Embed Size (px)
Citation preview

GASTROENTEROLOGY 1995;109:850-860
Differential Expression of Substance P Receptors in Patients With Crohn's Disease and Ulcerative Colitis
CHRISTOPHER R. MANTYH,* STEVEN R. VIGNA,* R. RANDALL BOLLINGER,*
PATRICK W. MANTYH, § JOHN E. MAGGIO, II and THEODORE N. PAPPAS* *Department of Surgery and tDepartments of Cell Biology and Medicine, Duke University Medical Center, Durham, North Carolina; ~Molecular Neurobiology Laboratory, University of Minnesota, Minneapolis, Minnesota; and ~lDepartment of Biological Chemistry and Molecular Pharmacology, Harvard Medical School, Boston, Massachusetts
Background & Aims: Although clinical and pathological differences exist between Crohn's disease (CD) and ulcerative colitis (UC), distinguishing features are often absent, making diagnosis and treatment problematic. This study evaluated the differences in the expression of substance P (SP) receptors in patients with CD or UC. Methods: Tissue samples from patients with in- flammatory bowel disease or control patients were ob- tained at surgery, processed for 12SI-SP binding, and analyzed by quantitative autoradiography. Results: Pa- tients with CD showed a massive increase in SP recep- tors in lymphoid aggregates, small blood vessels, and enteric neurons of the small and large bowel relative to controls. Six of 16 CD specimens had no pathological evidence of CD yet continued to express high concen- trations of SP receptors. Pathologically positive pa- tients with UC showed high concentrations of SP recep- tors on colonic lymphoid aggregates and small blood vessels but not enteric neurons. No increased SP bind- ing was evident in clinically and pathologically quies- cent UC colons and normal UC Ueostomy samples. Con- clusions: The increased expression of SP receptors on the enteric neurons of patients with CD distinguishes CD from UC. The persistent increased SP binding in pathologically normal CD tissue may indicate a subclini- cal disease state. SP receptor expression may have important diagnostic, etiologic, and therapeutic use- fulness in inflammatory bowel disease.
'nflammatory bowel disease (IBD) encompasses two , disease states, Crohn's disease (CD) and ulcerative co-
litis (UC), that have been separated by clinical, endo- scopic, radiological, and pathological differences. 1 Cur- rently, CD represents an inflammatory condition affecting any part of the intestine (but most commonly is found in the distal small bowel and proximal colon) with skip lesions, fissures, granulomas, and transmural inflammation as pathological features. UC by definition involves only the colon (although backwash ileitis may occur) and is usually uniform and continuous in mucosal
inflammation. 2 Although extensive diagnostic criteria ex- ist to differentiate CD and UC, no single, uniformly reliable diagnostic feature exists. 3 In addition, a signifi- cant percentage of patients with IBD are incorrectly diag- nosed or cannot be categorized into either CD or UC. It has been estimated that 5%-15% of patients with IBD have indeterminate colitis, a term used when macroscopic and microscopic examinations reveal both types of disease of the colon but are not diagnostic of either. 44 Further- more, misdiagnosis of colonic IBD may result in im- proper treatment because CD and UC have distinct medi- cal and surgical therapies/
Because of the potential difficulty in assigning a diag- nosis of CD or UC, several investigators have attempted to find a distinct marker for either disease state. These have included differential expression of cytokines and their receptors s-~2 and neutrophil autoantibodies.13 How- ever, the specificities and sensitivities of these methods are inconclusive, and the significance of neutrophil auto- antibodies in the pathogenesis of IBD remains obscure. 14
The cause of the uncontrolled inflammation in IBD is also unclear. Numerous alterations in the immune system are evident in CD and UC. Several cytokines and other proinflammatory mediators have been shown to be ele- vated in affected regions of CD and UC bowel. 15-1s How- ever, to our knowledge, no study has yet determined if unaffected, pathologically normal regions of IBD bowel show any up-regulation of proinflammatory substances. This observation may be particularly important in CD, in which skip lesions between affected regions occur. Additionally, CD has a recurrence rate of between 50% and 90% after surgical resection of one region of affected bowel. ~9 Potentially, changes in the receptor density of a proinflammatory mediator in pathologically normal tis- sue may provide a rational explanation for the indolent nature of CD.
© 1995 by the American Gastroenterological Association 0016-5085/95/$3.00

September 1995 SUBSTANCE P RECEPTORS IN IBD 851
In this report, we have examined substance P (SP)
receptor distribution in surgically resected specimens taken from patients with CD and UC. SP is an 1 I - a m i n o
acid neuropeptide belonging to the tachykinin family of
peptides that acts via a G protein-coupled seven trans-
membrane domain receptor designated the neurokinin 1 receptor. 2°'-~ SP has multiple effects throughout the cen-
tral nervous system and the periphery, including potent nociceptive and proinflammatory properties. 22 SP acts
both directly and indirectly on immune cascades and on
the vasculature to cause plasma extravasation, edema, and
pain. 23 We have previously shown that resected bowel
from both patients with CD and UC shows a > 1 0 0 0 -
fold increase over controls in SP receptor levels in active
CD and UC tissue in lymphoid aggregates and small blood vessels. 24 It was suggested that SP may contribute
to the inflammatory response in IBD via the dramatic
increase in its receptor density. However, in this study, no direct comparison of the regional distribution of the
SP receptor was performed. Additionally, we did not
examine asymptomatic patients with IBD or pathologi-
cally normal regions of resected IBD bowel for SP recep-
tor up-regulation.
The differential expression of SP receptors in IBD may be important not only for diagnostic and pathophysiolog-
ical purposes but also therapeutically. Recently, several
synthetic nonpeptide SP receptor antagonists have been developed that have been shown to block the inflamma- tory and nociceptive effects of SP in vitro and in vivo. 25
These antagonists have been shown to be nontoxic and
have been suggested for use in several human inflamma- tory diseases, including CD and UC. 26 Knowledge of the
gut SP receptor status of patients with CD and UC dur- ing active and quiescent disease would be crucial in de-
termining the t iming and duration of dosing of these
potential agents.
In the present study, we have examined 32 patients
with IBD with both active and quiescent disease states and 10 control patients. Regional differences in the local- ization of the ectopically expressed SP receptors were
compared in pathologically positive tissue samples from patients with CD and UC. In addition, we examined SP
receptor expression in pathologically negative surgical
specimens from patients who had a previous diagnosis
of CD or UC.
Materials and Methods
Patients
Tissue samples were taken from patients undergoing operative removal or reanastomotic procedures for IBD at Duke University Medical Center and the Durham Veterans Affairs
Hospital. A list of the patients with CD, patients with UC, and control patients studied is provided in Table 1. A total of 16 patients with a previous diagnosis of CD and 16 patients with diagnostically proven UC were evaluated for SP receptor expression. The CD and UC specimens were subdivided into groups whose final pathological diagnosis was either positive or negative for CD or UC. Thirteen patients with CD had pathological confirmation of CD, whereas 6 patients either had uninvolved regions or did not have any pathological evidence of CD in regions of resected bowel. Eleven patients with UC underwent a colectomy and were pathologically positive for UC. Eight patients with UC subsequently had an ileostomy takedown procedure and had pathologically normal specimens. Two asymptomatic patients with a previous diagnosis of UC had a colectomy performed to avoid the risk of carcinoma; in both specimens, the pathological diagnosis was quiescent UC. Several of the patients with CD and UC are included in both pathologically positive and negative groups because tissue was obtained during the primary (e.g., colectomy) and reanasto- motic (e.g., ileostomy takedown) procedures. The control spec- imens included six colon specimens, four resected for carci- noma and two for diverticulitis, in which the tissue samples were taken at least 4 cm from the primary disease site. Addi- tionally, four ileostomy samples were obtained in which the primary colonic diseases before the ileostomy takedown proce- dure included one with Ogilvie's syndrome, two with familial polyposis, and one with colovaginal fistulas. A gastrointestinal pathologist determined the pathological diagnosis for all tis- sues without knowledge of SP receptor expression.
Preoperative medications of all patients were obtained. Ta- ble 2 lists the CD- and UC-positive patients taking either steroids or other anti-inflammatory drugs before surgery. Ste- roid use was defined as any oral, parenteral, or rectal supposi- tory administration 1 week before surgery. Other anti-in- flammatory drugs included sulfasalazine (or its derivatives), azathioprine, or metronidazole. Nine of the 12 CD-positive patients and 7 of the 11 UC-positive patients were taking steroids preoperatively. One of the CD-negative patients and none of the UC-negative patients was taking steroids before surgery was performed. None of the control patients was receiv- ing either steroids or anti-inflammatory agents before surgery was performed.
T issue Preparat ion
Quantitative radioligand binding for the SP receptor was performed as previously described. 24 Briefly, surgically resected specimens from patients with CD, patients with UC, or control patients were obtained immediately after surgical removal. Once removed, the specimens were rapidly placed in a plastic mold, embedded in Tissue Tek O.C.T. compound (Miles, Elkhart, IN), and frozen on dry ice. The tissue was then stored at -80°C until sectioning. Specimens were sectioned at 20 t.tm using a Hacker-Bright microtome cryostat (Hacker Instruments, Fairfield, NJ) at -20°C, thaw mounted on Su- perfrost/Plus glass slides (Fisher Scientific, Pittsburgh, PA),

852 MANTYH ET AL. GASTROENTEROLOGY Vol. 109, No. 3
Table 1. Number of Patients Categorized by Sex, Age, and Specimen Site for Those Pathologically Positive for CD, Pathologically Positive for UC, Pathologically Negative for CD, Pathologically Negative for UC, and Controls
CD-positive CD-negative UC-positive UC-negative Control
Sex Male 3 2 5 4 9 Female 10 4 6 6 2
Mean age (SEM) 36.0 (3.3) 37.2 (6.1) 33.3 (4.2) 37.6 (2.8) 49.0 (4.8) Specimen site
Ileum 6 2 - - 1 - - Ileum and colon 2 . . . . Colon 4 1 11 2 6 Ileostomy 1 3 - - 7 5
and stored desiccated at - 80°C until the day of receptor bind- ing.
SP Radiolabeling and Receptor Binding Assay
125I-Bolton-Hunter SP was synthesized using a pre- viously published protocol. 2v On the day of the experiment, the slide-mounted tissue sections were thawed to room temper- ature. The slides were preincubated in 50 mmol/L Tris-HCl containing 0.005% (vol/vol) polyethylenimine, pH 7.4, at room temperature for 10 minutes. The sections were then
Table 2. Effects of Steroids or Other Anti-Inflammatory Agents on SP Receptor Density in Lymphoid Aggregates of Pathologically Positive Patients With CD and UC and Pathologically Negative Patients With CD
SP receptor Pathology n density a P value ~
Preoperative steroids CD-positive 10 9327 _+ 276 NS
CD-negative 2 8025 __ 18 UC-positive 8 9801 + 253
No steroids CD-positive 3 9321 _+ 601 NS CD-negative 4 9254 __ 289 UC-positive 3 9272 _+ 127
Other anti- infiammatories CD-positive 3 9089 _+ 519 NS
CD-negative 2 9205 __+ 276 UC-positive 4 9346 __ 167
NOTE. Patients were divided into groups that had been administered steroids (orally, intravenously, or rectally) within 7 days of their opera- tion (preoperative steroids), no steroids administered within 7 days of surgery (no steroids), or other anti-inflammatory agents within 7 days of surgery (other anti-inflammatories). Other anti-inflammatory medications included sulfasalazine or its derivatives, azathioprine, or metronidazole. A one-way analysis of variance of the densitometric values of the lymphoid aggregates in CD- or UC-positive patients showed no significant difference in SP receptor density among the groups. Similar not significant values were obtained among the three groups in SP receptor density in blood vessels (data not shown). aValues are expressed as mean _+ SEM. ~P > 0.10.
incubated at room temperature for 1 hour in a solution con- taining 100 pmol/L 125I-Bolton-Hunter SP containing 50 mmol/L Tris-HC1, 3 mmol/L MnCl2, 200 mg/L bovine serum albumin, 2 mg/L chymostatin, 4 mg/L leupeptin, and 40 mg/ L bacitracin; 1.5 mL of incubation solution was used for each tissue section. After incubation with the radioligand, the incu- bation medium was aspirated to waste, and the slides were rinsed four times for 4 minutes each in 50 mmol/L Tris-HCl, pH 7.4, at 4°C and then dipped twice in ice-cold, double- distilled water for 5 seconds each to remove salts. The slides were dried at 4°C under a stream of cold air and stored desic- cated overnight. The slides were then placed in apposition to high-resolution x-ray film (Hyperfilm-Betamax; Amersham, Arlington Heights, IL) for 1 week. An 125I-microscale standard (Amersham) (20-~tm thick) with increasing concentrations of '2~I was also exposed to the x-ray film with the labeled slides. After exposure to the film, the slides were fixed in 4% formal- dehyde for 10 minutes at room temperature and stained with H&E. Autoradiograms were quantitated by densitometric anal- ysis using the Bioquant Meg IV system (R&M Biometrics, Nashville, TN) with a solid-state camera (Dage-MTI Inc., Michigan City, MI) mounted on a Wild M5A stereomicroscope (Wild Leitz, Heerbrugg, Switzerland) with a light-field base. The autoradiographic image was displayed on a video monitor, and anatomic areas to be analyzed were outlined using a mouse and a digitizing pad (SummaSketch Plus; Summagraphics, Fairfield, CT). Densitometric analysis of the microscales was used to correct for the nonlinear response of the film as well as to compare different assays. Nonspecific binding (in the presence of 1 gtmol/L unlabeled SP) was negligible in all cases. Complete displacement of lzSI-SP by CP-96,345 (a nonpeptide SP receptor antagonist) established that the SP binding sites were authentic neurokinin 1 tachykinin receptors, e6 The con- centrations of SP receptors for all groups are shown in Table
3.
Statistical Analysis
A minimum of six densitometric values were obtained from the autoradiogram for each tissue area, and these numbers were then averaged. The averaged densitometric values from each group of patients (either CD-positive, CD-negative, UC-

September 1995 SUBSTANCE P RECEPTORS IN IBD 853
Table 3. SP Receptor Concentrations Expressed in Neurons, Blood Vessels, Lymphoid Aggregates, and Circular Muscle
Pathology Neurons Blood vessels Lymphoid aggregates Circular muscle
CD-positive 8646 (6817-10,216) 8047 (4016-9980) 9326 (7779-10,466) 4240 (1631-8365) CD-negative 8537 (7667-9537) 7903 (6316-9482) 8864 (8067-9950) 4236 (2829-5975) UC-positive 0 8775 (6427-10,068) 9633 (8565-10,883) 4246 (1329-6306) UC-negative 0 0 834 (0-2236) 2966 (1070-8447) Control 0 0 0 4336 (1034-7593)
NOTE. Values are expressed as the mean. Ranges of values are shown in ~arentheses (n = 6-13). All values are expressed as disintegrations per minute per milligram.
positive, UC-negative, or controls) were then pooled, and the SEM was calculated. To compare the differences in receptor densities among various pathological groups, an unpaired t test was performed to determine significance among the patient groups (i.e., CD-positive vs. UC-positive vs. controls) as well as receptor areas (i.e., neurons vs. lymphoid aggregates).
Results Pathologically CD-Positive Versus UC-Positive Specimens
The differential expression of SP binding between a representative tissue specimen from a pathologically positive CD specimen, pathologically positive UC speci- men, or control specimen of uninvolved colon taken from a patient with adenocarcinoma is shown in Figure 1. A moderate level of 125I-SP binding is observed in the circu- lar muscle of all tissues from patients with CD, patients with UC, and control patients. In the CD- and UC- positive specimens, very high concentrations of SP recep- tors were observed in submucosal and subserosal lymphoid aggregates. Small blood vessels scattered throughout the submucosa, muscularis, and serosal fat also contained ectopically expressed SP receptors in both the CD- and UC-positive patients. The CD-positive spec- imen also showed a high concentration of binding sites in enteric neurons in the myenteric plexus and the mus- cularis layer. The receptor distribution of the enteric neurons was discontinuous in nature, with large neurons and their respective arborizations containing receptors observed every few millimeters. Although the neurons expressing SP receptors were unevenly distributed in a tissue section of bowel, they could be identified in all CD-positive tissue. In contrast, although enteric neurons could be readily observed on H&E-stained sections of UC-positive and control tissue, no saturable binding of 125I-SP was found in neurons on any of the corresponding autoradiograms. SP receptor concentrations (expressed in disintegrations per minute per milligram tissue equiva- lents) in pathologically positive specimens from CD-posi- rive, UC-positive, and control patients are shown in Fig- ure 2. A large and statistically significant (P < 0.001)
increase in receptor density was noted in the small blood vessels and lymphoid aggregates in both the CD- and UC-positive patients when compared with control speci- mens. However, the enteric neurons of the CD-positive patients also showed a statistically significant (P < 0.001) increase in SP binding in comparison with the UC-positive patients and control patients. No difference in receptor concentration was found in the circular mus- cle in the CD-positive, UC-positive, and control groups (P > 0.1).
Pathologically CD-Negative Versus UC-Negative Specimens
Six patients with a history of CD underwent bowel resection and had negative pathological findings for CD. Three patients had ileostomy takedown after previous colonic resection for CD. One patient had pre- viously undergone multiple small and large bowel resec- tions and finally had a proctectomy performed after nu- merous coloenteric and colocutaneous fistulas. Two patients underwent removal of the terminal ileum and proximal colon; CD pathology was confined exclusively to the colon. In these 2 patients, both the terminal ileum and proximal colon were assayed for SP receptor expres- sion. In all 6 cases, the tissue that was processed for quantitative autoradiography was pathologically negative for any colitis. The pattern of SP receptor binding in the 6 cases of CD tissue was nearly identical to the active CD- positive tissues. As shown in Figure 3A and B, lymphoid aggregates, small blood vessels, and enteric neurons ex- press a high concentration of SP receptors similar to that observed in CD-positive tissue. The receptors on the enteric neurons on CD-negative tissues were again expressed discontinuously throughout the myenteric plexus and muscularis.
Ten patients with a previous pathological diagnosis of UC subsequently underwent further surgical therapy. Seven patients had an ileostomy takedown, 1 had recur- rent fistulas and bleeding after an ileoanal pull-through and required a Brooke ileostomy (where ileal tissue was obtained), and 2 who were asymptomatic for UC at sur-

854 MANTYH ET AL. GASTROENTEROLOGY Vol. 109, No. 3
Figure 1. A comparison of SP receptors in CD-positive, UC-positive, and control tissue. A, D, and G are bright-field photomicrographs of sections of resected bowel stained with H&E. B, E, and H represent an autoradiogram of the Hyperfilm that overlaid the tissue sections shown in A, D, and G, respectively. The sections were incubated with 100 pmol/L of ~251-SP and represent total binding (TB). C, G, and / represent serial sections adjacent to and treated identically to the corresponding total binding sections except for the addition of 1 #mol /L of unlabeled SP and therefore represent nonspecific binding (NSB). The CD-positive tissue was obtained from the ileum of a patient who underwent resection for disease that was refractive to medical management. The H&E-stained section in A shows extensive lymphocytic infiltration throughout the submucosa and to the serosa. (B) Saturable 1251-SP binding is found in the lymphoid aggregates (LA) in the submucosal and serosal regions, small blood vessels (BY) in the submucosa, circular muscle (CM), and myenteric plexus (arrowheads). (D-F) The UC-positive specimen was taken from the colon of a patient with medically intractable disease who underwent a colectomy and ileoanal pull-through. SP receptors are localized to the LA, BV, and CM. Note the lack of binding to the myenteric neurons (D, arrowheads). The control specimen was obtained from a patient with carcinoma who had a subtotal colectomy. Binding in the control specimen is confined only to the CM (bars: A, 1.00 mm; D, 1.01 mm; G, 1.08 ram).
gery had a colectomy with an ileoanal pull-through per- formed to avoid the risk of carcinoma. In the latter two cases, the pathological diagnosis was quiescent UC. All UC tissue from the pathologically normal ileostomy tis- sue and the two cases of quiescent UC showed no ectopic SP receptors. An example of a UC ileostomy takedown sample in which the only discernable SP receptors are found in the circular muscle is shown in Figure 3C and D. No receptor up-regulation was found in small submu- cosal blood vessels or lymphoid aggregates. The same pattern of receptor binding was found in the circular
muscle of the control ileostomy tissue (Figure 2D and E).
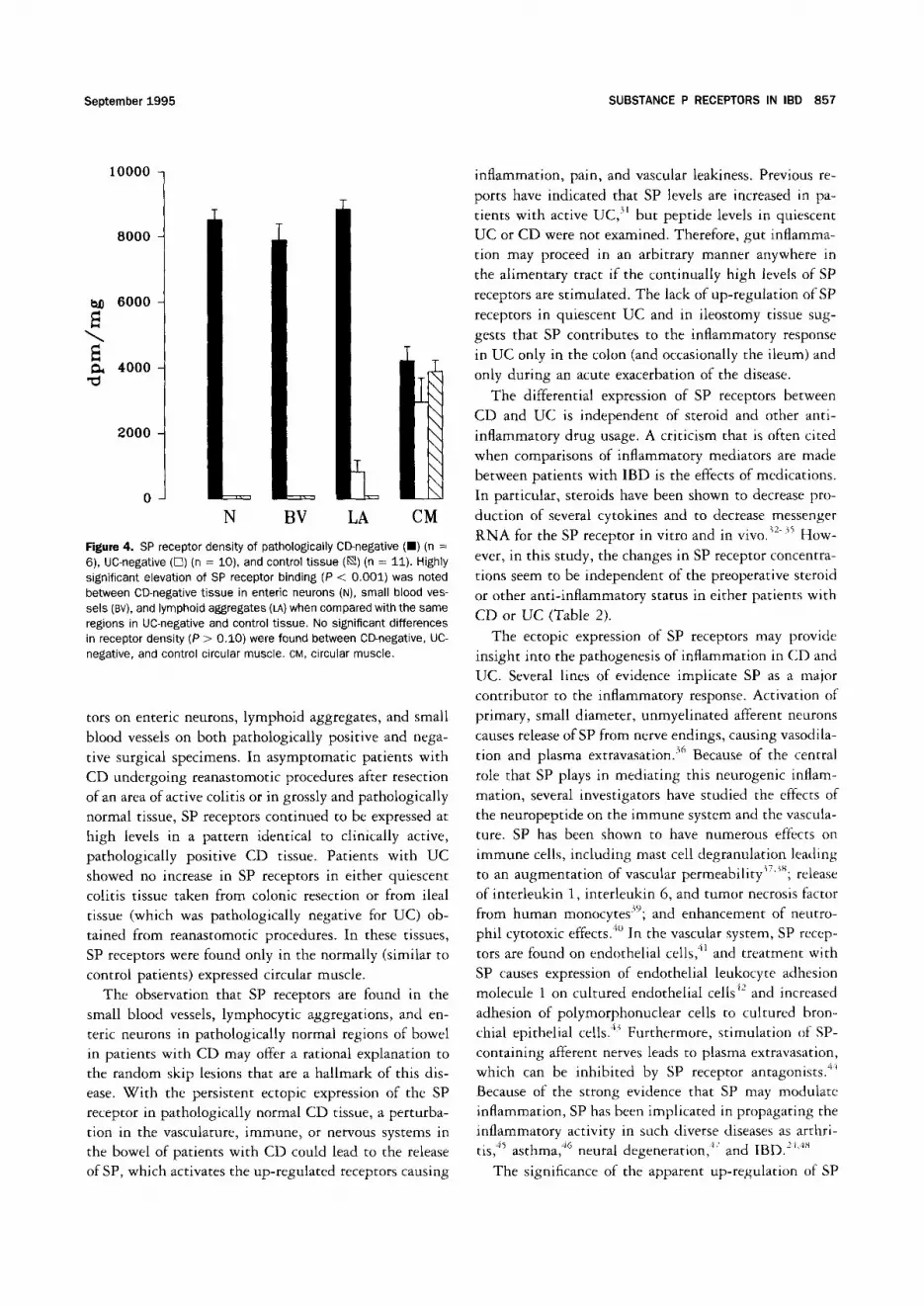
The increase in SP binding sites in pathologically neg- ative patients with CD on the enteric neurons, small blood vessels, and lymphoid aggregates in comparison with pathologically negative patients with UC or control patients is shown in Figure 4. A highly significant (P < 0.001) difference in SP receptors was found between the CD-negative tissue and the UC-negative and control tis- sue in enteric neurons, blood vessels, and lymphoid ag- gregates. However, the differences between the circular

September 1995 SUBSTANCE P RECEPTORS IN IBD 855
qV
10000
8000
6000
4000
2000
N BV LA
_ T
\ \ \ \ \ \ \ \ \ \
CM
Rgure 2. Graphic representation of the total SP receptor density of CD-positive (B) (n = 13), UC-positive (r-I) (n = 11), and control tissues ([ ]) (n = 11). The four regions analyzed in each group were enteric neurons (N), small blood vessels (BY), lymphoid aggregates (LA), and circular muscle (CM). The receptor density is expressed as disintegra- tions per minute per milligram tissue obtained from comparing tissue samples with radioactive microscale standards containing known amounts of 1251 cut at 20 Ilm. Error bars represent the SEM of all of the collected samples. Note that CD-positive tissue had a highly significant (P < 0.001) increase in SP receptor density in the enteric neurons in comparison with UC-positive and control tissue. Significant differences in binding were noted in CD- and UC-positive tissues and control specimens (P < 0.001) in the blood vessels and lymphoid aggregates, but no significant differences (P > 0.10) were found between CD- and UC-positive tissue in these areas. The circular mus- cle had nearly identical levels of SP receptor density in the CD-positive, UC-positive, and control tissues (P > 0.10).
muscle of the CD-negative, UC-negative, and control circular muscle were not significant (P > 0.10). No dif- ference in receptor density was noted between CD-posi- rive and CD-negative specimens in any region (P > 0.10).
Preoperative Steroid and Anti-inflammatory Medications
SP receptor concentrations of lymphoid aggre- gates of patients with CD and UC either receiving or not receiving preoperative steroids or other anti-in- flammatory medications are shown in Table 2. Nine of 12 CD-positive patients and 8 of 11 UC-positive patients were administered steroids preoperatively. No significant change in receptor density on the lymphoid aggregates was found between the CD and UC group that received preoperative steroids when compared with those that did not. Three of 12 CD-positive and 4 of 11 UC-positive
patients had received other anti-inflammatory drugs; again, no significant change in receptor density was noted when compared with patients not receiving these drugs.
Discussion
In this study, we have used quantitative receptor autoradiography to compare the SP receptor density and distribution on surgical specimens from patients with CD and UC that were either pathologically positive or negative for colitis. Several significant findings are re- ported. In all CD tissue examined, a high concentration of SP receptors was localized on lymphoid aggregates and small blood vessels and in enteric neurons in the myenteric plexus and throughout the muscularis. In con- trast, all pathologically positive UC tissue examined ex- pressed high concentrations of SP receptors on lymphoid aggregates and small blood vessels but showed minimal binding on neuronal tissue.
The differential expression of SP receptors in CD vs. UC may aid in the diagnosis of patients who do not fit clinically or pathologically into one disease state. Ap- proximately 5 %-15 % of patients are diagnosed with in- determinate colitis, a term used when no reliable diag- nostic feature categorizes a patient. 4 Although no clinical study has examined the rate of misdiagnosis of CD and UC, it is well known among gastroenterologists and sur- geons that a significant population of patients with IBD will have a change in their diagnosis. It is currently estimated that approximately 30%-50% of patients with CD will have disease in the colon. 28'29 Incorrect diagnosis of IBD in these patients could lead to improper medical and surgical therapy. Particularly hazardous in a patient with CD is a colectomy with construction of an ileal pouch reservoir because a significant number of these patients will have a recurrence of CD in the pouch, lead- ing to chronic inflammation and pouch failure. 7'3° Al- though we found that all patients with CD examined show continual ectopic SP receptor expression and have a unique receptor distribution in comparison with UC, the potential for diagnostic assistance is still problematic. In our assay, the enteric neurons expressing the SP recep- tors in CD are located in the muscularis and require a full-thickness sample of bowel, obviating endoscopic biopsy sampling. Thus, this test may be of greater use in examination of resected bowel from patients with IBD in which traditional pathological distinctions between CD and UC are not found or in full-thickness rectal biopsy specimens.
In addition to CD having a unique distribution of SP receptors in comparison with UC, CD tissue, unlike UC specimens, continued to express high levels of SP recep-

D
Figure 3. Comparisons of SP receptor binding among CD-negative, UC-negative, and control tissue. A, C, and Eare bright-field photomicrographs of the H&E-stained tissue sections, whereas B, D, and F are the corresponding autoradiograms that overlaid the tissue sections. (A and B) The CD-negative specimen was taken from the ileostomy of a patient who 10 weeks previous to the takedown procedure had a resection of the terminal ileum and proximal colectomy for CD. At the time of the ileostomy takedown, the patient was asymptomatic and the final pathological analysis was negative for CD. Similar to the CD-positive tissue seen in Figure 1, SP receptor up-regulation is observed on the lymphoid aggregates (LA) in the serosal region, small blood vessels (BY) in the submucosa, circular muscle (CM), and the myenteric plexus and its arborizations (arrowheads). (C and D) The UC-negative tissue was obtained from a patient undergoing a complete colectomy for carcinoma avoidance. The patient was asymptomatic at the time of surgery, and the pathological diagnosis was quiescent UC. Only a moderate amount of binding is observed in the circular muscle with no detectable receptors in the lymphoid aggregates, small blood vessels, or enteric neurons. (E and F) The control tissue was taken from the ileostomy of a patient with familial polyposis coli who had previously undergone a colectomy and was now undergoing a reanastomotic procedure. The patient was asymptomatic, and pathological analysis showed only normal ileum. SP receptors are present only on the circular muscle of the control tissue (bars: A, 0.89 mm; C, 0.90 mm; E, 0.83 mm).
September 1995 SUBSTANCE P RECEPTORS IN IBD 857
1 0 0 0 0
8 0 0 0
1~ 6 0 0 0
4 0 0 0
2 0 0 0
N BV LA CM
Figure 4. SP receptor density of pathologically CD-negative ( I ) (n = 6), UC-negative ([q) (n = 10), and control t issue (i~) (n = 11). Highly significant elevation of SP receptor binding (P < 0.001) was noted between CD-negative tissue in enteric neurons (N), small blood ves- sels (BY), and lymphoid aggregates (LA) when compared with the same regions in UC-negative and control tissue. No significant differences in receptor density (P > 0.10) were found between CD-negative, UC- negative, and control circular muscle. CM, circular muscle.
tors on enteric neurons, lymphoid aggregates, and small blood vessels on both pathologically positive and nega- tive surgical specimens, In asymptomatic patients with CD undergoing reanastomotic procedures after resection of an area of active colitis or in grossly and pathologically normal tissue, SP receptors continued to be expressed at high levels in a pattern identical to clinically active, pathologically positive CD tissue. Patients with UC showed no increase in SP receptors in either quiescent colitis tissue taken from colonic resection or from ileal tissue (which was pathologically negative for UC) ob- tained from reanastomotic procedures. In these tissues, SP receptors were found only in the normally (similar to control patients) expressed circular muscle.
The observation that SP receptors are found in the small blood vessels, lymphocytic aggregations, and en- teric neurons in pathologically normal regions of bowel in patients with CD may offer a rational explanation to the random skip lesions that are a hallmark of this dis- ease. Wi th the persistent ectopic expression of the SP receptor in pathologically normal CD tissue, a perturba- tion in the vasculature, immune, or nervous systems in the bowel of patients with CD could lead to the release of SP, which activates the up-regulated receptors causing
inflammation, pain, and vascular leakiness. Previous re-
ports have indicated that SP levels are increased in pa- tients with active UC, 3~ but peptide levels in quiescent UC or CD were not examined. Therefore, gut inflamma- tion may proceed in an arbitrary manner anywhere in the alimentary tract if the continually high levels of SP receptors are stimulated. The lack of up-regulation of SP
receptors in quiescent UC and in ileostomy tissue sug- gests that SP contributes to the inflammatory response in UC only in the colon (and occasionally the ileum) and only during an acute exacerbation of the disease.
The differential expression of SP receptors between CD and UC is independent of steroid and other anti- inflammatory drug usage. A criticism that is often cited when comparisons of inflammatory mediators are made between patients with IBD is the effects of medications. In particular, steroids have been shown to decrease pro- duction of several cytokines and to decrease messenger
RNA for the SP receptor in vitro and in vivo.~2-~ How- ever, in this study, the changes in SP receptor concentra- tions seem to be independent of the preoperative steroid or other anti-inflammatory status in either patients with
CD or UC (Table 2).
The ectopic expression of SP receptors may provide insight into the pathogenesis of inflammation in CD and UC. Several lines of evidence implicate SP as a major contributor to the inflammatory response. Activation of primary, small diameter, unmyelinated afferent neurons
causes release of SP from nerve endings, causing vasodila- tion and plasma extravasation) 6 Because of the central role that SP plays in mediating this neurogenic inflam- mation, several investigators have studied the effects of the neuropeptide on the immune system and the vascula- ture. SP has been shown to have numerous effects on immune cells, including mast cell degranulation leading to an augmentation of vascular permeability~7'~s; release of interleukin 1, interleukin 6, and tumor necrosis factor from human monocytes~9; and enhancement of neutro- phil cytotoxic effects. *° In the vascular system, SP recep- tors are found on endothelial cells, 4~ and treatment with SP causes expression of endothelial leukocyte adhesion molecule 1 on cultured endothelial cells 42 and increased adhesion of polymorphonuclear cells to cultured bron- chial epithelial cells. 43 Furthermore, stimulation of SP-
containing afferent nerves leads to plasma extravasation, which can be inhibited by SP receptor antagonists. <'* Because of the strong evidence that SP may modulate inflammation, SP has been implicated in propagating the inflammatory activity in such diverse diseases as arthri- tis, ~5 asthma, 46 neural . .47 IBD -'~'J'~ degeneration, and .
The significance of the apparent up-regulation of SP

858 MANTYH El" AL. GASTROENTEROLOGY Vol. 109, No. 3
receptors in the enteric neurons of patients with CD but not patients with UC is not clear; however, recent work may be insightful. Early studies have shown hyperplasia of ganglion cells in the submucosal or myenteric plexuses in CD, 49'5° and the presence of these enlarged neurons is now generally accepted as a pathological feature of CD. In addition, electron microscopy of CD tissue has shown extensive axonal degeneration and infiltration of the gut plexuses with mast cells, lymphocytes, and plasma cells.5~ Other investigators have examined alterations in motor activity in animal models of gut inflammation and have suggested that the motility changes are caused by pertur- bations in inflammatory mediators that subsequently in- fluence enteric neuron and epithelial function. 52 How- ever, it is not known if the increase in SP receptor density represents either ectopic expression, up-regulation, mi- gration of SP receptor-containing cells (in blood vessels or lymphoid aggregates), or a concentration of receptors after activation and endocytosis of the receptor. At least for neurons, we have recent evidence to indicate the lat- ter. We have shown that after endogenous SP release in either the spinal cord (stimulated by capsaicin or a pain- ful stimulus) or the ileum (by Clostridium difficile toxin A injection), the SP receptor is rapidly endocytosed and dramatic morphological changes occur in the cellular architecture. 53'54 In the ileum, the enteric SP receptor- expressing neurons appear swollen with thickened axons and dendrites. Therefore, it is conceivable that the in- crease in receptor density in CD may reflect the cellular concentration of SP receptors and subsequent morpho- logical changes after a toxin- or chemically induced SP release. The relationship of these observations to IBD must remain speculative until reproducible animal mod- els of chronic relapsing enterocolitis are examined for SP receptor changes.
Finally, the differential expression of SP receptors in CD and UC may have therapeutic implications. Recently, several specific, nonpeptide antagonists to the SP receptor have been developed. 25 These antagonists have been shown to block SP receptor activation both in vitro and in vivo. 55 Specifically, the antagonists inhibit SP-induced neurogenic inflammation, such as plasma extravasation in the lung 56'57 and plasma leakage in the knee joint, 25 as well as specific spinal pain pathways. 58 In the gut, the SP receptor antagonist CP-96,345 effectively blocked granuloma formation in a Trichinella spiralis mouse model of inflammation. 59 In addition, the same SP receptor an- tagonist inhibited the histological and physiological ef- fects of C. difficile toxin A-induced enterocolitis in the rat, 6° suggesting that the SP receptor modulates these inflammatory responses. Finally, our group has recently
shown that several of the nonpeptide SP receptor antago- nists effectively eliminate SP binding to CD and UC tissue at nanomolar concentrations. 26 Therefore, the non- peptide receptor antagonists are novel compounds that may potentially ameliorate the proinflammatory effects of SP in IBD and other inflammatory conditions such as asthma and arthritis. Based on our study, we hypothesize that SP receptor blockade may be beneficial in active (and presumably pathologically positive) CD and UC. Additionally, the antagonists may also be useful in quies- cent (and presumably pathologically negative) CD in which the continual up-regulation of SP receptors may indicate a subclinical disease state.
In conclusion, we have shown the differential distribu- tion of SP receptors in CD and UC. SP receptors are ectopically expressed in lymphoid aggregates, small blood vessels, and enteric neurons of CD in both active, pathologically positive surgical specimens as well as in quiescent, pathologically negative samples. In UC, the SP receptor up-regulation is confined to the blood vessels and lymphoid aggregates of active, pathologically posi- tive specimens. No SP receptor up-regulation was evident on quiescent, pathologically negative UC tissue. These findings may have significant diagnostic, etiologic, and therapeutic importance in IBD.
References 1. Riis P. Differential diagnosis, ulcerative colitis, Crohn's disease
and other disorders, including diverticular disease. In: Allan RN, Keighley MRB, Alexander-Williams J, Hawkins CF, eds. Inflamma- tory bowel disease. Edinburgh: Churchill Livingstone, 1990: 191- 198.
2. Geller SA. Pathology of inflammatory bowel disease: a critical appraisal in diagnosis and management. In: Targan SR, Shana- han F, eds. Inflammatory bowel disease: from bench to bedside. Baltimore: Williams & Wilkins, 1994:337-351.
3. Shepherd NA. Pathological mimics of chronic inflammatory bowel disease. J Clin Pathol 1991;44:726-733.
4. Price AB. Overlap in the spectrum of non-specific inflammatory bowel disease-- 'col i t is indeterminate.' J Clin Pathol 1978; 31:567-577.
5. Lee KS, Medline A, Shockey S. Indeterminate colitis in the spec- trum of inflammatory bowel disease. Arch Pathol Lab Med 1979; 103:173-176.
6. Kent TH, Ammon RK, DenBesten L. Differentiation of ulcerative colitis and regional enteritis of colon. Arch Pathol 1970 ;89 :20- 29.
7. Koltun WA, Schoetz D J, Roberts PL, Murray J J, Coller JA, Veiden- heimer MC. Indeterminate colitis predisposes to perineal compli- cations after ileal pouch-anal anastomosis. Dis Colon Rectum 1989; 32:653-658.
8. Mahida YR, Kurlac L, Gallagher A, Hawkey CJ. High circulating concentrations of interleukin-6 in active Crohn's disease but not ulcerative colitis. Gut 1991;32:1531-1534.
9. Mueller C, Knoflach P, Zielinski CC. T-cell activation in Crohn's disease. Increased levels of soluble interleukin-2 receptor in se- rum and in supernatants of stimulated peripheral blood mononu- clear cells. Gastroenterology 1990; 98:639-646.
September 1995 SUBSTANCE P RECEPTORS IN IBD 859
10. Mullin GE, Lazenby AJ, Harris ML, 8ayless TM, James SP. In- creased interleukin-2 messenger RNA in the intestinal mucosal lesions of Crohn's disease but not ulcertaive colitis. Gastroenter- ology 1992; 102:1620-1627.
11. Breese E, Braegger CP, Corrigan C J, Walker-Smith JA, MacDonald l-r. Intefleukin-2- and interferon-gamma-secreting T cells in nor- mal and diseased human intestinal mucosa. Immunology 1993; 78:127-131,
12. Sartor RB. Pathogenetic and clinical relevance of cytokines in inflammatory bowel disease. Immunol Res 1991;10:465-471.
13. Shanahan F, Landers C, Duerr R, Targan SR. Neutrophil autoanti- bodies as disease markers for ulcerative colitis. Immunol Res 1991; 10:479-484.
14. Shanahan F. Neutrophil autoantibodies in inflammatory bowel disease: are they important? Gastroenterology 1994; 107:586- 589.
15. Brynskov J, Tvede N, Andersen CB, Vilien M. Increased concentra- tions of interleukin 1-beta, interleukin-2, and soluble interleukin-2 receptors in endoscopical mucosal biopsy specimens with active inflammatory bowel disease. Gut 1992;33:55-58.
16. Youngman KR, Simon PL, West GA, Cominelli F, Rachmilewitz D, Klein JS, Fiocchi C. Localization of intestinal interleukin 1 activity and protein and gene expression to lamina propria cells. Gastro- enterology 1993; 104:749-758.
17. Matsuura T, West GA, Youngman KR, Klein JS, Fiocchi C. Immune activation genes in inflammatory bowel disease. Gastroenterol- ogy 1993; 104:448-458.
18. Matsuura T, West GA, Klein JS, Ferraris L, Fiocchi C. Soluble interleukin 2 and CD8 and CD4 receptors in inflammatory bowel disease. Gastroenterology 1992; 102:2006-2014.
19. Sutherland LR. Prevention of postoperative recurrence. In: Rach- milewitz D, ed. Inflammatory bowel disease: 1994. Dordrecht: Kluwer Academic, 1994:237-245.
20. Yokota Y, Sasai Y, Tanaka K, Fujiwara T, Tsuchida K, Shigemoto R, Kakizuka A, Ohkubo H, Nakanishi S. Molecular characteriza- tion of a functional cDNA for rat substance P receptor. J Biol Chem 1989; 264:17649-17652.
21. Hershey AD, Krause JE. Molecular characterization of a functional cDNA encoding the rat substance P receptor. Science 1990; 247:958-962.
22. Lembeck F. Substance P: from extract to excitement. Acta Physiol Scand 1988; 133:435-454.
23. Mantyh PW. Substance P and the inflammatory and immune re- sponse. Ann NY Acad Sci 1991;632:263-271.
24. Mantyh CR, Gates TS, Zimmerman RP, Welton ML, Passaro EP Jr, Vigna SR, Maggio JE, Kruger L, Mantyh PW. Receptor binding sites for substance P, but not substance K or neuromedin K, are expressed in high concentrations by arterioles, venules, and lymph nodules in surgical specimens obtained from patients with ulcerative colitis and Crohn disease. Proc Natl Acad Sci USA 1988; 85:3235-3239.
25. Watling K J, Krause JE. The rising sun shines on substance P and related peptides. Trends Pharmacol Sci 1993; 14:81-84.
26. Mantyh CR, Vigna SR, Maggio JE, Mantyh PW, Bollinger RR, Pap- pas TN. Substance P binding sites on intestinal lymphoid aggre- gates and blood vessels in inflammatory bowel disease corre- spond to authentic NK-1 receptors. Neurosci Lett 1994;178: 255-259.
27. Too H-P, Maggio JE. Radioimmunoassay of tachykinins. Methods Neurosci 1991;6:232-247.
28. Greenstein A J, Geller SA, Dreiling DA, Aufses AH. Crohn's dis- ease of the colon IV. Clinical features of Crohn's (ileo) colitis. Am J Gastroenterol 1975;64:191-199.
29. Lockhart-Mummery HE, Morson BC. Crohn's disease of the large intestine. Gut 1964; 5:493-509.
30. Hyman NH, Fazio VW, Tuckson WB, Lavery IC. Consequences of
ileal pouch-anal anastomosis for Crohn's colitis. Dis Colon Rec- tum 1991; 34:653-657.
31. Bernstein CN, Robert ME, Eysselein VE. Rectal substance P con- centrations are increased in ulcerative colitis but not in Crohn's disease. Am J Gastroenterol 1993;88:908-913.
32. Larsson E-V. Cyclosporin A and dexamethasone suppress T cell responses by selectively acting at distinct sites of the triggering process. J Immunol 1980; 124:2828-2833.
33. Reed JC, Abidi AH, Alpers JD, Hoover RG, Robb R J, Nowell PC. Effect of cyclosporin A and dexamethasone on interleukin 2 re- ceptor gene expression. J Immunol 1986; 137:150-154.
34. Schliemer RP. Effects if glucocorticosteroids on inflammatory cells relevant to their therapeutic applications in asthma. Am Rev Respir Dis 1990; 141:$59-$69.
35. Ihara H, Nakanishi S. Selective inhibition of expression of the substance P receptor mRNA in pancreatic acinar AR42J cells by glucocorticoids. J Biol Chem 1990;265:22441-22445.
36. Lembeck F, Holzer P. Substance P as a neurogenic mediator of antidromic vasodilatation and neurogenic plasma extravasation. Naunyn Schmiedebergs Arch Pharmacol 1979;310:175-183.
37. Hagermark O, HSkfelt T, Pemow B. Flare and itch induced by substance P in human skin. J Invest Dermatol 1978;71:233- 235.
38. Yano H, Wershil BK, Arizono N, Galli SJ. Substance P-induced augmentation of cutaneous vascular permeability and granulo- cyte infiltration in mice is mast cell dependent. J Clin Invest 1989; 84:1276-1286.
39. Lotz M, Vaughan JH, Carson DA. Effect of neuropeptides on pro- duction of inflammatory cytokines by human monocytes. Science 1988; 241:1218-1221.
40. Wozniak A, McLennan G, Betts WH, Murphy GA, Scicchitano R. Activation of human neutrophils by substance P: effect on FMLP- stimulated oxidative and arachidonic acid metabolism and on antibody-dependent cell-mediated cytotoxicity. Immunology 1989;68:359-364.
41. Greeno EW, Mantyh P, Vercellotti GM, Moldow CF. Functional neurokinin 1 receptors for substance P are expressed by human vascular endothelium. J Exp Med 1993; 177:1269-1276.
42. Nakagawa N, Iwamoto I, Yoshida S. Effect of substance P on the expression of an adhesion moecule ICAM-1 in human vascular endothelial cells. Regul Pept 1993;46:223-224.
43. DeRose V, Robbins RA, Snider RM, Spurzem JR, Thiele GM, Ren- nard SI, Rubenstein I. Substance P increases neutrophil adhe- sion to bronchial epithelial cells. J Immunol 1994;152:1339- 1346.
44. Louis SM, Jamieson A, Russell NJW, Dockray GJ. The role of substance P and calcitonin gene-related peptide in neurogenic plasma extravasation and vasodilatation in the rat. Neuroscience 1989; 32:581-586.
45. Levine JD, Clark R, Devor M, Helms C, Moskowitz MA, Basbaum AI. Intraneuronal substance P contributes to the severity of exper- imental arthritis. Science 1984; 226:547-549.
46. Barnes P J, Baraniuk JN, Belvisi MG. Neuropeptides in the respira- tory tract. Am Rev Respir Dis 1991; 144:1187-1198.
47. Mantyh PW, Johnson D J, Boehmer CG, Catton MD, Vinters HV, Maggio JE, Too H-P, Vigna SR. Substance P receptor binding sites are expressed by gila in vivo after neuronal injury. Proc Natl Acad Sci USA 1989;86:5193-5197.
48. Mantyh PW, Catton MD, Boehmer CG, Welton ML, Passaro EP Jr, Maggio JE, Vigna SR. Receptors for sensory neuropeptides in human inflammatory diseases: implications for the effector role of sensory neurons. Peptides 1989; 10:627-645.
49. Davis DR, Dockerty MB, Mayo CW. The myenteric plexus in re- gional enteritis: a study of the number of ganglion cells in the ileum in 24 cases. Surg Gynecol Obstet 1955; 101:208-216.

860 MANTYH ET AL. GASTROENTEROLOGY Vol. 109, No. 3
50. Siemers PT, Dobbins I. The Meissner plexus in Crohn's disease of the colon. Surg Gynecol Obstet 1974; 138:39-42.
51. Dvorak AM, Connell AB, Dickersin GR. Crohn's disease: a scan- ning electron microscopic study. Hum Patho11979; 10:165-177.
52. Cooke HJ. Neuroimmune signaling in regulation of intestinal ion transport. Am J Physiol 1994;266:G167-G178.
53. Mantyh PW, Demaster E, Malhotra A, Ghilardi JR, Rogers SD, Mantyh CR, Liu H, Basbaum AI, Vigna SR, Maggio JE, Simone DA. Receptor endocytosis and dendrite reshaping in spinal neu- rons after somatosensory stimulation. Science 1995;268: 1629-1632.
54. Lapp JA, Mantyh CR, Lyedy DM, Vigna SR, Pappas TN. Alterations in enteric neuron substance P receptors in Clostridium difficile toxin A-induced colitis (abstr). Gastroenterology 1995;108:A858.
55. Lowe JA III, Drozda SE, Snider RM, Longo KP, Zorn SH, Jackson ER, Morrone J, McLean S, Bryce DK, Bordner J, Nagahisa A, Kanai Y, Suga O, Tsuchiya M. Discovery of CP-96,345 and its characterization in disease models involving substance P. Regul Pept 1993; 46:20-23.
56. Lei YH, Barnes P J, Rogers DF. Inhibition of neurogenic plasma exudation in guinea-pig airways by CP-96,345, a new non-peptide NK1 receptor antagonist. Br J Pharmacol 1992;105:261-262.
57, Lembeck F, Donnerer J, Tsuchiya M, Nagahisa A. The non-peptide
tachykinin antagonist, CP-96,345, is a potent inhibitor of neuro- genic inflammation. Br J Pharmacol 1992; 105:527-530.
58. Radhakrishnan V, Henry JL. Novel substance P antagonist, CP- 96,345, blocks responses of cat spinal dorsal horn neurons to noxious cutaneous stimulation and to substance P. Neurosci Lett 1991; 132:39-43.
59. Blum AM, Metwali A, Elliott D, Sandor M, Lynch R, Weinstock JV. Substance P receptor antagonist blocks granuloma IgM produc- tion in vivo (abstr). Gastroenterology 1994; 106:A653.
60. Pothoulakis C, Castagliuolo I, LaMont JT, Jaffer A, O'Keane JC, Snider RM, Leeman SE. CP-96,345, a substance P antagonist, inhibits rat intestinal responses to Clostridium difficile toxin A but not cholera toxin. Proc Natl Acad Sci USA 1994;91:947- 951.
Received February 6, 1995. Accepted April 19, 1995. Address requests for reprints to: Christopher R. Mantyh, M.D.,
Department of Surgery, Duke University Medical Center, Box 3614, Durham, North Carolina 27710. Fax: (919) 286-5530.
Supported by Veterans Affairs grant 0010 and National Institutes of Health grant GM-15904.
The authors thank Evelyn Stimson and Kelly Van Koughnet for excellent technical support.





























