Embed Size (px)
Citation preview
LOUISIANA PSYCHIATRIC MEDICAL ASSOCIATION
LPMA IS A BRANCH OF THE AMERICAN PSYCHIATRIC ASSOCIATION SPRING 2006 • Vol. 41 • No. 1
ThS SSUE,
•Hcen:s [.,1essacie .............. 2
Drm Conference .................... 4
ature Article .......................... 5
7 1 Highlighgts......................... 8
Thmmittees Form................... 10
lembership ............................ 13
CPTCoding ............................ 22
DR. POST ELECTED DISTINGUISHED FELLOW Congratulations to Dr. David E. Post who was elected to the status of Distinguished Fellow of the American Psychiatric Association. His election reflects recognition by his peers of his outstand-ing abilities, talents and contributions. He will receive a special medallion at the Convocation of Fellows at the APA Annual Meeting in Toronto on May 22, 2006.
Dr. Post is currently the Medical Director of the Capitol Area Human Services District, a seven-parish region based in Baton Rouge, LA. In this position he led disaster relief after Hurricane Katrina hit Louisiana, and New Orleans was evacu-ated. Many of the New Orleans citizens relocated to Baton Rouge. His exceptional work is detailed in the Winter 2005 edition of the Newsletter.
Dr. Post graduated cum laude from Tulane University with a BS in Biology and received an MD from Tulane Medical School. He finished a psychiatric residency at LSU Health Sciences Center and then completed a subspecialty in fo-rensic psychiatry at Harvard Medical School. Dr. Post is board certified by the American Board of Psychiatry and Neurology and has added qualifi-cations in forensic psychiatry. He has maintained an academic link to two Louisiana medical schools holding the rank of Clinical Assistant Professor at both Tulane and LSU. He has provided lectures to residents at LSUMC on History and Overview of Forensic Psychiatry and has been instrumental in collaborating with Baton Rouge General Hospital in developing a Primary Care teaching program.
Dr. Post was the president of LPMA and served as president of the Baton Rouge Psychiatric Society for three years. He was president of the West Feliciana Parish Medical Society, a chapter of the Louisiana State Medical Society as well as a delegate to the LSMS Assembly from 1999 to the present.
Dr. Post founded a non-profit foundation (The Post Foundation) to present a more positive image of the Deep South. He works with universi-ties and students across the Deep South on this initiative.
Fellow and Distinguished Fellow Criteria If you are interested in applying for Distinguished Fellow or in nominating a member for this honor, call the LPMA office at 504-865-0030 or email Charlene Smith at [email protected] and ask for an application and guidelines. The LPMA deadline for receiving completed applications along with three support letters from Distinguished Fellows is June 1, 2006.
Criteria for APA Distinguished Fellowship:
General Membership in APA for at least eight years Primary designation as a psychiatrist Significant contributions in a least five of the areas shown below
Certification by ABP&N or an equivalent board Involvement in the work of the district branch or other APA components Involvement in other medical and profes-sional organizations Participation in non-compensated mental health and medical activities of social sig-nificance Participation in community activities unre-lated to income producing activities Clinical contributions Administrative contributions Teaching contributions Scientific and scholarly contributions
If you want to apply for Fellow, the eligibility criteria for this category is as follows.
General Member for at least five consecutive years Certification by the ABPN, the Royal College of Physicians and Surgeons of Canada or the American Osteopathic Association Three letters of recommendation from current Fellows, Distinguished Fellows, Life Fellows or Distinguished Life Fellows

EDITOR'S NOTEBOOK
THE SLIPPERY SLOPE
JULIANA FORT, MD, EDITOR
The italicized excerpt is reprinted from The Times (Shreveport), April 14, 2006, Pg. OlD, with the per-mission of Gannett Co., Inc. by NewsBank, Inc. The marriage and family therapist is David McMillian who can be heard on "Strategies for Living" every weekday from 11 a.m. to noon on www.strategies-forliving.com and from 6 a.m. to 7 a.m. Saturdays on Newsradio 710 KEEL.
If it were not for the qualifying remarks, it would appear that he is practicing medicine.
Dear David: I was prescribed Prozac fIve years ago, but lately am realizing I haven 't much will to do things. I sleep a lot and miss lots of opportunities that come my way So about two weeks ago, I stopped taking the Prozac to see ifthis would clear my head. I seem tofèel more empowered, but this may be a false mental perception. A lot of good things have been happening, like a good new job; however, I've had a TERRIBLE headache for about a week now. Pain pills have little to no effect. Am I experiencing withdrawal? Is it lack ofsome chemical? Any advice or counsel would be so helpful, because Idon i'know what to do. Shouldlstart the Prozac again or tough it out? - Wondering about Dependence.
Dear Wondering: First, it really important to never alter your medication without the supervi-sion ofyour physician. It can be dangerous to stop some medication abruptly. One of the symptoms of stopping Prozac too quickly is headaches. Prozac is not addictive so there really are not withdrawal symptoms per se, but stopping the medication too quickly can cause headaches, moodiness, irritabil-ity, insomnia, resumption of depression and, in rare cases, con fused thinking. Usually after two or three weeks these symptoms cease.
However, I wonder why you felt the medication wasn 't working as well as it did in the beginning. This can happen at times with any antidepressant, sometimes because the dosage is no longer sufficient. I'm glad you are feeling better except for the head-aches, but I think it would make sense to go back to your doctor and have a complete evaluation done. These decisions are too important to make without the assistance ofsomeone who specializes in manag-ing medications.
Louisiana is one of the first and only states where psychologists prescribe medication, who will ask to do this next? LPCs?
I personally like two of the psychologists that I know are prescribing. However I wonder if psy -chopharmacology by book is really enough. I saw one bipolar patient admitted to the hospital in an emergency situation who had a great rapport with his psychologist. It was evident from the patient's behavior that he had to have some medication for an episodic mania, which was quite disabling. The patient had graduated from a prestigious college and didn't believe his psychologist when he told the patient that the weight gain with Seroquel really is "not that much of a problem." The psychologist seemed to be missing a clinical experience similar to an intern's that would have given him a feel for and understanding of the different antipsychotics. Interestingly, the psychologist expressed to me his discomfort with prescribing mood stabilizers such as anticonvulsants although he seemed to have no issues with prescribing atypical antipsychotics.
It seems that much of the push for enlarging the scope of practice of various non-physicians has come from a Louisiana senator who as a fellow physician is familiar with the lack of care available in rural areas. He seems to feel that expanding the scope of practice of various persons such as psychologists, nurse practitioners, etc. is the answer, but I wonder if their training is really adequate.
It is frightening that some of the back and forth debate between psychiatrists on these topics such as the recent expansion of the role of psychiatric nurse practitioners seems to be occurring at the same time as these issues are being voted on as legislation. The expansion of scope of practice seems to be moving forward at a brisk pace in Louisiana without serious legislative efforts in regard to alternatives such as telemedicine.
The real question is if you or your child or partner had a serious mental illness but live in the rural equivalent of Louisiana Timbuktu, would you be delighted to have anyone with some training see you or would you want someone highly trained even if you had to travel hours to do so?
CONTRIBUTIONS WELCOME Contributions to the LPMA Newsletter are welcome. Both personal and professional items of interest in written or photograph form are sought. Every effort will be made to preserve the spirit and intent of the author when it is neces-sary to shorten or edit an article. Authors' opinions do not necessarily reflect the of-ficial opinion of the Louisiana Psychiatric Medical Associa-tion. Letters to the editor and responses to those letters are also welcome. Mail: LPMA,
P.O. Box 15765 New Orleans, LA 70175
E-mail: [email protected]
2 • Louisiana Psychiatric Medical Association • Spring 2006

PRESIDENT'S MESSAGE
Given the many difficult scenarios encountered this year, I would like to thank the executive council and our executive director, Ms. Charlene Smith of the LPMA for their availability and support. Crises are notorious for exposing vulnerabilities of any indi-vidual or organization, yet most impressive during my term, was the voice of our fellowship to stand strong in serving those individuals in need. Numer-ous members have consistently remained in contact with the LPMA via e-mails, phone calls, individual meetings, etc. Their passion for the psychiatric pro-
fession has set the pace for LPMA to begin rebuild-ing the necessary infrastructure that will highlight the strength of our association for years to come. As a final word, I would like to thank the membership of the LPMA for their vote that allowed me to serve you as President May 2005-May 2006. Membership will be receiving a ballot to elect incoming executive committee. I would like to wish for the newly elected executive committee to experience a productive and peaceful year.
Crises are notorious for exposing vulnerabilities of any individual or organization, yet most impressive during my term, was the voice of our fellowship to stand strong in serving those individuals in need.
ActceolralVle0/(e The Missing Piece of the New Orleans Disaster Response Plan - Support of Local Physicians and Medical Schools KENNETH SAKAUYE, MD
Disaster response involves four distinct phases: evacuation, emergency phase (first response), early post-impact phase and restoration. Disaster plans usually end with the evacuation and emergency phase. The question of how to restore services and how funds will be allocated remains a major un-planned part of recovery efforts. Over 6000 physi-cians were displaced after Hurricane Katrina in Louisiana and Mississippi. There have been no coordinated plans to restore hospitals, retain staff, or provide services beyond the first response efforts at the emergency shelters.
In New Orleans, estimates from informal phar -maceutical company surveys suggested only 40% of psychiatrists in the New Orleans area had returned by four months later. One city report estimated that only 30% of the population had returned and 10% of businesses had reopened by four months later. Only one general hospital and one free standing psychiatry unit had reopened within the city boundaries by four months later.
Contracts from FEMA and SAMHSA went to large emergency response groups with an adminis-trative infrastructure like the Red Cross or contrac-tors specializing in such services in Washington. No open bidding was allowed for local carriers for
funds. Volunteers were flown in from around the country to help in shelters while local physicians and programs working with other community agencies and services went unsupported. Loans, rather than grants, were all that was available to small busi-nesses, no longer taking into account the high risk for business failures and defaults in new businesses reopening in a disaster area. As of the writing of this abstract, FEMA was still rejecting money to rebuild the Charity Hospital or the University Hospitals lost in the post-Hurricane flooding.
The problems faced by local universities and training programs have been insurmountable. Hun-dreds of faculty members, including tenured profes-sors, have been let go. Many subspecialties have been closed down, including Geriatric Psychiatry. Without a timetable for return of major teaching hospitals in New Orleans, it will be hard to recruit our next generation of physicians.
The solution has always been simple - it in-volves planning and a willingness by government to support local physicians and programs to come back. The emphasis on funding outside contractors and outside volunteers, but not local programs or
CONT/NUED ON PAGE4
Spring 2006 Louisiana Psychiatric Medical Association 3
RESPONSE TO DISASTER
STORM CONFERENCE Recognizing Health and Mental Health Issues and Implementing Change in the Post-Katri na/ Rita Era July 14-18, 2006
This "Storm Conference" will be held at The Astor Crowne Plaza in New Orleans. It will focus on the hurricane's impact on medical and mental health ser-vices in the affected tn-state area of Texas, Louisiana and Mississippi. Presentations will focus on local response activities and how the local actions were, should have been and should be integrated into state and federal response efforts.
The perspective of the traditional first and early responders—police, fire, EMS, and American Red Cross will be compared and contrasted with initiatives taken by non-traditional early responders including the media, faith-based organizations, phar-maceutical representatives, academic institutions and medical facilities such as community-based hospitals and nationally-based health care delivery systems like the Veteran's Administration Medical Centers.
The goal of the conference is to identify strengths and weaknesses in the disaster responses in each of the three states and to discuss how to improve future cooperation, coordination, cornmu-nication and information for when the next natural or man-made disaster occurs. The United States National Response Plan and the Canadian National Framework for Health Emergency Management will be used as a model upon which the conference's recommendations will be discussed.
See page 21 for conference schedule. For more information email jofostormconfceJJce.com or visit www.stormconference.com. n.
DISASTER RECOVERY FUND FOR PSYCHIATRISTS The APA, together with its philanthropic subsidiary, the American Psychiatric Foundation, has launched the Disaster Recovery Fund to assist psychiatrists and psychiatric residents who have been adversely affected by disasters such as hurricanes Katrina, Rita and Wilma
Psychiatrists and psychiatric residents who have been affected by disasters may apply for grant funding up to $2,500. Grants will be made to allow psychiatric residents to continue their medical train-ing and to help psychiatrists rebuild their practice in order to serve the mental health needs of the people in their communities. Applications for recovery grants have been accepted since Jan. 1, 2006 and grant deci-sions will be made on an ongoing basis.
To download applications forms go to www. psychfoundation.org , click on Grants, scroll down to Disaster Recovery Fund and download Psychiatric Resident Application Form or Practicing Psychiatrist Application Form.
MISSING PIECE OF THE PLAN Continuted from page 3
physicians, has been poor planning. Failure to al-locate special funds for elderly, faculty retention, or hospital restoration has been poor planning. Let's hope things can be corrected before there is further attrition.
Note: This article was written on Januaiy 9for the last issue of the Newsletter but was received after it went to the printer. FIK
ASTRAZENECA GIVES $1 MILLION TO MCLNO AstraZeneca, a Wilmington, DE based pharmaceutical company presented $1 million to the Medi-cal Center of Louisiana at New Orleans (MCLNO) to help improve health care for citizens in the aftermath of Hurricane Katrina. The donation will help expand MCLNO's telemedicine system and support health care programs in six community-based health centers planned to open in the greater metropolitan New Orleans area this year.
The telemedicine system will play an integral role in providing patients with access to doc-tors not on staff in their local facility and will allow doctors on MCLNO's main campus to have two-way, real-time visual and verbal communication with the community-based sites.
4 Louisiana Psychiatric Medical Association Spring 2006
A CROSS-CULTURAL PSYCHIATRIC ODYSSEY: CHALLENGES FOR THE FEMALE PSYCHIATRIST'
Dr. Ullrich presented this paper in Vienna at the April 18-20, 2006 meeting of the World Psychiatric Association, the Transcultural Section.
Just as by chance I was born a USA citizen, so by chance a village in Karnataka State, South India, chose me. I say chose because I initially planned to do the research for my linguistics PhD dissertation in North India. When my undergraduate mentor, Ed-ward B. Harper, suggested that I work on the Havik dialect of Kannada, also known as 'old Kannada,' he arranged for my living with a Havik Brahmin family in the village where he had done his research. I told the family that I would stay three months, but stayed closer to two years. My last visit was 2005-06, more than forty years after my initial visit in 1964-66.
While analyzing the Havik dialect of Kannada, later published as a book 2 , I learned the rules of this culture. I also noted that many Brahmin women had been angry and depressed at the time of their mar-riage. They regarded themselves as a lower caste and were envious of their brothers who had more education than they. Some women learned to read when their children attended school; other women persuaded their husbands to teach them to read; but most of the older Brahmin women were illiterate in 1964. When I started to teach my hostess English, her mother-in-law told me there was no need to bother her daughter-in-law, as husbands talked for their wives. During my initial fieldwork I established rap-port while I learned their language. During this first field trip I developed the hypothesis that pre-pubertal marriage increased vulnerability to depression.
My second field trip occurred ten years later. The purpose of this trip was to analyze the caste dialects of non-Brahmins and the linguistic accommoda-tions when members of different castes conversed. To obtain cross-caste linguistic accommodation, I hung out in my host's store or left my tape recorder there. I focused on the Potter caste, two different agricultural castes (Vokkaligas and Divarus), the Harijans (untouchables), and the Girijans (former tribal people). I went to each hamlet where I worked on the caste dialects. Castes reside in different ham-lets, which are at a distance from each other. When Havik Brahmin women decided to accompany me to
the Divaru hamlet, this was their first visit to a non-Brahmin hamlet. The women of the non-Brahmin castes were more assertive than Brahrnin women. From observations made on this trip I developed the hypothesis that assertiveness might be a protective factor and socialized passivity a predisposing factor for depression.
Approximately twenty years after my first visit to the village, I decided to apply to medical school. After all, I had chosen my college to facilitate my admission into medical school and had majored in sociology-anthropology in college so that I would be more aware of my patients' cultural background and so become a more empathic physician. During my twenty-year detour I earned my PhD in linguistics and taught linguistics, cultural anthropology, Hindi-Urdu, Kannada, and Sanskrit at Michigan State University, Duke University, The State University of New Yark at Albany, and The University of Texas at Austin. I went to the medical school at the University of Texas Health Science Center at Houston.
My interest in cross-cultural psychiatry began during my last year in medical school. When Arthur Kleinrnan came to the University of Houston to lecture, a South Asia colleague, Pauline Kolenda, included me in the events. Then Dr. Kleinman ar-ranged for a rotation at Cambridge City Hospital which gave me an opportunity to explore cross-cul-tural psychiatry for my area of specialization within medicine. From this experience I realized that I could never formally test my hypothesis of the relationship between pre-pubertal marriage and depression, as pre-pubertal marriage was no longer the custom. Although a control group was impossible, a study of cohorts might suggest this as a predisposing fac-tor. Indeed, marriage might be a predisposing factor depending on the age of marriage and whether the woman had had a say as to whom she would marry. The more than two generation study of the Totagadde population would allow for this type of study. More-over, I had developed linguistic skills and had rapport with the community. A community study provides a better idea of incidence and prevalence of psychiatric illness as well as treatment.
During my last year of medical school I began
CONT/NUED ON PAGE 7
APA NEWS
EMPHASIZE TRAINING, EXPERIENCE, QUALIFICATIONS HERBERT S. PEYSER, MD
As we attempt to reach out to the public, industry and government to increase awareness of the depreda-tions of psychiatric illnesses, including substance use disorders, to educate them about our ability to deal with them and to decrease the stigmatization of these afflictions, we must be careful to avoid certain of the consequences where the ancillary professions and we are concerned. A guidelines idea is nice but I am not sure how much it will do under the real life financial circumstances. The dollar reigns.
The modern iteration of the professions arose in the 19th century when the professional organizations were created, the AMA, APA, ABA, etc, setting for each a scope of practice, standard of care, training requirements, ethical obligations, etc, and driving out the snake oil salesmen and their equivalents. Where medicine, including our psychiatry, was concerned the stage was set for the enormous growth and ef-ficacy of the profession over the next century and a half.
As the technology grew and the effectiveness of the health care product increased, its economic value as well as its costs increased. It attracted capital, which it needed, and as capital came in, seeking return on its investment, it progressively took over ownership and control of the product, its means of production, the distribution of the prod-uct, etc, The process commercialized the product and proletarianized the physician, just as it did a century or so earlier with other individual artisans, and it caused much of the alienation and discomfort we see in our field.
APA LIFERS The APA Lifers group was formed to represent
the views of older Members and Fellows who have achieved Life Status, as well as to address their spe-cific needs from APA. Each year the Lifers hold an evening reception and invite all newly elevated Life Members and Life Fellows to join them and meet other Senior Psychiatrists. They also have a breakfast business meeting/educational forum.
We physicians were oppressed by the process, but were also oppressed from another quarter. The ancillary professions also grew in the latter part of the 20th century as they saw the growth of the health care product's value, and they were drawn in to compete with us for the product, seeking their piece of the pie. They offered decreased labor costs, a kind of internal outsourcing. Hence psychology prescribing and hospital admitting efforts and other such activities in the rest of medicine.
As we physicians reach out to the public, indus-try and government, we must be on guard. Medicine all over is under attack, from all sides, and we can-not afford to be disinterested philanthropists. Each endeavor of ours, wherever it is done and whatever it is, must be accompanied by an emphasis on how better trained, experienced and qualified in all areas we are. If guidelines would help, well, so much the better. In any event, every initiative must have this part of it included and must be directed to that purpose, that we can do it much better. Our APA DBs and local membership as well as our state and national organizations must be integral parts of the initiatives.
Our members have not given us a mission to increase the activities and work of social workers, counsellors, psychologists, creative arts therapists, etc, etc.
Herbert S. Peyser MD is the APA Representative for the New York County District Branch anda Cor-responding Member of the Council on APA/Business Initiatives n
APA DUES DISCOUNT FOR RETIRED MEMBERS The APA board approved a reduction by 50% for the dues of those members who are at least 70 and are fully retired. This reduction would be applied on an ongoing basis to the member's stated dues until he/she reaches the point where no dues are owed.
You should initiate a request for the discount if you qualify. Contact Philip Pardee in the Office of Membership, 703-907-7351 or ppardee@psych. trg.
APA ELECTION RESULTS President-Elect: Carolyn B. Robinowitz, M.D. (76.1%)
Secretary-Treasurer: Donna M. Norris, M.D. (51.4%)
ECP Trustee-at-Large: Amy M. Ursano, M.D. (67.4%)
Member-in-Training Trustee-Elect: Abigail L. Donovan, M.D. (50.3%)
9,819 ballots were received, representing the votes of 32.4% of the eligible voting members. 28.3% were online ballots.
• Louisiana Psychiatric Medical Association • Spring 2006

A CROSS-CULTURAL PSYCHIATRIC ODYSSEY
my study of depression in Totagadde. Brahmin wom-en comprised the community for this study. I used the Schedule for affective disorders and Schizophrenia (SADS)4. The women were forthcoming although many commented that I already had the information. Some women answered one way when given the questionnaire and gave contradictory information in a conversational interview. One researcher told me I would avoid that difficulty if I never asked twice. But this glib approach assumes a static situation. As the culture evolves, the same symptoms may have a different meaning. An example is a woman who indicated she had no right to be depressed, but had experienced spirit possession as a presumed mani-festation of her depression. The following year when I asked her about depression, she said 'Of course I was depressed.'
After my internship I extended this research to an assertive non-Brahmin group. My instrument for this later trip included the Schedule for affective disorders and Schizophrenia (SADS), the Hamilton Anxiety Test, the Hamilton Depression Test, The Indian Psychiatric Survey Schedule (IPSS) 5 , and Paykel's life events scale. I asked the subjects to rate their expectations of life events as to their dif-ficulty of adjustment should those events occur. In 1994 I added The Duke Social Support Index 6 and a questionnaire to evaluate perception of change and their response to change.
Upon completion of my residency, Ijoined the faculty of the Psychiatry Department at Tulane Uni-versity Medical Center. Arranging trips to India was a bureaucratic challenge. Although Tulane faculty valued both my clinical skills and my cross-cultural psychiatric skills, the department gained more finan-cially from my clinical skills. Upon entry into private practice I had no such competing factors. While I miss the collegial interchange, faculty were already dispersed among different treatment facilities, as indeed I had been.
The Sapir-Whorf Hypothesis emphasized the interrelationship of language and culture. Each in-dividual has her own form of speech, which reflects personality and individual cultural experiences. As the culture changes, so the language changes. For example, when I first did field work in Totagadde, the term for widow was pra:Ni a homonym with 'ani-mal.'The only difference was in the plural. The word
for 'animals' is pra:NigaLu; the word for widows was pra:Ne:ru. Now that widows may remarry, their status has changed. No longer are they inauspicious. No longer does pra:Ni refer to a widow.
Another term no longer in use is ka:e banje 'crow barren' for a woman who had only one child. 'Crow barren' has disappeared from the language as many couples elected to limit their family size to one or two children. In 1964 the average number of children each couple had was 5.1 in 1984 it was 2.5; and in 2004 it was 1.6. Brothers or brothers-in-law may vociferously urge a couple to limit their family size—to the extent of calling the couple irresponsible and even 'crazy.' One woman and her husband who had four daughters and wanted a fifth child in an effort to have a son was the object of her brother's criticism. No longer does one need two sons, but one child—either son or daughter—is a frequent choice. This contrasts sharply with a discussion I overheard in 1965 where a woman's parents urged her to continue her family lest the lack of two sons would cause her husband to develop schizophrenia like his father. She completed her family with the birth of her two youngest children—both Sons.
Knowledge of the language allows one to overhear or to participate directly in conversations. To function in any given society one needs cultural competence. By the time I knew the language I had established rapport and the Totagadde inhabitants trusted me to follow the customs which they con-sidered essential. Until they felt I knew their cultural rules, they were uncomfortable. However, once they perceived that I knew the cultural rules, I could alter my observations of those rules.
In a society where women stayed in the back-ground, I stayed in the background as an observer. However, I had access to both men and women. In contrast, women would have been reluctant to speak with men. I could slip from a woman's group to a man's group at ceremonies in which the women tended to gather in the back by the kitchen and the men tended to gather in the front where the priests were. The men talked of 'exceptional women' who had access to professional opportunities. After Prime Minister Lal Bahadur Shastri died, the men discussed with me their idea that Indira Gandhi was the most qualified to become the next prime minister. I was indeed surprised when she became the prime minister.
CONTINUED ON PAGE 15
ia researcher told me I :uld avoid that difficulty
never asked twice. But s glib approach assumes static situation. As the iture evolves, the same mptorns may have a
; ,IjJI

I
SPRING MEETING
2006 GENERAL MEMBERSHIP MEETING HIGHLIGHTS
Left Photo: (L-R) Linda Hughes (Director of Ethis and District Branch Relations), Charlene Smith, James Scully, MD (Medical Director), and Therese Swetman. PhD (Chief Financial Officer). Right Photo: (L-R) Joseph Rubin, MD (Assembly Speaker), Eugene Cassel (Director, Advocacy), Mark Townsend, MD, Harold Ginzburg, MD and Dudley Stewart, MD.
The General Membership Meeting was held at the Royal Sonesta Hotel in New Orleans from 9 A.M. to 12 noon, March 18, 2006. It was held in conjunc-tion with the APA Area V Council and Public Affairs workshops, which met in the afternoon. When the meeting was called to order, Dr. Holloway intro-duced Dr. Steven Sharfstein, APA President, Ms. Linda Hughes, APA Director of Ethics and District Branch Relations, and Mr. Jason Pray, staff member of the APA Political Action Committee. Dr. Sharf-stein said APA was especially glad to be here to support New Orleans in its recovery from Hurricane Katrina. He regretted the storm related cancellation of the Southern Psychiatric Association meeting with LPMA in October 2005.
Dr. Holloway asked for a moment of silence for Drs. Arthur Epstein, Henry Miles, Vann Spruiell, John Stocks, and Burton White, who died after the last General Membership Meeting in March, 2005.
The members elected Dr. Harold Ginzburg and Dr. David Post as psychiatrists of the year for 2005. This was the first time two members were chosen for the honor. They will be officially recognized at the Fall Meeting in Shreveport on Oct. 13, 2006.
The Membership, Child & Adolescent, and Geriatrics committe reports can be found on pages 11-13 of this newsletter. Information about the July 2006 meeting on "Lessons Learned from the Storm" in on page 4.
Dr. Snow announced that she will be resigning as Governmental Affairs chair of state affairs and wants someone to be her apprentice.
Dr. Drell reported that the New Orleans Adoles-cent Hospital (NOAH) is again in danger of being closed. If it is closed, there will be no public child psychiatry beds in New Orleans. NOAH is approved by JCAH and is the model system of care for training
child psychiatrists. The population of New Orleans may be halved but there are now twice as many children with problems. NOAH hires more child psychiatrists than any other facility in the state.
Dr. Ginzburg reported that when Katrina hit, initially there were no psychiatric volunteers from Louisiana and no psychiatric medications except Valium. He praised the pharmaceutical representa-tives in St. Bernard Parish for playing a crucial role by donating urgently needed medications. Dr. Foulks commented that many patients stayed in the New Orleans area because they were too frightened to move. Many were without medications.
Dr. Glindmeyer informed members that physi-cians who patients cared for from the time of the hurricane through January 16 can bill Medicaid
Dr. Toups presented two scenarios for the LPMA Fall Meeting to be held Oct. 13-14 or 15, 2006 in Shreveport. The members approved Dr. Snow's motion that LPMA committee, Council and Gen-eral Membership meetings be held on Oct. 13, the scientific program on Oct. 14 and the Buprenorphine program on Oct. 15. (Buprenorphine program has been moved to Nov. 11, 2006 in Baton Rouge.)
The members approved Dr. Toups motion ask-ing Dr. Holloway to write a letter to the Louisiana State Board of Medical Examiners requesting formal rules to govern psychiatrists working with prescrib-ing psychologists.
Dr. Mancuso recommended that the LPMA directory be placed on the LPMA website with a separate document for information regarding where members could be reached in emergency situations. Dr. Ginzburg volunteered to work on this project.
Dr. Snow thanked Dr. Holloway for her effective leadership of LPMA in a very difficult year.
8 • Louisiana Psychiatric Medical Association • Spring 2006
Debra DePrato, MD
Dvigh: L. Evans, Ivid
MEMBERSHIP NEWS Fran Nixon Hagaman writes that she is enjoying partial retirement. She works on contract two days a week seeing kids at the Shreveport Mental Health Center and working on more mysteries. She is send-ing a synopsis of each of the four in the series, "Rub a Dub Dub Death in a Tub" plus the first 20 pages to an associate editor at Avalon publishers.
New Orleans City Business named Jodie Holloway in its seventh annual list of the Top 50 Women of the Year in New Orleans. The women are recognized for professional and community achievements. A luncheon honoring them took place on January 20 at the downtown Sheraton Hotel in the Grand Ballroom.
Daniel Winstead was elected president of the American Board of Psychiatry and Neurology.
At the APA Area V Council Meeting dinner in New Orleans on March 17, 2006, Dr. Steven Sharfstein, the president of the American Psychiatric Association, presented Dr. Christopher Meyers with a plaque for his article "On Homosexuality ... A Scientific Point of View," which was selected as the winner in the APANewsletter of the Year outstanding feature category. Dr. and Mrs. Meyers were guests at the diimer.
DR. DEPRATO CHOSEN AS JUVENILE JUSTICE GRANT PROJECT DIRECTOR The Louisiana Board of Regents was selected by the MacArthur Foundation as the lead agency for the administration ofa five-year, 57.5 million juve-nile justice reform grant. The Regents will partner with the LSU System to administer the "Models for Change" initiative, designed to identify and acceler-ate promising state models forjuvenile justice system reform. Pennsylvania, Illinois, and Washington will also participate. Dr. Debra DePrato was chosen as the project director for the grant.
The LSU System will provide personnel in ac-complishing the goals of the initiative, which seeks to hold young offenders accountable for their actions, provide for their rehabilitation, protect them from harm, increase their life chances and manage the risk they pose to themselves and to public safety.
After interviewing dozens of Louisiana stake-holders, Dr. DePrato was chosen as the project director. For the past six years Dr. DePrato has been the director of the medical, mental health and dental program that LSUHSC provides to the Office of Youth Development (OYD). She has resigned as OYD Program Director in order to dedicate her ef-forts to this initiative. She will remain an employee of the LSUHSC. The Board of Regents will contract for her services through LSU. n
11TH ANNUAL USDIN LECTURE GIVEN BY DR. EVANS Dr. Dwight L. Evans, Ruth Meltzer Professor and Chairman of Psychiatry and Professor of Psychia-try, Medicine and Neuroscience at the University of Pennsylvania School of Medicine and Health System, was the Ochsner Clinic Foundation's I 11h
Annual Gene L. Usdin, M.D. Distinguished Visiting Lecturer in Psychiatry on Friday, March 3.
Dr. Evans presented Psychiatry Grand Rounds at 12 noon on Clinical Management of Bipolar Dis-orders. At a dinner meeting that evening he spoke before an invited audience on Mood Disorders and Medical Illness: A Major Public Health Problem. In this presentation, he reviewed research studies, in-cluding his own findings. Essentially, he summarized that mood disorders are prevalent in patients with chronic medical illnesses and are more than simply a consequence of medical co-morbidity. The pres-ence of depression considerably worsens the medical
prognosis, primarily because it hinders adherence to treatment regimens. impairs physical and cognitive function, diminishes quality of life, increases mor-bidity and, in some cases, decreases survival. It also may be an etiologic factor for incident diseases.
Evans encourages additional studies to confirm that treating depression improves overall medical outcomes. Of consequence, for those using medica-tions for the treatment of depression and medical illness, is the finding that the utilization of tricy-clic antidepressants is relatively contraindicated because these drugs are Type I-A antiarrhythmics and might increase morbidity with ischemic heart disease (IHD). He cautions that additional studies are indicated to evaluate the effectiveness of SSRIs in general.
Spring 2006 Louisiana Psychiatric Medical Association . 9
COMMI1TEE REPORTS
LPMACOMMflTEESTRUCTURE : The LPMA committee structure is being reorganized to make it more effective. Only the Standing Committees are being retained. Retention or establishment of any other committee depends on the number of i
YOUR INPUT IS NEEDED members who demonstrate an interest and pledge to participate in it by circling or listing it on this u Retention or form. We also want to know who wants to retain their membership on the standing committees because as I
establishment of the politicians say we are going to "scrub" them.
any other committee depends on the number
i I would like to be considered for membership on one of the Standing Committees beginning n June, 2006. Circle the committee.
of members who demonstrate an interest Constitution & Bylaws Continuing Education Ethics
and pledge to participate Governmental Affairs Membership in it by circling or listing it on this form. Other committees I would like to have retained or established. Circle the committee and write in any new
committee.
Budget Child & Adolescent Business/Insurance
I Disaster Response Geriatrics Psychiatry & Law I I I
Psych. & Religion Public Affairs Public Psychiatry I
New committee___________________________________________________________________ I I I I I I I
Name I I
Address
Telephone FAX________________________________
Pleaseprint name_________________________________________________________________________
MAIL to LPMA, P0 Box 15765, New Orleans, LA 70175 or fAX to 504-865-0040.
HUGHES GETS APA AWARD NAMI AWARDS DR. POST Linda Hughes, the Director of the office of Ethics Dr. David Post received a 2006 Exemplary Psychia-and District Branch/State Association relations re- trist Award from the National Association for the ceived the Melvin Sabshin, M.D. Award, given to an APA staffer with a long-term record of the highest achievement and extraordinary dedication to APA members. Prior to serving in her current position, Linda spent many years in the Department of Gov-ernment Relations (DGR) at the APA. She has been very helpful to our Executive Director with both Ethics and District Branch concerns. Dudley Stewart spoke highly of her effectiveness when she was in the DGR. We congratulate her and APA.
Mentally Ill (NAMI). He was nominated by NAMI Louisiana for his work in the area of disaster psychia-try following the hurricanes and for his continued commitment to the community.
Established in 1992, the awards are given each year at a breakfast ceremony during the APA's an-nual convention. This award is especially significant because it comes from people living with mental illnesses and from their family members.
10 • Louisiana Psychiatric Medical Association Spring 2006
COMMI1TEE REPORTS
CHANGES MADE TO LPMA BYLAWS Several changes to the LPMA bylaws were approved at the General Membership Meeting on March 18, 2006 at the Royal Sonesta Hotel in New Orleans. They were presented by Dr. Daniel Winstead, Chair -man of the Constitution and Bylaws Committee.
The amendments are as follows. 1. Addition to Chapter I, Membership, Section
4, "Members of any category may be placed in inactive status by the Executive Council and ex-cused from paying dues to both the APA and the LPMA. Inactive members shall not receive credit toward the number of years of active member-
ship required for Life status for those years of inactive status. Active members may be granted a waiver of dues by the Executive Council for sufficient reason, and such members shall receive credit toward the number of years required for Life status for those years they are in the dues waiver status."
2. Chapter I'V Executive Council a. The first paragraph stated "The Council
shall meet monthly except in August and December." It now reads "The Council shall meet regularly no
CONT/NUED ON PAGE 14
CHILD AND ADOLESCENT COMMITFEE
DONALD A. SCHEXNAYDER, MD, PHD, CHJR
/
The committee discussed two bills, FDA reviews, the potential closure of NOAH and reimbursement for treatment provided in post-hurricane shelters.
House Bill 234, introduced by Rep. Cedric Rich-mond, would prevent teachers from recommending or requiring psychiatric treatment for children by making this a policy of the school system and pro-viding consequences for violating the policy. This is an issue which has frequently been discussed in our meetings, so it is gratifying to see the bill being introduced. Please support the bill by calling your representative. I worked with Kerry Cooley, an LSMS lobbyist.
The Federal Drug Administration will review the use of stimulants in children based on recent re-ports of deaths. There has been a trend to add a "black box" to medication descriptions in the Physicians' Desk Reference. The "Church of Scientology" has received money to represent their views against the use of stimulants. The APA will ask families to testif' about the benefits of stimulant treatments. Contact Liz Boroughs (703-489-5907) in the APA Depart-ment of Government Relations as she is available to help with national political issues.
Dr. Drell pointed out that there is again a move to close New Orleans Adolescent Hospital. Such closure would eliminate hospital beds as well as the NOAH crisis team and outpatient program. Due to Hurricane Katrina, increase demand is anticipated. LSU has relied on NOAH for their child psychiatry program, and in its absence patients would lose their
limited services. We have been promoting programs in the par-
ishes for children that utilize a dedicated millage to subsidize care. Aaron Levine met with me to discuss the program in Ascension Parish as a model for rural psychiatric care.
After the hurricanes, child psychiatrists and general psychiatrists provided whatever psychiatric care was needed in shelters throughout Baton Rouge and in Ascension Parish. Apparently, the media got the impression that there was not much of a response from psychiatrists, but there was in Baton Rouge where their efforts were organized by Dr. Post. Dr. Ginzburg is now organizing disaster response for LPMA. And, for those who provided care for unin-sured without payment, you can now get reimbursed at Medicaid rates.
There is currently a bill that specifies evalua-tions of mentally disabled and retarded people must be made by psychologists who have had special training in that area. It specifies utilizing a child psychiatrist who has specialized training in devel-opmental disabilities and mental retardation. This doesn't seem appropriate. Many of the individuals being treated are adults with head injuries. General psychiatrists who are board certified have trained in neurology and have been tested in their board exams for neurology. Therefore, any board certified psy-chiatrist should be qualified. However, the meaning of specialized training has not been specified. This is being addressed.
INTERNET RESOU RCES
LPMA www.11Dma.net
National Mental Health Association www.nmha.org
American Academy of Psychoanalysis and Dynamic Psychiatry www.aaosa.org .
National Alliance for the Mentally Ill www.nami.org
American Psychiatric Association www.psych.org
American Psychoanalytic Association www.apsa.org
Spring 2006 Louisiana Psychiatric Medical Association • 11

RESPONSE TO DISASTER
GERIATRIC PSYCHIATRY COMM I1TEE
KENNETH SAKAUYE, MD, CHAIR
I have been unable to find any reports on how geriatric patients in other parts of the state fared after Hurricane Katrina, which implies that central coordination is absent (no one is collecting data or giving orders).
Geriatric psychiatry must be rebuilt from the ground up in New Orleans. I am sorry that I will not be a part of rebuilding. I am a casualty of Katrina myself— it took a disaster to get me to accept a promotion. I will be available long distance in my new role as Vice Chair of Clinical Affairs and Director of Geriatric Psychiatry at the University of Tennessee in Mem-phis. I plan to start a Geriatric Psychiatry Fellowship and geriatric services with a core of three full-time geriatric psychiatrists and several Geriatric Board Certified voluntary faculty around a consortium of several teaching hospitals.
Geriatric Psychiatry services in New Orleans are severely damaged. I have been unable to find any reports on how geriatric patients in other parts of the state fared after Hurricane Katrina, which implies that central coordination is absent (no one is collect-ing data or giving orders). Although many physicians tried to come back, they encountered many obstacles. The list below is true for all ages, but the problems were most evident for the elderly because no resources were allocated for the special needs of the frail elderly or dementia patients, and there was no disaster plan for the elderly. The state "plan" for the elderly, to the best of my knowledge, was for each nursing home to have its own evacuation plan.
Obstacles: • Offices were destroyed • Small Business loans, but not grants, were avail-
able. (The safety net of being able to default without penalty without declaring bankruptcy was eliminated by congress in a bill supported by David Vitter.)
• Few had interruption of practice insurance poli- cies while rebuilding.
• Communication systems (including mail) were still not fully functional six months later.
• The hospital system was severely damaged —salaries attached to the hospitals were gone.
• Scrambling for space meant psych space was given to med-surg and emergency care. For example, the Geriatric Psych unit was lost at Ochsner because LSU leased the entire building that unit and SNF were housed in for a Trauma Center and medical beds. Nursing homes and rehab facilities for chroni-
cally ill could not reopen right away, even if undamaged, because support workers could not find housing and were unavailable (e.g. one home reopened on a limited basis in November with less than 20% of its original staff) Paper charts were lost (flooded). Electronic records with backups outside of the area seem essential now. The frail elderly and dementia patients did espe-cially poorly—safe houses rather than evacuation is clear for many. Specially trained staff are needed to avoid restraints or "snowing" patients. Post-disaster mourning of losses hits everyone. The elderly have marked increases in death rates (they just gave up). The depression that this represents fits the old label of "existential de-pression" which implied this was not effectively treated with medications alone. Non-specialists often have trouble doing psychotherapy with the elderly, partly due to communication styles, sensory impairments, cognitive impairment or at times conceptualization of the problem or countertransference. All of these issues are reduced by training and experience. There is no evidence based treatment approach (what works best). The best that can be done now are case reports and testimonials of what individuals tried to do, without outcome data. Disaster plans end with what first responders should do. Recovery plans need to be built in, such as where to get grant money and what the eligibility criteria are, and assigning who will coordinate so that all of the funds do not go to Washington firms to bring in volunteers months later while local physicians exit for lack of fund-ing for their efforts.
What is the next step? Some hospital or program must be the first to begin recruiting Board Certified Geriatric Psy-chiatrists to work with the elderly and provide a continuum of care that includes an inpatient geriatric psychiatry program and outpatient services. LPMA should be advocating for this. General psychiatrists must be willing to increase their knowledge base about geriatrics, especially
CONTINUED ON NEXT PAGE
12 • Louisiana Psychiatric Medical Association • Spring 2006
COMM flEE REPORTS
GENERAL MEMBERSHIP REPORT March 18, 2006
APA Records 1 Honorary Fellow 33 Distinguished Fellows 50 Distinguished Life Fellows 12 Fellows 188 General Members 7 Inactive Fellows 19 Inactive Members 35 Life Members 75 Members-in-Training
LPMA Records add 3 Affiliate Members
TOTAL -419
Changes in Membership Since April 15, 2005:
Deceased: Arthur Epstein, Henry Miles, Vann Spruiell, John Stocks, E. Burton White,
New Distinguished Fellow: David Post New Fellows: Robert Ellis, Calvin Walker New 50 year Distinguished Life Fellows: Wil-
liam McBride, Andrew Mullen, Max Sugar New Distinguished Life Fellows: Ann Ar-
retteig, Howard Osofsky, Ted Reveley, Daniel Winstead
New Life Member: Rennie Culver New General Members: Shelly Savant ofNew
Orleans New Members-in-training: Katherine Anders,
Michael Beason, Tony Hanna, Abid Nazeer, Syeda
Munir, Travis Phifers, John Turpin, John Wagner of LSUHSC, Shreveport, Laura Delulca, Jessica E. Hof. Schoener LaPrairie, Anh Le, Desiree Morrell, Pavan Pancholy of LSU/Ochsner, Indira Adapa of LSUHSC Child and Adolescent Program, NO., Nicole Mavrides of the Tulane Triple Board Pro-gram, Janet Bradley, Jaime Hook, Andrew Morson, Stephanie Vetere of Tulane
Reinstated: Cheryll Bowers-Stephens (GM) of New Orleans, Krishna Kambhampati (GM) of West Monroe, Gregory Khoury (GM) of New Or-leans, Kimberly Law (MT) of LSUHSC/Ochsner, Eben McClenahan (GM) of New Orleans, Michael Walsh (GM) of Covington, Lakisha Williams (MT) of LSUHSC/Ochsner
Transfers-in: Charlotte Hutton (GM) from Massachusetts,
Transfers-out: Jody Brown (GM) to Ohio, Martha Brown (GM) to Florida, W. Mark Dean (GM) to Oregon, Elizabeth Grigor to Southern California, Tara Hammond (GM) to Georgia, John Kluznik to Minnesota, Adelwisa Lizada (GM) to Nevada, Men Nisimova (GM) to New York, Omayra Nieves (MT) to Massachusetts, Sanjay Rao (MT) to San Diego, Aretta Rathmell (DLF) to Illinois, Ted Reveley (DLF) to Alabama, Samuel Rubin (LM) to Alabama, Eric Weinstock (MT) to Florida
Resigned: Lyn Goodin (DF), W. Douglas Goodin (LM), Helen Mason (GM), Mary C. Olmsted (GM), Paul Rodenhauser (DF)
GERIATRIC PSYCHIATRY COMMI1TEE Continued from previous page
dementia patients, medically ill frail elderly, and psychotropic medication use.
• The American Association for Geriatric Psy- chiatry may be tapped for educational materials and help. About 60% of the AAGP membership are members of the APA.
• On-line and other educational programs exist. • I appealed to AAGP for help and they have
created a Disaster Task Force that I will be co-chairing, with funding from its Foundation, and plans to seek a SAMSHA grant for a national meeting to specifically address the missing information about optimal approaches with the elderly. We hope that 100% of states will adopt special Disaster Plans for the elderly (less than 50% of states have this now).
AAGP, which will have its Annual Meeting in New Orleans from March 1-4, 2007, has asked me to approach LPMA regarding any use of volunteers of meeting participants to give educational or community programs, bilingual people for geriatric assessments, or other ideas. I would encourage any special requests or ideas from LPMAtoAAGP for this. Some of the most highly published experts in delirium, dementia, depression, and psychosis are members, such as Dilip Jeste, George Alexopoulos, Dan Blazer, Chip Reynolds, Jeff Cummings, and a host of other big names" are members. Although I cannot guarantee that these individuals would be available, many other big names (to me) have offered to help.
Spring 2006 • Louisiana Psychiatric Medical Association • 13

COMMI1TEE REPORTS
CHANGES IN BYLAWS Continued from page 11
less than six times per year." b. Section 3 states that the Treasurer shall
have responsibility for the collection and disburse-ment of all funds of the association subject to the approval of the Council and or membership, the words "collection and" were deleted because APA collects for LPMA.
c. Section 5 states that the President can-not hold elected office for four years thereafter. The words "except for the offices of APA Representa-tive or Deputy Representative" were added.
Chapter V, Elections stated, "The Nominating Committee must mail its slate of nominees to the general membership by January 15. Nominations by petitions signed by 10% of the membership must be received by the Secretary by February 15. Bal-lots will be mailed out after the Spring Meeting and must be returned to the Secretary two weeks after receipt. Since there may not always be a Spring meeting, these lines were amended to read, "The Nominating Committee must meet and mail its slate of nominees to the general membership. Nominations by petitions must be signed by 10% of the membership and received by the Secretary within one month of receiving the Nominating Committee slate. Ballots with the Nominating Committee slate and any nominations received by petition will be mailed to the members and must be returned to the Secretary two weeks after receipt."
Chapter V Elections, the following state-ments were added.
"If the office of President becomes vacant, the President Elect will become Acting President for the remainder of the year and then will begin his/her term as President.
If the office of President Elect becomes vacant, the President will request the Nominating Committee to meet at an early date for the purpose of selecting one or more candi-dates for President Elect. A mail ballot will be sent to the general voting membership to be returned to the Secretary two weeks after receiving it. The President Elect will be elected by a simple major-ity of those returning their ballots.
C. If the office of a Representative to the Assembly becomes vacant, the Deputy Rep-resentative will assume the duties of the office until a new Representative to the Assembly shall be elected.
d. In the event any other office becomes
vacant before expiration of a term, the Council shall elect a member to serve for the remainder of the term.
5. Chapter VI, Committees, Section 2 stated, "The Membership Committee consisting of six members shall be appointed by the President and approved by the Council. The first committee shall be appointed for terms of 1, 2, and 3 years. After the first committee is appointed, all appointments shall be for 3-year terms. The Chair shall be ap-pointed for 3 years and be eligible for another 3 year appointment at the discretion of the President and Executive Council. This section was amended to read, "The Membership Committee consisting of 6 members shall be appointed by the President and approved by the Council. The Chair shall be appointed for 3 years and be eligible for another 3 year appointment. One of its duties is to recom-mend members for Distinguished Fellowship. This committee should include an International Medical Graduate."
6. Chapter VI, Committees, Section 5 stated that the chair of Continuing Education will be selected from the members of the previous year's commit-tee and shall serve for one year. This statement was deleted and now reads, "The chair of Continuing Education may be reappointed."
7. A new chapter, Chapter VII, entitled Eth-ics Complaints and Disciplinary Procedures was added. It reads as follows.
All members of the District Branch shall be bound by the ethical code of the medical profession, specifically defined in the Principles ofMedical Ethics with Annotations Especial/yAp-plicable to Psychiatry.
Complaints charging members of the District Branch with unethical behavior or prac- tices shall be investigated, processed, and resolved in accordance with procedures approved by the As-sembly and the Board ofTrustees of the Association. The name of a nember who resigns during an ethics investigation will be reported to the membership.
8. Chapter VII, Chapters a. Section 2, Membership, stated, "Clas-
sification of membership and qualification for membership shall be the same as for the district branch. Persons applying for membership in the district branch from within the territorial jurisdiction of a chapter shall apply for membership through
CONTINUED ON PAGE 16
14 • Louisiana Psychiatric Medical Association • Spring 2006

A CROSS-CULTURAL PSYCHIATRIC ODYSSEY
By the time I studied medicine, the reaction of my Totagadde household was that 'there is now a doctor in the family.' With my choice of psychiatry they used me as a consultant for their psychiatric illnesses—depression, psychosis, spirit possession which has been redefined as a psychiatric illness. I found the community support which I had developed as a linguist transferred to my work as a cross-cul-tural psychiatrist.
Chae
Why did the people of Totagadde talk with me? Frankly, I don't know, Initially, I was embarrassed at their comments that I did not know Kannada and did not wear a sari properly. The grandmother in my household told me that her three-year-old granddaughter knew more than I did. When a person came to inform me that the Labor Party had won in my country, I was unable to convince him that the United States has no Labor Party. I wonder whether this initial adjustment gave Totagadde residents the opportunity to socialize me. Perhaps my willingness to leam and my acceptance that they were all my teachers contributed to the establishment of rapport. Perhaps I provided a safety valve, as they knew I kept each household's information to myself.
There have been challenges when people deny several years later what I saw for myself as well as information which they provided earlier. Whether this makes my data suspect or is an illustration of the limitation ofretrospective studies is for the audience to ascertain. An instance of this occurred when a mother-in-law invited me to dinner. Her daughter-in-law did not eat this mother-in-law's cooking nor did she cook for her mother-in-law. When I arrived for dinner, the mother-in-law and the daughter-in-law had prepared different meals. The mother-in-law praised her daughter-in-law's cooking and urged me to partake of her daughter-in-law's cooking as well. The daughter-in-law spoke not a word to her mother-in-law. After this mother-in-law's suicide, the daughter-in-law denied a conflictual relationship, as well as that they had cooked separately. But I was the one who had had two meals when invited for one. In addition, this daughter-in-law later denied that she had been depressed during her sole pregnancy. My field notes indicate otherwise.
Married at age twenty, she dreamed of having a son whom she would give every possible educational advantage. During her pregnancy she was depressed
for eight months. She worried that she might have a daughter. Her mother-in-law and her sisters-in-law teased her that she was carrying a daughter. She lost so much weight that the physician was concerned and told her she would have a son. She did not want a daughter because life is so difficult for a woman. She wanted to continue her studies, but after her P.U.C. (Pre University Course), the man who became her husband appeared as a marriage prospect. She wanted to refuse; however, she realized that her fam-ily would not be at peace until she married... While she was depressed, her father tried to comfort her as he could not let her sit without talking. She did some crying and had trouble sleeping—such was her worry about having a daughter. Until her son was born, she had no interest in anything.
Twenty years later and after her son has gradu-ated from college, she denies her depression during her pregnancy. This is a good example of the limita-tion of retrospective studies.
The Havik society and Totagadde residents, in general, provided me with hospitality. However, I have done all of my research alone. Although the members of the community believe that I visited each household regularly, this really applies to the Havik Brahmins. Indeed, they believed that I visited daily, but talking with approximately thirty households daily would have been impossible. Members of other castes question me as to why I do not visit them more frequently. When I do visit some non-Brahmin areas, I feel like a magnet in which all in the hamlet gather to talk with the 'America.' If relatives visit, I am an object of interest. Should I know that visitors plan to come, I may decide to visit elsewhere. Interviews of a confidential nature are impossible in a crowd.
There may be culture-specific challenges. Women are the source of pollution during their men-ses. As a woman, I was similarly subject to periods of pollution. I used this as a time to consult with other women and to develop a library for women. At times I counted on this time for writing, only to be inundated with visitors. One of the rules was that those who touched my desk when I had my coffee cup on the desk would become polluted and have to go home for a purificatory bath. I was thinking 'gotcha' when a crowd touched my desk. You can imagine my chagrin when my hostess silenced me before I could say anything.
In 1964 Totagadde had a population in which
CONTINUED ON PAGE 16
There have been challenges .ihen people deny several years later what I saw for myself as well as information which they
Sphng 2006 Louisiana Psychiathc Medical Association 15

INTERNET RESOURCES
LPMA www.lnma.net
National Mental Health Association www. n m ha. org
American Academy of Psychoanalysis and Dynamic Psychiatry www.aapsa.org .
National Alliance for the Mentally Ill www.nami.org
American Psychiatric Association www.psych.org
American Psychoanalytic Association www.aosa.org
A CROSS-CULTURAL PSYCHIATRIC ODYSSEY Continued from page 15
only the unsuccessful left. A visit to the state capitol two hundred miles away was rare. Now the suc-cessful and the educated generally leave the village for work throughout India and in other countries. Studying a population that has spread beyond the village is a challenge. What types of psychiatric ill-ness occur as a result of distance from one's support system? Does this enhanced autonomy enable greater self-realization? These are questions which I pose for those immigrating as well as those remaining in India or those residing at a distance from family.
Privacy in the field may be a valuable commod-ity. Children fascinated with the foreigner are hard to dissuade. I have resulted to the subterfuge that my computer needs recharging or that my tape recorder is broken. Then there was the time when I played
LPMA BYLAWS Continued from page 14
the chapter, and acceptance for membership in the district branch will be automatically followed by membership in the chapter. Members-in-training shall not be bound by this section. This paragraph with the exception of the first line was deleted.
b. Section 3, Officers, first line stated, "The officers of the chapter will consist of a President, President-Elect, Secretary, Treasurer or Secretary-Treasurer and up to three Councilors, one of whom shall be, after the first year, the immediate past-Presi-dent. This line was deleted. The line stating that the President of the chapter shall be a member of the Council of the Louisiana district branch was retained and the following lines were added. "A proposal for a recall election may be initiated by petition by 10% of the voting membership or by a majority vote of the Executive Council. A mail ballot shall then be sent to the general member-ship to be returned no later than 30 days upon its issuance. Recall shall be effected if two-thirds off the voting membership so indicates.
9. A new chapter, Chapter XII entitled Amend-ment of Bylaws, was added. It reads "Amend-ments to the bylaws shall be made by a majority of the Executive Council members voting for an amendment at a regularly scheduled meeting with a quorum being present. The Council members must be notified of the full text of the proposed amendments 20 days prior to the meeting. •
Bach and Mozart on my tape recorder. Upon hearing this the grandmother came into my room with the comment, 'tape recorder broken again'?' (Turn about is fair play—when I was playing village music, an American friend asked me if my tape recorder was broken!)
My decision to be solo in the village is a chal-lenge for a community study. Yet I believe that regu-lar visits allow for follow-up observations. Do the life events predicted as difficult turn out to precipitate depression? Does assertiveness provide protection against anxiety and depression? What are the psy -chiatric consequences of endorsing cultural beliefs when one resents those beliefs? Are there similar consequences if one follows one's own path when it is diametrically opposed to cultural values?
Other challenges include the time away from academia or private practice to spend in the field. I have found annual trips possible only after I entered private practice. This, however, has its limitations as one cannot stay a year or so and expect patients to continue with one.
Focus on Depression Time spent in Totagadde provided me with
hypotheses about depression and anxiety. The patri-archal Havik Brahmin culture predisposed women to passivity and dependence. The oldest male held all authority over the younger men who resided in the household, as well as over all the women. A hus-band held authority over his wife. For a wife to visit her parents, she needed the permission of both her husband and the household head. Without such per-mission she was at risk for physical abuse. Although women remained silent with others in the household, I both observed and listened to their humiliation at their invisibility and powerlessness.
When I went to Totagadde as a medical student to focus on depression, I focused on women and depression. They were willing to talk individually and in groups. I believe that they all knew the SADS by heart—some before I got around to interviewing them.
To decrease bias, I drew the names of the women out of a hat to determine the interviewing order. The goal of this initial study was to determine whether those who had married before puberty were more vulnerable to depression than those married later. The study included all the adult women.
CONT/NUED ON PAGE 20
16 • Louisiana Psychiatric Medical Association • Spring 2006

ATtOur VViiram Epstein, MD
IN MEMORIAM
ARTHUR WILLIAM EPSTEIN, MD 1923-2005
Arthur William Epstein, MD, Professor Emeritus of Psychiatry and Neurology at Tulane University School of Medicine, died in a hospital in Austin, TX on Nov. 8, 2005. The Epsteins had evacuated to Austin from New Orleans prior to Hurricane Katrina. Art was 82 years old.
Born in New York City on May 15, 1923, Dr. Epstein received his undergraduate degree from Co-lombia, and his MD from the College of Physicians and Surgeons of Colombia where he was AOA. Art was always interested in psychology and human behavior as it related to the brain. One of Art's pro-fessors at Colombia was Dr. Robert Heath who "was a model for me because he was one of the first to in-tegrate neuroscience and psychoanalytic concepts," said Dr. Epstein in a videotaped interview on June 28, 2004. During his residence in neurology at Mt. Sinai Hospital, Art attended a meeting in Atlantic City and ran into Dr. Heath, who at the time was Chairman of the Department of Psychiatry and Neurology at Tulane University School of Medicine. Bob invited Art to Tulane and in 1950 he accepted a position as a fellow. Because of Art's perspicacity and productiv -ity, he rapidly rose to the rank of full professor. Art spent his entire academic life at Tulane. In 1981-81, he served as Acting Chairman of the Department of Psychiatry and Neurology.
Correlating behavior with neurological phe-nomena was a lifelong goal of Dr. Epstein's. Early in his research, he observed that certain psychiatric syndromes were related to abnormal brain activity. He noted that anticonvulsants could be used to treat behavioral abnormalities, a fact that is well-known today. Going beyond the biological basis ofbehavior, Dr. Epstein underwent personal psychoanalysis and later became Director of the Tulane program in psy-choanalytic medicine. In 1986-87, he was President of the American Psychoanalytic Association. One of his early papers published in 1967 in the APA journal was titled, "The Role of the Arts in Leisure Time Planning," and another article written in 1990, was "The Creative Artist and Psychoanalysis." These articles illustrate Dr. Epstein's eclectic interests.
Dr. Epstein's involvement in biological psychia-try led to his studies of epilepsy, dream life and body image, and culminated in a book entitled "Dreaming and Other Involuntary Mentations," published in 1996. In 1981-82, he served as President ofthe Soci-ety ofBiological Psychiatry. The Louisiana Psychiat-ric Medical Association named him "Psychiatrist of the Year" in 1992. Art's publications included scores
of scientific articles for professional journals. Dr. Epstein's literary creativity resulted in the
publication of seven books. "A release of primary process thinking," is one of the ways Art described his poetry in a June 2004 videotaped interview. His first book, "An Anatomist's Dream of Love," was published over 40 years ago. The breadth of his poetic creativity is illustrated in his other works including: "The Lady and the Serpent" and "Faust Encounters Helen of Troy."
Those of us who knew Art were impressed not only by his intelligence and creativity but also by his willingness to share his knowledge with others. He was a professor who inspired others and, above all, was a warm and compassionate human being. Art loved to walk and was renowned for walking from the medical school downtown to his home in the uptown area. On occasion I accompanied Art and our conversations were memorable, enlightening and always engaging. We shall miss Art.
Dr. Epstein was a devoted husband and father. His successful marriage of over 50 years to Leona was blessed with two sons and two daughters: David Byron Epstein, James Jacob (Jack) Epstein, Nona Epstein Samuels and Emily Epstein Kobayashi, and a host of grandchildren.
Art's life was a full one. He was a physician, board certified neurologist, board certified psychia-trist, certified psychoanalyst, an excellent teacher, author of many scientific articles, and a poet. He was also a devoted family nian and a wan'n, genu-ine and caring colleague. He was without doubt, a renaissance man.
Perhaps the last few lines from his 1999 book, "Poems of Later Life," characterized Art's personal philosophy: ". ..at least to know it was inside me not a book or being shown but inside of me my very own."
Art was buried in Hebrew Rest Cemetery in New Orleans on Nov. 13, 2005 with a private grave-side service. A memorial service is to be scheduled this spring in New Orleans.
Submitted fri C. B. Scrignar, MD. •
Soring 2006 Louisiana Psychiatric Medical Association 17
N tV1iVñJRIAVi
HENRY HARCOURT WATERS MILES, MD 1916-2005
Henry Harcourt Waters Miles, MD, who passed away in the wake of Hurricane Katrina, was by every measure a gentleman's gentleman. All who knew him deeply feel the loss of this son of the culture of a genteel South, now long passed.
Born at the Houmas House plantation, built as he told me before the Civil War for Major General Wade Hampton, C.S.A., one of Lee's Lieutenants, Henry spent his first 1 5 or 20 years there until the sugar growing industry became economically unfea-sible, and the family moved to New Orleans which became his life-long home.
He had many stories to tell about Houmas House. At the begirming of the Civil War the title was conveniently passed to a Scottish businessman. In 1862 a Union patrol was dispatched to seize the property. The Scotsman acidly informed the officer that he was a British subject of H.M. Queen Victoria, and seizure of his property was a very serious matter in the eyes of the British government. The Yankees beat a hasty retreat.
On another occasion over breakfast coffee, we were talking about bird hunting. He mentioned that as a youth he and his friends would hunt quail from horseback. Impressed, I said that horses were too "spooky" and I had never dared hunting from a horse. In his very quiet and almost self demeaning way, he said, "Ahem, yes, well you see we would ride on horseback with the beaters and dogs ahead in the bush. When they spotted a covey we would
dismount, they would hold the horses, and we would hunt." A different world.
Henry received his MD from Tulane shortly before the outbreak of WWII. He was interested in Internal Medicine and had some training in that discipline. However, the army like Cowper's God "moves in mysterious ways." They needed psychiatrists and Henry became one. He served the war years as an officer in the Tulane Army Medical Unit in Africa and Italy. He was discharged with the rank of Major.
Following the war he maintained his interest in psychiatry and trained in Boston at the Psychoana-lytic Institute. He then returned to New Orleans.
In the 1950s following a "cardiac event" he joined the faculty of the Department of Psychiatry and Neurology at Tulane while continuing his association with the New Orleans Psychoanalytic Institute.
As a supervisor and director of the Hutchinson Adult Psychiatric Clinic, a generation of residents remembers his quiet, wise counsel, cogent inter-pretations of patients' dynamics and stature as a role model. Henry deeply grieved the death of his wife, Margaret, several years ago. I suppose his last publication was his memoirs which were the "recol-lections of a happy man."
Dr. H. H. W. Miles embodied in full measure that quality Sir William Osler deemed critical in the superior physician "Equanimity."
Submitted by Wallace K. Tomlinson, MD.
JOHN A. STOCKS, MD 1929-2006
John A. Stocks, MD died on Feb. 13, 2006 at his home in New Orleans. He was in full time practice as a child and adult psychoanalyst and psychiatrist. He co-founded and was medical director of River Oaks Hospital in the 1970s and 1980s.
Dr. Stocks served as Sergeant Major in the United States Army. He was educated at the Uni-versity of Chicago (BA), Tulane Medical School (MD), LSU (adult and child psychiatry), and the New Orleans Psychoanalytic Institute (adult and child psychoanalysis). He committed his life to the practice and teaching of a range of psychoanalytic therapies, including inpatient and outpatient psycho-therapy and psychoanalysis, both of individuals and of family systems.
VANN SPRUIELL, MD 1926-2005
Vann Spruiell, MD grew up in Leeds, AL. He was set on being a doctor from the age of four and never got far away from that aim. He did not know what kind of doctor he wanted to be until he was sixteen and read Freud for the first time. He was fascinated with the mind, not necessarily or always with Freud.
After serving in the army, he graduated from the University ofAlabama and later from Harvard Medi-cal School. He interned at Belleview, completed a residency at Payne Whitney and then moved to New Orleans. In 1964 he graduated from the New Orleans Psychoanalytic Institute. He served on various edito-rial boards, the longest period on the "Psychoanalytic Quarterly."
18 Louisiana Psyciatric Spring 2611

ERNEST BURTON WHITE, MD 1925-2005
Dr. Ernest Burton White, Jr. was born in Garyville, LA and lived in New Orleans after his graduation from LSU Medical School in 1948. He served as a Captain in the Medical Corps of the Army during the Korean Conflict, following which he trained in psychiatry at LSU Medical School and, subsequently as a psychoanalyst at the New Orleans Psychoana-lytic Institute. He played a principal advisory role in the development and eventual accreditation of the Dallas Psychoanalytic Institute. He is survived by his wife, Elizabeth Maught White, six children and 12 grandchildren.
In thinking about Burt (or E.B. as I sometimes called him), I always felt that I had been blessed with a dear friend and colleague all of my life. Actually, it was only since our days of residency during the '5 Os.
The last time we were together, he was his wonderful self as we enjoyed our Friday lunch. On
Monday morning, I was crushed by the tragic news of his sudden death during the night before. We weren't going to have our regular bridge game on Tuesday or ever again. We weren't going to have lunch together ever again. Months have passed, and the pain is no longer acute, but all of you who read this understand that deep mourning doesn't come to a sudden end.
Speaking of all of you who read this, I wonder how many of you feel that you have really known any of us old "codgers." If you were indeed fortunate to have known E.B. as a friend, colleague or profes-sor and supervisor at LSU and/or the Psychoanalytic Institute, you certainly remember him. What a warm, bright, insightful gentleman he was.
We sincerely extend our deepest sympathy and empathy to Burt's loving family and to all who share our loss.
Submitted by Jack WeisIer, MD.
BOOK REVIEW "FAMOUS MARRIAGES: WHATTHEYCAN TEACH US" byJerryM. Lewis, MD
Dr. Jerry M. Lewis, a gifted writer and speaker, is especially well known to LPMA members and other mental health professionals in our area, having lec-tured throughout our state. He has achieved national recognition as an author, scholar and organizational leader.
With this book, Lewis brings his extensive experience and expertise in the field of marital-fam-ily systems, pointing out the interrelationship of spouses, sometimes negatively, but often positively, with each partner utilizing the strengths of the other. He has conducted many evaluations of non-patients (e.g., applicants to residency and staff programs in psychiatry as well as the Episcopalian ministry). He has followed up with many of these. He stresses the importance of the continuing maturation of each partner's personality and the adjustments that each has to make in the marriage. The 10 couples in the
famous marriages are persons well known to read-ers, and Lewis has done extensive research regard-ing them. The couples are the Duke and Duchess of Windsor, Charles and Anne Morrow Lindbergh, Gertrude Stein and Alice Toklas, Eleanor and Frank-lin Roosevelt, Isaac and Rebekah, Henry and Clare Boothe Luce, Paul and Eslanda Robeson, Zelda and Scott Fitzgerald, Robert and Elizabeth Barrett Browning, and Will and Ariel Durant.
This volume is extremely readable for profes-sionals as well as laypersons and, as such, may be recommended to patients and others who are trying to better understand their marital relationships.
Submitted by Gene Usdin, MD *In New Orleans, this book is available at The
Maple Street Book Shop, 7523 Maple St., New Orleans, LA 70118; 504-866-4916.
Spring 2006 Louisiana Psjchlatr!c Medical Association 19

A CROSS-CULTURAL PSYCHIATRIC ODYSSEY
With globalizatior cultural psychiatry important. Since patterns and cultu patterns are automatL unless others questio one's culture individtk, have no way to unloi* cultural assurnitL:
Twenty years after my initial visit, Havik women attributed their difficulty in making decisions to the culture. They believed that their husbands would be-come angry if they assumed decision-making power. In some instances the women discovered that physi-cal abuse was the price for acting independently. These women explained in a group at a ceremony that nothing they did would bring praise. If anything went wrong, they received the blame—such as the time a husband ordered new clothes for the children using the prior year's measurements. Somehow, the husband was not upset, his wife was. She felt that this illustrated how little her husband valued her opinion. Yet when the women had accomplishments, the husband received the credit for accomplishments. This enhanced the husband's and the family reputa-tion. These same women wondered how they could have believed in their inferiority, when they later distinguished between their own beliefs and cul-tural beliefs. Even though cognitively these women realized their inferiority was a cultural artifact, they continued to feel inferior and to act on an emotional level as if they had no rights. Their daughters and granddaughters benefited from this change in culture, which acknowledged the ritual superiority of males, but ignored this in practice to the extent that there is no longer a need for sons to observe the father's death ceremonies. In the case of no Sons other kins-men perform the ceremonies.
One's career trajectory is a combination of op-portunity and planning. I was fortunate in having a mentor who provided me with a household where I could reside among those whom I have been study-ing. The community is multi-caste. The more than forty-year study of Totagadde has provided a long-term study of various cohorts. Among the changes that have occurred during this period is a later age of marriage, marriage after the bride has finished her education, the freedom of individuals to choose their bride or groom within the arranged marriage system, increased assertiveness among women, and increased nuclear families among younger couples. Family size is also smaller. Women as well as men may indicate that they wish one child or two. With these changes there has been a decrease in the incidence of depres-sion at marriage and decreased bitterness of the bride toward her father when he arranged her marriage without consulting her. These changes appear to start with the Brahmins and progress through the
castes—from higher to lower castes. With globalization cross-cultural psychiatry
is important. Since language patterns and cultural patterns are automatic, unless others question one's culture individuals have no way to unlock their cultural assumptions. After the hurricane, which col-lapsed the New Orleans levees, patients frequently reacted in dystonic ways. They questioned many of their assumptions and the foundations of their security. At times this resulted in their learning of their own racial prejudices. Before catastrophes assumptions about their culture were automatic. Similarly psychiatric illness may have a cultural focus. In Totagadde by the time I left in 1966 the men were telling me that they thought widows were treated unfairly. They may have instigated the reform for widows; however, the women also gave credit to the first widow who refused to shave her hair and to adapt the widow stigmata of a maroon or white sari, no jewelry, and no longer wearing the red dot signif'ing an auspicious woman. I will never know the impact that my questions had as a reflector for Totagadde residents to question and change their own cultural assumptions.
The anthropological approach of participant observation allows for reliable and valid inforniation versus the survey approach, which is not necessar-ily sensitive to emic cultural concepts. Similarly, psychiatrists attempt to learn the context and the underlying semantics of a patient's statements. This is akin to recognizing each patient as a cultural en-tity. The socialization of women into nurturing roles may contribute to their understanding each patient's culture. In this way the information obtained is more reliable and valid. Hence cross-cultural psychiatry plays an important role in challenging one's own as well as one's patient's assumptions about illness. When the patient feels that his psychiatrist listens, then there is an essential basis for the treatment of psychopathology. In my opinion this is the most important contribution of cross-cultural psychiatry.
I thank Eve Fortson, MD, Ann Lathrop, and Charlene Smith for their helpful comments.
This paper has been prepared for the 2006 annual meeting of the World Psychiatric Associa-
CONTINUED ON PAGE 24
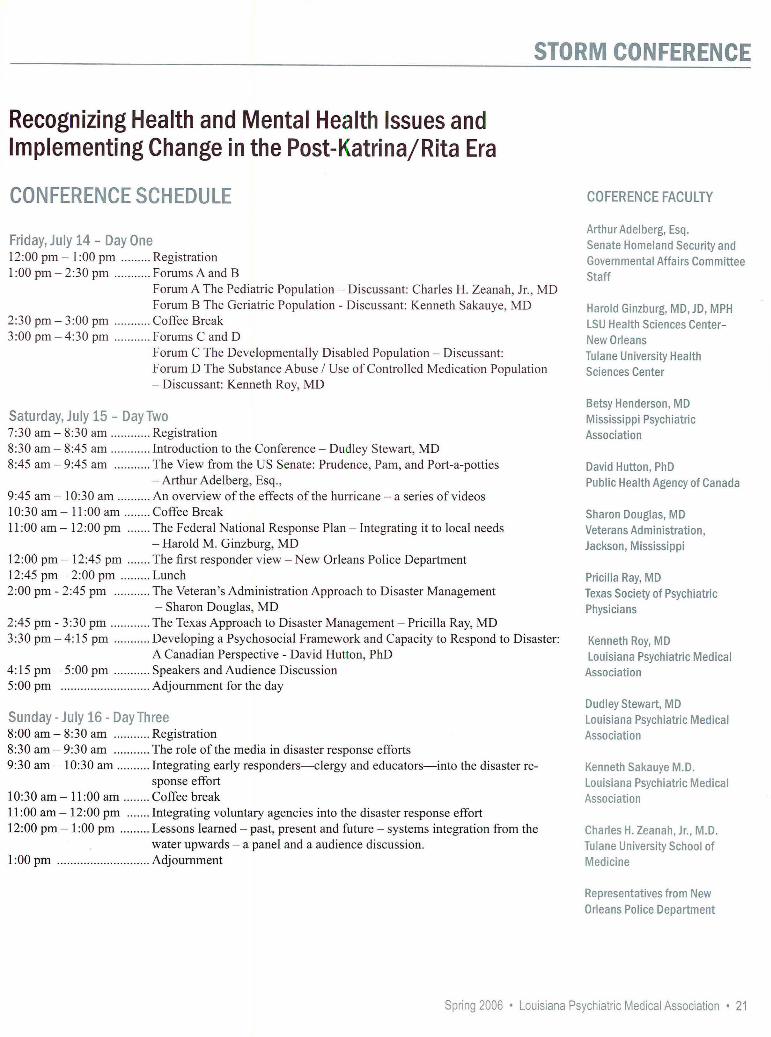
Oil
Recognizing Health and Mental Health Issues and Implementing Change in the Post- Katrina/ Rita Era
CONFERENCE SCHEDULE CUFERENCE FACULTY
Arthur Adelberg, Esq. Friday, July 14 - Day One Senate Homeland Security and 12:00 pm - 1:00pm ......... Registration Governmental Affairs Committee 1:00 pm-2:30 pm ........... Forums A and B Staff
Forum A The Pediatric Population - Discussant: Charles H. Zeanah, Jr., MD Forum B The Geriatric Population - Discussant: Kenneth Sakauye, MD Harold Ginzburg, MD,JD, MPH
2:30 pm - 3:00 pm ........... Coffee Break LSU Health Sciences Center- 3:00 pm - 4:30 pm ........... Forums C and D New Orleans
Forum C The Developmentally Disabled Population Discussant: Tulane University Health Forum D The Substance Abuse / Use of Controlled Medication Population Sciences Center - Discussant: Kenneth Roy, MD
Betsy Henderson, MD Satutciay. J i V if: - U Mississippi Psychiatric 7:30 am - 8:30 am ............ Registration Association 8:30 am - 8:45 am ............ Introduction to the Conference - Dudley Stewart, MD 8:45 am - 9:45 am ........... The View from the US Senate: Prudence, Pam, and Port-a-potties David Hutton, PhD
—Arthur Adelberg, Esq., Pubhc Health Agency of Canada 9:45 am - 10:30 am .......... An overview of the effects of the hurricane —a series of videos 10:30 am— 11:00 am ........Coffee Break Sharon Douglas, MD 11:00 am - 12:00 pm .......The Federal National Response Plan - Integrating it to local needs Veterans Administration,
- Harold M. Ginzburg, MD Jackson, Mississippi 12:00 pm - 12:45 pm .......The first responder view - New Orleans Police Department 12:45 pm - 2:00 pm ......... Lunch Pricilla Ray, MD 2:00 pm - 2:45 pm ........... The Veteran's Administration Approach to Disaster Management Texas Society of Psychiatric
- Sharon Douglas, MD °hysicians 2:45 pm - 3:30 pm ............ The Texas Approach to Disaster Management - Pricilla Ray, MD 3:30 pm - 4:15 pm ........... Developing a Psychosocial Framework and Capacity to Respond to Disaster: Kenneth Roy, MD
A Canadian Perspective - David Hutton, PhD Louisiana Psychiatric Medical 4:15 pm - 5:00 pm ........... Speakers and Audience Discussion Association 5:00 pm ........................... Adjournment for the day
Dudley Stewart, MD Stat :a - .tiy 16 Lay Thaee Louisiana Psychiatric Medical 8:00 am - 8:30 am ........... Registration Association 8:30 am - 9:30 am ........... The role of the media in disaster response efforts 9:30 am - 10:30 am .......... Integrating early responders—clergy and educators—into the disaster re- Kenneth Sakauye M.D.
sponse effort Louisiana Psychiatric Medical 10:30 am - 11:00 am ........ Coffee break association 11:00 am— 12:00 pm ....... Integrating voluntary agencies into the disaster response effort 12:00 pm - 1:00 pm ......... Lessons learned —past, present and future - systems integration from the Charles H. Zeanah, Jr., M.D.
water upwards - a panel and a audience discussion. Tulane University School of 1:00 pm ............................ Adjournment Medicine
Representatives from New Orleans Police Department
Spring 2006 • Louisiana Psychiatric Medical Association 21
2006 Changes to CPT Coding
The A iVIA CPT Editorial Panel made a number of changes to CPT coding for 2006 that are relevant to psi'chiatrisis. We encourage all psychiatrists to purchase ci cop1 of the A iVIA ('PT manucil each year in order to remain current with regard to CPT coding and documentation requirements. Copies can he obtained hr calling 800-621-8335. APA members with specifIc CPT coding questions should put iliem,i in writing and email /ist(Lpsv(_'h.or.) or/ax (703-907-1089) thein to APA 5 0//ice of Jiealihcare Systems and Financing for review by APA s CPT Coding Network.
Psychiatry Section
90871 - ECT multiple seizure. This code was deleted at the request of the APA. All visits for ECT should now be coded using CPT code 90870.
0018T - Delivery of high power, focal magnetic pulses for direct stimulation to cortical neurons. A parenthetical note was added regarding coding for repetitive transcranial magnetic stimulation (rTMS) for treatment of clinical depression. CPT now , directs clinicians to use Category Ill code 0018T.
95970, 95974, and 95975 - Neurostimulators, Analysis-Programming. The CPT Editorial Panel approved coding for vagus nerve stimulation (VNS) therapy for treatment-resistant depression. Clinicians performing VNS therapy should use codes 95970, 95974, and 95975 found in the neurology subsection of the CPT manual. A parenthetical to this effect will appear in the 2007 edition of the AMA CPT publication.
Evaluation and Management Section
Consultations New descriptive language has also been added to CPT in an effort to better define the use of the consultation codes.
• Consultations that are requested by a physician or other appropriate source should be noted in the patient's written record the consulting physician should also provide a written report of landings back to the requesting entity. In this instance the appropriate consultation CPT code should be used.
• A consultation initiated at the request of patient or family shotild not he reported using the consultation codes but rather the appropriate office visit codes.
• Mandated consultations (e.( , ., third-party payers) should be reported using the consultation codes along with modifier 32
If following the consultation the clinician assumes responsibility for the management of a portion or all of the patient's condition, the appropriate evaluation and management services code should be used after the initial consult.
99261-99263 - Follow-up inpatient consult codes. These codes were deleted from CPT. Instead clinicians should use the appropriate code from one of the following groups:
22 Louisiana Psychiatric Medical Association • Spring 2006
CPT CODING
For follow-up inpatient consultations see 9923 1-99233, Subsequent Care Codes in the Inpatient S ettinz.
For follow-up consultations in a nursing facility see 99307-993 10, Subsequent Nursing Facility Care
99311-99313 - Subsequent nursing facility care codes. These codes were deleted and replaced by the following new codes: 99307- 99310. There are now four levels of care rather than the previous three levels of care. Note that there are no typical unit times for the new subsequent care codes forrJnu facilities. The AMA CPT Editorial Panel has sent these codes to the AMA RVS Update Committee to be valued and have the times assigned. APA has asked CPT for a status report and for recommendations we can share with our members in those instances when time is supposed to drive the choice (when more than 50% of the visit is spent on counseling and coordination of care). Until those recommendations from the AMA are received code selection shoLild be based on the descriptors below.
New codes: These codes are the new subsequent nursing facility care codes
99307 - Subsequent nursing facility care, per day, for the evaluation and management of a patient. Requires at least two oftliese three key components: I. Problem focused interval history, 2. Problem focused exam, 3. Straightforward medical decision making. Counseling and/or coordination of care with other providers or agencies provided consistent with the nature of the problem(s) and the patient's and/or faniilv's needs. Usually the patient is stable, recovering, or improving.
99308 - SubseqUent nursing facility care, per day, for the evaluation and management of a patient. Requires at least two of these three key components: 1. Expanded problem focused interval history. 2. Expanded problem focused exam. 3. Medical decision making of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient's and/or family's needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication.
99309— Subsequent nursing facility care, per day, for the evaluation and management of a patient. Requires at least two of these three key components: I. Detailed interval history, 2. Detailed exam. 3. Medical decision making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient's and/or family's needs. Usually, the patient has developed a signilicant complication or signiflcant new problem.
99310— Subsequent nursing facility care, per day, for the evaluation and management of a patient. Requires at least two of these three key components: 1. Comprehensive interval history, 2. Comprehensive exam, 3. Medical decision making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient's and/or family's needs. Usually the patient is unstable or has developed a signiflcant new problem requiring immediate physician attention.
Central Nervous System Assessments/Tests Section There have also been extensive changes to the section on Central Nervous System Assessments/Tests (96100-- 96120) which are not included in this document. See AMA's 2006 CPT manual for complete details.
Spring 2006 Louisiana Psychiatric Medical Association • 23
EDITOR Juliana M. Fort, M.D., M.P.H. A CROSS-CULTURAL PSYCHIATRIC ODYSSEY
ASSISTANT EDITOR! EXECUTIVE DIRECTOR
Charlene Smith
LAYOUT EDITOR Wendy L. Schneider
LOUISIANA PSYCHIATRIC MEDICAL ASSOCIATION
P.O. Box 15765 New Orleans, LA 70175
Voice: (504) 865-0030 or Fax: (504) 865-0040
www.lpma.net E-mail: [email protected]
PRESIDENT Jodie S. Holloway, MD
PRESIDENT-ELECT Patricia A. Toups, MD
VICE PRESIDENTS Catherine McDonald, MD
Janet Johnson, MD Herman Soong, MD
Lee Stevens, MD
tion—Transcultural Psychiatry Section, April 18-20, 2006.
The author thanks the following for grants which made possible the research:
American Institute of Indian Studies Senior Research Fellowship, 1975-1976, 1986-1987,1994-1995.
American Philosophical Society (for research on depression in South India), 1985.
National Endowment for the Humanities (NEH) in conjunction with the 1994-1995 AIlS grant.
In addition, the author has visited the village,
MARK YOUR CALENDAR July 14-16, 2006
Astor Crowne Plaza, New Orleans
October 13-14, 2006
Totagadde by pseudonym, in 1984. 1998, 1999, 2000, 2001, 2002, 2003, 2005-6.
2 Clause Structure of Northern Havyaka Kan-nada (Dravidian): A Tagmemic Analysis. Dravidian Linguistics Association, 1980.
I gLfi refers to mountain andj.n refers to people: hence girijanru 'mountain people.'
Schedule for affective disorders and Schizo-phrenia (SADS). New York, New York. State Psy-chiatric Institute: Biometric Research, 1978.
Kapur, Ravi L., Kapur, M., and Carstairs, G. Morris. Indian Psychiatric Survey Schedule (IPSS) Social Psychiatry 9:71-76, 1974.
6 Hughes, Dana C., Blazer, Dan, Hybels, Celia. Duke Social support Index (DSSI), April 1990.
SECREIARY Marc Colon, MD
TREASURER Janet Johnson, MD
REPRESENTATIVE Dudley M. Stewart, Jr., MD
DEPUTY REPRESENTATIVE Harold Ginzburg, MD
IMMEDIATE PAST PRESIDENT
David M. Post, MD, MPH
FEDERAL LEGISLATIVE REPRESENTATIVE
Dudley M. Stewart, Jr., MD
STATE LEGISLATIVE REPRESENTATIVE Anita L. Snow, MD
EXECUTIVE ADVISERS Cheryll Bowers-Stephens, MD
Kathleen Crapanzano, MD Robert Fisher, MD
Paul Ware, MD
MEMBERS-IN-TRAINING REPRESENTATIVES
Andrew Morson, MD Jasjit Singh, MD
Andrew Williams. MD
are in 21st Century." This meeting coincides with the Red River Revel and the Louisiana State Fair. The Clarion Hotel, Shreveport
November 11, 2006
Petros LeVounis, MD, course director, Addiction Institution of NY Baton Rouge
LPMA Newsletter P.O. Box 15765 New Orleans, LA 70175 Address Seniice Requested





























