Embed Size (px)
Citation preview
92 30 WEITEREN Vol 49 Ndeg 3 1995 Quarterly
ISSN 0001 - 6497
ffiCClrffi OTOmiddotRHINOmiddotLARYNGOLOGICA [B[E~~CCffi
Publication of the Roya l Belgian Society for Ear Nase Throat Head and Neck Surgery
Acta olO-rhino-arynggico beg 1995 49 257-261
Complete Sphenoethmoidectomy and Computer-Assisted Surgery
A R Gunkel W Freysinger W F Thumarl amI C Puosehnig
ENT-Department Univers it y of lnnsbruck Innsbruck Austria
Key words Computer-assisted surgery endonasal endoscopic sphenoethmoidectomy
Abstract Camplele sphenoehmoideclOmy and campuler-assisled surgery M any surgical procedures in the rieJd of ENT take place in close proximity to vital structures like the orbit the skull base the internal carotid artery etc Ln our clinic we have decided to study two different computer-assisted navigation systems to reduce the risk 01 trauma to these structures during endonasal endoscopic procedures Such systems should be able to correlate the position 01 the surgical instrument ideally in the submillimeter range to CT- or MR-images The A RTM A Virtual Patient rM rinds the position of the instrument by permanently measuring magnetic field s The ISG-system uses a mechanical a rm to 10cali7e the probe in the patient Using Computer-Assisted-S urgery (CAS) does not significantly extend the time needed for surgery We found that it prevents the surgeon from inadvertently injuring structures Other groups have shown (I) that CAS-systems minimize the risk of complications of surgical procedures in the frontobasis arising from mishaps in the usage of the end oscope or the surgical tool If properly used CAS-systems can be a very helpful tool in the hand of an experienced surgeon but will never repl ace his expertise and knowledge
Introduction
Patients with chronic polyposis of the para nashysal sinuses who cannot be treated successfully by conservative therapy are normally operated upon using the functional endoscopic-endonashysal technique 1n cases of minor polyposis in the middJe meatus and the anterior ethmoid we usually perform a partial ethmoidectomy the Messerklinger operation (2) or infundibushylotomy For patients with massive polyposis of all paranasal sinuses though we use the complete functional sphenoethmoidectomy folshylowing the Wigand technique (3) Most of the time all paranasal sinuses can be clea red of polyps by using the suction-irrigation endoshyscope via the endonasal route Rarey and only in particular cases clearing the frontal sinus demands an external approach Typishycally this is indicated in cases of recurrent
polyposis inside the frontal sinus after previous endoscopic sinus operations or because of serious complications in acute sinusitis as for instance inflammatory processes of the orbit a subperiosteal abscess meningitis etc
Only recently various new techniques of computer-assisted 3D-navigation have been developed Details about CAS-systems in general (4) and the Viewing Wand in particular have been published elsewhere (5) Clinical tests of two of these systems a re under way in our ENT-department 1n principle every system correlates the actual position of the surgical instrument to the position in the corresponding slice of the CT- or the MRshyimages This is done by exploiting the inherent spatial information of the CT - MR-imaging modalities
Presented a t the meeting or the Belgian Socjety fo r Ea r Nose Throat Head and Neck Surgery Brussels December 1994
258
Materials and Methods
The two 3D navigation systems were used mainly in patients with chronic polyposis of the paranasal sinuses Preoperativey an axial CT-scan of the head was performed extending from the forehead to the hard palate demonshystrating in particular the paranasal sinuses The table increment was chosen to be 3 mm The helical scan was reconstructed to give non-overlapping slices of I mm thickness
The data to be used wirh the Viewing Wandtrade were transferred to a graphie workshystation and the 3D-reconstruction was pershyformed Regions of special interest for examshypie tumors of the skull base can be marked A magnetic tape was used to import the reshyconstruction into the Viewing WandTM located in the operating suite
Calibration is done by touching prominent points on the patients skull with a rigid probe flxed on the end of a high precision mechanical articulated arm Thus the CT-slices and the 3D reconstruction stored in the navigation system are linked to the patient Once this correlation has been established every moveshyment of the stylus is shown on the screen in relation to the axial coronal and sagittal CTshyscan planes in real-time Additionally the location of the probe can be displayed in a three-dimensional image on the screen
The accuracy of the calibration (following the protocol of ISO (6)) is defined as the difshyference between the actual anatomical position in the patient and the corresponding calculated point displayed on the screen (CT-scans)
The ARTMA Virtual Patient Vl (7) system
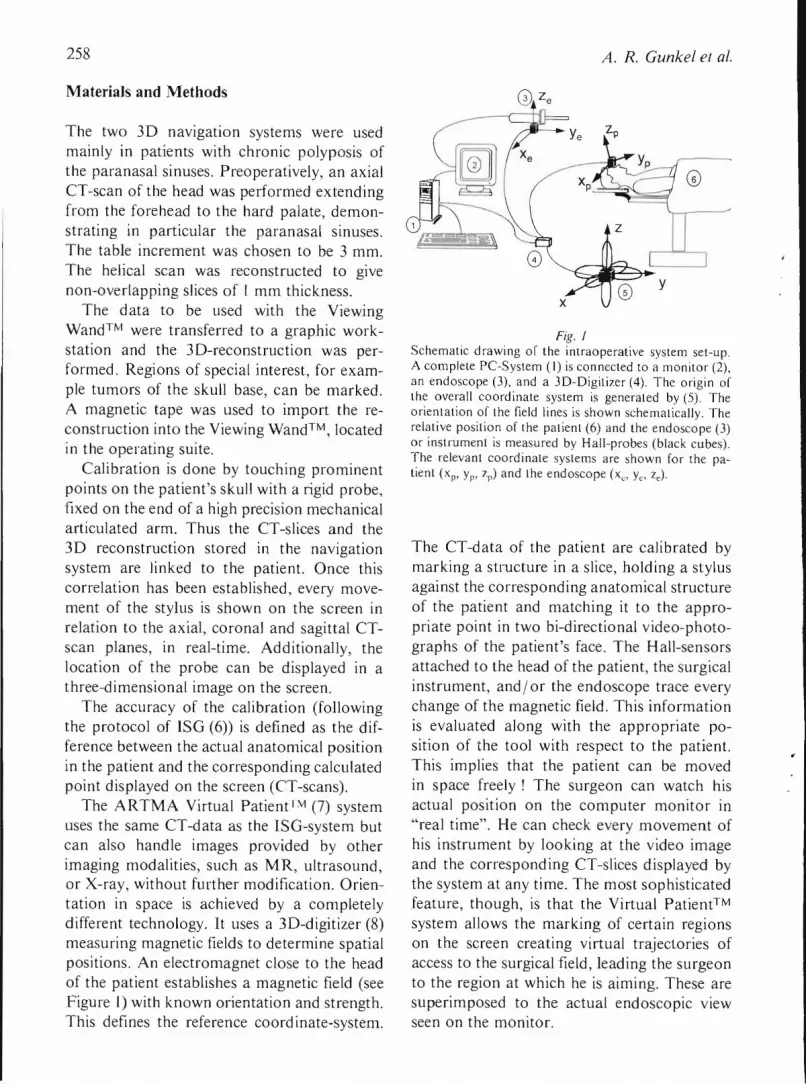
uses the same CT-data as the ISO-system but can also handle images provided by other imaging modalities such as MR ultrasound or X-ray without further modiflcation Orienshytation in space is achieved by a completely different technology It uses a 3D-digitizer (8) measuring magnetic fields to determine spatial positions An electromagnet close to the head of the patient establishes a magnetic field (see Figure I) with known orientation and strength This defines the reference coord inate-system
A R Gunkel el al
Fig I Schematic drawing of the intraoperative system set-up A complete Pe-System (I) is connected to a monitor (2) an endoscope (3) and a 3D-Digitizer (4) The origin of the overall coordinate system is generated by (5) The orientation of the field Iines is shown schematically The relative position of Ihe patient (6) and the endoscope (3) or instrument is measured by Hall-probes (black cubes) The relevant coordinate systems are shown for the pashytient (xp yp 7p) and the endoscope (xc ylt zc)
The CT-data of the patient are calibrated by marking a structure in a slice holding a stylus against the corresponding anatomical structure of the patient and matching it to the approshypriate point in two bi-directional video-photoshygraphs of the patients face The Hall-sensors attached to the head of the patient the surgical instrument and or the endoscope trace every change of the magnetic field This information is evaluated along with the appropriate poshysition of the tool with respect to the patient This implies that the patient can be moved in space freely The surgeon can watch his actuaJ position on the computer monitor in real time He can check every movement of his instrument by looking at the video image and the corresponding CT-slices displayed by the system at any time The most sophisticated feature though is that the Virtual Patienttrade system allows the marking of certain regions on the screen creating virtual trajecLories of access to the surgical field leading the surgeon to the region at wh ich he is aiming These are superimposed to the actual endoscopic view seen on the monitor
259 Compuler-assisled sphenoelhmoideclomy
The accuracy of the ARTM A System was assessed by visually judging the quality of the match between the actual anatomical location of the instrument and its calculated position as displayed on the video-image
Results
For a well-trained operating team (surgeon technician and nurse) the time necessary to calibrate the patient to his CT-data does not significantly increase the operating time
The properly calibrated ISG-system achieshyved an accuracy of I - 25 mm depending on whether we used radioopaque fiducial markers attached to the patients head or not Geneshyrally the accuracy determined was higher using these markers We found that it was of crucial importance which anatomicallocations were chosen for calibration lt is best to take landmarks that are immobile (ie spina nasalis anterior glabella teeth orbital rim) as comshypared to arbitrary locations on the skin (cheek lips lobule of helix etc) This is valid for both systems Working inside the nose towards the paranasal sinuses we found that only such anatomical sites could be accessed easily with the rigid and straight probe which are in direct sight These are structures like the anterior wall of the sphenoid cavity the posterior ethshymoid the posterior wall of the nasopharynx the posterior part of the frontal skuJl base Structures outside the direct approach though they can easily be seen with the appropriate endoscope (25deg 70deg optics) cannot practically be reached with the straight probe At most the opening of the maxillary sinus can barely be touched In some patients we were able to place the probe just inside the maxillary sinus Other very important structures such as the entrance to the frontal sinus the frontal part of the skull base the lateral aspect of the sphenoid cavity with the optic nerve could not be reached regularly
The Virtual Patienttrade system requires that the magnetic field not be influenced by large masses of metal near the operating area A custom-built wooden head rest gave the best
resulls After the caJibration procedure it was indeed possible to move the patients head without interfering with the calibration We found that the equipment did somehow natushyrally integrate ioto the usual operative proceshydure The surgeon was not hindered by the introduction of additional instruments like the measuring probe of the iSG-system This means that the normal endonasal instruments Ceg Blakesly forceps) serve both as an instrushyment and as a probe for the navigation system
Another feature of the system proved to be very helpful the surgeon could follow the preoperatively defined paths to the regions he had marked He is guided by coloured recshytangular frames floating in space superimposed to the live video-endoscopic images These rectangular frames form the path and lead to the region of interest It is important to note that these structures were not limited to lying on a straight line starting at the nostril and extending to the posterior parts of the nose and the paranasal sinuses But instead the Virtual P2-tienttrade System aHows us to define paths to measure distance and to work in any region inside the nose or the paranasal sinuses as is done normally during surgery
Discussion
Having calibrated the Viewing Wandtrade metishyculously it is possible to reach an accuracy of around 2 mm and with use of fiducial markers even an accuracy up to I mm But after the calibration proced ure the patients head has to be absolutely fixed and must not be moved any further This forms the main disadvantage of this system since movements destroy the calibration In most of the procedures under consideration the head of the patient has to be moved several times during the operation to achieve an optimal approach to different anatomical regions This implies that prior to each use of the system the calibration and accuracy have to be tested and if necessary re-established This is quite a cumbersome procedure for both the surgeon and the Viewshy
260
ing Wands operator Other limitations are the rigid mechanical arm and the probe which makes it very difficult to each anatomical regions located at an angle to the surgical approach Surgery in the region of the skull base and the paranasal sinuses frequently means working through small openings toshywards delicate structures Often the surgeon has to manipulate at an angle This is why he needs a tool supporting orientatio1 in these areas which are not directly accessible Thereshyfore the limitations of this system are soon attained
A word of caution seems to be appropriate here As the calibration of the patient to his 3D-reconstruction exploits only a few anatoshymicaJ Jandmarks it is not necessarily implied that the correJation between patient and reshyconstruction (CT-scan) is accurate throughout the whole operating field An accuracy of 2 mm in the antenor part of the nose can change enormously if approaching the outershymost borders of the operating field In these areas the surgeon no longer can rely on this system and he has to be very much aware of this fact
One of the major advantages of the ARTM A Virtual Patienttrade System is that both the patient and the instruments can be moved freely relative to each other without disturbing the calibration This means that the surgeon can operate in the normal manner moving the patients head as he deems necessary This system opens even more possibilities because other media can be used for correlation ie MRI images ultrasound images etc Many more tests are necessary to improve this system and introduce it into regular clinical routine The Virtual Patient System impleshyments the principles of lnterventional Video Tomography stating that the two-dimensional images supplied by the endoscope do have an exact correlate in the CT- or MR-slices The use of advanced image-processing algorithms and of the spatial information provided by the imaging modalities allows an exact orientashytion in space We would like to note that we worked with a first prototype of the ARTMA
A R Gunkel el al
Fig 2 Inlraoperalive pholograph of an endoscopic image some marked structures (full points) and the rectangles symshybolizing the preoperatively defined trajectory of approach (path)
Virtual Patienttrade System A second and more convenient software version is being developed
Conclusion
3D-navigation tools can be excellent aids during surgery for example endoscopic enshydonasaJ surgical procedures The ISG Viewing Wandtrade is a pure 3D-pointing device while the ARTMA Virtual Patienttrade System can be termed a 3D-video navigation system The advent of even more powerful computers and intelligent software will never replace the experience and the skill of a surgeon It is alshyways he who has to take the ultimate decision about the next step of a surgical procedure
Acknowledgement
We thank M VOGELE and R HAlF for their assistance in performing the 3D-reconstructions
References
1 KUI~ 7EJA A WE -LEI M KORVES B MOumlSGES R Dekompress ion des Nervus oplicus nach Frakturen des Riechschadeis mit Hilfe von CAS (ComputershyAssisted Surgery) Laryngo-Rhino-OIOI 73 274shy276 1994
2 MI SS ERKI1NG~ 1 W Endoscopy of the nose Urban amp Schwarzenberger Baltimore Muumlnchen 1979
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria

Acta olO-rhino-arynggico beg 1995 49 257-261
Complete Sphenoethmoidectomy and Computer-Assisted Surgery
A R Gunkel W Freysinger W F Thumarl amI C Puosehnig
ENT-Department Univers it y of lnnsbruck Innsbruck Austria
Key words Computer-assisted surgery endonasal endoscopic sphenoethmoidectomy
Abstract Camplele sphenoehmoideclOmy and campuler-assisled surgery M any surgical procedures in the rieJd of ENT take place in close proximity to vital structures like the orbit the skull base the internal carotid artery etc Ln our clinic we have decided to study two different computer-assisted navigation systems to reduce the risk 01 trauma to these structures during endonasal endoscopic procedures Such systems should be able to correlate the position 01 the surgical instrument ideally in the submillimeter range to CT- or MR-images The A RTM A Virtual Patient rM rinds the position of the instrument by permanently measuring magnetic field s The ISG-system uses a mechanical a rm to 10cali7e the probe in the patient Using Computer-Assisted-S urgery (CAS) does not significantly extend the time needed for surgery We found that it prevents the surgeon from inadvertently injuring structures Other groups have shown (I) that CAS-systems minimize the risk of complications of surgical procedures in the frontobasis arising from mishaps in the usage of the end oscope or the surgical tool If properly used CAS-systems can be a very helpful tool in the hand of an experienced surgeon but will never repl ace his expertise and knowledge
Introduction
Patients with chronic polyposis of the para nashysal sinuses who cannot be treated successfully by conservative therapy are normally operated upon using the functional endoscopic-endonashysal technique 1n cases of minor polyposis in the middJe meatus and the anterior ethmoid we usually perform a partial ethmoidectomy the Messerklinger operation (2) or infundibushylotomy For patients with massive polyposis of all paranasal sinuses though we use the complete functional sphenoethmoidectomy folshylowing the Wigand technique (3) Most of the time all paranasal sinuses can be clea red of polyps by using the suction-irrigation endoshyscope via the endonasal route Rarey and only in particular cases clearing the frontal sinus demands an external approach Typishycally this is indicated in cases of recurrent
polyposis inside the frontal sinus after previous endoscopic sinus operations or because of serious complications in acute sinusitis as for instance inflammatory processes of the orbit a subperiosteal abscess meningitis etc
Only recently various new techniques of computer-assisted 3D-navigation have been developed Details about CAS-systems in general (4) and the Viewing Wand in particular have been published elsewhere (5) Clinical tests of two of these systems a re under way in our ENT-department 1n principle every system correlates the actual position of the surgical instrument to the position in the corresponding slice of the CT- or the MRshyimages This is done by exploiting the inherent spatial information of the CT - MR-imaging modalities
Presented a t the meeting or the Belgian Socjety fo r Ea r Nose Throat Head and Neck Surgery Brussels December 1994
258
Materials and Methods
The two 3D navigation systems were used mainly in patients with chronic polyposis of the paranasal sinuses Preoperativey an axial CT-scan of the head was performed extending from the forehead to the hard palate demonshystrating in particular the paranasal sinuses The table increment was chosen to be 3 mm The helical scan was reconstructed to give non-overlapping slices of I mm thickness
The data to be used wirh the Viewing Wandtrade were transferred to a graphie workshystation and the 3D-reconstruction was pershyformed Regions of special interest for examshypie tumors of the skull base can be marked A magnetic tape was used to import the reshyconstruction into the Viewing WandTM located in the operating suite
Calibration is done by touching prominent points on the patients skull with a rigid probe flxed on the end of a high precision mechanical articulated arm Thus the CT-slices and the 3D reconstruction stored in the navigation system are linked to the patient Once this correlation has been established every moveshyment of the stylus is shown on the screen in relation to the axial coronal and sagittal CTshyscan planes in real-time Additionally the location of the probe can be displayed in a three-dimensional image on the screen
The accuracy of the calibration (following the protocol of ISO (6)) is defined as the difshyference between the actual anatomical position in the patient and the corresponding calculated point displayed on the screen (CT-scans)
The ARTMA Virtual Patient Vl (7) system
uses the same CT-data as the ISO-system but can also handle images provided by other imaging modalities such as MR ultrasound or X-ray without further modiflcation Orienshytation in space is achieved by a completely different technology It uses a 3D-digitizer (8) measuring magnetic fields to determine spatial positions An electromagnet close to the head of the patient establishes a magnetic field (see Figure I) with known orientation and strength This defines the reference coord inate-system
A R Gunkel el al
Fig I Schematic drawing of the intraoperative system set-up A complete Pe-System (I) is connected to a monitor (2) an endoscope (3) and a 3D-Digitizer (4) The origin of the overall coordinate system is generated by (5) The orientation of the field Iines is shown schematically The relative position of Ihe patient (6) and the endoscope (3) or instrument is measured by Hall-probes (black cubes) The relevant coordinate systems are shown for the pashytient (xp yp 7p) and the endoscope (xc ylt zc)
The CT-data of the patient are calibrated by marking a structure in a slice holding a stylus against the corresponding anatomical structure of the patient and matching it to the approshypriate point in two bi-directional video-photoshygraphs of the patients face The Hall-sensors attached to the head of the patient the surgical instrument and or the endoscope trace every change of the magnetic field This information is evaluated along with the appropriate poshysition of the tool with respect to the patient This implies that the patient can be moved in space freely The surgeon can watch his actuaJ position on the computer monitor in real time He can check every movement of his instrument by looking at the video image and the corresponding CT-slices displayed by the system at any time The most sophisticated feature though is that the Virtual Patienttrade system allows the marking of certain regions on the screen creating virtual trajecLories of access to the surgical field leading the surgeon to the region at wh ich he is aiming These are superimposed to the actual endoscopic view seen on the monitor
259 Compuler-assisled sphenoelhmoideclomy
The accuracy of the ARTM A System was assessed by visually judging the quality of the match between the actual anatomical location of the instrument and its calculated position as displayed on the video-image
Results
For a well-trained operating team (surgeon technician and nurse) the time necessary to calibrate the patient to his CT-data does not significantly increase the operating time
The properly calibrated ISG-system achieshyved an accuracy of I - 25 mm depending on whether we used radioopaque fiducial markers attached to the patients head or not Geneshyrally the accuracy determined was higher using these markers We found that it was of crucial importance which anatomicallocations were chosen for calibration lt is best to take landmarks that are immobile (ie spina nasalis anterior glabella teeth orbital rim) as comshypared to arbitrary locations on the skin (cheek lips lobule of helix etc) This is valid for both systems Working inside the nose towards the paranasal sinuses we found that only such anatomical sites could be accessed easily with the rigid and straight probe which are in direct sight These are structures like the anterior wall of the sphenoid cavity the posterior ethshymoid the posterior wall of the nasopharynx the posterior part of the frontal skuJl base Structures outside the direct approach though they can easily be seen with the appropriate endoscope (25deg 70deg optics) cannot practically be reached with the straight probe At most the opening of the maxillary sinus can barely be touched In some patients we were able to place the probe just inside the maxillary sinus Other very important structures such as the entrance to the frontal sinus the frontal part of the skull base the lateral aspect of the sphenoid cavity with the optic nerve could not be reached regularly
The Virtual Patienttrade system requires that the magnetic field not be influenced by large masses of metal near the operating area A custom-built wooden head rest gave the best
resulls After the caJibration procedure it was indeed possible to move the patients head without interfering with the calibration We found that the equipment did somehow natushyrally integrate ioto the usual operative proceshydure The surgeon was not hindered by the introduction of additional instruments like the measuring probe of the iSG-system This means that the normal endonasal instruments Ceg Blakesly forceps) serve both as an instrushyment and as a probe for the navigation system
Another feature of the system proved to be very helpful the surgeon could follow the preoperatively defined paths to the regions he had marked He is guided by coloured recshytangular frames floating in space superimposed to the live video-endoscopic images These rectangular frames form the path and lead to the region of interest It is important to note that these structures were not limited to lying on a straight line starting at the nostril and extending to the posterior parts of the nose and the paranasal sinuses But instead the Virtual P2-tienttrade System aHows us to define paths to measure distance and to work in any region inside the nose or the paranasal sinuses as is done normally during surgery
Discussion
Having calibrated the Viewing Wandtrade metishyculously it is possible to reach an accuracy of around 2 mm and with use of fiducial markers even an accuracy up to I mm But after the calibration proced ure the patients head has to be absolutely fixed and must not be moved any further This forms the main disadvantage of this system since movements destroy the calibration In most of the procedures under consideration the head of the patient has to be moved several times during the operation to achieve an optimal approach to different anatomical regions This implies that prior to each use of the system the calibration and accuracy have to be tested and if necessary re-established This is quite a cumbersome procedure for both the surgeon and the Viewshy
260
ing Wands operator Other limitations are the rigid mechanical arm and the probe which makes it very difficult to each anatomical regions located at an angle to the surgical approach Surgery in the region of the skull base and the paranasal sinuses frequently means working through small openings toshywards delicate structures Often the surgeon has to manipulate at an angle This is why he needs a tool supporting orientatio1 in these areas which are not directly accessible Thereshyfore the limitations of this system are soon attained
A word of caution seems to be appropriate here As the calibration of the patient to his 3D-reconstruction exploits only a few anatoshymicaJ Jandmarks it is not necessarily implied that the correJation between patient and reshyconstruction (CT-scan) is accurate throughout the whole operating field An accuracy of 2 mm in the antenor part of the nose can change enormously if approaching the outershymost borders of the operating field In these areas the surgeon no longer can rely on this system and he has to be very much aware of this fact
One of the major advantages of the ARTM A Virtual Patienttrade System is that both the patient and the instruments can be moved freely relative to each other without disturbing the calibration This means that the surgeon can operate in the normal manner moving the patients head as he deems necessary This system opens even more possibilities because other media can be used for correlation ie MRI images ultrasound images etc Many more tests are necessary to improve this system and introduce it into regular clinical routine The Virtual Patient System impleshyments the principles of lnterventional Video Tomography stating that the two-dimensional images supplied by the endoscope do have an exact correlate in the CT- or MR-slices The use of advanced image-processing algorithms and of the spatial information provided by the imaging modalities allows an exact orientashytion in space We would like to note that we worked with a first prototype of the ARTMA
A R Gunkel el al
Fig 2 Inlraoperalive pholograph of an endoscopic image some marked structures (full points) and the rectangles symshybolizing the preoperatively defined trajectory of approach (path)
Virtual Patienttrade System A second and more convenient software version is being developed
Conclusion
3D-navigation tools can be excellent aids during surgery for example endoscopic enshydonasaJ surgical procedures The ISG Viewing Wandtrade is a pure 3D-pointing device while the ARTMA Virtual Patienttrade System can be termed a 3D-video navigation system The advent of even more powerful computers and intelligent software will never replace the experience and the skill of a surgeon It is alshyways he who has to take the ultimate decision about the next step of a surgical procedure
Acknowledgement
We thank M VOGELE and R HAlF for their assistance in performing the 3D-reconstructions
References
1 KUI~ 7EJA A WE -LEI M KORVES B MOumlSGES R Dekompress ion des Nervus oplicus nach Frakturen des Riechschadeis mit Hilfe von CAS (ComputershyAssisted Surgery) Laryngo-Rhino-OIOI 73 274shy276 1994
2 MI SS ERKI1NG~ 1 W Endoscopy of the nose Urban amp Schwarzenberger Baltimore Muumlnchen 1979
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria
258
Materials and Methods
The two 3D navigation systems were used mainly in patients with chronic polyposis of the paranasal sinuses Preoperativey an axial CT-scan of the head was performed extending from the forehead to the hard palate demonshystrating in particular the paranasal sinuses The table increment was chosen to be 3 mm The helical scan was reconstructed to give non-overlapping slices of I mm thickness
The data to be used wirh the Viewing Wandtrade were transferred to a graphie workshystation and the 3D-reconstruction was pershyformed Regions of special interest for examshypie tumors of the skull base can be marked A magnetic tape was used to import the reshyconstruction into the Viewing WandTM located in the operating suite
Calibration is done by touching prominent points on the patients skull with a rigid probe flxed on the end of a high precision mechanical articulated arm Thus the CT-slices and the 3D reconstruction stored in the navigation system are linked to the patient Once this correlation has been established every moveshyment of the stylus is shown on the screen in relation to the axial coronal and sagittal CTshyscan planes in real-time Additionally the location of the probe can be displayed in a three-dimensional image on the screen
The accuracy of the calibration (following the protocol of ISO (6)) is defined as the difshyference between the actual anatomical position in the patient and the corresponding calculated point displayed on the screen (CT-scans)
The ARTMA Virtual Patient Vl (7) system
uses the same CT-data as the ISO-system but can also handle images provided by other imaging modalities such as MR ultrasound or X-ray without further modiflcation Orienshytation in space is achieved by a completely different technology It uses a 3D-digitizer (8) measuring magnetic fields to determine spatial positions An electromagnet close to the head of the patient establishes a magnetic field (see Figure I) with known orientation and strength This defines the reference coord inate-system
A R Gunkel el al
Fig I Schematic drawing of the intraoperative system set-up A complete Pe-System (I) is connected to a monitor (2) an endoscope (3) and a 3D-Digitizer (4) The origin of the overall coordinate system is generated by (5) The orientation of the field Iines is shown schematically The relative position of Ihe patient (6) and the endoscope (3) or instrument is measured by Hall-probes (black cubes) The relevant coordinate systems are shown for the pashytient (xp yp 7p) and the endoscope (xc ylt zc)
The CT-data of the patient are calibrated by marking a structure in a slice holding a stylus against the corresponding anatomical structure of the patient and matching it to the approshypriate point in two bi-directional video-photoshygraphs of the patients face The Hall-sensors attached to the head of the patient the surgical instrument and or the endoscope trace every change of the magnetic field This information is evaluated along with the appropriate poshysition of the tool with respect to the patient This implies that the patient can be moved in space freely The surgeon can watch his actuaJ position on the computer monitor in real time He can check every movement of his instrument by looking at the video image and the corresponding CT-slices displayed by the system at any time The most sophisticated feature though is that the Virtual Patienttrade system allows the marking of certain regions on the screen creating virtual trajecLories of access to the surgical field leading the surgeon to the region at wh ich he is aiming These are superimposed to the actual endoscopic view seen on the monitor
259 Compuler-assisled sphenoelhmoideclomy
The accuracy of the ARTM A System was assessed by visually judging the quality of the match between the actual anatomical location of the instrument and its calculated position as displayed on the video-image
Results
For a well-trained operating team (surgeon technician and nurse) the time necessary to calibrate the patient to his CT-data does not significantly increase the operating time
The properly calibrated ISG-system achieshyved an accuracy of I - 25 mm depending on whether we used radioopaque fiducial markers attached to the patients head or not Geneshyrally the accuracy determined was higher using these markers We found that it was of crucial importance which anatomicallocations were chosen for calibration lt is best to take landmarks that are immobile (ie spina nasalis anterior glabella teeth orbital rim) as comshypared to arbitrary locations on the skin (cheek lips lobule of helix etc) This is valid for both systems Working inside the nose towards the paranasal sinuses we found that only such anatomical sites could be accessed easily with the rigid and straight probe which are in direct sight These are structures like the anterior wall of the sphenoid cavity the posterior ethshymoid the posterior wall of the nasopharynx the posterior part of the frontal skuJl base Structures outside the direct approach though they can easily be seen with the appropriate endoscope (25deg 70deg optics) cannot practically be reached with the straight probe At most the opening of the maxillary sinus can barely be touched In some patients we were able to place the probe just inside the maxillary sinus Other very important structures such as the entrance to the frontal sinus the frontal part of the skull base the lateral aspect of the sphenoid cavity with the optic nerve could not be reached regularly
The Virtual Patienttrade system requires that the magnetic field not be influenced by large masses of metal near the operating area A custom-built wooden head rest gave the best
resulls After the caJibration procedure it was indeed possible to move the patients head without interfering with the calibration We found that the equipment did somehow natushyrally integrate ioto the usual operative proceshydure The surgeon was not hindered by the introduction of additional instruments like the measuring probe of the iSG-system This means that the normal endonasal instruments Ceg Blakesly forceps) serve both as an instrushyment and as a probe for the navigation system
Another feature of the system proved to be very helpful the surgeon could follow the preoperatively defined paths to the regions he had marked He is guided by coloured recshytangular frames floating in space superimposed to the live video-endoscopic images These rectangular frames form the path and lead to the region of interest It is important to note that these structures were not limited to lying on a straight line starting at the nostril and extending to the posterior parts of the nose and the paranasal sinuses But instead the Virtual P2-tienttrade System aHows us to define paths to measure distance and to work in any region inside the nose or the paranasal sinuses as is done normally during surgery
Discussion
Having calibrated the Viewing Wandtrade metishyculously it is possible to reach an accuracy of around 2 mm and with use of fiducial markers even an accuracy up to I mm But after the calibration proced ure the patients head has to be absolutely fixed and must not be moved any further This forms the main disadvantage of this system since movements destroy the calibration In most of the procedures under consideration the head of the patient has to be moved several times during the operation to achieve an optimal approach to different anatomical regions This implies that prior to each use of the system the calibration and accuracy have to be tested and if necessary re-established This is quite a cumbersome procedure for both the surgeon and the Viewshy
260
ing Wands operator Other limitations are the rigid mechanical arm and the probe which makes it very difficult to each anatomical regions located at an angle to the surgical approach Surgery in the region of the skull base and the paranasal sinuses frequently means working through small openings toshywards delicate structures Often the surgeon has to manipulate at an angle This is why he needs a tool supporting orientatio1 in these areas which are not directly accessible Thereshyfore the limitations of this system are soon attained
A word of caution seems to be appropriate here As the calibration of the patient to his 3D-reconstruction exploits only a few anatoshymicaJ Jandmarks it is not necessarily implied that the correJation between patient and reshyconstruction (CT-scan) is accurate throughout the whole operating field An accuracy of 2 mm in the antenor part of the nose can change enormously if approaching the outershymost borders of the operating field In these areas the surgeon no longer can rely on this system and he has to be very much aware of this fact
One of the major advantages of the ARTM A Virtual Patienttrade System is that both the patient and the instruments can be moved freely relative to each other without disturbing the calibration This means that the surgeon can operate in the normal manner moving the patients head as he deems necessary This system opens even more possibilities because other media can be used for correlation ie MRI images ultrasound images etc Many more tests are necessary to improve this system and introduce it into regular clinical routine The Virtual Patient System impleshyments the principles of lnterventional Video Tomography stating that the two-dimensional images supplied by the endoscope do have an exact correlate in the CT- or MR-slices The use of advanced image-processing algorithms and of the spatial information provided by the imaging modalities allows an exact orientashytion in space We would like to note that we worked with a first prototype of the ARTMA
A R Gunkel el al
Fig 2 Inlraoperalive pholograph of an endoscopic image some marked structures (full points) and the rectangles symshybolizing the preoperatively defined trajectory of approach (path)
Virtual Patienttrade System A second and more convenient software version is being developed
Conclusion
3D-navigation tools can be excellent aids during surgery for example endoscopic enshydonasaJ surgical procedures The ISG Viewing Wandtrade is a pure 3D-pointing device while the ARTMA Virtual Patienttrade System can be termed a 3D-video navigation system The advent of even more powerful computers and intelligent software will never replace the experience and the skill of a surgeon It is alshyways he who has to take the ultimate decision about the next step of a surgical procedure
Acknowledgement
We thank M VOGELE and R HAlF for their assistance in performing the 3D-reconstructions
References
1 KUI~ 7EJA A WE -LEI M KORVES B MOumlSGES R Dekompress ion des Nervus oplicus nach Frakturen des Riechschadeis mit Hilfe von CAS (ComputershyAssisted Surgery) Laryngo-Rhino-OIOI 73 274shy276 1994
2 MI SS ERKI1NG~ 1 W Endoscopy of the nose Urban amp Schwarzenberger Baltimore Muumlnchen 1979
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria
259 Compuler-assisled sphenoelhmoideclomy
The accuracy of the ARTM A System was assessed by visually judging the quality of the match between the actual anatomical location of the instrument and its calculated position as displayed on the video-image
Results
For a well-trained operating team (surgeon technician and nurse) the time necessary to calibrate the patient to his CT-data does not significantly increase the operating time
The properly calibrated ISG-system achieshyved an accuracy of I - 25 mm depending on whether we used radioopaque fiducial markers attached to the patients head or not Geneshyrally the accuracy determined was higher using these markers We found that it was of crucial importance which anatomicallocations were chosen for calibration lt is best to take landmarks that are immobile (ie spina nasalis anterior glabella teeth orbital rim) as comshypared to arbitrary locations on the skin (cheek lips lobule of helix etc) This is valid for both systems Working inside the nose towards the paranasal sinuses we found that only such anatomical sites could be accessed easily with the rigid and straight probe which are in direct sight These are structures like the anterior wall of the sphenoid cavity the posterior ethshymoid the posterior wall of the nasopharynx the posterior part of the frontal skuJl base Structures outside the direct approach though they can easily be seen with the appropriate endoscope (25deg 70deg optics) cannot practically be reached with the straight probe At most the opening of the maxillary sinus can barely be touched In some patients we were able to place the probe just inside the maxillary sinus Other very important structures such as the entrance to the frontal sinus the frontal part of the skull base the lateral aspect of the sphenoid cavity with the optic nerve could not be reached regularly
The Virtual Patienttrade system requires that the magnetic field not be influenced by large masses of metal near the operating area A custom-built wooden head rest gave the best
resulls After the caJibration procedure it was indeed possible to move the patients head without interfering with the calibration We found that the equipment did somehow natushyrally integrate ioto the usual operative proceshydure The surgeon was not hindered by the introduction of additional instruments like the measuring probe of the iSG-system This means that the normal endonasal instruments Ceg Blakesly forceps) serve both as an instrushyment and as a probe for the navigation system
Another feature of the system proved to be very helpful the surgeon could follow the preoperatively defined paths to the regions he had marked He is guided by coloured recshytangular frames floating in space superimposed to the live video-endoscopic images These rectangular frames form the path and lead to the region of interest It is important to note that these structures were not limited to lying on a straight line starting at the nostril and extending to the posterior parts of the nose and the paranasal sinuses But instead the Virtual P2-tienttrade System aHows us to define paths to measure distance and to work in any region inside the nose or the paranasal sinuses as is done normally during surgery
Discussion
Having calibrated the Viewing Wandtrade metishyculously it is possible to reach an accuracy of around 2 mm and with use of fiducial markers even an accuracy up to I mm But after the calibration proced ure the patients head has to be absolutely fixed and must not be moved any further This forms the main disadvantage of this system since movements destroy the calibration In most of the procedures under consideration the head of the patient has to be moved several times during the operation to achieve an optimal approach to different anatomical regions This implies that prior to each use of the system the calibration and accuracy have to be tested and if necessary re-established This is quite a cumbersome procedure for both the surgeon and the Viewshy
260
ing Wands operator Other limitations are the rigid mechanical arm and the probe which makes it very difficult to each anatomical regions located at an angle to the surgical approach Surgery in the region of the skull base and the paranasal sinuses frequently means working through small openings toshywards delicate structures Often the surgeon has to manipulate at an angle This is why he needs a tool supporting orientatio1 in these areas which are not directly accessible Thereshyfore the limitations of this system are soon attained
A word of caution seems to be appropriate here As the calibration of the patient to his 3D-reconstruction exploits only a few anatoshymicaJ Jandmarks it is not necessarily implied that the correJation between patient and reshyconstruction (CT-scan) is accurate throughout the whole operating field An accuracy of 2 mm in the antenor part of the nose can change enormously if approaching the outershymost borders of the operating field In these areas the surgeon no longer can rely on this system and he has to be very much aware of this fact
One of the major advantages of the ARTM A Virtual Patienttrade System is that both the patient and the instruments can be moved freely relative to each other without disturbing the calibration This means that the surgeon can operate in the normal manner moving the patients head as he deems necessary This system opens even more possibilities because other media can be used for correlation ie MRI images ultrasound images etc Many more tests are necessary to improve this system and introduce it into regular clinical routine The Virtual Patient System impleshyments the principles of lnterventional Video Tomography stating that the two-dimensional images supplied by the endoscope do have an exact correlate in the CT- or MR-slices The use of advanced image-processing algorithms and of the spatial information provided by the imaging modalities allows an exact orientashytion in space We would like to note that we worked with a first prototype of the ARTMA
A R Gunkel el al
Fig 2 Inlraoperalive pholograph of an endoscopic image some marked structures (full points) and the rectangles symshybolizing the preoperatively defined trajectory of approach (path)
Virtual Patienttrade System A second and more convenient software version is being developed
Conclusion
3D-navigation tools can be excellent aids during surgery for example endoscopic enshydonasaJ surgical procedures The ISG Viewing Wandtrade is a pure 3D-pointing device while the ARTMA Virtual Patienttrade System can be termed a 3D-video navigation system The advent of even more powerful computers and intelligent software will never replace the experience and the skill of a surgeon It is alshyways he who has to take the ultimate decision about the next step of a surgical procedure
Acknowledgement
We thank M VOGELE and R HAlF for their assistance in performing the 3D-reconstructions
References
1 KUI~ 7EJA A WE -LEI M KORVES B MOumlSGES R Dekompress ion des Nervus oplicus nach Frakturen des Riechschadeis mit Hilfe von CAS (ComputershyAssisted Surgery) Laryngo-Rhino-OIOI 73 274shy276 1994
2 MI SS ERKI1NG~ 1 W Endoscopy of the nose Urban amp Schwarzenberger Baltimore Muumlnchen 1979
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria

260
ing Wands operator Other limitations are the rigid mechanical arm and the probe which makes it very difficult to each anatomical regions located at an angle to the surgical approach Surgery in the region of the skull base and the paranasal sinuses frequently means working through small openings toshywards delicate structures Often the surgeon has to manipulate at an angle This is why he needs a tool supporting orientatio1 in these areas which are not directly accessible Thereshyfore the limitations of this system are soon attained
A word of caution seems to be appropriate here As the calibration of the patient to his 3D-reconstruction exploits only a few anatoshymicaJ Jandmarks it is not necessarily implied that the correJation between patient and reshyconstruction (CT-scan) is accurate throughout the whole operating field An accuracy of 2 mm in the antenor part of the nose can change enormously if approaching the outershymost borders of the operating field In these areas the surgeon no longer can rely on this system and he has to be very much aware of this fact
One of the major advantages of the ARTM A Virtual Patienttrade System is that both the patient and the instruments can be moved freely relative to each other without disturbing the calibration This means that the surgeon can operate in the normal manner moving the patients head as he deems necessary This system opens even more possibilities because other media can be used for correlation ie MRI images ultrasound images etc Many more tests are necessary to improve this system and introduce it into regular clinical routine The Virtual Patient System impleshyments the principles of lnterventional Video Tomography stating that the two-dimensional images supplied by the endoscope do have an exact correlate in the CT- or MR-slices The use of advanced image-processing algorithms and of the spatial information provided by the imaging modalities allows an exact orientashytion in space We would like to note that we worked with a first prototype of the ARTMA
A R Gunkel el al
Fig 2 Inlraoperalive pholograph of an endoscopic image some marked structures (full points) and the rectangles symshybolizing the preoperatively defined trajectory of approach (path)
Virtual Patienttrade System A second and more convenient software version is being developed
Conclusion
3D-navigation tools can be excellent aids during surgery for example endoscopic enshydonasaJ surgical procedures The ISG Viewing Wandtrade is a pure 3D-pointing device while the ARTMA Virtual Patienttrade System can be termed a 3D-video navigation system The advent of even more powerful computers and intelligent software will never replace the experience and the skill of a surgeon It is alshyways he who has to take the ultimate decision about the next step of a surgical procedure
Acknowledgement
We thank M VOGELE and R HAlF for their assistance in performing the 3D-reconstructions
References
1 KUI~ 7EJA A WE -LEI M KORVES B MOumlSGES R Dekompress ion des Nervus oplicus nach Frakturen des Riechschadeis mit Hilfe von CAS (ComputershyAssisted Surgery) Laryngo-Rhino-OIOI 73 274shy276 1994
2 MI SS ERKI1NG~ 1 W Endoscopy of the nose Urban amp Schwarzenberger Baltimore Muumlnchen 1979
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria
261 Computer-assisted sphenoethmoidectomy
3 WIGA NI) M E Endoskopische Chirurgie der Nasenshynebenhoumlhlen und der vorderen Schaumldelbasis Thieme Stuttgarl New York 1989
4 KAVAN AG H K T Applicalions of Image-Direcled Robolics in Ololaryngologic Surgery LarYl7goscope 104 283-293
5 ZINREICII S J TEilo S A LON( D M BRFM
H M An oc D E U )U R Y M E VANI)(I( KII K C A K OC H W M K [NNUW D W BI(YAN R N Frameless Slereotaxic Integralion of cr Imaging Dala Accuracy and Inilial Applicalions Radioag) 188 735-742 1993
6 Clinical Report Form ISG Technologies Missasshysauga Ontario Canada 1994
7 see eg M J Truppe Augmenled Realily in Endoshyscopic Surgery presenled at Medicine Meets Virtual Rea li ty JJI San Diego USA January 19-22 1995
8 HII I)EROIT C F VANNIER M W Three-Dimensional Measuremenl Accuracy of Skull Surface Landmarks Am 1 Phys Al7lhropol 76 497-501 1988
A R Gunkel ENT-Department Universi ly of lnnsbruck Anichstr 35 A-6020 Jnnsbruck Austria





























