Embed Size (px)
Citation preview
1980 55: 199-204
GA Omura, S Moffitt, WR Vogler and MM Salter randomized central nervous system prophylaxisCombination chemotherapy of adult acute lymphoblastic leukemia with
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom

Blood, Vol. 55, No. 2 (February), 1980 199
Combination Chemotherapy of Adult Acute Lymphoblastic LeukemiaWith Randomized Central Nervous System Prophylaxis
By George A. Omura, Steven Moffitt, W. Ralph Vogler, and Merle M. Salter (Writing Committee
for the Southeastern Cancer Study Group)
Although major progress has been made in the treatment of childhood leukemia. the optimal chemotherapy of acutelymphoblastic leukemia (ALL) in adults has been unclear. In addition. the value of central nervous system prophylaxis(CNS-P) in adults has been assumed. but not established in a systematic fashion. The Southeastern Cancer Study Grouphas completed a prospective study in which the use of vincristine plus low-dose methotrexate and high-dose prednisone in
adult acute Iymphoblastic leukemia has produced an 80% (79/99) complete remission rate in patients age 1 5 yr and over.
Younger patients had a significantly higher remission rate but no increase in remission duration. This induction regimenwas associated with minimal toxicity. Random assignment to CNS-P or to no prophylaxis. after a multidrug consolidationregimen. has demonstrated a significant prolongation of CNS relapse-free interval (p=.O.008) in favor of CNS-P. CNS-P did
not improve hematologic remission duration or survival. All complete remitters were maintained on mercaptopurine.
methotrexate, and cyclophosphamide with pulses of prednisone and vincristine; the median time from remission to eitherhematologic or CNS relapse was 19.3 mo after CNS-P. and survival for these patients was 26.1 mo. We conclude that ourcurrent induction regimen is highly effective in adult ALL and that CNS prophylaxis is indicated in such patients.
A MINORITY ofadults with acute leukemia have
morphological and other features of their disease
consistent with childhood lymphoblastic leukemia.
However, the response rate to “induction” chemother-
apy has been lower and the response duration has been
considerably shorter in adults.’ Although prophylaxis
against central nervous system (CNS) leukemia has
been a major advance in the management of childhood
leukemia, its value in adults has been unclear. In view
of multiple complications of CNS prophylaxis that
have been reported2 � and uncertainty about the
frequency of CNS leukemia in adults, the Southeast-
em Cancer Study Group began a controlled trial in
1972. We sought to confirm the promising results of
an earlier Group study that induced remissions with
vincristine plus low-dose methotrexate and high-dose
prednisone.6 A maintenance drug schedule, based on a
regimen used successfully in children,7 was to be
preceded by a multidrug consolidation regimen. In
anticipation of slow case accrual in this uncommon
disease, we chose to study only one question in a
prospective randomized fashion, namely, is cranial
radiation plus intrathecal methotrexate of value in
preventing leukemic meningitis in adults?
MATERIALS AND METHODS
Untreated patients age 15 yr and over with a diagnosis of ALL
were eligible after written informed consent. The morphological
diagnosis was made by the individual investigator using the follow-
ing criteria: Auer rods must not be present; megaloblastic erythro-
poiesis and cytoplasmic granules must be minimal: leukemic cells
must have no more than a moderate amount of cytoplasm; the
degree of marrow infiltration and the uniformity of leukemic cells
must be fairly high.
Eighty-eight of the cases evaluable for induction had slides
reviewed by the senior author, who agreed with each investigator
about the diagnosis; the other I I evaluable cases did not have slides
available for this review. Special histochemical stains were encour-
aged but not required: immunologic and other special studies were
not routinely done. No attempt was made to subclassify the ALL
cases morphologically.
From the Departments of Medicine and Radiation Oncology.
University of Alabama in Birmingham. and the Departments of
Medicine and Biometri’. Lmort’ University, and other institutions
of the Southeastern (‘ancer Studt Group.
Supported in part h3’ LLSPHS grants from the National (ancer
Institute. NIH.
Submitted April 18. 1979; accepted October 3. 1979.
The fdlowing members of the Southeastern Cancer Studt
Group participated in and the fi/lowing USPHS grants supported
this study; R. Burson. M. (‘amphell. J. (‘arpenter, J. Durant, R.
Gams, D. Lineberry. G. Omura, M. Poon, and J. Prchal (Universitt
ofA/abama in Birmingham. (‘A-030/3. (‘A /9657 and (‘A 24456);
H. Si/berman (Duke Universit�, CA-03/77); H. Cohen (Durham
V.A. Hospital. CA-05634); J. Butts, C. (‘orlet. L. Hefiner. (‘.
Huguley, H. Kann. J. Keller, M. Robertson, W. Vogler. and F.
Winton (Emory Universiti-. (‘A 03227 and (‘A 1/263); G. Faguet
and C. Wright (Medical College ofGeorgia. CA 06807); Y. Ahn. H.
Lessner and M. Troner (Universitt’ of Miami, (‘A 05641); S.
Fischer. R. Joseph. R. Smalley. and R. Wright (Temple University,
(‘A 0796/); V. Loeb (Washington University. (‘A 03376); N.
Ma/donado, F. Robert, and F. Vele:-Garcia (University of Puerto
Rico, CA /2223); S. Gregory and W. Knospe (Rush MedicalCollege, (A /2840); 5. Krauss and T. Sonoda (University of
Tennessee, Knoxville. (‘A /3237); K. Tornt’os (New Orlean.c V.A.
Hospital. (‘A /3249); W. Forman. R. Kellermever. A. Lubin. and A.
Rassiga (Case Western Reserve University, (‘A /5584); W. Arrow-
smith (Oschner Clinic. (‘A /5578); (‘. Nee/t (University of Tenne.c-
see, Memphis, (‘A /7027); G. Broun and P. Petruska (St. Lt.ui.c
University, (‘A 1 7214); P. De Simone and J. Gockerman (Ulniversit3-
ofKentucky. (‘A 20255); 0. Martelo (University of Cincinnati); W.
Hanson (Radiological Physics Center. M. D. Anderson Hospital.
Houston, Texas).
Presented in part to the American Society of (‘linical Oncology,
April 4. /978, Washington. D.C.
Address reprint requests to George A. Omura, M.D.. 638 Zeigler
Building. University Station. Birmingham. Ala. 35294.
© I 980 by Grune & Stratton, Inc.
0006-497//80/5502-00/6$01 .00/0
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom

200 OMURA ET AL.
Treatment Program Induction
The induction treatment was given in 20-day cycles, using a single
daily dose of prednisone, 350 mg/sq m orally for 10 days, then 70
mg/sq m every other day through day 20. Vincristine, I mg/sq m
intravenously once weekly, and methotrexate, 2 mg/sq m orally
every 6 hr for 4 doses repeated twice weekly, were started on day I.
The entire cycle was to be repeated as long as progressive improve-
ment continued. Allopurinol, hydration, blood products, and anti-
biotics were given as needed. A complete remission was diagnosed
when the marrow was normocellular with 0%-5% blasts, erythroid
activity at least 1 5%, granulocytic elements at least 25%, the blood
had more than 10 g/dl hemoglobin concentration, more than 2000
granulocytes and more than 100,000 platelets, and there were no
relevant physical findings. Spinal fluid examination was not
required to diagnose complete remission.
Consolidation
Once a complete remission (CR) was confirmed, ‘�consolidation”
treatment was given: arabinosyl cytosine (ARA-C), 100 mg/sq m
intravenously, plus 6-thioguanine, 100 mg/sq m orally, every 12 hr
times 10 doses; approximately 9 days later, asparaginase, 500 lU/sq
m, was given intravenously daily times 5, plus vincristine, I mg/sq
m on days I and 5, and prednisone, 50 mg/sq m daily times 5, as a
second consolidation.
At the end of the consolidation phase, a repeat bone marrow
examination was done to confirm continuing marrow remission. In
addition, a lumbar puncture was done with cytocentifugation of the
spinal fluid. If the lumbar puncture showed 10 or more mononuclear
cells or any definite blast cells, cranial radiation and intrathecal
methotrexate were given on a nonrandomized basis.
CNS Prophylaxis
If the spinal fluid was normal and the bone marrow normal,
patients were randomly assigned to 3 wk of systemic mercaptopu-
rine, 50 mg/sq m/day, plus cyclophosphamide, 200 mg/sq m
weekly, with or without intrathecal methotrexate and cranial radia-
tion, 2400 rad in 12 fractions over 2.5 wk through opposing lateral
ports to the head, with each field being treated each day. A shaped
port was used to include the extensions of the meninges. The
treatment portals were to include the whole brain, excluding the
ocular globes, which were to be adequately shielded. The anterior
superior and posterior boundaries of the field were to extend at least
to the external table of the bones of the calvarium and to the
posterior wall of the orbit. Inferiorly, the line was to extend to the
auditory canal, including the entire middle fossa (temporal lobes),
and from here to follow the clivus, extending posteriorly to the level
of C-2.
Shielding materials were to have at least five half-value layers for
megavoltage energies. Localization films on the treatment machine
were to be obtained on every patient. A supervoltage source was
required with the treatment distance being at least 70 cm to the skin
or to the isocenter. Preservative-free intrathecal methotrexate, 10
mg/sq m (no maximum dose), was given twice weekly for 5 doses
using Elliott’s B solution as diluent.
Maintenance
Nonrandomized maintenance therapy for 24 mo included 6-
mercaptopurine, 50 mg/sq m orally daily, cyclophosphamide, 200
mg/sq m orally or intravenously weekly, and methotrexate, 20
mg/sq m orally, intramuscularly, or intravenously weekly. “Inducer
dosing” with vincristine, I .5 mg/sq m intravenously weekly times 3,
plus prednisone 50 mg/sq m daily times 14, was repeated every 8
wk, after a follow-up bone marrow examination to confirm the
remission.
At the end of 24 mo maintenance, bone marrow examination and
lumbar puncture were repeated; if normal, no further treatment was
given as long as remission persisted, but monthly blood counts and
every 2 mo bone marrows were to be done thereafter. No additional
spinal taps were done except on clinical indication. Documentation
of a bone marrow relapse marked the end of the remission. If CNS
relapse occurred while still in hematologic remission, CNS therapy
was given as described above and the patient remained on study. All
patients were followed for the duration of remission and survival.
Dose Adjustment
Induction. Vincristine could be discontinued for disabling
paresthesias or weakness.
Consolidation. Asparaginase could be discontinued for anaphy-
laxis, abdominal pain, or an increased serum amylase.
CNS phase. If the granulocyte count was less than 2000 or
platelet count less than IOO,000/pl, the 6-MP and cyclophospha-
mide were omitted; if the granulocyte count was less than I 500 or
the platelet count less than 75,000/pl, the intrathecal methotrexate
was delayed until blood counts improved.
Maintenance phase. The doses of 6-MP, cyclophosphamide,
and methotrexate were to be titrated up or down proportionately to
maintain the white count at 3000-4000. Cyclophosphamide was to
be discontinued if hemorrhagic cystitis occurred. Hematologic
toxicity was graded according to SEG criteria.8 A granulocyte
toxicity score of I + equals fall from normal to 0.75-1 .5 x l09/liter
orfrom 1.5-3.0 x l09/litertoO.20-O.75 x 109/Iiter;2+ indicatesa
fall from normal to the range of 0.20-0.75 x 109/Iiter or from the
range of I .5-3.0 x I 09/liter to <0.20 x I 0’/liter. A platelet toxicity
score of I + equals fall from more than 130 x 109/liter to 50-100 x
lO’/liter or from 100-130 x 109/liter to 10-50 x 109/liter; 2+
indicates a fall from <130 x 10’/liter to the range of 10-50 x
109/liter or from the range of 100-130 x 109/liter to <10 x
lOt/liter. A score of 3 + toxicity indicates life-threatening infection
or bleeding associated with blood count depression.
Statistical Methods
Survival and remission curves were plotted according to the
technique of Kaplan and Meier.9 The curves were statistically
compared by the generalized Wilcoxon technique of Gehan.’#{176}
Table 1 . Pretreatment Characteristics
Age range 15-70 yr (median age, 23)
Sex: 53 male, 46 female
Race: 80 white, 1 9 black
Spleen: 54 palpable, 45 not palpable
Mediastinal mass: 3 present, 96 absent
Adenopathy: 30 present, 69 absent
WBC: �100,000, 75; �100,000, 24
Platelet < 1 00,000, 84; � 100,000, 15
Ta ble 2. Response
Percent
Eval CR PR NC Worse Dead CR
Induction 99 79 7 3 2 8 80%
Consolidation 77 7 1 5 1 92%
CNS-P + Chemo 28 27 1 96%
Chemo only 34 33 1 97%
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom

TREATMENT OF ADULT ALL 201
Granulocytes Platelets
1�- 2+ 3+1� 21 3+
Induction
Consolidation
Maintenance
(99evaluable)
(77 evaluable)
(54 evaluable)
17(17%)
1 3 ( 1 7%)
1 7 (3 1 %)
16(16%)
32 (42%)
1 1 (20%)
1 (1%)
2 (3%)
11 (11%)
22 (29%)
8 (1 5%)
4(4%)
19 (25%)
1 (2%)
2(2%)
For grading of toxic) ty see Materials and Met hods section.
Response rates were compared using a x2 test on proportions.
Prognostic factors were assessed for association with duration of
remission using a step-wise version of Cox’s regression analysis’ ‘ and
for association with achievement of remission using a logistic
regression analysis.’2
RESULTS
One-hundred-fourteen (I 14) patients were entered
from August 1972 through June 1978 and have had
their review completed. Nine were not eligible (prior
therapy, 3; acute myelogenous leukemia, 3, blastic
phase of chronic myelogenous leukemia, I � prior
lymphoma, 2), 3 had major protocol violations during
the induction phase, and 3 refused to continue therapy.
Thus, 99 were evaluable for induction. Their pretreat-
ment characteristics are shown in Table I.
Table 2 shows the outcome of induction, consolida-
tion, and the randomized treatment phase (chemo-
therapy plus or minus CNS prophylaxis). Seventy-
nine patients (80%) achieved complete remission, 27
within 4 wk; 30 took 4-6 wk, and 22 required more
than 6 wk of treatment. The induction regimen was
generally well tolerated. However, two patients died of
pneumocystis infection in complete remission after
requiring multiple cycles of induction therapy. One
patient developed urate nephropathy despite the use of
allopurinol. Two patients developed a transient steroid
psychosis, and five patients developed hyperglycemia
during induction. One patient had acute pancreatitis
attributed to asparaginase. One patient had transient
paraplegia after intrathecal methotrexate. During the
CNS phase, I 8% of patients receiving prophylaxis had
headaches; 30% had nausea compared with I 5� of
those receiving chemotherapy only. No late sequelae
of the cranial radiation have been noted to date on the
semiannual follow-up forms, although no specific
neurologic testing is called for in the protocol. One
patient developed hemorrhagic cystitis requiring
cessation ofcyclophosphamide. Several patients devel-
Table 4. Nonhem atologic Toxicity
Stomatitis
Nausea
�
Vomiting
Pares-
thesias
Induction
Consolidation
Maintenance
(99 evaluable)
(77 evaluable)
(54 evaluable)
14 (14%)
3 (4%)
8 (15%)
20 (20%)
1 1 (14%)
18 (33%)
21 (21%)
6 (7%)
14 (26%)
oped transient liver function abnormalities, but none
had drug toxicity established as the cause. Other
aspects of toxicity are shown in Tables 3 and 4.
Table 5 shows response by age for induction; in the
age group I 5-23, the complete remission rate was
90%; of the 5 failures, 3 achieved normal marrow and
blood counts, but 2 of them had persistent spleno-
megaly and the other had residual adenopathy. In
those aged 24 and older, the complete remission rate
was 67%, which is significantly lower (p = 0.01). If
one chooses age 20 as a break point, the CR rate was
92% (33/36) for those aged 15-20, and 73% (46/63)
for those aged 21 and over (p = 0.03).
Of 71 patients remaining in CR at the end of
consolidation, 2 were not randomized to the CNS
phase because of overt CNS leukemia; after CNS
therapy, one has had a CNS relapse and the other a
hematologic relapse. Of 69 who were randomized, 2
refused CNS prophylaxis and were lost to follow-up.
Two others who were randomized to no prophylaxis
were considered inevaluable because of poor com-
pliance and major medication errors early in this
phase of treatment; one subsequently had a CNS
relapse and the other a hematologic relapse. Two
patients had incomplete records. One other patient
was taken off protocol because of what was thought to
be intercurrent illness shortly after completing the
CNS prophylaxis but died in hematologic relapse.
Thus, there were 62 patients evaluable for the
randomized phase of the study.
Eleven of 34 evaluable patients in the no-prophy-
laxis group have had a CNS relapse. Of 28 evaluable
patients receiving cranial radiation and intrathecal
methotrexate as prophylaxis, 3 had a CNS relapse.
The difference between the two groups is significant at
the p = 0.03 level (x2 = 4.93). Since this calculation
does not take into account the time at risk for CNS
Table 5. Rasp onse by Age (lnducti on)
Number of Patients
15-23’ 24-30 31-40 41-50 51-60 60+
<CR
CR
Total
5
45
50
7
7
14
4
12
16
1
8
9
2
4
6
2
2
4
Age in years.
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom
1.
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
C0
00.00.
Total Fail In Rem Median
34 18 16 24.7 0NoCNSP28 16 12 21.2 ‘�s CNS P
0 ts V5 0�ts P=0.757
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
Total3428
C0
00.0
0.Fail Censrd11 23 oNoCNSP3 25 �CNSP
OE�iV5O�1� P=0.008
6 12 18 24 30 36 42 480
Total Fail Censrd Median34 14 20 32.2 0NoCNSP28 14 14 30.5 ACNS P
O� VSOeAPO.9890.9
0.8
0.7
.� 0.6
�. 0.50
0. 0.4
0.2
0.1
0.00 7 14 21 28 35 42 49 56
Months
Survival from Date on Study for PatientsEvaluable for CNS Phase
202 OMURA ET AL.
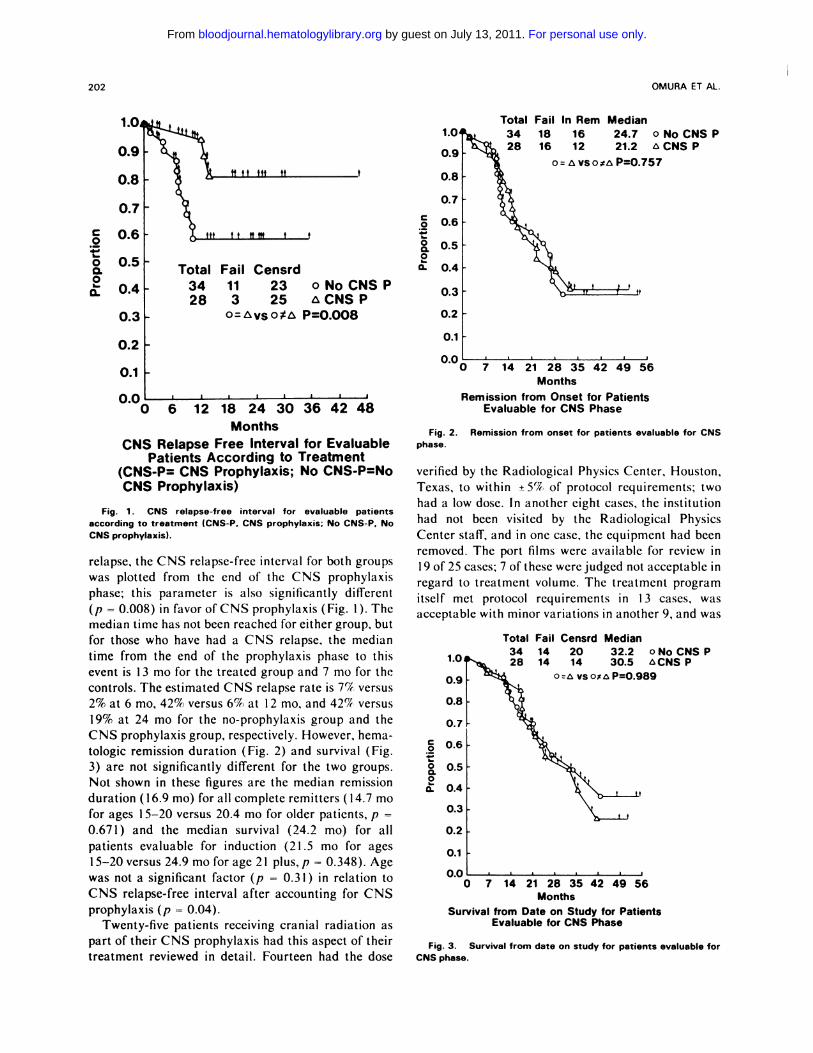
Fig. 3. Survival from date on study for patients evaluable forCNS phase.
Months
CNS Relapse Free Interval for EvaluablePatients According to Treatment
(CNS-P CNS Prophylaxis; No CNSPNoCNS Prophylaxis)
Fig. 1 . CNS relapse-free interval for evaluable patients
according to treatment (CNS-P. CNS prophylaxis; No CNS-P, NoCNS prophylaxis).
relapse, the CNS relapse-free interval for both groups
was plotted from the end of the CNS prophylaxis
phase; this parameter is also significantly different
(p = 0.008) in favor ofCNS prophylaxis (Fig. I). The
median time has not been reached for either group, but
for those who have had a CNS relapse, the median
time from the end of the prophylaxis phase to this
event is 1 3 mo for the treated group and 7 mo for the
controls. The estimated CNS relapse rate is 7% versus
2% at 6 mo, 42% versus 69� at 1 2 mo, and 42� versus
19% at 24 mo for the no-prophylaxis group and the
CNS prophylaxis group, respectively. However, hema-
tologic remission duration (Fig. 2) and survival (Fig.
3) are not significantly different for the two groups.
Not shown in these figures are the median remission
duration ( I 6.9 mo) for all complete remitters ( I 4.7 mo
for ages I 5-20 versus 20.4 mo for older patients, p -
0.671) and the median survival (24.2 mo) for all
patients evaluable for induction (21.5 mo for ages
1 5-20 versus 24.9 mo for age 2 1 plus, p = 0.348). Age
was not a significant factor (p = 0.3 1 ) in relation to
CNS relapse-free interval after accounting for CNS
prophylaxis (p = 0.04).
Twenty-five patients receiving cranial radiation as
part of their CNS prophylaxis had this aspect of their
treatment reviewed in detail. Fourteen had the dose
0.2
0.1
0.00 7 14 21 28 35 42 49 56
Months
Remission from Onset for PatientsEvaluable for CNS Phase
Fig. 2. Remission from onset for patients evaluable for CNSphase.
verified by the Radiological Physics Center, Houston,
Texas, to within ±5% of protocol requirements; two
had a low dose. In another eight cases, the institution
had not been visited by the Radiological Physics
Center staff, and in one case, the equipment had been
removed. The port films were available for review in
I 9 of 25 cases; 7 of these were judged not acceptable in
regard to treatment volume. The treatment program
itself met protocol requirements in I 3 cases, was
acceptable with minor variations in another 9, and was
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom

TREATMENT OF ADULT ALL 203
not acceptable in 3. In regard to the 3 patients who
had a CNS relapse in spite of CNS prophylaxis, the
port film in one showed an inadequate treatment
volume; the second had a low dose (2200 rad instead of
2400) and neither the dose nor the treatment volume
could be verified in the third. It should be noted that
all of these patients received intrathecal methotrexate
as well, so the relative importance of these protocol
deviations is unclear.
Of 54 evaluable patients in the maintenance phase,
16 completed 2 yr of maintenance treatment; of these,
5 have had a marrow relapse and I I remain in hema-
tologic remission from I to 27 mo posttreatment.
Thirty-eight have not completed the maintenance
phase, 25 because of relapse; I 3 remain in remission in
the maintenance phase. Of the 16 who completed
maintenance, 8 had received CNS prophylaxis with 2
marrow relapses (at I .5 and 6 mo); of the others, 3 had
a marrow relapse (at I , 1 .5, and 4 mo after completing
treatment). There have been no late CNS relapses in
either group.
Potential prognostic variables (age, sex, hemoglobin
level, platelet count, white count, splenomegaly, hepa-
tomegaly, mediastinal or other adenopathy) were
examined in multivariate fashion, but none were
predictive of remission rate or duration except age
versus remission rate (p = 0.01, x2 test of signifi-
cance).
DISCUSSION
In any large series of adults with ALL, prednisone
plus vincristine produces approximately a 509� remis-
sion rate,’ compared with over 90% in children.7
Several reports have indicated an improved remission
rate in adults by the addition of anthracyclines or
asparaginase. Woodruff’ has tabulated the results of
such trials, showing adult remission rates ofabout 759�.
for prednisone plus vincristine plus an anthracycline in
some recent studies, with median remission durations
ranging from 7.5 to 25 mo. In general, teenagers have
had a higher remission rate.
One of the larger trials was reported by Lister et
al.’3 in which 71% (36/51) of adults achieved CR
using prednisone plus vincristine plus adriamycin plus
asparaginase; the remission rate was 79% ( 1 5/ 1 9) in
those aged 15-20 and 66% (21/32) in older patients,
but there was no correlation between age and remis-
sion duration, as in the present report. The predicted
median remission duration was 18.5 mo and the
survival 27 mo. All patients in that trial were to
receive CNS prophylaxis; 3 of 30 who received it had
their initial relapse in the central nervous system.
Henderson and Glidewell’4 reported a study of pred-
nisone plus vincristine plus asparaginase in ALL
patients aged 20 and older, adding daunorubicin in
those not in remission by 4 wk. The CR rate was 72%
and median remission duration I 5 mo. Dowling et al.’5
used prednisone, vincristine, and adriamycin for
induction in 25 adults aged I 5 plus; 4 were considered
not evaluable; 20 achieved CR. Remission duration
after a multiple drug consolidation and maintenance
program appeared to be longer than with their
previous protocol. All patients in those studies received
CNS prophylaxis.
The present study indicates that the addition of
low-dose methotrexate to vincristine plus high-dose
prednisone can produce a high complete remission rate
(80%), especially in those aged 15-20 (92%), with
minimal toxicity. When this teenage group is
excluded, the median remission duration is actually a
bit longer, 20.4 mo, and the remission rate (73%) is
not inferior to the general experience cited by Wood-
ruff.’ It has been assumed that the benefits of CNS
prophylaxis in children would apply to adults, but this
has not been previously evaluated in a systematic
manner. The present study establishes that CNS
prophylaxis is of value in decreasing the occurrence of
CNS relapse in adults with lymphoblastic leukemia.
Although there is currently no advantage regarding
hematologic remission duration or survival, it is of
interest that the effect of CNS prophylaxis on hemato-
logic remission duration in children is not seen during
the first 24 mo of remission.7 It is likely that the full
impact of CNS prophylaxis on adult lymphoblastic
leukemia will not become apparent until better
systemic therapy is developed.
The relative importance of the consolidation
program and of the specific maintenance program that
we used cannot be stated. Further improvements are
clearly needed, especially in regard to remission induc-
tion in older adults, reduction in the CNS relapse rate
after CNS prophylaxis, and increased hematologic
remission duration. Identification of other poor-risk
factors, such as T-cell ALL, Burkitt-type leukemia,
blastic CML presenting as ALL, extreme leukocyto-
sis, or extensive tissue infiltration,’ may help to iden-
tify subcategories in which new approaches will be
required.
ACKNOWLEDGMENT
L-Asparaginase, preservative-free methotrexate for intrathecal
administration, and Elliot’s B solution were supplied by the Division
ofCancer Treatment, National Cancer Institute. The human inves-
tigations described herein were performed after approval by the
Human Investigations Committee of each participating institution
and in accord with assurances filed with and approved by the
Department of Health, Education and Welfare.
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom

204
REFERENCES
OMURA ET AL.
1. Woodruff R: The management of adult acute lymphoblastic
leukemia. Cancer Treat Rev 5:95, 1978
2. Kay HEM, Knapton P. O’Sullivan JP, Wells DG, Harris RF,
Junes EM, Stuart J, Schwartz FCM, Thompson EN: Encephalopa-
thy in acute leukemia associated with methotrexate therapy. Arch
Dis Child 47:344-353, 1972
3. Duttera Mi, Gallelli JF, Kleinman LM, Tangrea JA, Witt-
grove AC: Intrathecal methotrexate. Lancet I :540, 1972
4. Peylan-Ramu N, Poplack DG, Pizzo PA, Adornato BT,
DiChero G: Abnormal CT scan in asymptomatic children after
prophylactic cranial irradiation and intrathecal chemotherapy. N
EngI J Med 298:815-819, 1978
5. Pochedly C: Neurotoxicity due to CNS therapy for leukemia.
Med PediatrOncol 3:101, 1977
6. Huguley CM: Combination therapy for acute leukemia in
adults. Blood 30:889, 1967 (abstr)
7. Simone JV: Factors that influence haematological remission
duration in acute lymphocytic leukemia. Br J Haematol 32:465,
I 976
8. Kremer W, Volger WR, Chan YK: An attempt at synchroni-
zation of marrow cells in acute leukemia-relationship to thera-
peutic response. Cancer 37:390-403, 1976
9. Kaplan EL, Meier P: Non-parametric estimation from incom-
plete observations. J A Statist Assoc 53:457-48 1 , I 958
10. Gehan E: A generalized Wilcoxon test for comparing arbi-
trarily singly censored samples. Biometrika 52:203-223, 1965
I I . Cox DR: Regression models and life tables. J R Stat Soc (B)
34:187-220, 1972
I 2. Lee ET: A computer program for linear logistic regression
analysis. Comput Prog Biomed 4:80-92, 1974
13. Lister TA, Whitchouse JMA, Beard MEJ, Brearley RL,
Wrigley PFM, Oliver RTD, Freeman JE, Woodruff RK, Malpas
is, Paxton AM, Crowther D: Combination chemotherapy for acute
lymphoblastic leukemia in adults. Br Med J I : I 99, 1978
14. Henderson E, Glidewell 0: Combination therapy of adult
patients with acute lymphocytic leukemia. Proc AACR ASCO
15:102, 1974 (abstr 407)
15. Dowling MD, Kempin S, Gee T, Dufour M, Noble 5,
Clarkson B, Burchenal I: Improved survival in adult acute lympho-
cytic leukemia. Proc AACR ASCO I 8:337, 1977 (abstr C28 I)
For personal use only. by guest on July 13, 2011. bloodjournal.hematologylibrary.orgFrom


















![[Prophylaxis of cerebroascular diseases] Профилактика на мозъчно-съдовите заболявания](https://img.dokumen.tips/doc/110x75/6333389fce61be0ae50e8a82/prophylaxis-of-cerebroascular-diseases-profilaktika-na-mozchno-sdovite.jpg)






![[Venous thromboembolic prophylaxis. Guidelines for adults in Argentina]](https://img.dokumen.tips/doc/110x75/633aa650ad51ed758105c455/venous-thromboembolic-prophylaxis-guidelines-for-adults-in-argentina.jpg)



