Embed Size (px)
Citation preview

The Journal of Arthroplasty Vol. 21 No. 2 2006
Deep Vein Thrombosis Prevention in
Joint Arthroplasties
Continuous Enhanced Circulation Therapy vsLow Molecular Weight Heparin
Yael Gelfer, MD,*§ Hovav Tavor, MD,*§ Amir Oron, MD,*§ Amir Peer, MD,y§Nahum Halperin, MD,*§ and Dror Robinson, MD, PhDz§
From the *DepartmZeriffin, Israel, yDepMedical Center, ZerifMedical Center, CampSackler Medical Schoo
Submitted FebruNo benefits or fuReprint requests
Orthopedics, RabinTikwa, Israel.
n 2006 Elsevier0883-5403/06/19doi:10.1016/j.art
Abstract: Deep vein thrombosis prevention efficacy using a new, miniature, mobile,
battery-operated pneumatic system (continuous enhanced circulation therapy
[CECT] system) combined with low-dose aspirin was compared to enoxaparin.
One hundred twenty-one patients who underwent total hip or knee arthroplasty
were prospectively randomized into 2 groups. The study group was treated by the
CECT system starting immediately after the induction of anesthesia. Postoperatively,
a daily 100-mg aspirin tablet was added. The control group received 40 mg of
enoxaparin per day. Bilateral venography was performed at the fifth to eight
postoperative day. In the CECT group, as compared to the enoxaparin group, there
was a significantly lower overall rate of DVT and proximal DVT. Safety profiles were
similar in both groups. The combination of the CECT device with low-dose aspirin is
more effective than enoxaparin in preventing deep-vein thrombosis after lower limb
arthroplasties. Key words: deep vein thrombosis, low molecular weight heparin,
arthroplasty, total knee arthroplasty, total hip arthroplasty, aspirin, continuous
enhanced circulation therapy, intermittent pneumatic compression, compliance.
n 2006 Elsevier Inc. All rights reserved.
The ultimate goal of any prophylactic regimen in
joint arthroplasty surgery is to prevent the forma-
tion of DVT and postphlebitic syndrome, as well as
the occurrence of pulmonary emboli. Most authors
recommend routine prophylaxis for thromboem-
bolism prevention after total joint arthroplasty
[1,2]. The rationale is based on the high prevalence
206
ent of Orthopedics, Assaf Harofe Medical Center,artment of Invasive Radiology, Assaf Harofefin, Israel, zDepartment of Orthopedics, Rabinus Golda, Israel, and §Department of Orthopedics,l, Tel Aviv University, Tel Aviv, Israel.ary 23, 2004; accepted April 19, 2005.nds were received in support of this study.: Dror Robinson, MD, PhD, Department of
Medical Center, Campus Golda, Petah
Inc. All rights reserved.06-0004$32.00/0
h.2005.04.031
of venous thromboembolism among hospitalized
patients, the clinically silent nature of the disease in
most of the patients, and the potential morbidity
and mortality associated with thrombi. Both DVT
and pulmonary embolus (PE) produce few specific
symptoms, and clinical diagnosis is unreliable [2].
Prophylaxis can be either mechanical or chemical.
Although chemical prophylaxis, particularly with
use of low molecular weight heparin, effectively
reduces the frequency of DVT as diagnosed with
venogram after total joint arthroplasty, many
orthopedic surgeons are concerned about the
potential for soft-tissue side effects and hemorrhag-
ic complications, especially during the operation
itself and immediately after, and therefore, are
attracted to mechanical prophylactic methods [3].
Total hip arthroplasty (THA) and total knee arthro-
plasty (TKA) are associated with venous stasis,
which is an important etiologic factor in the

1 Patients were contributed by either Dr Halperin or Dr
Robinson. No benefits were received or will be received by the
authors in material or in kind in conjunction with this study.
DVT Prevention in Joint Arthroplasties: CECT vs LMWH ! Gelfer et al 207
development of DVT. The operative maneuvers
that are needed to implant prosthetic components
obstruct venous blood flow [4]; the patient is
relatively immobile for several days after the
operation, and the physiology of the venous system
appears to be altered for some weeks postopera-
tively [5]. Intermittent pneumatic compression
(IPC) devices cyclically inflate air-filled cuffs,
leading to an increase venous blood flow velocity.
Increased flow velocity overcomes venous stasis,
the primary DVT formation mechanism. Increased
fibrinolysis is the secondary mechanism by which
IPC decreases DVT formation [6-12]. However, the
major disadvantage of the currently available IPC
devices is their size, weight, and requirement for
continuous attachment to an external power
source. Poor compliance with proper use of the
current stationary devices by both patients and
nursing staff significantly limits their efficacy [13].
A recently developed device (WizAir continuous
enhanced circulation therapy [CECT] System, MCS
Ltd, Or-Akiva, Israel) is a miniature, battery
operated, and fully mobile pneumatic compression
system, thus, simplifying treatment and increasing
patient’s compliance [14,15]. Even though small,
this device was shown to provide state of the art
hemodynamic profile [16]. The high compliance
achieved with this device encouraged us to try a
new treatment protocol for DVT prophylaxis after
orthopedic surgery using a combination of me-
chanical prophylaxis and low-dose aspirin, that is, a
combination of a theoretically very potent me-
chanical device, with low-cost, low-risk, moderate-
ly effective chemical prophylaxis. The rationale for
the combination of treatment agents is the multi-
factorial nature of DVT. It has been more than a
century since Virchow [17] described his triad. The
proposed treatment affects both the stasis arm and
the antiaggregation arm of the triad. The CECT
system affects DVT rates by accelerating blood flow
and venous peak flow velocity. Aspirin’s main
effect on clot formation is achieved through
inhibition of platelet function. The combined
regimen of CECT and aspirin allows minimal drug
dosage, thus, decreasing the risk of gastrointestinal
side effects.
The aim of the current study was to compare the
frequency of thromboembolism after THA and TKA
in patients who were randomized to be managed
either with the CECT-based protocol (with aspirin)
or low molecular weight heparin, on the basis of
the Marder’s classification of DVT [18]. To the best
of our knowledge, a prospective randomized trial
that compared the combination of a pneumatic
device and low-dose aspirin with low molecular
weight heparin, on the basis of venogram-detected
DVT, was not previously published.
Materials and Methods
Study Design
This was a prospective randomized study con-
ducted at a single medical center. Blinding was not
considered feasible, because even if placebo injec-
tions were used, the pump action could not be
masked. Instead, comparison of 2 clinically applica-
ble DVT prevention protocols was performed. Both
TKA and THA were included in the study. Though
the incidence of DVT differs between these groups,
it was estimated that because of the randomization
process, similar numbers of each procedure would
be treated according to either protocol.
Patient Selection
All patients who were scheduled for unilateral
primary THA or TKA between April 2001 and
September 2002 at Assaf Harofe Medical Center
were considered for inclusion in the trial1. All
women included were postmenopausal. Exclusion
criteria were refusal of consent, long-term antico-
agulant therapy, treatment with antiaggregant
medication for the last 10 days, known hypersen-
sitivity to contrast medium or aspirin or low
molecular weight heparin, previously diagnosed
venous thromboembolism (VTE), concurrent
thrombosis process, and enrollment in another
clinical trial. One hundred forty-two patients were
screened. Six patients were dropped after screen-
ing. One hundred thirty-six patients were random-
ized to the study. Fifteen were dropped after
randomization (7 in the CECT group and 8 in the
enoxaparin group). All 15 dropouts were classified
as missing completely at random. One hundred
twenty-one patients completed the study—60 in
the enoxaparin group and 61 in the CECT group.
Randomization
Randomization was performed before the oper-
ation with the use of sealed envelopes containing a
slip indicating the allocation, which had been
derived from a computer-generated sequence.
Patients either received the enoxaparin or the
CECT-based protocol.

208 The Journal of Arthroplasty Vol. 21 No. 2 February 2006
Treatment Protocols
All patients were admitted either on the evening
before surgery or on the day of surgery. Because
patients were mobile (no fractures were included in
this series), pharmacological DVT prophylaxis was
not administered before surgery.
Patients randomized into the enoxaparin group
received 40 mg of enoxaparin (Clexane, Aventis
Pharma, Netanya, Israel) administered subcutane-
ously into the abdominal wall once daily. The first
injection was received within 12 hours (range, 6-12
hours) after the operation and then every 24 hours.
In the CECT-based protocol, the mechanical
prophylaxis was started before surgery, immediate-
ly after the induction of anesthesia. Sequential
pneumatic calf sleeves were used in candidates for
THA. In the case of TKA, the operated leg was fitted
with a foot sleeve for the operation time and then,
immediately after skin closure, switched to the calf
sleeve, as in the other leg. The patients, nurses, and
physiotherapists were advised to activate the pump
continuously, without any activity restrictions.
One hundred milligrams of aspirin was adminis-
tered to the CECT-based protocol patients within
12 hours (range, 8-12 hours) after the operation
and then every 24 hours.
The pneumatic device that was used in this study
(WizAir CECT System, MCS Ltd) is a new type of
device that is fully mobile and is designed to supply
CECT. The consol system of this device, weighing
only 690 g, is battery operated and can operate foot
sleeve, calf sleeve, thigh high sleeve, and any
desired combination of them on 1 or 2 legs.
Surgical Procedures
General anesthesia was used in most patients;
the operative approach was a transvastus approach
for TKA and anterolateral modified Hardinge
approach for THA. The THAs were all performed
with the patient in a lateral decubitus position. All
THAs were intended to be cementless unless
technical difficulties during the procedure pre-
vented such fixation. All TKA were cemented.
Primary Outcome
The primary outcome measure was the preva-
lence of DVT as determined by ascending venogram,
performed on both limbs on the 5th to 8th postop-
erative day; in addition, patients were followed for
3 months postoperation for clinical VTE events.
Venograms were performed using a modification
of Rabinov and Paulin technique with a nonionic
contrast medium (50 mL, Omnipaque, 180 mg of
iodine per milliliter). The patient was seated with
the leg in a dependent vertical position. The
contrast material was injected into a dorsal foot
vein. Frontal and lateral films of the lower leg were
obtained. The patient was then placed in a supine
position; a tourniquet was applied to the thigh to
occlude the greater saphenous vein. Another
50 mL of contrast material were injected through
the same dorsal vein, and films of the popliteal,
femoral, and iliac veins were obtained. A consul-
tant radiologist who had a special interest in
thromboembolism and unaware of the randomiza-
tion category of the patient (Dr Peer) interpreted
the results. A thrombus was diagnosed when there
was a filling defect surrounded by contrast medi-
um, or a deep vein was consistently nonvisualized.
Only thrombi located within the deep fascia were
considered deep vein thrombosis. The thrombi
were categorized and scaled according to the
Marder’s classification [18], which permits assess-
ment of the following 11 deep veins: common iliac,
external iliac, common femoral, superficial femo-
ral, and popliteal veins, and the 6 deep veins of the
calf (anterior tibials, posterior tibials, and pero-
neals). The classification was further detailed into
total occlusion, segmental occlusion, or filling
defects that were scored in accordance with the
degree of involvement severity. The maximum
possible score was 40 points. Proximal venous
thrombosis was defined as a thrombus in either
the popliteal, femoral, or iliac veins.
When thrombosis was suspected for clinical
reasons before the time of the scheduled venogram,
a duplex ultrasound scan of the proximal veins was
performed. In cases with proven DVT, venogram
was not performed. Venogram was considered as
inadequate if the amount of contrast medium
injected was too small or it was not possible to
inject contrast medium. In patients in whom
adequate venogram could not be performed be-
cause of technical reasons, a duplex ultrasound
scan was used to assess the proximal veins.
All thrombi detected were treated with full dose
enoxaparin and warfarin sodium until an interna-
tional normalized ratio value of between 2 and 3
was reached. Then, warfarin alone was adminis-
tered for a period of 6 months. Clinical symptoms
consistent with pulmonary embolism were ex-
plored and documented.
Secondary Outcome
The secondary outcome measures were adverse
events, blood loss index, and hospitalization days.
Adverse events were assessed and documented

Table 1. Demographic Characteristics and Risk Factorsin 121 Patients Who Underwent Total JointArthroplasty, According to Study Group
(Nonparametric Test—v2)
Enoxaparin CECTParameter (n = 60) (n = 61) Significance
Sex (Male) 23 (38%) 21 (34%) nsProcedure type
(THA)40 (67%) 33 (54%) ns
Duodenal ulcer 7 (12%) 3 (5%) nsIschemic heart
disease12 (20%) 5 (8%) P = .062
DVT Prevention in Joint Arthroplasties: CECT vs LMWH ! Gelfer et al 209
each day. The blood loss index, a validated measure
used in clinical studies to determine blood loss in
patients being managed with therapeutic antico-
agulation [19], was calculated with the following
equation: blood loss index = (preoperative hemo-
globin level � hemoglobin level before discharge) +
number of units transfused. The volume of blood
drained postoperatively was recorded. Other bleed-
ing-related parameters evaluated included: postop-
erative hemorrhage, wound hematoma, and
reoperation. Hemorrhage was classified as either
minor or major. Major hemorrhage was defined as
clinically overt bleeding that was associated with a
decrease in the hemoglobin level of 2 g/dL or more,
required 2 units of transfusion or more, was either
retroperitoneal or intracranial, or necessitated re-
operation. Our policy is transfusing patients having
a hemoglobin level of less than 9 g/dL. Hospitali-
zation period was documented for each patient.
Statistical Methods
The sample size calculation was based on the
assumption of 70% DVT rate without prophylaxis
and DVT rate of 20% in the enoxaparin group. For
a 2-tailed alpha error of 5% and power of 80%, we
estimated that at least 60 patients in each group
were required. All randomized patients who re-
ceived at least one dose of enoxaparin or used the
CECT were included in the safety analysis. Efficacy
analyses were performed on all patients completing
the study and who had a technically interpretable
venogram, as well as on all randomized patients.
Univariate analysis was used to compare the basic
characteristics and outcomes between the 2 groups.
The v2 test and the independent t test were con-
ducted for categorical and numerical variables,
respectively. Comparison in small subgroups was
performed by Fisher exact test and by Mann-
Whitney test for categorical and numerical varia-
bles, respectively. The study primary outcome,
incidence of DVT, was assessed using 95% confi-
dence interval (CI) with normal approximation to
binomial distribution. Multivariate analysis was
conducted using the logistic regression for the
prediction of DVT incidence, controlled for possible
confounders. A 2-tailed P value of less than .05 was
taken to be significant.
Hypertension 26 (43%) 26 (43%) nsDiabetes 10 (17%) 3 (5%) P = .037Malignancy 8 (13%) 5 (8%) nsOther diseases 35 (58%) 30 (49%) nsSmoking 6 (10%) 10 (16%) nsParametric test—independent t test (mean F SD)Age 67 (8.7) 68 (10.4) nsBMI 29 (4.8) 28 (4.0) ns
Results
Study Subjects
Between April 2001 and September 2002, 142
patients were screened and 136 patients were
randomized. One hundred twenty-one patients
finished the study protocol: 60 were treated by
enoxaparin and 61 by the CECT-based protocol.
The Institutional and National ethics committees
approved the study. All patients gave written
informed consent.
Dropouts were missing completely at random
and did not depend in any way on the treatment
response or protocol. The reasons for dropout were
the following: refused venography and Doppler
scanning (6 patients in the enoxaparin and
3 patients in the treatment group), late information
about old DVT event (1 patient in each group),
1 patient who had early dislocation of hip prosthe-
sis that led to revision in the enoxaparin group, and
3 patients with protocol violation (patients received
combined treatment with CECT plus enoxaparin).
There was a total of 15 dropouts, 8 in the
enoxaparin group and 7 in the treatment group.
The 2 groups were comparable in terms of baseline
characteristics of the patient and medical history,
except for a significantly higher number of dia-
betics in the enoxaparin group (Table 1). One
hundred thirteen patients were operated under
general anesthesia and 8 under epidural or spinal
anesthesia (3 in the enoxaparin group and 5 in the
CECT group). Duration of surgery was similar in
both groups. There were no statistically significant
differences between the 2 groups with regard to
postoperative drainage, the decrease in hemoglobin
levels, the transfusion requirements, or the blood-
loss index. Ascending venogram was performed
successfully in 107 patients. The remaining
14 patients (7 in the enoxaparin group and 7 in

Table 2. Adverse Events According to Study Group
Adverse Events Enoxaparin CECT
Soft-tissue problemsPressure ulcer 1 1Limb edema 3 1Serosanguineous discharge 0 1
Gastrointestinal eventsAbdominal pain 2 3Gastrointestinal bleeding 0 0Constipation 11 12
Bleeding-related eventsHb b 9 g/dL 4 7Wound drainage over 500 mL in 72 h 8 10More than 2 units of blood transfusion 29 34Platelets b 100000 2 1
GeneralWound infection 0 0Elevated temperature N 38.58C 6 3Chest pain 2 1Arrhythmia 0 1Dyspnea 0 1
210 The Journal of Arthroplasty Vol. 21 No. 2 February 2006
the CECT group), in whom complete venogram
was not performed because of technical reasons,
underwent additional bilateral duplex. In agree-
ment with the incomplete venograms, no DVT was
found in these patients and they were considered
DVT free.
Thromboembolism
No patient died during the follow-up period.
DVT was detected venographically in 17 of 60
patients in the enoxaparin group (28.3%; 95% CI,
17%-39%) compared to 4 of 61 in the CECT group
(6.6%; 95% CI, 0.4%-12.8%). Proximal DVT was
detected in 6 (10%) patients in the enoxaparin
group and 1 (1.6%) in the CECT group. The
differences between the groups are statistically
significant for both total DVT and proximal DVT
rates (v2 test, P = .002 and P = .049, respectively).
The average Marder’s severity score was 5.3 for
the DVTs in the enoxaparin group and 4.0 in the
CECT group. This difference is not statistically
significant (Mann-Whitney test, P = .52). In the
enoxaparin group, there were more proximal
DVTs (6/17 vs 1/4 in the CECT group) and more
contralateral side DVTs (4/17 vs 0/4 in the CECT
group); however, probably because of the limited
size of the study, the differences are not statisti-
cally significant.
One patient from the enoxaparin group devel-
oped a clinically important pulmonary embolism
1 month after the operation; the diagnosis was
confirmed by a ventilation-perfusion scan showing
a high probability of pulmonary embolism. No PE
was found in the CECT group. Logistic regression
analysis was carried out to determine the odds
ratio of DVT according to study group. Multivariate
analysis for prediction of DVT incidence revealed
significant superiority of the CECT protocol
over enoxaparin protocol (odds ratio, 6.5; 95% CI,
1.95-21.4, P = .002).
Despite adequate randomization, there was a
slight preponderance for more comorbidity in the
enoxaparin group. However, these multivariate
analysis results were obtained after controlling for
the potential effect of this minor mismatch. The
above logistic regression was done with DVT
incidence as the dependent variable, and prophy-
lactic treatment protocol, malignancy, diabetes,
and heart disease as the independent variables.
Treatment with CECT appears to be particu-
larly effective in prevention of DVTs after THA
(13/17 DVTs in the enoxaparin group were iden-
tified in patients with THA vs 0/4 in the CECT
group, P b .012).
Adverse Events
Adverse events were recorded on a daily basis. They
were classified as mild, moderate, or severe. Relation
to treatment was classified as possible, probable, or
definite. Each event was classified by one of the
authors (Dr Oron). There were 68 events in the eno-
xaparin group and 76 in the CECT group (Table 2).
Four events were possibly related to the treatment
by enoxaparin (1 moderate, 3 mild) vs 2 events
possibly related and one probably related to the
treatment in the CECT group.
Hospitalization
The length of hospital stay in the 100 patients
who did not develop DVT was found to be 9.1 F2.4 days compared with 10.7 F 2.4 days in the
21 patients who did develop DVT (P = 0.01).
Patients treated with the CECT system had a
shorter hospital stay (8.8 F 1.9 days) as compared
with patients treated by enoxaparin (9.9F 2.7 days).
The difference was statistically significant (P b .02)
and appears directly related to the higher rate of
DVT in the latter group.
Cost Analysis Comparing the 2 TreatmentGroups
Cost analysis was on the basis of current costs of
enoxaparin, DVT, and PE treatments in the US
hospitals as recently published by Botteman et al
[20] and Ollendorf et al [21]. The pricing of the

Table 3. Cost Analysis Comparing the Treatment Costof CECT-Based Protocol vs Enoxaparin (Prices in US$)
LMWH CECT + ASA*
Clinical resultsPostoperative hospital stay 9.95 8.88% of DVT 28.33 6.60% of PE 1.67 0.00
Cost analysis (per patient) in $Sleeves—direct cost 42.00Clexane direct cost
(cost per day,y 9.95 d)365.17
Aspirin direct cost(cost per day,y 8.88 d)
0.09
Direct cost per patient 365.17 42.09Cost of system per patient
($1500/108 = no. ofpatient in 3 years)
13.89
Direct cost per patientincluding cost of system
365.17 55.98
Average cost of DVT treatment 2200.96 512.75Average cost of PE treatment 152.93 0.00Cost of hospitalization
(cost per day,y no. ofdays per protocol)
4447.15 3968.92
Total 7166.21 4537.65Saving per patient 2628.56Total saving for 1000 patients $2628557
Assumptions: cost per day of hospitalization, $447.00y; cost ofCECT system, $1500.00; cost of pair of sleeves, $42.00; costof aspirin per day, $0.01; cost of enoxaparin, $36.70y; cost oftreatment of a patient diagnosed with DVT, $7769.00z; cost oftreatment of a patient diagnosed with PE, $9176.00z.
*ASA=Acetylsalicylic Acid.yBotteman et al [20].zOllendorf et al [21].
DVT Prevention in Joint Arthroplasties: CECT vs LMWH ! Gelfer et al 211
CECT system and pneumatic sleeves was calculated
according to manufacturer price list in the United
States. The overall analysis indicates a cost reduc-
tion using the CECT protocol compared to enox-
aparin. Savings to the hospital reached $2628557
per 1000 patients (Table 3).
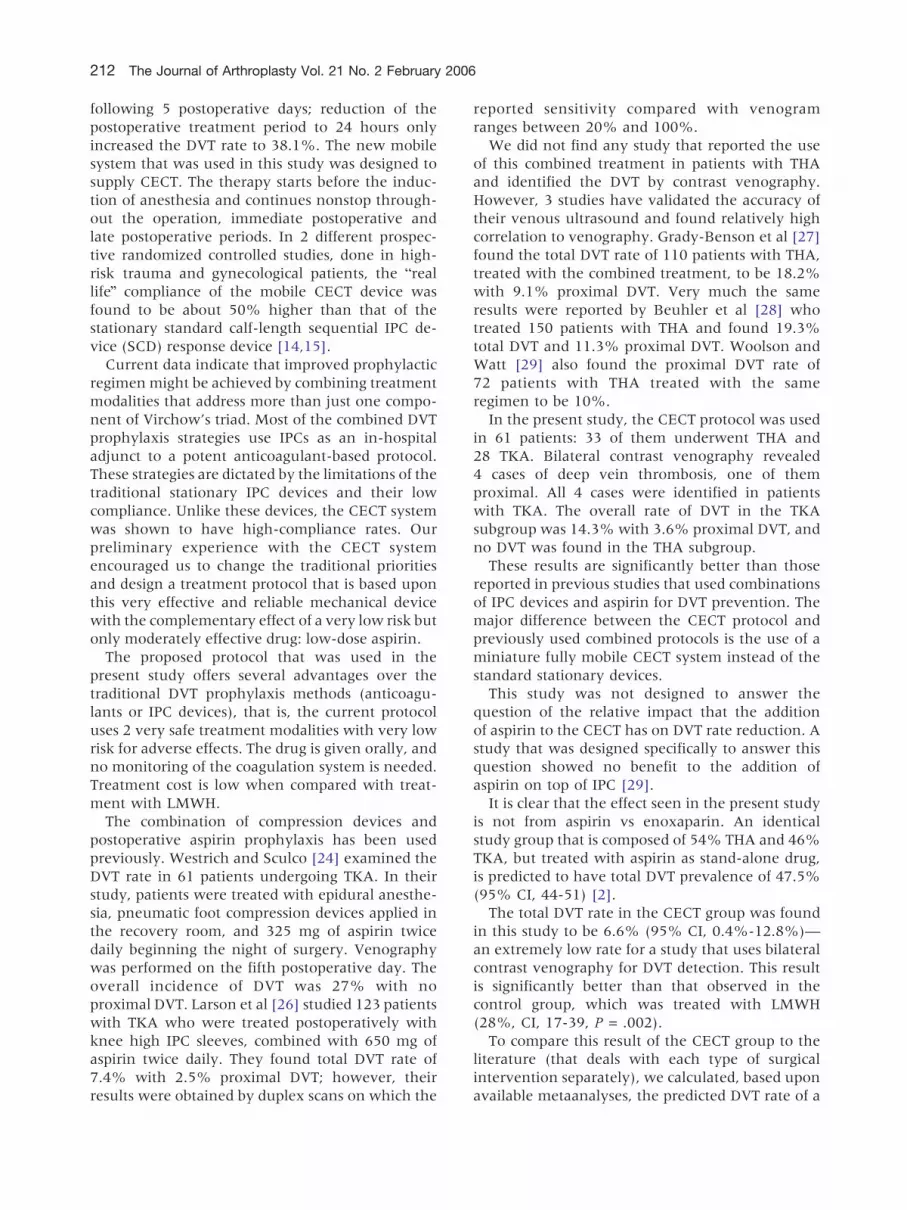
Fig. 1. Distribution of DVT cases during study period.
Note that most cases in the CECT group occurred at the
beginning of the study. Rectangle indicates CECT and
aspirin group; diamond, enoxaparin group.
Discussion
The current study indicates that the CECT
system combined with 100 mg of aspirin is more
effective than enoxaparin as a prophylactic agent
for DVT after joint arthroplasty in the lower limb.
Strong and significant evidence was found for the
advantage of the CECT protocol over the com-
monly used enoxaparin-based protocol. The inci-
dence of DVT was 4-fold in the univariant analysis
and in the enoxaparin group compared to the
CECT group. In multivariate analysis, the odds
ratio for incidence of DVT was 6.5 after controlling
for potential confounders. The significant differ-
ence in hospitalization days was probably due to
differences in DVT rates.
No DVTs were found in the patients using CECT
after THA, whereas in the enoxaparin group, most
of the DVT cases were found in patients after THA
(13 of 17). The difference is statistically significant
(P = .012).
The incidence of study dropouts was 11%. No
possible bias of dropouts was found.
Most of the DVTs in the CECT group (3 of 4)
appeared during the first 2 months of the study,
whereas the DVT in the enoxaparin group was
almost evenly distributed along the study period.
This difference may be due to bdevice learning
curveb of the clinical team (Fig. 1).
The study and control groups appear similar, and
the patients who eventually did not successfully
complete the venogram do not affect the primary
outcome measure and were evenly distributed
between the 2 treatment groups.
We monitored clinical symptoms possibly indi-
cating DVT or PE occurrence for 3 months after
discharge. No clinical signs of VTE occurred during
this period in the CECT group in our study;
however, one patient in the enoxaparin group
developed a clinically important pulmonary embo-
lism 1 month after the operation.
Compression therapy is effective when used
intraoperatively and continuously at least until
the patient is fully ambulatory [2,22]. The tradi-
tional IPC devices, being big, heavy, and dependent
on mounted electrical outlets for power, are
practically incompatible with round the clock use
and have reported compliance rate of 33% to 48%
[13,23]. Westrich and Sculco [24] were able to
demonstrate direct relationship between compli-
ance with the use of an IPC device and its efficacy.
Clark-Pearson et al [25] reported DVT rate of 9.1%
in a group of gynecological patients who were
treated with IPC devices during surgery and the
212 The Journal of Arthroplasty Vol. 21 No. 2 February 2006
following 5 postoperative days; reduction of the
postoperative treatment period to 24 hours only
increased the DVT rate to 38.1%. The new mobile
system that was used in this study was designed to
supply CECT. The therapy starts before the induc-
tion of anesthesia and continues nonstop through-
out the operation, immediate postoperative and
late postoperative periods. In 2 different prospec-
tive randomized controlled studies, done in high-
risk trauma and gynecological patients, the breal
lifeQ compliance of the mobile CECT device was
found to be about 50% higher than that of the
stationary standard calf-length sequential IPC de-
vice (SCD) response device [14,15].
Current data indicate that improved prophylactic
regimen might be achieved by combining treatment
modalities that address more than just one compo-
nent of Virchow’s triad. Most of the combined DVT
prophylaxis strategies use IPCs as an in-hospital
adjunct to a potent anticoagulant-based protocol.
These strategies are dictated by the limitations of the
traditional stationary IPC devices and their low
compliance. Unlike these devices, the CECT system
was shown to have high-compliance rates. Our
preliminary experience with the CECT system
encouraged us to change the traditional priorities
and design a treatment protocol that is based upon
this very effective and reliable mechanical device
with the complementary effect of a very low risk but
only moderately effective drug: low-dose aspirin.
The proposed protocol that was used in the
present study offers several advantages over the
traditional DVT prophylaxis methods (anticoagu-
lants or IPC devices), that is, the current protocol
uses 2 very safe treatment modalities with very low
risk for adverse effects. The drug is given orally, and
no monitoring of the coagulation system is needed.
Treatment cost is low when compared with treat-
ment with LMWH.
The combination of compression devices and
postoperative aspirin prophylaxis has been used
previously. Westrich and Sculco [24] examined the
DVT rate in 61 patients undergoing TKA. In their
study, patients were treated with epidural anesthe-
sia, pneumatic foot compression devices applied in
the recovery room, and 325 mg of aspirin twice
daily beginning the night of surgery. Venography
was performed on the fifth postoperative day. The
overall incidence of DVT was 27% with no
proximal DVT. Larson et al [26] studied 123 patients
with TKA who were treated postoperatively with
knee high IPC sleeves, combined with 650 mg of
aspirin twice daily. They found total DVT rate of
7.4% with 2.5% proximal DVT; however, their
results were obtained by duplex scans on which the
reported sensitivity compared with venogram
ranges between 20% and 100%.
We did not find any study that reported the use
of this combined treatment in patients with THA
and identified the DVT by contrast venography.
However, 3 studies have validated the accuracy of
their venous ultrasound and found relatively high
correlation to venography. Grady-Benson et al [27]
found the total DVT rate of 110 patients with THA,
treated with the combined treatment, to be 18.2%
with 9.1% proximal DVT. Very much the same
results were reported by Beuhler et al [28] who
treated 150 patients with THA and found 19.3%
total DVT and 11.3% proximal DVT. Woolson and
Watt [29] also found the proximal DVT rate of
72 patients with THA treated with the same
regimen to be 10%.
In the present study, the CECT protocol was used
in 61 patients: 33 of them underwent THA and
28 TKA. Bilateral contrast venography revealed
4 cases of deep vein thrombosis, one of them
proximal. All 4 cases were identified in patients
with TKA. The overall rate of DVT in the TKA
subgroup was 14.3% with 3.6% proximal DVT, and
no DVT was found in the THA subgroup.
These results are significantly better than those
reported in previous studies that used combinations
of IPC devices and aspirin for DVT prevention. The
major difference between the CECT protocol and
previously used combined protocols is the use of a
miniature fully mobile CECT system instead of the
standard stationary devices.
This study was not designed to answer the
question of the relative impact that the addition
of aspirin to the CECT has on DVT rate reduction. A
study that was designed specifically to answer this
question showed no benefit to the addition of
aspirin on top of IPC [29].
It is clear that the effect seen in the present study
is not from aspirin vs enoxaparin. An identical
study group that is composed of 54% THA and 46%
TKA, but treated with aspirin as stand-alone drug,
is predicted to have total DVT prevalence of 47.5%
(95% CI, 44-51) [2].
The total DVT rate in the CECT group was found
in this study to be 6.6% (95% CI, 0.4%-12.8%)—
an extremely low rate for a study that uses bilateral
contrast venography for DVT detection. This result
is significantly better than that observed in the
control group, which was treated with LMWH
(28%, CI, 17-39, P = .002).
To compare this result of the CECT group to the
literature (that deals with each type of surgical
intervention separately), we calculated, based upon
available metaanalyses, the predicted DVT rate of a

DVT Prevention in Joint Arthroplasties: CECT vs LMWH ! Gelfer et al 213
theoretical identical group that is composed of 54%
patients with THA and 46% patients with TKA, and
is treated with LMWH.
The pooled DVT rate after TKA and LMWH
prophylaxis, as determined by contrast venography
in 13 prospective studies for a total of 1740 patients,
was found to be 30.6% (95% CI, 29%-33%). For
THA and LMWH prophylaxis, the pooled DVT
prevalence of 30 studies with a total of 6216 patients
was 16.1% (95% CI, 15%-17%) [2].
Theoretically, a mixed group of patients com-
posed of 54% THA and 46% TKA that is treated
with LMWH is predicted to develop 22.8% DVT
(95% CI, 21.4%-24.4%). The lower limit of
this predicted DVT range (21.4%) is much higher
than the upper limit of the 95% CI that was found
in the CECT group in the present study (12.8%)—
suggesting, once again, significant reduction in DVT
rate that was caused by the application of the new
CECT protocol.
One of the potential shortcomings of the present
study is the fact that both the study group (CECT)
and the control group (LMWH) are composed of
combination of patients with THA and TKA.
In our department, we are using the same DVT
prophylaxis protocol for all types of arthroplasties.
Our standard of care was based upon administra-
tion of 40 mg of enoxaparin once daily, starting
12 hours after surgery, and the regimen is the same
for THA and TKA. The goal of this preliminary study
was to evaluate a new prophylaxis protocol and
compare its efficacy to that of our current standard
of care in our routine medical environment. To
achieve this goal, we chose not to separate in the
present study between the 2 types of arthroplasties.
From the thromboembolism perspective, TKA
differs from THA. Without prophylaxis, the total
DVT rate is greater in TKA than in THA, and the
relative proportion of proximal DVT out of total
DVT is higher in patients with THA.
The major question that has to be asked when
such inhomogeneous surgical groups are used
together in a study is whether the distribution of
TKA and THA between the study group and the
control group is significantly different.
It seems that the effect of the inhomogeneity in
our study is negligible: The difference between the
percent of THA in the enoxaparin group (67%) and
in the CECT group (54%) is not statistically
significant (P = .158). However, to further support
the validity of our study results, we add to our
multivariate analysis for prediction of DVT inci-
dence the type of surgery as a confounder variable.
The new calculated odds ratio for DVT incidence
while using enoxaparin was similar after this
manipulation: 6.85 (95% CI, 2.00-23.40) instead
of 6.50 (95% CI, 1.95-21.50).
These results actually discard the possibility that
uneven distribution of the surgical intervention is
the cause for the favorable results observed in the
CECT group. The differences in DVT rates observed
between the groups in our study are reflecting the
effect of treatment modality, and they cannot be
explained by differences in group combination in
terms of type of surgery.
Of 121 venographies performed in this study, 14
were considered incomplete. In accordance with
the study protocol, these patients underwent an
additional duplex scanning. In agreement with the
incomplete venograms, no DVT was found in these
patients and they were considered DVT free and
were included in the statistical analysis. Statistically,
the chance that their inclusion biased the study
results is extremely low. These patients were evenly
distributed between the treatment groups and
constituted less than 12% of the study population.
Subtraction of this group from the statistical anal-
ysis resulted in only minor effects on the calculated
total DVT rates (32.1% in the enoxaparin group and
7.4% in the CECT group, P = .001) and on the
proximal DVT rates (11.3% vs 1.9%, respectively,
P = .048). The study power was kept 90%.
Summary and Conclusions
Consensus of the American Association of Hip and
Knee Surgeons is that multimodality approach is the
standard of care [30]. However, the most appropriate
prophylactic regimen remains highly controversial.
The combination of the new CECT system and
low-dose aspirin was found to be both safe and
effective method of prophylaxis against thrombo-
embolism after THA and TKA. We found a signif-
icantly lower prevalence of deep vein thrombosis
with this combination than with the standard
enoxaparin prophylaxis. This combined prophylax-
is protocol has favorable risk-benefit and cost-
effectiveness profiles. Further research is needed
to establish the place of this prophylaxis protocol as
the treatment of choice in high-risk orthopedic
patients. Future studies will be designed to deter-
mine its specific efficacy in different orthopedic
surgical interventions.
References
1. Nicolaides AN, Breddin HK, et al. Prevention of venous
thromboembolism. International Consensus State-
ment (guidelines compiled in accordance with the
scientific evidence). Int Angiol 2001;20:1 [Review].

214 The Journal of Arthroplasty Vol. 21 No. 2 February 2006
2. Geerts WH, Heit JA, et al. Prevention of venous throm-
boembolism. Sixth ACCP Consensus Conference on
Antithrombotic Therapy. Chest 2001;119:132s.
3. Murray DW, Britton AR, Bulstrode CJK. Thrombo-
prophylaxis and death after total hip replacement.
J Bone Joint Surg 1996;78-B:863.
4. Warwick D, Martin AG, Glew D, et al. Measurement of
femoral vein blood flow during total hip replacement.
Duplex ultrasound imaging with and without the use
of a foot pump. J Bone Joint Surg 1994;76-B:918.
5. McNally MA, Mollan RAB. Total hip replacement,
lower limb blood flow and venous thrombogenesis.
J Bone Joint Surg 1993;75-B:640.
6. Hull RD, Raskob GE. Current concept review. Prophy-
laxis of venous thromboembolic disease following hip
and knee surgery. J Bone Joint Surg 1986;68-A:146.
7. Kaempffe FA, Lifeso RM, et al. Intermittent pneu-
matic compression versus Coumadin. Prevention of
deep vein thrombosis in lower-extremity total joint
arthroplasty. Clin Orthop 1991;269:89.
8. Bradley JG, Krugener GH, et al. The effectiveness of
intermittent plantar venous compression in preven-
tion of deep venous thrombosis after total hip
arthroplasty. J Arthroplasty 1993;8:57.
9. Salvati EA, Pellegrini DV, Sharrock NE, et al. Recent
advances in thromboembolic prophylaxis during and
after total hip replacement—Symposium. J Bone
Joint Surg 2000;80-A:252.
10. Jacobs DG, Piotrowski JJ, Hoppensteadt DA, et al.
Hemodynamic and fibrinolytic consequences of inter-
mittent pneumatic compression: preliminary results.
J Trauma 1996;40:710.
11. Knight MIN, Dawson R. Effect of intermittent
compression of the arms on deep venous thrombosis
in the legs. Lancet 1976;2:1265.
12. Comerota AJ, Chouhan V, Harada RN, et al. The
fibrinolytic effects of intermittent pneumatic com-
pression. Mechanism of enhanced fibrinolysis. Ann
Surg 1997;226:306.
13. Comerota AJ, Katz ML, White JV. Why does prophy-
laxis with external pneumatic compression for deep
vein thrombosis fail?. Am J Surg 1992;164:265.
14. Murakami M, McDill TL, Cindrick-Pounds L, et al.
Deep venous thrombosis prophylaxis in trauma: im-
proved compliance with a novel miniaturized pneu-
matic compression device. J Vasc Surg 2003;38:923.
15. Kahn M, Lord C, Murakami M, et al. Deep venous
thrombosis prophylaxis in gynecologic surgery: im-
proved compliance with a novel miniaturized pneu-
matic compression device. J Pelvic Med Surg 2003;
9(Suppl 1):S6.
16. Killewich LA. WizAirDVTk hemodynamics Projects
calf/thigh length. University of Galveston Texas
Medical Branch (UTMB); 2001.
17. Virchow RLK. Gesammele abhandlungen zue
wisscnschaftlicher medizin, von meidinger sohn.
Franfur-ann-Main; 1856.
18. Marder VJ, Soulen RL, et al. Quantitative venographic
assessment of deep vein thrombosis in the evaluation
of streptokinase and heparin therapy. J Lab Clin Med
1977;89:1018.
19. Landefeld CS, et al. Identification and preliminary
validation of predictors of major bleeding in hospi-
talized patients starting anticoagulant therapy. Am J
Med 1987;82:703.
20. Botteman MF, Caprini J, Stephens JM, et al. Results
of an economic model to assess the cost-effectiveness
of enoxaparin, a low molecular weight heparin,
versus warfarin for the prophylaxis of deep vein
thrombosis and associated long term complications in
total hip replacement surgery in the United States.
Clin Ther 2002;24:1960.
21. Ollendorf DA, Vera-Llonch M, Oster G. Cost of
venous thromboembolism following major orthope-
dic surgery in hospitalized patients. Am J Health Syst
Pharm 2002;59:1750.
22. Carrol P. Deep venous thrombosis: implications for
orthopedic nursing. Orthop Nurs 1993;12:33.
23. Haddad FS, Kerry RM, McEwen JA, et al. Unantic-
ipated variations between expected and delivered
pneumatic compression therapy after elective hip
surgery. J Arthroplasty 2001;16:37.
24. Westrich GH, Sculco TP. Prophylaxis against deep
venous thrombosis after total knee arthroplasty.
Pneumatic plantar compression and aspirin compared
with aspirin alone. J Bone Joint Surg Am 1996;
78:826.
25. Clarke-Pearson DL, Synan IS, Hinshaw WM, et al.
Prevention of postoperative venous thromboembo-
lism by external pneumatic calf compression in pa-
tients with gynecologic malignancy. Obstet Gynecol
1984;63:92.
26. Larson CM, MacMillan DP, Lachiewicz PF. Throm-
boembolism after total knee arthroplasty: intermit-
tent pneumatic compression and aspirin prophylaxis.
J South Assoc 2001;10:155.
27. Grady-Benson JC, Ohishi CS, Hanson PB, et al.
Routine postoperative duplex ultrasonography
screening and monitoring for the detection of deep
vein thrombosis. Clin Orthop Relat Res 1994;
307:130.
28. Beuhler KO, D’Lima DD, Colwell CW, et al. Venous
thromboembolic disease after hybrid hip arthroplasty
with negative duplex screening. Clin Orthop Relat
Res 1999;361:168.
29. Woolson ST, Watt JM. Intermittent pneumatic com-
pression to prevent proximal deep venous thrombosis
during and after total hip replacement. J Bone Joint
Surg 1991;73-A:507.
30. Mesko JW, Brand RA, Iorio R, et al. Venous
thromboembolic disease management patterns in
total tip arthroplasty and total knee arthroplasty
patients. A survey of the AAHKS membership.
J Arthroplasty 2001;16:679.





























