Embed Size (px)
Citation preview
Diagnosis: Psoriasis or Not? What are the Clues? Emily M. Altman and Hideko Kamino
Psoriasis is a common Inflammatory, hyperprolif- erative skin dlsorder that affects 1% to 2% of the population of Western Europe and the United States. Because the clinical presentation of psoria- sis is varied, many times the definitive diagnosis depends on the histological examination. How- ever, the hlstological changes of psorlasis are as varied as the cllnlcal presentatlons. Therefore, a combination of histopathologic features must be present for the diagnosis of psoriasis to be made. In this adlcle, we revlew the clues for the hlsto- pathologlc dlagnosls of each type and stage of psorlasls, such as psoriasis vulgaris, pustular pso- riasis, and erythrodermlc psoriasis, as well as the hlstopathologlc differential diagnosis of these entitles. Copyright �9 1999 by W.B. Saunders Company
p SORIASIS IS AN inflammatory, hyperproliferative skin disorder that affects 1% to 2% of the popula-
tion of Western Europe and the United States, but is infrequent in Africa and Asia and rare among the native North and South American populations. ~ Both genetic and environmental factors are thought to play a role in the initiation and progression of the disease. A family history for psoriasis is indicated by one third of the patients. Family studies, twin studies, and pedigree analyses point to a polygenic and multifactorial inheri- tance of psoriasis. 2 Among the documented environ- mental factors that affect the development and course of psoriasis are trauma and infection. 3 Other factors that may play a role in psoriasis are drugs, sunlight, stress, and HIV infection. Environmental factors such as streptococcal infection, stress, and colder climate are also associated with disease onset and/or severity. Earlier age of onset is thought to correlate with worse prognosis. 4 The strong association between psoriasis and certain human leukocyte antigen (HLA) types, namely HLA-B13, B175, and Cw66, the exocytosis of mononuclear cells prior to epidermal hyperplasia, and the efficacy of T cell-selective immunosuppressive treatments, such as cyclosporine, 7 FK506 s, and anti- CD4+ monoclonal antibody 9 in treating psoriasis, establish psoriasis as an immunologically-mediated dermatosis. The clinical course and prognosis of psoria- sis is unpredictable, characterized by exacerbations and remissions. There is a variety of clinical types of psoriasis ranging from mild, localized plaques to gener- alized pustular psoriasis or erythroderma.
PSORIASIS VULGARIS: CLINICAL FEATURES
In nonpustular psoriasis, lesions may erupt as acute guttate papules or appear as chronic plaques. Initial lesions of guttate or eruptive psoriasis appear as pinpoint erythematous papules with central scaling that enlarge rapidly. Numerous small (0.5 to 1.5 cm) lesions appear simultaneously over the upper trunk and proximal extremities, sparing the scalp and inter- triginous zones. Acute guttate psoriasis typically is charac- terized by an early age of onset and has a strong association with antecedent streptococcal throat infection. 1~
Psoriasis vulgaris (chronic plaque psoriasis) is the most frequent clinical form of psoriasis, ll In this form of psoriasis, the lesions develop slowly from erythema- tous macules to asymptomatic papules with a tendency to eventually become confluent, forming stable, ele- vated, sharply demarcated, erythematous plaques with a silvery, adherent (micaceous) scale. The sites of predilection include the scalp, elbows, knees, lower back, and umbilicus. The Auspitz sign is present in this type of psoriatic plaques. Psoriasis vulgaris may also involve the intertriginous zones (psoriasis inversa). The nails are frequently involved, with pitting, oil spots, and/or onychodystrophy. The lesions of chronic plaque psoriasis may remain stable for years, may occasionally involute, or may develop into erythroder- mic or pustular psoriasis. During severe flares, psoriatic plaques may become studded with pustules.
PUSTULAR PSORIASIS: CLINICAL FEATURES
Pustular and erythrodermic psoriasis are less stable, more severe for the patient and more difficult to treat than guttate and plaque psoriasis. Pustular psoriasis is subdivided into two categories: generalized and local. Generalized pustular psoriasis is usually seen in middle- aged persons. 12 Males and females are affected equally. There is abrupt onset of widespread fiery erythema that may eventuate in erythroderma, sheets of pustulation, and scarlatiniform desquamation, accompanied by fe-
From the Dermatopathology Section, Department of Dermatol- ogy, New York University Medical Center, New York, NY
E.M.A. supported by the Holtzman Fellowship. Address reprint requests to Emily M. Altman, MD, New York
University Medical Center, 530 First Ave, Suite 7J, New York, NY 10016.
Copyright �9 1999 by W.B. Saunders Company 1085-5629/99/1801-0007510.00/0
Seminars In Cutaneous Medicine and Surgery, Vol 18, No I (March), 1999: pp 25-35 25

26 ALTMAN AND KAMINO
ver, malaise, leukocytosis, and an elevated erythrocyte sedimentation rate. Sterile pustules, 2 to 3 mm in diameter are disseminated over the trunk and the extremities, including the nail beds, palms, and soles, as well as in the oral and genital mucosa. Pustules may be asymptomatic or associated with burning and may coalesce to form lakes of pus 1 to 2 cm in diameter. The disease characteristically occurs in waves of fever and pustules. Typical extensive psoriasis usually precedes the acute pnstular flare for several years. The factors implicated in the development of pustular psoriasis include excessive topical medications, infections, stress, and the discontinuation of systemic corticosteroids. Impetigo herpetiformis most likely represents general- ized pustular psoriasis precipitated by pregnancy, al- though some authors classify it as a separate and distinct disorder. 13 It is a superficial sterile pustular eruption on an erythematons base, accompanied by fever, toxicity, hypocalcemia, and sometimes tetany. 14 The eruption begins in flexural areas, as pustules at the periphery of erythematons patches, then becomes gen- eralized. Impetigo herpetiformis usually remits after childbirth and is likely to recur in subsequent pregnan- cies. Pustules may also arise in previously existing psoriatic plaques during exacerbations of the disease. In palmar/plantar pustular psoriasis, sterile pustules develop in erythematous scaling plaques localized to the palms and soles. This form of psoriasis is character- istically indolent and resistant to treatment. In acroder- matitis continua, there is a chronic, localized area of scaling and sterile pustules that begins acrally on a finger or toe and remains localized to one or more digits for months or years. Systemic signs and symp- toms are absent in localized forms of pustular psoriasis.
ERYTHRODERMIC PSORIASIS: CLINICAL FEATURES
Erythrodermic psoriasis (exfoliative erythroderma) is an acute condition that usually results from a progressive worsening of psoriasis in an acute or chronic fashion and affects 75% or greater of body surface area, including the face, trunk, and extremi- tiesJ 5 It frequently arises in patients with unstable psoriasis vulgaris. Erythrodermic psoriasis is clinically difficult to differentiate from erythroderma of other etiologies, such as pityriasis rubra pilaris, Sezary syn- drome, severe atopic or allergic contact dermatitis, or drug eruption. The skin becomes diffusely and in- tensely red, warm, edematous and profoundly scaling to the point of generalized desquamation. There is usually associated pruritus. Constitutional symptoms, such as fever, chills, shortness of breath, and myalgias, are often present. Patients may have leukocytosis, electro- lyte imbalances, high output cardiac failure, abnormal liver function tests and Staphylococcus aureus bacteremia. The
etiological agents of erythroderma in psoriasis have been ascribed to intercurrent infections, harsh topical treat- ments, and withdrawal of systemic steroids.
CLUES TO THE HISTOPATHOLOGIC DIAGNOSIS OF PSORIASIS
Clinical diagnosis of fully developed plaque psoriasis rarely presents a problem. However, because the clini- cal presentation of psoriasis is so varied, often the definitive diagnosis depends on the histological exami- nation. Histological changes of psoriasis are as varied in different types and at different stages of psoriasis as are the clinical presentations. Recognition of the various histological presentations of psoriasis is important in assisting the clinician in the diagnosis and treatment of this common skin disorder. Certain clues are present in the histopathologic specimens of psoriasis that in combination make the differentiation of psoriasis from other psoriasiform disorders possible.
Clues to the Diagnosis of Psoriasis (1) Dilated and tortuous capillaries in the papillary
dermis, that spiral to near the undersurface of the epidermis. These capillaries are frequently congested with erythrocytes, which may arrange themselves in stacks (the rouleau formation). Dilated papillary der- mal vessels are present in all types and stages of psoriasis, and are still present in clinically resolved plaques of psoriasis after treatment.
(2) Papillary dermal edema. (3) Superficial perivascular, predominantly lympho-
cytic infiltrate. Neutrophils appear in the dermal papil- lary infiltrate as the lesion of psoriasis matures.
(4) Epidermal hyperplasia with elongated, thin, club-shaped rete ridges of even lengths (psoriasiform hyperplasia). In early psoriasis, the epidermal hyperpla- sia is slight or absent, and the rete ridges are of uneven lengths. The typical psoriasiform hyperplasia is present in mature plaques of psoriasis.
(5) Increased number of mitotic figures in basal and suprabasal locations.
(6) Markedly thinned suprapapillary plates. (7) Pallor of keratinocytes in the upper portions of
the epidermis. (8) Hypogranulosis: the hypogranulosis is focal in
early lesions of psoriasis, then becomes confluent with eventual disappearance of the granular layer in mature plaques.
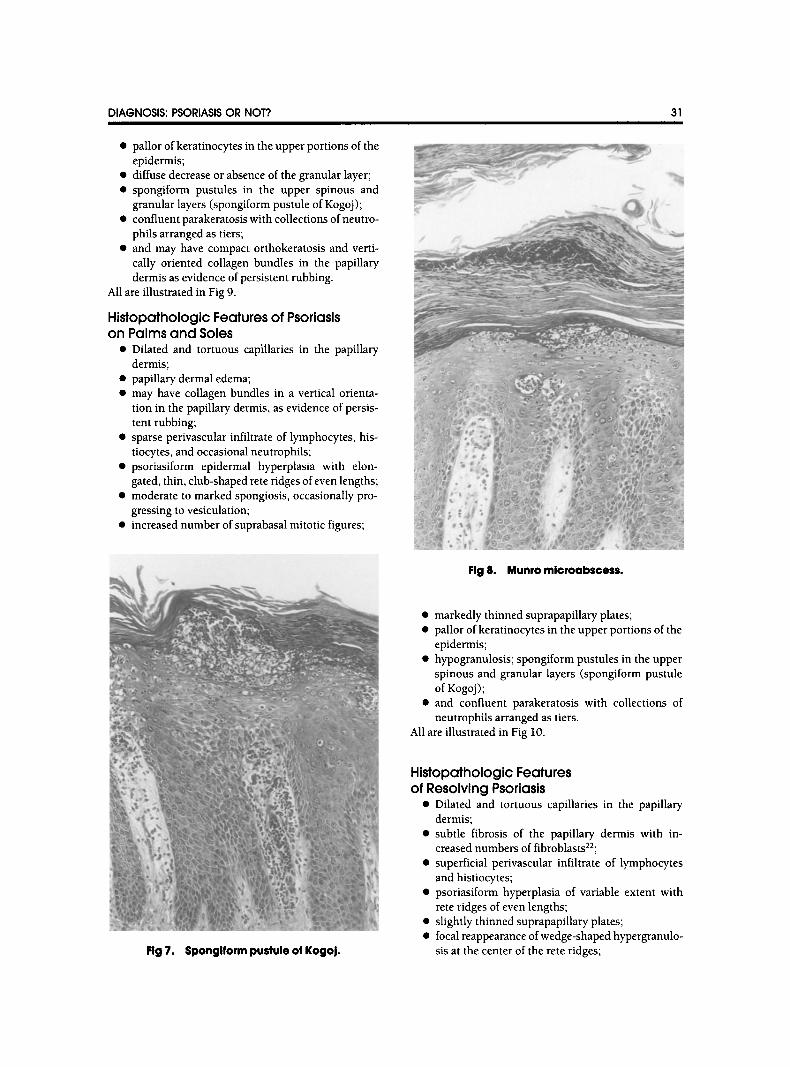
(9) Parakeratosis with neutrophils: in early and guttate/eruptive lesions of psoriasis, the parakeratosis is disposed in distinct mounds, which are staggered within an orthokeratotic cornified layer. Neutrophils accumulate at the summits of these mounds. In mature lesions, neutrophils are arranged in tiers within the confluent parakeratotic cornified layer. Munro microab-
DIAGNOSIS: PSORIASIS OR NOT? 27
scesses are collections of neutrophils within the para- keratotic cornified layer. The spongiform pustule of Kogoj is a collection of neutrophils in the upper spinous layer immediately beneath the parakeratotic scale. At the periphery of the spongiform pustule, neutrophils are present between compressed keratino- cytes. In pustular psoriasis, the accumulation of neutro- phils in a subcorneal location is so massive that it gives rise to macropustules. Of all histological features of psoriasis, only the spongiform pustule of Kogoj and the Munro microabscess are considered diagnostic but not pathognomonic of psoriasis, and the histological diag- nosis of psoriasis cannot be made with certainty in their absence. 16 However, spongiform pustules and neutro- phils in mounds of parakeratosis may be seen in dermatophytosis and candidiasis.
In different types and at different stages of psoriasis, the above histological manifestations are present in varying degrees, and often it is the combination of these manifestations that helps the pathologist arrive at the diagnosis of psoriasis.
PSORIASIS VULGARI$: HISTOPATHOLOGIC FEATURES
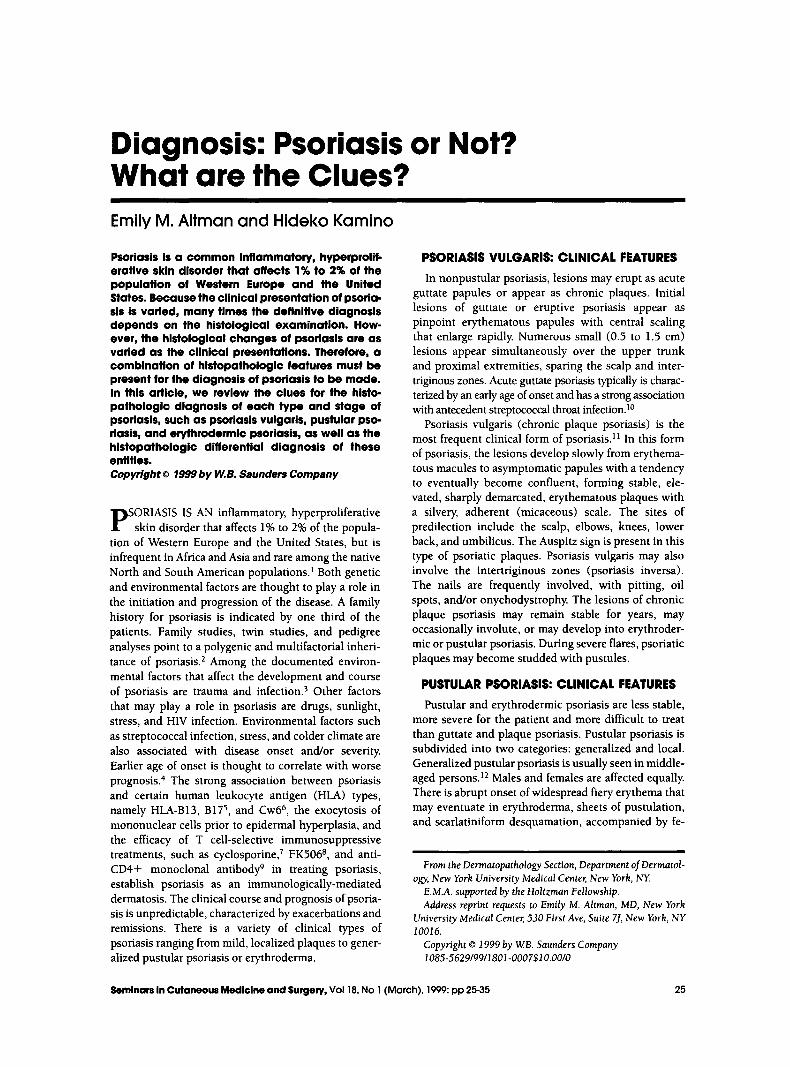
HJstopathologJc Features of Early Psoriasis Vulgarls
�9 Dilated and tortuous capillaries in the papillary dermislZ;
�9 papillary dermal edema; �9 superficial perivascular infiltrate of lymphocyteslS; �9 slight, irregular epidermal hyperplasia in the cen-
ter of the lesion; �9 exocytosis of lymphocytes into the epidermis; �9 spongiosis in the lower levels of the epidermis; �9 focal diminution and/or disappearance of the
granular layerlg; �9 small mounds of parakeratosis in the cornified
layer overlying the foci of hypogranulosis; �9 and neutrophils at the summits of the parakera-
totic foci (early Munro microabscesses).
All are illustrated in Fig 1.
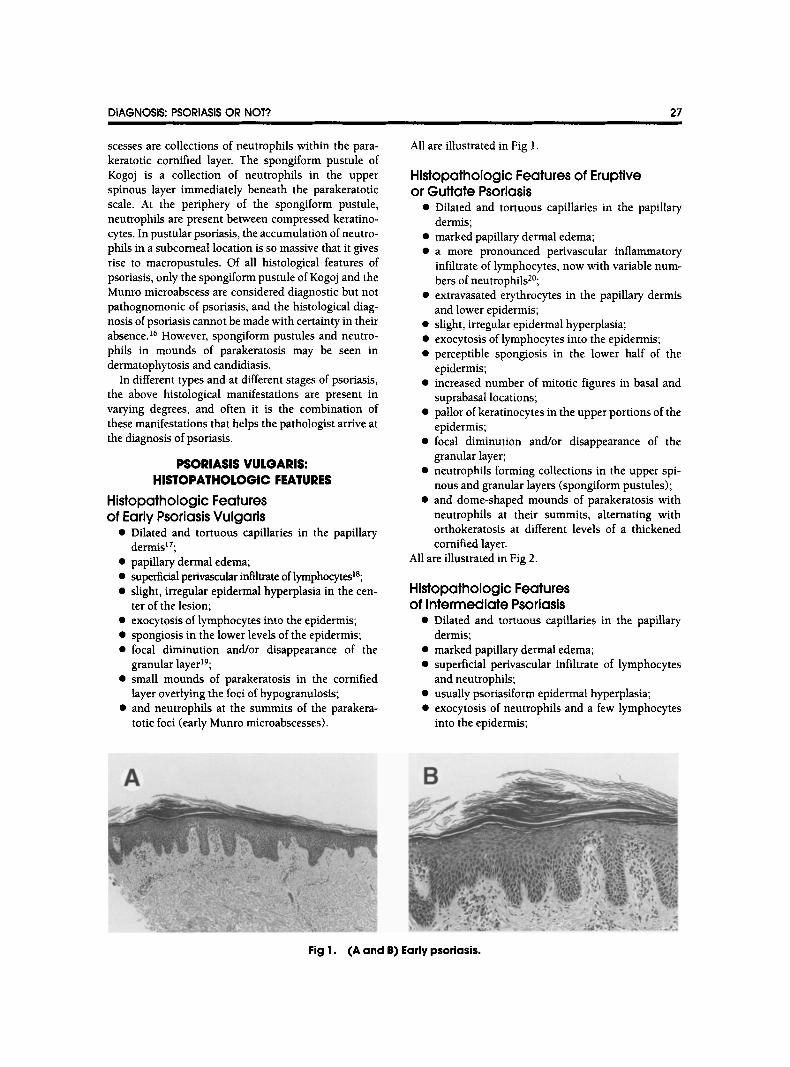
Histopathologic Features of Eruptive or Guttate Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 marked papillary dermal edema; �9 a more pronounced perivascular inflammatory
infiltrate of lymphocytes, now with variable num- bers of neutrophils2~
�9 extravasated erythrocytes in the papillary dermis and lower epidermis;
�9 slight, irregular epidermal hyperplasia; �9 exocytosis of lymphocytes into the epidermis; �9 perceptible spongiosis in the lower half of the
epidermis; �9 increased number of mitotic figures in basal and
suprabasal locations; �9 pallor of keratinocytes in the upper portions of the
epidermis; �9 focal diminution and/or disappearance of the
granular layer; �9 neutrophils forming collections in the upper spi-
nous and granular layers (spongiform pustules); �9 and dome-shaped mounds of parakeratosis with
neutrophils at their summits, alternating with orthokeratosis at different levels of a thickened cornified layer.
All are illustrated in Fig 2.
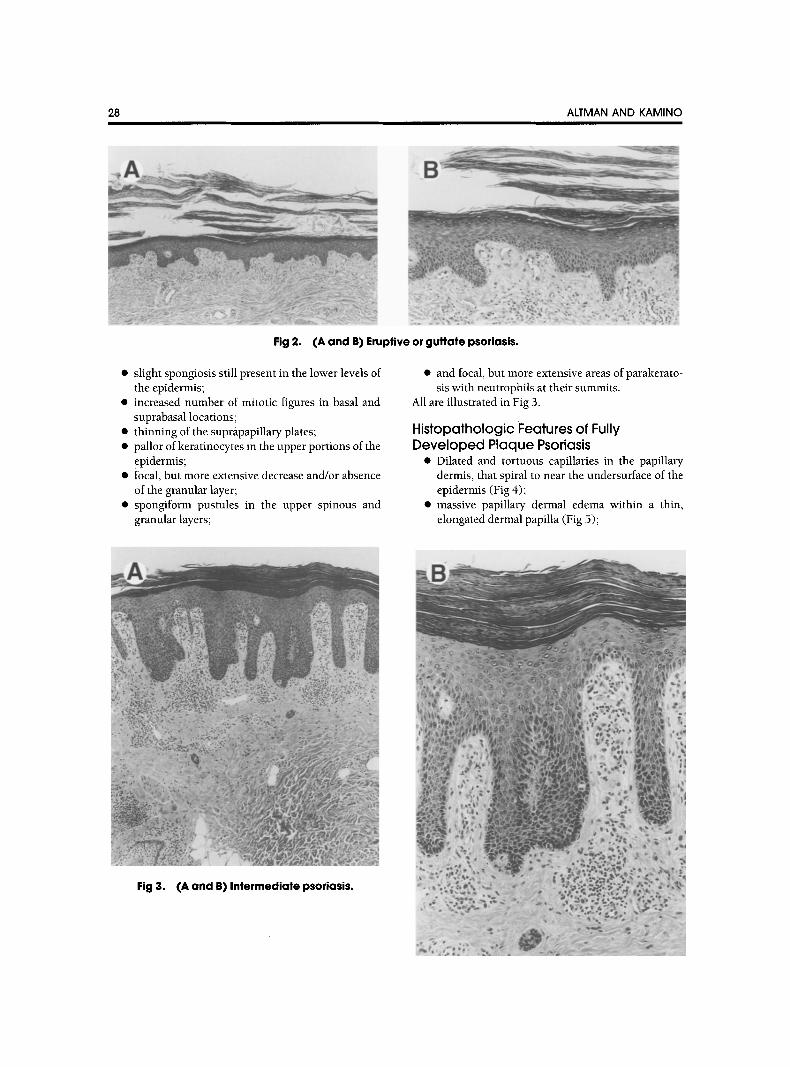
Hlstopathologic Features of Intermediate Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 marked papillary dermal edema; �9 superficial perivascular infiltrate of lymphocytes
and neutrophils; �9 usually psoriasiform epidermal hyperplasia; �9 exocytosis of neutrophils and a few lymphocytes
into the epidermis;
A
Fig I. (A and B) Early psoriasis.
28 ALTMAN AND KAMINO
Fig 2. (A and B) Eruptive or guttate psoriasis.
�9 slight spongiosis still present in the lower levels of the epidermis;
�9 increased number of mitotic figures in basal and suprabasal locations;
�9 thinning of the suprapapillary plates; �9 pallor of keratinocytes in the upper portions of the
epidermis; �9 focal, but more extensive decrease and/or absence
of the granular layer; �9 spongiform pustules in the upper spinous and
granular layers;
�9 and focal, but more extensive areas of parakerato- sis with neutrophils at their summits.
All are illustrated in Fig 3.
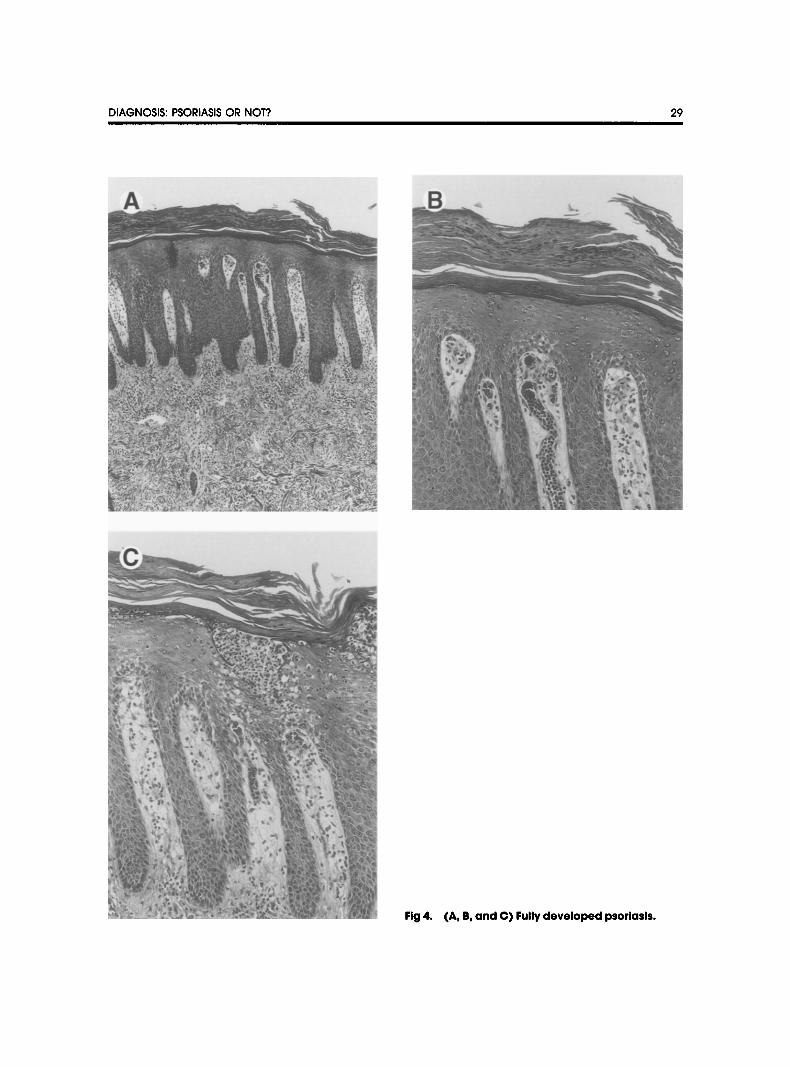
Histopathologic Features of Fully Developed Plaque Psoriasis
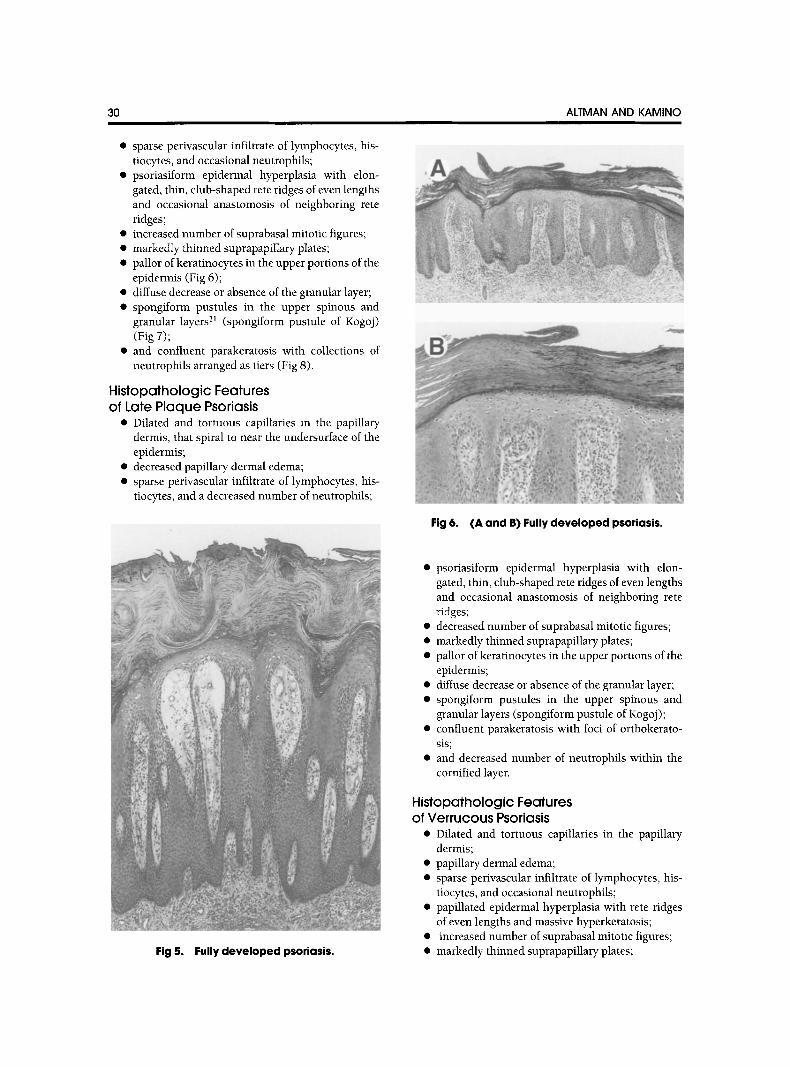
�9 Dilated and tortuous capillaries in the papillary dermis, that spiral to near the undersurface of the epidermis (Fig 4);
�9 massive papillary dermal edema within a thin, elongated dermal papilla (Fig 5);
Fig 3. (A and B) Intermediate psoriasis.
DIAGNOSIS: PSORIASIS OR NOT? 29
Jlt
Fig 4. (A, B, and C) Fully developed psoriasis.
30
�9 sparse perivascular infiltrate of lymphocytes, his- tiocytes, and occasional neutrophils;
�9 psoriasiform epidermal hyperplasia with elon- gated, thin, club-shaped rete ridges of even lengths and occasional anastomosis of neighboring rete ridges;
�9 increased number of suprabasal mitotic figures; �9 markedly thinned suprapapillary plates; �9 pallor of keratinocytes in the upper portions of the
epidermis (Fig 6); �9 diffuse decrease or absence of the granular layer; �9 spongiform pustules in the upper spinous and
granular layers 21 (spongiform pustule of Kogoj) (Fig 7);
�9 and confluent parakeratosis with collections of neutrophils arranged as tiers (Fig 8).
Histopathologic Features of Late Plaque Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis, that spiral to near the undersurface of the epidermis;
�9 decreased papillary dermal edema; �9 sparse perivascular infiltrate of lymphocytes, his-
tiocytes, and a decreased number of neutrophils;
i,!fiiii!i~ii!ii~ii!i!ii!ii~iiiii~ii!
Fig 5. Fully developed psoriasis.
ALTMAN AND KAMINO
�9 i ~ J
Fig 6. (A and B) Fully developed psoriasis.
�9 psoriasiform epidermal hyperplasia with elon- gated, thin, club-shaped rete ridges of even lengths and occasional anastomosis of neighboring rete ridges;
�9 decreased number of suprabasal mitotic figures; �9 markedly thinned suprapapillary plates; �9 pallor of keratinocytes in the upper portions of the
epidermis; �9 diffuse decrease or absence of the granular layer; �9 spongiform pustules in the upper spinous and
granular layers (spongiform pustule of Kogoj); �9 confluent parakeratosis with loci of orthokerato-
sis; �9 and decreased number of neutrophils within the
cornified layer.
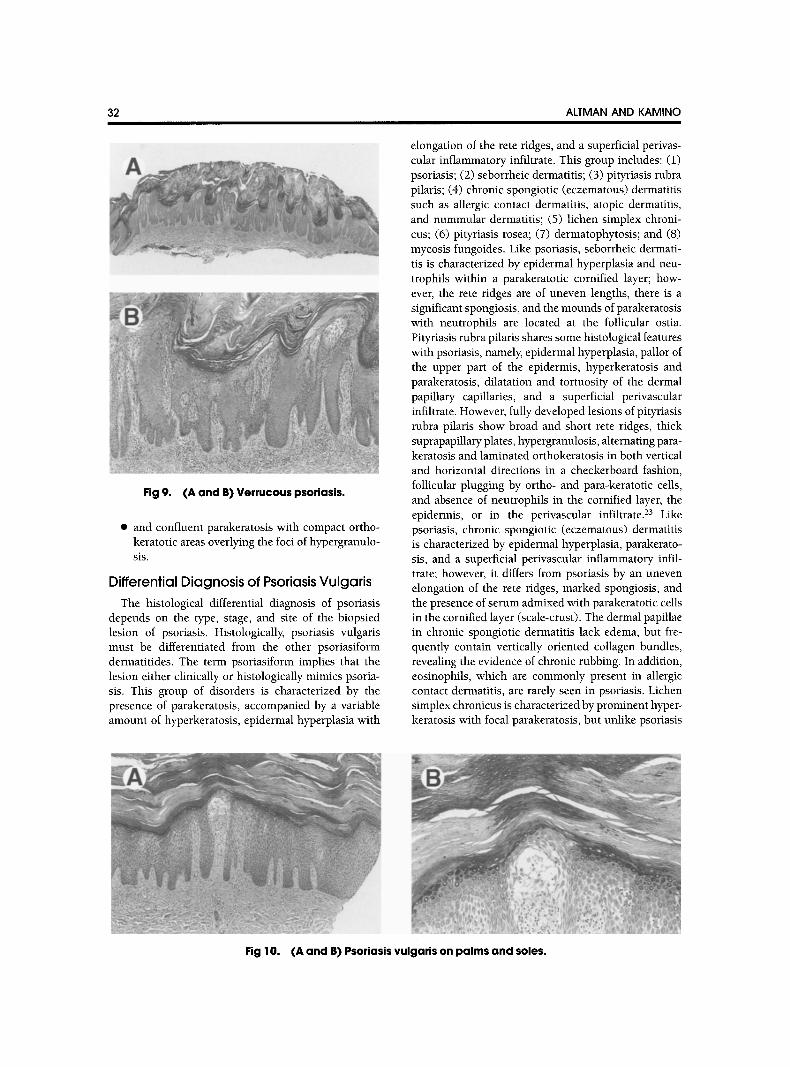
Histopathologic Features of Verrucous Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 papillary dermal edema; �9 sparse perivascular infiltrate of lymphocytes, his-
tiocytes, and occasional neutrophils; �9 papillated epidermal hyperplasia with rete ridges
of even lengths and massive hyperkeratosis; �9 increased number of suprabasal mitotic figures; �9 markedly thinned suprapapillary plates;
DIAGNOSIS: PSORIASIS OR NOT? 31
�9 pallor of keratinocytes in the upper portions of the epidermis;
�9 diffuse decrease or absence of the granular layer; �9 spongiform pustules in the upper spinous and
granular layers (spongiform pustule of Kogoj); �9 confluent parakeratosis with collections ofneutro-
phils arranged as tiers; �9 and may have compact orthokeratosis and verti-
cally oriented collagen bundles in the papillary dermis as evidence of persistent rubbing.
All are illustrated in Fig 9.
Histopathologic Features of Psoriasis on Palms and Soles
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 papillary dermal edema; �9 may have collagen bundles in a vertical orienta-
tion in the papillary dermis, as evidence of persis- tent rubbing;
�9 sparse perivascular infiltrate of lymphocytes, his- tiocytes, and occasional neutrophils;
�9 psoriasiform epidermal hyperplasia with elon- gated, thin, club-shaped rete ridges of even lengths;
�9 moderate to marked spongiosis, occasionally pro- gressing to vesiculation;
�9 increased number of suprabasal mitotic figures;
F *
q
k : ,%
\ , r
" ' - 1 .
Fig 8. Munro mlcroabscess.
�9 markedly thinned suprapapillary plates; �9 pallor of keratinocytes in the upper portions of the
epidermis; �9 hypogranulosis; spongiform pustules in the upper
spinous and granular layers (spongiform pustule of Kogoj);
�9 and confluent parakeratosis with collections of neutrophils arranged as tiers.
All are illustrated in Fig 10.
Fig 7. Spongiform pustule of Kogoj.
Histopathologic Features of Resolving Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 subtle fibrosis of the papillary dermis with in- creased numbers of fibroblasts22;
�9 superficial perivascular infiltrate of lymphocytes and histiocytes;
�9 psoriasiform hyperplasia of variable extent with rete ridges of even lengths;
�9 slightly thinned suprapapillary plates; �9 focal reappearance of wedge-shaped hypergranulo-
sis at the center of the rete ridges;
32 ALTMAN AND KAMINO
Fig 9. (A and B) Verrucous psoriasis.
�9 and confluent parakeratosis with compact ortho- keratotic areas overlying the loci of hypergranulo- sis.
Differential Diagnosis of Psoriasis Vulgaris The histological differential diagnosis of psoriasis
depends on the type, stage, and site of the biopsied lesion of psoriasis. Histologically, psoriasis vulgaris must be differentiated from the other psoriasiform dermatitides. The term psoriasiform implies that the lesion either clinically or histologically mimics psoria- sis. This group of disorders is characterized by the presence of parakeratosis, accompanied by a variable amount of hyperkeratosis, epidermal hyperplasia with
elongation of the rete ridges, and a superficial perivas- cular inflammatory infiltrate. This group includes: (1) psoriasis; (2) seborrheic dermatitis; (3) pityriasis rubra pilaris; (4) chronic spongiotic (eczematous) dermatitis such as allergic contact dermatitis, atopic dermatitis, and nummular dermatitis; (5) lichen simplex chroni- cus; (6) pityriasis rosea; (7) dermatophytosis; and (8) mycosis fungoides. Like psoriasis, seborrheic dermati- tis is characterized by epidermal hyperplasia and neu- trophils within a parakeratotic cornified layer; how- ever, the fete ridges are of uneven lengths, there is a significant spongiosis, and the mounds of parakeratosis with neutrophils are located at the follicular ostia. Pityriasis rubra pilaris shares some histological features with psoriasis, namely, epidermal hyperplasia, pallor of the upper part of the epidermis, hyperkeratosis and parakeratosis, dilatation and tortuosity of the dermal papillary capillaries, and a superficial perivascular infiltrate. However, fully developed lesions of pityriasis rubra pilaris show broad and short rete ridges, thick suprapapillary plates, hypergranulosis, alternating para- keratosis and laminated orthokeratosis in both vertical and horizontal directions in a checkerboard fashion, follicular plugging by ortho- and para-keratotic cells, and absence of neutrophils in the cornified layer, the epidermis, or in the perivascular infiltrate. 23 Like psoriasis, chronic spongiotic (eczematous) dermatitis is characterized by epidermal hyperplasia, parakerato- sis, and a superficial perivascular inflammatory infil- trate; however, it differs from psoriasis by an uneven elongation of the rete ridges, marked spongiosis, and the presence of serum admixed with parakeratotic cells in the cornified layer (scale-crust). The dermal papillae in chronic spongiotic dermatitis lack edema, but fre- quently contain vertically oriented collagen bundles, revealing the evidence of chronic rubbing. In addition, eosinophils, which are commonly present in allergic contact dermatitis, are rarely seen in psoriasis. Lichen simplex chronicus is characterized by prominent hyper- keratosis with focal parakeratosis, but unlike psoriasis
Fig 10. (A and B) Psoriasis vulgaris on palms and soles.
DIAGNOSIS: PSORIASIS OR NOT? 33
shows irregular epidermal hyperplasia with prominent hypergranulosis, vertically oriented collagen bundles in the papillary dermis, and a moderate, predominantly perivascular infiltrate of lymphocytes, histiocytes, and occasional eosinophils. 24 Pityriasis rosea, which is primarily in the differential diagnosis of early psoriasis vulgaris, shows a superficial perivascular lymphohistio- cytic infiltrate with occasional eosinophils. Lympho- cytes extend into a slightly and irregularly hyperplastic epidermis, where there is spongiosis, focally decreased or absent granular layer and mounds of parakeratosis with plasma. 25 There is extravasation of erythrocytes into a slightly edematous papillary dermis with exten- sion into the epidermis. In addition to the previously mentioned features, the herald patch may show a more psoriasiform epidermal hyperplasia, greater papillary dermal edema, and a deeper and denser perivascular inflammatory infiltrate. 26 Dermatophyte infection may histologically simulate all types and stages of psoriasis. Therefore, a special stain for fungal organisms should be performed in all cases of suspected psoriasis. Derma- tophyte infection usually shows a sparse to moderate lymphohistiocytic infiltrate, occasionally with neutro- phils around dilated vessels of the superficial plexus, a slight psoriasiform epidermal hyperplasia, orthokerato- sis with focal parakeratosis, and the presence of fungal hyphae "sandwiched" at the interface between normal and altered (compact orthokeratosis or parakeratosis) portions of the cornified layer. 2~ Neutrophils may be
A ~
present in the altered areas of the cornified layer, within the viable epidermis, and/or in the papillary dermal perivascular infiltrate. The fungal organisms are most easily detectable near the collections of neutrophils in the ortho- rather than para-keratotic areas. 2s Intraepi- dermal pustules and vesicles may also be seen in the histological picture of dermatophytosis. Mycosis fungoi- des may also show a psoriasiform epidermal hyperpla- sia, parakeratosis in the cornified layer, and a superfi- cial perivascular lymphocytic infiltrate. 29 However, the lymphocytes in the perivascular and band-like infiltrate and particularly those that extend into the epidermis show cytologic atypia with enlarged, hyperchromatic nuclei with irregular contors. In the papillary dermis there is fibroplasia, with collagen bundles arranged parallel to the overlying epidermis.
PUSTULAR PSORIASIS: HISTOPATHOLOGIC FEATURES
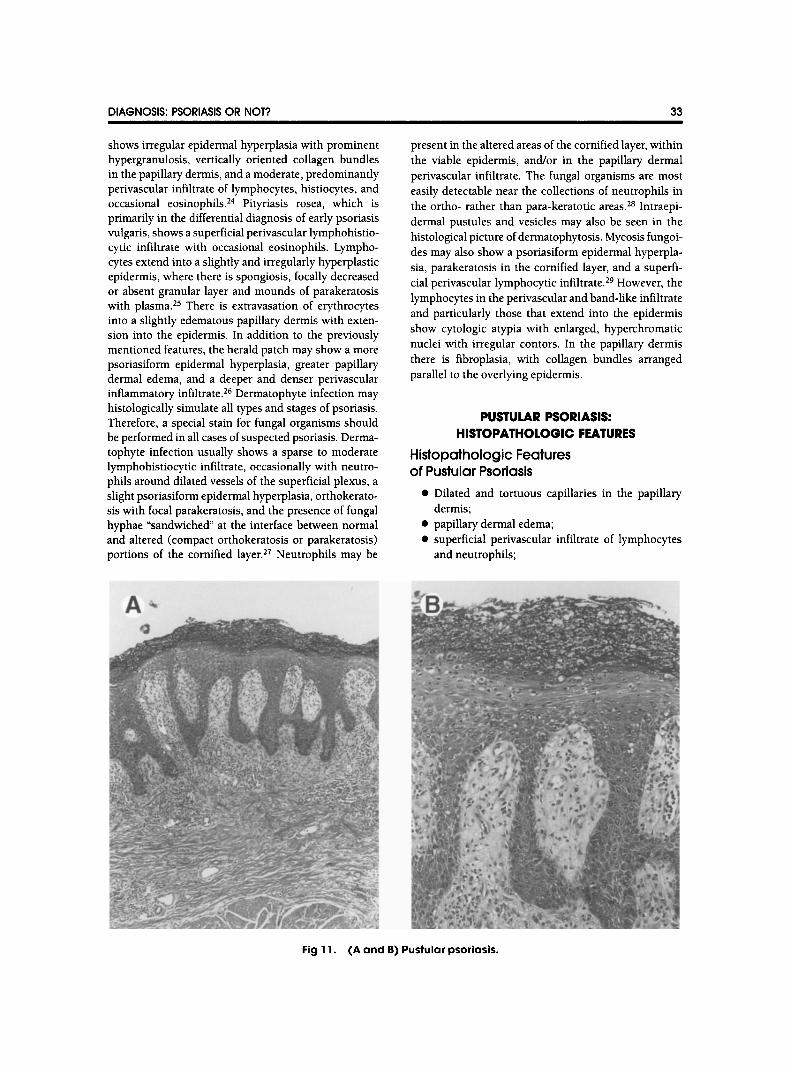
Histopathologic Features of Pustular Psoriasis
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 papillary dermal edema; �9 superficial perivascular infiltrate of lymphocytes
and neutrophils;
Fig 11. (A and B) Pustular psoriasis.
34 I
�9 slight, irregular epidermal hyperplasia--psoriasi- form hyperplasia present only in long-standing lesions;
�9 perceptible spongiosis, especially in acral sites; �9 increased number of mitotic figures in basal and
suprabasal locations; �9 and massive aggregation of neutrophils within a
lattice of degenerated keratinocytes in the upper spinous and subcorneal locations and formation of intraepidermal macropustules.
All are illustrated in Fig 11. Early lesions of pustular psoriasis on acral skin may
show spongiosis and a mononuclear cell infiltrate in the lower epidermis. 3~ This may be followed by the formation of an intraepidermal vesicle containing mostly mononuclear cells: Subsequently, as the vesicle ex- pands, neutrophils may be found scattered among keratinocytes at the periphery of the vesicle. Eventually neutrophils massively invade the cavity of the vesicle, forming a pustule.
Differential Diagnosis of Pustular Psoriasis In the differential diagnosis of pustular psoriasis are
the disorders that are characterized by intraepidermal and subcorneal pustules. The Kogoj spongiform pus- tule is highly characteristic of the psoriasis group of diseases, including pustular psoriasis, impetigo herpeti- formis, acrodermatitis continua, geographic tongue, and Reiter's syndrome. However, spongiform pustules may also be seen in dermatophytosis, candidiasis, bacterial impetigo, pustular drug eruptions, and other pustular conditions such as early lesions of pyoderma gangrenosum and halogenodermas.
ERYTHRODERMIC PSORIASIS: HISTOPATHOLOGIC FEATURES
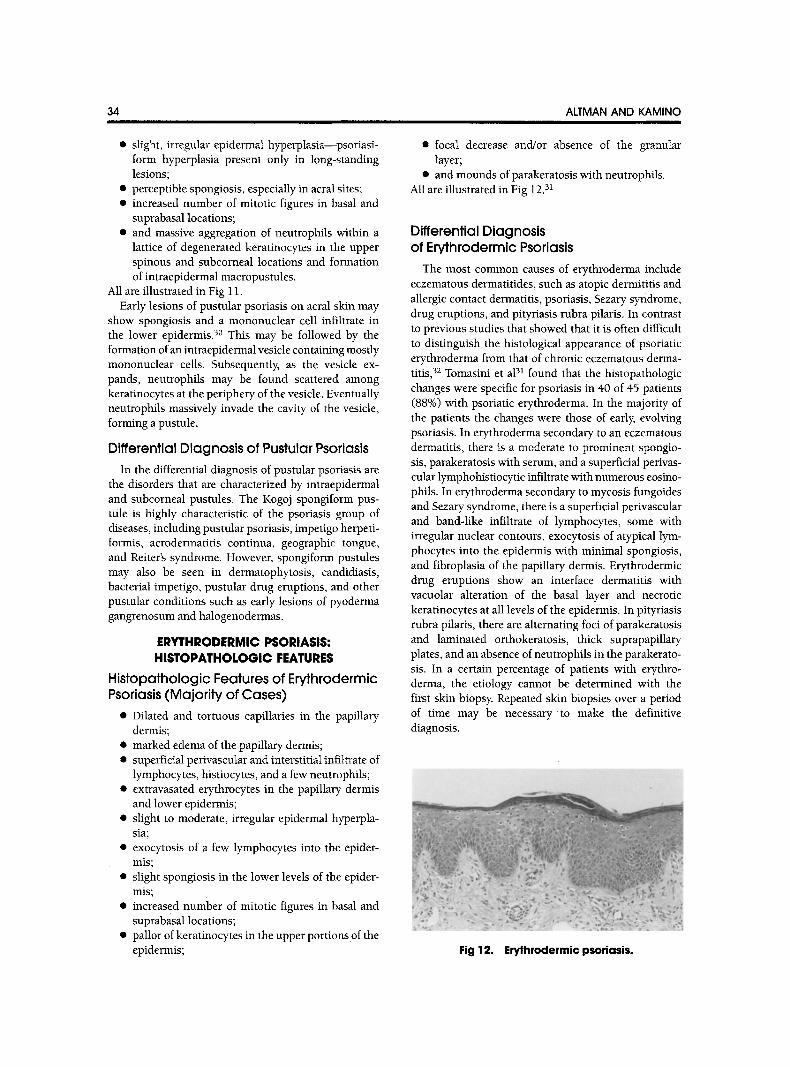
Histopathologic Features of Erythrodermic Psoriasis (Majority of Cases)
�9 Dilated and tortuous capillaries in the papillary dermis;
�9 marked edema of the papillary dermis; �9 superficial perivascular and interstitial infiltrate of
lymphocytes, histiocytes, and a few neutrophils; �9 extravasated erythrocytes in the papillary dermis
and lower epidermis; �9 slight to moderate, irregular epidermal hyperpla-
sia; �9 exocytosis of a few lymphocytes into the epider-
mis; �9 slight spongiosis in the lower levels of the epider-
mis; �9 increased number of mitotic figures in basal and
suprabasal locations; �9 pallor of keratinocytes in the upper portions of the
epidermis;
ALTMAN AND KAMINO
�9 focal decrease and/or absence of the granular layer;
�9 and mounds of parakeratosis with neutrophils. All are illustrated in Fig 12. 31
Differential Diagnosis of Erythrodermic Psoriasis
The most common causes of erythroderma include eczematous dermatitides, such as atopic dermititis and allergic contact dermatitis, psoriasis, Sezary syndrome, drug eruptions, and pityriasis rubra pilaris. In contrast to previous studies that showed that it is often difficult to distinguish the histological appearance of psoriatic erythroderma from that of chronic eczematous derma- titis, 32 Tomasini et a131 found that the histopathologic changes were specific for psoriasis in 40 of 45 patients (88%) with psoriatic erythroderma. In the majority of the patients the changes were those of early, evolving psoriasis. In erythroderma secondary to an eczematous dermatitis, there is a moderate to prominent spongio- sis, parakeratosis with serum, and a superficial perivas- cular lymphohistiocytic infiltrate with numerous eosino- phils. In erythroderma secondary to mycosis fungoides and Sezary syndrome, there is a superficial perivascular and band-like infiltrate of lymphocytes, some with irregular nuclear contours, exocytosis of atypical lym- phocytes into the epidermis with minimal spongiosis, and fibroplasia of the papillary dermis. Erythrodermic drug eruptions show an interface dermatitis with vacuolar alteration of the basal layer and necrotic keratinocytes at all levels of the epidermis. In pityriasis rubra pilaris, there are alternating foci of parakeratosis and laminated orthokeratosis, thick suprapapillary plates, and an absence of neutrophils in the parakerato- sis. In a certain percentage of patients with erythro- derma, the etiology cannot be determined with the first skin biopsy. Repeated skin biopsies over a period of time may be necessary to make the definitive diagnosis.
Fig 12. Erythrodermic psoriasis.
DIAGNOSIS: PSORIASIS OR NOT? 35
REFERENCES
1. Farber EM, Nall L: Epidemiology: Natural history and genetics, in Roenigk HH, Maibach HI, (eds): Psoriasis (ed 2) New York, NY, Marcel Dekker, Inc, 1991, pp 209-258
2. Henseler T: The genetics of psoriasis. J Am Acad Dermato137:S1-$11, 1997
3. Tagami H: Triggering factors. Clin Dermato115:677-685, 1997
4. Church R: The prospect of psoriasis. Br J Dermatol 70:139-145, 1958
5. Gottlieb AB, Krueger JG: HLA region genes and immune activation in the pathogenesis of psoriasis. Arch Dermatol 126:1083-1086, 1990
6. Tiilikainen A, Lassus A, Karvonen J, et al: Psoriasis and HLA-Cw6. BrJ Dermatol 102:179-180, 1980
7. Ellis CN, Gorsulowsky DC, Hamilton TA, et al: Cyclos- porine improves psoriasis in a double-blind study. JAMA 256:3110-3116, 1986
8. The European FK 506 muhicentre psoriasis study group. Systemic tacrolimus (FK 506) is effective for the treatment of psoriasis in a double-blind, placebo-controlled study. Arch Dermatol 132:419-423, 1996
9. Nicholas J-F, Chamchick N, Thivolet J, et al: CD4 antibody treatment of severe psoriasis (letter). Lancet 338: 321, 1991
10. Telfer NR, Chalmers RJG, Whale K, et al: The role of streptococcal infection in the initiation of guttate psoriasis. Arch Dermato1128:39-42, 1992
11. Christophers E, Sterry W: Psoriasis, in Fitzpatrick TB, Eisen AZ, Wolff K, et al (eds): Dermatology in General Medicine (ed 4). New York, NY, McGraw Hill, Inc, 1993, pp 489-514
12. Muller SA, Kitzmiller KW: Generalized pustular psoria- sis: Report of two cases. Acta Dermato-Venereologica 42:504- 512, 1962
13. Pierard GE, Pierard-Franchimont C, de la Brassinne M: Impetigo herpetiformis and pustular psoriasis during preg- nancy. AmJ Dermatopathol 5:215-220, 1983
14. Pregnancy and the menstrual cycle, in Braverman IM (ed): Skin Signs of Systemic Diseases (ed 3). Philadelphia, PA, Saunders, 1998, p 541
15. PrystowskyJH, Cohen PR: Pustular and erythrodermic psoriasis. Derm Clin 13:757-770, 1995
16. Toussaint S, Kamino H: Noninfectious erythematous, papular, and squamous diseases, in Elder D, Elenitsas R, Jaworsky C, et al (eds): Lever's Histopathology of the Skin (ed 8). Philadelphia, PA, Lippincott-Raven, 1997, pp 151-184
17. Telner P, Fekete Z: The capillary responses in psoriatic skin. J Invest Dermato136:225-230, 1961
18. Pinkus H, Mehregan AH: The primary histologic lesion of seborrheic dermatitis and psoriasis. J Invest Dermatol 46:109-116, 1966
19. Christophers E, Parzefall R, Braun-Falco O: Initial events in psoriasis: Quantitative assessment. Br J Dermatol 89:327-334, 1973
20. Brody I: Dermal and epidermal involvement in the evolution of acute eruptive guttate psoriasis vulgaris. J Invest Dermatol 82:465-470, 1984
21. Gordon M, Johnson WC: Histopathology and histo- chemistry of psoriasis. I. The active lesion and clinically normal skin. Arch Dermato195:402-407, 1967
22. Ragaz A, Ackerman AB: Evolution, maturation, and regression of lesions of psoriasis. Am J Dermatopathol 1:199- 214, 1979
23. Soeprono FF: Histologic criteria for the diagnosis of pityriasis rubra pilaris. Am J Dermatopathol 8:277-283, 1986
24. Barr RJ, Young Jr EM: Psoriasiform and related papulo- squamous disorders. J Cutan Pathol 12:412-425, 1985
25. Panizzon R, Bloch PH: Histopathology of pityriasis rosea of Gibert. Qualitative and quantitative light-microscopic study of 62 biopsies of 40 patients. Dermatologica 165:551- 558, 1982
26. Bonafe JL, Icart J, Perpere M, et al: Etude histo- pathologique, uhrastructurale, immunologique et virologique du pityriasis rosea de Gibert. Ann Dermatol Venereo1109:189, 1982
27. Gottlieb GJ, Ackerman AB: The "sandwich sign" of dermatophytosis. AmJ Dermatopathol 8:347-350, 1986
28. Ackerman AB: Subtle clues to diagnosis by conven- tional microscopy. Neutrophils within the cornified layer as clues to infection by superficial fungi. Am J Dermatopathol 1:69-75, 1979
29. Shapiro PE, Pinto FJ: The histologic spectrum of mycosis fungoides/Sezary syndrome (cutaneous T-cell lym- phoma). A review of 222 biopsies, including newly described patterns and the earliest pathologic changes. Am J Surg Pathol 18:645-667, 1994
30. Uehara M, Ofuji S: The morphogenesis of pustulosis palmaris et plantaris. Arch Dermatol 109:518, 1974
31. Tomasini C, Aloi F, Solaroli C, et al: Psoriatic erythro- derma: A histopathologic study of forty-five patients. Derma- tology 194:102-106, 1997
32. Abrahams I, McCarthy JT, Sanders ST: 101 cases of exfoliative dermatitis. Arch Dermatol 87:96, 1963





























