Embed Size (px)
Citation preview

Cardiovascular Pathology 17 (2008) 156–165
Original Article
Dedifferentiation of atrial cardiomyocytes in cardiac valve disease:unrelated to atrial fibrillation
Mien-Cheng Chena,⁎, Jen-Ping Changb, Shun-Chen Huangc, Hsueh-Wen Changd,Chien-Jen Chena, Cheng-Hsu Yanga, Wen-Hao Liua
aDivision of Cardiology, Department of Internal Medicine, Chang Gung Memorial Hospital-Kaohsiung Medical Center,Chang Gung University College of Medicine, Kaohsiung, Taiwan, R.O.C.
bDivision of Cardiovascular Surgery, Department of Surgery, Chang Gung Memorial Hospital-Kaohsiung Medical Center,Chang Gung University College of Medicine, Kaohsiung, Taiwan, R.O.C.
cDepartment of Pathology, Chang Gung Memorial Hospital-Kaohsiung Medical Center,Chang Gung University College of Medicine, Kaohsiung, Taiwan, R.O.C.
dDepartment of Biological Sciences, National Sun Yat-Sen University, Taiwan, R.O.C.
Received 26 March 2007; received in revised form 1 July 2007; accepted 23 July 2007
Abstract
Background: Valvular heart disease has become an important public health concern. The increased wall stress and underlying diseaseentity associated with mitral valve disease provide unfavorable circumstances for atrial cardiomyocytes. The expression of the α-smoothmuscle actin isoform is considered characteristic of cardiomyocyte dedifferentiation (embryonic cardiomyocyte), and cardiomyocytededifferentiation may indicate an adaptive state, enabling cardiomyocytes to survive despite unfavorable circumstances.Methods: This studycomprised 20 adult patients with symptomatic severe mitral valve disease and moderate to severe tricuspid valve disease and withoutcoronary artery disease undergoing valve operations for congestive heart failure. Ten patients had persistent atrial fibrillation and 10 patientshad never been in atrial fibrillation by history and electrocardiograms before surgery. Atrial tissues of the right atrial appendage were obtainedduring surgery. Results: Immunohistochemical study demonstrated that α-smooth muscle actin protein expression was not altered by atrialfibrillation, and α-smooth muscle actin protein expression in atrial tissues was higher in patients with sinus rhythm than in those with atrialfibrillation (the percentage of cells that were α-smooth muscle actin-positive was 51.5±34.9% for right atria from patients in sinus rhythm vs.16.2±15.0% for right atria from patients with atrial fibrillation) (Pb .03). Semiquantitation of α-smooth muscle actin by immunoblotting ofextracts from atrial tissues showed similar findings as in the immunohistochemical observations: that is, atrial fibrillation did not influence theexpression of α-smooth muscle actin protein. Interstitial fibrosis represented 43.2±13.9% of the right atrial tissue in the sinus group, whereasinterstitial fibrosis comprised 49.8±8.2% of the right atrial tissue in the atrial fibrillation group (P=.320). Conclusions: Dedifferentiation ofatrial cardiomyocytes occurs in patients with cardiac valve disease, even without atrial fibrillation. © 2008 Elsevier Inc. All rights reserved.
Keywords: Atrial fibrillation; Atrium; Cardiomyocytes; Dedifferentiation; Cardiac valve disease
This study was supported by program grants from the ChangGung Memorial Hospital-Kaohsiung Medical Center, Chang GungUniversity College of Medicine, Kaohsiung, Taiwan, Republic of China(CMRPG850031).
⁎ Corresponding author. Division of Cardiology, Department of InternalMedicine, Chang Gung Memorial Hospital-Kaohsiung Medical Center,Chang Gung University College of Medicine, Niao Sung Hsiang, KaohsiungHsien 83301, Taiwan, Republic of China. Tel.: +886 7 731 7123x8300;fax: +886 7 732 2402.
E-mail address: [email protected] (M.-C. Chen).
1054-8807/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1016/j.carpath.2007.07.008
1. Introduction
For many years, the prevalence of valvular heart diseasehas been underestimated, and valvular heart disease hasbecome a growing public health problem [1,2]. Valvularheart disease, though less prevalent than coronary arterydisease, is among the more important underlying causes ofheart failure and sudden death [3,4].
157M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
The expression of the α-smooth muscle actin isoform isconsidered a characteristic feature of cardiomyocyte ded-ifferentiation (embryonic cardiomyocyte) [5]. Dedifferentia-tion of cardiomyocytes was previously reported in patientswith chronic hibernating myocardium and a goat model ofchronic atrial fibrillation [5,6]. Previous studies havereported that dedifferentiated cardiomyocytes are moreischemia-tolerant, that is, better protected against ischemicinsults than normally structured cardiomyocytes [7]. Addi-tionally, previous studies have suggested that this structuralremodeling in chronic hibernating myocardium is at leastpartially responsible for the delay in function recovery afterrevascularization [8]. Consequently, these indirect observa-tions have indicated that dedifferentiation of cardiomyocytesmay indicate an adaptive state, permitting the cardiomyo-cytes to survive despite unfavorable circumstances [7]. Thechronic hemodynamic load, increased wall stress, and under-lying disease entity associated with mitral valve disease andtricuspid valve disease create unfavorable circumstances foratrial cardiomyocytes. Therefore, atrial myocardial stretch asa result of chronic increased wall stress due to mitral valvedisease and tricuspid valve disease may play a role in thetrigger for dedifferentiation of atrial cardiomyocytes. Noprevious investigations have examined whether dedifferen-tiation of atrial cardiomyocytes occurs in patients withmitra valve disease and tricuspid valve disease. This studyhypothesized that dedifferentiation of atrial cardiomyocytesoccurs in patients with mitral valve disease and tricuspidvalve disease, even without atrial fibrillation.
2. Materials and methods
2.1. Patient population
This study examined patients with symptomatic severemitral valve disease and moderate to severe tricuspid valvedisease undergoing valve operations for congestive heartfailure. Exclusion factors included coronary artery lesions,previous myocardial infarction, febrile disorder, infectious orinflammatory disease, autoimmune disease, malignancy,chronic renal failure (serum creatinine N2.5 mg/dl), acuteor chronic viral hepatitis, or taking immunosuppressivedrugs. Ten patients had persistent atrial fibrillation [mean(±S.D.) duration of 39.2±41.0 months; duration range, 1–107 months] before surgery (atrial fibrillation group). Thesample included three men and seven women, with a mean(±S.D.) age of 57±14 years (age range, 37–77 years). Allpatients had mitral valve disease: five patients had mitralregurgitation, one patient had mitral stenosis, and fourpatients had combined mitral stenosis and mitral regurgita-tion. Moreover, eight patients had concomitant severetricuspid regurgitation, and two patients had moderatetricuspid regurgitation, defined by echocardiography [9].None of the patients had aortic valve disease. Furthermore,seven patients had underlying rheumatic heart disease. Ten
patients who had never been in atrial fibrillation by historyand electrocardiograms before surgery had symptomaticsevere mitral valve disease (sinus group). The sampleincluded five men and five women, with a mean (±S.D.)age of 52±19 years (age range, 17–74 years). All patientshad mitral valve disease: nine patients had mitral regurgita-tion and one patient had combined mitral stenosis andmitral regurgitation. Furthermore, three patients had con-comitant severe tricuspid regurgitation, and seven patientshad moderate tricuspid regurgitation, defined by echocar-diography [9]. Additionally, two patients had concomitantaortic valve disease, and two patients had underlyingrheumatic heart disease. Informed consent was obtainedfrom all study subjects. The study protocol was approved bythe Institutional Review Committee for Human Research inour institution.
Normal adult atrial tissue samples (21 years old) werepurchased from BioChain Institute (Abcam, Cambridge,UK) for immunochemical studies and from G-Biosciences(St. Louis, MO, USA) for Western blotting. In addition, wealso examined normal right atrial appendage tissue from a25-year-old male patient with a prior history of infectiveendocarditis of the congenital bicuspid aortic valve andwithout heart failure. These normal atrial tissues were usedas normal controls.
2.2. Echocardiography
Transthoracic echocardiographic examinations were per-formed using a 2.5-MHz transducer attached to a commer-cially available echo Doppler machine (Sonos 7500;Hewlett–Packard; Palo Alto, CA, USA) on the day beforevalve surgery in all patients. M-mode measurements wereperformed according to the recommendations of theAmerican Society of Echocardiography. Left and right atrialareas were measured via planimetering in a four-chamberview, and the maximum areas of left and right atrial areaswere taken as the average of measurements (at the end of theT wave on the electrocardiogram) over five beats.
2.3. Hemodynamic measurements
Measurements of the left and right atrial pressures andpulmonary artery pressure were performed during the weekbefore surgery.
2.4. Specimen storage
In the atrial fibrillation group, small pieces of atrial tissuesof the right atrial appendage (apical portion) and left atrialappendage (apical portion) were obtained during surgery,while in the sinus group, owing to ethical concerns, onlyatrial tissue of the right atrial appendage was obtained. Someatrial tissues were fixed immediately following excision andmaintained in 4% buffered formalin overnight at roomtemperature, then embedded in paraffin and stored until later
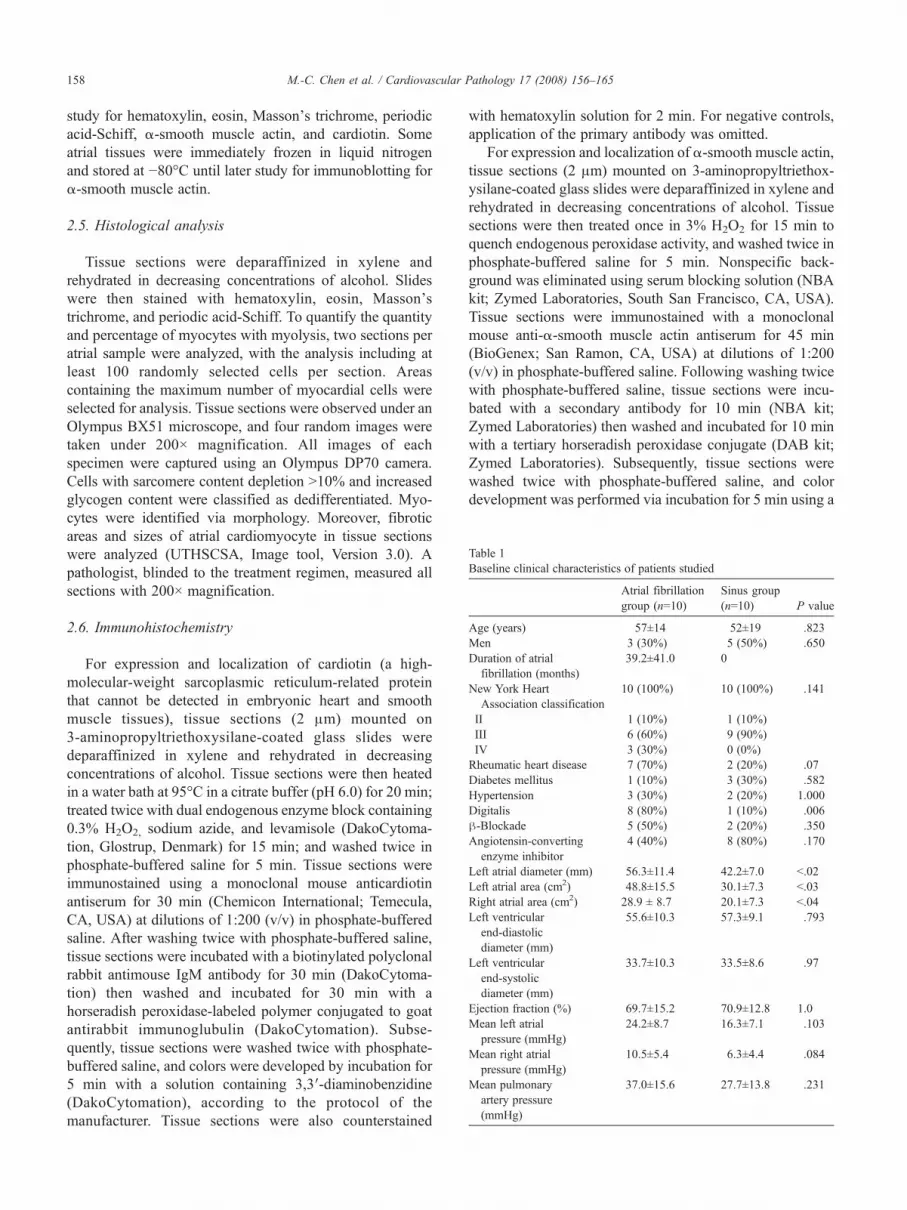
Table 1Baseline clinical characteristics of patients studied
Atrial fibrillationgroup (n=10)
Sinus group(n=10) P value
Age (years) 57±14 52±19 .823Men 3 (30%) 5 (50%) .650Duration of atrial
fibrillation (months)39.2±41.0 0
New York HeartAssociation classification
10 (100%) 10 (100%) .141
II 1 (10%) 1 (10%)III 6 (60%) 9 (90%)IV 3 (30%) 0 (0%)Rheumatic heart disease 7 (70%) 2 (20%) .07Diabetes mellitus 1 (10%) 3 (30%) .582Hypertension 3 (30%) 2 (20%) 1.000Digitalis 8 (80%) 1 (10%) .006β-Blockade 5 (50%) 2 (20%) .350Angiotensin-converting
enzyme inhibitor4 (40%) 8 (80%) .170
Left atrial diameter (mm) 56.3±11.4 42.2±7.0 b.02Left atrial area (cm2) 48.8±15.5 30.1±7.3 b.03Right atrial area (cm2) 28.9 ± 8.7 20.1±7.3 b.04Left ventricular
end-diastolicdiameter (mm)
55.6±10.3 57.3±9.1 .793
Left ventricularend-systolicdiameter (mm)
33.7±10.3 33.5±8.6 .97
Ejection fraction (%) 69.7±15.2 70.9±12.8 1.0Mean left atrial
pressure (mmHg)24.2±8.7 16.3±7.1 .103
Mean right atrialpressure (mmHg)
10.5±5.4 6.3±4.4 .084
Mean pulmonaryartery pressure(mmHg)
37.0±15.6 27.7±13.8 .231
158 M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
study for hematoxylin, eosin, Masson's trichrome, periodicacid-Schiff, α-smooth muscle actin, and cardiotin. Someatrial tissues were immediately frozen in liquid nitrogenand stored at −80°C until later study for immunoblotting forα-smooth muscle actin.
2.5. Histological analysis
Tissue sections were deparaffinized in xylene andrehydrated in decreasing concentrations of alcohol. Slideswere then stained with hematoxylin, eosin, Masson'strichrome, and periodic acid-Schiff. To quantify the quantityand percentage of myocytes with myolysis, two sections peratrial sample were analyzed, with the analysis including atleast 100 randomly selected cells per section. Areascontaining the maximum number of myocardial cells wereselected for analysis. Tissue sections were observed under anOlympus BX51 microscope, and four random images weretaken under 200× magnification. All images of eachspecimen were captured using an Olympus DP70 camera.Cells with sarcomere content depletion N10% and increasedglycogen content were classified as dedifferentiated. Myo-cytes were identified via morphology. Moreover, fibroticareas and sizes of atrial cardiomyocyte in tissue sectionswere analyzed (UTHSCSA, Image tool, Version 3.0). Apathologist, blinded to the treatment regimen, measured allsections with 200× magnification.
2.6. Immunohistochemistry
For expression and localization of cardiotin (a high-molecular-weight sarcoplasmic reticulum-related proteinthat cannot be detected in embryonic heart and smoothmuscle tissues), tissue sections (2 μm) mounted on3-aminopropyltriethoxysilane-coated glass slides weredeparaffinized in xylene and rehydrated in decreasingconcentrations of alcohol. Tissue sections were then heatedin a water bath at 95°C in a citrate buffer (pH 6.0) for 20 min;treated twice with dual endogenous enzyme block containing0.3% H2O2, sodium azide, and levamisole (DakoCytoma-tion, Glostrup, Denmark) for 15 min; and washed twice inphosphate-buffered saline for 5 min. Tissue sections wereimmunostained using a monoclonal mouse anticardiotinantiserum for 30 min (Chemicon International; Temecula,CA, USA) at dilutions of 1:200 (v/v) in phosphate-bufferedsaline. After washing twice with phosphate-buffered saline,tissue sections were incubated with a biotinylated polyclonalrabbit antimouse IgM antibody for 30 min (DakoCytoma-tion) then washed and incubated for 30 min with ahorseradish peroxidase-labeled polymer conjugated to goatantirabbit immunoglubulin (DakoCytomation). Subse-quently, tissue sections were washed twice with phosphate-buffered saline, and colors were developed by incubation for5 min with a solution containing 3,3′-diaminobenzidine(DakoCytomation), according to the protocol of themanufacturer. Tissue sections were also counterstained
with hematoxylin solution for 2 min. For negative controls,application of the primary antibody was omitted.
For expression and localization of α-smooth muscle actin,tissue sections (2 μm) mounted on 3-aminopropyltriethox-ysilane-coated glass slides were deparaffinized in xylene andrehydrated in decreasing concentrations of alcohol. Tissuesections were then treated once in 3% H2O2 for 15 min toquench endogenous peroxidase activity, and washed twice inphosphate-buffered saline for 5 min. Nonspecific back-ground was eliminated using serum blocking solution (NBAkit; Zymed Laboratories, South San Francisco, CA, USA).Tissue sections were immunostained with a monoclonalmouse anti-α-smooth muscle actin antiserum for 45 min(BioGenex; San Ramon, CA, USA) at dilutions of 1:200(v/v) in phosphate-buffered saline. Following washing twicewith phosphate-buffered saline, tissue sections were incu-bated with a secondary antibody for 10 min (NBA kit;Zymed Laboratories) then washed and incubated for 10 minwith a tertiary horseradish peroxidase conjugate (DAB kit;Zymed Laboratories). Subsequently, tissue sections werewashed twice with phosphate-buffered saline, and colordevelopment was performed via incubation for 5 min using a

Fig. 1. Light microscopic appearance of hematoxylin and eosin- (A and B; original magnification ×200), periodic acid-Schiff- (C and D; in purple, originalmagnification ×200), and Masson's trichrome-stained (E and F; in blue, original magnification ×200) sections of the right atria of atrial fibrillation patient (A, C,E, and G) and sinus patient (B, D, F, and H). There were numerous cardiomyocytes with perinuclear sarcomere depletion and glycogen accumulation(arrowheads) in both patients (C and D). The normal longitudinally orientated cardiotin arrays (in brown) can no longer be detected in dedifferentiatedcardiomyocytes with perinuclear sarcomere depletion (arrows) (G and H).
159M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
solution containing 3,3′-diaminobenzidine (Liquid DAB-Plus substrate kit; Zymed Laboratories), according to theprotocol of the manufacturer. Tissue sections were alsocounterstained using hematoxylin solution for 2 min.Application of the primary antibody was omitted for
negative controls, while a fetal heart atrium from autopsywas used for the positive controls.
For immunostaining quantification, two sections peratrial samples were analyzed, with at least 100 randomlychosen cells being analyzed per section. Areas containing
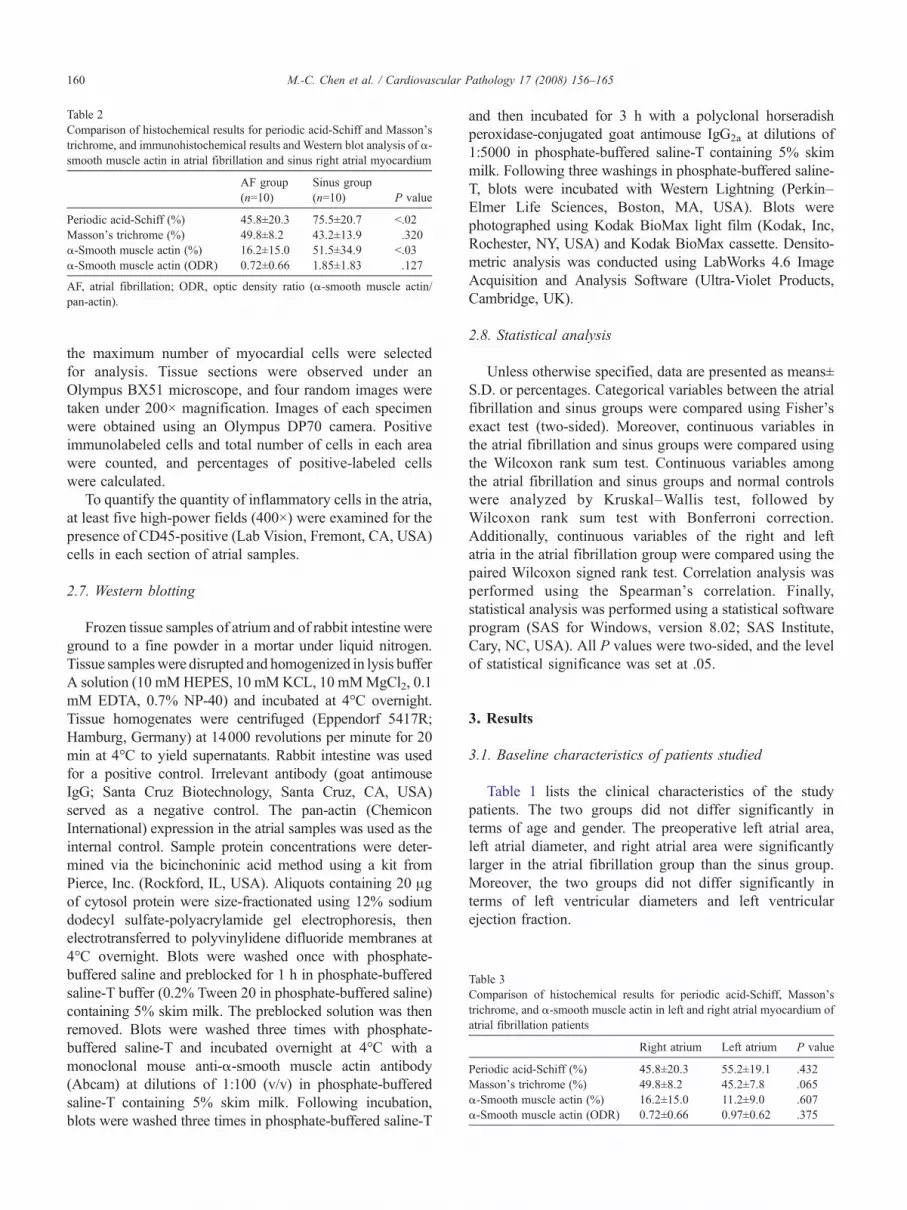
Table 2Comparison of histochemical results for periodic acid-Schiff and Masson'strichrome, and immunohistochemical results and Western blot analysis of α-smooth muscle actin in atrial fibrillation and sinus right atrial myocardium
AF group(n=10)
Sinus group(n=10) P value
Periodic acid-Schiff (%) 45.8±20.3 75.5±20.7 b.02Masson's trichrome (%) 49.8±8.2 43.2±13.9 .320α-Smooth muscle actin (%) 16.2±15.0 51.5±34.9 b.03α-Smooth muscle actin (ODR) 0.72±0.66 1.85±1.83 .127
AF, atrial fibrillation; ODR, optic density ratio (α-smooth muscle actin/pan-actin).
Table 3Comparison of histochemical results for periodic acid-Schiff, Masson'strichrome, and α-smooth muscle actin in left and right atrial myocardium ofatrial fibrillation patients
Right atrium Left atrium P value
Periodic acid-Schiff (%) 45.8±20.3 55.2±19.1 .432Masson's trichrome (%) 49.8±8.2 45.2±7.8 .065α-Smooth muscle actin (%) 16.2±15.0 11.2±9.0 .607α-Smooth muscle actin (ODR) 0.72±0.66 0.97±0.62 .375
160 M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
the maximum number of myocardial cells were selectedfor analysis. Tissue sections were observed under anOlympus BX51 microscope, and four random images weretaken under 200× magnification. Images of each specimenwere obtained using an Olympus DP70 camera. Positiveimmunolabeled cells and total number of cells in each areawere counted, and percentages of positive-labeled cellswere calculated.
To quantify the quantity of inflammatory cells in the atria,at least five high-power fields (400×) were examined for thepresence of CD45-positive (Lab Vision, Fremont, CA, USA)cells in each section of atrial samples.
2.7. Western blotting
Frozen tissue samples of atrium and of rabbit intestine wereground to a fine powder in a mortar under liquid nitrogen.Tissue sampleswere disrupted and homogenized in lysis bufferA solution (10 mMHEPES, 10 mMKCL, 10 mMMgCl2, 0.1mM EDTA, 0.7% NP-40) and incubated at 4°C overnight.Tissue homogenates were centrifuged (Eppendorf 5417R;Hamburg, Germany) at 14000 revolutions per minute for 20min at 4°C to yield supernatants. Rabbit intestine was usedfor a positive control. Irrelevant antibody (goat antimouseIgG; Santa Cruz Biotechnology, Santa Cruz, CA, USA)served as a negative control. The pan-actin (ChemiconInternational) expression in the atrial samples was used as theinternal control. Sample protein concentrations were deter-mined via the bicinchoninic acid method using a kit fromPierce, Inc. (Rockford, IL, USA). Aliquots containing 20 μgof cytosol protein were size-fractionated using 12% sodiumdodecyl sulfate-polyacrylamide gel electrophoresis, thenelectrotransferred to polyvinylidene difluoride membranes at4°C overnight. Blots were washed once with phosphate-buffered saline and preblocked for 1 h in phosphate-bufferedsaline-T buffer (0.2% Tween 20 in phosphate-buffered saline)containing 5% skim milk. The preblocked solution was thenremoved. Blots were washed three times with phosphate-buffered saline-T and incubated overnight at 4°C with amonoclonal mouse anti-α-smooth muscle actin antibody(Abcam) at dilutions of 1:100 (v/v) in phosphate-bufferedsaline-T containing 5% skim milk. Following incubation,blots were washed three times in phosphate-buffered saline-T
and then incubated for 3 h with a polyclonal horseradishperoxidase-conjugated goat antimouse IgG2a at dilutions of1:5000 in phosphate-buffered saline-T containing 5% skimmilk. Following three washings in phosphate-buffered saline-T, blots were incubated with Western Lightning (Perkin–Elmer Life Sciences, Boston, MA, USA). Blots werephotographed using Kodak BioMax light film (Kodak, Inc,Rochester, NY, USA) and Kodak BioMax cassette. Densito-metric analysis was conducted using LabWorks 4.6 ImageAcquisition and Analysis Software (Ultra-Violet Products,Cambridge, UK).
2.8. Statistical analysis
Unless otherwise specified, data are presented as means±S.D. or percentages. Categorical variables between the atrialfibrillation and sinus groups were compared using Fisher'sexact test (two-sided). Moreover, continuous variables inthe atrial fibrillation and sinus groups were compared usingthe Wilcoxon rank sum test. Continuous variables amongthe atrial fibrillation and sinus groups and normal controlswere analyzed by Kruskal–Wallis test, followed byWilcoxon rank sum test with Bonferroni correction.Additionally, continuous variables of the right and leftatria in the atrial fibrillation group were compared using thepaired Wilcoxon signed rank test. Correlation analysis wasperformed using the Spearman's correlation. Finally,statistical analysis was performed using a statistical softwareprogram (SAS for Windows, version 8.02; SAS Institute,Cary, NC, USA). All P values were two-sided, and the levelof statistical significance was set at .05.
3. Results
3.1. Baseline characteristics of patients studied
Table 1 lists the clinical characteristics of the studypatients. The two groups did not differ significantly interms of age and gender. The preoperative left atrial area,left atrial diameter, and right atrial area were significantlylarger in the atrial fibrillation group than the sinus group.Moreover, the two groups did not differ significantly interms of left ventricular diameters and left ventricularejection fraction.
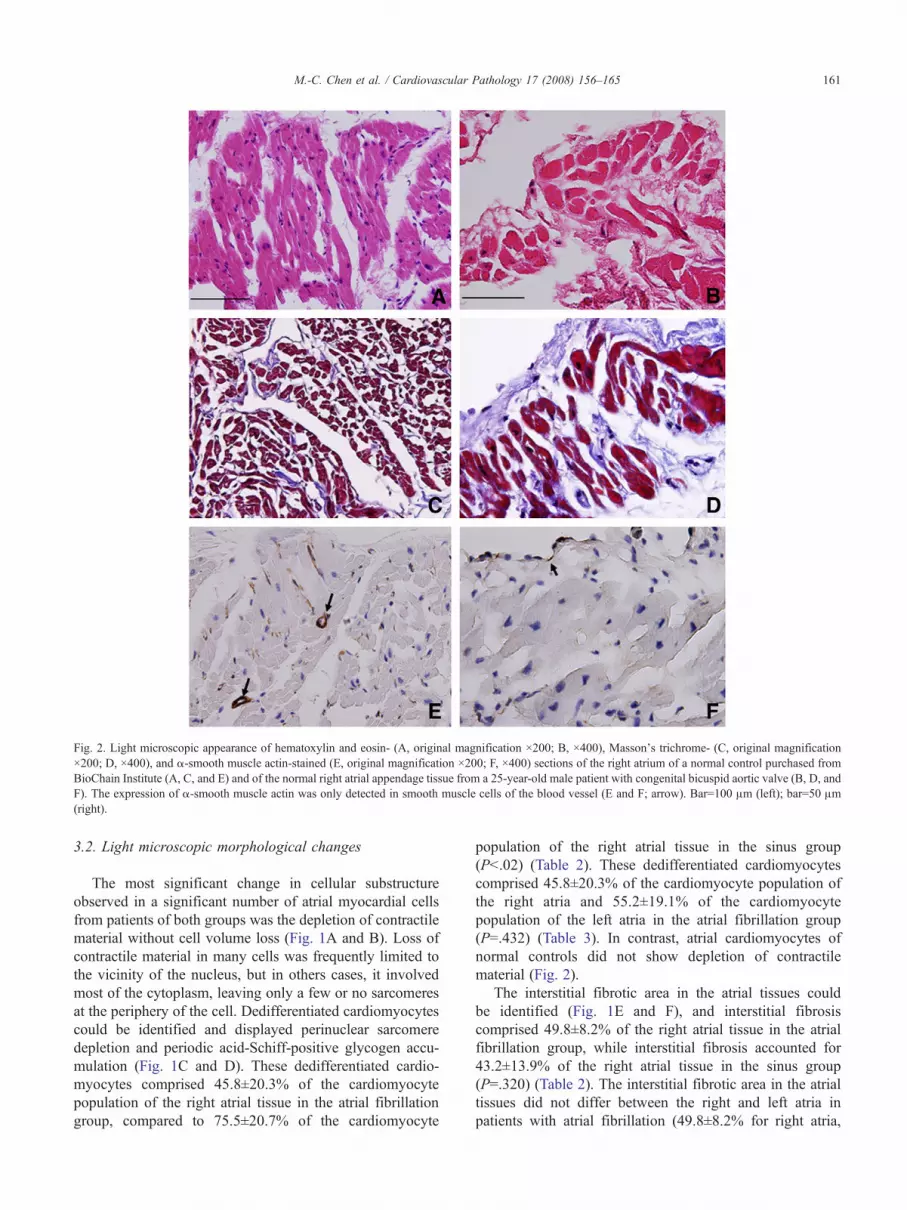
Fig. 2. Light microscopic appearance of hematoxylin and eosin- (A, original magnification ×200; B, ×400), Masson's trichrome- (C, original magnification×200; D, ×400), and α-smooth muscle actin-stained (E, original magnification ×200; F, ×400) sections of the right atrium of a normal control purchased fromBioChain Institute (A, C, and E) and of the normal right atrial appendage tissue from a 25-year-old male patient with congenital bicuspid aortic valve (B, D, andF). The expression of α-smooth muscle actin was only detected in smooth muscle cells of the blood vessel (E and F; arrow). Bar=100 μm (left); bar=50 μm(right).
161M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
3.2. Light microscopic morphological changes
The most significant change in cellular substructureobserved in a significant number of atrial myocardial cellsfrom patients of both groups was the depletion of contractilematerial without cell volume loss (Fig. 1A and B). Loss ofcontractile material in many cells was frequently limited tothe vicinity of the nucleus, but in others cases, it involvedmost of the cytoplasm, leaving only a few or no sarcomeresat the periphery of the cell. Dedifferentiated cardiomyocytescould be identified and displayed perinuclear sarcomeredepletion and periodic acid-Schiff-positive glycogen accu-mulation (Fig. 1C and D). These dedifferentiated cardio-myocytes comprised 45.8±20.3% of the cardiomyocytepopulation of the right atrial tissue in the atrial fibrillationgroup, compared to 75.5±20.7% of the cardiomyocyte
population of the right atrial tissue in the sinus group(Pb.02) (Table 2). These dedifferentiated cardiomyocytescomprised 45.8±20.3% of the cardiomyocyte population ofthe right atria and 55.2±19.1% of the cardiomyocytepopulation of the left atria in the atrial fibrillation group(P=.432) (Table 3). In contrast, atrial cardiomyocytes ofnormal controls did not show depletion of contractilematerial (Fig. 2).
The interstitial fibrotic area in the atrial tissues couldbe identified (Fig. 1E and F), and interstitial fibrosiscomprised 49.8±8.2% of the right atrial tissue in the atrialfibrillation group, while interstitial fibrosis accounted for43.2±13.9% of the right atrial tissue in the sinus group(P=.320) (Table 2). The interstitial fibrotic area in the atrialtissues did not differ between the right and left atria inpatients with atrial fibrillation (49.8±8.2% for right atria,
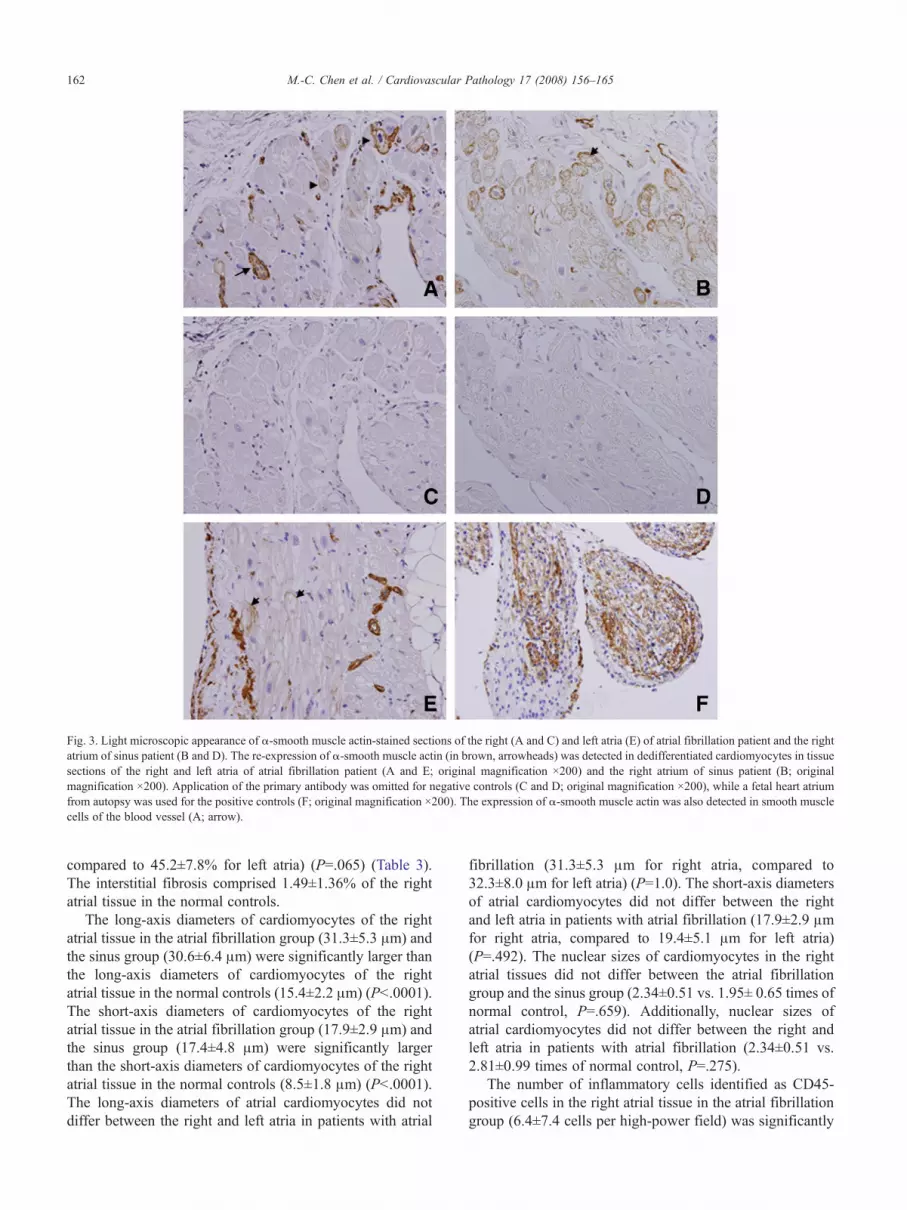
Fig. 3. Light microscopic appearance of α-smooth muscle actin-stained sections of the right (A and C) and left atria (E) of atrial fibrillation patient and the rightatrium of sinus patient (B and D). The re-expression of α-smooth muscle actin (in brown, arrowheads) was detected in dedifferentiated cardiomyocytes in tissuesections of the right and left atria of atrial fibrillation patient (A and E; original magnification ×200) and the right atrium of sinus patient (B; originalmagnification ×200). Application of the primary antibody was omitted for negative controls (C and D; original magnification ×200), while a fetal heart atriumfrom autopsy was used for the positive controls (F; original magnification ×200). The expression of α-smooth muscle actin was also detected in smooth musclecells of the blood vessel (A; arrow).
162 M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
compared to 45.2±7.8% for left atria) (P=.065) (Table 3).The interstitial fibrosis comprised 1.49±1.36% of the rightatrial tissue in the normal controls.
The long-axis diameters of cardiomyocytes of the rightatrial tissue in the atrial fibrillation group (31.3±5.3 μm) andthe sinus group (30.6±6.4 μm) were significantly larger thanthe long-axis diameters of cardiomyocytes of the rightatrial tissue in the normal controls (15.4±2.2 μm) (Pb.0001).The short-axis diameters of cardiomyocytes of the rightatrial tissue in the atrial fibrillation group (17.9±2.9 μm) andthe sinus group (17.4±4.8 μm) were significantly largerthan the short-axis diameters of cardiomyocytes of the rightatrial tissue in the normal controls (8.5±1.8 μm) (Pb.0001).The long-axis diameters of atrial cardiomyocytes did notdiffer between the right and left atria in patients with atrial
fibrillation (31.3±5.3 μm for right atria, compared to32.3±8.0 μm for left atria) (P=1.0). The short-axis diametersof atrial cardiomyocytes did not differ between the rightand left atria in patients with atrial fibrillation (17.9±2.9 μmfor right atria, compared to 19.4±5.1 μm for left atria)(P=.492). The nuclear sizes of cardiomyocytes in the rightatrial tissues did not differ between the atrial fibrillationgroup and the sinus group (2.34±0.51 vs. 1.95± 0.65 times ofnormal control, P=.659). Additionally, nuclear sizes ofatrial cardiomyocytes did not differ between the right andleft atria in patients with atrial fibrillation (2.34±0.51 vs.2.81±0.99 times of normal control, P=.275).
The number of inflammatory cells identified as CD45-positive cells in the right atrial tissue in the atrial fibrillationgroup (6.4±7.4 cells per high-power field) was significantly

Fig. 4. Western blot analysis of the α-smooth muscle actin (SMA) proteins inthe right (RA) and left atria (LA). Protein extracts from rabbit intestine wereused as positive controls for α-smooth muscle actin. The upper panel showstheWestern blot assay for α-smooth muscle actin, and the lower panel showsthe Western blot assay for pan-actin used as the internal control. NCindicates normal adult atrial appendage tissue; C, right atria from patients insinus rhythm; S, atria from patients with atrial fibrillation; P, positive control;N, negative control.
163M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
higher than the number of inflammatory cells in the rightatrial tissue in the normal controls (1.6±0.9 cells per high-power field) (P=.031). The number of inflammatory cellsin the right atrial tissues did not differ between the sinusgroup and normal control (2.5±1.8 cells vs. 1.6±0.9 cellsper high power field, PN.05). Additionally, the number ofinflammatory cells in the atrial tissues did not differbetween the right and left atria in patients with atrialfibrillation (6.4±7.4 cells per high-power field for rightatria, compared to 6.8±5.5 cells per high-power field forleft atria) (P=.275).
3.3. Dedifferentiation markers
Immunohistochemical identification of cardiomyocytededifferentiation was performed by analyzing proteinexpression patterns of cardiotin and α-smooth muscle actinin the atrial cardiomyocytes (Fig. 1G and H and Fig. 3).Cells, identified based on α-smooth muscle actin andcardiotin staining were counted to determine their reactivitywith monoclonal antibodies. In cells displaying perinuclearsarcomere depletion, the longitudinally oriented cardiotinarrays were less obvious or were even lost in dedifferentiatedcardiomyocytes (Fig. 1G and H). Re-expression of α-smoothmuscle actin was detected in the dedifferentiated cardio-myocytes in both groups of patients (Fig. 3). As Fig. 3shows, the expression of α-smooth muscle actin protein wasnot influenced by atrial fibrillation, and expression ofα-smooth muscle actin protein in atrial tissues was higherin patients with sinus rhythm than those with atrialfibrillation (percentage of cells that were α-smooth muscleactin-positive was 51.5±34.9% for right atria from patientsin sinus rhythm compared to 16.2±15.0% for right atriafrom patients with atrial fibrillation) (Pb.03) (Table 2). Theexpression of α-smooth muscle actin protein did not differbetween the right and left atria in patients with atrialfibrillation (percentage of cells that were α-smooth muscleactin-positive was 16.2±15.0% for right atria, compared to11.2±9.0% for left atria) (P=.607) (Fig. 3) (Table 3). Incontrast, atrial cardiomyocytes from normal controls did notshow the expression of α-smooth muscle actin (Fig. 2).
The changes in the expression of α-smooth muscle actinin the atrial myocardium were also analyzed using Westernblotting. Indeed, semiquantitation of α-smooth muscleactin via immunoblotting of extracts from atrial tissuesshowed similar findings as in the immunohistochemicalobservations (Fig. 4). As Fig. 4 shows, atrial fibrillation didnot influence the expression of α-smooth muscle actinprotein (P=.127) (Table 2). Furthermore, the expression ofα-smooth muscle actin protein did not differ between theright and left atria in patients with atrial fibrillation(P=.375) (Fig. 4) (Table 3).
3.4. Correlation between the expression of α-smooth muscleactin in the right atrial myocardium and hemodynamic andechocardiographic variables
In the atrial fibrillation group, correlation analysisrevealed no significant association between the expressionof α-smooth muscle actin in the right atrial myocardium viaWestern blotting and right atrial area (P=.829; r=−.079),and mean right atrial pressure (P =.290; r =−0.372).Additionally, correlation analysis revealed no significantassociation between the expression of α-smooth muscleactin in the right atrial myocardium based on cell counts byimmunohistochemistry and right atrial area (P =.533;r=.224), and mean right atrial pressure (P=.554; r=.213).In the sinus group, correlation analysis, based on Westernblotting, also showed no significant association between theexpression of α-smooth muscle actin in the right atrialmyocardium and right atrial area (P=.180; r=.571) andmean right atrial pressure (P=.200; r=.800). Similarly,correlation analysis, based on cell counts by immunohis-tochemistry, revealed no significant association between theexpression of α-smooth muscle actin in the right atrialmyocardium and right atrial area (P=.701; r=.139) andmean right atrial pressure (P=.577; r=−0.290).
4. Discussion
This study examined the structural changes of the atriain patients with severe mitral valve disease and moderateto severe tricuspid valve disease. This study yields severalimportant conclusions. First, dedifferentiation of atrialcardiomyocytes occurred in patients with cardiac valvedisease, even without atrial fibrillation. Second, the percen-tage of right atrial tissues with interstitial fibrosis wasthe same in patients with sinus rhythm and patients withatrial fibrillation.
4.1. Dedifferentiation of atrial cardiomyocytes in cardiacvalve disease
The expression of the α-smooth muscle actin isoform isconsidered characteristic of cardiomyocyte dedifferentiationand yields cardiomyocytes with structural hallmarks of fetal
164 M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
heart cells [5]. Cardiomyocyte dedifferentiation has pre-viously been reported in patients with chronic hibernatingmyocardium and in a goat model of chronic atrial fibrillation[5,6,10]. This study showed that, in adult patients withsevere mitral valve disease and moderate to severe tricuspidvalve disease, many atrial myocytes switched their differ-entiation program back to a state characteristic of fetalcardiac cells. Therefore, in the absence of atrial fibrillation,many atrial myocytes of patients with severe mitral valvedisease and moderate to severe tricuspid valve diseasededifferentiated to the point where an embryonic geneprogram that included the expression of the α-smoothmuscle actin gene was activated.
Atrial fibrillation generally results from profound changesin the functional properties and structure of the atrialmyocardium [11]. For instance, at the cellular level, atrialfibrillation is associated with a significant shortening of theaction potential. This study found structural changes in theatria, including adaptive (dedifferentiation of cardiomyo-cytes) and maladaptive (degeneration of cells with replace-ment fibrosis) features. This study thus proposed that, inpatients with mitral valve disease and sinus rhythm, thesestructural abnormalities could increase atrial vulnerability tothe future development of atrial fibrillation.
4.2. Potential mechanisms of structural remodeling incardiac valve disease
In this study, interstitial fibrosis comprised 49.8±8.2%and 43.2±13.9% of the right atrial tissue in the atrialfibrillation group and the sinus group, respectively. Dediffer-entiation of cardiomyocytes can be induced via coculturingadult rabbit cardiomyocytes with fibroblasts, and fibroblastproliferation prevents the cellular alteration from beingreversed [12,13]. These observations suggest that many ofthe structural changes accompanying dedifferentiation arenot, per se, dependent on reduced oxygen availability. Thehemodynamic load and increased wall stress of mitral valvedisease and tricuspid valve disease provide unfavorablecircumstances for dedifferentiation of atrial cardiomyocytesand for fibroblast proliferation, leading to interstitial fibrosis.Furthermore, fibroblast proliferation induces further dedif-ferentiation of cardiomyocytes and prevents reversal of thiscellular alteration.
4.3. Cardiomyocyte dedifferentiation as an adaptivemechanism capable of preserving myocardial viability
Dedifferentiated cardiomyocytes have been reported to beviable and more ischemia-tolerant, i.e., better protectedagainst ischemic insults than normally structured cardio-myocytes [7]. In the embolization-induced microinfarctedtissue model, the dedifferentiated cells are considered to bestable-surviving cells [14]. This structural remodeling, i.e.,dedifferentiation of the cardiomyocytes in chronic hibernat-ing myocardium, has been suggested to be at least partially
responsible for the delayed recovery of ventricular functionfollowing revascularization [8]. These indirect observations,thus, have suggested that cardiomyocyte dedifferentiationmight be an adaptive mechanism capable of prolongedpreservation of myocardial viability under unfavorablecircumstances [7]. This study identified structural changesin the atria, including adaptive (dedifferentiation of cardio-myocytes) features. Therefore, dedifferentiation of cardio-myocytes could result from common and nonspecificadaptive responses to changes in the working conditions ofthe atrial myocardium, including ischemia, rapid beating, orhemodynamic overload.
4.4. Cardiomyocyte dedifferentiation and recovery ofmyocardial function
Atrial fibrillation is mainly characterized by electricalremodeling and atrial functional deterioration. Both phe-nomena are reversible, but after prolonged duration of atrialfibrillation, there is a marked difference in the speed of thereversal, with rapid electrical remodeling but slow recoveryof atrial contractile function [15,16]. Recent studies haveshown that morphological remodeling might underlie thisincongruity, and dedifferentiation of atrial cardiomyocytes,myolysis, and atrial fibrosis is the proposed mechanismunderlying atrial stunning following cardioversion of atrialfibrillation [10,17]. In patients with atrial fibrillation,cardiomyocyte dedifferentiation does occur and may resultfrom underlying cardiac pathologies or longer atrial fibrilla-tion duration [10].
4.5. Clinical implication
Our findings indicate that atrial myocardial stretch as aresult of volume and pressure overload due to mitral valvedisease and tricuspid valve disease may play a predominantrole in the trigger for dedifferentiation of atrial cardiomyo-cytes. These subcellular adaptations represent a ratherstereotypic response of cardiomyocytes when the heart issubjected to unfavorable conditions, as seen in a variety ofother cardiac diseases such as chronic ischemia, dilatedcardiomyopathy, and atrial fibrillation [5–8]. These sub-cellular adaptations are not degenerative in nature but, rather,seem to be an act of programmed cell survival to theincreased cell stress [18]. Additionally, this structuralremodeling may be at least partially responsible for theatrial contractile dysfunction observed in patients withpressure and volume overload in the atria [19]. Whetherthis structural remodeling is partially responsible for the laterestoration of atrial function after valve surgery needs to beinvestigated in experimental studies [20].
4.6. Study limitations
The limitations of this study should be addressed. First,the exclusive focus on atrial appendage tissue was too

165M.-C. Chen et al. / Cardiovascular Pathology 17 (2008) 156–165
limited for investigating the presence of cardiomyocytededifferentiation in the whole atrium of the patients.However, it should not affect our major findings, i.e.,dedifferentiation of atrial cardiomyocytes occurred inpatients with cardiac valve disease, even without atrialfibrillation. Second, the possibility of paroxysmal atrialfibrillation in the sinus group could not be entirely excluded.However, patients in the sinus group had never been in atrialfibrillation by history and electrocardiograms before surgery,and the atrial tissues were obtained during sinus rhythm.Third, α-smooth muscle actin was constitutionally expressedin vascular smooth muscle cells in the vessel walls of theatria. Only positive immunolabeled atrial cardiomyocyteswere counted in immunohistochemical analysis; however,extracts of vascular smooth muscle cells in the vessel wallswere also included in Western blotting quantification. Theoptic density ratio of α-smooth muscle actin vs. pan-actin innormal adult atrial appendage tissue was 0.227. Additionally,atrial tissue sections of the atrial appendage used for Westernblotting were not from the same region as those forimmunohistochemical analysis. Therefore, it is not surpris-ing to observe that the expression of α-smooth muscle actinprotein in atrial tissues was significantly higher in patientswith sinus rhythm than patients with atrial fibrillation byimmunohistochemical analysis, not by Western blotting.Finally, atrial cardiomyocytes were under chronic hemody-namic load due to mitral valve disease and tricuspid valvedisease, not in acute model; therefore, we did not find anycorrelation between the expression of α-smooth muscle actinin the right atrial myocardium based on Western blotting andright atrial pressure in this study.
5. Conclusions
Dedifferentiation of atrial cardiomyocytes, as character-ized by the re-expression of the α-smooth muscle actinisoform, occurs in patients with cardiac valve disease, evenwithout atrial fibrillation.
References
[1] Supino PG, Borer JS, Yin A. The epidemiology of valvular heartdisease: an emerging public health problem. Adv Cardiol 2002;39:1–6.
[2] Supino PG, Borer JS, Yin A, Dillingham E, McClymont W.The epidemiology of valvular heart diseases: the problem is growing.Adv Cardiol 2004;41:9–15.
[3] Wilson PW. An epidemiologic perspective of systemic hypertension,ischemic heart disease, and heart failure. Am J Cardiol 1997;80:3J–8J.
[4] Grigioni F, Enriquez-Sarano M, Ling LH, Bailey KR, Seward JB,Tajik AJ, Frye RL. Sudden death in mitral regurgitation due to flailleaflet. J Am Coll Cardiol 1999;34:2086–7.
[5] Ausma J, Wijffels M, van Eys G, Koide M, Ramaekers F, Allessie M,Borgers M. Dedifferentiation of atrial cardiomyocytes as a result ofchronic atrial fibrillation. Am J Pathol 1997;151:985–97.
[6] Ausma J, Schaart G, Thone F, Shivalkar B, Flameng W, Depre C,Vanoverschelde JL, Ramaekers F, Borgers M. Chronic ischemic viablemyocardium in man: aspects of dedifferentiation. Cardiovasc Pathol1995;4:29–37.
[7] Ausma J, Thone F, Dispersyn GD, Flameng W, Vanoverschelde JL,Ramaekers FC, Borgers M. Dedifferentiated cardiomyocytes fromchronic hibernating myocardium are ischemic-tolerant. Mol CellBiochem 1998;186:159–68.
[8] Maes A, Flameng W, Nuyts J, Borgers M, Shivalkar B, Ausma J,Bormans G, Schiepers C, De Roo M, Mortelmans L. Histologicalalterations in chronically hypoperfused myocardium: correlation withpositron emission tomography findings. Circulation 1994;90:735–45.
[9] Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD,Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, RakowskiH, Stewart WJ, Waggoner A, Weissman NJ. Recommendations forevaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr2003;16:777–802.
[10] Ausma J, Litjens N, Lenders MH, Mast F, Wouters L, Ramaekers F,Allessie M, Borgers M. Time course of atrial fibrillation-inducedcellular structural remodeling in atria of the goat. J Mol Cell Cardiol2001;33:2083–94.
[11] Nattel S. New ideas about atrial fibrillation 50 years on. Nature 2002;415:219–26.
[12] Dispersyn GD, Geuens E, Ver Donck L, Ramaekers FCS, Borgers M.Adult rabbit cardiomyocytes undergo hibernation-like dedifferentia-tion when co-cultured with cardiac fibroblasts. Cardiovasc Res 2001;51:230–40.
[13] Rucker-Martin C, Pecker F, Godreau D, Hatem SN. Dedifferentiationof atrial myocytes during atrial fibrillation: role of fibroblastproliferation in vitro. Cardiovasc Res 2002;55:38–52.
[14] Dispersyn GD, Mesotten L, Meuris B, Maes A, Mortelmans L,Flameng W, Ramaekers F, Borgers M. Dissociation of cardiomyocyteapoptosis and dedifferentiation in infarct border zones. Eur Heart J2002;23:849–57.
[15] Mattioli AV, Bonatti S, Bonetti L, Mattioli G. Left atrial size aftercardioversion for atrial fibrillation: effect of external direct currentshock. J Am Soc Echocardiogr 2003;16:271–6.
[16] Nishino M, Hoshida S, Tanouchi J, Ito T, Kato J, Iwai K, Tanahashi H,Hori M, Yamada Y, Kamada T. Time to recover from atrial hormonal,mechanical and electrical dysfunction after successful electricalcardioversion of persistent atrial fibrillation. Am J Cardiol 2000;85:1451–4.
[17] Khan IA. Atrial stunning: determinants and cellular mechanisms.Am Heart J 2003;145:787–94.
[18] Thijssen VLJL, Ausma J, Borgers M. Structural remodelling duringchronic atrial fibrillation: act of programmed cell survival. CardiovascRes 2001;52:14–24.
[19] Tabata T, Oki T, Fukuda N, Iuchi A, Manabe K, Kageji Y, Sasaki M,Yamada H. Influence of left atrial pressure on left atrial appendage flowvelocity patterns in patients with sinus rhythm. J Am Soc Echocardiogr1996;9:857–64.
[20] Pascual JG, Pajuelo CG, Bodes RS, Perez IS, Casares SF, Romero FL,Meneses RT, Sanchez JJ, de la Calzada CS. Systolic left atrial failure inelderly women with severe aortic stenosis: mitral and pulmonary veinDoppler analysis by transesophageal echocardiography. Echocardio-graphy 2004;21:247–55.





























