Embed Size (px)
Citation preview
C
642 Original article
Compensatory or inappropriat
e left ventricular mass indifferent models of left ventricular pressure overload:comparison between patients with aortic stenosis andarterial hypertensionGian Francesco Mureddua, Giovanni Cioffib, Carlo Stefenellib, AlessandroBoccanellia and Giovanni de SimonecBackground Aortic valve stenosis and arterial hypertension
(AH) are two models of left ventricular (LV) pressure
overload, which commonly induce increase in LV mass.
Prevalence and predictors of excess of LV mass
(inappropriate LVM) has been recently investigated in AH
patients. Whether or not this phenomenon also exists in
patients with aortic valve stenosis has to be defined.
Objective To evaluate prevalence of and factors associated
with inappropriate LVM as a response to overload in aortic
valve stenosis compared to AH patients.
Design and methods One hundred patients with aortic
valve stenosis (mean valve area 0.67 W 0.18 cm2/m2) were
studied by Doppler echocardiography and compared to 200
patients with AH. Inappropriate LVM was diagnosed when
the measured LV mass exceeded by 28% the expected
value predicted from height2.7, sex and stroke work.
Results Prevalence of inappropriate LVM was similar in
aortic valve stenosis (n: 24 U 24%) and AH patients (n:
55 U 27.5%). Aortic valve stenosis had greater LVM (203 W 57
vs. 182 W 53 g, P U 0.001), more concentric LV geometry,
lower midwall shortening and higher left atrial systolic force
than AH. In both study groups, high LV mass, concentric LV
geometry and reduced systolic function emerged as
independent correlates of inappropriate LV mass.
opyright © Lippincott Williams & Wilkins. Unautho
0263-6352 � 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
Conclusion Although LV and left atrial geometric
adaptation in aortic valve stenosis is different from AH,
reflecting a near-pure pressure overload, aortic valve
stenosis patients have a prevalence of inappropriately high
LVM which is similar to those with AH. Geometric and
functional characteristics of inappropriate LVM do not differ
in aortic valve stenosis and AH, despite the different loading
conditions. J Hypertens 27:642–649 Q 2009 Wolters Kluwer
Health | Lippincott Williams & Wilkins.
Journal of Hypertension 2009, 27:642–649
Keywords: aortic stenosis, arterial hypertension, cardiac load, ventriculargeometry, ventricular hypertrophy, ventricular mass
Abbreviations: AH, Arterial hypertension; AS, Aortic stenosis; LA, Left atrial;LV, Left ventricular; LVH, Left ventricular hypertrophy; NYHA, New York HeartAssociation
aCardiology Unit S. Giovanni-Addolorata Hospital, Rome, bEchocardiographyLaboratory, Villa Bianca Hospital, Trento and cDepartment of Clinical andExperimental Medicine, Naples, Italy
Correspondence to Gian Francesco Mureddu, MD, Cardiology Unit, Departmentof Cardiocirculatory Diseases, San Giovanni-Addolorata Hospital, Via AmbaAradam 8, 00184 Rome, ItalyTel: +39 06 77055399; fax: +39 06 8177587; e-mail: [email protected]
Received 27 November 2007 Revised 15 September 2008Accepted 17 September 2008
IntroductionLeft ventricular (LV) pressure overload is common to both
aortic stenosis and arterial hypertension (AH). However,
whereas aortic stenosis is the paradigm of pure pressure
overload, AH is typically a combined pressure–volume
overload state [1,2]. The two conditions are, therefore,
haemodynamically different. Both in aortic stenosis and in
AH, LV overload is thought to initially increase wall stress
and stimulate parallel myocyte growth leading to LV
hypertrophy (LVH), which is typically concentric [3,4].
According to this postulate, LVH would be finalized to
reduce wall stress and preserve LV pump function but over
time it becomes an inconvenient adaptation mechanism
[4], determining an alteration of myocardial structure that
leads to impairment of LV performance and progression
from compensated LVH to heart failure [5–12]. LV geo-
metric adaptations in conditions of pressure overload are
also closely related to changes in left atrial (LA) size and
function [2,13,14].
More recently, values of sex-specific LV mass exceeding
those expected for individual body size and stroke work,
called ‘inappropriate LV mass’, have been interpreted as
a ‘maladaptive response’ to increased LV load, emerging
as an independent predictor of adverse prognosis [15–
19]. The magnitude and characteristics of this pathophy-
siological state have been studied in patients with AH
[15–19], whereas they are unknown in patients with
aortic stenosis.
Accordingly, this study has been conceived to assess the
prevalence and the characteristics of inappropriate LV
mass in patients with aortic stenosis, compared with
patients with AH.
rized reproduction of this article is prohibited.
DOI:10.1097/HJH.0b013e32831cec98

C
Ventricular mass growth in pressure overload Mureddu et al. 643
MethodsPatients aged more than 18 years with stable sinus
rhythm and any grade of aortic stenosis, defined as aortic
valve thickening on echocardiographic evaluation accom-
panied by a Doppler-measured peak flow velocity across
the valve of more than 2.5 m/s [20], were studied. They
were selected among patients consecutively referred to
the Echocardiography Laboratory of ‘Villa Bianca’ Hos-
pital in Trento by their general practitioners, for the
presence of cardiac murmur and suspected valve disease.
History of angina, syncope and/or worsening functional
status, as well as of AH, were not considered as
exclusion criteria.
A group of patients with AH was also included in the
study and compared with those with aortic stenosis,
matching the groups as explained below in the statistical
analysis section. These patients were consecutively
referred to the same echo-lab and during the same period
by their general practitioners, with AH as the indication
for the echocardiographic examination. AH was defined
as pharmacologically treated high blood pressure. The
same definition was used for those patients with aortic
stenosis who had these clinical characteristics, identifying
two subgroups of aortic stenosis patients (with and with-
out AH). In all AH and aortic stenosis patients, blood
pressure was well controlled for at least 6 months before
echocardiographic evaluation by pharmacological therapy
which was unchanged during that period.
For both groups the exclusion criteria were: previous
diagnosis of coronary heart disease (on the basis of history
of myocardial infarction, any procedure of coronary artery
revascularization and the results of exercise/echo-stress
test or coronary angiography), LV wall motion abnorm-
alities, any grade of mitral stenosis, moderate to severe
aortic and/or mitral regurgitation, and documented epi-
sodes of sustained atrial arrhythmias occurring within
3 months before the echocardiogram. Patients taking
medications to prevent recurrence of atrial arrhythmias
were also considered not eligible for this study.
EchocardiographyStandard transthoracic Doppler-echocardiographic stu-
dies were performed in a dimly light room with all
patients in partial left decubitus position using a Megas
Esaote Biomedica machine (Florence, Italy) equipped
with a 2.5–3.5 MHz annular-array transducer. LV
chamber dimensions, septum and posterior wall thick-
ness and mass were measured according to the American
Society of Echocardiography [21,22], using M-mode tra-
cings. LV dimension was normalized for body height and
LV mass for height to the 2.7 power [23]. LV hypertrophy
was defined as LV mass more than 51 g/m2.7 [23]. Relative
wall thickness was calculated as two times the posterior
wall thickness/LV diastolic diameter ratio in all patients
independently of the presence of LV hypertrophy and
opyright © Lippincott Williams & Wilkins. Unauth
used as index of LV geometry. Values of this index
greater than 0.44 were considered to be indicative of
concentric geometry, whereas eccentric geometry was
identified for values less than 0.44, as previously reported
[1]. Thus, four subgroups of patients were identified
according to LV geometric pattern: patients with normal
geometry (mass <51 g/m2.7 and relative wall thickness
<0.44), concentric remodeling (mass <51 g/m2.7 and
relative wall thickness >0.44), concentric hypertrophy
(mass >51 g/m2.7 and relative wall thickness >0.44) and
eccentric hypertrophy (mass >51 g/m2.7 and relative wall
thickness <0.44). Wall LV mechanics were assessed by
computation of midwall fractional shortening according
to previously reported methods [10,11]. Circumferential
end-systolic stress was calculated, on the basis of a
cylindrical model, as previously described [10,11].
Stress-corrected midwall shortening less than 88% in
men and less than 89% in women was considered depres-
sed [24] and used as cut-off for definition of LV systolic
dysfunction. The area–length method was used to gen-
erate maximal LA volume [25]. Both LA and LV volumes
were normalized for height to the third power, consistent
with expected allometric relations between variables
with volumetric dimensions. LA systolic force was used
as an index of LA function and calculated according to the
formula previously validated by Manning et al. [26].
Aortic valve area was measured by the continuity
equation method and normalized for body surface area.
LV stroke work loss was also measured to assess the
degree of aortic stenosis [27]. Valve disease severity
(mild, moderate and severe aortic stenosis) was identified
by maximizing between-cluster value of aortic valve area
using Euclidean distance metric. Patients were also stra-
tified according to the values of LV stroke work loss using
the frequency procedure of tertiles.
Appropriateness of LV mass was defined as the ratio
between observed and predicted value [28]. LV mass
was predicted from stroke work, sex and body size by the
following reference equation:
Predicted LV mass ¼ 55:37þ ð6:63� height 2:7Þ
þ ð0:64� stroke workÞ � 18:1
� sex
where stroke work was estimated as systolic blood pres-
sure times stroke volume (using the method of Teichholz
et al.) [29] and converted to g�m by multiplying by
0.0144; sex was assigned the value of 1 for men and 2
for women. In aortic stenosis patients, stroke work was
obtained by adding the CW Doppler transaortic peak
gradient to brachial systolic blood pressure. LV mass was
defined as inappropriate when higher than 28% of the
value predicted (95th percentile of normal distribution)
and adequate for values equal to or smaller than 28% [28].
orized reproduction of this article is prohibited.

C
644 Journal of Hypertension 2009, Vol 27 No 3
Table 1 General characteristics of study population: comparison between patients with systemic arterial hypertension and aortic stenosis(divided in two subgroups with or without hypertension)
VariablesHypertensives(200 patients)
Aortic stenosis withhypertension (37 patients)
Aortic stenosis withouthypertension (63 patients) P
Age (years) 74�7 78�7§ 74�10 0.02Male sex (%) 41 35 43 n.s.Body weight (kg) 72�13 70�16 70�14 n.s.Body height (m) 1.65�0.08 1.64�0.09 1.64�0.08 n.s.Body mass index (kg/m2) 26.6�4.2 26.5�4.0 26.4�4.0 n.s.Systolic blood pressure (mmHg) 151�19§ 160�15§ 132�13§ <0.0001Diastolic blood pressure (mmHg) 87�14§ 86�11§ 79�9§ <0.001Heart rate (beats min�1) 66�17 68�11 68�10 n.s.Medicationsa
Diuretics 32 (%) 38 (%) n.s.ACE inhibitors/AT1-RB 59 (%) 60 (%) n.s.Calcium antagonists 32 (%) 30 (%) n.s.Beta-blockers 30 (%) 28 (%) n.s.
RB, receptor blockers. a Patients with aortic stenosis without hypertension (n¼63) were off drugs. Medications (%) are calculated considering only the 37 patients withaortic stenosis and hypertension. § P<0.05 vs. all other groups.
Data on intraobserver/interobserver variability and
test/re-test variability for the assessment of LV mass
appropriateness measured by this method have become
available [30].
Statistical analysisData are reported as mean values� 1SD. Patients with
AH were statistically matched with their counterparts
affected by aortic stenosis for potential confounders
such as age, sex, body weight and height and body mass
index according to the following procedure: a Gower’s
generalized distance from each of the patients with aortic
stenosis was computed and ranked in ascending order.
The distance was calculated using the following vari-
ables: age, sex, body height, body weight, body mass
index. The AH group was then defined by taking for each
patient with aortic stenosis the two closest cases.
Unpaired Student’s test and x2 statistics were used for
descriptive statistics. Between-group comparisons of con-
tinuous and normally distributed variables were per-
formed by the analysis of variance (ANOVA). Least
squares linear regressions were used to investigate the
relation of observed/predicted LV mass and the indices of
LV and LA function. Stepwise multiple linear regression
was used to identify independent correlates of inap-
propriate LV mass both in aortic stenosis and AH
patients, entering variables significantly related to inap-
propriate LV mass in univariate analysis. SPSS 11.0
Release (SPSS Inc., Chicago, Illinois, USA) was used
for statistical analysis. A two-tailed value of P less than
0.05 was considered statistically significant.
ResultsStudy populationThe recruitment period lasted from March 2004 to March
2006. During this period, 100 patients with aortic stenosis
(63 without AH and 37 with AH) met the enrollment
criteria and entered the study. Among the 336 patients
with AH who were eligible during the same period, 200
opyright © Lippincott Williams & Wilkins. Unautho
were selected and matched with the aortic stenosis group
accordingly to the previously described procedure and
formed the final study group of AH patients. The main
characteristics of the study groups are listed in Table 1.
Among 100 aortic stenosis patients, only 4 declared
symptoms potentially due to aortic valve disease (1
had high threshold stable angina, 3 had reduced func-
tional NYHA class). The remaining 96 patients with
aortic stenosis and all 200 AH patients were free of
symptoms and physical signs of cardiac disease. Patients
with aortic stenosis exhibited greater LV mass and more
concentric LV geometry than those with AH. Prevalence
of LV hypertrophy, LA volume and systolic force were
significantly greater in the groups with aortic stenosis
(Table 2). Patients with aortic stenosis without AH had
reduced indices of LV systolic function in comparison
with the other two groups.
Prevalence of inappropriate left ventricular massEchocardiographic characteristics of the study groups are
shown in Table 2. Prevalence of inappropriate LV mass
was similar in patients with aortic stenosis and AH (24 and
27.5%, respectively, P¼NS), but some differences
emerged when examining LV geometric patterns
(Fig. 1). Prevalence of inappropriate LV mass was not
significantly different in aortic stenosis and AH when LV
geometry was normal – a condition more frequent in AH
than in aortic stenosis (51 and 31%, respectively;
P¼ 0.001). However, in the presence of LVH, inap-
propriate LV mass was more frequent in AH than in
aortic stenosis (P< 0.01), independent of LV geometric
pattern (P¼ 0.04 and 0.001 in concentric and eccentric
LVH, respectively). No difference was found in the
presence of concentric LV remodelling.
Inappropriate left ventricular mass in aortic stenosispatients with and without aortic hypertensionAmong 100 aortic stenosis patients, 37 (37%) also had AH.
These patients were older and had higher systolic and
rized reproduction of this article is prohibited.

C
Ventricular mass growth in pressure overload Mureddu et al. 645
Table 2 Echocardiographic characteristics of study population: comparison between patients with systemic arterial hypertension and aorticstenosis (divided into two subgroups with or without hypertension)
VariablesHypertensives(200 patients)
Aortic stenosis withhypertension (37 patients)
Aortic stenosis withouthypertension (63 patients) P
LV end-diastolic diameter (cm/h) 2.94�0.28 2.9�0.30 3.0�0.33 N.S.Relative wall thickness 0.42�0.07§ 0.45�0.08 0.44�0.08 0.02LV mass (g) 182�53§ 194�52 208�60 0.001LV mass index (g/m2.7) 52�12M 57�16 59�13 0.001LV hypertrophy [n (%)] 56 (28%)§ 52 (43%) 52 (57%) 0.001Cess (kdyn/cm2) 139�44y 133�44 120�44 0.02Stress-corrected MFS (%) 88�16y 85�11 79�14 0.002LV systolic dysfunction (%) 100 (50%)y 69 (55%) 69 (73%) 0.002LA maximal volume (ml/h3) 8.5�2.6§ 11.8�4.2 10.4�3.3 0.000001LA systolic force (kdyn/cm2) 9.2�6§ 16.0�10 17.2�10 0.00001Predicted LV mass (g) 159�37§ 189�48 177�48 0.00001Observed/predicted LV mass (g) 116�31 107�26 117�28 N.S.
Cess, Circumferential end-systolic stress; LA, left atrial; LV, left ventricular. LV systolic dysfunction, stress-corrected midwall shortening<88% in men and<89% in women;MFS, midwall fractional shortening. § P<0.05 vs. all other groups. yP<0.05 vs. aortic stenosis without HT. MP<0.05 vs. aortic stenosis with HT.
diastolic blood pressure at the time of study evaluation
than their counterparts without AH. All patients with
aortic stenosis and hypertension were receiving antihy-
pertensive medications at the time of study evaluation,
whereas those without hypertension were off drugs
(Table 1). The two subgroups of patients did not differ
for any other clinical and echocardiographic parameter.
Prevalence of inappropriate LV mass in aortic stenosis
patients with and without AH was similar (16 and 29%,
respectively, P¼NS).
Inappropriate left ventricular mass and severity of valvediseaseAortic stenosis patients were categorized into three sub-
groups according to the valve area measured by the
continuity equation method (mild aortic stenosis¼ area
>0.75 cm2/m2, moderate aortic stenosis¼ area between
0.74 and 0.56 cm2/m2, severe aortic stenosis¼ area
<0.56 cm2/m2). Prevalence of LVH was similar between
the three subgroups (50, 44 and 64%, respectively).
opyright © Lippincott Williams & Wilkins. Unauth
Fig. 1
Prevalence (%) of the different left ventricular geometric patterns in thewhole hypertensive and aortic stenosis groups (white and blackcolumns, respectively) and prevalence (%) of inappropriate leftventricular mass in each study subgroup (spotted columns).
Prevalence of inappropriate LV mass was marginally
higher in the subgroups with moderate (9 of 34¼ 26%)
and severe (9 of 28¼ 32%) aortic stenosis than in that
with mild grade of valvular obstruction (6 of 38¼ 16%), a
difference that did not achieve, however, statistical sig-
nificance. Similarly, no significant difference in preva-
lence of inappropriate LV mass emerged among the
tertiles of LV stroke work loss (22, 31 and 25% in tertiles
with low, moderate and high LV stroke work loss,
respectively, P¼NS).
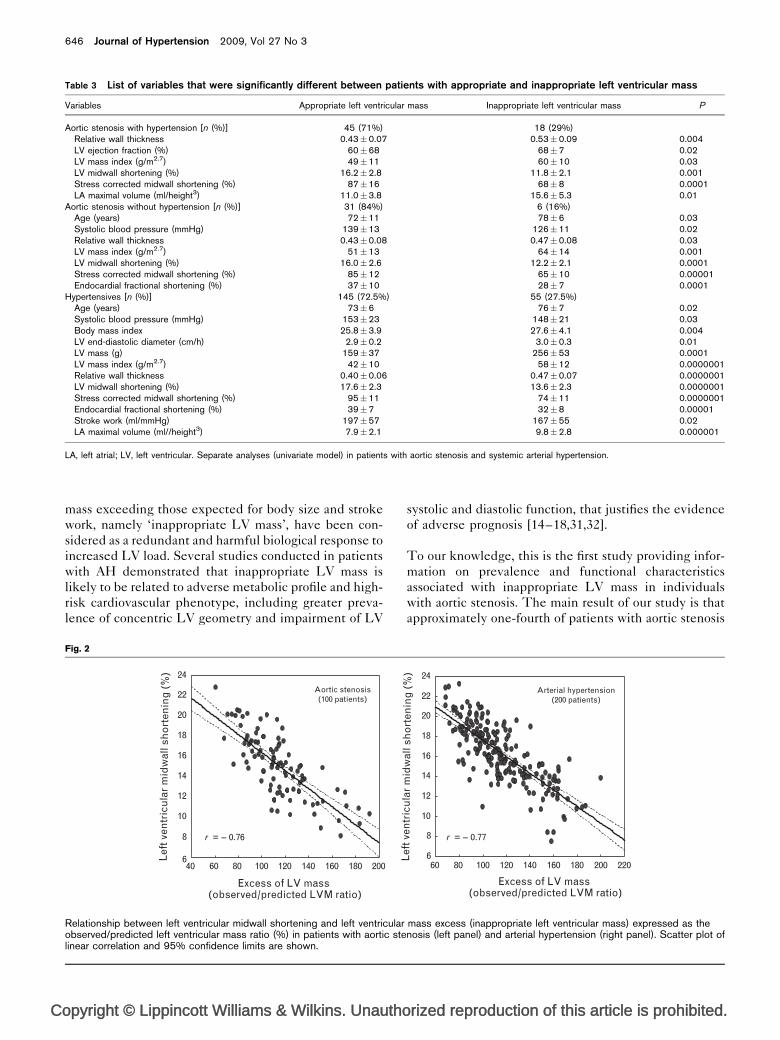
Characteristics of inappropriate left ventricular massTable 3 shows that, in the presence of inappropriate LV
mass, both patients with aortic stenosis and those with
AH were similarly characterized by high LV mass and
concentric LV geometry, reduced indexes of LV systolic
performance and higher LA volume as compared to those
with appropriate LV mass. Close negative linear relations
were found between excess of LV mass (expressed by the
observed/predicted ratio) and LV midwall shortening
both in aortic stenosis (r¼�0.76, P< 0.00001) and in
AH patients (r¼�0.77, P< 0.00001) (Fig. 2), whereas no
significant relation was found between excess of LV mass
and LA systolic force (r¼ 0.11 and 0.14 in aortic stenosis
and AH patients, respectively).
In multiple linear regression analyses run separately in
patients with aortic stenosis (with and without AH) and
AH (including age, systolic blood pressure, body weight,
body mass index, LV end-diastolic diameter and mass,
relative wall thickness, LV midwall shortening, stress-
corrected LV midwall shortening, LV endocardial frac-
tional shortening and LA maximal volume), reduced LV
systolic function (expressed as stress-corrected LV mid-
wall shortening) emerged as a variable mutually associ-
ated with LV mass excess in either study group (Table 4).
DiscussionEvaluation of the appropriateness of LV mass response to
cardiac load allows to investigate the nature of compen-
satory LV hypertrophy in AH. Values of sex-specific LV
orized reproduction of this article is prohibited.
C
646 Journal of Hypertension 2009, Vol 27 No 3
Table 3 List of variables that were significantly different between patients with appropriate and inappropriate left ventricular mass
Variables Appropriate left ventricular mass Inappropriate left ventricular mass P
Aortic stenosis with hypertension [n (%)] 45 (71%) 18 (29%)Relative wall thickness 0.43�0.07 0.53�0.09 0.004LV ejection fraction (%) 60�68 68�7 0.02LV mass index (g/m2.7) 49�11 60�10 0.03LV midwall shortening (%) 16.2�2.8 11.8�2.1 0.001Stress corrected midwall shortening (%) 87�16 68�8 0.0001LA maximal volume (ml/height3) 11.0�3.8 15.6�5.3 0.01
Aortic stenosis without hypertension [n (%)] 31 (84%) 6 (16%)Age (years) 72�11 78�6 0.03Systolic blood pressure (mmHg) 139�13 126�11 0.02Relative wall thickness 0.43�0.08 0.47�0.08 0.03LV mass index (g/m2.7) 51�13 64�14 0.001LV midwall shortening (%) 16.0�2.6 12.2�2.1 0.0001Stress corrected midwall shortening (%) 85�12 65�10 0.00001Endocardial fractional shortening (%) 37�10 28�7 0.0001
Hypertensives [n (%)] 145 (72.5%) 55 (27.5%)Age (years) 73�6 76�7 0.02Systolic blood pressure (mmHg) 153�23 148�21 0.03Body mass index 25.8�3.9 27.6�4.1 0.004LV end-diastolic diameter (cm/h) 2.9�0.2 3.0�0.3 0.01LV mass (g) 159�37 256�53 0.0001LV mass index (g/m2.7) 42�10 58�12 0.0000001Relative wall thickness 0.40�0.06 0.47�0.07 0.0000001LV midwall shortening (%) 17.6�2.3 13.6�2.3 0.0000001Stress corrected midwall shortening (%) 95�11 74�11 0.0000001Endocardial fractional shortening (%) 39�7 32�8 0.00001Stroke work (ml/mmHg) 197�57 167�55 0.02LA maximal volume (ml//height3) 7.9�2.1 9.8�2.8 0.000001
LA, left atrial; LV, left ventricular. Separate analyses (univariate model) in patients with aortic stenosis and systemic arterial hypertension.
mass exceeding those expected for body size and stroke
work, namely ‘inappropriate LV mass’, have been con-
sidered as a redundant and harmful biological response to
increased LV load. Several studies conducted in patients
with AH demonstrated that inappropriate LV mass is
likely to be related to adverse metabolic profile and high-
risk cardiovascular phenotype, including greater preva-
lence of concentric LV geometry and impairment of LV
opyright © Lippincott Williams & Wilkins. Unautho
Fig. 2
Lef
t ven
tric
ula
r m
idw
all s
ho
rten
ing
(%
)
2001801601401201008060406
8
10
12
14
16
18
20
22
24
Excess of LV mass (observed/predicted LVM ratio)
Aortic stenosis(100 patients)
r = -- 0.76
Relationship between left ventricular midwall shortening and left ventricularobserved/predicted left ventricular mass ratio (%) in patients with aortic stelinear correlation and 95% confidence limits are shown.
systolic and diastolic function, that justifies the evidence
of adverse prognosis [14–18,31,32].
To our knowledge, this is the first study providing infor-
mation on prevalence and functional characteristics
associated with inappropriate LV mass in individuals
with aortic stenosis. The main result of our study is that
approximately one-fourth of patients with aortic stenosis
rized reproduction of this article is prohibited.
22020018016014012010080606
8
10
12
14
16
18
20
22
24
Excess of LV mass (observed/predicted LVM ratio)
Lef
t ven
tric
ula
r m
idw
all s
ho
rten
ing
(%
)
Arterial hypertension(200 patients)
r = -- 0.77
mass excess (inappropriate left ventricular mass) expressed as thenosis (left panel) and arterial hypertension (right panel). Scatter plot of

C
Ventricular mass growth in pressure overload Mureddu et al. 647
Table 4 Multiple regression analyses applied in patients withhypertension, aortic stenosis with and without hypertension:variables independently associated with inappropriate leftventricular mass expressed as ratio observed/predicted leftventricular mass (%)
Arterial hypertension Exp (beta) P
Stress-corrected midwall shortening (%) �0.56 0.0000001Left ventricular end-diastolic diameter (cm) 0.49 0.000001
Relative wall thickness 0.46 0.000001Multiple r¼0.89; r2¼0.79; intercept¼�3.6; SEE¼12.6; F¼236;P¼0.0000001
Aortic stenosis with arterial hypertension Exp (beta)
Stress-corrected midwall shortening (%) �0.69 0.0000001Relative wall thickness 0.37 0.000001
Multiple r¼0.90 r2¼0.82 intercept¼132.2 SEE¼9.2 F¼58.1P¼0.0000001
Aortic stenosis without arterial hypertension Exp (beta)
Stress-corrected midwall shortening (%) �0.68 0.0000001Left ventricular mass (g/h2.7) 0.39 0.000001
Multiple r¼0.84, r2¼0.71, intercept¼175.0, SEE¼13.5, F¼51.4,P¼0.0000001.
exhibit inappropriately high LV mass, a prevalence which
is not statistically different from that found in our hyper-
tensive patients. A similar magnitude of inappropriate LV
mass was reported in other studies conducted on AH
patients [14–18,31]. This phenomenon does not seem to
be influenced by the coexistence of AH in aortic stenosis
patients, because the prevalence of inappropriate LV
mass was similar between the two study aortic stenosis
subgroups, with and without AH.
In the AH and aortic stenosis groups, inappropriate LV
mass was recognized in a small proportion of patients with
normal LV geometry. In these patients, evidently, the
simple measurement of LV mass could underestimate
the risk for cardiovascular events. Conversely, the preva-
lence of inappropriate LV mass was particularly high in
the subgroups of patients with LV hypertrophy, and this
behaviour was detected more frequently in patients with
AH than aortic stenosis. It is possible that the role of
nonhaemodynamic factors as determinants of LV mass
inappropriateness such as proto-oncogenes and other
growth factors, cytokines, plasma noradrenaline and other
neurohormones has more influence in AH than aortic
stenosis patients [33–35]. Recent studies documented a
significant increase in a member of the interleukin-6
superfamily, ‘cardiotrophin-1’, in patients with inap-
propriate LV mass. This finding was detected both in
patients with AH [36], in whom cardiotrophin-1 increased
or decreased according to the regression or persistence of
mass excess during the time, respectively, and in those
with aortic stenosis [37], whose plasma levels of cardio-
trophin-1 were proportional to the valvular severity.
These studies could support the hypothesis that a chronic
opyright © Lippincott Williams & Wilkins. Unauth
excess of cardiotrophin-1 may predispose hearts to pro-
gress to heart failure and/or other cardiovascular compli-
cations through the development of an excess of LV
mass, but data on the link between this biochemical
marker and clinical events are not yet available.
In this study, the prevalence of inappropriate LV mass
was similar in the three groups of patients with different
degrees of aortic stenosis, suggesting a possible appli-
cation of this bioassay for decision making. Whether the
presence of inappropriate LV mass might help identify
the time for aortic valve replacement and/or stratify the
risk of cardiovascular morbidity and mortality remains to
be clarified.
Also, interestingly, this study demonstrates that, despite
differences in LV overload between the two pathophy-
siological models, the cardiac characteristics associated
with inappropriate LV mass are identical in aortic stenosis
and AH patients. In both overload patterns, inappropriate
LV mass is associated with concentric LV geometry and
reduced systolic function, visible at both endocardial and
midwall levels, paralleling lower brachial systolic pres-
sure, as a possible indirect marker of LV pump failure.
However, differences between the two models of LV
overload exist that should be highlighted.
In aortic stenosis, LV systolic function appears to be more
severely reduced than in AH, and, on the basis of our
findings, to be relatively independent of myocardial after-
load, being most probably related to more impaired
myocardial contractility, as also suggested by the con-
comitant preserved LV chamber dimension (a raw index
of preload). This adverse cardiac phenotype in aortic
stenosis is amplified in the presence of inappropriate
LV mass. Aortic stenosis patients with inappropriate
LV mass exhibit the lowest level of LV systolic function
and the greatest LA volume (nearly twice the LA volume
found in the AH patients with appropriate LV mass),
strongly suggesting also a severe, albeit asymptomatic,
global LV dysfunction, also including LV diastolic dys-
function [38]. Merging this functional impairment with
the highly prevalent concentric LV geometric pattern and
LA dilatation (as a raw marker of LV diastolic dysfunc-
tion) [38] found in the aortic stenosis group, a cluster of
adverse characteristics emerges that was recently hypoth-
esized to potentially lead to cardiac decompensation,
even in the absence of coronary heart disease [16,39].
Abnormalities in LV size, geometric pattern and
performance, however, cannot completely explain the
magnitude of LV mass excess in aortic stenosis. Micro-
structural abnormalities including increased micro-
tubules, nuclear DNA mutations, ACE and TGF-ß1
up-regulation and apoptosis parallel LV hypertrophy
and dysfunction in aortic stenosis experimental models
[6,40]. Whether these alterations simply represent a
orized reproduction of this article is prohibited.

C
648 Journal of Hypertension 2009, Vol 27 No 3
negative ‘side effect ‘ of LV mass growth or, instead, an
important determinant has to be yet understood.
ConclusionAlthough LV and LA geometric adaptation in aortic
stenosis is quite different from AH, reflecting a near-pure
pressure overload, aortic stenosis patients have a similar
prevalence of inappropriately high LV mass to those with
AH and the variables associated with this condition are
analogous in the two groups. Particularly, as already
demonstrated in AH, the strong negative relationship
between LV mass excess and LV systolic function could
be of clinical relevance also in aortic stenosis patients.
Future studies should investigate whether inappropriate
LV mass may provide prognostic information also in
aortic stenosis patients, whose timing for surgery could
be better arranged.
References1 Ganau A, Devereux RB, Roman MJ, de Simone G, Pickering TG, Saba PS,
et al. Patterns of left ventricular hypertrophy and geometric remodeling inessential hypertension [see comments]. J Am Coll Cardiol 1992;19:1550–1558.
2 Chinali M, de Simone G, Liu JE, Bella JN, Oberman A, Hopkins PN, et al.Left atrial systolic force and cardiac markers of preclinical disease inhypertensive patients: the Hypertension Genetic Epidemiology Network(HyperGEN) Study. Am J Hypertens 2005; 18:899–905.
3 Grossman W, Jones D, McLaurin LP. Wall stress and patterns ofhypertrophy in human left ventricle. J Clin Invest 1975; 56:56–64.
4 Meerson FZ. The myocardium in hyperfunction, hypertrophy and heartfailure. Circ Res 1969; 25 (Suppl 163).
5 Devereux RB, de Simone G, Ganau A, Koren MJ, Mensah GA, Roman MJ.Left ventricular hypertrophy and hypertension. Clin Exp Hypertens 1993;15:1025–1032.
6 Hein S, Arnon E, Kostin S, Schonburg M, Elsasser A, Polyakova V, et al.Progression form compensated hypertrophy to failure in the pressure-overloaded human heart. Structural deterioration and compensatorymechanisms. Circulation 2003; 107:984–991.
7 Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Battistelli M, Barroccini C,et al. Adverse prognostic significance of concentric remodeling of the leftventricle in hypertensive patients with normal left ventricular mass. J AmColl Cardiol 1995; 15:871–878.
8 Krumholz HM, Larson M, Levy D. Prognosis of left ventricular geometricpatterns in the Framingham Heart Study. J Am Coll Cardiol 1995;879–884.
9 Shimizu G, Hirota Y, Kita Y, Kawamura K, Saito T, Gaasch WH. Leftventricular midwall mechanics in systemic arterial hypertension. Myocardialfunction is depressed in pressure-overload hypertrophy. Circulation 1991;83:1676–1684.
10 de Simone G, Devereux RB, Roman MJ, Ganau A, Saba PS, Alderman MH,Laragh JH. Assessment of left ventricular function by the midwall fractionalshortening/end-systolic stress relation in human hypertension. J Am CollCardiol 1994; 23:1444–1451.
11 de Simone G, Devereux RB, Koren MJ, Mensah GA, Casale PN, Laragh JH.Midwall left ventricular mechanics. An independent predictor ofcardiovascular risk in arterial hypertension. Circulation 1996; 93:259–265.
12 Aurigemma GP, Silver KH, McLaughlin M, Mauser J, Gaasch WH. Impact ofchamber geometry and gender on left ventricular systolic function inpatients >60 years of age with aortic stenosis. Am J Cardiol 1994;74:794–798.
13 Cioffi G, Mureddu GF, Stefenelli C, de Simone G. Relationship between leftventricular geometry and left atrial size and function in patients withsystemic hypertension. J Hypertens 2004; 22:1–8.
14 Cioffi G, Stefenelli C. Comparison of left ventricular geometry and left atrialsize and function in patients with aortic stenosis vs. those with pure aorticregurgitation. Am J Cardiol 2002; 90:601–606.
15 de Simone G, Verdecchia P, Pede S, Gorini M, Maggioni AP. Prognosis ofinappropriate left ventricular mass in hypertension: the MAVI Study.Hypertension 2002; 40:470–476.
opyright © Lippincott Williams & Wilkins. Unautho
16 Chinali M, De Marco M, D’Addeo G, Benincasa M, Romano C, Galderisi M,de Simone G. Excessive increase in left ventricular mass identifieshypertensive subjects with clustered geometric and functionalabnormalities. J Hypertens 2007; 25:1073–1078.
17 de Simone G, Palmieri V, Koren MJ, Mensah GA, Roman MJ, Devereux RB.Prognostic implications of the compensatory nature of left ventricular massin arterial hypertension. J Hypertens 2001; 19:119–125.
18 Palmieri V, Wachtell K, Gerdts E, Bella JN, Papademetriou V, Tuxen C, et al.Left ventricular function and hemodynamic features of inappropriate leftventricular hypertrophy in patients with systemic hypertension: the LIFEstudy. Am Heart J 2001; 141:784–791.
19 Mureddu GF, Pasanisi F, Palmieri V, Celentano A, Contaldo F, de SimoneG. Appropriate or inappropriate left ventricular mass in the presence orabsence of prognostically adverse left ventricular hypertrophy. J Hypertens2001; 19:1113–1119.
20 American College of Cardiology/American Heart Association Task Forceon Practice Guidelines; Society of Cardiovascular Anesthesiologists;Society for Cardiovascular Angiography and Interventions; Society ofThoracic Surgeons. Bonow RO, Carabello BA, Kanu C, de Leon AC Jr,Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT,O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK,Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL,Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guidelines for the management of patients with valvular heartdisease: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines (writing committee to revisethe 1998 Guidelines for the Management of Patients With Valvular HeartDisease): developed in collaboration with the Society of CardiovascularAnesthesiologists: endorsed by the Society for CardiovascularAngiography and Interventions and the Society of ThoracicSurgeons. Circulation 2006; 114:84–231. J Am Coll Cardiol 2006;48:1–148.
21 Sahn DJ, Demaria A, Kisslo J, Weyman A. The committee on M-Modestandardization on the American Society of Echocardiography:recommendations regarding quantitation in M-Mode echocardiography.Results of a survey study of echocardiographic measurements. Circulation1978; 58:1072–1083.
22 Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I,Reichek N. Echocardiographic assessment of left ventricular hypertrophy:comparison to necropsy findings. Am J Cardiol 1986; 57:450–458.
23 de Simone G, Devereux RB, Daniels SR, Koren MJ, Meyer RA, Laragh JH.Effect of growth on variability of left ventricular mass: assessment ofallometric signals in adults and children and their capacity to predictcardiovascular risk. J Am Coll Cardiol 1995; 25:1056–1062.
24 Bella JN, Palmieri V, Liu JE, Kitzman DW, Oberman A, Hunt SC, et al., TheHypertension Genetic Epidemiology Network (HyperGEN) Study.Relationship between left ventricular diastolic relaxation and systolicfunction in hypertension. Hypertension 2001; 38:424–428.
25 Lester SJ, Ryan EW, Schiller NB, Foster E. Best method in clinical practiceand in research studies to determine left atrial size. Am J Cardiol 1999;84:829–832.
26 Manning WJ, Silverman DI, Katz SE, Douglas PS. Atrial ejection force: anoninvasive assessment of atrial systolic function. J Am Coll Cardiol 1993;22:221–225.
27 Tobin JR Jr, Rahimtoola SH, Blundell PE, Swan HJ. Percentage of leftventricular stroke work loss. A simple hemodynamic concept forestimation of severity in valvular aortic stenosis. Circulation 1967; 35:868–879.
28 de Simone G, Devereux RB, Kimball TR, Mureddu GF, Roman MJ, ContaldoF, Daniels SR. Interaction between body size and cardiac workload.Influence of left ventricular mass during body growth and adulthood.Hypertension 1998; 31:1077–1082.
29 Teichholz LE, Kreulen T, Herman MV, Gorlin R. Problems inechocardiographic volume determinations: echocardiographic–angiographic correlations in the presence or absence of asynergy. Am JCardiol 1976; 37:7–11.
30 Muiesan ML, de Simone G, Ganau A, Longhini C, Verdecchia P, Mancia G,Agabiti-Rosei E, Working Group on Heart and Hypertension of ItalianSociety of Hypertension. Inappropriate left ventricular mass: reliability andlimitations of echocardiographic measurement for risk stratification andfollow-up in single patients. J Hypertens 2006; 24:2293–2298.
31 de Simone G, Kitzman DW, Palmieri V, Liu JE, Oberman A, Hopkins PN,et al. Association of inappropriate left ventricular mass with systolic anddiastolic dysfunction: the HyperGEN study. Am J Hypertens 2004;17:828–833.
32 Celentano A, Palmieri V, Esposito ND, Pietropaolo I, Crivaro M, MuredduGF, et al. Inappropriate left ventricular mass in normotensive andhypertensive patients. Am J Cardiol 2001; 87:361–363.
rized reproduction of this article is prohibited.
C
Ventricular mass growth in pressure overload Mureddu et al. 649
33 Strand AH, Gudmundsdottir H, Os I, Smith G, Westheim AS, BjornerheimR, Kjeldsen SE. Arterial plasma noradrenaline predicts left ventricular massindependently of blood pressure and body build in men who develophypertension over 20 years. J Hypertens 2006; 24:905–913.
34 Olsen MH, Wachtell K, de Simone G, Palmieri V, Dige-Petersen H,Devereux RB, et al. Is inappropriate left ventricular mass related toneurohormonal factors and/or arterial changes in hypertension? A LIFEsubstudy. J Hum Hypertens 2004; 18:437–443.
35 de Simone G, Pasanisi F, Contaldo F. Link of nonhemodynamic factors tohemodynamic determinants of left ventricular hypertrophy. Hypertension2001; 38:13–18; Review.
36 Lopez B, Castellano JM, Gonzalez A, Barba J, Diez J. Association betweenplasma cardiotrophin-1 and inappropriate Lift ventricular mass in essentialhypertension. Hypertension 2007; 50:977–983.
37 Talwar S, Downie PF, Squire IB, Davies JE, Barnett DB, Nq LL. PlasmaN-terminal pro-BNP and cardiothophin-1 are elevated in aortic stenosis.Eur J Heart Failure 2001; 3:15–19.
38 Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, Tajik AJ,Tsang TS. Left atrial size: physiologic determinants and clinicalapplications. J Am Coll Cardiol 2006; 47:2357–2363.
39 de Simone G, Gottdiener J, Chinali M, Maurer M. Left ventricular masspredicts heart failure not related to previous myocardial infarction: theCardiovascular Heart Study. Eur Heart J 2008; 29:741–747.
40 Zile MR, Green GR, Schuyler GT, Aurigemma GP, Miller DC, Cooper G4th. Cardiocyte cytoskeleton in patients with left ventricular pressureoverload hypertrophy. J Am Coll Cardiol 2001; 37:1080–1084.
opyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.




























