Embed Size (px)
Citation preview

CTW
A7cmtocaoPbymttc
CPvmfib
D
A
2
ontroversies in thereatment of Central Cord Injuriesinston Fong, MD, and Frank J. Eismont, MD
Central cord injury or central cord syndrome is an acute cervical spinal cord injurycharacterized by more extensive motor weakness of the upper extremities compared withthe lower extremities, usually with bladder dysfunction, and variable sensory loss below thelevel of the lesion. Central cord syndrome is the most common type of incomplete spinalcord injury pattern and is associated with a moderate to good prognosis. Over the last fivedecades, the role of surgical intervention, as well as the type and timing of surgery,continues to be the subject of considerable debate. These controversies are the focus ofthis article.Semin Spine Surg 19:260-271 © 2007 Elsevier Inc. All rights reserved.
KEYWORDS central, spinal, spine, cord, syndrome, injury
lw7hticnrawewsar
PSdsfctvvcr
pproximately 16 to 25% of patients with cervical spinalcord injuries present with central cord syndrome, while
0% of all incomplete cervical spinal cord injuries are centralord lesions.1,2 Multiple authors have demonstrated a bi-odal age distribution to the central cord syndrome popula-
ion.3-7 Schneider and coworkers3 were the first to note anlder age group (mean age, 59) with spondylotic changesompromising the canal but no bony damage, and a youngerge group (mean age, 31) with fractures and/or dislocationsf the cervical spine. Shrosbree,4 Roth and colleagues,5 andenrod and colleagues6 showed approximately equal num-ers of older and younger patients, with two peaks at 21 to 30ears and 61 to 70 years. Merriam and colleagues2 found thatore than half of the patients in their series were under age 30 at
he time of injury, whereas Hardy8 noted that older people sus-ain central cord syndrome more frequently. Motor vehicle ac-idents and falls are the most common causes of injury.
linical Courseatients with acute central cord injuries typically have a fa-orable prognosis for neurological and functional improve-ent. Recovery occurs in a predictable pattern beginningrst in the lower extremities and then progressing to theladder and upper extremities, with the hands improving
epartment of Orthopaedics and Rehabilitation, University of Miami, MillerSchool of Medicine, Miami, FL.
ddress reprint requests to Frank J. Eismont, MD, Department of Orthopae-dics and Rehabilitation, University of Miami, Miller School of Medicine,
oP.O. Box 016960, Miami, FL 33131. E-mail: [email protected]
60 1040-7383/07/$-see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1053/j.semss.2007.09.008
ast. In a retrospective review of 42 patients who presentedith acute central cord injury, Bosch and colleagues1 noted7% regained ambulatory skills, 56% regained functionalands, and 53% regained bowel and bladder control at long-erm follow-up, although 10/42 had late deterioration afternitial improvement in symptoms. Predictors of a better out-ome include younger age, absence of spasticity, and lesseurological deficit on admission.1,4-7,9-11 Central cord inju-ies with selective upper extremity involvement have beenssociated with better functional improvement than in thoseith both upper and lower extremity involvement.5,11 Inter-
stingly, preinjury employment and formal education levelere also found to correlate with better outcomes.5,10 The
trongest predictor of a poor functional outcome is advancedge, although the elderly may also experience significant neu-ological improvement.5-7,9
rimary Mechanisms of Injurychneider and coworkers reported that central cord syn-rome typically occurred in elderly patients with cervicalpondylosis and stenosis without bony damage, but they alsoound that it rarely occurred in patients with fracture-dislo-ations or compression fractures.12 They believed hyperex-ension to cause a pinching effect of the spinal cord betweenentral osteophytes anteriorly and a buckled ligamentum fla-um posteriorly. Subsequent studies have shown that centralord syndrome can occur in individuals of any age and canesult from fractures, dislocations, and hyperflexion injuries
f the cervical spine at a much higher rate than originally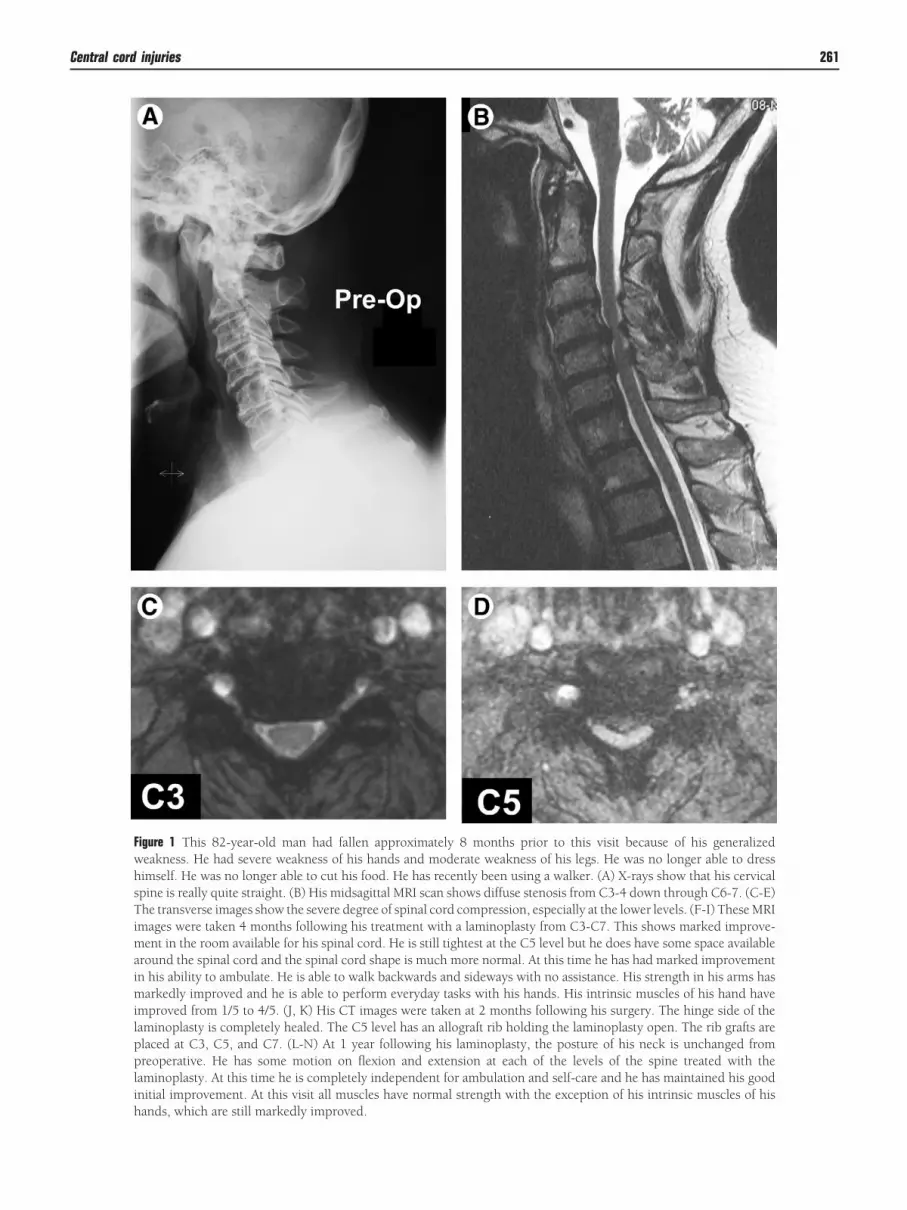
Central cord injuries 261
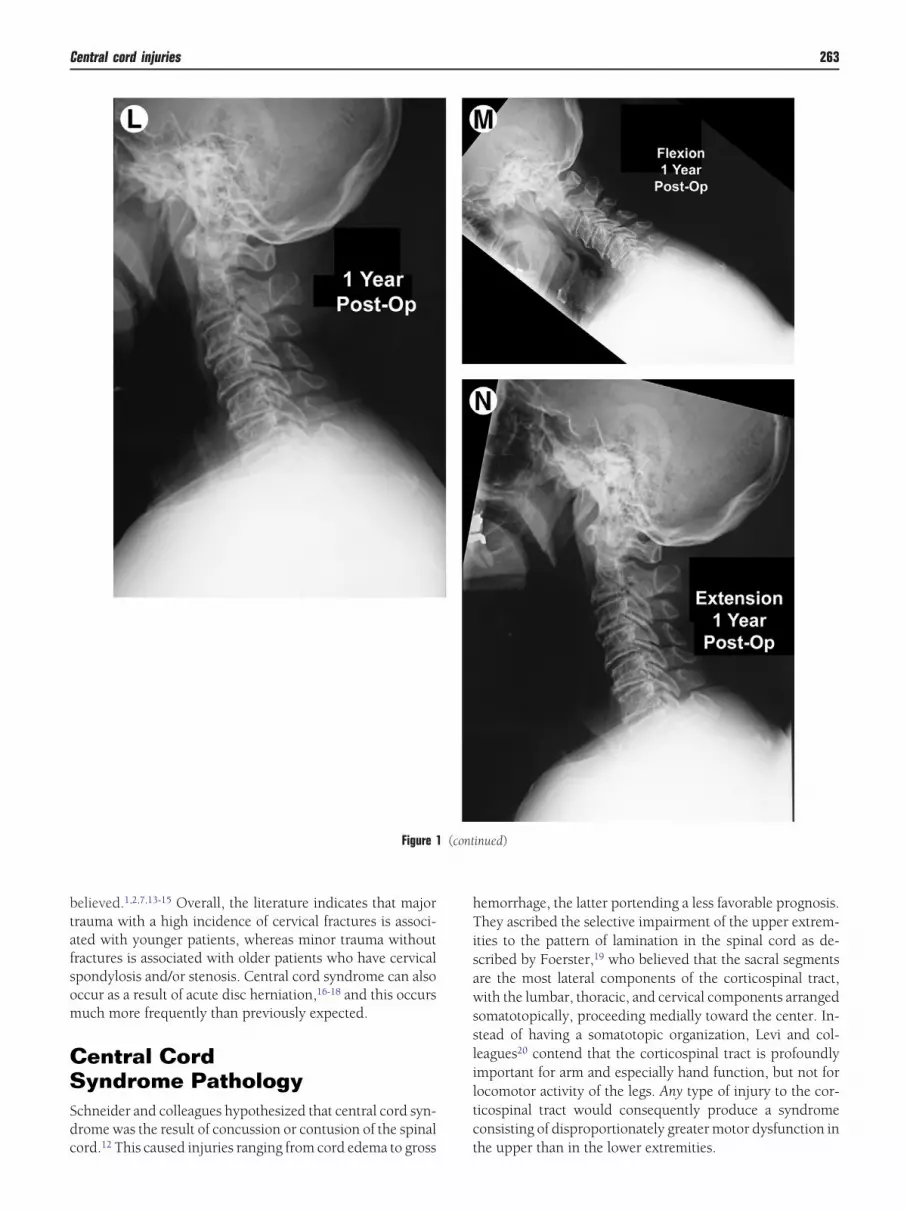
Figure 1 This 82-year-old man had fallen approximately 8 months prior to this visit because of his generalizedweakness. He had severe weakness of his hands and moderate weakness of his legs. He was no longer able to dresshimself. He was no longer able to cut his food. He has recently been using a walker. (A) X-rays show that his cervicalspine is really quite straight. (B) His midsagittal MRI scan shows diffuse stenosis from C3-4 down through C6-7. (C-E)The transverse images show the severe degree of spinal cord compression, especially at the lower levels. (F-I) These MRIimages were taken 4 months following his treatment with a laminoplasty from C3-C7. This shows marked improve-ment in the room available for his spinal cord. He is still tightest at the C5 level but he does have some space availablearound the spinal cord and the spinal cord shape is much more normal. At this time he has had marked improvementin his ability to ambulate. He is able to walk backwards and sideways with no assistance. His strength in his arms hasmarkedly improved and he is able to perform everyday tasks with his hands. His intrinsic muscles of his hand haveimproved from 1/5 to 4/5. (J, K) His CT images were taken at 2 months following his surgery. The hinge side of thelaminoplasty is completely healed. The C5 level has an allograft rib holding the laminoplasty open. The rib grafts areplaced at C3, C5, and C7. (L-N) At 1 year following his laminoplasty, the posture of his neck is unchanged frompreoperative. He has some motion on flexion and extension at each of the levels of the spine treated with thelaminoplasty. At this time he is completely independent for ambulation and self-care and he has maintained his goodinitial improvement. At this visit all muscles have normal strength with the exception of his intrinsic muscles of his
hands, which are still markedly improved.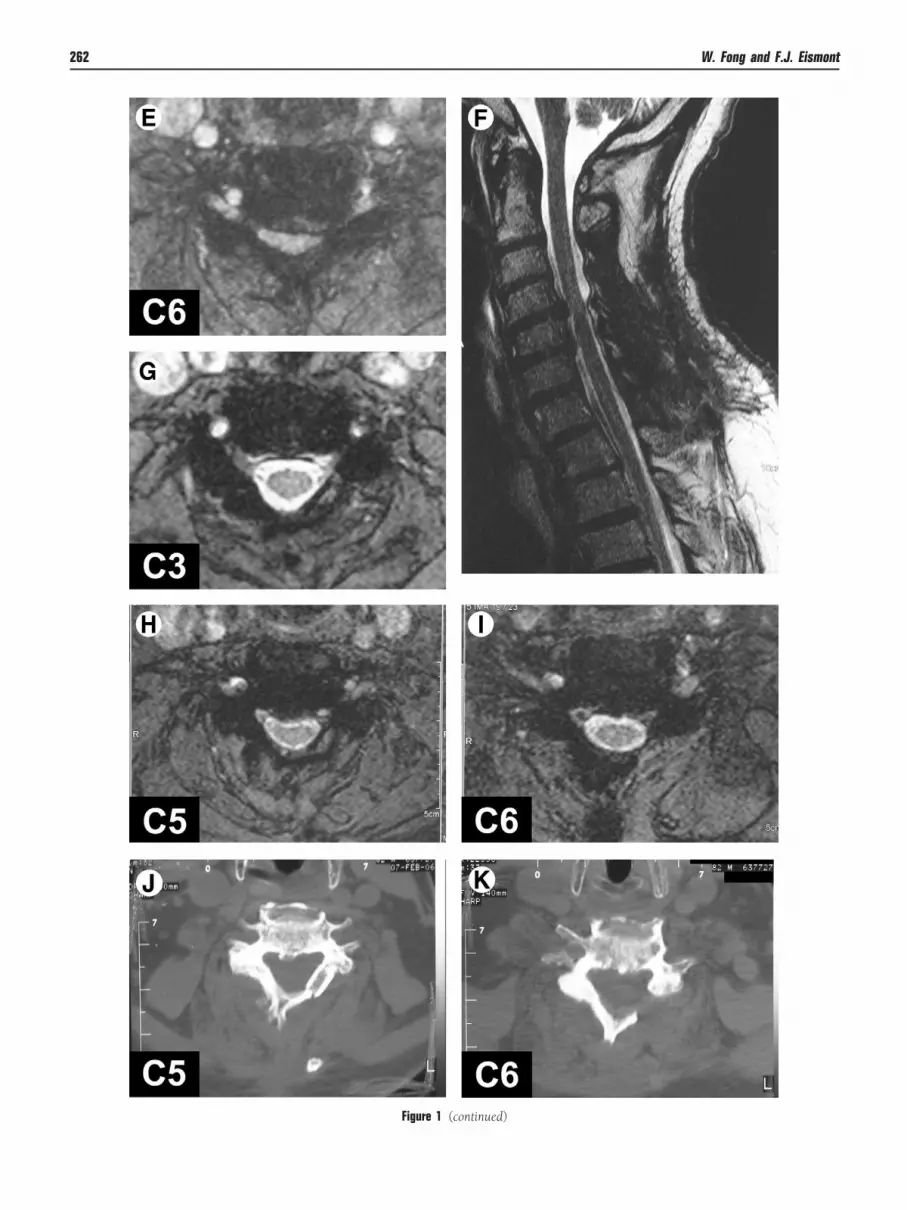
262 W. Fong and F.J. Eismont
Figure 1 (continued)
btafsom
CSSdc
hTisawssliltc
(cont
Central cord injuries 263
elieved.1,2,7,13-15 Overall, the literature indicates that majorrauma with a high incidence of cervical fractures is associ-ted with younger patients, whereas minor trauma withoutractures is associated with older patients who have cervicalpondylosis and/or stenosis. Central cord syndrome can alsoccur as a result of acute disc herniation,16-18 and this occursuch more frequently than previously expected.
entral Cordyndrome Pathology
chneider and colleagues hypothesized that central cord syn-rome was the result of concussion or contusion of the spinal
Figure 1
ord.12 This caused injuries ranging from cord edema to gross t
emorrhage, the latter portending a less favorable prognosis.hey ascribed the selective impairment of the upper extrem-
ties to the pattern of lamination in the spinal cord as de-cribed by Foerster,19 who believed that the sacral segmentsre the most lateral components of the corticospinal tract,ith the lumbar, thoracic, and cervical components arranged
omatotopically, proceeding medially toward the center. In-tead of having a somatotopic organization, Levi and col-eagues20 contend that the corticospinal tract is profoundlymportant for arm and especially hand function, but not forocomotor activity of the legs. Any type of injury to the cor-icospinal tract would consequently produce a syndromeonsisting of disproportionately greater motor dysfunction in
inued)
he upper than in the lower extremities.
csdn(adsns
ioicJfw
PTocTtfrTIctorosaA(mcOta
neStm
SSDs
cdtctmtliwlccis1dsaowld
aaswcacactjn(
aspoBs1twpafis8dscst
264 W. Fong and F.J. Eismont
Recent autopsy studies performed in 3 of 11 subjects withentral cord syndrome by Quencer and colleagues21 and in 1ubject by Martin and colleagues22 revealed diffuse axonalisruption and edema in the surrounding white matter, buto involvement of the gray matter. Magnetic resonance imagingMRI) studies of patients with acute central cord syndrome havelso revealed edematous changes within the cord but no evi-ence of hemorrhage within the gray matter.21-23 These studiesuggest that disruption of axons in the lateral white matter, andot hemorrhage of the gray matter, is most commonly respon-ible for the central cord syndrome.
Although less common than cord swelling and axonal edema,ntramedullary hemorrhage has been described in MRI reportsf central cord syndrome.24-26 Dai24 found hemorrhage on MRIn 3 of 32 patients with central cord syndrome, and Maroon andolleagues26 noted 1 of 10 cases had hemorrhage in their series.ust as Schneider and colleagues12 originally hypothesized, Dai24
ound that the presence of hemorrhage was associated with aorse prognosis.
harmacological Therapyhere has been a longstanding interest in the administrationf pharmacological therapies to improve neurological out-omes in patients suffering from acute spinal cord injury.hese pharmacological interventions are aimed at limiting
he secondary injury cascade. A substantial body of evidencerom animal models supports this concept, but effective neu-oprotection in humans has been difficult to demonstrate.he publication of the second National Acute Spinal Cordnjury Study (NASCIS II)27 in 1990 was heralded as the firstonvincing study to demonstrate pharmacological neuropro-ection in humans and became widely accepted as a standardf care for use in acute spinal cord injury. However, moreecent criticisms28-30 on the presentation and interpretationf this study and the subsequent NASCIS III study31 have ledome groups32,33 to speak out against methylprednisolone asguideline for the treatment of acute spinal cord injury.dditional pharmacological agents such as GM-1 ganglioside
Sygen),34 naloxone,27 thyrotropin releasing hormone,35 ni-odipine,36 and tirilazad mesylate31 have undergone human
linical trials but have not demonstrated significant efficacy.ther promising medications undergoing current investiga-
ion include riluzole, minocycline, erythropoietin, and rhontagonists.37
Various controversies have prompted a committee of Ca-adian neurosurgical and orthopedic spine specialists andmergency physicians as well as the Congress of Neurologicalurgeons to conclude that methylprednisolone cannot be es-ablished as a guideline and can only be regarded as a treat-ent option.32,33
urgical Decompressionurgery versus Nonoperative Careespite the numerous animal studies that suggest that early
pinal cord decompression improves neurological out- g
ome,38-42 controversy remains over the role of spinal cordecompression in humans. In their original description ofraumatic central cord syndrome in 1954, Schneider andolleagues12 recommended conservative management for pa-ients with these injuries. This was based on observations thatost patients in their series improved spontaneously and
hat one of two patients whom they treated surgically with aaminectomy and intradural exploration worsened neurolog-cally immediately after surgery. Their recommendation wasidely accepted until 1971 when Bosch and colleagues1 pub-
ished a review of patients with spinal cord injuries that in-luded 42 cases of central cord syndrome that were managedonservatively. While improvement in neurological functionn most patients was seen initially, long-term observationshowed that only 59% of patients retained functional skills at0-year follow-up. They noted a “chronic central cord syn-rome” in which patients who initially improved with con-ervative management later developed increased spasticitynd pyramidal tract involvement. This occurred in 10 (24%)f their 42 patients. Unfortunately, seven of these patientsho had been functional ambulators at the time of discharge
ater became wheelchair dependent because of neurologicaleterioration.After Bosch’s report of “chronic central cord syndrome”
nd the development of new surgical techniques, Brodkeynd colleagues14 revisited the management of central cordyndrome in 1980 in an article that reviewed their experienceith operative treatment of seven patients with traumatic
entral cord injuries. They performed surgery 3 to 6 weeksfter injury in these patients, all of whom had spinal cordompression. All patients had rapid improvement postoper-tively, which distinctly contrasted to their static clinicalourse immediately before surgery. The authors concludedhat decompression of the spinal cord after central cord in-ury may be beneficial if present in the setting of a stable pooreurological condition with residual neural compressionFig. 1).
Subsequent studies have suggested that surgery may bessociated with more rapid neurological recovery than con-ervative treatment in patients with persistent neural com-ression and either neurological deterioration or plateauingf neurological function at an unacceptably low level.13,16,43
ose and colleagues13 evaluated 28 patients with central cordyndrome paralysis with 14 patients managed medically and4 patients managed both medically and surgically. Al-hough no randomization was performed and the two groupsere not comparable, they found that operative interventionrovided better motor recovery than did conservative ther-py alone. In 1997, Chen and colleagues16 reported similarndings in a retrospective review of traumatic central cordyndrome that involved 28 patients managed surgically and6 patients managed medically. Later, Chen and colleagues43
escribed the management of 37 patients with preexistingpondylosis who sustained incomplete injuries after minorervical trauma without fracture, subluxation, or disc protru-ion. Many suffered acute central cord injuries. Patients werereated surgically if they did not improve more than one
rade within 3 to 14 days (mean 9 days) after injury. Al-
tocaiteo
cmndtiSfhttm
TTtpolstdhaovvnrcPvrnclcdsi
aacsopc
coias
cuccslfadedoit
icitdcpAcir
vmsligt
itdIr(sctf
SSpl
Central cord injuries 265
hough there were no statistically significant differences inutcome at 2-year follow-up, they found that surgical de-ompression was associated with more rapid improvementnd a shorter hospital and rehabilitation stay. Recent stud-es17,44 have suggested that surgical treatment is the optimalreatment for patients with central cord injury if MRI revealsvidence of spinal cord compression, even without fracturer dislocation.In 2002, Ishida and Tominaga11 identified a subset of the
entral cord syndrome population in which they recom-ended nonoperative treatment. They studied the course ofeurological recovery of 22 patients with central cord syn-rome with only upper extremity involvement and foundhat their motor and sensory deficits rapidly recovered dur-ng the first 3 weeks after injury and plateaued by 6 weeks.eventy-seven percent of patients had full recovery of motorunction. The remaining 23% had mild dysfunction of theands at 2-year follow-up. Based on the favorable outcome ofheir patients with isolated upper extremity involvement,hese authors recommended an initial nonoperative treat-ent course for this subset of central cord syndrome.
iming of Surgeryhe most appropriate timing of surgical intervention for all
ypes of acute spinal cord injury (both complete and incom-lete injuries) remains controversial. This subject is the topicf recent review articles.45,46 La Rosa and colleagues45 pub-ished a meta-analysis of the literature regarding the timing ofurgical decompression after spinal cord injuries in whichhey were able to extract data on 1687 patients. Patients wereivided into three treatment groups: early surgery (�24ours), delayed surgery (�24 hours), and conservative man-gement. Statistically, early decompression resulted in betterutcomes compared with both delayed surgery and conser-ative management. However, analysis of homogeneity re-ealed that only data regarding patients with incomplete spi-al cord injuries who underwent early decompression wereeliable. They concluded that early surgical decompressionan only be considered as a treatment option.45 Fehlings anderrin46 recently performed an evidence-based literature re-iew. They noted that, while there are currently no standardsegarding the role and timing of decompression in acute spi-al cord injury, there is evidence that supports urgent de-ompression in a patient with neurological deterioration fol-owing spinal cord injury and that early (�24 hours) surgeryan be performed safely. They thus recommended urgentecompression as an option following isolated acute cervicalpinal cord injury, provided that the patient is hemodynam-cally stable.46
Most studies investigating the role of surgical timing forcute spinal cord injury, including those reviewed by La Rosand colleagues45 and Fehlings and Perrin,46 involved bothomplete and incomplete injuries. The appropriate timing ofurgery in central cord injury, however, may be different thanther types of cervical spinal cord injuries given its distinctathophysiology. In fact, central cord syndrome was ex-
luded from analysis in some studies on the basis of its spe- lific pattern of injury and favorable prognosis for spontane-us recovery.47 Thus, data from these studies, althoughnformative, may not be relevant to central cord injury. Therere only a few studies that address the role of surgical timingpecifically in patients with central cord injury.18,48,49
In 2002, Guest and colleagues18 compared the clinical out-omes of patients with traumatic central cord syndrome whonderwent early (�24 hours) versus late (�24 hours) surgi-al decompression. They also compared the clinical out-omes of those patients with central cord syndrome paralysisecondary to acute disc herniations or cervical fractures/dis-ocations to those with spondylosis or stenosis. Early surgeryor both groups was found to be safe and was associated withdecreased intensive care and hospital stay compared withelayed surgery. With respect to neurological outcomes,arly surgery was associated with improved recovery of blad-er and ambulatory ability for patients with disc herniationsr fracture/dislocations. There was no difference in neurolog-cal improvement with respect to timing of surgery for pa-ients with spondylosis or stenosis.
In contrast, in a review of 412 patients with traumatic,ncomplete cervical spinal cord injuries of which 24% hadentral cord syndrome, Pollard and Apple48 found no signif-cant differences in neurological improvement for early (lesshan 24 hours) versus late (greater than 24 hours) surgicalecompression. This was true for both patients with anteriorord compression from fracture or disc herniation and foratients with cervical stenosis without fracture or instability.s expected, the authors did find that patients with a centralord syndrome or Brown–Sequard syndrome had relativelymproved outcomes compared with other incomplete inju-ies.
In 2005, Yamazaki and colleagues49 retrospectively re-iewed their experience with 47 patients who suffered trau-atic central cord injury, 23 of whom were treated with
urgery. They found that the only factors predictive of excel-ent recovery were the AP diameter of the spinal canal and thenterval from injury to surgery. Patients who underwent sur-ery within 2 weeks had more neurological improvementhan those who underwent surgery after 2 weeks.
The mixed results of these studies and their methodolog-cal limitations highlight the need for well-designed prospec-ive studies to evaluate the effect of early versus late surgicalecompression. The Surgical Timing in Acute Spinal Cordnjury Study is a multicenter, prospective trial that is cur-ently evaluating the effect of early (�24 hours) versus late�24 hours) decompressive surgery for patients with cervicalpinal cord injury.46 The appropriate timing of surgery inentral cord injury, however, may be different than otherypes of cervical spinal cord injuries and thus also requiresurther detailed investigation.
urgical Approachurgical decompression for central cord injury may be ap-roached either anteriorly or posteriorly and should be tai-
ored to the specific pathology involved. Guest and col-
eagues18 performed an anterior approach for patients with
dvdll(rp
ap
phdi
266 W. Fong and F.J. Eismont
isc herniation or significant anterior compression due toertebral body fracture, large focal spondylotic bars, or spon-ylotic stenosis confined to no more than three vertebral
evels. When spinal stenosis was present at three or moreevels, posterior laminectomy or laminoplasty was performedFig. 2). Their strategy was consistent with what others haveeported in the literature9,17,26,43,44,49 and what is typically
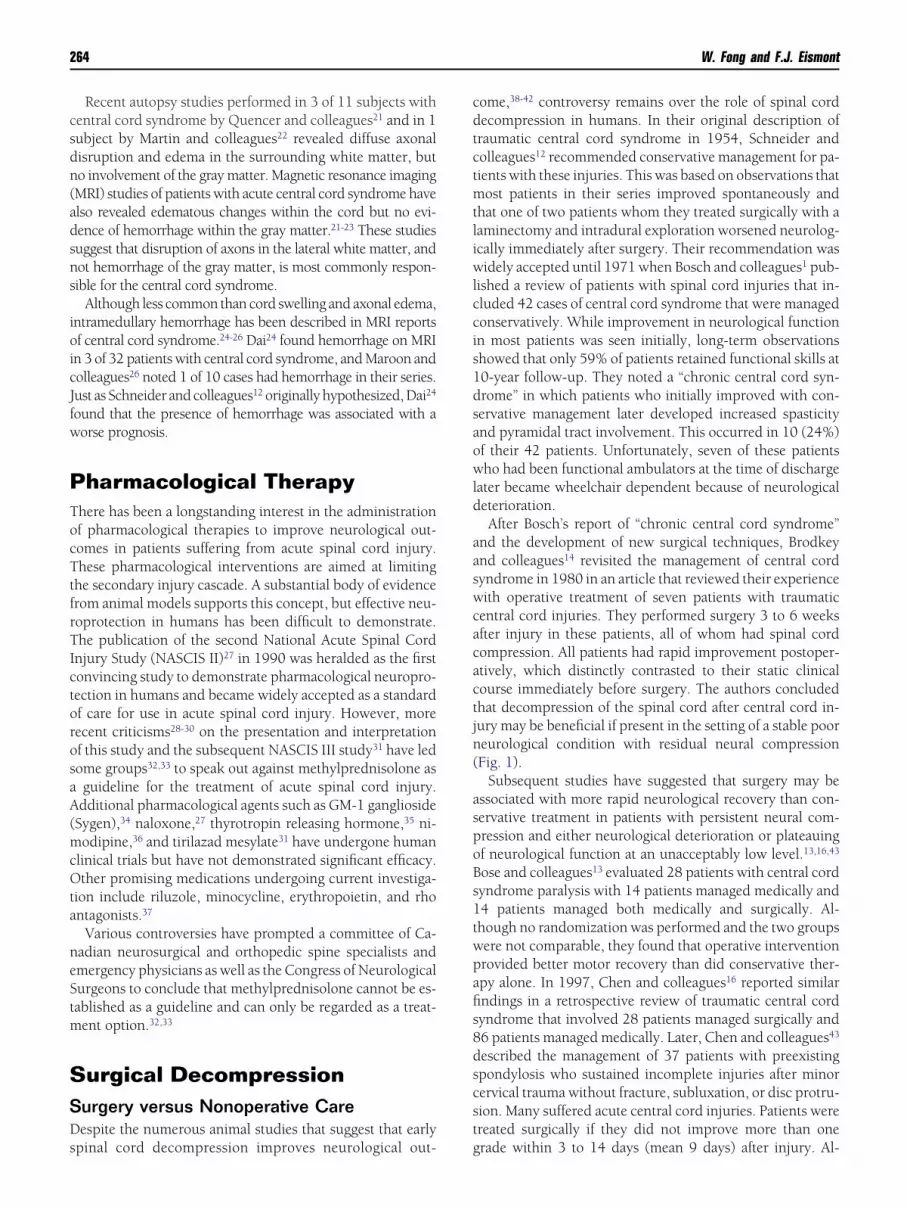
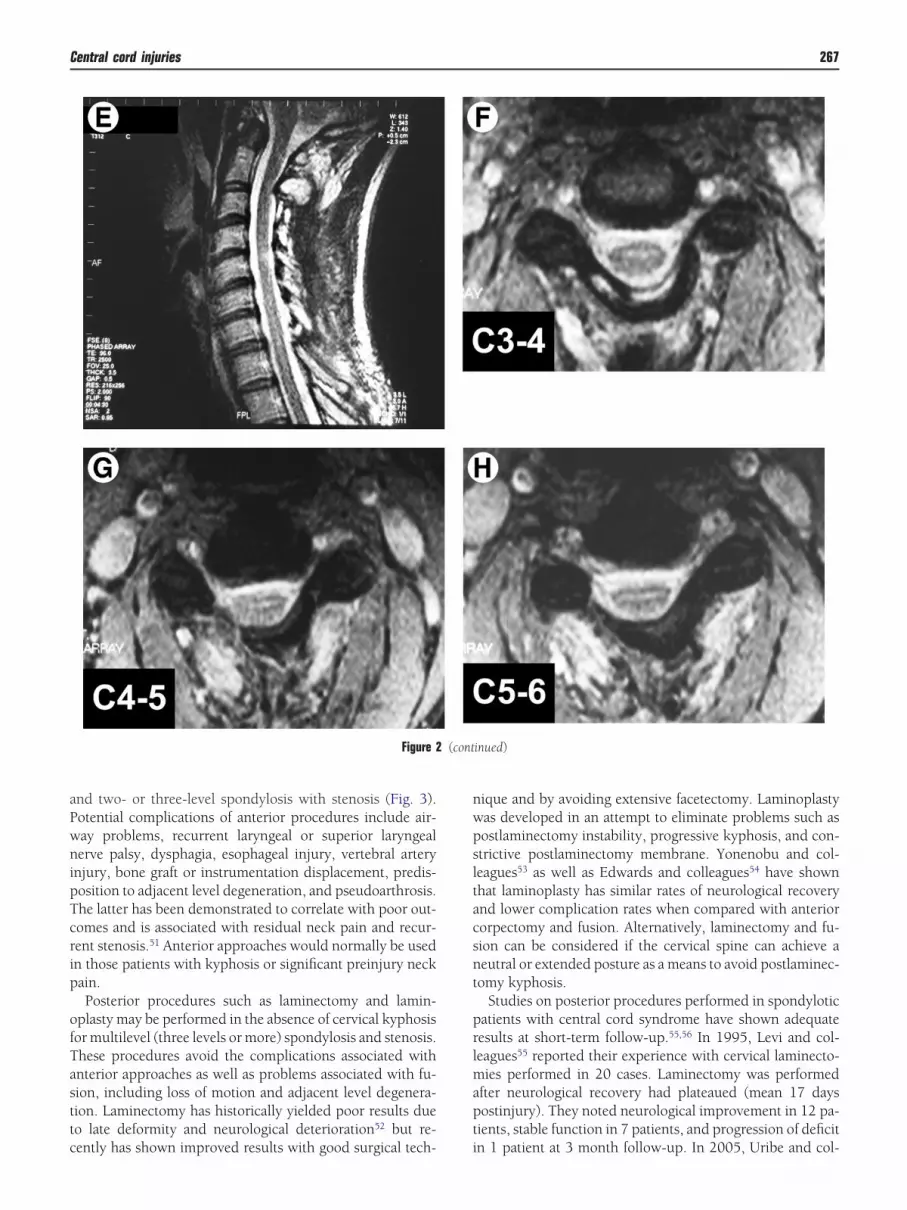
Figure 2 (A-H) This 44-year-old man was skiing and fellfalls, he had problems with severe weakness. He had impget off the mountain. He had some significant weakness owithout dropping them. In the past week he has had excimproved but he still has abnormal sensation in his habilaterally. His leg strength is normal. (A-D) The patienspinal canal and significant spinal cord compression at thcord at that level. Because of his young age and his desirbe treated with a posterior cervical laminoplasty from C3MRI scan shows that there is more than adequate room fthe spinal cord remains unchanged. The patient hasmarathons and high-level skiing. At this time he hashigh-energy and high-impact sports.
erformed for cervical myelopathy.50 There are advantages b
nd disadvantages to both the anterior and the posterior ap-roaches.Anterior cervical discectomy and fusion (ACDF) may be
erformed in cases of central cord injury secondary to discerniation or spondylotic degeneration that is limited to theisc level. The indications for corpectomy and strut grafting
nclude neural compression and instability due to vertebral
different times 1 week before this visit. After one of hisent after 15 minutes and was able to continue skiing toght hand; he was unable to hold things in his right handimprovement of his leg strength. His hand function hasthis time his biceps and wrist extensor strength is 4/5injury MRI scan shows that he has a congenitally small
level. He also has an abnormal signal within the spinalback to high-impact-type sports, it was advised that heh C7. (E-H) At 4 months following his laminoplasty hispinal cord at all levels. The area of myelomalacia withinble to return to high-level activities such as runningcleared for return to all types of activities including
threerovemf his riellentnd. Att’s poste C4-5
e to gothroug
or his sbeen abeen
ody fractures, the presence of any retrovertebral pathology,
aPwnipTcrip
ofTasttc
nwpsltacsnt
prlmapt
(cont
Central cord injuries 267
nd two- or three-level spondylosis with stenosis (Fig. 3).otential complications of anterior procedures include air-ay problems, recurrent laryngeal or superior laryngealerve palsy, dysphagia, esophageal injury, vertebral artery
njury, bone graft or instrumentation displacement, predis-osition to adjacent level degeneration, and pseudoarthrosis.he latter has been demonstrated to correlate with poor out-omes and is associated with residual neck pain and recur-ent stenosis.51 Anterior approaches would normally be usedn those patients with kyphosis or significant preinjury neckain.Posterior procedures such as laminectomy and lamin-
plasty may be performed in the absence of cervical kyphosisor multilevel (three levels or more) spondylosis and stenosis.hese procedures avoid the complications associated withnterior approaches as well as problems associated with fu-ion, including loss of motion and adjacent level degenera-ion. Laminectomy has historically yielded poor results dueo late deformity and neurological deterioration52 but re-
Figure 2
ently has shown improved results with good surgical tech- i
ique and by avoiding extensive facetectomy. Laminoplastyas developed in an attempt to eliminate problems such asostlaminectomy instability, progressive kyphosis, and con-trictive postlaminectomy membrane. Yonenobu and col-eagues53 as well as Edwards and colleagues54 have shownhat laminoplasty has similar rates of neurological recoverynd lower complication rates when compared with anteriororpectomy and fusion. Alternatively, laminectomy and fu-ion can be considered if the cervical spine can achieve aeutral or extended posture as a means to avoid postlaminec-omy kyphosis.
Studies on posterior procedures performed in spondyloticatients with central cord syndrome have shown adequateesults at short-term follow-up.55,56 In 1995, Levi and col-eagues55 reported their experience with cervical laminecto-
ies performed in 20 cases. Laminectomy was performedfter neurological recovery had plateaued (mean 17 daysostinjury). They noted neurological improvement in 12 pa-ients, stable function in 7 patients, and progression of deficit
inued)
n 1 patient at 3 month follow-up. In 2005, Uribe and col-

268 W. Fong and F.J. Eismont
Figure 3 (A) This 44-year-old gentleman had congenital stenosis with early myelopathy. Following a traumatic event,he had a transient quadriparesis. He regained his function to the point that he was ambulatory but with a significantmyelopathy. He had burning in his hands and more dysfunction in his hands than in his legs. (A, B) These X-rays weretaken after his traumatic event. (C-F) These MRI scans show severe stenosis and changes in signal within the spinalcord. (G, H) These X-rays were taken 5 years after his two level anterior cervical corpectomy and fusion. At this timehe still has residual myelopathy and persistent burning in his hands. The burning in his hands has persisted despiteposterior foraminotomies, which were performed 2[1/2] years following his anterior decompression procedure. (I-J)This MRI scan 4[1/2] years after his surgery shows that his decompression at the areas of severe stenosis remain open
but he is beginning to develop stenosis at the C3-4 level above his fusion.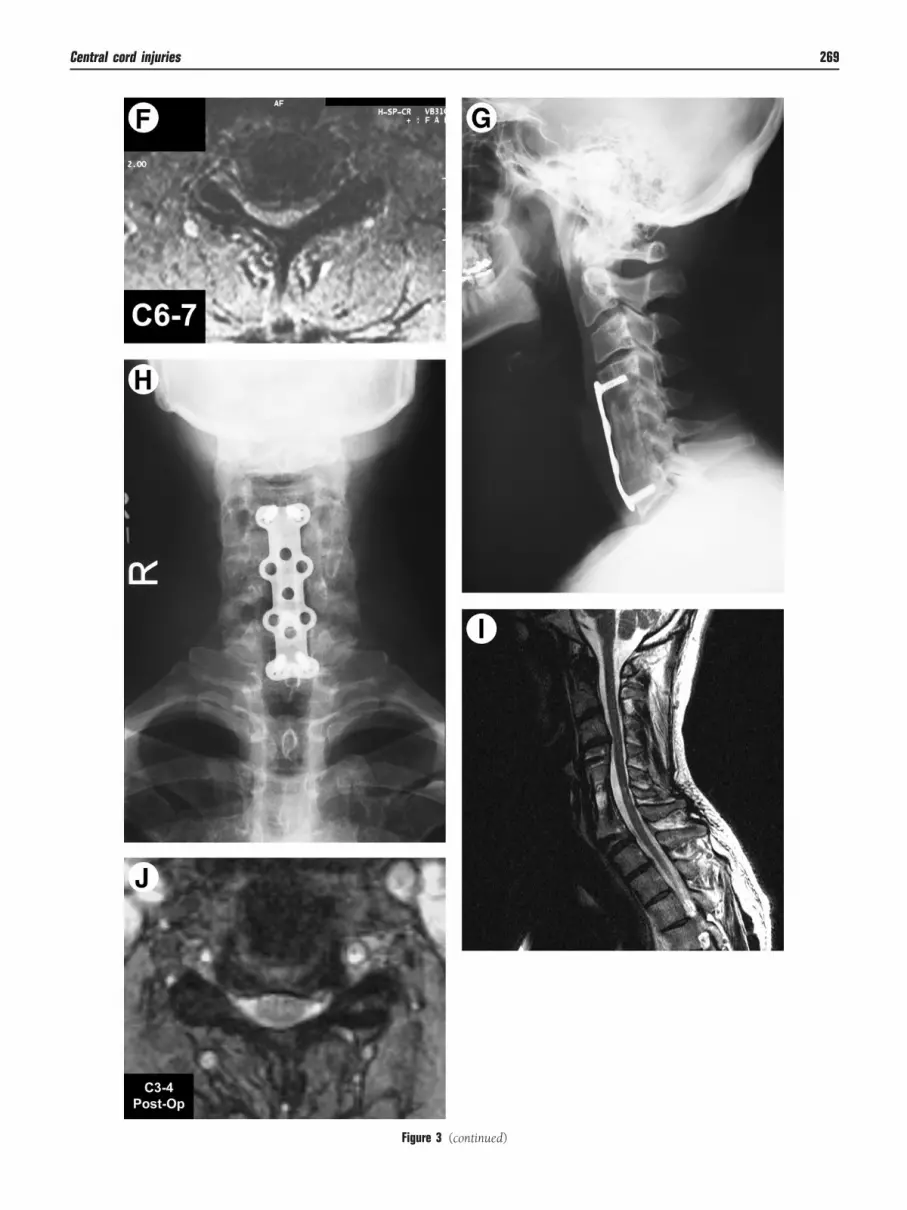
Central cord injuries 269
Figure 3 (continued)

losfplpg
SAew
nstop
ccrgls
warmc
lcp
wocatpocsudsp
STait
1cptmiTssrietcst
R
1
1
1
1
1
1
1
1
1
270 W. Fong and F.J. Eismont
eagues56 reviewed their experience using open-door lamin-plasty in 15 cases of central cord syndrome associated withpondylosis. Open-door expansile laminoplasty was per-ormed as soon as possible after injury (average, 3 daysostinjury). At 3 month follow-up, 10 patients had neuro-
ogical improvement; 4 patients had stable function, and 1atient had died due to respiratory failure unrelated to sur-ery.
enior Author Preferencesny patient with a central cord syndrome after a traumaticvent who has proven spinal cord compression is best treatedith surgical decompression.For those patients with multilevel (level 3 or 4) canal ste-
osis who have either a lordotic spine or at least a straightpine, a posterior C3-C7 cervical laminoplasty would be myreatment of choice. I would normally block the laminoplastypen with allograft rib at C3, C5, and C7 and immobilize theatient in a rigid orthosis for 8 weeks.For those patients with only one or two levels of spinal
ord compression and with the remainder of the cervicalanal being clearly normal in size, I would perform an ante-ior discectomy and/or corpectomy with fusion using allo-raft bone and titanium plate with screws. I would immobi-ize the patient in a rigid cervical collar until the fusion wasolid.
Another factor which should be considered includeshether the patient has kyphosis. If kyphosis is present, then
nterior decompression and fusion would be recommendedegardless of the numbers of levels involved. If it involvedore than three disc levels or two corpectomy levels, a con-
omitant posterior fusion would be recommended.If the patient has significant preinjury neck pain, the usual
aminoplasty would not be recommended. An anterior de-ompression and fusion or a laminoplasty combined with aosterior fusion would then be recommended.As regards the timing of surgery, the only patient who
ould benefit from an emergency decompression would bene who was deteriorating neurologically and who hadlearly demonstrated spinal cord decompression on MRI im-ging and who was medically stable enough to predictablyolerate the surgery. Other patients with stable or slowly im-roving neurologic status are best treated on an elective basisnce medically stabilized and when the optimal surgical teaman be assembled. There is also a role for late decompres-ion for those patients who have either stabilized at annacceptable neurologic/functional level or who are un-ergoing late neurologic deterioration. I would follow theame criterion as listed above considering anterior versusosterior approaches.
ummaryhe pathophysiology of central spinal cord injuries and mostppropriate treatment for patients who have sustained thesenjuries have been the subjects of considerable debate since
heir original description by Schneider and colleagues in954. Central cord injury occurs in all age groups and isaused by a variety of mechanisms that traumatically com-ress the spinal cord, resulting in cord swelling and dysfunc-ion. Multiple animal studies have shown evidence that phar-acological therapies and urgent surgical decompression
mprove neurological outcomes after spinal cord trauma.his has not been convincingly demonstrated in humantudies, although recent literature indicates that surgery isafe and may be associated with more rapid neurologicalecovery than conservative treatment. Currently, the admin-stration of methylprednisolone within 8 hours of injury andarly surgical decompression are regarded as treatment op-ions, not the standards of care, for patients suffering acuteentral cord injuries. Further investigation, including pro-pective, randomized controlled trials, is needed to establishhe roles and timing of these interventions.
eferences1. Bosch A, Stauffer ES, Nickel VL: Incomplete traumatic quadriplegia. A
ten-year review. JAMA 216:473-478, 19712. Merriam WF, Taylor TK, Ruff SJ, et al: A reappraisal of acute traumatic
central cord syndrome. J Bone Joint Surg Br 68:708-713, 19863. Schneider RC, Thompson JM, Bebin J: The syndrome of acute central
cervical spinal cord injury. J Neurol Neurosurg Psychiatry 21:216-227,1958
4. Shrosbree RD: Acute central cervical spinal cord syndrome—aetiology,age incidence and relationship to the orthopaedic injury. Paraplegia14:251-258, 1977
5. Roth EJ, Lawler MH, Yarkony GM: Traumatic central cord syndrome:clinical features and functional outcomes. Arch Phys Med Rehabil 71:18-23, 1990
6. Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for func-tional recovery in acute, traumatic central cord syndrome. Arch PhysMed Rehabil 71:963-968, 1990
7. Newey ML, Sen PK, Fraser RD: The long-term outcome after centralcord syndrome: a study of the natural history. J Bone Joint Surg Br82:851-855, 2000
8. Hardy AG: Cervical spinal cord injury without bony injury. Paraplegia14:296-305, 1977
9. Dai LY: Acute central cervical cord injury: the effect of age upon prog-nosis. Injury 32:195-199, 2001
0. Dvorak MF, Fisher CG, Hoekema J, et al: Factors predicting motorrecovery and functional outcome after traumatic central cord syn-drome: a long-term follow-up. Spine 30:2303-2311, 2005
1. Ishida Y, Tominaga T: Predictors of neurologic recovery in acute centralcervical cord injury with only upper extremity impairment. Spine 27:1652-1658; discussion 1658, 2002
2. Schneider RC, Cherry G, Pantek H: The syndrome of acute centralcervical spinal cord injury; with special reference to the mechanismsinvolved in hyperextension injuries of cervical spine. J Neurosurg 11:546-577, 1954
3. Bose B, Northrup BE, Osterholm JL, et al: Reanalysis of central cervicalcord injury management. Neurosurgery 15:367-372, 1984
4. Brodkey JS, Miller CF Jr, Harmody RM: The syndrome of acute centralcervical spinal cord injury revisited. Surg Neurol 14:251-257, 1980
5. Massaro F, Lanotte M, Faccani G: Acute traumatic central cord syn-drome. Acta Neurol (Napoli) 15:97-105, 1993
6. Chen TY, Lee ST, Lui TN, et al: Efficacy of surgical treatment in trau-matic central cord syndrome. Surg Neurol 48:435-440; discussion 441,1997
7. Dai L, Jia L: Central cord injury complicating acute cervical discherniation in trauma. Spine 25:331-335; discussion 336, 2000
8. Guest J, Eleraky MA, Apostolides PJ, et al: Traumatic central cordsyndrome: results of surgical management. J Neurosurg 97:25-32,
2002 (suppl 1)
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
Central cord injuries 271
9. Foerster O: Symptomatologie der Erkrankungen des Ruckenmarks undseiner Wurzeln. Bumke Foersters Handb Neurol 5:1-403, 1936
0. Levi AD, Tator CH, Bunge RP: Clinical syndromes associated withdisproportionate weakness of the upper versus the lower extremitiesafter cervical spinal cord injury. Neurosurgery 38:179-183; discussion183-185, 1996
1. Quencer RM, Bunge RP, Egnor M, et al: Acute traumatic central cordsyndrome: MRI-pathological correlations. Neuroradiology 34:85-94,1992
2. Martin D, Schoenen J, Lenelle J, et al: MRI-pathological correlations inacute traumatic central cord syndrome: case report. Neuroradiology34:262-266, 1992
3. Collignon F, Martin D, Lenelle J, et al: Acute traumatic central cordsyndrome: magnetic resonance imaging and clinical observations.J Neurosurg 96:29-33, 2002 (suppl 1)
4. Dai L: Magnetic resonance imaging of acute central cord syndrome:correlation with prognosis. Chin Med Sci J 16:107-110, 2001
5. Lagares A, Gomez PA, Ramos A, et al: Traumatic cervical central cordsyndrome due to intramedullary hemorrhage studied with MRI: casepresentation. Eur Spine J 11:294-297, 2002
6. Maroon JC, Abla AA, Wilberger JI, et al: Central cord syndrome. ClinNeurosurg 37:612-21, 1991
7. Bracken MB, Shepard MJ, Collins WF, et al: A randomized, controlledtrial of methylprednisolone or naloxone in the treatment of acute spi-nal-cord injury. Results of the Second National Acute Spinal CordInjury Study. N Engl J Med 322:1405-1411, 1990
8. Coleman WP, Benzel D, Cahill DW, et al: A critical appraisal of thereporting of the National Acute Spinal Cord Injury Studies (II and III)of methylprednisolone in acute spinal cord injury. J Spinal Disord13:185-199, 2000
9. Hurlbert RJ: Methylprednisolone for acute spinal cord injury: an inap-propriate standard of care. J Neurosurg 93:1-7, 2000 (suppl 1)
0. Nesathurai S: Steroids and spinal cord injury: revisiting the NASCIS 2and NASCIS 3 trials. J Trauma 45:1088-1093, 1998
1. Bracken MB, Shepard MJ, Holford TR, et al: Administration of methyl-prednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in thetreatment of acute spinal cord injury. Results of the Third NationalAcute Spinal Cord Injury Randomized Controlled Trial. National AcuteSpinal Cord Injury Study. JAMA 277:1597-1604, 1997
2. Con S: Pharmacological therapy after acute cervical spinal cord injury.Neurosurgery 50:S63-S72, 2002 (suppl 3)
3. Hugenholtz H: Methylprednisolone for acute spinal cord injury: not astandard of care. CMAJ 168:1145-1146, 2003
4. Geisler FH, Coleman WP, Grieco G, et al: The Sygen multicenter acutespinal cord injury study. Spine 26:S87-S98, 2001 (suppl 24)
5. Pitts LH, Ross A, Chase GA, et al: Treatment with thyrotropin-releasinghormone (TRH) in patients with traumatic spinal cord injuries. J Neu-rotrauma 12:235-243, 1995
6. Pointillart V, Petitjean ME, Wiart L, et al: Pharmacological therapy ofspinal cord injury during the acute phase. Spinal Cord 38:71-76, 2000
7. Fehlings MG, Baptiste DC: Current status of clinical trials for acutespinal cord injury. Injury 36:B113-B22, 2005 (suppl 2)
8. Dimar JR 2nd, Glassman SD, Raque GH, et al: The influence of spinalcanal narrowing and timing of decompression on neurologic recovery
after spinal cord contusion in a rat model. Spine 24:1623-1633, 19999. Dolan EJ, Tator CH, Endrenyi L: The value of decompression for acuteexperimental spinal cord compression injury. J Neurosurg 53:749-755,1980
0. Fehlings MG, Sekhon LH, Tator C: The role and timing of decompres-sion in acute spinal cord injury: what do we know? What should we do?Spine 26:S101-10, 2001 (suppl 24)
1. Tarlov IM: Spinal cord compression studies. III. Time limits for recov-ery after gradual compression in dogs. AMA Arch Neurol Psychiatry71:588-597, 1954
2. Tarlov IM, Klinger H: Spinal cord compression studies. II. Time limitsfor recovery after acute compression in dogs. AMA Arch Neurol Psy-chiatry 71:271-290, 1954
3. Chen TY, Dickman CA, Eleraky M, et al: The role of decompression foracute incomplete cervical spinal cord injury in cervical spondylosis. Spine23:2398-2403, 1998
4. Song J, Mizuno J, Nakagawa H, et al: Surgery for acute subaxial traumaticcentral cord syndrome without fracture or dislocation. J Clin Neurosci12:438-443, 2005
5. La Rosa G, Conti A, Cardali S, et al: Does early decompression improveneurological outcome of spinal cord injured patients? Appraisal of theliterature using a meta-analytical approach. Spinal Cord 42:503-512,2004
6. Fehlings MG, Perrin RG: The timing of surgical intervention in thetreatment of spinal cord injury: a systematic review of recent clinicalevidence. Spine 31:S28-S35; discussion S36, 2006 (suppl 11)
7. Papadopoulos SM, Selden NR, Quint DJ, et al: Immediate spinal corddecompression for cervical spinal cord injury: feasibility and outcome.J Trauma 52:323-332, 2002
8. Pollard ME, Apple DF: Factors associated with improved neurologic out-comes in patients with incomplete tetraplegia. Spine 28:33-39, 2003
9. Yamazaki T, Yanaka K, Fujita K, et al: Traumatic central cord syn-drome: analysis of factors affecting the outcome. Surg Neurol 63:95-99;discussion 99-100, 2005
0. Geck MJ, Eismont FJ: Surgical options for the treatment of cervicalspondylotic myelopathy. Orthop Clin North Am 33:329-348, 2002
1. Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompres-sion and arthrodesis for the treatment of cervical spondylotic myelop-athy. Two to seventeen-year follow-up. J Bone Joint Surg Am 80:941-951, 1998
2. Gregorius FK, Estrin T, Crandall PH: Cervical spondylotic radiculopa-thy and myelopathy. A long-term follow-up study. Arch Neurol 33:618-625, 1976
3. Yonenobu K, Hosono N, Iwasaki M, et al: Laminoplasty versus subtotalcorpectomy. A comparative study of results in multisegmental cervicalspondylotic myelopathy. Spine 17:1281-1284, 1992
4. Edwards CC 2nd, Heller JG, Murakami H: Corpectomy versus lamin-oplasty for multilevel cervical myelopathy: an independent matched-cohort analysis. Spine 27:1168-1175, 2002
5. Levi L, Wolf A, Mirvis S, et al: The significance of dorsal migration of thecord after extensive cervical laminectomy for patients with traumaticcentral cord syndrome. J Spinal Disord 8:289-295, 1995
6. Uribe J, Green BA, Vanni S, et al: Acute traumatic central cord syn-drome—experience using surgical decompression with open-door ex-pansile cervical laminoplasty. Surg Neurol 63:505-510; discussion
510, 2005




























