Embed Size (px)
Citation preview
INF
OR
MA
TIO
N
2006
Cases of PoisoningReported by Physicians
aerztl_mitteilungen_06_engl 21.09.2007 14:59 Uhr Seite u1

Cases of Poisoning Reported by Physicians in 2006Published by: BfR Press and Public Relations OfficeEditors: Centre for Documentation and Assessment of Poisonings at the BfRTranslation from German by Andrea Bartel, BerlinNo of copies printed: 1000Typesetting and printing: Werbedruck SchreckhasePrinted on chlorine-free paper
ISBN 3-938163-28-3ISSN 1435-4047
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite u2

Cases of Poisoning Reported by Physicians2006
Centre for Documentation and Assessment of Poisonings at the Federal Institute for Risk Assessment – 13th Report (2006)
A. Hahn, K. Begemann, R. Burger, J. Hillebrand, H. Meyer, K. Preußner
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 1

2
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 2
Table of Contents
1 Legislation on chemicals to serve the needs of people 5
2 Introduction 72.1 Legal basis and activities of the Centre 72.2 Processing of reports received 72.3 Product data bank (poison information data bank) 92.3.1 Figures 92.3.2 Collaboration between the BfR, industry and Poison Control Centres 9
3 Case reports by physicians 113.1 Evaluation of reports 113.2 Reports on cases of poisoning in 2006 113.2.1 Origin 113.2.2 Spectrum of cases reported 113.2.3 Causes of poisoning 133.2.4 Age structure and sex distribution 133.2.5 Degree of severity of health impairment 143.2.6 Outcome of cases 153.3 The product information system, PRINS 163.3.1 Rapid communications 163.3.2 Summary reports 18
4 Selected toxicological problems 204.1 Acute health impairment due to “Magic Nano” sealant sprays 204.2 Specific risks for the elderly – Poisoning by cleansers and disinfectants 264.3 Selected cases by cause of poisoning 284.3.1 Mistake 284.3.1.1 Descaling products 284.3.1.2 Dishwasher detergent 304.3.2 Health disorders caused by foods 314.3.2.1 Shiitake mushroom 314.3.2.2 “Butterfish” 334.3.3 Accidents 354.3.3.1 Chemical burns from sodium hydroxide 354.3.3.2 Fire breathing 364.3.4 Abuse 394.3.4.1 Slimming agent (2,4-dinitrophenol) 394.3.4.2 Sniffing agents (deodorant spray) 414.3.4.3 p-Nitroaniline 434.3.5 Suicides 45
3
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 3

4.3.5.1 Valproic acid 454.3.5.2 2,4-Dinitrophenol (DNP) 474.3.5.3 Dimethoate 48
5 Annex 505.1 Spectrum of cases reported during the 1 January – 31 December 2006 period 505.2 Notification form for cases of poisoning 555.3 Notification form for industrial accidents 565.4 Press releases on toxicological problems issued by the BfR in 2006 59
Cases of Poisoning Reported by Physicians
4
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 4

1 Legislation on chemicals to serve the needsof people
topicality with regard to toxicological issues,their proposals of measures and consistentpresentation of individual case reports. In addi-tion, ministries, companies and industrial asso-ciations are informed about adverse effects ofchemical products (technical term: toxicovigi-lance) either immediately (in severe cases) or atannual intervals through a well-working productinformation system.
Meanwhile, the data recorded on humans haveprovided a sound basis of facts and figures formeaningful regulatory measures. Before, casesof exposure to lamp oil and liquids for grill light-ing had been clearly underestimated based ontoxicological data from animals, and other sub-stances, in contrast, overestimated. Emotionsand concerns that had been associated for example with pyrethroid exposure could be re-duced to a technical level and replaced by amore objective assessment merely by facts froma consistent documentation of data on humans.In contrast to former expectations, frequentcomplications (aspiration) due to ingestion ofsolutions containing surfactants did not affectchildren and adults but instead, have proved aparticular risk for elderly and disoriented per-sons. Last but not least, given the fact that com-pulsory notification by physicians also refers tocases involving harmful substances from the en-vironment, a new basis has been formed by leg-islation to ensure that in the event of an industri-al accident not only the technological aspectsare taken into account but also the resultingcases of health impairment among exposedgroups of individuals are recorded.
From now on, the German regulatory frameworkon chemicals will be completed by the new European regulatory framework on chemicals,REACH (Registration, Evaluation, Authorization
5
On 1 August 1990, the requirement of compul-sory notification of poisonings by attendingphysicians within the framework of the Chemi-cals Act came into force. This compulsory notifi-cation is a meaningful counterpart, so to speak,to the reporting of adverse reactions to medici-nal products.
It has been the purpose and objective of this le-gal provision in the Chemicals Act to receivefrom physicians acting “on the scene” well doc-umented findings on human health complaintscaused by chemical products. In addition, it hasbeen the intent to obtain valuable data on the in-cidence of poisoning accidents, doses and ef-fects of chemicals as well as on product formu-lations involved in cases of poisonings which ata very early date may suggest effective preven-tive measures that could be taken. In this re-gard, it has been a special intent of legislationthat assessment of poisonings should not onlyrely on toxicological data from animal studiesbut as much as possible make use of knowl-edge gained from poisoning accidents thathave occurred in humans. If regrettably, suchaccidents occur, their evaluation should at leastbe useful to humans and in addition, contributeto animal welfare by reducing the number oftoxicological studies required for assessment.
Thus, legislation has resulted in a most usefulproject which is unique on the global level: The“Cases of Poisoning Reported by Physicians”have been compiled at the Federal Institute forRisk Assessment (BfR) in direct cooperationwith attending physicians and the German Poi-son Control Centres (PCCs) and subsequentlyevaluated as data derived from humans formore than 15 years now. The annual reportspublished (meanwhile also in English) have metwith a very affirmative response owing to their
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 5

and Restriction of Chemicals) which has comeinto force on 1 June 2007. Nevertheless, theGerman national legislation on chemicals hadalready achieved a very high level of consumerprotection as compared to that in other coun-tries. The reporting of cases of poisoning byphysicians is a good example for this. Hopefully,REACH will provide for such monitoring systemsbeing furthermore promoted and supported tothe benefit of consumers. Based on physicians’reports of cases of poisoning and the legallyfounded collaboration with the German PCCs,
the BfR could make an essential contribution toan effective identification of health risks posedby chemical substances and products bymeans of the documentation of accidents in-volving humans. Obviously, animal studies aloneare not sufficient for this purpose.
Horst Spielmann,Head of the Scientific Services Department(“Wissenschaftliche Querschnittsaufgaben“) atthe BfR
Cases of Poisoning Reported by Physicians
6
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 6

2 Introduction
2.1 Legal basis and activities of the CentreWith the Chemicals Act (ChemG), legislation inthe Federal Republic of Germany has provideda basis “to protect humans and the environmentfrom harmful effects of dangerous substancesand preparations, particularly to make them rec-ognizable, to avert and to prevent the develop-ment of such effects” (according to §1).
For a realistic assessment of risks for humanhealth, importance has been increasingly givento the knowledge of data on human toxicologythat can be obtained from the evaluation of cas-es of poisoning in humans. This is why legisla-tion has introduced compulsory notification ofpoisonings by attending physicians from 1 Au-gust 1990, by the first amendment to theChemG (§16e).
A physician who is consulted for treatment orevaluation of sequelae of diseases caused bychemical substances or products is obliged tosubmit essential data on poisonings to the Cen-tre for Documentation and Assessment of Poi-sonings at the Federal Institute for Risk Assess-ment (BfR).
According to the Chemicals Act, reportingrefers to illnesses or suspected poisonings thatare associated with the following substances:� Chemical substances and products used in
the household, e.g. detergents and cleansingagents, hobby and DIY articles;
� Cosmetics;� Pest control products;� Plant protection products;� Wood preservatives;� Chemicals used at the workplace;� Harmful chemical substances found in the
environment, also after industrial accidents;and
� Plants/animals.
Within the meaning of the Chemicals Act, theterm of poisoning designates all cases in whichhealth impairment has occurred, including sus-pected cases of poisoning. Under the Act, alsothe poison information and treatment centres(Poison Control Centres, PCCs) were subjectedto compulsory reporting of their knowledge (ofgeneral importance) gained in the context oftheir activities.
In 2006, the Poison and Product DocumentationCentre moved from Berlin-Dahlem to Berlin-Marienfelde. Of course, the aspects of secrecyand security with regard to formulation data willbe paid at least the same attention at the newpremises as formerly at the Dahlem site.
2.2 Processing of reports receivedReports received on health impairment associ-ated with chemicals are subjected to an assess-ment procedure resulting in the rating of a pos-sible causal relationship between the toxicantand the manifestations observed, as well as oth-er conclusions. Such relationship may be classi-fied as “possible”, “probable”, “confirmed”, “ab-sent” or “cannot be assessed”. The rules ap-plied in the assessment of individual caseshave been described in detail in earlier annualreports.
The estimation of toxic risks in humans is basedon differentiated analyses and evaluation of thedata on cases. For these purposes, the data oncases in humans are continuously documentedin the form of case data sets and case reports.Information on identified risks is passed on tothe responsible ministries, manufacturers andindustrial associations in the form of rapid communications or annual summarizing reportsby means of the product information systemPRINS (see Chapter 3.3). At the same time, theresponsible manufacturers or distributors arerequested to submit information on the meas-ures envisaged by them to improve productsafety.
7
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 7
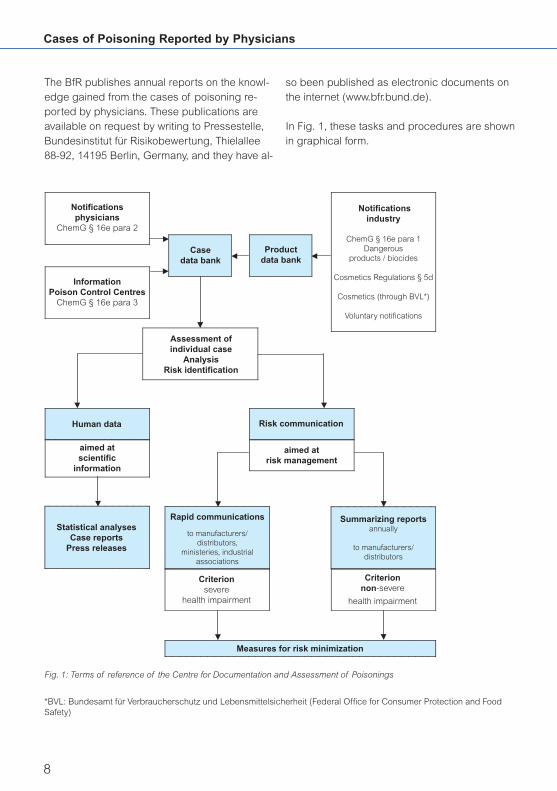
The BfR publishes annual reports on the knowl-edge gained from the cases of poisoning re-ported by physicians. These publications areavailable on request by writing to Pressestelle,Bundesinstitut für Risikobewertung, Thielallee88-92, 14195 Berlin, Germany, and they have al-
so been published as electronic documents onthe internet (www.bfr.bund.de).
In Fig. 1, these tasks and procedures are shownin graphical form.
Cases of Poisoning Reported by Physicians
8
Notificationsphysicians
ChemG § 16e para 2
Human data
InformationPoison Control Centres
ChemG § 16e para 3
Case data bank
Product data bank
Assessment of individual case
AnalysisRisk identification
aimed at scientific
information
Statistical analysesCase reports
Press releases
Rapid communications
to manufacturers/distributors,
ministeries, industrial associations
Criterionsevere
health impairment
Summarizing reportsannually
to manufacturers/distributors
Criterionnon-severe
health impairment
Measures for risk minimization
Risk communication
aimed atrisk management
Notificationsindustry
ChemG § 16e para 1Dangerous
products / biocides
Cosmetics Regulations § 5d
Cosmetics (through BVL*)
Voluntary notifications
Fig. 1: Terms of reference of the Centre for Documentation and Assessment of Poisonings
*BVL: Bundesamt für Verbraucherschutz und Lebensmittelsicherheit (Federal Office for Consumer Protection and FoodSafety)
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 8

2.3 Product data bank (poison informationdata bank)
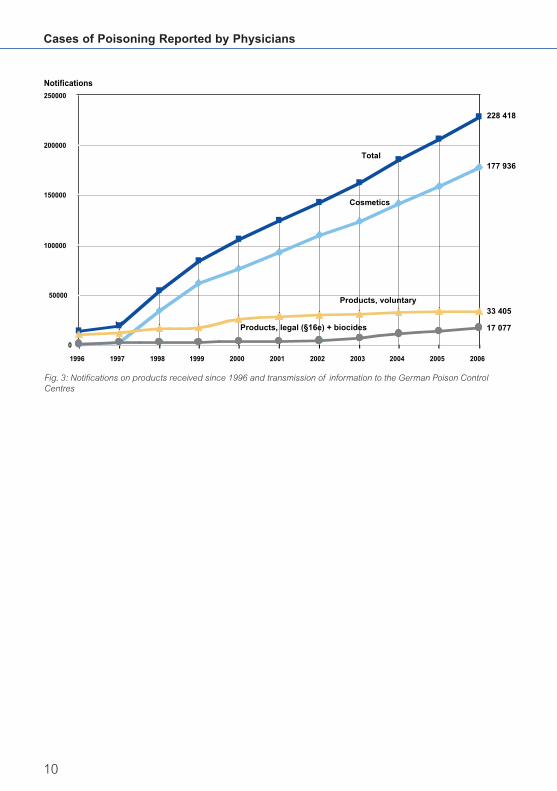
2.3.1 FiguresUntil late December 2006, 228 418 documentson individual products were recorded in the poi-son information data bank maintained by theBfR which can be accessed by the PCCs inGermany, thus supporting their activities in pro-viding consultation and treatment in cases ofpoisoning. Thus, the number of notifications onproducts submitted to the Poison and ProductDocumentation Centre at the BfR increased by22 469 in 2006. The structure of the data bankand the different types of product data setshave been described in detail in earlier reports.
2.3.2 Collaboration between the BfR, indus-try and Poison Control CentresThe major part of product data on dangerouspreparations and biocidal products as well as ofthe voluntary reports by manufacturers, distribu-tors and importers received by the BfR is still
submitted on paper forms. The recording of cos-metics, which until June 2005 had been enteredinto the poison information data bank at the BfRpredominantly in electronic form, is now carriedout at the Federal Office for Consumer Protectionand Food Safety (BVL), as a consequence of thesubdivision of the former Federal Institute forHealth Protection of Consumers and VeterinaryMedicine (BgVV) into the two successor insti-tutes, BfR and BVL. From the BVL, the data arereturned to the BfR at monthly intervals and fromthere, transmitted to the PCCs together with theother product data in the well-established way.
Of the dangerous preparations and biocidalproducts notifiable under §16e para 1 of theChemicals Act, 17 077 product data sets havebeen transmitted to the Poison Control Centresso far. Of these, 7 582 refer to dangerouspreparations and 9 495, to biocides. Due to re-structuring, the figures for voluntary and legallyrequired reports have slightly changed com-pared with the reporting year of 2005.
9
Fig. 2: Notifications under § 16e para 1 of the Chemicals Act: legal products and biocidal products (2002: entryinto force of the regulations on biocides)
Biocides9 495
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
1998 2000 2002 2004 2006
No
tifi
cati
on
s
Legal notifications
7 582
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 9
Cases of Poisoning Reported by Physicians
10
Fig. 3: Notifications on products received since 1996 and transmission of information to the German Poison Control Centres
0
50000
100000
150000
200000
250000
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Total
Cosmetics
Products, voluntary
Products, legal (§16e) + biocides
228 418
177 936
33 405
17 077
Notifications
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 10

During the period between 1 August 1990, i.e.the beginning of the compulsory notification,and 31 December 2006, altogether 48 705 re-ports on cases of health impairment, poisoningor suspected cases of poisoning were receivedby the BfR. In 2006, the reporting year consid-ered, 4 551 notifications were received (Fig. 4).
The increase in the number of notifications re-ceived in 2000 was due to an agreement withthe Berufsgenossenschaften. According to thisagreement, all notifications on cases of acutehealth impairment after contact with chemicalsor chemical products are directly reported bythe Berufsgenossenschaften to the BfR. Howev-er, since 2001, a continuous decrease has beenobserved in the number of reports by the Berufs-genossenschaften. According to the BG-Insti-tute for Occupational Safety and Health (Berufs-genossenschaftliches Institut für Arbeitsschutz –BGIA), the number of accidents is in fact on thedecrease. This is caused by a better occupa-
3.1 Evaluation of reports
tional safety and accident prevention, cam-paigns informing about accidents and changesin operational processes (in part automation).
3.2 Reports on cases of poisoning in 2006
3.2.1 OriginIn 2006, 4 069 cases, i.e. 89.4 % of all casesnotified, were reported by the Berufsgenossen-schaften. The remaining 482 notifications(10.6 %) were essentially submitted by hospi-tals, medical practitioners and PCCs. Single notifications were also received from the Arznei-mittelkommission der Deutschen Ärzteschaft(Drug Commission of the German Medical Profession) or the Arzneimittelkommission derDeutschen Apotheker (Drug Commission ofthe German Pharmacists) and others.
3.2.2 Spectrum of cases reportedFig. 5 provides a synoptic view of the spectrumof product groups involved in the cases report-
11
3 Case reports by physicians
Fig. 4: Cases reported (BG reports 100 % = 4 069; non-BG reports 100 % = 482) BG: Berufsgenossenschaften - institu-tions for statutory accident insurance and prevention for trade and industry in Germany
0
1 000
2 000
3 000
4 000
5 000
6 000
7 000
8 000
9 000
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06
Non-BG reports BG reports
Year
Number
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 11
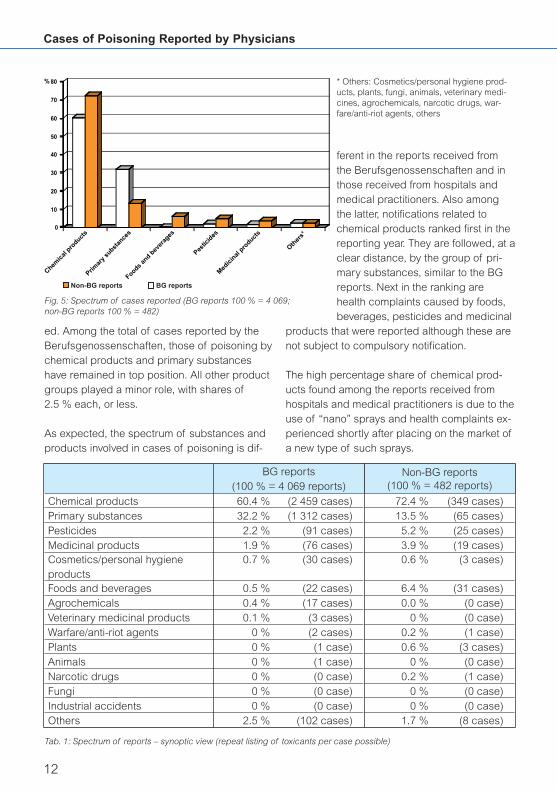
ed. Among the total of cases reported by theBerufsgenossenschaften, those of poisoning bychemical products and primary substanceshave remained in top position. All other productgroups played a minor role, with shares of2.5 % each, or less.
As expected, the spectrum of substances andproducts involved in cases of poisoning is dif-
ferent in the reports received fromthe Berufsgenossenschaften and inthose received from hospitals andmedical practitioners. Also amongthe latter, notifications related tochemical products ranked first in thereporting year. They are followed, at aclear distance, by the group of pri-mary substances, similar to the BGreports. Next in the ranking arehealth complaints caused by foods,beverages, pesticides and medicinal
products that were reported although these arenot subject to compulsory notification.
The high percentage share of chemical prod-ucts found among the reports received fromhospitals and medical practitioners is due to theuse of “nano” sprays and health complaints ex-perienced shortly after placing on the market ofa new type of such sprays.
Cases of Poisoning Reported by Physicians
12
* Others: Cosmetics/personal hygiene prod-ucts, plants, fungi, animals, veterinary medi-cines, agrochemicals, narcotic drugs, war-fare/anti-riot agents, others
BG reports(100 % = 4 069 reports)
Non-BG reports(100 % = 482 reports)
Chemical products 60.4 % (2 459 cases) 72.4 % (349 cases)Primary substances 32.2 % (1 312 cases) 13.5 % (65 cases)Pesticides 2.2 % (91 cases) 5.2 % (25 cases)Medicinal products 1.9 % (76 cases) 3.9 % (19 cases)Cosmetics/personal hygiene products
0.7 % (30 cases) 0.6 % (3 cases)
Foods and beverages 0.5 % (22 cases) 6.4 % (31 cases)Agrochemicals 0.4 % (17 cases) 0.0 % (0 case)Veterinary medicinal products 0.1 % (3 cases) 0 % (0 case)Warfare/anti-riot agents 0 % (2 cases) 0.2 % (1 case)Plants 0 % (1 case) 0.6 % (3 cases)Animals 0 % (1 case) 0 % (0 case)Narcotic drugs 0 % (0 case) 0.2 % (1 case)Fungi 0 % (0 case) 0 % (0 case)Industrial accidents 0 % (0 case) 0 % (0 case)Others 2.5 % (102 cases) 1.7 % (8 cases)
Tab. 1: Spectrum of reports – synoptic view (repeat listing of toxicants per case possible)
Fig. 5: Spectrum of cases reported (BG reports 100 % = 4 069;non-BG reports 100 % = 482)
0
10
20
30
40
50
60
70
80%
Chemic
al p
roduct
s
Primar
y su
bstan
ces
Pestic
ides
Foods an
d bev
erag
es
Med
icin
al p
roduct
s
Other
s*
Non-BG reports BG reports
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 12
For a detailed list of toxicants in tabular formsee Annex. In this table, the cases reported in2006 have been classified by product applica-tion groups (assignment of toxicants accordingto their intended use).
3.2.3 Causes of poisoningThe Berufsgenossenschaften almost exclusivelyreported cases of exposure to poisons in thecontext of occupational accidents (ca. 97 % ofcases). The remaining 3 % of cases referred toaccidents that had occurred during the com-mon use of a product or because a chemicalhad been mistaken for another substance, orthe cause of the accident was unknown.
Among the reports submitted by hospitals andmedical practitioners, exposure during commonuse was the predominant cause of poisoning(45.2 %) followed by poisoning accidents(42.5 %). The high share of cases where com-mon use was the cause of the health impairmentexperienced is due to the events associated with
“nano” sprays (see Chapter 4.1). Exposure dueto mistaking chemicals for other substances wasthe cause in 3.1 % of cases, suicidal actionswere reported in 2.3 % of cases. 0.4 % of caseswere associated with abuse of substances. Inthe remaining cases, the cause was unknown.
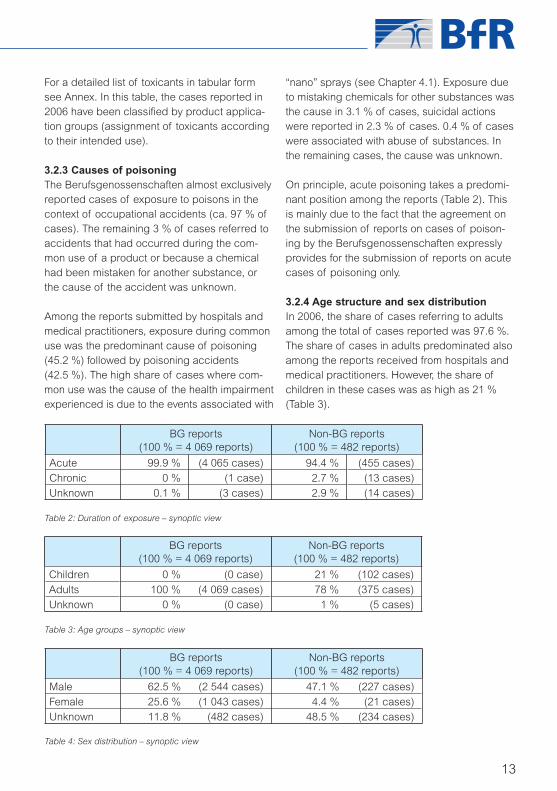
On principle, acute poisoning takes a predomi-nant position among the reports (Table 2). Thisis mainly due to the fact that the agreement onthe submission of reports on cases of poison-ing by the Berufsgenossenschaften expresslyprovides for the submission of reports on acutecases of poisoning only.
3.2.4 Age structure and sex distributionIn 2006, the share of cases referring to adultsamong the total of cases reported was 97.6 %.The share of cases in adults predominated alsoamong the reports received from hospitals andmedical practitioners. However, the share ofchildren in these cases was as high as 21 %(Table 3).
13
Table 2: Duration of exposure – synoptic view
BG reports(100 % = 4 069 reports)
Non-BG reports(100 % = 482 reports)
Acute 99.9 % (4 065 cases) 94.4 % (455 cases)
Chronic 0 % (1 case) 2.7 % (13 cases)Unknown 0.1 % (3 cases) 2.9 % (14 cases)
BG reports(100 % = 4 069 reports)
Non-BG reports(100 % = 482 reports)
Children 0 % (0 case) 21 % (102 cases)
Adults 100 % (4 069 cases) 78 % (375 cases)Unknown 0 % (0 case) 1 % (5 cases)
BG reports(100 % = 4 069 reports)
Non-BG reports(100 % = 482 reports)
Male 62.5 % (2 544 cases) 47.1 % (227 cases)
Female 25.6 % (1 043 cases) 4.4 % (21 cases)Unknown 11.8 % (482 cases) 48.5 % (234 cases)
Table 3: Age groups – synoptic view
Table 4: Sex distribution – synoptic view
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 13

3.2.5 Degree of severity of health impairmentAlso in 2006, the majority of cases reported referred to minor health impairment only, bothamong the cases reported by the Berufs-genossenschaften and among those reportedby hospitals and medical practitioners. Moder-ate and severe health impairment is more oftenreported by medical practitioners or physiciansworking in hospitals because they also deal withreports on suicide attempts (Table 5).
The product groups involved most frequently withregard to the degree of severity of health effectshave been listed in Table 6 for the cases reported
by the Berufsgenossenschaften and in Table 7, forthe cases reported by hospitals and medicalpractitioners. Of course, the toxicants reportedfrom occupational environments were differentfrom those reported from the private sphere be-cause the availability of certain product groupsdiffers, for example. One of the reasons for thehigh number of cases involving lamp oil may beseen in the specific ascertainment of such casesin collaboration with ESPED (Erhebungseinheit fürseltene pädiatrische Erkrankungen in Deutschland– clinical registration unit for rare paediatric ill-nesses in Germany), an organization cooperatingwith almost all paediatric hospitals in Germany.
Cases of Poisoning Reported by Physicians
14
Health impairmentProduct group Minor (3 528 cases) Moderate (285 cases) Severe (6 cases)
Primary substances 1 108 105 1
Cleansing products 622 47
Drain cleansers 11 1
All-purpose cleansers 50 1
Oven and grill cleansers 15 6
Descaling products 25 1
Industrial cleaners 39 3
Milking machine cleaners 35 4
Lavatory cleansers 19
Disinfectants/sterilizers 308 22
Waste gases 140 11 1
Paints and related materials
133 8 1
Accumulators 100 1 1
Building materials 101 17
Pesticides 83 3Glues 68 7
Table 6: Product groups involved most frequently, by degree of severity of health impairment (BG reports)
Table 5: Degree of severity of health impairment – synoptic view
BG reports(100 % = 4 069 reports)
Non-BG reports(100 % = 482 reports)
None 2.7 % (110 cases) 6.0 % (29 cases)
Minor 86.7 % (3 528 cases) 65.1 % (314 cases)
Moderate 7.0 % (285 cases) 16.0 % (77 cases)
Severe 0.1 % (6 cases) 5.4 % (26 cases)Cannot be assessed 3.4 % (140 cases) 7.5 % (36 cases)
aerztl_mitteilungen_06_engl 21.09.2007 15:37 Uhr Seite 14

3.2.6 Outcome of casesFor the notifications submitted by the Berufs-genossenschaften, the outcome has remainedunknown in ca. 59 % of cases. The reason forthis is that in the majority of cases, the reportsubmitted corresponds to that by the “Durch-gangsarzt” (“transition doctor” appointed by theBerufsgenossenschaft). The reporting form iscompleted after the patient’s first presentation.Therefore, such report does not contain any in-formation on the course of the patient’s illness. Inselected cases, enquiries were made to obtaininformation on the course of illness. In the majori-ty of cases on which information was available,patients had recovered completely.
Of the notifications submitted by hospitals andmedical practitioners, patients recovered com-pletely in 305 cases (63.3 %). In 153 cases(31.7 %), the outcome was unknown; in fourteencases (2.9 %), late sequelae could not be ex-cluded or partial recovery was reported.
Ten deaths were reported to the BfR in 2006:
Case No 1:An elderly patient died from the sequelae of as-piration pneumonia after accidental ingestion ofa detergent (see Chapter 4.2). The problem oforal ingestion of solutions containing surfactants,particularly in elderly persons, is again dealt within Chapter 4.2.
Case No 2:The patient had suffered chemical burns due toformaldehyde affecting 33 % of his body surfacein his working environment. He died from multipleorgan failure in spite of intensive therapy.
Case No 3:The patient had ingested, with suicidal intent, asolution containing dimethoate. Resuscitation attempts and antidote administration remainedunsuccessful (see Chapter 4.3.5.3).
Case No 4:A male adolescent died after ingestion ofp-nitroaniline. It was impossible to conclusivelyestablish whether the substance had been in-gested with suicidal intent in the sense of abuseor due to being mistaken for another substance(see Chapter 4.3.4.3).
Case No 5:A male adolescent had sniffed deodorant sprayand died from cardiac decompensation (seeChapter 4.3.4.2).
Case No 6:A young adult died after he had ingestedcannabinoids, atropine and scopolamine.
Cases 7 and 8Two patients died after ingestion of 2,4-dinitro-phenol: A young female had ingested the sub-
15
Table 7: Product groups involved most frequently, by degree of severity of health impairment (non-BG reports)
Health impairmentProduct group Minor (314 cases) Moderate (77 cases) Severe (26 cases)
Cleansing products 123 36 9
Glass cleaners 62 19 3
Lavatory cleansers 30 12 2
Primary substances 44 7 6
Lamp oil 28 15
Pesticides 21 1
Insecticides 12 1
Foods and beverages 16 4 5Medicinal products 11 3 2
aerztl_mitteilungen_06_engl 21.09.2007 15:37 Uhr Seite 15

stance as a fat burner with the intent to loseweight (see Chapter 4.3.4.1). The second pa-tient had ingested 2,4-dinitrophenol with suici-dal intent (see Chapter 4.3.5.2). Both patientsdeveloped malignant hyperthermia and respira-tory insufficiency; cardiopulmonary resuscita-tion was unsuccessful.
Case No 9:The patient had to check a propane gas tank athis workplace and therefore climbed into thetank. He lost consciousness and developed in-creasing respiratory insufficiency. Cerebraldeath was diagnosed. Neither the informationavailable from the description of the accidentnor that on the clinical course were sufficient toelucidate whether the patient’s death had to beattributed to propane gas.
Case No 10:The patient died after accidental ingestion of anindustrial dishwasher cleanser. Post-mortemfindings did not reveal any association betweenthe patient’s death and the toxicant (see Chap-ter 4.3.1.2).
3.3 The product information system, PRINSThe notifications by physicians in cases of poi-soning legally required under §16e para 2 ofthe Chemicals Act (Chemikaliengesetz –ChemG) are regularly evaluated to protect con-sumers from health risks posed by chemicalsand chemical products. Since 1994, the report-ing physicians, the responsible ministries and
the scientific community have been informed byannual reports on analyses of these notifica-tions and the corresponding results. In the con-text of these notifications, the term, poisoning, isused to designate any health impairment asso-ciated with chemicals, including for example al-so allergies.
Since 1998, manufacturers and distributors ofchemical products such as household chemi-cals and DIY products, cosmetics, plant protec-tion and pest control products and correspon-ding products for commercial use have been in-formed about cases of health impairment asso-ciated with their products that have becomeknown to the BfR through case reports.
3.3.1 Rapid communicationsIf reports on severe health risks (except thoserelated to suicides) are received by the BfR, itwill provide for immediate information of themanufacturer/distributor of the chemical prod-uct involved as well as the competent industrialassociation/federal trade association and the re-sponsible ministries, i.e. the Federal Ministry ofFood, Agriculture and Consumer Protection(BMELV), the Federal Ministry for the Environ-ment, Nature Conservation and Nuclear Safety(BMU), and the Federal Ministry of Health(BMG) as well as the Federal Office for Con-sumer Protection and Food Safety (BVL).
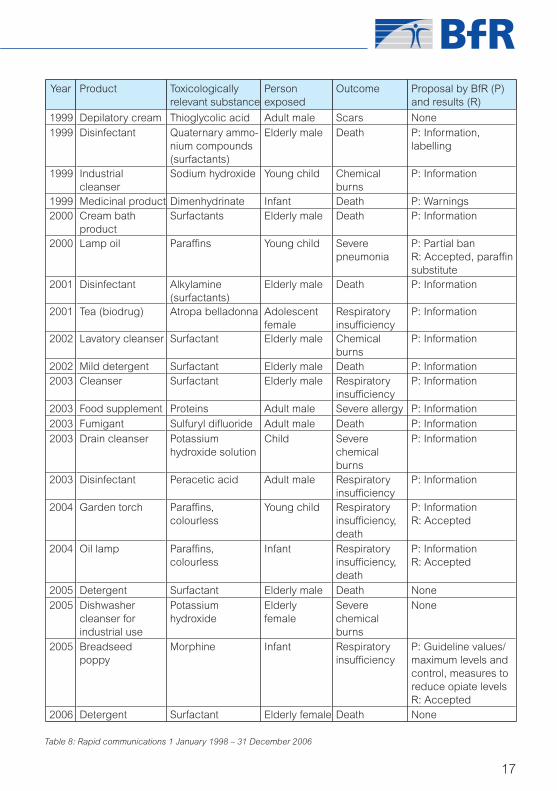
Between 1 January 1998 and 31 December2006, 25 rapid communications were prepared
Cases of Poisoning Reported by Physicians
16
Year Product Toxicologically relevant substance
Person exposed
Outcome Proposal by BfR (P) and results (R)
1998 Impregnating agent
Fluorinated hydrocarbons
Adult male Death P: Warnings for asthmatics R: Accepted
1998 Disinfectant Quaternary ammo-nium compounds (surfactants)
Elderly male Death P: Information, labelling Ñcorrosive“ R: Accepted
1999 Toilet drain cleanser
Sodium hydroxide Adult male Chemical burns
None
1999 Solvent Petrol Adult male Lung oedema None
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 16
17
Year Product Toxicologically relevant substance
Person exposed
Outcome Proposal by BfR (P) and results (R)
1999 Depilatory cream Thioglycolic acid Adult male Scars None1999 Disinfectant Quaternary ammo-
nium compounds (surfactants)
Elderly male Death P: Information, labelling
1999 Industrial cleanser
Sodium hydroxide Young child Chemical burns
P: Information
1999 Medicinal product Dimenhydrinate Infant Death P: Warnings2000 Cream bath
productSurfactants Elderly male Death P: Information
2000 Lamp oil Paraffi ns Young child Severe pneumonia
P: Partial ban R: Accepted, paraffi n substitute
2001 Disinfectant Alkylamine (surfactants)
Elderly male Death P: Information
2001 Tea (biodrug) Atropa belladonna Adolescent female
Respiratory insuffi ciency
P: Information
2002 Lavatory cleanser Surfactant Elderly male Chemical burns
P: Information
2002 Mild detergent Surfactant Elderly male Death P: Information2003 Cleanser Surfactant Elderly male Respiratory
insuffi ciencyP: Information
2003 Food supplement Proteins Adult male Severe allergy P: Information
2003 Fumigant Sulfuryl difl uoride Adult male Death P: Information2003 Drain cleanser Potassium
hydroxide solutionChild Severe
chemical burns
P: Information
2003 Disinfectant Peracetic acid Adult male Respiratory insuffi ciency
P: Information
2004 Garden torch Paraffi ns, colourless
Young child Respiratory insuffi ciency, death
P: Information R: Accepted
2004
Oil lamp Paraffi ns, colourless
Infant Respiratory insuffi ciency, death
P: Information R: Accepted
2005 Detergent Surfactant Elderly male Death None2005 Dishwasher
cleanser for industrial use
Potassium hydroxide
Elderly female
Severe chemical burns
None
2005 Breadseed poppy
Morphine Infant Respiratory insuffi ciency
P: Guideline values/ maximum levels and control, measures to reduce opiate levels R: Accepted
2006 Detergent Surfactant Elderly female Death None
Table 8: Rapid communications 1 January 1998 – 31 December 2006
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 17
Cases of Poisoning Reported by Physicians
18
First level Second level Third levelAgrochemicals 6Chemical products 419 Paints and related
materials5
Building materials, auxiliary products
8
Fuels, liquid 16 Lamp oil 16Dental materials 3Disinfectants/sterilizers 88Glues 7Metallurgy, auxiliary products
3
Cleansing products 221 All-purpose cleansers 3Washing-up detergent (manual use)
5
Dishwasher detergent 4Industrial cleansers 9Glass cleaners 86Milking machine cleansers
11
Shoe and leather cleansers
19
Lavatory cleansers 48Cosmetics/personal hygiene products
6 Oral care/dental products
3
Skin care products 3Pesticides 26 Herbicides 3
Insecticides 9Fungicides 3
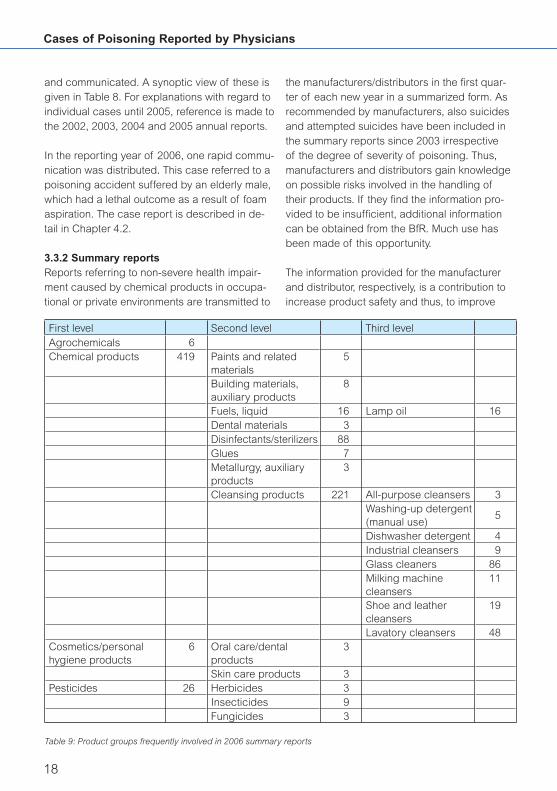
Table 9: Product groups frequently involved in 2006 summary reports
and communicated. A synoptic view of these isgiven in Table 8. For explanations with regard toindividual cases until 2005, reference is made tothe 2002, 2003, 2004 and 2005 annual reports.
In the reporting year of 2006, one rapid commu-nication was distributed. This case referred to apoisoning accident suffered by an elderly male,which had a lethal outcome as a result of foamaspiration. The case report is described in de-tail in Chapter 4.2.
3.3.2 Summary reportsReports referring to non-severe health impair-ment caused by chemical products in occupa-tional or private environments are transmitted to
the manufacturers/distributors in the first quar-ter of each new year in a summarized form. Asrecommended by manufacturers, also suicidesand attempted suicides have been included inthe summary reports since 2003 irrespective of the degree of severity of poisoning. Thus,manufacturers and distributors gain knowledgeon possible risks involved in the handling oftheir products. If they find the information pro-vided to be insufficient, additional informationcan be obtained from the BfR. Much use hasbeen made of this opportunity.
The information provided for the manufacturerand distributor, respectively, is a contribution toincrease product safety and thus, to improve
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 18

19
First level Second level Third levelAgrochemicals 1Chemical products 55 Building materials,
auxiliary products3
Fuels, liquid 4 Lamp oil 4Disinfectants/sterilizers 4Refrigerants 1Metallurgy, auxiliary products
1
Cleansing products 39 Dishwashing detergent 1Oven and grill cleansers
1
Glass cleaners 17Industrial cleansers 1Metal cleansers 1Soot removers 1
Lavatory cleansers 11Shoe and leather cleansers
4
No data 2Others 3
Cosmetics/personal hygiene products
1 Oral care/dental products
1
Table 10: Product groups associated with moderate health impairment listed in summary reports in 2006
consumer protection. There has been great in-terest in such information. For example, accidentanalyses have revealed that eye injuries causedby chemical products have frequently occurredin spite of wearing safety goggles. The safetydata sheet should therefore draw attention towearing “closely fitting safety goggles”.
In 2006, 451 cases of poisoning were reportedwith a specification of the products incriminat-ed. These cases referred to 244 different prod-ucts from altogether 131 manufacturers.
Table 9 provides a synoptic view of product application groups (minimum three listings) of the 2006 summary reports. Strikingly highnumbers have been recorded for disinfectants(88 cases) and cleansing products (221 cases).Attention has to be drawn to the relatively highnumber of accidents involving glass cleaners(86 cases) and lavatory cleansers (48 cases)
in the form of “nano” sealant sprays, see Chap-ter 4.1.
Table 10 shows the numbers of moderate healthdisturbances associated with the respectiveproduct groups in 2006. 57 cases have beenlisted. It may be concluded that ca. 13 % of re-ports requiring summary reports to manufactur-ers referred to cases of severe health impair-ment. For 29 cases, the degree of severity ofthe health impairment could not be assesseddespite further investigations.
The BfR also performs cumulative data analysesof case reports. If trends become apparent, themanufacturers of the products concerned areinformed. Manufacturers are requested by theBfR to, in turn, communicate comparable dataand trends that may serve to improve productsafety.
aerztl_mitteilungen_06_engl 21.09.2007 15:41 Uhr Seite 19

4.1 Acute health impairment due to “MagicNano” sealant sprays
At the end of March 2006, a series of rapidlydeveloping and in part, severe cases of healthimpairment such as lung oedema were ob-served after the correct use of “nano” sealantsprays intended for the treatment of glass andceramic surfaces. These sprays had been soldby discount shops as a special offer. On 27March 2006, the first case was reported to thePoison Control Centre in the city of Erfurt. Untilnoon of the following day, more than 10 caseswere reported to the Poison Control Centre ofthe city of Göttingen, and another day later, thenumber of cases recorded had increased to 69.So far, the Federal Institute for Risk Assessment(BfR) has received reports on a total of 150 cas-es, which are being processed and evaluated ina standardized and harmonized procedure andscreened for a uniform pattern of manifestations.The persons affected had used these water re-pellent sprays in their households in closedrooms that had been insufficiently ventilated(e.g. bathroom). Subsequently, they developed,in part severe, pulmonary manifestations andtheir general condition was affected in a similarway as from a common cold. The cardinal signwas a strong cough. Dyspnoea and, in severecases, lung oedema, were observed (8 cases).
Sealant sprays are used as impregnating agentsin the household to restore the water and dirt re-pelling properties of textiles and leather prod-ucts and for sanitary facilities to act as a sealingcoat. They are liquids commercially available inpressure-tight bottles with a pump mechanismor aerosol cans, which provide for an even distri-bution. These impregnating agents contain pro-pellants, solvents and the active substance. Pro-pellants used include propane, butane, dime-thylether and air. Typical solvents used includepetrol or short-chain alcohols, and in a few prod-
ucts, xylene. Active substances used include sil-icones (polysiloxanes), fluorocarbon andmelamine resins, beeswax or wool fat.
In the form of pump sprays, impregnating orsealant sprays have been considered as safe interms of health. In contrast, problems have beenassociated with aerosol sprays. The use of suchsprays in small and insufficiently ventilatedrooms may result in conjunctival irritation, dysp-noea or in rare cases, narcosis-like manifesta-tions due to the solvents contained. Based onsystematic animal studies in birds, a key role hasbeen attributed to fluorocarbon resins and/or re-active polysiloxanes in combination with sol-vents. In addition, improper use such as spray-ing for extended periods or failure to shake thecontents sufficiently etc. should also be taken in-to account. However, it is mainly the physicalproperties such as the droplet size of the spraysthat decide on whether and which toxic effectsare caused in the respiratory tract. Obviously,the persons affected had inhaled components ofthe atomized sprays that had remained in the in-door air as fine aerosols. Due to the smalldroplet size, these components may havereached the alveolar region causing accumula-tion of fluid, which resulted in an impairment ofthe oxygen and humidity exchange in the lungs.
The small droplet size is only achieved if the liq-uid applied contains a propellant and is appliedby means of a correspondingly small nozzle inthe spray head. If, in contrast, the same liquid isapplied by means of a pump mechanism, thedroplets are larger than 100 micrometres andtherefore, cannot penetrate into the alveolar tis-sue. This is probably the reason why productsapplied to surfaces by means of pump spraybottles have not caused any problems so far.Hence, toxic effects may only occur if the prod-uct itself, i.e. the entire substance mixture of theformulation is inhaled as a fine spray fog char-
Cases of Poisoning Reported by Physicians
20
4 Selected toxicological problems
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 20

on three meetings held at the BfR to which ex-perts had been called immediately. In addition,an extraordinary EU meeting involving Germanand Luxembourgian authorities was held inBrussels in early May 2006 because one of thesuppliers was resident in Luxembourg.
Investigations into the composition of the prod-uct were considerably complicated by the factthat the distributor had no knowledge at all con-cerning the composition of his products, andthe suppliers claimed trade secrets with regardto their component preparations. The suppliercompanies and the components provided bythese for the formulation of the final productcould only be established through investigationsby the BfR and information obtained from theLänder authorities. The basic component of theassumed “nanofluid” had been producedabroad.
Results and evaluation of the incidentsThe components responsible for the cases ofhealth impairment, some of which had been se-vere, were largely determined in the context ofan expert meeting held at the end of May 2006.
1. The products concerned did not containany nano-sized particles. The nano functionsuggested by the product name referredonly to the thickness of the film of the activesubstance remaining on the glass and ce-ramic surfaces treated.
2. Due to chemical changes during the pro-cessing to produce aerosol sprays, the ac-tive compounds contained in the share ofactive substances had obviously disap-peared to a large extent. Thus, the sprayapplied consisted only in a mixture of sol-vents which no longer contained anyshares of active substances.
3. With regard to their pattern, the manifesta-tions observed in the cases associated withnano sealant sprays were very similar to thehealth problems documented in a numberof earlier case clusters associated with
21
acterized by a correspondingly small dropletsize.
Risk communicationFollowing the receipt of initial information, theBfR, as required under § 16e of the ChemicalsAct, immediately contacted the German PCCsand the manufacturers involved, in an investiga-tive effort to establish as soon as possible theformulation of the incriminated products as wellas possible health problems associated with itsuse. In cooperation with the PCCs of Erfurt andGöttingen, the BfR could achieve a recall beinglaunched within a single day with the assistanceof the crisis unit of the distributor, the ReweGroup, thus preventing further cases of suchpoisoning and contributing to an effective con-sumer protection. In parallel, information wascommunicated to the responsible governmentauthorities of the German Länder, the FederalOffice for Consumer Protection and Food Safety(BVL) (EU rapid alert system for non-food prod-ucts – RAPEX), the Federal Ministry of Food,Agriculture and Consumer Protection (BMELV),the Federal Ministry for the Environment, NatureConservation and Nuclear Safety (BMU) and theWHO rapid information system (WHO INTOX).The public as well as authorities and ministrieswere informed about findings and results bytimely publication of three press releases inGerman and English which were mostly based
Fig. 6: Nano product
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 21

leather and impregnating sprays (Germany,USA, Netherlands, Denmark, Switzerland).As in the most recent series of cases attrib-uted to nano sealant sprays, repetitive se-ries involving 100–200 cases each, amongthem seriously ill patients, had been record-ed at that time.
Considerations regarding product safetyThe series of cases associated with nanosealant sprays and characterized by sometimessevere health impairment among consumershas shown considerable gaps to exist with re-gard to the documentation of formulations thatis available in the event of medical emergency.Where products not subject to compulsory noti-fication are involved, neither the distributor norany other party in the chain of supplier compa-nies is sufficiently informed about the formula-tion of the final product. Knowledge of the com-plete formulation of a product will considerablyenhance product safety. It is therefore requiredthat in the future, prior to placing on the marketof a product not subject to compulsory notifica-tion, sufficient information about the formulationof the final product is made available for casesof emergency at least at one point of the pro-duction chain or from a neutral party where ithas been deposited (e.g. at a lawyer’s office).
Especially for products which are applied byspraying and therefore may readily enter thelungs and be extensively absorbed, the follow-ing measures should be taken to enhance prod-uct safety:
1. Sprays tested according to acknowledgedcriteria (e.g. OECD) should be awarded alabel well recognizable for consumers.
2. Sprays containing defined nanoparticlesshould be recognizable as such for productsafety reasons.
3. For early identification of possible health effects, products containing definednanoparticles should be listed in a registersuch as the BfR poison information databank.
In the opinion of the BfR, further research is ur-gently required with regard to nanoparticles thatcan be absorbed by the inhalational route. Asfar as surface sealant sprays are concerned, anumber of research projects are under way atthe BfR: With regard to the case series in April2006, comprehensive studies should concen-trate on the manifestations observed, the spe-cial risk posed by the substances involved andthe risk involved for the individual persons af-fected. The next step to follow immediately willconsist in a review and analysis of case seriesreported from other countries. In parallel, achemical analysis will be carried out to examinethe respirable components of the aerosol frac-tions in the sprays that caused the health im-pairments reported. Proof-of-principle experi-ments on aerosol behaviour are conducted andstudies carried out using standardized animalmodels. The BfR will report on further progressmade in this matter.
Case reportToxic lung oedema following use of anano impregnation sprayIn an indoor environment with open window,the female patient aged 37 had applied anano impregnation foam to four pairs of shoesand used the entire contents of a 125 ml spraycan. For this purpose, she had drawn the highboots over her lower arm and tried to keep adistance of 20 cm as recommended by thespray manufacturer. During the operation,some of the foam also hit her glasses. Approx-imately 30 minutes after starting the operation,she experienced a sudden shortness ofbreath at rest which became more pro-nounced at work, and hacking cough, whichwas particularly intensive in her throat and ret-rosternally. For this reason, she sought assis-tance at the emergency unit of a hospital.
It should be added that the patient was asmoker with a daily consumption of some 10cigarettes.
Cases of Poisoning Reported by Physicians
22
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 22

herself for a control examination four weekslater. The BfR lacks information about the fur-ther course of this case.
Notes:As a first measure, patients showing a corre-sponding symptomatology are provided with afresh air supply. There should be an early in-halative therapy using topical steroids and thepatient be presented to a hospital, to exclude apresence of lung infiltrates. Onward therapy willbe oriented by the existing symptomatology.
In Germany, attention was directed to the pul-monary toxicity of impregnation sprays alreadyin 1981. Because of their inherent health risk,several sprays for the impregnation of leatherwere withdrawn from the market. Numerousmodifications of the respective formulations bythe manufacturers also contributed to a reduc-tion in the number of cases of poisoning show-ing relevant manifestations. This was followed, in2002, by another rise in the number of reportsconcerning impaired airway functions associat-ed with impregnation sprays for leather and textiles in the Netherlands and in Switzerland.
As a result of the introduction of new technolo-gies in consumer products, shoe leather im-pregnation sprays and sealant sprays for ce-ramic and glass surfaces containing nano parti-cles appeared in the market. It is unknownwhether also nano particles, which are hy-drophobic, are capable of penetrating into thelungs and have adverse effects on the alveolartissue. Therefore, it has to be clarified whetherthese particles may have contributed to the de-velopment of the health disorders observed.It has not yet been finally elucidated whethernano particles are among the components ofthe incriminated shoe impregnation spray.
23
Manifestations/courseOn admission, a weakened breathing soundand shortness of breath were found to bepresent while other physical findings werenormal.
Chest X-ray performed for completion of di-agnosis demonstrated the presence of a but-terfly-like interstitial lung oedema with an ini-tial alveolar component. The patient was ad-mitted as an inpatient for monitoring andtreatment. After having consulted a PCC, thepatient was treated by administration of a sin-gle i.v. dose of 500 mg glucocorticoid, inhala-tion of ipratropium bromide and salbutamol.Additional oxygen supply was continued. Un-der conditions of permanent monitoring, thistherapy led to a continued improvement ofthe patient’s complaints. Already on the nextday, control radiology showed an obvious re-gression of the toxic interstitial lung oedema.
Clinical chemistry revealed the presence of adiscrete leukocytosis (19.5/nl) while the otherparamaters routinely examined were found tobe within their normal ranges.
After 24 h of monitoring, the patient who hadbecome symptom-free could be dischargedand referred to her family doctor’s care.Steroid therapy was to be continued on anoutpatient basis by sytemic and topical ad-ministration, as was the administration of be-tamimetics. Eight days after the toxic event,the patient consulted a pulmonologist for acontrol examination. Residual lung oedemacould be demonstrated by radiology. Spirom-etry values had become completely normal-ized while the diffusion capacity was still im-paired. In contrast, blood gas values had re-mained stable also under conditions of exer-cise. In view of the good lung function results,systemic administration of steroids was dis-continued and the patient asked to present
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 23
Evaluation of the case describedBased on the data concerning a temporal asso-ciation between application of the impregnatingproduct in aerosol form and the appearance oftypical manifestations, a causal relationship isconsidered as confirmed. It remains openwhether also nano particles were involved in thecase of this product.
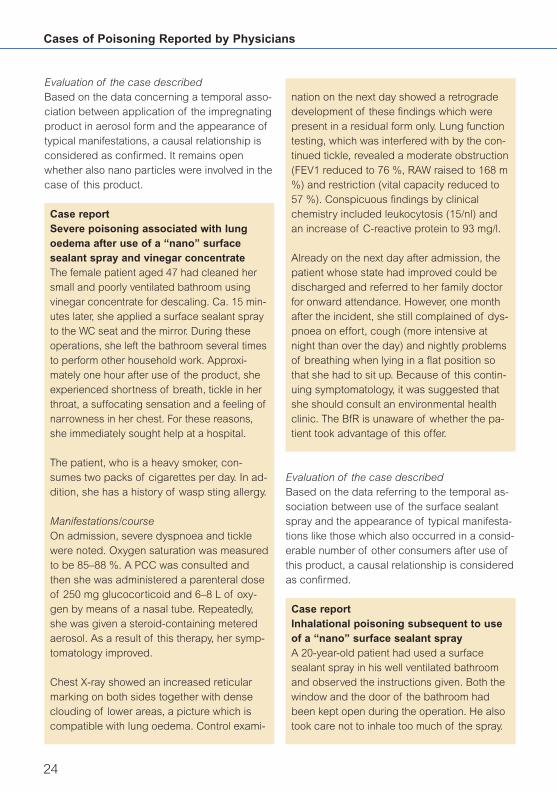
Case reportSevere poisoning associated with lungoedema after use of a “nano” surfacesealant spray and vinegar concentrateThe female patient aged 47 had cleaned hersmall and poorly ventilated bathroom usingvinegar concentrate for descaling. Ca. 15 min-utes later, she applied a surface sealant sprayto the WC seat and the mirror. During theseoperations, she left the bathroom several timesto perform other household work. Approxi-mately one hour after use of the product, sheexperienced shortness of breath, tickle in herthroat, a suffocating sensation and a feeling ofnarrowness in her chest. For these reasons,she immediately sought help at a hospital.
The patient, who is a heavy smoker, con-sumes two packs of cigarettes per day. In ad-dition, she has a history of wasp sting allergy.
Manifestations/courseOn admission, severe dyspnoea and ticklewere noted. Oxygen saturation was measuredto be 85–88 %. A PCC was consulted andthen she was administered a parenteral doseof 250 mg glucocorticoid and 6–8 L of oxy-gen by means of a nasal tube. Repeatedly,she was given a steroid-containing meteredaerosol. As a result of this therapy, her symp-tomatology improved.
Chest X-ray showed an increased reticularmarking on both sides together with denseclouding of lower areas, a picture which iscompatible with lung oedema. Control exami-
nation on the next day showed a retrogradedevelopment of these findings which werepresent in a residual form only. Lung functiontesting, which was interfered with by the con-tinued tickle, revealed a moderate obstruction(FEV1 reduced to 76 %, RAW raised to 168 m%) and restriction (vital capacity reduced to57 %). Conspicuous findings by clinicalchemistry included leukocytosis (15/nl) andan increase of C-reactive protein to 93 mg/l.
Already on the next day after admission, thepatient whose state had improved could bedischarged and referred to her family doctorfor onward attendance. However, one monthafter the incident, she still complained of dys-pnoea on effort, cough (more intensive atnight than over the day) and nightly problemsof breathing when lying in a flat position sothat she had to sit up. Because of this contin-uing symptomatology, it was suggested thatshe should consult an environmental healthclinic. The BfR is unaware of whether the pa-tient took advantage of this offer.
Evaluation of the case describedBased on the data referring to the temporal as-sociation between use of the surface sealantspray and the appearance of typical manifesta-tions like those which also occurred in a consid-erable number of other consumers after use ofthis product, a causal relationship is consideredas confirmed.
Case reportInhalational poisoning subsequent to useof a “nano” surface sealant spray A 20-year-old patient had used a surfacesealant spray in his well ventilated bathroomand observed the instructions given. Both thewindow and the door of the bathroom hadbeen kept open during the operation. He alsotook care not to inhale too much of the spray.
Cases of Poisoning Reported by Physicians
24
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 24

Immediately upon termination of the cleaningprocess, i.e. when leaving the bathroom, heexperienced episodes of coughing whichlasted for ca. 1 1/2 h, and of vomiting. A friendaccompanied him on his way to the familydoctor who prescribed a metered aerosolcontaining steroids. When taking a rest afterhe had returned to his home, frequency andintensity of the cough attacks became initiallyreduced. When after a few hours he made anattempt to rise, coughing attacks and vomitingreturned. For this reason, the patient decidedto seek help at a hospital.
Two days prior to having used the sealantspray, the patient had already experiencedepisodes of vomiting and diarrhoea after ex-cessive alcohol consumption. He also had ahistory of hypothyreosis compensated bymedication and was adipose.
Manifestations/courseOn admission, the patient exhibited markeddyspnoea and a vehement tickling in histhroat on deep inhalation. The adipose pa-tient’s general state of health was found to bemoderately reduced. Auscultation revealedspastic ronchi. He was admitted for inpatienttreatment at the intensive care ward underconditions of permanent monitoring. Becauseof the dyspnoeic symptomatology, the pro-nounced initial tickling and the presence oftachycardia, medication for the patient con-sisted of a steroid-containing metered aerosoland i.v. administration of prednisolone,furosemide and theophyllin. Ciprofloxacin wasadministered as antibiotic treatment. To con-trol his gastroenteric complaints, the patientwas administered pantoprazole and given flu-id supply with an addition of metoclopramide.As a result of this therapy, an obvious im-provement in the patient’s condition was seenon the next morning, so that he could betransferred to a normal ward.
Radiology revealed a discrete reduction oftransparency and a minor mesh-like increasein structures. Clinical chemistry showed high-degree leukocytosis, a reduced Quick’s valueand elevated values of hepatic parameters. Inview of the short latency period, changes inthe levels of hepatic parameters were not at-tributed to the acute inhalation trauma. Theremay have been an association with a historyof acute gastroenteritis two days ago or withthe preceding event of excessive alcoholconsumption. Due to the patient’s adiposity,the presence of chronic exogenous toxichepatitis and at least, of a considerable nutri-tive steatosis was suggested.
In the onward course, all laboratory parame-ters which had shown pathological changesexhibited an obvious tendency towards remis-sion. Continuation of antibiotic treatment witha supplementary dihydrocodeine medicationresulted in an increasing improvement of thepatient’s complaints, in particular of the ticklein his throat. After three days of inpatientcare, the patient, who was in a state of sub-jective well-being, could be discharged andreturned to his home.
Notes:During the period between 27 March and ca.10 April 2006, partially severe health complaintssuch as cough, shortness of breath and in sin-gle cases, toxic lung oedema appeared amonga considerable number of consumers. This hadbeen due to sales of two surface-sealing “nano”sprays by a major chain of discount shops inthe context of an advertising campaign. Alreadya few hours after these products had appearedin the market, they were removed from theshelves upon intervention by the BfR and thePCCs.
The pattern of manifestations resembled the se-ries of cases experienced in the past which had
25
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 25

occurred after the use of impregnating spraysin 1982/83 in Germany and 2002 in Switzerlandand the Netherlands. Extensive research intothe formulations of such surface sealant spraysrevealed a great similarity of the chemical spec-trum of the relevant components with that of theimpregnating sprays. This suggests that thesymptomatology seen after inhalational expo-sure may correspond to that of the known “im-pregnating agent syndrome”. Analysis of the“nano” sprays, however, demonstrated the ab-sence of nano particles as claimed by the ad-vertising campaign. The term “nano” was to re-fer to the ultra fine water and dirt repelling layerformed from silanes undergoing a chemicalprocess.
Evaluation of the case describedBased on the data referring to the temporal as-sociation between use of the surface sealantspray and the appearance of typical manifesta-tions like those which also occurred in a consid-erable number of other consumers after use ofthis product, a causal relationship is consideredas confirmed regarding the pulmonary manifes-tations. It is noted with interest that despite in-tensive efforts made by the patient to keep ex-posure as low as possible and to apply theproducts in a well-ventilated room, he devel-oped complaints.
4.2 Specific risks for the elderly – Poisoningby cleansers and disinfectantsShower gels, bubble baths, shampoos, all-pur-pose cleansers, disinfectants, liquid detergents,etc. may involve considerable risks for elderlypersons. In the context of cases of poisoningreported by physicians since 1990, a total of 23cases have come to the knowledge of the BfRwhere the ingestion of large amounts of house-hold cleansers and disinfectants resulted in se-vere manifestations of poisoning. A lethal out-come was recorded in 17 cases. All of thesecases referred to disoriented elderly persons.There has certainly been a considerable num-ber of undetected and unreported cases. As to
the possible causes, research and consultationof experts have revealed the following:� Frequently, the olfactory and gustatory per-
ception is reduced in old-age persons. Evenif their olfactory and gustatory senses havebeen preserved, disoriented patients oftenlack the ability of distinguishing between ac-ceptable (eatable, drinkable) and unaccepta-ble matter.
� Once started, they are unable to discontinuean action in a reflexive way like young per-sons do.
� Elderly people cannot call for help immedia-tely, or they keep silent about what has hap-pened, for reasons of shame or uncertainty.
� Things may be confounded due to impairedvision.
� Unlike young children, elderly persons are of-ten left by themselves for extended periodsand they are not under constant observation,as a rule.
In 2002, the BfR had launched a large-scalecampaign involving press releases, manualsand flyers in a variety of languages, pointing outthe risks for the elderly and addressing nursingand cleaning staff in hospitals, nursing homesand homes for the aged.
On account of the fact that fresh cases of thistype have been reported in 2005 and 2006, theBfR will conduct another concerted action to
Cases of Poisoning Reported by Physicians
26
Fig. 7: Elderly lady in need of care
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 26
draw public attention to the risks for the elderlyfrom such substances. By visits to the homes ofelderly persons, they may be alerted regardingthe risks of accidents which could be reducedby using special dispensers for detergents andcleansers. Such dispensers are being used ona large scale already now, for example in hotels,pensions and also hospitals.
Case reportLiquid detergentSevere health impairment with lethal out-come in an 82-year-old female temporallyrelated to the ingestion of ca. 100 ml of adetergentIn accordance with § 16e para 2 of the Chem-icals Act, the Rostock University Hospital re-ported a case of severe health impairmentwith lethal outcome in a female patient aged82 years who at her home due to her lack oforientation had ingested ca. 100 mL of a liq-uid detergent containing ca 25 % surfactants.
Although the course of her illness had beenfairly uncomplicated, the patient died after 11days from aspiration pneumonia associatedwith septicaemia.
Manifestations/courseBecause of her initial senile dementia, the pa-tient had been in need of care and was at-tended by her sister-in-law at her own home.In addition, an ambulant nursing servicelooked after her in the morning and in theevening. On the day of the accident, as usu-al, her sister-in-law had placed the supper forthe patient on the kitchen table and then leftthe flat. When the nursing service arrivedabout one hour later, they found the patient onthe kitchen floor, retching and with foam in hermouth. The patient vomited when the nursewas present. On the kitchen table, there weretwo opened bottles containing liquid deter-gent for fine textiles, side to side with a drink-ing glass which still contained residual detert-
ergent. Owing to the situation in which the pa-tient had been found, an oral intake of deter-gent was assumed to have taken place.
Obviously, the patient in her disoriented situa-tion had brought these bottles from the bath-room and poured some of the contents intothe glass. According to the nurse and the sis-ter-in-law, the bottle with the liquid detergenthad been unused and full, and the other onealso containing detergent was of less recentdate, probably dating back to GDR times.Since from the first mentioned bottle, theamount corresponding to that of a drinkingglass was missing, it can be assumed that thepatient had primarily ingested that. Whetheralso part of the contents of the other bottlewas missing, could not be clearly established.
Assuming that the patient had ingested deter-gent, the nursing service immediately calledfor emergency medical services. The patient,whose respiration was sufficient and cardio-vascular condition stable, was initially admittedto the ward for general internal medicine. Afterthree days with relatively little complications,the patient developed an increasing global res-piratory insufficiency which required her trans-fer to the intensive care ward for intubation andartificial respiration. Her circulation remainedstable and did not require any medication. Ra-diology demonstrated the presence of pneu-monia on the right side which in the furthercourse clearly aggravated despite a broad an-tibiotic therapy. There was complete cloudingof both sides on chest X-ray and an obvious in-crease in respiration intensity. In addition, therewas anuric renal failure. In spite of the inten-sive therapy, the patient died eleven days afteringestion of the detergent, from aspirationpneumonia. The pathologist stated that bothlungs had become completely destroyed.A post-mortem report in writing has not cometo hand.
27
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 27
EvaluationBased on the available data concerning a tem-poral association between the accidental intakeand appearance of manifestations and in theabsence of other causes for these, a causal re-lationship is probable.
4.3 Selected cases by cause of poisoning
4.3.1 Mistake
4.3.1.1 Descaling products
Oral intake of descaling solutionsCase No 1:The electric kettle in an office was descaled.The descaling solution remained in the kettle.A 25-year-old female clerk wanting to maketea added water to the descaling solution andtook one sip of the tea made with this diluteddescaling solution.
Manifestations/courseThe patient saw a physician. The BfR doesnot have information on the manifestations ob-served and the medical findings, so that acourse with a mild symptomatology is as-sumed.
Case No 2:The staff of a laundry business performeddescaling on their coffee machine. Thedescaling solution was used to make coffee;a male staff member aged 49 drank some ofthis coffee.
Manifestations/courseThe subsequent medical examination estab-lished a “chemical burn“ on his tongue. Thepatient did not state any other complaints.Other organs did not show any appreciabledisease so that there was no need for furthermeasures.
Case No 3:By mistake, a 45-year-old member of the staffof an industrial establishment drank descal-ing solution instead of coffee. Probably, thecoffee machine had undergone descalingand descaling solution had been left in themachine. Since the patient noticed his mis-take immediately, he spat out the solution anddid not swallow it. Immediately afterwards, hepresented at the accident surgery ward of ahospital from where he was referred to theENT department.
Manifestations/courseMedical examination by a specialist showedthat the patient’s tongue was reddened andslightly swollen in the front part, while all otherfindings were normal. The BfR lacks informa-tion about the further course of this case.
Case No 4:During a break, a 42-year-old nurse wanted todrink some coffee in the recreation room. Thecoffee machine had just undergone descalingand residual descaling solution was still in themachine. By mistake, the nurse drank half asip of the descaling solution. She soon realisedher mistake, spit out the remaining descalingsolution that was still in her mouth and rinsedher mouth with water. Afterwards, she present-ed to the ENT department of the hospital.
Manifestations/courseThe examination did not reveal any signs ofchemical burns, mucosae were free from irri-tation, there was no hypersalivation and thepatient had no complaints. Following consul-tation of a PCC she was discharged and re-turned to her home. A continued dilution ther-apy was recommended.
Case No 5:A merchant served himself with a cup of cof-fee from the coffee machine. However, he had
Cases of Poisoning Reported by Physicians
28
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 28

failed to notice that the machine still con-tained residual descaling solution. He inad-vertently drank a small sip of the diluteddescaling solution, noticed his mistake rightaway and spit out the rest of the diluted solu-tion he still had in his mouth. Later on, hecomplained of a retrosternal burning sensa-tion and also in his pharynx and throat. As afirst measure, he drank an ample helping ofwater immediately and then presented to aphysician on duty.
Manifestations/courseThe ensuing physical examination which in-cluded an inspection of mouth and pharynxdid not show anything appreciable. A consul-tation of the responsible PCC provided the in-formation that there was no further risk; drink-ing of water with an added antifoaming agentwas recommended.
Case No 6:A 22-year-old patient inadvertently drank asip of a descaling solution which in additionto surfactants contained up to 12.5 % hy-drochloric acid and phosphoric acid. After-wards, the patient had difficulties to swallowand a sensation of swelling and closing of hispharynx. As a self-help measure, he drankwater and then called for an emergencyphysician.
Manifestations/courseThe emergency physician administered threepuffs of a corticoid spray. He administered250 mg prednisolone by the i.v. route and hadthe patient transferred to a hospital.On admission, a reddening of the pharynxwas noted but there was no swelling. Else,medical findings and routinely establishedlaboratory parameters were normal.
The patient was to be admitted for stationarymonitoring and presentation to an ENT spe-cialist. Also, gastroscopy was envisaged todemonstrate or rule out chemical burns in theoesophagus. However, the patient shunned allthese measures by leaving the ward on hisown.
Notes:Descaling agents or cleansers for coffee ma-chines and electric kettles are specific cleans-ing products for the removal of scales fromhousehold appliances. The calcium carbonateis dissolved by acids. In most cases, descalingproducts for household use contain organicacids, e.g. citric acid in concentrations of up to100 %, malic acid up to 60 %, or formic acid upto 25 %. In contrast, products for industrial usepreferentially contain more aggressive inorganicacids like hydrochloric and/or phosphoric acidas in the present case.
For descaling, the household appliance is filledwith descaling solution. This solution will remainresident in the appliance. Frequently, personsperforming the descaling operation would forgetto remove the solution later on. Some time later,another person will use this inconspicuousdescaling solution for making tea or coffee.Such tea will often be only somewhat lighter incolour and have a strong lemon flavour. Like cof-fee, it may also have a bad taste and lead to mi-nor manifestations such as nausea and irritationof the gastrointestinal tract. For those affected,
29
Fig. 8: Household chemicals
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 29

it will mean nothing but a scare and an unpleas-ant sensation. This has been similar in most ofthe cases reported to the BfR. As a treatment,drinking of fresh water or some other well-tast-ing fluid that does not contain carbonic acidsuch as tea will be sufficient.
Inadvertently ingested descaling products forindustrial use will be more problematic. Due totheir aggressiveness and depending on theirdegree of dilution, they may produce chemicalburns. As a first measure in these cases, drink-ing of water is recommended and presentationto a physician is indispensable. Depending onthe medical findings, the patient must remainunder observation or the scheme for treatmentof chemical burns must be applied like that de-scribed in the last mentioned case.
Accidents involving descaling solutions mistak-en for drinks are a daily routine activity forPCCs. In 2005, more than 500 events of thistype were registered by the Berlin PCC, and thetendency is on the rise. Some relief may bebrought about by a conspicuous staining of thedescaling products to distinguish them easilyfrom coffee, tea, or water. In this way, confound-ing could be avoided in advance. Potential vic-tims would be spared discomfort and medicalconsultations with the associated expenditure.
Evaluation of the cases described Based on the data about a temporal relationshipbetween ingestion and appearance of manifes-tations fortunately involving only minor healthcomplaints and in the absence of other causes,causal relationships probably exist in these cases.
4.3.1.2 Dishwasher detergent
Death erroneously associated with a dish-washer detergentFrom a press report, we came to know aboutan alleged case of poisoning with lethal out-
come in a 54-year-old male inmate of a nurs-ing home. Due to negligence, the patient hadbeen offered a dishwasher detergent contain-ing sodium hydroxide instead of tea. Uponappearance of severe health disorders, thepatient was immediately transferred to a hos-pital where he died despite intensive caremeasures. Post-mortem findings, however,did not confirm the initially suspected effectsof oral intake of a highly caustic detergent ascause of death.
The course of the accident was described asfollows. In the large kitchen of a nursinghome, a female member of the cleaning staffhad filled a tea-making machine with a clean-ing agent and then left the machine for thedetergent to take effect. At the end of hershift, she left a written note for her colleaguewho was to continue the cleaning operationon the tea-making machine. No warning wasfixed to the machine proper. When the col-league arrived, she had other duties to fulfilfirst so that the tea-making machine contain-ing the detergent fluid was left unattended forsome time. In the meantime, a nurse arrivedand poured “tea” from the machine. The pa-tient who later died took medicines togetherwith this „tea”. Although he complained aboutthe bad taste of the “tea”, he drunk a few sipswhen again asked to do so. The nursing staffdid not have any qualms in this context. Fourother patients also drank the fluid but none ofthem developed severe health disturbances.Judging by the press release, it was assumedinitially that a descaling agent was involved.Further investigations, however, revealed thata dishwasher detergent had been used whichis known to contain the toxicologically rele-vant substances, sodium hydroxide, sodiummetasilicate and sodium polyphosphate. Thisformulation may cause severe chemicalburns.
Cases of Poisoning Reported by Physicians
30
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 30

Manifestations/courseOnly when the mix-up had become knownand the patient was in a very bad state, a pos-sible link to poisoning was seen. The patientwas admitted to the nearest hospital. He diedthere shortly afterwards. Unfortunately, the BfRlacks information about the clinical manifesta-tions in this patient. Autopsy did not reveal anysigns of chemical burns on the patient’s skinor mucous membranes so that the dishwasherdetergent can be ruled out as a cause ofdeath. According to the post-mortem report,the cause of death was of cardiac nature.
Notes:Even though in this case, the nursing home in-mate’s death had not been caused by the dish-washer detergent, the course of the accident isof general interest and suitable to draw attentionto the poisoning potential due to confusion andinsufficient labelling of detergents and cleansers.
Evaluation of the case describedOn account of the findings stated in the post-mortem report, no poisoning with detergentshad taken place.
4.3.2 Health disorders caused by foods
4.3.2.1 Shiitake mushroom
Flagellate dermatitis after consumption ofraw shiitake mushroomsIn February 2006, a 65-year-old patient cameto the BfR and reported a highly discomfort-able skin reaction after having consumedabout twelve raw shiitake mushrooms. He hadbecome aware of the BfR through the publi-cation of a similar case on the internet.
Manifestations/courseInspired by a holiday in Japan, he had pre-pared for himself a salad from raw shiitake
31
mushrooms in the evening. During the follow-ing night he complained of stomach disorderand an unpleasant burning sensation over hisentire back. Initially, there was no pronounceditch. On the next morning, he was the moresurprised about a massive reddening of theskin on his entire belly and back, with clearlyvisible whip-like weals. He described a sen-sation like that of a massive sunburn. Overthe following days, the burning sensation in-tensified and turned into a painful itch whilereddening spread over the entire body andthe skin changes became pale and then re-appeared. Since initially, the patient declinedto undergo a cortisone therapy, a first attemptwas made to treat his condition by homeo-pathic medication (a general remedy againstfungi) and sedatives on a vegetal basis. Un-der this treatment regimen, however, the pa-tient’s symptomatology deteriorated. Therewere a strong pruritus, headache, swolleneyelids and finger joints, bluish-pink spots onarms and legs and a formation of urticariaand papulae. Therapy including oral corti-sone (20 mg/day) and antihistamines fromday 10 of illness resulted in the healing ofskin changes within one week.
During the following weeks, the patient devel-oped an increased susceptibility to infections,with initial signs of allergic rhinitis and later
Fig. 9: Flagellate dermatitis after consumption of rawshiitake mushrooms
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 31
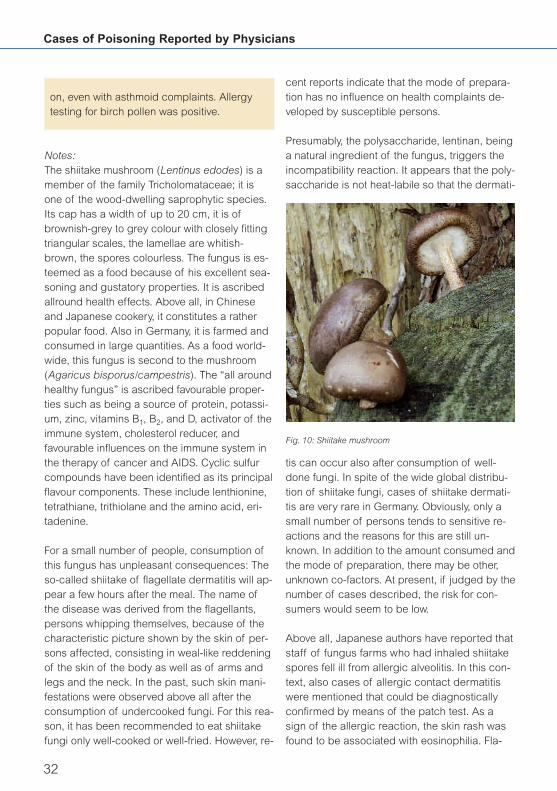
on, even with asthmoid complaints. Allergytesting for birch pollen was positive.
Notes:The shiitake mushroom (Lentinus edodes) is amember of the family Tricholomataceae; it isone of the wood-dwelling saprophytic species.Its cap has a width of up to 20 cm, it is ofbrownish-grey to grey colour with closely fittingtriangular scales, the lamellae are whitish-brown, the spores colourless. The fungus is es-teemed as a food because of his excellent sea-soning and gustatory properties. It is ascribedallround health effects. Above all, in Chineseand Japanese cookery, it constitutes a ratherpopular food. Also in Germany, it is farmed andconsumed in large quantities. As a food world-wide, this fungus is second to the mushroom(Agaricus bisporus/campestris). The “all aroundhealthy fungus” is ascribed favourable proper-ties such as being a source of protein, potassi-um, zinc, vitamins B1, B2, and D, activator of theimmune system, cholesterol reducer, andfavourable influences on the immune system inthe therapy of cancer and AIDS. Cyclic sulfurcompounds have been identified as its principalflavour components. These include lenthionine,tetrathiane, trithiolane and the amino acid, eri-tadenine.
For a small number of people, consumption ofthis fungus has unpleasant consequences: Theso-called shiitake of flagellate dermatitis will ap-pear a few hours after the meal. The name ofthe disease was derived from the flagellants,persons whipping themselves, because of thecharacteristic picture shown by the skin of per-sons affected, consisting in weal-like reddeningof the skin of the body as well as of arms andlegs and the neck. In the past, such skin mani-festations were observed above all after theconsumption of undercooked fungi. For this rea-son, it has been recommended to eat shiitakefungi only well-cooked or well-fried. However, re-
cent reports indicate that the mode of prepara-tion has no influence on health complaints de-veloped by susceptible persons.
Presumably, the polysaccharide, lentinan, beinga natural ingredient of the fungus, triggers theincompatibility reaction. It appears that the poly-saccharide is not heat-labile so that the dermati-
tis can occur also after consumption of well-done fungi. In spite of the wide global distribu-tion of shiitake fungi, cases of shiitake dermati-tis are very rare in Germany. Obviously, only asmall number of persons tends to sensitive re-actions and the reasons for this are still un-known. In addition to the amount consumed andthe mode of preparation, there may be other,unknown co-factors. At present, if judged by thenumber of cases described, the risk for con-sumers would seem to be low.
Above all, Japanese authors have reported thatstaff of fungus farms who had inhaled shiitakespores fell ill from allergic alveolitis. In this con-text, also cases of allergic contact dermatitiswere mentioned that could be diagnosticallyconfirmed by means of the patch test. As asign of the allergic reaction, the skin rash wasfound to be associated with eosinophilia. Fla-
Cases of Poisoning Reported by Physicians
32
Fig. 10: Shiitake mushroom
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 32

gellate dermatitis was described for the firsttime in 1977 by Nakamura. In 1985, he report-ed on 30 cases observed in Japan within a pe-riod of nine years. They referred to patientspresenting with severe erythema and pruritusafter ingestion of the mushrooms in traditionalAsian dishes. All of his patients exhibitedstrongly itching, linear, dense and very smallpapulae and stated that these stripes had ap-peared one or two days after consumption ofthe meal containing the mushrooms. The papu-lae had obviously formed by scratching in theform of stripes (Koebner phenomenon). Themanifestations receded after a period of 20–30days. Additional cases were recorded by Naka-mura later, until 1991. Other authors reportedon 58 patients presenting with shiitake dermati-tis during the 1997–2001 period. In 33 of thesecases, the disease had developed after theconsumption of sufficiently cooked fungi. InGermany, there have been quite sporadic cas-es of disease following consumption of this edible fungus.
So far, three cases involving health disordersdue to shiitake fungi were reported (one in 2004and two in 2005). In all cases, a typical whip-likereddening of the skin was present. The degreeof severity was rated as minor in all cases, butfor those affected, the general discomfort wasquite disagreeable.
In the case described above in detail, quite pro-nounced dermatitis was seen after consumptionof shiitake fungi which led to an appearance ofurticaria in the further course. However, therewas rapid healing as a result of therapy consist-ing in administration of cortisone and antihista-mines. Some weeks later, an allergic diathesisassociated with rhinitis (running nose) and asth-moid complaints became manifest for the firsttime. The clinical course seen has supportedthe hypothesis that proneness to allergy maybecome enhanced by consumption of shiitakefungi in persons with a latent allergic predispo-sition.
33
The mode of preparation, i.e. whether the fungiare raw or cooked, does not seem to have anyinfluence on the development of dermatitis. Shi-itake dermatitis has been observed also afterconsumption of well-cooked meals containingthe fungus.
It is recommended to pay attention to incompat-ibility reactions after the consumption of shiitakemushrooms and if first signs appear, to omitconsumption of this fungal species in the future.Since UV radiation may amplify the reaction,skin areas affected should not be exposed tosunlight.
Evaluation of the case describedIn the case described above, a causal relation-ship between the ingestion and the appearanceof manifestations has been rated as probableon the basis of the information given and in theabsence of other causes for the manifestations.
4.3.2.2 “Butterfish”
Intestinal haemorrhage in a 65-year-oldmale patient after consumption of “butter-fish”After surgical treatment of cancer of the largeintestine in 2005, the patient had been carrierof an anus praeter. Before consumption ofthe “butterfish”, he had felt well and did nothave any digestive disorder.
Manifestations/courseImmediately after the meal, the patient com-plained of an uncomfortable feeling in the up-per abdomen. One and a half day later, thepatients stool showed a bloody-liquid consis-tency. On account of this symptomatology,the patient was admitted to hospital and sub-jected to a detailed differential diagnosis.Findings revealed an initial ischaemic colitis.The intestinal haemorrhages spontaneouslycame to a halt so that the patient could bedischarged in a state of relative well-being.
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 33

marketed in Germany for a number of years aspieces of “butter mackerel” treated by hotsmoke and offered under the name of “smokedbutter mackerel”, formerly as “smoked butter-fish”. Also the oil or fat of such smoked fish mar-keted in Germany as “Butterfisch” and “Butter-makrele” consist of wax esters with a share of90 %, as established in a study conducted bythe Federal Research Centre for Fisheries, Ham-burg.
In an expert opinion dated 30 August 2004, theScientific Panel on Contaminants in the FoodChain stated the following regarding the toxicityof fishery products from fish of the Gempylidaefamily: EFSA (European Food Safety Authority)has stated that on the basis of the case reportsreceived, it is not possible to fix daily intake lev-els for fish which do not produce the side ef-fects reported. It may be possible to avoid anappearance of these manifestations by suitablepractices of preparation such as discarding ofthe oil that has become liberated from the food.
Evaluation of the case describedBased on the data about a temporal associationbetween ingestion and appearance of manifes-tations, a causal relationship is considered aspossible.
In view of the intestinal haemorrhage de-scribed, the case under reference has to be rat-ed as moderately severe while the extent of the
Cases of Poisoning Reported by Physicians
34
The attending physicians saw a possible as-sociation between the appearance of colitisand the consumption of “butterfish“. Differen-tial diagnosis also considered an adverse re-action to the short-term use of a vasodilativemedicine. In the medical press, there havebeen reports of vascular disease which inrare cases may occur after use of that partic-ular medicinal product.
Notes:In mid-2003, Australian health authorities report-ed health disorders associated with the con-sumption of escolar, also referred to as butter-fish, rudderfish, or butter mackerel. Since 1999,98 cases have been recorded in Australia. In apress release dated 30 April 2003, the BfR drewattention to the fact that after consumption ofmajor quantities of fish of the species Lepido-cybium flavobrunneum (escolar) and Ruvettuspretiosus (oil fish or escolar) of the Gempylidaefamily (German terms: Butterfisch or Butter-makrele) particularly sensitive persons may suf-fer health disorders such as diarrhoea, abdomi-nal cramps, vomiting and headache. Cautionwhen consuming these fish species was sug-gested. Experts assume that these disordersare caused by the presence of not readily or notat all digestible wax esters accounting for 90 %of the oil or fat of these two fish species. It hasnot yet been elucidated whether the wax estersalone can be held responsible for such healthcomplaints or whether there are other contribut-ing factors. One could think of certain fish pro-teins having allergenic activity or of biogenicamines (among these, histamine) which mayform in fish when stored over extended periods.Also, the quantities of fish are unknown whichwould have to be ingested to produce suchhealth disorders. “Butterfisch” and “Butter-makrele” (butter mackerel) are collective terms(trade names) for marketing a number of fishspecies which are rich in fat and come as a by-catch from deep-sea fishing. They have been
Fig. 11: “Butterfish”
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 34

associated health disorder depended on thepatient’s underlying disease as a co-factor.
Further cases involving “butterfish”For the first time, a similar report was publishedin the BfR brochure entitled Cases of PoisoningReported by Physicians in 2004. The patient in-volved had been alerted to this problem by theinternet publication of the respective BfR com-ments (No. 12/03) and had sought contact withthe BfR as somebody personally affected by thehealth disorder described. Also in the presentcase, the patient made reference to the com-ments cited. He pointed out that at his homeplace on the Baltic Sea, a number of personshad suffered from the manifestations described(diarrhoea, abdominal cramps, headache, vom-iting) after having consumed “butterfish”. In ad-dition to describing his own case, he had in-tended to draw attention to the fact that therehad been obviously more cases than those re-ported to the BfR.
Summary: During the reporting period,2004–2006, a total of 14 cases involving gas-trointestinal disorders after the consumption of“butterfish” were recorded at the BfR (5 cases in2004, 6 cases in 2005 and 3 cases in 2006). Inall cases recorded so far, health disorders wererated as minor. Nevertheless, these complaintsmeant an obvious impairment of the well-beingof the persons affected.
4.3.3 Accidents
4.3.3.1 Chemical burns from sodium hydroxide
Chemical burns from sodium hydroxide:Severe course A male patient aged 39 suffered severe dam-age to his eye. Causes of the accident arenot known. Examination by an ophthalmologi-cal practitioner resulted in findings of severechemical burn. The patient was admitted for
inpatient treatment. At the hospital, surgicalintervention was performed consisting in re-moval of the vitreous body (vitrectomy) andinsertion of an artificial lens (pseudophakia).
Manifestations/courseDetails of the accident situation and first aidmeasures applied are unknown. The patient’seye was accidentally hit by sodium hydroxide.Owing to the severe chemical burn whichpresented itself by the aspect of a “cookedfish eye”, the attending practitioner referredthe patient to a hospital. At the hospital, thevitreous body, which had suffered severeposttraumatic damage, was removed by sur-gery. An artificial lens had to be inserted anda corneal graft performed. As a result ofthese numerous complicated interventions,the patient’s visual acuity could be restored tosuch a degree that movements of the handcould be recognized by him. To obtain a fur-ther improvement of the patient’s sight, atransplantation of stem cells is envisaged.Nevertheless, partial recovery is expected inthis case.
Notes:In this case, the grave consequences of achemical burn by sodium hydroxide involvingdifficult surgical intervention followed by partialhealing become evident. Alkaline compoundssuch as sodium and potassium hydroxide andammonia produce local damage to skin andmucosae as well as the eye, resulting in soap-like liquefaction of tissue and colliquative necro-sis. Owing to the ability of alkalis to liquefy pro-tein and to dissolve it, alkalis have a greater in-depth effect than acids.
� In the event of a minor chemical burn, onlythe uppermost layer of the cornea will beco-me detached. The rim of the cornea will re-main. From there, the cornea can regenerateitself. No corneal clouding will develop later.
35
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 35

� In the event of a chemical burn of moderateseverity, also the conjunctiva is damaged inaddition to the outer layer of the cornea. Inthis case, reddening is a favourable sign be-cause this indicates that circulation is still in-tact.
� Most severe chemical burns are recognizedby the presence of a dense white opacificati-on of the eyeball. In this case, also deeperparts of the eye such as iris, lens, blood ves-sels and sclera have suffered irreparable da-mage. The eye will remain blind unless surgi-cal intervention is performed for correction.
If exposure to a corrosive substance has affect-ed the eyes, intensive rinsing with water (mini-mum 10 minutes) should be performed. For thispurpose, the eyelids must be ectropionizedwhich often is difficult to accomplish. A slippingof fingers may be prevented by the use of drycloth or swabs. If unsuccessful, 2 % lidocainefrom the emergency kit can be applied drop-wise to the edge of the eyelid to produce anal-gesia and thus opening of the eyelid. Ideally butimpossible in most cases for technical reasons,would be rinsing of the open eye under runningwater from the tap. As an alternative, repeatedpressing out of a piece of water-soaked clothmay be used.
In the case described, it is unknown which firstaid measures were taken. White opacification ofthe eyeball in the event of most severe chemical
burns is referred to, as in the present case, as“cooked fish eye”. Vitrectomy consists in surgi-cal removal of the damaged vitreous body andsubsequent replacement by Ringer’s solution,gas, or silicone oil while damaged cornea is re-placed by corneal grafting. Thus, a completeloss of sight could be prevented for the eye af-fected. It remains to be seen whether the envis-aged stem cell transplantation can improve thepatient’s visual acuity. Modern surgical tech-niques may be successful in such severe casesand perhaps partially cure amaurosis.
Evaluation of the case described Based on the data regarding the corrosive sub-stance that caused the damage and the mani-festations seen, and in the absence of othercauses, a causal relationship is probable.
4.3.3.2 Fire breathing
Severe health damage from aspirationpneumonia after amateur fire breathingThe male adult patient had performed firebreathing as a hobby. During this activity,some of the fire breathing fluid he kept in hismouth was aspirated. He was admitted to ahospital and then transferred to another hos-pital for onward treatment. There, bron-choscopy was performed, during which thepatient developed bronchospasm so that hehad to be intubated and respirated. Chestsonography revealed bilateral pleural effu-sions which, however, underwent regressionin the further course. After slightly more thantwo weeks which he spent at the hospital, thepatient could be discharged and referred toambulatory care.
Manifestations/course One day after the aspiration event, the patientwas transferred to another hospital. For rea-sons unknown to the BfR, it was decidedthere to perform bronchoscopy on the follow-ing day. When this was performed a compli-
Cases of Poisoning Reported by Physicians
36
Fig. 12: Severe chemical burn of the eye – “fish eye”(Copyright © Online Journal of Ophthalmology)
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 36

be achieved. Final radiology after terminationof antibiotic treatment also exhibited clearlyloosened infiltrates in the lower area left andan absence of fresh lesions which indicateda decisive improvement of findings. After a to-tal of 17 days of stationary monitoring andtreatment, the patient was discharged in aclearly improved general state and referred toambulatory care. A pulmonological practition-er was to check the patient’s lung function af-ter two or three weeks and to gradually re-duce the dosage of steroids. The patient wasstrongly recommended to abstain from nico-tine consumption.
Notes:Fire breathing (Fig. 13) is the act of creating aflame by spraying, with one’s breath, a flamma-ble substance upon the open flame of a torchthus lighting the fine spray fog. On principle, theflammable substances used are powders or liq-uids. Beginners are recommended to use pow-ders such as Lycopodium (club moss) sporesbecause the health risk involved is lower. Thissubstance is available in pharmacies as a natu-ral laxative. Liquid fuels used (e.g. PyrofluidTM)are mostly based on highly purified kerosene orlow-viscosity paraffinic preparations, as in thecase described above. The fire breather takesthis liquid into his mouth and blows it out againunder high pressure, using a special technique.During the performance, the fire breather needsto deeply concentrate and constantly control thenatural swallowing reflex in order to avoid acci-dental swallowing. Also, an inhalation ofdroplets of the liquid poses the risk of severelung damage. Due to certain physical proper-ties of the fire-breathing liquids such as lowvolatility, viscosity and surface tension, theyreadily “undercreep” the epiglottis and enter thelungs (aspiration). Even the smallest quantitiesinhaled may cause this effect. Owing to theirphysicochemical properties, these substancespenetrate further into the lungs thus reaching
37
cation arose in the form of a bronchospasmso that the patient had to be intubated and in-tensively respirated for some hours. Extuba-tion could be accomplished still on that day,without any complication. Bronchoscopy re-vealed an acute inflammation in the trachealarea and, in the bronchial area, the presenceof acute bronchitis with moderate formationof green mucus. Chest sonography revealedbilateral pleural effusions which, however,were clearly retrograde in the further courseof inpatient treatment. On admission, bloodgas analysis showed the presence of partialrespiratory insufficiency with values of paO2
61.5 mm Hg, paCO2 35.4 mm Hg and pH7.45. By lung function analysis, a mixed venti-lation disorder was observed, in particularwith obstruction but also with signs ofoverdistension of the lungs. Initially, infectionparameters were clearly elevated, with a CRP
level of 29 mg/dl and leukocytosis (17.9/nl).Therefore, the patient was administered anantibiotic over a period of 12 days which re-sulted in a clear decrease of the levels of in-fection parameters. Furthermore, he wastreated by systemic and inhalational adminis-tration of steroids. An obvious regressionfrom the initial levels of the pathological lungfunction and blood gas analysis values could
Fig. 13: Fire breather
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 37

the deep lung areas. This will result in a reduc-tion of gas exchange in the alveoli followed byoxygen deficiency (hypoxia). It has been as-sumed that the surfactant effect is impaired inthe alveolar region. The direct capillary damageis attributed to the development of chemicalpneumonia (pneumonitis), haemorrhagic bron-chopneumonia and lung oedema. In severecases, patients die presenting a clinical pictureof ARDS. Up to the present time, no promisingtherapy has become known. Since 1990, asmany as five children died in the Federal Re-public of Germany from the sequelae ofkerosene or paraffin aspiration.
Initial manifestations after aspiration such ascough and/or vomiting are experienced rapidlyafter exposure. The simultaneous presence ofnausea and vomiting are caused by the local ir-ritating effect of pyrofluids on the mucous mem-branes. Either initially or after a symptom-free in-terval, patients will develop, in addition tocough, other pulmonary manifestations of aspi-ration pneumonia. These may increase in inten-sity in the course of the first day and will, as arule, recede within two to five days. In severecases, lung oedema associated with haemopty-sis, pneumothorax or, as in the above case,pleuritis (pleural effusion) may develop. Radiolo-gy will reveal pneumonic infiltrates in the basalor perihilar regions, less frequently, a migratingpneumonia or pneumatoceles forming in the pe-riod between the 3rd and 15th day. The firstchanges may be demonstrated by radiology af-ter approximately two hours, as a rule, however,they should become evident within a period of12 hours. Other manifestations may include car-diac arrhythmia resulting from hypoxia, or CNSmanifestations indicating ingestion of majorquantities (which in fire breathing is rather im-probable to occur). Fever developed initially,which is unrelated to the clinical findings andwill in most cases recede within 24 hours, is afrequent occurrence and should be consideredas a “resorption fever”; there is no need fortreatment. Prophylactic administration of antibi-
otics is not recommended. However, if feverlasts for an extended period, a bacterial super-infection may be present and should be treatedaccordingly. Also prophylactic administration ofglucocorticoids will not result in any improve-ment of the clinical picture. In contrast, it willeven increase the risk of infection. It is only required for the treatment of lung oedema.Bronchial lavage should also be omitted be-cause it poses an additional risk of aspirationby shifting pyrofluid into deeper lung areas. Incases of pneumonitis, a reasonable therapyshould only be oriented by the manifestationsobserved and avoid any unnecessary manipu-lating measures.
An art related to that of fire breathing is referredto as fire eating (Fig. 14). The performer placesa specially prepared flaming torch into his/hermouth and extinguishes the flame. The „art“consists in placing the flame of the torch intothe mouth in an absolutely vertical position, i.e.with the head bent backwards. In this position,the oxygen supply for the upward-blazing flameis completely interrupted. Hence, use is onlymade of the laws of physics (hot air rises).There is no such thing as a “cold flame” nor isthere any special substance in the performer’smouth other than saliva. Unless having under-gone a special training, fire eating amateurscannot perform fire eating without running seri-ous risks.
Cases of Poisoning Reported by Physicians
38
Fig. 14: Fire eater
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 38

Evaluation of the case describedBecause the fluid used involved a high risk ofaspiration, the description of the accident (anamateurish attempt of fire breathing) and thetemporal relationship between aspiration andappearance of pulmonary manifestations, acausal relationship is considered as probable. Ithas remained unclear why the patient under-went bronchoscopy and was administeredsteroids. The bronchospasm requiring intuba-tion and artificial respiration has to be consid-ered as a complication arising during medicalintervention, i.e. bronchoscopy.
4.3.3 Abuse
4.3.4.1 Slimming agent (2,4-dinitrophenol)
Death after ingestion of 2.4-dinitrophenolfor weight reductionA 19-year-old healthy female had obtained2,4-dinitrophenol (DNP) from a friend. Neitherthe trade name of the product nor its originare known. In order to reduce her bodyweight, she took half a teaspoon of the sub-stance once in the evening. She did not takeany other medicines or narcotic drugs. Shereported that four hours later she had a sen-sation of heat, her heartbeat accelerated andshe felt sick and vomited. During the night,the patient vomited several times, she couldhardly retain any fluid supplied and wassleepless. In addition, she suffered from ex-cessive sweating and hyperventilation. On thenext morning, she saw her family physicianwho ordered her admission to a hospital. Inthe further course, a rapid increase in the pa-tient’s CK and a continuous increase of herheart frequency were observed. In addition,she developed lung oedema and a vehementrise in body temperature. In spite of massivemeasures of intensive medical treatmentsuch as cooling and artificial respiration, car-diac arrest occurred eventually leading to thepatient’s death.
39
Manifestations/courseOn admission to the hospital, the patient waswet with sweat, her symptomatology had re-mained unchanged since the last night andher body temperature was still normal(36.4 °C). Clinical chemistry showed leukocy-tosis (20 800/µl), a CK of 826 U/L and ablood sugar level of 183 mg/dL. Due to hy-perventilation, blood gas analysis showed acompensated respiratory alkalosis of pH7.45, pCO2 30 mmHg, pO2 79.7 mmHg, BE–2.7. In the further course, a rapid CK in-crease of up to 1067 U/L was seen. A strik-ingly vehement increase in body temperatureby ca. 0.1 °C/min was observed which couldnot be stopped in spite of external cooling bymeans of ice packs, administration of coolgastric lavage and cool infusions. In addition,a continuous increase of the heart rate froman initial value of 136/min to 180/min wasrecorded. Echocardiography revealed a hy-perdynamic left ventricle with a low filling sta-tus. Due to imminent respiratory exhaustion,the patient had to be intubated and respirat-ed. Blood gas levels deteriorated under con-trolled artificial respiration with an increase ofpCO2 to 68.3 mmHg and a BE of –9.9 associ-ated with a pO2 of 112 mmHg. The patientdeveloped a massive uncontrollable lungoedema. Shortly afterwards, cardiac arrestoccurred that required resuscitation meas-ures. These remained unsuccessful andtherefore, were discontinued after 45 min.Death occurred under the clinical picture ofmultiple organ failure. A striking observationwas seen in the fact that complete rigor mor-tis developed within a period of 15 minutes.
Notes:2,4-dinitrophenol is a lipophilic substance be-longing to the substance group of nitrophenols.All substances of this group are highly toxic andmay cause poisoning by the inhalational, dermaland oral routes. DNP, in particular, is assumed to
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 39

have embryotoxic, carcinogenic and mutageniceffects.
DNP was used for the first time already in 1919,namely in France to produce ammunition. Work-ers in factories producing explosives who suf-fered from health disorders such as attacks ofdizziness, sweating and headache were alsofound to lose body weight. This resulted in theidea that overweight might be treated by admin-istering DNP. However, in 1938, it becameknown that DNP administration involved consid-erable risks such as the formation of cataractassociated with a yellow-brownish discolorationof the ocular lenses. As a consequence, DNPwas withdrawn from the market in the USA as amedicinal product for weight reduction. Later,DNP was used as a wood preservative, a photo-chemical substance and a pest control agent.
In the 1980ies, a Texan physician rediscoveredthe substance: he sold a product for weight re-duction that contained DNP. The death of awrestler treated with this product was followedby an investigation which resulted in DNP beingbanned again as a medicinal product for weightreduction. Up to the present, no food supple-ment or medicinal product containing DNP hasbeen authorized by the US Food and Drug Ad-ministration (FDA).
DNP uncouples oxidative phosphorylation. Thehigh-energy molecules for ATP synthesis contin-ue to be delivered but they are converted toheat instead of ATP. This elicits a high thermo-genesis associated with a drastic increase inbody temperature. Because no more ATP isformed, the body uses other resources for ener-gy production and reduces body fat. The liverreleases glucose as an alternative ATP source.This anaerobic degradation process results inthe formation of lactate and ethanol as endproducts, which results in metabolic acidosis.
The lethal dose is stated to be of 1–3 g DNP(single dose). The details of pharmacokinetics
are unknown, however, the half-life period of thesubstance seems to permit its accumulation.This is suggested for example by the death of abodybuilder who took a daily dose of 600 mgDNP for four days and died on the fifth. Proba-bly, many deaths due to DNP have to be attrib-uted to the fact that the cumulative effect wasnot taken into account.
DNP is a highly toxic substance. Manifestationsof poisoning with this substance include hy-potension, tachycardia, cardiac arrhythmia,sudden cardiac death, dyspnoea, aspirationpneumonia, lung oedema, headache, agitation,cerebral oedema, coma, hyperthermia, dehy-dration, metabolic acidosis, rhabdomyolysis,thyroid dysfunction, hyperglycaemia, gastroin-testinal disorders, cyanosis, haemolyticanaemia, methaemoglobinaemia, agranulocyto-sis, yellowish discoloration of skin, sperm andthe ocular lenses associated with cataract for-mation, renal insufficiency, hepatic failure and fi-nally, multiple organ failure.
Results of investigations at the German SportUniversity, Cologne, have indicated that recently,DNP has been massively advertised as a fat-burner for effective weight reduction. The sub-stance is very cheap and can be obtained rela-tively easily from companies trading in chemi-cals. It might also be used as an anabolicsteroid to accentuate the muscles after body fatreduction. Therefore, a survey among all PCCswas initiated in order to find out whether an in-creasing number of inquiries referring to DNP orcases of poisoning involving the substance hadbeen recorded recently. Fortunately, it wasfound that no other cases of poisoning had oc-curred except for the two cases reported to theBfR. Information on the second case reported isgiven in the Section on suicides (Chapter4.3.5.2).
Evaluation of the case describedBased on the data concerning a temporal asso-ciation between the intake of a lethal dose of
Cases of Poisoning Reported by Physicians
40
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 40

occurring during intubation, aspiration wassuspected in addition.
When the patient was transferred from theambulance to the intensive care unit, oxygensaturation was 80 %. Clinical findings includ-ed a heart rate of 130–150/min with inade-quate circulation. Adrenaline was again ad-ministered and buffering with sodium bicar-bonate initiated. This resulted in a stabiliza-tion of circulation with beginning cardiac out-put and development of measurable bloodpressures. The patient was administered nor-epinephrine to support his circulation. In or-der to improve cardiac output, sodium nitro-prusside was administered for afterload re-duction and an appropriate volume replace-ment performed. These measures as well asadministration of a phosphodiesterase in-hibitor and intensive respiration therapy were intended to stabilize the patient’s circu-lation.
The first echocardiography performeddemonstrated a pronounced damage to theendocardium. Also the ECG revealed severerepolarization disorders. Ventricular contractil-ity was markedly impaired. This could becompensated initially. Transcranial dopplersonography soon revealed a reduced cere-bral perfusion which had to be interpreted asa consequence of the poor cardiac outputand of the development of progressive cere-bral oedema. Resistance indicators showedsometimes values of no more than 0.4, asso-ciated with a clearly elevated diastolic and re-duced systolic pressure. Repeated CT andMRI revealed a pronounced focal cerebraloedema.
Clinical chemistry showed a massive in-crease in creatine kinase levels including CK-MB as an indicator of myocardial dam-age. Increased levels were also found for
41
DNP (half a teaspoon corresponds to approxi-mately 2.5 grams) and the appearance of typi-cal manifestations, a causal relationship is con-sidered as confirmed in the case described.
4.3.4.2 Sniffing agents (deodorant spray)
Death of an 11-year-old boy after sniffingof deodorant sprayAn 11-year-old boy returned home fromschool. He complained of nausea and want-ed to take a shower. Shortly afterwards, hisgrandmother found him unconscious in theclosed shower cabinet. He was cyanotic andunresponsive and showed a gasping breath-ing. About one minute later, the mother’s part-ner arrived and started lay resuscitationmeasures. Next to the boy, an empty deodor-ant spray can was found which had been fullbefore. Therefore, inhalation of propellantswas strongly suspected. Later, the boy’smother reported that she had become awareof occasional sniffing among the boy’sfriends. She stated that also the boy himselfhad sniffed several times before. Otherwisehe had been a healthy and normally devel-oped boy.
Manifestations/courseThe emergency physician, who arrived tenminutes after the emergency call had beenmade, found ventricular fibrillation. The pa-tient was immediately intubated and defibrilla-tion administered with energies of 200 joulesinitially, followed by 240 and subsequently,360 joules. Because no spontaneous cardiacrhythm set in, cardiopulmonary resuscitationwas continued. After repeated administrationof atropine and adrenaline and of defibrilla-tion, a sinus rhythm set in with 130 beats/minwhich, however, was associated with broad-ened ventricular complexes and a aerody-namically insufficient cardiac output. Oxygensaturation measured at that time was approxi-mately 80 %. Because of repeated vomiting
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 41

LDH, AST and ALT. Also the initially normal re-nal parameters increased, showing a pro-gressive renal insufficiency. In the context ofterminal renal insufficiency, a gradual in-crease in phosphate levels was observed. El-evated levels were also found for ammoniawhile electrolytes and lactate remained withintheir normal ranges. Deep sedation was per-formed for cerebral protection. Under seda-tion, the EEG showed changes of short-termsegments of low-amplitude reflex activity andextended phases in the sense of an incipientburst suppression pattern. Circulation couldbe stabilized for a short period of time. Sub-sequently, however, a condition of increasingcardiac decompensation set in associatedwith a deformation of ventricular complexes,echocardiography showed almost no activity.Blood pressure levels could only be main-tained by means of maximum doses of nor-epinephrine and the phosphodiesterase in-hibitor. Doppler sonography showed a furtherdeterioration of cerebral perfusion. Given thestill persisting cerebral perfusion and low-am-plitude EEG pattern, transfer of the patient toa heart centre was decided in order to con-sider the option of using an assist device.
Prior to the envisaged transfer, a sudden in-crease in pCO2 occurred, pupils became un-round and showed no reaction to light at all.No spontaneous respiration at all could bedemonstrated by the apnoea test so that aclinical picture of cerebral death was seen.The latter was confirmed over the next 48hours by means of repeated apnoea tests, apositive doll’s eye sign and repeated isoelec-tric EEGs over a period of more than 30 min-utes. Doppler sonography showed the ab-sence of cerebral perfusion, and an unequiv-ocal oscillatory flow was seen in the carotidarteries. After completion of all criteria ofcerebral death and consultation of the boy’sparents, it was decided to discontinue all
therapy including dialysis that had been initi-ated because of progressive renal insuffi-ciency. The boy died ten days after the inci-dent.
Notes:Propellants used in sprays include butane andpropane. Both gases are characterized by acomparatively low toxicity. At higher concentra-tions (> 6 %) they have a weak narcotic effect.They displace oxygen because their volume in-creases by 250 times on transition from the liq-uid to the gaseous state.
Due to their euphoric effects, these as well asother substances are frequently used by ado-lescents as sniffing agents. According to epi-demiological studies, first experiences with nar-cotic drugs in the form of sniffing agents aremade as early as at the age of 9–10 years,3–10 % of all school children have alreadymade corresponding experiences. The childreninvolved mostly come from a difficult socialbackground. On the European level, severalhundreds of deaths have to be assumed to occur due to sniffing every year. Recently, thepredominant number of cases has been due topropane/butane mixtures like those used incamping stoves or in aerosol cans, as in thecase described. After three to six months ofsniffing, the desired effects will decrease. Thiswill inevitably be followed by increasing of thedoses or starting of narcotic drug abuse, whichis associated with a very poor rehabilitationprognosis. Sniffing agents have a considerablepsychological addiction potential, which essen-tially depends on the social situation of the per-sons affected.
Short-term accidental inhalational exposure topropane or butane does not result in poisoning.At sufficiently high concentrations and after ex-tended duration of exposure, the persons af-fected will rapidly develop reversible manifesta-
Cases of Poisoning Reported by Physicians
42
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 42

tions such as the desired euphoric feeling fromdrug abuse, but also effects ranging from seda-tion to coma, muscular tremor, dizziness andnausea. The „kick“ experienced from sniffing ordue to stress, panic etc. causes myocardialsensitization to endogenous catecholamines.This may result in severe cardiac arrhythmia orventricular fibrillation with a lethal outcome. Alsomyocardial infarction has been observed inadolescents with healthy hearts, which wereprobably due to vascular spasm after cate-cholamine action.
Due to the above-mentioned displacement ofoxygen, massive exposure may result in hypoxiaincluding all its consequences such as acidosis,shock, unconsciousness and suffocation. Thisplays a minor role in cases of abuse but mayoccur after exposure caused by a release fromdefective technical installations.
Therapy should include absolute physical immo-bilization because physical activity increasesthe imminent risk of ventricular fibrillation. If re-quired, the patient should be sedated by meansof a benzodiazepine. Catecholamine adminis-tration should be avoided because this couldpromote myocardial sensitization to exogenousand endogenous catecholamines and possiblytrigger severe cardiac arrhythmia. Onward ther-apy will be oriented by the existing symptoma-tology.
The above case provides an impressive de-scription of the tragic and typical picture of ad-diction to sniffing propellants from aerosol cans.Immediately after inhalation of butane/propane,patients will collapse under sudden cardiac ar-rhythmia, in particular ventricular fibrillation. Thecardiac damage causes cardiovascular insuffi-ciency associated with deficient perfusion of vi-tal organs such as brain and kidneys. In theabove case, the myocardial damage was sopronounced that the patient could probablyhave survived only by receiving a heart trans-plant.
Evaluation of the case describedBased on the case history, the characteristicmanifestations and the course, a causal rela-tionship between the inhalation of deodorantspray and poisoning is considered as con-firmed.
4.3.4.3 p-Nitroaniline
Death from nitroaniline poisoning in amale adolescent A 15-year-old male had attended a party withfriends and therefore spent the following nightat a friend’s home. Allegedly, neither drugsnor alcohol had been consumed at the party,however, the patient was said to have told afriend that he was taking drugs. The type ofdrugs could not be specified by the friend.On the following day, the patient returned tohis parents’ home at about 14:00 h. The nextevening was said to have passed in a “nor-mal” way, and the boy went to bed at about21:00 or 22:00 h. He was said to have beenwell and not having complained of any painor discomfort. In the night, the parents heardtheir son scream. They found him uncon-scious on the floor of his room in the base-ment and called for the fire brigade. On ar-rival at the hospital, respiratory arrest oc-curred. Resuscitation attempts remained un-successful, and the boy died at the emer-gency unit of the hospital. To elucidate thecause of death, a post-mortem was per-formed whose results provided indications ofnitroaniline poisoning.
Manifestations/courseThe emergency physician found the patient inhis room. He was unconscious and showedmydriasis. Since drug abuse was suspected,she injected naloxone. There were no injec-tion sites found suggesting narcotic drugconsumption, also the parents were notaware of any drug abuse by their son. No dis-eases or abnormal behaviour possibly associ-
43
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 43

ated with drug consumption had been ob-served. A small pharmaceutical bottle con-taining a yellow powder was found on thewindowsill of the boy’s room.
The patient was brought to a hospital byemergency ambulance. On arrival at theemergency unit, respiratory and cardiovascu-lar insufficiency occurred. Resuscitation at-tempts that had been initiated remained un-successful, the boy died at the emergencyunit. Except for a head laceration, no informa-tion has been available to the BfR regardingthe findings on admission. No blood was collected for toxicological analysis at the hos-pital.
To elucidate the cause of death, post-mortemwas performed at a forensic medical unit. Theabove-mentioned contused laceration wasfound in the temporal area, and in addition,abrasions in the region of the patient’s hips.These injuries may have resulted from fallingdown in his parent’s flat. They were, however,of no relevance for the cause of death. Find-ings included haemostasis of the internal or-gans, which can be considered as an indica-tion of heart failure. Both palms showed yel-low discoloration resembling a map whichcould have originated from contact with theyellow powder from the pharmaceutical bottlefound in the patient’s room. The contents ofthe stomach was interspersed with tiny yel-lowish powdery particles adhering to thestomach lining also in a map-like pattern. Thissuggested oral ingestion of the substance.Whether the cause of ingestion was a suici-dal intent, abuse or a mistake has remainedunclear. The post-mortem findings did not re-veal any cause of death that could have beenexpressed in morphological terms.
A toxicological-chemical analysis was ruled toexamine poisoning as a suspected cause of
death. Analysis detected p-nitroaniline andcorresponding metabolites in the venousblood, in the contents of the stomach and in aliver specimen. Also the yellow powder men-tioned in the case history contained p-nitroani-line as the main component. There were no in-dications found of the presence of other toxicsubstances (including ethanol) that might havebeen associated with the patient’s death. Thisapplies also to the special analysis to detect il-licit (narcotic) drugs in venous blood and hair.Since nitroaniline is a methaemoglobin pro-ducer, MetHb determination was performed af-ter death that revealed an elevated level of36.8 %. Repeat measurements performed inthis case found MetHb levels to have de-creased during extended periods of samplestorage. Hence, the level present at the time ofdeath may have been markedly higher andpossibly caused the boy’s death.
Notes:4-nitroaniline (p-nitroaniline) usually exists in theform of pale yellow needles and is used for theproduction of dyes, antioxidants and pharma-ceuticals. Nitroaniline is very toxic: the oral LD50
for mice is 750 mg/kg. It may be absorbedthrough the airways by means of inhalation ofdust, vapour or aerosols. However, due to therelatively low vapour pressure, absorption of rel-evant quantities seems to be hardly possible. Itis readily absorbed and may cause poisoning al-so on contact with the skin. No special data areavailable on dispersion, metabolism and excre-tion in humans. After ingestion or absorption byother routes, methaemoglobin is formed as aprimary toxic effect. Oxidation of the ferroushaemoglobin causes methaemoglobinaemia.The normal value for MetHb is 1–2 %, in smok-ers approximately 10–20 %. Oxidative stressmay denature haemoglobin resulting in haemoly-sis. Once the „normal“ haemoglobin has under-gone change, it is no longer available for oxygentransport. MetHb concentrations of 10–30 % will
Cases of Poisoning Reported by Physicians
44
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 44

result in isolated cyanosis. If a generalizedcyanosis in patients with a healthy cardiopul-monary system is unresponsive to oxygen sup-ply, methaemoglobinaemia should always beconsidered. Due to presence of oxidized iron,the blood has a dark brown colour. Therefore, asuitable bedside test consists in the filter papertest for which a single drop of poisoned patient’sblood is placed on dry white filter paper. AtMetHb concentrations of 10-15 % and higher,the colour of this drop will appear chocolatebrown while that from a healthy person is red.Anaemic patients will show a less pronouncedcyanosis but in turn, more severe clinical mani-festations. Concentrations of 30–40 % MetHbwill cause cardiovascular and central nervousmanifestations such as headache, dyspnoea,tachypnoea, tachycardia and discrete hyperten-sion; concentrations of 40–50 % MetHb will re-sult in disorientation, lethargy and metabolic aci-dosis; and concentrations exceeding 50 %MetHb will cause coma, convulsive seizures,cardiac arrhythmia and a drop in blood pres-sure. A lethal outcome has to be expected atlevels of 70 % MetHb and above.
The treatment of methaemoglobinaemia may in-clude administration of the antidotes, methyleneblue and toluidine blue, in addition to oxygensupply. Both substances will reduce MetHb tofunctional Hb and become oxidized during thisprocess. If a life-threatening methaemoglobi-naemia cannot be controlled by means of theabove-mentioned redox dyes, blood transfusionis indicated in order to supply functional redblood cells.
The high blood levels of methaemoglobin de-tected in the case described above have to beconsidered as a possible cause of respiratoryand circulatory depression with a lethal out-come.
However, it has remained unclear how poisoningdeveloped in this case. An assumption that can-not be excluded is that p-nitroaniline was mis-
taken for 2.4-dinitrophenol. This substance is al-so yellow in colour and has recently been thesubject of massive advertising as a fatburner,either to reduce weight or to accentuate mus-cles by reducing body fat.
Evaluation of the case describedBased on the facts that p-nitroaniline was de-tected in the patient’s body fluids, in his stom-ach, on his hands and that the substance wasfound in the pharmaceutical bottle, and afterother causes could be excluded by post-mortem findings, a causal relationship betweenthe ingestion of p-nitroaniline and poisoning isconsidered as confirmed.
4.3.5 Suicides
4.3.5.1 Valproic acid
Severe poisoning with valproic acid due tosuicidal attemptAfter a family quarrel with her mother, a 13-year-old girl ingested an unknown quantity ofvalproic acid tablets in a suicidal attempt.She had been stabilized on valproic acid be-cause of a seizure disorder. On admission tohospital she was suffering from severe mani-festations already which required aggressiveintensive therapy. Measures for primary andsecondary detoxification were performed, thegirl had to be respirated and was adminis-tered an antidote. Complications arose due tohepatic damage and pneumococcal septi-caemia. Owing to such maximal therapy, thegirl could be transferred to a normal ward in astable general condition after five days of in-tensive medical care, apparently without hav-ing suffered any recognizable long-term dam-age to her health. The BfR lacks informationabout the further course of this case.
Manifestations/courseOn admission to the hospital, the patient wasunresponsive and did not show any reaction
45
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 45

to pain stimulus. Her cardiorespiratory statewas initially stable, however, in the furthercourse, she had to be intubated and respirat-ed due to respiratory insufficiency associatedwith hypercapnia (pCO2 70.5 mm Hg) andacidosis (pH 7.133, bicarbonate 18.2 mmol/l,BE –5,3, lactate 40) (GCS 3). For primarydetoxification, she was administered charcoaland Glauber’s salt as a laxative by means ofa gastric tube. Due to the very high valproatelevel (>1000 mg/L), an initial haemodialysiswas required followed by haemoperfusionover charcoal as measures of secondarydetoxification, of which the latter was repeat-ed on the next day. When dialysis was initiat-ed, problems arose from a hypotonic circula-tory situation which could be controlled bymeans of continuous catecholamine infusion(norepinephrine) over a period of three days.After consultation of a PCC, also carnitinewas administered as an antidote in this se-vere case. The course became complicatedin addition due to pneumococcal septicaemiaand impaired liver function. Findings includedan increase of ammonia to a maximum of300.99 µmol/L and thrombocytopenia of up to31/nl. Another toxic effect seen was CK in-crease up to 1 280 U/L. Cerebral oedemacould be excluded by cranial CT scan. As ex-pected, EEG findings demonstrated severegeneral changes, however, without any signsof elevated predisposition to an attack.
The massive detoxification measures led to arapid improvement of the patient’s condition.Artificial respiration could be discontinuedquickly and subsequently, extubation wasperformed without any problems. She be-came increasingly more awake, was respon-sive again and showed improved sponta-neous motor functions. Valproate levels re-ceded, as did the elevated ammonia levels(on transfer, to 40.8 µmol/L). Only thrombo-cytes remained at a reduced level of 38/nl.
After five days, the patient, who was in a sta-ble general condition, was transferred to anormal ward for onward care.
Notes:Poisoning with medicinal products is not subjectto compulsory notification under § 16e of theChemicals Act or any other legal provision. Ac-cording to an arrangement, reports submittedto the BfR are transmitted to the Federal Institutefor Drugs and Medical Devices (BfArM).
We have reported on this case because theyoung patient’s life could be saved thanks to anadequate and consistent therapy. Attentionshould be drawn to the age of the 13-year-oldpatient because suicidal attempts are rather un-common among such young adolescents.
Valproic acid is an anticonvulsive agent. Thetherapeutic dose stated is 25–40 mg/kg bodyweight. After oral administration, it is readily andcompletely absorbed, however, absorption isdelayed in the case of tablets resistant to gas-tric juice. The maximum plasma level is reachedafter two hours, the half life of 10–17 hours isreduced to 6–9 hours in stabilized patients. Theplasma protein binding is 85–95 %, the sub-stance is metabolized in the liver and renalclearance takes place in a predominantly inac-tive, i.e. 3–10 % unchanged, state. The thera-peutic serum concentration is 50–100 mg/L.There is a poor correlation between the quantityingested and the serum concentration, respec-tively, and clinical manifestations observed.Manifestations at serum concentrations of < 450mg/L, if any, will be only minor to moderate innature. At levels of 450–850 mg/L, severe mani-festations may occur, as a rule, and at levels of> 850 mg/l, severe manifestations are probableto occur. Irrespective of the dose, an irre-versible and frequently lethal hepatic coma mayoccur under prolonged therapy.
Cases of Poisoning Reported by Physicians
46
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 46


type, quantity and mode of absorption, manifes-tations may occur within a few hours in cases ofminor poisoning, or within a few minutes in cas-es of severe poisoning. The cardinal signs con-sist in the classical triad of miosis, hypersaliva-tion and bradycardia. In cases of minor poison-ing they are seen in a milder form. In addition,the clinical picture of poisoning includes visualdisturbances, nausea, headache, vertigo, weak-ness of muscles and tremor. Findings of clinicalchemistry will include a reduced activity ofserum and erythrocyte cholinesterase, which insevere cases is below 10 % of the lower normalvalue or is not measurable. The renewed rise incholinesterase levels may extend over a periodof days or even weeks. Repeat determination ofcholinesterase is a good indicator of the courseof the poisoning and therefore may serve as atherapeutic criterion.
Therapy will be primarily focussed on thepreservation of the vital functions, i.e. resuscita-tion, intubation, respiration and stabilization ofthe circulatory condition. During all these meas-ures, self-protection of the helper is imperative.Atropine should be rapidly administered as anantidote in sufficiently high doses. The most ad-equate criterion for adequate dosage consistsin the normalization of bronchorrhoea and othersecretions such as sweating (dry armpits).Symptom-free patients need not be adminis-tered atropine. Administration of another anti-dote, namely oximes, is not required in cases ofaccidental or minor poisoning. However, in cas-es of severe poisoning, administration of thischolinesterase reactivator should be initiated(after atropine administration), if possible within
the first six hours. However, the efficiency ofobidoxime varies depending on theorganophosphate involved. First aid measuresand administration of antidote are followed bymeasures of primary detoxification. These in-clude excessive gastric lavage in cases of oralingestion, which is performed as long as thecharacteristic odour of the lavage fluid is stillperceptible, and repeated (continuous) admin-istration of charcoal and Glauber’s salt. Howev-er, attention should be paid to possible intestinalatonia or even paralytic ileus caused by a pro-longed administration of atropine. In such cas-es, charcoal administration should not be re-peated but high enemas administered instead.In cases of severe poisoning, atropine is “bio-logically titrated” as a continuous infusion whichis continued until a rise in cholinesterase to >30% of the lower normal value is achieved, andmay be discontinued abruptly at that point. De-pending on the severity of the clinical picture,this stage may last for several days or weeks (inextremely severe cases). Measures of second-ary detoxification are ineffective, they do not im-prove the prognosis.
As in the case described above, a quantity of100 mL may cause severe poisoning which can-not be controlled in spite of administration ofsufficiently high atropine doses.
Evaluation of the case describedBased on the case history data and the charac-teristic manifestations (coma, respiratory insuffi-ciency, bradycardia) and in the absence of oth-er causes, a causal relationship has been con-sidered as possible.
49
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 49
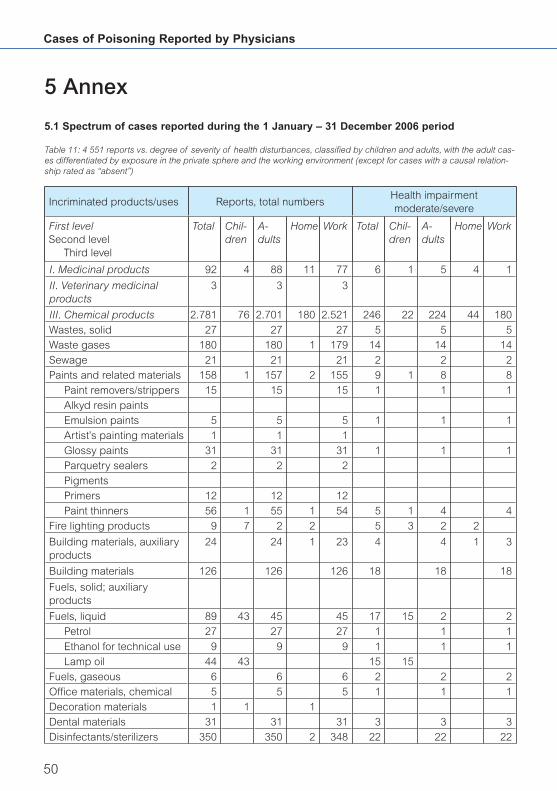
5.1 Spectrum of cases reported during the 1 January – 31 December 2006 period
5 Annex
Table 11: 4 551 reports vs. degree of severity of health disturbances, classified by children and adults, with the adult cas-es differentiated by exposure in the private sphere and the working environment (except for cases with a causal relation-ship rated as “absent”)
Incriminated products/uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
A-dults
Home Work Total Chil-dren
A-dults
Home Work
I. Medicinal products 92 4 88 11 77 6 1 5 4 1
II. Veterinary medicinal products
3 3 3
III. Chemical products 2.781 76 2.701 180 2.521 246 22 224 44 180
Wastes, solid 27 27 27 5 5 5
Waste gases 180 180 1 179 14 14 14
Sewage 21 21 21 2 2 2
Paints and related materials 158 1 157 2 155 9 1 8 8
Paint removers/strippers 15 15 15 1 1 1
Alkyd resin paints
Emulsion paints 5 5 5 1 1 1
Artist’s painting materials 1 1 1
Glossy paints 31 31 31 1 1 1
Parquetry sealers 2 2 2
Pigments
Primers 12 12 12
Paint thinners 56 1 55 1 54 5 1 4 4
Fire lighting products 9 7 2 2 5 3 2 2
Building materials, auxiliary products
24 24 1 23 4 4 1 3
Building materials 126 126 126 18 18 18
Fuels, solid; auxiliary products
Fuels, liquid 89 43 45 45 17 15 2 2
Petrol 27 27 27 1 1 1
Ethanol for technical use 9 9 9 1 1 1
Lamp oil 44 43 15 15
Fuels, gaseous 6 6 6 2 2 2
Offi ce materials, chemical 5 5 5 1 1 1
Decoration materials 1 1 1
Dental materials 31 31 31 3 3 3
Disinfectants/sterilizers 350 350 2 348 22 22 22
Cases of Poisoning Reported by Physicians
50
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 50

51
Incriminated products/uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
A-dults
Home Work Total Chil-dren
A-dults
Home Work
Deodorants for technical use 5 2 3 3
Diagnostic agents/reagents 2 2 2
Printing, auxiliary products 1 1 1
De-icing products 2 2 2 1 1 1
Fire extinguishing media 24 24 24
Flame retardants
Galvanic cells 115 115 115 2 2 2
Dry cells 3 3 3
Button batteries
Accumulators 112 112 112 2 2 2
Galvanizing agents 2 2 2
Galvanizing agents, auxiliary products
3 3 3
Gases for technical use
Antifreezes 4 4 1 3 2 2 1 1
Glass-working, auxiliary products
Rubber, production materials 1 1 1
Semiconductors, production materials
Household auxiliary products, chemical-technical
Hydraulic fl uids 31 31 31 4 4 4
Refrigerants 12 12 12 1 1 1
Ceramics, auxiliary products 1 1 1
Ceramic materials
Glues 82 1 81 1 80 7 7 7
Coolants 26 26 26 4 4 4
Plastics, starting materials 16 16 16 2 2 2
Plastics, formulating materials
4 4 4 1 1 1
Leather processing products
Luminophors 1 1 1
Solvents for technical use 57 57 57 3 3 3
Soldering and welding products (except welding fumes)
13 13 13 1 1 1
Measuring equipment, chemical-technical
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 51

Cases of Poisoning Reported by Physicians
52
Incriminated products/uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
A-dults
Home Work Total Chil-dren
A-dults
Home Work
Heating meters
Mercury thermometers
Thermometer fl uids
Metallurgy, auxiliary products 20 20 20 4 4 4
Dairy, auxiliary products
Paper-making, auxiliary products
Photography, auxiliary products
6 6 6
Radioisotopes, radionuclides 2 2 2
Cleansing products 879 19 858 145 713 91 3 88 38 50
Drain cleanser 14 1 12 12 1 1 1
All-purpose cleansers 52 52 1 51 2 2 1 1
Oven and grill cleansers 23 1 22 22 7 1 6 6
Cleansers for electronic products
Descaling products 29 29 1 28 1 1 1
Front wall and stone cleaners
8 8 8 1 1 1
Stain removers 1 1 1
Floor polishes 4 4 4
Washing-up detergents (manual use)
7 1 6 6
Dishwasher detergents 10 10 10 1 1 1
Dishwasher cleaners 4 4 4
Glass cleaners 97 4 93 89 4 22 1 21 21
Industrial cleansers 44 44 44 3 3 3
Rinse aid for dishwashers 11 2 9 9
Plastic cleansers
Glossy paint cleansers 2 2 2
Milking machine cleaners 42 42 42 4 4 4
Metal cleansers 24 24 24 2 2 2
Furniture polishes 1 1 1 1
Soot removers 1 1 1 1 1 1
Lavatory cleansers 66 66 45 21 14 14 14
Shoe and leather cleansers
21 3 17 17 5 5 5
Carpet/upholstery cleansers
1 1 1
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 52

53
Incriminated products/uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
A-dults
Home Work Total Chil-dren
A-dults
Home Work
Detergents 14 14 1 13 1 1 1
Detergents, auxiliary products
4 1 3 3
Joke articles
Lubricants 25 25 25 2 2 2
Welding fumes 35 35 1 34
Dust-laying oils
Toys 1 1 1
Textile, auxiliary products 3 1 2 3
Propellants/sprays 2 2 2
Water treatment products 3 3 3
Pet shop products
IV. Cosmetics/personal hygiene products
33 1 32 2 30 2 1 1 1
Hair care products 10 10 10
Permanent wave products 3 3 3
Depilatory products
Hair dyes/colorants 5 5 5
Hair conditioners
Hair tonics
Shampoos 2 2 2
Skin care products 16 1 15 15 1 1
Bath oils/salts 2 2 2
Tanning products
Creams/ointments 2 2 2
Deodorants 2 1 1 1 1 1
Face tonics
Make-up products 1 1 1
Oils
Perfumes/after shaves 2 2 2
Powders
Soaps 5 5 5
Sun blockers
Oral care/dental products 4 4 2 2 1 1 1
Nail care products 2 2 2
V. Pesticides 107 2 105 6 99 4 4 1 3
Acaricides
Fungicides 5 5 1 4
Herbicides 20 20 1 19
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 53

Cases of Poisoning Reported by Physicians
54
Incriminated products/uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
A-dults
Home Work Total Chil-dren
A-dults
Home Work
Wood preservatives 6 6 6
Insecticides 30 30 4 26 2 2 1 1
Carbamates
Chlorinated hydrocarbons 1 1 1
Phosphoric esters 11 11 1 10 1 1 1
Pyrethroids 4 4 2 2
Molluscicides
Repellents 1 1 1
Rodenticides 4 2 2 2
Anticoagulants
Phosphates 2 2 2
Seed dressings 1 1 1
VI. Agrochemicals other than pesticides
16 16 16 1 1 1
Fertilizers 6 6 6
Plant care products 1 1 1
Growth regulators
VII. Substances of abuse Narcotic drugs
1 1 1 1 1 1
VIII. Plants 4 4 3 1 1 1 1
IX. FungiX. Animals 1 1 1
XI. Foods and beverages 52 4 48 25 23 11 11 9 2
Alcoholic beverages 7 7 4 3 2 2 2
Food additives 4 4 1 3 1 1 1
Tobacco and tobacco products
Food supplements 10 10 9 1 4 4 4
XII. Warfare/anti-riot agents 3 3 3
Pyrotechnic products
Tear gas
XIII. Miscellaneous 109 1 108 5 103 13 13 2 11
Textiles 6 6 1 5
Clothing 5 5 1 4
Furnishing fabrics
XIV. Primary substances 1.371 5 1.366 8 1.358 119 2 117 5 112
XV. Industrial accidents
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 54
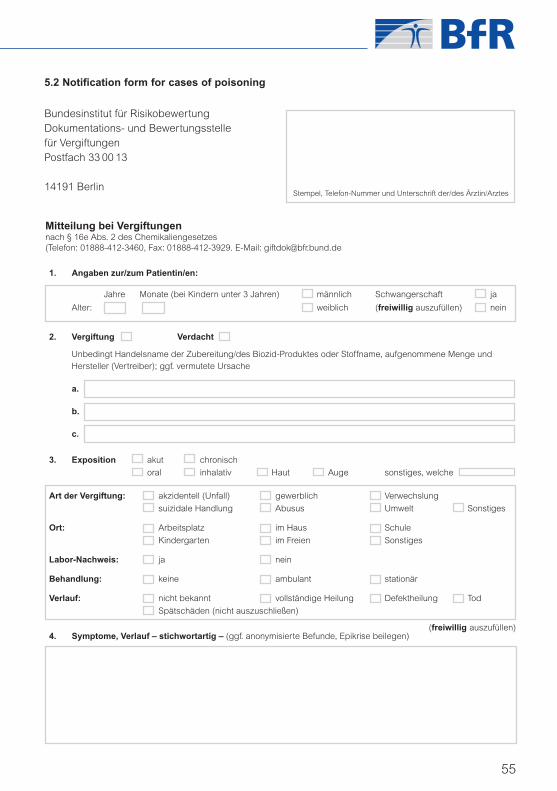
55
Bundesinstitut für RisikobewertungDokumentations- und Bewertungsstellefür VergiftungenPostfach 33 00 13
14191 BerlinStempel, Telefon-Nummer und Unterschrift der/des Ärztin/Arztes
Mitteilung bei Vergiftungennach § 16e Abs. 2 des Chemikaliengesetzes(Telefon: 01888-412-3460, Fax: 01888-412-3929. E-Mail: [email protected]
1. Angaben zur/zum Patientin/en:
Jahre Monate (bei Kindern unter 3 Jahren) männlich Schwangerschaft ja
Alter: weiblich (freiwillig auszufüllen) nein
2. Vergiftung Verdacht
Unbedingt Handelsname der Zubereitung/des Biozid-Produktes oder Stoffname, aufgenommene Menge und Hersteller (Vertreiber); ggf. vermutete Ursache
a.
b.
c.
3. Exposition akut chronisch
oral inhalativ Haut Auge sonstiges, welche
Art der Vergiftung: akzidentell (Unfall) gewerblich Verwechslung
suizidale Handlung Abusus Umwelt Sonstiges
Ort: Arbeitsplatz im Haus Schule
Kindergarten im Freien Sonstiges
Labor-Nachweis: ja nein
Behandlung: keine ambulant stationär
Verlauf: nicht bekannt vollständige Heilung Defektheilung Tod
Spätschäden (nicht auszuschließen)
4. Symptome, Verlauf – stichwortartig – (ggf. anonymisierte Befunde, Epikrise beilegen)(freiwillig auszufüllen)
5.2 Notification form for cases of poisoning
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 55

Cases of Poisoning Reported by Physicians
56
Pers. Nummer
weiblich männliich Erwachsene(r) Kind
Bereich I
Unmittelbar Betroffene(r)
(Bitte Eintrag in die Landkarte)
Direkt am Unfallort Arbeiter(in)
Nahe Unfallort Feuerwehr
m Polizei/Rettungsdienst
Privatperson
Sonstige(r)
Erstexposition Uhrzeit Datum
Dauer ständig nicht ständigStunden/Tage
Schutzmaßnahmen ja nein
Symptome ja nein
(Wenn ja, bitte Dokumentation auf dem Meldebogen)
Bereich II
Nicht unmittelbar Betroffene(r)
(Bitte Eintrag in die Landkarte)
Entfernung vom Unfallort Anwohner
m Beschäftigte(r)/Arbeitnehmer(in)
km Sonstige(r)
Erstexposition Uhrzeit Datum
Dauer ständig nicht ständigStunden/Tage
Schutzmaßnahmen ja nein
Symptome ja nein
(Wenn ja, bitte Dokumentation auf dem Meldebogen)
Biomonitoring Stoff:
Blutentnahme Datum Zeitpunkt Konzentration
Urinprobe Datum Zeitpunkt Konzentration
Spontanurin 24h Sammelurin Kreatinin
5.3 Notification form for industrial accidents
BfR-Fragebogen zur Expositionsermittlung bei Stör- und Transportunfällen
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 56

57
List of Poison Control Centres in Germany
Berlin BBGes – Giftnotruf Berlin Oranienburger 13437 Phone: +49-30-19240
Institut für Toxikologie Str. 285 Berlin Fax: +49-30-30 68 6721
Klinische Toxikologie und Germany [email protected]
Giftnotruf Berlin www.giftnotruf.de
Bonn Informationszentrale gegen Adenauerallee 53113 Phone: +49-2 28-19240
Vergiftungen 119 Bonn Fax: +49-2 28-2 873314
Zentrum für Kinderheilkunde Germany [email protected]
Universitätsklinikum Bonn www.meb.uni-bonn.de/
giftzentrale
Erfurt Gemeinsames Nordhäuser Str. 99089 Phone: +49-3 61-73 0730
Giftinformationszentrum der Länder 74 Erfurt Fax: +49-3 61-7307317
Mecklenburg-Vorpommern, Germany [email protected]
Sachsen, Sachsen-Anhalt und www.ggiz-erfurt.de
Thüringen
Freiburg Zentrum für Kinderheilkunde und Mathildenstr. 1 79106 Phone: +49-761-19240
Jugendmedizin Freiburg Fax: +49-761-270 44 57
Vergiftungs-Informations-Zentrale Germany [email protected]
www.giftberatung.de
Göttingen Giftinformationszentrum-Nord der Robert Koch-Str. 37075 Phone: +49-5 51-38 3180
Länder Bremen, Hamburg, Nieder- 40 Göttingen Fax: +49-5 51-3 8318 81
sachsen und Schleswig-Holstein Germany [email protected]
(GIZ-Nord) Universität Göttingen – www.giz-nord.de
Bereich Humanmedizin
Homburg Informations- und Behandlungs- 66421 Phone: +49-68 41-192 40
zentrum für Vergiftungen des Homburg/ +49-68 41-162 8314
Saarlandes Saar Fax: +49-68 41-162 84 38
Klinik für Kinder- und Germany [email protected]
Jugendmedizin www.uniklinikum-saarland.de/de/
einrichtungen/andere/giftzentrale
Mainz Klinische Toxikologie und Langenbeckstr. 55131 Phone: +49-6131-192 40
Beratungsstelle bei Vergiftungen der 1 Mainz +49-6131-23 24 66
Länder Rheinland-Pfalz und Hessen Germany Fax: +49-6131-23 24 69
Universitätsklinikum +49-6131-23 24 68
www.giftinfo.uni-mainz.de
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 57
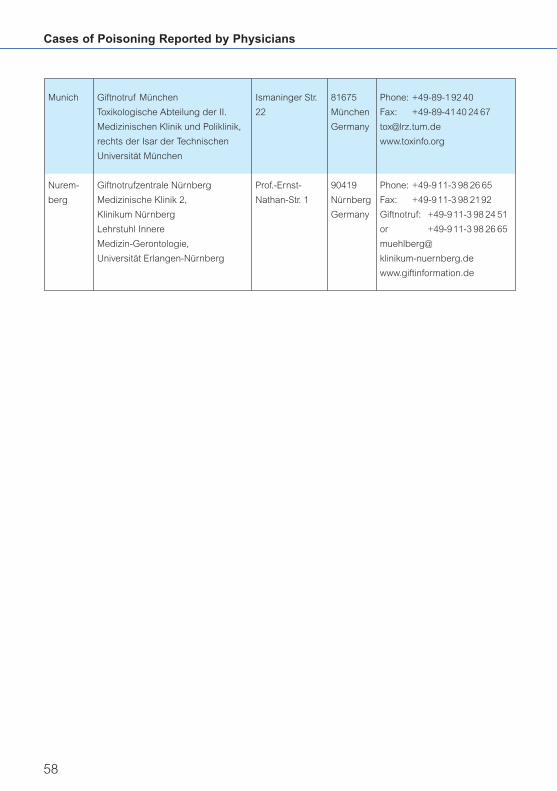
Cases of Poisoning Reported by Physicians
58
Munich Giftnotruf München Ismaninger Str. 81675 Phone: +49-89-192 40
Toxikologische Abteilung der II. 22 München Fax: +49-89-4140 24 67
Medizinischen Klinik und Poliklinik, Germany [email protected]
rechts der Isar der Technischen www.toxinfo.org
Universität München
Nurem- Giftnotrufzentrale Nürnberg Prof.-Ernst- 90419 Phone: +49-911-3 98 26 65
berg Medizinische Klinik 2, Nathan-Str. 1 Nürnberg Fax: +49-911-3 98 2192
Klinikum Nürnberg Germany Giftnotruf: +49-911-3 98 24 51
Lehrstuhl Innere or +49-911-3 98 26 65
Medizin-Gerontologie, muehlberg@
Universität Erlangen-Nürnberg klinikum-nuernberg.de
www.giftinformation.de
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 58

5.4 Press releases on toxicological problemsissued by the BfR in 2006
From welding fumes to sewage gas – Hidden risks for consumersNew brochure gives overview of poisoning cases in 200402/2006, 2006-01-12
Elevated morphine levels in poppy seeds:Risk to health not ruled outBfR recommends a guidance value and a dailyupper intake level05/2006, 2006-02-20
Exercise caution when using “nano-sealingsprays” containing a propellant!When used in confined spaces, they can causerespiratory problems08/2006, 2006-03-31
Nanotechnology – Applications, Trends andRisksBfR gathers up-to-date information on nano particles in consumer-related application areas09/2006, 2006-04-06
Cause of intoxications with nano spray not yetfully elucidatedScientific discussions at BfR did not produceany clear results10/2006, 2006-04-12
Nano particles were not the cause of healthproblems triggered by sealing sprays!Products did not contain any ultrafine particles 12/2006, 2006-05-26
Carcinogenic effect of inhaled formaldehydesufficiently documentedBfR presents results of scientific assessmentand recommends new classification14/2006, 2006-05-29
Health effects should be systematically recorded for industrial and transport accidentsinvolving chemicals!Standardised notification forms can now bedownloaded from the Internet19/2006, 2006-07-07
BfArM and BfR warn: Exercise caution whenbuying muscle-building productsJoint press release by BfArM and BfR24/2006, 2006-08-28
Indications that styrene has a tumorigenic effect in humansResults of experimental research at BfR are ofimportance for the reassessment of this existingsubstance25/2006, 2006-08-31
REACH: An opportunity for more consumer protectionThe success of the new European chemicalslegislation will depend on its practical implementation32/2006, 2006-12-18
59
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 59

Cases of Poisoning Reported by Physicians
60
List of abbreviations (German notation)
Used in the brochure
Meaning Common use
µmol/l Masse pro Volumen in Mikromol pro Liter µmol / l
136/min Herzfrequenz HF 136 / min
170/107 mmHg Blutdruck (Einheit: Millimeter Quecksilbersäule) RR 170 / 107 mm Hg
31/nl Menge pro Volumen 31 / nl
ALAT Alaninaminotransferase ALT
ALT Alaninaminotransferase ALT
ARDS Adult Respiratory Distress Syndrome (Atemnotsyndrom)
ARDS
ASAT Aspartataminotransferase AST
AST Aspartataminotransferase AST
ATP Adenonsintriphosphat ATP
BE Base-Excess (Basenüberschuss) BE
BfR Bundesinstitut für Risikobewertung BfR
BG Berufsgenossenschaften BG
BgVV Bundesinstitut für gesundheitlichen Verbraucher -schutz und Veterinärmedizin
BgVV
BMELV Bundesministerium für Ernährung, Landwirtschaft und Verbraucherschutz
BMELV
BMU Bundesministerium für Umwelt Naturschutz und Reaktorsicherheit
BMU
BVL Bundesamt für Verbraucherschutz und Lebensmittel BVL
ChemG Chemikaliengesetz ChemG
CK Creatinkinase CK
CK-MB Creatinkinase, Herzmuskeltyp CK-MB
CPK Creatinkinase CK
C-reaktives Protein Capsel-reaktives Protein CRP
CT Computertomographie CT
d Tag d
DNP Dinitrophenol DNP
EEG Elektroenzephalogramm EEG
EFSA European Food Safety Authority EFSA
EG Europäische Gemeinschaft EG
ESPED Erfassungsstelle für seltene Pädiatrische Erkrankungen
ESPED
EU Europäische Union EU
FEV1 Einsekundenkapazität FEV1
GCS Glasgow Coma Scale GCS
GIZ Giftinformationszentrum GIZ
GOT Glutamat-Oxalacetat-Transaminase GOTGPT Glutamat-Pyruvat-Transaminase GPT
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 60
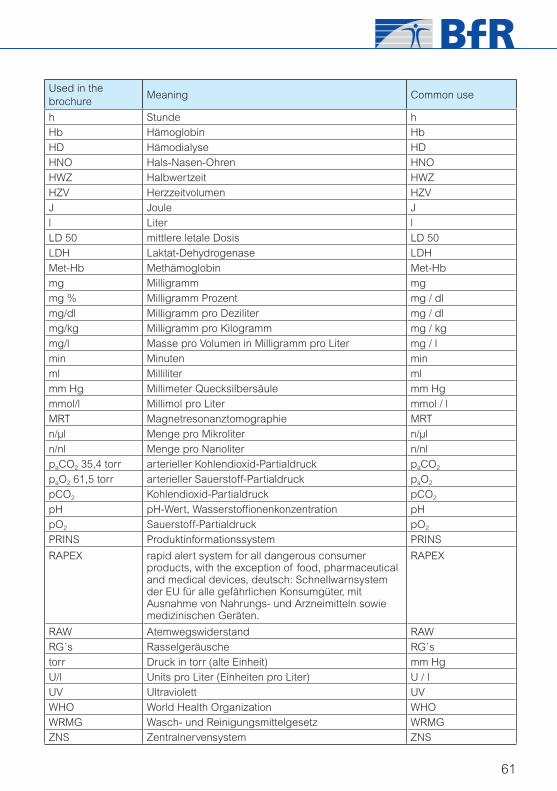
61
Used in the brochure
Meaning Common use
h Stunde hHb Hämoglobin Hb
HD Hämodialyse HD
HNO Hals-Nasen-Ohren HNO
HWZ Halbwertzeit HWZ
HZV Herzzeitvolumen HZV
J Joule J
l Liter l
LD 50 mittlere letale Dosis LD 50
LDH Laktat-Dehydrogenase LDH
Met-Hb Methämoglobin Met-Hb
mg Milligramm mg
mg % Milligramm Prozent mg / dl
mg/dl Milligramm pro Deziliter mg / dl
mg/kg Milligramm pro Kilogramm mg / kg
mg/l Masse pro Volumen in Milligramm pro Liter mg / l
min Minuten min
ml Milliliter ml
mm Hg Millimeter Quecksilbersäule mm Hg
mmol/l Millimol pro Liter mmol / l
MRT Magnetresonanztomographie MRT
n/µl Menge pro Mikroliter n/µl
n/nl Menge pro Nanoliter n/nl
paCO2 35,4 torr arterieller Kohlendioxid-Partialdruck paCO2
paO2 61,5 torr arterieller Sauerstoff-Partialdruck paO2
pCO2 Kohlendioxid-Partialdruck pCO2
pH pH-Wert, Wasserstoffi onenkonzentration pH
pO2 Sauerstoff-Partialdruck pO2
PRINS Produktinformationssystem PRINS
RAPEX rapid alert system for all dangerous consumer products, with the exception of food, pharmaceutical and medical devices, deutsch: Schnellwarnsystem der EU für alle gefährlichen Konsumgüter, mit Ausnahme von Nahrungs- und Arzneimitteln sowie medizinischen Geräten.
RAPEX
RAW Atemwegswiderstand RAW
RG´s Rasselgeräusche RG´s
torr Druck in torr (alte Einheit) mm Hg
U/l Units pro Liter (Einheiten pro Liter) U / l
UV Ultraviolett UV
WHO World Health Organization WHO
WRMG Wasch- und Reinigungsmittelgesetz WRMGZNS Zentralnervensystem ZNS
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite 61

Phone +49-30 - 84 12 -0Fax +49-30 - 84 12 [email protected]
Federal Institute for Risk AssessmentThielallee 88-92D-14195 Berlinwww.bfr.bund.de
aerztl_mitteilungen_06_engl 14.09.2007 14:37 Uhr Seite u4















![[Paraphenylenediamine poisoning in Morocco: report of 24 cases]](https://img.dokumen.tips/doc/110x75/634d082a7b55c75a3406d9f9/paraphenylenediamine-poisoning-in-morocco-report-of-24-cases.jpg)













