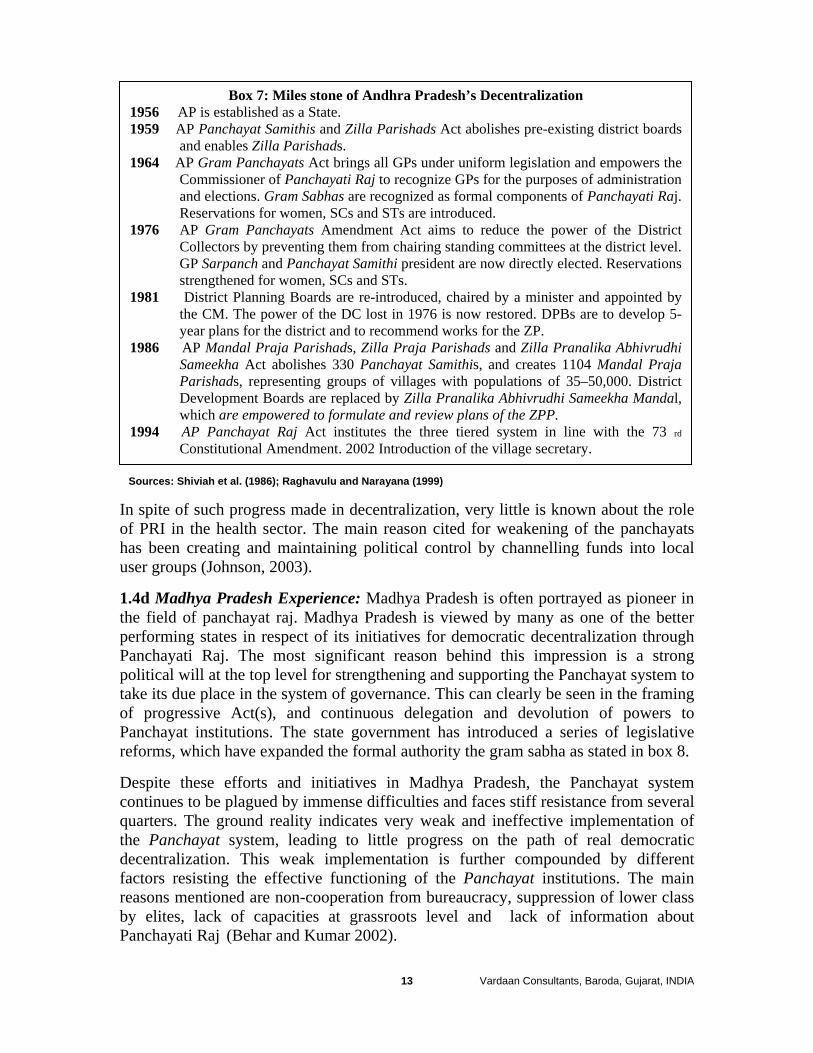
Box 7: Miles stone of Andhra Pradesh’s Decentralization 1956 AP is established as a State. 1959 AP Panchayat Samithis and Zilla Parishads Act abolishes pre-existing district boards
and enables Zilla Parishads. 1964 AP Gram Panchayats Act brings all GPs under uniform legislation and empowers the
Commissioner of Panchayati Raj to recognize GPs for the purposes of administration and elections. Gram Sabhas are recognized as formal components of Panchayati Raj. Reservations for women, SCs and STs are introduced.
1976 AP Gram Panchayats Amendment Act aims to reduce the power of the District Collectors by preventing them from chairing standing committees at the district level. GP Sarpanch and Panchayat Samithi president are now directly elected. Reservations strengthened for women, SCs and STs.
1981 District Planning Boards are re-introduced, chaired by a minister and appointed by the CM. The power of the DC lost in 1976 is now restored. DPBs are to develop 5-year plans for the district and to recommend works for the ZP.
1986 AP Mandal Praja Parishads, Zilla Praja Parishads and Zilla Pranalika Abhivrudhi Sameekha Act abolishes 330 Panchayat Samithis, and creates 1104 Mandal Praja Parishads, representing groups of villages with populations of 35–50,000. District Development Boards are replaced by Zilla Pranalika Abhivrudhi Sameekha Mandal, which are empowered to formulate and review plans of the ZPP.
1994 AP Panchayat Raj Act institutes the three tiered system in line with the 73 rd
Constitutional Amendment. 2002 Introduction of the village secretary.
Sources: Shiviah et al. (1986); Raghavulu and Narayana (1999) In spite of such progress made in decentralization, very little is known about the role of PRI in the health sector. The main reason cited for weakening of the panchayats has been creating and maintaining political control by channelling funds into local user groups (Johnson, 2003).
1.4d Madhya Pradesh Experience: Madhya Pradesh is often portrayed as pioneer in the field of panchayat raj. Madhya Pradesh is viewed by many as one of the better performing states in respect of its initiatives for democratic decentralization through Panchayati Raj. The most significant reason behind this impression is a strong political will at the top level for strengthening and supporting the Panchayat system to take its due place in the system of governance. This can clearly be seen in the framing of progressive Act(s), and continuous delegation and devolution of powers to Panchayat institutions. The state government has introduced a series of legislative reforms, which have expanded the formal authority the gram sabha as stated in box 8.
Despite these efforts and initiatives in Madhya Pradesh, the Panchayat system continues to be plagued by immense difficulties and faces stiff resistance from several quarters. The ground reality indicates very weak and ineffective implementation of the Panchayat system, leading to little progress on the path of real democratic decentralization. This weak implementation is further compounded by different factors resisting the effective functioning of the Panchayat institutions. The main reasons mentioned are non-cooperation from bureaucracy, suppression of lower class by elites, lack of capacities at grassroots level and lack of information about Panchayati Raj (Behar and Kumar 2002).
Vardaan Consultants, Baroda, Gujarat, INDIA
13
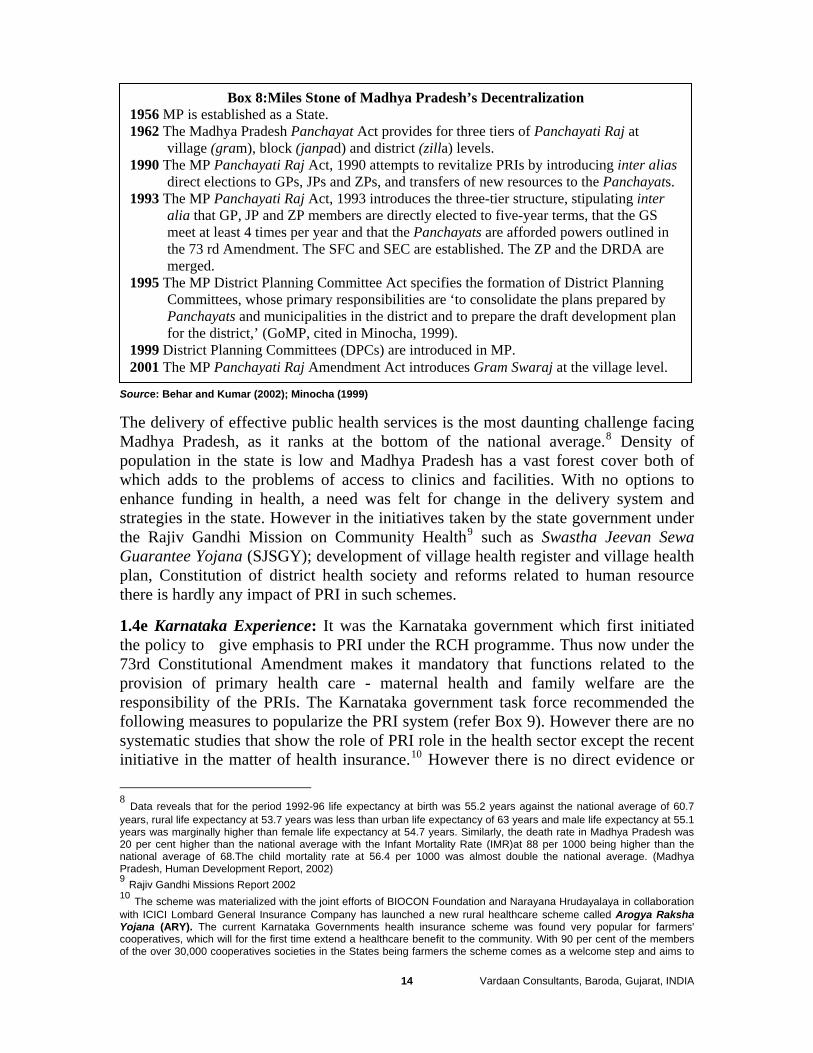
Box 8:Miles Stone of Madhya Pradesh’s Decentralization 1956 MP is established as a State. 1962 The Madhya Pradesh Panchayat Act provides for three tiers of Panchayati Raj at
village (gram), block (janpad) and district (zilla) levels. 1990 The MP Panchayati Raj Act, 1990 attempts to revitalize PRIs by introducing inter alias
direct elections to GPs, JPs and ZPs, and transfers of new resources to the Panchayats. 1993 The MP Panchayati Raj Act, 1993 introduces the three-tier structure, stipulating inter
alia that GP, JP and ZP members are directly elected to five-year terms, that the GS meet at least 4 times per year and that the Panchayats are afforded powers outlined in the 73 rd Amendment. The SFC and SEC are established. The ZP and the DRDA are merged.
1995 The MP District Planning Committee Act specifies the formation of District Planning Committees, whose primary responsibilities are ‘to consolidate the plans prepared by Panchayats and municipalities in the district and to prepare the draft development plan for the district,’ (GoMP, cited in Minocha, 1999).
1999 District Planning Committees (DPCs) are introduced in MP. 2001 The MP Panchayati Raj Amendment Act introduces Gram Swaraj at the village level.
Source: Behar and Kumar (2002); Minocha (1999)
The delivery of effective public health services is the most daunting challenge facing Madhya Pradesh, as it ranks at the bottom of the national average.8 Density of population in the state is low and Madhya Pradesh has a vast forest cover both of which adds to the problems of access to clinics and facilities. With no options to enhance funding in health, a need was felt for change in the delivery system and strategies in the state. However in the initiatives taken by the state government under the Rajiv Gandhi Mission on Community Health9 such as Swastha Jeevan Sewa Guarantee Yojana (SJSGY); development of village health register and village health plan, Constitution of district health society and reforms related to human resource there is hardly any impact of PRI in such schemes.
1.4e Karnataka Experience: It was the Karnataka government which first initiated the policy to give emphasis to PRI under the RCH programme. Thus now under the 73rd Constitutional Amendment makes it mandatory that functions related to the provision of primary health care - maternal health and family welfare are the responsibility of the PRIs. The Karnataka government task force recommended the following measures to popularize the PRI system (refer Box 9). However there are no systematic studies that show the role of PRI role in the health sector except the recent initiative in the matter of health insurance.10 However there is no direct evidence or 8 Data reveals that for the period 1992-96 life expectancy at birth was 55.2 years against the national average of 60.7 years, rural life expectancy at 53.7 years was less than urban life expectancy of 63 years and male life expectancy at 55.1 years was marginally higher than female life expectancy at 54.7 years. Similarly, the death rate in Madhya Pradesh was 20 per cent higher than the national average with the Infant Mortality Rate (IMR)at 88 per 1000 being higher than the national average of 68.The child mortality rate at 56.4 per 1000 was almost double the national average. (Madhya Pradesh, Human Development Report, 2002) 9 Rajiv Gandhi Missions Report 2002 10 The scheme was materialized with the joint efforts of BIOCON Foundation and Narayana Hrudayalaya in collaboration with ICICI Lombard General Insurance Company has launched a new rural healthcare scheme called Arogya Raksha Yojana (ARY). The current Karnataka Governments health insurance scheme was found very popular for farmers' cooperatives, which will for the first time extend a healthcare benefit to the community. With 90 per cent of the members of the over 30,000 cooperatives societies in the States being farmers the scheme comes as a welcome step and aims to
Vardaan Consultants, Baroda, Gujarat, INDIA
14

any studies which prove the role of PRI to be effective in public health system of the State.
Box 9: Recommendation of Karnataka task force for popularizing PRI system 1. The involvement of the Panchayat institutions and of the community in providing services
should be encouraged for improvement and enhancement of these services based on real needs:
2. Information should be made available to community and a forum need to be developed. 3. Amendment of sec61 to constitute a separate committee for health and sanitation and
education in the GP 4. Continuous training to be provided for health needs to orient Panchayat members of roles
and responsibilities. 5. Separate training to empower women members of Panchayat to be organized 6. A woman of the village to be appointed by the Panchayat to assist the auxiliary nurse and
midwife. 7. Model plan need to be formulated for adoption by Panchayats. 8. Health hierarchy needs to be orientated regarding its role in the Panchayat system.
Especially for the state funded activities supervision and inspection. 9. A system of monitoring and feed back of health activities need to be developed. 10. An inter-sectoral collaboration and monitoring, feed back and interactive system needs to
be established. 11. Village communities would be encouraged to form village health committees to address
the need of all section and should represent all sections including women’s group representative, youth, ANM’s and Anganwadi workers.
12. A pilot study project would be formulated to test the above.
Souce: Dr Sudarshan et al Task Force Karnataka 2001. 1.4f Gujarat Experience: Gujarat has decentralized development administrative machinery in the form of its Panchayati Raj institution The 73rd and 74th Amendments to the Constitution have raised hope for improving many services in rural areas by handling them over to panchayats. Gujarat was one of the first states to implement the panchayati raj system in 1963 and primary healthcare was handed over to district panchayats. Gujarat has achieved a degree of decentralization through delegation of functions from state government to the District Rural Development Authorities (DRDAs). The planning apparatus consists of two agencies – one responsible for rural development programmes run by local administrators called the District Rural Development Agency (DRDA), the other responsible for overall district planning run by local politicians called the zilla panchayat. Many NGOs in the state have participated with local village panchayat under water shed management programmes for providing drinking water to respective villages.
provide the best medical care and services to 25 lakh farmers co-operators in Karnataka. The scheme - Yeshasvini - entails that each member of farmer cooperative societies pays Rs.5 a month or Rs.60 per annum to get insured for surgeries and post-operative treatment at 67 identified private and government hospitals across the state. The first lot of 1.7 million farmers, who have paid the small amount, have created a corpus of Rs.150 million that has been further bolstered by the state government contributing an additional Rs.2.50 per farmer per month. The hospitals are paid from this amount once the cooperative society sends the bill to the state-run National Insurance. By Imran Qureshi, Indo-Asian News Service, October 2005.
Vardaan Consultants, Baroda, Gujarat, INDIA
15

One of the early attempts made by an NGO (SEWA Rural) in Jhagadia taluka of Bharuch district, was a partnership with GO and NGO model in health with the participation of the local village leaders and panchayat members. However, many attempts integrate the PRI in public health could not succeed various reasons. On the contrary, very few studies have been made to details role of PRI in health. The experience of PHC under the panchayat system is not very clear: whether the benefits of handing over the PHC system to panchayats out weight the risks. There are several problems and shortcoming in the PHC system which the district panchayats have not been able to address effectively in terms of participation and lack mechanism for devolution of power to panchayats (Mavalankar and Patel 1998). The overall picture that emerges is that panchayats have not paid very much attention to health function and hence PHCs are no better under Panchayat control as compared to possible scenario under state control. Recently the policy document for the interface between the Gujarat government and the Jan Swastha Abhiyan (GOG 2005) had showed the vertical approach by dividing various health initiatives into four levels11 without much importance given to the role of PRI in the decentralization process. The status of the health index is far better than other states because of the availability related infrastructure, which are easily accessible (rail, road, water supply, ..etc). Beside the per capita income of villages in Gujarat is high compared to other states and thus the status of public health in Gujarat is far better than other states of India.
11 1) PHC/UFWC/HP: Jan Swasthya Manch; 2) Taluka Level: Taluka Jan Swasthya Manch; 3) District level,: Jilla Jan Swasthya Manch, and 4) State level: the Rajya Jan Swasthya Manch
Vardaan Consultants, Baroda, Gujarat, INDIA
16
Chapter 2: Description of the Project After its detachment from the bigger state of Punjab, the Haryana economy has boomed. Haryana's geographical proximity to the national capital New Delhi and a well-developed transport infrastructure are two of its major strengths. The state has been able to attract sizable investment from multinational companies, large business houses, foreign investors, non-residents Indians and small scale entrepreneurs. In recent years Haryana has emerged as one of the three most progressive states of India with an impressive trail of achievements in the field of agriculture, automobile industry business, information technology, tourism, and overall development. However, rural transformation lacked the institutional scaffolding of the Panchayati Raj, a vital organ of participative democracy in the rest of India. The Haryana Panchayati Raj Act, 1994 has rectified this sorry state of affairs with regular elections to the new bodies being held since April 1995. Panchayati raj leadership in Haryana has projected their views and perceptions on a very wide range of issues ranging from empowerment of women to bureaucracy and prospects and problems of resource mobilization. The elected PRIs office-holder’s perceptions about the objectives and operational road-blocks in the working of PRIs have also been analyzed and their doubts and dismay about the ‘new’ constitutional Panchayati Raj in Haryana have been projected making the study useful for all those interested in making PRIs vibrant institutions of self–government.
“Haryana Panchayati Raj Act was enacted to provide for the constitution of three tier system of Panchayats in the State as Gram Panchayat at the village level, Panchayat Samiti at the block level Zila Parishads at the district level establish a Gram Panchayat at village level having a population of not less than 500 consisting minimum of 6 Panches and maximums 20 Panches”.
Gram Vikas Samiti (GVS), still in its infancy, is a seven-member committee constituted as per the directions of the Government of Haryana. The purpose of setting up GVS was to ensure more effective participation of the residents of the gram sabha in the execution of development works and also to bring more transparency and efficient utilization of funds and to minimize official intervention. GVS consists of the panchayat sarpanch who is the Chairperson of the committee, a woman elected member of the panchayat, an elected member of the panchayat belonging to the scheduled caste community, and another from the backward class, an ex-serviceman of the village, and two residents of the gram Panchayat.
Vardaan Consultants, Baroda, Gujarat, INDIA
17
Box 10: Miles stone of Haryana’s Panchayati Raj System 1952 Proposed to repeal Punjab Gram Panchayat Act, 1959 Stared after independence 1992 The 73rd and 74th Constitution Amendment Act, 1961 Punjab Panchayat Samitis Act, 1994 Formulate a single Act namely, The Haryana Act 1994. Received the assent of the President of India on the 21st of April 1994 1992 In accordance with the provision of the constitution (73rd amendment Act).
Later this was amended by, Act No. 19 of 1995; Act No 8 of 1997; and Act no. 10 of 1999;
Source: Jaiswal and Chawala (2000)
As per the PRI system of Haryana, roles and responsibilities of PRI to work in tandem with government health functionaries in all National Health Programmes are related with awareness generation to arrest communicable and non communicable diseases; participation in reproductive and child health programmes. So far there is no direct evidence or any systematic study that highlights the importance or significant role played by GVK or any PRI contributing to the improvement of public health. However to narrow down the gap of sex ratio, the Haryana government has started new schemes like devi rupak scheme and swasthya aapke dwar.
2.1 Description of the Project Area12: Historically, Gurgaon district derived its name from Guru Dronacharya; the village was given as gurudakshina to him by his students; the Pandavas and hence it came to be known as Guru-gram, which in course of time got distorted to Gurgaon. Thus the district has been existence since the times of Mahabharata. The district is surrounded by Delhi & Rajasthan. During Akbar's reign, the district fell within the subas of Delhi and Agra, and comprised, wholly or partly, the sikars of Delhi, Rewari, Suhar Pahari and Tijara. With the decay of the Mughal empire, it remained in a disturbed state as a consequence of fighting between the neighboring chiefs till 1803 AD when most of the territory came under British rule through the Treaty of Surji Arjungaon with Scindia. Till the beginning of the 90s, the Haryana economy was agrarian. Thereafter it slowly developed and it noe equally relies upon industry and agriculture as witnessed in several districts (Ambala, Faridabad, Gurgaon, etc). Looking at these developments, it was decided to select an area with a mix economy of both agriculture and industry. Gurgaon district was found ideal for the current study. It is the southern-most district of Haryana. The present Gurgaon district comprise three sub-divisions (Gurgaon, Ferozpur Jhirka, Nuh); seven tehsils (Gurgaon, Sohna, Pataudi, Nuh, Taoru, Punhana and F.P.Jhirka); two sub-tehsils; (Farukhnagar and Nagina); four municipal committees (Gurgaon, Sohna, Nuh & F.P.Jhirka) and nine blocks (Tauru, Nuh, Pataudi, Nagina, Punhana, F.P.Jhirka, Sohna, Gurgaon and Farrukhnagar). It had adopted three tier system of Panchayati Raj with total villages of 734 with the having 538 Panchayats as indicated in table 2.1. 12 The description has been from http://gurgaon.nic.in/f_administration.htm and http://haryana.gov.in/
Vardaan Consultants, Baroda, Gujarat, INDIA
18
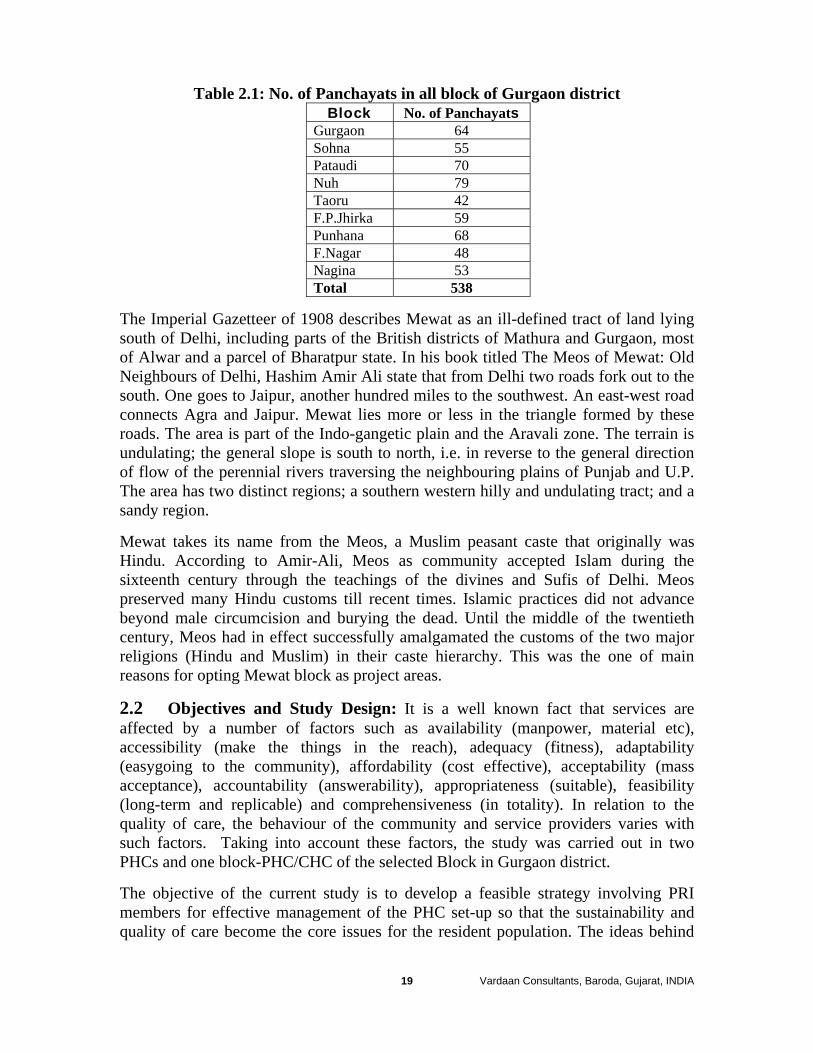
Table 2.1: No. of Panchayats in all block of Gurgaon districtBlock No. of Panchayats
Gurgaon 64 Sohna 55 Pataudi 70 Nuh 79 Taoru 42 F.P.Jhirka 59 Punhana 68 F.Nagar 48 Nagina 53 Total 538
The Imperial Gazetteer of 1908 describes Mewat as an ill-defined tract of land lying south of Delhi, including parts of the British districts of Mathura and Gurgaon, most of Alwar and a parcel of Bharatpur state. In his book titled The Meos of Mewat: Old Neighbours of Delhi, Hashim Amir Ali state that from Delhi two roads fork out to the south. One goes to Jaipur, another hundred miles to the southwest. An east-west road connects Agra and Jaipur. Mewat lies more or less in the triangle formed by these roads. The area is part of the Indo-gangetic plain and the Aravali zone. The terrain is undulating; the general slope is south to north, i.e. in reverse to the general direction of flow of the perennial rivers traversing the neighbouring plains of Punjab and U.P. The area has two distinct regions; a southern western hilly and undulating tract; and a sandy region.
Mewat takes its name from the Meos, a Muslim peasant caste that originally was Hindu. According to Amir-Ali, Meos as community accepted Islam during the sixteenth century through the teachings of the divines and Sufis of Delhi. Meos preserved many Hindu customs till recent times. Islamic practices did not advance beyond male circumcision and burying the dead. Until the middle of the twentieth century, Meos had in effect successfully amalgamated the customs of the two major religions (Hindu and Muslim) in their caste hierarchy. This was the one of main reasons for opting Mewat block as project areas.
2.2 Objectives and Study Design: It is a well known fact that services are affected by a number of factors such as availability (manpower, material etc), accessibility (make the things in the reach), adequacy (fitness), adaptability (easygoing to the community), affordability (cost effective), acceptability (mass acceptance), accountability (answerability), appropriateness (suitable), feasibility (long-term and replicable) and comprehensiveness (in totality). In relation to the quality of care, the behaviour of the community and service providers varies with such factors. Taking into account these factors, the study was carried out in two PHCs and one block-PHC/CHC of the selected Block in Gurgaon district.
The objective of the current study is to develop a feasible strategy involving PRI members for effective management of the PHC set-up so that the sustainability and quality of care become the core issues for the resident population. The ideas behind
Vardaan Consultants, Baroda, Gujarat, INDIA
19
such study is to prepare a strategy involving Panchayati Raj Institutions for an effective management of PHC set up and create a model PHC that not only sustains, but also provides quality of health and family planning services. The specific objectives of the project are as follows:
2.2a Beneficiaries Related: 1. To generate benchmark estimates for various indicators in the project area,
through which project performance could be monitored and effectiveness of intervention could be measured.
2. Measure the impact of the services among the resident community and their health seeking behaviour for public health services
3. Analyse the role of district health officials and the grassroot level voluntary organizations and civil societies
4. Understand the involvement of panchayati raj institution (PRI) members in the functioning and/or monitoring of the activities of rural health institutions
2.2b Providers Related 1. Measure the readiness of the centre in the matter of material, manpower,
methods (for providing services) and maintenance of the building. It also includes assessment of different types of services (curative, preventive and promotive) rendered through the PHC system;
2. Assess the working environment of the service centre in providing quality and sustainable services to the community
3. Understand the training needs of services providers and demand of the community in the matter of quality of care in PHC set-up
2.2c Policy and Programme Related: 1. Explain the process of decentralization and integration to seek participation of
PRI in the matter of effective management of the PHC through NGO collaboration
2. Develop a model involving PRIs for effective management of PHC set-up that can be replicated in other areas.
The reason for choosing Haryana is because PFI has already trained the PRI members on RCH issues and the state has achieved medium level performance in the family welfare programme. Keeping in view the objectives, it was proposed to cover one block-PHC/CHC and two PHCs from Gurgaon district. The selection of the PHCs was based on distance from the selected block-PHC/CHC at the block headquarter. It is proposed to have one PHC, which is located in the range of less than 20 km from the block head quarter and the second beyond 20 kms. Since the PHC system is connected with the sub-centre and part of the services are rendered through sub- centres, it was proposed to have at least two sub-centres from each PHC. A criterion for selecting sub-centre was based on the distance from the respective PHC. One sub-centre will be chosen at a distance of 3-5 km and the other beyond 10 kms from PHC. The entire project intervention is conducted in nine villages as indicated in Table 2.2 with sample classification as per the criteria adopted.
Vardaan Consultants, Baroda, Gujarat, INDIA
20
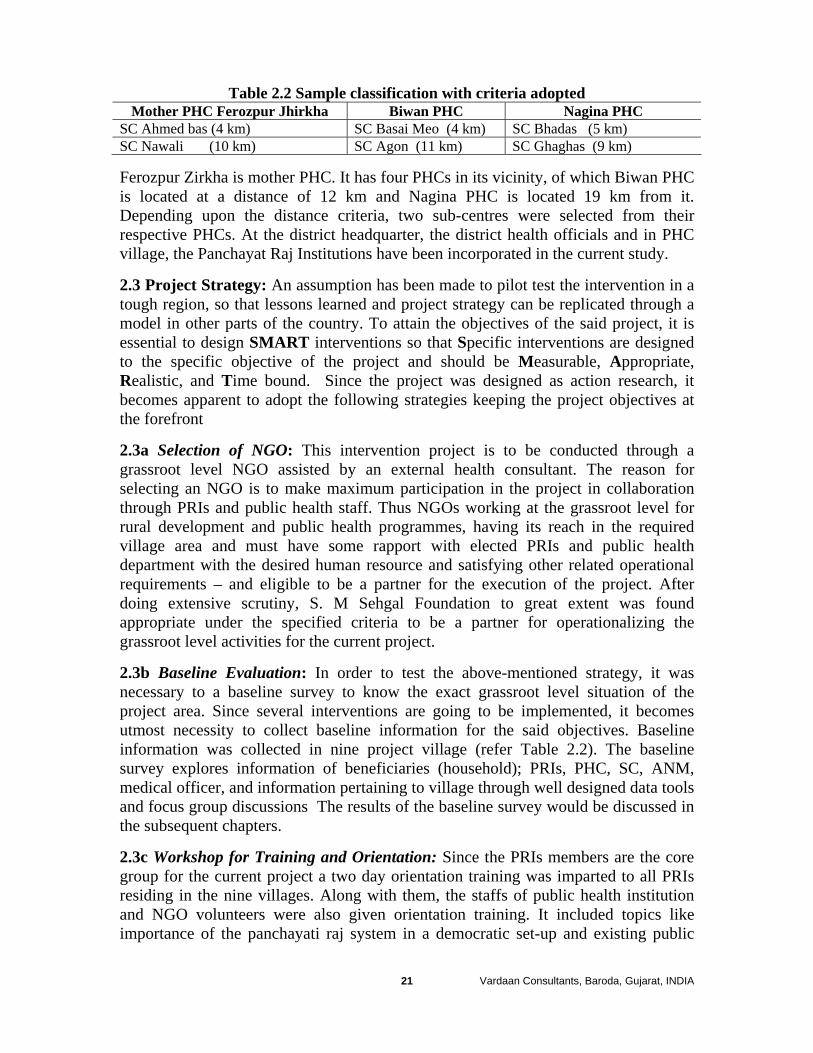
Table 2.2 Sample classification with criteria adopted Mother PHC Ferozpur Jhirkha Biwan PHC Nagina PHC
SC Ahmed bas (4 km) SC Basai Meo (4 km) SC Bhadas (5 km) SC Nawali (10 km) SC Agon (11 km) SC Ghaghas (9 km)
Ferozpur Zirkha is mother PHC. It has four PHCs in its vicinity, of which Biwan PHC is located at a distance of 12 km and Nagina PHC is located 19 km from it. Depending upon the distance criteria, two sub-centres were selected from their respective PHCs. At the district headquarter, the district health officials and in PHC village, the Panchayat Raj Institutions have been incorporated in the current study.
2.3 Project Strategy: An assumption has been made to pilot test the intervention in a tough region, so that lessons learned and project strategy can be replicated through a model in other parts of the country. To attain the objectives of the said project, it is essential to design SMART interventions so that Specific interventions are designed to the specific objective of the project and should be Measurable, Appropriate, Realistic, and Time bound. Since the project was designed as action research, it becomes apparent to adopt the following strategies keeping the project objectives at the forefront
2.3a Selection of NGO: This intervention project is to be conducted through a grassroot level NGO assisted by an external health consultant. The reason for selecting an NGO is to make maximum participation in the project in collaboration through PRIs and public health staff. Thus NGOs working at the grassroot level for rural development and public health programmes, having its reach in the required village area and must have some rapport with elected PRIs and public health department with the desired human resource and satisfying other related operational requirements – and eligible to be a partner for the execution of the project. After doing extensive scrutiny, S. M Sehgal Foundation to great extent was found appropriate under the specified criteria to be a partner for operationalizing the grassroot level activities for the current project.
2.3b Baseline Evaluation: In order to test the above-mentioned strategy, it was necessary to a baseline survey to know the exact grassroot level situation of the project area. Since several interventions are going to be implemented, it becomes utmost necessity to collect baseline information for the said objectives. Baseline information was collected in nine project village (refer Table 2.2). The baseline survey explores information of beneficiaries (household); PRIs, PHC, SC, ANM, medical officer, and information pertaining to village through well designed data tools and focus group discussions The results of the baseline survey would be discussed in the subsequent chapters.
2.3c Workshop for Training and Orientation: Since the PRIs members are the core group for the current project a two day orientation training was imparted to all PRIs residing in the nine villages. Along with them, the staffs of public health institution and NGO volunteers were also given orientation training. It included topics like importance of the panchayati raj system in a democratic set-up and existing public
Vardaan Consultants, Baroda, Gujarat, INDIA
21
health situation in India; identifying barriers and difficulties at community, village and institutional level; and exercise for the possible action plan in coordination of PRI members along with public health staff and NGO volunteers. Later looking at the objectives and action plan of the project, each group (PRI members, public health staff, and NGO volunteers) prepared a micro level action plan for all nine project villages.
2.3d Coordination Mechanism: The project needs coordination of PRI member, Public Health Staff, and NGO volunteers for executing the project objectives. Here the entire project was implemented through an NGO and thus NGO volunteers became the key link persons between PRI members and public health staff. This started with rapport building among each group, but NGO took a major initiative in narrowing the gap between PRI members and NGO staff. Later these NGO volunteers helped in preparing the intervention plan along with PHC staff and PRI members. Project execution involved routine activities related to resource mobilization, planning, and imparting health services and generating the desired data for monitoring the activity. In order to understand the process of decentralization in governance of health sector as well as technical intervention, efforts were made to attend the desired planned meetings at public health institutions and annual meetings in the zilla panchayats (two general - first meeting in the month of April and October of the each calendar year) especially related to the budget preparation of public health. All these intervention were planned putting the PRI members at the forefront and facilitated by NGO volunteers and supported by public health staff as shown in box 11.
Box 11: Planned Interventions for execution of project 1. Resource mobilization related activities 2. Interventions related to up scaling the public health services. 3. Intervention to provide safe water for drinking. 4. Intervention for proper Hygienic Sanitation 5. Intervention for providing Accessible Road 6. Intervention to Avert Epidemic 7. Interventions for Timely Birth and death Certificate 8. Expanding the reach of family welfare services 9. Strengthening Women Developmental Programmes 10. Strengthening effective referral services 11. Demand generating IEC activities 12. Organize the desired meetings at various levels of administrative hierarchy
2.3e Operating Strategy: As reported earlier that NGO volunteers would be playing a leading role in the execution of the project making PRI at the forefront. Out of total nine villages, one NGO volunteer was assigned for three villages. Thus a total of three NGO volunteers and senior female PIT members of the NGO have assisted the PRI members for execution of the planned interventions as described in box 11.
Vardaan Consultants, Baroda, Gujarat, INDIA
22

2.4 Limitation of the Study: Mewat region is very conservative and very tough for eliciting the desired support. In spite of having sound rapport (of NGO) with the resident community, the level of support from the female population was limited and confined to some project villages only. Since the panchayat elections came in between, lot of efforts were put again for the newly elected PRIs for the swift functioning of the project activities. The power hierarchy and administrative set-up of the democratic system restricted the grassroot level work and other advocacy items under the panchayati raj system to be conveyed to the policy makers. These missing links restricted some of the interventions to be pilot tested. One of the limitations in the project was related with duration of the project (eighteen months) and planned interventions. Thus efforts were restricted more to process building exercise and demand generating activities with the help of participations of PRIs in the effective management of PHCs and we could not analyzed the actual impact through indicators.
Vardaan Consultants, Baroda, Gujarat, INDIA
23
Chapter 3: Learning Experiences
The current description is provided keeping the role of PRIs at the forefront in the public health system. In doing so, importance was given to the structural integration among the three partners and the innovations made in the process of execution and coordination of the project activities. The numbers for success and failure were not given much importance as the process of coordination mechanism required to make the effective management of the public health institutions.
3.1 Understanding Partners: During the process of integration of NGO, PHC staff and PRIs members, it was essential to know about their perception, notion, and experience about each other. a) Reported by PRI members: The public health conditions in their respective regions are very pathetic. The absence of building and those exist requiring repair and maintenance were the major drawback, followed by absence of manpower and materials. This has led ignorance of among the resident villagers. The major complaints were spill of water; remains of stagnant water; over used or wrong use of water; short supply of water; spread of dirt in the village lead to the occurrence of various types of diseases (malaria, fever; TB, boils, itching, vomiting; diarrhoea; white discharge. etc) among the resident population. Absence of bathroom and latrine facilities also adds to the problem of cleanness and unhygienic conditions in the villages. Other issues pointed out by them were related with the administration. Several complaints regarding the absence of the PHC/SC staff were made to the higher authorities, but no action has been taken. This is because of the vested interest between the BDO, surpanches and some members of the health department. Corruption and regional politics restrict village level PRI members to do constructive work under in any development programme. Further, ignorance of different health problems makes the resident population live in pathetic conditions. Another reason is poor supervision about the functioning of public health services. The PRI members also reported that majority of the problems arose from lack of coordination among PWD, Public health and PRI institutions. Besides, no serious efforts were made to check the accountability of health workers and sarpanches for the work assigned to them: imparting desired health services and implement development programmes in the villages. b) Reported from PHC staff: Illiteracy among PRI members and their biased attitude restrict them to interact with public health institutions. They further pointed out that the PRI members we are confined to regional politics under the direction of sarpanches and the block development officer. The PRI members are least interested in development programmes and even if at all they take initiatives, their efforts are suppressed by corruption and regional politics. Nepotism and ignorance were supposed to be the major hurdles in coordination with the public health system. Strong restraints were shown against the illiterate and aged PRIs, because they have no idea either of the public health system or the panchayati raj system.
Vardaan Consultants, Baroda, Gujarat, INDIA
24
c) Reported by NGO: Since the NGO has to deal with PRI members, PHC staff and the resident community, its perceptions were given true weightage as it is the external representative of the panchayati raj system. One of the important points is related to the linkage between PRI members and public health staff. The PHC staff accused on panchayat members for misusing public health commodities and PRI members pointed out long absenteeism of the health staff in the assigned villages. They are always overloaded and work according to their convenience. The PHC staff are not willing to work sincerely. Frequent irregularities and poor supervision among the PHC staff had major contribution in degrading the public health services. The superiority feeling among the PHC have staff restrict NGO volunteers to work in collaboration. The PRI members are more influenced by village sarpanches and block development authorities. Party politics restricts them from taking initiatives on social services or development in their respective villages. Besides lack of knowledge about the developmental programmes and their roles and responsibilities are the major factors for the failure of the panchayati raj system in the region. The PRI members only work with vested interests and promote nepotism so that they could retain power in the family. Illiteracy and religious orthodox attitude among the resident community restrict them taking any initiative in developmental programmes. They are more concerned about their basic necessities rather thinking about development programmes in their villages. Wrong concept about NGO volunteers and more demands to satisfy their personal needs are the major constraints in popularizing health programmes in the region. Further village communities are not aware of their rights and have least knowledge about developmental programme through the panchayati raj system. Lack of interest and unity (because of culture; caste, religion, etc) prevents them to work under joint collaboration. d) Reported by Community: Based on our baseline survey, 34 per cent of household reported awareness about gram sabha meetings being organized in their respective villages. Among these, 98.9 per cent reported that politics and routine functions were usually carried out in the gram sabha meeting. Development and other social welfare schemes were discussed and approved among selected members of the village panchayat who are happened to be close to the village panchayat leader and BDO. Further, only 36.2 per cent of the households reported having knowledge about the responsibilities of the gram panchayat for public health. Among these, 90 percent reported that the GP is very irresponsible to public health issues. Further, majority (62%) of households reported demanding proper sanitation and water supply followed by proper functioning of public health institutions (32.4) and implementation of all developmental schemes.
Vardaan Consultants, Baroda, Gujarat, INDIA
25
About 40 per cent of household were aware the implementation of developmental activities by the gram sabha. Those who were aware were somehow linked to or benefited from with ongoing agriculture and social developmental schemes. The perception and attitude of the community about the PRI members and the panchayati raj system are very well narrated in the focus group discussions held at Biwan and Nagina village and are given below: Village Biwan
It was nice to know that all those present in the focus group discussion (FGD) had heard about the panchayati raj system. The question on development work done by the panchayat, provoked a sharp response. According to them their panchayat has not done much work. There are collections of water everywhere, which causes fever, malaria, diarrhea, boils and abscesses. “Hum sab aur humare bacche bhi bimaar padh jaate hain. Panchayat thodai na parwa karti hai. Humare yeh dikkate inke kaanon tak kahan pahuncti hai.” They reiterated that the Panchayat is not interested in village developmental activities at all. Rather they believe in “herapheri” and how to fill their pockets. No work on public health improvement has been done. It should first clean up the whole village, and ensure potable drinking water to all households. Water here is a big problem. People have to walk long distance to fetch water. A remarkable thing was reported by the women – that men also equally help out women in fetching water. Also the group said that the panchayat can easily help reviving the PHC if it put some pressure on the government. Definitely the panchayat can help improve, provided that it is interested. It is the elected representative of the village, so it is are authorized enough to do development work. “Unko chuna hi isliye tha ki kuch kaam karenge gaon ke bhalai ke liye. Lagon ke vote hai unke paas, hai na?” As discussed earlier, the group said that most panch members believe they have come to power and can do anything. However, their motive is now to make money. Otherwise they surely would have improved he health centre. “Elect hota hai yeh sochke ki ab to chandi hi chandi hoga. Swasthya ka kaam to sarkar ka hai. Hamara thodai na hai?” Also the present Sarpanch being from a lower caste, nobody is bothered to listen to what he says or does. “Panchayat ke paas to bahut kuch hai. Power bhi aur paisa bhi hai.” It is much within its power and it can get money from the government also. However it did
Vardaan Consultants, Baroda, Gujarat, INDIA
26
not know that resources can also be mobilized from other than government resources. “Public health mein Panchayat kay kar sakti hai? Centre khol de to maan lenge ki kaam kar diya.” They said they only know that the centre activities could be revived by the panchayat provided it is interested. At least get the heath centre started. Make sure the workers, doctors attending regulrly. They can allot a better land which can easily approachable by all villagers. “Dhalai hai na gaon mein, isliye dhyaan dena padhega is baat ke.”
Village Nagina
The group knew about the panchayat system. But the refrain was that the panchayat is functioning only on paper. “Sirf naam ka hi hai panchayat.” The group got very agitated on being asked about development work done by the panchayat. The collective answer was in negative: no work has been done in the last five years. “Har cheez ki kami hai – paani ka, safai ka, har cheez ka”. There is shortage of water, poor village hygiene and sanitation and in fact, gambling and ‘Satta’ is also rampant in the village. Women and young girls are not able to venture out of their houses after 7 PM in the evening. Some of the women present in the meeting said they belonged to those families where men indulge in ganbling. In their words: ‘Bhar pet khana to nahin milta, upar se aadmi raat ko sharaab pi ke sabko (including children) maarpeet karta hai’. The local authorities have also turned a blind eye to all these illegal activities. The panchayat is not serious at all. In fact, when trouble arises if always encourages and supports those who are financially well off. “Who to sirf unki sunte hain jiske paas paisa hai. Hum jaise gareeb ka kaun sunega?” As explained earlier the panchayat has not done any work for the village. “Karne ko to bahut kuch kar sakta hai. Paani ke bare main khas karke. Saaf safai dusra mudda hai. In cheezon pe sabse pehle dhyan dena chahiye. Aage satte ke bare mein kuch thos kadam uthaana chahiya.” What they can do is – Clean up the village roads, make arrangements for potable water for everybody, ensure that ANM visits the village regularly, stop all gambling activities, and puts a stop to all alcoholic outlets if possible.
Vardaan Consultants, Baroda, Gujarat, INDIA
27
“Kuch kaam bhi agar mil jaaye? Yeh bhi to panchayt kar sakti hai”. The women especially wanted that some work which would be a source of income for them should also be started. “Panchayat chahe to kaya nahi ho sakta?Par imaandar hona chahiye uske baad hi koi kaam kar payega.” They can. Provided they are dedicated and educated people. “Par sab to chor hain, isiliye to kaam nahi ho paata. Agar imaandar hote to har kisike dukh dard ko samjhte”. They are corrupt people that’s the reason why they are least bothered about any public health activities. “Paisa to panchayat ke paas bhi hai, baahar se bhi lekar humein kuch rozi roti dilwa sakta hai. Par unko pehle koi seek sikha de ki public health mein kya hota hai.” Yes definitely they can seek resources from outside. But then they have to be trained for that.
3.2 Exploring Ground realities: To strengthen the public health system of the region, problems identified by the public health staff were mostly related to the repair and maintenance of the building, operation theater, delivery room and short supplies of the manpower, materials and other related equipment. It appears that the public health staff restricted their needs to service oriented as described in the vertical health system. They were least concerned about community need and quality. This was much evident in the focus group discussions.
Ye! Sarkari doctors to hain, par hum jaate nahi – we do not go there as explained above. Most did not know that what services are available and on which days – ANC, immunization sessions, etc. Maternal and child health was poor. About 1 -2 mothers die every year. Reason: too many babies too soon. (‘Zyada bacche karne se sarir kamzor nahin hoga? They were not sure about children deaths – the groups put the figure at 5 – 6 per year. Reasons that they could identify were pneumonia and gastrointestinal disorders (mostly diarrhea). Otherwise they said children suffered mostly from fever, boils and abscess, and respiratory infections. On being asked about the government health services, ,they answered in unison – “hospital ki building tuti hui hai, bilkul bekaar hai”. Government health services they said are “highly insufficient and inefficient”. “pehle ek ANM aur doctor Sharmaji thae, to sithi thoda accha tha. Dawaii bhi militia thi, ab to kuch bhi nahin hai, aur uspare ye log dawaii bechte hain. RMPs ko dawaii bechte hain”.
Vardaan Consultants, Baroda, Gujarat, INDIA
28
Earlier when Dr. Sharma was available at the PHC, things were much better. Now that he is gone, things have gone from bad to worse. The ANM also used to come regularly for immunization and ante natal clinics and Dr. Sharma was always available. The group further said that complete doses of medicines were also given to the patients. Now, they said that most medicines are being sold to RMPs. On becoming ill the villagers go to the local doctors – “aur koi chaara nahinhai” was the prompt reply. The PHC is as good as defunct – “tuti building mein kaun baithega?” ,they said. None of the present workers come regularly. In fact, as they elaborated, – the PHC would only be opened on the days of pulse polio Immunization, Anganwadi workers’ meeting day and when the LHV would come to dispense anti-TB drugs. “Yeh sirf isliye taki koi complaint na kar sake ki dawaii bant jaati hai ya bachi jati hai”.
The demands of NGO and PRI volunteers are similar and are more confined to preventive measures in public health as summarized in Table 3.1. Their demands more toward maintaining healthy and hygienic condition, avert the epidemic, provide potable water and improve the related infrastructure for easy accessibility of health services. Besides, they have identified the felt need to regularize the basic health services in the community such as vaccination, pulse polio, birth and death registration, etc.
On being asked the reasons as to why do they not avail government health services, they said the PHC building was located in another place earlier. Only after it collapsed recently, has it been shifted to its current place. The previous place was located in such a way that everybody in the village could access it. Now people who live down the hill are not able to make it. Moreover they said that the panchayat has got a grant of a 60 lakh to build a new centre but nobody is bothered. The sarpanch is ‘Valmiki’ and hence has no say. So government apathy and public neglect are the reasons for this state of affairs. “Hamare is halat ko agar Panchayat chahe to sudhaar zarroor sakta hai. Par Panchayat bhi to waisa hona chahiye. Hamara ‘Valmiki Sarpanch to kuch bhi kar sakta”. The panchayat needs to be active and the Sarpanch someone whom everybody would look up to. A new PHC should be built. It is not as if there is no money, Money has been allotted as we have already said earlier, only that all Panch and Sarpanch are sitting and doing nothing. They pointedly said that the money could be with the ‘PHC people’ but the panchayat could at least put some pressure on them to make things happen. Ultimately they said –‘ab to aap log hi karo jo karna hai, par sudhar aani chaiye’. When
Vardaan Consultants, Baroda, Gujarat, INDIA
29

Vardaan Consultants, Baroda, Gujarat, INDIA
30
told that everybody has to do their bits as this is community responsibility, all present promised that they would fully cooperate.
Low cost of treatment was reported to be the reason for preferring government hospital; while effective treatment as the reason for preferring qualified private doctors. Focus group discussions revealed similar findings in village Biwan as narrated below:
Government health services are however still popular with the masses. The government provides most treatment free of cost including operations. Probably that’s why it is within the reach of every people and this could be the reason for its popularity. “Wahan operation to bina kharche ka hota hai. Hum to Alwar jake karwate hain – usme bahut paise kharch hota hai”.
For treating minor illness, the availability of the doctors from any private or government doctors were given preference. Another reasons the effectiveness and cost of treatment. Services in the vicinity and convenience reasons for opting any private and Government hospital.
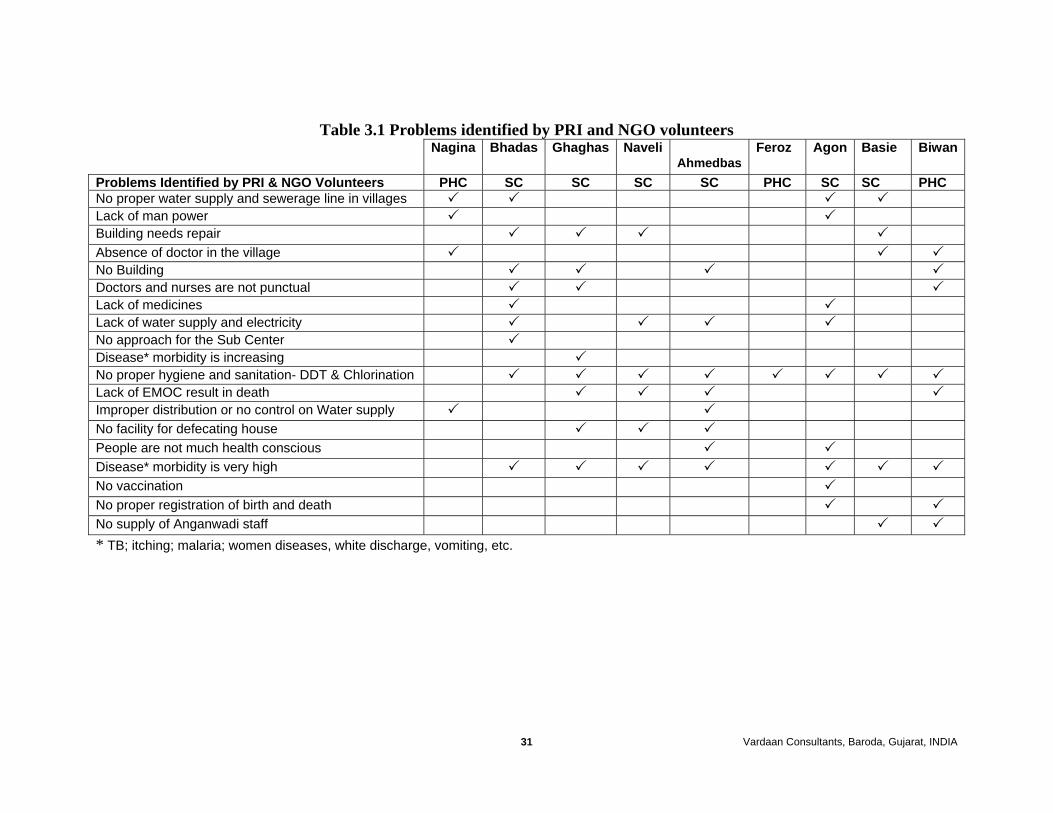
Vardaan Consultants, Baroda, Gujarat, INDIA 31
Table 3.1 Problems identified by PRI and NGO volunteers Nagina Bhadas Ghaghas Naveli
AhmedbasFeroz Agon Basie Biwan
Problems Identified by PRI & NGO Volunteers PHC SC SC SC SC PHC SC SC PHC No proper water supply and sewerage line in villages Lack of man power Building needs repair Absence of doctor in the village No Building Doctors and nurses are not punctual Lack of medicines Lack of water supply and electricity No approach for the Sub Center Disease* morbidity is increasing No proper hygiene and sanitation- DDT & Chlorination Lack of EMOC result in death Improper distribution or no control on Water supply No facility for defecating house People are not much health conscious Disease* morbidity is very high No vaccination No proper registration of birth and death No supply of Anganwadi staff * TB; itching; malaria; women diseases, white discharge, vomiting, etc.
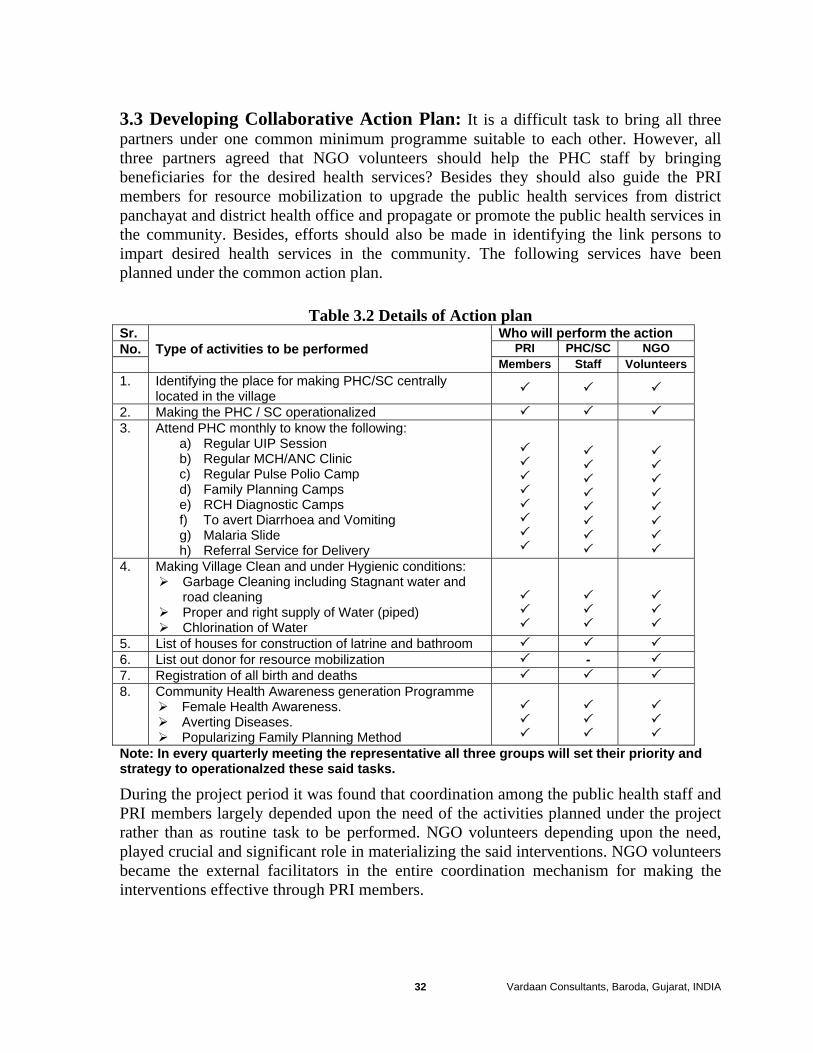
3.3 Developing Collaborative Action Plan: It is a difficult task to bring all three partners under one common minimum programme suitable to each other. However, all three partners agreed that NGO volunteers should help the PHC staff by bringing beneficiaries for the desired health services? Besides they should also guide the PRI members for resource mobilization to upgrade the public health services from district panchayat and district health office and propagate or promote the public health services in the community. Besides, efforts should also be made in identifying the link persons to impart desired health services in the community. The following services have been planned under the common action plan.
Table 3.2 Details of Action plan Sr. Who will perform the action No. Type of activities to be performed PRI PHC/SC NGO Members Staff Volunteers 1. Identifying the place for making PHC/SC centrally
located in the village
2. Making the PHC / SC operationalized 3. Attend PHC monthly to know the following:
a) Regular UIP Session b) Regular MCH/ANC Clinic c) Regular Pulse Polio Camp d) Family Planning Camps e) RCH Diagnostic Camps f) To avert Diarrhoea and Vomiting g) Malaria Slide h) Referral Service for Delivery
4. Making Village Clean and under Hygienic conditions: Garbage Cleaning including Stagnant water and
road cleaning Proper and right supply of Water (piped) Chlorination of Water
5. List of houses for construction of latrine and bathroom 6. List out donor for resource mobilization - 7. Registration of all birth and deaths 8. Community Health Awareness generation Programme
Female Health Awareness. Averting Diseases. Popularizing Family Planning Method
Note: In every quarterly meeting the representative all three groups will set their priority and strategy to operationalzed these said tasks.
During the project period it was found that coordination among the public health staff and PRI members largely depended upon the need of the activities planned under the project rather than as routine task to be performed. NGO volunteers depending upon the need, played crucial and significant role in materializing the said interventions. NGO volunteers became the external facilitators in the entire coordination mechanism for making the interventions effective through PRI members.
Vardaan Consultants, Baroda, Gujarat, INDIA 32
3.4 Interest and Participation: Health is no priority for every individual and this is true among the PRIs. During the project tenure, the PRIs were provided orientation and training about the panchayati raj system and the public health system of Haryana. Out of total 90 PRIs in the first phase, only 10 per cent were found interested in the subject matter and this was true in the second phase of training for newly elected PRIs. Most of the PRI have no knowledge of the panchayati raj system and its related schemes. On an average two PRIs from each village were willing to provide voluntary services for the said objectives of the project. In the baseline survey only 6 per cent of the PRIs were found having knowledge of panchayati raj system. The PRI members showed keen interest in motivating the cases for UIP and RCH sessions at the sub-centres. As regards IEC activities they became the catalyst in imparting education with the help of local ANM in hygiene and sanitation, immunization, and family planning methods. They also helped the PHC staff in doing survey for the entire village. Since the region is engulfed in illiteracy and orthodox, it was difficult to penetrate women issues and their demand generation activities. During the project tenure it was observed that if proper counselling was done, then one could expect positive action. Here, but at least two PRIs from each village have started contributing in the health programme. They do canvassing in the community and bring the beneficiaries to the desired health services. As a result the PHC/SC staff have changed their attitude and started contributing to the efforts of PRI and NGO volunteers. Such efforts could extened the reach and maintain desired quality in the health programme. Overall, it seems that the PRIs had helped in improving or upgrading public health infrastructure, canvassing and motivating the local residents to participate in health programme, improving health and sanitation, and averting epidemics. However it is also true that these activities are done by a handful PRIs interested in the health programme as indicated in Table 3.3
Vardaan Consultants, Baroda, Gujarat, INDIA 33
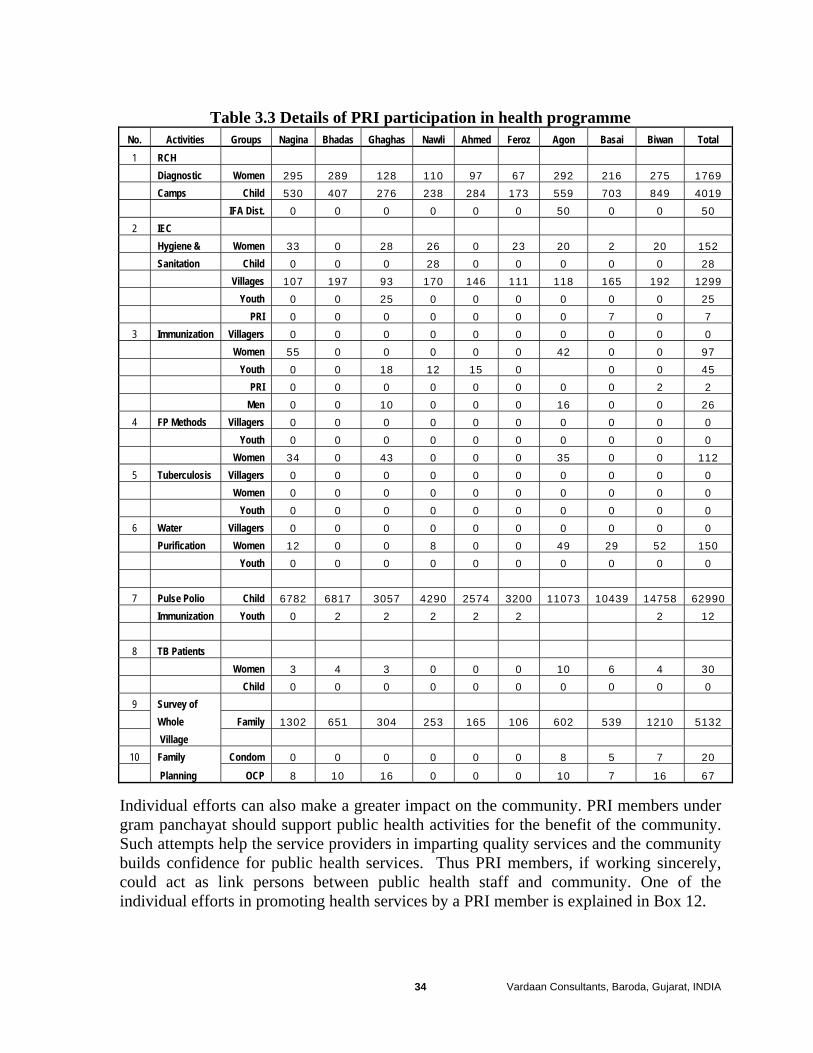
Table 3.3 Details of PRI participation in health programme No. Activities Groups Nagina Bhadas Ghaghas Nawli Ahmed Feroz Agon Basai Biwan Total 1 RCH Diagnostic Women 295 289 128 110 97 67 292 216 275 1769
Camps Child 530 407 276 238 284 173 559 703 849 4019
IFA Dist. 0 0 0 0 0 0 50 0 0 50
2 IEC
Hygiene & Women 33 0 28 26 0 23 20 2 20 152
Sanitation Child 0 0 0 28 0 0 0 0 0 28
Villages 107 197 93 170 146 111 118 165 192 1299
Youth 0 0 25 0 0 0 0 0 0 25
PRI 0 0 0 0 0 0 0 7 0 7
3 Immunization Villagers 0 0 0 0 0 0 0 0 0 0
Women 55 0 0 0 0 0 42 0 0 97
Youth 0 0 18 12 15 0 0 0 45
PRI 0 0 0 0 0 0 0 0 2 2
Men 0 0 10 0 0 0 16 0 0 26
4 FP Methods Villagers 0 0 0 0 0 0 0 0 0 0
Youth 0 0 0 0 0 0 0 0 0 0
Women 34 0 43 0 0 0 35 0 0 112
5 Tuberculosis Villagers 0 0 0 0 0 0 0 0 0 0
Women 0 0 0 0 0 0 0 0 0 0
Youth 0 0 0 0 0 0 0 0 0 0
6 Water Villagers 0 0 0 0 0 0 0 0 0 0
Purification Women 12 0 0 8 0 0 49 29 52 150
Youth 0 0 0 0 0 0 0 0 0 0
7 Pulse Polio Child 6782 6817 3057 4290 2574 3200 11073 10439 14758 62990
Immunization Youth 0 2 2 2 2 2 2 12
8 TB Patients
Women 3 4 3 0 0 0 10 6 4 30
Child 0 0 0 0 0 0 0 0 0 0
9 Survey of
Whole Family 1302 651 304 253 165 106 602 539 1210 5132
Village
10 Family Condom 0 0 0 0 0 0 8 5 7 20
Planning OCP 8 10 16 0 0 0 10 7 16 67
Individual efforts can also make a greater impact on the community. PRI members under gram panchayat should support public health activities for the benefit of the community. Such attempts help the service providers in imparting quality services and the community builds confidence for public health services. Thus PRI members, if working sincerely, could act as link persons between public health staff and community. One of the individual efforts in promoting health services by a PRI member is explained in Box 12.
Vardaan Consultants, Baroda, Gujarat, INDIA 34
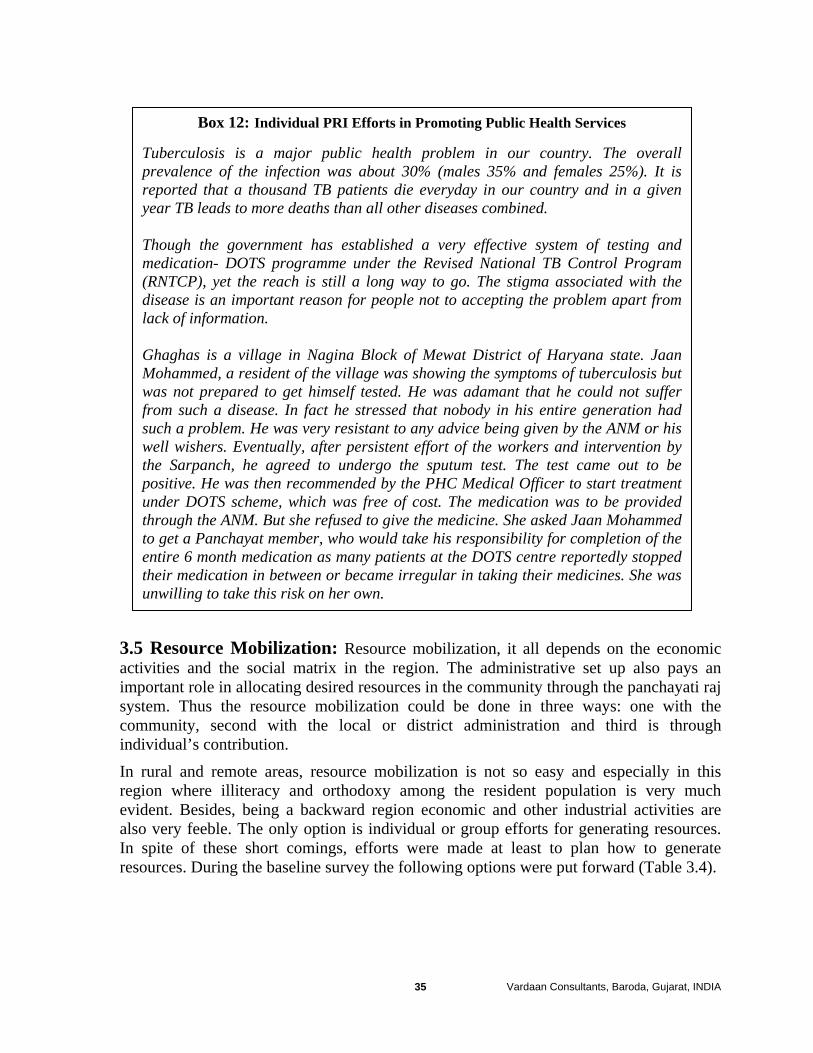
Box 12: Individual PRI Efforts in Promoting Public Health Services
Tuberculosis is a major public health problem in our country. The overall prevalence of the infection was about 30% (males 35% and females 25%). It is reported that a thousand TB patients die everyday in our country and in a given year TB leads to more deaths than all other diseases combined. Though the government has established a very effective system of testing and medication- DOTS programme under the Revised National TB Control Program (RNTCP), yet the reach is still a long way to go. The stigma associated with the disease is an important reason for people not to accepting the problem apart from lack of information. Ghaghas is a village in Nagina Block of Mewat District of Haryana state. Jaan Mohammed, a resident of the village was showing the symptoms of tuberculosis but was not prepared to get himself tested. He was adamant that he could not suffer from such a disease. In fact he stressed that nobody in his entire generation had such a problem. He was very resistant to any advice being given by the ANM or his well wishers. Eventually, after persistent effort of the workers and intervention by the Sarpanch, he agreed to undergo the sputum test. The test came out to be positive. He was then recommended by the PHC Medical Officer to start treatment under DOTS scheme, which was free of cost. The medication was to be provided through the ANM. But she refused to give the medicine. She asked Jaan Mohammed to get a Panchayat member, who would take his responsibility for completion of the entire 6 month medication as many patients at the DOTS centre reportedly stopped their medication in between or became irregular in taking their medicines. She was unwilling to take this risk on her own.
3.5 Resource Mobilization: Resource mobilization, it all depends on the economic activities and the social matrix in the region. The administrative set up also pays an important role in allocating desired resources in the community through the panchayati raj system. Thus the resource mobilization could be done in three ways: one with the community, second with the local or district administration and third is through individual’s contribution. In rural and remote areas, resource mobilization is not so easy and especially in this region where illiteracy and orthodoxy among the resident population is very much evident. Besides, being a backward region economic and other industrial activities are also very feeble. The only option is individual or group efforts for generating resources. In spite of these short comings, efforts were made at least to plan how to generate resources. During the baseline survey the following options were put forward (Table 3.4).
Vardaan Consultants, Baroda, Gujarat, INDIA 35
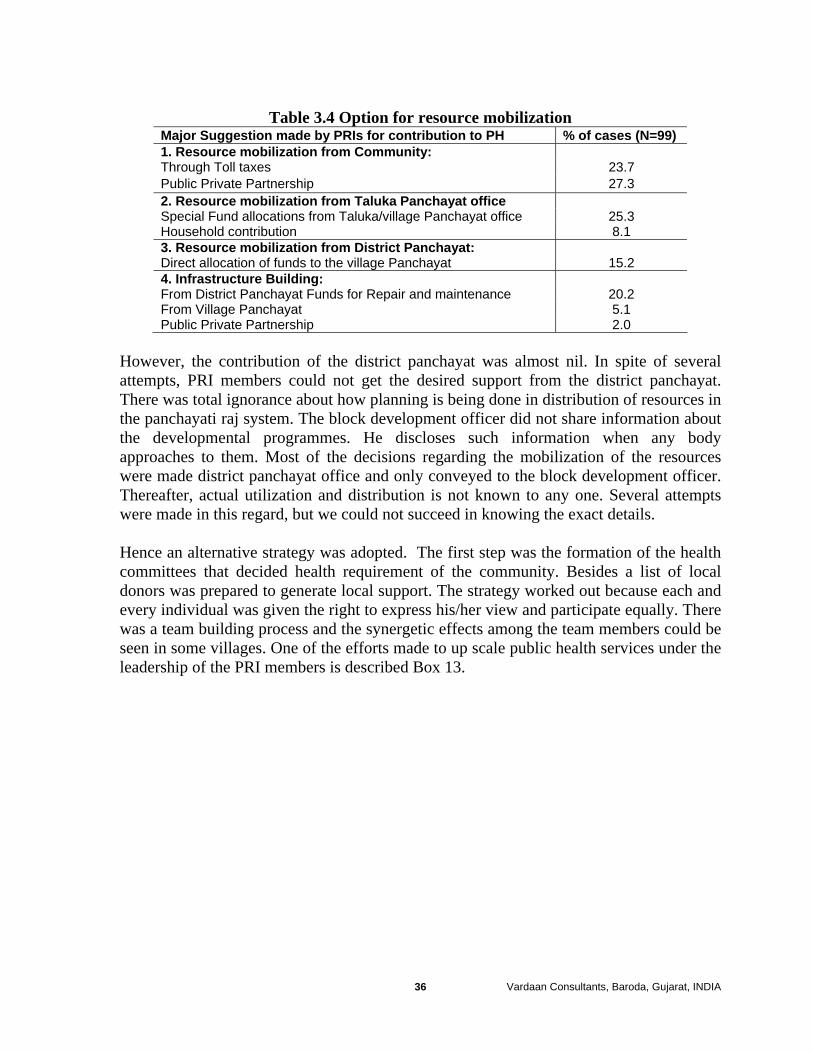
Table 3.4 Option for resource mobilization Major Suggestion made by PRIs for contribution to PH % of cases (N=99) 1. Resource mobilization from Community: Through Toll taxes 23.7 Public Private Partnership 27.3 2. Resource mobilization from Taluka Panchayat office Special Fund allocations from Taluka/village Panchayat office 25.3 Household contribution 8.1 3. Resource mobilization from District Panchayat: Direct allocation of funds to the village Panchayat 15.2 4. Infrastructure Building: From District Panchayat Funds for Repair and maintenance 20.2 From Village Panchayat 5.1 Public Private Partnership 2.0
However, the contribution of the district panchayat was almost nil. In spite of several attempts, PRI members could not get the desired support from the district panchayat. There was total ignorance about how planning is being done in distribution of resources in the panchayati raj system. The block development officer did not share information about the developmental programmes. He discloses such information when any body approaches to them. Most of the decisions regarding the mobilization of the resources were made district panchayat office and only conveyed to the block development officer. Thereafter, actual utilization and distribution is not known to any one. Several attempts were made in this regard, but we could not succeed in knowing the exact details. Hence an alternative strategy was adopted. The first step was the formation of the health committees that decided health requirement of the community. Besides a list of local donors was prepared to generate local support. The strategy worked out because each and every individual was given the right to express his/her view and participate equally. There was a team building process and the synergetic effects among the team members could be seen in some villages. One of the efforts made to up scale public health services under the leadership of the PRI members is described Box 13.
Vardaan Consultants, Baroda, Gujarat, INDIA 36
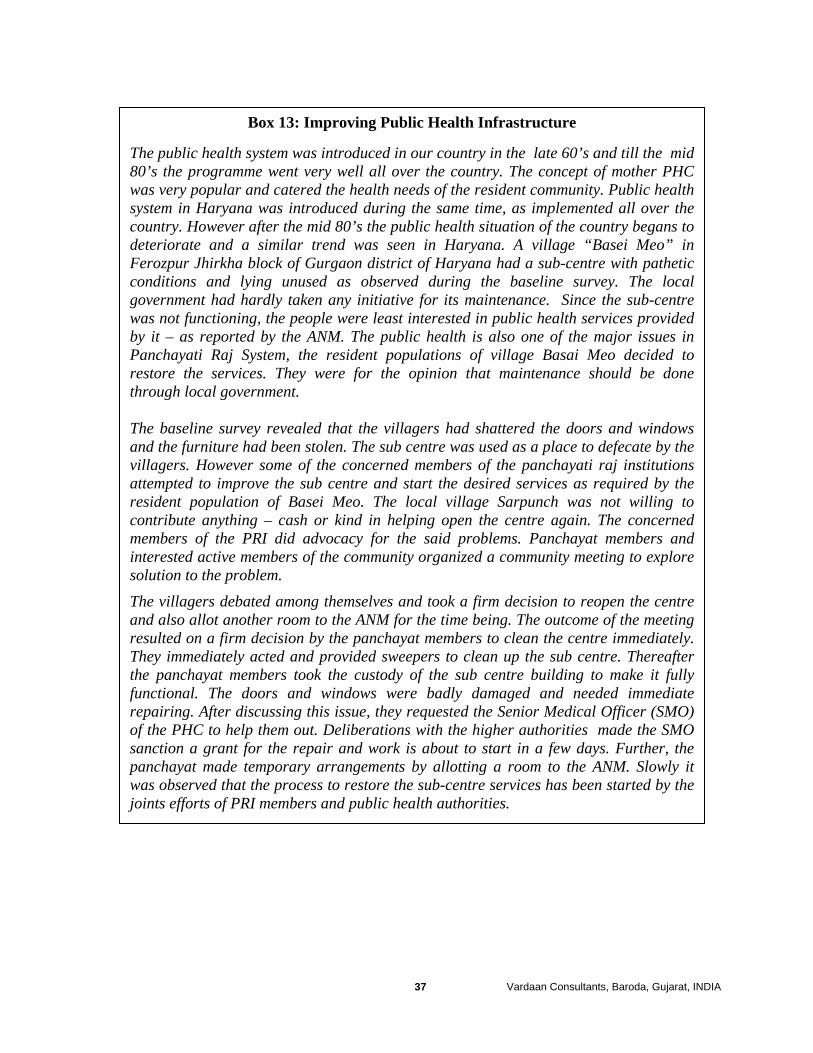
Box 13: Improving Public Health Infrastructure
The public health system was introduced in our country in the late 60’s and till the mid 80’s the programme went very well all over the country. The concept of mother PHC was very popular and catered the health needs of the resident community. Public health system in Haryana was introduced during the same time, as implemented all over the country. However after the mid 80’s the public health situation of the country begans to deteriorate and a similar trend was seen in Haryana. A village “Basei Meo” in Ferozpur Jhirkha block of Gurgaon district of Haryana had a sub-centre with pathetic conditions and lying unused as observed during the baseline survey. The local government had hardly taken any initiative for its maintenance. Since the sub-centre was not functioning, the people were least interested in public health services provided by it – as reported by the ANM. The public health is also one of the major issues in Panchayati Raj System, the resident populations of village Basai Meo decided to restore the services. They were for the opinion that maintenance should be done through local government. The baseline survey revealed that the villagers had shattered the doors and windows and the furniture had been stolen. The sub centre was used as a place to defecate by the villagers. However some of the concerned members of the panchayati raj institutions attempted to improve the sub centre and start the desired services as required by the resident population of Basei Meo. The local village Sarpunch was not willing to contribute anything – cash or kind in helping open the centre again. The concerned members of the PRI did advocacy for the said problems. Panchayat members and interested active members of the community organized a community meeting to explore solution to the problem.
The villagers debated among themselves and took a firm decision to reopen the centre and also allot another room to the ANM for the time being. The outcome of the meeting resulted on a firm decision by the panchayat members to clean the centre immediately. They immediately acted and provided sweepers to clean up the sub centre. Thereafter the panchayat members took the custody of the sub centre building to make it fully functional. The doors and windows were badly damaged and needed immediate repairing. After discussing this issue, they requested the Senior Medical Officer (SMO) of the PHC to help them out. Deliberations with the higher authorities made the SMO sanction a grant for the repair and work is about to start in a few days. Further, the panchayat made temporary arrangements by allotting a room to the ANM. Slowly it was observed that the process to restore the sub-centre services has been started by the joints efforts of PRI members and public health authorities.
Vardaan Consultants, Baroda, Gujarat, INDIA 37
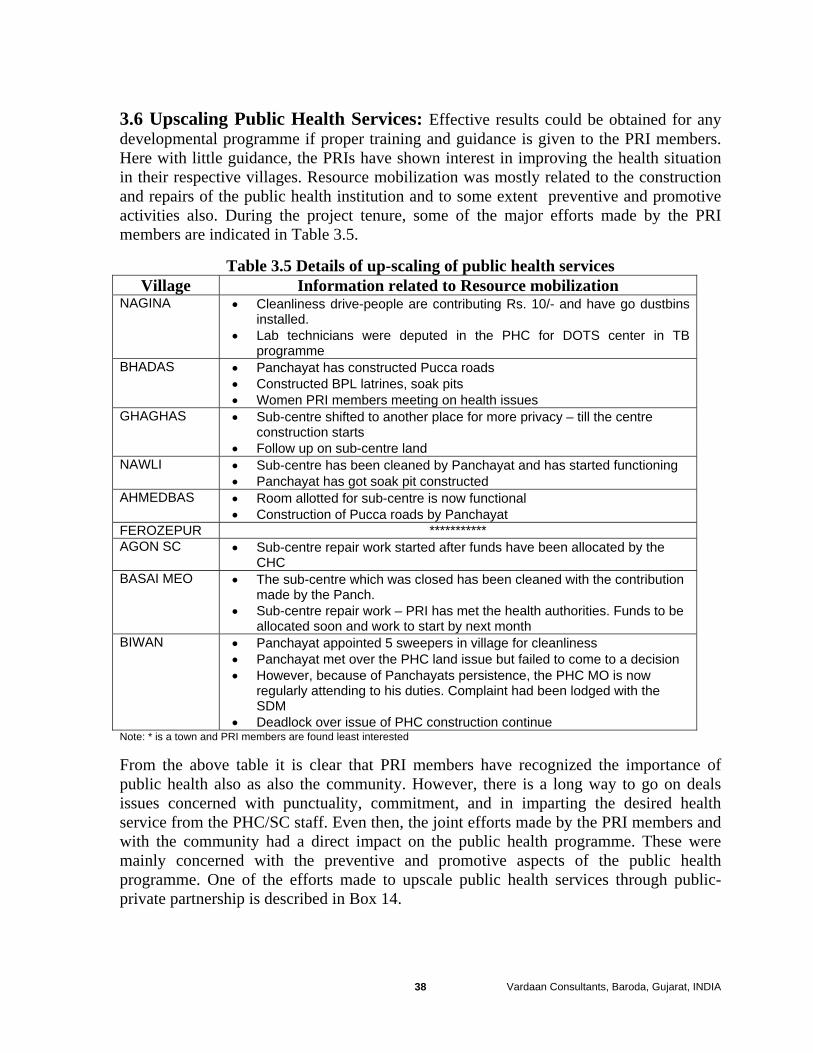
3.6 Upscaling Public Health Services: Effective results could be obtained for any developmental programme if proper training and guidance is given to the PRI members. Here with little guidance, the PRIs have shown interest in improving the health situation in their respective villages. Resource mobilization was mostly related to the construction and repairs of the public health institution and to some extent preventive and promotive activities also. During the project tenure, some of the major efforts made by the PRI members are indicated in Table 3.5.
Table 3.5 Details of up-scaling of public health services Village Information related to Resource mobilization
NAGINA • Cleanliness drive-people are contributing Rs. 10/- and have go dustbins installed.
• Lab technicians were deputed in the PHC for DOTS center in TB programme
BHADAS • Panchayat has constructed Pucca roads • Constructed BPL latrines, soak pits • Women PRI members meeting on health issues
GHAGHAS
• Sub-centre shifted to another place for more privacy – till the centre construction starts
• Follow up on sub-centre land NAWLI • Sub-centre has been cleaned by Panchayat and has started functioning
• Panchayat has got soak pit constructed AHMEDBAS • Room allotted for sub-centre is now functional
• Construction of Pucca roads by Panchayat FEROZEPUR *********** AGON SC • Sub-centre repair work started after funds have been allocated by the
CHC BASAI MEO • The sub-centre which was closed has been cleaned with the contribution
made by the Panch. • Sub-centre repair work – PRI has met the health authorities. Funds to be
allocated soon and work to start by next month BIWAN • Panchayat appointed 5 sweepers in village for cleanliness
• Panchayat met over the PHC land issue but failed to come to a decision • However, because of Panchayats persistence, the PHC MO is now
regularly attending to his duties. Complaint had been lodged with the SDM
• Deadlock over issue of PHC construction continue Note: * is a town and PRI members are found least interested
From the above table it is clear that PRI members have recognized the importance of public health also as also the community. However, there is a long way to go on deals issues concerned with punctuality, commitment, and in imparting the desired health service from the PHC/SC staff. Even then, the joint efforts made by the PRI members and with the community had a direct impact on the public health programme. These were mainly concerned with the preventive and promotive aspects of the public health programme. One of the efforts made to upscale public health services through public- private partnership is described in Box 14.
Vardaan Consultants, Baroda, Gujarat, INDIA 38
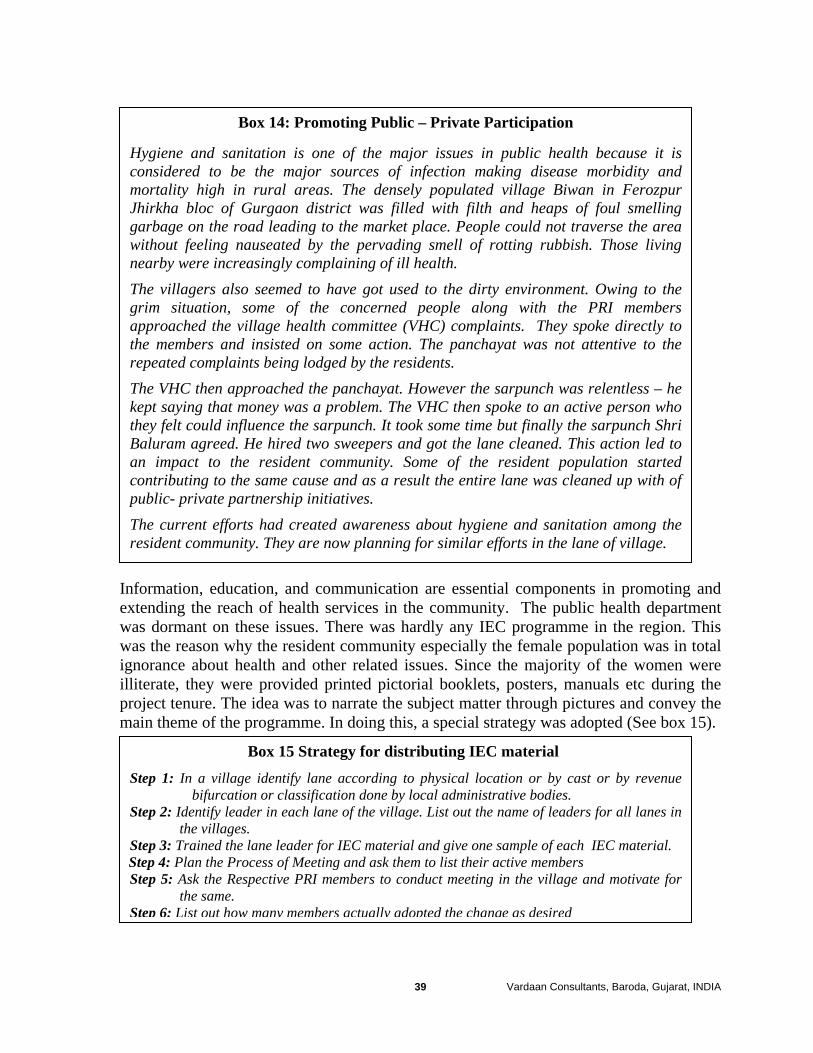
Box 14: Promoting Public – Private Participation
Hygiene and sanitation is one of the major issues in public health because it is considered to be the major sources of infection making disease morbidity and mortality high in rural areas. The densely populated village Biwan in Ferozpur Jhirkha bloc of Gurgaon district was filled with filth and heaps of foul smelling garbage on the road leading to the market place. People could not traverse the area without feeling nauseated by the pervading smell of rotting rubbish. Those living nearby were increasingly complaining of ill health.
The villagers also seemed to have got used to the dirty environment. Owing to the grim situation, some of the concerned people along with the PRI members approached the village health committee (VHC) complaints. They spoke directly to the members and insisted on some action. The panchayat was not attentive to the repeated complaints being lodged by the residents.
The VHC then approached the panchayat. However the sarpunch was relentless – he kept saying that money was a problem. The VHC then spoke to an active person who they felt could influence the sarpunch. It took some time but finally the sarpunch Shri Baluram agreed. He hired two sweepers and got the lane cleaned. This action led to an impact to the resident community. Some of the resident population started contributing to the same cause and as a result the entire lane was cleaned up with of public- private partnership initiatives.
The current efforts had created awareness about hygiene and sanitation among the resident community. They are now planning for similar efforts in the lane of village.
Information, education, and communication are essential components in promoting and extending the reach of health services in the community. The public health department was dormant on these issues. There was hardly any IEC programme in the region. This was the reason why the resident community especially the female population was in total ignorance about health and other related issues. Since the majority of the women were illiterate, they were provided printed pictorial booklets, posters, manuals etc during the project tenure. The idea was to narrate the subject matter through pictures and convey the main theme of the programme. In doing this, a special strategy was adopted (See box 15).
Box 15 Strategy for distributing IEC material
Step 1: In a village identify lane according to physical location or by cast or by revenue bifurcation or classification done by local administrative bodies.
Step 2: Identify leader in each lane of the village. List out the name of leaders for all lanes in the villages.
Step 3: Trained the lane leader for IEC material and give one sample of each IEC material. Step 4: Plan the Process of Meeting and ask them to list their active members Step 5: Ask the Respective PRI members to conduct meeting in the village and motivate for
the same. Step 6: List out how many members actually adopted the change as desired
Vardaan Consultants, Baroda, Gujarat, INDIA 39
However, in the short span of the project, its impact could not be evaluated. But, the interest of women and adolescent girls has been aroused as majority want to listen and become volunteers to help others. For long-term sustainability, most of the interventions should rely on public-private partnership. The community feels the ownership of the programme and therefore takes interest in solving the problem. Shortages of funds or manpower could be overcome through such partnerships. It also helps take timely decisions by persons assigned to solve the problems. Moreover, it also inculcates a sense of team sprit and group responsibility towards the problem that forbids any controversy, irrational behaviour and vested interest of an individual. Thus in any community programme, public – private partnership could provide strength in making it successful and sustainable at the grassroot level. Such a strategy could be a probable option to deal with issues pertaining to the panchayati raj system at grassroot level. 3.7 Status of Women and Gender Equalities: When India was under colonial rule only male members could vote and contest elections while women were totally absent from the political scene. For instance, the Bombay Village Panchayat Act 1920 categorically stipulated that no person could become an elected member who was a female and that the election was to be held in each village by the adult male residents at a meeting presided over by the assistant or deputy collector. Even after independence the Indian constitution did not mention or specifically provide reservation for women's' representation in parliament or state assemblies. It took nearly 40 years for women to find political representation in formal political institutions. As stated earlier, this was made possible through the 73rd Constitution Amendment Act, which introduced the landmark provision of reserving not less than one-third of the total number of seats in the local bodies for women (Goerge, 2003). It provided the much-needed opportunity for women to actively participate in the decision-making processes of their locality through the political right that was conferred on them through the central act. In this new era of panchayati raj, there are now more than one million women representatives elected to the three tiers of panchayats who give more meaning for democratic representation as they become spokespersons of the local community. However in the given social milieu, it is the rich who continue to hold the levers of socio-economic power. They get their women folk elected on the reserved seats for women while they themselves continue to function as de-facto representatives. Despite the constitutional guarantee of equality between the sexes the women in India face much discrimination which impinges on their right as human beings. They are still denied the basic right on equal education, food, nutrition, healthcare, and employment. This can be characterized by a system of domination and control – as a child, woman is under the control of her father, as a wife she is under the domination of her husband, and as a widow under the protection of her son. Women do not have any separate or independent existence of her especially in rural area, although few exceptions always
Vardaan Consultants, Baroda, Gujarat, INDIA 40
exist. Thus, unless specific conditions are met, women face multiple hurdles and find it difficult to participate in the political process that has hitherto been a male bastion (Poornima and Vinod, 1999). In Mewat too the situation is not different. Women panchayat members act only for names sake, their husbands or sons act as proxy representatives and unfortunately are being un-hesitantly entertained at all administrative levels as elected representatives. Women in Mewat are the most deprived and, live in utter ignorance and poverty, completely unaware of their potential and individuality. Meo women in particular surpass all Indians in illiteracy; most of the girls are either never sent to schools or are early dropouts who regress back into illiteracy. The average age of marriage among ‘meos’ is as low as 14years leading to unhealthy lives, burdened by too many and too frequent pregnancies. Being a closed society they neither go to a hospital nor consult doctors. As a result child mortality rate is high. Lack of information about basic hygiene coupled with low education and stronghold of traditional customs and practices put these women at higher risk. They are weakly represented in decisions making. It is the men folk who decide and make decisions. Like in any community, the gender inequality affects every aspect of culture and society of the Meos. The most prominently affected are the family structure, the education system and the economy. The baseline survey shows the low status of women. About 43.9 per cent of PRI members reported that women are illiterate and 31.7 per cent reported adopting ‘parda’ (covering forehead). Further about 19.5 per cent of PRI members are of the view that the domestic responsibilities restrict them to be efficient PRI members than male. However 75 per cent of PRI members reported agreeing that women could propagate better health programmes than males but illiteracy, suppression by males and domestic responsibilities had adverse affect in propagating health programmes. Each woman reported having at least five children. They shared the dual responsibility of doing domestic work and in the field. Women are only treated as object of enjoying sex and producing children. Only 6.25 per cent of household women reported using a contraceptive before the birth of first child. Below is a description of usage of contraceptives in the community (Box 16).
Vardaan Consultants, Baroda, Gujarat, INDIA 41

Box 16: Usage of Contraceptives
Lower use of contraceptive and higher fertility among Muslims is a proven fact. Various factors can be considered as contributing to this: lower socioeconomic status, the fundamentalist approach and greater opposition to family planning. Ghaghas is a village in Nagina block of Mewat district. Nessa, wife of Ramjaan, a resident of the village, has 10 children. She wanted to adopt method of family planning for quite some time but owing to lack of awareness and religious sanctions, she was not able to do so. Initially her husband also was not keen on her adopting the method. Frequent pregnancies have deteriorated her health to an extent that she was unable to do any work. She used to get tired soon. Household work is taken care by her daughter who herself is a small kid. During a visit, the husband met one of the PRI members and after listening about his work he shared the health problem of his wife. The husband realized that for the sake of his wife is health, family planning was essential. She cannot bear the burden of yet another pregnancy. The PRI with the help of the volunteer explained in detail all the methods of family planning. The couple decided to adopt Copper-T with the help ANM. The couples is completely satisfied and is helping to spread the word around. Trust is being developed. As a result people are themselves coming forward asking for support.
The baseline survey revealed that the mean age of marriage among females is 16 years. It all depends upon local customs and tradition. Since the majority of the population is Muslim marriages relies on several factors. The focus group discussion held in village Naginas support the fact:
The usual marriage age is 14-15 years for girls but some also get married at 16 years. As soon as the girl starts menstruating, she is considered eligible for marriage. “Pehli mahawari ke baad beti ko rakhna haraam manta hai Mussalmaan”. Par agar ghar mein behenein hain aur ek ka rishte ke saath dosra ka bhi mil jaata hai, to phir donon ke saath hi byah kar dete hain, chahe chhoti ki umar 10-12 saal hi kyon nah on.” The boys here are, however, younger than their bride. If the girl is 15 – 16 years at the time of marriage, the boy is usually 12 – 13 years. This is because the lure of dowry prompts the villagers to get their young boys married off – as they said “baad mein itna paisa miley na miley”. “Kabhi to Kondom aadmi ko pasand nahi aata, copper-T mein kabhi to bahut zyaada bleeding hota hai, goli to kabhi yaad hi nahi rehta, kaya Karen?”. Discontinuation of condom was due to no satisfaction of the malelerving no satisfaction, copper – T because of excessive bleeding and pain, pills is as not a favoured option anyway (as women will have to remember taking it daily) and injections have led to pregnancy in some cases. “Islam mein parhez hai aur agar ksisko pata chal jaata hai ki koi tarrek aistmaal kar raha hai koi to phir kair nahi”Most felt that using contraceptives would go against religious beliefs. However those who were
Vardaan Consultants, Baroda, Gujarat, INDIA 42
in favour, felt that fear of others knowing and their family members not agreeing were the main hindrances.
Out of total 274 deliveries, only 14.2 per cent got ANC care and a similar number also got post natal care. Pre and post care for women of the villages has no concern in their families especially among males. Thus it seems that the panchayat members are least bothered about the MCH programme in the community as witnessed in the focus group discussion in Nagina.
No precautions are taken during pregnancy. They had no idea about what we were taking. “Woho to kudrat ke dein hai, hai na. Par itna to hai ki ghar ki baaki mahilayein kabhi kabhi kaam mein madat kar deti hain.” The women of the household sometimes help out but the men do not. “Behenji ke paas to jaate hain jab bachha pet mein hota hai”. Yes. The ANM and local dai are consulted but the doctor only when any complications are identified. No prior arrangements for delivery are made. However the group also pointed out that in case the dai is not able to handle any delivery, the ANM is called or they make arrangements to go the PHC. Decision making is done by the local RMP who is also consulted during the labour time. “Ghar pe hi bachha hota hai”. The deliveries are conducted at home only or the place where they are most comfortable. In the hospital, the workers sometimes hold them to ransom – meaning they ask for some money (‘mithai ke liye’) before allowing them to leave the centre. No post- natal checkups are done. Nobody comes nor they do they think it is required.
Overall the status of the women in this region is very poor. The participation of women as PRI members has not made any difference in the their status or self-prestige. 3.8 Review and Follow up Mechanism: Since the project had three working partners, it was essential having review and regular follow-ups to trace the activities and their outcomes. Four types of meetings were regularly conducted as summarized below:
a) Village level/Gram Panchayat meetings: Village level or the gram level meetings of NGO volunteers with PRI members was routinely conducted. Not exactly as per the norms of the gram panchayat meeting, but PRI members started attending and discussing matters related to preventive and promotive aspects of the public health programme. Of nine villages, this activity was reported running swiftly in four villages. In a very informal manner the agenda was discussed and issues pertaining to health were given prime importance. Issues pertaining to improving the public health infrastructure through construction and repair; material and other supplies, etc are also now discussed. Activities related to this have been already discussed in the preceding section of this report (refer Table 3.5).
Vardaan Consultants, Baroda, Gujarat, INDIA 43
b) Lane Meetings: This is usually being conducted in the village lane in order to share information on various aspects of health issues. Usually the meeting is being conducted by senior women who explain various aspects of health. This meeting is specially organized to generate demand for health services among women through public health institutions. Such meetings also help to understand the morbidity pattern and related health services as desired by women.
c) PHC level Meetings: This is a routine meeting in the PHC where the PHC staff assemble data and plan activities. During the project tenure the NGO volunteers used to participate in such meetings and communicated the message to PRI for the forthcoming health programme in the villages. Active PRI members do further canvassing among the resident community for the desired support to make the health programme successful. Such collaboration has given fruitful results as shown in Table 3.3. In one village, PRI members have started attending monthly meetings organized in the PHC.
d) Monthly Review Meetings: Monthly review meetings are an essential component of this intervention project. Here the NGO volunteers and PRI members meet regularly and share their experiences and future planning. However the during the project tenure, the PRI members were found irregular as they had other commitments and most of them had a feeling that village level meeting are sufficient. However, compilation of data and future strategy is an essential element that makes this meeting a regular activity. Such meetings of made PRI members, PHC staff and NGO volunteers in the panchayati raj system should be made mandatory.
3.9 Shortcomings in System: It was not easy to generate support and linkage among PRI members, public health staff, and NGO volunteers. Though NGO volunteers were directly associated with project consultants, they were clear about the objectives. However lack of conceptual clarity and poor linkage among the public health staff and PRI members in the panchayati raj system led to total failure. During the project tenure, there were many unexplored issues:
(a) Forced Linkage: The project areas had a panchayati raj system linked with block development authority and the district panchayat. However, before the start of the project there was no linkage between PRI members and public health staff. Since the local NGO was working in rural development, there was some linkage with PRI members in the selected villages. Overall, it seems that they were forced to make linkages among themselves especially with PRI members and public health staff. However after seeing the result of working in TRIO combination, majority feel the need continue the process. Since project intervention was done in a very informal manner (without any mandatory process and administrative support of the public administration) a limited number of PRI members agreed to work in TRIO combination.
(b) Demand Generation Activities: One of the important thrusts of the public health system is demand generation activities for the desired health services. In spite of working in TRIO combination, the public health staff was found reluctant in conducting and
Vardaan Consultants, Baroda, Gujarat, INDIA 44
participating in IEC activities. Moreover, looking the fruitful project experience, they assume that canvassing and propagation of health programmes is the duty of PRI members and NGO volunteers only. They have to deliver health services to the community motivated by PRI members and NGO volunteers. One of the ideas proposed NGO volunteers to generate demand for the public health services was to introduce citizen charter of public health and distribute printed leaflets among the community. The idea could not work as the public health institutions were not well equipped with the desired infrastructure, manpower and other material supplies.
(c) Missing Information: Under the PRI system, there are several developmental schemes13 associated with different sectors. Such information was found reported missing among the PRI members as well as in the community. Looking the health sector, information pertaining to the development of the family welfare programme was totally missing. To improve the sex ratio, the schemes like “devi rupak and swastha aapke dwar” were major initiatives of the state government. However the desired information of the beneficiaries was missing. According to the baseline survey, only 5 per cent of the households have accurate knowledge of the development programme under the panchayati raj system. Project experience also reveals that there was total ignorance about the development programme not only among the community but also among the PRI members. (d) Budget: The project staff faced two bad experiences of the budget process. Since the NGO volunteers were taking the leading role in the implementation of the project, they visited district panchayat office to get budget details for last three years. The idea behind getting budget details was to know the allocation of budget to public health and other development programmes. None of the concerned authority could give the desired information. Mewat became an independent district in the middle of the tenure of the project. The concerned authorities were found busy setting up the district administrative system and directed the volunteers to get details from the respective block development authorities. At block level, this was not possible as the concerned BDO considered it a confidential matter and could only be shared with the consent of the higher district authorities. It was not possible to get details regarding participation and role of PRI members in the formulation of the budget. Overall, it seems that there is no transparency in the budget formulation. The budget and the process of budgeting remain confined between the BDO and the selected village panchayat. (e) Birth and Death Registration: During the project tenure, it was observed that at micro level there no coordination between the PHC and the gram panchayat level. The vital statistics available at the gram panchayat level is not reliable. This leads to the problem of assessing progress for different health programmes. According to the baseline survey, most (94.5%) deliveries are reported conducted through trained traditional birth attendants (TBAs) or dais. The chowkidaar of the village has the responsibility to collect information of all the births from the dai’s in the villages and deaths individually by the ANM who 13 Agriculture, wasteland development, sanitation, animal husbandry, social forestry, small scale industries, seed and fertilizer subsidy, drinking water, women and child development, family welfare, upgrading people under BPL, etc
Vardaan Consultants, Baroda, Gujarat, INDIA 45

submits details after filling a form at the PHC. The PHC then releases the certificate. However the practice of birth and death registration is very poor. The ANM collects the certificate from the PHC and distributes it to the respective parents. The process does not involve the panchayat at any point. (f) Inadequate Infrastructure of Public Health: This has become the universal problem all over the country, and was also found true in the project area. There was shortage of manpower, materials, and supplies, and poor infrastructure that has led to deterioration of public health services. In spite of several attempts of advocacy at the district level, PRI members were found helpless in this regard. According to the baseline survey, out of 99 PRI members, majority (40%) are in the age group of the 50 - 60 years and about 55 per cent of them are found to be illiterate. This leads to identity crisis among PRI members and feeling of superiority complex in district administration under the PRI system. This is the reason for the failure of every effort of advocacy for public health problems in the panchayati raj system.
Vardaan Consultants, Baroda, Gujarat, INDIA 46

Chapter 4: Conceptualizing the Model
The Tenth plan has prioritized reorganization and restructuring of the existing public healthcare infrastructure through a decentralized process with the existing structure of panchayati raj system so that quality services are delivered to the resident community at the grassroot level. Taking lead from this, an effective project strategy a TRIO management -model has been designed for the effective management of public health institutions. It includes a combination of PRI members, Public Health institution staff, and NGO volunteers. Project experience suggests that effective management of public health institutions can not be done through individual efforts of PRI members alone, but should involve public health staff and NGO volunteers as equal partners as indicated in the vein diagram.
PRI
NGO PHC/SC
A B
C
X
The project experience suggests interdependency among each other that would make effective management of public health institutions. There are certain common tasks (A) between PRI and PHC/SC which make their interdependency valid such as the building repair and maintenance; canvassing of health programmes; mobilization of desired resource from the district panchayat and district health office etc. A similar type of interdependency is also witnessed between PRI members and NGO volunteers (B) for doing advocacy, desired resource mobilization from the community, generating demand, promoting health programmes in the community etc. Inevitable combination of PHC/SC and NGO volunteers (C) in imparting the desired health services is also a important combination and very well pointed out by the National Rural Health Mission. The project experience shows that feeble team efforts between (NGO and PHC) do not mean a failure but needs a clear strategy. Here the X factor signifies the community for whom the desired health services could effectively be imparted through this “TRIO model” as the community dependency to a large extent depends on these three institutions. Table 3.6 gives the overlapping of health issues among PRI members, PHC/SC staff, and NGO volunteers to be resolved in partnership.
Vardaan Consultants, Baroda, Gujarat, INDIA 47
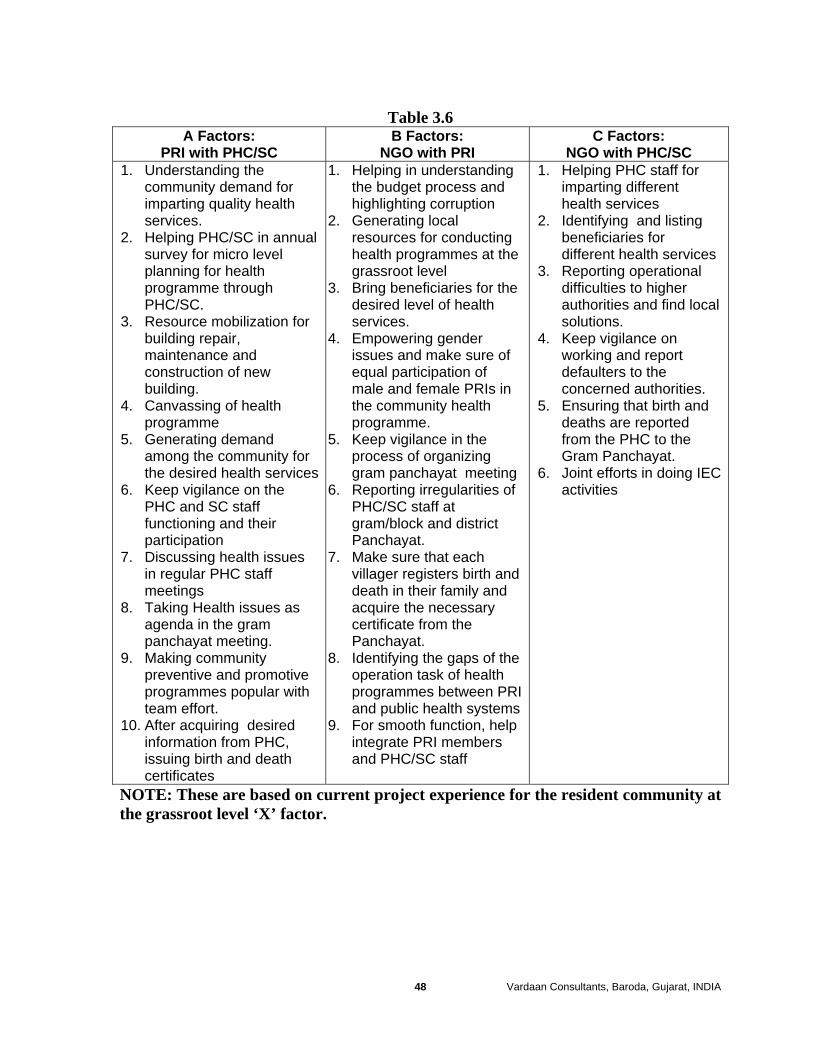
Table 3.6 A Factors:
PR C
NC Factors:
NGO C B Factors:
I with PHC/S GO with PRI with PHC/S1. Un
2. C/SC in annual
3. obilization for
d
4. g of health
5. Generating for
6.
ir
7. alth issues
8. alth issues as
9. tive
10. g desired
1. Help ding
2. ucting
3. s for the
4. Empowering gender of
in
5. e in the
ng 6.
istrict
7. at each and
8. gaps of the
I
9.
1.
2. listing
rvices 3.
cal
4. nce on
ities. 5.
6. g IEC
derstanding the community demand for imparting quality health services. Helping PHsurvey for micro level planning for health programme throughPHC/SC. Resource mbuilding repair, maintenance anconstruction of newbuilding. Canvassinprogramme
demand among the communitythe desired health servicesKeep vigilance on the PHC and SC staff functioning and theparticipation Discussing hein regular PHC staff meetings Taking Heagenda in the gram panchayat meeting. Making community preventive and promoprogrammes popular with team effort. After acquirininformation from PHC, issuing birth and death certificates
ing in understanthe budget process and highlighting corruption Generating local resources for condhealth programmes at the grassroot level Bring beneficiariedesired level of health services.
issues and make sure equal participation of male and female PRIsthe community health programme. Keep vigilancprocess of organizing gram panchayat meetiReporting irregularities of PHC/SC staff at gram/block and dPanchayat. Make sure thvillager registers birthdeath in their family and acquire the necessary certificate from the Panchayat. Identifying theoperation task of health programmes between PRand public health systems For smooth function, help integrate PRI members and PHC/SC staff
Helping PHC staff for imparting different health services Identifying and beneficiaries for different health seReporting operational difficulties to higher authorities and find losolutions. Keep vigilaworking and report defaulters to the concerned authorEnsuring that birth and deaths are reported from the PHC to the Gram Panchayat. Joint efforts in doinactivities
NO re based on current project experience for the resident community at TE: These athe grassroot level ‘X’ factor.
Vardaan Consultants, Baroda, Gujarat, INDIA 48
The benefits of adopting the “TRIO” model for effective management of public health institutions are numerous. Some of the benefits as experienced during the project tenure include resource mobilization, creating community volunteers to compensate shortage of manpower as observed in the national programmes as Jan Swasthya Rakshak, (JSR) or Community health worker schemes (CHWS) or Janmangal Yojana (JY) in Rajasthan and Swaasth Mangal Yojana (SMY) (Mavalankar, Sinha et al 2001) in Gujarat, and making local efforts to sustain and impart quality of health services. Besides, the preventive and promotive aspects of public health services could be best imparted through this combination as witnessed during the project tenure.
This model will make provision of health services accountable to the community and bring about transparency in various process of the panchayati raj system. It helps inculcate the problem solving attitude and the ability to work in a team. This will help to empower the community acquire desired health services in terms adequacy, quality, and accessibility. This will be possible, only if communities’ participation is empowered using this model. Tasks like resource identification and mobilization, local budgeting and plan formulation through GRAM Panchayat can be linked with this model in which the roles of NGO, PRI volunteers and public health staff are clearly identified. This will not only help conduct participatory monitoring but also help evaluate plans and social audit.
The TRIO model is based on the current project experience with little transparency in the system and without any mandatory process to a backward region of Haryana. The learning experience suggests that such a model could be sustained, if authorities at various levels narrate the individual role and responsibility as a mandatory process. The major drawback of the model is related to the operating system that largely depends upon the transparency made by the concerned authorities in the Panchayati Raj System and district officials. Earlier several studies have pointed out that bureaucracy; nepotism, corruption etc are some of the major conflicting factors and major hindrances that affect the decentralization process.
The current model has been is tested at the village level i.e.; at the gram Panchayat level only. The major challenges to integrating and synchronizing the inbuilt system and process to three tier Panchayati Raj system are yet to be operationalized. Thus under the 73rd Constitutional Amendment Act, there is great need to do necessary architectural correction using the TRIO model in the basic healthcare service delivery system for the forthcoming National Rural Health Mission Programme. This will provide more weightage to community participation and decentralize process the panchayati raj system for the effective management of public health institutions at the grassroot level.
Vardaan Consultants, Baroda, Gujarat, INDIA 49
Chapter 5: Conclusion and Recommendations These are certain cross cutting issues where policy interventions are very essential to make the system transparent and mandatory, so that the PRI system could effectively manage public health institutions at the grassroot level with the help of NGO volunteers and public health staff. The trio combination could be helpful to extend the reach of public health services among the resident population at the grassroot level and acquire desired health services in terms adequacy, quality, and accessibility. The following changes to be are made in the panchayati raj system and integrated to the National Rural Health Mission.
1. The model is a prime example of community participation and decentralized process. Thus structural integration of this model is required at all three levels of panchayati raj system and district administration. Thus under 73rd Constitutional Amendment Act, necessary architectural correction should be done such that to make all the processes related to resource identification and mobilization, local budgeting, and plan formulation become mandatory using the TRIO model at all three levels of the panchayati raj system. Further strict norms should be fixed to select grassroot level NGOs or self help group or any civil society.
2. It has been observed that about 50 per cent of PRI members are in the age group of
50 - 60 years having least knowledge of PRI system and are being used as proxy representatives in their family. Haryana panchayati raj system has adopted two child norms and now there is need to introduce qualifying conditions of maximum age limit (below 50 years) for contesting panchayat elections. This will help more number of youth and adolescent to be integrated into the PRI system. This will generate community participation as well as decentralize process.
3. In order to reduce corruption and nepotism, a separate provision should be made as
a mandatory process in the election that no family members in the same household and also close relations (uncle, aunty, cousins, etc) could consecutively be elected for second time as PRI members. A gap of minimum ten years should be made for one family or their relatives for contesting the second election so that power does not remain confined to some families or class of society.
4. There is no provision in budget for repairs and maintenance of public health
building. Even if the district panchayat authorities approve the budget for construction, delays in the construction of building demotivate the resident community and alienate them from the panchayati raj system as well as district administration. A separate provision should be made to allocate some funds for repair and maintenance of public health institutions at the gram panchayat level and more autonomy should be provided for construction under approved norms rather totally depending upon the PWD department. Besides, at GRAM Panchayat level provision should be made for a separate budget for bringing emergency
Vardaan Consultants, Baroda, Gujarat, INDIA 50
medicines at the time of shortage of materials and supplies at public health institutions and to avert epidemics in the village.
5. The problem of shortage of manpower and materials and supplies in public health
is becoming universal. There is an urgent need to tackle the problem at the gram panchayat level. However under NRHM, a major initiative has been taken by integrating the “ASHA” as a self help group for extending the reach of public health services and also mainstreaming AYUSH – revitalizing local health tradition. It is recommended that the SHG should have same provisions as observed in the Janmangal Yojana in Rajasthan and the Swastha Mangal Yojana, in Gujarat. Such a programme gives more weightage to voluntary couple per thousand population with basic training of public health. These voluntary couples in village can form a self help group that will generate more community participation and will help to take own decisions in the matter of health seeking behaviour.
6. Strict vigilance norms should be specified for organization, participation and
selection of agenda for the gram panchayat meetings. The project experience has a reveled that gram panchayat meetings are only on paper with least preferences given to public health issues and with no participation of the community or public health staff. The village sarpunch organizes meetings on paper and passes the resolution with the help of illiterate PRI members. Participation of NGO volunteers and member of civil society with public health staff will definitely have affirmative impact and will help in doing impartial vigilance in the process and participation, of Gram Panchayat meetings.
7. Birth and death registration is considered to be an important component of
panchayati raj system. Absence of roles and responsibility for PRI members’ birth and death registration creates lot of irregularities in the vital statistics. A mandatory process should made in such a way that all births and deaths are reported first in the GRAM Panchayat level. Special power should be assigned to the Gram Panchayat for issuing birth and death registration certificates as observed in Gujarat, Kerala, West Bengal etc.
8. Integration of NGO volunteers or members of civil society in the TRIO
management model at all levels of PRI system will be very helpful to check corruption and help to keep a watch on the work being done by PRI members and public health staff at grassroot level.
Vardaan Consultants, Baroda, Gujarat, INDIA 51
Conclusion: Panchayat raj existed in India since British rule but it gained momentum only after independence. Mahatma Gandhi had a vision to devolution power to the bottom – at village level to ensure people’s participations in the task of rural development in such a way that a every village ought to be a republic with local panchayat having power under the three – tier panchayat raj system. However in reality, The PRI system is based on age-old caste hierarchy and social status.
The PRI system has been found effective in a few states. While in other states, PRIs have not yet started participating in desired developmental programmes. The central report of the PRI task force had clearly pointed out that PRIs are bypassed in all centrally sponsored / central sector schemes. Further there are immense difference between states in the involvement of PRIs in the public health programme. The recommendation of the ICPD conference and the Agenda for Reforms (AFR) of the World Bank for providing quality services and to promote decentralization process, have forced the policy makers to give panchayati raj institutions prime importance. Thus the Tenth Plan has prioritized reorganization and restructuring of existing health care infrastructure at primary, secondary and tertiary levels through a decentralized process with the existing structure of the panchayati raj system so that for the resident population (especially the rural community) gets the desired level of health services. The challenge of providing affordable, available, accessible, acceptable and appropriate healthcare to over a billion people of India is daunting. The problems are many: limited resources, poor governance, skewed manpower, inadequate infrastructure, lack of accountability, misdirected investments, mounting hospital costs, monumental corruption, ignorance, and illiteracy. Hence to overcome such problems, it is essential to make the local government (such as panchayats) to be effective and strong. To generate public participation and make the decentralization process popular, it is recommended to integrate the TRIO management model for effective management of public health institutions. This would be the beginning of the new era - where all mandatory process of PRI system would be implemented with better transparency, as multiple agencies are now involved along with the PRI members. This will help keep track of the proper functioning of the PRI system with a greater option of flexibility and constant vigilance for the effective implementation as well as management of the health programme. Some interesting result could be obtained if the management model is integrated with the National Rural Health Mission in the three-tier system of the panchayati raj system through out the country.
Vardaan Consultants, Baroda, Gujarat, INDIA 52
References: Bajpai, N. and Goyal, S. (2004), “Primary Health Care in India: Coverage and Quality Issues, Center on Globalization and Sustainable Development (CGSD) Working Paper No. 15
Behar, A. and Kumar, Y. (2002) Process of Decentralization in Madhya Pradesh: Panchayati Raj to Gram Swaraj (1995–2000). Background report submitted to ODI Livelihood Options Project. London: Overseas Development Institute.
B. Ekbal (2000), “Decentralize Planning and Health Sector in Kerela”, Issue Paper at People Health Assembly, www.pha2000.org or www-sph.health.latrobe.edu.au/pha
Bruce, Judith (1990), “Fundamental Elements of the Quality of Care: A Simple Framework,” Studies in Family Planning, 21(2): 61-91.
Craig Johnson, (2003), Decentralization in India: Poverty, Politics and Panchayati Raj, Working Paper 199, Department of Political Science University of Guelph, Ontario, ODI, London.
George Mathew (1999), “Panchayati Raj Institutions and Human rights”, PUCL bulleting, March www.pucl.org/topics/law/2003/panchayati-raj.htm.
Crook, R.C. and Manor, J. (1998) Democracy and Decentralization in South Asia and West Africa. Cambridge: Cambridge University Press.
Gurgaon “District Profile” http://haryana.gov.in/; http://gurgaon.nic.in/f_administration.htm as on 15th November 2005
Ghatak, M and Ghatak, M (2002), “Recent Reforms in the Panchayat System in West Bengal Toward Greater Participatory Governance?”, Economic and Political Weekly, January 5, 2002 pp. 45-58.
Gore, C. (2000) “The Rise and Fall of the Washington Consensus as a Paradigm for Developing Countries”, World Development 28(5): pp.789–804.
Ghatak, M and Ghatak, M (1999), “Grassroots Democracy: A Study of the Panchayat System in West Bengal”, Paper Prepared for the Conference on Experiments in Empowered Deliberative Democracy, Wisconsin–Madison, January, 2000.
Johnson, C. and Start, D. (2001) ‘Rights, Claims and Capture: Understanding the Politics of Pro-Poor Policy,’ ODI Working Paper 145. London: Overseas Development Institute.
Madhya Pradesh, Human Development Report, 2002, Bhopal Govt. of Madhya Pradesh.
Mission Report (2002) “Rajiv Gandhi Missions: Eight Years 1994 – 2002” Report to the People, www.mpindustry.mp.nic.in
Vardaan Consultants, Baroda, Gujarat, INDIA 53
Meenakshisundaram, S.S. (1999) “Decentralization in Developing Countries,” in S.N. Jha and P.C. Mathur (eds.) (1999) Decentralization and Local Politics: Readings in Indian Government and Politics (2). London: Sage, pp. 54–69.
Minocha, A.C. (1999) “District Government in Madhya Pradesh: Laudable Objective, Inappropriate Mechanism,” Economic and Political Weekly, 9 July 1999.
Mavalankar D.V., Sinha Harshit, Dave J and Patel V (2001), SWASTHA MANGAL YOJANA, : An Innovative Method for Community Participation, Indian Institute of Management, Ahmedabad. Mavalankar D.V., Sharma B (1999), “The Quality of Care in Sterilization Camps: Evidence from Gujarat. In: Improving Quality of Care in India’s Family Welfare Programme: The challenges ahead. Ed Michael A. Koenig and M.E. Khan. Population Council, New York pp. 293-313.
Mavalankar D.V. (1998) “Need and Challenges of Management Education in Primary Health Care System in India, IIMA, Working Paper No.98-11-05, Indian Institute of Management, Ahmedabad.
Mavalankar DV, and Patel VM. (1998) “Primary Health Care under Panchayat Raj in Gujarat: Perceptions of Health Service Staff”. Social Change. Special issue edited by R. Balakrishnan of Council for Social Development, New Delhi, March; 28(1). Pp. 54-69.
National Rural Health Mission Report (NRHM) (2005-12) Mission Document, Ministry of Health and Family welfare, Government of India, New Delhi.
Planning Commission Report (2002-07), Family Welfare, Chapter 2.10, Planning Commission, 2002-07.
Panchayati Raj Institutions (PRIs) (2001) Report of the Task Force on Planning Commission, New Delhi, December 2001 Narayana, D. and Hari Krupa, K.K. (2000), “Decentralisation of the Health Care Sector in Kerala: Some Issues Working Paper No. 298, Centre for Development Studies, Thiruvananthapuram
Poornima and Vinod Vyasulu (1999) “Women in Panchayati Raj: Grassroots Democracy in India, Experience from Malgudi, Background Paper No. 4, Meeting on Women and Political Participation: 21st Century Challenges, United Nations Development Programme, New Delhi, 24-26 March 1999. Policy for Interface between the Gujarat Government health department and the Jan Swasthya Abhiyan-Gujarat www.phm-india.org/doc/gujarat/guj_jsa_policy.doc
Raghavulu, C.V. and Narayana E.A. (1999) “Reforms in Panchayati Raj: A Comparative Analysis of Andhra Pradesh, Karnataka and West Bengal,” in S.N. Jha
Vardaan Consultants, Baroda, Gujarat, INDIA 54
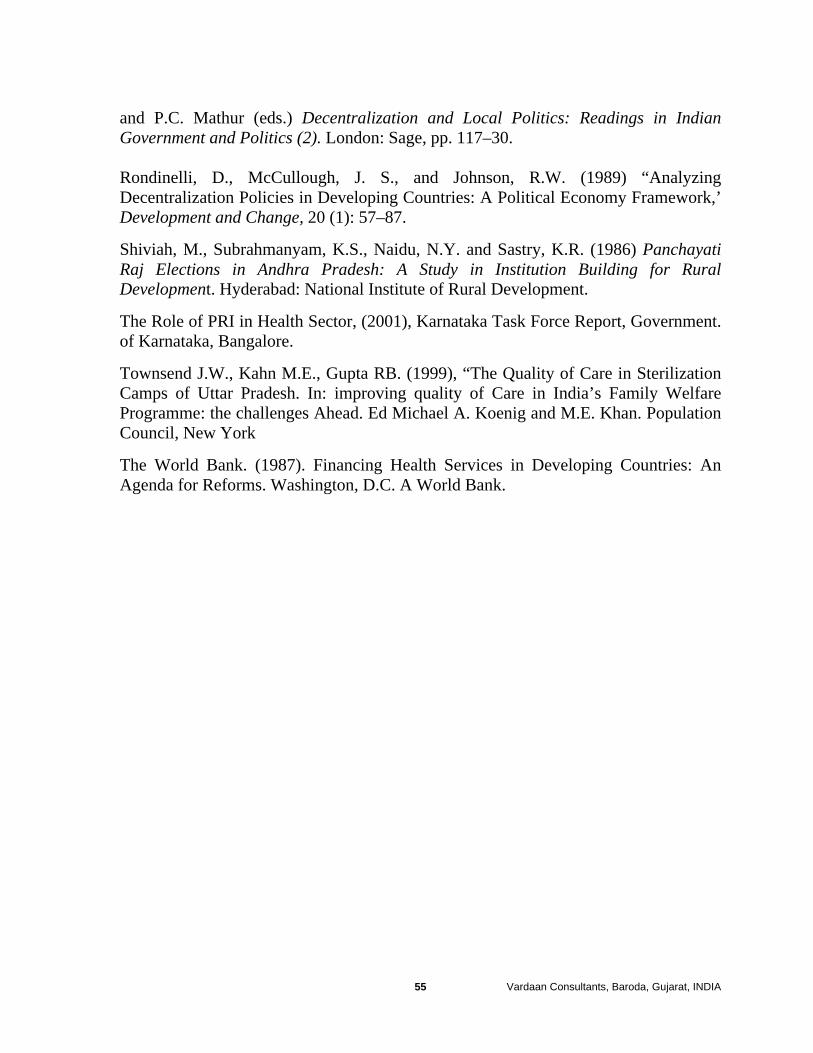
and P.C. Mathur (eds.) Decentralization and Local Politics: Readings in Indian Government and Politics (2). London: Sage, pp. 117–30. Rondinelli, D., McCullough, J. S., and Johnson, R.W. (1989) “Analyzing Decentralization Policies in Developing Countries: A Political Economy Framework,’ Development and Change, 20 (1): 57–87.
Shiviah, M., Subrahmanyam, K.S., Naidu, N.Y. and Sastry, K.R. (1986) Panchayati Raj Elections in Andhra Pradesh: A Study in Institution Building for Rural Development. Hyderabad: National Institute of Rural Development.
The Role of PRI in Health Sector, (2001), Karnataka Task Force Report, Government. of Karnataka, Bangalore.
Townsend J.W., Kahn M.E., Gupta RB. (1999), “The Quality of Care in Sterilization Camps of Uttar Pradesh. In: improving quality of Care in India’s Family Welfare Programme: the challenges Ahead. Ed Michael A. Koenig and M.E. Khan. Population Council, New York
The World Bank. (1987). Financing Health Services in Developing Countries: An Agenda for Reforms. Washington, D.C. A World Bank.
Vardaan Consultants, Baroda, Gujarat, INDIA 55

We are fast growing consultancy organization, providing diversified consulting services with highly qualified professionals and individuals associated with our group. Our company provides services with the motto to have competitive edge linked with professional standards. The experts of our company encourage our customers to be a part of our services with total satisfactions and long-term business dealing. The consulting group adopts inter-disciplinary scientific approach and latest technology to explore the assigned task. With the ideas and solution, we create data bank put information to a larger perspective for future expansion. The company specializes in training, internal change agent, quality control and strategic planning. For details visit www.vardaan.org email: [email protected]





























