Embed Size (px)
Citation preview

Dysnatremia in the ICU
Milap Pokaharela and Clay A. Blocka,baSection of Nephrology and Hypertension andbDartmouth Medical School, Dartmouth HitchcockMedical Center, Lebanon, New Hampshire, USA
Correspondence to Clay A. Block, MD, 1 MedicalCenter Dr., Lebanon, NH 03576, USATel: +1 603 653 3830; fax: +1 603 653 3991;e-mail: [email protected]
Current Opinion in Critical Care 2011,17:581–593
Purpose of review
Dysnatremias, disorders of sodium concentration, are exceedingly common in critically
ill patients and confer increased risk for adverse outcomes including mortality. The
physiology that underpins the diagnosis and management of these disorders is complex.
This review seeks to discuss current literature regarding the pathophysiology,
diagnosis, epidemiology, and management of these disorders.
Recent findings
The role of arginine vasopressin in the maintenance of normal and pathologic plasma
osmolality increasingly is refined, improving our ability to diagnose and understand
dysnatremia. Identified recent epidemiologic studies highlight the frequent hospital
acquisition or exacerbation of dysnatremia, confirm the recognized adverse
consequences and explore the potential causality. Despite the complex nature of these
disorders, simple consensus treatment strategies have emerged.
Summary
Dysnatremia remains a common disorder across the spectrum of critically ill patients. It
is frequently hospital acquired. Simplified treatment regimens are proposed and the
potential for prevention or earlier recognition and intervention is emphasized. Future
directions of interest include further exploration of how dysnatremia contributes to
adverse outcomes and new treatment strategies.
Keywords
dysnatremia, hypernatremia, hyponatremia, vasopressin
Curr Opin Crit Care 17:581–593� 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins1070-5295
Introduction
Disorders of sodium concentration, dysnatremias, are
among the most commonly encountered electrolyte
abnormalities in the ICU. They are disorders of relative
water excess or deficiency, resulting in alteration in effec-
tive plasma osmolality (Posm) (tonicity), leading to trans-
cellular shift of water, thereby altering cell volume. This
is in contradistinction to disorders of sodium excess or
deficiency, which produce changes in the extracellular
fluid (ECF) volume, namely edema or hypovolemia, res-
pectively. Hyponatremia is commonly defined as a plasma
sodium concentration (PNa) less than 136 mmol/l; hyper-
natremia, commonly as PNa greater than 145 mmol/l.
Both frequently develop or are exacerbated during
hospitalization and are associated with increased length
of stay (LOS) and mortality. Clinical manifestations may
range from absent to life threatening. Treatment may be
life saving but carries substantial risk of harm. Appropriate
management requires an understanding of underlying
pathophysiology and treatment principles.
PhysiologyUnderstanding dysnatremia starts with an appreciation
that water moves freely between the intacellular fluid
Copyright © Lippincott Williams & Wilkins. Unaut
1070-5295 � 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins
(ICF) compartment and the ECF compartment to main-
tain osmotic equilibrium. As the bulk of the intracellular
solute is accounted for by exchangeable potassium (Ke)
and extracellular solute by exchangeable sodium (Nae)
and their companion anions, the relationship between
these quantities and total body water (TBW) can be
described as [1]:
Posm ¼ Iosm � 2� Nae þ 2� Ke
TBW
Posm will fall as a result of potassium depletion, sodium
depletion, or an increase in TBW. Likewise, Posm will
increase if potassium or sodium is added or if TBW is
reduced. Changes in Posm are usually identified by
changes in PNa. TBW is estimated as a fraction of body
weight: 0.6 in children and healthy, nonelderly men, 0.5
in women and elderly men, and 0.45 in elderly women
[2].
Posm homeostasis, or osmoregulation, requires the integ-
ration of water intake and excretion to be precisely
balanced with salt intake and excretion. Challenges to
osmoregulation occur on a regular basis due to ingestion
of water, salt, exercise, and other routine activities. For
example, an elevation in Posm of approximately
horized reproduction of this article is prohibited.
DOI:10.1097/MCC.0b013e32834cd388

C
582 Renal system
Key points
� Even mild degrees of hyponatremia and hyperna-
tremia confer markedly increased risk for mortality
and increased length of stay.
� Hospital acquired or exacerbated dysnatremia con-
fers a worse prognosis than community acquired
dysnatremia.
� Severe hyponatremia, paradoxically, may have a
better prognosis than moderately severe hypona-
tremia, perhaps because it is more likely to occur
as a primary disorder without multiple comorbid
conditions.
� Acute, symptomatic hyponatremia should be trea-
ted with 3% saline given as 100 ml bolus(es) to
raise the plasma sodium concentration rapidly by
4–6 mmol/l.
� Correction of hyponatremia should be no greater
than 10 mmol/l in the first 24 h and no greater than
18 mmol/l in the first 48 h; correction of hyperna-
tremia should be no greater than 0.5 mmol/l per
hour and bolus therapy with isotonic saline should
be avoided unless there is circulatory collapse.
10 mOsm/kg may occur after 40 min of strenuous exercise
in a hot environment; ingestion of two large glasses of
water (850 ml) can lower Posm by 6 mOsm/kg in 30 min
[3]. Changes in Posm of as little as 1% result in activation
of homeostatic processes that are mediated via neuro-
endocrine pathways orchestrated in the hypothalamus.
Specialized neurons in the organum vasculosum laminae
terminalis (OVLT), supraoptic (SON), and paraventric-
ular nuclei of the hypothalamus sense changes in Posm,
possibly through mechanically sensitive cation channels.
A rise in Posm results in the activation of thirst and the
secretion of antidiuretic hormone [also known as arginine
vasopressin (AVP)]. AVP is synthesized by specialized
neurons in the SON and paraventricular nucleus that give
rise to long axons terminating in the posterior pituitary,
wherein AVP is stored. A fall in the Posm results in
suppression of thirst and suppression of AVP release.
Under normal conditions, AVP is maximally suppressed
at PNa of approximately 135 mmol/l. The hypothalamus
also participates in salt intake (craving) and renal
excretion (via natriuretic peptides). These homeostatic
mechanisms tend to maintain Posm within 1–3% of the
set point, a range compatible with health [4].
AVP exerts its effect by binding to a specific receptor
(V2R) on the basolateral membrane of principal cells of
the collecting tubule of the distal nephron, activating
adenyl cyclase production of cyclic adenosine mono-
phosphate, leading to activation of protein kinase A
(PKA). PKA phosphorylates water channels, aquaporin
2 (AQP2), which undergo exocytotic insertion into
the apical membrane, increasing water permeability.
Ultimately, reabsorbed water is returned to the systemic
circulation via the peritubular capillaries. In the absence
of AVP, AQP2 is internalized and distal nephron water
permeability is greatly reduced. The presence or absence
of AVP can be inferred by measuring the urine osmolality
(Uosm). A Uosm greater than maximally dilute (50–
100 mOsm/l) implies AVP activity. Other actions of
AVP include vasoconstriction, platelet aggregation, and
gluconeogenesis mediated by V1A receptors present on
smooth muscle cells, platelets, and liver. AVP activation
of V1B receptors on the anterior pituitary promotes
release of adrenocorticotropic hormone. AVP secretion
is also stimulated by a reduction in effective arteriolar
blood volume (EABV) mediated by baroreceptors dis-
tributed throughout the circulation. This effect overrides
the expected suppression of AVP and accounts for the
water retention observed in cases of hypovolemia and the
edematous disorders [congestive heart failure (CHF),
cirrhosis, and nephrosis] [1,5��].
The brain responds to hypotonic stress in two ways. First,
increased interstitial pressure caused by cerebral edema
results in movement of interstitial fluid into the cere-
brospinal fluid and ultimately into the circulation.
opyright © Lippincott Williams & Wilkins. Unauth
Second, brain cells extrude intracellular solutes, thus
limiting ingress of water and cerebral edema. This pro-
cess begins with extrusion of potassium and sodium
within several hours and continues with the extrusion
of organic osmolytes over several days. It is this adaptive
response that predisposes to osmotic demyelination
during correction of hyponatremia (discussed in detail
below). In the setting of hypernatremia, brain cells will
accumulate potassium and organic osmolytes, thus blunt-
ing cell shrinkage but predisposing the brain to edema if
hypernatremia is rapidly corrected [6–8].
Classification of hyponatremiaThe first step in classification of hyponatremia is to
confirm the presence or absence of a hypoosmolar/
hypotonic condition. Nonhypotonic hyponatremia has a
limited differential diagnosis that is discussed below.
Low Posm usually identifies hypotonic hyponatremia
although hypotonic hyponatremia can also be seen in
the setting of retention of an ineffective osmole (such as
urea or ethanol) that is able to permeate the cell mem-
brane. In these cases, the Posm may be normal or high,
but the plasma tonicity will be low and the clinical
consequences of hypotonic hyponatremia can occur,
including cerebral edema. Hypotonic hyponatremia
due to impaired water excretion can be distinguished
from excess water intake or inadequate solute intake by
determining the Uosm. Low Uosm identifies primary
polydipsia, beer potomania, or tea diet and toast diet.
Uosm greater than 100 mOsm/kg implies AVP activity.
Assessment of the volume status by clinical exam and
orized reproduction of this article is prohibited.

Dysnatremia in the ICU Pokaharel and Block 583
measurement of UNa can then establish if there is
reduction in EABV producing a physiologic AVP stimu-
lation. If euvolemia is identified, AVP activity is most
commonly due to the syndrome of inappropriate anti-
diuretic hormone (SIADH). Diagnostic criteria for
SIADH require hypoosmolality, Uosm greater than
100 mOsm/l, absence of diuretics, absence of edema or
clinical signs of volume depletion, UNa greater than
30 mmol/l, absence of renal impairment, and a clinical
response to water restriction with correction of hypona-
tremia and a reduction in UNa. SIADH has myriad causes
including malignant tumors (especially small cell lung
cancer), pulmonary disorders (infections, airways obstruc-
tion, respiratory failure), central nervous system (CNS)
conditions (masses, hemorrhage, infection, multiple
sclerosis, Guillain–Barre syndrome, etc.), drugs that
stimulate AVP secretion or enhance activity (serotonin
reuptake inhibitors, tricyclics, chlorpropramide, ifosfa-
mide, nonsteroidal anti-inflammatory drugs, cyclophos-
phamide, narcotics, psychotropics, etc.), drugs that have
AVP activity (vasopressin, desmopressin, and oxytocin),
and miscellaneous conditions including postoperative
state, stress, pain, and nausea. Adrenal insufficiency
and hypothyroidism are associated with euvolemic hypo-
natremia and measurement of these hormones is indi-
cated [5��,9��,10].
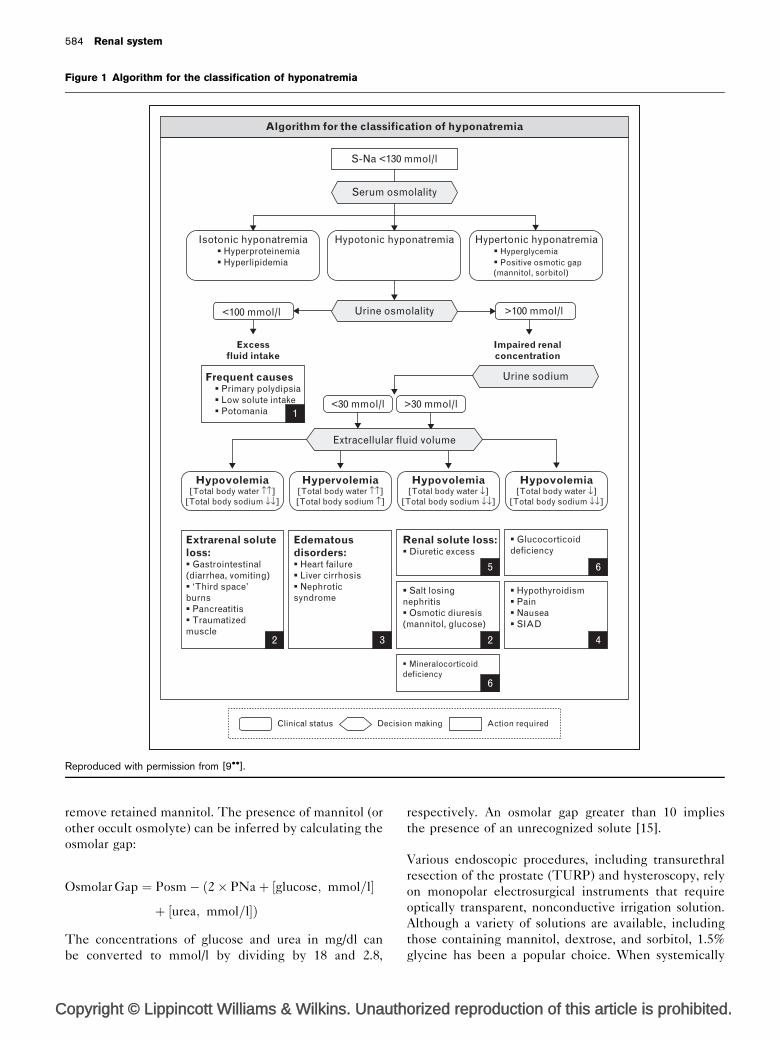
Algorithms have been developed to facilitate correct
classification (Fig. 1) [9��]. Application of such algorithms
improves the accuracy of classification compared with
clinical judgment by experienced physicians but may still
fail to arrive at the correct diagnosis as determined by
retrospective review by an expert. Confusion can occur
due to overlap in the laboratory findings in conditions of
diuretic use, renal salt wasting, and cerebral salt wasting
(CSW). In these conditions, clinical exam for hypovole-
mia is imprecise; UNa will be relatively high and can
result in misclassification as SIADH. As water excretion
may be subtly impaired in patients with primary poly-
dipsia, Uosm may not be less than 100 mOsm/kg, leading
again to misclassification as SIADH.
Renal salt wasting as a cause of hypovolemia is particu-
larly problematic as these patients have natriuresis by
definition. Renal salt wasting can occur in adrenal insuf-
ficiency that may be congenital or acquired. Renal tubular
injury by cisplatin can cause salt wasting within days to
weeks of exposure. As cisplatin is used to treat solid
tumors that can also cause SIADH, it is crucial to deter-
mine the presence or absence of volume depletion.
Autonomic dysfunction, which can accompany small cell
lung cancer, can further confuse the situation. CSW can
occur in the setting of neurosurgical conditions, such as
subarachnoid hemorrhage (SAH), that are also known to
be associated with SIADH. The diagnosis of CSW relies
on the simultaneous demonstration of unequivocal
Copyright © Lippincott Williams & Wilkins. Unaut
volume depletion and elevated UNa in an appropriate
clinical setting. Unfortunately, even direct hemodynamic
assessments sometimes fail to yield unequivocal results.
Such patients should be managed with hypertonic saline
or saline as necessary to ensure maintenance of normo-
natremia and adequate intravascular volume.
Saline infusion has been labeled the ‘gold standard’, as
volume expansion in a sodium-depleted patient should
suppress the hemodynamic stimulus for AVP secretion
and allow excretion of a dilute urine and correction of
hyponatremia. However, in clinical practice, this is not
always practical or effective, as up to 30% of patients
treated with 2 l of isotonic saline failed to elevate PNa by
greater than 5 mmol/l or lower their Uosm. Likewise,
some patients with SIADH will show an improved PNa
with isontonic saline infusion if their Uosm is less than
300 mOsm/l. The fractional excretions of Na, urea, and
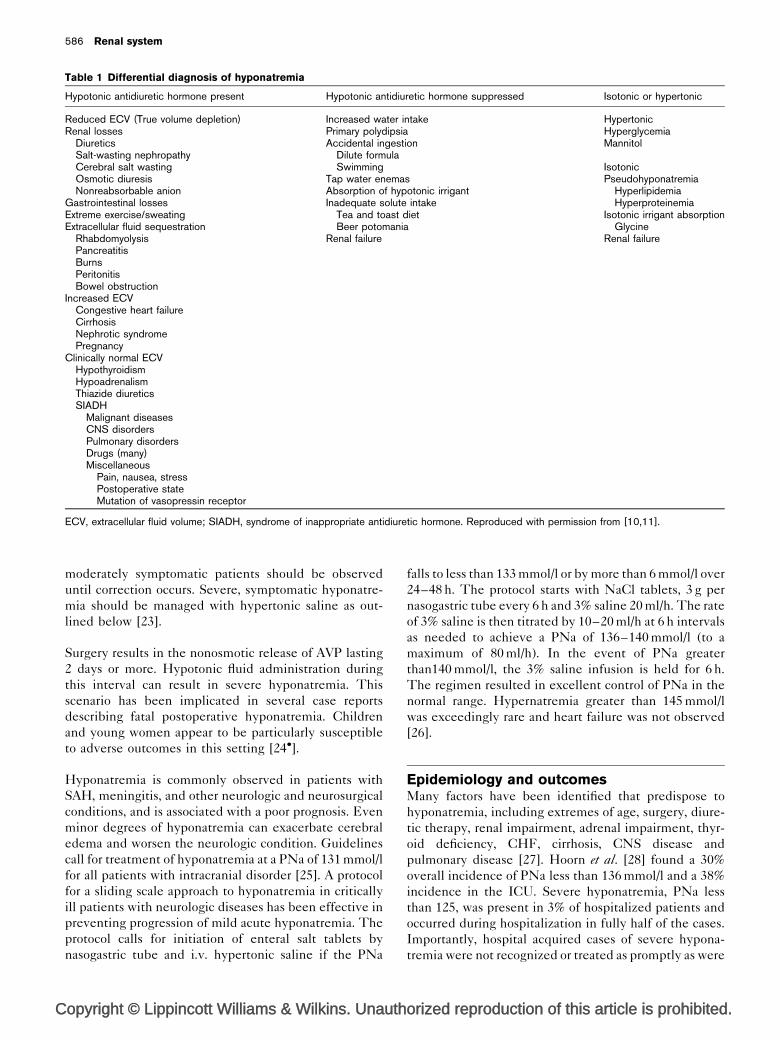
uric acid (Table 1) [10,11] have all been utilized to add
diagnostic accuracy. A fractional excretion of sodium
(FENa) greater than 0.15% or a fractional excretion of
urea (FEUrea) favors a diagnosis of SIADH. Plasma uric
acid level of less than 4 mg/dl and FEUric acid greater
than 16% also favor a diagnosis of SIADH [12].
Nonhypotonic hyponatremiaNonhypotonic hyponatremias include those that are
hypertonic due to the retention of a nonpermeable solute
resulting in translocation of water from the intracellular
to the extracellular compartment, thereby lowering the
PNa. The most common cause of this phenomenon is
hyperglycemia due to diabetes mellitus. An analysis
published in 1973 by Katz [13] predicted that the serum
sodium concentration would fall by 1.6 mmol/l for every
100 mg/dl increase in the glucose concentration above
normal. This prediction rule appears to be valid in the
setting of renal failure when there is no osmotic diuresis
to complicate the situation. However, when renal func-
tion is intact, some sodium loss occurs secondary to the
osmotic diuresis provoked by glucosuria leading to a
greater than expected fall in serum sodium concentration.
An average fall in PNa of 2.5 mmol/l was seen in experi-
mentally induced hyperglycemia in healthy patients and
a nonlinear change in PNa was observed (1.6 mmol/l for
glucose levels up to 400 mg/dl then as high as 4 mmol/l for
every 100 mg/dl of glucose concentration for glucose
exceeding 400 mg/dl) [14].
Exogenous solutes such as mannitol can also result in
hypertonic hyponatremia by similar mechanism. Manni-
tol is used therapeutically in a variety of settings to induce
an osmotic diuresis or to induce a hypertonic condition to
treat cerebral edema. If renal function is intact, the
mannitol will be excreted and PNa will recover to normal.
If renal function is impaired, dialysis may be used to
horized reproduction of this article is prohibited.
C
584 Renal system
Figure 1 Algorithm for the classification of hyponatremia
Algorithm for the classification of hyponatremia
Hypertonic hyponatremia � Hyperglycemia � Positive osmotic gap (mannitol, sorbitol)
Hypotonic hyponatremiaIsotonic hyponatremia � Hyperproteinemia � Hyperlipidemia
S-Na <130 mmol/l
Serum osmolality
>100 mmol/l<100 mmol/l
<30 mmol/l >30 mmol/l
Frequent causes � Primary polydipsia � Low solute intake � Potomania 1
2 3 2 4
6
65
Hypovolemia[Total body water ↑↑]
[Total body sodium ↓↓]
Extrarenal soluteloss:� Gastrointestinal(diarrhea, vomiting)� ‘Third space’burns� Pancreatitis� Traumatizedmuscle
Edematousdisorders:� Heart failure� Liver cirrhosis� Nephroticsyndrome
Hypervolemia[Total body water ↑↑][Total body sodium ↑]
Hypovolemia[Total body water ↓]
[Total body sodium ↓↓]
Renal solute loss:� Diuretic excess
Hypovolemia[Total body water ↓]
[Total body sodium ↓↓]
Urine osmolality
Urine sodium
Extracellular fluid volume
Excessfluid intake
Impaired renalconcentration
� Hypothyroidism� Pain� Nausea� SIAD
� Mineralocorticoiddeficiency
Clinical status Decision making Action required
� Salt losingnephritis� Osmotic diuresis(mannitol, glucose)
� Glucocorticoiddeficiency
Reproduced with permission from [9��].
remove retained mannitol. The presence of mannitol (or
other occult osmolyte) can be inferred by calculating the
osmolar gap:
Osmolar Gap ¼ Posm� ð2� PNaþ ½glucose; mmol=l�
þ ½urea; mmol=l�Þ
The concentrations of glucose and urea in mg/dl can
be converted to mmol/l by dividing by 18 and 2.8,
opyright © Lippincott Williams & Wilkins. Unauth
respectively. An osmolar gap greater than 10 implies
the presence of an unrecognized solute [15].
Various endoscopic procedures, including transurethral
resection of the prostate (TURP) and hysteroscopy, rely
on monopolar electrosurgical instruments that require
optically transparent, nonconductive irrigation solution.
Although a variety of solutions are available, including
those containing mannitol, dextrose, and sorbitol, 1.5%
glycine has been a popular choice. When systemically
orized reproduction of this article is prohibited.

Dysnatremia in the ICU Pokaharel and Block 585
absorbed, these solutions can cause hyponatremia and
volume overload. Glycine solutions can cause a constella-
tion of symptoms and signs including nausea, vomiting,
confusion, hypotension, cardiac dysfunction, bradycardia,
visual disturbance, and even coma and death [16]. This
constellation has been referred to as TURP syndrome
and correlates with postoperative glycine concentration.
As ammonia is an intermediate metabolite of glycine,
hyperammonemia can occur. The solution is isotonic
and initially is confined to the ECF compartment. PNa
will fall but tonicity and Posm will remain normal. As
glycine is taken up by muscle cells and metabolized, a
process that requires several hours, PNa will return
toward normal. In a single-center experience, hyponatre-
mia occurred equally frequently in patients randomly
assigned to either glycine or dextrose irrigant solution,
but TURP syndrome developed only in 17 of 120 (14%)
patients randomly assigned to glycine irrigation [17�].
The major risk factor for TURP syndrome appears to
be the volume of irrigant absorbed. Newer technology
incorporating bipolar electrosurgical instruments that are
compatible with use of isotonic saline as an irrigant
should eliminate the occurrence of hyponatremia and
TURP syndrome, but could still result in volume over-
load if systemic absorption is substantial. Glycine absorp-
tion can be recognized by the presence of an osmolal
gap in the appropriate clinical setting. The treatment of
TURP syndrome is supportive. Hypertonic saline
should not be used unless there is concomitant hypotonic
hyponatremia. Dialysis has been utilized in severe cases,
particularly those with hyperammonemia and renal
impairment [18].
Pseudohyponatremia is a relatively uncommon cause
of nonhypotonic hyponatremia that relates to the
measurement of PNa by instruments (chemical auto-
analyzers) that use indirect ion-specific electrodes
(ISEs). These devices dilute the plasma sample prior
to measurement of the sodium concentration and are
calibrated on the basis that normal plasma by volume
contains 93% water and 7% protein and lipid. The
sodium content of plasma is confined to the aqueous
phase. In the setting of hyperproteinemia or hyper-
lipidemia, the water content is actually less than 93%,
leading to an artifactually low PNa determination.
Instruments that use ISEs to measure sodium concen-
tration, such as blood gas analyzers, are not subject to
such artifact. Hyperlipidemia resulting from hypertrigly-
ceridemia causes the specimen to appear turbid;
hypercholesterolemia, on the contrary, does not produce
visibly lactescent serum. Hyperproteinemia can be seen
in cases of endogenous hypergammaglobulinemia, as
in the setting of hepatitis or HIV infection, or in the
setting of exogenous administration of intravenous (i.v.)
gammaglobulin. Although relatively uncommon, it is
important to recognize pseudohyponatremia so that such
Copyright © Lippincott Williams & Wilkins. Unaut
patients are not subjected to inappropriate interventions
[5��].
Acute hypotonic hyponatremiaAcute hypotonic hyponatremia, also known as ‘acute
water intoxication’, is seen most frequently in primary
polydipsia, exercise-associated hyponatremia (EAH),
drug ingestions (particularly of 3,4-methylenedioxy-
methamphetamine, ‘ecstasy’), and the administration
or consumption of hypotonic fluids in a medical setting.
Primary polydipsia is a common disorder among patients
with underlying psychiatric disorders, particularly those
with schizophrenia. This condition was found in up to
47% of psychiatry inpatients in series from Cuba, with
almost 7% developing hyponatremia [19]. Hyponatremia
occurs if the volume of water ingestion exceeds the
excretory capacity of the kidneys. The water excretory
capacity of normal kidneys is estimated to be approxi-
mately 10% of the glomerular filtration rate (GFR),
which, in adults, ranges from approximately 108 to
170 l per day depending on age. In the setting of reduced
GFR, hyponatremia may occur with less dramatic fluid
intake. Water intoxication due to excessive consumption
has also been reported in water drinking contests [20].
Endurance exercise is associated with the nonosmotic
release of AVP. EAH occurs when the ingestion of water
is in excess of losses due to sweat, and the excess water is
retained due to the presence of AVP. Sodium loss in
sweat and excessive water intake driven by fear of dehy-
dration appear to contribute to the problem. This
phenomenon has been identified in as many as 7% of
endurance athletes. PNa testing in the finish-line tent at
the Boston Marathon has identified hyponatremia in
4.8% of runners. Two percent had PNa less than 130.
Sixteen were treated with hypertonic oral solution and
10 were treated with i.v. 3% saline raising the PNa by
6–7 mmol/l in approximately 15–30 min and abolishing
symptoms [21,22].
Ecstasy is a popular recreational drug among college age
people, particularly in association with rave parties and
nightclub activities. It has been implicated as a cause of
hyponatremia resulting in seizures and death in numer-
ous case reports. The mechanism appears to be multi-
factorial including induction of AVP release, induction of
thirst, and ready access to water and other hypotonic
fluids. Hyperpyrexia and vigorous activity may contribute
to sodium loss via sweat and lead to volume contraction
that further induces AVP. Women appear to be more
susceptible to ecstasy-related hyponatremia accounting
for approximately 85% of reported cases. Hyponatremia
often corrects spontaneously as a water diuresis ensues as
the effect of the drug dissipates. Asymptomatic to
horized reproduction of this article is prohibited.
C
586 Renal system
Table 1 Differential diagnosis of hyponatremia
Hypotonic antidiuretic hormone present Hypotonic antidiuretic hormone suppressed Isotonic or hypertonic
Reduced ECV (True volume depletion) Increased water intake HypertonicRenal losses Primary polydipsia Hyperglycemia
Diuretics Accidental ingestion MannitolSalt-wasting nephropathy Dilute formulaCerebral salt wasting Swimming IsotonicOsmotic diuresis Tap water enemas PseudohyponatremiaNonreabsorbable anion Absorption of hypotonic irrigant Hyperlipidemia
Gastrointestinal losses Inadequate solute intake HyperproteinemiaExtreme exercise/sweating Tea and toast diet Isotonic irrigant absorptionExtracellular fluid sequestration Beer potomania Glycine
Rhabdomyolysis Renal failure Renal failurePancreatitisBurnsPeritonitisBowel obstruction
Increased ECVCongestive heart failureCirrhosisNephrotic syndromePregnancy
Clinically normal ECVHypothyroidismHypoadrenalismThiazide diureticsSIADH
Malignant diseasesCNS disordersPulmonary disordersDrugs (many)Miscellaneous
Pain, nausea, stressPostoperative stateMutation of vasopressin receptor
ECV, extracellular fluid volume; SIADH, syndrome of inappropriate antidiuretic hormone. Reproduced with permission from [10,11].
moderately symptomatic patients should be observed
until correction occurs. Severe, symptomatic hyponatre-
mia should be managed with hypertonic saline as out-
lined below [23].
Surgery results in the nonosmotic release of AVP lasting
2 days or more. Hypotonic fluid administration during
this interval can result in severe hyponatremia. This
scenario has been implicated in several case reports
describing fatal postoperative hyponatremia. Children
and young women appear to be particularly susceptible
to adverse outcomes in this setting [24�].
Hyponatremia is commonly observed in patients with
SAH, meningitis, and other neurologic and neurosurgical
conditions, and is associated with a poor prognosis. Even
minor degrees of hyponatremia can exacerbate cerebral
edema and worsen the neurologic condition. Guidelines
call for treatment of hyponatremia at a PNa of 131 mmol/l
for all patients with intracranial disorder [25]. A protocol
for a sliding scale approach to hyponatremia in critically
ill patients with neurologic diseases has been effective in
preventing progression of mild acute hyponatremia. The
protocol calls for initiation of enteral salt tablets by
nasogastric tube and i.v. hypertonic saline if the PNa
opyright © Lippincott Williams & Wilkins. Unauth
falls to less than 133 mmol/l or by more than 6 mmol/l over
24–48 h. The protocol starts with NaCl tablets, 3 g per
nasogastric tube every 6 h and 3% saline 20 ml/h. The rate
of 3% saline is then titrated by 10–20 ml/h at 6 h intervals
as needed to achieve a PNa of 136–140 mmol/l (to a
maximum of 80 ml/h). In the event of PNa greater
than140 mmol/l, the 3% saline infusion is held for 6 h.
The regimen resulted in excellent control of PNa in the
normal range. Hypernatremia greater than 145 mmol/l
was exceedingly rare and heart failure was not observed
[26].
Epidemiology and outcomesMany factors have been identified that predispose to
hyponatremia, including extremes of age, surgery, diure-
tic therapy, renal impairment, adrenal impairment, thyr-
oid deficiency, CHF, cirrhosis, CNS disease and
pulmonary disease [27]. Hoorn et al. [28] found a 30%
overall incidence of PNa less than 136 mmol/l and a 38%
incidence in the ICU. Severe hyponatremia, PNa less
than 125, was present in 3% of hospitalized patients and
occurred during hospitalization in fully half of the cases.
Importantly, hospital acquired cases of severe hypona-
tremia were not recognized or treated as promptly as were
orized reproduction of this article is prohibited.

Dysnatremia in the ICU Pokaharel and Block 587
cases present on admission. Stelfox et al. [29] reported
ICU acquired hyponatremia (defined as a SNa less than
133 mmol/l) in 11% of patients and that this was associ-
ated with an increase in in-hospital mortality from 16 to
28%. The population studied included medical, surgical,
trauma, and neurologic patients. Higher acute physiology
and chronic health evaluation (APACHE) II scores and
longer ICU LOS were found to be risk factors for hypo-
natremia. Funk et al. [30] defined borderline, mild, and
severe hyponatremia as 130–135 mmol/l, 125–129, and
greater than 125, respectively. They found an overall
incidence of hyponatremia in 17.7% of ICU admissions
with a breakdown of 13.8% classified as borderline, 2.7%
mild, and 1.2% severe. Hyponatremia at all levels was an
independent risk factor for mortality. Adjusted mortality
odds ratios (ORs) were significant at all levels ranging
from 1.3 for borderline to over 1.8 for moderate and
severe cases.
A recent analysis of over 50 000 patients admitted to a
single, large Boston teaching hospital utilizing a liberal
cutoff of PNa less than 138 mmol/l demonstrated a
remarkable 38% incidence of community acquired hypo-
natremia. The analysis was extended to show that hypo-
natremia of even this modest degree was associated with
multiple adverse outcomes including increased mortality
LOS, and discharge to a care facility. Hospital acquired
hyponatremia was equally as frequent, occurring in 38.2%
of patients and was associated with even higher ORs for
adverse outcomes. In this study, hospital aggravated
worsening of community-acquired hyponatremia con-
ferred an even higher mortality risk of hospital mortality
(OR 2.3 vs. 1.66 for hospital acquired vs. 1.5 for com-
munity acquired). In hospital-acquired hyponatremia,
PNa or less 127 mmol/l was associated with a 15-fold
increase in mortality, whereas community-acquired
hyponatremia to the same degree conferred only a
2.5-fold increase risk [31�].
A 2009 study that examined data from approximately
98 000 patients admitted to two large teaching hospitals
found an initial PNa of less than 135 mmol/l in 14.5% and
that an additional 5.2% acquired hyponatremia during
their hospitalization. Approximately half of these patients
underwent multiple determinations of PNa: 20% had
hyponatremia on at least one of the measurements. Of
these, hyponatremia resolved in 7.2%, developed in
3.8%, and persisted in 8.6%. Mild hyponatremia (defined
as 130–134 mmol/l) accounted for the majority of the
cases (83%), moderate (120–130 mmol/l) for 16.8%, and
severe (<120 mmol/l) for 0.2%. When this analysis
was adjusted for the presence of hyperglycemia,
approximately 12–19% of patients initially classified as
hyponatremic were reclassified as normonatremic or
hypernatremic. Compared with normonatremia, hospi-
tal-acquired and persistent hyponatremia each conferred
Copyright © Lippincott Williams & Wilkins. Unaut
an approximately three-fold increase in inhospital
mortality, a two-fold increase in 1-year mortality, and
1.3–1.4-fold increase in 5-year mortality. There was no
sex difference in the incidence of hyponatremia, but
women were more likely to have severe hyponatremia.
Patients with the most severe hyponatremia did not have
a statistically increased mortality rate 1.46 (0.73–2.91), a
surprising observation [32].
The relationship between the severity of hyponatremia
and mortality was examined by Chawla et al. [33��] in a
cohort of over 45 000 patients found to have at least one
SNa of less than 135 mmol/l admitted to a large teaching
hospital over an 11-year span ending in 2007. These
authors confirmed a three-fold increase in mortality for
hyponatremic patients vs. normonatremic patients (6.1
vs. 2.3%). They also found that mortality tended to
increase with lower SNa peaking at 11.2% for patients
with SNa of 120–124 mmol/l, but reversing at SNa less
than 120 mmol/l such that mortality fell to approximately
6.8% in the more severely hyponatremic group. The
authors analyzed 53 patients who died and had severe
hyponatremia (SNa <120 mmol/l) and found that 73% of
these patients had moderate or severe hyponatremia on
admission, whereas 27% had normal or mild hyponatre-
mia that worsened. Most patients had recovered to nor-
mal or near normal SNa when death occurred, which was
more than a week after the SNa nadir in most cases. They
found only three cases in which hyponatremia was felt to
play a causal role and only one case in which central
pontine myelinolysis (CPM) might have occurred.
Patients with severe hyponatremia who survived were
more likely have drug-induced hyponatremia (thiazides
and selective serotonin reuptake inhibitors) and were
unlikely to have severe comorbid conditions. The authors
theorize that severe hyponatremia occurs more often
secondary to drug toxicity and is likely to be acute and
treatable (or to resolve), whereas moderate hyponatremia
is more likely to accompany severe comorbid conditions
such as CHF, cirrhosis, and malignancy and therefore
strongly associated with mortality. An editorial that
accompanies this article proposes three clinical scenarios
based on these findings: (scenario 1) hyponatremia causes
mortality directly from cerebral edema or correction
provokes the osmotic demyelination syndrome (ODS);
(scenario 2) hyponatremia occurs secondary to a severe
underlying illness and it is the underlying illness that
causes death; or (scenario 3) hyponatremia exacerbates
organ system dysfunction and contributes to mortality
indirectly [34��]. Little is known about how hyponatre-
mia might affect organ system function but a recent
observation that hyponatremia predicts myocardial
infarction in community patients lends support to the
third scenario [35]. Acutely decompensated heart failure
is another setting in which hyponatremia confers an
independent increased risk for mortality [36�].
horized reproduction of this article is prohibited.

C
588 Renal system
Clinical effects of hyponatremia andtreatment
Chronic hyponatremia is often asymptomatic. Most
patients do not have overt clinical symptoms until the
PNa is less than 120 mmol/l. However, even a mild
degree of hyponatremia is associated with falls and
impaired attention and gait in a manner analogous to
an ethanol level of 0.6 g/l [37]. In addition, hyponatremia
has been associated with fractures and osteoporosis
[38�,39,40]. The third national health and nutritional
examination survey found an OR of nearly 3 for devel-
oping osteoporosis at PNa of 133 mmol/l compared with
normonatremic patients. PNa less than 135 mmol/l was
found to be an independent risk factor for hip fracture.
Thiazide diuretics, despite their known effect on
calcium balance, are associated with fractures in elderly
nursing home patients, although this finding has not been
shown to relate to low PNa. Selective serotonin reuptake
inhibitors, a known cause of hyponatremia, are also
associated with falls and fractures in the first 2 weeks
of therapy, a time course that corresponds to the usual
onset of SSRI-related hyponatremia. However, a direct
connection to hyponatremia remains to be established.
Patients with CHF, renal failure, or cirrhosis who also
have hyponatremia have a worse prognosis. Again, it is
not established whether the hyponatremia is simply a
marker of decompensated organ system disease or if
hyponatremia has a direct deleterious effect.
The major clinical concern of hyponatremia is encepha-
lopathy [41]. Initial symptoms are nonspecific and
include headache, lethargy, and nausea. Advanced symp-
toms include lethargy, depressed reflexes, seizures, and
coma followed by death. Although the optimal rate of
correction is often referred to as controversial, guidelines
have been established that recommend an increase in
PNa of less than 10 mmol/l over 24 h and less than
18 mmol/l over 48 h [1]. A rapid rate of correction has
been associated with the development of the ODS, a
potentially devastating neurologic condition. Initial
descriptions identified mainly pontine damage, whereas
subsequent reports have identified more widespread
demyelination, thus central pontine myelinolysis
(CPM) and extrapontine myelinolysis (EPM) can be
grouped as two manifestations of ODS [42]. The most
classic form of this condition presents 2–3 days after
correction of hyponatremia with evidence of neurologic
deterioration after a period of improvement. Symptoms,
depending on the location and severity of the lesions,
may include seizures, parkinsonism, dysarthria, quadri-
paresis, spastic hypertonia, coma, and death. Character-
istic changes may be present on MRI. Early reports
described a uniformly bad prognosis with either death
or persistent severe neurologic impairment. More recent
reports have documented a variable prognosis. The
opyright © Lippincott Williams & Wilkins. Unauth
adaptation by brain cells to hypotonic conditions predis-
poses to injury with rapid correction, which acts like an
acute hypertonic insult. Indeed, ODS has been described
in a patient with acute hypernatremia who never suffered
hyponatremia. Animal studies have confirmed that it is
the correction of hyponatremia, not hyponatremia itself,
that causes ODS. Relowering of PNa has been shown to
ameliorate early signs of ODS in multiple case reports.
The risk for ODS increases with rate of correction greater
than recommended. Although correction rates within
these guidelines are associated with lower risk, there
are case reports of ODS occurring in patients who were
corrected within these limits. More rapid reuptake of
previously extruded organic osmolytes, particularly myoi-
nositol, is also protective. There are regional differences
in the brain with regard to reuptake of osmolytes, perhaps
accounting for the predilection of ODS for the pons and
other structures. Uremia, which is associated with more
rapid reuptake of osmolytes, is protective against ODS.
Patient risk factors appear to include liver disease,
alcoholism, orthotopic liver transplant, female sex, and
postoperative state [5��].
The rate of correction also appears to impact the risk for
rhabdomyolysis. In a retrospective study of 22 patients
with self-induced water intoxication, rhabdomyolysis was
found to be associated with a more rapid rate of correction
of 2 vs. 0.9 mmol/l per hour. The rapid rate of correction
was attributed to spontaneous excretion of large volumes
of dilute urine shortly after presentation [43�].
Acute symptomatic hyponatremia, whether self-induced,
drug-related, or hospital-acquired, is a true medical emer-
gency that demands prompt intervention. In these
patients, hyponatremia has developed faster than brain
adaptation can keep pace resulting in cerebral edema.
Usually the PNa is quite low, often greater than
110 mmol/l, but patients with intracranial disorder, as
noted above, may be symptomatic with more modest
falls in PNa. The presence of symptoms of CNS dysfunc-
tion attributable to cerebral edema should guide the
decision to institute therapy. Even patients with primary
polydipsia or postoperative hyponatremia that is
expected to correct spontaneously should be treated so
as not to delay improvement in cerebral edema. The goal
of therapy for acute symptomatic hyponatremia is to raise
the PNa by 4–6 mmol/l, which according to consensus
has resulted in resolution of hyponatremia-related
seizures, and coma. This is best accomplished by boluses
of 3% saline of 100 ml or 2 ml/kg. This can be repeated
twice if necessary to abort seizures or reverse coma. Note
that the rate of correction in this instance is greater than
the conventional recommendation of 0.5 mmol/l per hour,
but the total correction is limited to approximately
6 mmol/l. Once this correction is achieved and the patient
is neurologically stabilized, further correction should be
orized reproduction of this article is prohibited.

Dysnatremia in the ICU Pokaharel and Block 589
delayed or minimized so as not to exceed a net correction
of greater than 10 mmol/l over 24 h or 18 mmol/l over 48 h
[5��]. Chronic hyponatremia, if severely symptomatic,
should initially be treated similarly to those with acute
symptomatic hyponatremia. Some authors have advo-
cated ‘a rule of sixes’ stating that correction should be
‘6 mmol/l in the first 6 h but also limiting correction to
6 mmol in the first day’. Correction should be targeted at
less than the upper desirable to avoid overshooting.
Patients with primary polydipsia, volume depletion, thia-
zide diuretic induced hyponatremia, or cortisol deficiency
related water retention are particularly predisposed to too
rapid correction as they will undergo a water diuresis once
the underlying cause is treated resulting in a rise in PNa
of up to 2 mmol/l per hour. Desmopressin can be used in
such circumstances to terminate or prevent a water diur-
esis, allowing slow, controlled correction of the PNa.
Desmopressin is given every 6 h to maintain consistent
urine concentration. Therapy with 3% saline can then be
titrated to achieve a rate of correction within the guide-
lines. Hypokalemia is another factor that will predispose
to overcorrection as the addition of potassium chloride
(KCl) provides effective osmoles and raises PNa [1,5��].
The contribution of both KCl and NaCl to raising PNa
can be estimated by the following formula from Adrogue
and Madias [10], which describes the anticipated effect of
the infusion of 1 l of a solution:
change in PNa ¼ ðinfusate Naþ infusate KÞ � PNa
TBWþ 1
When actively correcting hyponatremia, it is crucial to
utilize an infusate with an effective osmolality greater
than that of urine. The most common choice of fluid to
correct hyponatremia is 3% saline that has a Na concen-
tration of 513 mmol/l. Furosemide can be added to avoid
expansion of the ECF due to the saline load. As loop
diuretics usually cause a diuresis equivalent to half-
isotonic saline, they may also facilitate correction if the
Uosms are very high. Restriction of free water ingestion
must accompany the active management of hyponatre-
mia unless the stimulus for AVP and water retention has
been alleviated. Demeclocycline, which impairs the
action of AVP, has been used to treat persistent hypo-
natremia due SIADH but renal toxicity and other side
effects limit its acceptance. High salt diet, salt tablets,
high protein intake, and urea supplementation are all
adjunctive measures that can be useful in the manage-
ment of persistent hyponatremia due to SIADH out of
the acute phase [9��,11].
Patients with symptomatic hyponatremia and renal fail-
ure requiring renal replacement therapy are at risk for
rapid correction. Management options include infusion of
hypotonic fluid during dialysis or the use of continuous
Copyright © Lippincott Williams & Wilkins. Unaut
renal replacement therapy utilizing replacement fluid
calculated to correct PNa at slow rate [5��].
Vasopressin antagonists, vaptans, are an emerging option
for management of chronic hyponatremia. Vaptans com-
petitively inhibit the binding of AVP to its V2 receptor in
the collecting duct and thereby block the insertion of
aquaporins into the apical membrane. Convivaptan, an
intravenous form that inhibits V1a receptors on smooth
muscle cells, platelets, and liver in addition to V2 recep-
tors, was the first V2R antagonist to be approved by the
US Food and Drug Administration (FDA) for treatment
of euvolemic hyponatremia due to SIADH, hypothyroid-
ism, adrenal insufficiency, or pulmonary conditions. It is
also approved for treatment of hyponatremia associated
with CHF. The metabolism of convivaptan is by the liver
cytochrome system CYP3A4 making it prone to drug
interactions and contraindicated in the setting of potent
CYP3A4 inhibitors [44��]. When given to healthy adults, a
single 20 mg dose resulted in an increase in urine output
and fall in Uosm, peaking in 2 h and persisting for 6 h.
Therapeutically, it is given as a 20 mg bolus followed
by a 20 mg per day continuous infusion maintained for
1–4 days. It has been effective in clinical trials although
data are limited [45,46]. A single-center observational
study of 18 patients found that 67% improved by at least
4 mmol/l but that six patients with initial PNa less than
120 mmol corrected by greater than 10 mmol/l per 24 h, a
rate considered undesirable [47�]. Use of a single bolus of
20 mg in neurointensive care patients hyponatremia
resulted in a 4 mmol/l improvement within 12 h in 59%
of the patients. In this case series, no cases of infusion
vein phlebitis were identified, although this problem was
seen in earlier trials [48]. Finally, although antagonism of
VIa receptors might be problematic for patients with
cirrhosis (VIa agonism has been advocated as a treatment
for hepatorenal syndrome), convivaptan was utilized in
24 patients with end stage liver disease and PNa less than
130 mmol. All patients experienced a modest increase in
PNa (<6 mmol/l) and no complications of the underlying
liver disease were observed [49].
Tolvaptan is the first oral V2R antagonist to be approved
in the United States by the FDA. It has a much greater
affinity for the V2R than for the V1a receptor. The half-
life of tolvaptan is estimated to be 12 h. It is metabolized
in the liver by the CYP3A and, like convivaptan, should
not be used with potent inhibitors of this enzyme. The
onset of action is within 2–4 h [44��]. Multiple studies
have been conducted and now have been summarized
and analyzed including a meta-analysis. It has been
shown to raise PNa by approximately 4 mmol/l on day
4 and by approximately 6 mmol/l on day 30. When used to
treat CHF, it has resulted in weight losses around 2 kg.
Reported adverse effects have been thirst, dry mouth,
and polyuria. Effectiveness has been similar in patients
horized reproduction of this article is prohibited.

C
590 Renal system
with euvolemic hyponatremia (principally SIADH) and
CHF and somewhat less effectiveness has been demon-
strated with cirrhosis [50�,51�,52].
HypernatremiaHypernatremia occurs when there is an absolute or
relative deficit of free water. Hypovolemic hypernatremic
patients will display signs of volume depletion, but these
signs may be mild or minimal if there is a small water
deficit and no concomitant lost of solute. Hypervolemic
hypernatremia is caused by the addition of solute in
excess of water. Conditions that impair urinary concen-
tration include central diabetes insipidus, nephrogenic
diabetes insipidus (NDI), hypercalcemia, hypokalemia,
loop diuretics, and osmotic diuresis. Uncontrolled dia-
betes is the most common cause of osmotic diuresis, but a
high protein intake or protein catabolism can also pro-
duce diuresis due to the generation of urea. The latter
may occur in hospitalized patients receiving parenteral or
enteral nutrition with a high protein load. Nonrenal losses
of water are seen in the setting of excessive sweating,
emesis, diarrhea, burns, and tachypnea. Hypertonic
bicarbonate administration or hypertonic saline adminis-
tration is among the iatrogenic causes of hypernatremia.
As a rise in Posm is a potent stimulus of thirst that would
normally prevent or correct hypernatremia, almost all
cases display either impaired thirst (hypodipsia) or
impaired access to water [3,4,53].
The incidence of hypernatremia is approximately 1% in a
general hospital population. An incidence of 10–26% is
identified in ICU populations [54,55�]. In the majority of
cases, hypernatremia is hospital acquired. Community-
acquired hypernatremia is almost always hypovolemic in
nature, but hospital-acquired hypernatremia is frequently
not hypovolemic and some patients may even display
signs of volume overload. Causes of excess fluid loss in
cases of community-acquired hypernatremia include
fever (often from pulmonary infections), uncontrolled
diabetes mellitus, high ambient temperature, osmotic
diarrhea due to lactulose, and furosemide. In almost all
cases, water intake is inadequate due to impaired mental
status. Although emblematic of hypernatremia, diabetes
insipidus is relatively uncommon.
A Netherlands ICU study of 130 hypernatremic ICU
patients identified sepsis, renal impairment, hypokale-
mia, hypoalbuminemia, and the administration of
bicarbonate and mannitol as risk factors. Only 60% of
the patients had negative fluid balance during hyper-
natremia and some had positive fluid balance. Although
no patients received hypertonic saline, the conclusion
was that hypernatremia represented ‘too much salt and
not enough water’ [56]. A retrospective analysis of
approximately 8000 patients admitted to ICUs in France
opyright © Lippincott Williams & Wilkins. Unauth
found 901 individuals with mildly elevated PNa 145–
150 mmol/l and 344 with moderate to severely elevated
PNa greater than 150 mmol/l for an overall prevalence of
15%. The mild group had twice the in-hospital mortality
compared with normonatremic patients, whereas in the
more severe group mortality tripled. Independently
associated risk factors for ICU-acquired hypernatremia
present on ICU entry were male sex, great disease
severity, septic shock, acute respiratory failure, and coma
[55�].
The incidence of hypernatremia in cardiac surgery
patients has also been recently analyzed. A single-center
European experience found a 10% rate of ICU-acquired
hypernatremia that was associated with greater than a
two-fold increased mortality and a nearly six-fold
increased ICU LOS [57�]. A Canadian heart surgery
program found a 4% incidence of hypernatremia that
was also associated with an increased risk of mortality
compared with normonatremia (14 vs. 1.6%). Changes in
PNa greater than 12 mmol/l per day were associated with
an even greater mortality risk of 28%. Interestingly, in
this population the risk for hypernatremia tended to
accrue over time, whereas the risk for hyponatremia
was greatest in the first few days of ICU admission [58�].
Therapeutic hypernatremia has been utilized as an
alternative to mannitol to treat increased intracranial
pressure (ICP) associated with transtentorial herniation.
A 30–60 ml bolus of 23.4% saline (equivalent sodium
dose to 240–480 ml of 3% saline) successfully reversed
signs of herniation in 57 of 76 events (75%), 22 of
whom subsequently survived to discharge including five
who were reported to have only mild residual deficits.
ICP, when measured, fell significantly by 1 h. Clinical
improvement and fall in ICP correlated with a rise in PNa
by at least 5 mmol/l and PNa greater than 145 mmol/l
[59]. A 23.4% saline has also been used to treat cerebral
hypoperfusion to prevent elevation of ICP after SAH
[60]. Reviewers of the therapeutic use of 23.4% saline
point out that it can cause severe tissue injury in the
event of extravasation and that central venous access is
necessary. They also postulate that 3% saline given in
equivalent doses may be as effective, but that this com-
parison has not been done [61].
The clinical consequences of hypernatremia include
insulin resistance, impaired gluconeogenesis, and cardiac
dysfunction in addition to the neurologic consequences.
The brain injury that occurs with hypernatremia has been
postulated to result in part from shrinkage of the brain
away from the skull causing mechanical stress on vessels
that could lead to hemorrhage and or ischemia. As evi-
denced by multiple case reports, rapid, severe elevations
of PNa can result in ODS even in the absence of previous
hyponatremia [62�]. Hypernatremic patients may display
orized reproduction of this article is prohibited.

Dysnatremia in the ICU Pokaharel and Block 591
irritation, agitation, lethargy, depressed mental status,
seizures, and coma. Burn patients who develop hyper-
natremia have a higher mortality and there is evidence
that the hypernatremia may worsen the burn itself [63].
Treatment of hypernatremia in the ICU should start with
prevention. Predisposing conditions are recognizable;
for example, polyuria, diarrhea, fever, respiratory failure,
inability to take in water spontaneously, osmotic diarrhea,
and uncontrolled diabetes. Electrolytes are frequently
measured. Therefore, it is reasonable to identify a rising
PNa before severe derangement occurs. Indeed, the
occurrence of hypernatremia in the ICU has been
proposed as an indicator of quality of care [64]. Once
recognized, fluid therapy can be modified to prevent
progression and correct any adverse changes that have
already occurred. The optimal rate of correction of hyper-
natremia has not been extensively studied. A comparison
of patients treated for hypernatremia who developed
cerebral edema with similar patients who did not found
that initial isotonic saline bolus, a faster rate of fluid
administration, more severe hypernatremia at initiation
of treatment (PNa 167 mmol/l vs. 161 mmol/l), and a
faster rate of correction of PNa (1 mmol/l per hour vs.
0.5 mmol/l per hour) were all associated with the early
development of cerebral edema [65�]. The choice of
rehydration fluid did not appear to influence the
Copyright © Lippincott Williams & Wilkins. Unaut
Table 2 Differential diagnosis of hypernatremia
Pure water loss Hypotonic
Insensible losses Renal lossNo access to water Loop diu
OsmoticATN (poPostobsRenal im
GastrointeEmesisDiarrheaOsmotic
ExcessiveBurns
HypodipsiaInadequate replacement
Central (neurogenic) DITraumaSurgeryInfiltrative/infectious disorders
Sarcoid, tuberculosis, histiocytosisTumors, cystsEthanol
Nephrogenic DICongenitalAcquired
Renal damageCystic diseases, sickle cellHypokalemia, hypercalcemia
DrugsLithium, demeclocyclineAVP receptor antagonistsAmphotericin B, foscarnet
ATN, acute tubular necrosis; AVP, arginine vasopressin; DI, diabetes insipi
occurrence of neurologic complications. The authors
proposed that isotonic saline volume expansion be
avoided in the absence of severe circulatory impairment.
The overall rehydration should be limited to no more
than 6.8 ml/kg per hour and the rate of correction should
not be greater than 0.5 mmol/l per hour. Higher initial
PNa should be treated even more conservatively. The
Adrogue–Madias [53] formula described above can
be used to estimate the degree of correction that may
be achieved with administration of 1 l of a particular fluid
therapy. Alternatively, water deficit can be estimated as
follows:
Water deficit¼TBW (PNa/140�1).
Water can then be administered to correct the total
deficit gradually with a target rate greater than
0.5 mmol/l per hour. It is common for differences
between expected and achieved results to be substantial.
Ongoing losses must be considered in therapeutic
planning so that not only is the deficit addressed but
also further deficit will not occur. It is important to
measure PNa frequently and adjust therapy to maintain
the target rate of correction.
In the event of central or gestational diabetes insipidus,
desmopressin can be given to restore renal concentration
horized reproduction of this article is prohibited.
loss Hypertonic gain
es Hypertonic intravenous infusionsretics Sodium bicarbonatediuresis Hyperalimentation
lyuric phase) Salinetructive Hypertonic ingestionspairment Enteral feeding formulasstinal losses Sea water
Hypertonic saline enemasHypertonic intrauterine infusion
laxatives Hypertonic dialysatesweating Cushing’s syndrome
Primary hyperaldosteronism
dus. Reproduced with permission from [53].

C
592 Renal system
and abort polyuria. Renal failure that accompanies hyper-
natremia is often due to renal hypoperfusion and may
reverse with restoration of euvolemia. Renal failure
requiring renal replacement therapy is challenging, as
conventional dialysis will tend to rapidly correct hyper-
natremia, an effect that is undesirable unless it is known
that the hypernatremia is of very acute onset. Continuous
renal replacement therapy may be advantageous in this
setting as the replacement fluid composition and admin-
istration rate can be modified to achieve the desired rate
of correction.
ConclusionHyponatremia and hypernatremia are commonly encoun-
tered in ICU patients and are associated with adverse
outcomes including mortality and prolonged LOS. In the
minority of cases, dysnatremia results directly in death or
severe neurologic impairment. It remains uncertain
whether dysnatremia is a marker of poor prognosis or
an active contributor to adverse outcomes in the remain-
ing cases, but evidence of direct adverse effects on
multiple organ systems is emerging. Both hyponatremia
and hypernatremia frequently arise or worsen in the
hospital, representing an opportunity to identify and
address these disorders before derangement is severe.
A broad range of causes can be considered and attention
to underlying physiologic principles will aid in establish-
ing the correct diagnosis. Acute, severe hyponatremia
should be treated promptly with 3% saline to raise the
PNa by 4–6 mmol. Otherwise, both hyponatremia and
hypernatremia should be treated conservatively such that
PNa does not rise or fall by more than 8–10 mmol/l per
day. Many experts recommend targeting only a 6 mmol/l
change. Formulas can be used to estimate water excess or
deficit and to estimate the effect that intravenous
solutions will have on PNa, but there can be substantial
discrepancy between predicted and achieved results.
Therefore, the clinician must measure the PNa fre-
quently and adjust therapy accordingly to optimize the
chance for recovery (Table 2).
AcknowledgementsThe authors would like to thank Dr Howard Corwin for the opportunity tocontribute to this article.
Conflicts of interestThere are no conflicts of interest.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interestAdditional references related to this topic can also be found in the CurrentWorld Literature section in this issue (p. 668).
1 Verbalis JG, Goldsmith SR, Greenberg A, et al. Hyponatremia treatmentguidelines 2007: expert panel recommendations. Am J Med 2007; 120:S1–S21.
opyright © Lippincott Williams & Wilkins. Unauth
2 Oh MS, Carroll HJ, Regulation of intracellular and extracellular volume.In: Arieff AI, Defronzo RA, editors. Fluid, electrolyte and acid-base disorders.2nd ed. New York: Churchill Livingstone, 1995: 1–28.
3 Borque CW. Central mechanisms of osmosensation and systemic osmor-egulation. Nat Rev Neurosci 2008; 9:519–531.
4 Sharif-Naeini R, Ciura S, Zhang Z, Bourque CW. Contribution of TRPVchannels to osmosensory transduction, thirst, and vasopressin release. KidInt 2008; 73:811–815.
5
��Sterns RH, Emmett M. Fluid, electrolyte and acid-base disturbances.NephSAP 2011; 10:137–181.
Although intended as a self-assessment/board review aid for nephrologists, thisissue of NephSAP is an outstanding and comprehensive discussion of develop-ments in the field of dysnatremia over the past 2 years. Intensivists will find itreadable and rewarding.
6 Nguyen MK. Quantitative approaches to the analysis and treatment of thedysnatremias. Semin Nephrol 2009: 29: 216–226.
7 Lindner G, Kneidinger N, Holzinger U, et al. Tonicity balance in patients withhypernatremia in the intensive care unit. Am J Kid Dis 2009; 54:674–679.
8 Mount DB. The brain in hyponatremia: both culprit and victim. Semin Nephol2009; 29:196–215.
9
��Fenske W, Maier KG, Blechschmidt A, et al. Utility and limitations of thetraditional diagnostic approach to hyponatremia: a diagnostic study. Am JMed 2010; 123:52–657.
A novel evaluation of the classic diagnostic algorithm for the classification ofhyponatremia that identifies clinical pitfalls and recommends improvement stra-tegies.
10 Adrogue HJ, Madias NE. Hyponatremia. N Eng J Med 2000; 342:1581–1589.
11 Ellison DH, Berl T. The syndrome of inappropriate antidiuresis. N Eng J Med2007; 356:2064–2072.
12 Palmer BF, Sterns RH. Fluid, electrolytes, and acid-base disturbances.NephSAP 2009; 8:114–142.
13 Katz MA. Hyperglycemia induced hyponatremia: calculation of expectedserum sodium depression. N Engl J Med 1973; 289:843–844.
14 Hillier TA, Abbott RD, Barrrett EJ. Hyponatremia: evaluating the correctionfactor for hyperglycemia. Am J Med 1999; 106:399–403.
15 Tsai SF, Shu KH. Mannitol induced acute renal failure. Clin Nephrol 2010;74:70–73.
16 Collins JW, Macdermott S, Bradbrook RA, et al. The effect of the choice ofirrigation fluid on cardiac stress during transurethral resection of the prostate:a comparison between 1.5% glycine and 5% glucose. J Urol 2007;177:1369–1373.
17
�Yousef AA, Suliman GA, Elashry OM, et al. A randomized controlled trial ofthree types of irrigating fluids during transurethral resection in benign prostatichyperplasia. BMC Anesthesiol 2010; 10:7.
An interesting trial that confirms glycine as a cause of TURP syndrome andexplores the frequency and extent of irrigant absorptions.
18 Agarwal R, Emmett M. The posttransurethral resection of prostate syndrome:therapeutic proposals. Am J Kidney Dis 1994; 24:108.
19 Gonzalez I, Perez N, Penas-LLedo EM, et al. high risk of polydipsia and waterintoxication in schizophrenia patients. Schizophr Res 2008; 99:377–378.
20 ’Woman dies after being in water-drinking contest.’ Los Angeles TimesJanuary 14 2007. From the Associated Press News Agency.
21 Rosner MH. Exercise-associated hyponatremia. Semin Nephrol 2009;29:271–281.
22 Almond CSD, Shin AY, Fortescue EB, et al. Hyponatremia among runners inthe Boston Marathon. N Eng J Med 2005; 352:1550–1556.
23 Campbell GA, Rosner MH. The agony of ecstasy: MDMA (3,4 methylene-dioxymethamphetimine) and the kidney. Clin J Am Soc Nephrol 2008;3:1852–1860.
24
�Koczmara C, Wade AW, Skippen P, Campigotto MJ, et al. Hospital-acquiredacute hyponatremia and reports of pediatric deaths. Dynamics 2010; 21:21–26.
This paper confirms the risk of delivery of hypotonic fluids in postoperative patientsand emphasizes the greater safety of isotonic fluids in this setting.
25 Rahman M, Friedman WA. Hyponatremia in neurosurgical patients: clinicalguidelines development. Neurosurgery 2009; 65:925–935.
26 Woo CH, Rao VA, Sheridan W, Flint AC. Performance characteristics of asliding-scale hypertonic saline infusion protocol for the treatment of acuteneurologic hyponatremia. Neurocrit Care 2009; 11:228–234.
27 Upadhyhay A, Jaber BL, Madias NE. Epidemiology of hyponatremia. SeminNephrol 2009; 29:227–238.
orized reproduction of this article is prohibited.
Dysnatremia in the ICU Pokaharel and Block 593
28 Hoorn EJ, Lindemans J, Zietse R. Development of severe hyponatremia inhospitalized patients: treatment related risk factors and inadequate manage-ment. Nephrol Dial Transplant 2006; 21:70–76.
29 Stelfox HT, Ahmed SB, Khandwala F, et al. The epidemiology of intensive careunit-acquired hyponatremia and hypernatremia in medical-surgical intensivecare units. Critical Care 2008; 12:R162.
30 Funk GC, Lindner G, Druml W, et al. Incidence and prognosis of dysnatremiaspresent on ICU admission. Intensive Care Med 2010; 36:304–311.
31
�Wald R, Jaber BL, Price LL, et al. Impact of hospital associated hyponatremiaon selected outcomes. Arch Intern Med 2010; 170:294–302.
An impressively large analysis of a US teaching hospital population that empha-sizes the important role of nosocomial hyponatremia and also points out that long-term outcomes, as well as short-term mortality, are influenced by hyponatremia.
32 Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild,moderate, and severe hyponatremia. Am J Med 2009; 122:857–865.
33
��Chawla A, Sterns RH, Nigwekar SU, Cappucio JD. Mortality and serumsodium: do patients die from or with hyponatremia? Clin J Am Soc Nephrol2011; 6:960–965.
An intriguing and novel investigation of why and how hyponatremia contributes toexcess mortality.
34
��Hoorn EJ, Zietse R. Hyponatremia and mortality: how innocent is the by-stander? Clin J Am Soc Nephrol 2011; 6:951–953.
The companion editorial to [32] offers conjecture and a framework in which toconsider the mortality impact of hyponatremia.
35 Sajadieh A, Binici Z, Mouridsen MR, et al. Mild hyponatremia carries a poorprognosis in community subjects. Am J Med 2009; 122:679–686.
36
�Mohammed AA, van Kimmenade RR, Richards M, et al. Hyponatremia,natriuretic peptides, and outcomes in acutely decompensated heart failure:results from the international collaborative of NT-proBNP study. Circ HeartFail 2010; 3:354–361.
This study enhances and confirms our understanding that hyponatremia is a graveprognostic marker in CHF.
37 Renneboog B, Musch W, Vandemergel X, et al. Mild chronic hyponatremia isassociated with falls, unsteadiness, and attention deficits. Am J Med 2006;119:71.e1–71.e8.
38
�Ayus JC, Moritz ML. Bone disease as a new complication of hyponatremia:moving beyond brain injury. Clin J Am Soc Nephrol 2010; 5:167–168.
A consciousness raising discussion on the potential of hyponatremia to do harmoutside of the CNS.
39 Kinsella S, Moran S, Sullivan MO, et al. Hyponatremia independent ofosteoporosis is associated with fracture occurrence. Clin J Am Soc Nephrol2010; 5:275–280.
40 Verbalis JG, Barsony J, Sugimura Y, et al. Hyponatremia-induced osteoporo-sis. J Bone Miner Res 2010; 25:554–563.
41 Adroque HJ. Consequences of inadequate management of hyponatremia. AmJ Nephrol 2005; 25:240–249.
42 Brown W. Osmotic demyellination disorders: central pontine and extrapontinemyelinolyis. Curr Opin Neurol 2000; 13:691–697.
43
�Morita S, Inokuchi S, Yamamoto R, et al. Risk factors for rhabdomyolysis inself-induced water intoxication (SIWI) patients. J Emerg Med 2010; 38:293–296.
A brief report on a potentially underappreciated complication of the correction ofhyponatremia.
44
��Ferguson-Myrthil N. Novel agents for the treatment of hyponatremia. CardiolRev 2010; 18:313–321.
A comprehensive review of the physiology and literature regarding the use ofvasopressin receptor antagonists in the treatment of hyponatremia.
45 Li-Ng M, Verbalis JG. Convivaptan: evidence supporting its therapeutic use inhyponatremia. Core Evid 2010; 4:83–92.
46 Wright WL, Asbury WH, Gilmore JL, Samuels OB. Convivaptan for hypona-tremia in the neurocritical care unit. Neurocrit Care 2009; 11:14–19.
47
�Velez JC, Dopson SJ, Sanders DS, et al. Intravenous convivaptan for thetreatment of hyponatremia caused by the syndrome of inappropriate secretionof antidiuretic hormone in hospitalized patients: a single center experience.Nephrol Dial Transplant 2010; 25:1524–1531.
A report of the practical experience of the effectiveness of convivaptan in ‘real-world’ use.
Copyright © Lippincott Williams & Wilkins. Unaut
48 Murphy T, Dhar R, Diringer M. Convivaptan bolus dosing for the correctionof hyponatremia in the neurointensive care unit. Neurocrit Care 2009; 11:14–19.
49 O’leary JG, Davis GL. Convivaptan increases serum sodium in hyponatremicpatients with end-stage liver disease. Liver Transplant 2009; 15:1325–1329.
50
�Rozen-Zvi B, Yahav D, Gheorghiade M, et al. Vasopressin receptor antago-nists for the treatment of hyponatremia: systematic review and meta-analysis.Am J Kid Dis 2010; 56:325–337.
A current summary of the literature describing the use of vaptans for hyponatremicdisorders.
51
�Berl T, Quittnat-Pellitier F, Verbalis JG, et al. SALTWATER investigators: oraltolvapatn is safe and effective in chronic hyponatremia. J Am Soc Nephrol2010; 21:705–712.
An extension of the initial clinical trials of tolvaptan reporting on a larger number ofpatients.
52 Nemerovski C, Hutchinson DJ. Treatment of hypervolemic or euvolemichyponatremia associated with heart failure, cirrhosis, or the syndrome ofinappropriate antidiuretic hormone with tolvaptan: a clinical review. Clin Ther2010; 32:1012–1032.
53 Adrogue HJ, Madias NE. Hypernatremia. N Eng J Med 2000; 342:1493–1499.
54 Pavlevsky PM, Bhargrath R, Greenberg A. Hypernatremia in hospitalizedpatients. Ann Int Med 1996; 124:197–203.
55
�Darmon M, Timsit JF, Francais A, et al. Association between hypernatremiaacquired in the ICU and mortality: a cohort study. Nephrol Dial Transplant2010; 25:2510–2515.
A mirror of similar studies of hyponatremia annotated above that emphasizes thenosocomial nature of hypernatremia and its adverse impact.
56 Hoorn EJ, Betjes MG, Weigel J, Zietse R. Hypernatremia in critically illpatients: too little water and too much salt. Nephrol Dial Transplant 2008;23:1562–1568.
57
�Lindner G, Funk GC, Lassnigg A, et al. Intensive care-acquired hypernatremiaafter major cardiothoracic surgery is associated with increased mortality.Intensive Care Med 2010; 36:1718–1723.
A previously little reported segment of intensive care patients are shown to havesignificant risk for hypernatremia and adverse outcomes.
58
�Stelfox HT, Ahmed SB, Zygun D, et al. Characterization of intensive care unitacquired hyponatremia and hypernatremia following cardiac surgery. Can JAnaesth 2010; 57:650–658.
This report also identifies cardiac surgery patients as an at-risk population forhypernatremia.
59 Koenig MA, Bryan M, Lewin JL 3rd, et al. Reversal of transtentorial herniationwith hypertonic saline. Neurology 2008; 70:1023–1029.
60 Tseng MY, Kirkpatrick PJ. Enhancement of cerebral blood flow usinghypertonic saline therapy improves outcome in patients with poor-gradespontaneous subarachnoid hemorrhage. J Neurosurg 2007; 107:274–282.
61 Palmer BF, Sterns RH. Fluid, electrolytes and acid-base disturbances.NephSAP 2009; 8:146–147.
62
�Naik KR, Saroja AO. Seasonal postpartum hypernatremic encephalopathywith osmotic extrapontine myelinolysis and rhabdomyolysis. J Neurol Sci2010; 291:5–11.
A fascinating report of osmotic demyelination injury in a group of patients withhypernatremia of uncertain cause.
63 Namdar T, Siemers F, Stollwerck PL, et al. Increased mortality in hyperna-tremic burned patients. Ger Med Sci 2010; 8:Doc11.
64 Polderman KH, Schreudeer WO, van Schnijnedel RJM, Thijs LG. Hypern-tremia in the intensive care unit: an indicator of quality of care? Crit Care Med1999; 27:1105–1108.
65
�Fang C, Mao J, Dai Y, et al. Fluid management of hypernatremic dehydration toprevent cerebral oedema: a retrospective case control study of 97 children inChina. J Paediatr Child Health 2010; 46:301–303.
Although a retrospective analysis of a pediatric population, it offers firm sugges-tions on the fluid management of hypernatremia and points out the surprisingpotential risk of isotonic saline boluses in these patients.
horized reproduction of this article is prohibited.





























